
Suppl 3 to NRC Info Notice 86-106, "Feedwater Line Break ...
Upload
khangminh22Category
view
0download
0
Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-01Risk Factors and Prevention of Stroke
SIGLEC SNPs located at 19q13.41 (e.g., rs2034891) May Increase the Major Bleeding Riskin Patients on Direct Oral Anticoagulants
Tae-jin Song 1, Yee Jeong 2, Junbeom Park 3, Hye Sun Gwak 4
1 Neurology, Ewha University College of Medicine, Seoul, Korea2 Pharmacy, College of Pharmacy and Graduate School of Pharmaceutical Sciences, Seoul, Korea3 Cardiology, Ewha University College of Medicine, Seoul, Korea4 Pharmacy, College of Pharmacy and Graduate School of Pharmaceutical Sciences, Seoul, Korea
Purpose:Direct oral anticoagulants (DOACs), including dabigatran, rivaroxaban, apixaban, and edoxaban, are widely usedfor anticoagulation therapy. Despite of its efficacy, bleeding is the most serious and common complications ofDOACs. The purpose of this study is to identify the genetic factors associated with bleeding in Korean patientsreceiving DOACs.Methods:This study was a multicenter retrospective study of prospectively collected samples from June 2018 to October2019 using a case-cohort study design. A genome-wide association study (GWAS) was performed to identify thesingle nucleotide polymorphisms (SNPs) associated with the bleeding complications in the patients on DOACs.Multivariable logistic regression analysis was employed to investigate the independent risk factors for bleeding.Results:A total of 138 patients were included in the analysis; 27 cases for major bleeding, 7 cases for clinically relevantnon-major bleeding, and 104 controls. Old age (≥ 65 years), moderate or severe renal impairment (CrCl < 50 mL/min) and edoxaban treatment along with high CHA2DS2-VASc and modified HAS-BLED scores weresignificantly associated with major bleeding. The SIGLEC SNPs located at 19q13.41 were identified as thesuggestive signals for major bleeding. For rs2034891, the per-allele adjusted odds ratio was 3.6 (95% CI: 1.6–8.5,p-value = 0.003). The area under the receiver operating characteristic curve values of the multivariable modelfor major bleeding were approximately 0.8.Conclusions:This GWAS identified that the SIGLEC SNPs located at 19q13.41 (e.g., rs2034891) could increase the majorbleeding risk in patients on DOACs. Although this study is limited to a retrospective study design and relativelysmall sample size, this is the first GWAS for major bleeding in patients on DOACs.
1

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-02Prognosis/Outcome of Stroke
Machine Learning Model for The Prediction of Intracerebral Hemorrhage in Acute Ischemic Stroke PatientsReceiving Intravenous Thrombolysis
Poonnakarn Panjasriprakarn 1, Aurauma Chutinet 1
1 Medicine, Faculty of Medicine, Chulalongkorn University, King Chulalongkorn Memorial Hospital, Bangkok,Thailand
Purpose:Background: Pre-existing clinical risk scoring systems for the prediction of intracerebral hemorrhage (ICH) inpatients with acute ischemic stroke receiving with intravenous (IV) thrombolysis have low-to-moderateperformance and are mostly derived from western countries. Machine learning, considered a branch of artificialintelligence (AI), is a promising approach to predict clinical outcomes. Objective: To develop a model usingmachine learning to predict outcome in thrombolysis patients and assess its performance through comparisonwith a clinical predictive Symptomatic Intracranial Hemorrhage (SICH) score in Thai population.Methods:Patients with acute ischemic stroke and receiving intravenous tissue plasminogen activator (tPA) at KingChulalongkorn Memorial Hospital (KCMH), Bangkok between January 2009 and April 2016 and in PhrapokklaoHospital (PKH), Chanthaburi, Thailand between January 2019 and July 2019 were included. Patients who did notreceive follow-up brain imaging 24 hours post IV tPA or did not obtain a standard treatment dose of tPA wereexcluded. All patients received at least one follow-up CT brain imaging to evaluate complications after tPA.Classification models were used to predict ICH and internal validity was then analyzed. Predictive performanceof our supervised learning model and clinical SICH score was assessed by using the area under the receiveroperative characteristic curve (AUC).Results:After exclusion, 489 consecutive patients with acute ischemic stroke in KCMH (n = 362) and PKH (n = 127)received IV thrombolysis. Mean age was 64 year and 53% were male. Incidence of symptomatic ICH was 7.3%(36 of 489). Our machine learning model (AUC 0.80, 95%CI 0.79-0.81) performed better in predictive accuracythan SICH score (AUC 0.69, 95%CI 0.68-0.70). (Figure 1)
2

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:The machine learning model showed remarkable performance compared to clinical score in predicting ICH inpatients with acute ischemic stroke receiving IV thrombolysis. Our AI-based model should be considered as anadequate ICH predicting tool.
3

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-03Acute Management
The Significance of D-dimer Level in Acute Ischemic Stroke Patient with Active CancerTreated by Mechanical Thrombectomy
Kwang Hyun Pan 1, Jaeyoun Kim 1, Jong-won Chung 1, Keon Ha Kim 2, Oh Young Bang 1, Pyoung Jeon 2, Gyeong-moon Kim 1, Woo-keun Seo 1
1 Neurology, Samsung Medical Center, Sungkyunkwan University, Seoul, Korea2 Radiology, Samsung Medical Center, Sungkyunkwan University, Seoul, Korea
Purpose:The etiology of stroke due to cancer-related coagulopathy is thought to be different from conventional strokemechanisms and emerging etiology of stroke. We studied whether D-dimer might help to make decisionswhether to proceed mechanical thrombectomy(MT) and predict clinical outcomes in cancer stroke patients.Methods:Total of 369 stroke patients were screened as patients with active cancer from Samsung Seoul medical centerstroke registry(January to and February 2020). Patients were enrolled who was: age≥18years; a NIHSS score≥6; lesion vessel in the ICA, MCA; stroke onset within 24h.Results:A total of 68 cancer stroke patient’s mean age was 65.59 years, 52.9% were male, 47% had lung cancer, 52.9%had distant metastasis and the average NIHSS score was 14.17. Among the 68 patients, 36 patients were treatedby MT and 20 patients were successfully recanalized. The overall 3-month mortality was 50% and favorableoutcome(3-month mRS 0~2) was 26.5%. We divided patients in 2 groups by D-dimer level<4 group(N=25) and D-dimer level≥4 group(N=43). The D-dimer<4 group showed higher successful recanalization(mTICI 2b~3) rate than D-dimer>4 group(73.68% vs 35.29%) and higher rate of favorable outcome(63.16% vs 5.88%). The mortality ratewas higher in D-dimer>4 group(58.85% vs 10.53%). The multivariate logistic regression analysis showed the riskfactors of the 3-month mortality; MT(OR0.297,p=0.027) and D-dimer>4(OR 16.230,p<0.001). The factors ofclinical favorable outcomes were lesion volume(OR 0.936,p=0.009) and D-dimer<4(OR 0.098,p=0.005). Thesubgroup analysis showed, the favorable outcome was significantly poor in the patient D-dimer>4 treated byMT(OR0.06,p<0.01), and D-dimer<4 group showed a tendency to have favorable outcome(OR 1.71,p>0.05). Ifthe patient had D-dimer>4, the favorable outcome was significantly less either treated by MT or not(OR0.08,p<0.01 vs OR0.06,p<0.01) and there was significant interaction between D-dimer and MT(p-for-interaction<0.01). The 3-month morality risk was significantly high in the patients with D-dimer>4 and nottreated by MT (OR4.20,p<0.01, p-for interaction 0.47) but the risk was significantly low in the patients with D-dimer<4 and treated by MT(OR0.12,p<0.01).Conclusions:Our study showed the D-dimer level was an independent factor affecting clinical favorable outcomes andmortality in cancer stroke patients who treated by MT. Therefore, careful patient selection for MT in cancer strokepatient with high D-dimer level is considered.
4

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-04Epidemiology
Long-term Exposure to Air Pollution Increases The Mortality Rates by Subarachnoid Hemorrhagein Women; A Nationwide Analysis in South Korea
Jeongeun Hwang 1, Eun-jae Lee 2 , Hahn Yi 3 , Miso Jang 1 , Namkug Kim 4 , Sun Kwon 2
1 Medicine, University of Ulsan, College of Medicine, Seoul, Korea2 Neurology, Asan Medical Center, Seoul, Korea3 Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea4 Convergence Medicine, University of Ulsan, College of Medicine, Seoul, Korea
Purpose:Sex may be a modifier of the effects of air pollution on stroke mortality. We aimed to examine sex differences inassociations between air pollutant concentration and the morality for subarachnoid hemorrhage (SAH).Methods:We used data from nationwide databases between 2001 and 2018: mortality statistics from the Korean StatisticalInformation Service and air pollutant information (CO, SO2, NO2, PM10, and PM2.5 concentrations) via theAirKorea database. The SAH mortality was identified by using I60 code according to the InternationalClassification of Diseases, 10th revision. Mortality data were provided for 250 districts, while air pollution datawere captured from 332 stations across the nation. Distance-weighted linear interpolation was performed toassign average air pollutant concentrations for each district through the study period. Multivariable betaregression models for the SAH mortality rates were built with interquartile-range change of each air pollutant,adjusting for socioeconomic and meteorological factors.Results:During the study period, the mean annual age-adjusted mortality rates by SAH were 2.74 in males and 4.43 infemales (both per 100,000). With multivariate models, significant associations between NO2, SO2, and PM10concentrations and female SAH mortality rates were demonstrated, while no significant associations were shownin the analysis of the male SAH mortality rates (Figure 1). Female and male SAH mortality rates showedqualitatively different association patterns with air pollutant concentrations, that SAH mortality is moreprudently associated with NO2, SO2, and PM10 concentrations in females than in males.
5

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:The effect of air pollution on the SAH mortality may differ according to sex, suggesting the need for tailoredstrategies for air pollution in stroke management.
6

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-05Acute Management
Increase Futile Recanalization Rate without MRI Study During the COVID-19 Pandemic Period: A Single-center Experience
Do-sung Yoo 1, Kwan-wook Jo 2, Hae-kwan Park 1
1 Neurosurgery, Eunpyeong St. Mary’s Hospital, The Catholic University of Korea, College of Medicine, Seoul,Korea2 Neurosurgery, Bucheon St. Mary's Hospital, The Catholic University of Korea, College of Medicine, Bucheon,Korea
Purpose:Intravenous tissue plasminogen activator administration (IV-tPA) and additional intraarterial thrombolysis (IA-Tx)are regarded as standard treatments for ischemic stroke. The recanalization rate of IA-Tx is increasing, thanks tonew device development and greater interventional experience. Perfusion/diffusion mismatching (P/D-mismatch) on MRI is regarded as the best method for patient selection, but during the COVID-19 pandemicperiod, futile recanalization after IA-Tx increased without prior MRI studies.Methods:A total of 131 patients with anterior circulation larger vessel occlusion and treated with IA-Tx were included inthis study. In 81 cases, initial diagnostic imaging was performed using multimodal CT followed by stroke MRIstudies prior to IA-Tx. Another 50 cases admitted during the COVID-19 pandemic could not undergo MRI beforeIA-Tx. Recanalization, clinically significant intracerebral hemorrhagic (sICH) and neurologic outcomes werecompared in patients who underwent MRI studies and those who did not.Results:Recanalization occurred in 75.3% of the MRI group, and in 92.0% of the non-MRI group (p=0.013). More patientsin the MRI group had favorable neurologic outcomes (modified Rankin Score: 0~2, 69.7% vs. 32.0%, p=0.001),while fewer had sICH (22.2% vs. 44.0%, p=0.008), or reperfusion injury (2.5% vs. 44.0%, p=0.000) than the non-MRI group.Conclusions:During the CoVID-19 pandemic, futile recanalization may be contributing to increased complications and poorneurologic outcomes. Identification of P/D mismatch on MRI may be the best method to select patients for IA-Tx. In cases where an MRI study is not available, an appropriate CT-based program should be developed andimplemented.
7

Cerebrovasc Dis 2020;49(suppl 1):1-149
8

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-06Epidemiology
Association of Virological Status and Ischemic Stroke Subtypes among HIV-infected Inpatients: A 12-year Retrospective Study in Thailand
Akarin Hiransuthikul 1, Aurauma Chutinet 2, Nijasri Suwanwela 2
1 Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok,Thailand2 Chulalongkorn Stroke Center, Chula Neuroscience Center, King Chulalongkorn Memorial Hospital, Thai RedCross Society, Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University,Bangkok, Thailand
Purpose:Despite higher prevalence of ischemic stroke (IS) among HIV-infected individuals, information on IS subtypes islacking. We aimed to determine the prevalence of IS subtypes among HIV-infected patients and to determinethe differences in distribution of IS subtypes between virologically suppressed and unsuppressed HIV-infectedpatients.Methods:Medical records from patients who were hospitalized at the King Chulalongkorn Memorial Hospital, a tertiarycare center with a specialized stroke care multidisciplinary team, between 2008 and 2019 due to IS withdocumented HIV infection were retrospectively analyzed. IS subtypes were based on the Trial of Org 10172 inAcute Stroke Treatment (TOAST) and the Oxford Community Stroke Project (OCSP) classification. Virologicalsuppression was defined as plasma HIV RNA levels of <40 copies/mL (<1.6 log10).Results:Among 6,952 patients with IS, 50 (0.7%) were HIV-infected patients. The median (IQR) CD4 cell count was 294.5(186-485) cells/mL. The most common etiology of IS was small vessel occlusion (SVO) (48%), followed by strokeof undetermined etiology (UD) (26%), and stroke of other determined etiology (OD) (14%) based on TOASTclassification. Among 7 patients of OD, 5 were from infectious-related cause. Lacunar infarction (LACI) (64%) wasthe most common IS subtype based on OCSP classification. Among 46 patients with available plasma HIV RNAlevels, 28 (60.9%) were virologically suppressed. Virologically unsuppressed group had significantly higherproportion of OD (33.3% vs 3.6%) and UD (38.9% vs 17.9%) based on TOAST; and partial anterior circulationinfarction (PACI) (33.3% vs 3.6%) based on OCSP classification compared to virologically suppressed group.Whereas, virologically suppressed group had significantly higher proportion of SVO (60.7% vs 22.2%) and LACI(71.4% vs 50%). In multivariable regression analysis, unsuppressed viral status was associated with OD (aOR 10.6;95%CI 1.1 to 109.3, p=0.04) and PACI (aOR 16.6; 95%CI 1.4 to 193.1, p=0.03).Conclusions:SVO was the most common cause of IS among HIV-infected patients and was more likely to occur amongvirologically suppressed group, suggesting that traditional vascular risk factors may play a larger role indeveloping IS. Unsuppressed viral status was associated with OD; therefore, investigations including for infection,should particularly be performed among virologically unsuppressed HIV-infected patients who had IS.
9

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-07Acute Management
Network Mapping of Time to Antithrombotic Therapy among Patients with Ischemic Strokeand Transient Ischemic Attack (TIA)
Thanh Phan 1, Benjamin Clissold 1, Shaloo Singhal 1, John Ly 1, Andy Lim 3, Jason Vuong 2
Chelsea Matley 2, Talvika Kooblal 2, Henry Ma 1
1 School of Clinical Sciences, Monash University, Melbourne, Australia2 Neurology Department, Monash Health, Melbourne, Australia3 Emergency Department, Monash Health, Melbourne, Australia
Purpose:There is emphasis on timely administration of thrombolysis and clot retrieval but not antithrombotic therapywithin 48 hours for ischemic stroke (frequency of 64% in Australia and 97% in North America). We planned toassess the time metrics and variables associated with delaying antithrombotics (antiplatelet and anticoagulanttherapy) administration.Methods:This was a retrospective study at Monash Health over 12 months in 2015. We plotted the cumulative event andmapped the key drivers (dimensionless variable Shapley value/SV) of antithrombotics.Results:There were 42 patients with transient ischemic attack/TIA and 483 with ischemic stroke [mean age was 71.8±15.4;56.0% male; nil by mouth (NBM) 74.5% and 49.3% of patients received ‘stat’ dose antithrombotics]. The mediantime to imaging for the patients who did not have stroke code activated was 2.3 hours (IQR 1.4-3.7), from imagingto dysphagia screen was 14.6 hours (IQR 6.2-20.3), and from stopping NBM to antithrombotics was 1.7 hours(IQR 0-16.5). TIA patients received antithrombotics earlier than those with ischemic stroke (90.5% versus 86.5%,p=0.01). Significant variables in regression analysis for time to antithrombotics were time to dysphagia screen (β 0.20 ± 0.03, SV = 3.2), nasogastric tube insertion (β 19.8 ± 5.9, SV =-0.20), thrombolysis (β 8.6 ± 3.6, SV =-1.9), stat dose antithrombotic (β -18.9 ± 2.9, SV =-10.8) and stroke code (β -5.9 ± 2.5, SV =2.8). The partial correlation network showed that the time to antithrombotics increased with delay in dysphagia screen (coefficient=0.33)and decreased if ‘stat’ dose of antithrombotics was given (coefficient=-0.31).Conclusions:The proportion of patients receiving antithrombotics within 48 hours was higher than previously reported inAustralia but remained lower than the standard achieved in North American hospitals. Our process map andnetwork analysis show avenues to shorten the time to antithrombotic.
10

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-08Neurosonology and Neuroimaging
Influence of Ethnicity on Tmax Thresholds and Clinical Outcomes Post Stroke
Yohanna Kusuma 1, Paul Talman 2, Benjamin Clissold 2, Bernard Yan 3, Peter Riley 1, Lyna Soertidewi Kiemas 4,Melita Melita 4, Mursyid Bustami 4, Indah Aprianti Putri 4, M. Arief Rachman 4, Ricky Gusanto Kurniawan 4,Bambang Tri Prasetyo 4, Made Ayu Wedariani 4 , Yuli Felistia 4, Rizka Lydia Savitri 4, Paul Yielder 1
1 School of Medicine, Deakin University, Waurn Ponds, Australia2 Neurology, The University Hospital Geelong, Geelong, Victoria, Australia3 Neurology, The Royal Melbourne Hospital, Melbourne, Victoria, Australia4 Neurology, National Brain Centre, Prof.DR.dr. Mahar Mardjono-Univ Airlangga, Jakarta, Indonesia
Purpose:Penumbra, as estimated by CT perfusion utilizing a Tmax more than 6 seconds threshold, correlates well withfinal infarct volume in acute ischemic stroke (AIS) patients. However, thresholds correlation values are derivedfrom studies in Western populations have not been investigated and critically evaluated in Asian populations. Itis known that cerebrovascular reserve is etiological diverse with regard to different racial groups and it ismultifactorial. Other predictor factors. e.g. age, presentation stroke severity, NIHSS, premorbid functions andadmission are associated with the outcome post stroke. Tmax thresholds are likely variable across different ethnicpopulations in Asian and Western genotypes. It is important to establish an accurate Tmax threshold in Asianpopulation.Methods:Our prospective imaging registry study design investigates optimal ischemic thresholds of Tmax betweenAustralian and Indonesian ischemic stroke patients. Patient data was sourced from CT perfusion imaging (Tmax)at acute stroke presentation and MR Diffusion-Weighted Imaging (DWI) within 72 hours enabling modelledassessment of final infarct volumes. These data were then processed across a sequence of Tmax thresholdsproviding a basis for comparative matching across both populations.Results:To date, from January 2018 to June, 685 patients have been recruited. Data from 200 patients who had notundergone reperfusion therapy were included in this study: 100 in Jakarta (Indonesia), 100 in Geelong (Australia).In Jakartan, the mean age (IQR) was 59.71 ± 10.09 years, the median age was 60 (IQR 53-67), the median NIHSS(IQR) was 6 (3-11) and Geelong, the mean age 71.81± 15.17 years, the median age was 74 (IQR 63-84)years, themedian NIHSS was 3(1-5). The Tmax delays at 8 seconds (R coefficient 0.72) was the optimal threshold for Jakartapopulation. Bland-Altman plot of the Tmax at delay 8 seconds threshold against final infarct volume (FIV)calculated by DWI (Figure 1) demonstrated the smallest ranges compared with other Tmax thresholds.
11

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:Our preliminary analysis showed that Tmax threshold in Jakartan patients was potentially higher than Westernpopulations. Further analysis is planned to consolidate the validity of our initial findings.
12

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-09Epidemiology
Prevalence and Associated Factors of Premature discontinuation of Antiplatelet Therapyafter Ischemic Stroke: A Nationwide Population-based Study
Eung-joon Lee 1, Seung Jae Kim 2, Ho Chun Choi 3, Oh Deog Kwon 4
1 Department of Neurology, Seoul National University Hospital, Seoul, Korea2 Department of Family Medicine, Seoul St. Marys Hospital, Seoul, Korea3 Department of Family Medicine, Seoul National University Hospital, Seoul, Korea4 Department of Family Medicine Korea Navy 2nd Fleet Medical Corps, Seoul, Korea
Purpose:We tried to evaluate the prevalence of premature discontinuation of antiplatelets and its affecting factors afterischemic stroke using large-sized representative national claims data.Methods:4,621 patients aged 20 years or older with newly diagnosed ischemic stroke who started aspirin or clopidogrelfor the first time were selected from 2003-2010 National Health Insurance Service-National Sample Cohort(NHIS-NSC) of Korea, a randomly collected sample which accounts for 2.2% (N=1,017,468) of total population(N=46,605,433). The prevalence of discontinuation of antiplatelets was measured every 6 months until the 24months since the first prescription. Then we classified the subjects into 2 groups according to the discontinuationstatus at 12 months and assessed the factors influencing premature discontinuation of antiplatelets within 12months.Results:35.5% (n=1640) of total subjects discontinued antiplatelets within 12 months and 58.5% (n=2,704) discontinuedthem within 24 months. The remaining 41.5% (n=1,917) continued them for 24 months or more. In themultivariate logistic regression analysis, initiating treatment with aspirin monotherapy [adjusted OR (aOR), 2.66,95% CI 2.17-3.25] was the most prominent determinant of premature discontinuation within 12 months followedby CCI score ≥6 (aOR 1.50, 95% CI 1.31-1.98), and beginning treatment with clopidogrel monotherapy (aOR 1.41, 95% CI 1.15-1.72). Rural residence (aOR 1.36, 95% CI 1.14-1.62), < 4 total prescribed drugs (aOR 1.24, 95% CI1.05-1.47), lower income (aOR 1.20, 95% CI 1.03-1.40 for middle income class and OR 1.21, 95% CI 1.02-1.45 forlow income class), and ages ≥70 years (aOR 1.15, 95% CI 1.00-1.31) were also significantly associated with premature discontinuation of antiplatelets within 12 months.Conclusions:The prevalence of premature discontinuation of antiplatelets after ischemic stroke was quite high. Thus, morestrategic approach is required for the physicians to improve the persistence with antiplatelets by understandingfactors associated with premature discontinuation.
Figure A) Among the 4,621 newly diagnosed ischemic stroke patients who started antiplatelets for the first time,25.3% (n=1170) prematurely discontinued intake within 6 months. B) Among the 1,917 patients who continued
13

Cerebrovasc Dis 2020;49(suppl 1):1-149
antiplatelets for 24 months or more, those who began treatment with DAPT accounted for the highest proportion,followed by those who initiated with clopidogrel monotherapy, while the percentage of those who began withaspirin monotherapy was the lowest.
14

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-10Risk Factors and Prevention of Stroke
Cilostazol for Secondary Stroke Prevention: Systematic Review and Meta-analysis
Choon Han Tan 1, Andrew G R Wu 2, Bernard P L Chan 3 , Vijay K Sharma 3, Benjamin Y Q Tan 3, Leonard L L Yeo 3
1 Department of Medicine, Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore,Singapore2 Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore,Singapore3 Division of Neurology, Department of Medicine, National University Health System, Singapore, Singapore
Purpose:Stroke is one of the leading causes of death worldwide. Cilostazol, an antiplatelet and phosphodiesterase 3inhibitor, has not been clearly established for ischemic stroke use. We aim to determine the efficacy and safetyof cilostazol for secondary stroke prevention.Methods:MEDLINE, EMBASE, Cochrane Library, Web of Science, and ClinicalTrials.gov were searched from inception to 25September 2020, for randomized trials comparing the efficacy and safety of cilostazol monotherapy or dualtherapy to another antiplatelet regimen or placebo, in ischemic stroke patients. Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) was used to assess study quality. This meta-analysis was reported inline with the PRISMA statement.Results:Eighteen randomized trials comprising 11,429 participants were included in this meta-analysis. Most trialspossessed low risk of bias, and were of low heterogeneity. Cilostazol significantly reduced the rate of ischemicstroke recurrence (risk ratio, RR=0.69, 95% CI 0.58-0.81), any stroke recurrence (RR=0.64, 95% CI 0.54-0.74), andmajor adverse cardiovascular events (RR=0.67, 95% CI 0.56-0.81). Cilostazol did not significantly decreasemortality (RR=0.90, 95% CI 0.64-1.25) or increase the rate of good functional outcome (Modified Rankin Scalescore of 0-1; RR=1.07, 95% CI 0.95-1.19). Cilostazol demonstrated favorable safety profile, significantly reducingthe risk of intracranial hemorrhage (RR=0.46, 95% CI 0.31-0.68) and major hemorrhagic events (RR=0.49, 95% CI0.34-0.70).Conclusions:Cilostazol demonstrated superior efficacy and safety profiles compared to traditional antiplatelet regimens suchas aspirin and clopidogrel for secondary stroke prevention, but does not appear to affect functional outcomes.Future randomized trials can be conducted outside East Asia, or compare cilostazol to a wider range ofantiplatelet agents.
15

Cerebrovasc Dis 2020;49(suppl 1):1-149
16

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-11Epidemiology
Etiological Stroke Subtypes and Functional Outcomes in Chronic Kidney Disease: Japan Stroke Data Bank
Kaori Miwa 1, Masatoshi Koga 1, Sohei Yoshimura 1, Michikazu Nakai 2, Yusuke Sasahara 2, Junpei Koge 1, KazutakaSonoda 3, Yoshihiro Miyamoto 2, Kazuo Minematsu 4, Kazunori Toyoda 1
1 Department of Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Japan2 Center for Cerebral and Cardiovascular Disease Information, National Cerebral and Cardiovascular Center, Suita,Japan3 Department of Neurology, Saiseikai Fukuoka General Hospital, Fukuoka, Japan4 Hospital director, Iseikai Hosipital, Suita, Japan
Purpose:Chronic kidney disease (CKD) is a worldwide public health problem and is recognized as the risk factor for stroke.It remains largely understudied whether its stroke risk and clinical impact are consistent across stroke subtypes.We aimed to explore the association between CKD and acute stroke epidemiology, expressed in terms of theprevalence of stroke subtypes and functional outcome after stroke.Methods:Study subjects were 10067 patients aged 18 years or older who were hospitalized after the onset of an acutestroke with available baseline serum creatinine levels and were registered in the Japan Stroke Data Bank, ahospital-based multicenter stroke registration database, between October 2016 and December 2018. Allischemic stroke were classified by TOAST (Trial of ORG 10172 in Acute Stroke Treatment) criteria (cardioembolism,large artery disease, small vessel disease, undetermined, other etiology), and hemorrhage stroke was classifiedas hypertensive intracerebral hemorrhage and cerebral amyloid angiopathy-related intracerebral hemorrhage.Functional outcome was defined as modified Rankin Scale (mRS) 3-6 at discharge. Logistic regression was used to determine the relationship between CKD measures (defined as an estimated glomerular filtration rate [GFR]<60 mL/min per 1.73 m2, CKD stage [GFR <45, 45–59, ≥60 mL/min], and decreasing GFR levels) and outcomes adjusted for age, sex, hypertension, and premorbid mRS.Results:Among 8113 patients with ischemic stroke (n=3454) and intracerebral hemorrhage (n=1954), 3454 (42.6%) and628 (32.1%) had CKD for ischemic and hemorrhage stroke, respectively. Regarding the stroke subtype, CKD wasassociated with cardioembolism (CKD vs. no-CKD; odds ratio (OR), 1.40 [95% confidence intervals (CI), 1.24-1.57],
GFR <45 vs. GFR ≥60; OR, 1.57 [1.35-1.83], GFR 1SD decrease; OR, 1.22 [95% CI, 1.15-1.30]), undetermined(GFR
<45 vs. GFR ≥60; OR, 1.49 [95% CI, 1.05-2.12]), and hypertensive intracerebral hemorrhage (GFR <45 vs. GFR ≥60; OR, 1.53 [95% CI, 1.04-2.25], GFR 1SD decrease; OR, 1.18 [95% CI,1.05-1.33]). CKD was independently associatedwith increased risk of the worse functional outcome in cardioembolism (GFR <45 vs. GFR ≥60; OR, 1.30 [95% CI,1.02-1.66]), small vessel disease (GFR <45 vs. GFR ≥60; OR, 1.55 [95% CI, 1.09-2.22]), and hypertensive intracerebral hemorrhage (GFR <45 vs. GFR ≥60; OR, 1.57 [95% CI, 1.09-2.27]). Conclusions:CKD contributes to the risk and clinical impact of specific stroke subtypes, particularly cardioembolism andhypertensive intracerebral hemorrhage, possibly indicating shared mechanisms of susceptibility and potentialenhancing pathway.
17

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-12Prognosis/Outcome of Stroke
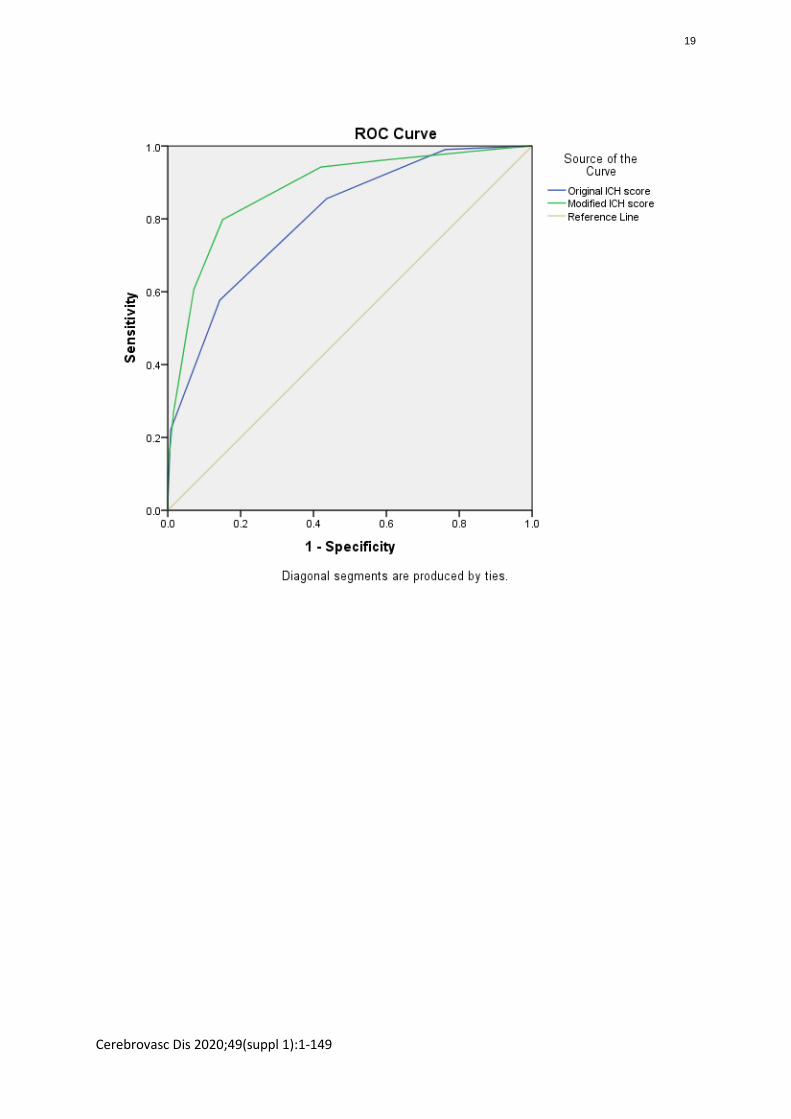
Evaluation of Original and Modified ICH Score for Predicting 30-day Mortality and Good Outcome for Non-Traumatic Intracerebral Hemorrhage
Andreas Soejitno 1, I Putu Eka Widyadharma 1, A. A. A. Putri Laksmidewi 1
1 Neurology, Faculty of Medicine Udayana University/Sanglah Hospital, Bali, Indonesia
Purpose:Intracerebral hemorrhage (ICH) score has been widely used as a consistent and reliable clinical grading scale forpredicting mortality. However, ICH score had not been used to predict good outcome or significant disability forthose who were alive. We intended to address whether any modifications would increase prediction accuracyfor mortalty as well as the extent of morbidity for those who survived.Methods:We conducted a retrospective cohort study, involving all non-traumatic ICH patients admitted to our hospitalbetween July 01 2019 to July 31 2020. Independent predictors of mortality (modified Rankin scale/mRS of 6) orgood outcome vs. significant disability (mRS≤2 vs. mRS 3-5, respectively) were identified by logistic regression. A modified ICH score was compared with the original ICH score for its diagnostic performance (DP). Overall DPswere graded and ranked according to Youden Index (YI).Results:As many as 230 patients were eligible with 45% and 32% 30-day mortality and good outcome, respectively.Factors independently associated with mortality were low GCS and high NIHSS score on admission (P 0.040,<0.001, respectively), and presence of respiratory failure (P 0.007). Independent factors for good outcome werelow NIHSS on admission (P<0.001) and mass effect (midline shift > 5 mm) [P 0.006]. A modification of ICH scorefrom the original was made by substituting GCS with NIHSS (0-10=1;11-20=2;>20=3) score, changing age cut-offpoint to >55 years old (=1), and adding respiratory failure (=1), and mass effect (=1). The modified ICH scoregenerally outperformed the sensitivity of the original ICH score with respect to mortality (sensitivity 79.81% vs.57.69%; specificity 84.92% vs. 85.71%; YI 0.63 vs. 0.43, respectively) and good outcome (sensitivity 78.38% vs.77.03; specificity 71.15% vs. 73.10%; YI 0.50 both, respectively). There was only one patient with original andmodified ICH score of 0 who died and none survived with original and modified ICH score of ≥5 and ≥7, respectively. The proportion of 30-day mortality and good outcome increased linearly with both scores.Conclusions:Both original and modified ICH score demonstrated good DP in terms of 30-day mortality and good outcome.The modified ICH score was slightly more sensitive for both indicators. This study provided evidence to encouragethe use of both scores for predicting not only mortality, but also good outcome after non-traumatic ICH.
18
Cerebrovasc Dis 2020;49(suppl 1):1-149
19

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-13Epidemiology
Stroke Epidemiology in Bangladesh
Narayanaswamy Venketasubramanian 1, Muzharul Mannan 2
1 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore2 Institute for Paediatric Neurodisorder & Autism, Bangabandhu Sheikh Mujib Medical University, Dhaka,Bangladesh
Purpose:Bangladesh, home to 165.6 million people, has a per-capita income of USD 1909, poverty rate of 20.5%, 73.2%literacy (7+ years), and life expectancy of 72.3 years. Stroke is the most common condition (47.5%) of neurologyin-patients. Approximately 23.9% of neurology out-patient prescriptions is for stroke. This paper describes theepidemiology of stroke in Bangladesh.Methods:A Medline search was made using the search terms ‘stroke AND Bangladesh’. Abstracts were reviewed and dataon stroke epidemiology extracted. The full publication was reviewed if available. Information on mortality,morbidity, incidence, prevalence, vascular risk factors, stroke subtypes and mechanisms are presented.Results:Stroke is a major cause of death and disability, with an age- and sex-standardised mortality rate of 54.8/100000,and DALYs lost of 888.1/100000. Stroke prevalence is 1.8% (among age >35yr), 1% (among age >20yr), similar inmales and females, urban and rural areas, higher among older people with a ratio of infarction to haemorrhageof 2.91 in the community. In a large multi-centre hospital study, 72% had ischemic stroke, 57.6% hypertension44.6% smoking, 24.3% tobacco use, 40% OCP use in females, 23% diabetes, 17.1% ischemic heart disease, 10.6%obesity, and 5.3% dyslipidaemia. Small artery occlusion accounts for 45.4% while large artery disease comprises32.5% of ischaemic strokes. Haemorrhagic stroke is more frequent during winter (62.2%) than summer (37.6%).The high stroke mortality among Bangladeshi populations, apart from the atherosclerotic risk factors especiallyof diabetes mellitus and smoking, has been attributed to squatting during defecation, vitamin D deficiency, andbetel nut chewing, with the latter OR of stroke death of 2.36 (95%C 1.45-3.80, P<0.001).Conclusions:Stroke is a major disease burden in Bangladesh, largely ischaemic, with vascular risk factors, and someuncommon mechanisms that may need further investigation.
20

