Performance of Bleeding Risk-prediction Scores in Patients with Atrial Fibrillation Undergoing...
7
Performance of Bleeding Risk-Prediction Scores in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Tuomas Kiviniemi, MD, PhD a, *, Marja Puurunen, MD, PhD b , Axel Schlitt, MD, PhD c , Andrea Rubboli, MD d , Pasi Karjalainen, MD, PhD e , Saila Vikman, MD, PhD f , Matti Niemelä, MD, PhD g , Heli Lahtela, MD a , Gregory Y.H. Lip, MD h , and K.E. Juhani Airaksinen, MD, PhD a The hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly, and drugs/alcohol (HAS-BLED); anti- coagulation and risk factors in atrial fibrillation (ATRIA); modified Outpatient Bleeding Risk Index (mOBRI); and reduction of atherothrombosis for continued health (REACH) schemes are validated bleeding risk-prediction tools, but their predictive performance in patients with AF receiving multiple antithrombotic drugs after percutaneous coronary intervention (PCI) is unknown. We sought to compare the predictive performance of bleeding risk-estimation tools in a cohort of patients with atrial fibrillation (AF) undergoing PCI. Management of patients with AF undergoing coronary artery stenting is a multicenter European prospective registry enrolling patients with AF undergoing PCI. We calculated HAS-BLED, ATRIA, mOBRI, and REACH bleeding risk-prediction scores and assessed the rate of bleeding complications as defined by Bleeding Academic Research Consortium at 12 months follow-up in 929 consecutive patients undergoing PCI. Increasing age, femoral access site, and previous peptic ulcer were independent determinants of bleeding. Low bleeding risk scores as determined by HAS-BLED 0 to 2, ATRIA 0 to 3, mOBRI 0, and REACH 0 to 10 were detected in 23.7%, 73.0%, 7.8%, and 5.7% of patients of the cohort, respectively. No significant differences were detected in the rates of any bleeding or major bleeding events for low versus intermediate/high scores with each risk-prediction tool. In conclusion, the performance of ATRIA, HAS-BLED, mOBRI, and REACH scores in predicting bleeding complications in this high-risk patient subset was useless. Ó 2014 Elsevier Inc. All rights reserved. (Am J Cardiol 2014;-:-e-) Patients with atrial fibrillation (AF) undergoing percuta- neous coronary intervention (PCI) are at high risk for bleeding complications and death due to the use of multiple antithrombotic drugs. 1e3 The hypertension, abnormal renal/ liver function, stroke, bleeding history or predisposition, labile international normalized ratio (INR), elderly, drugs/ alcohol (HAS-BLED) 4 ; anticoagulation and risk factors in atrial fibrillation (ATRIA) 5 ; modified Outpatient Bleeding Risk Index (mOBRI) 6,7 ; and reduction of atherothrombosis for continued health (REACH) 8 schemes are validated bleeding risk-prediction tools, but their predictive perfor- mance in this frail patient subset remains unknown. We sought to compare the predictive performance of bleeding risk-estimation tools for bleeding events and mortality in a cohort of patients with AF undergoing PCI. Methods Management of patients with AF undergoing coronary artery stenting is an observational, multicenter, prospective registry including patients with AF who are referred for PCI (Clinicaltrials.gov identifier NCT00596570). 2,9 Inclusion criteria were elective or acute PCI and (1) history of AF (paroxysmal, persistent, or permanent) or (2) ongoing AF during the index hospital stay. Because of the observational design, the only exclusion criterion was unwillingness/ inability to participate in the study or to give written informed consent. At each of the 17 centers, patients were treated according to local policies and were followed up for 12 months (phone call or outpatient clinic visit at 3, 6, and 12 months). The accuracy of the events and medications were checked using hospital and outpatient clinic records and mortality registries where appropriate. Patients were included from October 2008 to August 2010. Ethic a Heart Center, Turku University Hospital and University of Turku, Turku, Finland; b Hemostasis laboratory, Finnish Red Cross Blood Service, Helsinki, Finland; c Medical Faculty, Martin Luther University Halle-Wit- tenberg and Paracelsus-Harz-Clinic Bad Suderode, Halle-Wittenberg, Germany; d Division of Cardiology, Laboratory of Interventional Cardiol- ogy, Ospedale Maggiore, Bologna, Italy; e Heart Center, Satakunta Central Hospital, Pori, Finland; f Heart Center, Tampere University Hospital, Tampere, Finland; g Department of Medicine, Oulu University Hospital, Oulu, Finland; and h University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham, United Kingdom. Manuscript received January 12, 2014; revised manuscript received and accepted March 20, 2014. Dr. Tuomas Kiviniemi and Dr. Marja Puurunen are equally contributed authors. This study was supported by unrestricted grants from Novartis- Germany and Sanofi-Aventis-Germany and by grants from the Finnish Foundation for Cardiovascular Research, Helsinki, Finland, and the scholarship from the Finnish Cardiac Society, Finland (T.K.). See page 6 for disclosure information. *Corresponding author: Tel: (þ35) 8 2 313 1005; fax: (þ35) 8 2 313 2030. E-mail address: tuoski@utu.fi (T. Kiviniemi). 0002-9149/14/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. www.ajconline.org http://dx.doi.org/10.1016/j.amjcard.2014.03.038
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Performance of Bleeding Risk-prediction Scores in Patients with Atrial Fibrillation Undergoing...

