Personality Profiles in Young Adults with Subclinical ...
22
HAL Id: hal-03191814 https://hal.archives-ouvertes.fr/hal-03191814 Submitted on 7 Apr 2021 HAL is a multi-disciplinary open access archive for the deposit and dissemination of sci- entific research documents, whether they are pub- lished or not. The documents may come from teaching and research institutions in France or abroad, or from public or private research centers. L’archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des établissements d’enseignement et de recherche français ou étrangers, des laboratoires publics ou privés. Personality Profiles in Young Adults with Subclinical Obsessive-Compulsive Symptoms: Not just obsessionality Patrick Raynal, Tiffany Melioli, Henri Chabrol To cite this version: Patrick Raynal, Tiffany Melioli, Henri Chabrol. Personality Profiles in Young Adults with Subclinical Obsessive-Compulsive Symptoms: Not just obsessionality. Bulletin of the Menninger Clinic, Guilford Press, 2019. hal-03191814
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Personality Profiles in Young Adults with Subclinical ...
HAL Id: hal-03191814https://hal.archives-ouvertes.fr/hal-03191814
Submitted on 7 Apr 2021
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Personality Profiles in Young Adults with SubclinicalObsessive-Compulsive Symptoms: Not just
obsessionalityPatrick Raynal, Tiffany Melioli, Henri Chabrol
To cite this version:Patrick Raynal, Tiffany Melioli, Henri Chabrol. Personality Profiles in Young Adults with SubclinicalObsessive-Compulsive Symptoms: Not just obsessionality. Bulletin of the Menninger Clinic, GuilfordPress, 2019. �hal-03191814�

1
Running head: PERSONALITY AND OBSESSIVE-COMPULSIVE SYMPTOMS
Personality Profiles in Young Adults with Subclinical Obsessive-Compulsive Symptoms: Not
just obsessionality
Patrick Raynala*, Tiffany Meliolia, Henri Chabrola
a Centre d’Etudes et de Recherches en Psychopathologie et Psychologie de la Santé
Université de Toulouse, UT2J, France
* Corresponding author: Patrick Raynal, Centre d'Etudes et de Recherches en Psychopathologie
et Psychologie de la Santé, Université de Toulouse-Jean Jaurès, 5 allées Antonio Machado,
31058 Toulouse, France; Phone number : 33 561 50 35 59; Fax number : 33 561 25 70 93; E-
mail address: [email protected]
2
Abstract
Research is scarce regarding the personality profiles of individuals with subclinical obsessive-
compulsive symptoms. Cluster analysis based on personality disorders (obsessional, schizotypal,
borderline) and autism-spectrum features was conducted on 118 students scoring above cutoff
for the Obsessive Compulsive Inventory-Revised. This identified 4 groups (O, L, S and A). One
third of the sample was represented by individuals with obsessional traits (O) while another third
was composed of individuals with low traits (L); the last two profiles corresponded to a cluster
with autistic traits (A) and a group with schizotypal and borderline features (S), both clusters
representing altogether the remaining third. Significant differences were observed between
groups, both on personality traits and on psychopathological symptoms. The S cluster displayed
the highest scores of suicidality, depression or obsessive-compulsive symptoms, suggesting that
these individuals should require attention from clinicians. This study thus identified distinct and
meaningful personality profiles of individuals with subclinical obsessive-compulsive symptoms.
Keywords: Personality traits; Schizotypy; Borderline; Autism-spectrum; Cluster analysis.

3
1. Introduction
Obsessive-compulsive disorder (OCD) is a debilitating and chronic illness with an estimated
lifetime prevalence of 1.2-2.5%. It is a symptomatically heterogeneous condition in which
different kinds of compulsions and obsessions exist, including checking compulsions, symmetry
obsessions, washing rituals or repugnant obsessions (e.g., sex, violence…) (Abramowitz, Taylor,
& McKay, 2009; Ruscio, Stein, Chiu, & Kessler, 2010). Research has suggested the existence of
possible subtypes of OCD, based on the variety of symptom presentations and on different
responses to existing treatments (McKay et al., 2004; Steketee et al., 2011; Farris, McLean, Van
Meter, Simpson, & Foa, 2013; McKay et al., 2015), as well as on variations in
neuropsychological functioning (Glahn, Prell, Grosskreutz, Peschel, & Müller-Vahl, 2015).
Heterogeneity was also reported when studying the motivational dimensions of individuals with
OCD, as cluster analyses identified four subgroups with relatively high or low levels of harm
avoidance and incompleteness motivations (Bragdon & Coles, 2017).
Whether personality plays a role in OCD heterogenity remains unclear. Most individuals
with OCD display a comorbid personality disorder (PD) (Torres et al., 2006; Bejerot, Ekselius,
& Knorring, 1998; Baer & Jenike, 1992). Different types of PD can be associated with OCD,
notably obsessive-compulsive PD (OCPD). Clinicians have asserted for decades that a strong
relationship existed between OCD and OCPD but in fact there is a wide range (10-60%) of
comorbidity rate described in the literature (Wu, Clark, & Watson, 2006; Torres et al., 2006).
This fueled the debate about the nature of the link between OCD and OCPD. Researchers
suggested that obsessive-compulsive personality traits and OCD may exist along a continuum
(Mathews, Jang, Hami, & Stein, 2004; Pinto, Greene, Storch, & Simpson, 2015; Park, Storch,
Pinto, & Lewin, 2016). In contrast, other studies indicated that OCDP comorbidity might be
rather considered as a marker of OCD severity (Lochner et al., 2011; Wetterneck et al., 2011), or
that the comorbidity of OCD with OCPD could be a specific subtype of OCD (Garyfallos et al.,
2010).

