Phase I Study of ON 01910.Na, a Novel Modulator of the Polo-Like Kinase 1 Pathway, in Adult Patients...
7
Phase I Study of ON 01910.Na, a Novel Modulator of the Polo-Like Kinase 1 Pathway, in Adult Patients With Solid Tumors Antonio Jimeno, Jing Li, Wells A. Messersmith, Daniel Laheru, Michelle A. Rudek, Manoj Maniar, Manuel Hidalgo, Sharyn D. Baker, and Ross C. Donehower From the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Univer- sity, Baltimore, MD; and Onconova Ther- apeutics Inc, Newtown, PA. Submitted May 2, 2008; accepted July 25, 2008; published online ahead of print at www.jco.org on October 27, 2008. Supported by Onconova Therapeutics, Inc. Presented in part at the 98th Annual Meeting of the American Association for Cancer Research, April 14-18, 2007, Los Angeles, CA. Authors’ disclosures of potential con- flicts of interest and author contribu- tions are found at the end of this article. Corresponding author: Antonio Jimeno, MD, PhD, University of Colorado Cancer Center, PO Box 6511, Mail Stop 8117, Aurora, CO 80045; e-mail: [email protected]. The Appendix is included in the full-text version of this article, available online at www.jco.org. It is not included in the PDF version (via Adobe® Reader®). © 2008 by American Society of Clinical Oncology 0732-183X/08/2634-5504/$20.00 DOI: 10.1200/JCO.2008.17.9788 A B S T R A C T Purpose We conducted a first-in-man (to our knowledge) phase I study to determine the dose-limiting toxicities (DLTs), characterize the pharmacokinetic profile, and document any antitumor activity of ON 01910.Na, a new chemical entity that arrests cancer cells in G 2 /M by modulating mitotic regulatory pathways including polo-like kinase 1 (Plk1). Patients and Methods Patients had solid tumors refractory to standard therapy. ON 01910.Na was administered as a 2-hour infusion on days 1, 4, 8, 11, 15, and 18 in 28-day cycles. The starting dose was 80 mg, and an accelerated titration schedule (single-patient cohorts) was used for escalation. Pharmacokinet- ics were studied on days 1 and 15 of cycle 1. Results Twenty patients (11 women and nine men; age 46 to 73 years) were enrolled onto the study. Dose levels of 80, 160, 320, 480, 800, 1,280, 2,080, and 3,120 mg were evaluated in single-patient cohorts. A DLT and additional grade 2 toxicities made the 4,370-mg dose (n 6) not tolerable, and the next lower dose cohort (3,120 mg) was expanded to six assessable patients. Toxicities were skeletal, abdominal, and tumor pain; nausea; urge to defecate; and fatigue. Hematologic toxicity was infrequent and mild. ON 01910.Na pharmacokinetics were characterized by a rapid distribu- tion phase (distribution half-life, 1 hour) and a relatively slow elimination phase (elimination half-life, 27 hours). A refractory ovarian cancer patient had an objective response after four cycles and remained progression free for 24 months. Conclusion ON 01910.Na showed a distinct but moderate toxicity pattern. The recommended phase II dose of ON 01910.Na with this schedule of administration is 3,120 mg. Single-agent activity was documented in an ovarian cancer patient. J Clin Oncol 26:5504-5510. © 2008 by American Society of Clinical Oncology INTRODUCTION Cell cycle dysregulation is considered among the hallmark characteristics of cancer and thus consti- tutes a primary target for anticancer drug develop- ment. One key mediator in the intricate and overlapping control points into the mitotic phase is the polo-like kinase 1 (Plk1)– centered regulatory loop. 1,2 Plk1 is a key mitotic regulator that modu- lates the transition through the G 2 /M checkpoint by influencing the activation of the phosphatase CDC25C and cyclin B1. 3 Plk1 is overexpressed in non–small-cell lung cancer, 4 head and neck squa- mous cell cancer, 5 prostate cancer, 6 ovarian cancer, 7 and pancreatic cancer. 8,9 In non–small-cell lung cancer, head and neck squamous cell cancer, and ovarian cancer, high Plk1 expression was an inde- pendent prognostic factor of shorter survival. Sev- eral modalities targeting Plk1 have explored its role in cancer, including deletion mutants inducing apoptosis, 10 antisense oligonucleotides with anti- proliferative effect in lung 11 and pancreatic can- cer, 8 and interference RNAs on cervical and lung cancer. 12 This validated Plk1 as an anticancer tar- get, 13 but these approaches are difficult to translate to the clinic. ON 01910.Na is a small-molecule drug that disrupts Plk1-mediated G 2 /M cell cycle transi- tion and induces mitotic arrest and apoptosis. 14 Structurally, it is not an adenosine triphosphate mimetic and is believed, to compete for the substrate-binding site of the enzyme. ON 01910.Na JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T VOLUME 26 NUMBER 34 DECEMBER 1 2008 5504 © 2008 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission. Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Phase I Study of ON 01910.Na, a Novel Modulator of the Polo-Like Kinase 1 Pathway, in Adult Patients...
Phase I Study of ON 01910.Na, a Novel Modulator of thePolo-Like Kinase 1 Pathway, in Adult Patients WithSolid TumorsAntonio Jimeno, Jing Li, Wells A. Messersmith, Daniel Laheru, Michelle A. Rudek, Manoj Maniar,Manuel Hidalgo, Sharyn D. Baker, and Ross C. Donehower
From the Sidney Kimmel ComprehensiveCancer Center at Johns Hopkins Univer-sity, Baltimore, MD; and Onconova Ther-apeutics Inc, Newtown, PA.
Submitted May 2, 2008; accepted July25, 2008; published online ahead ofprint at www.jco.org on October 27,2008.
Supported by Onconova Therapeutics,Inc.
Presented in part at the 98th AnnualMeeting of the American Associationfor Cancer Research, April 14-18, 2007,Los Angeles, CA.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Corresponding author: Antonio Jimeno,MD, PhD, University of ColoradoCancer Center, PO Box 6511, Mail Stop8117, Aurora, CO 80045; e-mail:[email protected].
The Appendix is included in thefull-text version of this article,available online at www.jco.org.It is not included in the PDF version(via Adobe® Reader®).
© 2008 by American Society of ClinicalOncology
0732-183X/08/2634-5504/$20.00
DOI: 10.1200/JCO.2008.17.9788
A B S T R A C T
PurposeWe conducted a first-in-man (to our knowledge) phase I study to determine the dose-limitingtoxicities (DLTs), characterize the pharmacokinetic profile, and document any antitumor activity ofON 01910.Na, a new chemical entity that arrests cancer cells in G2/M by modulating mitoticregulatory pathways including polo-like kinase 1 (Plk1).
