Performance of valve-in-valve for severe para-prosthetic leaks due to inadequate transcatheter...
8
Performance of Valve-in-Valve for Severe Para-Prosthetic Leaks due to Inadequate Transcatheter Aortic Valve Implantation Massimo Napodano, 1 * MD, Valeria Gasparetto, 1 MD, Giuseppe Tarantini, 1 MD, PHD, Chiara Fraccaro, 1 MD, Ermela Yzeiraj, 1 MD, Gino Gerosa, 2 MD, Giambattista Isabella, 1 MD, and Sabino Iliceto, 1 MD Objectives: This study reports on mid-term safety and performance of valve-in-valve implantation as rescue strategy to overcome acute PPL after TAVI. Background. Mod- erate to severe para-prosthetic leaks (PPL) after transcatheter aortic valve implantation (TAVI) have been described with both self-expandable and balloon-expandable device.- Methods: We analyzed data regarding patients who underwent valve-in-valve implanta- tion, enrolled in the ongoing single-center prospective registry of TAVI, the Padova Uni- versity REVALVing experience Registry. All procedures were performed by a totally per- cutaneous approach, using the self-expanding Medtronic CoreValve (Medtronic, Minneapolis, MN). Results: Out of 87 patients who underwent TAVI, six received valve- in-valve implantation because of persisting severe PPL, due to prosthesis malposition. In all patients, the second device was successfully deployed, with a significant reduc- tion in aortic regurgitation: PPL was no longer appreciable in two of six patients, and it decreased from severe to mild or trivial in four patients. Four patients developed atrio- ventricular block requiring pace-maker implantation. At follow-up (6–24 months) two patients died, whereas no prosthesis-related death occurred. Transprosthesis pressure gradient, effective orifice area, and aortic regurgitation did not change at serial echo- cardiograms throughout the follow-up. Conclusions: Valve-in-valve implantation using self-expandable bioprosthesis seems safe and highly effective to overcome severe PPL due to prosthesis malposition early after TAVI. Moreover, the implantation of two valves does not affect the performance of prosthesis at follow-up. V C 2011 Wiley Periodicals, Inc. Key words: aortic stenosis; bioprosthesis; para-prosthetic leak; trans-catheter aortic valve implantation INTRODUCTION Recently, the feasibility and the safety of transcatheter aortic valve implantation (TAVI) have been reported for the treatment of degenerative aortic valve stenosis. In particular, self-expandable and balloon-expandable devi- ces have been successfully implanted over the last years with different transcatheter techniques, using both retro- grade and antegrade femoral transluminal approach [1–5] or direct transapical puncture of the left ventricle [6,7]. However, despite the high rate of successful implantation, residual para-prosthetic leaks (PPL) of variable degree have been reported in many cases [1–7], primarily because of stent misdeployment in highly calcified stenotic valves, accounting for variables gaps at commissure level between the stent external surface and the inner surface of native valve [8]. In addition, device malpositioning such as ‘‘too high’’ or ‘‘too deep’’ implan- tation may also occur, leading to acute failure of biopros- thesis because of extensive leak between the aortic annu- lus and the prosthetic frames. Recently, Piazza et al. have reported on the feasibility and safety of two self-expand- ing bioprosthetic valve implantation during the same pro- cedure in a small series to treat the acute failure of TAVI 1 Division of Cardiology, Department of Cardiac, Thoracic and Vascular Sciences, University of Padova, Italy 2 Cardiac Surgery, Department of Cardiac, Thoracic and Vas- cular Sciences, University of Padova, Italy Conflict of interest: Nothing to report. *Correspondence to: Massimo Napodano, MD, Division of Cardiol- ogy, Department of Cardiac Thoracic and Vascular Sciences, Univer- sity of Padova, 2 via Giustiniani, 35100 Padova, Italy. E-mail: mas- [email protected] Received 24 January 2011; Revision accepted 28 March 2011 DOI 10.1002/ccd.23181 Published online 5 October 2011 in Wiley Online Library (wileyonlinelibrary.com) V C 2011 Wiley Periodicals, Inc. Catheterization and Cardiovascular Interventions 78:996–1003 (2011)
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Performance of valve-in-valve for severe para-prosthetic leaks due to inadequate transcatheter...
