Outcomes of Sublobar Resection Versus Lobectomy for Stage I Non–Small Cell Lung Cancer: A 13Year...
9
GENERAL THORACIC SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS member or an individual non-member subscription to the journal. Outcomes of Sublobar Resection Versus Lobectomy for Stage I Non–Small Cell Lung Cancer: A 13-Year Analysis Amgad El-Sherif, MD, William E. Gooding, MS, Ricardo Santos, MD, Brian Pettiford, MD, Peter F. Ferson, MD, Hiran C. Fernando, MD, Susan J. Urda, BS, James D. Luketich, MD, and Rodney J. Landreneau, MD Department of Surgery, Heart, Lung, and Esophageal Surgery Institute, University of Pittsburgh Medical Center, Biostatistics Facility, and Cancer Registry, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania, and Department of Cardiothoracic Surgery, Boston Medical Center, Boston, Massachusetts Background. The appropriate use of sublobar resection versus lobectomy for stage I non–small cell lung cancer continues to be debated. A long-term analysis of the outcomes of these resections for stage I non–small cell lung cancer in a high-volume tertiary referral university hospital center was performed. Methods. The outcomes of all stage I non–small cell lung cancer patients (n 784) undergoing resection were analyzed from our lung cancer registry from 1990 to 2003. Lobectomy was the standard of care for patients with adequate cardiopulmonary reserve. Sublobar resection was reserved for patients with cardiopulmonary impair- ment prohibiting lobectomy. Predictors of overall sur- vival and disease-free survival were evaluated. Statistical analyses included Kaplan–Meier estimates of survival, log-rank tests of survival differences, and multivariate Cox proportional hazards models. Results. Lobectomy was used for 577 patients and sublobar resection for 207 patients. The median age was 70 years (range, 31 to 107 years). The median follow-up of patients remaining alive was 31 months. Compared with lobectomy, sublobar resection had no significant impact on disease-free survival, with a hazard ratio of 1.20 (95% confidence interval, 0.90 to 1.61; p 0.24). Sublobar resection had a statistically significant association with overall survival when compared with lobectomy, with an increased hazard ratio of 1.39 (95% confidence interval, 1.11 to 1.75; p 0.004). Twenty-eight percent of lobec- tomy patients experienced disease recurrence in that time compared with 29% of the sublobar patients. Seventy- two percent of the recurrences in the lobectomy cohort were distant metastasis versus 52% of the sublobar group recurrences (p 0.0204). Conclusions. Although sublobar resection is thought to be associated with increased incidence of local recur- rence when compared with lobectomy, we found no difference in disease-free survival between the two types of resection for stage IA patients but slightly worse disease-free survival for stage IB. (Ann Thorac Surg 2006;82:408 –16) © 2006 by The Society of Thoracic Surgeons S urgical resection remains the mainstay of therapy for stage I non–small cell lung cancer (NSCLC), provid- ing the best opportunity for cure. The extent of pulmo- nary resection required to achieve complete eradication of the malignancy has been a hotly debated issue [1]. Many patients presenting with resectable early stage disease are unable to tolerate pulmonary resection be- cause of compromised cardiopulmonary function. It has been suggested that more than 20% of patients who are diagnosed with stage I or II NSCLC do not undergo operation because of comorbid health factors [2]. The use of sublobar resection with adequate surgical margins in this setting may provide a comparable survival advan- tage to such patients along with preservation of pulmo- nary function [3]. Additionally, computed tomographic scan surveillance efforts directed to patients with a higher risk for lung cancer have identified small peripheral cancers amena- Accepted for publication Feb 4, 2006. Presented at the Forty-first Annual Meeting of The Society of Thoracic Surgeons, Tampa, FL, Jan 24 –26, 2005. Address correspondence to Dr Landreneau, Division of Thoracic and Fo- regut Surgery, Department of Surgery, Shadyside Medical Bldg, 5200 Centre Ave, Suite 715, Pittsburgh, PA 15232; e-mail: [email protected]. Dr Luketich discloses that he has a financial relation- ship with US Surgical, Stryker and Berchtold. © 2006 by The Society of Thoracic Surgeons 0003-4975/06/$32.00 Published by Elsevier Inc doi:10.1016/j.athoracsur.2006.02.029 GENERAL THORACIC
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Outcomes of Sublobar Resection Versus Lobectomy for Stage I Non–Small Cell Lung Cancer: A 13Year...
OfAABJDFC
vcolh
laLawmvalC
s7p
SinoMdc
A
PS
ArA
©P
GEN
ERA
LT
HO
RA
CIC
GENERAL THORACIC SURGERY:The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org.To take the CME activity related to this article, you must have either an STS member or anindividual non-member subscription to the journal.
utcomes of Sublobar Resection Versus Lobectomyor Stage I Non–Small Cell Lung Cancer: A 13-Yearnalysis
mgad El-Sherif, MD, William E. Gooding, MS, Ricardo Santos, MD,rian Pettiford, MD, Peter F. Ferson, MD, Hiran C. Fernando, MD, Susan J. Urda, BS,
ames D. Luketich, MD, and Rodney J. Landreneau, MDepartment of Surgery, Heart, Lung, and Esophageal Surgery Institute, University of Pittsburgh Medical Center, Biostatisticsacility, and Cancer Registry, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania, and Department of
ardiothoracic Surgery, Boston Medical Center, Boston, Massachusettslocroi1tctwr
brdod
Background. The appropriate use of sublobar resectionersus lobectomy for stage I non–small cell lung cancerontinues to be debated. A long-term analysis of theutcomes of these resections for stage I non–small cellung cancer in a high-volume tertiary referral universityospital center was performed.Methods. The outcomes of all stage I non–small cell
ung cancer patients (n � 784) undergoing resection werenalyzed from our lung cancer registry from 1990 to 2003.obectomy was the standard of care for patients withdequate cardiopulmonary reserve. Sublobar resectionas reserved for patients with cardiopulmonary impair-ent prohibiting lobectomy. Predictors of overall sur-
ival and disease-free survival were evaluated. Statisticalnalyses included Kaplan–Meier estimates of survival,og-rank tests of survival differences, and multivariateox proportional hazards models.Results. Lobectomy was used for 577 patients and
ublobar resection for 207 patients. The median age was0 years (range, 31 to 107 years). The median follow-up of
atients remaining alive was 31 months. Compared withbdoottn
ec
egut Surgery, Department of Surgery, Shadyside Medical Bldg, 5200 Centreve, Suite 715, Pittsburgh, PA 15232; e-mail: [email protected].