Performance of Bleeding Risk-Prediction Scores in Patients WithAtrial Fibrillation Undergoing Percutaneous Coronary Intervention
Tuomas Kiviniemi, MD, PhDa,*, Marja Puurunen, MD, PhDb, Axel Schlitt, MD, PhDc,Andrea Rubboli, MDd, Pasi Karjalainen, MD, PhDe, Saila Vikman, MD, PhDf, Matti Niemelä, MD, PhDg,
Heli Lahtela, MDa, Gregory Y.H. Lip, MDh, and K.E. Juhani Airaksinen, MD, PhDa
The hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition,
aHeart Center,Turku, Finland; bHHelsinki, Finland;tenberg and ParGermany; dDivisioogy, Ospedale MaHospital, Pori, FTampere, FinlandOulu, Finland; anSciences, City Hreceived JanuaryMarch 20, 2014.
Dr. Tuomas Kauthors.
This study wGermany and SanFoundation for Cscholarship from t
See page 6 for*Correspondin
2 313 2030.E-mail addres
0002-9149/14/$ -http://dx.doi.org/1
labile international normalized ratio, elderly, and drugs/alcohol (HAS-BLED); anti-coagulation and risk factors in atrial fibrillation (ATRIA); modified Outpatient BleedingRisk Index (mOBRI); and reduction of atherothrombosis for continued health (REACH)schemes are validated bleeding risk-prediction tools, but their predictive performance inpatients with AF receiving multiple antithrombotic drugs after percutaneous coronaryintervention (PCI) is unknown. We sought to compare the predictive performance ofbleeding risk-estimation tools in a cohort of patients with atrial fibrillation (AF) undergoingPCI. Management of patients with AF undergoing coronary artery stenting is a multicenterEuropean prospective registry enrolling patients with AF undergoing PCI. We calculatedHAS-BLED, ATRIA, mOBRI, and REACH bleeding risk-prediction scores and assessedthe rate of bleeding complications as defined by Bleeding Academic Research Consortiumat 12 months follow-up in 929 consecutive patients undergoing PCI. Increasing age, femoralaccess site, and previous peptic ulcer were independent determinants of bleeding. Lowbleeding risk scores as determined by HAS-BLED 0 to 2, ATRIA 0 to 3, mOBRI 0, andREACH 0 to 10 were detected in 23.7%, 73.0%, 7.8%, and 5.7% of patients of the cohort,respectively. No significant differences were detected in the rates of any bleeding or majorbleeding events for low versus intermediate/high scores with each risk-prediction tool. Inconclusion, the performance of ATRIA, HAS-BLED, mOBRI, and REACH scores inpredicting bleeding complications in this high-risk patient subset was useless. � 2014Elsevier Inc. All rights reserved. (Am J Cardiol 2014;-:-e-)
Patients with atrial fibrillation (AF) undergoing percuta-neous coronary intervention (PCI) are at high risk forbleeding complications and death due to the use of multipleantithrombotic drugs.1e3 The hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition,labile international normalized ratio (INR), elderly, drugs/
Turku University Hospital and University of Turku,emostasis laboratory, Finnish Red Cross Blood Service,cMedical Faculty, Martin Luther University Halle-Wit-acelsus-Harz-Clinic Bad Suderode, Halle-Wittenberg,n of Cardiology, Laboratory of Interventional Cardiol-ggiore, Bologna, Italy; eHeart Center, Satakunta Centralinland; fHeart Center, Tampere University Hospital,; gDepartment of Medicine, Oulu University Hospital,d hUniversity of Birmingham Centre for Cardiovascularospital, Birmingham, United Kingdom. Manuscript12, 2014; revised manuscript received and accepted
iviniemi and Dr. Marja Puurunen are equally contributed
as supported by unrestricted grants from Novartis-ofi-Aventis-Germany and by grants from the Finnishardiovascular Research, Helsinki, Finland, and thehe Finnish Cardiac Society, Finland (T.K.).disclosure information.g author: Tel: (þ35) 8 2 313 1005; fax: (þ35) 8
s: [email protected] (T. Kiviniemi).
see front matter � 2014 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2014.03.038
alcohol (HAS-BLED)4; anticoagulation and risk factors inatrial fibrillation (ATRIA)5; modified Outpatient BleedingRisk Index (mOBRI)6,7; and reduction of atherothrombosisfor continued health (REACH)8 schemes are validatedbleeding risk-prediction tools, but their predictive perfor-mance in this frail patient subset remains unknown. Wesought to compare the predictive performance of bleedingrisk-estimation tools for bleeding events and mortality in acohort of patients with AF undergoing PCI.