Performance of Valve-in-Valve for SeverePara-Prosthetic Leaks due to InadequateTranscatheter Aortic Valve Implantation
Massimo Napodano,1* MD, Valeria Gasparetto,1 MD, Giuseppe Tarantini,1 MD, PHD,Chiara Fraccaro,1 MD, Ermela Yzeiraj,1 MD, Gino Gerosa,2 MD,
Giambattista Isabella,1 MD, and Sabino Iliceto,1 MD
Objectives: This study reports on mid-term safety and performance of valve-in-valveimplantation as rescue strategy to overcome acute PPL after TAVI. Background. Mod-erate to severe para-prosthetic leaks (PPL) after transcatheter aortic valve implantation(TAVI) have been described with both self-expandable and balloon-expandable device.-Methods: We analyzed data regarding patients who underwent valve-in-valve implanta-tion, enrolled in the ongoing single-center prospective registry of TAVI, the Padova Uni-versity REVALVing experience Registry. All procedures were performed by a totally per-cutaneous approach, using the self-expanding Medtronic CoreValve (Medtronic,Minneapolis, MN). Results: Out of 87 patients who underwent TAVI, six received valve-in-valve implantation because of persisting severe PPL, due to prosthesis malposition.In all patients, the second device was successfully deployed, with a significant reduc-tion in aortic regurgitation: PPL was no longer appreciable in two of six patients, and itdecreased from severe to mild or trivial in four patients. Four patients developed atrio-ventricular block requiring pace-maker implantation. At follow-up (6–24 months) twopatients died, whereas no prosthesis-related death occurred. Transprosthesis pressuregradient, effective orifice area, and aortic regurgitation did not change at serial echo-cardiograms throughout the follow-up. Conclusions: Valve-in-valve implantation usingself-expandable bioprosthesis seems safe and highly effective to overcome severe PPLdue to prosthesis malposition early after TAVI. Moreover, the implantation of two valvesdoes not affect the performance of prosthesis at follow-up. VC 2011 Wiley Periodicals, Inc.
Key words: aortic stenosis; bioprosthesis; para-prosthetic leak; trans-catheter aorticvalve implantation
INTRODUCTION
Recently, the feasibility and the safety of transcatheteraortic valve implantation (TAVI) have been reported forthe treatment of degenerative aortic valve stenosis. Inparticular, self-expandable and balloon-expandable devi-ces have been successfully implanted over the last yearswith different transcatheter techniques, using both retro-grade and antegrade femoral transluminal approach [1–5]or direct transapical puncture of the left ventricle [6,7].However, despite the high rate of successful implantation,residual para-prosthetic leaks (PPL) of variable degreehave been reported in many cases [1–7], primarilybecause of stent misdeployment in highly calcifiedstenotic valves, accounting for variables gaps atcommissure level between the stent external surface andthe inner surface of native valve [8]. In addition, devicemalpositioning such as ‘‘too high’’ or ‘‘too deep’’ implan-tation may also occur, leading to acute failure of biopros-thesis because of extensive leak between the aortic annu-lus and the prosthetic frames. Recently, Piazza et al. have
reported on the feasibility and safety of two self-expand-ing bioprosthetic valve implantation during the same pro-cedure in a small series to treat the acute failure of TAVI
1Division of Cardiology, Department of Cardiac, Thoracic andVascular Sciences, University of Padova, Italy2Cardiac Surgery, Department of Cardiac, Thoracic and Vas-cular Sciences, University of Padova, Italy
Conflict of interest: Nothing to report.
*Correspondence to: Massimo Napodano, MD, Division of Cardiol-
ogy, Department of Cardiac Thoracic and Vascular Sciences, Univer-
sity of Padova, 2 via Giustiniani, 35100 Padova, Italy. E-mail: mas-
Received 24 January 2011; Revision accepted 28 March 2011
DOI 10.1002/ccd.23181
Published online 5 October 2011 in Wiley Online Library
(wileyonlinelibrary.com)
VC 2011 Wiley Periodicals, Inc.
Catheterization and Cardiovascular Interventions 78:996–1003 (2011)

[9], showing a satisfactory procedural outcome. However,the follow-up outcome of this procedure has beendescribed only anecdotally [10], and valve-in-valve per-formance at follow-up is still unknown. This study reportson mid-term safety and performance of valve-in-valve im-plantation as rescue strategy to overcome severe PPL dueto valve malpositioning after TAVI.
MATERIALS AND METHODS
We report procedural data as well as the outcome ofsix patients who underwent valve-in-valve implantationfor acute failure of TAVI using the Medtronic CoreValve(Medtronic, Minneapolis, MN) due to severe PPL, in thecontext of the ongoing single-center prospective registryof TAVI in aortic valve disease, the Padova UniversityREVALVing experience (PUREVALVE) Registry.
