
Pattern of Thyroid Function During Early Pregnancy in Women Diagnosed with Subclinical...
8
Pattern of Thyroid Function During Early Pregnancy in Women Diagnosed with Subclinical Hypothyroidism and Treated with L-Thyroxine Is Similar to That in Euthyroid Controls Christian De Geyter, 1 Sabine Steimann, 1 Beat Mu ¨ ller, 2 Marius E. Kra ¨ nzlin, 2 and Christian Meier 2 Background: Subclinical hypothyroidism (SCH) is associated with a higher miscarriage rate. It is unclear how the thyroid function in SCH differs from that in euthyroidism during early pregnancy. We intended to determine the regulation of thyroid function in women with SCH receiving constant L-thyroxine (T 4 ) replacement during early pregnancy as compared to euthyroid controls. Methods: This was a prospective cohort study with weekly serum sampling in eight women in early pregnancy with SCH and eight euthyroid women from week 5 to week 12 of pregnancy. Thyroid function was assessed before pregnancy. Women with SCH were treated with T 4 (50 mg daily) and continued on an unchanged dose until week 12. The following parameters were measured weekly: thyrotropin (TSH), thyroglobulin, thyroxine, triiodothyronine, free thyroxine (FT 4 ), free triiodothyronine (FT 3 ), estradiol, progesterone, human chorionic gonadotropin, and prolactin. Results: Although the pregestational levels of TSH were significantly higher among women with SCH as compared to euthyroid controls, the self-limited estrogen-induced increment of TSH during early pregnancy was similar in both groups. Conclusions: Although both SCH and ovarian hyperstimulation were associated with an intermediate rise in TSH, the pattern of thyroid function followed similar changes as in euthyroid controls and is unlikely to cause the higher miscarriage rate observed in SCH. Introduction S ubclinical hypothyroidism (SCH) is a laboratory di- agnosis, defined as a serum thyrotropin (TSH) concen- tration above the upper normal reference limit in the presence of normal free thyroxine (FT 4 ) or free triiodothyronine (FT 3 ) (1). As serum TSH levels rise logarithmically in the presence of minor deficiencies in the secretory output of the thyroid gland, the increase in TSH reflects preclinical hypothyroid- ism. If left untreated during pregnancy, even moderately re- duced serum levels of FT 4 may impair the later mental and motor development of the child (1–5). Although SCH is prevalent among women, routine screening of SCH is not recommended (1). On the other hand, more stringent refer- ence limits for normal TSH than those used previously (#4.5 mIU=L) were recommended recently (#2.5 mIU=L) (6). Abnormal thyroid function seems to be involved in early miscarriage and the detrimental role of antithyroidal anti- bodies in those events has been stressed, even in euthyroid women (7,8). At present it is unclear to what extent thyroid function in early pregnancy in women with SCH differs from that in early pregnancy in women without thyroid disorders. Early pregnancy, as defined from week 5 after the last menstruation to the end of the luteo-placental shift in week 12, involves a multitude of important adaptations to changes that occur in thyroid hormone clearance and compartmentaliza- tion and other factors that influence thyroid economy. The pregnancy-induced rise in estrogen levels is thought to in- crease the need for L-thyroxine (9), at least in part due to a rise in the serum levels of the thyroxine (T 4 )-binding globulin, thereby lowering the circulating concentration of unbound, free thyroid hormone. This increased demand for T 4 is in part compensated for by the rapid rise of the serum levels of the human chorionic gonadotropin (hCG), which has a weak but relevant affinity during early pregnancy for the TSH recep- tor (10–12). It is thought that the healthy thyroid gland is 1 Division of Gynecological Endocrinology and Reproductive Medicine at the Women’s Hospital, Basel, Switzerland. 2 Division of Endocrinology, Diabetes and Clinical Nutrition at the Department of Internal Medicine, University Hospital Basel, Basel, Switzerland. THYROID Volume 19, Number 1, 2009 ª Mary Ann Liebert, Inc. DOI: 10.1089=thy.2007.0355 53
Transcript of Pattern of Thyroid Function During Early Pregnancy in Women Diagnosed with Subclinical...

