Six Cultures of the PhD (on international styles or flavors of the PhD for artists)
Upload
khangminh22Category
view
0download
0
1
Aus der Abteilung für präventive Zahnmedizin
und Kinderzahnheilkunde
(Leiter: Prof. Dr. med. dent. habil. Ch. Splieth)
im Zentrum für Zahn-, Mund- und Kieferheilkunde
(Geschäftsführender Direktor: Univ.-Prof. Dr. Dr. med. habil. G. Meyer)
der Medizinischen Fakultät der Ernst-Moritz-Arndt-Universität Greifswald
Oral Health Awareness, Social Status, Caries and
Malocclusion among Schoolchildren
Inaugural – Dissertation zur Erlangen des Akademischen Grades
Doktor der Zahnmedizin (Dr. med. dent)
der Medizinischen Fakultät
der Ernst-Moritz-Arndt-Universität Greifswald
2010
Vorgelegt von
Samar Alsoliman
geb. am 31.03.1974 in Aleppo / Syrien

2
Dekan: Prof. Dr. rer.nat. Heyo K. Kroemer
1. Gutachter: Prof. Dr. Ch. Splieth (Betreuer)
2. Gutachter: Frau Prof. Dr. A. Borutta (Jena)
Ort, Raum: Hörsaal der HNO-Klinik, Walhenau-Straße 43-45
Tag der Disputation: 25. October 2010

3
Table of contents page
Chapter 1 Introduction and problem statement 5
Chapter 2 Aims and objectives 8
Chapter 3 Literature review 9
3.1 Impact of socioeconomic inequality on adult health 9
3.2 Models for health literacy 10
3.3 Health promoting school 12
3.3.1 Establishing health promotion in schools 13
3.3.2 Setting up oral health programs in schools 15
3.3.3 Process and out come evaluation 19
3.4 Polarisation of dental caries 20
3.5 Malocclusion impact on oral health and well being 21
3.6 Effect of tobacco on oral health 23
Chapter 4 Materials and methods 25
4.1 Sample and population 25
4.2 Study design 26
4.2.1 Survey approval and data protection 27
4.2.2 Questionnaire conception and planning approach 27
4.2.3 Questionnaire’s pre-test 28
4.2.4 Intra-examiner calibration 30
4.3 Variables and research tools 30
4.3.1 Children’s questionnaire 30
4.3.2. Parent’s questionnaire 34
4.3.3. Measuring instruments of dental and malocclusion examination 35
4.4 Statistical analysis 36
Chapter 5 Results 38
5.1 Response, sample characteristics and survey’s model 38
5.2 Dental awareness -related items and scale properties 40
5.2.1 Dental knowledge scale 41
5.2.2 Dental behaviour scale 42
5.2.3 Dental attitude scale 43
5.2.4 Association between dental awareness scales 45
5.2.5 Association between awareness and socio-economic status indicators 46
5.3 Caries experience distribution 46
5.3.1 Caries experience in deciduous teeth 47
5.3.2 Caries experience in permanent teeth 48
4
5.3.3 Distribution of sealants application 50
5.4 Oral health risk factors among different survey’s indictors 51
5.4.1 Caries experience in relation to socio-economic status (SES) 51
5.4.2 Caries experience, dental awareness in relation to self-esteem 52
5.4.3 Caries experience in relation to nutrition 52
5.4.4 Association between DMFT and the amount of daily television watching 54
5.4.5 Association between DMFT and smoking 54
5.4.6 Association between DMF and general health 56
5.4.7 Association between toothache and children’s performance at school 56
5.5 Association between caries experience and dental awareness 56
5.5.1 Association between caries experience and dental knowledge 57
5.5.2 Association between caries experience and dental behaviours 58
5.5.3 Association between caries experience and dental attitude 59
5.6 Distribution of malocclusion among the children 61
5.6.1 Relationships between different kinds of malocclusion 62
5.6.2 Relationship between prevalence of caries and malocclusion 62
5.6.3 Malocclusion in relation to dental awareness and socio-economic status 64
Chapter 6 Discussion 66
6.1 Dental awareness, knowledge, attitude and behaviour 66
6.2 Caries experience distribution 68
6.3 Caries experience in related to different survey’s indictors 70
6.4 Impact of dental awareness scales on caries experience 74
6.5 Malocclusion prevalence and distribution 76
Chapter 7 Conclusions and recommendations 80
7.1 Conclusions 80
7.2 Future perspectives according to situation of the survey’s region 81
7.3 Potential design of the future programs 82
Chapter 8 Summary 84
Chapter 9 References 86
Appendices

5
Chapter 1: Introduction and problem statement
Oral health affects people physically and psychologically and influences how they grow, enjoy life,
look, speak, chew, taste food and socialise, as well as their feelings of social well-being. Therefore,
the modern contemporary concepts of health suggest that oral health should be defined in general
physical, psychological and social well-being terms in relation to oral status [Acharya and Sangam,
2008; Sheiham, 2005; Petersen, 2003]. Oral diseases are the most frequent human infection
disease and are crucial public health problems especially because of their high treatment expense
[Yee, 2002]. In Germany, caries related problems cost approximately 10 billion € per year [KZBV,
2005]. However, the cost of neglect is even higher in terms of its financial, social and personal
impacts [Mouradian, 2000]. Oral disease is one of the most costly diet- and lifestyle-related
diseases [Sheiham, 2001]. Many oral health problems are preventable and their early onset
reversible. However, in several countries a considerable number of children, as well as their
parents and teachers have limited knowledge of the causes and prevention of oral disease
[Altamimi et al., 1998].
Malocclusion is one of the most common dental problems annoying mankind, together with dental
caries, gingival diseases [Dhar et al., 2007]. Maloccluded teeth particularly in younger subjects can
cause psychosocial problems related to impaired dento-facial aesthetics that may affect their
current quality of life influencing their social skills and education [Kenealy et al., 1989]. The
orthodontic features of several populations have been the object of several investigations in
different European countries with the purpose of recording the prevalence of malocclusions
[Josefsson et al., 2007; Manzanera et al. 2009; Tausche et al., 2004; Perillo ea al., 2009; Liepa et
al., 2003 and Chestnutt et al., 2006]. There is very high prevalence of malocclusions among the
children, with more than half of children being affected [Proffit et al., 1998; Stahl et al., 2004]. Many
epidemiological studies on prevalence of caries and malocclusion in children have been presented
in the literature. However, a causal relationship and possible interactions between malocclusion
and dental caries have not been convincingly demonstrated and even only a few have
simultaneously evaluated that in an adequate sample [McLain et al., 1985].
In industrialized countries, the prevalence of dental caries has clearly declined among children and
adolescents in the last few decades [Marthaler et al., 1996, Marthaler, 2004]. Survey data on
children’s oral health collected in Germany demonstrated that dental caries levels in Germany
followed this trend [Schulte et al., 2006; Pieper et al., 2004]. Nevertheless, the distribution of caries
has been very polarized. A group of approximately 25– 30% are the so-called “risk children”. This

6
group includes the majority of the decayed defects and fillings [Marthaler, 1996]. The conventional
mean values per child hide these inequalities of oral health statement and conceal the fact that not
all population groups have steadily profited from the caries decline [Marthaler, 1996]. For this
reason caries epidemiology will remain an indispensable part of dental public health [Marthaler,
2004]. Newer investigations show that the classical risk factors like plaque or diet are only loosely
correlated with the individual caries levels, but education and social status seem to have a stronger
correlation with caries [Splieth et al. 1997]. Thus, the improvement in oral health did not cover all
the socio-economic levels and children and young adults with a low social background are
generally more likely to suffer more from the health problems, particularly problems regarding oral
health [Quartey and Williamson, 1999; Strippel, 2001; Flinck et al., 1999; Pieper et al., 2004;
Splieth et al., 2005]. The difficulties arise in translating this knowledge of an unequal distribution of
oral health to a workable strategy for oral health professionals in order to target those children with
increased need for dental treatment and elevated risk of developing dental decay. While the
effectiveness and efficacy of many methods of caries prevention were scientifically examined in
detail, their effect in low socio-economic groups was not determined until the mid 80's in West
Germany [Schiffner and Belly, 1986]. It seems that conceptual movement away from the traditional
‘downstream’ approaches, to one addressing the ‘upstream’ underlying social determinants of oral
health is necessary, as dental health education programs alone will have only a marginal impact
and can indeed increase oral health inequalities [Sheiham et al., 2000].
Low functional health competence is associated with poor education, low income and low
occupational status of the parents [Schillinger et al., 2002; Shea et al., 2004]. Health competence is
defined as: "The degree to which individuals have the capacity to obtain, process, and understand
basic health information and services needed to make appropriate health decisions" [Ad-hoc-
Committee on Health Literacy, 1999]. Health competence is related to health status, health
outcomes, and health related behaviours [Gazmararan et al., 2006; Yin et al., 2007, Mancuso et al.,
2006]. However, according to the American Medical Association, poor health competence is "a
stronger predictor of a person's health than age, income, employment status, education level, and
race" [Ad-hoc-Committee on Health Literacy, 1999]. As the lack of health competence in turn
causes a number of health problems by detrimental behaviour such as malnutrition, caries, lack of
exercise, overweight and smoking among others [Goodman, 1999]. A central task of health
promotion is strengthening health competence to cope with risk factors particularly among children
and adolescents. As during childhood and early adolescence crucial health-related attitudes and
behaviours are shaped, children are developing the ability to think abstractly, to understand
consequences, to relate to their peers in new ways, and to solve problems. As they experience
more independence from parents and develop greater control over their own lives, the age around

7
puberty is considered the most influential stage of a child’s lives, and during this stage, lifelong
beliefs, attitudes and skills are developed [Mangrulkar et al.., 2001]. Schools could represent in this
situation an entry gate for all children, especially for those groups of children with a low socio-
economic background to decrease of oral health inequalities [Kraus et al., 2004]. Schools have a
powerful influence on child development and well-being and schools can effectively influence
students’ health, knowledge, beliefs, attitudes and behaviour [Freeman, 1999]. The European
Network of Health Promoting Schools announced that: every child and young person in Europe has
the right, and should have the opportunity to be educated in a health promoting school [HEN,
2006].
The Health Promoting Schools (HPS) concept has been introduced worldwide and recommended
by WHO as an important strategy for promoting the health and provides opportunities to tackle
health inequalities in society, not only of young people but also of the population at large [WHO,
1998]. The approach of HPS include efforts to improve health by reducing risks, promoting health
and strengthening possibilities to cope with ‘given’ risk factors – creating supportive environments
reducing the negative effects of certain risk factors and facilitating behaviour changes by making
healthy choices easier and unhealthy choices more difficult, as the poor effects of individualized
approaches for health prompting contrasts with more successful effects of environmental changes
[Sheiham et al., 0002]. Health Promoting Schools were effective in improving knowledge,
developing skills and promoting healthy behaviours [Denman et al., 2001].
Health promotion cannot and should not be compartmentalized to address problems and diseases
of specific parts of the body because the risk factors of dental diseases are common to a number of
chronic diseases [Dahlgren et al., 1986] and by directing the efforts to those risk factors (such as
diets high in sugars and low in fruit and vegetables, stress, smoking and TV consumption) a
number of major chronic diseases are tackled [Sheiham et al., 2000]. Moreover, there is a
significant relationship between having certain patterns of risk behaviours and socio-demographic
status [Wiefferink et al., 2006]. Therefore, incorporating oral health promotion into general health
promotion is becoming increasingly important, not only for the same risk factors, but also because
an integrated approach is likely to be more cost-effective than programs targeting a single disease
[Petersen, 2003].

8
Chapter 2: Aims and objectives
The main aim of this study is to establish background data for the development of an integrated
health promoting program including oral health and malocclusions aspects in Mecklenburg-
Vorpommern, a region of former East Germany. Prior to the planning or implementation of any
effective oral health promotion interventions or malocclusion preventions programs, it is important
to assess the current oral health status, hence, in this cross-sectional survey, data on the present
caries and malocclusion prevalence and their distribution patterns are analysed, especially in
context of the oral health knowledge, attitudes and behaviour assessed by structured
questionnaires for 5th grade children and their parents. These parameters where used to propose
new approaches for the specific problems and needs of caries risk children who lag behind in the
caries decline.
Data regarding oral health awareness including knowledge, attitudes and behaviours is imperative
to identify both positive and negative influences on oral health, such as, physical, cultural,
environmental, social, and economic factors that support or hinder the development of good oral
health practices. This could serve as a basis for health promotion in schools, based on a
strengthening of public health competencies. The needed information should answer on the
following questions:
1. How is the current oral health status of the schoolchildren?
2. How are oral health beliefs, knowledge, attitudes and behaviours distributed among the
children?
3. How are oral health related attitudes, knowledge, and behaviour associated with each other?
4. How are oral health beliefs, knowledge, attitudes and behaviours associated with caries?
5. How are these oral health related indicators and caries distributed across social status?
6. How are environmental and other factors related to oral health disease?
7. Are there any gender related differences in dental behaviour, knowledge and attitude?
8. How are the prevalence and the distribution of malocclusion in the representative sample?
9. Does prevalence of malocclusion differs significantly between caries-free and carious dentitions
nowadays?
10. Are there any differences between genders in malocclusion prevalence?
11. Is there a relationship between different kinds of malocclusion?
12. Is there a connection between dental awareness, socio economic status and malocclusion?
13. How can the observed associations be used to derive recommendations for oral health related
intervention strategies and malocclusion preventions programs?

9
Chapter 3: Literature review
3.1. Impact of socio-economic inequality on health
Health status is influenced by individual characteristics and behavioural patterns (lifestyles) but
continues to be significantly determined by the different social, economic and environmental
circumstances of individuals and populations [Kraus et al., 2004; Hart et al., 2002; Lin et al., 2007;
Seabra et al., 2008]. Recent epidemiological analysis of health, disease and disability in the
populations of most countries confirms the role of social, economic and environmental factors in
determining increased risk of disease and adverse outcomes from disease [Barefoot et al., 2001].
Societal inequality is a main public health issue in Germany and other Western industrialized
nations, as part of this problem, children and adolescents with a low social background suffer more
from health problems [Kraus et al., 2004]. In the industrialized countries an unparalleled increase in
health and prosperity could be noticed in the last century, which manifests itself e.g. in a reduced
child mortality rate and an increased life expectancy, however a clear polarisation in the distribution
of health, health risks, morbidity and mortality can be diagnosed, which is essentially associated
with socio-economic variables [Olshansky et al., 2005]. Inequalities in socio-economic status have
been shown to be of key importance to the health of adults and younger children [Marmot et al.,
1991]. The relationships between these social factors and health, although easy to observe, are
less well understood and much more difficult to act upon. WHO Regional Office for Europe [2004]
admitted that the health gap between socio-economic groups within countries should be reduced by
at least one fourth in all member states by substantially improving the level of health of
disadvantaged groups.
From a research perspective, differences in socio-economic status have been shown to have both
a direct and an indirect impact on health [Adler et al., 1994]. Health behaviour - dependent public
health sectors like diet and overweight, sporting activities, TV consumption, smoking, and teeth
brushing are directly linked to both socio-economic status and health outcomes [Verde et al., 2006;
Kraus et al., 2004]. There is also evidence that psychological characteristics, such as depression,
hostility, anxiety, poor self-esteem, psychological stress and lack of coping resources, are indirectly
associated with low socio-economic status [Barefoot et al., 2001].
This pattern poses the challenge of understanding how socio-economic status affects health. There
are two major trains of thought. The first takes a material view, suggesting that the health
disadvantage of the poor is due mainly to the direct physiological effects of lower absolute material

10
standards, such as bad housing, poor diet and inadequate heating. The second takes the
psychosocial perspective, suggesting that stress associated with being poorer than neighbours or
other relevant reference groups’ results in a health disadvantage. Having a lower social position
can lead to chronic mental and emotional illness resulting in direct physiological consequences, as
well as to indirect exposure to behavioural risks in the form of stress-relief strategies, such as
smoking, drinking and overeating [Harris, 1991].
In terms of ‘content’, efforts to improve people's health, should not only be directed at changing
personal lifestyle or the way in which people use the health services, but Health education could
also raise awareness of the social, economic and environmental determinants of health, and be
directed towards the promotion of individual and collective actions which may lead to modification
of these determinants [Nutbeam, 2000].
On the level of oral health, socio-economic inequality was clearly associated with polarisation of
caries prevalence, as despite of the dramatic decline in caries in the last two decades, there are
sections of the population who have relatively high caries rates [Marthaler, 1996]. Dental caries has
been considered a social class disease [Gratrix and Holloway, 1994]. In the developed and
increasingly also in developing countries studies have shown that the burden of dental caries and
the need for dental care is highest among the poor and disadvantaged populations [ Petersen,
2005]. The higher levels of caries in low socio-economic groups suggest that they may be exposed
to multiple risk groups and numerous adverse social and economic conditions therefore they are
likely to have other health problems [Fröhlich et al., 2008]. The current approaches to caries
prevention should be reoriented to a broad community perspective which tackles the causes; the
determinants of diseases, the environmental perspective, to make healthy choices easier and
unhealthy choices more difficult for most people [Sheiham et al., 2005].
3.2. Models for health literacy
The development of health literacy in socially disadvantaged children is of central importance and
consider as a keystone in health promotion, which may, at least partially compensate the effect of
socio-economic inequality on the health and to decrease the gap in health between socio-economic
groups [Schwarzer, 1994; Nutbeam, 2008]. Health literacy is a relatively new concept in health
promotion. The term has been commonly used in health literature for at least 30 years [Ad Hoc
Committee on Health Literacy, 1999]. Health literacy refers to the personal, cognitive and social
skills which determine the ability of individuals to gain access to, understand and use information to
promote and maintain good health. These include such outcomes as improved knowledge and
understanding of health determinants, and changed attitudes and motivations in relation to health
behaviour, as well as improved self-efficacy in relation to defined tasks [Nutbeam, 2000]. The

11
knowledge refers to a range of information and the understanding thereof. Attitudes lead people to
like or dislike something or to consider things good or bad, important or unimportant, worth caring
about or not worth caring about. Skills are abilities that enable people to carry out specific
behaviours, over several years [Denman et al., 2001]. Health literacy may be understood as a
composite term that comprises a range of outcomes. Nutbeam’s well-established model of health
literacy comprises three levels; functional, interactive and critical: ‘Functional health literacy’ is
directed towards improved knowledge of health risks and health services, and compliance with
prescribed actions, examples of this form of action includes traditional patient education.
‘Interactive health literacy’ reflects the outcomes to the approach to health education which have
evolved during the past 20 years. This is focused on the development of personal skills in a
supportive environment. This approach to education is directed towards improving personal
capacity to act independently on knowledge, specifically to improving motivation and self-
confidence to act on advice received, examples of this form of action can be found in many
contemporary school health education programs directed towards personal and social skill
development and behavioural outcomes. ‘Critical health literacy’ is directed towards provision of
information on a full range of determinants of health and assessment of opportunities to achieve
change in these determinants. This type of health literacy can be more obviously linked to
population benefits, alongside benefits to the individual. Health education in this case would be
directed towards improving individual and community capacity to act on these social and economic
determinants of health, which may benefit the health of whole populations [Nutbeam, 2000].
Health literacy is related to health status and health related behaviours [Gazmararan et al., 2006;
Yin et al., 2007, Mancuso et al., 2006]. Low functional health literacy is associated with poor
education, low income and low occupational status of the parents [Schillinger et al., 2002; Shea et
al., 2004]. The lack of health literacy in turn causes a number of health problems by detrimental
behaviour such as malnutrition, caries, lack of exercise, overweight and smoking among others
[Goodman, 1999]. Despite the high relevance attributed to health literacy, several deficits concern
the related empirical evidence. While there is increasing knowledge about health literacy in clinical
populations, especially in adults [Mancuso et al., 2006], less evidence is available from children and
adolescents [DeWalt et al., 2009]. In spite of the limited number of studies, a recent related
systematic review underlines the importance of health literacy in children, adolescents and their
parents [DeWalt et al., 2009]. Overall, it evidences that lower literacy levels in children and their
parents are associated with less knowledge about health outcomes, health behaviours and health
services. Targeting literacy levels in children and parents seems important to improve adolescent’s
and children’s health [Manganello, 2008]. In addition to the effects of low health literacy on the
individual patient, there are economic consequences of low health literacy to society. The National

12
Academy on an Aging Society estimated that additional health care costs due to low health literacy
were about $73 billion in 1998 [Ad Hoc Committee on Health Literacy, 1999].
Yet, available empirical evidence predominantly concerns the functional level in Nutbeam’s
taxonomy [DeWalt et al., 2009]. One important reason is the lack of instruments that focus beyond
print literacy skills and reading comprehension. Interactive and critical health literacy has largely
been neglected [Abel, 2008]. Measuring the functional level may be of a limited value in regions like
former East Germany (the study’s region), where a lack of basic literacy skills is no longer the main
concern. Rather, modifiable factors such as interpersonal communication, social skills, attitudes,
motivation and self-efficacy may need closer attention; based on these deficits, our study devised a
set of short scales related to oral health knowledge, attitudes and behaviours to measure oral
health literacy domains in children according to the Nutbeam’s framework [Nutbeam, 2000].
Education for health directed towards interactive and critical health literacy has formed part of
social mobilisation programs. There are many contemporary examples of education being used as
a powerful tool for social mobilisation with disadvantaged groups in both developed and developing
countries [St Leger and Nutbeam, 2000]. By the development of the individual interactive and
critical health literacy among socially disadvantaged children, the effect of socio-economic
inequality on Health, may, at least partially, be mediated [Nutbeam, 2008].
Pursuing the goal of improved health literacy will also require more overt alliances between health
and education sectors in pursuing the goal of improved literacy levels in the population [St Leger
and Nutbeam, 2000]. Schools provide an effective platform for promoting health literacy because
they reach a large group of people efficiently; schools are microcosms of the larger community. In
general, children are receptive to guidance and they are familiar with the learning environment
[Mangrulkar et al., 2001]. In schools, children are empowered to take control over their own health
early in their lives and are encouraged to develop positive attitudes toward preventive measures.
The school years, age (6–15), are critical moments for building skills and positive habits. Schools
can also provide an important network and channel to the local community. Similarly, through the
students, health promotion messages can be passed on to other members of the family. This
interaction between school-home-community is an important aspect of health promoting [Gregory et
al, 2000].
3.3. Health promoting school
The Health Promoting School HPS concept has been introduced worldwide as an important
strategy that provides opportunities to tackle health inequalities in society, not only of young people
but also of the population at large. The WHO Health Promoting Schools (HPS) program offers a
sound approach to tackling the problem of dental caries. The approach focuses on the influence of

13
the social and physical environment on health. The HPS approach aims to improve health for the
total school population by developing supportive environments conducive to the promotion of health
literacy as an effective method for the compensation of health inequality in disadvantaged children
groups (Fig.1.1).
The HPS concept embraces the principles that health of individuals can be advanced by both
health education and supportive physical and social environment conductive to making healthy
choices. A HPS can be characterised as a school constantly strengthening its capacity as a healthy
setting for living, learning and working [WHO, 1998]. All the HPS activities depend upon
collaborative working between staff, students, parents, education authorities, local government and
health professionals. In addition, through the interaction with external environments and alliances
with local community, school health promotion can be improved, and can positively influence the
community in which pupils' health choices are made [Sheiham et al., 2005].
Fig.1.1: Health literacy improvement among disadvantaged children through Health Promoting
Schools
3. 3.1. Establishing health promotion in schools
Since the 1950s, schools have been a popular setting for health promotion and health education.
Early programs focused on teaching children about health and its determinants, but the importance
Disadvantaged children
Socioeconomic Inequality
Improving of Health literacy
Modification of health
determinants
Environmental changes
Health Promoting School
Common Health Risk Factors

14
of enabling them to develop the skills to resist unhealthy lifestyles was soon recognized and most
programs now teach these skills based on the guiding principles of the Ottawa Charter for Health
Promotion [WHO, 2004]. The WHO Global School Health Initiative was launched in 1995 and
numerous technical reports have been published by WHO since 1995 to help schools to become
health-promoting schools.
Yet, the question is about the efficiency of school-based oral health promotion programs; There is
considerable evidence to support the effectiveness of well-conducted school-based oral health
promotion interventions worldwide, and a review of Health-Promoting Schools supports the claim
that a well designed and implemented program which links the curriculum with other health
promotion in school and the community is likely to produce health gains [Leger, 1999].
Thirty-seven countries have participated in the European Network of Health Promoting Schools
since 1997 [Leger, 1999]. In the United Kingdom have developed a National Healthy Schools
Standard based on the health promoting schools approach [HEN, 2006]. European Network of
Health Promoting Schools (ENHPS) announced that: every child and young person in Europe has
the right, and should have the opportunity, to be educated in a health promoting school [HEN,
2006].
The office for Europe’s Health Evidence Network reported that evidence of the effectiveness of an
intervention was obtained for programs that adopted a whole school approach and included key
elements of the health promoting schools approach, such as changing the school environment,
developing personal skills in class, involving parents and the wider community, and actively
involving the school. The review suggested that programs that fell short of a whole school approach
were more likely to be effective if they were implemented continuously for more than a year [HEN,
2006]. Interventions that involved families were more likely to be successful than those that did not.
With improved dental knowledge and attitudes, parents are more involved in caring for their
children’s oral health [Craft, 1981].
Several reviews found gender-sensitive results, with some intervention programs being more
effective with girls and others with boys. Some reviews found age effects, with some intervention
programs being more effective in older children and others in younger children [HEN, 2006].
The Danish Municipal Dental Health Service provides comprehensive oral health care to children
and adolescents in school, with strong emphasis on prevention and health education to students,
school staff and parents. Long-term epidemiological data show that dental knowledge, attitudes and
behaviour have improved over time, as has children’s oral health status [Petersen, 1999]. Health
promoting schools not only had reduced levels of caries but had lower levels of traumatic dental
injuries [Watt et al., 2007].