Inclusion and exclusion criteria were reported else-where [4]. Briefly, we included (1) severe aortic steno-sis defined as aortic valve area <1.0 cm2 (� 0.6 cm2/m2) with or without severe aortic regurgitation; and (2)age � 75 years with logistic EuroSCORE � 15%, orage � 65 years and one or more characteristics ofinoperability [4]. Patients were deemed high risk forsurgery on the basis of consensus among the cardiovas-cular team, including clinical cardiologists, interven-tional cardiologists, cardiac surgeons, and cardiacanaesthetists. All patients provided written consent tothe procedure. The local Ethic Committee approved thestudy protocol. To evaluate the eligibility to TAVIusing the CoreValve Revalving System, an accuratepatients selection was based on clinical profile, 2-dtransthoracic and transesophageal echocardiography,complete cardiac catheterization, and angiography [4].
Device Description and Procedure
The CoreValve Revalving system and proceduredescription have been reported elsewhere [4]. Briefly,the procedures were performed under general anaesthe-sia or mild sedation with local anaesthesia, accordingto patient’s condition and physician preference, bycompletely percutaneous femoral approach, using the‘‘preclosing’’ vascular device Prostar XL 10Fr (AbbottVascular. Redwood City, CA). Currently, the prosthesisis available in two sizes (26 and 29 mm). A 26-mmdevice was used when the diameter of aortic annuluswas >20 mm � 23 mm, and a 29 mm device wasimplanted when the diameter of aortic annulus was>23 mm � 27 mm. Prosthesis deployment was per-formed as step-by-step procedure under fluoroscopicand angiographic guidance. A careful evaluation ofprosthesis was then performed by aortic angiogram toassess the correct prosthesis position and stent-frame
expansion, as well as to evaluate the presence anddegree of residual PPL. Transprosthetic gradient wasassessed by contemporary pressure tracing in theascending aorta and left ventricle. We did valve-in-valve as rescue strategy in patients with evidence ofsevere (�3þ/4) PPL after first prosthesis implantation,as judged by angiography, and by hemodynamicassessment as elevated left ventricular filling pressure.However, since different mechanisms may lead tosevere PPL, such as inadequate prosthesis position (toohigh implantation, too deep implantation), underex-panded and/or asymmetrical stent frames expansion,and inadequate prosthesis to annulus size, we did dif-ferent back-up strategies according to the leak mecha-nism to reduce it [11]. In particular, in case of under-expanded or asymmetrical stent-frames expansion, asjudged by angiography, we did balloon postdilatation.In case of too high implantation, judged at angiographyas prosthesis ventricular end-frame lying <4 mmbelow the annulus plane, the strategy was to snare thedevice by using the Amplatz GooseNeck (ev3, Plym-outh, MN) in ascending aorta to avoid coronary ostiaobstruction, with a second valve implantation in thecorrect position. In case of too deep implantationjudged at angiography as prosthesis ventricular end-frame lying >12 mm below the annulus plane, anattempt to snare the device in the correct position byusing the Amplatz GooseNeck (ev3, Plymouth, MN)was made, however, when this was unsuccessful orwhen the prosthesis was implanted very deep in leftventricle, valve-in-valve was the strategy. The secondprosthesis was implanted inside the first one to reachthe correct match between prosthesis leaflet plane andaortic annulus plane. After valve-in-valve implantation,further re-dilatation was performed in case of incom-plete expansion of the prosthesis frames, and it wasleft to the judgment of operators. After the procedure,a dual antiplatelet regimen of aspirin 100 mg and clo-pidogrel 75 mg daily for six months, followed by aspi-rin 100 mg daily indefinitely, was prescribed.
Data Collection and Definition
Hemodynamic success was defined as effectiveprosthesis deployment across the native aortic valveannulus with a good performance of the bioprosthesis(i.e., aortic regurgitation �2þ/4; peak-to-peak gradient<20 mm Hg). Procedural success was defined ashemodynamic success without intraprocedural mortality[4,5]. Procedure-related events were defined as occur-ring during or as a direct result of the index procedure,and included death, neurological events (i.e., transientischemic attack and stroke), myocardial infarction, cor-onary flow impairment, cardiac perforation, aortic
Valve-in-Valve Implantation for PPL 997
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

dissection/rupture, access vascular complicationsrequiring percutaneous or surgical intervention and/orblood supply, need for urgent pace-maker, ventricularfibrillation/tachycardia, renal failure. The depth of bio-prosthesis implantation was measured as the distance(in millimeters) of the aortic prosthesis within the LVoutflow tract, from the lower edge of the non coronarycusp to the ventricular end of the prosthesis frame [12]using quantitative angiographic digital techniques(Allura, Philips Medical System, Best, The Nether-lands). Optimal prosthesis position was defined as im-plantation depth of 8–10 mm below the native non cor-onary cusp. Patients were followed up as part of anongoing prospective registry. Transthoracic echocardio-grams were obtained at baseline, 24–48 hr after proce-dure, at 1, 3, 6, and 12 month follow-up and yearlythereafter. Clinical conditions and adverse events,including death, heart failure, myocardial infarction,neurologic event, vascular access complication, andneed for permanent pace-maker, were collected atsame intervals.