Patients and MethodsPatients had solid tumors refractory to standard therapy. ON 01910.Na was administered as a2-hour infusion on days 1, 4, 8, 11, 15, and 18 in 28-day cycles. The starting dose was 80 mg, andan accelerated titration schedule (single-patient cohorts) was used for escalation. Pharmacokinet-ics were studied on days 1 and 15 of cycle 1.
ResultsTwenty patients (11 women and nine men; age 46 to 73 years) were enrolled onto the study. Doselevels of 80, 160, 320, 480, 800, 1,280, 2,080, and 3,120 mg were evaluated in single-patientcohorts. A DLT and additional grade 2 toxicities made the 4,370-mg dose (n � 6) not tolerable, andthe next lower dose cohort (3,120 mg) was expanded to six assessable patients. Toxicities wereskeletal, abdominal, and tumor pain; nausea; urge to defecate; and fatigue. Hematologic toxicitywas infrequent and mild. ON 01910.Na pharmacokinetics were characterized by a rapid distribu-tion phase (distribution half-life, 1 hour) and a relatively slow elimination phase (elimination half-life,27 hours). A refractory ovarian cancer patient had an objective response after four cycles andremained progression free for 24 months.
ConclusionON 01910.Na showed a distinct but moderate toxicity pattern. The recommended phase II doseof ON 01910.Na with this schedule of administration is 3,120 mg. Single-agent activity wasdocumented in an ovarian cancer patient.
J Clin Oncol 26:5504-5510. © 2008 by American Society of Clinical Oncology
INTRODUCTION
Cell cycle dysregulation is considered among thehallmark characteristics of cancer and thus consti-tutes a primary target for anticancer drug develop-ment. One key mediator in the intricate andoverlapping control points into the mitotic phase isthe polo-like kinase 1 (Plk1)–centered regulatoryloop.1,2 Plk1 is a key mitotic regulator that modu-lates the transition through the G2/M checkpointby influencing the activation of the phosphataseCDC25C and cyclin B1.3 Plk1 is overexpressed innon–small-cell lung cancer,4 head and neck squa-mous cell cancer,5 prostate cancer,6 ovarian cancer,7
and pancreatic cancer.8,9 In non–small-cell lungcancer, head and neck squamous cell cancer, and
ovarian cancer, high Plk1 expression was an inde-pendent prognostic factor of shorter survival. Sev-eral modalities targeting Plk1 have explored its rolein cancer, including deletion mutants inducingapoptosis,10 antisense oligonucleotides with anti-proliferative effect in lung11 and pancreatic can-cer,8 and interference RNAs on cervical and lungcancer.12 This validated Plk1 as an anticancer tar-get,13 but these approaches are difficult to translateto the clinic.
ON 01910.Na is a small-molecule drug thatdisrupts Plk1-mediated G2/M cell cycle transi-tion and induces mitotic arrest and apoptosis.14
Structurally, it is not an adenosine triphosphatemimetic and is believed, to compete for thesubstrate-binding site of the enzyme. ON 01910.Na
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 26 � NUMBER 34 � DECEMBER 1 2008
5504 © 2008 by American Society of Clinical Oncology
Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
decreases the activation/phosphorylation state of cell cycle effectorsdownstream of Plk1 such as CDC25C.14,15 ON 01910.Na showedefficacy against breast and pancreatic cancer xenografts.14,15
In an analysis of 33 investigational agents tested in phase Itrials from 1991 through 2001, body-surface area (BSA)– baseddosing only significantly reduced interpatient variability in drugclearance in five of the 33 agents, all five of them being conven-tional cytotoxics.16 On the basis of these results, the authors sug-gested that BSA need not be used to determine the doses ofinvestigational agents in phase I studies. Therefore, we chose flatdosing versus a BSA-based dose calculation.
The present phase I study represents the first-in-man (to ourknowledge) experience with ON 01910.Na. The primary objective wasto determine the maximum-tolerated dose (MTD) of ON 01910.Naadministered by 2-hour infusion on days 1, 4, 8, 11, 15, and 18 of a28-day cycle. The secondary objectives included determining the qual-itative and quantitative toxicity of ON 01910.Na and its reversibility;investigating the clinical pharmacology of ON 01910.Na, includingplasma pharmacokinetics; and documenting any antitumor activity.
PATIENTS AND METHODS
Patient Eligibility
Patients had histologically confirmed malignancy for which standardcurative or palliative measures did not exist; age � 18 years; Eastern Cooper-ative Oncology Group performance status � 2; life expectancy � 12 weeks;and adequate bone marrow, hepatic, and renal function (absolute neutrophilcount � 1,500/�L, platelets � 100,000/�L, bilirubin�1.5� the upper limit ofnormal [ULN], AST or ALT � 2.5� ULN, and creatinine � 1.5� ULN).Patients could have received any prior therapy ending � 28 days before studywithout residual toxicity. Measurable disease was not a requirement for studyentry. Patients with radiated, clinically stable brain metastases were allowed.Patients with severe, clinically significant, and/or uncontrolled medical condi-tions were excluded. Our institutional review board granted approval, andwritten informed consent was mandatory.
Treatment Plan
ON 01910.Na was supplied by Onconova Therapeutics Inc (Newton,PA). The drug was formulated in polyethylene glycol 400 and diluted withsaline for administration. Treatment consisted of ON 01910.Na administeredintravenously as a 2-hour infusion on days 1, 4, 8, 11, 15, and 18 of a 28-daycycle in an outpatient setting. This is based on similar divided dose schedulesthat showed higher efficacy in animal tumor models compared with shorterduration of administration. The starting dose of ON 01910.Na was 80 mg,which was approximately 10% of the lethal dose in 10% of treated rats for dailyadministration. No prophylactic antiemetics were administered. In the ab-sence of treatment delays as a result of adverse events, treatment was adminis-tered until disease progression, intercurrent illness, unacceptable adverseevent(s), or withdrawal of consent. Re-treatment required adequate labora-tory parameters on every evaluation and resolution of all nonhematologictoxicities (except alopecia and fatigue) to baseline or less than grade 1. In caseof a delay of more than 14 days, the patient was removed from the study.
Assessments, Follow-Up, and Monitoring
Toxic events were observed until resolution to baseline or less thangrade 1. Before study entry, patients underwent a clinical history andphysical examination, performance status assessment, CBC, platelet count,chemistries, urinalysis, stool for occult blood, pregnancy test (if applica-ble), chest x-ray, ECG, and disease assessment by computed tomography(CT) scan. Hematology was repeated before every infusion during the firstcycle and then weekly; chemistries were performed weekly (or when indi-cated). CT scan of disease sites was repeated every two cycles. Adverse
events were classified/graded according to the National Cancer InstituteCommon Terminology Criteria of Adverse Events (version 3). Responsewas evaluated by Response Evaluation Criteria in Solid Tumors.17 Patientswere considered assessable for toxicity once therapy started and assessablefor efficacy if at least one cycle was administered.