2006 by The Society of Thoracic Surgeonsublished by Elsevier Inc
obectomy, sublobar resection had no significant impactn disease-free survival, with a hazard ratio of 1.20 (95%onfidence interval, 0.90 to 1.61; p � 0.24). Sublobaresection had a statistically significant association withverall survival when compared with lobectomy, with anncreased hazard ratio of 1.39 (95% confidence interval,.11 to 1.75; p � 0.004). Twenty-eight percent of lobec-omy patients experienced disease recurrence in that timeompared with 29% of the sublobar patients. Seventy-wo percent of the recurrences in the lobectomy cohortere distant metastasis versus 52% of the sublobar group
ecurrences (p � 0.0204).Conclusions. Although sublobar resection is thought to
e associated with increased incidence of local recur-ence when compared with lobectomy, we found noifference in disease-free survival between the two typesf resection for stage IA patients but slightly worseisease-free survival for stage IB.
(Ann Thorac Surg 2006;82:408–16)
© 2006 by The Society of Thoracic Surgeonsurgical resection remains the mainstay of therapy forstage I non–small cell lung cancer (NSCLC), provid-
ng the best opportunity for cure. The extent of pulmo-ary resection required to achieve complete eradicationf the malignancy has been a hotly debated issue [1].any patients presenting with resectable early stage
isease are unable to tolerate pulmonary resection be-ause of compromised cardiopulmonary function. It has
ccepted for publication Feb 4, 2006.
resented at the Forty-first Annual Meeting of The Society of Thoracicurgeons, Tampa, FL, Jan 24–26, 2005.
ddress correspondence to Dr Landreneau, Division of Thoracic and Fo-
een suggested that more than 20% of patients who areiagnosed with stage I or II NSCLC do not undergoperation because of comorbid health factors [2]. The usef sublobar resection with adequate surgical margins inhis setting may provide a comparable survival advan-age to such patients along with preservation of pulmo-ary function [3].Additionally, computed tomographic scan surveillance
fforts directed to patients with a higher risk for lungancer have identified small peripheral cancers amena-
Dr Luketich discloses that he has a financial relation-
ship with US Surgical, Stryker and Berchtold.0003-4975/06/$32.00doi:10.1016/j.athoracsur.2006.02.029
brts
pesa2csaedisteasptultmNf
M
TBptrUUwm
snah
TCSssent
clpcs
dfrlnr
wpccFclmwc
Fb
Fo
409Ann Thorac Surg EL-SHERIF ET AL2006;82:408–16 SUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC
GEN
ERA
LT
HO
RA
CIC
le to sublobar resection with generous margins of pa-enchymal resection. Many surgeons have questionedhe necessity of total lobectomy for the management ofuch lesions [4–6].
The purpose of this investigation was to evaluate theatterns of recurrence, postoperative morbidity differ-nces, and survival differences between patients withtage I NSCLC treated by either sublobar resection ornatomic lobectomy. This period (from 1990 through003) of surgical experience with stage I NSCLC washosen for analysis as computed tomographic clinicaltaging and follow-up were routinely applied. Addition-lly, this was also a period of increased surgical experi-nce with patients having significant impairment in car-iopulmonary reserve as our group was actively involved
n the initial efforts with minimally invasive thoracicurgery, lung-volume reduction surgery, and the Na-ional Emphysema Treatment Trial [7]. These experi-nces influenced the nature of our lung cancer referral;ccordingly, many patients found to have peripheralmall lung cancers with significant cardiopulmonary im-airment were considered for surgical resection. Many of
hese cancer patients were thought to be at risk fornacceptable pulmonary functional loss associated with
obectomy, and thus sublobar resection was chosen ashe primary resectional therapy. The evaluation of this
ature experience with surgical resection of stage ISCLC by either lobectomy or sublobar resection
ollows.
aterial and Methods
he study was approved by the Institutional Reviewoard at the University of Pittsburgh (IRB 0408110), andatient consent was waived. We retrospectively analyzed
he outcomes of all stage I NSCLC patients undergoingesection between January 1990 and December 2003.sing the data from the Lung Cancer Registry at theniversity of Pittsburgh, 817 patients were identified, ofhom 784 had adequate recurrence and follow-up infor-ation. Lobectomy and mediastinal sampling was the
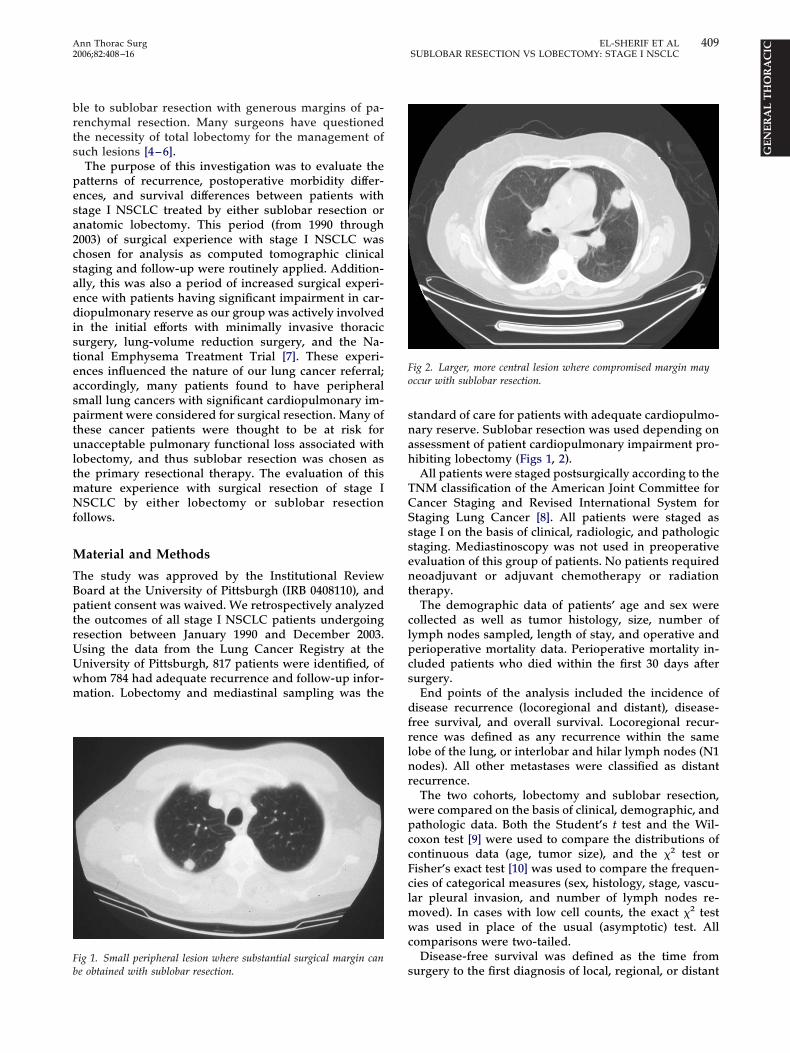
ig 1. Small peripheral lesion where substantial surgical margin can
se obtained with sublobar resection.tandard of care for patients with adequate cardiopulmo-ary reserve. Sublobar resection was used depending onssessment of patient cardiopulmonary impairment pro-ibiting lobectomy (Figs 1, 2).All patients were staged postsurgically according to the
NM classification of the American Joint Committee forancer Staging and Revised International System fortaging Lung Cancer [8]. All patients were staged astage I on the basis of clinical, radiologic, and pathologictaging. Mediastinoscopy was not used in preoperativevaluation of this group of patients. No patients requiredeoadjuvant or adjuvant chemotherapy or radiation
herapy.The demographic data of patients’ age and sex were
ollected as well as tumor histology, size, number ofymph nodes sampled, length of stay, and operative anderioperative mortality data. Perioperative mortality in-luded patients who died within the first 30 days afterurgery.