RESULTS
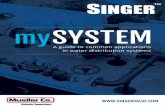
Out of 87 patients enrolled in the PUREVALVEregistry from June 2007 to November 2009, 31(35.6%) showed moderate to severe PPL after prosthe-sis deployment. Overall, of these, 22 showed an under-expanded prosthesis, and a balloon postdilatation wassuccessfully performed with PPL reduction to mild ormoderate degree; one patient had too high prosthesisimplantation, and the device was successfully snared inascending aorta by using the Amplatz GooseNeck(ev3, Plymouth, MN) and a second CoreValve prosthe-sis was implanted in the correct position. Eight patientshad too deep prosthesis deployment. Of these, twounderwent successfully prosthesis snaring with theAmplatz GooseNeck, obtaining an optimal and effec-tive prosthesis position with PPL reduction. Finally,six of 87 (6.9%) patients received a valve-in-valveimmediately after the first prosthesis implantation toovercome severe PPL (Fig. 1). Baseline clinical profileand co-morbidities are reported in Table I. Hemody-namic data are shown in Table II. All patients receivedvalve-in-valve because of too deep implantation of thefirst prosthesis (Table III). In two patients, we did valve-in-valve after unsuccessful prosthesis snaring by using theAmplatz GooseNeck. There was not difference in theoccurrence of inadequate prosthesis positioning (4/43patients vs 5/44patients) neither of valve-in-valve pro-cedure (3/43 patients versus 3/44 patients) between theinitial half and the second half of the experience. Afterthe second prosthesis implantation, in all cases an im-mediate hemodynamic improvement was observed
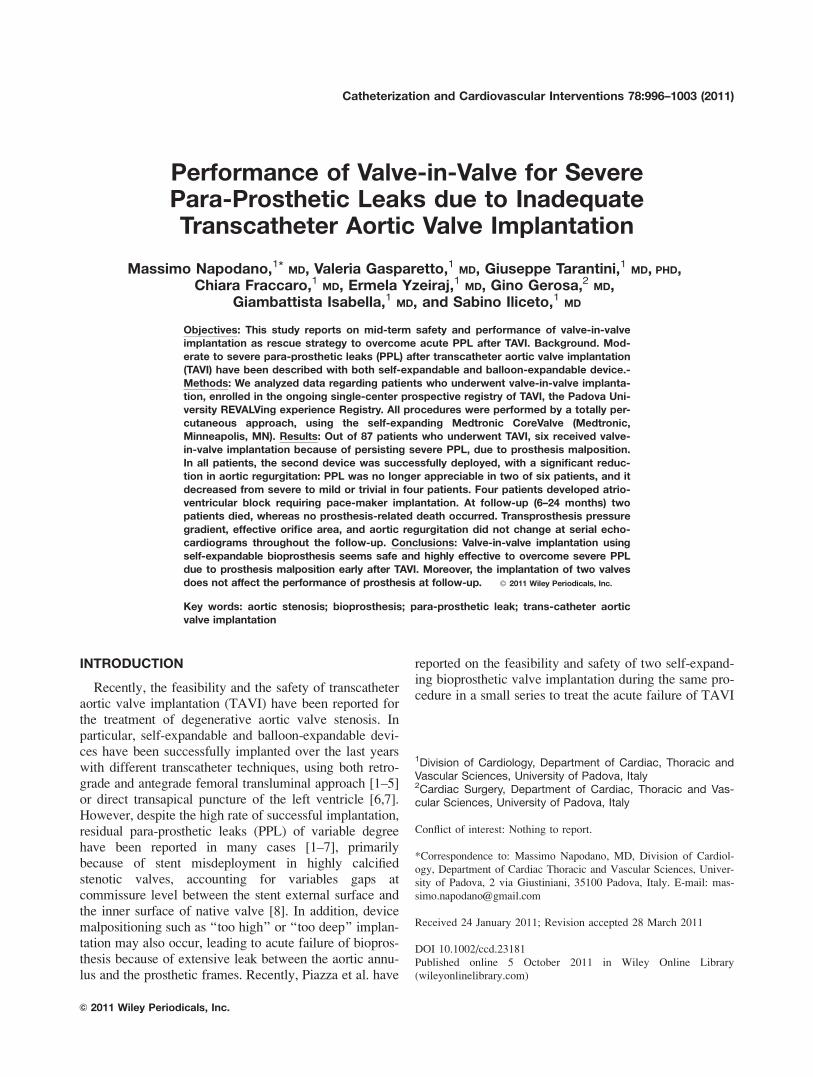
(Fig. 2). In particular, aortic regurgitation was no lon-ger appreciable by aortic angiography in two patients,and it decreased from severe to mild/trivial in theremaining four patients (Fig. 2); peak-to-peak trans-prosthetic gradient was 5 � 2 mm Hg. After therelease of the second prosthesis no case of early or lateprosthesis embolization was observed. Coronary ostiaocclusion or myocardial ischemia did not occur. Aftervalve-in-valve implantation procedural success wasreached in all patients. During the hospitalization, fourpatients developed conduction disorders requiring in-hospital permanent pace-maker implantation, no otherprocedure-related adverse events occurred. All patientswere discharged alive after 9.7 � 1.8 days. No deathnor cardiovascular and cerebrovascular event occurredat 30-day. One patient had heart failure at 2 monthsrelated to chronic anemia/atrial fibrillation and diedbecause of pneumonia complications at day 729; onepatient had gastrointestinal bleeding requiring bloodtransfusions at day 34 and died at day 122 because ofpulmonary surgery complications. One patient withsevere left ventricular dysfunction had heart failure at3-months follow-up, and was in NYHA class II at 1year follow-up. The remaining patients had uneventfulfollow-up, lasting 1 year in one and 2 years in twopatients, and were in NYHA class I. At 2-d transtho-racic echo after the procedure, mean transaortic gradi-ent decreased from 40.6 � 16.3 mm Hg to 10.7 �3.4 mm Hg, while aortic effective orifice areaincreased from 0.85 � 0.14 cm2 to 2.24 � 0.33 cm2,and remained stable throughout the follow-up in allpatients (Fig. 3A and B). At last