Definition of Dose-Limiting Toxicity, MTD, and
Dose-Escalation Plan
Dose-limiting toxicity (DLT) was defined as any drug-related grade 4hematologic toxicity (grade 4 neutropenia � 5 days), other toxicities � grade3, and grade 2 hemorrhage or neurologic toxicities. An accelerated titrationdesign was used for dose escalation, where one patient was treated at each doselevel until occurrence of � grade 2 toxicity, after which three patients weretreated per dose level. If no DLTs were encountered in any of the threepatients in cycle 1, dose escalation was allowed. If one of the three patientsexperienced a DLT, three more patients were to be enrolled at the samedose level, and if none of these three additional patients experienced a DLT,dose escalation was allowed. The MTD was defined as the highest feasible dosetested in which fewer than 33% of patients experienced DLT attributable to thestudy drug, when at least six patients were treated at that dose and wereassessable for toxicity.
Pharmacokinetic Sampling and Analytic Assay
Blood samples were collected in a tube with heparin anticoagulant at thefollowing time points on days 1 and 15 during the first cycle: before treatment;during infusion at 15, 30, and 60 minutes and 1 hour and 59 minutes; and afterthe infusion at 10, 20, and 30 minutes and 1, 2, 4, 8, 24, and 48 hours.Additionally, a pretreatment trough level was obtained on days 4, 8, 11, 18, and28. Samples were centrifuged at 1,000� g at 4°C for 10 minutes, and plasmawas stored at �80°C until analysis. ON 01910.Na plasma concentrations weredetermined using validated liquid chromatography/mass spectrometry/massspectometry, as described previously.18 The low and high calibration curveswere established at ON 01910.Na plasma concentrations of 10 to 2,000 ng/mLand 100 to 20,000 ng/mL, respectively. The low and high curves were crossvalidated, and a 1:100 dilution schema was also validated.18
Pharmacokinetic Data Analysis
ON 01910.Na pharmacokinetic parameters for individual patients wereestimated using compartmental analysis with WINNonlin version 5.2 (Phar-sight Corporation, Cary, NC). Individual patient ON 01910.Na plasma
Table 1. Patient Characteristics
CharacteristicNo. of Patients
(N � 20)
SexMale 9Female 11
Age, yearsMedian 63Range 46-73
Eastern Cooperative Oncology Group performance status0 81 112 1
Primary tumor siteColorectal 7Pancreas (adenocarcinoma) 3Ovary 3Biliary 2Hepatocellular 2Carcinoid 1Duodenal 1Endometrial 1
Phase I Study of ON 01910.Na
www.jco.org © 2008 by American Society of Clinical Oncology 5505Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.
Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
concentration-time data were fitted with two-compartment modeling with afirst-order elimination process from the central compartment. A t test wasused for the comparison of parameters on days 1 and 15. The a priori level ofsignificance was P � .05. Statistical analyses were performed with SPSS version10.0 (SPSS Inc, Chicago, IL).
RESULTS
Patient Characteristics
Between August 2004 and March 2007, 20 patients with ad-vanced solid tumors were enrolled onto the study. Nineteen patientswere assessable for toxicity, and response could be evaluated in 16patients. One patient in the 3,120-mg cohort developed rapid diseaseprogression before completing her first cycle, was considered notassessable, and was replaced. Response could not be assessed in three
additional patients (one was taken off study as a result of an unrelatedevent, one died, and a third withdrew consent). Demographic andclinical characteristics of the patients are listed in Table 1. A total of 33cycles of the study drug was delivered (median, two cycles; range, oneto four cycles).
Dose-Escalation Process
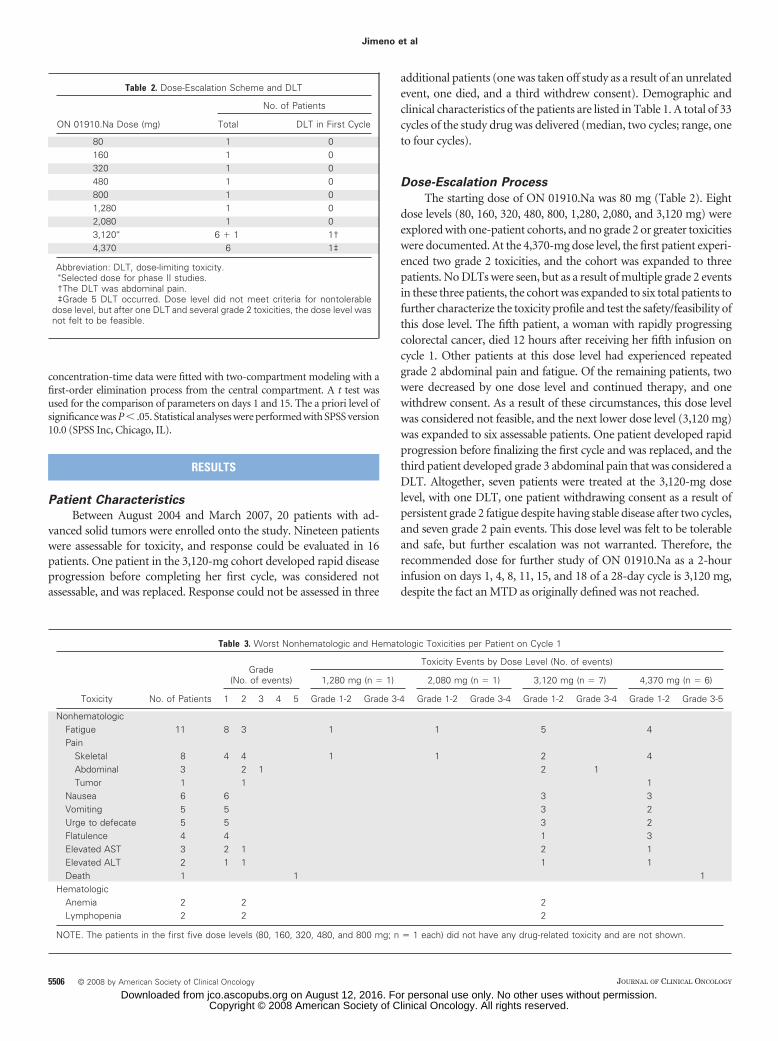
The starting dose of ON 01910.Na was 80 mg (Table 2). Eightdose levels (80, 160, 320, 480, 800, 1,280, 2,080, and 3,120 mg) wereexplored with one-patient cohorts, and no grade 2 or greater toxicitieswere documented. At the 4,370-mg dose level, the first patient experi-enced two grade 2 toxicities, and the cohort was expanded to threepatients. No DLTs were seen, but as a result of multiple grade 2 eventsin these three patients, the cohort was expanded to six total patients tofurther characterize the toxicity profile and test the safety/feasibility ofthis dose level. The fifth patient, a woman with rapidly progressingcolorectal cancer, died 12 hours after receiving her fifth infusion oncycle 1. Other patients at this dose level had experienced repeatedgrade 2 abdominal pain and fatigue. Of the remaining patients, twowere decreased by one dose level and continued therapy, and onewithdrew consent. As a result of these circumstances, this dose levelwas considered not feasible, and the next lower dose level (3,120 mg)was expanded to six assessable patients. One patient developed rapidprogression before finalizing the first cycle and was replaced, and thethird patient developed grade 3 abdominal pain that was considered aDLT. Altogether, seven patients were treated at the 3,120-mg doselevel, with one DLT, one patient withdrawing consent as a result ofpersistent grade 2 fatigue despite having stable disease after two cycles,and seven grade 2 pain events. This dose level was felt to be tolerableand safe, but further escalation was not warranted. Therefore, therecommended dose for further study of ON 01910.Na as a 2-hourinfusion on days 1, 4, 8, 11, 15, and 18 of a 28-day cycle is 3,120 mg,despite the fact an MTD as originally defined was not reached.
