
Anaesthetic considerations for interventional neuroradiology

CO-INFECTIONS (MA JACOBSON, SECTION EDITOR)
Oral Health Considerations in HIV-Infected Children
Francisco J. Ramos-Gomez & Morenike Oluwatoyin Folayan
Published online: 11 June 2013# Springer Science+Business Media New York 2013
Abstract Children with the human immunodeficiency virus(HIV) have a higher probability of hard and soft oral tissuediseases because of their compromised immune systems andsocioeconomic factors such as poor access to medical anddental care and limited availability of fluoridated water ortoothpaste. To improve health outcomes and help monitorthe progression of HIV, a preventive, child-specific oralhealth protocol for children with HIV that is easy to useand appropriate for all different resource settings should beestablished. Further, both medical and dental health practi-tioners should incorporate such a protocol into their careroutine for HIV-infected children. Using proactive oralhealth risk assessments complemented by scheduledfollow-up visits based on individual risk determination canprevent opportunistic infection, track the HIV disease tra-jectory, and monitor the effectiveness of highly active anti-retroviral therapy (HAART) while improving the quality oflife and longevity of children living with HIV.
Keywords Pediatrics . Oralhealth .HIV .Oralmanifestations .
Co-infections . HIV-infected children . Early childhood caries(ECC) . Cariesmanagement by risk assessment (CAMBRA)
Introduction
Globally, estimates show that 34 million people are livingwith the human immunodeficiency virus (HIV), including3.3 million children under the age of 15 [1•, 2•]. Of all newHIV infections among adults and children in 2011, 71 %
were from sub-Saharan Africa, totaling 90 % of prevalenceworldwide [1•, 2•]. In 2010, African Americans comprised12 % of the U.S. population but represented 44 % of newHIV infections [3]. Hispanic Americans were also dispro-portionately affected; although they made up only 16 % ofthe total U.S. population in 2010, they accounted for 21 %of new HIV infections that year [3]. In the U.S., the minorityof HIV cases are among children—a mere 15 of the 32,052cases in 2011 [2•].
The epidemiologic profile of early childhood caries(ECC), the single most common infectious, yet highly pre-ventable, disease among children, is very similar in HIV-infected and uninfected children. While there is evidenceindicating a global decline in caries for adults and olderchildren, it has increased in children under 5 years of age[4] primarily due to the lack of introduction of early andongoing effective interventions including systemic and top-ical fluorides, sealants, improved diet, oral health education,and dental care—all interventions highly endorsed by theAmerican Academy of Pediatricians (AAP) and theAmerican Academy of Pediatric Dentists (AAPD) [5, 6•].However, despite these improvements, ECC remains themost prevalent oral disease in much of Asia, Africa, andLatin America. In the U.S., it affects 60 %–90 % of children[7••], with children from poor homes twice as likely to beaffected by ECC when compared with their more affluentpeers. Furthermore, these low income, underserved childrenalso have a higher risk of not seeing a dentist or of receivingany disease treatment [8].
Oral Health Manifestations of HIV
Oral lesions are among the earliest and most common clin-ical signs of HIV among children and adults [9–11](Table 1). For effective management, early diagnosis andgood oral health and hygiene are paramount. Along with athorough medical/dental history, detection of oral lesions
F. J. Ramos-Gomez (*)UCLA School of Dentistry, 10833 Le Conte Avenue,Box 951668, CHS Room 23-020B,Los Angeles, CA 90095-1668, USAe-mail: [email protected]
M. O. FolayanObafemi Awolowo University, Ile-Ife, Nigeria
Curr HIV/AIDS Rep (2013) 10:283–293DOI 10.1007/s11904-013-0163-y

continues to be a low cost mechanism for diagnosing andtracking HIV [9, 12••]. Modeled after categories created bythe European Community (EC) Clearinghouse on OralProblems Related to HIV Infection and the World HealthOrganization (WHO) Collaborating Centre on OralManifestations of the Human Immunodeficiency Virus, orallesions for children are grouped as: (1) lesions commonlyassociated with pediatric HIV infection, (2) lesions lesscommonly associated with pediatric HIV infection, and (3)lesions strongly associated with HIV infection but rare inchildren [12••, 13].
Overall, oral candidiasis (OC) is the most common orallesion and often the first clinical manifestation in childrenwith HIV [9]. Oral diseases categorized by the above systeminclude: Group 1—OC, herpes simplex virus, linear gingivalerythema (LGE), parotid enlargement, recurrent aphthousulcers; Group 2—necrotizing stomatitis, necrotizing periodon-tal disease, human papillomavirus (HPV), xerostomia; Group3—Kaposi’s sarcoma (KS), non-Hodgkin’s lymphoma (NHL),and oral hairy leukoplakia (OHL) [12••, 14••].
Oral candidiasis often presents as 1 of the following 3types. The first type, pseudomembranous candidiasis, ischaracterized by non-adherent, creamy white plaques thatare wiped off easily to reveal underlying redness (Fig. 1).Erythematous candidiasis has flat, red patches showingmostly on the palate and top of the tongue, sometimesaccompanied by non-adherent filmy white plaques and/ortenderness and burning. Angular cheilitis displays as red orulcerated fissures radiating from the corners of the mouth,sometimes accompanied by red papules and/or OC, andoften causing pain (Fig. 2). Angular cheilitis has causesother than candida albicans, including infection fromStaphylococcus aureus or β-hemolytic streptococci or sim-ply recurrent dry skin or irritation from slobber due topacifier use. When diagnosing angular cheilitis, it is impor-tant to take a thorough medical history, and when possible, aculture to determine the cause and consequently right courseof treatment. Children with herpes simplex virus have afever, swollen, and tender lymph nodes, and lesions insideand around the mouth and lips that often ulcerate (Fig. 3).One of the most common forms of periodontal diseaseamong HIV-infected children, LGE, shows up as bands ofredness and/or lesions on the gums, particularly at the baseof the teeth, often accompanied by bleeding upon brushing.Parotid enlargement results in facial swelling and disfigure-ment and may cause pain or be seen with lymphoid intersti-tial pneumonitis (Fig. 4). Apthous ulcers range in size from5 mm (minor apthous ulcers) to 2 cm (major) and have a redborderline; major ulcers are often accompanied by pain andmay interfere with eating and speaking (Fig. 5).
