
Nutrition for the Childbearing Years
13
Nutrition for the Childbearing Years Elizabeth Reifsnider, RN, C, PhD, WHNP, Sara L. Gill, RN, PhD, IBCLC = Obiective: To review the literature on precon- ceptional nutrition and nutrition during pregnancy and lactation, focusing on recommendations from the Institute of Medicine. Data Sources: Computerized searches on MEDLINE, CINAHL, National Institutes of Health and Institute of Medicine web sites. Study Selection: Articles from indexed iour- nals and reports from government sources relevant to the topics of this review and published after 1990 (except for classic findings) were evaluated. Data Extraction: Data were analyzed under the headings of preconceptional nutrition, prenatal nutrition, nutrition during lactation, and nursing implications. Data Synthesis: The nutrition a woman receives before conception, during pregnancy, and during lactation affects her health and the health of her child. Information on the amount and timing of prenatal weight gain, recommended intakes of vita- mins and minerals, and nutrition and activity during lactation have been revised in the last 10 years. Conclusions: The health, size, and growth of the infant are dependent on the timing and amount of weight gain during pregnancy and on maternal nutrition during lactation. Prenatal weight gain also affects a woman‘s future risk of obesity. JOGNN, 29/43-55; 2000. Keywords: Lactation-Preconceptional nutri- tion-Prenatal nutrition. Accepted: July 1999 A woman’s nutritional status before and during pregnancy and during lactation helps determine the outcome of her pregnancy and the long-term health of herself and her child. A woman who enters pregnancy malnourished, with limited nutrient stores, is more likely to have a low-birth-weight (LBW) newborn who may con- tinue a poor growth trajectory during childhood. Everything consumed by the pregnant woman contributes to the fetal environment, which par- tially determines the newborn’s outcome. Retro- spective epidemiologic studies in England have shown that men with larger birth weights had lower rates of ischemic heart disease, obstructive lung disease, and hypertension (Barker & Osmond, 1992; Robinson, 1992). Barker (1994) hypothesizes that prenatal growth constraints have long-term effects on metabolic and physio- logic function that increase the risk for cardiovas- cular disease later. Maternal nutrition during preg- nancy and lactation may influence the development of the brain, the composition and size of the body, and the infant’s metabolic com- petence to handle nutrients (Jackson, Langley- Evans, & McCarthy, 1996). The mother’s future health likewise is affected by her nutritional status during pregnancy and lactation. Excess weight gained during pregnancy contributes to future obesity, which raises the risk of cardiovascular dis- eases and diabetes (Shaper, 1996). This article will review the nutrient requirements recommended before conception and during gestation and lacta- tion. The long-term outcomes of optimal versus poor nutrition before and during pregnancy and during lactation also are discussed. Researchers, both of animal and human sub- jects, have shown the effects of nutritional depri- vation before and during pregnancy. Underweight, malnourished females are less likely to conceive and more likely to have LBW newborns than are normal or overweight women (Pitkin, 1978). Studies conducted over a period of nearly 30 years in rural Guatemala have shown the impact of ade- quate nutrition during pregnancy and lactation (Allen, 1995; Martorell, 1995; Pollitt, Gorman, Engle, Rivera, & Martorell, 1995). The popula- tion studied was characterized by deficient diets, high rates of infection, and growth retardation of children. During this study, pregnant women received two nutritional supplements a day con- taining 11.5 g of protein and 163 kcal per 180 ml. ]anuary/February 2000 JOGNN 43
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Nutrition for the Childbearing Years

Nutrition for the Childbearing Years Elizabeth Reifsnider, RN, C, PhD, WHNP, Sara L. Gill, RN, PhD, IBCLC
= Obiective: To review the literature on precon- ceptional nutrition and nutrition during pregnancy and lactation, focusing on recommendations from the Institute of Medicine.
Data Sources: Computerized searches on MEDLINE, CINAHL, National Institutes of Health and Institute of Medicine web sites.
Study Selection: Articles from indexed iour- nals and reports from government sources relevant to the topics of this review and published after 1990 (except for classic findings) were evaluated.
Data Extraction: Data were analyzed under the headings of preconceptional nutrition, prenatal nutrition, nutrition during lactation, and nursing implications.
Data Synthesis: The nutrition a woman receives before conception, during pregnancy, and during lactation affects her health and the health of her child. Information on the amount and timing of prenatal weight gain, recommended intakes of vita- mins and minerals, and nutrition and activity during lactation have been revised in the last 10 years.
Conclusions: The health, size, and growth of the infant are dependent on the timing and amount of weight gain during pregnancy and on maternal nutrition during lactation. Prenatal weight gain also affects a woman‘s future risk of obesity. JOGNN, 29/43-55; 2000.
Keywords: Lactation-Preconceptional nutri- tion-Prenatal nutrition.
Accepted: July 1999
A woman’s nutritional status before and during pregnancy and during lactation helps determine the outcome of her pregnancy and the long-term health of herself and her child. A woman who enters pregnancy malnourished, with limited nutrient stores, is more likely to have a low-birth-weight (LBW) newborn who may con- tinue a poor growth trajectory during childhood. Everything consumed by the pregnant woman
contributes to the fetal environment, which par- tially determines the newborn’s outcome. Retro- spective epidemiologic studies in England have shown that men with larger birth weights had lower rates of ischemic heart disease, obstructive lung disease, and hypertension (Barker & Osmond, 1992; Robinson, 1992). Barker (1994) hypothesizes that prenatal growth constraints have long-term effects on metabolic and physio- logic function that increase the risk for cardiovas- cular disease later. Maternal nutrition during preg- nancy and lactation may influence the development of the brain, the composition and size of the body, and the infant’s metabolic com- petence to handle nutrients (Jackson, Langley- Evans, & McCarthy, 1996). The mother’s future health likewise is affected by her nutritional status during pregnancy and lactation. Excess weight gained during pregnancy contributes to future obesity, which raises the risk of cardiovascular dis- eases and diabetes (Shaper, 1996). This article will review the nutrient requirements recommended before conception and during gestation and lacta- tion. The long-term outcomes of optimal versus poor nutrition before and during pregnancy and during lactation also are discussed.
Researchers, both of animal and human sub- jects, have shown the effects of nutritional depri- vation before and during pregnancy. Underweight, malnourished females are less likely to conceive and more likely to have LBW newborns than are normal or overweight women (Pitkin, 1978). Studies conducted over a period of nearly 30 years in rural Guatemala have shown the impact of ade- quate nutrition during pregnancy and lactation (Allen, 1995; Martorell, 1995; Pollitt, Gorman, Engle, Rivera, & Martorell, 1995). The popula- tion studied was characterized by deficient diets, high rates of infection, and growth retardation of children. During this study, pregnant women received two nutritional supplements a day con- taining 11.5 g of protein and 163 kcal per 180 ml.
]anuary/February 2000 JOGNN 43

The short-term outcomes of this dietary supplementa- tion included larger newborns, reduced infant mortality rates, and improved growth rates for children up to age 3. The long-term outcomes included taller stature, greater muscle mass, increased capacity for work, and enhanced intellectual performance in children ages 10-20. Enhanced prenatal and early childhood nutri- tion is a benefit to society, and this benefit is not limit- ed to the 1st month of life.
A woman’s weight and height before
pregnancy and her stores of micronutrients
affect the health and size of her infant.
Prepregnancy weight i s a significant
determinant of newborn weight.
Preconceptional Nutrition Research on the relationship of preconceptional
nutrition to the outcome of pregnancy is limited. It is known that a woman’s weight and height before preg- nancy and her existing stores of micronutrients affect the health and size of her newborn. Weight before preg- nancy is a significant determinant of newborn weight. Women with lower prepregnancy weights and women who were underweight at conception are twice as likely to have a LBW newborn as women who were not underweight at conception (Krasovec, 1991). In devel- oping countries, low height is associated with LBW newborns because maternal shortness often is a marker of maternal malnutrition (Rivera, Martorell, Ruel, Habicht, & Haas, 1995). This association is weaker in developed countries where adequate food during child- hood is typical and prepregnancy weight is as accurate in predicting LBW newborns as is maternal weight-for- height (Allen, Hautvast, & Prentice, 1996). Maternal skeletal maturity also is of concern. Scholl and Hediger (1993) found that growing adolescents, both primi- parae and multiparae, had newborns who weighed less than did skeletally mature adolescents and older moth- ers. The developing fetus may compete with the grow- ing adolescent for nutrients.