Table 2. Dose-Escalation Scheme and DLT
ON 01910.Na Dose (mg)
No. of Patients
Total DLT in First Cycle
80 1 0160 1 0320 1 0480 1 0800 1 01,280 1 02,080 1 03,120� 6 � 1 1†4,370 6 1‡
Abbreviation: DLT, dose-limiting toxicity.�Selected dose for phase II studies.†The DLT was abdominal pain.‡Grade 5 DLT occurred. Dose level did not meet criteria for nontolerable
dose level, but after one DLT and several grade 2 toxicities, the dose level wasnot felt to be feasible.
Table 3. Worst Nonhematologic and Hematologic Toxicities per Patient on Cycle 1
Toxicity No. of Patients
Grade(No. of events)
Toxicity Events by Dose Level (No. of events)
1,280 mg (n � 1) 2,080 mg (n � 1) 3,120 mg (n � 7) 4,370 mg (n � 6)
1 2 3 4 5 Grade 1-2 Grade 3-4 Grade 1-2 Grade 3-4 Grade 1-2 Grade 3-4 Grade 1-2 Grade 3-5
NonhematologicFatigue 11 8 3 1 1 5 4Pain
Skeletal 8 4 4 1 1 2 4Abdominal 3 2 1 2 1Tumor 1 1 1
Nausea 6 6 3 3Vomiting 5 5 3 2Urge to defecate 5 5 3 2Flatulence 4 4 1 3Elevated AST 3 2 1 2 1Elevated ALT 2 1 1 1 1Death 1 1 1
HematologicAnemia 2 2 2Lymphopenia 2 2 2
NOTE. The patients in the first five dose levels (80, 160, 320, 480, and 800 mg; n � 1 each) did not have any drug-related toxicity and are not shown.
Jimeno et al
5506 © 2008 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
Toxicity
Treatment was generally well tolerated. The toxic events ex-perienced during cycle 1 and during all cycles of therapy andthought to be possibly, probably, or certainly related to ON01910.Na are listed in Table 3 and Appendix Table A1 (onlineonly), respectively. The most common adverse events were fatigue,pain, nausea, vomiting, an acute urge to defecate, and abdominalcomplaints best described as flatulence. Fatigue was mild duringthe first cycle but reached grade 3 in two patients on cycle 2.Nausea/vomiting, pain, and urge to defecate were infusion relatedand typically occurred during the second hour of the infusion andthe first 2 hours of the postinfusion period. Standard antiemeticsboth controlled and prevented subsequent occurrences of nausea/vomiting. Pain was categorized as skeletal (typically in the shoul-ders), abdominal (localized in the right upper quadrant), andrelated to tumor sites (in an ovarian cancer patient with skinmetastasis and a colorectal cancer patient with known bone metas-tases). Tumor pain did not increase in intensity but remainedstable with repeated infusions. Nonsteroidal anti-inflammatoryand opioid drugs only partially decreased established pain or pre-vented it in further infusions. As described earlier, these toxicities
clustered at the 3,120- and 4,370-mg dose levels, where most pa-tients had at least one event during the first cycle. Grade 2 eleva-tions in ALT/AST were documented in three patients, with noconcomitant alterations in functional liver tests. Hematologic tox-icity was mild.
A death occurred in a patient while on the study. A patient withrapidly progressing colorectal cancer died approximately 12 hoursafter receiving the fifth infusion on cycle 1. The administration hadbeen otherwise uneventful, but that day in the morning and promptedby the development of increased symptoms, the possibility of clinicalprogression had been discussed. An agreement to finalize the first cycleand re-evaluate the status of her disease had been reached. That night,the family reported that the patient vomited and became unrespon-sive. No resuscitation was attempted, necropsy was not performed,and therefore, the cause of death remains uncertain.
