Oral Abstract Sessions - Karger Publishers
66
© 2015 S. Karger GmbH, Freiburg Accessible online at: www.karger.com/tmh Fax +49 761 4 52 07 14 [email protected] www.karger.com Abstracts Transfus Med Hemother 2015;42(suppl 1):1–64 DOI: 10.1159/000438503 Oral Abstract Sessions Stem cell transplantation FV-01-1 Donor activating KIR2DS1/2/5 are associated with improved outcome of Haematopoietic stem cell transplantation in C1- ligand negative patients with myeloid malignancies Zollikofer C. 1 , Fürst D. 1 , Tsamadou C. 1 , Niederwieser D. 2 , Bunjes D. 3 , Wulf G. 4 , Pfreundschuh M. 5 , Wagner E. 6 , Stuhler G. 7 , Einsele H. 8 , Schrezenmeier H. 1 , Mytilineos J. 1 1 Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Ulm, Germany, 2 Abteilung für Hämatologie und Internistische Onkologie, Leipzig, Germany, 3 Innere Medizin III Universitätsklinikum, Ulm, Germany, 4 Institut für Hämatologie und Onkologie, Georg-August-Universität, Göttingen, Germany, 5 Klinik für Innere Medizin I, Universitätsklinikum des Saarlandes, Homburg, Germany, 6 III. Medizinische Klinik, Johannes Gutenberg-Universität, Mainz, Germany, 7 Deutsche Klinik für Diagnostik, Wiesbaden, Germany, 8 Medizinische Klinik und Poliklinik II, Würzburg, Germany Natural Killer cells (NK) are lymphocytes that have the potential to recog- nize and lyse cells with aberrant HLA expression profiles which escaped T-cell mediated lysis. Communication between NK and leukemic cells is facilitated, among others, by killer cell immunoglobulin-like receptors (KIR) on the surface of NK cells and their respective HLA-class I ligands. KIRs influence NK-cell activity by mediating activating or inhibitory sig- nalling, whereas activating signals and missing inhibition both lead to tar- get cell lysis. Activating KIRs may have an immune-modulatory effect on the outcome of HSCT. In this study we show that patients with myeloid malignancies that do not express a C1 Ligand suffer from impaired out- come aſter HSCT. Moreover, we demonstrate the beneficial influence of activating donor KIR2DS1/2/5 on this risk patient group. Patients and donors were high resolution HLA-typed. KIR-typing was performed through PCR-SSP. HLA-C alleles were grouped based on their amino acid pos 80 residue into C1 and C2 ligands. Patient malignancies were AML, CML or MDS. Clinical data for this study where obtained through the German Registry for Haematopoietic Stem Cell Transplan- tation (DRST). Previous studies showed that C1 negative patients have an inferior HSCT outcome. We could confirm these findings in our study by ana- lysing a group of 200 C1-negative. Overall survival (OS: HR = 1.41, CI = 1.14 - 1.74, p = 0.0012), disease free survival (DFS: HR = 1.27, CI = 1.05 - 1.53, p = 0.015), treatment related mortality (TRM: HR = 1.41, CI = 1.01 - 1.96, p = 0.04) and relapse incidence (RI: HR = 1.33, CI = 1.01–1.75, p = 0.04) were all inferior when compared to C1 car- riers (n = 1246). Within this risk patient group, however, OS was im- proved if a KIR2DS2 expressing donor with a single HLA mismatch was used (HR = 0.29, CI = 0.09–0.92, p = 0.03). In addition, transplanta- tion with KIR2DS1 (HR = 0.26, CI = 0.11–0.63, p = 0.003) or KIR2DS5 (HR = 0.31, CI = 0.12–0.81, p = 0.017) positive donors resulted in de- creased RI. Our findings can be explained by impaired donor derived NK-cell ac- tivity in C1-ligand negative patients. C2-restricted NK-cells form small- er populations, react slower to interferon γ secretion, and degranulate CD107a less potently. Activating signals derived from KIR2DS1/2/5 stim- ulation may overcome this impairment. We therefore suggest inclusion of KIR2DS1/2/5-genotyping in the unrelated donor search algorithm of C1-ligand negative patients with myeloid malignancies. FV-01-2 Identification of RUNX1 key target genes leading to clonal dominance in MDS Pignalosa D., Zickler A.M., Horn P.A., Heinrichs S. Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany Myelodysplastic syndromes (MDS) are a heterogeneous group of disorders of the hematopoietic system characterized by clonal expansion of stem cells and inefficient hematopoiesis due to partial inhibition of differentiation. Muta- tions of the RUNX1 gene, encoding a key hematopoietic transcription factor, occur at a high rate (>10%) in MDS patients. However, the mechanisms un- derlying mutant RUNX1-driven MDS pathogenesis are still unknown. Here we show the development of a mouse model to identify the pathomechanism of RUNX1 mutations. We reconstituted the hematopoietic system of recipi- ent mice using a transduction/transplantation approach with hematopoietic stem and progenitor cells (HSPCs) expressing a dominant-negative form of RUNX1 (dnRUNX1) and a green fluorescent protein (GFP). Of note, only 10–20% of the transplanted cells were genetically modified while the majori- ty was unaltered (competitive reconstitution). HSPCs expressing dnRUNX1 displayed a clear growth advantage over non-modified cells, as revealed by the significant expansion of GFP+ cells aſter 6 months. Moreover, the fre- quency of differentiated cells was skewed towards the myeloid lineage. Con- versely, HSPCs expressing only GFP did not show any clonal advantage (< 5%). e complete blood count analysis of the peripheral blood showed signs of leucopenia and anemia in experimental mice compared to controls. Dn- RUNX1-expressing cells were able to engraſt secondary recipients with an expansion phenotype. Interestingly, the onset of anemia occurred significant- ly earlier in those animals compared to primary transplanted mice (six weeks vs. six months). Histological examination of the spleen and the bone marrow of these secondary recipients showed signs of an abnormal bone marrow he- matopoiesis. Hence, the mouse model we successfully generated presented numerous MDS-like features. In the system we developed, dnRUNX1 ex- pression was maintained by doxycycline, provided in the diet. Withdrawal of doxycycline led to a 1000-fold decrease of dnRUNX1 expression within 48h. Hence, secondary recipients that had been transplanted from a single donor and harbored pre-malignant cells of the same oligo-clonal origin were divid- ed into two groups, one kept under a doxycycline-enriched diet and the other fed with normal food. Currently, we compare global gene expression profiles of HSPCs obtained from each group. In summary, our model will allow to identify RUNX1 molecular targets that play a key role in MDS pathogenesis. FV-01-3 Kindlin-2 enhances adhesion, migration and immune- regulation in induced pluripotent stem cell-derived mesenchymal-like cells Moslem M. 1,2 , Eggenschwiler R. 2 , Wichmann C. 1 , Buhmann R. 1 , Cantz T. 2 , Henschler R. 1,3 1 Abteilung für Transfusionsmedizin, Zelltherapeutika und Hämostaseologie, München, Germany, 2 Translational Hepatology and Stem Cell Biology, Hannover Medical School, Hannover, Germany, Hannover, Germany, 3 Blutspende Zürich SRK, Zürich, Switzerland Introduction: Kindlin-2, a scaffold protein which enhances Talin mediat- ed integrin activation, which binds to membranes enriched in phospho- inositides, and enhances integrin mediated cell adhesion and migration.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Oral Abstract Sessions - Karger Publishers

© 2015 S. Karger GmbH, Freiburg
Accessible online at: www.karger.com/tmh
Fax +49 761 4 52 07 [email protected]
Abstracts
Transfus Med Hemother 2015;42(suppl 1):1–64DOI: 10.1159/000438503
Oral Abstract Sessions
Stem cell transplantation
FV-01-1Donor activating KIR2DS1/2/5 are associated with improved outcome of Haematopoietic stem cell transplantation in C1-ligand negative patients with myeloid malignancies
Zollikofer C.1, Fürst D.1, Tsamadou C.1, Niederwieser D.2, Bunjes D.3, Wulf G.4, Pfreundschuh M.5, Wagner E.6, Stuhler G.7, Einsele H.8, Schrezenmeier H.1, Mytilineos J.1
1Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Ulm, Germany, 2Abteilung für Hämatologie und Internistische Onkologie, Leipzig, Germany, 3Innere Medizin III Universitätsklinikum, Ulm, Germany, 4Institut für Hämatologie und Onkologie, Georg-August-Universität, Göttingen, Germany, 5Klinik für Innere Medizin I, Universitätsklinikum des Saarlandes, Homburg, Germany, 6III. Medizinische Klinik, Johannes Gutenberg-Universität, Mainz, Germany, 7Deutsche Klinik für Diagnostik, Wiesbaden, Germany, 8Medizinische Klinik und Poliklinik II, Würzburg, Germany
Natural Killer cells (NK) are lymphocytes that have the potential to recog-nize and lyse cells with aberrant HLA expression profiles which escaped T-cell mediated lysis. Communication between NK and leukemic cells is facilitated, among others, by killer cell immunoglobulin-like receptors (KIR) on the surface of NK cells and their respective HLA-class I ligands. KIRs influence NK-cell activity by mediating activating or inhibitory sig-nalling, whereas activating signals and missing inhibition both lead to tar-get cell lysis. Activating KIRs may have an immune-modulatory effect on the outcome of HSCT. In this study we show that patients with myeloid malignancies that do not express a C1 Ligand suffer from impaired out-come after HSCT. Moreover, we demonstrate the beneficial influence of activating donor KIR2DS1/2/5 on this risk patient group. Patients and donors were high resolution HLA-typed. KIR-typing was performed through PCR-SSP. HLA-C alleles were grouped based on their amino acid pos 80 residue into C1 and C2 ligands. Patient malignancies were AML, CML or MDS. Clinical data for this study where obtained through the German Registry for Haematopoietic Stem Cell Transplan-tation (DRST). Previous studies showed that C1 negative patients have an inferior HSCT outcome. We could confirm these findings in our study by ana-lysing a group of 200 C1-negative. Overall survival (OS: HR = 1.41, CI = 1.14 - 1.74, p = 0.0012), disease free survival (DFS: HR = 1.27, CI = 1.05 - 1.53, p = 0.015), treatment related mortality (TRM: HR = 1.41, CI = 1.01 - 1.96, p = 0.04) and relapse incidence (RI: HR = 1.33, CI = 1.01–1.75, p = 0.04) were all inferior when compared to C1 car-riers (n = 1246). Within this risk patient group, however, OS was im-proved if a KIR2DS2 expressing donor with a single HLA mismatch was used (HR = 0.29, CI = 0.09–0.92, p = 0.03). In addition, transplanta-tion with KIR2DS1 (HR = 0.26, CI = 0.11–0.63, p = 0.003) or KIR2DS5 (HR = 0.31, CI = 0.12–0.81, p = 0.017) positive donors resulted in de-creased RI. Our findings can be explained by impaired donor derived NK-cell ac-tivity in C1-ligand negative patients. C2-restricted NK-cells form small-er populations, react slower to interferon γ secretion, and degranulate CD107a less potently. Activating signals derived from KIR2DS1/2/5 stim-ulation may overcome this impairment. We therefore suggest inclusion of KIR2DS1/2/5-genotyping in the unrelated donor search algorithm of C1-ligand negative patients with myeloid malignancies.
FV-01-2Identification of RUNX1 key target genes leading to clonal dominance in MDS
Pignalosa D., Zickler A.M., Horn P.A., Heinrichs S.Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany
Myelodysplastic syndromes (MDS) are a heterogeneous group of disorders of the hematopoietic system characterized by clonal expansion of stem cells and inefficient hematopoiesis due to partial inhibition of differentiation. Muta-tions of the RUNX1 gene, encoding a key hematopoietic transcription factor, occur at a high rate (>10%) in MDS patients. However, the mechanisms un-derlying mutant RUNX1-driven MDS pathogenesis are still unknown. Here we show the development of a mouse model to identify the pathomechanism of RUNX1 mutations. We reconstituted the hematopoietic system of recipi-ent mice using a transduction/transplantation approach with hematopoietic stem and progenitor cells (HSPCs) expressing a dominant-negative form of RUNX1 (dnRUNX1) and a green fluorescent protein (GFP). Of note, only 10–20% of the transplanted cells were genetically modified while the majori-ty was unaltered (competitive reconstitution). HSPCs expressing dnRUNX1 displayed a clear growth advantage over non-modified cells, as revealed by the significant expansion of GFP+ cells after 6 months. Moreover, the fre-quency of differentiated cells was skewed towards the myeloid lineage. Con-versely, HSPCs expressing only GFP did not show any clonal advantage (< 5%). The complete blood count analysis of the peripheral blood showed signs of leucopenia and anemia in experimental mice compared to controls. Dn-RUNX1-expressing cells were able to engraft secondary recipients with an expansion phenotype. Interestingly, the onset of anemia occurred significant-ly earlier in those animals compared to primary transplanted mice (six weeks vs. six months). Histological examination of the spleen and the bone marrow of these secondary recipients showed signs of an abnormal bone marrow he-matopoiesis. Hence, the mouse model we successfully generated presented numerous MDS-like features. In the system we developed, dnRUNX1 ex-pression was maintained by doxycycline, provided in the diet. Withdrawal of doxycycline led to a 1000-fold decrease of dnRUNX1 expression within 48h. Hence, secondary recipients that had been transplanted from a single donor and harbored pre-malignant cells of the same oligo-clonal origin were divid-ed into two groups, one kept under a doxycycline-enriched diet and the other fed with normal food. Currently, we compare global gene expression profiles of HSPCs obtained from each group. In summary, our model will allow to identify RUNX1 molecular targets that play a key role in MDS pathogenesis.
FV-01-3Kindlin-2 enhances adhesion, migration and immune-regulation in induced pluripotent stem cell-derived mesenchymal-like cells
Moslem M.1,2, Eggenschwiler R.2, Wichmann C.1, Buhmann R.1, Cantz T.2, Henschler R.1,3
1Abteilung für Transfusionsmedizin, Zelltherapeutika und Hämostaseologie, München, Germany, 2Translational Hepatology and Stem Cell Biology, Hannover Medical School, Hannover, Germany, Hannover, Germany, 3Blutspende Zürich SRK, Zürich, Switzerland
Introduction: Kindlin-2, a scaffold protein which enhances Talin mediat-ed integrin activation, which binds to membranes enriched in phospho-inositides, and enhances integrin mediated cell adhesion and migration.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts2
We have previously shown that human iPSCs can differentiate toward MSCs. In this study, we explored the role of Kindlin-2 to modulate ad-hesion, migration and immune-suppression properties of iPS-derived MSCs.Methods and Results: (i) After transfection (Lipofectamin LTX) with kindlin-2 shRNA and overexpressing constructs along with control plas-mids, iPSC-MSC had significantly higher attachment potential under shear stress to VCAM-1 co-coated with SDF1-α flow chamber slides. (ii) Post kindlin-2 overexpression, CD-90+ and CD105+ cells increased (~1.5 and 3 fold, respectively), accompanied by significantly increased transwell migration potential of iPSC-MSCs transfected with kindlin-2 after 24h and 36h compared to control group. (iii) kindlin-2 overexpress-ing iPS-MSCs significantly better dampened proliferation of CD4+ and CD8+ T-Lymphocytes in mixed lymphocyte reaction assays compared to iPSC-MSCs transfected by kindlin-2 shRNA, along with significantly decreased amount of IFN-γ and IL-2 production. Moreover, numbers of T-regulatory cells (CD25+/CD69+) were significantly increased in both CD4+ and CD8+ populations post transfection with kindlin-2 compared to controls. Discussion and conclusion: Here, we demonstrate that overexpression of kindlin-2 results in highly functional human iPSC-derived MSCs with increased expression of mesenchymal surface markers such as CD-90 and CD-105 and with higher proliferative potential. These MSCs could possibly be a suitable substitute for bona fide MSCs derived from bone marrow. Moreover, we were able to demonstrate that kindlin-2 trans-fected iPSC-MSCs significantly increase number of spreading cells and also their attachment to VCAM-1/SDF1-α under shear stress, pointing to improved homing ability after transplantation. Our results also exhib-ited that kindlin-2 over expression significantly increases the number of T-regulatory cells (CD4+/CD25+/CD69+ and CD8+/CD25+/CD69+) in mixed lymphocyte cultures, showing relevant potential of kindlin-2 sig-naling in immunomodulation of inflammatory reactions byiPSC-MSCs. These data indicate a potential relevance of kindlin-2 engineered MSCs in clinical conditions such GVHD and degenerative autoimmune diseases.
FV-01-4The activating NKG2C receptor is significantly reduced in NK cells after allogeneic stem cell transplantation in patients with severe Graft-versus-host disease
Rebmann V.1, Kordelas L.2, Beelen D.2, Horn P.A.1
1Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany, 2Universitätsklinikum Essen, Klinik für Knochenmarktransplantation, Essen, Germany
Introduction: Natural killer (NK) cells are important players of the innate immune system. The allo-reactivity of NK cells is regulated by a num-ber of receptors including the activating CD94/NKG2C or the inhibitory CD94/NKG2A receptors, both which are recognizing the non-classical human leukocyte antigen E (HLA-E). In allogeneic stem cell transplan-tation (allo-SCT) donor-derived allo-reactive NK cells are important effectors mediating killing of leukemia cells and patient’s dendritic cells thereby preventing leukemic relapses or graft-vs-host responses. Here we analyze the contribution of these receptors to NK cell allo-reactivity in 26 patients undergoing allo-SCT due to acute myeloid leukemia (n = 20), secondary AML (n = 4), myelodysplastic syndrome (n = 1) and T-Non Hodkgin-Lymphom (n = 1). Methods: EDTA samples were serially procured before and 1, 2, 3, 4, 5, 6, 9 and 12 month(s) after alloSCT. Receptor expression was analyzed by flow cytometer using specific antibodies against human CD56, NKG2A, CD94, NKG2C and correlated to acute or chronic GvHD. Results: The proportion of activating receptor CD94/NKG2C on NK cells was significantly reduced in 10 patients who had experienced a severe acute GvHD (aGvHD) grad 2–4 after alloSCT (p < 0.0001) compared to 16 patients without or mild aGvHD. Moreover, the proportion of CD94/NKG2C on NK cells was lower in patients with extended chronic GvHD (cGvHD) compared to patients without or limited cGvHD (n = 13,
p < 0.0001). No difference was detectable regarding the inhibitory NK-G2A receptor on NK cells and incidence of acute/chronic GvHD. Conclusion: Thus, these results provided substantial evidence that the CD94/NKG2C receptors contributes to the allo-reactivity of NK cells af-ter allo-SCT.
This study was supported by a research grant by the Deutsche José Carreras Leu-kämie-Stiftung e.V.
FV-01-5Quality of 74 autologous hematopoietic progenitor cell products after cryopreservation: Results are significantly dependent on dilution matrix
Humpe A., Trost B., Günther A., Gramatzki M., Buwitt-Beckmann U.Section of Stem Cell and Immunotherapy, University Clinic Schleswig-Holstein Campus Kiel, Second Department of Medicine, Kiel, Germany
Introduction: Harvest and transplantation of autologous hematopoietic progenitor cells (HPC) is a therapeutic option after high dose therapy for patients with different malignancies. Especially the quality of HPC prod-ucts after cryopreservation is a decisive factor for successful engraftment. Here, we analyzed the influence of the dilution matrix after cryopreserva-tion on viability and recovery of cells.Methods: Viability of CD45+ and of CD34+ cells and recovery of CD34+ cells were analyzed in satellite tubes of 74 autologous HPC products after cryopreservation and thawing. Products were generated from 38 aphere-ses of 29 patients (10 female, 19 male) with multiple myeloma (n = 20) or with nonHodgkin’s lymphoma (n = 9). Cells were thawed at +37 °C and rapidly diluted (1:10) in parallel in two different matrices, i.e. phosphate buffered saline with 10% AB serum (PBS) or Iscove’s Modified Dulbecco’s Medium without phenol red (IMDM). Cells were analyzed by FACS after shortened antibody staining but without lysis as published (Humpe et al., Transfusion,2005:1208).Results: The median viability of CD45+ cells after thawing was 68.0% (range: 34.5–89.5%) after dilution in PBS and significantly higher (p < 0.001) with 73.3% (range: 31.0–90.8%) after dilution in IMDM. With dilution in PBS, the median viability of CD34+ cells after thawing was 82.6% (range: 16.3–96.9%) and this was significantly higher (p < 0.001) at 93.5% (range: 29.8–98.8%) after dilution in IMDM. In addition, the me-dian recovery of CD34+ cells of cryopreserved products, defined as ratio between the number of CD34+ cells in the product after cryopreservation and the number of CD34+ cells in the product before cryopreservation, was significantly (p < 0.001) higher with 90.8% in the IMDM group com-pared with 83.5% in the PBS group.Conclusion: The presented results clearly show that a careful validation of quality control (QC) procedures for cellular products is mandatory. Espe-cially as parameters deduced from such measurements are decisive for the final release of a HPC graft. In addition, the aim of such QC after cryo-preservation should resemble the situation of the transplantation as close as possible. Since the patient’s blood serving as the best dilution matrix is not available and suitable for FACS QC after cryopreservation the in-vitro matrix should be optimized.
FV-01-6Indicators of obesity in healthy peripheral blood stem cell donors
Hauber D.1, Reinhardt P.1, Schauwecker P.1, Fürst D.1, Bunjes D.2, Mytilineos J.1, Schrezenmeier H.1, Wiesneth M.1, Körper S.1
1Universitätsklinik Ulm, DRK-Blutspendedienst Baden-Württemberg-Hessen, IKT Ulm, Ulm, Germany, 2Universitätsklinik Ulm, Medizinische Klinik III, Ulm, Germany
Body weight (BW) and male sex (MS) are established predictors for good mobilization of CD34+ cells. The reason for this finding is elusive. A more detailed analysis of markers of obesity might help to establish new hy-
Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 3
pothesis about the mechanisms that contribute to the better mobilization in these populations. We retrospectively analysed 316 healthy stem cell donors with respect to different factors that are related to BW and CD34+ blood cell count after G-CSF administration. A single platform assay was used to determine the CD34+ cell count/µl in peripheral blood after G-CSF mobilization (aim: 40 µg G-CSF per kg BW, divided in 8 dosages). The concentration of CD34+ cells was correlated with different parameters in all 316 healthy donors. Spearmans Test was used to determine significance (P ≤ 0.01) in these correlations. For further analysis groups poor (PM) and good mobilizers (GM) were defined by the 10 (28/µl) and 90 (132/µl) percentiles (n = 32 for each group). Body mass index (BMI), BW and ALT, and cholinesterase (obtained be-fore G-CSF administration) showed a weak but significant correlation with CD34+ mobilization in men and women. To compare the ultrasound examinations of the liver the presence of steatosis hepatis was examined in the PM and GM. Steatosis of grade 1 or 2 was present in 6% of the PM and 41% of the GM. A grade 2 steatosis was not seen in the PM but in 9% of GM. There was no significant difference in liver size between the groups. Correlation of other calculated measures depending on BW like blood volume (calculated by the Nadlers formula) or BMI or body surface area did not improve correlation compared to BW.
Tab. 1.
VariablePoor mobilizers (PM) n = 32 Median (range)
Good mobilizers (GM) n = 32 Median (range)
Spearmans Test n = 316 P-value
Weight (kg) 69 (46 to 110) 85 (62 to 140) <0.0001
Height (cm) 170 (150 to 186) 179 (158 to 205) 0.0476
BMI 23.4 (18.8 to 37.5) 27.2 (19.4 to 39.6) 0.0002
Body surface area (m2) 1.84 (1.38 to 2.33) 2.06 (1.76 to 2.61) 0.0002
Blood volume (l) 3.9 (3.1 to 5.1) 5.5 (4.9 to 7.2) 0.0001
ALT (U/l) 19 (6 to 80) 28 (12 to 79) <0.0001
ASAT(U/l) 29 (24 to 58) 32 (20 to 94) 0.0557
Cholinesterase 7176 (4438 to 9881)
8605 (5239 to 12217) <0.0001
Liver size (MCL) (mm) 137 (103 to 164) 141 (120 to 178) 0.4428
It is well known that BW is a positive predictive factor for good CD34+ mobilization. To our knowledge we show here for the first time a posi-tive association between ALT, cholinesterase, steatosis hepatis and CD34+ mobilization. In summary our findings link body fat to the quality of CD34+ mobilization.
FV-01-7Blood stem cell graft composition collected after various mobilization methods
Worel N.1, Greinix H.T.2, Agis H.3, Zojer N.4, Reisner R.5, Ruckser R.6, Fritsch G.7
1Medical University of Vienna, Transfusion Medicine, Vienna, Austria, 2Medical University Graz, Haematology, Graz, Austria, 3Medical University Vienna, Vienna, Austria, 4Wilhelminen Hospital, Vienna, Austria, 5Hanusch Hospital, Vienna, Austria, 6Donau Hospital, Vienna, Austria, 7Childrens Cancer Research Institute, Clinical Cell Biology & FACS Core Unit, Vienna, Austria
Introduction: Mobilized peripheral blood stem cells (PBSCs) are the pre-ferred graft for autologous stem cell transplantation. The use of cytokines, alone or in combination with chemotherapy, is the most common strategy to collect PBSCs. For hard-to-mobilize patients , plerixafor (P) has shown to enhance stem cell mobilization. However, limited data are available on graft content collected after various mobilization methods. The aim of this study was to assess the effects of different mobilization strategies on CD34+ cell and lymphocyte subsets.
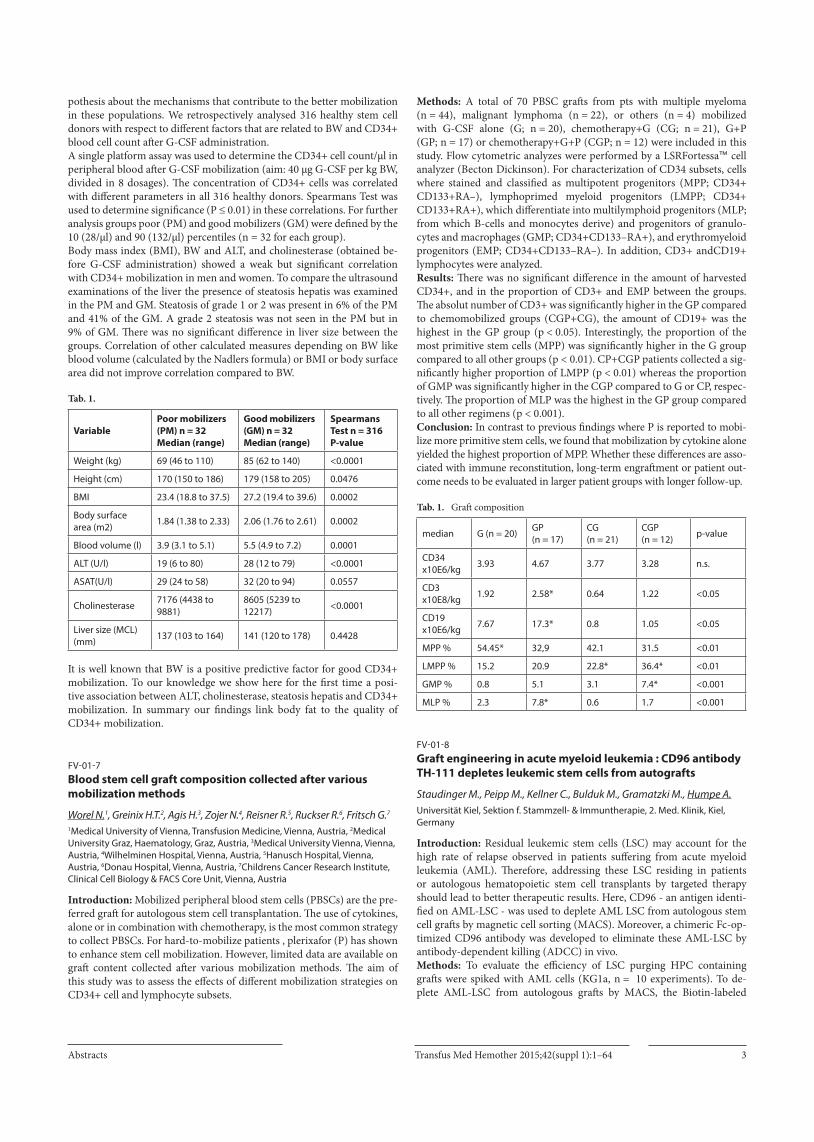
Methods: A total of 70 PBSC grafts from pts with multiple myeloma (n = 44), malignant lymphoma (n = 22), or others (n = 4) mobilized with G-CSF alone (G; n = 20), chemotherapy+G (CG; n = 21), G+P (GP; n = 17) or chemotherapy+G+P (CGP; n = 12) were included in this study. Flow cytometric analyzes were performed by a LSRFortessa™ cell analyzer (Becton Dickinson). For characterization of CD34 subsets, cells where stained and classified as multipotent progenitors (MPP; CD34+ CD133+RA–), lymphoprimed myeloid progenitors (LMPP; CD34+ CD133+RA+), which differentiate into multilymphoid progenitors (MLP; from which B-cells and monocytes derive) and progenitors of granulo-cytes and macrophages (GMP; CD34+CD133–RA+), and erythromyeloid progenitors (EMP; CD34+CD133–RA–). In addition, CD3+ andCD19+ lymphocytes were analyzed.Results: There was no significant difference in the amount of harvested CD34+, and in the proportion of CD3+ and EMP between the groups. The absolut number of CD3+ was significantly higher in the GP compared to chemomobilized groups (CGP+CG), the amount of CD19+ was the highest in the GP group (p < 0.05). Interestingly, the proportion of the most primitive stem cells (MPP) was significantly higher in the G group compared to all other groups (p < 0.01). CP+CGP patients collected a sig-nificantly higher proportion of LMPP (p < 0.01) whereas the proportion of GMP was significantly higher in the CGP compared to G or CP, respec-tively. The proportion of MLP was the highest in the GP group compared to all other regimens (p < 0.001).Conclusion: In contrast to previous findings where P is reported to mobi-lize more primitive stem cells, we found that mobilization by cytokine alone yielded the highest proportion of MPP. Whether these differences are asso-ciated with immune reconstitution, long-term engraftment or patient out-come needs to be evaluated in larger patient groups with longer follow-up.
Tab. 1. Graft composition
median G (n = 20) GP (n = 17)
CG (n = 21)
CGP (n = 12) p-value
CD34 x10E6/kg 3.93 4.67 3.77 3.28 n.s.
CD3 x10E8/kg 1.92 2.58* 0.64 1.22 <0.05
CD19 x10E6/kg 7.67 17.3* 0.8 1.05 <0.05
MPP % 54.45* 32,9 42.1 31.5 <0.01
LMPP % 15.2 20.9 22.8* 36.4* <0.01
GMP % 0.8 5.1 3.1 7.4* <0.001
MLP % 2.3 7.8* 0.6 1.7 <0.001
FV-01-8Graft engineering in acute myeloid leukemia : CD96 antibody TH-111 depletes leukemic stem cells from autografts
Staudinger M., Peipp M., Kellner C., Bulduk M., Gramatzki M., Humpe A.Universität Kiel, Sektion f. Stammzell- & Immuntherapie, 2. Med. Klinik, Kiel, Germany
Introduction: Residual leukemic stem cells (LSC) may account for the high rate of relapse observed in patients suffering from acute myeloid leukemia (AML). Therefore, addressing these LSC residing in patients or autologous hematopoietic stem cell transplants by targeted therapy should lead to better therapeutic results. Here, CD96 - an antigen identi-fied on AML-LSC - was used to deplete AML LSC from autologous stem cell grafts by magnetic cell sorting (MACS). Moreover, a chimeric Fc-op-timized CD96 antibody was developed to eliminate these AML-LSC by antibody-dependent killing (ADCC) in vivo.Methods: To evaluate the efficiency of LSC purging HPC containing grafts were spiked with AML cells (KG1a, n = 10 experiments). To de-plete AML-LSC from autologous grafts by MACS, the Biotin-labeled

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts4
CD96 antibody TH-111 raised in our laboratory was used in combination with anti-Biotin-MicroBeads. The efficiency of depletion was analyzed by flow cytometry. Colony assays were used to evaluate the differentiation and proliferation characteristics of hematopoietic progenitor cells (HPC). Chimeric CD96 antibodies optimized for Fc-receptor engagement were analyzed for purity by SDS page and specific binding by flow cytometry. Antibody-mediated effector functions were measured in 51Cr-release as-says or by flow cytometry.Results: Up to a 1000-fold depletion of target cells was achieved by MACS. The potential of HPC to proliferate and differentiate was not af-fected by the purging procedure. Chimeric CD96 antibodies combining a Fc optimized human IgG1Fc and wild type or affinity maturated variable regions were generated to recruit Fc-receptor bearing effector cells for ly-sis of CD96+ AML-LSC. The affinity maturated CD96 antibody efficiently recruited NK cell for lysis of CD96 positive target cells while HPCs’ viabil-ity was not impaired. The higher antigen binding affinity of the maturated antibody (EC50 0.6 vs. 2 µg/ml) may account for the elevated target cell lysis (EC50 0.02 vs. 0.15 µg/ml; E:T ratio 2.5:1).Conclusion: The efficient elimination of AML-LSC by MACS may be beneficial for the development of graft-engineering strategies to avoid re-transplantation of AML-LSC and provide rationale for autologous stem cell transplantation in certain patients with AML. In autologous as well as allogeneic situations the in vivo application of an Fc-optimized chimeric CD96 antibody targeting AML-LSC may possibly open additional thera-peutic avenues in eliminating residual disease.
FV-01-9Influence of HLA-C mismatch depends on recipients HLA-C encoded KIR ligand in allogeneic hematopoietic peripheral progenitor cell transplantation for high-risk myelodysplastic syndrome or secondary acute myeloid leukemia
Fischer J.C.1, Enczmann J.1, Uhrberg M.1, Groten A.2, Schröder T.2, Kondakci M.2, Kobbe G.2
1Medical Faculty, Heinrich Heine University, Institute for Transplantation Diagnostics and Cellular Therapeutics, Düsseldorf, Germany, 2Medical Faculty, Heinrich Heine University, Department of Hematology, Oncology and Clinical Immunology, Düsseldorf, Germany
HLA-C-encoded KIR ligands (C1 or C2) were identified as important factors for allogeneic transplantation (tpx): In a previous retrospective study CML recipients bearing at least one C2 ligand showed worse sur-vival when compared to C1C1 recipients (HR 5.9, p < 0.01), especially when peripheral blood progenitor cells (PBPC) were used or in patients at advanced disease stage. These initial findings were confirmed in a sec-ond cohort in advanced AML/CML, (but not in MDS or ALL/NHL) re-ceiving PBPC. Notably, HLA-C allele matching contributed differentially to the transplantation outcome: it was beneficial in C1 patients, but was detrimental in C2 recipients (increased TRM, HR 3.5, p < 0.012; increased relapse, HR 2.7, p = 0.06). In both cohorts no or only a small fraction of patients received ATG. The aim of the present retrospective study was to determine the influence of HLA-C allele matching on the background of HLA-C encoded KIR ligand status in a more recent patient cohort, using ATG in all unrelated transplantations. Within this single center cohort patients mostly suffering from high-risk myelodysplastic syndrome or secondary acute myeloid leukemia (n = 98, AML 43, MDS 18, MDS/MPS 6, MPS 3, sAML 28) were transplanted with allogeneic PBPC using a FLAMSA-based high-dose sequential condition-ing regimen between 2002 and 2011. Donors were either matched rela-tives (MRD, n = 38) or unrelated donors (MUD, n = 60). High resolution HLA typing (4 digit, HLA-A,B,C, DRB1. DQB1)) revealed that 12 of the transplant pairs showed HLA-C antigen mismatch (MM), 4 showed HLA DQB1 MM (3 combined with the HLA-C MM). Patients were predomi-nately at high risk for tpx (52% late, 30% intermediate, 18% early but with high risk phenotype). Mean estimates were used, when median survival rates were not reached.
Mean follow up of the total population was 2202 d (95% CI 1878–2526), with an EFS of 1303 d (95% CI 713–1893). MM of HLA DQB1 had no effect on EFS or OS, whereas HLA-C-MM lowered OS (mean 2407 vs 729 d, p < 0.01) and EFS (median 1391 vs 289 d, p < 0.01). Interestingly the detrimental effect of HLA-C-MM was more pronounced in recipients ho-mozygous for the KIR ligand C1C1 than in the others (OR OS: 10.2 (CI 1.8 - 57.0, p < 0.01) vs. 2.7 (CI .9 – 7.2, p < 0.06); OR EFS: 10.3 (1.8 – 57.8, p < 0.01) vs. 2.5 (0.9 – 6.4, p < 0.08)Using ATG based regimes HLA-C-MM should be avoided especially in recipients bearing the HLA-C encoded C1C1.
Infectious diseases and pathogen inactiviation
FV-02-1Clinical safety and efficacy of red blood cell components treated with the second generation s-303 pathogen and leukocyte inactivation system – a randomized controlled double-blind phase 3 study in patients requiring transfusion support of acute anemia
Brixner V.1, Kiessling A.-H.2, Madlener K.3, Leibacher J.1, Müller M.1, Geisen C.1, Henschler R.4, North A.5, Huang N.5, Mufti N.5, Ernst C.5, Rico S.5, Corash L.5, Seifried E.1
1German Red Cross Blood Donor Service Baden-Wuerttemberg-Hessen, Frankfurt, Germany, 2Department of Thoracic and Cardiovascular Surgery, Johann Wolfgang Goethe University, Frankfurt, Germany, 3Department of Haemostaseology and Transfusion Medicine, Kerckhoff-Klinik, Bad Nauheim, Germany, 4University Clinic Munich, Department for Transfusion Medicine, Cell Therapy and Hemostaseology, Munich, Germany, 5Cerus Corporation, Concord, United States
Introduction: The second generation S-303 pathogen and leukocyte in-activation system for red blood cells (RBC) is intended to improve blood transfusion safety by reducing the risk of transfusion transmitted infec-tions and transfusion-associated graft versus host disease. The clinical safety and efficacy in adult cardiovascular surgery patients requiring transfusion support for acute anemia was assessed in a random-ized, double-blind, controlled, multi-center clinical trial.Methods: Patients undergoing coronary artery bypass grafting, and/or valve replacement or repair were randomized to receive S-303 treated or conventional RBC during a 7-day treatment period. Clinical outcomes re-flective of tissue oxygenation were assessed: renal insufficiency, hepatic insufficiency; and cardiopulmonary function. Adverse events (AE) were collected throughout the study. Immunogenicity was assessed by testing patient serum against S303 treated RBCs using a gel card agglutination test prior to transfusion and at day 28 and day 90 postoperative. Results: Eighty-seven patients in two clinical centers were enrolled, and fifty-one patients (Test 25, Control 26) who received study RBC were eval-uable. A total of 73 S-303 treated RBC and 75 control RBC were trans-fused. Overall incidence of renal insufficiency was 15.7% (Test 5, Control 3; p = 0.41). None of the renal insufficiency events occurred in relationship to the administration of study RBC units. Incidence of hepatic insufficien-cy was 2% (Test 1, Control 0, p = 0.37). Most patients (84.3%) experienced an AE. There were no statistical differences in the overall incidence of AE rates (Test 22 vs. Control 21, p = 0.412), or in possibly related AEs (Test 5 vs. Control 3, p = 0.24). Overall, 22 (43.1%) patients experienced a serious adverse event (SAE), with similar distribution between groups (Test 13 vs. Control 9, p = 0.20). Three SAEs were considered possibly related to the transfusion of study RBC (Test 1 vs. Control 2). Five patients died during this study (Test 3 vs. Control 2, p = 0.53). Deaths were not considered re-lated to the administration of study RBC components. Observed AEs were within the expected spectrum for patients with advanced cardiovascular diseases undergoing cardiovascular surgery. No patients exhibited an im-mune response to S-303 treated RBCs.
Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts6
Results/Conclusions: Clinical safety and efficacy variables following the transfusion of S-303 treated RBC were comparable to conventional RBC.
FV-02-2The Intercept Blood System reduces platelet aggregation and in vivo platelet survival by inducing apoptosis
Stivala S.1, Gobbato S.1, Reiner M.F.1, Lüscher T.F.2, Meyer S.C.3, Infanti L.3, Buser A.3, Beer J.H.1,4
1University of Zurich, Laboratory for Platelet Research, Schlieren, Switzerland, 2University Hospital Zurich, Cardiology, Zürich, Switzerland, 3University Hospital Basel, Transfusion Center of the Swiss Red Cross, Basel, Switzerland, 4Cantonal Hospital Baden, Internal Medicine, Baden, Switzerland
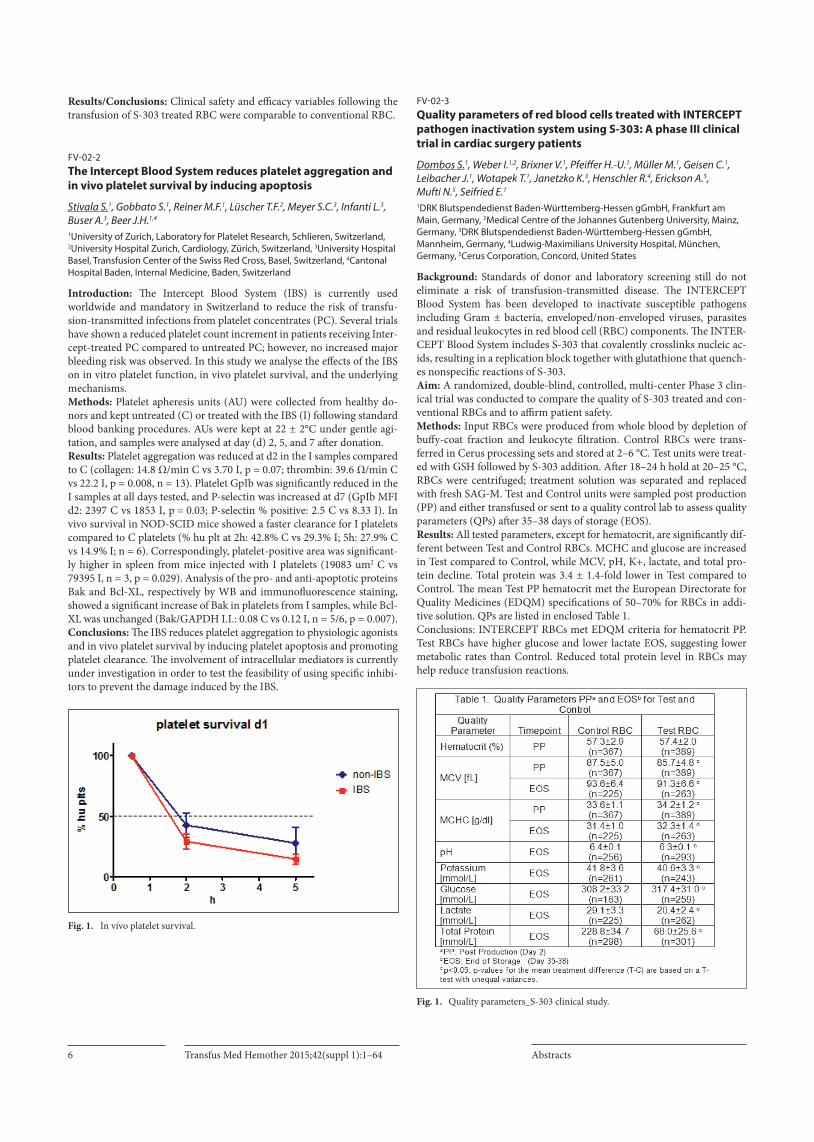
Introduction: The Intercept Blood System (IBS) is currently used worldwide and mandatory in Switzerland to reduce the risk of transfu-sion-transmitted infections from platelet concentrates (PC). Several trials have shown a reduced platelet count increment in patients receiving Inter-cept-treated PC compared to untreated PC; however, no increased major bleeding risk was observed. In this study we analyse the effects of the IBS on in vitro platelet function, in vivo platelet survival, and the underlying mechanisms.Methods: Platelet apheresis units (AU) were collected from healthy do-nors and kept untreated (C) or treated with the IBS (I) following standard blood banking procedures. AUs were kept at 22 ± 2°C under gentle agi-tation, and samples were analysed at day (d) 2, 5, and 7 after donation.Results: Platelet aggregation was reduced at d2 in the I samples compared to C (collagen: 14.8 Ω/min C vs 3.70 I, p = 0.07; thrombin: 39.6 Ω/min C vs 22.2 I, p = 0.008, n = 13). Platelet GpIb was significantly reduced in the I samples at all days tested, and P-selectin was increased at d7 (GpIb MFI d2: 2397 C vs 1853 I, p = 0.03; P-selectin % positive: 2.5 C vs 8.33 I). In vivo survival in NOD-SCID mice showed a faster clearance for I platelets compared to C platelets (% hu plt at 2h: 42.8% C vs 29.3% I; 5h: 27.9% C vs 14.9% I; n = 6). Correspondingly, platelet-positive area was significant-ly higher in spleen from mice injected with I platelets (19083 um2 C vs 79395 I, n = 3, p = 0.029). Analysis of the pro- and anti-apoptotic proteins Bak and Bcl-XL, respectively by WB and immunofluorescence staining, showed a significant increase of Bak in platelets from I samples, while Bcl-XL was unchanged (Bak/GAPDH I.I.: 0.08 C vs 0.12 I, n = 5/6, p = 0.007). Conclusions: The IBS reduces platelet aggregation to physiologic agonists and in vivo platelet survival by inducing platelet apoptosis and promoting platelet clearance. The involvement of intracellular mediators is currently under investigation in order to test the feasibility of using specific inhibi-tors to prevent the damage induced by the IBS.
Fig. 1. In vivo platelet survival.
FV-02-3Quality parameters of red blood cells treated with INTERCEPT pathogen inactivation system using S-303: A phase III clinical trial in cardiac surgery patients
Dombos S.1, Weber I.1,2, Brixner V.1, Pfeiffer H.-U.1, Müller M.1, Geisen C.1, Leibacher J.1, Wotapek T.1, Janetzko K.3, Henschler R.4, Erickson A.5, Mufti N.5, Seifried E.1
1DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Frankfurt am Main, Germany, 2Medical Centre of the Johannes Gutenberg University, Mainz, Germany, 3DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Mannheim, Germany, 4Ludwig-Maximilians University Hospital, München, Germany, 5Cerus Corporation, Concord, United States
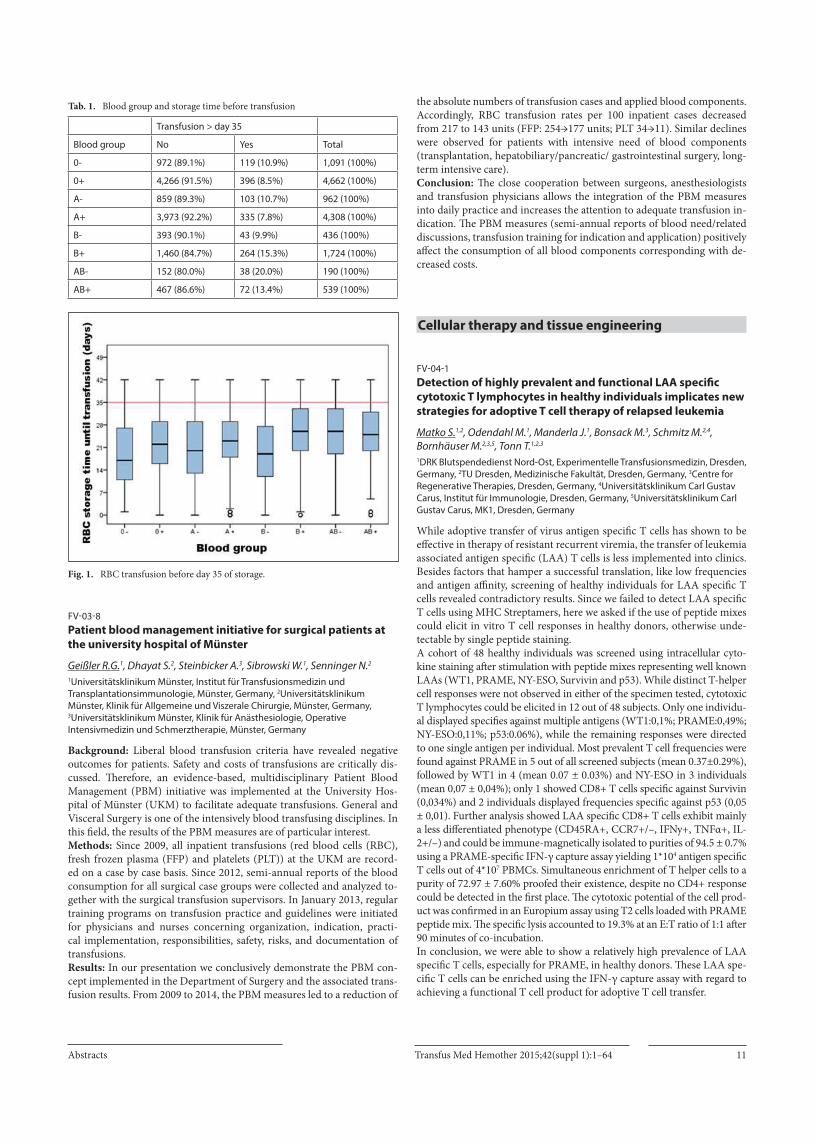
Background: Standards of donor and laboratory screening still do not eliminate a risk of transfusion-transmitted disease. The INTERCEPT Blood System has been developed to inactivate susceptible pathogens including Gram ± bacteria, enveloped/non-enveloped viruses, parasites and residual leukocytes in red blood cell (RBC) components. The INTER-CEPT Blood System includes S-303 that covalently crosslinks nucleic ac-ids, resulting in a replication block together with glutathione that quench-es nonspecific reactions of S-303. Aim: A randomized, double-blind, controlled, multi-center Phase 3 clin-ical trial was conducted to compare the quality of S-303 treated and con-ventional RBCs and to affirm patient safety. Methods: Input RBCs were produced from whole blood by depletion of buffy-coat fraction and leukocyte filtration. Control RBCs were trans-ferred in Cerus processing sets and stored at 2–6 °C. Test units were treat-ed with GSH followed by S-303 addition. After 18–24 h hold at 20–25 °C, RBCs were centrifuged; treatment solution was separated and replaced with fresh SAG-M. Test and Control units were sampled post production (PP) and either transfused or sent to a quality control lab to assess quality parameters (QPs) after 35–38 days of storage (EOS). Results: All tested parameters, except for hematocrit, are significantly dif-ferent between Test and Control RBCs. MCHC and glucose are increased in Test compared to Control, while MCV, pH, K+, lactate, and total pro-tein decline. Total protein was 3.4 ± 1.4-fold lower in Test compared to Control. The mean Test PP hematocrit met the European Directorate for Quality Medicines (EDQM) specifications of 50–70% for RBCs in addi-tive solution. QPs are listed in enclosed Table 1. Conclusions: INTERCEPT RBCs met EDQM criteria for hematocrit PP. Test RBCs have higher glucose and lower lactate EOS, suggesting lower metabolic rates than Control. Reduced total protein level in RBCs may help reduce transfusion reactions.
Fig. 1. Quality parameters_S-303 clinical study.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 7
FV-02-4Cytomegalovirus is efficiently inactivated in human plasma by the THERAFLEX MB-Plasma system
Gravemannn U.1, Handke W.1, Sumian C.2, Reichenberg S.3, Seltsam A.1
1DRK Blutspendedienst NSTOB, Springe, Germany, 2MacoPharma SA, Tourcoing, France, 3MacoPharma International, Langen, Germany
Introduction: Photodynamic treatment using methylene blue (MB) and visible light is in routine use for virus inactivation of human plasma. It has been shown to inactivate a broad range of different DNA and RNA viruses. Human cytomegalovirus (HCMV) is known to be transfusion transmissible and a recognized cause of morbidity and mortality in im-munocompromised individuals. Aims: Aim of the study was to investigate the efficacy of the THERAFLEX MB-Plasma system to inactivate HCMV in human plasma. Methods: Leukodepleted plasma was prepared from whole blood using standard blood banking technology. Donors were tested for anti-CMV antibodies using the Enzygnost Anti-CMV/ IgG+IgM test to exclude the presence of neutralizing antibodies in plasma. Only anti-CMV negative plasma units were included in the study. Plasma units (n = 4, 285 mL) were spiked with virus suspension (30 mL) to reach a final volume of 315 mL. MB/light treatment was done according to the manufacturer’s in-structions. Samples were taken after spiking (load and hold sample), after addition of MB and after illumination with different light doses. The titer of HCMV (strain AD-169, ATCC VR-538) was determined by endpoint titration and large volume plating in microtitre plate assays on MRC-5 cells (fibroblasts, ATCC CCL-171). Results: The results are summarized in the Table. HCMV was efficiently inactivated by more than 4.06 log steps. Already half of the standard light dose of 120 J/cm2 resulted in inactivation of HCMV to infectivity levels below the limit of detection.
Tab. 1. Inactivation kinetics
Sample/Time point mean titer [log10 TCID50/ mL]
mean log10 reduction factor
load 4.55 ± 0.58 0.00
after addition of MB 4.33 ± 0.54 0.22 ± 0.79
30 J/cm2 1.15 3.40
60 J/cm2 ≤ 1.19 ≥ 3.36
90 J/cm2 ≤ 0.49 ≥ 4.06
120 J/cm2 ≤ 0.49 ≥ 4.06
hold 4.37 ± 0.52 0.18 ± 0.78
Conclusions: It was shown that treatment of human plasma by THERAF-LEX MB-Plasma system efficiently inactivates HCMV and thereby signifi-cantly contributes to the viral safety of plasmas for transfusion.
FV-02-5Tick-borne encephalitis virus (TBEV) infection in Swiss blood donors – preliminary results
Eyer C.1, Gäumann R.2, Leib S.2, Niederhauser C.1
1Interregional Blood Transfusion SRC, Research & Development, Bern, Switzerland, 2SPIEZ LABORATORY, Spiez, Switzerland
Introduction: In Switzerland TBE is a notifiable disease. The number of reported cases ranges from approx. 100–200 cases per year, but the ma-jority of TBEV infections is thought to pass unnoticed, posing a potential risk to the safety of blood components. For this reason the IRB investigat-ed the seroprevalence of naturally acquired anti-TBEV IgG among Swiss blood donors. This data will be needed in future studies assessing the risk of TBEV contaminated blood components. Methods: The study was carried out with ethical clearance in endemic and non-endemic regions in the cantons BE, VD, SG, LU, BS and TI. The
sampling regions were selected according to the distribution of TBE cas-es reported by the Federal Office of Public Health (http://map.geo.admin.ch/?layers=ch.bag.zecken-fsme-faelle). Blood donors consenting to the study participation were asked to fill in a questionnaire with TBE-related questions. During the blood donation an additional tube of whole blood was collected from the pre-donation bag. Plasma samples were screened for IgG against TBEV using the Enzygnost anti-TBE virus ELISA (Sie-mens, Marburg). The TBEV vaccination status from donors reactive in screening ELISA (including grey zone) was checked with the question-naire. Selected samples from unvaccinated, initially reactive donors are currently being confirmed by indirect immunofluorescence test (Euroim-mun, Lübeck, Flavivirus Mosaic 2).Results: A total of 9’329 donations were tested in ELISA. 3’083 originated from TBEV endemic regions, 2’583 from regions neighbouring endemic foci and 3’663 from TBEV negative areas. 2’281 donors were reactive in IgG ELISA, 397 of which had not been vaccinated, whereas 27 had left the questionnaire blank resulting in a total of 424 reactive samples from potentially unvaccinated donors. Further investigation into the origin of these 424 samples, 136 came from TBEV endemic regions, 134 from bor-der regions and 154 from negative regions.Conclusion: We found roughly equal numbers of anti-TBEV reactive samples in endemic and non-endemic areas, as well as in regions in the vi-cinity of TBEV foci. This equal distribution probably reflects the mobility of people living in Switzerland. Further confirmatory tests and evaluation of the questionnaires will be carried out in order to confirm our results.
FV-02-6Experiences with the deferral of blood donors who returned from regions with continuous West Nile Virus transmission in Germany
Juhl D.1,2, Quandt T.1,2, Steppat D.1,2, Görg S.1,2, Hennig H.1,2
1Universitätsklinikum Schleswig-Holstein, Transfusionsmedizin, Lübeck, Germany, 2Universitätsklinikum Schleswig-Holstein, Transfusionsmedizin, Kiel, Germany
Background: Deferral of blood donors who spent time in North America during the summer months is mandatory in Germany already since 2003 to avoid transfusion-transmitted West Nile Virus (WNV) infections. But WNV became more and more endemic in Europe and neighbouring re-gions in the last years. Thus, since 2014, according to an enactment of the Paul-Ehrlich-Institut (PEI), donors must either be deferred for 28 days or tested for WNV RNA, if they have returned from such a region or a country with continuous WNV transmission. The aims of our study were to assess the donor loss due to donor deferral and the rate of donors being infected with WNV.Methods: Blood donors were deferred for four weeks after returning from a country with continuous WNV transmission in our institute between June 1 and November 30 2014. They have been tested for WNV RNA by NAT (Cobas TaqScreen West Nile Virus test, Roche diagnostics, Mann-heim) and for antibodies of the IgM and IgG class against WNV by ELISA (Anti-West Nile Virus ELISA, EUROIMMUN, Lübeck) if they returned to blood donation.Results: 16.908 donors were admitted to donate during the observation period. 49 donors (corresponding to 0,29% of the admitted donors) were deferred due to a stay in a region with continuous WNV transmission (Europe/neighbouring regions or North America). To date, 40 of these donors returned to blood donation after a mean time of 65 days. All the donors tested negative for WNV RNA and for anti-WNV IgM. 39 donors tested negative for anti-WNV IgG, one donor showed a borderline result for anti-WNV IgG.Summary: Donor deferral rate was very low and the majority of deferred donors returned to blood donation after the deferral period expired. Thus, donor and donation loss due to the PEI enactment were marginal in 2014 and donor deferral was a reasonable alternative to WNV RNA testing in that year. Infections in blood donors returning from regions affected by WNV seem to be a rare event: at least in 40 investigated blood donors, there was no evidence for a WNV infection.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts8
FV-02-7HIV-1 dual target NAT improves blood safety
Schmidt M.1, Hourfar K.2, Nübling M.3, Chudy M.3, Kress J.3, Gürtler L.4, Eberle J.4, Seifried E.2
1DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Spenderscreening, Frankfurt, Germany, 2DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Frankfurt, Germany, 3Paul Ehrlich Institute, Langen, Germany, 4Virologie LMU, München, Germany
Background: The introduction of nucleic acid amplification testing (NAT) into blood donor screening was able to reduce the diagnostic win-dow period to a minimum and to improve blood safety to a high level. Nevertheless RNA viruses are associated with a high frequency for mu-tations due to the missing proof- reading function of polymerases, as re-verse transcriptase. Between 2007 and 2010 six blood donations with false negative NAT results were reported in Germany. Therefore NAT-screen-ing in two genome regions was introduced by our blood donation service in 2010 on a voluntary basis and became mandatory in Germany since beginning of 2015.Material/Methods: Blood donor screening was done using in parallel the GRC HIV-1 CE ltr PCR kit and the GRC HIV-1 gag CE PCR kit. In total, 7 million blood donations were screened during the study period from 2010 to 2014 with the GRC dual target HIV-1 NAT system. In case of discrepant results between both assays samples were sequenced in the primer bind-ing regions (5´LTR and gag region) as well as in the hypervariable HIV-1 V3 region. Additionally those specimens were analysed by four single tar-get NAT assays and by four dual target NAT assays, respectively.Results: Three out of seven donations tested negative using the 5´LTR-PCR but positive if amplification was performed in the gag-region. HIV antibodies were detectable in all three donations . For two of these dona-tions sufficient plasma was available for sequence analysis and testing in additional NAT-assays. Nucleic acid sequence analysis identified a dele-tion of 24 base pairs within the 5´LTR probe binding region. Phylogenetic analysis revealed HIV-1 group M subtype B virus and excluded genetically identical viruses in both donors. 3 different ltr-based mono-target assays missed the two donations, with the exception of a low-reactive result ob-tained by one of the assays. In total the detection rates were 37.5% (3/8) for mono-target assays and 100% (10/10) for dual-target assays (p = 0.01).Discussion: Genetic modifications within the HIV-1 genome are very fre-quent during the transcription process from RNA into DNA. Although the primer and probe binding regions of screening assays are usually lo-cated in highly conserved genome regions mutations cannot be excluded. The current data demonstrate that dual target NAT systems reduce the risk of false negative NAT screening results significantly.
FV-02-8Rapid bacterial detection in platelet concentrates using the Bac-Detect System
Störmer M.1, Gielen J.2, Gathof B.S.1
1Transfusion Medicine, University Hospital of Cologne, Cologne, Germany, 2Institute for Medical Microbiology, Immunology and Hygiene, University Hospital of Cologne, Cologne, Germany
Background: In contrast to virus screening, bacterial testing of PCs is only performed as routine quality control in Germany since 1997 by using automated culture at the end of shelf-life or in order to prolong the shelf-life to 5 days since 2008 by using rapid methods on day 3 or 4 of storage. Here we present the first results of the evaluation of a new flow cytomet-ric assay using the Bac-Detect System (Blood Analysis) to detect bacterial contamination in PCs.Methods: Bacterial strains of the WHO International Repository for Platelet Transfusion Relevant Bacteria Reference Strains (S. pyogenes, SP; K. pneumonia, KP; E. coli, EC; S. epidermidis, SE) and spores of B. thuringiensis (BT) were inoculated separately in three replicates with 5–15 CFU/bag into expired buffy coat derived pooled PCs (PPCs) in ad-ditive solution and apheresis PCs (APCs) in plasma and stored under rou-
tine conditions. Bacterial detection was performed during storage using the Bac-Detect in comparison to the BactiFlow ALS (Biomerieux). Sterile PCs served as negative and artificial highly contaminated PCs as positive controls.Results: With the exception of SE who showed a prolonged growth, all strains were already detectable by using the Bac-Detect by sampling on day 2 if the artificial contamination was successful and if the strain did grow. Contrarily the BactiFlow detected the small numbers of SE on day 2. One additional PC contamination needed to be performed each for BT, SP and EC due to growth difficulties. The sample preparation for the Bac-De-tect system was easy to perform and showed advantages in comparison to the BactiFlow preparation process. Conclusion: Late sampling in combination with the BactiFlow currently represents a very good strategy for bacterial screening of PCs and is ac-cepted by the German national authority (Paul-Ehrlich-Institut) to extend the storage period of PCs from 4 to 5 days. Moreover the BactiFlow seems to present a higher sensitivity regarding slow growing organisms. But the first results of this study demonstrate comparable detection properties of both systems. Therefore and due to the superior application procedure the Bac-Detect presents a promising approach. Nevertheless there is a need for further studies regarding the applicability in a routine screening set-ting to fully evaluate the acceptance for routine bacterial screening of PCs.
Clinical hemotherapy and patient blood management
FV-03-1Indikationen zur Gabe von Blutprodukten in der Palliativmedizin unter Berücksichtigung ethischer Betrachtungen – gibt es wirklich Unterschiede zur kurativen Medizin?
Heim M.U.Universitätsklinikum Magdeburg A.ö.R, Institut für Transfusionsmediin, Magdeburg, Germany
Die palliative Gabe von Blut wird häufig allein unter ethischen Gesichts-punkten bewertet, obwohl in diesem Bereich auch eine normale teils Leit-linien-gerechte Indikationsstellung möglich und erforderlich ist. Da es für die Gabe von Blutprodukten keine durch große randomisierte Studien belegte Mindestgrenzwerte für die Indikation zur Transfusion gibt, ge-hen die meisten Empfehlungen in den Leitlinien auf Expertenmeinungen zurück, die auf jahrzehntelangen, wohlgemeinten Erfahrungen beruhen. Dies ist auch der Grund, dass in Deutschland keines der Blutprodukte «ordentlich» arzneimittelrechtlich zugelassen worden ist, sondern nur Gutachten aus Erfahrungsberichten nach 50 Jahren Transfusionsmedizin bei der Nachzulassung vorlagen. Allein aufgrund von Erfahrungsberich-ten von Ärzten, die vorwiegend Patienten behandeln, die aus vorwiegend religiösen Gründen Bluttransfusionen ablehnen, lassen sich Rückschlüsse auf absolut lebensnotwendige Grenzwerte ziehen. Trotzdem sind die Kri-terien für einen absoluten Verzicht auf die Gabe von Blutprodukten als eine der möglichen Therapiebegrenzungen sehr vage; ggf, auch ein Grund dafür, dass die Blutübertragung mit der künstlichen Beatmung und Flüs-sigkeitszufuhr zu den zuletzt abgesetzten Therapiemaßnahmen gehört. Bei der Indikationsstellung müssen vor allem die palliativen Therapiezie-le definiert und berücksichtigt werden, wie z.B. die effektive Linderung von Sterbesymptomen nach dem Hospiz-Gedanken: «Menschen helfen, gut zu leben, bis zuletzt». Dazu gehören auch die Grundgedanken bei der Indikationsstellung: Wohltun (Evidenz-basiert?), Selbstbestimmung (Pa-tienten-Autonomie ~ «manipulierte Aufklärung»?), Schaden vermeiden (Hinweise von transfusionsbedingter Verschlechterung bei der Mortali-tät) und Gerechtigkeit (Knappheit beim Blut – für alle ausreichend ?). Bei einer guten Strukturierung dieser Überlegungen begrenzt man «medizi-nisches Futility» (Oudenotherapie nach Bleuler) ohne dem «therapeuti-schen Nihilismus» zu erliegen.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 9
Schlussendlich sind die ethischen Grundsätze zur Indikationsstellung für die Gabe von Blut auf der kurativ konzipierten Intensivstation die gleichen wie in einem Hospiz.
FV-03-2Survey of patients receiving Leukocyte transfusions from 2012 until 2014, a one center retrospective analysis
Witt V., Pichler H.St. Anna Kinderspital, Department for Pediatrics, MUW, Vienna, Austria
Introduction: Infections continue to be a serious clinical challenge in pa-tients undergoing immunosuppressive therapies and/or stem cell trans-plantation for various reasons. In our institution since 1996 granulocyte transfusions (GT) from family and unrelated donors are fix therapeutic elements in neutropenic patients not or inadequately responding to the standard therapy with antibiotics and best supportive treatment. We now analysed the most recent treated cohort from 2012 to 2014 to evaluate the overall outcome of these patients.Methods: From 2012 to 2014 all documented GT were selected from the blut depot software program (datalabx, Bartels, Graz, A). 255 GT were performed in 24 patients, median age 9.5y (2.3–21), 10 male and 11 fe-male, 10 suffered from AML/MDS, 8 ALL, 3 solid tumours and 3 non-ma-lignant disease. The main indication was severe life threatening infection in neutropenia despite best supportive care, 9 Pseudomanas lesion +/– Sepsis, 4 local infection + sepsis of unknown origin, 5 SIRS . 3 Aspergil-lom, 1 Fusarium, 1 prophylactically (septic granulomatosis peri-SCTx).The reason for neutropenia were in patients with leukemia 10 under allo-geneic SCTx and 8 under chemotherapy.Results: 15/24 patients survived > than 1 year. Death were in 8/9 patients directly due to the infectious complication in combination with multiple organ failure (MOF). A subgroup analysis revealed, that in patients with Pseudomonas lesions even plus minus Sepsis the outcome was 79%, with unknown origin of the same clinical situation 62.5%, fungal infection had a overall survival of 50%, and 1 patients suffering from viral Sepsis did not survived. All patients with local infections +/– Sepsis had a 85% survival rate, whether patients with SIRS and/or MOF did all. Only a patient with fungal infection needed surgical treatment after recovery.Conclusion: Local infection with or without Sepsis treated with GT in addition to best supportive care showed an excellent overall outcome, whether severe MOF and/or SIRS had a fatal outcome. Whether this is due to the fact that immunosuppressed patients with MOF have a dismal prognosis per se could in our retrospective analysis not been stated. Fur-ther prospective studies are urgently warranted to give a clear answer for the urgent question when to administer and when not to administer GT in immunosuppressed paediatric patients with severe infectious compli-cations.
FV-03-3Longitudinal characterization of patients receiving blood transfusions in a 17 year period
Brockmann C.1, Hagen C.1, Busemann N.1, Schnell P.2, Gernhuber J.2, Görg S.1
1University Hospital of Schleswig-Holstein, Institute for Transfusionmedicine, Lübeck, Germany, 2University Hospital of Schleswig-Holstein, Institute for Transfusionmedicine, Kiel, Germany
While the total numbers of blood transfusions are collected nationwide in Germany, the epidemiological characteristics of individuals who receive transfusions have not been well described.In a retrospective analysis we analyzed data from our laboratory informa-tion system to characterize patients receiving red blood cell concentrates (RBC) in the University hospital of Lübeck between 1998 and 2014. Pa-tients with identical names, birthdays, sex, AB0 and Rhesus blood groups receiving RBCs within one year either while in a surgical ward or in a nonsurgical environment where defined as a case.
During the 17 years 64.312 patients received a total number of 353.053 RBCs. The annual total number of RBC units where 21361 in 1998, reach-ing 22669 in 2003 declining since then to 17183 in 2014. The decline was pronounced in 2013 and 2014 with a reduction of 7% in two consecutive years compared to the previous years. While 51.5% of the recipients were male they received 56.8% of the RBCs, and this was similar over the whole period. The average age of females receiving RBCs increased by 3.3 years from 64.5 to 67.8, whereas in males the average rose by 6.7 years from 60.3 to 67.0 years. The average numbers of RBC per female case decreased from 5.13 units in 1998 to 4.32 units in 2014, whereas in males the num-bers of RBCs declined from 6.64 to 5.63. The percentage of transfused RBCs within a surgical department decreased from 72% in 1998 to 60% in 2014 with a pronounced decline in the years 2013 and 2014, whereas the total numbers of RBCs given in nonsurgical Departments were stable over the time. In surgical cases the decline of the number of transfused RBC units was stronger in a subgroup receiving more than 10 units compared to patients receiving 10 or less units.In summary we observed an increase of age in patients receiving blood transfusions, whereas the total number of patients receiving RBCs was stable within the observed time period. Especially in the last two years a decline of given RBCs was observed mainly as a result of decreased num-bers of patients in surgical departments receiving more than 10 units and less as a result of patients receiving lower numbers of RBCs.
FV-03-4Healthy elderly and their lab Reference Intervals (RI) may influence transfusion strategy of Comprehensive Geriatric Assessment, CGA
Grebhardt C.1, Medina Escobar P.2, Nydegger U.1, Risch L.3, Risch M.4
1Labormedizinisches Zentrum Dr. Risch, Hämatologie, Liebefeld bei Bern, Switzerland, 2Labormedizinisches Zentrum Dr. Risch, Klinische Chemie, Liebefeld bei Bern, Switzerland, 3Labormedizinisches Zentrum Dr. Risch, Liebefeld bei Bern, Switzerland, 4Kantonsspital Graubünden, Zentrallabor, Chur, Switzerland
Introduction: Biologic variability in the elderly may lead to unexpected blood cell RIs in senior citizens. Even applying liberal transfusion strategy but more so with a restrictive schedule, the triggers are way below RIs of healthy elderly but may approach lower cut-offs of 10 or 9 g/dl.We therefore explored the data warehouse accumulated in the seniorlabor study (www.seniorlabor.ch) for RIs of Hb in healthy elderly ≥ 60 years.Methods: Apparently healthy 557 men and 722 women ≥ 60 years par-taking in the seniorlabor study (www.seniorlabor.ch) in whom CBC was assessed using an XE-5000 haematology analyzer (Sysmex-Digitana, Swit-zerland).Results: RIs were stratified according to age and gender. Double-sided 95% RIs for Hb for men were: 129–168 g/L (age 60–69), 125 - 168 g/L (age 70–79) and 118–169 g/L (age ≥80). The respective RIs of Hb for females were: 120–157 g/L (age 60–69), 116 - 156 g/L (age 70–79), 115–164 g/L (age ≥80) deviating from standards issued by WHO.We then evaluated possible associations of single Hb and plt values with RBC, Ht, MCV, albumin, haptoglobin, iron, ferritin, transferrin and IgG. For this purpose, we excluded 580 of 1467 participants for the following reasons: missing values (N = 40), C-reactive protein ≥ 10 mg/L (N = 46), > 5 p.o.drugs (N = 40), aggregation inhibitors and anticoagulants (N = 308), Ca++-blockers (N = 53), vitamin B12 and folic acid support (N = 89) and overt hemorrhage (N = 4).Among the remaining 887 healthy elderly subjects we first examined pos-sible associations with Hb concentrations and found significant correla-tions with RBC (p < 0.0001; r = 0.82), Ht (p < 0.0001; r = 0.94), MCV (p = 0.0254; r = 0.08), albumin (p = 0.0019; r = 0.10), iron (p < 0.0001; r = 0.31), ferritin (p < 0.0001; r = 0.37) and plt (p < 0.0001; r = -0.24).

