Nurse-led interventions in heart failure care: Patient and nurse perspectives
7
Nurse-led interventions in heart failure care: Patient and nurse perspectives Tialda Hoekstra a, ⁎ , Ivonne Lesman-Leegte a , Martje van der Wal a , Marie Louise Luttik a , and Tiny Jaarsma b a Department of Cardiology, University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB Groningen, The Netherlands b Department of Social and Welfare Studies, Faculty of Health Sciences, Linköping University, Norrköping, Sweden Received 22 June 2009; received in revised form 18 January 2010; accepted 28 January 2010 Available online 4 March 2010 Abstract Background: Perspectives of nurses and patients on the intensity and content of disease management programmes (DMPs) in heart failure are seldom addressed but are important in optimizing these programmes. Aim: To describe the perspectives of patients and nurses on delivered care in two DMPs. Methods: In total 442 patients (62% male; age 68 ± 12 years; LVEF 33% ± 14), assigned to the intervention groups of the Coordinating Study Evaluating Outcomes of Advising and Counselling in HF (COACH), and 32 registered nurses, completed questionnaires on satisfaction with the intensity and components of the DMPs. Results: In spite of large differences in intensity and components, patients were satisfied with the content of both DMPs. In patients (NYHA III–IV), treatment and educational goals were more often achieved in those who received intensive support, compared to patients who received basic support (85% vs. 70%). Patients and nurses perceived that most home visits were adding significant value to the HF care, while 12% of the home visits were perceived as unnecessary by the nurses. Conclusion: Patients and nurses did not perceive the intense DMP as an emotional and physical burden for themselves. Patients with severe HF might be in need of more support to achieve optimal treatment and educational goals. © 2010 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: Heart failure; Disease management programmes; Nurse perspectives; Patient perspectives; Satisfaction 1. Introduction Hospital readmission and mortality rates remain high in patients with heart failure (HF), despite improved pharmaco- logical interventions [1]. Reversible factors such as a lack of understanding of HF, poor treatment compliance, inadequate follow-up and difficulty in having access to specific HF care in-hospital are related to poor outcomes. As a consequence HF disease management programmes (DMPs) have been devel- oped. [2,3]. In the guidelines of the European Society of Cardiology (ESC), it is stated that a DMP should have several specific components defined as 9 key characteristics and every HF patient should have access to a DMP [1]. Recent meta-analyses support the finding that most DMPs are effective and reduce readmissions, length of hospital stay, costs of care, mortality and improve quality of life [4,5]. Although no studies are known to investigate the optimal model for specific patient groups, the ESC HF guidelines recommend to distinguish in intensity of DMPs between patients with mild HF (New York Heart Association (NYHA) functional class II) and patients with severe HF (NYHA functional class III–IV), in which the latter should receive more intensive counselling. Until now studies have identified effective components [6] but patient and nurse perspectives are not evaluated. It is unknown what the opinions of the nurses are about the different components in terms of effectiveness, invested time or emotional burden. Also, from a patient's point of view, it is unclear whether they perceive their care as being too intensive European Journal of Cardiovascular Nursing 9 (2010) 226 – 232 www.elsevier.com/locate/ejcnurse ⁎ Corresponding author. Tel.: +31 50 3612355; fax: +31 50 3614391. E-mail address: [email protected] (T. Hoekstra). 1474-5151/$ - see front matter © 2010 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejcnurse.2010.01.006
Transcript of Nurse-led interventions in heart failure care: Patient and nurse perspectives

European Journal of Cardiovascular Nursing 9 (2010) 226–232www.elsevier.com/locate/ejcnurse
Nurse-led interventions in heart failure care: Patient and nurse perspectives
Tialda Hoekstraa,⁎, Ivonne Lesman-Leegtea, Martje van der Wala, Marie Louise Luttika, andTiny Jaarsmab
a Department of Cardiology, University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB Groningen, The Netherlandsb Department of Social and Welfare Studies, Faculty of Health Sciences, Linköping University, Norrköping, Sweden
Received 22 June 2009; received in revised form 18 January 2010; accepted 28 January 2010Available online 4 March 2010
Abstract
Background: Perspectives of nurses and patients on the intensity and content of disease management programmes (DMPs) in heart failure areseldom addressed but are important in optimizing these programmes.Aim: To describe the perspectives of patients and nurses on delivered care in two DMPs.Methods: In total 442 patients (62% male; age 68±12 years; LVEF 33%±14), assigned to the intervention groups of the Coordinating StudyEvaluating Outcomes of Advising and Counselling in HF (COACH), and 32 registered nurses, completed questionnaires on satisfaction withthe intensity and components of the DMPs.Results: In spite of large differences in intensity and components, patients were satisfied with the content of both DMPs. In patients (NYHAIII–IV), treatment and educational goals were more often achieved in those who received intensive support, compared to patients whoreceived basic support (85% vs. 70%). Patients and nurses perceived that most home visits were adding significant value to the HF care,while 12% of the home visits were perceived as unnecessary by the nurses.Conclusion: Patients and nurses did not perceive the intense DMP as an emotional and physical burden for themselves. Patients with severeHF might be in need of more support to achieve optimal treatment and educational goals.© 2010 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
Keywords: Heart failure; Disease management programmes; Nurse perspectives; Patient perspectives; Satisfaction
1. Introduction
Hospital readmission and mortality rates remain high inpatients with heart failure (HF), despite improved pharmaco-logical interventions [1]. Reversible factors such as a lack ofunderstanding of HF, poor treatment compliance, inadequatefollow-up and difficulty in having access to specific HF carein-hospital are related to poor outcomes. As a consequence HFdisease management programmes (DMPs) have been devel-oped. [2,3]. In the guidelines of the European Society ofCardiology (ESC), it is stated that a DMP should have severalspecific components defined as 9 key characteristics and everyHF patient should have access to a DMP [1].