follow-up (6 monthsfor one patient, 1-year for two patients, 2-years forthree patients), mean transaortic gradient was 9.3 �5.8 mm Hg (Fig. 3A), aortic effective orifice area2.07 � 0.34 cm2 (Fig. 3B), aortic regurgitation wasabsent or mild for all patients (Fig. 3C); left ventricularejection fraction improved in four patients andremained unchanged in two (Fig. 3D). Before the pro-cedure, mitral valve regurgitation was trivial in twopatients, mild in three patients and moderate in onepatient; after valve-in-valve procedure it remained triv-ial in two patients, mild in three patients and moderatein one patient; and did not change at follow-up.
DISCUSSION
We describe early and mid-term outcome of valve-in-valve implantation in a small series of patients toovercome acute failure of TAVI. The main finding ofour report is that valve-in-valve implantation was feasi-ble in all attempted cases without major proceduralcomplications or adverse events related to double pros-thesis implantation. In particular, the deployment of a
998 Napodano et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

second device inside an already expanded valve wasreliable, since the first implanted prosthesis provided alandmark favoring the correct deployment of a seconddevice, and ensured its firm anchoring, avoiding therisk of early or late embolization or coronary occlu-sion. Furthermore, the deployment of valve-in-valvewas wide and symmetrical enough to guarantee a nor-mal leaflet excursion with an adequate effective orificearea. Indeed, mitral valve function seemed not affectedby deep position of the first prosthesis neither by dou-ble prostheses implantation. However, the incidence ofatrioventricular heart block and permanent pacemakerimplantation in our patients was higher than thosepreviously reported in TAVI [12,13]. We guess thismight be related to deep positioning of the first pros-thesis found in almost all reported cases [12,14], ratherthan to the deployment of two devices. In fact, a
deeper implantation of self-expandable prosthesisimplies a larger stent-frame surface forcing against theinterventricular septum, and may increase the risk ofinjury of the underlying conduction tissue [14]. Never-theless, valve-in-valve was highly effective in reducingsevere PPL acutely occurred as consequence of inad-equate positioning of transcatheter valve: aortic regur-gitation was no longer appreciable or only mild aftervalve-in-valve in all treated patients. Different mecha-nisms of PPL have been described, including mainlyincomplete stent-frame expansion [8,15] and prosthesisundersizing [16]. However, PPL may also occurbecause of bioprosthesis deployment in a suboptimalposition across the aortic annulus, particularly too-deepor too-high prosthesis deployment [17]. In fact, duringthe releasing process, the device ‘‘unloading’’ turnsinto forces directed forward that may lead to deep
Fig. 1. Valve-in-valve procedure—Panel A: severe aortic regurgitation early after CoreValveimplantation; Panel B: deployment of a second CoreValve inside and slightly upper the firstimplanted valve; Panel C: fluoroscopy of valve-in-valve implanted, showing the full expandedframe of second prosthesis; Panel D: aortic angiography after valve-in-valve implantationshowing a trivial aortic regurgitation.
