
The conserved translocase Tim17 prevents mitochondrial DNA loss
Upload
independentCategory
view
1download
0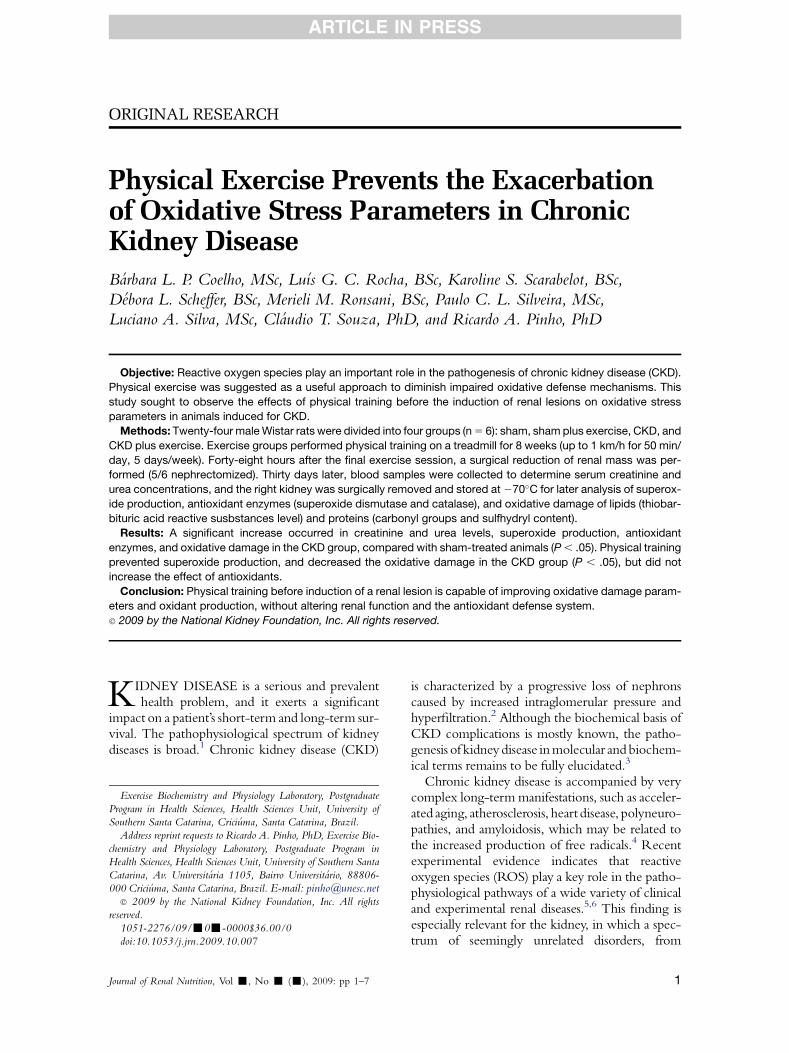
ARTICLE IN PRESS
ORIGINAL RESEARCH
Physical Exercise Prevents the Exacerbationof Oxidative Stress Parameters in ChronicKidney DiseaseBarbara L. P. Coelho, MSc, Luıs G. C. Rocha, BSc, Karoline S. Scarabelot, BSc,
Debora L. Scheffer, BSc, Merieli M. Ronsani, BSc, Paulo C. L. Silveira, MSc,
Luciano A. Silva, MSc, Claudio T. Souza, PhD, and Ricardo A. Pinho, PhD
Objective: Reactive oxygen species play an important role in the pathogenesis of chronic kidney disease (CKD).
Physical exercise was suggested as a useful approach to diminish impaired oxidative defense mechanisms. This
study sought to observe the effects of physical training before the induction of renal lesions on oxidative stress
parameters in animals induced for CKD.
Methods: Twenty-four male Wistar rats were divided into four groups (n 5 6): sham, sham plus exercise, CKD, and
CKD plus exercise. Exercise groups performed physical training on a treadmill for 8 weeks (up to 1 km/h for 50 min/
day, 5 days/week). Forty-eight hours after the final exercise session, a surgical reduction of renal mass was per-
formed (5/6 nephrectomized). Thirty days later, blood samples were collected to determine serum creatinine and
urea concentrations, and the right kidney was surgically removed and stored at 270�C for later analysis of superox-
ide production, antioxidant enzymes (superoxide dismutase and catalase), and oxidative damage of lipids (thiobar-
bituric acid reactive susbstances level) and proteins (carbonyl groups and sulfhydryl content).
Results: A significant increase occurred in creatinine and urea levels, superoxide production, antioxidant
enzymes, and oxidative damage in the CKD group, compared with sham-treated animals (P , .05). Physical training
prevented superoxide production, and decreased the oxidative damage in the CKD group (P , .05), but did not
increase the effect of antioxidants.