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts10
We then examined possible associations with plt concentrations and found significant correlations with RBC (p < 0.0001; r = –0.17), Ht (p < 0.0001; r = –0.22), MCV (p = 0.0462; r = –0.07), haptoglobin (p < 0.0001; r = 0.21), iron (p = 0.0009; r = –0.11), ferritin (p < 0.0001; r = –0.25) and transferrin (p < 0.0001; r = 0.16).Conclusion: Mild anemia in healthy elderly citizens sets the stage for overtransfusion.
FV-03-5Transfusion of pediatric patient with pathogen inactivated platelet concentrates
Schwarz F.1, Groß J.1, Gortner L.2, Graf N.3, Abdul-Khaliq H.4, Eichler H.1
1Universitätsklinikum des Saarlandes, Institut für Klinische Hämostaseologie und Transfusionsmedizin, Homburg, Germany, 2Universitätsklinikum des Saarlandes, Klinik für Allgemeine Pädiatrie und Neonatologie, Homburg, Germany, 3Universitätsklinikum des Saarlandes, Klinik für Pädiatrische Onkologie und Hämatologie, Homburg, Germany, 4Universitätsklinikum des Saarlandes, Klinik für Pädiatrische Kardiologie, Homburg, Germany
Background: Amotosalen inactivated platelet concentrates (PI-TK, IN-TERCEPT Blood System™, Cerus, USA) are licensed for the use in pe-diatric patients, but there are only few clinical data regarding the efficacy and safety in this patient group. Since 07/2012, a limited number of PI-TKs from apheresis donations are available for the treatment of pediatric patients at the Saarland University Hospital (pilot study), and all other pa-tients get transfused with non-inactivated apheresis platelet concentrates in ACD-A plasma (A-TK). Methods: In a single center approach, clinical and product data regarding pediatric PI-TK transfusions (period 02/2013 - 02/2014) were retrospec-tively analyzed and compared to pediatric patient receiving A-TK. All medical records were searched for documentation regarding the clinical effect of platelet transfusions (PLT counts pre/post transfusion, CCI) and signs of adverse events (AE). In addition, returned transfusion reports from the treating physicians were screened for the documentation of AE. Results: 24 children treated at one of the three pediatric departments of were transfused with overall 94 PI-TK (1–23 PI-TK per patient). The patients had a mean age of 5.8 years (0–13) and a mean weight of 28.3 kg (0.54–47.1). The PI-TK units showed a mean platelet content of 2.8 × 10E11 and had a mean storage time of 2.4 days (0–5) until delivery to the ward. All transfusions were well tolerated, and no AE were neither spon-taneously reported nor documented in the medical records. The clinical effects of PI-TK transfusions were not different compared to the use of standard A-TK. Conclusion: Due to our limited experience using PI-TK for preterm in-fants and children, this type of pathogen inactivated platelet concentrates is safe and efficient.
FV-03-6Blood donation of donors with disposition for hemochromatosis – Efficient prevention and gift for others in need
Gathof B., Ardin S., Biazik-Glaw H., Radojska S.Uniklinik Köln, Transfusionsmedizin, Köln, Germany
Background and aims: Hemochromatosis is the most prevalent genetic disposition (2–5/1000) in Caucasian populations. The genetically deter-mined increased iron absorption can lead to excessive iron accumulation with its respective consequences. Iron depletion by phlebotomy is the treatment of choice; (therapeutic) low normal iron levels (ferritin < 100 ug/L) are the target. Due to increased awareness for hemochromatosis in the medical profession and increased laboratory testing in the population persons with disposition for hemochromatosis are detected at an earlier stage of disease or even as asymptomatic carriers. Regular blood donation can help to maintain low iron levels and support the blood supply. If thera-
peutic goals are maintained Hemochromatosis patients even have a better life expectancy than the “normal” population due to decreased mortality related to cardiovascular disease (Bardou-Jaquet et al. J Hepatol 2015). For the update of the German guidelines target levels for the acceptance of a donation as a donation (in contrast to a therapeutic phlebotomy) are discussed, also in the “Arbeitskreis Blut” of the Robert Koch Institute. This study was to evaluate the results of the special program for donors with determination for hemochromatosis at our institute. Methods: Evaluation of the data of donors with disposition for hemo-chromatosis at our Institute for number of donations / phlebotomies, iron storage parameters.Results: Since 1998 a total of 70 hemochromatosis donors has been cared for at our institute. Weekly phlebotomies for iron depletion are performed until “normal” levels for iron storage parameters are reached. With each consecutive blood donation iron storage parameters are determined. The respective donation is only accepted for transfusion to patients if iron storage parameters are within the normal range. This resulted in 526 blood donations and 100 phlebotomies. 35 of presently 58 active donors not only maintain normal but low iron storage levels (ferritin < 100 ug/L).Conclusion: Blood donation can help persons with determination for hemochromatosis to maintain the recommended low iron levels. The do-nation as “gift” for patients in need can help to sustain the motivation for this long term prevention, which has been shown to increase survival even compared to the “normal” population.
The collaboration of the whole donation team represented by Mechthild Gerhard and Özlem Aylikci is highly appreciated.
FV-03-7The impact of the blood group on the time intervall from blood donation to RBC transfusion
Moog R.1, Tonn T.2
1DRK Blutspendedienst Nord-Ost, Institut Cottbus, Cottbus, Germany, 2DRK Blutspendedienst Nord-Ost, Dresden, Germany
Background: Current regulations permit the storage of red blood cells (RBCs) for up to 42 days. The impact of storage time of RBCs is still a mat-ter of debate in blood transfusion. Some studies report that RBC storage time prior to transfusion influences patient outcome with respect to mor-bidity and mortality while others do not. The aim was the present study was to analyse the time interval from blood donation to RBC transfusion stratified by blood groups.Materials and methods: 14,019 RBC units were followed up until trans-fusion. RBCs were stored in PAGGS-M additive solution up to 42 days. A focus was on the transfusion of the RBC units before day 35 of storage. Results: RBC Transfusion averaged on day 22.6 ± 9.4 (± SD). Details of the blood group distribution and the storage time before RBC transfu-sion are shown in figure 1. 12,649 (90.2%) units were transfused within 35 days of storage while 1,370 units (9.8%) were transfused thereafter. Table 1 shows details of the blood group distribution and transfusion before and after day 35 of storage.Conclusion: Our results demonstrate that most RBCs are transfused within 5 weeks after collection. There are differences in the time points of blood transfusions within the various blood groups. RBC units of blood group B and AB Rh positive as well as AB Rh negative were more often transfused after day 35 of storage.
Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 11
Tab. 1. Blood group and storage time before transfusion
Transfusion > day 35
Blood group No Yes Total
0- 972 (89.1%) 119 (10.9%) 1,091 (100%)
0+ 4,266 (91.5%) 396 (8.5%) 4,662 (100%)
A- 859 (89.3%) 103 (10.7%) 962 (100%)
A+ 3,973 (92.2%) 335 (7.8%) 4,308 (100%)
B- 393 (90.1%) 43 (9.9%) 436 (100%)
B+ 1,460 (84.7%) 264 (15.3%) 1,724 (100%)
AB- 152 (80.0%) 38 (20.0%) 190 (100%)
AB+ 467 (86.6%) 72 (13.4%) 539 (100%)
Fig. 1. RBC transfusion before day 35 of storage.
FV-03-8Patient blood management initiative for surgical patients at the university hospital of Münster
Geißler R.G.1, Dhayat S.2, Steinbicker A.3, Sibrowski W.1, Senninger N.2
1Universitätsklinikum Münster, Institut für Transfusionsmedizin und Transplantationsimmunologie, Münster, Germany, 2Universitätsklinikum Münster, Klinik für Allgemeine und Viszerale Chirurgie, Münster, Germany, 3Universitätsklinikum Münster, Klinik für Anästhesiologie, Operative Intensivmedizin und Schmerztherapie, Münster, Germany
Background: Liberal blood transfusion criteria have revealed negative outcomes for patients. Safety and costs of transfusions are critically dis-cussed. Therefore, an evidence-based, multidisciplinary Patient Blood Management (PBM) initiative was implemented at the University Hos-pital of Münster (UKM) to facilitate adequate transfusions. General and Visceral Surgery is one of the intensively blood transfusing disciplines. In this field, the results of the PBM measures are of particular interest.Methods: Since 2009, all inpatient transfusions (red blood cells (RBC), fresh frozen plasma (FFP) and platelets (PLT)) at the UKM are record-ed on a case by case basis. Since 2012, semi-annual reports of the blood consumption for all surgical case groups were collected and analyzed to-gether with the surgical transfusion supervisors. In January 2013, regular training programs on transfusion practice and guidelines were initiated for physicians and nurses concerning organization, indication, practi-cal implementation, responsibilities, safety, risks, and documentation of transfusions.Results: In our presentation we conclusively demonstrate the PBM con-cept implemented in the Department of Surgery and the associated trans-fusion results. From 2009 to 2014, the PBM measures led to a reduction of
the absolute numbers of transfusion cases and applied blood components. Accordingly, RBC transfusion rates per 100 inpatient cases decreased from 217 to 143 units (FFP: 254→177 units; PLT 34→11). Similar declines were observed for patients with intensive need of blood components (transplantation, hepatobiliary/pancreatic/ gastrointestinal surgery, long-term intensive care).Conclusion: The close cooperation between surgeons, anesthesiologists and transfusion physicians allows the integration of the PBM measures into daily practice and increases the attention to adequate transfusion in-dication. The PBM measures (semi-annual reports of blood need/related discussions, transfusion training for indication and application) positively affect the consumption of all blood components corresponding with de-creased costs.
Cellular therapy and tissue engineering
FV-04-1Detection of highly prevalent and functional LAA specific cytotoxic T lymphocytes in healthy individuals implicates new strategies for adoptive T cell therapy of relapsed leukemia
Matko S.1,2, Odendahl M.1, Manderla J.1, Bonsack M.3, Schmitz M.2,4, Bornhäuser M.2,3,5, Tonn T.1,2,3
1DRK Blutspendedienst Nord-Ost, Experimentelle Transfusionsmedizin, Dresden, Germany, 2TU Dresden, Medizinische Fakultät, Dresden, Germany, 3Centre for Regenerative Therapies, Dresden, Germany, 4Universitätsklinikum Carl Gustav Carus, Institut für Immunologie, Dresden, Germany, 5Universitätsklinikum Carl Gustav Carus, MK1, Dresden, Germany
While adoptive transfer of virus antigen specific T cells has shown to be effective in therapy of resistant recurrent viremia, the transfer of leukemia associated antigen specific (LAA) T cells is less implemented into clinics. Besides factors that hamper a successful translation, like low frequencies and antigen affinity, screening of healthy individuals for LAA specific T cells revealed contradictory results. Since we failed to detect LAA specific T cells using MHC Streptamers, here we asked if the use of peptide mixes could elicit in vitro T cell responses in healthy donors, otherwise unde-tectable by single peptide staining. A cohort of 48 healthy individuals was screened using intracellular cyto-kine staining after stimulation with peptide mixes representing well known LAAs (WT1, PRAME, NY-ESO, Survivin and p53). While distinct T-helper cell responses were not observed in either of the specimen tested, cytotoxic T lymphocytes could be elicited in 12 out of 48 subjects. Only one individu-al displayed specifies against multiple antigens (WT1:0,1%; PRAME:0,49%; NY-ESO:0,11%; p53:0.06%), while the remaining responses were directed to one single antigen per individual. Most prevalent T cell frequencies were found against PRAME in 5 out of all screened subjects (mean 0.37±0.29%), followed by WT1 in 4 (mean 0.07 ± 0.03%) and NY-ESO in 3 individuals (mean 0,07 ± 0,04%); only 1 showed CD8+ T cells specific against Survivin (0,034%) and 2 individuals displayed frequencies specific against p53 (0,05 ± 0,01). Further analysis showed LAA specific CD8+ T cells exhibit mainly a less differentiated phenotype (CD45RA+, CCR7+/–, IFNy+, TNFα+, IL-2+/–) and could be immune-magnetically isolated to purities of 94.5 ± 0.7% using a PRAME-specific IFN-γ capture assay yielding 1*104 antigen specific T cells out of 4*107 PBMCs. Simultaneous enrichment of T helper cells to a purity of 72.97 ± 7.60% proofed their existence, despite no CD4+ response could be detected in the first place. The cytotoxic potential of the cell prod-uct was confirmed in an Europium assay using T2 cells loaded with PRAME peptide mix. The specific lysis accounted to 19.3% at an E:T ratio of 1:1 after 90 minutes of co-incubation. In conclusion, we were able to show a relatively high prevalence of LAA specific T cells, especially for PRAME, in healthy donors. These LAA spe-cific T cells can be enriched using the IFN-γ capture assay with regard to achieving a functional T cell product for adoptive T cell transfer.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts12
FV-04-2Silencing MHC expression in the mouse cornea to prevent the risk of graft rejection
Börger A.-K.1, Mueller C.2, Wittig D.2, Blasczyk R.1, Engelmann K.2, Figueiredo C.1
1Hannover Medical School, Institute for Transfusion Medicine, Hannover, Germany, 2Technical University Dresden, Institute for Anatomy, Dresden, Germany
Introduction: Despite the immune privilege of the cornea, an increase number of studies have suggested that HLA mismatches are associated with a higher risk for rejection. Previously, we have developed a strategy to decrease the immunogenicity of cells and tissues by silencing HLA ex-pression. In this study we aim to evaluate the feasibility to downregulate the MHC class I and class II expression in mouse corneas in their 3D original structure. Material and methods: We used RNA interference (RNAi) to specifically knockdown MHC class I and class II expression by targeting the invariant β2-microglobulin (β2m) chain or the α-chain of MHC class II antigens, respectively. Lentiviral vectors were constructed to express those specif-ic short hairpin RNA (shRNA) sequences. The efficiency of the shRNA in knocking down MHC expression was evaluated in a mouse-derived cell line and analysed by real-time PCR and flow cytometry. In addition, mouse corneas were explanted and transduced with the lentiviral vectors to achieve a permanent silencing of the expression of MHC molecules in the corneal endothelium. Tissue transduction efficiencies and MHC ex-pression downregulation were evaluated by fluorescence microscopy and real-time PCR, respectively. T-cell proliferation assays were performed to determine the efficiency of MHC knockdown to prevent the activation of an allogeneic immune response. Results: The lentiviral vector-mediated delivery of RNAi cassettes encod-ing for shRNAs targeting either MHC class I or MHC class II transcripts caused a reduction of 65% at transcript and 60% MHC expression levels. Furthermore, we demonstrated the feasibility to transduce the corneal tis-sue in its 3D structure. Transduced corneas showed a downregulation of MHC expression by up to 70% at transcript level. Silencing MHC expres-sion in cells of a mouse-derived cell line resulted in a decrease in T-cell proliferation rates by up to 67%. Conclusion: We demonstrated that the downregulation of MHC class I and class II expression is feasible in mouse corneas and has the potential to abrogate the allogeneic immune response. Thus, reducing the immu-nogenicity of the cornea by genetic engineering might represent a robust strategy to prevent graft rejection after allogeneic keratoplasty.
FV-04-3Generation of EBV-specific human CD8+ cytotoxic T lymphocytes with stem cell memory and central memory properties by modulating glycolytic T cell metabolism
Weber I.1, Khan S.A.1, Henschler R.2, Theobald M.1, Hartwig U.F.1
1University Medical Center of Johannes Gutenberg-University Mainz, III. Dept. of Medicine - Hematology, Internal Oncology & Pneumology, Mainz, Germany, 2Medical Center of Ludwig-Maximilians-University München, Dept. of Transfusion Medicine, Cellular Therapeutics & Hemostaseology, München, Germany
Introduction: Adoptive transfer of virus-specific T cells has advanced as a valuable cellular therapy for opportunistic viral infections, EBV-mediat-ed lymphoma and leukemia relapse. However, durable clinical responses are frequently hampered by limited capability of terminally differentiat-ed effector T cells (TEFF) to establish sustained antileukemic immunity whereas less differentiated stem cell memory (TSCM) and central mem-ory (TCM) T cells could be shown to elicit potent antitumor responses, prolonged survival and memory. Moreover, TSCM and TCM depend less on glucose to drive oxidative phosphorylation (OXPHOS) whereas TEFF undergo additional aerobic glycolysis to generate more ATP. In the cur-
rent study, we therefore investigated means of modulating T cell metabo-lism to generate EBV-specific TSCM and TCM. Methods: Naïve CD8+CD45RA+ T cells isolated from PBMCs of healthy donors by MACS® and total CD8+ T cells were primed by autologous DC loaded with EBV-peptides and restimulated with peptide loaded PBMCs in the presence of 1mM glucose, glutamine, an optimized cytokine cock-tail and 1mM of 2-deoxy-glucose (2-DG). In addition to phenotypic and functional in vitro analyses by FACS, ELISPOT and 51Cr-release assay, we determined glucose uptake and lactate production. OXPHOS and aerobic glycolysis were assessed by measuring oxygen-consumption rate (OCR) and extracellular acidification rate (ECAR) using a Seahorse Analyzer. Results: Upon repetitive restimulation of naive T cells we obtained strong expansion of EBV-reactive CTL expressing a CD8+CD45RA+C-D45RO-CD95+CD27+CD28+CD62L+CCR7+ TSCM and CD8+C-D45RA-CD45RO+CD95+CD27+CD28+CD62L+ CCR7+ TCM pheno-type when compared to untreated CTL. Moreover, 2-DG treated TSCM and TCM as well as total CD8+ CTL showed less lactate production and ECAR, suggesting that differentiation to TEFF requires aerobic glycolytic ATP production. Functional assays in vitro revealed that EBV-TSCM and TCM treated with 2-DG for 20 days exhibited IFN-γ release and cytolytic activity comparable to untreated controls but elicited superior migration properties in a transwell migration assay. Conclusion: These studies demonstrate that modulating T cell metab-olism may be a promising approach to generate TSCM/CM in vitro for improved adoptive cellular therapy.
FV-04-4Stage-specific generation of T cells from pluripotent stem cells
Alzubi J.1, Mussolino C.1, Pallant C.2, Thrasher A.2, Cathomen T.1
1Institute for Cell and Gene Therapy/ University Medical Center Freiburg, Freiburg, Germany, 2Institute of Child Health/ University College of London, London, United Kingdom
Pluripotent stem cells (PSCs), such as embryonic stem cells (ESCs) and induced PSCs (iPSCs), are attractive cells to develop new approaches in regenerative medicine, drug discovery and disease modeling. PSCs have a self-renewal capacity and the ability to differentiate – at least in theory – into all somatic cell types, including blood and immune cells. Here we have established a differentiation protocol, which enabled us to generate mature T cells from murine ESCs in a stage-specific manner, and verified the potential of this protocol for disease modeling by utilizing ESCs pro-duced to generate a humanized mouse model for X-linked severe com-bined immunodeficiency (X-SCID). X-SCID is a rare, life-threatening im-mune disorder caused by mutations in the IL2RG locus, which codes for the common gamma chain (GC) present in several interleukin receptors needed for lymphocyte development and function. In our model, the mu-rine Il2rg locus was replaced with a human IL2RG version harboring the common G691A mutation in exon 5. To correct the underlying mutation, transcription activator-like effector nucleases (TALENs) were employed to introduce a corrective sequence in exon 5 of IL2RG. Next, both cor-rected and non-corrected ESC clones were differentiated to mature T cells in vitro. While all clones produced comparable levels of hematopoietic precursor cells, only corrected ESC clones could overcome the early block of differentiation and mature to CD4+/CD8+ double positive (DP) T cells expressing the T cell receptor (TCR). Further cultivation of these cells al-lowed us to produce mature single-positive CD8+ cells that showed re-stored IL-2 dependent signaling, hence confirming functional correction of X-SCID immunodeficiency in vitro. In conclusion, our study empha-sizes the significance of designer nucleases as a tool in generating isogenic disease models and demonstrates for the first time that pluripotent stem cells can be differentiated into mature T cells, with the prospect to pro-duce genetically modified autologous transplants for various applications in the clinic.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 13
FV-04-5MSC inhibit lymphocyte proliferation through AHR. Impact of inflammation and necrosis within tumor microenvironment
Grassl S.1, Rojewski M.1, Wiesneth M.2, Winkelmann M.1, Jahrsdörfer B.2, Schrezenmeier H.1,2,3, Lotfi R.1,2,3
1Universitätsklinikum Ulm, Institut für Transfusionsmedizin, Ulm, Germany, 2Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Ulm, Germany, 3DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Institut Ulm, Ulm, Germany
Introduction: Activation of the aryl hydrocarbon receptor (AHR) has been implicated in a variety of cellular processes such as embryogenesis, transformation, tumorigenesis and inflammation. AHR is expressed on various tumors but also on lymphocytes. A recently discovered endoge-nous ligand for AHR is kynurenine (Kyn) the metabolite of tryptophan which is converted by the enzyme indoleamine-2,3-dioxygenase (IDO). IDO is expressed in many tumors but also in tumor-associated mesenchy-mal stromal cells (MSCs). Deprivation of tryptophan and increased con-centration of Kyn suppress antitumour immune responses and promote tumor-cell survival and motility leading to a poor prognosis in various malignancies. S100A4 belongs to bioactive necrosis-associated factors found within advanced tumors. We sought to determine the impact of MSC-derived Kyn in the context of MSC-induced inhibition of lympho-cyte proliferation. Methods: Peripheral blood lymphocytes (PBL) from healthy donors were isolated by density gradient centrifugation using Ficoll. To obtain MSCs, bone marrow from healthy donors was cultured for 14 days in al-pha-MEM supplemented with 10% platelete lysate. Fibroblastoid-shaped adherent cells with capacity for chrondrogenic, ostegenic, and lipogenic differentiation and positive for CD73, CD90, CD105 and HLA-A, B, C and negative for CD34, CD3, CD45 were referred to as MSCs. MSCs and PBL were cocultured in the presence of anti-CD3/antiCD28-beads (to induce lymphocyte proliferation), IFNγ and S100A4 for 4 days and PBL proliferation was assessed by FACS analysis of CFSE-labeled lymphocytes. Results: In the presence of IFNγ (100ng/ml) in combination with S100A4 (1µg/ml), MSCs elevated their IDO expression leading to increased con-centration of Kyn within the culturing media and subsequent suppression of lymphocyte proliferation down to 35% compared to conditions without MSCs. Application of AHR-antagonist CH223191 (3µg/ml) to culturing media blocking the binding of Kyn to its receptor on lymphocytes, partial-ly abrogated the suppression of lymphocyte proliferation with 60% prolif-eration compared to conditions without MSCs. Conclusions: In the setting of inflammation (represented here by IFNγ) and necrosis (represented by S100A4) which are generally found within tumor tissue, Kyn plays a crucial role in MSC-induced inhibition of lym-phocyte proliferation and thus immunosuppression. Blocking AHR may partially antagonize the immunosuppressive nature tumor microenviron-ment.
FV-04-6Influence of hyperosmolaric injection media on the biodistribution and survival of human MSCs after systemic administration in mice
Leibacher J.1, Kollar K.1, Brixner V.1, Seifried E.1, Henschler R.1,2
1Institut für Transfusionsmedizin und Immunhämatologie, Produktion, Frankfurt/Main, Germany, 2Blutspende Zürich SRK, Zürich, Switzerland
Background: Human MSCs, because of their regenerative and immune modulatory potential, are currently deployed in a wide range of clinical applications and disease models. Unfortunately the fate of MSC after sys-temic administration and the related Interactions within the blood circu-lation are still not fully understood. The majority of i.v. or i.a administered MSCs accumulate in the lungs and loose traceability after 3–4 days in vivo.Aim: Since engraftment rate and long term persistence of injected MSCs seems rather low, we tried to improve in vivo kinetics by using hyperos-molaric Injection media (HyperHAES)) in order to describe the impact on biodistribution, cell morphology and survival rate.Methods: In vitro culture related changes in morphology and surface expression patterns were analysed using flow cytometry and brightfield morphology scan in correlation with a quanti bead system. In vivo track-ing of male PKH67 labeled human MSC in a Bl6/Cl57 mouse model were achieved using SRY-gene qRT-PCR analysis and flow cytometry/fluores-cence microscopy at different timepoints. Kinetics, viability and cell-cell interaction of HyperHAES were assessed with a combination of altering Mitochondrial Membrane Potential (MMP), Caspase 3/7-activity, addi-tional survival and surface markers in comparison to NaCl 0.9% injection media.Results: Incubation of hMSCs in hyperosmolaric injection media (Hy-perHAES) for ca. 30 min decreases average diameter of culture expanded MSC about 30% (from 48,7 µm ± 2,29 to 34,6 µm ± 2,04; means +/– SD) and improves survival rate of MSC injected in the host after 24h. Hyper-HAES decreases the loss of MMP and the signal intensity of the dead cell marker PI in comparison to MSC injected with NaCl 0.9%. Hyper-HAES treated MSCs are detected at higher frequencies in most murine tissues compared to controls incubated in NaCl 0.9%, but doesn`t result in alter-ations in interaction of injected MSCs with the host immune system or Caspase activation. HyperHAES also enables MSC to reach organs with smaller microcirculation like the spleen.Conclusion: Hyperosmolaric Injection media improves kinetics and per-sistence of injected MSCs in mice. However, HyperHAES cannot prevent clearance of injected MSCs by phagocytes and endothelial cells from the liver, kidney and lungs, but is still a possible tool for patient MSC graft engineering. Hyperosmolaric injection media might thus help to improve bioavailibilty of MSCs, e.g. in patients after allogeneic transplantations.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts14
FV-04-7The influence of mesenchymal stromal cells on platelet activation
Netsch P., Elvers-Hornung S., Uhlig S., Rink G., Klüter H., Bugert P., Bieback K., AG Prof. Bieback, AG Prof. BugertInstitute of Transfusion Medicine and Immunology, German Red Cross Blood Service of Baden-Württemberg-Hessen, University of Heidelberg, Faculty of Clinical Medicine, Mannheim, Germany
Mesenchymal stromal cells (MSCs) possess diverse promising therapeutic capacities like differentiation into different tissues, immunomodulation or trophic support. Therefore, they are being applied in numerous clinical trials already. Phase I trials proved the safety of systemic and local MSC injection with very few side effects. However, there were incidences sug-gesting a risk of thromboembolic events like lung embolism after MSC infusion. There are recent studies supporting these findings, however fo-cusing on MSC interactions with plasmatic coagulation suggesting both promoting and inhibiting influences of MSCs. As more evidence is needed to ensure the safety of MSC infusion we aimed to investigate possible in-teractions between platelets and MSCs asking whether MSC can promote or inhibit platelet activation. Effects of MSCs and MSCs supernatant were studied by assessing plate-let activation using flow cytometry (CD62P, CD63, PAC1-binding) and impedance aggregometry (Multiplate; Roche Diagnostics). Platelets were used unstimulated or stimulated with different agonists (ADP, TRAP)in the presence of MSCs (either from lipo aspirate (LA), cord blood (CB) or bone marrow (BM)), human umbilical vein endothelial cells (HUVECs) or HeLa tumor cells as a platelet inhibiting or activation promoting pop-ulation, respectively. In flow cytometry HeLa cells and CB-MSCs were capable of inducing activation of unstimulated platelets, whereas, activation marker expres-sion of stimulated platelets was either unaffected or increased compared to controls without cells. BM-MSCs, LA-MSCs and HUVECs caused a dose related decrease in activation marker expression only of stimulated platelets independent of the agonist used. The results from impedance ag-gregometry generally indicated a decrease in platelet aggregation in the presence of any cell type, which suggests that the method is probably not suitable in the present context. The data clearly demonstrate that MSC derived from BM and LA are able to inhibit platelet activation in a dose-dependent manner. This non-ac-tivation and even inhibition of primary hemostasis supports the clinical safety data. Interestingly, whereas both LA- and BM-derived MSC depict-ed this anti-coagulatory phenotype, CB-derived MSC differed in this re-spect. Further experiments are necessary to understand the underlying mechanisms to ensure safety of MSC therapies.
FV-04-8GMP-Process optimization to allow the clinical scale expansion of genetically modified, ErbB2-specific CAR expressing “off the shelf” natural killer (NK-92) cells
Nowakowska P.1, Odendahl M.2, Schönfeld K.3, Zhang C.3, Bönig H.1, Becker P.1, Grez M.3, Naundorf S.4, Seifried E.1, Wels W.3, Tonn T.2,5
1Institute for Transfusion Medicine and Immunohaematology, German Red Cross Blood Donation Service Baden Württemberg-Hessen, Frankfurt am Main, Germany, 2Institute for Transfusion Medicine, German Red Cross Blood Donation Service North-East, Dresden, Germany, 3Georg-Speyer-Haus, Institute for Tumor Biology and Experimental Therapy, Frankfurt am Main, Germany, 4EUFETS GmbH, Idar-Oberstein, Germany, 5Transfusion Medicine, Medical Faculty Carl Gustav Carus, TU Dresden and CRTD, Dresden, Germany
Introduction: Genetically modified NK-92 (NK-92#78), expressing an ErbB2-specific chimeric antigen receptor (CAR), efficiently and specifi-cally kill ErbB2(+) tumors in vitro and in vivo, without affecting ErbB2(–) cells. The clinical experience gathered with parental NK-92 cells encour-ages to use their more potent derivatives in the treatment
of NK-92-resistant, ErbB2-expressing malignancies. The clinical applica-tion of the cellular product is preceded by the optimization of the culture and cryopreservation protocols, enabling to obtain sufficient numbers of functional cells. The shipment isa challenging task considering the factors impacting the functionality and viability of the cells. Aim: Establishment of optimal expansion and cryopreservation protocols for genetically modified NK-92 cells, as well as finding shipping condi-tions not affecting notably the quality of the cells. Methods: Culture and cryopreservation media with different combi-nations of supplements (IL-2, hPlasma) were compared in terms of cell growth, viability, stability, functionality and recovery post-thaw. Cell via-bility and pH were tested over time in high density cell suspensions, pre-pared in different buffered solutions serving as a transport media. Results: X-Vivo 10 without Phenol red and Gentamicin containing rec-Transferrin, supplemented with 5% heat inactivated human plasma and 500U/ml of IL-2, enables efficient expansion of NK-92#78, as well as maintenance of long term functionality (specific cytotoxicity >50%) and stability (CAR expression >98%) of the cells.The established cryopreservation protocol is optimal for cell growth and recovery (> 50%) post-thaw. Parental NK-92 cells shipped from Frank-furt/Germany to Boston/USA in VueLife 750-C1 bag prefilled with sup-plemented X-Vivo 10 as a transport medium, retained high cytotoxicity toward K562 (>90%) and viability (>90%). Conclusion: Optimal protocols for expansion and cryopreservation of NK-92#78 were established. Long-distance transport of high cell numbers of NK-92 cells was successful with very promising results in terms of cell viability and functionality.
Infectious diseases special focus: Hepatitis E
FV-05-1Transfusion-transmitted Hepatitis E caused by a red blood cell concentrate
Reil A.1, Ochmann O.2, Rau E.3, Mueller B.1, Pichl L.1, Schottstedt V.1
1DRK-Blutspendedienst West, Hagen, Germany, 2DRK-Blutspendedienst West, Bad Kreuznach, Germany, 3Asklepios Südpfalzkliniken, Kandel, Germany
Introduction: Hepatitis E virus (HEV) usually causes an acute self-lim-iting hepatitis similar to hepatitis A, but may cause acute fulminant hep-atitis in the settings of pregnancy, underlying liver disease and immune compromise. HEV is a small non-enveloped RNA virus. There are four major genotypes of HEV and a single serotype. Genotypes 1 and 2 are considered human viruses, while genotypes 3 and 4 are primarily zoo-notic and have been isolated from humans and animals. In Europe, gen-otype 3 is the predominant genotype. The prevalence of HEV antibodies in the population is about 17%. Commonly, HEV is transmitted by the faecal-oral route through contaminated drinking water, foodborne trans-mission from consumption of undercooked or raw meat. Here, we report a case of HEV transmission by blood transfusion.Case report: One month after his last donation, a 63-year-old male do-nor informed our blood service about suffering from acute hepatitis. His symptoms had started 3 days after donation. Results of the laboratory ex-amination 11 days after donation were conclusive for acute HEV infection (anti-HEV IgM and IgG positive, HEV RNA positive; γ-GT, ALT and AST levels were 144, 1899 and 1553 U/l, respectively). The donor recovered within 2 months without sequelae. The whole blood donation had been processed to a red blood cell concentrate (RBC) and a fresh frozen plasma unit (FFP). Unfortunately, the RBC unit was transfused 2 weeks after do-nation, i.e. prior to the notification of the donor’s hepatitis. The FFP was still available in the blood service and tested positive for HEV RNA (Re-alStar HEV RT-PCR Kit, altona diagnostics). As this is a qualitative assay, viral concentration is estimated > 100,000 IU/ml according to a Crossing