⁎ Corresponding author. Tel.: +31 50 3612355; fax: +31 50 3614391.E-mail address: [email protected] (T. Hoekstra).
1474-5151/$ - see front matter © 2010 European Society of Cardiology. Publishdoi:10.1016/j.ejcnurse.2010.01.006
Recent meta-analyses support the finding that most DMPsare effective and reduce readmissions, length of hospital stay,costs of care, mortality and improve quality of life [4,5].Although no studies are known to investigate the optimalmodel for specific patient groups, the ESC HF guidelinesrecommend to distinguish in intensity of DMPs betweenpatients with mild HF (New York Heart Association (NYHA)functional class II) and patients with severe HF (NYHAfunctional class III–IV), in which the latter should receivemore intensive counselling.
Until now studies have identified effective components [6]but patient and nurse perspectives are not evaluated. It isunknown what the opinions of the nurses are about thedifferent components in terms of effectiveness, invested timeor emotional burden. Also, from a patient's point of view, it isunclear whether they perceive their care as being too intensive
ed by Elsevier B.V. All rights reserved.

Table 1Components of the COACH intervention groups.
Basic support Intensive support
Education and counselling on HFand HF related regimenaccording to protocol.
Education and counselling on HFand HF related regimenaccording to protocol.
At least 4 visits to a cardiologistat the outpatient clinic.
At least 4 visits to a cardiologistat the outpatient clinic.
A total of 8 visits to a HF nurseat the outpatient clinic during18 months.
Monthly visit to a HF nurseat the outpatient clinic during18 months.
In the first month, one telephonecontact with the HF nurse(nurse initiated).
In the first month, weekly telephonecontact with the HF nurse(nurse initiated).
Telephone availability of HFnurse during office hours.
Telephone availability of HF nurse24 h a day.
Two home visits (within 10 daysand 12 months after discharge).
227T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
or not intensive enough, whether it fits into their diseaseperception and whether it prevents symptomatic relapse.Additionally, we do not know if perspectives on DMPs aredifferent for patients with mild or severe HF. We recentlypublished the results of the COACH trial in which the effect oftwo DMPs that differed in intensity and components weredetermined [7]. The rationale for two DMPs was to evaluatehow much advising and counselling is required, assuming anoverall effect can be detected. If a basic programme will proveto cause most of the beneficial effect, a much more intensiveprogramme is unnecessary, and redundant (and too costly). Incontrast, if most of the effect can only be caused by intensiveadvising and counselling, a medium support fails to prove aneffect. The experiences of patients and nurses regarding thesetwo DMPs will be examined and therefore the objective of this(secondary) study is:
Multidisciplinary advice(physiotherapist, dietician,social worker, psychologist).
1) gain insight into the perspectives of patients on theirreceived treatment;2) gain insight into the perspectives of nurses on their
provided care;3) and examine similarities and differences in perspectives
of patients and nurses on the intensity of the programmesrelated to the severity of HF.
2. Methods
2.1. Research sample
All patients and nurses in the present study participated inthe COACH study (Coordinating Study Evaluating Outcomesof Advising and Counselling in Heart failure), a multicenterstudy on the effect of education and counselling in HF [8].Between November 2002 and February 2005, 1023 patientsfrom 17 Dutch hospitals were included in the COACH study.The study complied with the Declaration of Helsinki and wasapproved by the Committee for Ethics in Medical Investiga-tions of the University Medical Center of Groningen.
2.2.1. PatientsInclusion criteria for patients were hospitalisation for
symptomatic HF confirmed by the cardiologist, and structuralunderlying heart disease as the cause of HF. Exclusion criteriawere an invasive intervention within the last 6 months orplanned in the next 3 months, participation in a study requiringadditional visits to a research nurse, and evaluation for hearttransplantation. After written informed consent, patients werefollowed for a period of 18 months. Patients were randomizedto 1 of 3 study groups: basic support, intensive support or thecare as usual (Table 1). Since we were interested in theperspectives of patients on a HF programme, we includedpatients from the two support groups, who accomplished the18 month follow-up period.