Conclusion: Physical training before induction of a renal lesion is capable of improving oxidative damage param-
eters and oxidant production, without altering renal function and the antioxidant defense system.
� 2009 by the National Kidney Foundation, Inc. All rights reserved.
KIDNEY DISEASE is a serious and prevalenthealth problem, and it exerts a significant
impact on a patient’s short-term and long-term sur-vival. The pathophysiological spectrum of kidneydiseases is broad.1 Chronic kidney disease (CKD)
Exercise Biochemistry and Physiology Laboratory, Postgraduate
Program in Health Sciences, Health Sciences Unit, University of
Southern Santa Catarina, Criciuma, Santa Catarina, Brazil.
Address reprint requests to Ricardo A. Pinho, PhD, Exercise Bio-
chemistry and Physiology Laboratory, Postgraduate Program in
Health Sciences, Health Sciences Unit, University of Southern Santa
Catarina, Av. Universitaria 1105, Bairro Universitario, 88806-
000 Criciuma, Santa Catarina, Brazil. E-mail: [email protected]� 2009 by the National Kidney Foundation, Inc. All rights
reserved.
1051-2276/09/-0--0000$36.00/0
doi:10.1053/j.jrn.2009.10.007
Journal of Renal Nutrition, Vol -, No - (-), 2009: pp 1–7
is characterized by a progressive loss of nephronscaused by increased intraglomerular pressure andhyperfiltration.2 Although the biochemical basis ofCKD complications is mostly known, the patho-genesis of kidney disease in molecular and biochem-ical terms remains to be fully elucidated.3
Chronic kidney disease is accompanied by verycomplex long-term manifestations, such as acceler-ated aging, atherosclerosis, heart disease, polyneuro-pathies, and amyloidosis, which may be related tothe increased production of free radicals.4 Recentexperimental evidence indicates that reactiveoxygen species (ROS) play a key role in the patho-physiological pathways of a wide variety of clinicaland experimental renal diseases.5,6 This finding isespecially relevant for the kidney, in which a spec-trum of seemingly unrelated disorders, from
1

COELHO ET AL2
ARTICLE IN PRESS
minimal-change nephrotic syndrome to obstructivenephropathy, involves ROS.7
Patientswith CKDare subject to increased oxida-tive stress because of reduced antioxidant systemsand increased pro-oxidant stimuli.8,9 Vaziri5
suggested that pro-oxidant stimuli are caused bythe effects of uremic toxins, angiotensin 2, proin-flammatory cytokines, blood-dialyzer interactions,reactions to catheters and arteriovenous grafts, ironoverload, chronic infections, and underlying immu-nological or metabolic disorders, e.g., diabetes.
Routine therapeutic interventions, and espe-cially pharmacological and hemodialysis treat-ments, can significantly decrease the severity ofCKD. We hypothesized that physical trainingbefore induction of a renal lesion would exert a pos-itive effect on the oxidative parameters of the kid-ney. Although the benefits of physical exercise onrenal function are limited, physical training can bean important component in the treatment ofCKD.9 According to Pechter10 and Moinuddinand Leehey,11 exercise conditioning exerts a posi-tive influence on physical capacity, hypertension,left ventricular function, lipid and glucose metabo-lism, oxidative status, anemia, and quality of life inCKD patients and patients on renal replacementtherapy. Furthermore, no investigation has verifiedthe effects of physical training before renal disease,especiallyon oxidative stress parameters. Most stud-ies showed exercise to be a therapeutic resource inthe treatment of disease.10–12 Thus, this studysought to observe the effects of physical training be-fore induction of a renal lesion on the oxidativestress parameters in animals induced to CKD.
Table 1. Treadmill-Running Program Performedby Male Wistar Rats Before Induction of ChronicKidney Disease
Weeks Days
Velocity
(km/h) Inclination (%)
Time
(min)
Adaptation 1-5 0.6 0 10
1 1-5 0.8 0 302 1-5 0.8 0 30
3 1-5 0.8 0 40
4 1-5 0.8 0 505 1-5 1.0 0 50
6 1-5 1.0 0 50
7 1-5 1.0 0 50
8 1-5 1.0 0 50
Materials and Methods
Animals
Twenty-four male, 3-month-old Wistar rats,weighing 250 to 300 g, were used in this study,and were cared for according to the EuropeanCommunities Council Directive of November24, 1986. Food (Nuvilab CR1, NuvitalNutrientes S/A, Colombo, Parana, Brazil) andwater were available ad libitum, and the animalswere periodically checked to verify their patho-gen-free condition. Their room was kept at 70%humidity and at 20�C 6 2�C on a 12-hourlight/dark cycle, with lights on at 06:00 AM. Theanimals were randomly assigned to four groups(n 5 6 per group): sham, sham plus exercise,CKD, and CKD plus exercise.