15
There are a number of school-based oral health promotion initiatives undertaken in Ireland; the
program adopts the ethics of a Health-Promoting School and show promise. Children’s oral health
related knowledge, attitudes and behaviour, most notably healthy food choices, have been
improved [Friel et al, 2002]. The effect of a school-based oral health promotion program is more
apparent in Hungary [Szöke et al., 2000]. Similar findings have been reported in New Zealand; well-
designed school-based initiatives that aim at improving knowledge and social literacy are generally
effective, the school dental service is a valuable means of promoting health and equity [Wellington,
1998].
In Americas, schools that adopt and implement the principles of a Health-Promoting School
(‘supportive schools’) have a lower proportion of children with tooth decay and dental trauma
compared with ‘non-supportive schools’ ; the more comprehensive the curriculum, the better the
oral health outcomes and less inequalities in oral health within the school [Moysis,2003]. In general,
the cost per capita of community preventive programs is lower than that of treatment services.
Since the implementation of the nationwide school oral health program, the oral hygiene and oral
health of schoolchildren have improved, leading to a significant saving of 3.5 million US dollars
[Rockville, 2000].
In Brazil; the evaluation of the oral health aspects of HPS indicate that marked improvements in
oral health can be achieved. Food policies in state nurseries in a very deprived region not only
substantially reduced sugars consumption and improved the nutritional quality of the diet but also
successfully reduced caries increments over a one year period [Rodrigues, 1999].
3.3.2. Setting up oral Health programs in schools
In a health promoting school, depending on socio-cultural conditions and resources, oral health
promotion should target to provide:
1. Healthy School Environment: providing a supportive school environment determines the
effectiveness and sustainability of oral health promotion interventions, it enables students and
school staff to develop their physical, mental and social potential, enhancing the relationships
between members of the school community and encourages healthy lifestyles, making healthier
choice the easier choice. Healthy environment takes account of physical and psychosocial school
environments which support of each other. ‘Physical environment’ includes safe playgrounds and
buildings together with a smoke-free environment and the availability of healthy foods can help
reduce the risk to oral and general health and promote sustainable healthy lifestyles. Safe water
and sanitation facilities are essential for tooth brushing drills and for controlling cross-infection. And
children should be encouraged to use mouth guards in high-risk contact sports in order to reduce

16
the risk of oral trauma, initiatives that target improving environments in schools for children are
largely cost-effective, school environments have a significant impact on sustainable healthy
behaviours, which consider a key success factor [McLellan et al., 1999].‘Psychosocial environment’
refers to stress-free school, as stress may lead to poor diet, smoking, violent behaviours and the
consumption of sugary snacks and alcohol, which have serious oral health implications, This is
particularly relevant in today’s societies with prevailing social and family problems where stress can
affect all ages. A supportive social culture helps ameliorate the stress experience by students and
staff; which in turn improves their oral health. School programs that help children to develop self-
esteem and confidence are very important to equip children and school staffs with the skills that
help them prevent and, if unavoidable, deal with interpersonal conflicts, stress, peer pressure and
other social forces [Booth et al, 1997]. Based on a conceptual model of well-being in school in
Finland, it was found that social relationships both in and outside school play an important role in
schoolchildren's well-being. However, the most important correlates were connected with means for
self-fulfilment in school and well-being of children depending more on their relationship with their
teachers than with their friends, therefore health promotion aimed at supporting children's well-
being would benefit from focusing on this educational aspect [Konu et al., 2002]. Preventive
measures at an early stage of schooling may help to maintain the children’s mental health [Kraus,
et al., 2004]. Peer pressure can be beneficial. It can provide positive reinforcement among students
that healthy teeth are more socially desirable, emphasising the importance of good oral health; and
negatively reinforce tobacco use, sugary foods and drinks with or without alcohol which are
considered detrimental to oral health. Positive peer support promotes understanding and good
interpersonal relationships, preventing conflicts and violent behaviours that lead to craniofacial
injuries. Formal support can be obtained through school counselling and guidance service and
support groups [WHO, 2003].
2. Nutrition and food services: Children can be empowered to develop healthy dietary habits from
an early age through school health education and breakfast clubs, as eating behaviours adopted
during childhood are likely to be maintained into adulthood which underscoring the importance of
encouraging healthy eating as early as possible [Sheiham et al., 2000]. So students should be
educated about the harmful effects of isotonic drinks with high acidity and sugar content that can
lead to dental caries and erosion, a ban on selling unhealthy snacks in schools could be a starting
point, the canteens, tuck shops, kiosks and vending machines in schools are providing nutritious
meals and healthy snacks and put a ban on sugary foods and drinks [WHO, 2003]. Studying the
results of the programs which were done showed that most programs were effective, but effects
due to age and gender were observed, with greater benefits being observed in girls and older
students, also, peer-led interventions were effective, especially in terms of healthy eating [WHO,

17
2003].
3. School health services: The school health team works with the primary health care team to
provide: Dealing with dental emergencies, monitoring of oral health-related complaints, Working
closely with centre or local oral health service providers, training of school staff, Oral health
education, screening, diagnosis, needs assessment, preventive care, treatment, regular monitoring
and, for more complicated conditions, referral to other dental or medical specialists and secondary
care [Peterson et al 1999].
4. School oral health education: Providing education on oral health in schools helps children by
providing knowledge about oral health and promotes positive attitudes and healthy behaviours. In
short children should be able to practise proper oral hygiene care through the following healthy
components:
- Knowledge about the basic functions of the teeth, explain why each function is important, give
details of the two sets of teeth, describe the number and the importance of primary teeth, explain
why primary teeth are shed and replaced by permanent teeth, identify which permanent tooth
erupts first and its importance, name healthy and unhealthy foods related to teeth, describe how
and when to remove plaque, define dental plaque, describe the role of plaque and sugar in oral
health.
- Attitude and values which demonstrate a positive attitude towards oral health; demonstrate a
positive attitude towards the dental team, and appreciate the importance of teeth and oral
functioning.
- Behaviours by enhancing the daily tooth brushing and the use of fluoride, including affordable
fluoride toothpaste and fluoride rinsing programs with reducing the consumption and frequency of
sugary snacks and drinks; promoting the consumption of vegetables; promoting water or milk
fluoridation; promoting regular dental check-ups and care; preventing or reducing tobacco use;
preventing accidents, violence and anti-social behaviours [ENHPS, 2005].
Research shows that pupils that are more engaged in such a school are less likely to develop risky
behaviours because making young people aware of the pressures ahead of time gives them a
chance to recognise in advance the kinds of situations in which they may find themselves, and
teaching children resistance skills is more effective for reducing problem behaviours than just
providing information or provoking fear of the results of the behaviour, pointing toward early
prevention rather than later intervention focusing on skills for self-awareness and self-management
[ENHPS, 2005]. Skills-based health education will be most effective in influencing behaviour when
applied as part of a comprehensive, multi-strategy approach that delivers consistent messages
over time; for instance, research shows that a curriculum combined with youth community service

18
reduces risk behaviours more effectively than a curriculum alone [O’Donnell et al., 1999].
Skills are learned best when students have the opportunity to observe and actively practice them.
The most effective method of skill development is learning by doing – involving people in active,
participatory learning experiences rather than passive ones. Researchers argue that if young
people can practise the skills in the safety of a classroom environment, it is much more likely that
they will be prepared to use them in and outside of school [Tobler, 1992]. People learn what to do
and how to act by observing others, positive behaviours are reinforced by the positive or negative
consequences viewed or experience directly by the learner [Bandura, 1977].
Students play an essential role in the implementation of school oral health programs. Among many
other ways, oral health education can be delivered using peer teaching, a strategy that employs
students themselves to act as positive role models and educators for other students. Studies have
shown that the peer teaching method is effective in promoting healthy behaviours [Perry, 2003]. For
oral health education, peer leaders can help monitor other students’ oral hygiene and develop self-
care capacity in oral health. However, peer leaders must be properly trained to ensure that they
have adequate knowledge and skills to support other students and activities [Mellanby, 2000].
The importance of the teachers training: Teachers playing an important role in the oral health
education program, according to the results of a number of surveys, teachers are willing to teach
oral health education as part of their routine school activities, teachers are acutely aware of the
poor oral health conditions of their pupils and they are willing and happy to take a active role
because they suffered from toothache as children and wanted to help the children not to have the
same suffering [Wierzbicka et al, 2002].Teachers and school staff play a fundamental role in
carrying out day-to-day oral health promotion activities and interventions. Therefore guidelines for
teachers in monitoring and supervising tooth brushing drills should be developed. It is important to
engage them early in the design and planning stages, since teaching a practical skill such as tooth
brushing technique is necessary for the teachers to learn, and be competent on brushing their own
teeth effectively first. This is particularly important as teachers are often considered as role models
by students [Nyandindi et al 1994]. it is imperative for public health authorities and health
professionals to provide sustainable support, in terms of technical assistance, funding and/or
learning materials to facilitate the teacher’s task, as there a great deal of evidence that the good
school also is likely to be the healthy school and vice versa [Günther, 2006].
Systemic review of research in oral health education and health promotion involving 57 studies
found that oral health education can result in improved objective measures of oral health
behaviours and actual oral health measures but only limited success in changing attitudes towards
dental issues [Brown, 1994]. In another study in Manchester, the children had a higher level of

19
knowledge prior to the teaching program. Following the teaching program, children showed a
significant improvement in dental health knowledge, seven weeks later, the Manchester children
showed no significant loss of knowledge [Chapman et al., 2006]. Kay reported in an Oral health
training program for the elderly, that no changes in oral health practice resulted although the carer
training program was well received [Kay, 2002]. Another study for Kay and Locker [1996] showed
that dental health interventions have: a small positive, but temporary effect on plaque accumulation;
no discernible effect on caries increment and a consistent positive effect on knowledge levels.
The interaction between the school and the home is critical. Parental beliefs and attitudes play a
key role in moderating oral health related behaviour in young children and in determining whether
they develop caries [Splieth et al., 2004]. Hence, parents can be trained to reinforce oral health
messages at home and act as facilitators in outreach programs for children who do not attend
schools. It is important that both teachers and parents learn the same skills and provide nurturing
family and school environments, such programs can help promote oral health to these families and
may encourage them to become part of the school community [Booth et al, 1997].
Community support is crucial in lobbying for a healthy environment, clear food labelling and water
fluoridation. The media also offer a powerful channel for the delivery of oral health messages; the
media should be educated to refrain from targeting children and adolescents in tobacco advertising
campaigns and from the promotion of foods and drinks that are high in sugar, salt and fat [Friel et
al, 2002].
3.3.3. Process and out come evaluations
The costs of implementing health promoting schools programs should be considered alongside the
health benefits. This is a considerable challenge as costs are immediate and relatively easily
measured, but benefits in terms of changed behaviour and increased life chances are long-term
and may be difficult to attribute to a single intervention. Hence there is a need for a structured
approach to evaluation.
According to WHO, at least 10% of program resources should be allocated to evaluation [WHO,
1998]. Evaluation helps inform and strengthen school health programs and determines the extent to
which the program is being implemented as planned; it assesses processes and outputs, impact
and effectiveness of the program and, if any aspects have not worked well, identifies the key
lessons learned.
Evaluation can be used to reward the efforts of schools, students, teachers, parents and the
community and, by demonstrating the benefits, to encourage others to help more schools to
become Healthy School. Quality evidence can be used by schools to convince policy-makers,

20
sponsors and other stakeholders to provide continued support to, and to become involved in Health
promoting programs.
The targets for policy development to address the key components of the Healthy school can be set
for short-term evaluation, followed by evaluation of the effectiveness of various interventions, such
as oral health education in the classroom, exposure to fluoride, changes in knowledge about oral
health, attitudes, behaviours and lifestyles, as well as clinical outcomes and impact of interventions.
The sustainability of the Healthy school and its relationship with the wider community, partnerships
and networks should be considered in long-term evaluations [WHO, 1998].
3.4. Polarisation of dental caries
Caries is the most frequent human infection disease, which afflicts humans of all ages and in all
areas of the world. It is a disease of multifactorial nature including social, cultural, behavioural,
dietary and biological factors that can be associated with its initiation and progression [Fejerskov,
2004]. Several studies have been carried out to assess the dental caries prevalence among
children in different parts of the world [Marthaler, 2004; Szöke et al., 2000]. Since 1970, there has
been a significant reduction in the prevalence of dental caries in the majority of industrialized
countries [Stecksen-Blicks et al., 1999; Szöke et al., 2000; Marthaler et al, 1996 ; Bratthall et al.,
1996 and Astroth et al., 1998]. Different opinions exist regarding the reasons of the caries decline,
but there is agreement that the uses of fluorides are by far the most important factors of the decline
[Fejerskov et al., 1981]. In addition, the improvement of tooth brushing habits, would strengthen the
fluoride effect, and sealant application is also consider an important factor in lowering the DMFT
from 1.5 to 1.0 [Marthaler, 2004].
Concomitantly with the caries decline, a change in the distribution pattern have been observed as
polarisation of dental caries distribution occurred where a small group of children being social
disadvantaged has concentrated the majority caries burden [Pieper et al., 2004; IDZ, 1999]. This
group so-called “risk children” combines the mainstream of the decayed defects and fillings,
however the standard average values per child conceal these inequalities of the state of health and
hide the fact that not all population groups have steadily profited from the caries decline [Marthaler,
1996; Splieth et al., 2004]. Newer investigations show that with a single investigation or interview,
the classical risk factors like plaque, oral hygiene or indicated diet behaviour, are only loosely
correlated with the caries infestation, but another socio-economic factors appear to have a strong
correlation with caries initiation [Splieth et al. 1997]. Another study in Germany found that in the
youngsters (12 y.) 54% of Gymnasium school students have physically healthy dentition, but only
36% of the “Realschule” or “Hauptschule” pupils have the physically healthy dentition [IDZ,

21
1999].The effectiveness and efficacy of many methods of caries prevention were scientifically
examined in detail, whereby the effective in low social layers was not determined before the middle
of the 80's in West Germany [Schiffner, Belly, 1986]. In particular the prevention attempts which are
based on a "come" structure, e.g., in a dentist's practise did not show any effect here, except bad
cost efficacy [Splieth et al. 2005]. Simple outreach measures in schools based on plaque removal
and local fluoridation in comparison are more effective, and are cheaper because the application
take place in a group of schoolchildren simultaneously [Trummler, Weiss 2000; Splieth et al. 2004].
These measures offer a collective prophylaxis, and in addition the possibility of straight reaching to
the social risks groups with compliance problems and thereby they obtain equal chances for oral
health in society. Newer approaches offer additionally the required care by the stabilisation of the
health authority and the strength of the health competence for every child and youth [Jackson et al.,
2005; Anderson et al., 2005].
3.5. Impact of malocclusion on oral health and well being
Malocclusion is one of the most common dental problems apart from dental caries, gingival
diseases [Dhar et al., 2007]. Malocclusion is defined as an irregularity of the teeth or a
malrelationship of the dental arches beyond the range of what is accepted as normal [Walther et
al., 1994]. Maloccluded teeth can cause disturbances of oral function, such as mastication,
swallowing, and speech [Proffit and Fields, 2000] and greater susceptibility to trauma [Grimm et al.,
2004] and periodontal disease [Greiger, 2001] psychosocial problems related to impaired dento-
facial aesthetics [Kenealy et al., 1989]. Interest to orthodontic treatment has increased in recent
years, as a consequence of patients’ expectations as regards to oral impact on quality of life and
treatment opportunities. Moreover, the importance of oral health related quality of life is particularly
relevant for children and adolescents, since younger subjects are more sensitive to a variety of
impacts, such as appearance, that may affect their current quality of life and psychological
development and ultimately result in influencing their social skills and education [Acharya and
Sangam, 2008; Sheiham, 2005; Petersen, 2003]. Chen and Hunter [1996] found that psychological
impacts of oral health, such as avoiding laughing and being teased about teeth, were more
prevalent in children than in adults and elderly. Malocclusion or the variation of normal growth and
development affecting muscles and facial bones during childhood and adolescence can cause
psychological and social problems related mainly to impaired dental and facial aesthetics [Kenealy
et al., 1989]. Thus, an important aspect of orthodontic treatment is to improve dental aesthetics and
enhance well being [Shaw et al., 1991; Peres et al., 2008].
It is generally acknowledged that two major groups of aetiological factors for the development of

22
malocclusion may be distinguished, namely, genetic factors (inherited abnormalities) and non-
genetic (environmental) factors [Proffit et al., 1998]. A combination of both factors has often been
found in the same individual. Schopf [1981] highlighted the importance of environmental (non-
genetic) factors for the development of malocclusion and found that in 75% of the subjects, the
occurrence of anomalies had been encouraged by environmental factors such as biting habits,
abnormal pressure and sucking habits, abnormal swallowing, mouth breathing, caries in deciduous
teeth and early loss of teeth are among important environmental factors associated with
malocclusion. Many epidemiological studies on prevalence of caries and malocclusion in children
have been presented in the literature, as planning for orthodontic treatment within a public health
system requires information on the prevalence and distribution of malocclusion [Frazăo and Narvai,
2006]. Orthodontically relevant occlusal traits have been addressed in a number of cross-sectional
studies. Among German schoolchildren, Zeltmann et al. [1998] and among adults Jonsson et al.
[2007] determined that two groups of malocclusion traits were characterized by a particular high
prevalence that subsequently require orthodontic attention. These are space anomalies, in
particular anterior crowding [Zeltmann et al., 1998] and occlusal anomalies, such as distal molar
relationship and increased overjet. Tausche et al. [2004] showed that an increased overbite and
overjet were the most frequent malocclusions in the early mixed dentition period in Germany.
Although many epidemiological studies are available on the on prevalence of caries and
malocclusion, only a few have simultaneously evaluated dental and orthodontic findings in an
adequate sample and even fewer have analysed possible interactions between them. It has been
assumed by several authors that dental caries and premature loss of primary teeth are
predisposing factors for occlusal and space anomalies in mixed and permanent dentitions
[Pedersen et al., 1978; 2001; Stahl and Grabowski, 2004; Mitchell, 2005]. However, a causal
relationship between malocclusion and dental caries has not been convincingly demonstrated
[McLain et al., 1985]. Previous attempts to investigate a possible association of malocclusion and
dental caries have shown conflicting or inconclusive results [Helm et al., 1989; Ben-Bassat et al.,
1997; Frazăo and Narvai, 2006; Stahl and Grabowski, 2004; Gábris et al., 2006 and Nobile et al.,
2007]. This uncertain founds may be attributed to differences in caries experience of the study
sample, small sample sizes, or in unsuitable criteria used for defining ‘caries-free’ and ‘carious’
dentitions.
A notable increase in orthodontic treatment demand has occurred as a consequence of the high
perception rate of malocclusions, along with a greater attention to aesthetics. About one-third of all
children in different European country were with a need of urgent orthodontic treatment such as; in
Britani [ Burden and Holmes, 1994; Brook and Shaw, 1989; Holmes,1992]; in New Zealand
schoolchildren [ Crowther et al., 1997], in Northern Ireland [Burden, 1995], in Swedes [Josefsson et

23
al., 2007 ], in Spain [Manzanera et al. 2009],in Germany [Tausche et al., 2004], in Italy [Perillo ea
al., 2009] and in Britani [Liepa et al., 2003 and Chestnutt et al. , 2006].
3.6. Effect of tobacco on oral health
Tobacco use is a primary cause of many oral diseases and adverse oral conditions; smoking often
results discolouration of teeth and dental restorations, reduction of the ability to smell and taste,
development of oral diseases such as smokers palate, smokers melanosis, coated tongue and oral
candidosis, [Johnson et al., 2000]. People who start consuming these products at an early age may
have an increased risk of oral cancer in later life [Tomar et al., 1997]. Smoking and chewing
tobacco have a direct carcinogenic effect on the epithelial cells of the oral mucosa; a clear
association has been demonstrated between smoking and the prevalence and severity of
periodontal disease, suggesting smoking as an important risk factor for periodontal disease and is
responsible for more than half of the periodontal disease among adults in some industrialized
countries [Tomar and Asma, 2000]. Many investigators have discovered a correlation between
elevated smoking level and dental caries [Bruno-Ambrosius et al., 2005; Ide et al., 2002;
Kelbauskas et al., 2005; Hirsch et al., 1991 and Zitterbart et al., 1990]. Non-smokers reported more
frequent healthy oral health behaviour than did daily smokers and it is also seen that smokers have
ineffective brushing habits than non-smokers [Kelbauskas et al., 2005]. Studies indicate that
smokers not only had bad oral hygiene and less primitive outlook on health, but also had different
eating habits, presumably consuming high amount of sugar containing products like soft drinks and
snacks [Hirsch et al., 1991]. Prevention of smoking onset and support for cessation of smoking
could contribute to improved oral health status [Aguilar-Zinser et al., 2008]. There are many
evidence of the direct aetiological relationship between tobacco use and caries; as lower salivary
pH and buffer capacity is often found. A shift of bacterial population towards lactobacillus and the
cariogenic streptococci can be noticed in smokers [Johnson et al., 2000]. In natural tobacco, sugar
can be present in a level up to 20%wt. In addition, various sugars and sweeteners are added
intentionally during tobacco manufacturing process up to 4%wt or can be up to 13%wt of sugars.
The added sugars are usually reported to serve as flavour/casing and humectants. However,
sugars also promote tobacco smoking, because they generate acids that neutralize the harsh taste
and throat impact of tobacco smoke. Moreover, the sweet taste and the pleasant smell of
caramelized sugar flavours are appreciated in particular by starting adolescent smokers [Talhout et
al., 2006]. In terms of ‘content’, there are several ethical, moral and practical reasons why oral
health professionals should strengthen their contributions to tobacco-cessation programs; as they
are especially concerned about the adverse effects in the oral pharyngeal area of the body that are
caused by tobacco practices. Oral health professionals can build their patient’s interest in

24
discontinuing tobacco use by showing actual tobacco effects in the mouth.
The association between the low socio-economic class and the both off smoking and carries
prevalence is yet evidence [Soteriades et al., 2003]. In Germany and other industrial countries, a
huge number of investigations cover a very distinctive social polarisation of smoking behaviour.
People with lower school education, low professional status, are frequently smokers [Helmert et al.,
2001]. Smoking is considered like caries to be a risk factor related with behaviour pattern of the
youth, with continuous increasing rates of the youth smoker's. Besides that, the youth age has a
key position because at this age the habituations which take place are very hard to be dissolved
later. At the moment, in Germany, the average age of smoking the first cigarette is of 13.6 years
and the average age for the beginning of daily smoking is 15.6 years [BZgA, 2004]. In the group
that ranges 12-15 years of age, forty-one percent of them have actually already smoked and from
this group five percent are considered constant smokers, eleven percent of them are occasional
smokers, one percent of them are ex-smokers, twenty-four percent smoked just to try smoking, and
the remaining fifty-nine are non-makers [BZgA, 2004]. The youth smoke behaviour depends on
age, gender and education. Thus, the girls group that ranges from 12-17 years shows a smoker's
rate of thirty-five percent, in the East federal states while girls show a smoker's rate of twenty
percent in the West federal states. Similar figures exist among boys (32% versus 22%) [Kraus et al,
2004].

25
Chapter 4: Materials and methods
4.1. Sample and populations
The sample comprised children in fifth grade in schools in the city of Greifswald and West
Pomerania (age range 9-13 years). All schools with a fifth grade in the study region were invited to
participate in the study, but from all the 22 schools in this area 19 schools accepted to participate in
this survey, the number of children varied from 19 to 95 per school. Participating schools are listed
in (Table 4.1).
Table 4.1: Participating schools in survey
schools located in Greifswald city (HGW) schools located in East Pomerania(OVP)
Gymnasium, "Alexander von Humboldt" Regionale Schule, "Käthe Kollwitz" (Anklam)
Integrierte Gesamtschule, "Erwin Fischer" Regionale Schule Ostseeschule Ückeritz
Regionale Schule, "Ernst Moritz Arndt" Regionale Schule, "Heinrich Heine" (Karlshagen)
Regionale Schule, "Martin Andersen Nexö" Regionale Schule Lubmin
Evangelisches Schulzentrum Martinschule Regionale Schule mit Grundschule Wolgast
Gymnasium Ostsee Regionale Schule mit Grundschule Gützkow
Allgemeine Förderschule Regionale Schule mit Grundschule Ducherow
Johann Heinrich Pestalozzi Regionale Schule mit Grundschule Spantekow
Regionale Schule mit Grundschule Neuenkirchen Regionale Schule "Friedrich Schiller" (Anklam)
Freie Schule Zinnowitz
Regionale Schule, "Kosegarten" (Wolgast)
Greifswald is a town in north eastern Germany situated approximately 200 km north of Berlin in the
state of Mecklenburg-Vorpommern, bordering the Baltic Sea (Figure 4.1). The population of the
town and administrative district of East Pomerania is approximately 162.653 inhabitants, including
16.727 inhabitants younger than 15 years [Statistical Office MV, 2005]. The study region also
included around 57 inhabitants / km˛ in the rural region of East Pomerania (OVP), as well as an
urban area in Greifswald city (HGW) with around 1.058 inhabitants / km. The study region features
one of the highest rates of unemployment in Germany 2007 (Greifswald: 18.7%, West Pomerania:
21.5%) [Bundesagentur für Arbeit, 2009].