4
Schizotypal personality disorder (SPD) is also a frequent comorbidity in patients with OCD
or individuals with OCD living in the community, with comorbidity rates ranging from 5 to 30%
(Torres et al., 2006). In non-clinical samples, obsessive-compulsive symptoms were found to be
associated with schizotypy (Roth & Baribeau, 2000; Chmielewski & Watson, 2008; Fonseca-
Pedrero, Lemos-Giráldez, Paíno-Piñeiro, Villazón-García, & Muñiz, 2010). Not surprisingly,
patients with both OCD and SPD or schizotypal features were found to display poorer insight,
lower functioning and increased OCD severity in comparison with patients with OCD alone
(Poyurovski et al., 2008; Huang, Hwang, Huang, & Hwu, 2011). However other reports failed to
show that individuals with OCD and schizophrenia or high levels of schizotypy had a significant
increase in OCD severity (Brakoulias et al., 2014; Doyle, Chorcorain, Griffith, Trimble, &
O’Callaghan, 2014; Solem et al. 2015).
In this study, the occurrence of borderline traits in individuals with subclinical obsessive-
compulsive symptoms was explored, considering that borderline PD (BPD) is not a rare
comorbidity of OCD (rate range: 3-23%; Melca, Yücel, Mendlowicz, de Oliveira-Souza, &
Fontenelle, 2015; Bulli, Melli, Cavalletti, Stopani, & Carraresi, 2016). In addition our study took
into consideration autistic characteristics. Indeed overlaps between features of autism spectrum
disorders (ASD) and OCD were reported (Chasson et al., 2011; Wakabayashi, Baron-Cohen, &
Ashwin, 2012) and the prevalence of OCD in youth with ASD is not uncommon (Lewin, Wood,
Gunderson, Murphy, & Storch, 2011).
Research is scarce regarding the typology of individuals with subclinical obsessive-
compulsive difficulties. Yet having obsessions and compulsions is a matter of substantial
suffering and disability, as these subjects, even though they are not diagnosed with OCD, may
display similar consequences to patients with full-blown OCD (De Bruijn, Beun, De Graaf, Ten
Have, & Denys, 2010).

5
The present study had two objectives: a) to explore the typology of a nonclinical sample of
young adults with subclinical obsessive-compulsive symptoms based on schizotypal,
obsessional, borderline and autistic features and b) to examine the validity of clusters by
comparing them across variables potentially allowing to distinguish clusters (i.e., depressive
symptoms, frequency of cannabis use, academic performance). We hypothesized that clusters
will differ on both personality traits and psychopathological symptoms. This could allow to
identify relatively more homogeneous subgroups from a markedly heterogeneous sample of
individuals with subclinical obsessive-compulsive symptoms.
2. Methods
2.1. Participants
Potential participants (students in France universities) were informed about the study via social
networks and official website of several French universities. Informed consent was obtained
from all participants by ticking a box on the Internet website before completing the study.
Potential participants were provided with information regarding the study aims and were
informed that answers to the questionnaires would remain strictly confidential and be analyzed
according to scientific aims. No compensation was offered to participate in the study, following
a standard procedure of the institution. The participants were provided with the possibility to
contact the principal investigator (PR) via email for further information or to receive referral.
The questionnaires were anonymous. The study followed the ethical guidelines of the Helsinki
Declaration and its procedures were approved by the ethics committee of the research ward.
Inclusion criteria were also being aged over 18 years and having completed all the scales.
Personal information (age, gender, level of academic degree and academic results during the past
semester) was gathered. The initial sample was composed of 476 students (95 males; 381
females) aged between 18 and 25 (mean age of males = 21 ± 2.3; mean age of females = 20.7 ±
1.9; p = 0.32).
6
2.2. Measures
2.2.1. Obsessive-compulsive symptoms
Obsessive-compulsive symptoms were assessed using the French version of the Obsessive
Compulsive Inventory-Revised (OCI-R; Foa et al., 2002; Zermatten, Van der Linden, Jermann, &
Ceschl, 2006). It contained 18 items (e.g., "I check things more often than necessary") scored
from 0 ("Not at all") to 4 ("Extremely"). A cutoff score of 25 was chosen to identify individuals
with subclinical obsessive-compulsive symptoms as it provides high specificity (Foa et al.,
2002). Cronbach's α range was 0.81-0.93 in Foa et al.'s report.
2.2.2. Obsessional personality traits
Obsessional traits were measured using the French version of the Obsessional personality
disorder scale of the Personality Diagnostic Questionnaire-4 (Bouvard, 2002; Hyler, Rieder,
Williams, Spitzer, & Lyons, 1988). This scale contained 8 items (e.g., "I feel that my standards
and ethics are higher than those of my peers") scored 0 (false) or 1 (true). Cronbach's α range
was 0.46-0.66 in former studies (Hyler et al., 1988; Bouvard 2002).
2.2.3. Schizotypal traits
Schizotypal traits were assessed using the Schizotypal Personality Questionnaire-Brief (SPQ-B;
Raine & Benishay, 1995), a self-administered scale including 22 dichotomous items. We used a
French version of SPQ-B already described in previous studies (Raynal, Goutaudier, Nidetch, &
Chabrol, 2016; Raynal, Melioli, & Chabrol, 2016). Each item (e.g., "People sometimes find me
aloof and distant") was scored 0/1 (no/yes). Cronbach's α was 0.81 in a previous report (Fonseca-
Pedrero, Paino-Pineiro, Lemos-Giraldez, Villazon-Garcia, & Muniz, 2009).
