P ROJECT S TAFF
42
The Effectiveness of AIDS Prevention Efforts September 1995 OTA-BP-H-172
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of P ROJECT S TAFF

The Effectiveness of AIDS Prevention Efforts
September 1995
OTA-BP-H-172

P ROJECT S T A F F
Michael GluckEric RosenthalProject Directors
Hellen GelbandSenior Associate
Romulo ColindresResearch Assistant
Laura EsslingerResearch Assistant
Clyde J. BehneyAssistant Director, OTA
Sean R. TunisHealth Program Director
ADMINISTRATIVE STAFF
Louise StaleyOffice Administrator
Carolyn SwarmPC Specialist
Monica FinchWord Processing Specialist
Charlotte Y. BrownWord Processing Specialist
CONTRACTORS
Thomas J. Coates, Ph.D.Center for AIDS Prevention StudiesUniversity of California at San Francisco
Donald C. Des Jarlais, Ph.D.Chemical Dependency InstituteBeth Israel Medical CenterNew York, NY
Anke Ehrhardt, Ph.D.HIV CenterColumbia UniversityNew York, NY
Douglas Kirby, Ph.D.ETR AssociatesSanta Cruz, CA
Barbara VanOss Marin, Ph.D.Center for AIDS Prevention StudiesUniversity of California at San Francisco
Steve Rabin, J.D.Porter/NovelliWashington, DC
Jane E. Sisk, Ph.D.Columbia UniversitySchool of Public HealthNew York, NY
Marc A. Zimmerman, Ph.D.University of MichiganSchool of Public HealthAnn Arbor, MI

cONTENTS
Key Findings 1
Background 3
Trends in Numbers of AIDS Cases 5Gay and Bisexual Men 6Injecting Drug Users 8Ethnic and Racial Minorities 8Women 9Youth and Children 9
Approaches to AIDS Prevention--Changing Behavior 10Judging Effectiveness 12
General and Targeted Efforts 13Defining Groups 14
Counseling and Testing 14Evaluation of Counseling and Testing 16
Efforts Designed For the American People as a Whole 16Mass Communication Campaigns 17AIDS Prevention by Physicians 18
Preventing AIDS Among Injecting Drug Users 20Sexual Partners of Injecting Drug Users 22
Preventing AIDS in Racial and Ethnic Minority Populations 23
Preventing Heterosexual HIV Transmission to Women 24
Preventing AIDS Among School-Aged Youth 24
Preventing AIDS Among Children 25
Social Marketing 26
Economic Evaluation 28Findings From Economic Evaluations 28Potential For Greater Use of Economic Evaluation 29
REFERENCES 31

THE
EFFECTIVENESS
oTA first addressed the question,
How Effective Is AIDS Education? (91)in 1988. At that time, we concluded that“knowledge about the effectiveness ofparticular programs and of specificelements of programs has been slow toaccumulate. ” The Sub-committee onHealth and the Environ-ment of theHouse of Representatives Committee onCommerce asked OTA to take a freshlook at the question, and this backgroundpaper is the result. In 1995, there still isa need for additional research and fordevelopment and use of more carefully-refined research methods, but we knownow that certain inter-ventions cansuccessfully reduce the risk behaviorsl
associated with HumanImmunodeficiency Virus (HIV) trans-mission in certain groups at high risk ofAIDS. The details of what is known andstill unknown are reviewed in this back-ground paper.
Most of the information comes from aseries of commissioned papers writtenby experts on the following topics:
1 “Risk” and “risk behavior” are used in thispaper to mean behavior that may lead to thetransmission of HIV.
OF AIDSPREVENTION
EFFORTS
◆ HIV/AIDS Prevention for InjectingDrug Users
◆ Does HIV Prevention Work for MenWho Have Sex with Men?
◆ AIDS Prevention Among African-Americans and Latinos in the UnitedStates
◆ A Review of Educational ProgramsDesigned To Reduce Risk-TakingBehaviors Among School-Aged Youthin the United States
◆ A Review of HIV Interventions for At-Risk Women
◆ Applications of Social MarketingPrinciples to AIDS Education
◆ Economic Evaluation of HIV/AIDSEducation and Primary Prevention
◆ HIV / AIDS Education: NationalSurveys, Counseling and TestingPrograms and the Role of Physicians
KEY FINDINGS
◆ Much has been learned since 1988about which interventions areeffective in changing risk behaviorsrelated to HIV infection and AIDSamong certain key subpopulations.Adult gay and bisexual men who donot belong to ethnic minority groups

2 The Effectiveness of AIDS Prevention Efforts
have been the most intense focus ofAIDS prevention, and most is knownabout which interventions work inthis population.
◆ There still are major gaps in what isknown about interventions for certainhigh-risk populations. AfricanAmericans and Latinos account for adisproportionately large share ofpeople with AIDS, yet relatively littleresearch has been directed towardprevention in these populationgroups.
◆ Younger gay and bisexual men of allethnic groups still need to be reached,and continued efforts are required forthe entire population of gay andbisexual men, to make sure that thosewho have changed their behavior donot lapse back into early, riskybehaviors. Intravenous drug use isalso a very important risk factor forHIV transmission among gay andbisexual men.
◆ Interventions developed through in-depth preliminary work with thetarget population, that consist ofsmall-group programs that areinteractive and include skills de-velopment, have been among themost successful at reducing riskysexual and drug-related behaviors.
◆ The availability of sterile needlesdoes not increase the incidence ofillicit drug use and they can play animportant role in reducing thetransmission of HIV among injectiondrug users. Other approaches--including the increased availability ofdrug treatment and changes in
methadone prescribing policies--while not the focus of much research,also are potential tools for reducingHIV transmission in this population.
◆ Sex education and AIDS educationdirected at school-aged youth do notincrease sexual activity. Somespecific sex and AIDS educationprograms have been shown to reduceunprotected sexual activity, either bydelaying the onset of intercourse,reducing the number of sexualpartners, or increasing the use ofcondoms.
◆ Voluntary HIV “tes t ing andcounseling” --the combination of HIVblood tests and the informationprovided before and after testing--areof variable impact, possibly becausethey are done differently in differentplaces, in some cases more effectivelythan others. Done correctly, theyhave an important role in serving as abridge to appropriate AIDSpreventive, medical, and socialreferrals, and in some cases, alteringbehavior.
◆ Mandatory testing of certain low-prevalence populations (e.g., marriagelicense applicants) is an expensiveway of detecting HIV positiveindividuals, and there is no evidencethat interventions to change behaviorwould be effective with mandatorytesting.
◆ Maintaining safe sex and needle usebehavior over the long term once achange is made--perhaps over thecourse of one’s lifetime--is likely tobe important for individuals at risk of

The Effectiveness of AIDS Prevention Efforts 3
HIV, but little is known about theinterventions needed to maintainthese changes.
◆ The value of the research on AIDSprevention that has been conductedhas been diminished by poor studydesign. Flaws include poor basicdesign, small study groups, shortevaluation periods, and lack ofcontrol or comparison groups. (Thesesame flaws are common to asurprisingly high percentage ofresearch in all areas of medicine, andare not necessarily more problematicin the AIDS area than in others.)
◆ There is a gap between what is knownabout effective interventions and whatis actually delivered as prevention.Community-based organizations,which deliver a significant amount ofprevention, often are not able to orsimply do not take advantage ofcurrent knowledge about programeffectiveness.
◆ “Social marketing’’ --the application ofcommercial marketing strategies tosocietal issues--offers a possiblemethod of inducing behavior changeand maintaining non-risk behavior.Although social marketing has not bewidely applied to AIDS prevention inthe United States, it has demonstratedimpact on other health problems inthis country and on HIV transmissionin some other countries. Althoughpotentially very effective, socialmarketing programs can also be veryexpensive.
◆ Programs of voluntary, testing,counseling, referral, and partner
notification, as exemplified by sitesfunded by CDC, appear to be cost-saving in the long run, i.e., the costsof the programs are exceeded by thelong-term savings (discounted) inAIDS treatment costs averted. This istrue if only about 7 percent ofinfected people notified change theirbehavior to avoid further HIVtransmission. Needle exchange andbleach distribution programs forinjecting drug users also appear to becost-saving.
◆ AIDS prevention resources could beused much more effectively, evenwith current technology. In someinstances, soc ia l and culturalinfluences have impeded their use.Specifically, there has beenreluctance to encourage condom use,and there are societal and legalbarriers to making sterile needlesavailable to injection drug users.
BACKGROUND
H I V d i s e a s e a n d A I D S a r eprogressive conditions. They begin withinfection with HIV and conversion fromHIV seronegative to HIV seropositive.HIV may remain in the body for up toten years or more without causing anyapparent symptoms, and an individualmay be HIV seropositive for many yearswithout being diagnosed as having HIVdisease or AIDS. During this periodthey are infectious. A person who hasnot been tested for the presence of HIVantibodies or antigens is unlikely to beaware of the infection. All the whilethough, HIV attacks certain cells of theimmune system and causes the system to

4 The Effectiveness of AIDS Prevention Efforts
erode. Eventually, the body falls prey to“opportunistic” infections (e.g., bacterialand viral infections of the respiratoryand digestive tract) that are able to takehold due to the body’s weakenedimmune defenses. A formal diagnosis ofAIDS is not made until at least one of acertain group of infections occurs oruntil the immune system reaches acertain, critical level of deterioration. Inmost cases these infections--not HIVdirectly--incapacitate patients and causeillness and death.
HIV is transmitted in relativelyclearly defined and understood ways, allof which involve the transfer of blood,semen or certain other body fluids fromone individual to another (includingtransmission from infected woman tofetus). Transmission occurs in thecourse of certain behaviors, generallysexual or those associated with injectingdrug use. HIV also may be transmittedfrom a seropositive pregnant women toher fetus during pregnancy or birth and,in rare cases, to health care workersthrough needlesticks and other injuries.2
Rapid progress was made inidentifying HIV as the causative agent ofAIDS, in developing a test for antibodiesto it, and in finding prophylaxis andtreatment regimens for some of theopportunistic diseases associated withAIDS, but there is no short-termprospect for a preventive vaccine or anykind of cure. Currently availableantiviral treatments are of temporaryvalue at best. Consequently, the only
2 Through the end of 1994, there were 42documented cases of occupational transmissionof HIV to health care workers and 91 possiblecases (104).
viable method for stopping the spread ofAIDS is prevention, which dependsalmost entirely on individual behaviorchange (95).
Like other areas of medicine andhealth, public and private finding forHIV/AIDS has supported biomedicalresearch and development more heavilythan behavioral and social scienceresearch. It is noteworthy that the firstpreventive intervention shown throughrigorous evaluation to be efficaciouswas a device-based technology: theHIV-antibody test for blood.Moreover, development of the bloodtest responded to a pervasive fear thatpeople receiving blood products couldbecome infected independently of theirbehavior. Developers of the antibodytest could thus count on a large, securemarket among mainstream healthorganizations, such as hospitals andblood banks.
By contrast, behavioral and socialscience research has received lessemphasis and less funding, even thoughbehavior change could prevent almostall further HIV transmission. Thissituation at least partly reflects theconflicting views within fundingorganizations and society about thebehaviors associated with HIVtransmission, namely sex, reproduction,and drug abuse . It has alsocharacterized work on other sexually-transmitted diseases and drug abusegenerally. Only in recent years hasmore rigorous research usingexperimental designs become commonin behavioral and social scienceresearch, a development notable fromthe 1988 OTA report to the currentbackground papers. Many of the

The Effectiveness of AIDS Prevention Efforts 5
economic evaluations of the early 1990sin fact grew out of such research fundedby the Centers for Disease Control andPrevention (45,51,52).
The Federal Government has appro-priated funds primarily through theCenters for Disease Control andPrevention (CDC) for AIDS preventionand education. Beginning in 1985, theFederal Government appropriated $33million for AIDS prevention andeducation. The appropriated funds havegrown to $589 million, the estimatedexpenditure for Fiscal Year 1995.
Even where AIDS prevention pro-grams have been developed and tried,judging how effective they are remains adifficult task. It is challenging--particu-larly so when interventions are multi-faceted and community-wide--to designstudies that allow cause-and-effect to beinferred. Debate is ongoing about whattypes of studies and other types ofevidence are sufficiently rigorous thatthey can be relied on to provide evidenceof effectiveness, and some progress hasbeen made in developing methods toevaluate the effectiveness and cost-effectiveness of particular interventions.
Interventions have been studied morein some communities and populationsthan in others, and not necessarily inrelation to their importance to the currentspread of HIV. Much more is known,for example, about how to prevent HIVtransmission among white, gay andbisexual men over 30 than amongsexually active young people or hetero-sexual African American or Hispanicmen or women. And among injectingdrug users, efforts have been directedmainly at changing their drug-taking
behavior, but not their sexual behavior,through which they can infect others.Because this paper is largely a review ofliterature, it reflects the balance of whathas been done, which is not always theright balance for new efforts. It isparticularly important to recognize thatwomen and people of color are glaringlyabsent from much of the work on inter-ventions. It is these groups among whomtransmission is increasing the fastest,and they deserve higher priority inresearch and intervention programs thanthey have had up to now.
TRENDS IN NUMBERS OF AIDSCASES
The first cases of AIDS in the UnitedStates were reported in 1981. By the endof 1994, 442,000 Americans had beendiagnosed with AIDS and 271,000 haddied from symptoms related to thedisease. The number of AIDS cases inthe United States increased by about 3percent from 1992 to 1993 and another 3percent from 1993 to 1994.3 Women,African Americans, Hispanics, andpeople in the South and Northeastaccounted for higher proportions ofcases in 1994 than in 1993. The largestdecline in the proportion of reportedcases was among gay and bisexual men(figure 1).4
3 Because the AIDS surveillance case definitionwas expanded in 1993, AIDS incidence trendsfrom 1993 to 1994 are evaluated using theestimated incidence of AIDS-definingopportunistic illnesses (103) in order to makeaccurate comparisons over time.4 The term “gay and bisexual men” is used hereto refer to all men who have sexual relationshipswith other men regardless of their identificationor sexual orientation.