Valve-in-Valve Implantation for PPL 999
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

implantation. Indeed, the coaxial alignment of the pros-thesis in the left ventricular outflow tract as well as thestable position of the device during the step-by-stepdeployment in some patients is difficult to obtain, espe-cially in very unravelled aortas and in case of angu-lated aortic arch [17] and very tortuous iliac and femo-ral arteries. In such situations a careful realignment ofprosthesis during the deployment may be useful. Other-wise transubclavian approach may be preferable in thissetting, since the manipulation of the device and thepositioning of the valve seem more direct and reliable,
probably because of the shorter distance from the sub-clavian access to the aortic annulus and the straighterorientation requiring weaker forces of tension and tor-sion, which bind the delivery catheter [18]. Recently,Ruiz et al. [10] and Ussia et al. [19] respectivelydescribed two cases of valve misplacement successfullytreated by valve-in-valve implantation using the self-expandable CoreValve System. Moreover, Piazza et al.have reported in a small series on the effectiveness andsafety of two self-expanding bioprosthetic valve im-plantation during the same procedure to treat the acute
TABLE I. Clinical Characteristics
Variable Pt # 1 Pt # 2 Pt # 3 Pt # 4 Pt # 5 Pt # 6
Age (years) 86 76 74 84 72 76
Gender Female Male Male Male Male Female
Logistic EuroSCORE 25.65% 11.89% 24.90% 30.62% 5.90% 17.40%
NYHA class IV IV II III III IV
Coronary artery disease No No Yes Yes Yes Yes
Cerebrovascular disease No No No Yes Yes No
Previous myocardial infarction Yes No Yes No Yes Yes
Previous cardiac surgery No No Yes Yes No No
Severe obstructive pulmonary disease No Yes No Yes No No
Creatinine clearance (ml/min/1.73 m2) 32.1 46.1 42.4 46.2 72.2 50
Peripheral disease Yes No Yes No No No
Neurological dysfunction No No No No No No
Liver cirrhosis No No No No Yes No
Porcelain aorta No No No No No No
TABLE II. Baseline Hemodynamic Findings
Variable Pt # 1 Pt # 2 Pt # 3 Pt # 4 Pt # 5 Pt # 6
AVA (cm2/m2) 0.39 0.55 0.34 0.55 0.56 0.44
Peak-to-peak gradient (mm Hg) 50 30 80 85 30 20
LVEF (%) 57 34 44 58 72 26
AR (þ/4) 2 3 0 1 0 2
SPAP (mm Hg) 32 50 30 60 40 45
CI (L/min/m2) 2.8 2.4 2.8 2.1 3.1 2.1
AVA ¼ aortic valve area; AR ¼ aortic regurgitation; CI ¼ cardiac index; LVEF ¼ left ventricular ejection fraction; SPAP ¼ systolic pulmonary
artery pressure.
TABLE III. Procedural Data
Variable Pt # 1 Pt # 2 Pt # 3 Pt # 4 Pt # 5 Pt # 6
Aortic annulusa, mm 22.0 24.0 24.2 23.5 23.6 25.9
Sedation/anaesthesia GA GA S S None S
Oro-tracheal intubation Yes Yes No No No Yes
Transesophageal echo Yes Yes No No No No
BAV Yes No Yes Yes Yes No
1st CoreValve size (mm) 26 26 29 29 29 29
Implantation depth (mm) 14.4 14.9 14.8 12.7 22.3 15.7
Re-dilatation (1st prosthesis) No Yes Yes No No No
2nd CoreValve size (mm) 26 26 29 29 29 29
Re-dilatation (2nd prosthesis) No Yes No Yes Yes No
Procedural time (min) 76 76 97 80 130 152
Contrast amount (ml) 314 313 200 262 300 156
Procedural success Yes Yes Yes Yes Yes Yes
aAssesed by transthoracic or transesophageal echocardiogram.BAV ¼ balloon aortic valvuloplasty; GA ¼ general anaesthesia; S ¼ sedation.
1000 Napodano et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

failure of TAVI, due to valve malpositioning or valveundersizing [9]. Device repositioning by snaring hasbeen reported by Latib et al. in one case, and by Ussiaet al. in four patients respectively, as a feasible andeffective solution to PPL due to deep prosthesis im-plantation [20,11]. However, as suggested by theseauthors, this high-risk technique should be performedcautiously, because it might result in prosthesis emboli-zation in the ascending aorta, and only if the operatoris concerned about the risk of valve embolization,implanting another valve inside the first with valve-in-valve technique could be considered [20]. In our expe-rience valve snaring was useful in case of low but notvery deep implantation. In fact when the valve is verydeeply deployed in the left ventricle, it could be oflimited impact, since the snaring does not result in aneffective repositioning.
