Building evidence for peer-led interventions: assessing the cost of the Adolescent Asthma Action...
6
Building evidence for peer-led interventions: assessing the cost of the Adolescent Asthma Action program in Australia Michael E. Otim A,B,D , Ranmalie Jayasinha A , Hayley Forbes A and Smita Shah A,C A Poche Centre for Indigenous Health, Sydney Medical School, Edward Ford Building A27, University of Sydney, NSW 2006, Australia. B School of Allied Health, Faculty of Health Sciences, Australian Catholic University, PO Box 968, North Sydney, NSW 2059, Australia. C Primary Health Care Education and Research Unit, Western Sydney Local Health District, PO Box 533, Westmead, NSW 2145, Australia. D Corresponding author. Email: [email protected] Abstract. Asthma is the most common chronic illness among adolescents in Australia. Aboriginal and Torres Strait Islander adolescents, in particular, face substantial inequalities in asthma-related outcomes. Triple A (Adolescent Asthma Action) is a peer-led education intervention, which aims to improve asthma self-management and reduce the uptake of smoking among adolescents. The aim of this study was to determine the cost of implementing the Triple A program in Australia. Standard economic costing methods were used. It involved identifying the resources that were utilised (such as personnel and program materials), measuring them and then valuing them. We later performed sensitivity analysis so as to identify the cost drivers and a stress test to test how the intervention can perform when some inputs are lacking. Results indicate that the estimated cost of implementing the Triple A program in five schools was $41 060, assuming that the opportunity cost of all the participants and venues was accounted for. This translated to $8212 per school or $50 per target student. From sensitivity analysis and a stress test, it was identified that the cost of the intervention (in practice) was $14 per student. This appears to be a modest cost, given the burden of asthma. In conclusion, the Triple A program is an affordable intervention to implement in high schools. The potential asthma cost savings due to the program are significant. If the Triple A program is implemented nation-wide, the benefits would be substantial. Additional keywords: Aboriginal and Torres Strait Islander health, asthma self-management, economic assessment, health education, health promotion. Received 17 April 2014, accepted 19 August 2014, published online 18 September 2014 Introduction Asthma in Australia Asthma continues to be a significant health problem in Australia, accounting for 2.4% of the total burden of disease (Australian Institute of Health and Welfare 2009). In 2004–05, the total expenditure on asthma was ~$606 million, representing ~1.2% of all health expenditure (Australian Institute of Health and Welfare 2010). In 1989, the economic cost of asthma in New South Wales was estimated to be $209 million, which represented a cost to the Australian community of $769 per asthmatic (Mellis et al. 1991). The Boston Consulting Group (1992) estimated the cost of asthma in 1991 at $585–$720 million in Australia. Children aged 0 to 14 years disproportionately bear the largest share (61%) of the total burden of asthma (Australian Institute of Health and Welfare 2009). A study by Toelle et al.(1995) found that the mean annual cost of asthma to a family with an asthmatic child was $212.48 per asthmatic child and that 13.4 h was spent seeking treatment. The cost of absenteeism for parents has been estimated to be ~12.8 million child-care hours (Wang et al. 2005). Adolescent asthma self-management Asthma is the most common chronic illness among adolescents, who poorly understand it (Elizur et al. 2007; Jenkins et al. 2009; Yang et al. 2010). This is partly because adolescence can be a time for health-related risk-taking behaviour. This may lead to poor adherence to medications, which can result in school absences, poor social skills and lack of physical activity (Chen et al. 2007). Adolescents also have a significantly higher prevalence of near- fatal episodes of asthma, and episodes that require hospitalisation, incubation and cardiopulmonary resuscitation, compared with younger aged children (Elizur et al. 2007). Aboriginal and Torres Strait Islander adolescents, in particular, are twice as likely to have hospital visits for asthma, and three times as likely to die from asthma compared with non-Aboriginal adolescents (Jenkins et al. Journal compilation Ó La Trobe University 2014 www.publish.csiro.au/journals/py CSIRO PUBLISHING Australian Journal of Primary Health Research http://dx.doi.org/10.1071/PY14066
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Building evidence for peer-led interventions: assessing the cost of the Adolescent Asthma Action...
