
The History of Nurse Maude
204
District Nursing and Homecare in Canterbury The History of Nurse Maude Vivienne Allan
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The History of Nurse Maude

District Nursing and Homecare in Canterbury
The History of Nurse Maude
Vivienne Allan

‘The First 100 Years’ was published by the Nurse Maude Foundation in 1996
This electronic edition was updated in 2016
Copyright © Nurse Maude Association 2016
Author Vivienne Allan
All rights reserved
This book may not be reproduced in whole or in part, stored or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, photocopying, recording or otherwise) without permission in writing from the author,
copyright owner and the publisher of the book.

Twigs
It’s hard to walk on shaky ground. Feet slip on
fractured stone, cracks open where you least
expect. The signposts have all been washed away, the map’s a blur, you’ve lost
the guide.
You must depend on small signs: broken glass, a bird
that sings no no no, not that way, try this way,
this way.
Sometimes you find twigs laid out on a white page,
crisscross and up and down. You pause and puzzle. Then sidle off.
There is no option but to head straight into the sun, prodding as old women do with their irritable sticks,
feeling for solid spots.
By Fiona Farrell
Reprinted with her generous permission - May 2016

CONTENTS
Introduction .............................................................................................................. 1
Preface ...................................................................................................................... 6
Part One – Sibylla’s Story ........................................................................................ 7
Chapter One: The Early Years.......................................................................................... 8
The Family History ......................................................................................................... 8
Matron Maude .............................................................................................................. 13
Walking the Extra Mile ................................................................................................. 18
Nurse Maude and the Women’s Movement ................................................................. 22
Chapter Two: Tuberculosis – The Dreaded Disease ....................................................... 25
Christchurch – The Garden City ................................................................................... 25
The White Scourge ...................................................................................................... 26
Chapter Three: District Nursing Develops ....................................................................... 31
Breaking new ground ................................................................................................... 31
Taking a Break ............................................................................................................. 33
District Nursing Progresses .......................................................................................... 34
Chapter Four: The ‘Flu Epidemic ..................................................................................... 37
The War Years ............................................................................................................. 37
The Outbreak of ‘Flu .................................................................................................... 41
Chapter Five: Nurse Maude is Here to Stay .................................................................... 44
192 Madras Street ....................................................................................................... 44
Her Works do Follow Her ............................................................................................. 48
Part Two - The Winds of Change .......................................................................... 52
Chapter One: A New Matron Takes Charge .................................................................... 53
Adapting to Change ..................................................................................................... 53
New Directions ............................................................................................................. 55
Social Security ............................................................................................................. 57
Chapter Two: Shaking the Kaleidoscope ........................................................................ 61
A Golden Jubilee .......................................................................................................... 61
‘Fitzroy’ ........................................................................................................................ 62
Years of Progress ........................................................................................................ 65
Chapter Three: The Whispering Winds of Change.......................................................... 68
The Lady Superintendent ............................................................................................. 68
‘Freedom is Sweet’ ...................................................................................................... 70

Free Home Aid ............................................................................................................. 72
Chapter Four: Planning for the Future ............................................................................ 77
1967 – A New Act ........................................................................................................ 77
Community Care .......................................................................................................... 81
Consolidating Premises ............................................................................................... 83
Part Three - Health Reform .................................................................................... 86
Chapter One: The Best of Times ..................................................................................... 87
Severing Links with the Past ........................................................................................ 87
The White Paper .......................................................................................................... 89
New Services are Introduced ....................................................................................... 93
Averill House ................................................................................................................ 96
Chapter Two: Restructuring in the 1980s ...................................................................... 100
Health Reform Looms Large ...................................................................................... 100
Launching the Foundation .......................................................................................... 103
A New Order .............................................................................................................. 108
Chapter Three: The New Health Culture ....................................................................... 113
Health – the Hottest Topic in Town ............................................................................ 113
Working the Contract ................................................................................................. 114
A New Beginning ....................................................................................................... 117
Chapter Four: Managing Change ................................................................................. 119
1996 – A Year in Review ............................................................................................ 119
Hospice and Palliative Care ....................................................................................... 121
Part Four - A New Era for Nurse Maude ............................................................. 124
Chapter One: Grappling with the Nuances of Health Reform ......................................... 125
Unleashing the Potential of Nursing ........................................................................... 125
Approaching the new Millennium ............................................................................... 127
A Time of Transition ................................................................................................... 129
Partnering in Community Healthcare .......................................................................... 132
Expanding the Boundaries ......................................................................................... 137
Chapter Two: The Drive for Efficiency and Innovation .................................................. 141
110 Years On ............................................................................................................. 141
District Nursing – Aspirational, Competent and Responsive ....................................... 145
From Home Aid to Home Care ................................................................................... 148
Volunteering Builds Strong Communities ................................................................... 150
Marketing Nurse Maude ............................................................................................. 152

Chapter Three ............................................................................................................... 156
From Committee to Board – governing Nurse Maude ................................................ 156
Part Five: The Canterbury Earthquakes and Their Aftermath .......................... 162
Chapter One .................................................................................................................. 163
Priorities and Outcomes ............................................................................................. 163
CREST and TotalCare ............................................................................................... 167
Assessing the Damage .............................................................................................. 172
Chapter Two .................................................................................................................. 174
Revitalisation, Repair and Recovery .......................................................................... 174
A Blueprint for Community Nursing ............................................................................ 178
Chapter Three: .............................................................................................................. 184
Post-quake: The redefined normal ............................................................................. 184
Author’s Notes and Acknowledgements ............................................................ 191
Board and Management 2015 .............................................................................. 195
Board of Trustees .......................................................................................................... 195
Senior Management Team ............................................................................................ 195
Bibliography ......................................................................................................... 196
Index ...................................................................................................................... 198

[1]
Introduction
The earthquakes that struck Christchurch and Canterbury with overwhelming strength and
velocity began before daybreak on 4 September 2010 and continued almost without respite
through to the end of 2011, gradually tailing off in 2012 with the occasional aftershock in
2013, 2014, 2015 and 2016 as a grim reminder to the community of the disaster that had
happened. The quakes did not discriminate in street or suburb. They impacted on everyone
and every organisation, business, government agency and community group. No-one was
immune from their unremitting savagery. Keeping people safe was essential through the
early days and weeks after the worst of the quakes, particularly 4 September 2010 and 22
February 2011. Keeping people healthy was part of the continuum. It was that continuum
that Nurse Maude, as Canterbury’s long-established district nursing service, did
exceptionally well.
Since its inception, Nurse Maude had
been the public face of community
healthcare, visible first on foot, then cart
and horse, bicycle and eventually the
motor car. It had been an essential
service through the 1918 influenza
epidemic. Now it was an essential
service during the 2010 and 2011
sequence of earthquakes. Those early
20th century images of staunch women
in their floor-length, heavy-duty
uniforms, starched aprons and taut
caps, were replaced with high
visibility jackets and hard hats,
gumboots to withstand liquefaction, a
torch, gloves, mask and a bucket toilet. It was a representation in every respect of Nurse
Maude - the organisation doing what it did best – managing the situation, dealing with the
crisis, and providing quality healthcare regardless of, or in spite of, the circumstances.
The staff who talked later about their quake experiences were matter-of-fact about what they
did. They did not regard their contribution as exceptional, or different to any other
community health agency. ‘Health tends to be self-managing in a crisis,’ Chief Executive
Jim Magee said in the post-quake analysis. ‘In any emergency, healthcare workers have a
role to play. They just get on with it.’1
It was that ‘just getting on with it’ that sustained hundreds of Nurse Maude’s patients and
clients, waiting at home for the district nurse or the homecare worker to arrive on 4
September, 26 December, 22 February, 16 April, 13 June, 23 December and on all the other
days when a particularly nasty aftershock rattled doors and windows and shook already
1 Interview with Jim Magee November 2014
Nurse Maude and her horse and cart – Gyp, her faithful collie
would wait patiently for his mistress while she attended her patients

[2]
shaken foundations. ‘More than 90 per cent of our staff went about their duties on 23
February,’ Jim Magee said. ‘They put on their gumboots and did their job in spite of having
their own frightened families at home and damaged or wrecked property.’
It was confirmation that Nurse Maude’s staff, like the search and rescue teams that were
combing homes and buildings for injured people, like the police who were on cordon duty,
like the army that had set up posts around the inner city, had a job to do. They were trained
professionals, calm in their demeanour, careful in their observations, meticulous in their
care. There was a high risk of disease and infection due to failing sewerage systems,
inadequate supplies of clean water and a real risk of injury particularly in houses that had
sustained damage. Attending patients and clients with a pre-packed box of essentials to
cater for most needs was a priority. Manoeuvring their way around the ubiquitous orange
and white striped cones, stepping across cracked footpaths and driveways, avoiding sudden
slumps and hollows was part of the hazardous journeys that Nurse Maude staff made on a
daily basis. They needed to know who to contact if they believed their patients or clients
were in any danger, particularly in the worst affected suburbs. They needed to know where
the emergency shelters were located, the welfare centres, where portable toilets were going
to be situated and later where the chemical toilets delivered to households could be emptied.
These were days when emergency care was pivotal, taking over from routine procedures.
Having a well-honed disaster recovery plan stood Nurse Maude in good stead. It was part of
its business management strategy. As a result, both its hospital and hospice facilities were
able to carry on, with understandable limitations, but with adequate water and power
supplies. The Merivale premises became a hub for emergency supplies being available to
other community healthcare agencies and enabled them to continue to operate. Nurse
Maude was inundated with generous offers of help from hospices and eldercare agencies
throughout New Zealand. But, it coped without needing to send anyone out of the region and
was able to take additional people from rest homes in Christchurch that had been badly
damaged. There was an undoubted advantage being based in Merivale. Although the
property was damaged and buildings evacuated, later to be demolished and rebuilt, it was
not as bad as many others in the eastern suburbs and in the central city.
Inevitably, the earthquakes changed the face of health in Canterbury – the need for
improved homecare became more urgent. Over several decades, there had been a political
and social commitment to develop best-practice ways of enabling people to stay in their own
homes rather than be hospitalised or institutionalised in their later years. Nurse Maude was
at the innovation vanguard with emerging trends in such areas as telemedicine, streamlined
technology and highly qualified staff to lead the change. Now was not the time to reflect on
what had happened, instead time could be better spent on research and developing
opportunities. Working from temporary quarters, portacoms and rental premises, Nurse
Maude’s corporate teams looked at how its frontline staff could achieve better patient
outcomes.
There were always times in its history, when the Nurse Maude organisation had reviewed its
progress, and explored new opportunities. It was not necessarily about keeping up with
change, it was more about being innovative and recognising that quality care was critical to
business continuity. These analyses had resulted in the Memorial Hospital being built, the
Hospice being established, palliative care, dementia care, specialised wound care, stoma

[3]
services and a range of initiatives being developed that had kept Nurse Maude at the
forefront of community healthcare in Canterbury over successive decades. In 2016, the
pending introduction of CRM20162 will be its most significant technological success story to
date. Coupled with a major new child health initiative, and a revised building programme,
Nurse Maude will be well on its way to its next centennial jubilee.
In order to fully appreciate the Nurse Maude organisation in the 21st century, it is important to
understand and give due recognition to its history and its contribution to Christchurch and
Canterbury since the region’s pioneering days. Sibylla Maude’s family was part of the early
Canterbury establishment at a time when the streets of Christchurch were still dirt tracks and
when wooden shacks with tin roofs dotted the landscape. The town centre had yet to be
fully framed and formalised. Her parents were both well-connected and she was raised in a
privileged household which upheld the Christian principles and values of a predominantly
Anglican community. Sibylla took these ideals with her when she started her work as a
district nurse and they became as integrated in the development of her business as the
physical care of her patients.
There is no doubt that Sibylla Maude holds her place in Canterbury alongside Kate
Sheppard, Ettie Rout and other exemplary women who have shaped local history. Mabel
Howard, a notable Cantabrian and recognised as one of New Zealand’s more forthright
Members of Parliament, told the Nurse Maude Board at their 1949 Annual General Meeting
that she considered Sibylla Maude to have been one of the greatest citizens Christchurch
had ever known. She had enjoyed close contact with Sybil3 in the early days and was
familiar with the work she had achieved in the poorer parts of the city that were well-known
to Ms Howard. The Association must never lose its identity, she said.4
As an organisation, Nurse Maude has grown up alongside Christchurch and Canterbury. It
has become an integral part of Canterbury’s health landscape. It has lived and worked
through innumerable changes to health policies by successive governments, at all times
focused on patient care. Over decades, it has adapted to the nuances of health policies and
implemented initiatives that contribute to maintaining its public personae.
Resilience is an oft-quoted word to represent the tolerance and forbearance of Canterbury’s
residents through the worst of the earthquakes. Iconic is another oft-quoted and frequently
over-used word when referring to buildings that were damaged and have been demolished
in the post-quake period. Yet, both resonate when referring to Nurse Maude as an
organisation. Its staff showed remarkable resilience during the worst of times.
McDougall House, gifted to the organisation in 1949, was badly damaged in the February
2011 earthquake. It was rebuilt and refurbished and formally reopened in October 2015.
As one of only a few heritage buildings remaining in Christchurch, it is a treasured reminder
of the city’s history as well as providing a home to Nurse Maude’s administration team, and it
houses some of the organisation’s original art works including the marble bust of Sibylla
2 CRM2016 – Client Relationship Management system 3 Sibylla was also known as Sybil or Sibbie to her friends 4 Nurse Maude Archives: Annual General Meeting 1949

[4]
which, at the time it was crafted, she declared was to be put in a cupboard and never to be
on show.
In his address at the organisation’s 2015 annual meeting, Chair Murray Compton noted the
multiplicity of changes that have occurred over the last 120 years of the Association’s
existence. From walking and then cycling hundreds of miles in the early days, Nurse
Maude’s staff now cover more than 2.5 million kilometres every year, providing 100,000
houses of nursing care and more than 500,000 hours of homecare. The staff have access to
180 vehicles, carefully sign written to identify Nurse Maude caring for the community since
1896. At the same time, 330,000 hours of care are provided in the hospital, another 100,000
hours in the hospice and more than 300 volunteers give Nurse Maude 125,000 hours of their
time every year. ‘The community has always been an integral part of Nurse Maude and I am
proud to say Nurse Maude will always be an integral part of the community.’5
The original office building at 192 Madras Street, where Sibylla Maude and then Mona
Corkill lived in the upper-floor flat with their respective companions, was deemed unsafe by
structural engineers and therefore demolished after the earthquakes. But, the organisation’s
founding principles which were embedded in its structure by Sibylla and her original
Committee of three, remain intact. Reviewed and revitalised through the decades, they are
articulated in the organisation’s mission as: ‘providing our community with responsive and
effective community home care and nursing services in partnership with families and
professional or social agencies.’
Nursing as a profession has changed incrementally as health has changed. The education
model is very different. Registered nurses are trained to degree level and higher. Enrolled
nurses have an 18 month training period. Standards are rigorously imposed. Nurses are
more analytical. They are critical thinkers and they are technologically savvy. They provide
a different service to that of their forebears. Yet they retain the original philosophy that is part
of the job. The International Council of Nurses defines the profession thus: ‘Nursing
encompasses autonomous and collaborative care of individuals of all ages, families, groups
and communities, sick or well, in all settings. Nursing includes the promotion of health,
prevention of illness, and the care of ill, disabled and dying people. Advocacy, promotion of
a safe environment, research, participation in shaping health policy and in patient and health
systems management, and education are also key nursing roles.’6
In 2011, the New Zealand Nurses Organisation published its report: ‘2020 and Beyond: A
Vision for Nursing.’ It described nursing as an ‘exciting and dynamic profession with multiple
opportunities for every member of the profession to contribute towards achieving optimal
health outcomes for individuals, families, whanau, communities and populations.’ It said that
nursing in New Zealand faces a ‘set of challenges that are unprecedented in the history of
the profession in this country. New technology, a growing population, an aging workforce,
new treatment modalities, genetics, and the local and global context of healthcare are
emerging within a context of constant restructuring, a tightening economic climate, and
nursing workforce variability. The ability of nursing as a profession to achieve improved
health outcomes for people through effective nursing interventions is well known within
5 Murray Compton, address at the Annual Meeting 8 December 2015 6 International Council of Nurses 2002

[5]
nursing but poorly understood by the public, by other health professionals, and by
government. We must continue to meet these challenges head on if we are to enable the
profession of nursing to achieve its full potential.’
The New Zealand Report, like the International Council of Nurses definition, has resonance
for Nurse Maude because of the increasing emphasis on caring for people at home, for
making ‘wellness’ rather than ‘illness’ at the forefront of the care pathway and for improving
the profile of nursing. In Canterbury, the earthquakes unwittingly paved the way for greater
recognition of community healthcare, not at the expense of hospital care, but as an
opportunity for patients and clients to have greater involvement in their own care
programme. That it happened because hospitals were overloaded and there needed to be a
process and system in place that reduced hospital admissions to emergencies only, proved
beneficial to the individuals involved. The economic argument, if there was one, for
community healthcare, was outweighed by the post-quake imperative. Reverting to the
previous ways of working was never going to be an option.
Community or district nursing was also recognised as one part of the healthcare system that
involved specialist and support services. What could be achieved by itself in the early days,
was now separated by professionalism and expertise. As a result, the evolution of home
care has become as important as district nursing, recognised and understood by Nurse
Maude over successive decades and contributing to its integrated programme of services.
The financial imperative of this joint service remains a juggling act however. Women form
the major part of the workforce in both areas – district nursing and home care. As Nurse
Maude’s Chair Murray Compton points out, it is also an aging workforce caring for an aging
population. Predicting future requirements for both, needs intelligence and dedicated
planning. It also needs policy direction from national bodies which have the planning
resources to determine what will be required.
‘We are the delivery agency, dedicated to our community. We look to the funders and policy
makers to predict what will be required in the next century. In the meantime, we are here to
nurse, support and care for our patients and our clients, at home, in hospice, and in
hospital.’7
7 Interview with Murray Compton December 2014. Murray Compton stepped down as the organisation’s Chair at the 2015 Annual Meeting.

[6]
Preface
Emily Sibylla Maude OBE – known as Sybil, Syb or Sibbie to her friends – died in
Christchurch on 12 July 1935. Clad in her nurse’s uniform and watched over by the Anglican
Sisters from the Community of the Sacred Name, she lay in state at the Christchurch
Cathedral until her funeral two days later. Her death was mourned by thousands of people
who had known her, who had been nursed by her, and who had contributed to the
development of district nursing in Christchurch and Canterbury. The eulogies in the
language of the day were lengthy tributes, recounting her work, her indomitable spirit and
often feisty manner, and her dogged determination to succeed in her life’s work.
She had been a pioneer in district nursing, dedicating her life to serving the needs of the
elderly poor. A Christian woman who shunned publicity, Sybil rejected the upper middle-
class affluence she had been born into in favour of a more spartan existence closer to the
town’s needy folk.
Her death marked the end of a personality, of a lifetime during which the practice of caring
for people in their own homes had become firmly established. Her death also marked the
beginning of a broader organisation which was to develop into the first and most recognised
district nursing scheme in New Zealand. It was to become a living memorial for its founder.
While the shape of the Nurse Maude Association would inevitably change to accommodate
New Zealand’s health environment, the values and ethics espoused by Sibylla from
inception, would stay and flourish.

[7]
Part One – Sibylla’s Story
‘Let us in kindness covet for every man
One lovely memory at least in life-span
Fit to be locked up in Crystal reliquary
So all may see it, yet none see it, save he.’
‘Rock Crystal’ Mary Ursula Bethell

[8]
Chapter One: The Early Years
The Family History
Sibylla Maude was the eldest of eight children. She was born at the
family home of Hagley Lodge, in St Peter’s Parish, Riccarton Bush
Christchurch on 11 August 1862 and christened Emily Sibylla a
month later in St Michael’s Anglican Church. She was named after
her mother Emily Catherine and her paternal grandmother Sibylla
Jane (nee Green). Her father, Thomas William Maude came from a
strict Anglican family in the Suffolk village of Haskerton Woodridge
where his father Rev Thomas Maude was the rector at the historic
St Andrew’s Church. The eldest of five children,8 Thomas Jnr was a
bright student graduating with an MA from Balliol College Oxford.
While still in his early 20s, he and his younger brother Edmund set
sail for New Zealand in 1855 on board the Royal Stuart. They
walked down the gangway at the bustling port of Lyttelton in the
newly-established Canterbury colony with one thought in mind – to
head for the hinterland and become sheep farmers. It was a
familiar dream and one that was not destined to last.
The brothers took up a five-year lease on 8,000 acres of land, one of three large runs at Mt
Thomas Station which was situated at the fork of the Okuku and Ashley rivers in mid-
Canterbury.9 The land belonged to John Thomas Brown, a surveyor by profession who had
arrived in New Zealand in 1851 and started Mt Thomas as a cattlerun. John Brown and
Thomas Maude soon forged a strong friendship. They found they had much in common
intellectually if not necessarily related to farming. But Thomas was an entrepreneur, more
interested in the developing commercial interests of Lyttelton and Christchurch than the
slower pace of rural living. He easily found work in the Customs Department at Lyttelton
where waves of immigrants were regularly arriving and where there was potential and
opportunity for him to utilise his talents. He was able to keep a watching brief on the sale of
Canterbury runs and as a result he and Edmund secured several more properties in their
endeavours to achieve their original aim of becoming landowners.
Thomas soon made a name for himself in the growing settlement. He was appointed clerk
to the local court – John Hall was the resident magistrate at the time – and in February 1859
he was made Honorary Secretary of the Christchurch Cricket Club. In 1861, he accepted an
offer to become one of the directors10 of the Lyttelton Times newspaper. It was a significant
year for Thomas. Not only did he become a lay member of the first Anglican Diocesan
synod of Canterbury, but he was elected to the Provincial Council as the member for Ashley.
He was re-elected several times over the next decade taking his place at the Council table
with Robert Heaton Rhodes, Alfred Hornbrook, William Rolleston, Hugh Murray-Aynsley, and
8 Thomas, Cordelia, Edmund, Arthur and Charles Maude 9 Acland L.G.D. ‘The Early Canterbury Runs.’ (4th ed.) Whitcoulls Ltd Christchurch 1930 p 82. 10 During Thomas Maude’s tenure as a shareholder in the Lyttelton Times, the newspaper moved to Christchurch but retained its original name.
Sybil aged three years

[9]
William Sefton Moorhouse amongst others. Clearly, Thomas was destined to become a
familiar face in local government and potentially further afield. He was an affable man, well
liked and respected by his peers.
Thomas’s personal life changed at the same time as he grew his commercial and political
aspirations. In 1861, he married Emily Catherine, the daughter of his friend and business
colleague John Brown who was by now an active member of Canterbury’s fashionable
landed gentry. Born and raised in England, the son of the Anglican chaplain at Norwich
Castle, John Brown was an educated man with a keen business sense and more than a
passing interest in racehorses. He teamed up with his future son-in-law in land and property
deals including Ashwick, a large run which was further south than Mt Thomas, between the
Opihi and Opuha rivers. Ashwick, later reports suggest, was part of Emily’s dowry when she
married Thomas. Not limited to farming, John Brown expanded his interests further when he
bought the Albion brewery in Cashel Street Christchurch in partnership with his younger
brother Horace. He endorsed his daughter’s flourishing romance with Thomas Maude and
the couple were married at the Mt Thomas family homestead by the Archdeacon of Akaroa
Ven. Mathias on 3 April 1861.
The Brown family, like Thomas and Edmund Maude were keen to retain their investment in
Canterbury’s pastoral runs. Both John and Horace owned land and were considered to be
pioneering pastoralists, but they were also interested in the fast-developing urban life. By
August 1886, John Brown and Thomas Maude had decided to sell Ashwick. It was a
commercial decision but one that attracted a letter from John Hall to Thomas. The sale, he
wrote, created ‘a saddish feeling to see one of the old Pilgrims after another dropping away
from the old and staple industry of the country.’11 Regardless of any quasi-romantic notions
of land retention, the two men went on to sell all but the homestead block and the adjoining
flat land at Mt Thomas Station as well. Horace Jnr, one of Emily’s brothers, stayed to farm
the remaining acres, living in the large, comfortable, double-storeyed cob home until his
death in 1928. He was, by all accounts, a keen gardener and turned the homestead into
something of a showplace with more than a thousand different species of roses surrounded
by plantings of almost every forest tree available.12
Meanwhile Thomas Maude went from strength to strength in the world of commercial
business and local government politics. An early description of him by Crosbie Ward, a
partner in the Lyttelton Times, paints a picture of a young man who ‘lacks the experience
requisite to be the chief of an important department. But he has a suave deportment that
almost disarms criticism and his fresh, good-looking, good tempered face does as much to
make him friends as his industry, mild and obliging manner do to keep them.13
As his interest in public affairs flourished, so did his family with a second child Thomas Jnr
born in December 1863, Charles in May 1865, Mary in April 1868, Cordelia in August 1869,
and Arthur in June 1872. Six children in ten years was typical of the era. Sybil, as the eldest
was kept busy helping her mother with the growing family. It was an early introduction to
11 Pinney Robert. ‘Early South Canterbury Runs.’ A.H.& A.W. Reed Wellington 1971 p 39. 12 Acland L.G.D. ‘The Early Canterbury Runs.’ (4th ed.) Whitcoulls Ltd Christchurch 1930 p 82. 13 G.R. Macdonald. ‘Dictionary of Canterbury Biographies.’ Canterbury Museum NZ. Thomas Maude pp 1-7.

[10]
domestic duties and home care. Thomas strengthened his public profile by joining his father-
in-law’s brewing firm Brown & Co and was invited to serve on several commissions – one
inquiring into the civil service and another looking at the conduct and
organisation of the police force. From there it was a small stepping-
stone to national politics and when in 1871, William Reeves was
appointed Resident Minister of the Middle Island14 in the Fox
Government, Thomas became his private secretary. Less than a year
later he was elected unopposed to the Provincial Government and
took up the position of Provincial Secretary and later Secretary for
Public Works in 1874. It was a time of great commercial and
economic development in Canterbury particularly in the areas of
public works and Thomas greatly enjoyed the challenges that came
his way. As Provincial Secretary, he was in a powerful position – a
key decision-maker in such matters as the development of the
Lyttelton rail tunnel, harbour accommodation, provincial railways,
roads and bridges.
In his position, he also became involved in the decision to build a lunatic asylum in
Christchurch, to provide a more stable home for people with mental illnesses who were
previously retained in the Lyttelton gaol. Edward Seager was the driving force behind the
establishment of Sunnyside which was opened in 1863 and Thomas was named one of two
‘official visitors’ appointed by the Provincial Council. Their task was to regularly, and
comprehensively, inspect the premises and to observe every patient. They were then
required to furnish the Council with a detailed report. Thomas was appalled by the
conditions and roundly critical on many an occasion. ‘The continued keeping of patients in
these old15 buildings cannot be too strongly condemned,’16 he wrote after one particularly
lengthy and seemingly distasteful visit.
But in spite of his many activities and high community profile, Thomas hankered to be a
lawyer and in 1874, aged 44, he decided to sell his home and take his family to London
where he could study for the Bar. It was an unusual decision, particularly when he was
regarded as an up and coming politician. While many wealthy families regularly sailed back
‘home’ to visit relatives and friends, selling up and returning to England to study was
definitely different. Perhaps it signalled a restlessness in Thomas that he could achieve more
and do more if he had better qualifications, his earlier Oxford degree notwithstanding.
Introducing his wife and children to his parents and siblings was an added attraction
however and the family soon settled into their new routine.
Thomas and Emily moved in upper middle-class circles. They placed their children in good
schools, Sybil being sent to Linden which was recognised as a select establishment for the
daughters of gentlemen in Blackheath, south London. While they were living in London,
14 The South Island was known as the Middle Island. It was recognised as the South Island by 1907. 15 It can be assumed that he defined ‘old’ in the sense that they were stark and depressing, because they were scarcely old at the time. 16 Seager Madeleine. ‘Edward William Seager.’ The Heritage Press Waikanae. 1987. p 263.
Sybil – a young woman

[11]
Thomas met up with Leonard Harper, the son of Bishop Harper.17 Leonard had established
his own law firm in Christchurch and was on holiday in England. He invited Thomas to enter
his firm when he returned to New Zealand on payment of £2,000 which would give him a six
per cent profit share in the company. It was an offer Thomas accepted with enthusiasm. He
completed his law degree and was admitted to the Bar at Lincoln’s Inn before returning to
Christchurch.
By now, Sybil was fully occupied helping her mother with the family. Two more children
were born – Edward in January 1881 and Eva in May 1883. Like her parents and
grandparents, Sybil was a dedicated member of the Anglican Church and when time
permitted, she would visit the poor in the parish. Taking the lead from her good friend Fiona
Acland, the wife of a prominent Canterbury run-holder, Sybil was one of the first ‘visitors’ at
Christchurch Hospital and she soon encouraged two other friends Edith and Amy Rhodes18
to do likewise. Gradually, her interest expanded into a wish to become a nurse.
‘When I was a young girl, I used to be very fond of visiting among the poor and in hospital,
and I conceived the idea that by being trained as a nurse, I could best serve my fellow
creatures,’19 she wrote later.
Although two of her mother’s sisters (in England) were nurses, the profession was still in its
infancy in New Zealand. It was hard, tiring work; little was known of it outside the workplace
and it was considered to be not quite the right path for a young woman of good standing to
follow. If Sybil was going to make a career of anything other than marriage, it should be as a
governess or perhaps a lady’s companion. She was undeterred. She made inquiries but
soon realised there was no suitable training available in Christchurch. Her best option, she
decided, was to return to London. In 1889, aged 27, she sailed back to England on her own
and enrolled at Middlesex Hospital in central London as a paying Lady Probationer. Why
Middlesex Hospital? There is no specific historical fact that suggests any reason other than
it had an established reputation even in faraway New Zealand, having started as an infirmary
in 1745 with its medical school built in 1835. Sibylla’s intention to become a nurse was an
early indication of her fortitude and strength. It was a mark of her parent’s regard for her
personal resilience that she was permitted to travel on her own and to study and live so far
away from her immediate family.
Lady Probationers could enrol in London hospitals to train in medical and surgical nursing.
They were required to pay for their board and lodging and for uniforms. They paid for a
year’s intensive training including lectures with the intention of becoming qualified as nursing
Sisters. Not everyone lasted the distance. The hours were long and arduous and the
training strenuous, made cumbersome by thick serge uniforms which fell well below the
ankles and included a small train at the back. The probationers were also required to wear
frilly caps fastened with silk strings and tied in a bow under the chin. In spite of the dress
code and the paraphernalia which restricted movement, Sybil did well. In fact she thrived.
17 Bishop Henry John Chitty Harper was the first Bishop of Christchurch. Originally from Hampshire, England, he and his wife Emily (Woolridge) sailed to New Zealand in 1856. They had five sons and five daughters. 18 Macdonald C, Penfold M, Williams B (Eds) ‘The Book of New Zealand Women.’ Bridget Williams Books Ltd Wellington 1991 p 431. 19 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group, Christchurch 1950. p 25.

[12]
The only person from the antipodes in her group, she soon proved she was an excellent
worker and thoroughly dependable. ‘Temper and discipline exceedingly pleasant; always
loyal, true and obedient. For twelve months, she was acting Sister of Proderip and Percy
wards where she maintained complete discipline, managing patients and nurses with tact
and kindness.’20
Sybil completed her year and decided to stay at the hospital for an extra twelve months to
gain additional experience. She was assigned to a surgical ward where she worked with two
famous surgeons Sir Henry Morris and Sir J. Bland Sutton. Both men were pioneers in new
methods of surgical treatment and both had a life-long interest in anatomy. Sybil had a
rewarding and fulfilling year and returned home in November 1892 full of enthusiasm. Back
in Christchurch however, there were both changes and troubles within the Maude family.
Her brother Thomas had chosen to follow his father into law, studying at the University of
Canterbury, and he had established his own practice. As promised while still in England,
Thomas Snr had joined the firm of Harper & Co in partnership with the Harper brothers
Leonard and his younger brother George. But the arrangements were short-lived. The firm,
known as Harper & Maude, operated as three individual units. Leonard managed the
financial side, George took care of the court work and Thomas acted as general
conveyancer. Leonard proved to be secretive about his side of the business and reluctant to
discuss his external dealings with his partners. While Leonard was overseas in 1893, claims
of financial mismanagement resulted in both George and Thomas being taken to court and
the firm ultimately being declared bankrupt. The court case was not only lengthy, it attracted
considerable public interest. In July 1984, George Harper and Thomas Maude were struck
off the rolls. It was a terrible disgrace for both families.
Although both George and Thomas had nothing to do with the financial side of the business,
they had realised something was wrong and had tried to mitigate the situation without
success. The Press noted sombrely: ‘A large established firm in our midst of the highest
respectability and most honourable reputation has failed for something over a quarter of a
million… There is a large class at Home to whom New Zealand means Canterbury, and
Canterbury means Harper and Co…our honour as a colony stands impeached.’21
It took five years for both men to be allowed to practice law again and then only on the
condition that they were employed by someone else. Thomas went to work for his son.
Meanwhile Leonard Harper was brought back to New Zealand by the police and charged
with embezzlement. Although found not guilty, he too was struck off the rolls. It was a
humiliating situation for both the Harper and Maude families.22
Sybil, newly returned to her family, was keen to find work, to make use of her London
training and to immerse herself in activities that were not related to her father’s decline in
20 Macdonald C, Penfold M, Williams B (Eds) ‘The Book of New Zealand Women.’ Bridget Williams Books Ltd Wellington 1991 p 431. 21 Christchurch City Libraries/Heritage/Cemeteries: commentary on notable Canterbury figures. 22 Rhodes Jessie. Details of the Early History of Christchurch Nursing and Nurse Maude Association. (undated) pp 1-7.

[13]
fortunes. It did not take long. Within a few months she was offered the position of Matron at
Christchurch Hospital. Aged 32, her new career was about to begin.
Matron Maude
When it was built in 1862,
Christchurch Hospital was small
and lacking in many resources. It
was situated close to the Avon
River and its entrance was by the
Antigua street bridge. It
comprised a series of wooden
buildings which were not very
hygienic and which could
accommodate little more than 30-
40 patients at a time. There had
been plenty of arguments and
debates about the hospital’s
location, its intrusion onto Hagley Park, and whether there would be enough space for future
expansion. The first matron, Mrs Bunting, was so named simply because she was married
to the master (assumed to be the manager), a genial woman but with no knowledge of
nursing whatsoever. The hospital had no mortuary (known at the time as the ‘deadhouse’),
no operating theatre and inadequate kitchen facilities. It had no electricity and no sewerage
system. It was ‘purely a large house for the sick with a domestic outlook.’23
Over time, central government allocated more funds to improve the hospital, increase the
number of wards, to add a dispensary, a chapel and an operating theatre. Stringent rules
were imposed as to who was eligible to be admitted to hospital. Exclusions were more
common than admittances. The hospital expanded in size and in staff numbers over the
next two decades to accommodate the growing number of patients. In 1886, the hospital
was connected to the main Christchurch sewer lines, viewed as significant progress and
regarded as a ‘vast sanitary improvement.’24 A year later, the large fireplaces which
dominated the wards and which belched smoke and dust everywhere, were removed. Gas
lights replaced kerosene lamps in the wards. Thomas Maude organised a public appeal in
his capacity as the Provincial Secretary to fund a hospital library. The response was
generous resulting in sufficient money to buy more than 200 books.
By the time Sibylla was appointed matron in 1893, the North Canterbury Hospital Board had
been in place for nearly eight years. Its mandate stretched from Kaikoura, through Amuri,
Cheviot, Ashley, Akaroa and as far south as Selwyn County. Sibylla had several
predecessors. Miss Paton was the first trained nurse to be appointed matron in 1885. She
was succeeded by Miss Boys in 1888 and Miss Steele in 1890. Their individual tenures
were difficult and in spite of their nursing skills, they were subservient to both the doctors
and the Board. Like all new appointees, Sibylla believed she could achieve what the
23 Bennett F.O. ‘Hospital on the Avon.’ North Canterbury Hospital Board 1962 p 230 24 ibid p 73

[14]
previous matrons had been unable to. In many respects, the hospital was still fairly
primitive. The Board had decided to install electricity, but it took another five years for the
gas lighting to be replaced. Although the hospital had been training nurses for nearly three
years, there were still not enough who had the skills to do all that was required of them. As
the incumbent new matron, Sibylla had the added complication of older nurses who did not
understand modern practices. Many of them had trained on the job. They did not have the
benefit of overseas experience.
In many ways Sibylla was a reformist. She knew from her two years in London what nurses
could achieve and she wanted to instil the same professionalism and credibility in her staff
as she herself had grasped while working on the wards at Middlesex Hospital. Taking on the
position of matron was a challenge. Whether she could implement the necessary changes
remained to be seen.
She soon realised improvements were an immediate priority. She had two allies on whom
she counted. Rev Walter Averill, Vicar of St Michael’s parish was the recently appointed
hospital chaplain and Dr Murray Aynsley was the resident house surgeon. Both men
recognised the need for reform and supported their new matron in her endeavours. Dr
Aynsley argued for more wards to be built. The average age of the population was
increasing and there was a greater propensity for disease. Amongst his list of
recommendations was a proposal for women to be trained as district nurses so that poor
people could be looked after in their own homes.25
Less than a year after Sibylla’s appointment, a major public row developed when a letter to
The Star, one of Christchurch’s newspapers, charged the hospital authorities with gross
mismanagement, bad food, compulsory church services, bread and water for difficult
patients, crudity by the dresser, cruelty to and by the nurses, discrimination by religion and
incompetence of the house steward, adding up to 18 individual complaints.26 The Board
instigated an inquiry, headed by Dr McGregor who asked his assistant Grace Neill to make a
start. She observed and interviewed relevant staff and wrote her report which was handed
to the Board by Dr McGregor. The Board acknowledged the report including the comments
that there was some disharmony amongst the nurses organised, it was presumed, by one of
the long-standing staff members - Nurse Cameron.
As the hospital matron, Sibylla was then required to write to Nurse Cameron advising of her
dismissal with a follow-up letter telling her not to return to the hospital. A public meeting
about the report and Nurse Cameron’s dismissal was held on 8 April 1895. There was a
unanimous vote of no confidence in the Board. Lengthy meetings were held behind closed
doors with Board members in Christchurch and politicians in Wellington. A judicial inquiry
was set up and discovered amongst other matters, that the original letter sent under a
pseudonym to The Star had, in fact, been written by one of the hospital doctors. The internal
rumblings and factions within the Board and amongst the hospital staff were clearly part of
systems and processes that needed a radical overhaul. The final report described the North
Canterbury Hospital Board as ‘weak kneed’27 It recommended that some of the older nurses
25 Bennett F.O. ‘Hospital on the Avon.’ North Canterbury Hospital Board. p 55 26 ibid p 107 27 ibid p 11

[15]
should retire on the basis that they were continuing with outmoded practices. Food should
be of better quality, a housekeeper should be appointed, compulsory church services in
wards should be abolished, as should pauper funerals. All 18 original complaints were dealt
with in turn.
While all these issues festered in the media and stirred up negative public sentiment, Sibylla
continued to manage her nurses and introduce initiatives that would improve patient care.
As hospital matron, she was no doubt in a position to contribute her ideas to the construction
of the Nurse’s Home, the foundation stone of which was laid on 19 April 1894 and which was
completed and ready for its first intake in 1895. By all accounts, it was a lively institution
where the young women had their own rooms, a central dining room and separate recreation
areas. The doors were locked promptly at 10pm.28
But Sibylla was not happy in her job. She had a sense of frustration that everything required
someone else’s approval before it could be achieved. A firm believer in religious principles,
she asked permission for illuminated scripture texts to be placed on the walls between beds
in the wards.29 Her request was turned down. It was just something else to add to her
growing list of reasons why she should resign. She felt her real vocation lay with the elderly
poor who were sick, at home, and unable to get care. There was nowhere for them to go. If
they went to hospital they had to pay, but they had no money.
Since the 1850s when Christchurch was established, the sick poor were looked after by their
family members or by community groups like the Deaconesses from the Community of the
Sacred Name, an Anglican Order of nuns who lived in a small corrugated-iron building on a
large section which bordered Barbadoes and St Asaph Streets.30 The Community was
founded in 1893 by Edith Mellish under guidance from Rev Churchill Julius, Bishop of
Christchurch. Sister Edith had trained with the St Andrew Deaconess Community in
Westbourne Park London. The Sisters worked amongst the poor in Christchurch and
provided accommodation for unmarried women at St Mary’s Home in the city.
Constrained by a lack of nursing experience and knowledge, Sister Edith decided to send
one of her probationers Sister Rose Godfrey to Christchurch Hospital to be trained as a
nurse. It was a decision which would have long lasting effects for the Community of the
Sacred Name, for Sister Rose and for Sibylla Maude. The hospital could teach Sister Rose
the techniques of nursing but in the Sisters of the Community, Sybil recognised all that she
personally wanted to achieve. She toyed with the idea of becoming an Anglican nun, but it
was not to be.
‘She wanted to be a Sister, but she got turned down because the Reverend Mother felt her
vocation to nursing was so huge’.31
28 Campbell Helen. ‘Looking back, a history of the Christchurch School of Nursing 1891-1987’ Published 1997. 29 Bennett F.O. ‘Hospital on the Avon.’ North Canterbury Hospital Board. p 119 30 The buildings owned by the Anglican Order were demolished after the 2010 earthquakes. 31 Blakie Megan. ‘Anglican Life’, August/September issue. Interview with Sister Anne. 24 August 2012.

[16]
Through Rose Godfrey, Sybil developed a firm friendship with these quiet, gentle women,
visiting them frequently, staying for weekends and often calling in for tea after her day’s work
at the hospital was finished. She gave advice to them about health matters and in return
received the sisterly endorsement she needed for her work. But even this and her growing
friendship with Sister Rose was not enough to keep her contented as Matron Maude. The
hospital might be a training ground for nurses and a place where the sick could recover, but
there were constraints with rules and regulations which were more than the strong-willed
Sybil could take. The reforms she wanted to implement were too radical for the Board. With
never-ending disputes between the older untrained nurses and the new recruits and with
constant friction between herself and the Board, Sybil became the subject of an inquiry in
June 1895. Sister Rose was required to give evidence and Sybil appeared for a lengthy
examination. Afterwards, she was invited to tea with her friends at the Community of the
Sacred Name.
‘She is very brave,’ Sister Edith wrote later in her diary. Claims of mismanagement within
the hospital were proven groundless. Sybil was cleared of any charges and her ‘efficiency in
the nursing business…unquestioned’,32 but her mind was made up. Once the seeds of
mistrust were sown and some members of the medical profession were not prepared to
accept her professional opinion when it came to hospital nursing, why should she stay? The
lure of community work was becoming stronger and stronger, and determined to do
something about it, she went once again to see her friend and mentor Rev Walter Averill.
Was district nursing a possibility, she asked him? Could she set up something that would
meet the needs of the sick and poor people who could not afford to go to hospital and who
could be looked after in their own homes? Rev Averill expressed immediate interest and
discussed the concept with Jessie Heaton Rhodes, a parishioner at St Michael’s Church who
was well known for her philanthropy and support of community projects. Through her
marriage to Robert Heaton Rhodes, Jessie had become good friends with Sybil. His sisters
Emily, Edith and Amy were friends of Sybil’s from childhood which added to the connection.
The vicar of St Saviour’s in Sydenham, Rev Edwin Scott, was next to be brought into the
scheme. All agreed to support Sybil both financially and with the names of people who
needed care, with the proviso that she would only tend to people who were unable to pay for
the nursing services she would deliver.
In her written agreement, Sybil said: ‘I am aware of the tentative nature of the work and that
much must be left to circumstances as they develop, but I suggest for the consideration of
yourselves and Mrs Heaton Rhodes, who is so large a contributor to the funds required, one
or two leading features of the intended arrangement. That my services as a district nurse
within the parishes of St Michael and Sydenham be engaged for a period of twelve months
from the 5th day of October 1896, at an annual remuneration of £80 to be paid in monthly
instalments, and that after that time, the engagement be terminable on either side, by three
months’ notice in writing.’33
32 Rhodes Jessie Details of the Early History of Christchurch Nursing and Nurse Maude Association. (undated) pp 1-7. 33 Maude Sybil, District Nursing Kai Tiaki Nursing Journal 1908 p 118.

[17]
Sybil would undertake to work with financial support from her friends, particularly Jessie
Heaton Rhodes who had committed £100 per annum for the project. The agreement was
signed. Walter Averill and Edwin Scott wrote Sybil an official letter confirming her
appointment and with the blessing of her small band of supporters, Sybil handed in her letter
of resignation to the North Canterbury Hospital Board.
‘I beg to tender my resignation as matron, to take effect from the end of August,’ she wrote
on 27 May 1896. ‘My reason for leaving is simply that I feel the strain of responsibility too
much and believe that a change is necessary to enable me to carry on my work as a nurse.’
She went on to thank the Board for the ‘courteous way in which they have met my many
requests’ and gave three months’ notice instead of the usual one month.
Responding to the letter, the Chairman of the Hospital Board said Miss Maude had assured
him she was not leaving on account of any grievances, but because she meant to go in for
district nursing and give up hospital work.34 Sybil was leaving to go and live as an Associate
member with the Sisters of the Community of the Sacred Name and start her work as a
district nurse.
It was the beginning of a new journey. It was also a remarkably brave step for a woman at
that time. Notwithstanding the fact that women had been granted the vote three years
earlier under the stewardship of Kate Sheppard and the suffragists, Canterbury was still
positioning itself as a new and emerging colony with an emphasis on its pastoral bounty.
Less than 50 years old, the region was grappling with issues of infrastructure, commercial
and economic development, housing, and related social issues. But there was already a
distinct separation between the wealthier Christchurch citizens who preferred to live to the
north and west, and the poorer folk who lived on the south and the east sides of the town.
The ‘class’ to which the Maude family belonged, if ‘class’ was a term to be considered, did
not believe women should or could step beyond clearly identified boundaries. Training to be
a nurse working in a hospital was acceptable, but working alone?
What prompted Sibylla to shoulder such a responsibility and start out on a career that had no
local precedent? Perhaps she took her lead from her pioneering father, a man who
eschewed a career in industry and commerce in England following a successful university
education and opted instead to immigrate to New Zealand and settle in Christchurch. He
was a risk taker and accepted the inevitable rises and falls that went with his talent. Sybil
was a woman who had chosen a career path that was removed from her peers. In addition
to her formal nursing training, she empathised with the community’s less-fortunate. She had
the benefit of a strong Christian faith, and she was also well acquainted with influential
people who could help her with financial support. What she lacked in political nous, she
more than made up for in her connections with the right people.
As matron of Christchurch Hospital, she had learned how to manage her staff, how to plan
her budget and how to deal with the complicated nuances of health politics. That she did not
fully enjoy it, was more about her need for independence than her desire to walk away from
an important position. However, in her role as hospital matron, she was also able to observe
the operational decisions of the North Canterbury Hospital Board. They were to stand her in
34 Rhodes Jessie. Details of the Early History of Christchurch Nursing and Nurse Maude Association. (undated) pp 1-7.

[18]
good stead as she started her new life. Making a positive decision to tender her resignation
without rancour or criticism was an astute move because she was aware from her own
knowledge of Christchurch, that at some time in the future she might need the Board.
Walking the Extra Mile Nurse Maude, as Sybil quickly became known, was easily
recognisable as she walked briskly along the south Christchurch
streets, her black bag under one arm and a wash bowl or a
bedpan often tucked under the other. She was a short, rather
thickset young woman, somewhat inclined to stoop, with a stern
demeanour that belied a rather soft heart.
The design of her uniform had been the subject of much
discussion with her financial backers. It should be pale blue, they
agreed, with a stiff Eton collar35, stiff cuffs and belt and topped by
a stark white apron. To go over this she would wear a dark blue
cape which flowed to the ankles and a matching bonnet with navy
strings tied beneath the chin. It was indicative of the era and
similar to the style worn by the nurses she had observed in
London. Every morning she set out armed with her list of needy
families supplied by the vicars of St Michael’s and St Saviour’s.
She would go into a house, say a prayer and then get down to
business.
From the start, she realised her job would be more than simply nursing care. Poor people
who became ill generally lost their income. The average weekly wage was low, rents were
high and there was little in the house for food and clothing let alone anything left over in case
of sickness. Besides, the houses were often poorly ventilated, with little or no heating in the
bedrooms. The elderly poor who were sick did not have anywhere to go and frequently no
one to care for them. Some lived with their extended families; others had to make do with
what they had. Poverty, illness and disease tended to go hand in hand. Within a short
space of time, Nurse Maude had become a household word in the town’s poorer suburbs.
More and more people came to her for help and the town’s doctors soon realised they only
had to send word and she would be there. Before the year was out, Sybil had made over
1,100 visits on foot to those unable to afford hospital or private nursing care.
‘As this was almost the first work done here, I had to work it as nearly on English lines as I
knew how,’ she wrote later. ‘I first began district nursing from Deaconess House where I
had the use of a telephone and the space of a cupboard to keep necessaries of my work…’36
She quickly outgrew her little office in St Asaph Street and looked around for larger premises
where she could establish a dispensary and people could come for treatment. After an
inauspicious start, using part of an old stable in Winchcombe Street, she rented a little shop
35 The Eton collar was so named because of the stiff, broad buttoned collar designed for the shirts worn by the boys who attended Eton College, England in the late 19th century. 36 Fry Ruth. ‘Community of the Sacred Name. A Centennial History.’ Community of the Sacred Name, Christchurch 1993 p 25
Sybil Maude – District Nurse

[19]
in nearby Durham Street which had sufficient space to run a small clinic and store all her
supplies. Here people could come for minor treatment or be fitted for clothes. The rooms
would be open for half an hour at 9am and 2pm. At other times, messages could be left, and
anyone could call on the telephone – number 940. A sewing circle was formed. Second-
hand clothes were brought into the rooms and remade into garments for children. Footwear
and other clothing were sorted and stored in the little shop.
‘Well do I remember our circumstances,’ Jessie Heaton Rhodes wrote afterwards. ‘We had
only a table, chair and wooden cases to sit on.’37
As Sybil established her dispensary, she also moved house, going to live with Sister Rose in
1898 on the outskirts of Christchurch in a new suburb called Shirley. Rose had been put in
charge of St Mary’s Anglican Home for girls which had moved from its original site in
Addington to Stapleton Road which was semi-rural. The Home, managed by the Sisters of
the Community of the Sacred Name, could accommodate up to twenty young women at any
one time who were ‘rescued from the police court, the houses of ill-fame, or the cruelty of
unnatural or drunken parents’.38
The move to Shirley was a new beginning for both Rose and Sybil. Their friendship had
blossomed from the start. Rose Godfrey had joined the Sisters as a probationer in 1894.
Like Sybil, she came from a well-to-do family and the two shared an almost philanthropic
interest in their community. Rose was the quiet one, the nurturer; Sybil the stronger of the
two. St Mary’s was situated on four acres of windswept land in an area that was more of a
country district than a suburb. It was a considerable distance from her district nursing work
and before long Sybil decided she needed some form of transport. She owned a harness
but no horse. Undaunted, she put an advertisement in the local paper and almost
immediately found herself in possession of both a horse and a cart. It was an ideal mode of
transport. Each morning she packed her daily requirements in the cart and set off. Gyp, her
black collie ran at the back. A keen gardener, Sybil grew flowers on the property and picked
them fresh each morning to take to the market on her way to work. The money was added
to the collective fund.
A routine developed and with it a philosophy. Unwittingly, Nurse Maude was pioneering
district nursing in New Zealand, based on the English model of ‘services given to the sick
poor in their own homes regardless of the religious denomination of the sufferers.’39 As she
went on her rounds, she found more was required of her than just nursing care. She was
called on ‘sometimes to relieve, sometimes to heal, always to console.’40 She was the
provider of food and clothing, sometimes cleaning the house or instructing the family in the
principles of cleanliness. She was also aware of the community’s failure to recognise the
dangers of infection and a complete lack of knowledge about prevention measures. While
she never hesitated to interfere, albeit kindly, in the lives of her patients, she nevertheless
37 Macdonald C, Penfold M, Williams B (Eds) ‘The Book of New Zealand Women.’ Bridget Williams Books Ltd Wellington 1991 p 431. 38 ibid 39 Macdonald C, Penfold M, Williams B (Eds) ‘The Book of New Zealand Women.’ Bridget Williams Books Ltd Wellington 1991 p 431. 40 G.R. MacDonald Dictionary of Canterbury Biographies, Canterbury Museum New Zealand Thomas Maude pp 1-7.