6 The Effectiveness of AIDS Prevention Efforts
Figure 1: Trends in New AIDS Cases by Category
Gay and Bisexual Men
Year
SOURCE: OTA, 1995.
AIDS strikes the relatively young. In1993, it became the largest killer ofAmericans aged 25-44. This groupaccounts for about three-quarters of thecases. It also is the leading cause ofdeath in that age group in 79 out of the169 American cities with populationslarger than 100,000 (l). In 1992, AIDSwas responsible for the fourth greatestnumber of years of potential life lost forpeople under 65 years of age.5 AIDSwas the only major cause of years ofpotential life lost to show a significantincrease--1 1 percent--from the previousyear (102). An estimated one millionAmericans are infected with the humanimmune-deficiency virus (HIV), thevirus that causes AIDS. HIV is one ofthe most virulent human viruses known,with death rates exceeding 75 percent ofthose infected, and the ability to infectlarge numbers of people.
At the end of 1994, AIDS casesamong gay and bisexual men, the largestgroup of people with AIDS, constituted228,954 or 53 percent of the cumulativecase load (figure 2). An additional28,521, or 7 percent, of the cases are ingay and bisexual men who also injectillicit drugs (104) Gay and bisexual menrepresent a decreasing percentage ofnewly-diagnosed cases of AIDS, bothbecause their rate of increase has slowedin recent years6 (1989 through 1994) andbecause the epidemic is growing morerapidly in other segments of thepopulation (105). Gay and bisexual menhave reduced their sexual risk behavior,including reductions in multiple sexualpartners and reductions in incidence ofunprotected sex, since the start of theAIDS epidemic. But gay and bisexualmen continue to constitute the largest
5 Years of potential life lost is a public healthmeasure that reflects the impact of deathsoccurring in years preceding a conventional cut-off of age, in this case 65 years old. It is ameasure that takes into account number of deathsand age of decedents.
6 Because the AIDS surveillance case definitionwas expanded in 1993, AIDS incidence trends inthe study being discussed are evaluated using theestimated incidence of AIDS-definingopportunistic illnesses (103) in order to makeaccurate comparisons over time.

The Effectiveness of AIDS Prevention Efforts 7
Figure 2: Percentage of New AIDS Cases Represented
o% J-
5 9 % 5 9 %
1986 1987 1988 1989
SOURCE: OTA, 1995.portion of people with newly-diagnosedAIDS, so success in controlling theAIDS epidemic depends on preventingnew cases among this group.
The AIDS epidemic among gay andbisexual men, like the AIDS epidemicmore generally, is a composite ofepidemics among different groups, withdifferent times of onset and patterns ofspread. The rate of new cases amongcertain subcategories of gay and bisexualmen, especially white gay and bisexualmen, originally hardest hit by AIDS, isslowing (table 1). However, rates ofgrowth are increasing among othergroups less affected early in theepidemic (105). Rates of AIDS among
57% 55% 53%5 0 %
46%
1990 1991 1992 1993 1994
Year
African American gay and bisexual menwere highest in 1994 and showed thegreatest increase since 1989. The ratesof increase among other ethnic minority(Hispanic, Asian/Pacific Islander, andAmerican Indian/Alaskan Native) gayand bisexual men also exceeded that forwhites. In New York, Los Angeles, andSan Francisco, where 27 percent of theAIDS cases among gay and bisexualmen have occurred, the rate for whitemen decreased (20 percent, 16 percent, 3percent, respectively) and for AfricanAmerican men, it increased (49 percent,48 percent, 53 percent, respectively).
AIDS continues to spread beyondmajor metropolitan areas. The number
Table 1. Increases in the rate of newly diagnosed cases of AIDS among gay and bisexual men from1989 to 1994 and the rate of AIDS among gay and bisexual men per 100,000 men in mid 1994 areshown by race and ethnic group.
Race/Ethnicity Increase from 1989-94 Rate in Mid 1994 (per 100,000)African American 79 percent 37.3Hispanic 61 percent 22.6Native American/Alaskan 77 percent 6.9Asian/Pacific Islander 55 percent 6.2White 14 percent 12.2

8 The Effectiveness of AIDS Prevention Efforts
Table 2. Increases in the rate of newly diagnosed cases of AIDS among gay and bisexual men from1989 to 1994 and the rate of AIDS among gay and bisexual men per 100,000 men in mid 1994 areshown by size of area.
Size of Area (population) | Increase from 1989-94 I Rate in Mid 1994( per 100,000) I<50,000 69 percent 4.450,000-1 million 55 percent 10.2>2.5 million 19 percent 24.8
of cases continues to be greatest in the diagnosed among gay and bisexual menWest and Northeast and in urban areas, increased most in the Midwest (51but the highest rate of growth is percent) and in the South (49 percent)occurring in the South and Midwest, and and least in the West (21 percent) andin less populated areas (table 2 ). From the Northeast (13 percent) (105).1989
3 0 %
25%
2 0 %I
15%
1 0 %I
5%+II
0%
to 1994, the number of AIDS cases
Figure 3: Percentage of New AIDS Cases Represented by Injecting Drug Users
30% 29%
20% 20%
1986 1987
SOURCE: OTA, 1995.
Injecting Drug
As many asthe diagnosedthrough the endinjecting drug
Users
138,000AIDS
of 1994
26% 26% 26%27% 27%
1988 1989 1990 1991 1992 1993 1994Year
infections (43), which has implicationsfor the future course of AIDS cases.
(32 percent) ofcases reported Ethnic and Racial Minoritiesare the result of
use’ (figure 3) (104). Ethnic and racial minorities representEstimates of new HIV infections in the a disproportionate and increasing shareUnited States suggest that injecting drug of AIDS cases in the United Statesuse is associated with a plurality of new (figure 4). Fifty-one percent of all cases
have been among people of racial7 These figures include the categories “injecting minorities, which comprise only 23drug use” (109,393 cases) and “men who have percent of the population. One-third ofsex with men and inject drugs” (28,521 cases), as all cases are African Americans, 17used in the HIV/AIDS Surveillance Report.

The Effectiveness of AIDS Prevention Efforts 9
Figure 4: Trends in Cumulative AIDS Cases by Race
1986 1987 1988 1989 1990 1991 1992 1993 1994
Year
SOURCE:OTA,1995.
are Latinos,0.7 percent are Asian/PacificIslanders, and 0.2 percent are NativeAmericans, compared to 11 percent, 8percent, 3 percent, and 0.8 percent,respectively, in the population as awhole (104). Data fromHIVseroprevalence studies suggest thatthe proportion of racial minoritiesdiagnosed with AIDS will continue togrow in the coming years (38,75,93).
Ethnic minority groups are oftenviewed as homogeneous clans but, infact, there is enormous variety in thedemographic characteristics, immigra-tion history, and cultural values of ethnicsubgroups. HIV infection also is notspread evenly within these groups. Forinstance, there is a high concentration ofHIV among Latinos in the NortheastUnited States, who have come mainlyfrom Puerto Rico and the DominicanRepublic. Much lower incidence andprevalence rates are reported for Latinosfrom the West and Southwest, who havecome mainly from Mexico and Centraland South America.
Women
The proportion of AIDS cases amongwomen tripled from 1985 to 1994, risingto 18 percent of all new adult andadolescent cases (figure 5). Thirty-eightpercent of the 14,000 cases amongwomen diagnosed in 1994 werecontracted from heterosexual sexualpartners and 41 percent from injectingdrugs (106). Seventy-seven percent ofthe 1994 cases were among AfricanAmerican and Hispanic women.
Youth and Children
Many young people are at risk forHIV transmission through their sexualpractices. Through the end of 1994,68,000 males and 14,000 females age 20to 29 were diagnosed with AIDS (104).Because the period between HIVinfection and onset of AIDS may be upto ten years, it is likely that many ofthese people, who represent almost one-fifth of AIDS cases, were infected withHIV as teenagers. Most of these caseswere among gay and bisexual males,

10 The Effectiveness of AIDS Prevention Efforts
Figure 5: Percentage of New AIDS Casesby Women
20% T18% +
8%
11% 11%
1986 1987 1988 1989
SOURCE: OTA, 1995.
male and female injecting drug users,and heterosexual female sexual partnersof injecting drug users.
There were 6,000 pediatric AIDScases in the United States as of the endof 1994,8 representing just under 1.5percent of the cumulative cases. Therate of pediatric AIDS cases hasremained fairly constant at between 1percent and 2 percent of the total newcases of AIDS each year.
APPROACHES TOAIDS PREVENTION--CHANGING BEHAVIOR
More than 40,000 cases of new HIVinfection occur each year in the UnitedStates, despite a clear understanding ofhow the virus is transmitted. Although a
8 The CDC defines pediatric AIDS as AIDSoccurring in children less than 13 years old.
12%13%
Represented
18%
14%
16%
1990 1991 1992 1993 1994
Year
small number of infections arise fromaccidental transmission (i.e., bloodtransfusions, organ transplants, andneedlestick injuries), nearly all infectionsare potentially preventable if behaviorcould be changed. This does not mean,however, that prevention dependsentirely on persuading people to changetheir behaviors. It also involves accessto the necessary information andtechnologies, and structural changes thatmake it easy for people to practicepreventive behaviors.
With respect to Americans who aresexually active outside of a mutuallymonogamous relationship with anuninfected individual, behavior changemeans abstaining from certain sexualpractices, using condoms, or both.9 For
9 Although refraining from intercourse with aninfected individual remains the most effectiveway to prevent sexual transmission of HIV, theCenters for Disease Control and Prevention hasfound that consistent and correct use of latex

■
The Effectiveness of AIDS Prevention Efforts 11
individuals who inject illicit drugs,behavior change means ceasing to injectdrugs, using only sterile needles, or notsharing needles. 10
To be judged as effective, anintervention must reduce or eliminate thetransmission of HIV. No preventionmeasure for any disease is 100 percenteffective--many nowhere close to that--but they are still considered valuable.Likewise, attempts to change behaviorwill never stop all HIV transmission.But if an intervention even delaystransmission, there is a beneficial effectboth for the individual and for the courseof the epidemic. An individual whoavoids risk behavior even temporarilymay avoid becoming infected or avoidinfecting someone else. Partial successalso may have benefits in diminishingthe number of sexually transmitteddiseases, unwanted pregnancies, andabortions.
Most premature deaths in the UnitedStates spring from “choices” peoplemake--though not necessarily informedor “free” choices--and from socialconditions that promote health ordisease. These choices may be aboutsexual behavior, i l l icit drug use,smoking, drinking, diet, exercise, seatbelt use, or recreation. Like theseactivities, HIV transmission depends onindividual behavior choices. Similarly,HIV prevention is part of a spectrum ofdisease-fighting efforts that depend onrisk avoidance, long-term behavior
condoms is highly efficacious for preventingHIV transmission (107).10 For the purposes of this paper, “needlesharing” and “needle exchange” includes sharingor exchange of syringes and other drug injectionequipment.
change, and the development of policiesthat promote health and prevent disease.In most cases, simply telling anindividual that HIV is spread throughcertain sexual and drug-use behaviors isnot sufficient to alter that person’sbehavior, just as simply providinginformation on risk factors for heartdisease or cancer is not sufficient. To bemost effective, prevention strategiesshould provide information, motivation,skills, modification of perceived norms,and social or peer reinforcement. Just asimportant, long-term prevention requireslong-term prevention efforts, so thatpositive behavior changes are sustainedonce they begin.
At least some attempts to changebehavior to improve individual andpublic health historically have beenbeneficial, even though they haveachieved only partial success.Campaigns to reduce smoking, the mostimportant single cause of death in theUnited States, were initiated over threedecades ago, but still about a quarter ofAmericans smoke. Attempts to increaseexercise and improve dietary habits havefound far less than full acceptance. TheAmerican Cancer Society and theNational Cancer Institute recommendbreast cancer screening through bothmammography and clinical breastexaminations for asymptomatic womenaged 50 years or older. In a 1992 study,the CDC found that while 64 percent ofwomen in the previous year had at leastone of the exams, only 40 percent ofwomen c o m p l i e d w i t h therecommendation to have both (108).
Evidence shows that behavior changeis difficult for most people and sustainedbehavior change even more so. Public