Methods
Management of patients with AF undergoing coronaryartery stenting is an observational, multicenter, prospectiveregistry including patients with AF who are referred for PCI(Clinicaltrials.gov identifier NCT00596570).2,9 Inclusioncriteria were elective or acute PCI and (1) history of AF(paroxysmal, persistent, or permanent) or (2) ongoing AFduring the index hospital stay. Because of the observationaldesign, the only exclusion criterion was unwillingness/inability to participate in the study or to give writteninformed consent. At each of the 17 centers, patients weretreated according to local policies and were followed up for12 months (phone call or outpatient clinic visit at 3, 6, and12 months). The accuracy of the events and medicationswere checked using hospital and outpatient clinic recordsand mortality registries where appropriate. Patients wereincluded from October 2008 to August 2010. Ethic
www.ajconline.org

Table 1Baseline characteristics of patients with atrial fibrillation undergoing percutaneous coronary intervention according to bleeding status at 1 year
Variable Whole Cohort Bleeding p Value
(n ¼ 929) Yes (n ¼ 168) No (n ¼ 761)
Median age (years) 74.0 [11.0] 75.0 [9.0] 74.0 [11.0] 0.04Women 276 (29.7%) 61 (36.3%) 215 (28.3%) 0.04Body mass index (kg/m2) 27.8 [6.0] 27.8 [5.9] 26.9 [5.4] 0.07Periprocedural INR 1.9 [1.0] 1.9 [1.0] 1.9 [1.0] 0.82Treatment for hypertension 780 (84%) 136 (81.0%) 644 (84.6%) 0.25Treatment for hypercholesterolemia 618 (66.5%) 110 (65.5%) 508 (66.8%) 0.79Diabetes mellitus 337 (36.3%) 59 (35.1%) 278 (36.5%) 0.79Current smoker 93 (10.0%) 16 (9.5%) 77 (10.1%) 0.88Previous TIA/stroke 153 (16.5%) 26 (15.5%) 127 (16.7%) 0.82Previous myocardial infarction 237 (25.5%) 45 (26.8%) 192 (25.2%) 0.70Previous percutaneous coronary intervention 160 (17.2%) 31 (18.5%) 129 (17.0%) 0.65Previous coronary bypass 135 (14.5%) 23 (13.7%) 112 (14.7%) 0.81Previous hemorrhage 38 (4.1%) 9 (5.4%) 29 (3.8%) 0.39Previous peptic ulcer 44 (4.7%) 13 (7.7%) 31 (4.1%) 0.07Heart failure 186 (20.0%) 41 (24.4%) 145 (19.1%) 0.14Mechanical mitral valve 8 (0.9%) 3 (1.8%) 5 (0.7%) 0.16Mechanical aortic valve 14 (1.4%) 4 (2.4%) 10 (1.3%) 0.30Previous venous thromboembolism 30 (3.2%) 9 (5.4%) 21 (2.8%) 0.09Left ventricular ejection fraction (%) 50.0 [20.0] 50.0 [20.0] 50.0 [20.0] 0.89Pattern of AFPermanent 460 (49.5%) 87 (51.8%) 373 (49.0%) 0.55Persistent 108 (11.6%) 22 (13.1%) 86 (11.3%) 0.51Paroxysmal 354 (38.1%) 57 (38.1%) 297 (39.0%) 0.25
Indication for PCIAcute STEMI 126 (13.6%) 33 (19.6%) 93 (12.2%) 0.02NSTEMI 237 (25.5%) 45 (26.8%) 192 (25.2%) 0.70Unstable angina pectoris 166 (17.9%) 35 (20.8%) 131 (17.2%) 0.27Stable angina pectoris 399 (42.9%) 55 (32.7%) 344 (45.2%) 0.003
Drug-eluting stents 227 (25.0%) 35 (21.2%) 192 (25.8%) 0.23Femoral sheath 663 (71.4%) 137 (81.5%) 526 (69.1%) 0.001Medication at dischargeTriple 679 (73.1%) 119 (70.8%) 560 (73.6%) 0.50Dual antiplatelet 162 (17.4%) 33 (19.6%) 129 (17.0%) 0.43VKA and clopidogrel 73 (7.9%) 12 (7.1%) 61 (8.0%) 0.87VKA and aspirin 15 (1.6%) 4 (2.4%) 11 (1.4%) 0.33Statin 795 (85.6%) 143 (85.1%) 652 (85.7%) 0.85NSAID 10 (1.1%) 4 (2.4%) 6 (0.8%) 0.16Proton pump inhibitor 335 (36.1%) 68 (40.5%) 267 (35.1%) 0.32
Data are presented as mean � SD, median [IQR] and count (%).IQR ¼ interquartile range; NSAID ¼ nonsteroidal anti-inflammatory drugs; NSTEMI ¼ noneST-elevation myocardial infarction; STEMI ¼ ST-elevation
myocardial infarction; TIA ¼ transient ischemic attack; VKA ¼ vitamin K-antagonist.