[20]
believed implicitly that every family should maintain its independence. ‘The most cruel thing
a social worker can do,’ she often said, ‘is to take away a family’s self-respect.’41
In her second annual report which she presented to Jessie Heaton Rhodes, Walter Averill
and Edwin Scott; Sybil wrote: ‘The work has considerably increased outside the original
boundaries. I sincerely hope that it is now better understood that no question of creed is
considered as I have nursed patients of all creeds. St Michael’s parish heads the list, 800
visits having been paid during the year, in Sydenham 76, and 713 in other parishes making a
total of 1589. This number does not include those people who come to see me at
Deaconess House.
‘I cannot account for such a small number in Sydenham except that the district is too large to
expect all to grasp the fact that a nurse may be obtained without payment. I find that single
handed, I cannot go into other districts outside of Christchurch if the work increases as it has
done this year - that is 200 more than last year. A second nurse will be required, and I feel
sure the public will respond.’42
As was her habit, she signed herself simply as ‘Sybil Maude, District Nurse.’
Engrossed in her work, she had neither the time nor the inclination to bother with issues
other than health, although she retained her strong religious convictions, always attended
Sunday church services and was in regular contact with her family. Yet again, her siblings
had moved in different directions. Her brother Thomas was enjoying life as a lawyer. He
had married Georgina Branton-Day in 1895. Her brother Edward, nicknamed ‘Jogger’,
aspired to be a farmer, Arthur had qualified as an engineer and her sister Cordelia had
married a local brewer Charles Sloman. After the furore surrounding his involvement in the
Harper bankruptcy scandal, her father had remained in legal practice with his son. But it
was not easy. He was a man respected as a gentleman who had been involved in the early
development of the town and the province. He had mixed in social circles with John Hall,
William Moorhouse and William Rolleston and had been close friends with William Pember
Reeves who was godfather to Cordelia.
While Sybil was well aware of her father’s personal and financial disaster, she did not let it
affect her work. Caring for the poorer people in the community was her life’s calling. Even
so, she maintained close contact with influential friends who could help with fund-raising
efforts. In her District Nurse’s Report for 1899, she stated the number of visits had
increased once again this time to 1,683.
‘Relief has been given from a sick fund contributed to by different friends, also clothing which
is chiefly provided by the ladies who have met every week at Mrs Robison’s, Bank of New
South Wales, to mend and make for that purpose,’ she wrote. ‘Grateful thanks are due to
Mrs Heaton Rhodes for the use of the ‘Annie Clark’ bed and for various letters of admission
to the Convalescent Home also to others who have sent gifts throughout the year especially
at Christmas time.’43
41 Eldred Grigg, Stevan. ‘A New History of Canterbury.’ 1982. John McIndoe, Dunedin p 30. 42 Sibylla Maude Annual Report 1898 43 Nurse Maude District Nursing Association Annual Report 1899

[21]
Sybil’s report included a commentary about the success of a new sewing circle, led by Mrs
Izard, who accepted contributions of old linen and clothing to unpick, unravel, and recreate
into useful items for the poor and needy. She concluded with advice to the Board that her
district nursing work would be carried out by Nurse Annie Hickman Hiatt for the next twelve
months. Sybil had worked with Annie Hiatt at Christchurch Hospital and knew her to be an
experienced and conscientious nurse. Concerned at the lack of midwifery care in
Christchurch, Sybil thought that if she could gain her Obstetrics Diploma, she would be able
to offer more care and support. She had canvassed support for her decision from her three
benefactors before making her decision public.
Her role as matron of Christchurch Hospital had stood her in good stead when it came to
report writing and balancing budgets. Equally important was the care with which she
maintained her circle of friends, many of whom she had known from childhood, recognising
that their connections were important when it came to finding additional funds.
On 2 February 1900, Sybil and Sister Rose together with their close friend and poet Mary
Ursula Bethell, went to breakfast with the nuns at the Community of the Sacred Name. It
was a ‘talking’ meal instead of the usual silent fare, to say goodbye to Sybil as she left, once
again, for England. Annie Hiatt continued the rounds during Sybil’s absence. The visits
increased to nearly 1500, she reported to the Board at the end of the year. As had come to
be expected, more people from outside the parishes were turning to the district nurse for
help, as much for their social needs as for their medical ones.
Almost a year to the day, Sybil returned home and took over from Nurse Hiatt.44 But while
her newfound skills enabled her to do more, her midwifery training had the undesirable effect
of severely increasing her workload. She turned to her good friend Jessie Rhodes for advice
who suggested the original group should get together again and discuss progress. On 4
March 1901, Jessie Rhodes, Archdeacon Averill, Rev Scott, Rose’s father Charles Godfrey
and another local businessman Mr E.M. McDonald met with Sybil. They agreed to support
her financially on the understanding that she continue with her district nursing work without
including maternity care. It was a blow to Sybil, but she agreed with the collective decision.
She did not believe her midwifery training would be a wasted effort, particularly with the
increasing birth rate in the community.
Sybil’s supporters decided to form themselves into a committee and be responsible for the
funds to carry on the district nursing work and they promised that as funds became
available, they would appoint an assistant nurse to help Sybil. Rev Edwin Scott was elected
the first chairman and Charles Godfrey agreed to take on the role of secretary-treasurer. It
was a formalising of Sybil’s work and an acknowledgement of the principles by which her
work was being carried out. A week later, Charles Godfrey wrote a letter to the Lyttelton
Times with a public request for funds.
‘May I beg space in your paper under the notice of your readers the claim of this
institution (Christchurch District Nursing Fund) upon the public of Christchurch.
44 Annie Hickman Hiatt went to South Africa with five other New Zealand nurses during the time of the Boer War. (Ref: Women of the Waimakariri, Ch 7, p 69)

[22]
The services of the district nurse are given to the sick poor in their own homes
regardless of the religious denomination of the sufferers. The cases dealt with
are those that cannot be admitted to the hospital and where the means of the
patients are insufficient to enable them to pay a trained nurse – unfortunately,
there are many such cases.
‘The good work was begun about four years ago by one nurse, and was at first
confined to a limited area, but the calls soon came from outside those limits so
that now there is more work than can be undertaken by one nurse, and it is very
desirable that an assistant should be engaged. This, the committee has
determined to do when the funds will admit.
‘With this object, the present appeal is made to the public, and it is confidently
hoped that it will meet with a ready response. Those who are unable to give
much may of their little give some help, and the giver of ever so small a sum may
have the comfortable reflection that he has in a measure helped to smooth the
pillow and give ease to some poor sufferer.’
Donations, Mr Godfrey concluded, could be sent to him. The
appeal so successfully launched, placed the district nursing
programme on a firm footing and in 1902, Annie Holgate was
appointed as Sybil’s assistant nurse with a salary of £100 per
annum. Like Sybil, Nurse Holgate had trained at Middlesex in
London and like Sybil, also gained her obstetric diploma there.
Now she had returned to New Zealand and had become the
second formally qualified district nurse in New Zealand.
It had taken Sybil six years, albeit with one year’s absence to
undertake her midwifery training, to be recognised as a fully
functioning business. Nurse Maude, the District Nursing Fund,
was fully operational and ready to expand.
Nurse Maude and the Women’s Movement
The 1880s and 1890s were significant decades for New Zealand women. The issue of
women’s franchise had embraced many of their lives and Christchurch was recognised as
the centre of this early feminist movement. As far back as 1850, women were campaigning
vigorously throughout the country, writing articles, addressing public meetings and stating
the case for women to have the vote. The Women’s Christian Temperance Union while
dedicated to seeing something done about the ‘demon drink’, was also publicly advocating
the same cause. The issues stretched out to dress codes and other freedoms and became
the subject of much public debate.
Where was Sybil when hardy campaigners like Kate Sheppard and Ada Wells were fighting
for voter freedom? The very epitome of independence, Sybil embraced the right to self-
determination, freedom of speech and tolerance towards humanity – all the laudable

[23]
sentiments espoused by the growing band of suffragists. Yet she demonstrated no curiosity
in the developing furore that swirled around her, at least not publicly. If she commented
privately to Rose Godfrey about the need for women’s suffrage, or her concerns about the
extent of alcoholism amongst the families with whom she worked, she refrained from any
public involvement in the political struggle for universal suffrage.
Interested only in her work, Sybil clearly had little time for such activities. Yet, she could not
help but have been drawn into the discussions and debates on the topic as she was, like
many other committed Anglicans, keenly interested in helping her community. Often
confronted by the results of drunken behaviour during her rounds, she had learned to hold
her counsel while offering advice when asked. She was aware of abuse towards women as
a contributing factor to complex health issues in many of the cottages she visited, and from
the girls who lived at St Mary’s Home. Many of her family’s friends like politician John Hall,
advocated for women to have the right to vote. But Sybil’s interests lay in other directions –
actions rather than words. However, and somewhat reluctantly, she was drawn into a public
spat in the Lyttelton Times in response to a letter to the editor written by Kate Sheppard and
Ada Wells.45
The two campaigners described the situation of a woman who had been refused access to
Christchurch Hospital. The Charitable Aid Board had done all it could to help, they wrote.
The woman ‘had been lying prostrated from a disease of loathsome form.’ She had several
sons and the cottage she lived in was so small there was no way they could be separate
from their mother. Kate Sheppard and Ada Wells said they had checked out the facts and
had themselves paid a visit to the woman in the cottage. They then made a plea to the
public for financial support for the family, a request which was endorsed by the newspaper’s
editor.
Sibylla was not at all happy when she read the story. In her own letter to the newspaper
published two days later, she chastised the two suffragists for misrepresenting the facts.
The woman to whom they referred was not contagious, she was being properly treated and
the Charitable Aid Board was giving her all the help she needed, she stated. She went on to
quote from a letter the woman had written to the Board after she had seen the letter. ‘For
my children’s sake, I would be glad if you could give publicity to this fact,’46 she wrote. Sybil
added that the woman was not confined to the house and had been taken out for drives.
She did not want any public charity because she was already receiving sufficient help from
friends and from the authorities.
The editor, having said earlier that he had checked out, and agreed with, the facts as stated
by Kate Sheppard and Ada Wells, now reversed his opinion adding at the end of the
correspondence that if what Miss Maude said was true, the money already donated by the
public would be returned.
Mesdames Sheppard and Wells wrote again, explaining that they had ‘endeavoured to put
the case before the public in as careful and guarded manner as was consistent with the plain
statement.’ They had spoken with a medical expert and could not therefore modify their
original letter. They had intended to give the monies raised to Nurse Maude ‘or some other
45 Lyttelton Times Correspondence Columns 10-16 December 1898 46 ibid

[24]
responsible person’ but given that the patient herself did not wish to receive any charitable
aid, they felt they were forced to leave the responsibility of dealing with the issue to the
authorities.
Publicity about the issue did not end there. There were several other letters to the editor
from various members of the public supporting both Nurse Maude and the two women who
had made the issue so public. The correspondence ended abruptly however with another
rebuke from Sybil who cautioned Kate Sheppard and Ada Wells about their comments,
which, she said, had not been thoroughly researched. Then the final word came from ‘A
Piteous Case’ herself stating that neither of the two women had been to her house.47
The original letter and the correspondence that followed gave a public face to a common
problem of the era however. Caring for the poor and needy was a growing issue for
Christchurch. But the whole affair was an irritation to Sybil who did not like any politicisation
of her work. She had endured the political dimension when she was matron at Christchurch
Hospital because it was part of the job, but as a district nurse, her commitment was to her
patients and she was not about to have her profession used as part of a bigger campaign.
She preferred to fight her battles in a different way.
47 Lyttelton Times Correspondence Columns 10-16 December 1898

[25]
Chapter Two: Tuberculosis – The Dreaded Disease
Christchurch – The Garden City
As it approached the turn of the century, Christchurch was a fast developing town. It had a
population nearing 40,000 with clusters of communities springing up to the north, south, east
and west with the town’s centre starting to take its own shape and form. There were already
noticeable differences between the poorer people living in the lee of the Cashmere hills and
their wealthier neighbours on the other side of the retail and commercial area. Christchurch
was the chief industrial centre of New Zealand. Named after the early settler John Robert
Godley’s college in Oxford England, it had its roots in Anglican tradition – the cornerstone of
its Cathedral having been laid by Bishop Harper in the pouring rain on the province’s 14th
anniversary day – 16 December 1864.
It had the makings of a beautiful city and had already been given the title of New Zealand’s
garden city some years earlier. The streets were laid out squarely with plantings of double
rows of trees in European fashion. The Avon River meandered peacefully through the city
towards the estuary on the eastern side of Christchurch enabling a wide belt of grass to be
planted on either side as it did so. In the English tradition, areas of land were set aside for
development as public spaces. Hagley Park was already a botanical landmark.
Imposing buildings using local quarried stone, and architecturally designed by English
immigrant Benjamin Mountfort dominated the town’s centre. His Gothic-revivalist style
confirmed Christchurch as quintessentially English. Drapers, iron mongers, jewellers, boot
stores and the like, traded briskly alongside fruit and vegetable markets. Rural land and
farm agencies, banks, insurance companies and law firms were also established.
Pastoralists dominated the town, their wool cheques providing handsome returns for
investment in local development. Industrialisation was rapid – wool scours, lime kilns and
tanneries sprang up in swift succession, several in the southern suburbs like Woolston and
Sydenham where there was ready access to riverways. Cob coaches, some capable of
seating up to thirty people, provided transport as did the traditional horse and cart.
It was a time of evolution. The opening of the railway tunnel between Lyttelton and
Christchurch had resulted in a move away from river traffic. In earlier days, visiting ships off-
loaded their trade at Ferrymead and punts and barges used to sail up the Avon and
Heathcote Rivers stopping at various jetties to make their regular deliveries. Coal, firewood,
posts and rails as well as general cargo were easily transported this way. Sybil’s father
Thomas had been a central figure in the early days, overseeing progress.
Large homesteads had been built on the outskirts of Christchurch – areas like Riccarton
where Thomas and Emily Maude made their home were on the western side of Hagley Park
and therefore almost rural in aspect. Southwards, there were smaller cottages on smaller
sections. They were the cramped, meagre homes of the working classes, built from wood or
iron. With little or no drainage, they were harbingers of disease. The homes were situated
on land that was flat, swampy, marshy, and prone to flooding. In the 1860s, the Avon River
was seriously polluted and water-borne diseases were rife. It was not much better two

[26]
decades later, although with the establishment of the Christchurch Drainage Board, better
systems were soon put in place. Even so, for the poorer people of the city who had little or
no sanitation and who relied on the night-cart to remove waste, who were more prone to
infections than the more affluent residents in the north and north-west, Nurse Maude was
their Lady of the Lamp.
They were first and second generation residents, immigrants who had come out to New
Zealand, travelling steerage on the sailing ships, seeking greener pastures and the promise
of a better life. But under the exacting immigration policy of the day, once they had a roof
over their heads, they were expected to find work.48
To Sibylla Maude, they were people who needed help as they struggled to cope with
poverty, illness and frequently more children than they could afford. By modern standards,
her nursing skills and political knowledge were not enough to give her sufficient
understanding to fight for public health reform. But she was undisputedly a pioneer in district
nursing. In her philosophy, she possessed all the right attributes– a streak of iron,
inflexibility when required and a tough stance to achieve what she wanted. Although
disappointed at having to give up midwifery, Sybil realised the sensibility of her mentors’
proposals. However, on one point she was adamant, something had to be done about the
rapidly increasing numbers of tuberculosis sufferers in the city. It was a disease that did not
discriminate. John Deans recognised as the first settler in Christchurch died of tuberculosis.
John Robert Godley contracted the disease and died on his return to England.49 It was even
recommended in English medical journals of the day, that New Zealand, and in particular
Canterbury, was an ideal place to recuperate from TB because of the high levels of fresh air
compared with Great Britain.
The White Scourge
A universal problem amongst the Christchurch poor was superstitious ignorance of the way
diseases were treated. When this ignorance concerned a disease such as tuberculosis, it
became alarming. There was something dreadfully frightening about it. Referred to as the
‘white scourge’, it had a strange almost macabre effect on families and there were some
curious cures propounded. A piece of garlic or a lump of camphor tied around a child’s neck
was seen as a safeguard against infection. To the ordinary person, TB was a blow from
above – it was God’s will and must therefore be accepted with patient resignation.
Sibylla was determined to fight the fear and the superstition. She believed that as long as
she came up with an idea that was acceptable to the health establishment, the ways and
means would be found for it to continue. The general public would come to her aid as they
had done before. All they needed were the facts.
She discussed various options with two local doctors on whom she knew she could rely for
their advice and counsel. Dr Alice Moorhouse had graduated from Canterbury College in
Christchurch and Glasgow University in Scotland and had been the Medical Officer at the
48 Tolerton Jane. ‘Ettie.’ Penguin Books 1992 Auckland p 38. 49 Bennett F. O. ‘The Hospital on the Avon.’ North Canterbury Hospital Board. p 50

[27]
Hanmer Springs Sanatorium. Dr Leslie Crooke was a graduate from Edinburgh University
and was the Senior Medical Officer at Christchurch Hospital at the time. Both agreed with
the thesis of isolation and fresh air as part of a possible cure.
Sybil decided to set up open air camps, believing, as she did, in the ‘gospel of fresh air’.
She also realised that her first camp should be for men. Not that women did not suffer from
tuberculosis – it was simply a matter of what
was the easiest to begin with. She knew
that it was essential to get patients away
from their families to reduce the risk of the
disease spreading. But finding suitable land
might be more difficult. However, in 1903,
while she was still pondering on options and
potential sites, Sybil was offered a small piece of land on the sand hills near New Brighton
by its owner Mrs A.J. White. It was overgrown with broom, but Sybil could see its potential.
With the support of several local working men’s clubs, Sybil scouted around for tents. Four
were quickly provided. They were small – eight feet long by four feet wide with flies that
enabled the front flaps to be folded back and tucked over the supporting poles.
The tents were pitched facing the northwest to give their occupants the warmest possible
aspect and the wild broom, left in its natural state, provided shelter from the elements.
Prospective patients were asked to bring their own utensils and bedding. If possible, they
should pay seven shillings per week for expenses, but it was not obligatory. The Charitable
Aid Board agreed to provide the food and Dr Crooke gave his medical services free. The
primary idea was to treat the condition in its early stages to prevent infection spreading and
to build up the patients’ strength.
The camp started modestly with three men admitted. The wife of one of them, Mrs Reading,
agreed to be the matron responsible for cooking food and for the patients’ welfare and
wellbeing under Sybil’s instructions. Her husband had been advised by his doctor in
England that they should come to Christchurch to see whether the climate might cure his TB.
They had a small daughter who settled with her mother in a tent which was separated from
the men’s quarters. Mrs Reading was the ideal person for her new role. A former teacher in
England, she quickly adapted to her spartan surroundings. She was there from the first day
the camp was established. Her daughter, writing later of their experiences described the
camp in its raw state.
‘A piece of scrub land was obtained along the banks of the river near New Brighton, about
half-way between the New Brighton bridge and the Bower Hotel. A small, rough clearing
was made about a chain back from the road with a rough, stumpy, sand track connecting the
two… a larger tent was obtained for meals which were served on home-made tables and the
seats were ordinary forms. Camp beds or stretchers were the beds and any furniture the
men themselves possessed and could bring, was used in the tents. The floors were bare
sand at first, but after a while, someone suggested thatching them with the green tops of the
broom growing all around. This was a great improvement as it helped to keep the sand
under control.’50
50 Cocks E. Somers ‘A Friend in Need’ Printpac Print Group Christchurch 1950. p 69
[28]
Meal preparation was primitive, the daughter went on to explain. Her mother had lit the fire
on the first day watched by Sybil, Fred Hornibrook, the headmaster of Sydenham School Mr
Baldwin and Dr Crooke. Cooking was by way of a camp oven and a simple contraption of
saucepans suspended over the fire supported by two iron poles. After several months a
timber hut was built to act as a kitchen and storeroom.
Fred Hornibrook, who was the close friend, confidant and later the husband of safe sex
campaigner Ettie Rout, was also concerned about the increasing level of consumption in
Christchurch and offered Nurse Maude his support. He was a well-known public figure at the
Christchurch School of Physical Culture, who actively campaigned with Dr Cecil Greenwood
and raised money for the camp by organising a weight-lifting contest and a magic lantern
exhibition featuring famous athletes of the world.
Word spread, and before long, Nurse Maude’s camp had grown to such an extent that the
initial makeshift facilities were no longer suitable. Better accommodation and huts for food
preparation would have to be put in place. It did not take long. Ever vigilant, and knowing
the community would support her, Sybil soon had enough funds for a covered dining area
with donated tables and chairs. After three months, the camp was starting to look quite well
established. But winter was approaching and there were public expressions of concern
about the suitability of the camp and its site particularly after a few storms caused some
damage to the men’s tents. A neighbour whose land was considered more appropriate
offered nine acres with a cottage. It was an offer Sybil accepted with alacrity.
This time the camp was established in a more orderly fashion with three small groups of
eight tents in each. The cottage, where the matron lived, was the centre point with the
marquee and kitchen close by. A flag fluttering on a pole which was donated by men from
the Lyttelton wharf, marked the camp’s entrance. Very strict rules were imposed for the
disposal of sputum. Every patient was given a flask which was carried in his pocket. A
furnace was used to burn the contents daily and the flasks were boiled regularly. Any
patient who ignored these rules was likely to be expelled.
A year after Nurse Maude’s camp was established, another tent sanatorium was developed
at neighbouring Wainoni by Dr Greenwood. His father-in-law, Professor Bickerton, a
member of the New Brighton Borough Council owned the land and supported the venture.
Avon Pine Sanatorium was ready for occupancy in 1904 for fee-paying patients.
Then Sibylla mooted the idea of another camp, this time for women. She called a meeting of
Christchurch women to gauge their support. A local benefactor, Mrs Florance, offered four
acres of land some two miles from the men’s quarters at New Brighton. The land was
suitable and there was an existing cottage. The deal was struck and Sybil’s appeal for help
was met with its usual level of public enthusiasm. Tents, shelters and furniture were
donated by women’s organisations. Concerns for the patients’ safety at night were quickly
dealt with by putting up a high fence topped with barbed wire.
After a slow start with only two women patients, the camp began to grow. Sybil had found a
suitable housekeeper – Mrs Dunne - and persuaded her to take on the job, to live in the
cottage with her two daughters and to be responsible for managing the camp in the same
way that Mrs Reading was managing the men’s camp. Her two charges, Maggie and Molly

[29]
had a tent each. Like the male camp, the facilities were to say the least, spartan in design.
Mrs Dunne resigned after 18 months and was replaced by Mrs Murray. Trained at
Christchurch Hospital and a former ward Sister, Nurse Murray adopted a different approach
to her patients. More trained staff were engaged, and little wooden villas were built instead
of the canvas tents. More women arrived until the camp was full. The women were
encouraged to keep hens, grow their own vegetables and flowers, and like the men, were
given lessons in physical fitness by the ebullient Fred Hornibrook who supported not only
Sybil’s two camps but Cecil Greenwood’s as well. Rosters were introduced to help with the
chores and Mrs Murray followed Sybil’s regime of exercise combined with fresh air and good
food to aid recovery.
The three camps were the topic of much public discussion and not a little criticism by the
local medical profession. No-one volunteered a better solution and regardless of the
negative comments, everyone agreed that both Nurse Maude and Dr Greenwood were
doing something about a health issue that the authorities had consistently failed to deal with.
They were formally acknowledged when Sir Joseph Ward opened Avon Pine and Victoria
Plunket, the wife of the newly installed Governor General Lord William Plunket, opened
Nurse Maude’s camp for women.
Once a week Sybil visited her two camps, often bringing a member of the committee with
her. They would go on a tour of inspection and enjoy tea and a concert. More and more
men and women left the camps pronounced free of TB, proving to the sceptics that isolation,
as much as fresh air, was a contributing factor in the cure of the disease. With an ever-
increasing workload however, Sybil knew she could not continue with so many projects. She
appealed to the Christchurch Hospital Board to take over the TB camps, but it declined.
However, a growing public row over the state of the camps, including a major falling out with
their honorary medical officer, resulted in a general call for something more permanent to be
established. Not everyone approved of the primitive sand hill canvas huts, not least the
members of the Christchurch medical profession. They variously described the camps as
hovels which were grossly ill-equipped, and which had little or no real medical equipment.
It fell to the City Council to take the initiative. In July 1905, the Mayor of Christchurch Charles
Gray, called a public meeting with a view to building a sanatorium and two years later the
foundation stone was laid by the acting Prime Minister Hon William Hall-Jones on a site
gifted for the purpose by the Wilson estate in the Cashmere hills.51 Sibylla as the
‘philanthropic lady’ who had set up the first camps at New Brighton was invited to attend the
ceremony in recognition of her earlier work. She was then invited to be part of the
committee overseeing the construction and she agreed until ill-health forced her to resign.
Nonetheless, she continued to take a keen interest in the development of the sanatorium
designed by local architects Hurst Seagar, Wood and Mannings. Named the Cashmere
Sanatorium, it took another three years to build and was formally opened in March 1910 with
31 beds.52
51 Tuberculosis Institutions – original text by Winifred Norris digitised by Christchurch City Libraries (use as reference bibliography) 52 Silverson Alice: ‘The last 30 years: The history of the Canterbury Area Health Board.’ Canterbury Area Health Ltd, Christchurch 1995. p 167.

[30]
On two separate occasions during the construction, Sibylla asked for financial help from the
North Canterbury Hospital Board to maintain the hill camps until the Sanatorium was
completed and ready for patients. Both times, she was gratified that her requests were
granted. In a way, the formal if belated support of the camps, was a validation of her work
and her initiative in getting them established, proving to the local doctors and the Hospital
Board that fresh air was indeed a major part of treatment for TB sufferers.
If Sibylla had achieved nothing else, she had brought about positive change in an area of
health that had been sadly lacking. Always a good friend, she remained in contact with her
first camp matron Mrs Reading when she retired, regularly calling in to see her for a cup of
tea and a chat.

[31]
Chapter Three: District Nursing Develops
Breaking new ground
‘We look upon the district nurse, if she is what she should be, and if we give her the training
she should have, as the great civiliser of the poor, training as well as nursing them out of ill
health into good health, out of drink into self-control, but all without preaching, without
patronizing – as friends in sympathy.’ Florence Nightingale, December 1896
With the appointment of Nurse Annie Holgate, district nursing in Christchurch started to
develop in a more organised way. The two nurses continued their daily rounds and Mrs
Izard with her team of willing helpers spent many hours cutting down, altering and repairing
the bundles of clothes and old linen that were left by well-wishers at the Durham Street
premises. The wealthy society ladies began sending gifts to Nurse Maude – a wheelchair,
crutches and offers of food to be distributed to the sick and needy. The Post Office provided
a telephone rent free. Cheques arrived too. Sybil had an established routine. She would
drive into town from the St Mary’s Home in Shirley each weekday morning, her cart laden
with freshly cut flowers for the market. Then she would head to Durham Street and leave
the horse and cart well-guarded by her faithful Gyp.
Patients started arriving by nine o’clock. Sybil and Annie Holgate took it in turns to tend to
their needs while the other set off on her rounds. Surgery lasted for an hour and by ten
o’clock the rooms were locked up and both nurses were out and about the district. They
returned to Durham Street for lunch and an afternoon clinic followed by a brief tea break.
They would then head out again for another round of visits before the day was finished.
Saturday was similarly occupied although on a slightly reduced scale and Sunday remained
a day of rest – kept free except for emergencies.
In 1903 Nurse Holgate resigned and moved to Wellington.53 Once again Sybil was on her
own managing with voluntary, untrained support. It took several months to find a suitable
replacement but eventually Nurse Hay was appointed and quickly took up the supporting
reins. Together the two women became a team – nurses who were also social workers,
covering mile upon mile on a daily basis.
By now, their work was gaining more recognition and subscriptions started to flow in. The
management committee set up a bequest and donation list, carefully noting all the monies
that came their way. Acting on the advice of their erstwhile secretary Charles Godfrey,
Jessie Rhodes reduced her annual donation from £100 to £75. The committee also
approved a recommendation to have their annual reports printed. Clearly the organisation
was here to stay.
The year was 1904. The committee decided it had been in office for three years and being
self-elected, believed it was important that subscribers to the District Nursing Fund should
53 Annie Holgate became recognised as the pioneer of district nursing in Wellington just as Sibylla Maude was the pioneer in Christchurch and Canterbury.

[32]
have an opportunity to be nominated. On Sybil’s motion, the members voted to call a
meeting of subscribers at an early date to elect a new committee. It was an exciting move
and forward-thinking on behalf of the founding members. But it was also a sad time for the
Maude family with the death of their mother, Emily Catherine, while she and Thomas were
on a return visit to England. Sybil mourned her mother’s death, but as always, was stoic in
public.
Sybil and her supporters followed up their proposal to extend the group and have a properly
constituted fund-raising organisation which would keep minutes and accounts. They
formalised their operation under the name of the Christchurch District Nursing Fund and
called a public meeting on 27 May 1904. The result was a new committee of eight – the
original group plus four more. Meetings should be held on a regular basis, they decided,
details of the achievements of the organisation should receive greater publicity and the
nurses should be fully supported in their district work with progress reports being provided to
the committee.
Sybil was enthusiastic about the new management structure which enabled her to continue
her essential work. Her great love for the old, sick and helpless was an ‘overwhelming one;
one that overcame her horror of filth and the stuffy smells of unwashed bodies.’54 The
majority of cases she and Nurse Hay looked after were chronic, elderly invalids, often
partially or completely paralysed and forced to spend most or all of their time in bed. They
were poor people living in appalling conditions with sorry bedding and dilapidated beds
which were the old ‘brass-knobbed variety with a sagging wire mattress and a worn-out
powdery kapok one on top.’55 Death was common.
As if she did not have enough to do, Sybil took on the added responsibility of laying out fatal
accident victims, suicides and cases of sudden death which were admitted straight to the
morgue at Christchurch Hospital. It shocked her to think these tragic cases were left in the
hands of a hospital porter rather than a nurse. And the workload continued to increase. By
now, her district nursing service covered practically the whole of Christchurch and travelling
took up a great deal of time. Sybil’s strong team of supporters who had endorsed her from
the start agreed to another appointment. The staff grew to four – Nurse Maude, Nurse Hay,
a junior assistant and an office girl.
Again, family intervened with the death of Sybil’s father Thomas on 5 April 1905. He was 72
years old. He was buried alongside his wife Emily in the St Peter’s family plot. In
recognition of his services to the Anglican Church, the vestry decided to reduce the charge
for his grave from 15 to 10 guineas. Thus, another chapter in the Maude family history was
closed.
In a commentary written later for the Christchurch Press under the heading ‘Makers of
Canterbury’, Thomas Maude was described as having an exceedingly kindly disposition, was
always courteous and obliging in official life, and made no enemies and many friends.’ In
1893, the article continued, he had been the only person in New Zealand at the time to be
both a barrister and a solicitor as well as a Justice of the Peace. ‘An educationalist, he was
54 Cocks E Somers ‘A Friend in Need’ Printpac Print Group Christchurch 1950 p 91 55 The Christchurch Press, (undated) Makers of Canterbury, Pioneers of the Province. ‘Annalist’

[33]
a fellow of Christ’s College. From 1873 to 1876 he was a nominated member of the Board
of Governors of Canterbury College and from 1882 to 1893 an elected member. For nine
years, he was a member of the North Canterbury Education Board.’56
It was a fitting tribute in death that recognised some of his many achievements in life.
Taking a Break
Sybil was becoming weary. It was time to take a break. She had not stopped since she took
up the challenge of district nursing in November 1896. Apart from her trip to England in 1900
when she went to study for her Obstetrics Diploma, she had continued her daily rounds in
Christchurch’s poorer suburbs. In a rare article written in October 1908 for the nursing
journal Kai Tiaki, Sybil described some of her work.57
‘Nurse L arrived with her bag at the house of Mrs M, an old Irish woman with
internal malignant disease who had to be washed, dressed and a certain
treatment be gone through; her old man helps by warming her stays and doing
other minor duties to please her, for which he gets very little praise.’
‘Mrs M: “will you please nurse, ask Mr M to sleep in the kitchen as he snores and
I cannot sleep. Don’t mention it, but he gets up in the night and puts some
medicine into my mouth and in the mornin’ I wakes with such a bad taste, but
don’t say I told yer!” I don’t mention it, but explain how disturbing his snoring is
and will he please her by sleeping in the kitchen. Of course he will do so,
certainly, but he hasn’t yet.’
‘A few minutes later, nurse walks into another house where an old lady of 83
rents a room. She also has cancer, has to be dressed and put in her chair by the
fire; the sight of the nurse is often the signal to start her groaning and this keeps
up all the time with intervals of conversation. Her funeral was exercising her
mind one day, and nurse had to promise to arrange it. “Mrs R, the landlady was
not to interfere.” She said she would like “a nice hearse, one of them’s as you
slides in on” and “she is to be took to Cox’s church.”
‘After the poor old dear has been settled, and a little stimulant to keep things
going, and the landlady has had all her instructions for the day, nurse goes away
from this little pathetic scene out into the fresh air and sunshine, thankful for her
own healthy mind and body…’
‘All this doesn’t sound very inviting to any reader who may feel inclined for district
work but it has its fascinations and there is a large scope for teaching cleanliness
and fresh air. It is surprising too, to watch the improvement too, that will take
place during the nurse’s visits made regularly. Many a poor worried mother finds
great comfort in pouring out her difficulties and getting advice from the nurse.
56 The Press Obituary. 1895 57 Maude Sybil, 1908 District Nursing Kai Tiaki Nursing Journal pp 118,119

[34]
Even the children are threatened with “nurse will give you a nasty dose of
medicine” or “put you in her black bag” which is always a “bag of mystery.”
‘Let us for a brief space touch on the more serious side of nursing. There are
many whose lives are drawing to a close, and it falls to the nurse’s lot to tell them
so, then it is that so much lies in our power to comfort and strengthen them with
words of hope. A young man once said to me when he knew he could not
recover: “well nurse, I look upon death as an event in life.” And so it is. It makes
one feel a great responsibility in using aright the opportunities thus put in our
way. No-one comes near us, or across us, but it is through an intention of God,
that we may help, soothe, or cheer him.’
Sybil was keen to go back to England and she wanted Rose to go with her. It should be at least a year, they decided, and they would visit Palestine during their travels. Sybil approached her committee for leave of absence and made the necessary arrangements for three temporary staff to look after her patients. She took responsibility for the cost of the fares while Sister Rose sought permission from the Deaconesses to receive help from friends ‘at home’ to help with her expenses. On 17 December 1908 they set out on their travels. They were farewelled in some style. The Saturday before they left, an ‘At Home’ was held at the Alexandra Hall attended by the Mayor of Christchurch Charles Allison and the Anglican Bishop. Accepting the gift of a lady’s ‘travelling companion’ presented to her on behalf of ex-patients and friends of Nurse Maude, Sybil said she ‘did not think she deserved all the kindness as her work was a trust, remitted to her care for which she had to account.’58 On the day they left, Sybil and Sister Rose attended a special service in the Deaconesses’ private chapel. Prayers and the benediction were said for the two travellers and after dinner they left by train for Lyttelton to catch the boat.59 They set up house in a small flat in fashionable Chelsea as soon as they arrived. Sybil was no stranger to London and there were many family friends and relatives to visit. A visit to the Holy Land was planned. They particularly wanted to go to Jerusalem and the port of Haifa to see the missionary work. There were connections between the Community of the Sacred Name through Sister Edith, and the missionary schools in Palestine. It was a time of spiritual healing and restoration for both Sybil and Rose and they were reluctant to return home on their original date. Sybil wrote to the committee requesting another six month’s extension to her leave. Her request came before the committee on 22 December 1909 and although it was granted, it was agreed it should be without pay.
District Nursing Progresses Sybil and Rose arrived back in New Zealand early in 1910 – Sister Edith again recording their arrival in her diary. A welcoming party of Sister Edith, Nurse Savory (Sybil’s cousin) and Rose’s sister Dorothea were at the Lyttelton wharf to greet them as they stepped down from the gangway and the following day there was a celebration in the ChristChurch Cathedral with a thanksgiving service for Nurse Maude, Sister Rose and their fellow travellers. They were home again. Sybil was delighted to find the district work had been going ahead in her absence but saddened to learn that Archdeacon Walter Averill, one of her original supporters and a member of her committee was leaving Christchurch to become Bishop of Waiapu in the North Island.
58 Diaries of the Deaconess: Community of the Sacred Name 59 Cocks E Somers 1950 A Friend in Need. Printpac Print Group Christchurch p 92

[35]
Never one to dwell on the past however, she went back to work with renewed vigour. The committee had voted to increase her salary and she was now earning £150 a year. Jessie Rhodes appeared with a bicycle to replace the horse and cart Sybil had sold before she went abroad. It was an ideal mode of transport and she cycled around the town with her nurse’s bag strapped to the back and her other necessities strung about the handlebars. Gyp, faithful as ever, loped along behind. Cycling had become a fad in Christchurch as elsewhere in New Zealand and even the Deaconesses found it an easier way to get about. Sybil’s work embraced her life, but there was always time for the Sisters of the Community of the Sacred Name. They had moved to more spacious accommodation with the completion of their new three-storeyed brick house. Still on the original site, it now fronted onto Barbadoes Street and there were many visits not only for a cup of tea, but particularly for Sybil, more formal house calls as she tended to their various ailments. In recognition of her work, she was made an Associate Member of their Order. Rose and Sybil often joined the Sisters for their Sunday service, first in their tiny Oratory which was curtained off from the main room, and later in the wood-panelled Chapel with its stained-glass windows.60 There were changes too at St Mary’s Home in Shirley. It was closed in 1909 and reopened a year later after extensive renovations to convert it into an orphanage. Sister Rose remained in charge of the new Anglican establishment which was now named St Saviour’s. The orphanage accepted girls of all ages and boys between two and five years of age. It was challenging work and Sybil stayed with her, putting her nursing skills to good use with helpful advice when the children were sick. Towards the end of the year, Rose’s sister Dorothea became ill and died on 30 December. She had run a private school in Avonside for many years and was well known in the district. Her funeral on New Year’s Day at Avonside Church was a sad occasion, carefully documented yet again by Sister Edith. The good nun had a soft spot for both Sister Rose and Sibylla but remained ever anxious about their close relationship. If she voiced caution, her comments went unheeded. The two women went everywhere together, spending weekends at Sybil’s holiday bach at Redcliffs and occasionally going to Dunedin to see their young ward Lily Foster. Lily was an orphan whose mother Sybil had attended on her deathbed. The mother’s dying wish was for Sybil to take care of her daughter and never one to back down from a challenge, Sybil took Lily back to St Mary’s. There were no known relatives and Lily grew up in the care of her two new friends. She was lovingly cherished by the Sisters of the Community of the Sacred Name who often took her to concerts, visits to the circus and other delights. Mindful of the need for Lily to have a good education, Sybil sent her first to St Michael’s parish school and then, in 1908, to St Hilda’s Collegiate School in Dunedin, a private girls’ school, where Lily boarded full time while Sybil and Rose were overseas. There was a connection between St Hilda’s and the Deaconesses. The school was run by a group of Sisters from Kelburn in England who also took over the Anglican school for girls in Christchurch when Sister Edith declined an offer from the Bishop to take on the responsibility. Sybil later decided to send Lily to England to a Church school there, believing it would offer her a better chance in life. It was the last time the two saw each other. Lily, on
60 The building was designed by Christchurch architect Benjamin Mountfort

[36]
learning about her mother and her real family’s history, decided she would never return to New Zealand.61 Two other young girls received financial assistance from Sybil and the Deaconesses. Victoria Kort and Sara Taymour both lived in Palestine and attended St Mary’s, the English school for girls in Haifa which was run by the East Mission based in London. Sybil and Rose had been very impressed with the school when they visited it during their overseas travels and they began an ongoing correspondence with the pupils and their teachers, sending gifts and donations whenever possible. Although there was a long silence during World War 1 when nothing was heard of the two girls, the correspondence picked up again in 1918. The first decade of the new century was a period of progress for Sybil and her community work. Nursing still occupied most of her time, but increasingly, she became involved in organising fund-raising ventures to keep her projects alive. The early committee stalwarts, headed by her mentor Jessie Heaton Rhodes, kept a tight rein on the funds, finding prudent investments for the public donations that came their way. Sybil, always a firm believer in self-help, encouraged her patients to support the cause if they could. The funds swelled still further when she introduced fortnightly clothing sales. The clothes, refitted and meticulously cared for by the sewing circle, could be sold for a relatively small amount and still return a profit. It was a good idea and highly successful. The committee managed the money and gave Sybil half the proceeds of the clothing sales to spend as she saw fit. Jessie Heaton Rhodes had by this time reduced her personal annual donation to £50. All the while, the demands of district nursing increased. ‘Great difficulties have to be met in not knowing what to do with the chronic patients who are not welcome at the hospital,’ Sybil wrote in her annual report to the committee. ‘They are really more to be pitied than the more acute cases, as they are incurable and life must appear very grey indeed with no hope of recovery, and also of being a burden on those who have to support them. Then there are the helpless consumptives who are not eligible for the Sanatorium, nor for the shelters at the hospital, as they are capable of doing light work, but no one will employ them…’ ‘Old folk are still our special care. We have had a large number of a great age. One old lady of 85 years walked over the Bridle Path at 81 years of age, and although in our hands now, does not consider herself old. We have paid 8021 visits to 519 patients most of them suffering from either cancer, rheumatism, consumption or ulcerated legs.’62
61 Scotter, W. H. 1965. ‘A History of Canterbury.’ Whitcombe & Tombs Ltd Christchurch p 360 62 Maude Sibylla. Annual Report 1912. Nurse Maude District Nursing Association.

[37]
Chapter Four: The ‘Flu Epidemic
The War Years
The outbreak of World War 1 on 4 August 1914
had an immediate impact on Christchurch.
Within two weeks of the declaration by David
Lloyd George Prime Minister of Britain,
supported and endorsed by William Massey
Prime Minister of New Zealand, more than
1,000 men were in camp at Addington showgrounds. The Canterbury Patriotic Fund was
established to assist the dependents of men who went overseas and their rehabilitation
when they returned. Its stated objectives were to provide for the dependents of ‘our
volunteers’ (soldiers) to help them if they returned physically unfit and generally to ‘alleviate
suffering and distress caused by the present crisis’ (the outbreak of war). Donations would
be acknowledged in the Christchurch Press.63
Events to raise money for the patriotic fund were often considered a good excuse for parties
and illegal gambling to such an extent that churches and other organisations protested.
Less time should be given to ‘carnivals and local frivolity for the purpose of raising money
and more should be given to persuading the government that such funding should come
from taxation,’64 they decided. Effie Cardale was appointed the Fund’s inspector and visitor,
her main role being to investigate applications and visit the families of serving soldiers and
sailors. She was known to Sybil being a fellow member of St Michael’s Anglican Church and
one of its parish visitors.
News from the front was a daily worry in Christchurch, remote as it was from the trenches of
Europe. The German attack on Belgium had resulted in some crippling battles. Stories of
heroic efforts by the allies were superseded by tales of murder, rape and torture inflicted on
the defenceless Belgians by the German enemy. Determined to raise funds for the growing
numbers of Belgian refugees, Christchurch residents planned a Queen Carnival. It was to
be a grand affair and would be known as the Harvest Festival Carnival, being held in
autumn. Business houses, community groups and other organisations joined in the fun and
selected candidates for their ‘Queen’. The Tramway men chose Sybil Maude and agreed
her colours would be green and cream.
The carnival was soon the topic of conversation throughout the City. Sybil was a popular
choice. ‘I should like to convey to the Tramway staff my admiration for the way in which they
are working for the Queen Competition,’ she wrote to them mid-way through the carnival. ‘I
believe time, and even money, are being spent by them to make it a success and also I feel
grateful that they have chosen me to be their queen. I was feeling how little I had done for
the Belgians who had sacrificed so much for us, and I believe that between us, we shall
63 Christchurch Press. 10 September 1914 p 9 64 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group, Christchurch 1950. p 111.

[38]
draw the gold out of many pockets, and present a very substantial thank-offering to a gallant
nation.’65
Sibylla had predicted well. She was duly crowned Carnival Queen having attracted the most
donations to the cause. The Tramway men were jubilant at their victory. They had raised
£2,500 for the fund on their own. Overall, the carnival had raised £30,000 for the Belgian
refugees. The crowning ceremony was held at Lancaster Park66 in the afternoon followed by
a procession which moved slowly through the city’s central streets, crowds lining the route to
get a glimpse of the reigning queen.
‘There sat Nurse Maude, erect upon a raised dais, her sceptre in her hand, and attended by
the deposed queens who acted as her ladies-in-waiting. Nurse Maude wouldn’t dress as a
queen; she had on the old familiar nurse’s uniform, but behind she wore a long, glorious
scarlet train, held up by diminutive pages.’67
The ceremony was repeated again at the Coliseum68 in the evening, where the Mayor Henry
Holland and other local dignitaries were on hand to hear Sybil’s acceptance speech and to
enjoy the celebrations. The Deaconesses were seated in the audience.
65 ibid 66 Lancaster Park was established in 1881. It was used for many sporting and other events. 67 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group, Christchurch. 1950. p 111 68 New Regent Street is on the site of the original Coliseum built in 1888 as a roller skating facility between Armagh and Gloucester Streets. It was later used for private and public events, concerts and then a cinema.
Nurse Maude – Queen of the Harvest festival

[39]
‘Ladies and gentlemen, or better still, my dear people’, Sybil began. ‘Here I stand
– a nurse at the front and a queen at the back, but no doubt you will accept me
as a queen for the time being. I hardly know in what words I can best express my
deep appreciation of the honour you have conferred upon me in electing me
queen of the festival. I feel scarcely worthy of it.
‘To the Tramway staff, I cannot say enough in their praise. They have sacrificed
time and in some cases money to keep me at the top of the poll. They have
pushed and thrust me into everybody’s face and they have sold me again and
again. I have been sold even by children, but, for my own part, I have realised
the privilege of being used in such a splendid cause.
‘I am not unmindful of the opportunity you have taken advantage of to show me
your appreciation of my life’s work in Christchurch. I sincerely thank you all. May
I always prove worthy of the honour conferred upon me! Let me say a word of
praise for the other queens. All of them allowed themselves to be used for the
cause. They gave me a great run and they made the Tramway staff very anxious
at time, and without them there would not have been any £12,000 for the
Belgians…
‘Our hearts and pockets are open for the Belgians still. We are under an
obligation to them for all time. Not until their country has been restored to them
and full reparation has been made can we be relieved from our responsibilities.’
‘Nurse Maude voted for as Queen of the Festival,’69 was the diary note written by Sister
Edith and dated 17 April 1915.
Although Sybil’s sister May (Mary) served as a nurse, and two of her brothers, Thomas and
Edward, enlisted in the army and were also away, the war had little real impact on Nurse
Maude’s work as a district nurse. But, like everyone else, she followed the news and read
the lists of the men who were killed in action. Gallipoli was particularly harsh for New
Zealand families waiting anxiously for news. Sybil was particularly shocked to learn that one
of her nurses, Margaret Rogers, who had trained at Christchurch hospital and later joined
Sybil’s team, drowned when the troop ship H.T. Marquette was torpedoed in the Aegean
Sea on 23 October 1915. It was a terrible tragedy with 32 New Zealanders including ten
nurses listed among the 135 officers, nurses and soldiers who died. It was an event that yet
again brought home the savagery of war to the thousands of New Zealanders whose family
members were serving overseas.
In Christchurch, the district nurses carried on. Like Sybil, they had friends and family serving
overseas. Earlier in 1914, the committee had agreed to the Hospital Board’s proposal for a
subsidy of 24 shillings in the pound on the organisation’s whole income. Two months later, a
further letter from the Board set out its agreement to pay a subsidy on voluntary
subscriptions and later on ordinary income. For Sybil, the Board’s commitment was a
vindication of everything she had worked for and believed in. For her committee, it was
positive recognition at last and it created a platform for future development. The small trio of
nurses criss-crossed the city on a daily basis, their routine always included house calls and
69 Diaries of the Deaconess: Community of the Sacred Name

[40]
the traditional surgery in their rooms. Their visits continued to increase with over 13,000
calls made during 1915.
Sybil maintained her regular contact with the Deaconesses, entertaining them, joining them
for tea and, when her car arrived, taking them for drives. The car was a gift from
Christchurch businessmen following her success as Queen of the Carnival. Rose’s brother
Wilfred Godfrey, a member of the Federal Car Club had canvassed support from his fellow
car club members after seeing Sybil riding past
on her bicycle, one hand on the handlebars
which were, as usual, strung about with parcels,
and her other hand holding an umbrella high
above her head. The gift came with a stipulation
that her committee should be responsible for the
car’s maintenance and running repairs. The
committee agreed with their own requirement
that Sybil pay for the insurance.
It soon became apparent that Sybil was an
extrovert behind the wheel. She was an exuberant driver, reckless even, and thoroughly
enjoyed taking her friends for outings. She knew nothing about the mechanics of the car.
As long as it would go and travel fast, that was all she wanted.
‘Being short in the leg, she found it somewhat tiring to keep her foot pressed on the
accelerator all the time and soon hit upon the dodge of driving with an open throttle and not
bothering with her feet at all, but there were times when she forgot about the throttle being
open and pressed down her feet as well – and the car fairly leapt along.’70
‘She usually drove well in the middle of the road, throttle wide open, nodding and waving to
old friends and acquaintances as she passed by and wrenching wildly at the steering wheel
when the car showed the odd inclination to cross the road and mount the kerb. But she
never had an accident with any serious consequences and had a nerve of iron.’71
The car was exactly what she needed for her work. She was now in her early fifties; there
was always more to do than there were hours in the day and being able to drive from one
side of town to the other instead of cycling was a wonderful way to save time. Sybil
expanded her district work to develop a series of lectures for Mothers’ Unions and the Social
Hygiene Society72 where she was an active member. The Society had been established
during the war by a group of prominent Christchurch women. They had ‘ethical, education
and practical aims and actively campaigned for the elimination of venereal disease by
confining sexual contact to marriage.’73 Sybil was keen to teach young mothers the right
approach to health and her lectures emphasised the basics of home nursing and methods of
70 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group Christchurch. 1950. p 117 71 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group Christchurch. 1950. p 117 72 The Social Hygiene Society established in 1916. An advice and information centre which distributed pamphlets and books about venereal disease which had become a problem with troops returning home. Its members included doctors and nurses. 73 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group, Christchurch. 1950. p 117
Nurse Maude’s car which is on
display at Ferrymead Heritage Park

[41]
preventing disease. She explained to them the importance of cleanliness, fresh air and a
balanced diet.
The Outbreak of ‘Flu
I had a little bird
Its name was Enza
I opened the window
And in-flu-enza74
It was well known that Nurse Maude was the driving force behind the Christchurch District
Nursing Fund as the committee had decided to call itself in 1901. Without her, there would
be no district nursing. At its February meeting in 1918, the committee agreed unanimously
to include Sybil in its name in some way. After much discussion, the members decided on
‘The Nurse Maude Association for District Nursing.’ The war dragged itself to a sorry
conclusion with the armistice being signed on 11 November 1918. Early warnings of a
possible influenza pandemic were ignored as Canterbury prepared to enjoy the annual
carnival week. The ‘flu had already invaded much of Europe and the United States leaving a
terrible chaos in its wake. Said to have developed in the military camps in France,75 it was
described as the ‘black plague’ – a vicious disease that was indiscriminate in whom it
attacked.
The Lyttelton Times, like other newspapers around the country, did its best to warn the
public about the dangers of infection spreading in crowds, but few people took any notice.
Show Day and the annual race meetings traditionally attracted large crowds from all over the
country. Why should this year be any different? But within a week, Christchurch was in the
midst of a major crisis. Hundreds of people were falling sick on a daily basis. Schools
closed and the public health authorities moved in. A public meeting was called on 14
November and a central committee was elected. Sibylla Maude was asked to take control of
the nursing relief for Christchurch and the surrounding district. The authorities set up a
bureau in Cathedral Square next to the Post Office and the Red Cross shop and here Sybil
established her headquarters.
The city was divided into areas to try and control the spread and volunteers were called in to
help. Members of the public were encouraged to run through inhalation chambers which, it
was thought, might contain the ‘flu. The chambers were described as old converted trams
where ‘you entered at one end, ran through a fine spray, breathing deeply, and out at the
other end.’76 But nothing seemed to work. Factories closed down, mail deliveries were
reduced, the Municipal Baths closed their doors and the town virtually slowed to a halt as the
‘flu took hold. Christchurch became like a city of the dead. The volunteers worked all hours
74 Source: The 1918 Influenza Pandemic, Stanford. Cited: Crawford. 75 Research strongly suggests the factors contributing to the Spanish Influenza outbreak included the stress, fear, war gasses used for the first time in history in a massive and indiscriminate manner, life exposed to the elements, cold weather, humidity and contact with birds, pigs and other animals both wild and domestic. Source: Journal of Molecular and Genetic Medicine, online publication 30 November 2009 76 Rice Geoffrey. ‘Black November.’ Allen & Unwin Wellington 1988. pp 84-86

[42]
of the day and night but the ‘flu was relentless. The death toll grew higher each day; the
sextons dug graves like trenches and mass funerals were held. Even so, the epidemic was
not as bad in Christchurch as it was in Wellington or Auckland.
Amidst the chaos, order started to prevail. Nurse Maude organised lists of victims for
volunteers to visit. The Boy Scouts acted as messengers, directing the volunteers to the
cars which were lined up waiting in a roped-off part of Cathedral Square. The Red Cross
took responsibility for help in all the hospitals. St John’s Ambulance staff, and members of
the Automobile Association, worked tirelessly transporting patients and relief all over the city.
Although most of the volunteers had little or no nursing experience, Sybil’s careful
instructions were well heeded as they set out on their missions. Food was prepared by the
Women’s National Reserve77 at the Gas Company’s rooms and distributed the same way.
Newspapers ran regular columns reporting on different aspects of the epidemic as the days
wore on. Articles concentrated on what was happening, where food was required, what
businesses were closing and what services were being stopped. The reports were also
opportunities to call for volunteers and Sybil was quick to take advantage.
‘It is night workers in particular that are wanted,’ she said on one occasion. ‘I shall also want
all the motor car, motor cycle and bicycle assistance that can be given me. We are getting
along satisfactorily but there must be no relaxation of effort.’
But it was to Sybil herself that the people turned to for help, coming in their hundreds and
begging to see her. It became so bad that a guard was placed at the entrance to her
headquarters in the Square to prevent unauthorised entry. She worked with few breaks,
snatching sleep at Deaconess House in Barbadoes Street whenever possible. She headed
the city’s relief centre and also controlled the smaller depots, eleven of which had been set
up further out of town. It was exhausting work but it had to be done. Country districts were
desperate for help but the health authorities stipulated the city must come first and any spare
volunteers should go to the hospitals.
After two weeks, there were signs that the situation was starting to ease. Gradually the relief
organisation was wound down and slowly the city readjusted itself. The central bureau
finished its night shift on 2 December and the committees that had operated in each of the
block areas closed their books. Their toll was grim with 743 deaths recorded in Canterbury,
466 occurring in Christchurch. Just over half of the city’s ‘flu victims had died in hospital. ‘At
the last full meeting of the block committees on 3 December, a unanimous motion of censure
was passed on the Health Department’s handling of the pandemic.’78 Even in the midst of
tragedy however, it was also appropriate to recognise those who had volunteered their time
and energies during the crisis and in particular Sibylla Maude. The Christchurch City
Council voted an annual grant of £300 to the Association to enable two more nurses to be
appointed. The Automobile Association made Sybil a life member and they overhauled and
repainted her car. She was reported in the daily paper as the ‘hardest working woman of the
epidemic.’
77 The Women’s National Reserve was one of several organisations set up by women in Christchurch at the start of WW1 who wanted to do something that would contribute to the war effort. 78 Rice Geoffrey. ‘Black November.’ Allen & Unwin Wellington 1988. p 139

[43]
In a letter to the Editor of the Lyttelton Times on 10 December 1918, Sybil wrote: ‘Through
the intelligence and willingness of the nursing helpers, the splendid amount of well-cooked
food, the liberal loan of cars and ambulances and the admirable manner in which they were
handled, the distribution of food by girl and boy scouts, the work of the marshals, the able
management of the depot and the assistance of the telephone operators, we have managed
to cope with and overcome the most frightful menace which our dear city has ever been
called upon to face.’
Never one to ignore an opportunity to promote the work of her organisation, Sybil went on to
endorse an earlier publicly expressed belief that an extension of the district nursing scheme
would ‘do much to remedy the evil which the present epidemic has exposed.’

[44]
Chapter Five: Nurse Maude is Here to Stay
192 Madras Street
It was time for Christchurch to cast off the horrors of the Spanish influenza and for Sybil to
return to district nursing and the prospect of a new home. In 1917, Sir Heaton and Lady
Rhodes had presented her with a gift in recognition of her hard work. It was a plot of land in
Madras Street and sufficient money to establish a fund to build new rooms. Jessie Rhodes
had been Sybil’s friend and benefactor from the beginning, her generosity almost
immeasurable. The land was owned by Mrs J. W. Fleck and it was situated in a part of
Madras Street that had already been partially developed. Sybil was overwhelmed. Here at
last, she could have premises that were purpose built for her needs. Lady Rhodes had
donated £500 as the start-up fund. Now, at the start of 1919, a street collection was
organised to raise the balance of the money required. With one exception, it was the only
time while Sybil was alive, that the Association collected money this way.
The building should be two-storeyed with a flat above for
Sybil’s own accommodation and a garage beside it for her
car. The committee advertised for tenders and the
Christchurch firm of Head & Webb, with a price of £2,579,
was accepted. Gradually the building started to take shape.
The outside walls were to be brick and plaster, simply
designed with three six-paned windows on the street front.
The windows had curved decorative lintels – this design
being repeated over the main front door. Upstairs there was
a main window of single panes which stretched across the
central part of the building with two four-paned windows on
either side.
As was typical of the period, the interior walls were brick and
plaster downstairs and finished with wallpaper over lathe and
plaster on the second floor. The floors and staircase were
timbered as were the sash windows. There was a plain brick
fireplace and in a recess on the ground floor foyer there was
space for a memorial tablet to Lady Rhodes to be inserted.79
No foundation stone was laid on 21 March 1919 when work on the building actually started
because Sir Heaton and Jessie Rhodes were in London. The building would be formally
opened when they returned.
Construction work continued throughout the early months of the year. Downstairs the rooms
were starting to take shape. A dispensary, surgery, nurse’s room, storage space and an
office were built. The committee allocated £350 to be spent on furnishings and a sub-
committee of Sybil, Mrs Neville and Miss Tabart was set up to be responsible for what was
required. Sybil was now 57 years old. On 21 May 1919, before the furnishings were
79 Cocks E Somers. ‘A Friend in Need.’ Printpac Print Group, Christchurch. 1950
Two young collectors help raise
funds for the building project

[45]
completed, she moved into her new flat upstairs at Madras Street taking Sister Rose with
her. The move was a timely one, Rose having been forced to give up her position as matron
at St Saviour’s Orphanage due to ill-health.
They were frequent visitors at Deaconess House
which was just a short walk away, and sometimes
the Sisters came for dinner at the flat. A routine
developed with Sybil working during the week,
Rose taking care of the domestic arrangements
and in the weekends, the two women driving over
to Scarborough to Sybil’s cottage in the hills. Sybil
had built the cottage some years earlier after
selling the Redcliff’s house, as a retreat from her
overflowing, busy life in the city. Cut deep into
the hillside, part way up a zig-zag path, the
cottage was one of few properties in the area at
that time with an attached garage. Single-storeyed and built of timber, it enjoyed a
magnificent view of Christchurch and its expansive backdrop. The sunroom had double-
doors leading to the living room with a small dining alcove and a long, narrow kitchen. Two
bedrooms completed the house.
Towards the end of 1919, Sybil developed acute appendicitis and was admitted to Nurse
Turner’s Nursing Home for an operation. It was close to Christmas, but Sybil felt sufficiently
recovered to join Rose and the Deaconesses for Holy Eucharist at their little Chapel and
then dinner on Christmas Day.
Meanwhile, there were changes in Christchurch. As the men returned from the front,
unemployment rose, rents went up and the poorer areas of the city suffered as they had
always done. Sybil initiated relief, starting a soup kitchen at the Madras Street premises.
Local businesses offered help, the proprietor of the nearby hotel, Mr Coffey at the King
George, sent round the leftovers from the mid-day meals. The Charitable Aid Board and the
Farmers’ Co-op also lent support and it was not long before the soup kitchen had to be
enlarged. Sybil’s permanent store of second-hand clothing, usually well supplied, was run
down and she was obliged yet again to appeal to the generous public. Volunteers were
organised to go into homes where the mother was sick. They would prepare the mid-day
meal, clean the house and leave it ready for the family at night. Sybil
approached her committee for funds for this scheme, but while they
sympathised with the idea, they did not see it as part of their
responsibilities and suggested she should organise it herself, which
she did. She wrote and produced a booklet entitled ‘Nurse Maude’s
Household Book’80 which contained home nursing hints, gardening
ideas and simple recipes. It was an immediate success and all
proceeds went to the cause.
80 Nurse Maude’s Household Book: Published by Sibylla Maude for the District Nursing Association. Reprinted 2013
Nurses gather outside Madras Street

[46]
Sybil worked out her own programmes for her nurses as well, believing implicitly that a
patient responded to frequent changes of nurses. As a result, when the cases were
assigned each day, the nurses were nearly always sent to a different district with another
group of patients to attend. The system was not without its problems because while it might
improve the patient’s mental outlook, it created difficulties for the attending nurse not the
least of which was the need to establish a relationship between herself and the patient
particularly if the care was to be long term. But Sybil was adamant that her system was the
best and who was going to argue?
The new year dawned and with it Sybil’s determination to give prominence to district nursing
and its importance in the community. Sometimes her zeal got her into trouble as happened
when she was invited to address the Council of Churches on her favourite topic. She took
the opportunity to chastise the Hospital Board for not properly caring for its nursing staff.
The nurses were overworked and exhausted, she claimed, which had resulted in early
patient deaths. Unknown to Sybil, a reporter was present. The Board cried foul, but even
though Sybil later claimed her comments had been misrepresented, loyal members of the
public supported her, stating that ‘even if Miss Maude had not made the alleged statements,
it was time someone did.’81
The organisation’s work had extended beyond Christchurch by this stage, attracting the
interest of the Minister of Health James Parr, who paid a personal visit to Madras Street to
see for himself what was happening. In spite of this, however, or perhaps because the
Association appeared to be so well organised, the Department of Health decided to cancel
its subsidy the following year. The decision caused consternation within the committee.
Urgent discussions with the Christchurch Hospital Board resulted in the promise of an
annual subsidy of £400 with the agreement that Nurse Maude should take over the after-
care of patients leaving hospital. It was a major step for the organisation, but Sybil did not
hesitate.
The Association expanded and with it, the team of nurses. By now there were eight on the
staff. Each nurse had one day off per week plus part of Sunday and six weeks holiday – four
in summer and two in winter. It was considered generous but necessary. Each nurse was
allocated a bicycle for her travel. Home visits had increased to more than 12,000 per year
and as partial compensation, nurses were allotted five pounds cycle allowance. A brief
experience hiring a car twice a month to help with the rounds was stopped soon after it
started on the grounds that nurses spent too much time waiting for the car rather than
getting out and about their business. Their work was supported by the annual Hospital
Board grant, public subscriptions which usually ranged from between £500-£600 per year,
small donations from patients where possible and fees from the nurses’ work at the hospital
morgue, not to mention the jumble sales.
In the ‘Women’s Corner’ of the Christchurch Press in November 1920, tucked amongst the
social news of dances, travels and local events, was a paragraph about the Association’s
activities for the month. Nurses had paid 1293 visits in October including 187 out-patients
and 465 calls for various information and help had been made at the office. A number of
81 The Sun (Christchurch) undated. The Christchurch Sun was launched in 1914. It was modelled on the London Daily Mail. Source: New Zealand Yesterdays Hamish Hay 2001 David Bateman Ltd.