Of the oral lesions in Group 2, ulcers that may eat awayat the oral mucosa to the bone are characteristic of necrotiz-ing stomatitis. Similarly, necrotizing periodontal disease
causes tissue death. Necrotizing ulcerative gingivitis specif-ically eats away at the gingiva and may exhibit sloughingwith red, swollen, or sometimes yellowish-gray tissue andbleeding (Fig. 6). Necrotizing ulcerative periodontitis, how-ever, destroys tissue beyond the gingiva and may also causebleeding and pain, or in extreme cases, expose the jawbone.HPV can cause flesh-colored warts to erupt. Xerostomia is acondition where salivary flow rate is dramatically reducedor the consistency of saliva changed, resulting in dry mouth.Xerostomia commonly increases the thickness of saliva andmay lead to increased thirst, difficulty swallowing, mouthsoreness, halitosis, and dry, cracked lips as well increasedoral disease (Fig. 7).
Group 3 lesions are not often present in children, but mayoccur. Both KS and NHL are cancers associated with HIV.KS can cause lesions across the body (including inside themouth) and may range in color (often red or violet) andmorphology. NHL can cause symptoms such as fever, fa-tigue, and rash, along with swelling of the lymph nodes;however, it can also produce lesions on the body includingin the oral cavity. OHL consists of white lesions with cor-rugated surfaces commonly on the sides of the tongue.
Impact of Antiretroviral Treatment on Oral Health
Even when children are being treated for HIV with HAART,orofacial lesions may still present. But, the prevalence oflesions ranges from 31.4 % to 87.2 % depending on whetheror not and using which drug combination they are treated forHIV [15–17]. One study established an oral lesion preva-lence of 57.5 % in children treated with HAART [18].Another reported that, for children on HAART, 2.9 %presented with oral candidiasis, 2.9 % linear gingival ery-thema, 2 % bilateral parotid enlargement, and 1 % enlargedcervical lymph nodes [19]. However, other studies found nosignificant difference in HIV-related oral lesions in childrenon HAART compared with children not on therapy [20, 21].
Antiretroviral use has also been associated with softtissue lesions. For example, non-reverse transcriptase inhib-itors (NRTIs) have been linked to intra-oral ulcers in 3 %–30 % of patients receiving zalcitabine (ddC), mucocutane-ous hyperpigmentation in patients on zidovudine (AZT),and xerostomia in 30 % of patients taking didanosine (ddI)[22–25]. Xerostomia and/or oral ulcerations can also be seenin 7 % of patients taking protease inhibitors [26]. Otheradverse events include taste abnormalities in 20 % of patients,circumoral paraesthesia in a quarter of patients receivingritonavir, parotid lipomatosis or facial lipoatrophy (as a featureof generalized lipodystrophy) in patients receiving ritonavir,cheilitis in 57 % of patients taking indinavir, and erythemamultiforme with nevirapine treatment [27–32]. Although thisfinding has been inconsistent, long-term use of HAART
284 Curr HIV/AIDS Rep (2013) 10:283–293
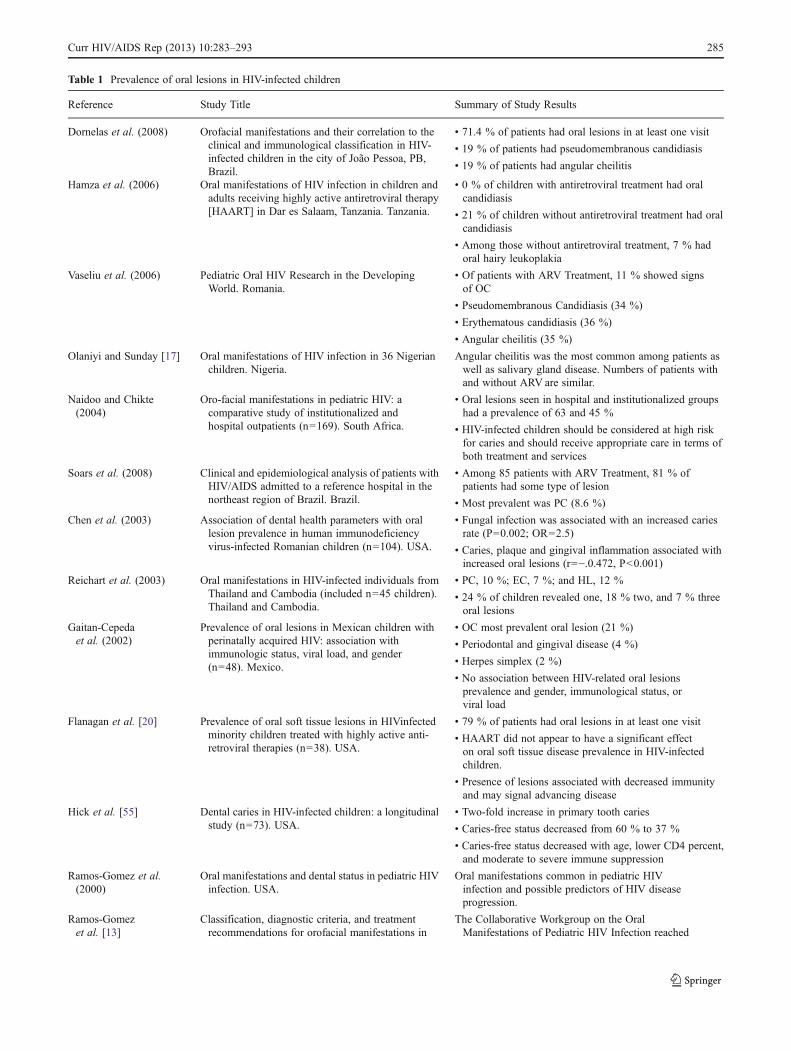
Table 1 Prevalence of oral lesions in HIV-infected children
Reference Study Title Summary of Study Results
Dornelas et al. (2008) Orofacial manifestations and their correlation to theclinical and immunological classification in HIV-infected children in the city of João Pessoa, PB,Brazil.
• 71.4 % of patients had oral lesions in at least one visit
• 19 % of patients had pseudomembranous candidiasis
• 19 % of patients had angular cheilitis
Hamza et al. (2006) Oral manifestations of HIV infection in children andadults receiving highly active antiretroviral therapy[HAART] in Dar es Salaam, Tanzania. Tanzania.
