Nurse-Focused Cultural Competency Education for Patients ...
92
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 1 Nurse-Focused Cultural Competency Education for Patients with Differences of Sex Development Tracy Lynn Pfeifer Hall An evidence-based doctoral project presented to the Department of Nursing at Mount St. Joseph University In partial fulfillment of the degree Doctor of Nursing Practice April 19, 2021 ________________________________________________ Dr. Nancy Hinzman, DNP Advisor
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Nurse-Focused Cultural Competency Education for Patients ...

DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 1
Nurse-Focused Cultural Competency Education for Patients with Differences of Sex
Development
Tracy Lynn Pfeifer Hall
An evidence-based doctoral project presented to the Department of Nursing at
Mount St. Joseph University
In partial fulfillment of the degree
Doctor of Nursing Practice
April 19, 2021
________________________________________________
Dr. Nancy Hinzman, DNP Advisor
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 2
Table of Contents
ABSTRACT .................................................................................................................................. 5
PROBLEM .................................................................................................................................... 9
Nomenclature ........................................................................................................................... 10
Incidence .................................................................................................................................. 12
Political Group Inclusions ......................................................................................................... 13
History of Care ......................................................................................................................... 15
Cultural Milieu/Life Experiences ............................................................................................... 17
PICOT QUESTION ...................................................................................................................... 19
REVIEW OF EVIDENCE ................................................................................................................ 19
Level of Evidence Results (LOE) ................................................................................................. 20
Evidence Table/Matrix .............................................................................................................. 21
SUMMARY OF LITERATURE ........................................................................................................ 21
Identifying needs ...................................................................................................................... 22
Cultural Competency ................................................................................................................ 26
Education, Evaluation, Outcomes.............................................................................................. 28
FRAMEWORKS ........................................................................................................................... 30
Evidence-Based Model.............................................................................................................. 31
Theoretical Framework ............................................................................................................. 32
Cultural Competency Framework .............................................................................................. 33
PROJECT PROPOSAL .................................................................................................................. 34
Population and Setting ............................................................................................................. 35
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 3
Intervention .............................................................................................................................. 36
Classroom Education ............................................................................................................ 36
PowerPoint. .......................................................................................................................... 38
Video. ................................................................................................................................... 38
Organization. ....................................................................................................................... 39
Data Collection Tools ........................................................................................................... 42
STRATEGIC PLANNING .............................................................................................................. 46
Ethical considerations .............................................................................................................. 46
Stakeholders ............................................................................................................................ 47
Driving Forces .......................................................................................................................... 47
Budget ...................................................................................................................................... 49
Milestone Timeline ................................................................................................................... 50
EVALUATION OF EVIDENCE-BASED PROJECT ............................................................................. 50
Clinical Knowledge Questionnaire ............................................................................................ 52
Health Belief Attitudes Survey Instrument (HBAS) Questionnaire ............................................... 54
SIGNIFICANCE AND IMPLICATIONS ............................................................................................ 56
PROJECT FUTURE ...................................................................................................................... 59
CONCLUSION ............................................................................................................................ 59
REFERENCES ............................................................................................................................. 62
APPENDIX A .............................................................................................................................. 71
APPENDIX B .............................................................................................................................. 72
APPENDIX C .............................................................................................................................. 73
APPENDIX D .............................................................................................................................. 74
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 4
APPENDIX E .............................................................................................................................. 75
APPENDIX F............................................................................................................................... 76
APPENDIX G .............................................................................................................................. 77
APPENDIX H .............................................................................................................................. 78
APPENDIX I ............................................................................................................................... 79
APPENDIX J ............................................................................................................................... 80
APPENDIX K .............................................................................................................................. 81
APPENDIX L............................................................................................................................... 82
APPENDIX M ............................................................................................................................. 83
APPENDIX N .............................................................................................................................. 84
APPENDIX O .............................................................................................................................. 85
APPENDIX P .............................................................................................................................. 86
APPENDIX Q .............................................................................................................................. 87
APPENDIX R .............................................................................................................................. 88
APPENDIX S............................................................................................................................... 89
APPENDIX T .............................................................................................................................. 90
APPENDIX U .............................................................................................................................. 91
APPENDIX V .............................................................................................................................. 92
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 5
Abstract
Hospitals are collecting Sexual Orientation and Gender Identity (SO/GI) data through the
Electronic Health Record (EHR). Although the SO/GI data is aimed at the lesbian, gay, bisexual,
and transgender (LGBT) patient (CDC, 2019), intersex (I) is also an option in the EHR. While
healthcare training exists for the LGBT population, nurses lack focused clinical training and
cultural competency for the intersex/Differences of Sex Development (DSD) patient. Nurse
education was implemented using a PowerPoint during Lunch-and-Learn sessions. Two
questionnaires were administered pre-and post-education, a clinical knowledge survey, and a
validated Health Belief Attitudes Instrument Survey (HBAS). Nineteen nurses attended the
education sessions. A Wilcoxon signed-rank test was used to compare survey data. Before
receiving education, 53% of healthcare workers surveyed for this project reported never having
heard the term DSD and 58% didn’t know intersex was not the same thing as transgender.
There were significantly improved knowledge scores after the education (median = 3 correct)
compared to before the education (median = 1 correct), Z=-3.62, p=0.0003. The percent of
nurses who had heard the term DSD increased from 47% pre-education to 100% post-
education. Nurses' scores on a DSD/intersex knowledge assessment increased from 33% pre-
education to 100% post-education. Finally, nurses’ Health Belief Attitudes Instrument scores
significantly increased from pre-education (M = 4.65, SD = 0.68) to post-education (M = 4.94,
SD = 0.66), p = .017. Qualitative feedback supported the need for this project. This work will
complement the existing SO/GI material in the hospital with the goal of enhancing patient
outcomes for patients with DSDs/intersex conditions.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 6
Keywords: Disorders of Sex Development, Differences of Sex Development, intersex,
sexual orientation and gender identity (SO/GI), nursing, cultural competency, attitudes, nursing
continuing education.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 7
Nurse-Focused Cultural Competency Education for Patients with Differences of Sex
Development
People with Disorders or Differences of Sex Development (DSD) have always existed.
Historically, they were called hermaphrodites or pseudohermaphrodites. The term intersex
began in the early twentieth century to replace older options (Dreger & Herndon, 2009). In
2005, the term Disorders of Sex Development (DSD) was created via the 2005 Chicago
Consensus Conference to replace intersex (Lee et al., 2016). The word differences, versus
disorders, is sometimes preferred to avoid pathologic stigma and is still called DSDs (Lee et al.,
2016). In addition to the terms intersex, and DSDs, some people prefer a karyotype-phenotype
in descriptive terms, such as Xy-female, but this requires users' knowledge (Barthold, 2011).
Others may prefer the actual condition name (Cools et al., 2018). DSD is an umbrella term
representing "congenital conditions within which the development of chromosomal, gonadal,
and anatomic sex is atypical" (Lee et al., 2016, p. 159). Terminology preferences remain
debated.
Having a DSD does not mandate having genital ambiguity. It may involve variations
involving chromosomes, hormone levels, gonads, and/or phenotype. Embryonic development is
still orderly but relying on a cascade of events not usually taught to nurses. Bygone cultures
attributed birth anomalies to an array of theories ranging from God’s will, size of the womb,
hereditary, illness, or even a demonic presence, to name a few (Bates, 2005). History
demonstrates cultural influence over babies born with birth anomalies when they referred to
them as monstrous births (Bates, 2005). Old nomenclature uses fit past eras that lacked basic
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 8
genetics. The knowledge of the double-helix deoxyribonucleic acid (DNA) strand did not exist
until the 1950s, which allowed for the explanation of human development. Atypical embryonic
events were no longer a mystery or curse, as doctors scientifically understood fetal
development. Specialty fields that did not exist came into being, fields like genetics, genetic
counseling, endocrinology, embryology, and molecular biology. Scientific terminology now had
the endless potential for redefining birth anomalies that were ever-present. People are not just
born into a world; they are born into social systems where cultures ascribe meaning onto them
from birth. Societal norms have always existed, as have people with DSDs. As science and
medicine continue to evolve, so must the civilization to which patients reside, which is the
essence of cultural competency.
People with DSDs have a painful history within the field of medicine (Dreger & Herndon,
2009). Optimistically, there have been changes to care approaches, but medical students are
still not receiving adequate attention for these patients (Liang et al., 2017). There is an ethical
burden to do better for this population. The nursing curriculum is finally recognizing this void
as well (Brennan et al., 2012). As hospitals continue to collect the Sexual Orientation and
Gender Identity (SO/GI) data as part of a government initiative for hospitals using the Electronic
Health Record (EHR), the unintentional confusion of transgender and DSD/intersex exists.
Nurses need to know what intersex is if it is an option in the EHR. It is timely to offer education
about what a DSD/intersex condition is, and is not, so nurses can provide appropriate care.
Patients with DSDs remain a vulnerable population (Liang et al., 2017).
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 9
Cultural awareness is a process of continuous improvement (Mitchell et al., 2018). It is
achieved gradually by educational interventions, like planting a seed that continues to receive
nourishment to grow. This DNP project aims to support better patient outcomes by adding
DSD/intersex cultural competency to nursing continuing education. Desired patient outcomes
are improved access and utilization of health care, patient satisfaction and perceptions of care,
better patient-provider relationships, health equity, bias-free care, and improved health
behaviors (Butler, 2016). Improving the patient experience is a goal nurses can impact. This
project will support nursing education for those caring for the patient with a DSD and expand
on the lifelong growth of becoming culturally competent nurses. Cultural competence includes
awareness, skill, knowledge, encounters, and desire (Campinha-Bacote, 2002). It complements
the SO/GI initiative. This project will focus on clinical knowledge, beliefs, and attitudes (aspects
of cultural competency) for caring for patients with DSDs. Nurses are gaining greater
responsibility to advocate for patients with DSDs/intersex conditions.
Problem
People with differences of sex development have clinical and cultural needs as patients.
The typical nursing curriculum lacks a core education on this subject matter (Brennan et al.,
2012). The burden of educating on DSDs/intersex is that it is complicated. Patients require
proper recognition (clinical knowledge) and understanding of life experiences that shape a
cultural context. For nurses to become literate of this population, they must be educated on
human development, current nomenclature options, history of care, incidence/perceived rarity,
lifespan milestones and experiences, and individualization of care. Educating nurses on this
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 10
topic is an arduous process comparable to using building blocks to form a structure, and each
layer of blocks is necessary for nurses to understand it. Even the selection of terminology for
literature searches requires a nurse to be familiar with the topic. The paucity of research
specific to the DSD/intersex patient is a barrier (Liang et al., 2017; Neff & Kingery, 2016). The
hospital-wide sexual orientation and gender identity (SO/GI) data collection has prompted
awareness that nurses lack discernment between transgender and DSD/intersex differences.
Medical students report knowing less about the patient with a DSD or transgender than the gay,
lesbian, or bisexual patient (Liang et al., 2017). While there are a growing number of capstone
projects on cultural competency for the lesbian, gay, bisexual, transgender patient, there is a
void for the DSD/intersex population. The following categories are common areas in which
nurses require education to shape culturally competent care.
Nomenclature
Nomenclature use is important legally and culturally, and nurses need to be aware of
currently acceptable terms. By definition, DSD/intersex are umbrella terms representing
"congenital conditions within which the development of chromosomal, gonadal, and anatomic
sex is atypical" (Lee et al., 2016, p. 159). Transgender is a term for “people who are born with
typical male or female anatomies but feel as though they’ve been born into the ‘wrong body’”
(Intersex Society of North America, 1993-2008). Although some individuals use these terms
interchangeably, they are not the same thing. Terminology is essential for correct
documentation and medical accuracy in the EHR as well as appropriate care. Terminology
ownership creates a boundary. Having a legal genetic basis of a condition and proper use of it
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 11
promotes access to insurance coverage, medical accuracy, and lack of confusion (Lee et al.,
2006).
The SO/GI data collection will impact future outcomes, which means there must be
integrity to the input. The target group for SO/GI data is the lesbian, gay, bisexual, and
transgender population (CDC, 2019). There is an option in the EHR to select transgender or
intersex as options (DSD verbiage is not an option at this particular hospital, and the diversity
team was not familiar with it). Terminology selection requires nurses to know the difference
between intersex and transgender. How this information is collected varies amongst hospital
systems. There are inherent challenges to this data collection, including if/how the patient
divulges the information and clinical knowledge of healthcare staff. This project can aid in
meaningful data entry into the EHR, which has long-term implications for several patient
groups. Patient outcomes could be understood through this data collection if gathered
correctly. Terminology use changes amongst specialties, impacting the patient (Miller et al.,
2018). Children’s hospitals have developed DSD clinics with multidisciplinary care teams, but
those specialized clinics cease to exist as patients enter adult care hospitals. When nurses have
insufficient knowledge of the pediatric setting's terminology options, it creates an immediate
communication barrier in the adult setting. Although the DSD nomenclature remains a
medicalized term over clinics, it is not without controversy with patients. Medical personnel
have generally adopted the DSD verbiage, while patients may still choose the word intersex
(Johnson et al., 2017). Friction remains on which term to use, with individuals often preferring
the condition's specific names instead of the DSD or intersex term (Cools et al., 2018). This use
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 12
requires that the nurse receive some clinical education on conditions under the DSD/intersex
label. Nurses should be aware of these options and allow the patient to guide the terminology
used. Involving the patient to provide tailored care is different than having the burden of fully
educating staff on DSDs/intersex to receive healthcare (Braun et al., 2017). The literate nurse
will be a nurse who has been exposed to this content and can distinguish the difference
between DSD/intersex and transgender and provide personalized nomenclature use.
Incidence
There is a perceived rarity to DSDs, which could make this nursing education seem easy
to dismiss. Perceived scarcity tends to be a stumbling block for recognition. Inclusion criteria
for what qualifies an individual as having a DSD, and estimates, can vary in the literature (Jones,
2016; Rosenwohl-Mack et al., 2020). A rule for health research is somatic variations, not
political identification (Jones, 2016). One broad method in which DSDs may be categorized can
be 46, Xy-DSDs, sex chromosome DSDs, and 46-XX-DSDs (Rothkopf & John, 2014). The
incidence of DSDs/intersex is not known, and inclusion criteria are a necessary discussion;
however, estimations exist (Lee et al., 2016). Sax (2002) challenged a statistic by Anne Fausto-
Sterling in her article The Five Sexes, which estimated intersex to occur at 1.7% of the
population (Fausto-Sterling, 1993), by arguing that some conditions should not be included in
this statistic (Klinefelter’s Syndrome and Turner’s Syndrome, for example) making the incidence
around 0.018%. Jones (2018) discussed DSD incidence rates’ estimates to range from 1.7% to
4% of the population, but calculations could be minimized since they require tests to diagnose
them. In the Consensus Statement of Global Disorders of Sex Development Update since 2006:
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 13
Perceptions, Approach, and Care, a statistical discussion is offered, endorsed by seven global
pediatric and endocrinology governing bodies (Lee et al., 2016), the following incidence rates
are provided: individual incidence of ambiguous genitalia is 1: 4,500 -5,500 live births, 46 Xy
DSDs are 1: 20,000, Ovo testicular DSDs 1:100,000 live births, testicular or mixed gonadal
dysgenesis is 1:10,000, 46, XX (mostly congenital adrenal hyperplasia [CAH]) is 1:14,000-
15,000 live births but can vary by geographic location (Lee et al., 2016). Males with CAH may
not even be included in the DSD category since sex differentiation is not an issue in this
scenario (Lee et al., 2016). Klinefelter’s Syndrome estimates are 1:500/1000 live births, and
Turner’s Syndrome to be 1:2,500 live births (Lee et al., 2016). They also offered that when
proximal hypospadias with cryptorchidism, Klinefelter’s Syndrome, and Turner’s Syndrome are
included, the overall incidence rate could be 1:200/300 (Lee et al., 2016). Jones (2018) added
that some researchers suggest that hormone-related disorders, such as polycystic ovarian
syndrome (PCOS), could qualify as a DSD. As a curriculum goal, all nurses require some
educational exposure to the conditions under DSD's umbrella term, not expertise. DSDs can be
diagnosed at all stages of life (Jones, 2018). This consensus statement will guide nurse literacy
on the topic and also demonstrates how complex this can be.
Political Group Inclusions
The framework to which patients are presented is something to be cognizant of (Jones,
2018). Aside from terminology confusion, it can be challenging to know how to approach
political group inclusions. Political classifications can also confuse the nurse from researching
the topic successfully when self-educating.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 14
The theoretical lens (patient, expert, theory, group) chosen in a study for patients can
impact health research (Jones, 2018). Media and research have a growing inclusion of the DSD
population among the lesbian, gay, bisexual, transgender communities by adding an I for
intersex and a "+" as an open-ended representation for advocacy (GLBTI+). The LGBTI+ is a
group construction and inclusion that requires consideration (Jones, 2018). Jones, 2018, states
that a less discussed political strain is that people with DSDs may not choose to be in this
group construction, which may distract from blurred goals. Jones (2018) articulates a sensitive
yet prominent undercurrent on this – indicating that adding intersex to the LGBT group should
not be assumed and that objectives need to align. Societal norms that are heteronormative can
create minority stress and stigma if a person has atypical sexual characteristics. Understanding
the root causes of health inequalities requires consideration, which can be political or cultural.
On the one hand, there may be political objectives to agree upon by LGBT inclusion. It is
feasible that the “+” can represent a broad ethical inclusion to which the DSD population can
find support (ANA Center for Ethics and Human Rights, 2019). Laws and ethics that determine
rights (marriage, adoption, vocation, etc.) may overlap with the LGBT community goals. On the
other hand, other advocates argue that inclusion could be political gain by inclusion (referred to
as pinkwashing) and can place added intolerance onto the DSD person (Jones, 2018). There is a
recommendation to ask permission to engage in such inclusion, emphasizing patient-centered
care (Jones, 2018). It is imperative to clarify that a person with a DSD could identify in many
ways, as anyone else in society can, because individuality still exists. Some people with DSDs
identify as gay, while others identify as heterosexual or bisexual. Gender identity may not be an
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 15
issue for some patients, while others may require more flexibility. Individualizing care is
recommended due to the assortment of phenotypic and psychosocial variances (Lee et al.,
2020). Nurses should be aware of political group construction but allow the patient to explain
what their perspective is on this topic.
It is also necessary for the nurse to be discriminating about research that includes the
intersex person. There are vague references to the LGBT+ or LGBTI+ titles in articles that imply
the patient deemed intersex is in a study, but not including them, which could be considered
exploitive (Jones, 2018). For nursing, it could mean the information is not-applicable. Newer
nomenclatures such as gender non-conforming and non-binary are catch-all terms that could
include DSDs or transgender. Growing vernacular and gender identities can sometimes appear
chaotic, with one study citing 13 genders/sexual orientations chosen by participants (Ross &
Setchell, 2019), making proficiency difficult and possibly creating learner fatigue. It is not easy
material to teach, nor is it done quickly. A call for discernment on this topic is in order, as
patients may not be accurately represented in research that has included them in the title. The
nursing implication is to become judicious about assessing research literature.
History of Care
The history of care is an essential part of the understanding of patient culture and
clinical knowledge. Approach to care since the 1950s involved picking a gender (psychologically
and/or physically) for babies with DSDs that often-included surgery (Thyen et al., 2014;
Rosenwohl-Mack et al., 2020). The purported evidence-based-practice for managing intersex
babies, which generally meant feminizing patients, primarily derived from the John/Joan case
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 16
involving the Reimer twins (Colapinto, 2004). The John/Joan case was the research used to
manage patients with intersex conditions and was eventually discredited at the twins' expense
and countless people with DSDs (Colapinto, 2004). During this era, medical records were often
concealed from patients (Dreger & Herndon, 2009). The ethical oath of not harming patients
was camouflaged in professional training that it was moral to lie to patients (Dreger & Herndon,
2009). In more recent decades, old care models have slowly been challenged, ushering in well-
intentioned replacement verbiage, multidisciplinary clinics, and increased visibility of
DSDs/intersex people through national support groups. Informed consent remains a critical
topic for patient care (Cools et al., 2018). Many patients have felt wronged by healthcare
professionals (Cools et al., 2018). A newer revelation has emerged that healthcare providers,
parents, and individuals with DSDs/intersex conditions differ in what is considered a priority of
care (Rosenwohl-Mack et al., 2020).