A woman’s intake of micronutrients, especially vitamins, affects the outcome of her pregnancy. Researchers (Czeizel & Dudas, 1992; MRC Research Group, 1991) have shown that an intake of at least 400 mcg of folate per day can decrease the incidence of neural tube defects (NTDs) by 71%. The Centers for
Disease Control and Prevention (1992) recommends that women of childbearing age who are capable of becoming pregnant should take 400 mcg of folic acid daily. Shaw, Schaffer, Velie, Morland, and Harris (1995) found that use of any vitamin supplement containing folic acid during the 3 months before conception reduced the risk of a NTD by more than one third. They also found that use of any vitamin supplement during the first 3 months after conception was associated with a lower NTD risk. A dietary intake of 230 mcg of folate also has been shown to be somewhat protective.
An excess of vitamin A is teratogenic (Worthing- ton-Roberts, 1996); the extreme case of this is the anti- acne drug isotretinoin (Accutane, Roche Laboratories, Nutley NJ), a vitamin A analogue. The Food and Drug Administration (FDA) has recommended that potential- ly childbearing women limit their intakes of vitamin A to 100% of the RDA, about 5,000 IU (FDA, 1995). The form of vitamin A that is toxic is retinol, not beta- carotene, so a high intake of fruits and vegetables rich in beta-carotene is not a concern (Worthington-Roberts, 1996).
The long-term use of oral contraceptives contain- ing high levels of ethinyl estradiol has been associated with lower levels of vitamin B, (Roepke & Kirksey, 1979) and has led to concern that maternal reserves of B, are low in women taking those contraceptives during early pregnancy. No data are available regarding the vit- amin B, status of women who are taking the lower estrogen oral contraceptives currently on the market (Institute of Medicine [IOM], 1990).
Intake of other substances that can be teratogenic is widespread in women of childbearing potential. Jack, Campanile, McQuade, and Kogan (1995) queried 70 women who had a negative pregnancy test about their preconception risk status. Nearly 60% smoked ciga- rettes, 17% were potential alcohol abusers (had at least one positive answer on an alcoholism screening ques- tionnaire), 55% were at nutritional risk, and 26% indi- cated recent use of an illegal substance. Alcohol, nico- tine, and other drugs, legal and illegal, can be teratogenic when used during early organogenesis, before a woman even knows she is pregnant. The women in the Jack et al. survey knew they were at risk for pregnancy since they sought a pregnancy test, yet they used potentially teratogenic substances.
Prenatal Nutrition Weight Gain
The amount of weight gain recommended for a pregnant woman has changed throughout the 20th cen- tury and remains controversial. Obstetric texts pub- lished at the beginning of the century recommended that pregnant women gain weight only during the 3rd
44 JOG” Volume 29, Number 1

trimester and that the weight gain be limited to 10 to 15 Ib total (Luke, Johnson, & Petrie, 1993). During the 1920s and 1930s, the amount of weight gain recom- mended varied from 15 to 25 Ib, with the warning that a higher gain could be associated with toxemia and a difficult delivery because of a large newborn (Luke et al., 1993). Recommending a weight gain of 20 lb or less was common even during the 1980s (Taffel & Keppel, 1986), even though research was emerging that a gesta- tional gain of 20 lb or less produced smaller newborns who had a poorer chance of survival (IOM, 1990).
The gaps and weaknesses in the research regarding maternal nutrition and its impact on infant outcomes led the Food and Nutrition Board of the National Institute of Medicine to study published data on nutrition during pregnancy and lactation (IOM, 1990). The resulting monograph is the recommended standard for maternal nutrition in the United States, but studies with pregnant women in other parts of the world have yielded different outcomes. European researchers recommend increasing calorie consumption by trimester, regardless of the preg- nant woman’s prepregnancy weight (Prentice et al., 1996). In the United States, the debate over optimal weight gain continues. For example, Bracero and Byrne (1998) recommend higher weight gains than the IOM, while Schieve, Cogswell, and Scanlon (1998) state that overweight women should not gain as much weight as the IOM recommends.
Generally, an overall gain of 27.5 lb (12.5 kg) is considered normal for pregnancy (Rossner, 1998). However, the recommended weight gain depends on the woman’s prepregnancy weight and height. The body mass index (BMI) is the preferred method to assess maternal nutritional status (IOM, 1990) because body
FIGURE 1 Chart for estimating body mass index (BMI) catego- ry and BMI. From Nutri- tion During Pregnancy and Lactation, an lmple- mentation Guide (p. 14). Copyright 1992 by the National Academy of Sci- ences, Washington, DC. Reprinted with permission.
mass is significantly correlated with total body fat con- tent (National Heart, Lung and Blood Institute, 1998). The BMI is based on weight (kg)/height (m)2 and is used internationally. A chart for determining BMI is shown in Figure 1. The BMI also can be determined with the following formula: [weight (lbs)/height ( i n ~ h e s ) ~ ] x 704.5. Table 1 shows the classification of overweight and obesity by BMI endorsed by the National Institutes of Health in June 1998. The BMI prepregnancy classifi- cations have not been altered since they were released in 1990 by the IOM. Table 2 shows the recommended weight gain for pregnancy based on prepregnancy BMI. Rossner (1998) demonstrated a significant correlation between mothers who had a prepregnancy BMI of less than 20 and LBW newborns. However, no relationship was found between mothers who had a prepregnancy BMI of 24 or higher and the birth weight of their new- borns. Women who are underweight before pregnancy need to gain enough weight to have a newborn with a normal birth weight.
Weight gain during pregnancy can be conceptual- ized by two methods: either (a) as the amount of energy necessary to produce a newborn of a normal birth weight or (b) as the components of the products of con- ception plus the maternal stores needed to sustain preg- nancy and lactation. The first method analyzes the ener- gy needs, calculated based on the basal metabolic rate (BMR). The BMR is increased for pregnant women. This increase is greater for women from developed countries than for women from developing countries. Allen et al. (1996) found that women with a high BMI (usually women from developed countries) experience an increase in their BMR from the beginning of preg- nancy. The BMR actually falls during the first half of
Height, cm 142 144 146 148 150 152 154 156 158 160 162 164 I66 168 170 172 174 176 178 180 182 184 186 188
22c I 00
2IC 95
ZOC 90
19C
18C
170 n c’ 160 c *f 150 ’ 140
I30
I20
I10
I00
90
56 5 7 50 59 60 61 62 63
85
80
75 2 r’
70 5 65
- 60
55
50
45
40
64 65 66 67 68 69 70 71 72 73 ‘ 7 4
Height, in
JanuarylFebruary 2000 JOG” 45

TABLE 1 Ckassi@tion of Overweight and Obesity by Body Mass Index (BMI) I
Obesity Class BMI (kg/m2)
Underweight c18.5 Normal 1 8.5-24.9 Overweight 25.0-29.9 Obesity 1 30-34.9
11 35-39.0 Extreme Obesity I11 2 4 0
Note. From Clitricd Gcridclitres otf the Identifinztion, Evidrrntiorr. and Trecitnient of Oi~ericwight und Obesity in Adults (p. 12), by the National Heart, Lung and Blood Institute. 1998, Washington, DC: National Institutes of Health.
pregnancy for women from Gambia, a developing nation in west Africa, and does not begin to rise until the latter half of pregnancy (Prentice et al., 1996). This may occur as an energy-sparing mechanism for women with fewer nutritional stores in that less energy is required for their basic metabolism and so can be used for the developing fetus. This energy-sparing mecha- nism is not wholly protective, however, because many women from developing countries gain less than 20 pounds during pregnancy and have LBW newborns (IOM, 1990).
