Rehabilitation plan and process of patient with heart failure
140
FACULTY OF MEDICINE Rehabilitation plan and process of patient with heart failure Bachelor's thesis Rana Mohammed Ismail Supervisor: Mgr. Michal Úlehla Department of physiotherapy and rehabilitation. Field physiotherapy Brno 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Rehabilitation plan and process of patient with heart failure

FACULTY OF MEDICINE
Rehabilitation plan and
process of patient with
heart failure
Bachelor's thesis
Rana Mohammed Ismail
Supervisor: Mgr. Michal Úlehla
Department of physiotherapy and rehabilitation.
Field physiotherapy
Brno 2022


2
Bibliographic record
Author: Rana Mohammed Ismail
Faculty of Medicine
Masaryk University
Hewlett-Packard Company
Title of Thesis: Rehabilitation plan and process of patient with heart failure
Nazev prace: Rehabilitační plán a postup u pacienta se srdečním selháním
Degree Programme: Bachelor programme
Field of Study: Physiotherapy
Supervisor: Mgr. Michal Úlehla
Year: 2022
Number of Pages: 140
Keywords: heart failure, cardiomyopathy, myocardial infarction, cardiovascular
rehabilitation, physiotherapy
Klicove slova: srdeční selhání, kardiomyopatie, infarct myokardu, kardiovaskulární
rehabilitace, fyzioterapie

3

4
Abstract
This bachelor’s thesis deals with rehabilitation and physiotherapy of patients after heart failure.
It is divided into three parts. As first, the theoretical part focuses on the definition of the disease
and basics of anatomy, physiology of the heart and pathophysiology of heart failure. It includes
brief classification and stages, diagnostic criteria of the disease, as well as diagnostic methods
and treatment, prevention and complications of heart failure. The second part of thesis focuses
on different type and possibilities of rehabilitation, physiotherapy approaches after heart
failure. The third and the last part contains a practical case report of a patient who suffered
from heart failure including examination, short-term rehabilitation plan, individual exercise
session by the author which lasted for 5 days, and finally recommendations for follow-up care.
Anotace
Tato bakalářská práce se zabývá rehabilitací a fyzioterapií pacientů po srdečním selhání. Je
rozdělena do tří částí. Teoretická část se nejprve zaměřuje na definici onemocnění a základy
anatomie, fyziologii srdce a patofyziologii srdečního selhání. Zahrnuje stručnou klasifikaci a
stadia, diagnostická kritéria onemocnění, dále diagnostické metody a léčbu, prevenci a
komplikace srdečního selhání. Druhá část práce je zaměřena na různé typy a možnosti
rehabilitace, fyzioterapeutické přístupy po srdečním selhání. Třetí a poslední část obsahuje
praktickou kazuistiku pacienta se srdečním selháním včetně vyšetření, krátkodobého
rehabilitačního plánu, individuálního cvičení autora v délce 5 dnů a nakonec doporučení pro
následnou péči.

5

6
Declaration
I hereby declare that this thesis with title Rehabilitation plan and process of patient with
heart failure I submit for assessment is entirely my own work and has not been taken from the
work of others save to the extent that such work has been cited and acknowledged within the
text of mine.
Brno March 22, 2022 .......................................
Rana Mohammed Ismail

7

8
Acknowledgements
At this point I would like to express my gratitude to my supervisor Mgr. Michal Úlehla, for his
time and guidance, valuable advice, comments, and help in processing the work. I would like
to thank prof. MUDr. Jarmila Siegelová, DrSc. for her prudent organizing and teaching. Lastly,
I would like to express my sincere gratitude to Mr. L.P., for his willingness and cooperation
throughout the whole rehabilitation process.

9

10
Table of Content
LIST OF FIGURES ................................................................................................... 14
LIST OF TABLES ..................................................................................................... 15
1 REVIEW OF THEORETICAL KNOWLEDGE ................................................ 21
1.1 GENERAL PART OF THESIS ...................................................................................................... 21
1.1.1 INTRODUCTION .................................................................................................................... 21
1.1.2 DEFINITION OF HEART FAILURE ..................................................................................... 23
1.1.3 INCIDENCE ............................................................................................................................. 23
1.1.4 CLASSIFICATION OF HEART FAILURE ............................................................................ 24
1.1.5 STAGES OF HEART FAILURE ............................................................................................. 27
1.1.6 ETIOLOGY AND RISK FACTORS OF HEART FAILURE .................................................. 28
1.1.7 PATHOPHYSIOLOGY OF HEART FAILURE ...................................................................... 31
1.1.7.1 SYSTOLIC DYSFUNCTION ........................................................................................... 34
1.1.7.2 DIASTOLIC DYSFUNCTION ......................................................................................... 35
1.1.8 ANATOMY OF THE HEART .............................................................................................. 36
1.1.8.1 THE HEART CHAMBERS ......................................................................................... 37
1.1.8.2 THE HEART VALVES .............................................................................................. 37
1.1.8.3 THE CONDUCTION SYSTEM .................................................................................. 38
1.1.8.4 THE CIRCULATORY SYSTEM................................................................................ 38
1.1.8.5 STRUCTURE AND FUNCTION ................................................................................ 39
1.1.8.6 EMBRYOLOGY .......................................................................................................... 40
1.1.8.7 BLOOD SUPPLY AND LYMPHATICS .................................................................... 40
1.1.8.8 INNERVATION OF THE HEART .............................................................................. 41
1.1.8.9 MUSCLES OF THE HEART ....................................................................................... 42
1.1.9 PHYSIOLOGY OF THE HEART ............................................................................................ 42
1.1.9.1 CARDIAC CYCLE ...................................................................................................... 42
1.1.9.1.1 PRESSURE AND FLOW ..................................................................................... 44
1.1.9.1.2 PHASES OF CARDIAC CYCLE ......................................................................... 45
1.1.9.1.2.1. ATRIAL SYSTOLE AND DIASTOLE ....................................................... 45
1.1.9.1.2.2. VENTRICULAR SYSTOLE ....................................................................... 45
1.1.9.1.2.3. VENTRICULAR DIASTOLE ..................................................................... 46
1.1.9.2 RESTING CARDIAC OUTPUT .................................................................................. 47
1.1.9.3 EXERCISE AND MAXIMUM CARDIAC OUTPUT ................................................. 48
1.1.9.4 HEART RATE ............................................................................................................. 48
1.1.10 DIAGNOSTIC CRITERIA OF HEART FAILURE .............................................................. 49
1.1.10.1 MEDICAL HISTORY AND PHYSICAL EXAMINATION .................................. 49
1.1.10.2 LABORATORY TESTS ........................................................................................... 49
1.1.10.3 CHEST RADIOGRAPHY ......................................................................................... 50
1.1.10.4 ELECTROCARDIOGRAPHY .................................................................................. 51
1.1.10.5 CLINICAL DECISION MAKING ........................................................................... 51
1.1.10.6 AN OVERVIEW OF HEART FAILURE EVALUATION AND DIAGNOSIS .... 52
11
1.1.11 WARNING SIGNS AND SYMPTOMS OF HEART FAILURE ......................................... 54
1.1.12 HEART FAILURE DIAGNOSIS ......................................................................................... 55
1.1.13 HEART FAILURE TREATMENT ...................................................................................... 57
1.1.14. PREVENTION OF HEART FAILURE ............................................................................... 59
1.1.15 COMPLICATIONS OF HEART FAILURE ......................................................................... 62
1.2 SPECIAL PART OF THESIS ......................................................................................................... 64
1.2.1 GENERAL PRINCIPLES OF EXERCISE TESTING IN CARDIAC REHABILITATION 64
1.2.1.1 INTRODUCTION ......................................................................................................... 64
1.2.1.2 CARDIOPULMONARY EXERCISE TEST (SPIROERGOMETRY) .................. 64
1.2.1.3 CARDIAC STRESS TEST .......................................................................................... 66
1.2.1.4. DYNAMOMETRY .................................................................................................... 68
1.2.1.5. COMPREHENSIVE MEDICAL REHABILITATION ............................................ 68
1.2.1.5.1 PERIOPERATIVE CARDIAC REHABILITATION .......................................... 69
1.2.1.5.2 POST-OPERATIVE CARDIAC REHABILITATION ...................................... 70
1.2.1.5.2.1 PHASE 1: ACUTE, IN HOSPITAL PATIENT PERIOD ......................... 70
1.2.1.5.2.2 PHASE 2: SUBACUTE OUTPATIENT CARE (POST-DISCHARGE,
PRE-EXERCISE PERIOD), (2-6 WEEKS POST-SURGERY) .............................................. 71
1.2.1.5.2.3 PHASE 3: SUBACUTE OUTPATIENT CARE (POST-DISCHARGE,
PRE-EXERCISE PERIOD), (7-12 WEEKS POST-SURGERY) ............................................ 72
1.2.1.5.2.4 PHASE 4: MAINTENANCE (13 WEEKS AND BEYOND POST-
SURGERY) ................................................................................................................. 73
1.2.1.5.3 OUTPATIENT CONTROLLED PROGRAM ..................................................... 74
1.2.1.5.3.1 SPA TREATMENT ...................................................................................... 75
1.2.1.5.3.2 HOME EXERCISE PROGRAM ................................................................. 76
1.2.1.5.4 THERAPEUTIC PHYSICAL EDUCATION ...................................................... 76
1.2.1.5.4.1 RESPIRATORY PHYSIOTHERAPY .......................................................... 76
1.2.1.5.4.2 RESISTANCE TRAINING .......................................................................... 82
1.2.1.5.4.3 ENDURANCE AEROBIC TRAINING ....................................................... 86
1.2.1.5.5 PHYSICAL THERAPY METHODS .................................................................. 88
1.2.1.5.5.1 CARBONIC BATH ...................................................................................... 89
1.2.1.5.5.2 LOW-FREQUENCY ELECTRICAL STIMULATION ............................... 90
1.2.1.5.6 ERGOTHERAPY ................................................................................................. 90
1.2.1.5.7 PSYCHOLOGICAL AND SOCIAL PROBLEMS OF THE DISEASES ........... 91
1.2.1.5.8 INDICATIONS AND CONTRAINDICATIONS OF CARDIAC
REHABILITATION ............................................................................................................................... 93
2 CASUISTICS ............................................................................................................ 94
2.1 BASIC DATA ................................................................................................................................. 94
2.2 PLACE OF HOSPITALIZATION .................................................................................................. 94
2.3 DIAGNOSIS UPON ADMISSION.................................................................................................. 95
2.4 PRESCRIBED REHABILITATION ............................................................................................... 96
2.5 ENGAGEMENT OF AUTHOR IN THE REHABILITATION PROCESS ................................... 96
2.5.1 ANAMNESIS ........................................................................................................................... 96
2.5.2 PHYSICAL EXAMINATION ................................................................................................. 99

12
2.5.3 INITIAL KINESIOLOGY EXAMINATION ....................................................................... 103
2.5.4 SHORT-TERM PLAN .......................................................................................................... 110
2.5.5 REHABILITATION PROCESS ............................................................................................ 112
2.5.6 KINESIOLOGICAL EXAMINATION AT DISCHARGE .................................................. 119
2.5.7 LONG-TERM PLAN ............................................................................................................ 120
3 CONCLUSION ..................................................................................................... 123
IBLIOGRAPHY ....................................................................................................... 125

13

14
List of Figures
FIGURE 1 ANATOMICAL PARTS OF THE HEART
26 ........................................................................................................ 36
FIGURE 2 THE FOUR VALVES OF THE HEART27 ............................................................................................................ 38
FIGURE 3 OVERVIEW OF CARDIAC CYCLE35 ................................................................................................................... 44
FIGURE 4 RELATIONSHIP BETWEEN THE CARDIAC CYCLE AND ECG35 ...................................... 47
FIGURE 5 MAJOR FACTORS INFLUENCING CARDIAC OUTPUT38 ........................................................................ 48
FIGURE 6 ALOGORITHM FOR EVALUATION AND DIAGNOSIS OF HEART FAILURE148 ........................... 53
FIGURE 7 BACK POSITION, POSTURAL DRAINAGE TECHNIQUE115 ................................................................... 78
FIGURE 8 SIDE LYING POSITION, POSTURAL DRAINAGE TECHNIQUE115 ..................................................... 79
FIGURE 9 STOMACH POSITION, POSTURAL DRAINAGE TECHNIQUE115 ......................................................... 79
FIGURE 10 DEPP BREATHING AND COUGHING TECHNIQUE117 ........................................................................... 81
FIGURE 11 OVERVIEW OF MAJOR CARDIOVASCULAR EFFECT OF EXERCISE131-132 .............................. 88

15
List of Tables
TABLE 1 FRAMINGHAM DIAGNOSTIC CRITERIA FOR HEART FAILURE ................................................ 53
TABLE 2 WARNING SIGNS AND SYMPTOMS OF HEART FAILURE .......................................................... 54
TABLE 3 SUBJECTIVE PERCEPTION OF EFFORT ACCORDING BORG SCALE ........................................ 67
TABLE 4 SUBJECTIVE EVALUATION OF DYSPNEA ...................................................................................... 67
TABLE 5 RESISTANCE TRAINING PROGRAMMING FOR CARDIAC PATIENTS ...................................... 84
TABLE 6 RESISTANCE TRAINING BENEFITS FOR CARDIAC PATIENTS .................................................. 84
TABLE 7 ABSOLUTE AND RELATIVE CONTRAINDICATIONS FOR RT IN CARDIAC PATIENTS ....... 85
TABLE 8 ANTHROPOMETRY, LENGTH AND CIRCUMFERENCE IN OF THE UPPER EXTREMITY ... 106
TABLE 9 ANTHROPOMETRY, LENGTH AND CIRCUMFERENCE IN OF THE LOWER EXTREMITY... 107
TABLE 10 PERIMETER DIMENSIONS OF THE ABDOMEN AND CHEST IN ............................................. 107
TABLE 11 DEEP TENDON REFLEXES AND SUPERFICIAL REFLEXES .................................................... 108
TABLE 12 PATHOLOGICAL REFLEXES ........................................................................................................... 108
TABLE 13 MUSCLE SHORTENING TEST ........................................................................................................ 109
16
Glossary
1-RM Repetition Maximum Approach
AACVPR Association for Cardiovascular and Pulmonary
Rehabilitation
ACC American College of Cardiology
ACD Arteria Coronaria Dextra
ACE Angiotensin Converting Enzyme
ADH Antidiuretic Hormone
ADHF Acute Decompensated Heart Failure
ADL Activity of Daily Living
AHA American Heart Association
AHF Acute Heart Failure
AKI Acute Kidney Insufficiency
ATP Adenosine Triphosphate
AV Atrioventricular
BNP B-Type Natriuretic Peptide
BP Blood Pressure
Bpm Beat Per Minute
CAD Coronary Artery Disease
CAGB Carbonic Acid Gas Bath
CHHF Chronic Heart Failure
CKTCH Cardio Surgery Clinic
CO Cardiac output
CO2 Carbon Dioxide
17
COPD Chronic Obstructive Pulmonary Disease
CPAP Continuous Positive Airway Pressure
CPB Cardiopulmonary Bypass
CPR Cardiopulmonary Resuscitation
CPX Cardiopulmonary Exercise Test
CR Cardiac Rehabilitation
CRP Cardiac Rehabilitation Program
CRT – Ds Cardiac Resynchronization Therapy Device
CT Computerized Tomography
CVD Cardiovascular Disease
CVVHD Continuous Veno-venous Hemodialysis
DCM Delated Cardiomyopathy
DS Dorsal Septum
DVT Deep Vein Thrombosis
dx Dexter
E deceleration time Early left Ventricular Filling
e NOS Endothelial Nitric Oxide Synthase
E/A ratio Ratio of Early Left Ventricular to Atrial Filling
ECG Electrocardiography
Echo Echocardiogram
ECM Extracorporeal Membrane Oxygenation
EDV End Diastolic Volume
EF Ejection Fraction
EGF Epidermal Growth Factor
EPC Endothelial Progenitor Cell

18
ESV End Systolic Volume
ET Exercise Test
HBP High Blood Pressure
HDL High Density Lipoprotein
HF Heart Failure
HFpEF Heart Failure with Preserved Ejection Fraction
HFrEF Heart Failure with Reduced Ejection Fraction
HR Heart Rate
HRSL Symptoms Limited Heart Rate
IADL Instrumental Activity of Daily Living
ICD Implantable Cardioverter Defibrillator
ICHD Ischemic Heart Disease
IEF Increased Expiratory Flow
IKAK First Internal Cardiology Clinic
IU International Unit
LA Left Atrium
LAD Left Anterior Descending Coronary Artery
LCA Left Coronary Artery
LCX Left Circumflex Coronary Artery
LDL Low Density Lipoprotein
LFES Low Frequency Electrical Stimulation
LK Left Kidney
LR- Negative Likelhood Ratio
LR+ Positive Likelhood Ratio
LV Left Ventricle

19
LVEF Left Ventricular Ejection Fraction
M2 receptor Muscarinic Acetylcholine Receptor
MI Myocardial Infarction
mmHg Millimeter of Mercury
MRI Magnetic Resonance Imaging
MVR Mitrals Valve Replacement
NO Nitric Oxide
NSIAD’s Non-Steroidal Anti-inflammatory Drugs
NYHA New York Heart Association
OTS Orthotopic Transplantation of Heart
PDA Posterior Descending Artery
QOL Quality of Life
RC Ramus Circumflexus
RCA Right Coronary Artery
RER Respiratory Exchange Ratio
Res Resume
RIA Ramus Interventricularis Anterior
RMS Ramus Marginalis Sinister
ROM Range of Motion
RPP Rate Pressure Product
RT Resistance Training
RV Ramus Ventricularis
SA node Sinoatrial Node
SCD Sudden Cardiac Death
sin Sinister

20
SKG Selective Coronarography
STEMI ST – Elevation Myocardial Infarction
SV Stroke Volume
TG Triglyceride
THR Training Hear Rate
VA ECMO Veno-Atrial ECMO (Extracorporeal Membrane
Oxygenation)
VCO2 Carbonic Dioxide Output
VE/VCO2 Minute Ventilation Per Unit Carbon Dioxide
Production
VLDL Very Low-Density Lipoprotein
VO2 Oxygen Consumption
VO2SL Volume of Oxygen Symptoms Limited
VSM Vascular Smooth Muscle
VT1 First Ventilatory Threshold
VT1 Second Ventilatory Threshold
WHO World Health Organization

21
1 REVIEW OF THEORETICAL KNOWLEDGE
1.1 General Part of Thesis
1.1.1 Introduction
Heart failure has been described by some authors as the cardiovascular epidemic of the
21st century, characterized by its increasing incidence and prevalence, as evidenced by the
increased number of hospitalizations. This is mainly due to an aging population, as well as
better and more accessible medical care, which has progressively reduced mortality due to
ischemic heart disease (ICHD) or myocardial infarction (MI). In the 1950s when Eisenhower
had his heart attack, the treating physician did not have many options, accordingly the mortality
rate averaged 50 % for those reaching hospital. Heart attack survivors at that time were prone
to developing heart failure or sudden death. Today we are much more successful in treating
patients with acute myocardial infarction. The mortality rate today is 5 % for those getting to
hospital and receiving appropriate treatment in a hospital with capability to perform primary
percutaneous coronary intervention. Another reason for the increase in hospitalizations due to
heart failure is the prevention of sudden death in patients with impaired left ventricular function
by the use of devices and antiarrhythmic drugs. Finally, the introduction of drugs and
interventions for the treatment of high blood pressure has reduced the occurrence of myocardial
infarction but has led to an increase in heart failure with preserved and reduced ejection
fraction.1-2-3
Heart failure is the end stage of all diseases of the heart and is a major cause of
morbidity and mortality. Roughly 670,000 people are diagnosed with heart failure each year. It’s
the main reason people older than 65 go into the hospital.
Despite significant advances in diagnosis and treatment, both acute and chronic heart failure
represent a clinical syndrome with a serious prognosis. According to the Framingham Study,
the 5-year mortality rate for chronic heart failure (CHHF) is 25 % for men and 40 % for women.
In patients classified as New York Heart Association (NYHA) III and IV, mortality can be as
high as 20-50 % in one year.2 In most cases, patients with heart failure die from cardiovascular
causes, particularly from sudden cardiac death (SCD) and exacerbation of heart failure.4
Heart failure and its symptoms significantly affect a patient’s quality of life.
Physical training and rehabilitative care are an integral part of the treatment procedure for
patients with heart failure. They not only help improve the patient’s quality of life, but also
help prevent and treat other comorbidities. In the case of heart attack or another heart problem,
22
cardiac rehabilitation is an important part of the recovery. Cardiac rehabilitation can help
prevent another heart attack, possibly a more serious one, and can help build heart-healthy
habits.
Generally, cardiac rehabilitation is an important program for anyone recovering from a
heart attack, heart failure, or other heart problem that required surgery or medical care.
Cardiac rehabilitation is a supervised program that includes physical activity. Education about
healthy living, including how to eat healthy, take medicine as prescribed, and quit smoking.
Counseling to find ways to relieve stress and improve mental health.
Anyone who has had a heart problem, such as a heart attack, heart failure, or heart
surgery, can benefit from cardiac rehabilitation. Studies have found that cardiac rehabilitation
helps men and women, people of all ages, and people with mild, moderate, and severe heart
problems.5
However, some people are less likely to start or finish a cardiac rehabilitation program,
including studies show that women, especially minority women, are less likely than men to
start or complete cardiac rehabilitation. This may be because doctors are less likely to suggest
cardiac rehabilitation to women. Older adults are also likely to join a cardiac rehabilitation
program following a heart problem. They may think they are unable to do the physical activity
because of their age, or they may have other conditions that can make exercising harder, such
as arthritis. The need to address other physical conditions makes cardiac rehabilitation
especially useful for older adults, since it can improve strength and mobility to make daily tasks
easier.
Cardiac rehabilitation can have many health benefits in both the short and long term,
including: strengthening the heart and body after heart complication, relieving symptoms of
heart problems such as chest pain, building healthier habits such as getting more physical
activity, quitting smoking, eating a heart-healthy diet, reducing stress, improving the mood,
lessen depression, increasing the energy and the strength to make daily activities like carrying
groceries and climbing stairs easier, preventing future illness and death from heart disease.
Studies have found that cardiac rehabilitation decreases the chance of death in the 5 years
following a heart attack or bypass surgery by about 35 %.6
The work itself is divided into a theoretical part, in which I focus on definition,
incidence, prevalence and etiology, pathophysiology, clinical manifestations, disease course,
diagnosis and, finally, treatment of heart failure, including comprehensive medical
rehabilitation. The second part is a case study, where I apply the theoretical knowledge

23
presented in the first part to a specific patient and focus mainly on the possibilities of
rehabilitation.
1.1.2 Definition of heart failure
Heart failure also known as congestive heart failure and congestive cardiac failure, is a
pathophysiological condition in which the heart, as a pump, is unable to meet the metabolic
requirements of the tissue for oxygen and substrates despite normal or increased venous return
to the heart, is a long-term condition that gets worse over time. Although the name sounds like
your heart has stopped working, from a pathophysiological point of view heart failure doesn’t
mean the heart stopped working. Rather, it means that the heart works less efficiently than
normal for various possible reasons, blood moves through the heart and body at a slower rate
and the pressure in the heart increases. As a result, the heart cannot pump enough oxygen and
nutrients to meet the body’s needs. The chambers of the heart may respond by stretching to
carry more blood to pump through the body or by hardening and thickening.
This helps keep the blood moving, but the walls of the heart muscle may eventually
weaken and become unable to pump blood efficiently. The kidneys may respond by making
the body retain fluid (water) and salt. If fluid builds up in the arms, legs, ankles, feet, lungs, or
other organs, the body becomes congested. The term congestive heart failure is used to describe
the condition.
In other words, we can say that is when the heart is not able to pump blood as well as
it should. When heart’s pumping power drops, it can damage your organs and fluid can collect
in your lungs.7
1.1.3 Incidence
Over the last 30 years we have gone from famine to feast in terms of the epidemiological data
now published for heart failure (HF). The field started with the seminal publication on the
natural history of HF from the Framingham study in 1971 showing a prevalence of HF of
0.8 % in those aged between 50 and 59, rising to 9.1 % in those over 80 years with incidence
rates of 0.2 % at age 54 and 0.4 % at age 85. This was followed by a large European study the
men born in 1913, which gave similar figures of a prevalence of 2.1 % at age 50 and 13 % at
age 67 and incidence rates of 0.15 % and 1 % respectively at ages 50 and 67.

24
These landmark studies relied on a clinical diagnosis of HF, based on symptoms, signs,
and scoring systems to identify cases. More modern epidemiological studies have used
definitions of HF which include objective measures of cardiac function in their definition, in
keeping with current European and United States guidelines for the diagnosis of HF. Initial
studies focused on systolic dysfunction because they reported at much the same time as the HF
treatment trials which also enrolled patients with systolic HF. More recently attention has
turned to describing the epidemiology of HF with preserved systolic function, in addition.
When describing the epidemiology of HF, it is worth bearing in mind that estimates of
incidence and prevalence will vary according to the definition of HF used and the type of cohort
being studied. This is especially important when assessing work which has objectively
measured left ventricular systolic function. Variables such as left ventricular ejection fraction
are normally distributed, so the cut point chosen is a critical determinant of the eventual results.
The present chapter aims to outline the contemporary epidemiology of HF by describing its
prevalence, incidence, etiology and mortality as well as describing the trends which are
occurring in the area. It will discuss hospitalization rates, prognosis and economic burden in
both Europe and the United States.8
1.1.4 Classification of heart failure
• Classification based on the course of the disease:
We classify heart failure from several perspectives. Depending on the rate of onset of
symptoms, it is acute and chronic heart failure. AHF is when symptoms appear suddenly, or a
person experiences rapid worsening of existing symptoms of heart failure, with AHF, you
experience a sudden, rapid decline in heart functioning and the amount of blood your heart can
pump to the rest of your body. AHF occurs in people with or without previous heart issues.
Acute decompensated heart failure (ADHF) occurs in people with heart conditions, such as
coronary artery disease. De novo acute heart failure occurs in people with no history of heart
disease.9 They have ongoing health conditions, like diabetes, that damage their heart.
The first manifestation of heart failure is AHF in approximately 20 % of cases. One of
the most common symptoms of AHF is shortness of breath (dyspnea), you may experience:
heavy breathing, sensation like suffocating, struggling to breath while laying down, tight chest.
Other symptoms may include: arrythmia, cough, chest pain, fluid retention (edema) in the arms
or legs. Health issues that strain the heart increase your risk of heart failure: advanced kidney
25
disease, alcoholism, blood clot in the lungs (pulmonary embolism), diabetes, hypertension,
hyperthyroidism, stroke, sleep apnea. Existing heart problems that cause ADHF include:
arrythmia, coronary artery disease, heart valve disease. CHHF otherwise known as congestive
heart failure, is manifested by a gradual development of symptoms. It can occur as a result of
AHF, but it can also occur in patients without a previous acute episode. The symptoms of
CHHF is quite similar to the AHF such as: shortness of breath, tiredness, swelling of the legs
and ankles, chest pain and a cough. In the long run, it is usually progressive in nature, with the
rate of progression varying for each patient. With adequate therapy, progression may be
stopped until the disease subsides. A typical feature is the intermittent and fluctuating nature
of the disease – periods of relative stability are alternated by periods of worsening cardiac
compensation, which often lead to hospitalization.
An estimated 15 % of patients are in the advanced CHHF phase in the NYHA category
III – IV.1 It most commonly affects older people and people with other heart conditions and is
typically treated with a combination of lifestyle and diet changes, and medications. Chronic
heart failure is typically a long-term condition that gradually worsens over time. This is the
feature that differentiates it from AHF, which develops very suddenly. It cannot typically be
cured, but symptoms can be managed effectively.
• Another classification:
Heart failure often only affects the left or right side of the heart but can affect both. Doctors
differentiate between three types of heart failure, accordingly:
Left-sided heart failure: The left ventricle of the heart no longer pumps enough blood around
the body. As a result, blood builds up in the pulmonary veins (the blood vessels that carry blood
away from the lungs). This causes shortness of breath, trouble breathing or coughing –
especially during physical activity. Left-sided heart failure is the most common type.
Right-sided heart failure: Here the right ventricle of the heart is too weak to pump enough
blood to the lungs. This causes blood to build up in the veins (the blood vessels that carry blood
from the organs and tissue back to the heart). The increased pressure inside the veins can push
fluid out of the veins into surrounding tissue. This leads to a build-up of fluid in the legs, or
less commonly in the genital area, organs or the abdomen (belly).

26
Biventricular heart failure: In biventricular heart failure, both sides of the heart are affected.
This can cause the same symptoms as both left-sided and right-sided heart failure, such as
shortness of breath and a build-up of fluid.
Left-sided heart failure is usually caused by coronary artery disease (CAD), a heart
attack or long-term high blood pressure. Right-sided heart failure generally develops as a result
of advanced left-sided heart failure and is then treated in the same way. It is sometimes caused
by high blood pressure in the lungs, an embolism in the lungs (pulmonary embolism), or certain
lung diseases such as chronic obstructive pulmonary disease (COPD).
• Classification based on pumping ability:10
Nowadays, heart failure is increasingly being classified based on the pumping ability of the
heart. This is because the pumping ability plays an important role when choosing the most
suitable medication. There are two different types of chronic heart failure:
Heart failure with reduced pumping ability: The medical term for this is “heart failure with
reduced ejection fraction (HfrEF), or systolic heart failure.” Systolic heart failure occurs when
the left ventricle loses its ability to contract, when the heart is too weak and doesn’t squeeze
normally. In people with systolic heart failure, blood fills the left ventricle at normal levels, but
it cannot be pumped in adequate amounts to support bodily functions. If the body’s tissues are
deprived of oxygen, organ failure may ensue. The most common causes of systolic heart failure
are coronary artery disease, hypertension, cardiomyopathy, myocarditis.10
Heart failure with preserved pumping ability: Doctors call this “heart failure with preserved
ejection fraction (HfpEF). Or diastolic heart failure.” Diastolic heart failure occurs when the
left ventricle loses its ability to expand due to stiffness. The heart chamber also is unable to fill
with enough blood normally during the resting periods of the cardiac cycle. As a result, there
is less blood available to pump out of the heart. Diastolic heart failure occurs when the left side
of the heart is too stiff to relax and fill normally with blood. The most common culprits of left-
sided heart failure are heart attack, coronary artery disease, hypertension. While the right side
of the heart is more commonly affected by: COPD, Rheumatic heart disease.10 As you get older,
the heart and blood vessels become less elastic, increasing the risk of developing diastolic heart

27
failure. Other causes of diastolic heart failure: diabetes, obesity, sedentary lifestyle, coronary
artery disease.10
It is also possible to be affected by a combination of these two types. Moreover, each
type of chronic heart failure can affect the left ventricle, right ventricle or both simultaneously.
The symptoms of chronic heart failure generally depend on the type of the condition being
experienced and its location, i.e. which ventricle is involved. The main symptom of left-sided
chronic heart failure is shortness of breath, which will generally become worse with activity or
when lying flat. A cough may also present. If the condition is affecting the right-side of the
heart, edema, a buildup of fluid causing swelling of the legs and ankles, is the most commonly
experienced symptom.10
1.1.5 Stages of heart failure
According to WebMD, in 2001, the American Heart Association (AHA) and American College
of Cardiology (ACC) described the “Stages of Heart Failure.” These stages, which were
updated in 2005, will help understand to that heart failure is often a progressive condition and
can worsen over time. They will also help to understand why a new medication was added to
the treatment plan and may also help understand why lifestyle changes and other treatments
are needed. The stages classified by the AHA and ACC are different than the New York Heart
Association (NYHA) clinical classifications of heart failure that rank patients as class I-II-III-IV,
according to the degree of symptoms or functional limits.11
• Stage A: Stage A is considered pre-heart failure. It means you’re at high risk of
developing heart failure because you have a family history of heart failure or you have
one or more of these medical conditions: hypertension, diabetes, coronary artery
disease, metabolic syndrome, history of alcohol abuse, metabolic syndrome, family
history of cardiomyopathy, history of taking drugs that can damage your heart muscle,
such as some cancer drugs. Simply, at high risk for heart failure but without structural
heart disease or symptoms of heart failure
• Stage B: Stage B is considered pre-heart failure. It means your healthcare provider has
given you a diagnosis of systolic left ventricular dysfunction, but you’ve never had
symptoms of heart failure. Most people with Stage B heart failure have an

28
echocardiogram (echo) that shows an ejection fraction (EF) of 40 % or less. This
category includes people who have heart failure and reduced EF (HF-rEF) due to any
cause. Simply structural heart disease but without signs or symptoms of heart failure.
• Stage C: People with Stage C heart failure have a heart failure diagnosis and currently
have or previously had signs and symptoms of the condition. Symptoms include
shortness of breath, fatigue, reduced ability to exercise, weak legs, waking up to urinate,
swollen feet, ankles, lower legs and abdomen.
• Stage D and reduced EF: People who have Stage D HF-rEF have advanced symptoms
that don’t get better with treatment. This is the final stage of heart failure.12
According to WebMD, The New York Heart Association (NYHA) clinical classifications
of heart failure rank people as class I-II-III-IV, according to the degree of symptoms or functional
limits.11
• Class I: Physical activity is not affected, and you have no unusual fatigue, shortness of
breath, palpitations, or pain during normal activities.
• Class II: Slight limitations on normal activities. You may have mild fatigue, shortness of
breath, palpitations, or pain during normal activities, no symptoms at rest.
• Class III: Marked limitation on normal activities. You have fatigue, shortness of breath,
palpitations, or pain during less than normal activities, no symptoms at rest.
• Class IV: You’re uncomfortable even at rest. Discomfort gets worse with any physical
activity.11
1.1.6 Etiology and risk factors of heart failure
Many other heart conditions can ultimately lead to heart failure. All of us lose some blood-
pumping ability in our hearts as we age, but heart failure results from the added stress of health
conditions that either damage the heart or make it work too hard. All of the lifestyle factors that
increase your risk of heart attack and stroke – smoking, being overweight, eating foods high in
fat and cholesterol and physical inactivity – can also contribute to heart failure.
Conditions that may lead to heart failure:13
1. Coronary artery disease. When cholesterol and fatty deposits build up in the heart’s
arteries, less blood can reach the heart muscle. This buildup is known as atherosclerosis.