12 The Effectiveness of AIDS Prevention Efforts
health messages must compete withnatural human desires, many of whichare pleasurable (e.g., sexual relations) aswell as with frequently appealingcounter messages from entertainmentmedia (e.g., to engage in sexual activity)or from peers (again, to engage in sexualactivity or to use illicit drugs). Thesecounter messages provide a constantchallenge to AIDS prevention.
Judging Effectiveness
The biggest barrier to knowing whichinterventions are most effective atpreventing the spread of HIV is that,considering the size of the problem andthe amount of effort that has gone intosolving it, too few interventions havebeen evaluated formally. And of thosethat have, many of the evaluations havenot been rigorous enough to providehighly reliable information.
Some interventions have been studiedin some locations and populations, butnot others. More studies of gay men(mostly white) have been carried outthan of any of the other important targetgroups, including women; younger, andnon-white gay and bisexual men;adolescents and young adults generally;people with other sexually transmitteddiseases; military personnel; prostitutes,and incarcerated populations. Inaddition, evaluation has, of necessity,focused on relatively short-term changes,in an area where the need is for changesthat persist over a lifetime.
Many individuals--especially those incommunities targeted for specialprevention efforts--are subject to manyinfluences on their behavior. If someoneis taking part in a formal study of an
intervention’s effectiveness, they willalmost always be exposed to information(e.g., news reports) or events (e.g., afriend or relative sick with or dying fromAIDS ) external to the study. The onlyreliable way to determine what effectsthe planned intervention had, versus theeffects of other influences, is to comparethe behavior of people who got theintervention with that of a “control”group which, other than the studyintervention, had similar inputs. Theintervention and control groups should,ideally, be allocated by a method thatgives an equal chance of getting into onegroup or the other, regardless of theindividual’s (or group’s) characteristics,and this requires some fo rm o frandomization. The “unit of randomi-zation” may be the individual, thecommunity, the school, or some otherunit. It is often difficult and expensive(and in some cases, not feasible) to applyrandomized controlled conditions to realworld intervention projects, but in fact, itis possible and the method should not beabandoned as facilely as it often is. Thisis not to say that other types of studiescan’t produce useful information, but theresults of other types of studies willnever be as reliable as the results ofrandomized studies. Even the strongly-held opinions of professionals aboutwhat does and doesn’t work in AIDSprevention are not, by themselves,reliable guides for further programs.
The methodological challenges instudying and validating interventions tochange behavior are even greater thanfor many other medical interventions(e.g., pharmaceuticals, surgical proce-dures). Trying to generalize the resultsof individual studies to the broaderpopulation is also more difficult.

The Effectiveness of AIDS Prevention Efforts 13
Interventions to change individualbehaviors can usually be considered“complex interventions,” wi th thefollowing features: Fi rs t , theintervention itself can be highly variable,depending on who actually conducts it.For example, the counseling portion of atesting program may vary substantiallyaccording to the style and knowledge ofthe provider. Much of this variabilitymay not be easily characterized or evendetected. Second, contextual factorsmay be important variables in theeffectiveness of the intervention. Forexample, an educational programdelivered to teenagers in a schoolroommay have a different impact than thesame program offered in a communitycenter. Third, complex interventions arecharacterized by a range of possibleendpoints that could be used todetermine effectiveness. The effects ofan educational leaflet could be measuredby how many are distributed, by surveysof how knowledge changes among thetarget population, by measuring changesin condom sales, or by tracking theprevalence of HIV.
In a practical sense, this means that anintervention found to be extremelyeffective in an individual study is notnecessarily transferable direct ly toanother population group or geographicarea. It may be that the key factor in itssuccess is the process by which thein te rven t ion was d e v e l o p e d a n d
(e gimplemented . ., with strongcommunity input), rather than the actualcontent of the intervention. In reviewingthe literature, therefore, it may not bepossible to make a list of interventionsthat work, but it may be possible to listthe characteristics of interventions andstudies that have been successful.
GENERAL ANDTARGETED EFFORTS
The overwhelming majority of newHIV infec t ions cont inues to beconcentrated in relatively fewgeographic areas (“communities”) anddemographic groups (“populations”),though some cases occur in everycommunity and population. Controversyhas surrounded the issue of whether totarget funds intensively to thecommunities and populations with thelargest number of new HIV infections orto stress universal risk to the entire U.S.population (19,86,96). The dilemmaarises for two reasons: first, concernsabout stigmati-zing people in targetedgroups, and second, because HIV caninfect anyone who engages in certainsexual or drug-related behaviors with aperson who is seropositive. It has thepotential to spread more widelythroughout society as it has, for example,in some African countries. In the UnitedStates, however, most people with AIDSare concentrated in small segments ofthe population1l which are largely self-contained in terms of risk behavior. IfHIV were spread exclusively withinclearly defined communities, it mightmake sense to concentrate efforts only inthese communities. However, riskbehavior is not completely confined inthis way and individuals outside thesecommunities may become infected.
11 For instance, at the end of 1994, 73.5 percentof the cumulative AIDS cases were in California,Florida, Georgia, Illinois, Maryland, NewJersey, Pennsylvania, New York ,Texas andPuerto Rico. In addition, at least 88.3 percent ofthe adult and adolescent cases were among gayand bisexual men, injection drug users and theirsexual partners.

14 The Effectiveness of AIDS Prevention Efforts
Effective AIDS prevention depends,therefore, on a combination of universaland targeted approaches. Universaleducation informs individuals who donot identify with a target population butmay be at risk for infection. It alsoserves as reinforcement for targetedefforts. In order to reduce the spread ofHIV, anyone, he terosexual orhomosexual, who is potentially sexuallyactive or who considers illicit drug useshould understand his or her risk andhow infection can be avoided. UniversalAIDS prevention programs also can helpreduce discrimination against peoplewith HIV infection or AIDS. However,most new HIV infections could beprevented by intensive efforts aimed atthe populations in which HIV isspreading, including gay and bisexualmen, in jec t ing drug users , andheterosexuals with high rates of sexuallytransmitted diseases (19). Intensiveefforts in certain groups also couldp r o v i d e t h e continuing supportindividuals would need to maintain non-risk behavior over time.
Defining Groups
People often are defined for thepurposes of AIDS education by thegroup or groups to which they belong--usually demographic or geographic.Many times, the groups are adoptedconveniently from the epidemiologicalperspective, i.e., the groups for whichdata are reported. But in fact, the UnitedStates is a “complicated patchwork ofbehaviors, incomes , and ethnicbackgrounds that confound simplecultural labeling” according to consumermarketers (85).
This suggests the need for a freshlook at how individuals are grouped forprevention efforts. Among AfricanAmericans, for example, there arevarieties of consumption patterns andhealth indices depending, among otherthings, on location and aspects ofheritage. In addition, many people fallinto several groups. The commercialsector relies on statistical clusters basedon geography, lifestyle, behavior,financial status, and attitudes more thanon race alone. African Americans,Hispanics, A s i a n s , a n d NativeAmericans should not automatically belumped together as “minorities” if AIDSprevention efforts are to be mosteffective. Traditional consumer market-ing also tends to segment the populationalong age lines rather than along the“r isk group” l ines sugges ted byepidemiological data. With half of thenew infections occurring in individualsunder 25, adolescents at risk may havemore in common with each other thanwith individuals of similar race,ethnicity, or sexual orientation, but ofdifferent ages.
COUNSELING AND TESTING
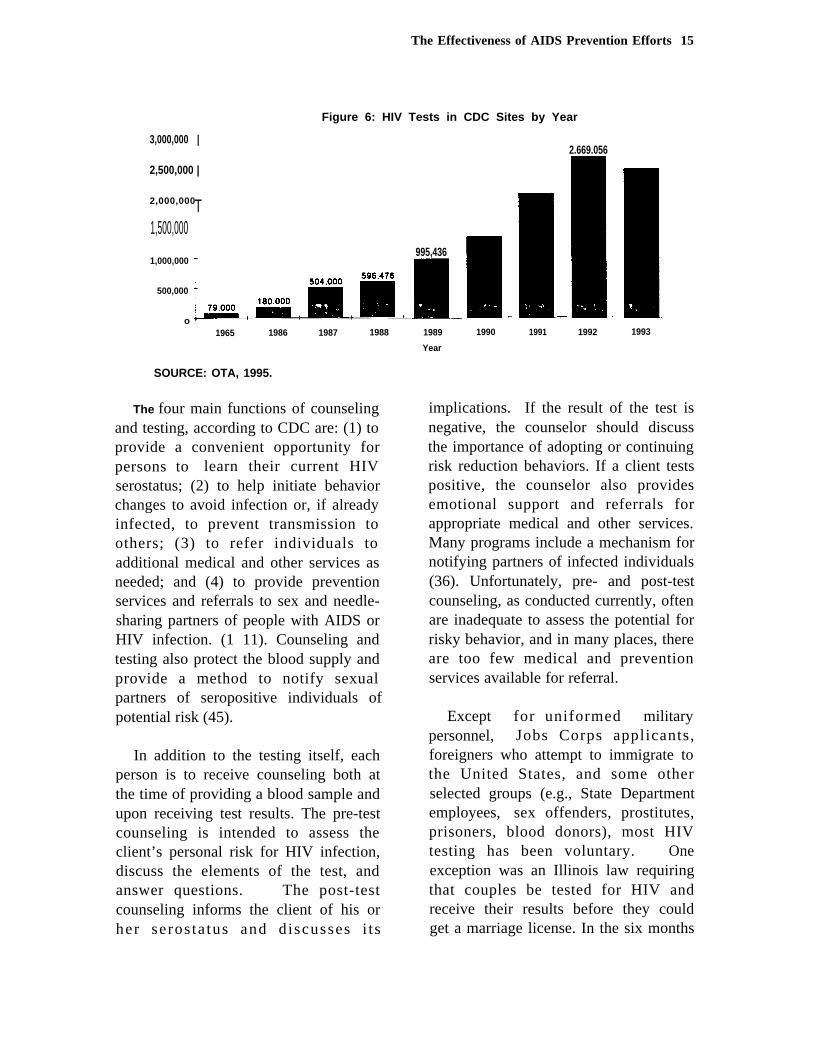
The CDC spends substantial funds onits program of counseling, testing,referral, and partner notification(CTRPN), much of which has beenmandated by Congress. The programbegan in 1985 with 79,000 people tested.By the end of 1993 11 million tests hadbeen performed (figure 6). Anadditional 5 million tests had beenperformed in private physicians’ officesand health maintenance organizationsthrough 1990 (101).
The Effectiveness of AIDS Prevention Efforts 15
Figure 6: HIV Tests in CDC Sites by Year
3,000,000 |2.669.056
2,500,000 |
2,000,000T1,500,000
995,4361,000,000
500,000
o ’1965 1986 1987 1988
SOURCE: OTA, 1995.
The four main functions of counselingand testing, according to CDC are: (1) toprovide a convenient opportunity forpersons to learn their current HIVserostatus; (2) to help initiate behaviorchanges to avoid infection or, if alreadyinfected, to prevent transmission toothers; (3) to refer individuals toadditional medical and other services asneeded; and (4) to provide preventionservices and referrals to sex and needle-sharing partners of people with AIDS orHIV infection. (1 11). Counseling andtesting also protect the blood supply andprovide a method to notify sexualpartners of seropositive individuals ofpotential risk (45).
In addition to the testing itself, eachperson is to receive counseling both atthe time of providing a blood sample andupon receiving test results. The pre-testcounseling is intended to assess theclient’s personal risk for HIV infection,discuss the elements of the test, andanswer questions. The post-testcounseling informs the client of his orher seros ta tus and d iscusses i t s
1989 1990 1991 1992 1993
Year
implications. If the result of the test isnegative, the counselor should discussthe importance of adopting or continuingrisk reduction behaviors. If a client testspositive, the counselor also providesemotional support and referrals forappropriate medical and other services.Many programs include a mechanism fornotifying partners of infected individuals(36). Unfortunately, pre- and post-testcounseling, as conducted currently, oftenare inadequate to assess the potential forrisky behavior, and in many places, thereare too few medical and preventionservices available for referral.
Except for uniformed militarypersonnel, Jobs Corps applicants,foreigners who attempt to immigrate tothe United States, and some otherselected groups (e.g., State Departmentemployees, sex offenders, prostitutes,prisoners, blood donors), most HIVtesting has been voluntary. Oneexception was an Illinois law requiringthat couples be tested for HIV andreceive their results before they couldget a marriage license. In the six months

16 The Effectiveness of AIDS Prevention Efforts
after the law took effect, only eight outof the 70 ,846 appl icants tes tedseropositive. During the same time,applications for marriage licensesdecreased by 22.5 percent, and licensesi s s u e d t o Illinois residents insurrounding states increased. Researchsuggests the possibility that residentsmost likely to test seropositive weremost likely to seek out-of-state licenses.Testing costs were paid by theapplicants, not by the state, but the costper case of HIV identified was estimatedto be $312,000, compared with $2,000per case identified through the state’svoluntary counseling and testingprogram. The law was repealed and theDirector of the Illinois Department ofPublic Health concluded that theexperience “provides a strong argumentagainst widespread mandatory orpublicly supported HIV antibody testingof low-prevalence populations” (100).
There also is evidence thatindividuals, especially high-riskindividuals, are more likely to comeforward if they have the option ofanonymous testing. In an Oregon study,anonymous HIV testing, as opposed toconfidential testing, increased thenumber of people who came in to betested and increased the proportionfound to be seropositive (28).
Evaluation of Counseling and Testing
Counseling and testing programs havebeen difficult to evaluate because of thevariety of study populations, researchdesigns, methodologies, analyses, andresults (42). In addition, testing is oftenperformed without counseling (thoughCDC’s guidelines require counselingwith testing) (41). There is evidence that
counseling and testing can lead toreduced sexual and drug risk behaviorassociated with viral transmission(42,45). The effects vary, however, byserostatus, population, and the quality ofthe counseling and testing service.
The single area with clear data forbehavior changes associated withreduced risk of HIV transmissionfollowing counseling and testingconcerns both gay and heterosexualdiscordant couples (one partner infectedwith HIV and the other not). It isimportant to note, however, that thisfinding comes from programs in whichthe counseling extended beyond thattypically received by most people whoare tested. In several studies ofdiscordant couples , there was asubstantial increase in condom use overtime. These results suggest thatintensive counseling over a sustainedperiod may be effective in reducing riskbehavior for individuals at high risk forHIV infection (21,53,81,98,1 14). Theymay point to ways to improvecounseling for other groups.
EFFORTS DESIGNED FORTHE AMERICAN PEOPLEAS A WHOLE12
Education and prevention effortsaimed at the American people as a wholehave several aims. In addition to theobvious aim of promoting safe practices,others are to reduce discriminationagainst infected people and to reduceanxiety among low-risk people by giving
12 This section is based largely on a paperprepared under contract to OTA by Zimmerman,Pham, and Steinman (120).