2.1.2. NursesRegistered nurses from all participating sites were asked
to complete a self report questionnaire on their satisfactionwith the care provided for each individual patient.
2.2. Study measurements
2.2.1. Patient satisfactionAt the end of the COACH study patients received a 19-item
self report questionnaire on patient satisfaction with the carereceived, which was constructed for this study. Nine itemswere about patients' satisfaction on the specific components(home visits, telephone consultations and multidisciplinaryteam), the intensity of the received treatment, and patients'future wishes. The other 10 items were about visits to theoutpatient clinic in general and not relevant to the currentstudy. Patients were asked to rate their satisfaction on a 5-pointLikert scale with a range from 0 to 4 (Appendix A). The itemsof the questionnaire were derived from previous patientsatisfaction questionnaires tailored to the specific componentsof this study. Content validity was assessed by a panel ofexperts including 3 nurse researchers in the areas of HF, onepatient communication expert and 2 HF nurses.
2.2.2. Nurse satisfactionAt the final study visit of each COACH patient, HF nurses
were asked to complete a self report questionnaire on nursesatisfaction with items on the intensity and on severalcomponents of the care provided (basic support or intensivesupport). The questionnaire was pilot-tested by the nursesworking at the initiating center and had six questions (twoopen, two 5-point Likert scales and two 4-point Likert scales).Nurses were asked to complete a questionnaire for each patientthey had advised and counselled during the study period. Thequestions addressed the intensity of the programmes (intensity,the emotional and physical burden for the nurses and whether
228 T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
the nurses had achieved their goals with the patients) and homevisits (whether and why it was meaningful) (Appendix A).
2.3. Statistical analyses
For purposes of data analyses and to improve themeaningfulness in the presentation of the results, the questionsof both nurse's and patient's satisfaction with a 5-point scalewere computed to 3-point scales and the questionswith 4-pointscales to 2-point scales. Statistical analyses consisted ofdescriptive statistics, using SPSS for Windows 16.0 software.Responses to close-ended questions were tabulated andanalysed with frequency distribution, percentages and cross-tabulations between study variables. Responses to open-endedquestions were summarized and categorized independentlyand agreed upon by two investigators.
3. Results
3.1. Demographic and clinical variables
3.1.1. PatientsA total of 1023 patientswere enrolled in the COACH study.
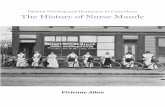
Patients assigned to the care as usual group (n=338) and thosewho died during the follow-up period (n=174), were excludedfrom the study. The final patient sample consisted of 511patients. From these 511 patients, 442 (86%) responded to thepatient satisfaction questionnaire. Respondents were signifi-
Fig. 1. Flowchart o
cantly younger than non-responders (68.5±12 vs. 74.5±10),but did not differ on other relevant variables like sex andNYHA functional class. Nurses completed 336 (66%)questionnaires on their satisfaction with the care providedfor a patient. Patients of which nurses completed theirquestionnaire (n=336) did not differ on relevant variablesfrom the final patient sample (n=511). In total, on 294 (58%)patients both a nurse and a patient satisfaction questionnaireswere completed (Fig. 1). Demographic and clinical character-istics of both patient groups are presented in Table 2.
3.1.2. Heart failure nursesIn total 32HFnurses (4men and 28women) completed 336
questionnaires of the 511 (66%) patients included in thepresent study. Nurses were all qualified for performing care onan outpatient clinic for HF patients. As part of the COACHstudy they all received a 4 day full time special education toperform the protocols of both the basic and intensive supports.
