Planning and strategy use in health behavior change: a life span view
12
Planning and Strategy Use in Health Behavior Change: A Life Span View Jochen P. Ziegelmann and Sonia Lippke Exercise-related strategy use and planning were investigated in younger (18–49 years) and older individuals (50–80 years) in orthopedic rehabilitation who were supposed to adhere to a strict exercise regimen. As part of a longitudinal study, N = 368 individuals completed questionnaires assessing the amount of physical activities performed pre-rehabilitation and 6 and 12 months after discharge. In addition, the ex- tent of strategy use (selection, optimization, and compensation) and planning after discharge was assessed. Planning was subdivided into two constructs: action plan- ning (planning when, where, and how to exercise) and coping planning (planning how to exercise in the face of barriers). Two-sample structural equation modeling was used. For both age groups, strategy use improved prediction of exercise goal attain- ment on top of planning, while strategy use mediated the relationship between coping planning and goal attainment. Interventions fostering strategy use as well as plan- ning might enhance exercise adherence across age groups. Key words: planning, implementation intentions, selection, optimization, and com- pensation (SOC), aging, interventions, relapse management Despite recent advances in research on health self- regulation such as the differentiation of self-efficacy (e.g., Schwarzer & Renner, 2000), and more elaborated planning concepts (Gollwitzer, 1996), Leventhal and Mora (2005) argue that there should be a greater em- phasis on the ongoing processes of self-regulation. We take the perspective that strategy use (Freund & Baltes, 2002) should provide us with insights as to how plans are being translated into behavior. Taking a life- span-view, we aim to investigate the interplay of plan- ning and strategy use in a sample of younger and older individuals undergoing orthopedic rehabilitation, who were recommended to adopt and maintain regular physical activity. Predicting Health Behavior Change Changing health behaviors such as regular physical exercise involves an initial motivation process that re- sults in intention formation, and subsequent self- regulation processes that address the pursuit of these goals. According to the Health Action Process Ap- proach (HAPA; Schwarzer, 1992; see Figure 1), in the motivation phase (where a person develops an inten- tion to act), risk perception sets the stage for further elaboration of thoughts about consequences (i.e., out- come expectancies) and competencies (i.e., self- efficacy). After intention formation, people enter the volition phase in which they pursue their goal by plan- ning, trying to act, investing effort, possibly failing, and finally recovering or disengaging. Within a self-regulatory cycle, self-efficacy can be subdivided in a phase-specific way (Luszczynska, & Sutton, 2006; Schwarzer & Renner, 2000). Task self-efficacy is the perceived capability of a person to implement a behav- ior. It facilitates goal setting and, thus, makes a differ- ence in the motivational phase whereas recovery self-efficacy describes optimistic beliefs in the volition phase to get back on track after being derailed (Scholz, Sniehotta, & Schwarzer, 2005). Schwarzer and Renner (2000) argue that, in the volition phase, self-efficacious individuals develop more strategies, effort, and persis- tence to overcome such barriers. In addition to self-efficacy, planning plays a major role in the volition phase. Concepts such as action planning (i.e., plans on “when”, “where”, and “how” to perform a behavior) and coping planning (i.e., plans how to pursue a behavior in the face of obstacles) can bridge the gap between intentions and behavior (Gollwitzer, 1996; Lippke, Ziegelmann, & Schwarzer, 2004; Sniehotta, Schwarzer, Scholz, & Schüz, 2005; Ziegelmann, Luszcynska, Lippke, & Schwarzer, 2007). While differentiating efficacy and goal concepts into more specific efficacy and goal units provides a more detailed view, Leventhal and Mora (2005) argue that International Journal of Behavioral Medicine 2007, Vol. 14, No. 1, 30–39 Copyright © 2007 by Lawrence Erlbaum Associates, Inc. 30 Jochen P. Ziegelmann and Sonia Lippke, Freie Universität Berlin. Correspondence concerning this article should be addressed to Dr. Jochen P. Ziegelmann, Health Psychology (PF 10), Freie Universitaet Berlin, Habelschwerdter Allee 45, 14195 Berlin, Ger- many. E-Mail: [email protected]
-
Upload
jacobs-university -
Category
Documents
-
view
0 -
download
0
Transcript of Planning and strategy use in health behavior change: a life span view

Planning and Strategy Use in Health Behavior Change:A Life Span View
Jochen P. Ziegelmann and Sonia Lippke
Exercise-related strategy use and planning were investigated in younger (18–49years) and older individuals (50–80 years) in orthopedic rehabilitation who weresupposed to adhere to a strict exercise regimen. As part of a longitudinal study, N =368 individuals completed questionnaires assessing the amount of physical activitiesperformed pre-rehabilitation and 6 and 12 months after discharge. In addition, the ex-tent of strategy use (selection, optimization, and compensation) and planning afterdischarge was assessed. Planning was subdivided into two constructs: action plan-ning (planning when, where, and how to exercise) and coping planning (planninghow to exercise in the face of barriers). Two-sample structural equation modeling wasused. For both age groups, strategy use improved prediction of exercise goal attain-ment on top of planning, while strategy use mediated the relationship between copingplanning and goal attainment. Interventions fostering strategy use as well as plan-ning might enhance exercise adherence across age groups.
Key words: planning, implementation intentions, selection, optimization, and com-pensation (SOC), aging, interventions, relapse management
Despite recent advances in research on health self-regulation such as the differentiation of self-efficacy(e.g., Schwarzer & Renner, 2000), and more elaboratedplanning concepts (Gollwitzer, 1996), Leventhal andMora (2005) argue that there should be a greater em-phasis on the ongoing processes of self-regulation. Wetake the perspective that strategy use (Freund & Baltes,2002) should provide us with insights as to how plansare being translated into behavior. Taking a life-span-view, we aim to investigate the interplay of plan-ning and strategy use in a sample of younger and olderindividuals undergoing orthopedic rehabilitation, whowere recommended to adopt and maintain regularphysical activity.
