Ocular choristomas
20
SURVEY OF OPHTHALMOLOGY VOLUME 33 - NUMBER 5. MARCH-APRIL 1989 MAJOR REVIEW Ocular Choristomas AHMAD M. MANSOUR, M.D.,’ JOHN C. BARBER, M.D.,’ ROBERT D. REINECKE, M.D.,’ AND FREDERICK M. WANG, M.D.3 Departments of Ophthalmology, ‘University of Texas Medical Branch, Galveston, Texas, 2Wills Eye Hospital, Philadelphia, Pennsylvania, and Montefzore Medical Center/Albert Einstein College of Medicine, Bronx, New York Abstract. Choristomas are congenital lesions representing normal tissue(s) in an abnormal loca- tion. They are the most common epibulbar and orbital tumors in children. Epibulbar choristo- mas affect the cornea, limbus or subconjunctival space, and range in appearance from a small, flat lesion to a large mass filling most of the epibulbar region. Astigmatism is often present. Choristo- mas may be associated with coloboma, Goldenhar syndrome or epidermal nevus syndromes; those associated with the latter are often bilateral and extensive. Choristomas are occasionally familial. Surgery may be indicated to improve vision or cosmesis, or to impede growth. Although choristomas most commonly involve the epibulbar area, they can affect many areas of the eye and orbit, and often affect more than one area. (Surv Ophthalmol 33:339-358, 1989) Kev words. astigmatism l choristoma l choroidal osteoma l dermoid l ectkpic tissue l 0 epidermal nevus syndromes l Goldenhar syndrome l lesion l lipodermoid Choristomas are the most common type of epi- bulbar and orbital tumors in the pediatric age group. in.14”~~1”L’ Choristomas (Greek choristos = sepa- rated, oma = tumor) represent congenital over- growth of normal tissues in an abnormal location. The predominant locations of ocular choristomas include the epibulbar region, the ocular adnexae, and the choroid (Fig. 1). They can be divided into four main histopathologic groups: dermoid, lipo- dermoid, single-tissue choristoma, and complex choristomas. Dermoids consist of collagenous con- nective tissue covered by epidermoid epithelium. Lipodermoids contain adipose tissue along with a dermis-like connnective tissue. Single-tissue choris- tomas consist of dermis-like tissue or ectopic tissues of mesoectodermal origin (lacrimal and other glands, fat, nerve, brain, cartilage, bone, and teeth). Complex or composite choristomas contain tissues of different origins. Other choristomatous growths include dermoid cysts, epiclermoid cysts, and ter- atomas. Dermoid cysts contain one or more dermal adnexal structures (hair follicle, sebaceous gland) and are lined by a keratinizing epithelium. Epi- dermoid cvsrs lack dermal adnexal structures. ep’dermo’d cyst l eyelid coloboma l l osseous choristoma Tissues derived from three germinal layers rep- resent teratomas, while those derived from two lay- ers are teratoid tumors. In this review, epibulbar and non-epibulbar choristomas will be considered separately. I. Epibulbar Choristomas A. HISTORICAL PERSPECTIVE According to Picque’?’ and Haye et al,‘“:’ Mau- chard and Samuels separately described epibulbar tumors with eyelashes in 1742. In 1853, RybaZ4” reviewed 24 published cases of epibulbar choristo- mas and used the term “dermoid” to group these similar tumors. PicqueZT7 presented a literature re- view of 94 cases of epibulbar dermoids in 1886. In 1937, Ida Mann’x’.‘x” established a three-grade clas- sification of cornea1 choristomas that is still in use (Fig. 2). In 1952, Goldenhar”‘” established the asso- ciation of epibulbar dermoids with auricular, facial, and vertebral anomalies. In 1972, Baum and Fein- goldI characterized further the ocular findings in Goldenhar syndrome. The present review clarifies the association of epibulbar choristomas with Gol- 339
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Ocular choristomas

SURVEY OF OPHTHALMOLOGY VOLUME 33 - NUMBER 5. MARCH-APRIL 1989
MAJOR REVIEW
Ocular Choristomas
AHMAD M. MANSOUR, M.D.,’ JOHN C. BARBER, M.D.,’ ROBERT D. REINECKE, M.D.,’ AND FREDERICK M. WANG, M.D.3
Departments of Ophthalmology, ‘University of Texas Medical Branch, Galveston, Texas, 2Wills Eye Hospital, Philadelphia, Pennsylvania, and Montefzore Medical Center/Albert Einstein College of
Medicine, Bronx, New York
Abstract. Choristomas are congenital lesions representing normal tissue(s) in an abnormal loca- tion. They are the most common epibulbar and orbital tumors in children. Epibulbar choristo- mas affect the cornea, limbus or subconjunctival space, and range in appearance from a small, flat lesion to a large mass filling most of the epibulbar region. Astigmatism is often present. Choristo- mas may be associated with coloboma, Goldenhar syndrome or epidermal nevus syndromes; those associated with the latter are often bilateral and extensive. Choristomas are occasionally familial. Surgery may be indicated to improve vision or cosmesis, or to impede growth. Although choristomas most commonly involve the epibulbar area, they can affect many areas of the eye and orbit, and often affect more than one area. (Surv Ophthalmol 33:339-358, 1989)
Kev words. astigmatism l choristoma l choroidal osteoma l dermoid l
ectkpic tissue l
0
epidermal nevus syndromes l
Goldenhar syndrome l lesion l lipodermoid
Choristomas are the most common type of epi-
bulbar and orbital tumors in the pediatric age
group. in.14”~~1”L’ Choristomas (Greek choristos = sepa-
rated, oma = tumor) represent congenital over- growth of normal tissues in an abnormal location.
The predominant locations of ocular choristomas
include the epibulbar region, the ocular adnexae,
and the choroid (Fig. 1). They can be divided into four main histopathologic groups: dermoid, lipo-
dermoid, single-tissue choristoma, and complex choristomas. Dermoids consist of collagenous con-
nective tissue covered by epidermoid epithelium. Lipodermoids contain adipose tissue along with a dermis-like connnective tissue. Single-tissue choris-
tomas consist of dermis-like tissue or ectopic tissues
of mesoectodermal origin (lacrimal and other glands, fat, nerve, brain, cartilage, bone, and teeth). Complex or composite choristomas contain tissues
of different origins. Other choristomatous growths include dermoid cysts, epiclermoid cysts, and ter- atomas. Dermoid cysts contain one or more dermal
adnexal structures (hair follicle, sebaceous gland) and are lined by a keratinizing epithelium. Epi- dermoid cvsrs lack dermal adnexal structures.
ep’dermo’d cyst l eyelid coloboma l
l osseous choristoma
Tissues derived from three germinal layers rep- resent teratomas, while those derived from two lay- ers are teratoid tumors. In this review, epibulbar
and non-epibulbar choristomas will be considered
separately.
I. Epibulbar Choristomas
A. HISTORICAL PERSPECTIVE
According to Picque’?’ and Haye et al,‘“:’ Mau- chard and Samuels separately described epibulbar tumors with eyelashes in 1742. In 1853, RybaZ4” reviewed 24 published cases of epibulbar choristo-
mas and used the term “dermoid” to group these similar tumors. PicqueZT7 presented a literature re-
view of 94 cases of epibulbar dermoids in 1886. In 1937, Ida Mann’x’.‘x” established a three-grade clas-
sification of cornea1 choristomas that is still in use (Fig. 2). In 1952, Goldenhar”‘” established the asso- ciation of epibulbar dermoids with auricular, facial, and vertebral anomalies. In 1972, Baum and Fein- goldI characterized further the ocular findings in Goldenhar syndrome. The present review clarifies the association of epibulbar choristomas with Gol-
339

340 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
Fig. I. Predominant locations of ocu- lar choristomas: Epibulbar region (cornea, limbus, subconjunctival space); eyelid (cartilaginous choris- toma; phakomatous choristoma in lower lid); orbit (dermoid cyst, tera- toma); iris; retina (ectopic ciliary body); choroid (osseous); optic nerve and tract. C = cornea; L = limbal; SC = subconjunctival; EL = eyelid, ch = choristoma; U = uvea; Ch = cho- roid; ON = optic nerve.
denhar syndrome, and further establishes the asso- ciation of epibulbar choristomas with linear skin nevi.
B. INCIDENCE
The incidence of epibulbar choristomas is be- tween 1/1O,OOO123 and 3/10,000.‘04 Ash found 7.5 cases of choristomas (7.5%) out of 1,016 epibulbar lesions studied at the Armed Forces Institute of Pa- thology.” By age distribution, Ash found choristo- mas to constitute 36% of epibulbar lesions in the first decade of life, 23% in the second decade, 7.2% in the third decade, and 0.9% in the fourth decade and beyond.6 At the Eye Pathology Laboratory of the Wilmer Institute, choristomas constituted 33% of epibulbar lesions in subjects below age 16 years,7g and 2.2% in subjects 16 years of age or older.“3
C. CLINICAL FEATURES
Epibulbar choristomas are solid tumors with a smooth or rough surface, and often with fine short or long hairs. The consistency may be hard, rub- bery, or soft, and the color may be whitish, yellow- ish, or pinkish. The size varies from a flat lesion of few millimeters to a large mass filling most of the epibulbar region. There may be more than one le- sion in the same eye (Fig. 3),253~2g’~*gQ*326 and lesions may be unilateral or bilatera1.76*2g2 They cover com- monly the cornea, 42~74~112~118,236.272 the limbus, or the
subconjunctival space. There is a wide clinical spec- trum for presentation of epibulbar choristomas, in- cluding epithelioma,‘j2 hemangioma,156 ‘foreign body granuloma, pterygium,‘j2 sclerocornea,24 ante- rior cornea1 dystrophy,‘25J85 staphyloma,24 and xanthoma. Rare presentations include multilobu- Iated lesions,273 annular perilimbal lesions,‘g4 corne- al cysts (Fig. 3),201 supernumerary caruncles,‘87v1g5 a
cutaneous horn overlying a conjunctival dermoid, and swelling of the caruncle by an epidermoid cyst (Fig. 4).
Of 82 epibulbar choristomas reported by Ash,‘j 43 (52%) were located in the bulbar conjunctiva, 24 (29%) in the limbus, 5 (6%) in the cornea, 3 (4%) each in the caruncle and the canthi, and 2 (2.5%) each in the conjunctival fornix and the palpebral conjunctiva. In a series of 100 choristomas,‘7g 94% of the lesions were temporal while 6% were nasal, and 83% were inferior while 17% were superior. Out of 25 epibulbar choristomas in Goldenhar syn- drome,‘s6 14% were nasal, 86% temporal, 16% su- perior, and 84% inferior.
Associated ocular findings in isolated epibulbar choristomas include scleral and cornea1 staphylo- mas 23*24,43 aniridia,74 congenital aphakia,‘ls cata- ract:lg5 miliary aneurysms of the retina,‘76 and mi- crophthalmia.“8~234~2*o~2g6 Epibulbar choristomas may be associated with choristomas of the eye- lid ‘32*‘85 osseous choristomas of the choroid,‘67.‘85 deimoid cysts of the orbit,2g5 systemic choristomas
I II III
Fig. 2. Grading of severity of epibuibar choristomas (modified from Mann’s classification). Grade 1: Superfi- cial cornea1 involvement. Grade II; Deep cornea1 involve- ment. Grade III: Involvement of the cornea and part of the anterior segment with associated ocular anomalies (i.e., microphthalmia).

OCULAR CHORISTOMAS
involving the face and scalp,74 and commonly with
cartilage choristomas in the preauricular region
(preauricular tags).
Astigmatism is common in eyes with epibulbar choristomas. In one series,18” the average degree of
astigmatism was 2.1 diopters for limbal choristomas
and 1.0 diopter for conjunctival choristomas. Cut- tone et al”’ have induced astigmatism by suturing
341
scleral sponges to the limbus of rabbits, mimicking
the effect of limbal choristomas.
D. ASSOCIATION WITH GOLDENHAR
SYNDROME
Van Duyse in 1882 described the association be- tween facial anomalies and ocular dermoids in
three of his cases and one case from the literature.‘“”
Fig. ?. Clinical appearance of epibulbar choristomas. Top kft: Multiple choristomas (limbal and subconjunctival). Top
right: Choristoma presenting as a limbal cyst. Middle right and bottom left: Subconjunctival choristoma filling the lowet- firnix. Bottom right: Limbal choristoma resembling a pterygium. Choristoma with lipid cornea1 ring and multiplr hairs protruding from the central portion of the mass.
342 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
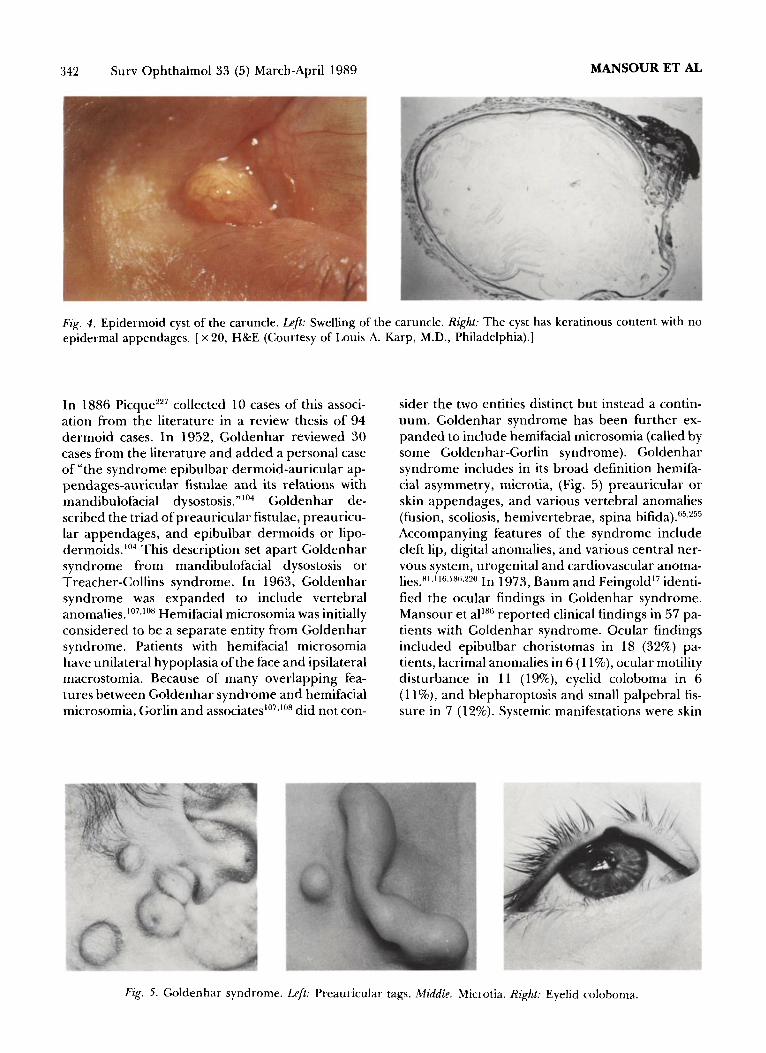
Fig. 4. Epidermoid cyst of the caruncle. Z@ Swelling of the caruncle. Right: The cyst has keratinous content with no
epidermal appendages. [X 20, H&E (Courtesy of Louis A. Karp, M.D., Philadelphia).]