29
The result may be chest pain (angina) or, if blood flow becomes totally obstructed, a
heart attack. Coronary artery disease can also contribute to having high blood pressure,
which may lead to heart failure over time.
2. Past heart attack (myocardial infarction). A heart attack occurs when an artery that
supplies blood to the heart muscle gets blocked. The denial of oxygen and nutrients
damages the heart’s muscle tissue – part of it essentially “dies.” The damaged heart
tissue does not contract as well, which weakens the heart’s ability to pump blood.
3. High blood pressure (hypertension or HBP). Uncontrolled HBP is a major risk factor
for developing heart failure. When pressure in the blood vessels is too high, the heart
must pump harder than normal to keep the blood circulating. This takes a toll on the
heart, and over time the chambers get larger and weaker. For those at risk of developing
heart failure, your doctor might prescribe medication to get your blood pressure below
130/80 mmHg.13
4. Abnormal heart valves. Heart valve problems can result from disease, infection
(endocarditis) or a defect present at birth. When the valves don’t open or close
completely during each heartbeat, the heart muscle has to pump harder to keep the blood
moving. If the workload becomes too great, heart failure results.
5. Heart muscle disease (dilated cardiomyopathy, hypertrophic cardiomyopathy) or
inflammation (myocarditis). Any damage to the heart muscle – whether because of drug
or alcohol use, viral infections or unknown reasons – increases the risk of heart failure.
6. Heart defects present at birth (congenital heart disease). If the heart and its chambers
don’t form correctly, the healthy parts have to work harder to compensate.
7. Severe lung disease. When the lungs don’t work properly, the heart has to work harder
to get available oxygen to the rest of the body.13
8. Diabetes. Diabetes increases the risk for developing heart failure. People with diabetes
tend to develop hypertension and atherosclerosis from elevated lipid level in the blood.
Both hypertension and atherosclerosis have been linked to heart failure.
9. Obesity. Obesity can cause the heart to work much harder than for a non-obese person.
Being obese is also a cause of sleep apnea and can cause cardiomyopathy.
10. Sleep apnea. Sleep apnea is a potentially life-threatening sleep disorder. Pauses in
breathing can contribute to severe fatigue during the day, increase your safety risks and
make it difficult to perform tasks that require alertness. Sleep apnea is also a risk factor
for medical problems like high blood pressure, heart failure, diabetes and stroke. In

30
some cases, people with heart failure may need to use a continuous positive airway
pressure machine (CPAP).13
Other conditions:
Less commonly, an otherwise healthy heart may become temporarily unable to keep up with
the body's needs. This can happen in people who have:
1. Low red blood cell count (severe anemia). When there aren't enough red blood cells to
carry oxygen, the heart tries to move the small number of cells at a faster heart rate. It
can become overtaxed from the effort.
2. An overactive thyroid gland (hyperthyroidism). This condition causes the body to work
at a faster pace, and the heart can be overworked trying to keep up.
3. Abnormal heart rhythm (arrhythmia or dysrhythmia). When the heart beats too fast, too
slow or irregularly, it may not be able to pump enough blood to meet all the body's
needs.
In these cases, the person may experience heart failure symptoms until the underlying problem
is identified and treated.13
According to WebMD, some drugs and natural supplements cause or worsen heart failure
because they: Are toxic to your heart, Affect the strength of heart muscle contractions, Make high
blood pressure worse, Prevent heart failure medications from working well.14
Prescription drugs: People with heart failure take an average of 6.8 prescription medicines
a day. The more drugs you take, the more likely you are to have a drug-drug interaction. This can
put your heart at risk.
These drugs can raise your risk of heart failure or related problems:
1. Nonsteroidal anti-inflammatory drugs (NSAIDs). Prescription NSIADs include
diclofenac, ibuprofen, indomethacin, and ketorolac. More than 70 million prescriptions
are written every year for this type of pain reliever. NSAIDs can boost heart failure odds
because they make you retain water and salt, make it harder for your blood to flow, and
make it tougher for diuretic drugs (often used to treat high blood pressure) to work
2. Diabetes medications. Your body gets rid of metformin through your kidneys, so it isn’t a
good choice if your kidneys don’t work like they should. Thiazolidinediones
(pioglitazone, rosiglitazone) cause fluid retention and weight gain in people with heart
31
failure and make people who don’t have it more likely to get it. Doctors aren’t sure why,
but dipeptidyl peptidase-4 inhibitors (alogliptin, linagliptin, saxagliptin, sitagliptin) seem
to send people with heart failure to the hospital.
3. Blood pressure medicine. Calcium channel blockers can worsen edema or fluid that stays
in your body’s tissues. Central agonists (clonidine, moxonidine) cause changes in the
way your body releases hormones that affect your heart.
4. Other types of drugs that can bring on heart failure include: Antifungal medications,
cancer medications, stimulants, antidepressants, tumor necrosis factor (TNF) inhibitor.
5. Natural supplements: There is no government regulation of natural supplements, so you
can't always be sure that a package contains what the label says. Some of them can
cause serious risks, especially if you have a health condition. That goes for vitamins, too.
They seem harmless because they occur naturally in food. But in pill form, it’s a different
story. More than 400 IU of vitamin E daily can increase your chances of developing heart
failure. Supplements can also interact with other drugs. One natural product may be fine
for your neighbor but put your health at risk.14
1.1.7 Pathophysiology of heart failure The primary pathophysiology of heart failure is decreased heart muscle efficiency as a result
of damage or overload. As a result, it can be caused by a variety of conditions, including
myocardial infarction (in which the heart muscle lacks oxygen and dies), hypertension (which
increases the force required to pump blood), and amyloidosis (in which it malfunctions).
During compression, proteins are deposited in the heart muscle, causing it to stiffen. Over time,
these increases in workload will cause changes in the heart.15
Because of the increased load on the ventricle, the heart of a person with heart failure
may have a lower force of contraction. An increase in ventricular filling causes an increase in
the force of contraction (according to Frank Starling's law of the heart) and thus an increase in
cardiac output in a healthy heart. This mechanism fails in heart failure because the ventricle
becomes so clogged with blood that contraction of the heart muscle becomes inefficient. This
is due to the dilated heart muscle's decreased ability to bind actin and myosin filaments.15
Reduced stroke volume can occur as a result of a failure of a systolic, diastolic, or both
failures. Reduced contractility is usually the cause of increased end systolic volume. End
diastolic volume is reduced as a result of impaired ventricular filling, which occurs when the

32
ventricle's compliance decreases (i.e., when the walls stiffen). As the heart works harder to
meet normal metabolic demands, the amount cardiac output can increase in times of increased
oxygen demand (e.g., exercise) is reduced. This contributes to the exercise intolerance
commonly seen in heart failure. This translates to the loss of one's cardiac nerve, or the ability
of the heart to work harder during strenuous physical activity. Since the heart has to work
harder to meet the normal metabolic demands, it is incapable of meeting the metabolic demands
of the body during exercise.
An increased heart rate, caused by increased sympathetic activity, is a common finding
in people with heart failure.16 In order to maintain adequate cardiac output. Initially, this helps
compensate for heart failure by maintaining blood pressure and perfusion, but it puts more
stress on the heart muscle, increasing coronary perfusion requirements, which can exacerbate
ischemic heart disease. Sympathetic activity may also cause an irregular heartbeat. An increase
in the physical size of the muscular layer of the heart may occur. This is caused by an increase
in the size of terminally differentiated myocardial fibers in an attempt to improve contractility.
This may contribute to an increase in rigidity and thus a reduced ability to relax during diastole.
Ventricular hypertrophy can also occur and contribute to an enlarged heart and the spherical
shape of a failing heart. An increase in ventricular volume also leads to a decrease in stroke
volume due to mechanical and ineffective contraction of the heart.17-18
The overall impact is a reduction in cardiac output and an increase in heart strain. This
raises the risk of cardiac arrest (due to irregular ventricular heart rhythms in particular) and
lowers blood flow to the rest of the body. Reduced cardiac output causes a variety of changes
in the rest of the body in chronic disease, some of which are physiological compensations and
others which are part of the disease process:23
1. Blood pressure in the arteries drops. Baroreceptors in the carotid sinus and aortic arch
that connect to the nucleus tractus solitarii are destimulated as a result. Catecholamines
are released into the bloodstream as a result of increased sympathetic activity in this
part of the brain. When alpha-1 receptors are binded, systemic arterial vasoconstriction
occurs. This helps to lower blood pressure, but it also raises total peripheral resistance,
which puts more strain on the heart. In an attempt to boost cardiac output, binding to
beta-1 receptors in the myocardium increases heart rate and makes contractions more
powerful. However, this increases the amount of work that the heart needs to do.
33
2. The posterior pituitary secretes vasopressin (also known as antidiuretic hormone or
ADH) in response to increased sympathetic activation, causing fluid retention in the
kidneys. Blood volume and blood pressure rise as a result of this.
3. Heart failure also limits the kidneys' ability to get rid of sodium and water, which
increases edema 19. Reduced blood flow to the kidneys stimulates the secretion of renin
- an enzyme that stimulates the production of powerful angiotensinogen that
compresses the vessels. Angiotensin and its metabolites cause further vasoconstriction
and stimulate increased secretion of the steroid aldosterone from the adrenal glands.
This promotes salt and fluid retention in the kidneys.
4. Chronically high levels of circulating neuroendocrine hormones including
catecholamines, renin, angiotensin, and aldosterone directly influence the myocardial,
producing long-term structural changes in the heart. Many of these remodeling effects
appear to be mediated by transforming growth factor beta (TGF-beta), which is a
common downstream target of the signal transduction cascade initiated by
catecholamines and angiotensin II,20-21and also by epidermal growth factor (EGF),
which is a target of the signaling pathway activated by aldosterone.22
5. Atrophy of muscle fibers occurs when skeletal muscle perfusion is reduced. This can
lead to weakness, fatiguability, and a loss of peak strength, all of which contribute to
exercise intolerance.23
Increased peripheral resistance and blood volume put additional load on the heart,
accelerating the deterioration of the myocardium. Vasoconstriction and fluid retention produce
an increased hydrostatic pressure in the capillaries. This shifts the balance of forces in favor of
interstitial fluid formation as the increased pressure forces additional fluid out of the blood,
into the tissue. Edema (fluid build-up) develops in the tissues as a result of this. Fluid
accumulation in right-sided heart failure often begins in the ankles, where venous pressure is
high due to gravity's effects (however if the patient is bed-ridden, fluid accumulation may begin
in the sacral area). It may also occur in the abdominal cavity, where the fluid buildup is called
ascites. In left-sided heart failure edema can occur in the lungs – this is called cardiogenic
pulmonary edema. This reduces spare capacity for ventilation, causes stiffening of the lungs
and reduces the efficiency of gas exchange by increasing the distance between the air and the
blood. The consequences of this are dyspnea (shortness of breath), orthopnea and paroxysmal
nocturnal dyspnea.

34
The symptoms of heart failure are largely determined by which side of the heart fails.
The left side pumps blood into the systemic circulation, whilst the right-side pumps blood into
the pulmonary circulation. Whilst left-sided heart failure will reduce cardiac output to the
systemic circulation, the initial symptoms often manifest due to effects on the pulmonary
circulation. In systolic dysfunction, the ejection fraction is decreased, leaving an abnormally
elevated volume of blood in the left ventricle. In diastolic dysfunction, the end-diastolic
ventricular pressure will be high. This increase in volume or pressure backs up to the left atrium
and then to the pulmonary veins. Increased volume or pressure in the pulmonary veins
interferes with normal alveolar drainage and encourages fluid flow from the capillaries to the
lung parenchyma, resulting in pulmonary edema. Gas exchange is hampered as a result of this.
As a result, shortness of breath, orthopnea, and paroxysmal nocturnal dyspnea are common
symptoms of left-sided heart failure. Patients with severe cardiomyopathy will experience cold
and clammy extremities, cyanosis, claudication, generalized weakness, dizziness, and fainting
as a result of decreased cardiac output and poor perfusion.
As a result of the low blood oxygen generated by pulmonary edema, the pulmonary
circulation becomes constricted, resulting in pulmonary hypertension. Since the right ventricle
generates lower pressures than the left ventricle (approximately 20 mmHg versus around 120
mmHg in a healthy individual) but produces cardiac output that is exactly the same as the left
ventricle, a small increase in pulmonary vascular resistance causes a large increase in the
amount of work the right ventricle must perform. However, the primary mechanism through
which left-sided heart failure leads to right-sided heart failure is unknown. Some theories
invoke mechanisms that are mediated by neurohormonal activation. 24
Mechanical effects may also play a significant role. As the left ventricle expands, the
intraventricular septum bends into the right ventricle, reducing the capacity of the right
ventricle.
1.1.7.1 Systolic dysfunction
Heart failure caused by systolic dysfunction is more easily identified. It can be described simply
as a failure of the heart's pump function. It is characterized by a lower ejection fraction (less
than 45 %). The strength of ventricular contraction is reduced, making it insufficient to generate
sufficient stroke volume, resulting in low cardiac output. In general, this is caused by
dysfunction or destruction of cardiac myocytes or their molecular components. Myocytes and

35
their components can be damaged by inflammation (such as in myocarditis) or by infiltration
(such as in amyloidosis). Toxins and pharmacological agents (such as ethanol, cocaine,
doxorubicin, and amphetamines) cause intracellular damage and oxidative stress.
The most common mechanism of damage is ischemia, which causes infarction and scar
formation. After a myocardial infarction, the dead muscle cells are replaced by scar tissue,
which detrimentally affects myocardial function. On an echocardiogram, this is manifested by
abnormal wall movement (hypokinesia) or absent wall movement (movement). The ventricular
diastolic end pressure and volumes rise as a result of insufficient ventricle emptying. This is
transmitted to the atrium. The increased pressure travels to the pulmonary blood vessels on the
left side of the heart, and the resulting hydrostatic pressure encourages fluid leakage into the
lung parenchyma, resulting in pulmonary edema. The increased pressure travels to the systemic
venous circulation and systemic capillary beds on the right side of the heart, causing fluid to
leak into the tissues of the target organs and extremities, resulting in associated peripheral
edema.25
1.1.7.2 Diastolic dysfunction
Heart failure caused by diastolic dysfunction is defined as the failure of the ventricle to
adequately relax in the backward direction and is characterized by a stiffer ventricular wall
during diastole. This leads in insufficient filling of the ventricle and, as a result, insufficient
stroke volume (SV). Final-diastolic pressures rise when ventricular relaxation fails, and the end
effect is the same as in the event of systolic dysfunction (pulmonary edema in left heart failure,
peripheral edema in right heart failure). Diastolic dysfunction can be generated by similar
processes as systolic dysfunction, especially those that impact heart remodeling.
Diastolic dysfunction may only appear in severe physiological states if systolic function
is maintained. The patient may be completely asymptomatic at rest. However, they are very
sensitive to increased heart rate, and may lead to sudden episodes of tachycardia (which can be
caused simply by physiological responses to stress, fever or dehydration, or by pathological
arrhythmias such as atrial fibrillation with ventricular response). Rapid flash of pulmonary
edema. Therefore, appropriate rate control (usually with a pharmacological agent that slows
AV conduction such as calcium channel blockers or beta-blockers) is critical to prevent acute
decompensation.
36
Echocardiography can determine left ventricular diastolic function by measuring
parameters such as the E/A ratio (ratio of early left ventricular to atrial filling), E deceleration
time (early left ventricular filling), and isovolumic relaxation time.25
1.1.8 Anatomy of the heart
According to Office of research administration at Texas Heart Institute.
The heart weighs between 7 and 15 ounces (200 to 425 grams) and is a little larger than the
size of your fist. By the end of a long life, a person’s heart may have beat (expanded and
contracted) more than 3.5 billion times. In fact, each day, the average heart beats 100,000
times, pumping about 2,000 gallons (7,571 liters) of blood.27-28-29
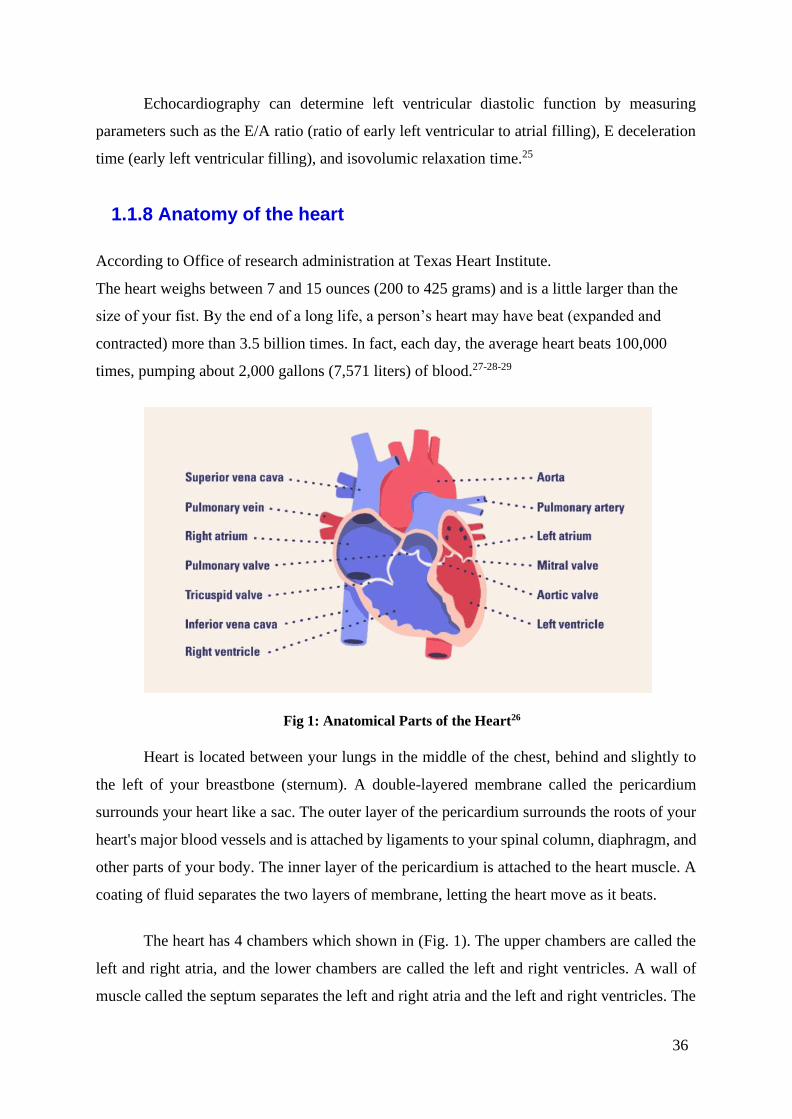
Fig 1: Anatomical Parts of the Heart26
Heart is located between your lungs in the middle of the chest, behind and slightly to
the left of your breastbone (sternum). A double-layered membrane called the pericardium
surrounds your heart like a sac. The outer layer of the pericardium surrounds the roots of your
heart's major blood vessels and is attached by ligaments to your spinal column, diaphragm, and
other parts of your body. The inner layer of the pericardium is attached to the heart muscle. A
coating of fluid separates the two layers of membrane, letting the heart move as it beats.
The heart has 4 chambers which shown in (Fig. 1). The upper chambers are called the
left and right atria, and the lower chambers are called the left and right ventricles. A wall of
muscle called the septum separates the left and right atria and the left and right ventricles. The

37
left ventricle is the largest and strongest chamber in your heart. The left ventricle’s chamber
walls are only about a half-inch thick, but they have enough force to push blood through the
aortic valve and into your body.
1.1.8.1 The Heart chambers
• The right atrium receives non-oxygenated blood from the body’s largest veins —
superior vena cava and inferior vena cava — and pumps it through the tricuspid valve
to the right ventricle.
• The right ventricle pumps the blood through the pulmonary valve to the lungs, where it
becomes oxygenated.
• The left atrium receives oxygenated blood from the lungs and pumps it through the
mitral valve to the left ventricle.
• The left ventricle pumps oxygen-rich blood through the aortic valve to the aorta and the
rest of the body.26
1.1.8.2 The Heart Valves
Four valves regulate blood flow through the heart, shown in (Fig. 2):
• The tricuspid valve regulates blood flow between the right atrium and right ventricle.
• The pulmonary valve controls blood flow from the right ventricle into the pulmonary
arteries, which carry blood to your lungs to pick up oxygen.
• The mitral valve lets oxygen-rich blood from your lungs pass from the left atrium into
the left ventricle.
• The aortic valve opens the way for oxygen-rich blood to pass from the left ventricle
into the aorta, your body’s largest artery.27

38
Fig 2: The Four Valves of the Heart27
Texas Heart Institute
1.1.8.3 The Conduction System
Electrical impulses from heart muscle (the myocardium) cause the heart to contract. This
electrical signal begins in the sinoatrial (SA) node, located at the top of the right atrium. The
SA node is sometimes called the heart’s “natural pacemaker.” An electrical impulse from this
natural pacemaker travels through the muscle fibers of the atria and ventricles, causing them to
contract. Although the SA node sends electrical impulses at a certain rate, your heart rate may
still change depending on physical demands, stress, or hormonal factors.28
1.1.8.4 The Circulatory System
The heart and circulatory system make up the cardiovascular system. The heart works as a
pump that pushes blood to the organs, tissues, and cells of the body. Blood delivers oxygen and
nutrients to every cell and removes the carbon dioxide and waste products made by those cells.
Blood is carried from your heart to the rest of your body through a complex network of
arteries, arterioles, and capillaries. Blood is returned to your heart through venules and veins.
If all the vessels of this network in your body were laid end-to-end, they would extend for about
60,000 miles (more than 96,500 kilometers), which is far enough to circle the earth more than
twice.29

39
1.1.8.5 Structure and Function
Three distinct layers comprise the heart walls, from inner to outer: endocardium, Myocardium,
Epicardium (inner layer of the pericardium).
The muscles of the heart, termed the myocardium, make up the middle and thickest
layer of the heart wall. This layer lies between the single-cell endocardium layer, which lines
the inner chambers, and the outer epicardium, which makes up part of the pericardium that
surrounds and protects the heart. Histologically, heart muscles are composed of cells called
cardiomyocytes that have unique structures and properties correlating to their contractile
function.30
Cardiomyocytes are striated, uninucleate muscle cells found exclusively in the heart
muscle. Unique cellular and physiological features of cardiomyocytes are intercalated discs,
which contain cell adhesions such as gap junctions, to facilitate cell-cell communication. These
discs reduce internal resistance and allow action potentials to spread quickly throughout the
entire heart muscle via the passage of charged ions. Thus, the heart muscle acts as a functional
syncytium with rapid synchronized contractions that are responsible for pumping blood
throughout the body. Functionally, the heart muscles rely on electrochemical gradients and the
potentials to generate contractile force for each heartbeat.
The sinus node, located within the right atrial myocardium, spontaneously depolarizes
and thus determines the heart rate. These depolarizations are currents of ion influx that are
carried from the sinus node to the heart muscle via conducting cells. When the depolarization
reaches the heart muscle, voltage-gated sodium channels open, allowing a rapid influx of
sodium ions into the cardiomyocytes, depolarizing the cells. The positive membrane potential
triggers voltage-gated potassium and then calcium channels to open, allowing potassium to
rush out and calcium to rush in. The initial influx of calcium is necessary for the second release
of calcium from the sarcoplasmic reticulum found within the heart muscle cells. The
accumulation of intracellular calcium ions binds to troponin C, moving tropomyosin aside to
allow actin-myosin binding and cross-bridge cycling responsible for muscle contraction.
The amount of calcium released is directly proportional to the amount of actin-myosin
interaction allowed and thus correlates with the contractile force of the heart muscle generated.
Physiologically, this corresponds with parameters such as stroke volume, ejection fraction, and
cardiac output used to assess heart function. At the end of each cycle, calcium gets restored to
the sarcoplasmic reticulum via SERCA (Sarco(endo)plasmic reticulum (SER) Ca2+ ATPase)

40
pumps while sodium-potassium and sodium-calcium ATPase pumps restore the cardiomyocyte
membrane potential so the cycle can repeat with the next incoming depolarization.30
1.1.8.6 Embryology
The heart muscle originates from the mesoderm layer and begins forming during the third week
of embryonic development. The mesoderm serves as the primary source for myocardial
precursor cells, which make up the cardiogenic or primary heart field during early
development. A primitive, horseshoe-shaped endothelial heart tube is formed and begins
contracting to facilitate the embryo’s early circulation system. Within the next several weeks,
the proliferation of cardiomyocytes is necessary for expanding the myocardial layer and
generating the multichambered system of the mature heart.
While existing cardiomyocytes contribute to the growth of the myocardium via
proliferation and organization, new heart muscle cells are also recruited from adjacent
mesenchymal layers that further expands the muscle layer.31
Following myocardial development, the heart walls undergo further maturation,
compaction, and trabeculation. Dilatations or swellings of the heart tube embryonic structures
along with neural crest cell migration facilitate the development of the chambers and
inflow/outflow tracts. These processes result in a mature and fully functional, contracting heart
by the eighth embryonic week and throughout adulthood.
1.1.8.7 Blood Supply and Lymphatics
The heart muscles’ blood supply comes directly from the system of coronary arteries that runs
within the epicardial layer. Two main coronary arteries, the left coronary artery (LCA) and the
right coronary artery (RCA), branch directly off the aorta via the coronary ostia. These arteries
and their branches supply tributary arteries that run perpendicular to the heart surface and
transverse from the epicardium, through the myocardium, and down to the endocardium.
The LCA quickly branches into the left anterior descending (LAD) coronary artery and
the left circumflex (LCX) coronary artery. The LAD runs vertically down the interventricular
groove towards the apex and supplies blood to the anterior left ventricular myocardium, the
anterior two-thirds of the interventricular septal myocardium, and the anterolateral papillary
muscle connecting the mitral valves. The LCX courses horizontally along the atrioventricular
groove and gives rise to the left obtuse marginal coronary artery, together supplying the lateral

41
and posterior left ventricular myocardium. The RCA runs horizontally along the right
atrioventricular groove and gives rise to the right acute marginal coronary artery, which
supplies the right ventricular myocardium. The RCA also gives rise to the posterior descending
artery (PDA) in about 90 % of the human population (the PDA comes from the LCX in the
other approximately 10 %), which supplies the posterior myocardium of both ventricles, the
posterior one-third of the interventricular septal myocardium, and the posteromedial papillary
muscle of the mitral valves.32
Blood flow via the coronary arteries to the myocardium occurs during diastole and
ventricular relaxation via the passive flow of blood into the aortic Ostia. During systole and
ventricular contraction, the coronary arteries become compressed, and thus impede myocardial
blood flow.
The venous system of the heart muscles runs parallel to the coronary arteries. Venous
drainage of the left ventricular myocardium is completed by the interventricular vein and the
great cardiac vein, which drains into the coronary sinus, found in the posterior right
atrioventricular groove, which then drains into the right atrium. The anterior cardiac veins are
responsible for draining blood from the right ventricular myocardium directly into the right
atrium.32
The cardiac lymphatic drainage system is comprised of lymphatic capillaries and pre-
collector vessels organized in plexuses within each of the heart wall layers. These lymphatic
vessels and plexuses flow from subendocardium, through the myocardium, up through the
subepicardium, into the mediastinal lymph nodes, and ultimately draining into both left and
right venous angles between the internal jugular veins and the subclavian veins. The source of
flow for lymphatic drainage comes from contractions of the myocardium, which generate force
to propel fluid movement through the system to the lymph nodes.33
1.1.8.8 Innervation of the heart
Heart muscles are innervated primarily by two nerves, the accelerans nerve and the vagus
nerve, which provide sympathetic and parasympathetic stimulation from the autonomic
nervous system, respectively. Intrinsic ganglia for the myocardium are present in the
epicardium, which receives signals from post-ganglionic sympathetic connections coming
from the accelerans nerve and pre-ganglionic parasympathetic connections from the vagus
nerve. Most post-ganglionic sympathetic connections synapse directly with the heart muscle
cells, releasing norepinephrine as the primary neurotransmitter.