Efficacy
Sixteen patients were assessable for response. In 14 patients, thebest response was progression of disease. One patient each had stabledisease and a partial response. The first patient had a previously pro-gressing hepatocellular cancer and withdrew consent after two cycles
CA12
5
050
100150200250300350400450
April 20,2005
August 20,2005
December 25,2005
April 20,2006
August 20,2006
December 20,2006
ON 01910.Na cycles
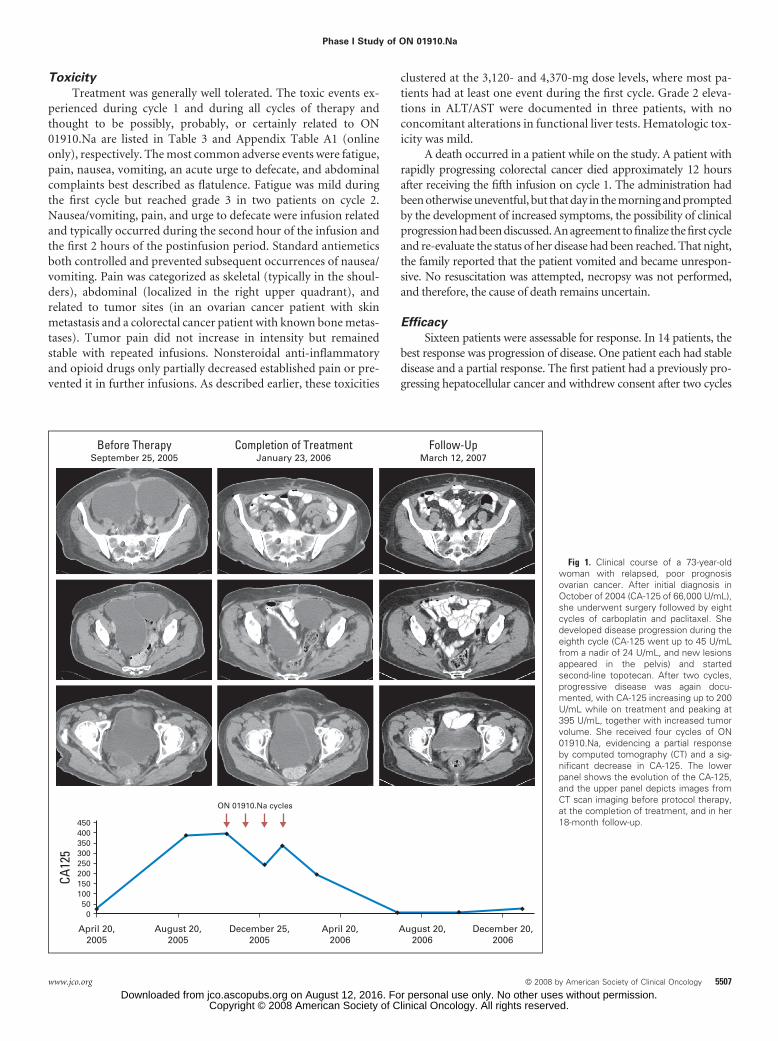
Before TherapySeptember 25, 2005
Completion of TreatmentJanuary 23, 2006
Follow-UpMarch 12, 2007
Fig 1. Clinical course of a 73-year-oldwoman with relapsed, poor prognosisovarian cancer. After initial diagnosis inOctober of 2004 (CA-125 of 66,000 U/mL),she underwent surgery followed by eightcycles of carboplatin and paclitaxel. Shedeveloped disease progression during theeighth cycle (CA-125 went up to 45 U/mLfrom a nadir of 24 U/mL, and new lesionsappeared in the pelvis) and startedsecond-line topotecan. After two cycles,progressive disease was again docu-mented, with CA-125 increasing up to 200U/mL while on treatment and peaking at395 U/mL, together with increased tumorvolume. She received four cycles of ON01910.Na, evidencing a partial responseby computed tomography (CT) and a sig-nificant decrease in CA-125. The lowerpanel shows the evolution of the CA-125,and the upper panel depicts images fromCT scan imaging before protocol therapy,at the completion of treatment, and in her18-month follow-up.
Phase I Study of ON 01910.Na
www.jco.org © 2008 by American Society of Clinical Oncology 5507Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.
Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
as a result of fatigue despite disease stabilization. The second patientwas an ovarian cancer patient diagnosed in October of 2004, with aCA-125 of 66,000 U/mL preoperatively. She underwent surgery fol-lowed by eight cycles of carboplatin and paclitaxel, with a CA-125nadir of 24 U/mL. During her eighth cycle, she developed diseaseprogression (CA-125 went up to 45 U/mL, and new lesions appearedin the pelvis) and started second-line topotecan. After two cycles,progressive disease was documented, with CA-125 increasing to 395U/mL plus increased tumor volume. She received four cycles of ON01910.Na at the 4,370-mg dose level. A minor response by CT and asignificant decrease in CA-125 (from 385 to 190 U/mL while ontherapy) were documented (Fig 1). The degree of the response in-creased in the observation period, meeting Response Evaluation Cri-teria in Solid Tumors for a partial response. The patient opted to stoptherapy, has been observed since then, and remained progression freefor 24 months.
Pharmacokinetics
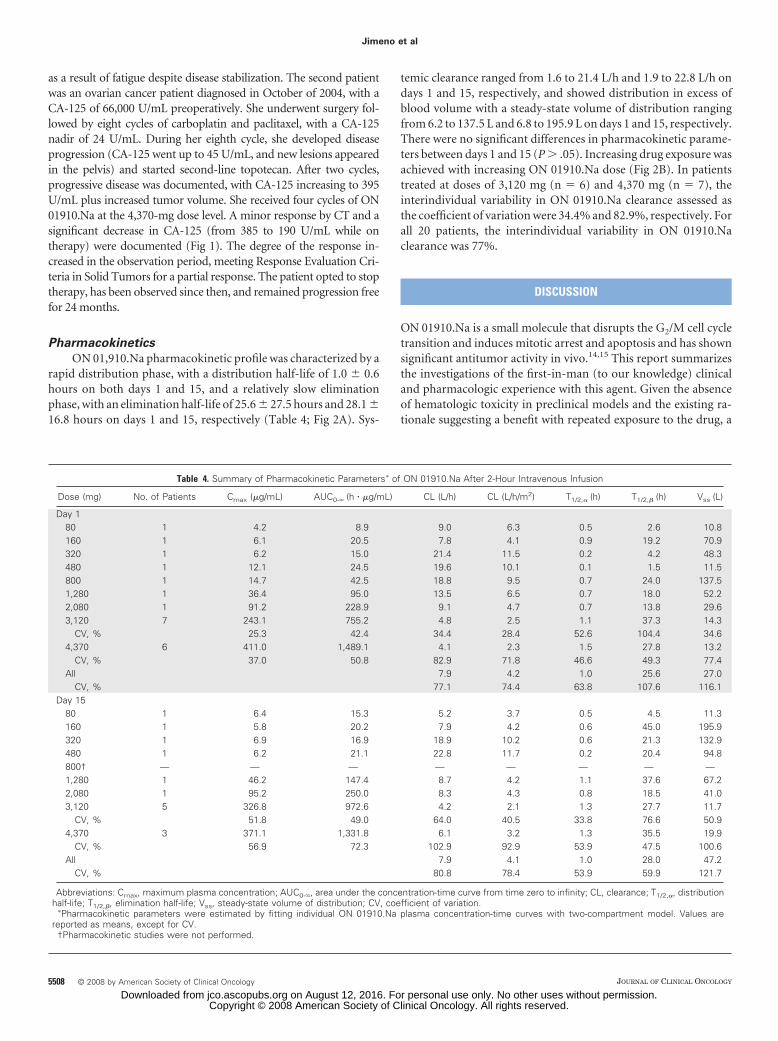
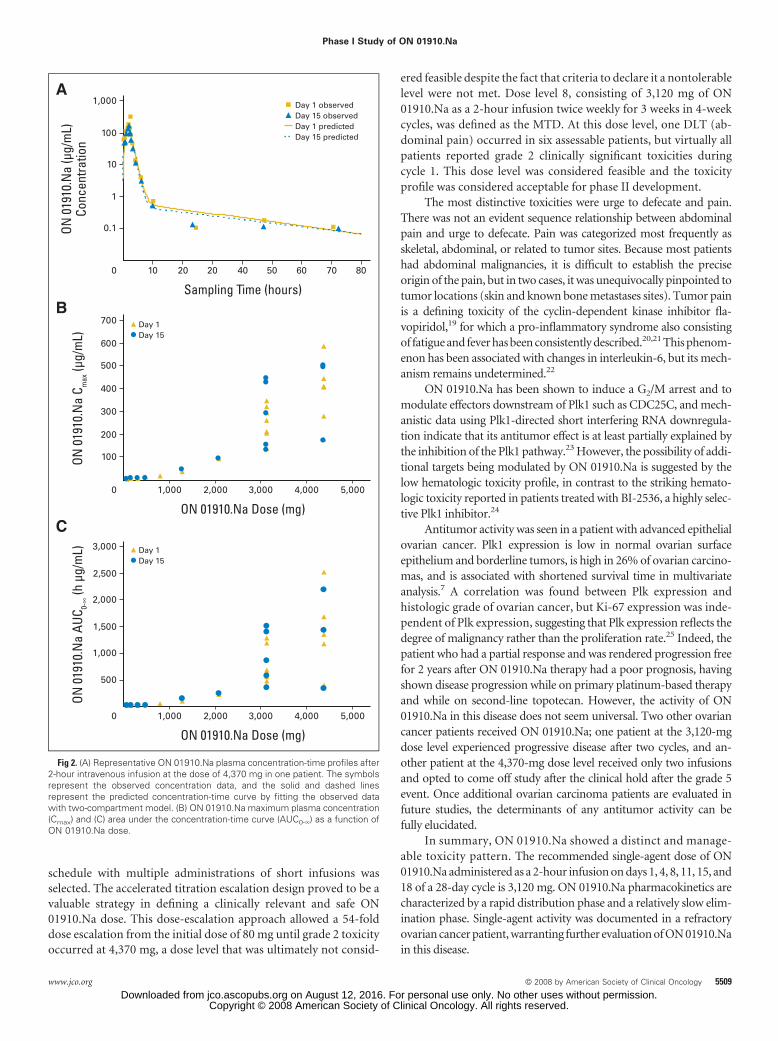