• 0 % of children with antiretroviral treatment had oralcandidiasis
• 21 % of children without antiretroviral treatment had oralcandidiasis
• Among those without antiretroviral treatment, 7 % hadoral hairy leukoplakia
Vaseliu et al. (2006) Pediatric Oral HIV Research in the DevelopingWorld. Romania.
• Of patients with ARV Treatment, 11 % showed signsof OC
• Pseudomembranous Candidiasis (34 %)
• Erythematous candidiasis (36 %)
• Angular cheilitis (35 %)
Olaniyi and Sunday [17] Oral manifestations of HIV infection in 36 Nigerianchildren. Nigeria.
Angular cheilitis was the most common among patients aswell as salivary gland disease. Numbers of patients withand without ARV are similar.
Naidoo and Chikte(2004)
Oro-facial manifestations in pediatric HIV: acomparative study of institutionalized andhospital outpatients (n=169). South Africa.
• Oral lesions seen in hospital and institutionalized groupshad a prevalence of 63 and 45 %
• HIV-infected children should be considered at high riskfor caries and should receive appropriate care in terms ofboth treatment and services
Soars et al. (2008) Clinical and epidemiological analysis of patients withHIV/AIDS admitted to a reference hospital in thenortheast region of Brazil. Brazil.
• Among 85 patients with ARV Treatment, 81 % ofpatients had some type of lesion
• Most prevalent was PC (8.6 %)
Chen et al. (2003) Association of dental health parameters with orallesion prevalence in human immunodeficiencyvirus-infected Romanian children (n=104). USA.
• Fungal infection was associated with an increased cariesrate (P=0.002; OR=2.5)
• Caries, plaque and gingival inflammation associated withincreased oral lesions (r=−.0.472, P<0.001)
Reichart et al. (2003) Oral manifestations in HIV-infected individuals fromThailand and Cambodia (included n=45 children).Thailand and Cambodia.
• PC, 10 %; EC, 7 %; and HL, 12 %
• 24 % of children revealed one, 18 % two, and 7 % threeoral lesions
Gaitan-Cepedaet al. (2002)
Prevalence of oral lesions in Mexican children withperinatally acquired HIV: association withimmunologic status, viral load, and gender(n=48). Mexico.
• OC most prevalent oral lesion (21 %)
• Periodontal and gingival disease (4 %)
• Herpes simplex (2 %)
• No association between HIV-related oral lesionsprevalence and gender, immunological status, orviral load
Flanagan et al. [20] Prevalence of oral soft tissue lesions in HIVinfectedminority children treated with highly active anti-retroviral therapies (n=38). USA.
• 79 % of patients had oral lesions in at least one visit
• HAART did not appear to have a significant effecton oral soft tissue disease prevalence in HIV-infectedchildren.
• Presence of lesions associated with decreased immunityand may signal advancing disease
Hick et al. [55] Dental caries in HIV-infected children: a longitudinalstudy (n=73). USA.
• Two-fold increase in primary tooth caries
• Caries-free status decreased from 60 % to 37 %
• Caries-free status decreased with age, lower CD4 percent,and moderate to severe immune suppression
Ramos-Gomez et al.(2000)
Oral manifestations and dental status in pediatric HIVinfection. USA.
Oral manifestations common in pediatric HIVinfection and possible predictors of HIV diseaseprogression.
Ramos-Gomezet al. [13]
Classification, diagnostic criteria, and treatmentrecommendations for orofacial manifestations in
The Collaborative Workgroup on the OralManifestations of Pediatric HIV Infection reached
Curr HIV/AIDS Rep (2013) 10:283–293 285

has also been connected with osteoporosis or osteodystrophywith implications for alveolar bone loss or periodontal disease[33, 34]. Similarly, HAART-induced diabetes mellitus anddyslipidemia may predispose patients to periodontal diseasein the long term [35, 36].
A disproportionate increase in the incidence and preva-lence of neoplasms from the persistent dysregulation of theimmune system has been hypothesized [37, 38]. In addition,a consistent observation has been an increase in benignHPV-associated oral neoplastic lesions (i.e., papillomas,condylomas, and focal epithelial hyperplasia) in patientson HAART [39–41]. This raises the possibility of an in-creased incidence of HPV-related oral malignancies withlong-term HAART, particularly if the HPV subtypes carriedare high-risk subtypes (such as HPV-16).
HIV and Hard Tissue Disorders
Nutrition has long been recognized to be important foroptimal growth and development [42]. HIV infection isknown to have a direct effect on worsening a child’s nutri-tional status, with protein-energy malnutrition being a majornutritional problem and a common complication of HIVinfection [43–45]. HIV infection, therefore, has a potentialimpact on the timing of tooth emergence due to its directinfluence on nutrition and growth. HAART also has the
potential to impact the formation of the teeth. In HIV infec-tion, there is a dysregulation of calcium homeostasis, whichresults in excessive increases of intracellular calcium in-duced by HIV viral proteins [46, 47]. Calcium is importantfor both tooth formation and tooth maturation and, thus,HIV infection may have a potential effect on tooth structureformation.
In addition, results suggest that COUP-TF interactingprotein 2 (Ctip2) functions as a critical regulator of epithelialcell fate and differentiation during tooth morphogenesis[48]. Tooth disruption has been demonstrated in Ctip2-/-
mice [48]. However, others have suggested that Ctip2 actu-ally recruits chromatin-modifying enzymes that promoteHIV-1 transcriptional silencing [49]. Thus, Ctip2-/- may beassociated with HIV-1 proliferation: a potential point ofrelationship between HIV-1 infection and disruption in toothdevelopment [48]. Although retroviruses do not interferewith the production of collagen I by odontoblasts inMoV13 mice, it does affect fibroblasts and other types ofcells [50].
With respect to tooth development and emergence, thereis some evidence to suggest that the use of antiretroviral
Table 1 (continued)
Reference Study Title Summary of Study Results
HIV-infected pediatric patients. CollaborativeWorkgroup on Oral Manifestations of PediatricHIV Infection. USA.
a consensus, and grouped orofacial manifestationsas: (1)those commonly associated with pediatricHIV infection; (2) those less commonly associatedwith pediatric HIV infection; and (3) thosestrongly associated with HIV infection but rarein children.