2 The American Journal of Cardiology (www.ajconline.org)
committees of participating centers approved the studyprotocol, and written informed consent was obtained fromevery patient. The study complied with the Declaration ofHelsinki. Coronary angiography and PCI were performedusing either radial or femoral approach for arterial access,and hemostasis was obtained according to the local practice.Lesions were treated according to the contemporary inter-ventional techniques. Low-molecular weight heparin(LMWH), unfractionated heparin, bivalirudin, and glyco-protein IIb/IIIa inhibitors were administered at the opera-tor’s discretion. Moreover, the choice of the combination ofantithrombotic treatment after the procedure was at thetreating physician’s discretion.
HAS-BLED, ATRIA, mOBRI, and REACH bleedingrisk scores were calculated for each patient based on thedefinitions used in their validation cohorts.4e6,8 In HAS-
BLED score, each risk factor (hypertension, abnormalrenal/liver function, stroke, bleeding history or predisposi-tion, labile INR, elderly, and drugs/alcohol) is calculated as1 point, and patients with scores �3 are considered to be atintermediate/high bleeding risk. In the HAS-BLED score,labile INR and impaired liver function could not beassessed, and these were therefore omitted so that amaximum of 7 points was used for a “modified HAS-BLED” analysis. For the ATRIA score, anemia (hemoglobin<13 g/dl in men and <12 g/dl in women) and renalimpairment (estimated glomerular filtration rate [eGFR]<30 or dialysis treatment) yield 3 point each; age �75 years2 points; and hypertension and previous bleeding episode 1point each. Patients with scores �4 are considered to be atintermediate/high bleeding risk. For mOBRI, age�65 years, previous stroke or gastrointestinal tract bleeding

Table 2Cox regression analysis of the HAS-BLED, ATRIA, mOBRI, and REACH scores for the outcomes of any bleeding (BARC 2 to 5), major bleeding (BARC>2), and all-cause mortality
Any Bleeding Major Bleeding All-Cause Mortality
HR (95% CI) p Value HR (95% CI) p Value HR (95% CI) p Value
HAS-BLEDScore 1.04 (0.84-1.28) 0.72 1.10 (0.84-1.45) 0.49 1.26 (0.97-1.63) 0.08Low <3 vs high �3 0.87 (0.62-1.23) 0.43 0.89 (0.56-1.40) 0.61 1.18 (0.74-1.88) 0.50
ATRIAScore 1.08 (0.98-1.18) 0.11 1.10 (0.97-1.24) 0.14 1.24 (1.10-1.39) <0.001Low <4 vs high �4 1.24 (0.86-1.78) 0.25 1.62 (1.01-2.61) 0.047 1.99 (1.24-3.17) 0.005
mOBRIScore 1.12 (0.91-1.39) 0.28 1.22 (0.92-1.61) 0.16 1.51 (1.16-1.97) 0.002Low 0 vs Hhgh �1 1.17 (0.86-1.58) 0.32 1.38 (0.93-2.06) 0.11 1.74 (1.18-2.57) 0.005
REACHScore 1.01 (0.95-1.07) 0.83 0.99 (0.92-1.07) 0.76 1.09 (1.01-1.18) 0.02Low <11 vs high �11 1.00 (0.73-1.36) 0.99 0.86 (0.57-1.28) 0.46 1.34 (0.89-2.01) 0.16
For each score, HRs were calculated as a continuous variable (per 1 unit of change) and as a dichotomous low vs. high score.CI ¼ confidence interval; HR ¼ hazards ratio.
Table 3C-indexes for HAS-BLED, ATRIA, mOBRI, and REACH scores
Any Bleeding Major Bleeding All-Cause Mortality
AUC 95% CI SE AUC 95% CI SE AUC 95% CI SE
HAS-BLEDScore 0.51 0.45-0.56 0.03 0.52 0.45-0.59 0.04 0.54 0.47-0.61 0.04Low <3 vs high �3 0.50 0.45-0.55 0.03 0.51 0.44-0.58 0.04 0.53 0.46-0.60 0.04
ATRIAScore 0.54 0.49-0.59 0.03 0.55 0.48-0.62 0.04 0.62 0.55-0.69 0.04Low <4 vs high �4 0.52 0.47-0.58 0.03 0.55 0.48-0.62 0.04 0.58 0.51-0.65 0.04
mOBRIScore 0.53 0.48-0.59 0.03 0.55 0.49-0.62 0.03 0.61 0.55-0.68 0.03Low 0 vs high �1 0.50 0.46-0.55 0.03 0.51 0.45-0.57 0.04 0.53 0.47-0.58 0.04
REACHScore 0.52 0.47-0.58 0.03 0.50 0.43-0.57 0.04 0.58 0.51-0.65 0.03Low <11 vs high �11 0.49 0.44-0.54 0.03 0.49 0.43-0.55 0.04 0.51 0.45-0.57 0.04
AUC ¼ area under curve; CI ¼ confidence interval; SE ¼ standard error.