Pattern of Thyroid Function During Early Pregnancyin Women Diagnosed with Subclinical Hypothyroidism
and Treated with L-Thyroxine Is Similarto That in Euthyroid Controls
Christian De Geyter,1 Sabine Steimann,1 Beat Muller,2 Marius E. Kranzlin,2 and Christian Meier2
Background: Subclinical hypothyroidism (SCH) is associated with a higher miscarriage rate. It is unclear howthe thyroid function in SCH differs from that in euthyroidism during early pregnancy. We intended to determinethe regulation of thyroid function in women with SCH receiving constant L-thyroxine (T4) replacement duringearly pregnancy as compared to euthyroid controls.Methods: This was a prospective cohort study with weekly serum sampling in eight women in early pregnancywith SCH and eight euthyroid women from week 5 to week 12 of pregnancy. Thyroid function was assessedbefore pregnancy. Women with SCH were treated with T4 (50 mg daily) and continued on an unchanged doseuntil week 12. The following parameters were measured weekly: thyrotropin (TSH), thyroglobulin, thyroxine,triiodothyronine, free thyroxine (FT4), free triiodothyronine (FT3), estradiol, progesterone, human chorionicgonadotropin, and prolactin.Results: Although the pregestational levels of TSH were significantly higher among women with SCH ascompared to euthyroid controls, the self-limited estrogen-induced increment of TSH during early pregnancy wassimilar in both groups.Conclusions: Although both SCH and ovarian hyperstimulation were associated with an intermediate rise inTSH, the pattern of thyroid function followed similar changes as in euthyroid controls and is unlikely to causethe higher miscarriage rate observed in SCH.
Introduction
Subclinical hypothyroidism (SCH) is a laboratory di-agnosis, defined as a serum thyrotropin (TSH) concen-
tration above the upper normal reference limit in the presenceof normal free thyroxine (FT4) or free triiodothyronine (FT3)(1). As serum TSH levels rise logarithmically in the presence ofminor deficiencies in the secretory output of the thyroidgland, the increase in TSH reflects preclinical hypothyroid-ism. If left untreated during pregnancy, even moderately re-duced serum levels of FT4 may impair the later mental andmotor development of the child (1–5). Although SCH isprevalent among women, routine screening of SCH is notrecommended (1). On the other hand, more stringent refer-ence limits for normal TSH than those used previously(#4.5 mIU=L) were recommended recently (#2.5 mIU=L) (6).Abnormal thyroid function seems to be involved in earlymiscarriage and the detrimental role of antithyroidal anti-
bodies in those events has been stressed, even in euthyroidwomen (7,8). At present it is unclear to what extent thyroidfunction in early pregnancy in women with SCH differs fromthat in early pregnancy in women without thyroid disorders.
Early pregnancy, as defined from week 5 after the lastmenstruation to the end of the luteo-placental shift in week 12,involves a multitude of important adaptations to changes thatoccur in thyroid hormone clearance and compartmentaliza-tion and other factors that influence thyroid economy. Thepregnancy-induced rise in estrogen levels is thought to in-crease the need for L-thyroxine (9), at least in part due to a risein the serum levels of the thyroxine (T4)-binding globulin,thereby lowering the circulating concentration of unbound,free thyroid hormone. This increased demand for T4 is in partcompensated for by the rapid rise of the serum levels of thehuman chorionic gonadotropin (hCG), which has a weak butrelevant affinity during early pregnancy for the TSH recep-tor (10–12). It is thought that the healthy thyroid gland is
1Division of Gynecological Endocrinology and Reproductive Medicine at the Women’s Hospital, Basel, Switzerland.2Division of Endocrinology, Diabetes and Clinical Nutrition at the Department of Internal Medicine, University Hospital Basel, Basel,
Switzerland.
THYROIDVolume 19, Number 1, 2009ª Mary Ann Liebert, Inc.DOI: 10.1089=thy.2007.0355
53

perfectly able to adapt to the increased demand during earlypregnancy, but that the impaired thyroid gland may not becapable of compensation necessitating exogenous supple-mentation with T4 (13–15).
The aim of this prospective study was to assess to whatextent the secretory capacity of the thyroid gland of womendiagnosed with SCH is different from that of women withoutSCH in early pregnancy. We hypothesized that if the observedhigher miscarriage in SCH is due to a derailment of the thy-roid function itself, major changes in TSH, FT4, or FT3 mustbecome apparent early during pregnancy. As it was consid-ered unethical to leave women with SCH without any sup-plementation with T4, we compared the changes in thyroidhormone regulation in SCH during constant substitution witha low dose of 50mg of T4 with those of age-matched pregnantwomen with normal thyroid function. That dose was found tobe sufficient to bring TSH levels into the normal range prior topregnancy. Because of the rapid biological and hormonalchanges typically occurring during early pregnancy, we de-cided to perform blood sampling at short intervals (i.e., everyweek). Based on the study design, the intent was to include atotal number of 62 women in this study. As a consequence ofthe findings published by Alexander and coworkers (14), whodemonstrated that the substitutional dose of T4 must be in-creased stepwise during early pregnancy according to theserum levels of TSH, the study was ended prematurely. Thefindings of the first 16 women enrolled are presented.
Material and Methods
During an infertility work-up in the Division of Gynecolo-gical Endocrinology and Reproductive Medicine at the Wo-men’s Hospital of the University of Basel, Switzerland, thethyroid function of infertile women is routinely examined.Women with SCH were recruited to participate in a prospec-tive study, in which weekly serum samples were collected untilthe 12th week of pregnancy. SCH was defined by a consistentlyelevated TSH concentration, i.e., above 4.5 mIU=L (1) in thepresence of normal FT4. Before the initiation of the infertilitytreatment and before establishment of pregnancy, the TSHserum values were normalized through exogenous L-thyroxinesupplementation. As an integral part of the study protocol, thisdosage was maintained until the 12th week of gestation. Inaddition to a fixed 50-mg dose of T4 daily (Eltroxin, GlaxoWellcome, London, U.K.), all women received folic acid (0.4 mgAndreafol, Andreabal, Basel, Switzerland).