Ramos-Gomezet al. [11]
Period Prevalence: N=276 perinatally exposedchildren; 6-year follow-up study. USA.
Among 91 HIV + children: oral candidiasis, 67 %;parotid enlargement, 4 %; Herpes simplex, 3 %
Fig. 2 Angular cheilitisFig. 1 Pseudomembranous candidiasis
286 Curr HIV/AIDS Rep (2013) 10:283–293

medication does delay dental development. One studyshowed that HIV positive children who were not on treat-ment presented practically no difference between the chro-nological age and dental age, while the children on antire-troviral treatment showed a difference of 10.67 months [51].This study built on evidence established by another studythat showed no significant difference between the chrono-logical age and the dental or the skeletal age of HIV-positiveand HIV-negative children over time; HIV-positive childrenpresented with delayed dental and bone development de-spite the administration of antiretroviral drugs [52].
Also, associated xerostomia with use of some antiretrovirals[53] and the high sugar content of HAART, formulated assweetened syrup or a suspension to make the drugs morepalatable for children [54], increases the risk of early childhoodcaries (Figs. 8 and 9). Since these drugs are taken continuouslyfor life, this further intensifies the caries risk for a child withHIV [55, 56]. An increase in caries prevalence has also beendirectly associated with a decrease in the absolute lymphocytecount of HIV-infected children [57••]. Some studies haveshown higher rates of caries and other oral diseases amongthose with HIV, while others have shown no difference or evenlower rates [7••, 58].
While there may not be a direct causative link between HIVand caries development, there is a symbiotic relationship for
risk and disease development. Untreated caries in primaryteeth has been clearly associated with pain, speech impedi-ment, difficulty eating, and being underweight. In HIV pa-tients, ECC may introduce infection into a compromisedimmune system and impact the ability to eat and maintainadequate nutrition. Compared with adults, the biologic mech-anisms of caries development differ in young children withnewly erupted teeth, continuous vertical and horizontal bacte-ria exposure, fragile tooth enamel, and immature immunesystems. In young children with HIV, transition from infectionto AIDS to death is compressed compared with adults [7••].Therefore, early detection and treatment are of particularimportance to maximize the quality of life and longevity ofchildren living with HIV. Because oral health disease and HIVare impacted by multiple and similar social, economic andbiological factors [8, 59], interventions for each disease mayhelp ameliorate both diseases.
Despite the potentially enhanced risk of hard and soft oraltissue diseases in HIV patients, findings reveal that a signif-icant number of patients who receive consistent medical
Fig. 3 Herpes simplex virus
Fig. 4 Parotid enlargement
Fig. 5 Apthous ulcer
Fig. 6 Ulcerative gingivitis
Curr HIV/AIDS Rep (2013) 10:283–293 287

care for HIV do not receive adequate dental care [60]. Inaddition, over two-thirds of persons living with HIV dwellin developing nations where there is a notable shortage oforal health personnel and where medical treatment capacityis generally limited to pain relief or emergency care [61]. Infact, the dentist-to-population ratio in Africa is approximately1:150,000 compared with about 1:2,000 in most developedcountries [62].
Although many studies have shown HIV to have a neg-ative impact on oral health, this association has not goneunchallenged. However, in the absence of more conclusivedata and because of the disparate impact of disease on thepoor and underserved, an oral health protocol that factors inHIV status and assumptions of increased disease risk isadvised.
Oral Health Protocol for Children Living With HIV
Targeted, multi-faceted approaches to prevent, diagnose,and manage HIV and oral disease among children is essen-tial. Infants and young children are almost wholly dependenton their caregivers, and both diseases can be transferred tochildren through close maternal contact [63•]. While a com-prehensive care program for both caregiver and child is
optimal, offering such a program relies upon access to care,which varies by country and socioeconomic conditions. At aminimum, an oral health protocol starting at infancy shouldbe instituted for HIV-infected children. An infant oral carevisit (IOCV) is a simple, easily administered, and effectiveprotocol for use with HIV-infected children that includes 6simple steps: a caries risk assessment, proper positioning ofthe child in a knee-to-knee posture to actively engage thechild's caregiver, a toothbrush prophylaxis, a clinical dentalexam, fluoride varnish application, and the establishment ofself-management behavior goals utilizing motivationalinterviewing techniques [64].
IOCVs do not need to be conducted in a dental clinic norby a dentist. They only require a simple light source such asa flashlight, and 2 chairs and personnel with basic training tocomplete the 6 steps of IOCV. Primary care practitioners andothers who are trained to work with infants and children canand have been taught to perform oral health risk assessmentsto identify risk factors for dental caries and other oral healthissues. In fact, research has shown that these pediatric prac-titioners accurately identified children with dental carieswith good specificity (92 %–100 %) and sensitivity(87 %–99 %) after receiving only 1 2-hour training in infantoral health [65]. This makes IOCVs ideal for deployment inconditions with limited resources.
The first step of the IOCV focuses on Caries Managementby Risk Assessment (CAMBRA). Currently being validatedfor use among children, CAMBRA is an easy-to-use methodof assessing risk for ECC among children aged 0–5 [66••].After considering the many determinants of oral health,CAMBRA hones in on the core risk and protective factorsfor ECC in conjunction with the clinical findings to bestdetermine a child’s risk for ECC (Table 2). Risk factors andbiological predispositions include active decay in the mother orprimary caregiver in the past 12 months, bottle use, diet, andsaliva-reducing factors (e.g., HAART medications), develop-mental problems, and level of health literacy. Protective factorsinclude individual, family, and community features, such aswhether or not the child lives in a fluoridated community, if the
Fig. 7 Dry lips
Fig. 8 Early childhood caries
Fig. 9 Severe early childhood caries
288 Curr HIV/AIDS Rep (2013) 10:283–293

child drinks fluoridated water, or whether the caregiver chewsproducts containing xylitol, which helps prevent ECC. Clinicalfactors include the presence of white spots and decay, restora-tions, plaque, inadequate saliva flow, and similarfactors—easily expanded to include the presence of oral le-sions. Depending upon the presence of these factors, a child israted to have low, moderate, or high risk for ECC. TheCAMBRA process assists the provider in explicitly consider-ing a child’s oral health condition and its relationship to HIVdisease indicators.