26
Fig. 4.1: Germany and the state of Mecklenburg-Vorpommern map
4.2. Study design
In conjunction with the compulsory community dental examinations, additional data were collected
using a self- completion questionnaire for the children (Appendix 1) and another for their parents
(Appendix 2) in autumn 2007. In German schools, the extended dental school examination is
routinely offered to the children in first, third, fifth or sixth and ninth grade. The school dental
examinations were performed by the community dentist. The schools provided facilities for the
medical examinations. The student’s questionnaire was completed at school under the supervision
of the scientific coordinator of the study. Parents filled out their questionnaires during parent–
teacher conferences, and for absent parents, a questionnaire was mailed to them. Most of the data
were obtained in September/October 2007, but the students who missed their appointment due to
illness or other reasons were examined in a second wave in November/December 2007. A total of
852 students participated in both the self-administered questionnaires and clinical examinations for
oral health, and 721 parents participated in the parental questionnaires. Parents’ questionnaire
contains questions on socio-economic status and child’s health. The parental questioning was
necessary because children of the 5th classes are unable to make valid statements concerning,
e.g., the education status and occupational status of the parents. To attain a high participation of
schools, principals were briefed about the research project by an invitation letter, telephone calls
and personal visits. All parents of fifth-grade students received a supporting letter of the Minister of
Education, Science and Culture of Mecklenburg–Western Pomerania, as well as detailed
information on the purpose of the study and data safety. It was clearly explained that the
participation of their child in health education and school examinations is mandatory, but the
participation in the additional scientific survey was voluntary and they could object to the survey

27
without any drawbacks for themselves or their children. The parents or guardians of the children
signed a written informed consent for study participation (Appendix 3). Students were selected for
the study based on inclusion and exclusion criteria. Students whose parents signed the written
informed consent form and who participated in the dental examinations met the inclusion criteria.
Students without signed parental informed consent or those who failed to appear on the
examinations days met the exclusion criteria. In addition, 25 students of Förderschule J.H.
Pestalozzi with special need were excluded from the study.
4.2.1. Survey approval and data protection
The survey was approved by the data protection commissioner of Mecklenburg–Pomerania, the
Ministry of Education, Science and Culture of Mecklenburg– Pomerania and the Ethics Committee
of the Ernst-Moritz-Arndt-University Greifswald (Appendix 4).
For ethical reasons the anonymity of each student must always be protected. To guarantee this, a
procedure was chosen to give each student a pseudonymity or code which is made from his or her
variables (Hash-code).
During investigation and through an encoding algorithm on the bases of date of birth, gender, name
and if necessary other variables, pseudonymity for each student was created. This will result in an
unequivocal code, which is highly secured from decoding.
A special software program was used during data exporting process from the record-keeping
system in the schools. This program allows the examiners extraction of all the relevant information
regarding the students; at the same time, it will create for each individual a specific pseudonym as
an individual key. The correct merging of data from different sources was ensured, and afterwards,
the encryption-key was deleted. The deletion of the algorithm after the last examination resulted in
a complete anonymization of the pupils’ data which agree with data privacy laws. This method was
successfully used by Hoffmann et al., [Hoffmann et al., 2004] in a big population-based study.
Parents have the right to refuse participation according to the authorization of the data protection
concept. Data were deleted when parents used their right to refuse.
4.2.2. Questionnaire conception and planning approach
There are in principle two ways for empirical research, qualitative and quantitative research
methods. Quantitative research applies a statistical analysis of observant reality segments,
whereas qualitative research methods focus on understanding the reaction types of the participants
by reconstructing their motives with non-numerical data [Bortz et al, 2002]. A quantitative survey

28
methodology was applied to achieve the objectives of this study. This selection was based
substantially on the special consideration of the investigation which was to analyze multiple
variables related to schoolchildren that qualitative methods could not address. Temporal resources
also played a roll in the determination of this method. In addition, quantitative procedures are
suitable for measuring facts objectively and testing the stated hypotheses that make it possible to
compare data and the resulting consequences.
To achieve cooperation, the questionnaire formulation was begun with "icebreaker questions," such
as “What is your name, how old are you?” These questions had little information value, but the
children could easily answer them. The composition of the questions and statements had clear
structuring of the item-blocks and covered paramount topic areas. In addition, it had consistent
logical formulation. The questions also were, simple, direct and linearly formulated. The duration of
the questionnaire was also considered, so it was designed to be completed with the 45 minute
period of one school lesson. With a longer questionnaire duration, negative consequences on the
information readiness were feared, for this reason, closed response possibilities were used. Most
questions could give the degree of approval or refusal on five level linear rating scales, and these
answer possibilities ranged from "absolutely true" to "rather correct" or "hardly correct" and
"absolutely incorrect". Such scaling is called “forced rating”, since the interviewees because of the
absence of an alternate category (such as “Do not know,” “No answer”), are forced to answer. For
some questions, two level answer scales were given; as the interviewees could her choose
between "yes" and "no". The front cover design was pleasant and printed in colour. The language
used for all the questionnaires were the German language.
4.2.3. Questionnaire’s pre-test
According to the questionnaire design, a pilot test was required. This challenge was necessary to
examine the fitness and the efficiency of the collection instrument. In this test, the comprehensibility
of the questions, the average questioning time and possible alternative question formulations could
be examined. In spring of 2007, the initial version of the students´ questionnaire was pilot tested on
36 schoolchildren. The dental examinations and the students’ questionnaire were tested to be
completed in 45 minutes. Based on the results, the children’s questionnaire was modified and
adjusted to meet the time 45 minute requirement. Some of the questions were deleted and others
were shortened. The final version of the questionnaire is in the appendix (1) and the following figure
summarises the sequential steps for the study methodology.

29
Fig.4.2. Flow chart of study methodology
914 5th grade students from 19 schools were conducted in September and October, 2007
Ethics Committee Approval
Pre.test for the Questionnaire
Inclusion and exclusion criteria
Primary Questionnaire Structure
Final Questionnaire Structure
Dental Clinical Examin
852 (93%) Attend both of the dental examination and self- administered questionnaire
Data Analyses and Evaluation
Data Entry
Schoolchildren’s Questionnaire
Parental Questionnaire
Data Collection

30
4.2.4. Intra-examiner calibration
Clinical examinations for recording dental caries were carried out by three examiners previously
trained on oral health examination following WHO diagnostic criteria guidelines [World Health
Organization, 1997] and the dmft/dmfs, DMFT/DMFS-indices. DMF indices were used in assessing
dental caries experience among schoolchildren in this study. The DMFT index is the simplest and
most commonly used measure in epidemiologic surveys of dental caries. Prior to the onset of the
study, a calibration course and training of the examiners were provided, including lectures and
clinical training. Inter-class correlation coefficient (ICC) was used to assess the inter examiner
reproducibility between examiners.
Poor reproducibility was assessed for ICCs below 0.40, fair reproducibility for ICCs between 0.40
and 0.59, good reproducibility for ICCs between 0.60 and 0.75, and excellent reproducibility for
ICCs between 0.75 and 1.00 [Altman, 1999].
Twelve students from the total sample size were selected randomly for assessment of examiners-
reproducibility and to enable the determination of the inter-class correlation (ICC). Cohen’s kappa
scores were calculated between each of the examiners and using the SPSS software package the
statistical analysis were done.
Inter-class correlation was carried out midway through the school dental examination on 12
randomly selected students by the examiners, and the ICC values for the first and final
examinations were 0.93 and 0.97 respectively. The interpretations of these ICC values give
excellent agreements between the examiners; the kappa statistics contained scores regarding
missing and fillings teeth.
4.3. Variables and research tools
4.3.1. Children questionnaire
The children questionnaire contained a series of questions that cover several topics on children’s'
general and oral health, nutrition, smoking, self-efficacy and health competence [ Duetz et al.,
2003; Nutbeam, 2000; Duetz, Abel, 2004; Ravens-Sieberer and Bullinger, 1998; Bisegger et al.,
2005; Roth-Isigkeit et al., 2002 and Thyrian et al., 2006 ].These particular domains have been
selected because they will be targeted by a health education program after the baseline survey.
The item selection was primarily based on consideration of item content. Scientists, participating in
the study, provided recommendations with respect to items in their specific field of expertise,
appendix (1). The questionnaire module was a standardized module of validated questionnaires
and compatible with the research tools of other big national studies, e.g., the German Health

31
Interview and Examination Survey for Children and Adolescents [Kurth and Robert-Koch-Institut,
2002; Thyen, 2007]. This gave us the opportunity for future comparison with other studies. All
questionnaires were well structured, standardized and designed to be self-administered by the
children and their parents. Data included children’s age, sex, school name, birth country, and
duration of residence in Germany. The children questionnaire could be divided depending on the
contents to oral health questionnaire and oral health risk factors questionnaire.
4.3.1. 1. Oral Health questionnaire
The questionnaire contained one big section for oral health competence/literacy. Which consisted
from 14 multiple choices; those 14 questions measured items on oral health-related knowledge,
attitudes and behaviour. Each was consisting of several questions (Table 4. 2).
Table 4.2: Oral health awareness related variables
Scale Questionnaire items Alternative score
Which toothpaste is the most effective for your age?
Adult toothpaste, children’s toothpaste, sea salt, toothpaste without fluoride
0-1
Which teeth need the most care while brushing?
Incisors, erupting teeth, milk teeth 0-1
Den
tal
kn
ow
led
ge
Is the dental check up free of charge? Yes, no 0-1
I eat only a few sweets to keep my teeth healthy
Absolutely untrue, hardly true, moderately true, exactly true
0-1
Healthy teeth are very important to me Absolutely untrue, hardly true, moderately true, exactly true
0-1
I pay extreme attention to my teeth Absolutely untrue, hardly true, moderately true, exactly true
0-1
Nothing will happen if I don’t brush my teeth once
Absolutely untrue, hardly true, moderately true, exactly true
0-1
My family makes sure that I brush my teeth Absolutely untrue, hardly true, moderately true, exactly true
0-1
I would avoid sweets, in order to keep my teeth good and healthy
Absolutely untrue, hardly true, moderately true, exactly true
0-1
Den
tal
Att
itu
de
Did you talk with your parents about what is good for your teeth?
Never, rarely, sometimes, often, always 0-1
How often do you visit your dentist every year?
Four times a year, three times a year, twice a year, once a year, didn’t go to the dentist at all
0-1
Do you brush your teeth in the evening? Every evening, most evenings, occasionally, did not brush my teeth at all in the evening.
0-1
Do you brush your teeth in the morning? Every morning, most mornings, occasionally, did not brush my teeth at all in the morning
0-1
How many times per day do you eat fruit and sweets?
2-3 times, 4-5 times, 6-7 times, or 8-9 times every day.
0-1
Den
tal
Beh
avio
ur
Do you brush your teeth with Elmex gelee Every day, Once per week, Occasionally, Not at all 0-1

32
Oral health knowledge items included questions about some valuable information such as; teeth
brushing should be concentrated on the erupting teeth; after the age of 6 children should start to
use adults tooth paste; the free dental check-up and preventive visit that the national health
systems provide for free. On other hand oral health attitude items were investigated to know if there
are communication between children and parents about what is good to keep healthy teeth or if the
parents pay attention to their children’s teeth brushing at home, in addition the children were asked
to give their personal impression on some statements such as; the avoiding of sweets eating to
keep teeth healthy, paying extreme attention to the teeth; healthy teeth are very important, eating
only a few sweets to keep teeth healthy and if the child consider that nothing will happen if he let
his teeth onetime without pushing. Finally, oral health behaviours items interested in evaluation of;
daily frequency of sugar and fruits consumption, evening and morning tooth brushing, the rate of
use fluoride gel, the frequency of children’s annual dental visits, in addition the number of sealed
teeth which was collected in the oral clinical examination considered an index of good oral health
behaviour.
The answers on the above questions, as we see in (Table 4. 2) had several choices such as;
absolutely untrue, hardly true, moderately true, and exactly true. Therefore, alternatives answers
were pooled into “positive” and “negative” or “right” and “wrong”, and then analyzed as categorical
data with rating scale format to improve scalability. The three groups were measured separately
with this newly generated scale and the sums of the three scales was created and called dental
awareness scale. This new scale on dental awareness was generated in order to measure the oral
health in a more comprehensive and specific way to our own sample population.
4.3.1. 2. Oral Health risk factors questionnaire
The questionnaire included several topics affected children’s' general oral health such as, nutrition,
smoking, TV watching, self-efficacy, (Table 4. 3). Regarding smoking the questionnaire included
several questions to obtain a broad picture of actual smoking behaviour status, gravity of nicotine
dependence using the Hooked on Nicotine Checklist [O'Loughlin et al., 2002, Wheeler et al., 2004];
temptation to smoke in certain situations; presence one or more smokers among the family
members; if the best friends of the child were smokers.
Self-efficacy was measured with three validated items taken from the German Health Interview and
Examination Survey for Children and Adolescents (KiGGS), aged 11–13 years [Thyen, 2007]. To
ascertain self-confidence level among the children, the child must give his/her impression about
three statements included the ability to solve most problems if the child invest the necessary effort.
If the child is in trouble, he can usually think of a solution. Finally, if the child can usually handle
whatever comes his way.

33
Table 4.3: Questionnaire items related different oral health risk factors
Scale Questionnaire items Alternative score
Do you smoke? Never, tried to smoke, used to smoke, occasionally, daily
0-1
Are your best friend’s smokers?
Yes, no 0-1
Are there smokers among your family members? Yes, no 0-1
Sm
okin
g
Do you felt nervous or worried if you had not smoked for a while?
Yes, no 0-1
I can find a solution for each problem
Not at all true, hardly true, moderately true, exactly true
1-4
If a new problem emerges, I can master it from my own ability
Not at all true, hardly true, moderately true exactly true
1-4
Self
-eff
ica
cy
Whatever happens, I can pass it well
Not at all true, hardly true, moderately true, exactly true
1-4
The health item is very important to me Never, rarely, sometimes, often, always 1–5
How did you feel last week? I was tired and worn-out
Never, rarely, sometimes, often, always 1–5
How did you feel last week? I had a lot of strength and endurance.
Never, rarely, sometimes, often, always 1–5
Ph
ys
ical-
he
alt
h
Did you have an earache /sore throat during the last three months?
Never, one time, more than one time 1–5
In the last week, learning in school was interesting
Never, rarely, sometimes, often, always 1–5
In the last week, I had anxiety from bad notes Never, rarely, sometimes, often, always 1–5
Men
tal
healt
h
In the last week I did all my homework Never, rarely, sometimes, often, always 1–5
Do you talk with parents about healthy food Never, rarely, sometimes, often, always 1–5
Most important in food is that it tastes to me Yes, no 0-1
Do you bring to drink in school? tea without sugar/ lemonade/iced tea/ water/ milk/ juice
Yes, no
0-1
N
utr
itio
n
What did you bring with you to eat in school? Chocolate/sweets/cakes/white bread/jam/honey/cereals/fruit/vegetables/salty snacks (chips, nuts).
Yes, no
0-1
TV
How many hours per day do you watch TV? Less than 1 hour 1-2. 2-3. more than 3 hour 1-4
Did you have toothache during the last three months?
Never, one time, more than one time 1–5
Because of this pain I could not attend school Never, rarely, sometimes, often, always 1–5
Because of this pain I couldn’t do my homework after school
Never, rarely, sometimes, often, always 1–5
Because of this pain I could only partially participate in the classroom
Never, rarely, sometimes, often, always 1–5
P
erfo
rman
ce a
t sc
ho
ol
Because of this pain my performance drop up to half of my normal capacity
Never, rarely, sometimes, often, always 1–5

34
Children’s general health category included physical wellness and mental health, physical wellness
registered by asking the child about the importance of the health item to him, and by giving his
feeling if he found himself tired and worn-out or had a lot of strength and endurance in the last
week, table 3. To evaluate mental health status, the child was asked to give his personal
impression on some statements such as; if he had anxiety from bad notes or if he did all his
homework in the last week. The child also was asked if learning in school is interesting to him.
Nutrition questionnaire included question about; communication between parents and children
about healthy food, the frequency of drinking lemonade /iced tea/ juice/ milk/ water / tea without
sugar, and which of them he used to take with him to drink in school.
children’s evaluation of healthy food was investigated by asking them about the importance of good
taste of food as most essential in food choosing, In addition the children were asked about the
frequency of eating chocolate/sweets/cakes/white bread/ jam, honey/ cereals/ fruit/vegetables/ salty
snacks (chips, nuts) and also which of them he bring with him to eat at school. The prolonged
television watching was assessed by asking the child about the amount of daily television watching.
The effect of toothache on children performance at school was also investigated.
4.3.2. Parent’s questionnaire
The questionnaire included questions about the children's health and family’s
socioeconomic status (Appendix 2). Socio-economic status in the parent’s questionnaire
was established by standardized instruments for the assessment of the socioeconomic
status [Schulte et al., 2006, Sofola et al., 2003; Lange et al., 2007; Thyen, 2007]. The
parents’ educational level, professional position and monthly net household income were
used as socioeconomic status indicators [Winkler-score index [Kurth and Robert-Koch-
Institut, 2002]. This index has been used in many other social studies, such as
[Vanobberge et al., 2001, Kumar et al., 2008, Saied-Moallemi et al., 2008]. Educational
level was computed as the highest educational level achieved by either father or mother.
Parent’s educational level was characterized as high (>10 years of education) or
medium/low (<10 years). Income was measured as net household income per month and
parents were dichotomized into a low (<1500V) and high (>1500V) income group.
Households with a low educational background of <9 years were not analysed as a
separate group because of their low frequency (n = 41). This low proportion is highly
specific to former Eastern German regions. Within this classification system, 21 social

35
classes were distinguished. For the purpose of the statistical analysis, these were reduced
to three categories, high, medium and low strata, low (3-8 points), middle socio-economic
status (9-14 points) and to high socio-economic status (15-21 points) based on Lange et
al., [2007] classification system.
4.3.3. Measuring instruments of dental and malocclusion examination
Clinical examinations for recording dental caries were carried out in both control and intervention
groups by following WHO diagnostic criteria guidelines [World Health Organization, 1997] and the
dmft/dmfs, DMFT/DMFS-indices. Orthodontic abnormalities (with or without therapy) were recorded
according to Klink-Heckmann and Bredy [1990]. After cleaning the teeth with sterile gauze, dental
examination was conducted by three examiners under natural indirect light with additional electric
light, using dental mirrors and explorers following WHO guidelines [World Health Organization,
1997]. Orthodontic assessment was recorded by visual inspection. All irregularities in the
anteroposterior, transverse and vertical planes were conducted with the children in upright positions
and the heads tilted back.
4.3.3.1. Caries measuring instruments
Caries occurrence in different populations can be described by mean values of caries indices, by
percentages of subjects attacked previously (DMFT>0) or currently (DT>0), and by the frequency
distributions of these subjects. Caries were recorded as present (d) when a lesion in a pit or fissure,
or on a smooth tooth surface, had a detectably softened floor, undermined enamel or softened wall.
A tooth with a temporary filling was also included in this category. On proximal surfaces, the
examiner was trying to be certain that the explorer had entered a lesion. Where any doubt existed,
caries were not recorded as present. Teeth were considered filled without decay (f) when one or
more permanent restorations were present and there was no secondary (recurrent) caries or other
area of the tooth with primary caries. If a tooth had both a caries lesion and a filling, it was
calculated as a decayed tooth only. Missing teeth (m) included permanent or primary teeth that had
been extracted because of caries. For missing primary teeth, premature loss of primary teeth due to
caries was considered when primary teeth were missing 2 years before their normal exfoliation.
Preventive fissure sealant application was counted in permanent and deciduous teeth using WHO
(1997) criteria. The fissure sealant was recorded for teeth in which a fissure sealant had been
placed on the occlusal surface. If a tooth with a sealant had decay, it was coded as decayed. No
radiological imagines were used because of technical difficulties. However, without radiographic
information, the need for restorative care would be underestimated. The extent of this

36
underestimation varied with disease prevalence and the number of restorations in the population. In
populations with very low, low, or moderate caries levels, the underestimation is likely to be of the
order of 3-5 %. Even in populations with high prevalence of disease, where a large amount of
restorative care had been provided, the underestimation would only be in the order of 10-15%
[WHO, 1997].
4.3.3.2. Malocclusion measuring instruments
Orthodontic abnormalities were classified according to its main symptom, as proposed by [Klink-
Heckmann and Bredy, 1990]. This classification was suitable to our visual inspection. All
irregularities in the anteroposterior, transverse and vertical planes were documented. Normal
overjet was defined as the horizontal overlap of the incisors in occlusion with the maxillary incisors
labially in contact with the mandibular incisors. Any deviations from normal overjet were measured
from the palatal surface of the most protruded, fully erupted maxillary incisor to the labial surface of
the corresponding mandibular incisor and defined as increased maxillary overjet. Mandibular
overjet was recorded when one or more maxillary incisors occluded lingually to the mandibular
incisors. Normal overbite was defined as covering the middle third of the mandibular incisors by the
maxillary incisors. An increased overbite was registered when more than two-thirds of the lower
incisors were covered by the upper incisors. A negative overlap in the vertical plane was recorded
as an anterior open bite. Occlusion of maxillary primary canines or molars lingually to the buccal
cusps of the opposing mandibular teeth was recorded as a posterior cross-bite. Crowding was
defined as any tooth rotated or out of line for which space would have to be created to allow
correction of malalignment. Spacing in mixed dentitions was recorded as a remarkable mismatch of
tooth and jaw sizes resulting in multiple spaces between the teeth. Mesial drift and missing of one
permanent tooth due to congenital missing, finger sucking as a wrong habit was registered.
However the another wrong habits such as nail biting, lip , tongue biting or functional disorders of
the tongue, speech disorders and incomplete mouth closure were not recorded.
4.4. Statistical analysis
Data management was done by transfer all data to the department of paediatric dentistry,
Greifswald University. The data of the extended dental examination including dmft/dmfs,
DMFT/DMFS-Indices, sealants and orthodontic abnormalities, were entered in a Microsoft Office
Excel 2003® database. The scanning of the questionnaires was conducted using the software
Teleform® (Version 10.2), and all the data were then finalized in a SPSS® (Statistical Package for
the Social Sciences, Version 15.0.1) database to be processed and analyzed. Before analysis, the

37
data were systematically reviewed by two independent research fellows to confirm that errors from
the files did not conflict with the true content of the examinations.
All the analyses were performed using the SPSS. In order to adequately describe the data two
approaches were used. First, the traditional approach was used, following the parametric model
and expressed with means, range, median and standard deviations (SD). The second, by
dichotomizing few variables into two groups (DMFT, DMFS and oral health competence variables)
and then expressed by proportions. With thus mixture of models a clear image about the samples
data would be provided.
Bivariate associations were calculated using Spearman correlation coefficients for all associations.
The Mann-Whitney was used to compare the oral health competence, malocclusion between caries
and non- caries cases and was used for every compensation between two groups. The Kruskal-
Wallis test was used to compare more than two groups. P-values and 95% confidence interval (CI)
were estimated for two-sided tests. In all the analyses, associations are labelled as being
‘significant’ if p < 0.05.

38
Chapter 5: Results
5.1. Response, sample characteristics and survey’s model
A total of 19 out of 22 schools in the target region participated in the survey. Within participating
schools, the fifth-grade students, mean age 10.4 years, participated in the survey. The
participation rate of the students in the dental examination was the highest among others surveys,
because of its obligatory nature. Out of 914 students 882 students (96.8%, 407 female, 475 male)
completed the school dental examination which performed by the community dentist. Only 93.2%
of the fifth-grade students completed the self-completion questionnaire (n = 852, Table 5.1). The
main reason for non-response among the children was illness at the day of the survey (4.2%), and
refusal of participation (2.6%). So, out of a total 914 children, 852 (93.2%) children had dental
checked ups and completed the self-completion-questionnaire.
In total, 721 out of 914 parents participated (78.8%). The single main reason for parental non-
response was failure to return the questionnaire because of lack of interest (18.9%), refusal
(1.7%), and moving out of the research region before the questionnaire was distributed (0.1%).
Table 5.1: Sample characteristics
N %
Response 852 93.2
Non-response: 89 6.8
Illness at day of survey 39 4.3
Refused participation 20 2.2
Moving away 30 0.3
Male 451 52.9
Female 401 47.1
Age in years 852 10.4 (9–13)
<=9 years 41 5.8
10 years 490 69.0
12 -13 years 179 25.2
Stu
den
ts
Migration background 29 3.4
Response 721 78.9
Non-response: 229 21.1
Questionnaire not returned 173 18.9
Refused participation 16 1.8
Moving away 4 0 0.4
High school education 178 24.7
par
ents
Monthly net income<1500V 196 27.2

39
The number of children who lived in Greifswald (HGW) or in the directly adjacent administrative
district of East Pomerania (OVP) was almost balanced, 48% (409 children) in Greifswald and 52%
(443 children) in the surrounding district. Additionally, the number of males and females was
almost balanced, 451 (52.9%) male and 401 (47.1%) female. The age range was 9-13 years, the
age means was a little bit more than ten years (10.34 ±0.56). Most of the children (93%) had
standard age 10 -11 years; eleven children were 9 years old and three children 13 years old.
The majority (67%) of children was living with their natural parents; 30% were living with their
mother. The remaining children were living with the father (2%), foster-parents (0.6%), in an
institution (0.3%) or with their grandparents (0.1%).
Parental education level, parental professional position and the monthly net household income
were used as social status indicators according to the Winkler-score index [Kurth and Robert-Koch-
Institut, 2002]. The children were divided into three socioeconomic groups, high, medium and low
socioeconomic level (Fig.5.1). The distribution of the socio-economic status among the total study
population shows an interesting pattern. In which equal distribution was found between the
students who belong to the high socio-economic status and those who belong to the low socio-
economic status (25% of the sample). And the majority of the students were in the middle socio-
economic status (48%).
Socio-economic status -Winkler (D2003)
High levelMidium levelLow level
Perce
nt 60
50
40
30
20
10
0
26
48
24
Fig.5.1: Children’s social
class distribution
About one-fourth of the parents had a high level of school education, while less than 6% reported a
low educational level. The majority of households (25%) reported a total net income a little less
than 1250€, which probably linked to social welfare or un- or underemployment in our study region.
23% had a total net income between 2250€ and 3000€; high household income, above 4000€,
was rare (6%).
Greifswald families reported significant more household income compared to the surrounding

40
Caries experience
Malocclusion
Socio-economic
status
Behaviours
Attitude
Knowledge
Dental
awareness
Gender
Smoking
Self -confidence
General Health
Nutrition
Rural-Urban
Occupation
Education
Income
district East Pomerania (Mann-Whitney Test p=0.03). The same thing was found regarding to the
socioeconomic status (SES), as the families in urban reported a significantly higher SES level
compared to families in rural (p=0.007). The following diagram illustrates the essential outlines of
the survey’s model:
Fig.5.2. Essential elements of the study model
5.2. Dental awareness-related items and scale properties
Dental awareness among the children was assessed according to the children’s knowledge about
oral health, the children’s attitudes towards oral health and the children’s oral health behaviour. The

41
children questionnaire included all of these three components in a shape of questions presented
the participants to determine their level of oral health awareness (Table 4.2).
5.2.1. Dental knowledge scale
Distribution of dental knowledge among the examined children was counted by giving one point for
each correct answer (the need of extra care for newly erupting teeth, children’s knowledge that the
dental examination is free of charge, use of adult toothpaste). It is noteworthy that only 30% of the
children were aware that newly erupting teeth need extra care, while most of them (46.3%) believed
that anterior teeth need extra care and 12% thought that deciduous teeth were the most important
(Fig.5.3).
Which teeth need the most care while brushing
deciduous teeth
newly erupting teeth
anterior teeth
Per
cent 50
40
30
20
10
0
12
30
46
Fig.5.3: Answers to the
question “Which teeth need the
most care while brushing?”
Interestingly, most of the children (70%) already knew that adult toothpaste was proper for
their age, but almost a fifth of them still thought that they should use children’s toothpaste.
Slightly more than half of the children (51.4%) knew that the dental examination visit was
free of charge. The children’s answers reflected a good level of dental knowledge; the values
for dental knowledge scale varied between 0-3 points (mean 1.9 ±1, Fig.5.4).
knowledge
3,02,01,00,0
Frequency
400
300
200
100
0
Fig.5.4: Level of dental
knowledge among the
schoolchildren

42
5.2.2. Dental behaviour scale
Distribution of dental behaviours among the examined children was also studied by giving
one point for each correct answer (tooth brushing every evening, tooth brushing every
morning, eating fruit and sweets only 2-3 times every day, four sealed permanent teeth).
The distribution of the evening brushing was highly polarised with most of the children
(74%, n=600) brushed their teeth every evening. Of the remaining children, 17% (135)
brushed their teeth most evenings. Very few children 6% (51) admitted to brushing their
teeth just occasionally in the evening, and 4% (11) did not even brush their teeth in the
evening at all. The morning brushing frequency showed a trend similar to the evening
brushing (Fig.5.5).
do you brush your teeth evening
every day
mostdays
occasionally
notime
missing
80
60
40
20
0
74
17
6
do you brush your teeth morning
everyday
most of days
occasionally
notime
missing
80
60
40
20
0
76
15
6
Fig.5.5: Answers to the question “Do you brush your teeth in the evening-morning?”
The majority of children eat sweets and fruit either 2-3 times a day (44%) or 4-5 times a day (41%).
Of the remaining children, slightly more than one-tenth eats fruit and sweets 6-7 times every day.
Whereas, very few (5%) eat fruit and sweets 8 to 9 times a day.
Half of the participants were evenly distributed between three visits and four visits to the dentist per
year, whereas 41% of them reported two visits yearly, less than one-tenth of them went once a year,
and just 1.7% of them did not go at all.
A normal distribution of dental behaviour among the children was counted; the values of dental
behaviour competence among the observed children varied from 0-4 points (mean 2.1 ±0.9, Fig.5.6).