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-14Acute Management
Endovascular Thrombectomy with and without Bridging Intravenous Tissue Plasminogen Activator in AcuteIschemic Stroke Patients with Basilar Artery Occlusion
Isabel Siow 1, Natalie Ong 1, Anil Gopinathan 2, Cunli Yang 2, Bernard Chan 3, Vijay Sharma 3 , Paul Bhogal 4 , LukasMeyer 5, Stefan Schob 6 , Seraphine Kutschke 7 , Qingyu Wu 8, Anastasios Mpotsaris 8, Volker Maus 9, BenjaminTan 3, Leonard Yeo 3
1 Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore2 Department of Neurodiagnostic Imaging, National University Health System, Singapore, Singapore3 Division of Neurology, Department of Medicine, National University Health System, Singapore, Singapore4 Department of Interventional Neuroradiology, St. Bartholomew's and The Royal London Hospital, London,Virgin Islands, British5 Department of Diagnostic and Interventional Neuroradiology, University Medical Centre Hamburg-Eppendorf,Hamburg, Germany6 Department of Neuroradiology, Leipzig University Hospital, Leipzig, Germany7 Department of Neuroradiology, University Hospital RWTH Aachen, Aachen, Germany8 Department of Neuroradiology, University Hospital Magdeburg, Magdeburg, Germany9 Department of Diagnostic and Interventional Neuroradiology, University Medical Centre Goettingen,Goettingen, Germany
Purpose:Endovascular thrombectomy (ET) is increasingly being performed in patients who present with basilar arteryocclusion (BAO) acute ischemic stroke. In patients with BAO who undergo ET, it is unclear whether priortreatment with bridging intravenous tissue Plasminogen Activator (IV-tPA) confers any benefit. In thisinternational multi-centre study conducted across five comprehensive stroke centres, we aimed to determine ifpatients who received bridging tPA therapy treatment prior to ET had better outcomes compared to patientswho received ET alone.Methods:In this real-world patient registry, we performed a retrospective analysis of all patients with BAO who hadundergone ET across 5 centres internationally (1 in Singapore, 1 in UK, and 3 in Germany) between 2015 and2019. Outcome measures included the discharge modified Rankin Score (mRS) of 0-2, in-hospital mortality, andsymptomatic intracranial haemorrhage (sICH). Multivariable logistic regression was used to compare outcomesof patients who had received bridging IV-tPA and ET versus those who received primary ET alone.Results:Of 212 consecutive patients analysed, 101 (47.6%) underwent bridging IV-tPA treatment prior to ET and 111(52.4%) underwent primary ET alone without bridging IV-tPA. Both groups were similar in baseline characteristicsincluding age (Mean = 68.9 ± 13.3 yrs vs 71.3 ± 12.9 yrs in bridging tPA group and primary ET group respectively),admission National Institute of Health Stroke Scale (NIHSS) score (Median = 14.00, IQR = 8.00 – 18.75 vs Median= 15.00, IQR = 7.00 – 24.75) and comorbidity profile. Both groups had similar rates of good functional outcomemeasured by mRS at 3-months (mRS 0 – 2 in 26.9% vs 21.1% in bridging tPA group and primary ET grouprespectively; OR = 1.38; CI = 0.72–2.63; p = 0.34), rates of in-hospital mortality (24.5% vs 33.3%; OR = 0.65; CI =0.35–1.20; p = 0.17), and sICH (4.5% vs 4.9%; OR = 0.92; CI = 0.20–4.25; p = 0.91).Conclusions:In patients with acute ischemic stroke due to BAO, the use of bridging IV-tPA treatment prior to ET is notassociated with improved outcomes. Randomized controlled trials are warranted to investigate this further.
21

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-15Risk Factors and Prevention of Stroke
The Association between Glucose Control and Composite Vascular Eventsaccording to The Subtypes of Ischemic Stroke
Jun Young Chang 1 , Moon Ku Han 2
1 Department of Neurology, Asan Medical Center, Seoul, Korea2 Department of Neurology, Seoul National University Bundang Hospital, Seong Nam, Korea
Purpose:There is a paucity of study regarding optimal target of HbA1c among patients with ischemic stroke and diabetes.We evaluated the association between admission HbA1c and composite vascular events including stroke,myocardial infarction, and vascular death among acute ischemic stroke with diabetes.Methods:Eighteen thousand five hundred sixty seven subjects with a transient ischemic attack or acute ischemic strokewithin 7 days after symptom onset, and history of diabetes were included. The association between HbA1c onadmission and composite vascular events over one year were estimated using gray and fine model. The risk ofevents and HbA1c according to the stroke subtype were explored using fractional polynomial and linear quadraticcurves.Results:During the follow up, 1395 patients developed composite vascular events. An adjsuted Hazard ratio (HR) for 1unit increase of HbA1c were 1.04 (95% CI 1.01-1.08) for composite vascular events. The risk significantlyincreased with a threshold of 6.8 to 7.0% after multivariable analysis using HbA1c as a prespecified categoricvariable. The optimal range of HbA1c associated with a minumum risk was the loweset for small vessel occlusionsubtype (6.4, 95% CI 4.8-7.9), while 7.5 (95% CI 7.0-8.0) for large artery atherosclerosis, and 7.8 (95% CI 6.7-9.0)for cardioembolism.Conclusions:The risk of composite vascular events was associated with HbA1c on admission in patients with ischemic strokeand diabetes. The optimal range of admission HbA1c were estimated to be below 6.8 to 7.0. More stringentglucose control may be justified in patients with small vessel occlusion subtype.
22

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-16Prognosis/Outcome of Stroke
Vertebral and Amygdala Glucose Uptake among Cerebral Infarction Patientsand Its Impact on Stroke Recurrence
Jeong-min Kim 1, Rhee Rhee Lee 2, Kwang-yeol Park 3, Ju Won Seok 4
1 Neurology, Seoul Nationl University Hospital, Seoul, Korea2 Nuclear Medicine, Chung-Ang University Hospital, Seoul, Korea3 Neurology, Chung-Ang University Hospital, Seoul, Korea4 Nuclear Medicine, Chung-Ang University Hospital, Seoul, Korea
Purpose:We investigated whether the glucose uptake of hematopoietic organs or internal carotid arterial (ICA) wall byfluorodeoxyglucose positron emission tomography (FDG PET) is related with future stroke recurrence amongcerebral infarction patients.Methods:Between August 2015 and March 2020 acute cerebral infarction patients with ICA stenosis who admitted toChung-Ang University Hospital underwent whole body FDG PET after patients had been stabilized. We comparedthe FDG uptake at the ICA, vertebrae, spleen and amygdala between the patients with stroke recurrence andthose without. Cox proportional hazards model was constructed to identify factors related to stroke recurrence.Results:A total of 110 stroke patients were included with mean age of 72 years (41 female). During the median follow-up period of 18 months, stroke recurred among 15 patients. Recurred stroke patients had more likely to havediabetes mellitus, lower estimated glomerular filtration rate and severe internal carotid artery stenosis. Thepatients with recurred stroke had significantly higher glucose uptake at vertebrae and amygdala from FDG PET,but uptake at liver, spleen and ICA were similar. Cox regression analyses including diabetes mellitus, estimatedglomerular filtration rate, ICA stenosis and FDG uptake at vertebrae and amygdala showed that stroke recurrencewas associated with higher FDG uptake at vertebrae (hazard ratio = 4.94, confidence interval = 1.29 – 18.9) andoverall vascular events with higher FDG uptake at amygdala (hazard ratio = 3.11, confidence interval = 1.11 –8.70). The FDG uptake at vertebrae is correlated with body mass index, bone mineral density and C-peptide. TheFDG uptake at amygdala is correlated with monocyte lymphocyte ratio and triglyceride.Conclusions:Increased FDG uptake from lumbar vertebrae is related to future stroke recurrence, suggesting detrimental roleof active bone glucose metabolism toward cerebral vasculature. Increased FDG uptake at amygdala is related tofuture vascular events after stroke, possibly due to exaggerated inflammation response.
23

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-17Prognosis/Outcome of Stroke
The Effects of Triglyceride-Glucose (TyG) Index on Leptomeningeal Collateral Status and Outcome ofReperfusion Therapy in Patients with Acute Ischemic Stroke
Minwoo Lee 1, Chul-ho Kim 1, Yerim Kim 1, Min Uk Jang 1, Jae-sung Lim 1, Kyung-ho Yu 1, Byung-chul Lee 1, Mi SunOh 1
1 Department of Neurology, Hallym Neurological Institute, Hallym University College of Medicine, Anyang, Korea
Purpose:The triglyceride glucose index (TyG index) is a simple and reliable surrogate marker of insulin resistance (IR). TyGindex is known to correlate with coronary collateral circulation (CC) and the outcome of myocardial infarction.However, it is not yet clear whether the TyG index predicts leptomeningeal CC and functional outcomes inpatients with stroke. Thus, we aimed to explore the prognostic value of TyG index on leptomeningeal CC andclinical outcomes of ischemic stroke patients who underwent reperfusion therapy.Methods:We retrospectively included consecutive patients with acute ischemic stroke with occlusion of either middlecerebral artery or internal carotid artery who were evaluated with multiphase CT Angiography (mCTA) andreceived reperfusion therapy. The TyG index was calculated as ‘ln(fasting glucose level[mg/dL] x triglyceridelevel[mg/dL])/2’ and dichotomized according to the cutoff points provided by previous studies. CC was evaluatedwith mCTA according to the University of Calgary Scale defined as good, intermediate or poor. Clinical outcomesincluded 3-month functional outcome represented as modified Rankin Scale (mRS). Multivariable logisticregression models were performed to determine the correlation of TyG index and the outcomes.Results:A total of 199 subjects from three university-affiliated hospitals were enrolled. The mean age was 70.2±12.7years and 114(57.3%) were male. Median initial NIHSS was 15.0 (IQR 11-18) and 25.6% received IV tissueplasminogen alone, 28.6% IA thrombectomy alone and 45.7% both IV tPA and IA thrombectomy. The median TyGindex was 4.81 (IQR, 4.63-5.062) and 167 patients had TyG level higher than 4.49 which represents the presenceof IR. On the univariate analysis, patients with high TyG index had higher initial NIHSS scores (15.0 versus 13.0,P=0.054), higher incidence of early neurological deterioration (23.1% vs 0% P =0.039), and worse functionaloutcomes at 3 months (mRS 4 versus 1, P<0.001). However, TyG level was not associated with CC status (P=0.858).After adjustment for age, sex, type of reperfusion therapies, initial stroke severity, stroke etiology, history ofdiabetes, and LDL cholesterol, high TyG index remained an independent predictor for poor 3-month functionaloutcome (adjusted OR,3.946; P=0.031).Conclusions:Our study revealed that insulin resistance represented as high TyG index might be a potential predictor of poor3-month functional outcomes in patients with acute ischemic stroke who received reperfusion therapy. However,high TyG index was not associated with poor pretreatment collateral status.
24

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-18Risk Factors and Prevention of Stroke
Stroke Riskometer for Predicting Internal Carotid Atherosclerotic Plaqueby Carotid Duplex Ultrasonography in Asymptomatic Thai Adults Older Than 45 Years
Teeraparp Kitjawijit 1
1 Neurology, Chulalongkorn hospital, Bangkok, Thailand
Purpose:This study aims to find the association between stroke risk calculated by stroke riskometer and the presence ofinternal carotid atherosclerotic plaque.Methods:Asymptomatic Thai adults older than 45 years old with no previous history of stroke were studied during Marchto December 2019. A stroke riskometer questionnaire was deployed using mobile phone application. Participantswith 10-years risk of stroke ≥ 10% by stroke riskometer were categorized as high risk group, whereas 10-years risk less than 10% were classified as low risk group. Carotid duplex ultrasound was performed to identify plaqueat the internal carotid arteries. Risks were compared by independent t test and Chi-square tests. Multiple logisticregression was used to assess the association between risk factors and plaque.Results:There were 169 subjects in this study, 87 in high risk and 82 in low risk group by stroke riskometer. Prevalence ofinternal carotid plaque was 52.1%. The prevalence of plaque was significantly higher in the high risk group (86.4%)than the low risk group (14.8%) (P < 0.001). In high risk group, plaque was more prevalent in participants withadvanced age, hypertension on medication, diabetes mellitus, history of myocardial infarction, atrial fibrillation,left ventricular hypertrophy, impaired memory and history of smoking. After multiple logistic regression, age,diabetes mellitus, hypertension, history of smoking and impaired memory were associated with atheroscleroticplaque.Conclusions:Stroke riskometer can predict atherosclerotic plaque in the internal carotid artery. Stroke riskometer factorsincluding age, diabetes mellitus, hypertension, history of smoking and impaired memory were associated withplaque.
25

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-19Basic Neuroscience in Stroke
Association of ELOVL6 Gene with Large Artery Atherosclerosis Stroke Risk through Nod-like Receptor ProteinInflammasome Pathway
Hua Liu 1, Xindong Liu 3, Danyang Luo 3, Yi Nie 2, Yifei Ji 2, Wei Liu 4
1 Department of Neurology, The Affiliated Hospital of Southwest Jiaotong University, Chengdu, Sichuan, China2 Neurology, North Sichuan Medical College, Nanchong, Sichuan, China3 Neurology, The Second Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, China4 Neurology, Nanbu County Peoples Hospital, Nanbu,Sichuan, China
Purpose:To investigate whether the elongase of very long chain fatty acids family member 6 (ELOVL6) gene affects thelarge artery atherosclerosis stroke (LAA) risk through the nod-like receptor protein 3 (NLRP3) inflammasomepathway.Methods:The Han Chinese patients with LAA and age- and sex-matched apparently healthy controls were included in thestudy and heparinized peripheral blood samples were acquired. We evaluated and compared the mRNA andprotein expression levels of ELOVL6 and NLRP3 genes, as well as the protein expression levels of inflammatorycytokines including interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor-α (TNF-α) in peripheral blood between LAA and health controls using small interfering RNA (siRNA) technology, real time polymerase chain reactionanalysis, and Western blotting. The two-tailed unpaired Student’s t-test or one-way analysis of variance wereused for comparisons of two or more groups. The correlations of the expression levels between genes wereanalyzed by Pearson’s correlation analysis.Results:The results demonstrated higher levels of mRNA (ELOVL6: 0.0011±0.0003 vs. 0.000 5±0.000 3, P<0.05; NLRP3:0.049±0.015 vs. 0.003±0.002, P<0.05) and proteins (ELOVL6: 0.801±0.347 vs. 0.451±0.193, P<0.05; NLRP3:0.897±0.346 vs. 0.406±0.339, P<0.05) of ELOVL6 and NLRP3 genes in LAA patients compared to the controls. Thedata also showed that the protein expression levels of IL-6 (1.087±0.178 vs. 0.507±0.094, P<0.05) and TNF-α (0.600±0.092 vs. 0.196±0.044, P<0.05) in LAA patients were significantly higher than those in the controls.However, the ELOVL6 gene had no effect on the expression change of inflammatory cytokines. The proteinexpression levels of IL-1β (r=0.937, P<0.001), IL-6(r=0.723, P=0.018), and TNF-α (r=0.672, P=0.033) were positively correlated with NLRP3 gene, and the protein expression levels of ELOVL6 gene was positivelycorrelated with that of NLRP3 gene (r=0.78, P=0.007). Meanwhile, the protein (0.399±0.081 vs. 0.897±0.346,P=0.002) and mRNA (0.002±0.001 vs. 0.049±0.015, P=0.010) expression levels of NLRP3 gene significantlydecreased after ELOVL6 gene silencing by siRNA in LAA samples.Conclusions:ELOVL6 gene is associated with LAA risk in Han nationality of Chinese population probably via regulating theELOVL6-NLRP3- inflammatory cytokines singling pathway.
26

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-20Acute Management
Predicting Significant Neurological Progression in Vertebrobasilar Artery Occlusion
Seungyon Koh 1, Mun Hee Choi 1, Sung Eun Lee 2, Jin Soo Lee 1, Ji Man Hong 1, Seong-joon Lee 1
1 Department of Neurology, Ajou University School of Medicine, Suwon, Korea2 Department of Emergency Medicine, Ajou University School of Medicine, Suwon, Korea
Purpose:Neurological progression occur in one-third acute stroke patients, and poor outcomes are associated with it.No established predictors of neurological progression have been identified among vertebrobasilar occlusion(VBO). Dynamic clinical course and its outcome in VBO patients are complicated by heterogeneous occlusionetiology and the mechanism of progression. This study aims to identify predictors of significant neurologicalprogression in VBO, with special focus on occlusion etiology and pathomechanism of the progression.Methods:From 2010 to 2018, vertebrobasilar artery occlusion (VBO) patients were selected from a prospective hospitalregistry. VBO was classified in the computed tomographic angiography (CTA) as an obvious filling defect in thebasilar artery, bilateral vertebral artery, or dominant vertebral artery with no contralateral vertebral artery flow.Occlusion etiology was classified according to occlusion types; a branching-site occlusion (BSO) was consideredembolic, and a truncal-type occlusion (TTO) was considered intracranial atherosclerosis. Degree of collateralswere measured based on CTA (the Basilar Artery on CTA score). Presenting infarct volume was classified basedon initial magnetic resonance (MR) diffusion weighted images (posterior circulation-ASPECTS). Significantneurological progression was defined based upon the difference of National Institutes of Health Stroke Scale(NIHSS) at the point of admission and discharge. The pathomechanism of the progression was classified into 3groups; lacunar progression, perfusion failure, and malignant transformation. Multivariate analysis was used toidentify factors predictive of significant neurological progression.Results:In total, 176 VBO patients could be identified. After excluding outliers showing futile outcome, 159 VBO patientswere selected for analysis. An increase in NIHSS of 3 or more at discharge was set as a definition of significantneurological progression, because of its prediction for poor outcome (3 months mRS 4-6) (OR: 63.074, 95% CI[11.347-350.612], p<0.001) after relevant covariables. 30 significant neurological progression were identified.When multivariate analysis was used, TTO type occlusion (OR:7.222, 95% CI [1.374-37.96], p=0.02), initial PC-ASPECTS (OR:1.725, 95% CI [1.136-2.619], p=0.01), BATMAN (OR:1.604, 95% CI [1.191-2.158], p=0.002) werepredictive of the progression. Subgroup analysis among progressive patients was performed. In TTO group, theBATMAN score was predictive of perfusion failure (OR:2.661, 95% CI [1.39-5.094], p=0.003).Conclusions:In posterior circulation stroke with VBO, atherosclerotic occlusion etiology, larger initial infarct volume, andpoorer collateral status appears to be predictive of significant neurological progression. Especially inatherosclerotic occlusion, collateral status measured by BATMAN score seems to predict the future perfusionfailure.
27

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-21Prognosis/Outcome of Stroke
Atherosclerotic Burden and Vascular Risk in Stroke Patients with Atrial Fibrillation
Jong-ho Park 1, Jong-won Chung 2, Oh Young Bang 2, Gyeong-moon Kim 2, Kang-ho Choi 3, Man-seok Park 3, Joon-tae Kim 3, Yang-ha Hwang 4, Tae-jin Song 5, Yong-jae Kim 6, Bum Joon Kim 7, Sung Hyuk Heo 8, Jin-man Jung 9,Kyung-mi Oh 10, Chi Kyung Kim 10, Sungwook Yu 11, Kwang Yeol Park 12, Jeong-min Kim 13, Jay Chol Choi 14, Woo-keun Seo 2
1 Department of Neurology, Hanyang University Myongji Hospital, Goyang, Korea2 Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea3 Department of Neurology, Chonnam National University Hospital, Gwangju, Korea4 Department of Neurology, Kyungpook National University Hospital, School of Medicine, Kyungpook NationalUniversity, Daegu, Korea5 Department of Neurology, Ewha Womans University Seoul Hospital, Ewha Womans University College ofMedicine, Seoul, Korea6 Department of Neurology, Eunpyeong St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea7 Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea8 Department of Neurology, Kyung Hee University College of Medicine, Seoul, Korea9 Department of Neurology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea10 Department of Neurology, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea11 Department of Neurology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea12 Department of Neurology, Chung-Ang University College of Medicine, Seoul, Korea13 Department of Neurology, Seoul National University Hospital, Seoul, Korea14 Department of Neurology, Jeju National University, Jeju, Korea
Purpose:Atrial fibrillation (AF) usually coexists with atherosclerotic vascular disease (ASVD). However, data on the effecton vascular outcomes of concomitant ASVD with AF after stroke are limited. This study aimed to evaluate theeffect of various ASVD burdens on the risk of vascular events among stroke patients with AF.Methods:We retrospectively analyzed a prospectively registered multicenter database from KATTENTION (Koreannationwide ATrial fibrillaTion EvaluatioN regisTry in Ischemic strOke patieNts) registry involving 3213 strokepatients with AF. ASVD included extracranial atherosclerosis (ECAS), intracranial atherosclerosis (ICAS) (all >/=50%stenosis), coronary artery disease (CAD), and peripheral artery disease (PAD), and was categorized into four stratadepending on the number of ASVD (0, 1, 2, and 3–4). The independent associations of ASVD with major adversecardiovascular events (MACE) defined as stroke, The primary endpoint was the first occurrence of major adversecardiovascular events (MACE), defined as a composite of stroke of any type, coronary heart disease, or vasculardeath. The secondary endpoint were stroke of any type and all-cause death. Cox proportional hazard regressionanalyses were performed to estimate the risk of outcome events after adjusting for covariatesResults:A total of 2670 patients were included (mean age, 73.5±9.8 years; median CHA2DS2-VASc score, 5; interquartilerange, 4‒6). During the follow-up (mean, 1.7 years), a total of 672 (25.2%) MACE, 170 (6.4%) stroke events, and 501 (18.8%) all-cause death were noted. The frequencies of ECAS, ICAS, CAD, and PAD increased with increasingASVD strata (all P<0.001). The adjusted hazard ratio for MACE versus no ASVD was 1.25 (95% CI, 1.00–1.56) forASVD 1, 1.34 (1.02–1.76) for ASVD 2, and 1.93 (1.24–2.99) for ASVD 3–4. The adjusted hazard ratio for all-causedeath versus no ASVD was 1.32 (1.01–1.74), 1.47 (1.06–2.03), and 2.39 (1.47–3.89), respectively. Among ASVDcomponents, the presence of ECAS was a more potent predictor of MACE (1.27 [1.05–1.54]) and all-cause death(1.45 [1.17–1.81]).Conclusions:ASVD burden with AF might be of prognostic value for identifying patients at a high risk for an untowardconsequence of worse vascular outcomes. Among ASVD components, the effect of the cerebral component wasgreater, especially for ECAS.
28

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-22Prognosis/Outcome of Stroke
Exploring the Usability of Wearable Devices for Early Predicting Strokewith Monitoring Patient’s Heart Rate Variability
Sih-wei Yun 1, Lung Chan 3, Ming-chin Lin 2
1 Graduate Institute of Biomedical Informatics, College of Medical Science and Technology, Taipei MedicalUniversity, Taipei, Taiwan2 Department of Neurosurgery, Shuang Ho Hospital, Taipei Medical University, New Taipei, Taiwan3 Department of Neurology, Shuang Ho Hospital, Taipei Medical University, New Taipei, Taiwan
Purpose:Cerebrovascular disease has been the second leading cause of death in Taiwan for many years. An ischemic strokehas an average of 50% chance that patients will have a stroke again. How to prevent or reduce stroke is animportant issue. Studies have shown that autonomic nervous system dysfunction is associated with increasedmorbidity and mortality after stroke. To provide affordable EEG equipment in the intensive care unit, we use alow-cost biosensor that uses the current standard Internet of Things technology.Methods:Studies have shown that the patient’s LF% or LF/HF when leaving the intensive care unit are significantly lowerthan when the patient enters the intensive care unit. The patient’s clinical manifestations of NIHSS scores, GCS,and limb muscle strength scores have also improved. HRV changes can not only know the best time to transferthe patient out of the intensive care unit, but also predict the risk of stroke.Results:A paired comparative analysis of HRV parameters before entering the ICU and leaving the ICU showed that therewere significant differences in LF, LF (%), and LF/HF during the ICU period (P <0.001). In addition, the correlationanalysis of HRV parameters during the ICU showed that HF entering the ICU was significantly correlated with LF,LF(%), and LF/HF (P <0.001), of which HF and LF were highly positively correlated; HF and LF (%) is low-degreenegative correlation; HF and LF/HF are low-degree negative correlation. There was a significant positivecorrelation between HF and LF, and LF (%) of patients leaving the ICU, of which HF and LF were highly positivelycorrelated (P <0.001); HF and LF (%) were lowly positively correlated (P = 0.015).Conclusions:Since the measurement of patient heart rate variability has the advantages of non-invasiveness, it has graduallybeen paid attention to by scientific researchers. The current research is mostly limited to the mortality predictionor prognosis results after the heart rate variability analysis. If the heart rate variability analysis can be instantlycompared with The combination of patient clinical characterization and widely used to monitor whether thestability of the patient's current condition is decreasing or increasing can be greatly helpful to the condition.
29

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-23Epidemiology
Changes in Stroke Patient’s Health-seeking Behavior by COVID-19 Epidemic Regions: Data from Korean Stroke Registry
Han-yeong Jeong 1, Min Kyoung Kang 1, Eung-jun Lee 1, Ki-woong Nam 1, Jeonghoon Bae 1, Kipyoung Jeon 1, TaeJung Kim 1, Keun-hwa Jung 1, Sang-bae Ko 1, Mi Sun Oh 2, Ji Sung Lee 3, Hee-joon Bae 4, Byung-woo Yoon 1, Jong-moo Park 5
1 Department of Neurology, Seoul National University Hospital, Seoul, Korea2 Department of Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea3 Department of Biostatistics, Asan Medical Center, Seoul, Korea4 Department of Neurology, Seoul National University Bundang Hospital, Seongnam, Korea5 Department of Neurology, Nowon Eulji Medical Center, Eulji University, Seoul, Korea
Purpose:With the wide spread of coronavirus disease 2019 (COVID-19) around the world, not only patients with COVID-19, but also patients with other disease such as stroke have undergone many changes in their health-seekingbehavior. Between late February and March 2020, COVID-19 was epidemic in the community of Daegu city andGyeongsangbuk-do region (D-G region) in Korea. We aimed to clarify the changes in the health-seeking behaviorsof stroke patients and stroke care services by region in Korea through analysis of data from Korean Stroke Registry(KSR).Methods:We retrospectively reviewed the data with acute stroke and transient ischemic attack (TIA) patients between2019 and 2020. We compared the stroke onset to hospital arrival (onset-to-door) time of these patients in theD-G region and other regions in Korea during the epidemic period in 2020 (post-COVID-19: February 18-March31, 2020) and the same period in 2019 (Pre-COVID-19). In addition, we investigated the in-hospital strokepathways with the patients.Results:1,792 patients in pre-COVID-19 and 1,555 patients in post-COVID-19 who visited KSR-registered hospitals wereanalyzed. Compared to pre-COVID-19, the number of patients registered in KSR decreased in most regions inpost-COVID-19. In the D-G region, the number of registered patients decreased by two thirds, and the proportionof patients with TIA decreased significantly. (9.97% to 2.91%). Unlike other regions, the median onset-to-doortime increased significantly in the D-G region (361 versus 526.5 minutes, p=0.0084). The proportion of patientswith onset-to-door time within 3 hours also decreased significantly (36.45% versus 28.16%, p=0.0485). Patientsin their 60s and 70s and mild symptoms (NIHSS score 0 to 3) came to the hospital later. As a result, the patientswho underwent thrombectomy also decreased, but the treatment time did not differ between the two periods.Conclusions:During the epidemic of COVID-19, the patients residing in the epicenter showed distinct changes in health-seeking behavior. Appropriate public education about stroke is needed during the COVID-19 pandemic.
30

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-24Neurosonology and Neuroimaging
Effect of Obstructive Sleep Apnea on Cerebral Microvascular Complianceand Cerebral Small Vessel Disease
Woo-jin Lee 1, Keun-hwa Jung 1, Yong-seok Lee 2
1 Neurology, Seoul National University Hospital, Seoul, Korea2 Neurology, Seoul National University Boramae Hospital, Seoul, Korea
Purpose:Reduced cerebrovascular compliance is the major mechanism of cerebral small vessel disease (SVD). Asobstructive sleep apnea (OSA) also promotes SVD development, we investigated whether the chronic vascularremodeling is involved in the association between OSA and SVD parameters.Methods:This retrospective study included individuals who were ≥ 50 years of age, underwent overnight polysomnographic (PSG) for the evaluation of OSA, and performed MRI and transcranial Doppler (TCD) within 12months of interval without development of a neurological event between the evaluations. TCD parameters forthe cerebrovascular compliance included middle cerebral artery pulsatility index (MCA PI) and mean MCAresistance index ratio (MRIR). SVD parameters included white matter hyperintensity (WMH) volume, number oflacunes, enlarged perivascular space (ePVS) score, and number of microbleeds.Results:Ninety-seven individuals (60.8% male, mean age 70.0±10.5 years) were included. The mean apnea-hypopneaindex (AHI) was 19.1±18.2 /h. AHI was not significantly associated with the MCA PI or MRIR. However, AHI wasassociated with the log-transformed total WMH volume (B=0.008; 95% confidence interval [CI] 0.001–0.016;P=0.020), subcortical WMH volume (B=0.015; 95% CI 0.007–0.022; P<0.001), total ePVS score (B=0.024; 95% CI0.003–0.045; P=0.026), and centrum semiovale ePVS score (B=0.026; 95% CI 0.004–0.048; P=0.019),independently from age, MCA PI, and MRIR.Conclusions:AHI was associated with the cerebral SVD parameters, especially with the subcortical SVD parameters,independently from the cerebrovascular compliance. A mechanism distinct from the dysregulated vascularremodeling might link the OSA and the pathogenesis of SVD.
31

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-25Prognosis/Outcome of Stroke
Immediate and Long-term Outcomes of Reperfusion Therapy in Patients with Cancer
Joonsang Yoo 2, Young Dae Kim 1, Hyungjong Park 3, Byung Moon Kim 4, Oh Young Bang 5, Hyeon Chang Kim 6,Euna Han 7, Dong Joon Kim 4, Joonnyung Heo 1, Minyoung Kim 1, Jin Kyo Choi 1, Kyung-yul Lee 8, Hye Sun Lee 9,Dong Hoon Shin 10, Hye-yeon Choi 11, Sung-il Sohn 3, Jeong-ho Hong 3, Jong Yun Lee 13, Jang-hyun Baek 12, Gyu SikKim 2, Woo-keun Seo 5, Jong-won Chung 5, Seo Hyun Kim 14, Tae-jin Song 15, Sang Won Han 16, Joong Hyun Park16, Jinkwon Kim 20, Yo Han Jung 8, Han-jin Cho 17, Seong Hwan Ahn 18, Sung Ik Lee 19, Kwon-duk Seo 2, Ji Hoe Heo1, Hyo Suk Nam 1
1 Neurology, Yonsei University College of Medicine, Seoul, Korea2 Neurology, National Health Insurance Service Ilsan Hospital, Goyang, Korea3 Neurology, Keimyung University School of Medicine, Daegu, Korea4 Radiology, Yonsei University College of Medicine, Seoul, Korea5 Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea6 Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea7 College of Pharmacy, Yonsei Institute for Pharmaceutical Research, Yonsei University, Incheon, Korea8 Neurology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea9 Research Affairs, Biostatistics Collaboration Unit, Yonsei University College of Medicine, Seoul, Korea10 Neurology, Gachon University Gil Medical Center, Incheon, Korea11 Neurology, Kyung Hee University Hospital at Gangdone, Kyung Hee University School of Medicine, Seoul, Korea12 Neurology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea13 Neurology, National Medical Center, Seoul, Korea14 Neurology, Yonsei University Wonju College of Medicine, Wonju, Korea15 Neurology, Seoul Hospital, College of Medicine, Ewha Woman's University, Seoul, Korea16 Neurology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea17 Neurology, Pusan National University School of Medicine, Busan, Korea18 Neurology, Chosun University School of Medicine, Gwangju, Korea19 Neurology, Sanbon Hospital Wonkwang University School of Medicine, Gunpo, Korea20 Neurology, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea
Purpose:Patients with acute stroke are often accompanied by comorbidities, such as active cancer. However, adequatetreatment guidelines are not available for these patients. The purpose of this study was to evaluate theassociation between cancer and the outcomes of reperfusion therapy in patients with stroke.Methods:We compared treatment outcomes in patients who underwent reperfusion therapy, using a nationwidereperfusion therapy registry. We divided the patients into three groups according to cancer activity: active cancer,non-active cancer, and without a history of cancer. We investigated reperfusion processes, 24-hour neurologicimprovement, adverse events, 3-month functional outcome, and 6-month survival and related factors afterreperfusion therapy.Results:Among 1,338 patients who underwent reperfusion therapy, 62 patients (4.6%) had active cancer, 78 patients(5.8%) had non-active cancer, and 1,198 patients (89.5%) had no history of cancer. Of the enrolled patients, 969patients received intravenous thrombolysis and 685 patients underwent endovascular treatment (316 patientsreceived combined therapy). Patients with active cancer had more comorbidities and suffered more severestrokes; however, they showed similar 24-hour neurologic improvement and adverse events, including cerebralhemorrhage, compared to the other groups. Although the functional outcome at 3 months was poorer than theother groups, 36.4% of patients with active cancer showed functional independence. Additionally, 52.9% of thepatients with determined stroke etiology showed functional independence despite active cancer. During the 6-month follow-up, 46.6% of patients with active cancer died, and active cancer was independently associatedwith poor survival (Hazard ratio 4.001; 95% confidence interval 2.548–6.283).Conclusions:
32

Cerebrovasc Dis 2020;49(suppl 1):1-149
In patients with active cancer, reperfusion therapy showed similar adverse events and short-term outcomes tothat of other groups. While long-term prognosis was worse in the active cancer group than the non-active cancergroups, many had good functional outcomes, especially those with determined stroke mechanisms.
33

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-26Acute Management
Clinical Diffusion Mismatch Predicts Early Neurological Improvementafter Late - Time Window Endovascular Revascularization
Bum Joon Kim 1, June Young Chang 1, Dong-wha Kang 1, Sun U. Kwon 1, Jong S. Kim 1
1 Neurology, Asan Medical Center, Seoul, Korea
Purpose:Clinical-diffusion mismatch (CDM) and diffusion-perfusion mismatch (DPM) is used to select patients eligible forendovascular thrombectomy (EVT) in the late-time window. As CDM well reflects true penumbra, wehypothesized that patients with CDM may better respond to EVT than those without.Methods:Acute ischemic stroke patients who received EVT between 6 to 24 hours from stroke onset were enrolled. Allpatients showed DPM (ratio of penumbra/ischemic core>1.8). CDM was defined according to the DAWN criteria;1) age≥80, National Institute of Health Stroke Scale (NIHSS) score≥10 and DWI lesion≤21 ml, 2) age<80, NIHSS score≥10 and DWI lesion≤31 ml and 3) age<80, NIHSS ≥ 20 and 31. Results:Among 94 patients enrolled, 44 (46.3%) patients showed CDM. ENI was observed from 48 (51.1%) of patients.Patients with CDM showed higher prevalence of hypertension (p=0.047) initial NIHSS score (14±4 vs. 8±4;p<0.001), more improvement of NIHSS after EVT (6±6 vs. 1±5; p<0.001) and a higher prevalence of ENI. From themultivariable analysis, ENI was associated with onset-to-door time (OR=0.998, 95% CI 0.997–1.000; p=0.042),complete recanalization (OR=23.912, 95 % CI 2.238–255.489; p=0.009), NIHSS score (OR=1.180, 95% CI 1.012–1.377; p=0.034) and CDM (OR=5.160, 95% CI 1.448–18.386; p=0.011). Interestingly, the correlation between DWIlesion volume and NIHSS score was strong in those without CDM (r=0.731), but only moderate in those withCDM (r=0.355).Conclusions:Patients with both CDM and DPM showed a better response to EVT in late-window than those with DPM only.
34