Previously infertile women with normal thyroid function,as defined by TSH levels between 1 and 4 mU=L, were re-cruited for control purposes. These women were also sub-jected to weekly serum sampling until the 12th week ofpregnancy, but they had no medication other than folic acid(0.4 mg, Andreafol). All serum samples were stored at �708Cuntil measurement. Iodine supplementation was not offered,because Swiss citizens are considered to receive adequatelysupplemented dietary iodine (16). Women with overt hypo-thyroidism, pre-existing endocrine diseases such as Addison’sdisease, or women with severe illness during earlier preg-nancies were excluded. None of the patients received pro-lactin (PRL)-lowering medications or antidepressants.
In five women pregnancies were achieved naturally with-out medical intervention other than T4 supplementation.Three pregnancies arose after the transfer of embryos result-
ing from previously frozen and thawed oocytes in the pro-nucleate stage (17) during mono-ovulatory cycles, duringwhich ovulation was induced with hCG (10,000 IU, Pregnyl,Organon, Pfaffikon, Switzerland). Eight pregnancies wereachieved with either conventional in vitro fertilization or withintracytoplasmic sperm injection after down-regulation witha long-acting gonadotropin-releasing hormone agonist (trip-torelin acetate, Decapeptyl Retard, Ferring, Wallisellen,Switzerland) followed by ovarian hyperstimulation with re-combinant follicle-stimulating hormone (Gonal F, Serono,Zug, Switzerland).
This study was presented to and approved by the localethics committee, and written informed consent was given byeach patient. Based on statistical power analysis the originalintent was to recruit 31 women with SCH and 31 euthyroidwomen for this study. While our study was in progressAlexander and coworkers (14) reported that in primary hy-pothyroidism, T4 must be adjusted to the serum levels of TSHduring early pregnancy. Therefore, it was considered uneth-ical to leave women with SCH with fixed (i.e., unadjusted) T4
supplementation until the 12th week of gestation, and ourstudy was ended prematurely.
Laboratory analyses
Serum samples were collected in the fasting state andstandardized with respect to sampling time (between 7:00 and8:00 A.M.). All samples were stored at �708C until batchanalysis. Circulating levels of thyroid hormones (TSH, FT4,FT3) thyroglobulin (Tg), anti-thyroid peroxidase (TPO) andTg antibodies, estradiol, progesterone, hCG, and PRL weremeasured by commercial immunoassays (Roche Diagnostics,Rotkreuz, Switzerland). The TSH assay used has no signifi-cant cross-reactivity with hCG at levels below 500,000 IU=L.The coefficient of variation was below 10% in all analyses.
Statistical analysis
As none of the hormone concentrations measured weredistributed normally, all statistical analyses were performedwith nonparametric tests, such as Mann Whitney U andKruskal Wallis. The concentrations of hCG were logarithmi-cally transformed. All data are presented with their medianvalues and with their respective 95% confidence intervals. Thelevel of statistical significance was set at 5%. All analyses werecalculated with the statistical software package StatgraphicsPlus Version 5.1 (Rockville, MA).
Results
Baseline characteristics
Before pregnancy 16 women were asked to participate inweekly blood samplings from early in their pregnancy untilthe 12th week: eight with SCH (i.e. TSH>4.5 mU=L) and eightwith confirmed euthyroid function (Table 1). As defined,pretreatment TSH levels were significantly higher amongwomen with SCH as compared with euthyroid women( p< 0.001). After the baseline visit all patients with SCH re-ceived 50mg of T4 daily and this dose was maintained until the12th week of pregnancy. The shortest interval between thebeginning of treatment with T4 and conception was 42 days,the longest 3 years and 10 months. None of the clinical char-acteristics were significantly different among both groups at
54 DE GEYTER ET AL.

baseline. In two cases, one in each group, miscarriage wasdiagnosed in the 10th week of pregnancy. All other womenwere delivered of healthy children after uncomplicatedpregnancies.