The DSD term remains an unsettled reference, but the initial goal was to distinguish
patients (Dreger & Herndon, 2009). This area of scientific expertise is still evolving (Lee et al.,
2016). Patients with DSDs can have health care needs related to sexual functioning, poor body
image, discontent with nomenclature, and social remoteness (Lee et al., 2016). Patients can and
should be offered the same mental health interventions as any other patient, including peer
support (Lee et al., 2016). The digital age has ushered in new opportunities for support group
opportunities that didn’t exist twenty years ago. There is still a lot of work that needs to be
done in DSDs/intersex care. In a 2020 study involving DSD/intersex adults, 179 individuals
completing the entire survey, 53% self-reported their mental health as fair or poor, and
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 17
diversified by age (p = 0.001), with younger people fairing worse than older individuals
(Rosenwohl-Mack et al., 2020). Approximately one-third of these individuals had prior suicide
attempts (Rosenwohl-Mack et al., 2020). The risk factors for suicidality are unknown but
speculated to be societal discrimination and possibly healthcare treatment (Rosenwohl-Mack et
al., 2020). When nurses are provided with some of the histories of care, it allows them to
empathize with current healthcare choices that might otherwise seem peculiar – such as
choosing not to have gender normalizing surgeries or the quest to retain sex organs that don’t
match phenotype. It also allows an understanding of generational differences nurses may
encounter between patients. Knowing the patient’s age (to understand the era of care they
received), history of care, supportive/cultural milieu, and perspective on their DSD/intersex will
help nurses offer personalized care.
Cultural Milieu/Life Experiences
Cultural challenges can impact someone with a DSD in ways not understood by those
who do not have DSDs. No two people with DSDs have precisely the same life experience; yet,
shared experiences often exist. Sex/gender impacts the entire life span– infancy, childhood,
adolescent milestones and development, marital rights, fertility and ability to adopt, military
eligibility/vocational options, religious participation, inheritance, discrimination laws, etc.
People with DSDs/intersex grow up conceptualizing how they fit into all of these scenarios.
People who are intersex grow up with a never-ending barrage of social conditioning. Pediatrics
can involve care decisions with surgery and gender assignment. Formative years generate self-
concept and self-esteem, choice of dress, and playmates. Classroom coursework usually does
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 18
not include them, such as an introductory biology class where two options for karyotypes and
sex/gender are often taught (which can even be at a collegiate level). Puberty may accompany
unintended changes differing from peers, such as unwanted virilization or lack of menses.
Adolescence may involve surgeries and transitional hormone replacement experimentation.
Dating and pair-bonding is another societal norm that people with DSDs navigate with
childbearing issues to follow. The cultural pressures never go away with age; they change
settings. Not having a menstrual cycle is revisited every time a nurse asks a phenotypic female
patient when their last menstrual cycle was. A milestone vaccination for the human
papillomavirus marketed to girls with cervixes creates new critical thinking for application with
a DSD/intersex condition where a cervix may be lacking. While brief examples of medical
scenarios can be given, the lifetime list of experiences can be exhaustive for someone with a
DSD/intersex condition.
Campinha-Bacote (2002) defines cultural competence as “the process in which the
healthcare professional continually strives to achieve the ability and availability to effectively
work within the cultural context of a client.” A compelling alternative label is diversity
competence (Butler, 2016). The need for education about the patient with a DSD/intersex
cannot be overstated (Alpert et al., 2017; Barthold, 2011; Braun et al., 2017; Brennan et al.,
2012; Cools et al., 2018; Jones, 2018; Kruse et al., 2018; Liang et al., 2017; Lindsay et al.,
2019; Rothkopf & John, 2014; Santori, 2018; Sherriff et al., 2019). This project aimed to
identify the problem statement as a lack of clinical education and nurses' cultural competency
with DSDs/intersex conditions. The advocacy of patients with DSDs, both culturally and
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 19
clinically, is resting in the fields of medicine. Nurse leaders are needed as DSD advocates in
legislation, hospital policy, hospital/unit education competencies, and caregivers. Although this
project cannot do this topic justice by covering every point that needs to be made, this
education will increase nurse literacy for patients with DSDs/intersex conditions. Nurses are not
equipped with DSD/intersex knowledge because it is generally missing from nursing and
hospital curricula.
PICOT Question
For registered nurses on a medical-surgical unit (P), how does an education module to
clarify the patient with a Disorders/Differences of Sex Development (DSD) condition (I),
compared to no education (C), effect clinical understanding and cultural competency (O) within
one month (T)?
Review of Evidence
A literature review was conducted to determine the evidence for support of this project
using five databases. An evidence matrix was implemented as a tool to organize research
information. The evidence matrix categorized the reference, purpose of the study, sample size
when applicable, independent and dependent variables if appropriate, the study's design, level
of evidence, critical results of the research, and a category to organize each article.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 20
Description of the Search
A literature review was completed in the Spring and Fall of 2020 to examine
DSDs/intersex, cultural competency, and nursing education. Five databases were utilized for
this review: Medline, Cochrane, Ovid, Cumulative Index of Nursing and Allied Health Literature
(CINAHL), and Academic Search. Search terms were intersex, disorders of sex development,
differences of sex development, nursing, genetics, diagnosis, nursing education, the attitude of
health personnel, clinical competence, cultural competence, gender, sex, health disparities,
education and patient outcomes, curriculum, evaluation or assessment. Inclusion and exclusion
criteria were 2010-2020, peer-reviewed, scholarly journals, references available, English
language, and academic journals. Search terms were combined using the options unique to
each database. A summary of this table is in Appendix A.
Level of Evidence Results (LOE)
The studies' levels of evidence vary on the topics for the problem, intervention, cultural
competency, and outcomes (nurse/healthcare provider and patient). Due to the emerging
research on DSDs, qualitative and expert opinions are prevalent and valuable.
After review of five databases, seven systematic studies were chosen (Butler, 2016;
Horvat et al., 2014; Jones, 2018; Lindsay et al., 2019; Reeves et al., 2013; Sani et al., 2019;
Sherriff et al., 2019), one randomized controlled trial (Carpenter et al., 2015); one prospective
study (Haider et al., 2018), six cross-sectional studies (Liang et al., 2017; Maragh-Bass et al.,
2017; Miller et al., 2018; 2018; Purnell et al., 2018; Ross & Setchell, 2019; Sanders et al.,
2017), two qualitative studies (Braun et al., 2017; Thyen et al., 2014), and fourteen expert
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 21
opinions (Amies-Oelschlager et al., 2015; Barthold, 2011; Beale & Creighton, 2016; Bomalaski,
2005; Brennan et al., 2012; Carpenter, 2018; Johnson et al., 2017; Kano et al., 2020; Kruse et
al., 2018; Lee et al., 2016; Lee et al., 2020; Mitchell et al., 2018; Rothkopf & John, 2014;
(Tamar-Mattis et al., 2014). A level of evidence table is in Appendix B.
Categories for the literature review were developed based on fundamental concepts;
however, many studies overlapped in subject areas. When synthesized, they support educating
nurses to strengthen nurses' cultural competency, such as beliefs and attitudes.
Evidence Table/Matrix
An Excel evidence table/matrix was used to organize the study, purpose, sample,
independent and dependent variables, level of evidence, design, results, reference, and what
category the research supports. The matrix was divided into two sections, one with the formal
literature search results and the other with resources used outside of inclusion/exclusion
criteria that included Google, textbooks, and websites for governing bodies. Thirty-one articles
were obtained from the formal literature search in Spring and Fall 2020 and placed in the Excel
matrix. The Excel table is used as a standardized method for organizing the research for this
project and allows for easy retrieval of information.
Summary of Literature
The literature summary provides a synopsis of how the research supports this project. It
was organized into three general content areas, though many research articles overlap on
topics. The summary threads critical concepts for this project, such as identifying this patient
population's needs and experiences that shape the cultural context. Cultural competencies of
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 22
awareness, knowledge, skill, encounter, and desire are intertwined within studies. The
intervention to educate staff is the universal recommendation to enhance the patient
experience/outcomes and impact nursing attitudes.
Identifying needs
Perceiving the patient’s life experience is the foundation of becoming conscious of
cultural sensitivity. The introduction of the patient to adult care begins as a person utilizes the
hospital system for healthcare. Amies-Oelschlager et al. (2015) offered expert opinions about
the challenges of transitioning from pediatric care to adult gynecology, reinforcing that a
congenitally-based condition will require an inevitable transition to adult management with
consideration. The relationship during pediatric care is vital to consider, and the transition goal
is for it to be as seamless as possible, but this requires preparation (Beale & Creighton, 2016).
Initial adult care appointments are litmus tests for ongoing services (Beale & Creighton, 2016)
and are considered a vulnerable time for them (Cools et al., 2018). Some of the long-term
health issues should be conceptualized, such as bone health, fertility issues, risk of
malignancies, endocrine management, cardiovascular health, and psychological well-being
(Beale & Creighton, 2016). Transitioning from pediatrics to adult care is not emphasized a lot in
literature and finding adult expertise is difficult (Cools et al., 2018). This period of time is also
when sexual orientation and gender identity discussions may occur (Cools et al., 2018).
Circularly, this links back to the original discussion of the SO/GI data collection. Being culturally
competent begins with awareness of the patient’s life experience, including a likely gap from a
specialized care team in pediatrics to the adult hospital setting in which this project was aimed.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 23
Terminology use is a prevalent topic of many studies (Barthold, 2011; Beale et al., 2016;
Braun et al., 2017; Carpenter, 2018; Johnson et al., 2017; Jones, 2018; Kano et al., 2020; Lee et
al., 2016; Lindsay et al., 2019; Miller et al., 2018). Some prefer intersex as a term, yet others
regard this term as too sensationalistic and confusing with the term transgender (Johnson et al.,
2017). Miller et al. (2018) highlighted the problem of discordant use of terminology, comparing
286 clinicians in different specialties regarding inconsistent uptake of nomenclature. They
examined frequency, comfort, why one term was used over another, and what words were
heard as urban language versus in a medical setting. Surveys asked what specific terms were
most comfortable to least comfortable. The term hermaphrodite was heard 68.2% in media by
provider users, but only 2.8% report using it to explain a patient’s condition to family. DSD
verbiage was the most often used term 60.9% of the time. The reasons for verbiage selection
were comfort, knowledge, confusion for patients/families, guidelines were lacking, or negative
branding with a term, all of which validate a barrier to communication exists for patients with
DSDs when they utilize different healthcare services. Johnson et al. (2017) recommended that
terminology use be approached with flexibility, as attitudes varied on existing options. They
interviewed 202 of 580 members of a national United States support group (AIS-DSDSG) and
found predominantly negative notions towards the term Disorders of Sex Development. Being
aware of current options and allowing the patient to guide the healthcare worker individualizes
care. While the DSD term was intended to create one term that was not offensive and assist in
medical legitimacy, it became unwittingly a possibly new offensive term (Johnson et al., 2017).
Medical personnel have had a quicker uptake to the DSD terminology (Johnson et al., 2017).
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 24
DSD is a formalized term used in literature and pediatric multidisciplinary clinics; therefore,
whether this term's uptake is agreed upon or not, nurses have to be familiar with it. The
selection of terms remains case-based to avoid unintentional psychological harm or deterrents
to care.
Sani et al. (2019) emphasized how preferred terminology use boosts confidence for a
patient. Sanders et al. (2017) considered interprofessional team members’ experiences,
utilizing 105 participants (professionals, pediatric patients, and parents) from 47 appointments.
Pertinent to this project, the questionnaires asked the name of the health condition and the
clinic's name. Participants, including team members, had inconsistent terminology for a DSD
clinic, using intersex, DSD, and specialists for sex disorders. Only 8% of professionals used
local or national guidelines even though they reported knowing them. Thyen et al. (2014) found
that a lack of care coordination was a problem for patients with DSDs. An updated consensus
statement supported by seven international governing bodies on DSD care provides occurrence
statistics, analysis of nomenclature use, and the importance of patient-centered care (Lee et al.,
2016).
To know the patient requires an approach and rationalization for why information is
sought. Maragh-Bass et al. (2017) discussed barriers to receiving care related to understanding
what the patient prefers when eliciting patient information. In another study, providers and
patients were surveyed, and eighty percent of providers thought the collection of sexual
orientation or gender identity would distress patients; eleven percent of patients reported it as
bothersome. In contrast, patients felt that providing this would provide personalized care,
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 25
whereas providers perceived enhanced patient-provider synergy as a benefit. This study has
implications for patient-focused care because the patients' feedback was different from what
the providers assumed, drawing on the fact that nurses must know their patients. Patients rated
sexual orientation and gender identity data as an essential topic to know (41.3% vs. 31.6%; p
<.001). Haider et al. (2018) also provided a patient-centered lens when they compared
approaches for how to best collect sexual orientation and gender identity data for sexual
gender minority patients verbally or nonverbally. The nonverbal collection was the preferred
method for sexual gender minority patients (mean [SD], 95.6 [11.9] vs. 89.5 [20.5]; p =.03),
which has implications for how to elicit information on sensitive topics with patients with DSDs
and provide patient-centered care.
Jones (2018) produced a unique collection on international intersex/DSD studies from
61 sources that examined nomenclature use, political group construction, and insight on the
lens through which patients are viewed, especially in research. Jones encouraged the
prioritization of patient-centered care, including terminology used (Jones, 2018). Regardless of
how one sees the inclusion of intersex in the LGBT political group, literature searches produced
some research articles with intersex included. Ross & Setchell (2019) examined LGBTI patients'
experiences while participating in physiotherapy, with 108 respondents. Surveys had themes to
them, such as feeling assumptions were made about them, unease with the observation and
proximity of their bodies, and lack of knowledge about their health issues. People with DSDs
can experience a lifelong focus of medical attention on genitals, sexuality, and genetics, which
requires some sensitivity training to consider the patient experience. Lindsay et al. (2019)
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 26
provided a review of 29 studies on gender-sensitive care, which involves training to alter
gender-based health inequalities, fourteen studies targeted gender-sensitivity, and 15 were
related to lesbian, gay, bisexual, transgender patients. The results did demonstrate that 37% of
the studies in review showed significant improvement in gender-understanding care. The
training content was terminology use, understanding gender issues, stigma, discrimination, and
increasing communication skills. Lee et al. (2016) emphasized the role of peer support and a
growing recognition of support groups as collaborative partners to healthcare professionals. It
is also essential to understand the ever-increasing legality of patient autonomy (Tamar-Mattis
et al., 2014).
Cultural Competency
According to the U.S. Health & Human Services, culturally competent nursing care
includes “personal attitudes, beliefs, biases, and behaviors” (Culturally Competent Nursing Care,
n.d., a). Cultural ingredients can impact family decisions for a patient with a DSD, including a
collaborative approach to gender (Ernst et al., 2020). Part of cultural competency is assessing a
patient’s unique cultural milieu in which they reside. A patient’s culture is vital in understanding
how a patient views having a DSD. The symbiotic relationship to this is realizing that nurses
need to become aware of their own attitudes to DSDs as patients are being assessed for how
they view having a DSD. Sanders et al. (2017) emphasized that attitudes are shaped by
education and experiences. Brennan et al. (2012) asked the nursing field to include LGBTI
patients in the definition of diversity and talk about attitudes and cultural awareness of these
populations. Butler et al. (2016) reviewed 56 studies, reporting that educational guidance was
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 27
the most common intervention to impact cultural competencies and that attitude towards a
population was most often measured.
Horvat et al. (2014) assessed cultural competence education effects, examining five
studies with 337 healthcare professionals and 8,400 patients. The studies focused on training
and outcomes. This project is useful because health behaviors improved (RR 1.53, 95% CI 1.03
to 2.27). Patient interpretation of healthcare workers was improved in the intervention group
(SMD 1.60 9%, CI 1.05 to 2.15), supporting training staff to increase patient satisfaction.
Zeeman et al. (2019) demonstrated, from reviewing 57 articles, that the LGBTI populations were
more likely to experience heteronormativity-related stressors and discriminations. The
recommendations were focused on improving the education and training of professionals and
reducing barriers to access care. Peer support is now considered a vital part of care yet not fully
developed for patient use (Lee et al., 2020). Whereas people with DSDs were once purposely
isolated in the belief that maintaining a secretive nature to the diagnosis was preferable, part of
culturally competent care is to extend the same supportive services to these patients as any
other patient would receive. Psychological support includes understanding the patient’s
response to care, procedures, or healthcare professionals. Nurses can assess the patient’s
support system – cultural norms, support groups, family, friends, and religion, to understand
what promotes resilience (Lee et al., 2020). The coping skills, attitudes, and socio-economics
should also be assessed (Cools et al., 2018). Care decisions are urged to be tailored because of
individual variations and cultural environments (Lee et al., 2020). Nurses are on the frontline of
patient advocacy and can support this by providing support group information to patients. Peer
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 28
support is an integral part of mental health, usually obtained through medical support groups,
which are quite visible today and can be located via the internet. Purnell et al. (2018) examined
1,220 physicians in ten departments at Johns Hopkins University School of Medicine for
perceptions of organizational cultural competence and teamwork for at-risk patients. Structural
workplace issues impacted the ability to recognize patient distrust, comparing major versus
moderate structural problems (OR: 2.01; 95% CI: 1.23-3.28, p <.0), and less than 50%
addressed cultural barriers (Purnell et al., 2018). Understanding workplace organization lends
itself to promoting workplace policies (structure) and educational training for cultural
competencies. Cultural competency is regarded as a virtuous cycle (Kruse et al., 2018), a
lifelong deconstruction and reconstruction (Mitchell et al., 2018), which challenges biases and
discriminatory tendencies.
Education, Evaluation, Outcomes
The need for education was a universal recommendation addressing this population.
Liang et al. (2017) demonstrated a critical vantage point looking at comparing knowledge and
training for medical students on transgender and intersex topics compared to lesbian, gay,
bisexual (LGB) curriculums. Knowledge and comfort with intersex health versus LGB health were
assessed. Of 713 students, 341 students answered one of two surveys that were offered. The
comfort with intersex health remained lower than LGB health for all four years. Self-reported
knowledge of LGB versus intersex was p < 0.001; self-reported comfort of LGB versus intersex
was p < .001. The conclusion was that knowledge of intersex health falls behind that of the LGB
population (Liang et al., 2017). Of the five patient categories, the intersex patient was most
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 29
requested to learn more about from free responses on the survey options: 25 for the intersex
patient compared to 6 for lesbian, 3 for gay, 1 for bisexual, and 22 for transgender patients
(Liang et al., 2017). This gap supports the need to offer focused education for the DSD/intersex
population.
Rothkopf & John (2014) provided nursing with a thorough DSD educational summary
and clarified the nurse's role as an advocate. Bomalaski (2005) provided clinical education to
urology nurses about DSDs with an evaluation tool. Braun et al. (2017) addressed educational
reform by considering a new approach to educating LGBTI. This study utilized four medical
schools, with 550 participants using Likert scales, to evaluate the course structure's impact and
effect. Results were that participants had improved comfort interacting with LGBTI (p <.01),
knowing where to find information (p <.01), and confidence in gathering medical history (p
<.01). Reeves et al. (2013) reviewed 15 studies and summarized that interprofessional
educational interventions produced positive outcomes in seven articles, including workplace
culture and patient satisfaction. Butler (2014) cited that provider education is a common
intervention for developing cultural competence and changing provider attitudes. Other
benefits were staff readiness to provide care (Braun et al., 2017), improved patient-provider
relationships, and improved health behaviors (Buter, 2014). Thyen et al. (2014) studied several
topics specific to a patient with a DSD, one of which was understanding patient satisfaction.
They studied 110 adults from Germany, Austria, and Switzerland using a Likert scale and the
type of DSD the patient had, which correlated to satisfaction. The Xy-females had less
satisfaction than women with congenital adrenal hyperplasia. Half of the women reported a low
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 30
quality of care. Poor patient satisfaction was reported as correlational to the rarest conditions.
As previously stated, initial appointments in adult care are an early indication of the utilization
of ongoing care and endocrine management (Beale & Creighton, 2016).