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-27Rehabilitation & Restorative Therapy in Stroke
Effects of Anodal Transcranial Direct Current Stimulation on Mobility and Balancein Post Stroke Patients
Mirza Obaid Baig 1, Sundas Akhter 2
1 Riphah College of Rehabilitation & Allied Health Sciences, Riphah International University, Rawalpindi, Pakistan2 Riphah College of Rehabilitation & Allied Health Sciences, Riphah International University, Rawalpindi, Pakistan
Purpose:To determine the effects of anodal transcranial direct current stimulation on mobility and balance in post strokepatients.Methods:A randomized control trial providing 6 weeks of anodal transcranial direct current stimulations, thrice a week onalternate days for 20 minutes in addition to conventional training. A sample of 35 patients of age 35 to 75 years,selected based on inclusion criteria. Participants were assessed at baseline, 3rd and 6th week. It took 5 monthsto complete from February 2019 to July 2019 at Pakistan Railway General Hospital. The tools used in this studywere 10 meter walk test(MWT), Dynamic gait index(DGI) and Fugyl-meyer assessment(FMA).Results:Mean age was reported as 54.71±11.38 years and 68.6% (n=24) were male whereas 31.4%(n=11) were female.Repeated Measure ANOVA shows significant improvement in 10MWT, DGI and FMA within groups. Whereasthere were significant improvement in DGI but there were no significant difference was observed in 10MWT andFMA on Independent T test between groups.Conclusions:Stroke patients who received a-tDCS along with conventional physical therapy shows a significant improvementin balance and mobility against control group.
35

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-28Pathophysiology of Stroke
Burden of Comorbidity Contributing Troponin Elevation Increases the Riskof Long-term Adverse Outcome inPatients with Acute Ischemic Stroke
Sung-ho Ahn 1, Young-hak Kim 3, Ji-sung Lee 4, Mi-sook Yun 5, Jung-hee Han 2, Soo-young Kim 2, Dong-wha Kang2, Jong S. Kim 2, Sun U. Kwon 2
1 Neurology, Pusan National University Yangsan Hospital, Yangsan, Korea2 Neurology, Asan Medical Center, Seoul, Korea3 Cardiology, Asan Medical Center, Seoul, Korea4 Clinical Research Center, Asan Medical Center, Seoul, Korea5 Division of Biostatistics, Pusan National University Yangsan Hospital, Yangsan, Korea
Purpose:Background: Cardiac troponin, as a biomarker for myocardial injury, frequently increases in patients with acuteischemic stroke (AIS), and is known to be associated with long-term outcome. Comorbid illnesses causingtroponin elevation even including minimally-elevated level below the 99th percentile of upper reference limitalso affect the outcome of AIS. Objectives: We aimed to evaluate the impact of predefined candidates,contributing to troponin elevation, on explanatory power of troponin elevation and long-term outcomes amongpatients with AIS, apart from the neurological status.Methods:Methods: Based on the prospectively-enrolled registry, ischemic heart disease (IHD), atrial fibrillation (AF),congestive heart failure (CHF), hypertrophic cardiomyopathy (HCM), chronic kidney disease (CKD) and activecancer were predefined as six-potential troponin-elevating comorbidities. Comorbidity burden, representingnumber of comorbidities, and composite neurological status, representing either moderate to severeneurological deficits, insular lesions or both, was newly-defined to estimate the relations among these factors.Area under the receiver operating characteristic curve (AUC) was used to assess the performance of model forexplanation of troponin elevation. Contribution of comorbidity burden to the rate of major adverse cardiac andcerebrovascular events (MACCE) and mortality was estimated.Results:Results: During 2-year of prospective enrolment, 145 (13.3%) and 335 (30.7%) out of 1,092 patients had anelevated (≥0.04 ng/mL) and minimally-elevated (0.040-0.010 ng/mL) troponin. Multivariable model based on the six comorbidities and one composite neurological status exhibited the AUC for elevated (0.789; 95% confidenceinterval [CI]: 0.748-0.830) and for elevated and minimally-elevated (0.720; 95% CI: 0.689-0.752) troponin. Overa median follow-up of 18 months, multivariable Cox model revealed rate of the MACCE and mortality wasincreased in proportion to the comorbidity burden even after adjusting clinically-relevant variables includingneurological status.Conclusions:Conclusions: Troponin elevation in AIS patients can be explained by overall burden of comorbidities withsynergistic combination of neurological status which, in turn, associated with proportionally-increased risk oflong-term outcomes.
36

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-29Prognosis/Outcome of Stroke
Left Ventricular Function and Covert Atrial Fibrillation Detected by Insertable Cardiac Monitorin Embolic Stroke of Undetermined Source
Hajime Ikenouchi 1, Junpei Koge 1, Tomotaka Tanaka 2, Eriko Yamaguchi 1, Kazuo Washida 2, Manabu Inoue 1,Satoshi Nagase 3, Kengo Kusano 3, Kazunori Toyoda 1, Masafumi Ihara 2, Masatoshi Koga 1
1 Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan2 Neurology, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan3 Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
Purpose:There are few studies regarding the association between left ventricle (LV) function and atrial fibrillation (AF)detection by implantable cardiac monitors (ICMs) in patients with embolic stroke with undetermined source(ESUS). We aimed to investigate the relationship between LV function and AF detection in ESUS patients withICMs implantation.Methods:We enrolled patients with ESUS who underwent ICMs implantation from September 2016 to September 2020using a single-center prospective registry. LV systolic function and diastolic function were assessed by leftventricular fractional shortening (LVFS) and average E/e’, respectively, on precordial echocardiography. Theassociation of LV systolic and diastolic function with AF detection by ICMs was analyzed.Results:98 patients (median age, 74 years; male, 65%) were enrolled. During median follow-up periods of 426 (IQR, 200–752) days, AF was detected in 24 (29%) patients. Median duration from ICM implantation to AF detection was75 (IQR, 15–151) days. When LVFS and E/e’ were divided into two groups by median values, both low LVFS (<36%; adjusted HR, 4.76, 95%CI 1.77–12.8) and high E/e’ (> 8.8; adjusted HR, 4.50, 95%CI 1.15–17.5) wereindependently associated with AF detection after adjustment for CHA2DS2-VASc score before index stroke. Whendivided into 4 groups according to the combination of dichotomized patients by LVFS and E/e’, low LVFS and highE/e’ had a significant low cumulative AF free rate compared with other 3 groups on Holm-Sidak multiplecomparisons test (p<0.05 each). Similarly, only low LVFS and high E/e’ group had significantly high hazard ratiofor AF detection compared with other 3 groups, which ranging from 7.72 to 21.9.Conclusions:In ESUS patients with ICMs implantation, the combination of low LVFS and high E/e’ was associated with AFdetection.
37

Cerebrovasc Dis 2020;49(suppl 1):1-149
38

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-30Prognosis/Outcome of Stroke
Recurrence Risk Stratification by Clinical Information for Acute Stroke Patientswith Atrial Fibrillation: Does It Suffice?
Beom Joon Kim 1, Eun Lyeong Park 2, Kanta Tanaka 3, Masatoshi Koga 3, Keon-joo Lee 1, Tadataka Mizoguchi 3,Sohei Yoshimura 3, Juneyoung Lee 2, Jae-kwan Cha 4, Byung-chul Lee 5, Kazunori Toyoda 3, Hee-joon Bae 1
1 Neurology and Cerebrovascular Center, Seoul National University Bundang Hospital, Seongnam-si, Korea2 Biostatistics, College of Medicine, Korea University, Seoul, Korea3 Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Japan4 Neurology, Dong-A University Hospital, Busan, Korea5 Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea
Purpose:Various risk stratification scores for subjects with atrial fibrillation have been developed and used in clinicalpractice. However, the validity of the prediction tool has not been evaluated in stroke survivors.Methods:A total of 5648 ischemic stroke patients with confirmed atrial fibrillation (admitted between 2011 and 2014)were used to develop a new model in the study (4483 from CRCS-K registry of Korea and 1165 from SAMURAI-NVAF registry of Japan). After harmonizing data elements of each registry, candidate predictors were selected byexpert’s consensus and literature searches. Vascular risk factors, laboratory values, and treatment informationwith interactions and transformations were used to build a new risk stratification model. We used the Fine-Gray'scompeting risk model for the multivariable analysis. Regression parameter estimates were re-estimated withbootstrapping with 999 replacements. External validation and re-calibration of the model was performed usinga single-center registry from Korea (admitted between 2015 and 2018). The performance of the developedmodel was compared to alleged risk stratification schemes.Results:Subjects included in the developmental set were mean 74.3±10.2 years old, 53.1% (n, 2998) male, NIHSS scoremedian 8 [IQR 3 - 15], and had newly diagnosed atrial fibrillation in 42.9% (n, 2425). Up to 1 year after the indexstroke, 6.0% (n, 338) had a recurrent stroke and 16.0% (n, 903) had died. A total of 26 variables were incorporatedin the final model (EAST-Af model), and its c-statistics was 0.67 [95% CI, 0.64 - 0.69]. Compared to alleged riskstratification tools, all four schemes did not show a dose-dependence relationship or sufficient riskdiscrimination except in the extreme score range (see Figure).
39

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:Risk stratification schemes for recurrent stroke based on clinical information did not effectively predict individualfuture risk.
40

Cerebrovasc Dis 2020;49(suppl 1):1-149
OP-31Risk Factors and Prevention of Stroke
Clinical Significance of Intracardiac Thrombus Identified by Transesophageal Echocardiographyin Atrial Fibrillation-associated Ischemic Stroke
Kanta Tanaka 1, Masatoshi Koga 1, Keon Joo Lee 2, Beom Joon Kim 2, Tadataka Mizoguchi 1, Eun Lyeong Park 3,Juneyoung Lee 3, Sohei Yoshimura 1, Jae Kwan Cha 4, Byung Chul Lee 5, Junpei Koge 1, Hee Joon Bae 2, KazunoriToyoda 1
1 Department of Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Japan2 Department of Neurology, Cerebrovascular Center, Seoul National University Bundang Hospital, Seongnam-si,Korea3 Department of Biostatistics, College of Medicine, Korea University, Seoul, Korea4 Department of Neurology, Dong-A University Hospital, Busan, Korea5 Department of Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea
Purpose:To clarify differences in clinical significance of intracardiac thrombi in nonvalvular atrial fibrillation (NVAF)-associated stroke as identified by transesophageal echocardiography (TEE) and transthoracic echocardiography(TTE).Methods:Using patient data on NVAF-associated ischemic stroke between 2011 and 2014 from the Clinical ResearchCollaboration for Stroke (CRCS-K) registry (15 South Korean stroke centers, n=4841) and the Stroke AcuteManagement with Urgent Risk-factor Assessment and Improvement (SAMURAI)-NVAF registry (18 Japanesestroke centers, n=1192), implementation rates of TEE/TTE and detection rates of intracardiac thrombi at eachcenter were correlated. The primary outcome was recurrent ischemic stroke at 1 year after the onset.Results:In this study, 5648 patients (median age, 75 years; 2650 women) were analyzed. Intracardiac thrombi weredetected in 75 patients (1.3%) overall. Thrombi were detected in 7.8% of patients with TEE (either TEE alone orTEE+TTE: n=679) and in 0.6% of those with TTE alone (n=3572). Thrombus detection rates varied between 0%and 14.3% among centers. As TEE implementation rates at each center increased from 0% to 56.7%, thrombusdetection rates increased linearly (detection rate [%] = 0.11 ´ TEE rate [%] + 1.09 [linear regression], P<0.01). TTEimplementation rates (32.3–100%) were not associated with thrombus detection rates (P=0.53). Intracardiacthrombi were associated with risk of recurrent ischemic stroke overall (adjusted hazard ratio [aHR] 2.35, 95%confidence interval [CI] 1.07–5.16). Thrombus-associated ischemic stroke risk was high in patients with TEE (aHR3.13, 95% CI 1.17–8.35), but not in those with TTE alone (aHR 0.89, 95% CI 0.12–6.51).Conclusions:Our data suggest clinical relevance of TEE for accurate detection and risk stratification of intracardiac thrombi inNVAF-associated stroke.
41

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-01Acute Management
Is Coil Embolization The Right Endovascular Treatment for Dissecting Aneurysms?
Hyung Jun Kim1, Pyoung Jeon1, Keon-ha Kim1
1 Radiology, Samsung Medical Center, School of Medicine, Sungkyunkwan University, Seoul, Korea
Purpose:Intracranial dissection occurs in the cerebral vessel of the vertebral artery, posterior inferior cerebellar artery,posterior cerebral artery, and anterior cerebral artery, and is accompanied by a dissecting aneurysm. A dissectinganeurysm is mainly formed in a fusiform shape; however, sometimes it can also be formed in a saccular shape.The treatment of dissecting aneurysms includes coil embolization, flow diverter, and multiple stenting. However,no clear endovascular treatment has been established. In this study, the outcome of coil embolization wasanalyzed in the treatment of dissecting aneurysm.Methods:We conducted a retrospective study of patients with dissecting aneurysms using digital subtraction angiography.The diagnosis of a dissecting aneurysm was classically represented as an angiographic pearl and string sign, withdilatation of the lumen adjacent to a stenotic segment, and sudden angiographic change when angiography wasfollowed up in a short term. The unfavorable outcome was defined as the occurrence of recanalization,hemorrhage, and infarction in dissecting vessels after endovascular treatment.Results:Of 72 dissecting aneurysm patients (mean age 53.9 ± 12.1 years, male 38.0%) with endovascular treatment, 26(36.1%) patients underwent multiple stents, 31 (43.1%) patients underwent coil embolization with (21 patients,29.2%) or without stent (10 patients, 13.9%), 8 (11.1%) patients deployed flow-diverters, and 8 (11.1%) patientsunderwent occlusion of the parent artery with or without bypass. Unfavorable outcome were significantly morecommon in the coil embolization group than in the other endovascular treatment groups (29.03% vs 7.32%,p=0.03). The presence of saccular aneurysm and coil embolization were independently associated withunfavorable outcomes.Conclusions:In the treatment of dissecting aneurysms, coil embolization has a unfavorable outcome compared to otherendovascular treatments. Therefore, when a dissecting aneurysm is suspected such as a saccular aneurysm, careshould be taken before performing coil embolization as a definitive treatment.
42

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-02Acute Management
Successful Intraarterial Thrombectomy with Direct Infusion of Arterial Nimodipinefor The Refractory Clot - Early Experience in A Single-center
Jong Wook Shin2, Hee-jung Song2, Hyon-jo Kwon3, Jeong-wook Lim4, Hye Seon Jeong1
1 Neurology, Chungnam National University Hospital, Dae-jeon, Korea2 Neurology, Chungnam National University Sejong Hospital, Sejong, Korea3 Neurosurgery, Chungnam National University Hospital, Dae-jeon, Korea4 Neurosurgery, Chungnam National University Sejong Hospital, Sejong, Korea
Purpose:Despite successful vascular access, refractory clots give rise to an unfavorable intra-arterial thrombectomy (IAT)in acute ischemic stroke treatment. We supposed that physical association between the clot and vessel might bethe cause of this refractoriness. We aimed to investigate the effect of intra-arterial nimodipine infusion for therefractory clots as rescue treatment during IAT.Methods:We defined refractory clot as the failure of clot retrieval more than four passes of any endovascular devices.Then, we administered intra-arterial nimodipine 1mg with an infusion pump over 10 minutes through amicrocatheter placed just in front of the refractory clot. After the nimodipine infusion, we attemptedthrombectomy again.Results:We tried intraarterial nimodipine assisted thrombectomy in a total of 5 patients. All the patients showed largecerebral vessel occlusion. (Patient No. 1,2,3, Terminal ICA; Patient No. 4,5, MCA M1) Four patients result incomplete recanalization of the occluded vessel showing TICI grade 3. Mean device passes and procedure durationbefore versus after the nimodipine infusion was 7.25 vs. 1.75 per patient and 66 vs. 24.3 minutes. Althoughsuccessful endovascular treatment, we concluded 2 patient as a futile recanalization. Characteristic brain imageafter IAT was the hemorrhagic transformation in patients No. 3 and 4 and vasogenic edema in patients No. 2 and4.Conclusions:There is still no clear strategy against refractory clots. In this study, we showed a synergistic effect of intraarterialnimodipine for the refractory clots during IAT. These findings imply considering the direct infusion of avasodilatory drug as a rescue strategy for the situation. However, we need further investigation for when to startthe drug and which one that affects the physical association between the vessel and clots could be a candidatefor the refractoriness.
43

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-03Acute Management
Outcomes of Endovascular Treatment for in Hospital Stroke: A Single Center Study
Jeonghoon Bae1, Eung-joon Lee1, Kipyoung Jeon1, Ki-woong Nam1, Min Kyoung Kang1, Keun-hwa Jung1, Byung-woo Yoon1
1 Neurology, Seoul National University Hospital, Seoul, Korea
Purpose:There are many differences between in hospital ischemic stroke(IHS) and community onset ischemic stroke(COS),and there are several comparative studies. Although the importance of mechanical thrombectomy(MT) in thetreatment of acute ischemic stroke is becoming increasingly important, there are not many studies on theeffectiveness of MT in IHS. We aimed to compare the clinical features and outcomes between IHS and COSpatients who received MT.Methods:We analyzed cases of MT performed at Seoul National University Hospital from January 2012 to June 2020. Weselected patients with previous mRS(modified Rankin Scale) 0-1 and then divided them into two groups: IHS andCOS, and compared successful recanalization, discharge mRS, 3month mRS, and 3month functionalindependence (mRS 0-2). In addition, the characteristics of the IHS group were analyzed in detail.Results:A total of 41 patients with IHS and 213 patients with COS were included. The baseline characteristics(age, sex,underlying disease, occlusion site) of the two groups were similar, but malignancy tended to be more commonin IHS than COS(19.5% vs 7.5%). The median/mean LNT(last normal time)-to-puncture time was 341min/399minin IHS and 370min/461min in COS. The percentages of successful recanalization (92% vs 89%), discharge mRS(mean, 2.19 vs 2.97), 3 month mRS (mean, 2.05 vs 2.56), 3 month functional independence (61% vs 49%) werecomparable between the two groups. In the multivariable analysis of the 3 month functional independence,initial NIHSS and successful recanalization were the most important predictors. In addition, a multivariableanalysis was performed on successful recanalization, and LNT to puncture time was the most important predictor.The most frequent departments in the IHS group were cardiology and thoracic surgery(TS). There were 8 casesof cancer related stroke(19.5%) and 7 cases of perioperative stroke(17.1%), all of which occurred in TS. Therewere 4 cases that occurred immediately after percutaneous coronary intervention(9.8%), and all showed goodoutcomes.Conclusions:The importance of MT is still high even in the in hospital stroke. IHS has more factors that can reduce the onsetto puncture time compared to COS such as well designed on-call system and patient transfer system, wellarrangement of nursing manpower. In addition, a significant proportion of patients undergoing MT in IHS is nota special group of patients, such as cancer patients or TS patients, but general patients. Therefore, more attentionis needed for MT in IHS.
44

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-04Acute Management
Decreasing Tendency of Blood Pressure during Successful Endovascular Treatmentof Acute Ischemic Stroke
Dong-hyun Shim1, Woo-chan Choi1, Jung-a Kwon1, Dong-seok Gwak1, Yong-won Kim1, Yang-ha Hwang1
1 Neurology, Kyungpook National University Hospital, Daegu, Korea
Purpose:Endovascular treatment (EVT) is now the main treatment for large vessel occlusion acute ischemic stroke (AIS)patients. However, patients with poor prognosis after successful EVT have been reported. Among various reasons,how to control blood pressure (BP) is one of an issue. For the purpose of determining the target of BP after EVT,we tried to investigate whether or not there is a characteristics of BP trend during EVT.Methods:We retrospectively collected data from patients with anterior circulation stroke who received EVT for fourmonths from April to July, 2020 who acquired TICI grade IIB or III. BP was measured every 5 minutes from thebrachial artery by NIBP (non-invasive blood pressure) method. All patients were treated under conscioussedation, and the calculated mean value before and after recanalization was analyzed based on the time pointof recanalization. Systolic BP, diastolic BP, mean arterial pressure (MAP), pulse pressure(PP) were measured.Results:A total of 14 patients were included in the analysis process. Statistically significant differences were observed insystolic BP (PV = 0.008), MAP (PV = 0.022), and PP (PV = 0.021). One of the patients showed hemorrhagictransformation, and his other BP parameters were also decreased after recanalization, except PP was increased.Conclusions:We found that there was a decreasing tendency of BP in successfully recanalized anterior circulation AIS patients.Further analysis on whether the reduced BP value can be used as a target value for BP is required.
45

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-05Acute Management
Endovascular Treatment of the Acute Basilar Artery Occlusion in Octogenarians
Jeong Jin Park1, Yoo Sung Jeon2, Hong Ghee Roh3
1 Neurology, Konkuk University Medical Center, Seoul, Korea2 Neurosurgery, Konkuk University Medical Center, Seoul, Korea3 Radiology, Konkuk University Medical Center, Seoul, Korea
Purpose:Basilar artery occlusion accounts for 1% all ischemic stroke. It iss related to a high mortality and poor outcome,despite the successful recanalization. Though multiple studies have shown a clinical benefit of thrombectomy inacute ischemic stroke, but most of them excluded octogenarians. It is still controversial whether age acts as adeterminant in performing mechanical thrombectomy. We compared the outcomes and safety betweenoctogenarians and younger patients with acute basilar occlusion undergoing the endovascular treatment.Methods:We retrospectively collected 47 patients with acute basilar artery occlusion who underwent mechanicalthrombectomy. Patients were divided into two groups, younger than 80 years(younger group) and older than 80years (elderly group). We analyzed baseline characteristics, functional outcomes, successful recanalization,complications (e.g., symptomatic hemorrhage, craniectomy), and mortality in both groups. Good functionaloutcome was defined as mRS ≤ 2 at 90-days and successful recanalization as Thrombolysis in Cerebral Infarction (TICI) grades 2b, 3.Results:In this study, 47 patients with acute BAO who underwent mechanical thrombectomy were enrolled. Among them,11 patients were octogenarians and 36 patients were younger than 80. There were no remarkable differences inthe gender, risk factors, initial National Institute of Health Stroke Scale (NIHSS) score, pre-mRS and site ofocclusion between two groups. Rates of functional independence (mRS score ≤ 2) after endovascular treatment in the octogenarians were slightly lower than younger group with no significant difference (54.6% vs. 58.3%,p=0.73). Successful recanalization( 100% vs. 94.4%, p>0.99) and incidence of complications showed no significantdifference between the two groupsConclusions:In our study, no significant difference in outcome, recanalization and complication in octogenarian, comparedwith younger group. However, there was tendency of lower chance of good clinical outcome in octogenarians,despite higher recanalization rate. The limitation of this study is the retrospective single-center design with smallsample size. More clinical data and randomized controlled trials are needed.
[Endovascular treatment of aBAO, age above 80 ]
Table. Baseline Characteristics of mechanical thrombectomy in Acute BAO
N=47Octogenarians
( n=11)Age below 80(n=36)
p-value
Gender (Male) 5 (45.45%) 23 (53.89%) 0.46*
Age +
Hypertension 5 (45.45%) 17 (47.22%) 1.00*
Diabetes mellitus 4 (36.36%) 10 (27.78%) 0.866*
Dyslipidemia 0 (0%) 2 (5.56%) 1.00*
46

Cerebrovasc Dis 2020;49(suppl 1):1-149
Smoker 0 (0%) 6 (16.67%) 0.351*
Atrial fibrillation 7 (63.64%) 11 (30.56%) 0.105*
Stroke Etiology 0.526*
- Large-arteryatherosclerosis
3 (27.27%) 14 (38.89%)
- Cardioembolism 6 (54.55%) 12 (33.33%)
- Other determinedetiology
0 (0%) 3 (8.33%)
- Undeterminedetiology
2 (18.18%) 7 (19.44%)
Initial NIHSS 10 (9.5. 15.5) 8 (5,16.25) 0.155+
Pre-mRS 0 (0,1) 0 (0,0.25) 0.611+
IV TPA 5 (45.45%) 16 (44.44%) 1.00*
Occlusion Site 0.226*
- Distal 9 (81.82%) 23(63.89%)
- Middle 1 (9.09%) 1 (2.78%)
- Proximal 1 (9.09%) 12 (33.33%)
Time Window- within 6hours- beyond 6hours
8(72.73%)3(27.27%)
30 (83.33%)6 (16.67%)
0.73*
Puncture to Recanalization(Minutes)
55min.(29, 68)
34.5min.(23, 58.25)
0.322+
Onset to Puncture(Minutes)
238min.(158.5, 374.5)
205min.(129, 265.5)
0.297+
*=Chi-square Test , +=Mann-Whitney U Test , mRS= Modified Rankin Score, NIHSS = National Institution of Health
Stroke Score
Table. Outcomes after mechanical thrombectomy in acute BAO
N=47Octogenarians
( n=11)Age below 80(n=36)
p-value
Good outcome(90 days mRS 0-2)
6 (54.55%) 21 (58.33%) 0.73*
Good recanalization(mTICI 2b-3)
11 (100%) 34 (94.44%) >0.99*
Number of Pass 1. (1.1.5) 1(1,2) 0.402+
Additional Procedure- Angioplasty- Stenting
2(18.18%)0(05%)2(18.18%)
14(38.89%)4(11.11%)9(25%)
0.366
47

Cerebrovasc Dis 2020;49(suppl 1):1-149
Symptomatic Hemorrhage 0(0%) 1(52.78%) >0.99*
Craniectomy 0(0%) 3(8.33%) >0.99*
Mortality 0(%) 2(5.56%) >0.99*
*=Fisher’s exact test, +=Mann-Whitney U test, mTICI=modified Treatment in Cerebral Infarction, min. =minute
48

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-06Acute Management
Intravenous Thrombolysis for Multi-ethnic Asians with Acute Ischaemic Stroke in Primary Stroke Centresversus Acute Stroke Ready Hospitals
: Comparison of Service Efficiency and Clinical Outcomes
Jie Ping Schee1, Chee Peng Hor2, Irene Looi2, Wan Chung Law3, Linda Yee Yen Then3, Anderson Steven3, Ding WeiHii3, Sin Hong Chew4, Zariah Abdul Aziz5, Khairul Azmi Ibrahim5, Mazlina Husin5, Yen Theng Chin5, Chun Fai Cheah6,Wee Kooi Cheah7, Ee Wen Loh8, Desmond Samuel9, Pravind Narayanan10, Aznita Ibrahim11, Zainura Che Isa11, ChaiLiang Ang12, Yuen Kang Chia4
1 Department of Medicine, Tawau Hospital, Tawau, Sabah, Malaysia2 Clinical Research Centre, Seberang Jaya Hospital, Seberang Jaya, Penang, Malaysia3 Department of Medicine, Sarawak General Hospital, Kuching, Sarawak, Malaysia4 Department of Medicine, Queen Elizabeth Hospital, Kota Kinabalu, Sabah, Malaysia5 Department of Medicine, Sultanah Nur Zahirah Hospital, Kuala Terengganu, Terengganu, Malaysia6 Department of Medicine, Raja Permaisuri Bainun Hospital, Ipoh, Perak, Malaysia7 Department of Medicine, Taiping Hospital, Taiping, Perak, Malaysia8 Department of Medicine, Bintulu Hospital, Bintulu, Sarawak, Malaysia9 Department of Medicine, Miri Hospital, Miri, Sarawak, Malaysia10 Department of Medicine, Sarikei Hospital, Sarikei, Sarawak, Malaysia11 Department of Medicine, Sultan Abdul Halim Hospital, Sungai Petani, Kedah, Malaysia12 Department of Medicine, Lahad Datu Hospital, Lahad Datu, Sabah, Malaysia
Purpose:Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator is beneficial in acute ischaemicstroke (AIS) even when administered by non-neurologists in non-stroke centres. We aim to compare theefficiency, effectiveness, and safety of IVT in Malaysian primary stroke centres (PSCs) equipped with in-houseneurologists versus acute stroke ready hospitals (ASRHs) without in-house neurologists.Methods:We conducted a multi-centre, periodic cross-sectional study involving 5 PSCs and 7 ASRHs in Malaysia. Throughreview of medical records, real world data was extracted for analysis. Consecutive adults with AIS who receivedIVT from 01 January 2013 to 31 May 2020 were included. Univariate and multivariate regression models wereemployed to evaluate the role of PSCs versus ASRHs in post-IVT outcomes and complications, adjusting fordemographics, clinical histories, and procedural parameters. Statistical significance was set at p<0.05.Results:A total of 301 multi-ethnic Asian adults, namely 225 (75%) from PSCs and 76 (25%) from ASRHs, were included.Both groups were matched in demographic, baseline clinical, and stroke characteristics. The efficiency of IVTdelivery, post-IVT clinical outcomes, and adverse events following IVT were comparable as well (refer Table 1).Regression analyses demonstrated that post-IVT outcomes and complications were independent of the role ofPSCs or ASRHs after adjustments.Conclusions:Our study may provide translational real-world evidence which suggests that IVT can be equally safe, effective,and efficiently delivered in both PSCs and ASRHs. This may encourage the establishment of such service in morehospitals without in-house neurologists, hence extending the benefits to a greater proportion of strokepopulations. Accordingly, development of ASRHs equipped with trained stroke teams should be advocated toenhance regional and international acute stroke care.
49

Cerebrovasc Dis 2020;49(suppl 1):1-149
50

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-07Acute Management
Association between Arterial Diameter and Procedural Outcome in The Acute M2 Occlusive Ischemic StrokePatients Treated with Endovascular Thrombectomy
Jun Yup Kim1, Keon-joo Lee1, Jihoon Kang1, Beom Joon Kim1, Moon-ku Han1, Hee-joon Bae1, Sung Hyun Baik2,Leonard Sunwoo2, Jae Hyoung Kim2, Cheolkyu Jung2
1 Department of Neurology, Seoul National University Bundang Hospital, Seoul National University College ofMedicine, Seongnam, Korea2 Department of Radiology, Seoul National University Bundang Hospital, Seoul National University College ofMedicine, Seongnam, Korea
Purpose:Several reports showed that clinical outcome was differed by the occluded location of M2 segment of middlecerebral artery in the endovascular thrombectomy (EVT). However, there is no report about the associationbetween arterial diameter and outcomes. We aimed to evaluate the relationship between arterial diameter ofacute ischemic stroke patients treated with EVT for M2 occlusion and the outcomes.Methods:Using a prospective single center endovascular thrombectomy registry, we identified acute M2 occlusion patientswho treated with EVT from 2011 to 2016. M2 diameter was measured at the proximal segment of occlusionusing axial source image of CT or MR angiography conducted before EVT. The association of M2 diameter withclinical and procedural outcome was assessed. Procedural complication was captured including extravasationduring angiography and hemorrhagic transformation on follow up image.Results:A total of 104 patients (age, 70.2 ± 11.9 years; male, 53.8%) was evaluated. Arterial diameter of M2 segment wasranged from 1.05 to 3.19 mm. Six patients were treated with intraarterial urokinase only, 90 with stent retriever,3 with aspiration thrombectomy, and 5 patients with both stent retriever and aspiration thrombectomy.Extravasation developed four times more frequently in the lowest quartile group (<1.63 mm) than the highestquartile group (≥2.29 mm) divided by M2 diameter. Hemorrhagic transformation occurred in 25% of patients and the half of them was subarachnoid hemorrhage. In the logistic regression analysis, the lowest quartile groupshowed positive association with hemorrhagic transformation (adjusted ORs 8.91 [95% CIs 1.50 – 52.93]), but noassociation with clinical outcome.Conclusions:This study demonstrated that the lowest quartile of M2 diameter was associated with procedural complicationin the acute M2 occlusion patients treated with EVT. However, clinical outcome was not differed.
51

Cerebrovasc Dis 2020;49(suppl 1):1-149
52

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-08Acute Management
Effectiveness of Interventions Done among Paramedics in Achieving Optimal Onset-to-door Time forThrombolysis in Patients with Acute Ischemic Stroke
: A Systematic Review and Meta-analysis
Amanda Ng1, Janice Iu1, Carissa Lee1, Jamuna Appalasamy1, Md Golam Hasnain2, Shazwani Shaharuddin1
1 School of Pharmacy, Monash University Malaysia, Selangor, Malaysia2 School of Medicine and Public Health, University of Newcastle, New South Wales, Australia
Purpose:The paramedics role is pivotal in ensuring eligible patients with stroke reaches the hospital within 4.5 hours asthis will increase the chance of patients being given recombinant tissue-plasminogen activator (rTPA) andimprove the outcome. However, given the lack of information as to which interventions are of the best practicein improving the thrombolysis rate, our study aims to identify the effectiveness of the interventions done amongparamedics.Methods:We searched PubMed, Embase, CINAHL, and RCN to identify studies that were published between 2010 and June30th, 2020. The primary outcome of this study is to investigate the impact of the interventions on the rate ofrTPA administration and onset to door timing. Other outcomes include improvement in door-to-needle (DTN)time, door-to-imaging (DTI) time, and onset-to-treatment (OTT) time. Random effect models were used toanalyze the effect of the intervention done.Results:We’ve gathered 621 papers of which 11 met eligibility criteria. Among interventions done include bypass (n=3),education (n=2), prenotification (n=4), and telemedicine (n=2). Based on the random effect model, rTPAadministration was significantly higher in the intervention arm of ischemic stroke patients (n=7) with an oddsratio of 1.45 (95% confidence interval [CI], 1.01-2.06). The trend was highest with bypass intervention: odds ratio2.23 (95% CI, 1.55-3.2), followed with education: odds ratio 1.51 (95% CI, 0.87-2.6).Conclusions:Interventions among paramedics have shown to have a considerable impact on the increasing rate of rTPAadministration. It is therefore encouraged for changes in policy to be made in the management of acute stroketo maximize the use of rTPA and improving the outcome of stroke patients.
53

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-09Risk Factors and Prevention of Stroke
Impact Factors for Early Arrival of Acute Ischemic Stroke Patients within 4.5 Hours
Hataichanok Lerdwarayut1, Aurauma Chutinet1, Nijasri C.Suwanwela1
1 Neurology, King Chulalongkorn Memorial Hospital, Bangkok, Thailand
Purpose:Background: Early thrombolytic therapy in acute ischemic stroke has proven to reduce stroke morbidity. Previousstudies showed a minimal rate of early arrival in the recommended <4.5 hours guideline. Delay in hospital arrivalafter acute stroke is the main reason for exclusion of Recombinant Tissue Plasminogen Activator (rt-PA) and isassociated with less favorable outcome. Objectives: To evaluate factors which are associated with early arrival ofacute ischemic stroke patients within 4.5 hours.Methods:Methods: An observational cross-sectional study included acute ischemic stroke patients who were admitted atKing Chulalongkorn Memorial Hospital, Bangkok, Thailand between July to December 2019. We excludedpatients who were referred from other hospitals, those who were unable to interview due to no relative presentor those who denied to participate in the study. The data was collected by direct interview using a questionnairedesigned to study factors such as demographic data, distances, transportation, stroke severity using the NationalInstitutes of Health Stroke Scale (NIHSS) for stroke awareness and knowledge of symptoms.Results:Results: There were 200 patients included in the study. 52% were male. Mean age was 63.37 years. 126 patients(63%) knew the symptoms of stroke but only 78 patients (39%) arrived at the hospital within 4.5 hours. Aftermultivariate analysis (Table 1), early arrival in less than 4.5 hours was significantly associated with 1) age < 45years (p = 0.03), 2) awareness (urgency) ( p < 0.001), 3) the use of ambulance transportation (p = 0.025) and 4)clear of symptoms onset (p < 0.001) .Conclusions:Conclusion: Age < 45 years, awareness (urgency), the use of ambulance transportation and clear of symptomsonset are associated with early arrival to the hospital in less than 4.5 hours in patients with acute ischemic stroke.
54