Predicting Health Behavior Change
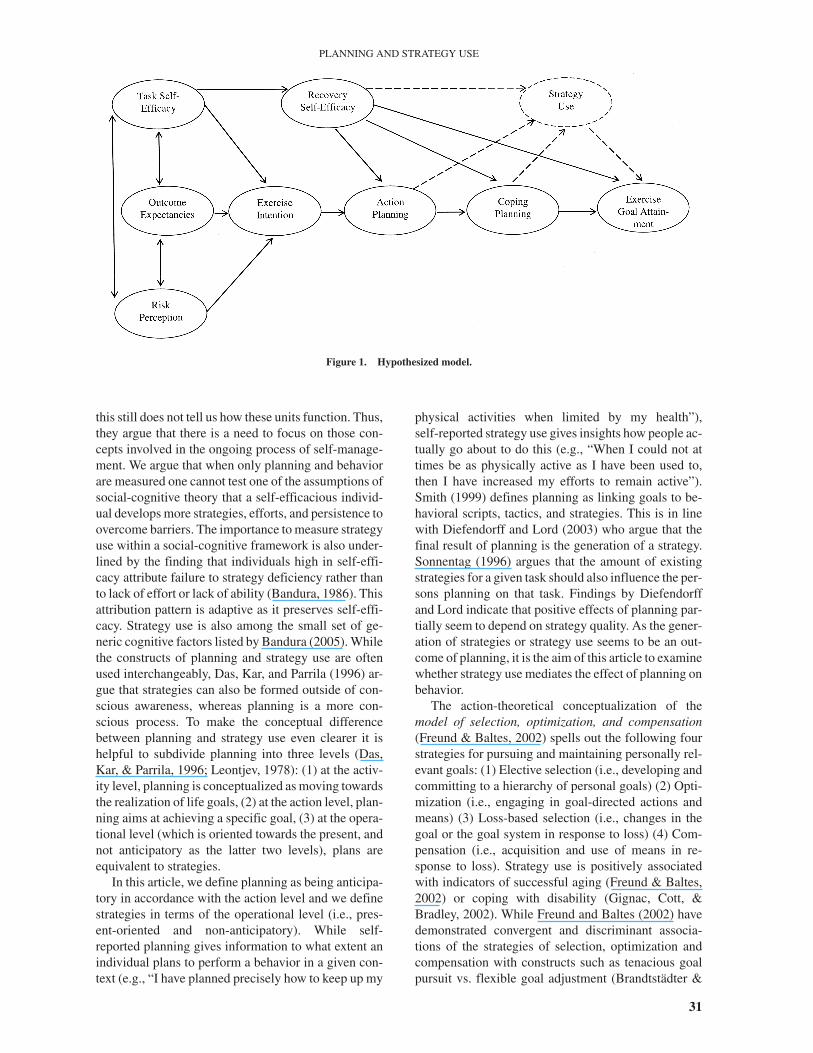
Changing health behaviors such as regular physicalexercise involves an initial motivation process that re-sults in intention formation, and subsequent self-regulation processes that address the pursuit of thesegoals. According to the Health Action Process Ap-proach (HAPA; Schwarzer, 1992; see Figure 1), in themotivation phase (where a person develops an inten-
tion to act), risk perception sets the stage for furtherelaboration of thoughts about consequences (i.e., out-come expectancies) and competencies (i.e., self-efficacy). After intention formation, people enter thevolition phase in which they pursue their goal by plan-ning, trying to act, investing effort, possibly failing,and finally recovering or disengaging. Within aself-regulatory cycle, self-efficacy can be subdividedin a phase-specific way (Luszczynska, & Sutton, 2006;Schwarzer & Renner, 2000). Task self-efficacy is theperceived capability of a person to implement a behav-ior. It facilitates goal setting and, thus, makes a differ-ence in the motivational phase whereas recoveryself-efficacy describes optimistic beliefs in the volitionphase to get back on track after being derailed (Scholz,Sniehotta, & Schwarzer, 2005). Schwarzer and Renner(2000) argue that, in the volition phase, self-efficaciousindividuals develop more strategies, effort, and persis-tence to overcome such barriers.
In addition to self-efficacy, planning plays a majorrole in the volition phase. Concepts such as actionplanning (i.e., plans on “when”, “where”, and “how” toperform a behavior) and coping planning (i.e., planshow to pursue a behavior in the face of obstacles) canbridge the gap between intentions and behavior(Gollwitzer, 1996; Lippke, Ziegelmann, & Schwarzer,2004; Sniehotta, Schwarzer, Scholz, & Schüz, 2005;Ziegelmann, Luszcynska, Lippke, & Schwarzer, 2007).While differentiating efficacy and goal concepts intomore specific efficacy and goal units provides a moredetailed view, Leventhal and Mora (2005) argue that
International Journal of Behavioral Medicine2007, Vol. 14, No. 1, 30–39
Copyright © 2007 byLawrence Erlbaum Associates, Inc.
30
Jochen P. Ziegelmann and Sonia Lippke, Freie UniversitätBerlin.
Correspondence concerning this article should be addressed toDr. Jochen P. Ziegelmann, Health Psychology (PF 10), FreieUniversitaet Berlin, Habelschwerdter Allee 45, 14195 Berlin, Ger-many. E-Mail: [email protected]
this still does not tell us how these units function. Thus,they argue that there is a need to focus on those con-cepts involved in the ongoing process of self-manage-ment. We argue that when only planning and behaviorare measured one cannot test one of the assumptions ofsocial-cognitive theory that a self-efficacious individ-ual develops more strategies, efforts, and persistence toovercome barriers. The importance to measure strategyuse within a social-cognitive framework is also under-lined by the finding that individuals high in self-effi-cacy attribute failure to strategy deficiency rather thanto lack of effort or lack of ability (Bandura, 1986). Thisattribution pattern is adaptive as it preserves self-effi-cacy. Strategy use is also among the small set of ge-neric cognitive factors listed by Bandura (2005). Whilethe constructs of planning and strategy use are oftenused interchangeably, Das, Kar, and Parrila (1996) ar-gue that strategies can also be formed outside of con-scious awareness, whereas planning is a more con-scious process. To make the conceptual differencebetween planning and strategy use even clearer it ishelpful to subdivide planning into three levels (Das,Kar, & Parrila, 1996; Leontjev, 1978): (1) at the activ-ity level, planning is conceptualized as moving towardsthe realization of life goals, (2) at the action level, plan-ning aims at achieving a specific goal, (3) at the opera-tional level (which is oriented towards the present, andnot anticipatory as the latter two levels), plans areequivalent to strategies.
In this article, we define planning as being anticipa-tory in accordance with the action level and we definestrategies in terms of the operational level (i.e., pres-ent-oriented and non-anticipatory). While self-reported planning gives information to what extent anindividual plans to perform a behavior in a given con-text (e.g., “I have planned precisely how to keep up my
physical activities when limited by my health”),self-reported strategy use gives insights how people ac-tually go about to do this (e.g., “When I could not attimes be as physically active as I have been used to,then I have increased my efforts to remain active”).Smith (1999) defines planning as linking goals to be-havioral scripts, tactics, and strategies. This is in linewith Diefendorff and Lord (2003) who argue that thefinal result of planning is the generation of a strategy.Sonnentag (1996) argues that the amount of existingstrategies for a given task should also influence the per-sons planning on that task. Findings by Diefendorffand Lord indicate that positive effects of planning par-tially seem to depend on strategy quality. As the gener-ation of strategies or strategy use seems to be an out-come of planning, it is the aim of this article to examinewhether strategy use mediates the effect of planning onbehavior.
The action-theoretical conceptualization of themodel of selection, optimization, and compensation(Freund & Baltes, 2002) spells out the following fourstrategies for pursuing and maintaining personally rel-evant goals: (1) Elective selection (i.e., developing andcommitting to a hierarchy of personal goals) (2) Opti-mization (i.e., engaging in goal-directed actions andmeans) (3) Loss-based selection (i.e., changes in thegoal or the goal system in response to loss) (4) Com-pensation (i.e., acquisition and use of means in re-sponse to loss). Strategy use is positively associatedwith indicators of successful aging (Freund & Baltes,2002) or coping with disability (Gignac, Cott, &Bradley, 2002). While Freund and Baltes (2002) havedemonstrated convergent and discriminant associa-tions of the strategies of selection, optimization andcompensation with constructs such as tenacious goalpursuit vs. flexible goal adjustment (Brandtstädter &
31
PLANNING AND STRATEGY USE
Figure 1. Hypothesized model.