43
behaviour
4,03,02,01,00,0
Freque
ncy 400
300
200
100
0
Fig.5.6: Level of dental
behaviour among the
schoolchildren
5.2.3. Dental attitude scale
Dental attitude were determined by the children’s personal impression of the following statements:
• I eat only a few sweets to keep my teeth healthy, about half of the children (45%) believed that
this is rather correct, another one-quarter considered that this is hardly correct; very few of them
(6%) considered it absolutely incorrect.
• I pay extreme attentions to my teeth, answers were almost evenly distributed between two
groups; the first group said that this statement was correct, and the second groups said that it
was rather correct. The few remaining children considered that it was hardly correct or
absolutely incorrect.
• Healthy teeth are very important to me, most of the children (72%) considered that healthy teeth
were very important to them; slightly more than one-fifth (23%) considered that was rather
correct. The very few remaining considered that this statement was hardly correct or absolutely
incorrect.
• My family makes sure that I brush my teeth, the distribution of the answers to this statement
was highly polarised, with most of the children (90%) saying that their parents took care of their
teeth brushing, and the rest said that their parents did not take care (Fig.5.7).
incorrect
hardly correct
rather correct
correct
80
60
40
20
0 47
18
72
Fig.5.7: Children’s impression
on the statement, “My family
makes sure that I brush my
teeth”
• Nothing will happen if I don’t brush my teeth once, slightly more than one quarter found that is

44
correct that nothing will happens, if they did not brush their teeth one time, 17% found that is it
rather correct, one quarter consider that it is hardly correct, whereas about third of the children
(32%) refused to keep their teeth one time without brushing.
• I would avoid sweets, in order to keep my teeth good and healthy, seventy percent of the
children said that they agreed with avoiding sweets to keep their teeth healthy, whereas the
remaining one-fifth said that they hardly agreed, and one-tenth absolutely didn’t agree.
• Did you talk with your parents about what is good for your teeth? This statement is considered
an indicator for family communication. Slightly more than one-quarter of the children often
talked with their parents about what was good for their teeth; 36% said that they occasionally
talked, one-fifth rarely talked, one-tenth did not talk at all, and just a few of participants (5%)
stated that they always talked with their parents about what is good for their teeth (Fig.5.8).
Did you talk with parents about your teeth?
alw ays
often
occasionally
rarely,
no
Percent 40
30
20
10
0
5
27
36
21
11
Fig.5.8: Children’s impression
on the question, “Did you talk
with your parents about what
is good for your teeth?”
Distribution of dental attitudes among examined children was evaluated by giving one point for
each of the above items (always talked with parents about what was good for teeth, avoided sweets
ate to keep teeth healthy, healthy teeth were very important to the child, paying extreme attention to
teeth, the family made sure that the child brushed his/her teeth, ate only few sweets to keep teeth
healthy). Normal distribution of dental attitude among the children was counted; its values varied
between 0-7 points (mean 2.9 ±1.6, Fig.5.9).
attitude
7,06,05,04,03,02,01,00,0
Frequency
300
200
100
0
Fig.5.9: Level of dental
attitude among the
schoolchildren

45
After studied each of dental awareness scales separately; a new variable representing the
sums of the three scales was created and called oral health awareness. Normal distribution
of oral health awareness among the children was counted. The values of this new
generated scale varied between 0-13 (mean 6.9 ±3.7, Fig.5.10).
20,018,016,014,012,010,08,06,04,02,00,0
200
100
0
Fig.5.10: Distribution of dental
awareness among children
Females performed better on all dental awareness related scales than males, with a mean
awareness of 9.8 ±3.8 and 0.8 ±3.5 for males, females, respectively (p=0.05, Fig.5.11). However,
the difference in dental attitude or dental knowledge was not significant. Only dental behaviour was
significantly different between the two gender with mean of 2.0 ±1.1, 2 ±0.8 for male and female,
respectively (p=0.004).
GirlsBoys
Den
tal awaren
ess 25
15
5
-5
Fig.5.11.Difference in
dental awareness
among boys and girls
(p=0.05)
5.2.4. Association between dental awareness scales
The association was evaluated by studying the correlation between the different components of
dental awareness (knowledge, attitude, behaviour), which illustrated that there was a direct
correlation between dental attitude and dental behaviour (Spearman correlation coefficient rs=0.32,
p<0.001). However, no correlations between the other components (knowledge vs. attitude,
knowledge vs. behaviour) were found. Thus, dental behaviour was independent of dental

46
knowledge, but dependent on dental attitude (Table 5.2).
Table 5.2: Correlation between dental knowledge, attitude and behaviour
r/p Spearman correlation
Dental Knowledge Dental Attitude Dental Behaviour
Dental Knowledge
_ -0.055 0.059
-0.018 0.3
Dental Attitude
-0.055 0.059
_ 0.320** 0.003
Dental Behaviour
-0.018 0.3
0.320** 0.003
_
Spearman correlation (* p< 0.05, ** p< 0.01)
5.2.5. Association between dental awareness and social status indicators
Educational level was more important in predicting the dental awareness related indicators
compared to net household income. Educational level was important in predicting dental knowledge
(rs=0.09, p=0.01, Fig.5.12) and communication skills (rs=0.06, p=0.04), but not for attitudes or
behaviour. Children with high educational background were more knowledgeable and
communicative about dental health topics.
Social score. (Winkler 2003)
High SESMedium SESLow SES
Whi
ch te
eth
need
mor
e ca
re w
hile
bru
shin
g?
,38
,36
,34
,32
,30
,28
,26
,24
,22
,35
,31
,24
Fig.5.12: Association between
SES and children’s Knowledge
that teeth brushing should be
concentrated on the erupting
teeth
In particular, the mother’s educational level was more important in predicting dental awareness
related indicators compared to the father’s educational level. The mother’s educational level was
associated with more evening tooth brushing (rs=0.08, p=0.01) and the child’s knowledge about
which teeth need more attention during brushing (rs=0.12, p=0.001) and sealant application
(rs=0.06, p=0.03).
5.3. Caries experience distribution
The general distribution of dental caries occurrence among the 5th grade students in Mecklenburg-
Vorpommern revealed a strong polarisation of caries with noticeable clear spike of extra zeros,

47
representing the caries-free students (Fig.5.13, Fig.5.14).
Seventy-one percent of permanent teeth and fifty two of deciduous teeth had DMFT and dmft
scores of zero. Thus, caries-free dentitions (DT=0, dt=0) were more common in permanent teeth
compared with deciduous teeth (91 vs. 75%). The dmft and DMFT mean values were 1.2 ±1.9 and
0.6 ±1.2, respectively. The difference between means was statistically significant (p<0.001). But in
the same time there was association between the prevalence of caries experience in permanent
and deciduous teeth (rs= 0.15, p=0.001). At any rate, the large number of students with no caries or
fillings in both dentitions is remarkable and seems to be a phenomenon for caries experience
distribution in most of the developed countries.
In order to adequately describe these data two approaches were used. One presents the traditional
approach, by following the parametric model and expresses the data with means and standard
deviations (SD). The second, by collapsing and pooling the populations into two groups; “caries
free” and “caries” subjects, the first group was recorded by number (0), the second group was given
number (1) and then analyzed as categorical data with rating scale format to improve scalability
and help for further comparisons.
The two histograms (Fig.5.13, Fig.5.14) show clearly that caries occurrence and distribution among
the samples of the study were a non-Gaussian distribution. In which both histograms are skewed to
the right (positively skewed) and caries experience variables considered as counting variables.
Therefore, a non-parametric tests and analysis were performed for these variables. Analysis of the
variables was initially performed through means and standard deviations (SD) for both of the
permanent and deciduous teeth.
5.3.1. Caries experience in deciduous teeth
A bout half of the children (52%) had a caries- and filling-free deciduous dentition. Of the remaining
children, 13% had just one affected tooth, and 11.4% had two affected teeth. The mean dmft/dmfs
were 1.2 ±1.9 and 3.1 ±5.5, respectively, and the values of the dmft/dmfs ranged from 0 to 11 and 0
to 47, respectively (Fig.5.13).

48
dmft
11109876543210
numbe
r of children 500
400
300
200
100
0 235160
97112
467
Fig.5.13: Distribution of the
dmft among the children,
(Ø 1.2 ±1.9)
• In relating to dt values, three-quarters of the children had caries-free deciduous dentition. Of
the remaining children, 13% had one decayed deciduous tooth, 5.6% had two decayed
deciduous teeth, and the dt values ranged from 0 to 10 with a mean dt of 0.47 ±1.01.
• Very few children had missing deciduous teeth; 3.5% of children had one missing
deciduous tooth, 2.3% of the children had two missing deciduous teeth, and the mt values
ranged from 0 to 9 with a mean mt of 0.13 ±0.63.
• A little more than half of the caries cases in the deciduous dentition had been treated with
fillings. Thus, the ft comprised more than the half of the dmft values (0.56%). Three-quarters
of the children were free of filled deciduous teeth. A little more than one-tenth of the children
had one filled tooth, and the ft values ranged from 0 to 9 with a mean ft of 0.68 ±1.29.
Of note, caries experience in deciduous dentition tended to be more prevalent among
males than females without attaining statistical significance (Mann-Whitney Test p=0.5)
with mean dmft values of 1.4 ±1.9, 1.3 ±1.8 for male and female, respectively.
5.3.2. Caries experience in permanent teeth
The distribution of the DMFT values was highly polarized, with Almost 71% of the children
exhibiting no carious defects, fillings or missing teeth in the permanent dentition (Fig.5.14). Of the
remaining children, most of them had just one affected tooth (12.6%). The overall DMFT and DMFS
values in the children ranged from 0 to 8/ 0 to19, respectively, with mean DMFT/DMFS of 0.6 ±1.2/
0.9 ±2.2, respectively.
• In regard to DT values, most of the children (91%) were caries-free. Only 5% of the children
had one decayed tooth; the rest (4%) had 2-4 decayed teeth. DT values ranged from 0 to 4
with a mean DT of 0.15 ±0.5. The number of caries lesions (DT) was a little bit higher in
males than females without statistical significance (p>0.05).

49
DMFT
8,07,06,05,04,03,02,01,00,0
num
ber of children 700
600
500
400
300
200
100
0 3361
104
612
Fig.5.14: Distribution of the
DMFT among the School
children (Ø 0.6 ±1.2)
• Only very few children had missing permanent teeth; 1% of children had one missing
permanent tooth and the MT values ranged from 0 to 3 with a mean of 0.01 ± 0.17.
• Most of the caries experience had been treated with fillings. Thus the FT comprised the
highest proportion of the DMFT (0.45%). Three-quarters of the children were free of filled
teeth; a little more than one-tenth had one filled tooth. The FT values ranged from 0 to 8
with a mean of 0.45 ±1.01. The number of filled teeth (FT) tended to be more prevalent
among females than males without attaining statistical significance (p>0.05).
A statistically significant, but weak positive correlation (rs=0.9, p=0.008) between age and DMFT
values were found. The DMFT, DMFS values tended to be more prevalent among females than
males, without attaining statistical significance Mann-Whitney test p>0.05 (Table 5.3).
Table 5.3: Caries distribution according to gender
DMFT DMFS DS MS FS
Female 0.72 ±1.28 1.09 ±2.35 0.23 ±0.83 0.11 ±0.97 0.76 ±1.73
Male 0.62 ±1.27 0.95 ±2.53 0.29 ±1.54 0.07 ±0.82 0.59 ±61
Total 0.68 ±1.29 1.04 ±2.45 0.26 ±1.25 0.10 ±0.92 0.68 ±1.67
Comparison was done between the schools located in Greifswald (HGW) versus those located in
East Pomerania (OVP) in regard to caries experience in both permanent and edacious dentition to
determine whether the place of residency had an impact on the caries prevalence. Both of the
DMFT and dmft were significantly lower in Greifswald compared to East Pomerania, with mean
DMFT values of 0.57 ±1.2 vs 0.71 ±1.2 and mean dmft values of 1.2 ±1.8 vs 1.5 ±2.0 (Mann-
Whitney Test p=0.05).
There was a significantly higher mean dmft in the children who were born in Germany than those

50
who were born in another country with a mean dmft of 1.4 ±1.9 vs 0.5 ±1.1 (Mann-Whitney Test
p=0.01). The difference in DMFT values between the children born in Germany or in another
country was found, but without attaining statistical significance (p=0.5).
5.3.3. Distribution of sealant
Slightly more than half of the children did not have any sealant, whereas approximately one-fifth of
them had sealants in all four first permanent molars. One-tenth of them had two sealed teeth, but
7.3% of them had only one sealed tooth; very few children had more than four sealants (Fig.5.15).
number of sealant teeth
11109876543210
60
50
40
30
20
10
0
Fig.5.15: Distribution of sealant
among schoolchildren
The DMFT and the number of sealed teeth were inversely correlated (Spearman correlation
coefficient rs=-0.13, p=0.001). Thus there was a significantly lower DMFT rate in the children who
had four sealed teeth than those with less than four sealants, with a mean DMFT of 0.15± 0.5 vs
0.8± 1.3 (Mann-Whitney Test p=0.004). The rate of sealant application was significantly lower in
Greifswald city (HGW) versus East Pomerania (OVP), with a mean sealants of 1.2 ±1.6 vs 1.7±1.8
(Mann-Whitney Test p=0.003, Fig. 5.16).
OVPHGW
seal
ants
in H
GW
. O
VP 12
10
8
6
4
2
0
-2
543
621452
Fig.5.16: Difference in the
sealant application between
Greifswald schools and East
Pomerania schools (p=0.004)

51
5.4. Oral health risk factors among different survey’s indictors
5.4.1. Caries experience in relation to socio-economic status (SES)
There was a significant reverse correlation between the DMFT and social class (rs=-0.19, p=0.001).
In our sample group; the higher the social class was, the lower the incidence of DMFT, with a mean
DMFT of 0.9 ±1.3, 0.6 ±1.1, 0.4 ±0.9 for the low, medium and higher social strata, respectively
(Fig.5.17).
Social score ( Winkler 2003)
high SESmedium SESlow SES
Mea
n-DMFT ,9
,8
,7
,6
,5
,4
,3
,4
,6
,9
Social score (winkler 2003)
3020100
Mea
n-DMFT 10
8
6
4
2
0
-2
Fig.5.17: Reverse correlation between carries experience and social class
The economic status of the family was negatively correlated with the DMFT incidence, with less
DMFT incidence in families with higher household income (rs=0.22; p=0.001, Fig.5.18).
>=5000 €
4000 - <5000 €
3000 - <4000 €
2250 - <3000 €
1750 - <2250 €
1250 - <1750 €
<1250 €
DMFT 1,0
,8
,6
,4
,2
0,0,1
,3
,3
,4
,6
,8
,9
Fig.5.18: correlation
between DMFT and family
income in Euros
By comparing the correlation strength between the DMFT and the socioeconomic status of the
mother and father, it was found that the correlation was stronger with the mother’s socioeconomic
status (rs mother=- 0.2, p=0.001, rs father =-1.4, p=0.001). This was obvious in both of the parent’s
education and professional positions, as the correlation between the parent’s education level and

52
the DMFT was stronger with the mother’s education level than with the father’s (rs mother =-0.14,
p=0.001, rs father =-0.68, p=0.04), parallel. The correlation between the parent’s professional
positions and the DMFT was stronger with the mother’s professional position than the father’s (rs
mother =-0.15, p=001, rs father =-0.08, p=0.01).
The rate of sealant application was significantly correlated to the socioeconomic status (rs=0.07,
p=0.04). The highest rate of sealant application was detected in the children who were from higher
socioeconomic status, with mean sealant application of 1.3 ±1.5/1.4 ±1.6/1.6 ±1 in the high,
medium and low social class, respectively.
5.4.2. Caries experience, dental awareness in relation to self-esteem
Self-efficacy of the child was associated with each of the DMFT incidence and oral health
awareness level among the schoolchildren of this age group. So there was found significant
correlation between the rate of the DMFT and the child’s ability to master the new problem alone
(rs=-0.9, p=0.02). Similarly, significant correlation was found between dental awareness and self-
esteem (rs=0.19, p=0.001, Fig.5.19). This association was particularly obvious between self-esteem
and the child’s desire to avoid sweets or eat only few sweets to keep his teeth healthy.
I can master problems alone
Absolutely untruehardly trueexactly true
Den
tal
awar
enes
s 1,2
1,1
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
Fig.5.19: Relationship
between dental awareness
and children’s impression on
the statement’ “If a new
problem emerges, I can
master it from my own ability.”
5.4.3. Caries experience in relation to nutrition
The questionnaire included several items about nutrition such as; communication between parents
and children about healthy food, the frequency of drinking lemonade /iced tea/ juice/ milk/ water /
tea without sugar, or eating chocolate/sweets/cakes/white bread/ jam, honey/ cereals/
fruit/vegetables/ salty snacks (Table 4. 2).
Consequently, analyzing the children’s answers on the above items illustrated some important
results as the frequency of drinking lemonade or iced tea showed clear correlations with the DMFT
(rs=0.16, p=0.01). Children who drank lemonade had higher caries levels with a mean DMFT of

53
1.2±1.9 vs 0.6±1.2 (Fig.5.16). The same was true for children who drank iced tea (rs=0.08, p=0.02).
Interestingly, the frequency of drinking lemonade or iced tea was associated negatively with the
level of socio-economic status (rs=0.2, p=0.01, Fig.5.20).
Do you take limonada to drinking in school?
YesNo
Mea
n DMFT 1,3
1,2
1,1
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
1,2
,6
Fig.5.20: Association between
DMFT and lemonade drinking
at school
Bringing water to drink at school was associated with less caries (rs=-0.13, p=0.001) with a mean
DMFT of 0.3 ±0.8 vs 0.7 ±1. The same thing was true for children who drank tea without sugar had
a lower DMFT rate than other children who did not, with a mean DMFT of 0.3± 0.9 vs 0.6±1 (rs=-
0.06, p=0.04).
Regarding eating habits, the frequency of eating salty snacks (chips, nuts) showed clear
correlations with the DMFT (rs=0.14, p<0.01). White bread (rs=0.07, p=0.05), sweets/cakes
(rs=0.07, p=0.06) and chocolate (rs=0.06, p=0.04) showed only a weak correlation. Items such as
jam, honey, cereals, fruit/vegetables, fruit juice and milk showed no association with caries at all.
Sosial score (Winkler 2003)
Low SESMidium SESHigh SES
Do
you
drin
k le
mon
ade
at s
choo
l?
4,5
4,0
3,5
3,0
2,5
2,0
1,5
1,0
,5
0,0
3,8
3,4
2,9
Fig.5.21: Association between
lemonade drinking and socio-
economic status
It worthy to reported that children’s evaluation of healthy food had an impact on the DMFT, as
children who rated good taste of food as most essential in food choosing had significantly higher
DMFT scores than children who did not, with a mean DMFT of 0.7 ±1.3 vs 0.4 ±1.0 (p=0.01). In
addition, the communication between parents and children about healthy food had an important

54
effect on the rate of the caries experience, as there was a significant correlation between the two
objects (rs=-0.09, p=0.006).
5.4.4. Association between DMFT and the amount of daily television watching
Interestingly, a significant correlation was detected between the DMFT and period spent watching
television per day (rs=0.1, p=0.002). As the children who spent more time watching TV were found
to have a higher incidence of DMFT than children who watched for shorter periods every day (Fig.
5.22). Moreover, there was a significant correlation between TV watching and socioeconomic
status (rs=-0.13, p=0.001) with mean TV daily viewing of 2.4 ±0.9/ 2.2 ±0.9/ 2.0 ±0.9 for the low,
medium and high social strata, respectively.
How many hours per day do you spend with T.V?
More than 3 hours2-31-2under 1
DMFT ,9
,8
,7
,6
,5
,4
Fig.5.22: Association between
the DMFT and duration of daily
television watching
5.4.5. Association between DMFT and smoking
The questionnaire included several questions to obtain a broad picture of actual smoking behaviour
status (Table.4.3). By studding the relationship between the actual caries smoking status, some
important information was detected as; a significant correlation was found between the prevalence
of each of caries and smoking among school children (rs=0.1, p=0.002). Smoking children had a
higher DMFT rate than children who weren’t smokers with a mean DMFT of 0.9 ±1.5 vs 0.6 ±1.2,
(p=0.004, Fig.5.23).
not smokersmoker
DMFT 1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
,6
,9
Fig.5.23: Association between
the DMFT and smoking

55
Age played an important roll in the prevalence of smoking and DMFT (rs for age/DMFT 0.094, rs for
age/smoking 0.18, p=0.001). Each age group was analysed separately and smokers in all age’s
groups registered more caries incidence (Fig.5.24).
Age
131211109
Mea
n D
MF
T 2,5
2,0
1,5
1,0
,5
0,0
Smoking
Not smoking
Fig.5.24: Relationship between
age, DMT and smoking
Interestingly, each of caries and smoking were correlated with the socioeconomic status level, as
smoking was negatively associated with socioeconomic status with higher rate of smoking
prevalence in the children from lower SES level (rs=0.17, p=0.001).
Moreover, there was a significant correlation between the rate of the DMFT and smoking addiction
(rs=-0.19, p=0.03, Fig.5.25). Addiction was defined as the child having formed an uncontrollable
dependence on tobacco to the point where stopping smoking would cause severe emotional,
mental, or physical reactions. This addiction was determined by asking the child smoker if he/she
felt nervous or worried if he/she had not smoked for a while.
Do you feel nervous if you have not smoked?
YesNo
DMFT 10
8
6
4
2
0
-2
Fig.5.25: Association between
the DMFT and smoking
addiction
There was also a significant correlation between the DMFT rate and the existence of one or more
smokers among the family members (rs=-0.13, p=0.00). The same correlation was found between
the DMFT rate and children whose their best friends were smokers (rs=-0.1, p=0.002).

56
5.4.6. Association between DMF and general Health
The survey’s questionnaire included several items about children’s physical and mental health
(Table 4.3). The children who considered that health item is an important thing to them, had
significant lower DMFT versus other children (Mann-Whitney Test p=0.05). Furthermore, a
significant correlation between the rate of the DMFT and ear / throat aches was detected (rs=0.08,
p=0.01), as the children who had ear / throat aches once or more times in the last three months
had higher DMFT rate than the children who did not complain at all, with a mean DMFT of 0.23
±0.4/ 0.3 ±0.46/ 0.4 ±0.48 in the three groups, respectively.
The children who found themselves in the last week tired and worn-out had more DMFT than other
(Mann-Whitney Test p=0.009). Similarly, the children who found themselves had a lot of strength
and endurance in the last week had lower DMFT versus other children (Mann-Whitney Test
p=0.008). In addition, DMFT incidence was negatively correlated with the child’s level of fear of
being marked badly (rs=0.08, p=0.01).
5.4.7. Association between toothache and children’s performance at school
Interestingly, toothache has a negative influence on children’s performance at school, as a
significant reverse correlation between toothache and the decline in the child’s participation in
school was found (rs=-0.11, p=0.003). Similarly, there was significant correlation between toothache
and the partial participation in the classroom (rs=-0.11, p=0.003) and the drop in the child’s
performance up to half of his/her normal capacity (rs=-0.09, p=0.007). Also, significant correlation
was detected between toothache and the inability to do home work after school (rs=-0.15, p=0.001).
5.5. Association between caries experience and dental awareness
Dental awareness scale as a new variable representing the sums of the three scales (dental
behaviour, dental attitude and knowledge) was reversely correlated with caries experience in
permanent and deciduous teeth (rs DMFT=-0.1, p=0.001 and rs dmft=- 0.64, p=0.04).
For a more knowledge of whether an increased dental awareness would result in fewer carious
defects, correlations between DMFT and each component of dental awareness were studied
separately.