In 1886 Picques7 collected 10 cases of this associ- ation from the literature in a review thesis of 94 dermoid cases. In 1952, Goldenhar reviewed 30 cases from the literature and added a personal case of “the syndrome epibulbar dermoid-auricular ap- pendages-auricular fistulae and its relations with mandibulofacial dysostosis.“‘n4 Goldenhar de- scribed the triad of preauricular fistulae, preauricu- lar appendages, and epibulbar dermoids or lipo- dermoids.‘04 This description set apart Goldenhar syndrome from mandibulofacial dysostosis or Treacher-Collins syndrome. In 1963, Goldenhar syndrome was expanded to include vertebral anomalies.‘07~‘0” Hemifacial microsomia was initially considered to be a separate entity from Goldenhar syndrome. Patients with hemifacial microsomia have unilateral hypoplasia of the face and ipsilateral macrostomia. Because of many overlapping fea- tures between Goldenhar syndrome and hemifacial microsomia, Gorlin and associates’“7l’08 did not con-
sider the two entities distinct but instead a contin- uum. Goldenhar syndrome has been further ex- panded to include hemifacial microsomia (called by some Goldenhar-Gorlin syndrome). Goldenhar syndrome includes in its broad definition hemifa- cial asymmetry, microtia, (Fig. 5) preauricular or skin appendages, and various vertebral anomalies (fusion, scoliosis, hemivertebrae, spina bifida).65,?55 Accompanying features of the syndrome include cleft lip, digital anomalies, and various central ner- vous system, urogenital and cardiovascular anoma- lies.n’~“6~‘xs~220 In 1973, Baum and Feingold17 identi- fied the ocular findings in Goldenhar syndrome. Mansour et alIS reported clinical findings in 57 pa- tients with Goldenhar syndrome. Ocular findings included epibulbar choristomas in 18 (32%) pa- tients, lacrimal anomalies in 6 (1 l%), ocular motility disturbance in 11 (19%), eyelid coloboma in 6 (1 l%), and blepharoptosis and small palpebral fis- sure in 7 (12%). Systemic manifestations were skin
Fig. 5. Goldenhar syndrome. Lpft: Preauricular tags. Middle: Microtia. Right: Eyelid coloboma.
OCULAR CHORISTOMAS 343
tags in Z-15 (61%) patients, microtia in 39 (68%),
hemifdciaj asymmetry in 45 (79%), and vertebral
anomaly in 17 (30%). The choristomas in Goldenhar syndrome are
limbal or subconjunctival, and few cases with corne-
al choristoma have been described.“2,‘““,S”fi A com-
prehensive listing of ocular findings reported in
Goldenhar syndrome are listed in Table 1.
E. ASSOCIATION WITH THE EPIDERMAL
NEWS SYNDROME
Bogel in 1886 reported “the association of a sub- conjunctival lipoma with ichthyosis hystrix.““’ Since
then a number of cases of choristomas associated
with the epidermal nevus syndrome have been re- ported, and these are summarized in Table 2. The
syndrome is manifested by skeletal, neurologic, vas-
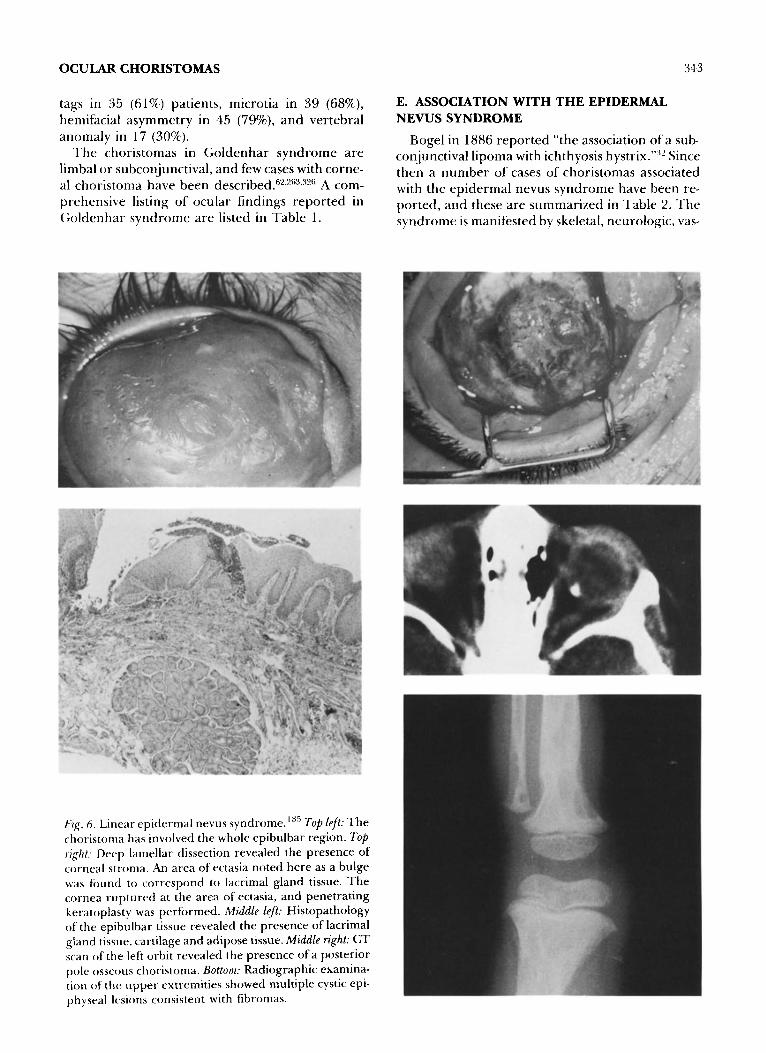
Fig. 6. Linear epidermal nevus syndrome.“” Top left: The choristoma has involved the whole epibulbar region. 7bp right: Deep lamellar dissection revealed the presence of cornea1 stroma. An area of ectasia noted here as a bulge was found to correspond to lacrimal gland tissue. The cornea ruptured at the area of ectasia, and penetrating keratoplasty was performed. Middle left: Histopathology of the epibulbar tissue revealed the presence of lacrimal gland tissue, cartilage and adipose tissue. Middle right: CT scan of the left orbit revealed the presence of a posterior pole osseous choristoma. Bottom; Radiographic examina- tion of the upper extremities showed multiple cystic epi- physral lesions consistent with fibromas.
344 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
TABLE 1 cular and dermatologic disorders.267-2”g
Ocular Findings in Goldenhur Syndrome
Epibulbar choristoma’2g~23g~304~s05 Eyelid & eyebrow colobomas**’ Lacrimal drainage anomalies’7~‘86*3” Duane’s syn&-ome2'9~226.228,294
Third nerve ophthalmoplegias* Microphthalmos50Jgz Neuroparalytic keratitis2”3~28s Orbital dermolipoma20s Facial neuropathy3 Partial cryptophthalmos24’ Eyelid choristoma214 Iris heterochromiag’ Aniridia227 Uveal coloboma230 Cataractlg5 Optic nerve hypoplasia53 Pseudopapilledema’5s Peripapillary hypopigmentation’86 Retinal vascular tortuosity’g2
Skeletal disorders include kyphoscoliosis, lor- dosis, hemihypertrophy and pathological frac- tures from cystic lesions of the long bones (Fig.
6). ‘70*‘72~284 Neurologic complications include con-
vulsions, mental retardation, and hemipare- sis '6~26~47~69~77~36~103.148.300~34~ Vascular anomalies in_
elude congenital cardiac malformations,8’ arteriovenous malformations of the brain, and hemangioma of the scapula.
The skin lesions are congenital, epidermal in character, linear, and usually do not cross the mid- line (Fig. 7). They have a predilection for the head and face. The lesions are of two types. Linear epider-
ma1 nevi (nevus unius lateris) are characterized by brown linear unilateral pap&es with increased bas- al cell hyperpigmentation and various degrees of hyperkeratosis. When the lesions have many seba- ceous glands, they are called sebacaeous nevi.
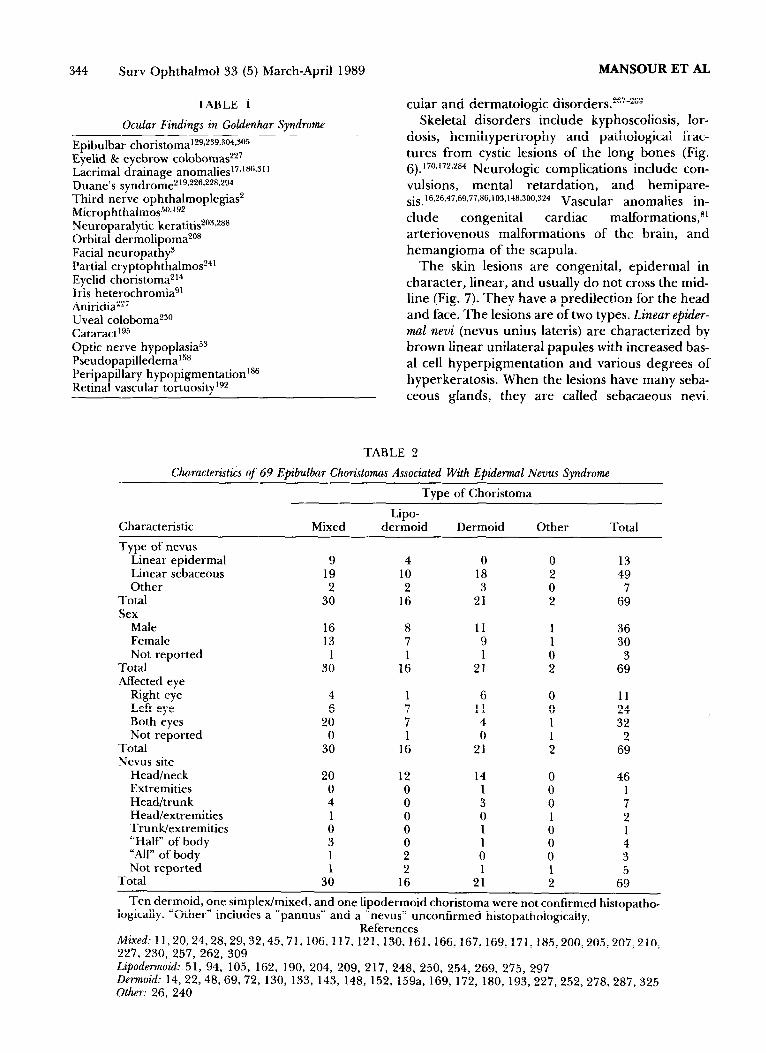
TABLE 2
Characteristics of 69 Epibulbar Choristomas Associated With Epidermal News Syndrome
Type of Choristoma
Lipo- Characteristic Mixed dermoid Dermoid Other Total
Type of nevus Linear epidermal 9 4 0 0 13 Linear sebaceous 19 10 18 2 49 Other 2 2 3 0 7
Total 30 16 21 2 69 Sex
Male 16 11 1 36 Female 13
r: 9 1 30
Not reported 1 1 1 0 3 Total 30 16 21 2 69 Affected eye
Right eye 4 1 6 0 11 Left 6 eye 7 11 0 24 Both 20 eyes 7 4 1 32 Not reported 0 1 0 1 2
Total 30 16 21 2 69 Nevus site
Head/neck 20 12 14 0 46 Extremities 0 0 1 0 Head/trunk 4 0 3 0 : Head/extremities 1 0 0 1 2 Trunk/extremities 0 0 1 0 1 “Half’ of body 3 0 1 0 4 “All” of body 1 2 0 0 3 Not reported 1 2 1 1 5
Total 30 16 21 2 69
Ten dermoid, one simplex/mixed, and one lipodermoid choristoma were not confirmed histopatho- logically. “Other” includes a “pannus” and a “nevus” unconfirmed histopathologically.
References Mixed: 11,20,24,28,29,32,45,71,106, 117, 121,130,161, 166, 167, 169, 171, 227, 230, 257, 262, 309
185,200,205,207,210,
Lipodermoid: 51, 94, 105, 162, 190, 204, 209, 217, 248, 250, 254, 269, 275, 297 Dermoid: 14, 22,48,69,72, 130, 133, 143, 148, 152, 159a, 169, 172, 180, 193, 227,252, 278,287, 325 Other: 26, 240
OCULAR CHORISTOMAS 345
Fig. 7. Nevus sebaceus involving the forehead.
These are yellowish verrucose cutaneous lesions;
sebaceous gland hyperplasia can be seen histopath- ologically.“?5 Unlike the linear epidermal nevus, the
sebaceus nevus is known to undergo malignant de-
generation into basal cell epithelioma and other skin tumors early in life.27~‘“x~‘7s~‘x~~‘g7 Systemic
malignancies in association with sebaceus nevi
include Wilms’ tumor of the kidney, adenocarci-
noma of the salivary glands, and rhabdomyosar- cOma “‘.70,X”.“l:i.‘.i’,1~~,~~!~
The choristomas found in epidermal nevus syn-
drome are most commonly the mixed (complex) type. These are most often bilateral and exten-
sive.‘x”,‘6” While bilaterality is less common in lipo- dermoid and dermoid lesions than in the mixed
type, it is more common in the choristomas associat- ed with epidermal nevus syndrome than in choris-
tomas not associated with this syndrome.
F. INHERITANCE
Transmission of choristomas through three gen-
erations was reported by Saebos”’ and Golden- bar.“‘” .4 literature review revealed six families with
choristomas in the context of Goldenhar syndrome, and five families with isolated choristomas (Table 4). The pattern of inheritance in isolated choristo-
mas was autosomal dominant in three fam- ilies Il)-I.?:ll .L’~5 sex-linked recessive in two, ‘25,“N.j and
probably autosomal recessive transmission in one.‘ls” The inheritance pattern in choristomas
with Goldenhar syndrome was multifactor- ial !)9,14l liJ.17i.IX~.“9!1
Eleven twin studies in epibulbar choristomas and/or Goldenhar-Gorlin syndrome were discor- dant for either t’.~.~~l..~~i,ll~~.lL’~.~Nti.~~~,L’5~ Frances&etti””
reported female bivitelline twins who had Golden-
har-Gorlin syndrome without choristomas. Ter-
haaP’ described the only monozygotic twins with
Goldenhar syndrome and epibulbar choristomas.