42
Upon binding, norepinephrine stimulates beta-adrenergic receptors to increase
contractility of the myocardium via increasing calcium influx. Preganglionic parasympathetic
fibers synapse first with the epicardial intrinsic ganglia and then post-ganglionic neurons
directly synapse with the myocardium. Acetylcholine is the primary neurotransmitter for
myocardial parasympathetic signals, acting on muscarinic (M2) receptors on the
cardiomyocytes.34
1.1.8.9 Muscles of the heart
The muscle layer of the heart is termed the myocardium and is made up of cardiomyocytes.
The myocardium is found in the walls of all four chambers of the heart, though it is thicker in
the ventricles and thinner in the atria. This disparity is due to the difference in the generation
of the force of contraction needed for propelling blood between the atria and the ventricles,
with ventricles requiring much more power.32
1.1.9 Physiology of the heart Cardiac physiology, often known as heart function, is the study of healthy, unaffected function
of the heart, including blood flow, myocardial shape, the heart's electrical conduction system,
the cardiac cycle, and cardiac output, as well as how they interact and depend on one another.
1.1.9.1 Cardiac Cycle
The period of time that begins with contraction of the atria and ends with ventricular relaxation
is known as the cardiac cycle, in other words is the beginning of one heartbeat to the beginning
of the next. It consists of two periods:
• The period of contraction that the heart undergoes while it pumps blood into circulation
is called systole (Fig. 3).
• The period of relaxation that occurs as the chambers fill with blood is called diastole.
Both the atria and ventricles undergo systole and diastole.35
After emptying, the heart immediately relaxes and expands to receive another influx of
blood returning from the lungs and other systems of the body, before again contracting to pump
blood to the lungs and those systems.
Assuming a healthy heart and a typical rate of 70 to 75 beats per minute, each cardiac
cycle, or heartbeat, takes about 0.8 seconds to complete the cycle.36

43
The heart relaxes and expands at the beginning of the cycle, during ventricular diastole-
early, while receiving blood into both ventricles through both atria; then, near the end of
ventricular diastole–late, the two atria contract (atrial systole), and each atrium pumps blood
into the ventricle below it.37 During ventricular systole, the ventricles contract and pulsate (or
expel) two distinct blood supplies from the heart - one to the lungs and the other to all other
bodily organs and systems - while the atria relax (atrial diastole).38 During ventricular diastole,
the mitral and tricuspid valves, often known as the atrioventricular or AV valves, open to allow
filling. The atria begin to contract (atrial systole) late in the filling period, forcing a final crop
of blood into the ventricles under pressure. The ventricles then begin to contract (ventricular
systole) in response to electrical signals from the sinoatrial node, and as back - pressure against
them increases, the AV valves are forced to close, preventing blood volumes in the ventricles
from flowing in or out; this is known as the isovolumic contraction stage.37
Pressures in the ventricles rise quickly as a result of systole contractions, exceeding
pressures in the aorta and pulmonary artery trunks and driving the requisite valves (the aortic
and pulmonary valves) to open, resulting in distinct blood volumes being ejected from the two
ventricles. The ejection stage of the cardiac cycle is represented by the ventricular systole–first
phase, followed by the ventricular systole-second phase. The aortic and pulmonary valves close
once ventricular pressures fall below their peaks and below those in the trunks of the aorta and
pulmonary arteries.
The isovolumic relaxation phase begins next, during which pressure within the
ventricles begins to diminish significantly, and the atria begin to refill as blood returns to flow
into the right atrium (from the vena cava) and left atrium (from the pulmonary veins). The
mitral and tricuspid valves open again as the ventricles relax, and the completed cycle returns
to ventricular diastole and a new "Start" of the cardiac cycle.37-39
Blood pressure rises and falls throughout the cardiac cycle. A series of electrical
impulses produced by specialized pacemaker cells found within the sinoatrial node and the
atrioventricular node coordinate the movements of heart muscle.40

44
Fig. 3: Overview of the Cardiac Cycle35 The cardiac cycle begins with atrial systole and
progresses to ventricular systole, atrial diastole, and ventricular diastole, when the cycle begins again.
Correlations to the ECG are highlighted.
1.1.9.1.1 Pressure and flow
Fluids flow from areas of high pressure to areas of low pressure. As a result, blood will flow
into the atria from the higher pressure of the veins while the heart chambers are relaxed
(diastole). Because the pressure in the atria rises as blood comes in, blood moves passively
from the atria to the ventricles at first. The pressure within the atria rises even further when the
action potential causes the muscles in the atria to contract (atrial systole), pump blood into the
ventricles. During ventricular systole, the pressure in the ventricles rises, pumping blood from
the right ventricle into the pulmonary trunk and from the left ventricle into the aorta.38
45
1.1.9.1.2 Phases of cardiac cycle
At the beginning of the cardiac cycle, both the atria and ventricles are relaxed (diastole). Blood
is flowing into the right atrium from the superior and inferior venae cava and the coronary
sinus. Blood flows into the left atrium from the four pulmonary veins. The two atrioventricular
valves, the tricuspid and mitral valves, are both open, so blood flows unimpeded from the atria
and into the ventricles. Approximately 70–80 percent of ventricular filling occurs by this
method. The two semilunar valves, the pulmonary and aortic valves, are closed, preventing
backflow of blood into the right and left ventricles from the pulmonary trunk on the right and
the aorta on the left.38
1.1.9.1.2.1. Atrial systole and diastole
Contraction of the atria follows depolarization, represented by the P wave of the ECG. As the
atrial muscles contract from the superior portion of the atria toward the atrioventricular septum,
pressure rises within the atria and blood is pumped into the ventricles through the open
atrioventricular (tricuspid, and mitral or bicuspid) valves. At the start of atrial systole, the
ventricles are normally filled with approximately 70-80 % of their capacity due to inflow
during diastole. Atrial contraction, also referred to as the "atrial kick," contributes the
remaining 20–30 percent of filling. Atrial systole lasts approximately 100 ms and ends prior to
ventricular systole, as the atrial muscle returns to diastole.38
1.1.9.1.2.2. Ventricular systole
The QRS complex in the ECG represents ventricular systole, which occurs after the ventricles
have depolarized (Fig. 4). It can be separated into two periods, each lasting 270 milliseconds.
At the end of atrial systole and just prior to ventricular contraction, the ventricles
contain approximately 130 mL blood in a resting adult in a standing position. This volume is
known as the end diastolic volume (EDV) or preload.38
The pressure of the blood within the chamber rises initially when the muscles in the
ventricle contract, but it is not yet high enough to open the semilunar (pulmonary and aortic)
valves and be ejected from the heart. Blood pressure, on the other hand, rapidly climbs above
that of the atria, which are now relaxed and in diastole. Blood flows back into the atria when
the pressure rises, sealing the tricuspid and mitral valves. The volume of blood within the

46
chamber remains constant since blood is not evacuated from the ventricles at this early stage.
As a result, isovolumic contraction, also known as isovolumetric contraction, is the name given
to the first phase of ventricular systole.38
The contraction of the ventricular muscle has elevated the pressure within the ventricle
to a point where it is larger than the pressures in the pulmonary trunk and the aorta during the
second phase of ventricular systole, the ventricular ejection phase. The pulmonary and aortic
semilunar valves are opened as blood is pushed out of the heart. Because the existing pressure
in the aorta is so much higher, the left ventricle will generate far more pressure than the right
ventricle. Despite this, the amount of blood pumped by both ventricles is the same.
Stroke volume is the name given to this quantity. In most cases, the stroke volume will
be in the 70–80 mL range. Since ventricular systole began with an EDV of around 130 mL of
blood, this suggests that there is still 50–60 mL of blood remaining in the ventricle following
contraction. This blood volume is referred to as the end systolic volume (ESV).38
1.1.9.1.2.3. Ventricular diastole
Ventricular relaxation, or diastole, follows repolarization of the ventricles and is represented
by the T wave of the ECG. It too is divided into two distinct phases and lasts approximately
430 ms.
During the early phase of ventricular diastole, as the ventricular muscle relaxes,
pressure on the remaining blood within the ventricle begins to fall. When pressure within the
ventricles drops below pressure in both the pulmonary trunk and aorta, blood flows back toward
the heart, producing the dicrotic notch (small dip) seen in blood pressure tracings. The
semilunar valves close to prevent backflow into the heart. Since the atrioventricular valves
remain closed at this point, there is no change in the volume of blood in the ventricle, so the
early phase of ventricular diastole is called the isovolumic ventricular relaxation phase, also
called isovolumetric ventricular relaxation phase.38
In the second phase of ventricular diastole called late ventricular diastole, as the
ventricular muscle relaxes, pressure on the blood within the ventricles drops even further.
Eventually, it drops below the pressure in the atria. When this occurs, blood flows from the
atria into the ventricles, pushing open the tricuspid and mitral valves. As pressure drops within
the ventricles, blood flows from the major veins into the relaxed atria and from there into the
ventricles. Both chambers are in diastole, the atrioventricular valves are open, and the
semilunar valves remain closed. The cardiac cycle is complete.38

47
Fig. 4: Relationship between the Cardiac Cycle and ECG.35 Initially, both the atria and
ventricles are relaxed (diastole). The P wave represents depolarization of the atria and is followed by
atrial contraction (systole). Atrial systole extends until the QRS complex, at which point, the atria
relax. The QRS complex represents depolarization of the ventricles and is followed by ventricular
contraction. The T wave represents the repolarization of the ventricles and marks the beginning of
ventricular relaxation.
1.1.9.2 Resting cardiac output
Cardiac output (CO) is a measurement of the amount of blood pumped by each ventricle in one
minute. To calculate this value, multiply stroke volume (SV), the amount of blood pumped by
each ventricle, by heart rate (HR), in contractions per minute (or beats per minute, bpm). It can
be represented mathematically by the following equation: CO = HR × SV.
There are several important variables influences cardiac output (Fig. 5), including size
of the heart, physical and mental condition of the individual, sex, contractility, duration of
contraction, preload or EDV, and afterload or resistance. Normal range for SV would be 55–
100 mL. An average resting HR would be approximately 75 bpm but could range from 60–100
in some individuals.41

48
Figure 5. Major Factors Influencing Cardiac Output.38 Cardiac output is influenced by
heart rate and stroke volume, both of which are also variable.
1.1.9.3 Exercise and maximum cardiac output
In healthy young individuals, HR may increase to 150 bpm during exercise. SV can also
increase from 70 to approximately 130 mL due to increased strength of contraction. This would
increase CO to approximately 19.5 L/min, 4–5 times the resting rate. Top cardiovascular
athletes can achieve even higher levels. At their peak performance, they may increase resting
CO by 7–8 times. Since the heart is a muscle, exercising it increases its efficiency. The
difference between maximum and resting CO is known as the cardiac reserve. It measures the
residual capacity of the heart to pump blood.41
1.1.9.4 Heart Rate
Heart rate (HR) differ significantly depending on age, as well as exercise and fitness levels.
The resting heart rate of a newborn can be as high as 120 beats per minute. HR falls gradually
until young adulthood, and steadily increases with age.
Maximum heart rates are usually between 200 and 220 beats per minute, though they
can go higher in extreme cases. The ability to generate maximal rates decreases with aging.
This can be calculated by subtracting the individual's age from the maximum value of 220 bpm.
So, a 40-year-old person's maximum rate would be around 180, whereas a 60-year-old person's
maximum rate would be around 160.41

49
1.1.10 Diagnostic criteria of heart failure
1.1.10.1 Medical History and Physical Examination
Patients with heart failure can have decreased exercise tolerance with dyspnea, fatigue,
generalized weakness, and fluid retention, with peripheral or abdominal swelling and possibly
orthopnea.42Patient history and physical examination are useful to evaluate for alternative or
reversible causes including, coronary artery disease, hypertension, idiopathic cardiomyopathy,
valvular heart disease.43-44
Nearly all patients with heart failure have dyspnea on exertion. However, heart failure
accounts for only 30 percent of the causes of dyspnea in the primary care setting.45
The lack of dyspnea on exertion reduces the risk of systolic heart failure only slightly,
while the presence of orthopnea or paroxysmal nocturnal dyspnea increases the risk of heart
failure slightly, (positive likelihood ratio [LR+] = 2.2 and 2.6).46-47
The presence of a third heart sound (ventricular filling gallop) indicates a drop in LVEF
and an increase in left ventricular end-diastolic pressure. A third heart sound and a displaced
cardiac apex, despite being relatively uncommon observations, are good predictors of left
ventricular dysfunction and essentially rule in diagnosis of systolic heart failure (LR+ = 11 and
16).46-47
The presence of jugular venous distention, hepatojugular reflux, pulmonary rales, and
pitting peripheral edema is indicative of volume overload and enhances the probability of a
heart failure diagnosis. Jugular venous distention and hepatojugular reflex have a moderate
effect (LR+ = 5.1 and 6.4), whereas the others, along with cardiac murmurs, have only a small
effect on the diagnostic probability (LR+ = 2.3 to 2.8). The absence of any of these findings is
of little help in ruling out heart failure.46
1.1.10.2 Laboratory Tests
Alternative and potentially reversible causes of heart failure can be identified by laboratory
testing. lists laboratory tests appropriate for the initial evaluation of heart failure and other
potential causes, includes: Arterial blood gases (hypoxia, pulmonary disease), Blood cultures
(endocarditis, systemic infection), Human immunodeficiency virus (cardiomyopathy), Lyme
serology (bradycardia/heart block), Serum ferritin level, transferrin saturation (macrocytic
50
anemia, hemochromatosis), Thiamine level (deficiency, beriberi, alcoholism), Troponin and
creatine kinase-MB levels (myocardial infarction, myocardial injury).
Other laboratory tests should be performed based on physician discretion to evaluate
further causes or identify comorbid conditions that require enhanced control. Includes: A1C
level (diabetes mellitus), Lipid profile (hyperlipidemia).44-48-49
The levels of B-type natriuretic peptide (BNP) and N-terminal pro-BNP (the cleaved
inactive N-terminal segment of the BNP precursor) can be used to evaluate patients for heart
failure who have dyspnea. The atria and ventricles secrete BNP in response to stretching or
increased wall tension.50
BNP levels rise with age, are higher in women and African Americans, and can be
elevated in renal failure patients.46-51
Especially in elderly populations, BNP appears to be more reliable than N-terminal pro-
BNP. 50-51
Monitoring BNP levels in the acute and outpatient settings is supported by limited
evidence. BNP levels were reduced by 30 to 50 percent after hospital discharge, which resulted
in increased survival and lower rehospitalization rates. Outpatient care for BNP levels less than
100 pg. per mL (100 ng per L) and N-terminal pro-BNP levels less than 1,700 pg per mL (1,700
ng per L) resulted in fewer decompensations, hospitalizations, and death occurrences. 52
1.1.10.3 Chest Radiography
Because chest radiography can detect pulmonary causes of dyspnea, it should be done first to
rule out heart failure (e.g., pneumonia, pneumothorax, mass). When a patient with dyspnea has
pulmonary venous congestion and interstitial edema on chest radiography, the diagnosis of
heart failure is more likely (LR+ = 12). Other abnormalities, such as pleural effusion or
cardiomegaly, may slightly raise the risk of heart failure (LR+ = 3.2 and 3.3), while their
absence only helps to reduce the risk of heart failure (LR– = 0.33 to 0.48).46

51
1.1.10.4 Electrocardiography
In individuals with suspected heart failure, electrocardiography (ECG) can help detect other
reasons. Changes such as left bundle branch block, left ventricular hypertrophy, acute or prior
myocardial infarction, or atrial fibrillation can be detected and may require additional study
through echocardiography, stress testing, or consultation with a cardiologist. Systolic heart
failure is only marginally less likely (LR– = 0.27) when ECG results are normal (or modest
anomalies).47 Other abnormalities, such as atrial fibrillation, new T-wave changes, or any
abnormality, have a minor impact on the diagnosis of heart failure (LR+ = 2.2 to 3.8).46
1.1.10.5 Clinical Decision Making
Although the concept of heart failure is still up for debate, it is nonetheless a clinical diagnostic.
Several organizations have produced diagnostic criteria, but the Framingham criteria are
widely accepted and include elements of the initial evaluation, which improves their accuracy.
And a more recent study analyzed them for systolic and diastolic heart failure. Both studies
found that systolic heart failure had a high sensitivity (97% vs. 89% for diastolic heart failure),
effectively ruling out heart failure when the Framingham criteria are not satisfied (LR– = 0.04).
The Framingham criteria have a minor impact in confirming a diagnosis of heart failure (LR+
= 4.21 to 4.57), but a considerable impact on excluding heart failure in general and diastolic
heart failure (LR– = 0.1 and 0.13).55-56

52
Table 1: Framingham Diagnostic Criteria for Heart Failure.55-56
(Heart failure is diagnosed when two major criteria or one major and two minor criteria are met)
Major Criteria Minor Criteria
Acute pulmonary edema Ankle edema
Cardiomegaly Dyspnea on exertion
Hepatojugular reflex Hepatomegaly
Neck vein distension Nocturnal cough
Paroxysmal nocturnal
dyspnea or orthopnea
Pleural effusion
Third heart sound gallop Tachycardia (> 120 beats per minute)
1.1.10.6 An Overview of Heart Failure Evaluation and Diagnosis
The most widely accepted and available approach for diagnosing systolic dysfunction is
echocardiography, which should be used after the initial evaluation to confirm the existence of
heart failure.44
Left ventricle ejection fraction (LVEF), left ventricular size, wall thickness, valve
function, and the pericardium can all be assessed using two-dimensional echocardiography
with Doppler flow studies. If high left atrial pressure, poor left ventricular relaxation, and
decreased compliance are observed, echocardiography can help diagnose diastolic heart
failure.44-57
Diastolic heart failure is frequently diagnosed clinically without conclusive
echocardiographic evidence. Transesophageal echocardiography, radionuclide angiography, or
cineangiography with contrast medium (during catheterization) can be performed to measure
heart function if echocardiography results are unclear or inadequate.58
Unless there is a contraindication to possible revascularization, the American Heart
Association and the American College of Cardiology suggest that the patient undergo coronary
angiography if angina or chest is present with heart failure. 3 In individuals with angina and a
low ejection fraction, coronary angiography has been demonstrated to improve symptoms and
survival.44
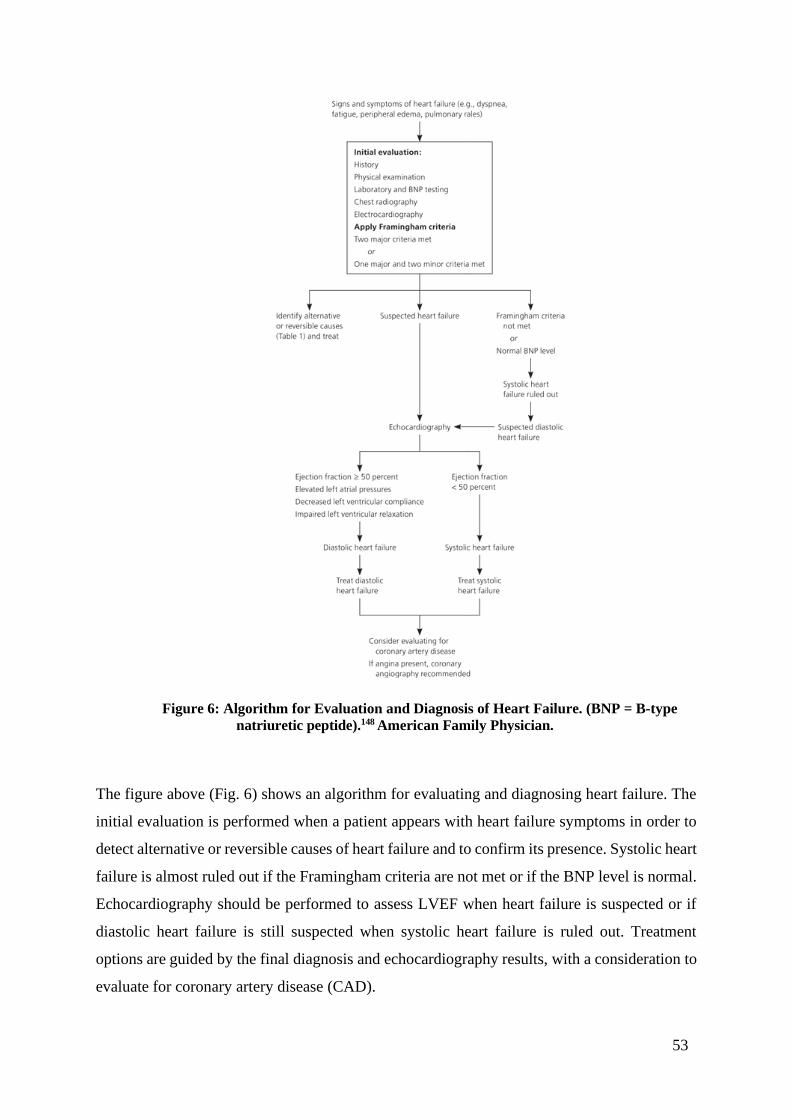
53
Figure 6: Algorithm for Evaluation and Diagnosis of Heart Failure. (BNP = B-type
natriuretic peptide).148 American Family Physician.
The figure above (Fig. 6) shows an algorithm for evaluating and diagnosing heart failure. The
initial evaluation is performed when a patient appears with heart failure symptoms in order to
detect alternative or reversible causes of heart failure and to confirm its presence. Systolic heart
failure is almost ruled out if the Framingham criteria are not met or if the BNP level is normal.
Echocardiography should be performed to assess LVEF when heart failure is suspected or if
diastolic heart failure is still suspected when systolic heart failure is ruled out. Treatment
options are guided by the final diagnosis and echocardiography results, with a consideration to
evaluate for coronary artery disease (CAD).

54
1.1.11 Warning signs and symptoms of heart failure
Table 2: Warning Signs and Symptoms of Heart Failure 59
Sign or Symptom People with Heart Failure
May Experience
Why It Happens
Shortness of breath (dyspnea) Breathlessness can occur
during activity, at rest, or while
sleeping, and can occur
suddenly, waking up. Patient
may need to prop up upper
body and head on two pillows
if there is trouble breathing
while sleeping flat. Patient
might frequently complain about waking up exhausted,
worried, or restless
Because the heart can't keep up
with the demand, blood "backs
up" in the pulmonary veins (the
vessels that return blood from
the lungs to the heart). Fluid
leaks into the lungs as a result
of this.
Persistent coughing or
wheezing
Coughing that produces blood-
tinged mucus that is white or pink in color.
Fluid builds up in the lungs
Buildup of excess fluid in body
tissues (edema)
swelling in the feet, ankles,
legs or abdomen or weight
gain. Patient may find that the
shoes feel tight.
As blood flow out of the heart
slows, blood returning to the
heart through the veins backs
up, causing fluid to build up in
the tissues. The kidneys are
less able to dispose of sodium and water, also causing fluid
retention in the tissues.
Tiredness, fatigue, dizziness a constant sense of exhaustion
and trouble performing routine
tasks such as climbing stairs,
carrying groceries, or walking
The heart can't pump enough
blood to meet the needs of
body tissues. The body diverts
blood away from less vital
organs, particularly muscles in
the limbs, and sends it to the heart and brain.
Lack of appetite, nausea a feeling of being bloated or
nauseous in the stomach
The digestive system receives
less blood, resulting in
digestion problems.
Confusion, impaired thinking Memory loss and
disorientation are common
symptoms. This may be
noticed first by a caregiver or relative.
Changing levels of certain
substances in the blood, such
as sodium, can cause
confusion.
Increased heart rate heart palpitation that feels like
your heart is speeding or
beating.
The heart beats quicker to
"make up" for the decrease of
pumping capability.

55
Although the body's ability to compensate for the failing heart initially is beneficial, in the long
run these adaptations contribute to the most serious cases of heart failure. For example:
• An enlarged heart eventually doesn't function as well as a normal heart, the increased
muscle mass adds stress to the entire circulatory system.
• Because of a lack of oxygen, the organ systems from which blood has been diverted
may eventually deteriorate.
• Blood vessel narrowing reduces blood flow and can lead to conditions like stroke, heart
disease, and clogged or blocked blood vessels in the legs and other parts of the body.
• Pumping blood too quickly over an extended period of time can harm the heart muscle
and disrupt its regular electrical signals, resulting in a dangerous heart rhythm
disorder.59
1.1.12 Heart Failure Diagnosis
The physician will take a full medical history, assess symptoms, and conduct a physical
examination to diagnose heart failure. Physician will also look for heart failure risk factors such
as high blood pressure, coronary artery disease, or diabetes.
Additionally, physician can listen to the lungs for signs of fluid buildup (lung
congestion) and to the heart for murmurs (whooshing sounds) that could indicate heart failure.
Veins in the neck may be examined, and fluid buildup in the abdomen and legs may be checked.
Following the physical examination, your physician may order some of the following tests:60
• Blood tests. Blood tests are performed to search for signs of heart disease.
• Chest X-ray. X-ray images can show the condition of the lungs and heart.
• Electrocardiogram (ECG). The electrical signals in the heart are recorded during this
quick and painless test. It can show the frequency and duration of heartbeats.
• Echocardiogram. Sound waves are used to produce images of the heart in motion. This
test reveals the heart's size, structure, and valves, as well as blood flow through the
heart. An echocardiogram can be used to measure ejection fraction, which reveals how
well the heart is pumping and helps diagnose heart failure and guides treatment.
• Stress test. Stress tests measure the health of the heart during activity. The patient might
be asked to walk on a treadmill while attached to an ECG machine, or might be given

56
an IV drug that boosts the effect of exercise on the heart. A stress test may be performed
while wearing a mask that monitors how well the heart and lungs get oxygen and exhale
carbon dioxide.
• Cardiac computerized tomography (CT scan). is used to find calcium deposits in plaque
of people with heart disease. They’re an effective way to spot atherosclerosis before
symptoms develop. The more coronary calcium, the more coronary atherosclerosis. That
gives a higher chance of cardiovascular problems in the future.
• Magnetic resonance imaging (MRI). MRI of heart shows damage by a heart attack or
if there is a lack of blood flow to the heart muscle due to constricted or clogged arteries.
A cardiac MRI may be done with a dye (contrast). It's important to tell the physician
about any problems with your kidneys before you receive a cardiac MRI because
Contrast can cause an uncommon but serious complication in people who have kidney
disease.60
• Coronary angiogram. This test involves inserting a thin, flexible tube (catheter) into a
blood vessel, commonly in the groin, and guiding it to the heart arteries. A dye
(contrast) is administered into the catheter to help the doctor locate blockages by
making the arteries appear more clearly on an X-ray.
• Myocardial biopsy. During this test the physician inserts a thin, flexible cord into a vein
in the neck or groin and takes very small pieces of the heart muscle for examination.
This test may be used to diagnose certain types of heart muscle diseases that cause heart
failure.
The results of tests used to detect heart failure assist doctors in determining the origin
of any signs and symptoms as well as determining a treatment plan. Doctors can use one of two
classification systems to select the appropriate treatment for heart failure:
• New York Heart Association classification. Heart failure is divided into four categories
on this scale:
- Class I heart failure. There are no heart failure symptoms.
- Class II heart failure. Everyday activities can be done without difficulty, but
exertion causes shortness of breath or fatigue.
- Class III heart failure. It's difficult to complete everyday activities.
- Class IV heart failure. Shortness of breath occurs even at rest. This category
includes the most severe heart failure.60

57
• American College of Cardiology/American Heart Association classification. This
stage-based classification system uses letters A to D and includes a category for those
at risk of developing heart failure:
- Stage A. There are several risk factors for heart failure but no signs or symptoms.
- Stage B. There is heart disease but no signs or symptoms of heart failure.
- Stage C. There is heart disease and signs or symptoms of heart failure.
- Stage D. Advanced heart failure requires special treatments.
Both classification systems used together to help determine the most appropriate
treatment options.60
1.1.13 Heart Failure Treatment
Heart failure is a chronic condition that requires lifelong treatment. However, the signs and
symptoms of heart failure might improve with treatment. Physicians sometimes can correct
heart failure by treating the underlying cause. For instance, repairing a heart valve or
controlling a fast heart rhythm may reverse heart failure. But for most people, treatment of
heart failure involves a balance of the right medications and, sometimes, use of devices that
help the heartbeat and contract properly. The main treatments are:61-65
• Medications:
- Angiotensin-converting enzyme (ACE) inhibitors. These drugs relax blood
vessels to lower blood pressure, improve blood flow and decrease the strain on the
heart. Examples include enalapril (Vasotec, Epaned), lisinopril (Zestril, Qbrelis,
Prinivil) and captopril.
- Angiotensin II receptor blockers. Losartan (Cozaar), valsartan (Diovan), and
candesartan (Atacand) are three medicines that offer many of the same benefits as
ACE inhibitors. They might be a great option for those who can't take ACE
inhibitors.
- Beta blockers. These drugs lower blood pressure and slow heart rate. Beta blockers
may help you live longer by reducing the signs and symptoms of heart failure,
improving heart function, and extending your life. Carvedilol (Coreg), metoprolol
(Lopressor, Toprol-XL, Kapspargo Sprinkle), and bisoprolol are among examples.
- Diuretics. Diuretics, often known as water pills, cause you to urinate more often
and prevent fluid from building up in your body. Diuretics like furosemide (Lasix)
help you breathe easier by reducing fluid in the lungs.

58
- Aldosterone antagonists. These drugs include spironolactone (Aldactone,
Carospir) and eplerenone (Inspra).
- Positive inotropes. People in the hospital with certain types of severe heart failure
may get these drugs by IV. Positive inotropes can help the heart pump blood more
effectively and maintain blood pressure.
- Digoxin (Lanoxin). This drug, commonly known as digitalis, makes heart muscle
contractions stronger. It also tends to slow the heartbeat. Digoxin reduces heart
failure symptoms in systolic heart failure.
- Hydralazine and isosorbide dinitrate (BiDil). This drug combination aids in the
relaxation of blood vessels. In severe heart failure symptoms and ACE inhibitors or
beta blockers haven't helped, it may be added given.61-65
• Devices for heart failure, implanted in the chest to control heart rhythm:
- Pacemaker. A pacemaker continuously monitors heart rate and provides electrical
pulses to the heart to keep it pumping at the proper rate. A cardiologist places the
device under the skin, usually under local anesthesia.
- Cardiac resynchronisation therapy. Cardiac resynchronization therapy (CRT) is
a form of pacemaker that can help by causing the left ventricle's walls to all contract
at the same time. This improves the efficiency of the heart's pumping.
- Implantable cardioverter defibrillators (ICDs). An ICD constantly monitors the
heart rhythm.
- CRT-Ds. Devices that combine cardiac resynchronization and defibrillation are
implanted into patients who need both.61-65
• Surgery for heart failure may include:
- Heart valve surgery. There are 2 types of valve surgery: valve replacement and
valve repair.
- Angioplasty or bypass. If your heart failure is caused by coronary heart disease,
your doctor may recommend one of the following treatments:
Coronary angioplasty – where a tiny balloon is used to stretch open a narrowed or
blocked artery. Coronary artery bypass graft (CABG) – where a blood vessel from

59
another part of the body is used to divert blood around narrowed or clogged parts
of an artery.
- Left ventricular assist devices. Left ventricular assist devices (LVADs) are
mechanical pumps that can help if your left ventricle isn't working properly, and
medication alone isn't helping. They can be used as a permanent treatment if a heart
transplant is not possible, or as a temporary solution while waiting for a transplant
- Heart transplant. Some people have heart failure that is so severe that surgery or
drugs are ineffective. These people's hearts might need to be replaced with a healthy
donor heart.61-65
1.1.14. Prevention of heart failure
According to Heart Information Center (Texas Heart Institute).69 Generally, heart disease is the
leading cause of death. It is also a significant contributor to disability. There are a variety of
factors that can increase your risk of heart disease. They're known as risk factors. You can't
control some of them, but you can control a lot of them. You can reduce your risk of heart
disease by learning about them.
The risk factors for heart disease that can't be changed:
• Age. As you become older, your chances of developing heart disease increase. Men and
women over the age of 45 and 55 are at a higher risk.
• Sex. Some risk factors may affect women's risk of heart disease differently than men.
For example, estrogen protects women from heart disease, but diabetes increases the
risk of heart disease in women more than it does in males.
• Ethnicity or race. Some people are at a higher risk than others. Heart disease is more
common in African Americans than in whites, whereas it is less common in Hispanic
Americans. East Asians, for instance, have lower rates, whereas South Asians have
greater rates.
• Family history. You have a greater risk if you have a close family member who had
heart disease at an early age.
To lower the risk of heart disease:
• Control your blood pressure. High blood pressure is a major risk factor for heart
disease. It is important to get your blood pressure checked regularly - at least once a

60
year for most adults, and more often if you have high blood pressure. Take steps,
including lifestyle changes, to prevent or control high blood pressure.
• Keep your cholesterol and triglyceride levels under control. High levels
of cholesterol can clog your arteries and raise your risk of coronary artery disease and
heart attack. Lifestyle changes and medicines (if needed) can lower your cholesterol.
Triglycerides are another type of fat in the blood. High levels of triglycerides may also
raise the risk of coronary artery disease, especially in women.
• Stay at a healthy weight. Being overweight or having obesity can increase your risk for
heart disease. This is mostly because they are linked to other heart disease risk factors,
including high blood cholesterol and triglyceride levels, high blood pressure, and
diabetes. Controlling your weight can lower these risks. Extra pounds can interfere with
blood circulation and put excess pressure and stress on the heart. Studies have shown
that even a modest weight loss of 5% to 10% can lead to significant improvements in
blood pressure, cholesterol, and co-morbidities associated with increased weight. A
healthy weight is defined as a body mass index (BMI) between 18.5 and 24.9.
Individuals with a BMI of 30 are considered obese.66-67
• Get regular exercise. Exercise has many benefits, including strengthening your heart
and improving your circulation. It can also help you maintain a healthy weight and
lower cholesterol and blood pressure. All of these can lower your risk of heart disease.
Aerobic activity in particular, such as high-intensity interval training (HIIT), which
alternates short stints of intense exercise with less vigorous ones, have been shown to
help strengthen and condition the heart so that it can function better. At least 30 minutes
per day (150 minutes per week) of moderate-intensity exercise, such as gardening, brisk
walking, dancing, or doubles tennis. This can be broken down into three 10-minute
sessions or two 15-minute sessions if that is easier to fit into a busy schedule.69
• Limit alcohol. Too much alcohol might cause your blood pressure to rise. It also adds
more calories, potentially leading to weight gain. Both of these factors increase your
chances of developing heart disease. Men should limit themselves to two alcoholic
drinks each day, while women should limit themselves to one.