[47]
minor accidents had been attended to and invalid chairs had proved very useful to those in
need of them.82
Local businessmen were beginning to take an interest in the Association, several offering to
serve on the committee. An endowment fund was set up and by the early 1920s it had
attracted over £1,600. It was more than the committee had hoped for, and clearly careful
and prudent investments were required.
On 25 May 1922, Mother Edith died. She had led her household of Anglican nuns since
1893. It was a sad day for the Sisters of the Community of the Sacred Name, especially so
for Sybil who helped nurse her old friend in the last days, and for Rose who, as one of the
first four probationers to join the order, had known her for nearly 40 years. The Deaconess
had welcomed Sybil into the Community House on Barbadoes Street, supported and
nurtured her through her problem days as matron of Christchurch Hospital and encouraged
her in the establishment of the district nursing service. Mother Edith had kept a diary in
which she had noted many of Sybil’s significant achievements. She had been a mentor as
well as a friend.
Like Rose, Sybil had a strong faith. Always dedicated to the Christian mission, she was
soon caught up in a spiritual revival that swept through New Zealand in 1923. A faith healer
from England named James Moore Hickson was touring the world attending church services
and, it was claimed, healing the sick through the ceremonial laying on of hands. For three
days, he joined the Bishop for services in ChristChurch Cathedral. People travelled long
distances to receive his blessing and to feel the touch of his hand on their heads.83 It was an
extraordinary experience and one that Sybil was anxious to share. She helped with the
services and promoted the Hickson mission84 by speaking to community groups not only in
Christchurch but in Dunedin and Wellington as well. If Sybil was at all sceptical about his
healing powers versus conventional medicine, she said nothing, at least nothing in public.
In 1925, Sybil became very ill. Aged 63, she had been district nursing for nearly 30 years.
She was worn out. She was sent to Queen Marys Hospital in Hanmer for a rest. The fresh
air did its duty as she had always prescribed, and she returned to Sister Rose in the Madras
Street flat, revitalised and refreshed. But reluctantly, she had to admit that her days of
travelling around the city, tending to the sick in their homes, was over. She could minister
them when they came to the rooms for treatment, but nothing else. She accepted the verdict
and continued with her community lectures speaking to women’s groups and nurses on a
regular basis.
Her household book was also a brisk seller in the city. Originally printed as a fund-raiser in
1919, it was another way in which Sybil could encourage mothers to be better homemakers.
‘As many lives are lost through ignorance,’ she wrote at the start, ‘I propose giving a few
hints for household use – especially for young mothers.’85 There were simple home nursing
82 Women’s Corner, The Press 4 November 1920 83 Eulogies of Nurse Maude 13 July 1935 The Press, Christchurch p 16 84 The Straits Times 11 December 1924 p 2. J M Hickson was quoted as saying he didn’t consider faith healers should dismiss medical science as unnecessary but should work in cooperation with doctors. 85 Maude Sibylla Emily: Nurse Maude’s Household Book (undated) p 3

[48]
notes starting with a paragraph on the benefits of fresh air, remedies, recipes, and general
cooking comments with a section at the back for gardeners. The booklet was interspersed
with plenty of advertising from supportive Christchurch businesses and sold for one shilling.
The committee decided to commission a marble bust of Nurse Maude in recognition of the
work she had done. It would be paid from the proceeds of the clothing fund. They
approached well-known Christchurch sculptor Francis Shurrock86 and for a fee of £110, he
agreed to take on the project. It was intended that the bust should be publicly displayed in
the foyer of the Madras Street rooms, but the committee had reckoned without Sibylla’s
opinion. She did not like it. It was too rigid, she said, too harsh, and although a good
likeness, would never, she said emphatically, be placed in a position of honour. The bust
was relegated to the Secretary’s cupboard.87
Her Works do Follow Her
The 1930s started without much hope or promise. Sybil was greatly saddened at the
sudden death of her long-time friend and mentor Jessie Heaton Rhodes from a cerebral
haemorrhage at her Otahuna home in Tai Tapu in October 1929. Although frequently
suffering poor health herself, Jessie had been a dedicated advocate for Sybil’s work. She
had supported Sybil not only with an indefinite financial commitment but with sage advice
from the day she had decided to leave Christchurch Hospital and start out on her own as a
district nurse. Always referring to her friend as ‘Sibbie’, she had encouraged other wealthy
benefactors to contribute to Sybil’s endeavours. It was a death that affected Sybil deeply.
Now the country was heading for a depression which would have long-lasting social
repercussions. Relief funds had been in operation in Christchurch for a decade, the
Canterbury Progress League having initiated the first in 1921. Unemployment had been
increasing since 1920. At that time, help came mainly from the Charitable Aid Board. Later
in the 1920s, a citizens’ unemployment committee was formed and chaired by the Mayor
John Archer. In 1927, the situation was becoming worse and the committee approached the
government for funding. The committee’s first food distribution depot was in Armagh Street.
It was not enough to meet demand and in 1928 three more depots were set up – one in
Bedford Row, another in Sydenham and a third in Linwood. The committee helped 1100
families that year.
The new Christchurch City Council demonstrating more of a social conscience than its
predecessor, adopted a proactive approach to the situation by raising loans and setting up
relief programmes. Street works were ideal for such projects, but the levels of
unemployment were becoming too much for even the Council to deal with. It was time for
the government to do something and it did, setting up the Unemployment Board late in 1930.
Under a new scheme, local bodies could develop work projects as well as the cost of
materials and the Board paid the wages. In February 1931, 600 men were given
86 Francis Aubrey Shurrock, English trained sculptor and artist, immigrated to New Zealand in 1924. Worked at the Canterbury College School of Art. Sculpted the bronze portrait statue of James FitzGerald in Rolleston Avenue Christchurch. Source: Encyclopaedia of New Zealand. 87 The bust was later given to the Director of the Society of Arts in Christchurch for safe keeping.

[49]
employment in Christchurch while the neighbouring boroughs and counties also contributed
with work programmes for several hundred more.
The Citizens’ Relief Association supplied food, clothing, paid for medical and dental bills
when necessary and generally assisted where it could. But there was no end in sight. By
1933, several thousand people were poverty stricken. They had nothing – no bedding, no
clothes, no food and no hope. Businesses crashed and Christchurch, like the rest of New
Zealand, was in the grip of a dreadful depression. Sibylla Maude, as ever, was there to help.
She was known to the most vulnerable families and could sympathise with their plight.
However badly the well-to-do were suffering, it was small compared to the poor and
destitute. Depression or not however, when Sybil asked for help, the public responded to
her plea and the dwindling shelves were filled up again. By now she had a staff of nine
trained nurses, all practising as she had taught them.
Sybil received a surprise letter in 1933 when the Governor General Lord Bledisloe wrote
asking for her consent to have her name placed on the New Year’s Honours List. Her first
response was to decline the invitation but family members and the close friends she
consulted, persuaded her to agree and she did so on the understanding that she must be
invested in private. The Community of the Sacred Name recorded the event with simple
dignity: ‘Nurse Maude made Officer of the Order of British Empire,’ was the diary note dated
1 January 1934.
The newspapers and the public were more jubilant. The inclusion of Nurse Maude in the
honour’s list ‘has been received with gratification,’ said the Sun newspaper the following day.
‘As the pioneer of district nursing, not only in this city but in the whole of New Zealand, as a
philanthropist, helper and healer, she has long been the most outstanding woman in the
Dominion.’88 It was high praise indeed for such a modest person.
As she had stipulated, Sybil was invested without fuss at the Madras Street headquarters by
Lord Bledisloe later that year. She was recognised again with the award of the King’s Silver
Jubilee Medal in 1935. King George V had approved the issue of 80,000 medals throughout
the British Commonwealth to mark the 25th jubilee of his reign on 6 May. They were to be
presented to men and women whose contributions to their communities were worthy of
special merit. Like the OBE, it was an honour so well deserved and yet there were only a
few months left for Sybil to enjoy it. Weary with it all, she had a sudden heart attack and
three days later on 9 July 1935 she died.
Word of her death spread quickly. Tributes started to flow in. Everyone had something to
say about this pioneer of district nursing who was acknowledged as the first registered nurse
in New Zealand.
‘The passing of Nurse Maude will be regretted by the entire community,’ said the Mayor of
Christchurch, Dan Sullivan. ‘Because of her wonderful social work among the poor and
distressed of the city, her name has become a household word.’ More eulogies were
reported in the local media in the days that followed. Everyone, it seemed, wanted to have a
88 The Christchurch Sun, 2 January 1934

[50]
say, to comment on the work she had done and what she had achieved during her 40 years
as the city’s district nurse.
Sibylla lay in state in ChristChurch Cathedral dressed in her familiar bonnet and pale blue
garments that ‘were her passport to the homes of the poor and distressed.’89 The Cathedral
was crowded to the doors for her funeral. Floral tributes were massed around her casket.
The service, conducted by Archbishop Julius, was a solemn one, and at the conclusion a
long procession left the Square for St Peter’s graveyard in Riccarton, passing thousands of
mourners who lined the streets to pay their last respects. At the graveside, Maori from the
city and from Tuahiwi honoured her name with a lament and service.
‘Her death left the city a poorer place,’ wrote Rev North in an obituary which well reflected
the feelings and emotions of the people of Christchurch. ‘In many homes, I have felt her
influence and have found that her name is honoured and revered. Again and again, one has
heard expressions of deep thankfulness for her untiring service. To many sufferers she was
a veritable ministering angel, and she leaves behind a name and an influence which will be
an enrichment to the life of the community. Let it always be true of her that her works do
follow her.’
89 The Waiapu Church Gazette, 1 September 1935
Nurse Maude’s funeral procession from ChristChurch Cathedral to St Peter’s graveyard in Riccarton

[51]
‘Hush! Everyone’s friend is sleeping –
Let her rest.
And they who know her best
Will know what she would wish.
No stately monument of stone,
But her work carried on;
Her sick and sad and lonely visited and helped,
Her old folks cheered and comforted,
Her hungry fed and not with bread alone,
But with the love and courage that she brought.
Then she, on waking, will look round,
And, smiling, see we loved her,
And the Lord Christ for whom in these she wrought.’90
90 The Waiapu Church Gazette, 1 September 1935

[52]
Part Two - The Winds of Change
‘O lovely time when bliss was taken
As the bird takes the nectar from the flower’
“Elements” by Arthur Fairburn

[53]
Chapter One: A New Matron Takes Charge
Adapting to Change
‘The death of Nurse Maude has left a blank that will long be felt,’ the Association noted
sombrely when it met the week after Sybil’s funeral. Recording a motion of respect, the
acting Chairman Mr J. W. Anderson said: ‘Her wonderful energy, her wholehearted
enthusiasm with the undertaking of the Association, and the response to her appeals by the
people of Canterbury, mark an outstanding character.’91
Sybil’s presence seemed to be everywhere. Her motto, carved in oak, hung in the foyer at
the Madras Street premises. ‘No man knoweth another’s burdens,’ it said simply. It had
been made in memory of Margaret Rogers’ death when the Marquette was torpedoed. For
Sybil, it was a symbol of all that the organisation represented. ‘To lift the burden of sickness
is what the district nurse tries to do,’ she would often say, and it was true.
The Maude family was distraught at her death. ‘We are all so thankful that Sibbie passed
away without any pain or discomfort,’ her sister May wrote to a friend in August. ‘She knew
nothing and never regained consciousness. We still cannot believe she has gone…I think it
was the love, admiration and all the tributes from the people that kept one up through it all.
At the end, a Maori man stepped forward and looking into the grave said in Maori: ‘well
done, thou good and faithful servant’…Sister Rose is very wonderful and bears up well but it
must be a great blow for her. She is just now living in Syb’s cottage at Scarborough which
has been left to her. They were both so fond of the cottage and the view was always a joy to
Syb…’
In fact, Sybil had left her Scarborough home to Rose’s niece Joyce Godfrey on the
understanding that Rose could have the use of everything for her remaining years. She had
vacated the little flat upstairs in Madras Street shortly after the funeral, taking little with her
but her memories, and, as was agreed, Sybil’s walnut writing desk. The Sisters of the
Community of the Sacred Name decided to commission a stained glass window in memory
of Nurse Maude to be installed in the little Chapel close to the pew where she preferred to
sit. They chose St Barnabas to be surrounded by Sybil’s favourite flowers, love-in-the-mist,
delphiniums and sweet roses.
For several months, the nurses continued about their duties under the direction of Sister Lily
Donahue. A dedicated nurse, she had been with the Association since her graduation from
Timaru Hospital in 1919. Familiar with the responsibilities of district nursing, she steadfastly
maintained the traditions which Sybil had initiated. Two other nurses, Irene Simpson and
Eileen Dagg worked with Lily to keep the services going. The Association’s committee was
in no hurry to find a replacement for Sybil, preferring to let everyone adapt to the changes
that must inevitably take place.
91 Nurse Maude District Nursing Association Board Minutes 22 July 1935

[54]
The end of the year approached and the committee agreed to dispense Christmas cheer to
the elderly poor and the needy as Nurse Maude had done for so many years. It was
important to maintain traditions. But it was also time to make some decisions about future
directions. The committee decided to meet as soon as possible in the new year. They
reconvened on 27 January 1936, welcomed Sybil’s younger sister May to the Board and set
about the business of appointing a successor to their founder.
They formed a special sub-committee comprising Sir Heaton Rhodes, Messrs W. G.
Jamieson and F. W. Anderson, May Maude and the Hon W. Hayward, and made contact
with Miss Mary Lambie and Miss Rose Muir to help them find the right person. Mary Lambie
was a Christchurch woman, whose early nursing training was at Christchurch Hospital. She
was well known throughout nursing circles in New Zealand for her work in public health and
was considered an idea person to give the committee the advice and information they so
badly needed. Rose Muir had been the matron of Christchurch Hospital since 1916 and was
highly regarded within medical circles.
The position of matron of Nurse Maude District Nursing Association was advertised in
Auckland, Wellington, Christchurch and Dunedin. In addition to the requisite tasks, the
position was to carry an annual salary of £225 with ‘comfortable rooms, fuel and lighting.’92
Applications were to be in the secretary’s hands by 1 July 1936.
As it happened, once applications were received, it took less than two weeks for the sub-
committee to arrive at a unanimous decision. Supported by their two advisors, Mary Lambie
and Rose Muir, and after carefully scrutinising the thirteen applicants, the sub-committee
recommended that Miss Mona Corkill be appointed ‘nurse in charge’. A week later, she
came to Christchurch to meet the full committee and on 27 July she was offered the position
with the amended title of Matron of the Association.
Born in New Plymouth in 1896, the year Sybil started district nursing in Christchurch, Mona
Corkill was one of five children. Her family was well known in the town and after completing
her secondary education, she accepted her first job with the Taranaki Education Board. But
she wanted to be a nurse and soon left her employer to start her training at New Plymouth
Hospital. She became the Red Cross nurse and social worker for New Plymouth and later
the public health nurse for the Taranaki district. During her early career, she had worked for
a time at Queen Mary Hospital in Hanmer, where, by strange coincidence, she had looked
after Sybil during her convalescence there in 1925. Sybil had invited her to visit Madras
Street if she was ever in Christchurch, an invitation she had taken up the following year. In
spite of a tempting offer to stay, Mona Corkill had returned to the North Island to continue
her public health work.
The decision to apply for the position with the Association was, as a consequence, more
than meaningful for her, and shortly after her appointment she moved into the upstairs flat,
much as her predecessor had done, with a companion, Lilian Priest. They had met following
an introduction through Lilian’s brother Alec who was a doctor in the city. Mrs Corkill,
Mona’s mother had come south to help Mona settle into the flat, and had suggested to Lilian
that she might like to move in with Mona as her companion. The idea appealed, particularly
92 Nurse Maude District Nursing Association Board Minutes 25 May 1936

[55]
as Alec was getting married and Lilian felt she should change her accommodation. She
agreed on one condition that ‘if we don’t get on we’ll tell each other.’ They lived together for
the next forty years.
‘I was in despair the first few weeks I was here,’ Mona confessed later. ‘Every patient I was
introduced to burst into tears and said: ‘You could never replace Nurse Maude.’ I was almost
in tears myself, when a very elderly woman patted my hand and said: ‘Never mind dear, you
have a nice face, and I’m sure you will do your best.’93 Sybil had become a legend. She
could never be replaced, but now it was time for the Association to move forward.
New Directions
The late 1930s were still years of comparative depression in Christchurch as elsewhere in
New Zealand and there was great poverty and hardship. It was an ‘uneven experience
which affected some groups far more adversely than others.’94 The better-established
members of the community were able to maintain their lifestyle although perhaps not as
obviously as in the past. But in the towns, the hardest hit were people who were unskilled
and unemployed, women and Maori. The Association under Mona Corkill’s careful
leadership sought to introduce new practices which would help those most in need. One of
the schemes was a weekly clothing sale, where clothes were sold at nominal prices to poor
people. The profits went into a comfort fund. The scheme was an extension of the first
clothing sales initiated by Sybil in the early days and was an endorsement of her exacting
principle that more than anything else, people should be allowed to retain their self-respect.
Significantly at this time, the Association finally passed its guiding rules. Many of them had
been set down and approved as principles during the previous twenty years, but it was not
until the Committee meeting on 30 November 1936, that they were formally endorsed and
written into the constitution. Seventeen carefully worded rules became embedded into the
organisation. ‘The name of the organisation shall be The Nurse Maude District Nursing
Association,’ was the first rule. Then followed the requirements as to financial membership
including subscriptions, the need to print and circulate membership lists and voting rights at
meetings.
The objectives of the Association were written in one breathless sentence as: ‘the care,
nursing and general welfare of poor, aged and sick persons in and about the City of
Christchurch, the relief of distress and investigation of deserving cases and generally all
such objects and activities as in the opinion of the Committee tend to further the same or
similar objects as far as possible according to the principles and methods adopted by the
Founder.’
Significantly also, the Association endorsed the earlier decision to separate the management
of the organisation from the work of the district nurses. Splitting the two functions enabled
93 The Press, Christchurch. October 1961 94 Brooking, Tom. ‘Economic Transformation.’ The Oxford History of New Zealand. Ed. W.H. Oliver with B.R. Williams 1981 Oxford University Press pp 247-248

[56]
the nurses to do their practical work and the Association to have a board of management
which could determine policy and raise funds.95
The new Board should consist of not more than twelve persons including ex officio members
of whom, not more than three shall be women, decreed the rules. Precise details were
outlined for the election of officers, criteria for eligibility and appointments for casual
vacancies if required. Finally, there were rules pertaining to the annual general meeting, the
need for an honorary auditor and what might be required should any of the rules be subject
to amendment or alteration. It was in all respects a very modern document embracing
contemporary business practices for an organisation that had started in such a humble way.
The organisation’s guidelines spelled out everything that its Board and staff believed in and
worked towards. At the same meeting, Mona sought approval from the Board for an
allowance of three shillings per month for those nurses without bicycles who travelled by
tram on their daily rounds, and five shillings petrol allowance for those who drove their own
cars.
The Board decided to trade in Sybil’s old car. They could get £130 for it and if they paid an
additional £129 they could buy a Ford with a 10HP engine. It was a tempting proposition
and did not take long for the approval to be given. Mona also broached the subject of a
uniform change and in March 1937, quotes were sought from Beaths96 department store for
‘costume coats’. They were priced at five guineas each. The pre-war styles and fashions
were changing even for nurses’ uniforms. They were lighter, a little shorter, and there was
more freedom of movement.
As she settled into her work, Mona began to appeal to the Board for better equipment and to
talk with them about the increasing workload. At a special meeting in July, she explained
she had been compelled to engage an additional nurse and asked what criteria might be
needed if similar circumstances occurred again. The Board unanimously agreed that such
matters should be left to the matron’s discretion. It was clearly a vote of confidence in
Mona’s ability. It was also an indication of the direction in which the Association was starting
to move. There should be a distinction between the Board which determined policy, and the
practical nurse management of the organisation. The latter could be safely left to matron.
During the year, the Chairman Mr Jamieson, who had led the Association through its most
difficult period following Sybil’s death, became ill himself and died. He was succeeded by J.
W. Anderson, also a long standing Board member. The Board had expanded to twelve in
the previous year, but there was no move to increase the requisite number of women. Mona
was busy establishing herself not only as matron but also within the community. She made
frequent use of the radio and would broadcast over 3YA, the Christchurch station. Sybil had
also used the new wireless to good effect when she felt it was necessary. The introduction
of new technology, such as it was, attracted an enthusiastic listening audience.
95 Although there is no documented evidence, it is assumed that the Committee changed its name to ‘Board at the same time as the guiding rules were formalised. 96 Beaths was one of the first department stores to be established in Christchurch. It was situated across the road from Ballantynes store and merged with DIC before the building was redesigned as Cashfields.

[57]
Mona joined the National Council of Women and encouraged the Association to pay
affiliation fees. She was more political than Sybil and recognised the benefits of an
organisation founded by Kate Sheppard that lobbied specifically for women. She also
regularly addressed community organisations particularly those who supported women. A
suggestion that she take one of the Board members with her was considered inadvisable
unless it was one of the women members. It might ‘restrict the subjects which they may
wish to discuss,’97 she said. Her work always came first though. She would frequently
phone her flatmate and say she was on her way home. Lilian would prepare the evening
meal and then wait for the second call that said she had been delayed. Mona installed a
second telephone by her bed and was permanently on call.
The Board held its regular meetings in the upstairs sitting room. Always hospitable, Mona
would prepare two large plates of thinly sliced bread and butter before the meetings.
Needless to say there was seldom if ever, anything left. As matron, she became
increasingly concerned at the lack of properly trained domestic help in Christchurch. It had
been an issue that had always irked Sybil as well, but there seemed to be no easy solution.
Mona reported regularly to the Board that much time was spent trying to find the level of
assistance in addition to the duties of the district nurse that she believed was necessary. ‘It
means so much in a home where sickness is present,’98 she said.
In 1938, the Association received its first substantial bequest when a local woman Annie Hill,
left her estate valued at £8,000 jointly to the Nurse Maude Association and St Saviour’s
Orphanage. There had been other bequests, one in particular had given Sybil £200 each
year to distribute amongst the poor. But it had been terminated when she died. The money
had been gifted to her personally and there was no way it could be continued. The Annie
Hill estate consisted of 75 acres on Mills Road Marshlands, and properly invested, would
return the Association considerable funds in interest. There was much discussion about how
the Association could benefit from such a generous donation and where the funds could be
best spent.
Social Security
On 3 September 1939, Britain’s Prime Minister Neville Chamberlain declared war on
Germany. There was a simultaneous declaration by New Zealand’s acting Prime Minister
Peter Fraser. It was not unexpected but it was a shock all the same. In every town, men
signed up to join the armed forces. Christchurch was the departure lounge for troops leaving
from the South Island. They marched in the central city and were farewelled by the Mayor
and other dignitaries before boarding the train to take them to Lyttelton. Women and
children lined the streets and waved handkerchiefs and scarves from the wharf side. Like
the years of the First World War, the women left at home would desert the kitchen in favour
of the factory. Everyone needed to do their bit. The Women’s Land Army was formed to
keep New Zealand farms operational while the men were away. Under the leadership of
Mary McLean, the land girls as they became known, grew produce for families whose
97 Nurse Maude District Nursing Association Board Minutes 15 August 1938 98 ibid

[58]
menfolk were fighting overseas and also supplied vegetables to those in need. In
Canterbury, they were generous in their support of Nurse Maude and a firm bond was soon
established between the two organisations.
Throughout the war years, the district nurses continued their daily rounds. Home visits
increased to 12,905 in 1940 with a total of 2234 outpatient visits and nearly 5000 calls at the
rooms for help of various kinds. In her monthly reports, Mona commented frequently about
the lack of domestic help. But the Board was facing other difficulties. The Madras rooms
were now 20 years old and repairs were required. There were other costs including
increases in nurses’ salaries as well as car and uniform allowances. Something had to be
done. A meeting with the North Canterbury Hospital Board resulted in an increase in the
annual subsidy from £400 to £600. Shortly afterwards, the Hospital Board requested a
meeting with the Association’s Finance Committee. It proposed to extend the services
offered by Nurse Maude including hospital visits and follow-up calls before patients were
discharged. In return, the Hospital Board would pay an additional £200 per annum. In her
annual report, Mona spoke positively about the new moves. ‘As time goes on,’ she said, ‘it
seems obvious that with complete cooperation between the Hospital and our Association, a
great deal more useful service in both nursing and social work must be accomplished.’99
The liaison between the two organisations did not stop there. Within a year, there were
further discussions about the possibility of more hospital visits and additional follow-up care.
The Hospital Board agreed to increase its annual grant to Nurse Maude, this time to £1500.
Another nurse was engaged. Community groups continued their welcome support by
providing clothes to be cut down and fitted for those most in need. The Tai Tapu
Wellwishers, a group of women who had banded together a decade earlier after an inspiring
address from Sybil, were also ready helpers – always willing to do what was asked of them.
In the winter of 1941, Rose Godfrey died and with her went one of the few remaining links
between the Sisters of the Community of the Sacred Name and the Nurse Maude District
Nursing Association. In spite of the age difference, a warm friendship had developed
between Rose, Mona Corkill and Lilian Priest. The three women would regularly get
together in the Scarborough cottage, chat about life and enjoy the view. Now the connection
was broken. Rose was buried alongside her former companions from Barbadoes Street in a
little walled plot which was part of Linwood cemetery. Sister Edith had bought the land for
the Deaconesses many years earlier, displaying an almost uncanny estimation of its
eventual level of use.
The war continued to rage overseas and life was increasingly stressful at home. Families
did their best to get on with their lives, always listening out for the dreaded knock on the door
and the telegram that spelt bad news. ‘We have many problems which would not ordinarily
arise in times of peace,’ Mona reported to the Board in 1943, and no wonder. Thousands of
New Zealanders were now serving in Europe and the Middle East and thousands more had
99 Nurse Maude District Nursing Association Board Minutes. March 1941

[59]
been recruited to manage essential services at home. The civil nursing reserve was
established which included registered nurses and VADs.100
Overseas, 362 New Zealand nurses were in the army nursing service and a further 3,600
Red Cross VADs were being trained. It was a sombre time with daily reports of casualties
and lists posted of the dead and wounded. Help for Nurse Maude came from many sources
particularly the Red Cross VADs who took it upon themselves to provide hot meals for
patients and to take care of housework and shopping for people who were housebound.
Mona was more than grateful. Always busy herself, she often visited difficult and needy
patients and as a medical social worker, she regularly attended outpatient clinics at
Christchurch Hospital. She was president of the Registered Nurses’ Association and
maintained her active interest in local women’s organisations.
At this time, the section beside the Madras Street headquarters was used as an air-raid
shelter. Often some of the men would miss the last train back to the Burnham military camp
at night and they used the shelter as a sleep-out. Frequently they entertained ‘lady
companions’. One night Nurse Donahue reported a great noise coming from the section.
Mona was dispatched to investigate. She returned smartly, donned her nurse’s uniform and
marched forth to put the ‘lady companions’ in a taxi. The inebriated soldiers watched in
stunned silence. When Mona Corkill spoke, it paid to listen.
The Board relied on Mona to make sound nursing and managerial decisions. In return, she
relied on the steadfastness and strength of the Board. In 1943, several members stood
down. Still a central figure within the Association in spite of his many other commitments, Sir
Heaton Rhodes was appointed Chairman. Denis Cotterill, a well-known lawyer in town,
Stewart Mair a prominent businessman and Eric Beaven joined the Board. The honorary
secretary/treasurer was Rod Compton, a Christchurch accountant.
In October 1944, the Social Security (District Nurses Services) Regulations were gazetted.
The implications for Nurse Maude were far reaching. They were a continuation of the earlier
welfare principles established by the government in the 1930s – the principle that ‘state
support was the just right of a citizen, not the reluctant gift of a government.’101 The new
regulations required all district nursing services to be provided free of charge, and a subsidy
from the Social Security Fund of an amount equal to two thirds of the direct nursing
expenditure to be paid through the local Hospital Board to reimburse the Association. Nurse
Maude was expected to find the remaining one third plus the cost of any other social
services provided from its own revenue. As a result, the annual grant from the North
Canterbury Hospital Board ceased on 30 September 1944 and was replaced by the
government subsidy.
During the year, the Association had also discussed the feasibility of a nurses’
superannuation scheme, and at the annual meeting in May 1945, Sir Heaton reported the
scheme had been arranged and would be introduced shortly. There were also changes on
100 The Voluntary Aid Detachment (VAD) was established in Britain 1909 with help from the Red Cross and the Order of St John. It spread to Commonwealth countries and was re-instigated when WW2 broke out. 101 Eldred Grigg Stevan. ‘A New History of Canterbury.’ John McIndoe Ltd Dunedin 1982. p 162

[60]
the Board. One of the outcomes of the new agreement with the North Canterbury Hospital
Board had been the appointment of two hospital representatives – Mrs Jessie Mackay and
Mr J.S. Barnett. The latter was replaced by Mr V.C. Lawn at the 1945 meeting.
The war officially ended on 8 May 1945. VE Day was celebrated in Christchurch as it was
everywhere else, with jubilation and thankfulness. Three months later on 15 August,
following the atomic bombing of Hiroshima and Nagasaki, VJ Day was acknowledged as the
final ending of a long and terrible world war. Soldiers had been returning home for several
months and families were re-establishing themselves. But this was not a return to life in pre-
war Christchurch. The community had changed.
By now, the Nurse Maude District Nursing Association had a firm foothold not only in
Christchurch City but in several of the neighbouring districts as well. The previous year,
ongoing discussions with the Hospital Board had resulted in the extension of the
Association’s operations to New Brighton, Heathcote, Sumner and Lyttelton. The port’s
small community was well spread out and it was often difficult for people needing care to
travel to the city. In fact, the idea of a district nursing service in Lyttelton had first been
mooted by the North Canterbury Hospital Board in a report presented in September 1939.
An earlier conference between the Medical Superintendent Dr Nelson, the Lyttelton GP
Doctor Gilmour and the Lyttelton Hospital matron Miss Houston had explored ways and
means of providing the service. They had discussed everything from operational matters to
the relationship between local doctors. ‘Primarily, the nurse will work amongst the poor
people, but it would be understood that she would not in any sense replace the doctor,’102
the report noted.
As it transpired, nothing happened until 5 June 1945, when a meeting was convened in the
Lyttelton Council Chambers. Chaired by Mona Corkill, it elected a local committee with Mrs
W. T. Lester agreeing to be its first Chairman. Clothes, food and equipment were the
immediate priorities and the Lyttelton fund received a kick-start of £20 from Nurse Maude
headquarters. The first district nurse was Marjorie Tait. Her daily routine included a two-hour
casualty clinic in the front room of an old house where the owner used to nurse seamen who
were sick.103 (This was the start of what would later become occupational and industrial
nursing.) Nurse Tait collected the doctor’s list of patients who needed home help and
walked from one end of Lyttelton to the other. Equipment and dressings were supplied by
the Madras Street office and all financial transactions went through Nurse Maude’s office. At
the end of her first year, Marjorie Tait had visited 1,722 patients in their homes and treated
243 in her clinic. The need was clearly established and the nurse was there to stay.
102 North Canterbury Hospital Report. 4 September 1939 (author unknown) 103 Stonehouse Eve A. ‘In the Name of Nurse Maude’ Nurse Maude District Nursing Association. 1972 p 30
[61]
Chapter Two: Shaking the Kaleidoscope
A Golden Jubilee
In 1946, two significant events occurred. Sibylla’s sister May Maude died on 21 July 1946.
She had been an active member of the Board for ten years, and had helped to keep the
memory of her sister alive within the organisation. In her will, May bequeathed her home at
Clifton to the Association’s nurses as a place for rest and recreation for as long as it was
needed. It was a generous and thoughtful gift and one that was readily taken up. Then, in
November, the Association celebrated its golden jubilee. It was a major event, not only
within the organisation but for many Christchurch people as well. It was a chance for them
to recall the early work of Sibylla Maude as the spirited founder of the Association, and to
recount stories and events that had happened in the intervening years. Some of them had
gained mythical status in the telling. A commemorative feature in the Christchurch Star-Sun
quoted one memorable occasion when Sybil on her 19th birthday had apparently received a
cheque and instead of spending it on herself she went out and bought an invalid chair for an
elderly man.104
The Board put together a programme that would do justice to the Association and to the
memory of its founder. A packed ChristChurch Cathedral attended the service on 10
November and listened to the lesson read by the Governor General Sir Bernard Freyberg. A
large garden party followed in the grounds of Christchurch Hospital to which not only current
members and friends of the Association were invited but also former committee members
and many old friends. Guests were welcomed by Mona Corkill and entertained by a pipe
band from St Andrew’s College. The five-tiered jubilee cake, which had been made by the
Association’s nurses, instead of being cut and distributed to the guests, was packed up and
send to the staff at Middlesex Hospital in London where Sibylla had graduated in 1893.105
‘The record of service which the Association has built up over this period is one of which we
can justly feel proud,’ Sir Heaton Rhodes told the assembled guests. ‘We feel sure that the
traditions of service which have grown around the life of our founder Nurse Maude, will
always be the ideals of the Association. We believe that the torch could not be placed in
better hands than in those of our present matron and nursing staff.’106
There were other highlights during the year. Emily Bashford retired after 34 years of service.
She had trained under Sybil and was one of the few remaining stalwarts of those early
years. Staff levels had increased and there were now 13 nurses in addition to the matron.
The jubilee year was also an opportunity to thank the clothing committee whose members
continued to work tirelessly behind the scenes, altering, repairing and remaking garments for
the needy. Irene Simpson, one of Mona’s trusted nurses took on the role of medico-social
worker at Christchurch Hospital. Irene had a good knowledge of the hospital and district
104 The Christchurch Star-Sun. 12 November 1946 105 Eve A. Stonehouse ‘In the Name of Nurse Maude’ A History of the Nurse Maude District Nursing Association. 1972 p 35 106 Nurse Maude District Nursing Association Annual Meeting Minutes. 31 March 1947

[62]
work and understood the role that was proposed. She already knew Maisie McNair, the
benevolent officer for the North Canterbury Hospital Board.
As it entered another new decade, the Association prepared to consolidate its position within
the community. The kaleidoscope was changing. Nurse Maude was an acknowledged
private health organisation with a high public profile. In its first 50 years, it had established
itself as the pre-eminent provider of district nursing services to the people of Christchurch
and surrounding districts including Lyttelton. It had developed a strong working relationship
with Christchurch Hospital and it had built a firm relationship with the public. It was
dedicated to improving the health and welfare of the elderly poor in the community, a calling
which prompted the more affluent members of society, particularly local businessmen to lend
their support by making themselves available to serve on the Association’s Board and its
growing number of committees.
Mona Corkill was widely recognised in Christchurch as a woman of substance – a nurse who
knew the clinical requirements of the job and who also had a solid understanding of what
was required to ensure good staff management. She was an excellent communicator who
believed in forging strong relationships with other hospitals and health organisations in the
city – private as well as public.
St George’s Hospital had been established in the 1920s – its belated contribution to the early
Anglican settler’s belief that a cathedral, a university college, a secondary school for boys
and a Church-based hospital and then a medical school should all be part of the emerging
colony. The first matron Rev Mother Alice and her assistant Margaret Thwaites were
installed in the hospital together with the first patient in 1928. After 20 years, both women
decided to retire back to England. A new Lady Superintendent was required and Mona
Corkill was invited to sit on the selection panel together with Dr Leslie Averill, Mr L.A.
Bennett, and Miss Widdowson, Matron-in-Chief at the North Canterbury Hospital Board. The
appointment of Edith Williams at St George’s was a unanimous decision and one Mona
completely endorsed.
‘Fitzroy’ From time to time, the Association was the beneficiary of generous gifts and bequests. In
1949, they received an offer which was to radically expand its services and change its
direction. A wealthy widow, Mrs Malvina McDougall107 and her three daughters suggested
they gift their eight acre property with its family home of ‘Fitzroy’ in McDougall Avenue
Merivale to the Association. The proposal came initially from Sybil’s niece Peg, who was in
Christchurch on a visit home from England. Mrs McDougall had indicated to her that the
homestead was becoming something of a burden and Peg suggested the Association might
be able to make use of it.
The proposal was welcomed enthusiastically by the Nurse Maude Board. It noted in its
minutes how grateful it was for such a generous gift. ‘Fitzroy’ was an elegant home with
large rooms and a magnificently plastered ceiling in the ballroom. The building could be
107 Malvina and Robert McDougall were well known benefactors in Christchurch. Robert loved the arts and donated money for the city’s art gallery which was named after him on its completion.
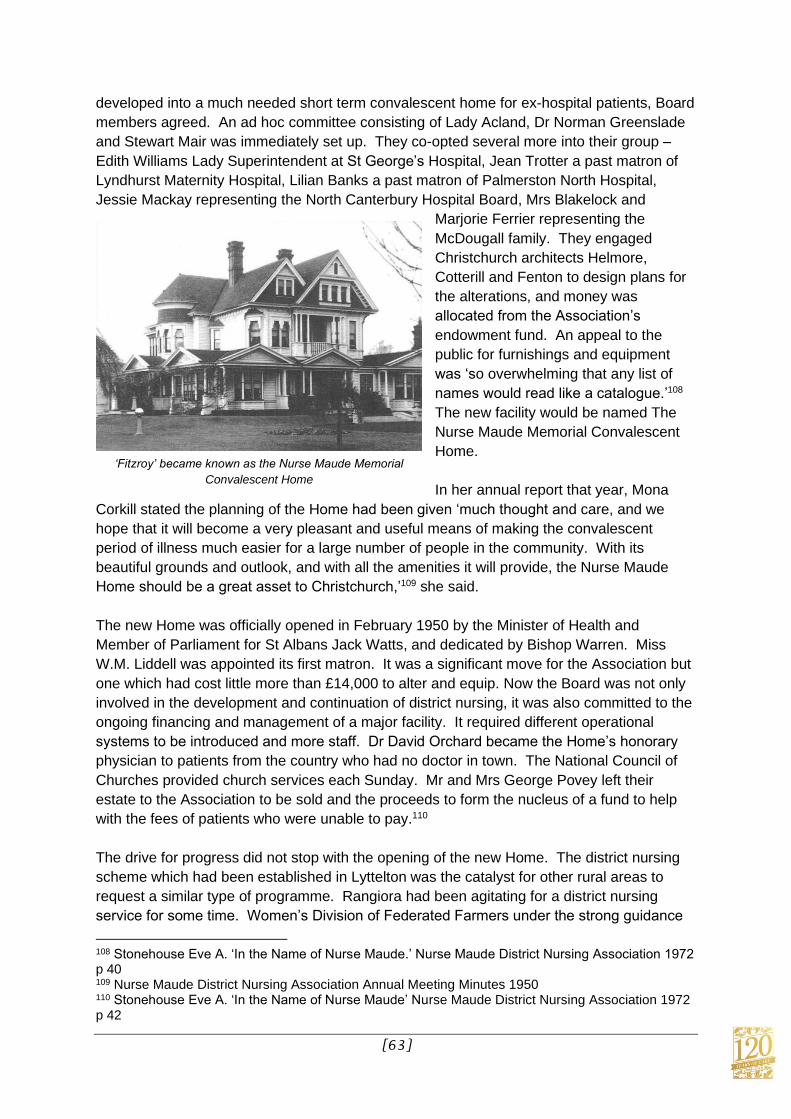
[63]
developed into a much needed short term convalescent home for ex-hospital patients, Board
members agreed. An ad hoc committee consisting of Lady Acland, Dr Norman Greenslade
and Stewart Mair was immediately set up. They co-opted several more into their group –
Edith Williams Lady Superintendent at St George’s Hospital, Jean Trotter a past matron of
Lyndhurst Maternity Hospital, Lilian Banks a past matron of Palmerston North Hospital,
Jessie Mackay representing the North Canterbury Hospital Board, Mrs Blakelock and
Marjorie Ferrier representing the
McDougall family. They engaged
Christchurch architects Helmore,
Cotterill and Fenton to design plans for
the alterations, and money was
allocated from the Association’s
endowment fund. An appeal to the
public for furnishings and equipment
was ‘so overwhelming that any list of
names would read like a catalogue.’108
The new facility would be named The
Nurse Maude Memorial Convalescent
Home.
In her annual report that year, Mona
Corkill stated the planning of the Home had been given ‘much thought and care, and we
hope that it will become a very pleasant and useful means of making the convalescent
period of illness much easier for a large number of people in the community. With its
beautiful grounds and outlook, and with all the amenities it will provide, the Nurse Maude
Home should be a great asset to Christchurch,’109 she said.
The new Home was officially opened in February 1950 by the Minister of Health and
Member of Parliament for St Albans Jack Watts, and dedicated by Bishop Warren. Miss
W.M. Liddell was appointed its first matron. It was a significant move for the Association but
one which had cost little more than £14,000 to alter and equip. Now the Board was not only
involved in the development and continuation of district nursing, it was also committed to the
ongoing financing and management of a major facility. It required different operational
systems to be introduced and more staff. Dr David Orchard became the Home’s honorary
physician to patients from the country who had no doctor in town. The National Council of
Churches provided church services each Sunday. Mr and Mrs George Povey left their
estate to the Association to be sold and the proceeds to form the nucleus of a fund to help
with the fees of patients who were unable to pay.110
The drive for progress did not stop with the opening of the new Home. The district nursing
scheme which had been established in Lyttelton was the catalyst for other rural areas to
request a similar type of programme. Rangiora had been agitating for a district nursing
service for some time. Women’s Division of Federated Farmers under the strong guidance
108 Stonehouse Eve A. ‘In the Name of Nurse Maude.’ Nurse Maude District Nursing Association 1972 p 40 109 Nurse Maude District Nursing Association Annual Meeting Minutes 1950 110 Stonehouse Eve A. ‘In the Name of Nurse Maude’ Nurse Maude District Nursing Association 1972 p 42
‘Fitzroy’ became known as the Nurse Maude Memorial
Convalescent Home

[64]
of its president Mrs Gibson, had gone to Wellington to lobby the Minister of Health. At a
public meeting in the town on 29 August 1950, a small committee was formed under the
chairmanship of the Mayor Charles Tyler and discussions began with the Health
Department.
By October, it was agreed a district nursing service should be initiated in Rangiora for a
year’s trial period. The local community was required to find a £400 contribution which was
easily achieved with a door to door collection. Elspeth Croy was appointed the district nurse.
As with Lyttelton, the administration was managed from the Christchurch headquarters,
directed by Mona Corkill. At the end of the first six months, she reported an excellent start to
the service with more than 1209 treatments given to 50 patients and a considerable number
of requests for nursing advice.
‘Judging by the interest taken in the service by the community, and the use being made of it
by the medical men and their patients, there appears little doubt that it is serving a long-felt
need, and that it will be a permanent service in Rangiora,’111 she told the Board.
The Association’s nursing staff now numbered 17 plus Mona Corkill. The nurses were
busier than ever. The Board agreed to buy a little corgi scooter for the nurses to use. It
could fit a suitcase on the back and had high handlebars, but it was not popular with the staff
– they preferred the regular bicycle. The Association also agreed to one of the nurses, Irene
Simpson, becoming the medico-social worker at Christchurch Hospital and there was the
ongoing issue of insufficient home help.
In 1952, the Board reluctantly decided to sell May Maude’s cottage at Clifton. It was seldom
used anymore and there were perhaps other ways in which May’s generosity could benefit
the nurses. Again considerable discussion ensued with the eventual decision that the ‘May
Maude Annexe’ should be built in the grounds of the Convalescent Home on McDougall Ave
to provide accommodation for retired staff members who themselves required nursing care.
The annexe opened on 24 July 1953 with two beds.
Several of the Board members believed there were community-oriented opportunities for the
Association to profile its business. Mr Pratt was an advocate of public subscriptions as
much for the money itself as the need to keep Nurse Maude in front of the Christchurch
people. He started to visit businesses and private homes with the result that annual
donations soared by 80 per cent that year and the number of subscribers increased from
294 to 698. The year also saw the introduction of a new community group – The Friends of
Nurse Maude. The 60 or so members busied themselves organising a stall in Cathedral
Square for the annual appeal in June and enthusiastically made themselves available for
voluntary aid whenever it was requested. The Tai Tapu Wellwishers continued their long-
time support with regular donations to the fund.
111 Nurse Maude District Nursing Association Annual Meeting Minutes 1951

[65]
Years of Progress
The 1950s were years of significant progress and development for Nurse Maude. The
organisation was moving forward at a rapid pace. Mona Corkill was now responsible for a
sizeable operation and there was more to come. Always a keen advocate of home help in
addition to nursing care, she convinced the Board in July 1953 of the need to establish a
service which could function alongside district nursing. ‘In many cases of sickness, the
inability to get any domestic assistance to carry on the necessary daily routine causes
almost as much worry as would the inability to get skilled nursing attention at such a time,’112
she told the Board.
The service started in a small way with one full-time home aid and then two part timers. The
value of the work could not be over-estimated for ‘apart from the work done in the homes,
much off-time duty has been spent by the aids in doing many acts of kindness which have
helped to make conditions easier for the patients.’113 Mona wanted to see the service
expand so that other sick people in the community could receive the service, and so it did.
Elsie Simpson had been given the task of organising this aspect of the Association’s work
and within a year the number of part time aids had doubled and other women had
volunteered their help.
District nursing services were still the prime ‘raison d’etre’ but there were several other
aspects to the business which were now just as significant and important. Board meetings
were becoming lengthy affairs as report after report focused on new developments, ongoing
projects and the state of the Association’s finances. The business was no longer the straight
forward operation Sibylla Maude had initiated. Her maxim of ‘soap, water and plenty of
God’s fresh air’ might still apply, but health was becoming more sophisticated. The
Convalescent Home was usually full to capacity, links with Christchurch Hospital were
maintained through the services of the medico-social worker and the home aid service
continued to flourish. Another sizeable property, this time at Governors Bay was gifted to
the Association by Miss Olive Redfern. Comprising some eight acres, ‘Waitahuna’ as the
home and grounds were known, were to be used for nurses for their holidays and their days
off. It was remarkable that the work of the Association still invoked strong feelings of pride
and ownership by the wider Canterbury community to the extent that such generous
bequests continued to be made.
The Association was not yet ready to stop. After five years, the Nurse Maude Memorial
Home was proving to be an outstanding success. The Board could see there was an
obvious need to establish another facility so that elderly men who required convalescent
treatment could be provided for in the same way as women were. However, the Association
did not want to commit itself to something without adequate finance. Finally, in 1955, the
increase in bequests to the endowment fund was such that Denis Cotterill and Stewart Mair
negotiated on behalf of the Association to buy a property at 85 Leinster Road in Merivale
which was just a few minutes’ walk from the Memorial Home in McDougall Ave. Architect’s
plans were drawn up to alter and extend the premises to accommodate 25 patients with
112 Nurse Maude District Nursing Association Annual Meeting Minutes 1954 113 ibid

[66]
support staff. It was a bold move supported by the Department of Health which agreed to
subsidise the requisite number of beds.
Irene Simpson’s role as the medico-social worker continued to expand and in 1954, Nancy
Tait was appointed as her assistant. At the same time, a new district nursing service began
in Kaiapoi. The resident doctor there, Dr C.F. McKee had been concerned for some years
about the increasing number of elderly sick people who lived in the district and their lack of
skilled care. He approached the Mayor Norman Kirk who agreed to call a public meeting.
Mona Corkill, together with Irene Simpson and the newly appointed secretary Mr Wellbrook,
attended on behalf of the Association. Community representatives from Country Women’s
Institute, Women’s Division of Federated Farmers, Returned Services Association, Rotary
and the local freezing works lent their support. Like Rangiora, there was a stipulation from
the Health Department that the community should endorse the scheme with an annual
subscription of £400 to go towards the cost. And, like Rangiora, the money was easily
raised with a door to door appeal. Permission was granted from the Department early in
1956 and Pauline Forrester was appointed the first district nurse.
Nurse Maude in keeping with its tradition of working with the elderly was an enthusiastic
supporter of the Advisory Council on the Care of the Aged in Christchurch, which was
formed the same year. The Council’s work was to coordinate all welfare work in the
community and to report on any proposals coming forward for consideration by the
government.
During this period of rapid development, the Association had been led by Sir Heaton
Rhodes. A lawyer by profession, he was a prominent political figure having been elected to
parliament in 1926. He had held various cabinet posts including tourism, defence and public
health. He was particularly recognised in Canterbury for his keen interest in agriculture and
horticulture. His country estate ‘Otahuna’ at Tai Tapu had become legendary for its annual
spring display of daffodils. Sir Heaton and his wife Jessie had played a significant role in the
60 year history of the Nurse Maude Association and therefore his death in July 1956 was
marked with genuine sorrow. A renowned community leader and business entrepreneur, he
had been involved in many commercial interests, yet he had retained his dedication to the
family friend of his youth – Sibbie Maude.
The Association’s new Chairman was Denis Cotterill. A member of the Board since 1943,
he was coming to the position at a time when the organisation was pushing ahead on all
fronts. Alterations to the Leinster Road property were well underway and it was hoped to
have them completed by the end of 1957. It was to be known as ‘Averill House’ in memory
of one of Sybil’s early mentors and vicar of St Michael’s parish, Archdeacon Walter Averill.
Under Mona Corkill’s direction a team of willing volunteers including many who had been
instrumental in organising the Memorial Home, bought all the necessary equipment for
Averill House.
With so much going on, could the Association take on any more? It could, and it did. For
many months, it had been negotiating with the Department of Health to establish a laundry
service which would be available to sick and disabled people who were incapable of
attending to their own laundry requirements and who were unable to pay for a commercial
laundry service. The Board wrote to the North Canterbury Hospital Board asking for its

[67]
cooperation in setting up such a service. The Association would be prepared to establish
and control the service plus pay for the transport if the Hospital Board would supply and
launder the linen. The Hospital Board sympathised but did not support the proposal. But, in
October 1956, Mr Horne the Hospital Board’s assistant secretary suggested a laundry
service could be set up that was similar to one he was knew about in Australia. It could be
achieved in Christchurch by working together with Nurse Maude. The Health Department
agreed at the end of September 1957. The Hospital Board gave its endorsement.
The Association bought a van and engaged Olive Innes as its driver. Elsie Simpson took on
the responsibility of managing the service in addition to her home help duties. The Hospital
Board supplied enough sheets, pillowcases, towels and blankets for 50 people. It was a
new, joint service. Its success was measured within the first six months by the capable
matron who said it was ‘impossible to speak too highly of the value of a laundry service such
as this, and we trust that it will be enabled to expand as the need grows.’114
Averill House on Leinster Road was officially opened on 9 May 1958 by His Excellency the
Governor General Viscount Charles Cobham.115 Marion Herrick was appointed matron.
While there was no intention to make a profit from either convalescent home, the Chairman
Denis Cotterill reaffirmed the Board’s policy of maintaining a watching brief on the finances
of both establishments. The Board soon realised however, that the organisation was
becoming too big for Mona Corkill to manage on her own.
In February 1959, Miss Marjorie Rae was appointed assistant matron, in charge of the
district nursing division. She had served overseas as a nurse during World War II and later
as a district nurse in England before working as a public health nurse for the Department of
Health in Christchurch. She was ideally suited to the position, Mona wrote to Denis Cotterill
from Hanmer Springs at the end of January.
‘I came up here yesterday for a few days and realised that I had not let you know that we
have at last managed to get an assistant matron,’116 she said, adding that she hoped he
would approve and not feel they should have waited for a meeting of the Board.
114 Nurse Maude District Nursing Association Annual Meeting Minutes 1958 115 Viscount Charles John Lyttelton Cobham had an historical association with Christchurch. Hagley Park was named after the family estate in England and the port of Lyttelton is named after his great- grandfather. 116 Corkill Mona. Letter to Denis Cotterill 20 January 1959. Nurse Maude Archives.

[68]
Chapter Three: The Whispering Winds of Change
The Lady Superintendent
By now, the Association was the owner of several substantial properties not only in
Christchurch but also in Wellington where two houses, a block of shops and a flat had been
acquired, mainly through bequests. Closer to home, there were four major properties all of
which required maintenance and upkeep. The headquarters remained at the Madras Street
premises and Mona continued to live upstairs with her companion Lilian Priest. Apart from
minor repairs, little had been done to it since it had been built 40 years or so earlier. The two
convalescent homes in Merivale with a total of 53 beds, were relatively new having been
substantially altered and upgraded before they were occupied. Even so, it was fast
becoming apparent they were not big enough to cope with the ever increasing demand for
bed space. The Governors Bay property remained a retreat for the 85 nurses and others
who made up the staff. In addition, the Association also owned an expanding fleet of 24
vehicles.
The Board approved a change in status for Mona Corkill who was now officially referred to
as ‘Lady Superintendent.’ It differentiated her from the matrons of both convalescent homes
and maintained her position as the head of the staff. She decided at this time, in
consultation with the district nursing division and the local Kaiapoi committee, that the
Kaiapoi service should be amalgamated with the city. Nurse Forrester, who had looked after
the Kaiapoi community from the outset, had announced her retirement. After careful
consideration, it was decided a full time nurse was not warranted in the area. One of the
nurses from Christchurch could visit three times a week at first on a trial basis, Mona said.
Both Kaiapoi and Rangiora had incorporated their original committees into a Friends of
Nurse Maude Group which took on the responsibility of caring for the sick and elderly who
wanted to stay in their own homes. It would later link with the organisation’s wider home aid
service.
In October 1961, Mona announced her retirement. After 25 years, it was time to step down.
She had led the Association through a period of dramatic development and change and
been a driving force in its growth from a district nursing oriented structure, to an organisation
with several different divisions. She had guided the Board and her staff through the period
of adjustment when the Association’s status changed from being purely voluntary to one
which was subsidised by the state. Her achievements during her tenure as matron had
earned her considerable plaudits from the community and an MBE from Queen Elizabeth.
‘When I came here first in the ‘bad’ years,’ she said in a media interview the year prior to her
retirement, ‘the rooms were crowded with people in distress. Many of them were in real
poverty.’117 People claimed there was nothing quite like the Nurse Maude Association
anywhere in the world. Mona was inclined to agree. She had taken on the position when
the country was at the tail end of the depression and there was still a great deal of hardship
about. She had worked in Christchurch through the war years and during the rehabilitation
117 The Press, Christchurch 20 October 1962

[69]
period that followed. The 1950s had been a decade of tremendous development for Nurse
Maude and Mona would leave an indelible mark on the Association with her departure.
In its annual report the following year, the Board acknowledged the work that Mona Corkill
had achieved with a special note of appreciation.
‘The energy and drive of Miss Corkill soon made itself felt, and she proved a
worthy successor to Nurse Maude as evidenced by the tremendous expansion of
the work of the Association during her term in office.
‘Her influence was felt far outside the Association itself. She is one of the
representatives of the Nurse Maude Association on the Aged People’s Welfare
Council and its only representative on the Executive. She is also a member of
the Council’s Admission Committee which controls admissions to Windsor House
and to Langford House, and as a member of this committee, Miss Corkill
interviews applicants for admission to these homes. She was a past president of
the Registered Nurses’ Association and has for many years been a member of
the council. For some years she was also on the committee of the Glenelg
Health Camp.
‘During recent years, she added greatly to her responsibilities in the keen interest
she has taken, and the positions she has filled, in connection with the care of the
sick, the frail and the aged, and the affection with which she is regarded by so
many of her old nurses, patients and friends is a fitting tribute to her 25 years of
selfless service in this field.’118
It was an eloquent tribute to Mona whose task had been made more difficult at the outset
having followed in the footsteps of Sibylla Maude. The new Lady Superintendent was to be
Marjorie Rae, currently assistant matron and in charge of the district nursing division. She
was assisted by Maude Billcliff, a former nurse who had joined the Association in 1952. She
had worked for four years as a district nurse when Mona Corkill asked her to set up a more
efficient office function. She was responsible for the district nurses’ daily reports and she
gave them their lists of duties, attended to relatives who needed equipment for sick patients,
made up and sterilised dressings, made up the Nurse Maude ointment and sorted clothing to
the sick and the needy. She was an invaluable help to Marjorie Rae.
Like Mona Corkill before her, Marjorie had a hard act to follow. One of her first major tasks
was to oversee the official opening of the extensions to Averill house. Four new single-bed
wards had been built during the year. A new patients’ lounge had also been added and the
original lounge converted into a patients’ dining room. For patients who were too ill to use
the main lounge, a small sunroom had been built at the end of the Blue ward. Then there
were extensions to the staff quarters – a new sitting room for nurses and a changing room
for non-resident nurses.
A Trust which had been set up by one of Sybil’s cousins on her mother’s side of the family,
Philip Brown, and which regularly gave generous support to the Association, provided funds
for a modern luminous call system as well as a television set, and the Christchurch Lions
118 Nurse Maude District Nursing Association Annual Report 1962

[70]
Club raised sufficient money to buy a piano. Averill House like the Nurse Maude Memorial
Home in McDougall Avenue, was now recognised as a hospital, still retaining the concept of
a private facility, but with an increasing subsidy from the state. Depending on requirements,
funding came into the Association from several sources – the Department of Health, the
North Canterbury Hospital Board, the Association’s bequest programme and still money
continued to flow in from the community. The annual appeal was a call to the people of
Christchurch and the surrounding districts to recognise and remember the unique qualities of
the organisation and the work it achieved.
‘Freedom is Sweet’
The Association continued to expand in the early 1960s. The main building programme was
now complete, but there were continual debates about the need for more beds. There was
an unresolved problem with the ‘mentally confused’ patients the hospital committee reported
to the Board in 1962. ‘The ideal solution would be a radical reorganisation of the hospital but
this would call for much building and alterations that would be too costly. The whole matter
is receiving the most anxious consideration…’119
In fact, there were endless financial problems. The Association was having quite a bit of
difficulty making ends meet, the chairman Denis Cotterill said as he introduced his report to
the 65th annual meeting. There was a deficit of more than £1,000 and although income had
risen by more than £3,000, total expenditure had risen by £6,000. Bequests had come in
from 19 different estates and had amounted to more than £5,000 which had helped the
organisation meet its obligations. The only way to decrease the cost of a bed was to
increase the number of beds, he said.120
At the Nurse Maude Memorial Hospital, bed occupancy for women was close to 93 per cent
while at Averill house it continued at 98 per cent proving Mr Cotterill’s point. On the other
side, there were major cost increases in district nursing, the home aid service and the
laundry service. Social services overall continued to be a significant part of the
organisation’s work but there was growing concern that other agencies were also starting to
enter the market with the resultant potential for overlap not to mention competition. It was
the subject of MP Jack Walker’s address to the Association at its annual meeting.
He deplored the lack of coordination between the many social welfare agencies that were
now operating in Christchurch. He told the meeting the duplication of services was resulting
in ‘unnecessary and wasted voluntary effort which could be better channelled through some
central agency.’ By pooling their resources to some central point of administration, the
organisations would operate more efficiently and the public would get better treatment. He
went on to comment that a group such as Nurse Maude, ‘which was not perhaps as well-
known as some other welfare groups with worldwide contacts, would in this way be better
enabled to carry on its mammoth task in the city without labouring under its present
difficulties.’121 Responding to Mr Walker’s speech, Denis Cotterill said he agreed with the
119 Nurse Maude Hospital Committee Report 1962 120 Nurse Maude District Nursing Association Annual Report 1962 121 Nurse Maude District Nursing Association Annual Report 1962

[71]
suggestion for more comprehensive use of social services. It was one that had given the
Board great concern.
At the same annual meeting, the death of Jessie Mackay was recorded. She had been
appointed by the North Canterbury Hospital Board to the Nurse Maude Association in 1941.
It was ‘mainly through her advocacy that the Hospital Board agreed to help the Association
in the formation of the laundry service to the sick and aged attended by the district nurses
and in all phases of our social service, she played a leading part,’ the obituary said. ‘As a
member of the Nurse Maude Memorial Hospital Committee since its inception, she saw both
the Nurse Maude Memorial Hospital and Averill House become invaluable parts of the work
of the Association and gave wise counsel and specialised knowledge to many of the
problems encountered in the management of the hospitals.’122
The Association’s work was beginning to gain a different community profile. It had always
enjoyed a high social standing, having been the recipient of many philanthropic bequests
from the more affluent members of Canterbury’s society. Now the Board had discovered the
benefits of using the media to report on special events and major activities. It also realised
the importance of inviting guest speakers to various functions, particularly notable people,
who could themselves generate publicity for the Association’s work. Sometimes the
Association enjoyed publicity without seeking it, as happened in October 1962 when the
Minister of Health, Don McKay came to Christchurch to attend the annual conference of the
Hospital Officers’ Association. The issue of domiciliary services, particularly home care for
those who were recovering from hospital treatment came in for special mention.
‘Freedom is sweet,’ Sybil used to say. To send elderly people to an institution meant
separation from those dear to them. By providing a district nursing service, they could stay
where they belonged and still get proper care and attention. Don McKay’s remarks were
prompted by an earlier report from his Department which recorded: ‘There is an urgent need
for recognition that adequate health services can and must be provided with fewer beds in
proportion to population than Hospital Boards and their executives have previously thought
necessary. All overseas opinion in recent years has come to this view…’123
The report went on to call for higher clinical efficiency in hospitals, maximum turnover of
patients and relief of institutions wherever possible through the home treatment of illness.
The total number of inpatients treated at all Hospital Board institutions in New Zealand had
increased from 127,000 in 1940 to 250,000 in 1960. The number of outpatient attendances
had increased from 567,000 to 1,809,000 over the same period. Of concern, also, according
to the Department of Health’s report, was the estimate of £45 million for the country’s current
hospital building programme.
The Christchurch media were quick to comment. ‘Current emphasis on the domiciliary
treatment of many kinds of illness reflects not only a change of attitude among health
authorities, but also the urgency of curbing increases in the capital and maintenance costs of
hospitals,’ reported the Christchurch Press. The Health Minister’s remarks were particularly
timely, continued the article, because they coincided with an appeal for funds from the Nurse
Maude District Nursing Association which had ‘pioneered a domiciliary nursing system in
122 ibid 123 The Press Christchurch 20 October 1962