2.2.4. Borderline personality traits
Borderline PD traits were assessed using the nine relevant items of the Personality Diagnostic
Questionnaire-4 under its French version (Bouvard, 2002; Hyler, Rieder, Williams, Spitzer, &
Lyons, 1988). Items (e.g., " I often question my personal identity and frequently change my
7
opinion of who I am") were scored from 1 (totally false) to 7 (totally true). Cronbach's α range
was 0.69 in a former study (Chabrol, Valls, van Leeuwen, & Bui, 2012)
2.2.5. Autism-spectrum characteristics
Autism-spectrum characteristics were measured using the Autism spectrum Quotient (AQ)
(Baron-Cohen, Wheelwright, Skinner, Martin, & Clubley, 2001) under its 10-item version. A
French version of AQ-10 was adapted from the French version of AQ by selecting the 10
relevant items that have been selected in AQ-10, as previously described (Booth et al., 2013;
Raynal, Goutaudier, Nidetch, & Chabrol, 2016). Items (e.g., "When I am reading a story, I find it
difficult to work out the characters intentions") were scored 0 (no) or 1 (yes), except for items 2-
6 and 9 that were scored inversely. Cronbach’s α was 0.85 in Tchanturia et al.’s study (2013).
2.2.6. Depression symptoms and suicidal ideations
Depression was evaluated using The Centre for Epidemiological Studies-Depression scale (CES-
D; Radloff, 1977) under its 10-item version (e.g., "My sleep has not been good"). The French
version of this questionnaire was used (Fuhrer & Rouillon, 1989). Responses were made on a 4-
point Likert scale, ranging from 0 to 3. Cronbach's α was 0.70 in Radloff's report (1977).
The suicidal ideation was assessed using the 3-item scale ("I felt life was not worth living";
"I felt like hurting myself"; "I felt like killing myself") proposed by Garrison, Addy, Jackson,
McKeown, & Waller (1991). A French version of this scale was already described (Chabrol,
Rodgers, & Rousseau, 2007). Responses to these items were made on the same scale as the CES-
D items. A suicidal ideation score (range 0–9) was calculated by summing responses on these
three items. Cronbach's α was 0.85 in an earlier report (Chabrol et al., 2007).
2.2.7. Cannabis use
Cannabis use was measured with the Cannabis Use Disorder Identification Test-Revised
(CUDIT-R; Adamson et al., 2010). The French version of this questionnaire was
found in Annaheim, Rehm, & Gmel (2008). Cronbach's α range was 0.84 in Adamson et al.'s
study.

8
2.3. Statistical analysis
A cluster analysis was performed on individuals displaying a score above the cut-off for the
OCI-R. This analysis was based on scores obtained on the following dimensions: obsessional,
schizotypal, borderline and autistic. This was achieved by standardizing as z-scores the
participants scores for each dimension. A hierarchical cluster analysis was then conducted
(Ward’s method with Euclidean distance). The dendrogram and the agglomeration schedule were
used to identify the number of clusters. Then, K-means clustering was used to assign each
individual to the identified clusters. Missing data was replaced with the item mean. Because the
distribution of scores on cannabis use and on suicidal ideations were positively skewed, a square
root transformation was used to reduce skewness. Statistical analyses were performed using
Statistica 10.
3. Results
3.1. Descriptive statistics
In the initial sample of 476 students, the mean score for the OCI-R was 18.23 (SD = 11.08).
SPQ-B and CES-D-10 mean scores were 8.46 (SD = 4.42) and 12.79 (SD = 4.07), respectively.
Table 1 displays Cronbach's α and score ranges. The obsessional and the autism scales showed
suboptimal Cronbach's α in the 0.5 range.
3.2. Comparison of participants with obsessive-compulsive symptoms with a control group
The participants scoring above cutoff on the OCI-R were considered as composing the group
with a significant level of obsessive-compulsive symptoms (OC; n = 112, 77.7% female, 22.3%
male). This group was compared to the rest of participants (control group; n = 364, 80.8%
female, 19.2% male). The proportion of male was not higher in the OC group compared with the
control group (p = 0.278, Fisher's exact test). The OC group had higher scores on all personality
traits and psychopathological symptoms (Table 1). Cohen’s d indicated large size effects except
for autistic traits and cannabis use which showed medium or small size effects. Students in the

9
control group had slightly higher academic degrees but academic performance was virtually
identical between the two groups.
3.3. Cluster analysis
A cluster analysis was performed on the participants from the OC group. This analysis was
conducted in two steps based on scores on the following dimensions: obsessional, schizotypal,
borderline and autistic. Absence of multicollinearity was evaluated through an analysis of the
correlations between the variables selected for the cluster analysis (all variables had tolerance
values > .60). In the first step, a hierarchical cluster analysis was conducted (Ward’s method
with Euclidean distance). Based on the dendrogram and the aggregation curve, a four-cluster
solution was identified. In the second step, K-means clustering was used to assign individuals to
one of the identified clusters. A discriminant analysis showed clear differences between clusters
(Wilks’ λ = 0.116, p < 0.001) with 94.6% of cases correctly classified. Data revealed a first
group with a score of obsessional traits higher than other clusters by more than one SD, while the
scores of this cluster regarding the other variables were close to the mean of the sample
(Figure 1; Table 1). This cluster was thus termed "Obsessional" (O, n = 39, [34.8%]). A second
cluster displayed scores on both schizotypal and borderline traits higher than other clusters by at
least one SD. It was thus named "Schizotypal-borderline" (S, n = 15 [13.4%]). A third group was
characterized with autistic traits higher than the other clusters by nearly one and a half SD and
was thus called "Autistic" (A, n = 19 [17%]). A fourth group, called "Low traits" (L, n = 39
[34.8%]) was characterized with scores below the sample mean for all dimensions.