Renner, 1990) and action vs. state orientation (Kuhl &Goschke, 1994), the relationship between those strate-gies and planning has not yet been examined empiri-cally. According to action-control theory (Kuhl &Goschke, 1994) it is assumed to be adaptive toself-monitor one’s behavior, and to execute regulativemeans when there is a discrepancy between one’s be-havior and one’s standards, which is in line with find-ings from Sniehotta, Scholz, and Schwarzer (2005)who have demonstrated that self-reported action con-trol is a mediator between action planning and behav-ior in the domain of physical exercise. While the strate-gies of selection, optimization and compensationinclude facets from action control (e.g., executing reg-ulative means when discrepancies occur between theaction standard and the behavior), the strategy ap-proach by Freund and Baltes (2002) has the advantagethat it describes how the actor can select and pursuegoals in accordance with changing (rather than stable)personal, biological or social contexts. Thus, the strat-egy approach is contextualized, which “refers to theknowledge about and mastery of the triangulation ofcontext, goals and means” (Freund & Baltes, 2002,p. 643).
Age Differences in the TheoreticalConstructs
There seems to be an age-related decrease in exer-cise self-efficacy and exercise-related outcome expec-tancies (Netz & Raviv, 2004) as well as in exerciseintentions (Booth, Macaskill, Owen, & Oldenburg,1993). In addition, impaired physical health statuscan negatively influence older adults’ exercise self-efficacy (e.g., Clark, 1999). In this line, Renner, Knoll,and Schwarzer (2000) argue that on the one handage-related poorer health might be associated with re-ductions in self-efficacy of performing a specifichealth behavior, whereas aging might be related tomore expertise in initiating and maintaining behaviorchange despite various obstacles. Schwarzer andRenner (2000) have shown that age and body weightmay be moderators in the adoption of healthy nutritionand argue that self-efficacy in the motivation phase be-comes more important when the task is personally rele-vant and intricate. In everyday problem-solving situa-tions that are of ecological relevance for them, olderadults, display higher self-efficacy expectations thanyounger ones (Artistico, Cervone, & Pezzuti, 2003).
Regarding risk perception, Weinstein (1987) hasshown that unrealistic optimism regarding one’s ownvulnerability to disease decreases with illness experi-ence. Thus, there might be an age-related increase inrisk-perception as illnesses become more common inolder age groups. In a study concerning optimis-tic health beliefs and nutrition Renner, Knoll and
Schwarzer (2000) demonstrated that an optimistic biasregarding health-related vulnerability exists through-out life. Prohaska, Leventhal, Leventhal, and Keller(1985) have shown that older adults feel more vulnera-ble to disease as compared to younger adults. Anotherfinding of this study was that, while older adults re-ported higher levels of health promoting activities suchas healthy nutrition or regularly attending medicalcheckups, they were less likely to exercise on a regularbasis. Thus, which age-related pattern emerges, seemsto depend on the particular health behavior understudy.
In generic (i.e., not domain-specific) measures ofstrategy use and planning seems to be an age-relateddecrease: Freund and Baltes (2002) argue that early inlife, individuals acquire and refine knowledge and useof strategies whereas age-related decline in resourcesmight limit the expression of strategies. They havefound, accordingly, that the strategies of loss-based se-lection, optimization and compensation increase fromyoung to middle adulthood and decrease in late adult-hood. Only for elective selection there was also an in-crease in late adulthood. Regarding self-reported plan-ning, Prenda and Lachman (2001) have found anage-related decrease. However, it remains to be seenwhether this age trend can also be replicated inhealth-related planning and strategy use. In addition tothe reported age differences in the levels of predictors,there might also be age-specific prediction patterns(Schwarzer & Renner, 2000).
Research Questions
This study investigates the interplay of planningand strategy use in younger versus older adults under-going orthopedic rehabilitation who were supposed toadhere to a strict exercise regimen. First, the invariantmeasurement and factorial structure of the psycho-metric instruments will be tested. Items comprising aparticular instrument should operate equivalentlyacross the two age groups, and factor loadings andcovariances should be invariant. Second, to investi-gate whether strategy use contributes to the explana-tory power and to examine whether it mediates the re-lationship between coping planning and exercise, wefirst examine a model without strategy use (see Fig-ure 1, solid lines only) and then a model includingstrategy use (see Figure 1, including dashed lines). Inaddition, we examine whether age-group membershipmoderates the interplay between social-cognitivevariables, planning, strategy use and behavior. Re-garding group differences in latent means, we investi-gate whether the general age-related decrease in plan-ning and strategy use can be replicated in the exercisedomain.
32
ZIEGELMANN AND LIPPKE

Method
Participants and Procedure
After providing informed consent, N = 637 personswere assessed at the beginning (Time 1) and the end(Time 2) of a three-week outpatient orthopedic rehabil-itation. There were two postal follow-up assessmentsat six months (Time 3, n = 495, 77.9%) and twelvemonths (Time 4, n = 371, 58.4%) after discharge. Thefinal longitudinal sample on which the analyses arebased consists of n = 368 participants who provideddata for all four measurement points in time. No signif-icant differences on baseline social-cognitive variableswere revealed when comparing participants who werelost at follow-up with those completing all assess-ments. Individuals were admitted to rehabilitation dueto musculoskeletal conditions such as joint diseases,disc disorders and injuries. At the conclusion of theirrehabilitation, all individuals were recommended toengage in regular physical exercise after discharge.
The sample had a mean age of 47.4 years (range18–80), consisted primarily of women (62.0%), 72.8%were living with a partner, and 70.9% were employed.In all subsequent analyses, the sample was subdividedinto two age groups: 18–49 years (Younger Adults; n =199) and 50–80 years (Older Adults; n = 169). TheOlder Adults reported a significantly higher number ofdiagnoses and risk factors than the Younger Adults. Incomparison to the Younger Adults, Older Adults wereless likely to be female and to be employed, and morelikely to have a partner (see Table 1).
