
Extended Use of Dabigatran, Warfarin, or Placebo in Venous Thromboembolism
Upload
independentCategory
view
0download
0
ORIGINAL RESEARCH
Phlebitis risk varies by peripheral venous catheter site and increases
after 96 hours: a large multi-centre prospective study
Giancarlo Cicolini*, Lamberto Manzoli*, Valentina Simonetti, Maria Elena Flacco, Dania
Comparcini, Lorenzo Capasso, Angela Di Baldassarre & Ghaleb Eltaji Elfarouki
Accepted for publication 1 March 2014
Correspondence to G. Cicolini:
e-mail: [email protected]
*These authors equally contributed to this
study.
Giancarlo Cicolini MSN PhD
Nurse Director
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
and ASL 02 Abruzzo, Italy
Lamberto Manzoli MD MPH
Associate Professor of Epidemiology and
Public Health
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
Valentina Simonetti MSN RN
PhD Student
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
Maria Elena Flacco MD
Graduate School of Public Health Intern
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
Dania Comparcini MSN RN
PhD Student
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
Lorenzo Capasso MD
PhD Student
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
C ICOL IN I G . , MANZOL I L . , S IMONETT I V . , F LACCO M.E . , COMPARC IN I
D . , CAPAS SO L . , D I BALDASSARRE A . & ELTA J I ELFAROUK I G . ( 2 0 1 4 ) Phle-
bitis risk varies by peripheral venous catheter site and increases after 96 hours: a
large multi-center prospective study. Journal of Advanced Nursing 00(0), 000–
000. doi: 10.1111/jan.12403
AbstractAims. This multi-centre prospective field study evaluated whether peripheral
venous catheter site of insertion influences the risk of catheter-related phlebitis.
Potential predictors of phlebitis were also investigated.
Background. Millions of patients worldwide use peripheral venous catheters,
which frequently cause local complications including phlebitis, infection and
obstruction. Although phlebitis predictors have been broadly investigated,
uncertainties remain on the potential effect of cannulation anatomical site,
duration and the appropriate time for catheter removal.
Design. A prospective cohort design was carried out from January–June 2012.
Methods. The clinical course of each patient who received a new peripheral
venous catheter for any cause in five Italian hospitals was followed by trained
nurses until catheter removal. The presence of phlebitis was assessed every
24 hours using the Visual Infusion Phlebitis score. Analyses were based upon
multilevel mixed-effects regression.
Results. The final sample consisted of 1498 patients. The average time for
catheters in situ was 65�6 hours and 23�6% of the catheters were in place beyond
96 hours. Overall phlebitis incidence was 15�4%, 94�4% of which were grade 1.
The likelihood of phlebitis independently increased with increasing catheter
duration, being highest after 96 hours. Compared with patients with catheter
placed in the dorsum of the hand (22�8% of the sample), those with the catheter
located in the antecubital fossa (34�1%) or forearm were less likely to have a
phlebitis of any grade.
Conclusions. Antecubital fossa and forearm veins may be preferential sites for
peripheral venous cannulation. Our results support Centers for Disease Control
and Prevention recommendations to replace catheters in adults no later than
96 hours. A relevant proportion of healthcare personnel did not adhere to such
guidelines – more attention to this issue is required.
© 2014 John Wiley & Sons Ltd 1
continued on page 2

Angela Di Baldassarre MD PhD
Professor of Motor Sciences
Department of Medicine and Aging
Sciences, University of Chieti-Pescara, Italy
Ghaleb Eltaji Elfarouki MPH PhD
Professor
Center for Research on Health and Social
Care Management, SDA Bocconi, Milan,
Italy
Keywords: catheter site, catheter time in situ, catheterization, iatrogenic events,
infusion-related phlebitis, nurses, nursing, peripheral venous catheter, phlebitis,
thrombo-phlebitis
Introduction
Peripheral venous catheters (PVCs) are used in the care of
millions of patients worldwide, usually for intravenous fluid
infusion and other vital, often life-saving, clinical interven-
tions (McCallum & Higgins 2012). It has been estimated
that as many as one in three hospital patients have a PVC
in place at any given time (Reilly et al. 2007).
The use of PVCs puts patients at risk for local and systemic
infective complications, including bloodstream infections
(Cicolini et al. 2009). While PVCs rarely cause systemic
complications (Maki et al. 2006), they are frequently associ-
ated with phlebitis, catheter-related infection and obstruction
of the catheter (Bregenzer et al. 1998); complications which
lead to longer admissions, additional healthcare costs and
discomfort and morbidity for patients (McCallum & Higgins
2012). This has evoked the need for thorough patient assess-
ment and careful catheter management and observation and
several studies sought to investigate the determinants of phle-
bitis to devise strategies and guidelines for risk reduction
(Maki & Ringer 1991, Lundgren et al. 1993, Bregenzer et al.
1998, Curran et al. 2000, Karadag & Gorgulu 2000, Cornely
et al. 2002, Karadeniz et al. 2003, Uslusoy & Mete 2008,
Rego Furtado 2011).
In addition to patient-related factors, which are often
resistant to modification, a significant relationship was doc-
umented, independently and in combination, between phle-
bitis risk and catheter material and size (needle gauge)
(Maki & Ringer 1991, Lundgren et al. 1993, Bregenzer
et al. 1998, Curran et al. 2000, Cornely et al. 2002, Abbas
et al. 2007, Singh et al. 2008, Uslusoy & Mete 2008, Cico-
lini et al. 2009, Forni et al. 2010). Cicolini et al. (2009),
for example, found that phlebitis incidence was significantly
lower in patients with 22 gauge vs. 16–18 gauge cannulas.
The frequency of catheter insertion and indwelling time
have also been found to be related to phlebitis risk (Maki
& Ringer 1991, Bregenzer et al. 1998, Webster et al. 2007,
2008, 2010, Uslusoy & Mete 2008, Lee et al. 2009, Rego
Furtado 2011, Mestre Roca et al. 2012, Rickard et al.
2012). Finally, the type of infused fluid was also found to
affect phlebitis risk and applying aseptic, non-touch, princi-
ples at insertion reduced the incidence of infective compli-
cations (Maki & Martin 1975, Melly et al. 1975, Sheth
et al. 1983, Maki & Ringer 1991, O’Grady et al. 2011).
Some major uncertainties remain on the relationship
between catheter anatomical site and risk of phlebitis: the
latest Centers for Disease Control and Prevention (CDC)
guidelines recommend the use of the upper extremities for
peripheral catheterization with no more detailed or specific
Why is this research needed?
• The latest Centers for Disease Control and Prevention
guidelines recommend the use of the upper extremities for
peripheral catheterization with no specification of preferred
anatomical site.
• There is a debate whether dwell times of intravenous cann-
ulae could be safely extended after 96 hours if clinically
indicated.
What are the key findings?
• Placing peripheral venous cannulae in the antecubital fossa
and forearm veins rather than in the dorsum of the hand
may reduce the risk of phlebitis by 30–50%.
• The incidence of phlebitis was highest for catheters left in
place more than 96 hours.
• Healthcare personnel often do not follow current recom-
mendations of catheter indwelling time.
How should the findings be used to influence policy/practice/research/education?