The Effectiveness of AIDS Prevention Efforts 17
them good information about how HIVis and is not transmitted. To a largeextent these efforts are intended to reachsexually active heterosexual youth andadults for whom there are few targetedcommunity-based programs. This groupaccounts for relatively few AIDS cases,but the percentage of heterosexualadolescents and adults among AIDScases who do not belong to a definedhigh-risk category is growing. From1988 to 1994, the percentage of newly-diagnosed AIDS cases in this groupincreased from 5 percent to 10 percent.AIDS is becoming a particular problemin some heterosexual subpopulations,particularly African-Americans andHispanic-Americans (7,74).
Knowledge about HIV transmissionhas increased from 1987 to 1992, thoughthere continue to be significant gaps(88). This increased knowledge may beexplained by a combination of severalinfluences, including media attention,high profile cases such as MagicJohnson and Ryan White, and school-based AIDS education. Americans aremore likely to understand how AIDS canand cannot be transmitted. However, in1992, 55 percent did not know whetherlatex condoms and natural-membranecondoms conferred the same protectionagainst HIV/AIDS, and 60 percent didnot know whether oil-based lubricantscan cause latex condoms to break, twoimportant factors in condomeffectiveness.
Knowledge usually is necessary forbehavior change, but there is no clearand consistent evidence that accurateAIDS knowledge alone necessarilychanges behavior (4). Many sexuallyactive heterosexual Americans may be at
modest risk for HIV transmissionbecause they engage in sexual activitywith more than one sexual partner, oftenwithout a condom (2,7,8,23).13 Despitethe risk for transmitting HIV throughheterosexual activity, few interventionshave been evaluated to determine theirimpact on this behavior.
Mass Communication Campaigns
National surveys indicate thattelevision is the most frequently citedsource of information about AIDS.Thus , the mass media are wel l -positioned to play the dual role ofinfluencing people who are not reachedby other interventions and serving toreinforce non-risk behavior for thosewho are. The CDC developed AmericaResponds to AIDS (ARTA), a nationalpublic service advertisement and publicrelations campaign designed to reach asmany Americans as possible withinformation about HIV and how toprevent its spread. The campaign ranfrom 1987 to 1991, using electronic andprint media, as well as public events.ARTA focused on providing informationabout AIDS rather than urging behaviorchange. It shied away from strongprevention messages, because thebehavior changes needed to reduce thespread of HIV involve controversialtopics such as sexual behavior and druguse. For instance, the public serviceannouncements usually failed directly toaddress risk-reduction behaviors such asthe use of condoms. In addition, there
*3 Most Americans who engage exclusively inheterosexual sexual activity are at less risk forinfection than most gay and bisexual men simplybecause the incidence of HIV is lower amongheterosexuals than among gay and bisexual men.

18 The Effectiveness of AIDS Prevention Efforts
are inherent limitations to public serviceannouncements as opposed to paidcommercials because television andradio station personnel determine if andwhen the commercials run. They aremotivated primarily by the needs of thestation, not b y p u b l i c healthconsiderations. Further, to be mosteffective, mass media campaigns mustbe implemented for a sustained period oftime and heard repeatedly, which is notlikely with public service announcementcampaigns. The media potentially offersan important source of AIDS preventionbecause of its reach, but the opportunityhas not yet been used effectively.
AIDS Prevention by Physicians
Physicians are seen by the public assources of reliable health care andprevention information (14,1 17) andphysician counseling can lead tohealthier behaviors (65). As yet,however, physicians have not played amajor role in informing people abouttheir risk of infection with HIV, orcounseling them about how to avoid it.They represent a potential source ofinfluence for the 60 percent ofAmericans who see a physician eachyear--though many of the people athighest risk may not see a physician.
The U.S. Surgeon General, the CDC,the Agency for Health Care Policy andResearch, and many professionalmedical associations have encouragedphysicians to assess their patients’ riskbehaviors and counsel them to preventH I V t r a n s m i s s i o n , b u t n o c l e a rguidelines about what steps to take withpatients have been put forth. It appearsthat most physicians do not counselabout HIV or AIDS (6 ,35,110) .
(Physicians often do a poor job withother prevention opportunities as well,e.g., influenza vaccines for older people,rubella screening for potentiallypregnant women.)
Lack of information about andtraining in AIDS, discomfort inaddressing sexual conduct, and incorrectassumptions about high risk behaviorsmay be holding back some physiciansfrom counseling. Some research hasshown that physicians are uncomfortablewith AIDS, at least partially becausemost people with AIDS are gay or aremembers of other stigmatized groups(1 19). Other barriers to effectivephysician prevention efforts includerushed visits and limited or nonexistentreimbursement for counseling andtesting. Finally some people cannotafford to visit doctors, choose not to seethem regularly, or see them in settingsnot conducive to prevention counseling(69) .
A nationwide program of AIDSEducation and Training Centers(AETCs), set up through the HealthResources and Services Administrationof the Public Health Service, began in1987 to train physicians, nurses, anddentists. Most AETC activities are fortraining health care personnel to care forpeople with AIDS, but about 25 percentof the training activities are directedtowards prevention (13), and there alsoare private sector continuing medicaleducation programs on the topic. Fewstudies have evaluated the effects oftraining physicians or other health careworkers, but some evidence suggestst h a t t r a i n i n g m a y i m p r o v e r i s kassessment and prevention counselingfor HIV (29,44). Any future efforts

The Effectiveness of AIDS Prevention Efforts 19
should be subjec ted to rigorousevaluation.
PREVENTING AIDS AMONGGAY AND BISEXUAL MEN14
Carefully designed studies havedemonstrated that interventions can beeffective in lessening risk behavioramong gay and bisexual men. Theinterventions studied included individualor small-group counseling, HIVcounseling and associated testing, andcommunity approaches. In these studies,reduction in risk behavior was defined asstatistically significant increases incondom use or reductions in analintercourse without a condom. Thestudies showed that positive behaviorchanges can be both short-term andrelatively long-term (greater than oneyear). Evidence suggests that interven-tions can be effective with gay andbisexual men generally, includingAfrican Americans and adolescents. Nostudies of Latinos have been published,however.
Multiple session, small groupcounseling can result in both short-termand long-term increase in condom usageand less unprotected sexual activity(57,112), including with AfricanAmerican gay and bisexual men (83).No controlled studies have beenconducted considering the effects ofcounseling on gay and bisexualadolescents, but in two uncontrolledstudies, reductions in risk behavior wereassociated with counseling interventions.
‘4 This section is based largely on a paperprepared under contract to OTA by Coates et al.(lo).
Data suggest that HIV counseling andtesting may play a role in HIV riskreduction for gay and bisexual men (42).Gay and bisexual men who have beentested tend to engage less often in sexualrisk behavior. However, it is difficult toisolate the effects of HIV counseling andassociated testing from other factors thatmay affect risk behavior, including thesame personal factors that cause somepeople to be tested and others not to be.
Community-level interventions seekto modify the norms of entire groups ofpeople in which there is a high level ofHIV infection, so that there can be socialand peer reinforcement for non-riskbehavior. Several projects included pre-and post-intervention evaluations thatsuggest that community interventionsmay have an effect on reducing riskbehavior (11,54,55). For example, theSTOP AIDS Project in San Franciscoconducts outreach and workshops forgay and bisexual men. An evaluation,conducted with the Center for AIDSPrevention Studies, revealed that of thelast 505 pre- and post-test evaluations,25.1 percent of the men reportedunprotected intercourse prior to theworkshop and 19.4 percent after, withgreater differences observed forseropositive individuals (9). (None ofthese studies have randomizedcommunities to have the intervention ornot, or have had control communities, soit is not clear how much of the changecan be attributed to the intervention.) Ina study of small-town gay men who goto bars, training a small group of“trendsetters” in non-risk sexualbehavior altered the norms of the group.“If risk reduction is an expected andaccepted norm within one’s peer andsocial network, individuals will be

■
20 The Effectiveness of AIDS Prevention Efforts
encouraged to adopt precautionarypatterns (58).”
Determining whether HIV infectionprevention is working “on the ground” isdifficult because of the small number ofcontrolled studies and the lack ofconsistent, established surveillancesystems to provide regular and reliableinformation about HIV transmissionrates. Studies have found sharp declinesin risk behavior among gay and bisexualmen in San Francisco, New York, andother cities during the 1980s. Reportedbehavior changes early in the AIDSepidemic among gay and bisexual menwere among the most profound in publichealth (11,27,71,72,73). There havebeen declines in seroconversion fromHIV negative to positive (50), declinesin potentially unsafe sexual relations(20,24), declines in other sexuallytransmitted diseases, and declines in therate of new AIDS cases. For example,the San Francisco Department of Healthprojects the number of people in that citywho will become infected with HIVbetween 1994 and 1997 at 1,000 per year(an estimated 650 among gay men),down from 8,000 in 1982. Thesechanges appear to have continued intothe 1990s (89) and cannot be explainedsimply by saturation of high-activitycore groups (50). They almost certainlyrepresent benefits gained throughbehavior change (but not necessarilyfrom particular programs).
It must be underscored that whilethere is evidence of improvement for gayand bisexual men as a group, therecontinues to be high rates of newinfections among some racial and ethnicgroups and among younger gay andbisexual men. Young gay and bisexual
men are forging another wave of HIVinfections. Existing interventionstrategies do not appear to be successfulin reaching these populations. Inaddition, there is some indication thatgay and bisexual men who initiallyadopted low-risk behaviors may havefailed to maintain these behaviors(11,27,56,94). These data collectivelydemonstrate a need to focus on and findmore effective interventions for youngerand non-white gay and bisexual men,while continuing to pursue preventionand maintenance strategies for all gayand bisexual men.
PREVENTING AIDS AMONGINJECTING DRUG USERS15
The exchange of blood throughsharing of injecting drug equipment bytwo or more people is the second mostcommon cause of HIV transmission afterunprotected sexual intercourse betweenmen. The major mechanism for thespread of HIV infection among injectingdrug users is injection with traces ofblood from contaminated needles orother paraphernalia previously used byan HIV infected individual. Providingpreviously used equipment to anotherinjection drug user is often seen as an actof solidarity or as a service for whichone may legitimately charge a small fee.
Transmission of HIV within thepopulation of injecting drug users maybe lessened by eliminating or reducingillicit drug injection, reducing needlesharing, or using sterile injectionequipment. Without intervention, HIV
‘5 This section is based largely on a paper pre-pared under contract to OTA by Des Jarlais (16).