61
• Quit Smoking. Cigarette smoking raises blood pressure. The chemicals in tobacco can
directly damage arteries and contribute to congestive heart failure. [John Hopkins
Medicine. Congestive heart failure: prevention, treatment and research.].
Secondhand smoke can be just as harmful, as carbon monoxide can take the place of
oxygen in the blood, forcing the heart to pump harder. Once you quit smoking, you'll
notice an almost instantaneous improvement in your health:
o Within 20 minutes, heart rate decreases.
o Within 12 hours, carbon monoxide levels in the blood decrease to normal.
o Within 3 months, the risk of a heart attack decreases and lung function
improves.
o After 1 year, the added risk of coronary artery disease is half that of someone
who smokes.68
• Eat a Heart Healthy Diet: Limit saturated fat, trans fats, sodium, fatty cuts of red meat
and other proteins, and soda, baked goods, and other foods and beverages with large
amounts of added refined sugar.69-70
• Reduce Salt Intake: High levels of sodium in the diet can cause accumulation of fluid
in the body that consequently puts excess stress on the cardiovascular system.71 If you
have hypertension (high blood pressure), a primary risk factor for heart failure, it may
be advisable to reduce your intake of table salt, processed foods, and high-sodium
foods, such as bacon, ham. The goal is to reduce sodium consumption to 2,300
milligrams (mg) per day or 1,500 mg for people at a high risk of hypertension.
• Manage stress. Stress is linked to heart disease in many ways. It can elevate blood
pressure. Extreme stress can be a "trigger" for a heart attack. Also, some common ways
of coping with stress, such as overeating, heavy drinking, and smoking, are bad for the
heart.
• Manage diabetes. Having diabetes doubles your risk of diabetic heart disease. That is
because over time, high blood sugar from diabetes can damage your blood vessels and
the nerves that control your heart and blood vessels. So, it is important to get tested for
diabetes, and if you have it, to keep it under control.
62
• Get enough sleep. Not getting enough sleep, raise your risk of high blood pressure,
obesity, and diabetes. Those three things can raise your risk for heart disease.
1.1.15 Complications of heart failure According to WebMD, if you have heart failure, your heart may not be strong enough to pump
out as much blood as your body needs. As it tries to move more blood, your heart gets larger. It
also pumps faster, and your blood vessels narrow to get more blood out to your body.
As your heart works harder, it may become weaker. Your body gets less oxygen, and you
might notice symptoms like shortness of breath, swelling in your legs, and fluid buildup.
Your body tries to keep the blood it has to supply your heart and brain. This leaves less for organs
like your kidneys and liver. A lack of enough blood can damage these organs.72
Common complications of heart failure:72
• Atrial fibrillation: is an irregular heart rhythm (arrhythmia), it can make heart failure
worse, and greatly increases risk of stroke, can cause palpitations.
• Ventricular fibrillation or tachycardia: Irregular heart rhythms (arrythmias), it can
cause syncope (fainting), palpitations, sudden death.
• Kidney failure: Reduced functioning of the kidneys, leading to decreased urine
output, fatigue, poor appetite, lethargy, ultimately life-threatening.
• Anemia: Decreased oxygen-carrying hemoglobin in red blood cells, causing weakness
and fatigue, may raise risk or problems linked to heart failure.
• Stroke: your brain is deprived of oxygen because its blood supply has been
significantly decreased or cut off, leading to loss of cognitive or motor function.

63
• Heart valve condition: A leaky or tight valve reduces the efficiency of the heart’s
pumping action, makes heart failure worse, can predispose to atrial fibrillation, may
need surgical intervention.
• Cardiac cachexia: is an unintentional weight loss, can require supplemental nutrition,
can be life-threatening.
• Leg venous stasis and ulcers: venous stasis: skin thickens and looks shiny or scaly,
your hair might also fall out, skin may also turn brown or reddish. Ulcers: Injuries to
your swollen legs cause fluid to constantly ooze out of cuts in your skin.
• Liver damage: breaks down toxins so your body can remove them. It also stores bile, a
fluid used to digest food. Heart failure might deprive your liver of the blood it requires to
function properly. The fluid buildup that comes with it puts extra pressure on the portal
vein, which brings blood to your liver. This can scar the organ to the point where it
doesn't work as well as it should.
• Lung problems: A damaged heart can't pump blood as effectively from your lungs out
to your body. Blood backs up, raising pressure in the veins inside your lungs. This
pushes fluid into your air sacs. As liquid builds up, it gets harder to breathe. This is
called pulmonary edema.
• Extreme weight loss and muscle loss: Muscle and fat metabolism can be affected by
heart failure. You may lose a lot of weight and muscular mass as the disease
progresses. Muscles can shrink and weaken over time.72

64
1.2 Special Part of Thesis
1.2.1 General Principles of Exercise Testing in Cardiac Rehabilitation
1.2.1.1 Introduction
Every patient must undergo a clinical assessment before being admitted to a cardiac
rehabilitation program (CRP), which includes a medical consultation, an evaluation of left
ventricle (LV) function (usually by echocardiography), a maximal exercise test (ET) limited
by symptoms, and blood tests to determine the cardiovascular disease (CVD) risk factor profile.
In some situations, patients require additional diagnostic testing after the clinical evaluation,
such as 24-hour Holter monitoring, an imaging technique to evaluate perfusion or coronary
anatomy, or bypass grafting.73-74
The ET is a very important part of this clinical assessment performed before admission
and repeated at the end of the CRP phase, because it gives data regarding functional capacity
and information regarding the adaptation to maximal and submaximal levels of exercise (HR
and BP), residual myocardial ischemia, and cardiac arrhythmias induced or worsened by
exercise and permits the identification of the training heart rate (THR) for the aerobic training.75
Besides the objective parameters mentioned above, the ET is very important from the
psychological point of view for many patients and partners, because they realize that the patient
usually has a better functional capacity than they could pre- dict. In the follow-up period, the
ET is very useful to detect or confirm eventual clinical status changes which occurred during
the program, update exercise intensity, measure the gains obtained after the CRP, and perform
global prognostic assessment.
1.2.1.2 Cardiopulmonary Exercise Test (Spiroergometry)
Cardiopulmonary exercise test (CPX) is the ideal ET to be used in all kinds of patients in the
setting of a CRP.76 Although it is almost mandatory to use it in heart failure patients, it is
frequently replaced in many CR centers, primarily in CAD patients with normal or near-normal
LV function, by the standard ET, which is more widely available and familiar to most
cardiologists, due to its higher cost, more complicated delivery, and interpretation.77 During the
CPX, peak VO2, ventilatory thresholds, VE/VCO2 slope, and O2 kinetics are measured beyond
all the parameters recorded in the standard ET, like maximal load reached, HR and BP changes
65
from rest to maximal exercise, and, during recovery, the eventual arousal of symptoms like
angina pectoris or ECG abnormalities (ST changes or arrhythmias).78 Considering the
parameters obtained from the CPX, peak VO2 is the most important because it is the gold
standard for functional capacity and it was identified as the strongest prognostic parameter in
CVD.79-80 Because continuous moderate aerobic training, the classic modality, is performed at
a percentage of peak VO2 ranging from 50 to 70 %, peak VO2 is therefore very significant
when prescribing exercise intensity.81 The first and second ventilatory thresholds (VT1 and
VT2), which are expected to occur at submaximal level during the CPX, are independent of
motivation, contrary to peak VO2. Due to this fact, they are considered good indicators of the
training effect of the program, if they occur at a higher percentage of VO2 max.
The determination of the ventilatory thresholds is also useful to calculate the training
intensity for moderate continuous aerobic training, which must start at the HR attained at the
level of VT1 and increased to HR reached at the VT2 moment.82-83
Simply, Spiroergometric stress testing is one of the most common types of stress
testing, and it should be done on every patient undergoing post-hospital cardiovascular
rehabilitation. This examination allows for a thorough evaluation of the cardiopulmonary
system's functionality. It's a requirement for suggesting safe and successful physical activity
and calculating the proper training load intensity. Most of the time, we use a bicycle ergometer.
During the assessment, we gradually increase the load until we reach the symptoms of the
patient's limited maximum, according to the ramp protocol. The load, heart rate, blood
pressure, and ECG are all recorded. We are currently monitoring different ventilation
parameters, including oxygen uptake (VO2), carbon dioxide output (VCO2), and minute
ventilation (VE), as well as parameters derived from them, such as respiratory exchange ratio
(RER), ventilation equivalent for oxygen (VE / VO2), and ventilation equivalent for carbon
dioxide (VE / VCO2). We also evaluate the maximum achieved, so-called peak values of
oxygen intake (VO2peak) and power (W peak) in spiroergometry, which provide information
on the patient's maximum aerobic capacity and performance.84-85

66
1.2.1.3 Cardiac stress test
Simply, a stress test involves walking on a treadmill while the heart works harder and harder.
The electrical rhythms of the heart are monitored using an electrocardiogram (ECG). The
doctor will also check the blood pressure and see if there are any symptoms like chest pain or
exhaustion. Abnormalities in blood pressure, heart rate, or ECG, as well as worsening clinical
symptoms, may indicate coronary artery disease (CAD). When performing stress tests, it's
important to remember that the results are impacted not only by the patient's physical, mental,
and behavioral features, but also by environmental factors like temperature, room airflow, and
time of day, as well as the medication the patient is taking. Equipment’s of a stress measuring
are, ergometers (treadmills, bicycle ergometer, rowing ergometer), devices to measure
circulation parameters (ECG, pressure meters), devices to measure ventilation parameters
(spirometers, gas analyzers), dynamometers. Before a stress test is taken it is necessary to
choose the right stress protocol which will further specify the intensity of workload, its
duration: single-grade stress test, graded stress test, graded test with pauses, ramp, continual,
combined.86 During the stress test, the patient performs a subjective assessment of his feelings
most often using Borg scales. The scale 6-20 is used to evaluate the perception of the intensity
and stress of the load. The 0-10 scale is then used to assess dyspnea, chest pain, and lower limb
pain (HD). Individual results are recorded in the protocol and use the self-description of other
physical activity and the patient for self-control.87
Absolute contraindications for stress testing include acute and active chronic diseases,
unstable angina pectoris acute or unresponsive to therapy, clinical signs of cardiac, respiratory,
metabolic insufficiency, advanced aortic stenosis, cardiovascular aneurysm, malignant
hypertension, severe pulmonary hypertension, severe dysrhythmia. The relative
contraindications are then as follows: less severe heart rhythm and conduction disorders, some
congenital or acquired valve defects, conditions after complicated MI, some uncontrollable
metabolic diseases, serious systemic diseases, mental disorders and unwillingness to
cooperate.86-88
Borg rating of perceived exertion (RPE) is an outcome measure scale used in
knowing exercise intensity prescription. It is used in monitoring progress and mode of
exercise in cardiac patients as well as in other patient populations undergoing
rehabilitation and endurance training.

67
Table 3: Subjective Perception of Effort According to Borg scale 6 – 20, Borg RPE Scale.85
Scoring Level of Exertion Scoring Level of Exertion
6 No Exertion 13 – 14 A little Hard
7 – 8 Extremely light 15 – 16 Hard
9 – 10 Very Light 17 – 18 Very Hard
11 – 12 Light 19 – 20 Extremely Hard
The original Borg scale ranges from 6 to 20, with a strong correlation to heart rate. Multiplying
each number by 10 gives the training heart rate at the moment of scoring. It was later
reconstructed into the Borg CR10 Scale or modified Borg Dyspnea Scale, which is primarily
used to diagnose breathlessness and dyspnea, chest pain, and musculoskeletal pain. The CR-
10 scale is best used when a sensation is felt in a specific location of the body, such as muscle
pain or pulmonary reactions.
Table 4: Subjective Evaluation of Dyspnea, Chest Pain and HD According to Borg Scale 0 – 10.86-87
Scoring Level of Exertion Scoring Level of Exertion
0 No Exertion 5 Severe
0.5 Extremely slight 6 Severe
1 Very Slight 7 Very Severe
2 Slight 8 Very Severe
3 Moderate 9 Extremely Severe
4 Somehow Severe 10 Maximal

68
1.2.1.4. Dynamometry
Skeletal muscle strength measurement is becoming more significant as an outcome parameter
in patients with chronic heart failure.89 Muscle strength can be measured using dynamometers
during isometric (muscle length doesn’t change), isotonic, or isokinetic contractions. Isokinetic
dynamometers test muscles during a movement within a joint range. The so-called handgrip
test, which uses a hand dynamometer, is commonly used in internal medicine and cardiology.
It must be implemented before the inclusion of the strength training, as it allows you to
check the reaction of blood pressure and other cardiovascular function indicators to static load.
We speak of a normal reaction when blood pressure does not rise above 180/120 mm Hg)
during extended static exercise, and the intensity of strength training is further established by
the one repetition maximum approach (1-RM). The 1-RM test is not conducted in the case of
pressure hyperreaction, and training begins with light loads that gradually rise during the
rehabilitation program.84-86-87
1.2.1.5. Comprehensive Medical Rehabilitation
Cardiovascular disease (CVD) is one of the leading causes of death worldwide.90-91 Cardiac
rehabilitation is an integral part of the treatment of patients with heart failure.
According to PubMed, cardiac rehab, is a complex, interprofessional intervention
customized to individual patients with various cardiovascular diseases such as ischemic heart
disease, heart failure, and myocardial infarctions, or patients who have undergone
cardiovascular interventions such as coronary angioplasty or coronary artery bypass grafting,
that aims to help patients with cardiovascular diseases, such as acute and chronic heart failure,
regain and maintain their optimal physical, mental, social, occupational, and emotional health.
It also includes adhering to secondary prevention guidelines and leading a healthy
lifestyle.92 Cardiac rehabilitation programs are designed to assist patients cope with the
psychological and physiological effects of CVD, minimize the risk of CVD-related mortality,
and enhance cardiovascular function in order to help them achieve their highest quality of life
possible and to enable patients to return to an active social life, to work and recreational
activities 93. Improving total heart function and capacity, preventing or reversing the
progression of atherosclerotic disease, and gradually enhancing the patient's self-confidence
are all goals that must be accomplished.94 Patients may develop some cardiovascular problems
during cardiovascular rehabilitation as a result of increased physical and mental exertion. As a

69
result, close collaboration with the attending physician is required, as is additional control by
a physiotherapist.84
Several organizations, including the American Heart Association (AHA), the American
Association for Cardiovascular and Pulmonary Rehabilitation (AACVPR), and the Agency for
Health Care Policy and Research, agree that a comprehensive cardiac rehabilitation program
should contain specific core components. These components should optimize cardiovascular
risk reduction, reduce disability, encourage active and healthy lifestyle changes, and help
maintain those healthy habits after rehabilitation is complete. Cardiac rehabilitation programs
should focus on95
• Weight management,
• Blood pressure management,
• Diabetes management,
• Lipid management,
• Patient assessment nutritional counseling,
• Tobacco cessation,
• Psychosocial management,
• Exercise training,
• Physical activity counseling.95
1.2.1.5.1 Perioperative Cardiac Rehabilitation
Pre-rehabilitation helps patients to overcome the stress of surgery by improving functional
capacity. Preoperative exercise decreases sympathetic over-reactivity, improves insulin
sensitivity, and increases the ratio of lean body mass to body fat. It also promotes physical and
psychological readiness for surgery, reduces postoperative complications and length of stay,
and improves the transition from the hospital to the community. Patient who were given
education regarding postoperative mobilization before surgery will respond more positively
and enthusiastically to the program.96

70
1.2.1.5.2 Post-Operative Cardiac Rehabilitation
There is no place for "bedrest" in the management of patients with cardiovascular disease after
surgery. Early patient mobilization following cardiac surgery has been shown to improve
patient recovery. Physical activity, particularly walking exercise, should be started as soon as
possible following cardiac surgery to prevent complications.97
1.2.1.5.2.1 Phase 1: Acute, In Hospital Patient Period
While remaining in the hospital, patients with acute heart issues, such as those recovering from
heart surgery, may be referred to a cardiac rehab team. Depending on patient physical state,
this period will likely last between 1-14 days. This phase includes the following:
• Assessment: The patient will be visited by cardiac rehab specialists during this phase,
and the cardiac rehab team may perform the following tests: Heart rate, Blood pressure,
Oxygen saturation, Upper and lower extremity function, including strength and range
of motion (ROM), Functional mobility such as walking and self-care tasks. They will
also take a full medical history to rule out any potential risk factors or comorbidities.
• Education: Patient can begin receiving education and training in the following areas:
The cardiac event itself, Specific aspects of diagnosis and condition, managing
psychological reactions to the event, Managing cardiac pain and other symptoms,
Monitoring.
• Physical Therapy: Patient may be referred to an acute care physical therapist, who will
devise a carefully monitored, gradual, and very limited activity program to help you
patient get back on feet. This could start with simply sitting up in bed, progressing to
standing and checking range of motion, and then taking short walks around the hospital
wing. The rehabilitation team might also concentrate on activities of daily living
(ADLs) and educate the patient how to manage stress. Patients are advised to stay as
rested as possible until the treatment of comorbid disorders or post-operative
complications is completed.
• Discharging Plan: A plan for leaving the hospital will also be provided by the cardiac
rehab team. Before patient leave, they will examine walking skills, requirement for
home oxygen, and any other training or medical needs.
Throughout this phase, a mix of low-intensity physical activity, stress management
approaches, and risk factor education is recommended. The main goal of this phase is
preventing deconditioning, thromboembolic, pulmonary, inflammatory, and other

71
complications, as well as reducing muscle strength and joint stiffness. Our aim is to get the
patient ready for normal daily activities and assist with stress management. The content is
simple active non-strenuous exercises in the bed or at the bedside, to gradually begin with
walking, while evaluation patient physical activity by measuring the blood pressure and
heart rate as well as monitoring patient clinical condition and subjective feelings.98
1-2 days post-surgery: bed exercise to prevent deep vein thrombosis, the first day includes a
simple extremity movement with the least impact of gravity. The second day, the extremities
can be elevated above the surface. These simple exercises are also performed by patients
connected to mechanical lung ventilation, if their current medical condition allows it.
3-4 days post-surgery: sitting in bed or standing by the bed, the patient is usually transferred to
the cardiac surgery.
5-6 days post-surgery: ambulation in the room.
7-10 days post-surgery: ambulation in the hallways.
11-14 days post-surgery: ambulation around the ward at faster speeds, stair negotiation.119
1.2.1.5.2.2 Phase 2: Subacute Outpatient Care (Post-discharge, Pre-Exercise Period),
(2-6 weeks post-surgery)
Outpatient cardiac rehabilitation takes place once the patient is stable and cleared by
cardiology. Phase 2 usually lasts three to six weeks, but it can last up to twelve weeks in
some cases. It takes the form of an outpatient rehabilitation program, spa treatment or an
individual home rehabilitation program. The focus throughout this stage of therapy will
be on patient education. Patient will be given instructions on how to manage heart issue
and further information on heart-healthy living. During this time, health will be
continuously examined to ensure that the patient is progressing toward recovery. Once
patient is ready to begin exercising, he can move onto the next phase of rehab. A more
comprehensive patient-centered therapy plan is created, including three modalities:
information/advice, a customized training program, and a relaxation program. The goal of
the therapy phase is to encourage independence and lifestyle modifications in order to
prepare patients to return to their homes.
The main goal of this phase is to increase patient physical fitness and performance
to integrate him into a full active life and to be able to progress to phase 3. Posthospital
rehabilitation is appropriate for stabilized patients in NYHA functional classes I, II, and
72
III. For patients in NYHA functional class IV, rehabilitation in the form of standard
endurance aerobic training is contraindicated.98-99-100
1.2.1.5.2.3 Phase 3: Subacute Outpatient Care (Post-discharge, Pre-Exercise Period),
(7-12 weeks post-surgery)
Those patients who have experienced a severe cardiac event or surgery will most likely need
to complete phases 1 and 2 before moving into phase 3, which is a full cardiac rehabilitation
program (CRP). Some patients with milder cardiac problems may proceed directly to phase 3.
Phase 2 is closely monitored and is intended for patients who are still significantly affected by
their heart problem, whereas phase 3 introduces more autonomous activities and self-
monitoring. The patient is usually ready to begin phase 3 cardiac rehab when the vital signs,
such as heart rate and blood pressure, remain stable while increasing activity and
workloads advised in the sub-acute phase of cardiac rehab.
A complete Phase 3 cardiac exercise and training rehab program typically consists
of 36 outpatient sessions, while some patients may need inpatient care or require less
sessions and/or monitoring.98
Phase 3 focuses on increasing flexibility, strengthening, and aerobic conditioning,
outpatient visits to specialist physicians are recommended to monitor cardiovascular
health and medication regimes, promote healthy lifestyle changes, and intervene as needed
to prevent relapse.99-101
Before patient begin, a physical therapist will assess range of motion, muscle strength,
resting heart rate, blood pressure, breathing, endurance levels, and any scar mobility difficulties
if you've had surgery. Warm-up, cardiovascular exercise (such as using a stationary bike or
treadmill), and cool-down are commonly included in the cardiac rehab exercise sessions.
Patient may also be encouraged to include some resistance training, depending on his physical
condition. Will be encouraged to keep track workout responses, such as heart rate, exertion
level, and blood pressure.
At this phase, the focus of training will most likely be on:
• Nutrition: For people with cardiovascular diseases, eating a heart-healthy diet is
critically important. To avoid putting excessive strain on the heart, a healthy weight
should be maintained as well. Heart-healthy diet includes fruits and vegetables, whole
grains, and lean proteins and is low in sodium, sugar, and trans fats.

73
• Lifestyle: With a cardiac condition, patient may need to undertake lifestyle changes,
such as quitting smoking and exercising regularly, to improve long-term quality of life.
During Phase 3 of cardiac rehab program, the team of rehab specialists will provide
an assistance and advise on making the essential changes permanent.
• Stress management: In case of cardiac condition, it is critical to learn how to manage
stress effectively. Stress management training, such as breathing techniques and
meditation, may be included in the cardiac rehab program to help maintain stress levels
low once rehab is over.
The primary goal for Phase 3 of cardiac rehab is to educate patient with the knowledge
and skills necessary to manage heart problem on patient own and live a longer, happier, and
healthier life. When the patient finish his rehab program, he should know how to manage
his symptoms, cope with chest pain, monitor his blood pressure and exertion levels, and
manage his medications, oxygen, and other therapies on his own. The patient should also be
familiar with the elements of a heart-healthy lifestyle, such as how to exercise safely, eat well,
and handle stress. Ideally and by following these he should have fewer symptoms from
his heart problem and be less likely to have another episode or need to return to the hospital in
the future.98-99-101
1.2.1.5.2.4 Phase 4: Maintenance (13 weeks and beyond post-surgery)
If the patient has gone through the first three stages of cardiac rehabilitation, he should have a
good understanding of his heart disease and how to best manage it. Phase 4 essentially
continues for the rest of your life. During Phase 4, the patient should continue to follow
his rehab team's recommendations for exercise, nutrition, and lifestyle. He can either proceed
on his own or chose to self-fund further training with a physical therapist to assist him as he
progresses. He should see his doctor on a frequent basis to ensure that he is adequately
managing his cardiac condition and avoiding any flare-ups. The goal of Phase 4 is to keep up
with the lifestyle adjustments that started in Phase 3, stay on track with exercise routine, avoid
tobacco, eat well, and manage stress.98
The following activities are not recommended:
• Lifting and carrying heavy objects,

74
• Prolonged upper extremity activities above the head,
• Sports that involve jumping/rebounding,
• Strengthening in the form of resistance training (this should only performed under
the guidance of an experienced physical therapist).
The following activities are recommended:
• Alternating appropriate activities with a sufficient rest period,
• To prevent mucous formation, the patient should continue pulmonary physical
therapy learned in the hospital, including breathing exercises,
• Attempt to perform at least half an hour of endurance physical activity every day
(walking, stationary ergometer, swimming when the incision has healed) with
gradually increased duration of exertion,
• Rest in the case of heart palpitations, dyspnea or anxiety,
• Acclimatize during transitions from warmer to cooler areas.
1.2.1.5.3 Outpatient Controlled Program
The length of the outpatient rehabilitation program depends on patient health condition.
Generally, and in the majority of cases a typical program lasts for 10-12 weeks of structured
exercise sessions, for 2-3 times a week, each training unit lasts about 60-90 minutes and
takes place in the form of group exercises. A typical exercise unit consists of several parts
and begins with a warm-up that lasts for about 15 minutes, warm up has a goal to warming
up and prepare the heart for activity by boosting or increasing and making the patient
slightly breathless to prepare the body and muscles to minimize the risk of injury, The
training is low to medium intensity, and the phase is dynamic - which include dynamic warm-
up, dynamic stretching, and walking, for instance.
This followed by the main exercise component and can be called an endurance
aerobic phase, which lasts for 30-40 minutes it occurs in the form of continuous or interval
training, another modality is then circulating training in which the patient alternates
between different types of trainers such as a bicycle ergometer, rowing and elliptical
trainer, stepper, or treadmill, the staff will come over to check how patient doing and check
his pulse to determine whether if his achieving the target heart rate. Finally, this followed
by cool down (strengthening phase) that takes 10-15 minutes long. After exercise, the body
gradually transitions from exertion to rest, reducing the risk of hypotension, arrhythmia,
or myocardial ischemia. Finally cool down restores the heart rate and breathing to their

75
pre-workout levels. We include in this phase the Jacobson's progressive muscle relaxation
or Schultz's autogenous training The advantage of outpatient rehabilitation program is that
the patient is constantly monitored by medical personnel. The heart rate, blood pressure,
and, in high-risk patients, the ECG are all monitored during the training unit, the subjective
perception of exertion is assessed according to the Borg scales, and the occurrence of
symptoms indicating exercise intolerance is monitored. Another advantage of an
outpatient program is the opportunity to meet with other patients who are dealing with
similar issues, which can be beneficial to the patient's mental health.
Cardiac rehabilitation program requires a team approach, which includes a
multidisciplinary team that includes: Cardiologist, physiotherapist, occupational therapist,
psychologist, social worker, clinical nurse specialist.
Eventually, Exercise training has been proven to improve myocardial reserve flow,
improve endothelial function, and raise maximal oxygen uptake (VO2max). Additionally,
cardiac rehabilitation can help to quit smoking, lose weight, lower cholesterol, and lower
blood pressure.99 Milani et al. found that cardiac rehabilitation decreased depression in heart
disease patients who suffered a major coronary event.102 In heart failure patients with intact
ejection fraction, cardiac rehabilitation reduced hospital admissions and exhibited a long-term
reduction in all-cause mortality, according to a Cochrane analysis.
1.2.1.5.3.1 Spa Treatment
It can follow the hospitalization directly, or the patient undergoes it after an outpatient program.
Controlled physical activity, physiotherapy procedures, nutritional measures, psychotherapy,
and health education are all part of the spa treatment, which is monitored by doctors and
medical staff on a regular basis. Teplice nad Bečvou, Poděbrady, Konstantinovy Lázně,
Františkovy Lázně, and Libverda are spas that provide treatment for people with
cardiovascular disease.84 Patients are separated into groups during regulated physical exercise
based on the results of a stress test. Group therapeutic exercise for 30 minutes at least four
times a week, progressive ergometric training for 30 minutes at least four times a week, field
training and Nordic walking, and pool therapy, including swimming, are all part of this activity.
We emphasize weight loss in obese individuals; therefore, we incorporate a reduced-calorie

76
diet as well as frequent physical activity. We include lectures on cardiovascular issues in the
cultural program as part of health education. Patients are educated on the basic anatomical,
physiological, and pathological understanding about the heart, blood arteries, and disorders that
affect them, as well as the major risk factors for these diseases and treatment options.85
1.2.1.5.3.2 Home Exercise Program
It is advised not only for patients who do not want or are unable to participate in an outpatient
program and spa treatment, but also for those who use it as a supplement to their therapy on
days when they do not participate in regulated training. The patient is instructed on the proper
workload type, intensity, and frequency. The basis is mainly endurance activity, patients are
recommended to walk, Nordic-walking, cycling on an ergometer or swimming. This activity
should be done 3-5 times a week for 45-60 minutes.
1.2.1.5.4 Therapeutic Physical Education
1.2.1.5.4.1 Respiratory Physiotherapy
Pulmonary complications after surgery prolong hospital stay and increase healthcare costs. We
performed a systemic review to determine to what extent respiratory physiotherapy prevents
such complications, and the best type of physiotherapy intervention. We chose the setting of
cardiac surgery for three reasons. Firstly, patients are prone to pulmonary complications after
surgery; up to 65 % of patients may have atelectasis, and 3 % may develop pneumonia.
Secondly, the prevalence of cardiac surgery is high; around 110 per 100 000 population
annually in the western world. Thirdly, the extra costs of pulmonary complications after cardiac
surgery exceed 28 000 € for each patient.103
Patients with heart diseases often develop changes in respiratory mechanisms and lead
to respiratory complications.104
Thus, physiotherapy in pre- and postoperative period have as main objectives the
pulmonary re-expansion, airway clearance, prevention of complications in the post-operative
period of cardiac surgery such as: atelectasis, pneumonia, pleural effusion, pneumothorax,
chylothorax, pulmonary hypertension, pulmonary hemorrhage, etc.105
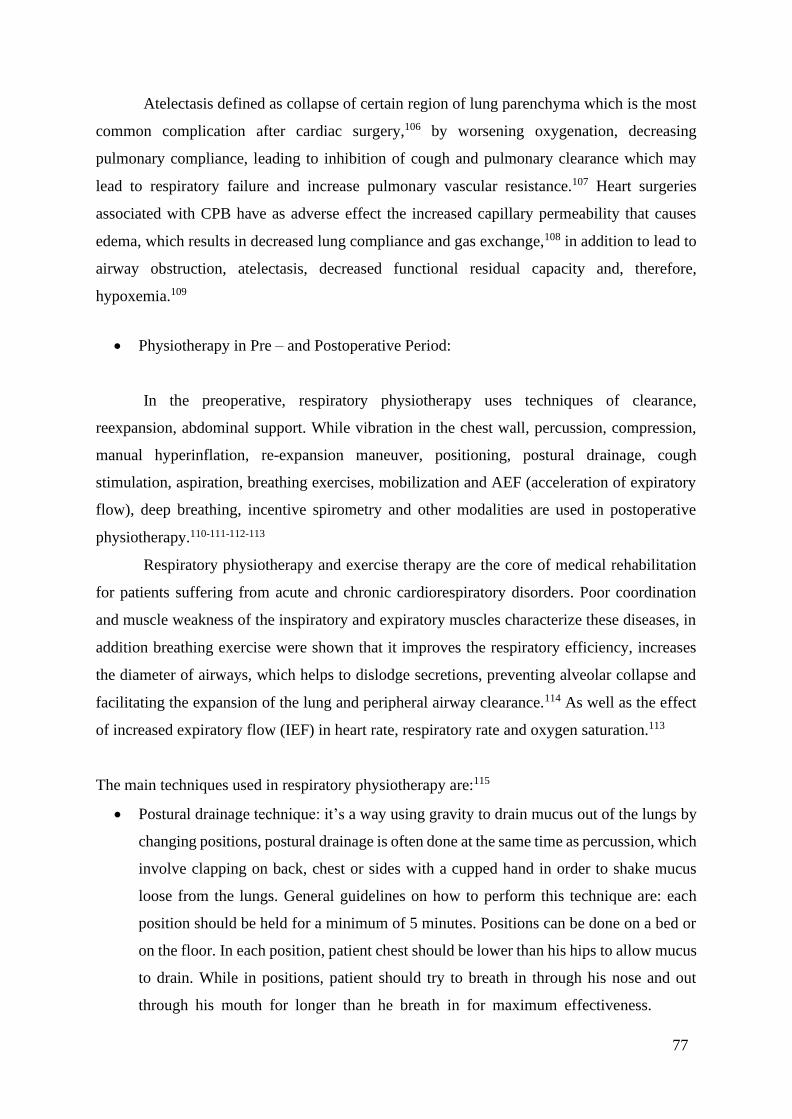
77
Atelectasis defined as collapse of certain region of lung parenchyma which is the most
common complication after cardiac surgery,106 by worsening oxygenation, decreasing
pulmonary compliance, leading to inhibition of cough and pulmonary clearance which may
lead to respiratory failure and increase pulmonary vascular resistance.107 Heart surgeries
associated with CPB have as adverse effect the increased capillary permeability that causes
edema, which results in decreased lung compliance and gas exchange,108 in addition to lead to
airway obstruction, atelectasis, decreased functional residual capacity and, therefore,
hypoxemia.109
• Physiotherapy in Pre – and Postoperative Period:
In the preoperative, respiratory physiotherapy uses techniques of clearance,
reexpansion, abdominal support. While vibration in the chest wall, percussion, compression,
manual hyperinflation, re-expansion maneuver, positioning, postural drainage, cough
stimulation, aspiration, breathing exercises, mobilization and AEF (acceleration of expiratory
flow), deep breathing, incentive spirometry and other modalities are used in postoperative
physiotherapy.110-111-112-113
Respiratory physiotherapy and exercise therapy are the core of medical rehabilitation
for patients suffering from acute and chronic cardiorespiratory disorders. Poor coordination
and muscle weakness of the inspiratory and expiratory muscles characterize these diseases, in
addition breathing exercise were shown that it improves the respiratory efficiency, increases
the diameter of airways, which helps to dislodge secretions, preventing alveolar collapse and
facilitating the expansion of the lung and peripheral airway clearance.114 As well as the effect
of increased expiratory flow (IEF) in heart rate, respiratory rate and oxygen saturation.113
The main techniques used in respiratory physiotherapy are:115
• Postural drainage technique: it’s a way using gravity to drain mucus out of the lungs by
changing positions, postural drainage is often done at the same time as percussion, which
involve clapping on back, chest or sides with a cupped hand in order to shake mucus
loose from the lungs. General guidelines on how to perform this technique are: each
position should be held for a minimum of 5 minutes. Positions can be done on a bed or
on the floor. In each position, patient chest should be lower than his hips to allow mucus
to drain. While in positions, patient should try to breath in through his nose and out
through his mouth for longer than he breath in for maximum effectiveness.