• Antecubital fossa and forearm veins may be the preferred
anatomical sites for peripheral intravenous cannulation.
• Peripheral venous catheters should remain in situ not more
than 96 hours after insertion.
• Operators should be sensitized to the clinical importance to
follow current recommendation on peripheral venous cann-
ulation management.
2 © 2014 John Wiley & Sons Ltd
G. Cicolini et al.

recommendation about the preferred site of insertion to
minimize risk of infection (O’Grady et al. 2011).
Background
Many authors investigated the influence of anatomical site
on phlebitis rate with contrasting results; a major source of
difficulty is the wide heterogeneity in defining and classify-
ing anatomical sites among studies (Maki & Ringer 1991,
Bregenzer et al. 1998, White 2001, Cornely et al. 2002,
Karadeniz et al. 2003, Kagel & Rayan 2004, Webster et al.
2007, Uslusoy & Mete 2008, Cicolini et al. 2009, Lee et al.
2009, Forni et al. 2010, Rego Furtado 2011, Mestre Roca
et al. 2012). Further, the definition of catheter-related infec-
tions remains unclear in the literature and clinical presenta-
tions vary. Thus, what constitutes the preferred catheter
site in terms of infection risk rather than convenience
remains an unresolved issue.
To our knowledge, only one study investigated and com-
pared, as its main objective, the relationship between differ-
ent anatomical sites and incidence of phlebitis with a view to
identifying the safest location (Cicolini et al. 2009). This
observational study was conducted on a sample of 427
patients from surgical and medical wards in one Italian hos-
pital; the incidence of phlebitis was found to be highest in
patients with cannulae inserted in the dorsal aspect of the
hand. The authors therefore advocated the use of antecubital
fossa veins rather than hand and forearm veins. Phlebitis was
assessed using the checklist from (Lundgren et al. 1993); all
insertions were carried out by nurses. A major limitation was
that the proportion of patients receiving catheters in the dor-
sal aspect of the hand was significantly lower than that of
other sites; furthermore, many patients were admitted to gen-
eral surgery wards where the lengths of stay were typically
shorter than for internal medicine units.
Another unsolved issue pertains to the effect of catheter
duration and the appropriate time for removal: prominent
national guidelines state that elective removal of peripheral
intravenous catheters should be considered if the PVC has
been in situ for 72–96 hours to reduce risk of complications
(Department of Health 2011). Other guidelines have been
more ambitious, suggesting replacement every 48–72 hours
(Tagalakis et al. 2002). In fact, some studies have been con-
ducted to investigate the possible merit of elective replace-
ment, i.e. in the absence of any clinical complications, of
peripheral intravenous catheters to prevent phlebitis occur-
ring. A systematic review conducted to search for relevant
randomized controlled trials identified three small trials,
with samples in two of the trials including patients requir-
ing parenteral nutrition (Idvall & Gunningberg 2006).
Although time intervals for elective replacement in the stud-
ies did vary, the overall conclusion was of limited scientific
evidence, suggesting but not confirming that elective
replacement of peripheral intravenous catheters reduces the
incidence (and severity) of phlebitis. In these studies, how-
ever, data collectors were not blinded as to whether the
patients were in intervention or control groups; and control
groups were those, where catheters were replaced on signs
and symptoms of complication and not merely on an elec-
tive scheduled basis.
The study
Aim
The primary objective was to evaluate whether PVC site of
insertion influences the risk of catheter-related phlebitis. We
also investigated other potential predictors of phlebitis with
a special emphasis on indwelling time (time in situ, i.e. dura-
tion between insertion and removal) for venous catheters.
Design
A prospective cohort design was carried out on a mixed
population of patients from five Italian hospitals (Ancona,
Chieti, Gallipoli, San Benedetto del Tronto, Vasto) based
on three different regions along the Adriatic coast (Marche,
Abruzzo and Puglia).
Participants
The criteria for inclusion were: patients admitted to medical
or surgical wards in an ordinary setting (no day-hospital or
day-surgery), age 18 years or above, written informed con-
sent. Patients were excluded if they had recognized cogni-
tive impairments, were on renal dialysis, were admitted or
had their catheter placed in an emergency department, were
known to be immune-compromised or had known blood
infections.
Sample size estimation
Sample size estimation was based on the following parame-
ters: 10% and 20% of phlebitis at the end of the follow-up
in the subjects with cannulae in the antecubital fossa and in
the dorsum of the hand, respectively (Cicolini et al. 2009);
alpha 0�05; 5% loss to follow-up. Using such parameters in
a two-tailed Chi-square test, 234 subjects were required in
each group to achieve 80% statistical power. Considering
multiple adjustments in multivariate modelling, we conser-
vatively decided to enrol at least 334 patients in each group.
© 2014 John Wiley & Sons Ltd 3
JAN: ORIGINAL RESEARCH Predictors of infusion-related phlebitis

Data collection
Study protocol and outcomes
Five trained nurses (one for each hospital), in coordination
with local personnel, took part in recruiting eligible
patients, collecting and recording their data up to the
96 hours after admission; it was presumed that all newly
inserted catheters would be removed by then. The 96-hour
rule has been violated in several cases and this is discussed
in detail in the results section. The recruiting nurses acted
as observers and could not make decisions to insert cathe-
ters or remove them; they did however remind local staff of
current CDC guidelines (O’Grady et al. 2011). This divi-
sion of labour was adopted both to simulate best routine
clinical practice conditions and to reduce the potential influ-
ence of local health personnel on data recording and collec-
tion. The primary outcome of interest was the occurrence
of phlebitis; the presence of phlebitis (and degree or grade)
was assessed at 24, 48, 72 and 96 hours following catheter
insertion. Thrombo-phlebitis is defined as the presence of at
least two symptoms/signs among erythema, swelling or pal-
pable venous cord (Maki & Ringer 1991).
The research nurses were trained to recognize and classify
infusion-related phlebitis implementing the Visual Infusion
Phlebitis score proposed by Gallant and Schultz (Gallant &
Schultz 2006) with grades of severity from 1–5. In addition
to the number of hours for catheters in situ and the ana-
tomical placement site, the following variables were
recorded at the time of catheter insertion for all partici-
pants: age, gender, body mass index (BMI), smoking status,
place of admission, category of admission, type of person-
nel inserting catheter, whether patient was on antibiotic
therapy, type of infusion, cannula needle gauge, catheter
material and type of dressing used.
In the previous single-site observational study, three
upper extremity venous access locations were defined: ant-
ecubital fossa, forearm veins and the dorsal aspect of the
hand (Cicolini et al. 2009). Both studies have similar
exclusion criteria and it was decided to use the same clas-
sifications for cannula position. More specifically, when
we refer to antecubital fossa veins, they include the med-
ian cubital vein, median cephalic vein, the cephalic vein
(along the lateral aspect of the antecubital fossa) and the
basilic vein (on the postero-medial aspect of the wrist);
forearm veins include the superficial median vein of the
forearm, the cephalic vein (along the radial aspect of the
forearm) and the part of the basilic vein posterior to the
ulnar border of the forearm; hand veins include the dorsal
metacarpal veins. The different factors mentioned thus far
were each considered as potential predictors of phlebitis or
confounders of the association between catheter site and
phlebitis.