Exercise Protocol
All groups were habituated to a nine-channel,motor-drive treadmill at a speed of 10 m/minfor 10 min/day for 1 week, to reduce stress in theirnew environment. The rats did not receive anystimuli to run. The exercise groups performedan incremental running program to achieve pro-gressive levels of intensity during 8 weeks for 5days/week, for a total of 60 days (Table 1). The un-trained animals were put on the switched-offtreadmill during the same 8 weeks as were theexercise-trained groups.
CKD Protocol
Forty-eight hours after the final exercise ses-sion, a surgical reduction of renal mass was per-formed in one step, under anesthesia withpentobarbital sodium (50 mg/kg, intraperitoneal),by removal of the right kidney and infarction oftwo thirds of the left kidney via the closure oftwo or three branches of the left renal artery.13
Sham-operated rats underwent anesthesia and ma-nipulation of the renal pedicles, without renal massreduction. After recovering from anesthesia, theanimals were returned to their original cages,which were heated for the subsequent 24 hours.
Sacrifice Protocol
Thirty days after renal ablation, the rats wereanesthetized with 50 mg/kg intraperitoneal pen-tobarbital sodium, and blood was collected fromthe abdominal aorta for the determination ofserum creatinine and urea concentrations. Theleft kidney was surgically removed, aliquoted,and stored at 270�C for later analysis.

EXERCISE AND ROS IN CKD 3
ARTICLE IN PRESS
Biochemical Assays
Creatinine and Urea
Creatinine and urea levels in serum were deter-mined using a kit from Labtest Diagnostica SA,Lagoa Santa, Minas Gerais, Brazil, according tothe manufacturer’s instructions. Concentrationswere expressed as mmol/L serum.
Superoxide Assay
Superoxide was measured in the kidney, usinga method previously described by Poderosoet al.14 The rate of adrenaline oxidation was deter-mined at an absorbance of 780 nm. Superoxidewas expressed as nmol/min/mg protein.
Superoxide Dismutase Activity Assay
The superoxide dismutase (SOD) activity of thekidney was determined according to the methodof Bannister and Calabrese.15 In brief, enzymaticactivity was estimated by adrenaline auto-oxidationinhibition, as determined by absorbance at 480nm. Enzyme activity was expressed as U/mgprotein.
Catalase Activity Assay
To determine catalase (CAT) activity, the kidneywas sonicated in 50 mM phosphate buffer, and theresulting suspension was centrifuged at 3000 3 gfor 10 minutes. The supernatant was used for theassay. Catalase activity was measured by the rateof decrease in hydrogen peroxide absorbance at240 nm.16 Enzyme activity was expressed asU/mg protein.
Lipid Peroxidation Assay
Levels of 2-thiobarbituric acid reactive species(TBARS) were measured according to Draperand Hadley,17 and were expressed as malondialde-hyde equivalent. Briefly, kidneys were mixed with1 mL 10% trichloroacetic acid and 1 mL 0.67%thiobarbituric acid. Subsequently, kidneys wereheated in a boiling water bath for 15 minutes.Levels of TBARS were determined by measuringthe absorbance at 532 nm, and the results are givenas nmol malondialdehyde/mg protein.
Carbonyl Assay
The protein concentration of soluble proteinfractions was determined according to the method
of Levine et al.18 Protein carbonyl content wasmeasured by forming labeled protein hydrazonederivatives, using 2,4-dinitrophenylhydrazide.These derivatives were sequentially extractedwith 10% (vol/vol) trichloroacetic acid, followedby treatment with 1:1 ethanol/ethylacetate (vol/vol), and re-extraction with 10% trichloroaceticacid. The resulting precipitate was dissolved in 6M urea hydrochloride. The spectrum differencefrom a 2,4-dinitrophenylhydrazide protein blankwas used to calculate the nmol of 2,4-dinitrophe-nylhydrazide incorporated per milligram of pro-tein. The results are shown for each sample readat 370 nm.
Sulfhydryl Content Assay
Total thiol content was determined using the5,50-dithiobis (2-nitrobenzoic acid) method(DTNB) (Sigma, St. Louis, MO). The reactionwas initiated by adding 30 mL of 10 mM DTNBstock solution to phosphate-buffered saline. Con-trol samples did not include DTNB. After 30 min-utes of incubation at room temperature, theabsorbance at 412 nm was measured, and theamounts of 5,5’-Dithiobis(2-nitrobenzoic acid),or TNB, formed were calculated (equivalent tothe amount of Sulphidril, or S,H groups), usingthe technique of Aksenov and Markesberya.19
Protein Measurement
Protein concentration was estimated by themethod of Lowry et al.,20 using bovine serum al-bumin as standard.