For a well-nourished woman, the average increase in energy requirements per trimester are 96, 265, and 430 kcal/day (Prentice et al., 1996). The IOM (1990) differs slightly and estimates the total energy require- ments to be 2,115 kcal during the 1st trimester; 2,275 kcal during the 2nd trimester; and 2,356 kcal during the 3rd trimester. Women who reduce their activity level may be able to reduce their calorie requirements, but women who are very active or engage in manual labor
TABLE 2 Recommended Wdght Gain fbr Pregnant Women
Recommended I
Prepregnancy Weight Total Gain Classification (BMZ) I6 k
Underweight (< 19.8) 28-40 12.5-1 8 Normal (19.8 to 26) 25-35 1 1.5-1 6 Overweight (26. I to 29) 15-25 7.0-1 1.5 Obese (>29) 215 2 7
Note. From Nutrition Dimring Pregmrnry und Lactation, nn Inaple- mctrtatiotr G i d e (p. 44), hy the Institute of Medicine, 1992, Wash- ington, I X : National Academy Press.
may need more calories. Women with a daily intake less than 1,900-2,000 kcal/day will most likely need dietary supplementation to gain weight during pregnancy. The total calorie intake needed across 9 months has been reported from 73,600 kcal (Prentice et al., 1996) to 80,000 kcal (Hytten & Chamberlain, 1980; Rossner, 1998), with 300 kcal/day as the average daily increase in calories needed across all three trimesters.
The second method for calculating maternal weight gain during pregnancy is based on the amount of weight needed for the products of conception and the maternal tissues gain. The products of conception are the fetus, representing 25% of the total maternal weight gain; the placenta, accounting for 5% of the gain; and the amniotic fluid, 6% of the gain (Hytten & Cham- berlain, 1980). The other 64% of the weight is account- ed for by the changes in maternal tissues. Approximate- ly 25% of the total maternal gain is fluid in the form of expanded blood volume and extracellular fluid. Increased total body water is associated with a larger newborn weight (Hytten & Chamberlain, 1980). Approximately 10% of the weight is protein gain, pri- marily in the breasts and uterus. The remaining 30% (approximately 7 to 8 lb [3.5 kg]) is maternal fat stores (Hytten, 1991; Hytten & Chamberlain, 1980). Howev- er, this estimate of fat accumulation has been called into question. Prentice et al. (1996) found that preg- nant women in Gambia gained only 2 lb of fat. Pren- tice et al. recommend a gain of 6.4 lb in maternal stores. The amount of fat stores necessary for a healthy pregnancy is important, because if the extra fat is not consumed during the postpartum period or during lac- tation, it may contribute to a woman’s increasing obe- sity. Most women are heavier 2 years after a pregnancy than women who have not been pregnant (Bray, 1998). For many women, pregnancy results in a sustained, pronounced weight gain (Rossner, 1998). Keppel and Taffel (1993) found that white women who gained the IOM-recommended amount of weight during pregnan- cy retained 1.6 lb 1 year after delivery, while black women who gained the recommended amount of weight retained 7.2 lb 1 year after delivery. Increasing parity may put black women at risk for obesity. Con- versely, women with high fertility (greater than six pregnancies) are at greater risk for poor nutritional sta- tus because of the stress of multiple pregnancies and lactations. Studies in the Philippines have shown that women with more than six children had poorer diets with lower intakes of energy, fat, and protein (Pol- hamus, 1996).
For women who are pregnant with more than one fetus, the IOM criteria apply as a baseline for comput- ing weight gain by BMI. A woman who was under- weight before pregnancy needs to gain more than a woman who was overweight before pregnancy. No spe-
46 JOGNN Volume 29, Number 1

cific dietary recommendations exist for a woman of normal BMI who becomes pregnant with multiple fetus- es. Researchers suggest that an optimal weight gain for twin pregnancy would be 24 lb by the 24th week of ges- tation and 1.25 lb weekly until delivery. For triplets and higher multiples, the weight gain would be 36 lb by the 24th week and 1.25 lb weekly until delivery (Luke, 1995). The caloric demand increases to 3,000 kcal/day. The recommended daily allowances (RDAs) for vita- mins and minerals increase as well during a multiple- fetus pregnancy, with the most notable increases being an RDA of 800 mcg of folic acid and 50 mg of iron. The need for most micronutients increases by SO-100 % (Luke, 1995). A woman with multiple fetuses should consult with a registered dietitian or nutritionist to achieve the weight gain and nutrition for an optimal outcome.
The rate and timing of weight gain for a singleton pregnancy also are important. For normal weight women (BMI = 19.8 to 25) a weight gain of 2 to 4 lb (1-2 kg) dur- ing the 1st trimester is recommended, with approximately 1 lb (.45 kg) per week during the 2nd and 3rd trimesters. Underweight women (BMI < 19.8) should gain S Ib (2.3 kg) during the 1st trimester and slightly more than 1 lb (.45 kg) per week during the 2nd and 3rd trimesters. Over- weight women (BMI > 26) should gain 2 Ib (1 kg) dur- ing the 1st trimester and then slightly less than 1 lb (.45 kg) per week during the 2nd and 3rd trimesters (Luke et al., 1993). Obese women who lose weight or who do
1 Weeks of I Date i Gestation i I
not gain weight are at increased risk of delivering a small for gestational age newborn. Obese women who gain more than 35 lb (16 kg) are at twice the risk for delivering a newborn who is large for gestational age (Edwards, Hellerstedt, Alton, Story, & Himes, 1996). A prenatal weight gain chart recommended by the IOM is shown in Figure 2.
Weight ~ Notes i
Smoking Smoking during pregnancy is a cause of low birth
weight in newborns. Hellerstedt, Himes, Story, Alton, and Edwards (1997) studied the birth outcomes of 1,343 pregnant women and found that obese smokers who gained less than 7 kg (15 lb), and normal weight smokers who gained less than 11.5 kg (25 lb) had the highest rate of LBW newborns. It had been thought that a higher gestational weight gain would protect against the risk of low birth weight from smoking, but retro- spective studies have demonstrated that it does not. Smoking was associated with lower birth weight, and increased gestational weight gain did not mitigate against the effects of smoking. Muscati, Koski, and Gray-Donald (1996) studied underweight pregnant smokers and found that even with a higher calorie intake they had a lower maternal weight gain and new- born birth weight. In the Muscati et al. study, 30% of the low birth weight of the newborns was attributable to smoking. The birth weights of the newborns were directly related to the amount of cigarettes their moth-
PreDreenancv BMI <19.8 ( * * * * * * * ), Prepregnancy BMI 19.8-26.0 (Normal Body Weight) (------ ), Prepregnancy BMI >26.0 (- - - )
Weeks of Pregnancy
FIGURE 2 Prenatal weight gain chart. From Nutrition During Pregnancy and Lactation, an Implementation Guide (p. 15). Copyright 1992 by the National Academy of Sciences, Washington, DC. Reprinted with permission.
JanuarylFebruary 2000 JOGNN 47

ers smoked. Women who smoked more than one pack per day had newborns with weight deficits of 458 g, those who smoked less than one pack per day had new- borns with weight deficits of 238 g, and women who were exposed to environmental tobacco smoke had newborns with weight deficits of 192 g (Murphy, Butler, Petersen, Heart, & Murphy, 1996; Nordentoft et al., 1996). Greater prepregnancy BMIs and greater mater- nal weight gain did not reverse the weight deficits of the newborns.
Macronutrients and Micronutrients The quality of the maternal diet is as important as
its quantity. The protein requirements for a pregnant woman are approximately 60 g a day, an increase of 20% over the nonpregnant level (Luke et al., 1993). Women in the United States routinely consume more than 60 g of protein a day, so protein deficiency is rare in this country (IOM, 1990). Vegetarian pregnant women also consume adequate amounts of protein (Mangels, 1997). Likewise, reports of riboflavin, vita- min BIZ, and niacin intake all exceed the RDAs for preg- nancy, perhaps because many breads and cereals are supplemented with these nutrients (IOM, 1990). Intakes also are reported at or above the RDA for vita- mins A (800 mcg) and C (70 mg). Intakes of vitamins B,, D, and E; folic acid; iron; zinc; calcium; and magne- sium have been reported at levels substantially below the RDAs (IOM, 1990). The RDAs are set at generous levels, so it is possible that the vitamin intake of the women studied was sufficient to promote normal preg- nancy (except for folic acid), even without meeting the RDA requirements. Of greater concern is the low intake of iron, calcium, zinc, and folic acid.