Ethical considerations
The study protocol received full approval from the institu-
tional review board and the local ethics committee of the
coordinating centre at the University of Chieti.
Data analysis
Initially the difference in the incidence of phlebitis of any
grade during follow-up according to the anatomical site of
the catheter was investigated using stratification per each
defined time-point: 24, 25–48, 49–72, 73–96 and 97–
120 hours. Kaplan–Meier survival estimates and log-rank
test by site were also used without stratification, including
the whole follow-up period. The validity of constant inci-
dence ratios over the follow-up period was checked using
Nelson-Aalen cumulative hazard estimates (Hosmer &
Lemeshow 1999).
The potential independent predictors of phlebitis were
evaluated using Cox proportional hazards analysis and then
multilevel mixed-effects regression, the latter to estimate the
potential impact of time (Rabe-Hesketh & Skrondal 2008).
In both analyses, all recorded covariates were included into
the final models a priori, although those that are continuous
or ordinal variables were tested for transformation into sev-
eral alternative dummy variables. Multicollinearity, interac-
tions and higher-power terms were tested for all covariates
in Cox analysis; Schoenfeld test was performed to check
the validity of proportional hazards assumption.
Although it is not specifically recommended in most guide-
lines to remove the catheter on the detection of grade 1 phle-
bitis (slight pain or redness close to the insertion site), this
was requested by the approving ethics committee. We there-
fore advised personnel in participating centres to remove
catheters on observing phlebitis of any grade. During the
study, catheters remained in situ despite a grade 1 phlebitis
in 32 cases, but only until one subsequent time-point. In the
analysis, all patients including the above 32 were censured at
the time-point where phlebitis was observed.
The mixed model was set as repeated regression analysis
(with one observation every 24 hours of follow-up), using a
patient’s identification number and hospital/centre as the
cluster levels, both cases assuming an independent correla-
tion structure. However, all models were repeated using an
exchangeable correlation structure, with marginal increases
in standard errors and no qualitative change. Time was
included in the model either as an ordinal variable or using
4 © 2014 John Wiley & Sons Ltd
G. Cicolini et al.
dummy variables for each 24-hour unit (0–24 hours being
the reference category). Given that all dummy odds ratios
(ORs) of time were significantly associated with phlebitis
and were quite linearly decreasing, time was treated as
ordinal in the final model: the OR of time is thus to be
interpreted as the variation in the odds of phlebitis for
every 24-hour increment (Parruti et al. 2010).
Given that the results of the survival and multilevel analy-
ses were substantially similar, we only reported the estimates
from the mixed model to avoid redundancy and include the
estimate of the effect of time. A two-tailed P value of 0�05was deemed significant for all analyses, which were per-
formed using Stata 10.1 software package (Stata Corp.,
College Station, TX, USA, 2007). Results with averages are
given along with 95% confidence intervals.
Validity and reliability
We followed participants’ clinical course using the Visual
Infusion Phlebitis (VIP) scale, that has shown content valid-
ity, inter-rater reliability higher than 85% and clinically
feasibility (Gallant & Schultz 2006) and it is recommended
in the Infusion Nursing Standards of Practice to determine
when an intravenous catheter should be removed (Infusion
Nurses Society 2006).
Results
Recruitment was carried out from January–June 2012,
inviting a total of 1539 (eligible) inpatients. Only 41 eligi-
ble patients did not consent to participate and thus the final
sample was 1498 patients (mean age 60�8, SD 20�7; 41�2%males – Table 1). Overall, 22�8% of the participants had
their catheter inserted on the dorsum of the hand, 34�1% in
the antecubital fossa and 41�1% in veins in the forearm.
The average time for catheters in situ was 65�6 hours (SD
34�5), a relatively lengthy period considering that many
patients had their cannulae removed due to phlebitis or no
longer requiring them. Although current guidelines recom-
mend that all peripheral catheters be removed and replaced
if necessary before reaching 96 hours, in 23�6% of cases the
same catheter was in place beyond the 96 hour of follow-
up (Table 1). Often this was not an oversight but due to
conscious decisions from personnel or resistance from
patients. In such cases, given that the study was not inter-
ventional in nature, the researchers’ role was confined to
strongly recommending the immediate removal of over-stay-
ing catheters to local health professionals. We subsequently
planned an additional visit at 120 hours postinsertion,
where was evaluated whether catheters were removed and
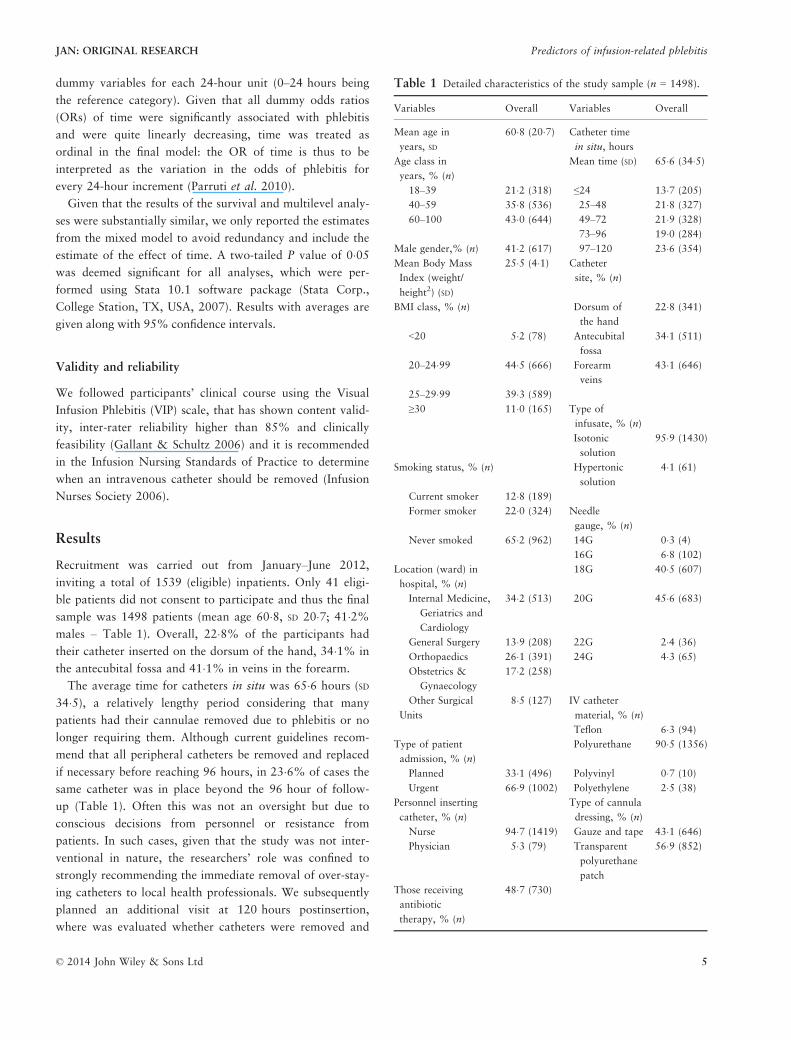
Table 1 Detailed characteristics of the study sample (n = 1498).
