
Patient Education in Cardiac Rehabilitation - TSpace
269
Patient Education in Cardiac Rehabilitation: the role of knowledge on behavior change and its mediators by Gabriela Lima de Melo Ghisi A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Graduate Department of Exercise Sciences University of Toronto © Copyright by Gabriela Lima de Melo Ghisi, 2014
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Patient Education in Cardiac Rehabilitation - TSpace

Patient Education in Cardiac Rehabilitation: the role of knowledge on behavior change and its mediators
by
Gabriela Lima de Melo Ghisi
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Graduate Department of Exercise Sciences University of Toronto
© Copyright by Gabriela Lima de Melo Ghisi, 2014
ii
Patient Education in Cardiac Rehabilitation: the role of knowledge on behavior change and its mediators
Gabriela Lima de Melo Ghisi
Doctor of Philosophy
Graduate Department of Exercise Sciences University of Toronto
2014
Abstract
The purpose of this series of studies was to investigate the relationship between patient education
and behavior change in CR and the role of knowledge on behavior change and its mediators in
the context of the Health Action Process Approach (HAPA). The first study was a systematic
review aimed to investigate the impact of education on patients’ knowledge and health behavior
change in cardiac patients. Findings from this review support the benefits of educational
interventions in CAD, through increases in patients’ knowledge and behavior change. The
second study aimed to develop and psychometrically-validate a tool to assess information needs
in CR patients. After a review by an expert panel, a pilot test, and a psychometric test in 203 CR
patients, the tool – called INCR – was demonstrated to have good reliability and validity. The
INCR was completed by 306 CR patients and 28 CR providers in the third study. Results showed
that CR patients desire information in many areas and that providers were highly cognizant of
those needs. The forth study aimed to develop and psychometrically-validate the second version
of the CADE-Q (Coronary Artery Disease Education Questionnaire), a tool to assess CR
patients’ knowledge. After a strict process, including a psychometric test in 307 CR patients, the
CADE-Q II was considered valid and reliable. Finally, the fifth study investigated: (1) changes in
knowledge and HAPA constructs among CR patients following participation in educational

iii
programs; and, (2) the theoretical correlates of exercise behavior change among CR patients
receiving educational interventions. There was a significant improvement in patients’ overall
knowledge, some HAPA constructs, and exercise from pre- to post-CR regardless of curriculum.
Path analysis revealed that knowledge was a significant motivational construct leading to
intention formation, and intentions to engage in physical activity were not directly related to
behavior, needing especially action planning, which was related to self-efficacy. Overall, results
from all five studies were valuable in the area of patient education in CR and showed the
importance of assessing patients’ information needs and knowledge as well as to identify
behavior determinants related to educational interventions.

iv
Acknowledgments
Every result described in this thesis was accomplished with the help and support of faculty,
colleagues, friends, students and family members, to whom I would like to express my gratitude.
First of all, I would like to only to thank but to dedicate this work to my husband and my very
best friend, Juliano. Your continual love, wisdom, commitment and support sustained me
throughout my phd and in my life. I feel truly blessed that you chose to share your life with me
as my partner. I love you. Thank you.
I would like to express my special appreciation and thanks to my advisors Professor Dr. Scott
Thomas and Dr. Paul Oh, whose expertise, understanding, and patience, added considerably to
my graduate experience. I would like to thank you two for encouraging my research, for giving
me freedom to pursue my independent work and never question my ability to rise to the
occasion, for believing in me and in my ideas, and for allowing me to grow as a research
scientist. Your advice on both research as well as on my career were extremely important for me
to become who I am now after four years of graduate studies. I would also like to thank my
committee members, professor Dr. Sherry Grace, professor Dr. Michale Evans, for serving as my
committee members and have generously given their time and expertise to better my work. I also
want to thank you for letting my defense be an enjoyable moment, and for your brilliant
comments and suggestions.
I am extremely grateful to the staff from the Toronto Rehabilitation Institute, including lab staff,
clinical staff, member of the Patient Education Committee, staff from the front office, other

v
trainees. A special thanks to Sabrina, Trish and Priscilla for all the help and support throughout
my four years at TRI.
I would especially like to thank physicians, nurses, and nurse aids in the brain injury
rehabilitation unit at University Medical Center. All of you have been there to support me when I
recruited patients and collected data for my Ph.D. thesis.
Apart from doing research I cannot imagine how my life would be going in Canada without my
friends. Thanks to all my friends, including Andresa, Flavia, Raquel and Pauline, who supported,
enlightened and entertained me over these years.
Lastly, my great gratitude is sent to my beloved family for all their love and encouragement. For
the members of Melo, Lima and Ghisi family my special thanks to all support. For my beloved
dog Jojoe, for his love, loyalty and patience to wait for me while I was studying hard. For my
sister who always encouraged me and served as a model. For my loving, supportive, and
encouraging parents who raised me with sacrifice to provide me the best of everything, including
the best education. Your prayers and your love was what sustained me thus far. Finally, to my
father-in-law and friend Zinaldo who passed away before I finished my PhD studies: I know you
are always around to support me during the hard times and I would like to thank you for you
support and encouragement.

vi
Table of Contents
Acknowledgments .................................................................................................... iv!Table of Contents ..................................................................................................... vi!List of Tables ......................................................................................................... xiii!List of Figures ........................................................................................................ xvi!List of Appendices ................................................................................................ xvii!
Chapter 1 OVERALL INTRODUCTION AND LITERATURE REVIEW ..... 1!
1! Introduction ........................................................................................................... 1!2! Review of Literature .............................................................................................. 3!
2.1!Patient Education in Cardiac Care .................................................................. 3
2.1.1! Factors Influencing Patient Education Effectiveness ........................... 5!2.2!Assessing Cardiac Patients’ Information Needs and Disease-related
Knowledge ...................................................................................................... 8
2.2.1! Patients' Information Needs .................................................................. 8!2.2.2! Patients' Disease-related Knowledge .................................................. 11!
3! Theoretical Orientation ....................................................................................... 15!3.1!Social Cognitive Theory ............................................................................... 18! 3.1.1 Self-Efficacy ........................................................................................ 19!3.2!Mediating Variable Framework .................................................................... 21!3.3!The Health Action Process Approach ........................................................... 22!
vii
3.4!Adult Education Theories ............................................................................. 26!4! Study Purpose, Objectives and Hypothesis ......................................................... 30!
Chapter 2 OVERALL RESEARCH DESIGN AND METHODOLOGY ........ 33!
1! Design and Procedure .......................................................................................... 33!2! Setting .................................................................................................................. 35!
2.1 Development of the New Education Curriculum .......................................... 36!2.1.1! Problem Definition ............................................................................. 37!2.1.2! Theoretical Foundation ....................................................................... 38!2.1.3! Needs Analysis ................................................................................... 39!2.1.4! Program Goals & Educational Objectives .......................................... 49!2.1.5! Sequencing Instruction ....................................................................... 50!2.1.6! Instructional Strategy and Design ....................................................... 50!2.1.7! Instructional Methods and Materials .................................................. 52!2.1.8! Evaluating Instruction and Materials .................................................. 53!2.1.9! Evaluating Learning for Health Outcomes ......................................... 54!2.1.10!Discussion ........................................................................................... 55!
Chapter 3 PAPER ONE: A systematic review of patient education in cardiac patients: do they increase knowledge and promote health behavior change? ............................................................................................... 59!
1! Introduction ......................................................................................................... 59!2! Methods ............................................................................................................... 61!
2.1 Search Methods for Identification of Studies ................................................ 61!
viii
2.2 Inclusion and Exclusion Criteria ................................................................... 61!2.3 Data Collection and Analysis ........................................................................ 64!
3! Results ................................................................................................................. 65!3.1 Characteristics of Included Studies ............................................................... 65!3.2 Nature of Education Interventions ................................................................ 77!3.3 Knowledge .................................................................................................... 82!3.4 Behavior Change and Psychosocial Well-Being ........................................... 83!
4! Discussion and Conclusion ................................................................................. 90!4.1 Discussion ..................................................................................................... 90!4.2 Conclusion ..................................................................................................... 92!4.3 Practice Implications ..................................................................................... 92!
Chapter 4 PAPER TWO: Development and psychometric validation of a scale to assess information needs is cardiac rehabilitation: The INCR tool ...................................................................................................................... 93!
1! Introduction ......................................................................................................... 93!2! Methods ............................................................................................................... 95!
2.1 Design and Procedure .................................................................................... 95!2.2 Participants .................................................................................................... 96!2.3 Measures ........................................................................................................ 97!2.4 Statistical Analysis ........................................................................................ 97!
3! Results ................................................................................................................. 98!3.1 Participants Characteristics ........................................................................... 98!3.2 Development of the Tool ............................................................................... 98!

ix
3.3 Pilot Testing .................................................................................................. 99!3.4 Psychometric Validation ............................................................................... 99!3.5 Information Needs ....................................................................................... 100!
4! Discussion and Conclusion ............................................................................... 105!4.1 Discussion ................................................................................................... 105!4.2 Conclusion ................................................................................................... 106!4.3 Practice Implications ................................................................................... 107!
Chapter 5 PAPER THREE: Healthcare providers’ awareness of the information needs of their cardiac rehabilitation patients throughout the program continuum ........................................................................................ 108!
1! Introduction ....................................................................................................... 108!2! Methods ............................................................................................................. 110!
2.1 Design and Procedure .................................................................................. 111!2.2 Participants .................................................................................................. 111!2.3 Measures ...................................................................................................... 112!2.4 Statistical Analysis ...................................................................................... 113!
3! Results ............................................................................................................... 114!3.1 Respondent Characteristics ......................................................................... 114!3.2 Information Needs ....................................................................................... 116!3.3 Education Delivery Formats and Gaps ........................................................ 119!3.4 Information Needs over the Course of CR .................................................. 120!
4! Discussion and Conclusion ............................................................................... 122!4.1 Discussion ................................................................................................... 122!

x
4.2 Conclusion ................................................................................................... 125!4.3 Practice Implications ................................................................................... 125!
Chapter 6 PAPER FOUR: Development and psychometric validation of the second version of the Coronary Artery Disease Questionnaire (CADE-Q II) .................................................................................................... 126!
1! Introduction ....................................................................................................... 126!2! Methods ............................................................................................................. 128!
2.1 Design and Procedure .................................................................................. 128!2.2 Participants .................................................................................................. 129!2.3 Measures ...................................................................................................... 129!2.4 Statistical Analysis ...................................................................................... 130!
3! Results ............................................................................................................... 131!3.1 Participants Characteristics ......................................................................... 131!3.2 Development of the Tool ............................................................................. 131!3.3 Pilot Test ..................................................................................................... 132!3.4 Psychometric Validation ............................................................................. 132!3.5 Knowledge Assessment ............................................................................... 136!
4! Discussion and Conclusion ............................................................................... 138!4.1 Discussion ................................................................................................... 138!4.2 Conclusion ................................................................................................... 139!4.3 Practice Implications ................................................................................... 139!

xi
Chapter 7 PAPER FIVE: Behavior determinants among cardiac rehabilitation patients receiving educational interventions: an application of the health action process approach ....................................... 140!
1! Introduction ....................................................................................................... 140!2! Methods ............................................................................................................. 144!
2.1 New Educational Curriculum Development ............................................... 144
2.2 Design and Procedure .................................................................................. 145!2.3 Participants .................................................................................................. 146!2.4 Measures ...................................................................................................... 146!
2.4.1 HAPA constructs ................................................................................ 148!2.4 Statistical Analysis ...................................................................................... 150!
3! Results ............................................................................................................... 153!3.1 Respondents Characteristics ........................................................................ 153!3.2 Knowledge .................................................................................................. 156!3.3 HAPA constructs ......................................................................................... 157!3.4 Exercise behavior ........................................................................................ 157!3.5 Knowledge and theoretical determinants of exercise behavior ................... 157!
3.5.1 Preliminary Analysis .......................................................................... 157!3.5.2 Path Analysis ...................................................................................... 165!
4! Discussion and Conclusion ............................................................................... 167!4.1 Discussion ................................................................................................... 167!4.2 Conclusion ................................................................................................... 170!4.3 Practice Implications ................................................................................... 170!

xii
Chapter 8 SUMMARY OF THE RESEARCH AND GENERAL DISCUSSION .................................................................................................. 171!
1! Summary of the Research ................................................................................. 171!2! General Discussion ............................................................................................ 176!3! Limitations ........................................................................................................ 180!4! Implications and Future Directions ................................................................... 180!
References ............................................................................................................ 184!
Appendices ........................................................................................................... 221!

xiii
List of Tables
Chapter 2
Table 2.1 – Responsibilities of the committee of CR and patient education experts ................................................................................................................. 37
Table 2.2 – Summary of the Literature review of best practice on CR patient education ............................................................................................................. 42
Table 2.3 – Main themes that emerged from patient’s focus group .................... 49
Table 2.4 – Education curriculum’s 5 program learning outcomes .................... 49
Table 2.5 – Sections of the new education curriculum for CR patients .............. 50
Chapter 3
Table 3.1 – Search Strategy ................................................................................. 63
Table 3.2 – Characteristics of the included studies describing the relationship between education knowledge and behavior change, N=42 ............................... 68
Table 3.3 – Characteristics of educational interventions (n=42) ......................... 85
Chapter 4
Table 4.1 – Sociodemographic/Clinical Characteristics of the Participants for the Psychometric Validation and INCR mean scores and differences among subgroups (N=203) .............................................................................................. 101
Table 4.2 – Mean and Standard Deviation of Clarity Rating by Experts (N=20) and Pilot Study Patients (N=20), INCR Score (N=203), and INCR Item Completion Rates ................................................................................................ 102

xiv
Table 4.3 – Mean and Standard Deviation of educational needs per subject area, N=203 ......................................................................................................... 104
Chapter 5
Table 5.1 – Sociodemographic and Clinical Characteristics of Patient Respondents (N=306), and Mean and Standard Deviation of Total Information Needs Scores by these Characteristics ................................................................ 115
Table 5.2 – Mean and Standard Deviation of Total Information Needs by Sample, and Mean Differences .......................................................................... 117
Table 5.3 – Preferences for Educational Delivery Formats by Sample .............. 120
Table 5.4 – Mean and Standard Deviation of Patient Information Needs by Subscale and Time in CR Program, N=306 ........................................................ 121
Chapter 6
Table 6.1 – Sociodemographic and Clinical Characteristics of Patient Respondents (N=307), and Mean and Standard Deviation of CADE-Q II Scores by these Characteristics ........................................................................... 133
Table 6.2 – Mean and Standard Deviation of Clarity Rating by Pilot Study Patients (N=30), CADE-Q II Score (N=307), CADE-Q II Item Completion Rates, Cronbach’s alpha per area, and Mean Score per area .............................. 134
Table 6.3 – Factor Structure of the CADE-Q II, sorted by loading .................... 137
Chapter 7
Table 7.1 – Sociodemographic and clinical characteristics of participants overall , and by curriculum ................................................................................................ 155

xv
Table 7.2 – Total, subscale and item knowledge scores at pre- and post-CR in overall sample and by curriculum ....................................................................... 159
Table 7.3 – HAPA constructs and exercise behavior at pre- and post-CR in overall sample and by curriculum ................................................................................... 162
Table 7.3 – Pearson’s correlation matrix for HAPA constructs and exercise behavior post-CR (n=173) ................................................................................... 164
*Chapters 1 and 8 do not have tables.

xvi
List of Figures
Chapter 1
Figure 1.1 – Structural paths of influence wherein perceived self-efficacy affects health habits (Bandura, 2004; p.146) ....................................................... 20
Figure 1.2 – Mediating variable model of behavior (Baranowski, Anderson & Carmack, 1998; p.282) .................................................................................... 21
Figure 1.3 – Health action process approach (Schwarzer, 1992; retrieved from http://userpage.fu-berlin.de/~health/hapa_figures.pdf) ....................................... 25
Chapter 2
Figure 2.1 – Infographic of the papers that comprise this thesis ......................... 57
Figure 2.2 – Development of the new education curriculum for CR patients (Infographic) ........................................................................................................ 58
Chapter 3
Figure 3.1 – Flow Diagram of Study Selection Process ...................................... 67
Chapter 7
Figure 7.1 – Model of the relationship between HAPA constructs, knowledge and exercise behavior ................................................................................................. 152
Figure 7.2 - Flow diagram of study participants (n=306) ................................... 154
Figure 7.3 - Modified model of the relationship between HAPA constructs, knowledge and exercise behavior ........................................................................ 166
*Chapters 2 and 4-8 do not have figures.

xvii
List of Appendices
Appendix 1 – The INCR Scale ............................................................................ 222
Appendix 2 – The CADE-Q II Questionnaire ..................................................... 226
Appendix 3 – Assessment Booklet for Paper 5 ................................................... 235

1
Chapter 1 OVERALL INTRODUCTION AND LITERATURE REVIEW
In this chapter an overall introduction and literature review characterizing coronary artery
disease as a chronic condition is presented to support the need for secondary prevention
strategies, including patient education. Furthermore, the theoretical orientation of this thesis is
described, as well as its rationale, purpose, objectives and hypothesis.
1 Introduction
The increasing incidence of chronic diseases has emerged as one of the most important health
issues in the 21st century. Cardiovascular Disease (CVD) - a chronic condition – is the leading
cause of mortality worldwide (World Health Organization [WHO], 2011) and a significant
contributor to morbidity and health-related costs (Neal, 2004; Law, Watt & Wald, 2002; Cardiac
Care Network [CCN], 2002). In Canada, CVD is also the leading cause of hospitalizations
(Statistics Canada, 2008) and, according to the Public Health Agency of Canada (2009), nine out
of ten Canadians over the age of 20 years have at least one of the following risk factors:
smoking, physical inactivity during leisure time, less than recommended daily consumption of
vegetables and fruit, stress, overweight and obesity, high blood pressure, or diabetes. Addressing
these risk factors through behavior change will not only reduce the risk of CVD, but also of
many other chronic conditions that share the same risk factors.
Coronary Artery Disease (CAD) – the most common type of CVD – is a chronic condition that
carries a high risk of recurrent events. Secondary prevention relies on early detection of disease
process and application of interventions to prevent progression of disease (Stone, Arthur, &
Suskin, 2009). These strategies to control CAD are highly effective, but multifactorial (i.e.

2
multiple interventions conducted over time may be employed to sustain outcomes, including
behavior change), necessitating patient awareness and adherence to optimize health outcomes
(Clark, Hartling, Vandermeer, & McAlister, 2005; Stone, Arthur, & Suskin, 2009; Heran et al.,
2011). Therefore, the treatment of CAD requires optimal medical management, including not
only drug therapy and revascularization, but also behavior change techniques (e.g. risk factor
modification, stress management, and physical activity promotion) and patient education. Indeed,
findings from recent systematic reviews demonstrate the importance of patient education in CAD
patients, in improving self-management behaviors, health-related quality of life and potentially
reducing healthcare costs (Mullen, Mains, & Velez, 1992; Dusseldorp et al., 1999; Aldcroft et
al., 2011; Schadewaldt & Schultz, 2011; Brown et al., 2012; Ghisi et al., 2014a). While most
CAD patients will receive some education if hospitalized, it is often forgotten, too brief, and
focused appropriately on acute recovery (which leaves no time to educate on chronic self-
management) (Mullen et al., 1992; Stone et al., 2009; Aldcroft et al., 2011; Berra, Miller, &
Jenning, 2011; Ghisi et al., 2014a).
Cardiac rehabilitation (CR), which is a comprehensive outpatient program of secondary
prevention and lifestyle counselling, has been shown to reduce mortality, improve functional
capacity, and decrease re-hospitalization and overall medical costs (Clark et al., 2005; Heran et
al., 2011; Lam et al., 2011; Lawler, Filion & Eisenberg, 2011). CR – which is often delivered by
a multi-disciplinary team of healthcare providers trained to be health educators – has several core
components: lifestyle and medical risk factor management, psychosocial health,
cardiopulmonary therapies, long term management, audit and evaluation, health behavior change
and patient education, this last topic being the focus of my studies (British Association for
Cardiovascular Prevention and Rehabilitation [BACPR], 2012).

3
Patient education has been formally defined as “the process by which health professionals and
others impart information to patients that will alter their health behaviors or improve their health
status” (Koongstvedt, 2001). As a facilitator of behavior change, patient education therefore
plays a key role in the management of CAD (Brown et al, 2012). While the important role of
patient education has been well-recognized in CR practice (e.g., clinical practice guidelines and
quality indicators), CR patients’ information needs, patient knowledge in CR, and the best way
to structure and deliver educational interventions has only poorly been investigated.
2 Review of Literature
2.1 Patient Education in Cardiac Care
The simple act of teaching cardiac patients has been identified as a prerequisite to create a sense
of well-being and optimism about the future and a positive influence to make healthy choices in
daily life, better manage their disease and avoid adverse outcomes (Karner, Goransoon &
Bergdahl, 2003; Alm-Roijet et al, 2006; Kayaniyil et al, 2009). Increased patient satisfaction and
perception of control, as well as reduced levels of psychological distress are all variables
associated with effective health information provision (Wingham et al., 2006; Parry et al., 2009).
There is a growing body of literature that contributes to our understanding of patient education
effectiveness. This literature includes many studies in which knowledge of CAD has been shown
to strongly influence symptom recognition (Zalesskaya et al., 2005; DeVon et al., 2010),
advocacy for physician screening (Bolman et al., 2005), attitudes towards the disease (Bellman et
al., 2009), and provide motivation for self-care and individual behavior change (Dickson, Tkas &
Riegel, 2008; Bellman et al., 2009). Likewise, inadequate understanding of the disease may

4
cause unwarranted emotional distress, inappropriate coping behavior, and non-compliance with
medical advice (Monane et al., 1994; Blyth et al., 1997), leading to unnecessary disease
progression (Zalesskaya et al., 2005, Sui et al., 2008).
Jolliffe et al. (2000) systematically compared the effectiveness of exercise-only CR versus more
comprehensive programs (including education and/or psychosocial counseling) on clinical
endpoints, such as rehospitalisation and mortality. Exercise-only CR reduced deaths by 31 per
cent versus 26 per cent in comprehensive CR programs. There was a significant net reduction in
total cholesterol and LDL cholesterol in the comprehensive cardiac rehabilitation group, but not
the exercise only rehabilitation group. Despite the fact that exercise-based CR appears to be
effective in reducing cardiac deaths, the evidence base is weakened by poor quality trials.
Moreover, it is not clear from this review whether exercise only or a comprehensive CR
intervention is more beneficial since the quality of reporting overall was poor, with generally
high losses to follow up.
A recent systematic review (Brown et al., 2012) assessed the effects of patient education on
mortality, morbidity, health-related quality of life (HRQoL) and healthcare costs in people with
CAD. This was the first study to find evidence to suggest that education can improve HRQoL
and decrease healthcare costs by reductions in downstream healthcare utilization. No evidence
that patient education reduced CAD-related morbidity, mortality, revascularization, compared to
no educational interventions was found. The ‘dose’ of the education intervention varied
substantially across the 13 studies included, and most studies had a relatively short follow-up
(Brown et al., 2012). However, effect size of the summative effects of education on mortality
(25% risk reduction) and morbidity (17- 42% risk reduction) are clinically important outcomes,
particularly in the context of the large number of individuals with CAD.

5
2.1.1 Factors Influencing Patient Education Effectiveness
The literature also provides some insight into a number of factors, which may influence patient
education effectiveness. Most often cited is educational level and how higher levels of education
may be a marker for higher levels of disease-specific knowledge (Potvin Richard & Edwards,
2000; Sui et al., 2008; Loucks et al., 2009; Lainscak, Farkas & Jaarasma, 2010). Education level
is a market of socioeconomic status (Kaplan & Keil, 1993; Fishella & Tancredi, 2008), and
patients with higher education may have better understanding and knowledge of their disease
process and treatment thereof (Sui et al., 2008). They also have easier access to high quality
health care (Feldman et al., 1989). Patients with lower education levels are less likely to have a
regular primary care physician (Rask et al., 1994), to see or consult a cardiologist (Rathore et al.,
2006), or be adherent to therapeutic recommendations (Jackson et al., 2005). In addition, lower
education level has been shown to be associated with poor quality of life, anxiety, physical and
emotional distress (Riedinger, Dracup & Brecht, 2000), and an inability to actively participate in
self-care recommendations (Vinson et al., 1990; Chin & Goldman, 1997; DeWalt et al., 2006;
Loucks et al., 2009). Results from these studies should be interpreted with caution, since other
factors may influence the relationship between patient education and socioeconomic level, such
as providers’ job execution and environment preventing learning.
Besides educational level, culture has been cited as an essential indicator that influences the way
patients interact with health systems, participate in prevention activities, choose health-related
lifestyle, and understand health and illness (London, 2008; Burns-Gibson & Koso, 2010). The
potential for misdiagnosis and mistreatments may increase significantly when the healthcare
provider is not culturally appropriate. Thus, the quality of care and patient education is also

6
impacted when the care provided is not culturally congruent (Niemeier, Burnett & Whitaker,
2003; Burns-Gibson & Koso, 2010).
Health literacy has been defined as a set of skills that people need to function effectively in the
health care environment (Berkman et al., 2011). It is also an important determinant of patients’
knowledge, and usually health knowledge is viewed as part of health literacy. According to U.S.
Department of Education (2006), approximately 80 million U.S. adults are thought to have
limited health literacy, which puts them at risk for poorer health outcomes. Thus, studies showed
that rates of limited health literacy are higher among elderly, minority, and poor persons and
those with less than a high school education. Low health literacy is associated with poorer health
outcomes and poorer use of health care services, including patient education (Berkman et al.,
2011).
Other factors that influence patient education include: age (Lane & Evans, 1979; Cranton, 1989;
Brown, 1992; Kirkland et al, 1999), and gender (Bubela et al., 1990; Stewart et al., 2004;
Kayaniyil et al., 2009). Chronological age can be an important factor to consider when
evaluating and planning instruction education and studies have shown that younger patients learn
more than older patients (Brown, 1992; Clark et al., 1992; Clark et al., 2006); however,
according to Cranton (1989) a statement of age only renders very general information since
individuals within the same age group may be completely different in other aspects, such as
educational level. Therefore, age should always be coupled with other information. Although the
role of gender in medical information seeking and decisional preferences is largely unexplored, a
few studies suggest that women may be better informed and more active in the decision process
than men (Mansell et al., 2000; Stewart et al., 2004).

7
While most CAD patients will receive some education if hospitalized, it is often forgotten, too
brief, and focused appropriately on acute recovery (which leaves no time to educate on chronic
self-management) (Aldcroft et al., 2011; Ghisi et al., 2014a). The real education in cardiac care
usually occurs during patients participation in CR programs, in which patient education is a core
component, as mentioned previously (BACPR, 2012). CR programs are offered over several
months permitting repeated patient contact with these providers, enabling fulsome education
regarding the numerous lifestyle changes and treatments shown to reduce risk over time (Berra et
al., 2011).
To deliver effective patient education, educators must understand what information needs
patients might have when they enter CR, and what they already know from health education
received at other points of their cardiac care journey (Ghisi et al., 2014a). Moreover, educators
should be aware of social determinants of health, which may impact patient’s health literacy.
They also need to consider the nature of the patient’s cardiac condition, risk factors, and their
health behaviors to tailor and optimize education delivery (Nutbeam, 2000). Unfortunately, much
previous literature on cardiac patient education has demonstrated that educators are often
unaware or inaccurately-perceive patients’ educational needs, as well as the characteristics
affecting patients’ ability to learn (Casey et al., 1984; Moynihan et al., 1984; Aldcroft et al.,
2011; Ghisi et al., 2013a). Clearly, this can result in less engaged and informed patients, and thus
potentially negatively impact not only their educational outcomes, but also their health outcomes.
Furthermore, patient education in coronary patients should be comprehensive, focusing not only
in the CR, but also in other phases of treatment (at the time of diagnosis, in hospital) (Cranton,
1989; Su, Herron & Osisek, 2011). Patient-centered education involves a commitment to
tailoring education to the needs and preferences of the patient, understanding factors that

8
influence this process and including family and friends’ needs (Furze et al., 2002). This
participatory approach may empower patients to change their behaviors and improve health
outcomes.
2.2 Assessing Cardiac Patients’ Information Needs and Disease-related Knowledge
A cardiac educational program comprises the individual’s interests, habits and socioeconomic
lifestyle (Egan, 1999). Active components of this program include the assessment of learning
needs and knowledge, which can be a useful tool to enhance patients’ experience in CR and
should be addressed in all cardiac educational programs during the early phase of development
(McLennan et al, 1996; Czar & Engler, 1997). Therefore, the assessment of cardiac patients’
information needs and knowledge are key factors for developing and delivering educational
programs. Particularly in CR this is problematic, since before this project there was no available
tool psychometrically validated to assess information needs in CR. In addition, few tools were
assessing cardiac patients’ knowledge, most of them not focusing on patient education
(McLennan et al, 1996; Czar & Engler, 1997).
2.2.1 Patients’ Information Needs
In regards to information needs, the “needs-based” approach, according to Timmins & Kaliszer
(2003) has been described as a means of educating cardiac patients, attempting to identify and
meet the needs of the individual. Analysis of the literature revealed a learning need to be a
personal item about which individuals required information. However, in its broadest sense, a
learning need can be defined as the gap between competencies specified and the present level of
development by the learner (Timmins, 2006). The crucial element in the assessment of this “gap”
is the learners’ own perception of the discrepancy between where they are now and where they

9
want to be. A learning need occurs as a result of the individual’s natural coping mechanism,
whereby they seek out information in response to a problem-focused approach (Czar & Engler,
1997). The information received helps them to adapt to their situation. Learning needs were
identified as unique to individuals and subjective in nature (Timmins & Kaliszer, 2003).
Studies suggest that after an acute event patients view different categories as areas where
learning needs exist. When patients are admitted to hospital, they experience a state of shock and
disbelief, the severity of illness is realized, and survival issues become grave concerns. During
this earliest stage of hospitalization, patients usually are motivated to learn and meet their
physiological requirements and satisfy their need for safety. Educational needs identified in this
phase included: when to call a doctor, signs and symptoms of MI, diagnostic procedures, among
others (Wang, 1994). After a while, patients improve and the need for information regarding diet,
physical activity, and follow-up arises (Ashton, 1997; Hughes, 2000). After hospital discharge,
patients’ needs change once more, and become related to resumption of regular activities and
prognostic, including information about the risk of recurrence, the level of heart muscle damage,
discharge medications, appropriate levels of physical activity and diet (Timmins & Kaliszer,
2003; Astin et al, 2008). Therefore, learning needs may change over time, depending on which
stage of treatment and/or recovery cardiac patients are in.
Furthermore, personal and sociodemographic characteristics appear to be related to different
needs (Stewart et al, 2004). Gender, age, and educational level are some examples of
characteristics associated with information needs and decisional preferences. Although some
studies have shown that higher information needs are associated with being a woman (Marcuccio
et al, 2003; Stewart et al, 2004), younger age (Arora et al, 2000) and higher educational status

10
(Degner & Sloan, 1992), there is contradictory evidence (Mahler & Kulik, 1991; Czar & Engler,
1997).
In addition, there is a difference between patients’ and health professionals’ perceptions of what
constitute priority educational needs. Turton (1998) showed that patients appear to favor
practical information about their condition, its cause and prevention, whereas health
professionals are more focused on medical aspects of care such as medications, anatomy and
physiology. These incongruities have implications for health care delivery and for the
development of educational programs.
The literature highlights the importance of a comprehensive understanding of patients’ health
information needs as a logical first step in the development of educational programs. Despite the
fact that there are tools to assess information needs of cardiac patients following
revascularization (Goodman, 1997; Brezynskie et al, 1998; Astin et al, 2008), acute coronary
syndrome (Czar & Engler, 1997; Nakano, Mainz & Lomborg, 2008), MI (Casey, O’Connel &
Price, 1984; Moynihan, 1984; Orzeck & Staniloff, 1987; Bubela et al, 1990; Chan, 1990;
Wingate, 1990; Moser, Dracup & Marsden, 1993; Mirka, 1994, Larson et al, 1996; Ashton,
1997; Hughes, 2000; Timmins & Kaliszer, 2003; Decker et al, 2007; Smith & Liles, 2007), and
heart failure (Wehby & Brenner, 1999; Lile, Buhmann & Roders, 1999), to my knowledge, there
were no validated tools to assess information needs in CR and a previous literature review (Scott
& Thompson, 2003) failed to identify any available and validated tool to assess information
needs in coronary patients in cardiac rehabilitation programs. Chapter 3 of this thesis describes
the development and psychometric validation of a scale to assess information needs in cardiac
rehabilitation.

11
2.2.2 Patients’ Disease-related Knowledge
In regards to patients’ knowledge, this measure has been usually assessed through investigator-
generated open-ended and closed-ended questionnaires. To date, there are different types of
questionnaires and studies assessing cardiac patients’ knowledge in the literature, most of them
are designed for heart failure patients. Despite well-established benefits from patient education in
the CR setting, there are few psychometric-validated questionnaires published in the literature
assessing cardiac patients’ knowledge applicable to CR programs or that could be integrated into
the routine management of this population. To my knowledge, only 5 studies aimed to develop a
psychometrically-valid measure of CR patients’ knowledge: the Cardiac Knowledge
Questionnaire (CKQ), the Coronary Heart Disease Knowledge Test, the Knowledge Inventory,
the Maugeri Cardiac Prevention Questionnaire (MICRO-Q), and the Coronary Artery Disease
Education Questionnaire (CADE-Q).
The CKQ consists of 3 subscales addressed to assess different aspects of CAD: the Basic Cardiac
Knowledge Scale (BCKS), a 30-item scale to measure knowledge about the cardiovascular
system and nature of CAD; the Cardiac Lifestyle Knowledge Scale (CLKS), a 15-item scale
about behavioral aspects of the cause and consequences of a heart attack; and, the Cardiac
Misconceptions Scale (CMS), a 10-tem scale about prognostic implications of MI. The CKQ
was developed by Maeland & Havik (1987) with input from expert panels of cardiologists,
cardiac nurses, and physical therapist. Cronbach’s alpha was 0.84 for the BCKS, 0.69 for the
CLKS, and 0.74 for the CMS. All scales were demonstrated to be sensitive to change in patients
groups after a CR. The CKQ scales have limitations. Firstly, the psychometric-validation was not
established in a group of patients; therefore its applicability to cardiac patients use is unknown.
Secondly, in a subsequent study (Lidell & Fridlung, 1996) the subscales showed lower internal

12
consistency (BCKS=0.78;CLKS=0.50;CMS=0.40), which may demonstrate the inability to use
the CKQ in other studies.
The Coronary Heart Disease Knowledge Test is a 40-multiple-choice item questionnaire
covering 10 areas of knowledge: program orientation, nature of heart disease, risk factors,
physical activity, diet, cardiopulmonary resuscitation, psychological factors associated with
CAD, type A and B behavior, stress management, and problems related to home and family. A
sample from this scale is “A risk factor of CAD that cannot change is”. Each item has 4 options
as answer, only 1 correct. Smith, Hicks & Heyward (1991) examined the psychometric
properties of this scale in a sample of 93 male subjects diagnosed with CAD, 48 (52%)
participating in CR programs. Cronbach’s alpha was 0.84 and construct validation indicated that
the average test score of CR participants was significantly higher than that of non-participants
(p≤0.01). Firstly, while Coronary Heart Disease Knowledge Test showed a valid difficulty rating
(DR=63%) of the questions, information about time to completion and clarity index is missing.
Secondly, despite the incorporation of relevant topics to CR education, the dimensional structure
was not tested. Finally, the criterion validity of this scale is questionable due to the lack of a
large and broad sample of cardiac patients.
The Knowledge Inventory is a 50-item scale (46 multiple-choice items and 4 open-answer ones),
described by the authors as a “criterion-referenced mastery test”, which means that each learner
should attain a certain score level to be successful. Items covered the following areas of
knowledge: coronary disease, cardiac surgery, diagnostic, physical exercise guidelines, smoking,
diet, drugs and stress. A sample from this scale is “Angina and chest pain is caused by”. The
scale was validated in a sample of 10 post-bypass surgery patients and pilot-tested in 54 patients,
either following home or structured CR at a single medical center in Ohio (Schuster, Wright &

13
Tomich, 1995). Cronbach’s alpha was 0.84. Subgroups analysis of total scores showed male
patients in structured CR programs with higher knowledge than their female counterparts
(P<0.001). Further details or an independent assessment of content and criterion validity is
needed, as well as factorial analysis. Thus, testing on a larger and more diverse population of
patients is necessary.
The Maugeri Cardiac Prevention Questionnaire (MICRO-Q) is a 26-item self-report
questionnaire, which asks patients to indicate for each statement the response “true”, “false”, or
“don’t know”. The questionnaire covers four areas of knowledge: 1) risk factors and lifestyle; 2)
diet; 3) pre-admission avoidable delay; and, 4) cardiac disease. A sample item from this scale is
“People who feel under stress cannot do anything to change this”. The scale was validated in a
sample of 250 MI patients at an in-hospital CR in Italy (Sommaruga et al, 2003). Preliminary
psychometric validation of this scale has been established: spearman Rho correlation coefficient
of 0.72, and a Cronbach’s alpha value of 0.68. Subgroup analysis of total scores showed patients
with higher education had significantly higher scores on the correct scale (p≤0.0001), while
patients with a lower level of education showed a higher score for misconceptions (p≤0.0001).
Overall, while this scale incorporates important topics related to CR (e.g. risk factors), it was
psychometrically-validated in a sample of MI inpatients only, and therefore its generalizability to
CR programs is unknown. Additionally, statistical evidence of a multifactorial structure was not
found and the subdivision into 4 areas is of clinical relevance only.
The Coronary Artery Disease Education Questionnaire (CADE-Q) is a 19- multiple-choice item,
self-administered questionnaire, which assesses patients’ knowledge about their disease and CR
related factors. A sample item from this scale is “Which description below is a typical symptom
of CAD?”. Each item has 4 alternatives or statements, that correspond to a knowledge level: a

14
correct statement showing “complete knowledge”; a correct statement showing “incomplete
knowledge”; an incorrect statement showing “wrong knowledge”; and, a ‘don’t know’ statement
showing a “lack of knowledge”. Each alternative has a score and the sum of final scores leads to
a classification of knowledge (excellent, good, acceptable, poor, and insufficient). This scale was
developed through a comprehensive review of the literature and feedback from a CR
multidisciplinary team and patients (Ghisi et al., 2010).
The CADE-Q was originally developed in Brazil by Ghisi et al (2010) in Portuguese, and
psychometrically-validated in a sample of 155 CR patients. It was later translated, and culturally-
adapted to English by De Melo Ghisi et al (2012). The latter version was then psychometrically-
validated in a sample of 200 Canadian patients enrolled in CR (Ghisi et al, 2012). In the
Brazilian version of the CADE-Q, Cronbach’s alpha was 0.68, intraclass correlation coefficient
(ICC) was 0.78, and factorial analysis revealed 6-internally-consistent factors related to CADE-
Q’s 4 areas of knowledge: 1) pathophysiology and signs and symptoms of the disease, 2) risk
factors and lifestyle habits, 3) diagnosis, treatment and medicines, and 4) exercise. In the English
version, Cronbach's alpha was 0.809, ICC was 0.846, and factorial analysis revealed five factors,
all internally-consistent and well-defined by the items. Thus, criterion validity was supported by
significant differences in mean scores by family income (p=0.02) and educational level
(p<0.001). Although both versions demonstrated good reliability and validity, the CADE-Q
presented lack of detailed assessment of all core components of cardiac rehabilitation (CR), such
as nutrition and psychosocial risk. Besides that, the development of CADE-Q started in 2004,
needing update. The availability of a more comprehensive and updated CADE-Q is important to
assess patients’ knowledge and to tailor the educational component of CR programs (Ghisi et al.,
2013a). Therefore, the second version of this instrument (called CADE-Q II) was developed and
psychometrically validated and this process is described in chapter 6 of this thesis.

15
3 Theoretical Orientation
Theories are a generalized set of rules, and according to Hochbaum, Sorenson, & Lorig, (1992)
they become important instruments to help understand, influence and assess patient learning and
motivation. A number of studies have shown that using theory in crafting interventions can lead
to more powerful effects than interventions developed without theory (Ammerman et al, 2002;
Legler et al, 2002; Glanz, Rimer, & Viswanath, 2008). In the context of patient education,
theories can provide us with a workable basis for an education action we wish to undertake. This
is especially important when teaching patients whose educational needs are less predictable or
more diverse (Doak, Doak, & Root, 2007).
The theoretical basis of chronic disease management (CDM) models typically involves
components of the medical and behavioral/lifestyle approaches to health promotion. The medical
approach is used to eliminate or treat disease and illness through the use of scientific and
technological innovation (Laverack, 2004). The behavioral and lifestyle approach often works
within this medical model framework. The underlying assumption to this approach is that
individuals, once educated about healthy lifestyle choices and risk of disease or illness, will
avoid high-risk behaviors and adopt health behaviors to reduce their disease risk. This approach
often uses the Transtheoretical Model of Behavior Change (TTM) in conjunction with health
education to assess and increase individuals’ readiness to change and capacity to adopt health
promoting behaviors (Prochaska & DiClemente, 1983). The TTM uses stages of change to
integrate processes and principles of change across major theories of intervention. The major
weakness in this approach is that it fails to recognize the broader contextual and structural issues
that may affect individual’s ability to adopt healthy behaviors (Betancourt & Quinlan, 2007).
TTM is also unable to address a number of issues beyond personal motivation for health

16
promoting behavior.
Offering a more comprehensive approach to health promotion that takes into account social and
structural impediments for behavior change, the Social Cognitive Theory (SCT) posits a
multifaceted causal structure in which self-efficacy beliefs operate together with goals, outcome
expectations, and perceived environmental impediments and facilitates the regulation of human
motivation, behavior, and well-being (Bandura, 2004). However, because this theory is so broad
and ambitious, it has not been tested comprehensively in the same way that other health behavior
theories have been tested. Thus, to test the theory more fully, different concepts and principles in
SCT need to be measured, and manipulated in systematic experiments replicated over diverse
behaviors and populations (Glanz, Rimer, & Viswanath, 2008). This could determine whether
some of SCT’s concepts and principles are more or less useful or feasible for particular
behaviors or types of behavior change.
According to Schwarzer (2008), changing health-related behaviors requires two separate
processes that involve motivation and volition, respectively. First, an intention to change is
developed, in part on the basis of self-beliefs. Second, the change must be planned, initiated, and
maintained, and relapses must be managed. In addition, self-regulation plays a critical role in
these processes. Social-cognition models of health behavior change should address these two
processes. One such model, the Health Action Process Approach (HAPA), is explicitly based on
the assumption that two distinct phases need to be studied longitudinally: one phase that leads to
a behavioral intention and the other one that leads to the actual behavior. Particular social-
cognitive variables may play different roles in the two stages; perceived self-efficacy is the only
predictor that seems to be equally important in the two phases (Schwarzer, 1992). A recent
overview covering seven empirical studies (Schwarzer, 2008), has demonstrated the universal

17
applicability of the HAPA for a number of health behaviors and for diverse samples from various
cultures, including physical exercise adherence after a CR program (Scholz, Sniehotta, &
Schwarzer, 2005).
Choosing a structural theoretical model to fit your objectives, however, does not prove that the
chosen model is the only one or the best one that fits your research. The question is whether this
model appears to be empirically superior to alternative models. According to Glanz, Rimer, &
Viswanath (2008) finding the best model for a particular research context requires consideration
of several questions, such as: Which model accounts for most of the criterion variance? Which
one provides the best insight into the causal mechanism of health behavior change? Is the model
that makes the best prediction also the best one for the design of interventions? Which is the
most parsimonious one?
Three different theories and models influenced the development of this thesis: the SCT, the
Mediating Variable Model (MVM), and the HAPA. The SCT was valuable to understand what is
needed for a patient to make a behavior change. Thus, this thesis investigates self-efficacy as a
focal determinant of patient knowledge, affecting behavior both directly and by its influence on
the other determinants. As will be discussed further, self-efficacy plays a crucial role at all stages
of the health behavior change process. The MVM is helpful to understand the importance of
mediators in predicting health-promoting behavior. Finally, the HAPA was used to design the
new educational curriculum, as well as to identify which variables should be measured and
compared. All three models are described below. In addition, Adult Education Theories are also
briefly described in order to provide the foundation of adult education practice.
18
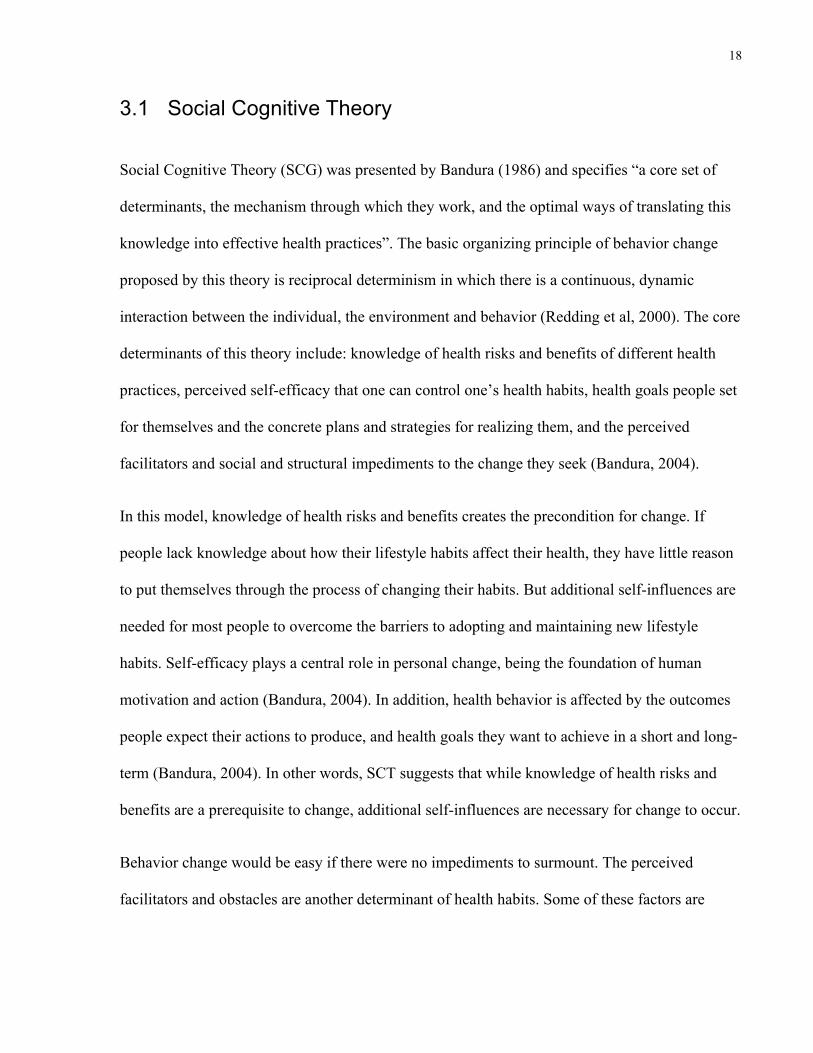
3.1 Social Cognitive Theory
Social Cognitive Theory (SCG) was presented by Bandura (1986) and specifies “a core set of
determinants, the mechanism through which they work, and the optimal ways of translating this
knowledge into effective health practices”. The basic organizing principle of behavior change
proposed by this theory is reciprocal determinism in which there is a continuous, dynamic
interaction between the individual, the environment and behavior (Redding et al, 2000). The core
determinants of this theory include: knowledge of health risks and benefits of different health
practices, perceived self-efficacy that one can control one’s health habits, health goals people set
for themselves and the concrete plans and strategies for realizing them, and the perceived
facilitators and social and structural impediments to the change they seek (Bandura, 2004).
In this model, knowledge of health risks and benefits creates the precondition for change. If
people lack knowledge about how their lifestyle habits affect their health, they have little reason
to put themselves through the process of changing their habits. But additional self-influences are
needed for most people to overcome the barriers to adopting and maintaining new lifestyle
habits. Self-efficacy plays a central role in personal change, being the foundation of human
motivation and action (Bandura, 2004). In addition, health behavior is affected by the outcomes
people expect their actions to produce, and health goals they want to achieve in a short and long-
term (Bandura, 2004). In other words, SCT suggests that while knowledge of health risks and
benefits are a prerequisite to change, additional self-influences are necessary for change to occur.
Behavior change would be easy if there were no impediments to surmount. The perceived
facilitators and obstacles are another determinant of health habits. Some of these factors are

19
personal ones, and others are related to external sources (health systems, culture, health
providers) (Bandura, 2002; 2004).
An example of SCT’s use is the self-management model, which has been shown to be effective
in cardiac patients (Clark et al, 1991; 1992; Haskell et al, 1994). This model operates through a
set of psychological subfunctions where people have to learn to monitor their health behavior
and the circumstances under which it occurs, including identifying proximal goals to motivate
themselves and to enlist social supports to sustain their efforts (DeBusk et al, 1994). Haskell et al
(1994) used the self-management system to promote lifestyle changes in patients suffering from
coronary artery disease. At the end of 4 years in self-management, patients achieved big
reductions in risk factors: decreased intake of saturated fat, weight lost, decrease of LDL
cholesterol, increase of HDL cholesterol, increase of exercise, and increase of cardiovascular
capacity. In contrast, those receiving regular medical care by their physicians showed no change
or they got worse.
Insights provided from this theory were helpful to understand what is needed for the patient to
make a behavior change. Using SCT it was understood that knowledge alone is not sufficient to
change and maintain behavior; but additional self-influence is needed for most people to
overcome the barriers to adopting and maintaining new lifestyle habits. Self-efficacy – a critical
determinant of behavior change – is described below.
3.1.1 Self-Efficacy
Self-efficacy is a fundamental component of the SCT and addresses the role of people’s
confidence that they could carry out the behavior asked of them. According to Bandura (1986),
all behavioral changes are mediated by self-efficacy. A person with low self-efficacy is less
20
likely to try to carry out a new health care behavior, or to change an ingrained behavior. Self-
efficacy influence goals and aspirations shape the outcomes people expect their efforts to
produce, and determine how obstacles and impediments are viewed (Bandura, 2004). A review
reported that self-efficacy could explain between 4% and 26% of variance in behavior (Keller et
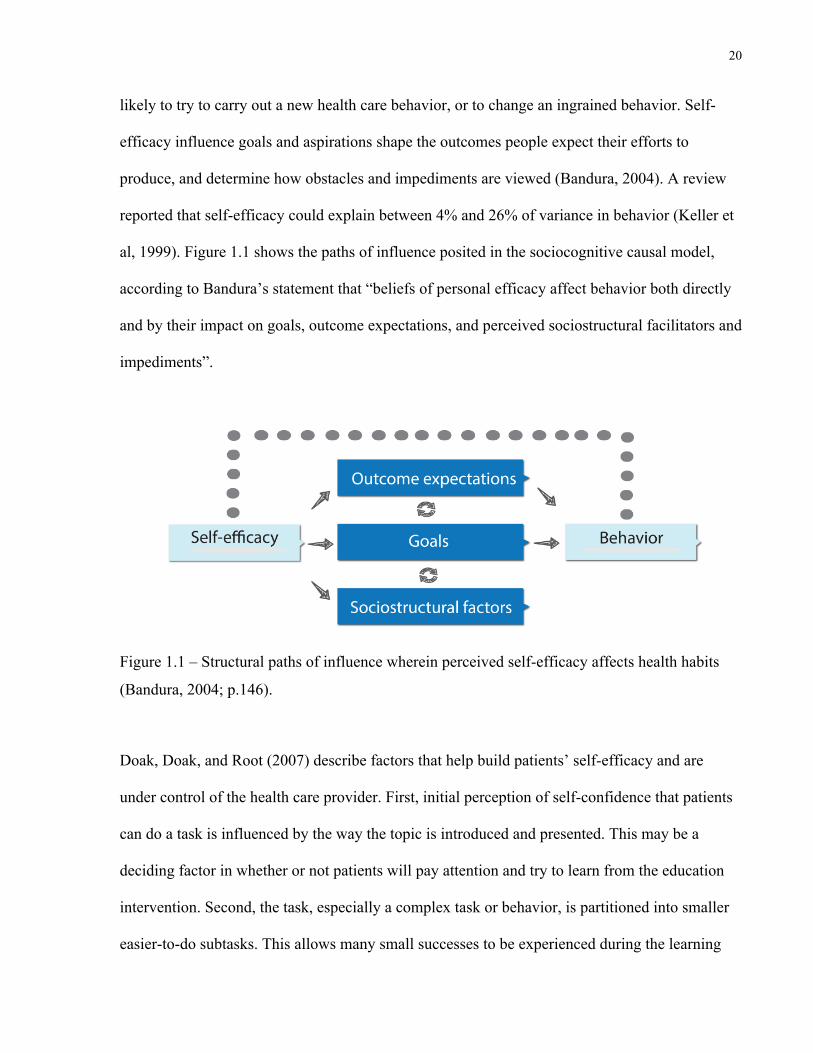
al, 1999). Figure 1.1 shows the paths of influence posited in the sociocognitive causal model,
according to Bandura’s statement that “beliefs of personal efficacy affect behavior both directly
and by their impact on goals, outcome expectations, and perceived sociostructural facilitators and
impediments”.
Figure 1.1 – Structural paths of influence wherein perceived self-efficacy affects health habits
(Bandura, 2004; p.146).
Doak, Doak, and Root (2007) describe factors that help build patients’ self-efficacy and are
under control of the health care provider. First, initial perception of self-confidence that patients
can do a task is influenced by the way the topic is introduced and presented. This may be a
deciding factor in whether or not patients will pay attention and try to learn from the education
intervention. Second, the task, especially a complex task or behavior, is partitioned into smaller
easier-to-do subtasks. This allows many small successes to be experienced during the learning

21
process. Third, there is repetition of the task or behavior, which builds self-confidence and skill,
and hence, self-efficacy. Finally, there is recognition, reward and reinforcement for doing the
task, which can build self-esteem and self-confidence.
3.2 Mediating Variable Framework
According to Baranowski, Anderson & Carmack (1998) interventions work by means of
mediating variables, such as: self-efficacy, self-motivation, knowledge, attitudes, expectations,
perceived barriers, positive/negative outcomes, benefits and barriers, processes of change and
social support. A mediating variable would account for the effect of an intervention if a positive
relationship between the intervention and outcome were rendered nonsignificant after
statistically controlling for the mediator (Baron & Kenny, 1986; MacKinnon & Dwyer, 1993).
Current theoretical models from which mediating variables are obtained often do not account for
substantial variability in the targeted outcomes. In addition, interventions have not been shown to
effect substantial change in the mediating variables (Baranowski, Anderson & Carmack, 1998).
These factors impose limits on the effectiveness of the interventions. As a result, the mediating
variable model can be applied to this thesis since it highlights the importance of theory in
understanding community intervention results, since the mediating mechanisms are the
theoretical variables used to design the interventions (see Figure 1.2 below).
Figure 1.2 – Mediating variable model of behavior (Baranowski, Anderson & Carmack, 1998;
p.282).