57
5.5.1. Association between caries experience and dental knowledge
There was a correlation between dental knowledge and caries experience (rs DMFT =0.09, p=0.003).
The correlation was stronger with DT (rs DT =0.2, p=0.03).
Two of three items concerning dental knowledge were associated significantly with the DMFT: The
child’s awareness that dental examination is free of charge was correlated positively with caries
(rs=0.13, p=0.001), as DMFT was higher in children who knew that the check-up by the dentist was
free of charge (1) than those who did not know (2), mean DMF (1)= 0.9 ±1.4, ; DMFT (2)= 0.5 ±0.9
(p=0.004, Fig.5.26).
Is the checkup by the dentist free?
YesNo
DMFT 12
10
8
6
4
2
0
-2
Fig. 5.26: Difference in the rate
of DMFT between children who
knew that the dental check-up
was free of charge and those
who did not (p=0.001)
It is noteworthy that the children who knew that new erupting teeth need the most care while
brushing (1) were with a significant lower DMFT rate than the another children who did not know
(2), mean DMFT (1)=0.25 ±0.46; DMFT (2)=0.32 ±0.43 (Mann-Whitney Test p=0.05, Fig.5.27).
However, there were no significant differences in the DMFT rate between children who knew the
suitable toothpaste for their age (adult toothpaste) and those who did not know (Mann-Whitney Test
p>0.05).
Which teeth need the must care while brushing?
Right replayWrong replay
Mea
n D
MF
T ,40
,30
,20
,10
0,00
,25
,32
Fig.5.27: Difference in the rate
of DMFT between children who
knew that the new erupting
teeth need more care during
brushing and those who did not
knew (p=0.05)

58
5.5.2. Association between caries experience and dental behaviours
In the present survey, a reverse correlation was detected between caries experience and dental
behaviour (rs=0.15, p=0.001, Fig. 5.28). So, four of four variables concerning oral health behaviour
scale were associated with caries prevalence, three of them was associated negatively and firths
positively.
Behaviour
4,003,002,001,00,00
Mea
n D
MF
T 1,2
1,0
,8
,6
,4
,2
0,0
,2
,6
,7
,8
1,0
Fig. 5.28: Relationship
between dental behaviour
and the DMFT rate
A reverse correlation between the evening brushing and dmft rate was found (rs=-0.11, p=0.001,
Fig.5.29), Kruskal-Wallis test showed significant differences in the dmft rate among the children in
the four groups who said definitely that they brushed their teeth 1) no time in evening, 2)
occasionally, 3) on most days, 4) every day, with mean dmft of 1.3 ±0.5/ 1.5 ±1.3/ 1.8 ±1,2 / 2.5
±1.2 in the four groups, respectively, p=0.002. Similarly, a reverse correlation was detected
between morning brushing and the DMFT rate (rs=-0.06, p=0.03).
Do you brush your teeth in the evening?
every day
most of days
occassionally
no time
Mea
n dm
ft 2,6
2,4
2,2
2,0
1,8
1,6
1,4
1,2
1,0
,8
,6
,4
,2
0,0
1,3
1,5
1,8
2,5
Fig.5.29: Negative association
between dmft and evening
brushing
The amount of daily sweets eating was correlated reversely with the dmft (rs=-0.07, p=0.01). The
Kruskal-Wallis test showed that the dmft was significantly differed between groups of children who
stated that they ate fruit and sweets daily: 1) 2-3 times 2) 4-5 times 3) 5-7 times 4) 7-9 times, with

59
mean dmft values of 1.1 ±1.7/ 1.5± 2.1/ 1.5± 1.9/ 1.6 ±1.6 in the previous four groups, respectively
((p=0.03, Fig.5.30). However, this difference was not significant with regard to DMFT average
(p>0.05).
how often do you eats fruits and sweets dially?
8-96-74-52-3
dmft 12
10
8
6
4
2
0
-2
Fig.5.30: Negative association
between dmft and the amount
of daily sweets consuming
One the other hand, the frequency of yearly dental visit was directly correlated with the DMFT rate
(rs=0.1 p=0.004). The Kruskal-Wallis test showed also that there was significant difference in the
DMFT between the five groups of children who go to the dentist 1) no times a year, 2) one time a
year, 3) two times a year, 4) three times a year, 5) four times or more a year with a mean DMFT of
0.5 ±1.1/ 0.6 ±1.1/ 0.5 ±1.1/ 0.7 ±1.3/ 0.9 ±1.5 in the five groups, respectively (p=0.04).
5.5.3. Association between caries experience and dental attitude
In general, no significant correlation was registered between dental attitude and the DMFT rate. But
by studying the correlations with the different items of dental attitude separately; a significant
reverse correlation was recorded between the families’ interest in their children’s tooth hygiene and
the DMFT/ dmft rate (rs DMFT=-0.06, p=0.03, and rs dmft=-0.1, p=0.005, Fig.5.31). Also, Kruskal-Wallis
test showed that dmft differs significantly among children depending on their family’s interest in
their tooth hygiene p=0.04, with the highest dmft among children who answered the question with
“hardly correct” (1) and the lowest among children who answered the question with “exactly correct”
(4), with mean (dmft) of 1.2±1.9/ 1.5±1.9, 1.7±1.8/ 1.8 ± 2.4 in the four groups, respectively. But this
difference was not significant with regard to DMFT average (p>0.05).

60
My family makes sure that i brush my teeth
not correct
hardly correct
rather correct
exactly correct
Mea
n dm
ft 2,0
1,8
1,6
1,4
1,2
1,0
,8
,6
,4
,2
0,0
1,8
1,7
1,5
1,3
Fig.5.31: Reverse correlation
between dmft and the family
confirmation on tooth brushing
of their children
Interestingly, the communication between children and parents about oral health items was of
essential importance, as there was detected a significant difference in the dmft rate among the
children who always talked with their parents about what is good for their teeth and those who
never talked with a mean dmft of 0.9 ±1.9 vs 1.6 ±1.7 (Mann-Whitney Test p=0.02).
Regarding, the children’s personal impression on the importance of controlling the amount of
sweets or absolutely avoiding sweets in their diet, to keep their teeth healthy; the Kruskal-Wallis
test illustrated that there were no significant differences in the DMFT rate among the different
impressions (p>0.05). Likewise, in the present survey, there was no significant difference in the
DMFT rate among children who admitted that they paid extreme attention to their teeth and those
who did not (p>0.05). Finally, Kruskal-Wallis test showed that there was a difference in the DMFT
rate among the different children’s impressions on the importance of healthy teeth, but this
deference was not strong enough to be a significance (p>0.05, Fig.5.32).
Healthy teeth are important to me
not correct
hardly correct
rather correct
exactly correct
DMFT 1,4
1,2
1,0
,8
,6
,4
1,3
,8
,7,6
Fig.5.32: Dissimilarity in the
DMFT rate among the
different children’s
impressions on the
importance of healthy teeth

61
5.6. Distribution of malocclusion among the children
When the distribution and the forms of malocclusion among schoolchildren in Greifswald and East
Pomerania were investigated, the results showed that 64 percent of the subjects had at least one
type of anomaly (Fig.5.33). Lack of space (crowding) represented the major percentage (28%) of all
children having any form of malocclusion; This was followed by maxillary overjet, happening in
23.4%; increased overbite (deep bite) 8.6%; posterior cross bite 8.4%; mandibular overjet (anterior
cross bite) 2.5%; open bite 1.7%; spacing 0. 9%; mesial drift 0. 3%. finger sucking was the lonely
wrong habits which was investigated in this survey and prevalent in 2.3% of all children. 30% of the
children were already undergoing orthodontic treatment.
Finger sucking
Mesial drift
Posterior cross-bite
Increased overbite
Open bite
Mandibular overjet
Maxillary overjet
Spacing
Crow
ding
Mea
n ,2
,1
0,0
Fig.5.33: Distribution of
malocclusion among
schoolchildren in Greifswald
and East Pomerania
The need for orthodontic treatment was found significantly greater in East Pomerania than in
Greifswald city (Mann-Whitney Test p=0.03).
In regard to gender differences, males recorded more malocclusion cases than female but this
difference wasn’t significant (p>0.05). By studding this gender difference in related to different kinds
of malocclusion separately, it was detected significant differences between girls and boys in
increased overbite and crowding. As males exhibited significantly higher increased overbite scores
than females (Mann-Whitney Test p=0.04). In contrast, the prevalence of crowding was more
common in females than in males (p=0.05, Fig.5.34).
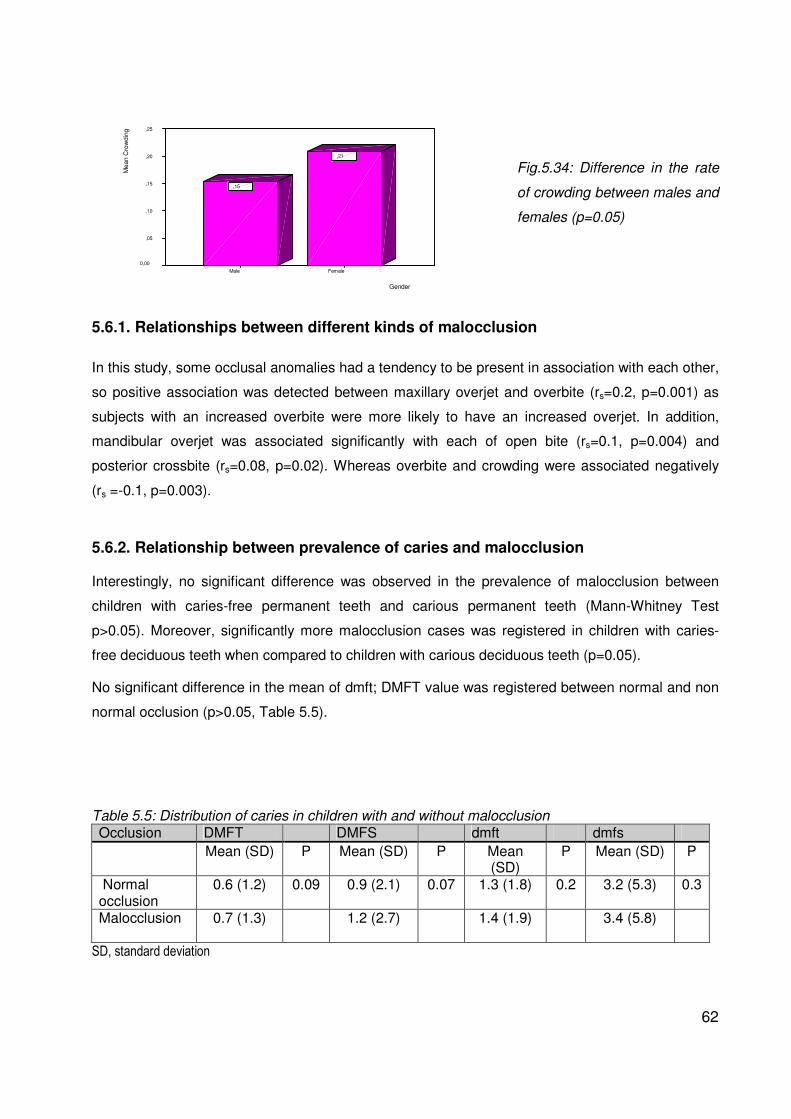
62
Gender
FemaleMale
Mea
n C
row
ding
,25
,20
,15
,10
,05
0,00
,21
,15
Fig.5.34: Difference in the rate
of crowding between males and
females (p=0.05)
5.6.1. Relationships between different kinds of malocclusion
In this study, some occlusal anomalies had a tendency to be present in association with each other,
so positive association was detected between maxillary overjet and overbite (rs=0.2, p=0.001) as
subjects with an increased overbite were more likely to have an increased overjet. In addition,
mandibular overjet was associated significantly with each of open bite (rs=0.1, p=0.004) and
posterior crossbite (rs=0.08, p=0.02). Whereas overbite and crowding were associated negatively
(rs =-0.1, p=0.003).
5.6.2. Relationship between prevalence of caries and malocclusion
Interestingly, no significant difference was observed in the prevalence of malocclusion between
children with caries-free permanent teeth and carious permanent teeth (Mann-Whitney Test
p>0.05). Moreover, significantly more malocclusion cases was registered in children with caries-
free deciduous teeth when compared to children with carious deciduous teeth (p=0.05).
No significant difference in the mean of dmft; DMFT value was registered between normal and non
normal occlusion (p>0.05, Table 5.5).
Table 5.5: Distribution of caries in children with and without malocclusion Occlusion DMFT DMFS dmft dmfs Mean (SD) P Mean (SD) P Mean
(SD) P Mean (SD) P
Normal occlusion
0.6 (1.2) 0.09 0.9 (2.1) 0.07 1.3 (1.8) 0.2 3.2 (5.3) 0.3
Malocclusion
0.7 (1.3) 1.2 (2.7) 1.4 (1.9) 3.4 (5.8)
SD, standard deviation

63
Crowding was found significantly most often in caries-free dentition (Mann-Whitney Test p=0.03).
Moreover, crowding was correlated negatively with caries experience with significantly greater dmft
values in non crowding cases (1) than in crowding cases (2), dmft (1) =1.4± 1.9/ dmft (2) =1.2±1.7
(rs=-0.07, p=0.04, Fig.5.35).
Crowding
CrowdingNo crowding
Mea
n dm
ft 2,0
1,5
1,0
,5
0,0
1,2
1,4
Fig.5.35: Negative correlation
between dmft rate and
Crowding
Maxillary overjet were a little bit more prevalence in caries-free dentition than in carious dentition
but without significant difference (p>0.05).
Subjects with maxillary overbite (1), had significantly lower dmft scores when compared with
children with normal occlusion (2); dmft (1) = 0,9±1.7; dmft (2) = 1.4± 1 (rs=-0.08, p=0.03).
In contrast, mesial drift of the first permanent molar combined with premature loss of primary teeth
in the posterior arches was associated directly with more dmft rate (p=0.03, rs=0.06). Posterior
cross-bite was also significantly more frequently in carious dentition than in caries-free dentition
(p=0.03). Subjects with posterior cross-bite were with significantly higher dmft scores when
compared with children with normal occlusion with mean dmft of 2.8±2.9 and 1.3±1.8 in the two
groups, respectively (p=0.003 Fig.5.36).
Posterior cross-bite
YesNo
Mea
n dm
ft 12
10
8
6
4
2
0
-2
Fig.5.36: Positive correlation
between dmft rate and posterior
cross-bite
Mandibular overjet correlated positively with more caries incidence (p=0.02, rs=0.07) and supjects
with Mandibular overjet had significantly higher mean dmft scores versus other supjects with mean
dmft of 1.7± 2.08 and 1.4±1.9 in the two groups, respectively (Fig.5.37).

64
Mandibular overjet
YesNo
Mea
n dm
ft 12
10
8
6
4
2
0
-2
Fig.5.37: Positive correlation
between dmft rate and
mandibular overjet
5.6.3. Malocclusion in relation to dental awareness and socio-economic status
When caries experience was studied among children who were with or without orthodontic
treatment, dmft scores was significantly lower among those who were seen and followed up by an
orthodontist versus other children with a mean dmft of 1. 5 ±1.9 vs 0.9 ±1.7 in the two groups,
respectively (Mann-Whitney Test p=0.003, Fig.5.38).
Orthodontic treatment
treated Untrated
Mean dmft 12
10
8
6
4
2
0
-2
Fig.5.38: significantly lower
dmft among children who
were undergoing to
orthodontic treatment
versus other children
(p=0.003)
A significant association was registered between undergoing to orthodontic treatment and dental
awareness level (rs=0.09, p=0.007), as the dental awareness scores was significantly higher among
the children who were undergoing to orthodontic treatment versus other children with mean dental
awareness of 6.7 ±2.3 vs 6.2 ±2.2 (Mann-Whitney Test p=0.01). This association was particularly in
dental knowledge and dental attitude. As the children who were undergoing to orthodontic
treatment had significantly higher knowledge scores in the aware of the importance of
concentrating on the new erupting teeth during brushing (rs=0.07, p=0.02, Fig.5.39).

65
Undergoing to orthodontic treatment
TreatedUntreated
Whi
ch te
eth
need
mor
e ca
re w
hile
bru
shin
g?,50
,40
,30
,20
,10
0,00
,38
,29
Fig.5.39: significantly higher
dental knowledge among
children who were
undergoing to orthodontic
treatment (p=0.02)
Similarly, children who were undergoing to orthodontic treatment recorded significantly higher
scores in dental attitude to keep their teeth healthy by pay extreme attention to it and manage the
amount of daily sweets eating (rs=0.09, p=0.01), in addition to the magnitude of the family’s role in
controlling the function of their children teeth brushing was also significantly higher among children
who were undergoing to orthodontic treatment (rs= 0.08, p=0.01).
Malocclusion was mostly independent of the socio-economic level (Kruskal-Wallis-Test p=0.3).
However by studying the association between socio-economic status and different kinds of
malocclusion, it was detected significant association between posterior cross bite and
socioeconomic status (rs=0.09, p=0.03); In addition, a significant correlation was found between
SES and increased maxillary overjet (rs=0.1, p=0.01).

66
Chapter 6: Discussion
6.1. Dental awareness, knowledge, attitude and behaviour
In this cross-sectional study, several noteworthy findings were provided by the dental awareness
scales analysis. While oral health knowledge is an important aspect of oral health awareness, its
association with the other two oral health-related indicators, attitude and behaviour, among
schoolchildren in this age group was of almost negligible magnitude. Our finding may also reflect,
as concluded by others, that knowledge may be neither a necessary nor a sufficient pre-requisite
for changes in attitudes and behaviour. For example, even if children know about healthy foods,
they may not like to eat them as taste and preference of certain food items were confirmed as
consistent influences in children's food classification [Hart et al., 2002]. In addition, social
circumstances play an important role. Restrictions by children’s parents are important factors on the
pathway to improved health behaviour as well as the behaviour of peers and social factors like
school community [Lin et al., 2007; Seabra et al., 2008]. Moyses et al., [2003] reported that health
education approaches alone have been found to be unsuccessful in achieving sustainable
improvements in oral health. On the other hand, Poutanen et al. [2005] demonstrated that poor
knowledge of oral health-related facts was one of the factors associated with a child's unfavourable
oral health behaviour. Possibly, the importance of knowledge may level off in a population with a
certain minimum level of literacy, but that would probably be of a limited value in regions like former
East Germany, where a lack of basic literacy skills is no longer the main concern.
The remaining two health scales on attitudes and behaviour were positively correlated with each
other. This means that the dental behaviour was mostly independent of dental knowledge, but
depended on dental attitude, which also suggests that targeting one specific aspect of oral health
competence in a campaign may exert only limited effects on other oral health related indicators.
Our result on the positive relation between dental behaviour and dental attitude supports the finding
of a statistically significant linear relationship between dental behaviour and dental attitude [Shard
et al., 2008].
The distribution of tooth brushing among schoolchildren seemed highly polarized. While most of the
children, about 90%, reported brushing their teeth every day or most of the time, one-tenth admitted
to brush their teeth only occasionally or did not brush their teeth at all. Theses results are slightly
better than the result of a nationwide representative German survey (KiGGS) which found that
about one-quarter of children and adolescents in Germany brush their teeth infrequently [Schenk et
al., 2007].

67
Dental awareness in relation to gender
There is an increased interest in looking at gender differences in health and disease, including
dental health. In our study, gender differences with regard to dental awareness were consistent.
Girls performed better on all of the three dental awareness related scales with the most pronounced
differences on the behaviour scale. Gender difference in oral health attitude and knowledge scales
were rather small but consistent. These significant behaviour gender differences particularly in
tooth brushing were similar to finding recently reported in a nationwide representative German
survey (KiGGS) among children and adolescents with regard to oral health behaviour [Schenk et
al., 2007]. Our result also is in line with other earlier publications by Campus et al. [2008], Honkala
et al. [2007], Poutanen et al. [2005], Vallejos-Sánchez et al. [2008], Kawamura et al [2008] and
Östbergť et al. [1999] indicating a trend of reporting better oral health care behaviour in girls than in
boys with higher scores in the desire and interest to improve oral care, concern over the number of
cavities and tooth brushing .
Dental awareness in relation to socio-economic status (SES)
The parents’ educational level, professional position and monthly net household income were used
as socio-economic status indicators according to Winkler-score index [Kurth and Robert-Koch-
Institut, 2002]. This index was used in many other social studies, such as [Vanobberge et al., 2001,
Kumar et al., 2008, Saied-Moallemi et al., 2008]. The largest group of households reported a total
net income slightly less than 1250€; and only about one fourth of the parents had higher levels of
education, which is probably linked to social welfare or un- or underemployment in the region of our
study.
Interestingly, parent’s educational level was more important in predicting the dental awareness-
related indicators than was net household income in this study. Children with higher socio-
economic status (SES) showed particularly better oral knowledge. The positive association
between the children’s oral health knowledge and the parents’ educational level is theoretically
reasonable and has been detected in other studies. Bozoni et al. [2006] found that the children of
higher SES were more knowledgeable on medications compared to those of to those of lower SES.
One explanation for this status dependency may be that children draw much of their information
from parents; consequently parents with a lower educational level have difficulties to provide
relevant health related knowledge to their children.
Amazingly, oral health behaviours showed only very weak associations with the parental socio-
economic status indicators in this study, although the actual caries levels differed significantly from
high to low SES. This highlights the complexities in the system of the underlying variables. Our
finding on the slight correlation between SES and the children’s oral health behaviour contrasts with

68
another study by Petersen et al [2008] which demonstrated that oral health-related behaviour
among adolescents was associated with the parental socio-economic status. It needs to be taken
into account that most studies were conducted under other social circumstances and the failure to
reproduce this aspect of social inequality might be due to a limited social variability reflected in
educational level in former Eastern Germany. Furthermore, social desirability bias might have
influenced the reporting of health behaviours, as; the questionnaire only collected the reported
behaviour and not the actual performed one, for instance, in another clinical study was undertaken
in Karlsruhe (Germany) with basis and high schoolchildren, both groups reported similar brushing
habits, but the high schoolchildren exhibited considerably less plaque and gingivitis compared to
the basic schoolchildren and during the supervised school brushing program, both groups achieved
comparable good oral hygiene scores [Einwag et al., 2006].
In the present study, the mother’s educational level was more important in predicting more dental
knowledge, behaviour and communication among schoolchildren in comparison to the father’s
educational level. The effect of the mother’s role as a propellant for their children’s behaviour was
also reported in the German survey (kOPS) among schoolchildren and with regard to obesity
[Plachta-Danielzik et al., 2007].
It is worthy to note that almost every fifth parent did not provide information on income. Therefore
associations concerning social status and oral health indicators might have been affected by some
bias. For this reason, multiple imputation was conducted to use as much of the available
information as possible.
6.2. Caries experience distribution
Several studies have been carried out previously to assess the dental caries prevalence among
children in Germany [Marthaler, 2004; Szöke et al., 2000]. In this cross-sectional study most of the
children exhibiting no carious defects, fillings or missing teeth in their permanent dentition
(DMFT=0.6). These high percentages of sound dentition reflects the severity reduction in the
prevalence of dental caries among children and young adults which has been achieved through
systematically organized dental care in Germany and in other industrialized countries for the last
two decades [Marthaler, 2004; Marthaler et al, 1996; Szöke et al., 2000; Stecksen-Blicks et al.,
1999; Bratthall et al., 1996; Astroth et al., 1998 and Al- Omiri et al., 2006]. Different opinions exist
regarding the reasons of caries decline, but there is agreement that the various and continued uses
of fluorides are by far the most important factors of this decline [Fejerskov et al., 1981]. It may be
also due to improved tooth brushing habits, as more frequent and more thorough tooth brushing
would strengthen the fluoride effect, lower the ‘aggressivity’ of dental plaque and remove

69
fermentable food remnants more thoroughly [Kay, Locker, 1998; Marthaler,2004]. Moreover,
sealant application considered although another important factor or even the main factor in lowering
the DMFT from say1.5 to 1.0 at school age [Marthaler, 2004]. The present questionnaire revealed
high tooth-cleaning frequencies among all the schoolchildren, with an average of 92% for morning
brushing and 93% for night brushing. According to the respondents, regular tooth-brushing was
already a prominent element which could explain the very low caries levels found in this study.
A closer look at the recent patterns of caries distribution shows that the distribution was highly
polarized; however, the conventional mean values per child hide these inequalities of oral health
statement and conceal the fact that not all population groups have steadily profited from the caries
decline, as a group of approximately 25– 30% are the so-called “high caries risk children”, this
group includes the majority of the decayed defects and fillings, this finding is supporting with other
representative surveys on children’s oral health in Germany [Marthaler, 1996; Splieth et al., 2004
and Pieper et al., 2004; IDZ, 1999].
Caries distribution with regard to place of residence
In this study, caries was slightly more prevalent among the children in rural areas in comparison to
others in urban areas. This result supports earlier findings of Sofola et al, [2003]; Muwazi et al,
[2005] and Smyth et al., [2005]. At the same time; families in urban areas reported higher scores in
monthly household income and socio-economic status compared to rural families. Possibly, this
socio-economic difference is responsible for the difference in caries detected in this study.
Interestingly, children who were born in Germany recorded higher caries experience rate than
those who were born in another country. This outcome corresponds to some earlier findings by
Bissar et al., [2007]; Sundby et al. and Kühnisch et al. [2003]. One explanation for this result
dependency might be that the proportion of foreigners is very low in the study region compared to
the federal national average (Greifswald: 4.3%, Ostvorpommern: 2.0%). In addition, most of the
immigrated children’s parents were well educated and they came to Germany to complete their
study or work at the university.
Caries distribution in regard to gender
The number of caries lesions in the permanent dentition (DT) was slightly higher in males than
females without reaching statistical significant level. On the other hand, the number of filled teeth
(FT) tended to be higher in females than in males. Thus, gender differences with regard to the total
caries experience in permanent dentition among this age group were of almost negligible
magnitude. Our results concur with another German study by Trinn et al. [2008] who found that DF-

70
T values were almost identical in boys and girls.
It is necessary to take into account that in this epidemiologic study, caries is defined as clearly
visible decay in the enamel with an analytical eye using penlight and without drying the tooth
surface, so the actual number of children with caries not visible yet could be higher and the white’
fillings have also become a problem, it is inevitable that part of them are not identified by the
examiner [Marthaler, 2004].
6.3. Caries experience in relationship to different survey’s indictors
Many multiple variable factors can contribute directly or indirectly to the increase in the incidence of
dental caries such as smoking, oral hygiene habits, eating habits, drinking habits, stress, socio-
economic standards etc. Due to these factors, the efforts in this section will be directed to define
and discuss different risk determinants of dental caries among school children in this age group.
Caries experience in relation to socio-economic status (SES)
It is worthy to note’ that this study showed social inequalities in oral health among schoolchildren,
as caries experience was significantly associated with the socio-economic status with more caries
prevalence in the lower socio-economic strata, which reflects the fact that the improvement in oral
health did not cover all the socio-economic levels and children from low socio-economic
backgrounds suffer more oral health problems, this finding was supported with many surveys
worldwide such as; Vanobberge et al., [2001] reported that the prevalence of caries-free children
was 2.5 times higher among the highest SES families compared with the lowest. The same result
was found in the KIGGS survey in Germany [2008] with children from socially disadvantaged
families having worse oral hygiene and fewer dental visits than the control group. Similarly, Sofola
et al. [2003]; Verde et al. [2006]; Kraus et al. [2004]; Frohlich et al. [2008]; Strippel, [2001]; Flinck et
al. [1999]; Splieth et al. [2005]; Quartey and Williamson, [1999]; Hobdell et al. [2003]; Gillcrist et al.
[2001] and Schulte et al. [2006] all detected poorer oral hygiene in children from a low social class.
Thus efforts to improve oral health, should be aware of the social, economic and environmental
determinants and should be directed towards the modification of these determinants by the
promotion of individual health literacy which considers of central importance to decrease the gap
and diminish disparities in health between socio-economic groups [Nutbeam, 2000 and Schwarzer,
1994].
In the present study, socio-economic status was determined for the two parents separately. The
impact of the mother’s professional position and education level played a slightly stronger role on

71
decreased caries incidence compared to the father’s. A possible reason for this difference is that
mothers generally spend more time with the children and have more contact than fathers. Our
results on the important role of mother’s socio-economic background in enhancement of children's
dental health agrees with other previous surveys; Kumar et al. [2008] reported that the education of
the mother was the single best predictor for oral hygiene status and explained 92% of the variance.
Vallejos-Sánchez et al. [2008] stated that the mothers' characteristics were associated with more
favourable patterns of tooth brushing in children. Saied-Moallemi et al. [2008] found that higher
level of oral health knowledge and better attitude scores of mothers were associated with children's
sound dentition. Moyses et al., [2003] and Smyth et al., [2005] found that mother’s education
appeared to be important predictors of the percentage of caries-free children in the schools. In
terms of ‘content’ it should take into account that certain characteristics of mothers are associated
with more desirable habits in their children; consequently, targeting the linkages between mothers'
characteristics and children's behaviours could lead to more effective health promotion efforts.
Future research should attempt to fully characterize these family linkages and determine how to
support them.
Caries experience in relation to self-esteem
The good development of children’s psychosocial competence and the capacity to cope with
challenges affected the ability to control the amount of sweets eaten and resulted in a lower rate of
caries incidence among those children. Moreover, the children who recorded higher self-efficacy
also registered better oral health awareness level. Such effects of self-esteem on health are logical
and have been observed earlier. For instance, Booth et al. [1997] reported that stress may lead to
poor diet, smoking and violent behaviours which are detrimental to health. Another survey in
Kuwait studied the association between life-satisfaction, school-satisfaction, self-esteem and oral
hygiene habits found that these variables seemed to be strongly associated together and
suggested that special emphasis should be placed on children who have personal problems in their
lives, school and self-esteem [Honkala et al., 2007]. The Institute for Medical Psychology at
Greifswald University developed the preventive program called, "I am I - health promotion by self-
esteem reinforcement”. This program was successful in improving the health competence among
children [Kraus et al., 2004]. Dumitrescu et al [2008] found that self-consciousness is negatively
correlated with anxiety, stress, depression, current non-treated caries, gingival bleeding and the
reason for the dental visit. In summary, our result supported other studies which suggest that self-
efficacy might be a psychosocial risk marker that influences self-reported oral health status and
should be an important aim in the future of oral health promoting programs.