Statistical Analyses
Means 6 SEM were calculated, and multiplecomparisons were performed using one-way anal-ysis of variance with Tukey post hoc tests. P ,.05was considered significant. The software used fordata analysis was the Statistical Package for theSocial Sciences, version 12.0 for MicrosoftWindows (SPSS, Inc., Chicago, IL).
Results
Effect of CKD Protocol and PhysicalTraining on Creatinine and UreaLevels
According to Table 2, the CKD protocol pro-duced a significant increase in creatinine andurea levels, compared with the control group
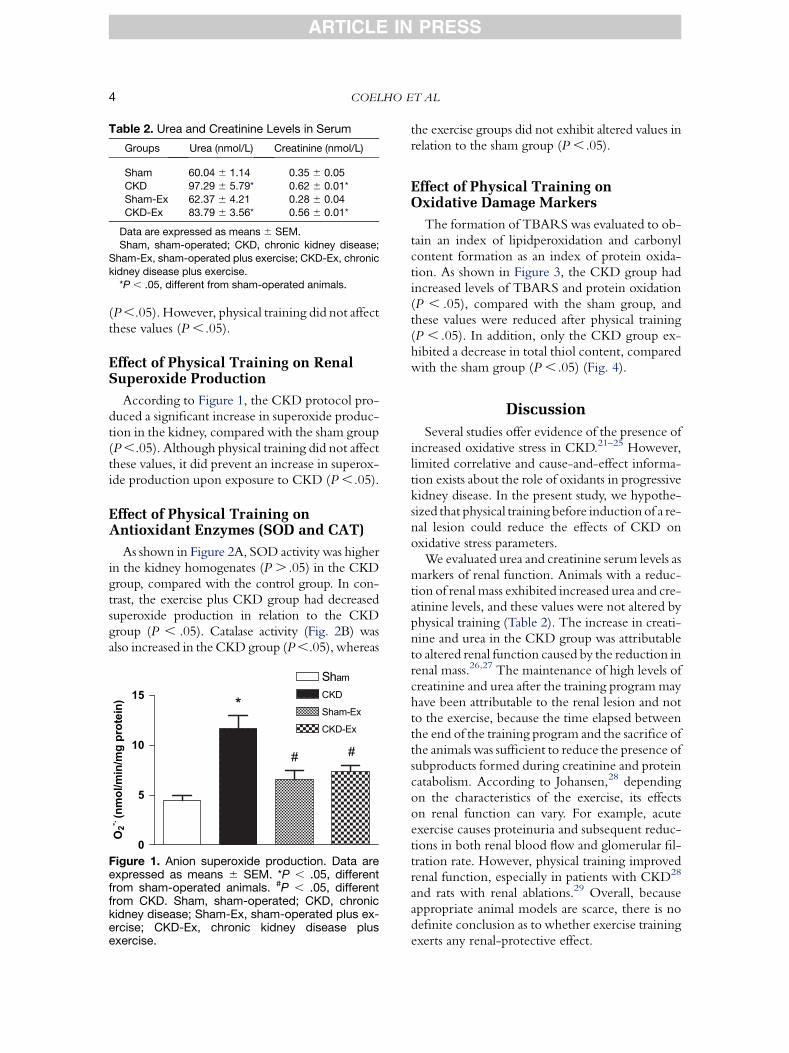
Table 2. Urea and Creatinine Levels in Serum
Groups Urea (nmol/L) Creatinine (nmol/L)
Sham 60.04 6 1.14 0.35 6 0.05
CKD 97.29 6 5.79* 0.62 6 0.01*
Sham-Ex 62.37 6 4.21 0.28 6 0.04
CKD-Ex 83.79 6 3.56* 0.56 6 0.01*
Data are expressed as means 6 SEM.
Sham, sham-operated; CKD, chronic kidney disease;
Sham-Ex, sham-operated plus exercise; CKD-Ex, chronic
kidney disease plus exercise.*P , .05, different from sham-operated animals.
COELHO ET AL4
ARTICLE IN PRESS
(P ,.05). However, physical training did not affectthese values (P , .05).
Effect of Physical Training on RenalSuperoxide Production
According to Figure 1, the CKD protocol pro-duced a significant increase in superoxide produc-tion in the kidney, compared with the sham group(P ,.05). Although physical training did not affectthese values, it did prevent an increase in superox-ide production upon exposure to CKD (P ,.05).
Effect of Physical Training onAntioxidant Enzymes (SOD and CAT)
As shown in Figure 2A, SOD activity was higherin the kidney homogenates (P . .05) in the CKDgroup, compared with the control group. In con-trast, the exercise plus CKD group had decreasedsuperoxide production in relation to the CKDgroup (P , .05). Catalase activity (Fig. 2B) wasalso increased in the CKD group (P ,.05), whereas
0
5
10
15
ShamCKD
Sham-Ex
CKD-Ex
*
# #
O2
-.