22
As shown, the independent variable (intervention) has its effects on the outcome (behavior) via
the mediator. Because of that, interventions can target change in critical antecedents of
behavioral engagement and these will follow a causal chain to ensuing behavior change. Thus,
Figure 1.2 is simplified, since there can be many mediating processes or cascading sequences of
mediating processes (Baranowski, Anderson & Carmack, 1998).
Reviews have identified that few studies have reported mediators’ analysis in experimental trials
(Baranowski et al, 1997; Baranowski, Anderson & Carmack, 1998). The MVM was helpful to
understand the importance of mediators to predict behavior, showing that studies aiming to
demonstrate the intervention effects on behavior should identify mediators, and test mediating
effects, not only outcomes.
3.3 The Health Action Process Approach
As described elsewhere, interventions need to be theory-guided to allow for meaningful
interpretations of empirical findings and to draw valid conclusions. Moreover, recommendations
for successful practice need a theory base. Studies of exercise behaviour of people with chronic
illness have been criticized for lacking a theoretical basis (Tulloch et al, 2009), leading to the
current interest in applying health behaviour change theories to improve our understanding of
exercise behaviour.
The traditional continuum models have been mainly criticized because of the intention–behavior
gap (i.e. the gap between wanting to make a behavior change and actually doing it). A model that
explicitly includes post-intentional factors to overcome this gap is the Health Action Process

23
Approach (HAPA), which integrates the health self-efficacy theory, the planned behaviour
theory, and stages of change to predict engagement in health behaviour (Schwarzer, Lippke &
Luszczynska, 2011). Thus, the HAPA model appears to have great potential as a motivational
model for physical activity self-management for people with chronic problems in a variety of
settings, in particular rehabilitation settings (Schwarzer, Lippke & Luszczynska, 2011).
The HAPA is designed as an open architecture that is based on principles rather than on specific
testable assumptions. It was developed in 1988 (Schwarzer, 1992) as an attempt to integrate the
model of action phases (Heckhausen & Gollwitzer, 1987) with social-cognitive theory (Bandura,
1986). It has 5 major principles that make it a distinct from other models and that help to apply
the HAPA to research and interventions
Principle 1: Motivation and volition. The first principle suggests that the health behaviour
change process should be divided into two phases: a motivational phase and a volitional phase.
The motivational phase is the one where people develop their intentions. Afterward, they enter
the volition phase.
Principle 2: Two volitional phases. In the volition phase, there are two groups of people: those
who have not yet translated their intentions into action, and those who have. There are inactive as
well as active persons in this phase. In other words, in the volitional phase one finds intenders as
well as actors who are characterized by different psychological states. Thus, in addition to health
behaviour change as a continuous process, one can also create 3 categories of people, depending
on their current location within the course of health behaviour change: preintenders, intenders
and actors.

24
Principle 3: Postintentional planning. Intenders who are in the volitional preactional stage are
motivated to change, but do not act because they may lack the right skills to translate their
intention into action. Planning is a key strategy at this point. It serves as an operative mediator
between intentions and behaviour.
Principle 4: Two kinds of mental simulation. Planning can be divided into action planning and
coping planning. Action planning pertains to the when, where, and how of intended action.
Coping planning includes the anticipation of barriers and the design of alternative actions that
help to attain one’s goal despite the impediments.
Principle 5: Phase-specific self-efficacy. Perceived self-efficacy is required throughout the entire
process; however, the nature of self-efficacy differs from phase to phase. This is because there
are different challenges that are not of the same nature. Therefore, it is important to distinguish
preactional self-efficacy (also called talk self-efficacy), coping self-efficacy (maintenance self-
efficacy), and recovery self-efficacy.
In addition to the five principles, the model suggests a distinction between (a) preintentional
motivation processes that lead to a behavioral intention, and (b) postintentional volition
processes that lead to the actual health behavior (Schwarzer, 1992). Thus, the model constitutes
an implicit stage model. Within the two phases or “stages”, different patterns of social-cognitive
predictors may emerge (see Figure 1.3, which appears on the next page).

25
Figure 1.3 – Health action process approach (Schwarzer, 1992; retrieved from http://userpage.fu-
berlin.de/~health/hapa_figures.pdf).
According to Schwarzer (1992), in the initial motivation phase, a person develops an intention to
act. In this phase, risk perception is seen as a distal antecedent (e.g. “I am at risk for
cardiovascular disease”). Risk perception in itself is insufficient to enable a person to form an
intention. Rather, it sets the stage for a contemplation process and further elaboration of thoughts
about consequences and competencies. Similarly, positive outcome expectancies (e.g. “If I
exercise five times per week, I will reduce my cardiovascular risk”) are chiefly seen as being
important in the motivation phase, when a person balances the pros and cons of certain
behavioral outcomes. Further, one needs to believe in one’s capability of performing a desired
action (perceived self-efficacy, e.g. “I am capable of adhering to my exercise schedule in spite of

26
the temptation to watch TV”). Perceived self-efficacy and outcome expectancies are seen as the
major predictors of intentions. Both beliefs are needed for forming intentions to adopt behaviors.
It is common knowledge that good intentions do not necessarily guarantee corresponding
actions. After a person develops an inclination towards a particular health behavior, the “good
intention” has to be transformed into detailed instructions on how to perform the desired action.
Once an action has been initiated, it has to be maintained. This is not achieved through a single
act of will, but involves self-regulatory skills and strategies. Thus, the postintentional phase
should be further broken down into more proximal factors, such as planning and recovery self-
efficacy (Schwarzer, 1992).
According to HAPA (Schwarzer, 1992), once an action has been initiated, it has to be controlled
by cognitions in order to be maintained. In this stage, self-efficacy determined the amount of
effort invested and the perseverance. People with self-doubts are more inclined to anticipate
failure scenarios, worry about possible performance deficiencies, and abort their attempts
prematurely. People with an optimistic sense of self-efficacy, however, visualize success
scenarios that guide the action and let them persevere in face of obstacles. Finally, barriers and
resources have to be considered, since actions are not only a function of intentions and cognitive
control, but are also influenced by the perceived and the actual environment.
3.4 Adult Education Theories
According to Cranton (1989): “no unified theory of instruction for adult learners exists”. It can
also be argued that no one theory of instruction is possible, given the diverse activities that are,
together, called adult education (Greenhalgh, 2000). However, several theoretical writers have
provided the foundations for adult education practice, even though they may not have been

27
writing directly about adult education. In this section, the foundations for adult education will be
provided briefly.
One of the earliest descriptions of adult education was provided by Dewey (1916, 1938) and
Lindeman (1926). Dewey argued that education must be thought of as a lifelong process, and
viewed learning as being based on life experience, emphasizing the importance of the scientific
method in learning. That is, an individual faced with a problem will develop hypotheses about it,
and then collect evidence to confirm or deny these hypotheses. The ways of describing learning
by Dewey and Lindemans’ works lead to a model of instruction in which the teacher’s role is one
of guide and facilitator rather than expert or formal authority.
Described as a critical theory, Freire’s (1973) work describes how things should or could be
rather than how things are. Freire worked in Brazil, in the area of health literacy, and believed
that lack of education, particularly literacy education, is a form of oppression. In order to
overcome this barrier, the educator becomes a learner, listening to and understanding the needs
of the individual. In this context, learners participate actively in the learning process, through
dialogue with the instructor. According to Freire (1973), educator and learner are mutually
responsible for the teaching and learning process.
The strongest influence on the practice of adult education has been the work done by Knowles
(1973,1980,1984). Although the term “andragogy” was used prior to Knowles work, he is
credited with popularizing the term, which is defined as “art and science of helping adults learn”.
Androgogy is based on five assumptions about how adults learn, and their attitude towards and
motivation for learning.

28
Most theorists agree that andragogy is not really a theory of adult learning, but they regard
Knowles’ principles as guidelines on how to teach learners who tend to be at least somewhat
independent and self directed (Kaufman, 2003). Knowles’s principles can be summarized as
follows:
- Establish an effective learning climate, both physical and psychological, where learners feel
safe and comfortable to express themselves;
- Involve learners in mutual planning of relevant methods and curriculum content;
- Involve learners in diagnosing their own needs, with the instructor acting as a guide and
resource person;
- Encourage learners to formulate their own learning objectives;
- Encourage learners to identify resources and devise strategies for using the resources to
achieve their objectives;
- Support learners in carrying out their learning plans; and,
- Involve learners in evaluating their own learning.
Despite the list presented above, Cranton (1989) warns about the over-simplification to
summarize the andragogy model. According to the author, “it must be remembered that the
teaching and learning process is a complex one and that individual learners and groups of
learners are very different from each other” (Cranton, 1989; page 34). In summary, there is no
single rule or principle of adult education, which could be applied in every situation.
In the context of adult education it is important to describe studies from theorists who have
contributed to the understanding of how adults learn, but not writing exclusively about adults.
Among them, Gagné (1977), Mezirow (1981), Rogers (1969), and Brundage & Mackeracher’s
(1980).

29
First, Gagné (1977) described a model of learning relevant to individuals of all ages. He
proposed that there are types of learning which form a hierarchy; that is, some types of learning
must precede others. The problem-solving cycle – proposed by this author – is related to the
design of educational curriculum for adult learning and includes: (1) the perception of the
problem; (2) collection of observations, thoughts, and ideas about the problem; (3) formulation
of hypothesis; (4) testing of hypothesis until the solution is found; (5) assimilation of the
solution; and (6) the situation no longer perceived as a problem. Second, Mezirow (1981)
described learning as “reflecting on experience” and proposes in her theoretical model of
learning that an individual learns during a life “crisis” or dilemma (i.e. divorce, promotion,
disease). The learning cycle described by the author includes: self-orientation, exploring options,
building confidence, planning a course of action, acquiring knowledge, experimenting with new
roles, and reintegration into society. Third, Rogers (1969) has provided useful insights into the
learning process, emphasizing the self-actualization of the learner as a goal of education. Finally,
Brundage & Mackeracher (1980) undertook the integration of the research and writing on adult
learning into a set of “learning principles” and their implications for educators. Examples of
some of these principles are listed below.
- Adults enter learning activities with an organized set of descriptions about themselves (self-
concept, self-esteem, self-efficacy), which influence their learning processes.
- Adult learning is facilitated when the learner's representation and interpretation of his own
experience are accepted as valid, acknowledged as an essential aspect influencing change,
and respected as a potential resource for learning.
- A certain degree of arousal is necessary for learning to occur, whereas stress acts as a major
block to learning.

30
- Adult learning is facilitated when teaching activities do not demand finalized, correct
answers and closure; express a tolerance for uncertainty, inconsistency, and diversity; and
promote question-asking and -answering, problem-finding and problem-solving.
- Adult skill learning is facilitated when individual learners can assess their own skills and
strategies to discover inadequacies or limitations for themselves.
- Adult learning is facilitated when the teacher can give up some control over teaching
processes and planning activities and can share these with learners.
Brundage & Mackeracher’s (1980) learning principles described above demonstrate the
complexity of the adult learning phenomenon. According to Cranton (1989) no set of adult
learning principles or guidelines can be regarded as definitive due to this complexity. Each
instructional situation should be adapted to the reality of the learners and instructors (Cranton,
1989).
4 Study Purpose, Objectives and Hypothesis
The purposes of this thesis were to investigate the relationship between patient education and
behavior change in CR and secondly examine the role of knowledge on behavior change and its
mediators in the context of the Health Action Process Approach.
This thesis combines five papers with specific objectives, as described below:
Paper 1: A systematic review of patient education in cardiac patients: do they
increase knowledge and promote health behavior change?
(1) To assess the published research which investigates the impact of education on patients’
knowledge about health and disease;

31
(2) To determine if the published evidence supports a relationship between educational
interventions and health behavior change in CAD patients; and,
(3) To describe the nature of the educational interventions offered to CAD patients.
Hypothesis: It was hypothesized that education significantly increased patients’ knowledge and
would be significantly correlated to behaviour change (physical exercise, medication adherence,
diet, smoking, response to symptoms, and psychosocial well-being).
Paper 2: Development and psychometric validation of a scale to assess
information needs in cardiac rehabilitation: The INCR tool
(1) To develop and psychometrically validate a new tool to assess information needs in CR
(INCR) patients.
Hypothesis: It was hypothesized that the INCR would have good psychometric properties (test-
retest reliability, internal consistency, criterion validity) and could be used to assess information
needs in CR patients.
Paper 3: Healthcare providers’ awareness of the information needs of their
cardiac rehabilitation patients throughout the program continuum
(1) To describe CR participant information needs;
(2) To investigate whether CR providers are cognizant of patient’s information needs and
preferred delivery formats; and,
(3) To investigate whether patient information needs change over the course of CR.
Hypothesis: It was hypothesized that CR providers were cognizant with patients’ information
needs and that these needs change over the course of CR.

32
Paper 4: Development and psychometric validation of the second version of
the Coronary Artery Disease Questionnaire (CADE-Q II)
(1) To develop and psychometrically validate the second version of the CADE-Q (CADE-Q
II).
Hypothesis: It was hypothesized that the CADE-Q II would have good psychometric properties
(internal consistency, criterion validity, factor structure, and content validity) and could be used
to assess CADE- related knowledge in CR patients.
Paper 5: Behavior determinants among cardiac rehabilitation patients
receiving educational interventions: an application of the health action
process approach
(1) To investigate changes in knowledge and related theoretical constructs (i.e., self-
efficacy, outcomes expectancies, risk awareness, intention, and planning) among CR
patients following exposure to a traditional or theoretically-informed educational
curriculum; and,
(2) To investigate the theoretical correlates of exercise behavior change among CR patients
receiving educational interventions.
Hypothesis: It was hypothesized that both groups of CR patients increased their knowledge of
cardiovascular health with education interventions and knowledge was correlated to intentions to
change behavior.

33
Chapter 2 OVERALL RESEARCH DESIGN AND METHODOLOGY
The proposed thesis involves five studies in order to understand the role of knowledge on
behavior change. To provide the reader with an overview of the proposal research, the overall
research design and how these studies are combined in a logical and interconnected sequence is
presented in this chapter, as well as a brief description of each phase. The appropriate methods
that are used in each study are described under each chapter. Furthermore, it is described in
detail the development of the new education curriculum for CR patients and their families, which
is an important piece of all studies described here.
1 Design and Procedure
All studies were reviewed and approved by the University Health Network Research Ethics
Board, in accordance with CNS’s resolution 196/96. All five papers presented in this thesis are
related as described below in four steps. The reader can also visualize this interaction through an
infographic at the end of this chapter (figure 2.1).
Step one: The initial step was to review systematically the literature in order to assess the state of
knowledge regarding the impact of education on patients’ knowledge about health and disease, to
determine if educational interventions are related to health behavior change in CAD patients, and
to describe the nature of the educational interventions offered to CAD patients. This step was
important to gain a clear picture of how these interventions are structured and how they impact
not only behaviour, but disease-related knowledge. To our knowledge, such a synthesis had not
been published previously. A literature search of five electronic databases was conducted for
published articles from database inception to August 2012. Eligible articles included cardiac

34
patients, and described delivery of educational interventions by a healthcare provider. Outcomes
were knowledge, smoking, physical activity, dietary habits, response to symptoms, medication
adherence, and psychosocial well-being. Articles were reviewed by two authors independently.
Results as well as a more detailed methodology are presented in chapter 3.
Step two: In this step the author as well as a group of researches and experts in CR (called
Patient and Family Education Committee) conducted a comprehensive review of existing
documents related to adult learning and patient education in order to develop a new education
curriculum for cardiac patients participating in the largest academic CR centre of Toronto. One
of the findings was that, within the context of CR, educational interventions based on patients’
needs are likely to be more effective. Therefore, a needs analysis was one of the first phases
included in the development of the education curriculum. Since a previous literature review
failed to identify any available and validated tool to assess information needs in coronary
patients in CR programs a new questionnaire was developed and psychometrically validated.
This questionnaire was called INCR and its development and validation are described in chapter
4. In addition, chapter 5 presents a study using the INCR to describe CR participant information
needs, investigate whether CR providers are cognizant of patient’s information needs and
preferred delivery formats, and whether patient information needs change over the course of CR.
Results from this study were important in the development of the new education curriculum for
CR patients.
Step Three: In this step a more comprehensive and updated questionnaire to assess CR patients’
knowledge was developed and psychometric validated. This questionnaire was called CADE-Q
II and the process of development involved a literature search, analysis of the information needs
assessment study results (chapter 5), focus group discussions with 15 CR experts, and a pilot

35
study with a convenience sample of 30 coronary patients who finished their CR programs. A
final version was generated and psychometrically tested in 307 CR patients. A detailed
methodology and results are described in chapter 6.
Step Four: After the development of the new education curriculum and the tool to assess
patients’ knowledge, the final step was to investigate changes in knowledge and behavior change
mediators pre and post CR in two groups of patients: one receiving a traditional education
curriculum and one receiving a new education curriculum. Another objective of this step was to
test the extent to which knowledge can predict behavior change mediators in the context of
education interventions. In summary, a sample of CR patients was divided into two groups based
on the type of education they were receiving (current or new education curriculum). Patients’
knowledge and behavior change mediators were assessed in the beginning of their CR program
and 6 months after discharge. A detailed methodology and results are described in chapter 7 of
this thesis.
2 Setting
All studies described in this thesis included participants recruited from the largest academic CR
centre of Toronto: Toronto Rehabilitation Institute (TRI). The cardiac rehabilitation and
secondary prevention program at TRI is a national leader in the provision of comprehensive,
long-term outpatient services involving medical evaluation, prescribed exercise training, cardiac
risk factor modification, education and counseling. These services are designed to limit the
physiological and psychological effects of cardiac illness, reduce the risk of sudden death, re-
infarction or new cardiovascular events, control or improve cardiac symptoms, stabilize or

36
reverse the atherosclerotic process, and enhance the psychosocial and vocational status of
patients (TRI, 2011).
The CR program in this location is 6-months in duration. The program benefits more than 1,650
patients each year, with a new cohort of 80 patients starting every third Monday of the month.
Upon starting CR, each patient undergoes a comprehensive assessment, they are provided a CR
education workbook and pamphlets as applicable to their educational needs. Participants then
come to the center for weekly classes that include exercise, education, counseling and support.
In addition they are encouraged to exercise on their own at home 4 other times and read an
applicable chapter in their education workbook. In conjunction with these weekly visits, an
interprofessional team provides approximately 15 hours of patient education over the course of
the 6-month program. This is delivered in large and small group education session.
A new educational curriculum was developed for these patients and it is described below. An
infographic illustrating these steps is presented in Figure 2.2, in the end of this chapter.
2.1 Development of the New Education Curriculum
This section describes the development of an education curriculum for CR patients and their
families, called in this thesis the “New Education Curriculum”. This development was based on
two education curriculum frameworks: the University Health Network (UHN) curriculum
framework (UHN, 2003) that guides the delivery of health education for patients and the Eastern
Region Community College ABC program (Eastern Region Community College, 2012) that
guides education delivery in public colleges within Ontario. A committee of 16 CR and patient
education experts – called Patient Education Committee (PEC) – was organized in order to
develop the education curriculum. The responsibilities of this committee are described below.

37
Table 2.1 – Responsibilities of the committee of CR and patient education experts
Responsibilities
1. Developing educational strategies to accelerate the translation of scientific discovery and knowledge to improve patient and family knowledge and skill about the prevention and treatment of cardiovascular disease. This includes a focus on areas that might improve clinician knowledge, attitudes for enhancing communication with patients and families including topics such as health literacy, cultural competence, group facilitation, motivational interviewing and the development and use of patient/family educational materials.
2. Providing oversight for the design, implementation, and evaluation of the new education curriculum activities and products.
3. Performing ongoing evaluations of the education curriculum for patients and families, as well as the general public, to determine that they are relevant, current, effective and cost-effective.
4. Overseeing the periodic development, updating and modification of the program’s educational portfolio for patients and families and conducts periodic strategic planning aimed at continued improvement.
5. Exploring ways to ensure that the patient and family perspective is incorporated into educational activities.
6. Ensuring that staff is best equipped to provide patient and family education and have the opportunity to provide education to other rehabilitation settings within the organization.
Although the word curriculum has its roots in the Latin word for “track” or “race course” its
definition is much wider and represents the expression of educational ideas in practice, including
all the planned learning experiences of an institution. Successful education curriculums are in a
form that can be communicated to those associated with the health learning (i.e. clinicians,
patients, family), are open to critique and are readily transformed into practice (Cranton, 1989).
The development of the curriculum involved a rigorous 3-year process with multiple stages of
research, analysis, and revision as following: (1) problem definition, (2) theoretical foundation,
(3) needs analysis, (4) program goals & educational objectives, (5) sequencing instruction, (6)
instructional strategy/design, (7) instructional methods/materials, (8) evaluation of
instruction/materials, and (9) evaluation of learning for health outcomes.
2.1.1 Problem Definition
According to literature and guidelines, health education should be delivered not only to increase
patients’ knowledge but to also achieve health behavior change (Mullen et al., 1992; Dusseldorp

38
et al., 1999; Thomas et al., 2007; Aldcroft et al., 2011; Schadewaldt & Schultz, 2011; Canadian
Cardiovascular Society [CCS], 2013; Ghisi et al., 2014a). Although studies have shown that
knowledge is insufficient for generating sustained behaviour change (Brown et al., 2011),
knowledge is an essential component of behaviour change because it informs patients of the
probable consequences and outcomes of their choices. PEC members identified a gap between
knowledge and behaviour change, so the new education curriculum was developed to
consciously improve knowledge to influence behaviour change.
2.1.2 Theoretical Foundation
Three different theories guided the committee to meet their objectives of developing an
education curriculum that increased knowledge and promoted and supported behaviour change:
constructivist learning theory, adult learning theory, and the HAPA model. Constructivist
learning theory and adult learning theory guided the education curriculum and the HAPA model
supported their efforts of incorporating behaviour change into the curriculum. Self-management
skills were incorporated to support the behaviour component of the new curriculum and
prescriptive model to support curriculum design.
Adult learning theory and the HAPA model were described on chapter 1 of this thesis. In regards
to constructivist learning theory, constructivism refers to the idea that learners construct
knowledge for themselves – each learner individually (and socially) constructs meaning – as he
or she learns. In this context, learning is active, constructive, social, and contextual. The learner
is an information constructor. People actively construct or create their own subjective
representations of objective reality. New information is linked to prior knowledge and
motivation is a key component in learning (Cole & Griffin, 1987).

39
In regards to self-management (SM) theory, current evidence indicates that individuals and
families who engage in self-management behaviours improve their health outcomes (Ryan &
Sawin, 2009). SM is a multidimensional, complex phenomenon that can be conceptualized as
affecting individuals or families across all the learning process. The SM theory consists of three
dimensions: context, process, and outcomes. In summary, the SM theory says that improvement
of individual and family outcomes translate to improved outcomes for health care practitioners
and systems (Meleis, 1997; Fawcett et al., 2001). Self-management strategies mediate self-
efficacy, which is an important component of patient education as described in chapter 1.
Finally, one other concept was useful in the development of the new curriculum: the prescriptive
model. Prescriptive models are concerned with the ends rather than the means of a curriculum.
The “outcomes based education” model is recent and starts from a simple premise: the
curriculum should be defined by the outcomes to be obtained by learners. Curriculum design
proceeds by working “backwards” from outcomes to the other elements (e.g. content, teaching
and learning experiences, assessment and evaluation) (Harden, Crosby, & Davis, 1991).
2.1.3 Needs Analysis
In order to plan and deliver an effective CR educational intervention, it is important to have
precise information about the educational needs of the patients (i.e. how patients want their
education to be structured and delivered) (Scott & Thompson, 2003; Ghisi et al., 2013a). Indeed,
the literature highlights the importance of a comprehensive understanding of patients’ health
information needs as one of the first steps in developing education curriculums (Cranton, 1989).
The needs analysis as part of the new curriculum development process included the following
five steps: (1) development of a tool to access CR patient information needs; (2) assessment of
CR patients’ information needs and CR clinical staff awareness of patients’ information needs;

40
(3) environmental scan of other CR programs; (4) literature review of best practice on CR patient
education; and, (5) patient focus group. Steps 1 and 2 are described in detail on chapters 4 and 5
of this thesis, respectively.
2.1.3.1 Environmental Scan of other CR programs
In order to understand how education is delivered in similar CR programs, an environmental
scan was performed. From 12 possible sources for this scan, 3 (25%) responded. Together, the
programs provide a variety of education topics including exercise, medical, risk factor
identification and modification and goal setting. Group and individual education is offered as
well as workshops in smoking cessation, stress and weight management. Two of the CR
programs involve patients in the process of developing the curriculum for their education
program (via feedback surveys). A patient needs assessment done in one CR program resulted in
their team revamping the content, amount of detail and comprehension level of the education
offered to their patients and family. Modes of delivery consist of power point presentations,
handouts, workbook and e-learning (for those with internet access). Nutrition education includes
use of food models, real packaging and grocery store demonstrations. Finally, evaluation of the
education programs includes some or all of the following: knowledge uptake, patient satisfaction
and change in behaviour. One program provides “game days” consisting of review of the
patients’ understanding of the educational material. Immediate feedback is given to the patients
and incorrect responses are then reviewed with the group.
2.1.3.2 Literature review of best practice on CR patient education
A literature search of CR guidelines was conducted for information regarding patient education.
Six guidelines were included (Globle & Worcester, 1999; Queensland Health, 2000; National

41
Heart Foundation of Australia [NHFA] & Australian Cardiac Rehabilitation Association
[ACRA], 2004; Ries et al., 2007; Stone et al., 2009; British Association for Cardiovascular
Prevention and Rehabilitation, [BACPR], 2012). Data was extracted and combined into 5
categories: content (educational topics and materials), special considerations (groups which
education should be adjusted), effectiveness (principles for effective teaching and learning),
mode (delivery format), and evaluation. Table 2.2 summarizes the results from this literature
review.
2.1.3.3 Patient focus group
Focus groups are collective discussions that are designed to explore a specific set of issues. They
are a qualitative technique appropriate for exploring patients’ knowledge and experiences,
examining not only what they think but why they hold a particular opinion. They can reveal
dimensions of understanding that often remain untapped by quantitative data methods. Thus,
focus groups explore people's understanding of issues by encouraging interaction between
research participants (Kitzinger, 1999).
Focus groups were used to determine patients’ experience with the education they were receiving
in the CR program prior to any changes made to the curriculum. Analysis of 9 CR patients’
narratives – composing 1 focus group – identified key themes and issues about previous patient
education. Using qualitative framework approach, participants’ narratives were coded and
grouped together under themes (Kitzinger, 1999). Main themes that emerged are described in
Table 2.3.

42
Table 2.2 – Summary of the Literature review of best practice on CR patient education
Source Content Special Considerations To be Effective Mode Evaluation
CACR (Canada)
Topics: − Risk factor target and risk factor
modification (weight reduction, smoking cessation, dietary and nutrition habits)
− Dietary habits to increase fibre, alpha-linolenic acid, fruits, nuts, vegetables, whole grains, monounsaturated fats, polyunsaturated fats, omega 3s, plant-based proteins and reduce saturated fats, simple carbohydrates and sodium)
− Adherence to life-enhancing and/or life-prolonging prescription and non-prescription drugs. (e.g. aspirin, clopidogrel, beta blockers, statins, ACE inhibitors and/or angiotensin receptor blockers)
− Health behaviour interventions including optimal dietary, physical activity strategies and weight control
− Develop self-management techniques (problem solving, decision making, resource utilization, partnership formation, action planning (SMART goal setting) and self-tailoring)
Elderly-cognitive function may be impaired; instructions need to be clear, concise and may need to be written down and frequently reviewed (often with family members) Hearing impaired-clear description by video Visually impaired-clear description by audio Heart failure-education (and counselling) to help them adjust to the psychological, physical and social effects of living with heart failure. Importance of weighing themselves daily and how to adjust diuretic usage in response to weight gain. Diabetes-foot care, proper footwear, medication adherence to diabetes meds, blood sugar monitoring and prevention/treatment of hypo and hyperglycemia. Sexual health- expert education and counselling in patients with congenital heart disease, heart failure or patients who have received information about their sexual health in relation to their cardiovascular condition.
− Voluntary participants − Mutual respect − Time for critical
reflection of material − Empowered to become
self-directed learners − Discuss specific health
goals − Is personalized − Explains the risks of not
changing, the benefits of changing
− Seeks to influence outcome beliefs regarding the outcome efficacy of interventions or behavioural changes
− Often emphasizes proximal risks and benefits over distal ones
− Seeks to heighten self-efficacy concerning possible effective self-regulation of specific behaviours
− May seek to elicit positive emotions, to increase optimism about the possibility of change and to heighten the salience of personal experience or other evidence supporting self-efficacy.
− Individual or group
− Collaborative learning activities
− Internet-based cardiac rehab education
− Efficacious dietary interventions include case management and group interventions combined with individual counselling
− Education outcomes are considered a core component of cardiac rehab
− Documentatio
n of the education plan and progress.

43
AACVPR
(USA)
Topics: − Improving cardiac risk (through a low-
fat diet, blood pressure management, lipid management, smoking cessation, diabetes management, depression/stress management and physical activity habits)
− Managing cardiac emergencies (angina, possible heart attack, pain or discomfort during exercise
− Understanding the disease process (atherosclerosis, high blood pressure, diabetes)
− Maintaining psychosocial health (addressing sexual function, social relationships, depression, anger, hostility
− Adapting to limitations imposed by the disease process (changing roles in the family, jobs at work, hobbies and recreational activities)
Materials should be: − Consistent with national guidelines − Developed by health care professionals − Developed from behaviour and
education programs with documented success
− Reviewed and commented on by patients and families
− Approved by the appropriate institutional administrative structure
− Dependent upon the needs and preferences of patient and families
− At appropriate reading level of patient and family
− Large print on nonglossy paper is more readable
− Translated into different languages
Elderly-address impaired senses(e.g., printed instruction for hearing impaired large-type print for poor vision), offer daylight times, small amounts of information repeated often and individualized to each person, involve family/care givers to reduce social isolation, emphasize nutrition principles adapted for this age group, identify barriers to learning) Multicultural-plan education sessions to last longer than usual, use simple sentences when giving instruction, speak clearly and avoid technical terms, sequence the material, have patient give a return demonstration on any skill you teach, include one or more significant family members, partner with faith-based organizations whenever possible, use health care providers from the patient’s culture where possible, respect the patient’s health beliefs or practices Transplant patients-medications, symptoms, specific diet changes (diet low in fat, cholesterol and sodium to prevent weight gain and hypertension), importance of regular exercise Diabetes-medications, exercise safety, diet, complications, blood sugar monitoring, prevention/treatment of hypoglycemia, foot care.
− Should be dependent upon the needs and preferences of the patient and family
− Individual or group
− Telephone,
internet based, books, audiotapes, videotapes, CD-ROMs, interactive computer programs (computer assisted instruction)
All programs should have written plans for providing education and a method for documenting implementation and patient progress.

44
The Heart Research Centre (Australia).
Medical topics: − Anatomy, physiology and pathology of
cardiovascular disease − Coronary heart disease/ischemic heart
disease − Acute cardiac events − Investigation and procedures − Symptoms and their management − Cardiac medications Modifiable risk factors: − Smoking, raised lipids, nutrition and
dietary fat, high blood pressure, overweight, obesity and diabetes, physical inactivity, other risk factors
Non modifiable risk factors: − Older age, male sex, positive family
history Behavioural and psychosocial topics: − Behaviour change and adherence to
medication and advice − Mood and emotions − Psychosocial risk factors and social
support − Impact upon the spouse and family − Sexual activity and activities of daily
living − Return to work (this is considered a
major aim of cardiac rehab. This is not consistently done in USA and Canada)
Low education levels, increasing age, and heightened anxiety all negatively impacts the cardiac patients’ ability to learn and retain information.
− The patients’ specific needs and their receptivity to information should be considered.
− Joint setting of priorities for educational content by the patient and educator is recommended to maximize learning.
− Information given needs to be repeated reinforced and be consistent amongst the healthcare providers.
Individual or group
Number (%) of patients whose knowledge level is assessed. Number (%) of patients with improved knowledge.
BACPR
(England)
Topics: − Attention to the common unhelpful
beliefs and misconceptions about cardiac illness that lead to increased disability
− Pathophysiology and symptoms − Physical activity, smoking, diet, blood

45
pressure, lipids, weight management and glucose
− Psychological issues − Occupational issues − Sexual dysfunction − Cardioprotective drug therapy, surgical
interventions and devices − Cardiopulmonary resuscitation
NHFA & ACRA
(Australia)
Topics: − Basic anatomy and physiology of the
heart, effects of heart disease, the healing process, recovery and prognosis, symptom management, medications, investigations and procedures, cardiac health beliefs and misconceptions,
− Risk factors for heart disease and their modification for secondary prevention (e.g. smoking cessation, physical activity, healthy eating, control of blood lipids, weight, blood pressure and diabetes)
− Supporting skill development to enable behaviour change and maintenance
− Resumption of physical, sexual and daily living activities including driving and return to work (emphasized),
− Psychological issues e.g. mood (depression), emotions, sleep disturbance, social factors e.g. family and personal relationships, social support/isolation
Queensland Health
(Australia)
Heart disease: − How the heart works, atherosclerosis,
angina, conduction disorders, valvular disease, diseases of the heart muscle, heart attack and the healing process
− Employ adult learning principles
− Encourage group disclosure and sharing of experiences
“Education involves more than the transfer of information. It is not confined
Regularly conduct process, impact and outcome evaluations

46
(causes and symptoms, difference between heart attack and cardiac arrest, myths and misconceptions), cardiac symptoms and their management, what to expect during recovery
Risk Factors: − Modifiable risk factors (smoking,
raised lipids, nutrition and diet, high blood pressure, overweight and obesity, management of type 2 diabetes, physical inactivity alcohol intake, stress)
− Non-modifiable risk factors (age, sex, diabetes, positive family history
Physical Activity/Exercise: − Definition of physical activity,
definition of exercise, type, durations, frequency, intensity, how to monitor the level of exertion, benefits, how to manage angina while doing activity, appropriate clothing and footwear, orthopedic and musculoskeletal problem avoidance-acute and chronic, barriers to exercise, co-morbidity impact on exercise (e.g. CVA, congenital heart disease, very low level of exercise capacity)
Activities of Daily Living: − Outline of recovery process and
anticipated timeframes, general principles regarding resumption of activity, self-monitoring of exertion and symptoms, how to resume general activities using (principles of energy conservation, principles of work simplification), guidelines for return to self-care, home, work and leisure
− Understand group work principles (group dynamics and participant behaviour to foster a positive learning environment for all)
− Encourage the group to generate their own solutions to encourage ownership of knowledge
− Use theories and strategies for behaviour change
− Tailor the education mode to suit individual needs
− Assess knowledge and learning style/preferences
− Address misconceptions − Establish/provide a
supportive learning environment
− Address knowledge, attitude, beliefs and skills of the individual
− Develop client-set, client- focussed learning objectives in collaboration with the health professional
− Provide written confirmation of information provided
to formal education sessions, but is an integral component of physical activity and exercise prescriptions, counselling sessions and informal gatherings such as morning teas. Individuals can benefit from the experiences of others in similar situations so time should be allowed for group members to share their experiences either in a formal or informal way.”

47
activities, use of assistive equipment Nutrition: − Healthy weight range, healthy eating,
modification of diet to achieve appropriate body weight and maintain micronutrient adequacy, dietary fats-types, role in heart disease, salt, fibre, other nutrients in food, cholesterol, food selection/shopping, eating habits/meal patterns, food preparation/cooking, eating out/takeaway, food labelling, recipe modification, hydration during exercise
Smoking Cessation: − Association of smoking and heart
disease, benefits of quitting, nicotine dependence, methods of quitting (behaviour change), resources available, medications available for nicotine addiction
Medications: − Knowledge and understanding of
medications, cost, method of administration, strategies for compliance with medications
Psychosocial Issues: − Mood and emotions (anxiety, denial,
depression, grief and loss), normalization of event, address areas of concern (job security, sexual activity), psychosocial risk factors, return to normal activities, financial concerns, social support, social isolation, impact on family

48
Stress Management: − Link between stress and heart disease,
resources available, stress management strategies (relaxation techniques, time management, setting priorities, balancing work, family and leisure, resources available)
Cardiac Investigations and Procedures: − Explanation of test they have had (e.g.
ECG, echocardiogram, stress test, blood tests, angiogram). Explanation of management (medical or intervention) e.g. thrombolytic therapy, heart surgery, angioplasty, pacemaker implantation. Address and discuss anxieties associated with the above.
CPR: − See heart disease topics, emergency
procedures, community resources
CR indicates cardiac rehabilitation; CACR Canadian Association of Cardiac Rehabilitation; AACVPR American Association of Cardiovascular and Pulmonary Rehabilitation; BACPR British Association of Cardiovascular Prevention & Rehabilitation; NHFA National Heart Foundation of Australia; ACRA Australian Cardiac Rehabilitation Association; ACE angiotensin-converting-enzyme; CVA cerebrovascular accident; ECG electrocardiogram; CPR cardiopulmonary resuscitation.

49
Table 2.3 – Main themes that emerged from patient’s focus group
Main Themes
The workbook is a valuable resource for patients.
The group setting for education delivery is an important part of the CR program. A greater number of participants could benefit from this aspect of the program if more opportunities for peer support and discussion were woven into the curriculum.
There was great value seen in the additional learning groups provided within the program including; the Eating Behaviours, Chronic Disease Self Management, Stress Management, and Post-Surgical clinic.
− The importance of promoting cardiac rehab program throughout the community to increase patient access.
− The CR program is holistic and customized for individuals within a group setting.
− More attention to goals, including follow-up throughout rehabilitation.
− The importance of the facilitator.
2.1.4 Program Goals & Educational Objectives
Program learning outcomes are statements that reflect what learners will know and be able to do
when they graduate from a program. In the development of an education curriculum, it is
important to ensure that program learning outcomes are clearly identified, which described what
graduates of the program will be able to do. This aligns well with the Prescriptive Model,
described earlier. After the previously described steps were completed, the results enabled the
development of the education curriculum’s 5 program learning outcomes, described in Table 2.4.
Table 2.4 – Education Curriculum’s 5 program learning outcomes
By the end of their 6-month CR program, patients will be able to:
1. Take charge of their medical condition and respond appropriately to changes in their health status;
2. Maintain an exercise program to improve their health and well-being;
3. Identify and develop strategies to decrease their risk factors for heart disease;
− 4. Incorporate healthy food choices and practices to manage their health and well-being; and,
− 5. Identify and develop strategies to manage their psychosocial risks for heart disease and improve their well-being.
CR indicates Cardiac Rehabilitation

50
2.1.5 Sequencing Instruction
Sequencing instruction is the order in which topics or objectives will be taught. The process of
determining which learning must precede which other learning is called instructional analysis
(Cranton, 1989). To summarize briefly, instructional analysis is simply a systematic procedure
for sequencing instruction in order to optimize learning. To develop this education curriculum a
type of instructional analysis called task analysis was used, which is based on the assumption
that learning is hierarchical in nature, and learners should be taught from simplest to most
complex topics. In addition, results from the needs assessment study described in chapter 5 were
important to determine in which stage of treatment patients wanted to know about a certain topic.
The education curriculum developed has 3 sections, which are described in Table 2.5.
Table 2.5 – Sections of the new education curriculum for CR patients
Period (weeks)* Section Description
Beginning (1–5 weeks)
Safety and Foundation Information about the CR program, their aerobic exercise prescription and safety, managing angina, irregular heartbeats, diabetes, exercising in cold and hot weather, the heart (anatomy, pathophysiology, diagnoses and treatment) and cardiac medications.
Middle (6-12 weeks)
Skill Development Information about the patient’s risk factor profile, goal setting and action planning, resistance training, nutrition (fats, fiber, reading food labels, sodium), psychosocial risk, and sexual intimacy
End (18-26 weeks) Preparing for Graduation
Information about how much physical activity is good, aerobic and resistance training progression, relapse planning, and graduation.
CR indicates Cardiac Rehabilitation.
* The CR program is 26 weeks long.
2.1.6 Instructional Strategy and Design
Once the content of the course was described in terms of expected learning and once that
learning has been sequenced, the next step in the curriculum development was the instructional

51
strategy and design, or the activities around the learner, which will facilitate his/her learning. In
this context, learning activities, learning assessments, and learning resources and materials were
developed.
Learning activities are designed, grouped and sequenced activities that help learners achieve the
course learning outcomes. Through these learning activities learners also receive feedback about
their progress and are prepared for evaluation where they can demonstrate their achievement of
the course learning outcomes (ERCC, 2012). In the end of each lesson, learning activities are
available for patients within their education workbook as well as in their group education class.
Activities included practical ones like taking their pulse, cognitive ones like reflecting on their
own thoughts and experiences depending on the topic and self-regulatory activities like action
planning and problem solving around a desired behaviour.
Learning assessments should be aligned with learning outcomes. Thus, well-planned assessments
allow learners to demonstrate that they have achieved the learning outcome or provide feedback
that identified the progress they are making towards their achievement (ERCC, 2012). Each
educational topic of the curriculum has learning assessments and assessments of patients’
motivation and confidence level to incorporate change into their lifestyle pertaining to the topic.
Finally, when developing an education curriculum it is important to ensure that learning
resources and materials support the learning activities and assessments. They also need to align
with the needs, interests and abilities of the learners (ERCC, 2012). In this context, the resources
and materials of the new education curriculum are:
- 24 educational weekly group education sessions strategically mapped and sequenced
to support the program learning outcomes. Education sessions are given by an
interprofessional team of CR experts and are usually 30 minutes in duration.

52
- A comprehensive education workbook for people living & thriving with
cardiovascular disease containing 22 chapters. Clinicians and patients reviewed the
material and a plain language and clear design review was completed. The
workbook’s chapters were mapped to correspond to the three topics of the education
curriculum described in Table 2.5.
2.1.7 Instructional Methods and Materials
2.1.7.1 Instructional Methods
For the new education curriculum a combination of four teaching methods were used: (1)
instructor-centered, (2) interactive, (3) individualized techniques, and (4) experiential learning.
Although in this curriculum lectures are included in each CR session, instead of learners being
passive receivers of information, interactive methods are used to promote communication among
learners, as well as between learners and the instructor (e.g. class discussion, peer-to-peer
learning and discussion groups). Individualized learning techniques are also included in the new
curriculum, based on the assumptions that individuals learn at different speeds and that regular
immediate feedback facilitates the learning process (Cranton, 1989). In this context, patients
have the opportunity to have a one-on-one consultation with health providers, including a
dietician, a social worker and a psychologist. Finally, experiential learning methods – learners
performing tasks – are also used in this curriculum, such as creating action plans.
2.1.7.2 Instructional Materials
Instructional materials are the tools used by the educator to help the learner retain, compare,
visualize and reinforce learning (UHN, 2003). As described elsewhere, the materials of the new
education curriculum are an education workbook and educational weekly lectures. Both
53
resources were strategically mapped and sequenced to support the program learning outcomes.
While the workbook comprises the full comprehensive explanation, the weekly lectures highlight
the important ideas of each topic, as well as check patients’ progress (assessments). Besides that,
there are individual care plans, in which patients can interact with staff while they are exercising.
In the future this educational curriculum will be multicultural (to ensure that information is
understood by patients from different cultures) and multimedia (internet and mobile resources
will be added in order to achieve a broader group of patients, in different countries).
2.1.8 Evaluating Instruction and Materials
2.1.8.1 Evaluating Instruction
Capacity building involves increasing knowledge, skills and resources of existing structures to
disseminate an idea (Jackson et al., 1994). During the development of the new education
curriculum each instructor participated in building capacity sessions, which involved information
about the new curriculum, including learning activities, assessments and outcomes in order to
enhance instructors’ skills essential to implementation of the new educational curriculum. In
these sessions, instructors met in small groups of 4-6 on a weekly basis over a course of 6
months. They had the opportunity to learn the new curriculum and the skills for group
facilitation. Furthermore, instructors also expressed their learning needs and used the time to
support one another during this implementation phase. The experience with the new education
curriculum indicates that building capacity sessions are a viable method for instruction
assessment, since an informal feedback is provided to instructor about their instruction.

54
2.1.8.1 Evaluating Materials
Three groups evaluated the new education workbook: patients, staff, and experts. In regards to
patients’ feedback, 8 focus groups (total of 24 patients and 1 spouse) were held. Sessions were
45 minutes long and a 21-item discussion guide was developed by the PEC to guide the
discussion. Positive features of the workbook identified by patients included: content covers their
needs, appropriate amount of information, and appropriate language and content. Negative
features included binding and weight. Overall, patients were very satisfied with the workbook.
Staff’s feedback was also collected during a focus group (n=10), and 13-item discussion guide
was developed by the PEC to guide the discussion. Staff identified that the workbook promotes a
better interaction with patients, and that it is a good resource for them too. However, they point
out that finding information is not always easy.
Finally, experts (editors, volunteers, patients with a medical or educational background) assessed
the content and outcomes of the workbook. Results were positive and reinforced the use of this
tool to educate patients.
2.1.9 Evaluating Learning for Health Outcomes
Chapter 7 of this thesis describes a study aimed to investigate the effects of patient education on
behavior change and its mediators in CR patients, before and after their participation in this new
education curriculum. CR patients were assessed at the beginning of their program and at the
end, through questionnaires. A cohort of CR patients participating in a traditional version of the
education curriculum was also assessed for comparison.