Changes in circulating hormone levels during earlypregnancy
During T4 supplementation with a fixed dose of 50mg daily(in SCH only), TSH levels remained higher throughout theobservation period in patients with SCH as compared to eu-thyroid controls (Fig. 1). For both groups the serum TSH levelsincreased during early pregnancy with peak levels at week 6.The differences among both groups were most prominentduring weeks 6 ( p< 0.06), 7 ( p< 0.03), and 8 ( p< 0.05). Two ofthe eight patients diagnosed with SCH had TSH levels ex-ceeding 4.5 IU=L during weeks 6 and 7 of their pregnancy (Fig.2). Thereafter, TSH levels declined reaching constant levelsfrom the ninth week of gestation onward, in parallel for wo-men with SCH and euthyroid controls. The rise in serum TSHlevels was more pronounced in SCH than in euthyroid wo-men, although the differences did not reach statistical signifi-cance (Fig. 3). When compared with the serum TSH levelsduring week 5 of gestation, a rise of the TSH concentration wasobserved during week 6 of pregnancy, similarly among eu-thyroid women and women diagnosed with SCH supple-mented with a constant dose of T4 (Fig. 3). Thereafter, the TSHlevels dropped, most significantly during week 12 of gestationin those women diagnosed with SCH ( p< 0.01).
During early pregnancy (up until week 9) serum hCGlevels increased progressively with stable values thereafter. Incontrast to hCG and TSH, however, circulating levels of thy-roid hormone (FT4, FT3) remained unchanged during thewhole sampling period both in women with SCH and in eu-thyroid controls (Fig. 1). The PRL levels increased with pro-gressing pregnancy. However, in week 11 and 12 of gestationthe concentration of PRL was significantly lower in the wo-men with SCH treated with 50 mg of T4 daily ( p< 0.03).
Role of preceding ovarian hyperstimulationon subsequent hormonal parameters duringearly pregnancy
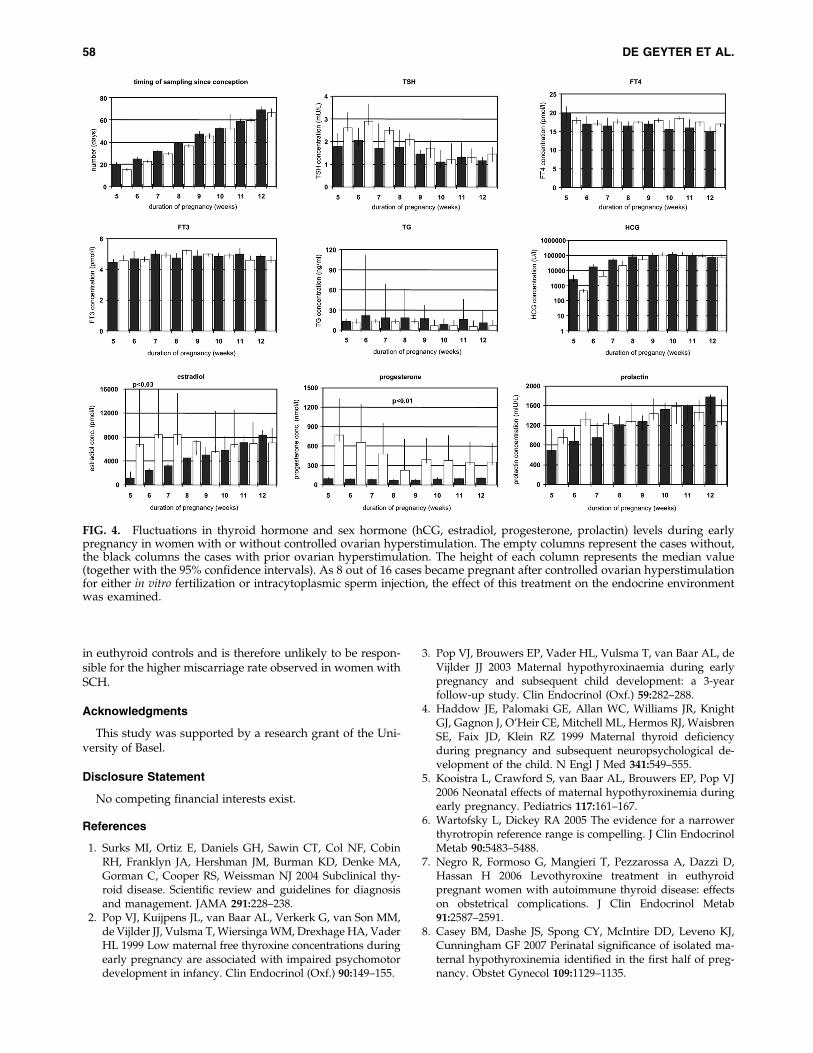
As a proportion of the pregnancies were induced aftercontrolled ovarian hyperstimulation with exogenous gonad-otropins, the role and the duration of the modified hormonalenvironment during early pregnancy on thyroid functionwere also evaluated (Fig. 4). In the women treated with con-trolled ovarian hyperstimulation, the mean number of pre-ovulatory ovarian follicles was eight (ranging between 2 and13). In the other group of women, not treated with controlledovarian hyperstimulation, we never observed more than onepre-ovulatory follicle per cycle. In the cases after controlledovarian hyperstimulation the sampling started significantlyearlier ( p< 0.05) leading to lower hCG concentrations in week5 of gestation ( p< 0.05). Thereafter, hCG levels were com-parable between both groups. The pregnancies arising aftercontrolled ovarian hyperstimulation were characterized bysignificantly higher estradiol levels from week 5 to 7 ( p< 0.03)and higher progesterone levels throughout the observationperiod ( p< 0.01) (Fig. 4). Whereas the concentration of TSHwas higher among women without previous ovarian hyper-stimulation (although the differences did not reach statisticalsignificance), the concentrations of FT4 and FT3 were notsignificantly altered by the hormonal environment inducedby controlled ovarian hyperstimulation, nor were those ofPRL and Tg.