Cluster group differences in levels of PD traits, depression symptoms, suicidality, cannabis
use and academic results were tested using an analysis of variance (ANOVA; Table 2). Firstly,
ANOVA showed that significant differences between clusters existed on all variables except
cannabis use and academic degree (column "F"). Tukey post-hoc test further confirmed the
importance of differences between clusters (column "Significant comparisons"). Indeed S was
more elevated than all other clusters when considering schizotypy and borderline traits. O scored
10
higher than the other groups regarding obsessionality. A was more elevated than all other
clusters for the autistic dimension. Further confirming this classification, significant differences
were also observed between clusters when analyzing depression symptoms, suicidal ideation and
academic results of past semester. Indeed S was more elevated than the other clusters on suicidal
ideas and it scored higher than O and L regarding depression symptoms. In addition, S displayed
higher obsessive-compulsive symptoms in comparison to L, and lesser academic results during
past semester, when compared with 0 or L. Of note, A scored higher than L on suicidality and
depression. Taken together these data allowed to identify four distinct profiles of individuals
with subclinical obsessive-compulsive symptoms.
4. Discussion
Regarding the validity of this study, our sample appeared to be very similar to other non clinical
samples described in the literature. For instance, in our initial sample of 476 participants, 112
individuals (24.4%) displayed a score suggesting obsessive-compulsive symptoms, which is
close to the rate of 28.2% of US adults reporting similar symptoms (Ruscio, Stein, Chiu, &
Kessler, 2010). Similarly, the mean OCI-R score of this study was 18.23, that is almost identical
to values reported earlier: 18.82 in Foa et al. (2002); 18.91 in Hajcak, Huppert, Simons, & Foa
(2004). On the same theme, the mean scores for SPQ-B and CES-D-10 in our whole sample
were 8.46 and 12.79 respectively, close to 9.6 and 12.9 reported in the general population (Raine
& Benishay, 1995; Radloff, 1977).
In this study we performed a cluster analysis based on PD traits and the autistic dimension
on individuals with subclinical obsessive-compulsive symptoms. To our knowledge, this is the
first study to propose a personality-based typology of individuals with this type of symptoms.
This resulted in 4 distinct profiles: one third of the sample was represented by individuals with
obsessional traits as core feature (O group), while another third was composed of individuals
with low traits (L); the last two profiles corresponded to a group of individuals with autistic traits
11
(A) and a group with schizotypal and borderline features (S), both groups representing altogether
the remaining third of the sample.
A noticeable finding provided by this study is that a significant heterogeneity prevails in the
personality profiles of individuals with subclinical obsessive-compulsive difficulties. Firstly
students with obsessional traits represented one third of these individuals, which is very close to
the prevalence rate of OCPD in individuals with OCD described in recent reports (33-34%;
Garyfallos et al., 2010; Lochner et al., 2011). The remaining two thirds of individuals with
obsessive-compulsive symptoms was thus composed of persons who did not display
obsessionality features. Hence it seems difficult to envision that obsessionality and subclinical
obsessive-compulsive symptoms are necessarily on the same continuum.
Those two thirds were constituted of 3 distinct profiles: A, S and a Low-trait group. The A
group is composed of individuals featuring an association between subclinical obsessive-
compulsive problems and autism-spectrum traits. Although OCD and ASD seem to be highly
disparate at first sight, links between these disorders have been recently established in terms of
shared social competence impairment (Chasson et al., 2011), and ASD symptoms were already
reported in OCD children (Arildskov et al., 2016). In support of this association, the same
polymorphism producing a gain-of-function of the serotonin transporter gene was identified in
individuals with OCD and ASD (Wendland et al., 2008). Further supporting this link, our data
indicates that, even when considering obsessive-compulsive symptoms at a subclinical level,
autistic features are not uncommon, reinforcing the notion that ASD comorbidity can be
significantly associated with OCD.
The S group was composed of individuals with high schizotypy and borderline traits, which
may reflect the high comorbidity between SPD and BPD (Pulay et al., 2009). This S group
appeared to share characteristics with patients displaying OCD and SPD or BPD comorbidity
(Melca, Yücel, Mendlowicz, de Oliveira-Souza, & Fontenelle, 2015). However the prevalence of
this association seems to be lower in individuals with subclinical obsessive-compulsive
12
symptoms than in those with full-blown OCD. Indeed individuals with SPD or BPD represented
altogether ≈34% of patients with OCD (Melca et al., 2015), while the S group constituted only
13.4% of individuals with subclinical obsessive-compulsive difficulties.
The individuals with the S group profile seem to require the most attention from clinicians,
with significant degradations when compared to other clusters. Indeed this group displayed the
highest scores of suicidality, depression or obsessive-compulsive symptoms. In agreement with
these observations, previous studies on patients with OCD and with SPD or BPD showed that
these individuals had the highest rates of several comorbid psychiatric disorders in comparison
with other types of patients with OCD (Melca, Yücel, Mendlowicz, de Oliveira-Souza, &
Fontenelle, 2015). Similarly other reports found that patients with OCD with the highest load of
schizotypal symptoms had increased general psychopathology, including greater depressive
symptomatology (Poyurovsky et al., 2008; Solem et al., 2015).
The S group also showed the highest score for cannabis use, even though large SD impaired
the significance of this difference. In addition this group displayed the lowest scores on academic
functioning, even though with a non significant difference for the variable "academic degree".
Former studies in patients with full-blown OCD and schizotypal features also reported a lower
functioning in these individuals in comparison with non-schizotypal patients with OCD (Huang,
Hwang, Huang, & Hwu, 2011; Brakoulias et al., 2014).
Therefore schizotypal and borderline traits appeared to be a detrimental element for
individuals with subclinical obsessive-compulsive symptoms, requiring particular attention from
clinicians, as these personality traits may aggravate the outcome of these symptoms, notably
through increasing depression and suicidality.
This study is not exempt from limitations. Firstly, the small sample size and the low
proportion of men may restrict the generalizability of the present findings, even though OCD
appears to be somewhat more frequent in women (Bebbington, 1998). In addition, the cross-
sectional nature of data collection and the use of self-report measures impaired the assessment of

13
causality in the results and can induce common bias in this type of study. Furthermore scales
showed suboptimal Cronbach's α in the 0.5 range, although this can be considered as an
acceptable level of consistency (Schmitt, 1996).