Building evidence for peer-led interventions: assessingthe cost of the Adolescent Asthma Action program in Australia
Michael E. OtimA,B,D, Ranmalie JayasinhaA, Hayley ForbesA and Smita ShahA,C
APoche Centre for Indigenous Health, Sydney Medical School, Edward Ford Building A27,University of Sydney, NSW 2006, Australia.
BSchool of Allied Health, Faculty of Health Sciences, Australian Catholic University, PO Box 968,North Sydney, NSW 2059, Australia.
CPrimary Health Care Education and Research Unit, Western Sydney Local Health District,PO Box 533, Westmead, NSW 2145, Australia.
DCorresponding author. Email: [email protected]
Abstract. Asthma is the most common chronic illness among adolescents in Australia. Aboriginal and Torres StraitIslander adolescents, in particular, face substantial inequalities in asthma-related outcomes. Triple A (Adolescent AsthmaAction) is a peer-led education intervention, which aims to improve asthma self-management and reduce the uptake ofsmoking among adolescents. The aim of this study was to determine the cost of implementing the Triple A program inAustralia. Standard economic costing methods were used. It involved identifying the resources that were utilised (such aspersonnel and program materials), measuring them and then valuing them. We later performed sensitivity analysis so as toidentify the cost drivers and a stress test to test how the intervention can perform when some inputs are lacking. Resultsindicate that the estimated cost of implementing the Triple A program in five schools was $41 060, assuming that theopportunity cost of all the participants and venues was accounted for. This translated to $8212 per school or $50 per targetstudent. From sensitivity analysis and a stress test, it was identified that the cost of the intervention (in practice) was$14 per student. This appears to be a modest cost, given the burden of asthma. In conclusion, the Triple A program is anaffordable intervention to implement in high schools. The potential asthma cost savings due to the program are significant.If the Triple A program is implemented nation-wide, the benefits would be substantial.
Additional keywords: Aboriginal and Torres Strait Islander health, asthma self-management, economic assessment,health education, health promotion.
Received 17 April 2014, accepted 19 August 2014, published online 18 September 2014
Introduction
Asthma in Australia
Asthma continues to be a significant health problem in Australia,accounting for 2.4% of the total burden of disease (AustralianInstitute of Health and Welfare 2009). In 2004–05, the totalexpenditure on asthma was ~$606million, representing ~1.2%of all health expenditure (Australian Institute of Health andWelfare 2010).
In 1989, the economic cost of asthma in New South Waleswas estimated to be $209million, which represented a cost to theAustralian community of $769 per asthmatic (Mellis et al. 1991).The Boston Consulting Group (1992) estimated the cost ofasthma in 1991 at $585–$720million in Australia. Childrenaged 0 to 14 years disproportionately bear the largest share(61%) of the total burden of asthma (Australian Institute ofHealth and Welfare 2009). A study by Toelle et al. (1995) foundthat the mean annual cost of asthma to a family with an asthmaticchild was $212.48 per asthmatic child and that 13.4 h was spent
seeking treatment. The cost of absenteeism for parents hasbeen estimated to be ~12.8million child-care hours (Wanget al. 2005).
Adolescent asthma self-management
Asthma is the most common chronic illness among adolescents,who poorly understand it (Elizur et al. 2007; Jenkins et al. 2009;Yang et al.2010). This is partly because adolescence canbe a timefor health-related risk-taking behaviour. This may lead to pooradherence to medications, which can result in school absences,poor social skills and lack of physical activity (Chen et al. 2007).Adolescents also have a significantly higher prevalence of near-fatal episodes of asthma, andepisodes that require hospitalisation,incubation and cardiopulmonary resuscitation, compared withyounger aged children (Elizur et al. 2007). Aboriginal and TorresStrait Islander adolescents, inparticular, are twice as likely tohavehospital visits for asthma, and three times as likely to die fromasthma comparedwith non-Aboriginal adolescents (Jenkins et al.