End points of the analysis included the incidence ofisease recurrence (locoregional and distant), disease-
ree survival, and overall survival. Locoregional recur-ence was defined as any recurrence within the sameobe of the lung, or interlobar and hilar lymph nodes (N1odes). All other metastases were classified as distantecurrence.
The two cohorts, lobectomy and sublobar resection,ere compared on the basis of clinical, demographic, andathologic data. Both the Student’s t test and the Wil-oxon test [9] were used to compare the distributions ofontinuous data (age, tumor size), and the �2 test orisher’s exact test [10] was used to compare the frequen-ies of categorical measures (sex, histology, stage, vascu-ar pleural invasion, and number of lymph nodes re-
oved). In cases with low cell counts, the exact �2 testas used in place of the usual (asymptotic) test. All
omparisons were two-tailed.Disease-free survival was defined as the time from
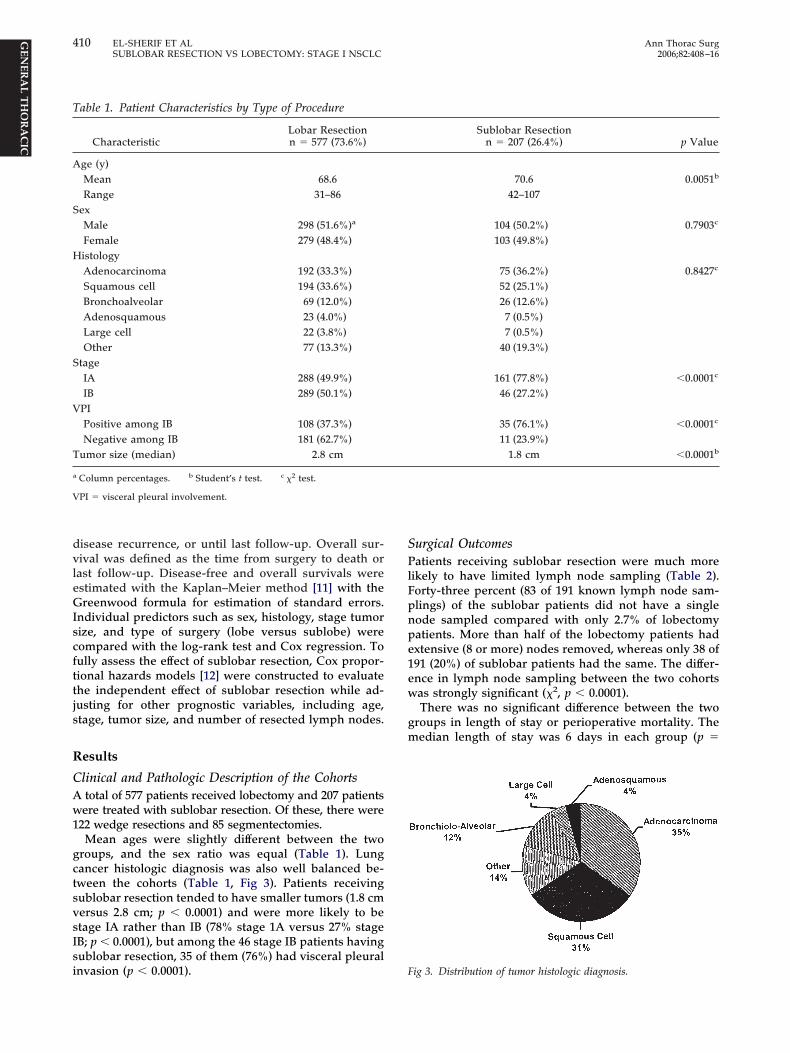
ig 2. Larger, more central lesion where compromised margin mayccur with sublobar resection.
urgery to the first diagnosis of local, regional, or distant
dvleGIscfttjs
R
CAw1
gctsvsIsi
SPlFpnpe1ew
gm
T
A
S
H
S
V
T
a
V
410 EL-SHERIF ET AL Ann Thorac SurgSUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC 2006;82:408–16
GEN
ERA
LT
HO
RA
CIC
isease recurrence, or until last follow-up. Overall sur-ival was defined as the time from surgery to death orast follow-up. Disease-free and overall survivals werestimated with the Kaplan–Meier method [11] with thereenwood formula for estimation of standard errors.
ndividual predictors such as sex, histology, stage tumorize, and type of surgery (lobe versus sublobe) wereompared with the log-rank test and Cox regression. Toully assess the effect of sublobar resection, Cox propor-ional hazards models [12] were constructed to evaluatehe independent effect of sublobar resection while ad-usting for other prognostic variables, including age,tage, tumor size, and number of resected lymph nodes.
esults
linical and Pathologic Description of the Cohortstotal of 577 patients received lobectomy and 207 patientsere treated with sublobar resection. Of these, there were
22 wedge resections and 85 segmentectomies.Mean ages were slightly different between the two
roups, and the sex ratio was equal (Table 1). Lungancer histologic diagnosis was also well balanced be-ween the cohorts (Table 1, Fig 3). Patients receivingublobar resection tended to have smaller tumors (1.8 cmersus 2.8 cm; p � 0.0001) and were more likely to betage IA rather than IB (78% stage 1A versus 27% stageB; p � 0.0001), but among the 46 stage IB patients havingublobar resection, 35 of them (76%) had visceral pleural
able 1. Patient Characteristics by Type of Procedure
CharacteristicLobar Resectionn � 577 (73.6%)
ge (y)Mean 68.6Range 31–86
exMale 298 (51.6%)a
Female 279 (48.4%)istologyAdenocarcinoma 192 (33.3%)Squamous cell 194 (33.6%)Bronchoalveolar 69 (12.0%)Adenosquamous 23 (4.0%)Large cell 22 (3.8%)Other 77 (13.3%)
tageIA 288 (49.9%)IB 289 (50.1%)
PIPositive among IB 108 (37.3%)Negative among IB 181 (62.7%)
umor size (median) 2.8 cm
Column percentages. b Student’s t test. c �2 test.