72
Caries experience in relation to television watching
Increased hours of television watching is a common lifestyle factor which is associated with chronic
diseases [Sheiham et al., 0002]. In the present study more TV viewing was also connected directly
to higher rates of caries. This result is in line with the earlier finding of Palmer [2005] and Basak et
al. [2008]. One explanation for this status dependency may be that the child viewers are exposed to
a TV environment that predominantly promotes unhealthy food, high in fat, sugar, and salt,
nutrients associated with obesity, dental caries, and other chronic diseases [Zuppa et al., 2003;
Rodd et al., 2005]. Amazingly, an inverse relationship was indicted between the increased hours of
daily TV watching and socio-economic status, with higher rate of daily TV watching among children
of lower SES. This interesting result on the interaction between SES and daily TV viewing parallels
the finding by Natsiopoulou et al., [2009] and may be another explanation for the higher caries
prevalence among low socio-economic children.
Caries experience in relation to nutrition
Nutrition is still considered as risk determinant of dental caries. This exploratory study found that
dietary pattern and eating habits especially convenience food and sweetened drinks (drinking
lemonade or ice tea) seem to influence caries-resistance or development among the
schoolchildren. This result reflects some earlier findings by Rehman et al., [2008] who reported that
caries experience was significantly more strongly correlated with frequency of snacking between
meals. Jerkovic et al. [2009] also found that high consumption of fruit juices and/or soft drinks and
the number of snacks consumed were associated with caries and are a significant risk factor for
caries prevalence. Similarly, MacIntyre et al., [2006] and Mazzocchi et al, [1993] found that caries
increased by drinking soft drink beverages. It is surprising that, children from a lower SES
consumed significantly more fruits juices than children from other SES groups. The same result
was observed by [Jerkovic et al., 2009]. At any rate, this association between the consummation of
fruits juices and lower SES can be one explanation for higher caries prevalence in children from low
socio-economic status.
Although dental caries is a sugar dependant disease, in the present study, sweets consumption
showed a weak association with caries prevalence. This finding is supported also by Vanobbergen
et al. [2001] and Jerkovic et al. [2009] who reported that the high intake of sweets was not found to
be a significant risk factor for caries and not responsible for the high number of caries in Western
European countries. On the other hand, this finding is in contrast with other older studies in less
developed countries [Freire et al., 1996; Irigoyen et al., 1999]. Possibly the frequency of sugar
consumption is the reason which hiding behind those conflicting reviews as most studies point at

73
frequency of eating as being of greater etiological importance for caries than the total consumption
of sugar [Sreebny, 1982; Karlsbeek and Verrips,1994].
Caries experience in relation to smoking
Smoking is considered to be one of the modifiable lifestyle related risk behaviours pattern of the
youth affecting more than one chronic disease [Sheiham et al., 0002]. In the present study
clustering between caries incidence and smoking was evidence even after adjusting to age. This
finding on the association between caries and smoking reflect some earlier findings by Vellappally
et al. [2007] and Aguilar-Zinser et al., [2008] who documented that smoking can present significant
risk factors for dental caries. Moreover, it has been reported by other recent studies that elevated
smoking level can be one of the causative factors for dental caries [Bruno-Ambrosius et al., 2005;
Ide et al., 2002; Kelbauskas et al., 2005] even though, a direct etiological relation between caries
incidence and smoking is lacking. One possible explanation suggests that smoking is associated
with bad oral hygiene and food habits and limited preventive dental visits. In addition, the high
amount of various sugars and sweeteners added during the commercial manufacturing of
smokeless tobacco products can be responsible for this association [Kelbauskas et al., 2005].
Furthermore, socio-demographic factors are expected, as it is clearly confirmed in this study that
caries and tobacco use were more prevalence among children with low socio-economic status. This
result is supported by Chew et al. [2006] and Mancuso et al. [2004] and underlines the necessity of
prevention in socially underprivileged classes.
It is interesting to know that the existence of a smoker in the family had an effect on the increase of
caries incidences among the children. This finding is supported by data from Aligne [2003] provided
strongest evidence of an increased risk of dental caries in the deciduous dentition of children who
have been exposed to passive smoking or environmental tobacco smoke. Similarly, another study
done in 2004 also confirmed that children residing in regularly smoking homes had significantly
higher prevalence of caries compared to non-smoking homes [Shenkin et al., 2004]. The reason for
this association is poorly understood. However, some experimental data might support the
biological role of passive smoking, as it is associated with decreased serum vitamin C levels in the
affected children which is associated with growth of cariogenic bacteria [Aligne et al., 2003].
Vellappally et al. [2007] stressed that young children may be particularly vulnerable to the harmful
effects of environmental tobacco smoke on the immune system and saliva flow. Finally, it seems
necessary to search in the area of prevention to find the more effective intervention methods to
prevent smoking and passive smoking amongst children with more incorporating of oral health
promotion programs into smoking prevention programs.

74
Caries experience in relation to general health
Oral health means more than just sound teeth, it is integral to overall health [Petersen, 2003].
Amazingly, in this study earaches and sore throats were connected with caries incidence. This
finding agrees with another study by Barclay [2008] who reported that dental disease is one of the
most common causes of secondary earache. Muratbegovic et al., [2007] detected that children with
high molar incisor hypo mineralization (MIH) suffered more often from various diseases, particularly
from tonsillitis and illnesses accompanied by high fever.
Furthermore, this thesis confirmed that diseases and conditions of the mouth have a direct impact
on the health of the entire body, as inverse relationship between general health and caries was
detected in the present study, this found is supported by the findings of Richmond et al. [2007] who
reported a statistically significant association between oral and general health in 11 year old
children. One explanation for this status dependency may be that the risk factors of dental diseases
(such as diets high in sugars and low in fruit and vegetables, stress, smoking and TV consumption)
are common factors to a number of chronic diseases [Dahlgren et al., 1986]. Furthermore, there is
a clrar relationship between having certain patterns of risk behaviours and socio-demographic
status [Wiefferink et al., 2006]. Hence, promotion of oral health lifestyles should be integrated with
other general health actions, this incorporation of oral health promotion into general health
promotion is becoming increasingly important, not only for the combined risk factors, but also
because an integrated approach is likely to be more cost-effective than programs targeting a single
disease [Petersen, 2003].
Caries experience in relation to performance at school
Notwothy, in the present study, toothache had a negative influence on children’s performance at
school. This is in line with the earlier finding of Gift et al. [1992] who reported that more than 50
million school hours in the US are lost annually because of oral health problems. The US General
Accounting Offices [2000] demonstrated that children who suffer from poor oral health are 12 times
more likely to have restricted-activity days than those who do not. Jiang et al. [2005] illustrated that
oral health-related behaviours were associated with poor school performance. So, the
establishment of school-based health promotion programs is urgently needed on all levels.
6.4. Impact of dental awareness scales on caries prevalence
The present study illustrated that higher oral health awareness score resulted in less caries

75
prevalence among children. In particular, oral health behaviour scale appeared to be the stronger
predict of the participants’ actual oral health status. Apart from sealants, reporting regular brushing
in the evening and in the morning were excellent predictors for the caries levels. Children with high
caries levels often showed a combination of brushing their teeth less than twice a day, a low
number of sealants, and a high frequency of sweets consumption. Our findings are in line with
earlier publications by Liran et al, [2004] who found that individuals with low levels of dental disease
had a positive oral health attitudes and behaviour. Nadanovsky et al. [1995] reported that the
changes in oral behaviour were considered to be one of the major contributions to improved caries
levels.
Interestingly, there was a significant difference in the number of sealants between high and low
socio-economic statuses, particularly regarding the mother’s SES. Sealants were also associated
with less caries as in other studies [systematic review Gillcrist et al., 2001]. On the other hand,
recording sealants and caries or fillings were mutually exclusive which means that sealants always
coincide with low caries levels in pits and fissures. All failed sealants which have been converted
into fillings are not detected.
This study found that about three-quarters of the children had a high knowledge on oral health
issues. Although most of the children already knew that adult toothpaste was the appropriate
toothpaste for their age, most of the children were not aware that newly erupting teeth needed extra
care during brushing which was directly associated with higher carries prevalence and low socio-
economic status. Thus, this point could be an important to concentrate on it in prospective
preventive programs. Half of the schoolchildren did not know that the examination in a dental
practice was free of charge which could also be addressed in future programs.
Amazingly, children with a higher number of fillings exhibited a higher level of dental knowledge
which indicated that the experience of dental treatment increased their knowledge. This finding is in
agreement with earlier study by Van Steenkiste et al, [1991] who reported a considerable
discrepancy between dental knowledge and caries experience among schoolchildren in Germany.
Talking with the parents about “what is good for healthy teeth” was an important aspect of oral
health attitudes which was associated with less caries, this result confirms the importance of
communication between children and parents in health related matters, and suggests that oral
health-related interventions could aim beyond the provision of facts to foster favourable attitudes as
well as a social ambient that strengthens adequate oral health communication between parents and
their children [Schmidt et al., 2010]. Of note, the information about the communication aspect in the
present survey has been assessed quantitatively; however qualitative aspects are likely to be of
importance as well.

76
6.5. Malocclusion prevalence and distribution
The findings of the present study showed that, as in other populations, malocclusion traits were
very common in this sample (64%). This high prevalence of malocclusion is comparable to other
studies in other European populations for instance; Proffit et al. [1998] stated that about 59 % of the
children from different ethnic groups required some kind of orthodontic treatment. A similar finding
was reported in Swedes by Josefsson et al, [2007], in Germans by Stahl et al, [2004] and Tausche
et al, [2004]. One explanation for this high prevalence of malocclusion may be the long-term effects
of unfavourable functional influences and hereditary factors [Proffit et al., 1998].
This survey’s data illustrated clearly very low prevalence of dental caries contrasted with wide
range of orthodontically relevant occlusal traits. Thus, the caries-reducing measures are not likely
to have a significant influence on the formation of malocclusion in the mixed dentition, which
underlines the need for orthodontic preventive programs in order to combat the high prevalence of
malocclusion by encouraging the early diagnosing of malocclusion problems to be intercepted and
treated before it become more complex. In addition, preventive programs are important to restraint
the faulty oral habits like thumb sucking, tongue thrusting, lip biting and mouth breathing which are
responsible of many types for malocclusion [Proffit et al., 1998].
With regard to the occlusal findings, crowding was the most frequent occlusal trait overall occurring
in 28% of all children having any form of malocclusion. This was followed by maxillary overjet,
happening in 23.4% of all children having any form of malocclusion. These findings serve as
reference data for the epidemiology of malocclusions at an age which is frequently considered as
the optimal time for treatment of many of these dento skeletal disharmonies [ Malmgren et al. ,
1987 ; Gianelly, 1995 ; Baccetti et al. , 2000 ; McNamara and Brudon, 2001]. It is interesting to
know that the findings of the present study concurred with the observation of another study in
Germany and other European populations. For instance, Stahl et al. [2003] stated that crowding
was the most prevalent malocclusion followed by maxillary overjet in mixed dentitions in Rostock,
Germany. A Šidlauskas et al., [2009] illustrated that the most common malocclusion was dental
crowding among Lithuanian schoolchildren. Perillo ea al., [2009] found that the highest prevalence
was for crowding in north Italian school children. Finally, Souames et al., [2009] found that crowding
and overjet were the most common malocclusions frequently forming among 9- to 12-year-old
French children. The aetiology of increased maxillary overjet, is known to be related to oral habits
such as finger, thumb or pacifier sucking, or myofascial dysfunctions of the craniomandibular
muscles [Farsi et al., 1999 Schopf, 1973 and Larsson, 1994].
Posterior crossbites were present in 8.6 percent of the subjects and mandibular overjet
malocclusions in 2.5 percent. The prevalence rates for these occlusal disharmonies appear to be

77
slightly high especially when early treatment in the primary or early mixed dentition has been
recommended for these types of malocclusions [ Thilander et al. , 1984 ; McNamara and Brudon,
2001 ; Franchi et al., 2004 ].
Regarding gender, males exhibited significantly higher overbite scores than females. This result is
in line with other studies such as; Lux et al. [2009] in Germany and Ciuffolo et al. [2005] in Italian.
The prevalence of crowding was more common in females than in males. Corresponding results
were reported by Borzabadi-Farahani et al., [2009] in Iran and by Thilander et al., [2009] in Central
Anatolia.
Relationships between different kinds of malocclusion
The occlusal anomalies tended to be present in association with each other, as subjects with
mandibular overjet were more likely to have an increased posterior crossbite. Whereas, subjects
with an increased overbite were more likely to have an increased overjet, these findings were
supported by another study in Italy [Ciuffolo et al 2005].
Malocclusion in relation to dental caries
The relationship between different kinds of malocclusion and dental caries was analysed in this
thesis. From the resulting data it is evident that caries experience in deciduous teeth was not an
important factor in formation of the most prevalent types of malocclusion, crowding and maxillary
overjet. It is not surprising therefore, that prevalence of malocclusion was found significantly more
often in caries-free dentitions when compared with carious dentitions. This found is supported by
[Helm and Petersen, 1989; Stahl and Grabowski, 2004]. On other hand, it contrasts with findings of
other studies which found positive association between the caries and malocclusion [Frazăo and
Narvai, 2006; Kolmakow et al. 1991; Alexander et al. 1997; Gábris et al., 2006 and Nobile et al.,
2007]. One explanation for this difference in results may be due to the differences in the age of the
subjects, differences in sample sizes, differences in criteria used for defining ‘caries-free’ and
‘carious’ dentitions, or possibly differences in caries prevalence as the role of caries as a
malocclusion risk factor is limited in a community such as Germany, where the caries is not more
so prevalent to the degree in which it can really predict malocclusion incidence. Perhaps in such
community the genetics, the oral habits or the dysfunctions dysfunctions play more of an essential
role than does caries. Hence, an individual examination in the presence of the parents and with
enough time available to determine oral habits and dysfunctions is recommended in the future
researches.

78
Crowding was the most prevalent malocclusion in this sample. The fact that crowding was found
more often in caries-free than in caries-affected dentitions indicates that non-caries-related factors
might have induced the formation of crowding. However, the general increase in the prevalence of
crowding cannot be explained by human evolutionary development and inherited characteristics
alone. Functional factors such as mouth breathing might conceivably contribute to crowding [Proffit
et al. 1993].
It is noteworthy that in spite of the difficulty in determining any correlation between caries and the
most prevalent kinds of malocclusion (crowding and overjet); increased caries incidence was
detected with some specific types of malocclusion dentitions when compared with prevalence of
caries in dentition without malocclusion. Mandibular overjet and posterior cross-bite were
significantly correlated with an increased caries risk. As there appears to be no causal relationship
between caries experience and these two types of malocclusion, the answer might be that there are
conditions which lead to dental caries and malocclusion independently in the same individual. For
instance, myofacial dysfunctions such as mouth breathing resulting in incomplete mouth closure or
dysfunction of the tongue could contribute to both the formation of caries and malocclusion. This
result is in line with another study by Stahl et al. [2004]. In addition, mesial drift of the first
permanent molar was even associated with increased caries experience. This result had been
assumed by several authors who considered that dental caries and premature loss of primary teeth
are predisposing factors for occlusal and space anomalies in mixed and permanent dentitions
[Mitchell, 2005 and Pedersen et al., 1978].
Malocclusion in relation to dental awareness and socio-economic status
The children who were undergoing orthodontic treatment had less caries experience and recorded
higher dental awareness scores particularly in knowledge and attitude versus other children. This
finding is in agreement with an earlier study by Agou et al. [2008]. One explanation for this status
dependency may be that orthodontist should be able sufficiently to motivate patients toward
maintaining an agreeable standard of oral hygiene because without good oral hygiene plaque
accumulates around the appliance, causing several problems for the neighbouring tissues. Hence,
the importance of paying special attention to oral hygiene in orthodontic patients was always
suggested. Another possible reason could be that dentally aware families seek orthodontic
treatment more often.
A Slightly more caries prevalence and more need for orthodontic treatment were found in rural
areas in comparison to urban areas. The evident increase of caries in rural areas could possibly
contribute although in more prevalence of malocclusion. This finding contrasts with the finding of

79
Liepa et al., [2003] in United Kingdom reporting no statistically significant differences in treatment
need between rural and urban settings.
It should be noted that socio-economic status was not a risk indicator for malocclusion in this
thesis, as no significant differences in prevalence of malocclusion between the different socio-
economic strata were observed. This result is supported with another recent study in Italy [Nobile et
al., 2007]. However this result contrasts with another study by Tickle et al. [1999] who found that
the normative need for orthodontic treatment was more common amongst deprived UK children
than among their affluent counterparts. Perhaps, the difference between socio-economic strata in
the United Kingdom is stronger and more obvious in comparison to (East) Germany.

80
Chapter 7: Conclusions and recommendations
7.1. Conclusions
In this population of 5th grade students in an area with low caries prevalence, clearly polarisation of
the remaining dental caries after the caries decline was confirmed. Gender differences with regard
to the total caries experience were of almost negligible magnitude. A set of short scales on oral
health awareness-related knowledge, attitude and behaviour were generated. Dental knowledge
was not associated with any other scale and rather moderate strength of associations between the
dental behaviour and dental attitude was found in this study. Therefore, enhancing oral health-
related knowledge does not seem to be a future way to improve the oral health situation of children,
as it did not improve the oral health behaviour in this study. Oral health related attitudes and
behaviours should be addressed directly.
Higher scores in dental behaviour and self-esteem resulted in lower caries incidence, as did socio-
economic status. However the impact of the mother’s socio-economic status played a slightly
stronger role than the father’s. Children with a higher socio-economic status reported a higher level
of dental knowledge and communicated with their parents more about health topics. Furthermore, a
low number of sealants, smoking, prolonged TV watching and wrong diet habits were associated
with low socio-economic status and high caries incidence. This clustering of risk factors in
individuals and groups, particularly those at the lower levels of the social class gradient suggests
that social inequalities are strongly linked with health inequalities. Hence, oral health-related
interventions in children sample should be directed at the social structures and aim to the provision
of social ambient that furthers adequate health communication, self-esteem and health behaviours
among the children. This cross-sectional study confirmed the multifactorial structure of dental
caries, as in addition to above determined risk factors, other factors such as general health,
earache and sore throat were direct predictors for caries. Thus, incorporating oral health promotion
programs into general health promotion programs is becoming of increasing importance.
Regarding malocclusion, as in other populations, malocclusion traits were very common in this
sample. The occlusal anomalies tended to be present in association with each other and the
prevalence of an increased overbite was higher in males than in females whereas more crowding
prevalence was observed in females than in males. An association between prevalence of
malocclusion and socio economic status could not be established. Furthermore, no generalised
conclusion could be drawn about the relationship between prevalence of caries and malocclusion.

81
However, with some specific types of malocclusion (posterior cross-bite and mandibular overjet),
there was a significant parallelism of high dental caries experience and malocclusion, but this does
not mean that there is a causal relationship between caries and malocclusion.
7.2. Future perspectives according to situation of the survey’s region
Our study and many investigations have found that inequalities in health cannot be explained with
children and young people by individual parameters but are essentially associated and conditioned
by the education and health authority lacking in the families and the lifestyle resulting from it. For
example, children who are at the highest risk of dental disease are associated in the majority with
low social family situation [Schulte et al., 2006; Hobdell et al., 2003; Gillcrist et al., 2001]. The
evidence available clearly indicates that the quality of our social life is a powerful contributing factor
to our health. Therefore, health promotion can help resolve some of the social problems in our
societies and contribute to the reduction of health inequalities [Sheiham, 2005]. From this point, the
essential aim of health promotion is strengthening health literacy among children and adolescents
to cope with health risk factors as poor health literacy is "a stronger predictor of a person's health
than age, income, employment status, education level, and race" [Ad-hoc-Committee on Health
Literacy, 1999]. By developing of the individual health literacy amongst socially disadvantaged
children, the effect of socio-economic inequality on health, may be at least partially, mediated
[Nutbeam, 2008]. Schools provide an effective platform for promoting health literacy among
children to compensate the negative influence of the family and the lack of parental health literacy
[Kraus et al., 2004; Splieth et al., 2005]. The concept of school-based health promoting programs is
supported by WHO and proved its effectiveness worldwide [Moyses et al., 2003; Petersen, 1999
Friel et al, 2002; Wellington, 1998 and Rodrigues, 1999]. It depends on decreasing health risks and
creating supportive environments to facilitate behaviour changes by making the healthier choice the
easier choice [Sheiham et al., 0002]. Initiatives which aim to improve the school’s environment are
largely cost-effective and have a significant impact on sustainable healthy behaviours which is
considered as a key success factor [McLellan et al., 1999]. The school stage is considered to be
the most influential phase of children's lives, as children develop greater control over their own lives
and crucial health-related attitudes and behaviours are moulded in this period [Mangrulkar et al.,
2001].
The study’s region included the city of Greifswald and the directly adjacent administrative district
East Pommerania. This region is characterised by a high prevalence of risk factors (e.g.,
adiposities), health-risky behaviours (e.g., smoking) and the socio-economic data in the region are
significantly below the federal national average. It is therefore important to establish preventative

82
measures in the structures of the schools, because only through this method all children,
particularly children from socially disadvantage families can be reached early. Besides the ethical
obligation for equal chances of health, there is high economic pressure for lowering the health risks
and the prevalence of illness in the socially conditioned risk groups on account of increasing the
cost pressure in the health systems and social systems, as the raised illness levels in individuals
with low socio-economic status results in a reinforced need of treatment and higher health costs
which are up until now cushioned by the whole social system. In Germany, caries related problems
cost alone approximately 10 billion € per year [KZBV, 2005]. Thus, an improvement of the health
literacy altogether seems urgently required.
Only cooperation of scientific expertise, local health authorities and, last but not least, the
educational sector should be able to tackle this difficult problem. The structural framework of
compulsory schooling, obligatory dental and medical screening in schools and kindergartens, the
existing solid data pool from these examinations and the networking with school physicians and
other community health workers allow for interdisciplinary projects and prospective interventions to
tackle the total burden of disease and improve health equality.
7.3. Potential design of the future programs
The recommended integrative future modular prevention program should aim to improve internally
controlled beliefs of children and increase the understanding of healthy behaviours to enable them
to make positive decisions and to take action to promote and protect their own health and the
health of others [Duetz et al., 2003]. These skills could be specifically distinguished in the cases of
oral hygiene, dental and orthodontic visits, nutrition and smoking. Teachers, students and parents
do not have to follow specific guidelines or instructions on how to act in these situations, but the
essential point of this program would be to develop and implement some effective elements of
health promotion in the school / family context, which will create an autonomy of health behaviour
that allows students to feel effective in their actions and to feel confident that they can initiate their
own behaviour. For the actual programs in schools, teachers should be aware to focus mainly on
the students’ psychological attitudes.
It has been proven that plaque removal and fluoride application are effective measures in caries
prevention [Kay, Locker, 1998]. In addition to improving the motivation for good oral hygiene,
strategies will be mapped out and implemented to impart to the students the necessary knowledge
and the essential skills which give them the ability to take care of their teeth more efficiently.
The prevention of malocclusion might be also possible as; some types of malocclusion, if

83
diagnosed early, can be intercepted and treated by simple appliances. In addition, many types of
malocclusion are caused by faulty oral habits like thumb sucking, tongue thrusting, lip biting and
mouth breathing. Consequently, the stopping of these wrong habits will result in improvement of the
malocclusion problem if it was done early enough, before to creation irreversible changes in the
skeletal structure. Therefore, these preventive efforts would be targeted on kindergarten children,
but this contrasts the current approach of late and massive orthodontic intervention in the German
health system. At any rate, parents, teachers and dentists would be able to make the child aware
about the danger of oral habits and encourage them to stop these habits as soon as possible. In
addition, parents and teachers should also be informed about the importance of a healthy
deciduous dentition, as the caries rates in primary teeth were higher and the care index was lower
compared to the permanent dentition among schoolchildren in this age group.
Most areas of health education, but especially nutrition, can often be successful if parents and
schools work together. Therefore, students will be taught the basics of a healthy lifestyle that
should also be emphasised also at home.
Smoking prevention could be a key element in a healthy school concept and it is usually carried out
on several levels. Educational intervention regarding smoking and non-smoking subjects and how
to deal with these problems were derived from the Federal Centre of Health Education database
[Meyer-Nurnberger, 2004]. It describes measures that can be carried out in schools and in different
classes for dealing with smoking and supports smokers in their efforts to quit smoking. Teachers
introduce the subject of "smoking/non-smoking" in the classes and parent-teacher conferences,
and they also develop a package of measures that can be applied in the class.
Such program would support and strengthen the individual decision-making and responsibility. In
addition, it seems to be promising to compensate dissimilarly and unequally conditioned health
chances in children and adolescents [Nutbeam, 2008]. However, a national long-term plan will be
required in order to achieve the goal of reducing differences in health according to the socio-
economic status.