Journal compilation � La Trobe University 2014 www.publish.csiro.au/journals/py
CSIRO PUBLISHING
Australian Journal of Primary Health Researchhttp://dx.doi.org/10.1071/PY14066

2009). Thus, Aboriginal and Torres Strait Islander adolescentsare particularly disadvantaged.
Asthma self-management takes on an additional dimensionduring adolescence, with the responsibility for health careshifting from parents to adolescents (Beal et al. 2001; Elizur et al.2007). This shift is commonly mediated through externalinfluences, with an increase in the importance of peer friendships(Bruzzese et al. 2004). Social support plays an important role inasthma self-management during adolescence and has aconsiderable influence on adolescent risky health behaviour(Beal et al. 2001; Chen et al. 2007; Yang et al. 2010). Despite theneed for greater social support and asthma awareness duringadolescence, there are a limited number of interventionsdesigned for this age group (Beal et al. 2001). Effective peer-ledinterventions that target asthma self-management could equipadolescents with the necessary skills to manage their asthma(Ayala et al. 2006). Schools are a suitable location to implementpeer-led interventions.
Peer-led education in schools
By facilitating the implementation of peer-led interventions inschools, it allows easy access to the target asthmatic students whoneed it most, allows intervention outcomes to be measured andallows contact with the wider community (Shah et al. 2001;Al-sheyab et al. 2013). It has also been noted as a key setting forpeer group influences on health behaviours in adolescence(Alexander et al. 2001).
Peer-led health education is a potential alternative to healthprofessional- or teacher-delivered health education in the schoolcontext (Mellanby et al. 2000). Peers are often seen byadolescents as more credible sources of information (Hardenet al. 2001). Peer-led education programs have been found to beeffective in a range of health behaviours (Campbell et al. 2008;Flay 2009). This paper focuses on theAdolescent AsthmaAction(Triple A) program, a peer-led school-based intervention, whichaims to improve asthma self-management and prevent smokinguptake by high school students.
The Triple A program
The Triple A program is based on psychosocial theory (Shahet al. 1998, 2001) and it is implemented in high schools locatedin low socioeconomic areas. As such, the intervention targets
disadvantaged students, such as Aboriginal and Torres StraitIslander peoples, and those with a refugee or migrantbackground. The intervention uses slightly older students todeliver the program.
The Triple A program has undergone rigorous scientificreview and testing (Gibson et al. 1998; Shah et al. 2001). Theresults show that participation in the program encourages a senseof personal responsibility. Furthermore, it leads to significantimprovement in quality of life of asthmatic students by an averageof 0.12 (95%CI = 0.05–0.18). Participating students experiencedfewer asthma attacks and reduced school absenteeism. A recentrandomised trial undertaken in Jordanian schools resulted insignificant improvement of asthmatic quality-of-life by ~1.35(95%CI = 1.15–2.19) (Al-sheyab et al. 2012). Thus, the Triple Aprogram is effective in improving asthma self-management andpreventing smoking in adolescents in high school settings (Shahet al. 2001; Al-sheyab et al. 2012).
The program follows a three-step process (Shah and Jayasinha2013). First, trained university students (Triple A Educators)coach senior high school students between the ages of15–16years to beTripleAPeerLeaders during a1-dayworkshop.The Peer Leaders learn about asthma and its management andacquire skills in facilitation and leadership. Second, the PeerLeaders deliver three Triple A lessons to their younger peers,between the ages of 12–13 years, the target group. Finally, widerdissemination of asthma information and prevention of smokingoccurs when the target students relay what they have learnt to thewider school community, through creative student actions suchas posters, songs, dances, drama and/or performances.
However, the cost of implementing Triple A has not beenestimated. This study estimates the cost of implementing theTripleAprogram inhigh schools inAustralia over a 1 year period.Ethics approval to use secondary data for this study was obtainedfrom the University of Sydney Human Ethics Committee.