3.2. Intensity of the programmes
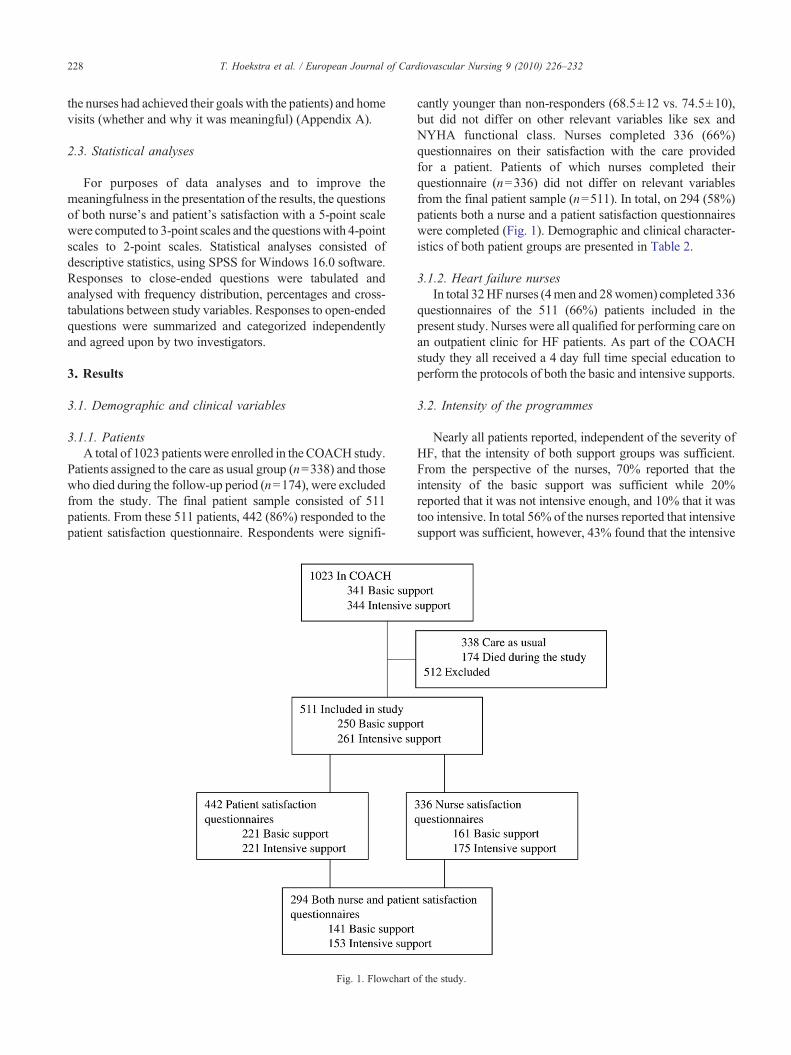
Nearly all patients reported, independent of the severity ofHF, that the intensity of both support groups was sufficient.From the perspective of the nurses, 70% reported that theintensity of the basic support was sufficient while 20%reported that it was not intensive enough, and 10% that it wastoo intensive. In total 56% of the nurses reported that intensivesupport was sufficient, however, 43% found that the intensive
f the study.
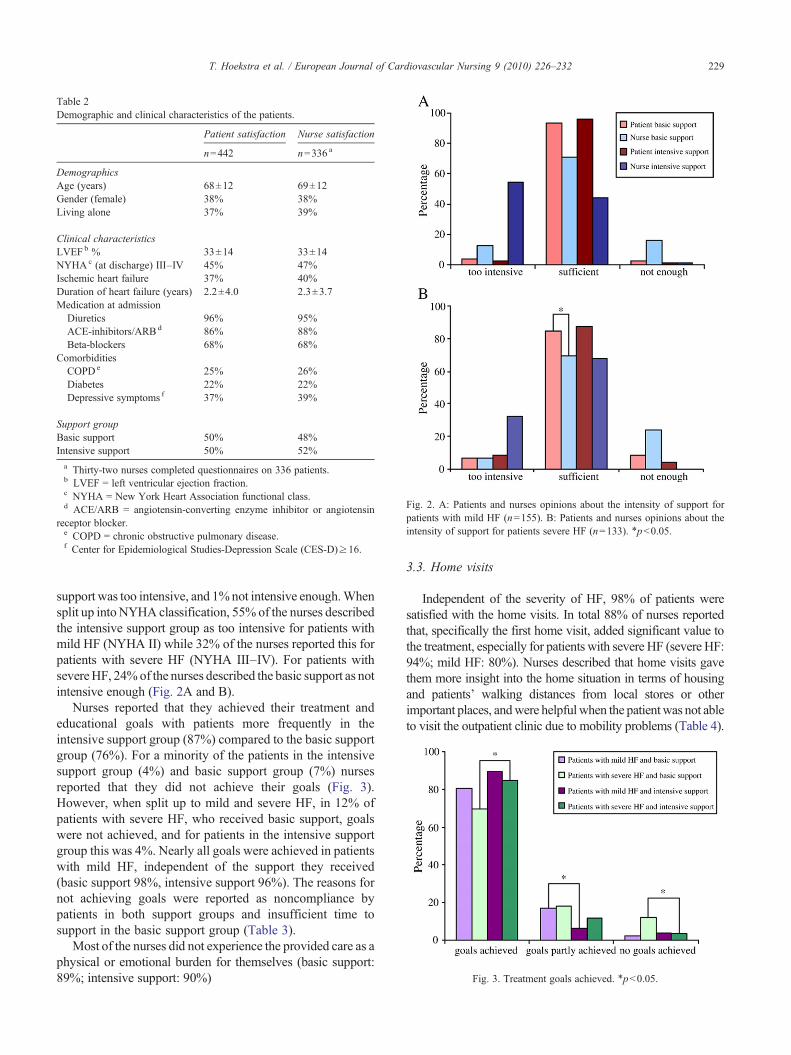
Table 2Demographic and clinical characteristics of the patients.