[72]
Christchurch more than 60 years ago. District nursing as a public institution nowhere enjoys
a higher status; partly this is attributable to the Nurse Maude Association’s retention of its
identity as a voluntary organisation, separate from, although subsidised by state
agencies.’124
The Christchurch Star went a step further, endorsing the Minister’s comments with its
editorial entitled ‘Care of the Sick.’ ‘Recovery in one’s own home, even after a comparatively
serious operation, in many instances has a distinct psychological advantage, encouraged by
the medical profession. With the pressure on hospital accommodation steadily growing
throughout New Zealand, every opportunity to free a bed for someone else needs to be
seized. It is not only a matter of placing the claims of the more seriously ill above those of
just sick or merely elderly.’125 With remarkable prescience, the Star editorial continued: ‘New
Zealand today, and in the foreseeable future, cannot hope to provide hospital treatment for
all those cases which in past years would have qualified. The simple truth is that, largely
because the life span is being extended for more people, the group of potential patients has
grown beyond the capacity of the hospitals to absorb them and the country’s capacity to
build more hospitals rapidly enough. A lot more will be heard in the future about domiciliary
services. Christchurch may consider itself well qualified to fit into the pattern. Indeed, over
the years, it has helped devise it. The devoted service of the Nurse Maude District Nursing
Association is very much to the point. Its’ honoured name has been not without zeal…the
city, in short, is already ‘sold’ on the idea.126
Free Home Aid
Politically, there were changes in the wind for health services generally in New Zealand.
What would that mean for Nurse Maude? The Association was dependent on government
subsidies for a large part of its work and accountability for services was becoming a catch
cry. The Board did not have long to wait. In June 1963, the Minister of Health Don McKay,
announced that home aid services would be provided free to patients for as long as they
required nursing care. It was good news and a recognition of the value of home aid services
for domestic work. Had Mona Corkill still been in office, she would have been delighted
having always been a keen advocate for the service. Hospital Boards were to pick up the
cost for the schemes under their care.
The announcement had an immediate impact on Nurse Maude which entered into an
agreement with the North Canterbury Hospital Board to provide the requisite service. The
Association employed 60 home aiders at the time and it was without doubt the biggest home
care service in the country. Nationally the statistics were climbing. In the previous year
(1962), 515,000 visits had been made to 65,000 cases in most instances under the auspices
of eleven different Hospital Boards around the country. ‘One area has reported that the
patients being treated in their own homes would fill a ward of 32 beds all year round,’127 Don
McKay said.
124 The Press Christchurch 20 October 1962 125 Christchurch Star Editorial 10 October 1962 126 ibid 127 Christchurch Star 5 June 1963

[73]
Apart from relieving the demand for hospital beds, home aid services cost considerably less
than keeping a patient in hospital. The Association saw the benefits of the government’s
scheme. Providing a service for all patients discharged from hospital depending on need,
meant more home aids and consequently more administrative assistance. Jill Harman was
taken on as a part time clerk and in 1964, Betty Gilmour was appointed in a full time
capacity. Within a short period, the number of home aiders increased to 98 and then to 152.
They worked not only in Christchurch but in Lyttelton, Kaiapoi and Rangiora as well. Their
pay packet included an hourly wage of five shillings and threepence plus an allowance for
bus fares or mileage if they owned a car. Home aiders were popular within the community.
They elevated their work beyond the menial to a task that fitted alongside nursing. They
were often the subjects of articles in women’s magazines and the women’s pages of daily
newspapers with their ready store of anecdotes about the homes they visited, always
mindful of the need for patient confidentiality.
The new government scheme provided for a six week home aid service at the conclusion of
which there was an assessment to check whether further help was needed. If it was decided
the patient needed more home help but not district nursing and was unable to pay, the
Social Security Department would make the judgement and pay for the service. For
geriatric, paraplegic and long term patients, needing both district nursing and home care
services, fees were paid by the Department of Health via the Hospital Board.128
With the home aid work steadily increasing, the Association needed to engage more clerical
staff in order to cope with the various government departments it had contact with: Social
Security, the War Pensions Department, the North Canterbury Hospital Board in addition to
Nurse Maude’s own complicated cross section of home aid services. It meant accurate
records had to be kept, a routine which was interrupted for two days every fortnight in order
to prepare over 200 time sheets which included not only the time worked, but the patient’s
category and area as well as the group the home aider herself was in – single, widowed or
divorced.129
Helen Doherty was employed as the Association’s full time clerk. To simplify the system,
time sheets were colour-coded – blue for hospital patients and white for paying or social
security patients. A map was set up on the superintendent’s office wall dividing the city into
east and west from Colombo Street. A blue or white pin on the map showed the home of
every patient. Another map alongside showed where each home aid lived and her available
mode of transport – black pins for cars, blue for bicycles and yellow for bus services.
By 1966, there were problems with parking outside the Madras Street premises. The
headquarters were originally designed for district nurses with parking in the side driveway for
eight cars at most. With the establishment of the home aid service and registered staff also
using their own cars, the Board bought the section next door when it was offered for sale.
But by 1968 the space was again inadequate. On pay days, the situation became
impossible, causing frustration and delays. The City Council’s traffic department was asked
if it could make an allowance for Nurse Maude, but although it was sympathetic to the cause,
128 Stonehouse Eve A. ‘In the Name of Nurse Maude’ Nurse Maude District Nursing Association 1972 p 82 129 Ibid p 79

[74]
it did not agree. Radley Brothers, produce auctioneers whose business was on the corner of
Madras and Lichfield Streets, rallied to the cause however, and supplied more parking on its
premises. It was a short term fix for a growing problem.
In spite of an increase in government subsidies, the Association went back to the community
with yet another plea for funds. In a delightful interlude, on the eve of the market day, the
morning paper printed an article written by a former neighbour of Sybil’s – Hazel Elmslie.
She described two incidents which by themselves were humorous, but also served to
underpin the unique qualities of the organisation which kept it at the forefront of the
community. Miss Elmslie had lived in Scarborough in the early 1900s when Sybil bought her
cottage there. They would swim together in the mornings.
‘Punctually at 8am she would appear running down the centre of the road, and I
mean running,’ Miss Elmslie wrote. ‘With her head help up and her peignoir
flying out behind her in the wind, she would come steadily down the hill. I would
fall in beside her as she rounded the steep turn and without stopping or speaking
we would carry on over the rocks and along the beach, fling down our robes and
plunge straight away into the waves. No shivering on the brink for us! A few
strokes in the water were enough and out we came to jog back along the sand
and up the road, exchanging a few remarks as we gasped for breath…I left her at
the corner as she turned and faced the long climb home, without any waste of
time.’
‘Later, about 9.15am, she sometimes picked me up in her two-seater on her drive
into Madras Street. There must be many who remember her notorious driving
habits. A drive with her into Christchurch had its exciting moments. She usually
drove well over the 30 miles an hour, and would scoot past the old electric trams
on the inside…I think it is true to say that never once was she summonsed for a
traffic offence. The traffic officers literally gave her the freedom of her home
town.’130
Recalling another incident, Miss Elmslie continued:
‘That same year, Lintz produced with local talent, a revue called the ‘Reveille’
which ran for several weeks in the Theatre Royal and made a lot of money for the
RSA. At, I think, the final performance, an unforgettable scene was introduced.
In her uniform of blue with white apron plus bonnet and strings, Nurse Maude
rode on her bicycle right across the stage from one side to the other where she
was safely caught in the wings. Thunderous applause from a full house broke
forth and she had to return to the stage again and again to acknowledge it, until
at last the cheering crowd was satisfied.’131
Hard work mixed with continuing progress were the hallmarks of 1964; implementing the
new changes in the home aid service, maintaining the extensive district nursing service and
keeping the two hospitals operating efficiently. In her annual report, Marjorie Rae said
130 The Press Christchurch 17 October 1963 131 The Press Christchurch 17 October 1963

[75]
nursing visits had increased by more than 17 per cent and home aid visits by more than 55
per cent. The laundry service had similarly doubled its output. It all meant staff increases of
nearly 29 per cent to meet the growing needs and a consequent increase in the amount of
money required for wages and salaries. But, because the domiciliary services had
expanded so much, many people were able to stay in their own homes rather than go into
hospital.
‘Numerous social problems are encountered in our work,’ Marjorie Rae reported. ‘It is
essential that members of the nursing staff have a sympathetic understanding and
knowledge of social services.’132 Nursing treatments in homes throughout the areas covered
by Nurse Maude totalled 77,107 in 1964 with an average of 740 patients being cared for
each month. District nursing and home care work in Lyttelton had expanded with the
opening of the road tunnel and the laundry and Red Cross Good Neighbour services were
now available to residents there.133 Meanwhile Friends of Nurse Maude continued to help
with sewing and mending at the Memorial Hospital. Street appeals and cake stalls
continued to generate revenue for them.
Although such publicly-spirited efforts helped with fund raising, the Association continued to
have financial difficulties. Eventually the position was outlined to the public in a series of
articles in June 1964. There was an anomaly in the payment system ever since the changes
had been introduced by the government which was disadvantaging both the Association and
the patients it served under the jurisdiction of the North Canterbury Hospital Board. Under
the new system, district nursing services were provided free on social security by Hospital
Boards. The district nursing scheme in Christchurch as provided by Nurse Maude was also
free to patients but the Association received reimbursement for only two-thirds of the direct
cost. The Association was required to find the balance as it had always done, through
donations and bequests. If the subsidy was raised to 80 per cent, the government’s
contribution to Nurse Maude would be raised by £6,000 per annum which would allow the
Association to stop asking patients for a contribution.134
The Association was embarrassed by the publicity, supportive as it was, and there was more
to come. In an editorial a week later, the Press continued the discussion. The Association
would be wise to seek an increased subsidy from the government. Why should the public be
penalised because Nurse Maude was a voluntary organisation and therefore only entitled to
a two-thirds subsidy?
‘Though, in some respects, an anachronism in the nursing system of New Zealand, the
Nurse Maude Association deserves official as well as public encouragement. The memory
of its founder, no less than the devoted efforts of her successors, has inspired a tradition of
voluntary service. This is measurable in hard cash as well as human endeavour: it saves
the taxpayer money.’ Better arrangements were surely possible, the article concluded. ‘An
increase in the government grant would enable the Association to relieve its district nurses of
collecting contributions from patients.’135
132 The Press Christchurch 12 June 1964 133 The Lyttelton Road Tunnel was officially opened by the Governor General Sir Bernard Fergusson on 27 February 1964 134 The Press Christchurch 12 June 1964 135 The Press Christchurch June 1964

[76]
But the Board was reluctant to make the move as explained by the acting Chairman Stewart
Mair at the annual meeting. The Association had a history of tackling issues in its own way
and now was not the time to change that. Both Nurse Maude Memorial Hospital and Averill
House had maintained their almost extraordinary high rates of occupancy with the result that
Averill House in particular was no longer able to cope with demand. More beds were
proposed which would take the total to 60.
In his annual report, the Chairman of the Association’s Hospital Committee, Mr Turner
Smith, said the facilities would benefit during the coming year from an increase in social
security payments to private hospitals, but as nursing salaries had also increased, it was not
yet clear what the final effect would be. He commented there would undoubtedly be a loss
of revenue particularly from Averill House with some beds out of use while the proposed
alterations were carried out.136
In August 1965, Marion Herrick stepped down as matron of Averill House. She had
supervised the all-male patients at the hospital since its opening seven years earlier, and it
was, in her own words, the happiest period of her 45 year nursing career.137 Interviewed on
the eve of her departure, she provided an interesting insight to nursing duties from the 1920s
to the present day. Christchurch Hospital had provided her basic training under Rose Muir’s
tutelage. From there, she had gone to Akaroa and Kaikoura hospitals, rural outposts which
in hindsight seemed very well equipped compared with the Chatham Islands which were her
next stop. There was no power on the Chatham’s in those days and home visits were made
on horseback. The nurses lived in a little cottage and were supplied with livestock by
grateful Islanders. After three years Marion left to travel overseas, going first to South Africa
where she worked in a private capacity and then to Europe accompanying patients. She
returned to New Zealand and after ten years back in Kaikoura, she joined Nurse Maude as a
district nurse.
Her subsequent appointment as matron of Averill House had been the culmination of her
career and when she finished her duties, tributes were paid by the former Superintendent
Mona Corkill and Marjorie Rae. ‘All nurses do what they can,’ Marion said in response to
presentations by both women. ‘My years at Averill House have been a great climax to my
nursing life.’138
Marion Herrick like so many of the Association’s former senior nurses, had enjoyed strong
links with Christchurch Hospital. Many of them had trained there or taken up positions in the
wards before joining Nurse Maude. Staff had come and gone, but the relationship between
the two organisations had stayed strong. Marion’s place at Averill House was taken by Miss
Shand, but she resigned after just six months to join a medical team in Vietnam. The new
arrival, Ethel Mazins, was appointed matron in May 1966.
136 Nurse Maude District Nursing Association Board Report 1964 137 Christchurch Star 26 August 1965 138 ibid
[77]
Chapter Four: Planning for the Future
1967 – A New Act
In November 1966, Denis Cotterill in his capacity as Chairman of the Nurse Maude Board,
wrote to a firm of constitutional law advisors – Watts & Patterson - in Wellington, seeking
their opinion about the Association’s constitution. He explained that while the Association
had drawn up rules early in its operation and had paid particular attention to the need for
careful financial scrutiny and investment, the rules themselves had never been registered.
The rules had been deposited with the District Land Registrar in 1964. The Association was
now contemplating building another facility adjacent to the Nurse Maude Memorial Hospital
on McDougall Ave which could then be converted into a suite of administration offices.
‘The Aged and Infirm Person’s Act does not provide machinery for elasticity,’139 Mr Cotterill
wrote. The Act gave the Board no power to borrow on mortgage and the Association
therefore had to apply to the court every time a loan was needed. In 1958, the Board had
looked into the possibility of setting up a new constitution, but the advice at the time had
been that the existing Act made no provision for the winding up of the existing Trust Board
and the substitution of another, even if everyone agreed. The Board now wondered whether
a private Act of Parliament to create a new constitution would enable it to continue with its
three principle objectives – district nursing, the home aid service and the two hospitals.
In fact, the Association was looking to the Act to solve a more immediate problem – the
growing rift between itself and the North Canterbury Hospital Board. There were increasing
disagreements between the two organisations – always kept in-house of course. In 1965,
there had been discussions about cementing relationships between them with the Hospital’s
Medical Superintendent Dr Patterson advocating the relocation of the district nursing office
to the Christchurch Hospital precincts. But it had not happened. Another suggestion from
the Hospital Board which was equally squashed was that Nurse Maude funds could be used
to build a home for the elderly people which the Hospital Board was being advised to
establish near Coronation Hospital in the Cashmere Hills. A Department of Health survey of
hospital accommodation for the elderly had pointed to the Hospital Board’s being short of
requirements by a total of 60 beds.
The response was swift and unequivocal – monies that had been gifted to Nurse Maude
could not be diverted to any state-owned institution. Furthermore any suggestion that legacy
monies could be diverted to subsidise investigation into various medical problems would also
be quite illegal.140 With three of its members on the Nurse Maude Association Board, the
Hospital Board had entré to the financial operations of the Association as well as intimate
knowledge of its assets. The Association, on the other hand, had no representation on the
North Canterbury Hospital Board. The Hospital Board was clearly trying to flex its muscles.
139 Cotterill Denis, Letter to Watts & Patterson, solicitors, Wellington 22 November 1966. Nurse Maude Archives 140 Note of talk with Dr Averill 5 February 1965, Author unknown. Nurse Maude Archives.

[78]
To make matters worse, it was suggested that the local branch of the New Zealand Medical
Association was also lobbying the Hospital Board for greater involvement in Nurse Maude.
A major point of disagreement was the Hospital’s contention that the district nurses should
report to a medical practitioner. There were other problems outlined by Norman Greenslade,
a medical specialist at Christchurch Hospital, in confidential memos to Denis Cotterill. This
time the Hospital Board complained about an apparent lack of cooperation between the
district nurses and local doctors. The problem, according to the Hospital Board, clearly lay
with Marjorie Rae’s lack of cooperation.141
But there were question marks about these claims. Within a week, the Association received
two letters – the first from the Canterbury faculty of the College of General Practitioners and
the second from the local branch of the British Medical Association. Both expressed their
appreciation of the Association’s work. ‘The feeling of the faculty is that the (Nurse Maude)
Association plays an integral part in the domiciliary care of the patient,’142 wrote Mr Louisson,
provost of the College. The president of the Medical Association, Mr Brockett, was more
effusive in his thanks to Nurse Maude for the ‘wonderful work it has done for the sick of this
town and district over the years. As a result of the continued selfless devotion of all the
members of the staff, both past and present, we now have a service which is an
indispensable factor and an integral part in the ever-increasing demand for domiciliary care
of the sick and convalescent patients.’143 The letter heaped praise upon Marjorie Rae and
her district nurses.
Nurse Maude’s Board could be forgiven for wondering what might be going on. The
Association had a strong ally in Norman Greenslade, who maintained a steady
correspondence with Denis Cotterill, keeping him up to date with what was happening. He
had a friend in high circles, Gordon Lee who was the national secretary of the Medical
Association and a close friend of the Minister of Health. Both were keen golfers and many a
discussion about health matters, including those concerning Nurse Maude, took place during
a round on the Wellington course.
The first real issue developed at the beginning of 1967 and centred on a report to the North
Canterbury Hospital Board that Nurse Maude home aids were looking after babies while
their mothers who required psychiatric care were being treated at Princess Margaret
Hospital. This was considered to be completely improper and should be stopped at once,
declared the Hospital Board’s Medical Superintendent in Chief Dr Lynton (Lyn) Berry.144
Norman Greenslade immediately contacted the home aid supervisor Eva Stonehouse who
told him that the service was being provided at the request of the North Canterbury Hospital
Board itself through its psychiatrist Dr John Dobson and, as it happened, consented by Dr
Berry. It was a political faux pas and demonstrated the extent to which the medical
profession was not entirely comfortable with the role of district nurses. Were they trying to
take over some of its work? More importantly, were they being successful?
141 Note of discussion between Norman Greenslade and Denis Cotterill 18 July 1967. Nurse Maude Archives 142 Letter from the Canterbury Faculty, College of General Practitioners 10 May 1966. Nurse Maude Archives 143 Letter from Canterbury Division, British Medical Association 17 May 1966. Nurse Maude Archives 144 Memorandum of a conversation with Norman Greenslade 26 January 1967 Nurse Maude Archives

[79]
To ease itself out of an apparent dilemma, the Hospital Board suggested the matter should
be referred to the Department of Health. Furthermore, could not the Department endorse
the idea of a crèche at Princess Margaret Hospital which would solve the perceived
problem? The Board argued the case back and forth with the last word going to Mr Corbett,
a Board member from Kaikoura, who said, as Norman Greenslade told Nurse Maude, that
the children and babies would be better kept in their own homes and that the home aid
‘could be getting on with a little housework while babysitting.’145
In Mr Greenslade’s opinion, Dr Berry and the Hospital Board’s secretary Gil Laurenson were
obviously opposed to Nurse Maude being ‘anything more than a servant of the Hospital
Board’. He went on to say that Dr Berry had gone so far as to say when the matter was first
raised, that it ‘illustrated the unsatisfactory situation over the Nurse Maude Association and
made it clear that it would be much more desirable to have the district nursing service under
the control of the North Canterbury Hospital Board.’146
By having its own legal constitution through an Act of Parliament, Nurse Maude could better
determine its own future. In this Norman Greenslade was again an ally. ‘Representatives’
rather than ‘members’ should be part of the wording in the Act when referring to people who
should be part of the new Nurse Maude Board, he suggested in another informative letter to
Denis Cotterill. In his view the North Canterbury Hospital Board was having its own
difficulties. ‘I have felt for some time that the Hospital Board is not adequately certificated to
deal with the many activities of the hospital which extend into the community a great deal
further than when hospital boards were first constituted,’ he wrote. ‘Socialised medicine
(state) now needs to involve the community and become social medicine,’147 he said. It
would be the subject of an address he would be making to the Private Hospitals’ Conference
later in the year.
Nurse Maude’s Board decided it should seek an independent opinion as to its operation and
it invited the Department of Health to conduct a complete investigation into its structure, its
aims, its management and its general activities.148 The purpose of the inquiry, as stated the
report in its introduction, was threefold. It should ascertain whether or not the Association
can best serve the public as an independent, private organisation or whether its functions
should be taken over and run as part and parcel of the service required by statute to be
provided by the regional hospital board. Secondly, to compare as far as possible, the
existing services of the Association with those provided by Hospital Boards in other parts of
New Zealand. Thirdly, to suggest improvements in any aspect that seemed desirable.149
The 46 page report was comprehensively detailed, observing every aspect of the
Association’s work including its governing rules. The conclusion was simple, straightforward
and a clear affirmation of Nurse Maude.
‘On the basis of the available evidence, there can be no doubt that the Nurse Maude
Association today is a viable and well-run institution, offering the Christchurch people a
145 Memorandum of a conversation with Norman Greenslade 26 January 1967 Nurse Maude Archives 146 ibid 147 Greenslade Norman: Letter to Denis Cotterill 16 June 1967. Nurse Maude Archives 148 Department of Health Investigation 1967. Nurse Maude Archives 149 ibid

[80]
service that is comparable with, and in several respects, more comprehensive than those
offered by regional Hospital Boards in other centres. It is, moreover, very doubtful if the
existing service could be run more efficiently or cheaply if it were incorporated into the
framework of the Hospital Board services at the present period of time. A partial take-over of
the services, e.g. district nursing, home aid and laundry would merely destroy a functioning
organisation leaving a ‘rump’ unable to carry on without increased outside help.’150
‘A truncated charity is worse than useless, it is obscene,’ the report continued. There were
several recommendations to the Board which would improve efficiencies particularly better
liaison not only at committee level, but more importantly, at senior nursing staff level. The
Hospital Board should be prepared to increase the annual subsidy if warranted, but even
then the service offered by Nurse Maude would be less of a cost to the Hospital Board than
if it operated the same itself. If the Hospital Board wanted to use its community nurses
more, it could be achieved by training them under the supervision of the district nurses. But,
‘a fairly long probationary period, say a year, might be required before the community nurse
could be safely entrusted with increased responsibilities involving decisions if the present
standard of service is to be maintained.’151
The report suggested some improvements to the management structure including
introducing a managing secretary who should have a background in accountancy rather than
medicine. It was a sound report and validated Nurse Maude’s decision to go to the
Department. It also put the Association in good standing with the Department, even if it
upset some members of the North Canterbury Hospital Board, in particular some of their
medical specialists. Within a few months, the Nurse Maude District Nursing Association Act
was going through the Parliament.
To facilitate its process, the Board decided it was inopportune to press for more funding. It
was better to wait until the Act passed into legislation and there was a return to a more
collegial relationship between themselves and the Hospital Board. The Association had a
credit balance after meeting the deficit for expenses the previous year and when the
government expenses were being heavily curtailed, it was not a suitable time to ask for more
money, Denis Cotterill told the annual meeting in June 1967.152
Regardless of the Act and its progression through the parliamentary process, the Board
continued with its plans to extend its facilities and through the generosity of the McDougall
family once again, it was able to buy adjacent land at low cost. ‘We will do our best to
extend our hospital facilities and keep within the finances. There is an urgent need for more
beds for the aged in Christchurch,’ Mr Cotterill said. The Board had to turn down between
15 and 20 applications for beds each month.153
For the first time in its history, the Association’s Board invited the Friends of Nurse Maude to
present an account of their activities during the year at the annual meeting. The president
Miss Simpson began with an explanation of their early beginnings. The Friends now
150 Department of Health Investigation Report 1967. Nurse Maude Archives 151 ibid 152 Nurse Maude District Nursing Association Annual Report June 1967 153 ibid

[81]
numbered 122 and up to the end of 1966, had raised over £6,000 for the Association.
Meetings were held where there no parking difficulties, she said with a touch of wry humour.
Lilian Priest was a keen member of the group and in keeping with Mona Corkill’s earlier
traditions, the group continued to end their meetings with a simple afternoon tea – plates of
thinly cut bread finely spread with butter.154
Meanwhile, the Act was into its second reading. The Bill had been introduced privately by
Robert McFarlane, MP for Christchurch Central. It set out the rules of the Association and
defined its powers. The existing Board would dissolve and be replaced with the newly
incorporated Association to be run by a new Board consisting of not more than 14 members
of which ‘not more than four shall be women.’155 It was an improvement on the previous
three, but for an organisation which had a predominantly female workforce, it was a
surprising inclusion in the Act. The North Canterbury Hospital Board could appoint up to
three people to the new Board and the Canterbury Branch of the Medical Association could
appoint one person. The Act was passed into law on 13 September 1967.
Community Care
The 1950s and 1960s were years of comparative affluence in New Zealand. Not-for-profit
organisations and independent health institutions relied on the state for annual subsidies
while maintaining the right to build and develop their own private resources. Nurse Maude
was no exception. It retained the right to independence by building on its past legacy and by
canvassing for funds from the public. At the same time it negotiated a growing subsidy from
the state for almost every aspect of its services. With representatives from the North
Canterbury Hospital Board and the local Medical Association attending meetings, and its
continuing high public profile, its increasing level of accountability for its operations was
regularly fed back to those who considered they had a stake in its business.
Not everybody was happy however. Occasionally letters to the local media commented on
the continual round of fund raising, asking why, in an era when the government provided a
free health system, were the people of Christchurch asked to make contributions to Nurse
Maude? Frequently, the Association came under scrutiny from other social service
operators and there was the constant cry for more community health planning.
Christchurch was the largest city in the South Island with a population fast approaching
300,000. It serviced a wealthy hinterland, affluent from the high prices received for its
agricultural industry, particularly meat and wool. Agriculture was still considered to be the
country’s biggest exporter and therefore the backbone of the country and what its produce
could not provide, the government did. These were the boom years and everyone should
benefit from the prosperity they offered. Unemployment was down to its lowest levels, yet
social services were continuing to gain in importance – at least at the planning level. It was
time to evaluate the machinery by which these services were delivered – to look more
closely at how they operated and what long term initiatives could be introduced which would
be more sustainable.
154 Friends of Nurse Maude Annual Report 1967. Nurse Maude Archives 155 The Nurse Maude District Nursing Association Act 13 September 1967. Nurse Maude Archives

[82]
As usual, Nurse Maude was at the forefront of change. The Association invited Dr T. K.
Williams, who was renowned for his opinions on the subject of health and community care,
to come and talk to the Board. Community health planning had been neglected and, he
believed, there was a vital need for a reassessment of both the work involved and the
helpers, he said. Because the people at the coalface had been busy coping with the
practical tasks that took precedence on a daily basis, little energy had been devoted to plan
for the future.
‘At present, hospitals are planning ways and means of extending their organisations into the
fields of community care. This is discharging the fringe of cure into the hands of others –
under the guidance and control of those inside – not a true planning for care. There is a
need to combine the services of the hospitals and the public health services to assist in such
planning. The government needs to provide money to support planning groups and to
accept the advice of such groups in improving community services.’156
Dr Williams went on to question the need for district nurses to always work under the
direction of doctors, and further, to ask whether there was a need for the nurses to perform
all the tasks identified in their daily lists. He concluded with a public plea for financial
assistance to investigate the best planning for community health, to coordinate the thinking
of public health planning, the hospital planner and then the educator.
Not long after Dr Williams’ address which had been fully covered in the media, the
Christchurch Star took a more probing look at Nurse Maude. Marjorie Rae outlined the
services offered including a summary of the recent analysis by the Department of Health.
She obligingly provided figures relating to the state subsidies for the previous year – the
district nursing subsidy of $78,790, home aid subsidy $70,994, laundry service subsidy
$3158, and hospital subsidy $80,918. Community donations included $15,740 for district
nursing patients and others, $3814 in subscriptions from members, $3120 in general
donations and $2870 raised from street, cake stalls and other such events. Then there were
special donations totalling $1000 and bequests of $24,752.157
The Association had developed a very successful working relationship with both the
government and its Canterbury community and was committed to its future. Yet the
complexities of an ever-changing and advancing health system created difficulties. During
the year, changes in the home aid service resulted in a reduction in the number of visits.
Unlike the district nursing service, home aid was fully paid by the state. As a result, the
number of free visits fell while the number of subsidised visits increased. There seemed to
be no adequate explanation other than the payment differential. In view of the increasing
workload on Superintendent Marjorie Rae, the Board advertised for an assistant and Mary
Renwick was duly appointed. The financial results for the year were once again a
disappointment with an overall deficit of $17,403 recorded. This was in spite of the
hospitals, the laundry service and the Trust fund showing surpluses. The deficit in district
156 The Press Christchurch 27 July 1967 157 Christchurch Star 28 October 1967. The amounts were now in dollars, New Zealand converted to decimal currency on 10 July 1967.

[83]
nursing was giving rise to more concern having increased to $27,488 over the year. The
Board agreed to look more closely at ways of reducing the load, caused by the constant
expansion of services and increases in nurses’ salaries. It was an ongoing problem.
Consolidating Premises
The new decade started promisingly. In spite of its financial concerns over the rising cost of
the district nursing services, the Association was going from strength to strength. The
previous year had seen major changes in the Board’s membership. Stewart Mair died in
December 1969. He had been involved with Nurse Maude since 1943, serving on the
general committee as well as the finance and hospital committees. Marjorie Ferrier also
died in the same month after active involvement with the Association for nearly 20 years.
She had been the direct link between the McDougall family, the Association and ‘Fitzroy’
renamed the Nurse Maude Memorial Hospital. Four new members joined the Board –
Campbell Ballantyne, Ralph Wylie, Dr Ross Fairgray (Medical Superintendent-in-Chief at
Christchurch Hospital) and Jean Taylor. Within the staff, Eve Stonehouse retired from the
home aid service she had managed since 1961 and Marjorie Rae stepped down as the Lady
Superintendent. She had been responsible for the overall management of Nurse Maude for
the previous eleven years.
The Board appointed Mary Renwick, who had been assistant Lady Superintendent under
Marjorie Rae, as Supervisor of the District Nursing Service and Amelia Slater as the
Manager of Home Aid and Laundry Services. In its 1970 annual report, the Board
announced its intention to appoint a Superintendent of Domiciliary Services who would be
responsible for coordinating and supervising the work of the staff. It was the first identified
separation within the management structure and part of the Board’s recognition that Nurse
Maude as a competent, efficient health organisation needed a structure that was built on
well-coordinated lines in keeping with modern business practice.
‘It is widely recognised that a major objective of domiciliary services is to relieve the burden
on public hospitals by enabling people to remain in their own homes whilst undergoing
treatment and to permit early discharge for those who must be admitted to hospital,’ the
report stated. ‘It is not widely recognised however, that the provision of these services, is, to
a considerable extent, an open-ended commitment particularly in district nursing, as the
service has to be ready to meet any demand that arises, as it arises. There can be no
question of putting people on a waiting list for the district nurse. It is becoming increasingly
apparent that suitable cases can be well and economically cared for at home, thus relieving
the pressure on hospital accommodation and providing for better care for those for whom
hospital treatment is urgently required.’158
During the year, nursing visits surged forward to a total of 120,378. At the same time, home
aid and laundry visits totalled 42,588, a six per cent increase on the previous year. It was
obvious the two services paralleled one another. Links with the Red Cross, Aged People’s
Welfare Council and Christchurch Hospital continued as before. The Board pursued its
plans for extensions to the Memorial Hospital which would take bed capacity over the two
facilities up to 95. It submitted its plans to the Department of Health for approval. Subject to
158 Nurse Maude District Nursing Association Annual Report 1970

[84]
basic planning requirements, the Department agreed to the proposed extension. The plans
included 40 new beds with new kitchens, a dining room, lounge, laundry and the most
modern facilities for the comfort and benefit of patients. The estimated cost was between
$130,000 and $140,000 of which $40,000 was a gift from Jack Ferrier159 and his family with
the promise of a further $20,000 when required. It was an exceptionally generous donation
which was gratefully accepted by the Association.
True to its word, the Board advertised for, and then appointed a Superintendent of
Domiciliary Services. Nancy Tait took up her position in August 1970. Educated at
Christchurch Girls’ High School, she had graduated from Christchurch Nursing School and
gone on to complete her maternity training in Nelson. After a two-year stint in the Australian
outback, she had joined the New Zealand Department of Health before returning to
Christchurch as the medico-social worker. During her 16 years there, she had covered both
Christchurch and The Princess Margaret Hospitals. Her personal philosophy mirrored that of
Nurse Maude.
‘Nursing must move out from hospitals more extensively into patients’ homes, as the
demand for hospital beds continues to increase,’ she was reported as saying prior to
beginning her new work. Many chronically sick patients could return to their own homes if
their relatives were given more help from ancillary medical services. Elderly patients who
could be discharged often had no available relatives to help them and as a result, they
became very worried about their future. It was an area familiar to Nancy Tait and the Board
was satisfied that in her appointment they had found the right person for the job.
In July 1971, the old premises at Madras Street were put up for sale. The land and buildings
were to be auctioned at the end of August. The Association was moving its entire
administrative operation to Merivale. It was a major change. While the deeper philosophy of
the organisation would always exist, the physical links with Sibylla Maude and the early days
of district nursing in Christchurch were about to be severed. Discussions about the possible
shift had been mooted several years earlier when the difficulties of having premises at either
ends of the city were first recognised. At the time though, the Association’s work was
predominantly in the poorer suburbs of Woolston and Sydenham. Time and the city’s growth
had changed that.
While there had been a definite separation between the administration and its actual
operations, it was time consuming nonetheless to go from McDougall Avenue to Madras
Street. Besides, the different services particularly home aid, had grown to such an extent
that car parking was becoming a major problem. The headquarters were to be shifted to
Mansfield Avenue. The block of land that backed onto the Memorial Hospital in McDougall
Avenue and alterations to the existing building would enable the facilities to be linked
together.
The move signalled the end of an era for the Nurse Maude District Nursing Association and
the beginning of another. It was not just a physical shift or the identified difference between
management and operational services. It was recognition that the Association in the 1970s
was very different from its origins. Yet, it was not a philosophical move away from the
159 Jack and Marjorie Ferrier were philanthropists and dedicated to supporting people in need.

[85]
principles and values that Sybil had espoused from the start, endorsed by Walter Averill,
Edwin Scott and her friend and mentor Jessie Heaton Rhodes. Its growth in all areas was
significant. It was recognised by an Act of Parliament. It had contracts with the North
Canterbury Hospital Board that required monitoring, reports and financial controls on a much
greater scale than before. It had accountabilities not only to the patients it served but to its
financial stakeholders. It was a different world.

[86]
Part Three - Health Reform
‘Sometimes to relieve
Sometimes to heal
Always to console’
Sibylla Maude

[87]
Chapter One: The Best of Times
Severing Links with the Past
The decision to sell 192 Madras Street effectively severed some of the closer links with the
past. Where would matron live? Gone was the upstairs flat with its homely sitting room, its
tiny attic which served as a washhouse and its flat roof where successive matrons had hung
their washing out to dry, hidden from street view. Gone too was the well-worn path past the
commemorative plaque honouring Jessie Heaton Rhodes, Sybil’s childhood friend and
mentor. Equipment and office furniture could be easily transported to the new premises, but
the memories were not so easy to shift. The relationship between the Sisters of the
Community of the Sacred Name who had lived so close to Sybil and Rose in Barbadoes
Street, and who had supported them in their hours of need had long gone, but there had
been a spiritual closeness between the two households living at both premises which had
remained.
What would it mean for the district nurses? They were the stalwarts of the organisation – its
public face. The hospitals might earn more money but it was district nursing that carried the
candle for Sybil’s ideals, her principles and her philosophy.
It was a question of economics however, and having a centrally based administration,
adjacent to the Nurse Maude Memorial Hospital and closer to Averill House had become a
necessity. There were several houses on the Mansfield Avenue property and the Board
intended altering and extending one of them to accommodate offices and meeting rooms.
This would become the new headquarters for the domiciliary services and there would be a
separate house for the matron of the hospital if she wished.
In December 1972, the extensions to the hospital finally started. An additional 42 beds were
to be accommodated including a new ward for psycho-geriatric patients as well as
physiotherapy and occupational therapy facilities. The Chairman of the North Canterbury
Hospital Board Dr Leslie Averill was invited to lay the foundation stone. There was some
symbolism in the act, Dr Averill being a son of Sybil’s great friend and early supporter
Archbishop Walter Averill.
‘In all other centres throughout New Zealand, the local Hospital Board has the direct
responsibility of organising and maintaining a district nursing service. In Christchurch,
although the Hospital Board is responsible for 75 per cent of the cost of the district nursing
service and 100 per cent of the cost of the home aid service, yet the Hospital Board has
been very happy to leave the management of both of these services in the capable hands of
the Nurse Maude Association,’160 he said. What he omitted to say was that in any other part
of New Zealand where a Hospital Board was responsible for the district nursing service, the
state paid the full 100 per cent subsidy. Only historical practice had prevented the same
happening in Canterbury.
160 The Press Christchurch Women’s Section 5 December 1972

[88]
The Mayor of Christchurch Neville Pickering also attended the ceremony. In his words, ‘a
great deal of foresight had gone into creating a haven for a large number of people in
need.’161
It was true, but it was not only planning; large sums of money were needed to complete the
double-storeyed extensions. The government was contributing $360,000 of the total cost
which was estimated at the time to be more than $650,000. While the fund had received a
considerable boost from the Jack Ferrier Trust, the Association still had a lot of money to
find. Of course, the other work continued and with it the necessary fund-raising just to make
ends meet. It was going to be a difficult year, made the more so by Denis Cotterill’s pending
retirement. He had been in the chair since 1947, often acting as Chairman during Sir Heaton
Rhodes’ tenure, who in his later years was frequently absent due to illness. Denis was then
elected Chairman following Sir Heaton’s death in 1956. The Association had experienced its
most prolific period of growth and development through these years and Denis was
attributed with playing a major role at the time. He was of course, ably supported by Mona
Corkill who was also intent on increasing Nurse Maude’s community profile. Together they
had been a formidable team pursuing projects that often seemed almost impossible to
achieve. The home aid service, the laundry and the establishment of the two hospitals were
all inaugurated in the 1950s.
More than this however, Denis had the capacity to steer a diplomatic path through what were
often rocky roads. He was familiar with the workings of the North Canterbury Hospital Board
and personal friends with some of the key decision makers. Being a partner in the
successful law firm of Duncan Cotterill also paid dividends for Nurse Maude, and his
knowledge and experience were critical during the lead-up to the Association’s Act of
Parliament. His wisdom and good counsel would be missed.
The Association recorded a deficit of nearly $28,000 that year. As in previous years, district
nursing continued to make a loss but this was off-set by the high occupancy rates at the
hospitals and an increasing number of bequests from an ever-supportive public. Much as
the Friends of Nurse Maude kept their raffles going however and maintained their cake
stalls, it was never enough. Unfazed, the organisation continued its work.
As always, the retirement of a long-serving nurse warranted public recognition and the local
media were only too happy to oblige. When Lorna Kilty left after 22 years as a district nurse,
it was an opportunity to highlight the work the nurses had done over that time and the
changes that they had observed. Sister Kilty had started when Mona Corkill was matron.
She was the twelfth nurse to be enrolled – there were now thirty. Her patch had covered
Shirley, Papanui and Fendalton and she had routinely attended an average of 15 patients a
day with tasks including sponging, bathing, injections and dressings. ‘I have always been
fond of elderly people,’ she commented. ‘They need help and are always so appreciative.’162
161 The Press Christchurch Women’s Section 5 December 1972 162 Christchurch Star 27 November 1973

[89]
The White Paper
Nationally, the health sector remained in the public eye. Earlier in 1972, changes to social
security benefits began to impact on the home aid service. A Royal Commission on Social
Security had recommended changes to the benefits which impacted on women who were
supplementing their benefit while employed by Nurse Maude as home aids. The women
were receiving benefits as deserted wives, widows or wives of beneficiaries. Their allowable
income was reduced by three dollars a week or by five dollars a week if they had dependent
children. Anyone on Social Security benefits who earned $25 or less suffered an abatement
of benefit of one dollar in every two over the ten dollar per week allowed. An income
exceeding $25 per week had an abatement rate of three dollars in every four over the $25
limit. The new regulations posed problems for home aiders who could only work for eleven
hours a week to earn ten dollars if they were on a benefit and had no other unearned
income. During that time, the aid might do three hours’ work three times a week and an
extra two hours duty.
‘Most of the women are capable of doing considerably more,’ said an irritated Nancy Tait.
As superintendent of the Association’s domiciliary services, she was faced with home aiders
having to stop work because of the new regulations. ‘Fit and vigorous women in their forties
can do about 20 hours a week for us and still be home before their school aged children, and
fulfil their other home obligations. They want to work longer hours and we need them – but
in many cases they feel it is not worth their while when restricted to earning $10 a week.’163
The issue did not stop there. While Nancy Tait agreed that a woman with no dependents
who was fit and who wished to work fulltime, did not need to claim the social security
benefits she might be entitled to, if the same woman became ill and could not work she
would have to wait months before she could get a benefit. In the meantime, she might be
living on a reduced pension and have no other money coming in.
'We know of such cases,’ she said. ‘As I see it, it is easy enough to give up a benefit but
difficult to get it fully reinstated.’ Although Nancy pleaded the case eloquently and publicly,
the Department of Social Welfare was unrepentant. A home aid earning $20 a week under
the new exemption rate would have a $5 per week deduction from her benefit. This would
leave her with $15 out of $20 a week. If she gave up work, she would lose that $15
altogether, was the Department’s response. It was a no-win situation for many of the home
aiders. Nancy was now the Superintendent of Domiciliary Services, a reviewed position
which carried with it overall responsibility for all areas of the Association’s domiciliary and
hospital work. In the Board’s collective opinion, the position considerably improved the
management control of the whole organisation. She had no hesitation in speaking out
publicly on a benefit system that, in her opinion, was flawed.
During 1974, the revenue from Nurse Maude’s two hospitals was greatly improved due
mainly to a special geriatric subsidy of $2.50 per person per day which had been introduced
in July. It applied to nearly all Nurse Maude’s inpatients resulting in some additional revenue
of $48,670 for the year. By November, the hospital’s extensions were nearly completed. In
keeping with tradition, the Governor General Sir Denis Blundell would officiate at the opening
163 The Press Christchurch Women’s News and Views 7 July 1972

[90]
ceremony. The Board appointed a new matron who would be responsible for 76 patients
compared with the existing 38.
‘It is only through the generosity of the public that Nurse Maude survives,’ said Matron-in-
Chief Kathleen Bland in the days preceding the official opening. ‘Every year, it is not the
amount of money that matters but the goodwill of all sections of the community to the
elderly.’164 Short term beds were an important part of care for the elderly, she said. They
were a wonderful help for those who had constant care of elderly relatives.
Praise was heaped on Nurse Maude at the official opening ceremony. Guest speakers took
it in turns to compliment the Association on its initiative and to refer yet again to the
spadework of its founder. New Zealand was fortunate in that the vast majority of people
accepted the formula of ‘love thy neighbour’ as being a normal part of the way of life, Sir
Denis told the assembled guests. Some people dedicated their lives to helping others.
Nurse Maude had been a ‘remarkable person who seemed to combine inspired
understanding of special needs that had been ignored by others, with devoted zeal for
putting that idealism into reality and practice. New Zealand, and Christchurch in particular,
had benefited from the district nurse at times when they had been needed.’165
It did not take long for the hospital staff to appreciate the difference made by having a
purpose-built facility. The settling in period over, it was time to consolidate services. The
maxim applied as much to the domiciliary services as it did to the hospitals. Everything with
the exception of Averill House was now operating from Mansfield Avenue. The Board met
regularly on site and with few exceptions, changed little in membership for the next three
years. Ably led by its new Chairman Rod Compton, it concentrated on getting the
Association’s finances in better order. In this, it was helped by an increase in the
Department of Health’s patient subsidy administrated by the North Canterbury Hospital
Board and which came into effect at the beginning of the following year.
But events were happening at a political level that signalled major changes in the health
system were on their way. In 1975, the Labour Government released its white paper A
Health Service for New Zealand which spelled out the need for a radical restructuring of all
aspects of health. New Zealand could no longer claim its former international leadership in
the provision of health care. ‘Hard though it may be to accept, New Zealand has never
attained a national health service, although such a service is often quoted,’166 stated the
government’s paper.
There were two references that interested Nurse Maude. In a special section devoted to the
voluntary sector, the paper commented on the integration that had taken place between
voluntary agencies and the state mainly through subsidies. Yet the state had been ‘reluctant
to assume responsibility for their provision in a coordinated and uniform manner.’167
164 News Advertiser 29 October 1974 165 The Press 20 November 1974 166 Government White Paper on Health 1974 p 83 167 ibid
[91]
In another section, the paper talked about private health services, identifying nursing in a list
of what it termed state-subsidised services. The Board was heartened by a comment in the
white paper which seemed written with the Association in mind. ‘It is not the government’s
intention to destroy the role of private organisations in the health and welfare fields…168
The proposed restructuring of the health sector would put people first. Hospitals, primary
care services and community care came next and the chart worked its way down through a
maze of functions with Regional Health Authorities reporting to the Minister of Health.
Regional Complaints Commissioners and an Ombudsman for Health completed a structure
that spelled the end of the existing system. New Regional Health Authorities would have a
mix of six appointed members and seven who were publicly elected but would not be
replacements for existing Hospital Boards. In essence, it was a split between the fund
managers and the service providers. Historically, there had always been apathy when it
came to local body elections and Hospital Boards were no exception. There were plenty of
statistics quoted in the white paper to prove the point. In many areas of the country there
were no elections because no nominations were received. Furthermore, in some parts of
New Zealand, government appointees were used to ensure the requisite number of people.
The date set for the introduction of the proposed changes was 1 April 1978. In the
meantime, consultative groups would be set up in February 1975 to discuss the issues
outlined in the paper. There were social and political ramifications which Nurse Maude as
an identified state subsidised service would need to come to grips with in order to make
submissions to the consultative groups. More importantly, the Association needed to know
where it might fit in the proposed new structure. Obviously the North Canterbury Hospital
Board would be substantially affected by any move to change the health system. What
would happen to Nurse Maude?
In fact, there was little if any impact on the day to day workings of Nurse Maude, because in
spite of consultative groups being set up and options proposed, there was a change in the
government of the day and the white paper effectively languished. It did send a message to
the health sector however, that even if change had not happened now, it would definitely do
so in the foreseeable future.
In his annual report to the Board in 1975, Rod Compton confirmed the Association’s long-
held belief that elderly people were better served by staying in their own homes than being
shifted into residential care or long-stay care. It depended on their health and the care that
was available. There was clearly a substantial financial advantage in addition to other
benefits in keeping people at home for as long as possible, he said. The margin was
sufficient to justify some expenditure by the state on houses to make them suitable for the
people concerned to live in them. Provision of ramps, handrails and wider doorways were
good examples.
‘In suitable cases an expenditure of a few hundred dollars might well save two or three
thousand dollars in hospital costs by postponing or eliminating the need for admission to a
residential home or hospital,’169 he said.
168 Government White Paper on Health 1974 169 The Nurse Maude District Nursing Association Annual Report 1974

[92]
As usual, the annual report was the vehicle by which the Association could tell its public
what it had achieved during the year. For the third year in succession, the two hospitals
could not meet the demand for beds and patients were regularly turned away every month.
As a result, the Association submitted a new application to the Minister of Health for
approval to build further extensions to the Nurse Maude Memorial Hospital. For the first time
in several years, the hospital revenue showed a surplus. While it was mainly due to the
increase in patient subsidies, it demonstrated well enough the benefits of appropriate
funding. The geriatric payment for patients in private medical hospitals which provided day
and night care, had increased to $4015 a year for each patient. But even so, it still did not
cover the full cost or the fees that had to be charged.
District nursing for the year had covered some 105,906 visits to over 3,000 patients with
4,000 of them receiving home help as well. The nursing service had cost $286,040 which
worked out at $90 per patient per year. If the home aid was included, the cost increased to
$114 per patient. In addition, more than 800 patients received home aid assistance under
the Association’s home-aid fee-paying service which cost $205 per patient. The overall
deficit for district nursing remained high at more than $48,000 but it was $4,000 less than the
previous year, the Board announced.170
Of special significance was the appointment of a part-time midwife. Sibylla Maude had
always hankered to provide a midwifery service from her first days as a district nurse and in
her impetuous way had rushed off to England to complete her training despite her
committee’s protestations. But her personal workload and her committee’s objections had
stymied the project and nothing had happened – until now. It was a proud moment for the
Association. Nancy Tait had correctly interpreted the new mother’s need for a service which
catered for her in much the same way as the Plunket Nurse looked out for the baby. There
was no other similar service in Christchurch and, like many another Nurse Maude initiative, it
was a pioneering start to domiciliary midwifery in the region. It was not without its critics
however, particularly from the Association’s ‘friendly foe’ – the medical profession who gave
it at best, wary approval.
In 1977 Ethel Mazins retired. She had been matron of Averill House for twelve years and
like her predecessor, had found the experience immensely rewarding. Occupancy at the
hospital remained extraordinarily high over the period and potential patients were frequently
turned away. Plans were well advanced to increase accommodation at the Leinster Road
premises which would enable an additional four beds to be completed by the end of the
year. While the costs of beds continued to rise, Averill House rates had increased by three
dollars during the year. Bed usage was high with the average length of stay up to 57 days.
It was clearly more than a short-stay hospital but then the problem became funding for the
longer term care they might require which was, of course, provided by the Hospital Board’s
own facilities at Jubilee, Coronation and Lyndhurst171 Hospitals. It would often take several
weeks for the subsidies to be approved. Nurse Maude’s Board sounded a warning that
continually rising costs would eventually force an increase in fees.
170 ibid 171 Lyndhurst was a private hospital from the 1920s to the mid-1950s. It was converted to a residential care facility for elderly women in 1969 by the North Canterbury Hospital Board.

[93]
New Services are Introduced
During the 1970s, the Nurse Maude Board had undergone several changes. Conservative
in its approach and outlook, it tended to attract a membership that stayed the long distance.
There were family connections that dated back several generations to its original Anglican
roots. Once appointed, members found they enjoyed the challenges and the genial
atmosphere that prevailed most of the time. Many of them were friends or acquaintances in
business and of course there were those who were appointed by the North Canterbury
Hospital Board. One of the long-term members was Jean Taylor. She had retired from
nursing in 1969 with an OBE for her services, and was well known in Christchurch health
circles having trained and nursed in the city in the 1930s and then returned as assistant
matron at Christchurch Hospital. She had been matron at Burwood Hospital and then The
Princess Margaret Hospital before taking up the position of Matron-in-Chief for the Auckland
Hospital Board. She brought a wealth of nursing knowledge and background to the Board at
a political as well as a management level and was well equipped to comment, not always
favourably, on a system that she said required changing. She could recall the district nurses
during her tenure at Burwood and Princess Margaret Hospitals and had some sympathy for
their issues. For her, the prospect of health reform was exciting. Hopefully it would enforce
the changes that were sorely needed particularly in hospitals.
‘A lot of money was wasted under the Hospital Board system,’ she said in retrospect.
‘Requests for complicated equipment were approved with very little discussion. The Board
members used to say they were only lay people and therefore could not refuse requests
from specialists. It was quite a different matter when nursing staff were ordering new
supplies of bed sheets and bed spreads. Much discussion took place and examinations
were made of every article.’172
A keen supporter of Nurse Maude, she applauded its efforts to work within the system often
against stringent criticism from others in the health sector, and commended the staff for their
initiatives of the 1980s became apparent. ‘We are very much a living organisation,’ she said.
‘Our strength is our social conscience which it has to balance with the economies of the
day.’173
At the beginning of 1978, Denis Cotterill died. He was remembered in a special tribute by
the Board. It was also a time to record the long and dedicated service of several other
former Board members and senior staff. Mr Wellbrook had died as had Kathleen Bland.
Elsie Simpson who had done so much sterling work in the formative years of the home aid
and laundry services had died just a month before Denis Cotterill. They had all maintained a
lively interest in Nurse Maude after retirement and were given due recognition by the Board.
From the beginning, its annual meetings were always faithful records of people who had
made a contribution to the Association.
Meanwhile staffing levels across the organisation continued to rise. By the end of March
1978, there were 59 district nurses, 227 home aiders and a further 104 people employed at
both hospitals. The administration had grown to a staff of 15. How different it all was from
172 Jean Taylor: Personal recollections: interview July 1996 173 ibid

[94]
the early days. While the hospital service remained dedicated to the care of the elderly,
there were changes in the district nursing services which now included Ellesmere in its rural
areas. The pending appointment of a coordinator of geriatric and domiciliary services was
announced to bring about a ‘more efficient use of available resources and a reduced reliance
on institutional care.’174 It was to be a Hospital Board appointment although the person
would be based at Mansfield Avenue. Nurse Maude had introduced a liaison service
between Christchurch Hospital and The Princess Margaret Hospital the year before and this
proved to be a bonus for patients who were being discharged.
As it had done in 1977, the Board used its annual meeting as an opportunity to comment on
the alarming increase in sporting injuries and motor accidents which were resulting in more
young people being disabled. In large measure, this was due to the Accident Compensation
Commission legislation. ‘We emphasise that this is laying an increasing and largely
unnecessary burden on the health services and at the same time seriously reducing the
capacity of the victims to play their part in supporting the community.’175 It was a comment
more pertinent to community health than district nursing and demonstrated the wider interest
the Association was starting to take in the health and welfare of the community at large.
During the year, two initiatives were successfully promoted by Nancy Tait. The ‘night sitter’
service was designed to give a night off to relatives and care givers who looked after
patients at home. Special training programmes were introduced for the women who put their
names forward. The service was free to the public and funded by a limited community
health grant to the Association. According to Nancy, health needs did not begin at 9am and
finish at 5pm. Patients often required care on a 24 hour basis.
The introduction of the cancer nurses was a further specialist nursing service. Their role
was to give supportive care to patients who were terminally ill and who wanted to stay at
home. The nurses were responsible for coordinating the other care and services they
needed and they liaised with the doctor involved and the hospital which provided the
treatment. They were an immediate success as much for their nursing skill as their ability to
give support to the relatives. The service was the small beginning of a wider palliative care
programme which would culminate in hospice facilities being built in the 1990s.
Like the new midwifery initiative, the introduction of the cancer nurse was looked upon with
some suspicion by the medical profession. Never overtly critical of Nurse Maude, it
nonetheless made it plain that doctors were there to give clinical advice and nurses were
there to follow the orders.
As it approached what was going to be a tumultuous decade in health, the Association was
still returning an annual deficit. It was only the continued income from bequests that kept it
from financial crisis. In its report for the year ending 31 March 1979, the Board recorded an
overall deficit of $102,831.00. It was substantially higher than in any previous year.
Bequests offset this amount by $105,690.00.176 It was a small profit but enough. Again the
district nursing service showed a loss and overall the hospitals did as well. Salaries, wages,
174 Nurse Maude District Nursing Association Annual Report 1978 175 ibid 176 Nurse Maude District Nursing Association Board Report 1979

[95]
car and travelling expenses accounted for the major part of the increased expenses.
Although occupancy rates at both hospitals remained high, costs per patient day had
increased, again due in part to wage increases but also due to unexpected increases in
power prices.
Clearly one of the major stumbling blocks to get to a break-even point financially, was the
amount of money paid by the North Canterbury Hospital Board for its contracted services.
Having to go cap in hand to the general public every year was not only a major exercise by
itself, it was simply not returning enough. Commenting (yet again), on the proposed
extensions to the Nurse Maude Memorial Hospital, Rod Compton said the government
subsidy still had not been approved and although preparatory work had been completed, the
main work could not start. Such delays were a frustration to the Board but the bureaucratic
machine did not always work in its favour.
Mary Renwick resigned during the year. Like many staff in the organisation before her, she
had devoted a large part of her working life to Nurse Maude, starting as a district nurse more
than 25 years earlier. The secretary Brian Johnstone also retired, but he was not leaving the
organisation having accepted an invitation to join the Board. Maybe because of its
constitution and the stipulation that there should only ever be four women members at any
one time, or maybe because no one had ever considered it, not one of the retiring senior
nurses was ever offered a place on the Board.
The Association had redefined its operating structure when Nancy Tait was appointed.
Based on an earlier recommendation from the Department of Health when it had
investigated the organisation prior to the Act being passed, a more streamlined management
system had been introduced. While still at Madras Street, Nancy was in charge with the title
of Superintendent, domiciliary services. Mary Renwick was responsible for the district
nursing services and Amelia (Millie) Slater was in charge of the home aid and laundry
services. Kathy Bland was Matron-in-Chief of the two hospitals and there was a matron at
each – Dorothy McLenaghen at Nurse Maude Memorial and Ethel Mazins at Averill House.
Operationally, it worked extremely well.
Nancy Tait, Mary Renwick and Millie Slater were initially based at Madras Street as was the
secretary Brian Johnstone. With the decision to move premises came the issue of where to
house the administration. It was decided, given the size of the land now owned, to use No
15 Mansfield Avenue as the new headquarters address. It became the base for all
domiciliary services and the secretary’s office. A separate entrance for the hospital was
accessed from McDougall Avenue. The two streets ran parallel to each other which was in
all respects, an added bonus to the organisation, staff, patients and visitors.
Mary Renwick’s retirement gave the Association the opportunity to streamline its
management a little further. The position of Matron-in-Chief had been disestablished in
1974 when Kathy Bland retired. Now Nancy Tait’s title was changed from Superintendent to
Supervising Principal Nurse. Coral Gardiner was appointed Supervisor of the district nursing
services and the home and linen (formerly laundry) services were supervised by three staff –
Val Houghton, Joy Bigwood and Ruth Wright. Joan Duffey was Matron of Nurse Maude
Memorial Hospital and Anne Lassen appointed as Matron at Averill House.