Discussion
Subclinical hypothyroidism is a common entity affectingapproximately 5% of the adult female population. It may berelated to infertility (18) but the pathogenetic factors involvedin infertility and pregnancy wastage are unknown (7,19,20).Still, widespread screening for thyroid disease based on TSHduring infertility work-up is common. If SCH is detected, itshould be supplemented with T4. However, what the uppernormal limits of TSH during early pregnancy should be iscontroversial (1,6,21). The presence of antithyroidal anti-bodies seems to be more relevant for the occurrence of earlymiscarriage (7,8). All statements about the relationship be-tween complications during early pregnancy and hypo-thyroidism are based on a retrospective analysis of theobservations made in women suffering from more severe (i.e.,overt) hypothyroidism including some after thyroid ablativetherapy (14). Prospectively collected data in women in earlypregnancy with mild thyroid abnormalities such as SCH arelacking.
Thyroid function is profoundly modified by the hormonalchanges occurring during early pregnancy. First, the thyroidgland is challenged to increase it secretory capacity because ofrising thyroxine binding globulin levels in the presence ofhigh estrogen levels (9). Second, the thyroid gland is alsostimulated by the rapidly rising hCG levels during earlygestation (10–12). The high circulating estrogen levels inpregnancies, in which controlled ovarian hyperstimulation isdone to assist reproduction, appears to increase thyroid hor-mone requirements (22). Davis and coworkers (23), however,concluded that hypothyroid patients who conceive after go-nadotropin stimulation or with oral medications for ovulationinduction do not need additional thyroid supplementation ascompared to those who conceive spontaneously.
Table 1. Clinical Characteristics
Subclinicalhypothyroidism Euthyroidism
Number of women 8 8Age (y) 34.9 (32.0–37.2) 37.4 (34.5–40.3)Baseline TSH (mU=L) 6.14 (5.53–6.75)a 2.20 (1.59–2.81)a
Daily dose ofL-thyroxine (mg)
50 0
Conception duringMono-ovulatory
menstrual cycle3 5
Controlledhyperstimulation
5 3
After ovarianhyperstimulationNo. of pre-
ovulatory follicles3.6 (2.2–5.0) 4.5 (2.7–6.3)
Singleton delivery 7 7Miscarriage 1 1
For age and baseline thyrotropin (TSH; before treatment withthyroxine) mean values are given together with their 95% confidenceintervals.
aStatistically significant difference p< 0.001 (Mann Whitney U).
HYPOTHYROIDISM DURING EARLY PREGNANCY 55
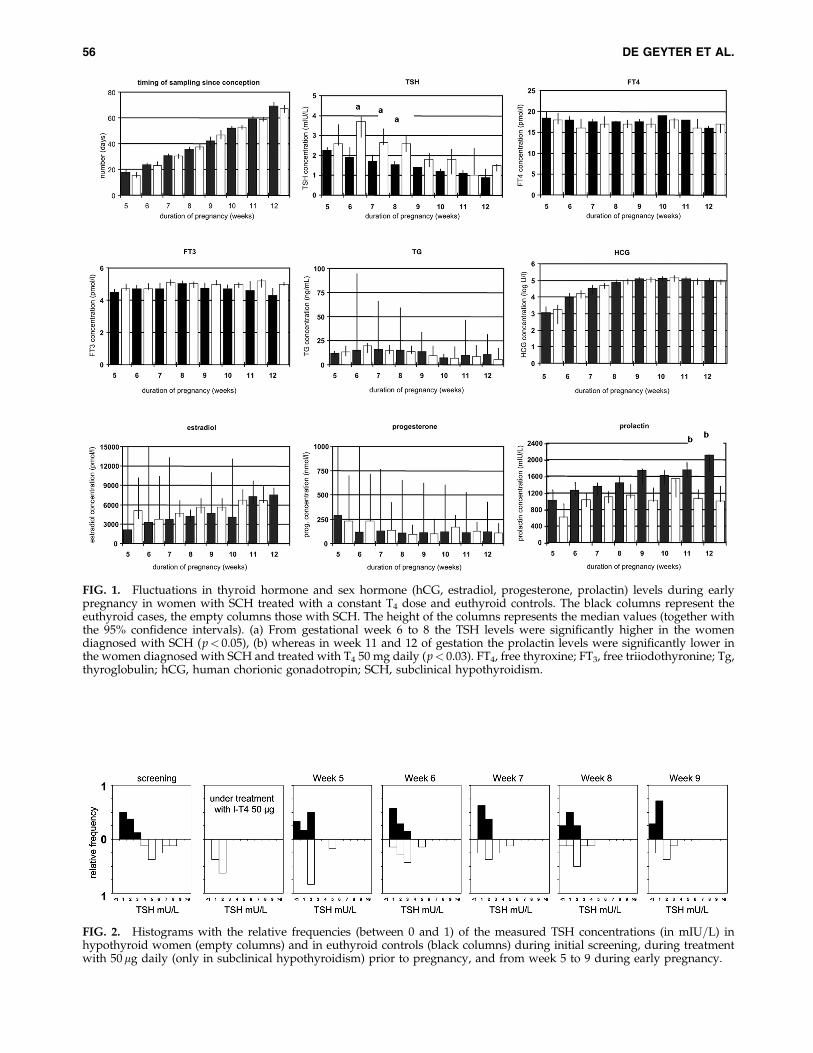
FIG. 1. Fluctuations in thyroid hormone and sex hormone (hCG, estradiol, progesterone, prolactin) levels during earlypregnancy in women with SCH treated with a constant T4 dose and euthyroid controls. The black columns represent theeuthyroid cases, the empty columns those with SCH. The height of the columns represents the median values (together withthe 95% confidence intervals). (a) From gestational week 6 to 8 the TSH levels were significantly higher in the womendiagnosed with SCH (p< 0.05), (b) whereas in week 11 and 12 of gestation the prolactin levels were significantly lower inthe women diagnosed with SCH and treated with T4 50 mg daily (p< 0.03). FT4, free thyroxine; FT3, free triiodothyronine; Tg,thyroglobulin; hCG, human chorionic gonadotropin; SCH, subclinical hypothyroidism.