Measures
Unless otherwise noted the following items weretaken from Fuchs (1996) and adapted to the rehabilita-tion context. Risk perception (Time 1; Cronbach’s α =.85) was measured by three items such as: “Comparedto other persons of your age and sex, how do you esti-
mate the likelihood that you will ever suffer fromchronic pain?” Task self-efficacy (Time 1; Cronbach’sα = .61) was composed of three items such as: “I amable to exercise at least twice per week for at leasttwenty minutes.” whereas recovery self-efficacy (Time2; Cronbach’s α = .92) was measured with six itemssuch as “I am confident that I can resume engaging inphysical activity, even when I feel weak after an ill-ness.” Positive outcome expectancies (Time 1;Cronbach’s α = .73) included six items such as “If Iwould engage in physical exercise on two or moredays, for at least 20 minutes, then I would be doingsomething good for my health” Exercise intentionswere assessed at Time 1 (Cronbach’s α = .63) with fiveitems such as “I intend to exercise for 20 minutes orlonger on at least two days per week on a regular ba-sis.” Action plans were measured at Time 3(Cronbach’s α = .94) with five items such as: “In thelast six months, I have planned precisely when I willperform my physical activities.” Coping planning wasmeasured at Time 4 (Cronbach’s α = .92) with fouritems such as: “In the last six months, I have plannedprecisely how to keep up my physical activities when Iam limited by my health condition.” All answers werescored on a four-point scale from not at all true (1), nottrue (2), a little true (3), to exactly true (4). A 12-itemmeasure of the strategies selection (both elective selec-tion and loss-based selection), optimization, and com-pensation was administered at Time 4 (Cronbach’s α =.90) to assess self-reported strategy use in the domainof physical activity. In contrast to the original generalquestionnaire of selection optimization and compensa-tion strategies (Freund & Baltes, 2002) this do-main-specific scale employs a single item format usinga five-point Likert scale. The previous general targetitems were slightly changed to become do-main-specific for physical activity, and the items wererephrased to assess strategy use retrospectively (seeAppendix). Physical exercise goal attainment wasmeasured with the following two items at Time 4
33
PLANNING AND STRATEGY USE
Table 1. Sample Characteristics
Younger Adultsa Older Adultsb Totalc
Characteristic M SD % M SD % M SD %
Chronological age in years 38.5 7.0 58.0 5.8 47.4 11.7SF12 physical functioningd 38.0 9.3 36.7 9.2 37.4 9.3SF12 psychological functioningd 49.7 10.1 51.4 11.1 50.5 10.6Number of diagnoses 2.4 1.3 3.1 1.5 2.7 1.5Number of risk factors 1.3 1.3 1.5 1.3 1.4 1.3Years of education 13.9 5.0 14.4 5.5 14.1 5.2Female 69.8 52.7 62.0Living with partner 62.8 84.6 72.8Employed 77.9 62.7 70.9German native speakers 96.0 97.6 96.7
Note. SF12 = 12 Item Short-Form Heath Survey (Ware, Kosinski, & Keller, 1996).a n = 199. b n = 169. c N = 368. dHigher scores indicate better health. Regression weights and a constant are added to transform the scores to have amean of 50 and a standard deviation of 10 in the 1998 general U.S. population.
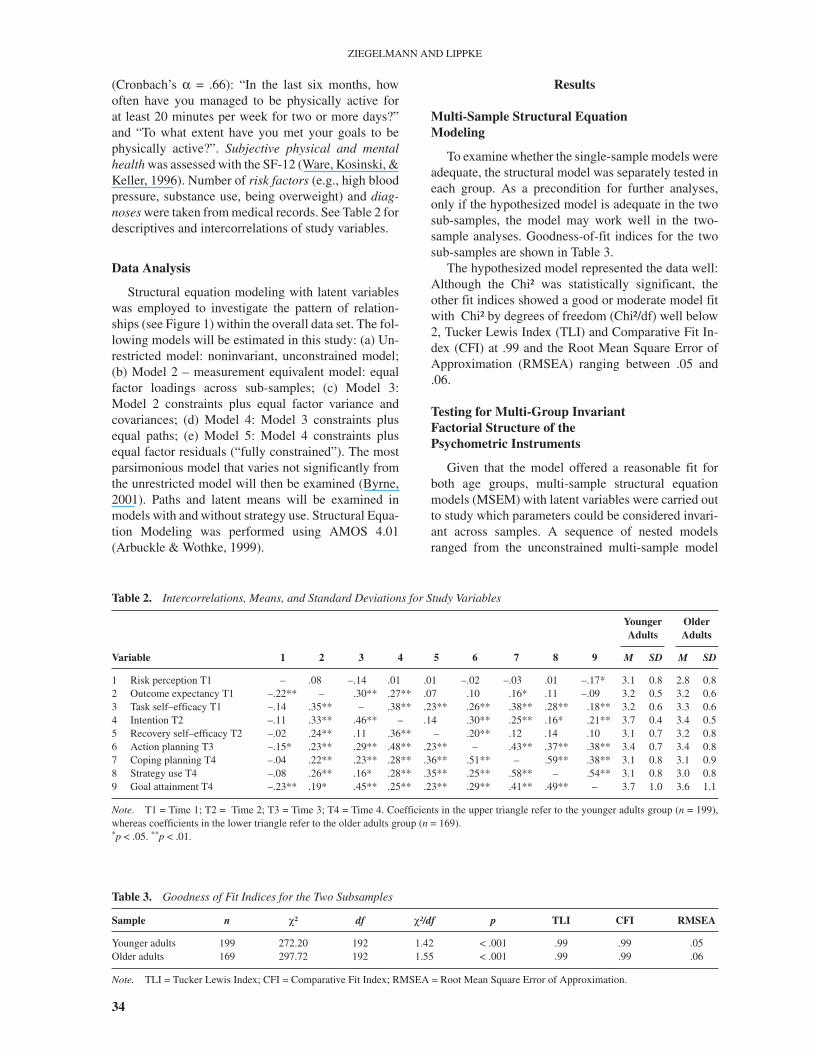
(Cronbach’s α = .66): “In the last six months, howoften have you managed to be physically active forat least 20 minutes per week for two or more days?”and “To what extent have you met your goals to bephysically active?”. Subjective physical and mentalhealth was assessed with the SF-12 (Ware, Kosinski, &Keller, 1996). Number of risk factors (e.g., high bloodpressure, substance use, being overweight) and diag-noses were taken from medical records. See Table 2 fordescriptives and intercorrelations of study variables.
Data Analysis
Structural equation modeling with latent variableswas employed to investigate the pattern of relation-ships (see Figure 1) within the overall data set. The fol-lowing models will be estimated in this study: (a) Un-restricted model: noninvariant, unconstrained model;(b) Model 2 – measurement equivalent model: equalfactor loadings across sub-samples; (c) Model 3:Model 2 constraints plus equal factor variance andcovariances; (d) Model 4: Model 3 constraints plusequal paths; (e) Model 5: Model 4 constraints plusequal factor residuals (“fully constrained”). The mostparsimonious model that varies not significantly fromthe unrestricted model will then be examined (Byrne,2001). Paths and latent means will be examined inmodels with and without strategy use. Structural Equa-tion Modeling was performed using AMOS 4.01(Arbuckle & Wothke, 1999).
Results
Multi-Sample Structural EquationModeling
To examine whether the single-sample models wereadequate, the structural model was separately tested ineach group. As a precondition for further analyses,only if the hypothesized model is adequate in the twosub-samples, the model may work well in the two-sample analyses. Goodness-of-fit indices for the twosub-samples are shown in Table 3.