Cerebrovasc Dis 2020;49(suppl 1):1-149
Table 1. Factors associated with early arrival (< 4.5 hours)
Variables Univariate analysis Multivariate analysis
OR (95%CI) p-value Adjust OR (95%CI) p-value
Age (>45) 0.36 (0.14-0.88) 0.026 0.18 (0.03-0.85) 0.030
Suspected 2.64 (1.47-4.73) 0.001 1.45 (0.60-3.47) 0.404
Awareness (urgency) 16.7 (8.09-34.82) < 0.001 14.94(5.86-38.1) < 0.001
Onset (Clear) 10.1 (5.05-20.22) < 0.001 11.5(4.44-29.85) < 0.001
Transported byambulance
5.59 (2.34-13.36) < 0.001 5.29(1.23-22.81) 0.025
Distances (<5 km) 1.89 (1.02-3.52) 0.043 1.14 (0.39-3.28) 0.807
Initial NIHSS (>15) 10.90 (2.37-50.21) 0.002 3.15(0.39-25.47) 0.280
Acute ischemic stroke- Cardioembolic
- Small vessel2.81 (1.23-6.38)0.42 (0.23-0.75)
0.0130.004
1.56 (0.4-6.02)0.69 (0.26-1.76)
0.5130.440
55

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-10Case Report
A Successful Thrombectomy in A Middle Cerebral Artery Stroke Secondary to Aortic Metallic ValveThrombus: How to Predict Post Thrombectomy Hematoma & Start Anticoagulant Early?
Kim Lim Koo1, Jackson Wee1, Jin Yi Goh1, Siew Kian Chow1, Hamdi Najman Achok1
1 Neurology, Hospital Sultanah Aminah , Johor Bahru, Malaysia
Purpose:There is no clear answer emerging to refine the optimal timing for initiation of anticoagulant after stroke causedby a cardiac thrombus. Although it is always risk and benefits weighing, the limited evidence breeds uncertaintywhen the infarct size is large and carries higher risk of bleeding. We analyse the predictors for postthrombectomy hematoma in our patient and share the management approach.Methods:Case report.Results:A 28-year-old man with aortic metallic valve for 2 year presented with left hemiparesis an hour before arrivalwith NIHSS 14. His CT showed ASPECTS 6 and angiogram showed high clot burden proximal M1 occlusion withunfavourable collaterals. His INR was 1.73. Door-to-groin puncture was 45 min and the clot was removed withTICI 2C & 2 passes at 60 min from groin puncture. NIHSS improved immediately on table to 5. He washemodynamically stable with normotensive. Echocardiogram after thrombectomy revealed a thrombus on thewall of aortic metallic valve. Due to a very high risk for further cardioembolic stroke, anticoagulation therapyseems mandatory but high risk of hematoma if anticoagulant initiated early in a major stroke is a matter ofdebate. We initiated i.v unfractionated heparin infusion at 9 hours post recanalisation (about 12 hours fromstroke onset) after repeating a CT plain. Serial daily CT plain brain later revealed worsening infarct and cerebraledema without obvious mass effect and no hemorrhagic transformation. His NIHSS was 0 at 72 hours post strokeonset. We initiated warfarin after 96 hours of stroke onset when repeated CT plain showed reduced cerebraledema without bleeding. I.V heparin infusion was stopped once INR was therapeutic and he was discharged wellwith mRS 0 at 90 days.Conclusions:Despite the risk of reperfusion hematoma is high in our patient due to a larger ischemic lesion (ASPECTS 6),unfavourable collaterals by angiogram and possible embolisation in new territory, the indication foranticoagulation is strong to prevent mortality. In addition, the young age, normotension and earlyrecanalisation are the factors for low risk of reperfusion hematoma. When risk of post thrombectomy hematomais high and the anticoagulant is mandatory, serial imaging guided monitoring for acute infarct evolution can beused to anticipate the subsequent bleeding risk after initiation of anticoagulants.
56

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-11Case Report
Intravenous Thrombolysis for Cerebral Infarction in Patients with Cardiac Myxoma
Hyoung-cheol LEE1, Byung-Kun KIM1, Jungju LEE1, Woong-woo LEE1, Kyusik KANG1, Ohyun KWON1
Jong-moo PARK1
1 Department of Neurology, Nowon Eulji Medical Center, Eulji University, Seoul, Korea
Purpose:Cardiac myxoma is a benign cardiac tumor and known as a rare cause of embolic stroke. Current guidelines donot recommend intravenous thrombolysis for cerebral infarction caused by cardiac myxoma for fear of cerebralhemorrhage. We report two cases who presented with cerebral infarction with cardiac myxoma and receivedintravenous thrombolysis.Methods:Case reportResults:A 66-year old male with hypertension and diabetes was referred to emergency department (ED) for suddenlydeveloped right side weakness. Neurologic examination revealed alert mentality with anarthria and right-sidedhemiplegia. The initial NIHSS score was 15. CT scan showed no hemorrhage or area of abnormal attenuation.The patient received recombinant tissue plasminogen (rtPA) intravenously at 1 hour and 29 minutes fromsymptom onset. DWI-MRI and MRA showed acute infarction in left MCA territory with non-visualized left ICA.Assuming chronic ICA occlusion, no further endovascular interventions were considered. Cardiac myxoma (1.24x 2.38 cm) in left atrium was detected on transthoracic echocardiogram (TTE). There was no neurologicaldeterioration with medication of aspirin 100mg, so he was transferred to tertiary hospital for the resection ofmyxoma on the 4th day. A 62-year old male was transported to ED for suddenly developed right side weakness.Neurologic examination revealed alert mentality but global aphasia, left gaze preponderance, right central typefacial palsy and right hemiplegia. The intial NIHSS score 21. Immediately after confirming the absence ofintracranial hemorrhage on CT scan, rtPA was infused intravenously at 53 minutes after symptom onset. DWI-MRI and MRA demonstrated left MCA infarction without vessel occlusion. We found Left atrial cardiac myxoma(1.34 x 2.42 cm). There was no neurologic deterioration on aspirin 300mg, but on the 7th day, he showed dyspneawith cyanosis, desaturation, and hypotension. Considering acute respiratory failure presumably due to left atrialmyxoma, he got endotracheal intubation and mechanical ventilation. His vital sign was stabilized quickly, and weextubated him on the next day. He was transported to tertiary hospital for the resection of myxoma on the 11thday.Conclusions:In most acute stroke associated with cardiac myxoma, it is hard to know accompanying cardiac myxoma beforeIV thrombolysis. In our patients, treated with intravenous thrombolysis, were not complicated with intracranialhemorrhage. It would not be necessary to delay IV thrombolysis for fear of potential cardiac myxoma.
57

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-12Acute Management
Inter-ankle Blood Pressure Difference Predicts Long-term Outcome in Patientswith Cryptogenic Stroke
Minho Han1, Minyoul Baik1, Young Dae Kim1, Junghye Choi1, Kangsik Seo1, Eunjeong Park2
Ji Hoe Heo1, Hyo Suk Nam1
1 Neurology, Yonsei University College of Medicine, Seoul, Korea2 Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul, Korea
Purpose:We investigated whether inter-ankle blood pressure (BP) difference (IAND) can predict major adversecardiovascular events (MACEs) in patients with cryptogenic stroke (CS) without peripheral artery disease (PAD).Methods:Consecutive patients with CS who underwent ankle–brachial index measurements were enrolled. Systolic anddiastolic IANDs were calculated as follows: right ankle BP − left ankle BP. MACEs were defined as stroke recurrence, myocardial infarction occurrence, or death. Survival analyses were conducted using the Kaplan–Meier method and Cox regression analysis.Results:A total of 612 patients with CS were enrolled. In the Cox regression analysis, systolic and diastolic IANDs ≥15 mmHg were independently associated with MACEs in patients with CS without PAD (hazard ratio [HR]: 2.131, 95%confidence interval [CI]: 1.242–3.659 and HR: 2.488, 95% CI: 1.060–5.657, respectively). In the subgroup analysis,systolic IAND ≥15 mmHg was independently associated with MACEs in older patients (age: ≥65 years) but not in younger patients (age: <65 years).Conclusions:Large IAND is independently associated with the long-term occurrence of MACEs in patients with CS without PAD.In particular, IAND is closely associated with outcomes in elderly patients with CS.
58

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-13Acute Management
The Impact of Relevant Artery Stenosis on Ischemic Stroke Patients with Atrial Fibrillation: Clinical andRadiological Implications
Jung Hoon Han1, Kyung Chul Noh2, Chi Kyung Kim1, Sun U. Kwon3
1 Neurology, Korea University Guro Hospital, Seoul, Korea2 Neurology, Kyung Hee University Hospital at Gangdong, Seoul, Korea3 Neurology, Asan Medical Center, Seoul, Korea
Purpose:The purpose of this study was to investigate the clinical and radiologic impact of significant stenosis on relevantartery in atrial fibrillation (AF)-related stroke.Methods:We included AF-related stroke patients with unilateral anterior circulation lesions who were admitted within 7days of symptom onset between September 2013 through March 2019. Initial severity of the ischemic strokewas measured by National Institutes of Health Stroke Scale (NIHSS) and was divided into mild severity (NIHSS <5) and moderate to severe severity groups (NIHSS ≥ 5). The degree of stenosis in the relevant artery was divided into two, without significant stenosis and significant stenosis groups. Lesion pattern was evaluated for size andlocation using diffusion weighted images (DWIs)Results:Among variables of demographical and clinical data, median NIHSS (2 [IQR 0-3] vs. 10 [IQR 7-15], p < 0.01) andhypertension (62% vs. 77%, p = 0.02) were higher in moderate to severe severity group which were statisticallysignificant. In univariate analysis, patients with hypertension (OR = 2.02; 95% CI [confidence interval] = 1.12 -3.66) and significant stenosis (OR = 1.79; 95% CI = 1.03 - 3.11) were more frequent in moderate to severe severitygroup which were statistically significant. After adjustment of possible confounders, only the presence ofsignificant stenosis was independently related to moderate to severe stroke severity (adjusted odd ratio [aOR] =1.87; 95% CI = 1.02-3.35). Size of lesions that are 2cm or larger were more frequent in significant stenosis groupwith trend toward significance (57% vs. 69%, p = 0.072). Location of lesions also showed difference in frequencybetween the groups(p=0.03).Conclusions:More severe initial stroke severity is related to residual significant stenosis on relevant arteries in patients withAF-related stroke
59

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-14Acute Management
Multivessel Occlusions in Patients who Received Endovascular Thrombectomy
Chiting Chung1, Chihhao Chen1, Yenheng Lin2, Chungwei Lee2, Sungchun Tang1, Likai Tsai1, Jiannshing Jeng1
1 Neurology, National Taiwan University Hospital, Taipei, Taiwan2 Medical Imaging, National Taiwan University Hospital, Taipei, Taiwan
Purpose:Acute ischemic stroke (AIS) caused by multivessel occlusions (MVO) is a rare but devastating condition. Multi-target endovascular thrombectomy (EVT) for MVO might be urgent and important. This study investigated theprevalence, risk factors and outcome of MVO in AIS patients who underwent EVT.Methods:Consecutive AIS patients who received EVT between September 2014 and August 2020 in a single medical centerwere included. Acute MVO was defined as simultaneous occlusions of 2 or more intracranial vessel in eitherbilateral anterior circulation, or ipsilateral anterior and posterior circulation, as documented by computedtomography angiography. Patients’ baseline characteristics, risk factors, and clinical courses of MVO wereanalyzed.Results:Of 345 AIS patients (mean age, 71 13 years; male, 53%) who received EVT, 7 patients (2.0%; 95% confidenceinterval [CI], 0.54%-3.5%) had acute MVO. The involved vessels included bilateral cervical internal carotid arteries(ICAs) in 1, bilateral distal ICAs in 1, bilateral middle cerebral arteries (MCAs) in 2, ipsilateral vertebral artery andMCA in 1, and ipsilateral ICA and distal PCA in 2. Although four of these cases had received mechanicalthrombectomy for at least two target vessels, only two of them achieved the optimal reperfusion of all attemptvessels successfully. Though none of the clinical or laboratory factors were independently associated with MVO,patient with poor pre-morbid modified Rankin scale (mRS) and high D-dimer had higher risk to develop MVO.The etiology of MVO included large vessel atherosclerosis in 3, atrial fibrillation related cardioembolic in 2, andcancer-related hypercoagulopathy in 2. None of these patients reached modified Rankin scale ≤2, and their mortality at 90 days were 71%. Acute MVO was independently associated with mortality (odds ratio 19.5; 95%CI 3.6-103.9; P<0.01).Conclusions:We found the prevalence of acute MVO in patients underwent EVT was 2%. Multi-target mechanicalthrombectomy to achieve reperfusion was difficult but still possible. Nevertheless, patients’ outcome was stilldevastating.
60

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-15Intracranial Atherosclerosis
Role of the RNF213 variant in vascular outcomes in patients with intracranial atherosclerosis
Hyung Jun Kim1, Jong-won Chung1, Woo-keun Seo1, Gyeong-moon Kim1, Oh Young Bang1
1 Neurology, Samsung Medical Center, School of Medicine, Sungkyunkwan University, Seoul, Korea
Purpose:The Ring Finger Protein 213 gene (RNF213) variant R4810K is a susceptibility allele not only for Moyamoyadisease (MMD) but also for intracranial atherosclerosis (ICAS) in East Asians. We hypothesized that this variantwould affect the distribution of ICAS and recurrence of cerebrovascular events.Methods:We conducted a prospective study of patients with ICAS and MMD using high-resolution MRI (HR-MRI) andRNF213 R4810K genotyping. Patients were included in the ICAS group when relevant plaques existed on HR-MRIand in the MMD group when they carried the variant and HR-MRI showed no plaques but characteristic featuresof MMD. We compared clinical and neuroimaging features of ICAS-RNF213+ patients with ICAS-RNF213− patients and of MMD patients.Results:Of 477 patients, 238 patients were the ICAS group and 239 were the MMD group. Among ICAS patients, 79patients (33.2%) were the ICAS-RNF213+ group and 159 (66.8%) the ICAS-RNF213− group. Vascular risk factors were more prevalent in ICAS patients than in MMD patients, but there was no statistically significant differencebetween the ICAS-RNF213+ and ICAS-RNF213− groups. Tandem lesions were significantly more common in the ICAS-RNF213+ group than in the ICAS-RNF213− group (40.3% vs. 72.2%, p<0.001), and their distributions were similar between the ICAS-RNF213+ and MMD groups. The presence of the R4810K variant (hazard ratio, 3.203;95% CI, 1.149-9.459, p=0.026) and tandem lesions ( ≥3) (hazard ratio, 8.315; 95% CI, 1.930-39.607, p=0.005) were independently associated with recurrent cerebrovascular events.Conclusions:ICAS patients carrying the RNF213 R4810K variant showed clinical and imaging features distinct from ICASpatients without the variant, suggesting that the R4810K variant plays a role in intracranial atherosclerosis in EastAsians.
61

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-16Intracranial Atherosclerosis
Intracranial Arterial Stenosis Is an Important Cause of Ischemic Strokein Takayasu’s Arteritis Patients
Kwan Young Park1, Yeon Jung Kim1, Min Hwan Lee1, Sun U. Kwon1
1 Neurology, Asan Medical Center, Seoul, Korea
Purpose:Takayasu’s arteritis (TA) is defined as granulomatous inflammation of the aorta and its major branches, and it hasbeen recognized as uncommon cause of cerebral infarction in young age patients. However, intracranial arterialstenosis (ICAS) has been reported as a cause of ischemic stroke in young patients with TA, still systematic studiesabout ICAS in TA patients is not yet sufficient. Through this research, we evaluated the prevalence of ICAS in TApatients to investigate the role of ICAS on the development of ischemic strokes.Methods:We retrospectively reviewed medical charts, laboratory findings and evaluated neuroimaging of 153 TA patientswho diagnosed as TA by the supra-aortic vascular imaging at Asan Medical Center, South Korea, between January2005 and December 2017. The recruited patients were classified according to the presence of history of acuteischemic stroke or TIA. Steno- occlusions in the intracranial arteries, distal to the C2 level of internal carotid arteryand V4 level of vertebral artery, were classified as ICAS. All images were analyzed independently by twoexperienced reviewers who were blinded to the patients’ clinical condition.Results:Among 153 TA patients, 32 patients (20.8%) were classified into acute stroke group. ICAS was identified in 10.4%(n=16) of total TA patients and located mainly at middle cerebral artery (10 of 16, 62.5%). Other ICAS site wereanterior cerebral artery (2 of 16, 12.5%), posterior cerebral artery (2 of 16, 12.5%) and vertebral artery (1 of 16,6.3%). Acute stroke group had significantly higher prevalence of ICAS (11 of 32, 34.3%) than non- acute strokegroup 5 of 121, 4.1%) (pConclusions:ICAS is not an uncommon finding in TA patients and more likely to exist in TA patients with acute stroke thannon-acute stroke patients with statistical significance.
62

Cerebrovasc Dis 2020;49(suppl 1):1-149
63

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-17Intracranial Atherosclerosis
Distribution and Efficacy of Antiplatelet Therapy after Endovascular Treatmentfor Atherothrombotic Stroke
Min-surk Kye1, Hee-joon Bae1, Dong Woo Shin1
1 Neurology, Seoul National University Bundang Hospital, Seungnam-si, Gyeonggi-do, Korea
Purpose:In patients with minor ischemic stroke or transient ischemic attack, clopidogrel plus aspirin combination therapyis known to be effective. However, there is no evidence in acute ischemic stroke caused by large arteryatherosclerosis in particular after endovascular treatment.Methods:Patients with acute ischemic stroke of large artery atherosclerosis after endovascular treatment within 72 hoursof symptom onset were identified from a Korean multicenter stroke registry database. We estimated thedistribution of combinations of antithrombotics. The primary outcomes were stroke recurrence. Secondaryoutcomes were stroke, myocardial infarction, vascular death.Results:Of 1178 patients enrolled in this study. We divided 6 groups according to the types of antithrombotics. Most ofpatients received aspirin plus clopidogrel (609, 51.7%) and aspirin monotherapy (226, 19.2%). Other groups wereother antiplatelet polytherapy (66, 5.6%), other antiplatelet monotherapy (41, 3.5%), anticoagulant only (17,1.4%) and no medical therapy (219, 18.6%). Each groups stroke recurrence rates were 4.6%, 4.0%, 6.1%, 4.9%,11.8% and 4.6%. Secondary outcome event rates were 10.8%, 13.7%, 16.7%, 9.8%, 23.5% and 21.9%. Strokerecurrence rate was comparable between the aspirin plus clopidogrel and the aspirin monotherapy groups. (4.6%versus 4.0%; relative risk 1.46: 95% confidence interval, 0.62-3.47; P=0.53). There were no differences insecondary outcomes between 2 groups, aspirin plus clopidogrel and aspirin monotherapy group.Conclusions:Many types of antithrombotics have been used for patients undergoing endovascular treatment in large arteryatherosclerosis. There was no difference between the group using the most frequently used aspirin plusclopidogrel and the aspirin mono therapy group.
64

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-18Intracranial Atherosclerosis
Profile Icad and Non-icad Ischemic Storke in Dr. Moewardi Hospital Indonesia
Dody Wahyu Lestya Nugraha1, Rivan Danuaji2, Subandi Subandi3
1 Neurology, Universitas Sebelas Maret, Surakarta, Indonesia2 Neurology, Universitas Sebelas Maret, Surakarta, Indonesia3 Intervensional Neurology, Universitas Sebelas Maret, Surakarta, Indonesia
Purpose:Intracranial atherosclerotic disease (ICAD) of the major arteries (intracranial internal carotid artery, middlecerebral artery, vertebral artery, and basilar artery) is the most common proximate mechanism of ischemic stroke.Traditional risk factors associated with ICAD include hypertension, smoking, diabetes mellitus, andhyperlipidemia. For diagnosis of ICAD, cerebral digital subtraction angiography (DSA) is the gold standard toidentify extent of stenosis.Methods:Case control study was conducted in Dr Moewardi Hospital in patients with ICAD in ischemic stroke underwentcerebral DSA procedure. The data taken from medical record between January 2018 until July 2020 and analyzedstatistically using chi square.Results:Total of 97 ischemic stroke patients underwent cerebral DSA procedure was collected and 57% of them had ICAD.They consisted of 40 (71,4 %) males and 16 (28, 6 %) females with ICAD was found in MCA 20 (31 %), ICA 19(30 %), ACA 10 (16 %), basilar artery 9 (14 %), PCA 4 (6%) and vertebral artery 2 (3 %). Forty-three percent ofthem were non ICAD patients, consist of normal DSA 12 (29%), vascular hypoplasia 12 (29%), cerebral smallvessel disease 8 (20%), cerebral venous thrombosis 5 (12%), extra cranial stenosis 4 (10%) respectively. Patientswith hypertension were at risk of experiencing ICAD 2.603 times greater than patients without hypertension (p=0.03)Conclusions:Fifty-seven percent of ischemic stroke patients who underwent DSA had ICAD with the most locations in MCAand the greatest risk factor was hypertension.
65

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-19Risk Factors and Prevention of Stroke
Preventive Effect of Statin on Cerebral Small Vessel Disease Progression
Jun-beom Lee1
1 Neurology, Hong-Ik Hospital, Seoul, Korea
Purpose:Statin decreases serum cholesterol and improves functional outcome in acute stroke. It is mainly due topreventive effect on large artery atherosclerosis. Cerebral small vessel is a broad term that pertain to smallervessels (5 μm to 2 mm). We aimed to investigate if statin has beneficial effect on preventing cerebral small vessel disease.Methods:One hundred forty three healthy elderly individuals who received brain MRI for health check-up and identifiedto have white matter hyperintensity were enrolled. Among them, 51 had moderate atherosclerosiscardiovascular disease risk factors and started moderate to high intensity statin according to Korean society oflipid and Atherosclerosis guideline 4th edition (Figure 1). Twenty nine individuals among 51 statin users (statingroup) and 22 in none users (control) took brain MRI again after 2 years and they were analyzed to compare lowdensity lipoprotein cholesterol (LDL-C) and cerebral white matter hyperintensity change using Fazekas gradingsystem.Table 1. Changes in LDL-C and Fazekas grade
LDL-C (mean SD)
P
Fazekas grade (mean SD)
PBaseline Follow up Change(%) Baseline
Followup
Change(%)
Control 129.3±32.8 124.7±35.6 3.6<0.0001
1.3±0.7 2.1±0.5 61.5<0.0001
Statin 156.7±27.5 78.2±19.7 50.1 1.4±0.3 1.5±0.5 7.1
LDL-C, Low density lipoprotein cholesterol.Results:Baseline demographics between control and statin group showed difference in LDL-C (Control, 129.3± 32.8mg/dL; Stain group, 156.7±27.5 mg/dL, p=0.024). The LDL-C change in statin group was significant compared tocontrol. (Control, 129.3±32.8mg/dL at baseline and 124.7±35.6mg/dL at follow up (3.6% decrease); Statin group,156.7±27.5mg/dL at baseline and 78.2±19.7mg/dL (50.1% decrease) at follow up, p <0.001). Fazekas grade instatin group remained stationary contrary to control which showed increased Fakekas grade in 2 years.(Control, 1.3±0.7 at baseline and 2.1±0.5 at follow up (61.5% increase); Statin group, 1.4±0.3 at baseline,1.5±0.5 at follow up (7.1% increase), p<0.001).Conclusions:This study identified statin prevents cerebral small vessel disease progression in health elderly populationswhich reflects statin can benefit both extreme of cerebral large and small vessel disease spectrum. However, inorder to determine whether this result is due to reduced serum LDL-C concentration or statin pleiotrophic effect,future study is needed whether non statin LDL-C lowering agent has same preventive effect.
66

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-20Intracranial Atherosclerosis
Stroke due to Basilar Artery Dissection: A Management Dilemma
Charles Chan Chung1
1 Neurology, National Neuroscience Institute of Singapore, Singapore, Singapore
Purpose:To discuss management of basilar artery dissection as a cause of stroke.Methods:N/AResults:We present a case of a 69 year old Chinese Male, with background of diabetes mellitus, hypertension andhyperlipidaemia, who presented with a right sensory transient ischaemic attack. He subsequently progressedduring his stay. Magnetic resonance imaging of the brain revealed the presence of a left hemipontine infarct andmagnetic resonance angiography showed presence of a basilar artery dissection. He was also noted to havebilateral severe internal carotid artery stenoses and his stay was complicated by a non-ST elevation myocardialinfarction.Conclusions:Basilar artery dissection is a rare cause of stroke. Early recognition allows for optimal management to minimisemortality and morbidity.
67

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-21Case Report
Acute Ischemic Stroke Due to Simultaneous Bilateral Internal Carotid Artery Occlusion
Bang-hoon Cho1, Kyung-hee Cho1, Sungwook Yu1
1 Neurology, Korea University Anam Hospital, Seoul, Korea
Purpose:Acute simultaneous bilateral internal carotid artery occlusion (ICAO) is a rare form of ischemic stroke withcatastrophic prognosis.Methods:We report a patient without any vascular risk factors including atrial fibrillation who had a rapidly aggravation ofneurological signs.Results:A 67-year-old male patient presented consciousness disturbance 6 hours ago. Initial brain computed tomography(CT) revealed hypodense lesion on both cerebral hemispheres. On CT angiography, bilateral ICA terminusocclusion was revealed. Initial diffusion weighted imaging showed acute infarction of bilateral hemispheresexcept right posterior cerebral arterial territory and both thalami. Because of unstable patient’s vital sign,transthoracic echocardiography could not be examined. Also, there is no abnormal heart rhythms on routineelectrocardiography monitoring in intensive care unit. Despite intensive management, his neurologicalsymptoms were aggravated and the cerebral edema with herniation progressed. After 3 day, the patient wasdead due to severe brain edema.Conclusions:This is a case report of a rare entity of acute ischemic stroke. A proper management for bilateral ICAO awaitsfurther investigation.
68

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-22Basic Neuroscience in Stroke
Exosomes from Cortical Neurons Subjected to Oxygen-glucose Deprivation/reperfusion Challenge PesentDifferentially Expressed miRNA Cargo and Blunt Neurite Outgrowth
Chien-sung Chiang1, Ssu-ju Fu2, Chia-lang Hsu3, Chung-jiuan Jeng4, Chih-yung Tang2, Yi-shuian Huang5, Sung-chunTang1
1 Neurology, National Taiwan University Hospital, Taipei, Taiwan2 Physiology, National Taiwan University, Taipei, Taiwan3 Medical Research, National Taiwan University Hospital, Taipei, Taiwan4 Anatomy and Cell Biology, National Yang-Ming University, Taipei, Taiwan5 Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan
Purpose:Ischemia/reperfusion is a common feature of acute ischemic stroke, which causes neuron dysfunction and death.Exosomes, small extracellular vesicles produced by most cell types, are implicated in the mediation of cellularinteractions with their environment. Here, we investigated the contents and functions of exosomes from neuronsunder ischemic reperfusion injury.Methods:First, rat cortical primary neuronal cell cultures were placed in an oxygen- and glucose-deprived (OGD) medium,followed by reperfusion in a normoxic conditioned medium (OGD/R) to mimic ischemia/reperfusion in vitro. Theneuron-derived exosomes were harvested from the conditioned medium under normoxia and OGD/R. Throughnext-generation sequencing, exosomal miRNA expression levels in normoxic and OGD/R condition werecompared. Their functional activity in terms of neuron viability and quantitative analysis of neurite outgrowthwere examined.Results:The expression levels of 45 exosomal miRNAs were significantly different between normoxic and OGD/Rconditions. Bioinformatics analysis of dysregulated exosomal miRNAs identified multiple pathways involved incell survival and death processes and neuronal signaling. Moreover, treatment with exosomes from OGD/R tocultured cortical neurons significantly impaired neuronal cell viability and reduced neurite outgrowth in termsof the number of primary or total neurites as well as length of primary neurites, compared with exosomes fromnormoxic conditions.Conclusions:MiRNA-packed exosomes released by neurons under OGD/R challenge may contribute to neuronal loss andprovide further understanding of the effect of stressed neurons on neighboring neuronal functions.
69

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-23Basic Neuroscience in Stroke
Reduction of Artery Re-occlusion after Low-dose Recombinant Tissue Plasminogen Activator by CombinationTreatment with Mouse iPSCs in A Rat Model of Acute Carotid Thrombosis
Tsong-hai Lee1, Cheng-yu Lu1
1 Neurology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
Purpose:Recombinant tissue plasminogen activator (rt-PA) has been known the standard treatment for acute arterialthrombosis. However, rt-PA treatment carries a high bleeding side effect and has high re-occlusion rate. Also,there is narrow therapeutic time window after ischemic stroke onset. The present study investigated thepotential effect of mouse iPSCs to reduce the re-occlusion rate after low-dose rt-PA treatment.Methods:Single irradiation with 6 mW/cm2 LED for 4 hours at rat common carotid artery was used as the thrombosismodel according to our previous study. Endothelin-1 (ET-1) was used as the marker of artery endothelial injury.Results:After LED irradiation alone, there was persistent occlusion from 2 hours to 7 days, suggesting the success ofthrombosis model. The administration of 0.9 mg/kg rt-PA could recanalize the thrombotic artery from 24 hoursto 7 days with stenotic degree ≤50%. When 0.45 mg/kg rt-PA or 1x10(-6) iPSCs was administrated, there was high re-occlusion rate with stenotic degree >50%. However, combined administration of 0.45 mg/kg rt-PA plus 1x10(-6) mouse iPSCs caused a significant reduction of re-occlusion from 2 hours to 7 days with improved expressionof ET-1.Conclusions:The present study suggested that iPSCs could recover the integrity of artery endothelia and reduce the re-occlusion rate after low-dose rt-PA against acute carotid artery thrombosis.
70

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-24Basic Neuroscience in Stroke
Effects of Pre-treatment with Tocovid on Oxidative Stress and Apoptosisin Ischemic Mouse Brain
Toru Yamashita1, Jingwei Shang1, Feng Tian1, Kota Sato1, Mami Takemoto1, Nozomi Hishikawa1, Koji Abe1
1 Neurology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama,Japan
Purpose:Dietary supplement is an attempt to reduce the risk of ischemic stroke (IS) in high risk population. A new mixedvitamin E-Tocovid which mainly contains tocotrienols other than tocopherol, attenuated the progression of whitematter lesions (WMLs) by oral in humans. However, the effect of Tocovid on IS has not been examined. In thepresent study, we assessed the therapeutic effects of Tocovid pre-treatment on transient middle cerebral arteryocclusion (tMCAO) in mice.Methods:After pre-treatment with Tocovid (200 mg/kg /day) or vehicle for 1 month (M), 60 min tMCAO was performed,and these mice were examined at 1, 3 and 7 days (d) after reperfusion. we histologically assessed the effects ofTocovid pre-treatment on the expressive changes of oxidative stress markers, cleaved caspase-3 and LC3-II aftertMCAO in mice.Results:We observed that Tocovid pre-treatment significantly improved the rotarod time, reduced infarct volume,decreased the number of 4-HNE, nitrotyrosine and 8-OhdG positive cells, inhibited advanced glycation endproducts (AGEs) biomarkers RAGE, CMA and CML expressions, and increased Nrf2 and MRP1 levels withGSSG/GSH ratio decrease.Conclusions:Furthermore, Tocovid pre-treatment greatly decreased cleaved caspase-3 and LC3-II expressions after tMCAO.The present study obviously demonstrated that Tocovid pre-treatment showed neuroprotective effects againstoxidative stress and at least in part by anti-apoptotic/autophagic cell death in ischemic mice brain.
71

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-25Basic Neuro Science in Strok
A Prospective Cohort Study to Develop and Validate a Multivariable Prediction Model for TransientIschaemic Attack (TIA) Diagnosis Using Proteomic Discoveryand Candidate Lipid Mass Spectrometry,
Neuroimaging and Machine Learning: Study Protocol
Austin G Milton1, Karlea L Kremer2, Sushma R Rao3, Emilie Mas4, Marten F Snel3, Paul J Trim3, Suzanne Edwards5,Stephan Lau6, Mark Jenkinson6, Erik Noschka7, Simon A Koblar2, M Anne Hamilton-Bruce1
1 Stroke Research Programme, Central Adelaide Local Health Network (CALHN), Adelaide, SA 5000, Australia2 Stroke Research Programme, Adelaide Medical School, Faculty of Health and Medical Sciences, University ofAdelaide, Adelaide, SA 5005, Australia3 Proteomics, Metabolomics and MS-imaging Core Facility, South Australian Health and Medical ResearchInstitute (SAHMRI), Adelaide, SA 5000, Australia4 Genetics and Molecular Pathology, SA Pathology, Women's and Children's Hospital, North Adelaide, SA 5006,Australia5 Data, Design and Statistics Service, Adelaide Health Technology Assessment (AHTA), School of Public Health,Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, SA 5005, Australia6 Australian Institute for Machine Learning, School of Computer Science, Faculty of Engineering, Computer andMathematical Sciences, University of Adelaide, Adelaide, SA 5005, Australia7 Equine Health and Performance Centre, School of Animal and Veterinary Sciences, Faculty, University ofAdelaide, Adelaide, SA 5005, Australia
Purpose:Urgent evaluation and diagnosis of TIA is important as early treatment can prevent subsequent strokes, but TIAis difficult to differentiate from small stroke and TIA mimics. Current advanced mass spectrometer (MS)technology allows quantification of many plasma proteins and lipids, resulting in large datasets needingsophisticated analysed. We aim to (1) identify and validate plasma protein, lipid and/or radiological biomarkersand develop a panel with the most significant biomarkers as a diagnostic tool to differentiate TIA from smallstroke and TIA mimics; (2) assess our results using different techniques including statistical analysis and machinelearning.Methods:Patients with TIA/small stroke/TIA-like symptoms who attend the TIA Clinic, Emergency Department or StrokeWard at the Royal Adelaide Hospital will be recruited consecutively (allowing for logistical limitations) for ourprospective cohort study of at least 518 patients (80% power, alpha=0.05 allowing 20% for potential mismatches).Patients will provide written informed consent to participate in this grant-funded ethics-approved study. Non-contrast CT and CT-angiography/multi-modal MRI (diffusion, T1, T2 and MR-angiography) will be performed oneach patient with images independently assessed by three stroke-neurologists. Venous blood samples will becollected within the first 48-hours of onset of symptoms along with demographic and clinical data: medicalhistory, modified Rankin Score and ABCD2 stroke-risk stratification score. Advanced MS will be used for discoveryplasma proteomic and candidate lipid analysis. Using MS-software, Principal Component Analysis andhierarchical cluster analysis will be undertaken and output files analysed for biomarker differences between thethree groups. We will also apply machine learning to the data, including deep learning with neural networks.Advanced radiological neuroimaging will be included and excluded in machine learning models to developalgorithms appropriate for medical centres with neuroimaging capabilities, and also for rural and remote regionswithout neuroimaging capacity.Results:Twenty-seven of 29 potential TIA candidates have been enrolled (range 48-94 years; 15 female), blood samplescollected and plasma frozen – these have not been analysed – the study is suspended due to COVID-19restrictions.Conclusions:We have designed a new TIA biomarker study protocol. Using plasma protein, lipid and radiological biomarkers,our study will develop and validate predictive algorithms for differentiating TIA, small stroke and TIA mimics,with analysis by conventional statistical methods and also machine learning.
72

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-26Pathophysiology of Stroke
Proteomic Analysies of Retrieved Clots in Acute Ischemic Stroke: Associationwith Antiplatelet Use
Min Kyoung Kang2, Eung-joon Lee1, Han-yeong Jeong1, Tae Jung Kim1, Sang-bae Ko1, Byung-woo Yoon1
1 Neurology, Seoul National University Hospital, Seoul, Korea2 Neurology, Nowon Eulji University Hospital, Seoul, Korea
Purpose:One-third of ischemic strokes occured while on antiplatelet therapy. Limited data exist on the composition anddetailed characteristics of arterial thrombi associated with large vessel occlusion in patient with antiplatelettherapy. We investigated retrieved clots with endovascular thrombectomy and its associations with antiplateletdrug uses.Methods:In this prospective study, we consecutively included 16 acute ischemic stroke patients treated by thrombectomy(2017–2019). We excluded patients with cancer or treated with intravenous thrombolysis. We collected clotsamples and stored frozen in liquid nitrogen tank during the thrombectomy procedure. Baseline characteristics,procedural and outcome data were analyzed. A proteomic analysis of clots was based on quantitative liquidchromatography-mass spectrometry.Results:Clots from eight patients (3 antiplatelet drug users, 5 antiplatelet drug never-users) were analyzed with the aimof obtaining a deep insight into the protein cargo and protein function of the thrombotic material isolated byendovascular thrombectomy. Among 3,499 clot-bound proteins identified in all clots, a total of 41 proteins werefound to have significant differences passing clustering tests: the cell adhesion response cluster and localizationsecretion transport cluster were significantly highly expressed in the antiplatelet drug never-user group than inthe antiplatelet drug user group, while the transcription factor cluster and response reactive oxidative clusterwere significantly highly expressed in the antiplatelet drug user group (all p < .05).Conclusions:This study is the first to show associations of retrieved clot properties with antiplatelet drug use, suggesting thatdifferent pathomechanism was involved in the thrombotic process according to antiplatelet therapy. The clotproteomics findings propose a rational and systematic approach for precision medicine.
73