Chromosomal studies were normal in several se- ries of patients with Goldenhar syndrome.‘:“.‘X”~‘“”
One patient had the combination of Goldenhar syn- drome and the cri-du-chat syndrome (deletion of
the short arm of one of the chromosomes in the 4-5 group).‘“’ Another patient with Goldenhar syn- drome and normal karyotype had a relative with the cri-du-chat syndrome.‘K”
Two uncommon forms of epibulbar choristomas
were noted to be familial: the annular limbal form
described by Mattos et al,‘“” and the cornea1 dystro-
phy form described by Henkind et al”” and Topi-
low et al.‘x” The latter form presented at birth as
bilateral superficial crocodile shagreen opacity of the cornea. Examination of family members dis- closed a more characteristic cornea1 choristoma
(Fig. 8).
TABLE 3
Ocular Findings in the Epidervnal NQWV Syndromr
Epibulbar choristomas Epidermal nevus of e Eyelid ,-horistomal”.I I 7
elid 152. I7:i. I i,i.L’4X.?.~L’.WI
.IX.i.L’62
Nystagmus’“” Ophthalmoplegia”” Coloboma of eyelid, optic nerve and choroid7’,““’ Osseous choristoma of the choroid”” Cortical blindness7’.‘2’,‘“x Microphthalmia’“’ Macrophthalmia”‘” Catdract’75
TABLE 4
Literature Rez&w of Favnilic~i Epihulhar Chorzstovna.\
Familial Goldenhar With Familial Lkvnoids Saraux”“’ Krause”” KirkeI”i
Terharr””
Baum”
Rollnick”“” isolated Favnilinl Choristomas
Saebo”4”
Two sisters Brother and sister Two sisters Male and female mono-
zygotic twins Paternal grandmother
and grandchild Three siblings
(irandmother, mother, and daughter
Father, son, and daughte’
Henkind 8c Topilow’Y5.“n” ‘I‘wo brothers and thei’ nephew
Pouliquen’:” Mother, fi~ur sons. grandson and grandaughte’
Mattes”” Mother, three daughters, and one grandson
Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
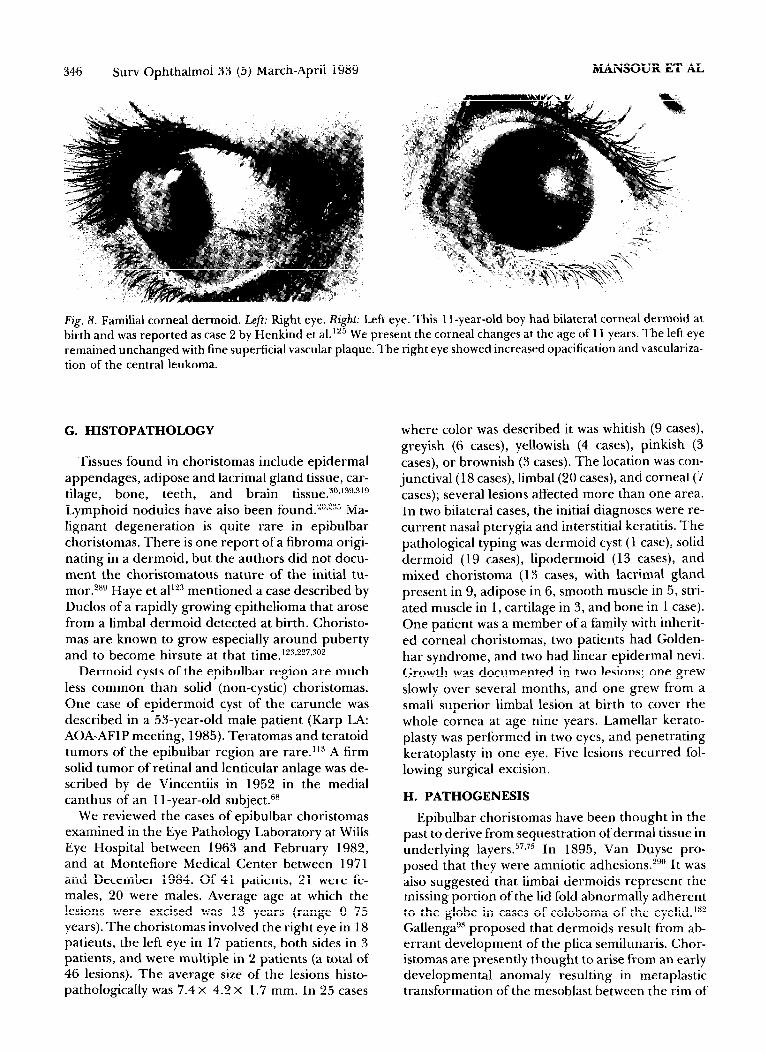
Fig. 8. Familial cornea1 dermoid. Left: Right eye. Right: Left eye. This 1 l-year-old boy had bilateral cornea1 dermoid at birth and was reported as case 2 by Henkind et al. lz5 We present the cornea1 changes at the age of 11 years. The left eye remained unchanged with fine superficial vascular plaque. The right eye showed increased opacification and vasculariza- tion of the central leukoma.
G. HISTOPATHOLOGY
Tissues found in choristomas include epidermal appendages, adipose and lacrimal gland tissue, car- tilage, bone, teeth, and brain tissue.3”*‘3g.“‘g Lymphoid nodules have also been found.20.235 Ma- lignant degeneration is quite rare in epibulbar choristomas. There is one report of a fibroma origi- nating in a dermoid, but the authors did not docu- ment the choristomatous nature of the initial tu- mor.28g Haye et alIz mentioned a case described by Duclos of a rapidly growing epithelioma that arose from a limbal dermoid detected at birth. Choristo- mas are known to grow especially around puberty and to become hirsute at that time.‘23.2?7~so’
Dermoid cysts of the epibulbar region are much less common than solid (non-cystic) choristomas. One case of epidermoid cyst of the caruncle was described in a 53-year-old male patient (Karp LA: AOA-AFIP meeting, 1985). Teratomas and teratoid tumors of the epibulbar region are rare.‘13 A firm solid tumor of retinal and lenticular anlage was de- scribed by de Vincentiis in 1952 in the medial canthus of an 1 l-year-old subject.6R
where color was described it was whitish (9 cases), greyish (6 cases), yellowish (4 cases), pinkish (3 cases), or brownish (3 cases). The location was con- junctival (18 cases), limbal (20 cases), and cornea1 (7 cases); several lesions affected more than one area. In two bilateral cases, the initial diagnoses were re- current nasal pterygia and interstitial keratitis. The pathological typing was dermoid cyst (1 case), solid dermoid (19 cases), lipodermoid (13 cases), and mixed choristoma (13 cases, with lacrimal gland present in 9, adipose in 6, smooth muscle in 5, stri- ated muscle in 1, cartilage in 3, and bone in 1 case). One patient was a member of a family with inherit- ed cornea1 choristomas, two patients had Golden- har syndrome, and two had linear epidermal nevi. Growth was documented in two lesions; one grew slowly over several months, and one grew from a small superior limbal lesion at birth to cover the whole cornea at age nine years. Lamellar kerato- plasty was performed in two eyes, and penetrating keratoplasty in one eye. Five lesions recurred fol- lowing surgical excision.
H. PATHOGENESIS
We reviewed the cases of epibulbar choristomas Epibulbar choristomas have been thought in the examined in the Eye Pathology Laboratory at Wills past to derive from sequestration of dermal tissue in Eye Hospital between 1963 and February 1982, underlying layers. 57.75 In 1895, Van Duyse pro- and at Montefiore Medical Center between 1971 posed that they were amniotic adhesions.2g0 It was and December 1984. Of 41 patients, 21 were fe- also suggested that limbal dermoids represent the males, 20 were males. Average age at which the missing portion of the lid fold abnormally adherent lesions were excised was 13 years (range O-75 to the globe in cases of coloboma of the eyelid.‘@ years). The choristomas involved the right eye in 18 Gallengag3 proposed that dermoids result from ab- patients, the left eye in 17 patients, both sides in 3 errant development of the plica semilunaris. Chor- patients, and were multiple in 2 patients (a total of istomas are presently thought to arise from an early 46 lesions). The average size of the lesions histo- developmental anomaly resulting in metaplastic pathologically was 7.4 x 4.2 x 1.7 mm. In 25 cases transformation of the mesoblast between the rim of
OCULAR CHORISTOMAS
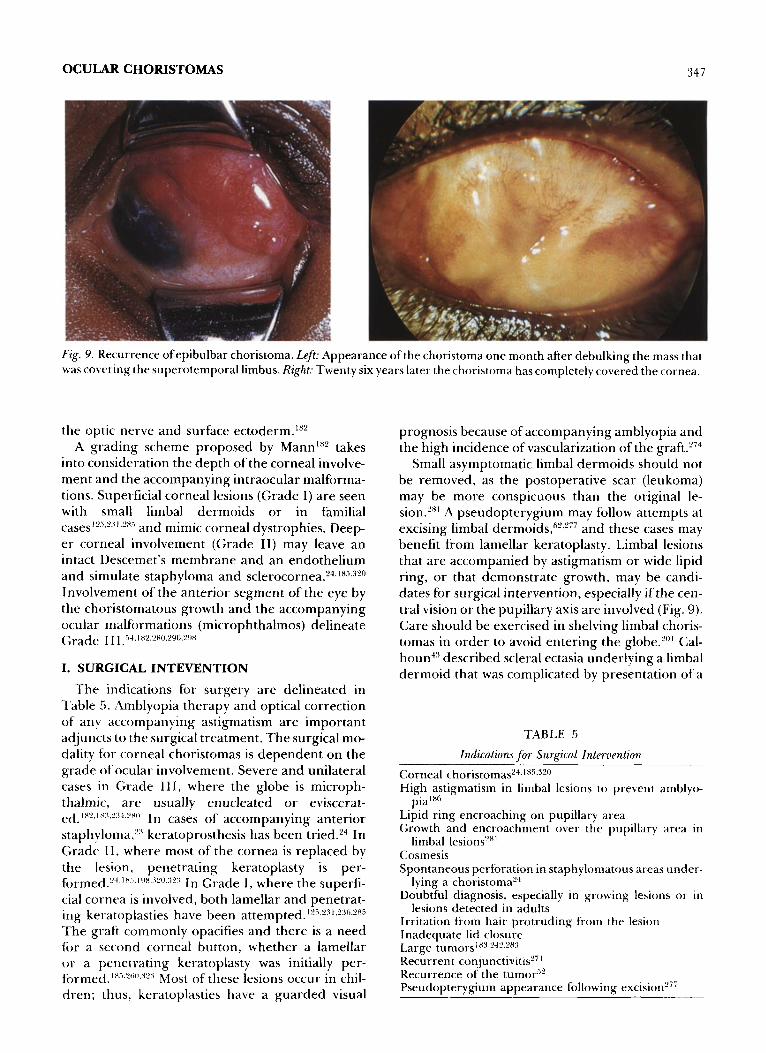
Fig. 9. Recurrence of epibulbar choristoma. Left: Appearance of the choristoma one month after debulking the mass that was covering the superotemporal limbus. Right: Twenty six years later the choristoma has completely covered the cornea.
the optic nerve and surface ectoderm.ix2 A grading scheme proposed by MannIx’ takes
into consideration the depth of the cornea1 involve- ment and the accompanying intraocular malforma- tions. Superficial cornea1 lesions (Grade I) are seen with small limbal dermoids or in familial cases’““~2”‘~SH” and mimic cornea1 dystrophies. Deep- er cornea1 involvement (Grade II) may leave an intact Descemet’s membrane and an endothelium and simulate staphyloma and sclerocornea.“4.‘X5~““o Involvement of the anterior segment of the eye by the choristomatous growth and the accompanying ocular malformations (microphthalmos) delineate Grade III: i.&. I X2.‘wJ.“L)6.2AX
I. SURGICAL INTEVENTION
The indications for surgery are delineated in Table 5. Amblyopia therapy and optical correction of any accompanying astigmatism are important adjuncts to the surgical treatment. The surgical mo- dality for cornea1 choristomas is dependent on the grade of ocular involvement. Severe and unilateral cases in Grade III, where the globe is microph- thalmic, are usually enucleated or eviscerat- ed. I XL’. I x:I,“:I-I.“xo In cases of accompanying anterior staphyloma,‘:’ keratoprosthesis has been tried.“4 In Grade I I, where most of the cornea is replaced by the lesion, penetrating keratoplasty is per- f~~rmed~L’-I.lXi.l!lX.‘~Yl~.:I”:~ In Grade I, where the superfi- cial cornea is involved, both lamellar and penetrat- ing ket-atoplasties have been attempted.‘“~,9”‘,‘““,‘X”
The graft commonly opacifies and there is a need fi)r a second cornea1 button, whether a lamellar or a penetrating keratoplasty was initially per- fol-mecl.‘xi~2”“~‘~~‘~ Most of these lesions occur in chil- dren; thus, keratoplasties have a guarded visual
prognosis because of accompanying amblyopia and the high incidence of vascularization of the graft.“”
Small asymptomatic limbal dermoids should not be removed, as the postoperative scar (leukoma) may be more conspicuous than the original le- sion.‘“’ A pseudopterygium may follow attempts at excising limbal dermoids,fi’,‘77 and these cases may benefit from lamellar keratoplasty. Limbal lesions that are accompanied by astigmatism or wide lipid ring, or that demonstrate growth, may be candi- dates for surgical intervention, especially if the cen- tral vision or the pupillary axis are involved (Fig. 9). Care should be exercised in shelving limbal choris- tomas in order to avoid entering the globe.““’ Cal- houn”’ described scleral ectasia underlying a limbal dermoid that was complicated by presentation of a
TABLE 5
Indications for Surgical Intervention
Cornea1 choristomas’4.‘X5-J’o High astigmatism in limbal lesions to prevent amblyo-
pia’s” Lipid ring encroaching on pupillary area Growth and encroachment over the pupillary area in
limbal IesionP’ Cosmesis Spontaneous perforation in staphylomatous areas under-
lying a choristoma’” Doubtful diagnosis, especially in growing lesions or in
lesions detected in adults Irritation from hair protruding from the lesion Inadequate lid closure Large tumOrSlH:i.“4B.‘H”
Recurrent conjunctivitis”’ Recurrence of the tumo? Pseudopterygium appearance following excision”’

348 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
vitreous bead during a superficial dissection. Spon- taneous collapse of the anterior chamber in a child with limbal choristomas (Spencer WM: Verhoeff Society Meeting, 1983) attests to the special care needed in excising limbal choristomas. Subcon- junctival lipodermoid choristomas are removed if there is a cosmetic blemish. The lesion may extend deep into the orbit, and no attempt should be made to remove the entire lesion. Such attempts in the past have led to distortion of the eyelids and diplo- pia from excessive surgical manipulation.z8’
II. Choristomas Outside the Epibulbar Region
A. EPISCLERAL OSSEOUS CHORISTOMAS
Episcleral osseous choristomas are detected in early infancyn5 or childhood and tend to increase in size in early childhood5’ or around puberty.“” They appear as whitish pea-sized raised lesions, 5 to 10 mm from the limbus. They have a pre- dilection for the superotemporal quadrant (30 out of 44 cases described in the litera- ture) 12,19,34,73,120.126.1~3,1~.233~237.259.63,30~~322 or the tem_
poral corner ( 10 out of 44 cases).34~~g*x3~85~‘zo~~37~265 They simulate a dermoid,‘gs34 a dermolipoma,‘g a granuloma,34 a pyogenic granuloma,*?’ a sea??’ or ivory teeth.221 They are composed of osseous tissue arranged in Haversian systems, and are enclosed by periosteum. The finding of a tooth-shaped opacity by skull X-rays helps in the preoperative diagno- sis.lg The majority are freely movable and easy to dissect. Adherence of the tumor to the sclera34*2”i9 and to the lateral rectus muscle sheathx5,221 is com- mon. Osseous choristomas seem to arise from or lie within Tenon’s tissue, either over the sclera in the superotemporal quadrant or in a reflection of the Tenon’s capsule that forms the sheath of the lateral rectus muscle in the temporal corner.22’
Fig. IO. Dermoid cyst of the orbit located in the supero- temporal quadrant.