In conclusion this study identified four distinct personality profiles of individuals with
subclinical obsessive-compulsive difficulties, among which those with significant obsessionality
represented no more than one third of the sample. This clearly emphasizes the importance of
other personality traits, notably schizotypal, borderline and autistic features. Further studies are
now required to explore how these profiles may influence the progression of obsessive-
compulsive symptoms.
Acknowledgements: We thank V. Loir and V. Nidetch for help in study design and data
collection.
5. References
Abramowitz, J. S., Taylor, S., & McKay, D. (2009). Obsessive-compulsive disorder. The Lancet,
374, 491-499.
Adamson, S. J., Kay-Lambkin, F. J., Baker, A. L., Lewin, T. J., Thornton, L., Kelly, B. J., &
Sellman, J. D. (2010). An improved brief measure of cannabis misuse: the Cannabis Use
Disorders Identification Test-Revised (CUDIT-R). Drug and Alcohol Dependence, 110, 137-
143.
Annaheim, B., Rehm, J., & Gmel, G. (2008). How to screen for problematic cannabis use in
population surveys. European Addiction Research, 14, 190-197.
Arildskov, T. W., Højgaard, D. R., Skarphedinsson, G., Thomsen, P. H., Ivarsson, T., Weidle,
B., ... & Hybel, K. A. (2016). Subclinical autism spectrum symptoms in pediatric obsessive–
compulsive disorder. European Child & Adolescent Psychiatry, 25, 711–723.
Baer, L., & Jenike, M. A. (1992). Personality disorders in obsessive compulsive disorder.
Psychiatric Clinics of North America, 15, 803-812.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The autism-
spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males

14
and females, scientists and mathematicians. Journal of Autism and Developmental Disorders,
31, 603-603.
Bebbington, P. E. (1998). Epidemiology of obsessive-compulsive disorder. The British Journal
of Psychiatry, 173, 2-6.
Bejerot, S., Ekselius, L., & Knorring, L. V. (1998). Comorbidity between obsessive-compulsive
disorder and personality disorders. Acta Psychiatrica Scandinavica, 97, 398-402.
Booth, T., Murray, A. L., McKenzie, K., Kuenssberg, R., O’Donnell, M., & Burnett, H. (2013).
Brief report: An evaluation of the AQ-10 as a brief screening instrument for ASD in adults.
Journal of Autism and Developmental Disorders, 43, 2997-3000.
Bouvard, M. (2002). Questionnaires et échelles d’évaluation de la personnalité. Masson. Paris.
Bragdon, L. B., & Coles, M. E. (2016). Examining heterogeneity of obsessive-compulsive
disorder: Evidence for subgroups based on motivations. Journal of Anxiety Disorders, 45, 64-
71.
Brakoulias, V., Starcevic, V., Berle, D., Milicevic, D., Hannan, A., Viswasam, K., & Mann, K.
(2014). The clinical characteristics of obsessive compulsive disorder associated with high
levels of schizotypy. Australian and New Zealand Journal of Psychiatry, 0004867414531831.
Bulli, F., Melli, G., Cavalletti, V., Stopani, E., & Carraresi, C. (2016). Comorbid personality
disorders in obsessive–compulsive disorder and its symptom dimensions. Psychiatric
Quarterly, 87, 365-376.
Chabrol, H., Rodgers, R., Rousseau, A. (2007). Relations between suicidal ideation and
dimensions of depressive symptoms in high-school students. Journal of Adolescence, 30, 587-
600.
Chabrol, H., Valls, M., van Leeuwen, N., & Bui, E. (2012). Callous-unemotional and borderline
traits in nonclinical adolescents: Personality profiles and relations to antisocial behaviors.
Personality and Individual Differences, 53, 969-973.
Chasson, G. S., Timpano, K. R., Greenberg, J. L., Shaw, A., Singer, T., & Wilhelm, S. (2011).
Shared social competence impairment: Another link between the obsessive-compulsive and
autism spectrums? Clinical Psychology Review, 31, 653-662.
Chmielewski, M., & Watson, D. (2008). The heterogeneous structure of schizotypal personality
disorder: item-level factors of the Schizotypal Personality Questionnaire and their
associations with obsessive-compulsive disorder symptoms, dissociative tendencies, and
normal personality. Journal of Abnormal Psychology, 117, 364-376.
De Bruijn, C., Beun, S., De Graaf, R., Ten Have, M., & Denys, D. (2010). Symptoms and
obsessive-compulsive disorder: evaluating the diagnostic threshold. Psychological Medicine,
40, 989-997.

15
Doyle, M., Chorcorain, A. N., Griffith, E., Trimble, T., & O’Callaghan, E. (2014). Obsessive
compulsive symptoms in patients with schizophrenia on clozapine and with obsessive
compulsive disorder: a comparison study. Comprehensive Psychiatry, 55, 130-136.
Farris, S. G., McLean, C. P., Van Meter, P. E., Simpson, H. B., & Foa, E. B. (2013). Treatment
response, symptom remission, and wellness in obsessive-compulsive disorder. The Journal of
Clinical Psychiatry, 74, 685-690.
Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G., & Salkovskis, P. M.
(2002). The Obsessive-Compulsive Inventory: development and validation of a short version.
Psychological Assessment, 14, 485-496.
Fonseca-Pedrero, E., Paino-Pineiro, M., Lemos-Giraldez, S., Villazon-Garcia, U., & Muniz, J.
(2009). Validation of the Schizotypal Personality Questionnaire-Brief form in adolescents.
Schizophrenia Research, 111, 53-60.
Fonseca-Pedrero, E., Lemos-Giráldez, S., Paíno-Piñeiro, M., Villazón-García, U., & Muñiz, J.
(2010). Schizotypal traits, obsessive-compulsive symptoms, and social functioning in
adolescents. Comprehensive Psychiatry, 51, 71-77.