Iron deficiency anemia is a serious condition dur- ing pregnancy. It is associated with preterm delivery and increased maternal mortality (Allen, 1997). The RDA for iron in pregnancy (30 mg) is twice as high as the non- pregnant RDA (15 mg) and the average daily intake of women, so it is rarely met solely by diet alone (IOM, 1990; Luke et al., 1993). Iron is needed for the rapid expansion of maternal blood volume and the deposition of iron in fetal tissues. Reduced oxygen-carrying capaci- ty of the maternal blood can cause poor oxygenation in the fetus. An average pregnancy demands up to 1,100 mg of iron total, with a daily demand of 3.5-4 mg. The average U.S. diet contains about 10 mg of iron per 1,000 calories (Winick, 1989). Heme iron, the kind found in food of animal origin, is absorbed at a rate of 15-30%, whereas nonheme iron, the kind found in foods of plant origin, is absorbed at a rate of 5% (Winick, 1989).
A pregnant woman meeting all her iron needs from her diet would need to consume nearly 3,000 calo- ries a day, with a large portion of the diet being com- posed of meat. This would lead to an excess of calories
and fat and high gestational weight gain. Consequently, routine supplementation of iron at a level of 30-60 mg per day is recommended for all pregnant women. Women who do not consume heme iron sources may need individual assessment of their iron status and treat- ment if iron deficiency anemia is found.
Women may consider themselves to be vegetarian if they fall into one of three categories: avoidance of red meat but consumption of fish and/or chicken; no meat consumption but intake of dairy products and eggs (lacto-ovo vegetarians); and no consumption of any food of animal origin (vegans). Women who follow a macrobiotic diet, which is based on grains with a small amount of vegetables, fall into the last category. Gener- ally, lacto-ovo vegetarians consume sufficient amounts of protein and only need the routine vitamin and min- eral supplementation offered to all pregnant women. Vegan women may need additional calcium and vita- mins D and B,, and should be referred for nutritional counseling (Mangels, 1997).
The IOM (1997) reported that all U.S. adults (ages 19-50) need to consume more calcium and increased the RDA for calcium from 800 mg/day to 1,000 mg/day. According to the IOM, pregnant women do not need more calcium than nonpregnant adults, unless the pregnant woman is an adolescent. Then the recommended amount is 1,300 mg/day. An intake of greater than 2,500 mg/day is not recommended because of an increased risk of developing kidney stones (IOM, 1997). However, Winick (1989) argues that the calcium requirement should be 1,000 mg per day during the first two trimesters and 2,000 mg per day during the last trimester to meet fetal skeletal demands, with enough left over to maintain a positive calcium balance in the pregnant woman’s bones. Assessments of U.S. women’s calcium consumption reveal that fewer women get sufficient calcium in their diets now than they did in 1990 and that overall calci- um intake has declined (IOM, 1997). Calcium is most commonly found in dairy products in amounts ranging from 400 mg for a cup of plain yogurt, to 170 mg for a cup of ice cream. Protein foods and some vegetables also can supply calcium. See Table 3 for a list of calci- um-rich foods. Women who do not consume many dairy products may need to supplement with 600-1,000 mg of calcium daily (Mangels, 1997). Vita- min B,, supplementation may be needed by vegetarian women who do not eat eggs or dairy products, because this vitamin is found naturally only in animal protein sources (Winick, 1989) and brewer’s yeast and is added to cereal and grain products.
Zinc is crucial for tissue growth, and zinc defi- ciency can cause poor fetal growth. The RDA for zinc during pregnancy is 20 mg, 5 mg more than for other adults (Winick, 1989). Zinc deficiency is common
48 JOGNN Volume 29, Number 1
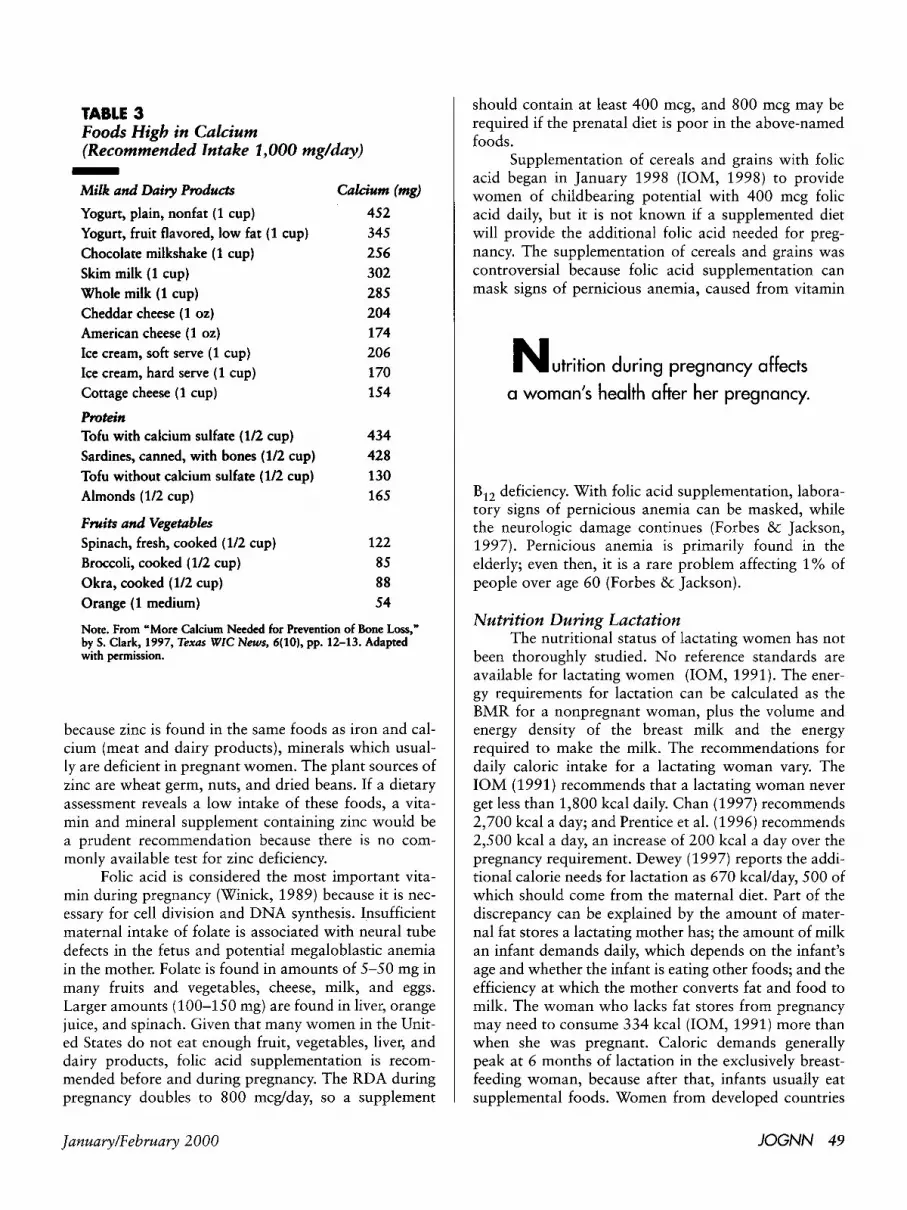
TABLE 3 Foods High in Calcium (Recommended lntake 1,000 mg/day)
Milk and Daily Ptvducts -
Calcium (mg) Yogurt, plain, nonfat (1 cup) Yogurt, fruit flavored, low fat (1 cup) Chocolate milkshake (1 cup) Skim milk (1 cup) Whole milk (1 cup) Cheddar cheese (1 oz) American cheese (1 02)
Ice cream, soft serve (1 cup) Ice cream, hard serve (1 cup) Cottage cheese (1 cup)
452 345 256 302 285 204 1 74 206 170 154
Ptvtein 434
Sardines, canned, with bones (112 cup) 428 Tofu without calcium sulfate (1/2 cup) 130 Almonds (112 cup) 165
Fwits and Vegetables
Tofu with calcium sulfate (1/2 cup)
Spinach, fresh, cooked (112 cup) Broccoli, cooked (1/2 cup) 85 Okra, cooked (1/2 cup) 88 Orange (1 medium) 54
122
Note. From "More Calcium Needed for Prevention of Bone Loss," by S. Clark, 1997, Texas WIC News, 6(10), pp. 12-13. Adapted with permission.
because zinc is found in the same foods as iron and cal- cium (meat and dairy products), minerals which usual- ly are deficient in pregnant women. The plant sources of zinc are wheat germ, nuts, and dried beans. If a dietary assessment reveals a low intake of these foods, a vita- min and mineral supplement containing zinc would be a prudent recommendation because there is no com- monly available test for zinc deficiency.