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 15
Point of 16 cycles. In spite of small plasma volume, we therefore expected the RBC unit to be infectious and informed the hospital of the recipi-ent. The recipient was a 52-year-old male suffering from gastrointestinal bleeding. He received 8 units of RBC during gastrectomy. Six weeks after transfusion, the recipient was tested positive for HEV infection (anti-HEV IgM and IgG positive; γ-GT, ALT and AST levels were 207, 160 and 40 U/l, respectively). The recipient recovered without sequelae. Ten weeks after transfusion, HEV RNA was not detectable anymore and ALT/AST levels were normalized. Conclusion: The clinical course clearly implicates HEV transmission with RBC transfusion. The source of infection of the donor could not be elu-cidated.
FV-05-2PCR-Screening of blood donations for hepatitis E with the cobas HEV test performed on the new Roche cobas 8800 platform in minipools of 6
Müller B.1, Koch H.2, Pichl L.1
1DRK-Blutspendedienst West, NAT-Labor, Hagen, Germany, 2Roche Diagnostics, Mannheim, Germany
Introduction: Hepatitis E virus (HEV) is a small single stranded non-en-veloped RNA virus which may lead to fulminant or chronic hepatitis E, especially in immunocompromised persons. The risk of transfusion-as-sociated HEV transmission by contaminated blood products still remains unknown but has been recognized in recent years as an emerging and potentially underestimated infection. Since infections in many cases are asymptomatic in blood donors, the disease often remains undiagnosed. Sensitive detection of HEV RNA is therefore crucial for diagnosis of HEV infected blood donors. Results: In order to gain a more detailed insight into the rate of HEV infections among german blood donors, we analyzed in a first step 6,108 blood donations in minipools of 6 of volunteer first time and repeat do-nors of the german red cross blood donation service West by the cobas HEV test performed on the fully automated cobas 8800 platform. The cal-culated sensitivity of this test in pools of 6 is 112 IU/ml for the individual donation. A total of 9 donors were identified as confirmed positive for HEV RNA, which is 1 out of 679 or a rate of 0.15%. Quantification of HEV RNA and antibody status of the individual donations are currently under investigation. Conclusion: The prevalence of blood donations containing HEV RNA was higher than anticipated based on the published data for german blood donors. The extent of transmission as well as the clinical relevance of transfusion-associated hepatitis E infection still require further inves-tigation.
FV-05-3Feasibility of routine Hepatitis E virus RNA screening of blood donors
Vollmer T.1, Diekmann J.1, Eberhardt M.2, Knabbe C.1, Dreier J.1
1Herz- und Diabeteszentrum NRW, Institut fuer Laboratoriums- und Transfusionsmedizin, Bad Oeynhausen, Germany, 2TMD Gesellschaft für transfusionsmedizinische Dienste mbH, Kassel, Germany
Background: Hepatitis E virus (HEV) infection is recognized as an emerging and often undiagnosed disease in industrialized countries, ac-tually with asymptomatic infections occurring in blood donors of vari-ous European countries. The clinical relevance of transfusion-associated HEV infection is insufficiently understood with an ongoing debate on the impact of blood safety. Routine screening for HEV RNA was recently introduced in our blood transfusion service to identify viraemic donors. Actually, we present the successful implementation of a 100% screening of therapeutic blood products for HEV RNA. Furthermore, we determined the distribution of viral RNA in the resulting blood products.
Methods: From January to April 2015, 23,182 donations from 18,822 in-dividual donors (whole blood, platelets) were routinely screened for the presence of HEV RNA using the RealStar HEV RT-PCR assay (Altona Diagnostics GmbH). Nucleic acids were extracted from 4.8 ml plasma us-ing the Chemagen MSM-I extractor (Viral 5k, Perkin Elmer Chemagen GmbH). The presence of HEV-specific IgM and IgG antibodies was deter-mined using the anti-HEV IgM/IgG ELISA (Euroimmun, Luebeck). HEV RNA concentrations were quantified using the first WHO international Standard for hepatitis E Virus RNA for NAT-based assays.Results: Screening was additionally performed to our routine screening procedure for HAV, HBV, HCV, HIV and Parvovirus B19 in a pool size of 96 samples without secondary pooling or extraction efforts. The 95% LOD of the assay was determined to 4.66 IU/ml (447 IU/ml per single donation). In total, 17 HEV RNA positive donors were identified (inci-dence: 0.09%). Only four donors already showed reactive IgM and/or IgG antibody titers (IgM+/IgG–, IgM+/IgG+). Quantification of viral RNA in resulting blood products is currently under way, showing decreasing con-centrations in concordance to the proportion of plasma in the respective blood product.Conclusion: Regarding the remaining controversy debate on the HEV safety of blood, we confirmed the feasibility of a routine sensitive NAT-screening method for the detection of HEV in blood donors. The incidence of HEV RNA in blood donors observed in this study period is comparable to previous results (0.08% summer 2011 vs. 0.09%)
Blood donors and blood components
FV-06-1Safety of whole blood donation in subjects aged 65–75 years: Results from 3 Swiss Blood Donation Centers
Pehlic V.1, Brassel Rodrigues A.2, Schnegg A.3, Müller O.1, Mauchle P.2, Buser A.1, Holbro A.1, Infanti L.1
1Blutspendezentrum SRK beider Basel, Basel, Switzerland, 2Interregionale Blutspende SRK, Bern, Switzerland, 3Interregionale Blutspende SRK, Epalinges, Switzerland
Introduction: Due to the current demographic developments, strategies for the long-term retention of active blood donors are essential. In 2012 the Swiss Blood Transfusion Service extended the upper age-limit for whole blood (WB) donation from 65 to 75 years. In 2013 notification of adverse events (AEs) of blood donation to the Haemovigilance author-ity (Swissmedic) became mandatory. Data on the incidence and type of AEs in donors aged 65–75 years were analyzed in 3 Swiss blood donation centers.Methods: Subjects aged ≥65-years who donated in 2013 and 2014 in the Bern, Waadt and Basel regions were included. Both males and females donated only WB with a minimal interval of 3 months. AEs were classified according to the modified ISBT-EHN 2008 classification in use in Switzer-land. Severe adverse events (SAEs) were grades 3–4 AEs and those grade 2 requiring outside medical care.Results: At the end of 2014 a total of 5’515 donors aged ≥65 were active in the 3 centers (4.9% of the blood donor population; 3.6% in Bern, 6.5% in Waadt and 8.6% in Basel). In the period 2013–14, 8’734 WB donations (3.9% of all WB donations; 2% in Bern, 4.3% in Waadt and 12.3% in Basel) were performed by older donors, with a mean of 1,0 donation/donor (0.6 in Bern and Waadt, 1.9 in Basel). 42 AEs were reported (2.1% of all AEs), with 21 local hematomas, 11 vasovagal reactions, 3 mild nerve injuries, 2 unspecific local pain, tendon injury, tachycardia and fatigue (1 case each). Two SAEs were observed: a delayed vasovagal reaction requiring outside medical care and persistent, unspecific local pain requiring specialist eval-uation.Conclusions: In the 3 Swiss centers, donors aged ≥65 years represent an important part of the active donor population and contribute significant-
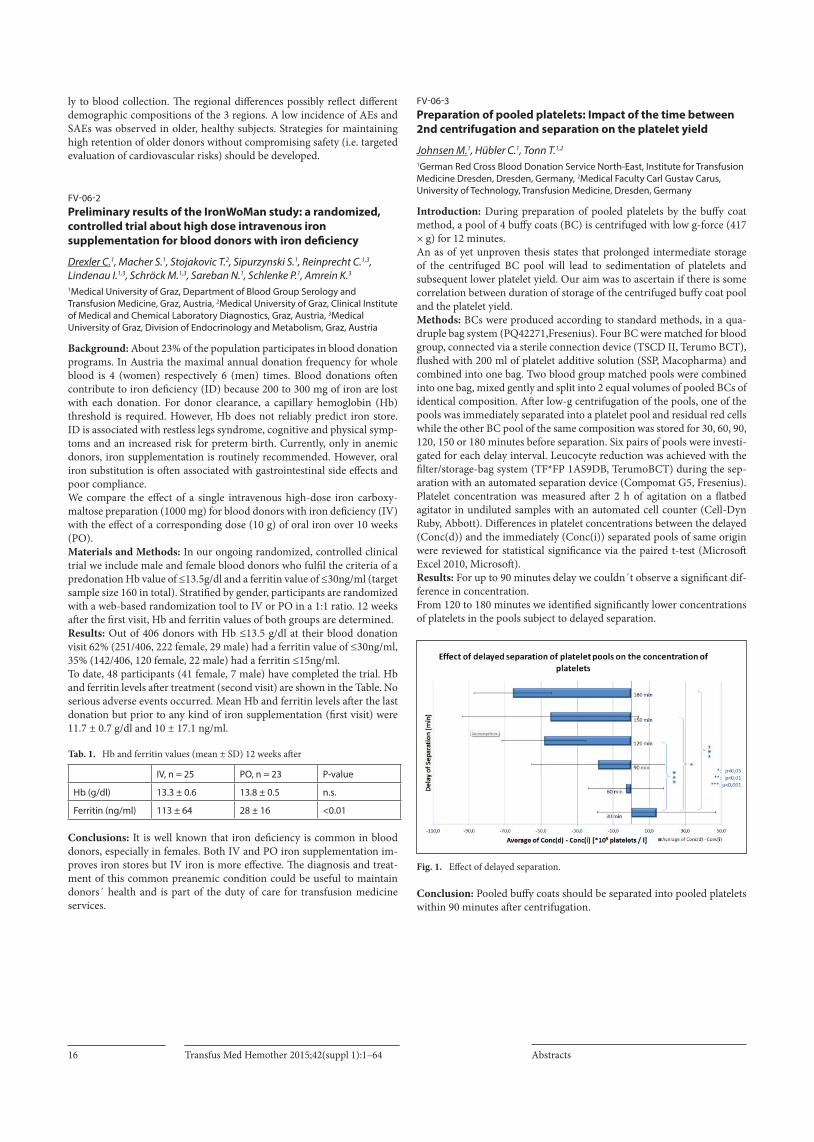
Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts16
ly to blood collection. The regional differences possibly reflect different demographic compositions of the 3 regions. A low incidence of AEs and SAEs was observed in older, healthy subjects. Strategies for maintaining high retention of older donors without compromising safety (i.e. targeted evaluation of cardiovascular risks) should be developed.
FV-06-2Preliminary results of the IronWoMan study: a randomized, controlled trial about high dose intravenous iron supplementation for blood donors with iron deficiency
Drexler C.1, Macher S.1, Stojakovic T.2, Sipurzynski S.1, Reinprecht C.1,3, Lindenau I.1,3, Schröck M.1,3, Sareban N.1, Schlenke P.1, Amrein K.3
1Medical University of Graz, Department of Blood Group Serology and Transfusion Medicine, Graz, Austria, 2Medical University of Graz, Clinical Institute of Medical and Chemical Laboratory Diagnostics, Graz, Austria, 3Medical University of Graz, Division of Endocrinology and Metabolism, Graz, Austria
Background: About 23% of the population participates in blood donation programs. In Austria the maximal annual donation frequency for whole blood is 4 (women) respectively 6 (men) times. Blood donations often contribute to iron deficiency (ID) because 200 to 300 mg of iron are lost with each donation. For donor clearance, a capillary hemoglobin (Hb) threshold is required. However, Hb does not reliably predict iron store. ID is associated with restless legs syndrome, cognitive and physical symp-toms and an increased risk for preterm birth. Currently, only in anemic donors, iron supplementation is routinely recommended. However, oral iron substitution is often associated with gastrointestinal side effects and poor compliance. We compare the effect of a single intravenous high-dose iron carboxy-maltose preparation (1000 mg) for blood donors with iron deficiency (IV) with the effect of a corresponding dose (10 g) of oral iron over 10 weeks (PO). Materials and Methods: In our ongoing randomized, controlled clinical trial we include male and female blood donors who fulfil the criteria of a predonation Hb value of ≤13.5g/dl and a ferritin value of ≤30ng/ml (target sample size 160 in total). Stratified by gender, participants are randomized with a web-based randomization tool to IV or PO in a 1:1 ratio. 12 weeks after the first visit, Hb and ferritin values of both groups are determined. Results: Out of 406 donors with Hb ≤13.5 g/dl at their blood donation visit 62% (251/406, 222 female, 29 male) had a ferritin value of ≤30ng/ml, 35% (142/406, 120 female, 22 male) had a ferritin ≤15ng/ml. To date, 48 participants (41 female, 7 male) have completed the trial. Hb and ferritin levels after treatment (second visit) are shown in the Table. No serious adverse events occurred. Mean Hb and ferritin levels after the last donation but prior to any kind of iron supplementation (first visit) were 11.7 ± 0.7 g/dl and 10 ± 17.1 ng/ml.
Tab. 1. Hb and ferritin values (mean ± SD) 12 weeks after
IV, n = 25 PO, n = 23 P-value
Hb (g/dl) 13.3 ± 0.6 13.8 ± 0.5 n.s.
Ferritin (ng/ml) 113 ± 64 28 ± 16 <0.01
Conclusions: It is well known that iron deficiency is common in blood donors, especially in females. Both IV and PO iron supplementation im-proves iron stores but IV iron is more effective. The diagnosis and treat-ment of this common preanemic condition could be useful to maintain donors´ health and is part of the duty of care for transfusion medicine services.
FV-06-3Preparation of pooled platelets: Impact of the time between 2nd centrifugation and separation on the platelet yield
Johnsen M.1, Hübler C.1, Tonn T.1,2
1German Red Cross Blood Donation Service North-East, Institute for Transfusion Medicine Dresden, Dresden, Germany, 2Medical Faculty Carl Gustav Carus, University of Technology, Transfusion Medicine, Dresden, Germany
Introduction: During preparation of pooled platelets by the buffy coat method, a pool of 4 buffy coats (BC) is centrifuged with low g-force (417 × g) for 12 minutes.An as of yet unproven thesis states that prolonged intermediate storage of the centrifuged BC pool will lead to sedimentation of platelets and subsequent lower platelet yield. Our aim was to ascertain if there is some correlation between duration of storage of the centrifuged buffy coat pool and the platelet yield.Methods: BCs were produced according to standard methods, in a qua-druple bag system (PQ42271,Fresenius). Four BC were matched for blood group, connected via a sterile connection device (TSCD II, Terumo BCT), flushed with 200 ml of platelet additive solution (SSP, Macopharma) and combined into one bag. Two blood group matched pools were combined into one bag, mixed gently and split into 2 equal volumes of pooled BCs of identical composition. After low-g centrifugation of the pools, one of the pools was immediately separated into a platelet pool and residual red cells while the other BC pool of the same composition was stored for 30, 60, 90, 120, 150 or 180 minutes before separation. Six pairs of pools were investi-gated for each delay interval. Leucocyte reduction was achieved with the filter/storage-bag system (TF*FP 1AS9DB, TerumoBCT) during the sep-aration with an automated separation device (Compomat G5, Fresenius).Platelet concentration was measured after 2 h of agitation on a flatbed agitator in undiluted samples with an automated cell counter (Cell-Dyn Ruby, Abbott). Differences in platelet concentrations between the delayed (Conc(d)) and the immediately (Conc(i)) separated pools of same origin were reviewed for statistical significance via the paired t-test (Microsoft Excel 2010, Microsoft).Results: For up to 90 minutes delay we couldn´t observe a significant dif-ference in concentration.From 120 to 180 minutes we identified significantly lower concentrations of platelets in the pools subject to delayed separation.
Fig. 1. Effect of delayed separation.
Conclusion: Pooled buffy coats should be separated into pooled platelets within 90 minutes after centrifugation.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 17
FV-06-4Intercept treatment of previously frozen and thawed plasma
Brys B.1, Jaster G.2, Ulrich E.2, Thierbach J.3, Zimmermann A.3, Baumann-Baretti B.I.1
1Haema Ag, Qualitätskontrolle, Leipzig, Germany, 2Haema Ag, Leipzig, Germany, 3Haema Ag, Herstellung und Vertrieb, Leipzig, Germany
Introduction: The INTERCEPT Blood System™ (IBS) for plasma is CE marked for use with fresh and previously frozen apheresis -derived plas-ma. In the case of pathogen reduction (PR) of thawed plasma using the Intercept System, the preservation of the coagulation factors and func-tioning are mandatory. This study investigated the clotting factor stability according to the varying previous time of storage until thawing and PR. Methods: n = 48 units of fresh-frozen plasma (FFP), collected from 16 apheresis procedures and stored for 6 (A, n = 12), 12 (B, n = 12), 15 (C, n = 12) and 18 (D, n = 12) months at < –30 °C were thawed within an average of 18 min using the plasma thawer (Plasmatherm Euro, Barkey). Subsequently 3 FFP of one donation were pooled and immediately under-went PR. After splitting in 3 units the FFP were frozen for a second time within 1 hour to a temperature below –30 °C and stored < –30 °C. FFP was tested for fibrinogen (fib), factor (F)V, F VIII, FXI and von Willebrand Factor(vWF), protein C (PC) and protein (PS) activity, prothrombin time (INR) and partial thromboplastin time (aPTT) using the BCS (Siemens). Samples were taken before and after PR and until the maximum of 24 months of shelf live. Results: A mentionable decrease of fib, F V, VIII after PR was seen. At the end of storage the mean recovery of F VIII showed 76% of the initial value while absolutely the mean F VIII dropped from 1,19 ± 0,26 U/ml after thawing to 0,99 ± 0,24 U/ml after PR and 0,91 ± 0,21 U/ml at the end of storage. The highest decrease was observed in FFP (D) which was stored 18 months prior thawing and PR. The retention of vWF and F VIIa were almost equivalent in all samples. aPTT and INR slightly increased within the norm: the mean aPTT from 31,49 ± 2,13 s to 35,85 ± 2,72 s and the mean INR from 1,02 ± 0,06 to 1,12 ± 0,07. Overall the retention after PR and during storage never dropped below 70% of the initial value. Independent of the time of storage (group A to D) prior PR no significant differences in the coagulation parameters were seen. Conclusion: Plasma stored at < –30 °C between 6 to 18 months prior thawing and PR showed an adequate preservation of coagulation factor activities and functionality during storage until end of shelf live. Therefore Intercept treatment of previously stored plasma represents an alternative approach to the use of FFP in quarantine in case of the unavailability of donors for testing.
FV-06-5Manual vs automated preparation of platelet concentrates from pooled buffy coats: qualitative and economic aspects
Madla W.1, Jungk H.2, Unnerstall B.3, Kischnick T.4, Zeiler T.5
1DRK-Blutspendedienst West, Zentrale Herstellungsleitung, Hagen, Germany, 2DRK-Blutspendedienst West, Bad Kreuznach, Germany, 3DRK-Blutspendedienst West, Münster, Germany, 4DRK-Blutspendedienst West, Hagen, Germany, 5DRK-Blutspendedienst West, Breitscheid, Germany
Introduction: A number of methods can be used to prepare platelet concentrates (PC) from pooled buffy coats (BC). Aside from manual techniques (M-PC), automated methods (TACSI (T-PC)) in particular promise high platelet yields, quality standardisation and time savings. The aim of this study was to examine the extent to which these claims can be corroborated when routinely producing M-PCs and T-PCs (>45 000 PCs per year), respectively.Methods: A total of 4 BCs were each pooled with PAS III-M. A Frese-nius kit was used for M-PC. The methods were compared by referring to quality control data. In each case the time and human resources expended in relation to the quantity of PCs to be produced were monitored over a minimum period of 2 weeks and separately recorded for each individual process step.
Results: The platelet content per unit of T-PC was found to be approx. 40×109 higher than that of M-PC, albeit with a slightly higher coefficient of variation and an outlier rate of 0.9% (M-PC = 0%). No significant dif-ferences could be found in the residual cell counts.The pH levels, as a sta-bility parameter, were slightly lower in the T-PCs but all the pH values met the defined specifications. At the end of the shelf life, a drop in the platelet number of 5–15×109/unit was noted both in the M-PCs and T-PCs. Pro-cess time analysis: per hour and operator, an average of 4 PCs could be produced using TACSI, and 3 PCs using a manual method. This difference only became noticeable, however, above a quantity of approx. 25 PCs. As the quantity of PCs being produced increases, the mean process time is decreased by up to 2 minutes per PC for M-PCs as well as T-PCs.Conclusion: The higher platelet yield from T-PCs, as demonstrated by the validation data, was confirmed in routine practice. A higher level of stan-dardisation could not be ascertained, however - neither in this case nor with the other parameters. Outlier rates were observed only with T-PCs. Purity and stability parameters revealed no significant differences. At the end of shelf life, the platelet content in the T-PCs was reduced to the same extent as in the M-PCs. The automated production of pooled PCs may be less time-consuming and thus less demanding of human resources, but only above a minimum production quantity of PCs. Hence, this compensates only minimally for the increase in material expenditure.
FV-06-6Transfusion with 0 RhD+ blood in emergencies does not increase mortality in RhD- patients and reduces the overall risk of anti-D immunization
Selleng K.1, Jenichen G.1, Dickau K.1, Selleng S.2, Westphal A.1, Müllejans B.3, Greinacher A.1
1Universitätsmedizin Greifswald, Inst. f. Immunologie und Transfusionsmedizin, Abt. Transfusionsmedizin, Greifswald, Germany, 2Universitätsmedizin Greifswald, Klinik für Anästhesiologie, Intensivmedizin, Notfallmedizin und Schmerzmedizin, Greifswald, Germany, 3Klinikum Karlsburg, Herz- und Diabetes- Zentrum, Klinik für Anästhesie und Intensivmedizin, Karlsburg, Germany
Background: Shortage of red blood cell concentrates (RBC) of the blood group 0 Rhesus D negative (0 RhD-) is a notorious problem, primarily caused by the widely used praxis to transfuse an unknown patient who requires emergency RBC transfusion with 0 RhD- blood until the blood group has been determined. This shortages requires transfusion of 0 RhD- patients with 0 RhD+ RBCs in case of semi-urgent surgery. We report a 10 year prospective study assessing the risks (in-hospital mortality and anti-D immunization) of providing only RBCs of blood group 0 RhD+ for the unknown patient in emergency situations. Methods: From 2001–2011 all emergency patients were transfused with RhD+ RBCs only. RhD- patients were followed for anti-D immunization every 3–5 days until death or hospital discharge within the first month after transfusion and then followed after 2, 3, 6 months up to 12 months by direct antiglobulin test, antibody screen (capture method or gel card) and differentiation. Results: A total of 336 patients received 4,454 RhD+ RBCs within 24 h after emergency admission (mean age 64 years; range 1–99) of whom 58 were RhD–. 166 patients survived (24 RhD–). None of the 58 RhD- pa-tients had an anti-D in the pre-transfusion blood sample (tested retro-spectively). In-hospital mortality did not differ between RhD+ and RhD- patients; 136/278 (48.9%) vs 34/58 (58.5%; p = 0.18). 11 RhD- patients developed an anti-D, but eight RhD- patients were lost during follow up. This results in an overall risk of inducing an anti-D between minimal 3.3% (11/336) and maximal 5.7% (19/336), assuming that all patients lost during follow up developed an anti-D. Providing 0 RhD+ RBCs for emer-gency transfusions of the unknown patient saved 2,016 RBCs BG 0 RhD-, which was 11–13% of the mean 0 RhD- RBCs needed annually in our hos-pital. This likely reduced the necessity to transfuse 0 RhD- patients with 0 RhD+ RBCs in semi-urgent situations because of RhD- blood shortage.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts18
As semi-urgent surgery patients likely have a lower mortality compared to patients admitted with major bleeding in the emergency room, they have a higher risk to survive with an anti-D. Conclusion: Providing 0 RhD+ RBCs in the emergency room does not increase mortality in RhD- patients. It bears a risk of about 3–6% to in-duce an anti-D but safes about 12% of the total demand of 0 RhD- RBCs.
Immunohaematology
FV-07-1Complement activation by anti-erythrocyte alloantibodies is interfered by eculizumab
Anliker M., von Zabern I., Höchsmann B., Schrezenmeier H., Weinstock C.Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Universität Ulm, DRK-Blutspendedienst Baden-Württemberg-Hessen, Ulm, Germany
Introduction: RBC destruction by allo- or autoantibodies may cause life-threatening disease occasionally requiring emergency treatment. Immune-mediated hemolysis involves complement activation and intra-vascular lysis or phagocytosis in the reticuloendothelial system. Not all antibodies activate complement; therefore, we tested a large number of different anti-erythrocyte alloantibodies with a sensitive assay to assess their complement activating capacity. As a potential means of therapy, we also investigated the interference of immune-mediated hemolysis by the C5 inhibitor eculizumab (ecu). Materials and Methods: Antibodies were incubated with RBC of patients with paroxysmal nocturnal hemoglobinuria (PNH) at 37 °C, thereafter human serum was added as a source of complement and incubation was continued for 2 h at 37 °C. RBC were then labelled with anti-CD59 and analyzed by flow cytometry. Ecu was added to a final concentration of 2.3 µM to inhibit lysis by pooled human serum. Results: PNH RBC clones are especially sensitive to lysis by complement because of a deficiency of all glycosylphosphatidylinositol (GPI)-linked proteins including the complement inhibitors CD55 and CD59.The prop-erties of PNH RBC were used to test the complement activating potency of antibodies. Examples of activating antibodies were: anti-A, -B, -H, -I, -P, -PP1Pk, -Vel, -Jra, -Lan, -Jk3, -Fy3, -Co3, -Ku, -Lea, some anti -Coa, -Kpb, -Jka, -Jkb as well as anti-Fya, -Fyb. Eculizumab interfered with com-plement lysis initiated by antibodies. Fig. 1 shows: (A) control without antibody (PNH RBC, 48% clone); (B) complement-mediated destruction of PNH RBC initiated by anti-Jra which (C) was inhibited by the comple-ment inhibitor ecu. Conclusion: Information about complement activation by alloantibodies is often derived from clinical data which are influenced by many variables. We here report a direct test system which allows to asses the complement activating capacity of anti-erythrocyte antibodies in a human system. This knowledge also provides information about a potential means of thera-py. The complement inhibitor ecu was found to interfere with comple-ment-mediated lysis by antibodies (Fig. 1).
Fig. 1.
FV-07-2Noninvasive fetal RHD typing with the use of targeted massively parallel sequencing of maternal plasma cell-free DNA
Wienzek-Lischka S.1, Dehl J.1, Fröhner V.1, Krautwurst A.1, Gattenlöhner S.2, Bräuninger A.2, Deisting C.3, Axt-Fliedner R.3, Degenhardt J.3, Santoso S.1, Sachs U.1, Bein G.1
1Institute of Clinical Immunology and Transfusion Medicine, Justus-Liebig-University, Gießen, Germany, 2Institute of Pathology, Justus-Liebig-University, Gießen, Germany, 3Division of Prenatal Medicine, Department of OB/GYN, Gießen, Germany
Introduction: In pregnant women immunized against RhD or with a his-tory of hemolytic disease of the newborn noninvasive fetal RHD typing is required to determine whether the fetus is at risk.Published methods for noninvasive RHD genotyping with the use of maternal plasma cell-free DNA do not provide internal controls for the presence of circulating fetal DNA for exclusion of false-negative results.Methods: Cell-free DNA was isolated from plasma of 3 RhD negative pregnant women. The gestational age at the time of blood sampling was 26 weeks (median, range 17–32). Exonic sequences of RHD, RHCE, SNPs coding for common blood group antigens KEL, DARC, SLC14A1, GYPA, GYPB and for common platelet antigens ITGB3, ITGA2B, ITGA2, CD109 furthermore SRY, DBY, TTTY2B and 14 anonymous autosomal SNPs were massively parallel sequenced by means of semiconductor technology (Ion Torrent, life technologies).Results: Non maternal RHD sequences of RHD exon 4, 5 and 7 were de-tected in all cases. Analysis of Y chromosome regions, SNPs coding for common blood group and platelet antigens and autosomal SNPs allowed detection of fetal DNA at 5 (median, range 3–5) additional loci. The frac-tional fetal DNA concentration was 12.76% (mean, range 4.4%–27.14%). Conclusion: Targeted massively parallel sequencing of plasma cell-free DNA from RhD negative pregnant women detected the paternal RHD de-rived sequences in all cases. Sequencing of polymorphic control regions serves as internal positive control and allows exact counting of the fetal DNA fraction. We propose this method also for noninvasive detection of other fetal blood group polymorphisms that are frequently involved in hemolytic disease of the newborn.
FV-07-3Accurate MNSs serotype prediction using MALDI-TOF MS based genotyping as shown in 5’743 Swiss blood donors
Meyer S.1, Vollmert C.2, Trost N.1, Gottschalk J.3, Ries J.3, Marcovic A.3, Infanti L.4, Buser A.4, Amar el Dusouqui S.5, Castelli D.6, Weingand T.7, Sarraj A.8, Braisch M.C.9, Thierbach J.9, Frey B.M.3, Gassner C.1
1Blood Transfusion Service Zürich, Swiss Red Cross, Department of Molecular Diagnostics and Research & Development (MOC), Zürich-Schlieren, Switzerland, 2Agena Bioscience, Hamburg, Germany, 3Blood Transfusion Service Zürich, Swiss Red Cross, Zürich-Schlieren, Switzerland, 4Blood Transfusion Service beider Basel, Swiss Red Cross, Basel, Switzerland, 5Blood Transfusion Service Genève, Swiss Red Cross, Geneva, Switzerland, 6Blood Transfusion Service Svizzera Italiana, Swiss Red Cross, Lugano, Switzerland, 7Blood Transfusion Service Zentralschweiz, Swiss Red Cross, Luzern, Switzerland, 8Blood Transfusion Service Neuchâtel-Jura, Swiss Red Cross, Neuchâtel, Switzerland, 9Blood Transfusion Service Ostschweiz, Swiss Red Cross, St. Gallen, Switzerland
Background: Antigenetic relevance of the MNSs blood group system may be implied by its low ISBT ID number 002. However, beside “genetically untouchable” ABO and pleiotropic RhD, and in comparison to K/k, Jk(a/b) and Fy(a/b) (Meyer S. et al., Transfusion 2014), published performance data for MNSs genotyping are underrepresented. The aim of the project was to estimate performance of MALDI-TOF MS based MNSs genotyping.Methods: SNPs were detected at coding nucleotides 59(C/T) and 72(T/G) for M/N and G59 for He (actually on GYPB), 140(C/T/A) for Vw/Hut and 230(C/T) for Mt(a+) on GYPA, and 143(T/C) for S/s, intron 4+5(g/t) for U+W on GYPB plus zygosity typing of the “GYPB deletional U- pheno-type”. The approach included 10 antigens of the MNSs blood group sys-

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 19
tem, encoded by 8 SNPs on 10 GYPA/B alleles, multiplexed into 1 reac-tion. All genotypes (GTs) were compared to existing standard-serological MNSs values of 5,743 Swiss donors. Generic and allele-specific PCR-SSPs and Sanger-DNA sequencing revealed genetic backgrounds in cases with confirmed pheno(PT)/genotype discordances.Results: Concordant MN PTs comprised into 1,711 MM (with 1Vw), 2,807 MN (with 1He, 4Vw and 10Mt(a)), and 1,208 NN (with 4Vw and 4Mt(a+)) all located on GYPA (PT/GT concordance 5,726/5,743, 99,88%). There were 10 serological mistypings. Sequencing of 7 MM GTs with MN PTs revealed GYPA/B hybrid genes of 1 Mur(GYP.504)-like and 6 Sch(G-YP.401)-like alleles, all known to encode N-like PTs, while GYPA*02(N) negative. Genotyping for Ss on GYPB was fully concordant in 619 SS, 2,416 Ss and 2,702 ss samples (concordance 5,737/5,743, 99,90%). Dis-crepancies were due to 3 serological mistypings and 3 “genotyping errors”. We identified 1 mutated primer binding-site and 2 new GYPB*03 null-al-leles, both with a G218A(Gly73Asp).Summary: MNSs serotyping errors had about the same frequency as “genotyping errors”, which could all be explained by rare GYPA/B gene variants, or new alleles. Consequently, “genotyping errors” may rather be interpreted as specific “indicators”, than profane “errors”, and were caused by Sch(GYP.401)-like alleles in about 1 per 1’000 typings, most frequently. Single, or multiple SNP-GT drop-outs were only observed in 0.98% of all GTs ( = “drop-out rate”, 57/5,800). MALDI-TOF MS based MNSs geno-typing proved to be extremely practical, robust and accurate, and - for donors - may well be considered as a valid stand-alone method and/or valuable addition for serotyping.
FV-07-4MiRNA regulation of blood group AB0 genes
Kronstein-Wiedemann R.1, Nowakowska P.2, Seifried E.2, Tonn T.1,3
1Medizinische Fakultät der TU-Dresden, Dresden, Germany, 2DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Institut für Transfusionsmediin, Frankfurt, Germany, 3DRK Blutspendedienst Nord-Ost, Institut für Transfusionsmediin, Dresden, Germany
The molecular genetic basis of the AB0 system has been known since 1990. More than 100 AB0 subgroup-related variations were detected in the cod-ing region of glycosyltransferases, consisting of seven exons, resulting in weak blood group antigen expressions. Beside introns and exons, two re-gions were found to be critical for transcriptional activity of AB0 genes: a promotor sequence upstream of the translation start site and a CBF/NF-Y-binding enhancer element. However, the molecular mechanisms under-lying some subgroups could not be explained by current methods. Here we asked whether microRNA´s may play a role in the regulation of blood group A and B antigens. In mature red blood cells from healthy donors ~ 200 miRNA’s are present with partially different expression patterns de-pending on the blood group genotype. Most of miRNA´s with potential binding sites for glycosyltransferases were not or only weakly expressed in mature red blood cells. Nevertheless miRNA-331–3p was significantly enhanced in red blood cells of Aweak variants. Sequencing of the 3´ un-translated region (3’UTR) of 6 Aweak variants revealed the presence of more miRNA binding sites for certain miRNAs (miRNA-1908) compared to normal controls. We identified glycosyl transferase A as a target gene for miRNA-331 and -1908 by cloning DNA sequences of the 3’UTR of the blood group A glycosyl transferase and of weak blood group A variants into a luciferase expression system and co-transfection with relevant miR-NA’s into K562 cells. Overexpression of these miRNAs was able to reduce the expression of the respective transgene by 25–40% and the 3’UTR of the Aweak variant leads to a further reduction of luciferase expression of 10% +/–6. qPCR at different time points of erythroid differentiation shows a significant down regulation of relevant miRNA´s in the first 5 days. Therefore we overexpressed miRNA-331 in primary hematopoietic stem cells resulting in 10% blood group A negative red blood cells at day 8 of culture and a reduction in mean receptor expression by ~40%, as deter-mined by flow cytometry. This new concept of microRNAs as regulators of blood group glycosyltransferase expression may for the first time pro-
vide an explanation of the molecular basis for weak blood group receptor expressions in previously unexplainable Aweak phenotypes and may also play a role in regulation of other blood group variants (Rhesus, KELL).
FV-07-5Serological and molecular screening for MAR (RH51) negative blood donors and the first case report of anti-MAR-like antibody in Germany
Scharberg E.A.1, Weber S.1, Kömürcü N.1, Richter E.1, Rink G.2, Burkhart J.3, Bugert P.2
1Institut für Transfusionsmedizin und Immunhämatologie, DRK-Blutspendedienst Baden-Württemberg-Hessen, Immunhämatologie, Baden-Baden, Germany, 2Institut für Transfusionsmedizin und Immunologie, Molekulardiagnostik, Mannheim, Germany, 3Institut für Transfusionsmedizin München, Blutspendedienst des Bayerischen Roten Kreuzes, Immunhämatologie, München, Germany
Introduction: MAR is a high prevalence Rh antigen (RH51). The original anti-MAR was found in 1994 in a Finnish woman whose red cells were Cx+ Cw+ D+ C+ c– E– e+. The antibody reacted with all red cells except Rhnull, D-- and Cx+/Cw+ and it was weakly reactive with Cw+/Cw+ and Cx+/Cx+ cells. Antibodies made by people with Cw+/Cw+ and Cx+/Cx+ show MAR-like specificity and do not react with Cw+/Cx+ red cells. An-ti-MAR is clinically significant. Because of a complete lack of MAR nega-tive blood donors in Germany we conducted a serological and molecular screening for homozygous Cw+ and Cw/Cx donors in our population. The red cells of these donors would be essential to provide compatible blood to patients with anti-MAR or anti-MAR-like and for antibody iden-tification panels with rare blood groups.Methods: Between March 2012 and November 2013 all blood donors of the daily routine in our center were tested for the Cw antigen on Beck-man Coulter PK 7200 analyzer using a monoclonal anti-Cw (MS110). The Cw+ donors of blood group O R1R1 were genotyped for the single nucle-otide polymorphisms (SNPs) in the RHCE gene encoding Cw (122A>G) and Cx (106G>A) by using PCR with allele-specific primers or TaqMan probes. The identified Cw+/Cw+ donors were tested with one anti-MAR serum from SCARF in the indirect antiglobulin test in the gel technique. The red cells of these donors were frozen to be used for antibody identifi-cation panels containing rare blood phenotypes.Results: 152.102 of the 378.273 tested blood donors had blood group O (40,2%) and 1.632 of the O group donors were R1R1 Cw positive (1,07%). The molecular testing of these donors revealed 8 Cw+/Cw+ individuals but none Cw+/Cx+. The Cw+/Cw+ donors were tested negative with a moder-ate reactive anti-MAR serum from SCARF. A few weeks after the produc-tion of the first antibody identification panel containing Cw+/Cw+ cells the first example of anti-MAR-like antibody in Germany was identified. Conclusion: Using serological and molecular methods 8 Cw+/Cw+ MAR-like negative blood donors could be identified among 152.102 do-nors with the blood group O. We found no single Cw+/Cx+ MAR negative donor in our study. The frequency of Cw+/Cw+ phenotype in our donor population is 1:19.000. The red cell units of these donors are currently used to create a stock of frozen units. Cw+/Cw+ red cells are also included in an antibody identification panel and made it possible to identify the first example of anti-MAR-like antibody in Germany.
FV-07-6Antibody titer and non-invasive prenatal blood group typing in 419 pregnancies with alloantibodies
Kühling E., Vogt C., Petershofen E.K., Doescher A.Blutspendedienst NSTOB, F & E, Oldenburg, Germany
Introduction: Fetal red blood cell (RBC) antigens are relevant in the pathologic involvement of maternal alloantibodies causing hemolytic disease of the fetus (HDF) or newborn (HDN). Diagnostic procedures include the determination of the fetal blood group from maternal plasma

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts20
or amniocentic fluid and maternal antibody screening. Here, we present data from 419 pregnancies with alloantibodies.Methods: Samples from 419 pregnancies with alloantibodies (< 20th week of gestation: n = 230; 21th to 30th: n = 143; ≥ 30th: n = 46) were tested. Screening for antibodies was done according to standard procedures and in cases of positive results titration of the antibody was performed. DNA from plasma samples was checked for the presences of blood group sequences with real-time PCR (RHD and KEL1) or SSP-PCR with fluorescent primer pairs (RHC, RHc, RHE, MNS, JK, FY) and the GeneScan method.Results: Detection of anti-D antibodies was positive in 222 samples (53%), followed by anti-K (n = 55), anti-E (n = 51) and anti-c (n = 38). The antibody-specifity of the remaining samples (n = 53) was heteroge-neous (anti-C, anti-Fy, anti-Jk, anti-M, anti-s). Titers for anti-D antibod-ies were up to >65000, while anti-c antibodies showed significantly lower values. Out of the pregnancies with anti-D antibodies, in 93 samples a second or third antibody was present. Additional antibodies were found in 42% of samples with an initial anti-c, developing further antibodies during pregnancy. However, anti-K was detected in 94% as single immu-nisation event. In about 95% of samples, fetal blood group typing showed the expected polymorphism and was in concordance with the detected maternal antibody.Conclusion: Identification and monitoring of alloantibodies combined with non-invasive blood group genotyping offers a useful diagnostic tool in pregnancies at risk. The main benefit of non-invasive prenatal diagno-sis is to avoid amniocentesis, which can include a subsequent minimal bleeding and/ or the risk to booster an antibody. Besides this, our results demonstrate a relatively high number of pregnancies with a second or third antibody.
FV-07-7Positive antiglobulin test - to perform or not to perform elutions?
Vogt M., Mansouri Taleghani B.Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Transfusionsmedizin, Bern, Switzerland
Background: The direct antiglobulin test (DAT) commonly detects im-munoglobulin G (IgG) and/or complement components on the red blood cell (RBC). Elution procedures may identify the specificity of bound IgG antibodies. We reviewed how frequently elutions contributed novel sero-logic information (“informative elution results”) under our current policy. Methods: In compliance to our national guidelines and deduced own al-gorithms we perform 1) DAT (BioRad, Switzerland) plus elutions (BAG, Germany) in case of transfusion reactions (performing elutions even without positive DAT); 2) elutions in all positive DAT for IgG with grade 3+ to 4+; 3) elutions in newly positive DAT for IgG with grade ± to 2+ in case of preceding transfusions in the last 14 days; 4) elutions if DAT shows a changing grade of positivity for IgG with preceding transfusions in the last 14 days; 5) elutions in newly positive DAT for C3d of patients having received RBC in the past 7 days (without positive cold agglutination). For antibody identification we used also a commercial gel-test (BioRad). Results: Main results are shown in table 1.
Tab. 1. Results of all 1776 elutions in 1357 patients
Results % patients
negative 81.1
AB0-antibodies (minor incompatible PLT-transfusions, i.v. IgG-treatment) 1.5
allo-antibodies in serum plus eluate 2.3
allo-antibodies in eluate only (“informative elution results”) 0.4
auto-antibodies 2.8
pan-reactivity 11.9
unclear 0.1
Conclusion: Our current national policy and deduced internal algorithms for performing elutions reveals only 0.4% informative elution results (numbers needed to test (NNT) = 270) and hence has very limited value. Therefore we made a suggestion to our responsible national working group to modify their recommendations in the planned version of 2016 accord-ingly. In particular we recommend to perform elutions more restrictively: 1) in case of transfusion reactions (even without positive DAT); 2) in all positive DAT for IgG with grade ± to 2+ in case of preceding transfusions in the last 14 days and when transfusion history is unknown; 3) elutions in newly positive DAT for C3d of patients having received RBC in the past 7 days (without positive cold agglutination). This will skip elutions in DAT IgG 3+ and 4+. Compared to our current policy we expect a reduction of NNT from 270 down to ca. 150.
FV-07-8Deglycosylated human monoclonal antibody against HPA-1a prevents anti-HPA-1a alloantibodies mediated endothelial apoptosis
Wihadmadyawati H.1, Burg-Röderfeld M.1, Werth S.1, Ruan C.2, We M.-W.3, Bein G.1, Sachs U.1, Santoso S.1
1Klinische Immunologie und Transfusionsmedizin, Giessen, Germany, 2Jiangsu Institute of Hematology, Jiangsu, China, 3Dongying Lida Pharmaceutical, Suzhou, China
Foetal/neonatal alloimmune thrombocytopenia (FNAIT) is caused by the destruction of fetal platelets by maternal platelet alloantibodies which crossed through the placenta during pregnancy. Antibodies against HPA-1a residing on the b3-integrin subunit on platelets are known to be re-sponsible for the development of FNAIT. Recently, we could demonstrate that the deglycosylated mouse mab SZ21 against HPA-1a is able to cross through placenta, and prevents the destruction of platelets in mouse mod-el (Bakchoul et al, Blood 2013). Meanwhile, this mab is humanized as chi-meric antibody (mab 813). It is known that the b3-subunit is abundantly expressed as vitronectin receptor (avb3 integrin) on endothelial surface. In this study, we sought to investigate the effect of deglycosylated mab 813 (deg-813) on endothelial cells. Surface Plasmon Resonance analysis showed similar binding activity of intact 813 and deg-813 with purified avb3 (Kd 7.43×10–11 and 6.67×10–11, respectively). To study the influence of mab 813 on endothelial function, apoptosis experiment with HUVEC was performed using Tunel and Caspase-3/7 assay. In both assays, endo-thelial apoptosis was not observed with intact 813 and deg-813. In con-trast, inhibitory mabs against avb3 receptor (23C6, LM609) and cyclic Arg-Gly-Asp peptide caused significant apoptosis of these cells. Similar results were obtained with brain endothelial cells (hCMEC/D3). Accord-ingly, deg-813 did not inhibit the adhesion of HUVEC on vitronectin ma-trix when compared to avb3 specific mabs.Furthermore, we asked the question whether maternal anti-HPA-1a aabs may induce endothelial apoptosis. Anti-HPA-1a aabs derived from FNAIT mothers giving birth of babies with ICH (n = 3) were purified by absorption/elution method using HUVEC. Analysis of the eluted mate-rial by antigen capture assay showed specific binding to avb3, but not to aIIbb3. This result could be confirmed by immunoprecipitation analysis. When avb3-reactive anti-HPA-1a antibodies were tested with endothelial cells, significant apoptosis was observed. Finally, incubation of HUVEC with deg-813 prevented cell death mediated by anti-HPA-1a antibodies.Taking together, our observation indicates that deg-813 can protect not only anti-HPA-1a aabs mediated platelet destruction but also endothelial disturbance without altering endothelial function. These results suggest that deg-813 may represent a novel drug to prevent ICH in severe FNAIT during pregnancy.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 21
FV-07-9Identification of a novel ABO allele caused by a deletion of 2169 base pairs including exon 2 and 3 of the ABO gene
Matzhold E.M., Drexler C., Schlenke P., Wagner T.Medizinische Universität Graz, Univ. Klinik für Blutgruppenserologie und Transfusionsmedizin, Graz, Austria
Introduction: Discrepant serological findings in ABO blood group typing are often caused by ABO gene variants, influencing the ABO transferase activity. Many A and B subgroup alleles responsible for ABO subgroup formation are due to single-nucleotide substitution leading to amino acid alteration. Here we describe a new mutation covering two exons and in-tronic sequences of the gene in a sample with aberrant ABO phenotype.Material and methods: ABO blood groups were determined with stan-dard serologic and gel matrix techniques (MicroTyping system, Bio-Rad, Vienna, Austria). Samples were ABO genotyped using the Ready Gene ABO diagnostic kit (inno train, Diagnostic GmbH, Gallneukirchen, Austria), which is based on sequence specific (SSP) PCR. Haplotype spe-cific sequence analyses of exons 2 to 7 including intermediate intronic regions by allele-specific long-range PCR (KAPA longrange) and direct sequencing (ABI PRISM 3130, Big Dye Terminator V 3.1 Applied Bio-systems) were performed. Regulatory regions including enhancer and promotor in 5´UTR, and +5.8-kb site in intron 1, as well as exon 1 were investigated by genomic PCR (SuperHot Mastermix, Bioron) and then sequenced. Results: Antigen typing indicated blood group O (negative reactions with both monoclonal and human anti-A and anti-B antibodies). The serum contained 4+ reactive anti-B, but no anti-A1 and anti-A2 isoagglutinins were found in reverse blood group typing. While genotyped as O1A by SSP PCR, allelspecific sequence analysis revealed a novel A101 like allele with a deletion of 2169 basepairs starting at nucleotide position 12880 in intron 1 up to 1214 in intron 3, according to the section of 15378 to 17546 in the reference sequence (NG_006669, GenBank). Gene sequences of exon 2 and exon 3 are completely absent. Additionally, the ABO*O011 allele was detected.Conclusion: Sequence analysis of regulatory regions and exon 1 did not reveal any known damaging variation. The identified deletion of intronic sequences 5´of exon 2 and 3´of exon 3 may cause erroneous splicing of the ABO gene transcript. As exon 2 and 3 encode the transmembrane domain as well as part of the luminal stem region, absence of these regions is supposed to have adverse effects on the function of the protein resulting in very weak protein activity.
Haemostasis
FV-08-1Prophylactic platelet transfusions to reverse antiplatelet therapy before surgery
Thiele T.1, Baschin M.1, Selleng S.2, Westphal A.1, Greinacher A.1
1Universität Greifswald, Transfusionsmedizin, Greifswald, Germany, 2Universität Greifswald, Klinik für Anästhesiologie und Intensivmedizin, Greifswald, Germany
Introduction: An increasing number of patients admitted for surgery re-ceive antiplatelet therapy for cardiovascular disease. Prophylactic platelet transfusions before surgery may reduce the bleeding risk by improving hemostasis but may in turn increase the risk for cardiovascular compli-cations. We report on the outcome of patients under antiplatelet therapy, who received prophylactic platelet transfusions before surgery. Methods: Consecutive patients between 01/2012–08/2014 under antiplate-let therapy who received at least two prophylactic platelet transfusions be-fore surgery were identified. Assessed were the risk for major adverse cardiac and cerebrovascular events (MACCE), American Society of Anesthesiolo-
gists (ASA)-score, perioperative bleeding, cardiovascular and thrombotic complications until day 30 after surgery. Risk factors for bleeding and addi-tional red cell transfusions were analysed using univariate analysis.Results: In total, 146 patients were analysed: 94 received mono and 52 dual antiplatelet therapy. MACCE-risk was high in 52, moderate in 80 and low in 14 patients. One acute coronary syndrome occurred (coronary supply/demand mismatch). Bleeding at the site of surgery occurred in 17 (11%) patients; in 7 (5%) surgical revision was necessary. Red cell trans-fusions were more likely in patients with high ASA-scores (p < 0.05). In contrast, the level of preoperative platelet inhibition (mono or dual) had no impact on the likelihood of bleeding or red cell transfusion. Conclusion: Prophylactic platelet transfusions for reversal of antiplatelet therapy before surgery are associated with a low risk of acute coronary syndromes. Red cell transfusions are more likely in patients with higher morbidity, but not influenced by the level of platelet inhibition. These data justify a prospective trial to evaluate prophylactic platelet transfusions be-fore surgery in patients with antiplatelet therapy.
FV-08-2Heparin level in blood plasma as sensitive marker for systemic mast cell activation
Vysniauskaite M.1, Hertfelder H.J.1, Haussels I.1, Ohlenforst S.1, Rühl H.1, Selbitz A.1, Unkrig S.1, Dreßen P.2, Brettner S.3, Homann J.4, Oldenburg J.1, Molderings G.J.5
1Institut für Exp. Hämatologie und Transfusionsmedizin, Universitätsklinikum, Bonn, Germany, 2St. Franziskus-Krankenhaus, Eitorf, Germany, 3Krankenhaus, Waldbröl, Germany, 4St.-Elisabeth-Krankenhaus, Bonn, Germany, 5Institut für Humangenetik, Universitätsklinikum, Bonn, Germany
Introduction: Systemic mast cell activation disease (MCAD) denotes a group of primary mast cell (MC) disorders comprising the idiopathic sys-temic mast cell activation syndrome (MCAS) and systemic mastocytosis (SM). MCAD is characterized by enhanced release of MC-derived medi-ators. Demonstrating increased MC mediator release is mandatory in the diagnostic algorithm of MCAD. Currently, only a few MC mediators are established as biomarkers of MCAD.Aims: To determine the sensitivity of plasma heparin levels as an indicator for MC activation and to compare with that of serum tryptase, chromogr-anin A (CgA) and N-methlyhistamine in a large cohort of MCAD patients (n = 285).Methods: For determination of plasma heparin levels blood sampling was done using CTAD Monovette® tubes. Samples were stored at +4°C until centrifugation in the cold. Mild non-pharmacological stimulation of MCs were achieved by venous occlusion (VO) of the upper arm for 10 min. Plasma heparin level was measured by chromogenic anti-factor Xa assay before (baseline) and prior ceasing VO.Results: Baseline heparin had a sensitivity for indicating increased MC activation of 41% in MCAS and 27% in SM patients. After VO elevated heparin levels were detected in 59% of MCAS and 47% of SM patients. In MCAS patients sensitivities of tryptase, CgA and N-methylhistamine levels were low (10, 12 and 22%, respectively) for indicating increased MC activation, but were higher for SM (73, 63 and 43%, respectively).Conclusion: These data suggest that elevated plasma heparin level is a useful indicator of increased systemic mast cell activation. In patients with MCAS its sensitivity is superior to the sensitivities of the other mediators investigated here. Elevated post-VO plasma heparin levels suggest pres-ence of pathologically activated MCs in the occluded compartment.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts22
FV-08-3Macrophages as modulators of wound healing in hemophilic arthropathy
Knowles L.M., Eichler H., Pilch J.Saarland University Hospital, Institute for Clinical Hemostaseologie and Transfusion Medicine, Homburg/Saar, Germany
Introduction: Hemophilic arthropathy is a major cause of morbidity in patients with severe hemophilia. The natural history of hemophilic ar-thropathy involves accumulation of ferrous iron from extravasating red blood cells (RBCs), which can induce synovial inflammation and cartilage damage. Macrophages on the other hand are known to sequester iron by phago-/endocytosing RBCs and heme. We propose that the overall re-duced clotting activity in hemophilia impairs recruitment of macrophages to wounds and, thus, prevents iron clearance after joint bleed.Methods: To study the role of the clotting system for macrophage hom-ing, monocytes isolated from the blood of healthy donors and hemophil-ia patients were embedded in a 3-dimensional matrix of clotted plasma, fibrin-fibronectin or fibrin compared to 2-dimensional cell culture on plastic plates. Macrophages were assessed for spreading (2D) or podo-some formation (3D cell invasion) after treatment with M-CSF to induce M2-polarization or GM-CSF and LPS/IFNγ to induce M1-polarization, respectively. Results: Podosome formation in clot-embedded macrophages was most extensive after treatment with M-CSF compared to GM-CSF and untreat-ed monocytes. Activation with LPS/IFNγ largely abolished spreading in M-CSF-treated macrophages suggesting that clotted plasma predomi-nantly supports adhesive interactions with M2-macrophages. These in-teractions depend on the presence of plasma fibronectin, which appears to be an obligatory co-factor for M-CSF-induced podosome formation in fibrin-embedded macrophages. Interestingly, while M-CSF caused ex-tensive and reproducible spreading in 2D- as well as 3D-cultured donor macrophages, the same cytokine was largely ineffective in macrophages from hemophilia patients, which maintained the round shape of M1 mac-rophages. Conclusion: Our results indicate that clot invasion predominantly occurs in M2-macrophages in a plasma fibronectin-dependent manner. More-over, they suggest that clot-associated plasma fibronectin is involved in maintaining M2 polarization in macrophages. Our ongoing research is geared towards understanding the role of blood clotting in invasion, po-larization and iron endocytosis of macrophages from patients with he-mophilia.
FV-08-4Pathway-specific monitoring of factor XIa generation induced by contact activation or thrombin in human plasma
Rühl H., Friemann A., Müller J., Oldenburg J., Pötzsch B.University Bonn, Institute for Experimental Hematology and Transfusion Medicine, Bonn, Germany
Background: The coagulation factors XII and XI (FXI) are both activated via the contact phase pathway, but only deficiencies of FXI are associated with a bleeding phenotype (hemophilia C). This finding, as well as the high interindividual variability in the clinical phenotype of hemophilia C patients, is believed to be due to feedback activation of FXI by thrombin. Methods: In order to selectively study contact activation or thrombin-in-duced activation kinetics of FXI in human plasma, we developed an acti-vated FXI (FXIa) generation assay. In this assay contact activation of FXI is achieved by addition of aPTT reagent (Actin FS) to citrated plasma in a final dilution of 1:5. For selective thrombin-induced FXI activation thrombin and dextran sulfate are added to defibrinated citrated plasma at a final concentration of 5 µg/mL each. In both preparations, FXIa genera-tion is stopped by sequential addition of benzamidine to subsamples and FXIa quantified using an enzyme capture assay.Results: In normal plasma a contact activation-induced FXIa generation curve was obtained with a peak concentration of 1.99 ± 0.11 (mean ± SD)
µg/mL, a median time to peak (TTP) of 4 min, and an area under the curve (AUC) of 34.15 ± 2.97 (µg · min)/mL after 120 min. For throm-bin-induced FXIa generation a peak concentration of 40.27 ± 2.40 ng/mL, a TTP of 10 min, and an AUC of 905.27 ± 41.83 (ng · min)/mL after 120 min was observed. Analysis of plasma samples with different levels of FXI, ranging between 9% and 131%, revealed a strong correlation between the AUC and FXI activity levels measured with an aPTT-based system (r = 0.97, n = 10 for contact phase-induced FXIa generation; r = 0.97, n = 7 for thrombin-induced FXIa generation).Conclusion: The thrombin-induced endogenous FXIa potential, corre-sponding to the AUC, seems to be substantially lower than that induced by contact activation. Further studies with a larger number of hemophilia C patients are warranted to investigate a potential association between FXIa generation assay results and the bleeding phenotype.
FV-08-5Plasma fibronectin promotes macrophage iInvasion in blood clot
Gurski L.A.1, Knowles L.M.2, Schwarz E.C.3, Eichler H.2, Pilch J.2
1University of Pittsburgh, Department of Urology, Pittsburgh, United States, 2Saarland University Hospital, Institute of Clinical Hemostaseology and Transfusion Medicine, Homburg/Saar, Germany, 3Saarland University, Biophysics – CIPMM, Homburg/Saar, Germany
Introduction: We previously showed that plasma fibronectin (pFN) sup-ports lung metastasis by promoting tumor cell invasion and survival in clotted plasma. Based on the role of clotting for macrophage homing, we set out to test if macrophages reiterate the clot-invasive mechanisms that have been established for tumor cells.Methods: To determine the contribution of pFN to macrophage homing, we analyzed lung tissue sections from transgenic, pFN-deficient mice for co-localization with intravenously injected B16F1 tumor cells. To inves-tigate the role of pFN for macrophage homing in vitro, we embedded freshly isolated monocytes from healthy blood donors in clotted plasma and assessed the capacity of these cells to form podosomes as a means to invade blood clot. Real-time PCR and gene silencing experiments were performed using the macrophage cell line THP-1.Results: Melanoma cells were injected into the tail vein of wild-type or transgenic C57BL/6-Fn(fl/fl) Mx-Cre mice that are deficient for pFN. Compared to wildtype lungs, which showed efficient recruitment of monocytes and later macrophages, this process was significantly delayed in absence of pFN. The same requirement for pFN existed for macro-phages cultured in clotted plasma or fibrin, which only generated podo-somes when pFN was present. In addition to pFN, we found that podo-some formation depends on integrin β3 and the receptor tyrosine kinase Tie2, which has been shown to be expressed on a pro-angiogenic sub-class of M2 macrophages. In agreement, we found that M2 polarization is associated with extensive podosome formation in clotted plasma while clot-embedded M1 macrophages stay largely round. Conclusion: Our results suggest that blood clotting plays an important role for the recruitment of macrophages to circulating tumor cells and that the underlying mechanism of macrophage recruitment involves pFN, integrin β3 and Tie2.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 23
Haemapheresis
FV-09-1Apheresis education for nurses/operators and physicians
Neyrinck M.M.1, Vrielink H.2, Joint Task Force for Apheresis Education and Certification1AZ Delta, Hematology, Roeselare, Belgium, 2Sanquin Blood Supply, Unit of Transfusion Medicine, Amsterdam, Netherlands
Introduction: To guarantee uniformity and quality, a modular training program for apheresis nurses was developed by a group of experienced apheresis nurses and physicians from Europe and the USA (JTFAEC). Learning objectives of identified themes related to apheresis (hematology, anatomy, physiology, calculations, adverse events, basics, nursing, qual-ity, collection of cells for cellular therapies, pediatrics, and therapeutic apheresis) were made. Based on this, a modular course with 13 lessons was build. In co-operation with authors and editors, ASFAs 5th edition “Principles of Apheresis Technology” was written to cover the majority of the learning objectives. Therefore, this book can be used as manual for the course developed by JTFAEC.Methods: In December 2013, the course was given in Indonesia in English to 39 nurses and 32 physicians. Participants came from Cambodia, Indo-nesia and Singapore. In March, September, October 2014, and January 2015 the course was given in Belgium and the Netherlands to 52 nurses and 23 physicians. In February 2015, 11 nurses from Austria, Italy, Spain, Sweden, Switzerland, The Netherlands, UK and USA participated in a course in Austria. Finally, 4 trainers from SANBS were trained in April 2015 to give the course. Following the train-the-trainer course the newly trained trainers gave, supported by the two authors, with success a course for 3 physicians and 10 apheresis nurses of SANBS in Johannesburg South Africa.Results: In the post-course tests, all nurses and physicians showed a sig-nificant increase of knowledge in apheresis compared to the results in the pre-course tests. All participating nurses and operators could be certified according to the requirements as agreed by JTFAEC. Conclusions: This educational program provides an approach to educate and certificate apheresis nurses. This can be of help in GMP/ISO/FACT/JACIE inspections/audits. It is also shown that also for physicians this course can be of value to increase their knowledge regarding apheresis. Up to now, all courses were given in English and Dutch. By giving this course in a train-the-trainer situation, courses like this with specified learning objectives can be given in local languages in order better understanding for persons working in the field of apheresis for whom English is not the native language. At present, training of apheresis nurses (and physicians) according to the concept of this course is discussed in various countries.
FV-09-2Comparison of two programs (Spectra Optia cMNC and MNC) for peripheral blood progenitor collection in autologous patients
Rox J.M.1, Kobbe G.2, Dienst A.2, Fischer J.C.1
1Universitätsklinik Düsseldorf, Institut für Transplantationsdiagnostik und Zelltherapeutika, Düsseldorf, Germany, 2Universitätsklinik Düsseldorf, Klinik für Hämatologie, Onkologie und Klinische Immunologie, Düsseldorf, Germany
Introduction: Treatment of patients with autologous peripheral blood progenitor cell (PBPC) rescue following high-dose chemotherapy requires PBPC apheresis. Since shortly, two programs are available to collect PB-PCs with the Spectra Optia apheresis device (Terumo BCT): the “MNC” (mononuclear cell) as well as the “cMNC” (continuous MNC) program. MNC combines continuous hard-spin centrifugation with subsequent cel-lular collection into a platelet elutriation chamber. PBPCs are harvested intermittently from this chamber. With cMNC the target cells are contin-uously harvested using soft-spin centrifugation conditions. Which pro-
gram to use for PBPC collection of autologous patients remains an open question.Methods: We investigated 255 autologous PBPC collections performed with the Spectra Optia device using the MNC- (n = 110) or the cMNC-pro-gram (n = 145). The performance of the two methods was compared with respect to collection efficiency (CE2, cells harvested/cells processed based on pre apheresis peripheral blood count), throughput (TP or collection rate per time, PBPC harvested/kg BW/run time [h]/PBPC pre apheresis count [CD34+ cells/µl]), and platelet loss.Results: There was no difference in CD34+ collection efficiency (CE2, 51 ± 15% for MNC vs 50 ± 11% for cMNC, p = 0.53) between both pro-grams. Due to the intermittent collection of the MNC program there is a substantial loss of effective collection time (average calculated flow rate 64 ± 16 ml/min for MNC vs 91 ± 22 ml/min for cMNC, p < 0.001). Be-cause procedure times were equal, significant more total blood volume was processed using the cMNC program (21 781 ± 7 185 ml for cMNC vs 14 593 ± 6 260 ml for MNC, p < 0.001). Therefore, TP was higher using the cMNC program (0.033 ± 0.009 for cMNC vs 0.025 ± 0.008 for MNC, P < 0.001). Although an additional elutriation platelet recovery process is implemented in the MNC program these procedures showed significant more platelet loss than the cMNC- procedures (platelet CE2: 10 ± 3% for cMNC vs 17 ± 7% for MNC, p < 0.001).Conclusion: The cMNC collects CD34+ cells with higher collection rate per time (TP), equal collection efficiency (CE2) and less platelet loss com-pared to MNC. It allows high flow rates that permit large-volume-leuka-pheresis which is especially useful in patients with low peripheral blood CD34+ cell counts.
FV-09-3MNC2 versus CMNC-program for autologous PBSC collection with Spectra Optia®
Mansouri Taleghani B.1, Vetsch G.2, Pfeuti S.2, Marbacher C.2, Besson N.3
1Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Transfusionsmedizin, Bern, Switzerland, 2Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Bern, Switzerland, 3Terumo BCT, Zaventem, Belgium
Background: A new continuous mononuclear cell collection protocol (CMNC) has been released on the Spectra Optia® platform (Terumo BCT, Belgium) for peripheral blood stem cell (PBSC) collections. Com-pared to MNC2, where MNC are collected by cycles, the CMNC offers a continuous collection & allows higher inlet-flow rates facilitating our “individualized high-flow, very-large-volume apheresis” (Transfusion 2006;46:1408–1416). We directly compared MNC2 vs CMNC. Methods: We investigated 20 autologous PBSC collections: 10/protocol. Performance was evaluated by Collection Efficiency (CE) and Throughput (TP). Data presented as mean, statistical differences evaluated by a t-test. Results: Data were comparable for BW, total body blood volume (TBV), WBC, PLT, Hct and CD34+ precounts. Despite lower BV processed on MNC2 (3.38 × TBV vs 5.19 × TBV; p = 0.011), they trended to take longer (340 vs 267 min, p = 0.051), while comparable CD34+ doses were col-lected (MNC2 17.8 × 106/kg vs CMNC 10.3 × 106/kg, p = 0.353). CE were high and comparable (MNC2 73.45% vs CMNC 66.69%, p = 0.47), but CMNC allowed a higher TP (58.96 vs 36.46; p = 0.005), a lower product volume (276.4 mL vs 450.8 mL; p = 0.0004), a higher product WBC con-centration (393 × 109/L vs 209 × 109/L; p = 0.002). PLT contamination and % PLT loss (patients) were comparable, while loss of PLT per L of processed blood was lower in CMNC (1.91% vs 3.22%, p = 0.038). Conclusion: MNC2 seems more efficient according CE and superior in reproducibility of yields (Fig 1).
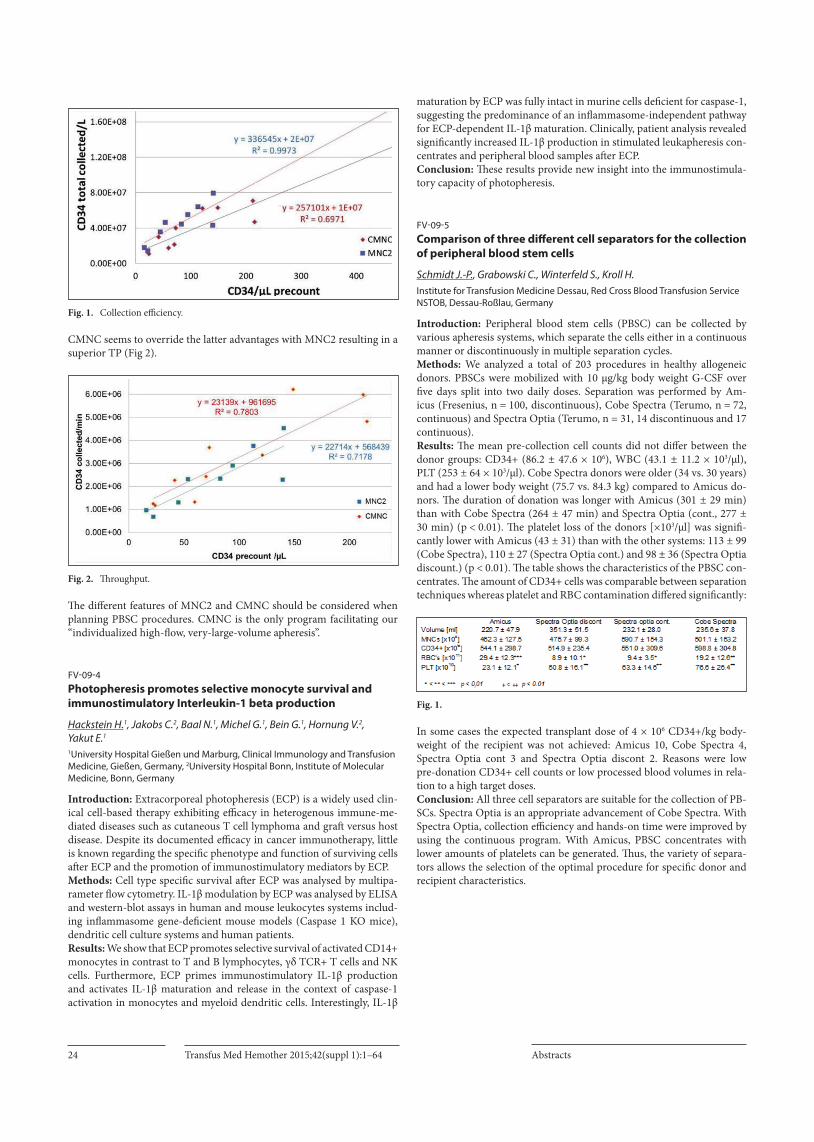
Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts24
Fig. 1. Collection efficiency.
CMNC seems to override the latter advantages with MNC2 resulting in a superior TP (Fig 2).
Fig. 2. Throughput.
The different features of MNC2 and CMNC should be considered when planning PBSC procedures. CMNC is the only program facilitating our “individualized high-flow, very-large-volume apheresis”.
FV-09-4Photopheresis promotes selective monocyte survival and immunostimulatory Interleukin-1 beta production
Hackstein H.1, Jakobs C.2, Baal N.1, Michel G.1, Bein G.1, Hornung V.2, Yakut E.1
1University Hospital Gießen und Marburg, Clinical Immunology and Transfusion Medicine, Gießen, Germany, 2University Hospital Bonn, Institute of Molecular Medicine, Bonn, Germany
Introduction: Extracorporeal photopheresis (ECP) is a widely used clin-ical cell-based therapy exhibiting efficacy in heterogenous immune-me-diated diseases such as cutaneous T cell lymphoma and graft versus host disease. Despite its documented efficacy in cancer immunotherapy, little is known regarding the specific phenotype and function of surviving cells after ECP and the promotion of immunostimulatory mediators by ECP.Methods: Cell type specific survival after ECP was analysed by multipa-rameter flow cytometry. IL-1β modulation by ECP was analysed by ELISA and western-blot assays in human and mouse leukocytes systems includ-ing inflammasome gene-deficient mouse models (Caspase 1 KO mice), dendritic cell culture systems and human patients.Results: We show that ECP promotes selective survival of activated CD14+ monocytes in contrast to T and B lymphocytes, γδ TCR+ T cells and NK cells. Furthermore, ECP primes immunostimulatory IL-1β production and activates IL-1β maturation and release in the context of caspase-1 activation in monocytes and myeloid dendritic cells. Interestingly, IL-1β
maturation by ECP was fully intact in murine cells deficient for caspase-1, suggesting the predominance of an inflammasome-independent pathway for ECP-dependent IL-1β maturation. Clinically, patient analysis revealed significantly increased IL-1β production in stimulated leukapheresis con-centrates and peripheral blood samples after ECP.Conclusion: These results provide new insight into the immunostimula-tory capacity of photopheresis.
FV-09-5Comparison of three different cell separators for the collection of peripheral blood stem cells
Schmidt J.-P., Grabowski C., Winterfeld S., Kroll H.Institute for Transfusion Medicine Dessau, Red Cross Blood Transfusion Service NSTOB, Dessau-Roßlau, Germany
Introduction: Peripheral blood stem cells (PBSC) can be collected by various apheresis systems, which separate the cells either in a continuous manner or discontinuously in multiple separation cycles. Methods: We analyzed a total of 203 procedures in healthy allogeneic donors. PBSCs were mobilized with 10 µg/kg body weight G-CSF over five days split into two daily doses. Separation was performed by Am-icus (Fresenius, n = 100, discontinuous), Cobe Spectra (Terumo, n = 72, continuous) and Spectra Optia (Terumo, n = 31, 14 discontinuous and 17 continuous).Results: The mean pre-collection cell counts did not differ between the donor groups: CD34+ (86.2 ± 47.6 × 106), WBC (43.1 ± 11.2 × 103/µl), PLT (253 ± 64 × 103/µl). Cobe Spectra donors were older (34 vs. 30 years) and had a lower body weight (75.7 vs. 84.3 kg) compared to Amicus do-nors. The duration of donation was longer with Amicus (301 ± 29 min) than with Cobe Spectra (264 ± 47 min) and Spectra Optia (cont., 277 ± 30 min) (p < 0.01). The platelet loss of the donors [×103/µl] was signifi-cantly lower with Amicus (43 ± 31) than with the other systems: 113 ± 99 (Cobe Spectra), 110 ± 27 (Spectra Optia cont.) and 98 ± 36 (Spectra Optia discount.) (p < 0.01). The table shows the characteristics of the PBSC con-centrates. The amount of CD34+ cells was comparable between separation techniques whereas platelet and RBC contamination differed significantly:
Fig. 1.
In some cases the expected transplant dose of 4 × 106 CD34+/kg body-weight of the recipient was not achieved: Amicus 10, Cobe Spectra 4, Spectra Optia cont 3 and Spectra Optia discont 2. Reasons were low pre-donation CD34+ cell counts or low processed blood volumes in rela-tion to a high target doses. Conclusion: All three cell separators are suitable for the collection of PB-SCs. Spectra Optia is an appropriate advancement of Cobe Spectra. With Spectra Optia, collection efficiency and hands-on time were improved by using the continuous program. With Amicus, PBSC concentrates with lower amounts of platelets can be generated. Thus, the variety of separa-tors allows the selection of the optimal procedure for specific donor and recipient characteristics.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 25
FV-09-6Changes in haemoglobin and ferritin levels in double red cell apheresis: a longitudinal analysis
Keshelashvili K.1, Stern M.2, O’Meara A.2, Jirout Z.1, Buser A.1, Holbro A.1, Sigle J.1, Infanti L.1
1Blutspendezentrum SRK Basel, Basel, Switzerland, 2Universitätsspital, Hämatologie, Basel, Switzerland
Background: Iron stores recovery is incomplete 4 months after double red blood cell (2RBC) apheresis [1, 2]. In Europe, the interval between 2RBC donations must be ≥4 months for males and ≥6 months for females, in Switzerland 6 months for both genders. Longitudinal changes of haemo-globin (Hb) and serum ferritin (SF) in 2RBC donors were retrospectively analysed in Swiss 2RBC donors.Methods: Requirements for 2RBC donation were Hb ≥140 g/l and body weight ≥70 kg; SF, determined in all donors at baseline and at each dona-tion, was not a selection criterion. Collections of 360 ml RBC with ALYX devices were made at a 6-months interval. Donor demographics were ana-lysed with descriptive statistics. Mean ± standard error of the mean (SEM) of Hb and SF were calculated in donors grouped by number of donations. The effect on SF and Hb levels of whole blood (WB), platelet (PLT) and plasma (PL) donations performed between 2RBC aphereses by the same donor was evaluated with generalized linear models. Results: From January 2003 to December 2013 4’140 2RBC aphereses were performed in 770 donors (758 males). Donors also gave 4’402 WB, 1’216 PLT and 424 PL donations. Median donor age was 57 years, median number of donations was 4 (range 1–20); 139 donors had baseline SF ≤30 ng/ml. Mean Hb and SF were 157 g/l (SEM 0.3) and 173 ng/ml (SEM 11) at baseline, and 156 g/l (SEM 2.7) and 54 ng/ml (SE 12) at the last dona-tion. Mean SF dropped to 50–70 ng/ml after 5 procedures and remained stable (Figure). No case of ID anaemia occurred. Conclusions: Male donors of 2RBC at a 6-months donation interval have low stable SF levels. No ID anaemia occurs, even with low baseline SF and when other types of donations are additionally performed. References: 1. Hogler W, Mayer W, Messmer C et al.: Prolonged iron depletion after allogeneic
2-unit RBC apheresis. Transfusion 2001;41:602–605.2. Mendrone A Jr, Arrais CA, Almeida Neto C et al.: Impact of allogeneic
2-RBC apheresis on iron stores of Brazilian blood donors. Transfus Apher Sci 2009;41:13–17.
New Technologies/new methods
FV-10-1Detection of changes in the miRNA expression profile during blood storage – a pilot study
Henke A.1, Pfaffl M.W.1, Henschler R.2, Wichmann C.2, Riedmaier I.1
1Technical University Munich, Physiology, Freising-Weihenstephan, Germany, 2Ludwig-Maximilians University Hospital, Department of Transfusion Medicine, Cell Therapeutics and Hemostaseology, München, Germany
Since 1986 illegal blood manipulation or transfer, commonly referred as “blood doping”, has been prohibited by WADA (World Anti-Dop-ing Agency) because of its serious health threats and fairness in sports. Whereas homologous blood doping can be detected using flow cytometry, there is still no reliable method to detect autologous blood transfer. MiR-NAs are already known as powerful biomarkers that can be used to detect a particular physiological condition or a disease status on the basis of a specific miRNA pattern. That supports the hypothesis that a similar anal-ysis of erythrocyte miRNAs can reveal changes in the miRNA expression between fresh and stored blood. The essential step to carry out autologous blood doping is to store the Red Blood Cells (RBCs) in blood bags for several weeks. In a pilot study, blood samples were taken from 10 healthy subjects before blood donation and from the respective blood bags at sev-
eral points in time during blood storage in order to evaluate changes in the miRNA profile caused by blood storage conditions. Up to now, the samples taken from six subjects were investigated using small RNA Se-quencing, a method that enables the detection of all existing small RNAs in a sample. Using the DESeq algorithm for normalization, it could be shown that the expression of 119 miRNAs is significantly affected either by the addition of a preservative solution or by changes in the blood cells physiology during time of storage. Using multivariate data analysis tools, on the basis of 10 upregulated miRNAs, two separate clusters could be visualized: one contains the fresh blood samples taken from the subjects and the second includes samples taken from the stored blood bags. These findings suggest the potential of creating a valid biomarker signature, containing a stable set of autologous blood doping-associated miRNAs in order to detect autologous blood doping.
FV-10-2Characterization of mouse hybridomas producing monoclonal antibodies against platelet aIIbb3 complex using ELISPOT
Maenner D., Werth S., Bein G., Santoso S.Klinische Immunologie und Transfusionsmedizin, Giessen, Germany
Antibodies against platelet aIIbb3 integrin are commonly found in pa-tients with immune mediated thrombocytopenia. The exact binding sites of these antibodies, however, are not known. Theoretically, antibodies may react with complex specific epitopes formed by the aIIb- and b3-sub-units or against antigenic determinants residing either on the aIIb or b3 subunit alone. Several evidences indicate that antibody against aIIbb3 complex may play an important role on the pathomechanism of immune thrombocytopenia. Recent studies indicated that B cell Enzyme-Linked ImmunoSpot (ELISPOT) assay is useful for the identification of antibody production of single B cell clone in patients with immune thrombocyto-penia. In this assay, however, aIIbb3 was isolated from outdated platelets by chromatography. Here, a novel ELISPOT approach using biotinylated recombinant aIIbb3, avb3 and b3 glycoprotein was established to char-acterize the specificity of mouse monoclonal antibodies (mabs) against human aIIbb3. Mabs produced by hybridomas were captured by secondary antibody im-mobilized on the PVDF membrane. Bound mabs were then detected with biotinylated recombinant proteins aIIbb3, b3, or avb3. Spots represent-ing antibody-antigen complex were then visualized by enzyme labelled streptavidin and substrate system. Hybridoma Gi5 producing mab against aIIbb3 complex developed only spot formation when recombinant aIIbb3 was used in our ELISPOT assay. In contrast, no reaction was found with b3 and avb3 proteins. To prove the immunoreactivity of both proteins used, solid phase ELISA was per-formed. Recombinant b3 and avb3 proteins reacted with mab SZ21 and 23C6 specific for b3 subunit and avb3 complex, respectively. Titration analysis showed that the number of spot correlated significantly with the number of seeded cells, and approximately 15 antibody producing B-cell clone could be identified among 103 non-producing B cells. Analysis of independent experiments resulted in good intra-assay (n = 9) and in-ter-assay value (n = 4). Our results indicate that ELISPOT can be used for the specific identifica-tion of small number of B-cell clone producing antibodies against aIIbb3 complex in high number of non-producing B cell clones. In the future, this approach may useful to dissect the diversity of B-cell clones in pa-tients developed platelet antibodies reacted against different b3-integrins.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts26
FV-10-3Evaluation of hepcidin as novel biomarker to reflect the actual human iron status
Enko D.1, Wagner H.2, Kriegshäuser G.1, Stolba R.1, Halwachs-Baumann G.1
1Institute of Laboratory Medicine, General Hospital Steyr, Steyr, Austria, 2Department of Applied Statistics, Johannes Kepler University Linz, Linz, Austria
Background: The purpose of the present study was to investigate, whether hepcidin is a useful additional clinical biomarker to reflect the actual hu-man iron status, especially functional ID. Methods: A total of 233 hospitalized adult patients with suspected ID were included. All subjects were investigated for hepcidin, reticulocyte haemoglobin content (CHr), soluble transferrin receptor (sTfR)/log fer-ritin ratio (i.e. Thomas plot), sTfR, ferritin, transferrin saturation (TSAT), C-reactive protein (CRP) and for complete blood cell count. The hepci-din measurements were performed with the recently launched European Community (CE)-marked enzyme-linked immunoabsorbent assay (ELI-SA) (Hepcidin-25 bioactive ELISA; DRG Instruments GmbH, Marburg, Germany). Functional ID was defined as a CHr < 28 pg. Separate logistic regression models were calculated with all potential biomarkers to eval-uate and compare the predictive performance with respect to functional ID in patients without (CRP ≤ 0.5 mg/dL) and with (CRP > 0.5 mg/dL) acute-phase reaction, respectively. Results: The hepcidin measurements correlated with parameters of iron metabolism. There was a positive correlation with serum ferritin (p < 0.001, Pearson correlation coefficient 0.261) and TSAT (p = 0.035, Pearson correlation coefficient 0.138), and a negative correlation with transferrin (p < 0.001, Pearson correlation coefficient –0.602), sTfR (p < 0.001, Pearson correlation coefficient –0.374), and iron (p = 0.162, Pear-son correlation coefficient -0.092). There was also a positive correlation between CRP and hepcidin (p < 0.001, Pearson correlation coefficient 0.258). One hundred seventeen patients with CRP > 0.5 mg/dL showed a distinctly higher hepcidin median value (35.60 [range: 4.27–80.03] ng/mL) as compared to 116 patients with CRP ≤ 0.5 mg/dL (18.55 [range: 3.77–73.01] ng/mL). With respect to functional ID, sTfR/log ferritin ratio and sTfR were of better positive predictive value (PPV) (sTfR/log ferritin ratio: 58.33 and 70.83%; sTfR: 60.00 and 60.00%) than when compared to hepcidin (PPV: 37.74 and 42.86%) and ferritin (PPV: 27.54 and 46.15%) in both subgroups. Conclusion: In the logistic regression modeling and when compared with the sTfR/log ferritin or the sTfR measurements, hepcidin as well as ferri-tin, both molecules are known as acute phase reactants, were only of low predictive value to reflect functional ID.
FV-10-4Automated microscopic evaluation of Red Blood Cell storage lesion
Sierra D.A.1, Janetzko K.2, Dobrinski C.2, Bieback K.2, Suhr H.1, Wiedemann P.3
1Department of Information Technology, Mannheim University of Applied Sciences, Mannheim, Germany, 2Institute of Transfusion medicine and Immunology, Medical Faculty Mannheim, Heidelberg University, German Red Cross Blood Donor Service Baden-Württemberg-Hessen, Mannheim, Germany, 3Department of Biotechnology, Mannheim University of Applied Sciences, Mannheim, Germany
Introduction: Red blood cells (RBC) can be stored refrigerated up to 6 weeks, until used for transfusion. During this period, RBC undergo changes, called RBC storage lesion. Biochemical alterations cause changes in rheological properties such as aggregability, deformability and osmotic fragility. Thus, some authors question whether older RBC units have an increased risk of causing medical complications in severely sick patients. Current methods to determine the quality of RBC-units focus on assess-ing biochemical parameters. These, however, are only indirectly related to the present status of the cells. Therefore, a simple automatable technique
appears advantageous. We propose in situ microscopy for directly diag-nosing RBCs in a flow chamber. Methods: Due to progressive cell degradation, morphology of RBCs changes noticeably over storage-time. We use an in situ microscope (ISM) to generate large statistics of RBC images from small extracted RBC sam-ples over the storage period of 13 weeks, validated by assessing a number of biochemical parameters in parallel. The ISM observes directly a flow of diluted samples from RBC-units through a flow chamber. A statistic feature extraction process is carried out with respect to size, roundness, roughness, texture homogeneity and orientation in the flow field classifying three defined morphology types (disc-shaped erythrocytes, acanthocytes and spherocytes). Results: Young RBC samples show insignificant amounts of acanthocytes and spherocytes. Progressively increasing over time (until week 10), flex-ible disc-shaped erythrocytes begin to adopt a spiky morphology (acan-thocytes). At late stages, the amount of detected spherocytes increases significantly. Interestingly, the speed of degradation differs very much be-tween different donors. Biochemical parameters, in contrast, do not reveal the same differences between donors.Conclusions: In situ microscopy is able to characterized RBC samples showing a high correlation between the elapsed time of stored RBC units and the proportion of acanthocytes and spherocytes. Variability between donors was encountered by the ISM evaluation, not registered by bio-chemical reference measurements. This observation hints at a sensitivity of the ISM technique with respect to relevant quality issues in RBC-units. We also expect fast ISM response to accidental damage of RBC units as caused for instance by time intervals with inappropriate temperature.
FV-10-5Computer-Aided-Facility-Management improves daily maintenance of laboratory instruments
Heinz-Senf P.1, Spyrantis A.1, Groß M.1, Capalbo G.1, Sireis W.2, Seifried E.1, Schmidt M.1, QM1DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Frankfurt, Germany, 2DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Kassel, Germany
Background: The German Red Cross blood donor service Baden-Würt-temberg-Hessen, North-East and its affiliates is represented at 18 institutes in six different states. Computer-Aided-Facility-Management (CAFM) is an integrated system, which unifies multiple functions. In consideration of the huge number of devices, technical facilities and buildings, which have to be proofed technical and to be documentated. To meet the legal requirements, a special software complies all these conditions.Aims: To guarantee the legal guidelines of the technical maintenances, monitoring of devices, technical facilities and buildings in an uniformed and electronical documentation at the different places with the same pro-cedure and to assure an archiving system for the documents over a long period. Furtheron CAFM gives the possibility, to link the devices- and building management of each department with the superior coast center, to control and check the economic efficiency and productivity. Method: Since 4,5 years CAFM is implementated at all 18 institutes of our blood donor services and supports the technical department as a monitor-ing module. With the program MTBT-Data according to the actual and legal specifications, the test data are archived in the SQL Data base. The software program „Maqsima TMS“ and EMTEC provide the info-types with the legal requirement for all devices, buildings and facilities. Each device, coming new in the institute, gets an own BSD-ID, which is given one-time systemic numbered consecutively. The devices keep this identi-fication the hole life time cycle. Even when a relocation will happen in-or outside the institute, nothing will change, but for location and room-num-ber. Results: Thitherto in the complete German Red Cross are until today already registered 17.295 devices and technical equipments, 3459 rooms and 99 buildings. This are 70–80% in BaWüHe and around 30% in North-