Positioning of the child is vital to ensuring that a child iscomfortable and cooperative as well as to enabling the exam-iner to clearly visualize the child’s oral cavity. Generally,infants and toddlers ages 6 months to 3 years, or up to age 5for children with special needs, should be placed in a knee-to-knee position. In this position, the examiner and the caregiversit facing each other, knee-to-knee. The child’s head lies in theexaminers lap with the child’s legs wrapped around the care-giver’s waist. The caregiver can then hold the child’s handsand stabilize the child’s legs and body with her arms. Childrenolder than 3 years can sit forward on their caregiver’s lap or sitalone in a chair. In this position, the examiner can now retractthe child’s lips and cheek to do a tooth brush prophylaxiswhile demonstrating the proper tooth-brushing technique tothe caregiver. The spongy handle of an age-appropriate sizedtoothbrush can be used to prop open the child’s mouth. This“Tell-Show-Do” encounter provides an opportunity to encour-age the caregiver to brush her own and her child’s teeth at leasttwice a day, especially before bed time, with fluoridatedtoothpaste. Children under the age of 2 should only use asmear of fluoridated toothpaste, while children over 2 shoulduse a small, pea-sized dab.
During the clinical examination, the examiner counts thechild’s teeth aloud, using the toothbrush handle as a mouthprop if necessary with the following information document-ed: visible plaque and location; chalky white spots; brownspots that indicate decay; tooth defects; deep pits/fissures;tooth anomalies; oral and other tooth abnormalities; missingand decayed teeth; existing restorations; untreated caries,and/or defective restorations; presence and location ofgingivitis; presence and location of soft tissue abnormali-ties; occlusal status; malocclusion or developmental pa-thology; and, indications of trauma. The provider shouldbe able to determine a caries risk level once theCAMBRA form and clinical exam is complete. Childrencategorized as moderate to high risk should be given afull-mouth topical fluoride varnish and be recommendedfor re-application every 3 months, and at a minimum ofevery 6 months, even if the child lives in a communitythat already receives the benefits of water fluoridation.
The sixth and final step of an IOCV should end on apositive note and proactively engage the caregiver and childinto making positive changes to improve their oral health. A
final discussion with the caregiver should include: results ofthe risk assessment interview and clinical exam; key mes-sages for good oral health (eat a healthy diet and limit thefrequency of sugary snacks and drinks); and a customizeddisease management plan or “care path” that includes treat-ment modalities and a recall frequency for follow-up aimedat reducing caries risk directly and other oral diseases indi-rectly [66••]. An effective care path helps to educate parentsabout healthy feeding habits, their own oral health risk, andwhat protective measures they can take to give their new-born a healthier start based on their current practices andability to take on new ones over time. The provider shouldalso establish a mutually-agreed upon self-management planwith the caregiver (self-management goals include providinghealthy snacks and brushing with fluoride to support positivebehavioral changes).
While the IOCVemphasizes screening children for caries,it also affords health care providers an opportunity to addressoral hygiene practices and techniques, dietary counseling, andoral health behaviors with the child's caregiver. These simplepractices are important for the oral health of children with HIVand can prevent their otherwise increased risk for caries andother oral health disease. With minimal startup and mainte-nance costs, IOCVs can improve oral health among HIV-infected children and can be applicable for children with highrisk for caries in the general population. For these children,IOCVs can provide the consistent disease management theymay not otherwise have access to by providing a lower cost,more accessible option in locations with limited resources.When more advanced services are required, personnel canrefer patients to trained dentists.
Discussion
The dental community has already recognized a need forconsensus guidelines for the dental treatment of personsliving with HIV and recommends the development of aspecialized oral health protocol for infants and young chil-dren with the disease [67]. Although definitive criteria canbe used to diagnose HIV, resource-poor countries often lackadequate laboratories and testing facilities to ensure earlydetection. Presumptive criteria incorporating the presence oforal soft tissue manifestations and lesions for the diagnosisof HIV in infected children have been widely documented[13, 68–70]. Oral lesions are among the earliest and mostcommon clinical signs of HIV [9], and can be used toascertain HAART efficacy [71]. For patients already onantiretrovirals, the presence of certain oral manifestationsmay suggest HIV progression and an increase in plasmaviral load. For example, oral manifestations such as oralhairy leukoplakia may suggest a failure in the current drugtherapy necessitating a change in the drug regimen [71].
Curr HIV/AIDS Rep (2013) 10:283–293 289

Table 2 Caries management by risk assessment (CAMBRA)
290 Curr HIV/AIDS Rep (2013) 10:283–293

In resource-limited countries, access and utilization ofdental services is inadequate. For the most part, even wheredental services are available, utilization is poor [72].Unfortunately, preventive and proactive early dental visitsare not perceived as a standard of care. Factors that impededental care services utilization in resource-limited settingsremain poorly understood. The main reason for dental ser-vice utilization and access continues to be for curativepurposes [73] with underutilization based on a lack ofperceived need for these services due to the absence of pain[10, 74]. Family structure also plays a crucial role in dentalservice utilization in these countries; those living with singlemothers or who had no parents would be less likely to utilizedental clinics [10, 75].
Empowering health care providers and families in all butespecially resource-limited settings to be able to early diag-nose, manage, and refer children with high risk for oraldiseases is very important, since obstetricians, physicians,nurses, and health care professionals are more likely to seenew mothers and infants than are dentists. Empowered withthis knowledge, they will be better prepared to make appro-priate decisions regarding timely and effective interventionsand to facilitate the establishment of dental homes for thesechildren. In the same vein, the majority of children with HIVwill be seen and managed by health care providers otherthan dentists. It is essential that providers be aware of theetiology and risk factors of ECC in a multidisciplinary andcollaborative approach. Empowering health care providersto use a simple risk assessment diagnostic tool likeCAMBRA will enhance the early diagnosis, managementand referral of children living with HIV for management oftheir oral health problems.
Conclusions
HIV-infected children are at higher risk for developing oralhealth diseases. Left undiagnosed and untreated, these dis-eases are likely to be deleterious to their long term healthoutcomes including HIV disease progression. Despite theirincreased risk and susceptibility, HIV-infected children arealso less likely to have access to dental care for prevention,early diagnosis, and treatment. In addition, although re-search is well established to address the oral health needsof adults living with HIV, established protocols remainnascent for pediatrics partially because of the differencesin the dentition and oral manifestations of young children.