Carpenter et al. (2015) conducted a randomized controlled study to use the Health
Beliefs Attitudes Survey with 180 medical students in a 2010 class in two formats: traditional
lecture or web-based. The results demonstrated the importance of asking the patients’
perspectives, beliefs, cultural context, and the concept of good health, which resonates with
application to the DSD population for this project. Student opinions and beliefs improved,
respectively (4.88, 5.10 p <.01; 4.49, 5.08, p <.001). This study aligns with patient-centered
care and provides an applicable survey to use for this project.
In summary, while the research on DSDs/Intersex has been maturing over the last 20
years, there are studies and expert opinions to guide advocacy for this vulnerable population.
By gathering the myriad research and synthesizing it to shape cultural experiences, nurses can
better understand their role in caring for patients. Workforce development is common
throughout articles; yet, few have focused solely on the DSD/intersex patient.
Frameworks
The frameworks for this project include The Iowa Model of Evidence-Based Practice to
Promote Quality of Care by Marita G. Title (Melnyk & Fineout, 2015), a nursing theory called
Twenty-One Nursing Problems by Faye Abdellah (Pitripin, 2016), and a cultural competency
model by Dr. Campinha-Bacote called Cultural Competence in Healthcare Delivery (Campinha-
Bacote, 2002). Each framework will guide different parts of the project. The evidence-based
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 31
model generates the basis for identifying the need for this intervention (an educational need),
and research was gathered to support this project. The nursing theory aligns with the approach
to care. There is a recommendation to know the patient and individualize care in research (Lee
et al., 2020). The cultural competency model guides the definition of culture in this context,
stating that it is a process of development (Campinha-Bacote, 2002). Each of the chosen
models is operational to this project.
Evidence-Based Model
The Iowa Model of Evidence-Based Practice to Promote Quality Care developed by Marita
G. Titler was applied to this project (Melnyk & Fineout-Overholt, 2015). A model provides a
guide to evaluating appropriateness to change in practice, implementing the change, evaluating
and monitoring the process, and gathering outcome data then disseminating results (Melnyk &
Fineout-Overholt, 2015). Titler’s model requires identifying a trigger, in this case, a
knowledge-focused trigger (Melnyk & Fineout-Overholt, 2015). Whether this is a priority for the
organization must be considered. Intersex was included in the SO/GI training for the LGBT
patient population but only given minimal reference; therefore, this additional training
complements the stakeholders' current educational aim. It supports accurate SO/GI data entry.
It strengthens and clarifies clinical and cultural knowledge to provide comprehensive care,
which could enhance outcomes for patients with intersex/DSD conditions. This model formed a
team to gather, develop, evaluate, and implement change. This model, as applied to this
proposed DNP project, is shown in Appendix C.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 32
Theoretical Framework
Faye Glenn Abdellah's conceptual framework, called Twenty-One Nursing Problems, is
applied to this project (Petripin, 2016). This theory was chosen to emphasize patient-centered
care and combine nursing's art and science (Petiprin, 2016). The physical, emotional, and
psychological needs of patients and interpersonal relationships between the nurse and patient
are accentuated (Petiprin, 2016). The model allows for individualized care, recognizing physical,
emotional, and sociological nursing care goals. It has a ten-point explanation of nursing as a
service and steps to identify the 21 nursing problems, which begin by learning to know the
patient (Petiprin, 2016). This theory recognizes poverty, race, pollution, education, and other
things influencing health care (Petiprin, 2016). It urges the development of nurse leaders to
advocate for underserved patients and to alter nursing education for these needs (Petiprin,
2016). This model is applied to the care of the DSD patient because it guides recognizing the
patient's nursing problems, sorting out relevant patient data, utilizing available research about
patients with DSDs, and identifying a therapeutic plan. It aims to reduce discomfort for the
patient, validates the patient’s conclusions about their health issues, and assesses the patient’s
attitudes and beliefs. It encourages nurses to know the patient, includes the patient/family in
care decisions, examines their attitudes and beliefs about the patient’s problems, and develops
a patient-centered nursing care plan.
The theory guides nurses to assess how the patient is responding emotionally to issues
of medical care. It includes cultural awareness principles, such as socioeconomics, education,
race, and miscellaneous things to influence care, gender, and sexuality. Most importantly, the
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 33
nurse is encouraged to know the patient and to include the patient and family in the care
(Petiprin, 2016). The model for this theory is shown in Appendix D.
Cultural Competency Framework
The cultural competency model chosen to guide this project is by Dr. Campinha-Bacote,
called The Process of Cultural Competence in the Delivery of Healthcare Services, (2002). It has
five domains - knowledge (educational base), awareness (of self), skill (to perform an
assessment), encounters (direct engagement), and desire to change (Campinha-Bacote, 2002).
An essential emphasis of this model is that cultural competence is a process (Camphina-Bacote,
2002). It is an applicable model to use with any number of validated tools. It includes one’s
attitudes, prejudices, biases, and stereotypes. The Health Belief Attitudes Instrument Survey
(HBAS) tool is operational to this project and is congruent with this conceptual framework and
patient-centered care plan. The nurse must have the desire to advocate for this patient
population and be driven to provide excellent care. Knowledge comes from educational training
and encounters, such as this project. Awareness and attitudes come from learning more and
doing self-examination. Skills are the focus of tactfully knowing the patient and finding out
what their definition of patient-centered care is, and demonstrating the art and science of
nursing for patients with DSDs. The history of care in this project is of western medicine in the
United States. Patients with DSDs are worldwide. Immigrants with different homeland norms
may require additional cultural awareness of how DSDs/intersex conditions are perceived within
a non-western context. All of the cultural implications of ethnicity, linguistics, folk medicine or
home remedies, and socioeconomics associated with cultural competency coursework still apply
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 34
but not the focus of this specialized training; instead, they would be additional layers of
consideration per patient.
Project Proposal
The project proposal was to educate registered nurses on a medical-surgical urology
unit about DSDs/intersex conditions and apply cultural competency concepts to be
incorporated into care of this patient population. Nursing beliefs and attitudes, as aspects of
cultural competency, will be evaluated. While nurses are often familiar with generalized cultural
competency coursework related to ethnic differences, linguistics, and religious beliefs, this
expands generalized coursework directly applied to the DSD/intersex population. The nursing
education consisted of (a) familiarizing staff to the SO/GI data collection; (b) recognition of
patients with DSDs/intersex and differences between DSDs/intersex versus transgender
patients (Lee et al., 2016; Liang et al., 2017), (c) identity politics (Jones, 2018), (d) history of
care and evolution of terminology (Barthold, 2011; Braun et al., 2017; Carpenter, 2018; Jones,
2018; Kano et al., 2020; Lee et al., 2016; Lindsay et al., 2019), (e) essential knowledge of
embryonic development and sex differentiation (Bomalaski, 2005; Rothkopf & John, 2014), (f)
incidence (Lee et al., 2016), (g) transition of care from pediatric to adult care (Amies-
Oelschlager et al., 2015, Beale & Creighton, 2016), (h) individuality of people with DSDs (Jones,
2018), and (i) patient-centered care (Maragh-Bass et al., 2017). There will be a video for a
simulated patient encounter (Quinn, 2016). The tenants of cultural competency are knowledge,
awareness, skill, encounters, and desire (Campina-Bacote, 2002). Knowledge involves clinical
training on DSDs, terminology inconsistencies, identity politics, occurrence rates, history of
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 35
care, and patient-centered approaches to care. Knowledge and cultural competency require
understanding the life experiences of this population. Awareness requires nurses to self-
analyze biases, incorrect assumptions, attitudes, and beliefs. Skill includes the ability to provide
tailored care and assessments. A skill could include knowing terminology but allowing the
patient to guide the preference to what is used, for example. Patient encounters are direct
engagement experiences with patients and will be simulated with the video of a person with a
DSD. Personal encounters challenge existing nursing beliefs. Desire means the nurse wants to
become becoming culturally sensitive and literate.
Nurses were educated on clinical information about DSDs/intersex conditions to clarify
this patient population. Nurses were provided with a broad overview of patients' life
experiences with DSDs/intersex to promote aspects of cultural competency (nursing beliefs and
attitudes) when caring for them. Pre-and post-evaluation was done using a validated tool called
the Health Belief Attitudes Instrument Survey (HBAS) and the Clinical Knowledge DSD/Intersex
Questionnaire. Evaluation sessions were provided at three intervals, pre-education, post-
education, and one-month post educations to measure knowledge retention. The evaluation
results were summarized to assess the effectiveness of the program.
Population and Setting
The setting was a large midwestern hospital in Cincinnati, Ohio. The population of
participants was 19 adult healthcare workers. Three participants were registered nurse
educators, six were medical-surgical registered nurses, one licensed practice nurse, seven were
senior nursing students, and two were personal-care-attendants (PCA). The setting was a
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 36
medical-surgical urology unit with a 22-patient accommodation. People with DSDs can have
urogenital anomalies and receive care on such a unit, which lends itself to this location's
appropriateness. An educator on the unit offered support for this project. The site was chosen
because of its applicability, support, and availability. The classroom to teach is in the same unit,
close to the staff nurses. A Lunch-and-Learn educational opportunity was offered in three
back-to-back sessions to allow for flexibility with the nursing workflow and comply with the
COVID-19 pandemic policies for gathering sizes. Incentives were provided for staff
participation (a meal and gifts) using personal funds. The unit educator posted advertisements
for the Lunch-and-Learn on the unit.
Intervention
Classroom Education. There are many pedagogical approaches considered in providing
education to this population of learners. There are lectures, simulations, online learning, role-
playing, case studies, discussion/debating, and problem-based learning methods to consider
(Xu, 2016). Patient panels are also an effective method to promote empathy (Brennan et al.,
2012). Selig (2006) demonstrated that discussion and interactive exercises had more impact on
participants in learning cultural competence Movies/videos and lectures were also useful
methods. The knowledge of andragogy implies that adult nurses will be inwardly motivated to
learn. This project was trialed with a small group of nurses in a classroom setting, and the aim
is a future expansion to an e-LEARN hospital-wide module and publication. There are
advantages and disadvantages to virtual and live classroom teaching. Virtual learning allows
nurses to do coursework at their own time and pace, reach more learners, and provide optimum
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 37
tracking and evaluation. One significant disadvantage of online learning is the lack of
interaction with learners. This pilot project used a live classroom setting with a PowerPoint that
guided the course. A live class allowed assessment of the program and feedback from
participants, allowing them to make changes before reaching a broader audience (such as an E-
LEARN). For example, at the beginning of the education, participants were asked to participate
by answering what they thought intersex was, whether it was the same thing as transgender,
and what they thought of when they thought of the word intersex. This spontaneous dialogue
allowed the educator insight into what the participants thought, and it demonstrated the need
for this project in real-time. An advantage of the live classroom session is elaborating on parts
of a topic and answering questions.
The body language of the instructor can be a useful classroom tool to emphasize
emotion. Non-verbal skills in instructors have influenced students' moods (Bambaeeroo &
Shokrpour, 2017). Students can receive non-verbal influences without even realizing it
(Bambaeeroo & Shokrpour, 2017). Speaking gives the instructor freedom for instinctual verbal
fluctuations or body language changes to inspire the learner (Bambaeeroo & Shokrpour, 2017).
It also allows the instructor to assess the learners’ body language, make adjustments, and
evaluate learner comprehension. This spontaneity cannot be achieved virtually. This project
aimed to teach new layers of scientific knowledge on DSDs/intersex. It was intended to inspire
nursing beliefs and attitudes for a vulnerable population who deserve advocacy. Teaching
cultural competency principles beckons a relationship to form between the instructor and the
learner. As Dr. Campinha-Bacote’s model for cultural competency depicts, desire must exist in
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 38
the process of becoming competent. Desire generates the will to provide better care to impact
the patient experience. The challenges or disadvantages to a live Lunch-and-Learn program
were minimal attendants and disjointed listening by nurses entering and exiting the room.
However, this was a minimal issue for all three sessions.
PowerPoint. A 30-minute PowerPoint with discussion guided the Lunch-and-Learn. The
PowerPoint topics that were covered were defining what DSD/intersex is, why it is a relevant
topic, introduction to SO/GI data collection and the electronic health record (EHR), the evolution
of terminology and why it matters, types of DSDs/intersex, essential embryonic development,
discussion of a few specific DSDs/intersex conditions, history of care, pediatric to adult care
gaps, political group inclusions, assessing a patient’s cultural milieu and nursing impact on
patient care, hospital policy, and legislation. The video of Emily Quinn, who has a DSD/intersex
condition, was embedded in the PowerPoint (Quinn, 2016). The closing portion was applying
the Campinha-Bacote model to the care of patients with DSDs/intersex conditions. The
discussion with the PowerPoint began after each participant turned in the initial pre-education
survey. The gender identity EHR screenshot used to collect SO/GI data that this hospital is
currently using can be found in Appendix E. The outline of the PowerPoint is in Appendix F.
Video. In collaboration with Emily Quinn, a woman with a DSD/intersex condition called
Androgen Insensitivity Syndrome (AIS), an online video was retrieved and used with permission
for the educational PowerPoint (Quinn, 2016). This short video was embedded in the PowerPoint
to serve as a simulated patient encounter. Dr. Campinha-Bacote’s cultural competency model
includes patient encounters as a tenant of the model. Since a patient encounter could not be
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 39
produced at whim for nurses, this served as a patient encounter. A video allowed for
DSD/intersex advocacy by providing a genuine experience for this stakeholder. The YouTube
video can be found at https://www.youtube.com/watch?v=5vDVUPjBJiM (Quinn, 2016).
Organization. In collaboration with the unit educator, preparation for the educational site and
method was planned for approximately six months. Planning including COVID-19 pandemic
policy-related adjustments. The following were organizational components: the date and time
frame for the room reservation, length of each session, incentives to use and obtaining them,
creation of an advertisement and a sign-in sheet for participants’ name and email, large manilla
envelopes to store the completed pre-and post-education surveys, food order and delivery
plans related to COVID-19 restrictions, creation of a Checkbox web-based survey and
preparation of the final email with instructions for the last survey with the link, one month after
the Lunch-and-Learn.
Due to emergent policy changes related to the COVID-19 pandemic, adjustments were
made. Training rooms were restricted to 50% of maximum occupancy, so classrooms hosted
about eight people at a time. This restriction required three back-to-back Lunch-and-Learn
sessions, with each being approximately 45-minute time blocks and 15 minutes between each
course to clean. The PowerPoint discussion was around 30 minutes, and the pre-and post-
education surveys, sign-in, and gift entries were allotted for about 10 - 15 minutes. Due to
COVID-19 policy, face masks were required, and individual pens were provided for sign-in and
survey completion. Hand sanitizers were in the room, and surfaces were disinfected between
users. The food was planned and ordered the day before the course for approximately 30
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 40
attendees. The food delivery was limited to the hospital lobby due to COVID-19 restrictions. A
medical assistant on the unit volunteered to transport it to the classroom. Drinks and desserts
were brought in with the rest of the supplies. The location of the classroom was located in the
medical-surgical urology unit. The course was scheduled for October 28, 2020, and the
classroom was reserved for that day. The classroom was small, and a projector was not
available, so a personal laptop computer using hospital wireless internet was utilized for
sharing the PowerPoint. The room was arranged to accommodate COVID-19 policy spacing,
create flow for signing in, entering their name for a prize, and viewing the PowerPoint. The
large whiteboard had the presentation's title, as attendants had no prior information on the
Lunch-and-Learn contents. Instructions were also located on the whiteboard to sign in, provide
an email address, and be aware that three surveys were being requested to complete this
program. Advertisements for the Lunch-and-Learn were posted on the unit walls with the date
and three available times. The educator actively recruited available nurses, medical assistants,
managers, and educators to attend in real-time. Participants used their meal breaks and/or
personal time without added cost to the hospital.
Incentives were offered for attendance. Lunch and individually wrapped cookies were
provided. Each participant was given the opportunity to enter their name into nine gift
drawings. Nurses were allowed one entry per gift package. The winning names were selected
after the last session, and gifts were distributed. Participants were instructed to sign in for
attendance upon coming to the classroom and providing an email. The email was required as a
means to contact them for the one-month final post-education questionnaire. Although
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 41
participant names are on a master list, the coding-maintained anonymity. They continued to
use the same coding for all three surveys. The project team researcher created a Checkbox
web-based survey (Checkbox Survey Incorporated, 2002-2020) that learners utilized for the
third survey. This option was chosen due to convenience for all and because some participants
were nursing students who would be more challenging to track down. The final survey one
month after the Lunch-and-Learn was used to measure retention, although there were risks of
a ceiling effect (Carpenter et al., 2015) or non-participation altogether.
One month after the Lunch-and-Learn, an email was sent to participants with
instructions and the link to the Checkbox web-based survey. They were offered a final $5
Starbucks gift card upon completing the last survey by replying with their mailing address, then
mailing the gift card to them.
The pre-and post-education questionnaires consisted of the clinical knowledge
questions created for this project and the validated HBAS tool. The only difference with the
post-education clinical education tool is the final question asking if the education changed
their knowledge and understanding regarding individuals born with Disorders or Differences of
Sex Development/Intersex. If the answer was yes, they were to explain how it changed their
knowledge and understanding with a space to write in whatever they wanted to. The
participants took the pre-education survey immediately after signing in to be efficient and
manage the time. After the PowerPoint presentation, they took the post-education survey.
The completed surveys were placed in manilla envelopes marked pre-and post-surveys.
The completed surveys were faxed to the project team researcher for scoring. The details of
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 42
this are found in the evaluation section of this paper. Upon completing the Lunch-and-Learn, a
$100 gift- thank-you card was provided to the educator for her assistance. An additional $100
gift card was provided to the team researcher upon completion of the survey scoring. The
advertisement for the Lunch-and-Learn is in Appendix G.
Data Collection Tools
The data collection tools included the following: (a) a validated cultural competency tool
called the Health Belief Attitude Survey (HBAS) (Dobbie et al., 2002) and (b) a brief questionnaire
measuring Clinical Knowledge DSD/intersex-specific content, with one open-ended question.
The two survey questionnaires are coded to track the same learner for all three submissions
while maintaining anonymity. The coding for the questionnaires is explained in the evaluation
section of this paper.
Cultural Competency – Health Beliefs Attitudes Instrument Survey Questionnaire Tool
(HBAS). The HBAS tool was chosen due to its operational fit for this project, the number of
questions it possesses, and its accuracy. It examines nursing beliefs and attitudes. It has
rigorous psychometric measures, with excellent reliability and validity, and is of an ideal length
for a 30-45 minutes allotment of time, consisting of 15 questions (Medrano & Dobbie, 2002;
Corley et al., 2015). While many cultural competency/attitude tools exist, other tools can have
25-100 questions. This project's tool had to be generalizable, operational, have validity, and
have a user-friendly number of questions. This scale has four domains to measure cultural
competency beliefs and attitudes: (a) opinion, getting to know the patient’s views, (b) belief,
knowing the patient’s belief toward treatment, (c) context, understanding the patient’s
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 43
psychosocial culture, (d) quality, knowing the patient’s perspective for what appropriate care is
(Carpenter et al., 2015). This tool aligns with the patient-centered care that is woven
throughout this project. It focuses on nurses' desired change: their beliefs/attitudes when
caring for patients and, in this case, applied to patients with DSDs/intersex conditions. Due to
the broadness of cultural competency and the expectation that cultural growth continues over
the nurse's life, this narrows the focus on changing nursing beliefs and attitudes and is
expected to be part of ongoing lifelong training. It was administered as a pre-and post-
education questionnaire, then again one month after the education via email to measure
retention. Each person had a coding system to thread their three evaluations together with
anonymity. This tool's 15 questions were scored using a 6-point Likert scale, one being the
lowest confidence score and six being the highest confidence score. The outcomes compared
the pre-and post-educational questionnaires to demonstrate whether nursing beliefs and
attitudes had changed. Final data collection compared the pre-and two post-education
questionnaires with summarization. The explanation of the evaluation technique is discussed in
the Evaluation section of this paper. The HBAS questionnaire is located in Appendix H.