55
2.1.10 Discussion
This section described the 9 phases of the development of an education curriculum for CR
patients and their families. The new curriculum consists of 24 educational weekly lectures
strategically mapped and sequenced to support the program learning outcomes and an
educational workbook with 22 chapters matching the weekly lectures. Individual care plans are
also provided. Each educational topic contains a background educational content, learning
activities, learning assessments, behavioral-based action planning related to the topic, and
assessment of patients’ motivation and confidence level to incorporate change into their lifestyle
pertaining to the educational topic. Positive aspects of the education curriculum include the
following: topics structured from simplest to most complex; instructional strategy and design
comprising learning activities, learning assessments and learning resources and materials; all 4
categories of teaching methods included (instructor-centered, interactive, individualized
techniques and experiential learning); capacity building sessions to increase knowledge, skills
and resources of instructors as well as to assess them; and evaluation of the materials by multiple
groups (patients, staff, and experts).
A key strength of the new curriculum is that it is empirically derived and conceptually congruent.
The new education intervention was developed on the principles of the following theories:
constructivist learning theory, the HAPA model, adult learning theory and prescriptive model. In
addition, because CAD is considered a chronic condition, the intervention was designed to
promote self-management, which is an important element for the management of chronic disease.
Reviews of effectiveness of chronic disease management interventions indicate that interventions
based on behavioral change models are more likely to be effective than those that are not (Jordan
& Osborne, 2007).

56
Another strength in the new curriculum was the needs analysis phase, with information gathered
from five activities to allow the CR expert committee to develop a vision for a patient and family
education curriculum and five program learning outcomes. These activities were very
comprehensive including information derived from patients (assessment of patient information
needs and patient focus group), health providers (staff survey of patient information needs), other
CR programs (environmental scan of other CR programs), and national guidelines (literature
review of best practice). Synthesizing the information gathered from the needs analysis allowed
the development of a vision for a patient and family education curriculum that includes: a variety
of topics and modes of delivery that are relevant to CR patients; information that help CR
patients to make informed decisions about their health; and information that is also consistent
across the team members and is supported by best evidence. In addition, based on results from
this phase the new curriculum is sensitive to potential barriers to learning, culture specific for
both patients and staff, and designed for special populations.
One of the greatest challenges of delivering educational interventions to cardiac patients is to
integrate multiple characteristics and cultures into clinical practice. In the future, the education
curriculum will be translated to different languages to address this issue. Besides being
multicultural, a multimedia set will be build, so patients can assess information in their mobile
and at home. Whether a software version of the curriculum would have similar efficacy in
delivering the message is unknown, but is worth investigated.
In conclusion, the new education curriculum developed in this study is a sequential and
theoretical strategy that could reach CR programs in order to support cardiac patients’ education.
This intervention may be a powerful tool to promote behaviour change in CR patients. CR
programs can use this model to implement education components into their practice.

57
Figure 2.1 - Infographic of the papers that comprise this thesis

58
Figure 2.2 – Development of the new education curriculum - Infographic

59
Chapter 3 PAPER ONE: A systematic review of patient education in cardiac
patients: do they increase knowledge and promote health behavior change?
In this chapter are presented results from a systematic literature search of several electronic
databases from database inception to August 2012 in order to: (1) investigate the impact of
education on patients’ knowledge; (2) determine if educational interventions are related to health
behavior change in cardiac patients; and (3) describe the nature of educational interventions.
Overall, 42 articles were included, of which 23(55%) were randomized controlled trials. This
paper was published in Patient and Education Counseling Journal, in 2014 (Ghisi et al., 2014a).
1 Introduction
Cardiovascular Diseases (CVDs) are the leading cause of mortality worldwide (WHO, 2012),
and are a significant contributor to morbidity and health-related costs (Cardiac Care Network
[CCN], 2002). Coronary Artery Disease (CAD) – the most common type of CVDs – is
considered a chronic condition and, therefore, requires a careful medical management with
multiple recommendations for patients to achieve optimal secondary prevention (Stone, Arthur,
& Suskin, 2009; Clark et al., 2005; Heran et al., 2011). As a consequence, patient education is a
necessary first step to promote patient understanding of the recommended therapies and behavior
changes, as well as to follow them (Alm-Roijer et al., 2006; Kayaniyil et al., 2009; Boyde,
Turnet, Thompson, & Stewart, 2011; Brown et al., 2011).
Patient education has been formally defined as “the process by which health professionals and
others impart information to patients that will alter their health behaviors or improve their health
status” (as cited in Koongstvedt, 2001, p. 788). Research is beginning to demonstrate a positive

60
effect of cardiac patient education on behavior change, including 4 reviews (Mullen, Mains, &
Velez, 1992; Dusseldorp et al., 1999; Aldcroft, Taylor, Blackstock, & O’Halloran, 2011;
Schadewaldt & Schultz, 2011). Of these, 3 demonstrated that educational interventions produce a
positive effect on behavior change. Although these reviews may be less subject to bias as they
included only randomized controlled trials, they included a small number of trials and focus on
outcomes, failing to describe the interventions in depth and aiming only to assess psycho-
educational strategies. It is important to gain a clear picture of how these interventions are
structured and how they impact not only behavior, but knowledge. To our understanding , such a
synthesis has not been published previously.
Cardiac rehabilitation (CR) is a comprehensive risk reduction program, of which patient
education is considered a core component (Buckley et al., 2013). Thus, American and Canadian
Cardiovascular Societies include education as a quality indicator of CR (Thomas et al., 2007;
Canadian Cardiovascular Society, 2013). According to the Canadian Association of CR
Guidelines (Stone et al., 2009), patient education should: be personalized; be led by a
professional staff, with regular contact between staff and patients; be delivered in individual or
group settings; discuss specific health goals; and seek to influence outcomes beliefs, to elicit
positive emotions, to increase optimism about the possibility of change, and to heighten the
salience of personal experience or other evidence supporting self-efficacy. However, the nature
of education delivery is not fully specified, and the impact of the education has not been often
considered.
The first objective of this systematic review was to investigate the impact of education on
patients’ knowledge about health and disease. The second objective was to determine if
educational interventions are related to health behavior change in CAD patients, namely

61
smoking, physical activity, dietary habits, response to cardiac symptoms, and medication
adherence, as well as psychosocial well-being. Finally, the third objective was to describe the
nature of the educational interventions offered, as per the Workgroup for Intervention
Development and Evaluation Research (WIDER) reporting guideline (Workgroup for
Intervention Development and Evaluation Research [WIDER], 2008).
2 Methods
2.1 Search Methods for Identification of Studies
Literature published from database inception until August 2012 was searched using the
MEDLINE, PsycINFO, CINAHL, EMBASE and EBM computerized databases, in conjunction
with a subject librarian. Search results were downloaded into bibliographic software. The search
strategy incorporated 3 concepts: (1) condition, which was divided into cardiac and rehabilitation
aspects (e.g. coronary disease, myocardial infarction, and rehabilitation); (2) education (e.g.
health education or patient education); and (3) outcomes (e.g. knowledge, health behavior,
lifestyle, and attitude toward health). Search terms were specific to each database. The search
strategy for 2 databases is shown in Table 3.1. A snowball hand-search was undertaken after the
first selection of articles.
2.2 Inclusion and Exclusion Criteria
The criteria for considering studies for this review were:
(1) Design: peer-reviewed studies were considered for inclusion. Primary or secondary studies
were included, whether they were observational or interventional in design. Qualitative studies
62
were not included, however they served to inform interpretation of quantitative findings.
Reviews were identified as a source of additional primary studies.
(2) Participants: cardiac patients with primary diagnosis of CAD, myocardial infarction, or who
have undergone coronary artery bypass graft surgery, or percutaneous coronary intervention.
These patients are indicated for CR in clinical practice guidelines (Stone et al., 2009). Heart
failure patients were excluded from this review as these patients require additional education
when compared to CAD patients.
(3) Education: any educational interventions about CAD and its management, delivered by a
healthcare provider. In order for the article to be included, the educational intervention had to be
described in accordance with the reporting guidelines for behavior change interventions
developed by WIDER (WIDER, 2008). Specifically, at least 3 of the 8 recommended elements
for intervention description had to be detailed: characteristics of those delivering the intervention
(i.e. type of healthcare professional), characteristics of the recipients, the setting (i.e. time and
place of intervention), mode of delivery, the intensity (i.e. contact time), the duration (i.e.
number of sessions), adherence to delivery protocols, and a detailed description of the
intervention content.
(4) Outcomes: Studies had to either report the impact on knowledge, behavior, or psychosocial
indicators (e.g., stress). The five behaviors were: smoking, physical activity, dietary habits,
response to cardiac symptoms, and medication adherence. These behavioral outcomes were
chosen because they are related to better health outcomes in cardiac patients (Clark et al., 2005;
Stone et al., 2009; Verril et al., 2009; Heran et al., 2011).
(5) Published in the English language.

63
Table 3.1 – Search Strategy
Concept Search Terms - MEDLINE Search Terms - EMBASE
1. Condition Aspect Coronary disease Coronary artery disease 1.1 Cardiac Aspect Heart disease Heart disease
1.2 Rehabilitation Aspect Cardiovascular disease Cardiovascular disease Coronary artery disease Heart infarction Myocardial infarction Myocardial infarction
Rehabilitation Rehabilitation Physical therapy modalities Rehabilitation research/
medicine/patient Rehabilitation Centers Rehabilitation Centers Physical medicine Physical Medicine Cardiac Rehabilitation Cardiac Rehabilitation
2. Education Aspects Health education Health education Educational status Educational status Education Education Education session/program/
support/target/patient/intervention Education session/program/ support/target/patient/intervention
Patient education as topic Teaching Health literacy Nurses role Teaching session Nurse-patient relations Nurse patient relationship
3. Outcomes Health behavior Health behavior Patient knowledge Patient knowledge Self care Self care Disease management Disease management Treatment outcome Treatment outcome Life style Lifestyle Self-efficacy Self concept Attitude to health Attitude to health Outcome assessment Outcome assessment Effect behavior change Effect behavior change Behavior modification Behavior modification Behavior change Behavior change Lifestyle modification Lifestyle modification Diet Diet Blood glucose Glucose blood level Sodium dietary Sodium intake Smoking Smoking Alcohol drinking Drinking behavior Exercise Exercise Physical fitness Fitness Vital signs Vital sign Body weights and measures Morphometrics Health attitudes, practice Attitude Lipids Lipid blood level Adherence Adherence Medication Medication Psychosocial Psychosocial Stress Stress Symptoms Symptoms

64
2.3 Data Collection and Analysis
Two reviewers independently screened the references identified by the search strategy by title
and abstract. In order to be selected, abstracts had to clearly identify cardiac participants,
educational interventions and one of the outcomes described previously. The full-text reports of
all remaining citations were obtained and assessed independently for eligibility by these 2
reviewers, based on the defined inclusion criteria. Any disagreements were resolved through
discussion between the two investigators and, if needed, consultation with a third author.
Data extraction was undertaken by a single reviewer and checked by a second reviewer. The
Downs and Black scale (Downs & Black, 1998) - a checklist used to assess the methodological
quality not only of randomized controlled trials but also non-randomized studies - was selected
to assess the quality of the studies, as it contained the highest number of relevant items for the
needs of this review. Given not all items were relevant to all study types included in this review,
2 modified versions of the checklist were created. The one for cohort / cross-sectional studies
consisted of 18 items with a maximum score of 18 points. The one for randomized controlled
trials (RCT) consisted of 25 items. This tool was used to rate article quality in 4 areas: reporting,
external validity, internal validity (bias), and internal validity (confounding). The total points for
each article were categorized as “good”, “fair”, or “poor” based on the United States Preventive
Services Task Force approach (Harris et al., 2001).
Given the nature of the literature, quantitative synthesis of data was not possible. The multiple
sources of heterogeneity observed across studies (in terms of interventions and outcomes) meant
that undertaking a formal meta-analysis was not considered appropriate. Heterogeneity amongst

65
included studies was explored qualitatively. Studies were grouped accordingly to intervention
characteristics (e.g., delivery format and education content) and the outcomes of interest.
3 Results
Initial searching yielded 6476 records, and 3 records were identified through the snowball hand-
search. After the screen, 343 full-articles were assessed for eligibility. Overall, 42 articles were
included in this systematic review. A flow diagram depicting the search results, reasons for
exclusion, and study selection is presented in Figure 3.1.
3.1 Characteristics of Included Studies
Table 3.2 summarizes the methodological characteristics of the 42 included studies. Thirty
(71.4%) were experimental: 23 (55%) RCTs (Horlick et al., 1984; van Elderen-van et al., 1994;
van Elderen et al., 1994; Oldenburg et al., 1995; Lidell & Fridlund, 1996; Moore & Dolansky,
2001; Jeong et al., 2002; Mayou et al., 2002; Otterstad, 2003; Leslie et al., 2004; Buckley et al.,
2007; Heidal et al., 2007; Jiang, Sit, & Wong, 2007; Giannuzzi et al., 2008; Kummel et al., 2008;
Cordasco et al., 2009; Lindsay et al., 2009; McKinley et al., 2009; Smith & Burgess, 2009;
Carlson et al., 2011; Wolkanin-Bartnik, Pogorzelska, & Bartnik, 2011; Chan et al., 2012;
Eckman et al., 2012) and 7 (16.7%) quasi-experimental (Linde & Janz, 1979; Dracup et al.,
1984; Marshall, Penckofer, & Llewellyn, 1986; Verges et al., 1998; Yoshida et al., 1999; Van
Elderen & Dusseldorp, 2001; Irmac & Fesci, 2010); and 11 (26.2%) observational: 6 (14.3%)
cross-sectional in design (Fletcher, 1986; Song & Lee, 2001; Frame et al., 2003; Pelletier,
Kundrat, & Hasler, 2003; Oliveira, Ribeiro, & Gomes, 2008; Froger-Bompas et al., 2009) and 5
(12%) were cohort studies - 4 prospective (Lisspers et al., 1999; Palomaki et al., 2002; Timlim,

66
Shores, & Reicks, 2002; Jensen, 2003) and 1 retrospective (Bellman et al., 2009). One (2.5%)
study used a mixed-methods design (Davidson et al., 2008).
The included studies involved 16,079 participants from 187 centers. Thirteen (35%) studies were
undertaken in the United States, 5 (12%) in the United Kingdom, 3 (7%) each in the Netherlands,
Sweden, Australia and Canada, 2 (5%) each in China, France, Korea and Finland, and 1 (2.5%)
each in Japan, Italy, Turkey and Portugal.
The quality ratings of the studies are also shown in Table 3.2. Overall, 16 (38%) studies were
considered “good”, 24 (57%) studies “fair”, and 2 (5%) studies were considered “poor” quality.

67
Figure 3.1: Flow Diagram of Study Selection Process.
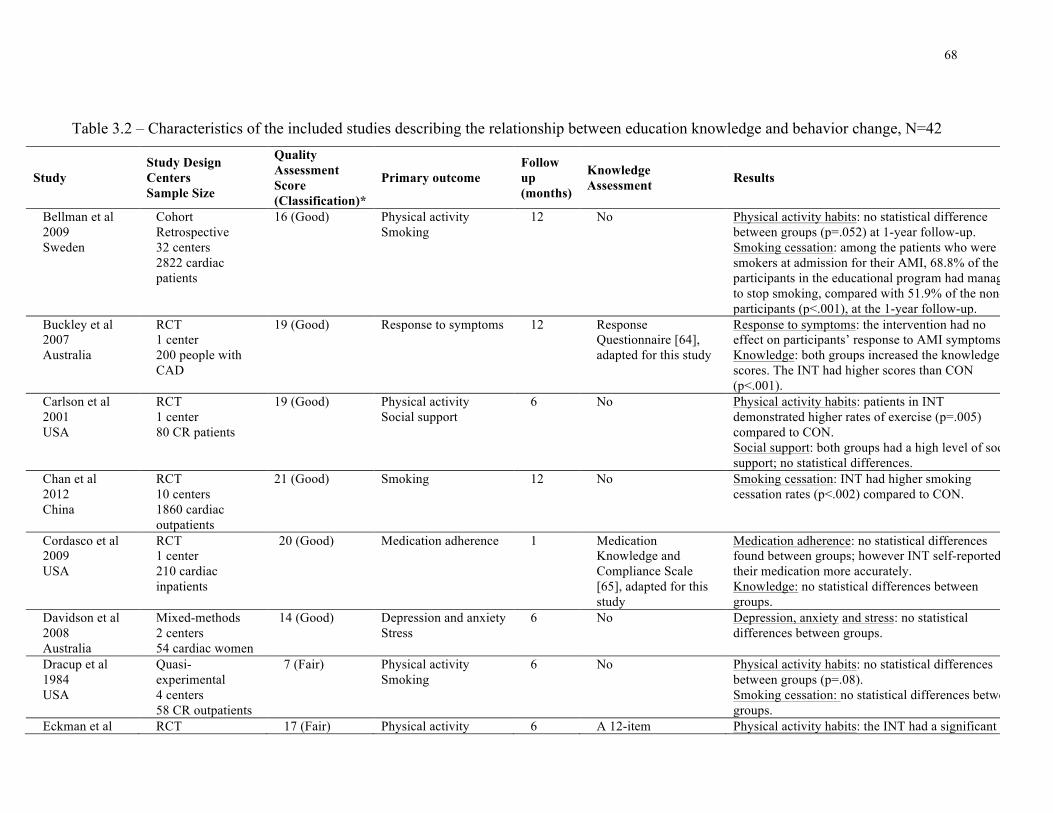
68
Table 3.2 – Characteristics of the included studies describing the relationship between education knowledge and behavior change, N=42!
Study Study Design Centers Sample Size
Quality Assessment Score (Classification)*
Primary outcome Follow up (months)
Knowledge Assessment Results
Bellman et al 2009 Sweden
Cohort Retrospective 32 centers 2822 cardiac patients
16 (Good) Physical activity Smoking
12 No Physical activity habits: no statistical difference between groups (p=.052) at 1-year follow-up. Smoking cessation: among the patients who were smokers at admission for their AMI, 68.8% of the participants in the educational program had managed to stop smoking, compared with 51.9% of the non-participants (p<.001), at the 1-year follow-up.
Buckley et al 2007 Australia
RCT 1 center 200 people with CAD
19 (Good) Response to symptoms 12 Response Questionnaire [64], adapted for this study
Response to symptoms: the intervention had no effect on participants’ response to AMI symptoms Knowledge: both groups increased the knowledge scores. The INT had higher scores than CON (p<.001).
Carlson et al 2001 USA
RCT 1 center 80 CR patients
19 (Good) Physical activity Social support
6 No Physical activity habits: patients in INT demonstrated higher rates of exercise (p=.005) compared to CON. Social support: both groups had a high level of social support; no statistical differences.
Chan et al 2012 China
RCT 10 centers 1860 cardiac outpatients
21 (Good) Smoking 12 No Smoking cessation: INT had higher smoking cessation rates (p<.002) compared to CON.
Cordasco et al 2009 USA
RCT 1 center 210 cardiac inpatients
20 (Good) Medication adherence 1 Medication Knowledge and Compliance Scale [65], adapted for this study
Medication adherence: no statistical differences found between groups; however INT self-reported their medication more accurately. Knowledge: no statistical differences between groups.
Davidson et al 2008 Australia
Mixed-methods 2 centers 54 cardiac women
14 (Good) Depression and anxiety Stress
6 No Depression, anxiety and stress: no statistical differences between groups.
Dracup et al 1984 USA
Quasi-experimental 4 centers 58 CR outpatients
7 (Fair) Physical activity Smoking
6 No Physical activity habits: no statistical differences between groups (p=.08). Smoking cessation: no statistical differences between groups.
Eckman et al RCT 17 (Fair) Physical activity 6 A 12-item Physical activity habits: the INT had a significant

69
2012 USA
3 centers 170 cardiac patients
Dietary habits Smoking
questionnaire developed and pilot tested for this study
improvement (p=.05). Dietary habits: significant improvement in diet, in both groups (p<.001). Smoking cessation: significant improvement in both groups (p<.001) Knowledge: significantly higher in INT (p<.001).
Fletcher 1986 USA
Cross-sectional, longitudinal 1 center 30 cardiac patients
4 (Poor) Physical activity Dietary habits Smoking
6 No Physical activity habits: 16 of 30 patients started exercising regularly. Dietary habits: 18 of 30 patients adhere to a fat-controlled diet. Smoking cessation: 18 of 30 patients stopped smoking.
Frame et al 2003 USA
Cross-sectional, longitudinal 1 center 118 CR patients
10 (Fair) Dietary habits 24 No Dietary habits: the reduction of dietary fat intake was sustained by patients 2 years after CR; and, little progress was observed in the increase intake of fruits and vegetables.
Froger-Bompas et al 2009 France
Cross-sectional 1 center 136 cardiac patients
11(Fair) Dietary habits 36 No Dietary habits: intervention patients had significantly higher consumption of fruits and vegetables (p<.001), global cardiovascular protective diet score (p<.001) and lower consumption of saturated fatty acids (p<.001).
Giannuzzi et al 2008 Italy
RCT 78 centers 3241 CR patients
20 (Good) Physical activity Dietary habits Smoking Stress
12 No Physical activity habits: significant differences between groups (p=.01) and time effect (p<.001). Dietary habits: significant differences between groups (p<.001) and time effect (p<.001). Smoking cessation: at 6 months after intervention, patients were more likely to stop smoking than control (p=.02). Stress: significant differences between groups (p<.001) and time effect (p<.001).
Heidal et al 2007 USA
RCT 1 center 36 cardiac patients
12 (Fair) Dietary habits 2 No Dietary habits: both groups increased n-3 FA intakes from baseline to 1 month (p<.001) and from baseline to 2 months (p<.014). No significant differences between groups after 2 months.
Horlick et al 1984 Canada
RCT 3 centers 116 MI patients
16 (Fair) Physical activity Smoking
6 No Physical activity habits: no statistical differences between groups. Smoking cessation: no statistical differences between groups.
Irmak & Fesci Quasi- 12 (Fair) Physical activity 3.5 No Physical activity habits: the proportion of patients

70
2010 Turkey
experimental 1 center 36 MI patients
Dietary habits Smoking Medication adherence
exercising regularly increased significantly (p<.001). Dietary habits: the proportion of patients who were careful about their nutritional intake before and after the program increased significantly (p<.001). Smoking cessation: the proportion of smokers decreased significantly (p<.001). Medication adherence: no statistical differences.
Jensen 2003 Canada
Cohort 3 centers 350 cardiac inpatients
12 (Fair) Medication adherence 4 Medication Knowledge Questionnaire, developed and validated for this study
Medication adherence: no statistical differences. Knowledge: significantly increased from admission to 16 weeks after discharge (p<.001). Medication knowledge scores were found to be significantly higher for subjects in the INT compared to CON (p=.003).
Jeong et al 2002 Korea
RCT 3 centers 45 MI patients
13 (Fair) Physical activity Smoking
12 No Physical activity habits: the number of subjects exercising at the INT was significantly higher (p=.001) compared to CON. Smoking cessation: after the education, the number of non-smokers had significantly increased, in both groups (INT p=.014, and CON p=.001). The number of non-smokers was significantly higher in the INT (p=.019).
Jiang et al 2007 China
RCT 3 centers 167 CAD patients
18 (Good) Physical activity Dietary habits Smoking Medication adherence
6 No Physical activity habits: compared with baseline, the INT demonstrated a significantly greater increase in the mean scores of walking performance, both at 3 months (p=.001) and 6 months (p=.002), compared to CON. Dietary habits: compared with baseline, the INT demonstrated a significantly greater increase in the mean scores of diet adherence, both at 3 months (p=.001) and 6 months (p=.002), compared to CON. Smoking cessation: no significant differences between the percentages of quitters in the INT and CON. Medication adherence: significant differences were found only at 3 months between groups (p=.029). The mean scores for medication adherence of both groups were decreased, but to a significantly lesser extent in INT.
Kummel et al 2008
RCT 1 center
15 (Fair) Physical activity Dietary habits
12 No Physical activity habits: the reported frequency of PE increased more among men in INT than in CON

71
Finland 117 CABG patients
(p<.001). A similar result was found, when men and women were analyzed together. At 3 months following operation, the change in PE was more favourable among women in CON than women in INT. At 6 months, the change was more favourable in INT, whereas at 12 months, women in CON exercise even more regularly than women in INT. These differences were significant between groups (p=.024). Dietary habits: in the 3-month follow-up, men in CON reported decreased frequency of eating fresh greens and vegetables, but they increased it by 12-month measurement. At 6 months, the frequency of eating vegetables increased among men in INT. Differences between groups were significant (p<.001).
Leslie et al 2004 UK
RCT 2 centers 85 CR patients
16 (Fair) Dietary habits 12 No Dietary habits: differences between groups were significant at 3 months on portions of fruits and vegetables (p=.006), and macronutrients composition (p<.001). Differences in food intakes between groups observed at 3 months were no longer evident at 12 months.
Lidell & Fridlund 1996 Sweden
RCT 1 center 97 MI patients
18 (Good) Physical activity Dietary habits
60 The Cardiac Health Knowledge Questionnaire [66]
Physical activity habits: differences between groups favouring the INT after 1 year (p<.001) and after 5 years (p<.001). Dietary habits: differences between groups favouring the INT after 5 years (p<.04). Knowledge: INT group presented statistical higher knowledge compared to CON 5 years after MI (misconceptions; p<.04 and basic cardiac knowledge; p<.005).
Linde & Janz 1979 USA
Quasi-experimental 1 center 48 cardiac patients
9 (Fair) Dietary habits 4 A 10-item questionnaire developed for this study
Dietary habits: significant differences were found pre and post education in both groups (p=.01). Knowledge: general cardiac knowledge increased significantly (p=.0038). No significant differences observed in knowledge on medication.
Lindsay et al 2009 UK
RCT 1 center 108 cardiac patients
11 (Fair) Physical activity Dietary habits Smoking
12 No Physical activity habits: patients in INT spent significantly more days per week exercising CON (p<.001). The CON also experienced a significant reduction in the number of days per week spent in
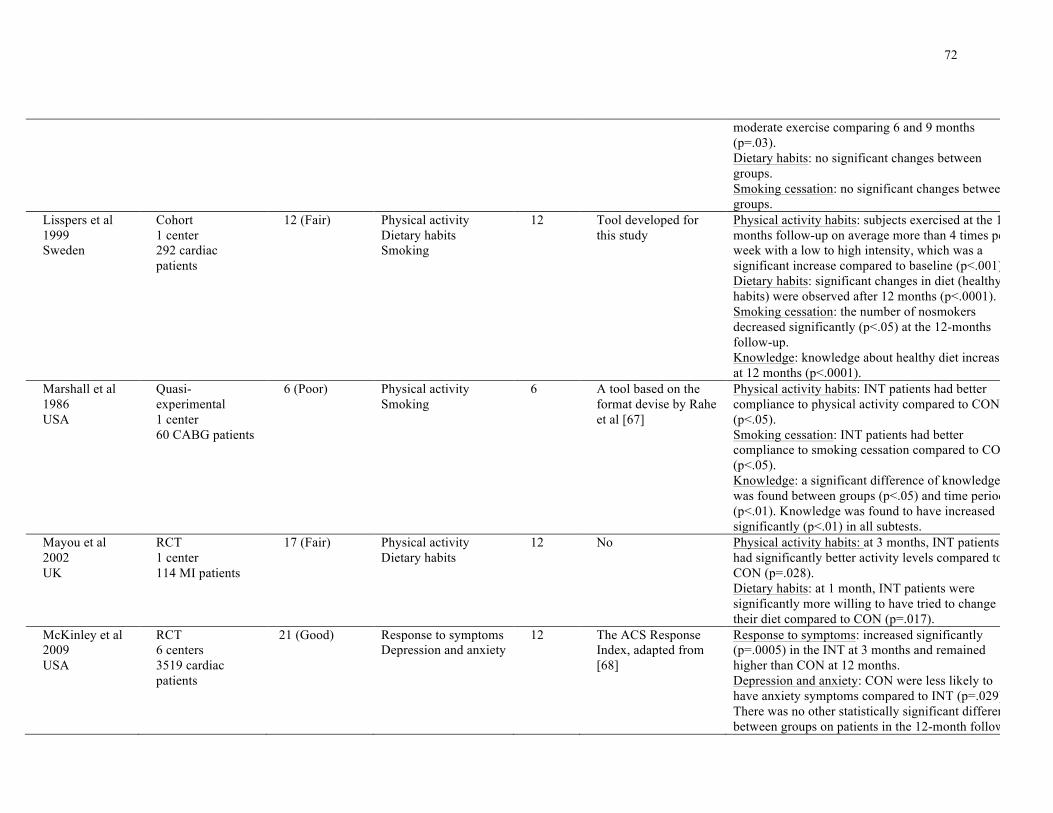
72
moderate exercise comparing 6 and 9 months (p=.03). Dietary habits: no significant changes between groups. Smoking cessation: no significant changes between groups.
Lisspers et al 1999 Sweden
Cohort 1 center 292 cardiac patients
12 (Fair) Physical activity Dietary habits Smoking
12 Tool developed for this study
Physical activity habits: subjects exercised at the 12-months follow-up on average more than 4 times per week with a low to high intensity, which was a significant increase compared to baseline (p<.001). Dietary habits: significant changes in diet (healthy habits) were observed after 12 months (p<.0001). Smoking cessation: the number of nosmokers decreased significantly (p<.05) at the 12-months follow-up. Knowledge: knowledge about healthy diet increased at 12 months (p<.0001).
Marshall et al 1986 USA
Quasi-experimental 1 center 60 CABG patients
6 (Poor) Physical activity Smoking
6 A tool based on the format devise by Rahe et al [67]
Physical activity habits: INT patients had better compliance to physical activity compared to CON (p<.05). Smoking cessation: INT patients had better compliance to smoking cessation compared to CON (p<.05). Knowledge: a significant difference of knowledge was found between groups (p<.05) and time periods (p<.01). Knowledge was found to have increased significantly (p<.01) in all subtests.
Mayou et al 2002 UK
RCT 1 center 114 MI patients
17 (Fair) Physical activity Dietary habits
12 No Physical activity habits: at 3 months, INT patients had significantly better activity levels compared to CON (p=.028). Dietary habits: at 1 month, INT patients were significantly more willing to have tried to change their diet compared to CON (p=.017).
McKinley et al 2009 USA
RCT 6 centers 3519 cardiac patients
21 (Good) Response to symptoms Depression and anxiety
12 The ACS Response Index, adapted from [68]
Response to symptoms: increased significantly (p=.0005) in the INT at 3 months and remained higher than CON at 12 months. Depression and anxiety: CON were less likely to have anxiety symptoms compared to INT (p=.029). There was no other statistically significant difference between groups on patients in the 12-month follow-
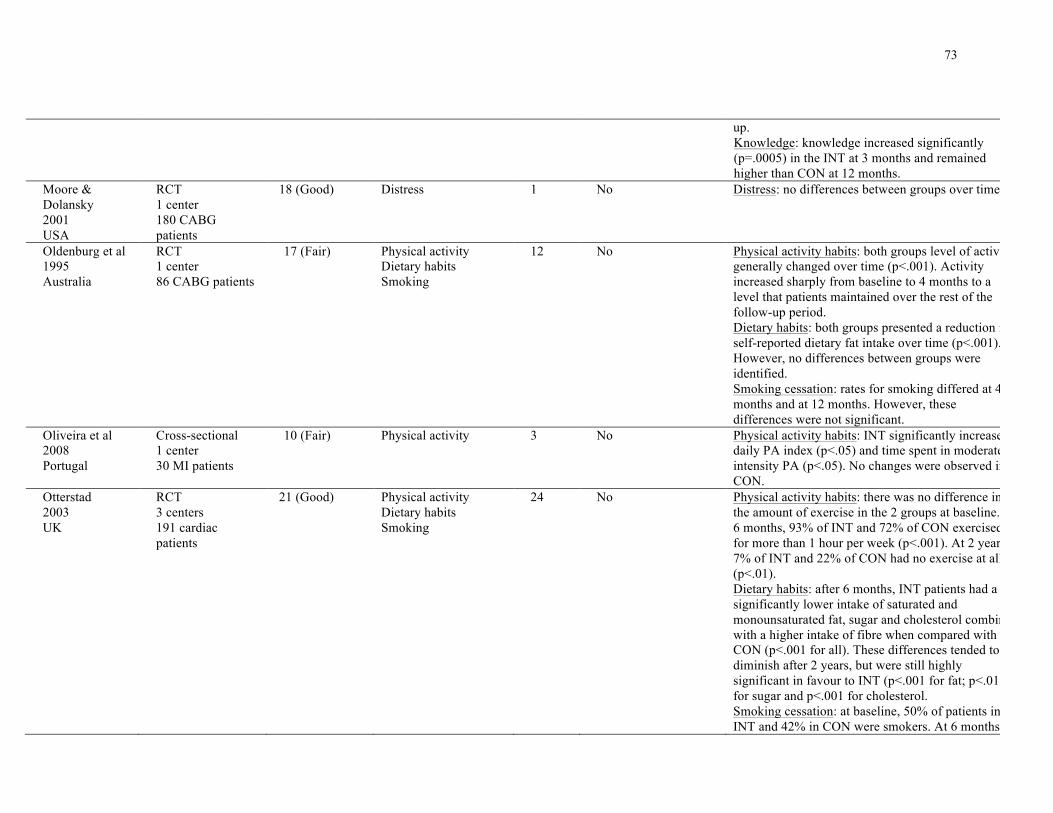
73
up. Knowledge: knowledge increased significantly (p=.0005) in the INT at 3 months and remained higher than CON at 12 months.
Moore & Dolansky 2001 USA
RCT 1 center 180 CABG patients
18 (Good) Distress 1 No Distress: no differences between groups over time.
Oldenburg et al 1995 Australia
RCT 1 center 86 CABG patients
17 (Fair) Physical activity Dietary habits Smoking
12 No Physical activity habits: both groups level of activity generally changed over time (p<.001). Activity increased sharply from baseline to 4 months to a level that patients maintained over the rest of the follow-up period. Dietary habits: both groups presented a reduction in self-reported dietary fat intake over time (p<.001). However, no differences between groups were identified. Smoking cessation: rates for smoking differed at 4 months and at 12 months. However, these differences were not significant.
Oliveira et al 2008 Portugal
Cross-sectional 1 center 30 MI patients
10 (Fair) Physical activity 3 No Physical activity habits: INT significantly increased daily PA index (p<.05) and time spent in moderate-intensity PA (p<.05). No changes were observed in CON.
Otterstad 2003 UK
RCT 3 centers 191 cardiac patients
21 (Good) Physical activity Dietary habits Smoking
24 No Physical activity habits: there was no difference in the amount of exercise in the 2 groups at baseline. At 6 months, 93% of INT and 72% of CON exercised for more than 1 hour per week (p<.001). At 2 years, 7% of INT and 22% of CON had no exercise at all (p<.01). Dietary habits: after 6 months, INT patients had a significantly lower intake of saturated and monounsaturated fat, sugar and cholesterol combined with a higher intake of fibre when compared with CON (p<.001 for all). These differences tended to diminish after 2 years, but were still highly significant in favour to INT (p<.001 for fat; p<.01 for sugar and p<.001 for cholesterol. Smoking cessation: at baseline, 50% of patients in INT and 42% in CON were smokers. At 6 months,

74
55% of smokers in INT and 33% in CON had stopped smoking (p<.05). At 2 years, 45% in INT and 23% in CON were non-smokers (p<.05).
Palomaki et al 2002 Finland
Cohort 3 centers 72 cardiac patients
16 (Good) Physical activity Dietary habits
12 No
Physical activity habits: the weekly leisure time increased significantly during 8 months in the INT (p=.002) without any change in the CON. At 12 months, the physical activity remained at a higher level in the INT, compared to baseline (p=.017). The total amount of physical activity in leisure time was significantly higher at 8 months compared to baseline (p=.046) in the INT. In the CON this variable remained unchanged. Dietary habits: did not change significantly during the 1-yeaqr follow-up.
Pelletier et al 2003 USA
Cross-sectional 2 centers 69 CR patients
9 (Fair) Dietary habits 2 No Dietary habits: all 4 functional foods consumption increased significantly from survey 1 and 2 (p<.001).
Smith & Burgess 2009 Canada
RCT 1 center 276 cardiac patients
22 (Good) Smoking 12 No Smoking cessation: more patients at INT than in CON reported not smoking at 3 months (p=.009), 6 months (p=.003), and 12 months (p=.007). The odds of quitting were 2 times greater for patients who received INT compared to CON in all endpoints. More patients at INT than in CON were confirmed nonsmokers at 12 months (p=.002).
Song & Lee 2001 South Korea
Cross-sectional 1 center 86 MI outpatients
12 (Fair) Physical activity Dietary habits
2 No Physical activity habits: after the INT, participants tend to significantly be more active than before (p<.001). Dietary habits: after the INT, participants tend to significantly eat better (p=.025) than before.
Timlin et al 2002 USA
Cohort study 2 centers 104 cardiac patients
16 (Good) Dietary habits 3 No Dietary habits: significantly improved in both groups from entry to discharge from the program (p=.0001), indicating overall dietary changes, but there was no effect related to group by time.
Van Elderen & Dusseldorp 2001 The Netherlands
Quasi-experimental 3 centers 339 CAD patients
15 (Good) Physical activity Dietary habits Smoking
12 No Physical activity habits: at the first follow-up, patients in INT had a higher risk of maintaining a sedentary lifestyle than patients in CON. Dietary habits: participants in INT decrease the odds of maintaining unhealthy eating habits by a factor 0.30 than patients in CON. Smoking cessation: at the first follow-up treatment

75
was not a significant predictor for smoking cessation. At the second follow-up, patients in INT1 had a higher risk of continuing smoking than patients in CON.
Van Elderen-van et al 1994 The Netherlands
RCT 1 center 30 MI patients
11 (Fair) Physical activity Dietary habits Smoking Depression and anxiety
12 No Physical activity habits: in the short term (8 weeks after discharge; p<.05) the INT resulted in an increase in physical exercise. Dietary habits: in the short term (8 weeks after discharge; p<.001) and long term (1-year after discharge; p<.05) the INT resulted in an increase in healthy eating habits. Smoking cessation: no statistical differences were found. Depression and anxiety: no statistical differences were found.
Van Elderen et al 1994 The Netherlands
RCT 1 center 217 CAD patients
15 (Fair) Physical activity Dietary habits Smoking
12 The Knowledge Questionnaire for Heart Patients [69]
Physical activity habits: no statistical differences were found between patients in CON and INT in both short and long term. Dietary habits: a significantly higher number of patients in INT compared to CON decreased their salt intake in the short-term (p=.009). In the long-term patients in INT maintained a tendency to consume less salt than CON (p=.107). In the short-term, there is a tendency of INT patients to consume less fat than CON (p=.08); however, this did not persist in the long term. Smoking cessation: the number of smokers who quit smoking was significantly higher in INT than in CON, in the short-term (p=.007) and in the long-term (p=.011). Knowledge: Patients in INT showed a higher knowledge than patients in CON in the short-term (4- month assessment) (p=.005). In the long term (1-year assessment) this difference was not maintained (p=.0704).
Verges et al 1998 France
Quasi-Experimental 1 center 52 CAD men
10 (Fair) Dietary habits Smoking
2 A 16-item questionnaire developed for this study
Dietary habits: consumption of fat and fried food reduced in 82% and 52%, respectively, in the INT. Smoking cessation: 12 patients in INT and 11 in CON quit smoking. Knowledge: pre and post analysis showed a

76
significant higher knowledge on the fat-content of the nutriments in 82% of the INT.
Wolkanin-Bartnik et al 2011 UK
RCT 1 center 115 cardiac patients
11 (Fair) Physical activity 12 No Physical activity habits: at baseline, self-reported physical activity did not differ significantly between CON and INT. At 3 months, it was observed a significantly increase in INT (p<.001). The improvement is leisure PA was maintained for the 12-month period for the INT.
Yoshida et al 1999 Japan
Quasi-Experimental 1 center 63 MI patients
11 (Fair) Physical activity Depression and anxiety
6 No Physical activity habits: there was no significant difference in the frequency of exercise between groups before the onset of MI. At the 6-month follow-up, the percentage of patients was: in the INT 74% had good physical activity, 4% had low, and 22% had very low, and in the CON, 31%, 24% and 45%, respectively (no p values reported). Depression status: before entry the program, the depression score in INT was significantly higher than CON (p=.02). At the 6-month follow-up, the score significantly decreased in INT (p=.02). In contrast, the depression score increased numerically in the CON, but it was not significant. At 6-months, there were no significant differences in SRQ-D score between the 2 groups (p=.75). Anxiety status: in INT, the anxiety scores improved significantly after the completion of the CR (p=.04). In the CON scores showed no change at the 6-month follow-up. However, there were no significant differences between groups (p=.59).
RCT: randomized controlled trial; CABG: coronary artery bypass grafting; CAD: coronary artery disease; MI: myocardial infarction; CR: cardiac rehabilitation; INT:
intervention or intervention group; CON: control or control group; PA: physical activity; MI: myocardial infarction.
* For RCT scores ranged from 0-25 (Poor: 0-8; Fair: 9-17; Good: 18-25). Other types of study, scores ranged from 0-18 (Poor: 0-6; Fair: 7-12; Good: 13-18).

77
3.2 Nature of Education Interventions
Table 3.3 summarizes the nature of educational interventions. The educational interventions
were categorised based on WIDER reporting guidelines (WIDER, 2008), and no study reported
complete characteristics. Seventeen studies (40.5%) reported 6 of the 8 WIDER intervention
description elements. None of the studies reported on fidelity or adherence to delivery protocols.
With regard to those delivering the intervention, nurses delivered the education in 15 (35.7%)
studies (Marshall et al., 1986; van Elderen-van et al., 1994; Lisspers et al., 1999; Moore &
Dolansky, 2001; Mayou et al., 2002; Jensen, 2003; Buckley et al., 2007; Jiang et al., 2007;
Davidson et al., 2008; Kummel et al., 2008; Cordasco et al., 2009; McKinley et al., 2009; Smith
& Burgess, 2009; Irmak & Fesci, 2010; Chan et al., 2012), a multidisciplinary team in 13 (31%)
studies (Horlick et al., 1984; Fletcher, 1986; van Elderen et al., 1994; Olderburg et al., 1995;
Lidell & Fridlund, 1996; Yoshida et al., 1999; Song & Lee, 2001; Van Elderen & Dusseldorp,
2001; Palomaki et al., 2002; Timlin et al., 2002; Otterstad, 2003; Bellman et al., 2009; Carlson et
al., 2011), dietitians in 6 (14.3%) studies (Verges et al., 1998; Frame et al., 2003; Pelletier et al.,
2003; Leslie et al., 2004; Heidal et al., 2007; Froger-Bompas et al., 2009), and a cardiologist in 1
(2.4%) study (Giannuzzi et al., 2008).
With regard to setting, most studies (n=22; 52.4%) delivered the educational intervention after
hospital discharge; of these, 11 (26.2%) were interventions in CR (Verges et al., 1998; Yoshida
et al., 1999; Timlin et al., 2002; Frame et al., 2003; Pelletier et al., 2003; Leslie et al., 2004;
Davidson et al., 2008; Giannuzzi et al., 2008; Oliveira et al., 2008; Carlson et al., 2011;
Wolkanin-Bartnik et al., 2011). Six (14.3%) studies provided the education intervention before
hospital discharge (Fletcher, 1986; Marshall et al., 1986; Jeong et al., 2002; Mayou et al., 2002;

78
Jensen, 2003; Smith & Burgess, 2009). A total of 8 (19%) studies (Linde & Janz, 1979; Lidell &
Fridlund, 1996; Lisspers et al., 1999; Horlick et al., 2007; Jiang et al., 2007; Kummel et al.,
2008; Froger-Bompas et al., 2009; Irmak & Fesci, 2010) delivered education interventions both
before and after hospital discharge, whereas 2 (4.8%) studies provided education only at
discharge (Moore & Dolansky, 2001; Cordasco et al., 2009). Four studies reported providing
education to ambulatory patients (Heidal et al., 2007; Lindsay et al., 2009; McKinley et al.,
2009; Eckman et al., 2012).
With regard to mode of delivery, group (n=37 studies; 88.1%) education was delivered by
lectures in 17 (40.5%) studies (Horlick et al., 1984; van Elderen-van et al., 1994; van Elderen et
al.,1994; Oldenburg et al., 1995; Verges et al., 1998; Lisspers et al., 1999; Yoshida et al., 1999;
Song & Lee, 2001; Palomaki et al., 2002; Timlin et al., 2002; Pelletier et al., 2003; Leslie et al.,
2004; Heidal et al., 2007; Kummel et al., 2008; Oliveira et al., 2008; Bellman et al., 2009;
Froger-Bompas et al., 2009), group discussions in 17 (40.5%) studies (Dracup et al., 1984;
Horlick et al., 1984; van Elderen-van et al., 1994; van Elderen et al., 1994; Oldenburg et al.,
1995; Lisspers et al., 1999; Song & Lee, 2001; Van Elderen & Dusseldorp, 2001; Frame et al.,
2003; Otterstad, 2003; Davidson et al., 2008; Kummel et al., 2008; Oliveira et al., 2008; Bellman
et al., 2009; Lindsay et al., 2009; Irmak & Fesci, 2010; Carlson et al., 2011), and question and
answer periods in 3 (7.1%) studies (Song & Lee, 2001; Frame et al., 2003; Bellman et al., 2009).
Individual education was used in 37 (88.1%) studies, including individual counselling in 21
(50%) studies (Linde & Janz, 1979; Fletcher, 1986; Marshall et al., 1986; Lidell & Fridlund,
1986; van Elderen-van et al., 1994; Verges et al., 1998; Lisspers et al., 1999; Yoshida et al.,
1999; Moore & Dolansky, 2001; Timlin et al., 2002; Frame et al., 2003; Leslie et al., 2004;
Buckley et al., 2007; Heidal et al., 2007; Jiang et al., 2007; Gianuzzi et al., 2008; Lindsay et al.,
2009; McKinley et al., 2009; Smith & Burgess, 2009; Carlson et al., 2011; Chan et al., 2012),

79
follow-up telephone contacts in 13 (31%) studies (Lidell & Fridlund, 1986; Marshall et al., 1986;
van Elderen-van et al., 1994; Lisspers et al., 1999; Van Elderen & Dusseldorp, 2001; Jeong et
al., 2002; Buckley et al., 2007; Heidal et al., 2007; Oliveira et al., 2008; McKinley et al., 2009;
Smith & Burgess, 2009; Wolkanin-Bartnik et al., 2011; Chan et al., 2012) and home visits in 3
(7.1%) studies (Jiang et al., 2007; Oliveira et al., 2008; Irmak & Fesci, 2010).
Few studies provided information regarding intensity. The contact time varied from 5-10 minutes
(Smith & Burgess, 2009) to 3 hours (Oldenburg et al., 1995) as well as a full day of education
(Song & Lee, 2001); 15 (35.7%) studies provided no duration information (Fletcher, 1986;
Marshall et al., 1986; Lisspers et al., 1999; Yoshida, 1999; Moore & Dolansky, 2001; Mayou et
al., 2002; Jensen, 2003; Jiang et al., 2007; Kummel et al., 2008; Oliveira et al., 2008; Bellman et
al., 2009; Cordasco et al., 2009; Lindsay et al., 2009; Carlson et al., 2011; Wolkanin-Bartnik et
al., 2011; Chan et al., 2012). With regard to duration, the average number of educational sessions
offered was 6 – range 1 (Moore et al., 2001; Cordasco et al., 2009) to 24 (Lidell & Fridlund,
1996; Van Elderen & Dusseldorp, 2001; Otterstad, 2003), however this was not described in 5
(12%) studies (Fletcher, 1986; Marshall et al., 1986; Lisspers et al., 1999; Lindsay et al., 2009;
Wolkanin-Bartnik et al., 2011). The frequency of contact varied from daily education (Jensen,
2003) to every 6 months (Gianuzzi et al., 2008); most studies (n=17; 40.5%) described weekly
education (Horlick et al., 1984; Dracup et al., 1984; van Elderen et al., 1994; Oldenburg et al.,
1995; Lidell & Fridlund, 1996; Verges et al., 1998; Van Elderen & Dusseldorp, 2001; Palomaki
et al., 2002; Frame et al., 2003; Leslie et al., 2004; Buckley et al., 2007; Heidal et al., 2007;
Davidson et al., 2008; Gianuzzi et al., 2008; Bellman et al., 2009; McKinley et al., 2009; Carlson
et al., 2011) and 12 (28.6%) studies provided no frequency information (Linde & Janz, 1979;
Fletcher, 1986; Marshall et al., 1986; van Elderen-van et al., 1994; Lisspers et al., 1999; Yoshida
et al., 1999; Mayou et al., 2002; Timlin et al., 2002; Gianuzzi et al., 2008; Lindsay et al., 2009;

80
Smith & Burgess, 2009; Wolkanin-Bartnik et al., 2011).
With regard to intervention content, the educational interventions described in the 42 studies
included 19 different topics, with an average of 3.3 topics per study (range from 1 to 7 topics).
One study did not describe the educational content of its intervention (Bellman et al., 2009).
Education content most-often concerned nutrition (n=26; 62%: Linde & Janz, 1979; Horlick et
al., 1984; Fletcher, 1986; Marshall et al., 1986; van Elderen-van et al., 1994; van Elderen et al.,
1994; Verges et al., 1998; Lisspers et al., 1999; Yoshida et al., 1999; Song & Lee, 2001; Van
Elderen & Dusseldorp, 2001; Jeong et al., 2002; Palomaki et al., 2002; Timlin et al., 2002;
Frame et al., 2003; Pelletier et al., 2003; Otterstad, 2003; Leslie et al., 2004; Heidal et al., 2007;
Jiang et al., 2007; Giannuzzi et al., 2008; Froger-Bompas et al., 2009; Lindsay et al., 2009; Irmak
& Fesci, 2010; Carlson et al., 2011; Eckman et al., 2012), exercise (n=19; 45.2%: Linde & Janz,
1979; Fletcher, 1986; Marshall et al., 1986; van Elderen-van et al., 1994; Verges et al., 1998;
Lisspers et al., 1999; Yoshida et al., 1999; Song & Lee, 2001; Jeong et al., 2002; Palomaki et al.,
2002; Otterstad, 2003; Jiang et al., 2007; Giannuzzi et al., 2008; Oliveira et al., 2008; Lindsay et
al., 2009; Irmak & Fesci, 2010; Carlson et al., 2011; Wolkanin-Bartnik et al., 2011; Eckman et
al., 2012), risk factors (n=17; 40.5%; Horlick et al., 1984; Fletcher, 1986; Marshall et al., 1986;
van Elderen-van et al., 1994; Oldenburg et al., 1995; Lidell & Fridlund, 1996; Verges et al.,
1998; Yoshida et al., 1999; Van Elderen & Dusseldorp, 2001; Jeong et al., 2002; Palomaki et al.,
2002; Otterstad, 2003; Giannuzzi et al., 2008; Oliveira et al., 2008; Irmak & Fesci, 2010; Carlson
et al., 2011; Eckman et al., 2012), psychosocial education (i.e. stress, anxiety, social support,
emotions, relaxation techniques and self-management; n=16; 38.1%: Dracup et al., 1984; Horlick
et al., 1984; van Elderen-van et al., 1994; van Elderen et al., 1994; Lidell & Fridlund, 1996;
Lisspers et al., 1999; Yoshida et al., 1999; Moore & Dolansky, 2001; Song & Lee, 2001; Van
Elderen & Dusseldorp, 2001; Otterstad, 2003; Buckley et al., 2007; Jiang et al., 2007; Giannuzzi

81
et al., 2008; McKinley et al., 2009; Carlson et al., 2011), and medications (n=13; 31%: Linde &
Janz, 1979; van Elderen-van et al., 1994; van Elderen et al., 1994; Song & Lee, 2001; Van
Elderen & Dusseldorp, 2001; Jeong et al., 2002; Jensen, 2003; Otterstad, 2003; Leslie et al.,
2004; Cordasco et al., 2009; Irmak & Fesci, 2010; Carlson et al., 2011; Eckman et al., 2012).
Other content topics were smoking cessation (n=8; 19%: Lisspers et al., 1999; Otterstad, 2003;
Jiang et al., 2007; Gianuzzi et al., 2008; Lindsay et al., 2009; Smith & Burgess, 2009; Irmak &
Fesci, 2010; Chan et al., 2012), responding to cardiac symptoms (n=7; 16.7%: Fletcher, 1986;
Lidell & Fridlund, 1996; Moore & Dolansly, 2001; Buckley et al., 2007; Jiang et al., 2007;
McKinley et al., 2009; Irmak & Fesci, 2010), behavior change strategies (n=6; 14.3%:
Oldenburg et al., 1995; Lisspers et al., 1999; Jiang et al., 2007; Davidson et al., 2008; Irmak &
Fesci, 2010; Carlson et al., 2011), surgical procedures (n=5; 11.9%: Linde & Janz, 1979;
Fletcher, 1986; Marshall et al., 1986; Moore & Dolansky, 2001; Kummel et al., 2008), return to
activities (n=4; 9.5%: van Elderen-van et al., 1994; van Elderen et al., 1994; Yoshida et al.,
1999; Mayou et al., 2002), management of CAD (n=4; 9.5%: Van Elderen & Dusseldorp, 2001;
Otterstad, 2003; Lindsay et al., 2009; Eckman et al., 2012), physiology of the heart (n=3; 7.1%:
Horlick et al., 1984; Marshall et al., 1986; Song & Lee, 2001), and nature of the disease (n=2;
4.8%: Fletcher, 1986; Jeong et al., 2002). Other topics were described only by 1 study: secondary
prevention (Mayou et al., 2002), quality of life (Oldenburg et al., 1995), metabolic syndrome
(Palomaki et al., 2002), sexual activity (van Elderen et al., 1994), health beliefs (van Elderen et
al., 1994), and shared decision-making (Eckman et al., 2012).
Finally, educational materials provided to patients included: teaching booklets in 11 (26.2%)
studies (Linde & Janz, 1979; Fletcher, 1986; Marshall et al., 1986; Moore & Dolansky, 2001;
Van Elderen & Dusseldorp, 2001; Jeong et al., 2002; Jiang et al., 2007; Giannuzzi et al., 2008;
Oliveira et al., 2008; Smith & Burgess, 2009; Eckman et al., 2012), cookbooks in 3 (7.1%)

82
(Verges et al., 1998; Leslie et al., 2004; Heidal et al., 2007), educational videos in 5 (11.9%)
(Fletcher, 1986; Yoshida et al., 1999; Smith & Burgess, 2009; Carlson et al., 2011; Eckman et
al., 2012), educational audio-recordings in 2 (4.8%) studies (Moore & Dolansky, 2001; Smith &
Burgess, 2009), medication education kits in 2 (4.8%) studies (Jensen, 2003; Cordasco et al.,
2009) and in 1 study (2.4%) medication and illustration cards (Linde & Janz, 1979), a checklist
(Marshall et al., 1986), heart models (Fletcher, 1986). Verbal orientation to educational materials
was described in 6 (14.3%) studies (Jeong et al., 2002; Jensen, 2003; Cordasco et al., 2009;
Lindsay et al., 2009; Smith & Burgess, 2009; Wolkanin-Bartnik et al., 2011).
3.3 Knowledge
Eleven studies (26%) reported the assessment of knowledge about their condition and 11
different tools were used to assess this knowledge. Six studies used tools developed by other
authors – Response Questionnaire (used by Buckley et al., 2007, and developed by BACPR,
2008), Medication Knowledge and Compliance Scale (used by Cordasco et al., 2009, and
developed by Brown, 1992), the Cardiac Health Knowledge Questionnaire (used by Lidell &
Fridlund, 1996, and developed by Lane & Evans, 1979), the Rahe et al. format model (used by
Marshall et al., 1986, and developed by Kirkland et al., 1999), the Acute Coronary Syndrome
Response Index (used by (McKinley et al., 2009, and adapted from Stewart et al., 2004), and the
Knowledge Questionnaire for Heart Patients (used by van Elderen et al., 1994, and developed by
Sui et al., 2008). In 3 studies the authors developed a questionnaire (Linde & Janz, 1979; Verges
et al., 1998; Lisspers et al., 1999), in 1 study the authors developed and pilot-tested a tool
(Eckman et al., 2012), and in 1 study the authors developed and psychometrically-validated their
tool (Jensen, 2003).