Methods
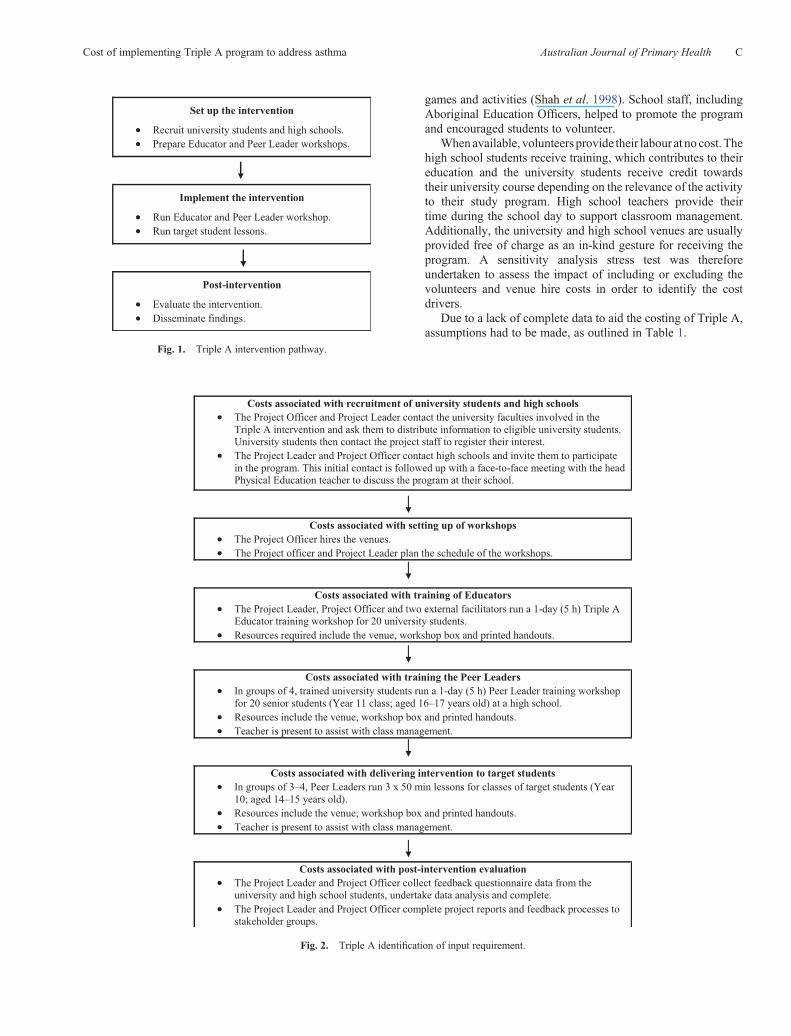
Standard economic costing methods were used to estimate thecost of implementing the Triple A program over a 1-year period,following three basic steps: identification of interventionactivities; measurement of resource use; and valuation of theresources (Drummond et al. 2005). To identify Triple A activitiesfor costing purposes, an activity pathway (Fig. 1) was used. Theindividual cost components of the interventions and unit costs ofthe activities were identified from the literature (Kernick 2000;Chapko et al. 2009; Doran et al. 2012).
Input costs were estimated according to the requirements foreach activity and their unit cost (Fig. 2).
Estimating the economic cost of the intervention involvedidentifying the opportunity costs (the best alternatives foregone)of the required inputs (Kernick 2000), including volunteer labourand venue hire costs. Typically, inputs include 20 universitymedical and pharmaceutical students who are trained as Triple Aeducators in a 1-day workshop. In collaboration with five highschools in Western Sydney, which have high numbers ofAboriginal students (10–20%), Triple A Educators in groups ofthree or four,mainly volunteer students fromYears 10or 11,weretrained as TripleA Peer Leaders. They learnt about asthma and itsmanagement, and how to resist smoking through videos,
What is known about the topic?* Asthma is the most common chronic illness amongadolescents in Australia. Triple A, a peer-led educationprogram, improves adolescent asthma self-management. An economic analysis has not yet beenundertaken.