84
Chapter 8: Summary
Dental caries and malocclusion are of the most common human problems presenting a crucial
public health problem especially because of their high treatment expense. Development of oral
health awareness is regarded as a keystone in oral health promotion. This thesis focussed on the
associations among oral health awareness, caries experience, malocclusion and socio-economic
parameters. In addition, the effect of self-esteem, general health, environmental health risk factors
such as; nutrition, smoking and other factors that support or hinder the development of good oral
health were studied.
Eight hundred and fifty two students with an age range 9-13 years (mean 10.34, SD±0.56, 48%
females) were recruited from the fifth grade students of different 19 primary schools in Greifswald
and East Pomerania. In conjunction with the compulsory dental community examination, additional
data were collected with two questionnaires for the children and their parents. Newly generated
items were taken from the children’s questionnaire to form short scales for oral health-related
knowledge, behaviour, attitudes. Parents’ questionnaire contains questions on socio-economic
status (SES) and child’s health. The response rate was 93.2%; 78.8% for children; parents,
respectively.
Results:
The distribution of DMFT values was highly polarized with most of the children (71%) exhibiting no
carious defects, fillings or missing teeth in the permanent dentition with a mean of 0.6 ±1.2. There
was a significant correlation between DMFT and social class levels (rs=-0.19, p=0.001) with mean
DMFT values of 0.9 ± 1.3, 0.6 ±1.1 and 0.4 ± 0.9 for the low, medium and higher social strata,
respectively. There was a clear correlation between the dental attitude and dental behaviour
(rs=0.32, p=0.003). However, correlations between knowledge vs. attitude and knowledge vs.
behaviour were loose. A statistically significant correlation between DMFT and dental behaviour
was found (rs=-0.15, p=0.003).
It should be noted that children with higher self-esteem were found to have significantly higher
dental awareness scores (rs=0.19, p=0.001). General health was a significant predictor for caries
incidence (rs=0.08, p=0.01). The frequency of drinking lemonade or ice tea and eating salty snacks
(chips, nuts) showed clear correlations with the DMFT (rs=0.17 and 0.13, p<0.01). Prolonged daily
TV watching was associated directly with DMFT values (rs=0.13, p=0.001). A significant correlation
was found between caries and smoking, even after adjusting for age (rs=0.1, p=0.002). Smoking
children had a significantly higher DMFT rate than children who were not smokers with a mean

85
DMFT of 0.9 ±1.5 vs 0.6 ±1.2 (p=0.004). Interestingly, each of prolonged TV watching, more
lemonade drinking and smoking were correlated directly with the low socioeconomic status
(Spearman correlation coefficient of 0.13, 0.2 and 0.17, respectively, p<0.05).
Regarding malocclusion, 64% the subjects had at least one type of anomaly. Crowding and
maxillary overjet represented the major proportion 28% and 23%, respectively. Males exhibited
significantly higher increased overbite scores than females p=0.04. Whereas the prevalence of
crowding was more common in females than males (p=0.05). Amazingly, more malocclusion was
registered in children with caries-free primary teeth when compared to children with carious primary
teeth (p=0.05). No significant differences in the mean of dmft or DMFT value were found between
normal and non normal occlusion (p>0.05). Undergoing to orthodontic treatment was associated
with significantly higher dental awareness scores (p=0.003). No correlation between socio-
economic status and malocclusion was registered.
Conclusion:
This thesis confirms the decline and polarisation of dental caries. Dental behaviour was mostly
independent of dental knowledge, but depended on dental attitude. Higher scores in dental
behaviour resulted in lower DMFT scores; possibly, oral health promotion should strengthen
attitude and actual behaviour instead of knowledge. Higher scores in self-esteem and general
health connected with lower caries incidence and higher score in dental awareness.
Social inequalities was strongly linked with health inequalities with more prevalence of caries,
smoking, prolonged TV watching, wrong diet habits and less sealants application among children of
low SES. Hence, oral health-related interventions in children sample should be directed at the
social structures with more incorporating of oral health promotion programs into other general
health promotion programs. This thesis suggests that; the establishment of healthy
behaviours such as a regular teeth brushing at school could be one of the most successful
ways to involve all children especially children of low SES in dental care.
Malocclusion traits were very common in this sample. This underlines the need for more
orthodontic preventive programs among children, in order to reducing the risk factors of
malocclusion. The association between prevalence of malocclusion and socio economic status
could not be established. No generalised conclusion could be drawn about the relationship between
caries and malocclusion.

86
Chapter 9: References
1. Abel T. Measuring health literacy: moving towards a health - promotion perspective. Int J Public Health.
2008;53:169-170.
2. Acharya S, Sangam DK. Oral health-related quality of life and its relationship with health locus of control
among indian dental university students. Eur J Dent Educ. 2008;12:208-212.
3. Ad-hoc-Committee on Health Literacy for the American Council on Scientific Affairs. American Medical
Association. JAMA. 1999;281:552-557.
4. Adler NE, Boyce T, Chesney MA, Cohen S, Folkman S, Kahn RL, Syme SL. Socioeconomic status and
health: the challenge of the gradient. Am Psychol. 1994;49:15-24.
5. Agou Sh, Malhotra M, Tompson B, Prakash P, Locker D. Is the Child Oral Health Quality of Life
Questionnaire Sensitive to Change in the Context of Orthodontic Treatment? J Public Health Dent.
2008;68:246-248.
6. Aguilar-Zinser V, Irigoyen ME, Rivera G, Maupomé G, Sánchez-Pérez L, Velázquez C. Cigarette
smoking and dental caries among professional truck drivers in Mexico. Caries Res. 2008;42:255-62.
7. Alexander S, Hedge S, Sudha P. Prevalence of malocclusion and periodontal status in Tibetan
schoolchildren of Kushalnagar, Mysore district. J Indian Soc Pedod Prev Dent. 1997;15:114-117.
8. Aligne CA, Moss ME, Auinger P, Weitzman M. Association of pediatric dentalcaries with passive
smoking. JAMA. 2003;289:1258-64.
9. AL-omiri MK, AL-wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behaviour among
school children in North Jordan. J Dent Educ. 2006;70:179-87.
10. Al-Tamimi S, Petersen PE. Oral health situation of schoolchildren, mothers and schoolteachers in Saudi
Arabia. Int Endod J. 1998;48:180-6.
11. Altman DG. Practical statistics for medical research. London, de, Chapman, Hall, 1999;30:141-54.
12. Anderson C, Longbottom C, Pitts NB, Robertson M. Integrated care approach to targeting caries
prevention in pre-school children. Caries Res. 2005;39;295-334.
13. Astroth J, Berg R, Berkey D, McDowell J, Hamman R. Dental caries prevalence and treatment need in
Chirique province, Panama. Int Dent J. 1998;48:203-209.
14. Baccetti T, Franchi L, Toth L R, McNamara J A. Treatment timing for twin block therapy. Am J Orthod
Dentofacial Orthop. 2000;118:159-170.
15. Barclay L. MD Diagnostic Methods to Treat Ear Pain in Primary Care Setting. Am Fam Physician.
2008;77:621-628.
16. Barefoot JC. Hostility pattern and health implications: correlates of Cook–Medley Hostility. Scale scores
in a national survey. Health Psychology. 1991;10:18-24.
17. Ben-Bassat Y, Harari D, Brin I. Occlusal traits in a group of school children in an isolated society in
Jerusalem. Br J Orthod. 1997;24:229-35.
18. Bisegger C, Cloetta B, Von rueden U, Abel T, Ravens-sieberer U. Health-related quality of life: gender
differences in childhood and adolescence. Soz Praventiv med. 2005;50:281-291.
19. Bissar AR, Oikonomou C, Koch MJ, Schulte AG. Dental health, received care, and treatment needs in
11- to 13-year-old children with immigrant background in Heidelberg, Germany. Int J Paediatr Dent.
2007;17:364-370.
20. Booth M, Samdal O. Health promoting schools in Australia: models and measurement. Aust N Z J Public
Health. 1997;21:365-370.
21. Bortz J, Döring N. Forschungsmethoden und Evaluation. Berlin, Heidelberg, New York: Springer.

87
Besonderheiten der Evaluationsforschung. 2003;3:101-136.
22. Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. Malocclusion and occlusal traits in an urban
Iranian population. An epidemiological study of 11- to 14-year-old children. Eur J Orthod. 2009;3:477-
484.
23. Bozoni K, Kalmanti M, Koukouli S. Perception and knowledge of medicines of primary schoolchildren:
the influence of age and socioeconomic status. Eur J Pediatr. 2006;165:42-49.
24. Bratthall D. Dental caries: intervened-interrupted-interpreted. Concluding remarks and cariography. Eur J
Oral Sci. 1996;104:486-491.
25. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod.
1989;11:309-320.
26. Brown LF. Research in dental health education and health promotion: a review of the literature. Health
Educ Q. 1994;21:83-102.
27. Bruno-Ambrosius K, Swanholm G, Twetman S. Eating habits, smoking and toothbrushing in relation to
dental caries: a 3-year study in Swedish female teenagers. Int J Paediatr Dent. 2005;15:190-6.
28. Bundeszentrale für gesundheitliche Aufklärung (BZgA): Die Drogenaffinität Jugendlicher in der
Bundesrepublik Deutschland 2004 - Teilband Rauchen. Köln: Bundeszentrale für gesundheitliche
Aufklärung, Köln 2004.
29. Burden DJ. Need for orthodontic treatment in Northern Ireland. Community Dent Oral Epidemiol.
2001;29:220-5. 1995;23:62-63.
30. Campus G, Lumbau A, Lai S, Solinas G, Castiglia P. Socio-economic and behavioural factors related to
caries in twelve-year-old Sardinian children. Caries Res. 2001;35:427-434.
31. Chapman A, Copestake SJ, Duncan K. Dental health and school-based health education among 15-
year-olds in Tehran, Iran. Int J Paediatr Dent. 2006;16:40-44.
32. Chen MS, Hunter P. Oral health and quality of life in New Zealand: a social perspective. Soc Sci Med.
1996;43:1213-22.
33. Chestnutt IG, Burden DJ, Steele JP, Pitts NB, Nuttall NM, Morris AJ. The orthodontic condition of
children in the United Kingdom, 2003. Br Dent J. 2006;200:609-612.
34. Chew LD, Bradley KA, Flum DR, Cornia PB, Koepsell TD. The impact of low health literacy on surgical
practice. Am J Surg. 2004;188:250-253.
35. Cinar B, Murtomaa H. Clustering of Obesity and Dental Health with Lifestyle Factors among Turkish and
Finnish Pre-Adolescents. Obes Facts. 2008;1:196-202.
36. Craft M. A programme of dental health education for adolescents in schools. Int Dent J. 1984;34:204-13.
37. Currie C, Hurrelmann K, Settertobulte W, Smith R, Todd J. Health and health behaviour among young
people. Copenhagen: WHO Regional Office for Europe. 2000;1:65-72.
38. Dahlgren G, Diderichsen F. Strategies for equity in health: Report from Sweden. Int J Health Serv.
1986;4:1-21.
39. De Walt DA, Hink A. Health literacy and child health outcomes: a systematic review of the literature.
Pediatrics. 2009;124:265–74.
40. Denman S, Moon A, Parsons C, Stears D. The health promoting school. Sozialmagazin. 2001;28:31-42.
41. Dhar V, Jain A, Van Dyke TE, Kohli A. Prevalence of gingival diseases, malocclusion and fluorosis in
school-going children of rural areas in Udaipur district. J Indian Soc Pedod Prev Dent. 2007;25:103-5.
42. Duetz MS, Abel T, Niemann S. Health measures: differentiating associations with gender and socio-
economic status. Eur J Public Health. 2003;13:313-9.
43. Dumitrescu AL, Kawamura M, Dogaru B, Dogaru C. Investigating the relationship between self-reported
oral health status, oral health-related behaviours and self-consciousness in Romania. Oral Health Prev

88
Dent. 2008;6:95-103.
44. Einwag J, Henkel R, Döhler B. Auswirkungen präventiver Maßnahmen auf die Zahngesundheit 14- bis
16-jähriger Jugendlicher. Oralprophylaxe, Kinderzahnheilkunde. 2006;28:68-75.
45. European Network of Health Promoting Schools (ENHPS). Fourth workshop on practice of evaluation of
the Health Promoting School - concepts, indicators and evidence held in Sigriswil, Switzerland, 17-20
November 2005.
46. Farsi NMA, Salama FS. Sucking habits in Saudi children: prevalence in contributing factors and effects
on the primary dentition. Pediatr Dent. 1997;19:28–33.
47. Fejerskov O, Thylstrup A, Larsen MJ. Rational use of fluorides in caries prevention. A concept based on
possible cariostatic mechanisms. Acta Odont Scand. 1981;39:241-249.
48. Fejerskov O. Changing paradigms in concepts on dental caries: consequences for oral health care.
Caries Res. 2004;38:182-91.
49. Flinck A, Kallestal C, Holm A K, Allebeck P, Wall S. Distribution of caries in 12-year-old children in
Sweden. Social and oral health-related behavioural patterns. Community Dent Health. 1999;16:160-165.
50. Franchi L, Baccetti T, McNamara J A. Post pubertal assessment of treatment timing for maxillary
expansion and protraction therapy followed by fixed appliances. Am J Orthod Dentofacial Orthop.
2004;126:555-568.
51. Frazăo P, Narvai PC. Socio-environmental factors associated with dental occlusion in adolescents. Am J
Orthod Dentofacial Orthop. 2006;129:809-16.
52. Freeman R. The psychology of dental patient care. 5. The determinants of dental health attitudes and
behaviours. Br Dent J. 1999;187:15-8.
53. Freire Mdo C, de Melo RB, Almeida S. Dental caries prevalence in relation socioeconomic status of
nursery school children in Goiania-Go.Brazil. Community Dent Oral Epidemiol. 1996;24:357-361.
54. French SA, Jeffery RW, Story M, Breitlow KK, Baxter JS.purchases: the CHIPS Study. Am J Public
Health. 2001;91:112-117.
55. Friel S, Hope A, Kelleher C, Comer S, Sadlier D. Impact evaluation of an oral health intervention
amongst primary school children in Ireland. Health Promot Internation. 2002;17:119-26.
56. Frohlich KL, Potvin L. Transcending the known in public health practice. The Inequality Paradox: The
Population Approach and Vulnerable Populations. Am J Public Health. 2008;98:216-221.
57. Gábris K, Márton S, Madléna M. Prevalence of malocclusions in Hungarian adolescents. Eur J Orthod.
2006;28:467-470.
58. Gazmararian JA, Kripalani S, Miller MJ, Echt KV, Ren J, Rask K. Factors associated with medication
refill adherence in cardiovascular-related diseases: a focus on health literacy. J Gen Intern Med.
2006;21:1215-1221.
59. Gianelly A. One-phase versus two-phase treatment. Am J Orthod Dentofacial Orthop. 1995;108:556-
559.
60. Gift HC, Reisine ST, Larach DC. The social impact of dental problems and visits. Am J Public Health.
1992;82:1663-68.
61. Gilbert L, Rudolph MJ, Moosa A. Social characteristics and oral health behaviour of families in Riverlea.
J Dent Assoc S Afr. 1989;44:461-63.
62. Gillcrist JA, Brmley DE, Blackford JU. Community socioeconomic status and children’s dental health. J
Am Dent Assoc. 2001;132:216-222.
63. Goodman E. The role of socioeconomic status gradients in explaining differences in US adolescents'
health. Am J Public Health. 1999;89:1522-1528.
64. Gratrix D, Holloway P J. Factors of deprivation associated with dental caries in young children.

89
Community Dent Health. 1994;11:66-70.
65. Gregory JR, Lowe S, Bates CJ, Prentice A, Smithers G, Clarker PC. National Diet and Nutrition Survey:
Young People Aged 4 to 18 Years. Report of the Diet and Nutrition Survey. London: HMSO, 2000;1:3-
14.
66. Greiger A. Malocclusion as an etiologic factor in periodontal disease: a retrospective essay. Am J Orthod
Dentofacial Orthop. 2001;120:112-115.
67. Grimm S, Frazao P, Antunes JL, Castellanos RA, Narvai PC. Dental injury among Brazilian
schoolchildren in the state of Săo Paulo. Dent Traumatol. 2004;20:134-138.
68. Harris TO. Life stress and illness: the question of specificity. Ann Behav Med. 1991;13:211-219.
69. Hart KH, Bishop JA, Truby H. An investigation into school children's knowledge and awareness of food
and nutrition. J Hum Nutr Diet. 2002;15:129-140.
70. Health Evidence Network (HEN), What is the evidence on school health promotion in improving health or
preventing disease and, specifically, what is the effectiveness of the health promoting schools approach?
WHO Regional Office for Europe’s Health Evidence Network (HEN) 2006.
71. Helm S, Petersen PE. Causal relation between malocclusion and periodontal health. Acta Odontol
Scand. 1989;47:223-228.
72. Helmert U, Borgers D, Bammann K. Soziale Determinanten des Rauchverhaltens in Deutschland.
Ergebnisse des Mikrozensus 1995. Sozial- und Präventiv medizin. 2001;46:172-81.
73. Hershey AD, Powers SW, Vockell AL, Lecates SL, Segers A, Kabbouche MA. Development of a patient-
based grading scale for PedMIDAS. Cephalalgia. 2004;24:844-9.
74. Hirsch JM, Livian G, Edward S, Noren JG. Tobacco habits among teenagers in the city of Goteborg,
Sweden, and possible association with dental caries. Swed Dent J. 1991;15:117-23.
75. Hobdell MH, Oliveira ER, Bautista R, Myburgh NG, Lallo R, Narendran S, Johnson NW. Oral diseases
and socio-economic status (SES). Br Dent J. 2003;194:91-96.
76. Hoffmann W, Munzinger H, Horstkotte E, Greiser E. A population-based evaluation of an intervention to
improve advanced stage cancer pain management. J Pain Symptom Manage. 2004;28:342-450.
77. Holmes A. The subjective need and demand for orthodontic treatment. British Journal of Orthodontics.
1992;19:287–297.
78. Honkala S, Honkala E, Al-Sahli N. Do life- or school-satisfaction and self-esteem indicators explain the
oral hygiene habits of schoolchildren? Community Dent Oral Epidemiol. 2007;35:337-347.
79. Ide R, Mizoue T, Ueno K, Fujino Y, Yoshimura T. Relationship between cigarette smoking and oral
health status. Sangyo Eiseigaku Zasshi. 2002 ;44:6-11.
80. IDZ; Institut der Deutschen Zahnärzte, Dritte Deutsche Mundgesundheitsstudie (DMSIII). Köln,
Deutscher Ärzte-Verlag, 1999.
81. Irigoyen MH, Mejia AM. Caries experience and treatment needs in 6-12.year-old urban population in
relation to socio-economic status. Community Dent Health. 1999;16:254-249.
82. Jackson RJ, Newman HN, Smart GJ, Stokes E, Hogan JI, Brown C, Seres J. The effects of a supervised
toothbrushing programme on the caries increment of primary school children, initially aged 5-6 years.
Caries Res. 2005;39:108-15.
83. Jerkovic K, Binnekade JM. Differences in oral health behaviour between children from high and children
from low SES schools in the Netherland. Community Dent Health. 2009;26:110-115.
84. Johnson NW, Bain CA. Tobacco and oral disease. Br Dent J. 2000;189:200-206.
85. Jonsson T, Arnlaugsson S, Karlsson KO, Ragnarsson B, Arnarson EO, Magnusson TE. Orthodontic
treatment experience and prevalence of malocclusion traits in an Icelandic adult population. American
Journal of Orthodontics and Dentofacial Orthopedics. 2007;131:8-18.
86. Josefsson E, Bjerklin K, Lindsten R. Malocclusion frequency in Swedish and immigrant adolescents -

90
influence of origin on orthodontic treatment need. Eur J Orthod. 2007;29:79- 87.
87. Kalnins IV, McQueen DV, Backett KC, Curtice L, Currie CE. Children, empowerment and health
promotion: some new directions in research and practice. Health Promotion International. 1992;7:53-59.
88. Karlsbeek H, Verrips GH. Consumption of sweet snacks and caries experience of primary school
children. Caries Res. 1994;28:477-83.
89. Kassenzahnärztliche Bundesvereinigung (KZBV): Jahrbuch 2004, Köln,2005.
90. Kawamura M, Takase N, Sasahara H, Okada M. Teenagers' oral health attitudes and behavior in Japan:
comparison by sex and age group. J Oral Sci. 2008;50:167-74.
91. Kay E, Locker D. A systematic review of the effectiveness of health promotion aimed at improving oral
health. Community Dent Health. 1998;15:132-44.
92. Kelbauskas E, Kelbauskiene S, Nedzelskiene I. The influence of smoking on oral health. Mil Medicina
(Kaunas). 2005;41: 8-26.
93. Kenealy P, Frude N, Shaw W. An evaluation of the psychological and social effects of malocclusion:
some implications for dental policy making. Soc SciMed. 1989;28:583-91.
94. Kersting M, Schoch G. Achievable guidelines for food consumption to reach a balanced fat and nutrient
intake in childhood and adolescence. J Am Coll Nutr. 1992;11:74-78.
95. Klink-Heckmann U, Bredy E . Kieferorthopdie. Johann Ambrosius Barth, Heidelberg, 1990; pp. 95-97.
96. Kolmakow S, Honkala E, Puranen M, Sainio P. Dento-facial morphology and caries experience: an
epidemiological study. Journal of Clinical Pediatric Dentistry. 1991;16:31-37.
97. Konu A, Rimpelä M. Well-being in schools: a conceptual model. Health Promot Int. 2002;17:79-87.
98. Kraus L, Heppekausen K, Orth B. Die Europäische Schülerstudie zu Alkohol und anderen Drogen
(ESPAD): Befragung von Schülerinnen und Schülern der 9. und 10. Klasse in Bayern, Berlin,
Brandenburg, Hessen, Mecklenburg-Vorpommern und Thüringen. MÜnchen, Germany: IFT, 2004.
Report No.141.
99. Kühnisch J, Senkel H, Heinrich-Weltzien R. Vergleichende Untersuchung zur Zahngesundheit von
deutschen und ausländischen 8- bis 10-Jährigen des westfälischen Ennepe-Ruhr-Kreises.
Gesundheitswesen. 2003;65:96-101.
100. Kumar S, Dagli RJ, Mathur A, Jain M, Duraiswamy P, Kulkarni S. Oral hygiene status in relation to
sociodemographic factors of children and adults who are hearing impaired, attending a special school.
Spec Care Dentist. 2008;28:258-64.
101. Kurth BM, Robert-Koch-Institut: Pretestbericht kinder-jugend-gesundheit21.De : Studie zur gesundheit
von kindern und jugendlichen in deutschland, ed Stand: 23.05.2002. Berlin, 2002.
102. Lampert T, Mensink GB, Romahn N, Woll A. Physical activity among children and adolescents in
Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents
(KiGGS). Bundesgesundheitsblatt- Gesundheitsforschung- Gesundheitsschutz. 2007;50:634-642.
103. Lampert T, Thamm M. Consumption of tobacco, alcohol and drugs among adolescents in Germany.
Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS).
Bundesgesundheitsblatt- Gesundheitsforschung- Gesundheitsschutz. 2007;50:600-608.
104. Lange M, Kamtsiuris P, Lange C, Schaffrath Rosario A, Stolzenberg H, Lampert T. [sociodemographic
characteristics in the german health interview and examination survey for children and adolescents
(KIGGS) - operationalisation and public health significance, taking as an example the assessment of
general state of health]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz
2007;50:578-589.
105. Larsson E. Artificial sucking habits: etiology, prevalence and effect on occlusion. Int J Orofacial Myology.
1994;20:10-21.
106. Leger LH. The opportunities and effectiveness of the health promoting primary school in improving child

91
health – a review of the claims and evidence. Health Educ Res. 1999;14:51-69.
107. Liepa A, Urtane I, Richmond S. Orthodontic treatment need in Latvia. Eur J Orthod. 2003;25:279-284.
108. Lin W, Yang HC, Hang CM, Pan WH. Nutrition knowledge, attitude, and behavior of Taiwanese
elementary school children. Asia Pac J Clin Nutr. 2007;16:534-546.
109. Liran Levin DM, Alon Shenkman M. The relationship between dental caries status and oral health
attitudes and behavior in young Israeli adults. J Dent Educ. 2004;68:1185-91.
110. Lowry R, Kann L, Collins JL, Kolbe LJ. The effect of socioeconomic status on chronic disease risk
behaviors among US adolescents. JAMA. 1996;276:792-797.
111. Lux Ch, Dcker B, Pritsch M, Komposch G, Niekusch U. Occlusal status and prevalence of occlusal
malocclusion traits among 9-year-old schoolchildren. Eur J Orthod. 2009;31:294-299.
112. MacIntyre UE, du Plessis JB. Dietary intakes and caries experience in children in Limpopo Province,
South Africa. SADJ. 2006;61:058-63.
113. Malmgren O, Ömblus J, Hägg U, Pancherz H. Treatment with an appliance system in relation to
treatment intensity and growth periods. Am J Orthod Dentofacial Orthop. 1987;91:143-151.
114. Mancuso CA, Rincon M. Impact of health literacy on longitudinal asthma outcomes. J Gen Intern Med.
2006;21:813-817.
115. Manganello JA. Health literacy and adolescents: a framework and agenda for future research. Health
Educ Res. 2008;23:840-847.
116. Mangrulkar L, Vince Whitman C, Posner M. Life skills approach to child and adolescent healthy human
development. Washington, D.C: Pan American Health Organisation. 2001;17:567-583.
117. Manzanera D, Montiel-Company J M, Almerich-Silla JM, Ganda JL. Orthodontic treatment need in
Spanish schoolchildren: an epidemiological study using the Index of Orthodontic Treatment Need. Eur J
Orthod. 2009;31:180-183.
118. Manzoli L, D'Attilio M, Tecco S, Muratore F, Festa F, Romano F. Prevalence and distribution by gender
of occlusal characteristics in a sample of Italian secondary school students: a cross-sectionalstudy. Eur J
Orthod. 2005;27:601-6.
119. Marmot MG. Health inequalities among British civil servants: the Whitehall II study. Lancet, Acta Obstet
Gynecol Scand. 1997;76:748-54.
120. Marthaler TM, O'mullane DM, Vrbic V. The prevalence of dental caries in Europe 1990-1995. ORCA
Saturday afternoon symposium 1995. Caries Res. 1996;30:237-255.
121. Marthaler TM. Change in dental caries1953-2003. Cries Res. 2004;38:173-81.
122. Mazzocchi A, Pasini S, Salgarello S. [Nutrition and carious pathology] Pediatr Med Chir. 1993;15:137-40.
123. McLain JB, Proffit WR. Oral health status in the United States: prevalence of malocclusion. J Dent Educ.
1985;49:386-396.
124. McLellan L, Rissel C, Donnelly N, Bauman A. Health behaviour and the school environment in New
South Wales, Australia. Soc Sci Med. 1999;49:611-19.
125. McNamara JA, Brudon WL. Orthodontics and dentofacial orthopedics. Needham Press, Ann Arbor,
2001 , pp. 264-272.
126. Mecklenburg-Vorpommern SL: Statistisches jahrbuch mecklenburg-vorpommern 2004, ed 1. Aufl.
Schwerin, Meckl, Statistisches Landesamt Mecklenburg-Vorpommern, 2004.
127. Mellanby AR, Reesa JB, Tripp JH. Peer-led and adult-led school health education: a critical review of
available comparative research. Health Educ Res. 2000;15:533-45.
128. Meyer-nurnberger M. Health information database system of the Federal, Center for Health Education
(FCHE). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. 2004;47:464-9.
129. Mitchell L. An introduction to orthodontics (3rd edn.). Oxford University Press, Oxford , 2005, pp 13-26.
130. Mouradian WE, Wehr E, Crall JJ. Disparities in children's oral health and access to dental care. JAMA.