83
Of these 11 studies assessing knowledge, 6 (14.3%) were RCTs and 3 (7.1%) quasi-
experimental. The majority (n=10; 91%: Linde & Janz, 1979; Marshall et al., 1986; van Elderen
et al., 1994; Lidell & Fridlund, 1996; Verges et al., 1998; Lisspers et al., 1999; Buckley et al.,
2007; Jensen, 2003; McKinley et al., 2009; Eckman et al., 2012) reported a significant increase
in knowledge associated with the educational interventions. Results are shown in Table 3.2.
3.4 Behavior Change and Psychosocial Well-Being
Behavior change and psychosocial well-being were assessed via self-report in all (n=42; 100%)
studies. In regards to behavior change, physical activity was measured in 26 studies (62%:
Dracup et al., 1984; Horlick et al., 1984; Fletcher, 1986; Marshall et al., 1986; van Elderen-van
et al., 1994; van Elderen et al., 1994; Oldenburg et al., 1995; Lidell & Fridlund, 1996; Lisspers et
al., 1999; Yoshida et al., 1999; Song & Lee, 2001; Van Elderen & Dusseldorp, 2001; Jeong et
al., 2002; Mayou et al., 2002; Palomaki et al., 2002; Otterstad, 2003; Jiang et al., 2007;
Giannuzzi et al., 2008; Kummel et al., 2008; Oliveira et al., 2008; Bellman et al., 2009; Lindsay
et al., 2009; Irmac & Fesci, 2010; Carlson et al., 2011; Wolkanin-Bartnik et al., 2011; Eckman et
al., 2012), while dietary habits were measured in 25 studies (60%: Linde & Janz, 1979; Fletcher,
1986; van Elderen-van et al., 1994; van Elderen et al., 1994; Oldenburg et al., 1995; Lidell &
Fridlund, 1996; Verges et al., 1998; Lisspers et al., 1999; Song & Lee, 2001; Van Elderen &
Dusseldorp, 2001; Mayou et al., 2002; Palomaki et al., 2002; Timlin et al., 2002; Frame et al.,
2003; Otterstad, 2003; Pelletier et al., 2003; Leslie et al., 2004; Heidal et al., 2007; Jiang et al.,
2007; Giannuzzi et al., 2008; Kummel et al., 2008; Froger-Bompas et al., 2009; Lindsay et al.,
2009; Smith & Burgess, 2009; Irmac & Fesci, 2010; Eckman et al., 2012). Twenty (48%) studies
measured smoking (Dracup et al., 1984; Horlick et al., 1984; Fletcher, 1986; Marshall et al.,
1986; van Elderen-van et al., 1994; van Elderen et al., 1994; Oldenburg et al., 1995; Verges et

84
al., 1998; Lisspers et al., 1999; Van Elderen & Dusseldorp, 2001; Jeong et al., 2002; Otterstad,
2003; Jiang et al., 2007; Giannuzzi et al., 2008; Kummel et al., 2008; Bellman et al., 2009;
Lindsay et al., 2009; Irmac & Fesci, 2010; Chan et al., 2012; Eckman et al., 2012) measured
smoking, 4 (9.5%) studies measured medication adherence (Jensen, 2003; Jiang et al., 2007;
Cordasco et al., 2009; Irmac & Fesci, 2010), and 2 (5%) studies measured response to symptoms
(Buckley et al., 2007; McKinley et al., 2009). Results are described in Table 3.2.
Of the 26 studies measuring physical activity, 20 (77%) reported a significant positive
relationship between education and physical activity, 5 (19%) reported no differences, and 1
(4%) reported a negative relationship. Of the 25 studies assessing dietary habits, 21 (84%)
reported a significant positive relationship between education and dietary habits. No negative
associations were found between dietary habits and educational strategies. Twenty studies
assessed the influence of educational strategies on smoking and 13 studies (65%) reported
significant and positive associations. No negative associations were found. With regard to
response to symptoms, 1 (50%) study reported a significant positive association to education,
and 1 (50%) study found no significant association. With regard to medication adherence, only 1
(25%) study reported a significant difference between educational and non-educational groups;
however, significant differences were only demonstrated at the 3-month assessment point (the
association did not persist).
Finally, 7 (16%) studies examined psychosocial well-being: 4 depression and anxiety (van
Elderen-van et al., 1994; Yoshida et al., 1999; Davidson et al., 2008; McKinley et al., 2009), 2
stress (Davidson et al., 2008; Giannuzzi et al., 2008), and 1 each general distress (Moore &
Dolansky, 2001) and social support (Carlson et al., 2011). Three (43%) studies reported
significant and positive associations; and the other studies presented null results.

85
Table 3.3 - Characteristics of educational interventions (n=42)
Study Health provider delivering the intervention
Setting Delivery Format
Intensity - Contact time - Frequency of each educational session
Mean number of educational sessions*
Education Content
Bellman et al 2009 Sweden
Multidisciplinary team
After D/C Lectures Group discussions Q and A
NR Weekly
5 Not described
Buckley et al 2007 Australia
Nurse After D/C Individual counselling Follow-up telephone contacts
45 minutes Weekly
5 Psychosocial education Symptoms
Carlson et al 2001 USA
Multidisciplinary team
After D/C, CR Group discussions Individual counselling Educational videos
NR Weekly
4 Behavior change strategies Exercise Medications Nutrition Psychosocial education Risk factors
Chan et al 2012 China
Nurse After D/C Individual counselling Follow-up telephone contacts
1 hour Baseline, 1 week and 1 month
3 Smoking cessation counselling
Cordasco et al 2009 USA
Nurse At D/C Medication education kit Verbal orientation
NR NA
1 Medications
Davidson et al 2008 Australia
Nurse CR Group discussions 1 hour Weekly
6 Behavior change strategies
Dracup et al 1984 USA
Not provided After D/C Group discussions
90 minutes Weekly
10 Psychosocial education
Eckman et al 2012 USA
Not provided Ambulatory patients
Teaching booklet Educational videos
NR NA
NA Exercise Management of CAD Medications Nutrition Risk factors Shared decision making
Fletcher 1986 USA
Multidisciplinary team
Before D/C Individual counselling Teaching booklet Educational videos Heart models
NR NR
NR Exercise Nutrition Risk factors Surgical procedures Symptoms

86
Frame et al 2003 USA
Dietician CR Group discussions Q and A Individual counselling
1 hour Weekly
12 Nutrition
Froger-Bompas et al 2009 France
Dietician Before D/C, After D/C
Lectures NR 2x/week
6 Nutrition
Giannuzzi et al 2008 Italy
Cardiologist CR Individual counselling Teaching booklet
NR Monthly and every 6 months
12 Exercise Nutrition Psychosocial education Risk factors Smoking cessation
Heidal et al 2007 USA
Dietician Ambulatory patients
Lectures Teaching booklet (cookbook) Follow-up telephone contacts Individual counselling
1 hour Weekly
5 Nutrition
Horlick et al 1984 Canada
Multidisciplinary team
Before D/C, After D/C
Lectures Group discussions
30-45 minutes Weekly
6 Nutrition Physiology of the heart Psychosocial education Risk factors
Irmak & Fesci 2010 Turkey
Nurse Before D/C, After D/C
Group discussions Home visits
30-40 minutes Monthly
5 Behavior change strategies Exercise Medications Nutrition Risk factors Smoking cessation Symptoms
Jensen 2003 Canada
Nurse Before D/C Medication education kit Verbal orientation
NR Daily
2 Medications
Jeong et al 2002 Korea
Not provided Before D/C Verbal orientation Teaching booklet Follow-up telephone contacts
20-25 min 3rd and 5th days hospitalization
3 Exercise Medications Nature of the disease Nutrition Risk factors
Jiang et al 2007 China
Nurse Before D/C, After D/C
Individual counselling Teaching booklet Home visits
NR Weekly
12 Behavior change strategies Exercise Medications Nutrition Psychosocial education Symptoms
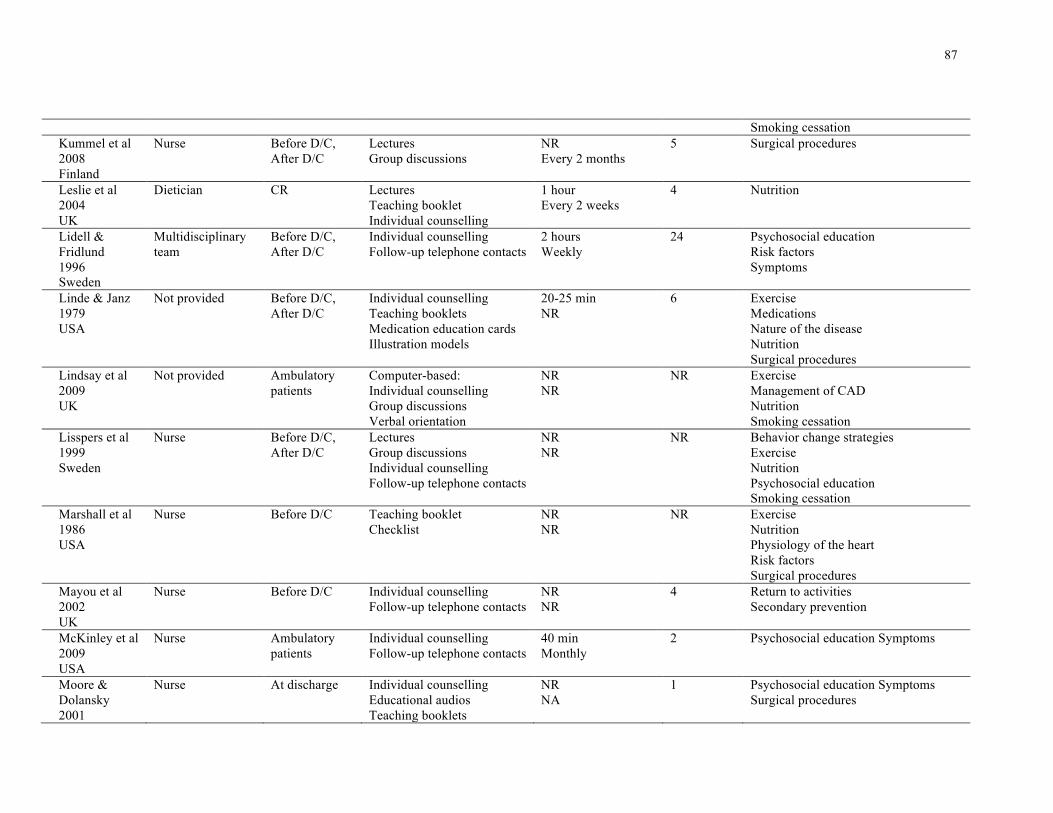
87
Smoking cessation Kummel et al 2008 Finland
Nurse Before D/C, After D/C
Lectures Group discussions
NR Every 2 months
5 Surgical procedures
Leslie et al 2004 UK
Dietician CR Lectures Teaching booklet Individual counselling
1 hour Every 2 weeks
4 Nutrition
Lidell & Fridlund 1996 Sweden
Multidisciplinary team
Before D/C, After D/C
Individual counselling Follow-up telephone contacts
2 hours Weekly
24 Psychosocial education Risk factors Symptoms
Linde & Janz 1979 USA
Not provided Before D/C, After D/C
Individual counselling Teaching booklets Medication education cards Illustration models
20-25 min NR
6 Exercise Medications Nature of the disease Nutrition Surgical procedures
Lindsay et al 2009 UK
Not provided Ambulatory patients
Computer-based: Individual counselling Group discussions Verbal orientation
NR NR
NR Exercise Management of CAD Nutrition Smoking cessation
Lisspers et al 1999 Sweden
Nurse Before D/C, After D/C
Lectures Group discussions Individual counselling Follow-up telephone contacts
NR NR
NR Behavior change strategies Exercise Nutrition Psychosocial education Smoking cessation
Marshall et al 1986 USA
Nurse Before D/C Teaching booklet Checklist
NR NR
NR Exercise Nutrition Physiology of the heart Risk factors Surgical procedures
Mayou et al 2002 UK
Nurse Before D/C Individual counselling Follow-up telephone contacts
NR NR
4 Return to activities Secondary prevention
McKinley et al 2009 USA
Nurse Ambulatory patients
Individual counselling Follow-up telephone contacts
40 min Monthly
2 Psychosocial education Symptoms
Moore & Dolansky 2001
Nurse At discharge Individual counselling Educational audios Teaching booklets
NR NA
1 Psychosocial education Symptoms Surgical procedures

88
USA Oldenburg et al 1995 Australia
Multidisciplinary team
After D/C Lectures Group discussion
3 hours Weekly
8 Behavior change strategies Quality of life Risk factors
Oliveira et al 2008 Portugal
Not provided CR Lectures Group discussions Teaching booklet Home visits Follow-up telephone contacts
NR NR
4 Exercise Risk factors
Otterstad 2003 UK
Multidisciplinary team
After D/C Group discussions 2 hours 2x/week
12 Exercise Management of CAD Medications Nutrition Psychosocial education Risk factors Smoking cessation
Palomaki et al 2002 Finland
Multidisciplinary team
After D/C Lectures
2 hours Weekly
6 Exercise Metabolic syndrome Nutrition Risk factors
Pelletier et al 2003 USA
Dietician CR Lectures 90 minutes Every 2 months
2 Nutrition
Smith & Burgess 2009 Canada
Nurse Before D/C Teaching booklets Verbal orientation Individual counselling Educational videos Educational audios Follow-up telephone contacts
1 (45-60 min) and 7 (5-10 min) NR
8 Smoking cessation
Song & Lee 2001 South Korea
Multidisciplinary team
After D/C Q and A Lectures Group discussions
Daily activity Every 2 months
2 Exercise Medications Nutrition Physiology of the heart Psychosocial education
Timlin et al 2002 USA
Multidisciplinary team
CR Lectures Individual counselling
1 hour NR
3 Nutrition
Van Elderen & Dusseldorp
Multidisciplinary team
After D/C Group discussions Follow-up telephone contacts
5 (2 hours) and 7 (NR)
12 Management of CAD Medications

89
2001 The Netherlands
Weekly Nutrition Psychosocial education Risk factors
Van Elderen-van et al 1994 The Netherlands
Nurse CR Individual counselling Lectures Group discussions Follow-up telephone contacts
90 minutes NR
2 Exercise Medications Nutrition Psychosocial education Risk factors Return to activities
Van Elderen et al 1994 The Netherlands
Multidisciplinary team
After D/C Lectures Group discussions
2 hours 8 weekly and 1 2 months after the 8th session
9 Healthy beliefs Medications Nutrition Psychosocial education Return to activities Sexual activity
Verges et al 1998 France
Dietician CR Lectures Individual counselling Teaching booklets
NR Weekly
8 Exercise Nutrition Risk factors
Wolkanin-Bartnik et al 2011 UK
Not provided CR Teaching booklets Verbal orientation Follow-up telephone contacts
NR NR
NR Exercise
Yoshida et al 1999 Japan
Multidisciplinary team
CR Lectures Educational videos Individual counselling
NR NR
7 Exercise Nature of the disease Nutrition Psychosocial education Return to activities Risk factors
* Including all types of intervention strategies
NA: not applicable (Only one intervention or no formal intervention – e.g., printed or audio/visual materials only); Q and A: Questions and answers; CAD: Coronary
Artery Disease; D/C: discharge; CR: cardiac rehabilitation; NR: not reported.
90
4 Discussion and Conclusion
4.1 Discussion
This systematic review investigated the impact of education on CAD patients’ knowledge and
health behavior change and described the nature of educational interventions delivered. Overall
results of this review suggest that educational interventions within cardiac care increase patients’
knowledge and facilitate behavior change. All studies assessing knowledge but one reported an
increase in patients’ knowledge, in areas including appropriate responses to cardiac symptoms
and medications. Analysis showed that educational interventions were related to increases in
physical activity, healthier dietary habits and smoking cessation, but revealed equivocal relation
to response to cardiac symptoms, medication adherence and psychosocial well-being.
Although the results were mainly positive, studies varied significantly with regard to educational
interventions characteristics. This can be considered a significant gap as no data exists to guide
healthcare providers on the optimal setting, mode of delivery, intensity, duration and content for
provision of patient education for cardiac patients. Indeed, no study described all 8
characteristics according to the WIDER reporting guidelines (WIDER, 2008), and less than half
of the studies reported 6 characteristics. WIDER also makes the recommendation that authors
articulate the assumed change process and design principles underlying their intervention, and
also that they provide access to manuals and protocols to enable reproducibility.
This review demonstrated that on average: nurses were the most frequent educator; most education
was delivered post-discharge; lectures and group discussions were the most common delivery
formats; most interventions also incorporated some form of follow-up telephone contact and

91
individual counseling; the average number of educational sessions delivered was 6; and, an average
of 3.3 topics per intervention were covered, with the most common ones being nutrition, exercise,
risk factors, psychosocial well-being, and medications. Few studies provided information regarding
education duration, but when reported it varied from 5-10 minutes to a day of education.
An underlying principle of patient education is that knowledge is necessary, but not sufficient to
change health behaviours. Patient education involves more than telling people what to do or
giving them instructional materials to read; age (Lane & Evans, 1979; Brown, 1992; Kirkland et
al., 1999), gender (Stewart et al., 2004; Kayaniyil et al., 2009), social and economic (Rathore et
al., 2006; Sui et al., 2008; Loucks et al., 2009), cognitive factors (Schwarz, Schoberberger,
Rieder, & Kunze, 1994; Dracup & Moser, 1997), and environmental factors (Stern, 2000) are
also important considerations. Studies suggest that younger patients learn more than older ones,
and women may be better informed and more active in the decision-making process than men.
Furthermore, economically-challenged patients will face additional barriers to learning. Even
with good access to providers, patients with cognitive impairments and low literacy will need
interventions tailored to their needs (Berckman et al., 2011). Different factors may affect
patients’ ability to learn or engage in interventions, and these factors should be addressed in
educational programs as well as studies assessing educational interventions (Michie et al., 2009).
The findings presented in this review should be interpreted with caution. First, the broad variety of
outcomes parameters across many time periods, and the variety of interventions mitigated the use of
meta-analysis. Indeed, it was impossible to compare the effects of the interventions based on their
characteristics as they were so poorly described. Second, the majority of the trials utilized self-
reported outcome measures, which can be subject to expectation bias. Third, multiple and
simultaneous interventions were often implemented, and thus it is difficult to ascertain what

92
components contribute to the outcomes. Fourth, generalizability is limited as only English articles
were included. Finally, studies in CR setting offer multiple interventions and so we cannot rule out
explanation of effect by these other interventions in uncontrolled studies. Potential biases in the
review process were minimal.
4.2 Conclusion
In conclusion, I was unable to identify the nature of effective educational interventions to cardiac
patients because it was poorly described in the studies. Yet, this systematic review supports the
benefits of educational interventions in CAD, through increases in patients’ knowledge, physical
activity, nutrition behavior and smoking cessation. It is recommended that future reporting of
education interventions should be more explicitly characterized.
4.3 Practice Implications
The weight of evidence suggests the need for comprehensive multidisciplinary education
programs offered in-hospital and post-discharge, through individual and group educational
activities delivered in discursive rather than didactic fashion (BACPR, 2008; Kayaniyil et al.,
2009; Stone et al., 2009; Boyde et al., 2011; Heran et al., 2011). Ensuring CAD patient have
access to comprehensive, evidence-based and manualized education programs may optimize the
benefits observed in relation to physical activity, diet and smoking cessation.

93
Chapter 4 PAPER TWO: Development and psychometric validation of a
scale to assess information needs in cardiac rehabilitation: The INCR tool
In this chapter the development and psychometric validation of a scale to assess information
needs in cardiac rehabilitation (CR) are described. This tool was called INCR (Information
Needs in Cardiac Rehabilitation), has 55 items and asks respondents to rate the importance of
each item to increase their knowledge about coronary artery disease. The INCR was tested in 203
CR patients. This paper was published at Patient and Education Counseling Journal, in 2013
(Ghisi et al., 2013a).
1 Introduction
Cardiovascular Diseases (CVDs) are the leading cause of mortality worldwide (WHO, 2001) and
are a significant contributor to morbidity and health-related costs (CCN, 2002). Moreover, up to
90% of risk for a myocardial infarction (MI) for instance, is due to modifiable behaviours (Yusuf
et al., 2004). A key aim to cardiac rehabilitation (CR), a comprehensive risk reduction program,
is not only to improve physical health and quality of life but to equip and support people to
develop the necessary skills to successfully self-manage (Stone, et al., 2009; BACPR, 2012).
According to the British Association of Cardiovascular Prevention and Rehabilitation, there are
seven core components of CR: health behaviour change and education; lifestyle risk factor
management; psychosocial health; medical risk factor management; cardioprotective therapies;
long-term management; and audit and evaluation (BACPR, 2012). Studies have shown that when
all core components of CR programs are applied in a comprehensive and systematic fashion,
including patient education, it has a significant impact on mortality, improved functional

94
capacity, and decreased re-hospitalization and overall medical costs (Clark et al., 2005; Heran et
al., 2011).
Knowledge of health and disease is necessary, although not sufficient, for successful patient self-
management of coronary artery disease (Potvin, Richard, & Edwards, 2000; Karner, Goransson,
& Bergdahl, 2003; Gazmararian et al., 2003). Studies have shown that patient education is
related to healthier patient choices in daily life, and to better management of cardiac disease. It
has also been shown to relate to fewer adverse outcomes, and even to regression of coronary
disease (Roter, Stashefsky-Margalit, & Rudd, 2001; Karner et al., 2003; Alm-Roijet et al., 2004;
Khan et al., 2006; Osborne, Elsworth, & Whitfield, 2007; Williams, Lindsell, Rue, & Blomkalns,
2007; Krannich et al., 2008; Michie et al., 2008; Kayaniyil et al., 2009).
In the CR population, it has been reported that some patients understand little of what has
happened to them or how to manage their lives in the aftermath of their treatments (Alm-Roijet
et al., 2004). Unfortunately, some patients also report that they would want and need more
information than they usually receive in the course of CR (Kayaniyil et al., 2009). In order to
plan and deliver an effective CR educational intervention, it is important to have precise
information about what patients know regarding cardiac disease and secondary prevention, and
also to identify their information needs (Scott & Thompson, 2003). Indeed, the literature
highlights the importance of a comprehensive understanding of patients’ health information
needs as a logical first step in developing educational programs.
Despite existing studies assessing information needs of patients following revascularization
(Goodman, 1997; Brezynskin, Pendon, Lindsay, & Adam, 1998; Astin et al., 2008), acute
coronary syndrome (Czar & Engler, 1997; Nakano, Mainz, & Lomborg, 2008), MI (Casey,
O’Connel, & Price, 1984; Moynihan, 1984; Orzeck & Staniloff, 1987; Bubela et al., 1990; Chan,

95
1990; Wingate, 1990; Moser, Dracup, & Marsden, 1993; Mirka, 1994; Larson, Nelson,
Gustafson, & Batalden, 1996; Ashton, 1997; Hughes, 2000; Timmins & Kaliszer, 2003; Decker
et al., 2007; Smith & Liles, 2007), and heart failure (Wehby & Brenner, 1999; Lile, Buhmann, &
Roders, 1999), to our knowledge, there are no validated tools to assess information needs in CR
patients. Given wait times to start CR are often upwards of two months (Russel et al., 2011),
patient information needs are likely very different at program inception than they were at the
time of hospitalization. In addition, a previous literature review failed to identify any available
and validated tool to assess information needs in coronary patients in cardiac rehabilitation
programs (Scott & Thompson, 2003). The objective of this study was to develop and
psychometrically validate a new tool to assess information needs in CR (INCR) patients.
2 Methods
2.1 Design and Procedure
This study was reviewed and approved by the Toronto Rehabilitation Institute Research Ethics
Board. The design consisted of a series of cross-sectional, observational studies.
First, a broad search of research in articles and books was performed to identify the most
important areas of information that coronary patients need to know about their disease and its’
management. A literature review of studies and tools examining information needs of coronary
patients was also undertaken. Based on this review, an inventory of these elements was
developed into a first version of the questionnaire and areas of information needs were identified.
This was then emailed to 20 healthcare professionals who were experts in CR. They performed a

96
content analysis, verifying if the new instrument was appropriate for administration in a CR
population and evaluating clarity of the questions. Items were refined based on the findings.
Second was a pilot study to verify the applicability of the INCR instrument, and to evaluate
patient understanding of the items (clarity). Here a convenience sample of coronary patients that
finished their CR programs and had previously-agreed to be contacted about research
opportunities were recruited. Results were used to further refine the INCR tool.
Third, a psychometric validation was performed. The refined tool was administered to a larger
sample of current CR participants from 2 CR programs. The questionnaire was re-administered
two weeks after the first application in 25 randomly selected participants to assess test-retest
reliability. Data were collected between January and April of 2012.
2.2 Participants
For the pilot test, graduates of the Toronto Rehabilitation Institute CR program were surveyed.
For the psychometric-validation of the INCR Tool, a convenience sample of current CR patients
from two institutions were recruited: Toronto Western Hospital and the Toronto Rehabilitation
Institute, both of the University Health Network in Toronto, Ontario, Canada. These programs
are 4-6 months in duration. The inclusion criteria were the following: confirmed coronary artery
disease diagnosis or multiple cardiovascular risk factors (such as hypertension and diabetes). The
exclusion criteria were the following: younger than 18 years old, lack of English-language
proficiency, any significant visual or cognitive condition or serious mental illness which would
preclude the participant’s ability to answer the questionnaire.

97
2.3 Measures
To assess clarity, the expert panel and pilot study patients were asked to rate each information
item Likert-type scale (Pasquali, 2003) ranging from 1 (not clear) to 10 (very clear). CR
participants from the pilot study and psychometric-validation were characterized according to
sex, age, educational level and family income, comorbidities, cardiac risk factors and history,
and duration of participation in CR. All characteristics were self-reported.
2.4 Statistical Analysis
To test the psychometric properties of the new tool, I investigated reliable measures of each one
of the areas of information needs. The first analysis was test-retest reliability, assessed through
the intraclass correlation coefficient (ICC). Since bad items were found they were eliminated. I
then proceed to internal consistency analysis of each area by Cronbach’s alpha. For this analysis,
values higher than 0.70 were considered acceptable, reflecting the internal correlation between
items of the same area (Hair & Anderson, 1998). The factor structure was an option of
assessment if the internal correlation between items in the areas was not confirmed.
Criterion validity was also assessed by comparing INCR scores by participant’s level of
education and duration in CR, using t-tests and Pearson’s correlation respectively. Item
completion rates were also described. As subjects are rating importance, ceiling and floor effects
are likely not applicable (Terwee et al., 2007).
Finally, a descriptive analysis of the INCR Tool was performed. A mean total score was
computed to reflect total information needs. T-tests, one-way analysis of variance and chi-square
tests were used as appropriate to assess differences in INCR scores based on patient’s socio-

98
demographic and clinical characteristics. SPSS Version 21.0 (IBM Corp, 2012) was used for
entering, cleaning and analyzing the data and the level of significance was set at 0.05 for all tests.
Where more than 10% of the items were missing, the data were excluded from further analysis.
3 Results
3.1 Participants Characteristics
For the content validation, there were 10 (50%) clinicians, and 10 (50%) researchers who
reviewed the items. For the pilot test, 50 CR graduates who agreed to be contacted were
contacted. Thirty-four (68%) responded, of which 15 (44%) were female. Respondents had a
mean age of 69.4±8.4, and had participated in a mean of 11±6.5 months of CR.
For the psychometric validation study, 290 coronary patients participating in CR (representing
approximately 25% of total annual CR patients) were approached to participate in this study
during the recruitment phase. Two hundred and three (70%) participants signed the consent form
and completed the INCR tool. The characteristics of these participants are presented in Table 4.1.
To assess test-retest reliability, 25 of these participants were randomly selected and ask to
complete the INCR.
3.2 Development of the Tool
Through the literature review, 11 areas of information needs – a total of 60 items - were
identified and comprised the first version of the INCR Tool. These areas are: the heart
(physiology, symptoms, surgical treatments), nutrition, exercise/physical activity, medication,
work/vocational/social, stress/psychological factors, general/social concerns, emergency/safety,
99
diagnosis and treatment, risk factors, and barriers/goal setting. The mean clarity rating by the
experts was 8.56±1.99. Item ratings are shown in Table 4.2. No changes were made in the scale
at this phase.
After this review, the items were formatted for patient administration with Likert-type response
options as follows: 1 = really not important; 2 = not important; 3 = neutral; 4 = important; and 5
= very important. On the top of the page, patients were asked to report their current educational
needs about each item following the Likert scale.
3.3 Pilot Testing
The 34 participants took a mean of 11.45±4.8 minutes to complete the INCR. Regarding the
evaluation of clarity, mean clarity of the items was 8.21 and no items had mean clarity scores
lower than 6 (ratings are shown in Table 4.2). These results indicated that the questionnaire was
understood by the target population.
3.4 Psychometric Validation
The INCR was administered to the CR participants from 2 programs, and the mean scores are
shown in Table 4.2. Item completion rates are also shown in Table 4.2.
The test-retest reliability was evaluated through the intraclass correlation coefficient (ICC) for
each area, and the ICCs for items 15, 25, 59, and 60 did not meet the minimum recommended
standard (Nunnally & Bernstein, 1994) and were eliminated. Since items 59 and 60 contribute to
the scale barriers/goal setting and this scale has 3 items, I could not compute the scale based on 1
item; therefore, item 58 also dropped.

100
After that, the reliability of each area was assessed by Cronbach’s alpha. All areas were
considered internally consistent (α > 0.7). Table 4.2 displays Cronbach’s alpha of each area.
With regard to criterion validity, total INCR scores were compared by education level and by
duration in CR. As shown in Table 4.2, patients with lower educational level had significantly
greater information needs than those with higher education (p<0.05). Regarding duration in CR,
there was a correlation between this characteristic and total needs (r=0.15; p<0.001): patients in
the first 4 months of the program had significantly higher needs compared to patients finishing
the program (5-6 months of duration). In addition, patients participating in the program for more
than 6 months had significantly higher needs compared to regular participants (at most 6
months).
3.5 Information Needs
The mean total score was 4.08±0.53. Forty-seven percent of patients identified all items as very
important. Analyses (t-tests, one-way analysis of variance and chi-square tests as appropriate)
were performed to evaluate differences in mean INCR scores by patients’ socio-demographic
and clinical characteristics. As shown in Table 4.1, scores were only related to gender (p=0.02),
educational level (p=0.03) and duration in CR (p<0.001).
Means and standard deviations of each item are reported in details in Table 4.2.
Regarding the 10 subject areas of the tool, participants rated emergency/safety
(mean=4.53±0.71), the heart (mean=4.32±0.63), and stress/psychological factors
(mean=4.29±0.7) as the areas with the greatest information needs; and work/vocational/social
(mean=3.61±1.09), general/social concerns (mean=3.83±1.13) and risk factors

101
(mean=3.83±0.79) as their lowest information needs. Mean and standard deviation of each area
is reported in Table 4.3.
Table 4.1 – Sociodemographic/Clinical Characteristics of the Participants for the Psychometric
Validation and INCR mean scores and differences among subgroups (N=203)
Characteristic INCR Score Sociodemographic (mean±SD) p Age (mean±SD) 64.2±11.8 Sex n(%) Male 154 (75.9) 4.04±0.53 0.02† Female 49 (24.1) 4.23±0.50 Educational Level n(%) Elementary School 2 (1.0) 3.30±0.36 0.03† High School 53 (26.1) 4.03±0.56 College 52 (25.6) 4.16±0.46 University 55 (27.1) 3.65±0.57 Postgraduate 40 (19.7) 4.29±0.45 Missing 1 (0.5) - Family Income per year n(%) Under $10.000 6 (3.0) 4.52±0.45 0.24
between $11.000 and $50.000 59 (29.1) 4.07±0.61 between $50.001 and $100.000 70 (34.5) 4.01±0.53 between $100.001 and $150.000 38 (18.7) 4.06±0.39 above $150.000 15 (7.4) 4.03±0.39 Missing 15 (7.4) - Clinical Risk Factors n(%) Hypertension 48 (23.9) 4.03±0.50 0.42 Dyslipidemia 5 (2.5) 4.74±0.24 0.50 Smoking History 41 (20.2) 4.12±0.72 0.80 Comorbidities n(%) Heart Failure 8 (3.9) 4.03±0.80 0.77 Diabetes Mellitus type I 6 (3.0) 4.24±0.75 0.48 Diabetes Mellitus type II 33 (16.3) 3.99±0.71 0.27 Peripheral Arterial Disease 12 (5.9) 4.11±0.91 0.86
Chronic Obstructive Pulmonary Disease 3 (1.5) 3.92±0.68 0.85
Acute Cardiac Event n(%) Acute Myocardial Infarction 39 (19.2) 4.18±0.51 0.20 Revascularization Coronary Bypass 1 (0.5) 3.95±0.59 0.10 Procedures n(%) Angioplasty 90 (44.3) 4.16±0.53 0.06 Duration in CR (mean±SD) 3.8±3.9 At most 2 months 66 (32.5) 4.04±0.51 <0.001†††
3 – 4 months 72 (35.5) 4.10±0.60 5 – 6 months 42 (20.7) 3.90±0.41 More than 6 months 10 (4.7) 4.68±0.18 Missing 13 (6.4) -
SD=standard deviation. Significant differences between groups: †p<.05; ††p<.01; †††p<.001. Note: Income shown in Canadian dollar

102
Table 4.2 – Mean and Standard Deviation of Clarity Rating by Experts (N=20) and Pilot Study Patients (N=20), INCR Score (N=203),
INCR Item Completion Rates and Cronbach’s alpha per area.
Clarity Rating by Expert Panela
Clarity Rating by Pilot Study Patientsa
INCR Scoreb
INCR Item Completion Rates
Cronbach’s alpha per area
Areas Item Mean±SD Mean±SD Mean±SD % The Heart 1. How does a healthy heart works? 8.17±2.17 7.44±2.58 4.32±0.74 100% 0.88 (physiology, 2. What is “coronary artery disease”? 9.00±2.33 8.44±2.28 4.41±0.75 100% symptoms, surgical 3. What is angina? 8.92±2.31 8.00±2.25 4.41±0.77 100% treatments) 4. What happens when someone has a heart attack? 9.33±1.50 8.06±2.24 4.55±0.65 98% 5. What is “bypass surgery”? 8.33±2.39 8.31±2.09 4.14±0.82 100% 6. What is an angioplasty 8.67±2.10 8.75±2.14 4.24±0.86 97.5% Nutrition 7. What foods should I eat for a healthy heart? 8.58±2.57 8.31±1.58 4.40±0.76 100% 0.87 8. How can I choose healthy foods at the grocery
store? 9.42±1.08 8.31±1.85 4.21±0.82 98.5%
9. How can I choose healthy foods when dining out? 9.25±1.42 8.50±1.46 3.99±0.80 100% 10. How do I read food labels? 8.75±2.14 8.25±1.98 4.18±0.75 99.5% Exercise/ Physical 11. How will exercise help my heart condition? 8.17±2.17 9.13±1.02 4.58±0.59 100% 0.88 Activity 12. What are the components of a safe exercise
program? 7.58±2.97 8.25±1.81 4.54±0.67 97%
13. What is cardiovascular or aerobic exercise? 8.42±2.75 8.31±1.54 4.27±0.83 99.5% 14. What can I do to improve of maintain flexibility? 7.92±2.35 8.00±2.00 4.19±0.76 100% *15. How do I check my heart rate (pulse)? 9.75±0.62 9.25±1.34 16. How should I exercise in hot or cold weather? 8.17±2.08 9.13±1.15 4.07±0.94 100% 17. If I have diabetes, how do I prevent low blood
sugar with exercise? 7.83±2.41 6.69±3.70 3.66±1.12 88.2%
18. How do I take care for my feet when in an exercise program?
8.33±2.42 6.75±3.24 3.72±0.99 99%
19. What is resistance training (i.e. exercise for strengthen)?
8.50±3.00 8.81±1.28 3.88±1.08 98.5%
20. What types of exercise equipment are available? (where?)
8.17±2.69 8.44±1.63 3.77±0.98 100%
21. How can I exercise at home safety? 9.92±0.29 8.69±1.35 3.94±1.00 100% 22. When should I stop physical exercise? 7.17±3.07 8.38±1.41 4.14±0.99 100% 23. Is sexual activity safe for me? 6.92±3.40 8.56±2.00 3.70±1.15 99% Medication 24. What medications do I need to help my heart? 9.42±1.00 8.69±1.62 4.28±0.99 100% 0.92

103
*25. What is the purpose of each of my medications? 8.00±2.04 7.69±2.36 26. How do I take my medication in the right way? 7.75±3.05 7.94±1.88 4.30±0.91 100% 27. What side effects are possible with my
medication? 9.58±0.90 7.06±2.98 4.22±0.95 98.5%
28. Do the medications I am taking interfere with each other?
8.58±2.61 7.44±2.55 4.23±0.99 98%
29. Are there foods I should avoid while taking these medications?
8.58±2.79 7.63±2.06 4.42±0.83 100%
30. What are the effects of complementary and alternative medications?
6.67±4.05 6.69±2.44 4.17±0.95 100%
Work/Vocational/ Social
31. When can I return to work and my old activities? 8.83±2.12 8.19±1.80 3.80±1.08 97% 0.85
32. Can I go back to my same job? 9.50±0.80 8.50±1.46 3.59±1.21 94.1% 33. When can I start driving again? 9.33±2.31 8.75±1.65 3.86±1.16 97.5% Stress/Psychological Factors
34. What feelings are common after a heart attack? 8.92±1.62 8.25±2.14 4.26±0.92 99.5% 0.87
35. How does stress affect my heart? 9.67±0.89 8.69±1.58 4.52±0.70 100% 36. How can I cope with stress? 8.83±1.99 8.31±1.58 4.42±0.75 97.5% 37. What can I do to reduce stress in my life? 8.50±2.07 8.44±1.63 4.36±0.87 98.5% 38. Do sleep problems affect my heart? 9.75±0.62 8.25±1.61 4.15±1.01 99.5% General/Social Concerns
39. What services, support organizations and groups are available?
8.17±1.9 8.63±1.26 4.04±0.94 97% 0.84
40. What support services are available to my family?
9.08±1.00 8.56±1.46 3.84±1.05 97%
Emergency/Safety 41. How do I recognize angina symptoms? 7.92±1.59 8.50±1.86 4.54±0.70 98.5% 0.90 42. What should I do if I feel angina or chest pain? 9.58±0.79 8.88±1.41 4.54±0.78 98.5% 43. When should I call the doctor? 9.17±1.47 8.50±1.37 4.61±0.65 99.5% 44. When should I call 911 or go to emergency
room? 7.58±2.97 8.13±1.67 4.61±0.79 100%
Diagnosis and treatment
45. What are the tests used to diagnosis my heart condition?
9.08±1.44 8.25±1.29 4.32±0.92 99.5% 0.86
46. What treatments are available for my condition? 8.50±2.28 8.44±1.67 4.50±0.89 99.5% Risk Factors 47. What are the risk factors for heart disease? 8.08±2.27 7.88±1.89 4.36±0.97 99.5% 0.87 48. What are the risk factors that I cannot control? 8.25±2.34 8.25±1.65 4.17±0.90 100% 49. What are the risk factors I can control? 8.08±2.57 7.88±1.86 4.63±0.60 100% 50. What can I do to bring my risk factors under
control? 9.42±1.44 8.88±1.15 4.60±0.70 98.5%
51. How does cholesterol affect my heart? 9.67±0.65 7.44±2.76 4.27±0.97 99.5% 52. How does diabetes affect my heart? 8.42±2.11 8.56±1.50 3.93±1.07 93.1% 53. How does physical inactivity affect my heart? 9.83±0.39 9.25±1.12 4.35±0.85 99.5%

104
54. How does smoking affect my heart? 9.58±0.79 8.94±1.47 3.33±1.45 93.6% 55. What are the benefits of quitting smoking? 9.50±1.17 9.13±1.26 3.28±1.52 92.6% 56. What supports are available to help me quit
smoking? 9.92±0.29 8.38±1.75 3.00±1.43 92.6%
57. How does alcohol affect my heart? 6.25±2.77 6.13±1.96 3.35±1.41 98% **Barriers/Goal Setting
*58. How do I identify and overdue barriers to start and maintain a healthy lifestyle?
7.92±2.94 8.19±1.33
*59. How can setting goals help me to be successful in my rehab program?
6.25±3.33 7.75±1.61
*60. How do I establish effective goals for my rehab program?
6.25±3.72 6.63±2.85
Total 8.56±1.99 8.21±1.82 4.08±0.53 98% - SD=standard deviation. aClarity rating out of 10 were 1 = not clear and 10 = very clear. bINCR response options were 1 = really not important; 2 = not important; 3 = neutral; 4 = important; and 5 = very important. *items dropped due to low ICC. **area excluded due to test-retest analysis
Table 4.3 – Mean and Standard Deviation of educational needs per subject area, N=203
Subject Mean±SD 1 – The Heart (physiology, symptoms, surgical treatments)
4.32±0.63
2 – Nutrition 4.18±0.67 3 – Exercise/ Physical Activity 3.99±0.63 4 - Medication 4.28±0.77 5- Work/Vocational/Social 3.61±1.09 6 – Stress/Psychological Factors 4.30±0.70 7-General/Social Concerns 3.83±1.13 8-Emergency/Safety 4.54±0.72 9-Diagnosis and treatment 4.39±0.90 10-Risk Factors 3.84±0.79 Total 4.08±0.53
SD=standard deviation

105
4 Discussion and Conclusion
4.1 Discussion
Education is a core component of CR, and is necessary to promote patient understanding of
secondary prevention strategies and adherence to these strategies. Herein, a new tool to assess
CR participant’s information needs has been developed and psychometrically-validated through
a rigorous process. Internal reliability, test-retest reliability, content and criterion validity as well
as factor structure were all established, and demonstrate the utility of this tool. In particular,
results should inform review of educational programs provided to patients within CR.
The overall mean, as well as many of the 10 subject areas means were all quite high,
demonstrating that CR participants consider most of the 55 information items to be “important”.
This also highlights the importance of CR, where patients have repeated contacts with the
program, so there is sufficient opportunity to provide such comprehensive education. Clearly, it
would be difficult to convey all the information patients deemed important in a clinic visit,
although written patient education materials can be provided.
Although the provision of education to patients with acute cardiac disorders has been a
predominant theme in the literature over the past 20 years, to our knowledge, there is no
available tool in the literature that addresses information needs during CR. Studies have being
assessed information needs of cardiac patients following different conditions; however timing is
an important framework in this context, and information needs may vary from when the patient
is at home, after discharge and during rehabilitation (Scott & Thompson, 2003; Decker et al.,
2007).

106
Results of the present study are generally consistent with those reported previously in MI
patients. In particular, the emergency/safety (Casey et al., 1984; Larson et al., 1996; Timmins &
Kaliszer, 2003) and medication (Casey et al., 1984; Chan, 1990; Timmins & Kaliszer, 2003;
Smith & Liles, 2007) subject areas were highly concordant. However, there are differences in the
present study compared to literature. Firstly, the present study revealed a stress/psychological
factor as a subject area, which is not well documented as a need in some studies (Timmins &
Kaliszer, 2003). Thus, knowing about risk factors is described as the highest information need in
different studies (Casey et al., 1984; Chan, 1990; Wingate, 1990) but, surprisingly, not in this
study.
There are some limitations to this study, which should be stated. First, a sample size of at least
50 patients is generally considered adequate for the assessment of test-retest reliability (Altman,
1991), yet only 25 were tested in the current study. There are some elements of the scale, which
require further assessment. Construct validity was not tested, and this should form the basis for
future study. Moreover, future research is needed to assess whether the scale is sensitive to
change, such as following participation in the education components of CR, or to test
implementation of new education materials. Finally, whether the INCR is a valuable and valid
tool to identify information needs in individual patients should be explored.
4.2 Conclusion
In conclusion, the INCR Tool proved to have strong psychometric properties, providing
preliminary evidence of the reliability and validity of the INCR Tool to assess information needs
in CR patients. It is hoped this tool can support CR evaluation of their program’s education
107
component, and promote greater provision of information consistent with patient’s identified
needs.
4.3 Practice Implications
Good patient education involves assessing needs (Kayaniyil et al., 2009; Roter et al., 2001; Scott
& Thompson, 2003; Timmins & Kaliszer, 2003), setting goals and objectives, implementing a
teaching plan, and evaluating outcomes (Cranton, 1989). Before implementing patient education
programs, it is prudent to evaluate what information is needed. The availability of this valid
needs assessment tool is essential to evaluate the information needs of CR patients and to tailor
the information component of these programs. Then tools such as the CADE-Q (Coronary Artery
Disease Educational Questionnaire) (Ghisi et al., 2010; de Melo Ghisi et al., 2013) can be
administered to determine whether patients have the learned the information they perceived as
important.