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 27
East. For the institute in Frankfurt are 4882 devices and 572 rooms regis-tered. Whereof 375 concern the mobile blood withdrawal.Conclusion: The introduction of CAFM allows a digital monitoring with electronic recording of the total history from a device, technical equip-ment or room. Statistical analyses of trends are easy to perform for techni-cal, medical or commercial questions and to oversee the total coast. And last not but least CAFM supports also the guidelines of the quality man-agement.
Presidential symposium best abstract
PSB-01-1Partially desulfated heparin modulates the interaction between anti-protamine/heparin antibodies and platelets
Jouni R., Zöllner H., Khadour A., Krauel K., Wesche J., Greinacher A., Bakchoul T.Universitätsmedizin Greifswald, Institute for Immunology und Transfusion Medicine, Greifswald, Germany
Introduction: Protamine (PRT) is the standard drug to neutralize hepa-rin. PRT/heparin complexes induce an immune response similar to that observed in heparin-induced thrombocytopenia (HIT). The presence of anti-PRT/heparin antibodies (Abs) has been suggested to be associated with postoperative complications. No therapeutic strategies are currently available to reduce the sensitizing properties of PRT/heparin complexes or to prevent complications that might be induced by anti-PRT/heparin Abs. Partially desulfated heparin (ODSH) was shown to interfere with anti-platelet factor 4/heparin Abs, which are responsible for HIT. In this study, we analyze the impact of ODSH on the interactions between an-ti-PRT/heparin Abs and platelets (PLTs).Methods: The ability of ODSH to prevent anti-PRT/heparin Ab-induced human (hu) PLT-destruction was investigated using the NOD/SCID mouse model. The interaction between PRT/heparin complexes and PLTs in the presence of ODSH was analyzed using flow cytometry (FC). The ability of ODSH to interfere with Ab-mediated PLT activation was inves-tigated using the functional assay HIPA.Results: ODSH improved the survival of huPLTs in the circulation of the NOD/SCID mice in the presence of PRT, heparin and anti-PRT/heparin Abs (median huPLT-survival after 5h: with ODSH 75%, range 70–81 vs. without ODSH 49%, range 44–59, p = 0.006). Interestingly, even when ODSH was administrated into the mice 1h after Ab injection PLT-sur-vival was higher compared to buffer (median huPLT-survival after 5h: with ODSH 83%, range 77–93% vs. without ODSH 59%, range 29–61%, p = 0.021). In HIPA, anti-PRT/heparin Abs activated PLTs only in the presence of PRT and heparin (median time to PLT aggregation: 10 min, range 5–25). ODSH prolonged the time to PLT activation (median time to PLT aggregation with ODSH: 45 min, range 20 - 45, p < 0.001). The FC analysis showed that ODSH did not only inhibit complex binding to PLTs (mean fluorescence intensity [MFI]: without ODSH 85±14 vs. with ODSH: 15±0.6, p = 0.013) but also displaced pre-bound complexes from the PLT surface (complex binding MFI: before addition of ODSH 324±43 vs. after addition of ODSH: 53±9, p < 0.001).Conclusion: Our study demonstrates the ability of ODSH to prevent anti-PRT/heparin Ab-mediated PLT-activation and -destruction by modulating complex binding to the PLT surface. These results suggest a therapeutic benefit of ODSH to reduce anti-PRT/heparin Ab-mediated complications.
PSB-01-2Protein modified magnetic nanoparticles for GMP conform production of magnetically labelled platelets from platelet concentrates
Aurich K.1, Wesche J.1, Scholz L.1, Medvidov M.2, Palankar R.2, Greinacher A.1,2, Bakchoul T.1,2
1Universitätsmedizin Greifswald, Transfusionsmedizin, Greifswald, Germany, 2Universitätsmedizin Greifswald, Innovation Center - Humoral Immune Responses in Cardiovascular Disorders, Greifswald, Germany
Background: Cell labelling is often required, such as in the context of reg-istration trials of novel platelet concentrates (PC) to distinguish between platelet populations or in platelet survival studies. Recently, we presented magnetic labelling of platelets by Resovist® nanoparticles. Here we report on a method for improved cell uptake of magnetic particles by modifying the particle shell and we show the feasibility of producing magnetically labelled platelets from PC according to EU good manufacturing practice (GMP) guidelines. Methods: Protein modified particles and magnetically labelled platelets were produced according to EU GMP guidelines under aseptic conditions in a cleanroom facility with subsequent sterility tests regarding Europe-an Pharmacopoeia. We used Ferucarbotran particles (Meito Sangyo), the raw material for Resovist®, and conjugated human serum albumin (HSA) covalently onto particles shell. Protein coupling was verified by measur-ing the increase of the hydrodynamic diameter due to cross-linking of HSA-Ferucarbotran particles by an anti-HSA-antibody (photon correla-tion spectroscopy). Platelets from PC were incubated with HSA-Ferucar-botran particles for 60 min. Particle uptake was detected by fluorescent and electron microscopy, and atomic absorption spectroscopy, and the impact on platelet function was determined by flow cytometry (activation marker CD62p). For in vitro re-isolation labelled platelets were spiked in whole blood. After 60 min labelled platelets were re-isolated by magnetic separation. Results: HSA conjugation particle uptake into cells increased tenfold compared to bare ferucarbotran particle or Resovist® uptake (incuba-tion iron concentration 0.5 mM; uptake: 0.002 vs. 0.021 pg iron/platelet, bare Ferucarbotran vs. HSA-Ferucarbotran respectively). Platelet imag-ing showed an adequate uptake of the particles into the open canalicular compartment. Determination of CD62p-expression after activation using TRAP-6 showed normal platelet function. Magnetic separation resulted in a yield of 55% of the HSA-Ferucarbotran labelled platelets from spiked whole blood. Conclusion: We demonstrate that magnetic labelling of platelets from PC can be improved by conjugation of human plasma proteins onto Ferucar-botran nanoparticles. We succeeded in in vitro reisolation of magnetically labelled platelets from whole blood and we are able to produce protein coupled particles and magnetically labelled platelets from PC under EU GMP conditions.
PSB-01-3First detailed molecular characterization of different Yus (GE*01.-02) alleles and description of a novel Gerbich (GE*01.-03) allele responsible for rare
phenotypes in the Gerbich blood group system
Gourri E.1, Scharberg E.A.2, Peyrard T.3,4, Frey B.M.1, Gassner C.1
1Blood Transfusion Service SRC, Zurich, Department of Molecular Diagnostics and Research & Development (MOC), Zürich-Schlieren, Switzerland, 2Red Cross Blood Service of Baden-Wuerttemberg-Hessen, Baden-Baden, Germany, 3Institut National de la Transfusion Sanguine (INTS), Centre National de Référence pour les Groupes Sanguins, Paris, France, 4Laboratory of Excellence GR-Ex, Paris, France
Introduction: The Gerbich blood group system consists of 11 antigens located on glycophorin C and D, proteins encoded by GYPC. Yus and Gerbich correspond to the rare Ge:-2,3,4 and Ge:-2,-3,4 types. Until now, their molecular background was only described approximately, with dele-

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts28
tions of exon 2 and 3 of the GYPC gene, for Yus and Gerbich, respectively. Serological determination of blood group Gerbich phenotypes is tedious and costly. Therefore, we aimed to design a rapid and cost-effective meth-od to screen them at the genetic level.Methods: 3 unrelated patients with anti-Ge had been reported to Blut-spende Zurich and were serologically defined as 2 Gerbich and 1 Yus phenotypes. Positional PCRs and sequencing of the GYPC gene allowed for the exact location of deletions. PCRs using Sequence Specific Prim-ing (PCR-SSP) were developed to detect the respective allelic breakpoints. They were used to genotype 5 additional samples from the Baden-Baden Red Cross Blood Service (BB), all with anti-Ge, but no phenotypic infor-mation, and 1 Gerbich sample from the SCARF exchange program.Results: All 3 Zurich samples were homozygous for 1 deletional GYPC al-lele, with 2 different molecular backgrounds. The genomic extent of both observed alleles was in line with the expected phenotypes, e.g. a deletion of exon 2 (i1–41 to i2+3511) in the Yus and a deletion of exon 3 (i2–2640 to i3+859) for the Gerbich phenotype. 4 BB samples were homozygous for one or the other of the previously observed Yus and Gerbich alleles as confirmed by PCR-SSP and sequencing. The SCARF sample was un-ambiguously recognized as Gerbich by our PCR-SSP. The 5th BB sample was compound heterozygous for two new Yus alleles, both with an exon 2 deletion (i1–1638 to i2+1917 and i1–778 to i2+2777). Supplementary PCR-SSPs were designed to detect them.Conclusion: A total of 9 investigated samples, 8 of them with anti-Ge al-lo-antibodies, were unambiguously genotyped for their Yus and Gerbich phenotypes using a diagnostic 10 reaction PCR-SSP approach. To our knowledge, this is the first report with a detailed molecular characteri-zation of 3 forms of the Yus allele, originally reported with the Gerbich allele in 1989 (Colin et al.). Another Gerbich allele have been described previously (Scott et al. 2008). Yus (i1–41 to i2+3511) seems to be most frequent. ISBT terminology for the alleles encoding the Yus (GE*01.-02) and Gerbich (GE*01.-03) phenotypes will likely need splitting into several alleles each, and revision.
PSB-01-4Manufacture, management and clinical application of pathogen-inactivated Ebola virus convalescent plasma
Geisen C.1, Kann G.2, Strecker T.3, Wolf T.2, Schüttfort G.2, van Kraaij M.4, MacLennan S.5, Rummler S.6, Weinigel C.6, Eickmann M.3, Fehling S.K.3, Krähling V.3, Seidl C.1, Seifried E.1, Schmidt M.1, Schäfer R.1
1Institute of Transfusion Medicine und Immunohaematology, German Red Cross Blood Service Baden-Wuerttemberg Hessen, University Hospital, Frankfurt am Main, Germany, 2Johann Wolfgang Goethe University, Department of Infectious Diseases, Frankfurt am Main, Germany, 3Philipps University, Institute of Virology, Marburg, Germany, 4on behalf of the European Blood Alliance, Amsterdam, Netherlands, 5NHS Blood & Transplant, Blood Centre, Leeds, United Kingdom, 6Institute of Transfusion Medicine, University Hospital, Jena, Germany
Introduction: Ebola virus disease is a public health emergency of interna-tional concern and enormous efforts are being made in the development of vaccines and therapies. Ebola virus convalescent plasma is a promising anti-infective treatment of Ebola virus disease, and programs are under-way to manufacture Ebola virus convalescent plasma on-site in African countries affected by Ebola virus disease. As standard screening tests cannot cover all transfusion transmissible pathogens that are prevalent in these regions, pathogen inactivation is suggested to maximize safety of blood products. Therefore, we developed and implemented a patho-gen-inactivated Ebola virus convalescent plasma concept assessing possi-ble impact on EBOV neutralizing antibodies. Methods: Ebola virus convalescent plasma manufacture and distribution was managed by collection centre, medical centres and an expert group co-ordinated by the European Blood Alliance. After process adjustments and regulatory approval, Ebola virus convalescent plasma was collected twice with an interval of 61 days from a donor recovering from Ebola virus disease in Germany. After amotosalen/UVA pathogen inactivation
the plasma was analysed for EBOV neutralizing antibodies and cryopre-served. Per request from clinicians treating an Ebola virus disease patient in Italy pathogen-inactivated Ebola virus convalescent plasma was re-leased and transfused without apparent adverse effects. Results: Convalescent plasma could be collected without adverse events. Notably, pathogen inactivation treatment did not reduce EBOV neutraliz-ing antibody titers in convalescent Plasma. Complex but highly functional management processes were required for successful production of patho-gen-inactivated Ebola virus convalescent plasma and its timely distribu-tion for patients worldwide.Conclusion: As proof-of-principle, we describe for the first time a con-cept and practical implementation of pathogen-inactivated Ebola virus convalescent plasma manufacture and its successful clinical application to an Ebola virus disease patient. The data of this case report are promising to achieve a safe and specific treatment option for the current Ebola epi-demic and in principle for other emerging pathogens. Therefore, clinical trials are eagerly awaited to demonstrate the clinical benefit of convales-cence plasma in the treatment of EVD.
PSB-01-5Efficacy and safety of a combined depletion/exchange procedure with a new cell separator in patients with sickle cell disease: a single centre experience
Wagner B., Karagianni M., Scheffler A., Wichmann C., Buhmann R., Frank J., Wittmann G.Klinikum der Universität München, ATMZH, München, Germany
Introduction: Sickle cell disease (SCD) is a hereditary hemoglobinopath-ia associated with severe vascular events such as pain attacks (“sickle cell crisis”), acute chest syndrome and stroke. For secondary prophylaxis therapeutic erythrocyte exchange by apheresis (TEA) has been well es-tablished. Here, we report on 59 TEA procedures 42 of them with an ad-ditional depletion step (DTEA) using a new apheresis device. In 1 patient the results are directly compared with the former device for efficacy (frac-tion of remaining cells, FCR) and safety (platelet loss, PL; side effects, SE). Methods: 4 patients with SCD were treated by (D)TEAs. In Patient (P)#1 15 TEAs with COBE Spectra (CS) were compared with 19 DTEAs with the new Spectra Optia (SO). Three others were treated primarily with SO: 1 TEA and 23 DTEAs. FCR was calculated from the percentage of hemoglo-bin S (HbS) after (D)TEA devided by HbS before (D)TEA. Vital param-eters, blood counts and procedure data were analyzed from the records. Results: In P#1 in 15 TEAs with CS device on average 2345 ml blood were processed in 67 min applying 4.3 RBCs while FCR was 0.49. With the new SO device the blood volume processed in 19 DTEAs averaged 3254 ml in 81 min using 4.7 RBCs and 183 ml HA 5%. This resulted in a sig-nificantly lower FCR of 0.39 but in a higher PL (0.45 vs. 0.34; p = 0.015). In P#2 in the mean 4719 ml blood were processed in 16 DTEAs during 86 min using 171 ml HA and 5.6 RBCs yielding a FCR of 0.38. PL was 0.59, but counts remained >120/nl after each procedure. P#3 received 4.8 washed RBCs because of former severe transfusion reactions. 5 DTEAs resulted in a FCR of 0.44. P#4 was pretreated 3 times applying irradiated RBCs in preparation for allogeneic BMT. A total of 4 mild to moderate SEs occurred: an increase of body temperature by 1.4°C (P#2), citrate re-lated paresthesia (P#3 on 2 occasions) and vasovagal reactions (P#4). All resolved rapidly on symptomatic therapy. Conclusion: The combined DTEA with SO yielded significantly lower FCR as compared to the TEA with CS. This permitted the extension of therapy intervals. Loss of platelets was significantly higher but not of clini-cal relevance. Thus, the DTEA procedure not only appears highly effective and safe, but also superior to TEA.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 29
PSB-01-6Forecasting blood supply and demand in Switzerland
Volken T.1, Schenk D.2, Koller A.2, Mansouri Taleghani B.3
1Zürcher Hochschule für Angewandte Wissenschaften, Department Gesundheit, Winterthur, Switzerland, 2Blutspende SRK Schweiz AG, Bern, Switzerland, 3Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Bern, Switzerland
Background: Several studies have raised concerns that the future demand for blood and blood products may not be met. The aging of the general population in Western countries and the fact that a large proportion of blood products is transfused to elderly patients has been identified as an important driver of blood shortages. The aim of this study is to collect for the first time nationally representative data of blood donors and transfu-sion recipients in order to predict the future development of blood dona-tions and red blood cell (RBC) use in Switzerland between 2014 and 2035. The forecasts account for demographic changes as well as for medium and long term trends of RBC use and blood donations.Materials and Methods: Blood donor and transfusion recipient data 1996–2013 by age and gender were derived from Regional Blood Services and 9 large acute hospitals in various regions of Switzerland. Population data and projections 1996–2035 were obtained from the Swiss Federal Of-fice of Statistics. We estimated trends of whole blood donations and RBC transfusions and projected corresponding age- and gender-specific rates up to 2035. Results: Between 2003 and 2013, the number of transfused RBCs de-creased from 309,000 to 280,000; respective transfusion rates declined from 43 to 34 per 1,000 population. Similarly, whole blood donations de-creased from 394,000 to 323,000 units; donation rates declined from 77 to 57 per 1,000 age-eligible donors in the population. If these secular trends, together with demographic change, are projected, the transfusion rates are expected to further decline and to reach 26 RBCs per 1,000 popula-tion by 2035. At the same time, the number of whole blood donations will decrease to 28 per 1,000 age-eligible donors in the population. This trend scenario suggests that demand will equal supply by 2018 and eventually cause an increasing shortfall of up to 77,000 RBCs by 2035. Conclusions: Our findings highlight the need for a continuous monitor-ing of national trends of blood transfusions and blood donations in order to proactively initiate and coordinate actions aimed at preventing blood shortages in Switzerland. Our currently derived forecast assures that ac-tions should be taken in order to prevent a further erosion of blood dona-tions and the blood donor base.
PSB-01-7Ectopic HOXB4 enforces hematopoietic development during transition from the hemangioblast to the hemogenic endothelium during pluripotent stem cell
differentiation
Teichweyde N., Horn P.A., Klump H.Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany
Generation of hematopoietic stem cells (HSCs) from pluripotent stem cells, in vitro, holds great promise for future somatic gene and cell thera-py. So far, HSCs capable of long-term multilineage reconstitution in mice have only been obtained when the homeodomain transcription factor HOXB4 was ectopically expressed during pluripotent stem cell differenti-ation. However, the primary “target” cell of HOXB4 during hematopoietic development, in vitro, is not yet known. Its identification is a prerequisite for unambiguously identifying the molecular circuits driving HSC devel-opment, at least in vitro. To pin down this cell, we retrovirally expressed HOXB4 or a Tamox-ifen-inducible HOXB4-ERT2 fusion protein in different reporter and knock-out mouse embryonic stem cell (ESC) lines. For these experiments, ESCs were differentiated for 6 days as embryoid bodies (EBs), dissociat-ed and subsequently cocultured on OP9 stroma cells for further 3 days. Use of a Runx1(–/–) ESC-line containing a doxycycline-inducible Runx1 coding sequence (“iRunx1”; kindly provided by G. Lacaud, Manchester) uncovered that HOXB4 acts during formation of the hemogenic endo-thelium (HE) from which HSCs arise. Without Runx1 induction, which arrests hematopoietic development at the HE-stage, ectopic HOXB4 ex-pression mediated an approximately 30-fold increase in the number of circular endothelial HE-sheets being Flk1+VE-Cadherin+Tie2+ and ex-pressing Sox17 and Lmo2. Limiting dilution experiments uncovered that this was due to a significant increase in the number of progenitors gener-ating hemogenic endothelial cells. After additional Runx1 induction, the endothelial cells morphologically underwent an Endothelial-to-Hemato-poietic Transition (EHT) as verified at the single cell level by time-lapse microscopy. Concomitantly, they upregulated transcription of Gfi1, Gfi1b and Pu.1, initiated surface expression of the pan-hematopoietic marker CD45 and generated hematopoietic colony forming cells, thus proving their identity as real hemogenic endothelial cells. So far, our results strongly suggest that HOXB4 acts by supporting the entry into the hematopoietic program during mouse pluripotent stem cell differentiation by increasing the number of HE-progenitors, most likely by biasing differentiation of the bipotent progenitor, the hemangioblast, towards hematopoiesis.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts30
Poster
Red blood cell, white blood cell and platelet physiology
P-01-1Promoter and 3’UTR dependent downregulation of AK1-Protein in lymphocytes may explain the immunophenotype of Reticular Dysgenesis (RD)
Waldmann R.1, Kuch S.1,2, Pannicke U.1, Högel J.3, Schwarz K.1,4
1Institute for Transfusion Medicine, Ulm University, Ulm, Germany, 2Biberach University of Applied Sciences, Biberach, Germany, 3Institute for Human Genetics, University Hospital of Ulm, Ulm, Germany, 4Institute for Clinical Transfusion Medicine and Immunogenetics Ulm, German Red Cross Blood Service Baden-Wuerttemberg-Hessen, Ulm, Germany
Reticular dysgenesis (RD), caused by defects in the adenylate kinase 2 gene (AK2), is the most severe form of inborn SCID. It is characterized by leukopenia and bilateral sensorineural deafness. A previous study in-dicates that leukocytes may be susceptible to defects caused by the lack of AK2, as they do not express adenylate kinase 1 (AK1) in sufficient amounts to compensate for the AK2 functional deficits (Pannicke et al., Nature Genetics 2009).Western blot and qRT-PCR analysis of AK1 expression in hematopoietic cell lines revealed, that human T lymphocytes, postfollicular B lympho-cytes and progenitor cells with myeloid surface markers have only mar-ginal AK1 RNA levels and do not express AK1 protein.Reconstitution experiments in an endogenously AK1 expressing cell line (K-562) and a cell line with no AK1 protein (Jurkat) with in vitro pro-duced AK1 mRNAs with varying 5’UTR and 3’UTR, showed that the 3’UTR of AK1 reduces AK1 protein production in Jurkat cells.The activity of the AK1 promoter were analysed in a Firefly/Renilla Lu-ciferase Assay and the AK1 promotor activity was lower in Jurkat cells compared to K-562 cells.Our conclusion is that the absence of AK1 protein in Iymphoid cells might be a combined effect of a repressed promoter activity and RNA degrada-tion induced by the 3’UTR of AK1.
P-01-2Formation of Red blood cell microparticles during storage of 49 days
Listopad J.J., Brys B., Dürrenfeld A., Baumann-Baretti B.I.Haema Ag, Leipzig, Germany
Background: Red blood cells microparticles (RMPs) recently have been shown as crucial indicator for evaluation of storage quality of red blood cell concentrates (RCC). Differentiation of RMPs can be influenced by collection systems, cell filtration, RCC storage kinetics and temperatures. How the diversity in conditions impacts the RMPs formation during stor-age progression is not precisely known. The content of RMPs during stor-age of RCC was investigated. Methods: 9 whole blood (WB) donations from normal volunteer donors were collected in CPD anticoagulant using the Composelect®4F-System (PQ 42271; 70 ml CPD, 110 ml PAGGS-M) manufactured by Fresenius. WB donations were centrifugated after intermediate storage (2 to 22 h) and separated using the automated Blood Component Separator (Com-poMat G5); leukoreduction was performed by RCC filtration within 24 hours after donation. Weekly samples for in vitro QC-parameters were taken during storage of 49 days. Additionally the RMP concentration was quantified by FACS analysis (Calibur, Becton Dickinson). Results: During storage an increase of hemolysis parameters, decrease of ATP and strong reduction of 2,3 DPG which is still detectable until day 21
were observed. RCC and RMPs concentrations demonstrate an unequal course during the storage kinetics: the RCC content altered insignificantly whereas the RMPs concentration started slightly to increase on day 28 and presents a significant rise until day 49. Conclusion: ATP, hemolysis parameters, 2,3 DPG, and RMPs are essential references for RCC storage quality. In contrast to the continuous decline of ATP and increase in hemolysis we observed a stable RCC/RMPs quan-tity until day 28 of storage and an exclusive increase of RMPs formation during storage progression until day 49 as a hint for impairment of RCC. Further analysis is necessary to determine the RMPs effects on RCC func-tionality.
Haemostasiology and coagulopathies
P-02-1Platelet transfusions to treat patients with intracranial haemorrhage under antiplatelet therapy
Baschin M.1, Selleng S.2, Westphal A.1, Schroeder H.W.3, Greinacher A.1, Thiele T.1
1Universitätsmedizin Greifswald, Institut für Immunologie und Transfusionsmedizin, Transfusionsmedizin, Greifswald, Germany, 2Universitätsmedizin Greifswald, Klinik für Anästhesiologie, Greifswald, Germany, 3Universitätsmedizin Greifswald, Klinik für Neurochirurgie, Greifswald, Germany
Introduction: Treatment of intracranial haemorrhage (ICH) in patients with antiplatelet therapy usually consists of prohemostatic platelet trans-fusions and neurosurgery to release intracranial pressure. As the cardio-vascular risk of these patients is also high, it is unclear, whether platelet transfusions increase the risk for new acute coronary syndromes. We re-port the outcome of patients with ICH under antiplatelet therapy receiv-ing platelet transfusions before neurosurgery. Methods: We identified consecutive patients under antiplatelet therapy with ICH receiving ≥ 2 platelet concentrates before neurosurgery between 2012–2014 and recorded the risk for major adverse cardiac and cerebro-vascular events (MACCEs), bleeding, thrombosis and acute coronary syn-dromes (ACS). Results: Seventy patients were included: 13 received dual (aspirin + clopi-dogrel) and 57 mono antiplatelet therapy (aspirin 53; or clopidogrel 4). MACCE-risk was high in 10, moderate in 49 and low in 11 patients. No ACS occured, but 15 (21.4%) postoperative ICHs developed between the day of surgery and the 11th postoperative day. Most bleedings occurred before restart of antiplatelet therapy. Preoperative platelet inhibition (dual or mono antiplatelet therapy) had no influence on postoperative bleeds.Conclusion: Platelet transfusion can reverse antiplatelet therapy in pa-tients with ICB without a substantial increase of cardiovascular compli-cations. The risk of re-bleeding remains high and justifies withholding antiplatelet drugs for at least one week after surgery.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 31
P-02-2Acquired factor V inhibitor after the administration of antibiotics
Stephan B.1, Hummel B.1, Hübner U.2, Peters C.3, Grabowy H.3, Pilch J.1, Gerber K.-D.3, Eichler H.1
1Saarland University Hospital, Institute of Clinical Hemostaseology and Transfusion Medicine, Homburg, Germany, 2Saarland University Hospital, Clinical Chemistry and Laboratory Medicine / Central Laboratory, Homburg, Germany, 3Knappschaftskrankenhaus, Department of Anaesthesiology and Intensive Care, Sulzbach, Germany
Purpose: An 83 year old man was hospitalised due to a symptomatic in-cisional hernia. He was treated by adhesiolysis, hernioplasty and mesh inlay (day 0). On day 7, a colon fistula was diagnosed and initially treated with vacuum assisted closure therapy, later with a surgical suture. From day 1, ceftriaxone and metronidazole were administered. On day 10, the lab results at the treating hospital showed prolonged prothrombin time (PT) and activated partial thromboplastin time (aPTT), the results for thrombin time, fibrinogen and antithrombin were normal. PT and aPTT could not be corected by application of vitamin K or transfusion of FFP or prothrombin complex concentrate (PCC). Bleeding signs appeared under enoxaparin, but stopped under tranexamic acid. Methods: Citrate blood samples were tested at the Central Laboratory of the Saarland Universitiy Hospital. Clotting factors II, V, VII and X, a pro-thrombin time based plasma mixing test including one hour incubation and inhibitor diagnostics by the Bethesda method were performed. Results: The patient’s PT and aPTT were 44 s and 42 s, respectively. The clotting factors II, VII and X were normal with 1.15, 0.79 and 1.25 IU, but factor V activity was < 0.01 IU. The plasma mixing test showed an inhibi-tor pattern: after addition of 50% patient’s plasma to normal plasma (NP), the PT of NP (10 s) was prolonged (28 s). Factor V inhibitor activity was detected showing 2.9 Bethesda units. Conclusion: An acquired factor V inhibitor is a rare coagulation disorder and sometimes seen after administration of antibiotics, especially ceph-alosporins. Clinical symptoms vary from asymptomatic to significant bleeding. An acquired factor V inhibitor should be excluded when PT and aPTT are abnormal and cannot be explained by anticoagulant therapy, liver disease or blood loss. It is not clear whether an acquired factor V inhibitor should be treated by immunosuppression. Bleeding may stop after treatment with tranexamic acid, platelet concentrates or eptacog alfa.
P-02-3TTP/HUS as initial manifestation of HIV infection
Lodemann P.1, Frey B.M.2, Peetz D.1, Bieringer M.3
1Helios Klinik Berlin Buch, Institut für Labormedizin, Berlin, Germany, 2Blood Transfusion Service SRC, Zurich, Zürich, Switzerland, 3HELIOS Klinik Berlin Buch, Kardiologie und Nephrologie, Berlin, Germany
Introduction: Hemolytic uremic syndrome (HUS) is a disease with rel-atively high mortality and belongs to the group of thrombotic microan-giopathies. It is characterized by hemolytic anemia, a low platelet count and endorgan damage like kidney-failure. First described by C. Gasser in Zürich/Switzerland 1955, meanwhile a variety of TTP/HUS-associated diseases are now identified, but their exact role in pathogenesis is still not always clear. Methods: We present a case of HUS as an initial manifestation of HIV Results: A patient with HUS in our clinic was at first successfully treated by plasmapheresis. Following our diagnostic routine standards in such cases, we tested the patient for HIV antibodies, but did not perform a HIV-PCR. Four months later, the patient presented with a pneumocystis carinii pneumonia, and HIV-antibodies were detected, as well as a high viral load. Anamnestic evaluation yielded no obvious cause for a HIV in-fection, so extensive lookback was performed, especially to rule out HIV transmission by variants not detected by standard donor PCR screening of the blood donation service. It showed, that the HIV infection was not due to transfusions for treating HUS (all donors were PCR negative and
antibody negative after >4 months control). Instead, retrospective sero-logic data strongly suggested, that HUS was associated with acute HIV infection, a phenomenon, which is described in some case-studies. Conclusion: The described case demonstrates that HUS may be the initial manifestation of a HIV infection. In all patients presenting with HUS of unclear cause, HIV antibody tests should be augmented by HIV-PCR to rule out an acute, antibody-negative infection.
P-02-4Acquired hemophilia – hard to diagnose, hard to therapy, and cost-intensive! Risk-benefit ratio and critical insights based on various complications associable with a factor VIII-dependent blood coagulation inhibitor
Stephan B.1, Lauer H.1, Groß J.1, Link A.2, Schenk J.F.1
1Saarland University Hospital, Institute of Clinical Hemostaseology and Transfusion Medicine, Homburg, Germany, 2Saarland University Hospital, Department of Cardiology and Angiology, Homburg, Germany
Introduction: To date there is a gap between estimated and actual num-ber of people known with bleeding disorders. Therefore registries are of benefit despite medical care depends on quality and experience of phy-sicians involved. It is a rarity that bleeding complications are associated with acquired hemophilia. Nevertheless these patients are at high risk for lethal outcome. Patient and Methods: A 86 y old patient with clinical signs of deep vein thrombosis (DVT) became hospitalized. Unfractionated heparin (iv) ad-justed on TT/reagent thromboclotin and aPTT/Actin FS - measured on BCS XP/Dade Behring was used. Instead expanded hematoma in the low-er leg was diagnosed. In the follow-up period surgical intervention was performed due to threatening compartment syndrome associated with polytransfusion based on massive bleeding (fig. 1–3). Besides Red blood cells, platelet concentrates and fresh frozen plasma, blood coagulation derivates (prothrombin complex, fibrinogen, and factor XIII concentrate) were applied. Results: Acquired hemophilia A was diagnosed by low levels of factor VIII (10–20%), plasma exchange in vitro and the presence of time depen-dent inhibitor in plasma (2,8 Bethesda Units). Since bleeding complica-tions could not adequately be managed two to four times daily given doses (adjusted to body weight: 90 micrograms / kg BW; totally amount applied: 818 mg) were successful. Algorithms defined by the GTH working group and own experience were reflected for eradication of the antibody by im-mune suppression. Wound healing problems became also evident in the postsurgical period (fig. 3,4). During intravenously given steroids (100 mg/d) renal failure worsened the clinical situation. Thus eradication of the inhibitor could not be achieved so that Rituximab was given. Six to eight weeks later factor VIII activity increased up to 15% as well as the titre of the autoantibody decreased to 0,5 BU (Fig. 5). At least antibiotics could not prevent lethal outcome of the exhausted patient due to pneumonia and respiratory distress. Discussion: In recent years rituximab proved its beneficial use in the therapy of acquired haemophilia, as well as RFVIIa was effective to stop critical bleedings. Early and proper diagnosis is mandatory. Otherwise cost-effectiveness should be taken into consideration.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts32
Haemovigilance
P-03-1Bedside washing of red blood cell concentrates with XTRA autotransfusion system (Sorin, Italy) in severe acute hypotensive transfusion reaction
Offner R.1, Seyfried T.2, Schelker R.3, Schmid S.4, Hutchinson J.5, Ahrens N.1
1Universitätsklinikum Regensburg, Abt. Transfusionsmedizin (IKCHLM), Regensburg, Germany, 2Universitätsklinikum Regensburg, Klinik für Anästhesiologie, Regensburg, Germany, 3Universitätsklinikum Regensburg, Klinik für Innere Medizin III, Regensburg, Germany, 4Universitätsklinikum Regensburg, Klinik für Innere Medizin I, Regensburg, Germany, 5Universitätsklinikum Regensburg, Klinik und Poliklinik für Chirurgie, Regensburg, Germany
Background: Acute hypotonic transfusion reactions (AHTR) are charac-terized by a drop in systolic and dyastolic blood pressure (BP) by at ≥30 mmHg within minutes of the transfusing blood components. Because the precipitating factors are still unknown, first-line treatment of acute ane-mia in patients with AHTR is transfusion of washed red cell concentrates (RBCC). This report concerns the emergency treatment of a 72-years-old man who presented to the Emergency Department with hemodynamic instability owning to gastrointestinal hemorrhage. Transfusion of < 10 ml RBC resulted in a severe AHRT (BP: 80/40 mmHg), despite prophy-laxis with fenistil, ranitidine and cortisone. Two days prior to admission he experienced a severe AHTR at another hospital resulting in asystole, requiring a cardiopulmonary resuscitation. With no short-term available washed RBCC a decision was made to use XTRA autotransfusion system (ATS) for the off-label purpose of washing RBCC for urgent transfusion.Study Design and Methods: Two RBCC were washed twice in isoton-ic saline, using of XTRA ATS, run on the pre-set ‘Popt’ program with a 225mL bowl. The bedside washed RBC-product was transfused (with antiallergic prophylaxis). The product volume, blood count, hematocrit, albumin and total protein were measured before and after washing. Results: Our patient has tolerated the transfusion of two bedside-washed RBCCs without any side effects. No AHRT or other clinical complications occurred. An increase of 1,9 g/dl Hb was observed. When the procedure was repeated two days later, it was similarly uncomplicated and final Hb of 9,5 g/dl was achieved. Conclusion: The emergency off-label use of an XTRA ATS to prepare washed RBCC for critically anemic patient with recurrent AHRT was suc-cessful. Depletion of residual plasma proteins by this method was effective and resulted in a clinically compatible blood product. The amount of total protein (0,382 g/RBCC) was well below the specified level (< 0,5 g/RBCC) in current German Hemotherapy Guidelines. Because saline was used for washing, the product contained no unwanted excipients (eg. SAGM) that might trigger AHTR. Under extenuating circumstances, washing RBCC at bedside can be an effective treatment for patients with recurrent AHRT. Further studies are planned.
P-03-2Transfusion related sepsis with Klebsiella pneumoniae: a case report
Zimmermann G.1, Sigle J.-P.1, Méndez A.2, Maurer S.2, Siderow A.1
1Stiftung Blutspende SRK Aargau-Solothurn, Aarau, Switzerland, 2Kantonsspital Aarau, Haemovigilance Department, Aarau, Switzerland
Background: There are very few reported cases of red blood cell concen-trate (RBC) transfusion related sepsis with K.pneumoniae. The course of the infection is usually severe with a high mortality.Case report: An 83 year old patient was admitted to the ER due to dys-pnoea and melaena; laboratory results showed anaemia (Hb 58 g/l). The patient had history of upper gastrointestinal bleeding and was under anti-coagulant treatment. In total nine RBC were administered during his hos-pitalization. 1h after transfusion of the third RBC the patient developed
fever. The immunohaematologic work-up showed no incompatibility; in the blood culture of the transfusion bag grew K. pneumoniae within 24h of transfusion. However, the patient’s blood cultures taken at the time of reaction remained negative. Because of the positive blood cultures of the transfusion bag and persistent fever, consecutive blood cultures of the pa-tient were taken which turned positive 72h after the transfusion reaction. The patient was transferred to the ICU due to progressively sepsis signs and haemodynamic instability. The sepsis treatment consisted, according to antibiotic spectrum, of Ceftriaxon i.v. und Bactrim forte p.o. The pa-tient recovered and was discharged 13 days after the transfusion reaction. Antibiogram and molecular typing showed that the two Klebsiella strains obtained from the RBC and patient were identical. The cultures of the se-rothek of the index blood donation remained negative; the cultures of the returned-back Q-Plasma remained also negative, as well as the eubacterial PCR conducted after centrifugation of this plasma. The donor of the RBC had no history of invasive interventions or symptoms of respiratory or urinary tract infections. Repeated blood cultures of the donor obtained one week and 5 months after the transfusion reaction remained negative. Conclusion: We present a case of severe transfusion-related sepsis with K.pneumoniae due to a RBC transfusion. In spite of thoroughly exam-inations the source of the contamination could not be identified. Of note, initial blood cultures of the patient remained negative which stresses the significance of repeated blood cultures if clinical symptoms persist or cul-tures of the blood bag turn positive.
Manufacturing blood products
P-04-1Evaluation of processing and storage conditions using a dinch-based blood bag system
Rach J.1, Gravemann U.1, Volgmann T.1, Handke W.1, Platenkamp K.2, Tijink M.2, Hakvoort K.2, Müller T.1, Seltsam A.1
1DRK Blutspendedienst NSTOB gGmbH, Springe, Germany, 2Fresenius Kabi - Transfusion Technology, Emmer-Compascuum, Netherlands
The plasticizer Hexamoll DINCH (1,2-cyclohexane dicarboxylic acid di-isononyl ester) is an alternative for DEHP (di-2-ethylhexyl phthalate) for medical devices as it may offer toxicological advantages over DEHP. How-ever, DEHP is known to have a protective effect on red blood cell (RBC) membranes and the use of DINCH might result in higher haemolysis rates of RBC units during storage. The aim of this study was to investigate the impact of a DINCH-based blood bag system (phthalate-free) on the quality of RBC units in PAGGS-M during storage of 49 days. In a five-arm study, whole blood units (WBU) were processed either within 4 or after approx. 22 hours after collection. In both groups, half of the RBC units was mixed weekly, while the other half was left untouched. RBC units prepared after more than 22 hours and stored in a conventional DEHP/PVC blood bag system without mixing served as controls. The quality of the RBC units was assessed by a set of in vitro quality parameters at different time points. Haemolysis measured on day 49 was higher in RBC units stored in DINCH bags than in RBC units stored in DEHP bags when processed and stored under the same conditions (preparation after 22 hours, no mixing). A shorter time interval between WB collection and RBC unit prepara-tion and regular mixing both had a positive effect on haemolysis in the DEHP-free test system. The mean haemolysis was lowest when WB was processed within 4 hours and RBC units were mixed regularly. The high-est rate of haemolysis was observed in DINCH RBC units prepared after more than 22 hours and not mixed during storage (mean 0.54% ± 0.17; day 49). Haemolysis rate in control units was similar to those test systems that were either prepared after 4 hours but not mixed or processed after 22 hours and mixed regularly (0.31% ± 0.12). For the other quality parame-ters only small and negligible differences were observed between groups.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 33
The unfavourable effect on haemolysis of DINCH as alternative plasticizer in blood bag systems might be compensated by regular mixing of the RBC units during storage. A shorter time interval between WB collection and RBC unit preparation also appears to have an additional positive effect on the haemolysis rate of RBC units stored in DINCH bags.
P-04-2Quality of leucoreduced Red Blood Cell Units - Evaluation of the TPL IMUFLEX CRC set including the new SepacellTM R-S01 leukoreduction filter
Störmer M., Radojska S., Gathof B.S.Transfusion Medicine, University Hospital of Cologne, Cologne, Germany
Introduction: Leukoreduction of red blood cell concentrates (RBCs) is a process by which leukocytes are removed to a certain threshold by the use of a filter to reduce the number of non-haemolytic febrile transfu-sion reactions, as well as the occurrence of alloimmunization in patients receiving multiple transfusions. In Germany the upper limit of residual WBCs in RBCs is ≤1 × 106/unit. Here we present the evaluation of the TPL IMUFLEX CRC blood collection set (TerumoBCT) including the new integrated soft SepacellTM R-S01 leukocyte removal filter for RBCs (Asahi Kasai Medical) for routine production and storage according to the German authorities’ requirements.Methods: Whole blood (WB) donations of 500ml were collected in CPD after donors gave informed consent. After separation (2–4 hours after WB collection) in SAGM, RBCs were filtered at room temperature through the SepacellTM R-S01 filter stored under usual conditions for 49 days. Quality parameters including volume, red cells, residual leukocytes and platelets, haematocrit, haemoglobin, %haemolysis, and sterility were assessed.Results: WB donations (n = 35) were performed on four different days. RBCs (volume 299 ± 22 ml) that were produced 1-hour post-collection showed the following quality data at the day of production: red cells (6.75 ± 0.47 × 106/µl), haemoglobin (57.84 ± 5.52 g/unit), haematocrit (0.59 ± 0.03l/l), haemolysis (0.10 ± 0.05%), residual leukocytes (0.004 ± 0.012 × 106/unit), residual platelets (0.41 ± 0.76 × 109/unit). At the end of storage on day 49 the following results were obtained: haematocrit (0.60 ± 0.03l/l), haemolysis (0.20 ± 0.06%), haemoglobin (28.95 ± 5.22g/unit). The mean filtration time was 41 ± 12 min.Conclusion: The suitability of the new TPL IMUFLEX CRC blood collec-tion set and the SepacellTM R-S01 leukocyte filter for RBC production in our Institute was evaluated. All quality parameters fulfilled German and European guideline requirements. In conclusion, the whole system has proven to be a reliable and efficient WBC-reduction system that consis-tently retains high-quality results of RBCs.
P-04-3Apheresis process data management systems of blood cell separators (Trima Accel, Spectra Optia and Amicus) from the user´s perspective
Offner R.1, Mages J.2, Skodnik K.2, Ahrens N.1
1Universitätsklinikum Regensburg, Abt. Transfusionsmedizin (IKCHLM), Regensburg, Germany, 2Universitätsklinikum Regensburg, IT-Abteilung (IKChLM), Regensburg, Germany
Background: There is a need for automated processes data management software in blood donation establishments with a wide spectrum of pre-parative and therapeutic apheresis. Such data should be recorded, trans-mitted, processed, displayed, archived, and submitted to the transfusion medicine information system (TMIS) in an automated manner. The legit-imate expectation of customers for user friendly integrable process data management solutions into the TMIS is contrary to the present diverse apheresis devices.
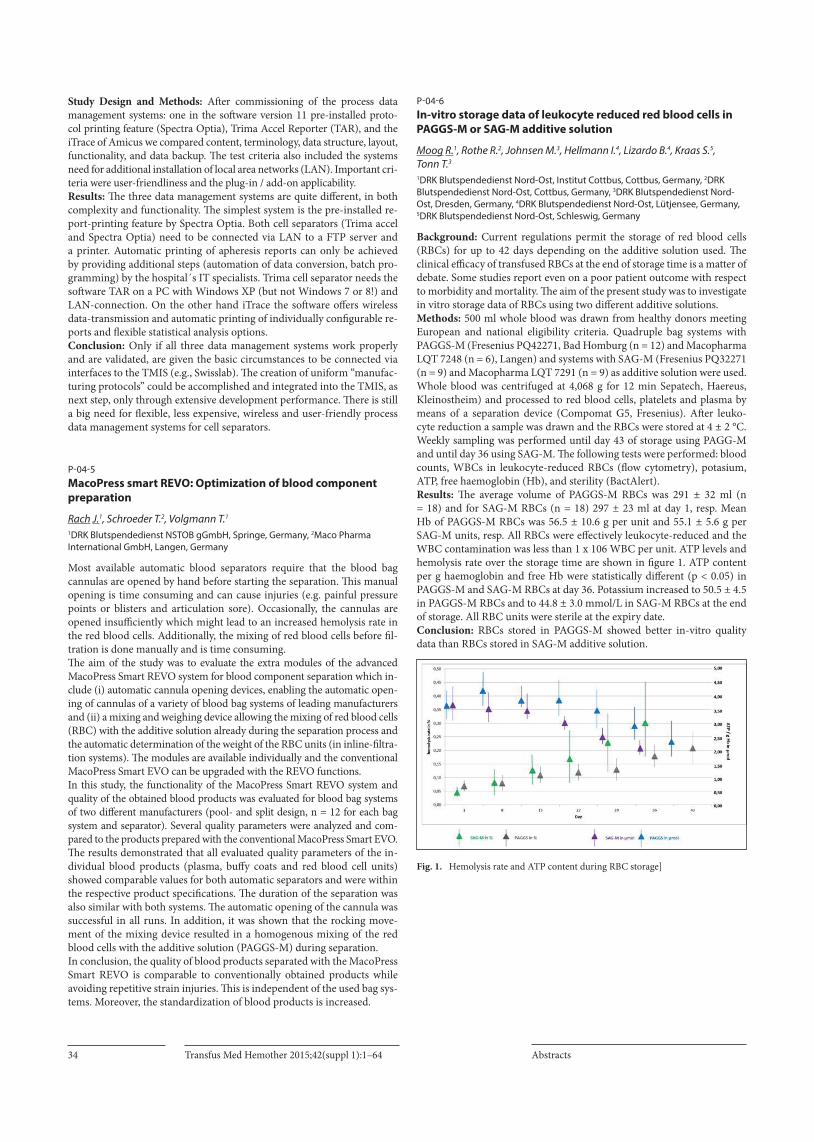
Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts34
Study Design and Methods: After commissioning of the process data management systems: one in the software version 11 pre-installed proto-col printing feature (Spectra Optia), Trima Accel Reporter (TAR), and the iTrace of Amicus we compared content, terminology, data structure, layout, functionality, and data backup. The test criteria also included the systems need for additional installation of local area networks (LAN). Important cri-teria were user-friendliness and the plug-in / add-on applicability.Results: The three data management systems are quite different, in both complexity and functionality. The simplest system is the pre-installed re-port-printing feature by Spectra Optia. Both cell separators (Trima accel and Spectra Optia) need to be connected via LAN to a FTP server and a printer. Automatic printing of apheresis reports can only be achieved by providing additional steps (automation of data conversion, batch pro-gramming) by the hospital´s IT specialists. Trima cell separator needs the software TAR on a PC with Windows XP (but not Windows 7 or 8!) and LAN-connection. On the other hand iTrace the software offers wireless data-transmission and automatic printing of individually configurable re-ports and flexible statistical analysis options. Conclusion: Only if all three data management systems work properly and are validated, are given the basic circumstances to be connected via interfaces to the TMIS (e.g., Swisslab). The creation of uniform “manufac-turing protocols” could be accomplished and integrated into the TMIS, as next step, only through extensive development performance. There is still a big need for flexible, less expensive, wireless and user-friendly process data management systems for cell separators.
P-04-5MacoPress smart REVO: Optimization of blood component preparation
Rach J.1, Schroeder T.2, Volgmann T.1
1DRK Blutspendedienst NSTOB gGmbH, Springe, Germany, 2Maco Pharma International GmbH, Langen, Germany
Most available automatic blood separators require that the blood bag cannulas are opened by hand before starting the separation. This manual opening is time consuming and can cause injuries (e.g. painful pressure points or blisters and articulation sore). Occasionally, the cannulas are opened insufficiently which might lead to an increased hemolysis rate in the red blood cells. Additionally, the mixing of red blood cells before fil-tration is done manually and is time consuming. The aim of the study was to evaluate the extra modules of the advanced MacoPress Smart REVO system for blood component separation which in-clude (i) automatic cannula opening devices, enabling the automatic open-ing of cannulas of a variety of blood bag systems of leading manufacturers and (ii) a mixing and weighing device allowing the mixing of red blood cells (RBC) with the additive solution already during the separation process and the automatic determination of the weight of the RBC units (in inline-filtra-tion systems). The modules are available individually and the conventional MacoPress Smart EVO can be upgraded with the REVO functions. In this study, the functionality of the MacoPress Smart REVO system and quality of the obtained blood products was evaluated for blood bag systems of two different manufacturers (pool- and split design, n = 12 for each bag system and separator). Several quality parameters were analyzed and com-pared to the products prepared with the conventional MacoPress Smart EVO. The results demonstrated that all evaluated quality parameters of the in-dividual blood products (plasma, buffy coats and red blood cell units) showed comparable values for both automatic separators and were within the respective product specifications. The duration of the separation was also similar with both systems. The automatic opening of the cannula was successful in all runs. In addition, it was shown that the rocking move-ment of the mixing device resulted in a homogenous mixing of the red blood cells with the additive solution (PAGGS-M) during separation. In conclusion, the quality of blood products separated with the MacoPress Smart REVO is comparable to conventionally obtained products while avoiding repetitive strain injuries. This is independent of the used bag sys-tems. Moreover, the standardization of blood products is increased.
P-04-6In-vitro storage data of leukocyte reduced red blood cells in PAGGS-M or SAG-M additive solution
Moog R.1, Rothe R.2, Johnsen M.3, Hellmann I.4, Lizardo B.4, Kraas S.5, Tonn T.3
1DRK Blutspendedienst Nord-Ost, Institut Cottbus, Cottbus, Germany, 2DRK Blutspendedienst Nord-Ost, Cottbus, Germany, 3DRK Blutspendedienst Nord-Ost, Dresden, Germany, 4DRK Blutspendedienst Nord-Ost, Lütjensee, Germany, 5DRK Blutspendedienst Nord-Ost, Schleswig, Germany
Background: Current regulations permit the storage of red blood cells (RBCs) for up to 42 days depending on the additive solution used. The clinical efficacy of transfused RBCs at the end of storage time is a matter of debate. Some studies report even on a poor patient outcome with respect to morbidity and mortality. The aim of the present study was to investigate in vitro storage data of RBCs using two different additive solutions. Methods: 500 ml whole blood was drawn from healthy donors meeting European and national eligibility criteria. Quadruple bag systems with PAGGS-M (Fresenius PQ42271, Bad Homburg (n = 12) and Macopharma LQT 7248 (n = 6), Langen) and systems with SAG-M (Fresenius PQ32271 (n = 9) and Macopharma LQT 7291 (n = 9) as additive solution were used. Whole blood was centrifuged at 4,068 g for 12 min Sepatech, Haereus, Kleinostheim) and processed to red blood cells, platelets and plasma by means of a separation device (Compomat G5, Fresenius). After leuko-cyte reduction a sample was drawn and the RBCs were stored at 4 ± 2 °C. Weekly sampling was performed until day 43 of storage using PAGG-M and until day 36 using SAG-M. The following tests were performed: blood counts, WBCs in leukocyte-reduced RBCs (flow cytometry), potasium, ATP, free haemoglobin (Hb), and sterility (BactAlert).Results: The average volume of PAGGS-M RBCs was 291 ± 32 ml (n = 18) and for SAG-M RBCs (n = 18) 297 ± 23 ml at day 1, resp. Mean Hb of PAGGS-M RBCs was 56.5 ± 10.6 g per unit and 55.1 ± 5.6 g per SAG-M units, resp. All RBCs were effectively leukocyte-reduced and the WBC contamination was less than 1 x 106 WBC per unit. ATP levels and hemolysis rate over the storage time are shown in figure 1. ATP content per g haemoglobin and free Hb were statistically different (p < 0.05) in PAGGS-M and SAG-M RBCs at day 36. Potassium increased to 50.5 ± 4.5 in PAGGS-M RBCs and to 44.8 ± 3.0 mmol/L in SAG-M RBCs at the end of storage. All RBC units were sterile at the expiry date.Conclusion: RBCs stored in PAGGS-M showed better in-vitro quality data than RBCs stored in SAG-M additive solution.
Fig. 1. Hemolysis rate and ATP content during RBC storage]