Patient satisfaction Nurse satisfaction
n=442 n=336 a
DemographicsAge (years) 68±12 69±12Gender (female) 38% 38%Living alone 37% 39%
Clinical characteristicsLVEFb % 33±14 33±14NYHAc (at discharge) III–IV 45% 47%Ischemic heart failure 37% 40%Duration of heart failure (years) 2.2±4.0 2.3±3.7Medication at admission
Diuretics 96% 95%ACE-inhibitors/ARBd 86% 88%Beta-blockers 68% 68%
ComorbiditiesCOPDe 25% 26%Diabetes 22% 22%Depressive symptoms f 37% 39%
Support groupBasic support 50% 48%Intensive support 50% 52%a Thirty-two nurses completed questionnaires on 336 patients.b LVEF = left ventricular ejection fraction.c NYHA = New York Heart Association functional class.d ACE/ARB = angiotensin-converting enzyme inhibitor or angiotensin
receptor blocker.e COPD = chronic obstructive pulmonary disease.f Center for Epidemiological Studies-Depression Scale (CES-D)≥16.
Fig. 2. A: Patients and nurses opinions about the intensity of support forpatients with mild HF (n=155). B: Patients and nurses opinions about theintensity of support for patients severe HF (n=133). ⁎pb0.05.
Fig. 3. Treatment goals achieved. ⁎pb0.05.
229T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
support was too intensive, and 1%not intensive enough.Whensplit up intoNYHA classification, 55% of the nurses describedthe intensive support group as too intensive for patients withmild HF (NYHA II) while 32% of the nurses reported this forpatients with severe HF (NYHA III–IV). For patients withsevereHF, 24%of the nurses described the basic support as notintensive enough (Fig. 2A and B).
Nurses reported that they achieved their treatment andeducational goals with patients more frequently in theintensive support group (87%) compared to the basic supportgroup (76%). For a minority of the patients in the intensivesupport group (4%) and basic support group (7%) nursesreported that they did not achieve their goals (Fig. 3).However, when split up to mild and severe HF, in 12% ofpatients with severe HF, who received basic support, goalswere not achieved, and for patients in the intensive supportgroup this was 4%. Nearly all goals were achieved in patientswith mild HF, independent of the support they received(basic support 98%, intensive support 96%). The reasons fornot achieving goals were reported as noncompliance bypatients in both support groups and insufficient time tosupport in the basic support group (Table 3).
Most of the nurses did not experience the provided care as aphysical or emotional burden for themselves (basic support:89%; intensive support: 90%)
3.3. Home visits
Independent of the severity of HF, 98% of patients weresatisfied with the home visits. In total 88% of nurses reportedthat, specifically the first home visit, added significant value tothe treatment, especially for patients with severe HF (severe HF:94%; mild HF: 80%). Nurses described that home visits gavethem more insight into the home situation in terms of housingand patients' walking distances from local stores or otherimportant places, andwere helpful when the patientwas not ableto visit the outpatient clinic due to mobility problems (Table 4).
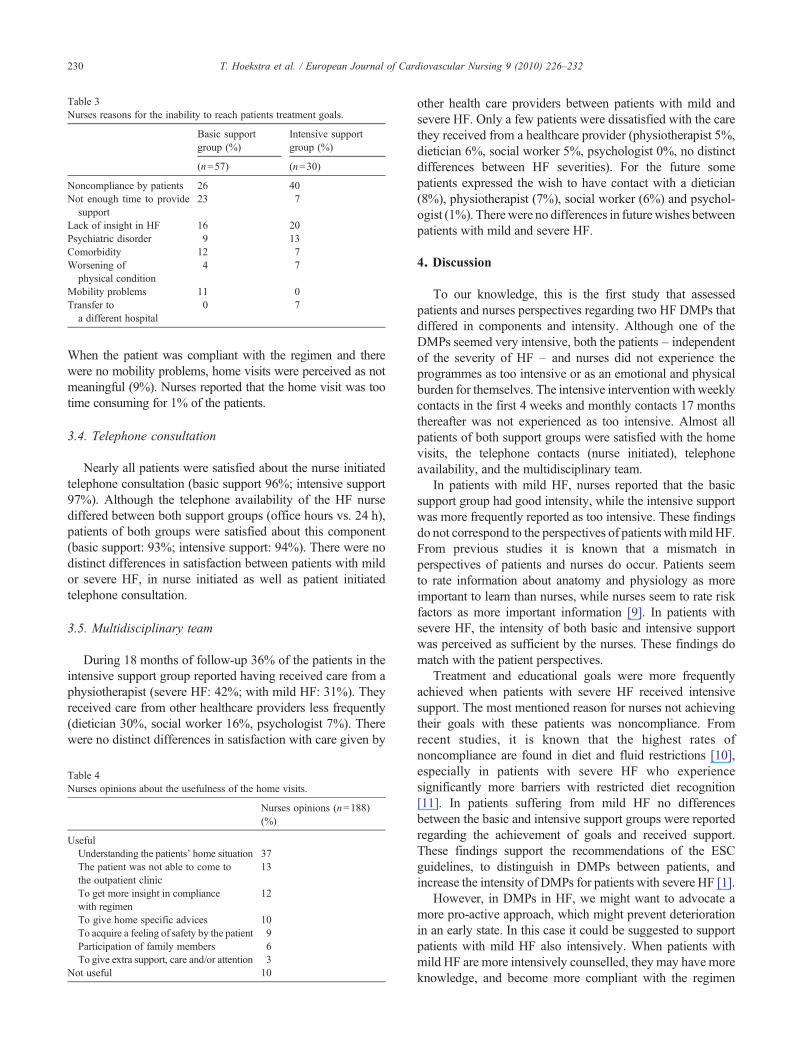
Table 3Nurses reasons for the inability to reach patients treatment goals.