denhar syndrome ‘7x214 or in the context of the linear epidermal nevus syndrome. 14,117,185,200,207,262,267 These
lesions have been mistaken for chalazia.“4 Ectopic lacrimal gland has been described in the upper eye- lid.154
A rare choristomatous growth involving the low- er eyelids is the phakomatous choristoma. The characteristic features of such tumors include: de- tection in early infancy, tendency for growth, in- volvement of the nasal part of the lower eyelid, and clinical resemblance to dermoid cysts. Of eight such lesions reported,g~“7~“‘~‘g”~‘s6~32s six were in males and two were in females. All were unilateral. By histo- pathology, the capsule-like bands and the enclosed material resemble respectively the lens capsule and the lens substance of cataractous lenses.328 The close resemblance of the tumor to lens structures has been further established by electron microscopic studies.‘g”.Z85 The tumor is thought to be of lenticu- lar anlage derivation.3zs
B. SCLERAL CHORISTOMAS D. ORBITAL CHORISTOMAS
The sclera can be replaced by ectopic lacrimal gland tissue4g,‘37 or by chondroosteomatous choris- tomatous growth,54,67,*'P,P'3,223*227,*48 usually in con_
tinuity with a choristoma or a coloboma of adjacent structures. Episcleral bone continuous with a peri- papillary choroidal coloboma was found in a case of D-trisomy with translocation.24s Intrascleral smooth muscle fibers occasionally have been noted in colo- bomas of the optic disc. 8g Ectopic retina in the sclera was found in a subject with triploidy.g?
C. EYELID CHORISTOMAS
Cartilage and complex choristomas of the eye- lids’“Z,?‘6 are single or multiple, and may occur in eyes having epibulbar choristomas as part of Gol-
Dermoid cysts represent the commonest choris- tomatous growth of the orbit. In a review of four large series totalling 358 cases of orbital tumors in children,78~‘4z~3?? dermoid cysts accounted for 37% of the cases. Some cysts enlarge to reach the size of the eyeball, giving them the designation of “giant dermoid cysts.“1’4 Dermoid cysts commonly arise superotemporally (Fig. 10) near the zygomatico- frontal suture line. They tend to be located superfi- cially in asymptomatic children,25” while in adults they are deeply located causing proptosis.“+“jx Haye et al’?? listed the location of the dermoid cysts in 125 patients as follows: superotemporal, 6 1 cases (49%); superonasal, 29 cases (23%); inferonasal, 14 cases (11%); inferotemporal, 7 cases (6%); orbital

OCULAR CHORISTOMAS
roof, 10 cases (8%); and deep in the orbit, 4 cases (3%). Yroptosis with mastication was encountered in one case of dermoid cyst communicating with the temporal fossa through a bony defect in the lateral orbital wall.“” Spontaneous rupture of the dermoid cyst with surrounding granulomatous inflamma- tion was present in 25% of the cases in one series.“’ Dermoid cysts are thought to result from an embry- onic displacement of the epidermis at the site of developmental fusion of bone. One case of dermoid cyst had accompanying epibulbar choristoma.2gj
Seven cases of “dermoid” cysts have been report- ed to be of conjunctival origin,‘47.P6” representing 5% of one series of orbital dermoid cysts.14’ Con- junctival adnexal cysts of the orbits tend to be locat- ed superonasally and represent sequestrations of conjunctival epithelium.
Dermolipomas account for 0.6% of orbital tu- mors in children.“” The subconjunctival lipoder- moid may be the forward lip of a large lipodermoid in the orbit.“x1 Extension of epibulbar dermolipo- mas deeply into the orbit is an indication for limited surgery to prevent such complications as motility restriction and obliteration of conjunctival fornicesZx’
Orbital ~~~~~~~a~4.1".l~.4~.':'".'"0.149,174 have been
considered choristomatous in nature because they arise from totipotential cells rather than from pluri- potential cells. 149~pJ5 They account for 1% of orbital tumors in children. 14:! There is a female-to-male ra- tio of 2: 1.“’ Most teratomas are cytologically be- nign, yet they frequently grow rapidly and cause severe proptosis and extensive destruction of the bony orbit. Most teratomas have three germinal lay- ers; those with two germinal layers are less common and are called “teratoid” tumors. Ectodermal (squa-
349
TABLE 6
Reports of Choristomas Containing Ectopic Tissues From Bmiu, L.acrimal Gland, and Cilia? Body
Ectopic Brain Tissue ~~~i~i.~~,Yl”.2~Y.‘“S.:“l) LimbusX”_ I SY
Ectopir Lacrimal Gland Epibulbar region 64.88.lOl.lOti.lI5.l:~,.IUO.L'III
~~~~~5.l~.56.41,110.14.5.1A1."0?.?11."4~3.~1?7
Evelid’FJ4 Ektraocular muscle”’ Sc]era4”J3’
9~.40.49.~~.ti:~.10(1.1 l(l.I:~i.L,~lli Iris and ciliary body.’ Ectopic Cilia9 Body2”
mous epithelium, adnexal structures) and meso- dermal (muscle, bone, cartilage, fat) derivatives are the commonest layers found, and endodermal de- rivatives (gastrointestinal and respiratory tissue) are the least common.‘*’ Transillumination of part of the lesion is secondary to cystic formation,‘“” and ossification or calcification may be evident on roent- genogram.’ Rapid proptosis is partly secondary to increase in the size of the cysts. Teratomas are con- sidered malignant when the tissue constituents are embryonal or immature. Six cases of malignant ter- atomas have been reported, and one patient died from metastasis.Y5,174,546.zc’j Twelve cases have been reported of successful preservation of the proptotic eye; 1y~4x.‘4”.‘44.‘74 exenteration was carried out in the remaining cases because of suspicion of malignant tumor or impending cornea1 perforation from ex- posure keratitis.‘” Optic anlages have been noted in one case of orbital teratomas and in several extraoc- ular teratomas.“” A tumor weighing 95 grams was
Fig. 11. Ectopic brain tissue in the or- bit. [X 16, Hematoxylin and eosin.
(Co1 urtesy of‘ Yue-Kong Au, MD, Was ihington, DC).]

350 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
removed in one case.14’ Teratomas are thought to
arise from loci of totipotential embryonic tissue
which have escaped the influence of primary
organizers.‘“5 Ectopic lacrimal gland tissues have been de-
scribed in the orbit in 17 cases (Table 6). Three
cases of ectopic lacrimal glands underwent malig-
nant transformation, one into adenocarcinoma”O
and two into pleomorphic adenoma.36*21’ Propto- sis35*3p7 from ectopic lacrimal glands is related to
inflammation of the gland tissue’9’ or to formation of ectopic gland cysts.4’J43
and thickened superior oblique muscle. Histopath-
ologically, connective tissue and hyaline cartilage
had replaced the muscle fibers. The choristoma had
occurred in the area of the trochlea and its presence could be attributed to an abnormal development of
the trochlea proper. A second case of fibrofatty in-
volvement of extraocular muscles in the context of the linear sebaceous nevus syndrome was de-
scribed.“j’ In a third case, ectopic lacrimal gland
involved the lateral rectus insertion.“’
F. OPTIC NERVE HEAD CHORISTOMA
Ectopic brain tissue has been described in six
cases (Fig. 11). One patient had Turner syn-
drome.3’0 Exophthalmos or eyelid swelling is usual- ly present at birth. ’ The orbital mass is circum-
scribed and has no direct connection with the central nervous system, in contrast to a meningoen-
cephalocele. 2’5 An intact dura mater has been noted
to separate the orbital lesion from the brain in the
region of a bony defect. 2’5 Striated muscle fibers connected to the ectopic nervous tissue were noted
in two cases.2’5,3’o Increasing proptosis in some
cases is due to intrinsic secretion of cerebrospinal fluid into the cystic orbital lesion.3’0
Heterotopic adipose tissue and smooth muscle have been detected in 29 optic nerve heads (Fig. 12).89.‘25,303,3’3 J-h e anomaly was accompanied by
distal enlargement of the optic nerve in the area of
the colobomatous malformation. The involved eyes were enucleated because of pain and blindness
from glaucoma or, less commonly, because of a sus-
picion of an ocular tumor (such as glioma) in a
seeing eye. The presence of smooth muscle in the optic nerve or peripapillary structures (choroid or
sclera) may partly account for the contractile behav- ior of some peripapillary staphylomas.‘0g~‘60~‘7g~3’4
One case of ectopic lymph node in the orbit has been described.3’s
Ectopic retina in the optic nerve head was noted in a subject with triploidy.g2
E. CHORISTOMAS OF THE EXTRAOCULAR MUSCLES
G. CHORISTOMA OF OPTIC NERVE AND CHIASM
Choristomas of the extraocular muscles are rare. In one patient, a choristomatous growth of the su-
perior oblique muscle presented as a trochlear pal-
sy and a palpable upper nasal orbital mass.46 At exploration, the palpable mass proved to be a hard
Choristomas involving the intracranial optic
nerve and the optic chiasm were mistaken for a glioma and a meningioma in two subjects3”0 Optic
atrophy on the involved side was present in both
cases, and accompanied by progressive visual loss in
one case. The two optic nerves were replaced by
Fig. 12. Choristoma of the optic nerve. Note the enlarged retrolam- inar portion of the optic nerve with replacement of the nerve substance by muscle and adipose tissue. [x4, Hematoxylin and eosin. (Courtesy of Richard O’Grady, MD, Northwestern University, Chicago).]

OCULAR CHORISTOMAS
Fig. 13. Prelenticular whitish membrane attached to the iris at 12 o’clock with inferotemporal limbal choristoma in a 4-year-old boy with Goldenhar syndrome.
smooth muscle and adipose tissue.
H. RETINAL CHOIUSTOMA
An accessory ciliary body has been reported in the dysplastic retina of a patient with anenceph- sly,“‘” and in a patient with trisomy 13 (Tso MOM: AOA-AFIP meeting 198’7).
I. ANTERIOR UVEAL CHORISTOMAS
Choristomas of the iris and ciliary body present as cysts or nodular masses. Dermoid cysts of the iris are acquired lesions and are not included in this discussion. Ectopic lacrimal gland tissue is a com- mon choristoma of the iris and ciliary body (Table 6). The similarity of the glandular structures in these intraocular lesions to those of the lacrimal glands have been substantiated by electron micro- scopic studies.““’ Ectopic lacrimal gland of the iris has been reported in an eye with an epibulbar chor- istoma.“” Cartilage has been found adjacent to anterior uveal colobomata,““’ often with trisomy 139’“. (::I or cyclopia,““l Heterotopic ciliary processes have been found attached to the iris in a case of’ triploidy. ““J
Six cases of choristomatous malformation of the iris, known as the prelenticular membrane, have been reported. lo.Ii.:~:i.4li.I(il’.L’it~ The membrane has been mistaken for intraocular spread of epibulbar choristomas.“” We have followed a 4-year-old boy since birth for a superior whitish avascular prelen- titular membrane not connected to an inferotem- poral limbal choristoma (Fig. 13).
J. CHOROIDAL CHORISTOMAS
The majority of choroidal choristomas are of the osseous variety, although heterotopic smooth mus- cle has been noted in the choroid in eyes with cryp- tophthalmos.‘“’ Most choroidal osteomas are XC-
Fig. I?. Choroidal osteoma covering the posterior pole. (Courtesy of-Lee M. Jampol, MD, Northwestern Univcr-- sky, (:hicago.)
quired lesions that occur adjacent to choroidal hemangiomas,“‘” and in phthisis bulbi or chronic intraocular inflammation. The origin of the os- teoma has been related to the proliferation and metaplasia of the retinal pigment epithelium:“” However, there is evidence that some choroidal os- teomas represent choristomatous growths accord- ing to the following criteria: detection in infancy’“’ or below six,h”~X.1~‘X5.‘?9” familial occurrence,“” and as- sociation with epibulbar choristomas. Io.;.llii.lx’,.“:~I) Of 27 choroidal osteomas reported in the litera- ture 7.iX.~~~l.X-1.!17.!1X,l~~,l~.~,l~7,~~~l~ ‘)3 were in women. Le_
sions were bilateral in seven patients,7.~~~l.‘17.1~i.l~!l
Eighteen lesions underwent growth and/or devel- opment of subretinal neovascular membranes. Pa- tient ages ranged from 6 months’“’ to 36 years.!” with a mean age of 19 years. Five patients’ ages were in the first decade, 10 in the second, 9 in the third, and 3 in the fourth. Several eyes were enucleated because of the suspicion of a malignancy.~“,““‘” The characteristic fundus appearance is a juxtapapillary flat yellow-white choroidal lesion with overlying pigmentary clumping; occasionally multiple short branching vascular trunks are present on the sur- face (Fig. 14).“’ Ultrasonographic and radiographic studies help to establish a definitive diagnosis. Symptoms develop when the osteoma grows to in- volve the fovea. A common presenting symptom is metamorphopsia from a subretinal neovascular membrane developing in the macular region.!‘!’