Clinical Knowledge-DSD/Intersex Questionnaire. A brief clinical knowledge of the
DSD/Intersex questionnaire was created for pre-and post-evaluation using a Likert scale, with
an open-ended question added to the post-evaluations. The pre-education has four questions,
and the post-education has five questions. The goal of this set of questions goes back to the
original PICOT question of being able to clarify the patient with a DSD/intersex condition. The
questions are as follows: (1) Intersex is the same thing as transgender (True, False, I don’t
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 44
know, as answer options), (2) Disorders, or Differences of Sex Development (DSD) are the same
as transgender (Yes, No, as answer options), (3) I have heard of the term Disorders or
Differences of Sex Development (Yes, No, I don’t know, as answer options), (4) All patients with
a DSD/Intersex condition identify as members of the Lesbian, Gay, Bisexual, Transgender
(LGBT) political group (True, False, I don’t know, as answer options), and (5) Did this education
change your knowledge and understanding regarding individuals born with Disorders or
Difference of Sex Development (DSD)/Intersex? (Yes, No, If yes, explain how with blank lines to
free-write in an answer. The questionnaires are identical until the last question on the two
post-education surveys, which allows the participant to personalize a response regarding how
the education did or didn’t change their knowledge of DSDs/intersex. Immediately after the
education session, the first post-education questionnaire was provided. Approximately one
month later, the final post-education questionnaire was sent to participants. The email
provided a link to the Checkbox online survey tool, with the same coding technique, and an
incentive gift provided to the learner upon completing it. Evaluations compared pre-and post-
education clinical knowledge to clarify the patient with a DSD/intersex content. The pre-
education questionnaire is in Appendix I. The post-education questionnaire is in Appendix J.
This project aimed to educate nurses and healthcare workers about DSDs/intersex and
introduce cultural competency applications for this patient population, focusing on nurses'
beliefs/attitudes. A newly developed educational PowerPoint (PPT) guided the teaching sessions.
Hospitals care for a growingly diverse community of people. Shifting societal norms and
scientific discoveries continually challenge the nurse’s personal beliefs and attitudes. Due to the
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 45
time constraints of this intervention, the essential points were summarized. The PowerPoint
included a definition of DSD/Intersex, Sexual Orientation/Gender Identity (SO/GI) introduction,
political group inclusions, examples of DSDs/intersex, history of care, cultural milieu/life
experiences, the transition from pediatrics to adult care hospitals, a simulated patient
encounter and cultural competency model with the application. A video of Emily Quinn, an
individual with Androgen Insensitivity Syndrome, was provided as a patient simulation (Quinn,
2016). Nurses were challenged to become self-aware of biases, beliefs, and attitudes. The
process of becoming competent begins with self-analysis. In this context, nurses were
challenged with the concept of ethnocentricity by realizing their life experiences are not
everyone’s life experiences. Awareness involves an awakening, realizing the cultural
attributions that others experience with having a DSD/intersex condition. A post-presentation
discussion to answer questions and offer additional resources concluded the teaching session.
The cultural competency model tenants were reinforced in the presentation – awareness,
knowledge, skill, encounters, and desire. The emphasis was on individualized care, becoming
literate on DSD/intersex conditions clinically and culturally, allowing the patient to guide the
medical visit, and being aware of nursing beliefs and attitudes.
Research shows that educating staff is an essential intervention to support patients with
DSDs/intersex conditions (Alpert et al., 2017; Barthold, 2011; Braun et al., 2017; Brennan et al.,
2012; Jones, 2018; Rothkopf& John, 2014; Kruse et al., 2018; Lee et al., 2020, Liang et al.,
2017; Lindsay et al., 2019; Santori, 2018; Sherriff et al., 2019). Education provides enhanced
readiness for patient care (Braun et al., 2017).
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 46
Strategic Planning
Upon analysis of strengths, weaknesses, obstacles, and threats to this project, strategic
planning was considered. The project planning required ethical considerations such as
obtaining the designation of this as a quality improvement project versus a research project by
Mt. St. Joseph University and the hospital where this project was conducted. The stakeholders
who would be involved in this project were identified. Driving forces were recognized, and
restraining forces that would hinder this project's progression needed to be addressed. This
project was active amid the COVID-19 pandemic.
Ethical considerations
Ethical considerations for this project included the nurses as the participants. The
Institutional Review Board (IRB) determination was sought through Mount Saint Joseph
University (MSJ) and hospital IRB, both of which were obtained and categorized as a quality
improvement project. Due to the rare patient population that this education is designed for,
patients will not be directly involved in any data collected in this project. The pre and post-test
questionnaires for the nurses do not have any identifiers on the forms to protect anonymity and
were voluntary, but with incentives, as already outlined. Nurses/staff were invited through
flyers posted on the unit walls. Team members for this project are the team leader, a research
nurse with a Ph.D., a unit educator with a DNP, and a student of this project, all of whom have
current Human Subject Protection (HSP) per training Citi Training. As mentioned, there were
incentives for meals and door prizes for attending the education class.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 47
The Citi Training certificate is located in Appendix K. The Mt. St. Joseph University IRB
letter stating this as a quality improvement project is in Appendix L. The hospital IRB letter
displaying this as a quality improvement project is in Appendix M.
Stakeholders
Key Stakeholders in this quality improvement project were those with interest or
influence with its success. The most important stakeholder is the patient with a DSD. Patients
are consumers, with many hospital choices in this midwestern area, and they will go where they
are most satisfied. This project's primary focus is to improve the patient experience by
educating and enhancing nurses' and staff members' cultural competency about DSDs/intersex
conditions. Additional stakeholders were the nurses on the unit where the education will occur,
senior nursing, and organizational leadership, including the diversity and inclusion team. This
project took place on a medical-surgical urology floor where adults with DSDs may be receiving
care; therefore, it supports physicians and hospitals' work to have educated staff. There were
governing bodies to consider as stakeholders. Accrediting bodies such as the Joint Commission
include cultural competency as a standard of quality (The Joint Commission, 2020). On a
national level, the United States Health and Human Services Office of Minority Health considers
cultural competency a national standard (National CLAS Standards, n.d., b).
Driving Forces
Several driving forces to this project existed - the ethical nature of advocating for a
vulnerable population, current work by the diversity team for SO/GI education, SO/GI data
collection, and cultural shifts with LGBTQI political activism. The project was designed to
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 48
complement the SO/GI education implemented by the hospital in 2020. Due to the pandemic,
the diversity team experienced job furloughs, and email correspondences ceased, but the
project was able to continue due to the support of the unit educator on the medical-surgical
unit where the project took place.
Restraining Forces
Restraining forces for this project have been the unplanned COVID-19 pandemic, with
the government placed restrictions on facilities that halted practicum hours. The diversity team
of the hospital experienced a lengthy work furlough and became unresponsive to inquiries. The
COVID-19 guidelines changed how the classes had to be conducted – room occupancy was
restricted to 50%, which meant multiple teaching sessions were required. Additional measures
were mandated, such as having individual pens, hand sanitizers, desks required disinfection
between users, and meal delivery required someone to retrieve the food from the lobby. The
national support group meeting was offered virtually this year due to the COVID-19 pandemic.
The IRB determination process required several explanations to obtain authorization to proceed
as a quality improvement project. The nature of the voluntary Lunch-and-Learn training risked
a fragmented learning session and a possible low turnout. Unfortunately, the school-based
grant funds that would generally support food and incentive gifts were denied due to a COVID-
19 rule pertaining to in-person meetings, which required personal funding. Despite obstacles,
none of them proved to be detrimental to the completion of this project.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 49
Budget
This project's budget involved nurse attendance incentives - nine gift packages
(toiletries from Bath and Body Works, including unisex items), a box of ink pens, a meal
estimated to be about $100, and thank you gifts for team members who helped with this
project which were $200 total. The meal was pizza, cookies, and drinks. Due to COVID-19
restrictions, the school presentation required a digital poster. The poster for display on the unit
and future conferences cost about $100.00. Using the adult learning theory of andragogy,
nurses who attended would show willingness and interest to participate in this program.
Personal drive is also part of the Campinha-Bacote model of having a desire to become better
(Campinha-Bacote, 2002). Nurses attended using their own time with no added cost to the
hospital. The educational flyers and questionnaire surveys were approximately $35.00 in
printing costs. The gift cards for the third survey were $5 each for 19 participants, with ten
participants. The remaining cards were gifted to the educators on the units for support of this
project. Two conference opportunities arose through the Sigma Theta Tau International Honor
Society, nationally and internationally. The national conference in November, 2021, was
supported by hospital funding costing $679.00. The cost to drive from to and from Cincinnati
to Indianapolis is approximately $60.00, food costs for the weekend are approximately $100.00
and one night at the conference hotel is approximately $180.00, which will be out-of-pocket
costs. The international (virtual) conference in Singapore in July, 2021, was funded by Mt. St.
Joseph University costing $300. The budget summary table is located in Appendix N.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 50
Milestone Timeline
The timeline of this project outlines requirements for milestone accountability. It began
in January 2020 and ends in April 2021. During Spring and Fall 2020, a literature review was
conducted. Faculty approval for the project and the IRB determination by Mt. St. Joseph
University and the hospital were also obtained in Spring 2020. Permission to use the Health
Belief Attitude Instrument Survey was obtained in Spring/Summer 2020. The approval to
proceed with the PowerPoint for the education session was obtained in Fall 2020. The Lunch-
and-Learn education on nursing cultural competency and DSD/intersex knowledge was
conducted in October 2020. Pre- and post-education questionnaires three intervals, before the
instruction and one immediately after the Lunch-and-Learn (October 2020) and a one-month-
after education evaluation (November 2020), with data collection completing fall 2020. The
final paper submission and poster/podium presentation will be in Spring 2021. The summary
timeline is in Appendix N.
Evaluation of Evidence-Based Project
The program's evaluation utilized two questionnaires, the Health Belief Attitudes
Instrument Survey (Dobbie et al., 2002) and the Clinical knowledge of DSD-specific
questionnaires. As stated, they were offered a total of three times as a pre-evaluation, post-
evaluation, and a one-month follow-up. The evaluations were anonymous, and a five-digit code
tracks each participant’s knowledge before and after the training session. It comprised the
following: the day of the learner’s birthday and the first three letters of their mother’s first
name. An example might be January 15, 1970, and a mother’s birthday is Catherine = 15cat. If
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 51
they chose not to use the mother’s name, they could use the letters ABC, but the code had to
remain consistent on all three evaluations. The emails were sent to all 19 participants with
instructions and the link for Checkbox web-based data management survey tool. The survey
collected the nurses’ five-digit code, answers to the four post-education knowledge questions,
and answers to the 15 HBAS questions. The purpose of tracking all three survey results was to
measure participants’ changes in knowledge, attitudes, and beliefs.
The scores were entered into a spreadsheet, one row per learner. The subject
identification had the code that the learner created. Each learner’s answers to the pre-and
post-question were entered in their identified row. The spreadsheet was scored after all three
completed surveys were collected. Reverse code scoring was used for questions that are
negatively worded (questions 3, 5, 7, 15). The overall average scores were calculated and
averaged for the four components of the scale: a. importance of assessing patients’
perspectives and opinions (opinions, questions 1,3,6,10,13); b. importance of determining
patients’ beliefs for history taking and treatment (belief, questions 2,4,8,11); c. importance of
assessing patients’ psychosocial and cultural contexts (context, questions 9,12,14); d.
importance of knowing patients’ perspectives for providing good health care (quality, 5,7,15).
A Wilcoxon Signed Ranks Test was used to determine any significant differences pre versus
post educations in the overall mean score or the mean score of any of the scale's four
components.
There were nineteen participants in the three sessions for the Lunch-and-Learn who
completed the pre-and post-evaluations. Ten of the learners were registered nurses (RN’s) – 3
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 52
were nurse educators, seven were nursing students, and two were personal care attendants
(PCA’s). A total of ten participants completed the survey one month after the education.
Clinical Knowledge Questionnaire
The clinical knowledge questions were to gauge what learners knew about terminology and
political group assumptions before and after the education. It also aimed to elicit what/if an
educational change of knowledge and understanding they gained from this in-service with a
chance to free-write an explanation. The question, “Have you heard of the term Disorders or
Differences of Sex Development (DSD)?” 47% (9 learners) answered yes, and 53% (10 learners)
marked no as a baseline before the education. After the instruction, 100% (19 learners) said
yes. One month later, the results were that 100% (ten learners) marked yes. The result was a
statistically significant increase in the percent of nurses who have heard of DSD after the
education (100%) compared to before the teaching (47%), Fisher’s Exact p=0.0004. The graph
for this is in Appendix P.
Three questions that offered true/false/I-don’t-know options were asked as a baseline
before, immediately after, and one month after the education. The questions were, “Intersex is
the same thing as transgender; Disorders or Differences of Sex Development (DSD) is the same
thing as transgender; and all patients with a DSD/Intersex condition identify as members of the
Lesbian, Gay, Bisexual, Transgender political group”. Before receiving education, 53% of
healthcare workers surveyed for this project reported never having heard the term DSD. Fifty-
eight percent of learners didn’t know intersex was not the same thing as transgender. The
baseline pre-education results were 32% (6) had none correct, 37% (7) had one right, 21% (4)
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 53
had two correct, and 11% (2) had all three correct. The post-education results were that 21% (4)
had two correct and 79% (15) had all three correct. A Wilcoxon signed-rank test was used to
compare the paired data. There were significantly improved knowledge scores after the
education (median = 1 correct) compared to before the education (median = 3 correct),
Z=3.62, p=0.0003. The graph for the clinical knowledge baseline, pre-and-post education
comparison is in Appendix Q.
Immediately after the education and at one-month after the education, 100% of the
respondents answered yes to whether this seminar changed their knowledge and understanding
of DSDs. Learners were given an option to free-write how their knowledge and understanding
had changed. The following were their responses:
• I better understand the make-up of someone with DSD and how I can help with their
care
• I learned things I didn't know before coming today
• I didn't realize all the different information and type of conditions
• Differences in the androgens/how they change to estrogens
• I had heard of DSD from LPN school, but this definitely expanded on the knowledge I
had on this subject
• A new topic for me gave me an insight on what they are… and what they go through
• Learned more about how hormones work in these conditions that I did not know of prior
• Yes, I never heard of intersex
• I had never heard of DSD before this education
• I had no idea this was something that even existed
• It's very interesting to learn about intersex. I never knew there was a term for it. I just
wonder how they learned about their differences
• I had no knowledge of this. I greatly appreciate this education as I want to be more
sensitive to all patients we care for.
• I didn’t really know what it was, and now I do and understand it now
• I was familiar with outdated terminology. I also did not realize the I individuals were
grouped with the LGBTQ community which could be difficult for some individuals based
on their individual values and beliefs
• I have a better understanding and awareness
• I was completely clueless on this topic and didn't know it existed
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 54
• Understand the physiology
Learners provided the following feedback at 1-month Post-Education:
• I didn't even know the definition of intersex, so yes.
• I learned something new. I had never heard of the term DSD.
• I now know that it is such a more complex diagnosing process than I originally believed.
• Yes, traditionally it has gay, lesbian, and bisexual, and now there is an alphabet soup
for the way individuals identify. When caring for patients I set the soup aside and ask
patients to help me understand how they identify. While this can be important with
intersex individuals it’s also important to know the biology taking place within their
body to fully understand the type of individualized care the patient needs. It is hard to
keep up with terminology that constantly changes and evolves, this presentation was
very beneficial in understanding individuals with disorders of sex development and how
important it is to understand the differences of all the letters in the alphabet soup.
• Very informative educational offering. Great education on androgen insensitivity and
how that affects development of sex organs.
It is worthwhile to point out that while this part of the assessment was for clinical
knowledge, within the feedback from learners were an array of cultural competency concepts
such as awareness, knowledge, skill, encounters and desire. When learners stated they wanted
to be more sensitive to patients, desire was illustrated. Learners said they gained knowledge
and awareness on topics, as other examples. This portion of the evaluation provided strong
support for this project.
Health Belief Attitudes Survey Instrument (HBAS) Questionnaire
The HBAS survey was administered to nurses at baseline, immediately post-education, and
at 1-month post-education. The researcher reverse-coded the questions that were negatively
worded (questions 3,5,7,15). Next, the researcher calculated the overall average score for each
participant at each time point (adding scores for all items and then dividing by the number of
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 55
items). The baseline mean (SD) was 4.65 (0.68), post-education was 4.94 (0.66), and the 1-
month post-education was 4.92 (0.78).
A Wilcoxon signed ranks test found that the post-education HBAS score (M-4.94, SD-0.66)
is significantly higher than the baseline HBAS score (M=4.65, SD-0.68), Z=2.39, p=0.017.
There is no significant difference between the post-education and the 1-month post-education
HBAS Score, W=15, p>0.05. The graph for this is in Appendix R.
The four subscales in the scale were averaged. The Opinion Subscale, which measured the
importance of assessing patients’ perspectives and opinions (questions 1,3,6,10,13) had a
baseline mean (SD) of 4.91 (0.69), post-education 5.12 (0.48), 1-month post-education 5.38
(0.67). The trendline shows improvement in the opinion subscale but not a statistically
significant difference using the Wilcoxon signed ranks test, W=39.5, p=0.05. The graph for this
is in Appendix S.
The Belief Subscale, which measured the importance of determining patients’ beliefs for
history taking and treatment (questions, 2,8,11), showed a baseline mean (SD) of 4.30 (1.03),
post-education 5.05 (0.98), and 1-month post-education 4.63 (1.28). A Wilcoxon signed ranks
test found that the post-education Belief Subscale score (M=5.05, SD-0.98) is significantly
higher than the baseline Belief Subscale score (M=4.30, SD=1.03), W-11, p=0.05. There is no
significant difference between the Post-education and the 1-month post-education Belief
Subscale, W=8.5, p>0.05. The graph for this is in Appendix T.
The Context Subscale, which measured the importance of assessing patients’ psychosocial
and cultural contexts (questions 9,12,14), showed a baseline mean (SD) of 5.40 (0.69), post-
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 56
education 5.70 (0.50), and 1-month post-education 5.77 (0.35). The trendline shows
improvement in the Context Subscale score, and the Wilcoxon signed ranks test found the
differences between time points were not statistically significant, W=27.5, p>0.05. The graph
for this is in Appendix U.
The Quality Subscale, which demonstrates the importance of knowing patients’ perspectives
for providing good health care (questions 5,7,15), had a baseline mean (SD) of 3.81 (1.64),
post-education 3.77 (1.81), and 1-month post-education 4.13 (1.77). The trendline shows an
improvement in the Quality Subscale score, and the Wilcoxon signed ranks test found the
differences between time points were not statistically significant, W-58, p>0.05. The graph for
this is in Appendix V.
The results of the questionnaires demonstrate improvement in clinical knowledge as well as
beliefs and attitudes of participants. For future programs, efforts would be to obtain a larger
pool of participants and consider methods to increase post-education participation when
learners are less engaged in doing the survey. Participants verbalized insightful concepts of
what they gained from the education via the surveys' free-written space, validating the course.
Survey results were placed into a graph for a formal display poster to satisfy the Mt. St.
Joseph University curriculum and the hospital as a quality improvement project.
Significance and Implications
This project has the potential to grow to utilize a hospital-wide e-Learn format based on the
optimistic results. Classroom engagement became more focused as learners started to grasp
the content and the ethical implications of not being prepared to care for this patient
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 57
population. While it was challenging to obtain a commitment from voluntary participation one
month later, the overall scores demonstrated an increase in clinical knowledge and changed
attitudes. The qualitative feedback and results were the most revealing. Limitations were a
small number of participants and a limited set of participants one-month later. The HBAS
scores decreased one month later, in part, to less participation and retention; therefore, it is
fair to recommend future work to layer further information they received. The hope is that
education will enhance patient outcomes. This course is a lesson in preparedness for the
intersex/DSD patient. As Cools et al., 2018, articulated so well, medical care could be deficient,
impacting outcomes. Patients need to feel comfortable seeking healthcare services, and if they
don’t, they aren’t going to want to utilize the care. Identifying problem areas allows attention to
be given to change those areas. Patients must have trust to use health services (Cools et al.,
2018). Young adults find it difficult to find subspecialty experts to help treat them, which can
cause cessation of medical care (Cools et al., 2018). Negative experiences with medical care
throughout pediatrics and adulthood make avoidance of care conceivable (Cools et al., 2018).
The perceived rarity and lack of understanding can undoubtedly work against this patient
population. Any potential adverse sequelae could result. Nurses need to receive exposure to
this content so that their time with patients is constructive.