Currently, there are interventions recommended by theAAP, the AAPD, the American Dental Association, and theAmerican Association of Public Health Dentistry. Theseinclude establishing a dental home and conducting a child’s
first dental visit by age 1 or within 6 months of the eruption ofa first tooth and a caries risk assessment [6•, 76•, 77•, 78, 79].Along with honing in on an effective assessment tool likeCAMBRA, it is important to find consensus on an oral healthprotocol to monitor the oral health of children infected withHIV. With consideration for regions impacted disproportion-ately by disease, this protocol must be comprehensive yetexecutable with limited resources and across a variety ofcultures. In the absence of more conclusive, consistent dataas to the increased risk for oral disease in HIV-patients, and inconsideration of the disproportionate burden of disease onunderserved populations, an oral health protocol that is basedon HIV status with assumptions of increased disease riskshould be used starting in infancy [80].
Acknowledgments The authors wish to recognize and thank Eric C.Chen, Eric Lan, Rebecca Pizzitola, and Debra L. Tom for their research,technical writing and editorial assistance.
Compliance with Ethics Guidelines
Conflict of Interest Franciso J. Ramos-Gomez declares that he hasno conflict of interest.
Morenike Oluwatoyin Folayan declares that he has no conflict ofinterest.
Human and Animal Rights and Informed Consent This articledoes not contain any studies with human or animal subjects performedby any of the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. • Joint United Nations Programme on HIV/AIDS. Global report:UNAIDS report on the global AIDS epidemic 2012. UNAIDS /JC2417E. 2012. Available at: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/20121120_UNAIDS_Global_Report_2012_en.pdf.Accessed April 4,2013. Summary of the state of HIV worldwide.
2. • Centers for Disease Control and Prevention. Monitoring selectednational HIV prevention and care objectives by using HIV surveil-lance data—United States and 6 U.S. dependent areas—2010. HIVSurveillance Report, Supplemental Report. 2012;17:1–27. Availableat: http://www.cdc.gov/hiv/surveillance/resources/reports/2010supp_vol17no3/index.htm. Accessed April 5, 2013. This is a summary ofthe state of HIV in the United States.
3. Petersen PE. The world oral health report 2003: continuous improve-ment of oral health in the 21st century—the approach of the WHOglobal health programme. Community Dent Oral Epidemiol.
Curr HIV/AIDS Rep (2013) 10:283–293 291

2003;31:3–24. Available at: http://www.who.int/oral_health/media/en/orh_report03_en.pdf. Accessed April 4, 2013.
4. Dye B, Arevalo O, Vargas C. Trends in paediatric dental caries bypoverty status in the United States, 1988–1997 and 1994–2004. IntJ Paediatr Dent. 2010;20:132–43.
5. America Academy of Pediatrics. Oral health risk assessmenttiming and establishment of the dental home. Pediatrics.2003;111:1113–6.
6. • American Academy of Pediatric Dentistry. Policy on early child-hood caries (ECC); classifications, consequences, and preventivestrategies. Pediatr Dent. 2011;33(Special Issue):24–5. This is apolicy statement.
7. •• Yengopal V, Bhayat A, Coogan M. Pediatric oral HIV researchin the developing world. Adv Dent Res. 2011;23:61–6. This is anexamination of caries and oral lesion risk and prevalence inHAART vs non-HAART subjects.
8. U.S. Department of Health and Human Services. Oral health inAmerica: a report of the Surgeon General. Rockville: U.S.Department of Health and Human Services, National Institute ofDental and Craniofacial Research, National Institutes of Health;2000.
9. Ranganathan K, Hemalatha R. Oral lesions in HIV infection indeveloping countries: an overview. Adv Dent Res. 2006;19:63–8.
10. Exposito-Delgado AJ, Valleio-Bolanos AE, Martos-Cobo E. Oralmanifestations of HIV infection in infants: a review article. MedOral Pathol Oral Cir Bucal. 2004;9:410–20.
11. Ramos-Gomez F et al. Risk factors for HIV-related orofacial softtissue manifestations in children. Pediatr Dent. 1996;18:121–6.
12. •• Patton L et al. Urban legends series: oral manifestations of HIVinfection. Oral Dis. 2013;10:1–18. This discusses HIV oral lesionidentification in children.
13. Ramos-Gomez F et al. Classification, diagnostic criteria, and treat-ment recommendations for orofacial manifestations in HIV-infected pediatric patients. J Clin Pediatr Dent. 1999;23:85–95.
14. •• Rwenyonyi C et al. Oral manifestations in HIV/AIDS-infectedchildren. Eur J Dent. 2011;5:291–8. HIV oral lesion identificationin children.
15. Miziara I, Filho B, Weber R. Oral lesions in Brazilian HIV-infectedchildren undergoing HAART. Int J Pediatr Otorhinolaryngol.2006;70:1089–96.
16. Adejuyigbe EO, Owotade FJ, Folayan MO, Adedigba M, AnyaboluH. Oro-facial lesion in human immunodeficiency virus infectedchildren in Ile-Ife, Nigeria. J Paediat Infect Dis. 2007;2:1–6.
17. Olaniyi TO, Sunday P. Oral manifestations of HIV infection in 36Nigerian children. J Clin Pediatr Dent. 2005;30:89–92.
18. Pongsiriwet S, Iamaroon A, Kanjanavanit S, Pattanaporn K,Krisanaprakornkit S. Oral lesions and dental caries status in peri-natally HIV-infected children in Northern Thailand. Int J PaediatrDent. 2003;13:180–5.
19. Okunseri C, Badner V, Wiznia A, Rosenberg M. Prevalence of orallesions and percent CD4+ T-lymphocytes in HIV-infected childrenon antiretroviral therapy. AIDS Patient Care STDs. 2003;17:5–11.
20. Flanagan MA, Barasch A, Koenigsberg SR, Fine D, Houpt M.Prevalence of oral soft tissue lesions in HIV-infected minoritychildren treated with highly active antiretroviral therapies. PediatrDent. 2000;22:287–91.
21. Khongkunthian P, Grote M, Isaratanan W, Piyaworawong S,Reichart PA. Oral manifestations in 45 HIV-positive children fromNorthern Thailand. J Oral Pathol Med. 2001;30:549–52.