(n
mo
l/m
in/m
g p
ro
te
in)
Figure 1. Anion superoxide production. Data areexpressed as means 6 SEM. *P , .05, differentfrom sham-operated animals. #P , .05, differentfrom CKD. Sham, sham-operated; CKD, chronickidney disease; Sham-Ex, sham-operated plus ex-ercise; CKD-Ex, chronic kidney disease plusexercise.
the exercise groups did not exhibit altered values inrelation to the sham group (P , .05).
Effect of Physical Training onOxidative Damage Markers
The formation of TBARS was evaluated to ob-tain an index of lipidperoxidation and carbonylcontent formation as an index of protein oxida-tion. As shown in Figure 3, the CKD group hadincreased levels of TBARS and protein oxidation(P , .05), compared with the sham group, andthese values were reduced after physical training(P , .05). In addition, only the CKD group ex-hibited a decrease in total thiol content, comparedwith the sham group (P , .05) (Fig. 4).
Discussion
Several studies offer evidence of the presence ofincreased oxidative stress in CKD.21–25 However,limited correlative and cause-and-effect informa-tion exists about the role of oxidants in progressivekidney disease. In the present study, we hypothe-sized that physical training before induction of a re-nal lesion could reduce the effects of CKD onoxidative stress parameters.
We evaluated urea and creatinine serum levels asmarkers of renal function. Animals with a reduc-tion of renal mass exhibited increased urea and cre-atinine levels, and these values were not altered byphysical training (Table 2). The increase in creati-nine and urea in the CKD group was attributableto altered renal function caused by the reduction inrenal mass.26,27 The maintenance of high levels ofcreatinine and urea after the training program mayhave been attributable to the renal lesion and notto the exercise, because the time elapsed betweenthe end of the training program and the sacrifice ofthe animals was sufficient to reduce the presence ofsubproducts formed during creatinine and proteincatabolism. According to Johansen,28 dependingon the characteristics of the exercise, its effectson renal function can vary. For example, acuteexercise causes proteinuria and subsequent reduc-tions in both renal blood flow and glomerular fil-tration rate. However, physical training improvedrenal function, especially in patients with CKD28
and rats with renal ablations.29 Overall, becauseappropriate animal models are scarce, there is nodefinite conclusion as to whether exercise trainingexerts any renal-protective effect.

0.00
0.05
0.10
0.15
0.20
0.25 *
##
TB
AR
S (
nm
ol/m
g p
ro
tein
)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7 Sham
CKD
Sham-Ex
CKD-Ex
Sham
CKD
Sham-Ex
CKD-Ex
##
*
Ca
rb
on
yl (n
mo
l/m
g p
ro
te
in
)
A
B
Figure 3. Levels of TBARS (A) and protein carbonyl(B). Data are expressed as means 6 SEM. *P , .05,different from sham-operated animals. #P , .05, dif-ferent from CKD. Sham, sham-operated; CKD,chronic kidney disease; Sham-Ex, sham-operatedplus exercise; CKD-Ex, chronic kidney diseaseplus exercise.
0.00
0.05
0.10
0.15
0.20
0.25
Sham
CKD
Sham-Ex
CKD-Ex*
##
SO
D (U
/m
g p
ro
tein
)
0.0
0.3
0.6
0.9
1.2
1.5
1.8
Sham
CKD
Sham-Ex
CKD-Ex
*
# #
CA
T (U
/m
g p
ro
tein
)
A
B
Figure 2. Superoxide dismutase (A) and catalase (B)activities. Data are expressed as means 6 SEM. *P, .05, different from sham-operated animals. #P ,.05, different from CKD. Sham, sham-operated;CKD, chronic kidney disease; Sham-Ex, sham-op-erated plus exercise; CKD-Ex, chronic kidney dis-ease plus exercise.
EXERCISE AND ROS IN CKD 5
ARTICLE IN PRESS
Several studies showed an increase in ROS inCKD.5,21,22,30 Renal sources for ROS include ac-tivated macrophages, vascular cells, and variousglomerular cells.6 This suggests that the kidneymay be particularly susceptible to oxidative stress.Additional studies demonstrated that physical ex-ercise improves the antioxidant defense systemand the resistance of tissue to oxidative dam-age.31–33 Thus, an efficient endogenous or exoge-nous antioxidant defense system is necessary toneutralize the deleterious effects of excessiveROS in CKD.