Variables Overall Variables Overall
Mean age in
years, SD
60�8 (20�7) Catheter time
in situ, hours
Age class in
years, % (n)
Mean time (SD) 65�6 (34�5)
18–39 21�2 (318) ≤24 13�7 (205)
40–59 35�8 (536) 25–48 21�8 (327)
60–100 43�0 (644) 49–72 21�9 (328)
73–96 19�0 (284)
Male gender,% (n) 41�2 (617) 97–120 23�6 (354)
Mean Body Mass
Index (weight/
height2) (SD)
25�5 (4�1) Catheter
site, % (n)
BMI class, % (n) Dorsum of
the hand
22�8 (341)
<20 5�2 (78) Antecubital
fossa
34�1 (511)
20–24�99 44�5 (666) Forearm
veins
43�1 (646)
25–29�99 39�3 (589)
≥30 11�0 (165) Type of
infusate, % (n)
Isotonic
solution
95�9 (1430)
Smoking status, % (n) Hypertonic
solution
4�1 (61)
Current smoker 12�8 (189)
Former smoker 22�0 (324) Needle
gauge, % (n)
Never smoked 65�2 (962) 14G 0�3 (4)
16G 6�8 (102)
Location (ward) in
hospital, % (n)
18G 40�5 (607)
Internal Medicine,
Geriatrics and
Cardiology
34�2 (513) 20G 45�6 (683)
General Surgery 13�9 (208) 22G 2�4 (36)
Orthopaedics 26�1 (391) 24G 4�3 (65)
Obstetrics &
Gynaecology
17�2 (258)
Other Surgical
Units
8�5 (127) IV catheter
material, % (n)
Teflon 6�3 (94)
Type of patient
admission, % (n)
Polyurethane 90�5 (1356)
Planned 33�1 (496) Polyvinyl 0�7 (10)
Urgent 66�9 (1002) Polyethylene 2�5 (38)
Personnel inserting
catheter, % (n)
Type of cannula
dressing, % (n)
Nurse 94�7 (1419) Gauze and tape 43�1 (646)
Physician 5�3 (79) Transparent
polyurethane
patch
56�9 (852)
Those receiving
antibiotic
therapy, % (n)
48�7 (730)
© 2014 John Wiley & Sons Ltd 5
JAN: ORIGINAL RESEARCH Predictors of infusion-related phlebitis
the timing; if a cannula was still in situ at this point, which
was the case in 5�3% of the sample, local health profession-
als were requested to have it removed immediately.
Overall, 231 patients (15�4%) were recorded as having an
episode of phlebitis, of which 94�4% were grade 1 phlebitis;
the most serious degree observed was grade 3. When univari-
ate analysis was conducted, the frequency of phlebitis sub-
stantially and significantly differed according to several
variables: age, smoking status, inpatient hospital ward, type
of admission, whether on antibiotic therapy or not, catheter
time in situ, catheter anatomical site, needle gauge and cath-
eter material (Table 2). However, at multivariate (multilev-
el) analysis, only catheter insertion site, length of time in situ
Table 2 Incidence of phlebitis (%) and selected variables
(n = 231 in the overall sample of 1498 patients).
Variables
Phlebitis,
% Variables
Phlebitis,
%
In overall sample 15�4 Catheter timein situ, hours≤24 2�6
Age category
in years
* 25–48 4�9
18–39 11�3 49–72 6�040–59 14�5 73–96 3�860–100 18�2 97–120 13�0
Gender Catheter
insertion site
*
Females 15�8 Dorsum of
the hand
19�0
Males 14�9 Antecubital
fossa
12�9
Forearm 15�5Body mass index
<20 16�7 Type of infusate
20–24�99 15�9 Isotonic
solution
15�2
25–29�99 14�1 Hypertonic
solution
19�7
≥30 17�6Needle gaugeused
*
Cigarette smoking
status
* 14G/16G 14�0
Current 9�5 18G 11�7Former 24�1 20G 16�2Never smoked 12�9 22G/24G 33�7
Admission hospitallocation (ward)
* Cathetermaterial
*
Internal Medicine,
Geriatrics and
Cardiology
24�6 Other
materials
26�1
General Surgery 16�3 Polyurethane 14�3Orthopaedics 5�6Obstetrics &
Gynaecology
13�9 Type of cannula
dressingOther Surgical
Units
10�2 Gauze and tape 14�0
Transparent
polyurethanepatch
16�5
Type of
admission
*
Planned 11�0Urgent 17�6
Personnel inserting
catheterNurse 15�6Physician 11�4
Whether on
antibiotic therapy
*
No 11�7Yes 19�5
*P < 0�05 – Chi-squared test.
Table 3 Results of the multivariate analysis predicting phlebitis
during follow-up period (mixed model with two cluster levels: hos-
pital and identification).
Variables OR (95% CI) P*
Catheter insertion site
Dorsum of the hand (Ref.) 1 –
Antecubital fossa 0�66 (0�46–0�95) 0�026Forearm veins 0�52 (0�32–0�84) 0�008
Catheter time in situ,
additional 24 hours
1�05 (1�03–1�07) <0�001
In-patient location (ward)
Internal Medicine,
Geriatrics, Cardiology (Ref.)
1 –
General Surgery 0�61 (0�38–0�98) 0�041Orthopaedics 0�53 (0�29–0�95) 0�034Obstetrics & Gynaecology 1�50 (0�80–2�78) 0�2Other Surgical Units 0�66 (0�35–1�25) 0�2
Age, 1 additional year 1�00 (0�99–1�01) 0�5Male vs. female gender 0�91 (0�66–1�24) 0�5Body Mass Index,
1 additional (kg/m2)
1�01 (0�98–1�04) 0�7
Cigarette smoking status
Current (Ref.) 1 –
Former 1�35 (0�98–1�85) 0�064Never smoked 0�88 (0�51–1�52) 0�7
Urgent vs. planned admission 1�21 (0�85–1�72) 0�3Physician vs. nurse
inserting catheter
0�73 (0�35–1�52) 0�4
Whether on antibiotic
therapy (yes vs. no)
1�09 (0�81–1�47) 0�6
Type of infusion:
Hypertonic vs. isotonic solution
1�16 (0�63–2�13) 0�6
Needle gauge, 1 level greater 1�11 (0�93–1�33) 0�2Catheter material:
Polyurethane vs. others
0�67 (0�42–1�07) 0�095
Type of cannula dressing:
Transparent polyurethane
patch vs. gauze and tape
0�97 (0�66–1�44) 0�9
6 © 2014 John Wiley & Sons Ltd
G. Cicolini et al.
and inpatient hospital ward were found to be significantly
associated with incidence of phlebitis (Table 3). In
particular, when compared to patients with a catheter placed
in the dorsum of the hand, those with the catheter located in
the antecubital fossa or forearm were less likely to have an
episode of phlebitis of any grade recorded (Adjusted ORs
0�66 and 0�52, respectively; both P < 0�05). Also, the proba-bility of having phlebitis was lower for patients admitted to
general surgery and orthopaedics wards compared with
patients admitted to the medical (internal medicine) units
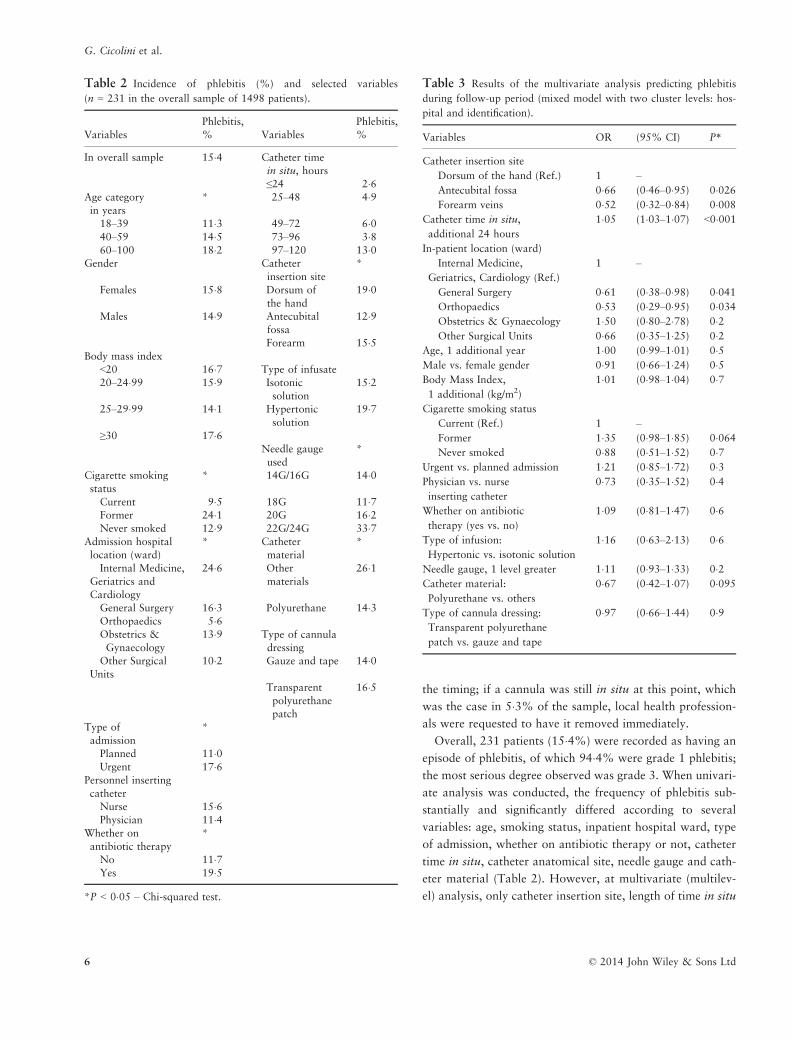
(ORs 0�61 and 0�51, respectively; both P < 0�05).Finally, the odds of having a recorded phlebitis episode
increased on average by 5% with every 24 hour increment
of catheter time in situ. All time-points were associated with
an independent and significant increase in the likelihood of
having phlebitis when compared with the first (0–24 hours –
Table 3). Notably, the frequency of phlebitis was highest for
those having the same catheter for 96–120 hours (Figure 1).
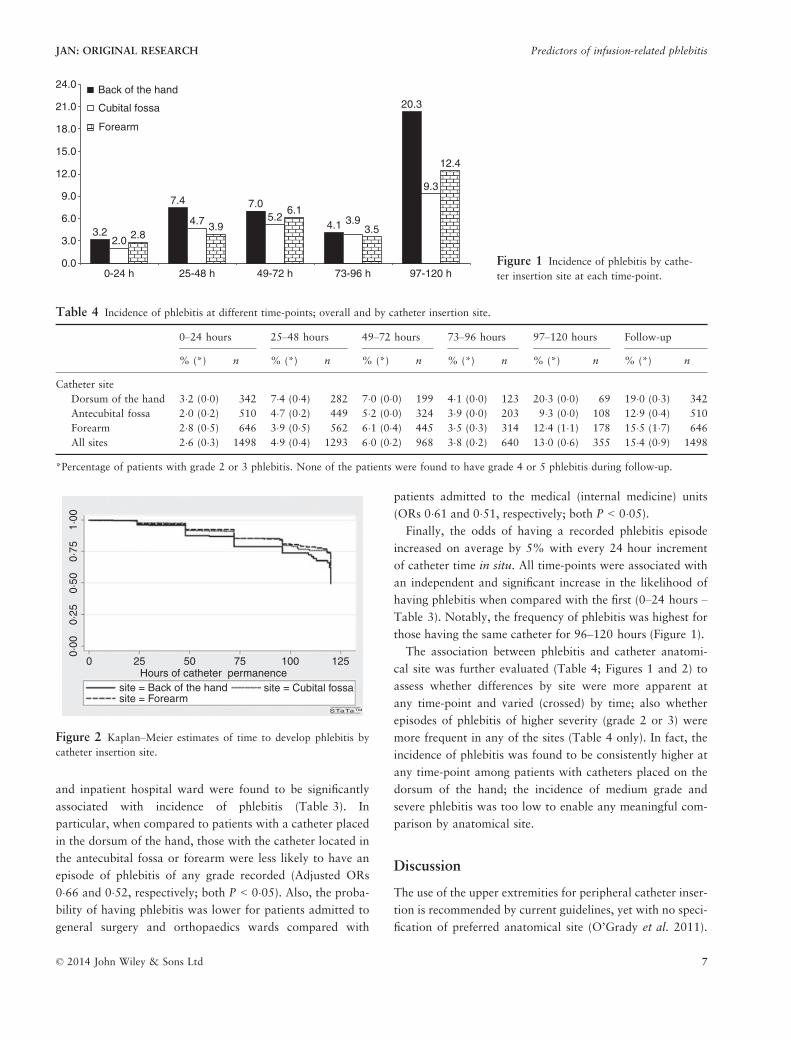
The association between phlebitis and catheter anatomi-
cal site was further evaluated (Table 4; Figures 1 and 2) to
assess whether differences by site were more apparent at
any time-point and varied (crossed) by time; also whether
episodes of phlebitis of higher severity (grade 2 or 3) were
more frequent in any of the sites (Table 4 only). In fact, the
incidence of phlebitis was found to be consistently higher at
any time-point among patients with catheters placed on the
dorsum of the hand; the incidence of medium grade and
severe phlebitis was too low to enable any meaningful com-
parison by anatomical site.
Discussion
The use of the upper extremities for peripheral catheter inser-
tion is recommended by current guidelines, yet with no speci-
fication of preferred anatomical site (O’Grady et al. 2011).
3.2
7.4 7.0
4.1
20.3
2.0
4.7 5.2
9.3
2.83.9
6.1
3.5
12.4
3.9
0.0
3.0
6.0
9.0
12.0
15.0
18.0
21.0
24.0
0-24 h 25-48 h 49-72 h 73-96 h 97-120 h
Back of the hand
Cubital fossa
Forearm
Figure 1 Incidence of phlebitis by cathe-
ter insertion site at each time-point.
Table 4 Incidence of phlebitis at different time-points; overall and by catheter insertion site.