Folic acid is considered the most important vita- min during pregnancy (Winick, 1989) because it is nec- essary for cell division and DNA synthesis. Insufficient maternal intake of folate is associated with neural tube defects in the fetus and potential megaloblastic anemia in the mother. Folate is found in amounts of 5-50 mg in many fruits and vegetables, cheese, milk, and eggs. Larger amounts (100-150 mg) are found in liver, orange juice, and spinach. Given that many women in the Unit- ed States do not eat enough fruit, vegetables, liver, and dairy products, folic acid supplementation is recom- mended before and during pregnancy. The RDA during pregnancy doubles to 800 mcg/day, so a supplement
should contain at least 400 mcg, and 800 mcg may be required if the prenatal diet is poor in the above-named foods.
Supplementation of cereals and grains with folic acid began in January 1998 (IOM, 1998) to provide women of childbearing potential with 400 mcg folic acid daily, but it is not known if a supplemented diet will provide the additional folic acid needed for preg- nancy. The supplementation of cereals and grains was controversial because folic acid supplementation can mask signs of pernicious anemia, caused from vitamin
N u t r i t i o n during pregnancy affects
a woman's health after her pregnancy.
B,, deficiency. With folic acid supplementation, labora- tory signs of pernicious anemia can be masked, while the neurologic damage continues (Forbes & Jackson, 1997). Pernicious anemia is primarily found in the elderly; even then, it is a rare problem affecting 1% of people over age 60 (Forbes &Jackson).
Nutrition During Lactation The nutritional status of lactating women has not
been thoroughly studied. No reference standards are available for lactating women (IOM, 1991). The ener- gy requirements for lactation can be calculated as the BMR for a nonpregnant woman, plus the volume and energy density of the breast milk and the energy required to make the milk. The recommendations for daily caloric intake for a lactating woman vary. The IOM (1991) recommends that a lactating woman never get less than 1,800 kcal daily. Chan (1997) recommends 2,700 kcal a day; and Prentice et al. (1996) recommends 2,500 kcal a day, an increase of 200 kcal a day over the pregnancy requirement. Dewey (1997) reports the addi- tional calorie needs for lactation as 670 kcal/day, 500 of which should come from the maternal diet. Part of the discrepancy can be explained by the amount of mater- nal fat stores a lactating mother has; the amount of milk an infant demands daily, which depends on the infant's age and whether the infant is eating other foods; and the efficiency at which the mother converts fat and food to milk. The woman who lacks fat stores from pregnancy may need to consume 334 kcal (IOM, 1991) more than when she was pregnant. Caloric demands generally peak at 6 months of lactation in the exclusively breast- feeding woman, because after that, infants usually eat supplemental foods. Women from developed countries
JanuarylFebruary 2000 JOG" 49

usually are 83% efficient at converting food to milk, but women from Gambia are 94% efficient in their con- version of food to milk (Prentice et al., 1996). Once again, the adaptability of a woman’s body in protecting the growth of her offspring is demonstrated.
Breast milk contains approximately 20 kcal per ounce regardless of the lactating mother’s BMI and despite maternal malnutrition. The difference is made up from maternal stores. The volume of milk usually is 750 to 800 ml/day, and this volume is not related to mater- nal weight, height, or fatness among women in the Unit- ed States, although thin women from developing coun- tries may not produce this volume of milk (IOM, 1991). The volume of milk produced does not vary with addi- tional dietary supplementation or with additional fluids (Morse, Ewing, Gamble, & Donahue, 1992). The fat content of human milk varies during a feeding, between feedings, between breasts, and at different months of lac- tation. The fat content of breast milk is similar from woman to woman. The quantity of fat in breast milk is not influenced by maternal diet; however, the fatty acid composition of human milk is influenced by the mater- nal diet (Nommsen, Lovelady, Heinig, Lonnerdal, & Dewey, 1991). Fatty acids are responsible for nerve and brain development in the infant.
Cigarette smoking can reduce the volume of milk through inhibition of prolactin or oxytocin levels (Hamosh, Simon, & Hamosh, 1979), and alcohol may inhibit the milk ejection reflex (IOM, 1991). The flavor of breast milk is altered when the breastfeeding mother consumes alcohol. Researchers have found that infants consume less milk for 3 to 4 hours after their mothers drink alcohol (Mennella & Beauchamp, 1993; 1998). Alcohol consumed by the lactating woman, in amounts that do not exceed one mixed drink, 8 oz. of wine, or two beers daily have not shown a detrimental effect on the breastfed infant (IOM, 1991). However, women should be encouraged to breastfeed their infants before consuming an alcoholic beverage.
The requirements for protein during lactation are the same as for pregnancy (20 g more a day, or 60 g total), so if the breastfeeding woman continues her pregnancy diet, she should have no trouble consuming adequate amounts of protein. Iron requirements drop back to what they were for a nonpregnant woman (15 mg/day). Any increase in iron in the diet is used to replace iron lost during pregnancy, through either blood loss and/or transfer to the fetus. If the woman was iron- deficient during pregnancy, iron supplementation can continue until her iron stores have returned to normal. Many women are amenorrheic during lactation, and this also helps to restore lost iron stores.
The concentrations of calcium, phosphorus, mag- nesium, sodium, and potassium in breast milk are not affected by maternal diet (IOM, 1991). Whatever min-
erals are lacking in the maternal diet will be taken from the mother’s stores. However, the vitamin content of the milk depends on maternal dietary intake, along with maternal stores of fat-soluble vitamins. Low intake of vitamins can result in a lower concentration of vitamins in the breast milk. It is recommended that all vitamins and minerals needed come from an adequate maternal diet, but if the maternal diet is not adequate, a vitamin and mineral supplement will ensure that all needed nutrients are present.
The minerals most likely to be deficient in a lac- tating woman’s diet are calcium, zinc, and magnesium (Chan, 1997). The amounts of these minerals are main- tained at a consistent level in the breast milk at the mother’s expense (IOM, 1991). Kalkwarf and Specker (1995) have shown that lactating women lose more bone in the total body and lumbar spine than do non- lactating women during the first 6 months postpartum, but gain more bone in the lumbar spine during the 6- month period after weaning their infants. Lactating women who were supplemented with calcium (1 g/day) lost less bone than did the unsupplemented lactating women and regained more bone during weaning (Kalk- warf, Specker, Bianchi, Ranz, & Ho, 1997). Thus, it appears that lactation may not result in net bone loss and that calcium supplementation can minimize any loss.
Zinc is poorly absorbed from dietary sources, but is absorbed at twice the level during lactation as before pregnancy (Fung, Ritchie, Woodhouse, Roehl, & King, 1997). The RDA for zinc during lactation is 4 to 13 times higher than the amount of zinc in breast milk. The amount of zinc in breast milk declines during the second 6 months of lactation, although this does not seem to impair infant growth (Robberecht, Benemariya, & Deelstra, 1995). Magnesium intake in most lactating women in the United States is low compared with the RDA, but low levels in the maternal diet are not associ- ated with low levels in breast milk. The long-term impact of low magnesium levels during lactation on a woman’s health has not been studied (IOM, 1991).
The vitamins most likely to be deficient in the maternal diet during lactation are B,, thiamine, and folic acid (Chan, 1997; IOM, 1991). Levels of vitamin B, in breast milk are directly correlated with maternal intake. A maternal diet low in B, causes breast milk to be low in this essential nutrient. Styslinger and Kirksey (1985) found that women who receive supplements of B, (2.5 mg/day) have breast milk levels of B, twice as high as unsupplemented women. Researchers in Finland found that low B, levels were associated with reduced growth in otherwise healthy infants (Heiskanen, Siimes, Salmenpera, & Perheentupa, 1995). Low dietary intake of thiamine results in low levels of thiamine in breast milk, and instances of beriberi have been reported in
50 JOGNN Volume 29, Number 1

infants who did not receive sufficient thiamine in breast milk (Winick, 1989). The IOM (1991) recommends an intake of 1.3 mg/day (an increase of .2 over the non- pregnant requirement of 1.1 mg/day) of thiamine for lactating women. Breads and cereals are fortified with thiamine at 10-100% of the nonpregnant RDA, so the lactating woman should be able to get sufficient thi- amine if she eats the recommended 6 to 11 servings of grain products a day. The need for folic acid increases by 140 mcg/day during lactation and as shown earlier, many women of childbearing age do not get sufficient folic acid in their diets to meet the RDA for nonpregnant women. Maternal reserves of folic acid will be depleted to maintain breast milk levels of folic acid. Researchers have shown that the folic acid stores accumulated by the fetus in utero are used by the infant to maintain serum folic acid levels (Salmenpera, Perheentupa, & Siimes, 1986; Smith, Picciano, & Deering, 1983). Because ade- quate folic acid is needed to prevent megaloblastic ane- mia, adequate folic acid intake protects both the moth- er’s and infant’s health.