PI � visceral pleural involvement.
nvasion (p � 0.0001). F
urgical Outcomesatients receiving sublobar resection were much more
ikely to have limited lymph node sampling (Table 2).orty-three percent (83 of 191 known lymph node sam-lings) of the sublobar patients did not have a singleode sampled compared with only 2.7% of lobectomyatients. More than half of the lobectomy patients hadxtensive (8 or more) nodes removed, whereas only 38 of91 (20%) of sublobar patients had the same. The differ-nce in lymph node sampling between the two cohortsas strongly significant (�2, p � 0.0001).There was no significant difference between the two
roups in length of stay or perioperative mortality. Theedian length of stay was 6 days in each group (p �
Sublobar Resectionn � 207 (26.4%) p Value
70.6 0.0051b
42–107
104 (50.2%) 0.7903c
103 (49.8%)
75 (36.2%) 0.8427c
52 (25.1%)26 (12.6%)7 (0.5%)7 (0.5%)
40 (19.3%)
161 (77.8%) �0.0001c
46 (27.2%)
35 (76.1%) �0.0001c
11 (23.9%)1.8 cm �0.0001b
ig 3. Distribution of tumor histologic diagnosis.

0lr
DAd(ayTdsfgdwrp
dtsotpsgii0cd
pgc2
sepodai(mddttwps
OWm5s5Fooi(hnocnntarrhstwt
T
LST
a
T
DLRDT
a
T
ASSLSVVN
a
C
411Ann Thorac Surg EL-SHERIF ET AL2006;82:408–16 SUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC
GEN
ERA
LT
HO
RA
CIC
.1149, Wilcoxon test). The perioperative mortality for theobectomy group was 2.6% versus 1.4% for the sublobaresection group (p � 0.42, Fisher’s exact test).
isease-Free Survivalll 784 patients were followed until disease recurrence oreath or until loss of follow-up in the tumor registry
Table 3). The median follow-up for patients who werelive and were disease-free at their last review was 2.7ears, with a range of less than 1 month to 14 years.wenty-eight percent of lobectomy patients experiencedisease recurrence in that time compared with 29% of theublobar patients. Although the proportion of patientsound with disease recurrence was the same in bothroups, there is a suggestion that the recurrence patternsiffer, as 72% of the recurrences in the lobectomy cohortere distant metastasis versus 52% of the sublobar group
ecurrences. This difference was significant (exact �2 test,� 0.0204).Sublobar resection was evaluated for association with
isease-free survival along with age, sex, histology, stage,umor size, visceral pleural invasion, and number ofample lymph nodes. Of these, tumor size as a continu-us variable and stage were the only significant predic-ors (Table 4). Because visceral pleural invasion was not aredictive factor, disease stage was substituted for tumorize. Table 4 shows individual proportional hazards re-ression coefficients and confidence intervals for these
ndividual covariates. Stage IB conferred a 50% increasen the risk of disease recurrence (hazard ratio, 1.51; p �.0023). The estimated hazard ratio for sublobar resectionompared with lobectomy was 1.20, with a 95% confi-ence interval of 0.90 to 1.61.The hazard ratios were also estimated with joint pro-
ortionate hazards models that included stage and sur-ery type. The hazard ratio for sublobar resection in-reased to 1.64, with a 95% confidence interval of 1.25 to.17. On further analysis this increase in risk as a result of
able 2. Number of Nodes Sampled by Type of Surgerya
Type of Surgery
Number of Nodes Sampled
Total0 1 2–7 8 or more
obectomy 14 12 186 303 515ublobar resection 83 23 47 38 191otal 97 35 233 341 706
�2 p � 0.0001.
able 3. Disease Recurrences
Recurrence Lobar Resection Sublobar Resection
isease-free 415 (71.9%)a 147 (71.0%)ocal 24 (4.2%) 15 (7.2%)egional 22 (3.8%) 14 (6.8%)istant 116 (20.0%) 31 (15.0%)otal 577 207
fColumn percentages.
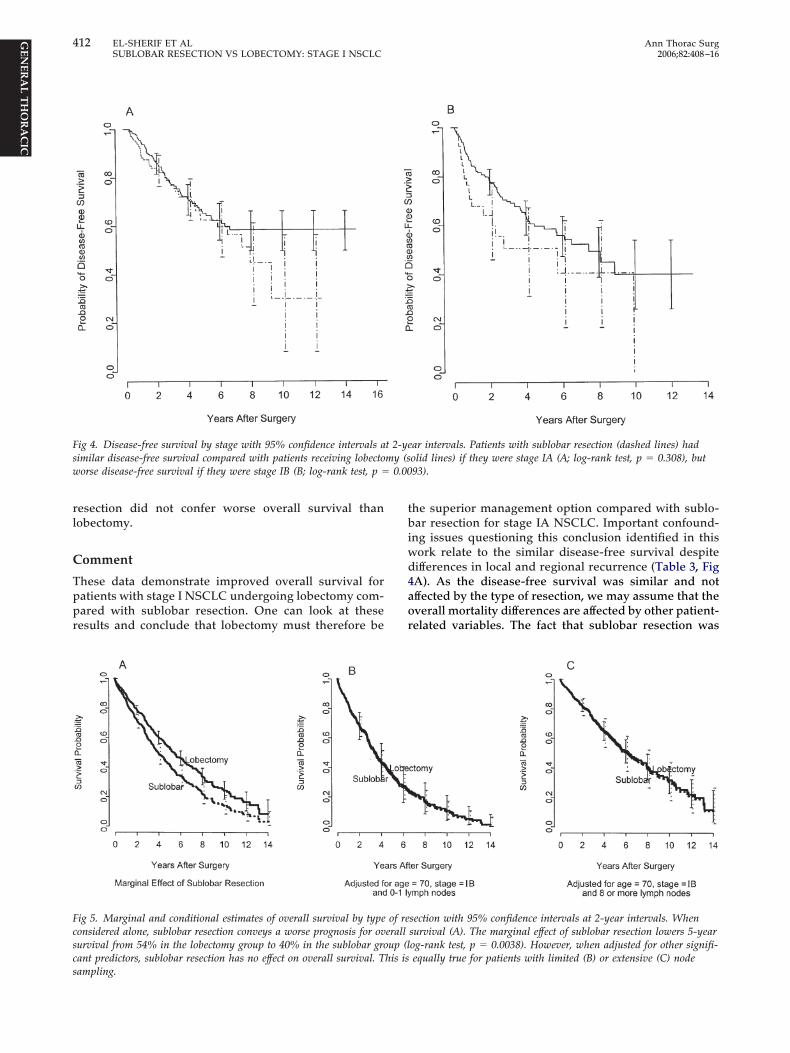
ublobar resection was caused solely by the greater thanxpected number of recurrences among the 46 stage IBatients with sublobar resection. To illustrate the effectsf sublobar resection by stage, Kaplan–Meier plots ofisease-free survival are shown in Figure 4 for stages IAnd IB. As shown in Figure 4A, stage IA patients haddentical disease-free survival in both cohorts for 7 yearslog-rank test, p � 0.308). Stage IB patients, although
ore likely to have lobectomy, did exhibit slightly worseisease-free survival after sublobar resection, with anecrease in 5-year disease-free survival from 58% (lobec-
omy) to 50% (sublobar, log-rank test, p � 0.0093). Thus,he risk of recurrence for sublobar resection in our cohortas equivalent to that of lobectomy among stage IAatients but slightly worse among the small number oftage IB patients with sublobar resection.