The Effectiveness of AIDS Prevention Efforts 21
can spread rapidly among injecting drugusers. In certain areas, the rate of infec-tion has increased from 10 percent to 40percent or more within just one or twoyears (17). In turn, HIV is often spreadfrom infected injecting drug users totheir sexual partners.
Successful drug detoxification andtreatment are the best methods of AIDSprevention among injecting drug usersbut are not a completely satisfactorysolution. Only 15 percent of active drugusers are in treatment on any given day,and there are not enough treatment slotsto meet the demand from drug users. Inaddition, many drug users do not want toenter treatment. Treatment programs canlead to substantial reductions in illicitdrug use (47), but treatment does notguarantee ending risk behavior or pre-venting a return to drug use. Educationat drug rehabilitation sites and “streetoutreach” to active drug users, includingeducation, needle exchange, and instruc-tion on needle sterilization were attempt-ed in some places.
The National Institute of Drug Abuse(National AIDS Demonstration Research/AIDS Targeted Outreach Model) fund-ed street outreach prevention efforts in41 projects in 50 cities. These programsoffered participants information aboutHIV and AIDS, personal risk assess-ment, and HIV counseling and testing.Results were somewhat mixed, but theinterventions were followed by a declinein needle sharing and an increase insterile needle use.
Needle Exchange
Needle exchange and bleachdisinfectant efforts have proven
controversial, with some critics assertingthey encourage illicit drug use or thatthey implicitly endorse the use of illicitdrugs. In the United States, unlike inseveral European countries, no Federalfunds may be used to support exchangesof needles or any distribution of sterileinjection equipment to illicit drug users.In addition, many states prohibit the saleof such equipment w i t h o u t aprescription. By contrast, providinglegal access to sterile injectionequipment, either through expandedpharmacy sales, needle exchange or bothis now a standard part of HIV preventionin many other industrialized countries.
Local needle exchange programs havebeen established in at least 102 U.S. sitesthrough at least 37 programs. Programsprovide a sterile needle in exchange for aused one. In addition, many of theprograms make referrals to drugdetoxification and treatment programsand distribute condoms, bleach, healthpamphlets, and other AIDS preventioninformation. About half of the needleexchange programs are legal under thelaw of the state in which they operate.About one-quarter are not legal butreceive support from a local electedbody. The remainder operate outside ofthe law and without such support (52).
Several U.S. needle exchangeprograms have been evaluated. In everypublished study, including oneconducted by the General AccountingOffice (GAO) in 1993, no evidence wasfound that the programs result in anyincrease in illicit drug use. In fact, oneprogram studied by GAO found adecrease in drug use in association withthe implementation of a local effort (52).In addition, there is evidence that

22 The Effectiveness of AIDS Prevention Efforts
outreach programs and needle exchangeprograms uncovered demand for drugdetoxification and treatment and were asignificant source of referrals to suchtreatment (3,49,79).
The National AIDS DemonstrationResearch/AIDS Targeted OutreachModel and other studies (18) have foundthat HIV infection rates are much lowerin areas that permit over-the-countersales of sterile injection equipment asopposed to areas that restrict them byrequiring prescriptions for theirpurchase. In one study, incidence ofHIV infection was lower by half in areaswith legal over-the-counter sales ofneedles (30). Studies of injecting drugusers participating in needle exchangeprograms in several U.S. cities also havefound a low rate of HIV transmissionamong participants (39,78,80,82).
A study of hepatitis B and hepatitis Cinfection in Tacoma, WA provides goodevidence for the effectiveness of needleexchange programs on reducingtransmission of blood-borne viruses,particularly because the study usedbiological outcomes and a controlledexperimental design. Failure to use thelocal needle exchange program wasstrongly associated with both hepatitis Band hepatitis C infection. Injecting drugusers who did not use needle exchangewere five times as likely to becomeinfected with hepatitis B and seven timesas likely to become infected withhepatitis C (1 8,40).
Taken together, these data and othersprovide evidence that access to sterile
injection needles has a beneficial effecton the drug-related behavior that putsindividuals at risk for contracting HIV.
In addition to attempts to prevent thesharing and reuse of needles, there areinterventions which involve teachingillicit drug users to clean their equipmentwith bleach which kills HIV. However,studies have raised questions about theeffectiveness of this type of intervention,and it is not clear there is a relationshipbetween self-reported use of bleachdisinfectant “in the field” and protectionfrom HIV infection.
Sexual Partners ofInjecting Drug Users
HIV also is transmitted from infectedinjecting drug users to their sexualpartners. By the end of 1994,heterosexual sexual activity betweeninjecting drug users and individuals whodo not inject drugs accounted for about16,000 cases of AIDS (104). Injectingdrug users have changed their sexual riskbehavior more than heterosexuals in theUnited States generally (62), but studieshave shown less success in persuadingthem to change their sexual risk behaviorthan their needle-sharing behavior (31).Thus, sexual relationships betweeninjecting drug users and their partnerscontinue to provide a route of HIVtransmission into larger populations.Finding effective ways to persuadeinjecting drug users to avoid riskbehavior during sexual activity is acritical challenge in slowing the spreadof AIDS.

The Effectiveness of AIDS Prevention Efforts 23
PREVENTING AIDSIN RACIAL AND ETHNICMINORITY POPULATIONS16
Research focus ing on AIDSprevention among minority populationshas lagged behind research on othergroups, despite the disproportionatelyhigh (and worsening) rate of HIVinfection among African Americans andLatinos. Before 1988, only one researchreport focusing on a minority populationhad been published. In 1995,41 reports,published (or accepted for publication)in peer reviewed journals, focusedentirely or m a i n l y o n AfricanAmericans, Latinos, or both. (There stillhave been no studies published onNative Americans or Asian/PacificIslanders.) Of these studies, 13 wererandomized trials. In four of those, theinterventions were very effective, and infive others, of moderate or mixedeffectiveness. Even from this smallliterature, however, some generalfindings emerge, and they are consistentwith interventions in other populations.
The most successful interventionswere developed through extensivepreliminary work wi th the ta rgetpopulation, and used formal behaviorchange theory in their development. Thepreliminary work consisted mainly offocus groups and individual interviews.These exchanges provided information,for instance, about the barriers to saferbehavior and about the level of skillsthat people had to deal with difficultsituations. They also served to helpdevelop and test the research
16This section is based largely on a paperprepared under contract to OTA by Marin (70).
questionnaires and role playing materialsbefore formal data collection began.
The four most effective interventionsemphasized behavioral skills andpractice (e.g., practice for teenagers inrefusing to engage in unsafe behavior,negotiating about condom use, andputting on condoms), and were generallymore interactive and less didactic thanthe less effective interventions. AfricanAmerican adolescents were the target oftwo of the particular programs that weremost successful, and the interventionswere, in one case, eight weekly groupmeetings of 90 minutes to two hourseach, focusing on behavioral skills,condom use skills, and refusal skills; andin the second case, a five-hour programof information, videos, games, exercises,and skills practice. A third successfulprogram, this one for high-risk mostlyAfrican American women, consisted of aseries of group sessions with a variety ofinformation, role playing, and otheractivities. The fourth program was forAfrican American and Latino sexually-transmitted-disease p a t i e n t s , a n dconsisted of culturally appropriatevideos, 20-minute group sessions, skillsbuilding, role playing, and discussions.
There are large gaps in the AIDSprevention research for minoritypopulations. Most strikingly, almost nowork has been done with AfricanAmerican and Latino drug users or gaymen, two groups affected heavily by theAIDS epidemic. Interventions targetingadult men who are not injection drugusers have been rare, except for studiesof STD patients. Adolescents have beenstudied to some extent in schools, butnot in neighborhoods or juvenile

24 The Effectiveness of AIDS Prevention Efforts
detention settings, where many of theseyouth are more likely to be.
Research has gone slowly withAfrican Americans and Latinos forseveral reasons. Funding agencies havenot specially targeted these groups, andresearchers may have shied away fromtaking on studies of high-risk, hard-to-reach populations. Few non-minorityresearchers have demonstrated interest inthese groups, and there are too fewminority researchers in positions toundertake the needed work.
PREVENTING HETEROSEXUALHIV TRANSMISSIONTO WOMEN17
Little is known a b o u t t h eeffectiveness of AIDS prevent ionactivities targeted towards women.Multiple counseling and skills sessionstargeted at female injecting drug users,female sexual partners of injecting drugusers, and inner-city or low-incomewomen seem to provide a benefit interms of increased condom use (26,87).A controlled study of a program of peeroutreach combined with distribution ofwritten material containing risk-reduction strategies increased condomuse among female sexual partners ofinjecting drug users living in publichousing (99)projects . Amethodologically sound HIV counselingand testing study found no benefit ateither two weeks or three months (48).
As with many other subpopulations,often studies enlisted very smallsamples, failed to provide enoughinformation to be assessed, had unclearor very short follow-up periods, were notrandomized, or did not use control orcomparison groups. This deficiency is aserious matter given the rate of increasein AIDS cases among women. Morework is needed in this area in order todevelop effective prevention programs.The variety of techniques studied mustbe expanded, especially to includecommunity-level interventions. Mainte-nance of non-risk behavior should bestudied as well.
PREVENTING AIDS AMONGSCHOOL-AGED YOUTH18
There have been various studiesevaluating school, community, andhealth clinic-based sex and AIDSeducation and prevention efforts targetedtowards youth. The weight of theevidence indicates that sex and AIDSeducation programs, in general, increasethe use of condoms (or other forms ofcontraception) by a small amount, andthat more targeted programs can increasecondom use by a greater amount. Still,overall, there are large gaps in knowinghow to prevent HIV transmission amongyoung people.
All 50 states either mandate orrecommend AIDS education in theirschools (15,34). Schools have theadvantage of reaching almost everyyoung person in society before he or shebegins potentially risk-associated
17 This section is based largely on a paperprepared under contract to OTA by Ehrhardt,Exner, and Seal (25).
l8 This section is based largely on a paperprepared under contract to OTA by Kirby (59).

behavior. There is widespread publicsuppor t for sexual i ty and AIDSeducation in the schools (32,33,67), butthere has been conflict in somecommunities over the content of sucheducation. Some believe that onlyabstinence until marriage should bediscussed, while others believe thatcontraception and other sexuality topicsshould be covered as well. Those whofavor only abstinence fear that furtherdiscussion would encourage youth toengage in sexual activity that theyotherwise would avoid, therebypotentially increasing HIV transmissionalong with other undesirable outcomes.People who favor discussion ofadditional topics along with abstinenceare concerned that abstinence alone isnot a sufficient lesson, because manyteenagers still would engage in sexualactivity.
Studies have found no evidence thatcurricula focusing only on abstinencehave an impact on delaying the onset ofsexual intercourse. However, limitationsin the design of these studies may haveobscured program impacts. On the otherhand, da ta s t rongly suppor t theconclusion that sexuality and AIDSeducation that include discussions ofabstinence and contraception incombination with other topics such asresistance skills do not hasten the onsetof sexual intercourse for students whohave not already initiated such activity(46,60,76,97,1 16). In fact, there isevidence that these more sexualeducational and AIDS preventionprograms result in a lower incidence ofsexual intercourse, and for individualswho do engage in sexual activity, fewersexual partners and greater use ofcontraception (46,60,64,68,1 15). At the
The Effectiveness of AIDS Prevention Efforts 25
same time, none of the interventionsresulted in increased or deceasedfrequency of intercourse for individualssexually active prior to the beginning ofthe study.
Some other methods also have beenfound to have at least marginal value inreducing HIV transmission. Multiple-session counseling (5), counselingconnected to other services (1 18), and awide-ranging program of communityprevention activities (61,1 13) all havesome promise, but need additionalrefinement and evaluation.
PREVENTING AIDSAMONG CHILDREN
HIV can be transmittedmother to her fetus during
from infectedpregnancy, at
birth, or during breast feeding. Anestimated 7,000 births occur each year toHIV-infected women in the UnitedStates. All of these children initially testseropositive because they carry certainelements of their mother’s immunesystem, though about three-quarters ofthem will become seronegative andsuffer no manifestations of HIV disease.In fact, about 25 percent of thesechildren are actually infected with HIV,and virtually all of them will developAIDS.
HIV transmission among thispopulation may be significantly reducedif the infected mother and newborn aretreated with Zidovudine (AZT). In arandomized clinical trial, only 8 percentof the children born to HIV-infectedmothers were born infected if the mothertook AZT during pregnancy and birth.(37). The effectiveness of this

26 The Effectiveness of AIDS Prevention Efforts
intervention in the community dependson the mother’s knowledge of herserostatus, her access to prenatal care,her confidence in her doctor, and herability and willingness to use AZT. Theeffect seen in the clinical trial also mightbe larger than it is likely to be in thecommunity.
Studies have shown that a program oftesting only pregnant women who appearto fall into a traditional exposurecategory for HIV infection will fail toidentify many of the women who in factare seropositive (22,37). Consequently,a program of voluntary testing might bea better method to screen for HIV amongpregnant women. Most pregnant womenwho may be at risk for HIV infectionwill agree to be tested if they are inprenatal care and the service is offered.In an eight-month pilot study done in1989 in six Los Angeles County publicclinics, 76 percent of 9,069 womenaccepted voluntary HIV testing. Resultsalso suggested that when the HIVantibody test was presented as a routinerather than a special, optional test,acceptance was nearly universal (12). In1987, routine prenatal HIV screeningwas offered as part of a battery of tests to3,472 women at Grady MemorialHospital, which serves a poor, intercitypopulation in Atlanta. The HIV test wassingled out from the others and thewomen received written informationabout the test and its implications, alongwith a consent form agreeing to the test.Even though at the time there was notreatment known to prevent transmissionfrom infected mother to child, 96 percentof the women agreed to be tested (66).Testing and counseling pregnant womencan be an effective part of reducingperinatal HIV transmission i f
seropositive women have access to AZTand to related medical care and supportservices.
SOCIAL MARKETING19
People and their needs changeconstantly, and th is inc ludes theinformation and stimulation they need topractice healthy behaviors. Even provenmethods may have to be tailored (e.g.,through community-based planning) tobe successful in different subpopulationsand over time. An effective approachmay be social marketing, which seeks toborrow consumer product marketingtechniques from the private sector anduse them for health promotion. Socialmarketing has been talked about butlittle used in AIDS prevention in theUnited States, though it has been used inother countries for AIDS prevention andfor other health promotion campaigns.Social marketing takes the approach thatprevention must be “sold” and that theremay be a need to “resell” it even to the“converted” in order to maintainbehavior change, just as there is withconsumer products. “No one at CocaCola would argue that selling Coke issomething you accomplish once andforever, especially when everyoneknows about Coke and likes it. SellingCoke is something you do every day, inever new ways, to meet an ever changingconsumer (92).”
Socia l market ing in an AIDSprevention context would use private-sector product marketing approaches to
19 This section is based largely on a paperprepared under contract to OTA by Rabin andPorter (84).