The hypothesized model represented the data well:Although the Chi² was statistically significant, theother fit indices showed a good or moderate model fitwith Chi² by degrees of freedom (Chi²/df) well below2, Tucker Lewis Index (TLI) and Comparative Fit In-dex (CFI) at .99 and the Root Mean Square Error ofApproximation (RMSEA) ranging between .05 and.06.
Testing for Multi-Group InvariantFactorial Structure of thePsychometric Instruments
Given that the model offered a reasonable fit forboth age groups, multi-sample structural equationmodels (MSEM) with latent variables were carried outto study which parameters could be considered invari-ant across samples. A sequence of nested modelsranged from the unconstrained multi-sample model
34
ZIEGELMANN AND LIPPKE
Table 2. Intercorrelations, Means, and Standard Deviations for Study Variables
YoungerAdults
OlderAdults
Variable 1 2 3 4 5 6 7 8 9 M SD M SD
1 Risk perception T1 – .08 –.14 .01 .01 –.02 –.03 .01 –.17* 3.1 0.8 2.8 0.82 Outcome expectancy T1 –.22** – .30** .27** .07 .10 .16* .11 –.09 3.2 0.5 3.2 0.63 Task self–efficacy T1 –.14 .35** – .38** .23** .26** .38** .28** .18** 3.2 0.6 3.3 0.64 Intention T2 –.11 .33** .46** – .14 .30** .25** .16* .21** 3.7 0.4 3.4 0.55 Recovery self–efficacy T2 –.02 .24** .11 .36** – .20** .12 .14 .10 3.1 0.7 3.2 0.86 Action planning T3 –.15* .23** .29** .48** .23** – .43** .37** .38** 3.4 0.7 3.4 0.87 Coping planning T4 –.04 .22** .23** .28** .36** .51** – .59** .38** 3.1 0.8 3.1 0.98 Strategy use T4 –.08 .26** .16* .28** .35** .25** .58** – .54** 3.1 0.8 3.0 0.89 Goal attainment T4 –.23** .19* .45** .25** .23** .29** .41** .49** – 3.7 1.0 3.6 1.1
Note. T1 = Time 1; T2 = Time 2; T3 = Time 3; T4 = Time 4. Coefficients in the upper triangle refer to the younger adults group (n = 199),whereas coefficients in the lower triangle refer to the older adults group (n = 169).*p < .05. **p < .01.
Table 3. Goodness of Fit Indices for the Two Subsamples
Sample n χ² df χ²/df p TLI CFI RMSEA
Younger adults 199 272.20 192 1.42 < .001 .99 .99 .05Older adults 169 297.72 192 1.55 < .001 .99 .99 .06
Note. TLI = Tucker Lewis Index; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation.
(Model 1) with the estimated parameters free to varyacross sub-samples as more parsimonious nested mod-els. These nested models included different levels ofequality constraints. The constrained models werespecified with equal factor loadings (Model 2), equalfactor loadings and factor covariances (Model 3), equalfactor loadings, covariances and variances (Model 4),equal factor loadings, covariances, variances, and fac-tor residuals (Model 5). The following results were ob-tained: The first two constrained models were tenable,with practical fit indices showing good model fit(RMSEA = .04). The Comparative Fit Index was lowerin Models 4 and 5 than in Models 2 and 3. This sug-gests that Models 2 and 3 account as well for the sam-ple’s variance/covariance as Model 1. For Models 4and 5 this indicates that factor loadings, variances, andfactor residuals were mostly sample specific. From apractical point of view, it could be maintained thatconstraints of Model 3 were best. Subsequently, allanalyses were based on this measurement-equivalencemodel.
Examining the Hypothesized CausalModel
To test the hypothesis that the paths in the specifiedcausal structure was unique (not invariant) across thetwo age groups, multi-group models were specified.The final optimal model (Model 3) was then tested, withconstrained factor loadings and factor covariances to beequal across samples. First Model 3 was tested withoutstrategy use and then including strategy use.
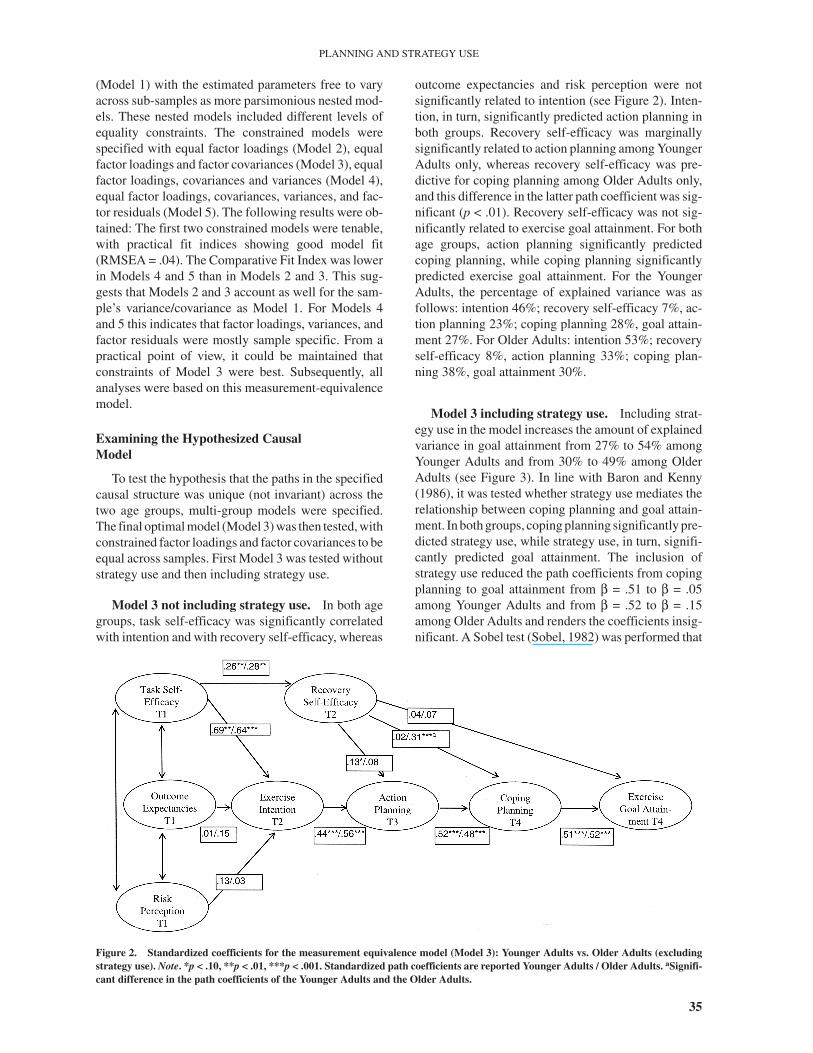
Model 3 not including strategy use. In both agegroups, task self-efficacy was significantly correlatedwith intention and with recovery self-efficacy, whereas
outcome expectancies and risk perception were notsignificantly related to intention (see Figure 2). Inten-tion, in turn, significantly predicted action planning inboth groups. Recovery self-efficacy was marginallysignificantly related to action planning among YoungerAdults only, whereas recovery self-efficacy was pre-dictive for coping planning among Older Adults only,and this difference in the latter path coefficient was sig-nificant (p < .01). Recovery self-efficacy was not sig-nificantly related to exercise goal attainment. For bothage groups, action planning significantly predictedcoping planning, while coping planning significantlypredicted exercise goal attainment. For the YoungerAdults, the percentage of explained variance was asfollows: intention 46%; recovery self-efficacy 7%, ac-tion planning 23%; coping planning 28%, goal attain-ment 27%. For Older Adults: intention 53%; recoveryself-efficacy 8%, action planning 33%; coping plan-ning 38%, goal attainment 30%.