verall Survivalith a median follow-up for surviving patients of 31onths, the cohort had a 5-year probability of survival of
1%. Sublobar resection was a strong predictor of overallurvival with a decreased 5-year survival of 40% versus4% for the lobectomy group (log-rank test, p � 0.0038;ig 5A). Age and number of lymph nodes also predictedverall survival. Hazard ratios for individual predictors ofverall survival are shown in Table 5. Owing to the
mbalance in lymph node removal between cohortsfewer nodes with sublobar resection), we estimated theazard ratios for resection type adjusting for age andumber of nodes, which were strongly associated withverall survival, and stage, which was only weakly asso-iated. As shown on Figure 5B and 5C, when simulta-eously adjusting for age, stage, and number of lymphodes, overall survival for lobectomy and sublobar resec-
ion was equivalent. Limited or no lymph node samplingppears to be a much stronger predictor than sublobaresection, such that when adjusting for the number ofesampled lymph nodes, patients with sublobar resectionad equivalent overall survival as lobectomy patients. Inummary, patients selected for sublobar resection tendedo be slightly older and to have limited node sampling,hich is a proxy variable for undocumented comorbidi-
ies that adversely affect overall health. When adjusting
able 4. Individual Predictors of Disease-Free Survival
Covariate Hazard Ratio 95% CI p Value
ge 1.00 0.85–1.19 0.9809tage IA reftage IB 1.51 1.16–1.97 0.0023obectomy refublobar resection 1.20 0.90–1.61 0.2429PI noa refPI yesa 1.0 0.68–1.48 0.998o. of nodes 1.08 0.93–1.25 0.341
VPI analysis limited to 335 stage IB patients.
I � confidence interval; VPI � vascular plueral invasion.
or the limited node sampling and for age, sublobar
rl
C
Tppr
tbiwd4aor
Fsw 0.00
Fcscs
412 EL-SHERIF ET AL Ann Thorac SurgSUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC 2006;82:408–16
GEN
ERA
LT
HO
RA
CIC
esection did not confer worse overall survival thanobectomy.
omment
hese data demonstrate improved overall survival foratients with stage I NSCLC undergoing lobectomy com-ared with sublobar resection. One can look at theseesults and conclude that lobectomy must therefore be
ig 4. Disease-free survival by stage with 95% confidence intervals aimilar disease-free survival compared with patients receiving lobectoorse disease-free survival if they were stage IB (B; log-rank test, p �
ig 5. Marginal and conditional estimates of overall survival by typeonsidered alone, sublobar resection conveys a worse prognosis for ovurvival from 54% in the lobectomy group to 40% in the sublobar groant predictors, sublobar resection has no effect on overall survival. T
ampling.he superior management option compared with sublo-ar resection for stage IA NSCLC. Important confound-
ng issues questioning this conclusion identified in thisork relate to the similar disease-free survival despiteifferences in local and regional recurrence (Table 3, FigA). As the disease-free survival was similar and notffected by the type of resection, we may assume that theverall mortality differences are affected by other patient-elated variables. The fact that sublobar resection was
ar intervals. Patients with sublobar resection (dashed lines) hadolid lines) if they were stage IA (A; log-rank test, p � 0.308), but93).
section with 95% confidence intervals at 2-year intervals. Whensurvival (A). The marginal effect of sublobar resection lowers 5-yearog-rank test, p � 0.0038). However, when adjusted for other signifi-equally true for patients with limited (B) or extensive (C) node
t 2-yemy (s
of reerallup (l
his is

eslcc
bswl
faaippiohcswDcgs(elttsEicasEpay
srddb
rlafswisbihstisol
smdpri0tfciFsaaldtpp
siertgMbNsfaa
T
ASSLSVV802
a
C
413Ann Thorac Surg EL-SHERIF ET AL2006;82:408–16 SUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC
GEN
ERA
LT
HO
RA
CIC
xclusively used by the operating surgeon to managetage I NSCLC patients thought to be poor candidates forobectomy because of cardiopulmonary physiologic con-erns can explain a possible greater risk of death fromomorbid diseases during follow-up.
Although we could not study this difference in comor-id conditions between the two groups given the retro-pective analysis and the limitations of the lung registry,e can only speculate based on our standard approach of
obectomy for stage I disease in patients with good risk.This effect of comorbid disease in evaluating survival
rom coronary artery disease has been recently analyzednd emphasized by a group from Duke [13]. In thisnalysis of coronary artery disease survival, the survivalnfluence of comorbidities such as chronic obstructiveulmonary disease or peripheral vascular disease in 1,471atients was equivalent to poor left ventricular function
n affecting patient survival. The effect of comorbidity onlder lung cancer patients’ survival after lung resectionas also been documented in a report by Birim andoworkers [14]. The authors assessed the risk factors ofurvival in 126 consecutive patients with NSCLC whoere older than 70 years of age and underwent resection.uring a period of 12 years, the patient survival was
ompared with the yearly expected survival rates of theeneral population. The study showed a 5- and 10-yearurvival rate of 37% and 15%, respectively. Smokingodds ratio, 2.3) and chronic obstructive pulmonary dis-ase (odds ratio, 2.1) were identified as risk factors forong-term survival. The observed survival was lower thanhe expected survival related to the natural history ofheir comorbid disease and the patient age. The recentubanalysis of the medical treatment arm of the Nationalmphysema Treatment Trial further emphasized the
mportance of the natural history of moderate to severehronic obstructive pulmonary disease [7]. The mortalitymong patients with predominant upper lobe emphy-ema and poor exercise tolerance was 34% at 2 years.ven among patients with the least chronic obstructiveulmonary disease limitations (lower lobe predominancend good exercise tolerance), the mortality was 13% at 2
able 5. Individual Predictors of Overall Survival
Covariate Hazard Ratio 95% CI p Value
ge 1.35 1.18–1.55 �0.0001tage IA reftage IB 1.18 0.96–1.45 0.124obectomy refublobar resection 1.39 1.11–1.75 0.0049PI noa refPI yesa 1.16 0.84–1.61 0.373� lymph nodes ref–1 lymph nodes 1.97 1.51–2.58 �0.0001–7 lymph nodes 1.02 0.71–1.31 0.907
VPI analysis limited to 335 stage IB patients.