The Effectiveness of AIDS Prevention Efforts 27
“sell” HIV prevention to the public. Itwould move beyond traditional healtheducation to provide a framework forconstantly adapting prevention efforts tonew audiences and audiences who arealways changing. It would employmarket research, segmentation, diversemarketing channels, measurableoutcomes, constant evaluation forcontinued efficacy and program redesignwhere needed. It would identify andattempt to meet a consumer need withthe goal of sustaining behavior changeover a period of time. In exchange foralterations in behavior, social marketingwould offer a desired benefit, one that isfound through rigorous consumer marketresearch. Social marketing research hasshown that desired benefits often havemore to do with social acceptance orstatus than “health.” For example, futurehealth benefits may be insufficient topersuade teens to avoid smoking, butthey may be willing to do so to escapecurrent social stigma. With respect toAIDS, social marketing would seek toaddress questions such as: What is thebenefit of abstinence for teenagers whensexual activity is considered a rite ofpassage by one’s peer group? How cancondom usage be increased whencondoms often are associated with gaypeople, a stigma for some, or a lack oftrust between partners? What is thebenefit of avoiding certain sexualactivities versus the risk of contracting avirus that may kill you in 10 to 15 years?
Social marketing considers perceivedbenefit, consumer acceptance, price(including monetary value, time, andsocial cost), sacrifice of behaviorpossibly considered pleasurable andconvenience of outlets. It takes as agiven that effective promotion requires a
wide array of creative tactics andrepetition involving professionalmessage design. For each AIDSprevention behavior, there is competingpressure to stray from that behavior, so asingle exposure to even the mosteffective message or adopting the “right”behavior may not be enough. Socialmarketing would “sell” prevention againand again to the same target audiences.
Social marketing approaches havebeen used in cardiovascular riskreduction, smoking cessation andpopulation planning, as well as in U. S.-funded AIDS prevention efforts in othercountries. For example, the NationalCancer Institute developed the 5-A-Daycampaign to increase fruit and vegetableconsumption. It employed marketingsegmentation to define target audiencesand f o l l o w e d a consumer-basedapproach to the design of mediamessages. Diverse marketing channelswere chosen to deliver messages to keygroups. Promotional materials wereplaced in over 30,000 retailestablishments. There were televisionappearances by Olympic gold medalists.
In April 1993, the CDC establishedthe Prevention Marketing Initiative(PMI), which uses a social marketingapproach. CDC has worked withcommunity-based organizations todevelop demonstration projects targetedto young people in Phoenix, AZ,Sacramento, CA, Northern Virginia,Nashville, TN, and Newark, NJ. It alsohas produced 12 publ ic serv iceannouncements for radio and televisionwith messages about abstaining from sexand using condoms. As yet, there hasbeen no outcome evaluation of PMI.The program entails considerable

28 The Effectiveness of AIDS Prevention Efforts
expense, and many questions remainabout whether i t can achieve anacceptable level of effectiveness to makeit worthwhile.
ECONOMIC EVALUATION20
A central question for policymakers iswhich strategies are most cost-effectivein preventing further HIV infection?
. The aim would, of course, be to choosethe mix of interventions that wouldprevent the largest number of infectionswith the amount of money available forAIDS prevention programs. As is thecase in most areas of medicine andhealth, the cost-effectivenessinformation that one would need ideallyto make “rational” choices is quitelimited. Only in recent years hassufficient evidence of the efficacy andeffectiveness of interventionsaccumulated to begin to support suchanalyses.
A total of 25 economic evaluations ofAIDS primary prevention interventionsmeeting minimum methodologicalcriteria were found in the publishedliterature in 1995 (90). Some of thesestudies look at interventions that are notbasically “educational,” such asscreening donated blood, and screeninghealth care workers, and are notdiscussed in this report. Interventionsthat do fall within the scope of thisreport and are the subjects of economicevaluations are:
◆ voluntary counseling and testing ofinjecting drug users, high- and low-
20 This section is based largely on a paperprepared under contract to OTA by Sisk (90).
risk populations (based on a model),the general public, pregnant women,and women age 13-44;mandatory testing of marriage licenseapplicants and premarital couples,notifying partners of infected peopleand injection drug users;bleach distribution to injection drugusers;needle exchange for injection drugusers; andtreatment of drug dependency.
Many of the interventions--even somefor which there is some evidence ofefficacy and effectiveness--discussedearlier in this report have not beensubject to economic analysis. Thisincludes the important category of smallgroup counseling (except as included inthe studies of injection drug users) andvirtually all the large-scale educationprograms aimed at the public and atvarious risk groups.
Findings From Economic Evaluations
The major types of economicevaluation--cost-effectiveness, cost-benefit, and cost-utility analyses--all takeinto account the costs and effects ofinterventions. In the case of AIDSprevent ion , as wi th many o therpreventive services, the costs ofintervening occur in the present, andmany, if not all, the benefits occursometime in the future. Discounting is atechnique used to allow all the costs andbenefits to be expressed in currentdollars, recognizing that money spenttoday is worth more than the sameamount of money spent 10 years fromnow. Having everything in the samecurrency is necessary for making

The Effectiveness of AIDS Prevention Efforts 29
comparisons, but money spent todaymust materialize in a particular budget,while money counted in the future neednot.
Programs of counseling, testing,referral, and partner notification, asexemplified by the CDC-funded sites,produce benefits greater than their costs.If only about 7 percent of the infectedpeople notified subsequently changedthei r behaviors to aver t fur thertransmission, savings in discountedlifetime AIDS treatment costs (about$85,000 in 1990 dollars, 6 percentdiscount rate) would more thancompensate for program costs . I fsavings in future earnings are added, netbenefits would exceed costs if onlyslightly more than 1 percent of infectedpeople notified averted further spread ofHIV.
A similar pattern emerges for severalinterventions targeted to injection drugusers. Savings in treatment costsavoided are likely to exceed programcosts for counseling and testing, partnernotification, and bleach distribution.Even using conservative assumptionsabout injection and sexual behavior formore controversial needle exchangeprograms, their savings in treatment.costs are likely to outweigh programcosts.
The results for testing marriagelicense applicants were less clear, partlybecause there is little information abouthow effective this type of testing wouldbe in changing sexual behavior. Testingwomen of childbearing age wouldproduce most benefits in preventinginfection among adult contacts, and lessin preventing the birth of infected
newborns, so it really reflects testing partof the adult population. Screeningwomen could potentially produce morebenefits than the costs of the program ifit were targeted at high-risk women andthe HIV prevalence were above a certainlevel.
Potential for Greater Useof Economic Evaluation
The use of cost-effectiveness analysisand other forms of economic evaluationin AIDS prevention policymaking islimited by the still meager literature onthe topic and by the variability inanalytic methods used. This situation ischanging, however, as the potentialvalue of this type of work is appreciatedand more is being undertaken byindependent academics and others. Inaddition, CDC is encouraging the use ofeconomic analysis by the HIVPrevention Community Planning Groupsthat it funds. Developments in the fieldof cost-effectiveness analysis itself mayalso help solidify this work. The U.S.Public Health Service has formulatedrecommendations for economic princi-ples to be applied in economic analyses,which should improve the rigor andcomparability of future work.

References
1.
2.
3.
4.
5.
6.
-7.
Altman, L. K., “AIDS is Now theLeading Killer of Americans from 25to 44,” New York Times, p. A7, Jan. 31,1995.Anderson, J.E. and Dahlberg, L.L.,“High-Risk Sex Behavior in theGeneral Population: Results from aNational Survey, 1988-1990,” SexuallyTransmitted Diseases 19(6):320-325,1992, cited in Zimmerman (120).Ashery, R. S., Davis, H., Davis, W. H.,et al.,’’ Entry into Treatment of IDUsBased on the Association of OutreachWorkers with Treatment Programs,”Handbook on Risk of AIDS, B.S.Brown and G.M. Beschner (eds.)(Westport, CT: Greenwood Press,1993), cited in Des Jarlais (16).Becker, M.H. and Joseph, J. G., “AIDSand Behavioral Change to ReduceRisk: A Review,” American Journal ofPublic Health 78:394-410, 1988.Berger, D.K., Perez, G., Kyman, W., etal., “Influence of Family PlanningCounseling in an Adolescent Clinic onSexual Activity and ContraceptiveUse,’’manuscript, no date, cited inKirby (59).Caretta, R.A., Mangione, T. W.,Marson, P.F., et al., “AIDS EducationPractices Among MassachusettsPhysicians,” Journal of CommunityHealth 15(3):147-162, 1990, cited inZimmerman (120).Catania, J. A., Coates, T.J., Stall, R., etal., “Prevalence of AIDS-Related RiskFactors and Condom Use in the United
States,” Science 258:1101-1106, 1992,cited in Zimmerman (120).
8. Choi, K.H., Catania, J.H., and Dolcini,M., “Extramarital Sex and HIV RiskBehavior Among U.S. Adults: Resultsfrom the National AIDS BehavioralSurvey,” American Journal of PublicHealth 84(12):2003-2007, 1994, citedin Zimmerman ( 120).
9. Coates, T., Director, Center for AIDSPrevention Studies, University ofCalifornia, San Francisco, CA,personal communication, Feb. 28,1995.
10. Coates, T. J., Faigle, M., Koijane, J., etal., Center for AIDS PreventionStudies, University of California, SanFrancisco, CA, “Does HIV PreventionWork for Men Who Have Sex withMen?,” unpublished contractor reportprepared for the Office of TechnologyAssessment, U.S. Congress,Washington, DC, September 1995.
11. Coates, T.J.,’’Strategies for ModifyingSexual Behavior for Primary andSecondary Prevention of HIVDisease,” Journal of Consulting andClinical Psychology 58(1):57-69,1990, cited in Coates (10).
12. Cozen, W., Mascola, L., Enguidanos,R., et al., “Screening for HIV andHepatitis B Virus in Los AngelesCounty Prenatal Clinics: ADemonstration Project,” Journal ofAcquired Immune DeficiencySyndromes 6:95-98, 1993.
3 1
32 The Effectiveness of AIDS prevention Efforts
14.
15.
16.
17.
18.
19.
20.
21.
Services, Rockville, MD, personalcommunication, June 1, 1995.David, A.K. and Boldt, J. S., “A Studyof Preventive Health Attitudes andBehaviors in a Family PracticeSetting,” Journal of Family Practice11 :77-84, 1980, cited in Zimmerman(120).DeMauro, D., “Sexuality Education1990: A Review of State Sexuality andAIDS Curricula,” SEICUS Report18(2):1-9, 1990, cited in Kirby (59).Des Jarlais, D. C., Beth Israel MedicalCenter, New York, NY, “HIV/AIDSPrevention for Injecting Drug Users,”unpublished contractor report preparedfor the Office of TechnologyA s s e s s m e n t , U . S . Congress,Washington, DC, September 1995.Des Jarlais, D. C., Friedman, S.R.,Choopanya, K., et al., “InternationalEpidemiology of HIV and AIDSAmong Injecting Drug Users,” AIDS6:1053-1068, 1992, cited in Des Jarlais(16).Des Jarlais, D. C., Goldberg, D.,Tunving, K., et al.,’’ Characteristics ofPrevented HIV Epidemics,” presentedat the Ninth International Conferenceon AIDS, Berlin, Germany, 1993, citedin DesJarlais(16).Des Jarlais, D. C., Padian, N. S., andWinkelstein, W., “Targeted HIV-Prevention Programs,” The NewEngland Journal o f Medicine331(21):1451-1453, Nov. 24, 1994,cited in DesJarlais(16).Detels, R., English, P., Visscher, B.R.,et al., “Seroconversion, SexualActivity, and Condom Use Among2915 HIV Seronegative Men Followedfor up to Two Years,” Journal ofAcquired Immune DeficiencySyndrome 2:77-83, 1989, cited inCoates (10).DeVincenzi, I. and Park, R. A.,“Heterosexual Transmission of HIV:Follow-up of a European Cohort ofcouples,” presented at the Sixth
22.
23.
24.
25.
26.
27.
28.
29.
International Conference on AIDS, SanFrancisco, CA, June 21, 1990, cited inZimmerman (120).DiFrancesco, E., “Routine PrenatalHIV Testing More Effective ThanRecommended Policy,” InfectiousDiseases in Children 3:3, 1990.Dolcini, M., Catania, J.A., Coates, T.J.,et al., “Demographic Characteristics ofHeterosexuals with Multiple Partners:The National AIDS BehavioralSurveys,” Family PlanningPerspectives 25(5):208-214, 1993,cited in Zimmerman (120).Doll, L. S., Judson, F.N., Ostrow, D. G.,et al., “Sexual Behavior Before AIDS:The Hepatitis B Studies ofHomosexual and Bisexual Men,” AIDS4:1067-1073, 1990, cited in Coates(lo).Ehrhardt, A. A., Exner, T. M., andSeal, D., Columbia University, NewYork, NY, “A Review of HIVInterventions for At-Risk Women,”unpublished contractor report preparedfor the Office of TechnologyAssessment , U.S. Congress,Washington, DC, September 1995.El-Bassel, N., and Schilling, R. F.,’’ 15-Month Followup of WomenMethadone Patients Taught Skills toReduce Heterosexual HIVTransmission,” Public Health Reports107(5):500-504, 1992, cited inEhrhardt (25).Ekstrand, M.L. and Coates,T.J.,"Maintenance of Safer SexualBehaviors and Predictors of Risky Sex:The San Francisco Men’s HealthStudy,” American Journal of PublicHealth 80:973-977, 1990, cited inCoates (1 O).Fehrs, L.J., Foster, L.R., Fox, V., et al.,“Trial of Anonymous VersusConfidential Human Immunodefi-ciency Virus Testing,” Lancet2(8607):379-382, Aug. 13, 1988..Feit, L. R., Metzler, S. M., Vermund,S. H., et al., “Impact of and AIDS