Coronary Artery Disease/Bleeding Risk Scores in AF Patients Undergoing PCI 3
within 2 weeks are assigned 1 point each; and any of thefollowing maximum of 1 point (recent myocardial infarc-tion, diabetes, hematocrit <0.30, creatinine >1.5 mg/dl, or133 mmol/L). Patients with �1 mOBRI points are at inter-mediate/high bleeding risk. For REACH score, age groups45 to 54, 55 to 64, 65 to 74, and �75 yield 0, 2, 4, and 6points, respectively. Peripheral arterial disease, diabetes, andhypercholesterolemia yield 1 point each; congestive heartfailure and hypertension 2 points each; oral anticoagulant 4points; aspirin 1 point, other antiplatelet 2, and combinationof 2 antiplatelet drugs 4 points; former smoking 1; andcurrent smoking 2 points. REACH scores >10 are consid-ered intermediate/high for the risk of bleeding.
The primary end points were bleeding complicationsdefined according to the bleeding academic researchconsortium (BARC) criteria as any (BARC 2, 3a, 3b, 3c,and 5) or major (BARC 3a, 3b, 3c, and 5)10 and all-causemortality.
Data are presented as mean � SD, median (interquartilerange) and frequencies (%), where appropriate. Continuous
variables were analyzed using independent samples t test.Categorical variables were analyzed using chi-square tests.Independent determinants of any bleeding complication wereassessed using univariate modeling and those associatedwith any bleeding event at p level <0.10 were entered into astepwise backward logistic regression analysis. Bleeding riskscores were analyzed in 3 ways: (1) as continuous variablesand (2) as dichotomous variables (low vs intermediate/highrisk); and (3) Cox proportional hazard analysis was usedwith each score assessed separately. Receiver operatingcharacteristic curves and c-indexes were constructed for anybleeding and major bleeding end points. Significance was setat p value <0.05. Analysis was performed with SPSSversion 16.0 (SPSS Inc., Chicago, Illinois).
Results
Overall, 929 patients were followed up for 1 year.Baseline characteristics according to any bleeding eventversus no bleeding event at 1-year follow-up are listed in

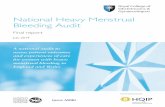
Figure 1. ROC curves according to HAS-BLED, ATRIA, mOBRI, andREACH scores for the outcomes of (A) any bleeding and (B) majorbleeding. ROC ¼ receiver operating characteristic.
4 The American Journal of Cardiology (www.ajconline.org)
Table 1. The use of drug-eluting stents was 25%. Themedian (interquartile range) duration of clopidogrel use inthe whole cohort was 3 (5) months.
At 12 months, the rates of any (BARC 2, 3a, 3b, 3c, and5), BARC 3, and major (BARC 3a, 3b, 3c, and 5) bleedingevents were 18.1%, 9.1%, and 10.4%, respectively. Mostbleeding events occurred early within the first month afterthe index PCI. INR level at the time of the first bleedingevent was 1.8 � 0.6 (range 1.0 to 3.0). Acute coronarysyndrome (ACS) as an indication for PCI appeared to
increase the rate of any bleeding and major bleeding eventscompared with stable angina (21.4% vs 13.8%, p ¼ 0.003,and 12.9% vs 7.3%, p ¼ 0.007, respectively). Comparedwith patients receiving bare metal stents, the rates of anybleeding and major bleeding events were similar in patientsreceiving drug-eluting stents (19.1% vs 15.4%, p ¼ 0.23,and 10.9% vs 9.3%, p ¼ 0.53, respectively). Increasing age(odds ratio 1.03, 95% confidence interval 1.01 to 1.06,p ¼ 0.009), previous peptic ulcer (odds ratio 2.32, 95%confidence interval 1.12 to 4.84, p ¼ 0.024), and femoralaccess site (1.86, 95% confidence interval 1.17 to 2.97,p ¼ 0.009) remained independent predictors of any bleedingevent in a multivariate logistic regression model includingalso renal impairment (eGFR <60), gender, body massindex, acute coronary syndromes versus stable angina as anindication for PCI, previous transient ischemic attack/strokeand the use of glycoprotein IIb/IIIa blockers during theindex procedure in the model.
HAS-BLED, mOBRI, and REACH scores were availablein all the 929 patients and ATRIA score in 748 patientsbecause of the lack of eGFR values in the rest of the cohort.C indexes and Cox proportional hazard ratios of the scoresfor the outcomes of any bleeding and major bleeding arelisted in Tables 2 and 3, respectively. Figure 1 showsreceiver operating characteristic curves for the outcomes ofany bleeding and major bleeding. Low bleeding risk scoresas determined by HAS-BLED 0 to 2, ATRIA 0 to3, mOBRI0, and REACH 0 to 10 were detected in 23.7%, 73.0%,7.8%, and 5.7% of patients of the cohort, respectively.