108
Chapter 5 PAPER THREE: Healthcare providers’ awareness of the information needs of their cardiac rehabilitation patients
throughout the program continuum
Results are presented from a cross-sectional study aimed to: (1) describe cardiac rehabilitation
(CR) participant information needs, (2) investigate whether CR providers are cognizant of
patient’s information needs and preferred delivery formats, and (3) whether patient information
needs change over the course of CR. The tool used to assess information needs was the INCR,
which development and validation was described in Chapter 4. This paper was published in
Patient and Education Counseling Journal, in 2014 (Ghisi et al., 2014b).
1 Introduction
Patient participation in cardiac rehabilitation (CR), a comprehensive outpatient risk reduction
program, mitigates the burden of cardiovascular diseases (Clark et al., 2005; Heran et al., 2011;
Lawler, Filion, & Eisenberg, 2011), the leading cause of mortality worldwide (WHO, 2011), and
a significant contributor to morbidity and health-related costs (CCN, 2002). Given the
complexity of CVD management, including physical activity, nutrition, medication adherence
and smoking cessation, education is necessary to support patients in achieving risk reduction and
ultimately secondary prevention (Alm-Roijer et al., 2006; Kayaniyil et al., 2009; Boyde et al.,
2011; Brown et al., 2011). Indeed, a core component of CR programs is patient education (Stone
et al., 2009; 2012).
Patient education has been formally defined as “the process by which health professionals and
others impart information to patients that will alter their health behaviors or improve their health
status” (Koongstvedt, 2001, p. 788). As a facilitator of behavior change, patient education

109
therefore plays a key role in the management of CVD (Brown et al., 2011). The effectiveness of
patient education has been demonstrated, such that patient CVD knowledge has been shown to
strongly influence their symptom recognition (Zalesskaya, Noruzbaeva, Lunegova, &
Mirrakhimov, 2005; DeVon, Rankin, Paul, & Ochs, 2010), advocacy for physician screening
(Bolman et al., 2005), attitudes toward their disease (Bellmanet al., 2009), promote their
motivation for self-care and ultimate behavior change (Dickson, Tkas, & Riegel, 2008; Bellman
et al., 2009), improve health-related quality of life, and decrease costs through reductions in
downstream healthcare utilization (Brown et al., 2011). Conversely, inadequate patient
understanding of their disease may cause unwarranted emotional distress, inappropriate coping
behavior, non-compliance with medical advice (Monane et al., 1994; Blyth et al., 1997), and
unnecessary disease progression (Sui et al., 2008; Zalesskaya et al., 2005).
To deliver effective patient education, educators need to address patients’ information needs. The
information needs of cardiac patients immediately following revascularization (Goodman et al.,
1997; Brezynskin et al., 1998; Astin et al., 2008), acute coronary syndrome (Czar & Engler,
1997; Nakano et al., 2008), myocardial infarction (MI) (Casey et al., 1984; Moynihan et al.,
1984; Ashton, 1997; Timmins & Kaliszer, 2003; Decker et al., 2007; Smith & Liles, 2007), and
heart failure (Wehby & Brenner, 1999; Lile et al., 1999), have been previously described, and
include knowing how to manage signs and symptoms, knowing how to modify or change risk
factors, and knowing the names, dosages and side-effects of medications. However, the
information needs of CR participants have only recently been described (Ghisi et al., 2013a).
This is a major gap, considering many CR participants understand or recall little of what
happened in hospital (due to anxiety and sedation for example), they would have received
information primarily related to acute recovery from their therapies (Kayaniyil et al., 2009; Alm-

110
Roijer et al., 2006; Boyde et al., 2011; Brown et al.,2011; de Melo Ghisi et al., 2013), and that
information needs change across the continuum of care (Cameron & Gignac, 2008).
To be effective, patient education should be comprehensive, planned, supportive and, in
particular, patient-centered (Koongstvedt, 2001; Su, Herron, & Osisek, 2001; Furze et al., 2002;
Brown et al., 2011). Unfortunately, much previous literature on cardiac and non-cardiac patient
education has demonstrated that healthcare providers’ are often unaware or inaccurately-perceive
patients’ educational needs (Casey et al., 1984; Moynihan, 1984; Gerard & Peterson, 1984;
Karlik & Yarcheski, 1987; Hagenhoff et al., 1994). Clearly, this can result in less engaged and
informed patients, and thus potentially negatively impact their health outcomes. Accordingly,
understanding what patients identify as information needs and concerns, especially early in CR,
can ensure that education provided is relevant to the learner. Thus, the objectives of this study
were to: (1) describe CR patient information needs and their relation to patient sociodemographic
and clinical characteristics, (2) investigate whether CR providers are cognizant of patient’s
information needs and preferred delivery formats, and (3) investigate whether patient
information needs change over the course of CR.
2 Methods
The framework for this study was based on Knowles’s assumptions regarding the nature of the
adult learning process (Knowles, 1973). Specifically, it was assumed that adults are able to
identify their own learning needs, and that they are motivated to learn when they see the content
as relevant.

111
2.1 Design and Procedure
This was a cross-sectional study. Ethics approval was obtained from the local review board, and
written consent to participate was provided by all respondents. Data was collected between
January and August, 2012.
CR patients were approached by a research team member at the beginning of their group classes
to participate in the study. They were provided the option to complete the survey while in the CR
center, or to take it home to complete, and bring it back at their next visit. The survey included
sociodemographic items, the Information Needs in CR (INCR) instrument (Ghisi et al., 2013a),
and items assessing patient preferences for educational delivery formats. Clinical data were
extracted from their medical charts. CR providers were asked to complete an adapted version of
the same survey.
2.2 Participants
This study included CR patients and healthcare providers recruited from a large academic CR
centre in Toronto, Canada. The CR program is 6-months in duration. Upon starting CR, each
patient undergoes a comprehensive assessment, they are provided a CR book, and are provided
pamphlets as applicable to their needs. Participants then come to the center for weekly exercise
classes, in addition to their home exercise. In conjunction with these weekly visits, an
interdisciplinary team provides approximately 15 hours of patient education including
information on exercise safety, nutrition, risk management, medications, stress management, and
lifestyle management. This is delivered in large and small group lectures.

112
A convenience sample of 500 CR patients was approached to participate in this study. Patients
from all CR classes were approached to solicit responses across all months of the program. The
exclusion criteria for patients were: age less than 18 years, lack of English language proficiency,
and any visual, cognitive or psychiatric condition that would preclude the participant from
completing the survey. All 59 healthcare providers from the CR centre were emailed the survey
to complete, including nurses, registered dietitians, exercise physiologists, kinesiologists,
physicians, physiotherapists, social workers, and psychologists. Administrative and exercise
testing staff were excluded from participation.
2.3 Measures
Patients’ clinical characteristics were obtained from the medical chart, and included cardiac
history, comorbidities, risk factors and months in CR. Patients and CR providers’
sociodemographic characteristics were also assessed: age, sex, educational level and family
income for patients; and age, sex and years working in CR for providers.
The INCR assessed CR patients’ information needs in 10 areas: the heart (physiology,
symptoms, and surgical treatments), nutrition, exercise/physical activity, medication,
work/vocational/social, stress/psychological factors, general/social concerns, emergency/safety,
diagnosis and treatment, and risk factors. Participants were asked to rate the importance of each
of the 55 information items in increasing their knowledge about CVD. Items were rated on a 5-
point Likert-type scale, that ranged from 1 = really not important to 5 = very important, and
accordingly higher scores indicated greater information needs. The INCR has been
psychometrically-validated in the CR setting, and demonstrated good reliability and validity
(Ghisi et al., 2013a). The INCR was adapted to be administered to CR providers, through minor

113
revision to the instructions. Providers were asked to rate the importance of each item to their
patients on the same 5-point scale.
Next, patients were asked to report their preferences for educational delivery formats, checking
their preferences from a list of options. There was also space to report “other” preferred formats,
in open-ended fashion. CR providers were similarly asked to denote their perceptions of their
patients preferred delivery formats. Finally, providers were also asked to describe the most
common questions asked by patients, to describe perceived education gaps in the program, in
open-ended fashion.
2.4 Statistical Analysis
SPSS Version 21.0 was used (IBM Corp, 2012). Descriptive statistics were used to describe
sociodemographic and clinical characteristics of patients and CR providers. To test the first
objective, INCR scores were explored. Pearson’s correlation, t-tests and ANOVAs (as
applicable) were computed to test for significant differences INCR scores based on patient and
provider characteristics. To determine whether outliers in the dataset influenced responses they
were removed and analyses repeated. If no difference is found between results excluding or
including these cases, all subsequent analyses will include outliers.
To test the second objective, a descriptive examination of mean total information needs scores
and mean item scores by sample (patients vs. CR providers) was performed. To test for
differences between samples, non-parametric tests (Mann-Whitney U) were applied, due to
difference in size between samples. A similar approach was also undertaken for preferred
delivery formats.

114
Open-ended questions (preferences for educational delivery formats, the most common questions
patients asked, and gaps in CR education curriculum) were coded (Silverman, 2000) and
described by sample. Responses from all open-ended questions were analyzed using the
following steps (Pope, Ziebland, & Mays, 1999): (1) consider the quality of the data; (2) focus
the analysis by topic; (3) categorize information, identifying themes or patterns and organize
them into coherent categories; (4) identify patterns and connections within and between
categories; and, (5) interpretation. Two researchers independently reviewed the data and met to
compare results. Any discrepancies in meaning were resolved by a third researcher.
Finally, to test the third objective, patients were categorized based on their month in the program,
as beginning (1-2 months), middle (3-4 months) and end (5 or more). INCR subscale scores were
compared across each time point using ANOVA.
3 Results
3.1 Respondent Characteristics
With regard to patients, 306 (response rate = 61.2%) returned and fully completed the INCR tool.
On average, patients had been in the program just over 4 of the 6 months. Table 5.1 displays
their sociodemographic and clinical characteristics, and how these characteristics were related to
their information needs. As shown, patients with lower income had significantly higher
information needs than those with higher income, despite outliers. When five individuals with an
income below CAD$10,000 that have disproportionally high information needs score were
excluded from the analysis, there is still a significant impact of income on information needs
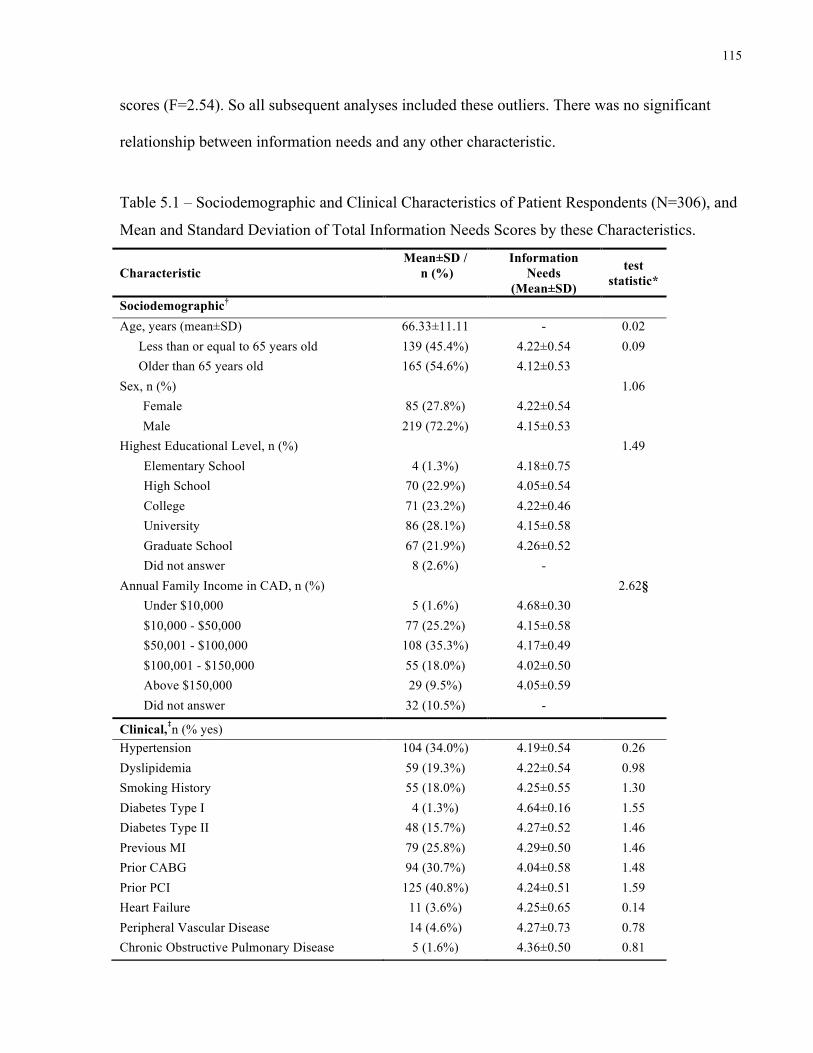
115
scores (F=2.54). So all subsequent analyses included these outliers. There was no significant
relationship between information needs and any other characteristic.
Table 5.1 – Sociodemographic and Clinical Characteristics of Patient Respondents (N=306), and
Mean and Standard Deviation of Total Information Needs Scores by these Characteristics.
Characteristic Mean±SD /
n (%)
Information Needs
(Mean±SD)
test statistic*
Sociodemographic† Age, years (mean±SD) 66.33±11.11 - 0.02
Less than or equal to 65 years old 139 (45.4%) 4.22±0.54 0.09 Older than 65 years old 165 (54.6%) 4.12±0.53
Sex, n (%) 1.06 Female 85 (27.8%) 4.22±0.54 Male 219 (72.2%) 4.15±0.53 Highest Educational Level, n (%) 1.49
Elementary School 4 (1.3%) 4.18±0.75 High School 70 (22.9%) 4.05±0.54 College 71 (23.2%) 4.22±0.46 University 86 (28.1%) 4.15±0.58 Graduate School 67 (21.9%) 4.26±0.52 Did not answer 8 (2.6%) -
Annual Family Income in CAD, n (%) 2.62§ Under $10,000 5 (1.6%) 4.68±0.30 $10,000 - $50,000 77 (25.2%) 4.15±0.58 $50,001 - $100,000 108 (35.3%) 4.17±0.49 $100,001 - $150,000 55 (18.0%) 4.02±0.50 Above $150,000 29 (9.5%) 4.05±0.59 Did not answer 32 (10.5%) -
Clinical,‡n (% yes) Hypertension 104 (34.0%) 4.19±0.54 0.26 Dyslipidemia 59 (19.3%) 4.22±0.54 0.98 Smoking History 55 (18.0%) 4.25±0.55 1.30 Diabetes Type I 4 (1.3%) 4.64±0.16 1.55 Diabetes Type II 48 (15.7%) 4.27±0.52 1.46 Previous MI 79 (25.8%) 4.29±0.50 1.46 Prior CABG 94 (30.7%) 4.04±0.58 1.48 Prior PCI 125 (40.8%) 4.24±0.51 1.59 Heart Failure 11 (3.6%) 4.25±0.65 0.14 Peripheral Vascular Disease 14 (4.6%) 4.27±0.73 0.78 Chronic Obstructive Pulmonary Disease 5 (1.6%) 4.36±0.50 0.81

116
CABG indicates coronary bypass artery graft surgery, CAD Canadian dollars, CR cardiac rehabilitation, MI myocardial infarction, PCI percutaneous coronary intervention, SD standard deviation. *F test, t-test or Pearson’s correlation, as appropriate. Significant differences between samples: §p<.05 †self-reported ‡extracted from medical chart Note. INCR scores range from 1-5, with greater scores denoting greater information needs.
With regard to CR providers, 28 (response rate = 47.5%) completed the survey. CR providers
were on average 43.64±13.56 years of age, and were primarily female (n=23, 82.1%). With
regard to tenure, 19 (68%) providers reported working in CR for more than 6 years, 7 (25%)
between 1 and 5 years, and 2 (7%) less than 1 year. There was no significant relationship
between total INCR scores and sex (p=0.30), age (p=0.25), or years working in CR (p=0.30).
3.2 Information Needs
The INCR performed reliably in both samples, with Cronbach’s alpha for the patients’ and CR
providers’ respondents being 0.98 and 0.89, respectively. Cronbach’s alpha for the subscales
ranged from .83 to .93 for the patients’ version, and from .75 to .91 for the CR providers’
version.
The mean total INCR for both samples was 4.38±0.44. Table 5.2 displays the mean total,
subscale and item needs scores for patients and CR providers. Both patients and CR providers
rated all items as “important” to learn (i.e., all item means above 3.0). The items where the mean
score was below 4 would generally not be applicable to all participants (i.e., diabetes, smoking,
return to work, driving); an observation which is supported by the generally higher standard
deviations for these items.
As shown in Table 5.2, CR providers rated the total information needs of patients significantly
greater than patients overall. Similarly, for 30 of 55 items and for 5 of 10 subscales, CR

117
providers rated the information needs significantly higher than patients did. There were only 2
items where patients scored the information importance as significantly higher than providers
rated them, specifically with respect to diagnosis and treatment. The greatest disparities in mean
item score between patients and providers were for again for specific items, which may not
pertain to all patients such as smoking (0.86 – 1.47) and diabetes (0.71-0.96).
CR providers were asked to report the topics that they perceived patients have more difficulty
learning. Using content analysis, responses were grouped into 9 categories: goal-setting and self-
care (identified by 12 providers; 43%), exercise (n=7; 25%), nutrition (n=6; 21%), the heart
(physiology, symptoms, surgical treatments; n=5; 18%), medication (n=5; 18%),
stress/psychological factors (n=3; 11%), risk factors (n=3; 11%), work/vocational/social (n=1;
4%), and diagnosis and tests (n=1; 4%).
Finally, based on their experiences with patients and their perceived information needs, providers
were asked to identify gaps in the education curriculum. They noted gaps in information related
to the heart (i.e., physiology, symptoms, surgical treatments), exercise, medication, sexual
activity, stress/psychological factors, sleep problems, different forms of physical activity (e.g. tai
chi, relaxation techniques), and risk factors. In addition, providers identified “other” topics,
including fall prevention, problem solving, and self-management.
Table 5.2 – Mean and Standard Deviation of Total Information Needs by Sample, and Mean
Differences.
Patients
(n=306; 91.6%) CR Providers (n=28; 8.4%)
Difference (CR providers needs –
patients needs) Subscale Item Mean±SD Mean±SD The Heart 1. How does a healthy heart work? 4.41±0.79 4.43±0.72 0.02 (physiology, 2. What is “coronary artery disease”? 4.46±0.79 4.79±0.57 0.33* symptoms, surgical
3. What is angina? 4.46±0.78 4.79±0.42 0.33*

118
treatments) 4. What happens when someone has a heart attack? 4.55±0.77 4.64±0.62 0.09 5. What is “bypass surgery”? 4.16±0.85 4.39±0.74 0.23 6. What is an angioplasty 4.28±0.85 4.46±0.69 0.18 Total Mean 4.39±0.65 4.58±0.50 0.19*** Nutrition 7. What foods should I eat for a healthy heart? 4.49±0.80 4.68±0.48 0.19 8. How can I choose healthy foods at the grocery
store? 4.32±0.87 4.54±0.58 0.22
9. How can I choose healthy foods when dining out?
4.16±0.85 4.50±0.51 0.34*
10. How do I read food labels? 4.32±0.78 4.64±0.56 0.32* Total Mean 4.32±0.68 4.59±0.50 0.27 Exercise/ Physical
11. How will exercise help my heart condition? 4.62±0.67 4.93±0.26 0.31*
Activity 12. What are the components of a safe exercise program?
4.54±0.69 4.86±0.36 0.32*
13. What is cardiovascular or aerobic exercise? 4.35±0.72 4.43±0.84 0.08 14. What can I do to improve or maintain
flexibility? 4.22±0.81 3.96±0.79 -0.26
15. How should I exercise in hot or cold weather? 4.20±0.85 4.61±0.57 0.41* 16. If I have diabetes, how do I prevent low blood
sugar with exercise? 3.83±1.13 4.79±0.42 0.96***
17. How do I take care for my feet when in an exercise program?
3.85±0.97 4.56±0.51 0.44***
18. What is resistance training (i.e. exercise for strengthening muscles)?
4.12±0.93 4.56±0.51 0.44*
19. What types of exercise equipment are available? (where?)
3.82±0.94 3.96±0.74 0.14
20. How can I exercise at home safely? 4.11±0.88 4.61±0.57 0.5*** 21. When should I stop physical exercise? 4.27±0.91 4.64±0.56 0.37* 22. Is sexual activity safe for me? 3.72±1.15 4.46±0.58 0.74*** Total Mean 4.09±0.59 4.51±0.41 0.42*** Medication 23. What medications do I need to help my heart? 4.41±0.93 4.75±0.52 0.34 24. How do I take my medication in the right way? 4.41±0.84 4.67±0.56 0.26 25. What side effects are possible with my
medication? 4.35±0.87 4.39±0.63 0.04
26. Do the medications I am taking interfere with each other?
4.41±0.87 4.39±0.69 -0.02
27. Are there foods I should avoid while taking these medications?
4.44±0.81 4.50±0.69 0.06
28. What are the effects of complementary and alternative medications?
4.24±0.89 4.25±0.80 0.01
Total Mean 4.37±0.69 4.51±0.55 0.14 Work/Vocational/ Social
29. When can I return to work and my old activities?
3.89±1.01 4.64±0.49 0.75***
30. Can I go back to my same job? 3.65±1.18 4.39±0.74 0.74** 31. When can I start driving again? 3.91±1.17 4.36±0.87 0.45 Total Mean 3.65±1.10 4.46±0.63 0.81*** Stress/Psychological Factors
32. What feelings are common after a heart attack? 4.24±0.95 4.68±0.48 0.44*
33. How does stress affect my heart? 4.50±0.76 4.75±0.44 0.25 34. How can I cope with stress? 4.41±0.80 4.75±0.44 0.34* 35. What can I do to reduce stress in my life? 4.39±0.86 4.79±0.42 0.40* 36. Do sleep problems affect my heart? 4.20±0.91 4.75±0.44 0.55** Total Mean 4.31±0.72 4.74±0.36 0.43

119
General/Social Concerns
37. What services, support organizations and groups are available?
4.04±0.92 4.54±0.58 0.50**
38. What support services are available to my family?
3.87±1.06 4.50±0.58 0.63**
Total Mean 3.92±0.99 4.52±0.54 0.60*** Emergency/Safety
39. How do I recognize angina symptoms? 4.57±0.75 4.93±0.26 0.36*
40. What should I do if I feel angina or chest pain? 4.59±0.80 4.89±0.32 0.30* 41. When should I call the doctor? 4.58±0.76 4.86±0.36 0.28 42. When should I call 911 or go to emergency
room? 4.63±0.80 4.79±0.42 0.16
Total Mean 4.58±0.70 4.87±0.26 0.29 Diagnosis and treatment
43. What are the tests used to diagnose my heart condition?
4.36±0.84 4.21±0.79 -0.15
44. What treatments are available for my condition? 4.48±0.80 4.44±0.75 -0.04 Total Mean 4.42±0.74 4.25±0.88 -0.17** Risk Factors 45. What are the risk factors for heart disease? 4.47±0.84 4.89±0.32 0.42* 46. What are the risk factors that I cannot control? 4.26±0.88 4.46±0.64 0.20 47. What are the risk factors I can control? 4.64±0.63 4.82±0.39 0.18 48. What can I do to bring my risk factors under
control? 4.64±0.70 4.86±0.36 0.22
49. How does cholesterol affect my heart? 4.40±0.90 4.75±0.44 0.35* 50. How does diabetes affect my heart? 3.97±1.12 4.79±0.42 0.82*** 51. How does physical inactivity affect my heart? 4.41±0.83 4.86±0.36 0.45** 52. How does smoking affect my heart? 3.46±1.46 4.93±0.27 1.47*** 53. What are the benefits of quitting smoking? 3.41±1.53 4.68±0.55 1.27*** 54. What supports are available to help me quit
smoking? 3.17±1.45 4.54±0.58 1.37***
55. How does alcohol affect my heart? 3.68±1.26 4.50±0.64 0.82** Total Mean 3.93±0.79 4.73±0.38 0.80** Total 4.17±0.53 4.59±0.34 0.42***
SD indicates standard deviation. Significant differences between samples: *p<.05; **p<.01; ***p<.001.
3.3 Education Delivery Formats and Gaps
Table 5.3 displays the preferences for education delivery formats by patients and CR provider’s
perceptions of patients’ preferences. Lecture, book and discussion with healthcare providers
were identified as the preferred formats by patients, and were also correctly perceived by CR
providers as patients’ preference. As with the information needs, providers endorsed each
delivery format more strongly than patients did. But contrarily, providers significantly under-
estimated patient preference for education delivered by their physician. However, this was the

120
least preferred format among patients. In addition, 10 (3.3%) patients reported as important the
inclusion of family or spouse during education delivery.
Table 5.3 – Preferences for Educational Delivery Formats by Sample
Format Patients (N=306)
CR Providers (N=28) p
Lectures 211 (69.0%) 25 (89.3%) 0.04 Book 206 (67.3%) 27 (96.4%) 0.004 Discussions with CR providers 198 (64.7%) 26 (92.9%) 0.004 Internet 162 (52.9%) 24 (85.7%) 0.001 Movies/videos 90 (29.4%) 11 (39.3%) 0.322 E-learning 71 (23.2%) 18 (64.3%) <.001 Audio 64 (20.9%) 10 (35.7%) 0.08 Peer 8 (2.6%) 6 (21.4%) 0.09 Physician only 13 (4.3%) 3 (1.0%) 0.04
3.4 Information Needs over the Course of CR
Table 5.4 displays patient’s information needs by area and by time in CR. Specifically, at the
beginning of the program, patients were most interested in learning about medications and
emergency/safety. Mid-program their greatest information needs related to diagnosis and
treatment, as well as nutrition. At the end of the program, participants reported their greatest
information needs related to emergency/safety, diagnosis/treatment and the heart. There was a
significant difference in information needs by time in program in the following areas:
general/social concerns (greatest mid-program), emergency/safety (greatest beginning of
program), and risk factors (greatest mid-program).
CR providers were asked to describe the most common questions patients asked them, when
during the program, and where (location inside the CR center) these were generally asked.
Content analysis revealed these questions corresponded to 9 of the 10 areas of the INCR, plus

121
questions related to the CR program itself. Questions related to the heart (physiology, symptoms,
and surgical treatments), work, vocational and social aspects of CR, and general and social
concerns were commonly asked in the beginning of the program, and usually on a one-on-one
basis. Questions related to exercise and physical activities were also usually asked in the
beginning of the program, in several places such as: in the exercise testing lab, on the exercise
track, during lectures, and one-on-one, among others. Furthermore, in the beginning of the
program overall questions about CR were mostly asked, in several locations inside the CR
center.
Table 5.4 – Mean and Standard Deviation of Patient Information Needs by Subscale and Time in
CR Program, N=306
Area of Information Need Beginning
Months 1 and 2 (n=86; 28.1%)
Middle Months 3 and 4 (n=93; 30.4%)
End More than 5 Months
(n=96; 26.8%) F
The heart 4.29±0.80 4.41±0.50 4.36±0.63 0.81
Nutrition 4.26±0.61 4.43±0.65 4.22±0.78 2.34
Exercise/Physical activity 3.98±0.65 4.12±0.60 4.10±0.52 1.59
Medication 4.47±0.58 4.36±0.75 4.30±0.75 1.26
Work/Vocational/Social 3.60±1.14 3.67±1.13 3.67±0.94 1.51
Stress/Psychological factors 4.22±0.70 4.38±0.71 4.35±0.72 1.19
General/social concerns 3.57±1.20 4.11±0.81 3.94±0.93 6.96***†‡
Emergency/safety 4.40±0.88 4.26±0.65 4.22±0.53 3.61*†
Diagnosis and treatment 4.32±0.69 4.53±0.75 4.38±0.80 1.92
Risk factors 3.81±0.83 4.08±0.82 3.86±0.74 2.90**†
SD indicates standard deviation. Significant differences by time: *p<.05; **p<.01; ***p<.001. † Significant differences between Beginning and Middle ‡ Significant differences between Beginning and End
Questions related to nutrition were asked in the beginning and middle of the program, mostly
during educational lectures or one-on-one. Questions about risk factors were most-commonly
asked in the middle of the program, in several places such as: the exercise testing lab, on the

122
exercise track, during lectures, and one-on-one, among others. Question regarding medication
were asked throughout the program and usually during lectures or during a one-on-one
consultation. Questions regarding diagnosis and tests were also asked throughout the program,
usually in the exercise testing laboratory, on the exercise track and during one-on-one
consultations. Although identified by CR providers, questions about stress and psychological
factors were not perceived to be common, and were usually asked to allied health professionals
and peers.
4 Discussion and Conclusion
4.1 Discussion
Both patients and CR providers generally reported all 55 informational items as “important” to
learn, suggesting that CR, which affords repeated contacts over time between patients and
providers, must play an important role in ensuring all patients’ information needs are met.
Overall, CR providers rated the total needs of patients significantly greater than patients, which
may be related to the fact that perhaps the providers were also considering the needs of those
who did not volunteer for this study. The greatest information needs identified by patients were
related to medication, emergency/safety, and diagnosis and treatment, and were perceived as
stress/psychological factors, emergency/safety, and risk factors by CR providers. CR providers
were quite aware of patient’s information needs, except in regard to diagnosis and treatment.
Finally, most additional questions CR providers reported they received by patients are included
in the INCR tool, supporting its validity and comprehensiveness.
123
Overall, patient’s desired information in areas that are vital to patient survival and ongoing
control of symptoms, and CR providers were quite aware of these information needs. In this
study, there was agreement between patients and CR providers that emergency/safety was one of
the highest information needs, which has also been observed in previous studies (Gerard &
Peterson, 1984; Czar & Engler, 1997; Ghisi et al., 2013a; de Melo Ghisi et al., 2013). Most of
the previous studies that compared patients and CR providers views of information needs, found
that providers considered medication information as a greater need than patients (Gerard &
Peterson, 1984; Ghisi et al., 2013a; de Melo Ghisi et al., 2013); however, this study did not
corroborate this, which may reflect an increasing awareness and interest of patients in their
pharmacological treatment. Moreover, in contrast to other studies (Gerard & Peterson, 1984;
Czar & Engler, 1997; Ghisi et al., 2013a; de Melo Ghisi et al., 2013), patients identified ‘risk
factors’ as one of their lowest information needs. Finally, providers should focus on educating
patients of lower income, as they identified significantly greater educational needs than their
high income counterparts (Kaplan & Keil, 1993).
In regards to delivery formats, lectures, books and discussions with healthcare providers were
identified as the preferred formats by patients, and were also correctly perceived by CR
providers as patients’ preference. These desired formats are congruent with what is offered in the
CR program evaluated. Surprisingly, patients did not desire to learn through electronic media
resources such as the internet, and e-learning. Despite patients’ preferences for non-electronic
resources, the effectiveness of this type of technology in patient education has been described in
the literature (Kuhn, Sears, & Conti, 2006). Moreover, there are some randomized controlled
trials of web-based CR currently underway (Lear, 2010). It will be important to test the user-
friendliness of the education modules, and the impact on patient knowledge, and subsequently
behavior. Indeed, the current research was intended to inform the development of online

124
education videos, to enable a broader reach to cardiac patients, and “on-demand” access right
when patients want particular information. Clearly, further consideration and assessment will be
needed prior to video development, to ensure the education content is learner-centered.
To our knowledge, this is the first study to have tested differences in patient information needs
over the course of CR. There were significant differences in information needs by time related to
general/social concerns, emergency/safety, and risk factors. Specifically, patients were
significantly most interested in learning about emergency/safety at the beginning of the program,
and about general/social concerns and risk factors mid-program. While replication is warranted,
these findings could inform efforts to “time it right” in CR education delivery.
Needs Assessment is considered an ongoing process of gathering data to determine what
information needs exist so that education can be developed to help the institution to accomplish
its patients’ goals. In this context, personal aspects, background, beliefs, previous knowledge
influence results. Thus, individual and group learning needs are different. The approach used by
this study is the group learning needs, which produce an average picture that fails to address
important needs and interests of individual members of the group—so a balance is required.
Individual learning needs assessment is best used in the context of learning that occurs on an
individual basis— which is not the case for most of the CR Programs, where the education is
delivered in group settings.
Caution is warranted when interpreting results. First, the generalizability of these finding to other
CR populations is somewhat limited, considering recruitment stemmed from a single centre.
Replication is warranted. Second, this was a convenience sample, and as such may be biased. For
instance, the sample could have been composed of patients with higher information needs than
the average CR participant. Third, the response rate for both samples (patients and providers)

125
was lower than 75%, which can also introduce bias. Finally, the design was cross-sectional and
therefore causal conclusions cannot be drawn. In particular, a longitudinal study of change in
patients’ information needs through the course of CR is warranted, to ascertain whether the
differences in information needs identified herein are robust.
4.2 Conclusion
CR patients desire information in many areas, but in particular they desire information regarding
emergency / safety and diagnosis / treatment. CR providers were highly cognizant of patient
information needs. Patients preferred information to be delivered via lectures, books or
discussions with CR providers. This is concordant with healthcare provider perceptions, and with
CR delivery in most instances. This is the first study to our knowledge to have documented
differences in patient information needs over the course of CR programs.
4.3 Practice Implications
The identification of needs using an instrument like the INCR could serve as a mechanism for
understanding patient information gaps. Moreover, CR staff could use the INCR to assess the
comprehensiveness of their education programming, and to consider whether the main focus of
their programming relates to the key information needs of patients at different stages of the
program. Programs should also consider whether the delivery format of their education program
is concordant with patient preferences.

126
Chapter 6 PAPER FOUR: Development and psychometric validation of the
second version of the Coronary Artery Disease Questionnaire (CADE-Q II)
The phases of development and psychometric validation of the second version of the Coronary
Artery Disease Education Questionnaire (CADE-Q II) are described in this chapter. CADE-Q
was originally developed and psychometrically validated to assess patients’ knowledge about
CAD in Brazil. It was later translated, cross-culturally adapted, and validated to English.
Although both versions demonstrated good reliability and validity, the CADE-Q presented lack
of detailed assessment of all core components of cardiac rehabilitation. In order to be used in the
study described on chapter 7, CADE-Q needed to be redesigned and updated. This paper was
submitted to Patient and Education Counseling Journal in May 2014 and is currently under
revision.
1 Introduction
Coronary Artery Disease (CAD) is a leading cause of morbidity worldwide (WHO, 2011). It is a
chronic condition that carries a high risk of recurrent events and, therefore, a significant
contributor to health-related costs. Secondary prevention strategies are highly effective, but
multi-factorial, necessitating patient awareness and adherence to optimize health outcomes
(Clark et al., 2005; Stone et al., 2009; Heran et al., 2011; Ghisi et al., 2014a). Indeed, findings
from a recent systematic review demonstrate the importance of patient education in CAD
patients, in improving self-management behaviors (Ghisi et al., 2014a), health-related quality of
life and potentially reducing healthcare costs (Brown et al., 2011). While most CAD patients will
receive some education if hospitalized, it is often forgotten, too brief, and focused appropriately

127
on acute recovery (which leaves no time to educate on chronic self-management) (Mullen et al.,
1992; Stone et al., 2009; Aldcroft et al., 2011; Berra, Miller, & Jenning, 2011).
Cardiac rehabilitation (CR) is a comprehensive secondary prevention program, delivered by a
multi-disciplinary team of healthcare providers. Patient education is considered a core
component of CR (Buckley et al., 2013). Programs are offered over several months permitting
repeated patient contact with these providers, enabling fulsome education regarding the
numerous lifestyle changes and treatments shown to reduce risk over time (Berra et al., 2011).
While the important role of patient education has been well-recognized in CR practice (e.g.,
clinical practice guidelines and quality indicators), patient knowledge in CR has only scantly
been investigated.
In order to plan and deliver an effective CR educational intervention, it is important to have
precise information of what cardiac patients know about their condition (Kayaniyil et al., 2009;
Brown et al., 2011). Patients’ knowledge of heart disease can strongly influence symptom
recognition, advocacy for physician screening, attitude towards the disease, and provide
motivation for individual behaviour changes. Likewise, inadequate understanding of the disease
may cause unwarranted emotional distress, inappropriate coping behaviour, non-compliance with
medical advice, and unnecessary disease progression (Alm-Roijer et al., 2006; Kayaniyil et al.,
2009; Brown et al., 2011).
In this context, the Coronary Artery Disease Education Questionnaire (CADE-Q) was previously
developed and psychometrically validated to assess patients’ knowledge about CAD in a
Portuguese speaking population of CR patients in Brazil (Ghisi et al., 2010). It was later
translated, cross-culturally adapted, and psychometrically validated to English (de Melo Ghisi et
al., 2013). It has been used to compare knowledge between a developed and a developing

128
country (Ghisi et al., 2013b). Although both versions demonstrated good reliability and validity,
the CADE-Q lacked detailed assessment of all core components of cardiac rehabilitation (CR),
such as nutrition and psychosocial risk. Besides that, the development of CADE-Q started in
2004, needing update based on new researches involving CR. The availability of a more
comprehensive and updated CADE-Q is important to assess patients’ knowledge and to tailor the
educational component of CR programs (Ghisi et al., 2013a). The aim of this study was to
develop and psychometrically validate the second version of the CADE-Q (CADE-Q II).
2 Methods
2.1 Design and Procedure
This study was reviewed and approved by the Toronto Rehabilitation Institute (TRI) Research
Ethics Board. The design consisted of a series of cross-sectional, observational studies.
First, results from a study using the Information Needs in Cardiac Rehabilitation tool (INCR)
(Ghisi et al., 2014b) were used to assess what information cardiac patients want to know and to
investigate whether CR providers are cognizant of patient’s information needs (Ghisi et al.,
2013a). In addition, a literature search on broad components of patient education in CR and
guidelines was performed to identify the most important information that coronary patients need
to know about their disease and its’ management. Based on an inventory of the results from these
studies, the review, and the development of a new education curriculum at the TRI, the first
version of the questionnaire was developed. This was then reviewed by a committee of 15 CR
experts (a multidisciplinary group of CR professionals with expertise in clinical and research

129
areas). They performed a content analysis, verifying if the new instrument was appropriate for
administration in a CR population. Items were refined based on the findings.
Second step was a pilot study to verify the applicability of the instrument, and to evaluate patient
understanding of the items (clarity). A convenience sample of coronary patients that finished
their CR programs (called graduates) and had previously-agreed to be contacted about research
opportunities were recruited. Results were used to further refine the CADE-Q II.
Third, a psychometric validation was performed. The refined tool was administered to a larger
sample of cardiac patients from a CR program in Toronto, Canada. Data were collected between
May and December 2013.
2.2 Participants
For the pilot test, graduate patients of the CR program were surveyed. For the psychometric-
validation, a convenience sample of cardiac patients from this institution was recruited before
their participation in CR or during their first week in the program. The inclusion criteria were the
following: confirmed CAD diagnosis or multiple cardiovascular risk factors (such as
hypertension and diabetes). The exclusion criteria were the following: younger than 18 years old,
lack of English-language proficiency, any significant visual or cognitive condition or serious
mental illness which would preclude the participant’s ability to answer the questionnaire.
2.3 Measures
To assess clarity, the pilot study patients were asked to rate each information item Likert-type
scale (Pasquali, 2003) ranging from 1 (not clear) to 10 (very clear).

130
CR participants from the psychometric-validation were characterized according to sex, age,
educational level, comorbidities, cardiac risk factors and history. All characteristics were
extracted from medical chart except educational level, which was self-reported.
2.4 Statistical Analysis
The sample size calculation for the psychometric analysis was based on Hair & Anderson (1998)
recommendation of a sample size of 10 subjects per item, and/or at least 100 participants. Since
the questionnaire has 31 items, a sample size of 307 is considered valid.
To investigate the psychometric properties of the new tool, the internal consistency, criterion
validity and the factor structure were assessed. The internal consistency was assessed by
Cronbach's alpha. Values higher than 0.60 were considered acceptable, reflecting the internal
correlation between items and factors (Hair & Anderson, 1998). Criterion validity was assessed
through t-tests, comparing CADE-Q II scores and participant’s level of education. Item
completion rates were also described.
The dimensional structure was analyzed through exploratory factor analysis. The main
component method for factor extraction was used, considering only those that presented
eigenvalues > 1.0. After the selection of the factors, a correlation matrix was generated, where
the associations between items and factors were observed through factor loadings greater than
0.30 on only one factor. The varimax method with Kaiser normalization was used to interpret the
matrix (Kaiser, 1960).
Finally, a descriptive analysis of the CADE-Q II was performed. A mean total score was
computed to reflect total knowledge. T-tests, one-way analysis of variance and chi-square tests

131
were used as appropriate to assess differences in CADE-Q II scores based on patient’s socio-
demographic and clinical characteristics.
SPSS Version 21 (IBM 2012) was used for entering, cleaning and analyzing the data and the
level of significance was set at 0.05 for all tests. Where more than 10% of the items were
missing, the data were excluded from further analysis.
3 Results
3.1 Participants Characteristics
For the content validation, there were 10 (75%) clinicians, and 5 (25%) researchers who
reviewed the items. For the pilot test, 50 CR graduates were contacted and 30 (60%) responded,
of which 8 (27%) were female. Respondents had a mean age of 68.7±8.4, and had participated in
a mean of 15±20.8 months of CR.
For the psychometric validation study, 307 coronary patients (representing approximately 26%
of total annual CR patients) were approached to participate in this study before starting CR,
signed the consent form and completed the CADE-Q II. The characteristics of these participants
are presented in Table 6.1.
3.2 Development of the Tool
First, results from a study using the INCR tool (Ghisi et al., 2014b) showed that CR participants
rated emergency/safety, the heart, and stress/psychological factors as the areas with the greatest
information needs. So, questions related to these needs were incorporated in the CADE-Q II. A
literature review on core content for a patient education program was performed and presented

132
consistency across sources, including the following topics: medical, risk factor target and
modification, nutrition, exercise, smoking cessation, and psychosocial risk. The best practice
guidelines’ review also provided suggestions for adapting an education program for special
populations attending CR programs, such as patients with diabetes and elderly and patients from
other nationalities and cultures.
Through these studies, 5 areas of knowledge – a total of 31 questions – were identified and
comprised the first version of the CADE-Q II. These areas were: medical condition, risk factors,
exercise, nutrition, and psychosocial risk. Overall, three items from the CADE-Q were retained.
As stated in the CADE-Q, each one of the questions had 4 alternatives, which generated a score.
The sum of scores was used to represent a mean total knowledge. The experts concluded that all
items were appropriate for administration in a CR population and no changes were made in the
scale at this phase.
3.3 Pilot Test
The 30 participants took a mean of 20±7 minutes to complete the CADE-Q II. Regarding the
evaluation of clarity, mean clarity of the items was 8.2 and no items had mean clarity scores
lower than 7 (ratings are shown in Table 6.2). These results indicated that the target population
understood the questionnaire.
3.4 Psychometric Validation
The CADE-Q II was administered to the CR participants from one CR program, and the mean
scores are shown in Table 6.2. Item completion rates are also shown in Table 6.2.

133
The reliability of each area was assessed by Cronbach’s alpha. All areas were considered
internally consistent (α > 0.7). Table 6.2 displays Cronbach’s alpha of each area.
With regard to criterion validity, total CADE-Q II scores were compared by education level. As
shown in Table 6.2, patients with lower educational level had significantly greater information
needs than those with higher education (p<.001).
Table 6.1 – Sociodemographic and Clinical Characteristics of Patient Respondents (N=307), and
Mean and Standard Deviation of CADE-Q II Scores by these Characteristics.
MI indicates myocardial infarction, CABG coronary bypass artery graft surgery, PCI percutaneous coronary intervention, SD standard deviation. aself-reported Significant differences between samples: *p<.05, **p<.01, ***p=<.001 Note. The maximum CADE-Q II score is 91, with higher scores indicating greater knowledge.
Characteristic CADE-Q II scores Sociodemographic (mean±SD) P Age (mean±SD) 63.78±11.9 - 0.72 Sex n (%) 0.24 Male 239 (77.9%) 63.87±18.6 Female 68 (22.1%) 65.50±15.9 Educational Levela n (%) <.001*** Less than high school 20 (6.5%) 53.45±18.8 High school/graduation certificate 40 (13%) 60.35±17.8 Trades certificate 11 (3.6%) 57.09±18.2 College certificate or diploma 61 (19.9%) 66.26±18.0 University 166 (54.1%) 67.39±16.0 Missing 9 (2.9%) - Clinical, n (% yes) Hypertension 143 (46.9%) 64.17±17.22 0.17 Smoking History 103 (33.6%) 63/67±18.2 0.90 Diabetes Type I 21 (6.8%) 57.57±21.5 0.35 Diabetes Type II 50 (16.3%) 63.58±16.1 0.34 Depression 9 (2.9%) 67.78±18.3 0.75 Sleep Apnea 26 (8.5%) 67.50±14.86 0.07 Fibrilation 28 (9.1%) 67.79±17.3 0.69 Angina 10 (3.3%) 60.10±15.9 0.97 Previous MI 114 (37.1%) 64.97±18.4 0.72 Transient Ischaemic Attack 8 (2.6%) 69.50±11.4 0.30 Prior CABG 71 (23.1%) 66.51±15.8 0.13 Prior PCI 118 (38.4%) 64.09±20.1 0.04* Heart Failure 18 (5.9%) 67.39±8.6 0.01* Cardiomyopathy 14 (4.6%) 71.79±9.2 0.04* Valvular Heart Disease 39 (12.5%) 58.79±18.4 0.98 Peripheral Vascular Disease 11 (3.6%) 65.55±13.4 0.25 Chronic Obstructive Coronary Disease 16 (5.2%) 63.75±16.8 0.51 Cerebral Vascular Accident 21 (6.8%) 57.52±20.4 0.72

134
Table 6.2 – Mean and Standard Deviation of Clarity Rating by Pilot Study Patients (N=30), CADE-Q II Score (N=307), CADE-Q II
Item Completion Rates, Cronbach’s alpha per area, and Mean Score per area.
Clarity Rating by Pilot Study Patientsa
CADE-Q II Scoreb
CADE-QII Item Completion Rate
Cronbach’s alpha per area
CADE-Q II Mean Score per Areac
Areas Question Mean±SD Mean±SD % α Mean±SD Medical condition 1. Coronary Artery Disease is: 8.6±2.4 2.92±0.7 96.7% 0.71 15.12±4.9
2. Angina (chest pain of discomfort) occurs: 8.9±2.1 2.12±0.6 97.7%
3. In a person with coronary artery disease, which of the following is a usual description of angina?
8.5±2.2 2.31±0.7 97.4%
4. A heart attack occurs: 8.8±1.6 2.78±0.8 98%
5. The best resources available to help someone understand his/her medications are:
8.5±2.2 1.72±1.1 99%
6. Medications such as aspirin (ASA) and clopidogrel (PlavixTM) are important because:
8.6±1.7 2.65±0.6 98%
7. The “statin” medications, such as atorvastatin (LipitorTM), rosuvastatin (CrestorTM), or simvastatin (ZocorTM), have a beneficial effect in the body by:
8.0±3.6 2.13±1.1 96.4%
Risk factors 1. The risk factors for heart disease that can be changed are: 8.7±3.2 2.55±0.9 96.7% 0.65 9.41±3.4
2. The actions that can be taken to control cholesterol levels include: 8.9±2.6 2.26±0.6 97.1%
3. The actions that can be taken to control blood pressure include: 8.7±2.2 2.91±0.5 98%
4. The first step towards controlling a risk factor (such as blood pressure or cholesterol) is:
7.4±4.2 2.51±1.0 97.7%
5. The actions to prevent developing diabetes include: 7.4±3.0 1.94±1.2 96.1%
Exercise 1. What are the important parts of an exercise prescription? 8.3±3.2 1.83±1.1 98.4% 0.77 15.59±5.3
2. For a person living with heart disease, it is important to do a cardiovascular warm-up before exercising because:
7.9±2.5 2.17±0.6 97.7%
3. The pulse can be found: 8.1±2.7 2.70±0.8 97.4%

135
4. Three things that one can do to exercise safely outdoors in the winter are:
7.8±2.2 2.21±1.0 98%
5. The benefits of doing resistance training (lift weights or elastic bands) include:
7.9±2.1 2.72±0.9 97.4%
6. If a person gets chest discomfort during a walking exercise session, he or she should:
8.2±2.1 2.87±0.5 98%
7. How does a person know if he/she is exercising at the right level? 8.6±1.9 1.64±1.1 98%
Nutrition 1. What is the best source of omega 3 fats in food? 8.6±4.2 3.03±0.7 98.4% 0.66 13.96±4.8
2. Trans fat are: 7.8±2.5 2.57±1.0 97.1%
3. What is one good way to add more fibre to your diet: 7.7±2.2 2.66±0.9 96.4%
4. Which of the following foods has the most salt: 8.2±3.8 2.12±0.6 99%
5. What combination of foods can help lower blood pressure? 8.3±2.2 2.93±0.5 98%
6. When reading food labels, what should one look at first? 8.3±3.2 1.76±1.1 98.4%
7. How many servings of fruits and vegetables should adults consume?
7.8±1.1 2.08±1.1 98%
Psychosocial risk 1. Which of the below are effective stress management techniques? 8.4±2.5 2.82±0.7 97.7% 0.67 10.15±3.7
2. What stresses have been related to increased risk for heart attacks? 8.1±0.28 1.93±1.2 97.4%
3. Which of the following describes your best option for reducing your risk from depression:
7.8±1.6 2.13±0.6 98.7%
4. It is important to recognize “sleep apnea” because: 7.9±0.29 2.61±0.9 98.4%
5. “Chronic stress” is defined as: 7.3±0.69 2.15±1.0 95.8%
Total 8.2±1.90 64.23±18.1 97.7% 0.91 - SD=standard deviation. aClarity rating out of 10 were 1 = not clear and 10 = very clear. bCADE-Q scores range from 0 to 3 in each question. The maximum total CADE-Q II score is 91. cThe maximum score for medical condition, exercise and nutrition’ areas is 21 and for risk factors and psychosocial risk.