0–24 hours 25–48 hours 49–72 hours 73–96 hours 97–120 hours Follow-up
% (*) n % (*) n % (*) n % (*) n % (*) n % (*) n
Catheter site
Dorsum of the hand 3�2 (0�0) 342 7�4 (0�4) 282 7�0 (0�0) 199 4�1 (0�0) 123 20�3 (0�0) 69 19�0 (0�3) 342
Antecubital fossa 2�0 (0�2) 510 4�7 (0�2) 449 5�2 (0�0) 324 3�9 (0�0) 203 9�3 (0�0) 108 12�9 (0�4) 510
Forearm 2�8 (0�5) 646 3�9 (0�5) 562 6�1 (0�4) 445 3�5 (0�3) 314 12�4 (1�1) 178 15�5 (1�7) 646
All sites 2�6 (0�3) 1498 4�9 (0�4) 1293 6�0 (0�2) 968 3�8 (0�2) 640 13�0 (0�6) 355 15�4 (0�9) 1498
*Percentage of patients with grade 2 or 3 phlebitis. None of the patients were found to have grade 4 or 5 phlebitis during follow-up.
0·00
0 25 50
site = Back of the handsite = Forearm
site = Cubital fossa
STaTaTM
75Hours of catheter permanence
100 125
0·25
0·50
0·75
1·00
Figure 2 Kaplan–Meier estimates of time to develop phlebitis by
catheter insertion site.
© 2014 John Wiley & Sons Ltd 7
JAN: ORIGINAL RESEARCH Predictors of infusion-related phlebitis

Therefore, the choice of anatomical site for catheterization is
determined by the operator on the basis of personal expertise,
habit, preferences and other factors such as the presence of
good quality veins. Several authors have suggested that the
anatomical site of insertion is a potential predictor of phlebi-
tis rate, yet no univocal consensus exists on anatomical site
selection (Maki & Ringer 1991, Bregenzer et al. 1998, White
2001, Cornely et al. 2002, Karadeniz et al. 2003, Kagel &
Rayan 2004, Webster et al. 2007, Uslusoy & Mete 2008,
Cicolini et al. 2009, Lee et al. 2009, Forni et al. 2010, Rego
Furtado 2011, Mestre Roca et al. 2012). To our knowledge,
this is the first multi-centre study specifically tailored to eval-
uate the relationship between site of insertion of PVCs and
risk of catheter-related phlebitis. Our results demonstrate
that, using the antecubital fossa and forearm veins, the risk
of phlebitis decreases by about 40%. This finding could be
expected, given that larger vessels may be less likely to
become inflamed than those with a narrow lumen and con-
firms previously published results that suggested that the ant-
ecubital fossa is a favoured site to minimize the risk of
phlebitis (Cornely et al. 2002). Furthermore, these results are
in accordance with others studies that showed an increased
risk of phlebitis when using veins in the (dorsum of the) hand
(Maki & Ringer 1991, Curran et al. 2000, Kagel & Rayan
2004, Lee et al. 2009, Forni et al. 2010). In an early study,
an increase in phlebitis incidence was observed when using
the hand and wrist as opposed to the forearm (RR: 0�71 and
0�60, respectively) (Maki & Ringer 1991). Another group
demonstrated a 1�5 risk ratio when the hand was used instead
of the forearms or lower extremities (Lee et al. 2009).
Nonetheless, the results of our study are in contrast to
those of other authors who reported higher phlebitis rates
for catheters inserted in the antecubital fossa (Uslusoy &
Mete 2008, Forni et al. 2010), or in the forearm (Bregenzer
et al. 1998, Karadeniz et al. 2003, Singh et al. 2008). A pos-
sible explanation given for the higher rate of phlebitis in the
antecubital fossa was excessive movement at the elbow joint
causing vessel wall traumas (Maki & Ringer 1991, Bregenzer
et al. 1998, White 2001, Cornely et al. 2002, Karadeniz
et al. 2003, Kagel & Rayan 2004, Webster et al. 2007, Uslu-
soy & Mete 2008, Cicolini et al. 2009, Lee et al. 2009,
Forni et al. 2010, Rego Furtado 2011, Mestre Roca et al.
2012). Furthermore, differences in study design (i.e. RCT vs.
observational), clinical setting (i.e. strictly general surgical or
also orthopaedic department) and sample size and character-
istics may help explain contrasting results across studies.
Another important consideration is the variation in classi-
fication and definition of different anatomical sites used.
For example, Bregenzer et al. (Uslusoy & Mete 2008) clas-
sified anatomical sites as ‘hand, forearm and other (includes
upper arm, leg)’; in contrast Karadeniz et al. (Bregenzer
et al. 1998) and Uslusoy and Mete (Karadeniz et al. 2003)
used ‘back of hand, wrist, antecubital area and forearm’.
Forni et al. (Uslusoy & Mete 2008) used ‘arm, antecubital
area, forearm, wrist, hand and leg’; Webster et al. (Forni
et al. 2010) used ‘hand, forearm, combination of sites and
others’; Lee et al. (Webster et al. 2007) used ‘hand, lower
extremity and forearm’ and finally Cicolini et al. (Lee et al.
2009) used the classification ‘cubital fossa, forearm and
hand’. This aspect should be taken into account when com-
paring results; it will certainly be advisable to use standard-
ized classification and terminology.
Clinical location
In addition to the particular anatomical site where can-
nulas are inserted, another factor proposed as being an inde-
pendent predictor of phlebitis incidence is the inpatient loca-
tion or hospital ward (Cicolini et al. 2009). We found a
reduced likelihood of developing phlebitis secondary to
peripheral intravenous cannulation for surgery or in the
orthopaedic wards when compared with the internal medi-
cine, geriatric and cardiology wards or services. Other stud-
ies found an increased risk of developing phlebitis associated
with medical (as opposed to surgical) wards (Lee et al.
2009, Mestre Roca et al. 2012). This has been attributed to
several factors such as the presence of underlying medical
conditions (e.g. cancer, immunodeficiency) or patient-spe-
cific risk factors related to hypercoagulability, including
inherited thrombophilias, which appear to increase the risk
of peripheral vein phlebitis. Other possible factors may be
operator-related, including the level of clinical staff experi-
ence (Maki & Ringer 1991, Mermel et al. 2001). One study
suggested that insertion in the emergency room, where
establishing venous access quickly is often necessary, could
be a risk factor for phlebitis (Tomford et al. 1984, Maki &
Ringer 1991, Soifer et al. 1998). In our study, we did not
consider the emergency room as a location.
Time in situ
Several research groups have concluded that a prolonged in
situ time for peripheral venous catheters is an independent
predictor of phlebitis incidence (Maki & Ringer 1991, Bre-
genzer et al. 1998, Lai et al. 1998). However, other studies
have challenged the need for routine re-sites, suggesting that
dwell times of intravenous cannulae may be safely extended
if clinically indicated (Tager et al. 1983, Maki & Ringer
1991, Bregenzer et al. 1998, Lai et al. 1998). Our results
support the recommendation of current CDC guidelines to
8 © 2014 John Wiley & Sons Ltd
G. Cicolini et al.

replace catheters in adults, at the latest, within 96 hours of
insertion (Bregenzer et al. 1998, Homer & Holmes 1998,
White 2001, Cornely et al. 2002, Webster et al. 2007,
2008, Van Donk et al. 2009, Hasselberg et al. 2010,
Rickard et al. 2010, 2012); most hospitals follow this rec-
ommendation.