Fuhrer, R., & Rouillon, F. (1989). French version of CES-D scale: description and translation of
self evaluation. Psychiatry and Psychology, 4, 163-166.
Garrison, C. Z., Addy, C. L., Jackson, K. L., McKeown, R. E., & Waller, J. L. (1991). A
longitudinal study of suicidal ideation in young adolescents. Journal of the American
Academy of Child and Adolescent Psychiatry, 30, 597-603.
Garyfallos, G., Katsigiannopoulos, K., Adamopoulou, A., Papazisis, G., Karastergiou, A., &
Bozikas, V. P. (2010). Comorbidity of obsessive–compulsive disorder with obsessive–
compulsive personality disorder: Does it imply a specific subtype of obsessive–compulsive
disorder? Psychiatry Research, 177, 156-160.
Glahn, A., Prell, T., Grosskreutz, J., Peschel, T., & Müller-Vahl, K. R. (2015). Obsessive-
compulsive disorder is a heterogeneous disorder: Evidence from diffusion tensor imaging and
magnetization transfer imaging. BMC Psychiatry, 15, 135.
Hajcak, G., Huppert, J. D., Simons, R. F., & Foa, E. B. (2004). Psychometric properties of the
OCI-R in a college sample. Behaviour Research and Therapy, 42, 115-123.
Huang, L. C., Hwang, T. J., Huang, G. H., & Hwu, H. G. (2011). c: a pilot study. Journal of the
Formosan Medical Association, 110, 85-92.
Hyler, S. E., Rieder, R. O., Williams, J. B., Spitzer, J. H., & Lyons, M. (1988). The Personality
Diagnostic Questionnaire: Development and preliminary results. Journal of Personality
Disorders, 2, 229-237.

16
Lewin, A. B., Wood, J. J., Gunderson, S., Murphy, T. K., & Storch, E. A. (2011).
Phenomenology of comorbid autism spectrum and obsessive-compulsive disorders among
children. Journal of Developmental and Physical Disabilities, 23, 543-553.
Lochner, C., Serebro, P., van der Merwe, L., Hemmings, S., Kinnear, C., Seedat, S., & Stein, D.
J. (2011). Comorbid obsessive–compulsive personality disorder in obsessive-compulsive
disorder (OCD): A marker of severity. Progress in Neuro-Psychopharmacology and
Biological Psychiatry, 35, 1087-1092.
Mathews, C. A., Jang, K. L., Hami, S., & Stein, M. B. (2004). The structure of obsessionality
among young adults. Depression and Anxiety, 20, 77-85.
McKay, D., Abramowitz, J. S., Calamari, J. E., Kyrios, M., Radomsky, A., Sookman, D., ... &
Wilhelm, S. (2004). A critical evaluation of obsessive-compulsive disorder subtypes:
symptoms versus mechanisms. Clinical Psychology Review, 24, 283-313.
McKay, D., Sookman, D., Neziroglu, F., Wilhelm, S., Stein, D. J., Kyrios, M., ... & Veale, D.
(2015). Efficacy of cognitive-behavioral therapy for obsessive-compulsive disorder.
Psychiatry Research, 225, 236-246.
Melca, I. A., Yücel, M., Mendlowicz, M. V., de Oliveira-Souza, R., & Fontenelle, L. F. (2015).
The correlates of obsessive–compulsive, schizotypal, and borderline personality disorders in
obsessive-compulsive disorder. Journal of Anxiety Disorders, 33, 15-24.
Park, J. M., Storch, E. A., Pinto, A., & Lewin, A. B. (2016). Obsessive-compulsive personality
traits in youth with obsessive–compulsive disorder. Child Psychiatry & Human Development,
47, 281-290.
Pinto, A., Greene, A. L., Storch, E. A., & Simpson, H. B. (2015). Prevalence of childhood
obsessive-compulsive personality traits in adults with obsessive-compulsive disorder versus
obsessive compulsive personality disorder. Journal of Obsessive-Compulsive and Related
Disorders, 4, 25-29.
Poyurovsky, M., Faragian, S., Pashinian, A., Heidrach, L., Fuchs, C., Weizman, R., & Koran, L.
(2008). Clinical characteristics of schizotypal-related obsessive-compulsive disorder.
Psychiatry Research, 159, 254-258.
Pulay, A. J., Stinson, F. S., Dawson, D. A., Goldstein, R. B., Chou, S. P., Huang, B., ... & Hasin,
D. S. (2009). Prevalence, correlates, disability, and comorbidity of DSM-IV schizotypal
personality disorder: results from the wave 2 national epidemiologic survey on alcohol and
related conditions. The Primary Care Companion to The Journal of Clinical Psychiatry, 11,
53-67.
Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the
general population. Applied Psychological Measurements, 1, 385-401.
17
Raine, A., & Benishay, D. (1995). The SBQ-B: A brief screening instrument for schizotypal
personality disorder. Journal of Personality Disorders, 9, 346-355.
Raynal, P., Goutaudier, N., Nidetch, V., & Chabrol, H. (2016). Typology of schizotypy in non-
clinical young adults: Psychopathological and personality disorder traits correlates. Psychiatry
Research, 246, 182-187.
Raynal, P., Melioli, T., & Chabrol, H. (2016). Personality profiles in young adults with
disordered eating behavior. Eating Behaviors, 22, 119-123.
Roth, R. M., & Baribeau, J. (2000). The relationship between schizotypal and obsessive-
compulsive features in university students. Personality and Individual Differences, 29, 1083-
1093.
Ruscio, A. M., Stein, D. J., Chiu, W. T., & Kessler, R. C. (2010). The epidemiology of
obsessive-compulsive disorder in the National Comorbidity Survey Replication. Molecular
Psychiatry, 15, 53-63.
Schmitt, N. (1996). Uses and abuses of coefficient alpha. Psychological Assessment, 8, 350-353.