Cerebrovasc Dis 2020;49(suppl 1):1-149
74

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-27Pathophysiology of Stroke
Neuroprotective Effect of Therapeutic Hypothermia against The Cognitive Impairmentin Ischemia-reperfusion Injury in Mice
Younghyurk Lee1, Jung-in Lee2, Hae Won Kim2, Hyungjong Park1, Sung-il Sohn1, Jeong-ho Hong1
1 Neurology, School of Medicine, Keimyung University, Daegu, Korea2 Nuclear Medicine, School of Medicine, Keimyung University, Daegu, Korea
Purpose:Cognitive impairment is one of most salient symptoms of ischemic stroke. Among the candidate, therapeutichypothermia (TH) is the best remedy for protecting ischemia/reperfusion (IR) injury. We evaluate the protectiveeffect TH on cognitive impairment after successful recanalization in acute stroke due to large cerebral arteryocclusion.Methods:Male, 9-week-old C57BL/6J mice were randomly assigned to sham group, unilateral transient middle cerebralartery occlusion (tMCAo), and unilateral tMCAo with hypothermia treatment. tMCAo was performed by insertinga nylon-6 monofilament into the internal carotid artery for 60 minutes followed by reperfusion. At one monthafter procedure, Y-Maze test, Western blots and positron emission tomography with fluorine-18fluorodeoxyglucose were evaluated retrospectively.Results:tMCAo induced learning and memory declines as well as ischemia and TH co-treatment significantly amelioratethat negative effect. The cerebral glucose metabolism of the hippocampus, striatum, and thalamus wassignificantly recovered in the TH group compared to that in the tMCAo group. The expression levels of amyloid-β(1-42) protein in the hippocampus, temporal cortex, and basal forebrain were significantly higher in the tMCAo group than those in the sham control group. TH reversed that effect. The tau and Cyclophilin A protein wererepresented similar tendency in the basal forebrain.Conclusions:These results indicate that IR induced damage was reduced TH treatment and may play a significant role toameliorate cognitive impairment.
75

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-28Risk Factors and Prevention of Stroke
Dysbiosis of Gut Microbiota in Patients with Large-Artery Atherosclerotic Stroke: A Pilot Study
Chatpol Samuthpongtorn1, Abhinbhen Saraya2, Nijasri Charnnarong Suwanwela2
1 6th year Medical student, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand2 Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok,Thailand
Purpose:One of the emerging risk factors of atherosclerosis is gut microbiota. Emerging evidence suggests that gutmicrobiota, their metabolites and immune response may play some roles in the pathophysiology of stroke. Short-chain fatty acids (SCFAs) produced by gut microbiota were found to have preventive effect on atherosclerosis.However, few studies have evaluated the association between gut microbiome especially SCFAs–producingbacteria and large-artery atherosclerotic ischemic stroke patients.Methods:A cross-sectional pilot study among patients with large-artery atherosclerotic ischemic stroke who were admittedat the stroke unit, King Chulalongkorn Memorial Hospital and asymptomatic subjects who presented at anoutpatient clinic were studied. Patients and controls were matched for age and sex. Fecal samples were collectedwithin 48 hours after stroke onset. Bacterial DNAs were extracted from the collected fecal samples, thenamplified and analyzed by using 16S ribosomal gene-specific methods Next-generation sequencing (NGS). SPSSversion 21 was used to perform all statistical analyses. Mann-Whitney U test was used to compare the differencesin gut microbiota profile.Results:There were 15 stroke patients and 15 controls in the study. The average age of patients and controls were62.07±8.1 and 61.67±8.5, respectively. 80% of the subjects were male. The most common traditional risk factorsof ischemic stroke were dyslipidemia (patients 4, controls 5) and hypertension (patients 5, controls 4). Incomparison to the control group, SCFAs-producing bacteria including Faecalibacterium spp. (p-value 0.04),Bifidobacterium spp. (p-value 0.04) and Eubacterium hallii (p-value 0.04) were significantly less abundant instroke patients. The quantities of Veillonella spp. (p-value 0.25) Roseburia spp. (p-value 0.18) and Anaerostipesspp. (p-value 0.33) in fecal samples were not significantly different between the two groups.Conclusions:Patients with acute ischemic stroke due to large artery atherosclerosis had significantly smaller amount ofFaecalibacterium spp.,Bifidobacterium spp., and Eubacterium hallii which are SCFAs-producing bacteria whencompared to controls. This confirms the relationship of gut microbiota and stroke due to large vesselatherosclerosis. These bacteria may be the therapeutic targets for stroke prevention in the future.
76

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-29Case Report
Diffusion Axonal Injury Induced Trochlear Nerve Palsy after Vehicle Accident
Ju-young Lee1, Yerim Kim1
1 Neurology, Kangdong Sacred Heart Hospital , Seoul, Korea
Purpose:Diffusion axonal injury (DAI) is intracranial injury caused by extensive axonal damage after a closed head injury.The damage is caused by deceleration or acceleration by the brain moving rapidly backward and forward withinthe skull. DAI showed multiple lesions those are characterized by imaging; grey-white matter junction, corpuscallosum and brainstems. This brain injury presented with various clinical symptoms due to these radiologicalfeatures. We reported a patient with binocular diagonal and vertical diplopia diagnosed with DAI after a bicycleaccident.Methods:Case A 54-year-old man presented with acute headache with dizziness in emergency room after bicycle accidentand developed binocular vertical diplopia after admission. The vertical diplopia had aggravated while lookingrightward and downward and left head tilt. Examination revealed a right hypotropia, a left hypertropia (7 prismdiopter) with left head tilt (8 prism diopter).Results:These findings were most consistent with isolated left superior oblique palsy. Magnetic resonance image (MRI)showed multiple small high signal intensity on diffusion weight image, but low signal intensity on gradient echoimage around right trochlear nucleus.Conclusions:DAI, as severe type of traumatic brain injury, is known to be caused by a variety of high energy traumas, especiallyvehicle accidents. The typical lesions showed punctuated microhemorrhage in MRI. These small lesions coulddevelop around the cranial nerve nuclei in the brainstem, with clinical symptoms that could be localized.
77

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-30Case Report
A Case of Cervical Spinal AVM Suspected of Brainstem Inaction
Sunjin Jin1, Joonyoung Ha1, Jiin Kim1
1 Neurology, Yonsei University Wonju Collage Of Medicine, Wonju, Kangwon, Korea
Purpose:Spine arteriovenous malformation (AVM) is a rare disease, about 2% of AVM occur around the cervical spine.Cervical spine AVM can caused brainstem dysfunction following progressive myelopathy caused by extension ofvenous congestion from the cervicothoracic cord to the medulla oblongata.Methods:.Results:A 71-year-old man visit hospital due to both leg weakness and respiratory difficulty. He had several repeatedurinary difficulty and gait disturbance from 2months ago. On neurologic exam, He had MRC G II weakness onboth lower extremities and decreased sense of touch and pinprick under C2-3 dermatome level. On T2 weightedspine MRI, high signal intensity lesion was observed in medullar, followed by a high signal along the C spine. Thepatient was refered neurologic department due to suspicious brain stem and spinal cord infarction. In CT branangiography, engorged premedullary vessel along the medullar to spinal cord was seen. There was no high signalintensity on diffusion-weighted MR images. Conventional angiography was done, BA perforator aneurysm andAVM from BA perforation to spinal vein was seen. He had been treated with corticosteroid and transarterialembolization with coil.Conclusions:We reported on a rare case of cervical AVM with venous congestion of medullar oblongata, that suspected ofbrainstem infarction.
78

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-31Case Report
Differential Histopathological Characteristics of Thrombi Retrieved from Arterial and VenousThromboembolism in A Patient with Cancer: Concomitant Phenomena with Distinct Origin?
Yeeun Soon1, Han Kyu Na1, Young Dae Kim1, Hyo Suk Nam1, Ji Hoe Hoe1
1 Neurology, Yonsei University College of Medicine, Seoul, Korea
Purpose:Although venous thromboembolism (VTE) and its association with cancer is well-known, arterialthromboembolism (ATE) under malignant condition has only recently begun to gain attention. Severalobservational studies have found that VTE tend to be associated with subsequent ATE, or vice versa. Althoughparadoxical embolism, or atherosclerosis including subclinical cases have been pointed out as potential commonpathologies, conclusion derived from such studies could be misleading as pathophysiology of cancer-associatedthrombosis are highly variable across individuals. In this regard, cases of concomitant arterial and venousthrombosis may be informative in disentangling the potential link between ATE and VTE.Methods:We report a cancer patient who presented with deep vein thrombosis (DVT) along with four separate events ofrecurrent acute ischemic stroke. Along with gross morphological features, composition of retrieved thrombi fromeach event was compared by using immunohistochemical staining (IHC).Results:A 73-year-old women with metastatic advanced gastric cancer visited our emergency room for aphasia and righthemiparesis, and her CT angiography revealed left middle cerebral artery (MCA) occlusion. Diffusion-weightedMRI performed after successful recanalization showed multifocal acute small and large infarctions widelydistributed over multiple territories. Trans-esophageal and trans-thoracic echocardiography (TTE) did not exhibitany abnormalities except for clinically insignificant small patent foramen ovale. She developed recurrent strokein right MCA territory followed by bilateral renal infarction, DVT, and two additional episodes of ischemic strokethereafter. Follow-up TTE revealed newly developed moderate mitral regurgitation due to thickened mitral valveand prolaptic motion of anteromedial valve without evidence of ischemic heart disease or chordae rupture.Pathological findings of arterial thrombi specimens retrieved from four stroke events were remarkably similarboth in terms of grossly highly friable white thrombi and microscopic IHC studies (platelet-rich and erythrocyte-poor composition without any heterogenous segments suggestive of VTE). By contrast, venous thrombus wasgrossly red of and its IHC studies showed fibrin- and erythrocyte-rich composition. Histopathological studies ofall specimens were not suggestive of culture-negative infective endocarditis.Conclusions:Our findings indicate that histopathology of cancer-associated ATE and VTE within a single patient may differsignificantly in composition, suggesting that antithrombotics against VTE may not be sufficient to prevent cancer-associated ATE. Although definite vegetation was not captured by echocardiography, her ATE may be associatedwith non-bacterial thromboembolism considering histopathological findings and acute mitral regurgitationassociated with thickened mitral valve.
79

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-32Pathophysiology of Stroke
Acute Cerebral Artery Occlusion by Cancer Embolus
Seong Hwan Ahn1, Dong Gun Lee1, Sang Woo Ha2
1 Neurology, Chosun University College of Medicine and Hospital, Gwangju, Korea2 Neurosurgery, Chosun University College of Medicine and Hospital, Gwangju, Korea
Purpose:In acute stroke, emboli are mostly composed of thrombi from artery, cardiac chamber, valve and vein. However,non-thrombotic emboli are sometimes difficult to identify the origin. According to the increased number ofcancer patients, now 10% of stroke patients have a cancer. However, the potential mechanism of stroke patientswith cancer is uncertain.Methods:We presented a case of serious acute arterial occlusion with a tumor embolus, which was revealed by histo-pathologic analysis of retrieved emboli.Results:Case: A 56-year-old female was presented with right hemiplegia and aphasia 3 hours from onset. Her familydenied any history of vascular risk factors. National institute of Health Stroke Scale score was 17.Electrocardiography showed prolonged QTc (528ms) with non-specific chest x-ray finding. Non-enhanced BrainCT showed subtle ischemic changes with ASPECT score 8. CT angiography revealed left distal internal carotidartery occlusion (carotid T) and right posterior cerebral artery occlusion. Immediately, mechanical thrombectomywas conducted for left internal carotid T occlusion (Fig. A). Although several procedures with stent retrievers andpenumbral aspiration catheters were tried, recanalization was not achieved (TICI 0). Retrieved some embolimaterials (Fig. B) was analyzed with histo-pathologic stains (Fig. C) because of non-thrombotic nature. Positiveimmunohistochemistry with vimentin (Fig. D) and desmin (Fig. E) suggested rhabdomyosarcoma with skeletalmuscle differentiation (Staining with actin, cytokeratin, and S-100 protein were all negative). However, after 12hours from admission, she died from cerebral edema.
Conclusions:Still, 40% of stroke patients are classified by embolic stroke with undetermined etiology. Our case showed thathistologic analysis can figure out a thromboembolic origin. Also, it is clear evidence that embolized tumor itselfcan obstruct intracranial artery directly.
80

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-33COVID19, Infections and Stroke
Stroke Care in Singapore during COVID-19 Pandemic
Narayanaswamy Venketasubramanian1
1 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore
Purpose:Stroke is a significant cause of admission to our acute care hospitals. Patients with suspected stroke who call fora public ambulance who meet criteria are taken directly to one of 3 thrombectomy centres for treatment; else,they are taken to one of the public hospitals for further management, including imaging, stroke unit care andrehabilitation, both in and out-patient, with follow-up reviews in the clinic. With the current COVID-19 pandemic,there have been major changes to our stroke care system. This paper describes these changes.Methods:Information was sought from ambulance staff, colleagues and publications on stroke care during COVID-19 fromthe various Singapore hospitals. This data was categorized and summarized into sections: pre-hospital,emergency room, imaging, revascularization, stroke unit(SU) care, rehabilitation, out-patient care. These findingsare reported below.Results:On calling for the public ambulance, those suspected to have COVID-19 infection are taken to the National Centerfor Infectious Diseases. Otherwise, on arrival at the emergency room, all cases with fever or respiratorysymptoms [possible COVID-19 patients(PCPs)] are evaluated separately, given face masks; staff wear full personalprotection equipment(PPE). Triage is not delayed. PCPs needing hyperacute therapies are sent to a separatescanner; otherwise, imaging is deferred to the latter part of the day. Interventional treatments are performed incarefully-prepared rooms. PCPs are managed in isolation rooms, and sent to the SU only after 2 consecutivelynegative COVID-19 swabs; urgent investigations and rehabilitation are done within the room. Those not felt tobe PCPs are given face masks, and managed in the usual manner. ASU rounds are attended by essential members,communications by electronic means. Multidisciplinary team rounds have ceased, discussions are via electronicplatforms. Patient transfer and staff movement are minimized. All hospital staff wear face-masks, safe-distancingand infection control are strictly enforced. Visitors are not allowed; staff call to update families daily.Rehabilitation is provided with safe-distancing; mild strokes may be sent home with advice. Out-patientrehabilitation centres are closed. Patients return for clinic visits only if needed; medications are sent to theirhome, nurses make essential home visits. Stroke support and rehabilitation activities have moved on-line.Conclusions:Evidence-based stroke care is delivered in a re-organised manner, with strict infection control.
81

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-34COVID19, Infections and Stroke
Characteristics of Acute Stroke in Patients with Coronavirus Disease 2019 and Challengesin Stroke Management during an Epidemic
Doo Hyuk Kwon1, Youngrok Do2, Mi-yeon Eun3, Jun Lee4, Hyungjong Park1, Sung-il Sohn1, Jeong-ho Hong1
1 Neurology, Keimyung University School of Medicine, Daegu, Korea2 Neurology, Catholic University of Daegu School of Medicine, Daegu, Korea3 Neurology, Kyungpook National University School of Medicine, Daegu, Korea4 Neurology, Yeungnam University School of Medicine, Daegu, Korea
Purpose:Coronavirus disease 2019 (COVID-19) is an ongoing pandemic characterized by high morbidity and mortality.Strokes in patients with COVID-19 have recently been reported, and for neurologists, strokes that occur duringpandemics are highly problematic. The mechanisms, phenotype, and optimal management of strokes in COVID-19 patients are unresolved. To determine how COVID-19 might cause or exacerbate ischemic stroke, we describefive patients with both diseases who were treated by us over the course of 3 months. We also discuss theproblems associated with stroke management during epidemics.Methods:The Korean city of Daegu endured the first large COVID-19 outbreak outside of China. The first confirmed casein Daegu was reported on February 18, 2020, and 6,880 confirmed cases were reported by May 29, 2020. Asearch of a retrospectively mainlined database identified five patients who were treated for both COVID-19 andischemic stroke at four tertiary hospitals in Daegu during this time period. COVID-19 was confirmed via real-timereverse transcription polymerase chain reaction. Stroke was diagnosed by clinical presentation and neurologicalexamination, and later confirmed by computed tomography and magnetic resonance imaging of the brain.Results:We compiled the demographic, clinical, radiological, and laboratory characteristics of the five patients. The D-dimer levels were high in all three patients in whom D-dimer blood testing was performed. Multiple embolicinfarctions were observed in three patients and suspected in one. The mean time from stroke symptom onset toemergency room arrival was 22 hours. As a result, acute treatment for ischemic stroke was delayed.Conclusions:The present case series report raises the possibility that the coronavirus responsible for COVID-19 causes orworsens stroke, perhaps by inducing inflammation. The control of COVID-19 is very important; however, earlyand proper management of stroke should not be neglected during the epidemic.
82

Cerebrovasc Dis 2020;49(suppl 1):1-149
83

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-35Epidemiology
Burden of stroke in Oceania
Narayanaswamy Venketasubramanian1
1 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore
Purpose:Oceania, located at the southern-easten-most part of the Asia-Pacific, is home to 42 million people living in 8.5million square km of land. It comprises the regions Australasia, Melanesia, Micronesia and Polynesia. There hasbeen no recent review of stroke in this part of the world. This paper reviews the burden of stroke in Oceaniancountries.Methods:Information on epidemiology of stroke in Oceanian countries was sought from data from the Global Burden ofDisease(GBD) study (incidence, mortality, incidence:mortality ratio, prevalence, disability-adjusted life-yearsDALYs lost due to stroke, subtypes), World Health Organisation(WHO) (vascular risk factors in the community),and PubMed (incidence, prevalence, stroke subtypes). Data were analysed by region to allow inter-countrycomparison within each region.Results:In 2010, age and sex-standardised stroke mortality rates were lowest in Australasia (29.85-31.67/100,000) andhighest in Melanesia and Micronesia (56.04-187.56/100,000), with wide ranges especially in Melanesia.Incidence rates were lowest in Australasia (101.36-105.54/100,000), similarly high elsewhere. Standardisedincidence:mortality ratio (IMR) (0.98-3.39) was the inverse of the mortality rates, and mirrored the prevalencerates (202.91-522.29/100,000). DALY rates (398.22-3781.78/100,0000) mirrored the mortality rates. Stroke riskfactors show a variable pattern - hypertension is generally the most common medical risk factor among males(18.0-26.6%), while among females, diabetes mellitus is the most common in Micronesia and Polynesia (21.5-28.4%). Among the life-style factors, current smoking is the most common in Melanesia among males, whileobesity is generally the most common factor among females. Ischaemic stroke comprises 70% of stroke subtypes.Conclusions:Stroke is a major healthcare problem in Oceania. Variations in stroke epidemiology are found between countriesin Oceania. Data are lacking in some; more research into the burden of stroke in Oceania is needed. Withexpected the increase in life expectancy and vascular risk factors, the burden of stroke in Oceania will likely rise.
84

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-36Epidemiology
Better Oral Hygiene is Associated with Lower Risk of Stroke
Yoonkyung Chang1, Tae-jin Song2
1 Neurology, Mokdong Hospital, Ewha Womans University College of Medicine, Seoul, Korea2 Neurology, Seoul Hospital, Ewha Womans University College of Medicine, Seoul, Korea
Purpose:Periodontal disease or poor oral hygiene may lead to local infection, inflammation and systemic inflammatoryreaction, which are important mediators of development of stroke. We aimed to investigate that association oforal hygiene with risk of stroke in nationwide population-based cohort.Methods:From Korean National Health Insurance System-Health Screening Cohort, 206,602 subjects who without missingdata regarding demographic information, medical history or blood/urine examination results were included. Thepresence of periodontal disease and indicators of oral hygiene, such as frequency of teeth brushing, visitinghistory of dental clinic, dental scaling, lost teeth and dental caries were evaluated. Occurrence of stroke includingcerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage was defined as newly registration ofInternational Classification of Diseases-10 codes from I60 to I64 accompanying brain CT and/or MR examinationat that time of diagnosis.Results:The 7,337 (3.6%) cases of stroke including 5,795 (2.8%) cases of cerebral infarction, 1,568 (0.8%) cases of cerebralhemorrhage, and 621 (0.3%) cases of subarachnoid hemorrhage were occurred during median 10.4 years followup. In multivariable analysis, frequent tooth brushing (≥3 times per day) was negatively associated with risk of occurrence for stroke (hazard ratio (HR): 0.78, 95% confidence interval (CI): 0.73–0.84). Number of dental caries(≥4) was positively related to occurrence for stroke (HR: 1.28, 95% CI: 1.13–1.44). Conclusions:Improved oral hygiene was negatively, and poor oral hygiene was positively associated with risk of occurrencefor stroke, respectively. Better oral hygiene may be associated with lower risk of stroke.
85

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-37Epidemiology
Prevalence of Infection in Stroke Patients Admitted to Intensive Care Unit
Nurotus Saniyah1, Baarid Luqman Hamidi1
1 Neurology, Sebelas Maret University, Surakarta, Indonesia
Purpose:Stroke is the third leading cause of death in developed countries and is the second leading cause of death inIndonesia. The prognosis is not only influenced by the severity of the stroke itself but also by its complications.Nosocomial infection is estimated to occur in one-third of patients with acute stroke, mainly affecting the urinarytract and respiratory tract. Stroke patients who are treated in the intensive care unit (ICU) have a higher risk ofinfection, associated with the severity of the disease itself and also the use of more medical devices. Theincidence of infection, especially in ICU patients, was also associated with severe disability, higher mortality,increased length of stay, and high cost of care. Therefore, the authors want to present data on the prevalence ofinfection in stroke patients, especially those who admitted to the ICU, as knowledge for clinicians who treatstroke patients, so that they can take preventive measures and manage infection in patientsMethods:This was an observational analytic study in which data obtained from the Clinical Microbiology laboratory andmedical records of Dr. RSUD Moewardi. Subjects were stroke patients who are treated in the intensive care unitat Dr. Moewardi Surakarta from January 2018 – December 2018Results:164 stroke patients were admitted to the ICU, and 79 patients had infections. Ischemic stroke patients had moreincidence of infection than hemorrhagic with a p-value = 0.013. The mean age of the infected group was 65 years,while the non-infected group was 59 years. The mean difference length of stay in the infected and non-infectedgroups was 6 days with a p-value <0.0001. The most common pathogen found is Klebsiella pneumonia. The mostsensitive antibiotics are tigecycline and gentamicin in our population. While the most antibiotic that causesresistance is ciprofloxacinConclusions:48.2% of stroke patients admitted to the ICU had an infection. Most are respiratory tract infection, with the mostcommon pathogen is Klebsiella pneumonia. Tigecycline is the most sensitive antibiotics
86

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-38Epidemiology
Description of Risk Factors for Stroke at Neurology Outpatient Service of Sanglah Hospital, Bali, March 2020 -August 2020
Maria Oktaviany Gabur1, Ida Bagus Kusuma Putra1
1 Neurology, Medical Faculty of Udayana University, Denpasar, Bali, Indonesia
Purpose:Stroke is the world's second-leading cause of death and a major factor in causing disabilities. This acute cerebralcirculatory disorder is caused by many risk factors, including those that can not be changed such as age and sex,and those that can be changed such as hypertension, diabetes, dyslipidemia, smoking. The epidemiology ofstroke based on their risk factors is still very varied and no data is reporting in Bali province. This study isconducted to describe the risk factors of stroke patients, specifically those who were treated at the Neurologyoutpatient service of Sanglah Hospital, Bali.Methods:This research used a descriptive study with a cross-sectional design. Data from the medical records of strokepatients in the Neurology outpatient service of Sanglah Hospital were taken retrospectively in March-August2020 using a total sampling method. Inclusion and exclusion criteria were applied during the process.Results:The study resulted in several findings with the 181 selected patients consisting of 100 males and 81 females,.The group of 45-54 years old (31.5%), high school-graduated (32.6%), and unemployed patients (47.5%) are thehighest prevalence of the study. The ischemic stroke had a higher prevalence (61.3%) than hemorrhagic stroke(38.7%). The highest risk factors were hypertension (40.9%), followed by Diabetes Mellitus Type 2(18.8%) andsmoking (17.2%). In both ischemic and hemorrhagic, hypertension plays the biggest risk role. It was 29.1% inischemic, while 89.3% in hemorrhagic.Conclusions:In conclusion, the incidence of stroke happens more frequently in the groups of men, adults in the productiveage, senior high school-graduated, and unemployed. Ischemic stroke is more common than hemorrhagic stroke.Hypertension is the most common risk factor, both ischemic and hemorrhagic stroke.
87

Cerebrovasc Dis 2020;49(suppl 1):1-149
88

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-39Epidemiology
Burden of Stroke in Myanmar
Yee Mon Khine1, Min Thit Win1, Ohnmar Ohnmar1, Myat Po Po Kyaw Khin2, NarayanaswamyVenketasubramanian3
1 Neurology, Yangon General Hospital/University of Medicine 1, Yangon, Myanmar2 Neurology, Yangon General Hospital, Yangon, Myanmar3 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore
Purpose:Myanmar is home to over 51 million people, a heterogeneous society of 135 ethnic groups living in 676,578square kilometers. Stroke comprises 20% of the work load of neurological disorders among inpatients andoutpatients in hospitals. With population per neurologist of 2.21 million, stroke cases are mainly managed bygeneral physicians. This paper describes the epidemiology of stroke in Myanmar.Methods:Medline was searched for publications using search terms ‘stroke’ AND ‘Myanmar’. The abstracts were reviewedand full papers obtained where possible. Data on stroke mortality, incidence, prevalence, disability and vascularrisk factors was extracted. The results are presented here.Results:Stroke is one of the leading causes of mortality according to the Ministry of Health’s report and morbidity andmortality according to annual reports of the largest Yangon General Hospital, Myanmar. The age and sex-standardised mortality rate due to stroke is 165.4/100,000, while age and sex-standardised disability-adjustedlife years lost due to stroke is 2971.3/100,000. The prevalence of stroke among adults aged 40 to 99 years is 1.5%.The high frequency of stroke has been attributed to hypertension due to eating very salty food and high use ofmonosodium glutamate. The age-standardised proportion of adults aged >18 years with systolic blood pressure>140/90mmHg or on medication for raised blood pressure is 24.9% among males and 24.2% among females;those with fasting blood sugar >7.0mmol/l or on medication for raised blood glucose is 6.9% and 7.9%respectively. Among adults aged >25 years, 5.1% of males and 7.9% of females have a fasting total cholesterol>6.1mmol/l. Among those aged >18 years, the frequency of insufficient exercise (<5 times 30 minutes ofmoderate activity per week, <3 times 20 minutes of vigorous activity per week, or equivalent) is 8.3% and 11.6 %,while obesity (body mass index BMI >30) is 2.0% and 5.5%; the frequency of smoking among those aged >15years is 31.5% and 6.4% respectively.Conclusions:Stroke is a major health burden in Myanmar. With the gradual aging of the population and the reduction ininfectious diseases, the burden due to stroke in Myanmar is likely to rise. Detection and control of vascular riskfactors and the provision of evidence-based treatments of stroke will be key in controlling this devastatingdisease.
89

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-40Epidemiology
Headache and Seizure Manifestation Related to Brain Arteriovenous Malformation Underwent DigitalSubtraction Angiography in Moewardi Hospital Periode
January 2018 to July 2020
Dyah Pranani1, Subandi Subandi2
1 Neurology, Universitas Sebelas Maret, Surakarta, Indonesia2 Interventional Neurology, Universitas Sebelas Maret, Surakarta, Indonesia
Purpose:The incidence of AVM in Indonesia, especially in Surakarta, is still not well and clearly described. This study triesto describe the incidence of clinical symptoms in AVM patients who had been done DSA examination.Methods:This study is a descriptive-analytic study with retrospective data collection. Patients with a history of seizurebefore, on antiepileptic drug therapy, were excluded. The data obtained were analyzed using the "Chi-Square"test.Results:The age at the time of diagnosis ranged from 12 years to 73 years (mean 40 ± 16,1 years). There were 21 malesand 25 females. The clinical manifestation was hemorrhage in 31 patients, the focal neurological deficit in 18patients, seizure in 19 patients, blurred vision in 14 patients, thunderclap headache in 2 patients, unspecifiedheadache in 16 patients, neuralgia trigeminal in 1 (2,2%) patient, migraine-like headache in 18 patients,exophthalmos in 3 patients. There were seven patients in frontal concerning AVM location, ten patients inparietal, 13 patients in temporal, 11 patients in occipital, one patient in the subcortex, and four patients ininfratentorial. There was a significant relationship between the AVM location and migraine-like headacheincidence in the occipital lobe (p=0.000). There was a significant relationship between seizure incidence at theAVM location in the temporal lobe (p = 0.037) and the frontal lobe (p = 0.003).Conclusions:The incidence of AVM in Moewardi hospital is more common in females than men. AVM location, which isassociated with the incidence of migraine-like headaches, was in the occipital lobe. AVM location whichassociated with the incidence of seizure were frontal and temporal lobes
90

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-41Rehabilitation & Restorative Therapy in Stroke
Post Stroke Patient Care During Covid-19 Pandemic
Sulistyani Sulistyani1
1 Neurology Department, Universitas Muhammadiyah Surakarta, Surakarta, Indonesia, Indonesia
Purpose:The purpose of this study was to identify the types of based home care for the post-stroke patient, both thosethat have been done and are being developed.Methods:A comprehensive search on PubMed, Science Direct, and Google Scholar databases was conducted with thekeyword was (home-based rehabilitation AND (“stroke” OR stroke) AND pandemic). Studies published in 2020about post-stroke care during pandemic were selected. The eligibility criteria of the articles were as follows:articles that mentioned the care of stroke patients during the Covid-19 pandemic, there were no age restrictions,no gender restrictions, no country or race restrictions, only articles in English, only research empirical (not areview article) and all quantitative research designs. Electronic searches conducted in September 2020 yieldeda total of 1290 after deduplicate. Sixty-one of these were deemed potentially relevant after the title and abstractreading. Forty-nine studies were excluded because they were not relevant after full-text reading. Thirteen studiesmet the inclusion criteria for this review.Results:Based-homed care innovations are a challenge for the physician during the new normal era. Studies showedvarious strategies for treating post-stroke patients from home. The most common type of post-stroke patientcare mentioned in the journal is telerehabilitation (11/13). The telerehabilitation program includes a homeexercise program, a virtual reality exercise, an augmented gaming reality device, and a home-based rehabilitation(HBR) system: a smartwatch and smartphone app equipped with a machine learning (ML) algorithm. Threejournals showed telemedicine to post-stroke patient care. It consists of virtual visits, virtual check-in, andtelemonitoring. Furthermore, ways to care post-stroke patients are home visits, Portable TranscutaneousElectrical Stimulation Device, and Mirror Therapy, each mentioned in 1 journal.Conclusions:The Covid-19 pandemic has indeed resulted in delayed patient care for the hospital. Recovery of stroke patientscannot be delayed and must be done from home as much as possible so that neurological functional declinedoes not occur. Studies showed various based-homed post-stroke patient care. These strategies are consist oftelerehabilitation (home exercise program), telemedicine, Portable Transcutaneous Electrical Stimulationdevices, mirror Therapy, and home-visit.
91

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-42Risk Factors and Prevention of Stroke
Anticoagulants Usage in Stroke Prevention among Patients with Severe COVID-19
Anvar Azimov1, Fakhriddin Azimov1, Gulnora Rakhimbayeva2
1 Neurology, Akfa Medline MC, Tashkent, Uzbekistan2 Neurology, Tashkent Medical Academy, Tashkent, Uzbekistan
Purpose:To determine more safe and effective anticoagulant in stroke prevention among patients with severe COVID19.Methods:Totally 520 patients participated in the study. All patients got treatment based on national COVID19 guideline atthe Akfa Medline MC in the period of March, 2020 up to September, 2020. Criteria for severe COVID19 werefollowing: SpO2 <92% on room air, PaO2/FiO2<300 mmHg, respiratory frequency >30 breaths per minute, lunginfiltrates >50% on CT. Eight patients died till to recheck time. 3 patients didn’t manage to come for recheck.Therefore, finally 509 patients are included in the study and divided into three groups. First group of patients gotHeparin in dosage 24000 –36000 IU per day. Second group took Enoxaparin 1mg/kgBM/day. Third group -Rivaroxaban 20 mg per day. Follow up done on 2nd-3rd-4th-5th-6th week after start of treatment. Brain CT orBrain MRI done when there was suspicious of stroke.Results:See Table 1 in the file "APSC2020 Azimov".
92
Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:Summing up, stroke prevalence is significantly higher in patients getting Heparin (p≤0,05). Enoxaparine and Rivaroxabane showed their safety and effectiveness in stroke prevention in severe COVID19. Further studies oncoagulation and aggregation tests analyzing in severe COVID19 patients are needed.
93

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-43Case Report
Petechial Hemorrhage Stroke in COVID-19 Patient with Seizureas First Neurologic Manifestation: A Case Report
Prysta Sitanggang1, Kumara Tini1, Ni Susilawathi1, Ida Wijayanthi1, Putu Dewi1, Dewa Samatra1
1 Neurology Department, Faculty of Medicine Universitas Udayana, Denpasar, Bali, Indonesia
Purpose:Coronavirus disease 2019 (COVID-19) is a systemic infection that is not only infected the respiratory tract or lungparenchymal but also the nervous system, especially stroke. The majority of COVID-19 patients presented withthe cerebrovascular disease had an ischemic stroke (83,7%) than hemorrhagic stroke (16.3%). Reports ofhemorrhagic stroke are still rare and usually related to the use of anticoagulation. We report a patient withpetechial stroke hemorrhage with COVID-19 with seizure as the first neurological presentation without any priormedication of anticoagulation.Methods:Medical charts were reviewed for significant history, physical examination findings, laboratory findings, andimaging. Due to the retrospective nature of this report, informed consent was not required. We used the CaseReport Guideline (CARE; https://www.care-statement.org/) checklist when writing this report.Results:A 62-years old male admitted to Hospital in Bali, Indonesia due to seizures for 2 minutes, and hard tocommunicate well. He had no symptoms of fever, cough, diarrhea before admission. The patient had a history ofischemic stroke and hypertension for the last 8 years. He was not regularly taking any antihypertensive orantiplatelet aggregation drugs to prevent any secondary stroke. Physical examination revealed body temperature36 C, blood pressure of 170/100 mmHg, pulse of 82 beats per minute, respiratory rate of 20 breath per minute,and blood oxygen saturation 99% on the nasal cannula. GCS E4V4M6; left central facial paresis, hemiparesisspastic on left extremities. National Institutes of Health Stroke Scale (NIHSS) is 10. Laboratory examinationrevealed: white blood cells (WBC) 8.76/L, Neutrophil-Lymphocyte Ratio 5.6; hemoglobin 19.3/L, platelets142/L,D-dimer 3,262 ng/ml. Blood glucose is 126 mg/ dL. RT-PCR from nasopharyngeal swab was positive for SARS-COV2. A chest x-ray showed left lung pneumonia. A Chest CT scan showed fibrotic on the right lung. The HeadNCCT scan showed a small parenchymal hematoma on the cortex of the left parietal lobe. Brain CTA revealednormals. He was treated with phenytoin 100mg every 8 hours, folic acid 1mg every 24 hours, and clobazam 10mg at night. The patient responded very well with the treatment and was discharged after 10 days ofhospitalization.Conclusions:The COVID-19 may damage blood vessels in the brain and cause bleeding. Hemorrhagic stroke with COVID-19 isnot always associated with a high risk of mortality. Early treatment can be very beneficial for good prognostic.
94