78
It is recommended to perform these positions in the morning to clear mucus that built
up overnight or night before bed to prevent coughing during night.
- On back position (Fig. 7): the chest should be lower than the hips, which can achieve
by lying on a slanted surface or propping the hips up about 18 to 20 inches with
pillows.
- This position is the best draining the bottom front parts of the lungs.115
Fig 7: Back Position, Postural Drainage Technique.115
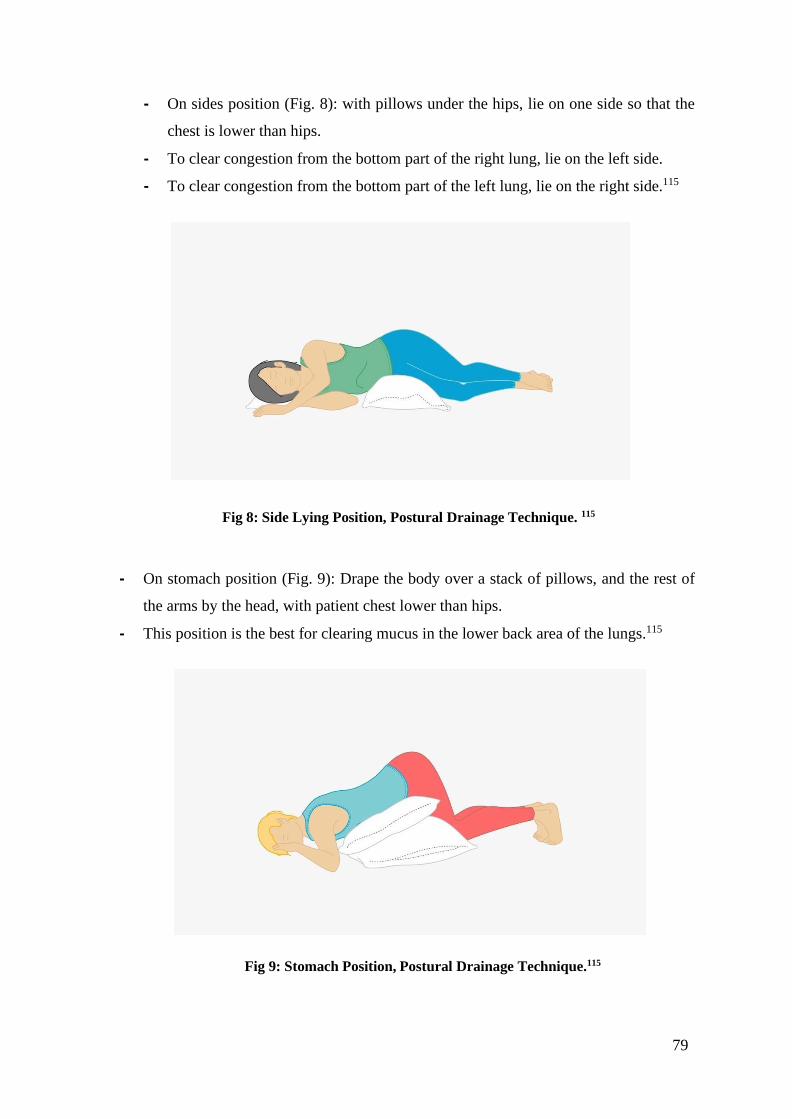
79
- On sides position (Fig. 8): with pillows under the hips, lie on one side so that the
chest is lower than hips.
- To clear congestion from the bottom part of the right lung, lie on the left side.
- To clear congestion from the bottom part of the left lung, lie on the right side.115
Fig 8: Side Lying Position, Postural Drainage Technique. 115
- On stomach position (Fig. 9): Drape the body over a stack of pillows, and the rest of
the arms by the head, with patient chest lower than hips.
- This position is the best for clearing mucus in the lower back area of the lungs.115
Fig 9: Stomach Position, Postural Drainage Technique.115

80
• Static and dynamic breathing exercise:116
Static breathing exercises:
- Diaphragmatic (abdominal) breathing - breathing is carried out mainly due to the work
of the anterior abdominal wall and diaphragm (for control, the patient's hands are
located on the anterior abdominal wall).
- chest breathing - breathing is carried out mainly due to work chest (for control, the
patient's hands are located on the chest).
- full breath - breathing is carried out due to the work of the chest and the anterior
abdominal wall (diaphragm), for control, one hand of the patient is located on the
anterior abdominal wall, the other on the chest.116
Dynamic breathing exercises:
- Are performed with the help of auxiliary respiratory muscles and consist of a
combination of breathing exercises and arm and leg movements. For instance,
spread arms to the sides and lean back while inhaling, then bring hands in front of
the chest and bend forward while exhaling. Exercise is utilized to expand the volume
of the lungs ventilated surface.
• Methodology:
- Start with 5-10 minutes of gymnastics. gradually increasing to 15-20 minutes,
eventually reaching 30-40 minutes.
- First, deep diaphragmatic breathing is taught (especially inhalation)
- The exhalation is carried out quickly, with the pronunciation of the sounds "he", "khe"
- Forced exhalation is combined with vibration massage in the drainage area.
- Cough movements are performed after several deep exhalations.

81
• Deep breathing and coughing technique:117
- Support the incision when coughing or sneezing by hugging your chest.
- Take 5 to 10 deep breaths followed by two double coughs four times a day for another
two weeks after you leave the hospital (Fig. 10).
Fig 10: Deep Breathing and Coughing Technique.117
The aim of each respiratory physiotherapy method is as following:118
• Deep breathing exercise: to encourage increased lung volume and prevent lung infection
and collapse.
• Hands-on technique and breathing facilitation exercises: to expand lung capacity.
• Percussions and vibrations: to help coughing and managing shortness of breath
• Breathing and circulation exercise: to prevent further respiratory and vascular
complications such as chest infection and deep venous thrombosis (DVTs).
• Uses of respiratory aids such as: flutter, acapella: reduce frequency of coughing.117

82
The goals of respiratory physiotherapy are:118-119
• To influence symptomatology such as shortness of breath, cough, and bronchial
secretion hyperproduction.
• Regular exercise improves respiratory muscle strength, chest wall mobility, airway
patency, ventilation parameters, and physical fitness.
1.2.1.5.4.2 Resistance Training
Resistance training (RT) has increasingly become a critical component of cardiac
rehabilitation, because of its significant health advantages and positive effects on cardiac
comorbidities.120 Increased muscular strength and endurance are the most well-known benefits
of RT. Overall muscle strength improvements of 25 % to 30 % are typical seen. Furthermore,
feeble persons who exercise RT have shown a 46 % increase in muscle power.121-122-123
This is important for cardiac patients because many daily activities require greater
muscular strength and endurance. These activities include the following: Getting out of a chair,
carrying groceries, ascending stairs, and holding/carrying children and grandchildren.
Resistance training can provide them gain the muscle strength and confidence they need to live
a more active and independent life. Resistance training reduces cardiac demands at specific
workloads by lowering the rate-pressure product (RPP) (systolic blood pressure vs. heart rate),
making tasks like lifting heavy things safer. Aerobic fitness has been shown to improve with a
combination of cardiorespiratory exercise and RT.124-125
• RT programming for cardiac patients:
A personalized program should be designed once a patient has been medically cleared
to begin RT. Other health issues should be taken into account while designing an RT program.
There should be a balance among major muscle groups trained. This will prevent muscle group
strength imbalances, which could lead to musculoskeletal injury. To save time, both lower- and
upper-body muscular groups should be trained on the same day. Multi-joint exercises should
be emphasized for their efficiency and functional effects, while single-joint exercises should
be used to supplement the RT program.126
83
Despite the fact that there are recommended 1RM (repetition maximum) percentages
for lower- and upper-body exercises for cardiac patients, 1RM testing is frequently avoided
due to safety concerns and a lack of RT experience, which is typical among cardiac patients.
On the Borg Scale, an RPE (rating of perceived exertion) of 11 to 13 (very light to slightly
hard) is a good place to start for calculating initial loads for RT exercises.127-128 Once the patient
can easily complete 12 to 15 repetitions, a gradual increase in resistance (5 %) should be
implemented. The following are a few training recommendations:
- Perform a warm-up before starting any RT session; A general warm-up would consist
of 5–10 minutes of light aerobic exercise; Gentle stretching and/or active range of
motion exercises with minimal or no resistance would be included in a specific warm-
up.129
- Resist the desired movements/synergies while keeping resistances (weights, bands,
tubes, medicine balls, etc.) parallel to the plane of motion and opposite the intended
direction of their movements.
- Always maintain proper body and joint alignment (e.g., ankles, knees, and hips in line
during a leg press or squat).126
- Machines usually allow for shorter RT sessions, are easier to perform with proper
technique, and stabilize the body, minimizing the need for balance (more muscle
isolation).126
- Free weights typically use more muscles for balance and stabilization, offer a variety
of technique manipulations (e.g., various hand positions), and work the muscles in a
more functional manner.126
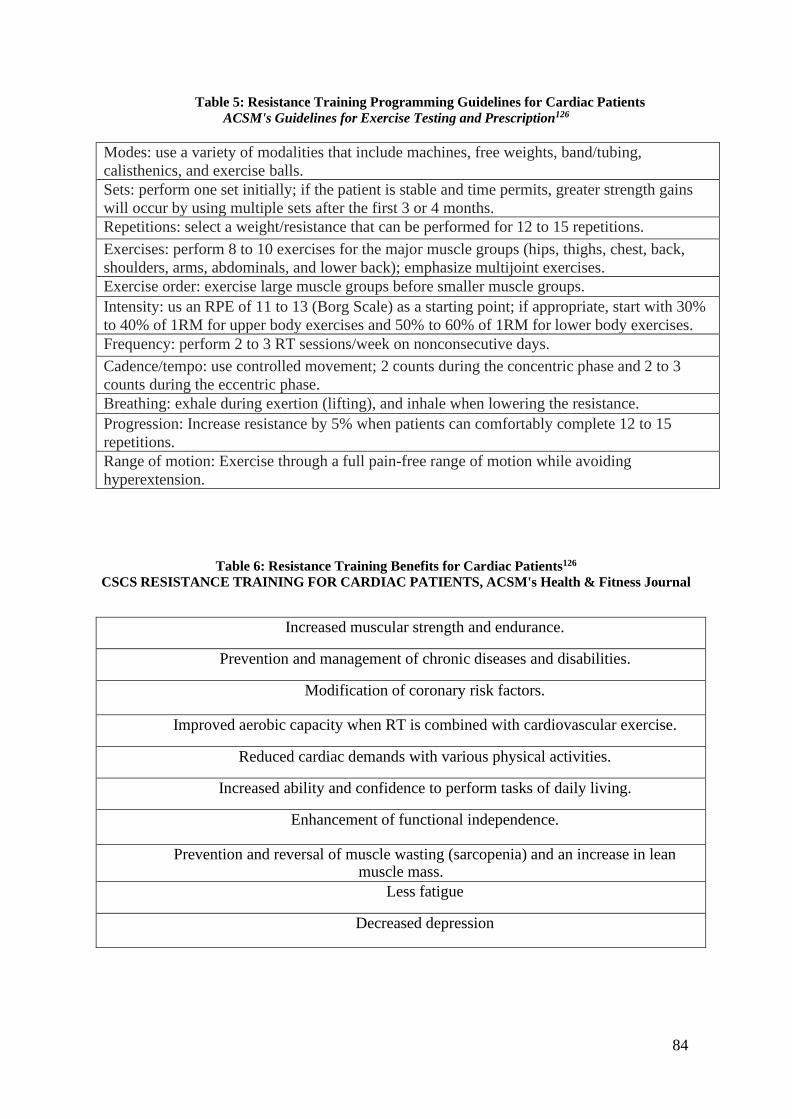
84
Table 5: Resistance Training Programming Guidelines for Cardiac Patients
ACSM's Guidelines for Exercise Testing and Prescription126
Modes: use a variety of modalities that include machines, free weights, band/tubing,
calisthenics, and exercise balls.
Sets: perform one set initially; if the patient is stable and time permits, greater strength gains
will occur by using multiple sets after the first 3 or 4 months.
Repetitions: select a weight/resistance that can be performed for 12 to 15 repetitions.
Exercises: perform 8 to 10 exercises for the major muscle groups (hips, thighs, chest, back,
shoulders, arms, abdominals, and lower back); emphasize multijoint exercises.
Exercise order: exercise large muscle groups before smaller muscle groups.
Intensity: us an RPE of 11 to 13 (Borg Scale) as a starting point; if appropriate, start with 30%
to 40% of 1RM for upper body exercises and 50% to 60% of 1RM for lower body exercises.
Frequency: perform 2 to 3 RT sessions/week on nonconsecutive days.
Cadence/tempo: use controlled movement; 2 counts during the concentric phase and 2 to 3
counts during the eccentric phase.
Breathing: exhale during exertion (lifting), and inhale when lowering the resistance.
Progression: Increase resistance by 5% when patients can comfortably complete 12 to 15
repetitions.
Range of motion: Exercise through a full pain-free range of motion while avoiding
hyperextension.
Table 6: Resistance Training Benefits for Cardiac Patients126
CSCS RESISTANCE TRAINING FOR CARDIAC PATIENTS, ACSM's Health & Fitness Journal
Increased muscular strength and endurance.
Prevention and management of chronic diseases and disabilities.
Modification of coronary risk factors.
Improved aerobic capacity when RT is combined with cardiovascular exercise.
Reduced cardiac demands with various physical activities.
Increased ability and confidence to perform tasks of daily living.
Enhancement of functional independence.
Prevention and reversal of muscle wasting (sarcopenia) and an increase in lean muscle mass.
Less fatigue
Decreased depression

85
Fig 7: Absolute and Relative Contraindications for RT in Cardiac Patients
American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical
Activity, and Metabolism
Absolutive Contraindications
Unstable coronary artery disease.
Severe pulmonary hypertension (mean pulmonary arterial pressure of 55 mmHg).
Severe symptomatic aortic stenosis.
Uncompensated congestive heart failure.
Uncontrolled dysrhythmias.
Acute myocarditis, endocarditis, or pericarditis.
Uncontrolled hypertension (<180/110 mmHg).
Dissecting aortic aneurysm.
Marfan syndrome.
High intensity RT (80 % to 100 % 1RM) in patients with active proliferative retinopathy or
non-proliferative diabetic retinopathy.
Relative Contraindications (Should Consult a Physician Before Participation)
Major coronary artery disease risk factors.
Diabetes.
Uncontrolled hypertension (<160/100 mmHg).
Low functional capacity (< 4 METs).
Musculoskeletal limitations (including but not limited to arthritis, osteoporosis, tendonitis,
etc.)
Implanted pacemakers and defibrillators.

86
1.2.1.5.4.3 Endurance Aerobic Training
Cardiovascular endurance training is the performed exercises involving the entire body at
moderate to high intensity for an extended period of time, which can effect on increasing the
heart and breathing rate. According to many experts, aerobic exercise is the most important
part of physical fitness. Cardiovascular endurance can be achieved by exercising aerobically
30 minutes per day, 3 to 7 days per week. Aerobic exercise is beneficial for cardiac patients
precisely in the following points:
- The heart pumps more efficiently.
- Lungs works better.
- Blood volume and delivery system are improved.
- Resting heart rate lower.
- Muscles, tendons, ligaments, bones get stronger.
- The body is more able to use fat as an energy source.
Based on the patient's fitness and condition, we can use three levels of training intensity:
low-intensity interval training, continuous training, and high-intensity interval training. Low-
intensity interval training is recommended for patients with significantly reduced EF LV (15-
20 %) in NYHA functional class III. The intensity of the exercise corresponds to 50-70 % of
the maximum power, as determined by a stress test performed to the patient's subjective
maximum. The load lasts 30 seconds, followed by a rest period. The intensity of the load is
gradually increased, and then exercises with a continuous form of load can be performed.
Continuous training is done in an aerobic zone of medium to high intensity. The first exercise
units last about 15 minutes and have a low intensity load of 40 - 50 % VO2peak. Depending
on the patient's medical condition and response to physical exercise, we gradually increase the
intensity of exercise to 70 % of the initial VO2peak, and the duration and frequency of exercise
can also be increased. Only patients in good clinical condition who are stable and very capable
can complete interval training at a high intensity of 85-95 % VO2peak. The load interval last
about 4 minutes, and the recovery time approximates 3 minutes.84-130
The overall effect and benefits of cardiovascular endurance training in post-cardiac
surgery patient are as following:
- Lower blood pressure.
- Higher insulin resistance.
- More favorable plasma lipoproteins profile.
- Increases cardiac output and blood pressure.

87
- Lower resting heart rate and cardiac hypertrophy.
- Improve overall stamina and the ability of the heart to pump oxygenated blood.
- Improving muscle strength and endurance.
In addition, these exercises include walking swimming, biking. Endurance exercise
keeps the heart, lung and circulatory system healthy. Increases in cardiac stroke volume and
heart rate during exercise raise cardiac output, which, combined with a transient increase in
systemic vascular resistance, raises mean arterial blood pressure.131
As it shown in (Fig. 11) long-term exercise, on the other hand, can promote a net
reduction in blood pressure at rest. A meta-analysis of randomized controlled interventional
studies discovered that 3-5 times per week of moderate to intense exercise lowers blood
pressure by an average of 3.4/2.4 mmHg.132
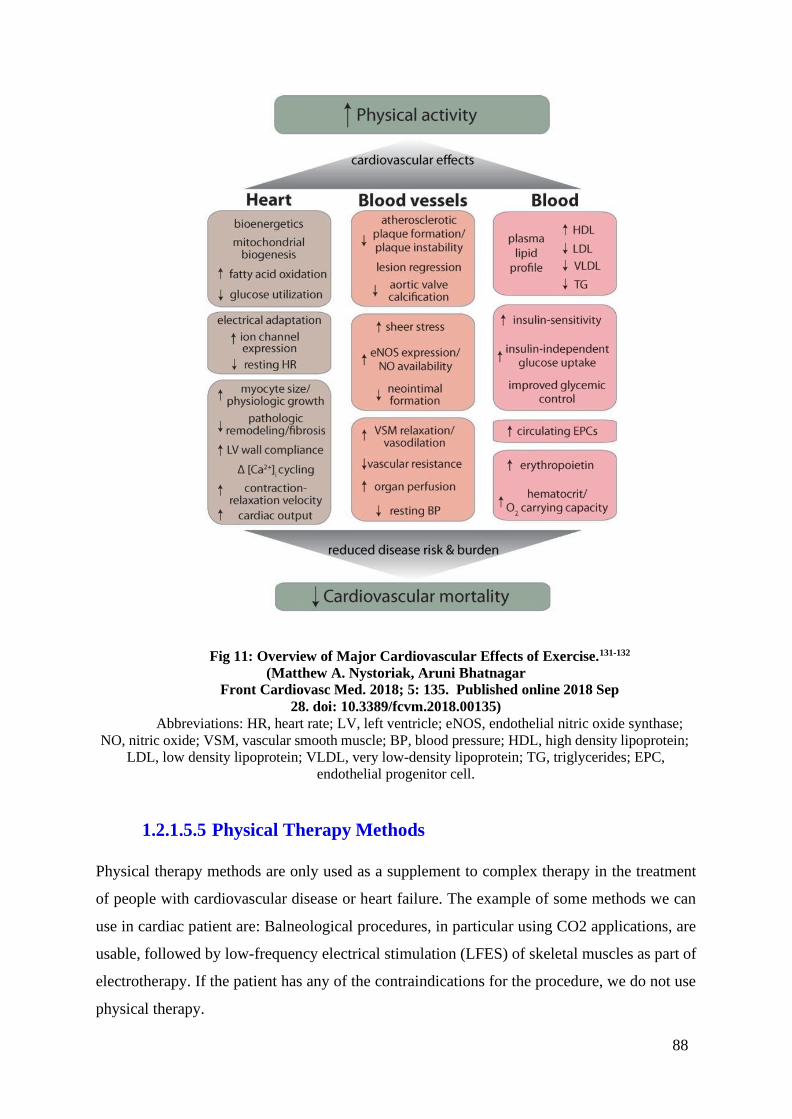
88
Fig 11: Overview of Major Cardiovascular Effects of Exercise.131-132
(Matthew A. Nystoriak, Aruni Bhatnagar
Front Cardiovasc Med. 2018; 5: 135. Published online 2018 Sep
28. doi: 10.3389/fcvm.2018.00135)
Abbreviations: HR, heart rate; LV, left ventricle; eNOS, endothelial nitric oxide synthase;
NO, nitric oxide; VSM, vascular smooth muscle; BP, blood pressure; HDL, high density lipoprotein;
LDL, low density lipoprotein; VLDL, very low-density lipoprotein; TG, triglycerides; EPC,
endothelial progenitor cell.
1.2.1.5.5 Physical Therapy Methods
Physical therapy methods are only used as a supplement to complex therapy in the treatment
of people with cardiovascular disease or heart failure. The example of some methods we can
use in cardiac patient are: Balneological procedures, in particular using CO2 applications, are
usable, followed by low-frequency electrical stimulation (LFES) of skeletal muscles as part of
electrotherapy. If the patient has any of the contraindications for the procedure, we do not use
physical therapy.

89
1.2.1.5.5.1 Carbonic Bath
The physiotherapy method of carbonic acid gas bath (CAGB) mediated through the effects of
carbon dioxide (CO2) is a minimally invasive treatment and prevention method of many human
disease. The carbonic bath has a reflective effect on the entire organism via the nervous system,
particularly on the cardiovascular system, and can therefore be used in the treatment of people
suffering from heart failure. We prepare it by saturating water under CO2 pressure in saturators,
with the bath containing at least 1000 mg of free CO2 per kilogram of water. The bath has the
greatest effect when the water temperature is low; in practice, a temperature of 34-28 °C is
often used. The rate of absorption is approximately 30 ml CO2/ min/m2 submerged skin
surface. Active hyperemia and skin erythema develop at the site of contact with the skin,
peripheral vasodilation and peripheral resistance decrease, and muscle blood flow improves.
There is a reduction in O2 consumption, overall metabolism, and as a result, the heart's
work is economized. In addition, the influence of a course of carbon dioxide baths,
hemodynamic parameters of cardiac output (cardiac and stroke volume) improved, rhythm
slowed, diastole become longer, and systolic and diastolic arterial pressures decreased. The
findings support the use of dry carbon dioxide baths during the recovery period for patients in
the I-III functional classes who have had a previous myocardial infarction or heart failure.
Additionally, diuresis is increased. The carbonic bath's result is determined by the
patient's reactivity, the time of application, the temperature of the bath, the size of the skin
surface that comes into contact with CO2, and the strength of the skin layer. The bath
duration should last between 8 and 25 minutes, with each positive step we gradually increase
the length by 2 minutes. The number of procedures should be in the range of 15. Furthermore,
it is best to start with partial baths and then progress to total baths after evaluating the effect on
the patient. We perform a dry wrap after the bath, and the patient rests on the bed for at least
30 minutes.133 Baths with carbonic dioxide are contraindicated in the following cases: cardiac
decompensation, epilepsy, tendency to hypertension, late-stage atherosclerosis, acute
inflammatory diseases, tachyarrhythmias, hypotension, coronary sclerosis, anemia.134

90
1.2.1.5.5.2 Low-frequency electrical stimulation
Low-frequency electrical stimulation (LFES) is an acupuncture technique that stimulates
muscle contraction to mimic the benefits of resistance exercise. Furthermore, the effects of
low-frequency electrical stimulation (LFES) on muscle strength and blood flow in patients with
advanced chronic heart failure (CHHF). As well as (LFES) has the potential to reduce
breathlessness and increase exercise capacity in people with chronic heart failure. This method
is specially used in patients with NYHA III and IV functional clinical classifications.
These patients develop global hypoperfusion, which affects the skeletal muscles, as a
result of the significantly reduced function of the cardiovascular system. Moreover, muscle
atrophy may be present in up to 70 % of cases, with a predominance of type IIB muscle fibers
and a decrease in the absolute amount of type I and IIA aerobic fibers. Muscle atrophies are
associated with low exercise tolerance and dyspnea, which leads to further physical inactivity.
For LFES, we use biphasic pacing with a frequency of 10Hz and a mode of 20 seconds "on"
and 20 seconds "off." The pulse duration is 200 ms, and the maximum intensity is 60 mA.
We use LFES for 60 minutes per day, and then we can increase it to twice a day for 60
minutes. LFES can also be used in combination with traditional physical training. Due to the
fact that the method does not cause hemodynamic changes, it is well tolerated by patients and
can thus be used in patients who are unable to engage in physical activity, based on this the
benefit of LFES is that it acts locally without increasing the demands on cardiac work; there is
no increase in cardiac output. During stimulation, the heart rate and blood pressure do not
change. LFES has a positive effect on increase muscle strength; with LFES, we can achieve
stronger muscle contractions than with free training because there is maximum synchronization
of the activation of all motor units during electrical stimulation. It enables patients to perceive
shortness of breath and exertion during normal daily activities as less intense, thereby
improving their quality of life as a result of illness.84-135-136-137
1.2.1.5.6 Ergotherapy
According to the World Health Organization (WHO), there are known correlations between
cardiac dysfunction and the incidence of cognitive impairment, with some studies estimating
its presence in more than 17 % of cardiac patients, potentially increasing to around 75 % of
patients with heart failure. Although the severity of cognitive deficit varies, among cardiac
patient groups, impairment is frequently classified as mild, which means that there is a

91
cognitive deterioration greater than expected for the person's age and education level, which
may impair their ability to engage in more complex activities and behaviors.135
Patients with cardiac dysfunction are more likely to experience mild cognitive
impairment, which can impair their ability to successfully engage in daily activities crucial for
home and community safety, as well as maintaining health and well-being. Ergotherapy plays
a role in chronic disease management by assessing and improving functional abilities affected
by physical, emotional, and cognitive domains. While the ability to independently complete
basic activities of daily living remain intact, the capacity to engage in more complex activities
requiring a higher level of cognitive function may be compromised, resulting in increased
difficulty completing instrumental activities of daily living (IADL), completing work activities,
and engaging in self-management behaviors. IADLs are more cognitively demanding task
behaviors required for independent living, and they include activities such as shopping, meal
preparation, driving, and financial management.136-137 Therefore, Occupational therapy is an
important part of the rehabilitation of people with cardiovascular disease.
It helps patients to maintain, use and improve the skills necessary for the day-to-day,
work, leisure and recreational activities through meaningful employment, promotes the active
integration of patients into society and contributes to maintaining an optimal quality of life.
Specifically, occupational therapy deals with the training of motor functions, sensory functions,
cognitive, communication and social functions, activities of daily living (ADL), the use of
compensatory aids are included if the patient's condition requires it. In addition to therapy it
deals with diagnostic methods for instance. The occupational therapist assesses the patient's
ability to return to their original job or assists in the selection of a new suitable job based on
the patient's condition and abilities.119Therefore, ergotherapy intervention can decrease risk of
further potential decline and injury to prevent risk of readmission to the hospital. As a result it
is an absolute essential to helping patients regain their independence and ability to do what they
love and enjoy in life.
1.2.1.5.7 Psychological and Social Problems of the Diseases
Heart failure (CHHF) is the terminal stage of many heart diseases and a major cause of
morbidity and mortality. The incidence of congestive carditis increases steadily as treatment of
its coronary antecedents, such as myocardial infarction.138
It's easy to see the effects of heart failure on your body - such as shortness of breath,
fatigue, and edema. What isn't obvious is the toll a weakened heart can take on your emotions.