What does this paper add?* Triple A is an affordable peer-led education program toimprove asthma self-management in adolescents.Investing in this intervention will most likely result insignificant cost savings in the long term.
B Australian Journal of Primary Health M. E. Otim et al.
games and activities (Shah et al. 1998). School staff, includingAboriginal Education Officers, helped to promote the programand encouraged students to volunteer.
Whenavailable, volunteers provide their labour at no cost.Thehigh school students receive training, which contributes to theireducation and the university students receive credit towardstheir university course depending on the relevance of the activityto their study program. High school teachers provide theirtime during the school day to support classroom management.Additionally, the university and high school venues are usuallyprovided free of charge as an in-kind gesture for receiving theprogram. A sensitivity analysis stress test was thereforeundertaken to assess the impact of including or excluding thevolunteers and venue hire costs in order to identify the costdrivers.
Due to a lack of complete data to aid the costing of Triple A,assumptions had to be made, as outlined in Table 1.
Fig. 1. Triple A intervention pathway.
Fig. 2. Triple A identification of input requirement.
Cost of implementing Triple A program to address asthma Australian Journal of Primary Health C

Results
Overall, the cost of implementing the Triple A program in fivehigh schools was ~$41 060, assuming the opportunity cost ofall the participants had been accounted for. This translated to~$8212 per school or $50 per target student. This estimate, asoutlined in Table 2, is the figure before sensitivity analysis andstress testing was undertaken.
Sensitivity analysis and stress testing of the results wasundertaken (Table 3). The effect of the volunteers and/or venuehire being included or excluded on the overall cost of theprogram was assessed. Results indicate that excluding both thecost of volunteers and venues more than halves the cost of theintervention per student, which translates to a cost of $14 perstudent, although there is still an opportunity cost, in spite of thefinancial savings.
Discussion
The primary aim of the study was to estimate the cost ofimplementing the Triple A program inAustralia. Results indicatethat high schools require an investment of $50 per target studentwith asthma.With such an investment, there are potential savingsthat can be achieved in terms of reduced school absenteeism andrelated costs of parental leave, as well as hospital admissions(Shah et al. 2001; Al-sheyab et al. 2012). This may, in turn,prevent further asthma-related costs among adults in the future
(Australian Institute of Health and Welfare 2010). This studyprovides evidence of the affordability of Triple A to improveadolescent asthma-self management.
The use of the activity pathway to identify and mapintervention activities allowed us to estimate the key componentcosts at each stage of the program (Chapko et al. 2009).Additionally, by using a sensitivity analysis and stress testing ofthe intervention, we were able to identify the key cost drivers thataffected the affordability of the program. As such, we were ableto determine that, while the intervention costs $50 per targetstudent in the study, in practise, the program financial costs is$14 per target student, which makes a significant difference interms of affordability. Such costing has important implicationsfor the future implementation of Triple A.
We had also planned to estimate the potential savings due tothe program using the reported improvement of health-relatedquality of life proposed by Shah et al. (2001) as the primaryoutcome measure of the effectiveness of the program. However,we were unable to do so due to a lack of recent estimates ofthe social cost of asthma data that used recent prevalence orincidence rates of asthma to reflect the current situation inAustralia. For example,Mellis et al. (1991) determined the socialcost of asthma to be $769 per person based on 1989 data and theBoston Consulting Group (1992) estimated the cost of asthmato be between $585 and $720million based on 1991 prevalencedata of 7%. Today, the prevalence of asthma in Australia among
Table 1. Assumptions for the costing of the Triple A intervention
Assumptions
Participants * The average number of student (11–12 year olds) was estimated to be 165 students, which was based on average class size at a typicalgovernment-funded high school in Western Sydney, New South Wales, Australia (Office of Education 2013).