[96]
For many years, the Association had included in its annual report a special section for The
Friends of Nurse Maude. A central part of its work from Mona Corkill’s time, it was these
women who maintained the link between the Community of the Sacred Name and retired
members of staff, many of whom became ‘Friends’ themselves. They were the social side of
Nurse Maude, keeping it in the public eye with well organised events and activities. Warm
and embracing, they worked untiringly and were responsible for the visitor service at both
the hospitals. Between them they had years of combined knowledge of the organisation and
could quote its journey from its earliest beginnings to the present day.
Averill House
Many of the long-term Board members were starting to look back nostalgically on the 1960s
and early 1970s which, in hindsight, seemed remarkably simple compared with the problems
which were now beginning to dog the Association. Although the practical work continued
and new ideas were always being considered, funding remained the critical issue. For
years, professional health care in New Zealand had been provided through public and
private funding. In the 1980s, the question of the proper balance between state and market
in health care became controversial.177 The questions were asked. Should the state concern
itself only with the access of poorer people to some basic level of care or should it seek
equal access for all? Should the state be in the business of providing health care or was it
something that could be better done through private firms competing in a health care
market?178 These were vexed questions and everyone had an opinion to offer.
The Minister of Health George Gair paid Nurse Maude a visit in 1981. Nancy Tait was
overseas at the time. On her return, she was greeted with the news that the government
subsidy could not continue at its present rate ad infinitum. The Minister had made it quite
plain that while the work of the Association was a valuable part of the health service
generally, it would have to learn to live within its budget. It was no surprise to Nancy but it
was a frustration for the Board. For years it had tried to have a funding system that was in
keeping with other district nursing services around New Zealand. Unfortunately, the legacy
of its founder, that her public could be counted on to help out in times of need, was a
stumbling block to change. At the same time, the Board recognised that the Minister was
not pointing the finger at Nurse Maude in particular. The cost of public health had leapt up to
unmanageable levels throughout the country. Everyone was grappling with similar
budgetary issues.
It took some doing, but two years later, Rod Compton announced the Association’s deficit
had been pared back to a mere $8,000, compared with a forecast loss of $200,000 the
previous year. It was a magnificent effort, he said. ‘It is not easy to decide who gets the
care we are funded to provide, but I am sure the public will understand the position the
Association is in.’179
177 Spoonley Paul, Pearson David, Shirley Ian. ‘New Zealand Society.’ Dunmore Press 1990 p 158 178 ibid 179 Nurse Maude District Nursing Association Board Report 1983

[97]
Under the prudent eye of the Board’s Finance Committee and with a tremendous effort by
Nancy Tait and her team, the budget was at last well under control. Visits by the district
nurses had been reduced during the year by more than 14,000 but importantly, the number
of visits from the district cancer nurse, the diabetes district nurse, the night sitter service and
the midwifery nurse had still increased. The latter had seen an astonishing leap from 2,180
the previous year to 7,100 visits. If ever there was justification for the service, this was it.
Similarly, there were ongoing supportive comments from the community for the cancer nurse
service. The Canterbury branch of the Cancer Society had been giving generous financial
assistance to the service since 1979 and had donated a car in 1981 as part of its
commitment to the initiative. It was this collaborative approach to district nursing that helped
not only the Association’s good relations with other non-governmental organisations, but
also contributed to sharing the budget burden.
There were some changes amongst the staff with Nora Kemp replacing Anne Lassen as
matron at Averill House and Barbara Stanton taking over the position of Supervisor of the
District Nursing Service following the untimely death of Coral Gardiner. She was
accidentally killed while climbing Mt Aspiring in the Southern Alps. Coral had been
instrumental in the introduction of the district cancer nurse and the night sitter services and
her death was a terrible shock to everyone.
Nancy Tait retired with a unanimous vote of appreciation for her achievements during her 13
year term as Supervising Principal Nurse. She was leaving at a time when the organisation
was maintaining its presence in the community and coming to grips with its contractual
obligations. Responsible for all nursing services, she had been at the forefront of the
turnaround Nurse Maude had experienced. Diane Barnes who had nursed at Burwood
Hospital was appointed as her replacement.
The new year saw an old family connection coming back to the Association. Colin Averill
was a grandson of Sibylla Maude’s great supporter and mentor Archbishop Walter Averill.
Colin’s father Leslie Averill had a long and distinguished career in medicine and had served
as the Chairman of the North Canterbury Hospital Board from 1956 to 1974. It was as if the
wheel had turned full circle. Colin took over as Nurse Maude’s Board Chairman just prior to
the end of the financial year in March 1984. Rod Compton remained on the Board as did
Campbell Ballantyne, Dr Calder Botting, Dr John Holmes, Roger Farrant, Tom McGuigan
and Ralph Wylie, the latter for only a brief period however. He resigned from the Board after
being appointed a judge of the Supreme Court. The four women members were Caroline
Cartwright, Jean Taylor, Betty Webb and Joyce McIvor.
As with the previous year, the Association’s finances continued to improve. For the first time
in many years, the Board reported it had achieved a surplus for the year’s operation. In its
notes to the financial statements attached to the report, was the usual summary of fixed
assets and the endowment fund. In 1983, the total amount in the fund had tipped the $2
million mark. In 1984, it passed $2.4 million. The improvement had not come easily, Colin
Averill said later.180 There were staffing issues to be resolved and the hierarchical structure
of the organisation needed some attention.
180 Interview with Colin Averill January 2015

[98]
In a low-key statement, Colin also announced that Averill House would close as soon as the
extensions to Nurse Maude Memorial Hospital were completed. A new floor was being
added to the hospital which would be able to accommodate all the male patients. The
advantage of having the entire hospital operation on one site, with the administration block
adjacent to it, would be significant for the organisation. It would streamline their operations.
There would be a period of transition while the changes were being made and it was
probable that Averill House would be sold, but in the meantime there would be ‘no diminution
in the hospital accommodation available.’181 The new ward on the top floor of the hospital
would be dedicated to Walter Averill.
The Friends of Nurse Maude recorded the death of Mona Corkill in their annual report. ‘She
leaves behind memories of an irrepressible sense of humour and a warmth of friendship and
caring. Our greatest tribute to her must surely be continuing to be good ‘Friends’ and loyal
to her ideals who in 1953, saw the need for our organisation.’182
The news that Averill House was going to close had a mixed reception. Not everyone was
happy about the proposed sale. It had been part of the organisation for 25 years. Not only
were patients fully satisfied with their care, the level of support for the hospital was
evidenced by its continuing high occupancy rates since its establishment. Seldom if ever,
had it dropped below 95 per cent. The idea of transferring patients to the McDougall Avenue
hospital had been first discussed during Nancy Tait’s tenure. While she heartily endorsed
the move, believing Averill House to be out on a limb in Leinster Road, she had recognised it
would not be a popular decision.
During the year, the Association began the mammoth task of replacing its aging vehicle fleet.
The Austin Minis had zipped around Christchurch’s and Canterbury’s roads for several years
and were as synonymous with Nurse Maude now as the black bicycles had once been.
Preparations for the 50th anniversary of Sibylla Maude’s death also began. The building
programme continued at the Memorial Hospital and plans were put in place to sell Averill
House. When the New Year’s honours list was posted, Rod Compton’s long association
with Nurse Maude was acknowledged with an OBE. As was the continuing trend, the Board
reported another surplus for the year ending 1985 albeit a small one. But the bigger problem
lay with district nursing. An essential service to the community with Lincoln now added to
the rural districts, it nevertheless continued to run at a substantial loss. The deficit now
exceeded $230,000. It was only the donations, the legacies and bequests that kept the
books balanced. The Board decided it was time to revisit the Act of Parliament under which
it operated. It would seek a legal opinion as to the amendments it wished to add.
On Friday 12 July 1985, a service of thanksgiving was held in ChristChurch Cathedral. It
was an appropriate choice as Sybil’s father Thomas Maude had been a founding member of
the Cathedral Chapter. The Maude family in Christchurch had stayed true to their Anglican
heritage dating back to their ancestors in England. Now, the service was a time to
remember Sybil’s early work as matron of Christchurch Hospital, the first registered nurse in
the city and the pioneer of district nursing. ‘The light kindled by her service over 50 years
ago is not extinguished. It burns brighter than ever, fuelled by the grateful and affectionate
181 Nurse Maude District Nursing Association Board Report 1984 182 Nurse Maude District Nursing Association Annual Meeting 1984

[99]
admiration of the people of Christchurch who honour her memory,’183 wrote Caroline
Cartwright in the Christchurch Press.
The memorial service was conducted by the Dean of Christchurch, the Very Rev Dr David
Coles. There, seated amongst the congregation, was a small group of Sisters from the
Community of the Sacred Name. Also in the Cathedral was the Vicar of St Michaels, Canon
Baker. It was a symbolic gesture, recognising the contribution the parish had made to
Sybil’s work in her early days under the leadership of Walter Averill.
‘What a remarkable woman she was,’ Rev Coles began. ‘When she made her will shortly
before she died, she tried to stipulate that having lived and worked among the poor, she
should have a pauper’s funeral. Her lawyer persuaded her to remove the clause for when
she died, rich and poor alike came in their thousands to her funeral in this Cathedral.’184
Others spoke of her work and the development of the service she had so enthusiastically
started. But, nothing made quite the impact that her old car did, displayed at the base of the
Cathedral’s steps. The freshly cleaned and polished Austin 7 had been secured for the
Association by the ever-dedicated group of ‘Friends’ who had raised the necessary $11,000
with the assurance from the Ferrymead Museum that it would be responsible for its
maintenance and upkeep.
183 Cartwright Caroline, The Press Christchurch. July 1985 184 David Coles, Memorial Service ChristChurch Cathedral 12 July 1985

[100]
Chapter Two: Restructuring in the 1980s
Health Reform Looms Large
The Nurse Maude District Nursing Association has ‘more patients than Christchurch public
hospital’ was the headline in a local paper in mid-1980. ‘With a staff of 85 nurses at charge-
nurse or ward-nurse level and a fleet of 30 cars, Nurse Maude is on duty 24 hours a day,
seven days a week. Full time district nurses visit between 8am and 5pm not only carrying out
doctors’ or surgeons’ instructions, but sharing their professional techniques and nursing
skills with relatives. When they go off duty they hand over to the evening team of part time
nurses who visit between 6.30pm and 10.30pm helping put patients to bed and completing
the treatment for the day. Through the night, there is always a nurse on call.’185
The article, while a positive, public affirmation of the many services offered by the
Association, unwittingly hit upon the very problem Nurse Maude was beginning to
experience. There were in fact too many nurses at charge or ward level and it was
beginning to impact on the wages and salaries the organisation had to pay.
‘Without our benefactors, there is little doubt that the Board would find it difficult to maintain
the high level of services which it endeavours always to provide.’ It was the perpetual theme
of the annual report throughout the first half of the 1980s and 1986 was proving to be no
different. Colin Averill said the Association had decided to review its services and future
directions. A special committee had been appointed for this purpose. Its brief would be to
make recommendations concerning possible extensions to the services currently provided
and in this context, the best use to which an existing plot of vacant land on the Mansfield
Avenue frontage could be used.
‘The Board is determined that the present and future needs in the community must be
thoroughly researched and the Association’s future role in meeting these needs must be
established before any building programme is contemplated,’186 Colin said. It was an
extraordinarily pre-emptive move. The new Labour Government had already signalled
radical change was on its way for the health sector. If the white paper of the 1970s had
failed to progress, its new proposals would. By reviewing its existing services and looking at
future trends, the Nurse Maude Association would be well placed to meet any changes that
were likely to be introduced.
In 1986, Nurse Maude began its emergency service. The Association’s executive secretary
Geoff Bradbury said the new service was designed to give home help to people who might
not have a medical reason for it, but whose social problems meant they might need help.187
The gap had been identified in 1983 by the Mayoress of Christchurch, Judith Lady Hay. She
called a series of home help meetings over the next three years with the aim of forming a
trust with a central office to coordinate all home help in the city. Although this did not
eventuate, an emergency telephone was installed at the Nurse Maude office to cope with
185 The Observer, Christchurch 18 August 1980 186 Nurse Maude District Nursing Association Board Report 1986 187 The Press Christchurch 1986

[101]
any crisis in the home help field. There was no intention of taking over existing services and
Nurse Maude would refer people to the other identified emergency services in the city where
it was appropriate. At the same time as he announced the service, Mr Bradbury also gave
details of the day care scheme which was to be expanded. A new 10-seater mini bus had
been bought to provide transport for elderly people to and from the Nurse Maude Memorial
Hospital. There would be an $8 cover charge which included meals.
While the Association was moving to increase its services, however, the North Canterbury
Hospital Board was suggesting cuts. The Medical Superintendent of Community Health
Services at Christchurch Hospital Dr John Holmes, a former Nurse Maude Board member,
was quoted as saying some patients might face a longer stay in public hospitals because
Nurse Maude would not be able to keep up with the demands placed on its district nursing
service.
‘The pressure has been increasing on the service but because it has to live within its budget,
the Association has, on occasion, been unable to do visits,’ he said. In the previous ten
months, the number of visits had increased 1.5 per cent but the number of referrals had
increased by 20 per cent. ‘At $17 an hour, another nurse working eight hours, five days a
week would cost $600 per week,’188 he said. Implications for hospitals were longer stays by
the patients, increasing cost bed occupancy and a decrease in throughput as a result.
One of the Hospital Board members David Close commented publicly: ‘It must be cheaper to
employ an extra nurse than to keep a person longer in hospital. I don’t accept that the
budget can’t be exceeded. Every month we are told we have exceeded our budgets at the
hospital.’189
But reform was just around the corner and the Hospital Board was not immune from the
changes about to be imposed by the government under Dr Michael Bassett. Budgets had
certainly been exceeded over many years and now a new way of working needed to be
introduced. True to its word, the government had come up with a proposal to deal with the
mounting health debt. Firstly however, the status of the existing Hospital Boards should be
changed. The North Canterbury Hospital Board began the formal process of becoming an
Area Health Board in February 1987 when it resolved to explore the concept and later in
June when it appointed a widely representative steering committee. In March 1988, the
committee reported to the Hospital Board which resolved to establish an Area Health Board
on 1 April 1989. The new organisation should come into effect over the next 12 to 18
months after that.
Nurse Maude began to deal with the pending health changes as the amendment to the
Nurse Maude District Nursing Association Act was passed on 16 December 1987. There
were two fundamental changes. Firstly the reference to the North Canterbury Hospital
Board was amended to mean ‘any Area Health Board or other body which assumes the
functions of the Canterbury Hospital Board.’190 This took into account the proposed changes
188 The Press Christchurch 1986 189 ibid 190 Nurse Maude District Nursing Association Act of Parliament September 1987

[102]
in the health sector. Secondly, the outmoded clause relating to the number of women who
could serve on the Board at any one time was removed.
On 5 April 1988, the report from the Gibbs task force hit the headlines. Produced for the
new Minister of Health David Caygill and Minister of Finance Roger Douglas, the report
entitled ‘Unshackling the Hospitals’ was a clear attempt to deal with the burgeoning
expenditure on health in New Zealand. The report was the work of Auckland business man
Alan Gibbs, together with Dame Dorothy Fraser and Sir John Scott supported by a team of
health and treasury staff headed by the Director General of Health Dr George Salmond and
Treasury Secretary Dr Graham Scott.
‘We have not tried to provide an ultimate solution. We consider the steps set out in this
report are critical for the evolution of the health service,’191 the report said in its introduction.
‘We have not endeavoured to provide an absolute blueprint, but we do believe there is
sufficient detail in our report to enable quick action. There is great confusion at present in the
hospital system about new directions and we consider that this uncertainty must be resolved
urgently.’192
The report commented in detail on long stay and community care, two issues which vitally
concerned the Nurse Maude Association. In the past, government policy had tended to
favour institutional care and there was therefore little funding given to services which allowed
people to remain in the community, even though in many situations institutional care was
more expensive and inflexible, the report said. ‘If this continues, it will not be possible to
provide for the needs of the elderly, mentally ill and handicapped people by the year 2000
without a massive increase in funding.’193
The report commented on the obvious reluctance of hospital staff to change their methods
and the ‘perverse incentive’ many Hospital Boards had for not providing extramural services.
‘Although it is more effective and costs less to treat many patients at home, it also frees up a
hospital bed for another patient on the waiting list thereby increasing the board’s total
expenditure.’194
The taskforce was roundly critical of the lack of liaison between the primary and secondary
health sectors – there was no incentive in the system to improve communications between
the hospital specialist, the general practitioner and the patient, for example. There was a
lack of management information in areas of accounting and costing systems and simply
operating statistics were difficult to obtain and often inconsistent and out of date. As an
inevitable consequence, there was also a lack of cost consciousness.
A radical reshuffling of the health sector was proposed with a Ministry of Health replacing the
Department that would be policy based only, a National Health Commission under whose
auspices the primary providers would fall, and the specific separation of the purchase and
provision of health services. Six Regional Health Authorities would be responsible for buying
191 ‘Unshackling The Hospitals: The Gibbs Taskforce 1988 pp 1-21 192 ibid 193 ibid 194 ibid

[103]
health services on behalf of the government and there would be a range of providers – area
health board, private hospitals and voluntary providers.
Internationally, health organisations both public and private, commented on the proposals.
The British Medical Journal was cautiously positive about the changes, particularly relating
to the suggestion that the new Ministry of Health would deal solely with policy advice to the
Minister. The rest of the system would be funded from central government through a Health
Commission to six Regional Health Authorities on a population basis. The Regional Health
Authorities would purchase publicly funded health services from hospitals and other
providers on behalf of the people in their region. They would not own or manage any
services but would contract with public, private and voluntary providers on a competitively
neutral basis.195
Canterbury moved relatively quickly to establish its new Area Health Board. It was the
second largest of the 14 new Health Boards in New Zealand with a staff in excess of 7,000.
Ron Parker was appointed its General Manager and Gordon Davies its Manager of
Corporate Services. There was yet another team of people with whom Nurse Maude
needed to liaise and engage to ensure its contracts were in place.
As a potential provider of health services in the new environment, the Nurse Maude
Association was extremely well placed, thanks in no small measure to the Board’s
determination to review its operation and endorse the introduction of new information
management systems alongside a revised strategic direction. Information technology was
advancing with speed and the Board recognised it was important not only to utilise what was
available in the market, but to strengthen its governance and management roles by
developing a strategic plan, identifying a new vision and a supporting mission statement. It
might be semantics to the old guard, but it was the new way of developing business acumen
in a more competitive world.
The Association produced an annual plan which would enable it to work alongside the new
Area Health Board. It created a new mission statement: ‘to provide quality community
nursing services, home-based support and hospital care for people within the Canterbury
region.’196
Launching the Foundation
While the Association’s administrative staff were coming to grips with new technology, more
business meetings and renewing its contracts, the work in the community continued to
flourish as before. Domiciliary services now extended to Diamond Harbour and the total
number of visits had increased by nearly 1000 compared with the year before. The work of
the district cancer nurses and the midwifery nurses had increased substantially and the sitter
service gained even greater recognition. At the Memorial Hospital the refurbishment for the
reception area was completed and further improvements to Wards 2 and 3 were due for
195 British Medical Journal Vol 297 12 November 1988 196 Nurse Maude District Nursing Association Annual Report 1988

[104]
completion at the end of winter. A new innovation was the central tray service with pre-
selected menus which would give a wider food choice to patients.
Total hours for home aid increased from 185,277 in 1988 to 202,580 in 1989. After 16
years, Joy Bigwood decided to retire and her place was taken by Helen Leonard in the new
position of Manager, Home Aid Department. Mrs Leonard also took over the role of
Secretary of the home-help liaison group replacing Belinda Lawrence who became the
group’s Chair when Diane Barnes stepped down. The group had continued to prosper since
its establishment in 1986 with 15 different interest groups and community organisations
regularly attending meetings.
In 1989, the Association launched the Nurse Maude Foundation which was designed to give
a more solid financial backing to the business. Announcing the decision, Colin Averill said
the Association ‘had considered its long term future funding requirements in light of the
increased demand on its services and the government-imposed cost restraints on the public
health sector. Nurse Maude’s work was assisted by bequests and donations from many
organisations and individuals, but the Association could not rely on ad hoc levels of financial
support under the current and economic conditions.’197
‘We have agreed we must place our funding requirements on a more secure and
dependable basis. For this reason, we have formed the Nurse Maude Foundation. Its task
will be to act as a controller of finances for all our operations in district nursing and
domiciliary support work. The Foundation will help by attracting and investing funds and by
ensuring that expenditure on Nurse Maude work in the community is undertaken as
effectively as possible.’198
What the Chairman did not say publicly, although the information was not confidential, was
that the Association now had investments totalling well over $4 million. There was always
the concern that the assets would be eaten into to top up funding shortfalls for the public
service Nurse Maude was providing. Bequests were often specified as going towards
identified projects or services, but just as often they were a general expression of gratitude
for the organisation and its work.
‘For many years, we were working with a comparatively inequitable system whereby Nurse
Maude was subsidising the Canterbury district nursing contract by a third of the total cost.
Other district nursing services around the country were fully funded. We realised that we
had to negotiate a better arrangement for our services and at the same time separate
bequests and donations from our contracts. That way we could demonstrate publicly what
we were being paid for and what we were paying for ourselves.’199
Establishing the Foundation, Murray Compton said later, was designed to develop a long
term fund for Nurse Maude’s activities outside of its health delivery contracts.
197 The Launch of the Nurse Maude Foundation. The Press Christchurch. September 1989 198 ibid 199 Interview with Colin Averill, January 2015

[105]
‘The Foundation had an unusually creative beginning,’ he said. ‘We had many art works that
had been donated over decades. We had them professionally valued and discovered that
one of them was a commissioned painting of the three McDougall daughters by the famous
New Zealand artist Sydney Lough Thompson. After some discussion with the McDougall
family we agreed the painting belonged in the city’s Art Gallery200 rather than hanging in the
original family homestead. We put a proposal to the Canterbury Community Trust Chair Ian
Howell, that it purchase the painting for $250,000 and that half of the proceeds act as the
start-up fund for the Foundation.’201
It was a noble idea, but it did not gain the approval of all the Community Trust’s members.
The Board, once again in discussion with the McDougall family, gave the painting to the
McDougall Art Gallery on permanent loan and started the Foundation itself. It was launched
with much public fanfare and supportive commentary from the new Canterbury Area Health
Board Chairman Tom Grigg and the Department of Health’s Programme Manager for the
Elderly, Disabled and Handicapped Margaret Guthrie who would later became a member of
the Nurse Maude Board.
The launch was an opportunity to promote some of the cost-effective measures the
Association had introduced. New initiatives included a computerised system of management
information which enabled Nurse Maude to constantly monitor statistical and financial data
across the whole spectrum of the organisation’s business. Data was now being
accumulated on diagnostic groups, length of stay, caseload, and the average length of visits.
This then enabled Nurse Maude to apply the results to expenditure according to individual
groupings or right across the community. Trends could be monitored from one year to the
next. New technology was being used and the results were exciting. More than that, other
similar community-oriented health groups were watching the Nurse Maude programme with
a view to introducing similar models. If reform was going to be an ongoing part of health
over the next few years, the Nurse Maude Association should be right at the pioneering
forefront as it had always been.
In 1990, the government changed hands. The Labour Party left the seat of power and a new
National Government took over. Health reform was still very much part of the political
agenda however, and another taskforce, chaired this time by Rod Carr, was set up to report
to the new Minister of Health Simon Upton in February 1991. The proposals that were
announced on budget night in July that year, were not too different from those of the earlier
report but there were some fundamental changes. Regardless of how it was phrased, this
time the report was intended to be the definitive blueprint for health in New Zealand as it
moved towards the next millennium.
The first stage was to appoint commissioners to take over existing Area Health Board
functions. As the Gibbs taskforce had recommended earlier, there would be a complete split
between the purchasing and provision of health services which were currently performed by
the Area Health Boards. Four Regional Health Authorities were to be set up to manage the
200 The McDougall Art Gallery was the Christchurch art gallery before the new one was built on the corner of Worcester Boulevard and Montreal Street. It was named after its benefactor Robert McDougall. 201 Interview with Murray Compton, December 2014

[106]
purchasing and contracting of health services and the new bodies would also take over
responsibility for funding primary care and hospital based care. Services could be bought
from the public, private or voluntary sector.
Hospitals would need to become more business-like in their management structure and
would be set up as Crown Health Enterprises. They would have appointed Boards of
Directors, not elected as before, who would combine a balance of health sector expertise
and business skills. There was an exhaustive list of changes which would be introduced
alongside these major initiatives all of which were designed to give the people of New
Zealand a better health system and, as a consequence, a more economical one.
The issues spelt out in the report were not new. New Zealand had an aging population, a
deteriorating economic position globally, and a blowout in its health budget. Earlier attempts
at health reform had failed at both local and national levels. Sometimes there was little
sound reasoning behind the health decisions that were made regionally, for example, many
hospital buildings were in a rundown state as a result of years of deferred maintenance, but
there was often an absolute reluctance to demolish them. Lobby groups frequently
paralysed Hospital Boards and rendered them incapable of making major strategic
decisions. The list went on. This time the government had no alternative but to act.
Hospital waiting lists had become a critical issue. They were not always well managed.
There was inadequate rehabilitation of long-stay facilities where people could be moved
once their condition improved. There were legislative constraints on the Area Health Boards
and conflict in their dual role of both the purchaser and the provider of services.
‘Underlying all the problems in the health system is the issue of fairness,’ stated the new
government report. ‘It must guarantee all New Zealanders reasonable access to an
adequate and affordable range, level and quality of services.’202 The report acknowledged
the work that had been achieved by Area Health Boards in the previous three years but
stated the key problem still facing them was that they were ‘expected to be both purchaser
and provider of services. These roles conflict, making it difficult for boards to carry out either
role effectively. This leads to other problems which are more visible to the public, such a
long waiting times for hospital care an lack of responsiveness to individuals’ needs.’203
There was a tight timeframe for implementation. Between July 1991 and June 1992, Area
Health Board Commissioners would be appointed as would a National Interim Provider
Board which would be responsible for identifying purchaser, provider, public health, and
education and training resources and services. Initial steps would be taken to establish the
Regional Health Authorities, Crown Health Enterprises and Community Trusts. Policy
issues, legislative and regulatory regimes would be worked on by a special Directorate set
up for the purpose and moves would be made to set up a National Advisory Committee on
Core Health Services for New Zealand.
Over the next 12 months, the establishment of the new hospital structures and community
trusts would be completed, the Interim Provider Board would be wound down as would the
role of the Commissioners. The Regional Health Authorities would begin contracting with
202 Government Health Policy Statement: ‘Your Health & The Public Health 1991 pp 18-23 203 ibid

[107]
the Crown Health Enterprises and other providers with support from the funding group and
the transfer of responsibility to the health authorities for primary care health funding would
begin. The Public Health Commission and Public Health Agency would also be established.
In the third year of transition, the Regional Health Authorities would be fully established and
responsible for primary, secondary and accident-related health care funding. They would
begin to develop and negotiate new payment contracts for health care providers and they
would implement further rationalisation of the user part-charge regime. Finally, people would
be given the opportunity to enrol in health care plans.
Community committees would be used as a conduit for submissions on the proposed new
structure, and the core health services group once it was established, would begin a process
of national consultation about what services, conditions or treatments should be part of the
core of health services New Zealanders wanted to see introduced.
Earlier in 1991, the Canterbury Area Health Board had produced its own strategic plan for
the next three years. While it recognised the need for health reform, it could not support the
idea of a non-elected Board and strongly favoured an internal separation between the funder
and the provider. However, it noted in its submission to the Government, in the event of a
clear separation between the purchaser and the provider, the Board favoured the second
option which was the creation of a new Regional Health Authority able to contract with a
variety of competing providers. In a section devoted to financial matters, the submission
stated: ‘The Board is currently in a critical financial situation, being overspent for the 1990-91
year by $7 million. The capital debt situation is likely to become critical by 1993. The heavy
debt incurred through the Christchurch Hospital rebuilding could make it difficult for the
Board to provide hospital services on a competitive basis if this is required.’204
The report went on to stress that reductions in expenditure would inevitably have an impact
on services over the next few years. ‘The rationing of health services has long existed
implicitly through waiting lists and other mechanisms. Where further restrictions in services
are needed, these will need to be done with clear justification and consultation. Resources
must be used as efficiently as possible to avoid such restrictions in service.’205 But for the
Canterbury Area Health Board, like other Health Boards around New Zealand, its new
strategic direction was almost too little too late.
In many ways, Canterbury was fortunate in the government’s decision to appoint Brian
Stokes as the regional Commissioner and Professor Don Beaven as his deputy. Both men
had a comprehensive knowledge of the health system and understood Canterbury’s unique
requirements. Following the two-year transition, the Southern Regional Health Authority was
formally instituted in 1993. Based in Dunedin, it included Canterbury, the West Coast, Otago
and Southland. Two new Crown Health Enterprises were established in Christchurch –
Canterbury Health which was responsible for acute care and disability support services, and
Healthlink South which was responsible for all other hospital care including geriatric care,
mental health and family health. Many Canterbury business and professional leaders were
surprised and unhappy that Dunedin had been selected as the base for the new Authority –
it should have been in Christchurch, they maintained, where the population was bigger and it
204 Canterbury Area Health Board Report 1991 205 ibid

[108]
was more central. The Authority created a second office in Christchurch but retained its
‘home’ in Dunedin.
A New Order
Where did Nurse Maude fit into this new health environment? The Association’s Board
diligently followed the reform process, watching and listening to the arguments for and
against the proposed changes. By 1990, it was almost ready to cope with any reforms. Not
only were changes in the management structure and the information systems well in place,
but more importantly, a programme for quality assurance and one for patient liaison was also
established.
Picking up on the reports that were circulating around the health sector, Colin Averill told the
Association at its annual meeting that one of the main changes in health services would be
an expansion in the numbers of elderly people remaining in their own homes for longer. ‘It is
also inevitable that shorter hospital stays for acute or chronic health problems will increase
demand for services in the home,’206 he said. Clearly, there was a definite role for Nurse
Maude in the new regional administration. Problematically though, the Association would be
dealing with the Southern Regional Health Authority and one or both of the two Crown
Health Enterprises for its contract renewals.
The Association was ready to accept the identified requirements and if necessary to expand
the range and volume of its domiciliary services. It was also undertaking research and
development in new skills for domiciliary health providers.
‘The circumstances which saw the beginnings of the Association appear to be turning full
circle,’ Colin Averill said. ‘Sibylla Maude in the 1890s, saw the need to provide home care in
a society which provided only hospital care for those in need of health services and who
could afford it. Now in the 1990s, there is an increasing trend towards keeping sick persons
in their own homes for longer if that is where they want to be, and providing that appropriate
health care services are available.’207
In addition to the management changes that had been introduced, the Board had also
improved its governance structure with the creation of two committees – Finance and
Planning which was chaired by Campbell Ballantyne, and Services and Community which
was chaired by Caroline Cartwright. ‘Our new structure should assist the Board in
concentrating on policy issues and delegating management decisions to our Chief Executive
and senior staff,’208 Colin Averill said.
During the previous year the organisation had developed a comprehensive new direction for
its future. It was a significant shift for Nurse Maude – a progressive move for a private
provider of health services in Canterbury, and in this, as in so many other areas, the
Association was a clear leader. While many other voluntary and private health organisations
were adopting a wait and see attitude, Nurse Maude under the direction of its new Chief
206 Nurse Maude District Nursing Association Annual Report 1990 207 ibid 208 Nurse Maude District Nursing Association Annual Report. 1990

[109]
Executive Anthea Bowden, was preparing to focus on the issues rather than the politics. It
must be prepared for whatever might eventuate when the two Canterbury Commissioners
handed over to the new Southern Regional Health Authority.
Management consultants were brought in to work with the Association during the year and a
final organisational structure was agreed to. The Board would devote its energies to policy
issues and the new management arrangements identified a clear distinction between patient
services and support services. The Chief Executive headed the management team.
Domiciliary services were restructured to take account of geographical areas and a quality
assurance programme as well as a fully computerised accounting information system was
introduced. A service liaison nurse role was proposed to deal with any patient and families’
concerns and also with issues that might arise from external agencies. The midwifery
service had expanded with two full time midwives and there were two continence advisors –
one full time and one part time. These additional services were paid for by grants from the
Canterbury Area Health Board. The domiciliary services with an extra $462,499 input from
the Association over and above the Area Health Board’s subsidy, had resulted in more than
200,000 visits, 259, 867 home aid and sitter hours and 8196 laundry van visits during the
financial year.
In the enlarged and refurbished Nurse Maude Memorial Hospital, the average bed
occupancy was 92.86 per cent. Computerised systems for payrolls, financial management
and statistics for service provision were introduced by the corporate services team. But it
was the constant support of patients, their families and the people of Christchurch that gave
strength to the organisation. The next year must be one of consolidation.
It was easier said than done. Reshaping Nurse Maude was an all-embracing task. If it was
going to be done at all, it should be done completely. It was not just a question of
introducing modern methods and techniques; training was required, new equipment was
needed, outdated systems needed to be upgraded. Technology was improving at a fast
pace. The benefits of computerisation were almost immediate. For the first time, the
Association was able to quantify the amount and type of service being provided with a
breakdown of the most intensive disease categories. The number of patients in each
grouping could be balanced against the number of nursing hours. That data could be
compared against age factors and, if required, against national trends and statistics. It was
valuable information. The Association was able to specify exactly what was required for
district nursing which would enable it to tender for services in the new health environment,
and to order supplies and equipment at a more precise level than before. Change, led by
Anthea Bowden was an imperative more than anything else.
In addition to the Association’s major funder, the (previous) Canterbury Area Health Board,
there were other agencies which gave generously to Nurse Maude although not on such a
large scale. The Canterbury West Coast Cancer Society which had made an initial
contribution when the cancer nursing service was first started a decade earlier, had
continued its financial support not only in Christchurch but in the rural areas as well. The
Society made an annual grant to Nurse Maude and its ever willing pool of volunteers worked
closely with the district nurses in the community. The benefits were mutual to both
organisations and the liaison which had, over the years, developed a routine of its own,

[110]
would be of considerable help to Nurse Maude as it broadened its scope to take on palliative
and hospice care in a more general way.
Service organisations in the region were ever generous and of course the ‘Friends’ remained
loyal to the Association. If large print books and magazines would make it easier for the
hospital patients to continue to read, the ‘Friends’ made it happen. If the knee rugs were
getting frayed and worn around the edges, the ‘Friends’ either darned them or made new
ones. If the music needed some improvement, they took care of it. Promotional days, open
days and with all the fundraising efforts, the ‘Friends’ were there to lend a willing hand. They
were an invaluable asset to Nurse Maude.
As the business was becoming more professional, so it was able to provide a more
comprehensive annual report to its interested public. The prudent investments of earlier
Boards had been wisely re-invested by succeeding members with the result that Nurse
Maude while almost always running at an operating deficit in some part of its operations, had
built up substantial reserves. The Foundation had established itself as an internal funder for
essentials that were not covered by contracted services. Also, the decision to move to
Mansfield Avenue when it outgrew Madras Street and to consolidate its operations on one
site had proven enormously beneficial with substantial rises in property valuations in
Merivale over the years.
True to its word, the government began to implement the new health reforms in 1992 and
the prospect of contracting for services became a reality. The Association would now be
contracting directly with the Southern Regional Health Authority for some services and
indirectly through the two Canterbury Crown Health Enterprises for others. It was a
complicated business which required more than a measure of skill in negotiation. In a
competitive environment, other providers could submit tenders for the services that
historically had been provided by Nurse Maude. Equally however, the Association could
tender for services it had not been previously involved with. The Association accepted it as
another challenge with its usual stoicism. Unlike many of its fellow organisations, it had
done its homework and was prepared for the challenges ahead.
Anthea Bowden was a forthright Chief Executive with a visionary perspective on health. She
was completely different to the previous women who had been engaged to lead the
organisation’s nursing and home care operations which by itself was always going to be a
challenge. She was something of a theorist and to that end, believed that not only should the
process of redesigning the internal workings of the organisation be completed, Nurse
Maude’s staff must be trained to grapple with the external environment and all its inherent
changes. While she continued to meet the organisation’s external obligations including
participating in a major Department of Health paper discussing the potential structure and
funding of hospice care, Anthea led the progression of a major cultural shift, something
which many staff were reluctant to accept. There was a philosophy of district nursing that
dated back to Sibylla’s first days amongst the elderly poor in Addington and Sydenham at
the turn of the century. The current mood did not favour sacrificing that heritage for modern
management practices, nor were many staff comfortable with the speed and direction of
decisions being made.

[111]
The first hint of internal conflict came in a newspaper report that staff had passed a
unanimous vote of no confidence in the Association’s Chief Executive. Anthea Bowden was
quick to refute any allegation but there were obvious problems. Part of the Association’s
restructuring had resulted in a high number of redundancies amongst the nurses, something
that was unheard of within the organisation. It was approaching its centennial year and in all
that time, the services had grown - not diminished. Worse however, was the proposal to
include two of the cancer nurses in the redundancy line-up. There was a mixed reaction
from the usually supportive public to the news. A letter-writing campaign began
accompanied by some intensive lobbying internally which resulted in some of the proposals
being modified.
‘Is humanity to be consigned to oblivion?’ asked the relative of one cancer patient. She
wrote movingly of the problems encountered when her husband was discharged from
hospital. ‘I was given no advice on how best to care for him. There were no follow up visits
from his GP. And then came the (Nurse Maude) cancer nurse. These nurses not only care
for the patient but give wonderful support and understanding to the family. They were the
ones who told me when it was time to notify distant family and friends. They were the ones I
called when the GP didn’t want to come out. They are very special people and should never
be discarded in favour of dollars and cents. I can only hope that the hierarchy of the Nurse
Maude Association never find themselves in the position of needing these wonderful
nurses.’209
And there were more letters. Former patients wrote about the quality of the nurses, their
warmth and humanity and their excellence service. Nurse Maude management responded
with a public statement in July announcing that a new palliative care service for the
terminally ill would be introduced that month. The service would replace and extend the
services offered by the three cancer nurses, the district nurses and the sitter staff who
relieved the family carers, all of whom had worked independently of each other under the old
structure. Palliative care case managers would provide counselling and education, help with
pain control and grieving, and medical liaison, supported by a team of enrolled nurses who
would provide the basic personal care. There were about 160 people receiving palliative
care although only 60 required intensive care at any one time. The new service would be
extended to include other terminally ill people.210
The issue, while seemingly resolved at least for the community, had soured relationships
internally. While the restructuring process which had gone on for three long months, had
resulted in a better organisation, it had also caused friction and disappointment. Staff
reductions were an inevitable consequence but for Nurse Maude it was anathema. The
financial result for the year made unhappy reading with the biggest deficit recorded in the
Association’s history. Added to the $585,724 operational loss, was the one-off cost of
restructuring which amounted to a further $318,014.
‘We simply can’t sustain operational deficits of this size, notwithstanding that we received
more public assistance through donations and legacies than ever before,’211 Colin Averill
209 The Press, Christchurch 27 April 1992 210 The Press, Christchurch 2 July 1992 211 Nurse Maude District Nursing Association Annual Report 1992

[112]
said in his annual report. As interest rates had fallen, so had the return on the Association’s
investments. The implementation of the health reforms had resulted in a decrease in funded
money from the government and for the first time in many years, there had been a fall in the
hospital occupancy rates from 93.51 per cent in the previous year to 82.44 per cent in the
1993 year.
‘Internally, the Association grappled with rising costs, outmoded industrial frameworks, an
inflexible structure, coupled with expectations from funders and the community at large to
continue providing the same amount of quality service which the Association is known for. In
order to remain viable in a new environment and survive in an uncertain future, the
Association needs to manage risk and its resources in a more business-like manner –
always being mindful that interest from charitable money allows us to go the extra mile.’212
In fact, the Association felt it had already reached the extra mile and by the end of 1993 a
new Chief Executive had been appointed. There was no doubt that with her intuitive
organisational and business management skills, Anthea Bowden had prepared Nurse
Maude for what was to come in the new world of health, but at a cost. Now the organisation
needed some reassurance that it was still the best provider of district nursing services in the
community.
212 ibid

[113]
Chapter Three: The New Health Culture
Health – the Hottest Topic in Town
Implementation of the Government’s new health regime began in earnest in 1992 with the
introduction of the split between the purchasers of services – the four Regional Health
Authorities, and the providers – Crown Health Enterprises and private health providers.
There was confusion at all levels. There was an entire new health dictionary of acronyms to
come to grips with and an explosion of a new health culture throughout New Zealand. In
spite of the Government’s best efforts, the changes were not well received. Never mind the
fact that everyone knew change had to happen, that the nation’s health budget had long
since blown out, that hospitals were chronically overspent and under-utilised. In fact, most
people who worked in the health sector agreed, at least privately, that health reform was
imperative.
Public dissatisfaction with the welfare state provision of hospital care had been an issue for
many years. In the late 1970s and during the 1980s it centred squarely on the problem of
waiting lists. Indulging in name changes now was not going to make the problem go away.
Area Health Boards like Hospital Boards before them may have been publicly elected bodies
but their level of public accountability had depended on whim. There were plenty of
journalists in New Zealand who would sigh in aggravated frustration at the number of times
important issues were discussed behind closed doors. For years, the system had been
overworked and overused. Greedy habits had developed. Yet, unhappiness with the public
hospital system tended to be accompanied by silence rather than public outcry.213
As the process of reform inched its way towards the start date, health became the hottest
topic in town. Everyone had an opinion to offer and another story to tell – most of it
negative. The fourth estate which, in the 1960s and 1970s had supported the call for better
hospital management, for increased home care services and for a reassessment of the
health vote, took a surprisingly reactionary approach to reform. It was a time when New
Zealanders, apparently, had never felt healthier. A Hillary Commission study quoted facts
indicating the country generally believed itself to be in good health. So why the continuous
clamour and why the daily headlines? Frustratingly for the new authorities, many of the
stories that were circulating spoke of old issues, of negligent treatment and lack of support
that had in fact happened prior to health reform. But who wanted to listen to the facts? The
stories were far more interesting.
There were problems with private health providers, particularly those who operated
throughout New Zealand rather than in specific regions. They now found themselves in the
impossible situation of negotiating with four different Regional Health Authorities all of whom
were establishing different criteria, processes and systems. It all created a strange
environment, politically charged, often promoted but more frequently condemned.
213 Spoonley Paul, Pearson David, Shirley Ian. ‘New Zealand Society’ Dunmore Press 1990 pp 158, 159

[114]
Christchurch and Canterbury had their own issues to deal with. Not only was there mounting
opposition to the location of the Southern Regional Health Authority in Dunedin rather than
Christchurch, but two Crown Health Enterprises – Canterbury Health and Healthlink South -
had been created for Canterbury instead of one as in the rest of the country. If there was
confusion in the community, there was more confusion within the two new structures.
Instead of giving the public a measure of confidence, the new system was instilling fearful
anticipation. It needed a settling in period, but there was not enough time. A rapport was
needed between the different providers but clearly that was not going to happen quickly.
The notion of market forces in the health sector was like a malignant cell. And the reality
was that it would not go away, at least not in the short term.
Working the Contract
In May 1993, Colin Averill stepped down after nine years as the Board’s Chairman and his
place was taken by Murray Compton, the son of an earlier Chairman - Rod Compton. It was
a change, like so many others, that had a certain symbolism for Nurse Maude. There was a
tradition, almost familial in its context, that at any one time, somewhere in the organisation,
there was a connection back to the old days. It leant a defined history to the organisation
that enabled its memory to remain in place. The fortunes of the Association had again been
reversed, this time with a profit recorded for the first time in three years. But the Board did
not consider this achievement to take priority over the provision of quality health care and
Murray Compton pointed this out in his first annual report. ‘We endeavour to achieve a result
that is financially prudent. This allows us to consider the development of new services as
these are justified.’214
Reference was made to the provision for the operation of contracts beyond the
organisation’s traditional areas should the appropriate opportunities occur. It was a signal to
those who needed to know that Nurse Maude was ready to expand into new areas if the
chance came its way.
There were other changes. Following Anthea Bowden’s resignation, the Association’s
Director of Operations, Stephanie Walmisley had been appointed acting Chief Executive.
Earlier, under her direction, the new case management system had been introduced.
Matching skills and competencies to the requisite task would result in a more appropriate
utilisation of nursing skills. There had been further assessment of the work undertaken at
the Memorial Hospital which resulted in a reduction in capacity to 88 beds. The organisation
now had to consider how to best utilise the facilities provided at the Hospital.
In her first annual report, Stephanie talked about the need to carefully read the external
environment to ‘enable us to plan and act upon threats and opportunities that are already
being evidenced.’ The next six months, she said, would require focus on cementing
relationship in the market place and being competitive in retaining contracts and piloting and
attracting new activities. ‘Currently a number of opportunities are being investigated by
management with a view to re-packaging or expanding on what we do well.’215
214 Nurse Maude District Nursing Association Annual Report 1993 215 Nurse Maude District Nursing Association Annual Report 1993

[115]
It was a year since the public outcry at the prospect of Nurse Maude changing the status of
the cancer nurses and the consequent introduction of the palliative care team. In the
intervening 12 months, the service had become well established. Each of the four teams
included a registered nurse, an enrolled nurse and there was a limited sitter service as well.
Palliative care was now funded through a contract with the Southern Regional Health
Authority and the team liaised directly with involved health professionals – oncology and
Ward 30 at Christchurch Hospital, the hospice at Burwood, general practitioners and the
Cancer Society. An independent survey of patient satisfaction was conducted earlier in the
year. It was an affirmation of the decision to revamp the service and extend it into the rural
areas of Rangiora and Kaiapoi through the appointment of an additional nurse, Debra
Wilson. Her position was confirmed through a seeding grant from the Canterbury-West
Coast Division of the Cancer Society.
The next twelve months were tumultuous ones for health and Nurse Maude was not exempt
from the impact. One of the greatest difficulties was the number of different contracts
required for services that had previously all come from one funding source – the North
Canterbury Hospital Board. Contestability had thrown everything into confusion. A
considerable amount of time was now taken up preparing tender documents, getting the
necessary statistics and costings and making sure there was a credible presentation to the
funding body. There were contracts for everything – diabetes, stoma services, continence,
hospital and district nursing – the list went on and on. If it was not a direct contract, it was a
sub-contract, and in some cases the Association might be in competition with one of the two
Crown Health Enterprises with whom it might have a direct contract for something else. It
was no wonder people often felt confused. There was competition too between Canterbury
Health and Healthlink South and an early sense that the Regional Health Authorities were
displaying too much muscle and not enough engagement. Understandably, they were also
feeling their way. Their Directors were independent appointments with predominantly
business backgrounds. They were responsible to the Minister of Health and as a result they
had no direct responsibility to their community.
There were fears that greenfields operators would move in, undercutting prices to get
contracts from the Regional Health Authorities but with no factual history or record of service
behind them. Nurse Maude, like many other private health providers, was well established
with a proven record of delivery. Yet, even that fact appeared to carry no weight with the
new health purchasers. The area of home care was particularly open to marginal operators
and the Association had to decide if it wanted to continue at perhaps a competitively lower
rate, or if it should move away from the service altogether. But care of the elderly had
always been part of its core service. It was the reason Sibylla Maude had begun the district
nursing service. It had history particularly in the poorer suburbs of the city. Services for the
elderly would increase as the population continued to age, reasoned the Association’s
Board. With its background of nearly a century of experience, it made sense to stay in the
business and to support the people who had always viewed Nurse Maude as its extended
family.
As another year ended, the Association reviewed its achievements with a sense of
accomplishment. In spite of the difficulties created by the political climate, Nurse Maude had
retained its position as a significant provider of its traditional services to the community. It
had been a challenge that Board and staff alike had taken up. There were some bright

[116]
moments, especially when renovations to McDougall House were completed. The
Foundation funded its alterations and with its usual diplomacy, the Board invited the new
Minister of Health Jenny Shipley to perform the official opening ceremony. In July, the first
Founder’s Day Service was held in the little red brick Nurses’ Chapel in the grounds of
Christchurch Hospital. It was an appropriate venue for a commemoration to one of the city’s
best known nurses. There was a stained glass window in the Chapel dedicated to Sibylla
Maude.
Not surprisingly, reform was starting to affect the Nurse Maude Memorial Hospital. After so
many years of profitable operation, it was disappointing to see a steady decline in residential
patients. Increasing the charge to patients was not an option because there was a fixed
contract with the Southern Regional Health Authority. It was obviously an issue the Board
would have to deal with in the coming year. In 1990, the Memorial Hospital had still enjoyed
a bed occupancy of 91 per cent. In 1992, recognising that the health reforms would have an
impact on occupancy, the Board decided to downsize the Hospital to 88 beds. However, the
introduction of needs assessment and income and asset testing in July 1993, had an
immediate effect and hospital bed occupancy had dropped to levels that were at times as
low as 67 per cent.
‘The sector is controlled by a tender process for fees, with eligible patients being directed to
the cheapest bed available in the area on the day,’ Stephanie Walmisley stated in her first
report to the Board as its appointed Chief Executive. ‘This has removed patient choice and
asset and income testing may have discouraged patients from choosing the most
appropriate level of care. Some clients appear to be choosing to spend less of their
resources, electing not to go into institutions.’216 Many elderly people were having to
reconsider their options particularly when it came to services they were previously entitled to,
but were now expected to pay for, partially or in full.
The government’s policy of income and asset testing for the elderly caused an uproar of
almost unprecedented proportions particularly amongst New Zealand’s fastest growing lobby
group – Grey Power. But their pleas went unheeded. If people could afford to pay for
services, why should the state pick up the tab? In Canterbury, there was a surplus of beds
not only for continuing care but for rest homes. Proposed changes to the Private Hospitals
Act 1957 would blur an already indistinct line and the future of the Nurse Maude Memorial
Hospital would have to be reviewed.
In line with its usual determination to find the best way to move forward, the Association had
welcomed the appointment of clinical advisor Dr John Musgrove to the Board in 1992. Now
it also began regular liaison with emerging health organisations like the Pegasus Medical
Group, one of the largest independent practitioner groups that had sprung up with the
implementation of the health reforms. Most of Canterbury’s GPs had joined the Pegasus
Group giving it a certain prestige within the health community. There were other
opportunities for Nurse Maude with more pilot projects for alternative service deliveries in
district nursing as part of primary community care.
………………………
216 Nurse Maude District Nursing Association Annual Report 1994

[117]
A New Beginning
In 1994, a social worker was appointed to the Association. Margaret Hockey’s task was to
work with other agencies and in particular to assist elderly clients who might be subject to
abuse. She was also involved in the ongoing training programme for staff. For all its
problems, the Association was as busy as ever in the community. The palliative care team
led by Liz Horn continued to have an increasing caseload. The extended continence clinic at
the Mansfield Avenue site was constantly busy due in large measure to a well organised
programme of public education. It was a contract acquired by Nurse Maude following a
decision to centralise all components of the service within a contract with the Southern
Regional Health Authority. In the rural areas – Rangiora, Kaiapoi, Lincoln and Ellesmere -
the many aspects of community and patient care continued as before. And the domiciliary
midwifery service continued amidst increasing rumours that new maternity services would be
introduced soon.
The government had signalled earlier that maternity services throughout New Zealand were
under review. In spite of providing a community midwifery service, the Association had not
been kept informed about the ongoing negotiations between the four Regional Health
Authorities, the New Zealand Medical Association representing doctors and the New
Zealand College of Midwives representing the different groups of practicing midwives. It
appeared there would be no easy outcome to any deliberations, the differences of opinion
amongst the various parties were too great. The prospect of losing the domiciliary midwifery
service brought a real sense of deja vue to Nurse Maude. Sybil had always wanted to set up
a domiciliary midwifery service in Christchurch and the Association had tried several times
before it was successful in the 1980s. No-one in the organisation wanted to see it stop now.
But in the current environment, with referrals coming from the competitive Crown Health
Enterprise, and with private health enterprises locally being invited to tender for maternity
services, Nurse Maude feared the worst.
Of even greater concern was the issue of palliative and hospice care in Christchurch. In
1995, the Southern Regional Health Authority announced it would tender both the hospice
services provided by Burwood hospice and the palliative care services provided by Nurse
Maude since the 1970s as a joint package. Failure to tender and win would mean the
automatic demise of the palliative care team from Nurse Maude’s services. The tender
price, according to the Health Authority, would be in line with that paid by the other three
Regional Health Authorities. The new contract was specifically designed to include
community funding – one of Nurse Maude’s great strengths. But this time, the project did
not receive universal support. Many people in Christchurch were appalled at the prospect of
the Burwood hospice closing and there were once again angry letters to the newspapers and
rebuttals issued from all sides. In spite of having a sound history in palliative care, the
Association found itself having to publicly defend its position and reaffirm its commitment to
the service it had dedicated itself to providing for 100 years.
When Sibylla Maude started her rounds in Sydenham in 1896, with her black bag under one
arm and a bedpan under the other, she was unwittingly staking her claim, her position, in the
town. Since then, the Nurse Maude Association had witnessed, and been a significant part
of, considerable social and economic change in Christchurch. The organisation had worked
through two world wars, the 1918 influenza pandemic, the clichéd good times and the bad.

[118]
It had been the beneficiary of some legislation, and been substantially affected by others
during that time, not always health oriented. Its own Act of Parliament and its subsequent
amendment had given Nurse Maude a status many another independent private health
provider lacked. More recently a raft of legislation including the Employment Contracts Act,
the Official Information Act and the Privacy Act all required the Association to revisit an
aspect of its business in some significant way.
In the end, the organisation did lose the midwifery contract. With a refocusing of its core
business, however, the Association was philosophical about the decision. At its best, it had
been extremely successful, taking the service into a high risk socio-economic grouping
which had very significant needs indeed. There were other opportunities for Nurse Maude to
consider, none-the-least of which was the service it delivered best – district nursing, the
emphasis of care on the community’s elderly people and new strategic alliances with other
health providers.
In 1996, its centennial year, Nurse Maude was recognised as the dominant provider of home
based care in the community. Its total revenue was in excess of $16.35 million and it
employed 1,700 staff. District nursing and specialist nursing visits made up a total of
195,109 visits and home support totalled more than 517,000 hours. It was a far cry from
Sybil’s solo operation 100 years earlier. Through all its changes, the Association never
forgot its roots. As many of the Board members and staff were still prone to ask: ‘What
would Nurse Maude have done about this?’