ON 01,910.Na pharmacokinetic profile was characterized by arapid distribution phase, with a distribution half-life of 1.0 � 0.6hours on both days 1 and 15, and a relatively slow eliminationphase, with an elimination half-life of 25.6 � 27.5 hours and 28.1 �16.8 hours on days 1 and 15, respectively (Table 4; Fig 2A). Sys-
temic clearance ranged from 1.6 to 21.4 L/h and 1.9 to 22.8 L/h ondays 1 and 15, respectively, and showed distribution in excess ofblood volume with a steady-state volume of distribution rangingfrom 6.2 to 137.5 L and 6.8 to 195.9 L on days 1 and 15, respectively.There were no significant differences in pharmacokinetic parame-ters between days 1 and 15 (P � .05). Increasing drug exposure wasachieved with increasing ON 01910.Na dose (Fig 2B). In patientstreated at doses of 3,120 mg (n � 6) and 4,370 mg (n � 7), theinterindividual variability in ON 01910.Na clearance assessed asthe coefficient of variation were 34.4% and 82.9%, respectively. Forall 20 patients, the interindividual variability in ON 01910.Naclearance was 77%.
DISCUSSION
ON 01910.Na is a small molecule that disrupts the G2/M cell cycletransition and induces mitotic arrest and apoptosis and has shownsignificant antitumor activity in vivo.14,15 This report summarizesthe investigations of the first-in-man (to our knowledge) clinicaland pharmacologic experience with this agent. Given the absenceof hematologic toxicity in preclinical models and the existing ra-tionale suggesting a benefit with repeated exposure to the drug, a
Table 4. Summary of Pharmacokinetic Parameters� of ON 01910.Na After 2-Hour Intravenous Infusion
Dose (mg) No. of Patients Cmax (�g/mL) AUC0-� (h � �g/mL) CL (L/h) CL (L/h/m2) T1/2,� (h) T1/2,� (h) Vss (L)
Day 180 1 4.2 8.9 9.0 6.3 0.5 2.6 10.8160 1 6.1 20.5 7.8 4.1 0.9 19.2 70.9320 1 6.2 15.0 21.4 11.5 0.2 4.2 48.3480 1 12.1 24.5 19.6 10.1 0.1 1.5 11.5800 1 14.7 42.5 18.8 9.5 0.7 24.0 137.51,280 1 36.4 95.0 13.5 6.5 0.7 18.0 52.22,080 1 91.2 228.9 9.1 4.7 0.7 13.8 29.63,120 7 243.1 755.2 4.8 2.5 1.1 37.3 14.3
CV, % 25.3 42.4 34.4 28.4 52.6 104.4 34.64,370 6 411.0 1,489.1 4.1 2.3 1.5 27.8 13.2
CV, % 37.0 50.8 82.9 71.8 46.6 49.3 77.4All 7.9 4.2 1.0 25.6 27.0
CV, % 77.1 74.4 63.8 107.6 116.1Day 15
80 1 6.4 15.3 5.2 3.7 0.5 4.5 11.3160 1 5.8 20.2 7.9 4.2 0.6 45.0 195.9320 1 6.9 16.9 18.9 10.2 0.6 21.3 132.9480 1 6.2 21.1 22.8 11.7 0.2 20.4 94.8800† — — — — — — — —1,280 1 46.2 147.4 8.7 4.2 1.1 37.6 67.22,080 1 95.2 250.0 8.3 4.3 0.8 18.5 41.03,120 5 326.8 972.6 4.2 2.1 1.3 27.7 11.7
CV, % 51.8 49.0 64.0 40.5 33.8 76.6 50.94,370 3 371.1 1,331.8 6.1 3.2 1.3 35.5 19.9
CV, % 56.9 72.3 102.9 92.9 53.9 47.5 100.6All 7.9 4.1 1.0 28.0 47.2
CV, % 80.8 78.4 53.9 59.9 121.7
Abbreviations: Cmax, maximum plasma concentration; AUC0-�, area under the concentration-time curve from time zero to infinity; CL, clearance; T1/2,�, distributionhalf-life; T1/2,�, elimination half-life; Vss, steady-state volume of distribution; CV, coefficient of variation.