Basic supportgroup (%)
Intensive supportgroup (%)
(n=57) (n=30)
Noncompliance by patients 26 40Not enough time to provide
support23 7
Lack of insight in HF 16 20Psychiatric disorder 9 13Comorbidity 12 7Worsening of
physical condition4 7
Mobility problems 11 0Transfer to
a different hospital0 7
230 T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
When the patient was compliant with the regimen and therewere no mobility problems, home visits were perceived as notmeaningful (9%). Nurses reported that the home visit was tootime consuming for 1% of the patients.
3.4. Telephone consultation
Nearly all patients were satisfied about the nurse initiatedtelephone consultation (basic support 96%; intensive support97%). Although the telephone availability of the HF nursediffered between both support groups (office hours vs. 24 h),patients of both groups were satisfied about this component(basic support: 93%; intensive support: 94%). There were nodistinct differences in satisfaction between patients with mildor severe HF, in nurse initiated as well as patient initiatedtelephone consultation.
3.5. Multidisciplinary team
During 18 months of follow-up 36% of the patients in theintensive support group reported having received care from aphysiotherapist (severe HF: 42%; with mild HF: 31%). Theyreceived care from other healthcare providers less frequently(dietician 30%, social worker 16%, psychologist 7%). Therewere no distinct differences in satisfaction with care given by
Table 4Nurses opinions about the usefulness of the home visits.
Nurses opinions (n=188)(%)
UsefulUnderstanding the patients' home situation 37The patient was not able to come tothe outpatient clinic
13
To get more insight in compliancewith regimen
12
To give home specific advices 10To acquire a feeling of safety by the patient 9Participation of family members 6To give extra support, care and/or attention 3
Not useful 10
other health care providers between patients with mild andsevere HF. Only a few patients were dissatisfied with the carethey received from a healthcare provider (physiotherapist 5%,dietician 6%, social worker 5%, psychologist 0%, no distinctdifferences between HF severities). For the future somepatients expressed the wish to have contact with a dietician(8%), physiotherapist (7%), social worker (6%) and psychol-ogist (1%). Therewere no differences in futurewishes betweenpatients with mild and severe HF.
4. Discussion
To our knowledge, this is the first study that assessedpatients and nurses perspectives regarding two HF DMPs thatdiffered in components and intensity. Although one of theDMPs seemed very intensive, both the patients – independentof the severity of HF – and nurses did not experience theprogrammes as too intensive or as an emotional and physicalburden for themselves. The intensive intervention with weeklycontacts in the first 4 weeks and monthly contacts 17 monthsthereafter was not experienced as too intensive. Almost allpatients of both support groups were satisfied with the homevisits, the telephone contacts (nurse initiated), telephoneavailability, and the multidisciplinary team.
In patients with mild HF, nurses reported that the basicsupport group had good intensity, while the intensive supportwas more frequently reported as too intensive. These findingsdo not correspond to the perspectives of patients withmildHF.From previous studies it is known that a mismatch inperspectives of patients and nurses do occur. Patients seemto rate information about anatomy and physiology as moreimportant to learn than nurses, while nurses seem to rate riskfactors as more important information [9]. In patients withsevere HF, the intensity of both basic and intensive supportwas perceived as sufficient by the nurses. These findings domatch with the patient perspectives.
Treatment and educational goals were more frequentlyachieved when patients with severe HF received intensivesupport. The most mentioned reason for nurses not achievingtheir goals with these patients was noncompliance. Fromrecent studies, it is known that the highest rates ofnoncompliance are found in diet and fluid restrictions [10],especially in patients with severe HF who experiencesignificantly more barriers with restricted diet recognition[11]. In patients suffering from mild HF no differencesbetween the basic and intensive support groups were reportedregarding the achievement of goals and received support.These findings support the recommendations of the ESCguidelines, to distinguish in DMPs between patients, andincrease the intensity of DMPs for patients with severe HF [1].
However, in DMPs in HF, we might want to advocate amore pro-active approach, which might prevent deteriorationin an early state. In this case it could be suggested to supportpatients with mild HF also intensively. When patients withmild HF are more intensively counselled, they may have moreknowledge, and become more compliant with the regimen

231T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
[12], resulting in a reduction of readmissions and mortality.For patients suffering from severe HF, the question arises as towhether it is possible to prevent them from hospital admissionor increased HF symptoms at that stage by a nurse-led DMP.Furthermore, the intensive support might feel as a burden tothese already very ill patients. However, the current studydemonstrated that patients, independent of the severity of HF,do not experience the intensive support as too intensive. At thismoment programmes are designed around similar sets ofconventional topics, but it is unclear how interventionsrespond to the needs, preferences, and values of patients [13].