[119]
Chapter Four: Managing Change
1996 – A Year in Review
‘To continue as leaders in the provision of valued home and hospital care for the
community.’
Nurse Maude District Nursing Association: Mission Statement 1996
Murray Compton stood before the Board to present his annual report for the end of the
Association’s centennial year. He was supported by people many of whom had
organisational memory, a significant and important aspect of Nurse Maude throughout its
100 years. They were complemented by new faces who brought fresh ideas to the table.
The year had been challenging, the Chairman reported. It was a polite synonym for
complex, difficult, worrying yet satisfying. While one door closed, another continued to open.
The Association had gained the contract for continence and stomal products. It was a
significant contract for hundreds of people who had major operations that removed all or part
of their bowel, either through cancer or other serious illnesses. It was a silent condition that
people did not like to talk about. Having a discreet service that took care of that essential
need was a blessing for many.
The changes to the midwifery service throughout New Zealand meant the loss of the
referrals from Healthlink South, one of the two Christchurch Crown Health Enterprises, but
the Association was philosophical about it. There was a new national maternity service that
would see a rapid change from the tradition of babies being delivered by GPs to qualified,
experienced midwives dominating the service, the introduction of a lead maternity carer and
a markedly improved service for expectant women before and after the birth of the baby.
One of the more positive aspects of the past year was the contract to provide a much
needed joint palliative care and hospice service for the Canterbury region. A hospice facility
in the Nurse Maude Memorial Hospital opened on 16 June 1996 with supporting palliative
community care. The Association was already planning to develop a purpose-built hospice
on the site adjoining the hospital as quickly as possible.
The centennial year had been one of celebration, of remembering the past and looking
forward to the future. The hospice, Murray Compton said, seemed to be a fitting project for
the Association in its centenary year because it reflected the philosophy that guided a true
pioneer in health care. Many events had been carefully and thoughtfully planned to
acknowledge the first 100 years. It was a time to reflect and a time to remember. It was
also a time to look to the future.
The Association successfully hosted the 5th National District Nursing Conference during the
year, and organised a Vice-Regal dinner for 270 guests in the Limes Room of the
Christchurch Town Hall as part of its celebratory events. A garden party and open day was
held on 2 November 1996 at the Mansfield Avenue headquarters that featured displays of

[120]
medical and nursing memorabilia while staff dressed in uniforms representing the decades
of change.
In spite of the positive results identified in its annual report, the Association was nevertheless
concerned at the future directions of the health sector under the new model of care, driven
by economics and managed by health authorities that were responsible to the government.
‘The purchasing prices of the CHEs and the RHA are often insufficient to meet the real costs
of our services,’ Murray Compton said. ‘Like so many non-profit groups, we rely heavily on
the generous support of the public. However, the public can only support so many causes,
and it is up to us to maintain Nurse Maude’s name and reputation. This can only be
achieved with the continuing support of a dedicated staff and loyal group of supporters who
have been responsible for the Association being held in such high regard over the past
century.’217
The Association was now the largest home care provider in Canterbury. Staff numbers rose
to 1700 in 1996 and the increase in the demand for disability support services was running
at between 20 to 30 per cent per month. The increase in staff was matched by training
programmes to ensure staff had the latest information and communication technology. A
new telephone system had been installed, and the organisation was now connected to the
internet and had email capabilities. A new inventory management system was also installed
to meet the Southern Regional Health Authorities reporting requirements. As the
organisation’s Chief Executive, Stephanie Walmisley was in frequent contact with the service
purchaser and she had no hesitation in telling her Board about the difficulties of both
securing and managing contracts.
‘The (SRH) Authority’s restricted financial position has, in turn, placed downstream
pressures on all service providers. The Authority’s service expectations have increased
across the board, but these expectations appear not to be matched by purchasing power.
As a result, the Association has been placed in a very difficult situation, where the level of
service provided has not always received the corresponding price required. There were
some major policy changes in terms of entitlement, particularly in the area of Disability
Support Services. In responding to these changes, the RHAs seem unprepared both
financially and managerially to predict the impact of their policies. As a result, they have
now been forced to bring demand back to manageable levels, using rather blunt strategies to
reverse the expectations of many people. No-one would argue with the concept of choice,
but one wonders whether the efficiencies are when clients are being visited by multiple
agencies, each responsible for a separate function and restricted through their contract from
doing what is sensible, efficient an effective for the purchases and especially for the
client.’218
Clearly the Regional Health Authorities still had some design faults to iron out in their
provider contracts.
217 Nurse Maude Association Annual Report June 1996 218 ibid

[121]
Hospice and Palliative Care
‘A service tailored to palliative rather than curative care…and a focus on the psychological
and social needs of the patient and family’ 219
The amalgamation of the existing Burwood hospice service with Nurse Maude’s palliative
care programme was welcomed by almost everyone although, as Murray Compton
remarked later, there were some people who were extremely unhappy at the change. ‘It was
up to us to prove the right decision had been made,’220 he said. It created a new and
seamless service for people with life-threatening illnesses. After a tight lead-in time of only
six weeks, the service was formally integrated on 16 June 1996. At the time, hospices
throughout New Zealand were funded to 50 per cent of their costs and they all relied heavily
on community support. It meant that although the Association had been successful with its
contract negotiations, it would still need to commit a significant amount of its donated funds
to ensure the service could be well maintained.
Hospice in New Zealand was still a fledgling movement although it was beginning to be
recognised for its different approach to end of life care. The very real connection between
hospice and palliative care was still open to debate however. The term ‘palliative care’ had
been coined by Canadian Professor Balfour Mount in 1975, but it was not considered an
interchangeable term with the concept of hospice where the goal was to ensure patients
were comfortable and free of pain. Nurse Maude was entering a new phase in its overall
nursing framework by bidding for and winning the hospice contract with the Southern
Regional Health Authority.
The existing hospice was transferred from Burwood to Merivale with surprising ease and
resulted in a steady stream of referrals from GPs and specialists. A new Medical Director Dr
Jan Whyte was appointed to head up the programme and Willem Vink a former palliative
care nurse with Nurse Maude took on the role of Unit Team Leader. Both were highly
trained and skilled in their respective specialist areas. Their priority, in addition to taking
care of their patients and managing their teams, was to contribute to the design and planning
of a new 11-bed hospice which would be available to people throughout Canterbury. As
Murray Compton had indicated, the building would be partially funded by a grant from the
Nurse Maude Foundation for the purchase of additional land adjacent to the administration
block in Mansfield Avenue.
A year after the amalgamation of the service, the benefits were obvious to everyone
involved. Dr Tony Stoop was engaged to support Jan Whyte. As the lead agency, Nurse
Maude adopted a cooperative style of networking, making sure other organisations and
agencies were well connected with the service. Doctors, clinical specialists, clergy and
social workers had open access to patients and families. Integrating on-site and community-
based services was essential; equally important was the integration of services beyond the
219 The hospice philosophy accepted worldwide, which recognises that for some people treatment strategies will not be appropriate. Introduction of a paper written by Pauline Barnett and Kay Smith, Health Research Services & Personal and Public Health Policy, Dept of Health June 1992 220 Interview with Murray Compton, December 2014

[122]
Association’s boundaries. A bereavement counsellor funded by the Pegasus Medical Group
for 30 hours a week added to the range of available services.
Final approval for the construction of the new hospice was given in May 1997 and work
began straight away. Funding for the building had come to the Association from several
grants including $350,000 from Trust Bank Canterbury, $1.8 million from the Nurse Maude
Foundation and donations from generous benefactors. Former National MP for Ilam, Philip
Burdon agreed to act as patron for the project. The team of six builders made solid progress
through the winter and the Association expected the facility would be completed on time and
on budget in time for Christmas.
While the palliative care programme was an important step forward it was not the only
project gaining momentum. Nurse Maude’s at-home intravenous therapy service had grown
steadily confirming the potential for freeing hospital beds and giving patients the option of
treatment at home. Established in 1994, referrals had increased particularly from the
infectious diseases and orthopaedic departments at Christchurch Hospital. The home-based
service was an internationally accepted practice; it used peripheral inserted central catheters
(PICs) and midlines which were placed by clinicians and enabled easy insertion.
The Association’s rural outreach programme continued to flourish. Volunteers in the
Ellesmere district, Rangiora and Kaiapoi raised funds locally to maintain the service. In
Ellesmere particularly, the local committee was able to invest $30,000 with the Foundation
on the condition that the funds were available for projects in the area. At the same time, the
Association stepped beyond Canterbury’s boundaries to form new relationships with several
different agencies. Exchanges had begun with Western Bay Health in the North Island in
1996. Nurse Maude had also established formal contract with two district nursing
organisations in Australia – Royal Melbourne District Nursing and the Perth-based nursing
organisation Silver Chain.
Progress was being made on many fronts. Stephanie Walmisley received full support from
Murray Compton and Campbell Ballantyne, Murray’s Deputy and Chair of the Finance and
Planning Committee. Caroline Cartwright was the Chair of the Services and Community
Committee. David Caygill had joined the Board as had Dr Margaret Guthrie. Stephanie’s
management team included Chris Shields as the Human Resources Manager, Adrian
Mouldey who was responsible for finance, Martine Iggo who managed the hospital, hospice
and palliative care, Helen Collie, responsible for home care services and Lorraine Webster
who managed operations. The Association had become a streamlined business in its
management with strong governance and a clinical team of advisors. Credit for the
introduction of improved technology, better systems and a more structured management
style, belonged as much to Anthea Bowden as it did to Stephanie Walmisley. Both had
brought considerable expertise to the Association at a time when many non-profit
organisations were baffled by the onslaught of health reforms.
The Association’s five year plan was to manage and grow its existing contracts and to
continue to explore new opportunities. ‘As a major provider of home-based services, we are
seeing increasing numbers of elderly and disabled people staying at home, sometimes
through choice, something through changing entry criteria for residential care and
sometimes through family pressure and self-interest. Income and asset testing for entry to

[123]
rest homes has created a situation where it is financially undesirable for a person to move
from home to residential care. Living at home can be a safe and desirable option if the need
is matched by community services, but it can also result in people remaining at home in very
marginal circumstances. The Association has identified these people and monitors
increasing numbers of ‘high risk’ clients within our service. The range of disability provision
carried out by the Association also includes some 300 people with psychiatric disability,
some of whom are at risk or subject others to risk in a number of ways.’221
Once again, Stephanie Walmisley used the annual report as a publicly available document
to discuss the ongoing issues within the health sector. ‘The new political environment and
the Coalition Agreement initially signalled a move away from obsessive competition and
market forces in health services, but towards the end of the financial period we were
confronted with the prospect of tendering for our District Nursing services in Christchurch
and all Disability Support Home Care Services – in effect, having to bid for the right to
continue serving the community. The Association’s Board made representations to
Southern Regional Health about the tender process which was then delayed for a number of
months. A modified tender process began earlier this year with the results effective from 1
October 1997. For Nurse Maude this means the retention of the right to provide District
Nursing services in Christchurch, the loss of DSS homecare work in North Canterbury, the
rural fringes, Lyttelton and Governors Bay; and the right to provide services in South
Canterbury and Southland. The organisation has exercised great care to ensure the
requirements of the Nurse Maude Act are observed and that activity outside Canterbury is
carried out through a separate company.’222
Stephanie concluded with: ‘The Association has noted comments by the Minister of Health
which acknowledge the fragmentation of health services. The Association views the key to
safe and effective services as being able to provide the best solution at the best price and at
the right time irrespective of service boundaries. The missing components of a true
brokerage system, rather than a service rationing system, and flexibility across boundaries,
would integrate a system into the sum of a number of fragmented parts. Initiatives such as
the age care integrated pilot will no doubt over time share these aims. New community
technologies, proposals to widen the clinical role of nurses, and prescribing rights, make the
position of the nurse in the community a vital one.’223
It was an intuitive, albeit political note on which to end one financial year and start another.
Not unexpectedly, many of the teething troubles first experienced with the changes in the
health system had yet to be ironed out.
221 Nurse Maude Association Annual Report 1997 222 ibid 223 ibid

[124]
Part Four - A New Era for Nurse Maude
‘Working in partnership with others in developing and implementing new services and
projects to advance community, nursing and hospice palliative care ensures that Nurse
Maude remains a relevant, dynamic and innovative force in the health sector.
E mahi whakahoa ana a matou ki etahi atu, kia whalahiato me whakarite nga ratonga hou
me nga kaupapa hei kokiritia nga mahi nehi-a-iwi-whanau me te tiakina tangata
whakahemohemo, kia noho tonu ana Nurse Maude, teropu pakari, hiranga, akiaki me auaha
I roto I te taha Hauora.’
Nurse Maude Mission Statement 2014

[125]
Chapter One: Grappling with the Nuances of Health Reform
Unleashing the Potential of Nursing
‘Nursing is a combination of many elements: knowledge, styles and models of care,
professional codes, clinical skills and attitude.’ Ministerial Taskforce 1998
The year 1998 began on a promising note when the new hospice was officially opened on
26 February by the Prime Minister Jenny Shipley. Her predecessor Jim Bolger had
ceremoniously planted a kowhai tree – the symbol of Hospice New Zealand - on the
Mansfield site before the construction work had started. Fundraising had been a mammoth
achievement. The committee led by Campbell Ballantyne had successfully canvassed
businesses and charities to meet the budget. Local Masonic groups promoted the hospice
to the Grand Lodge of Benevolence and to various other Lodges in Canterbury. The
Canterbury Plainsmen and The Sweet Adelines participated in the international B.T. Voices
for Hospice, the well-known Deans family organised an art exhibition entitled ‘Canterbury
Families for Hospice’ at Riccarton House. A large and attentive audience attended a
fundraising lunch with guest speaker Australian cricketer Merv Hughes. There were many
other equally inventive events including a triathalon where Nurse Maude was a joint
beneficiary, which together with substantial grants from the New Zealand Lotteries Board,
Trustbank Community Trust and of course the Nurse Maude Foundation helped with achieve
the overall goal. A public appeal in October 1997 raised more than $53,000.
The hospice was an immediate success. Patients were transferred from their temporary
wards at Nurse Maude Memorial Hospital following the issuing of a Medical Hospital Licence
and the confirmation visit by palliative care specialist Dr Ruth Redpath from Melbourne.
Pegasus Medical Group agreed to extend its funding support for a bereavement specialist
until March 1999. The opening of the new hospice allowed the Memorial Hospital to return
to its earlier 88- bed facility for short stay, post-operative, convalescence, specialised care
and long stay patients. Two lifting hoists were installed in the Hospital and three large
screen televisions. Outside, new planter boxes were added to the secure garden area
through the generosity of the ‘Friends’. Secure, electronic doors in the specialised care ward
were installed.
Local charities continued their support for special projects. The Griffin Charitable Trust
provided money to update the Association’s meal service vehicle and to install an additional
chiller to allow greater capacity and menu variety. The specialist nursing services
maintained its extensive community care programme. A third stomal therapist, Beth
Dunstan was engaged and Rachel Barton was sent to Britain and Israel to study the
development of continence related therapies. A new part time nurse joined the diabetes
team and Catherine Hammond was appointed as an additional wound care nurse. Part of
her role would be to promote the use of more research-based practices within the
Association.
Stephanie Walmisley could see the need for more fund-raising expertise in her management
team and she appointed Mary Pauwels in April 1998. Mary’s role was to create and

[126]
establish a permanent fund-raising programme which would meet the operational needs of
the hospice and supplement funds for other projects. A comprehensive plan was developed
which included appeals, bequests and events. Like most of the region’s voluntary
organisations, competition for the public’s generosity was keen and innovative ideas were
essential to ensure ongoing support.
The Nurse Maude Foundation under the capable direction of its Chair Colin Averill,
continued to make sound investments and even with its increased donation of $1.395 million
towards the hospice, it ended the 1998 financial year with funds totalling $5,295 million.
During the year, the Foundation had supported two of the Association’s research and
development initiatives with $10,000 to the wound care project and contributions to the Elder
Care Canterbury project for improvements in patient services. The Association was a
member of Elder Care Canterbury, an organisation that had started in 1997 to improve the
provision of health services to the region’s elderly people. Stephanie Walmisley was a firm
believer in working with other organisations which had similar interests and care of the
elderly had always been a significant part of Nurse Maude’s work. The Foundation had also
funded the engagement of a volunteer’s coordinator, a service development nurse and a
part-time social worker. Additional initiatives were being discussed including more research
into current technology, scientific and social trends in community-based health care.
Externally, the Association continued to grapple with the nuances of the health reforms.
Determined to stay on top of it all, Stephanie insisted her team contribute to as many
meetings as possible and make submissions in areas where, she believed, Nurse Maude
had an involvement. The development of national guidelines, health services in the southern
region, a special district nursing project, nurse prescribing, a Ministerial taskforce on nursing
– they were all essential to the organisation’s business. If Nurse Maude could make a
difference, it would. They continued the trend towards the standardisation of purchase
models through the development of clinical pathways and guidelines in an attempt to make
what is publicly purchased more explicit, she told the Board.224 She was complimentary
about the Ministerial taskforce on nursing.
‘It is the most thoughtful and significant report on nursing produced in this country for a
number of years. The report has the potential to remove many of the obstacles in front of
effective post-graduate nursing education and professional development which have been
established in other countries for many years.’225
The report was released in August 1998 by the Ministry of Health. In his foreword, the
Minister of Health Bill English said the taskforce had been established in response to calls
from nurses and nursing organisations. ‘I believe that there can be much smarter utilisation
of nursing skills. The nursing profession needs to continue to adapt to meet the challenge of
radically changing delivery of health care.’226
The taskforce, chaired by former Labour MP for Lyttelton, Dame Ann Hercus,227 was
charged with identifying barriers that prevented nursing from improving services to patients
224 Chief Executive’s Annual Report 1998. Nurse Maude Archives 225 ibid 226 ‘Releasing the potential of nursing’ The Ministerial Taskforce on Nursing August 1998 227 Dame Ann Hercus chaired the report until 30 June 1998. Toni Ashton took over the chair for the final month of the report – July 1998

[127]
and with devising strategies to remove them. In her preface, Dame Ann spelt out some of
the complications including the lack of consensus between the taskforce and the New
Zealand Nurses’ Organisation. Finding common ground in some areas was clearly a
complication. That said, the implementation of the recommendations in the report would be
the ‘first – but essential – step towards a more effective and innovative nursing workforce,’228
she wrote.
The list of recommendations included a request to address the current limitations of the
Nurses Act 1977, which, the taskforce believed, prevented the Nursing Council from
enforcing competency-based practising certificates, and specialist and advanced
competencies for practitioners. The taskforce had a list of recommendations specifically
directed at the Health Funding Authority, which, it believed should encourage primary-care
organisations to make more effective use of practice nurses and, re-prioritise in order to fund
and support the development of nurse-led services. Both these two recommendations were
particularly important to the Nurse Maude Association as was a suggestion directed to the
Clinical Training Agency that it should work with nursing organisations to develop and fund a
national framework for the first year of clinical practice.
The report highlighted the benefits of nurses taking a more proactive role in clinical care.
How, and to what extent, the recommendations could be effectively implemented would
depend on health politics across the spectrum. The establishment of nurse practitioners was
a few years away yet.
Approaching the new Millennium
In its introduction to the 1999 annual report, the Association discussed the speed with which
health care in New Zealand had changed in the previous century. It was not just changes
within the organisation from its simple origins in the poorer suburbs of Christchurch to the
multi-million dollar business it had become. ‘Life in New Zealand has altered dramatically
since the turn of the century, but certain human needs remain the same. The need for
compassion and support in a time of sickness and crisis, for a helping hand to ease the
burden of ill health or declining ability, and for someone to lead the way in a world
bombarded by change are the principles by which the Nurse Maude Association continues to
service the community. To say that the Association has witnessed great change in the 20th
century would be understating the case. The challenges and changes have become bigger,
more frequent, less predictable and more complex to manage. Whatever challenges lie
ahead, the Association will remain true to the vision of its founder yet alert to the emerging
needs of the community to ensure that people will always have someone to care for them in
their time of need.’229
It was almost impossible to quantify the rapidity of change over the previous decade, let
alone a century, or multiple centuries. And who was qualified to talk about the millennium in
general? There was nothing specific that marked the turning of the calendar from the 20th to
the 21st century, but there was a myriad of reports, pilot initiatives, studies and politically
driven policies to keep the health sector in front of the public. In part it was driven by
228 Preface to: ‘Releasing the Potential of Nursing’ The Ministerial Taskforce on Nursing August 1988 229 Nurse Maude District Nursing Association Annual Report 1999

[128]
technology and medical science, in part it was driven by an increasingly interested media
and in part it was driven by the public’s awareness of patient rights.
As Nurse Maude’s Chief Executive, Stephanie Waterfield230 maintained her feisty approach
to health reform commenting: ‘Health care in New Zealand continues to challenge, tantalise
with its possibilities and, paradoxically, to frustrate us with inertia as well as change.
Somehow the balance is never achieved, and this explains why health management is
compelling, complex and compulsive.’231
The impact of the Ministerial taskforce on nursing was still being analysed and with the new
millennium about to begin, the Association was confident the report would send a strong
message that the ways of the past would not be the ways of the future. The district nurses
continued their home visits, supported by a growing team of home care staff. The original
home aiders had developed into a comprehensive seven-day service which extended into
South Canterbury as well as the rural areas surrounding Christchurch. Training and
education for both district nurses and the home care teams was a priority for the Association.
Programmes were organised internally and staff were encouraged to attend seminars and
conferences. Workplace training and assessment for medical students and Christchurch
Polytechnic nursing students was also encouraged.
The Association’s specialist nursing services continued to expand. The stomal and
continence services were busier than ever and the team’s staffing levels rose from seven to
ten nurses. A continence outreach clinic was established in Kaiapoi and another at Age
Concern’s premises in Christchurch. The intravenous therapy service which had now been
operating for four years had adapted to technological advances with a corresponding
increase in teaching support for patients working with IV pumps. Infection control was on the
global radar. Hand hygiene had always been the poor relation although critically important
and more infections and consequent diseases were being identified by the World Health
Organisation. Guidelines were established in Canterbury for the management of MRSA232
and later published throughout New Zealand.
With the majority of the Association’s 1400 staff based in the community, safety was an
important issue. The client’s home was a work site and the Association took responsibility
for the hazards both inside and out, and how staff could be trained to deal with them. Nurse
Maude was now an accredited occupational health and safety employer. It was one of the
ongoing changes within the sector that was directed to the Association’s human resources
team to manage. The team was also responsible for leading the organisation through the
tentacles of the approaching new millennium.
Y2K preparedness was a government initiative that challenged every business, organisation
and individual to be ready. Almost bizarrely, there were some people in and out of
government departments who genuinely believed technology would explode. Bugs would
sneak into systems and create chaos. Sceptics ignored the rumours, suggesting people
should wind their clocks forward and wait to see if anything happened. New Zealand, as the
230 Stephanie Waterfield, formerly Stephanie Walmisley 231 Nurse Maude Association Annual Report 1999 232 MRSA: Methicillin-resistant Staphylococcus aurus infection. Most MRSA infections occur in people who have been in hospitals or other healthcare settings such as nursing homes and dialysis centres. (Mayo Clinic Definition of MRSA)

[129]
first country to turn over to the year 2000, was watched with interest by overseas
government agencies and private enterprise to see the outcome. Any perceived disruption
would be measured by the Department of Statistics. Being prepared was important
however, and it was an accepted part of the final year of the 20th century.
At Mansfield Avenue, the hospice had benefitted from the appointment of Dr Sandy
MacLeod as its Medical Director in December 1998. Dr Kate Grundy was appointed
palliative care physician in May 1999. Referrals to the palliative care and hospice service
continued to increase. There was greater emphasis on training and quality improvement.
New legislation covering standards for residential care facilities were introduced as was the
proposed Health and Disability Services (Safety) Bill which would introduce new national
standards and make consumer safety the responsibility of the service provider.
During the year, Campbell Ballantyne retired. A stalwart of the Board for many years and a
founding trustee of the Nurse Maude Foundation, the Campbell Ballantyne Fellowship was
established to honour his name and his contribution. The Fellowship would provide annual
funding to study the development in health services delivery and techniques overseas. The
Fellowship would be awarded in alternate years to the Association’s staff and local medical
professionals respectively. Importantly, in order to maintain a discreet separation from the
Association, the new Fellowship would be managed through the Nurse Maude Foundation.
The Foundation had become the investment arm of the Association, Murray Compton said.
One of its key objectives was to support the hospice which would never be fully funded by
the government.
As the year, the decade and the century drew to a close, the ‘Friends’ decided to disband.
Originally founded by Mona Corkill, they had been major contributors to Nurse Maude from
the beginning. As some friends retired or moved away, others came in. Former nurses,
care givers, home aid personnel and others had joined the ranks, willing helpers in the
community promotion of the organisation and its work. During the centennial year, the
‘Friends’ had paid for the refurbishment of Nurse Maude’s headstone in the St Peter’s
churchyard and for a plaque on the nave altar platform at the ChristChurch Cathedral. They
had paid for Nurse Maude’s car which was on permanent loan to the Ferrymead Historic
Park. Now the interest on the money they had invested was to be used to provide an
educational resource for the Association’s staff. The records of the ‘Friends’ would be safely
housed for all time.
A Time of Transition
By absolutely no quirk of fate, midnight came and went on New Year’s Eve, 31 December
1999. The hour ticked over without any disasters. The Y2K Readiness Commission
established by the government faded into oblivion in March 2000. There was more debate
about how to refer to any given year and what it might sound like than any anxieties about
perceived technology problems. New Zealand had spent more than $1billion to ensure it
was Y2K ready – money well spent according to the government. Paul Swain, the Minister
for Information Technology was quoted as saying that many businesses and public sector
agencies had updated their technology and had put business continuity plans in place to
manage future crises. ‘Many New Zealanders are better prepared to handle civil

[130]
disasters,’233 he said. ‘In fact, 80 per cent of New Zealanders surveyed said they had
prepared for any emergency on the changeover to the year 2000 – a huge achievement
relative to other disaster preparedness exercises.’234
The change from one year to another also heralded the change of one government to
another. ‘Externally, we are in transition,’ Stephanie Waterfield told the Board. ‘Our focus
has been on the establishment of the new District Health Boards and a move away from
competition towards population health, community representation, integration of services,
collaboration and transparent processes. The new ideologies have created a raft of
legislation and strategies, all of which have warranted careful consideration. With the health
sector in transition again, many of the Association’s contracts have been rolled over with
little or no adjustment to the prices offered.’235
The health sector was indeed once more in transition. The fifth Labour Government was
elected in 1999 under the leadership of Helen Clark. Inevitably, health was targeted for yet
another round of reforms. The most significant change politically and strategically, was the
dissolution of the Health Funding Authority, the introduction of the Primary Care Strategy
and the creation of District Health Boards. Under the Public Health & Disability Act (2000),
20 such Boards were established, 15 in the North Island and five in the South. The
governance was a combination of elected and selected members. Public voting for
membership would be included in the triennial local body elections. Chairs would be
selected by the Minister of Health. The Health Boards were to be responsible for primary
and secondary care. Importantly, they were both funder and provider of health services in
their region.
The new Canterbury District Health Board covered the geographical area of the original
North Canterbury Hospital Board and included the Ashburton district. Its first Chair was Syd
Bradley, a man well known in Christchurch. The former Chair of the now disestablished
Health Funding Authority, the Crown Health Industry Group and Canterbury Health Ltd, he
had an impressive background in local and central government. Jean O’Callaghan was the
Canterbury District Health Board’s new Chief Executive. Returning from Australia, she was
a welcome appointment to many of Nurse Maude’s staff who remembered her from Regional
Health Authority days, and was considered to have a good understanding of district nursing
and particularly disability support services.
In her 2000 Board report, Stephanie Waterfield talked about some of the difficulties Nurse
Maude was experiencing while the health sector reformed itself yet again. ‘Funding the
palliative care/hospice services is becoming increasingly difficult. The government
announced in July a further $3 million for palliative care services (nationally) but to date no
funding has been received by hospices. It is now 18 months since these providers first
indicated an urgent need for additional funding. Our own hospice/palliative care contract has
had one minimal increase in all of its four years and relies heavily on support from the Nurse
Maude Foundation to provide a service which is personalised and comprehensive.’236
233 Hon Paul Swain MP, media release 27 March 2000 234 ibid 235 Nurse Maude District Nursing Association Annual Report 2000 236 Chief Executive’s Report 2000 Nurse Maude Archives

[131]
Even so, a number of important appointments were made within the service during the year.
Dr Julia Holyoake was appointed Medical Officer, replacing Kate Grundy. Marie Glenys was
appointed as bereavement coordinator and Diana Gunn took on the job of service
coordinator for the integrated palliative/hospice service. Two separate teams were put in
place for palliative care, each working across half of the city, which created more efficiencies
and contributed to improved patient-focused care. Ongoing liaison with Pegasus Medical
Group contributed to greater collaboration between clinicians and the palliative care
programme.
While the Association’s community health service commitments continued unabated, its
internal management structures, strategic direction and the implementation of new
information and technology systems were also receiving attention. The whole focus was on
streamlining systems and processes to make it better. A new client management system
was introduced to enable the Association to better meet the changing needs of the funding
authorities. The new system maintained client identification and demographic information,
managed patient admission and discharges and managed the planning and implementation
of district nursing and home care visits. Ensuring client and patient confidentiality was
critical.
The new system was welcomed for many reasons, primarily though because it created a
sophisticated virtual roster which managed the complex task of planning the Association’s
home visit schedule up to four weeks in advance. At any one time, there were more than
1,000 staff actively working for more than 6,000 clients with up to 60,000 home care visits
every month. The scale of the task had magnified in the previous decade and creating an
information system that effectively managed the roster was essential. Technology also
meant special-purpose spaces being designed to house the equipment, ensuring off-site
access and putting in place business plans for disaster recovery. An off-site satellite
network was developed and new work stations organised for the administration staff. It was
an essential improvement to enable a smoother operational path for the Association.
Fundraising initiatives continued. A gold trail from Cathedral Square to Mansfield Avenue
raised more than $95,000 for the palliative care and hospice service. The annual envelope
appeal also raised money for the hospice and several businesses in the city contributed
financially during the year 2000. It was all part of raising Nurse Maude’s profile, thus
ensuring its place in the Canterbury region. The Foundation’s finances remained in good
shape. Its funds had risen to over $6.5 million with an additional $1.5 million in the hospice
fund. Its investments continued to be carefully managed at the same time providing seeding
grants to identified projects. Then there was the patient welfare fund. When every other
source of funds was explored and an urgent need still existed, this fund could be used for
extraordinary expenses, from language interpretation to spring cleaning, or individual client’s
whiteware repairs. It funded the annual Christmas event for patients and contributed to the
cost of bed hire and patient outings.
‘We know that our founder would be proud of the work that our management and staff have
continued in her name. We, on behalf of our patients, thank them for all the dedication and

[132]
kindness with which they continue to provide service,’237 Murray Compton said at the end of
the year.
Partnering in Community Healthcare
In May 2001, Stephanie Waterfield resigned and the Board appointed Ingrid Thomas a
month later. During her tenure, Stephanie had restructured the senior management team
and the Association’s annual turnover had doubled to $22.3 million. Assets had increased
from $10.6 million to $22.5 million. A more aggressive fund-raising strategy had been
developed and implemented. Now a new Chief Executive was in place.
Ingrid Thomas came from a strong health management background as the General Manager
of Family and Community Services for the South Auckland District Health Board based at
Middlemore Hospital. She was in all respects the steady, safe pair of hands that the Board
wanted to steer the organisation through the ongoing changes in the health sector and to
cement the organisation as one of pre-eminence in its field. Her role in Auckland had
included responsibility for community health, mental health and district nursing, all areas that
were essential to Nurse Maude. Her thesis for her Master’s degree was on alternatives to
hospitalisation. She was familiar with the Nurse Maude ethos and had met several of its
senior staff on different occasions. Now, the Board was looking for someone with Ingrid
Thomas’ tact and diplomacy to lead the Association’s negotiations with its major funder, the
Canterbury District Health Board and to manage its relationships with other key health
providers in the region.
In her first Board report she talked about the latest strategies to emerge from the Ministry of
Health that impacted on Nurse Maude. ‘These strategies have required the Association to
re-examine our own direction and operational procedures as we develop a new approach to
service delivery in which providers work together in the form of a Primary Health
Organisation. A key feature of the new model is the focus on increased community and
consumer participation. Hospital services, primary health and disability services will be
separated, with their own advisory committees on District Health Boards. The relationship
between Maori and the Crown, under the Treaty of Waitangi, will be embedded into
contracts.’238
In fact, the introduction of Primary Health Organisations created all sorts of pseudo political
issues in the health sector. They were explained as ‘not-for-profit organisations funded on a
capitation basis to provide a range of primary health services to an enrolled population.’239
They were formalised on 1 July 2002 and within two years, 53 such organisations were set
up covering about two thirds of the New Zealand population. They comprised groups of
doctors, nurses and other community-based health providers working together under an
organised umbrella. The emphasis was on improving poor health or poor access to primary
health services. The idea was to break away from the traditional fee-for-service treatment-
based system in which the GPs were the main providers.
237 Nurse Maude Association Annual Report 2000 238 Chief Executive’s Annual Report 2001 239 Health Policy Monitor. Toni Ashton, Jackie Cumming 2004

[133]
In Canterbury, there was confusion and some scepticism that the new approach would work.
Ingrid Thomas had a lot to contend with. The new Labour Government had introduced a raft
of new policies and health-related papers that all impacted on the Association. The broad-
based New Zealand Health Strategy, Primary Health Care Strategy, Positive Aging Strategy
and a new paper devoted to improving Maori health were all essential reading. The much-
vaunted Palliative Care Strategy was published in February 2001. Its foreword, by Health
Minister Annette King stated the case for the new plan. ‘This government is concerned to
ensure that all people who are dying and their family/whanau have access to palliative care
services, provided in a coordinated and culturally appropriate way.’240
As the major provider of hospice and palliative care in Canterbury, Nurse Maude had many
reasons for being involved in the strategy’s development. It made early submissions while
Stephanie Waterfield was the Chief Executive, and several of the staff - Margaret Hockey,
Shona Lawson, Diana Gunn, Martine Iggo, Julia Holyoake, Marie Glenys, and Neroli Iles had
attended the many regional meetings organised while the strategy was being developed.
The strategy’s aim was to ‘set in place a systematic and informed approach to the provision
and funding of palliative care services.’241 It would put in place a more responsive system to
support the person’s wish to die at home. The strategy was specific in its reference to care
coordination which was of particular importance to Nurse Maude. The care coordinator
should be responsible for ensuring that the dying person and their family were provided with
information about palliative care options and services. In addition, the care coordinator
should also take the lead in ensuring access to other available services.
Under Ingrid Thomas’s guidance, the Association accepted the new strategy in its entirety,
establishing an alliance with Pegasus Medical Group and inviting fourth year students from
the Otago University’s Christchurch School of Medicine to gain experience in community-
based palliative care by working alongside the Association’s palliative care nurses as part of
their general practice attachment. Nurse Maude was looking after about 300 patients in its
community-based palliative care programme in addition to the patients in the hospice.
‘We needed to show that our nursing service was just as important as the service provided
by GPs,’ Ingrid Thomas said later. ‘Our district nurses were out in the field visiting patients
in their homes every day. As a result, they had a much better understanding of the patient’s
needs and of their home life. It was a completely different service to a patient going to see a
GP in their medical rooms.’242
Ingrid Thomas told the Board that the implementation of so many government-initiated
strategies required the Association to review its own direction and operational procedures.
‘A key feature of the new model (Primary Health Organisations), is the focus on increased
community and consumer participation. Hospital services, primary health and disability
services will be separated, and with their own advisory committees on District Health
240 The New Zealand Palliative Care Strategy February 2001 Ministry of Health 241 Ibid 242 Interview with Ingrid Thomas, January 2015

[134]
Boards. The relationship between Maori and the Crown, under the Treaty of Waitangi, will
be embedded into contracts.’243
The needs of the community were becoming more complex, Ingrid reported. This was due
mainly to the aging population and the number of ‘older olds aged more than 85.’244 Funding
for these patients, many with dementia-related illnesses, was lagging behind their actual
needs. A similar situation existed with wound care, continence advisory services and the
community dietician. Waiting lists had developed and the Association had been required to
call on financial reserves through the Nurse Maude Foundation. At the same time, the
Association had to absorb a number of cost increases for wages, travel allowances, fuel,
dressings and drugs without any corresponding increases in the prices received for core
services. In many respects, the issues were similar to those faced by the organisation’s
earlier management teams – funding existing services and establishing new ones to meet an
expanding demand.
Yet, 2001 had been a positive year for the Association. District nursing had enjoyed an
exceptional year with a huge growth in numbers to a total of 75,214 hours. Total visits had
increased by more than 16,000 which required an additional six full time equivalent staff.
Relationships between Nurse Maude, Pegasus Medical Group and the Canterbury District
Health Board had been strengthened in all areas of district nursing and community care.
The Canterbury Elder Care programme remained high on the staff’s agenda and the
Association had contributed to the development of an Elder Abuse Resource Manual with its
social worker being a member of the Aged Care Forum.
Homecare remained an essential part of the Association’s services. Staff reported an
increase in the number of clients with mental health disabilities, particularly dementia in the
elderly and attention deficit disorders in children. The homecare caseload had increased by
3.43 per cent to 5,771. It was another area, according to the Chief Executive, where
demand outstripped supply.
Although the Rangiora Committee had voted to go into recess in September 2000, the
Association’s district nursing and homecare services in the town and its surrounding
countryside continued to expand as it had done in other parts of rural Canterbury. A
homecare clerk had been engaged to coordinate local activities and a new nurse Gaylene
Clegg appointed to the district nursing team. The Ellesmere and Lincoln areas combined
during the year based at Lincoln with another clerk engaged to help replicate the services
provided in Rangiora and Kaiapoi.
The most significant advancement of the year however was the completion of the new Nurse
Maude Memorial Hospital. The purpose-built 80-bed facility included the Lady Rhodes
Ward, named to honour Jessie Heaton Rhodes, comprising 40 beds for dementia patients.
The Hospital team now comprised registered nurses, nurse aids, a social worker, counsellor,
pastoral care workers, multi-disciplinary diversional therapists and regular support from a
psycho-geriatrician. The Association was hoping to be able to appoint an in-house psycho-
geriatric specialist to complement the services of its Medical Director John Musgrove. With
nursing care and general management facilities based at the Association’s Merivale
243 Nurse Maude Annual Report 2001 244 ibid

[135]
premises, it was undeniably easier for staff and volunteers to feel part of the growing
organisation.
Sibylla Maude’s spirit was always in evidence particularly with the patient welfare fund. Her
philosophy of caring for patients who were unable to pay for health services remained a
central part of the Association’s work. As a result, the fund was called upon to help when a
family needed support for overnight palliative care at home, or night sitters, or pay for special
pain relief medications when there was no public funding available.
The Association’s total staff had once again topped 1,400. In fact, during the previous
decade, staffing levels had fluctuated as a result of several management reviews and the
streamlining of its service provision.
In addition to the ongoing contractual negotiations with the Canterbury District Health Board
and various other health providers, there were annual employment negotiation rounds under
the new regime of the Employment Relations Act. Finding staff particularly for the homecare
service remained problematic. It was not well paid and yet the care needed to be
professional and well managed. Training was instrumental with the emphasis on evidence-
based practice. Nurses needed to be prepared for competency-based practice certificates.
The nurse’s skills and knowledge must meet the needs of the patient, contemporary nursing
practice and the Association’s contractual standards. In fact, the Association demanded the
highest standards from its staff regardless of their role and position. Everyone in the
organisation knew and understood the Sibylla Maude ethos. Behind her philosophy however
was the importance of developing and maintaining the Association’s technology
requirements, keeping up with the latest advancements and becoming a fully computerised,
modern organisation that was fit for purpose.
Ingrid Thomas followed her predecessors’ leads in ensuring the Association had a priority
place within the Canterbury health community. In addition to the Canterbury District Health
Board, Nurse Maude was now working closely with Pegasus Medical Group, Richmond New
Zealand, Te Runanga o Ngai Tahu and key advocacy groups like Elder Care Canterbury and
Age Concern.
A new Nursing Director position was created. Prior to Ingrid’s appointment, the Chief
Executive had incorporated the chief nurse’s job description. The organisation’s strength
had always been its district nursing portfolio and now was the time to give it greater profile.
Ingrid convinced the Board that a Director of Nursing was essential for the organisation’s
professional development and recognition within the health sector. Sheree East was
appointed and almost immediately linked the Association with the New Zealand Nurses’
Organisation, the College of Nurses Aotearoa and started working towards quality
accreditation for Nurse Maude. It was at a time when nurses still accessed their professional
information and news from magazines, journals and other publications. On-line access was
still to be made available. An information library was needed and the ‘Friends of Nurse
Maude’ willingly helped to create a suitable room in McDougall House. Computers were
required, furniture and furnishings were bought. The ‘Friends’ accepted the challenge and
funded the new facility.

[136]
Changes to the Board’s membership the following year gave impetus for new thinking while
maintaining the strong continuity brought by Murray Compton, Caroline Cartwright, John
Drayton and David Caygill amongst others. Colin Averill, the grandson of Walter Averill who
had been Sibylla’s long-standing friend and supporter, retired. Appointed to the Board in
1983, he had chaired the Association as well as the Nurse Maude Foundation from its
inception. Jennie Hamilton, a Board member since 1998 also stepped down as did Derry
Lee. Like all Board members before them, they had made a significant and welcome
contribution to the Association.245
In October 2003, funding for Disability Support Services devolved from the Ministry of Health
to District Health Boards and because a significant part of Nurse Maude’s nursing service
was funded through this service, Ingrid Thomas was particularly careful to involve her
organisation in the pilot programme to be initiated by the Canterbury and Northland District
Health Boards. The imperative was to develop an integrated continuum of care model for
older people’s health services as outlined in the government’s paper The Health of Older
People Strategy 2002.
Canterbury had been selected not only because it had the highest population of older people
in the country but because of the work already achieved by the Elder Care Canterbury
Project of which Nurse Maude was a partner. The name of the pilot project was LinkAGE –
Leading Integration for the Elderly (Te Huarahi Oranga mo nga Kaumatua). The overall aim
was to identify what worked well and what the gaps and barriers were. Then it should review
options for funding and contracts to support an integrated continuum of care model. Ingrid
Thomas was named a member of the steering committee whose key function was to provide
advice to assist the District Health Board in its analysis of what was needed to improve
health and support services for older people.
Ingrid Thomas noted that Nurse Maude had been concerned for some time at the artificial
barriers created by multiple funding streams with different criteria for access and multiple
providers. Simplifying the process was long overdue. At the same time creating a seamless
service required cooperation and collaboration between healthcare providers. While the
days of commercial competition appeared to have gone, she said there continued to be
considerable positioning occurring within the community health sector. It was not helped by
the ongoing controversy over the establishment of the Primary Health Organisations. ‘The
watering down of the intent of a PHO, with very little emphasis being given beyond the need
of general practice, marginalises other health professionals who could add considerable
value to the continuum of care,’246 she told her Board.
Under Ingrid’s guidance, Nurse Maude maintained its smooth operation while recognising
the need for change. It was awarded Quality Accreditation in 2004, presented by Health
Minister Annette King, a significant milestone in the organisation’s ongoing drive for greater
quality systems, controls and measures in all its service delivery.
It was a finalist in the Champion Canterbury Awards and the winner of the Charity Award
instituted by a local insurance company. The launch of the country’s biggest Primary Health
245 Interview with Murray Compton 2015 246 Nurse Maude District Nursing Association Annual Report 2003

[137]
Organisation - Partnership Health Te Kei o Te Waka - was another health milestone for
Christchurch. Its first Chair was Dame Ann Hercus who consulted with Christchurch-based
community groups to assess the views of local stakeholders. The result was the expansion
of the new PHO’s Board of Trustees to include other health providers. Nurse Maude was
one of the additional members.
Greater issues were giving the Nurse Maude Board and its senior staff ongoing headaches.
Funding was becoming a real problem. The Canterbury District Health Board was
considerably overfunded by some $42 million according to the population based formula.
This created tension between the Health Board and its many contracted service providers.
Nurse Maude struggled with the lack of contract price improvements with the district nursing
service not having received a price increase in four years. The Association was in the
difficult situation of bolstering its contracts with support from the Nurse Maude Foundation.
Although the Health Board expressed sympathy for the situation, it did not see how it could
do anything. Its biggest costs were always with its hospitals. ‘It is disappointing that the
very services that could assist with reducing pressures on the hospital service, community
and primary health, are being impacted by financial stresses in other areas of the sector,’
Ingrid explained to the Board. ‘One cannot help but conclude that the hospital services may
well be supported at the expense of the community sector.’247
By 2004, Nurse Maude had consolidated its range of services and expanded others. Home
care remained the largest of its clinical services while district nursing remained central to the
organisation. A range of other clinical and support services backed up these frontline staff.
Care volumes were changing with new technologies like keyhole surgery, blister packs for
medications and new wound-care techniques. The continence and stomal service was
driven by a multi-disciplinary team working in the rural areas as well as in the city. District
nurses were trained in IV delivery which remained in high demand. Referrals to Nurse
Maude’s diabetes service was gaining momentum with referrals from the Diabetes Centre,
the District Health Board and GPs. The wound care team specialised in leg ulcer
management supported by Professor Justin Roake, the vascular surgeon at Christchurch
Hospital. The palliative care service worked alongside the district nurses in a pilot
programme to explore how to better share the care programme. Then there was the
ongoing bereavement service, the creation of an allied health group within the organisation,
the outreach programme in the rural areas and the volunteer programme. A new nurse
practitioner role was recommended and a Maori projects coordinator engaged for a year to
help Nurse Maude implement its Maori health plan.
Behind the scenes, the administration staff acted as the support crew, developing
fundraising opportunities, managing the budgets, keeping up with new personnel and
employment practices and exploring the latest information technology advances. It was a
new way of working in many respects with a more corporate service structure in place. The
Nurse Maude health and mobility shop continued to make a profit and its range of products
included essentials such as walking frames, over-bed tables and lightweight wheelchairs.
Expanding the Boundaries
247 Nurse Maude District Nursing Association Annual Report 2004

[138]
In March 2005, the Association won the contract to develop and manage a new Wellington-
based Care Coordination Centre. It was the start of Nurse Maude’s work outside
Canterbury. Funded by the Capital and Coast District Health Board, it was to be based in
Porirua and modelled on the programme that had been established in Christchurch the year
before.
The main objective was to develop a practical referral management and screening process
that could enable people who would otherwise need residential care, to stay in their own
homes. A key factor in winning the Wellington contract was the development of a new
management information technology system that had proven to be exceptionally effective in
Christchurch. There had been 11,000 referrals in the Care Coordination Centre’s first year
locally which meant appointing more staff.
The time taken to confirm the contract had been a challenge for the organisation which was
not used to negotiating with a different Health Board and its different ways of working. Now
Nurse Maude was branching out and the Wellington office would mean engaging an
additional team of 30 people plus more vehicles and preparing for the opening date of 1
September. The new Centre was to become the single point of entry for clients, referrers and
provider agencies. Like the Christchurch operation, it would screen, triage and coordinate
the care for clients as well as make access easier for rehabilitation services, district nursing,
short and long term home support and residential care for people living in the Capital and
Coast Health Board’s Wellington region. If Nurse Maude could make a success of the
contract, it had the potential to open doors for other opportunities outside Canterbury.
The year was a bright one in spite of the Canterbury District Health Board’s decision not to
support pay parity for the Association’s district nurses who faced a 20 per cent remuneration
gap compared with all other district nursing services which were provided by secondary
hospital services. A similar gap existed for staff providing inpatient services. ‘It is simply not
sustainable for the Association to match the CDHB rates without a commensurate increase
in revenue,’ Ingrid Thomas wrote in her annual report. ‘We are extremely concerned that our
staff are disadvantaged in this way.’
It was no surprise therefore when rumours of industrial action became reality. On 9
September 2005 there was a 24 hour shut down. The strike had been notified well in
advance which enabled Nurse Maude to make alternative arrangements for its hospice
patients who were transferred to Christchurch Hospital for the day. The Nurse Maude
Memorial Hospital was staffed by a skeleton crew of registered nurses for each shift, and
several non-union nurse aides, administration staff and volunteers contributed to caring for
the patients. District nursing provided essential care only. The need to press for the
organisation’s nursing staff to receive pay parity was essential. This required an appropriate
increase in government funding via the Canterbury District Health Board. It was in all
respects a less than satisfactory situation where district nurses employed directly by District
Health Boards could be paid at a higher level than those employed by Nurse Maude. It
disadvantaged nurses who wanted to work for Nurse Maude and was a real frustration for
Ingrid Thomas and the Board. How could they continue to attract professional, highly
qualified and well trained nurses at a lower pay scale than their Health Board counterparts?

[139]
Pay matters aside, Nurse Maude continued to flourish with its services expanding. Home
care, district nursing, continence services, diabetes support, intravenous therapy, a nutrition
programme, stomal therapy, specialist wound care, the hospice and palliative care, meals
service, linen service, and the Memorial Hospital were all part of the organisation’s growing
business. A Memorandum of Understanding was established between Nurse Maude,
Pegasus Medical Group and the Rural Canterbury Primary Health Organisation. Coming to
grips with the PHOs and their role in the health sector had earlier been identified by Ingrid
Thomas as a critical success factor, and the organisation was already working closely with
the Pegasus Medical Group.
While the front line staff maintained the public face of Nurse Maude, significant progress was
being made behind the scenes. Keeping up with the rapid increase in technological
advancement was essential and the introduction of the Association’s first virtual server
enabled it to host a new mail server on existing hardware and to take the first step towards
an improved disaster recovery solution. Having effective IT systems and processes in place
was essential to secure funding contracts. It also allowed the organisation to improve its
ethnicity data collection. Nurse Maude’s Client Management System and Central
Coordination Centre System were modified to enable the recording of multiple Iwi for clients
and carers. Both systems were also modified so that when the National Health Index248
numbers were entered, their validity could be checked. It was all designed for a more
stream-lined service.
An important aspect of Nurse Maude’s corporate services was the preparation and delivery
of meals to identified patients in the community. Surveys had resulted in packaging and
presentation being redesigned. Similar surveys were carried out to improve the laundry and
linen service. As a result new contracts had been secured for other healthcare providers,
sports organisations and bed and breakfast businesses.
Fundraising and events management were now part of the corporate services portfolio with
an emphasis on speaking engagements to raise the Nurse Maude profile, and fundraising
that effectively added $418,000 to the Association’s finances. Nurse Maude also worked
together with the New Zealand Fire Service to install free smoke alarms in patients’ and
clients’ homes. Of special significance was the celebration of the Kaiapoi Committee’s
golden jubilee in 2005. The committee had become the ‘face’ of Nurse Maude in Rangiora
and Kaiapoi and had devoted its 50 years to raising the organisation’s profile in the district,
fundraising and making sure the visiting nurses were looked after.
In its annual statement, the Nurse Maude Foundation reported its capital had now reached
$7,352,713 million. It supported the annual grants from the Campbell Ballantyne Fellowship
and the year’s major projects included a research initiative to address overcrowding at
Christchurch Hospital’s Emergency Department and a proposal to examine the
hospital/community interface and identify alternative strategies for the care of non-urgent
patients.
The Association was about to celebrate its 110th anniversary. It was time to take stock.
There would be more changes to the Board with the resignation of long serving members
248 The National Health Index (NHI) was introduced in NZ in 1993.

[140]
Caroline Cartwright and John Drayton and the announced resignation of Chief Executive
Ingrid Thomas. ‘She has provided us with an excellent basis on which to continue to pursue
and implement best practices to attract, retain and develop talented people, making the
Nurse Maude Association an employer of choice,’ Murray Compton said.
Ingrid was leaving after five years at the helm. During her tenure, she had participated in
some major changes within the health sector. Internally, she said her success rested with
her staff. ‘I always attended staff orientations. It was important for new staff to know from
the outset that Nurse Maude was a wonderful organisation.’249
Accreditation had been achieved through the dedicated efforts of all her staff. Being
involved in the creation of the Primary Health Organisations had been a major achievement.
Monthly meetings with Pegasus Medical Group’s Chief Executive Paul McCormack and his
senior managers had been invaluable. Her time as Nurse Maude’s Chief Executive had
been extremely rewarding, she wrote. She was particularly pleased with the establishment
of the Director of Nursing position and Sheree East’s ability to review and reorganise the
nursing structure within the organisation.
‘I believe the role of the CEO is a little like a relay runner; you run as fast as you can for as
long as it takes, and at full speed, then hand the baton to the next runner. It is the joint
efforts of the entire Association that enables it to be a winning team. We have some
outstanding team members and I feel confident that as the Nurse Maude Association
celebrates its 110th year in the Canterbury community, it is well placed to continue for
another 110 years.’250
249 Interview with Ingrid Thomas, January 2015 250 Nurse Maude District Nursing Association Annual Report 2006

[141]
Chapter Two: The Drive for Efficiency and Innovation
110 Years On
‘Sibylla Maude was innovative,’ Murray Compton told the Board at its 2006 Annual General
Meeting. In a retrospective commentary, he wrote: ‘She was aware that the community did
not understand the danger of infection and lacked knowledge of prevention measures. In
1903 when the city was faced with a rapidly increasing number of tuberculosis cases, she
organised TB camps in an attempt to ease the spread of infection. She was also the driving
force behind the nursing relief centre and controlled smaller depots and was later reported in
the daily paper as the ‘hardest-working woman of the epidemic. 110 years on, the name of
Nurse Maude is still easily recognised as a leading provider of community healthcare.’251
The Association had moved with the decades in all respect, modernising its business,
adapting to the ever-changing political environment, recognising technological advances,
adopting clinical improvements and taking every opportunity to meet and extend its
commitments to its community. It had never wavered from Sibylla’s original premise of
helping the sick poor and tending to the frail elderly. What had changed however was the
need to forward plan, to invest in innovation and to manage risk. Expanding the business
while managing the constant financial outflow was essential and to achieve this, the Board
needed to make sure financial pressures were manageable and sustainable.
As it acknowledged its new milestone, the Board began its search for a new Chief Executive.
Originally from Britain, Jim Magee came to Nurse Maude with an impressive record in health
management, strategic planning and organisational development. His previous 20 years in
the health sector included senior leadership and management roles at Dunedin,
Christchurch Women's and Christchurch hospitals. He was familiar with health politics and
understood the need to maintain and strengthen relationships with the District Health
Boards, Ministry of Health and other public health organisations as well as the voluntary
groups and agencies that existing in Canterbury.
There were some immediate priorities. Nurse Maude had aging software that was unreliable
in a world where technology was a prerequisite to successful business practice. It had
resulted in complicated record keeping which was costing the organisation more than it was
achieving. Better financial structures were therefore essential and David Hackston was
appointed as the Association’s first Chief Financial Officer. His immediate task was to take
a broad look at financial disciplines and to implement change. The workload involving care
coordination was increasing at a rapid rate and there was scope to achieve more with the
potential for contracts to be initiated outside Canterbury using the Care Coordination Centre
initiative as the model.
251 Nurse Maude District Nursing Association Annual Report 2006

[142]
Changing his management team to bring a more comprehensive level of professionalism
and expertise to the organisation was the central tenet of Jim Magee’s thesis that there
needed to be a more cohesive level of strategic planning at the helm. He believed that
efficiencies were easier to find when the organisation was in growth mode and that growth
itself was the reward for success. He needed a team which could balance the imperatives of
finance with the development of business and information technology. He needed
professional people with the right qualifications. Relationships with existing and potential
funders, he said, were essential.
There were two key areas that Jim Magee recognised as important for Nurse Maude’s
growth and development – the Canterbury District Health Board as its principal funder and
Pegasus Medical Group as a long-term partner. He went to the Nurse Maude Board at the
end of his first year with his strategic planning process well defined and based on an
internationally recognised business excellence model – the Malcolm Baldridge suite of
principles designed to stretch the ISO 9000 model to a higher level. Its performance criteria
centred on innovation management, intelligent risk and strategic priorities, operational
effectiveness, work systems and core competencies.
More new appointments to the senior management team were made. Sue Bramwell was
engaged as the Marketing and Communications Manager, charged with reviewing the
organisation’s brand and image, identifying where improvements could be made and ways in
which the Nurse Maude profile could be enhanced. She would be responsible for exploring
ways in which fundraising could be updated and modernised.
There were changes too, around the Board table with David Caygill resigning to take up an
appointment as Chair of the New Zealand Electricity Commission. Alongside ongoing
internal management improvements, Jim Magee worked with Board Chair Murray Compton
to introduce separate committees dealing with the governance of finance, audit, fundraising,
ethics, community services and quality.
There were strategic and governance issues that needed to be dealt with, Murray Compton
explained later. Nurse Maude was operating in a very different environment compared with
the terms of previous Chief Executives. The precise nature of business management was
different. As a result, pay scales were different.
‘We engaged external consultants to benchmark Nurse Maude with other similar charitable
organisations in the not-for-profit and NGO environment. We didn’t want to over-emphasise
the difference in roles, but we didn’t want to under-estimate them either. It was unrealistic to
expect our staff to perform with professionalism and to the highest level of expertise and yet
to expect our Board as the overseeing governance body to be amateurs.’252 The concept of
governance and management had changed over time, he said. There were formalised rules
in place that Nurse Maude must adhere to. ‘We used to shoulder tap the people we thought
would make a contribution to our Board. We couldn’t do that any longer. We needed to look
for skills that would enhance our organisation.’253 The result, he said, was a decision to pay
252 Interview with Murray Compton, December 2014 253 ibid
[143]
Board members for their work. ‘We consulted with staff who were unanimous in their
agreement.’254
Alongside these Board changes, two other important infrastructure and management
systems were reviewed and assessed. A team of consultants reviewed community nursing
and homecare to look at how these two essential services could be more efficient. The
process for rostering staff and allocating work were the areas highlighted and cost
reductions could be made in back office activities by improving work flows and computer
systems. At the same time, business continuity planning in the event of any catastrophic
event came under scrutiny. Core systems needed to be replicated to a secure off-site facility
with servers maintained as stand-by operations. In addition, it was proposed to develop an
offsite business continuity facility with telephones, computers and printers for up to 15
administrative staff. Everything was designed for immediate implementation in the event of
a serious emergency.
For two years, the Association had contributed to the Canterbury-wide pandemic planning
programme. It was one of the outcomes of the H151 avian flu epidemic in 2005 which had
followed on from the virulent SARS255 outbreak that had occurred two years earlier. Being
prepared for a potential disaster was an essential component of the Baldridge criteria and it
make sense therefore that Nurse Maude should commit to the ongoing regional planning
within the health sector and at the same time develop and embed the Association’s own
disaster recovery plan. Identifying potential risks and making sure there were adequate
systems and processes in place in the event of an emergency or major disaster were
absolutely essential.
During the year, the Association was part of the Canterbury District Health Board’s project to
develop and implement a new model of homecare service for older adults. The proposed
restorative model had already been adopted by other Health Boards including the two with
which Nurse Maude had existing contracts – Capital and Coast Health and Hutt Valley
Health. The aim of the model was to maximise the independence of older people who
required support by providing more integrated and flexible home based services. Integrated
care that extended across primary, community, hospital and social care was a goal for the
health sector internationally and Canterbury was no exception. Although the project was not
yet completed and it was not fully known what changes would be required, the Association’s
Director of Nursing Sheree East was clear that high level information systems support would
be required in addition to increased training and professional development for the front line
staff.
After extensive lobbying the pay disparity between nurses employed by District Health
Boards and community organisations was resolved and Nurse Maude successfully
negotiated a contract price increase for its district nursing staff. It was a red letter day.
Of all the nursing initiatives that occurred during the organisation’s 110th anniversary year,
the opening of the Referral Management Centre took top billing. It enabled all referrals to be
254 Interview with Murray Compton, December 2014 255 SARS: Severe acute respiratory syndrome

[144]
checked, processed and logged into the Client Management System with the referrals then
forwarded to the relevant department.
Jim Magee identified several major projects for the 2008-2009 financial year that required
additional budget. It was essential to improve the financial viability of the district nursing and
homecare support services, create a strong procurement system based on best practice and
ensure ongoing quality and excellence in service delivery for the Care Coordination Centre
in Wellington, he told the Board. A call centre for Nurse Maude needed to be set up that
would cover all of the Association’s services except care coordination. And, he insisted on
documentation of the Association’s policies and procedures not only for the staff but for the
Board.
As part of a review of the Campbell Ballantyne Fellowship, the Director of the New Zealand
Institute of Community Care Chris Hendry suggested tighter application criteria be
implemented. She also proposed that the Fellowship be managed by the Institute as Nurse
Maude’s research arm, and that the selection process remain with the Nurse Maude
Foundation. It was a proposal that found favour with the Board, particularly the decision that
the Fellowship remain open to staff and related providers.
In 2008, the Association received a grant of $50,000 from the Sutherland Self Help Trust to
go towards building a roof garden on the Memorial Hospital. It was a generous donation
from a national organisation dedicated to helping community groups.256 It was also reflective
of the ongoing bequest programme that enabled the Nurse Maude Foundation to grow. At
the same time however, the Board recognised that it could not rely on the Foundation’s
investments to subsidise its government contracts. It needed to have more efficient systems
in place which included adopting international finance and accounting standards.
But no one had predicted the global financial crisis that was about to impact on the New
Zealand economy. The recession that followed was, as Jim Magee told the Board, a
defining characteristic of the 2009 and 2010 years. In real terms, he said, the government
health spend had continued to increase but at a lesser rate than previous years and certainly
behind the drivers of cost including wages, population growth and population ageing. The
result for Nurse Maude was a two-year period of no price increases in most of its contracts.
‘In a world recession, such as we are experiencing, no organisation can claim exemption or
opt out of the effort to lessen the impact. At Nurse Maude we have increased our focus on
efficiency and cost control, particularly on administrative and support functions.’
It had been a challenging year for Nurse Maude with an incurred deficit of around $1 million
offset by gains in the value of its investments. ‘We have taken the view that the Nurse
Maude investment fund is there to benefit future as well as present generations of
Cantabrians and that to spend capital, as distinct from income, would be irresponsible.
Therefore the level of service we provide is determined by contract revenue, income from
fundraising and investment income. As an efficient provider and with no requirement to
256 The Sutherland Self Help Trust, established in 1962 by the owners of New Zealand’s first chain of grocery stores – the Self Help Co-op.

[145]
provide for shareholders, we are in a position to provide an exemplary level of service but
most also accept the fact that financial and economic realities impose their limits,’ he said.
Such administrative challenges had become normal business for the organisation to be
managed in the office while the district nursing and home care services continued in the
community. There were now 225 district nurses working in the community. The vehicle fleet
had grown to 145 to enable the staff to travel around the region. The acute demand service,
developed in collaboration with Pegasus Medical Group continued to provide the equivalent
of hospital care in the patient’s own home.
Nurse Maude’s specialist hospice and palliative care programme provided a 24 hour service.
The team included nurses, doctors, bereavement counsellors, researchers, educators,
chaplains and volunteers and covered the Canterbury area from Kaikoura to Ashburton,
Banks Peninsula and the West Coast. In the hospice itself, patients were admitted in order
to better manage complex health symptoms and for terminal care.
As the community healthcare programme had expanded and developed with the emphasis
on enabling people to stay in their own homes for as long as possible, admissions to Nurse
Maude Hospital had changed with patients now coming in at a much later stage of their lives.
Their care was managed by the nursing team supported by a physiotherapist, occupational
therapist, family support counsellors and a chaplain. Volunteers helped with meals,
entertainment and organised visits.
The Care Coordination programme had grown exponentially in Canterbury and Wellington
since the additional contracts with the Capital & Coast, and Hutt Valley District Health
Boards had been implemented. The service was different in each location depending on the
contracted service, according to Deb Nind Nurse Maude’s General Manager for Care
Coordination. The emphasis in both the Wellington region’s services was on people over 65
years and on chronic health conditions. A new electronic clinical management system had
been introduced which had improved and streamlined the service. It enabled trends to be
identified with evidence-based outcomes that would benefit the client.
The Canterbury service had expanded with the introduction of a care team for non-complex
clients, a two-year initiative to reassess long term non-complex clients who received long
term care in the community. It was all part of Nurse Maude’s intention to maintain its
permanent position as a high performing, quality care provider.
District Nursing – Aspirational, Competent and Responsive
‘The district nurse role is the foundation of a system which should be able to manage
conditions and keep sick and frail people at home.’ Royal College of Nursing June 2014
Under Nurse Maude’s first two Chief Executives, Anthea Bowden and Stephanie Waterfield,
nursing retained its high profile position in part because both women had nursing
backgrounds. They understood the sector and could easily identify with the nursing
hierarchy and its variances. When Ingrid Thomas came into the role, her background was in
health management. She recognised the need for effective clinical services management.

[146]
In 2005, the key development had been the integration of palliative care into the district
nurse’s role. It was designed to increase the scope of practice and to provide a more
comprehensive service to patients. Nurse Maude’s palliative care handbook was reprinted
and gained in popularity with orders coming in from around the country.
In conjunction with the Christchurch Hospital’s urology department, Nurse Maude’s
continence team conducted a detailed internal assessment of treatment outcomes. The
study looked at quality of life, evaluation of outcomes and the effectiveness of the treatment
process. At the same time, there were ongoing discussions with the gynaecology service
and the colorectal ward at Christchurch Hospital to share information about stomal therapy.
It was a health contract that Nurse Maude had transformed into a high quality, personalised
service. District nurses caring for diabetes patients worked alongside the Diabetes Centre
and other providers to share information.
Specialist care had increased incrementally over the previous five years, and through
Ingrid’s determination to ensure Nurse Maude enjoyed positive relationships with other
providers and interest groups, new and existing links were forged and strengthened.
In 2008, Nurse Maude’s Director of Nursing Sheree East developed a comprehensive
nursing strategy designed to take the organisation through to 2015. It was the first time a
dedicated long-term strategy for Nurse Maude’s district nurses had been created giving
goals and objectives that were based on contemporary nursing methods and technologies
while remaining faithful to its founder’s principles. It took into account government policies
and plans that related to Nurse Maude’s work together with staff satisfaction surveys and a
community nursing cultural climate survey. The outcome, Sheree believed, should be a
competent and responsive workforce with a service model that could meet community’s
changing needs. Her appointment in 2001 had been one of Ingrid Thomas’ initiatives. Until
then, the women who had headed the operational side of the business had all come from a
nursing background whereas now it was clear the role should be separate. Under Sheree
East’s direction, Nurse Maude could become a magnet organisation, attracting and retaining
well-trained professional nurses and contributing to the end goal to be a leader of community
nursing in New Zealand. It was a visionary and aspirational aim to give district nursing and
the Association a higher profile.
The Liverpool Care Pathway was introduced to improve patient care in the hospital and the
hospice. Developed by the Royal Liverpool University Hospital and the Marie Curie
Palliative Care Institute in Liverpool in the late 1990s, it was universally accepted as an
improved approach to help doctors and nurses provide quality for people at the end of their
lives. It would become internationally recognised as the gold standard of care for the dying
patient by 2014. Its identified purpose was to standardise and manage the quality of care
that a patient received and it included guidelines for the control of symptoms, ongoing
assessment and then care for the family after death.257
257 In New Zealand, the Liverpool Care Pathway national office was established at Arohanui Hospice in New Plymouth. In 2006, there were 12 sites in New Zealand registered to use the Care Pathway. By March 2011 there were 278.