FIG. 2. Histograms with the relative frequencies (between 0 and 1) of the measured TSH concentrations (in mIU=L) inhypothyroid women (empty columns) and in euthyroid controls (black columns) during initial screening, during treatmentwith 50mg daily (only in subclinical hypothyroidism) prior to pregnancy, and from week 5 to 9 during early pregnancy.
56 DE GEYTER ET AL.

The present study was designed to examine in detail thefluctuations of the regulatory components of the thyroidgland during week 5 to 12 of early gestation in both womenwith SCH and euthyroid controls. We were interested in thatparticular period of pregnancy only, because the hCG levelsreach constant levels after the luteo-placental shift. It wasthought that weekly serum sampling starting immediatelyafter the first diagnosis of pregnancy would provide thenecessary information about the balance of both stress andsupportive mediators of thyroid function during early gesta-tion. Women presenting with SCH were supplemented with afixed daily dose of T4 (50 mg), initiated before the beginning ofthe pregnancy and kept constant until the 12th week of ges-tation. Leaving women with SCH without T4 supplementa-tion until the 12th week of pregnancy for the purpose ofthis study was considered unethical after Alexander and co-workers (14) published their results claiming that an early risein T4 dose is already needed during early pregnancy in hy-pothyroid women, and our study was ended prematurely.Consequently, the number of cases in this study is limited anddid not reach the numbers needed for an analysis with solidstatistical power. Another limitation of our study is the sup-plementation of women diagnosed with SCH with a constantdose of T4, which may have reduced possible differences be-tween both groups. However, such a close follow-up of thehormonal parameters among women with SCH during veryearly gestation has not been performed yet and the observeddifferences with euthyroid controls shed some light on thepossible mechanisms involved in early pregnancy loss de-scribed in these patients.
The TSH concentration was found to be higher throughoutthe entire period of observation in women with SCH ascompared to euthyroid controls, but the difference was sta-tistically significant only between week 6 and 8 of gestation( p< 0.05). In women receiving T4, and in euthyroid controls,
TSH levels peaked during week 6. This closely paralleled therising estrogen levels during the same period of pregnancy.However, the apparent estrogen-induced change in the TSHlevel during week 6 of pregnancy was similar in both groupsas was their slow decline after week 8 of pregnancy under theinfluence of hCG (Fig. 3). Obviously, both in euthyroid wo-men and in women diagnosed with SCH receiving a constantsupplementation with T4, the rapidly rising hCG levels wereable to stimulate the thyroid gland to such an extent that FT4
and FT3 levels remained within their normal limits.SCH is often, but not always, associated with the presence
of thyroidal autoantibodies. In the two cases, in which anti-TPO antibodies were detected, the serum levels of TSH and ofFT4 were higher than those with euthyroid women and bothwere diagnosed with SCH. This corresponds well to recentevidence (8,22), claiming that the presence or absence of anti-TPO antibodies may have a bigger impact on pregnancy thanSCH itself.