The Effectiveness of AIDS Prevention Efforts 33
28.
29.
30.
31.
32.
33.
34.
35.
36.
Fehrs, L.J., Foster, L. R., Fox, V., et al.,“Trial of Anonymous VersusConfidential Human Immunodefi-ciency Virus Testing,” Lancet2(8607):379-382, Aug. 13, 1988..Feit, L. R., Metzler, S. M., Vermund,S. H., et al., “Impact of and AIDSSymposium on Attitudes of Providersof Pediatric Health Care,” AcademicMedicine 65:461-463, 1990, cited inZimmerman (120).Friedman, S.R., Jose, B., Neaigus, A.,et al, “Over-the-Counter Syringe Salesand HIV Among Drug Injectors in theUnited States,” manuscript, no date,cited in Des Jarlais (16).Friedman, S.R., Des Jarlais, D. C.,Ward, T.P., et al., “Drug Injectors andHeterosexual AIDS,” AIDS and theHeterosexual Population , L. Sherr(cd.) (Chur, Switzerland: HarwoodAcademic Publishers, 1993), cited inDes Jarlais (16).Gallup, G., Gallup Poll Public Opinion1935-1971 (New York, NY: RandomHouse, 1972), cited in Kirby (59).Gallup, A., “The 19th Annual GallupPolls of the Public’s Attitudes Towardthe Public School,” Gallup Poll69(l): 1987, cited in Kirby (59).Gambrell, A. E. and Haffner, D.,Unfinished Business: A SEICUSAssessment o f State SexualityEducation Programs (New York,NY: SEICUS, 1993), cited in Kirby(59).Gemson, D. H., Colombotos, J.,Elinson, J., et al., “AcquiredImmunodeficiency SyndromePrevention. Knowledge, Attitudes, andPractices of Primary Care Physicians,”Archives o f Internal Medicine151:1102-1108, 1991, cited inZimmerman (120).Giesecke, J., Ramstedt, K., Granath, F.,et al., “Efficacy of Partner Notificationfor HIV Infection,” Lancet
338(8775):1096-100, Nov. 2, 1991,cited in Zimmerman (120).
37. Goedert, J.J. and Cote, T.R., “Editorial:Public Health Interventions to ReducePediatric AIDS,” American Journal ofPublic Health 84(7):1065-1066, 1994.
38. Gwinn, M., Pappaiaonou, M., George,R., et al., “Prevalence of HIV Infectionin Childbearing Women in the UnitedStates,” Journal of the AmericanMedical Association 265(13):1704-1708, 1991, cited in Marin (70).
39. Hagan, H., Des Jarlais, D. C.,Friedman, S.R., et al., “Risk for HumanImmunodeficiency Virus and HepatitisB Virus in Users of the TacomaSyringe Exchange Program,”Proceedings: Workshop on NeedleExchange and Bleach DistributionPrograms (Washington, DC:NationalAcademy Press, 1994), cited in DesJarlais (16).
40. Hagan, H., Des Jarlais, D. C.,Friedman, S.R., et al., “Reduced Riskof Hepatitis B and Hepatitis C AmongInjecting Drug Users Participating inthe Tacoma Syringe-ExchangeProgram,” American Journal of PublicHealth, in press, cited in Des Jarlais(16).
41. Henry, K., Maki, M, Willenbring, K.,et al., “The Impact of Experience withAIDS on HIV Testing and CounselingPractices: A Study of U.S. InfectiousDisease Teaching Hospitals andMinnesota Hospitals,” AIDSPrevention and Education 3(4):313-321, 1991, cited in Zimmerman (120).
42. Higgins, D.L., Galavotti, C., O’Reilly,K. R., et al., “Evidence for the Effectsof HIV Antibody Counseling andTesting on Risk Behaviors,” Journal ofthe American Medical Association266:2419-2429, 1991, cited in Coates(lo).
43. Holmberg, S. D., “EmergingEpidemiological Patterns in the USA,”unpublished paper presented at theSixth Annual Meeting of the National

34] The Effectiveness of AIDS Prevention Efforts
45,
46.
47.
48.
49.
50.
51.
Association 80(1):31-35, 1990, cited inZimmerman (120).Holtgrave, D. R., Valdiserri, R. O.,Gerber, A. R., et al., “HumanImmunodeficiency Virus Counseling,Testing, Referral, and PartnerNotification Services--A Cost-BenefitAnalysis,” Archives of InternalMedicine 153(10):1225-1230, 1993.Howard, M. and McCabe, J., “HelpingTeenagers Postpone SexualInvolvement,” Family PlanningPerspectives 22: 253-263, 1990, citedin Kirby (59).Hubbard, R.L., Marsden, M. E., Rachel,J. V., et al., Drug Abuse Treatment: ANational Study of Electiveness(Chapel Hill, NC: University of NorthCarolina Press, 1989), cited in DesJarlais (16).Ickovics, J.R., Merrill, A. C., Beren,S. E., et al., “Limited Effects of HIVCounseling and Testing for Women,”Journal of the American MedicalAssociation 272(6):443-448, 1994,cited in Ehrhardt (25).Jackson, J. and Rotkiewicz, L., “ACoupon Program: AIDS Education andDrug Treatment,” presented at theThird International Conference onAIDS, Washington, DC, 1987, cited inDes Jarlais (16).Jacquez, J.A., Koopman, J. S., Simon,C.P., et al., “Role of the PrimaryInfection in Epidemics of HIVInfection in Gay Cohorts,” Journal ofAcquired Immune DeficiencySyndromes 7:1169-1184, 1994, cited inCoates (10).Kahn, J.G., Washington, A. E.,Showstack, J.A., et al., UpdatedEstimates of the Impact and Cost ofHIV Prevention in Injection DrugUsers, Prepared for the U.S. Centersfor Disease Control, Division ofSTD/HIV Prevention, Institute forHealth Policy Studies, University ofCalifornia, San Francisco, CA,September 30, 1992, cited in Sisk (90).
52.
53.
54.
55.
56.
57.
58.
Kahn, J. G., “Are NEPs Cost-Effectivein Preventing HIV Infection?” Lurie,P., and Reingold, A.L. (eds.) ThePublic Health Impact of NeedleExchange Programs in the UnitedStates and Abroad, Prepared for theCenters for Disease Control andPrevention, School of Public Health,University of California, Berkeley,CA, and Institute for Health PolicyStudies, University of California, SanFrancisco, CA, 1993, cited in Sisk(90).Kamenga, M., Jingu, K., Hassig, S., et
al., “Condom Use and Associated HIVSeroconversion Following IntensiveCouples Counseling of 122 MarriedCouples in Zaire with Discordant HIVSerology,” presented at the FifthInternational Conference on AIDS,Montreal, Canada, June 6, 1989, citedin Zimmerman (120).Kegeles, S. M., Hays, R. B., and Coates,T.J., “Mobilizing Young Gay andBisexual Men for HIV Prevention: ATwo-Community Study,” manuscript,1995, cited in Coates (10).Kegeles, S. M., Hays, R. B., and Coates,T.J., “The Mpowerment Project: ACommunity-Level HIV PreventionIntervention for Young Gay andBisexual Men,” American Journal ofPublic Health, in press, cited in Coates(lo).Kelly, J.A., St. Lawrence, J. S., andBrasfield, T. L., “Predictors ofVulnerability to AIDS Risk BehaviorRelapse,” Journal of Consulting andClinical Psychology 57:60-67, 1991,cited in Coates ( 10).Kelly, J.A., St. Lawrence, J. S., Hood,H.V., et al., “Behavioral Interventionto Reduce AIDS Risk Activities,”Journal of Consulting and ClinicalPsychology 57:60-67, 1989, cited inCoates (10).Kelly, J.A., St. Lawrence, J. S.,Stevenson, L.Y., et al., “CommunityAIDS/HIV Risk Reduction: The

The Effectiveness of AIDS Prevention Efforts 35
57.
58.
59.
60.
61.
62.
63.
Kelly, J. A., St. Lawrence, J. S., Hood,H. V., et al., “Behavioral Interventionto Reduce AIDS Risk Activities,”Journal of Consulting and ClinicalPsychology 57:60-67, 1989, cited inCoates (10).Kelly, J.A., St. Lawrence, J. S.,Stevenson, L.Y., et al., “CommunityAIDS/HIV Risk Reduction: TheEffects of Endorsements by PopularPeople in Three Cities,” AmericanJournal of Public Health 82(11):1483-1489, Nov., 1992, cited in Coates (10).Kirby, D., “A Review of EducationalPrograms Designed to Reduce SexualRisk-Taking Behaviors AmongSchool-Aged Youth in the UnitedStates,” unpublished contractor reportprepared for the Office of TechnologyAssessment, U.S. Congress,Washington, DC, September 1995.Kirby, D., Barth, R., Leland, N., et al.,“Reducing the Risk: A NewCurriculum to Prevent Sexual Risk-Taking,” Family Planning Perspectives23(6):253-263, 1991, cited in Kirby(59).Koo, H.P., Dunteman, G.H., George,c., et al., “Reducing AdolescentPregnancy Through School andCommunity-Based Education:Denmark, South Carolina Revisited,1991,” Family Planning Perspectives26(5):206-217, September/October,1994, cited in Kirby (59).Laumann, E.O., Gagnon, J.H.,Michael, R.T., et al., The SocialOrganization of Sexuality:SexualPractices in the United S t a t e s(Chicago, IL: University of ChicagoPress, 1994), cited in Des Jarlais (16).Leigh, B.C., Temple, M. T., and Trocki,K. F., “The Sexual Behavior of U.S.Adults: Results from a NationalSurvey,” American Journal of PublicHealth 83(10):1400-1408, 1993.
64. Levy, S. R., Perhats, C. Weeks, K., et al.,“Impact of a School-Based AIDSprevention Program on Risk and
65.
66.
67.
68.
69.
70.
71.
72.
Protective Behavior for Newly SexuallyActive Students,” Journal of SchoolHealth 65(4):145-151, 1995, cited inKirby (59).Li, V. C., Coates, T.J., Ewart, C. K., etal., “The Effectiveness of SmotingCessation Advice Given During RoutineMedical Care: Physicians Can Make aDifference,” American Journal ofPreventive Medicine 3:81-86, 1987,cited in Zimmerman (120).Lindsay, M. K., Peterson, H.B.,andFeng, T. I., “Routine AntepartumHuman Immunodeficiency VirusInfection Screening in an Inner-CityPopulation,” Obstetrics andGynecology 74(3):289-94, 1989.Louis Harris and Associates, PublicAttitudes Towards Teenage Pregnancy,Sex Education and Birth Control (NewYork, NY: 1988), cited in Kirby (59).Main, D. S., Iverson, D.C., McGloin, J.,et al., “Preventing HIV InfectionAmong Adolescents: Evaluation of aSchool-Based Education Program,”Preventing Medicine 23:409-417,1994, cited in Kirby (59).Makadon, H.J. and Saline, J., “AReview of HIV Prevention in PrimaryCare: Current Practices, FuturePossibilities,” Annals of InternalMedicine, in press.Marin, B.V., “Analysis of AIDSPrevention Among African-Americansand Latinos in the United States,”unpublished contractor report preparedfor the Office of TechnologyAssessment, U.S. Congress,Washington, DC, September 1995.Martin, J., “The Impact of AIDS onGay Male Sexual Behavior Patterns inNew York City,” American Journal ofPublic Health 77:578-581, 1987, citedin Coates (1 O).Martin, J., Dean, L., Gracie, M., et al.,“The Impact of AIDS on a GayCommunity: Changes in SexualBehavior, Substance Use, and MentalHealth,” American Journal o f