Home visits were perceived as adding significant value tothe treatment. Nurses gained more insight into the patient'shome situation and in compliance with regimen. However, for12% of the patients, nurses believed the home visit was notmeaningful. A single home visit by a HF nurse reducesmortality and morbidity significantly in a HF population [14],but at the same time home visits are known to be timeconsuming. Future research needs to distinguish whichpatients might benefit optimally by a home visit.
Of the healthcare providers present in the multidisciplinaryteam, patients were most frequently referred to a physiother-apist and a dietician. Since all patients with severe HF shouldrestrict their sodium and fluid intake according to recentguidelines, the number of patients with severe HF referred tothe dietician, was relatively low. Patients who have contactwith a dietician have more knowledge about restrictions [15],are significantly more compliant to these restrictions [16], andimproved in their quality of life [17].
Additionally, almost no patients were referred to apsychologist. Considering the high prevalence of depressivesymptoms within HF populations [18], it was expected thatthe percentage of patients referred to a psychologist would behigher. Because HF nurses were not questioned about theirmotives for (not) referring a patient to other healthcareproviders, it is unclear why only a minority of the patientsvisited the dietician or a psychologist. Additionally, wefound that only 1–8% of the patients wish to have contactwith other health care providers in the future. This might bedue to the fact that patients are not aware of what can beoffered or lack of knowledge on heart failure and itstreatment and lifestyle recommendations, and lack of skillsof HF nurses to recognize and assess depressive symptoms inHF patients [19].
The limitations of this study should be considered. Firstly,the questionnaires used in this study were marginallyvalidated. However, this is one of the first studies that assessedpatient and nurse perspectives regarding HF DMPs and novalidated questionnaires are available at this moment. We areaware of floor and ceiling effects, however we deliberatelychoose to ask patients on a very detailed level for theirsatisfaction with the components of the support instead of anoverall number for satisfaction. This is tested in other patientsatisfaction researches, however we did not test this furtherthan only on face validity. Secondly, the questions of the nursesatisfaction questionnaire did not comprise questions about all
the components of the support groups. Further research issuggested to look more in depth on patient and nurseperspectives. Thirdly, the responders were significantlyyounger than the non-responders.
To conclude, patients and nurses did not perceive the nurse-led HF programmes of the COACH study as an emotional andphysical burden for themselves. In spite of the large differencesin intensity and components patients were satisfied with theintensity and components of the two DMPs. In these intensiveDMPs, the severity of HF should be taken into account;patients with severe HF should receive more support includinga home visit, whichmight result in an increase of treatment andeducational goals achieved within this patient population.However, the costs and benefits of home visits have to bestudied more thoroughly.
Appendix A
Patient satisfaction questionnaire
1 Did the nurse pay a home visit during the past 18 months?aHow satisfied were you about the home visit?b
2
Did the nurse initiate telephone counselling during the past 18 months?aHow satisfied were you about the telephone counselling?b
3
Did you have the possibility to contact the nurse by telephone in case ofproblems or questions?aHow satisfied were you about the possibility?b
4
During the past 18 months, did you have contact with a physiotherapist?aHow satisfied were you about the physiotherapist?b
5
During the past 18 months, did you have contact with a dietician?aHow satisfied were you about the dietician?b
6
During the past 18 months, did you have contact with a social worker?aHow satisfied were you about the social worker?b
7
During the past 18 months, did you have contact with a psychologist?aHow satisfied were you about the psychologist?b
8
What is your opinion about the intensity of the received treatment?c9
For future treatment, what would you like to receive? (More optionsapplicable)dNurse satisfaction questionnaire
1 What is your opinion about the intensity of the patients' receivedtreatment?c
2
To what extent was providing the treatment an emotional or physicalburden?e3
To what extent was the home visit meaningful?f4
Describe in one phrase why the home visit was meaningful or notmeaningful.5
To what extent did you achieve your goals with the patient?g6
What was the most important reason for not achieving your goals?Answer categories:aYes/no.bVery satisfied – satisfied – not satisfied, not dissatisfied – dissatisfied –very dissatisfied.cToo intensive – intensive – sufficient – not sufficient – not sufficient at all.dVisit to the cardiologist, education by a HF nurse, visit to the HF nurse atthe outpatient clinic, information about HF, home visit, telephoniccounselling, possibility to contact the HF nurse by telephone, contact witha physiotherapist, contact with a dietician, contact with a social worker,contact with a psychologist.eNot a burden at all – not a burden – a burden – a heavy burden – notapplicable.fVery meaningful – meaningful – not meaningful – not meaningful at all –not applicable.gAchieved all goals – achieved a majority – goals partly achieved –achieved a minority – no goals achieved.