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 35
P-04-7Comparison between leukapheresis systems in regard to buffy coat volume optimization
Müller I.1, Groß J.2, Stephan B.2, Eichler H.2
1Universität des Saarlandes, Institut für Klinische Hämostaseologie und Transfusionsmedizin, Homburg/Saar, Germany, 2Universitätsklinikum des Saarlandes, Institut für Klinische Hämostaseologie und Transfusionsmedizin, Homburg/Saar, Germany
Background: For GMP compliant preparation of autologous, activated dendritic cells (DC), monocytes must initially be harvested by an apher-esis procedure. Two apheresis systems were compared in regard to the monocyte yield and the red blood cell count, because the following step of monocyte enrichment by elutriation needs an hematocrit of less than 5% (PEV < 7.5 mL). Methods: Peripheral blood monocytes were obtained by leukapheresis from four test donors within an interval of > 3 months using the cell sep-arators TrimaOptia® (TerumoBCT) and Amicus® (Fresenius). Each do-nor (1 women, 3 men) performed two apheresis donations, one on each device, and the settings on the cell separators were standardized as far as possible (e.g. processed blood volume,) The derived cells and others on the expression of typical surface antigens examined, in addition on the purity of the population (CD14+ CD45+ CD3/CD19-), cell number, vi-tality, immune phenotype (CD14/CD80/CD86/CD83/HLA-DR; Residual content of T - and B-, NK-cells) and sterility. Cell counts were measured with the hemocytometer as well as with the single platform analysis based on cytometry measurement.Results: Collections (product volume 95±25 mL (TrimaOptia®) and 99±3 mL (Amicus®) ) yielded sufficient CD14+monocytes as output quantity for the production of DC with a yield of >1x109. The packed erythro-cyte volume (PEV) was 5±2 mL (TrimaOptia®) and 11±4 mL (Amicus®). Results on immunophenotyping of the extracted cells were comparable between the devices. The hematocrit of the cell suspension from Amicus® was high on average which counteracts the elutriation output.Conclusion: More collection cycles and enhanced collection volume could potentially lead to an increased yield by the Amicus® device. An optimization of the collection parameters concerning the haematocrit yield by Amicus® is additionally necessary which can be implemented by reduction of buffy coat volume.
Immune genetics
P-05-1The combined impact of amino acid polymorphism at HLA-DPB1 on T cell alloreactivity defines a functional distance between patient and donor independently predictive of survival after 10/10 matched unrelated HSCT for AML, ALL and MDS
Crivello P.1, Beelen D.2, Heinold A.3, Heinemann F.M.3, Rebmann V.3, Lindemann M.3, Ottinger H.2, Horn P.A.3, Fleischhauer K.1
1Universitätsklinikum Essen, Institut für Zelltherapeutische Forschung, Essen, Germany, 2Universitätsklinikum Essen, Klinik für Knochenmarktransplantation, Essen, Germany, 3Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany
We have previously experimentally determined the differential impact of individual amino acid polymorphisms on the alloreactive T cell response to HLA-DPB1*09:01, translated these findings into numeric “functional distance” (FD) scores for all HLA-DPB1 alleles, and showed that these FD scores correlate with T cell epitope groups determining non-permissive mismatches in unrelated HSCT (Fleischhauer et al., Lancet Oncol 2012; Crivello et al., Biol Blood Marrow Transplant 2014).
A cohort of 379 consecutive patients (pts) (age median 56 yrs [18 - 73 yrs]), who underwent high-resolution HLA-A,B,C,DRB1,DQB1 matched, but DPB1 mismatched unrelated HSCT for AML (n = 272 [72%]), ALL (n = 58 [15%]), or MDS (n = 49 [13%]) at the University Hospital of Essen were included in the analysis. FD scores of HLA-DPB1 alleles were calcu-lated as previously described, and the deltaFD scores for each transplant were calculated as the absolute number of [FDpatient-FDdonor]. Receiver Operator Curves (ROC) were constructed to calculate the best cut-off val-ues for the endpoint of overall survival (OS). With a median follow-up of 4 yrs for surviving pts, the 5-yrs OS for pts in early disease stages (n = 158 [42%]) was 56% (95%-confidence interval [CI] 48–64%). For pts in advanced disease stages (n = 221 [58%]) this estimate was 38% (95%-CI 31% - 45%) (p< 0.0005). deltaFD score dis-tribution ranged from 0.01 to 7.46 with a median of 2.12. ROC analysis indicated stratification into 2 subgroups with deltaFD scores < =2.665 (n = 252 [66%]) and >2.665 (n = 127 [44%]) as the best predictor. In these subgroups, the 5-yrs OS were 51% (95%-CI 44% - 57%) and 37% (95%-CI 28% - 46%), respectively (p< 0.008). In multivariate analysis, independent predictors of OS were time-dependent aGvHD (p< 0.0002) and cGvHD (p< 0.0001), the use of anti-thymocyte globulin (p< 0.0001) patient age (p< 0.004), and the stratified deltaFD score (p< 0.03).In this monocenter study cohort, the stratified DPB1 deltaFD score was a significant independent risk factor for OS after 10/10 matched unre-lated HSCT, possibly owing to the strength of the alloimmune response to mismatched HLA-DPB1 in this setting, which was also reflected by an independently increased non-relapse mortality in pts with deltaFD scores >2.665. These findings could pave the way for the identification of non-permissive DPB1 mismatches in unrelated HSCT based on an exper-imentally defined numerical weighting system for amino acid sequence polymorphism.
P-05-2Regulation of CD163 expression in human macrophages in diabetic conditions
Matuschik L., Riabov V., Moganti K., Gudima A., Klüter H., Kzhyshkowska J.Medical Faculty Mannheim, University of Heidelberg and German Red Cross Blood Service Baden-Württemberg – Hessen, Institute of Transfusion Medicine and Immunology, Mannheim, Germany
Scavenging function of monocytes and macrophages is essential for the clearance of both exogenous components and unwanted self-products and the control of inflammatory reactions. The monocyte- and macro-phage-specific scavenger receptor CD163 is responsible for the internal-ization and degradation of haemoglobin-haptoglobin complexes. These haemoglobin-haptoglobin complexes are built due to intravascular hae-molysis, a circumstance which particularly occurs in inflammatory con-ditions. Inflammation is an essential pathological process supporting the development of micro- and macrovascular diabetic complications, such as atherosclerosis. CD163 can actively be shed from the cell surface in inflammatory conditions. This leads to an impaired ability to scavenge the haemoglobin-haptoglobin complexes and consequently increases the risk of vascular oxidative damage. The project aims to examine how high glucose conditions affect the CD163-mediated scavenging of human primary differentially activated macrophages. CD14+-monocytes were isolated from the peripheral blood of healthy donors by density gradi-ent centrifugation and magnetic separation. M0 (non-stimulated), M1 (IFNgamma-stimulated) and M2 (IL-4-stimulated) macrophages were differentiated within 6 days in low (5mM) and high (25mM) glucose con-ditions. CD163-mRNA expression was quantified by qRT-PCR. CD163 surface expression was analysed by flow cytometry. Increased glucose had a suppressing effect on CD163 mRNA expression in 8 out of 10 donors in M1; and in 7 out of 10 donors in M2. The suppressive effect of glucose was more pronounced in M2 compared to M1. Regarding surface expression, the effect of high glucose was donor-dependent in M0 and M2, whereas the expression of CD163 uniformly decreased in M1. Our data suggest that elevated glucose levels affect both transcriptional and posttranscrip-

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts36
tional mechanisms of CD163 production in a donor-specific manner. We concluded that the suppression of CD163 expression in macrophages by high glucose can contribute to the development of inflammation-mediat-ed complications in diabetic patients.Funding: DFG GRK1874 DIAMICOM
Immunohaematology
P-06-1Five-minute simultaneous multi-parameter blood group typing of Fya, Fyb, Jka, Jkb, S, s, P1 and k antigens using lateral flow technique (MDmulticard)
Caesar A., Schwind P.Medion Grifols Diagnostics AG, Düdingen, Switzerland
Introduction: A lateral flow assay for rapid simultaneous typing of ABO, RhD, Rh phenotype and K (MDmulticard) is in routine use since several years. The objective of this study was to evaluate the performance charac-teristics of additional parameters with this technique: Fya, Fyb, Jka, Jkb, S, s, P1 and k.Methods: In 120 fresh blood samples, comprising 108 samples of blood donors, 10 authentic clinical samples and 2 samples of newborns, Fya, Fyb, Jka, Jkb, S, s, P1 blood groups were tested; k (Cellano) was tested addition-ally with 12 samples from k negative donors. The lateral flow based assay containing these parameters (MDmulticard, Medion Grifols Diagnostics, Duedingen, Switzerland) was compared with established CE marked re-agents: Anti-Fya,-Fyb,-Jka,-Jkb for DG Gel, Anti-S, Anti-P1 forte, Anti-k (Cellano) Mono-Type (Medion Grifols Diagnostics) and ID-Anti-s (Bio-Rad, Cressier, Switzerland).The credit-card sized lateral flow test device consists of a membrane, which is embedded in a cassette housing. Two detection areas containing antibody reagents against Fya, Fyb, Jka, Jkb, S, s, P1 and k and internal controls are at both sides of a central application zone. For blood group typing, 100 µl of diluted whole blood or erythro-cyte sediment are pipetted to the application zone, followed by 300 µl of a rinsing solution. Results may be interpreted after 5 minutes. Positive results clearly impose as distinct red bands, whereas negative results lack the respective bands.Results: All results of the blood samples tested were in full accordance with those of the CE certified comparative methods.Conclusions: MDmulticard lateral flow technique was presented earlier with unique features, e. g. simultaneous multiparameter testing with sta-ble end-point results within 5 minutes without a centrifiugation step. In this study, the same characteristics are reproduced also in the detection of Fya, Fyb, Jka, Jkb, S, s P1 and k. Moreover, for the first time, simultaneous determination of these blood groups, without the need of different phases and incubation times / temperatures in one single, homogeneous 5 minute assay is demonstrated, which entails significantly reduced testing times for certain parameters compared to currently available technology.
P-06-2Experience with a combined serologic and molecular antigen determination approach
Wagner F., Schmandt S., Bittner R.DRK Blutspendedienst NSTOB gGmbH, Springe, Germany
Background: Serologic antigen determination is unreliable in chronically or massively transfused patients. This problem is best documented for pa-tients with inherited anemia like sickle-cell disease and for patients after massive transfusion. The impact on routine antigen determination in a hemato-oncologic and preoperative setting as represented in our labora-tory is less well documented. To detect serologic failures, we devised a policy to complement serologic typing by a molecular check of a diagnos-
tic SNP in the case of recent transfusion, positive direct antiglobulin test (DAT) or positive results for all antigens (Jka, Jkb, Fya, Fyb, S, s). Methods: Serologic antigen determination was done with commercial antisera. In the case of a positive direct agglutination test or recent trans-fusion, monoclonal direct agglutinating reagents were used for Jka, Jkb, S and s. A result was considered positive if a 2+ agglutination was seen or a 1+ agglutination was documented for both antithetical antigens. Weak-ened reactivity or mixed field patterns were considered doubtful positive. For molecular typing, DNA was extracted using QIAAmp Blood Mini kit, and the polymorphisms for FY, JK and S/s were checked using pooled capillary electrophoresis. Results: For 344 of 660 serologic antigen determinations, a molecular check was performed. Full concordance with normal antigen strength (if positive) was seen for Jka in 304 cases (Jkb 306, Fya 273 Fyb 281 S 302 s 332), representing 80%(Fya) to 97% (s) of all cases. Discrepant results were seen for Jka in 10 cases (Jkb 9, Fya 18, Fyb 13, S 7, s 6). Serologically doubtful positive results were obtained for Jka in 35 cases (Jkb: 29; Fya: 52; Fyb:49; S:34; s: 4), representing 1% to 15% of the suspicious and 1% to 8% of all cases. The proportion of antigen negative samples among those with doubtful positive result were similar to the probabilities expected from the antigen distribution: For Jka, 20% of Jk(a?) samples were molecularly predicted to be antigen negative (Jkb: 21%; Fya: 64%, Fyb: 35%; S: 47%, s: 25%). Conclusion: In a routine setting in Germany, previous transfusions - of-ten not reported or even negated - and a positive DAT interfere with an-tigen determination. Initial serologic antigen determination may be mis-leading in 1 to 5%. Weakened results and mixed field patterns are frequent and may both represent antigen positive and antigen negative status, thus giving few information. .
P-06-3A blood donor with a predicted Kn:-8 allele detected by a weak positive antibody screen
Mardt I.1, Döscher A.2, Wagner F.1
1DRK Blutspendedienst NSTOB gGmbH, Springe, Germany, 2DRK Blutspendedienst NSTOB gGmbH, Institut Bremen-Oldenburg, Oldenburg, Germany
Background: The characterization of an irregular antibody in a blood do-nor may help to identify a blood donor with a rare phenotype. Red blood cells from such blood donors may be used for diagnostic purposes or transfusion support in patient in need of the respective rare phenotype. Historically, the ability of a laboratory to identify an antibody to an an-tigen of high frequency heavily depended on the availability of test cells, which are often scarcely availabe. Aims: Here, we report a case delineating how the combination of neutral-ization with recombinant proteins and sequencing allowed for the detec-tion of a blood donor with a rare KN allele. Methods: A serologic work-up of a blood donor with a weakly positive antibody screen was performed. Blood group serology was performed in BioRad ID and Immucor Capture technique. Recombinant blood group proteins (Imusyn, Hannover, Germany) used for neutralization included C4A, C4B, CR1 (KN) , INB, CROM, DOA, DOB, YT ; 2.5 µg soluble rBGP was mixed with 80 µL plasma and incubated for 15 min at 37°C; the mix-ture was then tested in IAT on the ID column agglutination system. CR1 Exon 37 was sequenced from genomic DNA on an ABI 310. Results: The donor was O Rh positive. A weakly positive antibody screen was first determined in 2009, but all attempts to identify the weak reactiv-ity failed. In a recent donation, weak positive reactions were observed with about half of the screening and identification cells. No correlation to one of the major blood group antigens could be established. Using a panel of recombinant proteins, the antibody was shown to be neutralized by CR1 protein carrying the antigens of the Knops blood group system, but not by C4A, C4B, CD44, CROM, DOA, DOB or YT. Sequencing of the CR1 exon containing the Kna/b polymorphism revealed a homozygous c.4828 T>A

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 37
substitution, and homozygosity for A at positions c.4801 and c.4843. This allele is presumed to be negative for Kn8 (Sl3) and Kn9 (KCAM) antigens. Conclusion: The combination of neutralization with recombinant pro-teins and sequencing of the target gene allowed to identify a donor homo-zygous for the Kn:4,-8,-9 allele, suggesting that the antibody could repre-sent an anti-Kn8 or anti-Kn9.
P-06-4Molecular genetic investigations of a D-homozygous sample habouring weak D type 1 and type 4.1 alleles
Gnoth S.1, Conradi R.2, Petershofen E.K.1, Doescher A.1
1Blutspendedienst NSTOB, F & E, Oldenburg, Germany, 2Medical Centre of the Johannes Gutenberg University, Transfusion Centre, Mainz, Germany
Introduction: Today, 84 different weak D types are listed in the rhesus base. The most common weak D types are detectable with commercial kits, while identification of rare or new types usually has to be analyzed by sequencing of the RHD gene. Detection of several polymorphisms by sequencing of D-homozygous samples is rather difficult to interpret due to possible cis-or trans-configurations. Here, we present a case with weak D-phenotype and suspect for the presence of weak D type 1 and type 4.1.Methods: SSP-PCR was performed for RHD exons, D-partial, weak D and D-zygosity (BAG and InnoTrain, Germany). Sequencing of RHD gene, including exons 1 to 10 and intron/exon borders, was done by direct taq cycle-sequencing using BigDye-terminators v.1.1. Haplotype specific sequencing of cDNA has been performed with a weak D type 1-specific sequencing primer, determination of antigen density with the extended partial RhD typing set (BioRad, Germany).Results: SSP-PCR showed positive reactions with weak D type 1 and type 4.1 primers and was confirmed by sequencing of genomic DNA. Deter-mination of zygosity gave a homozygous constellation for the RHD gene. Haplotype specific sequencing gave confirmation for one weak D type per allele. Estimation of antigen density was 2083 antigens/cell.Conclusion: Generic sequencing of DNA samples with two or more poly-morphisms offer no information about cis- or trans-constellation of mu-tations. To obtain this information, amplification or sequencing of at least one haplotype is necessary. Our results demonstrate the occurrence of two variant D alleles. Regarding the number of antigens per cell the antigen density of the sample lies between weak D type 1 and type 4.1.
P-06-5Repeating antibody screening tests every 4 days – Necessity or nuisance?
Weiland T., Hahn J.MEDILYS Laborgesellschaft mbH, Hamburg, Germany
Introduction: Current German regulationa require pretransfusional tests such as antibody screening tests (ABSC) and crossmatches to be repeat-ed, if the sample of the previous test is older than three days in order to detect irregular antibodies that have newly been formed or boosted in the meantime. This short validity time generates high workload for laborato-ries and clinicians and causes additional waiting time and blood loss for patients. However, the additional gain of information is subjectively felt to be very low by laboratory staff. Hence, this requirement often is considerd too conservative. Other countries provide different, sometimes less strict regulations. The aim of this study was to validate this subjective impression against objective numbers by determining the number of potentially missed ir-regular antibodies in our institiution, if the maximum time between two tests had been prolonged.Methods: Retrospective analysis of all ABSC performed at our institu-tion between March 2009 and February 2014. Detailed review of all pa-tients who showed ABSC conversion from negative to positive at any time during the study period.
Results: Among 323.302 ABSC in 179.924 patients, seroconversion oc-curred in 793 patients. After exclusion of nonsignificant specificities and incomplete datasets, 737 patients with 994 antibodies remained. Of these, 37 antibodies were detected within four days of the last negative ABSC. This equals the number of potentially missed irregular antibodies that might have caused hemolytic transfusion reactions if the ABSC-validity had been extended. 88% of patients with newly detected antbodies had a record of previous red cell transfusion in our institution. Taking into account the total number of negative ABSC repeated within 4 to 7 days, the rate of “informative” tests (new antibody) was 1 in 320.
Tab. 1. Newly detected antibodies since last ABSC
No. of days since last negative ABSC
< = 4 < = 5 < = 6 < = 7 < = 14 < = 21 < = 28 >28
No. of new significant AB (cumula-tive)
37 65 87 118 273 358 403 994
Conclusion: Seroconversion from negative to positive ABSC with demon-stration of significant antibodies within a short period of time was a rela-tively rare event in our study population. However, the absolute number of events was much higher than subjectively estimated by laboratory staff. These results leave us less critical of the three-day-validity of antibody screening tests in Germany, particularly in previously transfused patients.
P-06-6Fetal and neonatal alloimmune thrombocytopenia in adult female monozygotic twins and their offsprings
Cooper N.1, Axt-Fliedner R.2, Degenhardt J.2, Hackstein H.1, Santoso S.1, Sachs U.1, Bein G.1
1Justus-Liebig-Universität Giessen, Klinische Immunologie und Transfusionsmedizin, Giessen, Germany, 2Justus-Liebig-Universität Giessen, Obstetrics and Gynecology, Giessen, Germany
Background: Fetal and neonatal alloimmune thrombocytopenia (FNAIT) is caused by maternal alloantibodies against paternally-inherited human platelet antigens (HPAs) on fetal platelets. Maternal HPA alloantibodies can cross the placenta, resulting in fetal thrombocytopenia. The most devastating consequence of FNAIT is intracranial hemorrhage, which may lead to death or severe neurological disability. Intravenous Immu-noglobulin (IVIG) is currently commonplace as secondary prophylaxis in the management of FNAIT during a subsequent pregnancy. This is based on findings of observational studies since randomized controlled stud-ies comparing any intervention with no treatment are not available. Data on the efficacy of IVIG in the primary prophylaxis of FNAIT are lacking. Here, we describe the natural history of FNAIT in adult female monozy-gotic twins without and with primary prophylaxis of FNAIT with IVIG.Twin 1: A 30-year-old women delivered a preterm baby at 35 weeks of gestation by cesarean section. The baby presented with multiple hema-toma and severe thrombocytopenia of 8 G/l. After five days of treatment with random donor platelets (n = 3), corticosteroids and IVIG, the child was discharged with a normal platelet count. Monoclonal antibody immo-bilization of platelet antigens (MAIPA) assay revealed antibodies against HPA-1a in the serum of the mother. The genotype of the mother was HPA-1bb and the genotype of the child was HPA-1ab. Twin 2: The monozygotic twin sister contacted our outpatient service be-fore her first pregnancy and was typed HPA-1bb, her husband HPA-1aa. No platelet antibodies were detectable by MAIPA assay at presentation. After diagnosis of pregnancy, antibody screening was repeated every four weeks from 14th week of gestation. At 30th week of gestation HPA-1a an-tibodies were identified by MAIPA assay. Primary prophylaxis consisting of IVIG 1g/kg/week was started at 32th week of gestation. The baby was

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts38
delivered vaginally after an uneventful pregnancy with no signs of bleed-ing and a platelet count of 291 G/l.Conclusion: This study in monozygotic twins demonstrates the efficacy of IVIG in the primary prophylaxis of FNAIT.
P-06-7Identification of underlying Anti-G in primarily Anti-C+D positive tested sera by a modified adsorption plus elution approach
Vogt M., Rindlisbacher I., Mansouri Taleghani B.Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Transfusionsmedizin, Bern, Switzerland
Background: The G antigen (Rh12) is expressed on red blood cells that carry D and/or C antigen. In routine testing, anti-G antibodies are difficult to distinguish from anti-D in combination with anti-C (anti-C+D). But discrimination is particularly important during pregnancy, because 1) on rare occasions anti-G can cause haemolytic disease of newborns and 2) if there is a true anti-G antibody and no anti-D antibody, Rh-prophylaxis has to be administered (RhIG). We re-analysed collected sera (2012–2014, from own and several other laboratories, frozen at –20°C), being primarily interpreted as anti-C+D positive, in order to detect an eventually missed mix of different specificities. Additionally we tested, if there was a correla-tion between the titres of the antibodies and their presence in the sera. Methods: A total of 46 samples were available. For separation of poten-tially different antibodies we used the adsorption-elution method. As pe-culiarity we performed two parallel adsorptions using R2R2 cells (D+, C-, G+) and r’r cells (D-, C+, G+), facilitating antibody identification with R2R2, r’r and rr test cells (D-, C-, G-), the latter serving as negative con-trol. For elution we used an acid based method (BAG, Germany). All ad-sorption/identification tests and antibody-titrations were run with a com-mercial gel centrifugation system (BioRad, Switzerland). Results: The adsorption-elution tests showed that 30/46 samples (65%) contained an anti-G antibody (10× anti-C+D, 5× anti-C+G, 7× anti-D+G, 17x anti-C+D+G, 1x anti-G, 6× anti-D), including 13% clinically relevant antibodies (5× anti-C+G, 1x anti-G), i.e. in case of being eventually de-tected in Rh neg. pregnant females. The titration tests revealed that in sera with antibody constellations being relevant during pregnancy all reveal a higher anti-C than anti-D titre. In case of high anti-C and low anti-D titres the presence of anti-G or anti-C+G without anti-D seems to be more likely (5/17 samples = 30%). Conclusion: Our modified adsorption (using 2 test cells in parallel) plus elution test uncovered that with routine antibody screen/identification the majority of antibodies being primarily interpreted to be anti-CD are not correctly diagnosed and hence anti-G antibodies not detected. We recom-mend that during pregnancy high anti-C titres should always be further investigated to make sure that clinically relevant antibody constellations (anti-G or anti-C+G) are not missed.
P-06-8Scianna 4 genotyping: Diagnosis of materno-paternal incompatibility and of haemolytic disease of the foetus
Weinstock C.1, Ritgen J.2, Anliker M.1, von Zabern I.1, Schrezenmeier H.1, Rauch S.3
1Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, DRK-Blutspendedienst Baden-Württemberg-Hessen, Universität, Ulm, Germany, 2Praenatal.de, Ärztliche Partnerschaftsgesellschaft für Praenatal-Medizin und Genetik, Köln, Germany, 3Labor Enders, Prof. Dr. med. Gisela Enders & Kollegen, MVZ GbR, Stuttgart, Germany
Introduction: Maternal blood group antibodies may cause haemolytic disease of the foetus (HDF) and the newborn. The antigen Rd (Radin, SC4; Scianna system) is very rare (<0.01%), only very few reports on anti-Rd in pregnancy exist. We here report the diagnosis by molecular
methods of materno-paternal incompatibility caused by anti-Rd for two pregnancies. In one case severe HDF developed.Materials and Methods: Case 1: Anti-Rd was found by chance in routine antibody screen. Case 2: The foetus of an anaemic woman had an haemoglobin concentra-tion of 3.0 g/dl. Repeated intra-uterine transfusions (IUT) were required. Direct antiglobulin test (DAT) and antibody testing were done by column agglutination technique. SC4 genotyping was done by in-house SSP PCR. Results: Case 1: The maternal titre of anti-Rd was 8. The father’s red cells (RBC) were found to be Rd positive with only one antiserum available. Genotyp-ing confirmed the presence of the SC4 allele. Unfortunately no samples after birth were available, but a negative DAT was reported by the hospital.Case 2: The foetus was tested negative for viral infections known to cause anaemia. A strong reactive DAT was found. The maternal antibody screen was negative in the first place, extended testing disclosed an anti-Rd, ti-tre 64. ABO groups of mother (B) and father (AB) prohibited testing for materno-paternal incompatibility. In addition, serological testing for Rd was not possible for the father (no group AB antiserum available) and the foetus (DAT positive). Genotyping eventually revealed that father and foetus carried the SC4 allele. From a postnatal cord blood sample anti-Rd was eluted, confirming diagnosis HDF.Conclusion: Diagnosis of HDF caused by antibodies directed against rare antigens may be hampered by a positive DAT of the foetal RBC or by a lack of ABO-compatible antisera for typing the foetal or paternal RBC. Distinc-tion between immune haemolytic anaemia and infectious anaemia may be important for therapy of the foetus. In addition, identification of the caus-ative antibody is necessary for serological monitoring of future pregnancies. In both cases reported here, the specificity of materno-paternal incompat-ibility was confirmed by genotyping of the SC4 allele. In the case of HDF molecular testing confirmed the diagnosis of immune haemolysis.
P-06-9New reagent for the reliable detection of duffy x (Fyx) using lateral flow technique
Meyer S.1, Caesar A.2, Trost N.1, Neuenschwander K.1, Frey B.M.1, Gassner C.1, Schwind P.2
1Blood Transfusion Service Zurich, Swiss Red Cross, Department of Molecular Diagnostics and Research & Development (MOC), Zürich-Schlieren, Switzerland, 2Medion Grifols Diagnostics AG, Düdingen, Switzerland
Introduction: Fyx is a weak Fyb phenotype with a pronounced quantita-tive reduction of the number of Fyb antigens on the erythrocyte surface, thus provoking the risk of false-negative results in blood group pheno-typing [1]. Sensitivity of a novel Anti-Fyb reagent should be evaluated, especially focusing on the ability to detect Fyx in a selected cohort with Fyx positive individuals.Methods: Fresh EDTA samples were from 42 random individuals with standard Fy serotypes, and 45 samples with standard Fy serotypes and additional FY* genotypes detected by MALDI-TOF MS blood group ge-notyping [2]. The 45 samples included 9 samples with previously identi-fied phenotypic Fyx positivity and 13 previously serologically “overseen” Fyx cases (see table). All samples were tested by one person without prior knowledge of the existent phenotypes. Fyb serology was performed using a MDmulticard lateral flow blood grouping device (Medion Grifols Diag-nostics, Duedingen, Switzerland). Briefly, 100 µl of diluted whole blood were transferred to the application zone of the MDmulticard cassette, followed by 300 µl of a rinsing solution. Results were interpreted after 5 minutes. Positive results were interpretable as distinct red bands.Results: All samples with genotypic Fyx positivity were correctly rec-ognized as Fyb positive by the MDmulticard technique. All 42 random phenotype-only samples except one were concordant with the serologi-cal pre-values (see table). The discrepant sample had a recorded Fy(a+b-) phenotype (routine serology), but showed a Fy(a+Fybweak+) phenotype (MDmulticard).

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 39
Tab. 1. Observed Duffy genotypes and phenotypes
Conclusion: The MDmulticard Anti-Fyb reagent seemed to reliably de-tect all Fyb and Fyx positive phenotypes. Technically, the combination of well selected clones with appropriate diagnostic techniques may lead to novel methods with increased diagnostic sensitivity. As shown previously, genotyping may serve as a valuable tool to create more specific and better characterized testing panels [3].References:1. Murphy MT, et al: Trans Med 1997;7:135–141.2 Meyer S, et al: Transfusion 2014;54:3198–3207.3 Gassner C, et al: Transfus Med Hemother 2009;36:219–225.
P-06-10The first case report of an RhG negative phenotype in a cDE haplotype with RHD-CE(2)-D genotype
Leo A.1, Laier S.1, Weinstock C.2, Stürtzel A.3, Albrecht B.1, Scharberg A.E.3
1Institut für Klinische Transfusionsmedizin und Zelltherapie Heidelberg gGmbH, Heidelberg, Germany, 2Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Ulm, Germany, 3DRK-Blutspendedienst Baden-Württemberg-Hessen gGmbH, Institut Baden-Baden, Baden-Baden, Germany
Introduction: The RhG antigen is associated with the presence of the amino acid serine at position 103 on RHCE and RHD proteins expressing RhC and RhD antigens. Thus, individuals who are RhD or/and RhC pos-itive, are usually RhG positive. In very rare cases RhC and RhD negative red cells can express the RhG antigen (rGr or rGr´´ phenotypes). There are few known different molecular backgrounds of this unusual RhG an-tigen expression. The lack of the RhG antigen on RhD positive red cells is also extremely rare. It is mostly linked to the ccD.ee phenotype with RhD category IIIb which is caused by an exchange of exon 2 of the RHD gene versus exon 2 of the RHCE gene (RHD-CE(2)-D). We describe the first case of an RhG negative individual with the ccD.EE phenotype and RhD category IIIb. Methods: Antibody identification was performed in the IAT with untreat-ed/papain-treated red cells in the gel agglutination technique (BioRad, Switzerland). For serological RhD typing two sets of monoclonal anti-D reagents were used (Diagast, France and BioRad, Switzerland). The RhG antigen was tested in the IAT using different patient anti-G sera. The RHD gene of the serologically RhG negative individual was analyzed by exon amplification and direct sequencing.Results: A female patient (Rh phenotype D–,C–,c+,E+,e+) with known anti-D and anti-C unexpectedly did not react with one ccD.EE test cell in an antibody identification panel (BioRad, Switzerland) indicating that the test cell was RhG negative and the true antibody specificity was anti-G and not anti-D plus anti-C. Serological RhG antigen typing of the negative reacting ccD.EE red cell showed negative results confirming the G nega-tive phenotype. Serological RhD typing of this test cell with 15 different monoclonal anti-D reagents was positive with all test sera. Sequence based
typing revealed the RHD-CE(2)-D hybrid gene in an R2r´´ (ccDdEE) in-dividual. Conclusions: RhG negative phenotype associated with the RhD catego-ry IIIb was previously found only in persons with ccD.ee phenotype. We describe the first example of an RhG negative blood donor with the ccD.EE phenotype and RhD category IIIb in a cDE haplotype. The red cells of this donor have a significant diagnostic value to distinguish directly between anti-G and anti-C plus anti-D avoiding time consuming absorp-tion/elution studies performed otherwise. This is important in perinatal diagnostics, because women with anti-G without anti-D need prenatal anti-D prophylaxis.
P-06-11Rhnull phenotype caused by two novel mutations of RHAG
Just B.1, Strathmann K.2, Luetjens P.3, Grimsley S.4, Thornton N.4, Doescher A.5
1DRK-Blutspendedienst West, Zentrum für Transfusionsmedizin, Hagen, Germany, 2Uniklinik RWTH Aachen, Institut für Transfusionsmedizin, Aachen, Germany, 3MVZ Synlab GmbH, Laboratoriumsmedizin / Immunhämatologie, Leverkusen, Germany, 4NHSBT, IBGRL, Bristol, United Kingdom, 5DRK-Blutspendedienst NSTOB, Institut Oldenburg, Oldenburg, Germany
Introduction: Rhnull/Rhmod phenotypes may be caused by inactivating mutations in RHAG, the gene which encodes the Rh-associated glycopro-tein (RhAG). This protein forms a complex with other proteins including RhD and RhCcEe and is required for the expression of Rh antigens. Here we describe a case of the Rhnull phenotype caused by two heterozygous novel mutations of RHAG found in a patient suffering from congenital spherocytosis.Methods: Phenotypes were established by standard serological methods using both tube and gel-column agglutination techniques. Antibody-tests were carried out by indirect antiglobulin test (IAT) in the gel-card tech-nique (Bio-Rad) and the solid phase technique (Capture-R, Immucor). Eluates were prepared by acid elution method from autologous and RhD-negative red blood cells (RBC) following adsorption with poly-clonal anti-D. Genomic DNA was isolated from whole blood and SSP-PCR was carried out with CE-marked testkits of BAG. RHD, RHCE and RHAG were directly sequenced by taq cycle-sequencing in an ABI310. RHAG sequence was confirmed by bidirectional direct sequencing using an ABI3130xl.Results: No expression of D, C, c, E, e, Rh17 and Rh29 could be detect-ed on the patient’s cells by standard phenotyping methods and a potent monoclonal anti-RhAG (LA18.18) was also negative. Adsorption and elu-tion studies with polyclonal anti-D were inconclusive therefore very weak expression of D could not be ruled out. Expression of s and U was de-creased. A very weak IgG antibody was detected in the patient’s plasma by IAT/gel-card, reacting with most cells. In contrast only very few cells were reacting by Capture-R. The antibody was too weak to determine the spec-ificity. The patient’s RH genotype was RHD*D, RHCE*Ce/cE. Genomic DNA sequencing of all ten exons of RHAG revealed two novel heterozy-gous mutations, one in exon 3: c.465T>A causing p.N155K and the other in exon 4: c.620C>G causing p.S207STOP.Conclusion: Compound heterozygosity for two novel RHAG alleles, RHAG*465A and RHAG*620G is assumed due to the patient’s Rhnull phenotype. Further studies are required to explore the possibility of some expression of RhD and RhCcEe which will provide further information with regard to the risk of immunization. Supplying the patient with ap-propriate blood products is extremely difficult due to the global rarity of Rhnull donors. Among other options supply may be improved by cryo-preservation of autologous blood.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts40
P-06.12Evaluation of LABScreen® multi for granulocyte antibody detection
Reil A.1, Bux J.2, Kiefel V.3, Schulz U.4
1DRK-Blutspendedienst West, Hagen, Germany, 2Ruhr-Universität, Bochum, Germany, 3Universität Rostock, Institut für Transfusionsmedizin, Rostock, Germany, 4DRK-Blutspendedienst Nord-Ost, Cottbus, Germany
Introduction: To mitigate the risk of Transfusion-associated acute lung injury (TRALI), female plasma donors with a history of pregnancy have to be tested for HLA and HNA antibodies. For HNA antibody detection, the current gold standard is a combination of Granulocyte Immunofluores-cence Test (GIFT) and Granulocyte Agglutination Test (GAT). However, these tests are not suitable for high throughput testing. The fluorescence conjugated bead-based assay LABScreen® Multi (One Lambda) is suitable to screen up to 96 samples in one run. The first generation of this test was designed for the detection of HNA-1 and -2 antibodies. After elucidation of the molecular structure of the HNA-3 antigens, now a new test was introduced comprising the detection of HNA-1, -2, -3 and -4a antibodies. Here we report the results of our initial study evaluating the new gener-ation of LABScreen® Multi with focus on the recovery of known HNA antibodies.Methods: In total, 97 sera with HNA antibodies previously confirmed by GIFT, GAT and the antigen-specific MAIGA assay were tested by LAB-Screen® Multi for the presence of antibodies to HNA-1a, -1b, -1c, -2, -3a, -3b, and -4a. Results were expressed as a normalized background value ratio (NBG).The cutoff value was set for the beads HNA-1a, HNA-1b, HNA-1c, HNA-3a, HNA-3b and HNA-4a to 5. The bead for HNA-2 was evaluated with cutoff values 10 and 20, respectively.Results:
Tab. 1. Results HNA antibodies
SpecificityNumber of positive sera
Cutoff value (NBG)
True positive
True negative
False positive
False negative
HNA-1a 15 5 14 82 0 1 (IgM)
HNA-1b or -1c or -1d 21 5 21 76 0 0
HNA-2 16 20 / 10 16 / 16 72 / 65 9 / 16 0 / 0
HNA-3a 38 5 34 57 2 4
HNA-3b 6 5 2 62 29 4
HNA-4a 1 5 1 96 0 0
Conclusion: Compared to the first generation, the new LABScreen® re-acts highly specific for the specificities HNA-1a, -1b, -2 and -3a required to prevent TRALI. 100% of the HNA-1a, -1b, -1c, -1d and -2 IgG anti-bodies could be detected as true positive. 89% of the HNA-3a antibodies (34/38) were correctly identified. However, some HNA-3a antibodies were still not recognized and this means that GAT is still necessary for TRA-LI prevention. HNA-2 antibodies yield the highest NBG values and even with elevated cutoff (20), there are some false positives. The HNA-3b bead needs improvement, 4 out of 6 antibodies were not detected, but a lot of false positive reactions occurred.
P-06-13Anti-K antibodies in a pregnancy after artificial insemination: A case report
Vogt C., Petershofen E.K., Doescher A.Blutspendedienst NSTOB, F & E, Oldenburg, Germany
Introduction: Determination of HDN-relevant fetal blood groups in am-niocentic fluid is a routinely used method while examination of mater-nal plasma is increasingly utilized as an additional diagnostic tool. Next to RHD, typing of fetal KEL1 is most common in non-invasive prenatal
genotyping. In this report we present a case where interpretation solely based on the diagnostic results can lead to a wrong interpretation.Case report: External samples of a 43-year old pregnant mother (week of gestation: 18) were sent to our institute. In a first serologic test for irregu-lar antibodies an anti-K antibody (titer 1024) was detected. Clinical signs of HDN were not found at this stage. In addition, serological typing of the putative father was mentioned and showed a K-k+ phenotype. On request we received the following additional data: In the first successful pregnancy the woman gave birth to female twins, one being k+k+ phenotype, the other K+k+. At time of birth an anti-K was not detected. Transfusions had not been applicated in the past, as a means of immunization. After intense discussion with the obstetricians it came out that the wom-an had undergone artificial insemination with an egg-donor from abroad in the actual and previous pregnancy. According to the national regula-tions for egg-donations in that country, typing of KEL1 was not requested. Since cell samples from the egg-donor female were not available, samples from the 3 year old twins were examined for the presence of KEL 1.Methods: Maternal plasma was prepared according to Lo et al. and ex-tracted DNA was examined for KEL1 specific sequences with real-time PCR. Genomic DNA had been genotyped with SSP-PCR (Ready Gene KDK Kit, InnoTrain, Germany).Results and conclusion: KEL1 positive results were obtained in real-time PCR with ffDNA. Parallel KEL1 genotyping with DNA samples from the twins showed a positive results for one child, while the other was KEL1 negative, suggesting that the egg-donor inherits a K+k+ phenotype.Prenatal genotyping of HDN-relevant fetal blood groups is a useful tool in pregnancies with antibodies already present in maternal serum from a previous pregnancy but can lead to a wrong interpretation when the corresponding gene that leads to immunization, does not come as usually from the father, but from another genomic mother as given in this case.
P-06-14The Upper Austrian contribution to the heterogeneous RHCE allele repertoire
Polin H.1, Reiter A.1, Brisner M.1, Suessner S.2, Danzer M.2, Gabriel C.2
1Blutzentrale Linz, Molekulare Immunhämatologie, Linz, Austria, 2Blutzentrale, Linz, Austria
Introduction: The RHCE gene located on chromosome 1 encodes the red blood cell (RBC) membrane protein RhCE. A diminished expression of antigens C, c, E and e was associated with different molecular back-grounds causing for weak or partial phenotypes. Aim: During a one-year period, the molecular bases of blood donor sam-ples with diminished or discrepant RhCE typing results were determined. Materials and Methods: Molecular work-up comprised real-time PCR and DNA sequencing of RHCE exons 1–10 and adjacent intronic se-quences. Novel alleles were further characterised by flow cytometry and hemagglutination. Results: Among a total of 11 samples with questionable RhCE status, the well known RHCE*Ce.08.01 (n = 2) and RHC*cE.01 (n = 4) alleles were identified beside the less frequent RHCe*667T gene formation (n = 2) and the rare c.1–10C>T (n = 1). A novel variant, c.487–5T>G, was determined in two unrelated blood donors with decreased antigens C and e. This base change located at the end of intron 3 occured on RHCE*02 backbone with proper RHCE*03 in trans. Conclusion: The heterogeneity of the RHCE allele pool was proven for the Upper Austrian population and supplemented by a novel gene formation.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 41
P-06-15Vancomycin-dependent antibodies and mild hemolysis in a patient with hemodialysis
Sümnig A.1, Baschin M.1, Mayer B.2, Bakchoul T.1, Greinacher A.1, Salama A.2
1Universitätsmedizin Greifswald, Transfusionsmedizin, Greifswald, Germany, 2Charité – Universitätsmedizin Berlin, Institut für Transfusionsmedizin, Berlin, Germany
Background: Vancomycin is a widely used antibiotic. We report the first case of a patient with vancomycin-induced immune hemolysis. Patient and Method: A 63 year old patient undergoing dialysis due to renal failure developed mild hemolysis and was positive for the antibody screening test, and weak positive for the C3d-direct antiglobulin test. These findings were observed 3 days following commencement of treat-ment with vancomycin. Serological testing was performed using standard techniques in the presence and in the absence of vancomycin. Results: The antibody-screening test was initially found to be negative, and there was no evidence of the presence of autoantibodies to red blood cells (RBCs). Three days later, the patient’s serum was found to be reac-tive with all of the RBCs analyzed. The direct antiglobulin test was weak positive with anti-C3d only. The eluate from the patient RBCs was found to be negative. The patient received two positive crossmatched RBC units without complications. The haemoglobin concentration did not increase adequately, and mild signs of hemolysis were observed. Reexamination of the patient’s serum revealed vancomycin-dependent reactions. Discussion: Drug-dependent antibodies to RBCs usually cause severe hemolysis. Vancomycin has been implicated in the development of im-munothrombocytopenia and in RBC agglutination, but not in immune hemolysis. Despite the presence of drug-dependent (vancomycin-depen-dent) antibodies, the mild hemolysis described in the patient here may be explained by the limited immune response due to renal failure and dialysis. Conclusion: Vancomycin should be considered as a potential causative agent in patients who develop RBC agglutination in the presence or ab-sence of hemolysis.
P-06-16Analysis of positive IgM cross matches: non-specific or relevant?
Flommersfeld S.1, Ertl B.1, Marschall R.1, Bein G.2, Sachs U.J.2
1UKGM, Transfusionsmedizin, Marburg, Germany, 2UKGM, Transfusionsmedizin, Giessen, Germany
Background: Since 2014, type and screen as well as RBC cross match-ing (CM) are fully automated using Galileo NEO devices (Immucor, Rö-dermark, Germany) in our laboratory. In order to detect a possible AB0 incompatibility between RBCs and the recipient’s plasma in the absence of Anti-A, Anti-B of the IgG type, each cross match consists of two tests: an IgG cross match (on Capture Select plates) and an IgM cross match (CM-IgM) on microwell plates. Positive results of unknown relevance are sometimes observed in CM-IgM only, despite AB0 compatibility. Material and Methods: During the study period of 6 months, 14,006 CMs were performed. A total of 54 CM-IgM positive results only were observed (0.4%), which could be traced back to 27 patients. Material from these patients was further investigated for AB0 incompatibility. In addition, we performed Capture Ready Screen (Immucor), direct (DAT) and indirect antiglobulin test (IAT) by column agglutination (CA) (BioRad, Dreieich, Germany), cold-reactive antibody screens by CA (22°C) and tube (4°C) technique. Cold-reactive antibodies were titrated; DAT IgG-positives were eluated. In plasma of A2 recipients, we searched for Anti-A1. Results: No AB0 incompatibility was detected. A total of 17/27 patients (63%) had findings potentially explaining CM-IgM reactivity: 10× cold autoantibodies of Anti-I/-HI specificity with titers between 8 and 1,000; 2× cold reactive antibodies with Anti-M (n = 1) and Anti-Ch/Rg (n = 1) specificity, respectively; 3 patients with week, non-specific reactions in CA
at 22°C; and 2 patients with a positive DAT (IgG) with negative eluates. In-terestingly, in 2/27 samples Anti-K identified in addition to Anti-HI either by Capture screen or in the DAT. In 10/27 patients, all tests performed were without findings. Conclusions: Autoantibodies reactive in the cold are the most frequent reason for a positive CM-IgM. Clinically relevant specific antibodies are rarely detectable (2/27). As a consequence, in addition to AB0 typing of the RBC unit, we recommend to perform DAT and Capture antibody screen in patients with positive IgM cross matches.
P-06-17Monocyte migration under chronic inflammatory conditions is regulated by IL4-induced transcription factor FOXQ1
Riabov V.1, Ovsij I.2, Manousaridis I.2, Avdic A.2, Goerdt S.2, Kremmer E.3, Krenning G.4, Harmsen M.4, Gratchev A.2, Kzhyshkowska J.1,5
1Institute of Transfusion Medicine and Immunology, Medical Faculty Mannheim, Heidelberg University, German Red Cross Blood Donor Service Baden-Württemberg-Hessen, Mannheim, Germany, 2Department of Dermatology, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany, 3Helmholtz Center Munich, Institute of Molecular Immunology, Munich, Germany, 4Department of Pathology and Laboratory Medicine, Medical Biology Section, University of Groningen Medical Center, Groningen, Netherlands, 5German Red Cross Blood Service Baden-Württemberg-Hessen, Mannheim, Germany
Transmigration of monocytes through endothelium requires coordinat-ed receptor/ligand interactions. However, little is known about molecular pathways and a transcriptional control of transmigration in monocyte sub-types under chronic inflammatory conditions. We have recently demon-strated that monocytes respond to IL-4 by strong induction of FOXQ1 gene expression and observed its upregulation in monocytes of patients with atopic dermatitis. However, function of FOXQ1 in monocytes was unknown. Here, we investigated the regulation of FOXQ1 gene expression and its functions in human monocyte-derived macrophages (MDM).Analysis of FOXQ1 expression in human MDM revealed that its expres-sion was upregulated by IL-4. In addition, TGF-β1 in combination with dexamethasone amplified the effect of IL-4. A microarray analysis of mac-rophage-like RAW264.7 cells stably transfected with FOXQ1 demonstrat-ed that FOXQ1 target genes are involved in the monocyte motility. Indeed, FOXQ1-expressing RAW264.7 cells showed increased migration activity which correlated with suppressed expression of receptor PLXNC1 known to inhibit monocyte migration. Moreover, PLXNC1 was downregulated in human monocytes upon IL-4 stimulation and in patients with atopic dermatitis.Our data indicate that FOXQ1 is upregulated by IL-4 and TGF-β1 and stimulates monocyte migration in response to inflammatory stimuli by suppression of PLXNC1. FOXQ1 might support increased monocyte ex-travasation through the activated endothelium in chronic inflammation.
P-06-18Effect of increased glucose on the expression of TLRs in human macrophages: potential mechanism of chronic inflammation in diabetes
Balduff M.1, Moganti K.1, Li F.1, Harmsen M.2, Escobedo G.3, Gratchev A.1, Kzhyshkowska J.1
1Medizinische Fakultät Mannheim der Universität Heidelberg, Institut für Transfusionsmedizin und Immunologie. German Red Cross Blood Donation Service Baden-Württemberg-Hessen, Angeborene Immunität und Toleranz, Mannheim, Germany, 2Cardiovascular Regenerative Medicine, University Medical Centre Groningen, University of Groningen, Dept. Pathology and Medical Biology, Groningen, Netherlands, 3Medical Faculty , National University of Mexico, Unit of Experimental Medicine, Mexico City, Mexico
Diabetic patients suffer from chronic inflammation regulated primarily by macrophages. M1 and M2 represent two major directions of macrophage functional polarisation. Toll-like receptors (TLR)-mediated response to