No differences were observed in the rate of triple(vitamin K antagonist þ clopidogrel þ aspirin), vitamin Kantagonist þ clopidogrel or dual antiplatelet (aspirin þclopidogrel) therapy use according to low versus interme-diate/high HAS-BLED, ATRIA, and mOBRI scores. For theREACH score, triple therapy was used only in 9.4% ofpatients in the low risk score category versus 76.9% in theintermediate/high risk scores. Yet, no differences in theBARC bleeding rates were noted between patients with lowversus intermediate/high REACH scores.
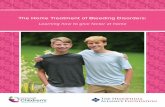
Figure 2 shows the incidence of any bleeding duringvarious antithrombotic treatment regimens according toHAS-BLED, mOBRI, ATRIA, and REACH categories lowversus intermediate/high bleeding risk. Triple therapy wasassociated with a higher absolute rate of any bleeding eventscompared with other regimens, regardless of the bleedingrisk.
None of the established bleeding-risk prediction toolsperformed well in the detection of intracranial bleeding(BARC 3c) as reflected by poor C indexes 0.42, 0.35, 0.58,and 0.41 for HAS-BLED, ATRIA, mOBRI, and REACHscores, respectively.
Discussion
The reports on the value of bleeding risk prediction toolsin predicting bleeding in patients with AF undergoing PCIare scarce. Previously, bleeding risk prediction by REACHor ATRIA scores has not been tested in patients with AFundergoing PCI and receiving multiple antithromboticmedications. In an earlier cohort study with patients withAF, intermediate/high HAS-BLED scores—calculated on a

Figure 2. Incidence (number of events per 100 months of treatment with clopidogrel) of any bleeding (upper panel) and BARC major bleeding (lower panel)during various antithrombotic treatment regimens according to HAS-BLED, mOBRI, ATRIA, and REACH categories low versus intermediate/high bleedingrisk. Triple refers to the use of vitamin K antagonist þ aspirin þ clopidogrel; VKA þ clopidogrel refers to the use of vitamin K antagonist þ clopidogrel; anddual antiplatelet therapy refers to the use of clopidogrel þ aspirin. VKA ¼ vitamin K-antagonist.
Coronary Artery Disease/Bleeding Risk Scores in AF Patients Undergoing PCI 5
post hoc basis—were associated with an increased risk ofall-cause death, major adverse cardiovascular events, andmajor bleeding episodes compared with low scores.11 In theAFCAS registry, the discriminatory capacity of HAS-BLED, ATRIA, mOBRI, and REACH bleeding risk pre-diction tools was weak as seen with relatively low Cindexes. Overall, bleeding risk prediction is complicateddespite including many clinically important determinantsinto scores as seen with low C-indexes already in theoriginal validation studies.4e6,8 In our study, increasing age,femoral access site, and previous peptic ulcer were inde-pendent determinants of bleeding. Compared with radialroute, femoral access site was associated with 1.9-fold riskof bleeding complications, which mainly occurred duringthe in-hospital phase. The risk of bleeding was 2.3 fold inthose with previous peptic ulcer. Strikingly, mean INRlevels at the time of bleeding events were subtherapeutic,and maximal INR level was 3.0. This indicates that
clinically relevant bleeding events may occur even at ther-apeutic INR levels in these patients receiving multipleantithrombotic medications. The clinical implication of ourfindings is that bleeding risk cannot be reliably anticipatedwith these established bleeding risk prediction tools in pa-tients receiving multiple antithrombotic medications due toAF and PCI. In line with previous reports, the use of radialaccess appears safer in terms of lower rate of local accesssite complications also in the AFCAS cohort.12,13 Therefore,choosing an optimal PCI strategy is pivotal in minimizingbleeding complications.
In a study by Ruiz-Nodar et al,11 the rate of majorbleeding was slightly lower to that of AFCAS registry at 1year (7.8% vs 10.4%, respectively) probably reflectinganother bleeding definition.14 Recently published WOESTtrial used the same BARC definition of bleeding events.3
In patients on triple therapy, the rate of BARC 3 majorbleeding events was higher in the WOEST trial compared

6 The American Journal of Cardiology (www.ajconline.org)
with AFCAS cohort patients on triple therapy (12.7% vs8.5%, respectively). The frequency of proton pump inhibitoruse was similar in AFCAS and WOEST (36% vs 34% to39%). As clopidogrel was being used by 78.9% of patientson triple therapy group in the WOEST trial at 12 months, apossible explanation for lower bleeding rates is the mark-edly shorter duration of clopidogrel therapy in patients in theAFCAS registry (median [interquartile range] 3 [5] months).