* The Shah et al. (2001) and Al-sheyab et al. (2012) studies on the Triple A intervention did not specify the number of health workers andproject staff used to train the senior high school students (15–16 year olds). As such, we contacted the Triple A intervention leader inAustralia to determine participant numbers for the current implementation of the program in Sydney.
* Twenty university students (Triple A Educators) are required to coach 20 senior high students (15–16 year olds) as Peer Leaders in eachschool (n = 100) in a 5-h workshop.
* Twenty senior school students (15–16 year olds) train ~165 junior students (11–12 year olds) in each school over three lessons. As there arefive schools that participated, with an average of 165 junior students, there was a total of 825 junior students (11–12 year olds).
* One teacher was present at each Peer Leader workshop and at each of the junior student lessons to assist with class management.* Four facilitators are required to train 20 university students in a 5-h workshop.* The possibility of drop-outs from the program was not accounted for.
Salary All salaries for Triple A project staff were based on 2013 professional salaries at The University of Sydney (2013):* The salary of the Project Officer was $35 per hour, Level 5/Step 1, pro rata (2 days per week).* The Salary of the Project Leader was $44 per hour, Level 7, Step 1.* The wage of the two external facilitators was $44 per hour, Level 7, Step 1.* On-cost of salaries were calculated at 30% as per University of Sydney standard practice.* In principle, the labour and time given by the volunteers, the university, senior high school students and teachers, should be costed because
there is an ‘opportunity cost’ to each of them.* An average wage for student volunteers was based on the Australian Department of Labour website. The estimated wage per hour for
university and senior high school students was $16.37 and $9.46 respectively (Fair Work Ombudsman 2013).* Teacher salary was based on a graduate starting salary of $60 000, which translates to approximately $35 per hour (NSW Teachers
Federation 2013).* In practise, volunteers are usually provided at no cost during the intervention, which was accounted for in the stress test, because in remote
areas, such volunteers may not be present.
Resources * In theory, the venues for the workshops used in the Triple A intervention should be costed, as there is an ‘opportunity cost’ to each of them.However, in practise, venues are usually provided at no cost during the intervention as an in-kind gesture.
* Where venue hire charge was costed in the sensitivity analysis, the $88 per hour room charge was based on advice regarding the base perhour hire fee of a tutorial room at the University of Sydney, Camperdown campus.
* 20% for incidentals includes the cost of office resources and transport.
D Australian Journal of Primary Health M. E. Otim et al.

adolescents is ~17% (Australian Centre for Asthma Monitoring2011), which means that the social cost of asthma may havesignificantly changed. Additionally, a study by Toelle et al.(1995), based on 1991–92 data from NSW, calculated the costof asthma to a family with a child with asthma as $212. Thus,available historic data require updating in order for the savingsdue to the Triple A program and other interventions to beaccurately estimated.
With increased need for efficient approaches in the healthsystem to address increasing healthcare needs, determining theeconomic cost of interventions is important for ensuringsustainability of interventions (Kernick 2000). Furthermore,outlining the intervention costs and comparisons with otherinterventions (such as adult- or expert-led interventions) can beundertaken to demonstrate the cost benefits of implementingschool-based peer-led education to improve adolescent asthmaself-management.
Conclusion
Asthma is the most common chronic illness among adolescents,especially among Aboriginal and Torres Strait Islanderadolescents, in Australia. Effective peer-led interventions thattarget asthma self-management are therefore urgently needed toequip adolescents with the skills to manage their asthma. Theschool context has also been noted as a key setting for peer groupinfluences on health behaviours in adolescence or peer-ledinterventions.
This study demonstrates that the Triple A program couldlead to significant savings in asthma costs. If the Triple Aintervention is implemented nationwide, the benefits would
be substantial. However, more updated figures on theeffectiveness of the Triple A program and the social costs ofexisting asthma programs is needed for potential savings to beachieved.
Conflicts of interestNone declared.