This project's significance can be recognized on an individual patient level or a national
level. To attain a broader audience - through conferences, poster-presentations, publication,
and a hospital-system engagement - there is a potential to change the society in which the
patient resides. For it to be effective on any level, it needs to be relentless in effort. Education
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 58
of nursing staff could support patient empowerment. Patients need to be able to trust
healthcare personnel and utilize appointments. Patients could ask for and receive psychological
support. Families of patients could receive help to support the cultural milieu surrounding the
patient. Patient comorbidities could be treated. Healthcare decisions would involve shared-
decision-making. When the LGBT population is represented, the intersex/DSD population
should receive equal, yet distinct, support.
The timeline was successful, despite the COVID-19 pandemic restrictions. The budget
demonstrated added self-pay costs (food, incentive gifts, paper, ink). Future work may benefit
from grant opportunities when the pandemic is no longer impacting in-person meeting
regulations.
This project implies that the nursing workforce will be better prepared for patients with
DSDs/intersex conditions. Nurses who participated in the course stated that they had little to
no knowledge before the Lunch-and-Learn and understood how the knowledge gap could
adversely affect patient outcomes. The qualitative feedback from learners demonstrated that
intersex/DSD education was clarifying to them. Stakeholders (diversity team, hospital
leadership, patients, etc.) will benefit from this project's supportive and complementary work.
The primary stakeholder is ultimately the patient. An additional pursuit of measuring patient
outcomes would be to utilize patient satisfaction scores, verbal feedback of providers and
patients, and data from the EHR.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 59
Project Future
Current scientific knowledge and political activism imply long sustainability and the need
for this project to grow and continue. As hospitals advance the nursing curriculum on LGBT, the
intersex/DSD patient should also be distinguished and given equal attention. This curriculum
could be generated through ongoing in-person learning sessions, digital e-Learn, conferences,
and published articles. Publishing would allow the broadest advocacy, allowing a trickle-down
effect within hospital systems. Resources for this project are unit educators in the hospital,
hospital researchers, support groups, staff diversity leaders, specialty physicians, and
knowledgeable team members. Future projects could explore other validated tools for
measuring attitudes.
Dissemination of this project was through a formal poster presentation. The poster was
provided to the unit educator for display on the unit where the education took place.
Dissemination through publishing via credible sources is a long-term goal by submitting
abstracts for conferences and submitting proposals to nursing publications. The Sigma Theta
Tau Nursing Honor Society accepted an abstract of this work for their 2021 conferences, both
nationally and internationally. This project will continue to be disseminated as opportunities
present themselves.
Conclusion
Nurses are required to care for diverse patients appropriately. People with DSDs/intersex
conditions remain a vulnerable population, often confused with transgender patients and not
recognized because of lack of representation in the nursing curriculum. Hospitals are a visiting
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 60
place for people throughout the lifespan. There isn’t an area of the hospital system where this
education isn’t needed – from labor-and-delivery units, medical-surgical floors, primary care,
outpatient services, to hospice. They can be burdened with others’ discomfort and judgment
about their sexual orientation or gender identity. While SO/GI may not be an issue for some
people with intersex/DSD conditions, for others, it may be a process of human development
given the variables they are sorting out. How to elicit that information is a separate quality
improvement area. Terminology is inconsistently used in society and within healthcare which
impacts the clarity of the patient. Incorrect understanding of intersex/DSDs can mean that
detrimental biases and ignorance can negatively impact patient outcomes. Incorrect EHR
documentation, and therefore inaccurate SO/GI data collection, can also mean wrong
conclusions could be formed about people with transgender or intersex/DSD conditions.
Conversely, the correct use of the EHR can also serve to collect useful information on patient
outcomes, making this a cyclic discussion.
Focused cultural competency awareness applied to patients with DSDs/intersex
conditions has been lacking in nursing. Advocacy requires a workplace champion for the
DSD/intersex population to promote optimum care, both clinically and culturally. This project
intended to further the rudimentary nursing work on DSDs/intersex conditions, ignite ethical
conviction to advocate for this population, generate self-awareness and examination of
personal attitudes, and enhance skills for patient encounters. It is a national standard to be
culturally competent for all patients, but there has been little modeling of what this entails for
patients with DSDs/intersex conditions. This training clarified intersex/DSD patients from LGBT
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 61
and provided clinical knowledge as a means to advocate for them. This project is by no means
all-encompassing. Given the complexity of the topic and limitations of a single Lunch-and-
Learn session, a goal would be to implement this project in a digital e-Learn format to all
hospital staff with mandatory participation for a broader audience. It would also be far more
significant to educate nationally by submitting abstracts to conferences and authoring journals
for reputable nursing organizations. Gratefully, this project’s abstract has been selected for the
Sigma International Honor Society national conference in Indianapolis, Indiana and international
conference in Singapore, 2021. One of the values of this hospital is respect for people, and this
educational intervention exemplified this. With fervent hope, nurses will lead in amending gaps
in care and positively impact healthcare experiences and outcomes for these valued patients.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 62
References
Amies Oelschlager, A., Muscarella, M., & Gomez-Lobo, V. (2015). Transition to adult care in persons
with disorders of sexual development. Obstetrics & Gynecology, 126 (4), 845–849.
https://doi.org/10.1097/AOG.0000000000001034
ANA Center for Ethics and Human Rights. (2019). ANA position statement: Nursing advocacy for
lesbian, gay, bisexual, transgender, questioning, + populations. OJIN: The Online Journal of
Issues in Nursing, 24(1).
Bambaeeroo, F., & Shokrpour, N. (2017). The impact of the teachers' non-verbal communication on
success in teaching. Journal of Advances in Medical Education & Professionalism, 5(2), 51–59.
Barthold, J. S. (2011). Disorders of sex differentiation: A pediatric urologist’s perspective of new
terminology and recommendations. Journal of Urology, 185(2), 393–400.
https://doi.org/10.1016/j.juro.2010.09.083
Bates, A. W. (2005). Good, common, regular, and orderly: Early modern classifications of monstrous
Births. Social History of Medicine, 18(2), 141–158. https://doi.org/10.1093/sochis/hki029
Beale, J. M., & Creighton, S. M. (2016). Long-term health issues related to disorders or differences in
sex development/intersex. Maturitas, 94, 143-148. https://doi:10.1016/J.
Maturitas.2016.10.003
Bomalaski, M. D. (2005). A practical approach to intersex. Urology Nursing, 25(1), 11–24.
Braun, H. M., Ramirez, D., Zahner, G. J., Gillis-Buck, E. M., Sheriff, H., & Ferrone, M. (2017). The
lesbian, gay, bisexual, transgender, queer, intersex health forum: An innovative
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 63
interprofessional initiative to support curriculum reform. Medical Education Online, 22(1),
1306419. https://doi.org/10.1080/10872981.2017.1306419
Brennan, A. M. W., Barnsteiner, J., Siantz, M. L. de L., Cotter, V. T., & Everett, J. (2012). Lesbian, gay,
bisexual, transgendered, or intersexed content for nursing curricula. Journal of Professional
Nursing, 28(2), 96–104. https://doi.org/10.1016/j.profnurs.2011.11.004
Butler, M., McCreedy. E., Schwer, N., Burgess, D., Call, K., Przedworski, J., Rosser, S., Larson, S.,
Allen, M., Fu, S., Kane, R. (2016). Improving Cultural Competence to Reduce Health Disparities.
Agency for Healthcare Research and Quality (U.S.).
Campinha-Bacote, J. (2002). The process of cultural competence in the delivery of healthcare
services: A model of care. Journal of Transcultural Nursing, 13(3), 181-184.
https://doi.org/10.1177/104365960201300303
Carpenter, R., Estrada, C. A., Medrano, M., Smith, A., & Stanford Massie, F., Jr. (2015). A web-based
cultural competency training for medical students: A randomized trial. The American Journal of
the Medical Sciences, 349(5), 442-446. https://doi:10.1097/MAJ.0000000000000351
Carpenter, M. (2018). Intersex variations, human rights, and the international classification of
diseases. Health and Human Rights, 20(2), 205–214
Centers for Disease Control and Prevention. (2019). Collecting sexual orientation and gender identity
information. https://www.cdc.gov/hiv/clinicians/transforming-health/health-care-
providers/collecting-sexual-orientation.html
Checkbox Survey Incorporated. (2002-2020). Secure data collection and real-time reporting
solutions for teams and enterprises. https://www.checkbox.com/.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 64
Citi Training Program Institutional Course. (n.d.), Institutional courses.
https://www.citiprogram.org/members/index.cfm?pageID=50
Colapinto, J. (2004) As nature made him: The boy who was raised as a girl. Harper Collins.
Congressional Research Service. (2019). Diversity, Inclusion, and Equal Opportunity in the Armed
Services: Background and Issues for Congress. https://fas.org/sgp/crs/natsec/R44321.pdf
Cools, M, Nordenstrom, A, Robeva, R, Hall, J, Westerveld, P., Fluck, C., Kohler, B., Berra, M., Springer,
A, Schweizer, K, Pasterski, V. (2018). Caring for individuals with a difference of sex
development (DSD): A Consensus Statement. https://www.nature.com/articles/s41574-018-
0010-8
Corley, J. E., Jr., F. S. M., Medrano, M., & Estrada, C. A. (2015). Medical students’ cultural attitudes:
The health belief attitudes survey. Journal of Education and Training Studies, 4(2).
https://doi.org/10.11114/jets.v4i2.1201
Ernst, M. M., Kogan, B. A., & Lee, P. A. (2020). Gender identity: A psychosocial primer for providing
care to patients with a disorder/difference of sex development and their families [individualized
care for patients with intersex (Disorders/differences of sex development): Part 2]. Journal of
Pediatric Urology. https://doi-org.msj.idm.oclc.org/10.1016/j.jpurol.2020.06.026
Dreger, A. D., & Herndon, A. M. (2009). Progress and politics in the intersex rights movement:
Feminist theory in action. GLQ: A Journal of Lesbian and Gay Studies, 15(2), 199–224.
https://doi.org/10.1215/10642684-2008-134
Fausto-Sterling, A. (1993). The Five Sexes. The Sciences, 33(2), 20-24.
https://doi.org/10.1002/j.2326-1951.1993.tb03081.x
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 65
Haider, A., Adler, R. R., Schneider, E., Uribe Leitz, T., Ranjit, A., Tan, C., Levine, A., Harfouch, O.,
Pelaez, D., Kodadek, L., Vail, L., Snyder, C., German, D., Peterson, S., Schuur, J. D., & Lau, B. D.
(2018). Assessment of patient-centered approaches to collect sexual orientation and gender
identity information in the emergency department. JAMA Network Open, 1(8), e186506.
https://doi.org/10.1001/jamanetworkopen.2018.6506
Horvat, L., Horey, D., Romios, P., & Kis-Rigo, J. (2014). Cultural competence education for health
professionals. Cochrane Database of Systematic Reviews.
https://doi.org/10.1002/14651858.CD009405.pub2
Intersex Society of North America. (1993-2008). What’s the difference between being transgender or
transsexual and having an intersex condition? https://isna.org/faq/transgender/.
Iowa Model Collaboration. (2017). Iowa Model of evidence-based practice: Revisions and
validation. Worldviews on Evidence-Based Nursing, 14(3), 175-182.
https://doi:10.1111/wvn.12223.
Johnson, E. K., Rosoklija, I., Finlayson, C., Chen, D., Yerkes, E. B., Madonna, M. B., . . . Cheng, E. Y.
(2017). Attitudes towards “disorders of sex development” nomenclature among affected
individuals. Journal of Pediatric Urology, 13(6), 608.e1-608.e8.
https://doi:10.1016/JPUROL.2017.03.035
Jones, T. (2018). Intersex studies: A systematic review of international health literature. SAGE Open,
8(2), 215824401774557. https://doi.org/10.1177/2158244017745577
Kano, M., Sanchez, N., Tamí-Maury, I., Solder, B., Watt, G., & Chang, S. (2020). Addressing cancer
disparities in sexual gender minority populations: Recommendations for a national action plan
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 66
to increase sexual gender minority health equity through researcher and provider training and
education. Journal of Cancer Education, 35(1), 44–53. https://doi.org/10.1007/s13187-018-
1438-1
Kruse, S. D., Rakha, S., & Calderone, S. (2018). Developing cultural competency in higher education:
an agenda for practice. Teaching in Higher Education, 23(6), 733–750.
https://doi.org/10.1080/13562517.2017.1414790
Lee, P. A., Fuqua, J. S., Houk, C. P., Kogan, B. A., Mazur, T., & Caldamone, A. (2020). Individualized
care for patients with intersex (disorders/differences of sex development): part I. Journal of
Pediatric Urology, 16(2), 230-237. https://doi:10.1016/J.JPUROL.2020.02.013
Lee, P. A., Nordenström, A., Houk, C. P., Ahmed, S. F., Auchus, R., Baratz, A., Baratz Dalke, K., Liao,
L.-M., Lin-Su, K., Looijenga 3rd, L. H. J., Mazur, T., Meyer-Bahlburg, H. F. L., Mouriquand, P.,
Quigley, C. A., Sandberg, D. E., Vilain, E., & Witchel, S. (2016). Global disorders of sex
development update since 2006: Perceptions, approach, and care. Hormone Research in
Paediatrics, 85(3), 158–180. https://doi.org/10.1159/000442975
Liang, J. J., Gardner, I. H., Walker, J. A., & Safer, J. D. (2017). Observed deficiencies in medical student
knowledge of transgender and intersex health. Endocrine Practice, 23(8), 897–906.
https://doi.org/10.4158/EP171758.OR
Lindsay, S., Rezai, M., Kolne, K., & Osten, V. (2019). Outcomes of gender-sensitivity educational
interventions for healthcare providers: A systematic review. Health Education Journal, 78(8),
958–976. https://doi.org/10.1177/0017896919859908
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 67
Maragh-Bass, A. C., Torain, M., Adler, R., Schneider, E., Ranjit, A., Kodadek, L. M., Shields, R.,
German, D., Snyder, C., Peterson, S., Schuur, J., Lau, B., & Haider, A. H. (2017). Risks, benefits,
and the importance of collecting sexual orientation and gender identity data in healthcare
settings: A multi-method analysis of patient and provider perspectives. LGBT Health, 4(2), 141–
152. https://doi.org/10.1089/lgbt.2016.0107
Medrano, M. & Dobbie A., (2002). Appendix B: Health belief attitude instrument survey. A guide to
cultural competence in the curriculum (p. 56). University of Texas Health Science Center at San
Antonio. http://cirrie-sphhp.webapps.buffalo.edu/culture/curriculum/guides/pt.pdf.
Miller, L., Leeth, E. A., Johnson, E. K., Rosoklija, I., Chen, D., Aufox, S. A., & Finlayson, C. (2018).
Attitudes toward ‘disorders of sex development’ nomenclature among physicians, genetic
counselors, and mental health clinicians. Journal of Pediatric Urology, 14(5), 418.e1-418.e7.
https://doi.org/10.1016/j.jpurol.2018.08.009
Mitchell, O., Malatzky, C., Bourke, L., & Farmer, J. (2018). A modified, continuous quality
improvement approach to improve culturally and socially inclusive care within rural health
services. Australian Journal of Rural Health, 26(3), 206–210. https://doi.org/10.1111/ajr.12409
Neff, A., & Kingery, S. (2016). Complete androgen insensitivity syndrome: A problem-based learning
case. MedEdPORTAL. https://doi.org/10.15766/mep_2374-8265.10522
Pitripin, A. (2016). Nursing Theory. Faye Abdellah: Nursing theorist, biography, and career of Faye
Glenn Abdellah. https://nursing-theory.org/nursing-theorists/Faye-Abdellah.php
Polit, D. F., & Beck, C.T. (2017). Nursing research:
Generating and assessing evidence for nursing practice (10th ed.). Wolters Kluwer.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 68
Purnell, T. S., Marshall, J. K., Olorundare, I., Stewart, R. W., Sisson, S., Gibbs, B., Feldman, L. S.,
Bertram, A., Green, A. R., & Cooper, L. A. (2018). Provider perceptions of the organization’s
cultural competence climate and their skills and behaviors targeting patient-centered care for
socially at-risk populations. Journal of Health Care for the Poor and Underserved, 29(1), 481–
496. https://doi.org/10.1353/hpu.2018.0032
Quinn, E. (2016, October 26). Intersex explained! Complete androgen insensitivity.
https://www.youtube.com/watch?v=5vDVUPjBJiM
Reeves, S., Perrier, L., Goldman, J., Freeth, D., & Zwarenstein, M. (2013). Interprofessional education:
effects on professional practice and healthcare outcomes. Cochrane Database of Systematic
Reviews. https://doi.org/10.1002/14651858.CD002213.pub3
Ross, M. H., & Setchell, J. (2019). People who identify as lesbian, gay, bisexual, transgender, intersex
queer+ can experience assumptions, discomfort, discrimination, and a lack of knowledge while
attending physiotherapy: a survey. Journal of Physiotherapy, 65(2), 99–105.
https://doi.org/10.1016/j.jphys.2019.02.002
Rosenwohl-Mack, A., Tamar-Mattis, S., Baratz, A., Dalke, K., Ittelson, A., Zieselman, Ki., & Flatt, J.
(2020). A national study on the physical and mental health of intersex adults in the U.S. PLOS
ONE, 15(10). https://doi.org/10.1371/journal.pone.0240088.
Rothkopf, A., & John, R. (2014). Understanding disorders of sexual development. Journal of Pediatric
Nursing, 29(5), e23–e34. https://doi.org/10.1016/j.pedn.2014.04.002
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 69
Sanders, C., Edwards, Z., & Keegan, K. (2017). Exploring stakeholder experiences of
interprofessional teamwork in sex development outpatient clinics. Journal of Interprofessional
Care, 31(3), 376–385. https://doi.org/10.1080/13561820.2016.1272559
Sani, A. M., Soh, K. L., Ismail, I. A., Arshad, M. M., Mungadi, I. A., Yau, S. L., & Soh, K. G. (2019).
Experiences of people living with disorders of sex development and sex reassignment: Meta-
ethnography of qualitative studies. Journal of Advanced Nursing, 75(2), 277–290.
https://doi.org/10.1111/jan.13833
Sax., L. (2002). How common is intersex? A response to Anne Fausto-Sterling. Journal of Sex
Research, 39(3), 174-178.