In the AFCAS cohort, HAS-BLED, ATRIA, and mOBRIscores did not influence the choice among triple, dual anti-platelet, or vitamin K-antagonist þ clopidogrel treatments asthese were used similarly in patients with low versus inter-mediate/high scores. In contrast, patients with low REACHscore had very seldom triple therapy compared withthose with intermediate/high risk scores. Nevertheless,no differences in the BARC bleeding rates were notedbetween patients with low versus intermediate/high REACHscores. ACS appeared to increase bleeding risk. One plau-sible explanation is that patients with ACS, especiallyST-elevation myocardial infarction, have more aggressiveantithrombotic/anticoagulation treatment during the indexprocedure compared with elective stable patients (data notshown). In contrast, the use of drug-eluting stents was 25% inthe cohort and was not associated with increased rates ofbleeding events. The choice of stent was entirely at theoperator’s discretion, and therefore, selection bias is inevi-table, as many clinical variables such as patients’ frailty couldnot be systematically assessed. Nevertheless, it seems thatclinical evaluation by experienced physicians may be at leastas good as using these scores. In addition, it seems that theprothrombotic risk outweighs the bleeding risk in most pa-tients even when the bleeding risk scores are high. The samephenomenon has been addressed in a recent European HeartRhythm Association position paper on bleeding risk assess-ment in patients with AF.15
Higher mortality rates have been previously reported inpatients with intermediate/high mOBRI scores7 as well asHAS-BLED scores.11 However, in the AFCAS cohort,ATRIA appeared better predictor of mortality comparedwith HAS-BLED, mOBRI, and REACH. Overall, ATRIAscore was a better predictor of mortality rather thanbleeding. Major bleeding and mortality are endpoints knownto be closely related in populations on anticoagulationtherapy.7,11
This study has all the inherent limitations of an obser-vational study including individual risk-based decision-making in the treatment choices. The choice of stent andantithrombotic treatment has been entirely at the treatingphysician’s discretion. The bleeding risk scores werecalculated on a post hoc basis because HAS-BLED,ATRIA, and REACH scores were published after theenrollment of the patients. Comprehensive information onliver function or labile INR was not available, and thus, theywere omitted in the calculation of the “modified” HAS-BLED score. This may diminish the value of applyingHAS-BLED to this population. However, the lack ofknowledge of labile INR levels probably did not have majorimpact on the results because the mean INR was only 1.8(range 1.0 to 3.0) at the time of the first bleeding event, andthus the majority of bleeding events was not causedby supratherapeutic INR levels. Moreover, a number of
patients with significant liver failure are likely to be verylow because in many of them the decision to undergo PCIwith stenting would be deferred due to presumed highbleeding risk. GFR values were not available in 181 patientsdue to the lack of creatinine level, and therefore, ATRIAscore was unavailable in these patients. Nevertheless, Cindexes and Cox proportional hazard ratios with HAS-BLED, mOBRI, or REACH scores were no differentwhen only patients with GFR were included (data notshown). Despite these limitations, we believe that these dataare of value to guide the treatment of patients with AFundergoing PCI. This is largest dataset so far analyzingpatient with AF undergoing PCI and also including a sub-stantial amount of patients with ACS. The strength of ourstudy is the inclusion of “real-world” patients with PCI. Endpoints were defined according to the latest recommendationswith BARC bleeding criteria. Centers participating in theAFCAS registry mainly enrolled consecutive patient withthe only exclusion criteria being unwillingness/inability toparticipate in the study. In this sense, the population rep-resents ”real-world” patients with PCI with AF.
In patients with AF undergoing PCI, increasing age,femoral access site, and previous peptic ulcer were signifi-cant predictors of BARC bleeding events. The performanceof HAS-BLED, ATRIA, mOBRI, and REACH scores inpredicting bleeding complications was useless.
Acknowledgment: We thank our study coordinator TuijaVasankari, RN, for her input in data management.
Disclosure
The authors have no conflicts of interest to disclose.
1. Lip GYH, Huber K, Andreotti F, Arnesen H, Airaksinen JK, Cuisset T,Kirchhof P, Marín F. Antithrombotic management of atrial fibrillationpatients presenting with acute coronary syndrome and/or undergoingcoronary stenting: executive summary—a Consensus Document of theEuropean Society of Cardiology Working Group on Thrombosis,endorsed by the European Heart Rhythm Association (EHRA) and theEuropean Association of Percutaneous Cardiovascular Interventions(EAPCI). Eur Heart J 2010;31:1311e1318.
2. Schlitt A, Rubboli A, Lip GH, Lahtela H, Valencia J, Karjalainen PP,Weber M, Laine M, Kirchhof P, Niemelä M, Vikman S, Buerke M,Airaksinen KEJ; for the AFCAS (Management of patients with AtrialFibrillation Undergoing Coronary Artery Stenting) study group. Themanagement of patients with atrial fibrillation undergoing percutaneouscoronary intervention with stent implantation: in-hospital-data from theatrial fibrillation undergoing coronary artery stenting (AFCAS) study.Catheter Cardiovasc Interv 2013;110:525e532.