22. McNeely MC, Yarchoan R, Broder S, Lawley TJ. Dermatologic com-plications associated with administration of 2_,3_- dideoxycytidine inpatients with human immunodeficiency virus infection. J Am AcadDermatol. 1989;21:1213–7.
23. GreenbergRG,Berger TG.Nail andmucocutaneous hyperpigmentationwith azidothymidine therapy. J Am Acad Dermatol. 1990;22(2 Pt 2):327–30.
24. Poizot-Martin I, Lafeuillade A, Dhiver C, Xeri L, Bouabdallah R,Gamby T, et al. Cutaneo-mucosal hyperpigmentation in AIDS. 4cases. Presse Med. 1991;20:632–6.
25. Allan JD, Connolly KJ, Fitch H, Jackson-Pope L, McLaren C,Canetta R, et al. Long-term follow-up of didanosine administeredorally twice daily to patients with advanced human immunodefi-ciency virus infection and hematologic intolerance of zidovudine.Clin Infect Dis. 1993;16 Suppl 1:S46–51.
26. Danner SA, Carr A, Leonard JM, Lehman LM, Gudiol F, GonzalesJ, et al. A short-term study of the safety, pharmacokinetics, andefficacy of ritonavir, an inhibitor of HIV-1 protease. European-Australian Collaborative Ritonavir Study Group. N Engl J Med.1995;333:1528–33.
27. Schiffman SS, Zervakis J, Heffron S, Heald AE. Effect of proteaseinhibitors on the sense of taste. Nutrition. 1999;15:767–72.
28. Scully C, Diz Dios P. Orofacial effects of antiretroviral therapies.Oral Dis. 2001;7:205–10.
29. Olive A, Salavert A, Manriquez M, Clotet B, Moragas A. Parotidlipomatosis in HIV positive patients: a new clinical disorder asso-ciated with protease inhibitors [letter/case report]. Ann Rheum Dis.1998;57:749.
30. Calista D, Boschini A. Cutaneous side effects induced by indinavir.Eur J Dermatol. 2000;10:292–6.
31. Wetterwald E, Le Cleach L, Michel C, David F, Revuz J.Nevirapine-induced overlap Stevens-Johnson syndrome/toxicepidermal necrolysis. Br J Dermatol. 1999;140:980–2.
32. Fagot JP, Mockenhaupt M, Bouwes-Bavinck JN, Naldi L, ViboudC, Roujeau JC, et al. Nevirapine and the risk of Stevens-Johnsonsyndrome or toxic epidermal necrolysis. AIDS. 2001;15:1843–8.
33. Madeddu G, Spanu A, Solinas P, Calia GM, Lovigu C, Chessa F, etal. Bone mass loss and vitamin D metabolism impairment in HIVpatients receiving highly active antiretroviral therapy. Q J NuclMed Mol Imaging. 2004;48:39–48.
34. Yoshihara A, Seida Y, Hanada N, Miyazaki H. A longitudinalstudy of the relationship between periodontal disease and bonemineral density in community-dwelling older adults. J ClinPeriodontol. 2004;31:680–4.
35. Cutler CW, Iacopino AM. Periodontal disease: links with serumlipid/triglyceride levels? review and new data. J Int AcadPeriodontol. 2003;5:47–51.
36. Renvert S. Destructive periodontal disease in relation to diabetesmellitus, cardiovascular diseases, osteoporosis and respiratory diseases.Oral Health Prev Dent. 2003;1 Suppl 1:341–57. discussion 358–9.
37. Manfredi R, Calza L, Chiodo F. Multiple AIDS-related malignan-cies just in the era of potent antiretroviral therapy. A rare butintriguing finding. Infez Med. 2003;11:153–6.
38. Manfredi R, Calza L, Chiodo F. Multiple opportunistic AIDS asso-ciated disorders strictly related to immunodeficiency levels in a girlwith congenital HIV infection. Int J STD AIDS. 2003;14:638–9.
39. Patton LL, McKaig R, Strauss R, Rogers D, Eron Jr JJ. Changingprevalence of oral manifestations of human immuno-deficiencyvirus in the era of protease inhibitor therapy. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2000;89:299–304.
40. Schmidt-Westhausen AM, Priepke F, Bergmann FJ, Reichart PA.Decline in the rate of oral opportunistic infections following intro-duction of highly active antiretroviral therapy. J Oral Pathol Med.2000;29:336–41.
41. Greenspan D, Canchola AJ, MacPhail LA, Cheikh B, GreenspanJS. Effect of highly active antiretroviral therapy on frequency oforal warts. Lancet. 2001;357:1411–2.
42. Abiona TC. Growth patterns of exclusively breastfed infants in IfeCentral Local Government Area, Osun State: implications for timingof complimentary feeding. Dissertation, National PostgraduateMedical College, Nigeria, submitted. 2001.
43. Nalwoga A, Maher D, Todd J, Karabarinde A, Biraro S,Grosskurth H. Nutritional status of children living in a community
292 Curr HIV/AIDS Rep (2013) 10:283–293

with high HIV prevalence in rural Uganda: a cross-sectionalpopulation-based survey. Trop Med Int Health. 2010;15:414–22.
44. Enwonwu CO. Interface of malnutrition and human immunodefi-ciency virus infection in sub-Saharan Africa: a critical review. NutrRes. 1992;12:1041–50.
45. Kottler DP. Nutritional support in AIDS. Am J Gastroenterol.1990;86:539–41.
46. Kasyanov A, Tamamura H, Fujii N, XiongH. HIV-1 gp120 enhancesgiant depolarizing potentials via chemokine receptor CXCR4 inneonatal rat hippocampus. Eur J Neurosci. 2006;23:1120–8.
47. Lipton SA. AIDS-related dementia and calcium homeostasis. AnnN YAcad Sci. 1994;747:205–24.
48. Golonzhka O, Metzger D, Bornert J-M, Bay BK, Gross MK,Kioussi C, et al. Ctip2/Bcl11b controls ameloblast formation dur-ing mammalian odontogenesis. PNAS. 2009;106:4278–83.
49. Marban C, Suzanne S, Dequiedt F, deWalque S, Redel L, Van Lint C,et al. Recruitment of chromatin-modifying enzymes by CTIP2 pro-motes HIV-1 transcriptional silencing. EMBO J. 2007;26:412–23.