36 The Effectiveness of AIDS Prevention Efforts
74.
75.
76.
77.
78.
79.
80.
81.
Michael, RT., Gagnon, J.H., Laumann,E., et al., Sex in America: A DefinitiveSurvey (New York, NY: Little Brown& co., 1994).Miller, H., Turner, C., and Moses, L.E.(eds.), AIDS: The Second Decade(Washington, DC:National AcademyPress, 1990), cited in Marin (70).Moberg, D.P. and Piper, D. L., “AnOutcome Evaluation of Project ModelHealth: A Middle School HealthPromotion Program,” HealthEducation Quarterly 17(1):37-51,spring, 1990, cited in Kirby (59).Nicholas, S. W., Bateman, D. A.,Stephen, K. C., et al., “Maternal-Newborn Human ImmunodeficiencyVirus Infection in Harlem,” Archives ofPediatric and Adolescent Medicine148:813-819, 1994.O’Brien, M., Murray, J. R., Rahemian,A., et al., “Three Topics From theChicago Needle Exchange CohortStudy: Seroconversion; the Behavior ofHIV-Positive NX Users; and the Needfor Additional Prevention AroundNon-Needle Injection Risks,”presented at The Annual Nor thAmerican Syringe ExchangeConference, Santa Cruz, CA,1994,cited in DesJarlais(16).O’Keefe, E., Kaplan, E., andKhoshnood, K., Preliminary Report:City of New Haven Needle ExchangeProgram (New Haven, CT:New HavenHealth Department, July, 1991), citedin Des Jarlais ( 16).Oliver, K., Maynard, H.,Friedman,S. R., et al., “Behavioral andCommunity Impact of the PortlandSyringe Exchange Program,”Proceedings of the Workshop onNeedle Exchange and BleachDistribution Programs (Washington,DC:National Academy Press,1994),cited in Des Jarlais (16).Padian, N. S., O’Brien, T.R., Chang,Y. C., et al., “Prevention ofHeterosexual Transmission of Human
82.
83.
84.
85.
86.
87.
88.
Immunodeficiency Virus ThroughCouple Counseling,” Journal ofAcquired Immune DeficiencySyndromes 6(9):1043-1048, 1993, citedin Zimmerman (120).Paone, D., Des Jarlais, D. C., Caloir, S.,et al., “New York City SyringeExchange: An Overview,”Proceedings: Workshop on NeedleExchange and Bleach DistributionPrograms (Washington, DC:NationalAcademy Press, 1994), cited in DesJarlais (16).Peterson, J. L., Coates, T.J., Hauck, W.,et al., “An HIV Prevention Strategy forAfrican American Gay and BisexualMen,” manuscript, no date, cited inCoates (10).Rabin, S.A. and Porter, R. W.,“Application of Social MarketingPrinciples to AIDS Education,”unpublished contractor report preparedfor the Office of TechnologyAssessment , U.S. Congress,Washington, DC, September 1995.Rabin, S.A., “A Private Sector View ofHealth, Surveillance, and Communitiesof Color,” Public Health Reports109(1):42-45, 1994.Rogers, D.E. and Osborn, J. E., “AIDSPolicy: Two Divisive Issues,” Journalof the American Medical Association270(4):2436, July 28, 1993.Schilling, R.F., El-Bassel, N., Schinke,S.P, et al., “Building Skills ofRecovering Women Drug Users toReduce Heterosexual AIDSTransmission,” Public Health Reports106(3):297-304, 1991, cited inEhrhardt (25).Schoenborn, C.A., Marsh, S.L., andHardy, A. M., “AIDS Knowledge andAttitudes for 1992: Data from theNational Health Interview Survey, “Advance Data from Vital and HealthStatistics, No. 243, Public HealthService, U.S. Department of Healthand Human Services, DHHS Pub. No.

The Effectiveness of AIDS Prevention Efforts 37
88.
89.
90.
91.
92.
93.
Schoenborn, C.A., Marsh, S.L., andHardy, A. M., “AIDS Knowledge andAttitudes for 1992: Data from theNational Health Interview Survey, “Advance Data from Vital and HealthStatistics, No. 243, Public HealthService, U.S. Department of Healthand Human Services, DHHS Pub. No.(PHS) 94-1250 (Hyattsville, MD:Feb.23, 1994).Silvestre, A.J., Kingsley, L. A.,Wehrman, P., et al., “Changes in HIVRates and Sexual Behavior AmongHomosexual Men,” American Journalof Public Health, 83:578-580, 1993,cited in Coates ( 10).Sisk, J. E., “Economic Evaluation ofHIV/AIDS Education and PrimaryPrevention,” unpublished contractorreport prepared for the Office ofTechnology Assessment, U.S.Congress, Washington, DC, September1995.Sisk, J.E., Hewitt, M., and Metcalf,K. L., How Effective is AIDSEducation?--staff paper #3 in OTA’sSeries on AIDS-Related Issues(Washington, DC: Office ofTechnology Assessment, U.S.Congress, May 1988).Smith, W., Strand, J., and Smith, R.,“Social Marketing: Two Approaches toHIV/AIDS Prevention,” presented atTranslating International Experiencesinto National HIV/AIDS PreventionObjectives: Lessons for the Future,conference sponsored by the Henry T.Kaiser Family Foundation, Centers forDisease Control and Prevention, andthe U.S. Agency for InternationalDevelopment, Washington, DC, Oct.20, 1994.St. Louis, M., Conway, G., Hayman,C.,et al., “Human ImmunodeficiencyVirus Infection in DisadvantagedAdolescents,” Journal of the AmericanMedical Association 266(17):2387-2391, 1991, cited in Marin (70).
94.
95.
96.
97.
98.
99.
Stall, R., Elkstrand, M., Pollack, L., etal., “Relapse from Safer Sex: The NextChallenge for AIDS PreventionEfforts,” Journal of Acquired ImmuneDeficiency Syndromes 3: 1181-1187,1990, cited in Coates (10).Stryker, J., Coates, T.J., DeCarlo, P., etal., “Prevention of HIV InfectionLooking Back, Looking Ahead,”Journal of the American MedicalAssociation 273(14):1143-1148, 1995.Stryker, J. and Bayer, R., “AIDSPolicy: Two Divisive Issues,” (letter),Journal of the American MedicalAssociation 270(20):2436, Nov. 24,1993.Thomas, B., Mitchell, A., Devlin, M.,et al., “Small Group Sex Education atSchool: the McMaster Teen Program,”Preventing Adolescent Pregnancy B.Miller, J. Card, R. Paikiff, J. Peterson(eds.) (Newbury Park, CA:SagePublications, 1992), cited in Kirby(59).Tice, J., Allen, S., Serufilira, A., et al.,“Impact of HIV Testing onCondom/Spermicide Use Among HIVDiscordant Couples in Africa,”presented at the Sixth InternationalConference on AIDS, San Francisco,CA, June 23, 1990, cited inZimmerman (120).Tress, S., Abdul-Quader, A. S., Simons,P. S., et al., “Evaluation of a PeerOutreach HIV Prevention Program forFemale Partners of Injecting DrugUsers (IDUs) in New York City(NYC),” presented at the NinthInternational Conference on AIDS,Berlin, Germany, June 6-11, 1993,cited in Ehrhardt (25).
100. Turnock, B.J. and Kelly, C. J.,“Mandatory Premarital Testing forHuman Immunodeficiency Virus,”Journal of the American MedicalAssociation 261:3415-3418, 1989.
101. U.S. Department of Health and HumanServices, Public Health Service, AIDSKnowledge and Attitudes for April-

.
38 The Effectiveness of AIDS Prevention Efforts
103.
104.
105.
106.
107.
Prevention, National Center for HealthStatistics, Health United States, 1994,DHHS Pub. No. (PHS) 95-1232(Hyattsville, MD:1995).U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “Update: Trends in AIDSDiagnosis and Reporting Under theExpanded Surveillance Definition forAdolescents and Adults --UnitedStates, 1993,” Mortality and MorbidityWeekly Report 43(45): 826-831, Nov.,18, 1994.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, National Center forPrevention Services, Division ofHIV/AIDS Prevention, HIV/AIDSSurveillance Report 6(2):1995.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “Update: Trends in AIDSAmong Men Who Have Sex with Men--United States, 1989- 1994,” Mortalityand Morbidity Weekly Report44(21):401-404, June 2, 1995.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “Update: AIDS AmongWomen--United States, 1994,”Mortality and Morbidity WeeklyReport 44(5):81-84, Feb. 10, 1995.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, Background Informationon The Morbidity and MortalityWeekly Report: The Effectiveness ofCondoms Update, Aug. 3, 1993,including “Update: Barrier ProtectionAgainst HIV Infection and OtherSexually Transmitted Diseases,”Mortality and Morbidity WeeklyReport 42(30):589-597, Aug. 6, 1993.
108.
109.
110.
111.
112.
113,
114.
U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “Mammography andClinical Breast Examinations AmongWomen Aged 50 Years and Older--Behavioral Risk Factor SurveillanceSystem, 1992,” Mortality andMorbidity Weekly Report 42(38):737-741, Oct. 1, 1993.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “Surveillance forOccupationally Acquired HIVInfection,” Mortality and MorbidityWeekly Report 41:823-825, 1992.U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, “HIV Prevention Practicesof Primary Care Physicians--U. S.,1992,” Mortality and Morbidity WeeklyReport 42(51-52):988-992, Jan. 7,1994, cited in Zimmerman (120).U.S. Department of Health and HumanServices, Public Health Service,Centers for Disease Control andPrevention, 1992 HIV PreventionProgram Guidance, cited inZimmerman (120).Valdiserri, R. O., Lyter, D. W., Leviton,L.C., et al., “AIDS Prevention inHomosexual and Bisexual Men:Results of a Randomized TrialEvaluating Two Risk-ReductionInterventions,” AIDS 3:21-26, 1989,cited in Coates (10).Vincent, M., Clearie, A., andSchluchter, M.,’’ Reducing AdolescentPregnancy Through School andCommunity-Based Education,”Journal of the American MedicalAssociation 257(24):3382-3386, 1987,cited in Kirby (59).Volger, M., Dugan, T., and Seidlin, M.,“Changes in Sexual and ReproductiveBehavior in Heterosexual CouplesAfter HIV Testing,” presented at the

The Effectiveness of AIDS Prevention Efforts 39
Community-Based Education,” Congress, Washington, DC, SeptemberJournal of the American Medical 1995.Association 257(24):3382-3386, 1987,cited in Kirby (59).
114. Volger, M., Dugan, T., and Seidlin, M.,“Changes in Sexual and ReproductiveBehavior in Heterosexual CouplesAfter HIV Testing,” presented at theFifth International Conference onAIDS, Montreal, Canada, June 5-9,1989, cited in Zimmerman (120).
115. Walter, H.J. and Vaughn, R.D., “AIDSRisk Reduction Among a Multi-EthnicSample of Urban High SchoolStudents,” Journal of the AmericanMedical Association 270(6):725-730,1993, cited in Kirby (59).
116. Warren, W.K. and King, A. J. C.,Development and Evaluation of anAIDS/STD/Sexuality Program forGrade 9 Students, Social ProgramEvaluation Group (Kingston,Canada: 1994), cited in Kirby (59).
117. Weaver, F.J., Herrick, K.L., Ramirez,A.G., et al., “Establishing aCommunity Base for CardiovascularHealth Education Programs,” HealthValues 2:249-256, 1978, cited inZimmerman (120).
118 Winter, L. and Breckenmaker, L. C.,“Tailoring Family Planning Services tothe Special Needs of Adolescents,”Family Planning Perspectives23(1):24-30, January-February, 1991,cited in Kirby (59).
119. Yedidia, M.J., Barr, J. K., and Berry,C. A., “Physicians’ Attitudes TowardAIDS at Different Career stages: AComparison of Internists,” Journal ofHealth and Social Behavior 34:272-284, 1993.
120. Zimmerman, M. A., Pham, C. T., andSteinman, K.J., “HIV/AIDS Education:National Surveys, Counseling andTesting Programs and the Role ofPhysicians,” unpublished contractorreport prepared for the Office ofTechnology Assessment, U.S.

Judy Auerbach, Ph.D.National Institutes of HealthBethesda MD
Lourdes Baezconde-Garbanati, Ph.D.Institute of Preventive ResearchUniversity of Southern California School ofMedicineLos Angeles, CA
Barbara Cambridge, Ph.D.Department of Obstetrics and GynecologyUniversity of Texas Southwestern MedicalCenterDallas, TX
James W. Curran, M.D. M.P.H.Centers for Disease Control and PreventionAtlanta, GA
Theresa Exner, Ph.D.College of Physicians and SurgeonsColumbia UniversityNew York, NY
Nicholas Freudenberg, Dr.Ph.Center on AIDS, Drugs, and Community HealthSchool of Health SciencesHunter CollegeNew York, NY
Robert Fullilove, Ed.D.HIV Center for Clinical and Behavioral StudiesColumbia University School of Public HealthNew York, NY
David HoltgraveCenter for AIDS Intervention ResearchMedical College of WisconsinMilwaukee, WI
ACKNOWLEDGEMENTS
Jeffrey Kelly, Ph.D.Department of PsychiatryMedical College of WisconsinMilwaukee, WI
Ronald KingWhitman-Walker ClinicWashington, DC
David L. Kirp, LL.B.Graduate School of Public PolicyUniversity of California at Berkeley
Len McNally, M.P.H.The New York Community TrustNew York, NY
Walt Odets, Ph.D.Berkeley, CA
Randy PopeMichigan Department of Public HealthLansing, MI
Mark Schuster, MD, PhDSenior Natural Scientist, RANDAssistant Professor of PediatricsUniversity of California at Los Angeles
Jane SilverAmerican Foundation for AIDS ResearchWashington, D.C.
Jeff StrykerCenter for AIDS Prevention StudiesUniversity of California at San Francisco
Ron Valdiserri, M. D., M.P.H.Division of STD and HIV PreventionCenters for Disease Control and PreventionAtlanta, GA