92
Therefor psychosocial issues are important variables that need to be addressed in patients with
heart failure. Unfortunately, these issues are frequently overlooked. Depression and a lack of
social support have been shown to negatively impact HF patients. Patients with HF who are
depressed or lack social support have higher morbidity and hospital readmission rates are less
adherent to their medical regimen and have a higher overall cost of care.139 Living with this
condition can elicit a wide range of emotions, including fear and sadness, as well as anxiety,
depression, and even anger. By letting them simmer, they can wreak even more damage on
the heart, making it more difficult to treat. According to research, people who have a positive
outlook are more likely to take their medication. They also maintain heart-healthy habits such
as eating nutritious foods and exercising.
When a long-term disease, such as heart failure, is diagnosed, it is normal to experience
a wide range of emotions, including fear about the future, worry to lose control over the health,
anger, stress over the ability to manage the condition, loneliness.
By letting all these feelings to build up, could make matters worse. Stress and anger
can raise the BP (blood pressure) and make the heart work even harder. Both can be as bad for
the heart as high BP and cholesterol. Depression for at least two weeks affect up to 70 % of
people with heart failure, along with depression and sadness patient might have fatigue, lack
of energy, loss of appetite, feeling of emptiness, loss of interest in activities, trouble sleeping
or sleeping too much.140
As patients with heart failure experience various physical and emotional symptoms,
these symptoms limit patient’s daily physical and social activities and result in poor QOL
(quality of life), therefore maintaining QOL in these patients should be assessed appropriately
to determine its impact on patients daily life.141 One of the best ways to handle these
psychological issues is psychological support, rehabilitation helps to overcome the fear of
physical activity and thus manage the newly created stressful situation. The patient's closest
environment should be the one that helps him change his lifestyle. Relaxation training,
education to influence risk factors, including dietary recommendations, and breaking down
unhealthy habits should all be included.
Psychological rehabilitation aids in the suppression of the patient's psychosocial factors
and personality traits that may contribute to the development of heart failure. It aims to improve
patients' ability to respond optimally to crisis life situations, which is important for lowering
the cardiovascular system's reactivity. It also aids in the treatment of any depression, anxiety,
or emotional stress caused by the disease.

93
On the matter of Social Services, social rehabilitation aims to achieve individuals
independence, self-sufficiency, by developing their specific abilities and skills, strengthening
habits, and practicing normal performance for independent living.
Cooperation with occupational therapists and social workers is used in the process of
social rehabilitation. Try to enable the patient to make the most of his remaining work potential
and reintegrate him into society.142
1.2.1.5.8 Indications and Contraindications of Cardiac Rehabilitation
Indications of cardiac rehabilitation are:143
• Recent myocardial infarction,
• Acute coronary artery syndrome,
• Chronic stable angina,
• Congestive heart failure,
• After coronary artery bypass surgery,
• After a percutaneous coronary intervention,
• Valvular surgery,
• Cardiac transplantation.
Contraindications of cardiac rehabilitation are:144
• Unstable angina,
• Acute decompensated congestive heart failure,
• Complex ventricular arrhythmias,
• Severe pulmonary hypertension (right ventricular systolic pressure greater than 60 mm
Hg),
• Intracavitary thrombus,
• Recent thrombophlebitis with or without pulmonary embolism,
• Severe obstructive cardiomyopathies,
• Severe or symptomatic aortic stenosis,
• Uncontrolled inflammatory or infectious pathology,
• Any musculoskeletal condition that prevents adequate participation in exercise.

94
2 CASUISTICS:
2.1 Basic Data Name: L.P.
Age: 62.
Height: 171 cm.
Body weight: 78 kg.
Gender: Male
BMI: 26.67
Marriage status: Married.
Occupational status: Janitor.
Data provider: In Person
Admission date: 1st of October 2021.
Data record date: 26th of October 2021.
2.2 Place of Hospitalization
On the 1st of October 2021 Mr. L.P. was transferred unconscious to Saint Ann’s hospital
ambulance, to the Department of Internal Cardio-angiology, University Hospital at St. Anna in
Brno. In the morning of the 1st of October 2021, Mr. L.P. was found by his wife on the floor
conscious and he was experiencing pressure, tightness sensation in his chest, shortness of
breath and he had a feeling of fast beating (palpitations). After that his wife immediately called
the emergency medical help and the ambulance came and transferred him to the hospital.
He suffered from dilated cardiomyopathy and on this basis, he was transplanted by a
new heart on the 25th of March 2017, and more physiological findings occurred in 2017, diffuse
calcification of brachial artery. Unfortunately, about month ago he suffered from heart attack
(myocardial infarction) and he is waiting for the new heart transplantation for the second time.
Upon admission, diagnosis of Delated cardiomyopathy (DCM) was confirmed by
Echocardiogram and this examination allowed the doctor to see that there was left ventricle
and also right ventricle wall motion abnormalities, and severe depression of systolic function.
95
2.3 Diagnosis upon admission
Upon admission the patient was diagnosed with Cardiorenal syndrome with oliguria on the
base of serious right ventricle dysfunction, tricuspid valve regurgitation, and signs of
hypervolemia, accumulation of fluid in the pleural cavity in an amount of 400 ml (Fluidothorax
bilateral) were confirmed.
Furthermore diagnosis were identified upon admission, they are as following:
– Acute kidney insufficiency AKI (acute on chronic)
– Continuous veno-venous hemodialysis (CVVHD) introduced from the 5th of November 2021,
anuria.
– from the 8th of November 2021 the patient is on the urgent waiting list for heart
transplantation.
– The State after Cardiopulmonary Resuscitation (CPR) for 5 minutes which took place on the
11th of November 2021, the patient was inserted with veno-arterial extracorporal membrane
oxygenation (VA ECMO).
– Subacute ST elevation myocardial infarction (STEMI) of the bottom wall and ramus
ventricularis selective coronarography (RV, SKG) on the 1st of October 2021 was diagnosed,
serious vasculopathy of graft with arteria coronaria dextra (ACD) obturation on the base of
massive thrombosis, additionally peripheral obturation of ramus interventricularis anterior
(RIA), ramus circumflexus (RC), ramus marginalis sinister (RMS), were identified.
– Furthermore, an ejection fraction of left ventricle (EFLV) of about 45 %- 35 % was diagnosed.
– The patient was implanted with implantable cardioverter defibrillator (1D-ICD) on the 21st
of October 2021.
– The patient underwent a heart transplantation surgery on the 25th of March 2017.
– Irregular, fast heart rate (Atrial fibrillation) was confirmed.
– Antireflux uretero-intestinal anastomosis procedure was introduced on the 15th of May 2019.
– Acneiform exanthema was identified.

96
2.4 Prescribed Rehabilitation
It is recommended to customize a rehabilitation program of exercise and education, to help the
patient improve his health, recover and treat heart disease and decrease the risk of other heart
disease, the cardiac rehabilitation should involve exercise training such as resistance training,
endurance aerobic training with a minimal load which can be gradually increased over the time.
Emotional support and education about lifestyle changes such as eating a heart-healthy diet,
maintaining a healthy weight and quitting smoking, to reduce the symptoms and the
progression of the disease, help regaining strength. Thus, will improve and keep independence,
self-sufficiency and physical abilities of the patient.
2.5 Engagement of Author in the Rehabilitation Process
2.5.1 Anamnesis
I was introduced to my patient at the Department of Internal Cardio-angiology 4th floor,
University Hospital at St. Anna in Brno. The anamnesis was taken on the 26th of October 2021,
in a conversation form. The patient Mr. L.P had the full ability to respond to my questions
fluently, and he was fully responsive and cooperative, and in a very good mental status.
Current Complaint:
Unfortunately, Mr. L.P about month ago suffered from Acute transmural myocardial infarction
of the bottom wall, and now he’s hospitalized, and in the waiting list for a donor organ. In more
details, and according to the medical documents, the patient acceded the cardiac clinic, ward
32 on the 1st of October 2021, and this is because he suffered from a heart attack of the bottom
wall, which was confirmed by coronarography. The patient Kidney’s function has deteriorated
and there was a tendency to bradycardia. Exanthema also appeared at the patient chest.
The patient suffered from paroxysmal atrial fibrillation, and application of amiodarone
(sodium channel blockers) had no effect on him, after that he underwent electrical
cardioversion to restore a normal heart rhythm, and it didn’t show any effect too. After that his
renal function got worse, complex QRS spread and on this basis he was transferred to coronary
unit. After a period of time when the patient’s condition has stabilized, he was transferred back

97
to ward 32. What happened day by day since he was admitted to the hospital according to the
medical documents:
On the 1st of October 2021, the patient was implanted with implantable cardioverter
defibrillator (ICD). Then on 2.11.202, his condition worsened with a signs of right-sided heart
failure, oliguria, and renal insufficiency progression. Then on the 4th of November 2021 the
patient returned back to the coronary unit, where he required dialysis and parenteral nutrition.
Then an oncologist was consulted, and the patient was classified on the 8th of November in the
urgent waiting list for heart transplantation.
Furthermore, on the 11th of November 2021, the patient needed cardiopulmonary
resuscitation (CPR) that took about 5 minutes long, but intubation was not necessary. After that
he was transferred to the cardio-surgery-clinic (CKTCH) for veno-arterial extracorporeal
membrane oxygenation (VA ECMO) insertion as bridge to transplant, and as a temporary
solution to be stable and safe until getting new heart.
Family History:
Mr. L.P is married and lives with his family. Parents of the patient are not alive, his father
suffered from acute myocardial infarction and he died at the age of 49. Mother of the patient
suffered from diabetes mellitus type 2 and died because of diabetic complications at the age of
63. The patient has six siblings, one brother died from esophagus cancer at the age of 56, and
all the other siblings are healthy. The patient has one son and one daughter and they’re healthy
too.
Personal-History:
In 2004 the patient was diagnosed with an insufficiency of a valve in the heart, and that was
the beginning of the journey, on this basis after four years the patient was implanted with ICD
(implantable-cardioverter-defibrillator). The patient after that continued his life normally for a
ten years long without any disturbances or health problems, and unfortunately in 2014 the
patient was diagnosed with cancer of urinary bladder (Urothelial Carcinoma – high grade), and
he underwent chemotherapy as a treatment and it went unsuccessfully, on this basis the patient
had a surgery of urinary bladder removal (cystectomy) in January 2017 and now he is living
with a urostomy which is placed in a small, spout like a hole on he’s abdomen as a new passage
where urine will leave his body.
98
In a meantime he also suffered from pulmonary embolism. Then in 2017 the patient
underwent the heart transplantation, because of cardiac decompensation, complicated by
hematuria and hemorrhagic shock, and an extracorporal membrane oxygenation (ECMO) was
inserted temporarily. And the patient got an injury of the right lung during surgery. And also
the patient was diagnosed by Muscle venous thrombosis of the right lower extremity which
was confirmed by sonography. The patient was diagnosed by a heart failure due to
arrhythmogenic left ventricular cardiomyopathy. Additionally, the patient suffered from
hypertension. The State after implantation of ICD in April 2014. The patient underwent
appendectomy surgery in 1969. And has an injury of ruptured tendon of the left hand.
Occupational History:
The patient used to work as a janitor, and now he is in pension. He has been working for 35
years long.
Social History:
The patient is married and lives with his wife, and he has two children, one girl and one boy.
He’s living in a flat and has about five stairs to climb.
Pharmacological-History:
The patient takes the following medications:
Envarsus 1.5 mg -0-0, Cetican 1mg -0-0.75 mg, Betaloc zok 200 mg tbl. 1-0-0,
Detralex 2-0-0, Magnosolv 1-0-1, Anopyrin 100 mg 0-1-0, Procoralan 7,5 mg tbl. 1-0-1, Furon
40 mg tbl. 1/2-0-0, Agen 5 mg tbl. 0-0-1, Alopurinol 100 mg tbl. 1-0-0 4x per week, Rocatrol
0.25 mg tbl. 1-0-0, Atoris 20 mg tbl. 0-0-1, Omnic 0.4 mg 0-0-1, Algifen gtt.d.p.d.p.
Medication at transfer:
Dobutrex 250mg ad FR 50 ml 10 ml/hod, Noradrenalin 5-amp ad FR 50 ml 0.10 ml/hod (stř.
TK > 65 mmHg), Smofkabiven 1970 ml + 1 amp. Cernevit + 1 amp. Tracutil 60 ml/hod, opak.,
FR 250 ml + Natriumglycerolphosphate 2amp=40 ml=40 mmol 80 ml/hod od 10h, s.c. Clexane
(enoxaparin) 0,4 ml 10 - 22, i.v. Torecan 1amp d.p. při nauzee, Certican (everolimus) snižuji
na 0,50mg tbl. 1 - 0 - 1, Advagraf (tacroimus) 0,5mg tbl. 1 - 0- 0, Rocatrol 0,25mgt bl. 1 - 0-
0, Trombex (clopidogrel) 75mg tbl ode dneška ex, Controloc (pantoprazol) 40 mg tbl dostal v
6,00, zítra v 6,00, Diazepam 5mg tbl 1/noc d.p.

99
Abuses:
The patient drinks one small beer daily, and once a day the patient drinks coffee, other than
this the patient denies that he has any addictive habitudes, including alcohol, drugs and
smoking.
Allergic History:
Negate, the patient is not allergic to anything.
Sport History:
The patient doesn’t do any sports now; his job was the only activity he has ever done.
At home he is just resting, sometimes goes for walks and from time to time does some cycling
but irregularly. These are all his activities.
Rehabilitation History:
The patient had the rehabilitation only once in the hospital while he was waiting for the heart
transplantation in 2017 and then after he got transplanted, he went to Poděbrady spa and he
spent there about a month long.
Physiological Function:
The patient has got a urostomy after the removal of urinary bladder, and that’s why he doesn’t
need to urinate (urination by stomia) and has a regular formed defecation without admixture.
The patient negates sweating, he doesn’t sweat even at night, and he sleeps well without any
disturbances, and he’s weight is stable.
Operation History:
The patient also underwent an operation of appendectomy and the operations that were
mentioned before, heart transplant and urinary bladder removal.
2.5.2 Physical Examination The patient was lucid, cooperative and responsive, well oriented to person, place and time.
The patient weight is about 78 kg, and height 171 cm. The body structure corresponded to the
Ectomorphs somatotype which is characterized by long and lean, with little body fat and little
muscles.
The patient was able to actively change a position where the transition from lying down to
sitting and standing positions and he haven’t experienced any dizziness. The patient did not
have shortness of breath at rest. The heart rate measured by pulse oximetry was 85 beats per
minute, O2 saturation reached 97 %, Blood pressure was about 138/90 mmHg measured by a
blood pressure monitor (sphygmomanometer), and when he needed to visit the toilet or have

100
some walk in the corridor he used to have the support from the walker. So, he can mobilize
with a walker independently and walk under assistant. The patient used to have a normal habit,
without shortness of breath and without cyanosis as well. There was no sign of surface injury,
and without neurological lateralization, no skin pathology, and normal coloring and turgor,
without swelling, unicteric.
Skin and mucosa:
Exposed skin and superficial mucosa are not completely normal with rashes and small raised
acne like bumps which can be observed in patients chest and upper back, due to an existence
of acneiform exanthema. Additionally, for the chest and neck, the skin was slightly red and dry
as a result of the insertion of the central venous catheter for medication administration; the skin
is otherwise normal in color, and with good elasticity, temperature, and moisture, and no
swelling. Surgical scars after the operations that the patient underwent can be observed clearly,
the scar along the chest bone (sternum) after the previous heart transplantation surgery, and the
scar that runs from just below the bellybutton to the pubic bone, can be clearly seen as well.
Lymph nodes:
Superficial lymph nodes were examined in the cervical region, axillary region, and abdominal
area. Lymph nodes were round in shape, medium in size, mobile, soft and palpable, and easy
to move, no abnormal magnification was found.
Head and face:
The head of the patient is slightly in a forward position. The pupils of both eyes are the same
size (isochoric pupils), no abnormal eyeballs protuberance. The eyes are symmetrical, no
conjunctival congestion, no edema, no icteric sclera, the cornea is transparent.
The patient could perfectly stick his tongue out in the middle line. No coating. The
shape of both ears is normal, the patient has got an oval shaped ear, bilateral asymmetry was
observed in the shape of the ear with no abnormal exudation. The sense of hearing is very good.
The nose is in center of the face with normal symmetry, length and width so the shape is normal
without edema on the nose mucosa. Functionally such as nasal breathing or ventilation function
is normal, without blockages, he can smell and taste very well, without inflammation. The
shape of the mouth is normal there wasn’t lip cyanosis or ulcer. Oral mucosa is normal. Uvula
located in the middle. Bilateral tonsils are normal.

101
Neck:
The shape and length of the neck are normal and symmetrical. Lymphoid nodules and veins
are impalpable. The carotid pulse is normal, symmetrical and palpable, and there is no visible
bulging of the jugular vein. Bilateral thyroids are normal, soft, symmetrical, and non-tender
and it slides upwards slightly when swallowing, without visible enlargement.
Chest:
The shape of the chest cage is normal and symmetrical. The sternum located in the middle of
the chest, without pain upon percussion. Breathing rhythm is quite normal. There are a surgical
scars after the operations that the patient underwent which can be observed clearly, the scar
along the chest bone (sternum) after the previous heart transplantation surgery which is named
as (post sternotomy scar). The patient had a skin condition in which the hair follicles become
inflamed - follicular exanthema. There is alveolar breathing without special phenomena.
Tapping on the chest is clear and full without abnormalities.
Abdomen:
There was confirmed peristalsis (positive). There was no pain with percussion and resistance,
and no pain or tenderness on palpation in the hepatic and spleen region. Percussion is bilaterally
negative. As the patient underwent surgical removal of the bladder then, there is a stomia in
the right hypogastric area, stomia is where the urine collects and leave the body.
Spine and Extremities:
The spine is located in the middle of the body and extended from the base of the skull to the
tailbone. The patient has a slight thoracic kyphosis. No scoliosis observed. The spinal
movement is normal, within the normal range of physiological movement. The upper extremity
looked normal in length and in shape with no rash nor edema or any other abnormality, The
patient got an injury a ruptured tendon in the left hand. The range of motion was within the
normal range. In the lower extremity the patient is diagnosed with muscular vein thrombosis
and, edema on the left lower extremity above the ankle, with no sign of phlebitis. Peripheral
pulsation was palpable. The patient had a calm varicose vein. There are weak pulses felt in the
extremities.
Electrocardiogram (ECG) findings:
RS reg 85/min, PQ = 0,16, QRS = 0,08, STE 1,5mm III, aVF, 0,5mm I, STD 1mm al, aVL,
V3-5, rsrV1-2, T flat, PZ V5, osa – 30. Without ES. Elevation of DS.
102
Additional Examination:
– On the 1st of October 2021:
1. FIRST INTERNAL CARDIOLOGY CLINIC – Coronarography findings:
Acute coronary syndrome: no stenosis of strain, inequalities in proximal ramus intermedius
artery, in ramus interventricularis anterior (v RIA-RD) there is 50 % bifurcated stenosis, in the
middle part of ramus interventricularis anterior (RIA) – there is multiple cascade stenosis to
90 %, and obturation of peripheral part of ramus interventricularis anterior (RIA), ramus
circumflexus (RC) and ramus marginalis sinister (RMS) can be observed.
Arteria Coronaria Dextra (ACD): massive thrombosis in the full length of the artery.
RLVG: hypokinesis DS, ejection fraction (EF) of the left ventricle 47 %.
Resume: serious vasculopathy of the graft with arteria coronaria dextera (ACD) obturation on
the basis of massive thrombosis, peripheral obturation of RIA, RC and RMS. EF of the left
ventricle LK 47 %.
The state after orthotopic transplantation of heart (OTS) on the 25th of March 2017 because of
decompensated cardiomyopathy (DCMP) and thrombotizatin of mitral valve replacement
(MVR).
– On the 4th of November 2021:
1. FIRST INTERNAL CARDIOLOGY CLINIC – findings of Sonography heart examination
by Vivid q, PACS 1443/17:
Left ventricle (LV): 45/37, interventricular septum (IVS) 10, dorsal septum (ZS) 10 – LV
without dilation or hypertrophy, dyskinesis of the large part of septum, akinesis of DS, ejection
fraction (EF) of 35 %.
Left atrium (LA): 39 Aorta: anulus 19 aorta ascendens 38.
Right ventricle (RV): 30 z PLAX, very serious dysfunction or akinesis found and, septal
dyskinesis, TAPSE 3 mm. there wasn’t pericardial effusion. Valve with physiological
morphology existed, and few congestions in hepatal vein existed too.
– Valves:
Mitral valve: asymmetric position, without pathological gradient, mitral valve regurgitation to
2nd degree, where the heart mitral valve doesn’t close tightly.
Aortic valve: without pathological gradient and regurgitation.
Tricuspid valve: there was a regurgitation of 2-3 degree.
Pulmonary valve: without regurgitation.
Resume: Serious dysfunction of the right ventricle, ejection fraction of left ventricle
(EFLV) of 35%. Fluidothorax I. sin. 300 ml, I. dx. 500-600 ml.

103
– On the 4th of November 2021:
Clinical imaging method of X-ray examination of the heart and lungs findings:
Invisible line of pneumothorax, there is the central vein catheter on the left side in situ.
Congestive lung drawing. Wore bilateral transparency of the lung parenchyma – effusion.
Bilaterally unbounded diaphragm observed.
– On the 10th of November 2021:
1. FIRST INTERNAL CARDIOLOGY CLINIC: findings of Sonography heart examination
Vivid S7, Control:
Resume: Serious dysfunction of the right ventricle, ejection fraction of left ventricle (EFLV)
of 35%, Significant Tricuspid valve regurgitation. Ascites stationary. Accumulation of fluid in
the pleural cavity in an amount of 400 ml (Fluidothorax bilateral). Were diagnosed.
– Operation performance:
On the 21st of October 2021, primo-implantation of implantable cardioverter defibrillator
(ICD).
2.5.3 Initial Kinesiology Examination
I performed the following kinesiological examination on Mr. L.P with his consent, under the
assistance and supervision of my supervisor Mgr. Michal Úlehla:
1. Inspection.
2. Goniometry.
3. Anthropometry.
4. Neurological Examinations.
5. Muscle shortening test.
6. General movement stereotype.
7. Gait Examination.
8. Spinal Development Test.
Inspection:
Inspection is a visual examination, which was performed from 3 views, from the posterior view
(the behind), form the lateral view (from the side), and finally from the anterior view (from the
front). The aim of this examination is to check or look at or inspect specific areas in the patient
body, for normal colour, shape and consistency. Certain findings on inspection may alert the

104
health care provider. For instance, the legs of the patient may be swollen. The health provider
will then pay attention to the common things that can cause leg swelling, such as extra fluid
caused by heart problems. Common areas which were inspected include the following:
1. The skin: to look for colour, bruising, cuts, moles or lumps.
2. Face and eyes: to see if they’re even and normal.
3. Neck and veins: to look for bulging or swollen.
4. Chest and abdomen: to see if there are any masses or bulges.
5. The legs: to see if there is any swelling.
6. The muscles: to check for good muscle tone.
7. The elbows and the other joints: check for swelling and inflammation, and if any
deformities are present.
I firstly asked the patient to take off his clothes and to stand in upright position with
both upper limbs aligned along the side of the body. Then I began my observation from the
posterior view. I tried to look for head, neck and shoulder position, if there is elevation or drop
of the shoulder, if there is head tilt or rotation, the spine if there is lateral deviation (scoliosis),
the scapula if there’s winging, pelvis and hip if there’s lateral pelvic tilt/shift, the knee if there’s
genu varum or genu valgum, ankle and foot to look for pes planus or pes cavus.
Posterior view findings as follow: shoulder elevation was observed on the patient as well as
scapula alata (winging). Non asymmetry of the chest found. Muscles of the neck in the right
side are more prominent. Varicose vein can be seen clearly in the back of both thighs. The hip
muscles are not asymmetry and shifting forward or anteversion of the pelvis was observed. The
patient has flat foot, and lower leg swelling (around the ankles). The patient knees are bowing
outward (genu varum) and the lower leg is angled inward (medially) in relation to the thigh
axis. The feet of the patient is pointing outward with tibia external rotation and knee facing
forward even when he walks can be seen clearly named as (Duck-footed or out-toeing).
I made an examination with the plumb line which was placed on the posterior of the
head and should pass through the occipital protuberance, spinous process of the vertebrae and
through gluteal cleft, between the legs. In the patient the plumb line wasn’t in a straight line
along the midline of the body, it was more to the lateral side. Hyper kyphosis the thoracic spine
was clearly observed as well.
And then I asked the patient kindly to turn, to make the next observation from the lateral
view, I tried to check for or to inspect for, head and neck, if there’s forward head position, and
if there’s flattened lordotic cervical curve or excessive lordotic curve (cervical lordosis). The
shoulder, if there’s forward shoulder, abducted/adducted shoulder. Thoracic spine, if there’s
105
kyphosis. Lumbar spine, if there’s lordosis or flat back. To check for the chest, if there’s pectus
excavatum (funnel chest) is when there’s depression in the sternum, and to look also for pectus
carinatum (pigeon chest) is when part of chest bone is pointing outwards. Pelvis and hip, if
there is anterior pelvic tilt or posterior pelvic tilt. Knee to look for genu recurvatum (knee
extension greater than 5 degree).
Lateral view findings as follow: the head of the patient is in forward position. Thoracic
kyphosis was observed. The ribs cage of the patient is slightly uneven, or protruding might be
due to abdominal muscle weakness that causes the ribs to stick out. Prominence on the belly of
the patient. I made a plumb line examination as well, and the plumb line from the lateral view
should pass through the ear lobe to acromion process (shoulder) to the lateral malleolus. But in
my patient the plumb line didn’t follow the shoulder it was slightly in front of the shoulder as
the patient has a forward head position, and it followed the hip, and it was aligned before the
lateral malleolus as I mentioned because of forward head as well as hyper-kyphosis.
Finally, I asked the patient to turn to make the last observation from the anterior view.
I tried to look for head and neck, if there’s tilt of the head or rotation. The shoulder, if there’s
elevation or drop and also if the shoulder is abducted/adducted. The chest how it looks like,
especially the position of the clavicle, if it’s dropped, and if there’s any prominence in the ribs,
as well as the position of the sternum as the patient underwent an open-heart surgery. The hip,
if there’s rotation or lateral tilt/shift. The elbow if there’s cubitus valgus or cubitus varus. The
knee to look for genu varum or genu valgum, and if there’s external or internal tibial torsion.
To check for the ankle and the feet, if there’s hallux valgus (hammer toe).
Anterior view findings as follow: funnel chest was clearly observed, as well as post-sternotomy
scar was visible clearly as the patient underwent an open-heart surgery for heart transplantation
in 2017. ICD prominence. Elevation of the shoulder. Patient knees were marked by outward
bowing. It could be seen also that the lower legs (around the ankles) are swelled, bluish, black
coloured.
Goniometry:
As the patient is after a heart complication we tried to be in the safe side and didn’t went to
prone position (on the abdomen). And we tried to make it more general to not exhaust the
patient.

106
Goniometry of the upper extremity:
The upper extremity overall was quite active in both right and left upper extremity. So, the
range of movement in the upper extremity is physiological, and no disturbance has been found
in the shoulder, elbow wrist joints all of them were in a very good status.
Goniometry of the lower extremity:
As a general examination of the lower extremity, the range of movement in both hip and knee
joint were active and around the physiological range and without any restriction or limitation.
While the ankle joint range of movement was limited and restricted in flexion, extension and
rotation, because of the swelling the patient has.
Anthropometry:
Then, we went for the third examination which is the (anthropometry) is to measure the length
and the circumference in (cm) of the upper extremity and the lower extremity. So
anthropometry is a systemic measurement of the physical properties of the human body, like:
the length of the arm and forearm, and the arm circumference, and the same for the lower
extremity. We performed anthropometry examination while the patient is in lying position to
make it convenient for him and to not to exhaust him as much as we can, and the patient was
fully cooperative so we went through it easily and without difficulties.
Table 8: Anthropometry, Length and Circumference in (cm) of the Upper Extremity.
Left Right
Arm and forearm 52 cm 54 cm
Arm 28 cm 29 cm
Forearm 25 cm 26 cm
Hand 18 cm 18 cm
Arm circumference (Relaxed) 26 cm 24 cm
Arm circumference
(Contracted)
28 cm 27 cm
Elbow joint circumference 24 cm 23 cm
Forearm circumference 23 cm 24 cm
Wrist circumference 17 cm 17 cm
Circuit over the metacarpus 21 cm 19 cm

107
Table 9: Anthropometry, Length and Circumference in (cm) of the Lower Extremity.
Left Right
Functional length of the
lower extremity (spina iliaca
anterior superior to lateral
malleolus)
91 cm 85 cm
Anatomical length of the
lower extremity (umbilicus
to medial malleolus)
91 cm 91 cm
Thigh length 38 cm 37 cm
Lower leg length 38 cm 41 cm
Leg length 24 cm 25 cm
Thigh circumference 47 cm 44 cm
Circumference above the
knee
41 cm 40 cm
Knee circumference 40 cm 38 cm
Circuit through tuberositas
tibiae
35 cm 36 cm
Calf circumference 41 cm 40 cm
Circumference over the
ankles
31 cm 30 cm
Circumference over the
insteps
33 cm 33 cm
Circuit over the metatarsus 26 cm 26 cm
Table 10: Perimeter Dimensions of the Abdomen and Chest in (cm).
Abdominal circumference 93 cm
Chest circumference (Inhalation) 96 cm
Chest circumference (Exhalation) 92 cm
Findings of the anthropometry test for upper and lower extremities:
Luckily, we have succeeded to make the anthropometry test in both upper and lower extremities
by using the meter while the patient is in lying position, as well as the perimeter dimensions of
the abdomen and chest during inhalation and exhalation while the patient is in sitting position.
As indicated in the tables above, these are the patient measures that were taken. All of them
were within the physiological range. There was no difference in the length of the upper
extremities, as well as the lower extremities.
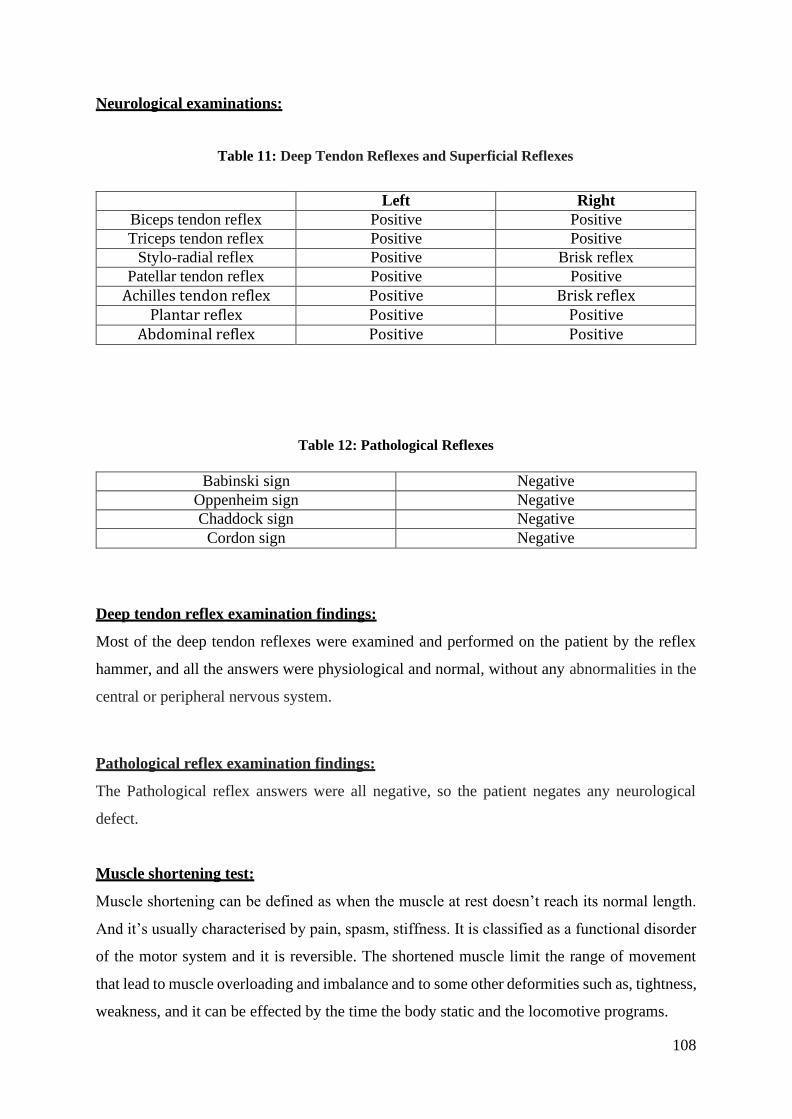
108
Neurological examinations:
Table 11: Deep Tendon Reflexes and Superficial Reflexes
Left Right
Biceps tendon reflex Positive Positive
Triceps tendon reflex Positive Positive
Stylo-radial reflex Positive Brisk reflex
Patellar tendon reflex Positive Positive
Achilles tendon reflex Positive Brisk reflex Plantar reflex Positive Positive
Abdominal reflex Positive Positive
Table 12: Pathological Reflexes
Babinski sign Negative
Oppenheim sign Negative
Chaddock sign Negative
Cordon sign Negative
Deep tendon reflex examination findings:
Most of the deep tendon reflexes were examined and performed on the patient by the reflex
hammer, and all the answers were physiological and normal, without any abnormalities in the
central or peripheral nervous system.
Pathological reflex examination findings:
The Pathological reflex answers were all negative, so the patient negates any neurological
defect.
Muscle shortening test:
Muscle shortening can be defined as when the muscle at rest doesn’t reach its normal length.
And it’s usually characterised by pain, spasm, stiffness. It is classified as a functional disorder
of the motor system and it is reversible. The shortened muscle limit the range of movement
that lead to muscle overloading and imbalance and to some other deformities such as, tightness,
weakness, and it can be effected by the time the body static and the locomotive programs.