In the present study, the increase in superoxideproduction evident in the CKD group (Fig. 1)was accompanied by a significant increase inSOD (Fig. 2A) and CAT (Fig. 2B) activities.However, the exposure of animals to physicaltraining led to a decrease in superoxide production
and antioxidant enzyme activities. Studies of hu-mans24,34–36 and animals37,38 showed that renaldisease increases oxidant production, suggestingan involvement of oxidants in the progression ofdisease.39 These studies also suggest a low levelof antioxidant enzyme activity in renal disease.5,25
It is possible that the evident differences betweenvarious studies are associated with the methodolo-gies used to determine enzymatic activity. Inaddition, we believe that the increase in bothCAT and SOD in rats with CKD in the presentstudy was attributable to the response of the anti-oxidant defense system to superoxide production.Nevertheless, the increase in antioxidant enzymeswas not sufficient to prevent oxidative damage tolipids and proteins (Fig. 3), or to decrease the thiolcontent (Fig. 4). Because physical exercise did notalter the renal enzymatic defense system, thereduction in superoxide production may havebeen related to the upregulation of uncouplingmitochondrial proteins (UCPs), or simply to an
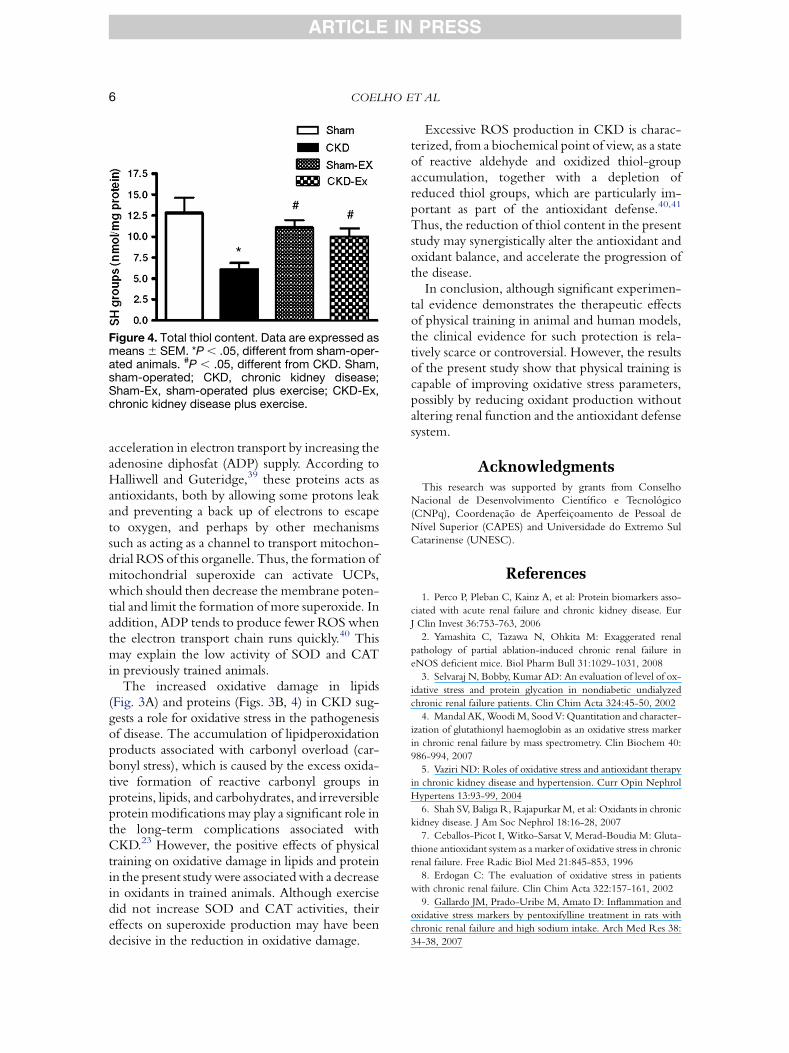
Figure 4. Total thiol content. Data are expressed asmeans 6 SEM. *P , .05, different from sham-oper-ated animals. #P , .05, different from CKD. Sham,sham-operated; CKD, chronic kidney disease;Sham-Ex, sham-operated plus exercise; CKD-Ex,chronic kidney disease plus exercise.
COELHO ET AL6
ARTICLE IN PRESS
acceleration in electron transport by increasing theadenosine diphosfat (ADP) supply. According toHalliwell and Guteridge,39 these proteins acts asantioxidants, both by allowing some protons leakand preventing a back up of electrons to escapeto oxygen, and perhaps by other mechanismssuch as acting as a channel to transport mitochon-drial ROS of this organelle. Thus, the formation ofmitochondrial superoxide can activate UCPs,which should then decrease the membrane poten-tial and limit the formation of more superoxide. Inaddition, ADP tends to produce fewer ROS whenthe electron transport chain runs quickly.40 Thismay explain the low activity of SOD and CATin previously trained animals.