I � confidence interval; VPI � vascular plueral invasion.
ears. t
The possible effect of erroneous “understaging” of aignificant number of the patients undergoing sublobaresection related to the thoracic lymph node samplingifferences observed in this study could have also led toisparate survival results between lobectomy and sublo-ar resection patients.The Lung Cancer Study Group conducted the only
andomized study comparing sublobar resection withobectomy for stage IA NSCLC patients [15]. Importantly,ll patients considered for the study had to be consideredunctional candidates for lobectomy if necessary. In thistudy, the intraoperative nodal staging requirementsere limited to sampling a single mediastinal, hilar and
nterlobar node before randomization to the mode ofurgical resection. Distant recurrence rate was unaffectedy the method of resection used. There was no difference
n hospital mortality between the two groups of patients;owever, patients who underwent lobectomies did haveignificantly more postoperative pulmonary complica-ions requiring mechanical ventilatory support. A signif-cant threefold increase in local recurrence was seen withublobar resection; however, there was no difference inverall survival or cancer-related survival between sub-
obar resection and lobectomy.Although all patients in this report were staged as
tage I on the basis of pathologic staging, we think thereay be an artificial tumor understaging of patients un-
ergoing sublobar resection as a consequence of dispro-ortionate dissection between lobectomy and sublobaresection techniques. Our analysis showed a 2% decreasen the risk of dying for every node that was resected (p �.0075); this resulted in a bias in survival favoring lobec-omy. Our results are consistent with the recent datarom the ACOSOG (American College of Surgeons On-ology Group) Z0030 trial presented at the Annual Meet-ng of The Society of Thoracic Surgeons in Tampa,lorida, in January 2005, and published in 2006 [16]. Thistudy included 1,111 randomized patients undergoingnatomic resection of stage I NSCLC. The report showed4% increase in number of positive lymph nodes when
ymph node sampling was compared with lymph nodeissection. Interestingly, an 18% stage shift from stage I
o stage II and III was seen when one compares thereoperative clinical staging to the intraoperative orostoperative pathologic staging.Recent investigations from Japan comparing extended
egmentectomy with thorough thoracic lymph node stag-ng for small peripheral stage I lesions have reportedquivalent survival to that of lobectomy [17]. Theseeports may be considered an expected consequence tohe lung cancer computed tomographic screening pro-rams begun in that country more than a decade ago.any thoracic surgeons began to selectively use sublo-
ar resection as the primary therapy for small peripheralSCLC in lieu of lobectomy. An interesting report of
ublobar management of small peripheral NSCLC camerom Swanson and coworkers [18] and Mery and associ-tes [19]. These investigators reported their experiencemong patients undergoing wedge resection as primary
herapy for subcentimeter peripheral lung cancers.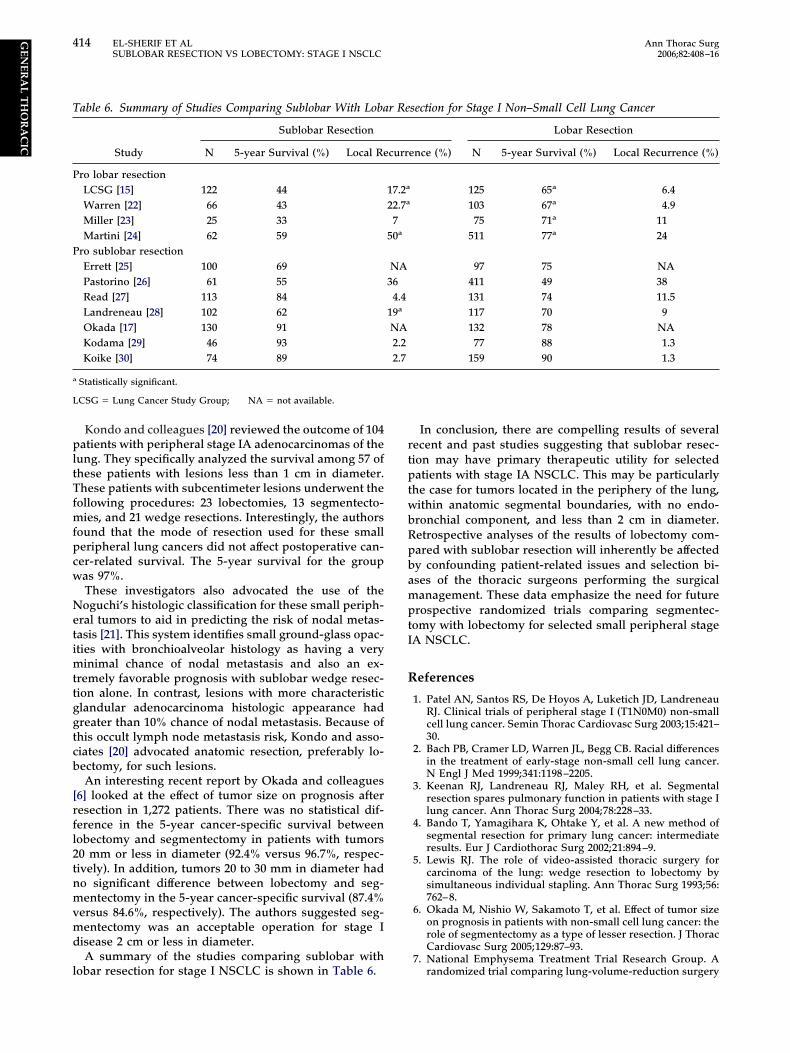
pltTfmfpcw
Netimttggtcb
[rfl2tnmvmd
l
rtptwbRpbamptI
R
T
P
P
a
L
414 EL-SHERIF ET AL Ann Thorac SurgSUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC 2006;82:408–16
GEN
ERA
LT
HO
RA
CIC
Kondo and colleagues [20] reviewed the outcome of 104atients with peripheral stage IA adenocarcinomas of the
ung. They specifically analyzed the survival among 57 ofhese patients with lesions less than 1 cm in diameter.hese patients with subcentimeter lesions underwent the
ollowing procedures: 23 lobectomies, 13 segmentecto-ies, and 21 wedge resections. Interestingly, the authors
ound that the mode of resection used for these smalleripheral lung cancers did not affect postoperative can-er-related survival. The 5-year survival for the groupas 97%.These investigators also advocated the use of theoguchi’s histologic classification for these small periph-
ral tumors to aid in predicting the risk of nodal metas-asis [21]. This system identifies small ground-glass opac-ties with bronchioalveolar histology as having a very
inimal chance of nodal metastasis and also an ex-remely favorable prognosis with sublobar wedge resec-ion alone. In contrast, lesions with more characteristiclandular adenocarcinoma histologic appearance hadreater than 10% chance of nodal metastasis. Because ofhis occult lymph node metastasis risk, Kondo and asso-iates [20] advocated anatomic resection, preferably lo-ectomy, for such lesions.An interesting recent report by Okada and colleagues
6] looked at the effect of tumor size on prognosis afteresection in 1,272 patients. There was no statistical dif-erence in the 5-year cancer-specific survival betweenobectomy and segmentectomy in patients with tumors0 mm or less in diameter (92.4% versus 96.7%, respec-ively). In addition, tumors 20 to 30 mm in diameter hado significant difference between lobectomy and seg-entectomy in the 5-year cancer-specific survival (87.4%
ersus 84.6%, respectively). The authors suggested seg-entectomy was an acceptable operation for stage I
isease 2 cm or less in diameter.A summary of the studies comparing sublobar with
able 6. Summary of Studies Comparing Sublobar With Loba
Study
Sublobar Resection
N 5-year Survival (%) Local Re
ro lobar resectionLCSG [15] 122 44Warren [22] 66 43Miller [23] 25 33Martini [24] 62 59
ro sublobar resectionErrett [25] 100 69Pastorino [26] 61 55Read [27] 113 84Landreneau [28] 102 62Okada [17] 130 91Kodama [29] 46 93Koike [30] 74 89
Statistically significant.