109
It is divided into 3 degrees:
0 – No shortening.
1 – Small shortening.
2 – Large shortening.
X – Not measured.
Table 13: Muscle Shortening Test
Muscle/muscle group Left Right
Sternocleidomastoid X X
Levator scapulae X X
Trapezius (upper part) X X
Quadratus lumborum X X
Piriformis 0 0
Hip adductors 0 0
Hip flexors X X
Hamstring 1 1
Triceps surae 2 2
Findings of the shortening muscle test:
We didn’t succeed to do most of the shortening muscle tests, due to that the patient situation
didn’t allow us to be in some specific positions for performing the test, such as the muscles in
the neck area (sternocleidomastoid, levator scapulae, trapezius) the test of these muscles
require lateral flexion of the neck in a position that the patient cannot be in, because of the
central venous catheter that it inserted in the patient neck for medicaments administration. As
well as quadratus lumborum couldn’t be performed due to that the patient situation didn’t allow
him to be in a prone position nor in a lateral position (second testing method), would be
inconvenient for him.
Luckily, we’ve succeeded to perform some of the lower extremity muscles such as
piriformis, hip adductors, hamstrings, triceps surae, and I didn’t manage to perform the test for
hip flexors as it was difficult for the patient to be in a position that the test requires. And the
rating is on the table above, some shortening been found.
General movement stereotype:
The test was fully performed by the patient actively, by instructing the patient to do what I’m
doing. The patient did the test while he was in a sitting position. We were focused on the
sequencing and activation of all the synergists involved in the movement. And luckily no

110
abnormal movement have been found or observed. All the movements were normal and around
the physiological range. As I mentioned above, we managed to do some of the movements
which can be done in a sitting position as the patient situation required.
Gait Examination:
Gait examination was carried out in the corridor by using the observation method. When
walking, the patient employed compensating aids. The patient was able to walk independently
with no dizziness, but not in a straight line, instead diverging to the right (for his safety I walked
next to him). Furthermore, findings were observed: the right and left lower extremities were
found to be in external rotation. His feet drag on the floor during walking phases, and he misses
the heel strike. The patient was able to walk on both his left and right legs' heels and toes. There
was no trunk rotation found, and the trunk was rigidly held during walking. After halfway down
the corridor, the patient had already experienced muscle weakness and pain in his lower leg, as
well as fatigue.
Spinal development test:
Finally, the last examination in my list. The spinal development test, schober test, thomayer’s
test, side bending test, OTTA’S test. Unluckily, due to the patient condition we didn’t succeed
to do any of them, as all of these tests required fully bending forward.
2.5.4 Short-term Plan
It was planned that the authors 10-12 sessions rehabilitation maximum and it was supposed to
be that we can make it maximally in 4 weeks, but unfortunately our plan didn’t went as we
planned it. Through all the examinations that I’ve went through with my patient Mr. L.P. I
realized that the patient had a few issues that we might need to focus and work on, in order to
see a little improvement after I finish with him the period of short-term plan rehabilitation.
And also to recommend the patient to focus on them when he begins with the long rehabilitation
plan.
The rehabilitation presented by the author was carried out in accordance with the
recommendations of my supervisor Michal Úlehla, as well as a personally created short
rehabilitation plan (exercise unit).

111
Based on the examinations findings, I have set the following short-term goals:
1. To improve the overall motion and strength.
2. To improve the range of movement in the ankle joint and relieve the swelling.
3. As he’s using the walker, we needed to focus on some gait training to stabilize the patient
while he’s walking.
4. Improving the postural balance of the patient.
5. Increasing the lung capacity by doing some breathing exercises.
6. Improve the blood circulation by cardiovascular exercises.
7. Patient education as part of self-treatment with simple exercises.
And as I released from the first session my patient is active and didn’t need any assistance in
all activities but only in some of them, during walking for instance he needed some support.
The following exercises were used on my patient Mr. L.P.:
1. Cardiovascular exercises (circulatory) of the lower extremity, in lying, sitting and few in
standing position. Vascular gymnastics to prevent atherosclerotic plaques, thromboembolism
and Edema, to improve the cardiovascular system.
2. Cardiovascular exercises (circulatory) of the upper extremity.
3. Breathing gymnastics to improve ventilation.
4. Exercising using some adds like overball, theraband, balance disc.
5. Isometric and post-isometric exercises.
6. Exercising on bar in the corridor
7. Mobilization of the knee joint, balling for the swelling around the ankle joint, by using the
small spongy ball.
8. Gait training exercise. Training of mobility, and training walking by the walker. Exercises
to improve stability and reduce fear of unassisted walking (without the walker).
9. Passive and active exercise (with or without resistance).
10. Spinal stabilization training and posture improvement.
11. Flexibility exercises include stretching.
The main outcomes expected from my short motor plan were:
1. Better balance, range of motion and better movement in the joints.
2. Lower the blood pressure, lower the heart rate and better breathing. Improved circulation
and the way the body uses oxygen.
3. Better posture, better flexibility.
4. To be more active without getting tires or short of breath easily.

112
5. More toned and stronger muscles.
6. Reduced stress, anxiety and depression.
7. Improved self-esteem of the patient.
8. Reduced the edema and the swelling around the ankle joint.
9. To be able to start walking without using the walker.
2.5.5 Rehabilitation Process
Mr. L.P used to have the stomia in the right hypogastric area, as well as the central venous
catheter which was placed on his neck, throughout the entire rehabilitation process. The first
visit took place in the afternoon, and after that we realized that it’s better to change our session
time to be before the noon around 11:00, as it was more convenient for the patient, due to that
he used to feel unwell somehow, after the lunch.
Session 1 – 26th of October:
In the afternoon of the 26th of October, the first session took place. In the Department of Internal
Cardio-angiology, University Hospital at St. Anna in Brno. Once I arrived there, me and my
supervisor discussed for about 15 minutes about my patient diagnosis in more details, and then
we moved together to the patient room. I introduced myself by the assistance of my supervisor,
and after the introduction, I explained to him why I have been assigned to him.
And what we are going to be doing in the upcoming days. Then I asked for his approval, to
make sure that I could go ahead and start taking the data. He gave us the oral consent that he
will be able to only share us he’s medical history and no more for that day.
We made it till the end and it took us almost 45 minutes. After I took the anamnesis/medical
history of the patient in the conversation/oral form under the supervision and the assistance of
my supervisor we made a deal with the patient that we will come the next day to start with the
kinesiological examinations.

113
Session 2 – 27th of October:
Before the noon around 11:00 o’clock of the 27th of October, the second session took place.
The aim of this session was to conduct all the kinesiological examination, at the very beginning
before I start working with the patient, I asked him if he suffers from some troubles, if there
are any palpitations (quick beating of the heart), if he has any pain nor fatigue, these are the
subjective signs. And then we have also the objective signs such as the oxygenation of the
blood, heart rate and blood pressure. Also the exercise shouldn’t lead to extreme raise of the
blood pressure and heart rate too. The maximum of the heart rate during exercise shouldn’t go
over 120 bpm, also the blood pressure, the systolic BP shouldn’t raise more than 20 mmHg,
and the diastolic not more than 10 mmHg, and also the systolic blood pressure should not
decrease about 10-15 mmHg. The oxygenation of the blood should be at least 90 % that’s the
minimum. And also some limitations that depend on the patient physic.
Specially with the heart patients the deep bend over is contraindicated, and that’s the
reason why we weren’t able to perform the spinal development tests. The patient was
cooperative and continued actively until the end of the session, and while we’re conducting the
examination from time to time I kept asking the patient if everything is alright and if he became
exhausted or not. I conducted all the kinesiological examinations needed successfully without
any difficulties, in supine position such as anthropometry and some of the goniometry, in sitting
position we were able to conduct the neurological examination and the general movement
stereotype, in standing position we made the inspection by observing the patient in 3 views
(posterior, lateral, anterior).
The session has ended with a little walk in the corridor for about 5 minutes long with a
support of the walker, and that was for observing the way the patient walks (gait examination).
All the values and the measurements have been written down accurately.
This session was a bit exhausting for me and for the patient as well, but we ended having all
the remarks, values and the measurements that examinations required. The entire process took
us about one and half hour with a few breaks in between.
Session 3 – 28th of October:
The 3rd session took place around the noon of the 28th of October. As we’ve conducted the
medical history as well as the kinesiological examinations, we’ve started with the exercise unit.
At the very beginning I asked my patient how he’s feeling today, and if he’s willing physically
to exercise with me, after he gave me his consent. I continued with taking the oxygenation of
the blood by using pulse oximetry placed on the patient index it was around the physiological

114
range 97 %, and then I placed the tonometer cuff on the patient arm in order to measure the
blood pressure as well as the heart rate before we start exercising, the patient had a low blood
pressure which was about 76/48 mmHg, and the heart rate was around the normal range 88
bpm. After we took all these values we started exercising. I planned to start with the patient
slowly and gradually increase the difficulty and the set of the exercises day by day more
exercises were added to the list. As the first day we began with the warm-up, cardiovascular
exercises for the lower extremity in lying (supine) position such as flex and extend the toes and
then I applied a small resistance, and flex and extend the ankle, rotation of the ankle, elevation
of the leg and return it back to the bed, flex the knee and extend it, move the leg to the side and
return it back, elevate the pelvis, bicycle, etc. The aim of the conditional training of vascular
gymnastics is to improve the blood flow. And then next we moved to the upper extremity, we
made cardiovascular exercises such as open and close the hand, rotate the wrist, flex and extend
the elbow. Hand to the shoulder and back to the bed, rotate or shrug the shoulder, bring the arm
to the side and return it back, internal and external rotation of the shoulder, put the right hand
on the left elbow and the left hand on the right elbow and bring it up above the head and down,
push by both hand (palms) into the bed hold and release, etc...
Then we moved to sitting position, we made some exercises of the lower extremity, like
extend and flex the leg while sitting, step on your toes and on your heel. Next, we tried some
breathing exercises, I instructed the patient to breath in deeply through the nose and count 1,2,3
and then breath out by the mouth and count 1,2,3,4,5,6. Abdominal breathing (breath in to the
abdomen from the nose while my hand are on patient belly and when he breaths out through
the mouth I put a little pressure on his belly), diaphragmatic breathing. Breathing exercises has
a positive impact on blood pressure, lung capacity and muscle tension, and as the patient breath
the cardiovascular system works to transport and circulate oxygen to every cell in his body.
Then, we tried to stand from the bed while I’m standing next to the patient and holding him as
a support and corrected his stand position, we exercised in standing position, like make a step
forward and a step backwards, etc.., then while the patient is standing, we made Romberg
examination, there was an imbalance. Next, I went to bring the walker, we walked in the
corridor for about 5 minutes, and we went back to the patient room. Lastly, I measured the
oxygenation of the blood, blood pressure and heart rate, with values of Blood O2: 100 %. Blood
pressure: 90/60 mmHg. Heart rate: 101bpm. That was all for this day, we tried to make it that
every day I prepare about 15-20 minutes exercise unit for the patient, and every new day some
new exercises were added. The whole process took us about 45 minutes.
Summary of the exercise unit (28th of October):

115
Cardiovascular exercises for the lower extremity in supine position:
1. Flex and extend the toes (5x)
2. Flex and extend the ankles (5x)
3. Rotate the ankles (5x)
4. Elevate the leg and back (5x)
5. Flex the knee and back (5x)
6. Move the leg to the side (5x)
7. Elevate the pelvis (5x)
8. Bring the knee to the chest (3x)
9. Role the knee to the side (5x)
10. Bicycle (5x)
11. Hip rotation (5x)
Cardiovascular exercises for the upper extremity in supine position:
1. Close and open the hands (5x)
2. The hands to front and back (5x)
3. Rotate the wrist (5x)
4. Flex and extend the elbow (5x)
5. Elevate both arms up above the head breath in and bring it back breath out (5x)
6. Bring both hands to the shoulders and return it back to the bed (5x)
7. Put the right hand on the left elbow and the left hand on the right elbow and bring it up above
the head and down.
8. Rotate or shrug the shoulder (5x)
9. Boxing.
10. Stick both palms together and elevate up above the head then bring it back, do the same but
to the right and left side (5x)
11. Bring the arm to the side of the bed and back (5x)
12. Shoulder external rotation (5x)
13. Elevate both arms towards the sealing and elevate the shoulder away from the bed (5x)
Exercises in sitting position:
1. Exercises to strengthen the leg muscles.
2. Flexion and extension of the ankle (5x)
3. Step on the toes and then on the heels (5x)
4. Elevate one knee and then then the other towards the sealing (5x)
Breathing gymnastics in sitting position:

116
1. Breath in deeply from the nose and count 1,2,3 and then breath out from the mouth and count
1,2,3,4,5,6. (5x)
2. Elevate your both arms up towards the sealing and breath in from the nose and then return
both arms back and breath out through the mouth. (5x)
3. Abdominal breathing (breath in into the abdomen from the nose while my hand are on patient
belly and when he breath out through the mouth I put a little pressure on his belly)
4. Diaphragmatic breathing. (5X)
Exercises in standing position:
1. Make a step forward and step backwards. (5x)
2. Elevate one knee and then the other towards the sealing as if you’re running bot slowly. (5x)
3. Bring one leg to the side and then the other. (5x)
Passive and active movements of the ankle joint for the swelling and the edema, as well as
balling technique.
Walking for 5 minutes in the corridor with the walker.
Session 4 – 29th of October:
The 2nd day of exercising took place in the afternoon, as my supervisor has told me that the
patient has been taken to some imaging method examination. I firstly measured the blood
oxygenation which was about 93 % before the exercise. The blood pressure was 78/65 mmHg
(low). The heart rate was 98 bpm. Every day we followed the same exercise unit which I have
in my plan and each day I added some new exercises as well as an exercise adds, and I increased
the set form 5x to 6x.
We started with the vascular gymnastics for the upper and lower extremities in supine position
and in sitting position.
As a second we moved to the isometric exercises, like squeeze the thigh (quadriceps
femoris), squeeze the glutes, push both knees against the bed, push both hands (palms) against
the bed, pushing both heels against the bed then relax, partially flex both knees and put both
hand on the abductors and push into abduction while putting resistance, do the same but into
adduction. As a third, isometric exercise for the upper extremity. Then, breathing gymnastics.
Next, we moved to an exercises with the overball in the lower extremity in supine position,
like, squeeze it and release between the knees, put it between the knees and extend one leg and
the other leg, squeeze it and release under the knees, put it under the heel and go forward and
117
backwards, hold the ball with both hands and pass it under the knee while the knee is flexed,
Then we moved with the overball to the upper extremity, hold the ball between the palms and
squeeze it and relieve, hold the ball and go to the front and back to the chest, and to the left and
right sides, hold the ball with both hands and put it above the head and raise up towards the
sealing and back down. Every exercise has 6 sets.
Passive and active movements of the ankle joint for the swelling and the edema, as well as
balling technique.
The session has ended with a small walk with a walker in the corridor for about 5 minutes. And
then after we returned back to the patient room I again measure the Blood O2: 96 %. Blood
pressure: 115/84. Heart rate: 109 bpm. The whole process took us about 45 minutes.
Session 5 – 1st of November:
The 5th session was the 3rd day of exercising, today Mr. L.P was more attentive and cooperative
throughout the entire session. The edema located around the ankles looked much better than
the previous days. The range of movement in the ankle joints increased and improved.
As always, it’s very important to start with taking the values of the blood oxygenation
which was about 92 %. The blood pressure: 98/73 mmHg. The heart rate: 86 bpm. After that,
we started training with the same exercise unit of the previous day, and I added more exercises
using an exercise adds at the end, so we started with the vascular gymnastics in supine, sitting
and standing position, then some isometric exercises for both upper and lower extremity were
performed, and after that we made some breathing exercises, then we moved to the exercising
unit using the overball. For today we added a new exercise adds which was the TheraBand, in
supine position patient secure the TheraBand around his hand and extend his elbow in a neutral
position and me as a therapist stood at the foot of the patient while holding the other side of the
TheraBand, and asked the patient to flex his shoulder with elbow extended for about (8x), next
the patient abduct his arm out to the side with forearm supinated (8x), then the patient placed
his arm extended and supinated on the bed and flex and extend his elbow (8x), then me as a
therapist I stood next to the patient head and the client and the patient flexes his shoulder to 90
degree, pulls down in extension (8x), the patient secure the TheraBand by both hands and
stretch it away from the body center and back (8x), etc..
Then, we practiced again active and passive movement in the ankle joint and I
performed balling technique. After that we went for gait training with an assistance using
walking aid (walker), before we began to walk I’ve adjusted the patient posture to be in an
upright position, with head and spine positioned correctly, we could walk today for about 8

118
minutes long, without getting tired. Finally, the session has ended by measuring again the blood
O2: 109 %. The blood pressure: 117/79 mmHg. Hear rate: 120 bpm. The whole process took
about 45 minutes.
Session 6 – 2nd of November:
The 6th session was the 4rth day of exercising, the patient was fully cooperative and energetic,
but unluckily, my supervisor has got the information that they will take the patient for some
imaging method examination in 30 minutes, and for that reason the session lasted for
25 minutes only. As usual I firstly took the values of the blood oxygenation: 92 % measured
by oximetry. Blood pressure: 106/78 mmHg. Heart rate: 72 bpm measure by tonometer.
The exercise unit began with vascular gymnastic of the upper and lower extremity.
After that we made some breathing exercises in supine position, on that day we didn’t use any
exercising adds. Then the breathing exercises were followed by an active and passive exercises
for the ankles and then I performed balling technique for the edema around the ankles. Then I
asked Mr. L.P to move into sitting position and instructed him for some isometric exercises of
the upper extremity.
Then I asked the patient if he’s willing to have a small walk and he agreed, with the
walking aid we walked for about 9 minutes long and also we tried to climb the stairs, and the
patient was able to climb about 4 stairs up and down with assistance and support of me and my
supervisor as well, and while we’re on the way back to the patient room, we made some
exercises on the bar for about 4 minutes, I was instructing the patient, to face the bar and step
on your toes and back on your heel. Face the bar and elevate your leg to the side and with the
2nd leg as well. Keep the bar on your left or right side hold it and walk like a ballerina. Face the
bar and make a circle with your feet to the side.
We ended the session with taking the values of the blood O2: 102 %. Blood pressure:
118/82 mmHg. Heart rate: 127 bpm.

119
Session 7 – 3rd of November:
The 7th session was the 5th day of exercising, the patient showed a great improvement
physically, and the edema around his ankles was getting better and better day by day. At the
beginning of the session, I took the measurements of blood oxygenation by oximetry placed on
patient index and it was about 94%. Blood pressure: 116/78 mmHg. Heart rate: 99 bpm, were
measured by tonometer.
Then we’ve started training in spine position, sitting and standing position vascular gymnastics
for the upper and lower extremities, for about 8 minutes long.
Next, we exercised using the overball for upper and lower extremities, for 6 minutes of time.
After that, for 3 minutes long we trained some isometric exercises. Then we worked on the
ankles we made some active and passive exercises for the edema and swelling around the
ankles and then I performed balling technique using the soft ball.
Next, we’ve added a new exercising adds, the (balance disc) for today’s exercise unit,
which has the aim of promoting the postural balance. I explained to the patient what is this
equipment for and how it will be used, and I asked him if he’s willing to move with us outside
in the corridor to exercise in front of the bar, he agreed. The exercise last for about 5 minutes
of time and then we went back to the room. As a final exercise unit for today we made some
breathing gymnastics as a form of relaxation. And as usual, the session has ended with taking
the measurements of the Blood O2: 107 %. Blood pressure: 123/83 mmHg. Heart rate:
135 bpm. The whole process took about 45 minutes long.
2.5.6 Kinesiological Examination at Discharge
The patient was transferred to cardio-surgery clinic for the heart transplantation. Before, we
conducted a brief kinesiological examination. The overall patient’s kinesiological examination
since the onset of our rehabilitation process haven’t improved, there were changes in patient’s
swelling (edema) around his ankles. There were not found any specific improvement in the
physical condition of the patient. Later the patient was transplanted with the heart of the donor.

120
2.5.7 Long-term Plan
The patient condition hasn’t progressed much at that time, although his condition changed
continuously day by day during my therapy, these were rather slight deviations which are
minimal in comparison with his general health condition.
As he wasn’t fully independent when he left to the cardio-surgery clinic, there were still evident
symptoms remained, edema around his both ankles which aimed to achieve full recovery, or at
least a remarkable improvement, this includes an increase in the function and motion of the
legs.
Unfortunately, the time with the patient was short due to his deteriorating health
condition, we had to end the therapy, and urgently he went for the heart transplant.
So, medical rehabilitation now and specially after he will get transplanted plays a key role in
treating the patient. Its main goal is to maintain the functional state of the patient and thus lead
the patient to the maximum possible self-sufficiency.
A long-term rehabilitation plan should always adapt to his current physical and mental
condition.
Mr.L.P. after he got transplanted will continue his rehabilitation in outpatient care.
In a long-term rehabilitation plan, it is recommended that the patient continue regular training,
which may include exercises performed in hospital rehabilitation.
It is appropriate to gradually increase the intensity, density and length of this exercise according
to the current condition of the patient.
The exercise unit should be complex and consist of a warm-up phase, when it is appropriate to
include warming up in bed or walking, a relaxation phase, when we can use elements of
respiratory physiotherapy or stretching.
Gradually, it is appropriate to include the endurance phase, for example, with training walking
on stairs or riding a bicycle ergometer, and a strengthening phase, where we use dumbbells,
overballs or therabands. Interval training is also suitable, during which the phases of exercise
and relaxation alternate between exhalation.
To improve the patient's condition and health, I also recommend regular walking, including the
possibility of using Nordic walking sticks or swimming. Furthermore, we direct the patient to
inappropriate physical activities, such as excessive strength exercises with breath-holding, and
teach him to recognize symptoms resulting from excessive physical activity.
The patient should be actively involved in doing normal daily and leisure-time activities, such

121
as cooking or gardening. We constantly motivate the patient to adopt the right lifestyle, reduce
risk factors, and try to create a positive relationship with his regular physical activity.
A prerequisite for successful rehabilitation is the active participation of the patient.
Within one year after the heart transplant, the patient also has the opportunity to undergo
treatment at the spa. It combines not only physiotherapy procedures, group or individual
therapeutic physical education, advice on a healthy lifestyle, but also has an undeniably positive
effect on the mental state of patients. In the Czech Republic, for example, Teplice nad Bečvou,
Poděbrady, Konstantinovy Lázně, Františkovy Lázně, Libverda or Hodonín Spa focus on
treating patients with cardiovascular diseases. Possible collaboration with an occupational
therapist, social worker, or psychologist is also important.
The aim of the long-term hospital rehabilitation program up to heart transplantation is to
prevent deconditioning of the patient, maintain the highest possible muscle strength and overall
performance, range in the joints, prevention of inflammatory, thromboembolic, respiratory and
other complications and preparation of the patient for return to normal daily activities and
employment.
After transplantation, the patient should be acquainted with the possibilities of
posthospital rehabilitation, i.e. with an outpatient controlled program, spa treatment, individual
home training, risk factors and primary, secondary and tertiary prevention. The aim of this
post-hospital rehabilitation is to increase the patient's physical fitness and performance, adjust
the lifestyle, integrate the patient into a full active life and improve the overall quality of life.
In most patients, it is recommended to start outpatient rehabilitation immediately after
discharge from the hospital, no later than 3 weeks. In patients after extensive procedures, it is
recommended to wait with certain activities for 6 weeks, which is the time required for the
bone to heal and to prevent unstable sternum due to early overload. After a sternotomy, it is
important to wear a chest strap (most often an elastic rib) because it allows the sternum to be
immobilized and thus facilitates the healing process.
Aerobic muscle training is generally considered to be the most suitable method of muscle strain
for patients with cardiac disease, with medium-intensity physical activity (40-60 % of
maximum O2 consumption) being the most effective. The recommended safe intensity is below
the anaerobic threshold or 60 % VO2SL and 70 % SFSL.
Unsuitable activities in the first 2 months after surgery are lifting weights over 3 kg, sharp
changes in position, holding your breath, manual housework, long-term work with your hands
over your head, extreme endurance performance exceeding the anaerobic threshold, activities

122
causing stress or with a possible risk of shocks on the chest and also some sports (tennis,
squash, strengthening, rebound and contact sports).
Therefore, it is important to find an appropriate aerobic physical activity to keep the patient
entertained and to run it at least three times a week for 30 minutes. This will make him take
care of himself regularly and not lose interest in the chosen activity.

123
3 CONCLUSION
Throughout the entire process of writing this thesis, I have expanded my knowledge across
several aspects of cardiovascular system, including the anatomical and physiological concepts
of the heart as well as a brief pathophysiological overview of heart failure and implementation
of physiotherapy and rehabilitation for patient after the incidence of heart failure. At the end of
general part, the basic diagnostic criteria, methods and treatment procedures in the case of heart
failure were described. In the special part of the thesis, I provided information on the various
stages of cardiovascular rehabilitation, exercise testing in cardiac rehabilitation, as well as the
principles of aerobic endurance training, resistance training and physical therapy procedures.
Issues of social and psychological problems of patient with cardiovascular disease were also
briefly mentioned. The last part of the thesis is the case report of rehabilitation of Mr. L.P.
which took place in the Department of Internal Cardio-angiology, University Hospital at St.
Anna in Brno.
Comprehensive cardiovascular rehabilitation is an indispensable part of the therapy of
both acute and chronic heart failure. Preoperative rehabilitation was implemented on the patient
by me for 5 days long, and there was a minimal gradual improvement of the patient’s physical
condition. I would have liked to continue with my patient for a longer period of time to see a
significant improvement, but the patient’s condition was critical, and he was transferred to
cardio-surgery clinic for the heart transplantation. The patient had a significant deconditioning
and reduced functional capacity of cardiovascular system he was confined to bed for long
period of time and the doctor allowed only a minimal load during exercise.
During his stay complications arose that put the patient first on the waiting list for a
heart transplant. Therefore, after finding suitable donor, the transplant was performed without
delay. During my visits and day-to-day of exercising I can say that the patient himself was
satisfied and pleased with the rehabilitation procedure, he assessed cardiovascular
rehabilitation positively. It improved his physical and mental health performance, increase self-
sufficiency and independence, and thus makes it easier for him to return to a normal life. It is
crucial for the prevention of further disease progression or the prevention of other
comorbidities. Heart failure is a serious disease that not only significantly reduces a patient's
life expectancy but also greatly reduces his quality of life. For these reasons, I believe that more
programs to prevent this disease should be established, including improving and adhering to
the principles of a healthy lifestyle, which is closely related to the proper functioning of the

124
cardiovascular system. I also believe it is essential to improve education of patient, which will
allow for earlier recognition of disease symptoms and diagnosis.
I hope that the heart transplant operation went successfully and without any
complications, to continue with the postoperative comprehensive cardiovascular rehabilitation
which is absolutely an indispensable part of the therapy of both acute and chronic heart failure
and plays a crucial role in the improvement of patient’s physical and mental state.
Eventually, I am grateful to have completed the second half of my thesis. This entire
experience exposed me to a clinical environment and prepared me for my future practice, and
career.
125
Bibliography
1. KAUTZNER, Josef a Vojtěch MELENOVSKÝ. Srdeční selhání: aktuality pro
klinickou praxi. Praha: Mladá fronta, 2015. 338 str. Edice postgraduální medicíny.
ISBN 978-80-204-3573-6.
2. WIDIMSKÝ, Jiří Srdeční selhání. 4., rozš. a přeprac. vyd. Praha: Triton, 2013. 203 str.
ISBN 978-80-7387-680-7.
3. (European Heart Journal (2015) 36, 395–397:10. doi 1093/eurheartj/ehv004).
4. ŠPINAROVÁ, Monika. Klinické klasifikace a skórovací systémy u srdečního selhání.
Kardiol Rev Int Med. 2015, 17(2), 131-135.
5. Servey JT, Stephens M. Cardiac rehabilitation: Improving function and reducing
riskexternal icon. Am Fam Physician 2016;94(1):37–43.
6. Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al.
Heart disease and stroke statistics-2020 update: a report from the American Heart
Associationexternal icon. Circulation 2020;141:e139-596.
7. American Heart Association. Heart Failure. (https://www.heart.org/en/health-
topics/heart-failure) Accessed 1/21/2022.
8. Theresa A. McDonagh, Roy S. Gardner, Andrew L. Clark and Henry Dargie, Oxford
Textbook of Heart Failure, 2011, ISBN-13: 9780199577729.
9. Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology.
Curr Heart Fail Rep. 2017;14(5):385-392. doi:10.1007/s11897-017-0351-y.
10. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV),
Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften
(AWMF). Nationale Versorgungsleitlinie Chronische Herzinsuffizienz. AWMF-
Registernr.: nvl-006. October 22, 2019.
11. WebMD, Congestive Heart Failure and Heart Diseases, Stages of Heart Failure,
https://www.webmd.com/heart-disease/guide-heart-failure.
12. Cleveland clinic, Heart Failure, https://my.clevelandclinic.org/health/diseases/17069-
heart-failure-understanding-heart-failure.
13. Hear Attack and Stroke Symptoms, Etiology of hear failure,
https://www.heart.org/en/health-topics/heart-failure/causes-and-risks-for-heart-
failure/causes-of-heart-failure.