136
With regard to criterion validity, total CADE-Q II scores were compared by education level. As
shown in Table 6.2, patients with lower educational level had significantly greater information
needs than those with higher education (p<.001).
The dimensional structure was evaluated through exploratory factor analysis. The results from
the Kaiser-Meyer-Olkin index (KMO=0.859) and Bartlett’s Sphericity tests (X²=2073.98;
p<0.001) indicated that the data were suitable for factor analysis. Four factors were extracted,
representing 62.2% of the total variance. Table 6.3 shows the factor loadings for each item.
Factor 1 reflected medical condition items, factor 2 risk factors and exercise, factor 3 nutrition,
and factor 4 psychosocial risk.
3.5 Knowledge Assessment
The mean total score was 64.23±18.1. Forty-seven percent of patients scored higher than 68,
which indicates a knowledge of 75% or higher. Analyses (t-tests, one-way analysis of variance
and chi-square tests as appropriate) were performed to evaluate differences in mean CADE-Q II
scores by patients’ socio-demographic and clinical characteristics. As shown in Table 6.1, scores
were only related to educational level (p<.001), heart failure (p=0.01), cardiomyopathy (p=0.04)
and history of PTCA (p=0.04). In this context, patients with higher educational level, history of
heart failure, cardiomyopathy and PTCA presented significantly higher knowledge compared
with their counterparts.
Means and standard deviations of each item are reported in details in Table 6.2. The questions
with higher scores were the following: “What combination of foods can help lower blood
pressure?” (2.93±0.5), “Coronary Artery Disease is:” (2.92±0.7), “The actions that can be taken

137
to control blood pressure include:” (2.91±0.5), and “If a person gets chest discomfort during a
walking exercise session, he or she should:” (2.87±0.5).
Regarding the 5 areas of the questionnaire, exercise and medical condition are the areas with the
greatest knowledge; and risk factors’ area is the one with the lowest knowledge. Mean and
standard deviation of each area are also reported in Table 6.1.
Table 6.3 – Factor Structure of the CADE-Q II, sorted by loading
Areas Items Factor 1 Medical
Condition
Factor 2 Risk factors/ Exercise
Factor 3 Nutrition
Factor 4 Psychosocial risk
Medical Q1 .454 Condition Q2 .425 Q3 .499 Q4 .573 Q5 .399 Q6 .506 Q7 .559 Risk Factors Q1 .534 Q2 .638 Q3 .637 Q4 .499 Q5 .549 Exercise Q1 .626 Q2 .582 Q3 .442 Q4 .566 Q5 .642 Q6 .541 Q7 .595 Nutrition Q1 .570 Q2 .518 Q3 .447 Q4 .433 Q5 .537 Q6 .330 Q7 .307 Psychosocial Q1 .584 Risk Q2 .491 Q3 .412 Q4 .610 Q5 .538

138
4 Discussion and Conclusion
4.1 Discussion
This study sought to develop and validate the CADE-Q II. Since patient education is a core
component of CR programs, this tool can be useful to help healthcare providers to understand
what information cardiac patients know about their condition, as well as to promote educational
strategies to these patients. The psychometric validation of the CADE-Q II followed strict rules,
since the development of the instrument required a greater effort including a needs assessment
study (Ghisi et al., 2013a), and a literature search on broad components of patient education in
CR and guidelines.
When a new version of a questionnaire is developed it should not only be updated, and better on
theoretical basis, but must also be shown to be at least as good as the original instrument in terms
of validity and reliability. In this context, results of the CADE-Q II were consistent with those
presented in the original instrument (Ghisi et al., 2010) and the English adapted version of the
CADE-Q (de Melo Ghisi et al., 2013), particularly in relation to criterion validity (correlation to
educational level) and all areas being considered internally consisted (α > 0.70). The overall
mean, as well as the means of the areas were high, reinforcing the idea that CR patients are
knowledgeable of the information that is important for them. It may also suggest that individuals
with low socioeconomic levels are not participating in these programs and strategies to eliminate
barriers to access CR should be implemented (Daly et al., 2002; Grace et al., 2008).
There are some limitations to this study, which should be stated. There are some elements of the
scale, which require further assessment. First, test-retest reliability was not evaluated, and this

139
should form the basis for future study. A sample size of at least 50 patients should be considered
to promote adequate assessment of this psychometric property (Altman, 1991). Second, future
research is needed to assess whether the scale is sensitive to change, such as following
participation in CR, or to test implementation of new education materials. Finally, whether the
CADE-Q II is a valuable and valid tool to identify knowledge differences in non-CR patients
should be explored.
4.2 Conclusion
In this study I have proved the CADE-Q II has strong psychometric properties, providing
preliminary evidence of its reliability and validity to assess patients’ knowledge about CAD in a
more comprehensive format. It is hoped this tool can support CR evaluation of their program’s
education component, and promote greater provision of information consistent with patient’s
educational needs.
4.3 Practice Implications
Good patient education involves assessing needs and knowledge, setting goals and objectives,
implementing a teaching plan, and evaluating outcomes (Cranton, 1989). Before implementing
patient education programs it is prudent to evaluate what patients know about their condition.
The assessment of CR patients’ knowledge is, therefore, relevant. The CADE-Q II can be
especially useful in the evaluation of comprehensive educational interventions, and can provide
valuable information to clinicians, and researchers regarding the content of educational
programming in CR.

140
Chapter 7 PAPER FIVE: Behavior determinants among cardiac rehabilitation patients receiving educational interventions: an application of the
health action process approach
This chapter presents the results from paper five, an observational prospective study assessing
knowledge, behavior and theory-driven constructs pre- and post-CR in two groups of patients
receiving different educational interventions. One of these interventions is the new educational
curriculum, which development was described in chapter 2 and its content was strategically
sequenced based on the needs assessment study described in chapters 5. Knowledge was
assessed in this study using the CADE-Q 2 questionnaire, which development is also described
in this thesis (chapter 6).
1 Introduction
For people with chronic conditions, behavior change can be an effective strategy to prevent
further morbidity and mortality (Schwarzer et al., 2011). When people are enrolled in secondary
prevention programs (e.g. cardiac rehabilitation), there is a good chance that these patients can
learn how to improve their health behaviors and maintain them after discharge. For persons with
Coronary Artery Disease (CAD), secondary prevention strategies are highly effective to promote
behavior change, but multi-factorial, necessitating patient awareness and adherence to optimize
health outcomes (Clark et al., 2005; Stone et al., 2009; Heran et al., 2011; Ghisi et al., 2014a).
Therefore, patient education is an essential part of the rehabilitation of CAD patients targeting
self-management behavior to reduce risk factors and subsequent cardiac events (Dusseldorp et
al., 1999; Balady et al., 2007; Stone et al., 2009).

141
Cardiac rehabilitation (CR) is a comprehensive risk reduction program, of which patient
education is considered a core component (Buckley et al., 2013). Thus, American and Canadian
Cardiovascular Societies include education as a quality indicator of CR (Thomas et al., 2007;
Grace et al., 2014). Findings from meta-analyses provide evidence of the effectiveness of patient
education in CAD patients, in improving self-management behaviors (Mullen et al., 1992;
Dusseldorp et al., 1999; Aldcroft et al., 2011), health-related quality of life, and potentially
reducing healthcare costs (Brown et al., 2011) and recurrence of acute events (Dusseldorp et al.,
1999). Furthermore, a recent systematic review demonstrates the benefits of educational
intervention in CAD, through increase in patients’ knowledge and behavior change (physical
activity, dietary habits, and smoking cessation) (Ghisi et al., 2014a). However, patient
knowledge in CR has only scantly been investigated, and the impact of the education on behavior
change has not been often considered.
To explain, predict, and effectively improve behavior change of individuals and to optimize
treatment, theories of health behavior change are needed (Noar, Benac, & Harris, 2007; Dunn &
Elliot, 2008). In this context, the Health Action Process Approach (HAPA) has received attention
from researchers, because it is considered as a useful integration of the basic concepts of current
social cognitive health behavior models and as a valuable theoretical framework for identifying
postintentional factors leading to behavior adoption (Schwarzer, 1992; Lippke, Ziegelmann, &
Schwarzer, 2004; Renner & Schwarzer, 2005; Schwarzer et al., 2011).
According to this model, changing health-related behaviors requires two separate processes that
involve motivation and volition, respectively. First, an intention to change is developed, in part
on the basis of self-beliefs. Second, the change must be planned, initiated, and maintained, and
relapses must be managed. In addition, self-regulation plays a critical role in these processes

142
(Schwarzer, 1992). A recent overview covering seven empirical studies (Schwarzer, 2008), has
demonstrated the universal applicability of the HAPA for a number of health behaviors and for
diverse samples from various cultures, including physical exercise adherence after a CR program
(Scholz, Sniehotta, & Schwarzer, 2005).
For CR patients, no standardized and evaluated educational program has so far been available for
routine use. Moreover, many CR education programs still lack certain quality requirements, such
as the use of manuals, patient-oriented didactics, small-group format and evaluation of
effectiveness (Ghisi et al., 2014a). To date, theory-based techniques to foster health behavior are
only rarely employed and, although the HAPA model has proven to be a valid framework for the
prediction of behavior change, existing studies within this framework have focused on
heterogeneous sample and no studies have specifically considered its predictive value among CR
patients in educational programs. In addition, few studies have compared different educational
approaches applied within a multidisciplinary rehabilitation program in an outpatient CR setting.
Therefore, the present study draws upon the HAPA model to investigate: (1) changes in
knowledge and related theoretical constructs (i.e., self-efficacy, outcomes expectancies, risk
awareness, intention, and planning) among CR patients following exposure to a traditional or
theoretically-informed educational curriculum; and, (2) the theoretical correlates of exercise
behavior change among CR patients receiving educational interventions. The chosen behavior
was exercise, which is associated with lower mortality, lower recurrence rates and reduced
symptoms in cardiac patients (Blair et al., 1995; Thompson et al., 2003; Taylor et al., 2004;
Nocon et al., 2008; Lawler, Filion, & Eisenberg, 2011).
To specifically analyze the second objective, theory-implied constructs of the HAPA model were
investigated. In the pre-intentional motivational phase, it was hypothesized that risk awareness,
143
outcome expectancies and task self-efficacy are determinants of intention formation. According
to Sniehotta, Scholz, & Schwarzer (2006) the starting point for the motivational phase is some
level of risk awareness, for example feeling vulnerable to a (recurring) cardiac event. Positive
and negative outcome expectancies are deliberated: if the pros outweigh the cons of a behavior
change, one prerequisite for an intention is accomplished. Task self-efficacy – the perceived
capability to implement successfully alternative behaviors – is recognized as the major
determinant of intention formation (Renner & Schwarzer, 2003; Ziegelmann & Lippke, 2007).
Finally, it was also hypothesized that knowledge would be positively correlated with intention,
which is reported in previous studies with cardiac patients (Meischke et al., 2002; Clark et al.,
2005; Petter et al., 2009).
A second set of hypothesis concerned the post-intentional volition phase. Social-cognitive
models of behavior propose that intention is the most proximal and powerful predictor of
subsequent behavior (Ajzen, 1991; Conner & Armitage, 1998; Sheeran, 2002). However, good
intention does not necessarily guarantee corresponding actions and is seldom successful alone
(Sutton, 1994). In the current study it was hypothesized that intention would be correlated with
planning, which may lead to behavior change. Planning was divided into two sub-constructs:
action planning and coping planning (Sniehotta, Scholz, & Schwarzer, 2006). It was also
hypothesized that task and scheduling self-efficacy could influence planning, and maintenance
self-efficacy could influence directly behavior. Figure 7.1 presents the proposed model under
investigation, illustrating the relationships described above.

144
2 Methods
2.1 New Educational Curriculum Development
The new education curriculum was developed by a multi-disciplinary committee of 16 experts
from the CR program. The aim of this curriculum was to enable patients to take charge of their
medical condition and respond appropriately to changes in their health, and in developing
strategies to improve their risk factors.
The development of the curriculum consisted of the following phases: problem definition,
theoretical foundation, needs analysis (including a literature search and environmental scan),
program goals/educational objectives, sequencing instruction, instructional strategy/design and
methods/materials development, and evaluation of instruction/materials and learning for health
outcomes (which is presented in this study). Constructive theory (Cole & Griffin, 1987) and
adult learning principles (Knowles, 1980;1984) were the foundations for curriculum
development and delivery. The HAPA model (Schwarzer, 1992) was embedded in the
curriculum to promote behavior change.
The curriculum includes: 24 educational weekly group education sessions strategically
sequenced in accordance with the CR program learning outcomes, a comprehensive education
workbook, and individual care plans. Each topic contains educational content, learning activities,
learning assessments, behavioral-based action planning, and assessment of patients’ motivation
and confidence to incorporate change into their lifestyle. It was provided by an interdisciplinary
team of on-site exercise leaders, nurses, nutritionist, psychologist, psychiatrist and physicians.

145
2.2 Design and Procedure
This study was quasi-experimental in design, with assessments undertaken pre and post-CR.
Random assignment of study participants was not possible, because patients were allocated to
educational curriculum based on their choice of class (i.e. the class they choose based on their
preferences). Ethics approval was obtained from the review board at the hospital where the CR
program was located. Data was collected between April 2013 and May 2014.
Patients were informed about the study during their first cardiopulmonary exercise stress test by
a technician. They were also provided with information to take home and consider if desired.
Consenting patients were then allocated to an education curriculum based on their choice of class
(i.e. the class they choose based on their preferences).
Participants were invited to complete a self-administered confidential survey in paper format
(pre-CR survey). The survey included sociodemographic items, and psychometrically-validated
scales to assess exercise and related theoretical constructs (self-efficacy, outcomes expectancies,
risk awareness, intention, and planning), and a knowledge scale, namely the Coronary Artery
Disease Education Questionnaire II (CADE-Q II) (Ghisi et al., 2014c). Clinical data were
extracted from electronic patient records.
CR participants are offered weekly supervised exercise classes for 24 weeks, and provided a
home exercise prescription for the other days of the week. The traditional educational program
was provided by another interdisciplinary team of on-site health providers. Topics covered
include exercise safety, nutrition, risk management, medications, stress management, and
lifestyle management, presented in a less comprehensive way when compared to the new

146
curriculum. Education was delivered in large and small group sessions, lectures, a workbook,
online videos, and in pamphlet form.
Between the 22nd and 24th weeks of CR, patients were approached during their CR class to
complete the post-CR survey. It again assessed exercise, HAPA constructs, and knowledge as
per the initial survey. Electronic patient records were reviewed to ascertain degree of CR
participation and completion.
2.3 Participants
This study included CR patients (with heart disease or multiple cardiovascular risk factors)
recruited from the largest CR program in Toronto, Canada. The exclusion criteria were: lack of
English-language proficiency, and any visual, cognitive or psychiatric condition that would
preclude the participant from completing the surveys.
Sample size was based on the Ding, Velicer & Harlow (1995)’s rule of a minimum of 100
participants to run structural equation modeling. Anticipating a retention rate of 70%, a
minimum of 145 participants per group were required to achieve a final sample size of 100 per
group. Patients were approached consecutively until the required sample size was achieved.
2.4 Measures
Clinical characteristics extracted from medical records included: CR referral indication,
comorbid conditions, and cardiac risk factors. Patients self-reported their sociodemographic
characteristics, which included highest educational attainment.
147
Health literacy – which is the ability to obtain, read, understand and use healthcare information
to make appropriate health decisions and follow instructions for treatment – was measured pre-
CR using two questionnaires: the Medical Term Recognition Test (METER; Rawson et al, 2009)
and the Newest Vital Sign (NVS; Weiss et al, 2005). The METER consists of 40 medical terms
and 30 non-words. Respondents are instructed to mark which words they recognize as actual
words. Scores are based on the number of “true hits”, or actual medical terms the respondent
correctly identified, and can range from 0-40. Score ranges from 0-20, 21-34, and 35-40 indicate
low, marginal and functional health literacy, respectively. The METER was shown to have good
reliability (Cronbach’s alpha = 0.93), and strong construct and predictive validity (Rawson et al,
2009). The NVS consists of six questions regarding the information found on an accompanying
nutrition label. Each correct response is worth one point. Scores greater than four are considered
to be evidence of adequate health literacy. In initial validation studies, the NVS was shown to be
internally consistent (Cronbach’s alpha = 0.76).
Knowledge was assessed at pre- and post-CR using the CADE-Q II (development described on
chapter 4), which assesses patients’ knowledge about CAD in 5 domains: (1) medical condition,
(2) risk factors, (3) exercise, (4) nutrition, and (5) psychosocial risk. Each of the 31 items has 4
alternative response options, of which 1 is most correct (scored 3), 1 is somewhat accurate
(scored 1), and 2 are incorrect (scored 0). These scores are summed, with a maximum score of
93.
The target behavior was exercise, measured at pre- and post-CR. Exercise behavior was self-
reported by 2 questions: “How often do you usually walk in a week?” (never, less than 3-4 times,
more than 3-4), and “How much time do you spend exercising per week? (in hours)”. Guidelines

148
recommend cardiac patients engage in exercise most days of the week, and accumulate 150
minutes (or 2.5 hours) (Stone et al., 2009).
2.4.1. HAPA constructs
All constructs from the HAPA model were assessed pre- and post-CR using the
psychometrically-validated scales outlined below.
Risk awareness. Risk awareness refers to the quality and quantity of an individual’s perceived
susceptibility to a health threat; it is usually assessed along the dimensions of vulnerability and
severity (Schwarzer, 1992). Accordingly, risk awareness was measured as follows: 4 items
assessing vulnerability with the stem of “If I keep my lifestyle the way it was prior to my heart
problem”; and, 4 items assessing severity with the stem of “How severe (serious) are the
following health-related problems if I don’t exercise regularly?”. For the vulnerability items,
response ranges from 1= “very unlikely” to 7= “very likely”. For the severity items, response
ranges from 1= “not severe at all” to 7= “very severe”.
Outcome expectancies. Outcome expectancies are subjective beliefs about contingencies of an
individual’s behavioral consequences. These outcomes were evaluated with regard to their
favorableness for the individual, as positive or negative. Outcomes expectancies were considered
in 3 domains (social, psychological, and physical), assessed by a total of 15 items. All items had
the stem “If I exercise regularly…”, followed by positive consequences such as “I will simply
feel better afterwards”, or “my cholesterol level will improve”. Response options ranged from 1=
“very unlikely” to 7= “very likely” (Renner & Schwarzer, 2005).
Intentions. Intention is the person’s motivationtowards a goal or target behavior in terms if
direction and intensity. Intentions related to physical exercise were assessed with 2 questions

149
starting with “I will try” and “I intend”, which was followed by “to do my exercise prescription
over the next 6 months”. Response options ranged from 1= “definitely false” to 7= “definitely
true” (Renner & Schwarzer, 2005).
Self-efficacy. Three types of self-efficacy were measured: task, scheduling, and maintenance.
Task self-efficacy is the perceived capability of a person to implement a certain behavior and
facilitates goal-setting. The stem of a task self-efficacy item contains a statement about the target
behavior or the behavior change. In this study, task self-efficacy was measured by asking
patients “Assuming you were very motivated, how confident are you that you could physically
do the following amounts of exercise in one session without stopping over the next 6 months”?
The alternatives varied from 10 to 60 minutes and response options ranged from 1= “not
confident at all” to 7= “very confident”. Scheduling self-efficacy relates to managing one’s
schedule to accommodate the behavior. The scale that measured scheduling self-efficacy asked
patients “Assuming that you are very motivated, in the next 6 months, how confident are you that
you can fit your exercise prescription into your weekly schedule”? The alternatives varied from
once per week to more than 5 times per week and response options ranged from 1= “not
confident at all” to 7= “very confident”. Finally, maintenance self-efficacy describes optimistic
beliefs about one’s capability to deal with barriers that arise while continuing exercise.
Maintenance self-efficacy was measured by 13 items identifying barriers to adherence to
exercise with the stem “Assuming you were very motivated, how confident are you that you will
do your exercise prescription over the next 6 weeks”. Response options also ranged from 1= “not
confident at all” to 7= “very confident” (Maddux, 1995; Bandura, 1997; Rodgers & Sullivan,
2001; Rodgers et al, 2002; Blanchard et al, 2003; Schwarzer, 2008).

150
Planning. Action planning and coping planning were assessed. Action planning refers to
concrete plans about when, where, and how to implement the intended behavior and has be
proven to be a useful strategy in health behavior change (Scholz, Sniehotta and Schwarzer,
2005). For action planning, the item stem “I already have concrete plans…” was followed by the
items (a) “where to exercise”, (b)”when to exercise”, (c)”how to exercise”, (d)”how often to
exercise”, (e)”with whom to exercise”, and (f) what types of activities to do. Coping planning
includes the anticipation of barriers and the design of alternative actions that help to attain one’s
goal despite impediments (Renner & Schwarzer, 2005). For coping planning, the item stem “I
already have concrete plans regarding…” was followed by the items (a)”what to do if someone
interferes with my exercise schedule”, (b)”what to do if I miss an exercise session”, (c)”what to
do in difficult situations in order to stick to my exercise schedule”, and (d)”if something gets in
the way of my plans to exercise”. Both scales had response options that ranged from 1=
“strongly disagree” to 7= “strongly agree”.
2.5 Statistical Analysis
SPSS Version 21.0 (IBM Corp, 2012) was used for entering, cleaning and analyzing the data,
and the level of significance was set at 0.05 for all tests. Firstly, descriptive statistics were used
to describe participants’ sociodemographic and clinical characteristics by educational curriculum
type, to ascertain if there were any differences which may impact the subsequent findings.
Frequency tables were used for categorical variables and descriptives (mean, standard deviation,
minimum and maximum) for continuous variables.
To test the first objective, the mean CADE-Q II scores were examined by item, subscale and
overall. Next, paired sample t-tests and ANOVA were computed to investigate changes in all
151
overall knowledge before and after exposure to each educational curriculum. Where significant,
changes in subscales and individual items were tested. Pre- and post-CR scores for each variable
were considered as a within-factor and groups as a between-factor.
Finally, to test the second objective, the exercise variable was examined. Outliers were identified
and excluded from the descriptive and path analysis. The program IBM SPSS AMOS 20
(Arbuckle, 2011) was used to conduct the path (regression) analysis, to establish the best-fitting
model for the relationship among the HAPA variables under study. A maximum likelihood
estimation procedure was used to generate the parameter estimates (e.g. regression weights).
Model fit was evaluated by consulting various indices: chi-square (χ²); root mean square error of
approximation (RMSEA); comparative fit index (CFI); and goodness-of-fit index (GFI).
According to Hu & Bentley (1999) CFI and TLI values above .90 and RMSEA values less than
.08 indicate an adequate fit. Where the fit indices indicated that the hypothesized model did not
provide an adequate fit to the data, the modification indices (MI) were consulted to identify any
areas of misfit in the model. The value of a modification index represents the expected drop in
chi-square value if a fixed parameter were to be freely estimated. The parameter with the largest
MI value was freed only if it made substantive sense; if it was not meaningful then the parameter
with the next largest MI value was considered. The regression coefficients were examined only
after a good-fitting model was identified.
The path analysis was used as a full structural equation model (SEM) (measurement + structural
model). The use of a SEM including a measurement model would have required a substantial
increase in the number of parameters to be estimated, and hence to an insufficient ratio of
participants : parameters.

152
Figure 7.1 – Model of the relationship between HAPA constructs, knowledge and exercise
behavior. SE indicates self-efficacy, OE outcome expectancies, e- errors.

153
3 Results
3.1 Respondents Characteristics
A flow diagram of study participation is presented in Figure 7.2. Overall, significantly more
males (77.8%) agreed to participate in this study than females (22.2%; p<.001), as well as
subjects with a university degree compared to other educational status (p<.001).
Three hundred and six patients consented to participate in this study, of which 146 (47.7 %) were
exposed to the new curriculum. Sociodemographic and clinical characteristics of the sample
overall and by curriculum are shown in Table 7.1. There were no significant differences in
participant characteristics by curriculum. METER and NVS mean scores showed that both
groups presented functional and adequate health literacy, respectively.
Overall, 173 (56.5%) participants completed the post-CR survey. Participants who completed the
post-CR survey were significantly older than the ones who completed only the pre-CR survey
(p=0.002). Reasons for not completing the post-CR survey are also presented in Figure 7.2.

154
Figure 7.2 – Flow diagram of study participants

155
Table 7.1 – Sociodemographic and Clinical Characteristics of Participants, and by Educational Curriculum.
Characteristic Overall (N=306)
Traditional (n=160; 52.3%)
New (n=146; 47.7%)
p*
Sociodemographic Age, years (mean±SD) 63.92±11.83 63.58±11.66 64.30±12.04 0.23
Sex, n (%) 0.51
Female 68 (22.2%) 37 (23.1%) 31 (21.2%)
Male 238 (77.8%) 123 (76.9%) 115 (78.8%)
Highest Educational Attainment, n (%)§ 0.31
Less than high school 20 (6.5%) 14 (8.8%) 6 (4.1%)
High School 40 (13.1%) 24 (15.0%) 16 (11.0%)
Trades Certificate 11 (3.6%) 5 (3.1%) 6 (4.1%)
College 62 (20.3%) 32 (20.0%) 30 (20.5%)
University 166 (54.2%) 80 (50.0%) 86 (58.9%)
Health Literacy, (mean±SD)†
METER 35.19±5.83 35.64±5.31 34.69±6.35 0.42
NVS 4.50±1.72 4.29±1.81 4.74±1.58 0.26
Clinical,!n (% yes)‡
Referral Indication
Heart Failure 18 (5.9%) 9 (5.6%) 9 (6.2%) 0.84
Cardiomyopathy 14 (4.6%) 8 (5.0%) 6 (4.1%) 0.71
Stroke/Transient Ischemic Attack 29 (9.5%) 16 (10.0%) 13 (8.9%) 0.38
Valvular Heart Disease 39 (12.7%) 21 (13.1%) 18 (12.3%) 0.84
Peripheral Vascular Disease 11 (3.6%) 5 (3.1%) 6 (4.1%) 0.65
Chronic Obstructive Pulmonary Disease 16 (5.2%) 8 (5.0%) 8 (5.5%) 0.85
Angina 10 (3.3%) 3 (1.9%) 7 (4.8%) 0.16
Arrhythmia 28 (9.2%) 14 (8.8%) 14 (9.6%) 0.80
Myocardial Infarction 113 (36.9%) 60 (37.5%) 53 (36.3%) 0.83
Coronary Artery Bypass Graft Surgery 71 (23.2%) 43 (26.9%) 28 (19.2%) 0.11
Percutaneous Coronary Intervention 117 (38.2%) 56 (35.0%) 61 (41.8%) 0.23
Risk factors
Hypertension 144 (47.1%) 72 (45.0%) 72 (49.3%) 0.45
Type I Diabetes 21 (6.9%) 13 (8.1%) 8 (5.5%) 0.68
Type II Diabetes 51 (16.7%) 24 (15%) 27 (18.5%) 0.42
Depression 9 (2.9%) 5 (3.1%) 4 (2.7%) 0.85
Sleep Apnea 26 (8.5%) 15 (9.4%) 11 (7.5%) 0.56

156
Smoking history 104 (34.0%) 54 (33.8%) 50 (34.2%) 0.93
Smoking, years (mean±SD) 7.95±13.92 7.90±14.2 8.01±13.6 0.31
SD indicates standard deviation, METER Medical Term Recognition Test (maximum = 40), NVS Newest Vital Sign (maximum = 5). *Chi-square or t-tests as appropriate for differences between groups (p<.05 for significant differences between traditional and new educational curriculum, if any). §Self-reported. †Assessed via pre-survey (pre-CR). ‡Extracted from electronic patients records.
3.2 Knowledge
Knowledge pre-CR did not differ significantly by curriculum. There was a significant increase
(p<.001) in overall knowledge from pre- to post-CR in the overall sample, as well as in
participants exposed to both curricula. As shown in Table 7.2, the increase in knowledge
appeared on all subscales overall and by curriculum. There were no significant differences by
curricula in any type of knowledge (overall, domains or items).
In regards to individual items, knowledge scores improved on 22 items in the overall sample (6
items from medical condition, 6 from exercise, 4 from risk factors, 3 from nutrition, and 3 from
the psychosocial risk subscale). Participants exposed to the traditional curriculum improved their
knowledge significantly on 16 items, particularly related to exercise (6 items), risk factors and
medical condition (3 items each). Finally, participants exposed to the new curriculum improved
their knowledge significantly on 17 items, particularly related to risk factors, nutrition, and
exercise (4 items each).

157
3.3 HAPA constructs
Table 7.3 displays mean HAPA theoretical constructs scores at pre- and post-CR, overall and by
curriculum. Results show significant increases in risk awareness, psychological and physical
outcomes expectancies, task self-efficacy, and action and coping planning, overall and
curriculum from pre to post-CR. Patients exposed to the traditional curriculum also significantly
improved scheduling self-efficacy and patients exposed to the new curriculum improved social
outcome expectancies. Significant differences among groups at post-CR were observed in social
outcome expectancies, with patients exposed to the new curriculum showing significant higher
scores.
3.4 Exercise behavior
As described elsewhere, the chosen behaviour for this study was physical exercise, which was
self-reported by 2 questions at pre- and post-CR. Results are presented in Table 7.3. Participants
reported a significant increase in hours of physical exercise per week from pre- to post-CR,
overall and by groups. In addition, the frequency of walking per week increased significantly
from pre- to post-CR, again overall and by groups.
3.5 Knowledge and theoretical determinants of exercise behavior
3.5.1 Preliminary Analysis
The means and standard deviations of the theoretical variables in the study are presented in Table
7.3. Overall, Pearson correlations confirmed the expected pattern of associations as proposed in
Figure 1. Specifically, risk awareness (r=0.20, p<0.05), psychological outcome expectancies
(r=0.21; p<0.05), task self-efficacy (r=0.27, p<0.01), and total knowledge (r=0.28, p<0.01) were

158
positively related to intention. Task self-efficacy (r=0.46, p<0.01), scheduling self-efficacy
(r=0.43, p<0.01), intention (r=0.48, p<0.01) and total knowledge (r=0.26, p<0.01) were
positively related to action planning. Task self-efficacy (r=0.33, p<0.01), scheduling self-
efficacy (r=0.44, p<0.01), and intention (r=0.43, p<0.01) were positively related to coping
planning. Scheduling self-efficacy (r=0.27, p<0.01), maintenance self-efficacy (r=0.20, p<0.01),
and action planning (r=0.20, p<0.05) were positively correlated to behavior. A correlation matrix
is presented in Table 7.4.

159
Table 7.2 – Total, subscale and item knowledge scores at pre- and post-CR in overall sample, and by curriculum
Knowledge scores (mean±SD)
Overall (N=306) Traditional (n=160) New (n=146)
Maximum possible
score
Pre-CR Post-CR p* Pre-CR Post-CR p* Pre-CR Post-CR p* p§
Total Knowledge 93 64.72±17.35 75.68±12.27 <.001 65.14±17.65 75.29±13.27 <.001 64.25±17.08 76.12±11.11 <.001 0.90
Subscales
Medical Condition 21 15.24±4.77 17.12±3.98 <.001 15.31±4.89 17.09±4.09 <.001 15.15±4.65 17.15±3.88 0.001 0.77
Risk Factors 15 9.49±3.32 11.26±2.66 <.001 9.43±3.43 11.08±2.87 <.001 9.56±3.20 11.47±2.41 <.001 0.73
Exercise 21 15.70±5.18 18.57±3.05 <.001 15.79±5.21 18.63±2.93 <.001 15.60±5.14 18.51±3.20 <.001 0.75
Nutrition 21 14.07±4.66 16.84±3.39 <.001 14.27±4.66 16.69±3.42 <.001 13.84±4.65 17.01±3.37 <.001 0.43
Psychosocial Risk 15 10.23±3.64 11.86±2.56 <.001 10.34±3.70 11.80±2.69 <.001 10.10±3.60 11.93±2.42 0.001 0.25
Items
Medical Condition
1. Coronary Artery Disease is: 3 2.17±1.27 2.49±1.07 0.004 2.13±1.28 2.54±1.06 0.01 2.22±1.27 2.43±1.10 0.14 0.52
2. Angina (chest pain or discomfort) occurs:
3 2.58±1.00 2.75±0.77 0.02 2.62±0.95 2.87±0.16 0.007 2.53±1.05 2.62±0.94 0.31 0.46
3. In a person with coronary artery disease, which of the following is a usual description of angina?
3 2.42±1.09 2.53±0.95 0.53 2.49±1.02 2.46±1.01 0.33 2.33±1.16 2.62±0.94 0.06 0.19
4. A heart attack occurs: 3 2.36±1.10 2.66±0.82 0.001 2.38±1.10 2.58±0.90 0.07 2.35±1.11 2.75±0.72 0.007 0.84
5. The best resources available to help someone understand his/her medications are:
3 2.29±1.06 2.45±0.93 0.02 2.32±1.09 2.42±0.97 0.15 2.27±1.04 2.49±0.90 0.09 0.67
6. Medications such as aspirin (ASA) and clopidogrel (PlavixTM) are important because:
3 1.90±1.13 2.18±1.06 0.01 1.79±1.15 2.07±1.05 0.06 2.02±1.09 2.31±1.07 0.09 0.08

160
7. The “statin” medications, such as atorvastatin (LipitorTM), rosuvastatin (CrestorTM), or simvastatin (ZocorTM), have a beneficial effect in the body by:
3 1.51±1.27 2.08±1.19 <.001 1.59±1.25 2.15±1.16 <.001† 1.43±1.29 1.99±1.21 0.02 0.28
Risk Factors
1. The risk factors for heart disease that can be changed are:
3 2.30±1.08 2.55±0.91 0.03 2.24±1.09 2.42±1.00 0.42 2.36±1.06 2.70±0.77 0.009 0.36
2. The actions that can be taken to control cholesterol levels include:
3 2.45±1.05 2.77±0.74 0.003 2.40±1.09 2.71±0.83 0.02 2.51±1.00 2.83±0.63 0.07 0.37
3. The actions that can be taken to control blood pressure include:
3 2.48±1.01 2.73±0.76 <.001 2.51±1.02 2.73±0.80 0.01 2.45±1.00 2.74±0.70 0.02 0.60
4. The first step towards controlling a risk factor (such as blood pressure or cholesterol) is:
3 0.55±0.94 0.78±1.11 0.07 0.59±0.94 0.81±1.11 0.22 0.49±0.93 0.75±1.11 0.19 0.35
5. The actions to prevent developing diabetes include:
3 1.72±1.34 2.42±1.11 <.001 1.69±1.35 2.41±1.12 <.001 1.76±1.33 2.44±1.11 <.001 0.63
Exercise
1. What are the important parts of an exercise prescription?
3 2.63±0.95 2.85±0.62 0.01 2.63±0.94 2.86±0.61 0.02 2.62±0.96 2.84±0.64 0.33 0.94
2. For a person living with heart disease, it is important to do a cardiovascular warm-up before exercising because:
3 2.12±1.16 2.44±0.95 <.001 2.09±1.20 2.41±0.95 0.003 2.15±1.11 2.47±0.95 0.04 0.67
3. The pulse can be found: 3 2.32±1.12 2.49±0.97 0.25 2.28±1.16 2.56±0.91 0.05 2.37±1.08 2.41±1.03 0.67 0.46
4. Three things that one can do to exercise safely outdoors in the winter are:
3 1.94±1.30 2.73±0.73 <.001 1.99±1.28 2.71±0.75 <.001 1.89±1.32 2.75±0.72 <.001 0.49
5. The benefits of doing resistance training (lift weights or elastic bands) include:
3 2.17±1.19 2.59±0.87 <.001 2.21±1.16 2.59±0.91 0.002 2.13±1.23 2.59±0.83 0.04 0.55
6. If a person gets chest discomfort during a walking
3 2.35±1.08 2.77±0.68 <.001 2.31±1.11 2.88±0.51 <.001 2.40±1.05 2.65±0.81 0.29 0.46

161
exercise session, he or she should:
7. How does a person know if he/she is exercising at the right level?
3 2.16±1.24 2.70±0.81 <.001 2.28±1.18 2.62±0.93 0.02 2.03±1.30 2.79±0.65 <.001 0.09
Nutrition
1. What is the best source of omega 3 fats in food?
3 2.33±1.20 2.51±1.03 0.18 2.34±1.19 2.53±1.05 0.11 2.32±1.22 2.49±1.01 0.74 0.87
2. Trans fat are: 3 1.67±1.41 2.41±1.12 <.001 1.73±1.41 2.43±1.11 <.001 1.61±1.41 2.38±1.15 0.004 0.48
3. What is one good way to add more fibre to your diet:
3 2.19±1.17 2.47±0.95 0.10 2.26±1.13 2.42±1.00 0.69 2.11±1.20 2.53±0.90 0.04 0.25
4. Which of the following foods has the most salt:
3 2.66±0.91 2.82±0.65 0.40 2.66±0.91 2.82±0.63 0.14 2.66±0.91 2.81±0.67 0.58 0.99
5. What combination of foods can help lower blood pressure?
3 2.55±0.96 2.77±0.72 0.09 2.58±0.96 2.77±0.72 0.05 2.52±0.97 2.77±0.73 0.90 0.58
6. When reading food labels, what should one look at first?
3 1.48±0.99 2.22±1.01 <.001 1.47±0.98 2.18±1.05 <.001 1.50±0.99 2.26±0.97 <.001 0.78
7. How many servings of fruits and vegetables should adults consume?
3 1.18±1.40 1.62±1.40 0.02 1.23±1.42 1.49±1.41 0.70 1.12±1.37 1.77±1.39 0.006 0.50
Psychosocial Risk
1. Which of the below are effective stress management techniques?
3 2.48±1.03 2.66±0.84 0.16 2.42±1.07 2.69±0.81 0.08 2.55±0.98 2.63±0.87 0.85 0.25
2. What stresses have been related to increased risk for heart attacks?
3 1.79±1.40 2.29±1.22 0.001 1.86±1.38 2.26±1.23 0.02 1.71±1.43 2.32±1.21 0.02 0.33
3. Which of the following describes your best option for reducing your risk from depression:
3 2.67±0.91 2.84±0.62 0.04 2.69±0.89 2.81±0.71 0.34 2.66±0.93 2.88±0.48 0.04 0.77
4. It is important to recognize “sleep apnea” because:
3 2.01±1.37 2.63±0.91 <.001 2.06±1.35 2.60±0.95 <.001 1.95±1.40 2.67±0.87 <.001 0.46

162
5. “Chronic stress” is defined as: 3 1.27±1.26 1.43±1.22 0.46 1.31±1.29 1.43±1.26 0.71 1.23±1.22 1.43±1.18 0.48 0.58
SD indicates standard deviation.
* Paired t-test
§ Independent sample t-test (between groups at post-CR)
Table 7.3 – HAPA constructs and exercise behavior at pre- and post-CR in overall sample, and by curriculum
Overall (n=306) Traditional (n=160) New (n=146)
Maximum possible
score
Pre-CR Post-CR p* Pre-CR Post-CR p* Pre-CR Post-CR p* p§
Constructs (mean±SD)
Risk Awareness 7 5.16±1.36 5.62±1.17 <.001 5.16±1.41 5.62±1.23 0.001 5.15±1.31 5.63±1.10 0.003 0.95
Outcome Expectancies
Social 7 4.45±1.51 4.65±1.48 0.13 4.48±1.55 4.34±1.58 0.94 4.42±1.47 4.95±1.30 0.005 0.006
Psychological 7 5.68±1.32 6.07±1.03 <.001 5.70±1.44 6.01±1.14 0.01 5.66±1.18 6.13±0.88 0.009 0.41
Physical 7 5.14±1.32 5.58±1.81 0.001 5.16±1.44 5.39±1.36 0.05 5.12±1.18 5.79±2.19 0.008 0.16
Self-efficacy
Task 7 5.09±1.72 5.75±1.49 <.001 4.97±1.80 5.67±1.56 <.001 5.21±1.64 5.84±1.42 0.002 0.46
Scheduling 7 5.20±1.68 5.61±1.48 0.02 5.13±1.70 5.63±1.46 0.02 5.27±1.65 5.58±1.51 0.35 0.80
Maintenance 7 5.20±1.26 5.44±1.27 0.31 5.15±1.37 5.30±1.28 0.77 5.25±1.14 5.60±1.24 0.13 0.12
Intention 7 6.30±1.17 6.34±1.08 0.60 6.35±1.24 6.26±1.19 0.74 6.32±1.09 6.42±0.93 0.64 0.33
Planning

163
Action 7 4.81±1.57 6.03±1.00 <.001 4.68±1.60 6.00±0.88 <.001 4.96±1.45 6.07±1.04 <.001 0.61
Coping 7 4.27±1.62 5.18±1.42 <.001 4.27±1.73 5.10±1.58 <.001 4.27±1.50 5.27±1.21 <.001 0.43
Behavior
Weekly physical exercise, hours (mean±SD)
- 4.91±5.90 8.05±13.24 <.001 5.26±6.97 7.45±6.01 0.03 4.55±4.52 8.73±13.35 <.001
Walking 3-4 times per week or more, n(%)
- 204 (68.7%) 147 (85.5%) <.001 104 (67.5%) 82 (89.1%) 0.001 100 (69.9%) 65 (81.3%) 0.04 0.15
SD indicates standard deviation.
* Paired t-test
§ Independent sample t-test (between groups at post-CR)

164
Table 7.4 - Pearson’s correlation matrix for HAPA constructs and exercise behavior post-CR (n=173)
Constructs 1 2 3 4 5 6 7 8 9 10 11 12
1. Risk Awareness 1 0.32** 0.33** 0.37** 0.27** 0.20*§ 0.17*
2. Outcome
Expectancies Social 1 0.38** 0.40** 0.18* 0.23** 0.18*
3. Outcome
Expectancies
Psychological
1 0.47** 0.21* 0.30** 0.22**§ 0.26** 0.20** 0.19*
4. Outcome
Expectancies Physical 1 0.17* 0.20* 0.17*
5. Task Self-efficacy 1 0.44** 0.41** 0.27**§ 0.46**§ 0.33**§ 0.37** 0.27**
6. Scheduling Self-
efficacy 1 0.45** 0.44** 0.43**§ 0.44**§ 0.27**§
7. Maintenance Self-
efficacy 1 0.52** 0.58** 0.53** 0.19*§ 0.32**
8. Intention 1 0.48**§ 0.43**§ 0.28**§
9. Action Planning 1 0.61** 0.20*§ 0.26**§
10. Coping Planning 1
11. Behavior 1
12. Total Knowledge 1
Only significant correlations are shown: *p<0.05 **p<0.01
§ Correlation included in our hypothesis model

165
3.5.2 Path Analysis
The proposed model illustrated in Figure 7.1 was tested, and results demonstrated unsatisfactory
fit (chi-square = 323.14, df = 50, CFI = 0.31, GFI = 0.68, RMSEA = 0.20 [0.18, 0.22]. The
model was then modified, guided by theory and modification indices. All types of self-efficacy
and outcome expectancies, and action and coping planning were correlated with each other,
which has been previously described as a way to simplify the model (Schwarzer, 1992). In
addition, knowledge was correlated to task and maintenance self-efficacy, since self-efficacy has
emerged as a highly effective mediator of motivation and learning (Zimmerman, 2000).
Knowledge was also correlated to action planning (Sniehotta et al., 2006) since the educational
programs assessed in this study had a strong action planning component. As self-efficacy is a key
factor influencing intention, the other factors from the motivational phase – risk awareness and
all types of outcome expectancies – were correlated.
This modified model (see Figure 7.3) yielded satisfactory fit across indices (chi-square = 66.98,
df = 34, CFI = 0.92, GFI = 0.93, RMSEA = 0.084 [0.05, 0.11]). All new correlations were
significant (p<.001): task self-efficacy with knowledge (r=0.20), scheduling self-efficacy
(r=0.41), and maintenance self-efficacy (r=0.39); scheduling self-efficacy with maintenance
self-efficacy (r=0.42); maintenance self-efficacy with knowledge (r=0.26), risk perception with
social (r=0.32), psychological (r=0.33), and physical (r=0.40) outcome expectancies, physical
outcome expectancies with psychological (r=0.47) and social (r=0.40), psychological and social
(r=0.38), and action and coping planning (r=0.45).
In the modified model the following associations were significant: knowledge was positively
related to intention (β=0.23, p=0.04), task self-efficacy to action planning (β=0.30, p<0.001) and

166
behavior (β=0.30, p=0.002), intention to action planning (β=0.32, p<0.001) and coping planning
(β=0.28, p<0.001), and scheduling self-efficacy to coping planning (β=0.25, p=0.003).
Figure 7.3 – Modified model of the relationship between HAPA constructs, knowledge and
exercise behavior. SE indicates self-efficacy, OE outcome expectancies, e- errors.

167
4 Discussion and Conclusion
4.1 Discussion
The present study provides evidence that education interventions in CR are effective strategies to
improve knowledge, change theory-implied constructs of behavior and enhance physical
exercise. Despite the fact that the sample was highly educated and health-literate, there was a
significant increase in patients’ overall knowledge from pre- to post-CR in the overall sample.
Knowledge improved significantly across all domains. However, contrary to expectation, the
revised educational curriculum did not result in improvements in knowledge, HAPA-related
constructs or behavior when compared to the traditional curriculum. This may be related to the
fact that patients were already knowledgeable, and the traditional curriculum was effective.
In the pre-intentional motivation phase it was hypothesized that, among CR patients receiving
educational interventions, task self-efficacy, followed to a lesser extent by risk awareness and
outcome expectancies would be positive predictors of intention. None of these associations were
supported. Although this analysis failed to identify these relations, positive correlations were
found between all these mediators and intention formation. This predictive pattern differs from
the one observed by Renner et al., (2007), on which was observed that middle-aged and older
adults are motivated to engage in physical activity only due to task self-efficacy. Results from
our study are similar to those reported by Caudroit, Stephan, & Le Scanff (2011) who identify
risk awareness as a determinant of intention formation to exercise among older adults. According
to these authors, older adults become motivated to engage in physical activity because they feel
at risk for future health problems and disease. This can be translated to our sample of CR patients

168
receiving educational interventions, who are strongly driven by a secondary prevention program,
aimed to decrease health risks and avoid new events.
A second and complementary set of hypothesis concerned the post-intentional volition phase. It
was hypothesized that, intention would be correlated to planning (action and coping), which may
lead to behavior change. It was also hypothesized that task and scheduling self-efficacy could
influence planning and maintenance self-efficacy could influence directly behavior. The results
partially confirmed this hypothesis and revealed that intention was positively related to action
and coping planning, which was correlated to behavior. These findings suggest that when CR
patients become motivated to engage in physical exercise, their intentions are not directly
translated into action. This result is in line with Reuter et al. (2010) who found that planning is
necessary to bridge the intention-behavior gap, but stands in contrast with research conducted by
Renner et al. (2007) and Caudroit et al. (2011) among older individuals where intentions directly
translated into action without preparatory strategies of approaching the activity.
Furthermore, it was hypothesized that knowledge was related to intentions. This hypothesis was
confirmed via regression analysis and knowledge was also positively correlated to action
planning, task and maintenance self-efficacy. According to health behavior models, knowledge
of the negative health consequences of a behavior is a necessary condition for behavior change
(Janz & Becker, 1984; Rosenstock, 1990). However, knowledge alone is not sufficient to
promote behavior change. It is generally thought that individuals who perceive themselves to
have an increased risk of CVD are more like to change their intentions and adopt behaviors that
reduce their risk (Dishman et al., 2004; Segan, Borland, & Greenwood, 2004; Lynch et al.,
2006).

169
Caution is warranted when interpreting these results. The chief limitation is potential selection
bias. The results are specific to a small, well-educated sample of cardiac patients who attend a
comprehensive CR program at a single-centre. They do not apply to cardiac patients with lower
educational status, which raises doubt about the possibility of generalizing the results. Low
retention was also observed (however, not compared to other CR programs). Future research
should examine the interplay of theory-implied constructs described in the HAPA in a larger
cohort of cardiac patients with lower educational levels to confirm results obtained in the present
study. Moreover, given the fairly low rate of program completion observed, it is not likely the
sample was biased towards highly-adherent patients. Second, results are only generalizable to
patients who are referred and attend CR programs, which are a low proportion of cardiac
outpatients (Suaya et al., 2007). Third, because both educational programs assessed were similar,
and usually educational programs for cardiac patients are not highly standardized (Ghisi et al.,
2014), whether the relationship between program completion and knowledge would be replicated
in other communities of practice is not known. Fourth, the behavior used in the model was self-
reported, which can introduce social desirability bias and over-reporting. The use of objective
assessment tools such as accelerometers should be undertaken. In addition, there are other
behavior that should be changed are not included in this study (e.g. diet, medication use,
smoking habits). Fifth, multiple comparisons were undertaken, which inflates error rates. Finally,
a study assessing CR patients not receiving education is warranted, to ascertain whether the
differences in knowledge identified herein are robust.

170
4.2 Conclusion
Knowledge, behavior, and theory-implied constructs of behavior improve in post-CR programs
with educational interventions. Although it was found positive correlations based on our
hypothesis, path analysis revealed that only knowledge was a significant motivational construct
leading to intention formation, and intentions to engage in physical activity were not directly
translated into behavior, needing especially action planning, which is related to self-efficacy.
The present study contributes to existing knowledge as the first to apply the HAPA for the
prediction of behavior among CR patients receiving educational interventions. It confirms that it
provides a useful framework for the understanding of the social cognitive processes underlying
this behaviour for this group of patients.
4.3 Practice Implications
Innovative educational strategies are needed for cardiac patients not only to increase knowledge
but also enhance intentions, self-efficacy, and action planning. This included the provision of
education and skill training for CVD prevention based on a better understanding of the
individuals’ social and cultural characteristics.