Weight loss is experienced by approximately 80% of lactating women. Most women will lose 1-2 lb a month, beginning as early as 15 days postpartum (Fornes & Dorea, 1995). Women who breastfeed for a year lose more weight during the second 6 months than during the first 6 months. Weight loss is related to breastfeeding style; the woman who breastfeeds fre- quently tends to lose more weight (Dewey, Heinig, & Nommsen, 1993). A sustained weight loss of more than 4 lb a month through dieting alone is not recommend- ed because it requires a dietary intake of less than 1,800 kcal/day. Nutrients from maternal stores are then mobilized to make breast milk, potentially affecting the mother’s health (Prentice et al., 1996). The energy costs of lactation are supported by the maternal diet and fat stores.
Aerobic exercise was not found to affect breast milk volume or composition (Dewey, Lovelady, Nommsen-Rivers, McCrory, & Lonnerdal, 1994). Lactating women in an aerobic exercise group expend- ed 400 kcal/day in aerobic exercise, but ate about 300 more kcal than did lactating women who did not exer- cise. No differences were found between the groups of lac- tating women in regard to maternal weight, infant weight gain, volume or composition of breast milk, or produc- tion of prolactin. A study of well-nourished, lactating women who restricted their energy intake for 11 days through diet alone or a combination of diet and exercise, showed a weight loss of more than 2 lb per week, which did not adversely affect their lactation (Dewey, 1998). Prolactin increases with a negative energy balance (expending more energy than consumed), increasing the amount of milk produced (Dewey, 1998). Physical activity levels are reported to be lower for lactating
N u r s e s can contribute to the health of
women and children by addressing nutritional
issues with their clients of childbearing age.
women who do not exercise than for nonlactating women (Van Raaij, Schonk, VermaatMiedema, Peek, & Hauvast, 1990), and lactating women reported being more tired during the 1st month postpartum than before pregnancy. The reduced activity level may con- serve energy needed for lactation. Further research is needed on the long-term effects of dieting before it can be recommended as a weight-loss strategy for lactating women.
Nursing Implications Nurses can improve the health of women and chil-
dren by addressing nutritional issues in their clients of childbearing age. At a routine gynecology or precon- ceptional visit, a nutrition screen can be conducted to gather the following data: the woman’s BMI; iron sta- tus; whether she is a vegetarian or practices pica (eating of any nonfood substance); any history of an eating dis- order or special, prescribed diet; any foods she cannot tolerate or avoids; intake of alcohol, tobacco, and pre- scription medications; illicit drug use; and current dietary intakes through diet history (Cefalo ik Moos, 1995). These items can be included on a patient history form, completed by patients in the waiting room. The nurse can then focus on the responses that deviate from normal.
Nurses also need to focus on food avoidances. Many women do not consider themselves vegetarian, but restrict their intake of meat because of fears of weight gain. They may see themselves as too busy to eat regular meals and so do a great deal of snacking. These women are often anemic or borderline malnourished, but appear healthy and deny malnutrition if asked. It also is helpful to ask how many servings of protein and milk products were consumed the previous day. If no special nutritional circumstances are discovered, the nurse can review a basic good diet (perhaps available in a pamphlet) that will supply nutrients needed to main- tain stores for a future pregnancy and recommend an intake of 400 mcg of folic acid daily via an over-the- counter vitamin supplement. If women are already con- suming vitamins, it is important to alert them that an excess of vitamin A is teratogenic and that they should avoid ingesting more than the RDA for any vitamin.
January/February 2000 JOGNN 51

Encouraging a daily intake of unsweetened breakfast cereal, fortified with iron, will improve the vitamin and mineral intake of most women. Posters are available that provide information on a basic diet and the need for increased folate for pregnant women. Such posters can be placed in the examination rooms for women to study while they wait.
The nurse’s role includes teaching women about the nutrition requirements for a healthy pregnancy, monitoring the pregnant woman’s dietary intake, and teaching about lactation. Women, and especially obese women, need to be reminded that they need to gain weight and never intentionally lose weight during preg- nancy. Whenever a weight loss or lack of weight gain is encountered, the nurse should inquire further. Lack of weight gain can occur from increased activity, such as manual labor; from a gastrointestinal illness; or from a desire to “get back into her jeans.” If an obese woman is losing weight, it is important to determine whether the weight loss is from eating less, or from eating less calorie laden foods and more fruits, vegetables, and lean meats. In either case, the nurse should review the caloric demands of pregnancy to ensure the woman is consum- ing what she needs.
Research on the importance of the prenatal envi- ronment (Clemetson, 1999) can be shared with expectant women. Pregnant women who eat well, exercise, and avoid excess stress may reduce their children’s risk for obesity, hypertension, and hyperlipidemia. Researchers are discovering that the intrauterine environment, includ- ing the nutrients available, is as important to the future development and health of the fetus as is its genetic makeup (Nathanielsz, 1996). Women may be willing to adhere to a recommended diet when they realize they are programming their child’s health for years to come.
Cultural practices may influence a woman’s diet while seeking pregnancy, and certain foods are recom- mended or forbidden to pregnant women in various cul- tures. Additionally, some foods are viewed as galacta- gogues that will increase a lactating woman’s milk supply. Nurses should be knowledgeable about the cul- tural practices of their clients and know which are ben- eficial, which are neutral, and which are harmful. The beneficial and the neutral ones should be encouraged, and the harmful ones discouraged. If, for example, a pregnant or lactating woman wants to take an herbal supplement, the nurse should ask the woman to bring it to the office before taking it. If the ingredients are not listed, the nurse should consult a pharmacist or herbal- ist. Herbal or natural supplements may contain heavy metals or potent herbs that can be toxic to a fetus or infant.
Education about easy ways to enhance nutrition, like snacking on fortified breakfast cereals, cheese cubes, or skim milk fruit smoothies, can encourage an appro-
priate weight gain. All women should be offered infor- mation about WIC (Supplemental Nutrition Program for Women, Infants and Children), available at local health departments and health centers. At her first visit to the WIC clinic, the patient needs to supply proof of pregnancy, income, and residency. The nurse also should be familiar with the food assistance network in the com- munity, including emergency food supplies, food banks, soup kitchens, and how to obtain food stamps. The nurse can consult with these resources to maximize their effectiveness for clients who need these services.
Education and support are necessary for successful breastfeeding. The nurse can review the lactating woman’s diet and inform her of the vitamins and miner- als that are essential for adequate milk production. The weight loss typical of lactation and the calorie require- ments of lactation should also be discussed.
Myths abound regarding foods to avoid during lactation. Most women do not need to avoid specific foods. For example, women often are told not to eat gar- lic while breastfeeding. However, garlic has been shown to make breast milk taste sweeter and infants were found to consume more milk when their mothers ingest- ed garlic capsules (Mennella & Beauchamp, 1991). Some infants may be sensitive to a certain food in their mothers’ diets. That food can be restricted from the mother’s diet for a week to see if the sensitivity resolves.
Some women may hesitate to breastfeed, fearing that their diets are inadequate. No woman should feel that she should not breastfeed because she likes to eat chips and drink soft drinks, but just reminded that mod- eration in all foods is preferred. Nurses should provide reassurance that most women will make adequate milk, assess each woman’s diet, and provide praise for appro- priate food choices. When necessary, diet changes should be identified and examples provided of better food choices.