It is important to note that many patients (13%) kept the
same catheter in situ beyond the maximum recommended
limit of 96 hours despite our pressure on local personnel
towards removal. Our researchers were more vigorous
towards removal when time exceeded 120 hours and after
phlebitis was observed. It appears that there is a need for
additional education of both healthcare personnel and
patients to raise awareness of the risks. On the other hand, a
strict epidemiological view may not be most apt at deciding
the cut-off; patient’s desires and comfort should also be con-
sidered, seeking a balance between danger and tolerability.
Our findings steer us towards recommending the use,
whenever possible, of antecubital fossa veins for peripheral
intravenous cannulation; future research efforts could seek
to confirm the reduced risk of phlebitis. Notably, the rate
of phlebitis (15�4%) was consistent with previous studies
that showed a range of phlebitis rate between 2�3% and
35% (O’Grady et al. 2011).
Limitations
In this study, as in most previous ones, the diagnosis of
phlebitis was made according to clinical signs at catheter
site, thus subject to operator-dependent variation (and
consequent variable investigators’ diagnosis). It is to note,
however, that blinding study subjects and operators to cath-
eter insertion site is practically very difficult and objective
criteria were strictly followed for phlebitis recognition and
classification.
Conclusions
Millions of catheter-related phlebitis worldwide may be
prevented by placing peripheral intravenous catheters into
the antecubital fossa or forearm veins rather than in the
dorsum of the hand and removing the cannulae within
96 hours. Educational campaigns on such issues are there-
fore urgently needed for healthcare professionals. A stan-
dardized classification of anatomical sites is warranted.
Acknowledgements
The authors acknowledge the collaboration of the following
nurses and nursing students, whose support was essential
for data collection: Dayana Di Vincenzo, Antonio Monteo-
dorisio, Andrea Cataldo, Valeria Rita Viva, Dunia Benl-
loch.
Funding
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
No conflict of interest has been declared by the author(s).
Authors contributions
All authors participated in all phases of the study (design,
data collection and interpretation of the results). LM and
MEF made the statistical analysis; VS, DC, ADB and LC
contributed to data collection; GC, GEE and LM wrote
the manuscript. All authors had full access to data and
are responsible for the integrity and the accuracy of the
data.
The authors have confirmed that all authors meet the IC-
MJE criteria for authorship credit (www.icmje.org/ethi-
cal_1author.html), as follows:
� substantial contributions to conception and design of,
or acquisition of data or analysis and interpretation of
data,
� drafting the article or revising it critically for impor-
tant intellectual content, and
� final approval of the version to be published.
References
Abbas S.Z., de Vries T.K., Shaw S. & Abbas S.Q. (2007) Use and
complications of peripheral vascular catheters: a prospective
study. British Journal of Nursing 16(11), 648, 650, 652.
Bregenzer T., Conen D., Sakmann P. & Widmer A.F. (1998) Is
routine replacement of peripheral intravenous catheters
necessary? Archives of Internal Medicine 158(2), 151–156.
Cicolini G., Bonghi A.P., Di Labio L. & Di Mascio R. (2009)
Position of peripheral venous cannulae and the incidence of
thrombophlebitis: an observational study. Journal of Advanced
Nursing 65(6), 1268–1273.
Cornely O.A., Bethe U., Pauls R. & Waldschmidt D. (2002)
Peripheral Teflon catheters: factors determining incidence of
phlebitis and duration of cannulation. Infection Control and
Hospital Epidemiology 23(5), 249–253.
Curran E.T., Coia J.E., Gilmour H., McNamee S. & Hood J.
(2000) Multi-centre research surveillance project to reduce
infections/phlebitis associated with peripheral vascular catheters.
Journal of Hospital Infection 46(3), 194–202.
© 2014 John Wiley & Sons Ltd 9
JAN: ORIGINAL RESEARCH Predictors of infusion-related phlebitis

Department of Health (2011) Peripheral Intravenous Cannula Care
Bundle. System, U. N. H., London.
Forni C., Loro L., Tremosini M., Trofa C., D’Alessandro F.,
Sabbatini T., Kapron M., Genco R., Schiavone M., Borri C.,
Bombino C., Notarnicola T., Amodeo A., Boschi R., Capezzali
D., Mosci D. & Mini S. (2010) Cohort study of peripheral
catheter related complications and identification of predictive
factors in a population of orthopedic patients. Assistenza
Infermieristica e Ricerca 29(4), 166–173.
Gallant P. & Schultz A.A. (2006) Evaluation of a visual infusion
phlebitis scale for determining appropriate discontinuation of
peripheral intravenous catheters. Journal of Infusion Nursing 29
(6), 338–345.
Hasselberg D., Ivarsson B., Andersson R. & Tingstedt B. (2010)
The handling of peripheral venous catheters–from non-
compliance to evidence-based needs. Journal of Clinical Nursing
19(23–24), 3358–3363.
Homer L.D. & Holmes K.R. (1998) Risks associated with 72- and
96-hour peripheral intravenous catheter dwell times. Journal of
Intravenous Nursing 21(5), 301–305.
Hosmer D. & Lemeshow S. (eds) (1999) Applied Survival Analysis.
John Wiley & Sons, New York.
Idvall E. & Gunningberg L. (2006) Evidence for elective
replacement of peripheral intravenous catheter to prevent
thrombophlebitis: a systematic review. Journal of Advanced
Nursing 55(6), 715–722.
Infusion Nurses Society (2006) Infusion nursing standards of
practice. Journal of Infusion Nursing 29(Suppl 1), S1–S92.
Kagel E.M. & Rayan G.M. (2004) Intravenous catheter
complications in the hand and forearm. Journal of Trauma 56
(1), 123–127.
Karadag A. & Gorgulu S. (2000) Effect of two different short
peripheral catheter materials on phlebitis development. Journal
of Intravenous Nursing 23(3), 158–166.
Karadeniz G., Kutlu N., Tatlisumak E. & Ozbakkaloglu B. (2003)
Nurses’ knowledge regarding patients with intravenous catheters
and phlebitis interventions. Journal of Vascular Nursing 21(2),
44–47; quiz 48–49.
Lai L.P., Lin J.L., Chen T.F., Ko W.C. & Lien W.P. (1998)
Clinical, electrophysiological characteristics and radiofrequency
catheter ablation of atrial tachycardia near the apex of Koch’s
triangle. Pacing and Clinical Electrophysiology 21(2), 367–374.
Lee W.L., Chen H.L., Tsai T.Y., Lai I.C., Chang W.C., Huang
C.H. & Fang C.T. (2009) Risk factors for peripheral intravenous
catheter infection in hospitalized patients: a prospective study of
3165 patients. American Journal of Infection Control 37(8),
683–686.
Lundgren A., Jorfeldt L. & Ek A.C. (1993) The care and handling
of peripheral intravenous cannulae on 60 surgery and internal
medicine patients: an observation study. Journal of Advanced
Nursing 18(6), 963–971.