50. Kratochwil K, von der Mark K, Kollar EJ, Jaenisch R, MooslehnerK, Schwarz M, et al. Retrovirus-induced insertional mutation inMov13 mice affects collagen I expression in a tissue-specificmanner. Cell. 1989;57:807–16.
51. Trigueiro M et al. An assessment of adverse effects of antiretroviraltherapy on the development of HIV positive children by observation ofdental mineralization chronology. J Oral Pathol Med. 2010;39:35–40.
52. Holderbaum RM, Veeck EB, Oliveira HW, da Silva CL, Fernandes A.Comparison among dental, skeletal and chronological development inHIV-positive children: a radiographic study. Braz Oral Res. 2005;19.http://dx.doi.org/10.1590/S1806-83242005000300010 AccessedAugust 15, 2011.
53. Turner M, Ship J. Dry mouth and its effects on the oral health ofelderly people. JADA. 2007;138:15S–20S.
54. Nahirya-Ntege P, et al. Young HIV-infected children and their adultcaregivers prefer tablets to syrup antiretroviral medications in Africa.Plos One. 2012. RetrievedApril 12, 2013 from http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0036186.
55. Hick M et al. Dental caries in HIV-infected children: a longitudinalstudy. Pediatr Dent. 2000;22:359–63.
56. Howell R et al. Oral soft tissue manifestations and CD4 lymphocytecounts in HIV-infected children. Pediatr Dent. 1996;18:129–36.
57. •• Beema J. Prevalence of dental caries and its correlation with theimmunologic profile in HIV-infected children on antiretroviraltherapy. Eur J Paediatr Dent. 2011;12:87–90. This reference founda decrease in the absolute lymphocyte count associated with anincrease in caries prevalence.
58. Ramos-Gomez F et al. Orofacial manifestations and managementof HIV-infected children. Oral Maxillofac Surg Child Adolesc.1994;6:37–47.
59. Fisher-Owens SA et al. Influences on children’s oral health: aconceptual model. Pediatrics. 2007;120:e510–20.
60. Shapiro M, et al. Access to HIV care: initial results from the HIVCost and Services Utilization Study. Santa Monica, CA: RANDCorporation. 2000. RetrievedApril 8, 2013 from http://www.rand.org/pubs/research_briefs/RB4530.
61. Peterson PE. Policy for prevention of oral manifestations in HIV/AIDS: the approach of the WHO Global Oral Health Program.Advances in Dental Research. 2006;19:17–20. Retrieved April 8,2013 from http://www.who.int/oral_health/action/communicable/Policy.pdf.
62. EC Clearinghouse on Oral Problems Related to HIV Infection andWHO Collaborating Centre on Oral Manifestations of the HumanImmunodeficiency Virus. Classification and diagnostic criteria fororal lesions in HIV infection. J Oral Pathol Med. 1993;22:289–91.
63. • Ramos-Gomez F et al. Mother and youth access (MAYA) mater-nal chlorhexidine, counseling and pediatric fluoride varnish ran-domized clinical trial to prevent early childhood caries. Int JPaediatr Dent. 2011;22:1–11. This discusses the transmission ofmaternal bacteria strains to newborn infants of high risk, lowincome mothers.
64. Ramos-Gomez F, Ng M. Six step protocol for a successful infantoral care visit. Pediatr Dent Today. 2009;2009:38–40.
65. Pierce K, Rozier R, Vann Jr W. Accuracy of pediatric primary careproviders’ screening and referral for early childhood caries.Pediatrics. 2002;109:e82–2.
66. •• Ramoz-Gomez F, Ng M. Into the future: keeping healthy teethcaries free: pediatric CAMBRA protocols. J Calif Dent Assoc.2011;38:723–33.Caries risk assessment and infant oral care protocol.
67. Petersen P et al. The global burden of oral diseases and risks to oralhealth. Bull World Health Organ. 2005;83:661–9.
68. Ramos-Gomez F, Greenspan D, Greenspan J. Orofacial manifes-tations and management of HIV-infected children. Oral MaxillofacSurg Clin N Am. 1994;6:37–47.
69. Kline M. Oral manifestations of pediatric human immunodeficiencyvirus infection: a review of the literature. Pediatrics. 1996;97:380–8.
70. Reznik D. Oral manifestations of HIV disease. Top HIV Med.2005;135:143–8.
71. Hodgson T, Greenspan D, Greenspan J. Oral lesions of HIVdisease and HAART in industrialized countries. Adv Dent Res.2006;19:57–62.
72. Oredugba FA. Use of oral health care services and oral findings inchildren with special needs in Lagos, Nigeria. Spec Care Dentist.2006;26:59–65.
73. Denloye O, Ajayi D, Bankole O. A study of dental caries preva-lence in 12–14 year old school children in Ibadan, Nigeria. PediatrDent J. 2005;15:147–51.
74. Folayan MO, Ozeigbe EO, Oyedele T, Ola D. Factors limitingdental service utilization by pupils in Ile-Ife, Nigeria. Unpublishedwork.
75. Ola D et al. Family structure, socio-economic position and oralhealth services utilization in Nigerian senior secondary schoolpupils. J Public Health Dent. 2012. doi:10.1111/j.1752–7325.2012.00362.x.
76. • American Academy of Pediatric Dentistry. Policy on the dentalhome. Pediatr Dent. 2011;33(Special Issue):24–5. This is a policystatement.
77. • American Academy of Pediatric Dentistry. Guideline on caries riskassessment and management for infants, children, and adolescents.Pediatr Dent. 2011;34(Special Issue):118–25. Retrieved April 11,2013 from http://www.aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf. This is a policy statement.
78. American Dental Association. ADA statement on early childhoodcaries. 2004. Retrieved April 11, 2013 from http://www.ada.org/2057.aspx.
79. American Association of Public Health Dentistry. First oral healthassessment policy. 2004. Retrieved April 11, 2013 from http://aaphd.org/default.asp?page=FirstHealthPolicy.htm.
80. Ramos-Gomez F. Oral aspects of HIV infection in children. OralDis. 1997;3:S31–5.
Curr HIV/AIDS Rep (2013) 10:283–293 293
Copyright © 2022 FDOKUMEN




