126
14. WebMD, Medications That Can Cause Heart Failure, https://www.webmd.com/heart-
disease/heart-failure/meds-cause-heart-failure.
15. Boron, Walter F.; Boulpaep, Emile L. (2005). Medical Physiology: A Cellular and
Molecular Approach (Updated ed.). Saunders. p. 533. ISBN 978-0-7216-3256-8.
16. Rang HP (2003). Pharmacology. Edinburgh: Churchill Livingstone.
p. 127. ISBN 978-0-443-07145-4.
17. Cardiac pathophysiology of heart failure. GPnotebook.
18. Richard E. Klabunde, PhD, Cardiovascular Physiology Concepts, 3rd edition, 2021,
ISBN-13: 9781975150075.
19. Tamparo, Carol (2011). Fifth Edition: Diseases of the Human Body. Philadelphia, PA:
F.A. Davis Company. p. 329. ISBN 978-0-8036-2505-1.
20. Shigeyama J, Yasumura Y, Sakamoto A, et al. (December 2005). "Increased gene
expression of collagen Types I and III is inhibited by beta-receptor blockade in patients
with dilated cardiomyopathy". Eur. Heart J. 26 (24): 2698–705.
doi:10.1093/eurheartj/ehi492. PMID 16204268.
21. Tsutsui H, Matsushima S, Kinugawa S, et al. (May 2007). "Angiotensin II type 1
receptor blocker attenuates myocardial remodelling and preserves diastolic function in
diabetic heart". Hypertens. Res. 30 (5): 439–49. doi:10.1291/hypres.30.439. PMID
17587756.
22. Krug AW, Grossmann C, Schuster C, et al. (October 2003). "Aldosterone stimulates
epidermal growth factor receptor expression". J. Biol. Chem. 278 (44): 43060–66.
doi:10.1074/jbc.M308134200. PMID 12939263.
23. Systemic pathophysiology in heart failure. GPnotebook.
24. Hunter JG, Boon NA, Davidson S, Colledge NR, Walker B (2006). Davidson's
principles & practice of medicine. Elsevier/Churchill Livingstone. p. 544. ISBN 978-
0-443-10057-4.
25. Federmann M, Hess OM. Differentiation between systolic and diastolic dysfunction.
Eur Heart J. 1994 Dec;15 Suppl D:2-6. doi: 10.1093/eurheartj/15.suppl_d.2. PMID:
7713107.
26. MICHIGAN HEALTH, Anatomy of a Human Heart,
https://healthblog.uofmhealth.org/heart-health/anatomy-of-a-human-heart.
27. Texas Heart Institute, Heart Valves, https://www.texasheart.org/heart-health/heart-
information-center/topics/the-heart-valves/.
127
28. Teach Me Anatomy. The Conducting System of the Heart.
(https://teachmeanatomy.info/thorax/organs/heart/conducting-system/) Accessed
9/8/2021.
29. Cleveland Clinic, Circulatory System of the heart,
https://my.clevelandclinic.org/health/body/21775-circulatory-system.
30. Ge Z, Li A, McNamara J, Dos Remedios C, Lal S. Pathogenesis and pathophysiology
of heart failure with reduced ejection fraction: translation to human studies. Heart Fail
Rev. 2019 Sep;24(5):743-758. [PubMed]
31. Eisenberg LM, Markwald RR. Cellular recruitment and the development of the
myocardium. Dev Biol. 2004 Oct 15;274(2):225-32. [PubMed].
32. Goodwill AG, Dick GM, Kiel AM, Tune JD. Regulation of Coronary Blood Flow.
Compr Physiol. 2017 Mar 16;7(2):321-382. [PMC free article] [PubMed]
33. Norman S, Riley PR. Anatomy and development of the cardiac lymphatic vasculature:
Its role in injury and disease. Clin Anat. 2016 Apr;29(3):305-15. [PubMed]
34. Huang WA, Boyle NG, Vaseghi M. Cardiac Innervation and the Autonomic Nervous
System in Sudden Cardiac Death. Card Electrophysiol Clin. 2017 Dec;9(4):665-679.
[PMC free article] [PubMed].
35. OpenStax, Anatomy and physiology, cardiac cycle,
https://openstax.org/books/anatomy-and-physiology/pages/19-3-cardiac-cycle.
36. Gersh, Bernard J (2000). Mayo Clinic Heart Book. New York: William Morrow. pp.
6–8. ISBN 0-688-17642-9.
37. Topol, Eric J (2000). Cleveland Clinic Heart Book. New York: Hyperion. pp. 4–5.
ISBN 0-7868-6495-8.)
38. Betts, J. Gordon (2013). Anatomy & physiology. pp. 787–846. ISBN 978-1-938168-
13-0. Retrieved 11 August 2014.
39. Hall, John E., PhD, Guyton and Hall Textbook of Medical Physiology, 14th Edition,
2020, ISBN 0323597122.
40. Walter F. Boron, Emile L. Boulpaep (2016) Medical Physiology (3rd Edition) Elsevier
ISBN 978-1-4557-4377-3.
41. OpenStax, Cardiac physiology, https://openstax.org/books/anatomy-and-
physiology/pages/19-4-cardiac-physiology)
42. Hunt SA, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the
ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults:
a report of the American College of Cardiology Foundation/American Heart
128
Association Task Force on Practice Guidelines: developed in collaboration with the
International Society for Heart and Lung Transplantation [published correction appears
in Circulation. 2010;121(12):e258]. Circulation. 2009;119(14):e391–e479.).
43. Dosh SA. Diagnosis of heart failure in adults. Am Fam Physician. 2004;70(11):2145–
2152.), (Institute for Clinical Systems Improvement (ICSI). Heart failure in adults.
Bloomington, Minn.: Institute for Clinical Systems Improvement (ICSI); 2009:95.).
44. Hunt SA, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the
ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults:
a report of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines: developed in collaboration with the
International Society for Heart and Lung Transplantation [published correction appears
in Circulation. 2010;121(12):e258]. Circulation. 2009;119(14):e391–e479.
45. Mulrow CD, Lucey CR, Farnett LE. Discriminating causes of dyspnea through clinical
examination. J Gen Intern Med. 1993;8(7):383–392.
46. Wang CS, FitzGerald JM, Schulzer M, Mak E, Ayas NT. Does this dyspneic patient in
the emergency department have congestive heart failure? JAMA. 2005;294 (15):1944–
1956.
47. Madhok V, Falk G, Rogers A, Struthers AD, Sullivan FM, Fahey T. The accuracy of
symptoms, signs and diagnostic tests in the diagnosis of left ventricular dysfunction in
primary care: a diagnostic accuracy systematic review. BMC Fam Pract. 2008;9:56.
48. Institute for Clinical Systems Improvement (ICSI). Heart failure in adults.
Bloomington, Minn.: Institute for Clinical Systems Improvement (ICSI); 2009:95.
49. Remme WJ, Swedberg K; Task Force for the Diagnosis and Treatment of Chronic Heart
Failure, European Society of Cardiology. Guidelines for the diagnosis and treatment of
chronic heart failure [published correction appears in Eur Heart J. 2001;22(23):2217–
2218]. Eur Heart J. 2001;22(17):1527–1560.
50. Chen WC, Tran KD, Maisel AS. Biomarkers in heart failure. Heart. 2010;96(4):314–
320.
51. Ewald B, Ewald D, Thakkinstian A, Attia J. Meta-analysis of B type natriuretic peptide
and N-terminal pro B natriuretic peptide in the diagnosis of clinical heart failure and
population screening for left ventricular systolic dysfunction. Intern Med J.
2008;38(2):101–113.
52. Balion C, Santaguida PL, Hill S, et al. Testing for BNP and NT-proBNP in the diagnosis
and prognosis of heart failure. Evid Rep Technol Assess (Full Rep). 2006;(142):1–147.

129
53. Battaglia M, Pewsner D, Jüni P, Egger M, Bucher HC, Bachmann LM. Accuracy of B-
type natriuretic peptide tests to exclude congestive heart failure: systematic review of
test accuracy studies. Arch Intern Med. 2006;166(10):1073–1080.
54. Latour-Pérez J, Coves-Orts FJ, Abad-Terrado C, Abraira V, Zamora J. Accuracy of B-
type natriuretic peptide levels in the diagnosis of left ventricular dysfunction and heart
failure: a systematic review. Eur J Heart Fail. 2006;8(4):390–399.
55. Maestre A, Gil V, Gallego J, Aznar J, Mora A, Martín-Hidalgo A. Diagnostic accuracy
of clinical criteria for identifying systolic and diastolic heart failure: cross-sectional
study. J Eval Clin Pract. 2009;15(1):55–61.
56. Jimeno Sainz A, Gil V, Merino J, García M, Jordán A, Guerrero L. Validity of
Framingham criteria as a clinical test for systolic heart failure [in Spanish]. Rev Clin
Esp. 2006;206(10):495–498.
57. Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR, Rodeheffer RJ.
Burden of systolic and diastolic ventricular dysfunction in the community: appreciating
the scope of the heart failure epidemic. JAMA. 2003;289(2):194–202.
58. Naik MM, Diamond GA, Pai T, Soffer A, Siegel RJ. Correspondence of left ventricular
ejection fraction determinations from two-dimensional echocardiography, radionuclide
angiography and contrast cineangiography. J Am Coll Cardiol. 1995;25(4):937–942.).
59. UCSF, health Heart failure signs and symptoms,
https://www.ucsfhealth.org/conditions/heart-failure/symptoms
60. MAYO CLINIC, Heart failure diagnosis, https://www.mayoclinic.org/diseases-
conditions/heart-failure/diagnosis-treatment/drc-20373148.
61. NHS, Heart failure treatment, https://www.nhs.uk/conditions/heart-failure/treatment/
62. National Heart, Lung, and Blood Institute Heart failure.
https://www.nhlbi.nih.gov/health-topics/heart-failure. Accessed Oct. 22, 2020.
63. Heart Failure Clinics. Dooley DJ, et al. The role of positive inotropic drugs in the
treatment of older adults with heart failure and reduced ejection fraction. 2017;
doi:10.1016/j.hfc.2017.02.008.
64. American Heart Association. Ejection fraction heart failure measurement.
https://www.heart.org/en/health-topics/heart-failure/diagnosing-heart-failure/ejection-
fraction-heart-failure-measurement. Accessed July 9, 2021.
65. Verquvo (approval letter). New Drug Application 214377. U.S. Food and Drug
Administration.
https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&
130
ApplNo=214377. Accessed July 8, 2021.), (Brown AY. Allscripts EPSi. Mayo Clinic.
Oct. 8, 2020.).
66. Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: Differences at
5%, 10%, 15%, and over. Curr Obes Rep. 2017;6(2):187-194. doi:10.1007/s13679-017-
0262-y
67. Ahmad F, Ning H, Rich J, et al. Hypertension, obesity, diabetes, and heart failure–free
survival. JACC: Heart Failure. 2016;4(12):911-919. doi:10.1016/j.jchf.2016.08.001.
68. Texas Heart Institute, Smoking and Your Heart, https://www.texasheart.org/heart-
health/heart-information-center/topics/smoking-and-your-heart/.
69. American Heart Association. The American Heart Association diet and lifestyle
recommendations.
70. Minelli P, Montinari MR. The mediterranean diet and cardioprotection: Historical
overview and current research. J Multidiscip Healthc. 2019;12:805-815.
doi:10.2147/JMDH.S219875.
71. Gupta D, Georgiopoulou VV, Kalogeropoulos AP, et al. Dietary sodium intake in heart
failure. Circulation. 2012;126(4):479-85.
doi:10.1161/CIRCULATIONAHA.111.062430.
72. WebMD What Problems Can Heart Failure Cause, https://www.webmd.com/heart-
disease/heart-failure/heart-failure-complications
73. Giannuzzi P, Mezzani A, Saner H, Björnstad H, Fioretti P, Mendes M, Cohen-Solal A,
Dugmore L, Hambrecht R, Hellemans I, McGee H, Perk J, Vanhees L, Veress G,
Working Group on Cardiac Rehabilitation and Exercise Physiology European Society
of Cardiology. Physical activity for primary and secondary prevention. Position paper
of the Working Group on Cardiac Rehabilitation and Exercise Physiology of the
European Society of Cardiology. Eur J Cardiovasc Prev Rehabil. 2003;10:319–27.).
74. Wenger NK. Current status of cardiac rehabilitation. J Am Coll Cardiol. 2008;51:1619–
31.).
75. American Association for Cardiovascular and Pulmonary Rehabilitation. Guidelines
for car- diac rehabilitation and secondary prevention programs. 4th ed. Champaign:
Human Kinetics Publishers; 2004.), (Balady GJ, Williams MA, Ades PA, Bittner V,
Comoss P, Foody JM, Franklin B, Sanderson B, Southard D. Core components of
cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific
statement from the American Heart Association Exercise, Cardiac Rehabilitation, and
Prevention Committee, the Council on Clinical Cardiology; the Councils on
131
Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical
Activity, and Metabolism; and the American Association of Cardiovascular and
Pulmonary Rehabilitation. Circulation. 2007;115:2675–82.
76. Mezzani A, Agostoni P, Cohen-Solal A, Corra U, Jegier A, Kouidi E, Mazic S, Meurin
P, Piepoli M, Simon A, Laethem V, Christophe, Vanhees L. Standards for the use of
cardiopul- monary exercise testing for the functional evaluation of cardiac patients: a
report from the Exercise Physiology Section of the European Association of
Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil.
2009;16:249–67.).
77. Corrà U, Giannuzzi P, Adamopoulos S, Bjornstad H, Bjarnason-Weherns B, Cohen-
Solal A, Dugmore D, Fioretti P, Gaita D, Hambrecht R, Hellermans I, McGee H,
Mendes M, Perk J, Saner H, Vanhees L; Working Group on Cardiac Rehabilitation and
Exercise Physiology of the European Society of Cardiology. Executive summary of the
position paper of the Working Group on Cardiac Rehabilitation and Exercise
Physiology of the European Society of Cardiology (ESC): core components of cardiac
rehabilitation in chronic heart failure. Eur J Cardiovasc Prev Rehabil 2005;12:321–325.
78. Myers J, Arena R, Franklin B, Pina I, Kraus WE, McInnis K, Balady GJ, on behalf of
the American Heart Association Committee on Exercise, Cardiac Rehabilitation and
Prevention of the Council on Clinical Cardiology, the Council on Nutrition, Physical
Activity and Metabolism, and the Council on Cardiovascular Nursing.
Recommendations for Clinical Exercise Laboratories: A Scientific Statement from the
American Heart Association. Circulation. 2009;119:3144–61.
79. Prakash M, Myers J, Froelicher VF, Marcus R, Do D, Kalisetti D, Atwood JE. Clinical
and exercise test predictors of all-cause mortality: results from > 6,000 consecutive
referred male patients. Chest. 2001;120:1003–13.
80. Guazzi M, Adams V, Conraads V, Halle M, Mezzani A, Vanhees L, Arena R, Fletcher
GF, Forman DE, Kitzman DW, Lavie CJ, Myers J. EACPR/AHA Joint Scientific
Statement. Clinical recommendations for cardiopulmonary exercise testing data
assessment in specific patient populations. Eur Heart J. 2012;33:2917–27.
81. Fletcher GF, Balady GJ, Amsterdam EA, Chaitman B, Eckel R, Fleg J, Froelicher VF,
Leon AS, Piña IL, Rodney R, Simons-Morton DA, Williams MA, Bazzarre T. Exercise
standards for testing and training: a statement for healthcare professionals from the
American Heart Association. Circulation. 2001;104:1694–740.

132
82. Carvalho VO, Mezzani A. Aerobic exercise training intensity in patients with chronic
heart failure: principles of assessment and prescription. Eur J Cardiovasc Prev Rehabil.
2011;18:5–14.
83. Mezzani A, Hamm LF, Jones AM, McBride PE, Moholdt T, Stone JA, Urhausen A,
Williams MA, European Association for Cardiovascular Prevention and Rehabilitation;
American Association of Cardiovascular and Pulmonary Rehabilitation; Canadian
Association of Cardiac Rehabilitation. Aerobic exercise intensity assessment and
prescription in cardiac rehabilitation: a joint position statement of the European
Association for Cardiovascular Prevention and Rehabilitation, the American
Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian
Association of Cardiac Rehabilitation. Eur J Prev Cardiol. 2013;20:442–67.).
84. VYMAZALOVÁ, Lucie. MÍFKOVÁ, Leona. Standard fyzioterapie doporučený
UNIFY CR - FYZIO/10 - Kardiovaskulární rehabilitace. UNIFY CR, 2016. Dostupné
z: http://www.unify-cr.cz/obrazky-soubory/4-1-10-rtf-8fcc1.pdf?redir.
85. CHALOUPKA, Václav aj. Rehabilitace u nemocných s kardiovaskulárním
onemocněním. Cor et Vasa. 2006, 48(7-8)., (PLACHETA, Zdeněk, Jarmila
SIEGELOVÁ aj. Praktická cvičení z klinické fyziologie: pro bakalarske stadium
Specializace ve zdravotnictví. Brno: Masarykova universita, 2010. 57 str. ISBN 978-
80-210-3620-6.).
86. PLACHETA, Zdeněk. Zátěžové vyšetření a pohybová léčba ve vnitřním lékařství.
Brno: Masarykova univerzita, 2001. 179 str. ISBN 80-210-2614-6.
87. PLACHETA, Zdeněk, Jarmila SIEGELOVÁ aj. Praktická cvičení z klinické fyziologie:
pro bakalárke stadium specializace ve zdravotnictví. Brno: Masarykova universita,
2010. 57 str. ISBN 978-80-210-3620-6.
88. PLACHETA, Zdeněk. Zátěžová funkční diagnostika a preskripce pohybové léčby ve
vnitřním lékařství. 2., přeprac. vyd. Brno: Masarykova univerzita, 1998. 156 str. ISBN
80-210-1170-X.).
89. Bandy W D, McLaughlin S. Intramachine and intermachine reliability for selected
dynamic muscle performance tests. J Orthop Sports Phys Ther. 1993; 18 609-613),
(Burdett R G, Van Swearingen J. Reliability of isokinetic muscle endurance test. J
Orthop Sports Phys Ther. 1987; 8 484-488)
90. Tarride JE, Lim M, DesMeules M, Luo W, Burke N, O'Reilly D, Bowen J, Goeree R.
A review of the cost of cardiovascular disease. Can J Cardiol. 2009 Jun;25(6):e195-
202. [PMC free article] [PubMed])

133
91. Forecasting the future of cardiovascular disease in the United States: a policy statement
from the American Heart Association. Circulation. 2011 Mar 01;123(8):933-44.).
92. Servey JT, Stephens M. Cardiac Rehabilitation: Improving Function and Reducing
Risk. Am Fam Physician. 2016 Jul 01;94(1):37-43.
93. Dalal HM, Doherty P, Taylor RS. Cardiac rehabilitation. BMJ. 2015 Sep
29;351:h5000.
94. Braverman DL. Cardiac rehabilitation: a contemporary review. Am J Phys Med
Rehabil. 2011 Jul;90(7):599-611.
95. Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, Franklin B,
Sanderson B, Southard D., American Heart Association Exercise, Cardiac
Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology.
American Heart Association Council on Cardiovascular Nursing. American Heart
Association Council on Epidemiology and Prevention. American Heart Association
Council on Nutrition, Physical Activity, and Metabolism. American Association of
Cardiovascular and Pulmonary Rehabilitation. Core components of cardiac
rehabilitation/secondary prevention programs: 2007 update: a scientific statement from
the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention
Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular
Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and
Metabolism; and the American Association of Cardiovascular and Pulmonary
Rehabilitation. Circulation. 2007 May 22;115(20):2675-82.
96. Kehler DS, Stammers AN, Tangri N., et al. 2017. Systematic Review of Preoperative
Physical Activity and Its Impact on Postcardiac Surgical Outcomes. BMJ Open.
7:e015712, pp 1-12.
97. Alexiev A, Terziev A, Gotcheva N. 2017. Effect of an Early Cardiac Rehabilitation
Following Heart Surgery In Patients Over 70 Years. SM J Clin Med 3(1):1019)
98. REHAB SELECT, Cardiac rehab: a guide for patients and families book, The four
cardiac rehab phases.
99. McMahon SR, Ades PA, Thompson PD. The role of cardiac rehabilitation in patients
with heart disease. Trends Cardiovasc Med. 2017 Aug;27(6):420-425.
100. Physiopedia, Cardiac rehabilitation, https://www.physio
pedia.com/Cardiac_Rehabilitation#cite_note-:7-1.
101. Achttien RJ, Staal JB, van der Voort S, Kemps HM, Koers H, Jongert MW, Hendriks
EJ., Practice Recommendations Development Group. Exercise-based cardiac

134
rehabilitation in patients with chronic heart failure: a Dutch practice guideline. Neth
Heart J. 2015 Jan;23(1):6-17.
102. Milani RV, Lavie CJ, Cassidy MM. Effects of cardiac rehabilitation and exercise
training programs on depression in patients after major coronary events. Am Heart
J. 1996 Oct;132(4):726-32.
103. Pasquina, Patrick, Martin R. Tramèr, and Bernhard Walder. “Prophylactic Respiratory
Physiotherapy After Cardiac Surgery: Systematic Review.” BMJ: British Medical
Journal 327, no. 7428 (2003): 1379–81. http://www.jstor.org/stable/25458019.
104. Stayer AS, Diaz LK, East DL, Gouvion JN, Vencill TL, Mckenzie ED et al. Changes
in respiratory mechanics among infants undergoing heart surgery. Anesth Analg.
2004; 98(1): 49-55.
105. Felcar JM, Guitti JCS, Marson AC, Cardoso JR. Fisioterapia pré-operatória na
prevenção das complicações pulmonares em cirurgia cardíaca pediátrica. Rev Bras
Cir Cardiovasc. 2008; 23(3): 383-8.
106. Kavanagh BP. Perioperative atelectasis. Minerva Anestesiol. 2008; 74(6): 285-7.
107. Goraieb L, Croti UA, Orrico SRP, Rincon OYP, Braile BM. Alterações da função
pulmonar após tratamento cirúrgico de cardiopatias congênitas com hiprefluxo
pulmonar. Arq Bras Cardiol. 2008; 91(2): 77-84.
108. Nina RVAH, Gama MEA, Santos AM, Nina VJS, Figueiredo NETO JA, Mendes
VGG, et al. O escore de risco ajustado para cirurgia em cardiopatias congênitas
(RACHS-1) pode ser aplicado em nosso meio? Rev Bras Cir Cardiovasc. 2007; 22(4):
425-31.
109. Undern-Sternberg BS, Petak F, Saudan S, Pellegrini M, Erb TO, Habre W. Effect of
cardiopulmonary bypass and aortic clamping on functional residual capacity and
ventilation distribution in children. J Thorac Cardiovasc Surg. 2007; 134(5): 1193-8.
110. Felcar JM, Guitti JCS, Marson AC, Cardoso JR. Fisioterapia pré-operatória na
prevenção das complicações pulmonares em cirurgia cardíaca pediátrica. Rev Bras
Cir Cardiovasc. 2008; 23(3): 383-8.
111. Balachandran A, Shivbalan S, Thangavelu S. Chest physiotherapy in pediatric
practice. Indian Pediatrics. 2005; 42(6): 559-68.
112. Silva NLS, Piotto RF, Barboza MAI, Croti UA, Braile DM. Inalação de solução salina
hipertônica como coadjuvante da fisioterapia respiratória para reversão de atelectasia
no pós-operatório de cirurgia cardíaca pediátrica. Rev Bras Cir Cardiovasc. 2006;
21(4): 468-71

135
113. Campos RS, Couto MDC, Albuquerque CLR, Siqueira AAF, Abril LC. Efeito do
aumento expiratório ativo-assistido em crianças com pneumonia. Arq Med ABC.
2007; 32(Supl 2): 38-41.
114. Main E, Castle R, Newham D, Stocks J. Respiratory physiotherapy vs. suction: the
effects on respiratory function in ventilated infants and children. Intensive Care Med.
2004; 30(6): 1144-51
115. Basics of postural drainage and percussion. (n.d.). cff.org/Life-With-CF/Treatments-
and-Therapies/Airway-Clearance/Basics-of-Postural-Drainage-and-Percussion/
116. yogagorod, Complex of static and dynamic breathing exercises,
https://yogagorod.ru/en/kompleks-staticheskoi-i-dinamicheskoi-dyhatelnoi-
gimnastiki/
117. health science center Sunnybrook, https://sunnybrook.ca/content/?page=schulich-
heart-coronary-artery-bypass-exercises)
118. Cardiorespiratory physiotherapy, active rehabilitation physiotherapy,
https://activerehab.com.au/services/rehabilitation/cardiorespiratory-physiotherapy/)
119. Kolar, P. et al. Clinical rehabilitation. (2013). ISBN:978-80-9054380-5
120. Spencer, J.L. Resistance training in outpatient cardiac rehabilitation. Strength and
Conditioning Journal 29(1):18-23, 2007.
121. Ades, P.A., P.D. Savage, M.E. Cress, et al. Resistance training on physical
performance in disabled older female cardiac patients. Medicine & Science in Sports
& Exercise® 35(8):1265-1270, 2003.
122. Volaklis, K.A., and S.P. Tokmakidis. Resistance exercise training in patients with
heart failure. Sports Medicine 35(12):1085-1103, 2005.
123. Williams, M.A., W.L. Haskell, P.A. Ades, et al. Resistance training in individuals
with and without cardiovascular disease: 2007 update. A scientific update from the
American Heart Association Council on Clinical Cardiology and Council on
Nutrition, Physical Activity, and Metabolism. Circulation 116:572-584, 2007.
124. Adams, J., M.J. Cline, M. Hubbard, et al. A new paradigm for post-cardiac event
resistance exercise guidelines. American Journal of Cardiology 97:281-286, 2006.
125. Pollock, M.L., B.A. Franklin, G.J. Balady, et al. Resistance exercise in individuals
with and without cardiovascular disease: benefits, rationale, safety, and prescription.
An advisory from the Committee on Exercise, Rehabilitation, and Prevention, Council
on Clinical Cardiology, American Heart Association. Circulation 101:828-833, 2000.
136
126. Sorace, P., and T. LaFontaine. Resistance training muscle power: design programs
that work. ACSM's Health & Fitness Journal® 9(2):6-12, 2005.
127. ACSM's Guidelines for Exercise Testing and Prescription. 7th ed. Whaley, M.H., P.H.
Brubaker, and R.M. Otto (Editors). Baltimore: Lippincott Williams & Wilkins,
2005:176-177, 189-191, 199-200, 223-225.
128. American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines
for Cardiac Rehabilitation and Secondary Prevention Programs. 4th ed. Human
Kinetics, 2004:36, 119, 182.
129. ACSM's Guidelines for Exercise Testing and Prescription. 7th ed. Whaley, M.H., P.H.
Brubaker, and R.M. Otto (Editors). Baltimore: Lippincott Williams & Wilkins,
2005:176-177, 189-191, 199-200, 223-225.
130. TUKA, Vladimír a Martin MATOULEK. Kardiovaskulární rehabilitace. Med Sport
Boh Slov. 2013, 22(4), 198-205.)
131. Shepherd JT. Circulatory response to exercise in health. Circulation (1987) 76(Pt
2):VI3–10.
132. Fagard RH. Exercise characteristics and the blood pressure response to dynamic
physical training. Med Sci Sports Exerc. (2001) 33(Suppl. 6):S484–92; discussion
S493–484. 10.1097/00005768-200106001-00018.
133. PODĚBRADSKÝ, Jiří a Radana PODĚBRADSKÁ. Fyzikální terapie: manuál a
algoritmy. Praha: Grada, 2009. 218. ISBN 978-80-247-2899-5.
134. CAPKO, Ján. Základy fyziatrické léčby. Praha: Grada, 1998. 396 s. ISBN 80-7169-
341-3.
135. ANCÍK, Jiří, Jarmila SIEGELOVÁ, Pavel HOMOLKA, Hana SVACINOVÁ,
Zdeněk PLACHETA, Leona VÁRNAYOVÁ, Lucie KOŽANTOVÁ, Petr DOBŠÁK,
Jiří DUŠEK, Bohumil FIŠER, Lenka ŠPINAROVÁ, Jiří TOMAN and J.C. EICHER.
Low-FREQUENCY ELECTRICAL STIMULATION OF SKELETAL MUSCLES
IN PATIENTS WITH CHRONIC HEART FAILURE. Scripta medica. Brno:
Masaryk University, Medical Faculty, 2002, vol. 75, No 4, p. 203-208. ISSN 1211-
3395.
136. Ennis S, McGregor G, Hamborg T, et al Randomised feasibility trial into the effects
of low-frequency electrical muscle stimulation in advanced heart failure patients BMJ
Open 2017;7:e016148. doi: 10.1136/bmjopen-2017-016148.
137. Dobšák P, Tomandl J, Spinarova L, Vitovec J, Dusek L, Novakova M, Jarkovsky J,
Krejci J, Hude P, Honek T, Siegelova J, Homolka P. Effects of neuromuscular
137
electrical stimulation and aerobic exercise training on arterial stiffness and autonomic
functions in patients with chronic heart failure. Artif Organs. 2012 Oct;36(10):920-
30. doi: 10.1111/j.1525-1594.2012.01474.x. Epub 2012 Aug 6. PMID: 22882472.
138. Leto L, Feola M. Cognitive impairment in heart failure patients. J Geriatr Cardiol.
2014;11:316-328. doi:10.11909/j.issn.1671-5411.2014.04.007), (McLennan SN,
Mathias JL, Brennan LC, Russell ME, Stewart S. Cognitive impairment predicts
functional capacity in dementia-free patients with cardiovascular disease. J
Cardiovasc Nurs. 2010;25:390-397.
139. Bell-McGinty S, Podell K, Franzen M, Baird AD, Williams MJ. Standard measures
of executive function in predicting instrumental activities of daily living in older
adults. Int J Geriatr Psychiatry. 2002;17:828-834.
140. Jefferson AL, Paul RH, Ozonoff A, Cohen RA. Evaluating elements of executive
functioning as predictors of instrumental activities of daily living (IADL). Arch Clin
Neuropsychol. 2006;21:311-320.
141. Davis RCHobbs FDRLip GYH ABC of heart failure: history and
epidemiology. BMJ. 2000;32039- 42).
142. Richardson LG. Psychosocial issues in patients with congestive heart failure. Prog
Cardiovasc Nurs. 2003 Winter;18(1):19-27. doi: 10.1111/j.0889-7204.2003.00835.x.
PMID: 12624569.
143. American Psychological Association: "Mind/Body Health: Heart Disease."), (Anxiety
and Depression Association of America: "Symptoms.
144. Health perceptions of primary care patients and the influence on health care
utilization.Connelly JE, Philbrick JT, Smith GR Jr, Kaiser DL, Wymer A Med Care.
1989 Mar; 27(3 Suppl):S99-109.
145. Allen RScheidt S Heart and Mind: The Practice of Cardiac
Psychology. Washington, DC American Psychological Association1996;), (Frasure-
Smith NLesperance FGravel G et al. Social support, depression, and mortality
during the first year after myocardial infarction. Circulation.2000;1011919- 1924).
146. Balady GJ, Ades PA, Bittner VA, Franklin BA, Gordon NF, Thomas RJ, Tomaselli
GF, Yancy CW., American Heart Association Science Advisory and Coordinating
Committee. Referral, enrollment, and delivery of cardiac rehabilitation/secondary
prevention programs at clinical centers and beyond: a presidential advisory from the
American Heart Association. Circulation. 2011 Dec 20;124(25):2951-60.

138
147. Mampuya WM. Cardiac rehabilitation past, present and future: an
overview. Cardiovasc Diagn Ther. 2012 Mar;2(1):38-49.
148. King M, Kingery J, Casey B. Diagnosis and evaluation of heart failure. Am Fam
Physician. 2012 Jun 15;85(12):1161-8. PMID: 22962896.