Solem, S., Hagen, K., Wenaas, C., Håland, Å. T., Launes, G., Vogel, P. A., ... & Himle, J. A.
(2015). Psychotic and schizotypal symptoms in non-psychotic patients with obsessive-
compulsive disorder. BMC psychiatry, 15, 1.
Steketee, G., Siev, J., Fama, J. M., Keshaviah, A., Chosak, A., & Wilhelm, S. (2011). Predictors
of treatment outcome in modular cognitive therapy for obsessive–compulsive disorder.
Depression and Anxiety, 28, 333-341.
Tchanturia, K., Smith, E., Weineck, F., Fidanboylu, E., Kern, N., Treasure, J., & Cohen, S. B.
(2013). Exploring autistic traits in anorexia: a clinical study. Molecular autism, 4, 1.
Torres, A. R., Moran, P., Bebbington, P., Brugha, T., Bhugra, D., Coid, J. W., ... & Prince, M.
(2006). Obsessive-compulsive disorder and personality disorder. Social Psychiatry and
Psychiatric Epidemiology, 41, 862-867.
Wakabayashi, A., Baron-Cohen, S., & Ashwin, C. (2012). Do the traits of autism-spectrum
overlap with those of schizophrenia or obsessive-compulsive disorder in the general
population? Research in Autism Spectrum Disorders, 6, 717-725.
Wendland, J. R., DeGuzman, T. B., McMahon, F., Rudnick, G., Detera-Wadleigh, S. D., &
Murphy, D. L. (2008). SERT Ileu425Val in autism, Asperger syndrome and obsessive–
compulsive disorder. Psychiatric Genetics, 18, 31-39.
Wetterneck, C. T., Little, T. E., Chasson, G. S., Smith, A. H., Hart, J. M., Stanley, M. A., &
Björgvinsson, T. (2011). Obsessive–compulsive personality traits: How are they related to
OCD severity? Journal of Anxiety Disorders, 25, 1024-1031.

18
Wu, K. D., Clark, L. A., & Watson, D. (2006). Relations between obsessive–compulsive
disorder and personality: Beyond Axis I–Axis II comorbidity. Journal of Anxiety Disorders,
20, 695-717.
Zermatten, A., Van der Linden, M., Jermann, F., & Ceschl, G. (2006). Validation of a French
version of the Obsessive-Compulsive Inventory-Revised in a non-clinical sample. European
Review of Applied Psychology, 56, 151-155.

Figure 1. Four-cluster solution based on the four dimensions indicated on the x-axis. Cluster names: Obsessional (O); Autistic (A); Schizotypal-borderline (S); Low traits (L).
O
S
Mean(z-scores)
L
ObsessionalAutisticSchizotypy Borderline
Cluster:
A
0.5 -
1 -
0 -
-0.5 -
-1 -
1.5 -
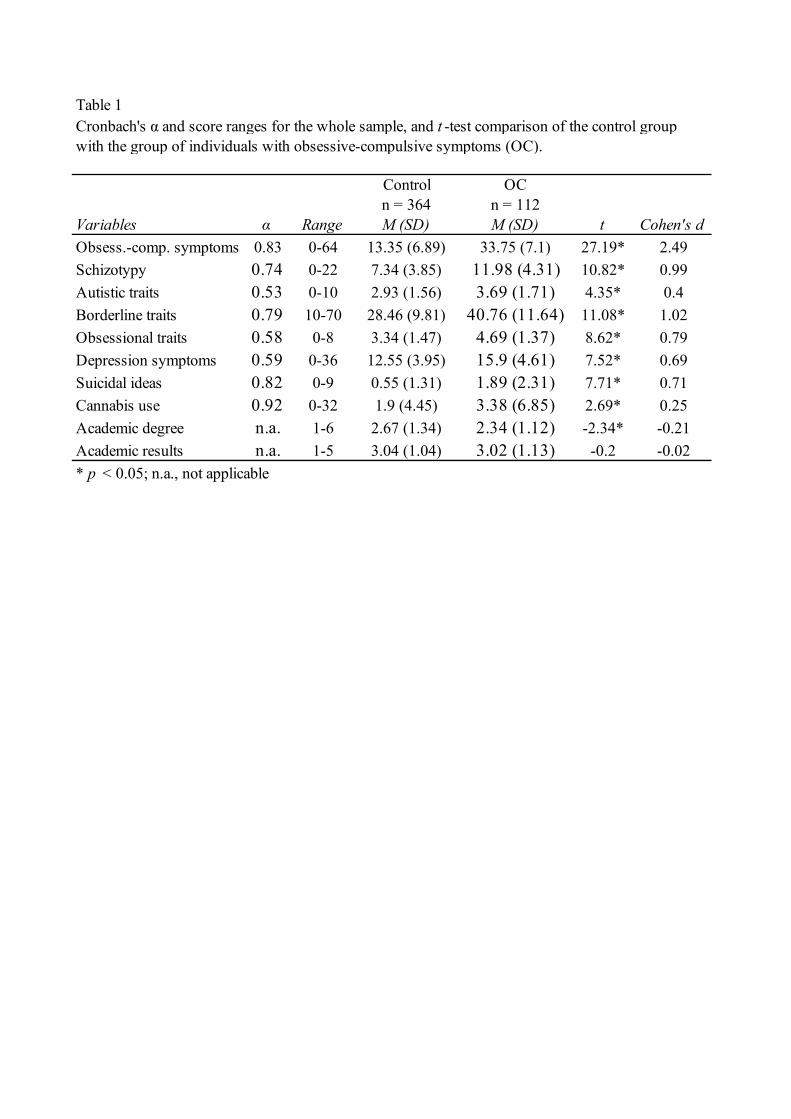
Table 1Cronbach's α and score ranges for the whole sample, and t -test comparison of the control group
Control OCn = 364 n = 112
Variables α Range M (SD) M (SD) t Cohen's dObsess.-comp. symptoms 0.83 0-64 13.35 (6.89) 33.75 (7.1) 27.19* 2.49Schizotypy 0.74 0-22 7.34 (3.85) 11.98 (4.31) 10.82* 0.99Autistic traits 0.53 0-10 2.93 (1.56) 3.69 (1.71) 4.35* 0.4Borderline traits 0.79 10-70 28.46 (9.81) 40.76 (11.64) 11.08* 1.02Obsessional traits 0.58 0-8 3.34 (1.47) 4.69 (1.37) 8.62* 0.79Depression symptoms 0.59 0-36 12.55 (3.95) 15.9 (4.61) 7.52* 0.69Suicidal ideas 0.82 0-9 0.55 (1.31) 1.89 (2.31) 7.71* 0.71Cannabis use 0.92 0-32 1.9 (4.45) 3.38 (6.85) 2.69* 0.25Academic degree n.a. 1-6 2.67 (1.34) 2.34 (1.12) -2.34* -0.21Academic results n.a. 1-5 3.04 (1.04) 3.02 (1.13) -0.2 -0.02* p < 0.05; n.a., not applicable
with the group of individuals with obsessive-compulsive symptoms (OC).