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts42
exogenous and endogenous factors results in pro-inflammatory activation of macrophages. Increased TLR expression in monocytes is associated with diabetic in-flammation and complications. The aim of our study was to examine how elevated glucose levels affect expression of TLRs in M1 and M2. Monocytes were isolated from healthy donors and cultured in serum-free medium in the presence of 5mM or 25mM glucose for 6 days. M1 and M2 differentiation was driven by IFN-γ and IL-4. Quantification of TLR mRNA expression was performed by RT-PCR and demonstrated that mRNA of TLR1, 2, 4, 6 and 8, but not TLR5 and 9, were expressed in M1 and M2. All identified TLRs were expressed on higher levels in M1 com-pared to M2 in low and high glucose conditions. Increased glucose had a most pronounced stimulatory effect on the ex-pression of TLR2 and less on TLR6. In the individual M1 cultures high glucose stimulated up to 8-fold increase of TLR2 and up to 28% increased of TLR6 expression. In M2, TLR2 expression was up to 6-fold higher in the presence to high glucose. High glucose had suppressive effect on the expression of TLR4 (in 5 of 8 donors up to 65%) in M1 and M2. Comparative analysis of expression profiles of fat tissue samples and blood parameters from patients with metabolic syndrome revealed a negative correlation between TLR2 expression and ALAT and between TLR6 and HDL. TLR2 expression correlates positively with TNF-α plasma levels. Reduced TLR expression can be linked to the protective role of HDL in cardiovascular diseases.We conclude that glucose regulates TLR2, TLR4 and TLR6 expression in a donor-specific way. Such individual responses suggest new glucose-me-diated mechanism for the development of patient-specific inflamma-tion-mediated complications in diabetes.
P-06-19Evidence of trace amounts of IgM autoantibodies at core temperature in patients with cold autoimmune haemolytic anaemia
Bartolmäs T., Yürek S., Mayer B., Salama A.Institut für Transfusionsmedizin/ Charité Berlin, Berlin, Germany
Background: It is unclear why the direct antiglobulin test (DAT) remains always positive in patients with cold autoimmune haemolytic anaemia (cAIHA) and why haemolysis does not completely abolish, when patients are kept warm. Patients and Methods: Unselected patients (n = 7) with cAIHA were in-cluded in this study. Serological testing (including thermal amplitudes) was performed using standard techniques. Pre-warmed patients’ RBCs were tested by the direct antiglobulin test (DAT), dual antiglobulin test (DDAT) and flow cytometry (FC). Temperature-dependent complement binding was determined by incubation of patients’ serum samples with group O RBCs and fresh donor serum as a source of complement. Results: All patients had serum cold aab with a thermal amplitude from 22–28 °C. The DAT remained always strongly positive with anti-C3d in all cases, whereas trace amounts of IgM aab were infrequently detectable on patients’ RBCs at 37 °C. Haemolysis usually improved in summer, but per-sisted throughout the year. In addition, strong complement activation was demonstrated following incubation (strictly at 37 °C) of group O RBCs with patients’ sera in the presence of fresh donor serum. The results indi-cate binding of IgM aab at 37 °C in patients with cAIHA.Conclusions: Binding of trace amounts of IgM aab may provide an expla-nation for the durable C3d-positive DAT and haemolysis in patients with cAIHA. The question whether the aab in cAIHA may be composed of two populations with different temperature amplitudes remains obscure.
P-06-20A retrospective single-centre study on the efficacy and tolerability of repeated treatment with IVIg in patients with ITP
Ringel F., Bal G., Salama A.Charite Universitätsmedizin Berlin, Institut für Transfusionsmedizin, Berlin, Germany
Background: Treatment with intravenous immunoglobulin (IVIg) for immune thrombocytopenia (ITP) is well established. The majority of ITP patients respond to IVIg treatment, and platelet counts increase for a period of 2 to 4 weeks. There is little information on the efficacy and tolerability of repeated treatment with IVIg in ITP. We present data from ITP patients that were repeatedly treated with IVIg in our clinic between 2002 and 2014.Methods: Thirty adult patients (23 females, 7 males) with chronic ITP were included in this study (mean age, 47 years; females, 43 years; males, 59 years). All patients received at least three independent treatment cycles with IVIg. Two patients were splenectomized prior to IVIg treatment, 8 women were pregnant, and 3 patients were splenectomized during ob-servation. Results: All patients achieved at least one partial response to treatment with IVIg. Responses were not found to correlate with IVIg cycles, gen-der, or duration of disease. Response to treatment with IVIg was consis-tently observed in 67% of patients including the 8 pregnant women. The response of the remaining patients was variable. Responses were observed to be independent of IVIg cycles, duration of treatment, and disease. IVIg administration was well tolerated in all patients, and no severe side effects were observed. None of the patients had a bleeding score higher than WHO grade 1 during observation.
Tab. 1. IVIg response
total female male
Duration of disease (years) 5.3 ± 6.3 5.5 ± 6.8 4.7 ± 4.4
Duration of IVIg treatment (months) 20.3 ± 25.1 21.4 ± 28.3 16.7 ± 9.3
Number of IVIg cycles 7.4 ± 5.4 8.4 ± 5.8 4.1 ± 1.1
Complete response (CR) 11 (37%) 8 (35%) 3 (43%)
Partial response (PR) 19 (73%) 15 (65%) 4 (57%)
Response (PR, CR) to every cycle of IVIg 20 (67%) 15 (65%) 5 (71%)
Conclusion: Durable response to repeated treatment with IVIg occurred in over 65% of patients, and was found to be independent of gender, IVIg cycles, duration of disease, and previous treatment. Interestingly, all preg-nant women consistently responded well to treatment, and bleeding com-plications were not observed in a single mother or baby. There appears to be no memory effect over time or amount of IVIg treatment leading to the loss of efficacy. Multiple administrations of IVIg were not associated with increased side effects.
P-06-21Newly detected irregular erythrocyte antibodies in a Northwest German centre laboratory within the year 2014
Schenck P., Stolle S., Kühling E., Doescher A., Petershofen E.K.DRK Blutspendedienst NSTOB, Bremen-Oldenburg, Oldenburg, Germany
Introduction: According to German guidelines for clinical hemotherapy all patients with newly detected irregular erythrocyte antibodies receive a passport for emergency cases including blood groups and specificity of these antibodies. During the year 2014 we collected data from our soft-ware system to evaluate the number and specificity of newly detected antibodies.Our institute serves as a regional reference centre, including a university hospital, 2 city hospitals with maximum support, 24 regional

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 43
hospitals and 16 outpatient centres in private practice, e.g. Hematology & Oncology, Nephrology, Gynaecology, MVZ, etc..Methods: Antibodies were detected using reference cells and reagents from commercial companies (BioRad, Grifols, Immucor, Biolith, Optima, Sifin, SD-nostik, all Germany). In rare cases we used frozen cells and plas-ma that were collected over the years or provided by colleagues from the Rare Donor Support of the German DGTI, Section 5. Antibody detection has been done in several milieus (LISS-ICT, NaCl, Enzyme, PEG-ICT) and techniques (gel-column and tubes). Results: During a one year period we collected data from the immuno-hematology laboratory. Only new antibodies showing a coombs-relevant reaction with at least 3 test cells, including a check for corresponding an-tigens, were used for this evaluation.The result of 490 samples is given in the following table format:
Tab. 1. Alloantibodies in North West Germany
specificity number specificity number specificity number
Anti-E 77 Anti-Jk(a) 28 Anti-Co(b) 4
Anti-K 57 Anti-Cw 19 Anti-Le(a) 4
Anti-D 56 Anti-Kp(a) 14 Anti-Le(b) 2
Anti-M 41 Anti-c 13 Anti-H (37°C) 2
Anti-Lu(a) 41 Anti-Jk(b) 12 Anti-s 1
Anti-Wr(a) 34 Anti-S 11 Anti-P1 1
Anti-C 31 Anti-Fy(b) 5 Anti-Ch(a) 1
Anti-Fy(a) 29 Anti-e 5 Anti-f 1
Conclusion: With regard to published data of antigenicity the frequency of antibodies shows a different picture in Northwest Germany. An unex-pected high number of new anti-Lu(a), anti-M and anti-Wr(a) immuni-zations has been found. Approx. 22% of emergency passports had more than 1 historic antibody, and 3% more than 2 antibodies. The reason for Anti-D immunisation has to be further evaluated (including women born before 1955 with suspected pregnancy and some RhD-neg. patients after emergency support with D-positive red blood cells). Remarkable is the high number of patients with anti-Lu(a) and anti-Wr(a) in Northwest Germany.
P-06-22Autoimmune hemolytic anemia induced by T- cryptantigen activation after gastointestinal and pulmonary infection in a three years old boy: a case report
Höppner S., Kasprzik-Diehl A., Müller-Steinhardt M., Janetzko K., Klüter H.Blutspendedienst Baden-Württemberg-Hessen GmbH, Institut für Transfusionsmedizin und Immunologie, Mannheim, Germany
Background: Specific infectious agents, for example pseudomonas aeru-ginosa and the influenza virus, are able to clear cryptantigen T on the surface of erythrocytes, by releasing neuraminidase. This may lead to a severe complement-mediated hemolysis triggered by the presence of non-immune anti-T antibodies. The application of plasma derivatives, for example FFPs, in case of coagulation disorders, may increases an exist-ing hemolysis by adding donor anti-T. Administration of this supplement must therefore be restricted. In contrast, the administration of plasma de-pleted supplements, such as platelet concentrates and red blood cells con-centrates, are preferential. In case of life-threatening hemolysis or severe complications caused by T-activation, the administration of washed sup-plements are recommended. Therapeutic measures consist in the treat-ment of the infection, e.g antibiotic therapy or neuraminidase inhibitors in case of viral infections. Clinical findings: A three year old boy was presented at the children`s hospital showing signs of severe autoimmune hemolytical anemia after an infection of the upper respiratory tract followed by a gastroenteritis caused by adenovirus infection. Additionaly a moderate thrombocytope-nia was seen. Transfusion of a plasma reduced red blood cell concentrate at haemoglobin levels of 4,9 g/dl was uneventful and the hemoglobin level
increased considerably to 6,8 g/dl. After treatment with corticosteroids and antibiotics the boy recovered quickly. Laboratory findings: Immunohematological assessment showed un-spe-cific reactions in the papain phase of the indirect antiglobulin test without indication for a specific alloantibody. The direct antiglobulin-test was pos-itive with C3c and C3d, suggesting complement activation. Donath-Land-steiner-antibodies were excluded. In contrast, the polyagglutination-test, was positive, proving the diagnosis of T-activation and explaining the cause of the hemolysis. In the microbiological tests Adenovirus was detected in stool specimen. Conclusion: This is another case-report of a severe haemolytic disease in childhood with T-activation. Particularly in infants with pneumo-nia, bronchopulmonary infections, septic diseases as well as abdominal infections combined with anemia, a T-activation should be considered. Polyagglutinatibility may be misdiagnosed as novel AHG sera lack anti-T. A fast diagnosis of the disease can reduce severe complications caused by T-activation.
P-06-23Detection of platelet reactive autoantibodies using the LuminexTM based Pak Lx™ immunoassay
Meyer O., Möckel M., Salama A.Institut für Transfusionsmedizin, Charité - Universitätsmedizin, Berlin, Germany
Purpose: Fetal/neonatal alloimmune thrombocytopenia and post-trans-fusion purpura are related to antibodies (abs) directed against human platelet alloantigenes (HPA). The LIFECODE Pak Lx assay is a Luminex based, qualitative immunoassay designed to detect and differentiate such abs to HPA-1, HPA-2, HPA-3, HPA-4, HPA-5, GPIV and Class I HLA, but not autoantibodies (aabs) directed against platelet glycoproteins (GP). Recently, Porcelijn and co-workers described GP-reactive abs detectable by the Pak Lx™ without any identifiable HPA-specificity. These reactions might be related to aabs. However, the clinical relevance of such abs re-mains unclear.Methods: We investigated 160 consecutive patient blood samples sent to our laboratory. The Pak Lx was applied as recommended by the manu-facturer. Additionally, the samples were investigated by the monoclonal antibody-specific immobilization of platelet antigens assay (MAIPA) us-ing monoclonal abs directed against GPIIb-IIIa, GPIb-IX, and GPIa-IIa. If possible, these experiments were complemented by the detection of plate-let bound GP-specific aabs (MAIPA) and elution experiments.Results: Using the Pak Lx, we identified only two serum samples in this series that contained abs against HPA-1a and HPA-5b, respectively. Both reactions were confirmed by the standard MAIPA. In 25 cases, the Pak Lx showed positive reactions against GPIIb-IIIa and in 6 cases against GPIa-IIa without any identifiable HPA-specificity. Therefore, aabs were suspect-ed, but only 7 of the reactions against GPIIb-IIIa could be confirmed by the MAIPA. In 24 of these cases, we were able to investigate the autolo-gous platelets. However, only six of these patients showed platelet bound aabs directed against GPIIb-IIIa and none against GPIa-IIa. In three of these patients, the aabs directed against GPIIb-IIIa could be confirmed by elution experiments. Interestingly, in 3 serum samples we identified free and platelet bound aabs directed against GPIb-IX by the MAIPA and confirmed by elution experiments, but none of these aabs could be using the PAK Lx.Conclusion: The PAK Lx is fast and easy to perform and a helpful tool for the detection of abs against HPA-1, HPA-2, HPA-3, HPA-4, HPA-5, GPIV and Class I HLA. However, this assay frequently detects GP-reactive abs that might be misinterpreted as aabs. To our hands, such GP-reactive abs should be confirmed by a glycoprotein-specific investigation for platelet bound aabs (e.g. MAIPA and/or elution experiments).

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts44
P-06-24Rhesus incompatibility in a Rh D-negative child, born after 31 weeks of gestation: a case report
Dahse K.1, Doescher A.2, Trestyanszki I.1, Dierks N.1, Petershofen E.K.2
1DRK-Blutspendedienst NSTOB, Institut Bremen-Oldenburg, Standort Bremen, Bremen, Germany, 2DRK-Blutspendedienst NSTOB, Institut Bremen-Oldenburg, Standort Oldenburg, Oldenburg, Germany
Introduction: Serological blood group typing of a newborn is a common and simple examination, but after intrauterine transfusion it may be im-possible.Case report: In the context of a transfusion reaction (single symptom: fe-ver of 38,5°C) blood samples of a preborn-child (31+3/7 w.o.g.) were sent to our laboratory approx. 5 weeks after birth. The informed diagnosis was Rhesus-incompatibility and the blood group of the child was documented as 0 Rh negative. After finishing the relevant tests with the child´s blood, we found a blood group 0, ccddee, K- (no mix field reactions), a negative DAT, but irregular antibodies for anti-D. For a Rhesus-incompatibility these results do not seem to fit together.While searching for more detailed anamnesis we received information, that the child had received three intra-uterine transfusions and one trans-fusion after birth. The mother´s blood group was A, Rh D-negative, show-ing an anti-D titer highest at 4096, and anti-C, titer 32.To further evaluate the constellation we performed an acid elution test (BAG, Germany) to detect maternal antibodies on very limited patient cells. Since the result from the eluat was positive for anti-D in the gel technique (Liss-AHG), we further examined the child´s blood group using molecular genetic typing, resulting in ABO*A201 and RHD *01, RHCE*01/02 to be interpreted as a phenotype A2, CcD.ee.With these additional findings our test results were in accordance with each other. The transfusions suppressed the haematopoiesis and the child’s erythrocytes were destroyed due to the strong maternal antibody. The concentration of the patients anti-D coated erythrocytes in circulation was too low to cause a positive DAT, but strong enough for the detection of anti-D in the eluate.Conclusion: False results in serological blood group typing after intra-uterine transfusion are possible due to a suppression of haematopoiesis of the fetus or newborn especially mix field reactions are not detectable. Only molecular genetic typing can give exact results. In addition, a nega-tive DAT does not always implicate a negative result in antibody detection from eluate in any case. The concentration of the patient´s anti-D coated erythrocytes in circulation can be too low to cause a positive DAT. When-ever antibody coated patient erythrocytes are suspected, detection of an antibody in eluate should be tried, even in case of a negative DAT.
P-06-25A real time qPCR assay for the screening of serological Rhesus D negative or doubtful laboratory findings
Boehm W., Ahrens N., Kissel K., Marell R.-R.BAG Health Care GmbH, Lich, Germany
Introduction: Serological testing for Rhesus D antigens is mandatory for blood donors in clinical diagnostics. However, in case of the presence of weak D, partial D and DEL phenotypes those serological tests have lim-itations in detecting Rhesus D and cannot ensure a sufficient accuracy. Therefore the use of the qPCR technique as a safeguarding check to detect doubtful negative samples represents an adequate technique besides the conventional serological testing (ICT). In this study the developed qPCR Assay was designed to detect the RHD Exons 5, 7 and 10. This Approach allows the examination of RHD positive and negative samples even the rare phenotypes with a high accuracy and sensitivity. Methods: A qPCR assay was developed to determine the Rhesus D status from blood donors. After gDNA-isolation, the presence of the RHD gene was tested with fluorescent-labeled dye hydrolysis probes for RHD exon 5, 7 and 10. The qPCR tests were performed using the BioRad CFX 96 touch cycler and the Bioline SensiFast Probe NO-ROX kit. The RHD genotyping
was achieved by using a BAGene-SSP-Kits (RH-TYPE, Partial D-TYPE, Weak D-TYPE and D Zygosity-TYPE). Results: To test the performance of the qPCR Assay 100 serological nega-tive pre-typed blood samples provided by a blood transfusion department were screened. After qPCR-RHD-screening, 3 of 100 samples showed a positive RHD result. 2 of 3 samples were positive on exon 5, 7 and 10. In one sample the RHD-exon 5 signal was missing. To cross-check the qPCR results the 100 samples were reanalyzed by a CE-marked PCR-SSP meth-od. The subsequent RhD-genotyping allowed the characterization of the present RHD variants in all examined test samples. After the SSP screen-ing the identical three samples were positive on RHD gene. Furthermore we could verify that sample 1 was clearly RHD positive, while in the other two test samples, a weak D type 1 and a RhD psi gene was detected. In case of exon 5 the primer/probe was designed to determine the RHD psi gene. The lack of exon 5 in the mentioned sample indicates the presence of the RHD psi gene. Conclusion: The results of this study show that the qPCR assay is a very sensitive and accurate tool to determine the presence of RHD gene en-coding sequences in case of unclear rhesus D serological findings. It rep-resents a suitable method for preselecting samples for further automated or semiautomated genotyping (e.g. MR.SPOT® SSO, SSP).
P-06-26Lack of the Cellano blood group antigen due to a non-sense mutation in the Kel gene
Strobel J.1, Rink G.2, Wieckhusen C.2, Kuta P.1, Eckstein R.1, Bugert P.2
1Friedrich-Alexander-Universität Erlangen-Nürnberg, Transfusionsmedizinische und Hämostaseologische Abteilung, Erlangen, Germany, 2Universität Heidelberg, Medizinische Fakultät Mannheim, Institut für Transfusionsmedizin und Immunologie, Mannheim, Germany
Introduction: The lack of expression of blood group antigens is most of-ten caused by null alleles of the corresponding blood group gene. For the Kell blood group system (KEL; 006) more than 20 different non-sense mu-tations and 8 frame-shift mutations leading to a lack of antigen expression (K0) are listed in the dbRBC database. Here, we describe a female patient with a Kell-positive and Cellano-negative (K+k-) phenotype but KEL1/KEL2 heterozygous genotype.Methods: Exon-resequencing of the KEL gene was performed by a next-generation-sequencing method. For the DNA sequence variations in exon 13 (1474C>T) and intron 7 (IVS7–10C>T/-11A>C) we developed PCR-SSP methods for rapid genotyping. Inheritance of the KEL alleles was investigated in the patient’s family using serological and molecular methods. Results: DNA sequencing revealed heterozygosity for the 1474C>T mu-tation in exon 13 of the KEL gene leading to a truncated KEL protein (Arg492stop). At the 3’-end of intron 7 we found heterozygosity at two ad-jacent positions (IVS7–10T>C and -11A>C) both listed in the SNP data-base. The 1474C>T mutation has been described very recently in a Dutch study in a subject with a K0 phenotype and compound heterozygosity for two null alleles. In our patient’s family we could identify inheritance of a normal KEL*01.01 allele encoding the K antigen and a KEL*02N null allele with altered nucleotides 1474T and IVS7–10C/-11C. Molecular screening for the 1474T allele in 11,800 blood donors with regular Kell phenotypes was negative.Conclusions: The rare 1474C>T mutation in the KEL gene encodes a truncated protein that is presumably not present in the cell membrane (lack of k antigen). The identification of null alleles of the Kell and other blood group systems in patients and blood donors helps clarifying geno-type-phenotype discrepancies, might prevent possible alloimmunization and significantly contributes to providing compatible blood supply.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 45
P-06-27Molecular screening for Vel-negative blood donors in Southwestern Germany
Wieckhusen C.1, Rink G.1, Rothenberger S.2, Kömürcü N.2, Scharberg E.A.2, Bugert P.1
1Institut für Transfusionsmedizin und Immunologie, Mannheim, Germany, 2Institut für Transfusionsmedizin und Immunhämatologie, DRK-Blutspendedienst Baden-Württemberg-Hessen, Baden-Baden, Germany
Background: The SMIM1 protein carries the Vel blood group antigen and homozygosity for a 17 bp deletion in the coding region of the SMIM1 gene represents the molecular basis of the Vel-negative blood group phenotype. We developed PCR-based methods for typing the SMIM1 17 bp (64–80 del) gene deletion and performed a molecular screening for the Velnega-tive blood type in German blood donors.Methods: For SMIM1 genotyping TaqMan-PCR and PCR-SSP methods were developed and validated using reference samples. Both methods were used for screening of donors with blood group O from southwestern Germany. Heterozygotes and homozygotes for the SMIM1 64–80 del al-lele were serologically typed for the Vel blood group antigen. In addition, the rs1175550 SNP in SMIM1 was typed and correlated to the results of the phenotyping. Results: Both genotyping methods, TaqMan-PCR and PCR-SSP, represent reliable methods for the detection of the SMIM1 64–80 del allele. Screen-ing of 10,598 blood group O donors revealed 5 individuals homozygous for the deletional allele. They were confirmed Vel-negative by serological typing. Heterozygotes for the 64–80del allele showed different antigen ex-pressions ranging from very weak to regular positive. Conclusions: Molecular screening of blood donors for the Vel-negative blood type is feasible and avoids the limitations of serological typing which might show false negative results with heterozygous individuals. The identification of Vel-negative blood donors significantly contributes to the adequate blood supply of patients with anti-Vel.
P-06-28A novel autoimmune hemolytic anemia with negative DAT but detectable Gerbich autoantibodies in patient’s plasma
Mayer B.1, Walkenhorst R.2, Just B.3, Yürek S.1, Bartolmäs T.1, Salama A.1
1Charité - Universitätsmedizin Berlin, Institut für Transfusionsmedizin, Berlin, Germany, 2Klinikum Westfalen GmbH, Klinik am Park, Lünen, Germany, 3DRK-Blutspendedienst West, Institut Hagen, Hagen, Germany
Background: Serological characteristics of warm autoimmune hemo-lytic anemia (AIHA) usually comprise a positive direct antiglobulin test (DAT), detectable autoantibodies (aab) in the eluate, and sometimes in the serum of the affected patients. Some of the aab show blood group specificity, mainly against antigens of the Rh blood group system. Au-toantibodies resembling Gerbich specificity have only been described in isolated cases. Here, we report on a patient with AIHA and negative DAT caused by auto-anti-Gerbich. Case report: A 69 year old female was admitted to hospital with suspect-ed pulmonary infection, which could not be confirmed. Since laboratory investigation revealed a decompensated hemolysis (Hb 7,3 g/dl, bilirubin 3,65 mg/dl, LDH 446 U/l, low haptoglobin), AIHA was suspected. Howev-er serological investigation showed a negative DAT and a broadly reactive antibody in patient’s serum. Initially, an antibody against a high frequency antigen was suspected, but there was no evidence for a hemolytic trans-fusion reaction. Methods: Serological tests including acid elution and antibody titers were performed using standard gelcard and tube techniques, respectively. Results: Despite negative DAT, the eluate performed from the patient’s red blood cells (RBCs) was strongly positive. Serum and eluate agglutinated untreated (reactivity 3+ to 4+), but not papain treated RBCs. In addition, no or only weak (+/–) reactions were observed with Gerbich-negative cells. Subsequently, the patient was typed as Gerbich positive. Treatment
with steroids (100 mg Prednisolon daily) was commenced and hemolysis ceased gradually. Conclusions: The fact that the auto-anti-Ge did not react with the pa-tient’s RBCs is most likely related to a temporary suppression of Gerbich antigens during the acute attack of hemolysis. Coombs-negative AIHA should be considered in all patients with unclear hemolysis. In such cases the causative aab are usually detectable in eluate and in isolated cases also in serum.
P-06-29An automated SSO based genotyping method for HPA alleles on MR.SPOT®System
Kissel K., Rahn H., Kirchgessner K., Albrizio M., Heiliger M., Mueller S., Schaffert T., Walter L., Marell R.-R.BAG Health Care GmbH, Lich, Germany
Introduction: HPA-matched platelets are needed in situations as alloim-mune thrombocytopenic syndrome, post-transfusion thrombocytopenic purpura, multiple transfusions and neonatal alloimmune thrombocyto-penia. Therefore, screening for platelet apheresis donors to provide com-patible platelets and the identification of an HPA-incompatibility between the parents platelets are of highest interest. Genotyping is the standard method for platelet typing which provides a useful tool for diagnosis and therapy of these patients, but automated systems are needed. Aim of the current study was the evaluation of a new sequence-specific oligonucle-otide (SSO-) -assay to determine clinical relevant HPA alleles, especial-ly HPA-1 and HPA-5, in a safe and fast workflow using the automated MR.SPOT® system. Methods: DNA isolation was performed on buffy coat and whole blood samples using column based DNA extraction methods. Molecular typing of HPA molecules as reference was performed using a CE-marked SSP-PCR method (BAGene kit, BAG Health Care). To assess the sensitivity of the system, different DNA concentrations were tested. To evaluate the re-producibility, SSO genotyping was performed by different users and with different thermal cyclers. Results: The SSO molecular investigation performed using MR.SPOT® system revealed 100% concordance with SSP results, verifying the spec-ificity of the test. Testing of sensitivity and reproducibility gave the ex-pected and correct results. An automated and standardized workflow fa-cilitated the test procedure allowing high throughput in a short time with low efforts. That means 96 samples can be processed in 4h 30 from DNA extraction to results. User-friendly software was developed to support the results analysis and assist in the generation of a clear results report. Conclusion: This work presents a new genotyping method for typing of clinical relevant HPA alleles using the MR.SPOT® system. Results for SSO based HPA typing showed full concordance with the SSP reference method. All tested parameters determined the expected results indicating that the system is robust and precise. The test was easy to han-dle because of the standardized workflow provided by the MR.SPOT® technology. Taking all findings into account, the new SSO genotyping method on MR.SPOT® system provides a precise, fast and automated tool for high throughput typing of HPA alleles.
P-06-30Screening for Vel and Jr(a) negative donors in Switzerland
Henny C.1, Fasler M.2, Graber J.1, Hustinx H.1, Lejon Crottet S.1, Infanti L.3, Rüfli T.3, Niederhauser C.1
1Interregionale Blutspende SRK, Bern, Switzerland, 2Medi, Zentrum für medizinische Bildung, Biomedizinische Analytik, Bern, Switzerland, 3Blutspendezentrum SRK beider Basel, Basel, Switzerland
Introduction: Although the Vel antigen was already discovered in 1952 the molecular background remained unknown until 2013 [Ballif et al. 2013, Storry et al. 2013, Cvejic et al. 2013]. Vel-negativity is caused

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts46
by a homozygous 17 nucleotide deletion in exon 3 of SMIM1, allele SMIM1*64_80del. Another blood group system for which the molecular background was discovered recently is the JR blood group system (Ze-linski et al. 2012, Saison et al. 2012). The Jr(a) antigen is a high prevalence antigen with a frequency of more than 99.9% in most populations [Reid et al. 2012]. Several alleles have been reported to silence the expression of the Jr protein. The most prominent ones are JR*01N.01 (376C>T) and JR*01N.02 (706C>T). We developed a donor screening test for alleles SMIM1*64_80del, JR*01N.01 and JR*01N.02 using multiplex SSP-PCR and pools of up to 94 donations. Methods: Donor screening was performed in pools using in-house prim-ers in a multiplex-SSP-PCR. Pools positive for the VEL and/or JR negative alleles were resolved down to the individual donation. Samples positive for the VEL or JR negative alleles were tested for zygosity using published [Reil et al. 2013] and in-house primers.Results: A total of 564 donations in 24 pools with up to 24 donations per pool were tested for the allele SMIM1*64_80del. Twelve pools were posi-tive. These were resolved to the individual donation. Fourteen donations were found to harbour allele SMIM1*64_80del. Zygosity testing revealed a heterozygous state for all fourteen donations. In 30 pools of 94 donations 2820 donors were screened for the alleles JR*01N.01 and JR*01N.02. No donor with variant JR*01N.01 was found, but three pools were positive for allele JR*01N.02. The pools were resolved and zygosity testing revealed a heterozygous state for all three donations. Conclusion: Screening of donors for alleles responsible for the Vel and Jr(a) negative phenotype using a multiplex-SSP-PCR is feasible. Screen-ing for the VEL negative allele using pools of 24 donations led to a posi-tive result in 50% of the pools. No homozygous VEL negative donor was revealed, but 14 heterozygous donors were found. For further screening using pools with fewer donations should be considered. Screening of JR negative alleles in pools of 94 donations is suitable as the allele frequency showed to be very low.
P-06-31A case of red blood cell multi-alloimmunisation, also against compound antigen in a patient with MDS
Trestyanszki I.1, Doescher A.2, Dierks N.1, Dahse K.1, Petershofen E.K.2
1DRK-Blutspendedienst NSTOB, Institut Bremen-Oldenburg, Bremen, Germany, 2DRK-Blutspendedienst NSTOB, Institut Bremen-Oldenburg, Oldenburg, Germany
Background: Patients with Myelodysplastic Syndrome (MDS) exhibited an enhanced risk of transfusion-induced red cell allo-immunisation. This depends on multiple factors but foremost on the presentation of foreign antigens to the immune system, e.g. by heterologous transfusion of red blood cells (RBC).Antibodies against compound antigens occur rather infrequently. Here, we present a case of anti-ce (also known as anti-f) as-sociated with other irregular antibodies.Case report: A 62-year-old male patient (blood group 0, Rh CcD.Ee, K-) with MDS was substituted with 2 RBC units, compatible for Rh and K. At this time, the antibody screening was negative. 18 month later, positive results for anti-Fy(a) and anti-S antibodies were obtained using indirect antiglobulin techniques.Autocontrol and direct antiglobulin test (DAT) were negative. Transfusion was then performed using RBC units compati-ble for Rh, K, S and Fy. Another 3 month later, additional antibodies were identified: anti-Jk(a), anti-Cw and anti-Kp(a). To avoid the induction of additional antibodies, genotyping of FY, JK, MNS, LU and DO was per-formed. The interpreted phenotypes were Fy(a-b+), Jk(a-b+), S-, s+, M+, N+, Lu(a+b+), Lu8+, Lu14-, Do(a-b+).The following transfusions were done with RBC units compatible for K, Fy, Jk, S, Kp(a), Cw and Rh ccd-dee. Two weeks later the tests for irregular antibodies showed additional positive reactions with no apparent specificity. But on the next hospital stay an anti-ce (anti-f) antibody was clearly identified.Over the last 2 years we found 6 new anti-f (mostly with other antibodies) in our reference lab-oratory. Three individuals with CcD.Ee, two with CCD.ee and one with ccD.EE.
Conclusion: (A) In this case a patient with MDS, presenting as a high responder to transfusion-induced red cell alloimmunisation shows a necessity for prophylactic matched RBC units. Compatibility should be given for the blood group systems Rh, K, Fy, Jk and MNS. (B) Patients with a Rhesus constellation CcD.Ee and having several positive reactions may also develop an anti-f. These patients should be transfused with units of blood lacking either the c or e antigens.We assume, that anti-f often remains undetected due to existing additional anti-c or anti-e antibodies.
P-06-32SSO based genotyping for common and rare blood group alleles on the MR.SPOT® System
Kissel K., Albrizio M., Heiliger M., Kirchgessner K., Mueller S., Schaffert T., Walter L., Marell R.BAG Health Care GmbH, Lich, Germany
Introduction: Molecular methods are well established in the blood group diagnostic field. The need of a deep analysis of the blood group specific-ities is based on the knowledge that incompatible transfusions can cause severe hemolytic transfusion reactions. To guarantee a safe and fast blood group typing a new SSO genotyping method on MR.SPOT® System was established to detect clinical relevant common and rare blood group al-leles. Methods: For the Kell, Kidd, Duffy and MNSs systems, serological meth-ods were used as reference. Molecular typing was performed using a CE-marked SSP-PCR system (BAGene, BAG Health Care) or sequence based typing. DNA was isolated from buffy coat and whole blood samples, using column based or beads based DNA extraction methods. To assess sensi-tivity and the accuracy of the system, different DNA concentrations were analysed. To evaluate reproducibility, SSO genotyping was performed by different operators and use of different thermal cyclers. Results: The SSO technique revealed 100% concordance with SSP results. Conversely, a few discrepancies were seen compared to serological typing. In particular, six of the tested alleles were different determined by serol-ogy (Kell, Kidd, MNS) and in one case (Kell) it was impossible to predict the phenotype of the sample. However, further investigation is required to prove the serological findings. Test performance was not affected by different DNA concentrations, different types of DNA extraction meth-ods, different operators and different thermal cyclers showing demanded stability, reproducibility and sensitivity. 1 to 96 samples can be processed in 4h 30 from DNA extraction to results facilitated by automated and stan-dardized workflow, allowing high throughput in a short time with low efforts. Result analysis was supported by user-friendly software and assist in the establishment of a clear results report. Conclusion: All tested parameters gave the expected results indicating that the system is sensitive, robust and precise. The automatized and stan-dardized workflow ensured an easy and comfortable handling. Taking all findings into account the new SSO genotyping method on MR.SPOT® system provides a precise, fast and automated tool for high throughput typing of common and rare blood groups alleles.
P-06-33Studies on performance of a modified MAIPA
Stüpmann A.S., Kiefel V.Institut für Transfusionsmedizin der Universitätsmedizin, Rostock, Germany
Background: The MAIPA (monoclonal antibody immobilization of plate-let antigens assay) developed in 1987 is a widely accepted technique for detection of platelet antibodies. It has proved to be a reliable method of-fering high sensitivity and specificity. However, the assay is time-consum-ing and requires a certain amount of technical expertise. To date several variations of this assay have been published in an attempt to simplify the technique without losing its reliability. One of these studies was published by Hou et al. (Eur J Haematol. 2003; 70:353–357). These authors modified

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 47
the initial platelet incubation and washing steps. The aim of this study was to compare the MAIPA-protocol-modified by Hou et al. with the orginal assay (Kiefel V; Transfus Med 1992; 2:181–188).Materials and Methods: A series of 34 patient sera containing previously defined platelet-reactive antibodies was tested in both assays (anti-HPA-1a (n = 10), anti-HPA-1b (n = 5), anti-HPA-5a (n = 1), anti-HPA-5b (n = 5), anti-HPA-15b (n = 1), HLA-I antibodies (n = 5) and autoantibodies (n = 8)). HLA antibodies were allowed to react with pooled platelets and with individual cell suspensions.Results: Using the modified assay, optical densities were equal or greater with alloantibodies against glycoproteins (GPs) IIb/IIIa, Ia/IIa, HLA-I and autoantibodies against GP IIb/IIIa. ELISA signals in the modified assay were lower with tests of allo- and autoantibodies against GP Ib/IX, where-as an alloantibody against CD109 yielded a negative result.Conclusion: The modified MAIPA assay appears to be an acceptable al-ternative method for detecting platelet antibodies. It seems reliable with alloantibodies against GP IIb/IIIa, IaIIa, HLA-I. The causes for the differ-ences observed with antibodies against GP Ib/IX and CD109 remain to be further analyzed.
P-06-34Harmless diclofenac-induced IgG-autoantibodies to red blood cells
Mayer B., Herziger A., Salama A.Charité – Universitätsmedizin Berlin, Institut für Transfusionsmedizin, Berlin, Germany
Background: Until now, diclofenac has been reported to cause immune hemolytic anemia due to the production of drug-dependent antibodies (ddab) with and without “bystander” autoantibodies (aab) to red blood cells (RBCs). The production of clinically insignificant autoantibodies alone has not yet been described.Case report: A 75 year old woman was readmitted to hospital for total knee replacement. Serological examination revealed strongly detectable IgG autoantibodies to RBCs in serum and eluate. Due to these findings and the positive cross-match, the operation was cancelled.Later on, labo-ratory investigation showed normal hemoglobin and no signs of hemoly-sis (bilirubin, LDH and haptoglobin within normal limits). Re-question-ing of the patient revealed that she had been frequently taking diclofenac within the last few weeks. Though drug-dependent antibodies against di-clofenac or its ex-vivo metabolites were excluded, drug-induced aab were suggested. Diclofenac was stopped and the operation was performed as planned. Due to postoperative anemia (Hb 6,0 g/dl), the patient received 2 units of RBCs without any adverse effects.During observation, the reac-tivity of the aab gradually ceased without any treatment. Six months later, the aab were completely abolished.Conclusion: Diclofenac may rarely also lead to the production of autoan-tibodies against RBCs alone.
Transfusion transmitted infections and pathogen inactivation
P-07-1Ebolavirus – a challenge for transfusion medicine
Strobel E.1,2, Betten S.1,2
1Städtisches Klinikum München GmbH, Department Medizinische Mikrobiologie, München, Germany, 2Städtisches Klinikum München GmbH, Department Klinische Chemie, München, Germany
Introduction: Hemorrhagic fever caused by Ebola virus (EboV) is life-threatening and highly contagious. Beginning in early 2014, the cur-rent outbreak in West Africa has caused 26 628 cases and 11 020 deaths
(WHO, 03.05.2015). The virus is transmitted human-to-human by direct contact with blood and other body fluids of infected persons. In Germany 8 hospitals provide isolation units for such patients, including the Klini-kum Schwabing, Munich.Methods: Already existing concepts for blood supply in patients with dangerous infections had to be actualized and adapted to the special situ-ation of EboV infection. Results: Two situations had to be distinguished for planning: First, the handling of suspicious blood samples, that arrive at our routine labo-ratory, from patients in the emergency room with fever and a relevant travel history to West Africa. Here, the samle container is kept safe and not opened until the suspicion of EboV infection is rejected. Second, the examination of blood samples from EboV infected patients in the isola-tion unit for providing the blood products they need because of anemia, thrombocytopenia and/or coagulation disorders. Generally, the safety of the staff and prevention of spreading the virus to the public is most important. Therefore all laboratory tests including blood group serology and coagulation studies are done in the isolation unit by staff members wearing the special protection clothing. A first blood grouping of the pa-tient is done by the clinician in the unit using a lateral-flow chart. In an urgent case, blood products are now applied according to the principles of emergency transfusion. For the further blood supply of the patient, a member of the hospital transfusion service enters the unit and performs blood grouping, antibody screening and cross-matching with the routine method using gelcards. By transfusing only red blood cell concentrates of blood group O the ABO bedside test is omitted to avoid formation of aerosols. All materials and equipement remain in the unit until they are disinfected after discharge of the patient.Conclusion: EboV infection is a great challenge for the hospital trans-fusion service, as blood products are needed for supportive treatment of patients with viral hemorrhagic fever. Moreover, it is a challenge for transfusion medicine in general as viral safety of blood products must be guaranteed by excluding donors at risk and, if available, by pathogen inac-tivation of the blood products.
P-07-2THERAFLEX MB-Plasma treatment does not interfere with the antibody integrity in human plasma
Handke W.1, Gravemann U.1, Sumian C.2, Reichenberg S.3, Seltsam A.1
1DRK Blutspendedienst NSTOB, Springe, Germany, 2MacoPharma SA, Tourcoing, France, 3MacoPharma International, Langen, Germany
Introduction: Convalescent plasma therapy is used to treat emerging infections which cannot yet be cured by drugs or prevented by vaccina-tion. Using plasma from patients who survived such incurable infection it is of special interest to ensure that the donated plasma is pathogen-free. THERAFLEX MB-Plasma treatment is used to inactivate pathogens in human plasma. For plasma intended to be used as convalescent plasma for treatment of acute infections, it is essential that the functionality of antibodies is preserved after the MB treatment procedure. It is known that MB/light treatment can influence the integrity of labile plasma proteins (e.g. plasma factor VIII and fibrinogen) but does not grossly reduce the function and life span of proteins in fresh frozen plasma. Aim: The aim of the study was to investigate whether antibody binding in human plasma is affected by the THERAFLEX MB-Plasma treatment. For this purpose exemplarily the reactivity of anti-HCMV and anti-HAV antibodies was tested prior to and after MB/light treatment.Methods: Plasma units were preselected for the presence of anti-HCMV antibodies (n = 6) and anti-HAV antibodies (n = 3). Pathogen inactivation was done using the THERAFLEX MB-Plasma system and the MacoTron-ic B2 illumination device and samples were taken before and after illumi-nation. In order to detect changes in antibody binding different dilutions of plasma samples were tested for reactivity of anti-HCMV and anti-HAV antibodies by ELISA. Results: Reactivity of anti-HCMV and anti-HAV antibodies in human plasma was not reduced after MB/light treatment.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts48
Conclusion: THERAFLEX MB-Plasma treatment does not negatively af-fect the binding of anti-HCMV and anti-HAV antibodies in human plas-ma. Pathogen inactivation by MB/light treatment therefore could contrib-ute to the safety of convalescent plasma without deteriorating its quality.
P-07-3Microbial contamination of allogeneic Cord Blood Units (CBU): Species and factors
Sauer A., Aurich A.-C., Nessel K., Platz A., Schmidt A.H.DKMS Nabelschnurblutbank, Dresden, Germany
Background: Microbiological control of blood and stem cell products is required by law in order to avoid transmissible infections. Testing con-ditions are described in the European Pharmacopoeia. Published con-tamination rates vary from 0 to 48%. Several factors appearing during collection, transport and processing might have impact on incidence and specificity.Methods: 3383 cord blood units collected in utero following delivery either vaginal or after cesarean section were processed and tested for microbial contamination between 2012 and 2014. Positive results were confirmed and specificities determined by subcultivation. Aerobic and anaerobic germs were assigned to the blood fractions. Red blood (RB) represented the initial product and transplant (TR) the final product. These groups were correlated with factors like mode of delivery and age of the unit at time of processing.Results: 188/3383 (5,6%) processed CBU were tested positive for microbi-al contamination of which 89% had been collected after vaginal delivery. The overall proportion of vaginal deliveries was 66% compared to 34% of cesarean sections. 38% cases showed contaminated TR only and 36% a combination of TR and RB. Elapsed time over 24h between collection and processing was found in 77,1% of contaminated CBU. 444 germs were de-tected and confirmed. The biggest proportions were Staphylococcus epi-dermidis (13%), Enterococcus faecalis (9%) and not specified Cocci (8%).Conclusion: The overall contamination rate of DKMS CBB products is low compared to previously published data. Positive results in RB were classified as primary contaminations with a higher incidence after vaginal delivery compared to cesarean section. Different ambient conditions and staff behavior might be the background of these findings. Positive results in TR and/or RB were considered as either primary or secondary contam-ination but were not differentiated. Specificities of bacteria did not allow conclusions about the mode of infection. Increased training efforts of col-lecting staff might lead to decreased contamination rates. Further studies will focus on discrimination of primary and secondary contaminations.
P-07-4Frequency of adverse events in transfusion of pathogen inactivated platelet concentrates
Gross J.C., Lauer H., Stephan B., Eichler H.Universitätsklinikum des Saarlandes, Institut für Klinische Hämostaseologie und Transfusionsmedizin, Homburg, Germany
Introduction: In platelet transfusion, bacterial contamination remains a serious risk which can be reduced by integration of pathogen inactivation (PI) in the manufacturing process of platelet concentrates (PC). Never-theless, only little is known about adverse events (AE) in transfusion of PI-PCs. Methods: For platelet apheresis, the COM.TEC as well as the TRIMA cell separator was used by routine in our blood donation center. PI was introduced for the PCs manufactured with the TRIMA device and was performed by the intercept method (CERUS) with addition of amoto-salen followed by UVA illumination. AEs were registered by the return of transfusion reports, which had to be given by routine on each platelet transfusion.
Results: A total of 9.498 PCs was transfused in a 29,5 month period, of which 1.017 (10,7%) were PI-PCs and 8.481 (89,3%) non PI-PCs. PI-PCs were predominantly transfused to hemato-oncological patients (75,3% vs. 44,8% in non PI-PCs), and no AEs occured during their manufacturing process. AEs were reported in 0,49% of transfused PI-PCs and in 0,43% of non – PI-PCs, respectively. Of the five AEs occuring in the PI group, four were reported as not-serious and associated with fever, shivering fit, urticaria and dizziness, while one potential serious AE was described as allergic reaction in this group. All five AEs occuring in the PI group were related to hemato-oncological patients (75% in the non - PI-PC group), who suffered from acute myeloic leucemia (2), B-cell-lymphoma, T-cell-lymphoma or testicle teratoma. Conclusion: There was a tendency to more common AEs associated with the transfusion of PI-PCs in the two different patient groups, nevertheless their frequency seems to be overall low.
P-07-5Dual-temperature microbiological control of cellular products: a potential impact for bacterial screening of platelet concentrates
Vollmer T., Knabbe C., Dreier J.Herz- und Diabeteszentrum NRW, Institut fuer Laboratoriums- und Transfusionsmedizin, Bad Oeynhausen, Germany
Background: An experimental study by the Paul-Ehrlich institute (PEI) demonstrated that temperatures between 35–37°C, are too high for the growth of some bacterial strains (e.g. Pseudomonas fluorescens). There-fore, the PEI passed a statement including the requirement of a dual-tem-perature microbiological control of haematopeotic stem cell preparations which was further assumed in a draft manuscript regarding the amend-ment of chapter 2.6.27 of the European pharmacopoeia in 2013. We ana-lyzed the growth kinetics of several bacteria in platelet concentrates (PCs) under standard storage conditions and compared the results of the micro-biological control at incubation temperatures of 25 °C and 35 °C.Methods: In total, PCs were inoculated with 37 strains (3–6 donors per strain) from different origins (PC isolates, reference strains) and stored for 3 days at 20–22°C under constant agitation. Subsequently, inoculated PCs were split to inoculate aerobic and anaerobic culture bottles (BacT/Alert AST/NST), each with 5 mL of sample and culture bottles were incubat-ed at 25 °C and 35 °C using the automated BacT/Alert Dual temperature system.Results: All tested strains of Staphylococcus spp. (n = 10), Streptococcus spp. (n = 4), Bacillus spp. (n = 4) and Pseudomonas aeruginosa (n = 5) showed bacterial proliferation within three days in most inoculated PCs, revealing a faster growth kinetic at an incubation temperature of 35 °C. Tested P. putida (n = 3) strains showed a noticeable reduced capability to grow in PCs. Nonetheless, those having a growth capability revealed faster growth kinetics at an incubation temperature of 35 °C. Exclusively one of four tested P. fluorescens strains (strain ATCC 13525) was able to grow in PCs showing a faster growth kinetic at an incubation temperature of 25 °C but also detection at 35 °C.Conclusion: The commonly detected bacteria involved in bacterial con-tamination of PCs showed no reduced detectability at 35°C incubation for microbiological control. Only one P. fluorescens strain showed an en-hanced growth at 25°C, but the microbiological control at 35°C did not fail to identify this contamination. In conclusion, screening of PCs using a dual-temperature setting for the microbiological control impresses at the moment as “using a sledgehammer to crack a nut”.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 49
P-07-6Evaluation of different strategies and test systems for anti-core specificity-testing (according V42 German National Advisory Committee Blood)
Hourfar K.1, Dengler T.2, Seifried E.1, Schmidt M.1
1DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Frankfurt am Main, Germany, 2DRK-Blutspendedienst Baden-Württemberg-Hessen gGmbH, Institut Baden-Baden, Baden-Baden, Germany
Introduction: The prevalence of Anti-HBc reactive blood donors among first time donors of our blood donor service is approximately 1,7%. Ad-ditionally approximately 0,19% of our multiple time donors show repeat reactive results for anti-core. However it is known that anti-HBc tests tend to unspecific reaction. Background: With the new resolution (V42) of the German National Advisory Committee ‘Blood’ recommendations for anti-HBc testing have changed, especially regarding first-time donors and multiple-time donors seroconverting to core-reactive. V42 allows to determine ‘non-specificity’ of the anti-HBc screening result. The repeatedly reactive screening result can be proven as being unspecific if testing in two additional anti-HBc tests (or a neutralisation test) and ID NAT for HBV-DNA give negative results. The decision which tests would be most suited to be used as sec-ond and third serologic test-system was difficult, because there was the assumption, that tests from the same manufacturers may show unspecific reactivity on same samples. Methods: In our blood donor service screening for anti-core is done using the Abbott PRISM system using the PRISM HBcore assay. Samples repeat reactive with this test were retested on four additional serologic tests from Abbott (ARCHITECT Anti-HBc II, AxSYM Core) and Siemens (ADVIA Centaur HBc Total, Enzygnost Anti-HBc monoclonal). Although the ADVIA test is now distributed by Siemens iHealthcare it was originally developed by Bayer diagnostics. Therefore the test can be considered as a non-Siemens test.Results: During the study period 130 repeat-reactive samples have been observed. These samples have been retested with the four additional an-ti-HBc tests. Results have shown, that the use of Enzygnost and ADVIA tests after initial screening with Abbott PRISM was much more effective in reducing the donor-loss. With the two Siemens tests as second and third test system 22 out of 130 initially reactive samples could be confirmed as being non-specific according to V42. In contrast using the two Ab-bott-tests only 4 donors could be allowed to reenter the donor population. Discussion: The assumption that tests from same manufacturers show unspecific reactivity on same samples could be confirmed. However es-tablishing test systems from manufacturers different than the supplier of the screening test may be uneconomic. On the other hand sending the samples to external laboratories is associated with logistical effort.
P-07-7Primary human macrophages cytokine responses to high glucose
Moganti K.1, Li F.1, Riemann S.1, Klüter H.1,2, Harmsen M.3, Gratchev A.1, Kzhyshkowska J.1,2
1Medical Faculty Mannheim, Heidelberg University, Institute of Transfusion Medicine and Immunology, Mannheim, Germany, 2German Red Cross Blood Service Baden-Württemberg-Hessen, Institute of Transfusion Medicine and Immunology, Mannheim, Germany, 3University Medical Center Groningen, University of Groningen, Cardiovascular Regenerative Medicine, Dept. Pathology and Medical Biology, Groningen, Netherlands
Hyperglycaemia is a factor for the induction and progression of micro- and microvascular diabetic complications. Macrophages are key innate immune regulators of inflammation, can be classified in to two major types: classically (M1) and alternatively (M2) activated macrophages. Both populations play a role in diabetes. M1 are involved in the estab-lishment and progression of insulin resistance in diabetes and diabe-tes-associated inflammation, whereas M2 contribute to the decrease hy-
perglycaemia. However, the effect of hyperglycaemia on differentiation and functional programming of macrophages is poorly understood. We established unique model system based on primary human monocyte-de-rived macrophages to examine the effects of hyperglycaemia on M0, M1 and M2 differentiation. Human peripheral blood monocytes were isolated from buffy coats by magnetic cell sorting using CD14 beads. Monocytes were cultivated in the presence of 5mM and 25mM glucose for 6 days under stimulation with IFNgamma, IL4 and Non stimulation (without cytokine) in serum free medium. In order to identify the effect high glu-cose on the development of M0, M1 and M2 phenotypes, cytokines were selected as key regulatory biomarkers. Using RT-PCR and ELISA the ex-pression and release of TNF-alpha and IL-1beta (M1 cytokines) and IL1ra and CCL18 (M2 cytokines) were quantified. RT-PCR analysis revealed that high glucose induced mRNA of TNF-alpha, IL-1beta, and IL1Ra only in part of donors. However, in all analysed donors the increased secre-tion of all three cytokine release was demonstrated by ELISA. RT-PCR showed that high glucose supressed the M2 marker CCL18 mRNA levels, and this corresponded to the ELISA-measured suppression of CCL18 re-lease. Our data indicated that increase glucose levels stimulates expression of TNF-alpha, IL-1beta and IL1Ra and suppresses release of CCL18 in a donor-specific way. High glucose stimulates production of TNF-alpha, IL-1beta and IL1Ra both in gene expression and secretion levels. Our data suggest that individual profile of vascular complications can be influenced by the individual spectrum of inflammatory responses of monocyte-de-rive macrophages to high glucose concentrations. Funding: DFG GRK1874 DIAMICOM
P-07-8Results of Syphilis screening in deceased organ donors in comparison to blood donors
Juhl D.1,2, Glessing P.1,2, Hennig H.1,2, Görg S.1,2, Ziemann M.1,2
1Universitätsklinikum Schleswig-Holstein, Transfusionsmedizin, Lübeck, Germany, 2Universitätsklinikum Schleswig-Holstein, Transfusionsmedizin, Kiel, Germany
Background: Deceased donor organs are scarce. Thus, exclusion criteria are not as strict as for blood donors. It is unknown, whether there are dif-ferences in the prevalence of Syphilis or in the rate of confirmed infections among repeatedly reactive donors between blood and organ donors.Methods: Between October 1st 2012 and April 1st 2015, 192 deceased organ donors were screened for antibodies against Treponema pallidum using chemiluminescent microparticle immunoassay (CMIA, Abbott AR-CHITECT) and compared to blood donor testing. Repeatedly reactive re-sults were confirmed by Western Blot (WB, Fujirebio) for all blood donors and for organ donors if feasible.Results: Out of 32,669 blood donors, 95 (0.29%) were repeatedly reactive in the CMIA, and 6 (0.018%) of those tested positive for anti-Trepenoma pallidum by WB. Of 192 deceased organ donors, 5 (2.6%) tested repeated-ly reactive for anti-Treponema pallidum by CMIA and 2 (1.0%) of those positive by WB. WB-results for two donors are pending, and in one organ donor, there was no material available for WB. According to the high ratio in the CMIA of 15.5 S/CO units, one of these donors presumably had a Syphilis infection. Taken together, Syphilis was confirmed in at least 2 out of 5 organ donors with repeatedly reactive results (40%), but in only 6 out of 95 blood donors (6%). All confirmed positive organ donors had not been eligible for blood donation, but only one had a risk factor for sexually transmitted infections (STI, man having sex with men). Summary: At our institute, the seroprevalence of Syphilis in deceased organ donors was considerably higher (≈ factor 50 - 100) compared to blood donors. Additionally, repeatedly reactive results in the screening as-say were confirmed more frequently by WB in organ donors than in blood donors. This is at least partly due to stricter exclusion criteria for blood donors. As deceased individuals with risk factors for STI are admitted to organ donation, there is also a higher risk for Syphilis. If a deceased organ donor tested repeatedly reactive in the Syphilis screening assay confirma-tory assays should be performed immediately after transplantation.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts50
Clinical haemotherapy and patient blood management
P-08-1Non-invasive determination of hemoglobin content in packed red blood cells
Netz U.J., Cappius H.-J., Gersonde I.Laser- und Medizin-Technologie, Berlin, Germany
Introduction: Implementation of controlled processes and strict compli-ance with various parameters from donation to manufacture of packed red blood cells (RBC) effectively ensures that hemoglobin (Hb) and hema-tocrit values lie within a predetermined range. No method currently exists to non-invasively determine the Hb content in the finished blood product. It is not possible to carry out direct quality control of a unit or quantify the administered dose between completion of the unit and its administration. We present an optical method with which the hemoglobin content of a unit can be exactly determined.Method: The RBC will be irradiated through the bag film in the label-free area of the bag with light from selected wavelengths. As bag films from different manufacturers have very different light penetration properties, a dynamic method will be used in which the measurement will be carried out several times, and the influence of the bag film will subsequently be eliminated by an algorithm. The Hb content will be calculated from the determined Hb concentration and the known weight / volume of the unit. The method is to be initially tested in the laboratory using RBCs from different donors for a range of Hb concentrations from 15 - 30 g / dL in bags from different manufacturers.Results: First results show it is possible with this method to effectively eliminate the influence of the bag film on the optical measurement. A Hb value can be determined with a relative accuracy of better than 5%. The optical method can be modified to determine Hb and lipid content for the quality control of plasma units.Conclusion: A new optical method allows the non-invasive determina-tion of the Hb content in the closed RBC with bags from different man-ufacturers. This will open up new possibilities worldwide in the quality control of RBC and facilitate the dosimetry of hemoglobin administration for transfusion.
P-08-2Influence of preoperative hemoglobin levels on the number of transfused blood products in cardiac surgery
Hagen C., Görg S., Brockmann C.Universitätsklinikum Schleswig-Holstein, Transfusionsmedizin, Lübeck, Germany
Introduction: Elective surgery raises the question which number of red blood cell concentrates (RBC) should be ordered. The German Guidelines for hemotherapy recommend the usage of a list of procedures and their probability of transfusion. Estimating the expected blood transfusion re-quirement various factors should be taken into account, including patient specific factors like the preoperative hemoglobin level (Hb). We would assume that in average a ten g/l lower Hb level should result in 1 more RBC given. Therefore we evaluated retrospectively the preoperative he-moglobin levels and the number of transfused RBC concentrates in aorto-coronary bypass procedures in cardiac surgery.Methods: The analysis is based on data of the hospital information System including the german classification of procedures (“Operationen- und Prozeduren-Schlüssel (OPS)), an adaption of the International Classifi-cation of Procedures in Medicine (ICPM) of the WHO. We matched the procedures, documented transfusions and preoperative hemoglobin lev-els by means of database-queries, considering the association between the number of RBC and the preoperative haemoglobin level in patient-groups
with rounded Hb-levels: Hb 80 g/l, Hb 90 g/l, Hb 100 g/l et cetera. For ex-ample: Group Hb 80 represents patients with an Hb between 75 and 84 g/l.Results: The transfusion probability related to all aortocoronary bypass procedures is 58,63%. 41,37% of all patients with ACVB-procedures re-ceived no RBCs. 8,16% received one, 18,22% received two, 10,15% re-ceived three, 6,64% received four, 3,8% received five, 3,23% received six and 8,35% received seven and more RBCs . The median number of trans-fused RBCs in the patient-group with Hb 80 was 5, with Hb 90 was 3, with Hb 100 was 4, with Hb 110 was 4, with Hb 120 was 2, with Hb 130 was 1and with Hb >140 was null RBC concentrates. The proportion of trans-fused patients decreased with a higher Hb level from 100% with Hb 80 to 0% with Hb >=170. Approximately a 10 g/l higher Hb resulted in a 10% decreased rate of transfused patients and 0,5 RBCs less were transfused.Conclusion: The preoperative Hb level should be considered in the deci-sion about the number of ordered red blood cell concentrates. However, the influence of the hemoglobin level seems to be smaller than expected in the resulting transfusion practice in cardiac surgery.
P-08-3Case reports of irregular Rhesus allo- and autoantibodies after D-mismatched allogeneic hematopoietic stem cell transplantation
Nowak-Harnau S., Enkel S., Starke U., Northoff H.Zentrum für Klinische Transfusionsmedizin, Tübingen, Germany
We retrospectively analyzed patients who underwent D-mismatched al-logeneic stem cell transplantation between 01.01.2010 and 15.04.2015. All recorded patients were D negative recipients receiving a D positive stem cell transplant. Red blood cell transfusions before and after trans-plantation for these patients were D negative red blood cells. If red blood cells were requested the antibody screen was performed every third day. We calculated the follow up time for antibody screening from the date of transplantation to the last available antibody screen after transplantation. 624 stem cell transplantations were performed during this time. From these transplantations 57 D negative patients received a stem cell graft from a D positive donor. 32 of these patients received an ABO identical graft, 26 patients had a major or minor ABO-mismatched donor. Anti-body screens were performed for a period of 1 to 1520 days after trans-plantation in our patient collective.Two patients showed an irregular Anti-E after transplantation in the anti-body differentiation, without any transfusion of E positive red blood cells or donor transplant specific Anti-E. In one patient anti-D was present in the recipient before transplantation, with negative antibody screening in follow up. Another patient with a CML and anti-D and anti-C present in the recipient before transplantation had high titers of anti-D and an-ti-C after first transplantation of a DC positive unrelated stem cell do-nor. A second transplantation from the same allogeneic unrelated donor had been done because of graft failure 3 months after first transplanta-tion. Anti-D and anti-C titers augmented once again. Seven month after transplantation with hematopoietic regeneration but relapse of the CML in peripheral blood anti-D and anti-C titers had the same values as before first transplantation. Another CML patient with D mismatched unrelat-ed stem cell donor transplantation showed a positive antibody screening and was DAT positive. Autoantibodies could be detected with acid elution 6 month after transplantation. Autoantibodies were differentiated as au-to-anti-D and auto-anti-C for a DC positive donor. One year after trans-plantation the autoantibodies persisted with clinical autoimmunhemoly-sis and decreasing levels of haemoglobin. Corticosteroid and Rituximab therapy were unsucssesful so a splenectomy was done May 2015. Further screenings of the autoantibodies after splenectomy could not be done yet.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 51
P-08-4Where did the blood go? Blood use in haematological fields at the University Hospital of Cologne
Behrens L.1, Störmer M.1, Hellmich M.2, Gathof B.S.1
1Universitätsklinikum Köln, Transfusionsmedizin, Köln, Germany, 2Universitätsklinikum Köln, Institut für Medizinische Statistik, Informatik und Epidemiologie, Köln, Germany
Background: Blood products such as red blood cell concentrates (RBC) are precious and restricted due to their short shelf-lifetime and the sus-tained clinical demand. Indices such as the C/T ratio (cross matched RBC/transfused RBC) help to evaluate the quality of the process of RBC order and use and should not exceed 2.5.Aims: Unnecessary order of blood products can result in restricted re-sources for other patients or even increased outdating. To prevent this, a standard ordering catalogue for surgical subjects had been established > 20 years ago and revised regularly. In this study the actual use in compar-ison to the orders was evaluated. The data might disclose trends in certain medical subjects with respect to future demands in blood products. Methods: Standard request forms were collected for Nov. 2013 including RBCs, platelets and fresh frozen plasma as well as age, gender, haemoglo-bin, platelet count and the indication for transfusion. Missing data has been accomplished via electronic health records in ORBIS®. Later da-ta-sets have been processed with Excel® and SPSS®. To indicate changes in certain fields, data was compared to previous studies performed at the same institute and further references. Results: In total, 2398 order forms were evaluated leading to 6874 cross-matched RBCs and 3040 transfused RBCs. 1658 RBCs were ordered for surgical, 1382 for non-surgical indications. Haemato-oncological diagno-sis was the predominant non-surgical use for RBCs (767/1382, 55.50%). Acute leukaemia was the leading indication with 355 doses, 11.68% of the total use [355/3040] following lymphoma (244/3040, 8.03%). The C/T ra-tio for these were within the recommended range (acute leukaemia = 1.7, lymphoma = 2.2). Besides the non-surgical demand of blood products, there is of course a high need in surgical fields as well. These data had been reported elsewhere and have shown higher results regarding the C/T ratio.Conclusion: In general most of the results concerning the C/T ratio were satisfying in haematological subjects. Continuous evaluation and education can improve the logistics of blood use in quality and economical issues.
P-08-5Severe mixed warm and cold autoimmunohemolytic anemia in a patient with EBV-associated aggressive Non Hodgkin lymphoma
Strathmann K., Angert K., Hutschenreuter G.Uniklinik RWTH Aachen, Institut für Transfusionsmedizin, Aachen, Germany
Introduction: We report a case of an 72-year old female patient with a severe autoimmune hemolytic anemia. The patient was admitted because of poor general condition, dyspnea and dizziness. The initial diagnostic showed anemia and progressive lymphadenopathy with high suspicion of a lymphoma. The laboratory tests initially showed a pronounced hemolyt-ic anemia with a hemoglobin decrease to 3.2 g/dl. Methods: Blood groups ABO, RhD, RhCE and K phenotyping, direct coombstest and antibody diagnostic, gel card technique (Bio-Rad GmbH, Munich).Results: In den immunhematologic diagnostic the blood group was typed as 0 Rh negative, ccddee, K neg. The direct coombs test for IgG, IgM and C3d was strong reactive. Warm and cold reactive autoantibodies with pan-reactivicity were detectable. Because of anamnestic pregnancies and red cell transfusions we performed differential absorption with detection of an anti-D and anti-E antibody. The initial therapy was prednisone with 1 mg/kg in combination with compatible warmed red cell concentrates. Among slowly succeeded in the course of a hemodynamic stabilization of the patient, so that diagnostic lymph node resection could be performed.
The positive result of the EBV-PCR suggested the association of the lym-phoma. When initially not clearly clarified entity of aggressive non-Hodgk-in´s lymphoma of B or T cell number assignment a preliminary phases of chemotherapy analogous Burkitt protocol with a prednisolone and cyclo-phosphamide was initiated. Although initially was still no clear association with the B-cell lineage, but was administered rituximab for the treatment of severe hemolysis because of the cold autoantibody. The completion of the first cycle R-CHOP was performed sequentially and the next share with doxorubicin and vincristin acutely well tolerated. Following the initiation of chemotherapy already showed a significant improvement of hemolysis.Conclusion: In this case of serious autoimmune hemolytic anemia with the immunohematological entities of warm and cold reactive autoanti-bodies the treatment with initial corticosteroids, rituximab and the start of chemotherapy to treat the underlying disease in combination with the administration of compatible packed red blood cells was the essential course to manage this life-threatening haemolytic event. The interdisci-plinary cooperation between hematologist and transfusion medicine phy-sician is crucial for the quickest possible rescue of these patients.
New technologies in laboratory diagnostics
P-09-1Six month experience with the cobas® MPX test on the cobas® 8800 System in a routine screening setting
Stolz M., Gowland P., Niederhauser C.Interregional Blood Transfusion SRC, Berne, Switzerland
Introduction: In January 2015 the Procleix® Ultrio assay on the Procleix® Tigris system was replaced by the cobas® MPX test run on a cobas® 8800 system. The new platform is used for routine screening of Swiss blood do-nors for HIV-1, HIV-2, HCV and HBV in an individual donation format (ID-NAT). Methods: For every blood donation a 9 ml EDTA plasma tube is especially taken for the screening with the cobas® MPX test on the cobas® 8800 sys-tem. The samples are tested for blood-borne viruses in an ID-NAT format according to the instructions in the package insert. Confirmation of re-peat reactive samples was performed serologically and with an alternative NAT assay (Abbott Real Time PCR Assay). Results: A total of 56’115 donations were tested in ID NAT format since January 2015. On average 703 samples were tested daily. Seventy nine do-nations (0.14%) were reactive in the initial screen. From these 7 samples (0.012%) were repeat reactive (2 HCV, 5 HBV) and were confirmed sero-logically and with the other NAT assay. One donation remained inconclu-sive. 3’030 samples were initially invalid (5.4%), the majority (2’241 sam-ples, 4.0%) due to invalid runs (50 from a total 1’213 runs). The remaining 789 samples (1.4%) had an invalid single test result (74% impaired ampli-fication plot, 21% detected clot and 5% various other reasons). The invalid runs were void for the following reasons: 22 invalid run controls (44%), 19 hardware failures (38%) and 7 clotting events (14%). Conclusion: The performance of the cobas® MPX test compares favour-ably with the data provided by the manufacturer and was supported by our own extensive validation data. The rate of initial positives, 0.12% with the cobas® MPX test, is very similar to our previous Procleix® Tigris sys-tem (0.11%), both having a test specificity of > 99.88%. The number of in-valid samples is similar to that observed with the Procleix® Tigris system (4.2% Procleix® Tigris vs 5.4% cobas® 8800). The initially observed higher number of invalid results (3.0%) was mainly linked to the larger volume demand required for the cobas® 8800. This could be reduced when mea-sures were introduced to economise sample volume (currently lies be-tween 0.6 - 1.3%). The stability of the cobas® 8800 system (4.1%) rivals the performance of the Procleix® TIGRIS system (3.6%) which is impressive for such a complex instrument shortly after its marked launch and further developments to improve stability have been recently announced.
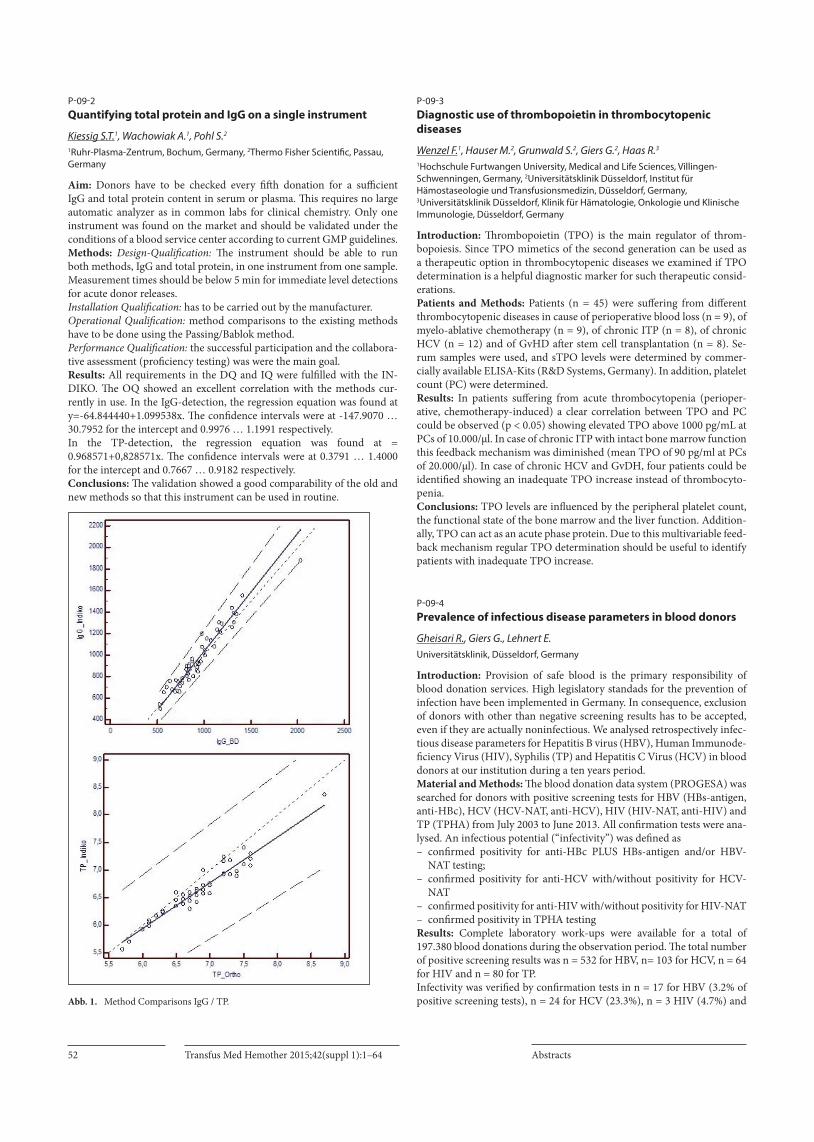
Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts52
P-09-2Quantifying total protein and IgG on a single instrument
Kiessig S.T.1, Wachowiak A.1, Pohl S.2
1Ruhr-Plasma-Zentrum, Bochum, Germany, 2Thermo Fisher Scientific, Passau, Germany
Aim: Donors have to be checked every fifth donation for a sufficient IgG and total protein content in serum or plasma. This requires no large automatic analyzer as in common labs for clinical chemistry. Only one instrument was found on the market and should be validated under the conditions of a blood service center according to current GMP guidelines. Methods: Design-Qualification: The instrument should be able to run both methods, IgG and total protein, in one instrument from one sample. Measurement times should be below 5 min for immediate level detections for acute donor releases. Installation Qualification: has to be carried out by the manufacturer. Operational Qualification: method comparisons to the existing methods have to be done using the Passing/Bablok method. Performance Qualification: the successful participation and the collabora-tive assessment (proficiency testing) was were the main goal. Results: All requirements in the DQ and IQ were fulfilled with the IN-DIKO. The OQ showed an excellent correlation with the methods cur-rently in use. In the IgG-detection, the regression equation was found at y=-64.844440+1.099538x. The confidence intervals were at -147.9070 … 30.7952 for the intercept and 0.9976 … 1.1991 respectively. In the TP-detection, the regression equation was found at = 0.968571+0,828571x. The confidence intervals were at 0.3791 … 1.4000 for the intercept and 0.7667 … 0.9182 respectively. Conclusions: The validation showed a good comparability of the old and new methods so that this instrument can be used in routine.
Abb. 1. Method Comparisons IgG / TP.
P-09-3Diagnostic use of thrombopoietin in thrombocytopenic diseases
Wenzel F.1, Hauser M.2, Grunwald S.2, Giers G.2, Haas R.3
1Hochschule Furtwangen University, Medical and Life Sciences, Villingen-Schwenningen, Germany, 2Universitätsklinik Düsseldorf, Institut für Hämostaseologie und Transfusionsmedizin, Düsseldorf, Germany, 3Universitätsklinik Düsseldorf, Klinik für Hämatologie, Onkologie und Klinische Immunologie, Düsseldorf, Germany
Introduction: Thrombopoietin (TPO) is the main regulator of throm-bopoiesis. Since TPO mimetics of the second generation can be used as a therapeutic option in thrombocytopenic diseases we examined if TPO determination is a helpful diagnostic marker for such therapeutic consid-erations.Patients and Methods: Patients (n = 45) were suffering from different thrombocytopenic diseases in cause of perioperative blood loss (n = 9), of myelo-ablative chemotherapy (n = 9), of chronic ITP (n = 8), of chronic HCV (n = 12) and of GvHD after stem cell transplantation (n = 8). Se-rum samples were used, and sTPO levels were determined by commer-cially available ELISA-Kits (R&D Systems, Germany). In addition, platelet count (PC) were determined.Results: In patients suffering from acute thrombocytopenia (perioper-ative, chemotherapy-induced) a clear correlation between TPO and PC could be observed (p < 0.05) showing elevated TPO above 1000 pg/mL at PCs of 10.000/µl. In case of chronic ITP with intact bone marrow function this feedback mechanism was diminished (mean TPO of 90 pg/ml at PCs of 20.000/µl). In case of chronic HCV and GvDH, four patients could be identified showing an inadequate TPO increase instead of thrombocyto-penia.Conclusions: TPO levels are influenced by the peripheral platelet count, the functional state of the bone marrow and the liver function. Addition-ally, TPO can act as an acute phase protein. Due to this multivariable feed-back mechanism regular TPO determination should be useful to identify patients with inadequate TPO increase.
P-09-4Prevalence of infectious disease parameters in blood donors
Gheisari R., Giers G., Lehnert E.Universitätsklinik, Düsseldorf, Germany
Introduction: Provision of safe blood is the primary responsibility of blood donation services. High legislatory standads for the prevention of infection have been implemented in Germany. In consequence, exclusion of donors with other than negative screening results has to be accepted, even if they are actually noninfectious. We analysed retrospectively infec-tious disease parameters for Hepatitis B virus (HBV), Human Immunode-ficiency Virus (HIV), Syphilis (TP) and Hepatitis C Virus (HCV) in blood donors at our institution during a ten years period. Material and Methods: The blood donation data system (PROGESA) was searched for donors with positive screening tests for HBV (HBs-antigen, anti-HBc), HCV (HCV-NAT, anti-HCV), HIV (HIV-NAT, anti-HIV) and TP (TPHA) from July 2003 to June 2013. All confirmation tests were ana-lysed. An infectious potential (“infectivity”) was defined as– confirmed positivity for anti-HBc PLUS HBs-antigen and/or HBV-
NAT testing; – confirmed positivity for anti-HCV with/without positivity for HCV-
NAT– confirmed positivity for anti-HIV with/without positivity for HIV-NAT– confirmed positivity in TPHA testing Results: Complete laboratory work-ups were available for a total of 197.380 blood donations during the observation period. The total number of positive screening results was n = 532 for HBV, n= 103 for HCV, n = 64 for HIV and n = 80 for TP. Infectivity was verified by confirmation tests in n = 17 for HBV (3.2% of positive screening tests), n = 24 for HCV (23.3%), n = 3 HIV (4.7%) and