Although in pregnancies arising after controlled ovarianhyperstimulation the estradiol levels remained significantlyelevated until week 7 of gestation and the progesterone levelsup to week 12 of gestation, the effect of this altered hormonalenvironment had little impact on thyroid function duringearly pregnancy. Initially, the concentrations of TSH in thewomen previously treated with ovarian hyperstimulationexceeded those of the control women. From week 9 of gesta-tion onward the TSH normalized again. Despite higher serumlevels of estradiol after controlled ovarian hyperstimulation,the concentrations of FT4, FT3, and Tg were not signifi-cantly different from those without controlled ovarian hy-perstimulation.
During gestational weeks 11 and 12 the serum levels of PRLwere significantly lower in women with SCH treated with T4
than in the nontreated euthyroid controls ( p< 0.03). Theselower levels of PRL can certainly not be attributed to differ-ences in the estradiol levels, because these were actuallyhigher after ovarian hyperstimulation. Alternatively, thelower levels of PRL might be caused by the exogenous T4 (24).
Despite the hormonal upheaval of early pregnancy anddespite unaltered supplementation with T4 all women diag-nosed with SCH remained euthyroid. Even the impressiverise of both estradiol and progesterone after ovarian hyper-stimulation failed to produce any effect on thyroid function.Obviously, the rapidly rising hCG levels were sufficient toensure normal thyroid function in both groups. The clinicalsituations presented in this study are different from thosewith primary hypothyroidism (14), characterized by pro-found abnormalities of the thyroid gland, unable to respondto the compensatory action of hCG. Recently, a higher inci-dence of both miscarriage and obstetrical complications weredescribed in the presence of anti-TPO antibodies, even inpreconceptional euthyroidism (7). Therefore, it is conceivablethat the numerous reports on pregnancy-related complica-tions observed in women with SCH, such as miscarriage andlate obstetrical complications, are not caused by hypothyr-oxinemia, but rather by additional contributing factors, suchas age and antithyroidal antibodies.
We conclude that although both SCH and ovarian hy-perstimulation were associated with an intermediate risein circulating TSH, the pattern of thyroid function duringearly pregnancy followed similar changes as those observed
FIG. 3. Changes in TSH level with reference to the TSHlevel measured during week 5 of pregnancy as calculated byTSH level measured later during early pregnancy minus TSHlevel during week 5 of pregnancy, both in euthyroid controls(black columns) and in women diagnosed with SCH butsupplemented with a constant daily dose of T4 (50mg). Theheight of each column represents the median value (togetherwith the 95% confidence intervals). All values were compa-rable in both groups except during week 12 of gestation,when the drop in the TSH concentration of women withsubclinical hypothyroidism treated with T4 was more pro-nounced than in euthyroid women ( p< 0.01).
HYPOTHYROIDISM DURING EARLY PREGNANCY 57
in euthyroid controls and is therefore unlikely to be respon-sible for the higher miscarriage rate observed in women withSCH.
Acknowledgments
This study was supported by a research grant of the Uni-versity of Basel.
Disclosure Statement
No competing financial interests exist.
References
1. Surks MI, Ortiz E, Daniels GH, Sawin CT, Col NF, CobinRH, Franklyn JA, Hershman JM, Burman KD, Denke MA,Gorman C, Cooper RS, Weissman NJ 2004 Subclinical thy-roid disease. Scientific review and guidelines for diagnosisand management. JAMA 291:228–238.
2. Pop VJ, Kuijpens JL, van Baar AL, Verkerk G, van Son MM,de Vijlder JJ, Vulsma T, Wiersinga WM, Drexhage HA, VaderHL 1999 Low maternal free thyroxine concentrations duringearly pregnancy are associated with impaired psychomotordevelopment in infancy. Clin Endocrinol (Oxf.) 90:149–155.
3. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, deVijlder JJ 2003 Maternal hypothyroxinaemia during earlypregnancy and subsequent child development: a 3-yearfollow-up study. Clin Endocrinol (Oxf.) 59:282–288.
4. Haddow JE, Palomaki GE, Allan WC, Williams JR, KnightGJ, Gagnon J, O’Heir CE, Mitchell ML, Hermos RJ, WaisbrenSE, Faix JD, Klein RZ 1999 Maternal thyroid deficiencyduring pregnancy and subsequent neuropsychological de-velopment of the child. N Engl J Med 341:549–555.
5. Kooistra L, Crawford S, van Baar AL, Brouwers EP, Pop VJ2006 Neonatal effects of maternal hypothyroxinemia duringearly pregnancy. Pediatrics 117:161–167.
6. Wartofsky L, Dickey RA 2005 The evidence for a narrowerthyrotropin reference range is compelling. J Clin EndocrinolMetab 90:5483–5488.
7. Negro R, Formoso G, Mangieri T, Pezzarossa A, Dazzi D,Hassan H 2006 Levothyroxine treatment in euthyroidpregnant women with autoimmune thyroid disease: effectson obstetrical complications. J Clin Endocrinol Metab91:2587–2591.