Acknowledgements
We acknowledge the funding support received from the Poche Centre ofIndigenous Health, Sydney Medical School, University of Sydney toundertake this project.We thank theAsthma Foundation ofNewSouthWalesfor their support of the Triple A program in high schools. We acknowledgeMsKylieGwynne, Professor Stephen Jan andShifraWaks for their commentson this manuscript.
References
Australian Institute of Health and Welfare (2009) Burden of disease due toasthma in Australia 2003. Cat. no. ACM 16. AIHW, Canberra.
Australian Institute of Health and Welfare (2010) Health system expenditureon disease and injury in Australia, 2004–05. Health and welfareexpenditure series. AIHW, Canberra.
Al-sheyab N, Gallagher R, Crisp J, Shah S (2012) Peer-led education foradolescents with asthma in Jordan: a cluster-randomized controlled trial.Pediatrics 129, e106–e112. doi:10.1542/peds.2011-0346
Al-sheyab N, Gallagher R, Gallagher P, Shah S (2013) Cigarette smoking inadolescents with asthma in Jordan: impact of peer-led education in highschools. Journal of Nursing and Practice 3(9), 13–22. doi:10.5430/jnep.v3n9p13
Alexander C, Piazza M, Mekos D, Valente T (2001) Peers, schools, andadolescent cigarette smoking. The Journal of Adolescent Health 29,22–30. doi:10.1016/S1054-139X(01)00210-5
Australian Centre for Asthma Monitoring (2011) Asthma in Australia 2011.AIHW Asthma Series no. 4. Cat. no. ACM 22. AIHW, Canberra.
Ayala GX,Miller D, Zagami E, Riddle C,Willis S, King D (2006) Asthma inmiddle schools:what students have to say about their asthma.The Journalof School Health 76, 208–214. doi:10.1111/j.1746-1561.2006.00098.x
Beal AC, Ausiello J, Perrin JM (2001) Social influences on health-riskbehaviors among minority middle school students. The Journal ofAdolescent Health 28, 474–480. doi:10.1016/S1054-139X(01)00194-X
Boston Consulting Group (1992) Report on the cost of asthma in Australia.National Asthma Campaign. National Asthma Council Australia,Melbourne.
Bruzzese JM, Bonner S, Vincent EJ, Sheares BJ, Mellins RB, Levison MJ,Wiesemann S,DuY, ZimmermanBJ, EvansD (2004)Asthma education:the adolescent experience. Patient Education and Counseling 55,396–406. doi:10.1016/j.pec.2003.04.009
Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N,Hughes R, Moore L (2008) An informal school-based peer-ledintervention for smoking prevention in adolescence: a cluster randomisedtrial. Lancet 371, 1595–1602. doi:10.1016/S0140-6736(08)60692-3
ChapkoMK,LiuC-F,PerkinsM,LiY-F,FortneyJC,MaciejewskiML(2009)Equivalence of twohealthcare costingmethods: bottom-up and top-down.Health Economics 18, 1188–1201. doi:10.1002/hec.1422
Chen E, Chim LS, Strunk RC, Miller GE (2007) The role of the socialenvironment in children and adolescents with asthma. American Journalof Respiratory and Critical Care Medicine 176, 644–649. doi:10.1164/rccm.200610-1473OC
Doran CM, Einfeld SL, Madden RH, Otim M, Horstead SK, Ellis LA,Emerson E (2012) How much does intellectual disability really cost?First estimates for Australia. Journal of Intellectual & DevelopmentalDisability 37, 42–49. doi:10.3109/13668250.2011.648609
Table 2. Cost of intervention
Cost
Salary $20 563Venue $11 660Resources $1994Subtotal $34 217Incidentals $6843Grand total $41 060Per school $8212Per student $50
Table 3. Sensitivity and stress tests
Full costA Withoutvolunteers
Withoutvenue
Withoutvolunteersand venueA,B
Salary $20 563 $8694 $21 838 $8694Venue $11 660 $11 660 $0 $0Resources $720 $720 $720 $720Subtotal $32 943 $21 074 $22 558 $9414Incidentals $6589 $4215 $4512 $1883Grand total $39 532 $25 288 $27 069 $11 296Per student $50 $31 $33 $14Per school $8212 $5058 $5414 $2259
AValues used in economic analysis.BUsual practise.