[147]
Nurse Maude’s specialist hospice palliative care programme provided a 24 hour service.
The team included nurses, doctors, bereavement counsellors, researchers, educators,
chaplains and volunteers and covered the Canterbury area from Kaikoura to Ashburton,
Banks Peninsula and the West Coast. In the hospice itself, patients were admitted in order
to better manage complex health symptoms and for terminal care.
Developing a practice handbook for nurses was essential, Sheree believed. She had
launched it in November 2006 and at the same time started a nurse practitioner trainee role
at the Memorial Hospital. Preliminary results showed a reduction in infection rates and the
number of falls since the role had been established. It augured well for the future of the
position which had been funded by the Nurse Maude Foundation and supported by the
Christchurch Polytechnic Institute of Technology’s nursing programme.
As a member of the senior management team, Sheree East was ideally placed to push for
centres of nursing excellence to be developed. ‘We aspire to be a leader in community
healthcare in Canterbury and beyond,’258 she wrote when she presented her paper to
develop a new institute for community health care. ‘For the Association to truly lead in the
community, this must be underpinned by evidence of the outcomes of our care. Our
success will be dependent on our ability to be a magnet to the best workforce who are
knowledgeable and have opportunities to develop, grow professionally and contribute.’
In her paper, she outlined what was required to develop centres of excellence. It required
research, evidence-based practice, education, partnership with other institutions to develop
new techniques and initiatives. The emphasis should be on interdisciplinary research,
encourage scholarship in nursing and link the clinical environment with the academic world.
The best way to achieve this was to create a separate institute. Nurse Maude was proud of
its professional staff who played an invaluable and crucial role in the delivery of high quality,
evidence-based patient care. For some time, the Association’s clinical staff and the Capital
& Coast Central Coordination Centre had been undertaking ground-breaking work and a
number of new initiatives had been trialled to strengthen community care. Research and
development opportunities were being generated at an ever-increasing rate but were often
restricted to the individual clinical area and at times Nurse Maude found itself under pressure
to further explore and explain these opportunities without being able to establish the
associated intellectual property. Creating a research institute would help resolve these
issues.
The institute would form an entity similar to the Nurse Maude Foundation with a clearly
defined mission, goals and objectives. It would integrate education, research and clinical
practice, raise the profile of community care, provide opportunities for partnerships to be
developed, create career opportunities and provide a means for developing knowledge
about the results of Nurse Maude’s care. In essence, the institute would work across the
health sector engaging with other community organisations to develop joint research and
learning opportunities. And, it would strengthen Nurse Maude’s capacity to fully benefit from
its research and development.
258 Board Paper presented by Sheree East July 2006

[148]
Sheree East also believed an institute would be able to work closely with such established
health organisations as the Victorian Royal District Nursing Service in Australia and its
associated Helen Macpherson Smith Institute of Community Health. Nurse Maude already
had well established links with the Christchurch Polytechnic Institute of Technology through
the provision of specialist nursing educators and the development of the Nurse Practitioner
role. Summer studentships had been established working with the University of Canterbury.
Joint research projects and shared appointments could be developed under an institute.
Nurse Maude’s Board approved the concept and a full business case was prepared. Under
Professor Ian Town’s direction, the new institute took shape. It was to be a separate entity,
fully funded by the Nurse Maude Foundation in its start-up phase, and with its own Board.
Dr Chris Hendry was appointed in 2007 as the inaugural Director. A nurse and midwife, Dr
Hendry had worked as a post-graduate lecturer at Victoria University and the Otago
Polytechnic and was an Adjunct Associate Professor at the University of Canterbury’s
School of Health Sciences. She came with impressive qualifications and experience. Rose
Laloli, Jim Magee and Sheree East joined Ian Town on the Institute’s Board. It was the
Director of Nursing’s highest achievement in her quest to put Nurse Maude on the map as a
centre of excellence in health research and educational knowledge.
Reflecting on the institute’s success, Murray Compton said later it was one of the
Association’s greatest achievements. ‘We wanted it to have a mandate that was broader
than Nurse Maude and Canterbury,’ he said. ‘The Foundation provided the seeding funds to
get it started. We believed it could be self-sustaining and we made the right decision.’259
The institute was fully functioning in its own right, at the same time, giving Nurse Maude the
validation it required to maintain its position as the major provider in district nursing for
Christchurch and Canterbury.
In a comprehensive report on district nursing services in 2010, the Ministry of Health
identified the service’s key objectives as preventing avoidable hospitalisation and enabling
early hospital discharge, providing support at home for patients with short and long term
health conditions, promoting patient self-care and independence, and, providing identified
palliative care in the community. The report profiled district nurses as providing a viable
alternative to hospitalisation for patients. This previously ‘invisible’ workforce, provided a
wide range of increasingly complex care in the community for people who would otherwise
have required hospital treatment or admission. The district nurses had developed
collaborative relationships with both hospital services and primary care teams, particularly
GP-based services.260 The report was recognition in all respects of the district nursing
service provided by Nurse Maude.
From Home Aid to Home Care
The separation between home care and district nursing was a gradual process. The two
were almost inseparable in Sibylla Maude’s day. Her duties covered the full range of care
259 Interview with Murray Compton, December 2014 260 District Nursing Services in New Zealand: Ministry of Health Report 2010

[149]
mainly because she had a strong view that her care was all encompassing and if there were
some additional duties that were apparent to her intuitive eye, then she dealt with them
promptly. Her household book was more than her home nursing suggestions of fresh air,
sleep and wholesome food. She wrote about the beauty and bounty of a home garden –
what fertilisers should be applied and when vegetables should be planted. She stopped
short of good housekeeping suggestions although she included notes about disinfectants.
Mona Corkill raised the issue of domestic duties in the early 1940s. She was concerned that
her nurses were doing more than they could cope with. Increasing the number of nurses
was not the solution, she believed. Throughout the decade and into the early 1950s, Mona
continued to press the point. There were now 17 district nurses but the issue of insufficient
home help was not yet resolved. In 1953, she was successful at last. The service started
with one full-time home aid followed with two additional part-time staff. Elsie Simpson was
appointed to organise the home help service and by the end of the year two more part-timers
were appointed and several volunteers had offered help.
In 1963, the government announced that home aid services would be free to patients for as
long as they required nursing care. Nurse Maude was contracted by the North Canterbury
Hospital Board to provide domestic help. More administration staff were required to manage
the increased number of home aiders up to 152. Their pay packet was slim however with an
hourly wage of five shillings and threepence. Women who entered the home aid service
tended to have young children at school or were older. They were often beneficiaries who
depended on social security for their income which they supplemented by taking on
additional work like housekeeping or home aid. In fact, it was a comparatively low paid job
and one that was not destined to change regardless of the respect felt by the care recipients
and the value Nurse Maude put on the workload. It frustrated the organisation but it was
totally reliant on the state subsidy. By 1978, the home aid teams numbered 227 and were
capably managed by Millie Slater. Rapid expansion of the service continued and a new
department was created within Nurse Maude to manage the growing need.
As the home aid service expanded, so did recognition of its contribution to the health reforms
with more emphasis on people being cared for in their own homes rather than being
hospitalised for long periods. Under Stephanie Waterfield, the service was reviewed and
revamped. Its new title of Healthcare Home Services better reflected its work, she
recommended, and engaged Sandra Lockwood as its manager.
By the time Nurse Maude had achieved its centennial year, home care was firmly
established as a complementary service to its district nursing companion. Clinical services
were the district nurses’ responsibility. Home care included domestic assistance and
personal care, plus numerous other services to enable people to remain independent and
stay in their own homes. It enabled patients to leave hospital earlier, or to be supported at
home rather than be admitted to hospital. Demand outstripped supply. In line with its
partnership philosophy, Nurse Maude liaised regularly with other similar services in
Canterbury and was represented on the Elder Care Canterbury Forum.
In 2002, the home care service celebrated its Golden Jubilee. Ingrid Thomas had initiated a
call centre to improve access to home care services. Clients included adults and children,
the elderly, people with physical or age-related disabilities and those recovering from

[150]
surgery. The annual statistics told the story with 553,696 home care visits covering 8493
clients. By 2005, home care was identified as the largest of Nurse Maude’s clinical
services.261 Remuneration continued to be a national issue however. The Association made
submissions to the Select Committee reviewing the level of carers’ wages, and there was
welcome news in March the same year when carers received a pay rise. There was
increased emphasis on improving the recruitment process for new carers, increasing the
range of training programmes and providing more opportunities for permanent contracts to
be initiated. It was all designed for staff retention and employment sustainability.
Successfully managing the contract to ensure the number of home visits could match the
increased demand was essential. When Jim Magee was appointed Chief Executive, one of
his early tasks was to review the programme. He realised that home care was under-valued
in funding terms compared with the high level of success it achieved. However, he said, it
would remain one of the lower paid services because of the way it was funded. Even so, it
was highly appreciated by patients and clients. Personal care included mobility needs and
meals, personal grooming and bathing seven days a week if required. Domestic help
covered laundry, cleaning, bed making and essential shopping from Monday to Friday.
In 2008, Nurse Maude was part of the Canterbury District Health Board’s project to develop
and implement a new model of home care service for older adults. It took two years for the
pilot project to be successfully implemented and resulted in significant gains in both the
health and function of Nurse Maude’s patients including better utilisation of existing and
specific services like the Arthritis Society, which enabled patients to enjoy increased
independence for longer in their own homes. The combination of the pilot and the increasing
complexity of care demanded the home care staff be available seven days a week including
evenings. This in turn required Nurse Maude to ensure it had a skilled, responsive team to
meet the challenge. Its staff started to work towards the New Zealand Qualifications
Authority Level 2 Foundation skills Certificate. It was an added bonus to attract and retain
staff particularly when demand was constantly outstripping supply.
The integration of home care and district nursing was essential for Nurse Maude to create a
seamless service in Canterbury. At the same time, the two operations were different, albeit
complementary. By encouraging greater emphasis on qualifications for its home care staff,
the organisation could broaden the range of services being delivered with the emphasis on
helping patients retain their independence.
‘Freedom is sweet’, Sibylla Maude used to say when she attended her patients. Although
she would give as much help as possible, her mantra was always to encourage
independence. The cruellest thing a social worker could do was to take away a family’s self-
respect.
Volunteering Builds Strong Communities
Ma nga huruhuru te manu ke rere (with feathers the bird can fly)262
261 Nurse Maude Association Annual Report 2005 262 Report of the Ministerial Reference Group for International Year of Volunteers 2001

[151]
From its earliest beginnings, Nurse Maude was blessed with benefactors and supporters.
Community-spirited individuals who believed in what Sybil was doing made financial
contributions to her work or, if they could not afford to donate money, they gave their time in
kind. They endorsed her district nursing by organising jumble sales and cake stalls, forming
sewing circles or simply calling themselves ‘Friends.’
As part of its 2000 annual report, the Board decided to formally recognise this generosity by
naming the people and the organisations who made donations to the Association or to
different aspects of the organisation’s work. The names ran to several closely typed pages.
Donations to district nursing, donations to continence supplies and the stomal department.
Donations to the home care service, donations to the Foundation, donations to the Memorial
Hospital, donations to palliative care and donations to the hospice, the latter generating a list
containing hundreds of names. They were a validation of the Association’s work,
representing people who had benefitted from Nurse Maude’s services and they identified
people and organisations who recognised more than a century of commitment to
Christchurch and Canterbury.
These donations and bequests enabled the Association to continue its work especially in
areas where its health contracts did not cover all its costs. Acknowledging these
contributions was an essential component of Ingrid Thomas’ role as Chief Executive and
also of the Board. Recognising the growing number of volunteers remained a priority and
the following year, the annual report included the names of its volunteers, its subscribers and
its members. Once again, the lists ran into several pages of names in alphabetical order.
The size and scope of the volunteers covered the full range of services – helping in the
hospital, in the community or working on a fund-raising mailout. Email was still to come, and
filling envelopes was a time-consuming task.
A team of 10 volunteers was selected to assist with Nurse Maude’s bereavement services.
They were trained in telephone skills, basic information about disease processes and
effective communication. This initiative was established with a grant from the New Zealand
Lottery Grants Board as part of the International Year of the Volunteer. Ingrid Thomas, like
Stephanie Waterfield and Anthea Bowden before her, was very aware of the need for not
only developing a highly skilled volunteer force, but for taking full advantage of available
external funding. Other volunteers were chosen to provide a diversity of cultural
perspectives, skills and life experiences. With the United Nations designating 2001 as a
global recognition of volunteers, it was an opportunity to give a special vote of thanks to the
Canterbury people who supported Nurse Maude.
They were the bridge between the political budget and the defined need. Fundraising
remained core to the management team’s ability to balance its books. As part of the year’s
programme, Nurse Maude contributed to a national project called ‘A Night to Remember’ in
which hospice supporters invited guests into their homes for a fundraising meal. Each
dinner guest was invited to make a financial donation. It was a great success.
Other highly innovative funding events took place during the year including several
Christchurch business people agreeing to appear before Christchurch mayor Garry Moore
as the ‘sentencing judge’ to raise $36,000 for the Hospice’s operational costs. Sentenced
for ‘dubious crimes’, the group raised the funds as part of their ‘bail’ conditions. The Hospice
also benefitted from monies raised at a variety concert in the Theatre Royal.

[152]
In September 2000, the Rangiora Committee went into recess. It had been in existence for
50 years, a volunteer group instrumental in organising the first rural district nurse for the
area. While a long-time contributory to the Association, it had been overtaken by modern
communications, new technology and a highly efficient administration team working from the
Mansfield Avenue offices. Ongoing training for volunteers was a central part of the whole
operation. They contributed in every aspect of Nurse Maude’s work from providing
companionship in the hospital and hospice to bereavement services, visiting patients in the
community and supporting the administrative staff.
Less than a decade later, a pool of 265 volunteers was available to keep the hospice shops
operational, work in the laundry, in the Nurse Maude grounds, the hair salon and support
fund-raising events. In 2010, they recorded nearly 20,000 hours of support, therapy and
comfort to patients in both the hospital and the hospice. The volunteer programme was
acknowledged nationally as an example of best practice in recruitment, orientation, training,
support and retention.
Marketing Nurse Maude
‘Caring for the people of Canterbury since 1896’
In 1896 when Sibylla Maude stepped out on her own, she instinctively knew that she was
her own best marketing tool, even if the terminology was not so defined during her tenure.
The Nurse Maude image was an imprint for the sick and the needy in the poorer suburbs of
Christchurch. The careful selection of her uniform was not just for comfort (not that it was
necessarily so) or its long-lasting abilities, it was designed to make a statement, so that
Sibylla stood out from the rest. She had learnt this from her working experience in London.
The impression that she left with her patients and her response to their needs ensured it was
a badge of honour to have been tended to by Sibylla and later by one of her nurses and it
generated respect from her patients. In death, as she lay in state at ChristChurch Cathedral,
she was dressed in that same time-honoured, starched, blue uniform.
As the organisation grew and its structure developed, two strands were created to work side
by side. The operational arm of the business was capably managed by Sybil and her team
and endorsed in their turn by Mona Corkill and Marjorie Rae. They accepted the mantle of
public relations as part of their work, attending evening meetings, accepting speaking
engagements and generally promoting Nurse Maude every time. They did it without the
luxury of marketing aids or an increase in their pay packet. They spoke off the cuff – their
uniform acting as the demonstration model rather than banners and posters.
When Sibylla produced her household book it was a cleverly conceived fund-raising tool for
the Association, supported with judiciously placed and carefully worded advertisements.
Whether it was intentional or not, the book with its recipes and helpful hints for the home
ensured the name Nurse Maude remained a household word. The district nurses
maintained the Nurse Maude image out of respect rather than duty. They wore the uniform
with pride and embraced the organisation’s unspoken values of care and empathy. They
had a shared ownership of everything Nurse Maude represented.

[153]
Because the Association was so much a part of the community, it contained all the elements
of positive charity that was recognised by the more affluent members of the Christchurch
society who were encouraged by Jessie Heaton Rhodes and her influential friends to
contribute financial support. People who could not make moneyed donations gave their time
and commitment with dressmaking, donating goods, serving on committees and parish
giving. It helped that Sybil came from a privileged background and through her family and
friends, knew who to turn to when required. It helped too, that her backers were well known
and knew who to contact when the need arose. It also helped that she had left her position
as matron of Christchurch Hospital with goodwill rather than rancour.
Keeping the community informed was also a task for the Board and the pool of volunteers
right from the start. Speaking about their work to friends, neighbours and colleagues gave
substance and gravitas to the organisation. The Tai Tapu Wellwishers initiated in Sybil’s day
through Jessie Rhodes, the ‘Friends’ started by Mona during her tenure, all gave the
Association a broader canvas upon which to advocate for its purpose and to generate funds.
Exploring the more strategic benefits of fund-raising, marketing and public relations did not
feature highly on the Association’s agenda until the era of the Chief Executive entered the
realm of health politics. Anthea Bowden recognised the need, Stephanie Walmisley initiated
it, Ingrid Thomas extended it, and Jim Magee took affirmative action.
Annual reports became more formalised, polished, professional documents that could be
used when meeting with funders, potential partners and other health organisations. They
served their financial purpose at the same time giving a public face to the many aspects of
the Association’s work. Before the advent of the internet and web-based publishing, the
annual report was the main tool to highlight the year’s achievements and to thank volunteers
and staff for their support. It could be distributed to funders, backers and supporters, given
to politicians and visiting guests.
Nurse Maude like many similar organisations, took stock of the prevailing marketing
environment and regularly changed colour-schemes, brand names, logos and straplines.
From its inception, it went from being recognised as the Christchurch District Nursing Fund
in 1901, to the Nurse Maude Association for District Nursing in 1918, the Nurse Maude
District Nursing Association in 1936 as its first constitutional rule, abbreviated to Nurse
Maude Association, NMA as an acronym in the 1990s, and eventually, at Sue Bramwell’s
insistence, it settled on simply being known as Nurse Maude. It moved with the times from
stepping out on foot, to bicycles, the corgi scooters, the occasional motor car and eventually
a fleet of cars with Nurse Maude’s signature slogan signwritten on its doors. The cars, like
the earliest horse and cart, followed by the black bicycles would become Nurse Maude’s
visual presence in the community.
Sue Bramwell, adopted a firm view on how the organisation should be perceived by its
public. ‘We have been caring for our community since 1896. It is an honour that no other
community health organisation can claim. It is part of our mantra and our organisational
culture and we are incredibly proud of our history and our founder. However, the market is a
crowded place in the 21st century and we need to reaffirm our points of difference. We need

[154]
to be able to continue our healthcare programmes and maintain our community presence,
meet our contractual obligations and fundraise to cover the balance.’263
Fundraising was inherent in Nurse Maude from the start but it needed to be sustainable for
the long term. Mary Pauwels had been the first person appointed specifically to put
fundraising on the organisation’s agenda. Sue Bramwell took the task several steps further.
She proposed the first Nurse Maude hospice shop which opened in 2008. It was an
immediate success. Located in Merivale, it took its lead from similarly designed outlets in
London’s more affluent suburbs where some of the biggest voluntary organisations had well-
stocked shops of pre-loved high fashion clothing and accessories. Over the next two years,
as the shop flourished, there was discussion about the potential to open more shops, to put
them on a commercial footing and to engage permanent staff. It all augured well for
increasing Nurse Maude’s image in the community.
By 2013, there were six hospice shops operating in Merivale, Avonhead, Sumner, Shirley,
Bishopdale and Kaiapoi with a seventh due to open in Beckenham in 2014. Locations were
carefully selected and professionally branded. An overall manager was engaged and retail
assistants supported by volunteers worked at all the stores. They all specialised in clothing
but Sue Bramwell realised the organisation could develop another outlet for the many
additional household items that it received.
‘We established ‘Maude’s on Trade Me’, which sells everything other than clothing. It is now
in its second year and is proving to be very successful. The best thing is that it gives Nurse
Maude a strong community profile.’264
The suburban shops coupled with on-line retail could give Nurse Maude an edge with
fundraising and contribute substantially to the organisation’s activities that were not covered
by its health contracts. Sue Bramwell also recognised that the Association’s fleet of white
cars could provide the organisation with ongoing affordable and sustainable marketing and
value-added fundraising. They were, she said, ‘large mobile billboards.’265 She put a
proposal to the real estate firm Harcourts (Holmwood) which resulted in half the fleet of cars
carrying the Harcourts brand on their back window. ‘It has resulted in significant income for
Nurse Maude every year since,’266 she noted.
Sue Bramwell was clear about the organisation’s marketing priorities. ‘Its public face is
essential and is led by its district nursing and homecare staff, its hospital and hospice teams.
The back office staff work to keep the public face fully operational. Our website is intuitive
and well-structured. All information is easily accessible. Branding and image are faithfully
maintained to ensure immediate recognition.’267
‘We changed the organisation’s name from NMA to Nurse Maude not long after I took up my
post,’ she said. ‘There was an era when organisations, businesses, even government
agencies believed a short snappy abbreviation or acronym would suffice, but it said nothing
263 Interview with Sue Bramwell, November 2014 264 Interview with Sue Bramwell, November 2014 265 Interview with Sue Bramwell, January 2016 266 Ibid. NB: In 2014, Harcourts Holmwood renewed the sponsorship on an indefinite basis. 267 Interview with Sue Bramwell, November 2014

[155]
to us as an essential health agency. NMA could have meant anything, and it didn’t conjure
any image in people’s minds about Nurse Maude and its role. So we went back to our roots
but with a difference. We decided on the simple name of ‘Nurse Maude’ with the strapline
caring for the people of Canterbury since 1896. And it works. It explains what we are, how
long we have been here, and we can expand depending on whether we are talking about
community care, hospital and hospice care, or any of the many other services we provide.’268
268 ibid

[156]
Chapter Three
From Committee to Board – governing Nurse Maude
‘Governance and leadership are the yin and the yang of successful organisations.’
Mark Goyder
From the beginning, Sibylla Maude, Jessie Rhodes, Walter Averill and Edwin Scott agreed
on the ground rules that would shape district nursing in Christchurch. They knew from their
own backgrounds and experience that there was a distinct separation between the physical
nursing role that Sybil would adopt and the financial and support role that her three friends
and mentors would take on. They would be the committee. Sybil would be the district nurse.
Walter Averill and Edwin Scott wrote Sybil an official letter confirming her position and
setting out the terms of her engagement including her annual salary. They provided her with
her lists of patients. Jessie provided the necessary start-up funds.
As Sybil’s workload increased and her reputation flourished, so did benefactors begin to
offer more financial resources to help out. By the time Rose Godfrey’s father Charles and
Mr E. M. McDonald joined the small committee, Nurse Maude was already on her way to
becoming a popular name amongst the poorer Christchurch suburbs and amongst the
establishment which had the money to back her endeavours. It had taken five years to
create the first district nursing organisation in New Zealand that was financially supported
and that had a committee which understood the need for good management and
governance. Not that the word itself had any mana at the time. Organisations like Nurse
Maude were fledgling operations, small by any measure and outflanked by local hospitals
and doctors who tended to their private patients.
The need for organised structures came with the Association’s expansion. Businessmen
offered to sit on the committee. There was an increasing bank of regular subscribers. In
1904 the original committee decided to formalise its operation. It would invite its subscribers
to a meeting to elect another four members to sit on the committee which would be
responsible to promote Nurse Maude’s work. Sybil would provide the committee with regular
progress reports and minutes would be formalised. The Association would operate on the
same business lines as the men who volunteered for the committee dealt with their individual
interests. There were no rules by which the Association should manage its business other
than the committee’s own intention to break even or better still make a profit and invest the
balance.
This careful risk management and understanding of thrift coupled with a sensible savings
regime became embedded in the Association’s modus operandi. Successive committees
planned for the future as they managed the present. If they were benefactors with a
philanthropic sense of public duty to begin with, they quickly became stalwarts of the Sibylla
Maude ethos. By the time Mona Corkill became the Lady Superintendent, the committee’s
role was assured and it had become more than just a committee. Its members were co-
opted through friends and colleagues rather than for any expertise they might bring to the
table. At the same time, because they were known to existing committee members, they

[157]
tended to share the same values, principles and usually similar careers. They were
ambassadors for Sybil and her nurses.
There was little differentiation between governance and management in the early days.
Both were seen as the committee’s responsibility which allowed Sybil and then Mona Corkill
to get on with the business of caring for the poor and frail elderly. When Sir Heaton and
Jessie Rhodes gifted the plot of land at 192 Madras Street to Sybil to build new rooms, it
was the committee that took responsibility for organising the construction. Sybil detailed
what she needed for her work; her committee advertised for the tenders, supervised the
building programme and paid the bills.
By 1920, the committee had entered into its first structured contract with the North
Canterbury Hospital Board. With eight nurses on its staff and an established endowment
fund, the organisation was substantially bigger than it was when it started. The original
committee expanded to manage the increasing demands of the organisation and gradually
morphed into a fully functioning Board. The Association’s guiding rules were formalised on
30 November 1936 and written into its constitution.
Although there is no record that formalised the name change from ‘committee’ to ‘Board’, it
can be assumed that this took place at the same time. The Board should consist of not
more than 12 people including ex officio members of whom ‘not more than three shall be
women.’ Details about the election of officers, criteria of eligibility and appointments for
casual vacancies were written down. Mona Corkill was responsible for determining her staff
numbers while the Board concentrated on policy matters and managed the Association’s
finances. The improved structure of the Board together with its business-oriented
membership enabled committees to be set up covering the essential matters of finance and
facility development.
By the time the Association ventured into convalescent and hospital care with first the Nurse
Maude Memorial Home and then Averill House, the Board was a well-established functioning
structure. Denis Cotterill became the Board’s Chairman at a time when health was changing
at a rapid rate. Well connected in Christchurch and a lawyer by profession, he led the
Association’s drive to change its constitution and the creation of the Nurse Maude District
Nursing Association Act which was passed in 1967. There were administrative staff
engaged to help manage the growing contingent of nurses but essentially the Board
remained the organisation’s managers.
A gradual internal separation between the Board and the nursing and support staff occurred
during the 1970s and 1980s with the Association’s expansion and the ever changing health
legislation. Colin Averill, a grandson of Sybil’s great friend and mentor Rev Walter Averill,
was the Board Chair.269 He had taken over from Rod Compton and, as he remarked later,
the time was ripe for change. There were two formally constituted committees – Finance
and Planning chaired by Campbell Ballantyne, and Services and Community chaired by
Caroline Cartwright. Rod Compton remained on the Board as did several other long-term
members. Like so many decades in the past, it was an era of rapid change, Colin Averill
269 In New Zealand, as a result of the feminist movement, the term ‘Chairman’ was changed to ‘Chair’ or ‘Chairperson’ during the 1980s.

[158]
said.270 The Board was intent on modernising the organisation’s management structure
which meant challenging some of the organisation’s long-held and institutionalised beliefs.
When Anthea Bowden was appointed as the Association’s first Chief Executive in 1989, the
Board became responsible for policy. Anthea led the management team and was also in
overall charge of patient services and corporate services. She had a team of managers as
well as clinical staff. One of the critical changes was the Chief Executive’s responsibility for
selecting and appointing staff. The Board was only responsible for appointing the Chief
Executive. It created a very distinct separation between the Board and the staff.
Colin Averill stepped down as the Board’s Chairperson in 1993 and Murray Compton took
his place. He led the Board through the radical health changes of the 1990s and into the
second millennium, thanking former Board members for their voluntary commitment to Nurse
Maude and inviting new people to come to the table. By the time Nurse Maude celebrated
its first centenary in 1996 the Board comprised men and women with financial or clinical
expertise and detailed knowledge of governance and management responsibilities like John
Drayton, Caroline Cartwright and Margaret Guthrie. Their combined expertise enabled them
to make policy decisions that had longevity for the organisation. An important added
component was their understanding of health politics.
Murray Compton realised there needed to be changes around the Board table that better
reflected the increasing level of professionalism and expertise within Nurse Maude’s staff.
‘We needed Board members with qualifications and skills to define long term policies for the
betterment of our organisation.’271 Information technology was starting to drive more change
within the health sector. Government contracts were more comprehensive and Nurse
Maude was working in a highly competitive environment. The Association’s Foundation had
become Nurse Maude’s investment arm. Board members, Murray Compton said, had to be
aware of the health industry and at the same time to appreciate and value the Association’s
history and its place in Christchurch and Canterbury.
Rose Laloli who chaired the Board for 18 months during Ingrid Thomas’ five year tenure as
Chief Executive, said the imperatives of good governance could not be overstated. Under
her stewardship the Board had undertaken a full review of its membership. She had invited
members of the New Zealand Institute of Directors to talk with the Board and to explain the
complexities of good governance required by legislation.
‘We had a highly skilled nursing workforce dealing with complex issues, greater demands on
our staff and by 2010 we were clearly influenced by legislation,’272 she said. It all added up
to a more professional Board which could understand the separation between governance
and management.
‘When Ingrid Thomas resigned and we started our search for a new Chief Executive, we
knew we needed someone who understood the health environment and who had a depth of
knowledge and experience of working in Canterbury. The person needed to know how we
270 Interview with Colin Averill, January 2015 271 Interview with Murray Compton, December 2014 272 Interview with Rose Laloli, January 2015

[159]
could survive in an information rich world and who could focus on better information
systems,’273 she said.
Now Murray Compton talked with the Board members and with their agreement, engaged a
specialist firm in 2013 to review their role and to compare it with other similar organisational
structures. The outcome was an affirmation of the Board’s responsibilities, and a proposal to
pay the Board members for their work.274 It was not a decision that came easily to anyone.
Most of the Board members had been there as volunteers for several years. The former
Committee members saw their role as an act of charity, contributing their expertise to the
Association’s development. Accepting payment for their services seemed almost misplaced.
However, Murray Compton discussed the proposal with senior staff and received their
unanimous approval.
Changes were made within the Board’s structure; its committees were reviewed and
redefined. A new Community Services and Quality Committee was set up with Rose Laloli
as its Chair. The Finance and Planning Committee was chaired by Dave Spence. There
were two sub-committees covering audit, fundraising and human resources. Strategic
planning workshops involving senior staff and the Board were an accepted part of the annual
planning process.
In 2010, the Board, like its predecessors, was an impressive group, selected for individual
skills, to provide the leadership Nurse Maude required. Several of its members had been on
the Board for a number of years – Murray Compton, Rose Laloli, Jane Parfitt, Reg Garters,
David Spence, Diana Sullivan and Ian Town. The comparative newcomers – Jane
Cartwright, David Lang and Mark Marshall were there to bring additional expertise to the
table.
The sequence of earthquakes in 2010 and 2011 challenged the Board to rethink its priorities,
to focus on what was important and to develop long-term policies for the Association that
would see it through one of the most difficult periods in its history. Its decision to remain in
Merivale rather than move to another suburb was a defining one.
‘Everyone understood our history and our heritage and our place in Canterbury,’ Murray
Compton said. ‘We had to decide what we could achieve given our insurance settlement,
what needed to be rebuilt and what we would repair. Most importantly, we needed to make
sure our staff were work safe. There was no argument about McDougall House. It will
always be part of our heritage. We used the time during our insurance negotiations to talk
with senior managers about the future direction of Nurse Maude and health priorities. This
confirmed our view that the need for dementia care and for hospice care will grow in the
future and Nurse Maude has a strong role to play in both areas.’
Advances in health technology had long been a priority for Jim Magee and the Board. The
decision to invest in a new system that would bring greater efficiencies and financial benefits
for Nurse Maude was positively received by everyone.
273 Interview with Rose Laloli, January 2015 274 The Board’s Foundation work remained on a voluntary basis. Interview with Colin Averill, January 2015

[160]
‘The introduction of CRM2016 will give the best possible business solution to Nurse
Maude,’275 Board member Mark Marshall said. Health contracts were by their very nature,
both tight and competitive. For Nurse Maude to achieve greater efficiencies in its operation,
it needed to have an IT system that was creatively designed and easy to use. CRM2016
would enable a cultural shift within the organisation as nurses and homecare staff started to
use technology as a key part of their daily work. Data governance like clinical governance
was an imperative of modern business practice, he said. By mid-2016, the new system
would be operational across the organisation.
Dr Cathy Andrew agreed that technology was critical, but she insisted that it is the district
nurse who is the priority for Nurse Maude. ‘District nursing is our core business. It needs a
long term vision that ensures nursing is sustainable for the foreseeable future. It is our
imperative. It is our reason for being. District nursing and healthcare services are the
means by which aging-in-place will flourish. We are the support network by which people
will be able to stay in their own home and in their own community rather than be encouraged
or forced to shift somewhere else.’276 She was clear that there was a place for both
registered and enrolled nurses and that training was essential as well as ongoing
management.
Dr Andrew made the point that syphoning older people into gated villages where everyone is
of the same or similar age, reduced choices and options. ‘For a community to thrive, it
needs variety and diversity,’277 she said. Nurse Maude needed to have the vision and the
integrity to foster these choices and make them real for people.
Along with the aging community, one of the biggest challenges for the Board however, would
continue to be its permanent workforce. Although homecare staff continued to increase, the
emphasis in the medium term would be to encourage greater awareness of the value of
nursing as a profession. There was strong competition from engineering, legal, accountancy,
architecture and other career options that were steering particularly young women away
from what had always been perceived as their traditional role.
‘Nurse Maude must attract a younger workforce,’ Deputy Chair David Lang said. ‘Nursing is
a brilliant career and there is long term potential for nurses to gain higher education and to
specialise in different areas of healthcare. We will need them for Nurse Maude to succeed
in the future.’278
Fellow Board member and Chair of the Institute of Community Health Care Jane Cartwright
shared his view.
‘By the time Nurse Maude celebrates its 125th year in 2021, it will be an organisation with
agility, a leading provider of community health services, with nursing and palliative care as
its priorities. Its post-quake building programme will be complete at its Merivale campus and
it will be recognised as the provider of choice to work with in the disability sector. In every
275 Interview with Mark Marshall, January 2015 276 Interview with Cathy Andrew, February 2015 277 ibid 278 Interview with David Lang, January 2015

[161]
respect, Nurse Maude will retain its strong reputation in Canterbury and in other parts of
New Zealand where it has health contracts.’279
Defining the Board’s role and giving it the professional leadership it needed was a critical
step forward. Nurse Maude was an established part of Canterbury’s landscape with a
history dating back to the earliest pioneers. Staying the course and being a leading provider
of community healthcare was not in doubt, according to Murray Compton. Having the
wisdom and the knowledge, the level of expertise and the political nous at the Board table
would be a major contributing factor to chart the organisation’s course and steer it into the
future. Health, he said, was a challenging world.
279 Interview with Jane Cartwright, January 2015

[162]
Part Five: The Canterbury Earthquakes and Their Aftermath
‘Christchurch isn’t supposed to have big earthquakes’280
280 Bennett Barnaby, Dann James, Johnson Emma, Reynolds Ryan. ‘Once in a Lifetime: City-building after Disaster in Christchurch.’ Freerange Press 2014. p18

[163]
Chapter One
Priorities and Outcomes
On Saturday 4 September 2010, Canterbury was woken in the early hours of the morning by
a heaving, unrelenting, magnitude 7.1 earthquake, centred near Darfield and later identified
as the most damaging earthquake in New Zealand since the Hawkes Bay earthquake in
1931.281 Its noise was horrendous, its movement more so and it lasted for 45 long and
terrifying seconds. Yet, in spite of extensive property and land damage and substantial
liquefaction especially in Christchurch’s eastern suburbs and in Kaiapoi, no deaths occurred
and there were comparatively few injuries. Even so, it was chaotic and ghastly in every
respect. The ongoing after-shocks rattled people’s nerves as much as they shook doors and
windows. Water supplies failed and many sewers were damaged. Much of the city was
without electricity for the day. Kaiapoi was badly affected. Several thousand homes and
commercial properties were badly damaged.
Canterbury’s emergency services immediately swung into gear ahead of a state of civil
defence emergency being announced first in Christchurch at 9.50 that morning, and ten
minutes later in the Waimakariri and Selwyn Districts. Search and rescue teams were flown
into Christchurch with sniffer dogs to search damaged buildings. Welfare centres were
established where tankers delivered drinking water. Engineers moved from one building to
the next leaving red, yellow or green stickers denoting the safety or otherwise of the
structure.
Like other health sector organisations, voluntary agencies and services, Nurse Maude’s first
priority was to check on patients and clients, to make sure they were safe and that their care
could be maintained. In many respects, because the earthquake had occurred on a
Saturday, the weekend gave the organisation breathing space. Its management team could
initiate its disaster recovery plan while confirming its staff members were unharmed. Road
access to many of the worst affected areas was limited in the first few days and created
problems for people who were housebound and for the district nurses and home care
workers who needed to visit them. But as soon as the phone lines and electricity were
restored, Nurse Maude could make contact. Making sure medical supplies were available
and that treatments could be continued, were priorities. Many roads especially those in the
country had buckled under the strain of the earth’s movement and there were deep fissures
along and beside rural roads.
Over the next two months as Christmas approached, the psychological effect of the quakes
and the ongoing aftershocks created problems for many people being cared for in their own
homes. Being mindful of their individual needs was an essential part of Nurse Maude’s
community care programme at the best of times. Now, it was even more important.
‘Our services were severely tested over the weeks that followed 4 September,’ Rose Laloli
said later. ‘Client visits became necessarily longer as we worked around homes and streets
281 GNS science report 2010

[164]
that had been compromised by the earthquake and we spent more time with patients and
clients who had a higher than usual need for reassurance and contact.’282
There were several major aftershocks in the months that followed in addition to the hundreds
of smaller quakes that continued to upset community nerves. Boxing Day was particularly
gruelling. There seemed no end to the ground movement and although people were
cautious, and authorities stressed another substantial earthquake might still occur, there was
little appreciation that the worst might be still to come. But it was.
On Tuesday 22 February 2011, at 12.51pm, Christchurch was ravaged by a magnitude 6.3
earthquake of such velocity and strength that buildings crumbled, homes were destroyed
and worst of all, 185 people were killed and more than 6,600 people were injured. It was
another shallow quake, this time centred in the Heathcote Valley, and later described as one
of New Zealand’s deadliest peacetime disasters. Power and water supplies were instantly
affected, creating chaos for emergency services. Roads and bridges were severely
damaged and the city was grid-locked as thousands of motorists tried to get home. People
were dazed and shocked. Fires created columns of grey smoke clouds. Sirens wailed
across the city. Water spouted from sudden streams. Grey sludge and liquefaction coursed
through concrete floors, pathways and roads. There was panic and anxiety everywhere as
people tried to escape the central city, to make contact with family members, to check on
children. The mobile phone system was overloaded. Roads were blocked. People left their
cars and columns of individuals trudged solidly towards the suburbs. Everyone’s thoughts
were turned inwards – family, friends, neighbours – were they safe?
For the second time in less than six months, an emergency command centre was set up by
the Christchurch City Council in the Christchurch Art Gallery. All emergency services and
the New Zealand Army stationed at Burnham, were there within hours. Military personnel
worked with police to set up road blocks and to create a shield around the inner city.
Marquees that had been put up in advance of the garden festival in Hagley Park, were
hastily converted into emergency shelters for hundreds of anxious and homeless people.
Triage centres were set up in Latimer Square and at the Bealey Avenue Medical Centre
staffed by St John and army personnel. In Lyttelton, the HMNZS Canterbury in port from
manoeuvres, was an immediate help to the town’s emergency.
Health services throughout Christchurch were critically affected. The hundreds of
earthquakes that had shaken Canterbury since 4 September 2010 were nothing compared
with the horror of 22 February 2011. Every business, organisation, government department,
private agency and community service had twin responsibilities – to their staff and to their
clients. A coordinated response was essential and the Government announced a state of
national civil defence emergency the next day. The task was too great for local authorities to
cope with on their own.
For Nurse Maude based in Merivale, localised property damage at first glance was not so
severe. The organisation had a well-developed emergency response strategy. Now it was to
be fully tested. Its command and control structure was immediately initiated and remained in
place for the duration of the main crisis period. The Nurse Maude Memorial Hospital and the
282 Nurse Maude Annual Report 2010

[165]
hospice were checked for any signs of damage. All patients were moved into the centre of
wards for safety and in case they needed to be relocated.
‘We had no concept of what was happening in the central city or anywhere else in
Christchurch,’283 Sheree East said afterwards. ‘Our immediate priority was the welfare of our
patients, our clients and our staff. We activated our emergency plans and established our
‘war’ room in the hospital. An engineer came to check the buildings and to confirm we
weren’t in any immediate danger. We did a stocktake to make sure we had sufficient
medical supplies on hand. We had emergency water and an emergency generator but we
also initiated contingency plans in case the lifts stopped operating. Mercifully, our phones
were still working and we contacted the District Health Board which had activated its own
emergency plan.’
‘It was frightening for everyone,’ Jim Magee said. ‘We all knew what it was because of the
September quake and we were probably better prepared as a consequence. We had to
make sure our buildings were safe for our patients and our staff. It was important that we
concentrated on the practicalities to reduce the hype from the situation.’
Everyone on the Merivale campus was sent home except for essential staff who were
needed to take care of the patients. It was part of Nurse Maude’s emergency plan.
The other critical factor was the patient at home, in the suburbs, waiting for a Nurse Maude
car to pull up outside the house regardless of the damaged water pipes, the twisted door-
frame, the broken furniture, and surrounding ponds of liquefaction. Many of Nurse Maude’s
district nurses and homecare workers had been on the road when the earthquake happened,
or tending to patients and clients in their homes – doing what they did in any normal day.
They needed to continue with their visits and at the same time maintain contact with the
office and also with their own families.
‘It was remarkable and a sign of the commitment staff gave to their patients and clients that
93 per cent of our nurses and homecare workers were out on the road the next day braving
damaged roads, liquefaction and client homes that had lost all their amenities,’ Jim Magee
said. ‘If they couldn’t drive to the patient’s door, they left the car on the corner and walked.
The hospital and the hospice remained operational in spite of burst pipes, broken windows,
loss of power and water. Administrative staff maintained their own essential activities as well
as supporting their clinical colleagues.’284
The first days and weeks were exhausting for everyone. The emphasis was on keeping
routines in place, maintaining the visiting schedule, ensuring medicines and clinical supplies
were available. In retrospect, it was a nightmare of organisational intelligence that had to be
dealt with regardless of the heaving earth, the lack of clean water, the lack of power, the
worries about food supplies, the slumps in the roads and the unending potholes. Yet, like all
other essential services Nurse Maude carried on. Pallets of water were delivered to the
Merivale office to be distributed around the city. The office became the distribution centre -
working with other homecare services - for clinical supplies as well as bucket toilets that
283 Interview with Sheree East, December 2014 284 Interview with Jim Magee November 2014

[166]
were a gift from some ‘good Samaritans’ in Rangiora. They were a godsend, Sheree East
said, ahead of portaloos being delivered and later chemical toilets. Parts of the city were
soon dotted with portable toilets but they came with their own sets of problems particularly in
high use areas. Older people and people with disabilities struggled with the portable toilets
many of which were not placed within easy access. The chemical toilets were too heavy for
some people to be able to empty at the identified stations. Tap water had to be boiled to
prevent an outbreak of disease. After testing the city’s water supply over several days, the
Community & Public Health section of the Canterbury District Health Board confirmed all
local water would be chlorinated. Nurse Maude’s staff reported concerns expressed by
clients and patients who were living on their own, that many immediate neighbours had left
Christchurch and they were worried about their personal safety as a result.
Nurse Maude was an essential service – there were hundreds of patients and clients
requiring different levels of care and every one of them had to be accounted for, checked on,
contact made with family members where possible and alternative arrangements organised
for those who could not remain in their own homes. At the same time, district nurses and the
home care staff, like everyone else, had their own private issues to cope with – family and
home disruptions, changes to schooling, suburban services changed or disappeared, roads
and bridges that were either impassable or severely damaged. Everyone knew someone
who was injured or worse who was missing or had been killed. Yet the patient visits must
continue, the medications and dressings checked. Situations varied according to the suburb
and it soon became apparent that a more collaborative approach to community care was
urgently needed.
As many of Nurse Maude’s staff as possible were rostered onto the nursing and homecare
programme. Many of them had personal worries with wrecked or damaged properties, the
need to shift house, liquefaction, lack of power, water and sewerage, but even so, they knew
there were priority patients and clients who could not be neglected no matter how severe the
situation was. Nurses and homecare workers donned gumboots to cope with the mud, the
water and the damage. Nurse Maude contacted the New Zealand Army and asked for help
to check on some of the families that the staff could not access. A small team of military
personnel went out with a list of names and addresses.
‘All staff cars were stacked with water supplies and bucket toilets, masks and gloves. It was
particularly difficult trying to do wound dressings without clean water, but we coped,’285 Fran
Cook said. ‘Our staff worked very long hours. Almost everyone turned up to help. We had
enough problems trying to negotiate the streets and the road blocks in some of the suburbs,
but our biggest problems were with clients on the hills. There were some we just couldn’t get
to.’ There were concerns that many patients who lived in their own homes or elderly clients
who suffered a disability were unable to protect themselves when aftershocks threatened
more damage. The mantra of ‘drop, cover and hold’ did not or could not apply to people for
whom quick or sudden movement was impossible.
Lanyard tags were made for support workers with emergency details that included ensuring
their safety first, checking on priority clients, and only contacting the Merivale headquarters if
285 Interview with Fran Cook, October 2014

[167]
it was absolutely necessary. Staff at the frontline needed to know they could take the lead
and make critical decisions rather than referring back to the central office.
In the first few weeks, finding patients and clients was the biggest challenge. Many had
gone. Their families had turned up and either moved them away from Christchurch or taken
them to stay with them. Nurse Maude’s administration staff telephoned medical centres and
next of kin to see if the clients were with them and if they needed any help. Then there
were the new clients who had been in residential care and were now living with their families
because the rest home was damaged or destroyed. It created stress and difficulties for
families particularly if their property was also damaged, if they had to use portable toilets and
if access to essential services was limited.
Some of Nurse Maude’s staff resigned because their partners either wanted to leave
Christchurch or they were transferred out of the city. They were ‘quaked out.’
‘It was a very complicated time. Staff were operating on adrenalin. We organised group
sessions on resilience where people could share their own experiences. But two to three
weeks on and exhaustion started to set in. The pace didn’t settle. The staff on the frontline
had an incredibly challenging time. We were working in emergency mode for months, long
after the Civil Defence Emergency had finished. It was about redesigning ‘normal’,286 Fran
Cook said.
Throughout the first three weeks, Sheree East acted as the contact between Nurse Maude
and the Canterbury District Health Board’s emergency operation centre, providing status
reports and receiving welcome updates in return. ‘We liaised with Civil Defence, Primary
Health and the DHB, teleconferencing on a regular basis. We were contacted by hospitals
and other hospices throughout New Zealand offering help with staff or taking patients. We
took some patients into our hospital ourselves to relieve the pressure on rest homes in the
city.’287
Having a specific person delegated to liaise between Nurse Maude and the emergency
operation centre was central to be able to identify the needs of the wider residential care
needs. The need for information, to identify priority patients, assist with emergency
accommodation arrangements and general coordination. Nurse Maude took the lead in
coordination. It established a ‘hospital in the home’ model of care with the support of
Help4U288 who were able to provide data about the extensive damage and human health
needs caused by the quakes.289
CREST and TotalCare
Yet the work must go on. In April 2011 while the national civil defence emergency was still
in place, Nurse Maude was part of a new system to expedite hospital discharges. The
286 Interview with Fran Cook, October 2014 287 Interview with Sheree East, December 2014 288 Help4U: an innovative data system developed by Christchurch entrepreneur Kay Poulson 289 Earthquake Preparedness in an Ageing Society: Learning from the experience of the Canterbury Earthquakes. Davey Judith, Neale Jenny February 2013

[168]
Community Rehabilitation and Enablement Support Team (CREST) involved Nurse Maude,
Health Care New Zealand and Access Homehealth – all Canterbury organisations. It was
designed to ease pressure on hospitals in the region that were stretched beyond capacity as
a result of the earthquakes. It was launched ahead of its planned start date due to the acute
shortage of hospital and aged residential care beds caused by the earthquakes. Staff from
each organisation worked together as a community-based discharge team to facilitate early
discharges from hospitals into home-based rehabilitation services. This freed up hospital
beds by reducing the length of hospital stays and supporting people at home.
One of the features of CREST was to assist people in a way that restored independence:
‘doing with, rather than doing for.’290 The project’s success was such that it was extended
beyond the emergency period to accept referrals directly from general practice enabling
older people to be rehabilitated in their own homes and therefore avoiding hospital
admissions altogether.
Associate Health Minister Jo Goodhew, who came to see the service in operation a year
later, praised the proactive approach adopted by the Canterbury providers. ‘We all know
from talking to our own parents that the key thing they want is to be healthy and stay as long
as possible in their own home. This service helps ensure that happens. Many people think
good health care is solely focussed around hospital care. It’s true that hospitals are critically
important, but it’s vital that we use them properly. If we overload hospitals with people able
to be better cared for at home or in their own community we will end up providing a poorer
service overall.’291
Canterbury reeled yet again when twin earthquakes hit the region with incredible force on 13
June. It was early afternoon. Once again, power and phone lines were affected. Once
again people were injured. Buildings that were already damaged from the previous quakes
were destroyed. Once again, Nurse Maude’s staff were out on the road, tending to patients
and caring for clients at the same time worrying about the safety of their own families.
Almost incredibly, barely a month later one of the worst snow storms New Zealand had ever
experienced, blanketed everything in the city and the region. Up to 30 centimetres covered
Christchurch and deeper falls were recorded elsewhere in Canterbury. Nurse Maude’s car
fleet was well equipped with chains but even so, only essential care could be delivered.
‘We were inundated with offers from people with four-wheel drive vehicles which helped,’
Sheree East said. ‘It was very important that we maintained our visits but we had to ration
our services for the duration. We also rescheduled our staff so that they could get sufficient
breaks as well.’ Coming on top of months of working in extreme circumstances, the winter
of 2011 was challenging and difficult. There was little change to individual clients’ and
patients’ circumstances particularly in the worst affected suburbs. Yet, as the nurses and
homecare workers noted, the earthquakes did not discriminate. North, south, east and west,
in the city, in the suburbs and in the surrounding rural areas, everyone they visited had their
own story to tell about what they had experienced and what they were still going through.
290 ‘Caring Counts’ Report of the Inquiry into the Aged Care Workforce: Impact of the Christchurch Earthquake. Human Rights Commission. p141 291 Associate Health Minister Jo Goodhew: Press release 19 April 2012

[169]
Administration staff were moved into temporary accommodation, frequently changing offices
as space demanded. It was very obvious that nothing would ever be the same again.
On 23 June 2011, new residential land zones were announced based on defined geo-
technical categories that determined whether the land was stable and therefore safe for
people to live. The zones were green, orange, red and white. Green properties were
deemed to be safe. Red zoned properties were unsafe and orange meant a decision was
yet to be made. White zones, predominantly in the hill areas of Christchurch and Banks
Peninsula, were still to be assessed. The red zones were mainly in the eastern suburbs of
Christchurch, in Kaiapoi and in small, isolated pockets in other parts of the city. Ultimately,
more than 7,800 properties would be affected. Several thousand people would need to
leave their homes permanently and find somewhere else to live. Their homes would be
demolished. Where once whole communities lived and worked, there would be nothing.
Many of Nurse Maude’s patients and clients lived in homes that were now red zoned; many
of Nurse Maude’s staff were similarly affected. The announcements created their own kind
of chaos particularly for older people who soon realised they were faced with some
unpalatable options. It was a severely disruptive time and for many people, especially those
who had lived in their neighbourhoods for decades, the Government’s announcements were
traumatic. Home owners would have a specific timeframe to accept the Government’s offer
to buy them out or they could negotiate a settlement with their individual insurers. Few
people at the time had any concept of the long term impact on well-established communities,
schools, local shops and businesses, sporting and cultural groups. Coming on top of
everything else, the news was an unwelcome shock. It was traumatic and it contributed to a
sense of unease particularly amongst the elderly.
Nurse Maude’s Business Development Manager Mary-Anne Stone was succinct in her
comments. The quakes and their impact, she said, were a massive interruption to the
concept of business as usual. It was like an amnesty on everything. ‘There was an
overwhelming sense that the job had just got that much harder.292
It was in all respects an extraordinary year of complexity, of challenge and change. The new
land zones affected different people in different ways. For some, being red zoned was a
relief. For others being green zoned was a disaster. It was an extraordinarily tumultuous
time and yet throughout it all, mainstream business had to continue. Nurse Maude’s
operations at the Merivale campus and out in the field had to be maintained and at an
increasingly high level. In addition to participating in the District Health Board’s CREST
initiative, Nurse Maude had introduced a complex restorative care service - TotalCare – in
May 2011. The aim was to provide a responsive community-based health service to patients
who would otherwise have required hospitalisation and/or early admission to a rest home.
More than 600 rest home beds had been destroyed in the earthquakes that the service was
‘effectively a response to the loss. Now we were delivering residential care services in the
person’s own home – seven days, invariably four visits a day, putting other types of services
in place around the client,’ Fran Cook said.
292 Interview with Mary-Anne Stone, September 2014

[170]
The service, funded by the Canterbury District Health Board was based on the Integrated
Community Services model, with care coordinated by a registered nurse who assessed and
case managed the patient’s service care needs, then oversaw support workers who provided
the majority of personal care for the patient. Through the service, patients would also have
access to occupational and physiotherapy, respite beds for crisis care, laundry and meal
services.
When it was evaluated a year later by the New Zealand Institute of Community Health Care,
the service was being provided to 53 patients living in their own homes. The aim of the
study was to identify the impact and effectiveness of the activities provided by the TotalCare
service; to identify patient profile characteristics and to identify patient outcomes related to
service utilisation and perceived health status; to identify the perceptions and satisfaction
levels of clients. The important result of the study was to provide the effectiveness of the
service by the reduction in the number of people who would have otherwise been admitted
to hospital.
The report noted that the service was provided by a nurse manager, three registered nurse
coordinators, five enrolled nurses and several support workers. A service manager was
responsible for receiving the referrals and for making sure the patient details were entered
into the Nurse Maude Patient Management System. As the programme progressed, nurses
were able to enter data on their patients using mobile devices. It was one of the
technological advances that Nurse Maude was activating in the post-quake period. The
patients ranged in age from over 65 to over 95 – the majority in the 85 to 95 age group.
Most of the patients lived in their own homes – some were in flats, some in houses, some
rented flats and a few lived in residential villages. For patients living on their own, there
were some identified risks which included allergies to drugs, hearing impairment, the risk of
falling, cognitive ability and the overall risk of living alone.
The study used internationally accepted methodologies for assessing levels of dependency,
pain, medications, and quality of life. It also surveyed patients and families’ perceptions of
the service which showed that they wanted to be involved in both care and decision making.
Part of the study included surveying Nurse Maude’s staff who were involved in the
programme. Most of them said the service was successful in meeting the needs of patients
and families; that it offered safe care in the home for patients who had been assessed earlier
as needing either resthome or hospital level care. The service was particularly good for
married couples to be able to live in their own home together rather than be separated due
to individual illness.
‘Indications are that this service is also achieving efficiencies through more efficient use of
staff, more economical medication management and a reduction in Emergency Department
and Hospital admissions. The service has also enabled the development of a patient-centric
electronic record used at the point of care which has subsequently provided significant data
to inform this evaluation,’293 Dr Chris Hendry noted in the report.
293 TotalCare Evaluation Report 1 October 2012. New Zealand Institute of Community Health Care.

[171]
The resilience and dedication of the Nurse Maude staff throughout the first six months after
22 February 2011 was awe-inspiring, Jim Magee commented later. They had their own
private worries particularly if they were in an identified red zone or if they were in an orange
zone and had no way of finding out what their future might be. Their children were now co-
located into different schools with different timetables; after school activities were either
curtailed or changed depending on whether the school could make alternative
arrangements. No-one knew the political timetable. There was no sense that anything would
improve in the short term or even in the medium term. It was a complex time for healthcare
professionals who had their own personal worries to contend with that were similar to those
being experienced by their patients and clients. By tradition, they could listen
dispassionately to what their patients told them and have a completely clinical response. But
the earthquakes had affected everyone regardless of their lifestyle, their health, their age
and their circumstances.
As the largest provider of domiciliary care in the region, Nurse Maude had been able to take
a leading role in contributing to services which would enable older people to stay in their own
homes or be moved to a family’s home. Many rest homes and residential care homes
including dementia units had been severely damaged beyond repair. Some families had
opted to move their older relatives to a safer location elsewhere in New Zealand. But for
many who remained and who lived in their own homes, they had been either red zoned, or
were waiting to be told if their orange zoned properties would become red or green. Nurse
Maude’s specialist nursing services including wound care, stomal therapy, continence care,
diabetes education and school based nursing were all in demand. A new serious injury
support team was set up to help patients with spinal injuries resulting from the earthquakes.
It was very clear in the immediate aftermath of the February earthquake that health services
in Canterbury had changed and would never be the same as before. It was impossible to
function in a business-as-usual mode. Meeting health and homecare needs in a greatly
changed environment meant adopting a different way of operating; of sharing services.
The ‘Better, Sooner, More Convenient Health Care in the Community’294 strategy was
launched by the Ministry of Health in Wellington in June 2011. It demonstrated that while
Canterbury was still reeling from its ongoing sequence of earthquakes, it was business-as-
usual for the rest of the country. Nurse Maude embraced the new concept of community
healthcare in part because it dovetailed so completely with its own care ethos, and in part
because everyone recognised that the new health world particularly in Canterbury would
thrive better by connecting the different services rather than operating separately and in
silos. It heralded the beginning of a collaborative approach to health services. Former
competitors recognised they could create an enhanced community service by sharing
knowledge and expertise.
The intent of the new policy was to create a better relationship between primary and
secondary care providers to share patient information and work together to improve health
outcomes for the patient. From the patient’s perspective, it was not necessarily important to
know who the health professional was employed by, but more important to know that the
care being received was as good as it could be. That patient-centred approach was central
294 ‘Better, Sooner, More Convenient Health Care in the Community. Ministry of Health Policy June 2011.