Cerebrovasc Dis 2020;49(suppl 1):1-149
95

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-44Case Report
Stroke and COVID-19 Patient in Indonesia: A Case Report
Sulistyani Sulistyani1, Immaculata Widiasmaningrum2, Titian Rakhma3, Hanindya Prabaningtyas4
1 Neurology Department, Universitas Muhammadiyah Surakarta/PKU Muhammadiyah Kartasura Hospital,Surakarta, Indonesia2 Neurology Department, Dr. Suyoto Hospital, Jakarta, Indonesia3 Neurology Department, Universitas Muhammadiyah Surakarta/Dr. Sayidiman Hospital, Magetan, Indonesia4 Neurology Department, Universitas Negeri Sebelas Maret (UNS)/UNS Hospital, Surakarta, Indonesia
Purpose:To report stroke cases with Covid-19 patients in Indonesia.Methods:We recorded several hospitals that treated stroke patients with Covid-19 during August 2020. We got 3 strokepatients with Covid-19 in the two hospitals we recorded. The other two patients were excluded because therewas no data regarding laboratory, imaging, therapy, and outcomes.Results:A 43-years-old man with the chief complaint was the weakness of the right extremity. He had simple focalseizures on the admission and couldn't speak and understand the other person's conversation. Before admission,he only felt a headache. No complaint about a cough, fever, and gastrointestinal syndromes. His history of illnesswas hypertension. He lives in the Covid-19 red zone area. On the examination, blood pressure: 110/60, the pulserate: 79 beats/minute, temperature 36.4ᵒ C and respiration rate: 20 times/minute, NIHSS score: 17. His head, cor, pulmonary, and abdomen were within normal. Neurologic examinations were somnolent, global aphasia, rightfacials, and hypoglossal nerves paralyze, bi hemiparesis. Laboratory findings were hyperglycemia, elevated ofHbA1C (8,8), and elevated of D dimer (2407). The pulmonary x-ray was left side pneumonia. A brain CT scanshowed a right pons and multifocal infarct. The rapid test was reactive and the nasopharyngeal swab was positive.The patient was hospitalized as a COVID-19 patient. After treatment, the patient improved with the stroke sequel.Conclusions:The case report shows on Covid-19 patients with signs and symptoms of a stroke. The stroke patient in this casewas a 43-year-old male in a Covid-19 patient. Clinical symptoms based on NIHSS was severe and had elevated D-dimer. Previous literature shows that most of the Covid-19 patients with stroke were young males (63.2%).Hypertension is the most common comorbid in Covid-19 (56.3%) as well as being a risk factor for stroke. A Covid-19 with stroke mostly had severe clinical symptoms (41.9%). Increased D-dimers are a sign of hypercoagulationdue to a systemic inflammatory process due to Covid-19 infection and can lead to stroke. Coagulation factorsdue to infection (sepsis-induced coagulopathy) are a risk factor for stroke in Covid-19. The SARS-CoV-2 virus bindsto angiotensin-converting enzyme 2 (ACE2) present on brain endothelial and smooth muscle cells. The virus tothe brain can be via the vascular route or directly (through the cribriform plate). A decrease in ACE2 by SARS-CoV-2 causes ACE1 / angiotensin II axis imbalance and results in tissue injury (stroke).
96

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-45Prognosis/Outcome of Stroke
The Effect of Hyponatremia on Length of Stay and Hospital Mortality in Patients with Stroke
Niawati Rokhaniah1, Baarid Luqman Hamidi1
1 Neurology, Sebelas Maret University, Surakarta, Indonesia
Purpose:Evaluating the effect of hyponatremia on lenght of stay and hospital mortality in patients with strokeMethods:This study is a retrospective study by analyzing the medical records data of stroke patients for 1 year (2018 -2019). In this study, stroke is classified into ischemic and hemorrhagic strokes. The collected data were analyzedusing the mann whitney and chi-square test while the effect of hyponatremia status to length of stay wasanalyzed using the kaplan meier survival curve and the log rank test.Results:In this study, data were obtained for a total of 424 patients with a proportion of 241 (57%) patients experiencingischemic stroke and 183 (43%) patients experiencing a hemorrhagic stroke. When analyzed from their sodiumstatus, it was found that 249 (59%) patients were in the non-hyponatremic category and 175 (41%) patients werein the hyponatremic category. Using the mann whitney test, there was a significant difference betweenhyponatremia and non-hyponatremia status on the length of stay of stroke patients (p = 0.028). In this study, theanalysis was also carried out using the chi-square test and found that there was no difference betweenhyponatremia and non-hyponatremia on the incidence of hospital mortality (p = 0.237). Based on the kaplanmeier survival curve and the log rank test (p = 0.018) in stroke patients with hyponatremia status, it was foundthat there was a difference in the survival curve where the probability of length of stay in hyponatremic patientswas higher than non-hyponatremic patients. Based on logistic regression analysis, it was found that the tendencyof mortality in hemorrhagic stroke patients was 2.32 times compared to an ischemic stroke which was statisticallysignificant (p <0.001), while hyponatremia status had no significant effect on hospital mortality (p = 0.166).Conclusions:Hyponatremia affects the length of stay in stroke patients but does not affect to hospital mortality. Patients withhemorrhagic strokes had a mortality tendency of 2.32 times compared to ischemic stroke patients.
97

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-46Prognosis/Outcome of Stroke
The Presence of Pre-diabetes Predicts Short-term Prognosis, But Not Long-term Outcome in Acute IschemicStroke using IV Thrombolysis
Jae-kwan Cha1, Byeol-a Yoon1, Dae-hyun Kim1
1 Stroke Center, Dong-A University Hospital, Busan, Korea
Purpose:Diabetes mellitus is a well-known predictor of poor outcome in acute ischemic stroke (AIS). However, there hasbeen debated whether pre-diabetes might influence on short and long-term outcomes after AIS. In this study,we investigated the association between short-and long-term outcomes in AIS using IV thrombolysis.Methods:We recruited patients with AIS using IV thrombolysis prospectively registered CRCS-K database in Dong-Auniversity stroke center from 2015 into 2019. According to their HbA1C levels, patients were divided into threegroups: normal, pre-diabetes, and diabetes. We assessed early neurologic deterioration, in-hospital death, pooroutcome at 90 days, and 1-year (mRS score 3-6) after using IV thrombolysis in AIS.Results:: Total 661 AIS patients using IV thrombolysis enrolled in this study. Among those subjects, pre-diabetes wasdiagnosed in 197 patients (29.8%) and diabetes in 210 patients (31.8%). In multiple logistic regression analysis,pre-diabetes was an independent predictor of END (OR, 1.79; 95% CI, 1.01 to 3.22; p<0.05) and of in-hospitaldeath (OR, 3.31; 95% CI, 1.12 to 9.80; p=0.03). Compared to this result, the presence of diabetes was anindependent predictor of 90 days (OR, 1.77; 95% CI 1.09 to 2.85; p<0.05) and 1-year (OR, 1.83; 95% CI 1.13 to2.95; p<0.05) poor outcomes.Conclusions:Pre-diabetes influences on short-term prognosis in AIS with IV thrombolysis. However, the presence of diabetesis associated with poor long-term prognosis after AIS using IV thrombolysis.
98

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-47Prognosis/Outcome of Stroke
Characteristics of Cervicocephalic Dissecting Occlusions
Seong-joon Lee1, Mun Hee Choi1, Sung Eun Lee2, Ji Man Hong1, Jin Soo Lee1
1 Neurology, Ajou University Medical Center, Suwon, Korea2 Emergency Medicine, Ajou University Medical Center, Suwon, Korea
Purpose:The diagnosis of cervicocephalic dissections is based on identification of pathognomic imaging findings, andtemporal changes observed in serial angiographic images. Recently, the use of high resolution MRI has resultedin detection of dissecting flaps and intramural hematoma that had previously been difficult to visualize.Furthermore, the diagnosis of occlusions presumed to be dissection in etiology is still difficult. Through analysisof computed tomography (CT), transfermoal cerebal angiography (TFCA), and high resolution magneticresonance imaging (HR MRI) findings, We evaluated the characteristics of cervicocephalic dissecting occlusions.Methods:Consecutive patients diagnosed as cervicocephalic dissections were included from a single center from 2001 to2019 June. From this database, patients with vascular occlusions that were clinically diagnosed as dissections, orpatients that were presumed to be of other etiology, yet performed CT angiographiy with either TFCA or HR MRI,or both, were included. From this database, patients were classified stepwise as 1) confirmed dissections basedon CTA or TFCA findings identifying pseudolumen or dissection flaps, 2) confirmed dissections on HR MRIidentifying peudolumen, dissection flaps, and intramural hematoma, 3) probable dissections that show over 50%recanalization, or recanalization with dilatations, 4) suspicious dissections, and 5) dissection unlikely.Results:Among 425 patients clinically suggestive of cervicocephalic dissections, potential 88 dissecting occlusion patientswere identified (age: 51±13, male: 66/88 [75.0%]). Occlusions were most commonly located in theintra+extracranial vertebral artery (29.5%) followed by intracranial vertebrtal artery (20.5%) and middle cerebralartery (10.2%). Acute neurointervention was performed in 13 (14.8%), delayed neurointervention in 1 (1.1%) andbypass surgery in 4 (4.5%). Medical management was performed in the rest, and resulted in a modified RankinSacle of 0 ~2 in 71.3%. Through a stepwise classification, 6 (12.6%) was confirmed the diagnosis of dissectingocclusions by baseline TFCA. Thirty-one (35.6%) could be confirmed the diagnosis of dissecting occlusions bybaseline HR MRI. Twenty (22.7%) could be considered probable dissections by identification of recanalization onserial angiography. Among 30 (34.1%) patients that dissections could not be confirmed, the occlusion etiologywas presumed to be dissections in another 22 patients.Conclusions:With current diagnostic criteria of cervicocephalic dissections, the etiology of occlusions can be confirmed asdissections in 65.9% of patients suspected. The best methods for accurate diagnosis of dissecting occlusions needto be further evaluated.
99

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-48Prognosis/Outcome of Stroke
The Relationship between Neutrophil-Lymphocyte Ratio (NLR) Dan Platelet- Lymphocyte Ratio (PLR) with Nihss on Acute Phase Thrombotic Ischemic Stroke Patients
Priyanka Ganesa Utami1, Diah Kurnia Mirawati1
1 Neurology, Universitas Sebelas Maret, Surakarta, Indonesia
Purpose:Stroke is the second leading cause of death and the highest cause of disability in adults in the world. Manyinflammatory mediators play a role during the ischemic process in acute ischemic stroke and are associated withtheir poor condition. Blood count examination using the neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) is a simple method and has the ability to detect increased inflammatory mediators inischemic stroke. This study aims to assess the relationship between the neutrophil-lymphocyte ratio (NLR) andplatelet-lymphocyte ratio (PLR) as proinflammatory parameters with NIHSS in acute phase thrombotic ischemicstroke patients.Methods:This study retrospectively reviewed the medical records of thrombotic ischemic stroke patients undergoingtreatment in Dr. Moewardi Surakarta from September 2019 - August 2020. The NIHSS was assessed at the timeof admission in the emergency room. We excluded patients with embolic and lacunar stroke; infarction on thewatershed area; infarction secondary to trauma, infection, and tumour; and known hematologic disorder. TheNLR and PLR values were obtained from blood lab tests taken during admission to the emergency room. The NLRand PLR values were analyzed for their relationship to the NIHSS using non-parametric Spearman Rho analysiswith a confidence level of 95% and p <0.05.Results:Of the 578 stroke patients hospitalized at Dr. Moewardi Hospital, 392 of them were ischemic stroke patients, and151 of them met the inclusion and exclusion criteria of this study. Based on statistical tests, there was astatistically significant relationship between NLR and NIHSS in acute phase thrombotic ischemic stroke patientsat admission (P = 0.03). Hence there was no statistically significant relationship between PLR and NIHSS in acutephase thrombotic ischemic stroke patients on admission (P = 0.552).Conclusions:NLR has a positive relationship with the condition of acute-phase thrombotic ischemic stroke patients assessedby NIHSS. Meanwhile, PLR did not have a positive relationship with the condition of acute-phase thromboticischemic stroke patients based on NIHSS.
100

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-49Rehabilitation & Restorative Therapy in Stroke
Transcutaneous Laryngeal Ultrasonography in Hemiplegic Stroke Patientswith Dysphagia - Pilot Study
Seung Min Baek1, Taehwan Kim1, Kwang Jae Lee1
1 Rehabilitation Medicine, Presbyterian Medical Center (Jesus Hospital), Jeon-Ju, Korea
Purpose:Dysphagia after stroke is a common and disabling condition that can cause significant clinical complications, suchas aspiration pneumonia and malnutrition. A videofluoroscopic swallowing study (VFSS) with or withoutendoscopy is a gold standard for evaluating dysphagia. In addition, Transcutaneous laryngeal ultrasonography(TLUS) can be applied to evaluate various laryngeal structures. We evaluated vocal cord movement andcompared the VFSS grade with incompletion in vocal cord closure presented by angle degree in hemiplegic strokepatients with dysphagia.Methods:Six hemiplegic stroke patients with dysphagia were recruited. VFSS and TLUS were conducted with the consentof the patients. VFSS was done for all patients, and for the TLUS, patients lied on their back with neck extensionand the ultrasound probe was applied on the centerline of the the thyroid cartilage to find the vocal cords. Themovement of the vocal cords was observed while the patient made an 'Ah' sound. We checked the vocal cordparalysis and captured the moment of maximal adduction to midline of them and the angle from the center linewas measured.Results:Five men and one woman were enrolled (age: 74.17±8.97 years old, 3 infarction and 3 hemorrhagic stroke, 3 leftand 3 right hemiplegia). Two patients were grade 8 in fluid 2 ml with 25.03⁰±5.55 of the difference between normal side and hemi-side vocal cord adduction angle, and 4 patients were grade 5 in fluid 5 ml with 8.66⁰±8.88 of it. So patients with grade 8 in fluid 2 ml were greater difference in vocal cord adduction angle than that inpatients with grade 5 in fluid 5 ml in VFSS.Conclusions:TLUS could be the additional evaluation tool to check the adduction movement of the vocal cords and then mightbe expected the severity of the dysphagia.
101

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-50Rehabilitation & Restorative Therapy in Stroke
Effects of Cerebrolysin Combined with Rehabilitation on Motor Recovery in Stroke Patients with SevereMotor Involvement
Won Hyuk Chang1, Jungsoo Lee1, Yong-il Shin2, Myoung-hwan Ko3, Deog Young Kim4, Min Kyun Sohn5, Jinuk Kim1,Yun-hee Kim1
1 Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular and StrokeInstitute, Samsung Medical Center, Sungkyunkwan Univ, Seoul, Korea2 Rehabilitation Medicine, Pusan National University College of Medicine, Pusan National University YangsanHospital, Pusan, Korea3 Physical Medicine and Rehabilitation, Research Institute of Clinical Medicine of Chonbuk National University,Biomedical Research Institute of Chonbuk Nationa, Jeonju, Korea4 Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea5 Rehabilitation Medicine, Chungnam National University, Deajeon, Korea
Purpose:Although there is some evidence that medications may help improve motor recovery after stroke, larger, well-controlled trials are needed to confirm that specific medications can facilitate motor recovery after stroke. Theobjective of this study was to evaluate whether Cerebrolysin on top of rehabilitation therapy provides additionalmotor recovery in subacute stroke patients with severe motor impairment.Methods:This phase IV trial was designed as a prospective, multicenter, randomized, double-blind, placebo-controlled,parallel-group study. Stroke patients with severe motor function impairment (Fugl-Meyer assessment (FMA) 0-50) were included within 7 days after stroke onset. They were randomized to receive a 21-day treatment course(Days 8-28) of either Cerebrolysin or placebo, given in addition to standardized rehabilitation therapy.Assessments for motor function with FMA were performed at baseline, immediately after treatment, and 3months after stroke onset. The plasticity of the motor system was assessed by diffusion tensor imaging (DTI) andresting-state functional magnetic resonance imaging (rsfMRI).Results:A total of 122 patients (Cerebrolysin n=62, placebo n=60) were enrolled, and 110 patients completed the studyprotocol (Cerebrolysin n=59, placebo n=51). Each group showed significant motor recovery over time. Repeatedmeasures ANOVA showed a significant interaction effect between time and type of intervention as measured byFMA (p<0.05). rsfMRI analysis also showed a significant interaction between intervention time and type inipsilesional functional connectivity. In DTI analysis, patients treated with Cerebrolysin demonstrated lessdegenerative white matter changes in major vertical, longitudinal, and lateral white matter tracts over time thanthe control group (Fig. 1).
102

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:Cerebrolysin treatment as an add-on to a rehabilitation program is a pharmacologic approach that is worthconsidering to improve motor recovery in ischemic stroke patients with severe motor impairment (This studywas funded by EVER Neuro Pharma GmbH and by a National Research Foundation of Korea (NRF) grant fundedby the Korean government (NRF-2020R1A2C3010304).
103

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-51Rehabilitation & Restorative Therapy in Stroke
Exploratory Study of Using Fourier M2 Upper Limb Rehab Robotics for Individualswith Chronic Stroke in Singapore: A Case Series
Alvin Lim1, Xue Su1
1 Rehabilitation, Woodlands Health Campus, Singapore, Singapore2 Rehabilitation Centre, Khoo Teck Puat Hospital, Singapore, Singapore
Purpose:It is widely accepted that individuals with chronic stroke demonstrate neural plasticity and the ability to improveboth upper limb function and activities of daily living (ADL). Emergent therapies such as robotic assisted therapyhad proven to have evidence to assist these individuals with chronic stroke, on top of the conventionalOccupational Therapy trainings. The aim of this trial is to explore the usability and effects of a novel roboticsdevice - Fourier M2 (Upper Limb Rehab Robotics) on individuals with chronic stroke.Methods:2 participants were included in this study. Both had residual upper limb deficits from previous stroke and theaverage age was 51. They underwent 30 minutes of robotics training with Fourier M2 per session, on top ofconventional Occupational Therapy training for a total of 15 sessions. Fugl Meyer Upper Extremity (FMA- UE)Scale and Quick Disability of Arm, Shoulder and Hand (QuickDASH) were selected as the primary outcomemeasures. System Usability Scale (SUS) was used as a secondary outcome to evaluate the usability of Fourier M2.Results:The study demonstrated improvement in both participants in terms of upper limb gross motor function in FMA-UE and participants’ own perception on the level of disability when performing ADL under QuickDASH. Nonoteworthy improvement was found in both participants’ upper limb fine motor function. Fourier M2demonstrated fair usability in SUS with an average score of 70.83 out of 100 points.Conclusions:This study shows positive effects of Fourier M2 in assisting individuals even with chronic stroke to improve theirupper limb gross motor function and ADL. It also showed some limitation of Fourier M2 in robotic rehabilitationin terms of system interphase and consistency. Further study is warranted to determine the effects of FourierM2 on larger population with chronic stroke and the long- term effects on them.
104

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-52Rehabilitation & Restorative Therapy in Stroke
Wearable Ankle-assist Robot for Enhancing Gait Symmetry of Stroke Patients
Hwang-jae Lee2, Su-hyun Lee1, Jinuk Kim2, Won Hyuk Chang1, Gyu-ha Ryu3, Yun-hee Kim1
1 Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Samsung Medical Center, Seoul,Korea2 Health Sciences and Technology (SAIHST), Sungkyunkwan University, Seoul, Korea3 Medical Device Management and Research, Sungkyunkwan University, Seoul, Korea
Purpose:The purpose of this study was to investigate the effect of wearable ankle-assist robot on spatiotemporalparameters and lower limb muscle activation during gait in stroke patients.Methods:Forty-five stroke patients participated and divided into three groups according to their gait pattern; 17 patientswith foot drop gait group, 17 with ankle spastic gait group, 11 with circumduction gait group. The Gait Enhancingand Motivating System-Ankle (GEMS-A, Samsung Electronics Co., Ltd., Korea), which functions as a wearableankle-assist robot was used in this experiment. All participants performed randomly assigned sessions of threeconditions; free gait without robot assistance [FG], robot-assist gait with zero torque [RAG-Z], and robot-assistgait [RAG]. In all conditions, spatiotemporal parameters of gait function were also determined by 3D motioncapture system (Motion Analysis Corporation, USA). Lower limb muscle activation patterns and symmetry duringwalking were analyzed using the 12-channel surface electromyography system (Desktop DTS system, Noraxon,USA) at preferred speed on 8 m walkway.Results:The RAG condition, the foot drop gait group demonstrated significantly greater gait speed and stride length thanthe FG and RAG-Z (P<0.05). The abnormal lower limb muscle activation patterns in medial gastrocnemius, soleus,and tibialis anterior muscles of the affected side were changed in close proximity to normal pattern in the RAGcondition. In addition, the compensatory activation of the affected hip flexor muscle due to foot drop and anklespasticity was significantly reduced (P<0.05). Significantly improved muscle activation symmetry in bilateraltibialis anterior, gastrocnemius, and hip flexor muscles were also demonstrated in RAG condition of all groups(P<0.05).Conclusions:This study demonstrated that the GEMS-A is a potentially useful robotic device for improving gait function byimproving the muscle activation patterns and symmetry of the lower limbs during walking in stroke patients.Further study to confirm the rehabilitation effect of GEMS-A in stroke patients will be performed in the nearfuture. Acknowledgements This study was supported by a grant from the Korea Health Technology R&DProject through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health &Welfare, Republic of Korea (HI17C1501), and a National Research Foundation of Korea (NRF) grant funded by theKorean government (NRF-2020R1A2C3010304, NRF-2020R1I1A1A01069227 and NRF- 2017M3A9G5083690).
105

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-53Case Report
Repetitive Seizure Attack and Loss of Consciousness Causedby Delayed Sinking Skin Flap Syndrome: A Case Report
Yeong-il Na1, Jyul-lee Choi1
1 Rehabilitation Medicine, Presbyterian Medical Center, Jeonju, Jeollabuk-do, Korea
Purpose:Sinking skin flap syndrome (SSFS) is defined as serious disabling neurologic deficits and impairment of generalstatus with concave deformity and relaxation of the skin flap. The pathophysiology include cerebrospinal fluid(CSF) hypovolemia and development of an atmospheric pressure gradient that may be aggravated by CSFdiversion, dehydration, and position change. Cranioplasty is the principal surgical treatment that could improvesthe neurological deficits by a decrease in local intracranial pressure, and correction of abnormal CSF dynamics.We found a case of repetitive convulsion and loss of concentration whose craniectomy was delayed because ofpatient’s high operation risk.Methods:We describe the case of 56-year-old man who had subarachnoid hemorrhage due to ruptured A-com aneurysmrupture. Patient didn’t undergo cranioplasty due to underlying chronic obstruction pulmonary disease, and hischief complaint was general weakness, memory loss, dysphagia, and aphasia. He was alert, mini-mental stateexamination (MMSE) score was 17. He can walk on his own, 4-extremities manual muscle testing (MMT) gradewas 4/5, and his initial Modified Barthel index (MBI) score was 27. Our team started comprehensiverehabilitation, but he had to transfer to pulmonology department due to asphyxia and aspiration pneumonia. Hetransferred to other hospital for rehabilitation 1 month after transfer. He was transferred to our hospital 5months after discharge and started convulsion right after admission. Antieplieptics were added to control hissymptoms, and he transferred to our rehabilitation center for rehabilitation care. The brain CT scan showedsinking skin flap syndrome with mild midline shifting to right side, which was “paradoxical herniation”. He wastransferred to Neurosurgery department. There were several seizure attacks although antiepileptic drugs wereadded, and cranioplasty was done despite high operation risks. Though successful cranioplasty was done, his lossof consciousness was not resolved, and his last MBI score was 0.Results:Repetitive seizure attacks can be present at patients who had brain injury. Although we changed our antiepilepticdrug regimen by consulting to neurosurgery and neurology department, there’s a chance of seizure attack causedby brain injury only.Conclusions:We report a case of repetitive seizure attack and cognitive impairment caused by SSFS and paradoxical hernia.Cranioplasty consultation to neurosurgery department should be done before neurologic symptoms of SSFSappears, because those symptoms can affect to patient’s high operation risk, eventually getting harder toperform cranioplasty.
106

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-54Case Report
Neuroleptic Malignant Syndrome following Reduction of Amantadine in A Patientwith Thalamus and Basal Ganglia ICH: A Case Report
Yu-mi Kim1, Jong-hoo Lee1
1 Rehabilitation Medicine, Presbyterian Medical Center (Jesus Hospital), Jeonju, Jeollabuk-do, Korea
Purpose:Neuroleptic malignant syndrome (NMS) is a fatal neurologic emergency of the use of dopamine-receptor blockeror withdrawal from a pre-dopaminergic drug, resulting of a 10-20% mortality. It is clinical syndromes includingtypical symptoms, hyperthermia, extrapyramidal symptoms, autonomic nervous symptoms, and mental change.Neuroleptic malignant syndrome by withdrawal of amantadine has been often reported, however, there havenot been cases due to reduction of amantadine, and in stroke patient.Methods:We report a 57-year-old female patient who had been admitted to our department because of intracranialhemorrhage on right thalamus and basal ganglia with intraventricular hemorrhage. She had been taking the
amanta ™ 100mg (amantadine) 1t BID and madopar™ 125mg (levodopa 100㎎ + benserazide hydrochloride 28.5
㎎) 0.5t BID for about 3 months. Because the state of consciousness improved, we planned to reduce the pre-
dopamine drugs. The amantadine was reduced 100mg BID to 100mg QD. After the reduction, the fever occurredon the same day and the consciousness fell. As infection was suspected, we started empiric antibiotics therapy.On the next day, body temperature became normal. On the fifth day thereafter, the body temperature reached
38.4℃, with rigidity of 4 extremities, tachycardia and mental deterioration. Under the consultation of Infectious
internal medicine, antibiotics were changed but hyperthermia was continued. Chest and abdomen-pelvic CTwere done but could not find reason of fever, and also serum inflammation markers were normal. Theelectroencephalogram and brain magnetic resonance imaging were done but had still not determined the cause.After 13 days upon occurrence of the first fever, suspecting NMS, bromocriptine and diazepam were taken.Results:Immediately, the continuous hyperthermia, rigidity and decreased mentality were improved.Conclusions:From this case we consider that even a small decrease in amantadine may cause NMS to a patient withimpairment in dopaminergic pathway and we suggest that such patients should be paid more attention whenreducing dopaminergic drug.
107

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-55Case Report
Large Cavernous Carotid Aneurysm: Report of Unruptured Case
Naomi Ditya Sari1, Subandi Subandi2, Suroto Setijorumekso3
1 Neurology Department, Universitas Sebelas Maret, Surakarta,Central Java, Indonesia2 Neuro-intervention Division, Department of Neurology, Universitas Sebelas Maret, Surakarta,Central Java,Indonesia3 Neurovascular Division, Department of Neurology, Universitas Sebelas Maret, Surakarta,Central Java, Indonesia
Purpose:The large cavernous carotid aneurysm (CCA) is a rare case. It accounts for between 3% and 5% of all intracranialaneurysms. CCA often remain asymptomatic and is detected incidentally. It can make some manifestations suchas diplopia, ptosis, ophthalmoplegia, or pain or paresthesia along with the trigeminal nerve distribution. Theappropriate treatment is required in this case. Therefore, we present a large cavernous carotid aneurysm caseso that all of the clinicians can make the correct assessment and decision for CCA.Methods:We obtained one case of the large cavernous carotid aneurysm with the occlusion of the aneurysms. The patientmanifestations were recorded and all of the imaging data were documented. Informed consent was obtainedfrom the patient.Results:A 57-years-old woman complained that she couldn't open the right eye, get diplopia and pain on the rightophthalmic and maxillary division of trigeminal nerve distribution since two years ago. It happened suddenly.She had no headache or seizure before. There is no hypertension, traumatic history, and family history with asimilar manifestation. From the neurology examination, we got right total ophthalmoplegia, right ptosis, andpain on the right ophthalmic and maxillary division of trigeminal nerve distribution. From the Digital SubtractionAngiography, there is an aneurysm of the internal carotid artery in the cavernous segment with a diameter of17.04 mm x 9.81 mm, neck 4.77 mm. She got the coiling treatment by using eight of Axium 14 mm x 40 cm. Twoweeks after coiling the diplopia and pain on the right trigeminal nerve distribution are subsided, but the ptosisis still minimally maintained. Since the last angiography, the aneurysm categorized with class IIIa of the ModifiedRaymond-Roy ClassificationConclusions:Patient neurological deficits after coiling are improved, but the ptosis manifestation is still minimally maintained.
108

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-56Rehabilitation & Restorative Therapy in Stroke
Longitudinal Changes in Multi-faceted Functional Assessment up to Four Yearsafter the First-ever Stroke in Korea: The KOSCO Study
Yu Min Bang1, Min Kyun Sohn2, Jongmin Lee3, Deog Young Kim4, Sam-gyu Lee5, Yong-il Shin6, Gyung-jae Oh7, Yang-soo Lee8, Min Cheol Joo9, So Young Lee10, Junhee Han11, Jeonghoon Ahn12, Young-hoon Lee7, Min-keun Song5,Won Hyuk Chang2, Soo Mi Choi13, Jin Ha13, Yun-hee Kim14
1 Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart VascularStroke Ins, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea2 Department of Rehabilitation Medicine, School of Medicine, Chungnam National University, Daejeon, Korea3 Department of Rehabilitation Medicine, Konkuk University School of Medicine, Seoul, Korea4 Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul,Korea5 Department of Physical and Rehabilitation Medicine, Chonnam National University Medical School, Gwangju,Korea6 Department of Rehabilitation Medicine, Pusan National University School of Medicine, Pusan NationalUniversity Yangsan Hospital , Busan, Korea7 Department of Preventive Medicine, Wonkwang University, School of Medicine, Daegu, Korea8 Department of Rehabilitation Medicine, Kyungpook National University School of Medicine, KyungpookNational University Hospital, Daegu, Korea9 Department of Rehabilitation Medicine, Wonkwang University School of Medicine, Iksan, Korea10 Department of Rehabilitation Medicine, Jeju National University Hospital, Jeju National University School ofMedicine, Jeju, Korea11 Department of Statistics, Hallym University, Chuncheon, Korea12 Department of Health Convergence, Ewha Womans University, Seoul, Korea13 Division of Chronic Disease Prevention, Center for Disease, Korea Centers for Disease Control and Prevention,Cheongju, Korea14 Department of Health Science and Technology, Department of Medical Device Management and Research,Department of Digit, SAIHST, Sungkyunkwan University, Suwon, Korea
Purpose:There is no definite consensus on the courses of long-term multi-facet functional level in stroke patients after 6months, although these are very important for a rehabilitation plan and national policies for disables. Thepurpose of this study was to analyze the functional recovery patterns from 7 days to 4 years after stroke onsetand the time point to reach the plateau and decline of each function for the total, ischemic and hemorrhagicstroke.Methods:This study was an interim analysis of the Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO)designed as 10 years long-term follow-up study of stroke patients. All patients who admitted to therepresentative hospitals in 9 distinct areas of Korea with their acute first-ever stroke (from August 2012 to May2015) were recruited. Both ischemic and hemorrhagic strokes were included, but transient ischemic attacks wereexcluded. Out of 10,636 screened first-ever stroke patients, 7,858 patients agreed and gave consents for long-term follow up assessment. Of these, 4,564 patients completed face-to-face assessments at 4 years after strokeonset. Functional assessments included Korean modified Barthel Index (K-MBI), Korean Mini-Mental StateExamination (K-MMSE), Fugl-Meyer Assessment (FMA), Functional Ambulatory Category (FAC), the AmericanSpeech-Language-Hearing Association National Outcome Measurement System Swallowing Scale (ASHA-NOMS),and Short Korean Version of Frenchay Aphasia Screening Test (Short K-FAST). We demonstrated functionalrecovery pattern for subsets grouped by their baseline stroke severities and age.Results:Among 4,564 patients, 79.3% (n=3,619) of patients suffered from ischemic and 20.7% (n=945) hemorrhagicstroke, respectively. Their mean age was 63.1 years, and the ratio of male to female was 1.48. K-MBI reached theplateau at 12 months after stroke onset and showed no decline up to 4 years after stroke onset. Patients showed
109

Cerebrovasc Dis 2020;49(suppl 1):1-149
different patterns of recovery according to their initial stroke severity. Especially, in the patients with more than65 years old, K-MBI showed a significant decline from 2 years to 4 years (p<0.05).Conclusions:The results of this study demonstrated functional decline after the 24 months in the first-ever stroke patientswho were older than 65 years. Therefore, the proper rehabilitation strategies should be considered in olderstroke patients to maintain their long-term functional level (This study was supported by the Research Programfunded by the Korea Centers for Disease Control and Prevention (2019E320200)).
110

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-57Prognosis/Outcome of Stroke
Frequency and Clinical Impact of Serious Adverse Events (SAEs) on Post-strokeRecovery - Effect of MLC601 Compared to Placebo: The CHIMES Study
Narayanaswamy Venketasubramanian1, Rajesh B Moorakonda2, Qingshu Lu2, Christopher Chen3
1 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore2 Singapore Clinical Research Institute, Singapore Clinical Research Institute, Singapore, Singapore3 Pharmacology, National University of Singapore, Singapore, Singapore
Purpose:Serious adverse events (SAEs) during hospital admission may impact upon patients, course of disease, and thehealthcare team. Since SAEs may be intervention- or drug-related, we conducted an analysis comparing thefrequency of SAEs and their clinical impact on subjects who received MLC601 compared to placebo during thefirst 3 months post-stroke onset in the CHIMES trial.Methods:CHIMES was a 3-month multi-centre, randomised, double-blind, controlled trial of MLC601 versus placebo insubjects with acute ischemic stroke of intermediate severity (Clinicaltrials.gov - NCT00554723). SAEs as reportedby investigators were analysed for their frequency and clinical impact (ie. death, life-threatening condition, newand/or prolonged hospitalization, disability).Results:Of the 1087 as-treated subjects included in the CHIMES study safety analysis, 135 experienced SAEs (MLC601=60,placebo=75). The number of SAEs in individual subjects was significantly reduced in the MLC601 arm, especiallyfor subjects with >2 SAEs (6.7% vs. 29.3%; p<0.001). Other positive trends were observed in favour of MLC601vs. placebo: the percentage of subjects with SAEs resulting in >2 impacts was reduced by 65% (0.7% vs. 2.0%;p=0.12), and the rate of SAEs recovery with sequelae reduced by 25% (31.7% vs. 42.7%; p=0.19).Conclusions:This exploratory analysis shows that a 3-month course of MLC601 reduced the frequency of SAEs and their ratesof harmful clinical impacts. These findings could translate into a benefit in term of patient quality of life. If thisreduction could be applied to the millions of stroke survivors annually, this could also represent huge savings interm of SAE burden and costs for patients and the community.
111

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-58Prognosis/Outcome of Stroke
Characteristics of Postoperative Stroke in Patients in Ajou University Hospital
Sung-jun Lee1, Joonho Lee1
1 Neurology, Hospital of ajou university, Suwon, Korea
Purpose:Ischemic stroke after general surgery are a rare complication that occurs about 1%, but when it occurs, it is knownto extend the postoperative treatment period and lead to poor prognosis. We compared the characteristics ofpostoperative stroke patients in Ajou University Hospital and thought about what we should be careful about inpostoperative stroke.Methods:From 2008 to 2016, we collected patients who had surgery at Ajou University Hospital and had a neurologicalconsultation within 1 month after surgery. And, among them, we collected patients who were diagnosed withAcute Stroke by conducting imaging tests including MRI.Results:From 2008 to 2016, 61 patients were diagnosed with stroke after surgery at Ajou University Hospital. Amongthem, there were 22 patients with department of cardiothoracic surgery. This was the highest PostoperativeStroke rate compared to the number of surgeries. Large artery disease was the most common cause of strokewith 15, followed by cardiogenic embolism. However, as many as 16 patients were not assessed for causes suchas death after postoperative stroke or hospitalization in other departments. The age of patients averaged 62.1years, showing no significant difference compared to control groups.Conclusions:There was no meaningful difference in the percentage of postoperative strokes at Ajou University Hospitalcompared to other studies. There was a high rate of postoperative stroke in cardiothoracic surgery, but it isthought to be sufficiently understandable considering that cardiovascular disease, atrial fibrillation, andatherosclerosis are typical risk factors of postoperative stroke. There were only two small artery disease patients,less than expected. We considered the possibility that the symptoms were mild and could not be assessed duringother departments hospitalization. It has also been confirmed that 12 out of 61 people have not been assessedfor etiology, which is important to evaluate actively even if they are hospitalized at other departments.
112