The Joint Commission. (2020). Health Equity.
https://www.jointcommission.org/en/resources/patient-safety-topic
Tamar-Mattis, A., Baratz, A., Baratz Dalke, K., & Karkazis, K. (2014). Emotionally and cognitively
informed consent for clinical care for differences of sex development. Psychology &
Sexuality, 5(1), 44–55. https://doi-org.msj.idm.oclc.org/10.1080/19419899.2013.831215
Thyen, U., Lux, A., Jürgensen, M., Hiort, O., & Köhler, B. (2014). Utilization of health care services
and satisfaction with care in adults affected by disorders of sex development (DSD). Journal of
General Internal Medicine, 29 (53), 752–759. https://doi.org/10.107/s11606-014-2917-7
United States Department of Health and Human Services Office of Minority Health (n.d., a). Culturally
competency nursing care: A cornerstone of caring.
https://ccnm.thinkculturalhealth.hhs.gov/Content/Introduction/Introduction1.asp
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 70
United States Department of Health and Human Services Office of Minority Health. (n.d., b). National
CLAS Standards. https://thinkculturalhealth.hhs.gov/clas
Xu, J. (2016). Toolbox of teaching strategies in nurse education. Chinese nursing research, 3(2), 54-
57. https://doi-org/10.1016/j.vnre.2016.06.002
Zeeman, L., Sherriff, N., Browne, K., McGlynn, N., Mirandola, M., Gios, L., Davis, R., Sanchez-
Lambert, J., Aujean, S., Pinto, N., Farinella, F., Donisi, V., Niedźwiedzka-Stadnik, M., Rosińska,
M., Pierson, A., Amaddeo, F., Taibjee, R., Toskin, I., Jonas, K., … de Sutter, P. (2019). A review of
lesbian, gay, bisexual, trans, and intersex health and healthcare inequalities. European Journal
of Public Health, 29(5), 974–980. https://doi.org/10.1093/eurpub/cky226
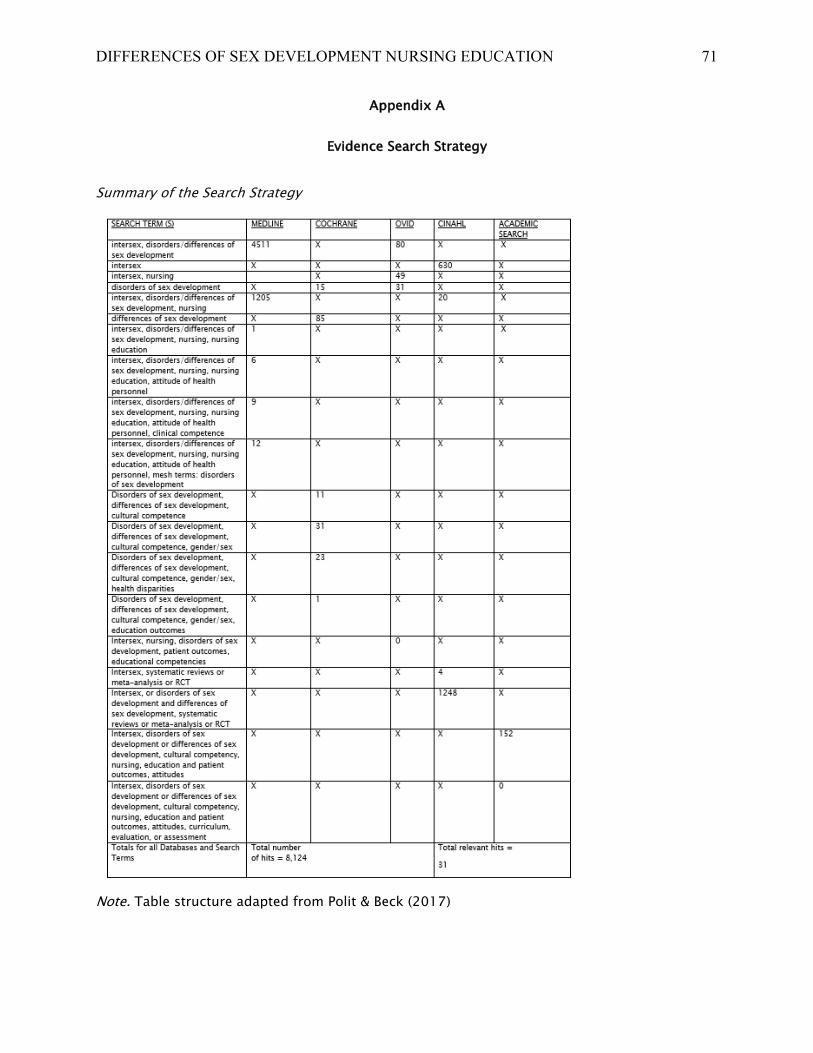
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 71
Appendix A
Evidence Search Strategy
Summary of the Search Strategy
Note. Table structure adapted from Polit & Beck (2017)
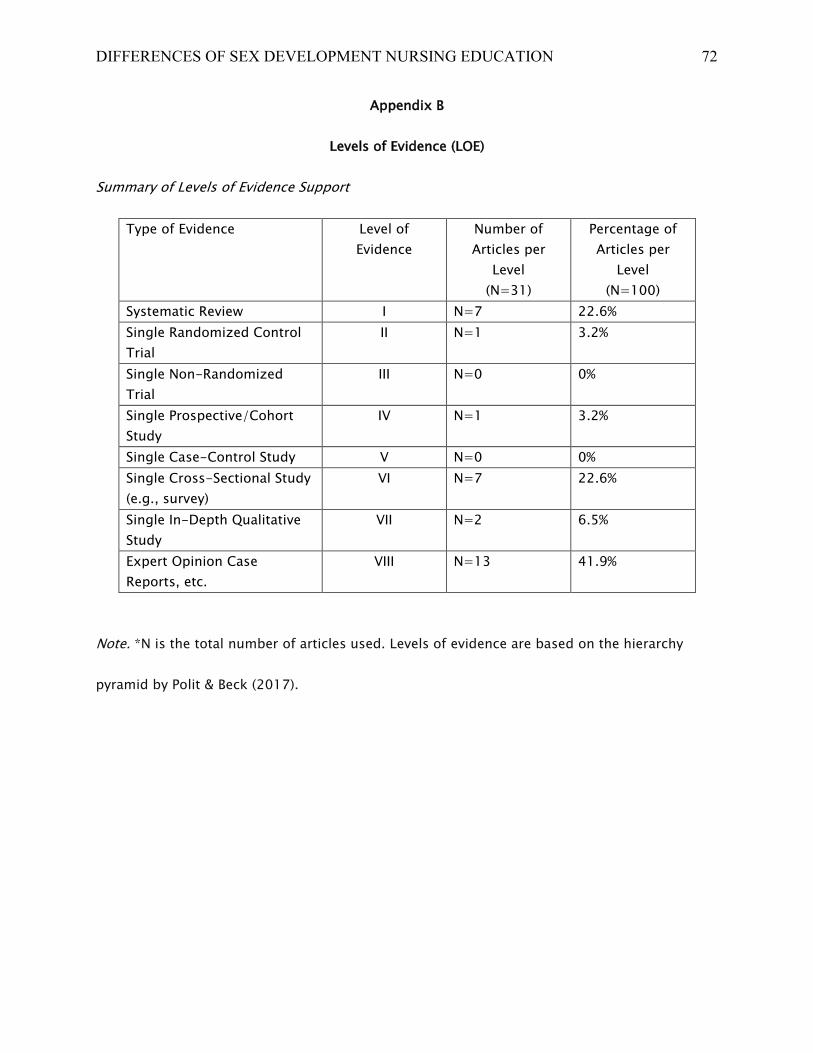
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 72
Appendix B
Levels of Evidence (LOE)
Summary of Levels of Evidence Support
Note. *N is the total number of articles used. Levels of evidence are based on the hierarchy
pyramid by Polit & Beck (2017).
Type of Evidence
Level of
Evidence
Number of
Articles per
Level
(N=31)
Percentage of
Articles per
Level
(N=100)
Systematic Review I N=7 22.6%
Single Randomized Control
Trial
II N=1 3.2%
Single Non-Randomized
Trial
III N=0 0%
Single Prospective/Cohort
Study
IV N=1 3.2%
Single Case-Control Study V N=0 0%
Single Cross-Sectional Study
(e.g., survey)
VI N=7 22.6%
Single In-Depth Qualitative
Study
VII N=2 6.5%
Expert Opinion Case
Reports, etc.
VIII N=13 41.9%
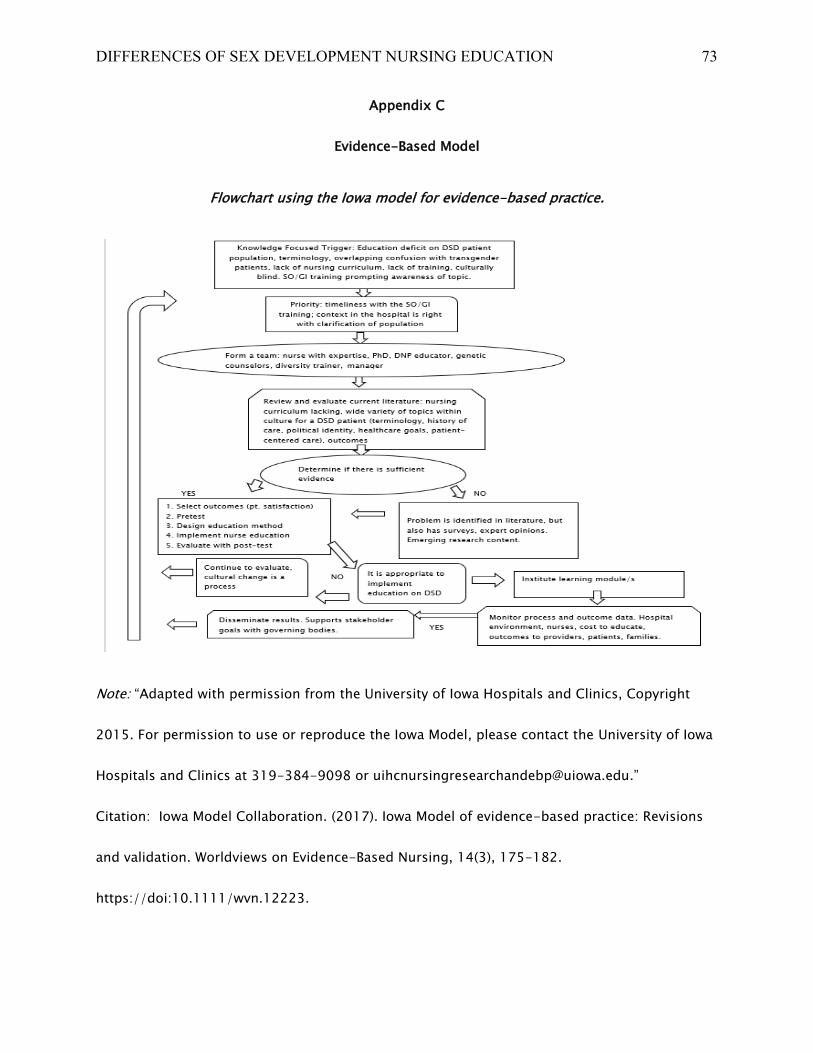
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 73
Appendix C
Evidence-Based Model
Flowchart using the Iowa model for evidence-based practice.
Note: “Adapted with permission from the University of Iowa Hospitals and Clinics, Copyright
2015. For permission to use or reproduce the Iowa Model, please contact the University of Iowa
Hospitals and Clinics at 319-384-9098 or [email protected].”
Citation: Iowa Model Collaboration. (2017). Iowa Model of evidence-based practice: Revisions
and validation. Worldviews on Evidence-Based Nursing, 14(3), 175-182.
https://doi:10.1111/wvn.12223.
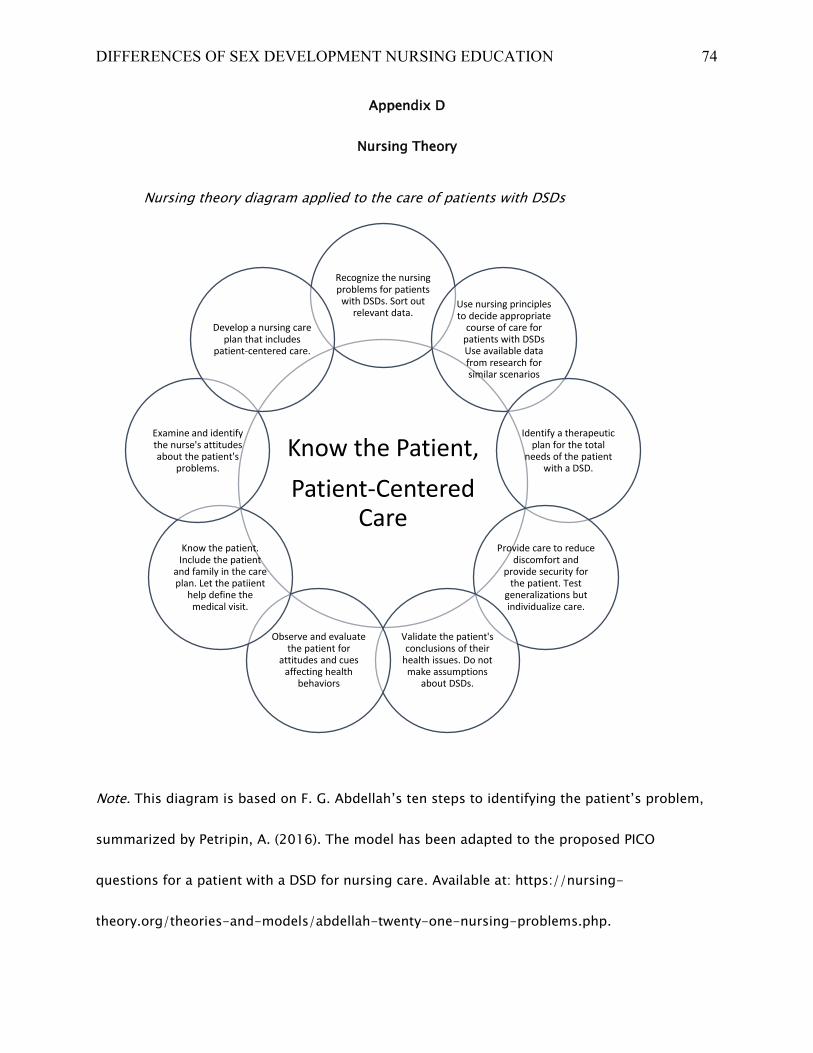
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 74
Appendix D
Nursing Theory
Nursing theory diagram applied to the care of patients with DSDs
Note. This diagram is based on F. G. Abdellah’s ten steps to identifying the patient’s problem,
summarized by Petripin, A. (2016). The model has been adapted to the proposed PICO
questions for a patient with a DSD for nursing care. Available at: https://nursing-
theory.org/theories-and-models/abdellah-twenty-one-nursing-problems.php.
Know the Patient,
Patient-Centered Care
Recognize the nursing problems for patients
with DSDs. Sort out relevant data.
Use nursing principles to decide appropriate
course of care for patients with DSDs Use available data from research for similar scenarios
Identify a therapeutic plan for the total
needs of the patient with a DSD.
Provide care to reduce discomfort and
provide security for the patient. Test
generalizations but individualize care.
Validate the patient's conclusions of their
health issues. Do not make assumptions
about DSDs.
Observe and evaluate the patient for
attitudes and cues affecting health
behaviors
Know the patient. Include the patient
and family in the care plan. Let the patiient
help define the medical visit.
Examine and identify the nurse's attitudes about the patient's
problems.
Develop a nursing care plan that includes
patient-centered care.
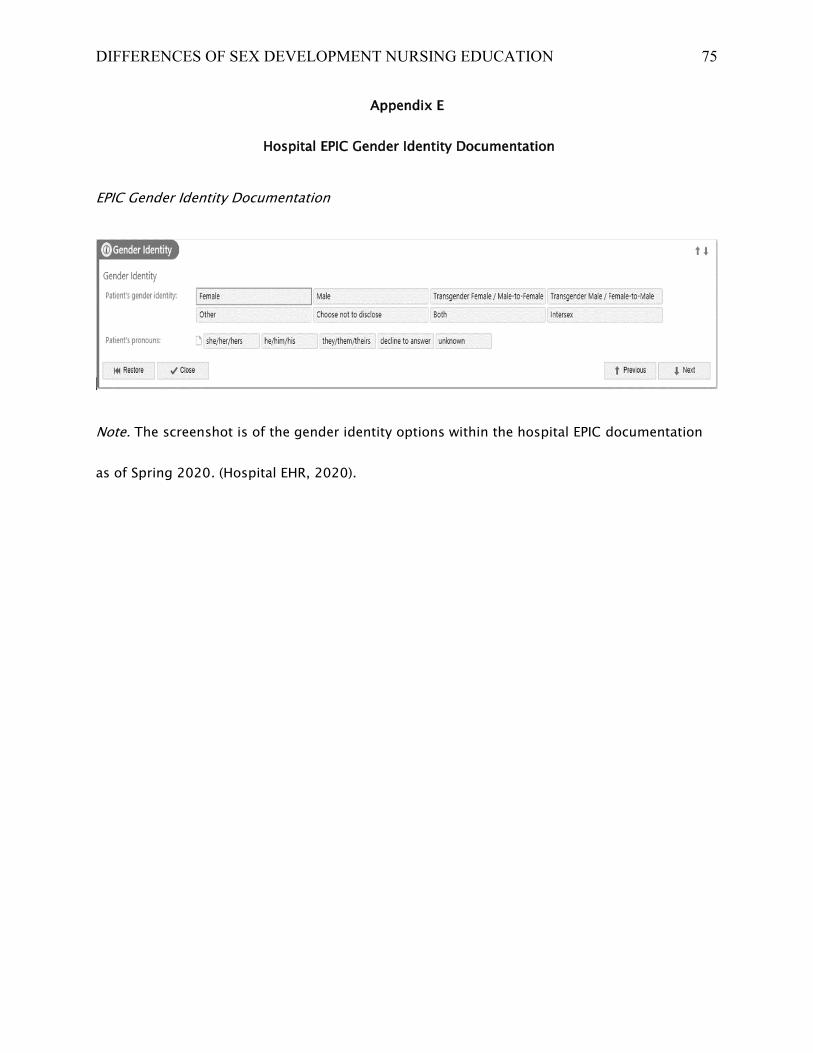
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 75
Appendix E
Hospital EPIC Gender Identity Documentation
EPIC Gender Identity Documentation
Note. The screenshot is of the gender identity options within the hospital EPIC documentation
as of Spring 2020. (Hospital EHR, 2020).
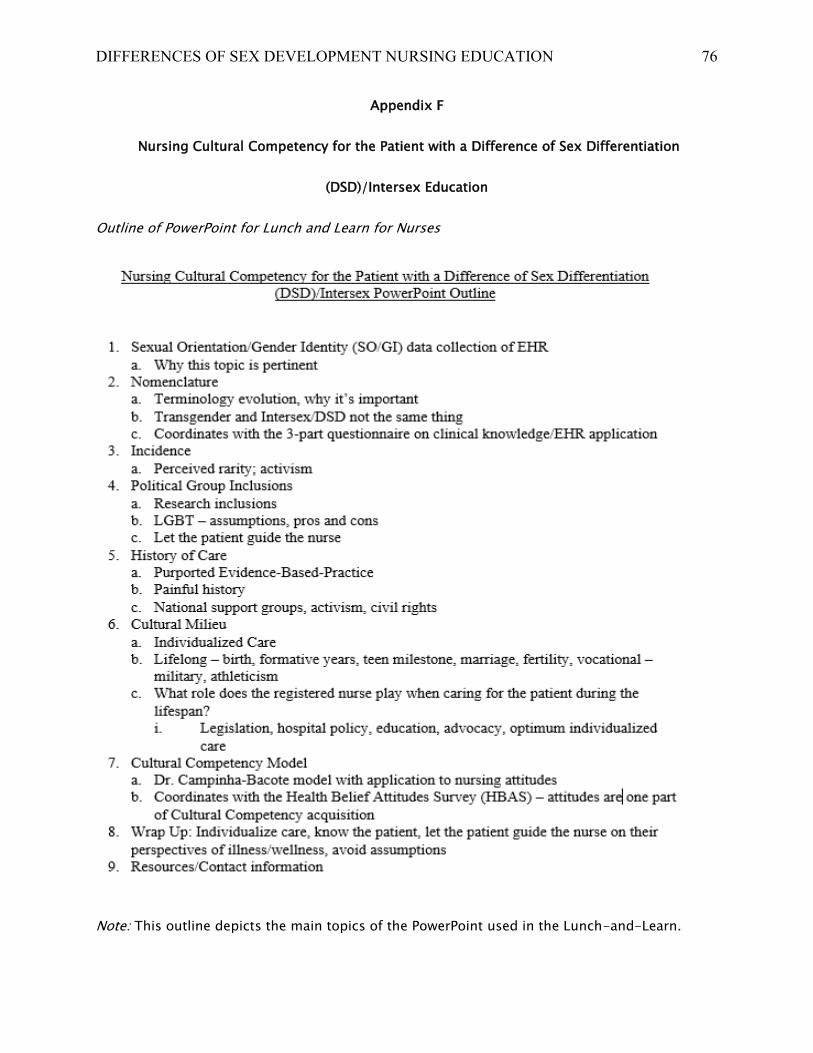
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 76
Appendix F
Nursing Cultural Competency for the Patient with a Difference of Sex Differentiation
(DSD)/Intersex Education
Outline of PowerPoint for Lunch and Learn for Nurses
Note: This outline depicts the main topics of the PowerPoint used in the Lunch-and-Learn.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 77
Appendix G
Advertisement for the Lunch-and-Learn
Promotional advertisement for the Lunch-and-Learn
Note: This was the promotional advertisement posted on the medical-surgical unit to alert
nurses to an educational opportunity that included food and gifts.