171
Chapter 8 SUMMARY OF THE RESEARCH AND GENERAL DISCUSSION
This chapter presents a summary of the 5 studies that composed this thesis, plus general
discussion, implications, future directions and limitations.
1 Summary of the Research
As described elsewhere, this thesis involved 5 studies divided into 4 steps: (1) a systematic
review; (2) information needs assessment; (3) knowledge assessment; and (4) assessment of
behavior determinants.
The initial step was to review systematically the literature in order to: (1) investigate the impact
of education on patients’ knowledge about health and disease, (2) determine if educational
interventions are related to health behavior change in CAD patients, and (3) describe the nature
of the educational interventions offered to CAD patients. This step was important to gain a clear
picture of how these interventions are structured and how they impact not only behaviour, but
disease-related knowledge. To our knowledge, such a synthesis had not been published
previously. A literature search of several electronic databases was conducted for published
articles from database inception to August 2012. Eligible articles included cardiac patients, and
described delivery of educational interventions by a healthcare provider. Measures were
knowledge, smoking, physical activity, dietary habits, response to symptoms, medication
adherence, and psychosocial well-being. Articles were reviewed by 2 authors independently.
Overall, 42 articles were included, of which 23 (55%) were randomized controlled trials, and 16
(38%) were considered “good” quality. Eleven studies (26%) assessed knowledge, and 10
showed a significant increase with education. With regard to measures, educational interventions

172
were significantly and positively related to physical activity, dietary habits, and smoking
cessation. The nature of interventions were poorly described and most frequently delivered post-
discharge, by a nurse, and in groups. In conclusion, findings from this study support the benefits
of educational interventions in CAD, though increase in patients’ knowledge and behavior
change. Furthermore, future reporting of education interventions should be more explicitly
characterized, in order to be reproducible and assessed.
Step two refers to the information needs assessment. In this step the author as well as a group of
researches and experts in CR conducted a comprehensive review of existing documents related
to adult learning and patient education in order to develop a new education curriculum for
cardiac patients participants in the largest academic CR centre of Toronto. One of the findings
was that, within the context of CR, educational interventions based on patients’ needs are likely
to be more effective. Therefore, needs analysis was one of the first phases included in the
development of the education curriculum. Since a previous literature review failed to identify
any available and validated tool to assess information needs in coronary patients in CR programs
a new questionnaire was developed and psychometrically validated. This questionnaire was
called INCR (Information Needs in Cardiac Rehabilitation). After a literature search, 60
information items divided into 11 areas of needs were identified. To establish content validity,
they were reviewed by an expert panel (N=10). Refined items were pilot-tested in 34 CR patients
on a 5-point Likert-scale from 1 “really not helpful” to 5 “very important”. A final version was
generated and psychometrically-tested in 203 CR patients. Test-retest reliability was assessed via
the intraclass correlation coefficient (ICC), the internal consistency using Cronbach's alpha, and
criterion validity was assessed with regard to patient’s education and duration in CR. Results
showed that 5 items were excluded after ICC analysis as well as one area of needs. All 10 areas
were considered internally consistent (Cronbach's alpha > 0.7). Criterion validity was supported

173
by significant differences in mean scores by educational level (p<0.05) and duration in CR
(p<0.001). The mean total score was 4.08±0.53. Patients rated safety as their greatest information
need. In conclusion, the INCR Tool was demonstrated to have good reliability and validity. This
is an appropriate tool for application in clinical and research settings, assessing patients’ needs
during CR and as part of education programming.
In addition to step two, another study was conducted using the INCR to describe CR participant
information needs, investigate whether CR providers are cognizant of patient’s information
needs and preferred delivery formats, and whether patient information needs change over the
course of CR. In this cross-sectional study, 306 CR patients and 28 CR providers completed a
survey. The survey consisted of the INCR questionnaire, and items about preferred education
delivery formats. Results showed that low-income CR participants had significantly greater
information needs than high-income participants. CR providers were cognizant of patient
information needs, except patients did desire more information on diagnosis and treatment than
providers perceived (p<.01). Books, lectures and discussion were identified as the preferred
delivery formats by both patients and providers. There were significant differences in patient
information needs over the course of the program, particularly in relation to exercise safety
concerns and risk factors. In conclusion, CR patients desire information in many areas,
particularly regarding emergency/safety and diagnosis/treatment. CR providers were highly
cognizant of patient information needs; however, these do change over time. These findings
could inform evaluation and improvement of CR education programming, to ensure programs
are meeting patient information needs across all stages of recovery. In addition, results from this
study where important in the development of the new education curriculum for CR patients.

174
Step three refers to knowledge assessment and the development and psychometric validation of a
more comprehensive and updated questionnaire to assess CR patients knowledge, called
Coronary Artery Disease Education Questionnaire version II (CADE-Q II). After an information
needs assessment study, a literature search and a focus group discussions with CR experts (n=15)
a 31-item pilot questionnaire was developed. Overall, three items from the CADE-Q were
retained. The questionnaire underwent pilot testing in 30 patients, in which clarity was provided.
A final version was generated and psychometrically tested in 307 CR patients. The internal
consistency was assessed using Cronbach's alpha, the dimensional structure through an
exploratory factor analysis, and criterion validity was assessed with regard to educational level.
Results showed a Cronbach's alpha of 0.91. Criterion validity was supported by significant
differences in mean scores by educational level (p<.001). Factor analysis revealed four factors,
which were all internally-consistent and well-defined by the items. The mean total score was
64.23±18.1. Patients with history heart failure (p=0.01), cardiomyopathy (p=0.04) and history of
PTCA (p=0.04) presented significantly higher knowledge compared with their counterparts.
Knowledge about exercise and medical condition was significantly higher than knowledge about
risk factors, nutrition and psychosocial risk. In conclusion, the CADE-Q II was demonstrated to
have good reliability and validity. This tool will provide valuable information to clinicians and
researchers about the value of patient education in CR.
Finally, step four refers to the assessment of behavior determinants among CR patients receiving
educational interventions. This final step draws upon the HAPA model to investigate: (1)
changes in knowledge and related theoretical constructs (i.e., self-efficacy, outcomes
expectancies, risk awareness, intention, and planning) among CR patients following participation
in one of two educational programs; and, (2) the theoretical correlates of exercise behavior
change among CR patients receiving educational interventions. This quasi-experimental study

175
assessed CR patients before and after exposure to an existing or new HAPA and evidence-based
education curriculum. Patients were allocated to an educational program based on their
preferences of time and day of the week, not knowing which type of education they would be
receiving. Consenting patients were invited to complete a self-administered survey assessing
sociodemographic characteristics, and including scales to assess exercise and HAPA constructs
(e.g., self-efficacy, outcome expectancies, risk awareness, intention, and planning), and
knowledge, namely the Coronary Artery Disease Education Questionnaire II (CADE-Q II).
Clinical data were extracted from charts. In the last weeks of their 6 month program, patients
were asked to complete a similar post-test survey. Three hundred and six patients consented to
participate, of which 146 (47.7%) were exposed to the new educational curriculum. There was a
significant improvement in patients’ overall knowledge from pre- to post-CR regardless of
curriculum (p<.001). With regard to the HAPA constructs, significant increases in risk
awareness, psychological and physical outcomes expectancies, task self-efficacy, and action and
coping planning were observed (p<0.05), regardless of curriculum. With regard to objective 2,
participants reported a significant increase in exercise from pre- to post-CR, again regardless of
curriculum. Path analysis revealed that knowledge was a significant motivational construct
leading to intention formation, and intentions to engage in physical activity were not directly
related to behavior, needing especially action planning, which was related to self-efficacy. In
conclusion this step showed that educational interventions in CR effectively improve knowledge,
change HAPA constructs and enhance physical exercise. Educational strategies are needed for
cardiac patients not only to increase knowledge but also enhance intentions, self-efficacy, and
action planning.
176
2 General Discussion
Patient education is a core component of CR (Buckley et al., 2013). Thus, Canadian
Cardiovascular Societies include education as a quality indicator of this practice (Grace et al.,
2014). According to the Guidelines of the Canadian Association of Cardiac Rehabilitation
(CACR; Stone et al., 2009) patient education should: be personalized; be led by a professional
staff, with regular contact between staff and patients; be delivered in individual or group settings;
discuss specific health goals; and seek to influence health beliefs, to elicit positive emotions, to
increase optimism about the possibility of change, and to heighten the salience of personal
experience or other evidence supporting self-efficacy. In addition, the problem of educating low-
literate patients cannot be ignored: health organizations should provide instruction
understandable to patients, assess patients' knowledge based on their literacy, and document such
educational efforts (Weiss et al., 1995; Williams et al., 1995; Doak, Doak, & Root, 2007). To
achieve this, a coordinated approach to developing an educational curriculum for patient
education is recommended and some “rules” should be followed.
In this thesis I have explored some of these rules, including needs and knowledge assessments,
and the need of CR educational interventions to be theory-driven and to aim behavior change. In
fact, two of our studies (the systematic review and the assessment of behavior determinants)
identify a positive relationship between education and behavior change. The systematic review
(study 1) supports the benefits of educational interventions in CAD, through increases in
patients’ knowledge, physical activity, nutrition behavior and smoking cessation. Furthermore,
the assessment of behavior change in study five showed that participants reported a significant
increase in hours of physical exercise per week from pre- to post-CR, overall and by groups. In
177
addition, the frequency of walking per week increased significantly from pre- to post-CR, again
overall and by groups.
The literature highlights the importance of a comprehensive understanding of patients’ health
information needs as a logical first step in developing and implementing educational programs
(Cranton, 1989; Scott & Thomspon, 2003; Timmins & Kaliszer, 2003). The availability of a
valid needs assessment tool is essential to evaluate the information needs of CR patients and to
tailor the information component of these programs. In this context, the Information Needs in CR
(INCR) scale was developed and psychometrically validated to assess information needs in CR
patients. Furthermore, we’ve also investigated whether CR providers are cognizant of patient’s
information needs using the INCR tool. Results showed that CR patients desire information in
many areas, particularly regarding emergency/safety and diagnosis/treatment, and that CR
providers are highly cognizant of patient information needs. However, patients’ information
needs change over time and healthcare providers should be aware of these change and
accurately-perceive patients’ needs in order to have engaged and informed patients, which can
positively impact their health outcomes (Karlik & Yarchesk, 1987; Hagenhoff et al., 1994; Ghisi
et al., 2014b).
In order to plan and deliver an effective CR educational intervention, it is important to have
precise information of what cardiac patients know about their condition (Kayaniyil et al., 2009;
Brown et al., 2011). Patients’ knowledge of heart disease can strongly influence symptom
recognition, advocacy for physician screening, attitude towards the disease, and provide
motivational for individual behaviour changes. In this context, the Coronary Artery Disease
Education Questionnaire (CADE-Q) was previously developed and psychometrically validated
to assess patients’ knowledge about CAD in a Portuguese speaking population of CR patients in

178
Brazil (Ghisi et al., 2010). It was later translated, cross-culturally adapted, and psychometrically
validated to English (de Melo Ghisi et al., 2013). It has also being used to compare knowledge
between a developed and a developing country (Ghisi et al., 2013b). Although both versions
demonstrated good reliability and validity, the CADE-Q presented lack of detailed assessment of
all core components of cardiac rehabilitation (CR), such as nutrition and psychosocial risk.
Therefore, a new version – CADE-Q II – was developed and psychometrically tested in this
thesis.
According to literature and guidelines, health education should be delivered not only to increase
patients’ knowledge but to also achieve health behavior change (Mullen et al., 1992; Dusseldorp
et al., 1999; Aldcroft et al., 2011, Schadewaldt & Schultz, 2011; Ghisi et al., 2014a). A number
of studies have shown that using theory in crafting interventions can lead to more powerful
effects than interventions developed without theory (Ammerman et al., 2002; Legler et al., 2002;
Glanz et al., 2008). In the context of patient education, theories can provide us with a workable
basis for an education action we wish to undertake. This is especially important when teaching
patients whose educational needs are less predictable or more diverse (Laverack, 2004; Doak,
Doak, & Root, 2007). Theories such as the HAPA model (Schwarzer, 1992; Schwarzer, Lippke,
& Luszynska, 2011), social cognitive theory (Bandura, 1986), and adult learning principles
(Knowles, 1978; 1980; 1984) are examples of useful theories that may be incorporated in
educational interventions to CR patients. In particular, the use of HAPA framework for
predicting physical exercise change after a comprehensive educational intervention in cardiac
rehabilitation patients was tested in Study 5, and results reinforce the use of HAPA model as an
important theory to guide development, delivery and assessment of patient education strategies.

179
Finally, it is important to describe how the term patient education was used throughout my
thesis. As described previously, patient education is defined as the process by which health
professionals or others impart information to patients with the purpose to improve their
knowledge, and consequently promote behavior change or improve outcomes. Although many of
the educational efforts described in my thesis incorporated strategies derived from psychosocial
and psycho-educational interventions (i.e. education offered to individuals to help empower them
and deal with a certain condition in an optimal way) I’ve decided to use the term patient
education because this is the term used in cardiac rehabilitation guidelines as a core component
and usually in clinical practice. I see psycho-education as a subtype of patient education, and in
my opinion patient education is a broader concept which involves not only social and
psychological aspects, but also learning principles and knowledge. Psychosocial or psycho-
educational interventions may affect rehabilitation outcomes in two ways. First, they can
facilitate psychosocial recovery, including the patient's return to everyday activities. Second,
they can play an important role in secondary prevention, by encouraging compliance with
medical advice and behavior change related to risk factor modification. Most interventions of the
first type can be characterized as stress management (SM) programs, and interventions of the
second type focus on behavior modification and health education (HE). Patient education can
incorporate these strategies but is a broader term, reflecting all types of learning that leads to
behavior change (increase in knowledge regarding different topics) (Dusseldorp et al., 1999).
Both patient education and psychosocial interventions may influence mediators. Studies should
be performed to find a way to usefully distinguish the two interventions.

180
3 Limitations
Caution is warranted when interpreting results from this thesis. Limitations from each study are
described in each chapter. Overall, the generalizability of these findings to other CR populations
is somewhat limited, considering recruitment stemmed from a single-centre, which has a strong
educational component in CR programs (impact of setting on findings and generalizability is
warranted). Results from these studies were not compared to people that do not attend formal CR
or populations, such as patients with low general or health literacy. I limited my studies to those
of the coronary artery disease population, which may have eliminated unique methods that could
be conducted in other populations such as patients with heart failure. Replication is warranted.
In regards to the instruments used to assess HAPA construct at study 5, HAPA creator
recommends these instruments; however, only partial descriptions of the methods used to
develop these tools are available.
4 Implications and Future Directions
Results from all 5 papers are valuable in the area of patient education in CR. Firstly, the weight
of evidence in the systematic review suggests the need for comprehensive multidisciplinary
education programs offered in-hospital and post-discharge, through individual and group
educational activities delivered in discursive rather than didactic fashion. Ensuring CAD patient
access to comprehensive, evidence-based and education programs may optimize the benefits
observed in relation to physical activity, diet and smoking cessation. Furthermore, this review
suggested that there was a need for valid and reliable tools to assess patients’ knowledge, since
few studies assess this measure. This gap was addressed in chapter 6, in which a new tool to

181
assess CR patients’ knowledge was developed and tested. Secondly, this thesis showed that good
patient education involves assessing needs, setting goals and objectives, implementing a teaching
plan, and evaluating outcomes. Before implementing patient education programs, it is prudent to
evaluate what information is needed and what patients know about their condition. The
availability of valid tools (such as the INCR and CADE-Q II) is essential to not only evaluate
these measures, but to tailor educational programs. Thus, these tools can be administered to
determine whether patients have changed their information needs or learned the information they
perceived as important. Furthermore, the identification of needs using an instrument like the
INCR could serve as a mechanism for understanding patient information gaps. CR staff could
use the INCR to assess the comprehensiveness of their education programming, and to consider
whether the main focus of their programming relates to the key information needs of patients at
different stages of the program. Programs should also consider whether the delivery format of
their education program is concordant with patient preferences. Finally, innovative educational
strategies are needed not only to increase knowledge but also enhance intentions, self-efficacy,
and action planning. This included the provision of education and skill training for CVD
prevention based on a better understanding of the individuals’ social and cultural characteristics.
Of the current health promotion models, the HAPA model appears to hold the most promise in
predicting health-related outcomes and informing subsequent interventions. It possesses an
integrative framework that addresses the variables associated with motivation, intention, and
action toward engaging in health-promoting behaviors (Schwarzer et al., 2011). In regards this
model, results from this dissertation support the usefulness of this model for prediction of
behavior change in CR patients. Although testing the HAPA model was not an objective of the
fifth study, results showed that the distinction of preintentional and intentional stages was
confirmed (principles 1 and 2 of the theory), as well as the importance of action planning to

182
change exercise behavior in this population. Results also showed that CR patients require
educational interventions targeting specific HAPA-constructs (e.g. intentions, action planning).
Future directions include: assess educational needs, knowledge and behavior determinants in
multicultural settings, and compare these measures to those who are not in CR programs or are in
non-comprehensive CR programs. In addition, due to the lack of evidence demonstrating benefit
of comprehensive CR programs in lower-resource settings future directions will include the
investigation of whether participation in educational programs CR in middle-income countries
results in better disease-related knowledge, behavior determinants and behavior in cardiac
patients when compared to usual care. A single-blinded pragmatic RCT with 3 parallel arms:
comprehensive CR vs. usual care vs. control group (no CR) is planned to occur in Brazil, where
CVDs are also a leading cause of death and responsible for 29% of total mortality in 2010
(approximately 37,000 deaths/year) (Brazil, 2010). Considering that most of these deaths occur
prematurely, the economic impact is devastating. To lessen the impact of CVDs on individuals
and societies, a comprehensive approach is needed.
In addition, future research should focus on developing guidelines on patient education for
special cardiac populations (e.g. low health literacy subjects, older patients, patients with
psychological impairments). As described in my thesis, guidelines usually mention that patient
education should be designed based on the characteristics of the recipients (including special
populations); however, there is no data to guide on how this education should be structured,
delivered, tested and which outcomes should be evaluated. Another future research direction
might focus on cost-effectiveness of comprehensive cardiac rehabilitation. Including patient
education in cardiac rehabilitation programs involves time, training, efforts and, consequently,
money. Although studies have shown that cardiac rehabilitation is more cost-effective than other

183
post-MI treatments (Ades, Pashkow & Nestor, 1997; Briffa et al., 2005) (e.g. thrombolytic
therapy, coronary bypass surgery and cholesterol lowering drugs), there are no studies comparing
cardiac rehabilitation programs versus comprehensive cardiac rehabilitation programs (i.e. with a
structured education intervention).
184
References
Ades, P.A., Pashkow, F.J., Nestor, J.R. (1997) . Cost-effectiveness of cardiac rehabilitation after
myocardial infarction. Journal of Cardiopulmonary Rehabilitation and Prevention, 17,
222-231.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision
Processes, 50, 179–211.
Aldcroft, S. A., Taylor, N. F., Blackstock, F. C., & O’Halloran, P. D. (2011) . Psychoeducational
rehabilitation for health behavior change in coronary artery disease: a systematic review of
controlled trials. Journal of Cardiopulmonary Rehabilitation and Prevention, 31, 273-281.
Alm-Roijer, C., Fridlund, B., Stagmo, M., & Erhardt, L. (2006) . Knowing your risk factors for
coronary heart disease improves adherence to advice on lifestyle changes and medication.
Journal of Cardiovascular Nursing, 21, E24-E31.
Altman, D. G. (1991) . Practical statistics for medical research. London: Chapman and Hall.
Ammerman, A. S., Lindquist, C. H., Lohr, K. N., & Hersey, J. (2002) . The efficacy of behavioral
interventions to modify dietary fat and fruit and vegetable intake: A review of the
evidence. Preventive Medicine, 35, 25-41.
Arbuckle, J.L. (2011) . Amos (version 20.0). Chicago: SPSS.
Arora, N., & McHorney, C. (2000). Patient preferences for medical decision making: who really
wants to participate? Medical Care, 38, 335-341.

185
Ashton, K. C. (1997) . Perceived learning needs of men and women after myocardial infarction.
Journal of Cardiovascular Nursing, 12, 93-100.
Astin, F., Closs, S. J., McLenachan, J., Hunter, S., & Priestley, C. (2008) . The information needs of
patients treated with primary angioplasty for heart attack: an exploratory study. Patient
Education and Counseling, 73, 325-332.
Bandura, A. (1986) . Social foundations of thought and action: A social cognitive theory. Englewood
Cliffs, New Jersey: Prentice-Hall.
Bandura A. (1997). Self-efficacy: The exercise of control. (pp. 24; 415-420). New York: Freeman.
Bandura, A. (2002) . Social cognitive theory in cultural context. Journal of Applied Psychology, 51,
269-290.
Bandura, A. (2004) . Health promotion by social cognitive means. Health Education & Behavior, 31,
143-164.
Baranowski, T., Lin, L. S., Wetter, D. W., Resnicow, K., & Davis, M. (1997) . Theory as mediating
variables: why aren’t community interventions working as desired? Annals of
Epidemiology, 7, 589-595.
Baranowski, T., Anderson, C., & Carmack, C. (1998) . Mediating variable framework in physical
activity interventions: How are we doing? How might we do better? American Journal of
Preventive Medicine, 15, 266-297.
Baron, R. M., & Kenny, D.A. (1986) . The moderator-mediator variable distinction in social
psychological research: conceptual, strategic, and statistical considerations. Journal of
Personality and Social Psychology, 51, 1173-1182.

186
Bellman, C., Hambraeus, K., Lindback, J., & Lindahl, B. (2009) . Achievement of secondary
prevention goals after myocardial infarction: A comparison between participants and
nonparticipants in a routine patient education program in Sweden. Journal of
Cardiovascular Nursing, 24(5), 362-368.
Berra, K., Miller, N.H., & Jenning, C. (2011) . Nurse-based models for cardiovascular disease
prevention: From research to clinical practice. European Journal of Cardiovascular
Nursing, 10, S42-S50.
Berckman, N.D., Sheridan, S.L., Donahue, K.E., Halpern, D.J., & Crotty, K. (2011) . Low health
literacy and health outcomes: an updated systematic review. Annals of Internal Medicine,
155, 97-107.
Betancourt, J. R., & Quinlan, J. (2007) . Personal responsibility versus responsible option: Health
care, community health promotion, and the battle against chronic disease. Preventing
Chronic Disease: Public Health Research, Practice and Policy, 4, A41.
Blair, S.N., Kohl, H.W., Barlow C.E., Paffenbarger, R.S., Gibbons, L.W., & Macera, C.A. (1995) .
Changes in physical fitness and all-cause mortality. A prospective study of healthy and
unhealthy men. Journal of the American Medical Association, 273, 1093-1098.
Blanchard, C. M., Courneya, K. S., Rodgers, W. M., Fraser, S. N., Murray, T. C., Daub, B., & Black,
B. (2003). Is the theory of planned behavior a useful framework for understanding exercise
adherence during phase II cardiac rehabilitation? Journal of Cardiopulmonary
Rehabilitation, 23, 29-39.

187
Blyth, F., Lazarus, R., Ross, D., Price, M., Cheuk, G., & Leeder, S. (1997) . Burden and outcomes of
hospitalization for congestive heart failure. Medical Journal of Australia, 157, 99-104.
Bolman, C., Brug, J., Bar, F., Martinali, J., & Borne, B. (2005) . Long-term efficacy of a checklist to
improve patient education in cardiology. Patient Education and Counseling, 56, 240-248.
Boyde, M., Turner, C., Thompson, D. R., & Stewart, S. (2011) . Educational interventions for
patients with heart failure: a systematic review of randomized controlled trials. Journal of
Cardiovascular Nursing, 26(4), E27-E35.
Brazil, Ministerio da Saude (2010). Sistema de Informações de Mortalidade (SIM) e IBGE. Retrieved
from: http//tabnet.datasus.gov.br/CGI/idb2006/matriz.htm
Briffa, T.G., Eckermann, S.D., Griffiths, A.D., Harris, P.J., Health, M.R., Freedman, S.B., … Keech,
A.C. (2005). Cost-effectiveness of rehabilitation after an acute coronary event: a
randomised controlled trial. Medical Journal of Australia, 183, 450-455.
British Association for Cardiovascular Prevention and Rehabilitation (2012). The BACPR standards
and core components for cardiovascular disease prevention and rehabilitation, 2nd edition.
Retrieved from: http://www.bacpr.com/resources/15E_BACPR_Standards_FINAL.pdf
Brezynskie, H., Pendon, E., Lindsay, P., & Adam, M. (1998) . Identification of the perceived learning
needs of balloon angioplasty patients. Canadian Journal of Cardiovascular Nursing, 9, 8-
14.
Brown, J. P. R., Clark, A. M., Dalal, H., Welch, K., & Taylor, R. S. (2011) . Effect of patient
education in the management of coronary heart disease: a systematic review and meta-

188
analysis of randomized controlled trials. Cochrane Database of Systematic Reviews, (12):
CD008895.
Brown, S.A. (1992) . Meta-analysis of diabetes patient education research: variations in intervention,
effects across studies. Research in Nursing & Health, 15, 409-19.
Brundage, D., & Mackeracher, D. (1980) . Adult Learning Principles and their Application to
Prgram Planning. Toronto: Ontario Institute for Studies in Education.
Bubela, N., Galloway, S., McCay, E., McKibbon, A., Nagle, L., Pringle, D., ... Shamian, J. (1990) .
The Patient Learning Needs Scale: reliability and validity. Journal of Advanced Nursing,
15, 1181-1187.
Buckley, T., McKinley, S., Gallagher, R., Dracup, K., Moser, D.K., & Aitken, L.M. (2007) . The
effect of education and counselling on knowledge, attitudes and beliefs about responses to
acute myocardial infarction symptoms. European Journal of Cardiovascular Nursing, 6,
105–11.
Buckley, J.P., Furze, G., Doherly, P., Speck, L., Connolly, S., Hinton, S., & Jones, J.L. (2013) .
BACPR scientific statement: British standards and core components for cardiovascular
disease prevention and rehabilitation. Heart, 99:1069-1071.
Burns-Gibson, S., & Koso, C. (2010) Developing cultural competence: caring for our diverse
community. Rehab Magazine, (winter edition), 24-25.
Cameron, J.I., & Gignac, M.A. (2008) . “Timing It Right”: a conceptual framework for addressing
the support needs of family caregivers to stroke survivors from the hospital to the home.
Patient Education and Counseling, 70, 305-314.

189
Campbell, N., Ritchie, L., Thain, J., Deans, H., Rawles, J., & Squair, J. (1998) . Secondary
prevention in coronary heart disease: a randomised trial of nurse led clinics in primary
care. Heart, 80, 447-452.
Canadian Cardiovascular Society. (2013) . The Canadian Cardiovascular Society quality indicators
e-catalogue: quality indicators for cardiac rehabilitation and secondary prevention.
Retrieved from: http://ddqi.ccs.ca/index.php/quality-indicators/cardiac-rehabilitation-
secondary-prevention-quality-indicators-chapter
Cardiac Care Network. (2002) . The Ontario cardiac rehabilitation pilot project: Report and
recommendations. Retrieved from: http://hdl.handle.net/1873/4971
Carlson, B. A., Neal, D., Magwood, G., Jenkins, C., King, M. G., Hossler, C. L. (2006) . A
community-based participatory health information needs assessment to help eliminate
diabetes information disparities. Health Promotion Practice, 7, 213S-222S.
Carlson, J.J., Norman, G.J., Feltz, D.L., Franklin, B.A., Johnson, J.A., & Locke, S.K. (2001) . Self-
efficacy, psychosocial factors, and exercise behavior in traditional versus modified cardiac
rehabilitation. Journal of Cardiopulmonary Rehabilitation, 21, 363–373.
Casey, E., O’Connel, J. K., & Price, J. H. (1984) . Perceptions of educational needs for patients after
myocardial infarction. Patient Education and Counseling, 6, 77-82.
Caudroit, J., Stephen, Y., & Le Scanff, C. (2011) . Social cognitive determinants of physical activity
among retired older individuals: an application of the health action process approach.
British Journal of Health Psychology, 16, 404-417.

190
Chan, S.S., Leung, D.Y., Wong, D.C., Lau, C.P., Wong, V.T., & Lam, T.H. (2012) . A randomized
controlled trial of stage-matched intervention for smoking cessation in cardiac-outpatients.
Addiction, 107, 829-837.
Chan, V. (1990) . Content areas for cardiac teaching: patients' perceptions of the importance of
teaching content after myocardial infarction. Journal of Advanced Nursing, 15, 1139-1145.
Chin, M. H., & Goldman, L. (1997) . Factors contributing to the hospitalization of patients with
congestive heart failure. American Journal of Public Health, 87, 643–648.
Clark, A. M., Hartling, L., Vandermeer, B. & McAlister, F.A. (2005) . Meta-analysis: Secondary
prevention programs for patients with coronary artery disease. Annals of Internal Medicine,
143(9), 659–672.
Clark, N. M., Becker, M. H., Janz, N. K., Lorig, K., Rakowski, W., Anderson, L. (1991) . Self-
management of chronic disease by older adults: A review and questions for research.
Journal of Aging and Health, 3, 3-27.
Clark, N. M., Janz, N. K., Becker, M. H., Schork, M. A., Wheeler, J., Liang, J., ... Santinga, J. T.
(1992) . Impact of self-management education on the functional health status of older
adults with heart disease. Gerontologist, 32, 438-443.
Cole, M., & Griffin, P. (1987) . Contextual factors in education. Madison: Wisconsin Center for
Educational Research.
Conner, M. (2008). Initiation and maintenance of health behaviors. Applied Psychology, 57, 42–50.

191
Cordasco, K.M., Asch, S.M., Bell, D.S., Guterman, J.J., Gross-Schulman, S., Ramer, L., ...
Mangione, C.M. (2009) . A low-literacy medication education tool for safety-net hospital
patients. American Journal of Preventive Medicine, 37, S209–S216.
Cranton, P. (1989) . Planning instruction for adult learners. Toronto: Wall and Emerson.
Czar, M. L., & Engler, M. M. (1997) . Perceived learning needs of patients with coronary artery
disease using a questionnaire assessment tool. Heart & Lung, 26, 109-117.
Daly, J., Sindone, A.P., Thompson, D.R., Hancock, K., Chang, E., & Davidson, P. (2002) . Barriers
to participation in and adherence to cardiac rehabilitation programs: a critical literature
review. Progress in Cardiovascular Nursing, 17, 8-17.
Davidson, P., Digiacomo, M., Zecchin, R., Clarke, M., Paul, G., Lamb, K., ... Daly, J. (2008) . A
cardiac rehabilitation program to improve psychosocial outcomes of women with heart
disease. Journal of Womens Health, 17, 123–134.
De Busk, R. F., Miller, N. H., Superko, H. R., Dennis, C. A., Thomas, R. J., Lew, H. T., … Taylor,
C. B. (1994). A case-management system for coronary risk factor modification. Annals of
Internal Medicine, 120, 721-729.
Decker, C., Garavalia, L., Chen, C., Buchanan, D. M., Nugent, K., Shipman, A., & Spertus, J.A.
(2007) . Acute myocardial infarction patient’s information needs over the course of
treatment and recovery. Journal of Cardiovascular Nursing, 22, 459-465.
Degner, L., & Sloan, J. (1992) . Decision making during serious illness: what role do patients really
want to play? Journal of Clinical Epidemiology, 45, 941-950.

192
De Melo Ghisi, G. L. M., Oh, P., Thomas, S., & Benetti, M. (2013) . Development and validation of
an English version of the Coronary Artery Disease Education Questionnaire (CADE-Q).
European Journal of Preventive Cardiology, 20(2), 291-300.
DeVon, H.A., Rankin, S.H., Paul, S.M., & Ochs, A.L. (2010) . The Know & Go! Program improves
knowledge for patients with coronary heart disease in pilot testing. Heart & Lung, 39, S23-
S33.
DeWalt, D. A., Malone, R. M., Bryant, M. E., Kosnar, M. C., Corr, K. E., Rothman, R. L., et al.
(2006) . A heart failure self-management program for patients of all literacy levels: a
randomized, controlled trial. BMC Health Services Research, 6, 30.
Dewey, J. (1916). Education and Democracy. New York: McMilliam.
Dewey, J. (1938). Experience and Education. London: Collier McMilliam.
Dickson, V. A., Tkas, N., & Riegel, B. (2008) . Social cognitive influences on self-care decision
making in persons with heart failure. American Heart Journal, 154, 424-431.
Ding, L., Velicer, W. F., & Harlow, L.L. (1995). Effects of estimation methods, number indicators
per factor, and improper solutions on structural equation modeling fit indices. Structural
Equation Modeling: A Multidisciplinary Journal, 2, 119-144.
Dishman, R.K., Motl, R.W., Saunders, R., Felton, G., Ward, D.S., …, Pate, R.R. (2004) . Self-
efficacy partially mediates the effect of a school-based physical activity intervention
among adolescent girls. Preventive Medicine, 38, 628-636.
Doak, C. C., Doak, L. G., & Root, J. H. (2007) . Teaching patients with low literacy skills (2nd ed).
Philadelphia: JB Lippincott.

193
Downs, S.H., & Black, N. (1998) . The feasibility of creating a checklist for the assessment of the
methodological quality both of randomised and non-randomised studies of health care
interventions. Journal of Epidemiology & Community Health, 52, 377-384.
Dracup, K., Meleis, A.I., Clark, S., Clyburn, A., Shields, L., & Staley, M. (1984) . Group counseling
in cardiac rehabilitation: effect on patient compliance. Patient Education and Counseling,
6, 169–177.
Dracup, K., & Moser, D.K. (1997) . Beyond sociodemographics: factors influencing the decision to
seek treatment for symptoms of acute myocardial infarction. Heart & Lung, 26, 253-262.
Dunn, D. S., & Elliott, T. R. (2008). The place and promise of theory in rehabilitation psychology
research. Rehabilitation Psychology, 53, 254–267.
Dusseldorp, E., van Elderen, T., Maes, S., Meulman, J., & Kraaij, V. (1999) . A meta-analysis of
psycho-educational programs for coronary heart disease. Health Psychology, 18, 506-519.
Eastern Region Community College. (2012) . ABC Curriculum Resources Framework. Retrieved
from: http://www.gototheexchange.ca/index.php/curriculum-resources-home
Eckman, M.H., Wise, R., Leonard, A.C., Dixon, E., Burrows, C., Khan, F., & Warm, E. (2012) .
Impact of health literacy on outcomes and effectiveness of an educational intervention in
patients with chronic diseases. Patient Education and Counseling, 87, 143–151.
Egan, F. (1999) . Cardiac rehabilitation into the new millennium. Intensive and Critical Care
Nursing, 15, 163-168.
Fawcett, J., Watson, J., Neuman, B., Walker, P.H., & Fitzpatrick, J.J. (2001) . Nursing Theories and
Evidence. Journal of Nursing Scholarship, 33, 115–119.

194
Feldman, J. J., Makuc, D. M., Kleinman, J. C., & Cornoni-Huntley, J. (1989) . National trends in
educational differentials in mortality. American Journal of Epidemiology,129, 919–933.
Fiscella, K., & Tancredi, D. (2008) . Socioeconomic status and coronary heart disease risk prediction.
Journal of American Medical Association, 300, 2666-2668.
Fletcher, G.F. (1986) . Rehabilitation after coronary angioplasty--is it effective? Archives of Physical
Medicine and Rehabilitation, 67, 517–519.
Frame, C.J., Green, C.G., Herr, D.G., Taylor, M.L. (2003) . A 2-year stage of change evaluation of
dietary fat and fruit and vegetable intake behaviors of cardiac rehabilitation patients.
American Journal of Health Promotion, 17, 361–368.
Freire, P. (1973). Education for Critical Consciousness. London: Sheed and Ward.
Froger-Bompas, C., Laviolle, B., Guillo, P., Letellier, C., Ligier, K., Daubert, J.C., & Paillard, F.
(2009) . Sustained positive impact of a coronary rehabilitation programme on adherence to
dietary recommendations. Archives of Cardiovascular Disease, 102, 97–104.
Furze, G., Roebuck, A., Bull, P., Lewin, R. J. P., & Thompson, D. R. (2002). A comparison of illness
beliefs of patients with angina and their peers: a questionnaire study. BMC Cardiovascular
Disorders, 2(4),1-5.
Gagné, R.M. (1977). The Conditions of learning. New York: Holt, Rinehart and Winston.
Gazmararian, J. A., Williams, M. V., Peel, J., & Baker, D. W. (2003) . Health literacy and knowledge
of chronic disease. Patient Education and Counseling, 51, 267-275.

195
Gerard, P.S., & Peterson, L.M. (1984) . Learning needs of cardiac patients. Cardiovascular Nursing,
20, 7-11.
Ghisi, G. L. M., Durieux, A., Manfroi, W. C., Herdy, A. H., Carvalho, T., Andrade, A., & Benetti,
M. (2010) . Construction and validation of the CADE-Q for patient education in cardiac
rehabilitation programs. Brazilian Archives of Cardiology, 94(6), 813-822.
Ghisi, G.L., Grace, S.L., Thomas, S., Evans, M.F., & Oh, P. (2013a) . Development and
psychometric validation of a scale to assess information needs in cardiac rehabilitation:
The INCR Tool. Patient Education and Counseling, 91, 337-343.
Ghisi, G.L., Oh, P., Thomas, S., & Benetti. M. (2013b) . Assessment of patient knowledge of cardiac
rehabilitation: Brasil vs Canada. Brazilian Archives of Cardiology, 101, 255-262.
Ghisi, G.L.M., Abdallah, F., Grace, S.L., Thomas, S., & Oh, P. (2014a) . A systematic review of
patient education in cardiac patients: Do they increase knowledge and promote health
behavior change? Patient Education and Counseling, 95, 160-174.
Ghisi, G.L.M., Grace, S.L., Thomas, S., Evans, M.F., & Oh, P. (2014b) . Healthcare providers'
awareness of the information needs of their cardiac rehabilitation patients throughout the
program continuum. Patient Education and Counseling, 95, 143-150.
Ghisi, G.L.M, Grace, S.L., Thomas, S., Evans, M.F., & Oh, P. (2014c) . Development and
psychometric validation of the second version of the Coronary Artery Disease Education
Questionnaire (CADE-Q II). Article under review.
Giannuzzi, P., Temporelli, P.L., Marchioli, R., Maggioni, A.P., Balestroni, G., Ceci, V., ... Vanuzzo,
D. (2008) . Global secondary prevention strategies to limit event recurrence after

196
myocardial infarction: results of the GOSPEL study, a multicenter, randomized controlled
trial from the Italian Cardiac Rehabilitation Network. Archives of Internal Medicine, 168,
2194-2204.
Glanz, K., Rimer, B. K., & Viswanath, K. (2008) . Health behavior and health education: theory,
research, and practice. Danvers, MA: Josey-Bass.
Globle, A.J., & Worcester, M.U.C. (1999) . Best practice guidelines for cardiac rehabilitation and
secondary prevention. Retrieved from: www.health.vic.gov.au/
nhpa/downloads/bestintr.pdf
Goodman, H. (1997) . Patients’ perceptions of their education needs in the first six weeks following
discharge after cardiac surgery. Journal of Advanced Nursing, 25, 1241-1251.
Grace, S.L., Gravely-Witte, S., Brual, J., Monette, G., Suskin, N., Higginson, L., ... Stewart, D.E.
(2008) . Contribution of patient and physiciam factors to cardiac rehabilitation enrollment:
a prospective multilevel study. European Journal of Cardiovascular Prevention and
Rehabilitation, 15, 548-556.
Grace, S.L., Poirier, P., Norris, C.M., Oakes, G.H., Somanader, D., & Suskin, N. (2014) . Pan-
Canadian development of cardiac rehabilitation and secondary prevention quality
indicators. Canadian Journal of Cardiology. In press.
Greenhalgh, T. (2000) . Changes and the individual 1: Adult Learning Theory. The British Journal of
General Practice, 50, 76-77.

197
Hagenhoff, B.D., Feutz, C., Conn, V.S., Sagehom, K.K., & Moranville-Hunziker, M. (1994) . Patient
education needs as reported by congestive heart failure patients and their nurses. Journal of
Advanced Nursing, 19, 685-690.
Hair, J. F., & Anderson, R. E. (1998) . Multivariate data analysis. New Jersey: Prentice Hall.
Harden, R., Crosby, J., & Davis, M. (1991) . Outcome based education: part 1—an introduction to
outcomes-based education. Medical Teacher, 21, 7-14.
Harris, R. P., Helfand, M., Woolf, S. H., Lohr, K. N., Mulrow, C. D., Teutsch, S. M., & Athinks, D.
(2001) . Current methods of the US Preventive Services Task Force: a review of the
process. American Journal of Preventive Medicine, 20, 21-35.
Haskell, W. L., Alderman, E. L., Fair, J. M., Maron, D. J., Mackey, S. F., Superko, H. R., ... Krauss,
R. M. (1994) . Effects of intensive multiple risk factor reduction on coronary
atherosclerosis and clinical cardiac events in men and women with coronary artery disease.
Circulation, 89, 975-990.
Heckhausen, H., & Gollwitzer, P.M. (1987) . Thought contents and cognitive functioning in
motivational versus volitional states of mind. Motivation and Emotion, 11, 101-120.
Heidal, K.B., Lewis, N.M., Evans, S.M., & Boeckner, L. (2007) . Nutrition education intervention
increases total -3 fatty acid intakes in heart patients living in the Midwest. Nutrition
Research, 27, 33–37.
Heran, B. S., Chen, J. M., Ebrahim, S., Moxham, T., Oldridge, N., Rees, K., ... Taylor, R.S. (2011) .
Exercise-based cardiac rehabilitation for coronary artery disease. Cochrane Database of
Systematic Reviews, (7), CD001800.

198
Hochbaum, G. M., Sorenson, J. R., & Lorig, K. (1992) . Theory in health education practice. Health
Education Quartely, 19, 295-313.
Horlick, L., Cameron, R., Firor, W., Bhalerao, U., & Baltzan, R. (1984) . The effects of education
and group discussion in the post myocardial infarction patient. Journal of Psychosomatic
Research, 28, 485-492.
Hu, L., & Bentler, P.M. (1999) . Cutoff criteria for fit indexes in covariance structure analysis:
Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-55.
Hughes, M. (2000) . An instrument to assist nurses identify patients’ self perceived information needs
post myocardial infarction. Ireland Journal of Nursing Midwifery, 1, 13-17.
IBM Corp. (2012) . IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.
Irmak, Z., & Fesci, H. (2010) . Effects of nurse-managed secondary prevention program on lifestyle
and risk factors of patients who had experienced myocardial infarction. Applied Nursing
Research, 23, 147–152.
Jackson, C., Fortmann, S.P., Flora, J.A., Melton, R.J., Snider, J.P., & Littlefield, D. (1994) . The
capacity-building approach to intervention maintenance implemented by the Stanford five-
city project. Health Education Research, 9, 385–396.
Jackson, L., Leclerc, J., Erskine, Y., & Linden, W. (2005) . Getting the most out of cardiac
rehabilitation: A review of referral and adherence predictors. Heart, 91, 10-14.
Janz, N.K., & Becker, M.H. (1984) . The health belief model: a decade later. Health Education, 11,
1-47.

199
Jensen, L. (2003) . Self-administered cardiac medication program evaluation. Canadian Journal of
Cardiovascular Nursing, 13, 35–44.
Jeong, H.S., Chae, J.S., Moon, J.S., & Yoo, Y.S. (2002) . An individualized teaching program for
atherosclerotic risk factor reduction in patients with myocardial infarction. Yonsei Medical
Journal, 43, 93–100.
Jiang, X., Sit, J.W., & Wong, T.K. (2007) . A nurse-led cardiac rehabilitation programme improves
health behaviours and cardiac physiological risk parameters: Evidence from Chengdu,
China. Journal of Clinical Nursing, 16, 1886–1897.
Jolliffe, J. A., Rees, K., Taylor, R. S., Thompson, D., Oldridge, N., Ebrahim, S. (2000) . Exercise-
based rehabilitation for coronary heart disease. Cochrane Database Systematic Review, (4):
CD001800.
Jordan, J.E., & Osborne, R.H. (2007) . Chronic disease self-management education programs:
challenges ahead. Medical Journal of Australia, 186, 84-87.
Kaiser, H.F. (1960) . The application of electronic computers to factor analysis. Educational and
Psychological Measurement, 20, 141-151.
Kaplan, G. A., & Keil, J. E. (1993) . Socioeconomic factors and cardiovascular disease: a review of
the literature. Circulation, 88, 1973–1998.
Karlik, B.A., & Yarcheski, A. (1987) . Learning needs of cardiac patients: A partial replication study.
Heart & Lung, 16, 544-551.
Karner, A., Goransoon, A., & Bergdahl, B. (2003) . Patients’ conceptions of coronary heart disease a
phenomenographic analysis. Scandinavian Journal of Caring Sciences, 17(1), 43-50.

200
Kaufman, D. M. (2003). ABC of learning and teaching in medicine: Applying educational theory in
practice. British Medical Journal, 326, 213-216.
Kayaniyil, S., Winstanley, J., Parsons, C., Brister, S., Oh, P., Stewart, D. G., ... Grace S.L. (2009) .
Degree and correlates of cardiac knowledge and awareness among cardiac impatiens.
Patient Education and Counseling, 75, 99-107.
Khan, M.S., Jafary, F.H., Jafar, T.H., Faruqui, A.M., Rasool, S.I., Hatcher, J., & Chaturvedi, N.
(2006) . Knowledge of modifiable risk factors of heart disease among patients with acute
myocardial infarction in Karachi, Pakistan: a cross sectional study. BMC Cardiovascular
Disorders, 6, 18-27.
Kirkland, S.A., MacLean, D.R., Langille, D.B., Joffres, M.R., MacPherson, K.M., & Andreou, P.
(1999) . Knowledge and awareness of risk factors for cardiovascular disease among
Canadians 55 to 74 years of age: results from the Canadian Heart Health Surveys, 1986-
1992. Canadian Medical Association Journal, 161, S10-S14.
Kitzinger, J. (1999) . Introducing focus groups. In: Mays, N., & Pope, C. (Ed.). Qualitative research
in health care (pp.36-45). London: BMJ Publishing Group.
Knowles, M. (1973) . The adult learner: A neglected species. Houston: Gulf Publishing Co.
Knowles, M. S. (1980) . The modern practice of adult education. New York: Association Press.
Knowles, M. S. (1984) . Andragogy in action: applying modern principles of adult learning. San
Francisco: Jossey-Bass.
Koongstvedt, P. (2001) . The managed health care handbook. Gaithersburg: Aspen Publishers.

201
Krannich, J. H., Wevers, P., Lueger, S., Faller, H., Schimmer, C., Deeq, P., ... Leyh, R. (2008) . The
short- and long-term motivational effects of a patient education programme for patients
with coronary artery bypass grafting. Rehabilitation, 47, 219-225.
Kuhn, E. A., Sears, S. F., & Conti, J.B. (2006) . Internet-based behavioral change and psychosocial
care for patients with cardiovascular disease: a review of cardiac disease-specific
applications. Heart Lung, 35, 374-382.
Kummel, M., Vahlberg, T., Ojanlatva, A., Karki, R., Mattila, T., & Kivela, S.L. (2008) . Effects of an
intervention on health behaviors of older coronary artery bypass (CAB) patients. Archives
of Gerontology and Geriatrics, 46, 227–244.
Lainscak, M., Farkas, J., & Jaarasma, T. (2010) . Education, knowledge, and self-management
strategies in patients with chronic heart failure. International Journal of Cardiology, 144,
90-91.
Lam, G., Snow, R., Shaffer, L., La Londe, M., Spencer, K., & Caulin-Glaser, T. (2011) . The effect
of a comprehensive cardiac rehabilitation program on 60-day hospital readmissions after an
acute myocardial infarction. Journal of American College of Cardiology, 57, 597.
Retrieved from http://content.onlinejacc.org/data/Journals/JAC/23261/05974.pdf
Lane, D.S., & Evans, D. (1979). Measures and methods in evaluating patient education programs for
chronic illness. Medical Care, 17, 30-42.
Larson, C. O., Nelson, E. C., Gustafson, D., & Batalden, P. B. (1996) . The relationship between
meeting patients’ information needs and their satisfaction with hospital care and general
health status outcomes. International Journal for Quality in Health Care, 8, 447-456.

202
Laverack, G. (2004). Health promotion practice: Power & empowerment. London: Sage
Publications.
Law, M. R., Watt, H. C., & Wald, N. J. (2002) . The underlying risk of death after myocardial
infarction in the absence of treatment. Archives of Internal Medicine, 162, 2405-2410.
Lawler, P. R., Filion, K. B., & Eisenberg, M. J. (2011) . Efficacy of exercise-based cardiac
rehabilitation post-myocardial infarction: A systematic review and meta-analysis of
randomized controlled trials. American Heart Journal, 162, 571-584.
Lear, S. (2010) . Trial of a cardiac rehabilitation program delivered remotely through the internet
(vCRP). Retrieved from:
http://clinicaltrials.gov/ct2/show/NCT00683813?term=cardiac+rehabilitation&rank=31
NLM Identifier: NCT00683813
Legler, J., Meissner, H. I., Coyne, C., Breen, N., Chollette, V., & Rimer, B. K. (2002). The
effectiveness of interventions to promote mammography among women with historically
lower rates of screening. Cancer, Epidemiology, Biomarkers and Prevention, 11: 58-71.
Leslie, W.S., Hankey, C.R., Matthews, D., Currall, J.E.P., & Lean, M.E.J. (2004) . A transferable
programme of nutritional counselling for rehabilitation following myocardial infarction: a
randomised controlled study. European Journal of Clinical Nutrition, 58, 778–786.
Lidell, E., & Fridlund, B. (1996) . Long-term effects of a comprehensive rehabilitation programme
after myocardial infarction. Scandinavian Journal of Caring Sciences, 10, 67–74.