Our report confirms the feasibility of valve-in-valveimplantation to overcome acute TAVI failure usingself-expandable device, due to inadequate valve
Fig. 2. Evolution of para-prosthetic leaks (PPL)—angio-graphic assessment of aortic regurgitation due to PPL afterfirst prosthesis implantation (on the left); after prosthesis re-dilatation when performed, and after the second prosthesisimplantation (on the right). Dash lines indicate patients whodid not received first prosthesis re-dilatation. [Color figurecan be viewed in the online issue, which is available atwileyonlinelibrary.com.]
Fig. 3. Prosthesis performance of valve-in-valve at follow-up echocardiographic assessmentbefore transcatheter aortic valve implantation and at serial follow-up evaluation. Panel A:Mean transvalvular gradient; Panel B: Aortic effective orifice area; Panel C: Aortic regurgita-tion; Panel D: Left ventricular ejection fraction. [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
Valve-in-Valve Implantation for PPL 1001
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

positioning. In fact, valve misplacement across the aor-tic annulus (particularly too deep implantation), maylead to large PPL between the not-skirted part of theprosthesis stent frame and the native valve annulus [9].In this situation, the deployment of a second prosthesis,which overlaps the first one in a slightly upper ordeeper position, correctly matching the annulus plane,may ensure effective PPL sealing, without compromis-ing leaflet function. Valve-in-valve implantation mayrepresent an effective bail-out strategy to overcomeacute TAVI failure due to valve misplacement, althougha significantly fall in TAVI failure could be expectedwith increasing operator experience, improvement inreleasing system, and more appropriate patients selec-tion. Furthermore, the rate of TAVI success could beimproved in the future through development of newtranscatheter heart valves, such as retrievable and reposi-tionable devices, and new imaging technologies capableto better locate aortic valve landmark.
The other relevant finding of our report is thatvalve-in-valve deployment seems not to compromisethe performance of bioprosthesis leaflets over time. Infact, serial echocardiographic data showed the persist-ence of low transprosthetic gradient and large effectivearea, without leaflet incompetence at up to 2-year fol-low-up. This result, along with the safety of the proce-dure, could suggest the reliability of redo-TAVI, usingself-expandable prosthesis to treat late transcatheterprosthesis failure. In fact, since life expectancy isgrowing and therefore the prevalence of aortic stenosisin octogenarians and sicker patients is expected toincrease, the use of transcatheter bioprosthesis is likelyto expand and a larger number of devices will beimplanted in the future [21]. In this scenario, the dem-onstration of safety and effectiveness of valve-in-valvetechnique represents a useful acquisition to guidefuture intervention in late percutaneous bioprosthesisdysfunction. However, larger studies assessing long-term follow-up, are necessary to further evaluate theclinical impact of this procedure.
REFERENCES
1. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Nerco-
lini D, Tapiero S, Litzler PY, Bessou JP, Babaliaros V. Treat-
ment of calcific aortic stenosis with the percutaneous heart
valve: Mid-term follow-up from the initial feasibility studies:
The French experience. J Am Coll Cardiol 2006;47:1214–1223.
2. Webb JG, Pasupati S, Humphries K, Thompson C, Altwegg L,
Moss R, Sinhal A, Carere RG, Munt B, Ricci D, Ye J, Cheung
A, Lichtenstein SV. Percutaneous transarterial aortic valve
replacement in selected high-risk patients with aortic stenosis.
Circulation 2007;116:755–763.
3. Grube E, Schuler G, Bullesfeld L, Gerckens U, Linke A, Wena-
weser P, Sauren B, Mohr FW, Walther T, Zickmann B, Iversen
S, Felderhoff T, Cartier R, Bonan R. Percutaneous aortic valve
replacement for severe aortic stenosis in high-risk patients using
the second and current third generation self-expanding Core-
Valve prosthesis. Device success and 30-day clinical outcome.
J Am Coll Cardiol 2007;50:69–76.
4. Piazza N, Grube E, Gerkens U, den Heijer P, Linke A, Luha O,
Ramondo A, Ussia G, Wenaweser P, Windecker S, Laborde JC,
de Jaegere P, Serruys PW. Procedural and 30-day outcome fol-
lowing transcatheter aortic valve implantation using the third
generation (18Fr) CoreValve Revalving System: Results from
the multicentre, expanded evaluation registry 1-year following
CE mark approval. Eurointervention 2008;4:242–249.
5. Webb JG, Altwegg L, Boone RH, Cheung A, Ye J, Lichtenstein
SV, Lee M, Masson JB, Thompson C, Moss R, Carere R, Munt
B, Nietlispach F, Humphries K. Transcatheter Aortic Valve
Implantation. Impact on clinical and valve-related outcomes.
Circulation 2009;119:3009–3016.