[172]
to Nurse Maude’s community care programme, backed by its specialist hospital and hospice
facilities.
‘It is only by fully involving patients and their families in the planning and provision of their
care and support that they are able to work in a more active partnership with those caring for
them,’295 Sheree East commented in her annual report. ‘Innovation and partnership in the
provision of nursing and homecare services have defined the past year. With the ‘Better,
Sooner, More Convenient Primary Health Care strategy ramped up several fold, post-quake,
the use of information technology and partnership with other health providers was not just
desirable, it was essential.’
‘Assessing and meeting the rapidly changing needs of a community in crisis these past 12
months has required an extraordinary level of motivation, innovation and understanding. It
has also meant a commitment to a new level of caring,’ Sheree wrote.
For many clients and patients, Nurse Maude’s support workers had been the only regular
contact they had with their community during the worst period. ‘This year, they not only went
to extraordinary lengths to reach our clients, but they provided the vital link needed between
Nurse Maude and the wider community, advising of any changes in living conditions that
may have compromised their client’s health or well-being and any additional care they
needed.’
Even with the compounding workload and greater emphasis on home-based community
care, technological advances were maintained and the move into more specialist areas
continued. E-learning was introduced to the organisation’s nursing staff and Nurse Maude
moved into serious spinal and head injury care. Nurse Maude initiated a collaboration with
Christchurch Hospital to introduce palliative outpatient clinics and palliative motor neurone
disease clinics and a Diabetes Nurse Specialist team also started work. At the same time
support workers continued to gain their National Foundations Certificate and Level 3
qualifications.
Assessing the Damage
It was in all respects a traumatic year with more to come. Nurse Maude’s staff, its systems
and its premises were all severely tested over the next 12 months as engineers and
insurance assessors moved in to confirm what buildings could be repaired, what should be
demolished and what the extent of the organisation’s claim might be. None of these major
issues however could be allowed to impact on the organisation’s ability to meet its
obligations to its clients and patients in the community and in its residential care. At the
same time, the global financial crisis continued its relentless impact and although the
government’s health funding was spared any major reductions, existing contracts were
renewed without any increases taking into account pay changes.
Engineering assessments showed that the Clinical Services building on McDougall Avenue
which had housed most of the organisation’s administration staff, the Health and Mobility
295 Nurse Maude Annual Report 2011 Nursing and Homecare Overview. p 8

[173]
shop and the supply department was no longer safe. The news came as a total surprise,
Jim Magee said later. ‘The building was checked by structural engineers after the
September earthquake and declared safe. But there was incremental damage with so many
quakes in the months afterwards and when it was reassessed, the engineers told us the
building would need to be demolished.’
There was a rush to shift everything out. Finding other premises was a real issue. There
was a severe accommodation squeeze in Christchurch not only for residential housing but
for commercial businesses as well. Everywhere space was at a premium. Nurse Maude’s
strong relationship with the Christchurch Polytechnic Institute of Technology stood it in good
stead however with the Institute’s offer of temporary premises in its vacated Information
Technology Department.
Portacoms were set up on the Merivale properties and staff also took more space in the
leased Brougham Street premises. The large building on Brougham Street adjoining the
city’s ice skating rink, had been part of the organisation’s move to establish hubs around the
city so that nurses and homecare staff could more easily relate to the local community in
which they worked.
‘Before the February earthquake, we had considered sub-leasing part of the office space in
Brougham Street because we didn’t think we would make use of it all. It was a good thing
we didn’t because as it happened we needed it all, and more,’ Jim Magee said.
Because McDougall House was also badly damaged and fenced off for safety purposes,
different rooms were required for Board meetings. The first post-quake meetings were held
in the Clinical Services Building across the road, but when that was declared unsafe,
meetings were held at the Brougham Street premises. It was a similarly short-lived shift but
for different reasons.
‘We needed all the space we could get for our staff,’ Jim Magee said. ‘We were lucky in
that the Bank of New Zealand offered their Board rooms in Sir William Pickering Drive. It
was an ideal replacement for us.’

[174]
Chapter Two
Revitalisation, Repair and Recovery
‘No man knoweth another’s burdens’
Sibylla Maude
How could anyone know the full impact of the earthquakes? On individuals? On
businesses? On communities? By 2012, according to estimates determined by the newly
constituted Ministry for Business, Innovation and Employment, there had been ‘severe
housing deprivation’ following the earthquakes with people living precariously in cars, tents,
camping grounds or crowding in with other households.296 Organisations like Nurse Maude
must continue to operate and at the same time to be more aware of their patients’ worries, of
their vulnerability due to the upheavals in their lives, all or some of which could have a
negative effect on their health. Research later noted that a particularly vulnerable part of the
population was people with chronic illnesses and disabilities297 – these were the people who
looked to Nurse Maude for help.
Managing the organisation’s staff time was complicated by the extended distances to be
travelled, by the relocation of patients and clients, and the challenges of negotiating road
works marked by never-ending lines of orange and white striped cones. There appeared to
be more cones than people in some of Christchurch’s worst affected suburbs. Large orange
and black signs warned motorists of merging cyclists. Driving had become a hazard. But
there was a job to be done regardless of the road conditions and the time delays.
‘Health is a very resilient service,’ Jim Magee observed. ‘In a crisis, it tends to be self-
managing, and it is always testing itself.’
Nurse Maude had a reputation to carry on regardless of what might be happening outside of
its sphere of influence. Its clinical teams pursued their projects in partnership with general
practitioners, hospitals and other homecare providers. It launched a new ACC Injury
Recovery Service and continued to work alongside Burwood Hospital to provide the nursing
and homecare needed to support injury recovery. And, now firmly embedded into the
community, was the Nurse Maude school-based nursing service which provided access to
youth-focused health services in Deciles 1 and 2 secondary schools, alternative education
facilities and teen patient units. In addition to health campaigns, Nurse Maude was now
providing universal health, disability and youth development checks which included hearing
and vision screening.
Its reputation was such that bequests to the Nurse Maude Foundation a year after the
earthquakes totalled over $804,500. The Foundation had made a strategic decision to focus
on how it could best support the organisation through the post-quake period. Already
funding the Patient Welfare Fund and contributing substantially to the hospice, the
296 Bennett B, Dann J, Johnson E, Reynolds R: Once in a Lifetime: City-building after Disaster in Christchurch. p 195 297 ibid

[175]
Foundation would need to invest in the organisation’s capital works when its insurance claim
was settled and it could decide what buildings could be repaired and what would be rebuilt.
In 2012, Nurse Maude launched its ACC Injury Recovery Service. The telemedicine project
which it had established in partnership with the Canterbury District Health Board prospered
with nurses and GPs in remote rural communities now able to access the information and
support required for patients who received palliative care.
The organisation’s investment in nursing and homecare was paying dividends in terms of its
quality and its community profile. At the same time there was an increasing large investment
in infrastructure and the latest technological systems. ‘Over the past two years, that
infrastructure has been tested on a grand scale,’ Sheree East reported. ‘Where there were
gaps, it was the professionalism and commitment of our people and the support of our
contractual partners and the community that allowed us to close them.’298
Based in part on its experiences through the worst of the earthquakes and their interminable
aftershocks, Nurse Maude utilised the New Zealand Institute of Community Health Care to
review its model of care and in 2012 it announced its new vision. While the concept of the
person at the centre of service development and delivery was not new, the revised model
put more emphasis on Nurse Maude’s core purpose of providing excellent clinical and
support services with compassion and skill to the community. The model reinforced the
organisation’s commitment to integrate with other services within the community, working
alongside clients, patients and their families so that they could receive the best possible
care. Restorative services, according to Jim Magee, aligned very positively with the model
of care.
In a paper presented to the Nurse Maude Board in October 2012, the Institute’s Director
Chris Hendry discussed the importance of the Nurse Maude model of care and what set it
apart from other healthcare providers. It was blessed with a ‘caring before cost’ approach,
she wrote. Its services were well respected and it had achieved a level of integration of
volunteers and charitable giving. As a result of its alignment of nursing and care, Nurse
Maude had built up a large population of highly complex service users. It had developed a
workforce of health and homecare providers skilled and available to provide flexible services
to meet the unique and varied needs of clients.
‘Nurse Maude remains one of the few and currently one of the largest non-DHB District
Nursing service providers in the country,’299she wrote. ‘Over the years, the visibility of the
service as distinct from a hospital-based service can work to the advantage of the
organisation give the future predominantly community based health service vision.’
Chris Hendry’s review gave impetus to Nurse Maude’s Board that it had acted with foresight
in creating a research organisation that was part of the business but that acted
independently and was in every sense the research and development arm that was needed.
The Institute’s Chairperson and Nurse Maude Board member Jane Cartwright was succinct
in her comments. ‘The Institute follows a competitive process for health research. At the
same time it facilitates the process for the annual Campbell Ballantyne Fellowship which is
298 Nurse Maude Annual Report 2012 299 Hendry Chris, ‘The Nurse Maude Model of Care’ October 2012

[176]
more focused now on research opportunities for clinicians in Canterbury. It is a mark of
respect to be nominated as a Fellow in any given year.’300
There were other significant signs of progress during the 2012 year. A pilot programme was
developed for children with cystic fibrosis so that treatment could move out of secondary
care into the community. Telemedicine had become commonplace in Nurse Maude’s
palliative care programme with clinical expertise being shared with the West Coast using
video links. Advanced wound imaging technology had been in practice for some time and
had joined the telemedicine system providing virtual consultation to remote rural areas. All
the time, staff were challenged in their routines, in their ability to get to patients who had
become isolated due to neighbours moving away, communities changing, and the fear factor
that another quake might happen.
While nurses and homecare workers maintained their schedules and kept their
appointments, Jim Magee’s management team wrestled with the dynamics of the
organisation’s insurance claim.
It took almost a year for Nurse Maude’s insurance negotiations to reach a satisfactory
settlement. It was not perfect, as Deputy Board Chair David Lang commented later, but it
was acceptable. A three-year rebuild and repair programme was anticipated which would
involve repairs to the Nurse Maude Hospital, a new hospice and a major repair and
refurbishment to McDougall House. This heritage homestead was one of few listed buildings
not to be demolished in the city’s post-quake environment. In its day, it had been one of the
city’s leading homes, architecturally designed with a large ballroom, drawing rooms and
separate living quarters for staff. Discussion around the Board table was enthusiastic about
the restoration albeit with concerns about the cost.
‘We all agreed the house should be reconstructed. It was as much about retaining our
heritage and our history as it was about contributing to the Christchurch recovery,’301 Murray
Compton said. The restoration programme would be carefully managed using original
photographs and drawings. When completed, it would incorporate office space and suitable
areas for functions.
Miraculously, the hospice shops had survived the quakes with minimal damage and
continued to attract welcome customers. The Health and Mobility shop which had been
located in the now demolished Clinical Services building had a permanent new home at 285
Wairakei Road.
‘Our overall rebuild will enable an increase in the number of hospital beds and provide
permanent accommodation for our long-suffering staff who have patiently endured the
inconvenience of very confined office space over the past two years,’ Jim Magee said.
‘Partnership,’ he said, ‘is a continuing and prominent theme in our thinking. Our most
important partnership engagement starts at referral and defines our relationship with
patients, clients and their families. Our partners in the provision of care are GPs and
300 Interview with Jane Cartwright, January 2015 301 Interview with Murray Compton, December 2014

[177]
practice nurses, the three District Health Boards with whom we have contracts and their
staff, ACC, the Ministry of Health and many others.’302
Eighteen months after the 22 February 2011 earthquake, Chris Hendry and Sheree East
completed a staff survey to assess the wellbeing of Nurse Maude’s elderly patients and
clients. They surveyed both district nurses and home care staff who had worked in the
community through the worst of the earthquakes and in their aftermath.
‘Community care staff have first-hand knowledge of the impact of the earthquakes on people
receiving health care services in the home. These people are often the most fragile in our
community with multiple, chronic health problems,’ they said later. ‘We needed better
information rather than relying on ad hoc reports so that we could check that we were
meeting clients’ needs and putting our resources in the right places. At the time, we couldn’t
wait for a well-resourced and planned approach. The staff survey seemed a simple solution
given the conditions we were working under. We had continual issues with service delivery,
broken roads, broken buildings – multiple sites and many moves on the part of both staff and
services. And, we were continuing to experience ongoing quakes…’
Dr Hendry and Sheree East decided to invite staff to volunteer to complete a survey form. It
was not intended to be scientific research, more to gain an overall impression of what had
happened, what staff had experienced and how they felt later.
They found five key issues – mental health, anxiety and depression, which were symptoms
similar to post-traumatic stress disorder; unsafe environments; loneliness and isolation;
difficulty coping with change; and poor access to mainstream services. Issues that impacted
on meeting the needs of patients and clients related to the staff needing more time to care
including calming people who had become more cautious and slower. Damaged and
blocked roads, compounded by many people moving house overnight without warning,
added to the time it took to deliver care in the home.303
Specifically, the survey found that nurses’ patients needed more medication, chronic disease
management and more end of life care. There were issues relating to damaged properties,
insurance worries, uncertainty regarding their living situation, home heating problems which
had increased the severity of chronic conditions and social isolation. The stress of dealing
with the Earthquake Commission, the Canterbury Earthquake Recovery Authority, and
insurance companies, coupled with financial worries caused by the costs of heating
damaged houses, transport, rent and additional healthcare needs were identified as major
problems.
Many patients and clients had moved house and some were having difficulty adapting to this
change and at the same time worrying about overcrowding if they were living with relatives.
Relocated patients and clients had lost access to their regular community services and they
worried about having to navigate new and different services. The staff observed that there
were issues that weren’t covered by Nurse Maude yet were immediately obvious, like
302 Interview with Jim Magee, December 2014 303 The survey was later published in the New Zealand Nursing Journal Kai Tiaki Vol 4 Issue 1 August 2013.

[178]
companionship and few visitors during and after the earthquakes. There were problems with
getting to the shops not just because the shops were no longer in the neighbourhood, but
because transport had become such an issue. Social isolation had grown to become a
bigger problem than it was before the earthquakes, often as a result of less people living in
the neighbourhood, problems with family being able to visit. In many instances, the district
nurse had become a comfort to come and a lifeline to others. It was a sad and often
unreported outcome of the disaster.
‘Anxiety is on the increase,’ one staff member commented. ‘Loneliness results in greater
attention on health stress.’
Nurse Maude’s staff commented on the wellbeing of their patients and clients who were over
80, whose health, in the opinion of some, were the most badly affected. Many commented
that those with mild dementia had deteriorated more quickly since the earthquakes. Chris
Hendry and Sheree East noted that isolation in the aftermath of a major disaster increased
the adverse impact on the elderly and contributed to their health deterioration particularly
people with chronic health conditions.
The results conformed with the annual wellbeing surveys conducted by the Canterbury
Earthquake Recovery Authority and other social and health related organisations. They also
provided Sheree East, her nursing staff and healthcare workers with formal evidence to
support more initiatives that would improve their patients’ and clients’ needs.
A Blueprint for Community Nursing
On 1 March 2013, the Christchurch PHO Partnership Health, formalised its merger with
Pegasus Medical Group. The new organisation would be known as Pegasus Health. It was
an important step forward for primary care and community health and a valuable one for
Nurse Maude which had strengthened its relationship and partnering opportunities with both
organisations since inception. The year was seen as one of revitalisation, repair and
recovery. In the immediate post-quake environment, greater collaboration had developed
between primary and homecare services, including a shared electronic patient record. The
newly formed Canterbury Clinical Network was an added bonus not only for patients and
clients but for all organisations involved in community health care. Patients with complex
needs should have a single care plan that all providers could access.
In an interview for nursing journal Kai Tiaki, Sheree East talked about Nurse Maude’s
specialist palliative care service as ‘integration at its finest.’304
‘Two years ago, the service began working more collaboratively with the hospital’s palliative
care team – now the teams work together as one. The service’s clinical director works out of
the hospital, but sometimes the hospital’s clinical nurse specialists will join our team to work
in the community. We do case reviews, triaging and strategic planning together…’
304 Nurse Maude Champions Community Care, Anne Manchester. Kai Tiaki Nursing New Zealand Vol 20 no 7. 2014

[179]
Nurse Maude’s community care programme was hailed as ‘leading the way in community-
based collaborative care in Christchurch. Its nurse-led model could become a blueprint for
other community-based services in New Zealand,’305 wrote Anne Manchester.
‘The community patients we care for are increasingly older, sicker and more complex to look
after,’ Sheree told the journal. ‘This has meant developing new service models to help them
remain safely in the community and to avoid unnecessary hospital admissions.’306
Under Sheree East’s careful direction, the nursing service was now managed across eight
geographical areas in Canterbury including two rural hubs with each area coordinated by a
district nurse and its own clinical nurse manager. Some reconfiguration had occurred as a
result of population shifts following the earthquakes with many of Nurse Maude’s clients
moving away from the eastern suburbs and into homes in the north and south of the city.
This shift would continue as houses in the identified red zones were demolished.
Reviewing the 2013 year, Jim Magee said Nurse Maude had increased its patient and client
visits by five per cent and several new services had been introduced including an infusion
centre for administering intravenous treatments. As in other years, government funding had
been substantially augmented with charitable income. The hospice had benefitted from an
additional $1.3 million generated from the hospice shops, fundraising and grants from the
Nurse Maude Foundation.
Telemedicine had developed to the extent that Nurse Maude’s palliative care programme
was being shared with the West Coast via video link. Advanced wound imaging technology
had moved into telemedicine enabling virtual consultation to remote and rural areas of
Canterbury. School based nursing had now extended into Decile 3 schools and included a
new relationship with Halswell Residential School.
The pool of volunteers continued to make a valuable contribution to the organisation.
Although numbers had slipped during the earthquakes and for several months afterwards, by
2013 there were more than 280 volunteers available to back up staff in the hospital, the
hospice and in the shops.
‘Our volunteers work alongside the nursing staff. They help with meals, read and talk with
patients. They contribute to the hospital’s Te Ora programme.307 They have initiated a
biography service and often go to people’s homes to interview families and write the
patient’s life story,’ Volunteer Manager Linda Mace said. ‘We have a gardening group and a
walking group. Volunteers help with filing and with bookwork. They work shift hours in our
seven hospice shops and help organise goods to go on the Nurse Maude Trade-Me site.’308
‘Volunteering in the 21st century is highly structured and efficiently managed,’ she said.
‘When people contact us to become volunteers, they are interviewed and screened before
being invited to become part of the Nurse Maude organisation. They attend an orientation
305 ibid 306 ibid 307 Te Ora Programme covers the range of therapies, occupational and recreational activities at the Nurse Maude hospital and hospice. 308 Interview with Linda Mace, December 2014

[180]
session and regular training days are planned in any given year. Many of our volunteers
have been here for several years. They are a necessary and essential part of our
organisation and we couldn’t achieve as much as we do without them. We value their
contribution and invite them to attend events as well as hosting an annual ‘thank you’
function.’309
Keeping the frontline services operating efficiently was one of Nurse Maude’s imperatives in
line with its target to become a world class organisation and achieving a gold award by 2018.
‘In many respects the earthquakes were the catalyst for change because we couldn’t go
back to what we were,’ Business Improvement Manager Wayne Hutchinson said. ‘The
priorities of the pre-quake world are not necessarily our priorities now. Having an
emergency generator and a back-up emergency generator are essential. We have
emergency water supplies. Who would have thought they were so critical in 2009?’310
In 2013, bequests to Nurse Maude increased further to over $1million boosting the
Foundation’s finances at a time when it was most needed. The community’s generosity was
an affirmation of the organisation’s home and residential care and recognition that in spite of
the earthquakes and the consequent upheavals, Nurse Maude had continued to travel the
distance to care for its patients. Its contribution to the earthquake recovery was recognised
by the Mayor of Christchurch Bob Parker and acknowledged in health circles throughout the
country.
Changes were made across the organisation. The vehicle fleet which was essential to
Nurse Maude’s community care programme was moved to a lease model. ‘We are in the
health care business not the vehicle trade so leasing is a much better option for us. We have
175 cars on the road in Christchurch and 15 based in Wellington. We need cars for our staff
to get out to patients. They need to have the Nurse Maude brand, they need to be functional
and easy for our staff to manage regardless of weather and road conditions,’311 Wayne
Hutchinson said.
‘The same principles apply to food preparation and laundry and to ground and facilities
management. Outsourcing these important functions to enterprises which make it their
business is the way of the future,’312 he said.
By far the biggest investment in the two years after the earthquakes however, was
CRM2016313 - the new business management system - using a locally developed technology
platform. It would be technology at its most advanced, Jim Magee said. The old manila
filing system would not work in the 21st century. Smart technology was the way of the future
to enable district nurses and home care workers to do their jobs more effectively and with
greater efficiency.
‘District nurses will have tablets and will be able to input notes while they are with the
patient. Support workers will have smart phones. Evidence-based decision making will
309 ibid 310 Interview with Wayne Hutchinson, August 2014 311 ibid 312 Interview with Wayne Hutchinson, August 2014 313 Crista: Community Record Information Systems for Teams

[181]
contribute to providing detailed reports for Nurse Maude’s funders. The new technology will
enable better planning and improved time allocation.’
CRM2016 would revolutionise Nurse Maude’s work, according to Clinical Services General
Manager and project lead Fran Cook. ‘It incorporates clinical documentation, contracts
management and includes scheduling and electronic time sheets. Currently, client records
are kept in the individual person’s home. It is a paper-based system and nurses have to
drive back to the office to input their notes. There is duplication of work and a lower than is
needed access to computers.’
‘The business continuity of the new system is exceptional. It will be hosted externally, with
appropriate back-ups in place. It is designed for disaster management, something that we
have all experienced here in Canterbury.’314
Migration from the old system to the new had started in mid-July 2014. A dedicated staff
training programme was developed as well as information for clients. Contingency and
emergency planning was integrated throughout the testing regime giving Fran Cook
confidence the new system would prove to be a high level success.
‘Nurse Maude will be more reliable and responsive,’ she said. ‘When there is a district nurse
referral, the system will find capacity and will automatically create a schedule to optimise the
requisite staff. There will be a more streamlined workflow to enable nurses and care
workers to get out to their clients with a more efficient travel time.’315 Of great importance to
Nurse Maude based on its earthquake experiences, the organisation would be able to see
immediately where its staff were located in an emergency situation.
Alongside the business improvement and new technology initiatives, Nurse Maude was also
exploring new opportunities. It was part of the organisation’s philosophy, driven from the
start by Sibylla herself with her interest in enterprise and service expansion.
‘We are a leading care model,’316 Business Development Manager Mary-Anne Stone said.
‘We have the ability to be New Zealand’s premiere health care support service. We are a
community health sector leader in terms of needs assessment, service coordination and
complex case management aligned to general practice and integrated community care. It is
what we do best.’
‘Our history proves we have developed specialist nursing services, general district nursing,
home support care and coordination in the community. It gives us a special understanding of
our patients and we follow the principles that Sibylla Maude instilled in her teams over a
century ago.’
Mary-Anne Stone said there were opportunities for the Nurse Maude model to be developed
and established in other regions where district nursing was undertaken by the District Health
Boards themselves. She visualised a developing need in the long term care for the elderly.
314 Interview with Fran Cook, August 2014 315 ibid 316 Interview with Mary-Anne Stone, September 2014

[182]
‘Not everyone can live in their own homes until the end of life.’ But, she said, people could
stay at home longer provided there was a safely managed high level of care when and as it
was needed.
‘People who stay in their own home will have high-end acute needs. Providing long term
care for elderly people at home is one strand, another is having the best available facilities
for dementia care. The Lady Rhodes facility planned for Mansfield Avenue will cater for this
need.’317
The New Zealand Institute of Community Health Care had played a key role behind the
scenes during 2011 and 2012. It had continued to work on research projects that explored
and evaluated activities that could support people receiving health care in the community.
They included medical practitioners from Nurse Maude, Christchurch Hospital and the
community, researchers from the Christchurch Polytechnic Institute of Technology, and
nurses working in palliative care and wound care as well as nurses undertaking post-
graduate study. The research programme covered the gamut of community health care.
In October 2013, Professor Ian Town stepped down as the Institute’s Chair and Jane
Cartwright took his place. Under Chris Hendry, the research programme had continued to
grow with 14 current projects involving 13 District Health Boards, residential care service
providers, community based clinicians and Nurse Maude. There was increasing emphasis
on electronic health initiatives focusing on the use of technology for recording, monitoring
and evaluating care provided to clients in the community.
In its 2013 annual report, the Nurse Maude Foundation praised the foresight and generosity
of its benefactors – individuals and organisations who had nominated Nurse Maude as the
recipient of a bequest or donation. Since the Foundation had been established 25 years
earlier, it had received more than $30 million in bequests. With wise investments the money
had been used to continue supporting the Nurse Maude Hospice, administer the Patient
Welfare Fund, contribute to research via the New Zealand Institute of Community Health
Care and fund the Campbell Ballantyne Fellowship. Now it would also continue to meet the
costs of Nurse Maude’s rebuilding programme not covered by its insurance settlement.
‘We must never forget that we have been charged by those who have left us a bequest, to
ensure that every cent we spend will directly benefit our patients, clients and their families. It
is the guiding principle in our decision-making and the benchmark by which we measure the
effectiveness of the work with which we have been entrusted,’318 Murray Compton said.
There was an inevitability about district nursing and community care in Canterbury’s post-
quake environment. Change in all its rapid manifestations, driven in part by the necessity
that had resulted from the region’s loss of residential care beds and the squeeze on bed
space in mainstream hospitals, had forced institutions and organisations both public and
private to work together for the greater good. Competition was useful but collaboration was
better. The patient-centred approach adopted through the CREST project and then
TotalCare had proven to be hugely successful. The financial imperatives of the public health
317 ibid 318 Murray Compton, Annual Report 2013

[183]
system to reduce the numbers of patients staying in hospital had given Nurse Maude the
opportunity to demonstrate as never before, its purpose of caring for people in their own
homes.
The effectiveness of Nurse Maude’s district nursing and community care programmes was
discussed in a 2014 paper produced by the Bay of Plenty District Health Board when it
looked at various international and New Zealand innovative service models. The report
noted that: ‘the governance and structure of Nurse Maude is unique in New Zealand as the
Association is established under its own Act of Parliament. The core focus of Nurse Maude
remains the same which is to support people to stay out of hospital and remain living as
independently as possible in their own homes, with an emphasis on self-care.’319
It was this aim, in place for more than a century that was severely challenged and tested by
the impact of the earthquakes from 4 September 2010 through the terrible year that followed
and well into 2012. No-one had predicted the aftershocks would continue to ravage people’s
lives for such an extended period, and no-one had expected there would be such a
prolonged time of worry about insurance, repairs and what the future might hold. For a
substantial percentage of Nurse Maude’s community-based patients, age was going to be a
defeating exercise.
319 Bay of Plenty District Health Board 2014

[184]
Chapter Three:
Post-quake: The redefined normal
Accepting the changed environment was an essential part of Nurse Maude’s ability to adapt
to what was recognised as a new normal. It was a quaint phrase, part of the new lexicon in
post-quake Canterbury. Normalisation occurred gradually and often without realisation. The
way of the world before 4 September 2010 was not the way of the world in 2016. It had
been redefined, reshaped and influenced by the earthquakes and their aftermath.
‘Nurse Maude’s development as an organisation reflects the professionalism of its workforce
and the increasing coverage and institutionalisation of the public health sector,’ Jim Magee
said in May 2014. ‘Our strengths lie not in advocacy or campaigning but in the practical
delivery of health care. We are a mainstream provider of services, running a large and
complex organisation requiring competencies in business systems, contracting, people
management and stakeholder relationships. Our vision is that Nurse Maude will be
recognised as a leading provider of community based healthcare services through customer
satisfaction, effectiveness of services outcomes and efficiency of processes. Nurse Maude
will be financially viable and noted for its all-round business excellence. Our mission is that
the frail and unwell in our community will receive affordable, high quality care and support
which will enable them to remain as long as possible in their home and family environment.’
‘The origins and culture of Nurse Maude motivate us to make a contribution over and above
the delivery of fully funded, specification based contracts. The best example of this is the
provision of hospice care which at present is only 70 per cent government funded. Emerging
areas of need which could benefit from the skills and resources of Nurse Maude are the care
of children with life limiting conditions, domiciliary dementia care and the use of telemedicine
for home based care of complex patients.’
Outlining his strategic direction for Nurse Maude through until 2018, Jim Magee said the
Christchurch earthquakes had generated costs well above the organisation’s insurance
cover, due mainly to the ongoing nature of their impact. Nurse Maude had rented additional
office space in Brougham Street while the repairs were continuing, but the inefficiencies of
working across two sites reinforced by the constraints on travel had added significant
operational costs. Space in the Memorial Hospital which should be available for patients
was still required for office accommodation. The completion of the Merivale site rebuild
programme would help alleviate this situation.
Merivale, he said, would remain ‘home’ for Nurse Maude. It was a decision that had not
been taken lightly. The Board had discussed the merits of retaining the Nurse Maude
presence in Merivale versus the profitability of selling its existing land and shifting to a new
location. It was a common sense outcome, he said, based as much on location, recognition
and heritage as on economics and finance.
The Baldridge model had provided Nurse Maude with a set of key performance areas which
were considered to be the drivers of business success in the medium to long term. In every
respect, Nurse Maude was a business. It was customer focused, provided high quality,

[185]
affordable services, financial viability, leadership and direction, and most importantly,
employed highly motivated staff. However, the organisation could not afford to be
complacent. A detailed customer and stakeholder-focused workplan would be part of the
next four years’ programme. Business development and growth were essential for the
organisation’s longevity. There were opportunities to increase market share for district
nursing, specialist nursing and home care in Christchurch and Canterbury alongside
promoting the care coordination programme, community nursing and home care services
throughout New Zealand.
Adversity and challenge had played a key role in Nurse Maude’s ability to survive the worst
of the earthquakes and had energised everyone in the organisation. There were several
major initiatives planned for the next five years which included new hospital and hospice
facilities. Together with ongoing financial viability, the improvements to the organisation’s
information technology systems and the ongoing quality care delivered to patients and
clients in residential care and the community would provide the organisation with the impetus
to achieve a New Zealand Business Excellence Gold Award by 2018.
Recognition of efficient management was important, Jim Magee said, however it was the
strength and profile of the organisation in its totality that gave it gravitas in the community.
Identifying one particular strength did not do justice to the ethos of Sibylla Maude.
As an organisation, Nurse Maude had come a long way since its founder had walked the
streets of Addington and Sydenham. Its community programme had extended beyond the
immediate care of the frail elderly and the sick poor. Supporting people with dementia to
stay in their own homes was growing in importance, Jim Magee said. ‘Dementia is rapidly
becoming one of New Zealand’s most significant healthcare challenges. Estimates show
that the numbers of New Zealanders living with dementia is approximately 41,000. This is
expected to increase to 77,000 by 2026. There is a well-recognised need to better support
those who care for people with dementia at home. It is critical that Nurse Maude is well
positioned to meet this need which includes educating the workforce, greater use of
technology and developing an excellent care model.’
Telehealth would play a vital part in home care, he said. ‘It has both a social and business
efficiency impact enabling a prolonged and safer stay in the client’s own home. It extends
the geographical access to care, improves data management and helps communication
between the patient and the health care provider. It extends the range of available clinical
services which in turn improves health outcomes.’
At the organisation’s 2014 meeting, Jim Magee reconfirmed his strategic direction for the
organisation. ‘The future augers well for Nurse Maude,’ he said. In addition to its ongoing
care programme, the organisation had taken delivery of its new clinical management system
due to go live in 2016. ‘The new system vastly reduces the amount of paperwork currently
required by both clinical and support staff. It gives our nurses instant access to information
within the patient’s home by way of tablet computers. It provides us with a very efficient
scheduling system which will result in clients having much more certainty about the arrival
time of arrival of their district nurse or care giver. It will set a new standard for community
based systems in New Zealand.’

[186]
Nurse Maude was a major healthcare provider in Canterbury, well recognised and
appreciated by its patients and clients. ‘This is due in no small measure to the quality care
we provide,’ he said. ‘We are slightly different from most providers in that we go out there
and run business operations to generate funding for mainstream healthcare. This includes
selling frozen meals from our kitchen, using spare laundry capacity to provide services for
rest homes, GP practices and even motels, running our seven hospice shops, our TradeMe
operation and our Health and Mobility shop. Even without our clinical services, we would
rank amongst the bigger business operations in Christchurch.’ The two existing hubs in
Halswell and on Brougham Street would continue to provide premises from which nursing
and homecare staff could readily drive to see patients and clients.
‘The state of the roads over the course of the year has continued to present a very real
challenge for our nurses and support workers. Many of our office staff are still working in
very restricted temporary conditions. But, I’m proud to say, people are just getting on with it
and you never hear complaints.’
‘Health services are constantly evolving under the influence of growing demand, changing
expectations, technical advances and economic conditions. As a provider, we need to be
able to respond to them as early and as effectively as possible. One of the biggest
challenges facing this country and others is how to respond to the health and economic
issues associated with the needs of an ageing population. We believe our contribution will
be to keep people as healthy and as independent in their own homes for as long as
possible.’
‘Working with the New Zealand Institute of Community Health Care, we have undertaken a
series of research projects that relate specifically to people being able to stay in their own
homes including home-based dementia care, the use of tele-monitoring technology and best
practice ways for maximising the contribution of volunteer visitors in the home environment.
We believe all of these activities will have relevance for the work that we do, but we want our
approach to be carefully planned and evidence-based.’
One of the Institute’s major projects, completed in February 2015, explored respite
requirements for children and young people with high level, complex, health-related support
needs. The project which was commissioned by Nurse Maude and endorsed by needs
assessors, care providers and parent representatives, was designed to quantify and qualify
the needs in the identified group and to describe current gaps in existing service delivery.
The study included structured focus groups involving parents, interviews, and discussions
with other healthcare providers together with research and analysis. The outcome was a
substantial report on an area of the health sector which included a potential model of respite
care for children and young people in the identified group.
Explaining the rationale for the study, the Institute’s Director Chris Hendry said it was
because anecdotal evidence had suggested families were struggling to find the best
resources for their children, that the challenges of caring could be overwhelming and that
finding their way through the mass of available services was confusing; that there was
limited suitable respite and carer support options available, and that access to support was
highly variable. She said the study had identified 256 children and young people in
Canterbury who met the study criteria of which 28 per cent lived in single parent households,

[187]
95 per cent had siblings and 12 per cent had four or five siblings. The range of identified
health-related need covered palliative care, physical and intellectual disability including
autism, mental health, long-term medically complex issues, and accidental disability.
‘Our aim was to find respite solutions by quantifying the need, identifying the underlying
issues and describing the type of support families need.’ The study found that many parents
said finding high quality carers was difficult and they were difficult to keep; there was a
mismatch between what parents believed was important and traditional respite care
solutions. Access to funding and high quality respite care was varied and inconsistent.
Many parents said they didn’t have the resources to navigate complex healthcare systems.
The study proposed several options to improve the situation including raising awareness,
improving current assessment and access and developing appropriate respite options in
Canterbury.
Respite care for older people remained a significant and important aspect of Nurse Maude’s
work in the post-quake environment. In 2014, three years after the February earthquake, a
large proportion of Christchurch people continued to report being affected by the event.
There was no age differentiation. The impacts were felt across the community. Everybody
experienced it; writing it down gave it a permanence that was important.
In her 2015 annual report, Sheree East commented on the substantial progress made with
the Care Coordination programme in Canterbury and in the Wellington region. The local
team of registered nurses and administrators managed an average of 500 referrals a week
for community based health services in the Canterbury area. ‘The Capital and Coast Care
Coordination Centre is the largest of the care coordination services, providing a single point
of entry for referrals for community based services,’ she said. The Hutt Valley Service
Coordination Centre worked in partnership with clients, their families, healthcare and support
services and had a presence in the Hutt Valley hospital supporting timely discharge from
hospital.
She talked about the numbers of patients who had been nursed over the previous 12
months. Of the 14,000 patients, 40 per cent were aged over 85 and 55 per cent had multiple
comorbidities.
‘This is the future of nursing and homecare. A future where in just 25 years those aged 65
years and over is predicted to double to number some 1.3 million. This places particular
demands on those of us providing care in the community,’ she wrote. ‘It’s very much about
meeting the wishes of those who want to stay in their own home and community and
reducing, as much as possible, the social isolation of those living alone through regular
contact with our nurses and home support staff. With 263 nurses and 477 home support
workers in people’s homes across Canterbury, we are better placed than most to see the
implications of a health and home care system that is already under strain.’
Sheree East’s comments were aligned with national predictions that by 2021, 90 per cent of
adults over 65 years are expected to be living at home and 28 per cent to be living alone.
(Statistics New Zealand, 2004). A Massey University study completed in 2015, delved
further into the predictions, stating that ‘faced with the greater number of older adults living in

[188]
the community, there is a need to recognise this group as being at-risk prior to a disaster
event.’320
For Nurse Maude’s staff, what had been achieved within a remarkably short timeframe was
testament to the organisation’s to deliver on its contracts and to give added value to clients
and patients. Its ability to deliver was due in no small measure to the ongoing efforts of the
Nurse Maude Foundation. In the five years that followed the earthquakes, the Foundation
had continued to provide background support to the organisation, to top up funds and to
underwrite exceptional spending including capital works, necessary infrastructure, research
and development.
‘This provision of critical financial support to areas which are under-funded and projects
which require substantial capital is essential for maintaining the quality of care we provide in
our hospice, hospital, speciality clinics and the community. Nurse Maude’s wish that the
most vulnerable in our community would always be cared for has been met because of our
benefactors who are our perpetual partners in care. It is they, along with our donors and
sponsors who make possible the sometimes seemingly impossible, which is to continue
meeting the increased demand to provide care to those who need it most.
It is an extraordinary gift to be able to make such a profound and positive effect on the lives
of others,’321 Foundation Chair Murray Compton said.
‘We are proud of our past and continue to draw inspiration from our founder; at the same
time we take pride in what Nurse Maude is today, our role during the worst of the
earthquakes, and what we achieved during that time of great crisis in our community. We
have a progressive approach to health and we can look forward to our organisation’s next
centennial celebration in the knowledge that we continue to make a valuable contribution to
the wellbeing of people in Canterbury and beyond.’
Murray Compton said the organisation had proactively adapted to the changing world of
health politics and healthcare. It had potential to expand its services in Canterbury and to
achieve similar results elsewhere. ‘We operate in a highly competitive market,’ he said,
‘particularly in the homecare sector. It is challenging and we must ensure we maintain our
position. We do this by always providing the best care possible. Everyone in our
organisation is passionate about Nurse Maude. Our professionalism is demonstrated in our
district nursing, in the care of patients in our hospice and hospital and with our homecare
programmes. It is our intention to ensure Nurse Maude retains its position at the forefront of
community health care and that it continues to grow and flourish.’
‘As we move towards our organisation’s second century, we want to be able to look back on
our achievements with pride and look forward to the challenges ahead with enthusiasm.
Health is an invigorating environment to work in. It is always changing to meet peoples’
needs. We are an aging population which means we have a tendency towards an aging
320 Tracking the Health & Wellbeing of Older New Zealanders affected by the Canterbury Earthquakes. Brendan Stevenson & Sally Keeling. Health & Ageing Research Team, School of Psychology, Massey University 2015. P 6. 321 Murray Compton 2015

[189]
workforce. It is not restricted to the health sector; it is generic across the community. We
have a responsibility to find the most effective way of resolving this and other issues in the
best way possible.
Preserving the memory of Sibylla Maude as the first district nurse in New Zealand was
important. Strengthening her resolve and her values was essential. ‘We are an organisation
which is part of Canterbury’s history dating back to 1896. We have a legacy that is unique in
New Zealand. Reflecting on the last four years, the earthquakes have shown us that we are
purposeful in our commitment to the people for whom we have a responsibility whether it is
in our hospital and hospice or whether it is in the community and we are challenged to
ensure we give them the best care possible.’
On 13 October 2015, on time and on budget, as was the organisation’s practice over its
approaching 120 years, the fully restored McDougall House was officially reopened.
‘One would be forgiven for wondering, looking at McDougall House immediately after the
February (2011) earthquakes, whether it could ever be successful restored. But the Nurse
Maude Board was very clear, very early in the piece, that restoration was the only option.
We particularly wanted to ensure that the Ballroom, the beautiful entrance hall and stairs,
and the Boardroom were returned as closely as possible to their original state,’322 Murray
Compton said at the opening ceremony. It was a tribute to the architects, Daryl Partridge of
Trengrove Architects, builders Armitage Williams and the two foremen Bruce Smart and
Bruce Harrington, their teams and sub-contractors and the Association’s staff who had
overseen the project. The project had earned a Christchurch Civic Trust Heritage Award for
their efforts.
‘Of course, none of this would have been possible without the magnificent gift of the
McDougall family home in 1949 which was originally known as ‘Fitzroy’, Murray Compton
remarked. ‘Today the paintings of Robert Ewing McDougall and the McDougall sisters are
back in place in the Boardroom,’323 he confirmed. The House had been fully restored and
new offices created upstairs and downstairs, with new supporting facilities. It was a
landmark building for Christchurch at a time when few heritage buildings remained standing.
In keeping with Sybil’s determination, her marble bust was carefully tucked into a corner of
the new Boardroom. Would it ever see the light of day?
McDougall House was a major part of the Association’s rebuilding programme which was
reconfirmed at the December 2015 annual meeting. Retiring Chair Murray Compton
acknowledged everything that had been achieved by the staff in the five years since the 4
September 2010 earthquake and looked forward to what would be achieved in the lead up to
the Association’s 120th year in 2016.
‘I have nothing but admiration for the work of our nursing and home support staff who, in the
community, in our speciality clinics, hospital and hospice have individually and collectively
for those who need us most.’324
322 Address by Murray Compton at the official opening of McDougall house, 13 October 2015 323 ibid 324 Chairman’s Report, Nurse Maude Annual Meeting 8 December 2015

[190]
‘Technology, along with our significant investment in research and development has seen
Nurse Maude provide a diverse and specialist range of nursing and homecare services to an
increasingly ageing population. What hasn’t changed however, is the skill and compassion
of those who provide that care, forging strong relationships in our community.’
‘Operating in a post-earthquake environment in a time of economic austerity, is, at times, a
challenge,’ Jim Magee observed. ‘Our administrative and support activities are still split over
two sites and our district nurses and support workers are (still) hampered daily by road
works and diversions. These, and other constraints, motivate us to search continually for
efficiencies in the way we work.’325
The previous twelve months had seen progress on replacing the quake-damaged hospital
and hospice. ‘Construction of the new 75-bed hospital based on the site of the former
Clinical Services Building will begin shortly. The first stage is the utilities block – the laundry
and the kitchen, both of which will be finished in July 2016. The hospital should be
completed by 2018. We are still not sure whether we will rebuild the hospice or give it a
radical refit to be finished in 2019. We want a hospice where the needs of the patient can be
fully met.’326
The ‘greenshoots of the rebuild are starting to appear.’327
325 Chief Executive’s Annual Report, Nurse Maude Annual Meeting 8 December 2015 326 ibid 327 ibid

[191]
Author’s Notes and Acknowledgements
As I was nearing the completion of this revised edition in February 2016, Christchurch was
once again struck by a severe earthquake. It was a grim reminder that the tectonic plates
beneath us are still lurching around trying to get comfortable. It is at these times that the
healthcare teams come into their own. They know what to do.
The history of the Nurse Maude Association is one of dedication and commitment to the
community it has served since 1896. District nursing has a well-established place in New
Zealand, thanks in no small measure to pioneers like Sibylla Maude. She fought for the
rights of nurses even before the Nurses Registration Act came into effect in 1901. In a way,
the Act, which was the first of its kind in the world, mirrored Nurse Maude’s early efforts to
put into practice standardised training for nurses that would give them the professionalism
and expertise they so badly needed.
In researching this book, some interesting facts were uncovered, particularly the tradition
that nurses were usually referred to by their surname. It was a tradition which the district
nurses inherited. As a result, trying to find the first names of early employees became
something of a problem. It was not restricted to nurses either. Most of the references to the
Nurse Maude Association’s early Board members were similarly restricted. In later years, it
became acceptable practice to identify people by their full name, however references to
many of those early friends and staff remains as they were known – by their initials and
surname.
Sibylla Maude’s family and friends referred to her as ‘Syb’ or ‘Sibbie’. She was more often
known as Sybil than Sibylla. For this reason, I have used ‘Sybil’ when talking more
personally about her, and ‘Sibylla’ when the more professional name was more appropriate.
There was some confusion surrounding the different Port Hills cottages both Sybil and her
sister May Maude owned. Sybil bought her first holiday home at Redcliffs which she
subsequently sold in order to buy a more substantial cottage at Scarborough. It was a
favourite retreat for Sybil and her companion Sister Rose, and when she died, Sybil left it to
Rose’s niece Joyce Godfrey. There was a stipulation that Rose should live there for as long
as she wished. May Maude owned another cottage at Clifton which she left to the Nurse
Maude District Nursing Association for the nurses to use for recreation and holiday breaks.
In 2015, I was given a late reference to the Sisters of the Community of the Sacred Name
who had supported and cared for Sybil in the early days. I had visited their Christchurch
convent on the corner of Barbadoes and St Asaph Streets in 1995 as part of my research for
the Centennial History of Nurse Maude. At the time, Sister Anne had allowed me access to
the diaries where Sybil’s achievements had been so carefully noted down. Their beautiful
brick building was severely damaged in the 2011 earthquake and had to be demolished. An
article in the Press (31 January 2015) commented that the original building remained intact
and would be sold to the Home and Family Society (formerly the Society for the Protection of
Women and Children). There was no reference to Sybil, but the connection was there
nonetheless.

[192]
The first two books that were written about Nurse Maude – ‘A Friend in Need’ by E. Somers
Cocks, and ‘In the name of Nurse Maude’, by Eve A. Stonehouse, covered some of the early
history and development of the Association. It was a fascinating exercise to revisit many of
these stories and to discover not only more about the Maude family, but to put into context
much of Sibylla’s own work. It became apparent, reading some of the later comments, that
while she paved the way for many new health initiatives, her endeavours did not always
have the results she wanted. She frustrated the health system as much as it frustrated her.
She was fortunate to have life-long friends like Jessie Heaton Rhodes who was well
connected in the Anglican Church and in the Christchurch community. As a result, Sybil
often benefitted from her friend’s energy in encouraging friends and acquaintances to
support the fledgling district nursing enterprise.
‘Freedom is sweet,’ Sybil said in a radio broadcast just one month before she died. She was
talking about the importance of older people staying in their own homes. It was one of her
most passionate concerns, and one that through district nursing, has been well and truly
realised in the years that have followed. This book tells the story of a unique organisation,
rich in history and with a philosophy of caring for people that has taken it through more than
a century of community nursing experience. It describes the people who have contributed to
the success of the organisation, the decisions that were made and the impact of those
decisions. In the 1996 centennial book, I found a poem by Sybil’s close friend Mary Ursula
Bethell which seemed appropriate to include. In researching this revised edition, I read
Fiona Farrell’s ‘The Broken Book’ which included her poem ‘Twigs’, such apt verses that
perfectly represent the extent to which Cantabrians have trudged an often lonely path since
2010.
When the Board decided that a revised edition was necessary in the wake of the
earthquakes that destroyed much of Canterbury’s physical and social fabric, it was an
opportunity to explore the challenges and changes that have contributed to keeping Nurse
Maude at the forefront of community healthcare in its home region and at the same time to
extend its services through its care coordination programme to the Wellington district.
Interviewing many people who are part of Nurse Maude in the 21st century has once again
proven that the philosophy and values of its founder remain as true in 2016 as they did in
1896. Her belief in patients retaining their dignity and their independence was a powerful
legacy for everyone. Her motto that hung in the Madras Street building remains as true
today as it was nearly 120 years ago. ‘No man knoweth another’s burdens.’
Revising and writing the new edition of Nurse Maude’s history was also an opportunity to
review ‘Nurse Maude: The first 100 Years’ partly because technology has enabled greater
access to old papers, and, some of the earlier books, documents and government policies
that pre-date 1996 are now digitised. There are websites accessible for research that did
not exist in the early 1990s and some of them proved to be very useful in updating records
and confirming or discounting what had previously been accepted as historical fact.
Attending two important events in 2015 was once again a validation of the organisation’s
strength and place in Canterbury. The official opening of McDougall House on 13 October
was attended by two of the founder’s family – Mrs Angela Moss and Mr Tim Seay, together

[193]
with many former staff and long-time friends of the Association. It is a superbly restored
building and one which can claim its rightful place in the city’s heritage listings. Its former
owner Robert Ewing McDougall was a philanthropist whose donations to many charities and
organisations in Christchurch were highly valued in their day.
Nurse Maude’s 2015 annual meeting was also held in McDougall House on 8 December
2015. It closed a chapter on Murray Compton’s long career as the Board’s Chair, although
he will remain on the Board. It also signalled the retirement of several Board members who
gave generous time and commitment to Nurse Maude over many years. Rose Laloli who
joined the Board in 2003 and who acted as Chair for 18 months, Diana Sullivan who also
became a Board member in 2003 and Reg Garters who served on the Board since 1998.
There are several people who have contributed to this revised edition of Nurse Maude’s
history in addition to those already mentioned in the first book. Jim Magee, the
organisation’s Chief Executive, Fran Cook General Manager of Clinical Services, Mary-Anne
Stone Business Development Manager, Wayne Hutchinson Business Improvement
Manager, Sheree East Director of Nursing, Deb Nind General Manager of Care
Coordination, Mark Nicklin the Chief Financial Officer, Linda Mace Manager of Volunteer
Services and Sue Bramwell the General Manager of Marketing have all given generous time
to enable Nurse Maude’s challenges and progress as an organisation to be documented
here. The current senior managers between them have a wealth of knowledge of the health
sector and a keen understanding of the imperatives that drive the business. They have a
firm belief in the principles and values of Nurse Maude as a major participant and contributor
to healthcare in New Zealand.
Former Chief Executive Ingrid Thomas took time to explain to me the nuances of Primary
Health Organisations when they were established and their impact on the health sector
particularly in Canterbury. Interviews with former Board Chair Colin Averill and former Board
member John Drayton helped enormously to better understand the contribution Board
members have made during some of the more complex upheavals in health and to gain a
more comprehensive insight into the governing body that has existed almost from day one.
They both commented on the enormity of change in health now, compared to the latter
stages of the 20th century.
Having access to the Nurse Maude Archives, its policy and strategy papers, was extremely
helpful to enable research for this book. And, the Christchurch libraries, temporary though
they are still, were a valuable source of information and data.
When I talked with the current Board members – Rose Laloli, Diana Sullivan, Mark Marshall,
Reg Garters, Jane Cartwright, David Lang, Cathy Andrews and Murray Compton - Nurse
Maude’s longest-standing Chair – in 2014 and 2015, every one of them gave me valuable
insights into the changing face of governance and the Board’s responsibilities. They know
their organisation, its progressive approach to health in general and its commitment to
helping people stay in their own homes for as long as practicable and possible. They are
fully aware of the complexities of health politics in the 21st century and of rapid change.
They have brought unique strengths to the Board table which will be invaluable in the next
few years as the post-quake environment in Canterbury enters a more consolidated period.

[194]
Everyone I interviewed, Board members and staff, talked about the earthquakes with
compassion for their patients, clients and fellow staff members. They all demonstrated an
individual belief that they simply did what had to be done at the time. They did not expect
medals. They were grateful for public recognition and appreciative of individual thanks but
being an essential service meant exactly that. Staff particularly commented that there was
no time for soul searching, and in the immediate post-quake period there was no time for
reminiscing. It was all about recovery, reconstruction and simply getting on with the job.
Everyone was also extremely positive about the future and of the imperative of keeping
Nurse Maude as the pre-eminent district nursing organisation in New Zealand.
Cathy Andrew was perhaps the most succinct in her view that for Nurse Maude to flourish in
the modern world of health politics, it must put its emphasis on nursing. A firm advocate for
enabling people to stay in their own homes for as long as possible, she considers the
organisation needs to act as the advocate for this philosophy, to convince the decision
makers that this is the best way of the future. Not to make decisions for people however, but
to act on their behalf. ‘We have a role to play working with age care organisations like Grey
Power which have the political will to speak on behalf of their members.’328
Sibylla Maude’s philosophy of helping people but not taking away their self-respect remains
the organisational mantra. The next decade will see enormous progress in health technology
much of which will contribute to people being able to stay at home longer.
Communities are, after all, a reflection of the people who live in them.
328 Interview with Cathy Andrew, February 2015

[195]
Board and Management 2015
Board of Trustees
Dr Cathy Andrew RN, BA, MA (Hons), PhD. 2013 - present
Jane Cartwright BSc, PGDipSci, NZRD, MBA (Otago). 2007 – present
Murray Compton – Chair, B.Com, C.A., C.M.C., FNZIM, Inst.D., QSM. 1988 – present
Reg Garters FNZIM, Dip Mgt. 1988 –2015
Dr John Hudson MB ChB, DRCOG, FRNZCGP, Dip Trav Med. 2013 – present
Tim Keenan BCM (Lincoln), CA. 2013 – present
David Lang – Deputy Chair, LLB. 2008 – present
Rose Laloli - 2003 - 2015
Mark Marshall Grad Dip App Mgt. 2010 – present
Diana Sullivan NZRN. 2003 – 2015
Senior Management Team
Jim Magee, Chief Executive
Sue Bramwell, General Manager Marketing
Sheree East, Director of Nursing
Murray Hendy, Site Development Manager
Wayne Hutchinson, Business Improvement Manager/Acting Chief Information Officer
Mark Nicklin, Chief Financial Officer
Deb Nind, General Manager Care Coordination & Specialist Services
Kim O’Keefe, Human Resources Manager
Sam Powell, General Manager Community Services
Mary-Anne Stone, Business Development Manager

[196]
Bibliography District Nursing Kai Tiaki Nursing Journal 1908 pp 118,119
Acland L.G.D. ‘The Early Canterbury Runs.’ (4th ed.) Whitcoulls Ltd Christchurch 1930 p 82
The Waiapu Church Gazette 1 September 1935
Cocks E. Somers: ‘Nurse Maude – Her Life and Work’. Nurse Maude District Nursing Association. Christchurch 1950
Rhodes Jessie. Details of the Early History of Christchurch Nursing and Nurse Maude Association. (undated) pp 1-7
Bennett F.O. ‘Hospital on the Avon.’ North Canterbury Hospital Board 1962 p 230
Letter from the Canterbury Faculty, College of General Practitioners 10 May 1966. Nurse Maude Archives.
G.R. Macdonald. ‘Dictionary of Canterbury Biographies.’ Canterbury Museum NZ. Thomas Maude pp 1-7.
Scotter, W. H. ‘A History of Canterbury.’ Whitcombe & Tombs Ltd Christchurch 1965. p 360
Note of talk with Dr Averill 5 February 1965 (Author unknown.)
Letter from Canterbury Division, British Medical Association 17 May 1966
Cotterill Denis, Letter to Watts & Patterson, solicitors, Wellington 22 November 1966
Note of discussion between Norman Greenslade and Denis Cotterill 18 July 1967
Memorandum of a conversation with Norman Greenslade 26 January 1967
Bennett Barnaby, Dann James, Johnson Emma, Reynolds Ryan. ‘Once in a Lifetime: City-building after Disaster in Christchurch. Freerange Press 2014
Pinney Robert. ‘Early South Canterbury Runs.’ A.H.& A.W. Reed Wellington 1971 p 39
Stonehouse Eve A: ‘In the Name of Nurse Maude’. Nurse Maude District Nursing Association. Christchurch 1972
Government White Paper on Health 1974 p 83
Brooking, Tom. ‘Economic Transformation.’ The Oxford History of New Zealand. Ed. W.H. Oliver with B.R. Williams Oxford University Press 1981.pp 247-248
Eldred Grigg, Stevan. ‘A New History of Canterbury.’ John McIndoe, Dunedin 1982. p 30
Seager Madeleine. ‘Edward William Seager.’ The Heritage Press Waikanae. 1987. p 263
Rice Geoffrey. ‘Black November.’ Allen & Unwin Wellington 1988. pp 84-86
‘Unshackling The Hospitals: The Gibbs Taskforce 1988 p 1-21
British Medical Journal Vol 297 12 November 1988
Spoonley Paul, Pearson David, Shirley Ian. ‘New Zealand Society.’ Dunmore Press 1990 p 158
Government Health Policy Statement: ‘Your Health & The Public Health 1991 p 18-23
Macdonald Charlotte, Penfold Merimeri, Williams Bridget: ‘The Book of New Zealand Women Ko Kui Ma Te Kaupapa.’ Bridget Williams Books Ltd Wellington 1991
Parker Bob. ‘Ripped Apart.’ Antares Publishing 2012
Farrell Fiona. ‘The Broken Book’ Auckland University Press 2011

[197]
Rogers Anna. ‘Christchurch – the city in literature.’ Exisle Publishing Ltd 2003
Tolerton Jane. ‘Ettie.’ Penguin Books 1992 Auckland p 38.
Fry Ruth. ‘Community of the Sacred Name. A Centennial History.’ Community of the Sacred Name, Christchurch 1993 p 25
Silverson Alice: ‘The last 30 years: The history of the Canterbury Area Health Board.’ Canterbury Area Health Ltd, Christchurch 1995. p 167.
Campbell Helen. ‘Looking back, a history of the Christchurch School of Nursing 1891-1987’ Published 1997.
Ministry of Health: ‘ Releasing the Potential of Nursing.’ The Ministerial Taskforce on Nursing 1998
Ministry of Health: The New Zealand Palliative Care Strategy 2001
Ashton Toni, Cumming Jackie: Health Policy Monitor 2004
Ministry of Health: District Nursing Services in New Zealand Report 2010
Ministry of Health: Better, Sooner, More Convenient Health Care in the Community 2011
Blakie Megan. ‘Anglican Life’, August/September issue. Interview with Sister Anne. 24 August 2012.
Diaries of the Community of the Sacred Name (undated)
Nurse Maude’s Household Book: Published by Nurse Maude for the District Nursing Association. Reprinted 2013.
Kai Tiaki Nursing New Zealand Vol 20 no 7 2014
Nurse Maude Annual Reports from 1898 to 2014
Nurse Maude Archives
The Press, Christchurch
The Christchurch Star
The Observer, Christchurch

[198]
Index
Andrew Cathy, Dr
Averill Colin
Averill Leslie, Dr
Averill Walter, Rev
Aynsley Murray, Dr
Ballantyne Campbell
Barnes Diane
Bashford Emily
Bassett Michael, Dr
Beaven Eric
Berry Lynton, Dr
Bethell Mary Ursula
Bland Kathleen
Bowden Anthea
Bradbury Geoff
Bramwell Sue
Brown John Thomas
Cartwright Caroline
Cartwright Jane
Caygill David
Compton Murray
Compton Rod
Cook Fran
Corkill Mona
Cotterill Denis
Crooke Leslie, Dr
Donahue Lily, Sister
Drayton John
Duffey Joan
East Sheree
Elmslie Hazel
Fairgray Ross, Dr
Foster Lily
Gair George
Gardiner Coral
Garters Reg
Godfrey Charles
Godfrey Rose, Sister
Goodhew Jo
Greenslade Norman, Dr
Greenwood Cecil, Dr
Grigg Tom
Grundy Kate, Dr
Gunn Diana
Guthrie Margaret, Dr
Hackston David
Harper Leonard
Hendry Chris, Dr
Herrick Marion
Hiatt Annie
Hickson James Moore
Hockey Margaret
Holgate Annie
Holland Henry, Mayor
Holmes John, Dr
Holyoake Julia, Dr
Horn Liz
Hornibrook Fred
Johnstone Brian
Kitty Lorna
Laloli Rose
Lambie Mary
Lang David
Lassen Anne
Mackay Jessie
Magee Jim
Mair Stewart
Marshall Mark
Maude May
Maude Sibylla
Maude Thomas
Mazins Ethel
McDougall Malvina
McDougall Robert
McIvor Joyce
McLenaghen Dorothy
McLeod Sandy, Dr
Mellish Edith, Sister
Moorhouse Alice, Dr
Muir Rose
Musgrove John, Dr
O’Callaghan Jean
Parfitt Jane
Pauwels Mary
Pickering Neville, Mayor
Priest Lilian
Rae Marjorie
Renwick Mary
Rhodes Heaton, Sir
Rhodes Jessie Heaton,
Lady
Scott Edwin, Rev
Sheppard Kate
Simpson Elsie
Simpson Irene
Slater Amelia
Slater Millie
Spence David
Stanton Barbara
Stone Mary-Anne
Stoop Tony, Dr
Sullivan Dan, Mayor
Sullivan Diane
Tait Nancy
Tait Marjorie
Taylor Jean
Thomas Ingrid
Town Ian, Prof
Walmisley Stephanie
Watts Jack, MP
Webb Betty
Wells Ada
Whyte Jan, Dr
Williams T.K. Dr
Wylie Ralph




