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-59Prognosis/Outcome of Stroke
Evaluation of The Effectiveness of Saftstraw® in Patients with Dysphagia after Stroke ThroughVideofluoroscopic Swallowing Study
Si-yun Kim1, Yu-mi Kim1, Jong-hoo Lee1
1 Presbyterian Medical Center (Jesus Hospital), Department of Rehabilitation Medicine, Jeonju-si, Jeollabuk-do,Korea
Purpose:A spoon is commonly used for small amounts of fluid(5ml) in patients with dysphagia after stroke. Safestraw®has recently been used for fluid intake in patients with dysphagia. We would like to confirm the effectiveness ofsafestraw® by comparing the method of using spoon and safestraw® in small fluid intake though VFSS(videofluoroscopic swallowing study)Methods:This study was conducted on ten patients who had been confirmed with aspiration (Grade 7) in the test ofdrinking 5ml fluid in VFSS using spoon. They had the ability to suck liquid using a straw and fulfill the instructions.We performed the same test in VFSS using safestraw® to the same patients. We used penetration-aspirationscale (PAS) to assess swallowing function.Results:Six out of ten patients who were observed aspiration when using spoon had no aspiration with safestraw®.Among those, one patient, penetration (Grade 1), and five patients, penetration (Grade 3) were observed.Comparing using safestraw® to using spoon when drinking fluid, it is thought that the bolus formation of thefluid in the oral preparatory phase is more advantageous, and to have the effect of preparing for the nextswallowing action.Conclusions:Based on the results of this study, it is believed that safestraw® is safer than spoon when drinking a small amountwater. Therefore, it is considered safer to apply safestraw® rather than spoon from the beginning for the patientssuspected to dysphagia after stroke even if the VFSS has not been performed.
113

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-60Prognosis/Outcome of Stroke
Are There Patent Foramen Ovale-attributable Risks of Stroke Recurrence in Patientswith Determined Etiology of Ischemic Stroke?
Minyoul Baik1, Hyo Suk Nam1, Young Dae Kim1, Ji Hoe Heo1
1 Neurology, Yonsei University College of Medicine, Seoul, Korea
Purpose:Medically treated patients with patent foramen ovale (PFO) experience recurrent ischemic stroke frequently,however it still remains unclear whether PFO is causally related to recurrent ischemic stroke or an innocentbystander. We investigated whether there are differences in long-term recurrence of ischemic stroke by thepresence of PFO in patients with ischemic stroke of determined etiology.Methods:Consecutive patients with acute ischemic stroke who underwent transesophageal echocardiography fromJanuary 2010 to December 2017 were considered eligible. Patients who underwent PFO closure were excludedfrom this study. Ischemic stroke of determined etiology was defined as large artery atherosclerosis,cardioembolic and lacunar infarction. The association of PFO with long-term ischemic stroke recurrence wasinvestigated using Cox proportional hazard models.Results:Among 1813 ischemic stroke patients of determined etiology, there were 666 (37%) patients with PFO. During amedian follow-up of 4.1 years, the cumulative ischemic stroke recurrence was observed in 8.7%. On multivariateanalyses, patients with ischemic stroke of determined etiology and PFO did not have a higher risk of ischemicstroke recurrence (hazard ratio 0.85, 95% confidence interval 0.61−1.20, p=0.352) in comparison with those without PFO.Conclusions:This study showed that medically treated patients with ischemic stroke of determined etiology and PFO did nothave a higher risk for ischemic stroke recurrence, compared with those without PFO during long-term follow-up.
114

Cerebrovasc Dis 2020;49(suppl 1):1-149
115

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-61Prognosis/Outcome of Stroke
Association between Serum Insulin-Like Growth Factor-1 and Neurological Severityin Acute Ischemic Stroke
Jeeun Lee1, Minwoo Lee2, Jae-sung Lim2, Kyung-ho Yu2, Mi Sun Oh2, Byung-chul Lee2
1 Neurology, Seoul National University Hospital, Seoul, Korea2 Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea
Purpose:Serum insulin-like growth factor-1 (IGF-1) is known to have a neuroprotective effect. This study aimed to evaluatethe effect of serum IGF-1 on stroke severity and the clinical outcome of acute ischemic stroke.Methods:Four hundred and forty-six patients with acute ischemic stroke admitted to Hallym University Sacred HeartHospital within 7 days of stroke onset from February 2014 to June 2017 were included in this study. Serum IGF-1 levels were measured within 24 hours of admission. Stroke severity was measured using the National Institutesof Health Stroke Scale (NIHSS) score at admission, and functional outcome at 3-month after symptom onset wasassessed using the modified Rankin Scale (mRS) score. The effect of serum IGF-1 levels on stroke severity and 3-month functional outcomes was analyzed using multivariate logistic regression analysis.Results:A total of 379 patients with acute ischemic stroke (mean age: 67.2±12.6, male: 59.9%) were evaluated afterexcluding 67 patients because of a history of previous stroke (n=25) or loss to follow-up at 3 months (n=42). Afteradjusting for clinically relevant covariates, higher serum IGF-1 levels were associated with a lower NIHSS scoreat admission (adjusted odds ratios, 0.44; 95% confidence interval, 0.24–0.8; p=0.01). However, there was nostatistically significant association between serum IGF-1 levels and functional outcomes at 3 months.Conclusions:This study showed that higher serum IGF-1 levels are associated with a lower NIHSS at admission. However, therewas no significant relationship with functional outcomes at 3 months. Further studies are required to clarify theusefulness of serum IGF-1 levels as a prognostic marker.
116

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-62Prognosis/Outcome of Stroke
Importance of White Matter Hyperintensities Load in Ischemic Strokewith Mild Neurological Deficit
Wi-sun Ryu1, Dong-eog Kim1, Hee-joon Bae2
1 Neurology, Dongguk University Ilsan Hospital, Korean Brain MRI Data Center, Goyang, Korea2 Neurology, Seoul National University Bundang Hospital, Seongnam, Korea
Purpose:White matter hyperintensities (WMHs) are associated with recurrent stroke and functional outcome afterischemic stroke. The severity of WMHs represents a vulnerability to and impaired capacity to withstand acuteischemic injury. Even in mild stroke, a considerable proportion of patients suffer from neurological deteriorationand eventually become disabled. A few studies have highlighted the clinical importance of WMHs on outcomesafter ischemic stroke mild stroke. However, these studies are limited due to the small sample size, insufficientadjustment for covariates potentially associated with stroke outcome, and unavailable information about thelong-term outcome. In this big neuroimaging–clinical data comprised of 5,245 patients with mild stroke, weinvestigated the impact of WMHs on the short-term (3-month) and long-term (1-year) clinical outcome.Methods:From May 2011 to Feb 2014, we screened 14,497 patients who visited participating centers within 7 days ofstroke onset. We defined mild stroke as imaging confirmed ischemic stroke with the National Institute of HealthStroke Scale (NIHSS) scores of 3 or less. We quantitatively measured WMH and infarct volume on diffusion-weighted images. To examine the independent association between WMH quintiles and uncategorized 3-monthand 1-year mRS scores, we used multivariable ordinal logistic regression analysis.Results:Of 5,245 patients included, mean age was 64±12 years, and 37% (n = 1,918) women. Compared with those inthe lower WMH quintiles, patients in the higher quintiles were likely to have higher mRS scores at 3-month and1-year after ischemic stroke (both P < 0.001 by χ2 test). Even in patients with NIHSS of 0, nearly 35% in the highest quintile of WMH had a disability, and 20% remained to be dependent at 3-month after ischemic stroke. Afteradjusting for covariates, odds ratios of the highest quintiles compared with the lowest quintile were 2.1 (1.8 –2.6) and 2.3 (1.9 – 2.8) at 3-month and 1-year, respectively. The association between WMH quintiles and 3-monthmRS scores were significantly modified by NIHSS score (P for interaction = 0.024). When we divided patients intoeach point of NIHSS (0, 1, 2, and 3), the highest quintile of WMH was independently associated with a highermRS score at 3-month in all NIHSS strata.Conclusions:In this study from the large multi-center image-based data, we found that WMHs are associated with higher mRSscore at 3-month and 1-year after ischemic stroke with a dose-dependent manner.
117

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-63Prognosis/Outcome of Stroke
Multimodal Imaging Biomarker-based Stratification Model for Predicting Motor Recoveryin Stroke Patients
Jungsoo Lee1, Heegoo Kim2, Jinuk Kim2, Won Hyuk Chang1, Yun-hee Kim1
1 Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart VascularStroke Inst, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea2 Department of Health Sciences and Technology, Department of Medical Device Management & Research,Department of Digital H, SAIHST, Sungkyunkwan University, Seoul, Korea
Purpose:Understanding recovery mechanism and predicting recovery pattern after stroke are important to makeindividually tailored rehabilitation plans. Various prognostic biomarkers for upper extremity (UE) motor recoveryafter stroke have been reported. However, most of them had relatively low predictive power in severe strokepatients. This study suggests imaging biomarker-based prediction models for UE motor recovery, including severestroke patients.Methods:Forty-two first-ever ischemic stroke patients with severe motor impairment, who had multimodal imaging dataat two weeks and clinical assessments at two weeks and three months after onset, were included. Patients weredivided by their recovery pattern based on the proportional recovery rule; Fitter or Non-fitter (i.e., their recoveryfit or did not fit the proportional recovery rule). The proportional recovery rule means most patients recoverapproximately 70% of their initial UE impairment within three to six months. Important neuroimaging biomarkersin motor recovery were investigated. Fractional anisotropy (FA) values of the corticospinal tract (CST), corpuscallosum (CC), superior cerebellar peduncle (SCP), lesion volume, lesion load of the CST, interhemispherichomotopic connectivity, and whole brain connectivity were extracted from multimodal imaging data.Results:Patients with severe motor impairment showed diverse recovery patterns. Multimodal imaging biomarkers wereinvestigated to improve the predictive accuracy for UE motor recovery in patients. Different imaging biomarkersexisted depending on the recovery pattern. The SCP FA was only a significant biomarker in the Fitter. In contrast,the splenium of CC FA was only a significant biomarker in the Non-fitter. Also, the left Heschl’s gyrus (HES) andright superior occipital gyrus (SOG) functional connectivity (HES-SOG FC) was the strongest biomarker amongthe examined functional connections in the Non-fitter. These biomarkers were reevaluated in patients withdifferent motor-evoked potential (MEP) responses. Finally, the prediction models were established using astratification strategy according to initial severity and MEP response. The proposed prediction modeldemonstrated high predictive accuracy (R2=0.853, RMSE=5.28).Conclusions:Most of all, the imaging biomarker-based prediction model proposed in this study could improve the predictiveaccuracy of UE motor recovery in patients with severe motor impairment. This model may also provide suggeststhe optimal use of imaging biomarkers for predicting UE motor recovery after stroke.
118

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-64Prognosis/Outcome of Stroke
Total Small Vessel Disease Burden and Functional Outcome in Patients with Ischemic Stroke
Wi-sun Ryu1, Sang-wuk Jeong1, Dong-eog Kim1
1 Neurology, Dongguk University Ilsan Hospital; Korean Brain MRI Data Center, Goyang, Korea
Purpose:Cerebral small vessel disease (SVD) is comprised of lacune, cerebral microbleeds (CMBs), white matterhyperintensities (WMHs), and enlarge perivascular space (EPVS). We examined the cumulative effect of SVD on3-month functional outcome after ischemic stroke using the total SVD score.Methods:We included 477 acute ischemic stroke patients who had adequate brain MRI to assess the total SVD score. Weused multivariable ordinal logistic regression analysis to investigate an independent impact of total SVD score onordinal modified Rankin Scale score at 3-month after ischemic stroke.Results:Mean age was 66±14 years, and 61% were men. The distribution of the total SVD score from 0 to 4 was 27%,24%, 26%, 16%, and 7%, respectively. As an increase in the total SVD score, the proportion of higher mRS scoreincreased (Figure 1, P < 0.001). In multivariable ordinal logistic regression analysis, compared with the total SVDscore of 0, total SVD scores of 2, 3, and 4 were independently associated with higher mRS scores with adjustedodds ratios (95% confidence intervals) of 1.68 (1.02-2.76), 2.24 (1.25-4.00), and 2.00 (1.02-4.29). Lacune, CMBs,WMHs but not EPVS were associated with unfavorable outcomes. However, the impact of each SVD subtype onstroke outcome was smaller than that of the total SVD score.
Conclusions:We found an independent association between total SVD score and functional outcome at 3-month afterischemic stroke. The total SVD score may be helpful for the stratification of patients who are at a high-risk ofunfavorable outcome.
119

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-65Case Report
A Growing Pseudoaneurysm of Middle Cerebral Artery That Caused RecurrentAcute Infarctions
Kayeong Im1, Hakjae Roh1, Sung-tae Park2, Beom-jun Kim3, Kyung Bok Lee1
1 Neurology, Soonchunhyang University Seoul Hospital, Seoul, Korea2 Radiology, Soonchunhyang University Seoul Hospital, Seoul, Korea3 Neurology and Cerebrovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea
Purpose:Intracranial pseudoaneurysm is rarely reported and usually caused by traumatic or infectious etiology, howeverintracranial pseudoaneurysm followed by no discernible history of major head injury is not reported. We describea growing spontaneous pseudoaneurysm on the proximal middle cerebral artery (MCA) which caused recurrentepisodes of ischemic strokes.Methods:A 28-year-old man had experienced recurrent acute infarctions 3 times over the last 5 months even though takingantithrombotics. He had no previous history of trauma, infection or vascular risk factors. In comparison to thefirst visit, gradient echo and CT of the last visit presented an enlarged perivascular hematoma. Vessel wall MRIand digital subtraction angiography revealed a blister-like pseudoaneurysm on the middle cerebral artery.Results:The formation of spontaneous pseudoaeurysm on proximal MCA can obliterate the blood flow throughlenticulostriate artery, and induce recurrent ischemic strokes.Conclusions:To prevent further infarction and intracranial bleeding, surgical isolation of pseudoaneurysm for cerebralcirculation by trapping excision can be a valid treatment option.
120

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-66Case Report
Cerebral Infarction Associated with Multiple Aortic Thrombi in Hypercoagulable Condition
Ho Geol Woo1
1 Neurology, Kyung Hee University College of Medicine, Seoul, Korea
Purpose:Introduction Embolic stroke due to aortic thrombus without atherosclerosis is uncommon. Here, we report acase of a patient with cerebral embolic infarction associated with multiple aortic thrombi without atherosclerosisaccompanying IDA, protein S deficiency, and huge uterine fibroids.Methods:Case report A 51-year-old woman visited emergency department with acute onset vertigo. Her neurologicexamination revealed limb ataxia at right side. Sensory for pain and temperature was declined in the right face(3/10). Initial National Institutes of Health Stroke Scale (NIHSS) score was 4. Diffusion-weighted magneticresonance image of brain showed an acute ischemic lesion at the left ventral lateral thalamus and left occipital
cortex. Head and neck CT angiography showed large protruding thrombus in ascending aorta (1.1 ⅹ 1.5 ⅹ
2.2 cm3). No steno-occlusive lesion in the basilar artery and both posterior cerebral arteries and vertebralarteries. Multiple small additional protruding thrombi in descending thoracic aorta and suprarenal abdominalaorta observed from CT angiography of aorta. Laboratory examinations revealed IDA (hemoglobin: 7.7 g/dL,mean corpuscular volume: 67.6 fL, ferritin: 11.1 ng/mL, and serum iron: <15 μg/dL). The activities of protein S was decreased (48 %). There was a negative work up for other hypercoagulable condition. On ultrasoundexamination, there was no evidence of deep vein thrombosis in the lower extremities or thrombus of intracardiac
chambers except huge uterine fibroids (8.5 ⅹ 7.5 ⅹ 4.2 cm3).
Results:.Conclusions:Discussion Previous study for 27,855 patients with recent arterial embolic events reported that only 23 cases(0.08%) was found in patient accompanying aortic thrombus without atherosclerosis. Also, previously, there areother report of young female patient with severe IDA and cerebral embolic infarction caused by aortic thrombus.However, the patient had no protein S deficiency, uterine fibroids, and multiple aortic thrombi. To date,thrombosis in arteries with uterine fibroids and IDA was rarely reported. In the current report, we thought thatprofound IDA, uterine fibroids, and protein S deficiency may have promoted a hypercoagulable state and causemultiple aortic thrombi that lead to cerebral embolic infarction.
121

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-67Case Report
A 32-year-old Female with Bilateral Septic Cavernous Sinus Thrombosis Complicatedby Septic Embolic Stroke and Narrowing of the Internal Carotid Artery
Kevin Paul Enriquez1, Muktader Kalbi1, Salip Nastra Jumaani1
1 Internal Medicine, Zamboanga City Medical Center, Zamboanga City, Philippines
Purpose:Cavernous sinus thrombosis (CST) is a rare, life threatening condition. Expert opinion guides therapy since norandomized controlled trials are available. Antibiotics have long been the mainstay of treatment whileanticoagulation remains controversial. Antibiotics while suggested by guidelines to be given for 4-6 weeks is stillan open subject of interest and research. Recent retrospective reviews revealed anticoagulation to have potentialmortality reduction.Methods:We report a case of a 32-year-old female with CST who presented with complete bilateral ophthalmoplegia andbilateral orbital cellulitis.Results:Magnetic resonance venography results were diagnostic of CST. Specimen from eye and blood isolated MRSA.Nuchal rigidity along with CSF abnormalities suggest meningitis which may be present in one third of patients.Septicemia resolved early but on the 5th hospital day, patient had aphasia and right-sided hemiplegia. Furtherworkup revealed multiple intracranial infarcts and flow void in the intracavernous segment of the left internalcarotid artery. The mechanism likely involves inflammation, septic embolism, and arteritis of the arterial wallleading to thrombosis and stenosis. Low Molecular Weight Heparin (Enoxaparin) was started, shifted to warfarinupon discharge. The duration of anticoagulation and vancomycin were 8 and 3 weeks, respectively. Althoughwith residual deficit, patient was reassessed after 2 months to have improved motor strength and return ofspeech.Conclusions:While no prospective trials are unavailable, timely diagnostic evaluation and identification of the condition iscrucial. An adequate knowledge of the disease process with good clinical judgement is vital in the managementto avoid fatal complications.
122

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-68Risk Factors and Prevention of Stroke
Real-world Oral anticoagulants for Asian patients with Non-valvular Atrial Fibrillation: A Systematic Review and Network Meta-analysis
Seung Min Kim1, Eun-tae Jeon2, Seong Hwan Kim2, Ji-sung Lee3, Jin-man Jung2
1 Neurology, Veterans Health Service Medical Center, Seoul, Korea2 Neurology, Korea University Ansan Hospital, Ansan, Korea3 Clinical Research Center, Asan Medical Center, Seoul, Korea
Purpose:The burden of AF and subsequent stroke in Asian may actually exceed that in Western because elderly personsin most Asian countries are rapidly increasing and their annual risk of stroke was higher than Westerns. Our studyaimed at evaluating the comparative efficacy and safety of 4 non-vitamin K antagonist oral anticoagulants(NOACs) and warfarin among Asians with non-valvular AF (NVAF) in a real world setting.Methods:We searched multiple comprehensive databases (PubMed, EMbase, and Cochrane library) for eligible studiesuntil April 2020. Studies were included if they were observational studies using multivariable analysis with orwithout propensity score matching. Pooled estimate was hazard ratio and 95% confidence interval. Efficacyoutcomes included ischemic stroke and stroke/systemic embolism and safety outcomes included major bleeding,gastrointestinal (GI) bleeding and intracerebral hemorrhage (ICH). P-score was calculated as ranking probabilities.A “total dose” includes total population regardless of dosage of 4 NOACs. Subgroup analyses were performed inaccordance with the dosage range of NOACs ("standard and low dose").Results:A total of 11 studies were included in total population and six studies were allocated to standard dose group,and eight studies to low dose group. In total study population, edoxaban ranked the best option in terms ofischemic stroke and ICH, apixaban in terms of stroke/systemic embolism, major and GI bleeding. In patients withstandard dose, apixaban ranked the best in ischemic stroke and stroke/systemic embolism. For the major and GIbleeding and ICH, edoxaban ranked the best. In patients with low dose NOACs, edoxaban ranked the best inprevention of ischemic stroke, stroke/systemic embolism, GI bleeding and ICH. For the prevention of majorbleeding, apixaban ranked the best.Conclusions:Our study demonstrates that all 4 NOACs had better effectiveness and safety profiles compared to warfarin intotal study population, however they could confer different effects on efficacy and safety outcomes according totype and dosage of them. Edoxaban and apixaban was considered as better option than other NOACs or warfarinfor Asian patients with NVAF.
123

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-69Risk Factors and Prevention of Stroke
The Positive Correlation of Ischemic Stroke Recurrence and Burden of Lacunar Infarctsin Patients under Anticoagulation for Non-valvular Atrial Fibrillation after Acute Ischemic Stroke
Kipyoung Jeon1, Jaseong Koo2, Kwang-soo Lee2, Keun- Hwa Jung1, Sang- Bae Ko1, Seung- Hoon Lee1, Yong- SeokLee3, Byung- Woo Yoon1
1 Neurology, Seoul National University Hospital, Seoul, Korea2 Neurology, Seoul St. Mary's Hospital, Seoul, Korea3 Neurology, SMG-SNU Boramae Medical Center, Seoul, Korea
Purpose:We sometimes observe that some patients experience recurrent ischemic stroke as lacunar infarction underanticoagulation for non-valvular atrial fibrillation (NVAF) after acute ischemic stroke (AIS). We hypothesize thatischemic stroke recurrence positively correlates with burden of lacunar infarcts in patients under anticoagulationfor NVAF after AIS.Methods:We conducted a retrospective observational study of one hundred fifty ischemic stroke patients with NVAF whovisited Seoul St. Mary’s Hospital from March 2014 to May 2018. We compared patients with recurrent ischemicstroke under anticoagulation for NVAF after AIS and those without it by analyzing their stroke risk factors,atherosclerosis burden in CT or MR angiographic images and cerebral small vessel disease (SVD) burden in brainMRI. We counted the number of lacunar infarcts in brain MRI and graded the burden of lacunar infarcts as follows:0(no lacunar infarct), 1(one or two lacunar infarcts), 2(three to five lacunar infarcts), 3(more than five lacunarinfarcts)Results:From one hundred and fifty patients from the registry composed of ischemic stroke patients with NVAF in SeoulSt. Mary’s Hospital. Thirty patients showed the recurrence of ischemic stroke under anticoagulation for NVAFafter AIS. One hundred and three patients showed no recurrence of ischemic stroke. Remaining seventeenpatients were excluded from analysis because some of their clinical and radiological information were missing.The burden of lacunar infarcts positively correlated with ischemic stroke recurrence in patients underanticoagulation for NVAF after AIS. Interestingly, we found out that the burden of lacunar infarcts showed astrong positive correlation with intracranial atherosclerosis (ICAS) burden in this study.Conclusions:The positive correlation between the burden of lacunar infarcts and ischemic stroke recurrence in patients underanticoagulation for NVAF after AIS implicates that these two different stroke etiologies should be treated withdifferent strategies for secondary prevention. On the contrary, the strong positive correlation between theburden of lacunar infarcts and ICAS burden suggests that lacunar infarcts and ICAS could be prevented with thesame strategy.
124

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-70Risk Factors and Prevention of Stroke
Aortic Atheroma and Ankle-brachial Index Predict Cardiovascular Outcomein Acute Ischemic Stroke Patients
Jaewook Jeong1, Minyoul Baik1, Young Dae Kim1, Ji Hoe Heo1, Hyo Suk Nam1
1 Neurology, Yonsei University College of Medicine, Seoul, Korea
Purpose:Aortic atheroma (AA) is associated with the occurrence and recurrence of acute cerebral infarction. Ankle-brachial index (ABI), a noninvasive marker of peripheral artery atherosclerosis, is a predictor of ischemic strokeand is associated with increased cardiovascular risk. In this study, we aim to investigate whether considering bothAA and ABI is better in predicting the occurrence of major adverse cardiac events (MACE) in stroke patientsduring long-term follow-up.Methods:We reviewed acute ischemic stroke patients admitted to a tertiary hospital from January 2012 to December 2018who had undergone both transesophageal echocardiography (TEE) and ABI measurements. After discharge, thepatients were regularly interviewed at the clinic or through the telephone for the occurrence of MACE, whichwas defined as ischemic stroke recurrence, the occurrence of hemorrhagic stroke, acute coronary syndrome,hospitalization due to heart failure, and all-cause mortality. Kaplan-Meier survival analysis and Cox regressionanalysis was performed to reveal independent factors associated with MACE.Results:Among the 2452 patients enrolled in the study, 750 patients had AA (-) and ABI≥0.9; 24 had AA (-) and ABI<0.9; 1515 had AA (+) and ABI≥0.9; 163 had AA (+) and ABI<0.9. Univariate Cox regression analysis showed that the occurrence of MACE was associated with AA (HR, 1.47; 95% confidence interval [CI], 1.18-1.82; p=0.001) andABI< 0.9 (HR, 2.21; 95% CI, 1.68-2.93; p<0.001), respectively. However, after adjusting for age, sex, history ofcongestive heart failure, diabetes mellitus, previous stroke, and the National Institutes of Health Stroke Scale(NIHSS) score at admission, AA was no longer a significant predictor of MACE (HR, 1.06; 95% CI, 0.85-1.34;p=0.598) while ABI was still one of the significant predictors (HR, 1.62; 95% CI, 1.21-2.16; p=0.001). Whencompared to AA (-) and ABI≥0.9, AA (-) and ABI <0.9 (HR, 1.17; 95% CI, 0.48-2.89; p=0.728) or AA (+) and ABI≥0.9 (HR, 1.02; 95% CI, 0.80-1.29; p=0.878) did not show significant difference. In contrast, the patients with both AA(+) and ABI <0.9 showed significant association with MACE occurrence (HR, 1.71; 95% CI, 1.20-2.45; p=0.003).Conclusions:We found that AA and ABI are associated with long-term outcomes in acute ischemic stroke patients. Especially,the patients who have both AA and peripheral artery disease showed a significant association with the long-termoccurrence of MACE. Our findings suggest that ABI measurements may help in predicting cardiac risks in strokepatients with aortic atherosclerosis.
125

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-71Risk Factors and Prevention of Stroke
Impact of Statin Pretreatment according to Statin Dose on The Periprocedural Complications of CarotidStenting in Asymptomatic Patients
Seong Hwa Jang1, Doo Hyuk Kwon2, Moon-ku Han3, Hyungjong Park4, Sung-il Sohn4, Jeong-ho Hong4
1 Radiology, Samsung medical center, Seoul, Korea2 Neurology, Daegu Dongsan Hospital, Daegu, Korea3 Neurology, Seoul National University Bundang Hospital, Seongnam, Korea4 Neurology, Keimyung University Dongsan Hospital, Daegu, Korea
Purpose:We aimed to investigate whether different doses of statin pretreatment can reduce periprocedural complicationsof carotid artery stenting in patients with asymptomatic carotid artery stenosis.Methods:Between July 2003 and June 2013, 276 consecutive patients were performed carotid artery stenting (CAS) forasymptomatic carotid stenosis. Periprocedural complications included the outcome of stroke, myocardialinfarction, or death within 30 days after CAS. Statin pretreatment was categorized into no-statin (n=87, 31.5%),standard-dose (<40 mg, n=139, 50.4%), and high-dose statin (≥40 mg, n=50, 18.1%) according to the atorvastatin equivalent dose. Cochran-Armitage (CA) trend test was performed for periprocedural complications toinvestigate the association with statin dose.Results:The overall periprocedural complication rate was 3.3%. There was no significant difference in the risk ofperiprocedural complications between the 3 groups (no statin: n=3 (3.4%); standard-dose: n=4 (2.9%); high-dosen=2 (4.0%) p = 0.923). CA trend test did not demonstrate a trend in the proportion of periproceduralcomplications across increasing statin equivalent dose (p = 0.919).Conclusions:Statin pretreatment before CAS showed neither absolute nor dose-dependent effects against periproceduralcomplications in asymptomatic patients with CAS
126

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-72Risk Factors and Prevention of Stroke
Inter-arm Blood Pressure Difference is Associated with Recurrent Strokein Non-cardioembolic Stroke Patients
Tae-jin Song1
1 Neurology, Seoul Hospital, Ewha University College of Medicine, Seoul, Korea
Purpose:Recurrent stroke increases mortality and aggravates the disability of stroke patients. We hypothesized thatincreased inter-arm systolic blood pressure difference and inter-arm diastolic blood pressure difference wouldbe related to recurrent stroke in non-cardioembolic stroke patients.Methods:Recurrent stroke increases mortality and aggravates the disability of stroke patients. We hypothesized thatincreased inter-arm systolic blood pressure difference and inter-arm diastolic blood pressure difference wouldbe related to recurrent stroke in non-cardioembolic stroke patients.Results:Inter-arm systolic and diastolic blood pressure differences ≥10 mmHg were noted in 9.7% (120/1226) and 5.0% (62/1226) of patients, respectively. During a median 24 months of follow-up, 105 (8.5%) patients experiencedrecurrent stroke. Patients who had inter-arm systolic blood pressure difference ≥10 mmHg showed increased risk of recurrent stroke (hazard ratio:1.77, 95% confidence interval: 1.04-3.00, p = 0.033). Moreover, inter-armdiastolic blood pressure difference ≥10 mmHg was also independently associated with increased risk of recurrent stroke (hazard ratio:2.92, 95% confidence interval: 1.59-5.34, p = 0.001).Conclusions:In conclusion, inter-arm blood pressure difference ≥10 mmHg may be associated with increased risk recurrent stroke in non-cardioembolic stroke patients.
127

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-73Risk Factors and Prevention of Stroke
Embolic Pattern Silent Brain Infarction Elevates The Risk of Stroke Recurrence in Patientsof Acute Ischemic Stroke with Atrial Fibrillation
Do Yeon Kim1, Han-gil Jeong1, Keon-joo Lee1, Beom Joon Kim1, Moon-ku Han1, Kang-ho Choi2, Joon-tae Kim2,Dong-ick Shin3, Jae-kwan Cha4, Dae-hyun Kim4, Dong-eog Kim5, Wi-sun Ryu5, Jong-moo Park6, Kyusik Kang6, JaeGuk Kim7, Soo Joo Lee7, Mi-sun Oh8, Kyung-ho Yu8, Byung-chul Lee8, Hong-kyun Park9, Keun-sik Hong9, Yong-jinCho9, Jay Chol Choi10, Sung Il Sohn11, Jeong-ho Hong11, Moo-seok Park12, Tai Hwan Park12, Sang-soon Park12, KyungBok Lee13, Jee-hyun Kwon14, Wook-joo Kim14, Jun Lee15, Ji Sung Lee16, Juneyoung Lee17, Hee-joon Bae1
1 Neurology and Cerebrovascular Center, Seoul National University Bundang Hospital, Seoul National UniversityCollege of Medicine, Seongnam, Korea2 Neurology, Chonnam National University Hospital, Gwangju, Korea3 Neurology, Chungbuk National University Hospital, Cheongju, Korea4 Neurology, Dong-A University Hospital, Dong-A University College of Medicine, Busan, Korea5 Neurology, Dongguk University Ilsan Hospital, Goyang, Korea6 Neurology, Eulji General Hospital, Seoul, Korea7 Neurology, Eulji University Hospital, Eulji University, Daejeon, Korea8 Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea9 Neurology, Ilsan Paik Hospital, Inje University, Goyang, Korea10 Neurology, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea11 Neurology, Keimyung University Dongsan Medical Center, Daegu, Korea12 Neurology, Seoul Medical Center, Seoul, Korea13 Neurology, Soonchunhyang University Hospital, College of Medicine, Seoul, Korea14 Neurology, Ulsan University Hospital, Ulsan University College of Medicine, Ulsan, Korea15 Neurology, Yeungnam University Hospital, Daegu, Korea16 Clinical Research Center, Asan Medical Center, Seoul, Korea17 Biostatistics, Korea University College of Medicine, Seoul, Korea
Purpose:The significance of silent brain infarction (SBI) for stroke recurrence in acute ischemic stroke (AIS) patients withatrial fibrillation (AF) has yet to be elucidated. This study aims to evaluate SBI as an independent predictor forstroke recurrence and which subtypes of SBI are associated with stroke recurrence in AIS patients with AF.Methods:A multicenter prospective cohort recruited AIS patients with non-valvular AF from 14 stroke centers and werefollowed for 1 year for ischemic stroke recurrence, all types of stroke and TIA, and all-cause mortality. Comparisonof cumulative incidences and adjusted hazards in three patient groups: stroke patients with prior stroke history(PS), first-ever stroke with SBI [F-SBI(+)] and first-ever stroke without SBI [F-SBI(-)] were made with log-rank testand frailty model according to predetermined covariates including demographics, vascular risk factors, CHA2DS2-VASc score, and discharge antithrombotics. SBI subtypes including embolic-appearing pattern (EAP) and non-EAP,and SBI characteristics including size, numbers, and vascular territory involvements were also assessed.Results:Among 978 AF-AIS patients, PS group was 269 (27.5%), F-SBI(+) was 285 (29.1%), and F-SBI(-) was 424 (43.4%).The proportion of EAP SBI (N=230, 80.7%) were higher than non-EAP SBI (N=55, 19.3%). Cumulative incidence ofischemic stroke recurrence in F-SBI(+) [6.41 (95% confidence interval (CI) 3.44-9.38)] was higher than F-SBI(-)[1.69 (0.45-2.92)], however, there was no significant difference compared to PS [6.83 (3.57-10.08), p=0.860].Adjusted hazards for ischemic stroke recurrence and all kinds of stroke and TIA in F-SBI(+) were shown to beelevated [Hazard ratio 3.87 (95% CI 1.53-9.16) and 2.60 (1.21-5.56)], and similar to PS [4.20 (1.73-10.24) and 2.90(1.36-6.18)] when compared to F-SBI(-), respectively. While non-EAP SBI [2.38 (0.49-11.62), p=0.280] were lackof association, a 4-fold increase of hazards in EAP SBI was observed [4.07 (95% CI 1.63-10.13)]. Other SBIcharacteristics including size, numbers and vascular territory involvements were not found to be associated withstroke recurrence. SBI and SBI features were not related to all-cause mortality.Conclusions:
128

Cerebrovasc Dis 2020;49(suppl 1):1-149
SBI and, specifically, EAP SBI elevated stroke recurrence in AF-AIS patients as much prior stroke increases the risk.Necessity of considering SBI to predict recurrence was suggested likewise prior stroke is scored in AFthromboembolic risk estimation tools.
129

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-74Risk Factors and Prevention of Stroke
Antiphospholipid Syndrome and Recurrent Ischemic Stroke: A Systematic Reviewand Meta-Analysis
Yerim Kim1, Soo Young Kim2
1 Neurology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea2 Family Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Purpose:Antiphospholipid syndrome (APS) is a multiorgan autoimmune disease, characterized by arterial and/or venousthrombi, recurrent miscarriages, and circulating antiphospholipid antibodies (aPLs). Although aPLs are known tobe associated with thrombotic event, especially in young patients, the role of aPLs on recurrent ischemic strokes(ISs) is unclear. Given that appropriate treatment based on stroke etiology might affect a patient’s outcome, it isessential to determine whether aPLs are the cause of recurrent ISs. Therefore, the aim of this study is to evaluatethe association between aPLs and recurrent ISs.Methods:We performed a systematic review and meta-analysis to analyze publications concerning aPLs and ischemicstrokes. The research was conducted by a computer-assisted search of literature in PubMed, EMBASE, andCochrane library published in English or Korean from 1990. All of the abstracts that fit the category were selectedby two researchers (SY Kim and Y Kim) and any discrepancies were resolved through consensus. Meta-analyseswere conducted using the fixed-effect model to estimate the relative risk for recurrent stroke with 95%confidence interval. Review Manager 5.3 software was used for statistical analyses.Results:Of the 2,272 identified articles, 8 studies were included (2,510 subjects; 844 aPLs positive). Meta-analysisdemonstrated that the relative risk of aPLs for recurrent IS was 1.41 (95% CI, 0.91-2.17; I2=54%). In the subgroupanalysis, ages under 50 years, ethnicity, and types of aPLs did not increase the risk of recurrent IS.Conclusions:We found that aPLs are not an independent predictor for recurrent IS in adults. However, most of the studies areretrospective and had a small sample size. Further well-designed prospective trials with a large population shouldbe considered to confirm these findings.
130