Women often are eager to lose weight after the birth of their children. The nurse should advise breast- feeding mothers about safe weight loss. Portion size and the importance of reading labels should be discussed. Often women attempt to lose weight by severely limiting calories or omitting foods from one food group. The nurse may suggest moderate exercise to enhance weight reduction. Breastfeeding before exercise will decrease the weight of the breasts, making exercise more comfort- able.
Nurses providing nutrition counseling should be aware of appropriate breastfeeding management. Slow weight gain in an infant may be related to breastfeeding management rather than poor maternal diet. Informa- tion should be obtained about feeding frequency and duration. Limiting the duration of a feeding prevents the infant from receiving the fat laden hind milk respon- sible for weight gain.
52 JOG” Volume 29, Number 1

Whether providing preconception, pregnancy, or lactation counseling, the nurse must have a thorough understanding of the caloric and nutrient requirements for each stage. The nurse must be able to guide the woman to culturally specific, correct food choices that are affordable and easy to prepare. Nurses can be cre- ative in integrating nutrition education into their prac- tices and consult the resources listed in the appendix for additional information. When a registered dietitian is available, the nurse can refer patients with nutrition problems that are outside the nurse’s expertise. The dietary changes made during pregnancy and lactation may last the lifetime of the pregnant or breastfeeding woman and the lifetime of her child.
REFERENCES
Allen, L. (1995). Malnutrition and human function: A com- parison of conclusions from the INCAP and Nutrition CRSP studies. Journal of Nutrition, 125 (4 Suppl.),
Allen, L. (1997). Pregnancy and iron deficiency: Unresolved issues. Nutrition Reviews, 55(4), 91-101.
Allen, L., Hautvast, J., & Prentice, A.M. (1996). Report of the working group on energy requirements for pregnancy and lactation. European Journal of Clinical Nutrition,
Barker, D. (1994). Mothers, babies and disease in later life. London: British Medical Journal.
Barker, D., & Osmond, C. (1992). Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. In D. Barker (Ed.), Fetal and infant origins of adult diseases (pp. 23-34). London: British Medical Journal.
Bracero, L., & Byrne, D. (1998). Optimal weight gain during singleton pregnancy. Gynecologic & Obstetric lnvesti- gation, 46( l), 9-16.
Bray, G. (1998). Classification and evaluation of the over- weight patient. In G. Bray, C. Bouchard, & W. James, Eds., Handbook of obesity (pp. 831-854). New York: Marcel Dekker, Inc.
Cefalo, R., & Moos, M.K. (1995). Preconceptual health care, a practical guide (2nd ed.). St. Louis: Mosby.
Centers for Disease Control and Prevention. (1992). Recom- mendations for the use of folic acid to reduce the num- ber of cases of spina bifida and other neural tube defects. Morbidity and Mortality Weekly Report, 41 (No. RR-
Chan, G. (1997). Lactation, the breastfeeding manual for
Clemetson, L. (1999). Our daughters, our selves. Newsweek,
Czeizel, A., & Dudas, I. (1992). Prevention of the first occur- rence of neural tube defects by periconceptional vitamin supplementation. New England ]ournu1 of Medicine,
Dewey, K. (1997). Energy and protein requirements during lactation. Annual Review of Nutrition, 17, 19-36.
Dewey, K. (1998). Effects of maternal caloric restriction and
11 19s-1126s.
50, (1 Suppl.) S190-S191.
14), 1-6.
health professionals. Chicago: Precept Press.
133(9A), 14-17.
327, 1832-1835.
exercise during lactation. Journal of Nutrition, 128(2 Suppl.), 3 86s-3 89s.
Dewey, K., Heinig, M., & Nommsen, L. (1993). Maternal weight-loss patterns during prolonged lactation. Ameri- can Journal of Clinical Nutrition, 58(2), 162-166.
Dewey, K., Lovelady, C., Nommsen-Rivers, L., McCrory, M., & Lonnerdal, B. (1994). A randomized study of the effects of aerobic exercise by lactating women on breast-milk volume and composition. New England Journal of Medicine, 330, 449-453.
Edwards, L., Hellerstedt, W., Alton, I., Story, M., & Himes, J. (1996). Pregnancy complications and birth outcomes in obese and normal-weight women: Effects of gestational weight changes. Obstetrics & Gynecology, 87(3) ,
Food and Drug Administration. (1995, October 6). Vitamin A and birth defects (press release). Rockville, MD: Author.
Forbes, C., &Jackson, W. (1997). Clinical medicine (2nd ed.). London: Mosby-White.
Fornes, N., & Dorea, J. (1995). Subcutaneous fat changes in low-income lactating mothers and growth of breast-fed infants. ]ournu1 of the American College of Nutrition,
Fung, E., Ritchie, L., Woodhouse, L., Roehl, R., & King, J. (1997). Zinc absorption in women during pregnancy and lactation: A longitudinal study. American Journal of Clinical Nutrition, 66, 80-88.
Hamosh, M., Simon, M., & Hamosh, P. (1979). Effect of nicotine on the development of fetal and suckling rats. Biology of the Neonate, 35, 290-297.
Heiskanen, K., Siimes, M., Salmenpera, L., & Perheentupa, J. (1995). Low vitamin B, status associated with slow growth in healthy breast-fed infants. Pediatric Research, 38(5), 740-746.
Hellerstedt, W., Himes, J., Story, M., Alton, I., & Edwards, L. (1997). The effects of cigarette smoking and gestational weight changes on birth outcomes in obese and normal- weight women. American Journal of Public Health,
Hytten, F. (1991). Weight gain in pregnancy. In F. Hytten & G. Chamberlain (Eds.), Clinical physiology in obstetrics (pp. 173-203). Oxford: Blackwell Scientific Publica- tions.
Hytten, F., & Chamberlain G. (1980). Clinical physiology in obstetrics. Oxford: Blackwell Scientific Publications.
Institute of Medicine. (1990). Nutrition during pregnancy. Washington, DC: National Academy Press.
Institute of Medicine. (1991). Nutrition during lactation. Washington, DC: National Academy Press.
Institute of Medicine. (1997). Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and fluo- ride. Washington, DC: National Academy Press.
Institute of Medicine. (1998). Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B,, folate, vitamin B,,, pantothenic acid, biotin, and choline. Washington, DC: National Academy Press.
Jack, B., Campanile, C., McQuade, W., & Kogan, M. (1995). The negative pregnancy test. An opportunity for pre- conception care. Archives of Family Medicine, 4(4),
3 89-394.
14, 61-65.
87(4), 591-596.
340-345.
January/February 2000 /OGNN 53

Jackson, A., Langley-Evans, S., & McCarthy, H. (1996). Nutritional influences in early life upon obesity and body proportions. In D. Chadwick & G. Cardew, (Eds.), The origins and consequences of obesity (pp. 118-137, Ciba Foundation symposium 201). Chi- Chester: Wiley.
Kalkwarf, H., & Specker, B. (1995). Bone mineral loss during lactation and recovery after weaning. Obstetrics & Gynecology, 86(1), 26-32.
Kalkwarf, H., Specker, B., Bianchi, D., Ranz, J., & Ho, M. (1997). The effect of calcium supplementation on bone density during lactation and after weaning. New Eng- land Journal of Medicine, 337, 523-528.
Keppel, K., & Taffel, S. (1993). Pregnancy-related weight gain and retention: Implications of the 1990 Institute of Med- icine guidelines. American Journal of Public Health,
Krasovec, K. (1991). The implications of poor maternal nutri- tional status during pregnancy for future lactational per- formance. Journal of Tropical Pediatrics, 37, (Suppl. l),
Luke, B. (1995). Maternal characteristics and prenatal nutri- tion. In L. Keith, E. Papiernik, D. Keith, & B. Luke (Eds.), Multiple pregnancy: Epidemiology, gestation and perinatal outcome (pp. 299-308). New York: Parthenon Publishing Group.
Luke, B., Johnson, T., & Petrie, R. (1993). Clinical maternal- fetal nutrition. Boston: Little, Brown and Co.
Mangels, A. (1997). Vegetarian nutrition during pregnancy and lactation. Perinatal Nutrition Report, 4(1), 12.
Martorell, R. (1995). Results and implications of the INCAP follow-up study. Journal of Nutrition, 125, (4 Suppl.),
Mennella, J., & Beauchamp, G. (1991). Maternal diet alters the sensory qualities of human milk and the nursling’s behavior. Pediatrics, 88(4), 737-744.