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 53
n= 31 for TP in (38.8%), respectively. Anamnestic HBV-infection (con-firmed anti-HBc and anti-HBs, HBs-antigen and HBV-NAT negative) was found in n = 280 donors (52,6%).Exclusions from further donations without confirmed infection occurred in n = 204 HBV cases (38,3% of positive screening tests) , n = 64 HCV-cas-es (62,1%), n= 53 HIV-cases (82,8%) and n = 39 syphilis cases (48,8%), respectively.Conclusions: Overall, for the exclusion of one truly infectious blood do-nor n = 4,8 donors will be excluded from further blood donations. This exclusion rate reflects the nonspecificity of highly sensitive screening tests. We tend to accept this loss of donors in favour of blood product safety.
P-09-5Comparison of two different flow cytometers. Method: Enumeration of residual leucocytes
Rothe R., Arlt N., Moog R.German Red Cross Blood Donor Service North- East, Cottbus, Germany
Background: To prevent severe side effects like febrile transfusion reac-tions through the presence of white blood cells (WBCs) in blood products, leuco-reduced blood products were used for blood transfusion. So quality control analysis for leuco-reduced blood products is a daily procedure in blood donor service departments for quality control investigations. The counting method for evaluating leuco-reduced blood products is still flow cytometry as already recommended by the FDA1. The following summary shows a comparison between Becton Dickinson (BD Heidelberg) FACS Calibur and Beckman Coulter (BC Krefeld) FC500 for the method residu-al white blood cell counting in leuco-reduced blood products. Methods: The BD Leucocount Kit was used at BD FACS Calibur and the BC Leucosure Kit at BC FC500. Every following described investigation was performed in both manufactures. Linearity: At first a double filtered leuco-reduced red blood cell concen-trates were constructed and spiked with a defined concentration buffy coat. 5 defined concentrations stock solutions were measured 3 times in series and linear regression analysis were performed. Precision: Red blood cell- and platelet samples were prepared and mea-sured 5 times in series and the coefficients of variation were calculated compared with manufactures declarations. Accuracy: In count 90 residual white cell enumerations were compared in red blood cell -, platelet- and plasma samples. Results: The BD Leucocount kit provides linearity from 1 to 350 WBCs/µl and the BC Leucosure kit a dynamical range from 0 to 400 WBCs/µl. We tested a sensitive range of 0- 5 WBCs/µl were the manufactures pro-vides a coefficients of variation of 19–43% (BD) or 16–33% (BC) for red blood cell concentrates and received for FACS Calibur 0,9807x - 0,0563 and for FC500 1,0114x + 0,0207. On precision analysis both manufac-tures achieved coefficients of variation in a similar manner under their declarations. During the parallel measurements comparable results were analysed. Conclusions: The counting of residual white blood cells in leuco-reduced blood products can be performed in a comparable way with BD FACS Calibur and BC FC500. Reference: 1 Center for Biologics Evaluation and Research. Recommendations and Licensure
Requirements for Leukocyte-Reduced Blood Products. Rockville, MD: Food and Drug Administration;1996.
Patient blood management
P-10-1Preoperative anaemia management: Which haemoglobin level should be of diagnostic and therapeutic consequence?
Enko D.1, Kriegshäuser G.1, Stolba R.1, von Goedecke A.2, Auersperg V.3, Halwachs-Baumann G.1
1Institute of Laboratory Medicine, General Hospital Steyr, Steyr, Austria, 2Institute of Anaesthesiology and Intensive Care Medicine, General Hospital Steyr, Steyr, Austria, 3Department of Orthopaedic Surgery, General Hospital Steyr, Steyr, Austria
Preoperative anaemia management is one essential part of patient blood management. Low preoperative haemoglobin (Hb) levels are well known as major predicting factors in requiring perioperative blood transfusion in major surgery. Patients with preoperative Hb levels between 10 and 13 g/dL may be more often transfused than those with Hb level >14 g/dL [1].In order to implement standard operation procedures for preoperative anaemia management in our Hospital (Steyr, Austria), we established an interdisciplinary group consisting of specialists for laboratory and trans-fusion medicine, internal medicine, anaesthesiology, surgery and ortho-paedics. Own observation studies [2] demonstrated, that 44% of women with elective hip or knee arthroplasty with a preoperative Hb level ≥12 < 13 g/dL showed a Hb nadir <9 g/dL within the first postoperative week, if they were not substituted with intravenous (i.v.) iron/erythropoietin stim-ulating agents (ESA). If women with a preoperative Hb level ≥12 < 13 g/dL were substituted with i.v. iron/ESA before elective surgery, only 22% of these showed a Hb level <9 g/dL within the first postoperative week. Therefore in our Hospital we implemented a preoperative threshold Hb level of 13 g/dl for diagnostic and therapeutic intervention for men as well as women based on published data [1, 2, 3].Using the definition of the World Health Organisation, Hb levels below the cut-off for men (13 g/dL) and for women (12 g/dL) are diagnostic. Nevertheless these criteria are questionable in preoperative anaemia management. In the preoperative setting, we suggest, that Hb levels below 13 g/dL should be considered as diagnostic and therapeutic cut-off value for men as well as women.References: 1. Monk TG. Preoperative recombinant human erythropoietin in anemic surgical
patients. Crit Care 2004; 8 Suppl 2:S45–48.2. Enko D, Wallner F, von Goedecke A, et al.: The impact of an algorithm-guided
management of preoperative anemia in perioperative hemoglobin level and transfusion of major orthopedic surgery patients. Anemia 2013;2013:641876.
3. Kumar A. Perioperative management of anemia: limits of blood transfusion and alternatives to it. Cleve Clin J Med 2009; 76 Suppl 4:S112–118.
Donor and therapeutic apheresis
P-12-1Routine quality controls comparison between products of two plateletpheresis systems: TRIMA Accel® (Terumo BCT ) and MCS®+ (Haemonetics)
Otto J.BZD Gesellschaft für Transfusionsmedizin Duisburg mbH, Duisburg, Germany
Background: Plateletpheresis devices and protocols have been optimized over the recent years. However, in a routine collection setting, differences in collected product qualities may occur between apheresis technologies. To study this hypothesis, we investigate the differences between routine quality controls of platelet concentrates re-suspended in plasma (SDP) produced by two different apheresis technologies: Terumo TRIMA Accel® (Software Version 6.0) and Haemonetics MCS®+ (UPP Rev.A).

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts54
Methods: Following the German „Richtlinien zur Gewinnung von Blut und Blutbestandteilen und zur Anwendung von Blutprodukten (Hä-motherapie)“ (Guidelines Hämotherapy) routine quality controls were performed on at least 1% of products of our monthly production. Cellular content of routine SDP units was measured by flow cytometry (Beckman-coulter FC 500).Results: Over a time of 22 months between July 2013 to April 2015, 104 platelet units produced with the TRIMA Accel® and 106 units produced with the MCS®+ were introduced into routine QC. Platelet product vol-umes for components collected on Trima Accel® and MCS®+ were: 235.7 ± 8.6 ml/unit (mean ± SD) and 243.7 ± 8.8 ml/unit (mean ± SD) respec-tively; platelet content for both devices 2.38± 0.30 1011/unit (mean ± SD) and 2.64 ± 0.48 1011/unit (mean ± SD) respectively. The SDP units produced on TRIMA Accel® contained approximately three times more red blood cells (4.36 ± 1.24 x 108 /unit (mean ± SD) than the SDP units produced on the MCS®+ system (1.50 ± 0.76 x 108 /unit (mean ± SD)). In addition SDP units produced on the TRIMA Accel® also contained more white blood cells (0.16 ± 0.37 x 106 /unit) than units produced with on MCS®+-system (0.04 ± 0.14 x 106 /unit). The residual white cell content of SDP units produced on the TRIMA Accel®-system in 3.8% of tested units exceeded the required specification (WBC < 1x106/unit) whereas only 0.9% of the tested products from the MCS®+-system failed this spec-ification.Conclusions: While platelet components produced on the TRIMA Ac-cel® as well as on the MCS®+ system overall complied with the require-ments specified in the German Guidelines Hämotherapy, there have been measurable differences in contents of undesired cellular contaminants. A clinical impact of the differences cannot be excluded and may warrant further studying.
P-12-3Long term follow up after granulocyte transfusions
Fischer I., Kreissig C.DRK-Blutspendedienst West, Zentralbereich Stammzelle, Ratingen, Germany
Introduction: Indication for granulocyte transfusion is put seldom, be-cause collection of products is complex, time consuming and costly. That’s why only very ill patients get granulocyte transfusions. We wanted to de-termine, if big effort is justified not only by the fact, that patient survive acute infection, but also by long term survival and good health. Material and method: We performed a retrospective analysis of one year follow up after granulocyte transfusions. Via a questionnaire we deter-mined patient status at four time points: when stopping transfusions, 4 weeks, 6 month and one year after last granulocyte transfusion. In this abstract we correlate one year survival with age, underlying disease, in-dication for granulocyte transfusion, number of granulocyte transfusions and dose of transfused granulocytes. Results: We treated 28 patients, 11 female, 17 male. They were 2 to 69 years old, 17 patients were pediatric, 11 adult. Underlying disease was in 17 patients leukemia, in 7 patients inborn diseases, in 2 patients lym-phoma, in one patient solid tumor, in one patient unwanted side effect of Novamin taking. Reasons for granulocyte transfusion were in 12 patients localized infection, in 10 patient septicemia and in 6 patients fever of un-known origin. Number of transfusions was 1 till 23. Dose of transfused granulocyte ranged from 0,4 till 5,5x10E9 per kg bodyweight. 7 out of 28 patients died during granulocyte transfusion series. In 5 of 21 surviv-ing patients follow up data were not available. One year after granulocyte transfusions 4 patients were alive and well. Surviving patients were 2, 10, 16 and 20 years old. They suffered from leukemia (2 Patients) or inborn disease (2 patients). Reason for granulocyte transfusion was septicemia (1 patient), fever of unknown origin (1 Patient) and localized infection (2 patients). Patients were given 3 till 23 transfusions, doses ranged from 0,7 till 4,6 x10E9 granulocytes per kg bodyweight. Discussion: 4 out of 15 patients were alive and well one year after gran-ulocyte transfusion. So we conclude, granulocyte transfusion is a useful treatment opportunity for seriously ill patients. We could not find any cor-
relation of one year survival with age, underlying disease, indication for granulocyte transfusion, number of granulocyte transfusions and dose of transfused granulocytes.
P-12-4Collection of sufficient quantities of T-cells from healthy donors for therapeutic use
Heuft H.-G.1, Goudeva L.1, Martens J.1, Krettek U.1, Priesner C.2, Aleksandrova K.2, Blasczyk R.1
1Medizinische Hochschule Hannover, Transfusionsmedizin, Hannover, Germany, 2Medizinische Hochschule Hannover, Cellular Therapy Centre, Hannover, Germany
Introduction: The collection of lymphocytes, in particular T-cells (CD3+ cells), for both unmanipulated donor lymphocyte infusions (DLI) and specifically designed T-cell products, e. g. virus-specific T-cells, is of grow-ing interest. Few data are available for T-cell collections with the Optia IDLapheresis system. Material and Methods: From 01/2014 to 05/2015 we compared 26 T-cell aphereses on the Spectra (26 donors, aged 41 [24–69] years, 83 [53–128] kg, 5.4 [3.5–7.4] L blood volume) versus 10 T-cell aphereses on the Optia system (10 donors, aged 42 [26–59] years, 92 [79–130] kg, 5.5 [4.7–6.9] L donor blood volume [DBV]). Both machines were run semiautomatically (Spectra, software version (SV) 4.7, WBC apheresis set; Optia, SV 11, IDL apheresis set with a donor blood process volume (BVproc) of 2.5 times DBV, an inlet flow of 60 mL and an apheresis time < 300 min to obtain a T-cell dose ≥ 1×108 CD3+ cells/kg of the recipient as target values.Results: Based on comparable preapheresis values for donor WBC, per-centage of lymphocytes and platelets (PLT), Spectra vs Optia run with largely identical apheresis parameters: BVproc 13.5 (3.7–17.4) L vs 13.4 (11.2–16.8) L, inlet flow 60 (30–65) vs 60 (50–65) mL, apheresis time 257 (103–302) vs 262 (213–295) min, product volume 247 (89–301) vs 267 (227–374) mL. Although both systems collect T-cells to the same concen-tration around 55%, the Optia appears to yield higher numbers of T-cells as shown by the total number collected per apheresis and by the collection rate (CR) per minute (see Table).
Tab. 1. T-cell yields with different apheresis sytems
WBC (×10E8) CD3+ (%) CD3+ (×10E8)
CD3+ (×108/kg)
CD3+CR (×10E6/min)
Spectra 192.2 (37.7–335.6)
55.8 (35.4–70.9)
100.1 (20.4–186.8)
1.39 (0.31–8.57)
38.5 (12.3–67.6)
Optia 213.4 (150.7–434.1)
56.4 (43.6–66.0)
131.8 (76.8–193.7)
1.49 (1.13–297.8)
49.6 (32.9–75.8)
p NS NS 0.11 NS 0.15
Donor PLT loss was 41.9 (23.1–54.7) %, Spectra vs 36.2 (19.6–38.4) %, Optia; p ≤ 0.03. Despite a higher admixture of ACD-A with the Optia at 1:12 (Spectra 1:14), PLT macroaggregates occurred with every Optia T-cell collection. Conclusions: The Optia showed a trend to higher T-cell yields at a re-duced PLT loss for the donor. Despite higher ACD-A admixture, PLT macroaggregate formation was common in Optia T-cell apheresis.
P-12-5Hyperleukocytosis induced lung insufficiency with immediate response to leukapheresis
Engels J.1, Mansouri Taleghani B.2
1Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Bern, Switzerland, 2Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor, Transfusionsmedizin, Bern, Switzerland
Introduction: Hyperleukocytosis (WBC > 100G/L) can lead to leukosta-sis (LS) – a medical emergency often involving lung & central nervous system. LS often occurs in acute or chronic myeloid leukemia (CML).

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 55
Treatment consists of supportive care & cytoreduction. Rapid cytoreduc-tion is achieved by leukapheresis (LA). However, data on LA in CML are rare, the benefit of prophylactic LA remains unclear. Case report: An 18 Y old male patient presented with syncope, weight loss and dry cough at a local emergency department. Dyspnea was negat-ed, the clinical examination showed distinct splenomegaly. Blood count revealed anemia, thrombo- & leukocytosis of WBC 179,7G/L with myeol-cytes, promyelocytes and blasts (4%). He was transferred to our university hospital. Supportive treatment for hyperleukocytosis and cytoreductive therapy with hydroxyurea were started. Diagnosis of CML was confirmed by bone marrow biopsy and molecular detection of bcr-abl1. Treatment with the TKI Nilotinib was established. Within 3 days WBC decreased to 121.5G/L and he was discharged in good general condition. Two days later he presented at a local emergency department with fatigue & dyspnea. WBC had raised to 164,8G/L, blood gas analysis showed partial respira-tory insufficiency. A CT-scan showed new bilateral pulmonary infiltrates. Antibiotic treatment was started and he was transferred to our ICU for non-invasive ventilation (NIV). Nilotinib was discontinued, considering a possible rare drug side effect. Further laboratory and radiological findings strongly suggested pulmonary LS and emergency LA was performed via peripheral venous access. During 197min ca. 3 patient blood volumes were processed and 982 ml WBC-concentrate was withdrawn without compli-cations. WBC declined from 138,1 to 82,3 G/L. Dyspnea and oxygenation improved rapidly, NIV was no longer required. Therapy with hydroxyurea was continued, resulting in a further decline of WBC. The patient left the ICU 2 days after LA. Nilotinib was reestablished, hydroxyurea stopped and the patient discharged after 8 days in good condition. Ambulatory monitoring showed a major molecular response after 6 month. Discussion: In the era of TKI CML is associated with an excellent progno-sis. LS in hyperleukocytosis is one of the acute complications, associated with early morbidity and mortality. Our case confirms the safety and effi-cacy of LA in clinical overt LS and challenges to use LA even as prophy-laxis in patients at risk (i.e. WBC > 100 G/L).
P-12-6An alternative mini buffy coat preparation method for adult patients with extracorporeal photopheresis contraindications
Grabmer C.1, Schlager S.1, Mayer G.1, Streif D.2, Lener T.1,2, Schallmoser K.1,2, Rohde E.1,2
1Univ. Klinik für Blutgruppenserologie und Transfusionsmedizin, Paracelsus Medizinische Privatuniversität Salzburg, Salzburg, Austria, 2Spinal Cord Injury and Tissue Regeneration Center Salzburg (SCI-TReCS); Paracelsus Medical University (PMU), Salzburg, Austria
Introduction: Extracorporeal photopheresis (ECP) is an important cell-based therapy for various diseases but is limited to patients eligible for apheresis. We developed a novel mini buffy coat preparation method which uses the bone marrow (BM) processing program of the Spectra Op-tia apheresis system (Terumo BCT, Lakewood, CO, USA) for white blood cell (WBC) collection and compared its efficacy of WBC recovery with the standard technique done with a separator device.Methods: Whole blood (450 ± 45 mL) of 30 randomly selected healthy volunteer blood donors was collected and subdivided into two groups (15 units each). In the first group, WBCs were separated with a separator device (Compomat G4, Fresenius, Bad Homburg, Germany). In the second group, buffy coats were separated with the BM processing program of the Spectra Optia apheresis system. Counts of RBCs, WBCs and lymphocytes as well as hemoglobin and hematocrit (Hct) of the final product were measured.Results: There was no significant difference in leukocyte count per prod-uct between the two groups. In contrast, lymphocyte count per product was significantly higher (p < 0.001) in apheresis derived buffy coats. Mean Hct of final products after dilution was <2% in both groups.Conclusion: Our modified technique results in higher lymphocyte yields than the classical mini buffy coat preparation method. Compared to WBC collection by classical ECP this method may enable the treatment of adult patients unsuitable for apheresis.
P-12-7F VIII: C in plasma donors and the corresponding products
Weber K., Fischer T., Laitinen T., Taborski U.Octapharmaplasma, Langenfeld, Germany
The aim of this study is to compare the F VIII:C in plasma donors with the activity in the donated plasma unitsMaterial and Methods: Immediately before starting the automated plas-ma donation (PCS 2;Express-software;Admixture of 4%citrate-solutionto the whole-blood in a ratio of 1:16 ;plasma donation volume 650 up to 850 ml depending on the donor’s body weight; donation time between 34 and 77 min) in 22 donors (12 male, 10 female) the F VIII:C was determined by a one-step-test. Within 6 h after donation the FVIII:C in the donated plasma was determined.Results: FVIII:C in the donors was dependent on the ABO blood group: in donors of blood group O it was 100.1% (n = 9); blood group A 142.1% (n = 8); blood group B 139.7% (n = 3); blood group AB 146% (n = 2). FVIII: C in the plasma units were 88.5% (blood group O); 90.6% (blood group A); 64.7% (blood group B) and 72% (blood group AB). In all 22 units a good recovery of FVIII: C was seen in comparison to the donor’s FVIII:C.Discussion: we interpret the reduced FVIII:C in the plasma units com-pared with the donor’s FVIII:C to that effect that the withdrawed intra-vascular volume by the plasma donation in the donor’s circulation is compensated by an influx of interstitial fluid into the vascular system. The synthesis of FVIII within this relatively short time of donation seems to be negligible.
P-12-8Comparison of two different hemoglobin (Hb) measuring techniques in plasma donors in routine operations
Ziyaie-Hochstrat O.1, Krull M.2, Kießig S.3, Alvermann G.1
1Plasma Service Europe, Köln, Germany, 2Plasma Service Europe, Rostock, Germany, 3Ruhr-Plasma-Zentrum, Bochum, Germany
Introduction: After internal qualification and validation the “non-inva-sive hb measurement” (NiHbM) via OrSense-NBM-200 was introduced to all plasmapheresis centers of PSE-GmbH in the second half of 2014 after regulatory approval. A comparative analysis of hb data in a group of qualified donors collected via NiHbM in the first quarter of 2015 against the hb values in the same donor group collected in the first quarter of 2014 via Haemo-Cue devices (“invasive hb detection”) was performed. Material and Method: Computerized test results for these two compar-ison groups (388 qualified donors at PSE in one pool) were included if plasma donation occurred at least ten times in one center in both quarters mentioned above allowed range (>4300 “double measured values” in an associated random sample). The calculated mean values were compared to one another by means of the statistical comparison method “Pass-ing-Bablok regression”.Discussion: The statistical analysis via the “non-parametric method of Passing-Bablok” revealed good comparability of the two measuring tech-niques for the measured hb values; deviations of the measured hb values were within the accepted limits and defined standard deviations.Conclusion: The results prove good comparability of the newly intro-duced “non-invasive method” with the previous standard procedure of the “bloody capillary” hb measurement. Donors with hemoglobin values outside of the allowed range could be easily identified and excluded. The device is accepted very well by the donors and the personnel due to the painless measurement and the simple manageability. Minimization of the danger of infection for the personnel that collects the blood samples – at the reception – (also applicable for pregnant employees) is a very desirable and positive “side effect”.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts56
Legal basis and quality assurance
P-13-1Validation of sterility testing for cornea organ culture medium containing antibiotics using blood culture bottles with penicillinase and acetylcystein as additives
Skenderi Z., Pruß A., Schroeter J.Universitätsmedizin Charité Berlin, Institut für Transfusionsmedizin / Universitätsgewebebank, Berlin, Germany
Background: Since tissue preparations are under pharmaceutical regula-tions in Germany since 2007, a validation of sterility testing according to the European Pharmacopoeia is mandatory. Inhibitory effects on sterility testing due to antibiotics used for the conservation of donor tissues, e.g. cornea, can occur. The use of blood culture bottles for sterility testing of cornea organ culture medium is a well-established standard. Our further investigations showed that the sensitivity of the resin consisting system is enhanced by Penicillinase an Acetylcystein. Methods: Blood culture bottles containing resins to inactivate antibiotics (BacTec Plus, aerobic/ anaerobic F medium, Becton Dickinson) were sup-plemented with 1 ml Penase (10 million units, Becton Dickinson) and 1 ml Acetylcystein (100 mg) (ACC inject, Hexal). 5, 7.5 and 10 ml of cornea organ culture medium (Modified Eagle’s Medium MEM with 2% fetal calf serum, penicillin (60 µg/ ml), streptomycin (130 µg/ ml) and amphotericin B (2.5 µg/ ml)) were added directly followed by 10 to 100 colony forming units of the test microorganism: Bacillus subtilis (BS), Stapylococcus au-reus (SA), Clostriduium sporogenes (CS), Pseudomonas aeroginosa (PA), Staphyloccocus epidermidis (SE), Enterobacter cloacae (EC) and Candida albicans (CA). The blood culture bottles were incubated in an automated system (BD Bactec 9120-FX System, Becton Dickinson) until a positive reading or a maximum of 14 days. Positive controls contained only the microorganisms, negative controls only the medium and the additives. Results: All microorganisms could be detected in the modified blood cul-ture bottles. Compared to the positive controls there was no significant delay for BS (control 10.5 vs. test 13.2 hours), SA (control 14.9 vs. test 13.2 hours), CS (control 15.2 vs. test 14.8 hours), SE (control 16.5 vs. test 19.0 hours), EC (control 11.2 vs. test 14.2 hours) and CA (control 14.9 vs. test 13.2 hours) up to 10 ml of medium. PA could only be detected up to 6 ml of medium (control 13.3 vs. 16.5 hours). Summary: Blood culture bottles enhanced with Penicillinase and ACC for the testing of cornea organ culture medium could be successfully vali-dated according to European Pharmacopoeia.
P-13-2Development and acceptance of an electronic document management system after 5 years
Spyrantis A., Capalbo G., Gross M., Gubbe K., Sireis W., Seifried E., Schmidt M.German Red Cross Blood Donor Service Baden-Württemberg-Hessen, Frankfurt am Main, Germany
Introduction: The German Red Cross blood donor service in Baden-Wuerttemberg-Hessen and its affiliates comprise of 18 indepen-dent institutes spread around six districts in Germany. In 2009 we de-signed and developed a customized document management system in order to replace our paper-based document control system. Features such as workflow-based functions and archiving capabilities are essential ele-ments for document control or replacing paper-based processes. Methods: Over the past 5 years we have developed five electronic modules within the Saperion DMS platform. Initially, a workflow-based module for the control and release of SOPs was developed. Due to the wide accep-tance of this platform, additional paper-based processes such as our Risk- and Deviation Management (2012) as well as our internal Audits (2013) were implemented as workflow-based electronic modules. In addition, the
development of archiving modules (non-workflow) for Haemovigilance and external audits were also developed in 2013. Results: All staff within our Organisation have access to our DMS plat-form. Accessibility is controlled by assigning each user into one of three existing user-categories: Group 1: Readers (69%), Group 2: Authors/Ap-provers (30%) and Group 3: QM-staff (1%). In our SOP module, all us-ers have access to released documents, while only the Author/Approver group can create new or revise and approve documents. Our Risk and deviation management module is structured in a similar way: All users within our organisation can report a deviation, while the assessment and analysis of these events is carried out by two separate subgroups of groups 2 and 3 (Group leaders and QA Staff). Similarly, the internal Audit mod-ule is accessible only by a panel of qualified internal auditors as well as group leaders and QA Staff.Conclusion: Overall, the advantages of switching ton an electronic man-agement system for SOP handling are plenty. The archiving capabilities enable traceability and a significant reduction of paper copies and storage requirements. Considering the size of our organisation, workflow-based functions have significantly accelerated the processing time required for documents, deviations as well as audit reports. Moreover, data exporting enables statistical analyses to be conducted in a reliable and time-saving manner. Finally, the fact that all additional modules were introduced in an existing DMS, the acceptance was greatly enhanced and the training expenditures minimized.
Recruitment, motives and safety of donors
P-14-1Incidence of vasovagal dysregulation during blood donation - What can we do better?
Scheffels B., Störmer M., Gathof B.S.Universitätsklinikum Köln, Transfusionsmedizin, Köln, Germany
Background: The increasing demand of blood products such as red blood cell concentrates (RBCs) in clinical practice makes it more and more im-portant to provide blood donors safety and well-being. Although blood donation is a safe procedure, some donors experience unpleasant symp-toms such as dizziness, nausea and vasovagal syncope but data about va-sovagal reaction (VVR) during blood donation in Europe, especially in Germany, is missing. In this study the amount and type of vasovagal reac-tions for our clientele should be evaluated in a prospective study. Methods: The present prospective study implies all blood donors who give whole blood in our blood donation centre between 01.04.2015 and 31.07.2015. Demographic data and clinical measurements will be col-lected and referenced to the count of VVR. Data collection will be per-formed on a purpose-made form to gather the occurrence of symptoms and generate an anonymized data bank. Moreover donors will complete a designed questionnaire after donation to examine if psychical or physical stress has an influence on the blood donors´ well- being after blood dona-tion. Data sets are processed with Excel® and SPSS®.Results: Prior to the prospective study a data baseline was generated by a retrospective examination of 6522 blood donations incidences between 01.01.15 and 15.03.15. In total 343 (5.26%) blood donors suffered from symptoms of vasovagal dysregulation. In the prospective study 2746 do-nors were observed between 01.04.15 and 30.04.15. Risk factors for com-plications included female sex (60.3% female, N = 85), young age (73.8% 18-26 years old, N = 104) and first- time donor status (51.1%, N = 72). Symptoms of vasovagal dysregulation such as paleness, dizziness or loss of consciousness occurred in 141 cases (5.14%).Conclusion: Symptoms during blood donation may occur in around 3-5% according to previously published data. Once the percentage rate of incidences during blood donation is proven true during our observing period, an appropriate intervention for our blood donators to reduce the

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 57
contemplated quantity of incidents should be introduced. Several studies already demonstrated that applied muscle tension is an effective tool to prevent donors from vasovagal reactions. Therefore this might be applied to our donors during this examination as well.
P-14-2Evaluating the cooperation between the institute of transfusion medicine at the university hospital Magdeburg and the friends´ association for blood donation in Magdeburg
Schulze S., Becker E., Heim M.U.1Universitätsklinikum Magdeburg A.ö.R, Institut für Transfusionsmedizin u. Immunhämatologie mit Blutbank, Magdeburg, Germany
Introduction: In 1995 the Friends´ Association for Blood Donation in Magdeburg was founded at the Institute for Transfusion Medicine at the University Hospital Magdeburg. This paper analyses the results of the twenty years lasting cooperation between the institute and an honorary association.Methods: Every year the executive committee of the association writes the annual report concluding the activities and finances (incomes and ex-penses). All the annual reports up to 2014 were broadly analysed and the benefit for the Institute of Transfusion Medicine was evaluated.Results: In the period from November 1995 until December 2014 the friends´ association for blood donation of Magdeburg received altogether about 159 000 €. Only 7 600 € (less than 5%) of the incomes are member-ship fees. About 114 000 € (i.e. near 72%) of the incomes are divided in donations as well as allowances (e.g. monetary fines). The expenses of the friends´ association for blood donation of Magdeburg from 1995 to 2014 amount to about 151 000 € in total. Promotion campaigns for blood do-nation like poster campaigns, advertisements in newspapers, banner ads as well as advertisements on public transport vehicles were funded with
121 000 €. Events happening in the institute like the „Vampires Night“ or barbecue parties for the blood donors were supported with 6 700 €. The friends´ association for blood donation invested about 9 300 € for the in-terior of the donation area, for instance for book shelves, picture frames and magazines. The expense for administrating and operating the associa-tion was mainly limited to the organisation of the members´ meetings and were equal to about 2 600 € for the evaluation period.Conclusions: An active friends´ association provides an efficient oppor-tunity to support a blood donation institution especially in blood donor recruitment.
Transplantation and biology of stem cells
P-15-1Identification of key regulators of symmetric versus asymmetric cell divisions during human hematopoietic lineage specification
Görgens A.1, Radtke S.1, Vitoriano S.1, Murke F.1, Möllmann M.2, Dürig J.2, Hanenberg H.3, Horn P.A.1, Giebel B.1
1Universitätsklinikum Essen, Institut für Transfusionsmedizin, Essen, Germany, 2Universitätsklinikum Essen, Klinik für Hämatologie, Essen, Germany, 3Universitätsklinikum Essen, Klinik für Kinderheilkunde III, Essen, Germany
Hematopoietic stem cells (HSCs) contain lifelong potentials to self-re-new and to create progenitors of all mature blood cells. According to the current view, HSC homeostasis is controlled by both, HSC-niches as well as asymmetric cell divisions. Our previous studies linked the process of asymmetric cell division of human hematopoietic stem and progenitor

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts58
cells (HSPCs) to the expression kinetics of the stem cell surrogate antigen Prominin 1/CD133 (1). Furthermore, by characterizing human HSPCs subpopulations by means of their CD133 surface expression we gained evidence that CD133+ multipotent progenitors (MPPs) create CD133+ lymphomyeloid (LMPP) and CD133low erythromyeloid (EMP) daughter cells. The LMPP lineage was shown to contain lymphoid and neutrophil potentials, while the EMP lineage mainly creates eosinophils and baso-phils as well as erythrocytes and megakaryocytes (1). Regarding lineage specification, we showed for the first time that under conventional cul-ture conditions almost all MPPs divide asymmetrically to create a set of LMPP and EMP daughter cells, resulting in a loss of MPPs after the first cell division (3). Thus, our data suggest that under conventional culture conditions asymmetric cell divisions are rather lineage instructive than self-renewing (4). To identify key factors regulating the MPP division mode, we now studied whether conditions reported to promote HSC/MPP expansion interfere with the outcome and symmetry of the HSC/MPP cell division. In this context we co-cultured human MPPs with murine and primary human stromal lines (human bona fide MSCs) and surprisingly observed that LMPPs are maintained and expanded but not MPPs. This contrary find-ing can be attributed to the former experimental definition of multipotent cells based on the classical model of hematopoiesis, according to which cells with dual lymphocyte and granulocyte (conventionally neutrophil) potentials can insufficiently be considered as multipotent. Currently, we test other culture conditions reported to expand human HSCs/MPPs in vitro. After confirming any of these conditions as HSC/MPP expansion condition, we will analyze its impact on the division mode of HSCs/MPPs using multi-parametric flow cytometry, live-cell im-aging and functional differentiation assays at the single cell level. (1) Beckman et al, Blood 2007 (2) Görgens et al, Cell Reports 2013 (3) Görgens et al, Stem Cell Reports 2014 (4) Görgens et al, Cell Cycle 2013
P-15-2Differences of post-thaw recovery within lymphocyte subpopulations and CD34+ cells in cryopreserved apheresis products for allogeneic transplantation
Berens C., Müller J., Oldenburg J., Pötzsch B., Rühl H.University Bonn, Institute for Experimental Hematology and Transfusion Medicine, Bonn, Germany
Background: Peripheral blood stem cells (PBSC) and peripheral blood mononuclear cells (PBMC) for allogeneic transplantation are often cryo-preserved to allow white blood cell infusions at a later date. Differences in the post-thaw recovery of CD34+ and CD3+ cells in these products have been hypothesized to depend on liquid storage time or, in case of CD3+ cells, if a donor has underwent G-CSF mobilization. Methods: In order to evaluate how well lymphocyte subpopulations tol-erate freezing and thawing compared to hematopoietic stem cells, recov-eries of CD3+CD4+, CD3+CD8+, CD19+, CD16+CD56+, and CD34+ cells from 43 allogeneic apheresis products were analyzed, thereof 28 from G-CSF-mobilized donors. All measurements were performed with aliquots that had been cryopreserved in parallel with the products using a controlled-rate freezer and 8% dimethyl sulfoxide and were stored in liquid nitrogen.Results: The post-thaw recovery was 79.1±16.2% (mean±SD) for CD3+CD4+ cells, 78.1 ± 13.9% for CD3+CD8+ cells, 94.3 ± 17.4% for CD19+ cells, 82.9 ± 22.9% for CD16+CD56+ cells, and 96.1 ± 23.7% for CD34+ cells. In G-CSF mobilized products higher recoveries were ob-served than in non-mobilized products, reaching statistical significance for CD3+CD4+ cells (85.3 ± 15.4 vs 69.9 ± 13.0%, p = 0.0023) and for CD16+CD56+ cells (95.1% ± 20.2% vs 65.0 ± 12.5%, p = 2.6×10-6). The differences of post-thaw recovery within the lymphocyte subpopulations were statistically significant for CD3+CD4+ vs CD19+ (p = 5.4×10-7 in G-CSF mobilized products, p = 0.0011 in non-mobilized products), CD3+CD8+ vs CD19+ (p = 8.6×10-5 in G-CSF mobilized products, p = 0.0046 in non-mobilized products), CD3+CD8+ vs CD16+CD56+ in
G-CSF mobilized products (p = 0.014), and CD16+CD56+ vs CD19+ in non-mobilized products (p = 0.0025). Any influence of the liquid storage time (35 ± 18 h for G-CSF mobilized products, 20 ± 8 h for non-mobi-lized products) on post-thaw recoveries was excluded by ANCOVA (p = 0.0022).Conclusion: G-CSF mobilization and longer liquid storage time does not seem to impair post-thaw recovery of lymphocytes compared to products from non-mobilized donors. Our results suggest that lymphocyte subpop-ulations tolerate freezing and thawing differently well, which may have clinical implications for cellular therapies.
P-15-3Erythrocyte depletion of bone marrow in stem cell transplantation in a pediatric center comparison of two systems
Witt V., Beiglböck E., Ritter R., Pichler H.St. Anna Kinderspital, Department for Pediatrics, MUW, Vienna, Austria
Introduction: ABO incompatible stem cell transplantation has an inci-dence of about 20–50%. To avoid side effects from hemolysis bone marrow is erythrocyte depleted. . In our center we use the erythrocyte depletion with conventional apheresis systems for ABO incompatible bone marrow transplants, for volume reduction if the bone marrow amount is too high. Recently the OPTIATM System was introduced with a predefined pro-gram for bone marrow volume and erythrocyte depletion. We compared the data from our old system (Cobe spectraTM) with the new OPTIATM System in the framework of our JACIE quality system.Methods: We retrospectively analysed our erythrocyte depletion proce-dures from 2008 to 2015. In total 36 procedures were performed in 32 patients with various diagnosis undergoing allogeniec stem cell trans-plantation with HPC-BM as the stem cell source. 21 were performed with the Spectra and 15 with the OPTIA. In 9 cases the bone marrow was prediluted with recipient and donor compatible pRBCs due to the very small volume of the original harvested bone marrow. The mean age of the recipients for both systems was comparable (8.64 +/– 2.58y Spectra; 8.76 +/– 4.74y OPTIA). Samples were taken pre and post procedure to perform HPC, leukocyte, erythrocyte, platelet, and lymphocyte counts. For all this parameters the collection efficiency was calculated. The charts were reviewed for engraftment data. For comparison of the groups the T-Test was applied. Results: The calculated collection efficiencies were statistically not differ-ent between Spectra and OPTIA for HPC 98% v. 103%, ns; Monocytes 96% v. 82%, ns; B-Lymphocytes 98% v. 96%, ns; T-lymphocytes 104% v. 99%, ns;) but significant different in platelets 49% v. 79%, *; Leukocytes 40% v. 50%, *; Granulo 21% v. 35%, *) erythrocytes (5.5% v. 1.4%, * re-sulting in a lower erythrocyte volume after the OPTIA procedures in the products (14.5 ml v. 3.7 ml, *). 20/21 patients (1 died) in the COBE Spec-tra group showed regular engraftment and 14/15 in the (1 died). The day to reach > 1 G/l leukocyte count in the PB was not different (d +20 versus d +19, ns). Conclusion: The erythrocyte depletion of bone marrow with OPTIA is regarding the leukocytes and leukocyte subpopulations as efficient as the procedure with the COBE spectra, even in pediatric patients. The OPTIA system showed lower erythrocyte contamination, which is superior to the older system.
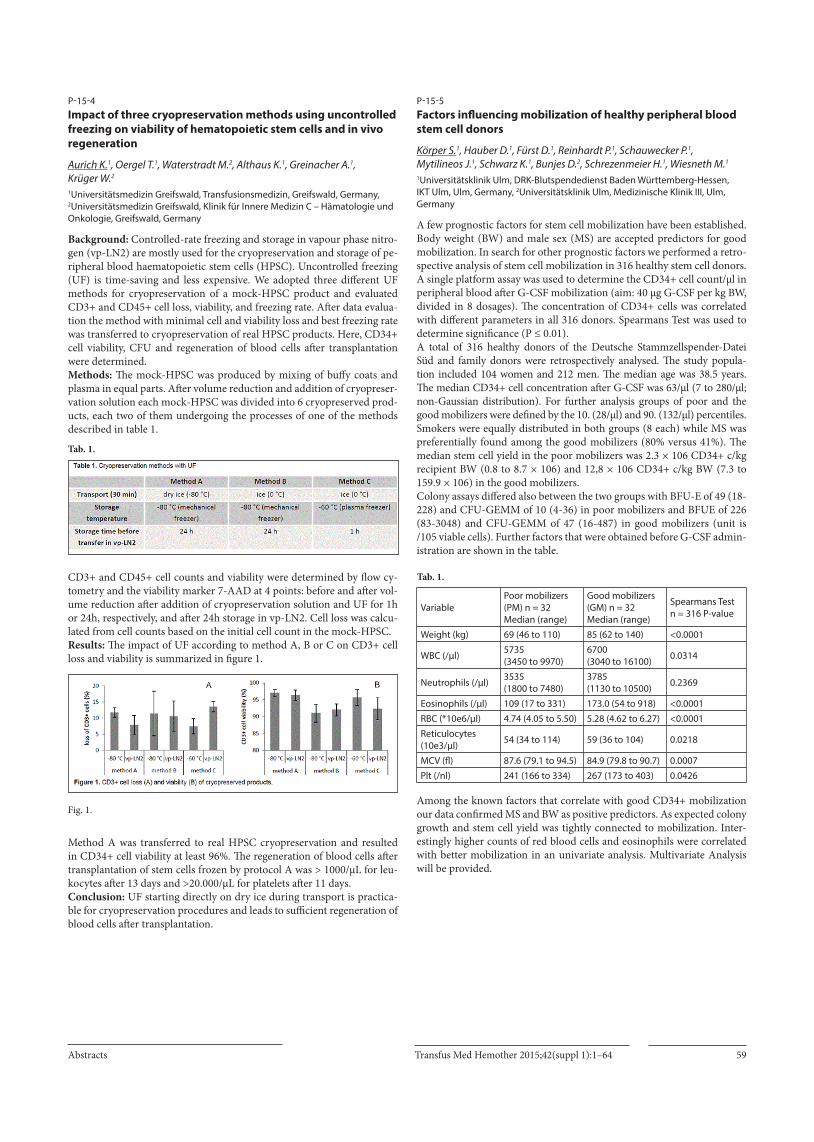
Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 59
P-15-4Impact of three cryopreservation methods using uncontrolled freezing on viability of hematopoietic stem cells and in vivo regeneration
Aurich K.1, Oergel T.1, Waterstradt M.2, Althaus K.1, Greinacher A.1, Krüger W.2
1Universitätsmedizin Greifswald, Transfusionsmedizin, Greifswald, Germany, 2Universitätsmedizin Greifswald, Klinik für Innere Medizin C – Hämatologie und Onkologie, Greifswald, Germany
Background: Controlled-rate freezing and storage in vapour phase nitro-gen (vp-LN2) are mostly used for the cryopreservation and storage of pe-ripheral blood haematopoietic stem cells (HPSC). Uncontrolled freezing (UF) is time-saving and less expensive. We adopted three different UF methods for cryopreservation of a mock-HPSC product and evaluated CD3+ and CD45+ cell loss, viability, and freezing rate. After data evalua-tion the method with minimal cell and viability loss and best freezing rate was transferred to cryopreservation of real HPSC products. Here, CD34+ cell viability, CFU and regeneration of blood cells after transplantation were determined.Methods: The mock-HPSC was produced by mixing of buffy coats and plasma in equal parts. After volume reduction and addition of cryopreser-vation solution each mock-HPSC was divided into 6 cryopreserved prod-ucts, each two of them undergoing the processes of one of the methods described in table 1.
Tab. 1.
CD3+ and CD45+ cell counts and viability were determined by flow cy-tometry and the viability marker 7-AAD at 4 points: before and after vol-ume reduction after addition of cryopreservation solution and UF for 1h or 24h, respectively, and after 24h storage in vp-LN2. Cell loss was calcu-lated from cell counts based on the initial cell count in the mock-HPSC. Results: The impact of UF according to method A, B or C on CD3+ cell loss and viability is summarized in figure 1.
Fig. 1.
Method A was transferred to real HPSC cryopreservation and resulted in CD34+ cell viability at least 96%. The regeneration of blood cells after transplantation of stem cells frozen by protocol A was > 1000/µL for leu-kocytes after 13 days and >20.000/µL for platelets after 11 days.Conclusion: UF starting directly on dry ice during transport is practica-ble for cryopreservation procedures and leads to sufficient regeneration of blood cells after transplantation.
P-15-5Factors influencing mobilization of healthy peripheral blood stem cell donors
Körper S.1, Hauber D.1, Fürst D.1, Reinhardt P.1, Schauwecker P.1, Mytilineos J.1, Schwarz K.1, Bunjes D.2, Schrezenmeier H.1, Wiesneth M.1
1Universitätsklinik Ulm, DRK-Blutspendedienst Baden Württemberg-Hessen, IKT Ulm, Ulm, Germany, 2Universitätsklinik Ulm, Medizinische Klinik III, Ulm, Germany
A few prognostic factors for stem cell mobilization have been established. Body weight (BW) and male sex (MS) are accepted predictors for good mobilization. In search for other prognostic factors we performed a retro-spective analysis of stem cell mobilization in 316 healthy stem cell donors. A single platform assay was used to determine the CD34+ cell count/µl in peripheral blood after G-CSF mobilization (aim: 40 µg G-CSF per kg BW, divided in 8 dosages). The concentration of CD34+ cells was correlated with different parameters in all 316 donors. Spearmans Test was used to determine significance (P ≤ 0.01). A total of 316 healthy donors of the Deutsche Stammzellspender-Datei Süd and family donors were retrospectively analysed. The study popula-tion included 104 women and 212 men. The median age was 38.5 years. The median CD34+ cell concentration after G-CSF was 63/µl (7 to 280/µl; non-Gaussian distribution). For further analysis groups of poor and the good mobilizers were defined by the 10. (28/µl) and 90. (132/µl) percentiles.Smokers were equally distributed in both groups (8 each) while MS was preferentially found among the good mobilizers (80% versus 41%). The median stem cell yield in the poor mobilizers was 2.3 × 106 CD34+ c/kg recipient BW (0.8 to 8.7 × 106) and 12,8 × 106 CD34+ c/kg BW (7.3 to 159.9 × 106) in the good mobilizers.Colony assays differed also between the two groups with BFU-E of 49 (18-228) and CFU-GEMM of 10 (4-36) in poor mobilizers and BFUE of 226 (83-3048) and CFU-GEMM of 47 (16-487) in good mobilizers (unit is /105 viable cells). Further factors that were obtained before G-CSF admin-istration are shown in the table.
Tab. 1.
VariablePoor mobilizers (PM) n = 32 Median (range)
Good mobilizers (GM) n = 32 Median (range)
Spearmans Test n = 316 P-value
Weight (kg) 69 (46 to 110) 85 (62 to 140) <0.0001
WBC (/µl) 5735 (3450 to 9970)
6700 (3040 to 16100) 0.0314
Neutrophils (/µl) 3535 (1800 to 7480)
3785 (1130 to 10500) 0.2369
Eosinophils (/µl) 109 (17 to 331) 173.0 (54 to 918) <0.0001
RBC (*10e6/µl) 4.74 (4.05 to 5.50) 5.28 (4.62 to 6.27) <0.0001
Reticulocytes (10e3/µl) 54 (34 to 114) 59 (36 to 104) 0.0218
MCV (fl) 87.6 (79.1 to 94.5) 84.9 (79.8 to 90.7) 0.0007
Plt (/nl) 241 (166 to 334) 267 (173 to 403) 0.0426
Among the known factors that correlate with good CD34+ mobilization our data confirmed MS and BW as positive predictors. As expected colony growth and stem cell yield was tightly connected to mobilization. Inter-estingly higher counts of red blood cells and eosinophils were correlated with better mobilization in an univariate analysis. Multivariate Analysis will be provided.