Model 3 including strategy use. Including strat-egy use in the model increases the amount of explainedvariance in goal attainment from 27% to 54% amongYounger Adults and from 30% to 49% among OlderAdults (see Figure 3). In line with Baron and Kenny(1986), it was tested whether strategy use mediates therelationship between coping planning and goal attain-ment. In both groups, coping planning significantly pre-dicted strategy use, while strategy use, in turn, signifi-cantly predicted goal attainment. The inclusion ofstrategy use reduced the path coefficients from copingplanning to goal attainment from β = .51 to β = .05among Younger Adults and from β = .52 to β = .15among Older Adults and renders the coefficients insig-nificant. A Sobel test (Sobel, 1982) was performed that
35
PLANNING AND STRATEGY USE
Figure 2. Standardized coefficients for the measurement equivalence model (Model 3): Younger Adults vs. Older Adults (excludingstrategy use). Note. *p < .10, **p < .01, ***p < .001. Standardized path coefficients are reported Younger Adults / Older Adults. aSignifi-cant difference in the path coefficients of the Younger Adults and the Older Adults.
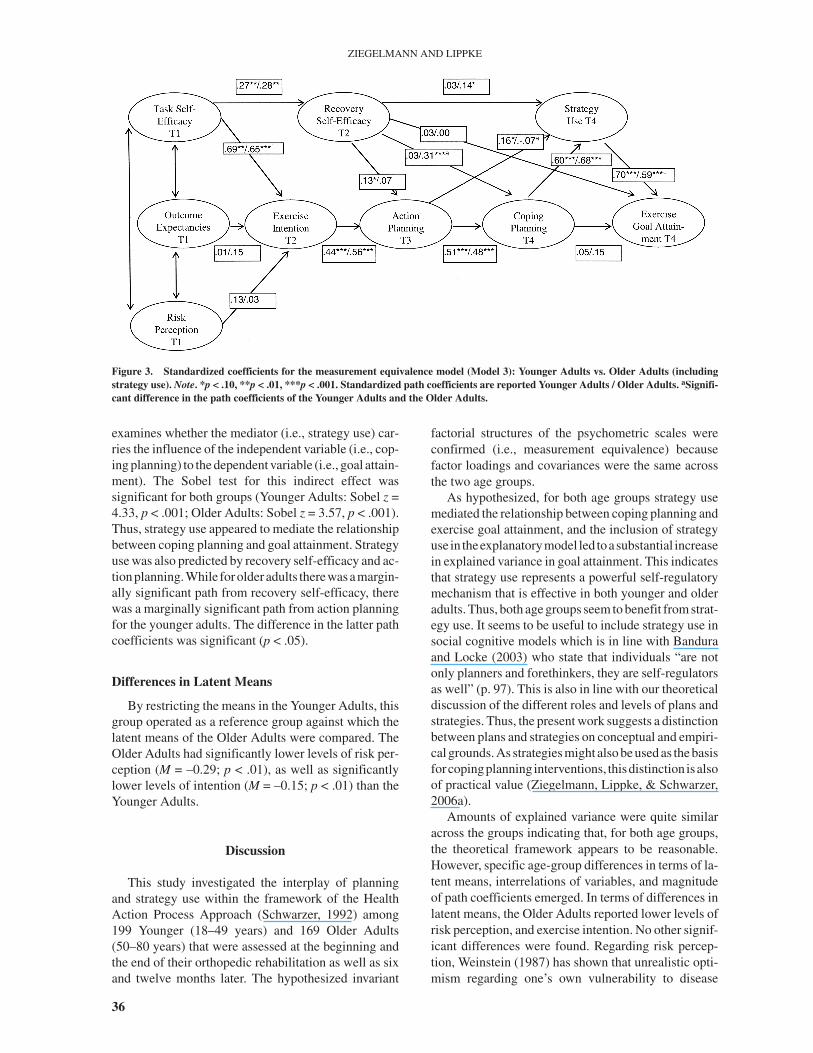
examines whether the mediator (i.e., strategy use) car-ries the influence of the independent variable (i.e., cop-ing planning) to the dependent variable (i.e., goal attain-ment). The Sobel test for this indirect effect wassignificant for both groups (Younger Adults: Sobel z =4.33, p < .001; Older Adults: Sobel z = 3.57, p < .001).Thus, strategy use appeared to mediate the relationshipbetween coping planning and goal attainment. Strategyuse was also predicted by recovery self-efficacy and ac-tionplanning.While forolderadults therewasamargin-ally significant path from recovery self-efficacy, therewas a marginally significant path from action planningfor the younger adults. The difference in the latter pathcoefficients was significant (p < .05).
Differences in Latent Means
By restricting the means in the Younger Adults, thisgroup operated as a reference group against which thelatent means of the Older Adults were compared. TheOlder Adults had significantly lower levels of risk per-ception (M = –0.29; p < .01), as well as significantlylower levels of intention (M = –0.15; p < .01) than theYounger Adults.
Discussion
This study investigated the interplay of planningand strategy use within the framework of the HealthAction Process Approach (Schwarzer, 1992) among199 Younger (18–49 years) and 169 Older Adults(50–80 years) that were assessed at the beginning andthe end of their orthopedic rehabilitation as well as sixand twelve months later. The hypothesized invariant
factorial structures of the psychometric scales wereconfirmed (i.e., measurement equivalence) becausefactor loadings and covariances were the same acrossthe two age groups.
As hypothesized, for both age groups strategy usemediated the relationship between coping planning andexercise goal attainment, and the inclusion of strategyuse in theexplanatorymodel led toasubstantial increasein explained variance in goal attainment. This indicatesthat strategy use represents a powerful self-regulatorymechanism that is effective in both younger and olderadults. Thus, both age groups seem to benefit from strat-egy use. It seems to be useful to include strategy use insocial cognitive models which is in line with Banduraand Locke (2003) who state that individuals “are notonly planners and forethinkers, they are self-regulatorsas well” (p. 97). This is also in line with our theoreticaldiscussion of the different roles and levels of plans andstrategies. Thus, the present work suggests a distinctionbetween plans and strategies on conceptual and empiri-cal grounds. As strategies might also be used as the basisforcopingplanning interventions, thisdistinction isalsoof practical value (Ziegelmann, Lippke, & Schwarzer,2006a).