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-75Risk Factors and Prevention of Stroke
Clinical Study on Three Patients with Infarction of The Vermis/tonsil in The Cerebellum
Katsuhiko Ogawa1, Takayoshi Akimoto1, Akihiko Morita1, Makoto Hara1, Yutaka Suzuki2, Hirokazu Yoshihashi3,Hideto Nakajima1
1 Neurology, Department of Medicine, Nihon University School of Medicine, Tokyo, Japan2 General Medicine, Department of Medicine, Nihon University School of Medicine, Tokyo, Japan3 Neurology, Kobari General Hospital, Chiba, Japan
Purpose:Infarction of the vermis and the tonsil in the cerebellum presents as truncal and gait ataxia. Acute rotatory vertigois often present in infarction of the nodulus in the caudal vermis, which is closely associated with the vestibularpathway, but is minor in infarction of the rostral vermis. The rostral vermis receives input from the dorsalspinocerebellar tract (DSCT) which conveys unconsciousness proprioceptive signals from the ipsilateral lowertrunk and leg. The present study investigated the neurological characteristics for infarction of the vermis and thetonsil in the cerebellum, based on neuroradiological findings in patients whose lesions were located in theseareas.Methods:We analyzed neurological and MRI findings of two patients with infarction of the vermis and one patient withinfarction of the tonsil in the cerebellum (age, 22-86 years; male, n = 1).Results:Infarcts were located in the anterior lobe in the rostral vermis, the nodulus in the caudal vermis, and the tonsil.Truncal and gait ataxia were exhibited by 3 patients. Lateropulsion to the opposite side of the lesion was apparentin a patient with infarction of the tonsil. Three patients exhibited acute vertigo at onset. Rotatory vertigo wasexhibited by 2 patients whose lesions were located in the nodulus and the tonsil. Dizziness was noted in a patientwith infarction of the anterior lobe in the rostral vermis. Gaze-evoked nystagmus when looking to the side of thelesions was observed in 2 patients with infarction of the nodulus and the tonsil. Neck pain on the ipsilateral sideof the lesion as well as nausea/vomiting were presented by a patient whose lesion was located in the nodulus.No patients had ataxia of the extremities or ataxic speech.Conclusions:The present study indicated the difference in impaired fibers between the rostral and caudal vermis, andsuggested a close relationship of the vestibular pathway with the nodulus. Infarction of the tonsil causedlateropulsion to the opposite side of the lesion and rotatory vertigo, which suggested that the tonsil exerted aninhibitory effect on the vestibular nucleus on the ipsilateral side, similar with the nodulus. Absence of rotatoryvertigo in infarction of the rostral vermis indicated impairment of the DSCT.
131

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-76Risk Factors and Prevention of Stroke
Abdominal Obesity and Recurrent Vascular Risk After an Ischemic Stroke
Kyusik Kang1, Tai Hwan Park2, Kyung Bok Lee3, Dong-eog Kim4, Keun-sik Hong5, Juneyoung Lee6, Hee-joon Bae7,Jong-moo Park1
1 Neurology, Nowon Eulji Medical Center, Seoul, Korea2 Neurology, Seoul Medical Center, Seoul, Korea3 Neurology, Soonchunhyang University Hospital, Seoul, Korea4 Neurology, Dongguk University Ilsan Hospital, Goyang,, Korea5 Neurology, Ilsan Paik Hospital, Goyang, Korea6 Biostatistics, Korea University College of Medicine, Seoul, Korea7 Neurology, Seoul National University Bundang Hospital, Seongnam-si, Korea
Purpose:Most of the epidemiological studies showing that obesity is a risk factor for stroke incidence and mortality weredone in the general population without illness. The waist circumference is superior to body mass index (BMI) forprediction of primary ischemic stroke incidence. However, previous studies have found that patients with highBMI who survive the first cerebrovascular event tend to have improved subsequent cerebrovascular diseaseburden and mortality. The objective of this study was to evaluate whether abdominal obesity is associated withrecurrent vascular risk after stroke.Methods:This study was a retrospective analysis of a nationwide prospective, multicenter, stroke registry (Clinical ResearchCollaboration for Stroke in Korea) database, which is a web-based database of consecutive patients with acuteischemic stroke or transient ischemic attack admitted to 17 hospitals in South Korea. We restricted our analysisto 16206 stroke patients who were free of a prior history of stroke and admitted to 6 hospitals within 7 days ofonset from January 2011 to November 2019. Patients had their waist circumference measured on admissionand the waist circumference was divided into sex-specific quintiles. Follow-up was conducted at 3 and 12months. Primary outcome was time to stroke, myocardial infarction, or vascular death and secondary outcometime to first recurrent stroke. The independent association of obesity with outcome was assessed by controllingfor other known risk factors.Results:Of 16206 patients enrolled in the registry, waist circumference or BMI measurements were unavailable in 1425patients, leaving 14781 (91.2%) patients for this analysis. Patients in the second quintile of waist circumferencehad a lower risk of a major vascular event compared with patients in the lowest quintile (adjusted hazard ratio(HR) =0.72, 95 % confidence interval (CI) 0.60-0.86). Compared with patients in the lowest quintile of waistcircumference, patients in the highest quintile had an adjusted HR of 0.77 (95% CI 0.63-0.92). Patients in thesecond quintile of the waist circumference had a lower risk of stroke compared with men in the lowest quintile(adjusted HR =0.73, 95% CI 0.59-0.91); comparing extreme quintiles, the adjusted HR was 0.87 (95% CI 0.70-1.08).Conclusions:Presence of abdominal obesity was a predictor of neither recurrent stroke risk nor overall vascular risk over aone-year follow-up period. Obese patients with stroke had lower risk for a major vascular event than did leanpatients.
132

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-77Case Report
A Case of Rhombencephalitis Mimicking Ischemic Stroke
Joonyoung Ha1, Ji-yong Lee1
1 Neurology, Yonsei University Wonju College of Medicine, Wonju, Gangwon-do, Korea
Purpose:Rhombencephalitis refers to inflammatory diseases affecting the hindbrain (brainstem and cerebellum).Rhombencephalitis has a wide variety of etiologies, including infections, autoimmune diseases, andparaneoplastic syndromes. Clinical courses can vary depending on the cause. Differential diagnosis betweenrhombencephalitis and stroke can be challenging, especially in the case of sudden onset neurologic deficits, andno sign of meningism or fever.Methods:Case ReprotResults:A 70-year-old man was admitted because of a one-day history of dysarthria. Brian MRI showed bilateral pontinelesions in DWI with Gd enhancement, which were read by a radiologist as cerebral infarction. He was treatedwith clopidogrel. However his symptom was not improved. A repeat MRI scan after 3 month revealedconsiderable further developed high signal intensity in the bilateral pons extending into the right midbrain in thediffusion and FLAIR - weighted image with strong gadolinium enhancement. Cerebrospinal fluid (CSF) proteinwas 50.6 mg/dL, with 251 cells/uL. He was treated with steroid pulse therapy followed by oral prednisolone.After 3 months of steroid treatment, brain MRI demonstrated lobulated T2/FLAIR high and T1 low signal intensitywithout contrast enhancement at right anterior aspect of pons.Conclusions:We report a case of rhombencephalitis mimicking ischemic stroke. Rhombencephalitis should be included in thedifferential diagnosis in patients with an acute onset brainstem dysfunction showing contrast enhancement inthe brain MRI.
133

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-78Case Report
Case Report: Good Outcome in a Pontine Hemorrhage Patient with a Classic Presentationof Fovile Millard-Gubler Syndrome
Baarid Luqman Hamidi1, Befrie Mahaztra Sudarman2
1 Neurology, Universitas Sebelas Maret, Surakarta, Central Java, Indonesia2 Neurology-Resident, Universitas Sebelas Maret, Surakarta, Central Java, Indonesia
Purpose:Primary Pons hemorrhage occurs in about 5-10% of all intracranial hemorrhages, and the mortality rate reaches40-50%. In this case report, Shows good clinical outcomes after adequate treatment of non-operative care inpatients with pons hemorrhage.Methods:Case Report.Results:A woman, 49 years old, with a history of previous hypertension had a sudden decrease in consciousness. Onarrival at the Emergency Unit, we found a Glasgow coma scale E2M3V2 accompanied by high blood pressure.CT-Scan results showed there is bleeding on the left side of the Pons area. Patients undergoing treatment at theNeurointensive Care Unit and get observation strictly related to vital signs and neurological deficits. Patientsreceive “Total care” while in the intensive room including diet control, bed rest management and physiotherapy,personal hygiene care, and infection controls. After the improvement of consciousness on day 6 of treatment,there are additional clinical findings. Patients had ipsilateral facial nerve palsy accompanied by hemiparesis andHemiparaesthesia contralateral of the lesion. On day 15 of treatment, patients exit from the hospital with amodified Rankin Scale (mRS) value is 4.Conclusions:This patient gets good care with intensive periodic monitoring so that she have a good clinical outcome. Theprimary goal of the management of pontine hemorrhage is the prevention of secondary brain injury whileawaiting the resolution of the hematoma. The strict control of blood pressure and fluid balance is necessary toensure adequate Cerebral Blood Flow while controlling intracranial pressure.
134

Cerebrovasc Dis 2020;49(suppl 1):1-149
135

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-79Case Report
A Case Series of Stroke in Young Adults: Public Health Concerns
Valentina Tjandra Dewi1, I Gusti Ngurah Budiarsa2, Ida Bagus Kusuma Putra2, Anak Agung Ayu Putri Laksmidewi2
1 Neurology Resident, Department of Neurology , Udayana University, Sanglah General Hospital, Denpasar, Bali,Indonesia2 Neurologist, Department of Neurology, Udayana University, Sanglah General Hospital, Denpasar, Bali, Indonesia
Purpose:Epidemiological studies suggest that there is a substantial increase in the incidence of ischemic stroke in youngadults. Dealing with stroke in young adults is challenging, not only on its socioeconomic and productivity impactbut also in terms of etiology. There are various, often rare, causes of strokes in younger population which requirespecific diagnostic approach and treatment. The purpose of this report is to emphasize the diversity ofuncommon stroke etiologies in young adults, its prognosis, and how to deal with strokes of undeterminedetiology.Methods:We report 4 selected cases of stroke in young adults aged under 40 years old with the youngest case of an 18-year old female patient.Results:The first case was an 18-year old female with 12 hours onset of left-sided weakness, categorized as moderateischemic stroke. History taking and examination indicated nephrotic syndrome and breast malignancy suspicionas the potential underlying etiologies in this patient. The second patient was a 34-year old obstetric patient withsudden confusion. Examination revealed sensory aphasia, cranial nerve palsy along with several otherneurobehavioral disorders. She was in the puerperium stage, 4 days after labour with severe preeclampsia andclass II obesity. Brain CT revealed left temporal lobe infarction under the left middle cerebral artery (MCA)territory. The third case was a 33-year old female who underwent intravenous recombinant Tissue PlasminogenActivator (rTPA) diagnosed with non-hemorrhagic stroke coming within 30 minutes of onset. Obesity anddyslipidemia were found to be apparent risk factors. The patients' weakness improved significantly overhospitalization. The last case was a 34-year old male with minor ischemic stroke although traditional risk factorswere absent. He was diagnosed with hebephrenic schizophrenia and took conventional antipsychotics regularlyfor 5 years. Several cohort and case-control studies have been conducted in the elderly, suggesting exposure toantipsychotics may become a proximal trigger for stroke. However, to the best of our knowledge, designatedstudy in the younger population on this relationship is lacking.Conclusions:Stroke in young adults possesses a wide variety of different and uncommon etiologies. Insufficient timing andresources of the investigations might explain the high number of stroke with undetermined etiology amongyoung patients. Primary prevention, early recognition of stroke and special precaution in people withcomorbidities are crucial. Given the increase of physical and socioeconomic burden, further studies andrecommendations are indispensable. Keywords: stroke, young adults
136

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-80Neurosonology and Neuroimaging
Feasibility of Monitoring Basilar and Middle Cerebral Arteries of Transcranial DopplerUsing Agitated Saline Injection for The Detection of Right-to-left Shunt
Min Kim1, Ji Man Hong1
1 Neurology, Ajou University School of Medicine, Suwon/Yeongtong-gu, Korea
Purpose:Transcranial Doppler (TCD) has been applied as an easy, non-invasive, and real-time monitoring apparatus forthe detection of right-to-left shunt (RLS). Nonetheless, this technique has been limited if the patient has poortemporal window. Therefore, the purpose of this study is to investigate whether basilar artery (BA) is as effectiveas middle cerebral artery (MCA) in the TCD monitoring using agitated saline injection to detect RLS.Methods:A total of 252 patients with headaches or dizziness were registered in the study, which was conducted with anewly manufactured headset monitoring both MCA and BA. The patients were categorized into 4 grades (Grade0, 1, 2, and 3) according to the International Consensus Criteria. They were also dichotomized to 2 groups; noneto mild (Grade 0-1) and moderate to severe (Grade 2-3).Results:The agreement between MCA and BA for the test of agitated saline TCD was 86.7% (226/252). The sensitivityand specificity were 93.6% and 81.5%, respectively. There was a significant correlation (p<0.001) between BAand MCA monitoring in term of RLS detection (Table 2). As compared to the discordance rate (15.2%, 28/184) inGrade 0 and 1, there was little discordance rate (1.4%, 1/68) in Grade 2 and 3. The sensitivity and specificity were98.5% and 98.9% respectively, when the patients were classified none to mild (Grade 0-1) and moderate tosevere (Grade 2-3).Conclusions:Our data suggest that the BA is as effective as MCA in the TCD monitoring using agitated saline injection to detectRLS.
137

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-81Neurosonology and Neuroimaging
Morphologic Remodeling of Left Atrial Appendage of Atrial Cardiopathy in Patientswith Embolic Stroke of Undetermined Source
Dong-seok Gwak1, Woo-chan Choi1, Jung-a Kwon1, Dong-hyun Shim1, Yong-won Kim1, Yang-ha Hwang1
1 Neurology, Kyungpook National University Hospital, Daegu, Korea
Purpose:The left atrial appendage (LAA) is a major source of thrombus in atrial fibrillation (AF), and non-chicken wing(CW) LAA morphology is a risk factor for embolic events. Non-CW morphology may also be associated with atrialcardiopathy (AC) in patients with embolic source of undetermined source (ESUS), which, however, had rarelybeen investigated.Methods:We included consecutive patients with ischemic stroke who underwent a cardiac computed tomographyangiography to assess LAA morphology from 2013 to 2016. Patients with ESUS or AF admitted within 24 hoursafter onset were enrolled in this study. Patients with ESUS were divided into two groups: AC and non-AC. AC wasdiagnosed if the echocardiography reported increased left atrial diameter (>40 mm for men and >38 mm forwomen), atrial high rate episodes were present at cardiac monitoring during hospitalization, or spontaneousechogenic contrast was seen in LAA. LAA morphologies were classified into CW versus non-CW types. Theprevalence of non-CW LAA morphology were compared among patients with AF, AC, or non-AC.Results:A total of 524 patients were identified (AF, n=331; AC, n=98; non-AC, n=95). The prevalence of non-CW type LAAwas 51.7%, 44.9%, and 40.0% in the AF, AC, and non-AC groups, respectively. Patients with AF wereindependently associated with non-CW LAA morphology than did patients with non-AC (adjusted odds ratio [aOR]1.67, 95% confidence interval [CI]: 1.02-2.73, p = 0.040). Patients with AC tended to have more non-CW LAAmorphology than did those with non-AC, although statistically not different (aOR 1.22, 95% CI: 0.69-2.17, p =0.50).Conclusions:Presence of AF was associated with a higher prevalence of non-CW type LAA. AC may also be associated withnon-CW LAA morphology. Our analyses suggest that remodeling of LAA in patients with AF and AC may lead to achange in LAA morphology. Larger studies are needed to confirm the associations.
138

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-82Neurosonology and Neuroimaging
Hemorrhagic Foci in The Lacunar Infarct Which was Revealed on Long-term Follow-up Gradient-echo MRI(PICASSO Substudy)
A-hyun Cho1, Hyuk Sung Kwon2, Min Hwan Lee6, Jong-ho Park3, Sung Hyuk Heo4, Sungwook Yu5, Sun U. Kwon6
1 Neurology, Catholic University of Korea, College of Medicine, Seoul, Korea2 Neurology, Hanyang University, College of Medicine, Seoul , Korea3 Neurology, Myongji hospital, Hanyang university, Koyang, Korea4 Neurology, Kyung Hee University, College of Medicine, Seoul, Korea5 Neurology, Korea university of Korea, College of Medicine, Seoul, Korea6 Neurology, Asan Medical Center, Ulsan university, College of Medicine, Seoul, Korea
Purpose:Through gradient-echo MRI (GRE), hemorrhagic change of lacunar infarcts can be observed as dark signals inlacunar lesions. Sometimes, hemorrhagic foci with lacunar infarcts might be confused with a sequela of primaryintracerebral small hemorrhage. In this context, we aimed to demonstrate hemorrhagic transformation of acutelacunar infarcts and investigate the prevalence, related factors, and clinical significance through long-term follow-up exam of acute lacunar infarction in the population of PICASSO study.Methods:Among PICASSO (PreventIon of CArdiovascular events in iSchemic Stroke patients with high risk of cerebralhemorrhage) trial subjects, patients with acute single subcortical ischemic lesions on penetrating arterialterritories without a definite cause of cardioembolism and large vessel disease were included. The follow-up MRI(FLAIR, GRE) was performed at the end of clinical trial. Initial DWI (lesion diameter), GRE and follow-up FLAIRand GRE were interpreted. Interpretation of follow-up GRE was focused on the presence of hemorrhagic darksignal at the lacunar lesion. Cavitation status of lacunar lesion were also observed on follow-up FLAIR.Demographics and other clinical outcomes were obtained. White matter hyperintensity (Fazeka), number ofcerebral microbleeds, presence of ICH were analyzed.Results:Total of 364 were analyzed in this study. Mean age was 63.59±10.6 and 238 (65.4%) were male sex. Lesionlocations of ischemic stroke were anterior circulation in 219 (60.2%) and posterior circulation in 145. Mediantime interval between initial MR and follow-up GRE MR was 33.5 months. Among 364, 38 (10.4%) showedhemorrhagic dark signal in lacunar lesion on follow-up GRE MR. In 40 patients, cerebral microbleeds wereobserved within or adjacent to the ischemic lesion on both initial and follow-up GRE. Age, sex, risk factors, timeinterval between initial and follow-up MRI, medication, cavitary change and initial stroke severity were notassociated with the hemorrhagic transformation of lacunar infarct. The number of cerebral microbleeds, historyof intracerebral hemorrhage (by history and also by radiological) were not associated with the hemorrhagictransformation. However, the large lesion size (OR 1.15, 95% CI, 1.07 to 1.24, p <0.001) and anterior circulationlocation (2.38, 1.05 to 5.4, p=0.038) were associated with hemorrhagic transformation of lacunar infarct.Conclusions:In 10.4% of acute lacunar infarcts, they revealed hemorrhagic transformation in their chronic stroke period ongradient echo MRI. Lacunar infarcts of larger size and anterior circulation location were prone to develophemorrhagic foci.
139

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-83Neurosonology and Neuroimaging
Association between Kidney Function and Cerebral Arterial Stiffness
Eung-joon Lee1, Hae Bong Jeong2, Byung-woo Yoon1
1 Neurology, Seoul National University Hospital, Seoul, Korea2 Neurology, Chung-Ang University Hospital, Seoul, Korea
Purpose:Chronic kidney disease (CKD) is known to have affected the systemic vasculature and its remodeling, whicheventually led to the systemic arterial stiffness. However, the relationship between cerebral circulation andimpaired renal function is poorly understood. To evaluate the effect of renal dysfunction to increase systemicand intracranial arterial stiffness, we assessed the relation between renal resistive index (RRI) and pulsatilityindex (PI) of the middle cerebral artery.Methods:We included patients with acute small lacunar infarction. Demographic and clinical data were collected byretrospective chart review. Bilateral transcranial Doppler ultrasound (TCD) examination of the MCAs wasperformed using the ST3 Ultrasound system (Spencer Technologies) and PI were calculated. RRI was obtainedthrough kidney Doppler sonography. Subjects with occlusion or significant stenosis of MCA, atrial fibrillation,bilaterally absent transtemporal sonographic windows were excluded.Results:Of the 283 included subjects (mean age 67.8 ± 10.2), 74 patients had renal dysfunction (eGFR <60ml/min/1.73m2 at admission) and 49 patients underwent kidney Doppler ultrasound within 1 year since theiracute stroke. Renal dysfunction was significantly associated with higher arterial stiffness (median PI 1.12, IQR0.85 to 1.57 vs. controls PI 0.84, IQR 0.54 to 1.22 [p<0.0001]). There was a proportional relationship betweenthe degree of renal dysfunction and the distal vascular resistance. In multivariate adjusted regression analysis,renal function was related to high PI (p<0.001). Furthermore, there is strong correlation between RRI and PI(r=0.65, p<0.001).Conclusions:In patients with lacunar infarction, renal impairment is an independent predictor of increased arterial stiffnessin cerebral circulations.
140

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-84Neurosonology and Neuroimaging
Vessel Wall Characteristics on High-Resolution Mri of Ischemic Stroke Associatedwith Intracranial Stenosis
Quyen Pham Thi Ngoc1, Chien Phan Cong2, Duy Doan Thai3, Khoa Dao Duy4, Thang Nguyen Ba5
1 Neurology, Hochiminh City University Medical Center, Ho Chi Minh City, Vietnam2 Diagnostic Imaging, Hochiminh City University Medical Center, Ho Chi Minh City, Vietnam3 Diagnostic Imaging, Hochiminh City University Medical Center, Ho Chi Minh City, Vietnam4 Neurology, Hochiminh City University Medical Center, Ho Chi Minh City, Vietnam5 Neurology, Hochiminh City University Medical Center, Ho Chi Minh City, Vietnam
Purpose:Using high-resolution magnetic resonance imaging (HR-MRI), our aim was to investigate the vessel wallcharacteristics of intracranial artery stenosis in ischemic stroke patients.Methods:This is a retrospective observational study including 38 patients with diagnosis of ischemic stroke associated withintracranial stenosis referred to the Neurology Department of Hochiminh City University Medical Center-Vietnam from January 2020 to July 2020.Results:Eccentric stenosis was observed in 32 (84.2%) patients and concentric stenosis in 6 (15.8%) patients. Eccentricstenosis was more frequently reported in the patients > 45 years old and concentric stenosis was more commonin the patients ≤ 45 years old (P=0.008). All concentric stenosis (6/6, 100%) had enhanced images on HR-MRI, as compared with eccentric stenosis (24/32, 75%; P=0.309). Mean degree of stenosis was 48.7± 21.7%. Meanremodeling ratio was 0.88±0.26. Constrictive artery remodeling was observed in 23 patients (62.2%), expansiveartery remodeling in 9 (24.3%). In 7 patients with intracranial artery dissection, 3 patients had positive dissectionfindings such as string sign and double lumen on MRA; the remainder were diagnosed dissection based on HR-MRI fndings of double lumen and hemorrhage in false lumen.Conclusions:Eccentric stenosis was observed more frequently in our study suggesting that atherosclerosis is the importantcause of intracranial stenosis. Concentric stenosis was more common in young patients suggesting of non-atherosclerosis disease as an important etiology in youth stroke. HR-MRI can help find the vessel wallcharacteristics of intracranial artery dissection such as double lumen and intimal flap.
141

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-85Neurosonology and Neuroimaging
Comparison between Intima Media Thickness (IMT) And Carotid Plaque as Predictors of Tia And IschemicStroke in Diabetes Mellitus Patients And Non Diabetes Mellitus Patients
Wahyu Agung Susilo1, Diah Kurnia Mirawati1, Rivan Danuaji1
1 Neurology, Universitas Sebelas Maret, Surakarta, Indonesia
Purpose:Stroke is one of the causes of death and disability, which is relatively high in the world. The incidence of strokeincreases over time, especially in patients with history of diabetes mellitus. Intima Media Thickness (IMT) is theonly trusted indicator of a cardiovascular event in neurosonology. Another indicator that can be examined inneurosonology is carotid plaque. This study aims to compare the two indicators in patients with TIA and ischemicstroke with history of diabetes mellitus and patients without history of diabetes mellitus.Methods:Samples in this study were taken from TIA patients and ischemic stroke patients who underwent Carotid Duplexexamination in the neurosonology unit of Dr. Moewardi Hospital Surakarta during January 2018 - September2020. Criteria for patients with history of DM and without history of DM was taken from the patient's medicalrecord data. Stroke in the young ages and patients who had sign and symptom of central vertigo were excluded.Thickening of IMT and carotid plaque as predictors of TIA and ischemic stroke in both groups were subjected tostatistical analysis using non-parametric Chi-Square test and cross-tabulation to assess the odds ratio.Results:There were 168 patients who underwent duplex carotid examination at the neurosonology unit of Dr. MoewardiHospital. Among them, 85 patients with TIA and ischemic stroke met the inclusion and exclusion criteria of thisstudy. Based on statistical anlyisis tests, there was no statistically significant difference between IMT thickeningin the presence of carotid plaque as a predictor of TIA and ischemic stroke in DM patients and without a historyof DM (p = 0.116). However, thickening of IMT was a stronger predictor of TIA and stroke than carotid plaque(OR 2.003 vs 1.350).Conclusions:There was no statisticaly difference between IMT thickening and carotid plaque as a predictor of TIA or ischemicstroke in both with and without DM patients Patients with thickening of IMT have a higher risk of developing TIAor stroke than patients with carotid plaque.
142

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-86Neurosonology and Neuroimaging
The Effect of Intracranial Stenosis with The Events of Ischemic StrokesAnd Transient Ischemic Attacks
Nuryanti 1 , Pepi Budianto1
1 Neurology, Sebelas Maret University, Surakarta, Indonesia
Purpose:Stroke is the leading cause of disability and the second leading cause of death in the world. Transient IschemicAttack (TIA) often progresses to ischemic stroke. The presence of intracranial stenosis is often associated withthe incidence of ischemic stroke and TIA. Intracranial stenosis can be detected with a noninvasive TranscranialDoppler (TCD) tool. This study aims to assess the effect of intracranial stenosis on the incidence of ischemic strokeand TIA.Methods:This study retrospectively reviewed the medical records of patients with a diagnosis of ischemic stroke and TIAwho underwent treatment in the neurology department of Dr. Moewardi Surakarta in the period of January 2018- August 2020. The inclusion criteria were patients who were tested for TCD during treatment. Data wereanalyzed using the contingency coefficient test. The results were considered statistically significant if the p-valuewas <0.05.Results:There were 96 patients obtained according to the inclusion criteria. Of the 70 ischemic stroke patients, 35 hadintracranial stenosis. Of the 26 TIA patients, 6 patients developed intracranial stenosis. Based on the analysis, itwas found that there was a statistically significant relationship between intracranial stenosis and the incidenceof ischemic stroke (p = 0.018). Patients with intracranial stenosis had a 1,341 greater relative risk of developingischemic stroke than those without intracranial stenosis. Patients with intracranial stenosis have a lower relativerisk of developing a TIA 0.402 than those without intracranial stenosis.Conclusions:There is a statistically significant relationship between intracranial stenosis and the incidence of ischemic stroke.Patients with intracranial stenosis had a 1,341 greater relative risk of developing ischemic stroke than thosewithout intracranial stenosis.
143

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-87Others
Gears of Stroke: Proposed Model of Stroke Care
Jasmyn De Leon1, Soon Pang Goh1, Carol Tham1
1 General Medicine , Khoo Teck Puat Hospital, Singapore, Singapore
Purpose:The Gears of Stroke concept aims to show the standard management that potentially decreases the burden ofthe disease.Methods:The Model is composed of 5 Gears which include: Early Recognition and Access, Early Revascularization, EarlyRestoration, Early Rehabilitation and Early Reintegration to community.Results:Early Recognition and Access reflects the public awareness and the urgency to seek medical attention for stroke.This may be monitored by the onset-to-door time and the number of stroke activations. Early Revascularizationinvolves thrombolysis and thrombectomy. The performance indicators are : thrombolysis rate, thrombectomyrate, door-to-needle time (DTN), door-to-groin time. Early Restoration involves stroke management in AcuteStroke Unit (ASU). The ASU utilization, initiation of antithrombotic therapy and statin are key indicators. EarlyRehabilitation involves collaboration with therapist. This stage also includes screening for post stroke depressionand cognitive impairment. Early Reintegration to community is a joined effort of allied health rehabilitation teamand the community support groups. This encourages our stroke patients to manage and cope with the life afterstroke.Conclusions:The future of the GEARS OF STROKE will be dependent on the collaboration of different stakeholders. Eachprogram should lend strength to the gears of stroke, thereby enhancing successful recovery and long-termsurvival among stroke patients.
144

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-88Case Report
Intracranial Dural Arteriovenous Fistulas with Increased Haemorrhage Risk: The Importance of Clinical & Imaging Characteristics
Kim Lim Koo1, Khairul Azmi Abd Kadir2, Mei-ling Sharon Tai1, Kay Sin Tan1
1 Neurology, Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia2 Biomedical Imaging, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Purpose:Intracranial dural arteriovenous fistulas (DAVF) are pathological shunts between dural arteries and dural venoussystem. Diagnostic dilemma may arise between DAVF and cerebral venous sinus thrombosis (CVST) due to thesimilar clinical and imaging manifestations. A high-flow DAVF with venous reflux has higher haemorrhagic risk.We present two cases of DAVF with clinical and imaging characteristics to differentiate DAVF from CVST.Methods:Case series.Results:Patient 1, a 70-year-old man who presented with headache and visual disturbances of 3 weeks duration. Anenlarged blind spot and right homonymous hemianopia was found. Patient 2 a 79- year-old lady presented withheadache, tinnitus, dysphasia, cognitive decline for a month and seizure on day of admission. CT-brain plain forpatient 1 showed features of left occipital venous infarct. Both CTA and MRI suggested a DAVF with engorgementof cortical veins (Figure 1). Patient 2 had left parieto-temporal infarct on her CT-brain plain and CTA only showedfew dilated vessels. Though it was not straightforward, MR-angiography is suspicious of a DAVF (Figure 2). Digitalsubtraction angiography in both patients confirmed an isolated left transverse sinus DAVF with cortical venousreflux. Both DAVFs are fed by left occipital artery and petrosquamous branch of the left middle meningeal artery.Endovascular liquid embolisation was performed to patient 1 and complete occlusion was achieved.
145

Cerebrovasc Dis 2020;49(suppl 1):1-149
146

Cerebrovasc Dis 2020;49(suppl 1):1-149
Conclusions:Cortical venous reflux in a DAVF has higher rate of haemorrhage and it is associated with malignant clinicalpresentations (haemorrhage, seizure, dementia) in our series. Imaging characteristics of both DAVF and CVSTneed to be studied thoroughly in a venous stroke in order to pick up DAVF and to prevent catastrophiccomplication secondary to anticoagulant therapy.
147

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-89Case Report
Transcranial Color-Coded Duplex (TCCD) Ultrasonography for Assessmentof Cerebrovascular Reserve
Narayanaswamy Venketasubramanian1
1 Raffles Neuroscience Centre, Raffles Hospital, Singapore, Singapore
Purpose:Impaired cerebrovascular reserve (CVR) carries an almost 4-fold odds of stroke among those with significantocclusive disease. There are many modalities for the assessment of CVR – positron emission tomography, single-photon emission computed tomography (SPECT), perfusion and nuclear CT, perfusion magnetic resonanceimaging (MRI), and transcranial Doppler (TCD); vasodilator challenges include carbon dioxide and acetazolamide.A Breath-Holding Index (BHI) of <0.69 as measured by TCD is associated with an increased stroke risk by morethan 3-fold. Transcranial color-coded duplex (TCCD) ultrasound combines TCD with B-mode imaging and color-coding of Doppler flow. Its use in assessing CVR in stroke patients has not been previously reported. This is thefirst reported case of intracranial stenosis with reduced CVR diagnosed by TCCD ultrasound.Methods:The patient is a 38 year old lady who presented with a 2-month history of nausea then feeling faint whenevershe got up suddenly. On the day of admission, she had gotten up to walk, felt nauseous, left upper limb felt‘funny’, after which she lost consciousness. Clinical and neurological examination was normal. MRI brain wasnormal. MR Angiogram and subsequent CT Angiogram showed flow attenuation in the M1 segment of the rightmiddle cerebral artery (RMCA), with a possible flap. Catheter angiography was suggestive of a dissection with2.7 mm pseudoaneurysm. She underwent TCCD of her MCAs with breath-holding to assess her cerebrovascularreserve.Results:TCCD at baseline showed very high velocities in the RMCA with reduced pulsatility index, normal in LMCA. TheBHI in RMCA was 0.56, suggestive of reduced cerebrovascular reserve in the RMCA territory; it was 0.78 in LMCA.Subsequent acetazolamide-SPECT showed confirmatory reduced right frontal cerebrovascular reserve. She wasgiven clopidogrel for secondary prevention, and has remained well.Conclusions:BHI as measured by TCCD ultrasound is a new method for assessing CVR in those with cerebral ischaemia
148

Cerebrovasc Dis 2020;49(suppl 1):1-149
PO-90Case Report
Asymptomatic Internal Jugular Vein Thrombosis Found Accidentally During Preoperative Examination
Yeonggeun Choi1, Woo-kyung Kim1, Yerim Kim1, Jong Seok Bae1, Ju-hun Lee1, Hong-ki Song1
1 Neurology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Purpose:Venous thrombosis is a vascular disease which is a consequence of Virchow’s traid: hypercoagulability, venousstasis, and endothelial injury. While lower extremity deep venous thrombosis (LEDVT) is common, jugular veinthrombosis is a rare. And even if it occurs, it usually caused by a complication of central venous catheterizationor malignancy-related paraneoplastic syndromes.Methods:Here, we present a case of a 63-year-old male who was found to have idiopathic internal jugular vein thrombosiswithout any symptom.Results:A 63-year-old male was admitted to hospital for surgery due to a rupture of the right shoulder rotator cuff. Hisphysical or neurological examination were all normal. He had no past medical history of intravenous drug use,thrombophilia, malignancies or other hormone replacement therapy. He worked as a construction worker andhe was a heavy smoker of about 40 pack years. Before surgery, ultrasonography with doppler was performed asa preoperative examination. In ultrasonography, a 2.1cm well defined focal thrombus was identified in the distalportion of left internal jugular vein thrombus. While he was hospitalized, basic blood test was performedincluding tumor markers to find out hypercoagulability and everything was normal. To treat his asymptomaticintravenous jugular thrombosis, warfarin was administered orally with the international normalized ratio (INR)of the treatment is adjusted to 2.0 – 3.0. Two months after he was discharged, ultrasonography was taken byfollow-up, and the existing thrombus from the previous sonography successfully disappeared.Conclusions:In conclusion, Spontaneous internal jugular vein thrombosis is a rare condition. Usually, internal jugular veinthrombosis appears asymptomatic. Nevertheless, neurologists should evaluate symptoms such as swelling ortenderness on the side of the neck. Furthermore, secondary etiologies of internal jugular vein thrombosis mustbe ruled out by investigating hidden malignancy, hypercoagulability or infections for recurrence prevention.Anticoagulation therapy is the treatment of choice for patients without contraindications. The oralanticoagulants should be taken for 4 to 12 weeks. Imaging follow-up is necessary before discontinuinganticoagulants
149
Copyright © 2022 FDOKUMEN




