Maki D.G. & Martin W.T. (1975) Nationwide epidemic of
septicemia caused by contaminated infusion products. IV.
Growth of microbial pathogens in fluids for intravenous
infusions. Journal of Infectious Diseases 131(3), 267–272.
Maki D.G. & Ringer M. (1991) Risk factors for infusion-related
phlebitis with small peripheral venous catheters. A randomized
controlled trial. Annals of Internal Medicine 114(10), 845–854.
Maki D.G., Kluger D.M. & Crnich C.J. (2006) The risk of
bloodstream infection in adults with different intravascular
devices: a systematic review of 200 published prospective studies.
Mayo Clinic Proceedings 81(9), 1159–1171.
McCallum L. & Higgins D. (2012) Care of peripheral venous
cannula sites. Nursing Times 108(34–35), 12, 14–15.
Melly M.A., Meng H.C. & Schaffner W. (1975) Microbiol growth
in lipid emulsions used in parenteral nutrition. Archives of
Surgery 110(12), 1479–1481.
Mermel L.A., Farr B.M., Sherertz R.J., Raad I.I., O’Grady N.,
Harris J.S. & Craven D.E. (2001) Guidelines for the management
of intravascular catheter-related infections. Infection Control and
Hospital Epidemiology 22(4), 222–242.
Mestre Roca G., Berbel Bertolo C., Tortajada Lopez P., Gallemi
Samaranch G., Aguilar Ramirez M.C., Cayla Buqueras J.,
Rodriguez-Bano J. & Martinez J.A. (2012) Assessing the
influence of risk factors on rates and dynamics of peripheral vein
phlebitis: an observational cohort study. Medicina Cl�ınica 139
(5), 185–191.
O’Grady N.P., Alexander M., Burns L.A., Dellinger E.P., Garland
J., Heard S.O., Lipsett P.A., Masur H., Mermel L.A., Pearson
M.L., Raad I.I., Randolph A.G., Rupp M.E. & Saint S. (2011)
Summary of recommendations: guidelines for the Prevention of
Intravascular Catheter-related Infections. Clinical Infectious
Diseases 52(9), 1087–1099.
Parruti G., Tontodonati M., Rebuzzi C., Polilli E., Sozio F.,
Consorte A., Agostinone A., Di Masi F., Congedo G., D’Antonio
D., Granchelli C., D’Amario C., Carunchio C., Pippa L.,
Manzoli L. & Volpi A. (2010) Predictors of pain intensity and
persistence in a prospective Italian cohort of patients with herpes
zoster: relevance of smoking, trauma and antiviral therapy. BMC
Medicine 8, 58.
Rabe-Hesketh S. & Skrondal A. (ed.) (2008) Multilevel and
Longitudinal Modelling using Stata. Stata Press, College Station,
TX.
Rego Furtado L.C. (2011) Incidence and predisposing factors of
phlebitis in a surgery department. British Journal of Nursing 20
(14), S16–S18, S20, S22 passim.
Reilly J., Stewart S., Allardice G., Noone A., Robertson C., Walker
A. & Coubrough S. (2007) NHS Scotland national HAI
prevalence survey. Final Report 2007, Health Protection
Scotland.
Rickard C.M., McCann D., Munnings J. & McGrail M.R. (2010)
Routine resite of peripheral intravenous devices every 3 days did
not reduce complications compared with clinically indicated
resite: a randomised controlled trial. BMC Medicine 8, 53.
Rickard C.M., Webster J., Wallis M.C., Marsh N., McGrail M.R.,
French V., Foster L., Gallagher P., Gowardman J.R., Zhang L.,
McClymont A. & Whitby M. (2012) Routine versus clinically
indicated replacement of peripheral intravenous catheters: a
randomised controlled equivalence trial. Lancet 380(9847),
1066–1074.
Sheth N.K., Franson T.R., Rose H.D., Buckmire F.L., Cooper J.A.
& Sohnle P.G. (1983) Colonization of bacteria on polyvinyl
chloride and Teflon intravascular catheters in hospitalized
patients. Journal of Clinical Microbiology 18(5), 1061–1063.
Singh R., Bhandary S. & Pun K.D. (2008) Peripheral intravenous
catheter related phlebitis and its contributing factors among
10 © 2014 John Wiley & Sons Ltd
G. Cicolini et al.

adult population at KU Teaching Hospital. Kathmandu
University Medical Journal (KUMJ) 6(24), 443–447.
Soifer N.E., Borzak S., Edlin B.R. & Weinstein R.A. (1998)
Prevention of peripheral venous catheter complications with an
intravenous therapy team: a randomized controlled trial.
Archives of Internal Medicine 158(5), 473–477.
Tagalakis V., Kahn S.R., Libman M. & Blostein M. (2002) The
epidemiology of peripheral vein infusion thrombophlebitis: a
critical review. American Journal of Medicine 113(2), 146–151.
Tager I.B., Ginsberg M.B., Ellis S.E., Walsh N.E., Dupont I.,
Simchen E. & Faich G.A. (1983) An epidemiologic study of the
risks associated with peripheral intravenous catheters. American
Journal of Epidemiology 118(6), 839–851.
Tomford J.W., Hershey C.O., McLaren C.E., Porter D.K. & Cohen
D.I. (1984) Intravenous therapy team and peripheral venous
catheter-associated complications. A prospective controlled study.
Archives of Internal Medicine 144(6), 1191–1194.
Uslusoy E. & Mete S. (2008) Predisposing factors to phlebitis in
patients with peripheral intravenous catheters: a descriptive
study. Journal of the American Academy of Nurse Practitioners
20(4), 172–180.
Van Donk P., Rickard C.M., McGrail M.R. & Doolan G. (2009)
Routine replacement versus clinical monitoring of peripheral
intravenous catheters in a regional hospital in the home
program: a randomized controlled trial. Infection Control and
Hospital Epidemiology 30(9), 915–917.
Webster J., Lloyd S., Hopkins T., Osborne S. & Yaxley M. (2007)
Developing a Research base for Intravenous Peripheral cannula
re-sites (DRIP trial). A randomised controlled trial of hospital in-
patients. International Journal of Nursing Studies 44(5), 664–
671.
Webster J., Clarke S., Paterson D., Hutton A., van Dyk S., Gale C.
& Hopkins T. (2008) Routine care of peripheral intravenous
catheters versus clinically indicated replacement: randomised
controlled trial. British Medical Journal 337, a339.
Webster J., Osborne S., Rickard C. & Hall J. (2010) Clinically-
indicated replacement versus routine replacement of peripheral
venous catheters. Cochrane Database Systematic Review (3),
CD007798.
White S.A. (2001) Peripheral intravenous therapy-related phlebitis
rates in an adult population. Journal of Intravenous Nursing 24
(1), 19–24.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal, with an Impact Factor of 1·527 – ranked 14/101 in the 2012 ISI Jour-
nal Citation Reports © (Nursing (Social Science)).
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 3,500 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Rapid online publication in five weeks: average time from final manuscript arriving in production to online publication.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
© 2014 John Wiley & Sons Ltd 11
JAN: ORIGINAL RESEARCH Predictors of infusion-related phlebitis
Copyright © 2022 FDOKUMEN




