Cost of implementing Triple A program to address asthma Australian Journal of Primary Health E

Drummond M, Sculpher M, Torrance G, O’Brien B, Stoddard G (2005)‘Methods for the economic evaluation of health care programmes.’(Oxford University Press: Oxford)
Elizur A, Bacharier LB, Strunk RC (2007) Pediatric asthma admissions:chronic severity and acute exacerbations. The Journal of Asthma 44,285–289. doi:10.1080/02770900701340445
Fair Work Ombudsman (2013) National minimum wage. Available at http://www.fairwork.gov.au/pay/national-minimum-wage/pages/default.aspx[Verified 27 October 2013]
Flay BR (2009) The promise of long-term effectiveness of school-basedsmoking prevention programs: a critical review of reviews. TobaccoInduced Diseases 5, 7. doi:10.1186/1617-9625-5-7
Gibson PG, Shah S, Mamoon HA (1998) Peer-led asthma education foradolescents: impact evaluation. The Journal of Adolescent Health 22(1),66–72. doi:10.1016/S1054-139X(97)00203-6
Harden A, Oakley A, Oliver S (2001) Peer-delivered health promotion foryoung people: a systematic review of different study designs. HealthEducation Journal 60, 339–353. doi:10.1177/001789690106000406
Jenkins CR, ChangAB, Poulos LM,Marks GB (2009) Asthma in IndigenousAustralians: so much yet to do for Indigenous lung health. The MedicalJournal of Australia 190, 530–531.
Kernick D (2000) Costing interventions in primary care. Family Practice 17,66–70. doi:10.1093/fampra/17.1.66
Mellanby AR, Rees JB, Tripp JH (2000) Peer-led and adult-led school healtheducation: a critical review of available comparative research. HealthEducation Research 15, 533–545. doi:10.1093/her/15.5.533
Mellis CM, Peat JK, Bauman A, Woolcock AJ (1991) The cost of asthma inNew South Wales. The Medical Journal of Australia 155, 522–528.
NSW Teachers Federation (2013) Graduate teachers survival kit 2013. NewSouth Wales Teachers Federation, Sydney.
OfficeofEducation (2013)Average class sizes.NewSouthWalesDepartmentof Education and Communities, Sydney.
Shah S, Jayasinha R (2013) ‘Triple A peer leader manual.’ (Western SydneyLocal Health District: Sydney)
Shah S, Mahmoon AH, Gibson PG (1998) Peer led asthma education foradolescents: development and formative evaluation. Health PromotionJournal of Australia 8, 177–182.
Shah S, Peat JK, Mazurski EJ, Wang H, Sindhusake D, Bruce C, Henry RL,Gibson PG (2001) Effect of peer led programme for asthma education inadolescents: cluster randomised controlled trial. British Medical Journal322, 583doi:10.1136/bmj.322.7286.583
The University of Sydney (2013) The University of Sydney enterpriseagreement 2013–2017. The University of Sydney, Sydney.
Toelle BG, Peat JK, Mellis CM, Woolcock AJ (1995) The cost of childhoodasthma to Australian families. Pediatric Pulmonology 19, 330–335.doi:10.1002/ppul.1950190604
Wang LY, Zhong Y, Wheeler L (2005) Direct and indirect costs of asthma inschool-age children. Preventing Chronic Disease 2, A11
Yang TO, Sylva K, Lunt I (2010) Parent support, peer support, and peeracceptance in healthy lifestyle for asthma management among earlyadolescents. Journal for Specialists in Pediatric Nursing 15, 272–281.doi:10.1111/j.1744-6155.2010.00247.x
F Australian Journal of Primary Health M. E. Otim et al.
www.publish.csiro.au/journals/py