Mennella, J., & Beauchamp, G. (1993). Effects of beer on breast-fed infants. Journal of the American Medical Association, 269, 1635-1 636.
Mennella, J., & Beauchamp, G. (1998). Early flavor experi- ence: Research update. Nutrition Reviews, S6( 7), 205-211.
Morse, J., Ewing, G., Gamble, D., & Donahue, P. (1992). The effect of maternal fluid intake on breast milk supply: A pilot study. Canadian Journal of Public Health, 83(3),
MRC Research Group. (1991). Prevention of neural tube defects: Results of the medical research council vitamin study. Lancet, 338, 131-137.
Murphy, N., Butler, S., Petersen, K., Heart, V., & Murphy, C. (1996). Tobacco erases 30 years of progress: Preliminary analysis of the effect of tobacco smoking on Alaska Native birth weight. Alaska Medicine, 38( l), 31-33.
Muscati, S., Koski, K., & GrayDonald, K. (1996). Increased energy intake in pregnant smokers does not prevent human fetal growth retardation. Journal of Nutrition,
Nathanielsz, P. (1996). Fetal and neonatal environment has influence on brain development. Lancet, 347, 314.
National Heart, Lung and Blood Institute. (1998). Clinical
83( 8), 1100-1103.
3-10.
1 127s-113 8s.
213-216.
126,2984-2989.
guidelines on the identification, evaluation, and treat- ment of overweight and obesity in adults. Washington, DC: National Institutes of Health.
Nommsen, L., Lovelady, C., Heinig, M., Lonnerdal, B., & Dewey, K. (1991). Determinants of energy, protein, lipid and lactose concentration in human milk during the first 12 months. American Journal of Clinical Nutrition, 53, 457-465.
Nordentoft, M., Lou, H., Hansen, D., Nim, J., Pryds, O., Rubin, P., & Hemmingsen, R. (1996). Intrauterine growth retardation and premature delivery: The influ- ence of maternal smoking and psychosocial factors. American Journal of Public Health, 86(3), 347-354.
Pitkin, R. (1978). Nutrition in pregnancy. WIC Currents, 4(2), 1-10.
Polhamus, B. (1996). A profile of high-fertility women in the Philippines. Chapel Hill, NC: Carolina Population Cen- ter, University of North Carolina at Chapel Hill.
Pollitt, E., Gorman, K., Engle, P., Rivera, J., & Martorell, R. (1995). Nutrition in early life and the fulfillment of intel- lectual potential. Journal of Nutrition, 125, (4 Suppl.), 11 11s-1118s.
Prentice, A., Spaaij, C., Goldberg, G., Poppitt, S., van Raaij, J., Totton, M., Swann, D., & Black, A. (1996). Energy requirements of pregnant and lactating women. Euro- pean Journal of Clinical Nutrition, SO, (Suppl. I),
Rivera, J., Martorell, R., Ruel, M., Habicht, J.-P., & Haas, J. (1995). Nutritional supplementation during the preschool years influences body size and composition of Guatemalan adolescents. Journal of Nutrition, 225, (4 Suppl.), 1068s-1077s.
Robberecht, H., Benemariya, H., & Deelstra, H. (1995). Daily dietary intake of copper, zinc, and selenium of exclusive- ly breast-fed infants of middle-class women in Burundi, Africa. Biological Trace Element Research, 49(2),
Robinson, R. (1992). Introduction, summary of contents. In D. Barker (Ed.), Fetal and infant origins of adult diseases (pp. 4-20). London: British Medical Journal.
Roepke, J., & Kirksey, A. (1979). Vitamin B, nutriture during pregnancy and lactation. 11. The effect of long-term use of oral contraceptives. American Journal of Clinical Nutrition, 32, 2257-2264.
Rossner, S. (1998). Obesity and pregnancy. In G. Bray, C. Bouchard & W. James (Eds.), Handbook of obesity (pp. 775-790). New York: Marcel Dekker, Inc.
Salmenpera, L., Perheentupa, J., & Siimes, M. (1986). Folate nutrition is optimal in exclusively breast-fed infants but inadequate in some of their mothers and in formula-fed infants. Journal of Pediatric Gastroenterology and Nutrition, 5, 283-289.
Schieve, L., Cogswell, M., & Scanlon, K. (1998). An empiric evaluation of the Institute of Medicine’s pregnancy weight gain guidelines by race. Obstetrics & Gynecolo-
Scholl, T., & Hediger, M. (1993). A review of the epidemiology of nutrition and adolescent pregnancy: Maternal growth during pregnancy and its effect on the fetus. Journal of the American College of Nutrition, 22(2), 101-107.
S82-S 1 1 1.
151-159.
gy, 92(6), 878-884.
54 JOGNN Volume 29, Number 1

Shaper, A. (1996). Obesity and cardiovascular disease. In D. Chadwick & G. Cardew (Eds.), The origins and conse- quences of obesity (pp. 90-107, Ciba Foundation sym- posium 201). Chichester: Wiley.
Shaw, G., Schaffer, D., Velie, E., Morland, K., & Harris, J. (1995). Periconceptual vitamin use, dietary folate, and the occurrence of neural tube defects. Epidemiology,
Smith, A., Picciano, M., & Deering, R. (1983). Folate supple- mentation during lactation: Maternal folate status, human milk folate content, and their relationship to infant folate status. Journal of Pediatric Gastroenterolo- g y and Nutrition, 2, 622-628.
Styslinger, L., & Kirksey, A. (1985). Effects of different levels of vitamin B, supplementation on vitamin B, concentra- tions in human milk and vitamin B, intakes of breastfed infants. American Journal of Clinical Nutrition, 41,
Taffel, S., & Keppel, K. (1986). Advice about weight gain dur- ing pregnancy and actual weight gain. American Journal of Public Health, 76, 1396-1399.
Van Raaij, J., Schonk, C., Vermaat-Miedema, S., Peek, M., & Hautvast, J. (1990). Energy cost of physical activity throughout pregnancy and the first year postpartum. Part I Dutch women with sedentary lifestyles. American Journal of Clinical Nutrition, 51, 158-161.
Winick, M. (1989). Nutrition, pregnancy and early infancy. Baltimore: Williams & Wilkins.
Worthington-Roberts, B. (1996). The role of maternal nutri- tion in the prevention of birth defects. Perinatal Nutri- tion Report, 2(3), 12.
6(3), 205-207.
11 16-1 117.
Elizabeth Reifsnider is an associate professor in the School of Nursing, University of Texas Health Science Center at Sun Antonio.
Sara L. Gill is an assistant professor in the School of Nursing, University of Texas Health Science Center at Sun Antonio.
Address for cowespondence: Elizabeth Reifsnider, RN, C, PhD, WHNC Associate Professor, University of Texas Health Science Center at Sun Antonio School of Nursing, 7703 Floyd Curl Drive, Sun Antonio, TX 78227-3900. E-mail: [email protected].
Appendix
Resources on Nutrition and Lactation American Dietetic Association Consumer Hotline
http://www.eatright.org Supplemental Nutrition Program for Women,
1-800-366-1655
Infants and Children (WIC) 1-800-545-2200 http://www. fns.usda.gov/wic
National Dairy Council
http://www. whymilk.com
United Dairy Industry of Michigan
International Lactation Consultant Association
http://www. ilca. com Food and Nutrition Information Center
http://www.nal. usda.gov/fnic Children’s Nutrition Research Center
http://www. bcm.tmc.edu/cnrc
Veggies Unite!, P.O. Box 5312, Fort Wayne, IN 46895- 5312 http://www.vegweb.com
The Sugar Association, Inc., 1101 15th St. N.W., Suite 600, Washington, DC 20005 Egg Nutrition Center, 1819 H St. N.W., Suite 520, Washington, DC 20006
Childbirth Graphics, a division of WRS Group, Inc., Waco, TX 76702-1207
For posters: Celestial Arts, P.O. Box 7327, Berkeley CA
1-800-426-8271
1 - 800-24 1 -MILK
1-919-787-51 8 1
1-30 1-504-571 9
1-713-798-7017
94707 1-510-559-1600
JanuarylFebruary 2000 JOGNN 55




