The increased oxidative damage in lipids(Fig. 3A) and proteins (Figs. 3B, 4) in CKD sug-gests a role for oxidative stress in the pathogenesisof disease. The accumulation of lipidperoxidationproducts associated with carbonyl overload (car-bonyl stress), which is caused by the excess oxida-tive formation of reactive carbonyl groups inproteins, lipids, and carbohydrates, and irreversibleprotein modifications may play a significant role inthe long-term complications associated withCKD.23 However, the positive effects of physicaltraining on oxidative damage in lipids and proteinin the present study were associated with a decreasein oxidants in trained animals. Although exercisedid not increase SOD and CAT activities, theireffects on superoxide production may have beendecisive in the reduction in oxidative damage.
Excessive ROS production in CKD is charac-terized, from a biochemical point of view, as a stateof reactive aldehyde and oxidized thiol-groupaccumulation, together with a depletion ofreduced thiol groups, which are particularly im-portant as part of the antioxidant defense.40,41
Thus, the reduction of thiol content in the presentstudy may synergistically alter the antioxidant andoxidant balance, and accelerate the progression ofthe disease.
In conclusion, although significant experimen-tal evidence demonstrates the therapeutic effectsof physical training in animal and human models,the clinical evidence for such protection is rela-tively scarce or controversial. However, the resultsof the present study show that physical training iscapable of improving oxidative stress parameters,possibly by reducing oxidant production withoutaltering renal function and the antioxidant defensesystem.
AcknowledgmentsThis research was supported by grants from Conselho
Nacional de Desenvolvimento Cientıfico e Tecnologico
(CNPq), Coordenacao de Aperfeicoamento de Pessoal de
Nıvel Superior (CAPES) and Universidade do Extremo Sul
Catarinense (UNESC).
References
1. Perco P, Pleban C, Kainz A, et al: Protein biomarkers asso-
ciated with acute renal failure and chronic kidney disease. Eur
J Clin Invest 36:753-763, 2006
2. Yamashita C, Tazawa N, Ohkita M: Exaggerated renal
pathology of partial ablation-induced chronic renal failure in
eNOS deficient mice. Biol Pharm Bull 31:1029-1031, 2008
3. Selvaraj N, Bobby, Kumar AD: An evaluation of level of ox-
idative stress and protein glycation in nondiabetic undialyzed
chronic renal failure patients. Clin Chim Acta 324:45-50, 2002
4. Mandal AK, Woodi M, Sood V: Quantitation and character-
ization of glutathionyl haemoglobin as an oxidative stress marker
in chronic renal failure by mass spectrometry. Clin Biochem 40:
986-994, 2007
5. Vaziri ND: Roles of oxidative stress and antioxidant therapy
in chronic kidney disease and hypertension. Curr Opin Nephrol
Hypertens 13:93-99, 2004
6. Shah SV, Baliga R, Rajapurkar M, et al: Oxidants in chronic
kidney disease. J Am Soc Nephrol 18:16-28, 2007
7. Ceballos-Picot I, Witko-Sarsat V, Merad-Boudia M: Gluta-
thione antioxidant system as a marker of oxidative stress in chronic
renal failure. Free Radic Biol Med 21:845-853, 1996
8. Erdogan C: The evaluation of oxidative stress in patients
with chronic renal failure. Clin Chim Acta 322:157-161, 2002
9. Gallardo JM, Prado-Uribe M, Amato D: Inflammation and
oxidative stress markers by pentoxifylline treatment in rats with
chronic renal failure and high sodium intake. Arch Med Res 38:
34-38, 2007

EXERCISE AND ROS IN CKD 7
ARTICLE IN PRESS
10. Pechter U: Regular low-intensity aquatic exercise im-
proves cardiorespiratory functional capacity and reduces protein-
uria in chronic renal failure patients. Nephrol Dial Transplant
18:624-625, 2003
11. Moinuddin I, Leehey DJ: A comparison of aerobic exercise
and resistance training in patients with and without chronic kidney
disease. Adv Chronic Kidney Dis 15:83-96, 2008
12. Adams G, Zhan C, Haddad F: Voluntary exercise during
chronic renal failure in rats. Med Sci Sports Exerc 37:557-562,
2005
13. Fujihara CK, Antunes GR, Mattar AL, et al: Chronic inhi-
bition of nuclear factor-B attenuates renal injury in the 5/6 renal
ablation model. Am J Physiol Ren Physiol 292:92-99, 2007
14. Poderoso JJ, Carreras MC, Lisdero C, et al: Nitric oxide in-