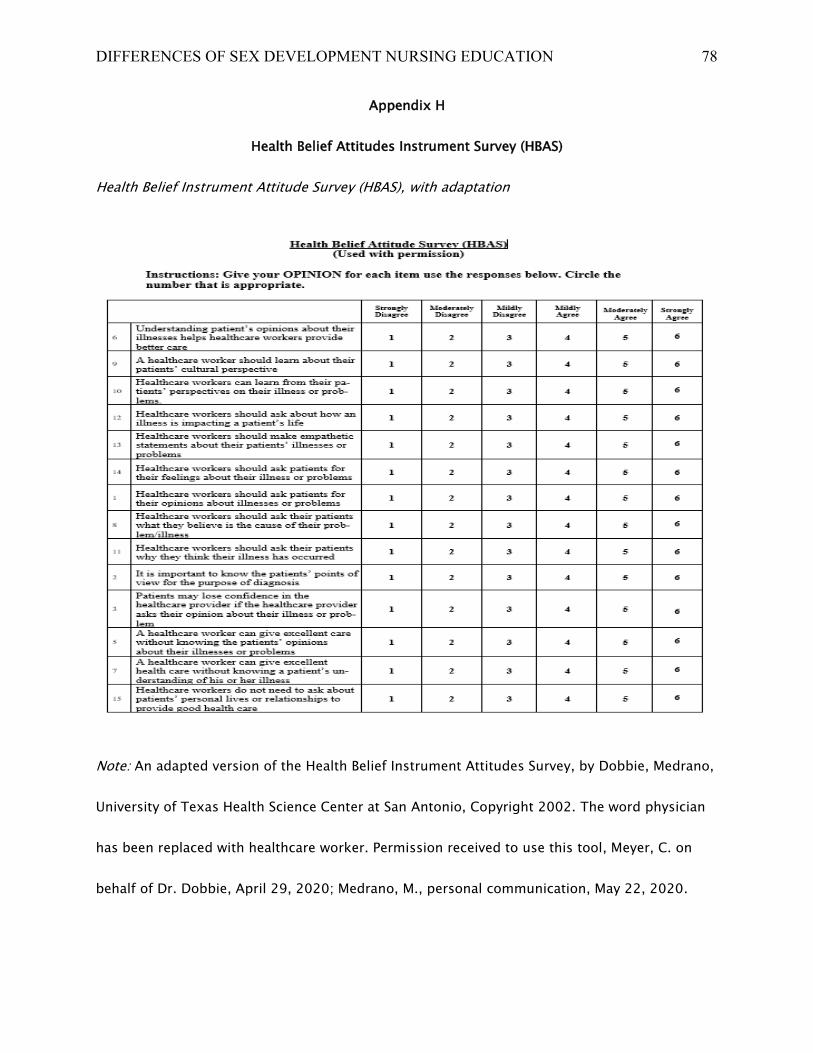
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 78
Appendix H
Health Belief Attitudes Instrument Survey (HBAS)
Health Belief Instrument Attitude Survey (HBAS), with adaptation
Note: An adapted version of the Health Belief Instrument Attitudes Survey, by Dobbie, Medrano,
University of Texas Health Science Center at San Antonio, Copyright 2002. The word physician
has been replaced with healthcare worker. Permission received to use this tool, Meyer, C. on
behalf of Dr. Dobbie, April 29, 2020; Medrano, M., personal communication, May 22, 2020.
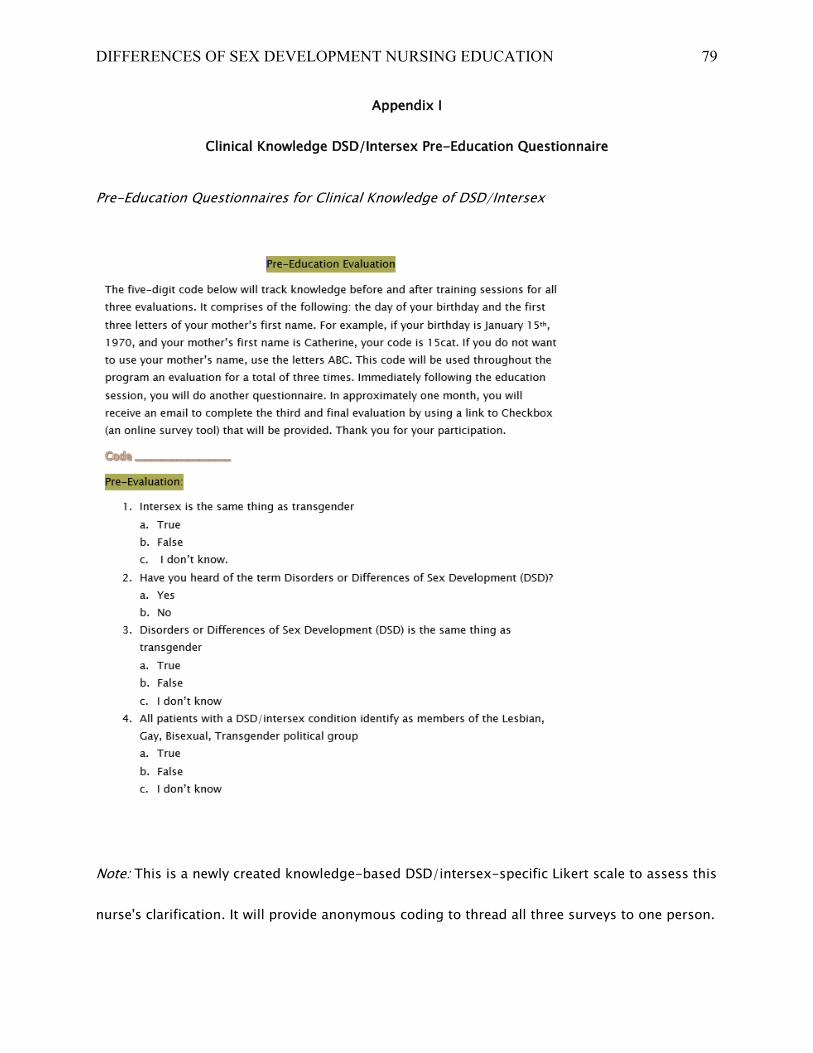
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 79
Appendix I
Clinical Knowledge DSD/Intersex Pre-Education Questionnaire
Pre-Education Questionnaires for Clinical Knowledge of DSD/Intersex
Note: This is a newly created knowledge-based DSD/intersex-specific Likert scale to assess this
nurse's clarification. It will provide anonymous coding to thread all three surveys to one person.
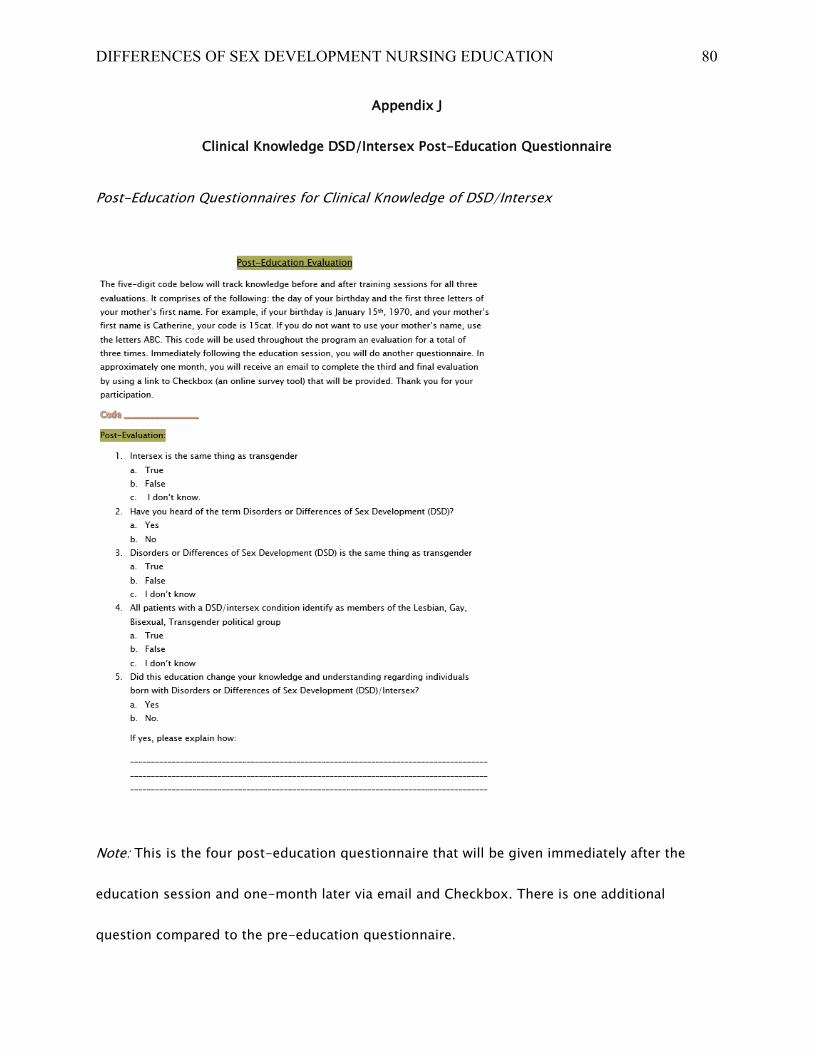
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 80
Appendix J
Clinical Knowledge DSD/Intersex Post-Education Questionnaire
Post-Education Questionnaires for Clinical Knowledge of DSD/Intersex
Note: This is the four post-education questionnaire that will be given immediately after the
education session and one-month later via email and Checkbox. There is one additional
question compared to the pre-education questionnaire.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 81
Appendix K
Citi Training Collaborative Institutional Training Initiative
Citi Training Certificate of Completion
Note: Certificate of completion of Citi Training Program course GVARHC-AAFP-(MARKED OUT)
Refresher Course, which expires April 2022.
https://www.citiprogram.org/members/index.cfm?pageID=50
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 82
Appendix L
Mt. St. Joseph University IRB Determination
Mt. St. Joseph University IRB Determination Record
Note: This is the IRB determination letter from Mt. St. Joseph University IRB, stating it is a
quality improvement project and not a research project. McDonough, T., personal
communication, April 1, 2020.
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 83
Appendix M
Hospital Institutional Review Board (IRB) Determination
Hospital IRB Determination of Project as a Quality Improvement Project
Note: This is a formal letter from the hospital IRB designating this as a quality improvement
project and is not a research project. (Gonzales, Y., personal communication, March 27, 2020).
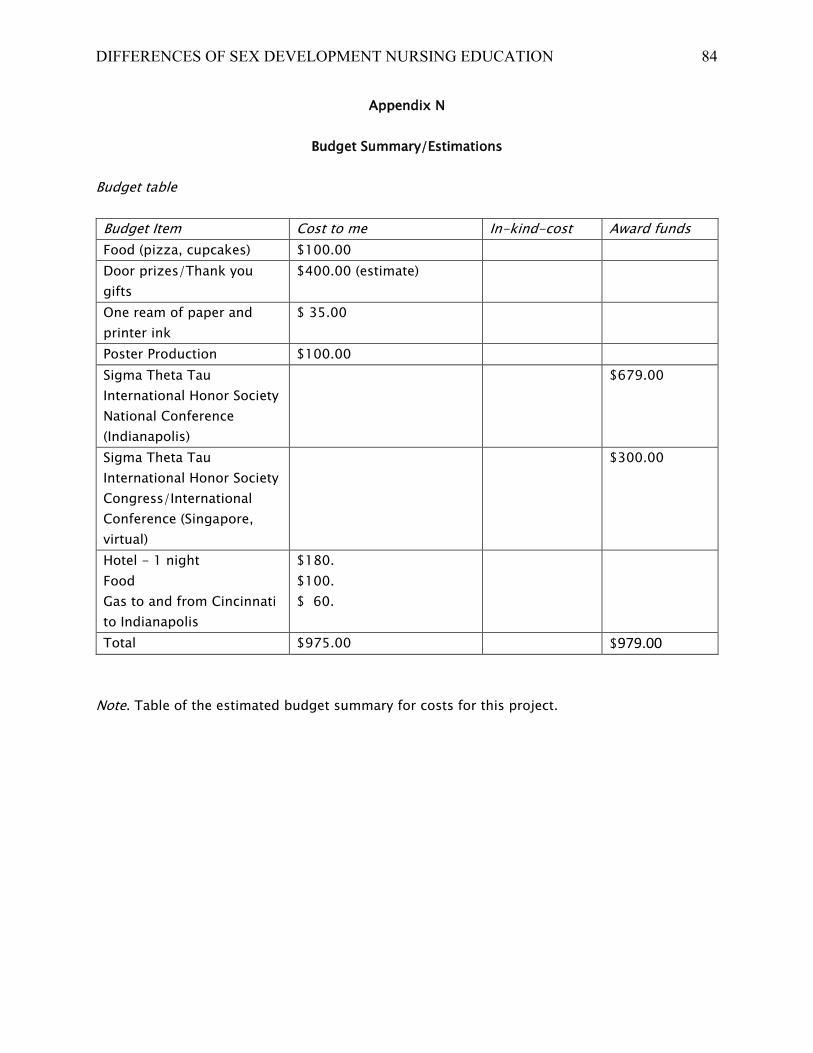
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 84
Appendix N
Budget Summary/Estimations
Budget table
Budget Item Cost to me In-kind-cost Award funds
Food (pizza, cupcakes) $100.00
Door prizes/Thank you
gifts
$400.00 (estimate)
One ream of paper and
printer ink
$ 35.00
Poster Production $100.00
Sigma Theta Tau
International Honor Society
National Conference
(Indianapolis)
$679.00
Sigma Theta Tau
International Honor Society
Congress/International
Conference (Singapore,
virtual)
$300.00
Hotel - 1 night
Food
Gas to and from Cincinnati
to Indianapolis
$180.
$100.
$ 60.
Total $975.00 $979.00
Note. Table of the estimated budget summary for costs for this project.
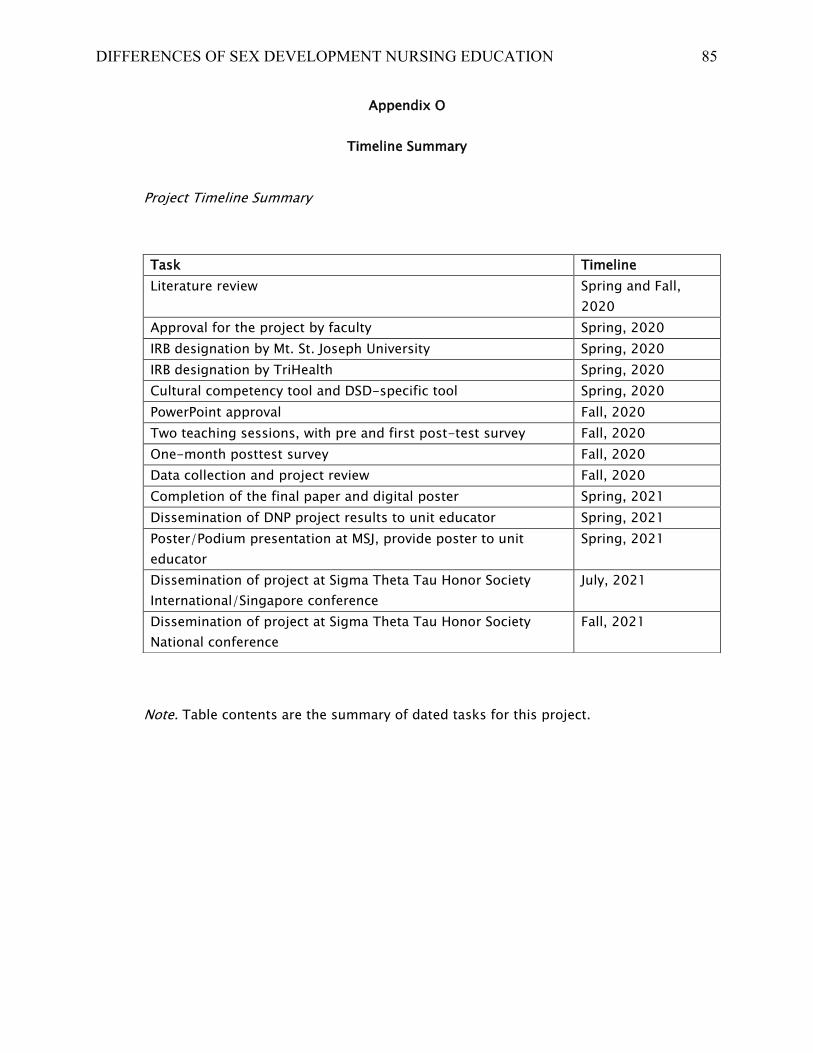
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 85
Appendix O
Timeline Summary
Project Timeline Summary
Note. Table contents are the summary of dated tasks for this project.
Task Timeline
Literature review Spring and Fall,
2020
Approval for the project by faculty Spring, 2020
IRB designation by Mt. St. Joseph University Spring, 2020
IRB designation by TriHealth Spring, 2020
Cultural competency tool and DSD-specific tool Spring, 2020
PowerPoint approval Fall, 2020
Two teaching sessions, with pre and first post-test survey Fall, 2020
One-month posttest survey Fall, 2020
Data collection and project review Fall, 2020
Completion of the final paper and digital poster Spring, 2021
Dissemination of DNP project results to unit educator Spring, 2021
Poster/Podium presentation at MSJ, provide poster to unit
educator
Spring, 2021
Dissemination of project at Sigma Theta Tau Honor Society
International/Singapore conference
July, 2021
Dissemination of project at Sigma Theta Tau Honor Society
National conference
Fall, 2021
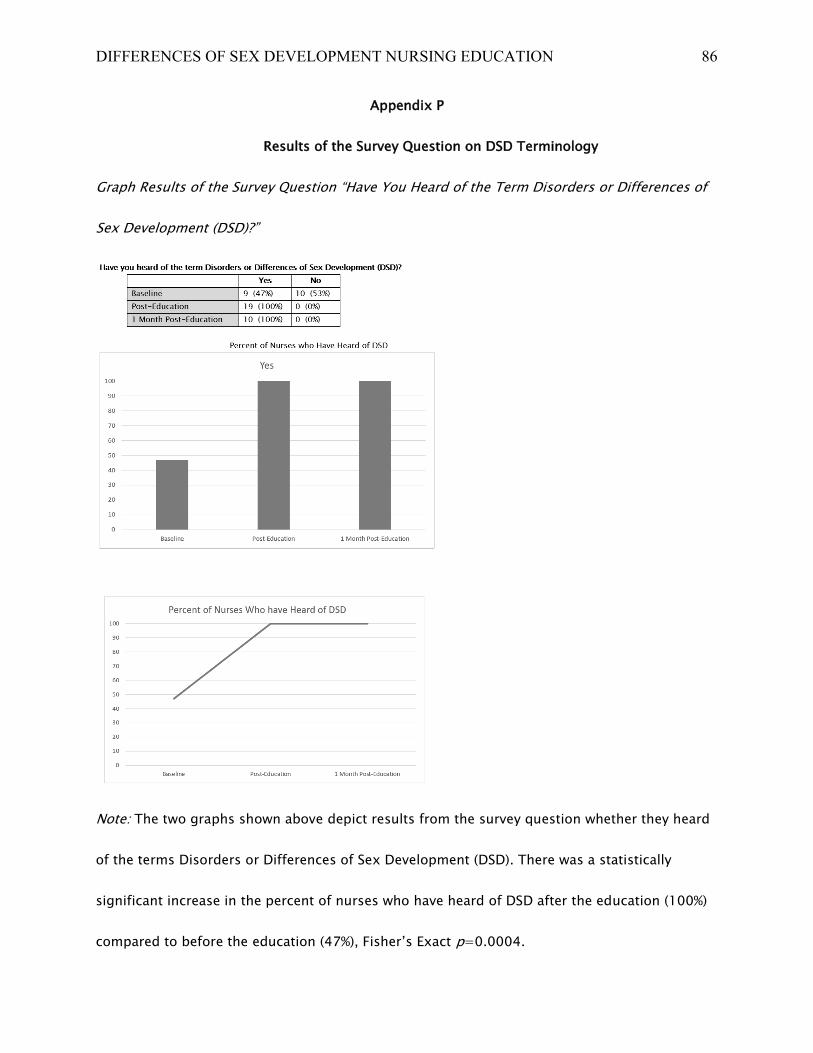
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 86
Appendix P
Results of the Survey Question on DSD Terminology
Graph Results of the Survey Question “Have You Heard of the Term Disorders or Differences of
Sex Development (DSD)?”