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts60
Cellular therapy and tissue engineering
P-16-1In vitro generation of HLA-universal granulocytes to reduce the risk of transfusion associated alloimmunisation and increase therapeutic efficacy
Figueiredo C., Zhang H., Goudeva L., Eiz-Vesper B., Blasczyk R.Hannover Medical School, Institute for Transfusion Medicine, Hannover, Germany
Introduction: Granulocyte transfusion is a promising adjuvant therapy to control infections during profound and prolonged neutropenia. How-ever, alloimmunization against HLA antigens may compromise posterior therapies such as transplantation. Functional HLA class I-deficient granu-locytes might cross histocompatibility barrier and constitute ideal sources for granulocyte transfusion. In this study, we have combined the concept of blood pharming with the possibility to regulate gene expression using RNA interference technology to generate HLA-universal granulocytes.Material and Methods: A short hairpin RNA (shRNA) targeting ß2-mi-croglobulin (ß2m) transcripts (shß2m) was used to silence the expression of HLA class I molecules on CD34+ hematopoietic stem and progenitor cells (HSPCs). Differentiation of HSPCs towards neutrophils and baso-phils was performed by culturing cells in the presence of specific cytokine cocktails. Morphology, phenotype, proliferation potential and functions of HLA-silenced and non-silenced neutrophils and basophils were com-pared. Allogeneic immune responses including allogeneic T cell prolifer-ation, T cell cytokine secretion and complement dependent cytotoxicity (CDC) were analyzed. Results: HLA class I expression was stably downregulated by up to 70%. Neutrophils and basophils maturation, cell morphology, phenotype, pro-liferation potential and functions remained unaffected by HLA-silencing. HLA-expressing and silenced HSPC derived neutrophils demonstrated similar phagocytic rates (51.08% ± 15.57 vs. 49.78% ± 7.79) and che-motactic functions (36.88% ± 17.92 vs. 39.80% ± 14.66), and both could form neutrophil extracellular trap upon PMA stimulation. Importantly, HLA-silenced granulocytes abrogated allogeneic T cell proliferation and cytokine secretion. Also, the susceptibility of HLA-silenced granulocytes to undergo HLA antibody-mediated CDC was significantly reduced com-pared with HLA non-silenced cells (45 ± 7% vs. 92 ± 8%, p < 0.0001). Conclusion: This study demonstrates the feasibility of using HLA univer-sal HSPCs as cell source for the differentiation of functional granulocytes. In vitro pharmed HLA-universal granulocytes prevented allogeneic hu-moral and cellular immune responses. HLA-universal cell products may become an alternative therapeutic option for the management of patients in need of multiple transfusions.
P-16-2Granzyme B is a key determinant of plasmacytoid dendritic cell immunogenicity
Trzaska T.1, Beyer T.1, Schrezenmeier H.1, Debatin K.-M.2, Fabricius D.2, Jahrsdörfer B.1
1IKT Ulm, Ulm, Germany, 2Klinik für Kinder- und Jugendheilkunde, Universitätsklinikum, Ulm, Germany
Despite their low frequency of approximately 0,5% in the peripheral blood, human plasmacytoid dendritic cells (pDC) are important modulators of adaptive immune responses and have meanwhile taken the step from the bench to promising initial tumor vaccination studies. PDC express high levels of the IL-3-receptor CD123, MHC class II and blood dendritic cell antigens (BDCA)-2 and -4. Apart from secretion of IFN-alpha and their capacity to rapidly initiate antigen-specific CD8+ T cell responses by cross-presentation, they produce large amounts of the serine protease gran-zyme B (GrB). GrB exhibits various non-cytotoxic functions including T cell regulation and the support of antigen processing and phagocytosis. We therefore hypothesized that pDC may use their GrB for both T cell regula-
tion and for antigen uptake and processing. PDC were isolated using mag-netically labeled antibodies against BDCA-4, and cultured in the presence of various stimuli. Here, we demonstrate that pDC are potent producers of enzymatically active GrB, which reached maximal concentrations up to two logs higher than those produced by cytotoxic cells including CTL and NK cells. The strongest inducers of GrB in pDC were IL-3 and IL-10, whereas toll-like receptor (TLR)-7 or TLR-9 ligands such as CpG ODN or imiqui-mod as well as CD40 ligand suppressed GrB induction. We demonstrate that pDC-derived GrB can suppress effector T cell proliferation by GrB-me-diated degradation of the T cell receptor zeta-chain. Moreover, we tested the uptake of fluorescently labeled antigenic material into pDC after lysis of tumor cells by freeze-thaw cycles and irradiation. These studies revealed a correlation between pDC GrB expression and antigen uptake, with GrBhigh pDC taking up significantly more antigenic material than GrBlow pDC, and GrB inhibition strongly interfering with antigen uptake. Our data support a novel concept, in which pDC acquire their maximal immunogenic poten-tial via a two-step activation process: First, high levels of GrB are induced by IL-3 and IL-10, thereby supporting antigen processing and uptake into pDC, while preventing precocious activation of T cells. Subsequently, TLR agonists and CD40 ligand turn off GrB in pDC and initiate the transfer of MHC-antigen complexes and co-stimulatory molecules to the pDC surface, resulting in highly immunogenic pDC. Our data may be of translational relevance for the further development of novel DC vaccination strategies in tumor therapy.
P-16-3MHC streptamer based selection and depletion to generate alloreactive KIR-2/3DL negative primary NK cell subsets
Becker P., Klemm D., Stricker N., Hennecke J., Seifried E., Seidl C.Institut für Transfusionsmedizin und Immunhämatologie, DRK Blutspendedienst Baden Württemberg-Hessen, Frankfurt, Germany
Natural killer (NK) cells mediate graft versus leukaemia (GvL) effects in hematopoietic stem cell transplantation (HSCT) and are used in clinical trials as adoptive immunotherapy after HSCT. The GvL effect is supported by NK cells that solely express inhibitory killer cell immunoglobulin-like receptors (KIR) missing their corresponding HLA ligand in the patient (KIR-HLA mismatch). In the present study, we developed a technique for the isolation of pa-tient specific alloreactive KIR positive donor-NK subsets at GMP level by MHC Streptamers for adaptive immunotherapy. KIR ligand specific MHC streptamers, with specific binding affinity to KIR2DL1, KIR2DL2/L3 or KIR3DL1 positive NK-cells (HLA-C*04:01-CMV, HLA-C*01:02-TIMP, HLA-B*57:01-HIV) respectively, were generated. Following neg-ative isolation of NK cells from peripheral blood, functional activity was assessed by the CD107 degranulation assay against the HLA negative cell line L721.221 transfected with HLA-C1, HLA-C2 and HLA-Bw4 ligands for the respective KIR expressing NK cells.Results obtained by flow cytometry showed a mean staining of 83% for KIR2DL1 positive NK cells, 71% for KIR2DL2/L3 positive NK cells, and 63% for KIR3DL1 positive NK cells. Following magnetic assisted cell sorting we obtained a mean purity of 89% KIR2DL1 positive and 73% KIR2DL3 positive cells indicating a specific and reproductive ligation of MHC streptamers to KIR on the NK cell surface. Importantly, sorted KIR positive NK cells showed lytic activity and higher degranulation activity against KIR-HLA matched target cells compared to bulk NK cells.In conclusion, this technology allows sorting of alloreactive KIR positive NK cell populations by negative isolation of all KIR expressing NK cells that will be inhibited by the patient´s HLA and only select the alloreactive NK cell subset for direct adoptive cell therapy or ex vivo NK cell expansion.

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 61
P-16-4Immunomonitoring of DC treated GBM patients by quantification of tumor antigen specific T cells
Müller I.1, Altherr D.1, Schwarz E.2, Flesch B.3, Urbschat S.4, Ketter R.4, Oertel J.4, Hoth M.2, Eichler H.1
1Universitätsklinikum des Saarlandes, Institut für Klinische Hämostaseologie und Transfusionsmedizin, Homburg/Saar, Germany, 2Universität des Saarlandes, Institut für Biophysik, Homburg/Saar, Germany, 3DRK-Blutspendedienst West, Labor für Immungenetik / HLA, Bad Kreuznach, Germany, 4Universitätsklinikum des Saarlandes, Klinik für Neurochirurgie, Homburg/Saar, Germany
Background: CD8+ T-cells (cytotoxic T-lymphocytes, CTL) of adaptive immunity are responsible for the elimination of tumor cells. Following ac-tivation by professional antigen-presenting cells e.g. by dendritic cell vac-cination, the effector CD8+ T-cells mediate the active immunotherapeutic potency against the aggressive glioblastoma multiforme (GBM). Missing immunomarker assays complicates an assessment of the effectiveness of the DC treatment strategy in GBM patients.Methods: Tumor antigen-pulsed- DC from healthy HLA-A2+ blood do-nors were generated to stimulate autologous CTL over a 12d culture period. The ability of CTL to express IFN-γ served as a measure of a successfully primed CTL response. The IFN-γ response was quantified with the sensi-tive real time PCR for expression level, while protein level was detected by flow cytometry. Cytometry determination of T cells with a peptide-specific multimer staining procedure allowed us a statement of antigen specific CTL activation. The presence of analysed proteins in the tumor was compared to healthy human brain cDNA by SSP-PCR characterization.Results: In runs with CTL from conventionally treated GBM-patients (n = 5), an upregulated IFN−γ mRNA level, intracellular IFN−γ expression and positively identified tumor antigen-specific CTL after stimulation with pep-tide-pulsed DC confirmed the application potential of the developed assays. Moreover, the peptide-specific CD8+T-cell response from the flow cytome-try measurement correlated to the specific protein expression.Conclusion: Our data show that the formation of antigen-specific CTL can be immuno-monitored in vitro using the presented assays. The effect of an in vivo stimulation of GBM patients by a DC vaccination can now be examined. These results are encouraging to further establish a real-time killing assay as test system for determining the effectiveness of tumor-spe-cific adaptive immune response in immunotherapies of GBM-patients. Accurate detection of CD8+-T cell response to antigen-pulsed DC as im-munomarker is not only for the acute treatment of medical importance, but can contribute important insights in the future for the concept of im-mune therapy.
P-16-5Similarities and differences in differentiation capacities of clinical grade human platelet lysate-expanded and fetal bovine serum-expanded human bone marrow-derived multipotent mesenchymal stromal cells by monitoring a broad range of differentiation markers using quantitative PCR
Erle A., Lotfi R., Schrezenmeier H.Universitätsklinikum Ulm, Institut für Transfusionsmedizin, Ulm, Germany
Introduction: Multipotent mesenchymal stromal cells (MSC) experience a rising interest in several fields of regenerative medicine. Especially bone marrow-derived MSC (BMMSC) show a profound capacity to differen-tiate into adipogenic, chondrogenic, and osteogenic lineages. To replace fetal bovine serum (FBS)-expanded cells in clinical applications, we are currently using platelet lysate (PL)-expanded BMMSC in clinical trials within the European project REBORNE, focused on healing of long non-union bone fractures. For this study we have subsequently compared the differentiation capacities of FBS- vs. PL-expanded BMMSC. Methods: Human BMMSC were in vitro expanded until cell culture pas-sage 1, using 10% FBS, respectively 5% and 8% PL. Following expansion, adipogenic, chondrogenic, and osteogenic differentiation capacities were examined using conventional histochemical staining methods. Accompa-
nying a qPCR marker panel was applied, consisting of 7 adipogenic, 10 chondrogenic, and 23 osteogenic differentiation markers. Differentiations were monitored every third day for 16–25 days. Results: FBS- and PL-expanded BMMSC behaved different during adi-pogenic, chondrogenic, and osteogenic differentiation. During adipogen-ic differentiation, FBS-expanded BMMSC showed a faster and stronger formation of lipid droplets. This was accompanied by a three days earlier onset of all adipogenic differentiation markers. PL-expanded BMMSC showed an earlier and stronger enclosure of aggrecan during chondro-genic differentiation. Spheres derived from PL-expanded BMMSC dra-matically increased in size, as typically for hypertrophic cartilage. Chon-drogenic marker gene expression was generally higher in PL-expanded BMMSC. In addition, PL-expanded BMMSC also showed an earlier calci-fication and ALPL activity during osteogenic differentiation. In contrast to adipogenic and most of chondrogenic markers, osteogenic markers were all already expressed at the end of cell expansion. Conclusion: FBS-expanded BMMSC occur to have a certain benefit for adipogenic differentiation. Whereas PL-expanded BMMSC occur to have a certain benefit for chondrogenic and osteogenic differentiation. This is most probably due to a pre-differentiation caused by PL. Together with the high basal expression of osteogenic markers, this supports that in par-ticular PL-expanded BMMSC are strong candidates for bone repair and chondrogenic medicinal indications.
P-16-6Surface modifications of polylactic acid-based biomaterials induce donor-specific reactions in macrophages: perspectives for personalized medicine
Gudima A.1, Stankevich K.S.1,2, Filimonov V.D.2, Klüter H.1,3, Mamontova E.M.2, Tverdokhlebov S.I.2, Kzhyshkowska J.1,4
1Universität Heidelberg, Medizinische Fakultät Mannheim, Institute for Transfusion Medicine and Immunology, Mannheim, Germany, 2National Research Tomsk Polytechnic University, Tomsk, Russian Federation, 3German Red Cross Blood Service Baden-Württemberg-Hessen, Mannheim, Germany, 4Tomsk State University, Tomsk, Russian Federation
Introduction: Monocytes and monocyte-derived macrophages are prom-ising cells for immune cell therapy in regenerative medicine. Macrophages are the first cells that recognize foreign bodies and therefore regulate re-action to implant materials. In order to improve implant acceptance and minimize inflammatory complications, polylactic acid (PLA) is used as a promising synthetic biodegradable polymer for the manufacturing of implants and coatings. PLA has been widely used in resorbable sutures, clips, plates and screws and in drug delivery devices. Advantages of using PLA as a biomaterial are that it provides high biocompatibility, processi-bility and good mechanical properties. However, degradation of PLA in the body into lactic acid can cause chronic inflammation and implant in-tolerance due to accumulation of acid in tissues. Surface modifications of PLA-based biomaterials may provide a solution to this problem. As mac-rophages play a central role in regulation of inflammation, their response to unmodified and modified PLA-based materials was analysed. Methods: Human peripheral blood monocytes were isolated from buffy coats by magnetic cell sorting using CD14 beads. M1 and M2 macrophages have been generated by cultivating human monocytes in the presence of IFNgamma and IL-4, correspondingly, for 6 days in serum-free medium. Cytokine production on days 1, 3 and 6 of incubation was measured by ELISA. On day 6, cells were fixed, stained by immunofluorescence and analysed by confocal microscopy. Results: We found that PLA samples modified with Brilliant Green dye (BG1, BG2, BG3) had a stimulatory effect on the production of inflam-matory cytokines TNFα and CCL18 released by both M1 and M2 hu-man primary monocyte-derived macrophages in a donor specific way. Additionally we analysed whether modified or unmodified PLA samples can induce an M2 tolerogenic phenotype in monocytes by studying the expression of macrophage mannose receptor CD206 and Stabilin-1. We show that unmodified PLA samples increase the expression of both mark-

Transfus Med Hemother 2015;42(suppl 1):1–64 Abstracts62
ers, while the modified PLA modulate their expression in a donor specific way. Conclusions: These results show that modification of PLA material sur-face can change the inflammatory responses of macrophages. A mono-cyte-based in-vitro system for testing individual responses to the implant-ed material is useful for selecting personalized implant variant.Funding: IMMODGEL project, Grant No (602694)
P-16-7A GMP-grade standard protocol for exclusively human mesenchymal stromal cell-derived extracellular vesicles
Lener T.1,2, Streif D.2, Pachler K.2, Desgeorges A.2, Somogyi-Dunai Z.2, Rohde E.1,2, Gimona M.1,2
1Salzburger Landeskliniken – Paracelsus Medizinische Privatuniversität, Department of Blood Group Serology and Transfusion Medicine, Salzburg, Austria, 2Spinal Cord Injury and Tissue Regeneration Center Salzburg (SCI-TReCS); Paracelsus Medical University (PMU), Salzburg, Austria
Introduction: Production and application of extracellular vesicles (EVs) for regenerative, immune-modulatory or neuroprotective therapies re-quires stringent control of identity, purity and potency. EVs present in FBS containing growth media lead to heterogeneous EV preparations. Alternatively, human platelet lysate (HPL) can be used as a growth medi-um supplement for the propagation of human mesenchymal stromal cells (MSCs). However, the fibrinogen present in HPL negatively affects the immune-modulatory functions of MSCs and high Ca2+ concentrations, commonly used for fibrinogen clotting and removal negatively influence osteogenic differentiation. Moreover, heparin (used to prevent fibrin clot-ting) impairs the uptake of EVs into recipient cells and the trilineage dif-ferentiation of MSCs under HPL conditions. Here we present a method for the production of heparin and fibrinogen-reduced growth media de-void of serum-derived EVs.Methods: We have developed a method to avoid heparin and to physically remove fibrin without addition of Ca2+ that results in a clear and stable growth medium, which supports MSC growth comparable to formula-tions containing heparin. HPL-derived vesicles are depleted from the me-dium in a single ultracentrifugation step. EVs are purified from the con-ditioned growth medium by sequential ultracentrifugation and filtration.Results: Applying minimal physical interventions we were able to gen-erate a growth medium suitable for human MSC in vitro culture. MSCs retain their in vitro potential for adipogenic and osteogenic differentia-tion, and surface marker expression, cell morphology, migration, con-tractility and cell death rate are unaltered compared with cells grown in heparin-containing medium. The proliferation rate is decreased by 15% +/– 0.3%. Bioanalyzer-based miRNA profiling revealed significant differ-ences between EVs from cells grown in heparin-free and fibrinogen-re-duced growth media compared to EVs isolated from cells propagated in standard HPL- or FBS-containing media. Conclusions: We present a GMP-grade protocol for the purification of exclusively human MSC-derived EVs from cells propagated in hepa-rin-free and fibrinogen-reduced growth medium avoiding FBS and lack-ing contaminating serum-derived EVs. With this protocol a thorough characterization and establishment of protein and miRNA profiles from MSC-derived EVs can now be achieved to identify the active components of therapeutic EVs for future clinical application.
P-16-8ATP, HMGB1 and S100A4 promote immunosuppressive mesenchymal stromal cells (MSCs) by enhancing their kynurenine production. Impact of necrosis on tumor-associated MSCs
Hang R.1, Rojewski M.1, Wiesneth M.2, Yildiz T.1, Jahrsdörfer B.2, Schrezenmeier H.1,2,3, Lotfi R.1,2,3
1Universitätsklinikum Ulm, Institut für Transfusionsmedizin, Ulm, Germany, 2Institut für Klinische Transfusionsmedizin und Immungenetik Ulm gGmbH, Ulm, Germany, 3DRK Blutspendedienst Baden-Württemberg-Hessen gGmbH, Institut Ulm, Ulm, Germany
Introduction: Mesenchymal stromal cells (MSCs) are known to act as immuosuppressive cells, partially due to the expression of the enzyme in-doleamine dioxygenase (IDO) which converts tryptophan to kynurenine. Accumulation of MSCs within tumor tissue is associated with tumor pro-gression and poor prognosis. Necrosis with subsequent release of damage associated molecular patterns (DAMPs) is found in advanced solid tu-mors. ATP, HMGB1 and S100A4 belong to DAMPs family members We have already shown that DAMPs act as chemoattractants on MSCs also influencing their proliferation. We now sought to determine if DAMPs have any impact on immunosuppressive capacities of MSCs with specific regard to IDO-activity. Methods: MSCs were obtained from bone marrow from healthy donors cultured in alpha-MEM supplemented with 10% platelete lysate. Fibro-blastoid-shaped adherent cells with capacity for chrondrogenic, ostege-nic, and lipogenic differentiation and positive for CD73, CD90, CD105 and HLA-A, B, C and negative for CD34, CD3, CD45 were referred to as MSCs. To mimic a proinflammatory setting, IFNγ was added at a concen-tration of 100ng/ml. In the presence of ATP, HMGB1, or S100, MSCs were cultured for 4 days in DMEM containing 10% human serum and 100µg tryptophan/ml. Supernatants were tested for kynurenine in a coloromet-ric assay, as described previously. Metabolism was assessed by measuring WST-1 cleavage. MSC proliferation was measured by using CyQuant de-tecting DNA-content. Results: In the presence of ATP at concentrations between 62 to 2000 µM, HMGB1 ranging from 250 to 1000 ng/ml and S100 with 125 to 500 ng/ml, the expression of IDO in MSCs was enhanced in a dose dependent manner with increased kynurenine concentration within culturing media up to 60%, 30% and 100%, respectively. Of note, ATP-stimulated MSCs doubled their metabolism without any change in proliferation. Neither S100A4 nor HMGB1 enfluenced the metabolism of MSCs. Observed ef-fects could be almost entirely inhibited by adding apyrase, anti-TLR2, an-ti-TLR4 and anti-RAGE to antagonize ATP, HMGB1, and S100A4. Conclusions: We characterized ATP, HMGB1 and S100 as DAMP family members responsible for necrosis-induced immunomodulation. Given the increased concentration of DAMPs within tumor tissue and the fact that necrotic material / DAMPs can act as chemotattractants to MSCs, our results have implications for therapeutic strategies targeting the tumor microenvironment.
P-16-9Ducest-therapy, an innovative treatment for therapy of refractory chronic lower leg ulcers
Leitner G.C.1, Hofmann I.2, Szeles J.C.2
1Medizinische Universtät Wien, Klinik für Blutgruppenserologie und Transfusionsmedizin, Wien, Austria, 2Univ. Klinik für Chirurgie, Wien, Austria
Background: Lower extremity ulcers due to a variety of disorders are of-ten refractory to standard treatment. Various systemic and local cellular, infectious and vascular, factors can result in non-healing wounds. Beside the pain and the influence on quality of life (QuOL) amputation of the lower extremity is often the only resolution for this problem in these pa-tients. Platelet rich fibrin (PRF, Vivostat) is already known to have a wound healing capacity due to growth factor release. In the present retrospective investigation patients from our special surgical ambulance, treated with a

Transfus Med Hemother 2015;42(suppl 1):1–64Abstracts 63
combination therapy consisting of Dual cell stimulation (DUCEST) and PRF, were evaluatedMaterial and Methods: PRF was prepared from 120ml autologous blood using the Vivostat system, DUCEST is a punctual stimulation (P-Stim) of the vagus nerve at the ear. Stimulation of the vagus has analgesic and circulation stimulating properties. The patients suffered from vascular (venous and arterio-venous) diseases (n = 18), traumatic injuries (n = 9), osteomyelitis (n = 13), erysipelas (n = 1), phlegmone (n = 5) and others (n = 5). The combined treatment with or without additional antibiotics was applied in weekly intervals. Duration of treatment was between 3 months and 1 year. The size of the wounds was documented in length, deepness, necrosis and the extent of bacterial contamination. Additional photo documentation was performed.Results: A response to this treatment was seen in all patients. In 55.5% (n = 28) a complete wound healing was acheived. Amputation of the lower extremity was avoided in all patients. Some of them were already suffering from chronic ulcers since several years.Conclusion: The combination of DUCEST and PRF is a promising ther-apeutic option in patients with chronic ulcers, resistant to conventional treatment. Amputation can be avoided in the majority of these patients accompanied by a significant increase in QuOL
P-16-10Modifications of pooled human platelet lysate for efficient expansion of mesenchymal stem cells without Fibrinogen
Öller M.1,2, Feichtner M.2, Dunai Z.A.2, Raninger A.2,3, Laner-Plamberger S.1,2, Lener T.1,2, Gimona M.2, Hartl A.4, Bieback K.5, Rohde E.1,2, Strunk D.2,3, Schallmoser K.1,2
1Univ. Klinik für Blutgruppenserologie und Transfusionsmedizin, Paracelsus Medizinische Privatuniversität Salzburg, Salzburg, Austria, 2Spinal Cord Injury and Tissue Regeneration Center Salzburg (SCI-TReCS); Paracelsus Medical University (PMU), Salzburg, Austria, 3Institut für Experimentelle und Klinische Zelltherapie, Paracelsus Medizinische Privatuniversität Salzburg, Salzburg, Austria, 4Institut für Physiologie und Pathophysiologie, Paracelsus Medizinische Privatuniversität Salzburg, Salzburg, Austria, 5Institut für Transfusionsmedizin und Immunologie, Mannheim Medizinische Fakultät, Universität Heidelberg, Deutsches Rotes Kreuz Blutspendedienst Baden-Württemberg-Hessen, Mannheim, Germany
Efficient expansion of human mesenchymal stem/progenitor cells (MSCs) is a prerequisite for cellular and regenerative therapies. Previous studies have shown that pooled human platelet lysate (pHPL) can replace fetal bovine serum (FBS). After large scale expansion and cryopreservation characteristic phenotype, in vitro differentiation capacity and genomic stability of cells were maintained, considering animal serum-free cell cul-ture protocols as safe. pHPL preparation is not standardized and various protocols are used. Whether cell biology is affected by plasmatic human fibrinogen or by porcine heparin (hep) added to prevent pHPL medium clotting is unclear.We tested different fibrinogen depletion procedures: Clotting pHPL in medium (mcpHPL) or adding CaCl2 (pHPLS [serum]), both enabling heparin avoidance. All pHPL preparations were tested for fibrinogen content. Bone marrow- and adipose tissue (AT)-derived MSCs were cultured in medium supplemented with pHPL+hep, mcpHPL±hep, pHPLS±hep, or FBS±hep for up to 3 passages. Cell proliferation and clo-nogenicity were analyzed. AT-MSC surface markers were tested by flow cytometry. Differentially supplemented media (d0 vs d5) were tested for 45 growth factors and cytokines using a multiplex immunoassay. Fibrino-gen was depleted from mean 776 µg/ml in pHPL to < 1 µg/ml in mcpHPL and pHPLS. Cell proliferation and clonogenicity declined similarly over passages in pHPL media but we observed constantly exceeding reduced cell yields and colonies in FBS media. AT-MSCs in all media showed char-acteristic marker pattern. PDGF-BB (265–290 pg/ml), EGF (123–140 pg/ml) and BDNF (772–849 pg/ml) were similar in all different pHPL media and were consumed until d5, but never detectable in FBS media. MSC-de-rived VEGF-A increased until d5 in all pHPL media to 14,858–15,990 pg/ml compared to 7,514–9,668 pg/ml in FBS media.In conclusion, MSC culture is feasible in a completely animal-component free system without
fibrinogen and heparin. Effects on MSC function need to be determined. Our results may help to optimize efficient and safe cell expansion proto-cols for future clinical application.
P-16-11Innovative multi-dosage form enhances microbiological safety and user convenient application of autologous serum eye drops
Jochheim-Richter A.1, Siwy J.2, Bönig H.1, Schrott M.3
1German Red Cross Blood Service Baden-Württemberg-Hessen and Institute for Transfusion Medicine and Immunohematology of the Goethe University, Frankfurt, Germany, 2Mosaiques diagnostics and therapeutics AG, Hannover, Germany, 3Central Apotheke, Steinbach, Germany
Objective(s): Aqueous tear deficiencies lead to ocular surface disease like sicca syndrome. Beside conventional treatment that mainly consists of the use of preservative-free artificial eye drops and punctual occlusion, autologous serum eye drops contain essential tear components that are beneficial for corneal and conjunctival integrity. Autologous serum eye drops have been reported to be effective for the treatment of ocular sur-face disorders but are vulnerable to microbiological contamination. Due to the resulting short expiry of serum eye drops an adequate packaging is essential.Method: To evaluate the effectiveness of the multidose 3K®-System (Aero Pump GmbH), autologous blood was collected from 10 volunteers, bot-tled and stored under various conditions for up to six months. Microbi-ological testing (Ph.Eur.) was performed intermittently as well as protein patterning analysis by means of CE/MS to identify substances that may serve as quality markers of stability. Results: The preservative free system (fig.1) showed a high dose consis-tency and was free of microbial contamination to at least 7 days post-thaw and for the frozen batch of at least 6 months.
Fig. 1.]
3K® Ophthalmic Multidose SystemPreservative free multidose eye care medication, easy to use side actuation combined with the advantages of a high accuracy dosing pump system with exactly defined drop size and single dose delivery control prevents waste of valuable product In summary, we are presenting a novel packaging system for serum eye drops which provides high microbial safety and hence extends the shelf-life of individual vials of serum eye drops to at least 7 days post-thaw while providing shelf-life for the frozen batch of at least 6 months. The benefits for the patient include increased safety, reduced frequency of blood col-lection and better accessibility of serum eye drop therapy in all relevant indications. The benefit for the health care system is markedly reduced annual cost. Last both authors contributed equally.
© 2015 S. Karger GmbH, Freiburg
Accessible online at: www.karger.com/tmh
Fax +49 761 4 52 07 [email protected]
Transfus Med Hemother 2015;42(suppl 1):65–68
Author Index
Abdul-Khaliq H. FV-03-5Agis H. FV-01-7Ahrens N. P-03-1, P-04-3, P-06-25 Albrecht B. P-06-10Albrizio M. P-06-29, P-06-32Aleksandrova K. P-12-4Althaus K. P-15-4Altherr D. P-16-4Alvermann G. P-12-8Alzubi J. FV-04-4Amar el Dusouqui S. FV-07-3Amrein K. FV-06-2Angert K. P-08-5Anliker M. FV-07-1, P-06-8 Ardin S. FV-03-6Arlt N. P-09-5Auersperg V. P-10-1Aurich A.-C. P-07-3Aurich K. P-15-4, PSB-01-2Avdic A. P-06-17Axt-Fliedner R. FV-07-2, P-06-6
Baal N. FV-09-4Bakchoul T. P-06-15, PSB-01-1, PSB-01-2Bal G. P-06-20Balduff M. P-06-18Bartolmäs T. P-06-19, P-06-28Baschin M. FV-08-1, P-02-1, P-06-15 Baumann-Baretti B.I. FV-06-4, P-01-2Becker E. P-14-2Becker P. FV-04-8, P-16-3 Beelen D. FV-01-4, P-05-1 Beer J.H. FV-02-2Behrens L. P-08-4Beiglböck E. P-15-3Bein G. FV-07-2, FV-07-8, FV-09-4,
FV-10-2, P-06-6, P-06-16 Berens C. P-15-2Besson N. FV-09-3Betten S. P-07-1Beyer T. P-16-2Biazik-Glaw H. FV-03-6Bieback K. FV-04-7, FV-10-4, P-16-10 Bieringer M. P-02-3, P-02-5Bittner R. P-06-2Blasczyk R. FV-04-2, P-12-4, P-16-1 Boehm W. P-06-25Bönig H. FV-04-8, P-16-11 Bonsack M. FV-04-1Börger A.-K. FV-04-2Bornhäuser M. FV-04-1Braisch M.C. FV-07-3Brassel Rodrigues A. FV-06-1Bräuninger A. FV-07-2Brettner S. FV-08-2Brisner M. P-06-14Brixner V. FV-02-1, FV-02-3, FV-04-6Brockmann C. FV-03-3, P-08-2 Brys B. FV-06-4, P-01-2
Eiz-Vesper B. P-16-1Elvers-Hornung S. FV-04-7Enczmann J. FV-01-9Engelmann K. FV-04-2Engels J. P-12-5Enkel S. P-08-3Enko D. P-10-1, FV-10-3Erickson A. FV-02-3Erle A. P-16-5Ernst C. FV-02-1Ertl B. P-06-16Escobedo G. P-06-18Eyer C. FV-02-5
Fabricius D. P-16-2Fasler M. P-06-30Fehling S.K. PSB-01-4Feichtner M. P-16-10Figueiredo C. FV-04-2, P-16-1Filimonov V.D. P-16-6Fischer I. P-12-3Fischer J.C. FV-01-9, FV-09-2Fischer T. P-12-7Fleischhauer K. P-05-1Flesch B. P-16-4Flommersfeld S. P-06-16Frank J. PSB-01-5Frey B.M. FV-07-3, P-02-3, P-02-5, P-06-9,
PSB-01-3 Friemann A. FV-08-4Fritsch G. FV-01-7Fröhner V. FV-07-2Fürst D. FV-01-1, FV-01-6, P-15-5
Gabriel C. P-06-14Gassner C. FV-07-3, P-06-9, PSB-01-3Gathof B. FV-03-6Gathof B.S. FV-02-8, P-04-2, P-08-4, P-14-1Gattenlöhner S. FV-07-2Gäumann R. FV-02-5Geisen C. FV-02-1, FV-02-3, PSB-01-4Geißler R.G. FV-03-8Gerber K.-D. P-02-2Gernhuber J. FV-03-3Gersonde I. P-08-1Gheisari R. P-09-4Giebel B. P-15-1Gielen J. FV-02-8Giers G. P-09-3, P-09-4Gimona M. P-16-7, P-16-10Glessing P. P-07-8Gnoth S. P-06-4Gobbato S. FV-02-2Goerdt S. P-06-17Görg S. FV-02-6, FV-03-3, P-07-8, P-08-2Görgens A. P-15-1Gortner L. FV-03-5Gottschalk J. FV-07-3
Bugert P. FV-04-7, FV-07-5, P-06-26, P-06-27
Buhmann R. FV-01-3, PSB-01-5Bulduk M. FV-01-8Bunjes D. FV-01-1, FV-01-6, P-15-5Burg-Röderfeld M. FV-07-8Burkhart J. FV-07-5Busemann N. FV-03-3Buser A. FV-02-2, FV-06-1, FV-07-3,
FV-09-6Buwitt-Beckmann U. FV-01-5Bux J. P-06.12 Caesar A. P-06-1, P-06-9Cantz T. FV-01-3Capalbo G. FV-10-5, P-13-,Cappius H.-J. P-08-1Castelli D. FV-07-3Cathomen T. FV-04-4Chudy M. FV-02-7Conradi R. P-06-4Cooper N. P-06-6Corash L. FV-02-1Crivello P. P-05-1
Dahse K. P-06-24, P-06-31Danzer M. P-06-14Debatin K.-M. P-16-2Degenhardt J. FV-07-2, P-06-6Dehl J. FV-07-2Deisting C. FV-07-2Dengler T. P-07-6Desgeorges A. P-16-7Dhayat S. FV-03-8Dickau K. FV-06-6Diekmann J. FV-05-3Dienst A. FV-09-2Dierks N. P-06-24, P-06-31Dobrinski C. FV-10-4Doescher A. FV-07-6, P-06-4, P-06-11,
P-06-13, P-06-21, P-06-24, P-06-31 Dombos S. FV-02-3Döscher A. P-06-3Dreier J. FV-05-3, P-07-5Dreßen P. FV-08-2Drexler C. FV-06-2, FV-07-9Dunai Z.A. P-16-10Dürig J. P-15-1Dürrenfeld A. P-01-2
Eberhardt M. FV-05-3Eberle J. FV-02-7Eckstein R. P-06-26Eggenschwiler R. FV-01-3Eichler H. FV-03-5, FV-08-3, FV-08-5,
P-02-2, P-04-7, P-07-4, P-16-4 Eickmann M. PSB-01-4Einsele H. FV-01-1
Author IndexTransfus Med Hemother 2015;42(suppl 1):65–6866
Goudeva L. P-12-4, P-16-1Gourri E. PSB-01-3Gowland P. P-09-1Graber J. P-06-30Grabmer C. P-12-6Grabowski C. FV-09-5Grabowy H. P-02-2Graf N. FV-03-5Gramatzki M. FV-01-5, FV-01-8Grassl S. FV-04-5Gratchev A. P-06-17, P-06-18, P-07-7Gravemann U. FV-02-4, P-04-1, P-07-2Greinacher A. FV-06-6, FV-08-1, P-02-1,
P-06-15, P-15-4, PSB-01-1, PSB-01-2Greinix H.T. FV-01-7Grez M. FV-04-8Grimsley S. P-06-11Groß J. FV-03-5, P-02-4, P-04-7Gross J.C. P-07-4Gross M. P-13-2Groß M. FV-10-5Groten A. FV-01-9Grunwald S. P-09-3Gubbe K. P-13-2Gudima A. P-05-2, P-16-6Günther A. FV-01-5Gurski L.A. FV-08-5Gürtler L. FV-02-7
Haas R. P-09-3Hackstein H. FV-09-4, P-06-6Hagen C. FV-03-3, P-08-2Hahn J. P-06-5Hakvoort K. P-04-1Halwachs-Baumann G. FV-10-3, P-10-1Handke W. FV-02-4, P-04-1, P-07-2Hanenberg H. P-15-1Hang R. P-16-8Harmsen M. P-06-17, P-06-18, P-07-7Hartl A. P-16-10Hartwig U.F. FV-04-3Hauber D. FV-01-6, P-15-5Hauser M. P-09-3Haussels I. FV-08-2Heiliger M. P-06-29, P-06-32Heim M.U. FV-03-1, P-14-2Heinemann F.M. P-05-1Heinold A. P-05-1Heinrichs S. FV-01-2Heinz-Senf P. FV-10-5Hellmann I. P-04-6Hellmich M. P-08-4Henke A. FV-10-1Hennecke J. P-16-3Hennig H. FV-02-6, P-07-8Henny C. P-06-30Henschler R. FV-01-3, FV-02-1, FV-02-3,
FV-04-3, FV-04-6, FV-10-1Hertfelder H.J. FV-08-2Herziger A. P-06-34Heuft H.-G. P-12-4Hilge A. P-12-2Hilger K. P-12-2Höchsmann B. FV-07-1Hofmann I. P-16-9Högel J. P-01-1
Holbro A. FV-06-1, FV-09-6Homann J. FV-08-2Höppner S. P-06-22Horn P.A. FV-01-2, FV-01-4, P-05-1, P-15-1,
PSB-01-7Hornung V. FV-09-4Hoth M. P-16-4Hourfar K. FV-02-7, P-07-6Huang N. FV-02-1Hübler C. FV-06-3Hübner U. P-02-2Hummel B. P-02-2Humpe A. FV-01-5, FV-01-8Hustinx H. P-06-30Hutchinson J. P-03-1Hutschenreuter G. P-08-5
Infanti L. FV-02-2, FV-06-1, FV-07-3, FV-09-6, P-06-30
Jahrsdörfer B. FV-04-5, P-16-2, P-16-8Jakobs C. FV-09-4Janetzko K. FV-02-3, FV-10-4, P-06-22Jaster G. FV-06-4Jenichen G. FV-06-6Jirout Z. FV-09-6Jochheim-Richter A. P-16-11Johnsen M. FV-06-3, P-04-6Jouni R. PSB-01-1Juhl D. FV-02-6, P-07-8Jungk H. FV-06-5Just B. P-06-11, P-06-28
Kann G. PSB-01-4Karagianni M. PSB-01-5Kasprzik-Diehl A. P-06-22Kellner C. FV-01-8Keshelashvili K. FV-09-6Ketter R. P-16-4Khadour A. PSB-01-1Khan S.A. FV-04-3Kiefel V. P-06.12, P-06-33Kießig S. P-12-8Kiessig S.T. P-09-2Kiessling A.-H. FV-02-1Kirchgessner K. P-06-29, P-06-32Kischnick T. FV-06-5Kissel K. P-06-25, P-06-29, P-06-32Klemm D. P-16-3Klump H. PSB-01-7Klüter H. FV-04-7, P-05-2, P-06-22, P-07-7,
P-16-6 Knabbe C. FV-05-3, P-07-5Knowles L.M. FV-08-3, FV-08-5Kobbe G. FV-01-9, FV-09-2Koch H. FV-05-2Kollar K. FV-04-6Koller A. PSB-01-6Kömürcü N. FV-07-5, P-06-27Kondakci M. FV-01-9Kordelas L. FV-01-4Körper S. FV-01-6, P-15-5Kraas S. P-04-6Krähling V. PSB-01-4
Krauel K. PSB-01-1Krautwurst A. FV-07-2Kreissig C. P-12-3Kremmer E. P-06-17Krenning G. P-06-17Kress J. FV-02-7Krettek U. P-12-4Kriegshäuser G. FV-10-3, P-10-1Kroll H. FV-09-5Kronstein-Wiedemann R. FV-07-4Krüger W. P-15-4Krull M. P-12-8Kuch S. P-01-1Kühling E. FV-07-6, P-06-21Kuta P. P-06-26Kzhyshkowska J. P-05-2, P-06-17, P-06-18,
P-07-7, P-16-6
Laier S. P-06-10Laitinen T. P-12-7Laner-Plamberger S. P-16-10Lauer H. P-02-4, P-07-4Lehnert E. P-09-4Leib S. FV-02-5Leibacher J. FV-02-1, FV-02-3, FV-04-6Leitner G.C. P-16-9Lejon Crottet S. P-06-30Lener T. P-12-6, P-16-7, P-16-10Leo A. P-06-10Li F. P-06-18, P-07-7Lindemann M. P-05-1Lindenau I. FV-06-2Link A. P-02-4Listopad J.J. P-01-2Lizardo B. P-04-6Lodemann P. P-02-3Lotfi R. FV-04-5, P-16-5, P-16-8Luetjens P. P-06-11Lüscher T.F. FV-02-2
Macher S. FV-06-2MacLennan S. PSB-01-4Madla W. FV-06-5Madlener K. FV-02-1Maenner D. FV-10-2Mages J. P-04-3Maier K. P-12-2Mamontova E.M. P-16-6Manderla J. FV-04-1Manousaridis I. P-06-17Mansouri Taleghani B. FV-07-7, FV-09-3,
P-06-7, P-12-5, PSB-01-6Marbacher C. FV-09-3Marcovic A. FV-07-3Mardt I. P-06-3Marell R. P-06-32Marell R.- R. P-06-25, P-06-29Marschall R. P-06-16Martens J. P-12-4Matko S. FV-04-1Matuschik L. P-05-2Matzhold E.M. FV-07-9Mauchle P. FV-06-1Maurer S. P-03-2Mayer B. P-06-15, P-06-19, P-06-28, P-06-34
Transfus Med Hemother 2015;42(suppl 1):65–68Author Index 67
Mayer G. P-12-6Medina Escobar P. FV-03-4Medvidov M. PSB-01-2Méndez A. P-03-2Meyer O. P-06-23Meyer S.C. FV-02-2Meyer S. FV-07-3, P-06-9Michel G. FV-09-4Möckel M. P-06-23Moganti K. P-05-2, P-06-18, P-07-7Molderings G.J. FV-08-2Möllmann M. P-15-1Moog R. FV-03-7, P-04-6, P-09-5Moslem M. FV-01-3Mueller B. FV-05-1Mueller C. FV-04-2Mueller S. P-06-29, P-06-32Mufti N. FV-02-1, FV-02-3Müllejans B. FV-06-6Müller B. FV-05-2Müller I. P-04-7, P-16-4Müller J. FV-08-4, P-15-2Müller M. FV-02-1, FV-02-3Müller O. FV-06-1Müller T. P-04-1Müller-Steinhardt M. P-06-22Murke F. P-15-1Mussolino C. FV-04-4Mytilineos J. FV-01-1, FV-01-6, P-15-5
Naundorf S. FV-04-8Nessel K. P-07-3Netsch P. FV-04-7Netz U.J. P-08-1Neuenschwander K. P-06-9Neyrinck M.M. FV-09-1Niederhauser C. FV-02-5, P-06-30, P-09-1Niederwieser D. FV-01-1North A. FV-02-1Northoff H. P-08-3Nowak-Harnau S. P-08-3Nowakowska P. FV-04-8, FV-07-4Nübling M. FV-02-7Nydegger U. FV-03-4
Ochmann O. FV-05-1Odendahl M. FV-04-1, FV-04-8Oergel T. P-15-4Oertel J. P-16-4Offner R. P-03-1, P-04-3Ohlenforst S. FV-08-2Oldenburg J. FV-08-2, FV-08-4, P-15-2Öller M. P-16-10O'Meara A. FV-09-6Ottinger H. P-05-1Otto J. P-12-1Ovsij I. P-06-17
Pachler K. P-16-7Palankar R. PSB-01-2Pallant C. FV-04-4Pannicke U. P-01-1Peetz D. P-02-3, P-02-5Pehlic V. FV-06-1
Peipp M. FV-01-8Peters C. P-02-2Petershofen E.K. FV-07-6, P-06-4, P-06-13,
P-06-21, P-06-24, P-06-31 Peyrard T. PSB-01-3Pfaffl M.W. FV-10-1Pfeiffer H.-U. FV-02-3Pfeuti S. FV-09-3Pfreundschuh M. FV-01-1Pichl L. FV-05-1, FV-05-2Pichler H. FV-03-2, P-15-3Pignalosa D. FV-01-2Pilch J. FV-08-3, FV-08-5, P-02-2Platenkamp K. P-04-1Platz A. P-07-3Pohl S. P-09-2Polin H. P-06-14Pötzsch B. FV-08-4, P-15-2Priesner C. P-12-4Pruß A. P-13-1
Quandt T. FV-02-6
Rach J. P-04-1, P-04-5Radojska S. FV-03-6, P-04-2Radtke S. P-15-1Rahn H. P-06-29Raninger A. P-16-10Rau E. FV-05-1Rauch S. P-06-8Rebmann V. FV-01-4, P-05-1Reichenberg S. FV-02-4, P-07-2Reil A. FV-05-1, P-06.12Reiner M.F. FV-02-2Reinhardt P. FV-01-6, P-15-5Reinprecht C. FV-06-2Reisner R. FV-01-7Reiter A. P-06-14Riabov V. P-05-2, P-06-17Richter E. FV-07-5Rico S. FV-02-1Riedmaier I. FV-10-1Riemann S. P-07-7Ries J. FV-07-3Rindlisbacher I. P-06-7Ringel F. P-06-20Rink G. FV-04-7, FV-07-5, P-06-26, P-06-27 Risch L. FV-03-4Risch M. FV-03-4Ritgen J. P-06-8Ritter R. P-15-3Rohde E. P-12-6, P-16-7, P-16-10Rojewski M. FV-04-5, P-16-8Rothe R. P-04-6, P-09-5Rothenberger S. P-06-27Rox J.M. FV-09-2Ruan C. FV-07-8Ruckser R. FV-01-7Rüfli T. P-06-30Rühl H. FV-08-2, FV-08-4, P-15-2Rummler S. PSB-01-4
Sachs U. FV-07-2, FV-07-8, P-06-6Sachs U.J. P-06-16
Salama A. P-06-15, P-06-19, P-06-20, P-06-23, P-06-28, P-06-34
Santoso S. FV-07-2, FV-07-8, FV-10-2, P-06-6
Sareban N. FV-06-2Sarraj A. FV-07-3Sauer A. P-07-3Schäfer R. PSB-01-4Schaffert T. P-06-29, P-06-32Schallmoser K. P-12-6, P-16-10Scharberg A.E. P-06-10Scharberg E.A. FV-07-5, P-06-27, PSB-01-3Schauwecker P. FV-01-6, P-15-5 Scheffels B. P-14-1Scheffler A. PSB-01-5Schelker R. P-03-1Schenck P. P-06-21Schenk D. PSB-01-6Schenk J.F. P-02-4Schlager S. P-12-6Schlenke P. FV-06-2, FV-07-9Schmandt S. P-06-2Schmid S. P-03-1Schmidt A.H. P-07-3Schmidt J.-P. FV-09-5Schmidt M. FV-02-7, FV-10-5, P-07-6,
P-13-2, PSB-01-4Schmitz M. FV-04-1Schnegg A. FV-06-1Schnell P. FV-03-3Scholz L. PSB-01-2Schönfeld K. FV-04-8Schottstedt V. FV-05-1Schrezenmeier H. FV-01-1, FV-01-6,
FV-04-5, FV-07-1, P-06-8, P-15-5, P-16-2, P-16-5, P-16-8
Schröck M. FV-06-2Schröder T. FV-01-9Schroeder H.W. P-02-1Schroeder T. P-04-5Schroeter J. P-13-1Schrott M. P-16-11Schulz U. P-06.12Schulze S. P-14-2Schüttfort G. PSB-01-4Schwarz E. P-16-4Schwarz E.C. FV-08-5Schwarz F. FV-03-5Schwarz K. P-01-1, P-15-5Schwind P. P-06-1, P-06-9Seidl C. P-16-3, PSB-01-4Seifried E. FV-02-1, FV-02-3, FV-02-7,
FV-04-6, FV-04-8, FV-07-4, FV-10-5, P-07-6, P-13-2, P-16-3, PSB-01-4
Selbitz A. FV-08-2Selleng K. FV-06-6Selleng S. FV-06-6, FV-08-1, P-02-1 Seltsam A. FV-02-4, P-04-1, P-07-2Senninger N. FV-03-8Seyfried T. P-03-1Sibrowski W. FV-03-8Siderow A. P-03-2Sierra D.A. FV-10-4Sigle J. FV-09-6Sigle J.-P. P-03-2Sipurzynski S. FV-06-2Sireis W. FV-10-5, P-13-2
Author IndexTransfus Med Hemother 2015;42(suppl 1):65–6868
Siwy J. P-16-11Skenderi Z. P-13-1Skodnik K. P-04-3Somogyi-Dunai Z. P-16-7Spyrantis A. FV-10-5, P-13-2Stankevich K.S. P-16-6Starke U. P-08-3Staudinger M. FV-01-8Steinbicker A. FV-03-8Steinke T. P-12-2Stephan B. P-02-2, P-02-4, P-04-7, P-07-4Steppat D. FV-02-6Stern M. FV-09-6Stivala S. FV-02-2Stojakovic T. FV-06-2Stolba R. FV-10-3, P-10-1Stolle S. P-06-21Stolz M. P-09-1Störmer M. FV-02-8, P-04-2, P-08-4, P-14-1Strathmann K. P-06-11, P-08-5Strecker T. PSB-01-4Streif D. P-12-6, P-16-7Stricker N. P-16-3Strobel E. P-07-1Strobel J. P-06-26Strunk D. P-16-10Stuhler G. FV-01-1Stüpmann A.S. P-06-33Stürtzel A. P-06-10Suessner S. P-06-14Suhr H. FV-10-4Sumian C. FV-02-4, P-07-2Sümnig A. P-06-15Szeles J.C. P-16-9
Taborski U. P-12-7Teichweyde N. PSB-01-7Theobald M. FV-04-3Thiele T. FV-08-1, P-02-1Thierbach J. FV-06-4, FV-07-3Thornton N. P-06-11Thrasher A. FV-04-4Tijink M. P-04-1Tonn T. FV-03-7, FV-04-1, FV-04-8,
FV-06-3, FV-07-4, P-04-6Trestyanszki I. P-06-24, P-06-31Trost B. FV-01-5Trost N. FV-07-3, P-06-9Trzaska T. P-16-2Tsamadou C. FV-01-1Tverdokhlebov S.I. P-16-6
Uhlig S. FV-04-7Uhrberg M. FV-01-9Ulrich E. FV-06-4Unkrig S. FV-08-2Unnerstall B. FV-06-5Urbschat S. P-16-4
Van Kraaij M. PSB-01-4Vetsch G. FV-09-3Vitoriano S. P-15-1Vogt C. FV-07-6, P-06-13Vogt M. FV-07-7, P-06-7Volgmann T. P-04-1, P-04-5Volken T. PSB-01-6Volkholz S. P-12-2Vollmer T. FV-05-3, P-07-5Vollmert C. FV-07-3Von Goedecke A. P-10-1Von Zabern I. FV-07-1, P-06-8Vrielink H. FV-09-1Vysniauskaite M. FV-08-2
Wachowiak A. P-09-2Wagner B. PSB-01-5Wagner E. FV-01-1Wagner F. P-06-2, P-06-3Wagner H. FV-10-3Wagner T. FV-07-9Waldmann R. P-01-1Walkenhorst R. P-06-28Walter L. P-06-29, P-06-32Waterstradt M. P-15-4We M.-W. FV-07-8Weber I. FV-02-3, FV-04-3
Weber K. P-12-7Weber S. FV-07-5Weiland T. P-06-5Weingand T. FV-07-3Weinigel C. P-12-2, PSB-01-4Weinstock C. FV-07-1, P-06-8, P-06-10Wels W. FV-04-8Wenzel F. P-09-3Werth S. FV-07-8, FV-10-2Wesche J. PSB-01-1, PSB-01-2Westphal A. FV-06-6, FV-08-1, P-02-1Wichmann C. FV-01-3, FV-10-1, PSB-01-5Wieckhusen C. P-06-26, P-06-27Wiedemann P. FV-10-4Wienzek-Lischka S. FV-07-2Wiesneth M. FV-01-6, FV-04-5, P-15-5,
P-16-8Wihadmadyawati H. FV-07-8Winkelmann M. FV-04-5Winterfeld S. FV-09-5Witt V. FV-03-2, P-15-3Wittig D. FV-04-2Wittmann G. PSB-01-5Wolf T. PSB-01-4Worel N. FV-01-7Wotapek T. FV-02-3Wulf G. FV-01-1
Yakut E. FV-09-4Yildiz T. P-16-8Yürek S. P-06-19, P-06-28
Zeiler T. FV-06-5Zhang C. FV-04-8Zhang H. P-16-1Zickler A.M. FV-01-2Ziemann M. P-07-8Zimmermann A. FV-06-4Zimmermann G. P-03-2Ziyaie-Hochstrat O. P-12-8Zojer N. FV-01-7Zollikofer C. FV-01-1Zöllner H. PSB-01-1