8. Casey BM, Dashe JS, Spong CY, McIntire DD, Leveno KJ,Cunningham GF 2007 Perinatal significance of isolated ma-ternal hypothyroxinemia identified in the first half of preg-nancy. Obstet Gynecol 109:1129–1135.
FIG. 4. Fluctuations in thyroid hormone and sex hormone (hCG, estradiol, progesterone, prolactin) levels during earlypregnancy in women with or without controlled ovarian hyperstimulation. The empty columns represent the cases without,the black columns the cases with prior ovarian hyperstimulation. The height of each column represents the median value(together with the 95% confidence intervals). As 8 out of 16 cases became pregnant after controlled ovarian hyperstimulationfor either in vitro fertilization or intracytoplasmic sperm injection, the effect of this treatment on the endocrine environmentwas examined.
58 DE GEYTER ET AL.

9. Arafah BM 2001 Increased need for thyroxine in womenwith hypothyroidism during estrogen therapy. N Engl JMed 344:1743–1749.
10. Pekonen F, Alfthan H, Stenman U-H, Ylikorkala O 1988Human chorionic gonadotropin (hCG) and thyroid functionin early human pregnancy: circadian variation and evidencefor intrinsic thyrotropic activity of hCG. J Clin EndocrinolMetab 66:853–856.
11. Kimura M, Amino N, Tamaki H, Mitsuda N, Miyai K, Ta-nizawa O 1990 Physiologic thyroid activation in normalpregnancy is induced by circulating hCG. Obstet Gynecol75:775–778.
12. Ballabio M, Poshyachinda M, Ekins RP 1991 Pregnancy-induced changes in thyroid function: role of human chorionicgonadotropin as putative regulator of maternal thyroid. J ClinEndocrinol Metab 72:824–831.
13. Mandel SJ, Larsen PR, Seely EW, Brent GA 1990 Increasedneed for thyroxine during pregnancy in women with pri-mary hypothyroidism. N Engl J Med 323:91–96.
14. Alexander EK, Marqusee E, Lawrence J, Jarolim P, FischerGA, Larsen PR 2004 Timing and magnitude of increases inlevothyroxine requirements during pregnancy in womenwith hypothyroidism. N Engl J Med 351:241–249.
15. Glinoer D 1998 The systematic screening and managementof hypothyroidism and hyperthyroidism during pregnancy.TEM 9:403–411.
16. Zimmermann MB, Aeberli I, Torresani T, Burgi H 2005 In-creasing the iodine concentration in the Swiss iodized saltprogram markedly improved iodine status in pregnantwomen and children: a 5-y prospective national study. Am JClin Nutr 82:388–392.
17. Senn A, Vozzi C, Chanson A, De Grandi P, Germond M 2000Prospective randomized study of two cryopresevation pol-icies avoiding embryo selection: the pronucleate stage leadsto a higher cumulative delivery rate than the early embryocleavage stage. Fertil Steril 74:946–952.
18. Bohnet HG, Fiedler K, Leidenberger FA 1981 Subclinicalhypothyroidism and infertility. Lancet 5:1278.
19. Bals-Pratsch M, De Geyter C, Muller T, Frieling U, Lerchl A,Pirke KM, Hanker JP, Becker-Carus C, Nieschlag E 1997Episodic variations of prolactin, thyroid-stimulating hor-mone, melatonin and cortisol in infertile women with sub-clinical hypothyroidism. Hum Reprod 12:896–904.
20. Poppe K, Velkeniers B, Glinoer D 2007 Thyroid diseaseand female reproduction. Clin Endocrinol (Oxf.) 66:309–321.
21. Brabant G, Beck-Peccoz P, Jarzab B, Laurberg P, Orgiazzi J,Szabolcs I, Weetman AP, Wiersinga WM 2006 Is there a needto redefine the upper normal limit of TSH? Eur J Endocrinol154:633–637.
22. Poppe K, Glinoer D, Tournaye H, Schiettecatte J, Devroey P,Van Steirteghem A, Haentjens P, Velkeniers B 2004 Impactof ovarian hyperstimulation on thyroid function in womenwith and without thyroid autoimmunity. J Clin EndocrinolMetab 89:3808–3812.
23. Davis LB, Lathi RB, Dahan MH 2007 The effect of infertilitymedication on thyroid function in hypothyroid women whoconceive. Thyroid 17:773–777.
24. Meier C, Christ-Crain M, Guglielmetti M, Huber P, Staub J-J,Muller B 2003 Prolactin dysregulation in women with sub-clinical hypothyroidism: effect of levothyroxine replacementtherapy. Thyroid 13:979–985.
Address reprint requests to:Christian De Geyter
University Women’s HospitalSpitalstrasse 21CH-4031 Basel
Switzerland
E-mail: [email protected]
HYPOTHYROIDISM DURING EARLY PREGNANCY 59





