III. Summary
Choristomas represent the commonest epibulbar lesions in childhood. They have predilection for the
352 SW-V Ophthalmol 33 (5) March-April 1989
subconjunctival space, the limbus, and the cornea. They present a wide clinical spectrum, mimicking cornea1 dystrophies and epibulbar malignancies. They are benign tumors, and rarely grow. About 10% of epibulbar choristomas are associated with either Goldenhar syndrome or linear epidermal nevus syndrome. Epibulbar choristomas are occa- sionally familial. Cornea1 choristomas are managed by a lamellar or a penetrating keratoplasty. Surgical excision of limbal choristomas should be performed with caution because of an associated limbal ectasia. Limited excision is indicated in subconjunctival choristomas that extend posteriorly into the orbit. Epibulbar choristomas are associated with choroi- da1 osteomas, cartilaginous choristomas of the eye- lids, dermoid cysts of the orbit, and various systemic choristomas. Choristomas may also occur in non- epibulbar areas, e.g., sclera, eyelid, or orbit, extra- ocular muscle, optic nerve head, retina, uvea, and choroid.
1. 2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
References Acers TE: Encephalocele. Arch Ophthalmol 73:84-85, 1965 Aleksic S, Budzilovich G, Choy A, et al: Congenital ophthal- moplegia in oculoauriculovertebral dysplasia-hemifacial microsomia (Goldenhar-Gorlin syndrome). A clinicopath- ologic study and review of the literature. Neurology 26: 638-644, 1976 Afeksic S, Budzilovich G, Ruben R, et al: Congenital facial neuropathy in oculoauriculovertebral dysplasia-hemifacial microsomia (Goldenhar-Gorlin syndrome). Bull Los Angeles Neural Sot 41:68-V, 1976 Alkemade PPH: Congenital teratoma of the orbit. Ophthal- mologica 17?:274-285, 1976 Appel N, Som PM: Ectopic orbital lacrimal gland tissue.] Comput Assist Tomogr 6:1010-1012, 1982 Ash JE: Epibulbar tumors. Am J Ophthalmol33: 1203-1219, 1950 Augsburger JJ, Shields JA, Rife CJ: Bilateral choroidal os- teomas after nine years. Can J Ophthalmol18:28 l-284,1979 Aurell C, Kornerup T: On glandular structures at the cor- neo-scleral junction in man and swine; the so-called “Manz’ glands.” Acta Ophthalmol 27: 19-45, 1948 Baggesen LH, Jensen OA: Phakomatous choristoma of lower eyelid. A lenticular anlage tumor. Ophthalmologica 175:231-235, 1977 Ballantyne AJ: Two cases of epibulbar osteoma. Ophthalmo- logica 99:87-95, 1940 Baker RS, Ross PA, Baumann RJ: Neurologic comphca- tions of the epidermal nevus syndrome. Arch Neural 44: 227-232, 1987 Ballantyne AJ: A case showing multiple congenital anoma- lies. Proc R Sot Med 26~313-315, 1933 Barber JC, Barber LF, Guerry D, et al: Congenital orbital teratoma. Arch Ophthalmol 91:45-48, 1974 Bardelli AM, Malandrini F, Fois A, et al: A proposito di una rara sindrome oculo-neuro-cutanea: Problemi diagnostici e di classificazione. Annali Ottat Ctin Ocul 100:727-738, 1974 Barishak YR, Mashiah M: Congenital teratoma ofthe orbit.
J Pediatr Ophthalmol 14:217-220, 1977 Barth PG, Valk J, Kalsbeek CL, et al: Organoid nevus syndrome (Linear nevus sebaceus of fadassohn): Clinical and radiological study of a case.-Neuropaediatrics 8: 418-428, 1977 Baum JL, Feingold M: Ocular aspects of Goldenhar’s syn-
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
MANSOUR ET AL
drome. Am J Ophthalmol 75:259-256, 1973 Beth K, Jensen OA: Mixed tumor of the lower orbital re- gion. Arch Ophthalmol 74:226-228, 1965 Beckman H, Sugar HS: Episcleral osseous choristoma - resport of two cases. Arch Ophthalmol 71:377-378, 1964 Benjamin SN, Allen HF: Classification for limbal dermoid choristomas and branchial arch anomalies: Presentation of an unusual case. Arch Ophthalmol 87:305-314, 1972 Berkeley WT: Nevus sebaceus (Jadassohn) complicated by bilateral salivary gland adenocarcinoma. Plast Reconstr Surg 23:55-63, 1959 Berkman MD, Feingold M: Oculo-auriculovertebral dys- plasia (Goldenhar’s syndrome). Oral Surg 25:408-417, 1968 Bernheimer S: Angeborenes totales Hornhautstaphylom mit Dermoidbildung. Arch Augenheilkd 18: 171-l 79, 1888 Bernuy A, Contreras F, Maumenee AE, et al: Bilateral, congenital, dermis-like choristomas overlying cornea1 staphylomas. Arch Ophthalmol 99: 1995-1997, 1981 Berthelon S, Cremer N: Syndrome de Goldenhar avec malformations associees. Bull Sot Beige Ophtalmol 149: 509-513, 1968 Besser FS: Linear sebaceous naevi with convulsions and mental retardation (Feuerstein-Mims’ syndrome). Vita- min-D-resistant rickets. Proc R Sot Med 69:5 18-520, 1976 Bianchine JW: The nevus sebaceous of Jadassohn. A neu- rocutaneous syndrome and a potentially premalignant le- sion. Am J Dis Child 120:223-228, 1970 Bittencourt AL, Marback R, Peralta MJ, et al: Neuro-oculo- cutaneous syndrome with multiple sebaceous nevi. Presen- tation of a case. Med Cutan Ibero Lat Am X1:375-382, 1983 Bitter K: Uber Die Erstbeobachtung eines angeborenen Naevus sebaceus im Trigeminusbereich mit GehirnmiBbil- dungen und Riesenzellgeschwulsten des Ober-und Unter- kiefers. Dtsch Zahn Mund-und Kieferheilk 56: 17-24, 197 1 Bock E: Beitrag zur pathologischen Anatomie der Carun- cula lacrymalis. Klin Monatsbl Augenheilkd 23:487-491, 1885 Bock RH: Ein Fall von epibulbarem Dermolipom mit Mif- bildung einer Gesichtschalfte diskordantes Vorkommen bei einem eineiigen Zwillingspaar. Ophthalmologica 122: 86-90, 1951 Bogel G: Ueber das subconjunctivale Lipom und Combi- nation desselben mit Ichthyosis hystrix. Graefes Arch Clin Exp Ophthalmol32:129-150, 1886 Bollack J, Offret G: Corectopie et kystes dermoides de l’oeil et de l’oreille. Bull Sot Ophtalmol (Paris) 9:705-714, 1937 Boniuk M, Zimmerman LE: Epibulbar osteoma (episcleral osseous choristoma). Am J Ophthalmol _53:290-296, 1962 Boudet C, Maisongrosse M, Malan P: Ectopie lacrymale dans le corps cillaire. J Fr Ophtalmol 4~677-678, 1981 Boudet C, Bertezene M: Exophtalmie par adenome lacry- mal en position ectopique (angiographie de l’orbite). Bull Sot Ophtamol Fr 64:624627, 1964 Bowen JH, Christensen FH, Klintworth GK, et al: A clini- copathologic study of a cartilaginous hamartoma of the orbit. A rare cause of proptosis. Ophthalmology 88: 1356-1360, 1981 Braun-Vallon S: Une curieuse anomalie du muscle droit externe. Bull Sot Ophthalmol Fr 4r212, 1955 Breinin GM: The eye in teratomas. Report of a case and review of the literature. Arch Ophthalmol43:482-499, 1950 Bruce G: Aberrant glandular tissue in the iris. Trans Am Acad Ophthalmol Otolaryngol 56:47-5 1, 1952 Bullock JD, Fleishman JA, Rosset JS: Lacrimal ductal cysts. Ophthalmotogy 931: 1355-l 360, 1986 Butler TH: A dermoid of the cornea. Arch Ophthalmol 52:469-171, 1923 Calhoun FP: Dermoid tumor of cornea-conjunctiva associ- ated with scleral ectasia. Am I Ophthalmol 7:669-670, 1924 Call NB, Baylis HI: Cerebella; heterotopia in theorbit. Arch Ophthalmol 98:717-719, 1980 Casanovas R, Trigueros M: Coristomas oculares bilaterales con hidrocefalia y nevus sistematizado. Arch Sot Esp Oftal-
OCULAR CHORISTOMAS
46.
47.
48.
49.
50.
51.
.52. 53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70
71
72
mol 32: 137-144, 1972 Castren JA, Tarkkanen A: Malformation of the superior oblique muscle simulating orbital tumor. Acta Ophthalmol ?2:975-979, 1964 Chalhub EG, Volpe JJ, Gado MH: Linear nevus sebaceous syndrome associated with porencephaly and nonfunction- ing major cerebral venous sinuses. Neurolog?r 25:857-860, 1975 Chang DF, Dallow RL, Walton DS: Congenital orbital tera- toma: report of a case with visual preservation. J Pedialr Ophthalmol Strabismus 17:88-95, 1980 Christensen L, Anderson ED: Aberrant intraocular adeno- mata and epithelization of the anterior chamber. Arch Ophthalmol -/X:19-29, 1952 Christiaens L, Walbaum R, Farriaux JP, et al: A propos de deux cas de dysplasie oculo-auriculo-vertebrale. P~diatrie 21.935-942. 1966 Clancy RR, Kurtz MB, Baker D, et al: Neurologic manifes- tations of the organoid nevus syndrome. Arch Neural -12: 236-240, 1985 Cohen C: Dermoid of conjunctiva. MedJ Aust 2t360, 1924 Collier MM: Dysostose mandibulo-faciale et hypoplasie pa- pillaire. Bull Sac Ophtnlmol Fr 11:873-878, 1961 Collins El‘: X. Congenital abnormalities. 1. Microphthal- mos with cystic protrusion from the globe. Tram Ophthalmol Sot UK 17:254-266, 1897 Conway VH, Brownstein S, Chisholm IA: Lacrimal gland choristoma of the ciliary body. Ophthalmology 92:449-453, 1985 Cordier J. Stricker M, Reny A, et al: Syndrome de France- shetti-Goldenhar discordant chez deux jumelles monozy- gotes. Arrh Ophtalmol (Paris) 30:321-328, 1970 Cosmettatos GF: Ueber einen Fall von epibulbarem der- moid Nebst einigen bemerkungen uber seine Pathogenie. Kiln Monntsbl Augenheilkd 44:252-256, 1906 Coston TO, Wilkinson CP: Choroidal osteoma. AmJ Oph- thalmol 86:368-372, 1978 Critchett A: Bony tumor of the conjunctiva. Truns Ophthal- mol Sor UK 2t254, 1882 Cunha SL: Osseous choristoma of the choroid. A familial disease. .4rch Ophthalmol 102:1052-1054, 1984 Cuttone JM, Durso F. Miller M, et al: The relationship between soft tissue anomalies around the orbit and globe and astigmatic refractive errors: A preliminary report. J Ppdintr Ophthalmol Strabismus 17:29-36. 1981 Dailey EG, Lubowitz RM: Dermoids of the limbus and cor- nea. .4m,/ Ophthalmol 53:661-665, 1962 Dallachy R: Ectopic lacrimal glandular tissue within the eyeball. Hr J [~phthu~rno~ -I 5:808-8 15, 1972 Dame LR: Accessory lacrimal gland of the cornea. Am J Ophthalmol 29:579-582, 1946 Darling DB, Feingold M, Berkman M: The roentgenologic aspects of Goldenhar’s syndrome (oculoauriculovertebral dysplasia). Kndiolop 91:254-259, 1968 Dayal Y. Hameed S: Periorbital dermoid. AmJ Ophthalmol 53:1013-1015, 1962 DC Lapersonne F: Sur un cas de microphtalmie double aver kystes orbitaires. .4rr,h Ophtnlmol (Paris) 11:207-223, 1x91 1)~ Vincentiis M: Sur les proprietes morphogenetiques et organisatrices de la vesicule optique humaine a la lumiere d’lm cas particulier de teratologie oculaire. Acta Ophthalmol 30:255-“79 195” -1 - Dcnk R: Schimmelpenning-Syndrom. Naevus sebacrus mit Augcnfehlbildungen Anfallsleiden und geistiger Retar- dierung. Med Welt 22:666-668, 1971 Dimond RL, Amon RB: Epidermal nevus and rhabdomyo- sarcoma. ,4rch Dermutol 1121424-1426, 1976 Diven DC:, Solomon AR, McNeely MC, et a!: Nevus seba- ceus associated with major ophthalmologic abnormalities. .Arrh DPrmatol 123:383-3X6, 1987 Donders, cited by Wilkes SR, Campbell RJ, Wailer RR: ocular malformation in association with ipsilateral nevus 01 Jadasrhon. Am J Ophthalmol 92:344-352, 1981
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87
88
89
90.
91.
92.
93.
94. 95.
96.
97.
98.
99
100.
101.
102.