3. Dewilde WJ, Oirbans T, Verheugt FW, Kelder JC, De Smet BJ,Herrman J, Adriaenssens T, Vrolix M, Heestermans AA, Vis MM,Tijsen JG, van ’t Hof AW, ten Berg JM. Use of clopidogrel with orwithout aspirin in patients taking oral anticoagulant therapy andundergoing percutaneous coronary intervention: an open-label, rando-mised, controlled trial. Lancet 2013;381:1107e1115.
4. Lip GYH, Frison L, Halperin JL, Lane DA. Comparative validation ofa novel risk score for predicting bleeding risk in anticoagulated patientswith atrial fibrillation: the has-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR,elderly, drugs/alcohol concomitantly) score. J Am Coll Cardiol2011;57:173e180.
5. Fang MC, Go AS, Chang Y, Borowsky LH, Pomernacki NK,Udaltsova N, Singer DE. A new risk scheme to predict warfarin-associated hemorrhage: the ATRIA (anticoagulation and risk factorsin atrial fibrillation) study. J Am Coll Cardiol 2011;58:395e401.

Coronary Artery Disease/Bleeding Risk Scores in AF Patients Undergoing PCI 7
6. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of anindex for predicting the risk of major bleeding in outpatients treatedwith warfarin. Am J Med 1998;105:91e99.
7. Airaksinen KEJ, Suurmunne H, Porela P, Niemelä M, Vikman S,Puurunen M, Annala A, Biancari F, Karjalainen PP. Usefulness ofoutpatient bleeding risk index to predict bleeding complications inpatients with long-term oral anticoagulation undergoing coronarystenting. Am J Cardiol 2010;106:175e179.
8. Ducrocq G, Wallace JS, Baron G, Ravaud P, Alberts MJ, Wilson PWF,Ohman EM, Brennan DM, D’Agostino RB, Bhatt DL, Steg PG. Riskscore to predict serious bleeding in stable outpatients with or at risk ofatherothrombosis. Eur Heart J 2010;31:1257e1265.
9. Lahtela H, Rubboli A, Schlitt A, Karjalainen PP, Niemelä M, VikmanS, Puurunen M, Weber M, Valencia J, Biancari F, Lip GYH,Airaksinen KEJ; for the AFCAS (management of patients with atrialfibrillation undergoing coronary artery stenting), study group. Heparinbridging vs. uninterrupted oral anticoagulation in patients with atrialfibrillation undergoing coronary artery stenting. Results from theAFCAS registry. Circ J 2012;76:1363e1368.
10. Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J,Kaul S, Wiviott SD, Menon V, Nikolsky E, Serebruany V, ValgimigliM, Vranckx P, Taggart D, Sabik JF, Cutlip DE, Krucoff MW, OhmanEM, Steg PG, White H. Standardized bleeding definitions for cardio-vascular clinical trials: a consensus report from the bleeding academicresearch consortium. Circulation 2011;123:2736e2747.
11. Ruiz-Nodar JM, Marín F, Roldán V, Valencia J, Manzano-FernándezS, Caballero L, Hurtado JA, Sogorb F, Valdés M, Lip GYH. Should werecommend oral anticoagulation therapy in patients with atrial fibril-lation undergoing coronary artery stenting with a high has-BLEDbleeding risk score? Circ Cardiovasc Interv 2012;5:459e466.
12. Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, BudajA, Niemelä M, Valentin V, Lewis BS, Avezum A, Steg PG, Rao SV,Gao P, Afzal R, Joyner CD, Chrolavicius S, Mehta SR. Radial versusfemoral access for coronary angiography and intervention in patientswith acute coronary syndromes (RIVAL): a randomised, parallel group,multicentre trial. Lancet 2011;377:1409e1420.
13. Karjalainen PP, Vikman S, Niemelä M, Porela P, Ylitalo A, VaittinenM, Puurunen M, Airaksinen TJ, Nyman K, Vahlberg T, AiraksinenKEJ. Safety of percutaneous coronary intervention during uninter-rupted oral anticoagulant treatment. Eur Heart J 2008;29:1001e1010.
14. Prism-plus investigators. Inhibition of the platelet glycoprotein IIb/IIIareceptor with Tirofiban in unstable angina and noneQ-wave myocar-dial infarction. N Engl J Med 1998;338:1488e1497.
15. Lip GYH, Andreotti F, Fauchier L, Huber K, Hylek E, Knight E, LaneDA, Levi M, Marin F, Palareti G, Kirchhof P, Document reviewers;Collet J, Rubboli A, Poli D, Camm J. Bleeding risk assessment andmanagement in atrial fibrillation patients: a position document from theEuropean Heart Rhythm Association, endorsed by the EuropeanSociety of Cardiology Working Group on Thrombosis. Europace2011;13:723e746.