CSG � Lung Cancer Study Group; NA � not available.
obar resection for stage I NSCLC is shown in Table 6.
In conclusion, there are compelling results of severalecent and past studies suggesting that sublobar resec-ion may have primary therapeutic utility for selectedatients with stage IA NSCLC. This may be particularly
he case for tumors located in the periphery of the lung,ithin anatomic segmental boundaries, with no endo-ronchial component, and less than 2 cm in diameter.etrospective analyses of the results of lobectomy com-ared with sublobar resection will inherently be affectedy confounding patient-related issues and selection bi-ses of the thoracic surgeons performing the surgicalanagement. These data emphasize the need for future
rospective randomized trials comparing segmentec-omy with lobectomy for selected small peripheral stageA NSCLC.
eferences
1. Patel AN, Santos RS, De Hoyos A, Luketich JD, LandreneauRJ. Clinical trials of peripheral stage I (T1N0M0) non-smallcell lung cancer. Semin Thorac Cardiovasc Surg 2003;15:421–30.
2. Bach PB, Cramer LD, Warren JL, Begg CB. Racial differencesin the treatment of early-stage non-small cell lung cancer.N Engl J Med 1999;341:1198–2205.
3. Keenan RJ, Landreneau RJ, Maley RH, et al. Segmentalresection spares pulmonary function in patients with stage Ilung cancer. Ann Thorac Surg 2004;78:228–33.
4. Bando T, Yamagihara K, Ohtake Y, et al. A new method ofsegmental resection for primary lung cancer: intermediateresults. Eur J Cardiothorac Surg 2002;21:894–9.
5. Lewis RJ. The role of video-assisted thoracic surgery forcarcinoma of the lung: wedge resection to lobectomy bysimultaneous individual stapling. Ann Thorac Surg 1993;56:762–8.
6. Okada M, Nishio W, Sakamoto T, et al. Effect of tumor sizeon prognosis in patients with non-small cell lung cancer: therole of segmentectomy as a type of lesser resection. J ThoracCardiovasc Surg 2005;129:87–93.
7. National Emphysema Treatment Trial Research Group. A
section for Stage I Non–Small Cell Lung Cancer
Lobar Resection
ence (%) N 5-year Survival (%) Local Recurrence (%)
125 65a 6.4103 67a 4.975 71a 11
511 77a 24
97 75 NA411 49 38131 74 11.5117 70 9132 78 NA
77 88 1.3159 90 1.3
r Re
curr
17.2a
22.7a
750a
NA364.4
19a
NA2.22.7
randomized trial comparing lung-volume-reduction surgery

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
D
Diytyg
D1rtofisrabcrto
Dpa
415Ann Thorac Surg EL-SHERIF ET AL2006;82:408–16 SUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC
GEN
ERA
LT
HO
RA
CIC
with medical therapy for severe emphysema. N Engl J Med2003;348:2059–73.
8. Mountain CF. Revisions in the International System forStaging Lung Cancer. Chest 1997;111:1710–7.
9. Daniel WW. Applied nonparametric statistics. Second Edi-tion. Boston: PWS-KENT, 1990:150–5.
0. Mehta CR, Patel NR. A network algorithm for the exacttreatment of Fisher’s exact test in RxC contingency tables.J Am Stat Assoc 1983;78:427–34.
1. Kaplan E, Meier P. Non-parametric estimation from incom-plete observations. J Am Stat Assoc 1958;53:457–81.
2. Peto R, Peto J. Asymptotically efficient rank invariant proce-dures (with discussion). J R Stat Soc Series A 1972;135:185–207.
3. Sachdev M, Sun JL, Tsiatis AA, Nelson CL, Mark DB, JollisJG. The prognostic importance of co-morbidity for mortalityin patients with stable coronary artery disease. J Am CollCardiol 2004;43:576–82.
4. Birim O, Zuydendorp HM, Maat AP, Kappetein AP, Eijke-mans MJ, Bogers AJ. Lung resection for non-small-cell lungcancer in patients older than 70: mortality, morbidity, andlate survival compared with the general population. AnnThorac Surg 2003;76:1796–801.
5. Ginsberg RJ, Rubinstein LV, for the Lung Cancer StudyGroup. Randomized trial of lobectomy versus limited resec-tion for T1 N0 non-small cell lung cancer. Ann Thorac Surg1995;60:615–23.
6. Allen MS, Darling GE, Pechet TT, et al. Morbidity andmortality of major pulmonary resections in patients withearly-stage lung cancer: initial results of the randomized,prospective ACOSOG Z0030 trial. Ann Thorac Surg 2006;81:1013–20.
7. Okada M, Yoshikawa K, Hatta T, Tsubota N. Is segmentec-tomy with lymph node assessment an alternative to lobec-tomy for non-small cell lung cancer of 2 cm or smaller? AnnThorac Surg 2001;71:956–61.
8. Swanson SJ, Jaklitsch MT, Mentzer SJ, Bueno R, LukanichJM, Sugarbaker DJ. Management of the solitary pulmonarynodule: role of thoracoscopy in diagnosis and therapy. Chest
1999;116(Suppl):523S–4S.bout a third as many as the lobectomy patients, and I’m
wat
pcphtslr
Dspiplvas
ma
9. Mery CM, Pappas AN, Burt BM, et al. Diameter of non-smallcell lung cancer correlates with long-term survival: implica-tions for T stage. Chest 2005;128:3255–60.
0. Kondo D, Yamada K, Kitayama Y, Hoshi S. Peripheral lungadenocarcinomas: 10 mm or less in diameter. Ann ThoracSurg 2003;76:350–5.
1. Noguchi M, Morikawa A, Kawasaki M, et al. Small adeno-carcinoma of the lung. Cancer 1995;75:2844–52.
2. Warren WH, Faber LP. Segmentectomy versus lobectomy inpatients with stage I pulmonary carcinoma. J Thorac Cardio-vasc Surg 1994;107:1087–94.
3. Miller DL, Rowland CM, Deschamps C, et al. Surgicaltreatment of non-small cell lung cancer 1 cm or less indiameter. Ann Thorac Surg 2002;73:1545–51.
4. Martini N, Bains MS, Burt ME, et al. Incidence of localrecurrence and second primary tumors in resected stage Ilung cancer. J Thorac Cardiovasc Surg 1995;109:120–9.