353
Dreizen NG, Schachat AP, Shields JA, et al: Epibulbar osse- ous choristoma. J Pediatr Ophthalmol 20:247-249, 1983 Duke-Elder S: System of Ophthalmology, Vol. 1. London, Hen- ry Kimpton, 1958, pp 403, 450 t&ke-E’lder S: Syst& if Ophthalmology, Vol llipt 2. St. Louis, CV Mosby, 1963, pp 488-495, pp 820-826 Dunnington JH: Bilateral multiple ocular dermoids. Arch Ophthalmol 1:669-671, 1929 Ebhard EG, Jaeger W: Schwerste Augenbeteiligung bei einem cerebralparetischen Kind mit ausgedehnten epider- malen Naevi (Schimmelpenning-Feuerstein-Mims-Syn- drome?). Ber Dtsch Ophthalmol GPS 78:857-859, 1981 Eldrup-Jorgensen P, Fledelius H: Orbital tumours in in- fancy. An analysis of Danish cases from 1945-1962. .4cta Obhthalmol53:887-893, 1975 Eisas FJ, Green WR: Epibulbar tumors in children. Am ,/ OBhthalmol 79:1001-1007. 1975 Gamy H, Ahmadian H: Limbal dermoid with ectopic brain tissue. Report of a case and review of the literature. 4rch Ophthalmol 95:220!-2202, 1977 Emerit 1. Vernant P: Syndrome de Goldenhar et malfor- mation complexe du coeur. Presse Med 74:507-510, 1966 Enjolras 0, Guerin D, Hewitt J: Contribution a la connais- rance du syndrome du naevus epidermique de Solomon. 4nn Derrnatol Venereal 106:673-680, 1979 Fanta H: Choristoma osseum orbitae. Ophthalmologira 174: 176-178, 1977 Fava GE, Brown GC, Shields JA, et al: Choroidal osteoma in a 6-year-old child. J Pediatr Ophthalmol Strabismus 17: 203-205, 1980 Ferry AP, Hein HF: Epibulbar osseous choristoma within an epibulbar dermoid. Am J Ophthalmol 70:764-766, 1970 Feuerstein RC, Mims LC: Linear nevus sebaceus with con- vulsions and mental retardation. Am .I Dt\ Chdd 104: 675-679, 1962 Filipic M, Silva M: Phakomatous choristoma of the eyelid. A tumor of lenticular anlage. Arch Ophthalmol88: 171-175, 1972 Firat I‘, Emuler U: Two cases of aberrant lacrimal gland. .4nn Ophthalmol 3:50-5 I, 197 1 Font RL, Zimmerman LE: Intrascleral smooth muscle in coloboma of the optic disk. Electron microscopic verifica- tion. Am I Obhthalmol 72:452%457. 1971 Franchesche‘tti A, Klein D, Brother JEW: La dysostose mandibulo-faciale dans le cadre des syndromes du premier arc branchial. Schweiz Med Wochenschr 89:47X-483, 1959 Franceschetti A, Klein D: Dysmorphie cervico-oculo-facial avec surdite familiale. / Genet Hum 3:176-l 83. 1954 Fulton AR, Howard Rh, Albert DM, et al: Ocular fmdings in triploidy. .4m J Ophthalmol 8-/:859-867, 1977 Gallenga C: Contribution a I’Ctude des tumeurs congeni- tales de la conjunctive et de la cornee. Considerations sur leur genese. ,4rzn Ocul (Paris) 94:215-224, 1885 Galloway: Society intelligence. Br J Dermatol 14t.57, 1902 Garden JW, McManis JC: Congenital orbito-intracranial reratoma with subsequent malignancy: case report. Br J Ophthalmol 70: I 1 l-l 13, 1986 earner LL: Dermoid of the limbus involving the iris angle and rhe lens. Arch Ofihthalmol 4669-72 1951 Gass JDM: New observations concerning cchoroidal osteo- mas. Int Ophthalmol /:71-84, 1979 Gass JMD, Guerry RK, Jack RL. et al: (:horotdal osteoma.
.4rrh Ophthalmol 96428435, 1978 Gayral I., Gayral J: Contribution a I’&ude de !a dysostose mandibulo-faciale (Nouveaux cas et asperrs neurologiques et psychiatriques). J Genet Hum Jtll7-142. 1955 Ghadially FN, Chisholm IA, Lalonde JM: Ultrastructure of an intraocular lacrimal gland choristoma.,/ Suhmrrrorc @to/ I&189-198, 1986 GinsbergJ, Ballard ET. Buchino JJ, et al: Further observa- tions of ocular pathology in Down’s syndrome. ,I fed&r Ophthalmol 17: 166 17 1. I 980 Ginsberg J, Ballard ET. Soukup S: Pathologic features of rhe eve in triploidy. ,/ Prdicitr Ophthnlmol /8.4X-55, 1981
354 Surv Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
103. Gobling-Ebhard E, Jaeger W: Schwerste Augenbeteiligung bei einem cerebralparetischen Kind mit ausgedehnten epi- dermalen Naevi (Schimmelpenning-Feuerstein-Mims- Syndrome?). Ber Dtsch Ophthalmol Ges 78:857-859, 1981
104. Goldenhar M: Associations malformatives de I’oeil et de l’oreille, en particulier le syndrome dermoide epibulbaire- appendices auriculaires-listula auris congenita et ses rela- tions avec la dysostose mandibulo-faciale. J Genel Hum 1:243-282, 1952
105. Gooskens RH, Veiga-Pires JA, Van Nieuwenhuizen 0, et al: CT of sebaceous nevus syndrome (Jadassohn disease). Am J Radio1 Nucl 1:203-205, 1983
106. Gorduren S: Aberrant lacrimal gland associated with other congenital abnormalities. Br J Ophthalmol 46:277-280, 1962
107. Gorlin RJ, Jue KL, Jacobsen U, et al: Oculoauriculoverte- bra1 dysplasia. J Pediatr 63:99 l-999, 1963
108. Gorlin RJ, Pindborg JJ, Cohen MM, Jr: Syndromes of the Head and Neck. New York, McGraw-Hill, 1976, ed 2, pp 546-552
109. Graether JM: Transient amaurosis in one eye with simulta- neous dilatation of retinal veins. In association with a con- genital anomaly of the optic nerve head. Arch Ophthalmol 70:342-435, 1963
110. Green WR, Zimmerman LE: Ectopic lacrimal gland. Arch Ophthalmol 78:318-327, 1967
111. Greer CH: Phakomatous choristoma in the eyelid. Aust J Ophthalmol 3:106-107, 1975
112. Gronholm V: Birkhausers neue Scalae typographicae. Dermoid im Zentrum der Kornea. Klin Monatsbl Augen- heilkd 70:771, 1923
113. Grossniklaus HE, Green WR, Luckenbach M, et al: Con- junctival lesions in adults. A clinical and histopathologic review. Cornea 6:78-l 16, 1987
114. Grove AS: Giant dermoid cysts of the orbit. Trans Am Acad Ophthalmol Otol 86: 1513-1520, 1979
115. Gruntzig J: Ektopische Tranendruse unter der Conjuncti- va bulbi. Klin Monatsbl Augenheilkd 176t4501152, 1980
116. Gupta JS, Gupta SD, Prashar SK: Oculo-auricular cranial dysplasia. Br J Ophthalmol 52:346-347, 1968
117. Haberland C, Peron M: Encephalocraniocutaneous lipo- matosis. Arch Nero-01 22:144-155, 1970
118. Hanke V: Dermoid der cornea Microphthalmos Aphakia congenita. Endobulbares Lipom. Graefes Arch Ophthalmol 57:38-52, 1904
119. Harman NB: Multiple anomalies in a child. Trans Ophthal- mol Sot UK 24:325-329, 1904
120. Hartridge G: Osteoma of the conjunctiva. Tram Ophthalmol Sot UK 15:51-55, 1895
12 1. Haslam RHA, Wirtschafter JD: Unilateral external oculo- motor nerve palsy and nevus sebaceous ofJadassohn. Arch Ophthalmol87:293-300, 1972
122. Haye C, Haut J, Romain M: A propos des kystes dermoides de I’orbite. Arch Ophtalmol 26:471-480, 1966
123. Haye C, Haut J, Sander JP: Les dermoides epibulbaires. Arch Ophtalmol Fr 29: 193-204, 1969
124. Heimann K: Beitrag zur Klinik des Goldenhar-Syndroms. Klin Monatsbl Augenheilkd 152:686-692, 1968
125. Henkind P, Marinoff G, Manas A, et al: Bilateral cornea1 dermoids. Am J Ophthalmol 76:971-977, 1973
126. Heustis JW: Osteoma of the conjunctiva. Ann Ophthalmol 8:18-19, 1899
127. Hirsch C: Ueber enkanthoschisis und andere augeborene anomalien des auges. Klin Monatsbl Augenheilkd 50:1-16, 1912
128. Hoffman ME, Sorr EM: Photocoagulation of subretinal neovascularization associated with choroidal osteoma. Arch Ophthalmol 105:998-999, 1987
129. Hoffman-Egg L, Velissaropoulos P: Malformations oculo- auriculaires (lipodermoide epibulbaire appendice pre- auriculaire colobome de la paupiere superieure) et leurs relations avec la dystsostose mandibulo-faciale. Ann Ocul 186:155-169, 1953
130. Holden KR, Dekaban AS: Neurological involvement in ne-
vus linearis sebaceus. Neurology 22:879-887, 1972 131. Hollwich F, Verbeck B: Zur dysplasia oculoauricularis
(Franceschetti-Goldenhar-Syndrom). Klin Monatsbl Augen- heilkd 154:430-443, 1969
132. Horner WD, Cordes FC: Congenital coloboma of the up- per eyelid with dermoids on cornea. Report of a case. Am J Ophthalmol 12:959-964, 1929
136. Hughes WL, Ballen PH: Ectopic lacrimal gland. Arch Ophthalmol55:271-273, 1956
137. Hunter WS: Aberrant intra-ocular lacrimal gland tissue. Br
133. Hornstein L, Bove KE, Towbin RB: Linear nevi, hemihy-
J Ophthalmol 44:619-625, 1960
pertrophy, connective tissue hamartomas, and unusual neoplasms in children. J Pediatr 110:4041108, 1987
134. Hornstein OP, Knickenberg M: Zur Kenntnis des Schim-
138. Hurwitz S: Epidermal nevi and tumors of epidermal ori-
melpenning-Feuerstein-Mims-Syndroms (organoide nae- vus-phakomatose). Arch Dermatol Forsch 250:33-50, 1974
135.
gin. Pediatr Clin North Am 30:483-494, 1983
Hoyt WE, Joe S: Congenital teratoid cyst of the orbit. Arch
139.
Ophthalmol 68: 19620 1, 1962
Hutchison DS, Green WR, lliff CE: Ectopic brain tissue in a limbal dermoid associated with a scleral staphyloma. Am J Ophthalmol 76:984-986, 1973
140. Ide CH, Davis WE, Black SPW: Orbital teratoma. Arch Ophthalmol 96:2093-2096, 1978
141. Ide CH, Miller GW, Wollschlaeger PB: Familial facial dys- plasia. Arch Ophthalmol 84t427-432, 1970
142. Iliff WJ, Green WR: Orbital tumors in children, in Jakobiec FA (ed): Ocular and Adnexal Tumors. Birmingham, Aescula- pius, 1978, pp 669-684
143. Insler MS, Davlin L: Ocular findings in linear sebaceous naevus syndrome. Br J Ophthalmol 71:268-272, 1987
144. Itani K, Traboulsi EI, Abdul Karim FW, et al: Conservative surgery in orbital teratoma. Orbit 5:61-65, 1986
145. Jacobs L, Sirkin S, Kinkel W: Ectopic lacrimal gland in the orbit identified by computerized axial transverse tomog- raphy. Ann Ophthalmol 9:591-593, 1977
146. Jadassohn J: Bemerkungen zur histologie der systemati- sierten naevi and uber “talgdrusen naevi”. Arch Dermatol Syphilol 33:355-394, 1895
147. Jakobiec FA, Bonanno PA, Sigelman J: Conjunctival ad- nexal cysts and dermoids. Arch Ophthalmol 96:1404-1409, 1978
148. Jancar J: Naevus syringocystadenomatosus papilliferus with skull and brain lesions, hemiparesis, epilepsy, and mental retardation. Br J Dermatol 82:402-405, 1970
149. Jensen OA: Teratoma of the orbit. Acta Ophthalmol 47: 317-327, 1969
150. Joffe L, Shields JA, Fitzgerald JR: Osseous choristoma of the choroid. Arch Ophthalmol 96:1809-1812, 1978
151. Jones EW, Hey] T: Naevus sebaceus. A report of 140 cases with special regard to the development ofsecondary malig- nant tumours. Br J Dermatol82:99-117, 1970
152. Kalis B, Degos R, Harmel L, et al: Naevus sebace verru- queux avec manifestations neurologique-oculaire-osseuse (Naevus de Solomon). Ann Dermatol Syphilol (Paris) 100: 380-381, 1973
153. Kaufer G, Plater GJ: Coristoma oseo epiescleral. Arch Oftal- mole Buenos Aires 43:12-13, 1968
154. Kaushik NC: Ectopic lacrimal gland in the eyelids (a case report). Indian J Ophthalmol 33t65-66, 1985
155. Kelinske M, Weinstein GW: Bilateral choroidal osteomas. Am J Ophthalmol 92:676-680, 1981
156. Kessing SV: Ectopic lacrimal gland tissue at the cornea1 limbus (gland of Manz?). Acta Ophthalmol (Copenh) (Kbh) 46:398-403, 1968
157. Kirke DK: Goldenhar’s syndrome: Two cases of oculo-au- riculo-vertebral dysplasia occurring in full blood Austra- lian aboriginal sisters. Aust Pediatr J 6:2 13-2 14, 1970
158. Kirkham TH: Cervico-oculo-acusticus syndrome with pseudopapilledema. Arch Dis Child 44:504:508, 1969
159. Kline LB, Skalka HW, Davidson JD, et al: Bilateral choroi- dal osteomas associated with fatal systemic illness. Am J

OCULAR CHORISTOMAS
0,bhthalrnol 93: 192-197, 1982 159a.Knoth W. Kleinhans D, Boepple D, et al: Systematisierter
Naevus sebaceus partim Verrucosus mit Augenbeteili- gung. D~rmatol Monntsschr 158:668-689, 1972
160. Kral K, Svarc D: Contractile peripapillary staphyloma. Am ,] Ophthnlmol 71:1090-1092. 1971
16 1. Kranz HW: Uber eine seltene angeborene Missbildung der Haut mit doppelseitigem Lipodermoid der Conjunctiva bulbi. Grcrrf~s Arch Clin Exp Ophthalmol 118: 167-174, 1927
16Q. Krause Li: I‘he syndrome of Goldenhar affecting two sib-
lings. Acts Ophthnlmol -/8:494-499, 1970 169. Krcibig W. Nehm 0: Uber die episklerale Knochenlamelle.