92
2000;284:2625-31.
131. Moyses ST, Moyses SJ, Watt RG, Sheiham A. Associations between health promoting schools’ policies
and indicators of oral health in Brazil. Health Promot Int. 2003;18:209-18.
132. Müller MJ, Danielzik S, Pust S. School- and family-based interventions to prevent overweight in children.
Proc Nutr Soc. 2005;64:249-254.
133. Muratbegovic A, Markovic N, Ganibegovic Selimovic M. Molar incisor hypomineralisation in Bosnia and
Herzegovina: aetiology and clinical consequences in medium caries activity population, Eur Arch
Paediatr Dent. 2007;8:189-94.
134. Muwazi ML, Rwenyonyi CM, Tirwomwe JF, Ssali C, Kasangaki A, Nkamba EM, Ekwaru P. Prevalence of
oral diseases/conditions in a Uganda. Afr Health Sc. 2005;5:227-233.
135. Nadanovsky P, Sheiham A. The relative contribution of dental services to the changes in caries levels of
12 year-old children in 18 industrialized countries in the 1970s and early 1980s. Community Dent Oral
Epidemiol. 1995;23:231-239.
136. Natsiopoulou T, Melissa-Halikiopoulou Ch. Effects of socioeconomic status on television viewing
conditions of preschoolers in northern Greece. Early Child Dev Care. 2009;179:407-423.
137. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and
orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17:637-641.
138. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and
communication strategies into the 21st century. Health Promot Int.2000;15:259-267.
139. Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67:2072-2078.
140. Nyandindi U, Palin-Palokas T, Milen A, Robison V, Kombe N, Mwakasagule S. Participation, willingness
and abilities of school-teachers in oral health education in Tanzania. Community Dent Health.
1994;11:101-104.
141. O’Donnell L, Stueve A, San Doval A. Violence prevention and young adolescents’ participation in
community youth service. J Adolesc Health. 1999;24:28-37.
142. O'loughlin J, Tarasuk J, Paradis G. Reliability of selected measures of nicotine dependence among
adolescents. Ann Epidemiol. 2002;12:353-362.
143. Östberg AL, Halling A, Lindblad U. Gender differences in knowledge, attitude, behavior and perceived
oral health among adolescents. Acta Odontol Scand. 1999;57:231-236.
144. Palmer CA. Dental caries and obesity in children: different problems, related causes. Quintessence.
2005;36:457-461.
145. Pedersen J, Stensgaard K, Melsen B. Prevalence of malocclusion in relation to premature loss of
primary teeth. Community Dent Oral Epidemiol. 1978;6:204-209.
146. Peres KG, Barros AJ, Anselmi L, Peres MA, Barros FC. Does malocclusion influence the adolescent's
satisfaction with appearance? A cross sectional study nested in a Brazilian birth cohort. Community Dent
Oral Epidemiol. 2008;36:137-143.
147. Perillo L, Apicella D, Ferro F. Prevalence of orthodontic treatment need in southern Italian schoolchildren
Eur J Orthod. 2010;32:49–53.
148. Perry CL, Komro KA, Veblen-Mortenson S, Bosma LM, Farbakhsh K, Munson KA, Stigler MH, Lytle LA.
A randomized controlled trial of the middle and junior high school D.A.R.E. and D.A.R.E. Plus Programs.
Arch Pediatr Adolesc Med. 2003;157:178-184.
149. Petersen PE, Jiang H, Peng B, Tai BJ, Bian Z. Oral and general health behaviours among Chinese
urban adolescents. Community Dent Oral Epidemiol. 2008;36:76-84.
150. Petersen PE, Torres AM. Preventive oral health care and health promotion provided for children and
adolescents by the Municipal Dental Health Service in Denmark. Int J Paediatr Dent. 1999;9:81-91.
151. Petersen PE. Sociobehavioural risk factors in dental caries-international perspectives. Community Dent

93
Oral Epidemiol. 2005;33:274-9.
152. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st
century--the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol.
2003;31:3-23.
153. Pieper K, Schulte AG. The decline in dental caries among 12-year-old children in Germany between
1994 and 2000. Community Dent Health. 2004;21:199-206.
154. Plachta-Danielzik S, Pust S, Asbeck I. Four-year follow-up of school-based intervention on overweight
children: the KOPS study. Obesity (Silver Spring). 2007;15:3159-3169.
155. Poutanen R, Lahti S, Hausen H. Oral health-related knowledge, attitudes, and beliefs among 11 to 12-
year-old Finnish schoolchildren with different oral health behaviors. Acta Odontol Scand. 2005;63:10-6.
156. Proffit WR, Fields HW, Ackerman JL, Sinclair PM, Thomas PM, Tulloch JFC. Contemporary
Orthodontics. Mosby-Year Book, St. Louis. 1993; pp 76-85.
157. Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the
United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg.
1998;13:97-106.
158. Quartey, JB., Williamson DD. Prevalence of early childhood caries at Harris County clinics. ASDC J Dent
Child. 1999;66:127-31.
159. Ravens-Sieberer U, Bullinger M. Assessing health-related quality of life in chronically ill children with the
German KINDL: first psychometric and content analytical results. Qual Life Res. 1998;7:399-407.
160. Richmond S, Chestnutt I, Shennan J, Brown R. The relationship of medical and dental factors to
perceived general and dental health. Community Dent Oral Epidemiol. 2007;35:89-97.
161. Rodd HD, Patel V. Content analysis of children’s television advertising in relation to dental health. Br
Dent J. 2005;199:710-712.
162. Rodrigues C, Watt R, Sheiham A. The effects of dietary guidelines on sugar intake in 3 year olds
attending nurseries. Health Promotion Int. 1999;14:329-335.
163. Roth-isigkeit A, Ellert U, Kurth BM. Assessment of pain in The Child and Adolescent Health Survey.
Gesundheitswesen. 2002;64:125-9.
164. Saied-Moallemi Z, Virtanen JI, Ghofranipour F, Murtomaa H. Influence of mothers' oral health knowledge
and attitudes on their children's dental health. Eur Arch Paediatr Dent. 2008;9:79-83.
165. Schenk L, Knopf H. Oral health behaviour of children and adolescents in Germany. First results of the
German Health Interview and Examination Survey for Children and Adolescents (KiGGS).
Bundesgesundheitsb-Gesundheitsforsch-Gesundheitsschutz. 2007;50:653-658.
166. Schiffner U, Bauch J. Das Kindergartenbetreuungsprogramm ist in erster Linie bei der Mittelschicht
effective. Zahnärztl Mitt. 1986;76:938-941.
167. Schiffner U, Hoffmann T, Kerschbaum T, Micheelis W. Oral health in german children, adolescents,
adults and senior citizens in 2005. Community Dent Health. 2009;26:18-22.
168. Schillinger D, Grumbach K, Piette J. Associations of Health Literacy with Diabetes Outcomes. JAMA.
2002;288:475-482.
169. Schmidt CO, Fahland R, Franze M, Splieth CH, Jochen Rene´ Thyrian JR, Plachta-Danielzik S,
Hoffmann W, Kohlmann T. Health-related behaviour, knowledge, attitudes, communication and social
status in school children in Eastern Germany. Health Educ Res. 2010:12
170. Schopf P. Der Anteil Exogener Faktoren an der Entstehung von Dysgnathien. Fortschr. Kieferorthop.
1981;42:19-28.
171. Schopf P. Der Einfluß habitueller Faktoren auf das jugendliche Gebiß. Fortschr. Kieferorthop.
1973;34:408-432.
172. Schulte AG, Momeni A, Pieper K. Caries prevalence in 12-year-old children from germany. Results of
94
the 2004 national survey. Community Dent Health 2006;23:197-202.
173. Schwarzer R. Optimistische Kompetenzerwartung: Zur Erfassung einer personellen
Bewältigungsressource. Diagnostica. 1994;40:105-123.
174. Seabra AF, Mendonca DM, Thomis MA. Associations between sport participation, demographic and
socio-cultural factors in Portuguese children and adolescents. Eur J Public Health. 2008;18:25–30.
175. Sharda AJ, Shetty S. A comparative study of oral health knowledge, attitude and behaviour of first and
final year dental students of Udaipur city, Rajasthan, India. Int J Dent Hyg. 2008;6:347-53.
176. Shaw WC, O'brien KD, Richmond S. Quality control in orthodontics: factors influencing the receipt of
orthodontic treatment. Br Dent J.1991;170:66-8.
177. Shea JA, Beers BB, McDonald VJ, Quistberg DA, Ravenell KL, Asch DA. Assessing Health Literacy in
African American and Caucasian Adults: Disparities in Rapid Estimate of Adult Literacy in Medicine
(REALM) Scores. Fam Med. 2004;36:575-581.
178. Sheiham A, Watt RG. The common risk factor approach: a rational basis for promoting oral health.
Community Dent Oral Epidemiol. 2000;28:399-406.
179. Sheiham A. Oral health, general health and quality of life. Bull World Health Organ. 2005;83:644.
180. Shenkin JD, Broffitt B, Levy SM, Warren JJ. The association between environmental tobacco smoke and
primary tooth caries. J Public Health Dent. 2004;64:184-6.
181. Šidlauskas A, Lopatienë K. The prevalence of malocclusion among 7–15-year-old Lithuanian
schoolchildren, Medicina (Kaunas). 2009;45:147-52.
182. Smyth E, Caamańo F. Factors related to dental health in 12-year-old children: a cross-sectional study in
pupils. Gac Sanit. 2005;19:42-53.
183. Sofola OO, Shaba OP, Jeboda SO. Oral hygiene and periodontal treatment needs of urban school
children compared with that of rural school children in Lagos State. Nigeria. Odontostomatol Trop.
2003;26:25-9.
184. Soteriades ES, DiFranza JR. Parent's socioeconomic status, adolescents' disposable income, and
adolescents' smoking status in Massachusetts. Am J Public Health. 2003;93:1155-1160.
185. Souames M, Bassigny F, Zenati N, Riordan PJ, Boy-Lefevre ML. Orthodontic treatment need in French
schoolchildren: an epidemiological study using the Index of Orthodontic Treatment Need. Eur J
Orthod.2006;28:605-609.
186. Splieth Ch, Hensel E, Kocher T, Schwahn C. Zusammenhänge zwischen Kariesrisikoparametern und
den dmfs-Werten bei Greifswalder Einschülern. Prophylaxeimpuls. 1997;1:74-79.
187. Splieth Ch, Meyer G. Factors for Changes of Caries Prevalence among Adolescents in Germany. Eur J
Oral Sci. 1996;104:444-451.
188. Splieth CH, Nourallah AW, König KG. Caries prevention programs for groups: out of fashion or up to
date? Clin Oral Investig. 2004;8:6-10.
189. Splieth CH, Steffen H, Welk A, Schwahn C Responder and nonresponder analysis for a caries
prevention program. Caries Res. 2005;39:269-72.
190. Sreebny LM. Sugar and human dental caries. World Rev Nutr Diet,1982, pp. 19–65.
191. Sreebny LM. Sugar and human dental caries. World Rev Nutr Diet. 1982;3:19-65.
192. St Leger L, Nutbeam D. Finding common ground between health and education agencies to improve
school health: mapping goals, objectives, strategies, and inputs. J Sch Health. 2000;70:45-50.
193. Stahl F, Grabowski R. Malocclusion and caries prevalence: is there a connection in the primary and
mixed dentitions? Clin Oral Invest. 2004;8:86-90.
194. Stecksen-Blicks C, Borssn E. Dental caries, sugar eating habits and tooth brushing in groups of 4-year-
old children 1967–1997 in the city of Ume, Sweden. Caries Res. 1999;33:409-414.
195. Strippel H. Sociodental indicators in children and adolescents. Gesundheitswesen. 2001;63:93-97.

95
196. Sundby A, Petersen PE. Oral health status in relation to ethnicity of children in the Municipality of
Copenhagen, Denmark. Int J Paediatr Dent. 2003;13:150-157.
197. Sussman S. School-based tobacco use prevention and cessation: where are we going? Am J Health
Behav. 2001;25:191-199.
198. Szöke J, Petersen PE. Evidence for dental caries decline among children in an East European Country
(Hungary). Community Dent Oral Epidemiol. 2000;28:155-160.
199. Talhout R, Opperhuizen A, van Amsterdam JG. Sugars as tobacco ingredient: effects on mainstream
smoke composition. Food Chem Toxicol. 2006;44:1789-1798.
200. Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic
treatment need. Eur J Orthod. 2004;26:237-244.
201. Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res.
1973;81:12-20.
202. Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic
treatment need in children and adolescents in Bogotŕ, Colombia. An epidemiologic study related to
different stages of dental development. Eur J Orthod. 2001;23:153-167.
203. Thyen U. The German Health Interview and Examination Survey for Children and Adolescents (KiGGS)
2003-2006-a milestone in paediatrics. Bundesgesundheitsblatt Gesundheitsforschung-
Gesundheitsschutz. 2007;50:529-530.
204. Thyrian JR, Hannover W, John U, Tagmat D, Wolff J. Smoking behavior in adolescents: a comparison of
population-representative, regional or selectively assessed data and implications for prevention.
Gesundheitswesen. 2006;68:566-570.
205. Tickle M, Kay EJ, Bearn D. Socio-economic status and orthodontic treatment need. Community Dent
Oral Epidemiol. 1999;27:413-418.
206. Tobler NS. Drug prevention programmes can work: Research findings. J Addict Dis. 1992;11:1-28.
207. Tomar SL, Asma S. Smoking attributable periodontitis in the United States: findings from NHANES III. J
Periodontol. 2000;71:743-751.
208. Tomar SL, Winn DM, Swango PA, Giovino GA, Kleinman DV. Oral mucosal smokeless tobacco lesions
among adolescents in the United States. Eur J Orthod. 1997;76:1277-1286.
209. Trinn CR, Reinhardt H, Wehrbein N, Willershausen B. University Hospital Mainz, Germany Caries
prevalence in children: implications for orthodontic treatment need? Dtsch Zahnarztl Z. 2008;63:555-563.
210. Trummler A, Weiss V. DMFT scores in 12 year old school children in the city of St. Gallen. Oral
prophylaxe. 2000;22:206-208.
211. ur Rehman MM, Mahmood N, ur Rehman B. The relationship of caries with oral hygiene status and
extra-oral risk factors. J Ayub Med Coll Abbottabad. 2008;20:103-8.
212. US General Accounting Offices. Oral health: Dental Disease Is a Chronic Problem Among Low-Income
Populations. Report to Congressional Requesters. Washington, 2000.
213. Vallejos-Sánchez AA, Medina-Solis CE, Maupomé G, Casanova Rosado JF, Minaya-Sánchez M,
Villalobos-Rodelo JJ, Pontigo-Loyola AP. Socio-behavioral factors influencing tooth brushing frequency
in schoolchildren. J Am Dent Assoc. 139:743-9.
214. Van Steenkiste M, Wagner T, Einwag J. Influence of ignorance of caries prevention on tooth health and
behavior of junior high students. Oralprophylaxe. 1991;13:70-5.
215. Vanobberge JN, Martens LC, Lesaffre E, Declerck D. Parental occupational status related to dental
caries experience in 7-year-old children in Flanders(Belgium). Community Dent Health. 2001;18:256-62.
216. Vellappally S, Fiala Z, Smejkalová J, Jacob V, Shriharsha P. Influence of tobacco use in dental caries
development. Cent Eur J Public Health. 2007;15:116-21.
217. Verde PE, Dragano N. Education and health in 22 European countries. Soc Sci Med. 2006;63:1344-51.

96
218. Villalobos-Rodelo JJ, Pontigo-Loyola AP. Socio behavioural factors influencing toothbrushing frequency
among schoolchildren, J Am Dent Assoc. 2008;139:743-9.
219. Walther DP, Houston WJB, Jones ML, Oliver RG. Walther and Houston's orthodontic notes. Wright,
Oxford. 2004;5:57-90.
220. Watt RG. From victim blaming to upstream action; tackling the social determinants of oral health
inequalities. Community Dent Oral Epidemiol. 2007;35:1-11.
221. Wheeler KC, Fletcher KE, Wellman RJ, Difranza JR. Screening adolescents for nicotine dependence:
the Hooked On Nicotine Checklist. J Adolesc Health. 2004;35,225-30.
222. Wiefferink CH, Peters L, Hoekstra F, Dam GT, Buijs GJ, Paulussen TG. Clustering of health-related
behaviors and their determinants: possible consequences for school health interventions. Prev Sci.
2006;7:127-149.
223. Wierzbicka M, Petersen PE, Szatko F, Dybizbanska E, Kalo I. Changing oral health status and oral
health behaviour of schoolchildren in Poland. Community Dent Health. 2002;19:243-50.
224. World Health Organisation WHO: Oral health promotion: an essential element of a health-promoting
school. Geneva: World Health Organization; WHO Information Series on School Health. 2003;
Document 11.
225. World Health Organisation WHO; Global Oral Health Data Bank. Geneva: World Health Organization;
2004.
226. World Health Organisation: WHO's Global School Health Initiative. Health-promoting Schools. A healthy
setting for living, learning and working. Geneva: World Health Organization; 1998.
227. World Health Organization. Healthy Environment for Children. Initiating an Alliance for Action. Geneva:
WHO, 2002.
228. World Health Organization: Oral health surveys: basic methods, Geneva, World Health Organization
(WHO)1997; 4: pp. 13 -15,47-50.
229. World Health Organization: Oral health: action plan for promotion and integrated disease prevention.
Report by the Secretariat. 2007: Document A60/16.
230. Yee R, Sheiham A. The burden of restorative dental treatment for children in third world countries.
International Dental Journal. 2002;52:1-9.
231. Yin HS, Forbis SG, Dreyer BP. Health Literacy and Pediatric Health. Curr Probl Pediatr Adolesc Health
Care. 2007;37:258-286.
232. Zeltmann S, Ingeborg K, Gernot G. Malocclusion and the Need for Orthodontic Treatment in 9-Year-Old
Children. J Orofac Orthop/Fortschr Kieferorthop. 1998;59:193-201.
233. Zenker C. Addiction and gender. Bundesgesundheitsblatt- Gesundheitsforschung- Gesundheitsschutz.
2005;48:469-76.
234. Zitterbart PA, Matranga LF, Christen AG, Park KK, Potter RH. Association between cigarette smoking
and the prevalence of dental caries in adult males. Gen Dent. 1990;38:426-31.
235. Zuppa JA, Morton H, Mehta KP. Television food advertising: counterproductive to children’s health? A
content analysis using the Australian Guide to Healthy Eating. Nutrition and Dietetics. 2003;60:78–84.

97
Appendix 1
98
Appendix 2

99
Appendix 3

100
Appendix 4

101
Appendix 5

102
Eidesstattliche Erklärung
Hiermit erkläre ich, daß ich die vorliegende Dissertation selbständig verfaßt und keine ande-
ren als die angegebenen Hilfsmittel benutzt habe.
Die Dissertation ist bisher keiner anderen Fakultät vorgelegt worden.
Ich erkläre, daß ich bisher kein Promotionsverfahren erfolglos beendet habe und daß eine
Aberkennung eines bereits erworbenen Doktorgrades nicht vorliegt.
Datum
Unterschrift

103
Curriculum Vitae (CV.)
Personal Detail
Name Samar Alsoliman
E-Mail Address [email protected]
Date of birth, place of birth 31.03.1974 in Derzor , Syrien
Nationality Syrian
Marital Status Married, have three children
Education
Elementary school 01.09.1979 – 15.06,1988
Secondary school 01.09.1988 – 28.07.1991 (Note: 85 %)
Faculty of dentistry, Aleppo University 15.09.1991 – 17.08.1996
(Note first graduate: 75%)
Department of Orthodontic,
Damascus University 16.10.1996 – 24.10.1999 (Note: 76 %)
Greifswald University
Promotion since 01.4.2007
Postgraduate student in since 01.4.2009
Paediatric dentistry
Scientific Qualifications
-License in dentistry / Aleppo University,Syria-1996 (Note first graduate: 75%).
-Diploma (Specialization) in Orthodontic / Damascus University, Syria-1999 (Note: 76%).
Practical Experience
-Practiced in Damaskus University in Department of Orthodontics 1996 – 1999
-Practiced in my private Orthodontic clinic 2000 – 2003
-Practiced in Alwan Alnakhil Orthodontic Centrum in Riyadh, Saudi Arabia 2003 – 2004
-Practicum in private-Orthopaedic clinic; Dr. Riedel, Greifswald, Germany 2005 –
2006
Member in:
Deutsche Gesellshaft für Kinderzahneheilkunde DGK
Syrian Dental Association
Syrian Association of Orthodontic

104
The following price is based on this PHD-thesis:
Wrigley price 2010 for Oral Prophylaxis
• A Treuner , S Alsoliman, CO Schmidt , CH Splieth;
Mundgesundheitskompetenz bei Schulkindern – Reicht Wissen allein für gute Zähne?
Earn of Wrigley price 2010 for Oral Prophylaxis in 1.06.2010.
The following abstracts are based on this PHD-thesis:
• S Alsoliman*, A Treuner, M Alkilzy, C. Splieth;
Oral Health Awareness-related Behaviour, Knowledge, Attitudes and Social Status among
German Schoolchildren.
Abstract No. 17 56th ORCA Congress, July 1-4, 2009, Budapest.
• S Alsoliman*, A Treuner, M Alkilzy, C. Splieth;
Oral Health Awareness-related Behaviour, Knowledge, Attitudes and Social Status among
German Schoolchildren.
Caries Res. 2009;43: 184 .
• M Alkilzy*, J Wittmeiera, S Alsoliman, S Plachta-Danielzik b, MJ Müller b, C. H. Splieth;
Correlation between Caries and Nutrition among Fifth Grade German School Children.
Abstract No. 66 56th ORCA Congress, July 1-4, 2009, Budapest.
• M Alkilzy*, J Wittmeiera, S Alsoliman, S Plachta-Danielzik b, MJ Müller b, C. H. Splieth;
Correlation between Caries and Nutrition among Fifth Grade German School Children.
Caries Res. 2009;43:202 .

105
Acknowledgements
I thank the Almighty God for keeping me strong and healthy to complete my study.
My heartfelt gratitude is due to my supervisor Prof. Dr. Ch. Splieth for unlimited
encouragement and support throughout my study period, for his valuable advice and for his
time spent supervising the study progress, step by step, and reviewing this thesis.
My honest appreciation goes to Prof. Dr. G. Meyer for his continuous support and assistance
whenever needed.
My utmost appreciation goes to Dr. Roth and the DAAD (Deutscher Akademischer
Ausländer-Dienst) for the financial support.
I would like to thank everyone who contributed to the survey; in particular, Members of
GEKO team and many thanks also go to the parents and children who participated in the
survey.
I am forever indebted to my husband Mohamad for his understanding, uncomplaining
support, for sacrifices he made to further my career.
This thesis is dedicated with love to my children Raghed, Omar and Sedra who continued to
love me and encouraged me; I am blessed to have them in my life.
I would like to acknowledge with great appreciation and love; my mother for her help and
extraordinary commitment to my education, my father who was his short life as a bridge for
our successes, he continue to encourage me in spite of his died.
I would like to express a special thanks to all my brothers Modar, Firas, Yaser, Yaman,
Hothaifa who still give me the confidence and strengthen my belief in the important of my
work.
Samar Alsoliman
Copyright © 2022 FDOKUMEN