232 T. Hoekstra et al. / European Journal of Cardiovascular Nursing 9 (2010) 226–232
References
[1] Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, PonikowskiP, Poole-Wilson PA, et al. ESC guidelines for the diagnosis andtreatment of acute and chronic heart failure 2008: the Task Force forthe diagnosis and treatment of acute and chronic heart failure 2008 ofthe European Society of Cardiology. Eur J Heart Fail 2008;10:933–89.
[2] Rich MW. Heart failure in the elderly: strategies to optimize outpatientcontrol and reduce hospitalizations. Am J Geriatr Cardiol 2003;12:19–24.
[3] Hunt SA, Baker DW, Chin MH, Cinquegrani MP, Feldman AM, FrancisGS, et al. ACC/AHA guidelines for the evaluation and management ofchronic heart failure in the adult: executive summary: a report of theAmerican College of Cardiology/American Heart Association Task Forceon Practice Guidelines (Committee to Revise the 1995 Guidelines for theEvaluation and Management of Heart Failure). Circulation 2001;104:2996–3007.
[4] McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinarystrategies for the management of heart failure patients at high risk foradmission: a systematic review of randomized trials. J Am Coll Cardiol2004;44:810–9.
[5] Gonseth J, Guallar-Castillón P, Banegas JR, Rodríguez-Artalejo F. Theeffectiveness of disease management programmes in reducing hospitalre-admission in older patients with heart failure: a systematic reviewand meta-analysis of published reports. Eur Heart J 2004;25:1570–95.
[6] Yu DS, Thompson DR, Lee DT. Disease management programmes forolder people with heart failure: crucial characteristics which improvepost-discharge outcomes. Eur Heart J 2006;27:596–612.
[7] Jaarsma T, van der Wal MH, Lesman-Leegte I, Luttik ML, HogenhuisJ, Veeger NJ, et al. Effect of moderate or intensive disease managementprogram on outcome in patients with heart failure. The Coordinatingstudy evaluating Outcomes of Advising and Counselling in Heartfailure (COACH). Arch Intern Med 2008;168:316–24.
[8] Jaarsma T, van der Wal MH, Hogenhuis J, Lesman I, Luttik ML, VeegerNJ, et al. Design and methodology of the COACH study: a multicenterrandomised Coordinating Study Evaluating Outcomes of Advising andCounselling in Heart failure. Eur J Heart Fail 2004;6:227–33.
[9] Hagenhoff BD, Feutz C, Conn VS, Sagehorn KK, Moranville-HunzikerM.Patient education needs as reported by congestive heart failure patientsand their nurses. J Adv Nurs 1994;19:685–90.
[10] Van der Wal MH, Jaarsma T, van Veldhuisen DJ. Non-compliance inpatients with heart failure; how can we manage it? Eur J Heart Fail2005;7:5–17.
[11] Van der Wal MH, Jaarsma T, Moser DK, van Gilst WH, van VeldhuisenDJ. Unraveling the mechanisms for heart failure patients' beliefs aboutcompliance. Heart Lung 2007;36:253–61.
[12] Van der Wal MH, Jaarsma T, Moser DK, Veeger NJ, van Gilst WH,van Veldhuisen DJ. Compliance in heart failure patients: theimportance of knowledge and beliefs. Eur Heart J 2006;27:434–40.
[13] Clark AM, Thompson DR. The future of management programmes forheart failure. Lancet 2008;372:784–6.
[14] Stewart S, Pearson S, Horowitz JD. Effects of a home-based interventionamong patients with congestive heart failure discharged from acutehospital care. Arch Intern Med 1998;158:1067–72.
[15] Neily JB, Toto KH, Gardner EB, Rame JE, Yancy CW, Sheffield MA,et al. Potential contributing factors to noncompliance with dietarysodium restriction in patients with heart failure. Am Heart J 2002;143:29–33.
[16] Arcand JA, Brazel S, Joliffe C, Choleva M, Berkoff F, Allard JP, et al.Education by a dietician in patients with heart failure results inimproved adherence with a sodium-restricted diet: a randomized trial.Am Heart J 2005;150:716.
[17] Kuehneman T, Saulsbury D, Splett P, Chapman DB. Demonstratingthe impact of nutrition intervention in a heart failure program. J AmDiet Assoc 2002;102:1790–4.
[18] Lesman-Leegte I, Jaarsma T, Coyne JC, Hillege HL, van VeldhuisenDJ, Sanderman R. Quality of life and depressive symptoms in theelderly: a comparison between patients with heart failure and age- andgender-matched community controls. J Card Fail 2009;15:17–23.
[19] Lesman-Leegte I, Jaarsma T, Sanderman R, Linssen G, Van VeldhuisenDJ.Depressive symptoms are prominent among elderly hospitalised heartfailure patients. Eur J Heart Fail 2006;8:634–40.