Note: The two graphs shown above depict results from the survey question whether they heard
of the terms Disorders or Differences of Sex Development (DSD). There was a statistically
significant increase in the percent of nurses who have heard of DSD after the education (100%)
compared to before the education (47%), Fisher’s Exact p=0.0004.
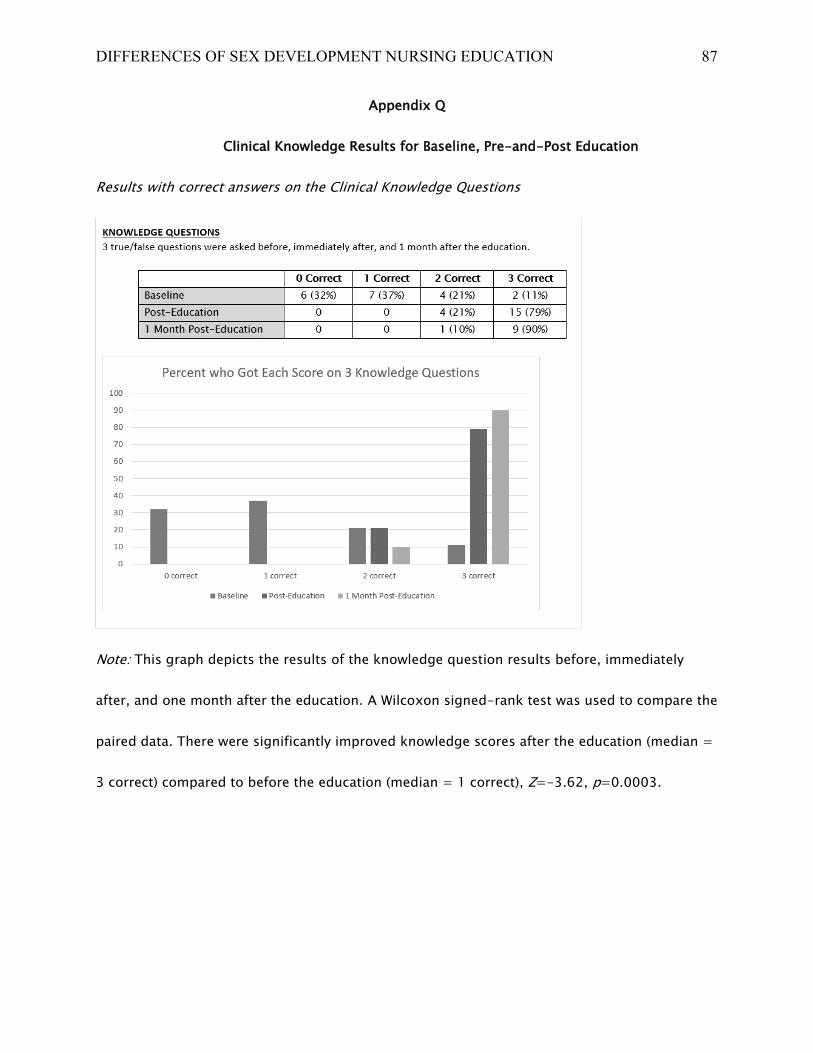
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 87
Appendix Q
Clinical Knowledge Results for Baseline, Pre-and-Post Education
Results with correct answers on the Clinical Knowledge Questions
Note: This graph depicts the results of the knowledge question results before, immediately
after, and one month after the education. A Wilcoxon signed-rank test was used to compare the
paired data. There were significantly improved knowledge scores after the education (median =
3 correct) compared to before the education (median = 1 correct), Z=-3.62, p=0.0003.
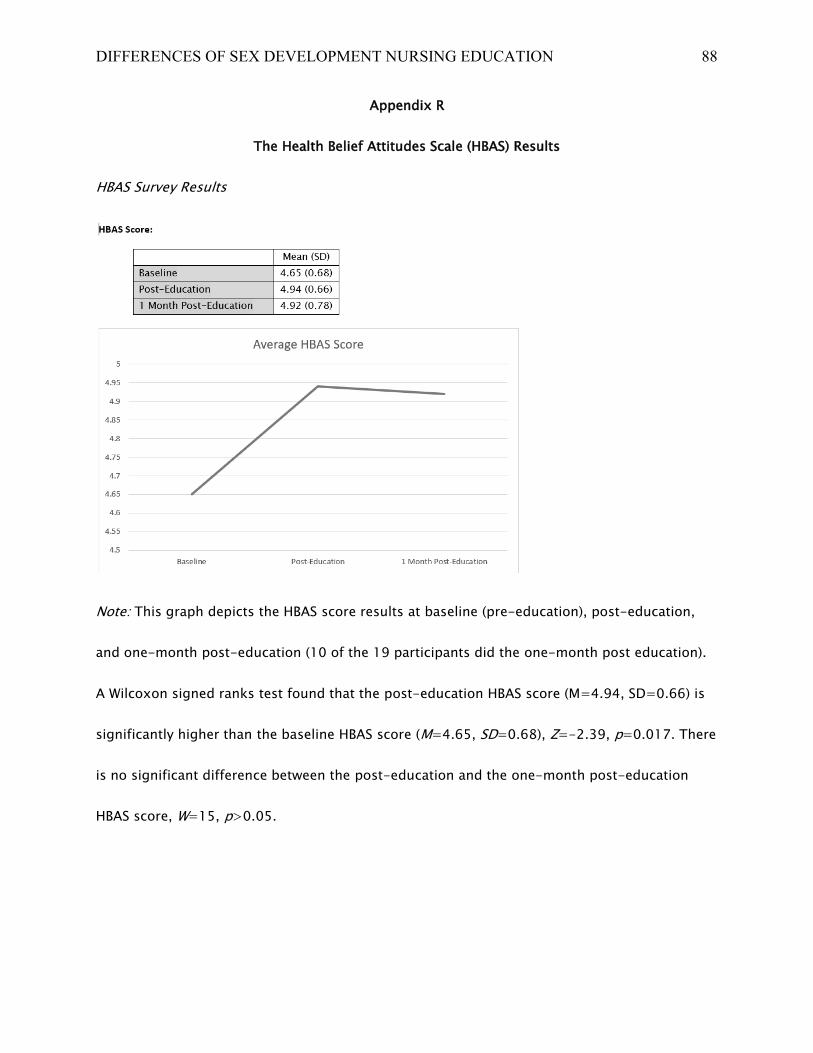
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 88
Appendix R
The Health Belief Attitudes Scale (HBAS) Results
HBAS Survey Results
Note: This graph depicts the HBAS score results at baseline (pre-education), post-education,
and one-month post-education (10 of the 19 participants did the one-month post education).
A Wilcoxon signed ranks test found that the post-education HBAS score (M=4.94, SD=0.66) is
significantly higher than the baseline HBAS score (M=4.65, SD=0.68), Z=-2.39, p=0.017. There
is no significant difference between the post-education and the one-month post-education
HBAS score, W=15, p>0.05.
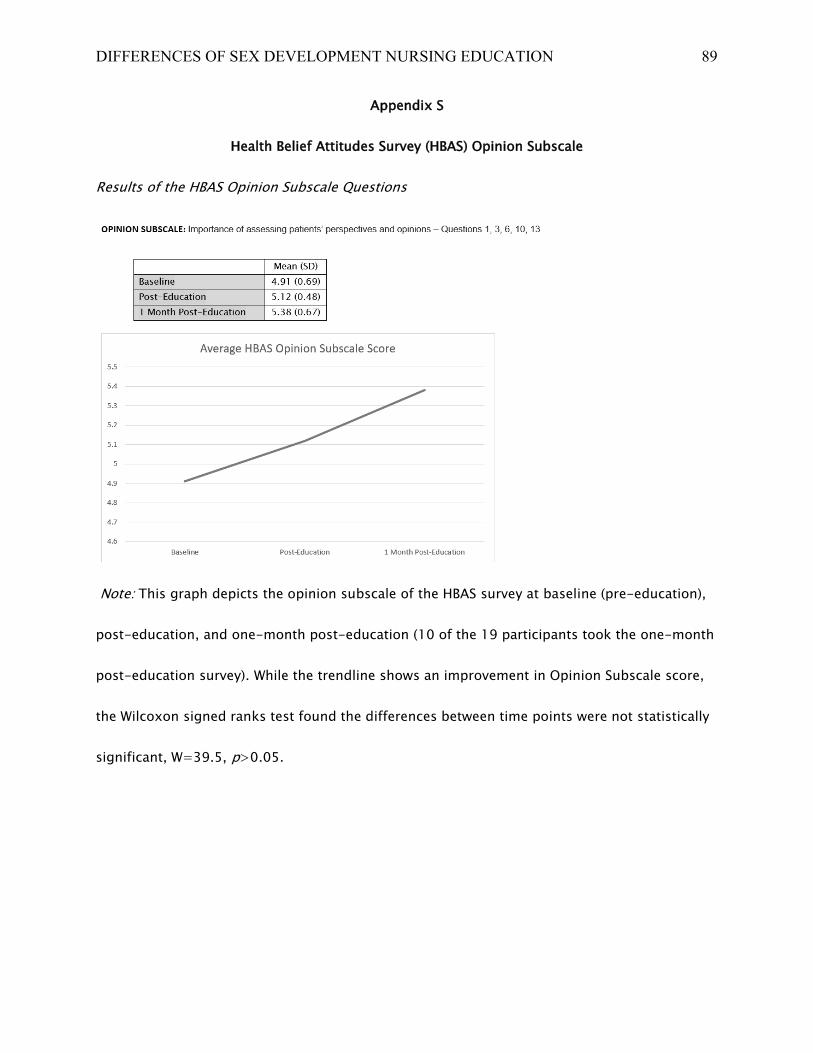
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 89
Appendix S
Health Belief Attitudes Survey (HBAS) Opinion Subscale
Results of the HBAS Opinion Subscale Questions
Note: This graph depicts the opinion subscale of the HBAS survey at baseline (pre-education),
post-education, and one-month post-education (10 of the 19 participants took the one-month
post-education survey). While the trendline shows an improvement in Opinion Subscale score,
the Wilcoxon signed ranks test found the differences between time points were not statistically
significant, W=39.5, p>0.05.
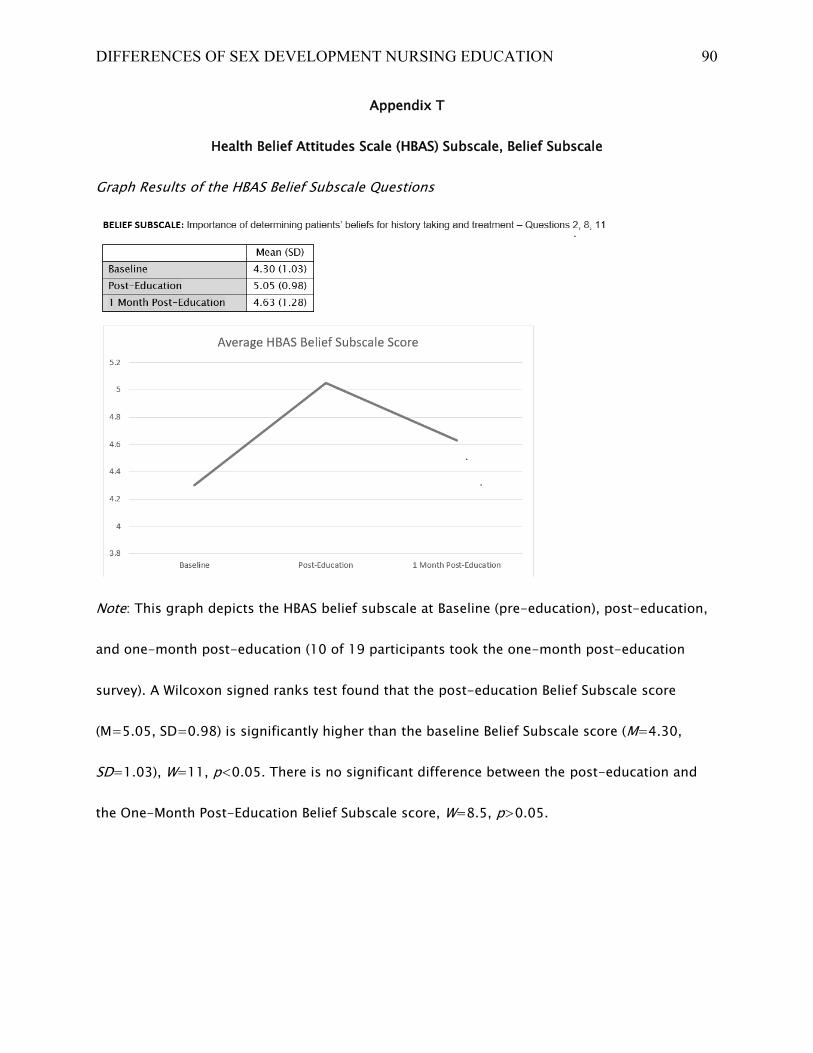
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 90
Appendix T
Health Belief Attitudes Scale (HBAS) Subscale, Belief Subscale
Graph Results of the HBAS Belief Subscale Questions
Note: This graph depicts the HBAS belief subscale at Baseline (pre-education), post-education,
and one-month post-education (10 of 19 participants took the one-month post-education
survey). A Wilcoxon signed ranks test found that the post-education Belief Subscale score
(M=5.05, SD=0.98) is significantly higher than the baseline Belief Subscale score (M=4.30,
SD=1.03), W=11, p<0.05. There is no significant difference between the post-education and
the One-Month Post-Education Belief Subscale score, W=8.5, p>0.05.
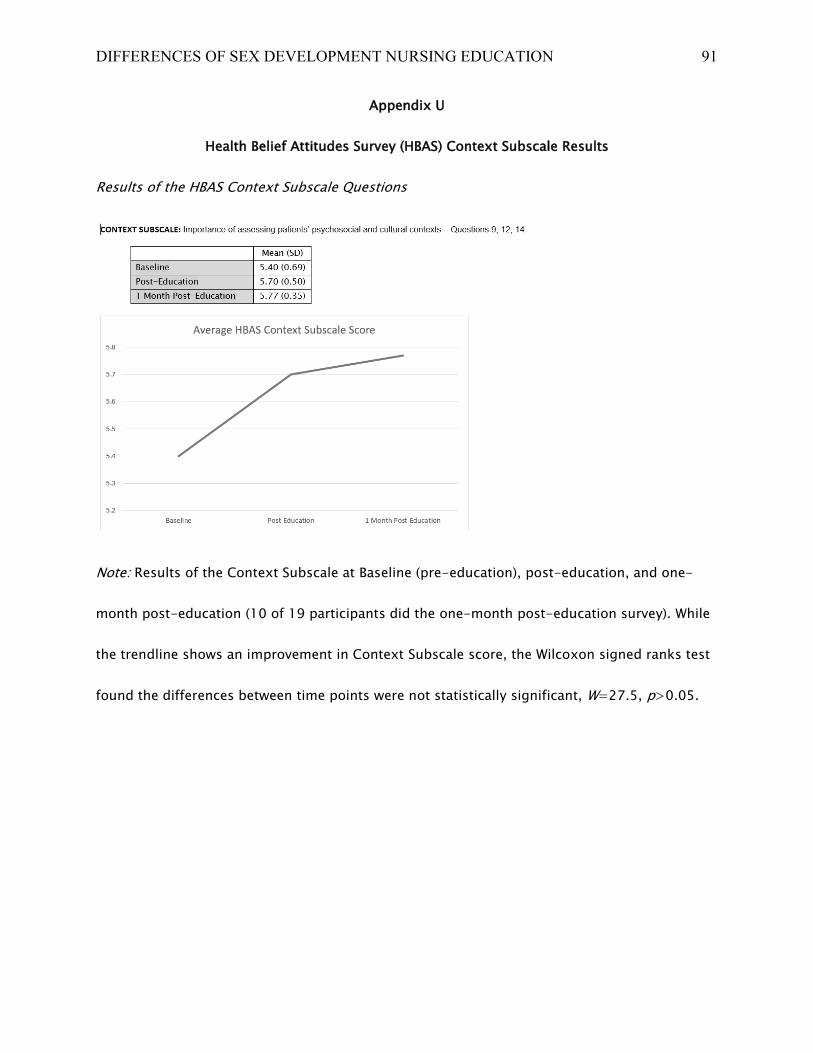
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 91
Appendix U
Health Belief Attitudes Survey (HBAS) Context Subscale Results
Results of the HBAS Context Subscale Questions
Note: Results of the Context Subscale at Baseline (pre-education), post-education, and one-
month post-education (10 of 19 participants did the one-month post-education survey). While
the trendline shows an improvement in Context Subscale score, the Wilcoxon signed ranks test
found the differences between time points were not statistically significant, W=27.5, p>0.05.
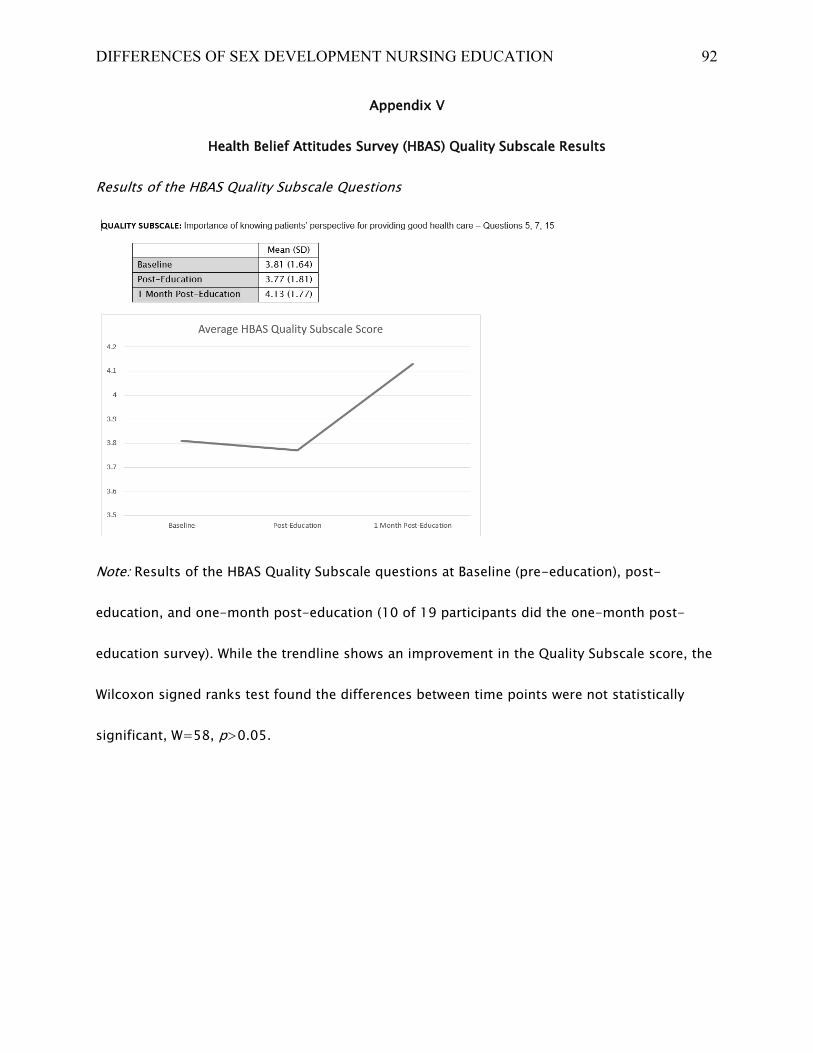
DIFFERENCES OF SEX DEVELOPMENT NURSING EDUCATION 92
Appendix V
Health Belief Attitudes Survey (HBAS) Quality Subscale Results
Results of the HBAS Quality Subscale Questions
Note: Results of the HBAS Quality Subscale questions at Baseline (pre-education), post-
education, and one-month post-education (10 of 19 participants did the one-month post-
education survey). While the trendline shows an improvement in the Quality Subscale score, the
Wilcoxon signed ranks test found the differences between time points were not statistically
significant, W=58, p>0.05.