5. Errett LE, Wilson J, Chiu RC-J, Munro DD. Wedge resectionas an alternative procedure for peripheral bronchogeniccarcinomas in poor-risk patients. J Thorac Cardiovasc Surg1985;90:656–61.
6. Pastorino U, Valente M, Bedini V, Infante M, Tavecchio L,Ravasi G. Limited resection of stage I lung cancer. Eur J SurgOncol 1991;17:42–6.
7. Read RC, Yoder G, Schaeffer RC. Survival after conservativeresection for T1N0M0 non-small cell lung cancer. Ann Tho-rac Surg 1990;49:242–7.
8. Landreneau RJ, Sugarbaker DJ, Mack MJ, Hazelrigg SR, et al.Wedge resection versus lobectomy for stage I (T1 N0 M0)non-small-cell lung cancer. J Thorac Cardiovasc Surg 1997;113:691–700.
9. Kodama K, Doi O, Higashiyama M, Yokouchi H. Intentionallimited resection for selected patients with T1 N0 M0 non-small cell lung cancer: a single-institution study. J ThoracCardiovasc Surg 1997;114:347–53.
0. Koike T, Yamato Y, Yoshiya K, Shimoyama T, Suzuki R.Intentional limited pulmonary resection for peripheral T1N0 M0 small-sized lung cancer. J Thorac Cardiovasc Surg
2003;125:924–8.ISCUSSION
R SCOTT J. SWANSON (New York, NY): That was a verynteresting paper. I wonder if you can clarify a point for me. Didou show that the local recurrence was similar until 10 years andhen it diverged, and if that’s true, can you explain that? Also, ifou understaged the patients, why wouldn’t you expect to see areater local recurrence in the sublobar resection group?
R EL-SHERIF: Thank you, Dr Swanson, we analyzed the0-year follow-up period as a means of evaluating overallecurrence. Accordingly, we did not find a difference betweenhe sublobar resection and lobectomy groups with regard toverall tumor recurrence. Most local recurrences will be identi-ed within the first 2 years after resection. The relative under-taging seen between lobectomy and sublobar resection patientselated to the difference in lymph node yield may confound theccuracy in comparing tumor recurrence. This would potentiallyias against the sublobar resection patients who had signifi-antly fewer lymph nodes sampled as a group. These sublobaresection patients also were physiologically more impaired thanhe lobectomy patients, which would also potentially affect theverall survival time owing to death from unrelated disease.
R FRANK C. DETTERBECK (Chapel Hill, NC): I was sur-rised by the number of sublobar resections you had. It was
ondering what your criteria for poor cardiopulmonary reservere that preclude lobectomy. They seem to be fairly liberal, Ihink.
Secondly, I think that in comparing the patients, what wouldrobably be best is if you could compare the same patients bylinical stage and tumor size, in other words, clinical stage I,eripheral 2-cm tumor, in both groups as opposed to what weave here, which are probably discrepant stages and, of course,
he whole issue of the accuracy of your postoperative pathologictaging, which is obviously different in the two groups. So if youook at clinical staging, can you give us a subset of your lobeesection patients and compare those two groups?
R EL-SHERIF: Thank you, Dr Detterbeck, our standard ofurgical care for the good risk stage I non–small cell lung canceratient was lobectomy during the entire period reviewed for this
nvestigation. However, we do see many patients with poorreoperative functional reserve for whom we do not recommend
obectomy but who could potentially obtain an important sur-ival advantage with a sublobar resection that they could toler-te. The criteria to utilize sublobar resection was variable amongurgeons in our group.
There were multiple factors affecting the decision to recom-end sublobar resection. The patient’s pulmonary function was
primary determinant for many patients; however, other im-
pat
rtf
Dbymtcif
te
D
DlssW
Dr
O
ETrcuTdt
itwwiiWevW
416 EL-SHERIF ET AL Ann Thorac SurgSUBLOBAR RESECTION VS LOBECTOMY: STAGE I NSCLC 2006;82:408–16
©P
GEN
ERA
LT
HO
RA
CIC
ortant medical comorbidities and advanced patient age werelso important variables leading to the decision to perform lesshan lobectomy for these stage I lung cancer patients.
We did not look at the patterns of recurrence betweenesection groups among patients with small, less than 2-cmumors. We will be investigating this subset of patients in theuture.
R SUDISH C. MURTHY (Cleveland, OH): This is just to getack to Dr Swanson’s question. You must be careful whenou’re comparing a group of very high-risk patients from aedical standpoint to a group of more fit patients. Because of
his type of analysis, you often have to normalize the data for theompeting risk of non-cancer death (which is likely much highern the patients undergoing limited resection). By not accounting
nline Discussion Forum
eb site.
A
Ra
GVPM
TTUP5SPFe
2006 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ion. This is just a suggestion for your additional analyses. Injoyed your presentation.
R EL-SHERIF: You are absolutely correct.
R DAVID RICE (Houston, TX): You alluded to the Japaneseiterature, and I think a point that I would make is that aignificant number of patients in these trials have very early-tage bronchoalveolar cancer (BAC) or ground-glass opacities.
hat was the percentage of BAC in both groups in your study?
R EL-SHERIF: Twelve percent, without a differential betweenesection groups.
or this, you may be overestimating the impact of your interven- DR RICE: Thank you.
ach month, we select an article from the The Annals ofhoracic Surgery for discussion within the Surgeon’s Fo-um of the CTSNet Discussion Forum Section. The arti-les chosen rotate among the six dilemma topics coverednder the Surgeon’s Forum, which include: Generalhoracic Surgery, Adult Cardiac Surgery, Pediatric Car-iac Surgery, Cardiac Transplantation, Lung Transplan-
ation, and Aortic and Vascular Surgery.Once the article selected for discussion is published
n the online version of The Annals, we will post a no-ice on the CTSNet home page (http://www.ctsnet.org)ith a FREE LINK to the full-text article. Readersishing to comment can post their own commentary
n the discussion forum for that article, which will benformally moderated by The Annals Internet Editor.
e encourage all surgeons to participate in this inter-sting exchange and to avail themselves of the otheraluable features of the CTSNet Discussion Forum and
For August, the article chosen for discussion under thedult Cardiac Dilemma Section of the Discussion forum is:
eduction Ascending Aortoplasty: Midterm Follow-Upnd Predictors of Redilatation
ianluca Polvani, MD, Fabio Barili, MD, Luca Dainese, MD,eli K. Topkara, MD, Faisal H. Cheema, MD, Eleonoraenza, MD, Sandro Ferrarese, MD, Alessandro Parolari,D, PhD, Francesco Alamanni, MD, and Paolo Biglioli, MD
om R. Karl, MDhe Annals Internet EditorCSF Children’s Hospitalediatric Cardiac Surgical Unit05 Parnassus Ave, Room S-549an Francisco, CA 94143-0118hone: (415) 476-3501ax: (212) 202-3622
-mail: [email protected]Ann Thorac Surg 2006;82:416 • 0003-4975/06/$32.00