Amounts of explained variance were quite similaracross the groups indicating that, for both age groups,the theoretical framework appears to be reasonable.However, specific age-group differences in terms of la-tent means, interrelations of variables, and magnitudeof path coefficients emerged. In terms of differences inlatent means, the Older Adults reported lower levels ofrisk perception, and exercise intention. No other signif-icant differences were found. Regarding risk percep-tion, Weinstein (1987) has shown that unrealistic opti-mism regarding one’s own vulnerability to disease
36
ZIEGELMANN AND LIPPKE
Figure 3. Standardized coefficients for the measurement equivalence model (Model 3): Younger Adults vs. Older Adults (includingstrategy use). Note. *p < .10, **p < .01, ***p < .001. Standardized path coefficients are reported Younger Adults / Older Adults. aSignifi-cant difference in the path coefficients of the Younger Adults and the Older Adults.

decreases with illness experience. Probably, in oursample, this only holds true for the younger ones, andone might speculate that for younger adults it is lessnormative to have severe health problems, and, thus,being at risk is more salient. In the context oforthopedic rehabilitation, there seems to be no age-related decrease in exercise planning and strategy usewhich is in contrast to general planning and strategyscales (e.g., Prenda & Lachman, 2001; Freund &Baltes, 2002). Thus, both age groups seem to be en-dowed with those important self-regulation skills (i.e.,planning and strategy use) that can lead to success-ful development in selected domains (Ziegelmann &Lipke, in press). Regarding the finding that in both agegroups only task-self efficacy but neither risk percep-tion nor outcome expectancies predict intention, onehas to bear in mind that individuals in rehabilitation arelimited by their physical health conditions. Harboringoptimistic self-beliefs that one is able to perform thebehavior might be a more important factor in intentionformation than simply perceiving that one is at risk orthat physical exercise has advantages. This is in linewith Schwarzer and Renner (2000) who argue that itcan depend on the particular context which construct ismore central for intention formation.
Regarding coping planning and strategy use, age-group specific prediction patterns emerged: Recoveryself-efficacy was predictive of coping planning onlyamong Older Adults. For action planning, this findingwas reverse (however without a significant difference inthe path coefficients). One might speculate that, foryounger adults, harboring self-efficacious thoughtsabout getting back on track after being derailed is moreclosely related to action planning (i.e., adhering to astrict when-where-how plan) whereas for older adults,harboring those self-efficacious thoughts is moreclosely related to coping planning (i.e., having an alter-native plan). As planning can be facilitated by perceivedself-efficacy, one might conclude from the age-groupdifferences that younger adults are better action plan-ners and older adults are better coping planners. How-ever, the lackofage-groupdifferences inplanning levelsspeaks against this interpretation. Another age-groupspecific prediction pattern emerged: Only for YoungerAdults, action planning was related to strategy use,which leads to speculate that they seem to adhere moreto their action plans than older ones do. To summarize,there seems to be an age-group specific pattern in the in-terplay of self-efficacy, planning, and strategy use thatneeds to be replicated in future studies.
Potential limitations of the study should also be dis-cussed. First, the exercise data are based on self-reports. However, there is evidence for the validity ofphysical exercise self-reports (Miller, Freedson, &Kline, 1994). Second, the cause-and-effect relation-ships found are based on theory or time lag and not onexperimental manipulation. The final model need not
necessarily represent the only true model, despite thefinding that it was applicable to two age groups.Finally, for the structural equation models, larger sam-ple sizes would have been favorable, which would haveallowed to subdivide the sample into more fine-grainedage groups. Regarding the reported age-related find-ings, one has to bear in mind that cross-sectional agedata are unable to unconfound chronological age, co-hort, and selective mortality (Baltes, Reese, & Nessel-roade, 1988). In addition, proximity to death might bea more prominent variable for the determination ofadult age variance than distance from birth (Ziegel-mann, Lippke, & Schwarzer, 2006b).
While previous research has demonstrated that indi-viduals benefit from coping planning (Sniehotta,Schwarzer, Scholz, & Schüz, 2005), the current studyprovides evidence for potential mediating mechanisms(i.e., strategy use) between coping planning and behav-ior. As there is a strong relationship between planningand knowledge of strategies (Sonnentag, 1996), wewould suggest to employ the strategies of selection,optimization, and compensation as outlined in Freundand Baltes (2002) as a source for planning interven-tions (Ziegelmann, et al., 2006a). This would representa resource communication approach, where knowl-edge and use of adaptive strategies could be acquired.
References
Arbuckle, J. L., & Wothke, W. (1999). Amos 4.0 user guide. Chicago,IL: SmallWaters.
Artistico, D., Cervone, D., & Pezzuti, L. (2003). Perceivedself-efficacy and everyday problem solving among young andolder adults. Psychology & Aging, 18, 68–79.
Baltes, P. B., Reese, H. W., & Nesselroade, J. R. (1988). Life-spandevelopmental psychology: Introduction to research methods.Hillsdale, NJ, England: Lawrence Erlbaum Associates.
Bandura, A. (1986). Social foundations of thought and action. A so-cial cognitive theory. Englewood Cliffs, NJ, Prentice-Hall.
Bandura, A. (2005). The primacy of self-regulation in health promo-tion. Applied Psychology: An International Review, 54,245–254.
Bandura, A., & Locke, E. A. (2003). Negative self-efficacy and goaleffects revisited. Journal of Applied Psychology, 88, 87–99.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator vari-able distinction in social psychology research: Conceptual,strategic and statistical considerations. Journal of Personalityand Social Psychology, 51, 1173–1182.
Booth, M. L., Macaskill, P., Owen, N., & Oldenburg, B. (1993). Pop-ulation prevalence and correlates of stages of change in physi-cal activity. Health Education Quarterly, 20, 431–440.
Brandtstädter, J., & Renner, G. (1990). Tenacious goal pursuit andflexible goal adjustment: Explication and age-related analysisof assimilative and accommodative strategies of coping. Psy-chology & Aging, 5, 58–67.
Byrne, B. M. (2001). Structural equation modeling with Amos: Ba-sic concepts, applications, and programming. Mahwah, NJ:Lawrence Erlbaum Associates.
Clark, D. O. (1999). Physical activity and its correlates among urbanprimary care patients aged 55 years or older. Journals of Geron-
37
PLANNING AND STRATEGY USE
tology: Series B: Psychological Sciences & Social Sciences, 54,S41–S48.
Das, J. P., Kar, B. C., & Parrila, R. K. (1996). Cognitive planning:The psychological basis of intelligent behavior. New Delhi, In-dia: Sage.
Diefendorff, J. M., & Lord, R. G. (2003). The volitional and strategiceffects of planning on task performance and goal commitment.Human Performance, 16, 365–387.
Freund, A. M., & Baltes, P. B. (2002). Life-management strategies ofselection, optimization and compensation: Measurement byself-report and construct validity. Journal of Personality & So-cial Psychology, 82, 642–662.
Fuchs, R. (1996). Causal models of physical exercise participation:Testing the predictive power of the construct “Pressure tochange”. JournalofAppliedSocialPsychology,21,1931–1960.