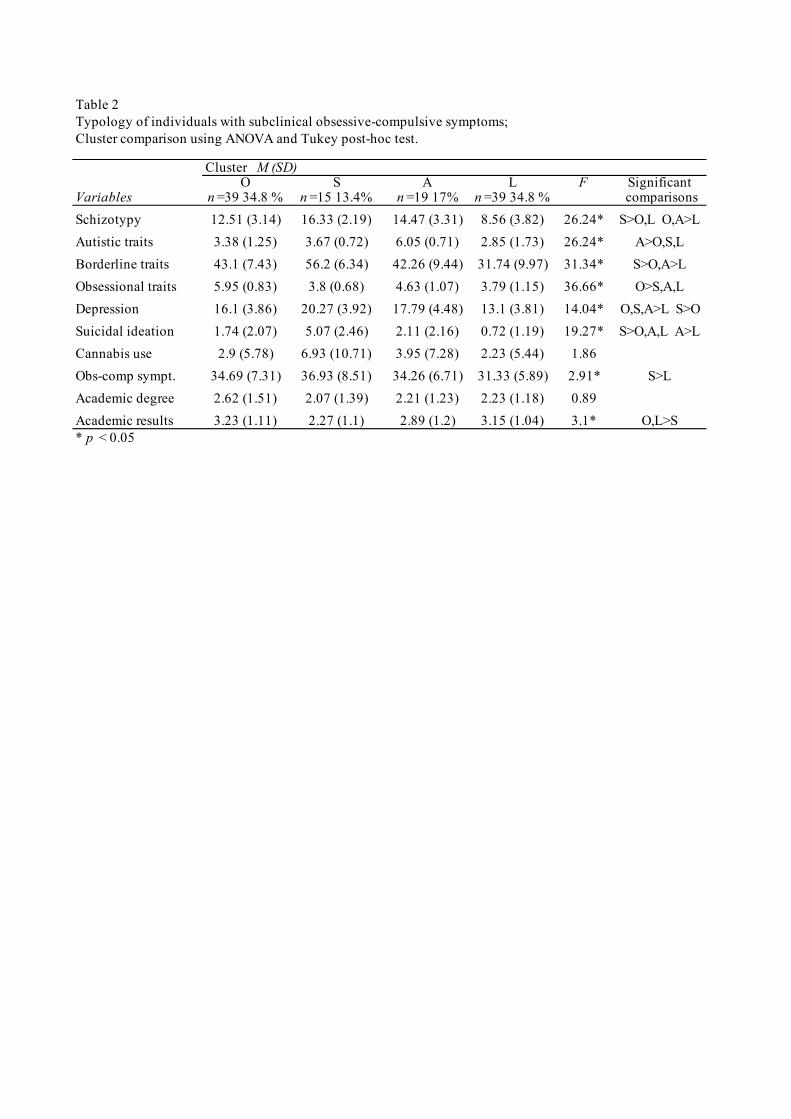
Table 2Typology of individuals with subclinical obsessive-compulsive symptoms; Cluster comparison using ANOVA and Tukey post-hoc test.
Cluster M (SD)O S A L F Significant
Variables n =39 34.8 % n =15 13.4% n =19 17% n =39 34.8 % comparisonsSchizotypy 12.51 (3.14) 16.33 (2.19) 14.47 (3.31) 8.56 (3.82) 26.24* S>O,L O,A>LAutistic traits 3.38 (1.25) 3.67 (0.72) 6.05 (0.71) 2.85 (1.73) 26.24* A>O,S,LBorderline traits 43.1 (7.43) 56.2 (6.34) 42.26 (9.44) 31.74 (9.97) 31.34* S>O,A>LObsessional traits 5.95 (0.83) 3.8 (0.68) 4.63 (1.07) 3.79 (1.15) 36.66* O>S,A,LDepression 16.1 (3.86) 20.27 (3.92) 17.79 (4.48) 13.1 (3.81) 14.04* O,S,A>L S>OSuicidal ideation 1.74 (2.07) 5.07 (2.46) 2.11 (2.16) 0.72 (1.19) 19.27* S>O,A,L A>LCannabis use 2.9 (5.78) 6.93 (10.71) 3.95 (7.28) 2.23 (5.44) 1.86Obs-comp sympt. 34.69 (7.31) 36.93 (8.51) 34.26 (6.71) 31.33 (5.89) 2.91* S>LAcademic degree 2.62 (1.51) 2.07 (1.39) 2.21 (1.23) 2.23 (1.18) 0.89Academic results 3.23 (1.11) 2.27 (1.1) 2.89 (1.2) 3.15 (1.04) 3.1* O,L>S* p < 0.05