�Pharmacokinetic parameters were estimated by fitting individual ON 01910.Na plasma concentration-time curves with two-compartment model. Values arereported as means, except for CV.
†Pharmacokinetic studies were not performed.
Jimeno et al
5508 © 2008 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.Copyright © 2008 American Society of Clinical Oncology. All rights reserved.
schedule with multiple administrations of short infusions wasselected. The accelerated titration escalation design proved to be avaluable strategy in defining a clinically relevant and safe ON01910.Na dose. This dose-escalation approach allowed a 54-folddose escalation from the initial dose of 80 mg until grade 2 toxicityoccurred at 4,370 mg, a dose level that was ultimately not consid-
ered feasible despite the fact that criteria to declare it a nontolerablelevel were not met. Dose level 8, consisting of 3,120 mg of ON01910.Na as a 2-hour infusion twice weekly for 3 weeks in 4-weekcycles, was defined as the MTD. At this dose level, one DLT (ab-dominal pain) occurred in six assessable patients, but virtually allpatients reported grade 2 clinically significant toxicities duringcycle 1. This dose level was considered feasible and the toxicityprofile was considered acceptable for phase II development.
The most distinctive toxicities were urge to defecate and pain.There was not an evident sequence relationship between abdominalpain and urge to defecate. Pain was categorized most frequently asskeletal, abdominal, or related to tumor sites. Because most patientshad abdominal malignancies, it is difficult to establish the preciseorigin of the pain, but in two cases, it was unequivocally pinpointed totumor locations (skin and known bone metastases sites). Tumor painis a defining toxicity of the cyclin-dependent kinase inhibitor fla-vopiridol,19 for which a pro-inflammatory syndrome also consistingof fatigue and fever has been consistently described.20,21 This phenom-enon has been associated with changes in interleukin-6, but its mech-anism remains undetermined.22
ON 01910.Na has been shown to induce a G2/M arrest and tomodulate effectors downstream of Plk1 such as CDC25C, and mech-anistic data using Plk1-directed short interfering RNA downregula-tion indicate that its antitumor effect is at least partially explained bythe inhibition of the Plk1 pathway.23 However, the possibility of addi-tional targets being modulated by ON 01910.Na is suggested by thelow hematologic toxicity profile, in contrast to the striking hemato-logic toxicity reported in patients treated with BI-2536, a highly selec-tive Plk1 inhibitor.24
Antitumor activity was seen in a patient with advanced epithelialovarian cancer. Plk1 expression is low in normal ovarian surfaceepithelium and borderline tumors, is high in 26% of ovarian carcino-mas, and is associated with shortened survival time in multivariateanalysis.7 A correlation was found between Plk expression andhistologic grade of ovarian cancer, but Ki-67 expression was inde-pendent of Plk expression, suggesting that Plk expression reflects thedegree of malignancy rather than the proliferation rate.25 Indeed, thepatient who had a partial response and was rendered progression freefor 2 years after ON 01910.Na therapy had a poor prognosis, havingshown disease progression while on primary platinum-based therapyand while on second-line topotecan. However, the activity of ON01910.Na in this disease does not seem universal. Two other ovariancancer patients received ON 01910.Na; one patient at the 3,120-mgdose level experienced progressive disease after two cycles, and an-other patient at the 4,370-mg dose level received only two infusionsand opted to come off study after the clinical hold after the grade 5event. Once additional ovarian carcinoma patients are evaluated infuture studies, the determinants of any antitumor activity can befully elucidated.
In summary, ON 01910.Na showed a distinct and manage-able toxicity pattern. The recommended single-agent dose of ON01910.Na administered as a 2-hour infusion on days 1, 4, 8, 11, 15, and18 of a 28-day cycle is 3,120 mg. ON 01910.Na pharmacokinetics arecharacterized by a rapid distribution phase and a relatively slow elim-ination phase. Single-agent activity was documented in a refractoryovarian cancer patient, warranting further evaluation of ON 01910.Nain this disease.
A
0
Day 1 observedDay 15 observedDay 1 predictedDay 15 predicted
ON 0
1910
.Na
(µg/
mL)
Conc
entra
tion
Sampling Time (hours)
1,000
100
10
1
0.1
10 2020 5040 60 8070
B
0
Day 1Day 15
ON 0
1910
.Na
C max
(µg/
mL)
ON 01910.Na Dose (mg)
700
600
500
400
300
200
100
1,000 2,000 3,000 4,000 5,000
C
0
ON 0
1910
.Na
AUC 0-
∞ (h
µg/
mL)
ON 01910.Na Dose (mg)
3,000
2,500
2,000
1,500
1,000
500
1,000 2,000 3,000 4,000 5,000
Day 1Day 15
Fig 2. (A) Representative ON 01910.Na plasma concentration-time profiles after2-hour intravenous infusion at the dose of 4,370 mg in one patient. The symbolsrepresent the observed concentration data, and the solid and dashed linesrepresent the predicted concentration-time curve by fitting the observed datawith two-compartment model. (B) ON 01910.Na maximum plasma concentration(Cmax) and (C) area under the concentration-time curve (AUC0-�) as a function ofON 01910.Na dose.
Phase I Study of ON 01910.Na
www.jco.org © 2008 by American Society of Clinical Oncology 5509Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.
Copyright © 2008 American Society of Clinical Oncology. All rights reserved.

AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Although all authors completed the disclosure declaration, the followingauthor(s) indicated a financial or other interest that is relevant to the subjectmatter under consideration in this article. Certain relationships markedwith a “U” are those for which no compensation was received; thoserelationships marked with a “C” were compensated. For a detaileddescription of the disclosure categories, or for more information aboutASCO’s conflict of interest policy, please refer to the Author DisclosureDeclaration and the Disclosures of Potential Conflicts of Interest section inInformation for Contributors.Employment or Leadership Position: Manoj Maniar, OnconovaTherapeutics Inc (C) Consultant or Advisory Role: None StockOwnership: Manoj Maniar, Onconova Therapeutics Inc Honoraria:None Research Funding: Antonio Jimeno, Onconova Therapeutics Inc;Michelle A. Rudek, Onconova Therapeutics Inc; Sharyn D. Baker,Onconova Therapeutics Inc; Ross C. Donehower, OnconovaTherapeutics Inc Expert Testimony: None Other Remuneration: None
AUTHOR CONTRIBUTIONS
Conception and design: Antonio Jimeno, Jing Li, Sharyn D. Baker,Ross C. DonehowerAdministrative support: Ross C. DonehowerProvision of study materials or patients: Antonio Jimeno, Jing Li, WellsA. Messersmith, Daniel Laheru, Michelle A. Rudek, Manuel Hidalgo,Sharyn D. Baker, Ross C. DonehowerCollection and assembly of data: Antonio Jimeno, Jing Li, Wells A.Messersmith, Daniel Laheru, Michelle A. Rudek, Manuel Hidalgo,Sharyn D. Baker, Ross C. DonehowerData analysis and interpretation: Antonio Jimeno, Jing Li, Wells A.Messersmith, Daniel Laheru, Michelle A. Rudek, Manoj Maniar, ManuelHidalgo, Sharyn D. Baker, Ross C. DonehowerManuscript writing: Antonio Jimeno, Jing Li, Michelle A. Rudek, SharynD. Baker, Ross C. DonehowerFinal approval of manuscript: Antonio Jimeno, Jing Li, Michelle A.Rudek, Sharyn D. Baker, Ross C. Donehower
REFERENCES
1. Nigg EA: Polo-like kinases: Positive regulatorsof cell division from start to finish. Curr Opin Cell Biol10:776-783, 1998
2. Smits VA, Klompmaker R, Arnaud L, et al:Polo-like kinase-1 is a target of the DNA damagecheckpoint. Nat Cell Biol 2:672-676, 2000
3. Jackman M, Lindon C, Nigg EA, et al: Activecyclin B1-Cdk1 first appears on centrosomes inprophase. Nat Cell Biol 5:143-148, 2003
4. Wolf G, Elez R, Doermer A, et al: Prognosticsignificance of polo-like kinase (PLK) expression innon-small cell lung cancer. Oncogene 14:543-549,1997
5. Knecht R, Elez R, Oechler M, et al: Prognosticsignificance of polo-like kinase (PLK) expression insquamous cell carcinomas of the head and neck.Cancer Res 59:2794-2797, 1999
6. Weichert W, Schmidt M, Gekeler V, et al:Polo-like kinase 1 is overexpressed in prostate can-cer and linked to higher tumor grades. Prostate60:240-245, 2004
7. Weichert W, Denkert C, Schmidt M, et al:Polo-like kinase isoform expression is a prognosticfactor in ovarian carcinoma. Br J Cancer 90:815-821,2004
8. Gray PJ Jr, Bearss DJ, Han H, et al: Identifi-cation of human polo-like kinase 1 as a potentialtherapeutic target in pancreatic cancer. Mol CancerTher 3:641-646, 2004
9. Weichert W, Schmidt M, Jacob J, et al: Over-expression of polo-like kinase 1 is a common andearly event in pancreatic cancer. Pancreatology5:259-265, 2005
10. Mundt KE, Golsteyn RM, Lane HA, et al: Onthe regulation and function of human polo-like ki-
nase 1 (PLK1): Effects of overexpression on cellcycle progression. Biochem Biophys Res Commun239:377-385, 1997
11. Spankuch-Schmitt B, Wolf G, Solbach C, et al:Downregulation of human polo-like kinase activityby antisense oligonucleotides induces growth inhi-bition in cancer cells. Oncogene 21:3162-3171,2002
12. Spankuch B, Matthess Y, Knecht R, et al:Cancer inhibition in nude mice after systemic appli-cation of U6 promoter-driven short hairpin RNAsagainst PLK1. J Natl Cancer Inst 96:862-872, 2004
13. Barr FA, Sillje HH, Nigg EA: Polo-like kinasesand the orchestration of cell division. Nat Rev MolCell Biol 5:429-440, 2004
14. Gumireddy K, Reddy MV, Cosenza SC, et al:ON01910, a non-ATP-competitive small moleculeinhibitor of Plk1, is a potent anticancer agent. CancerCell 7:275-286, 2005
15. Jimeno A, Chan A, Kulesza P, et al: Preclinicalevaluation of the novel Plk1 inhibitor ON-01910.Nain pancreatic cancer xenografts: Development ofbiomarkers predicting response. 98th Annual Meet-ing of the American Association for Cancer Re-search, Los Angeles, CA, April 14-18, 2007 (abstr2943)
16. Baker SD, Verweij J, Rowinsky EK, et al: Roleof body surface area in dosing of investigationalanticancer agents in adults, 1991-2001. J Natl Can-cer Inst 94:1883-1888, 2002
17. Therasse P, Arbuck SG, Eisenhauer EA, et al:New guidelines to evaluate the response to treat-ment in solid tumors: European Organization forResearch and Treatment of Cancer, National CancerInstitute of the United States, National Cancer Insti-tute of Canada. J Natl Cancer Inst 92:205-216, 2000
18. Li J, Zhao M, Jimeno A, et al: Validation andimplementation of a liquid chromatography/tan-
dem mass spectrometry assay to quantitate ON01910.Na, a mitotic progression modulator, inhuman plasma. J Chromatogr B Analyt TechnolBiomed Life Sci 856:198-204, 2007
19. Tan AR, Headlee D, Messmann R, et al: PhaseI clinical and pharmacokinetic study of flavopiridoladministered as a daily 1-hour infusion in patientswith advanced neoplasms. J Clin Oncol 20:4074-4082, 2002
20. Burdette-Radoux S, Tozer RG, Lohmann RC,et al: Phase II trial of flavopiridol, a cyclin dependentkinase inhibitor, in untreated metastatic malignantmelanoma. Invest New Drugs 22:315-322, 2004
21. Van Veldhuizen PJ, Faulkner JR, Lara PN Jr, etal: A phase II study of flavopiridol in patients withadvanced renal cell carcinoma: Results of South-west Oncology Group Trial 0109. Cancer ChemotherPharmacol 56:39-45, 2005
22. Messmann RA, Ullmann CD, Lahusen T, et al:Flavopiridol-related proinflammatory syndrome is as-sociated with induction of interleukin-6. Clin CancerRes 9:562-570, 2003
23. Jimeno A, Wheelhouse J, Chan F, et al: Agene expression-based approach to devise combi-nations with gemcitabine in pancreatic cancer iden-tifies polo-like kinase 1 as a rational target. 99thAnnual Meeting of the American Association forCancer Research, San Diego, CA, April 12-16, 2008(abstr 1597)
24. Hofheinz R, Hochhaus A, Al-Batran S, et al: Aphase I repeated dose escalation study of the Polo-like kinase 1 inhibitor BI 2536 in patients withadvanced solid tumors. J Clin Oncol 24:88s, 2006(suppl 18S, abstr 2038)
25. Takai N, Miyazaki T, Fujisawa K, et al: Expres-sion of polo-like kinase in ovarian cancer is associ-ated with histological grade and clinical stage.Cancer Lett 164:41-49, 2001
■ ■ ■
Jimeno et al
5510 © 2008 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on August 12, 2016. For personal use only. No other uses without permission.Copyright © 2008 American Society of Clinical Oncology. All rights reserved.