hibits electron transfer and increases superoxide radical production
in rat heart mitochondrial and submitochondrial particles. Arch
Biochem Biophys 328:85-92, 1996
15. Bannister JV, Calabrese L: Assays for SOD. Methods
Biochem Anal 32:279-312, 1987
16. Aebi H: Catalase in vitro. Methods Enzymol 105:121-126,
1984
17. Draper HH, Hadley M: Malondialdehyde determination as
index of lipid peroxidation. Methods Enzymol 186:421-431,
1990
18. Levine RL, Garland D, Oliver CN, et al: Determination of
carbonyl content in oxidatively modified proteins. Methods Enzy-
mol 186:464-478, 1990
19. Aksenov MY, Markesberya WR: Changes in thiol content
and expression of glutathione redox system genes in the hippo-
campus and cerebellum in Alzheimer’s disease. Neurosci Lett
302:141-145, 2001
20. Lowry OH, Rosebough NG, Farr AL, et al: Protein
measurement with the Folin phenol reagent. J Biol Chem 193:
265-275, 1951
21. Goeddeke-Mericke CM: Oxidative stress in chronic
kidney disease. Rev Adv Chronic Kidney Dis 12:326-334, 2005
22. Campesea VM, Sindhub RS, Yea S, et al: Regional expres-
sion of NO synthase, NAD(P)H oxidase and superoxide dismutase
in the rat brain. Res Rep 1134:27-32, 2007
23. Miyata T, Ueda Y, Izuhara Y: Accumulation of carbonyls
accelerates the formation of pentosidine, an advanced glycation
end product: carbonyl stress in uremia. J Am Soc Nephrol 9:
2349-2356, 1998
24. Oberg BP, McMenamin E, Lucas FL, et al: Increased prev-
alence of oxidant stress and inflammation in patients with moder-
ate to severe chronic kidney disease. Kidney Int 65:1009-1016,
2004
25. Sindhu RK, Ehdaie A, Farmand F, et al: Expression of cat-
alase and glutathione peroxidase in renal insufficiency. Biochim
Biophys Acta 1743:86-92, 2005
26. Fujihara CK, Sena CR, Malheiros DM, et al: Short-term
nitric oxide inhibition induces progressive nephropathy after re-
gression of initial renal injury. Am J Physiol Ren Physiol 290:
632-640, 2006
27. Fujihara CK, Antunes GR, Mattar A: Chronic inhibition
of nuclear factor-KB attenuates renal injury in the 5/6 renal abla-
tion model. Am J Physiol Ren Physiol 292:92-99, 2007
28. Johansen KL: Exercise and chronic kidney disease current
recommendations. Sports Med 35:485-499, 2005
29. Kanazawa M, Kawamura T, Li L, et al: Combination of ex-
ercise and enalapril enhances renoprotective and peripheral effects
in rats with renal ablation. Am J Hypertens 19:80-86, 2006
30. Agarwal R: On the nature of proteinuria with acute renal
injury in patients with chronic kidney disease. Am J Physiol
Ren Physiol 288:265-271, 2005
31. Pinho R, Andrades ME, Oliveira MR, et al: Imbalance in
SOD/CATactivities in rat skeletal muscles submitted to treadmill
training exercise. Cell Biol Int 30:848-853, 2006
32. Radak Z, Kumagai S, Taylor AW, et al: Effects of exercise
on brain function: role of free radicals. Appl Physiol Nutr Metab
32:942-946, 2007
33. Himmelfarb J, McMonagle E, McMenamin E: Plasma pro-
tein thiol oxidation and carbonyl formation in chronic renal fail-
ure. Kidney Int 58:2571-2578, 2000
34. Lin JL, Lin-Tan DT, Hsu KH, et al: Environmental lead ex-
posure and progression of chronic renal diseases in patients with-
out diabetes. N Engl J Med 348:277-286, 2003
35. Descamps-Latscha B, Witko-Sarsat V, Nguyen-Khoa T,
et al: Early prediction of IgA nephropathy progression: proteinuria
and AOPP are strong prognostic markers. Kidney Int 66:
1606-1612, 2004
36. Agarwal R: Proinflammatory effects of oxidative stress in
chronic kidney disease: role of additional angiotensin II blockade.
Am J Physiol Ren Physiol 284:863-869, 2003
37. Kuo HT, Kuo MC, Chiu YW, et al: Increased glomerular
and extracellular malondialdehyde levels in patients and rats with
focal segmental glomerulosclerosis. Eur J Clin Invest 35:245-250,
2005
38. Haugen E, Nath KA: The involvement of oxidative stress in
the progression of renal injury. Blood Purif 17:58-65, 1999
39. Halliwell B, Gutteridge JMC: Free Radicals in Biology
Medicine. New York: Oxford University Press, 2007
40. Himmelfarb J, Macmenamin E: Plasma aminothiol oxida-
tion in chronic renal failure. Kidney Int 61:705-716, 2002
41. Galli F, Floridi AG, Floridi A, et al: Accumulation of vita-
min E metabolites in the blood of renal failure patients. Clin Nutr
23:205-212, 2004
Copyright © 2022 FDOKUMEN




