203
Lile, J. B., Buhmann, J., & Roders, S. (1999) . Development of a learning needs assessment tool for
patients with congestive heart failure. Home Health Care Management & Practice, 11, 11-
25.
Linde, B.J., & Janz, N.M. (1979) . Effect of a teaching program on knowledge and compliance of
cardiac patients. Nursing Research, 28, 282–286.
Lindeman, E. (1926). The meaning of adult education. Montreal: Harvester House.
Lindsay, S., Smith, S., Bellaby, P., & Baker, R. (2009) . The health impact of an online heart disease
support group: a comparison of moderated versus unmoderated support. Health Education
Research, 24, 646–654.
Lippke, S., Ziegelmann, J. P., & Schwarzer, R. (2004). Initiation and maintenance of physical
exercise: Stage-specific effects of a planning intervention. Research in Sports Medicine,
12, 221–240.
Lisspers, J., Hofman-Bang, C., Nordlander, R., Ryden, L., Sundin, O., Ohman, A., & Nygren, A.
(1999) . Multifactorial evaluation of a program for lifestyle behavior change in
rehabilitation and secondary prevention of coronary artery disease. Scandinavian
Cardiovascular Journal, 33, 9–16.
London, F. (2008) . Meeting the challenge: patient education in a diverse America. Journal for
Nurses in Staff Development, 24, 283-285.
Loucks, E.B., Lynch, J.W., Pilote, L., Fuhrer, R., Almeda, N.D., Richard, H., ... Benjamin, E.J.
(2009). Life-course socioeconomic position and incidence of coronary heart disease – The
Framingham Offspring Study. American Journal of Epidemiology, 169, 819-826.
204
Lynch, E.B., Liu, K., Kiefe, C.I., & Greenlan, P. (2006) . Cardiovascular disease risk factor
knowledge in young adults and 10-year change in risk factors: the Coronary Artery Risk
Development in Young Adults (CARDIA) study. American Journal of Epidemiology, 164,
1171-1179.
MacKinnon, D. P. & Dwyer, J. H. (1993) . Estimating mediating effects in prevention
studies. Evaluation Review, 17, 144–158.
Maddux, J.E. (1995). Self-efficacy, adaptation, and adjustment: Theory, research, and application.
New York: Plenum.
Maeland, J. G., & Havik, O. E. (1987) . Measuring cardiac health knowledge. Scandinavian Journal
of Caring Sciences, 1, 23-31.
Mahler, H., & Kulik, J. (1991) . Health care involvement preferences and social-emotional recovery
of male coronary-artery-bypass patients. Journal of Health Psychology, 10, 399-408.
Mansell, D., Poses, R. M., Kazis, L., & Duefield, C. A. (2000). Clinical factors that influence
patients’ desire for participation in decisions about illness. Archives of Internal Medicine,
160, 2991-2996.
Marcuccio, E., Loving, N., Bennett, S. K., & Hayes, S. N. (2003) . A survey of attitudes and
experiences of women with heart disease. Women’s Health Issues, 13, 23-31.
Marshall, J., Penckofer, S., & Llewellyn, J. (1986) . Structured postoperative teaching and knowledge
and compliance of patients who had coronary artery bypass surgery. Heart & Lung, 15,
76–82.

205
Mayou, R.A., Thompson, D.R., Clements, A., Davies, C.H., Goodwin, S.J., Normington, K., ... Price,
J. (2002) . Guideline-based early rehabilitation after myocardial infarction: A pragmatic
randomised controlled trial. Journal of Psychosomatic Research, 52, 89–95.
McKinley, S., Dracup, K., Moser, D.K., Riegel, B., Doering, L.V., Meischke, H., ... Pelter, M. (2009)
. The effect of a short one-on-one nursing intervention on knowledge, attitudes and beliefs
related to response to acute coronary syndrome in people with coronary heart disease: a
randomized controlled trial. International Journal of Nursing Studies, 46, 1037–1046.
McLennan, M., Anderson, G. S., & Pain, K. (1996) . Rehabilitation learning needs: patient and
family perceptions. Patient Education and Counseling, 27, 191-199.
Meischke, H., Kuniyuki, A., Yasui, Y., Bowen, D.J., Andersen, R., & Urban, N. (2002).
Information women receive about heart attacks and how it affects their knowledge, beliefs,
and intentions to act in a cardiac emergency. Health Care Women International, 23, 149-
162.
Meleis, A.I. (1997) . Theoretical Nursing: Development and Progress. Philadelphia: Lippincott.
Mezirow, J. (1981) . A critical theory of adult learning and education. Adult Education Quarterly,
32(1), 3-24.
Mirka, T. (1994) . Meeting the learning needs of post-myocardial infarction patients. Nurse
Education Today, 14, 446-456.
Michie, S., Rumsey, N., Fussell, A., Hardeman, W., Johnston, M., Newman, S., & Yardley, L.
(2008). Improving health: changing behaviour - NHS health trainer handbook. Retrieved
from: http://www.healthcheck.nhs.uk/document.php?o=621

206
Michie, S., Fixsen, D., Grimshaw, J.M., & Eccles, M.P. (2009) . Specifying and reporting complex
behaviour change interventions: the need for a scientific method. Implementation Science,
4, 40-46.
Moore, S.M., & Dolansky, M.A. (2001) . Randomized trial of a home recovery intervention
following coronary artery bypass surgery. Research in Nursing & Health, 24, 93–104.
Monane, M., Bonn, R., Gurwitz, J., Glynn, R., & Avorn, J. (1994) . Noncompliance with congestive
heart failure therapy in the elderly. Archives of Internal Medicine, 154, 433-437.
Moynihan, M. (1984) . Assessing the educational needs of post-myocardial infarction patients.
Nursing Clinics of North America, 19, 441-447.
Moser, D. K., Dracup, K. A., & Marsden, C. (1993) . Needs of recovering cardiac patients and their
spouses: compared views. International Journal of Nursing Studies, 30, 105-114.
Mullen, P.D., Mains, D.A., & Velez, R. (1992) . A meta-analysis of controlled trials of cardiac
patient education. Patient Education and Counseling, 19, 143-162.
Nakano, A., Mainz, J., & Lomborg, K. (2008) . Patient perception and assessment of admission to
acute cardiac care unit. European Journal of Cardiovascular Nursing, 7, 10-15.
National Heart Foundation of Australia & Australian Cardiac Rehabilitation Association. (2004).
Recommended framework for cardiac rehabilitation. Retrieved from:
www.heartfoundation. org.au/SiteCollectionDocuments/Recommended-framework.pdf
Neal, B. (2004) . Secondary prevention of cardiovascular disease: fixed dose combinations. In:
Kaplan, W., & Laing, R. (Eds), Priority medicines for Europe and the world. Geneva:
World Health Organization.

207
Niemeier, J. P., Burnett, D. M., & Whitaker, D. A. (2003) . Cultural competence in the
multidisciplinary rehabilitation setting: Are we falling short of meeting needs? Archives of
Physical Medicine and Rehabilitation, 84, 1240-1245.
Noar, S. M., Benac, C., & Harris, M. (2007). Does tailoring matter? Meta-analytic review of tailored
print health behavior change interventions. Psychological Bulletin, 133, 673–693.
Nocon, M., Hiemann, T., Muller-Riemenschneider, F., Thalau, F., Roll, S., & Willich, S.N. (2008) .
Association of physical activity with all-cause and cardiovascular mortality: a systematic
review and meta-analysis. European Journal of Cardiovascular Prevention and
Rehabilitation, 15, 239-246.
Nunnally, J.C., & Bernstein, I.H. (1994) . Psychometric theory. New York: McGraw-Hill.
Nutbeam D. (2000) . Health literacy as a public health goal: a challenge for contemporary
health education and communication strategies into the 21st century. Health
Promotion International,15, 259-267.
Oldenburg, B., Martin, A., Greenwood, J., Bernstein, L., & Allan, R. (1995) . A controlled trial of a
behavioral and educational intervention following coronary artery bypass surgery. Journal
of Cardiopulmonary Rehabilitation, 15, 39–46.
Oliveira, J., Ribeiro, F., & Gomes, H. (2008) . Effects of a home-based cardiac rehabilitation program
on the physical activity levels of patients with coronary artery disease. Journal of
Cardiopulmonary Rehabilitation and Prevention, 28, 392–396.

208
Orzeck, S. A., & Staniloff, H. M. (1987) . Comparison of patients' and spouses' needs during the
posthospital convalescence phase of a myocardial infarction. Journal of Cardiopulmonary
Rehabilitation, 7, 59-67.
Osborne, R.H., Elsworth, G.R., & Whitfield, K. (2007) . The Health Impact Questionnaire: An
outcomes and evaluation measure for patient education and self-management interventions
for people with chronic conditions. Patient Education and Counseling, 66, 192-201.
Otterstad, J.E. (2003) . Influence on lifestyle measures and five-year coronary risk by a
comprehensive lifestyle intervention programme in patients with coronary heart disease.
European Journal of Cardiovascular Prevention and Rehabilitation, 10, 429–437.
Palomaki, A., Miilunpalo, S., Holm, P., Makinen, E., & Malminiem, K. (2002) . Effects of preventive
group education on the resistance of LDL against oxidation and risk factors for coronary
heart disease in bypass surgery patients. Annals of Medicine, 34, 272–283.
Parry, M., Watt-Watson, J., Hodnett, E., Tranmer, J., Dennis, C. L., & Brooks, D. (2009) . Cardiac
home education and support trial (CHEST): A pilot study. Canadian Journal of
Cardiology, 25, e393-e398.
Pasquali L. (2003) . Psychometrics: Theory testing in psychology and education. Rio de Janeiro:
Vozes.
Pelletier, S., Kundrat, S., & Hasler, C.M. (2003) . Effects of a functional foods nutrition education
program with cardiac rehabilitation patients. Journal of Cardiopulmonary Rehabilitation,
23, 334–340.
209
Petter, M., Blanchard, C., Kemp, K.A., Mazoff, A.S., & Ferrier, S.N. (2009) . Correlates
of exercise among coronary heart disease patients: review, implications and future
directions. European Journal of Cardiovascular Prevention and Rehabilitation, 16, 515-
526.
Pope, C., Ziebland, S., & Mays, N. (1999) . Qualitative Research in Health Care. London: BMJ.
Potvin, L., Richard, L., & Edwards, A. C. (2000) . Knowledge of cardiovascular disease risk factors
among the Canadian population: relationships with indicators of socioeconomic status.
Canadian Medical Association Journal, 162, S5-S11.
Prochaska, J. O., & DiClemente, C. C. (1983) . Stages and processes of self-change of smoking:
toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51,
390-395.
Public Health Agency of Canada (2009) . Tracking Heart Disease and Stroke in Canada. Retrieved
from: www.phac-aspc.gc.ca/publicat/2009/cvd-avc/pdf/cvd-avs-2009-eng.pdf
Queensland Health. (2000) . Best practice guidelines for outpatient cardiac rehabilitation. Retrieved
from: http://www.health.qld.gov.au/publications/best_practice/9115cardiac_doc.pdf
Rask, K. J., Williams, M. V., Parker, R. M., & McNagny, S. E. (1994) . Obstacles predicting lack of
a regular provider and delays in seeking care for patients at an urban public hospital. The
Journal of the American Medical Association, 271, 1931–1933.
Rathore, S.S., Masoudi, F.A., Wang, Y., Curtis, J.P., Foody, J.M., Havranek, F.P., & Krumholz, H.
M. (2006) . Socioeconomic status, treatment, and outcomes among elderly patients
210
hospitalized with heart failure: findings from the National Heart Failure Project. American
Heart Journal, 152, 371–378.
Rawson, K. A., Gunstad, J., Hughes, J., Spitznagel, M.B., Potter, V., Waechter, D., et al. (2009). The
METER: A brief, self-administered measure of health literacy. Journal of General Internal
Medicine, 25(1), 67-71.
Redding, C. A., Rossi, J. S., Rossi, S. R., Velicer, W. F., & Prochaska, J. O. (2000) . Health behavior
models. International Electronic Journal of Health Education, 3, 180-193.
Renner, B., & Schwarzer, R. (2003). Social-cognitive factors in health behavior change. In J. Suls &
K. Wallston (Eds.), Social psychological foundations of health and illness (pp. 169–196).
Oxford: Blackwell.
Renner, B., & Schwarzer, R. (2005). The motivation to eat a healthy diet: How intenders and
nonintenders differ in terms of risk perception, outcome expectancies, self-efficacy, and
nutrition behavior. Polish Psychological Bulletin, 36, 7–15.
Renner, B., Spivak, Y., Kwon, S., & Schwarzer, R. (2007) . Does age make a difference? Predicting
physical activity of South Koreans. Psychology and Aging, 22, 482–493.
Reuter, T., Ziegelmann, J. P., Wiedemann, A. U., Lippke, S., Schuz, B., & Aiken, L. S. (2010) .
Planning bridges the intention–behavior gap: Age makes a difference and strategy use
explains why. Psychology and Health, 25, 873-887.
Riedinger, M. S., Dracup, K. A., & Brecht, M. L. (2000). Predictors of quality of life in women with
heart failure. The Journal of Heart and Lung Transplantation, 19, 598-608.

211
Ries, A.L., Bauldoff, G.S., Carlin, B.W., Casaburi, R., Emery, C.F. Mahler, D.A. … Herrerias, C.
(2007) . Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical
Practice Guidelines. Chest, 131, 4S-42S.
Rodgers, W.M. & Sullivan, M.J.L. (2001). Task, coping, and scheduling self-efficacy in relation to
frequency of physical activity. Journal of Applied Social Psychology, 31(4), 741–753.
Rodgers, W.M., Hall, C.R., Blanchard, C.M., McAuley, E., & Munroe, K.J. (2002). Task and
Scheduling Self-efficacy as Predictors of Exercise. Behavior, Psychology & Health, 17(4),
405-416.
Roger, V. L., Go, A. S., Lloyd-Jones, D. M., Benjamin, E. J., Berry, J. D., Borden, W. B., ... Turner,
M. B. (2012) . Heart disease and stroke statistics – 2012 update: A report from the
American Heart Association. Circulation, 125, e2-e220.
Rogers, C.R. (1969) . Freedom to learn. Columbus: Merrill Publishing.
Ronis, D.L., Yates, J.F., & Kirscht, J.P. (1989) . Attitudes decisions and habits as determinants of
repeated behavior. In A.R. Pratkanis, S.J. Breckler, & A.G. Greenwald (Eds.), Attitude
structure and function (pp. 213-239). Hillsdale, NJ: Erlbaum.
Rosenstock, I.M. (1990) . The health belief model: explaining health behavior through expectancies.
In: Glanz K, Marcus Lewis F, Rimer BK, eds. Health Behavior and Health Education. San
Francisco, CA: Jossey-Bass Publishers.
Roter, D.L., Stashefsky-Margalit, R., Rudd, R. (2001) . Current perspectives on patient education in
US. Patient Education and Counseling, 44, 79-86.

212
Russel, K,L., Holloway, T.M., Brum, M., Caruso, V., Chessex, C., Grace, S.L. (2011) . Cardiac
rehabilitation wait times: effect on enrollment. Journal of Cardiopulmonary Rehabilitation
and Prevention, 31, 373-377.
Ryan, P., & Sawin, K.J. (2009) . The Individual and Family Self-management theory: background
and perspectives on context, process, and outcomes. Nursing Outlook, 57, 216-225.
Schadewaldt, V., & Schultz, T. (2011) . Nurse-led clinics as an effective service for cardiac patients:
results from a systematic review. International Journal of Evidence-Based Healthcare, 9,
199-214.
Scholz, U., Sniehotta, F. F., & Schwarzer, R. (2005) . Predicting physical exercise in cardiac
rehabilitation: The role of phase-specific self-efficacy beliefs. Journal of Sport and
Exercise Psychology, 27, 135–151.
Schwarz, B., Schoberberger, R., Rieder, A., & Kunze, M. (1994) . Factors delaying treatment of
acute myocardial infarction. European Heart Journal, 15, 1595-1598.
Schwarzer, R. (1992) . Self-efficacy in the adoption and maintenance of health behaviors: Theoretical
approaches and a new model. In R. Schwarzer (Ed.), Self-efficacy: Thought control of
action (pp. 217-242). Washington, DC: Hemisphere.
Schwarzer, R. (2008) . Modeling health behavior change: how to predict and modify the adoption and
maintenance of health behaviors. Applied Psychology, 57: 1-29.
Schwarzer, R., Lippke, S., & Luszczynska, A. (2011) . Mechanisms of health behavior change in
persons with chronic illness or disability: The health action process approach
(HAPA). Rehabilitation Psychology, 56, 161-170.

213
Shuster, P.M., Wright, C., & Tomich, P. (1995) . Gender differences in the outcomes of participants
in home programs compared to those in structured cardiac rehabilitation programs.
Rehabilitation Nursing, 20, 93-101.
Scott, J. T., & Thompson, D. R. (2003) . Assessing the information needs of post-myocardial
infarction patients: a systematic review. Patient Education and Counseling, 50, 167-177.
Segan, C.J., Borland, R., & Greenwood, K.M. (2004) . What is the right thing at the right time?
Interactions between stages and processes of change among smokers who make a quit
attempt. Health Psychology, 23, 86-93.
Sheeran, P. (2002) . Intention-behavior relations: A conceptual and empirical review. European
Review of Social Psychology, 12, 1-36.
Silverman, D. (2000) . Doing Qualitative Research - A Practical Handbook. London: Sage
Publications Ltd.
Smith, J., & Liles, C. (2007) . Information needs before hospital discharge of myocardial infarction
patients: a comparative, descriptive study. Journal of Clinical Nursing, 6, 662-671.
Smith, M. M., Hicks, V. L., & Heyward, V. H. (1991) . Coronary heart disease knowledge test:
Developing a valid and reliable tool. The Journal for Nurse Practitioners, 16, 35-38.
Smith, P.M., & Burgess, E. (2009) . Smoking cessation initiated during hospital stay for patients with
coronary artery disease: a randomized controlled trial. Canadian Medical Association
Journal, 180, 1297-1303.

214
Sniehotta, F.F., Schwarzer, R., Scholz, U., Scholz, U., & Schuz, B. (2005) . Action planning and
coping planning for long-term lifestyle change: Theory and assessment. European Journal
of Social Psychology, 35, 565-576.
Sniehotta, F.F., Scholz, U., & Schwarzer, R. (2006) . Action plans and coping plans for physical
exercise: A longitudinal intervention study in cardiac rehabilitation. British Journal of
Health Psychology, 11, 23-37.
Sommaruga, M., Vidotto, G., Bertolotti, G., Pedretti, R. F., & Tramarin, R. (2003) . A self
administered tool for the evaluation of the efficacy of health education interventions in
cardiac patients. Monaldi Archives of Chest Disease, 60, 7-15.
Song, R., & Lee, H. (2001) . Managing health habits for myocardial infarction (MI) patients.
International Journal of Nursing Studies, 38, 375–380.
Stern, P.C. (2000) . New Environmental Theories: Toward a Coherent Theory of Environmentally
Significant Behavior. Journal of Social Issues, 56, 407-424.
Stewart, D.E., Abbey, S.E., Shnek, Z.M., Irvine, J., & Grace, S.L. (2004) . Gender differences in
health information needs and decisional preferences in patients recovering from an acute
ischemic coronary event. Psychosomatic Medicine, 66, 42-48.
Stone, J. A., Arthur, H. M., & Suskin, N. (Eds.) (2009) . Canadian guidelines for cardiac
rehabilitation and cardiovascular disease prevention: Translating knowledge into action
(3rd ed). Winnipeg, MB: Canadian Association of Cardiac Rehabilitation.

215
Su, W. M., Herron, B., & Osisek, P. J. (2011). Using a competency-based approach to patient
education: Achieving congruence among learning, teaching and evaluation. Nursing
Clinics of North America, 46, 291-298.
Suaya, J.A., Shepard, D.S., Normand, S.L., Ades, P.A., Prottas, J., & Stason, W.B. (2007) . Use of
cardiac rehabilitation by Medicare beneficiaries after myocardial infarction or coronary
bypass surgery. Circulation, 116, 1653-1662.
Sui, X., Gheorghiade, M., Zannad, F., Young, J.B., & Ahmed, A. (2008) . A propensity-matched
study of the association of education and outcomes in chronic heart failure. International
Journal of Cardiology, 129, 93-99.
Sutton, S.R. (1994). The past predicts the future: interpreting behaviour-behaviour relationships in
social-psychological models of health behaviour. In: D.R. Rutter & L. Quine (Eds). Social
psychology and health: European perspectives (pp 47-70). Aldershot, England: Avebury.
Taylor, R.S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani, H., Rees, K., … , Oldridge, N. (2004).
Exercise-based rehabilitation for patients with coronary heart disease: systematic review
and meta-analysis of randomized controlled trials. American Journal of Medicine, 116,
682-692.
Terwee, C.B., Bot, S.D., de Boer, M.R., van der Windt, D.A., Knol, D.L., Dekker, J., … de Vet, H.C.
(2007) . Quality criteria were proposed for measurement properties of health status
questionnaires. Journal of Clinical Epidemiology, 60(1), 34-42.

216
Thomas, R.J., King, M., Lui, K., Oldridge, N., Pina, I.L., Spertus, J., … Whitman G.R. (2007) .
AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to
and delivery of cardiac rehabilitation/ secondary prevention services. Journal of American
College of Cardiology, 50, 1400-1433.
Thompson, P.D., Buchner, D., Pina, I.L. Balady, G.J., Williams, M.A., Marcus, B.H., …, Wenger,
N.K. (2003). Exercise and physical activity in the prevention and treatment of
atherosclerotic cardiovascular disease. Circulation, 107, 3109-3116.
Timlin, M.T., Shores, K.V., & Reicks, M. (2002) . Behavior change outcomes in an outpatient
cardiac rehabilitation program. Journal of American Dietetic Association, 102, 664–671.
Timmins, F., & Kaliszer, M. (2003) . Information needs of myocardial infarction patients. European
Journal of Cardiovascular Nursing, 2, 57-65.
Timmins, F. (2006) . Exploring the concept of ‘information need’. International Journal of Nursing
Practice, 12, 375-381.
Toronto Rehabilitation Institute (2011) . Toronto Rehab Opening Plan 2011-2012. Toronto, Canada.
Tulloch, H., Reida, R., D’Angeloa, M. S., Plotnikoff, R.C., Morrina, L., Beatona, L., … Pipe, A.
(2009) . Predicting short and long-term exercise intentions and behavior in patients with
coronary artery disease: A test of protection motivation theory. Psychology & Health, 24,
255-269.
Turton, J. (1998) . Importance of information following myocardial infarction: a study of the self-
perceived information needs of patients and their spouse/partner compared with the
perceptions of nursing staff. Journal of Advanced Nursing, 27, 770-778.

217
U.S. Department of Education, National Center for Education Statistics. (2006) . The Health Literacy
of America’s Adults: Results From the 2003 National Assessment of Adult Literacy
(NCES 2006-483). Retrieved from http://nces.ed.gov/pubs2006/2006483.pdf
University Health Network, 2003. Evidence based best practice guidelines for delivering patient
education curriculum. University Health Network’s Patient Education Task Force and
Curriculum Committee. Retrieved from: http://documents.uhn.ca/sites/uhn/
Patient_Education_Intranet/Materials/Guidelines_for_Effective_PtEd_Teaching.pdf.
Van Elderen-van, K.T., Maes, S., & van den Broek, Y. (1994) . Effects of a health education
programme with telephone follow-up during cardiac rehabilitation. British Journal of
Clinical Psychology, 33, 367-378.
Van Elderen, T.M., Maes, S., Seegers, G., Kragten, H., & Relik-Can Wely, L. (1994) . Effects of a
post-hospitalization group health education programme for patients with coronary heart
disease. Psychology & Health, 9, 317–330.
Van Elderen, T., & Dusseldorp, E. (2001) . Lifestyle effects of group health education for patients
with coronary heart disease. Psychology & Health, 16, 327–341.
Verges, B.L., Patois-Verges, B., Cohen, M., & Casillas, J.M. (1998). Comprehensive cardiac
rehabilitation improves the control of dyslipidemia in secondary prevention. Journal of
Cardiopulmonary Rehabilitation, 18, 408–415.
Verril, D., Graham, H., Vitcenda, M., Peno-Green, L., Kramer, V., & Corbisiero, T. (2009) .
Measuring behavioral outcomes in cardiopulmonary rehabilitation: an AACVPR statement.
Journal of Cardiopulmonary Rehabilitation and Prevention, 29(3), 193-203.

218
Vinson, J. M., Rich, M. W., Sperry, J. C., Shah, A. S., & McNamara, T. (1990) . Early readmission of
elderly patients with congestive heart failure. Journal of American Geriatrics Society, 38,
1290–1295.
Wang, W. W. (1994) . The educational needs of myocardial infarction patients. Progress in
Cardiovascular Nursing, 9, 28-36.
Wehby, D., & Brenner, P. S. (1999) . Perceived learning needs of patients with heart failure. Heart &
Lung, 28, 31-40.
Weiss, B.D., Reed, R.L., & Kligman, E.W. (1995). Literacy skills and communication methods of
low-income older persons. Patient Education and Counseling, 25, 109-119.
Weiss, B. D., Mays, M. Z., Martz, W., Castro, K. M., DeWalt, D. A. , Pignone, M. P., et al. (2005).
Quick Assessment of Literacy in Primary Care: The Newest Vital Sign. Annals of Family
Medicine, 3(6), 514-522.
Wingate, S. (1990) . Post-MI patients’ perceptions of their learning needs. Dimensions of Critical
Care Nursing, 9, 112-118.
Wingham, J., Dalal, H. M., Sweeney, K. G., & Evans, P. H. (2006) . Listening to patients: choice in
cardiac rehabilitation. European Journal of Cardiovascular Nursing, 5, 289-294.
Wolkanin-Bartnik, J., Pogorzelska, H., & Bartnik, A. (2011) . Patient education and quality of home-
based rehabilitation in patients older than 60 years after acute myocardial infarction.
Journal of Cardiopulmonary Rehabilitation and Prevention, 31, 249–253.

219
Workgroup for Intervention Development and Evaluation Research, WIDER Group. (2008) . WIDER
Recommendations to Improve Reporting of the Content of Behaviour Change
Interventions. Retrieved from: http://interventiondesign.co.uk/?page_id=9
Williams, M.V., Parker, R.M., Baker, D.W., Parikh, N.S., Pitkin, K., Coates, W.C., & Nurss,
J.R. (1995). Inadequate functional health literacy among patients at two hospitals. Journal
of the American Medical Association, 274, 1677-1682.
Williams, S., Lindsell, C., Rue, L., & Blomkalns, A. (2007) . Emergency Department education
improves patient knowledge of coronary artery disease risk factors but not the accuracy of
their own risk perception. Preventive Medicine, 44, 520-525.
Wingate, S. (1990) . Post-MI patients’ perceptions of their learning needs. Dimensions of Critical
Care Nursing, 9, 112-118.
World Health Organization. (2011). Global status report on noncommunicable diseases 2010.
Retrieved from: http://www.who.int/nmh/publications/ncd_report_full_en.pdf
Yoshida, T., Kohzuki, M., Yoshida, K., Hiwatari, M., Kamimoto, M., Yamamoto C, ... Sato, T.
(1999) . Physical and psychological improvements after phase II cardiac rehabilitation in
patients with myocardial infarction. Nursing & Health Sciences, 1, 163–170.
Yusuf, S., Hawken, S., Ounpuu, S., Dans, T., Avezum, A., Lanas, F., ... INTERHEART Study
Investigators. (2004). Effect of potentially modifiable risk factors associated with
myocardial infarction in 52 countries (the INTERHEART study): case-control study.
Lancet, 364, 937-952.

220
Zalesskaya, J. V., Noruzbaeva, A. M., Lunegova, O. S., Mirrakhimov, E. M. (2005) . Evaluation of
the economic efficiency of educational programs for patients with coronary heart disease
and dyslipidemia. Prevention and Control, 1, 297-304.
Ziegelmann, J. P., & Lippke, S. (2007). Planning and strategy use in health behavior change: A life
span view. International Journal of Behavioral Medicine, 14, 30–39.
Zimmerman, B.J. (2000). Self-efficacy: as essential motive to learn. Contemporary Educational
Psychology, 25, 82-91.

221
Appendices

222
Appendix 1: The INCR Scale

223

224

225

226
Appendix 2: The CADE-Q II Questionnaire

227
Domain: Medical Condition
Question 1 Coronary Artery Disease is:
a) A disease of the heart’s arteries that occurs only in older age and is mainly caused by deposits of calcium in the arteries.
b) A disease of the arteries of the heart which occurs in older age in people with high cholesterol or who smoke.
c) A disease of the arteries of the heart that starts silently at a young age. It is influenced by poor life style habits, genetics, and involves inflammation in the arteries.
d) I don’t know. Question 2 Angina (chest pain of discomfort) occurs:
a) When the heart muscle is working too hard. b) When the heart muscle is not getting enough blood and oxygen to work properly. c) When the brain is not getting enough oxygen. d) I don’t know.
Question 3 In a person with coronary artery disease, which of the following is a usual description of angina?
a) Headache after meals. b) Chest pain or discomfort, at rest or during physical activity, which can also be felt
in the arm and/or back and/or neck. c) Chest pain or discomfort during physical activity. d) I don’t know.
Question 4 A heart attack occurs:
a) If an artery in the heart becomes blocked. b) If the heart suddenly races in response to stress. c) If the flow of oxygen-rich blood to an area of heart muscle suddenly becomes
blocked. If blood flow is not restored quickly, the area of heart muscle begins to die. d) I don’t know.
Question 5

228
The best resources available to help someone understand his/her medications are:
a) The doctor, the cardiac rehab team, the pharmacist and recommended resources on the internet.
b) What someone reads on the internet. c) The doctor and the cardiac rehab team. d) I don’t know.
Question 6 Medications such as aspirin (ASA) and clopidogrel (PlavixTM) are important because:
a) They lower blood pressure. b) They “thin” the blood. c) They reduce the “stickiness” of platelets in the blood so that blood flows more
easily through coronary arteries and past coronary stents. d) I don’t know.
Question 7 The “statin” medications, such as atorvastatin (LipitorTM), rosuvastatin (CrestorTM), or simvastatin (ZocorTM), have a beneficial effect in the body by:
a) Lowering LDL cholesterol in the blood stream. b) Blocking the production of LDL cholesterol in the liver, lowering LDL cholesterol
in the blood stream, and encouraging cholesterol to move out of plaques from the arteries.
c) Reducing the absorption of cholesterol from food. d) I don’t know.
Domain: Risk Factors
Question 1 The risk factors for heart disease that can be changed are:
a) Blood pressure, cholesterol, and smoking. b) Age, family history of heart disease, ethnicity and sex. c) Blood pressure (systolic and diastolic), LDL + HDL cholesterol, smoking and
second hand smoking, waist size, and reaction to stress. d) I don’t know.
Question 2
229
The actions that can be taken to control cholesterol levels include:
a) Knowing the total cholesterol level, becoming a vegetarian and avoiding eggs. b) Knowing the LDL and HDL levels, taking cholesterol medication as prescribed,
increasing soluble fibre intake and reducing saturated fat in the diet, and participating in aerobic exercise 5 times per week.
c) Knowing the cholesterol levels and taking cholesterol medication as prescribed. d) I don’t know.
Question 3 The actions that can be taken to control blood pressure include:
a) Increasing calcium in the diet. b) Reducing the amount of salt in the diet, and taking blood pressure medication. c) Reducing the amount of sodium in the diet to <2000 mg per day, exercising,
taking blood pressure medication regularly and learning relaxation techniques. d) I don’t know.
Question 4 The first step towards controlling a risk factor (such as blood pressure or cholesterol) is:
a) Knowing if someone has the risk factor. b) Knowing the level of the risk factor. c) Setting a goal or action plan to control the risk factor. d) I don’t know.
Question 5 The actions to prevent developing diabetes include:
a) Follow a heart healthy diet, do 150 minutes of aerobic exercise weekly and twice weekly resistance exercises with weights and therabands.
b) Reduce the amount of fats and carbs in the diet. c) With a family history of diabetes, a person is bound to develop diabetes because
diabetes is not a preventable disease. d) I don’t know.
Domain: Exercise
Question 1
230
What are the important parts of an exercise prescription?
a) Replacing calories and salt during a light workout. b) How hard to exercise, how long to exercise, how often to exercise and what type
of exercise to do. c) How hard to exercise, and how long to exercise. d) I don’t know.
Question 2 For a person living with heart disease, it is important to do a cardiovascular warm-up before exercising because:
a) It gradually increases the heart rate, it may reduce muscle soreness and can reduce the risk of developing angina.
b) It adds more time to the total amount of minutes of exercise. c) It prepares the body for exercise. d) I don’t know.
Question 3 The pulse can be found:
a) In the wrist below the base of the thumb. b) In the wrist below the base of the pinky finger or on the neck on the Adam’s
apple. c) At the radial artery (wrist) or at the carotid artery (neck). d) I don’t know.
Question 4 Three things that one can do to exercise safely outdoors in the winter are:
a) Check the temperature and wind-chill, and wear layers of clothing. b) Check the temperature and wind-chill and make sure it is not below -10 degrees
C, wear 3-4 layers of clothing and adjust the pace of walking so that the level of exertion and heart rate are on target.
c) Check the temperature and wind-chill and make sure it is not below -15 degrees C, wear a winter coat and jog if one gets too cold.
d) I don’t know. Question 5 The benefits of doing resistance training (lift weights or elastic bands) include:
a) Builds up strength and muscles.

231
b) Lowers resting heart rate. c) Increases strength, improves the ability to carry out day to day activities,
improves blood sugar levels and increases muscle. d) I don’t know.
Question 6 If a person gets chest discomfort during a walking exercise session, he or she should:
a) Speed up to see if the discomfort goes away. b) Slow down and stop exercising. c) Slow the walk pace and if it does not go away within 1 minute, stop exercising. If
it still does not go away within the next 1 minute, take nitro-glycerine as prescribed. If the pain continues, get help.
d) I don’t know. Question 7 How does a person know if he/she is exercising at the right level?
a) The heart rate is in the target zone, the exertion level is no higher than “some-what hard”, and the person can exercise and talk.
b) The heart rate is in the target zone. c) Working up a sweat, breathing heavy and the heart rate is going fast. d) I don’t know.
Domain: Nutrition
Question 1 What is the best source of omega 3 fats in food?
a) Ground flaxseed. b) Pasta. c) Fatty fish (e.g. trout, salmon). d) I don’t know.
Question 2 Trans fat are:
a) Found in nuts and seeds.

232
b) Partially hydrogenated vegetable oils (e.g. vegetable shortening). c) Margarine. d) I don’t know.
Question 3 What is one good way to add more fibre to your diet:
a) Add nuts and seeds to a salad. b) Drink juice. c) Eat plant proteins (e.g. legumes/beans, lentils). d) I don’t know.
Question 4 Which of the following foods has the most salt:
a) Bread. b) Frozen dinners. c) Fruits and vegetables. d) I don’t know.
Question 5 What combination of foods can help lower blood pressure?
a) Red meat, poultry, fish. b) Vegetables and fruits. c) Vegetables and fruits, whole grains, low fat dairy, nuts and seeds. d) I don’t know.
Question 6 When reading food labels, what should one look at first?
a) Fat content. b) Brand name. c) Serving size. d) I don’t know.
Question 7 How many servings of fruits and vegetables should adults consume?
a) 7 to 10 servings a day. b) 5 servings a day.

233
c) As many as possible. d) I don’t know.
Domain: Psychosocial Risk
Question 1 Which of the below are effective stress management techniques?
a) Deep breathing. b) Avoid communication. c) Meditation, progressive muscle relaxation, making social connections,
stretching/exercise, deep breathing. d) I don’t know.
Question 2
What stresses have been related to increased risk for heart attacks?
a) Chronic stresses, major life events, disrupted sleep, and feelings of distress. b) Chronic stress at home or at work and feeling depressed. c) Stresses that you do not feel in control of. d) I don’t know.
Question 3 Which of the following describes your best option for reducing your risk from depression:
a) Take an antidepressant, and do your exercise prescription. b) Do your exercises, take better care of yourself, and if required take medications. c) The risk of heart attack due to depression cannot be reduced. d) I don’t know.
Question 4
It is important to recognize “sleep apnea” because:
a) It leads to long term lung disease. b) It is associated with high blood pressure, abnormal heart rhythms, and higher
risk of future heart attack.

234
c) It leads to further heart problems. d) I don’t know.
Question 5 “Chronic stress” is defined as:
a) Ongoing persistent stressful events in one area of your life. b) Events at work or at home that make you feel irritable, anxious, or sleepless. c) The stresses that are out of a person’s control. d) I don’t know.
Thanks for your participation!

235
Appendix 3: Assessment Booklet for Paper 5

236
Initial Survey
Instructions for completing the survey questions appear at the beginning of each section.
Please seal your completed questionnaire in the envelope provided and return it to the TRI
Version #2: 22 April 2013
Participant #_______
!!
Patient
Education Study

237
General Instructions
We need your help to make our study a success. Your candid answers to the items in this survey
are very important to us. The survey will take about 30 minutes to complete.
REMEMBER:
• We want to know what you think. • There are no right or wrong answers. • Everything you tell us will be kept strictly confidential. • Please provide only one answer for each item.
SESSIONS:
This survey has 3 sessions.
• Session A - About you: information needed to understand the characteristics of the people participating in this study. In this session you will be asked to provide your educational level, and we will assess health literacy and physical activity.
• Session B - Assessment of Mediators: mediators are characteristics that may influence your behaviour change
• Session C - Knowledge Assessment: CADE-Q 2 Questionnaire will be used to assess your knowledge about heart disease and related factors.
If, at any time, you have questions as you complete this questionnaire, or regarding your
participation in this study, please call:
Gabriela L. Melo Ghisi, PhD Candidate

238
Please answer the questions about physical activity, physical exercise and exercise prescription with the following definitions in mind: Physical Activity: any type of activity/movement produced by muscles that results in energy expenditure. Physical Exercise: physical activity that is planned, structured, and repetitive for the purpose of conditioning any part of the body. Exercise Prescription: physical exercise based on your medical history, your current level of fitness, the results from your cardiopulmonary assessment, and your specific goals.

239
Instructions: The information within this session is needed to help understand the characteristics of the people participating in this study. For this reason, it is very important information. Be assured that it will remain confidential.
1. Educational Level
What is the highest level of education you have completed?
2. Physical Activity
How often do you usually carry out the following physical activities?
(Almost) every day
3-4 times a week
Once a week
1-3 times a month
Less or never
Bicycling (also stationary exercise bike) 1 2 3 4 5
Walking, hiking, running 1 2 3 4 5
Calisthenics, gymnastics, aerobics, dancing 1 2 3 4 5
Endurance sports (swimming, rowing, skiing) 1 2 3 4 5
Resistance training (weight training) 1 2 3 4 5
(Almost) every day
3-4 times a week
Once a week
1-3 times a month
Less or never
1 Less than high school (no certificates, diplomas or degrees)
2 High school graduation certificate
3 Trades certificate
4 College certificate or diploma
5 University: a certificate below the bachelor’s level, bachelor’s degree, certificate above the bachelor’s level, master’s level, earned doctorate or a professional degree.

240
Martial arts 1 2 3 4 5
Team sport games (baseball, soccer, volleyball, etc) 1 2 3 4 5
Other? Please specify: ________________________ 1 2 3 4 5
How much time do you spend on the above mentioned activities? __________________ hours per week. Have you been exercising on a regular basis during the last 6 months?
3. Health Literacy
3.1.The Medical Term Recognition Test (METER)1
The following list (see next page) contains some real medical words. For example, some of the words have to do with body parts or functions, kinds of diseases, or things that can make your health better or worse. The list also contains some items that may look or sound like medical words but that are not actually real words.
As you read through the list, put an “X” next to the items that you know are real words.
You should not guess. Only put an “X” next to an item if you’re sure it’s a real word.
_______ Irrity _______ Astiringe _______ Infarth
_______ Arthritis _______ Nutral _______ Dose
1 No
2 Yes, with longer interruptions
3 Yes, with short interruptions
4 Yes, without interruptions

241
_______ Obesity _______ Asthma _______ Hemorrhoids
_______ Flu _______ Inflammatory _______ Testicle
_______ Behaviose _______ Anemia _______ Eye
_______ Syphilis _______ Allagren _______ Midlocation
_______ Potassium _______ Prognincy _______ Insomniate
_______ Hormones _______ Stress _______ Bloodgatten
_______ Nerves _______ Ellargic _______ Sexually
_______ Pilk _______ Inlest _______ Pelvince
_______ Rection _______ Pollent _______ Vaccilly
_______ Blout _______ Malories _______ Prescription
_______ Boweling _______ Cancer _______ Germs
_______ Exercise _______ Alcoheliose _______ Gonorrhea
_______ Pustule _______ Antibiotics _______ Tumic
_______ Cerpes _______ Antiregressant _______ Fatigue
_______ Kidney _______ Colitis _______ Osteoporosis
_______ Emergency _______ Diabetes _______ Constipation
_______ Potient _______ Occipitent _______ Hepatitis
_______ Menopause _______ Nausion _______ Fam
_______ Diagnosis _______ Impetigo
_______ Depretion _______ Menstrual
_______ Jaundice _______ Abghorral
_______ Gallbladder _______ Seizure
_______ Miscarriage _______ Appendix
3.2.The Newest Vital Sign (NVS)2

242
See the food label below and answer the questions on next page.

243
Based on the information in the nutritional label (see last page), please answer the following questions: a. If you eat the entire container of ice cream, how many calories will you eat? b. If you are allowed to eat 60 grams of carbohydrates as a snack, how much ice cream could you have? c. Your doctor advises you to reduce the amount of saturated fat in your diet. You usually have 42 grams of saturated fat each day, which includes 1 serving of ice cream. If you stop eating ice cream, how many grams of saturated fat would you be consuming each day? d. If you usually eat 2500 calories in a day, what percentage of your daily value of calories will you be eating if you eat one serving? e. Pretend that you are allergic to the following substances: penicillin, peanuts, latex gloves, and bee stings. Is it safe for you to eat this ice cream? YES NO f. If you answered 'no' to the last question, explain why it would not be safe to eat this ice cream. 1 Rawson, K. A., Gunstad, J., Hughes, J., Spitznagel, M.B., Potter, V., Waechter, D., et al. (2009). The METER: A
brief, self-administered measure of health literacy. Journal of General Internal Medicine, 25(1), 67-71.
2 Weiss, B. D., Mays, M. Z., Martz, W., Castro, K. M., DeWalt, D. A. , Pignone, M. P., et al. (2005). Quick Assessment of Literacy in Primary Care: The Newest Vital Sign. Annals of Family Medicine, 3(6), 514-522.

244
Section B: Mediators
Instructions: Mediators are characteristics that may influence your behaviour change and how
your knowledge can influence this behaviour. We are assessing 8 types of mediators (M1-M8).
M1: Risk Awareness
1. Using the scales provided, please circle the most appropriate response (from 1 to 7) to show
your agreement with each statement.
a) If I keep my lifestyle the way it was prior to my heart problem I will suffer from an elevated cholesterol level.
1 2 3 4 5 6 7 Very
unlikely Moderately
likely Very likely
b) If I keep my lifestyle the way it was prior to my heart problem I will suffer from a heart attack.
1 2 3 4 5 6 7 Very
unlikely Moderately
likely Very likely
c) If I keep my lifestyle the way it was prior to my heart problem I will suffer from high blood pressure.
1 2 3 4 5 6 7 Very
unlikely Moderately
likely Very likely
d) If I keep my lifestyle the way it was prior to my heart problem I will suffer from cardiovascular disease.
1 2 3 4 5 6 7 Very
unlikely Moderately
likely Very likely
2. Using the scales provided, please circle the most appropriate response (from 1 to 7) for each question.
a) How severe (serious) is obesity if I don’t exercise regularly? 1 2 3 4 5 6 7
Not severe at all
Moderately severe
Very severe
(can be ignored) (as if someone has the flu) (life threatening)

245
b) How severe (serious) is heart attack if I don’t exercise regularly?
1 2 3 4 5 6 7 Not severe
at all
Moderately severe
Very severe
(can be ignored) (as if someone has the flu) (life threatening)
c) How severe (serious) is high blood pressure if I don’t exercise regularly? 1 2 3 4 5 6 7
Not severe at all
Moderately severe
Very severe
(can be ignored) (as if someone has the flu) (life threatening)
d) How severe (serious) is cardiovascular disease if I don’t exercise regularly? 1 2 3 4 5 6 7
Not severe at all
Moderately severe
Very severe
(can be ignored) (as if someone has the flu) (life threatening) M2: Outcomes Expectancies 1. Using the scale provided below, please circle the most appropriate response (from 1 to 7) for the question: What do you think will be the consequences if you exercise regularly?
1 2 3 4 5 6 7 Very
unlikely Moderately
likely Very likely
a) Social Outcomes: If I exercise regularly… …I will be able to socialize with others. 1 2 3 4 5 6 7
…others will appreciate my willpower. 1 2 3 4 5 6 7
…I will take a lot of my time. 1 2 3 4 5 6 7
... I will spend time with others. 1 2 3 4 5 6 7
b) Psychological Outcomes:

246
If I exercise regularly… …I will reduce my stress. 1 2 3 4 5 6 7
…I will feel more energized. 1 2 3 4 5 6 7
…I will be more balanced in my daily life 1 2 3 4 5 6 7
... my quality of life will increase. 1 2 3 4 5 6 7
… I will look more attractive. 1 2 3 4 5 6 7
c) Physical Outcomes:
If I exercise regularly… …I will simply feel better afterwards. 1 2 3 4 5 6 7
…I won’t have weight problems (anymore). 1 2 3 4 5 6 7
…my cholesterol level will improve. 1 2 3 4 5 6 7
…I will prevent a heart attack. 1 2 3 4 5 6 7
… it will be good for my blood pressure. 1 2 3 4 5 6 7
... it will help me cope with medication side effects.
1 2 3 4 5 6 7
M3: Task Self-efficacy 1. For the following questions, please indicate how confident you are on a scale from 1 (not confident at all) to 7 (completely confident). Assuming you were very motivated, how confident are you that you could physically do the following amounts of physical activity in one session without stopping over the next 6 months. Please answer for each amount of time.
Not Confident At All Neutral Completely
Confident
10 minutes 1 2 3 4 5 6 7
20 minutes 1 2 3 4 5 6 7
Not Confident At Neutral Completely

247
All Confident
30 minutes 1 2 3 4 5 6 7
40 minutes 1 2 3 4 5 6 7
50 minutes 1 2 3 4 5 6 7
60 minutes 1 2 3 4 5 6 7
M4: Intention 1. Using the scales provided, please circle what extent (from 1 to 7) is the following statement true for you. a) “I will try to do my exercise prescription over the next 6 months.”
1 2 3 4 5 6 7 Definitely
False Definitely
True
2. Using the scales provided, please circle what extent (from 1 to 7) is the following statement likely for you. b) “I intend to do my exercise prescription over the next 6 months.”
1 2 3 4 5 6 7 Extremely Unlikely
Extremely Likely
M5: Action Planning 1. Using the scales provided, please rate the extent to which you agree with each statement. Do you already have concrete plans with regard to exercising?
a) I already have concrete plans about WHERE to exercise.
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
b) I already have concrete plans about WHEN to exercise.

248
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
c) I already have concrete plans about HOW to exercise.
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
d) I already have concrete plans about HOW OFTEN to exercise.
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
e) I already have concrete plans about WITH WHOM to exercise.
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
f) I already have concrete plans about WHAT TYPES OF ACTIVITIES I will do.
1 2 3 4 5 6 7
Strongly Disagree
Neutral Strongly Agree
M6: Coping Planning 1. Using the scales provided, please rate the extent to which you agree with each statement. Do you already have concrete plans for your new exercise schedule (habits)?
a) I already have concrete plans about what to do if something interferes with my exercise schedule.
1 2 3 4 5 6 7
Strongly Disagree
Neutral Strongly Agree
b) I already have concrete plans about what to do if I miss an exercise session.
1 2 3 4 5 6 7
Strongly Disagree
Neutral Strongly Agree
c) I already have concrete plans about what to do in difficult situations in order to stick
to my exercise schedule.

249
1 2 3 4 5 6 7 Strongly Disagree
Neutral Strongly Agree
d) I already have concrete plans if something gets in the way of my plans to exercise.
1 2 3 4 5 6 7
Strongly Disagree
Neutral Strongly Agree
M7: Scheduling Self-Efficacy 1. Using the scales provided, please answer each statement. Assuming that you are very motivated, in the next 6 months, how confident are you that you can fit your exercise prescription into your weekly schedule…
Please answer for each frequency
Not Confident At All
Neutral Completely Confident
…Once per week? 1 2 3 4 5 6 7
…Twice per week? 1 2 3 4 5 6 7
…Three times per week? 1 2 3 4 5 6 7
…Four times per week? 1 2 3 4 5 6 7
…Five times per week? 1 2 3 4 5 6 7
…More than 5 times per week? 1 2 3 4 5 6 7
M8: Maintenance Self-Efficacy 1. Using the scales provided, please answer each statement. Assuming you were very motivated, how confident are you that you will do your exercise prescription over the next 6 months…
Please answer for each frequency Not Confident At All
Neutral Completely Confident

250
…even if it takes you a long time to make it a habit? 1 2 3 4 5 6 7
…even if you are worried and troubled? 1 2 3 4 5 6 7
…even if you don’t see success at once? 1 2 3 4 5 6 7
…even if you are tired? 1 2 3 4 5 6 7
…even if you are stressed out? 1 2 3 4 5 6 7
…even if you feel tense? 1 2 3 4 5 6 7
…even if you do not have the support of others around you? 1 2 3 4 5 6 7
…even if you feel slow? 1 2 3 4 5 6 7
…even if your partner or family isn’t physically active? 1 2 3 4 5 6 7
…even if you don't feel well? 1 2 3 4 5 6 7
…even if you don't know where to go to engage in physical activity? 1 2 3 4 5 6 7
…even if you don't know what types of physical activity to do? 1 2 3 4 5 6 7
…even if you are physically sore or in pain? 1 2 3 4 5 6 7

251
Section C: CADE-Q 2 Questionnaire
CADE-Q 2
Coronary Artery Disease Education Questionnaire
You are being invited to fill out this questionnaire because you are in a cardiac
rehabilitation program. Knowledge about your condition, treatments and risk factors is
an important component about management. We would like to have a sense of the
information that you have acquired thus far as you have been treating your heart
problem or risk factor.
About the questionnaire:
The purpose of this questionnaire is:
• to assess patients’ overall knowledge about heart disease and related factors; and,
• to assess specific areas/domains of knowledge (medical condition, risk factors, exercise, nutrition, and psychosocial risk,).
Questions are structured as followed:
• multiple choice
• each question has 4 possible answers/alternatives
• each answer corresponds to a knowledge level:
- a correct statement showing “complete knowledge”
- a correct statement showing “incomplete knowledge”
- an incorrect statement showing “wrong knowledge”
- a don’t know statement showing “lack of knowledge”
• each alternative has a score and the sum of final scores lead to a classification on knowledge.

253
Instructions for completing this survey:
• Questions are grouped in domains (areas of knowledge);
• Please answer as many questions as you can;
• Check the alternative you think that is the most correct one;
• If you don’t know the answer, mark the “don’t know” statement (do not leave the question blank);
• After completing the questionnaire, please return to the researcher or to the reception;
This questionnaire is confidential and completely voluntary.
It should take around 20 minutes to complete.
Thanks for your time!
CADE-Q 2’s Version (April 9 2013)
For CADE-Q 2 please refer to Appendix 2




