Hit, Monatshl Augenhedkd 155:707-7 12, 1969 164. Ladekarl S: Combination of Goldenhar’s syndrome with
cri-tin-chat syndrome. ,4cftr Ophthalmol %:605-610, 1968 165. Laihovitz RA: An unusual cause ofintraocular calcification:
choroidal ostemoa. Ann 0~kthrrlmol 1 I; 1077-1080, 1979 166. Lall K: .I‘cratoma of the conjunctiva associated with nexus
systematic us and epilepsia symptomatica. Acln Oplhn/mt~/ 40:555-558, 1962
167. Lambert HM, Sipperley JO, Shore J W, et al: Lineal- nexus sebaceous syndrome. Ophthnlmolog?j ‘#:27%2X2, 19X7
16X. Lansky 1.1~. Funderburk S. Cuppage FE, et al: Linear seba- ceous nexus syndrome. A hamartoma variant. .4m ,/ D/s Child l-73:587-590, 1972
169. Lantis S. Leyden J,‘l‘hcw M. et al: Nexus sebaceus ofJadas- s&n. .-ln+ Dwrnxtol Y8:l 17-123, 1968
170. Laplanchc G. Grosshans E. Gabriel-RobeL 0, et al: Hyper- plasie epidermique et Hemidysplasie corporellc hypopla- siquc congenitales homolaterales (Demembrement du syn- drome de Solomon). .-Inn l~fvn~to/ Ibnrrol 107:729-739, 19x0
17 I. Larregue M. (Ioscas G. Masclef P, et al: Le Syndrome du naevus epidermique de Solomon. .-lrrn D~rmntol ,$yphilol (f’(/T/.\j 101.~45-55. 1974
172. Leonidas JC, Wolpert SM, Feingold M, et al: Radiographic features (if the linear nexus sebaceous syndrome. ,4rn,/ Ko- dial I32:277-279. I979
173. Levvn L: Systematisierrer haevus sebaceus bei gleichLeiti- gem Vorhandensein einer Prosis. LI~rmutol Monuta.trhr Yl: 14‘40-1442, 1990
174. Lenin ML, Leone (:R, Kincaid MC: Congenital orbital tera- tomas. .4rrr ,/ 0phthnlmol 102:476-48 1, I986
175. Lcvh F. Loewel R: Ein Fall van Schimmelpenning-Feuer- stein-Mims-SyntiroI11 mit allmahlicher Kataraktentwick- lung. % ffuutkr #:695-69X. 1973
176. Lichter- PR: Multiple corncal dermoids associated with mil- iarT .meurysms ofthe retina.,/ f’rdi&r Ophthalmol 4::‘~ l-.72. 19ii7
177. Lievre JA: Dysostose rnandibulo-faciale chez le frere et la soeur. F&T Khum Mnl O.stmtrrlir X:916-919, 1953
17X. Lillis I’J, Ceilley RI: Multiple tumors arising in nexus seba- ceous. C,‘at/.\ 23::s 1 O-3 14, 1979
179, Longfellow DW, Davis FS, I\‘alsh FB: Unilateral intermit- tent blindness with dilation ofretinal veins. Undetermined etiology. .4rrh Ophthalmol h7:554-55.5, 1962
180. Malik SR. Sood (X:, Cupta DK: Limbal derrnoid with ne- vus flammeus and neurofibromatosis. E~P Ear Nosr Throrrt Mon/hlr &?:612-614. 1967
181, Mamajis N. (;arland PE, At-gyle .JC. Apple DJ: Congenital orbital teratoma: A review and report of two cases. SICIX~ Ophthnlmol 30.4 l-46, 1985
182. Mann I (ed): Drrvlopmrnfn1 .-lhr/ormtd&u.\ ~4 thr EYY. Philadel- phia. Lippincott, 1957. 2d rd. pp 357-:lti4
I X:4. Mann I: A rare congenital abnormality of the eye. Hr J 0ph/hn/mnl IJ:321-SW, 1930
1x4. Matl\our AM, El Baba I;. Jar-udi N, et al: Association of epibulbat- c horistomas with linear cutaneous nevi: Review ofthc literature. Ophthalmrr f’urdmlr C;rnrt 4.25 l-256, 19X-1
185. Manaou~- AM, Laibson PD. Keinecke RD, et al: Bilateral total ~OI-nenl and conjunctival choristomas associated with rpidcrmal nevus. :lrrh Ophthc~lmol lO-f:245-248. I986
186. .Manx)ur rlM. Wang F. Henkind P. et al: Ocular findings in the ],I,-io;llll-iculc)~~rtchral \cqueuces (Goldenhar-Gorlin
syndrome). ,4m J Ophphthnlmol 100:555-559. 19% 187. Mansour K, van Busterveid OP: Supernumerary carunclc.
Report of a case. Ann Ophthalmol 17:677-67X. 1984 18X. ManL HJ, Rosen DA, Macklin RD, et al: Neuroectodermal
tumor of anterior lip of the optic cup. Glioneuroma transi- tional to teratoid medulloepithelioma. .-lrc// Of,h//m/nw/ NY:382-S9 1, 197:1
189. Marcus MD. Wooldridge WE: Sebaceous nexus and nexus syringoadenomatosus papilliferus. .4&z Drrmn/o/ .~yphdo/ 62: 105-I 08, 1950
190. Marden PM, Venters HD: A new neu~-o( utaneous svn- drome. ,4m J 1)i.c ChiM 11-7:79-X 1, I966
91. Margo CE, Naugle ‘IX;, Karcioglu %A: &topic lacrimal gland tissue of the orbit and s&r-osing datryoadenitis. Ophthalmir Sutg 1 h: 17X-l X I, I985
92. Margolis S, Aleksic S, Charles N, et al: Retinal and optic nerve tindings in Coldenhar-<;orlin syndrome. fl~~h/hnlmo/- ‘IQ 9/:13?7-135:1. 19x4
93. Marks JG. ‘I‘omasovic JJ: Linear net us sehaccom Hun- drome. J ATI> .4cttd Dwmntol 2::%1-:%‘L. 19X0
194. Mattes J, (Zontreras F. O’Donnell FE: Ring drrmoid syta- dromc. A new syndrome ofautosomal dominant inherited bilatel-al annular limbal dermoids with cornea1 and con- junctival extension. .4rch Ophthnlmol YK: 10.59- IO6 I. IWO
19.5. Mattson R: Bilateral epibulbar lipodrrmoids and eyelid coloboma, caruncular malformation. anterior polar cata- ract, abductional insufficiency. and acquired conjunctival c\ St in the same patient. ,I& f~phth~r/mo/L?5::‘12 I-Zl27, 1917
196. McMahon RI‘. Font RL, McLean IW: Phakomatous chat-is- toma of eyelid: Electron microscopical cxmfirmation oflen- ticulal- derivation. .-lrrh 0ph/hnlmo/ YJ: I7iH- I iX I, 1976
197. Mehrcgan AH, Pinkus H: Lile histol-y of’ organoid nevi. Special reference to nexus sehaceus ot,Jadassohn. ,‘I).c/I I)r,- m///o/ Yl:574-588. I965
198. Mehta K: A case of congenital librolipoma 01 cornea. Rr /blmJ 17:6X1, I947
109. Mcttier SK: Aberrant lacrimal gland. Itch O/~/t~/~dv~o/ hOc
W-4!) I, 19% 200. Mevthaler H: Augenbeftlnde beim Syndrom nnch Schim-
melpenning-Feuerstein und Minis. k//r/ ,‘Llot~~/th/ .-l~gr+ hrrlkd lhh:244-246. I975
201. Miller M: (:ongenital dermoid cyst of c~~rnra in condunc- tion with dermoliporna. .4nzJ O$hthn/mol 7:7O:i-704, 1921
202. Mindin A, l.amberts I), Barsky D: Mixed IatI-meal gland tumor ar-ising from ectopic lacrimal glmtl tirslie in tht, orbit. ,J f’rdialr Ophthalmol l-/:-&-47, I977
203. Mohandecsan MM, Roman0 PE: Ncuroparalytic keratitis in (;ol~lenhar--<;orlin syndl-omr. ltn / Oph/h~~lmol Ki: II l-l 1:s. 197x
204. Mollica F. Pavonr I.. Nucifel-o (;: Linear sebaccou\ nevll syndrome in a newborn. ,im/ Dr.\ Child 128:X68-X7 I, IN-l
20.5. Monahan RH. Hill CW’, Venters HD: Multiple chori\tomas t-onvulhions and mental retardation as a new ncurot ul;l- ncous syndrome. .4m J 0phtfmlmol hl:52%5SL’. I967
206. Morgan (;. Mushin A: Ectopic intraocular- lacrimal gland tissue. Hr./ Of,/rfhn/mo/ iht690-694. I972
207. Mori/allc H. Uemura I’. Shimi/u K: ‘I‘hrer USES of a new congenital o(11lo-cutaIle01,s syndrome. Abbcranr lacrimal glar~tl. abberant cartilage, upper lid coloboma, gap in eve- brow, alopecia and mews. :icltl .Ycrc, O~~l~thtrlr~d ./O/J /:i: I3 16-l 350. 197 1
208. Mortada A: Orbital dermo-lipoma with (;oldcnhat ‘5 syn- dt-ome and tsophthalmos. N,- ,/ Oph/h~~lmo/ i ?:7XfiL7XX. I WI
209. ,Moskowit/. R, Honig 1’1: Ne\us sebac eouh in .tssociation with an intracranial ma&.,/ ,l,r/ .dcrt// Dprnrcrlol /I: I 07X-I 0X0. I OX”
2 10. Moynaha,, E:J, Wolff OH: A new ,leut.ocl,tillleolls \\‘,I- tll-ome. Hi- / Dprmuto/ 79:651-652. I967
21 I. Mueller Et:. Borit A: .\berrant lacrimal gland and pleo- morphic adrnoma within the muscle cont. :I,(?/ f~@/hnlmol 11:66-66J, 1979
21 2. Mullanc\; I: (;omples sporadic colobomata. Hr/ fI/~h/holmol />_‘??X‘1..:IXX, 197X

356 SUN Ophthalmol 33 (5) March-April 1989 MANSOUR ET AL
213. Mullaney J, Coffey VP, Fenton M: Atavistic ocular ossicle. Br J Ophthulmol55:243-247, 1971
214. Natarajan R, Mathew H: Goldenhar syndrome. J Pediatr Ophthulmol 10: 192-l 96, 1973
215. Newman NJ, Miller NR, Green WR: Ectopic brain in the orbit. Ophthalmology 93:268-272, 1986
216. Nikhil KC: Ectopic lacrimal gland in the eyelids (a case report). Indian J Ophthalmol33:65-66, 1985
2 17. Novak: Symmetrische Lipodermoid an beiden Augen. Klin Monatsbl Augenheilkd 65:424, 1920
2 18. Nover A: Uber ektopisches Tranendrusengewebe. Ein Bei- trag zur Diagnose epibulbarer Geschwulste. Klin Monutsbl Augenheilkd 130:483-488, 1957
219. O’Malley ER, Helveston EM, Ellis FD: Duane’s retraction syndrome-Plus. J Pediatr Strabismus 19:161-165, 1982
220. Opitz JM, Faith GC: Visceral anomalies in an infant with the Goldenhar syndrome. Birth Defects Original Article Series 5:104-105, 1969
221. Ortiz JM, Yanoff M: Epipalpebral conjunctival osseous choristoma. Br J Ophthalmol 63:173-176, 1979
222. Papp Z, Gardo S, Walawska J: Probably monozygotic twins with discordance for Goldenhar syndrome. Clinical Genet 5:86-90, 1974
223. Patrinely JR, Green WR, Connor JM: Bilateral posterior scleral ossification. Am J Ophthalmol 94:351-356, 1982
224. Pe’er J, BenEzra D: Heterotopic smooth muscle in the choroid of two patients with cryptophthalmos. Arch Oph- thalmol 104:1605-1670, 1986
225. Pedler C: Unusual coloboma of the optic nerve entrance. Br J Ophthalmol 45:803-808, 1961
226. Pfaffenbach DD, Green WR: Ectopic lacrimal gland. Int Ophthalmol Clin 11(3):149-159, 1971
227. Picque L: Anomalies de Developpement et Maladies Congbitales du Globe de l’oeil. These d’agregation, Paris, G Chamerot, 1886
228. Pieroni D: Goldenhar’s syndrome associated with bilateral Duane’s retraction syndrome. J Pediutr Ophthalmol6: 16-l 8, 1969
229. Pinkus H: Organoid Nevus. Mod Probl Paediat 20:50-57. 1978
230. Pittke EC, Marquardt R, Mohr W: Cartilage choristoma of the eye. Arch Ophthalmol 101:1569-1571, 1983
23 1. Pouliquen Y, Dhermy P, Cotinat I, et al: Dermoide bilater- , al h&sditaire (Etude clinique histologique et ultrastructur-
ale). I Fr Ofihthalmol 1:443-450. 1978 232. Pro& F, &llica L: Contributo silo studio della ereditarieta
dei dermoidi epibulbari. Acta Genet Med Gemellol 15: 351-363, 1966
233. Prout JS: A case of osteo-fibro-lipoma of the conjunctiva. Am J Ophthalmol 5:173-174, 1888
234. Raiford M, Dixon JM: Cystic dermoid tumor replacing the anterior segment of the eye with microphthalmos. Am J Ophthalmol36:508-5 10, 1953
235. Reese AB: Tumors of the Eye. Hagerstown, Harper and Row, 1976, ed 3, pp 318-330,416-422
236. Rizzuti AB: Dermoides solides de la cornee traites par kera- toplastie lamellaire. Bull Sot Ophthalmol Fr 65:867-878, 1965
237. Roth LM, Milauskas AT: Epibuihar osteomas. Arch Oph- thalmol 79:578-579, 1968
238. Rodrigues M, Shannon G: Orbital meningoencephalocele in a healthy adult. Can J Ophthalmol 12:63-65, 1977
239. Rollnick BR, Kaye CI: Hemifacial microsomia and var- iants. Pedigree data. Am J Med Genet 15:233-253, 1983
240. Roscher: Krankendemonstration. Verh Berlin Dermatol Ges Arch Dermutol Syphilol 86:302-303, 1907
241. Rousseau MR: Dysostose mandibulo-faciale avec dermoide de la cornee (syndrome de Franceschetti). Rev Otoneuroph- talmol27:220-229, 1955
242. Rumbaur W: Beitrage zur klinik und anatomie einiger seltener tumoren des auges und der orbita. K&n Mona&b1 Augenheilkd 64:790-801, 1920
243. Rush A, Leone CR: Ectopic lacrimal gland cyst ofthe orbit. Am J Ophthalmol92: 198-201, 198 1
244. Ryba JE: Ueber Dermoidgeschwulste der Bindebaut. Vier- teljahresschtift f die Praktische Heilkunde 3: l-3 1, 1853
245. Saebo J: Lipoma conjunctivae in three generations. Acta Ophthalmol26:447-450, 1948
246. Sgradarian AV: Malignant teratoma of the orbit: six and one half vears’ observation. Arch Obhthalmol37:253. 1947
247. Saraux G, Dhermy P: La trisomie’l3: etude histologique des anomalies oculaires. J Genet Hum Ii(Suppl):303-310, 1968
248. Saraux H, Hudelo J, Levy JP: Un nouveau syndrome: La dysplasie ectodermique oculocutanee. Ann Ocul (Paris) 206:121-126, 1973
249. Saraux H, Grigon JL, Dhermy P: Apropos d’une observa- tion familiale de syndrome de Franschetti-Goldenhar’s. Bull Sot Ophthalmol Fr 63:705-707, 1963
250. Schieck F: Eine bislang unbekannte Missbildung des Auges. Ber Versamml Ophthalmol Ges 36:311, 1910
251. Schiess-Gemuseus: Dermoid der Karunkel. Klin Monatsbl Augenheilkd 15: 135-137, 1877
252. Schimmelpenning GW: Klinischer Beitrag zur Symptoma- tologie der Phakomartosen. Fortschr Rontgenstr 87:716- 720, 1957
253. Schultz GR, Wendler PF, Weseley AC: Ocular dermoids and auricular appendages. Am J Ophthalmol 63:938-942, 1967
254. Sehgal VN, Ramesh V, Ghorpade A: Naevus sebaceous associated with ocular dermolipoma. J Dermatol 11:97-98, 1984
255. Sen DK, Mohan H, Gupta DK: The syndrome of Golden- har. Acta Ophthalmol 47: 1044, 1969
256. Setzer ES, Ruiz-Castaneda N, Sevem C, et al: Etiologic heterogeneity in the oculoauriculovertebral syndrome. J Pediatr 98:88-g 1, 198 1
257. Sherman AR: Teratoid tumor of coniunctiva and other developmental anomalies with naevus ;errucosus of scalp. Arch Ofihthalmol 29:441-445. 1943
258. Sherman RP, Rootman J, iapointe J: Orbital dermoids: Clinical presentation and management. Br J Ophthalmol 68:642-652, 1984
259. Sheth KL, Mathur RN, Sheth JJ: Episcleral osseous choris- toma. Indian J Ophthalmol 26.49-50, 1978
260. Shields JA, Augsburger JJ, Donoso LA: Orbital dermoid cyst of conjunctival origin. Am J Ophthalmol lOlt726729, 1986
261. Shields JA, Laibson PR, Augsburger JJ, et al: Central cor- neal dermoid: a clinicopathologic correlation and review of the literature. Can J Ophthalmol 21:23-26, 1986
262. Shochot Y, Roman0 A, Berishak YR, et al: Eye findings in the linear sebaceous nevus syndrome: A possible clue to the pathogenesis. J Craniofac Genet Dev Biol 2:289-294, 1982
263. Sihota GS: Epibulbar osteoma. BrJ Ophthalmol48:504-506, 1964
264. Sinha PN, Mishra S: Cornea1 dermoid. Am J Ophthalmol 33:1137-l 141, 1950
265. Snell S: Bony tumour of conjunctiva (microscopical sec- tion). Trans Ophthalmol Sot UK 4:31-32, 1884
266. Soares EJ, Lopes KDS, Andrade JDS, et al: Orbital malig- nant teratoma. A case report. Orbit 4~235-242, 1983
267. Solomon LM: Epidermal nevus syndrome. Mod Probl Pae- diat I7:27-30, 1975
268. Solomon LM, Esterly NB: Epidermal and other congenital organoid nevi. Curr Probl Pediatr 6t3-56. 1975
269. Solomon LM, Fretzin DF, Dewald RL: The epidermal ne- vus syndrome. Arch Dermatol 97:273-285, 1968
270. Spencer WH, Jesherg DO: GEoneuroma (choristomatous malformation of the optic cup margin). Arch Ophthalmol 89:387-391, 1973
271. Stallard HB, Martin PP: A case of dermo-fibro-lipoma of the conjunctiva associated with other congenital abnor- malities. Br J Ophthulmol 15;580-584, 1931
272. Stark HH: Congenital tumor of the cornea of doubtful classification. Am J Ophthalmol 2:5-13, 1919
273. Stall KL: A case of multiple double lipodermoids of the conjunctivae and cornea accompanied by intrabulbar and

OCULAR CHORISTOMAS 357
274.