Gignac, M. A. M., Cott, C., & Badley, E. M. (2002). Adaptation todisability: Applying selective optimization with compensationto the behaviors of older adults with osteoarthritis. Psychology& Aging, 17, 520–524.
Gollwitzer, P. M. (1996). The volitional benefits of planning. In P. M.Gollwitzer, & J. A. Bargh (Eds.), The psychology of action:Linking cognition and motivation to behavior (pp. 287–312).New York: Guilford.
Kuhl, J., & Goschke, T. (1994). A theory of action control: Mentalsubsystems, modes of control, and volitional conflict resolutionstrategies. In J. Kuhl & J. Beckmann (Eds.), Volition and per-sonality: Action versus state orientation (pp. 93–124).Göttingen: Hogrefe.
Leventhal, H., & Mora, P. A. (2005). Is there a science of the pro-cesses underlying health and illness behaviors? A comment onMaes and Karoly. Applied Psychology: An International Re-view, 54, 255–266.
Leontjev, A. N. (1978). Activity, consciousness, and personality.Englewood Cliffs, NJ: Prentice-Hall.
Lippke, S., Ziegelmann, J. P., & Schwarzer, R. (2004). Behavioral in-tentions and action plans promote physical exercise: A longitu-dinal study with orthopedic rehabilitation patients. Journal ofSport & Exercise Psychology, 26, 470–483.
Luszczynska, A., & Sutton, S. (2006). Physical activity after cardiacrehabilitation: The evidence that different types of self-efficacyare important in maintainers and relapsers. Rehabilitation Psy-chology, 51, 314–321.
Miller, D. J., Freedson, P. S., & Kline, G. M. (1994). Comparison ofactivity levels using the Caltrac accelerometer and five ques-tionnaires. Medicine and Science in Sports and Exercise, 26,376–382.
Netz, Y., & Raviv, S. (2004). Age differences in motivational orienta-tion toward physical activity: An application of social-cognitivetheory. Journal of Psychology: Interdisciplinary & Applied,138, 35–48.
Prenda, K. M., & Lachman, M. E. (2001). Planning for the future: Alife management strategy for increasing control and life satis-faction in adulthood. Psychology & Aging, 16, 206–216.
Prohaska, T. R., Leventhal, E. A., Leventhal, H., & Keller, M. L.(1985). Health practices and illness cognition in young, middleaged, and elderly adults. Journal of Gerontology, 40, 569–578.
Renner, B., Knoll, N., & Schwarzer, R. (2000). Age and body weightmake a difference in optimistic health beliefs and nutrition be-haviors. International Journal of Behavioral Medicine, 7,143–159.
Scholz, U., Sniehotta, F. F., & Schwarzer, R. (2005). Predictingphysical exercise in cardiac rehabilitation: The role ofphase-specific self-efficacy beliefs. Journal of Sport & ExercisePsychology, 27, 135–151.
Schwarzer, R. (1992). Self-efficacy in the adoption and maintenanceof health behaviors: Theoretical approaches and a new model.In R. Schwarzer (Ed.) Self-efficacy: Thought control of action(pp. 217–243). Washington, DC: Hemisphere.
Schwarzer, R., & Renner, B. (2000). Social-cognitive predictors ofhealth behavior: Action self-efficacy and coping self-efficacy.Health Psychology, 19, 487–495.
Smith, J. (1999). Anticipating future life goals and managing per-sonal development. In J. Brandstäfer & R. M. Lerner (Eds.),Action & self-development: Theory and research through thelife span (pp. 223–255). Thousand Oaks: Sage.
Sniehotta, F. F., Scholz, U., & Schwarzer, R. (2005). Bridging the in-tention-behaviour gap: Planning, self-efficacy, and action con-trol in the adoption and maintenance of physical exercise. Psy-chology and Health, 20, 143–160.
Sniehotta, F. F., Schwarzer, R., Scholz, U., & Schüz, B. (2005). Ac-tion plans and coping plans for long-term lifestyle change: The-ory and assessment. European Journal of Social Psychology,35, 565–576.
Sobel, M. E. (1982). Asymptotic intervals for indirect effects instructural equations models. In S. Leinhart (Ed.), Sociologicalmethodology 1982 (pp.290–312). San Francisco: Jossey-Bass.
Sonnentag, S. (1996). Planning and knowledge about strategies:Their relationship to work characteristics in software design.Behaviour & Information Technology, 15, 213–225.
Ware, J. Jr., Kosinski, M., & Keller, S. D. (1996). A 12-ItemShort-Form Health Survey: construction of scales and prelimi-nary tests of reliability and validity. Medical Care, 34, 220–233.
Weinstein, N. D. (1987). Unrealistic optimism about susceptibility tohealth problems: Conclusions from a community-wide sample.Journal of Behavioral Medicine, 10, 481–500.
Ziegelmann, J. P., Lippke, S., & Schwarzer, R. (2006a). Adoptionand maintenance of physical activity: Planning interventions inyoung, middle-aged, and older adults. Psychology & Health,21, 145–163.
Ziegelmann, J. P., & Lippke, S. (in press). Use of Selection, Optimi-zation, and Compensation strategies in health self-regulation:Interplay with resources and successful development. Journalof Aging and Health.
Ziegelmann, J. P., Lippke, S., & Schwarzer, R. (2006b). Subjectiveresidual life expectancy in health self-regulation. Journals ofGerontology: Psychological Sciences, 61B, 195–201.
Ziegelmann, J. P., Luszczynska, A., Lippke, S., & Schwarzer, R.(2007). Are goal intentions or implementation intentions betterpredictors of health behavior? A longitudinal study in orthope-dic rehabilitation. Rehabilitation Psychology, 52, 97–102.
38
ZIEGELMANN AND LIPPKE
Appendix
Optimization (Items 1-3), and ElectiveSelection (Items 4-6):
In the following, we would like to know how youbehaved in the last six months regarding your physicalactivities.
1. I have thought carefully about how I could bestput my intentions to be physically active intoaction.
2. I have done everything possible to make myplans to be physically active come true.
3. In order to achieve advances in my level ofphysical activities, I have looked for new meth-ods and means. (new item)
4. Regarding my physical activities, I havecommitted myself to one or two importantgoals.
5. Regarding my physical activities, I have care-fully considered what is important to me.
6. Regarding my physical activities, I have de-fined my goals exactly and have stuck tothem.
Compensation (Items 7-9), andLoss-Based Selection (Items 10-12):
In the following, we would like to know how youbehaved in the last six months when facing difficultiesregarding your physical activities. Within the last sixmonths, when I could not at times be as physically ac-tive as I have been used to…
7. …then I have looked for alternative ways to ac-complish this.
8. …then I have increased my efforts in order toremain active.
9. …then I have applied more time and energy toremain active nevertheless.
10. …then I have thought about which other physi-cal activities I could practice instead.
11. …then I have reduced, for the time being, mylevel of physical activity to very little.
12. …then I have carefully considered which phys-ical activities I could still perform under thegiven conditions.
Note. Items are adapted from Freund and Baltes(2002) except otherwise noted.
39
PLANNING AND STRATEGY USE