6. Lichtenstein SV, Cheung A, Ye J, Thompson CR, Carere RG,
Pasupati S, Webb JG. Transapical transcatheter aortic valve im-
plantation in humans: Initial clinical experience. Circulation
2006;114:591–596.
7. Walther T, Falk V, Kempfert J, Borger MA, Fassl J, Chu
MWA, Schuler G, Mohr F. Transapical minimally invasive
aortic valve implantation—The initial 50 patients. Eur J Cardio-
thoracic Surg 2008;33:983–988.
8. Zegdi R, Ciobotaru V, Noghin M, Sleilaty G, Lafont A, Latre-
mouille C, Deloche A, Fabiani JN. Is it reasonable to treat all
calcified stenotic valves with a valved stent? Results from a
human anatomic study in adults. J Am Coll Cardiol 2008;51:
579–584.
9. Piazza N, Schultz C, de Jagere PT, Serruys P. Implantation of
two self-expanding aortic bioprosthetic valves during the same
procedure. Insights into valve-in-valve implantation (‘‘Russian
Doll concept’’). Catheter Cardiovasc Interv 2009;73:530–539.
10. Ruiz CA, Laborde JC, Condado JF, Chiam PTL, Condado JA.
First percutaneous transcatheter aortic valve-in-valve implanta-
tion with three year follow-up. Catheter Cardiovasc Interv
2008;72:143–148.
11. Ussia GP, Barbanti M, Imme S, Scartabelli M, Mule M, Cam-
malleri V, Aruta P, Pistritto AM, Capodanno D, Deste W,
Di Pasqua MC, Tamburino C. Management of implant failure
during transcatheter aortic valve implantation. Catheter Cardio-
vasc Interv 2010;76:440–449.
12. Piazza N, Onuma Y, Jesserun E, Kint PP, Maugenest AM,Anderson RH, de Jagere PP, Serruys PW. Early and persistentintraventricular conduction abnormalities and requirements forpacemaking after percutaneous replacement of the aortic valve.J Am Coll Cardiol Interv 2008;1:310–316.
13. Jilaihawi H, Chin D, Vasa-Nicotera M, Jeilan M, Spyt T, AndreG, Bence J, Logtens E, Kovac J. Predictors for permanent pace-maker requirement after transcatheter aortic valve implantationwith the CoreValve bioprosthesis. Am Heart J 2009;157:860–866.
14. Fraccaro C, Buja G, Tarantini G, Gasparetto V, Leoni L, Raz-zolini R, Corrado D, Bonato R, Basso C, Tiene G, Gerosa G,Isabella G, Iliceto S, Napodano M. Conduction abnormalitiesafter transcatheter aortic valve implantation for calcific aorticvalve disease. Am J Cardiol 2011;107:747–754.
15. Masson JB, Kovac J, Schuler G, Ye J, Cheung A, Kapadia S,Tuzcu ME, Kodali S, Leon MB, Webb JG. Transcatheter aorticvalve implantation. Review of the nature, management, andavoidance of procedural complication. J Am Coll Cardiol Interv2009;2:811–820.
16. Detaint D, Lepage L, Himbert D, Brochet E, Messika-Zeitoun
D, Iung B, Vahanian A. Determinants of significant paravalvu-
lar regurgitation after transcatheter aortic valve implantation.
J Am Coll Cardiol Interv 2009;2:821–827.
1002 Napodano et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

17. Sherif MA, Abdel-Wahab M, Stocker B, Geist V, Richardt D,
Tolg R, Richardt G. Anatomic and procedural predictors of par-
avalvular aortic regurgitation after implantation of the Med-
tronic CoreValve bioprosthesis. J Am Coll Cardiol 2010;56:
1623–1629.
18. Ussia GP, Mule M, Tamburino C. The valve-in-valve technique:
Transcatheter treatment of aortic bioprosthesis malposition.
Catheter Cardiovasc Interv 2009;73:713–716.
19. Fraccaro C, Napodano M, Tarantini G, Gasparetto V, Gerosa G,
Bianco R, Bonato R, Pittarello D, Isabella G, Iliceto S,
Ramondo A. Expanding the eligibility for transcatheter aortic
valve implantation the trans-subclavian retrograde approach
using the III generation corevalve revalving system. J Am Coll
Cardiol Interv 2009;2:828–833.
20. Latib A, Michev I, Laborde JC, Montorfano M, Colombo A.
Post-implantation repositioning of the CoreValve percutaneous
aortic valve. J Am Coll Cardiol Interv 2010;3:119–121.
21. Webb JG. Percutaneous aortic valve replacement will become a
common treatment for aortic valve disease. J Am Coll Cardiol
Interv 2008;1:122–126.
Valve-in-Valve Implantation for PPL 1003
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).