275.
276.
277.
278.
279.
280.
281.
282.
283.
284.
2x5.
286.
2x7
288
289
290
291.
292.
293.
294.
295.
296.
297
298
299
300
other anomalies. Am] Ophthalmol 3&l-14, 1913 Stulting RD, Sumers KD, Cavanagh HD, et al: Penetrating keratoplasty in children. Ophthalmology 91:1222-1230,
1984 Streiff‘ EB, Zografos L: Association d’un lipodermoide epi- bulbaire a une alopecic et un naevus verruqueux sebace: syndrome malformatif congenital a h&edite hologyne. Oph&halmologica I90:67-7 1, 1985 Sugar HS: An unusual example of the oculoauriculoverte- bra1 dysplasia syndrome ofGoldenhar./ Pediatr Ophthalmol
1.9-12, 1967 Sugar HS: The oculoauriculovertebral dysplasia. Syn- drome of Goldenhar. Am_/ Ophlhalmol 62:678-682, 1966 Sugarman Gl, Reed WB: Two unusual neurocutaneous disorders with facial cutaneous signs. Arch Neural 21:
242-247, 1969 Summitt RL: Familial Goldenhar’s syndrome. Birth Deferbv
Or$nnl Article Se% 5: 106-I 09, 1969 Svoboda JR, Madge G, Geeraets WJ: Cornea1 lipodermoid with microphthalmos. Am] Ophthalmol 65:36-42, 1968 Swan KC, Christensen L: Elxperiences with tumors of the limbus. Trnns Am Acad Ophthalmol Otol52:458-469, 1948
Terhaar B: Oculo-auriculo-vertebral dysplasia (Golden- har’s syndrome) concordant in identical twins. At/a Genrt
Mrd Gemeollol 21: 116-l 24, 1972 rimm VG: Zur Morphologie des Auges bei Mifbildunssyn- dromen. Klin Monatshl Augenheilkd 137:557-571, 1960 Tobias N: Nevus unius lateris with unilateral herniatrophy of left side of body. Arch Drrnu~lol Syphilol 15:83-84, 1927 Topilow HW, Cykiert RC, (Goldman K, et al: Bilateral cor- neal dermis-like choristomas: AX chromosome-linked dis- order. ,4rrh Ophlhalmol 99: 1387-l 39 I, 198 1 Tripathi RC, Tripathi BJ, Ringus J: Phakomatous choris- toma of the lower eyelid with psammoma body formation. A light and electron microscopic study. Ophthalmology X8:
119%1206, 1981 Tripp.jH, Joseph MC, Reay HA: A new “neurocutaneous” synclrome (skin, eye, brain and heart syndrome). ProcR Sac
Mrd 64:23-34, 197 I Van Bijsterveld OP: Unilateral cornea] anesthesia in ocu- loauriculovertcbral dysplasia. Arch Ophthalmol82: 189-I 90, 1969 Van Duyse, Bribosia: Fibroma epibulbaire. Arch Ophthalmol
(Pnrrs) 15:657-663, 1895 Van Duyse: Macrostomes congenitaux avec tumeurs pre- auriculaires et dermoide de l’oeil. Ann Sor A4ed de Gnnd
60:141-168, 1882 Vannas S: La dysostose mandibulo-faciale associee a des malfi,rmations oculaires particulieres. J Genet Hum 4.
234-255, 1955 Van Rier LJ, Stewart DM, Jr: Bilateral ocular dermoids preauricular appendages and canthal malocclusion associ- ated with facial asymmetry. / Pediatr Ophthalmol 6: 150-l 52, 1969 Vaquero J, Cabezudo JM, Leunda G, et al: lntraorbital and Intracranial glial hamartoma. Case report. J Neurosurg
53:l 17-120, 1980 VeleL G: Duane’s retraction syndrome associated with Goldenhar’s syndrome. AmJ Ophthalmol 70;945-946, 1970 Volmer W: Em Zahn in einer epibulbaren “komplizierte Dermoidzyste”. K/in Monntshl .4ugPnheilkd 72:181-187.
1924 Van Hippel E: Epibulbares Dermoid, Lidcolobom und Mi- crophthalmus. Cmcfe.s Arrh Ophthalmol 63:38-45, 1906 Waelsh L: Systematisierter ichthyosiformer Naevus. A)-rh
Dermalol .Syphilo( I I-1: 237-246, 19 12 Wagenmann A: Ueber einen merwurdigen Fall von Der- moiclgeschwulst mit rudimentarer Entwickelung des Auges. G-o+ .4rch Ophthalmol 35: 11 I-146. 1889 Wagenmann A: Uber multiple Lipodermoide an einem Auge. C;rarfec Arch Ophthalmol 76.5 1 l-5 I9, 19 10 Wauschkuhn J, Rohde B: SystematisierteTalgdrusen- Pig- ment- und epitheliale Naevi mit neurologischer Sympto- matik: Fellerstein-Mimssches Neuroektodermales Syn-
301.
302.
303.
304.
305.
306.
307.
308.
309.
310.
311.
312.
313.
314.
315.
316.
317.
318.
319.
320.
321.
322.
323.
324.
325.
326.
327.
drom. Hautarzt 22~10-13, 1971 Weinstein JM, Roman0 PE. O’Grady RB: Bone formation in association with a limbal dermoid. .4rch Ophthalmol
97:1121-1122, 1979 Werner L: Dermo-lipoma of con.junctiva. 7‘ran.j Ophthalmol
sac UK 24:216-219, 1904 Wexler D, Last M: Coloboma of the optic nerve and of the macula. A microscopic study. .4rch Ophthalmol20:7X7-796,
1938 Weyers H, Thier CJ: Malformations mandibulofaciales et delimitation d’un syndrome oculo-vertebral. ,/ Cpnrt Hum
7~143-173, 1958 Weyers H, Their CJ: Un cas de dermoides de la cornee et de la conjonctive associes a des oreilles rervirales. ,/ Gvnr/ Hum 8:76-78, 1959 White,JH: Oculo-nasal dysplasia.,/ &n~t tfum I7: 107-I 14. 1969 Whitney CE, Leone CR, Kincaid MC: Proptosis with masti- cation: an unusual presentation of an orbital dermoid cyst. Ophthalmic Surg 17.295-298, 1986 Wiesinger H, Guerry D: Two cases of epibulbar osteoma. Khn Monatsbl Augenheilkd 131:28 l-284, 1962 U’ilkes SR, Campbell RJ, Waller RR: Ocular malformation in association with ipsilateral nexus of Jadassohn. .-lm ,/
Ophthalmol 92:344-352, 1981 Wilkins RB, Hofmann RJ. Byrd WA, et al: Heterotopic brain tissue in the orbit. ,4rch Ophthnlmol 105:390-392,
1987 Wille-Jorgensen A: Dysostosis mandibulofacialis (Frances- chetti) report of two typical cases. .-lrtrc Ophtholmol -10. 348-357 1962 . . , Williams AT, Font RL, Van Dyk HJ, et al: Osseous choris- toma of the choroid simulating a choroidal melanoma. .4rrh
Ophthalmol 96:428--135, 1979 Willis R, Zimmerman LE, O’Grady R, et al: Heterotopic adipose tissue and smooth muscle in the optic. disc. ,4n.h
Ophthalmol 88: 139-I 46, 1972 Wise JB, Maclean AL, Gass JDM: Contractile peripapillar! staphyloma. ,4rrh Ophthalmol 75:626-630, 1966 Witschel H, Font RL: Hemangioma of the choroid. A clini- copathologic study of 71 cases and a review of the litera- ture. Sun) Ophthalmol 20:41543 1, 1976 Wolff H: Eine Dermoigeschwulst der Karunkel. E;/in Mon-
nhhl,4ugenheilkd 29:430435, 1891 Walter JR, Mesaros MP: Epidermoid cyst of. the eyelid in the nevoid basal cell carcinoma syndrome. ,/ Prdia/r (@/I- thalmol Strabismus 14:48-50, I977 Wolter JR. Roosenberg RJ: Ectopic lymph node ofthe orbit simulat’ing a lacrimal gland tumor. .4rn ,/ Ophthnlmol 83:
908-914, 1977 WolterJR. Walters PV, Judd DR: Unilateral episc-Iera tera- toma. ,/ Peduztr Ophthalmol 10: 197-199. 1073 Wood DJ, Scott RS: Dermolipoma of the cornea. Tran,\
Ophthalmol Sor lJK 45: 1 12-l 15. 1925 Yanoff M. Font RL: Intraocular cartilage in a microphthal- mic eye of an otherwise healthy girl. .Iwh Ophfhalmol
KI:‘~Y8-“40 1969 . -. Youssefi B: Orbital tumors in children.,/ Ppdwtr Ophthnfmol
6tl77-181. 1969 Zaidman GW, Johnson B, Brown Sl: Cornea1 transpianta- tion in an infant with cornea1 dermoid. Am ,/ Oph/hnlmol
93:78-X3. 19x2 Zaremba J. Wislawski J, Bidzinski J, er al: Jadassohn‘s nae- vus phakomatosis: A report of two cases. / iZl~n/ Drfir RP\
22:91-102, 1978 Zaremba J: Jadassohn’s naevus phakomatosis: A study based on a review of thirty seven cases. ,/ Mrnt De/zr Re\
22.~103-1”‘~ 1977 -... . Zentmaver W: A case of multiple dermoids of the eyeball with other anomalies of development. Trnn\ Am Ophthalmol
sot 17.34 I-344, 19 19 Zilkha A: Ectopic lacrimal gland and exophthalmos. Case report with emphasis on value oforbital venography. Radi- olo,q 103.~275-276, I972

358 Surv Ophthalmol 33 (5) March-April 1989
328. Zimmerman LE: Phakomatous choristoma of the eyelid. A tumor of lenticular anlage. Am J Ophthalmol 71: 169-177, 1971
329.
330.
331.
332.
Zimmerman LE: Verhoeff s “terato-neuroma.” A critical reappraisal in light of new observations and current con- cepts of embryonic tumors. The fourth Frederick H Ver- hoeff lecture. Am J Ophthalmol 72:1039-1057, 1971 Zimmerman LE, Arkfeld DL, Schenken JB, et al: A rare choristoma of the optic nerve and chiasm. Arch Ophthalmol 101:766-770, 1983 Zimmerman LE, Font RL: Congenital malformations of the eye. Some recent advances in knowledge of the patho- genesis and histopathological characteristics. JAMA 196: 684-692, 1966 Zografos L, Uffer S: Osteome epi-bulbaire. J Fr Ophtalmol 7:625-626, 1984
Outline
I Epibulbar choristomas A. Historical perspective B. Incidence
E. Association with the epidermal nevus syndrome
C. Clinical features D. Association with Goldenhar syndrome
MANSOUR ET AL
F. Inheritance G. Histopathology H. Pathogenesis I. Surgical intervention
II. Choristomas outside the epibulbar region A. Episcleral osseous choristomas B. Scleral choristomas C. Eyelid choristomas D. Orbital choristomas E. Choristomas of the extraocular muscles F. Optic nerve head choristomas G. Choristomas of optic nerve and chiasm H. Retinal choristomas I. Anterior uveal choristomas J. Choroidal choristomas
III. Summary
Supported by a research grant from UNlCEF, Paris, France (Dr. Mansour).
Reprint requests should be addressed to Ahmad Mansour, M.D., Department ofophthalmology, University ofTexas Medi- cal Branch, Galveston, TX 77550.