Does Your Child Have Asthma? Filled Prescriptions and Household Report of Child Asthma
10
Does Your Child Have Asthma? Filled Prescriptions and Household Report of Child Asthma Jutta M. Joesch, PhD, Hyoshin Kim, PhD, Gail M. Kieckhefer, PhD, ARNP, April A. Greek, PhD, & Nazli Baydar, PhD ABSTRACT Introduction: Surveys are central for information on asthma prevalence. Recently, the validity of parental reports of pediatric asthma has been questioned. Confi- dence is examined in the report of asthma for children, obtained in a sur- vey from the adult household member most knowledgeable about household health care (MKA). Method: MKA reports of asthma are compared with pharmacy records of prescriptions beneficial in asthma treatment (“asthma medications”) for children 0 to 17 years old in the 1996 Medical Expenditure Panel Survey. Results: “Asthma medications” were filled for 6.5% of children, yet the MKA did not report asthma for 47.3% of them. However, for 61.2% of these children, the MKA reported plausible alternative medical conditions. For 9.0%, diagnosis information was miss- ing. Among children with an “asthma medication,” the MKA was less likely to report either asthma or a plausible al- ternative diagnosis for girls and for children 0 to 5 years of age. Reporting was not statistically different by child race/ethnicity, household income, ed- ucation level, and MKA English lan- guage proficiency. Discussion: Surveys do not overlook as many children with asthma as pre- viously reported. Among children with “asthma medications,” only sex and age appear to be different for children whose MKA reported either asthma or a plausible alternative diagnosis versus those whose MKA did not report ei- ther. J Pediatr Health Care. (2006) 20, 374-383. Asthma is one of the most com- mon chronic illnesses among chil- dren younger than 18 years in the United States (Adams, Hendershot, & Marano, 1999; American Lung Association, 2004). The burden of asthma for affected children and their families can be high, as are health care costs resulting from asthma (National Heart, Lung, and Blood Institute [NHLBI], 2003; Smith et al., 1997). It is therefore of interest to know how many chil- dren have asthma and how the prevalence and impact of asthma change over time. Survey responses from parents are an important source of infor- mation about the prevalence and Jutta M. Joesch is Principal Health Research Scientist at Battelle Centers for Public Health Research & Evaluation, Seattle, Wash. Hyoshin Kim is Principal Health Research Scientist at Battelle Centers for Public Health Research & Evaluation, Seattle, Wash. Gail M. Kieckhefer is Professor, the Department of Family and Child Nursing, School of Nursing, University of Washington, Seattle, Wash. April A. Greek is Principal Health Research Scientists at Battelle Centers for Public Health Research & Evaluation, Seattle, Wash. Nazli Baydar is Visiting Associate Professor, Koç University, Istanbul, Turkey. This research was supported by grant No. RO1-HS 13110 from the Agency for Healthcare Research and Quality (AHRQ). Dr. Kieckhefer’s work also was supported in part by Project T 72 MC 00007 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration, Department of Health and Human Services. Reprint requests: Jutta M. Joesch, PhD, Battelle Centers for Public Health Research and Evaluation, 1100 Dexter Avenue N, Suite 400, Seattle, WA 98109-3598; e-mail: [email protected]. 0891-5245/$32.00 Copyright © 2006 by the National Association of Pediatric Nurse Practitioners. doi:10.1016/j.pedhc.2006.02.003 374 Volume 20 • Number 6 Journal of Pediatric Health Care Original Article www.jpedhc.org
Transcript of Does Your Child Have Asthma? Filled Prescriptions and Household Report of Child Asthma
Original Article www.jpedhc.org
Does Your ChildHave Asthma?Filled Prescriptionsand HouseholdReport of ChildAsthmaJutta M. Joesch, PhD, Hyoshin Kim, PhD, Gail M.Kieckhefer, PhD, ARNP, April A. Greek, PhD, &Nazli Baydar, PhD
ABSTRACT
Introduction: Surveys are central for information on asthma prevalence. Recently,the validity of parental reports of pediatric asthma has been questioned. Confi-
Jutta M. Joesch is Principal Health Research Scientist at Battelle Centers for PublicHealth Research & Evaluation, Seattle, Wash.
Hyoshin Kim is Principal Health Research Scientist at Battelle Centers for PublicHealth Research & Evaluation, Seattle, Wash.
Gail M. Kieckhefer is Professor, the Department of Family and Child Nursing, School ofNursing, University of Washington, Seattle, Wash.
April A. Greek is Principal Health Research Scientists at Battelle Centers for PublicHealth Research & Evaluation, Seattle, Wash.
Nazli Baydar is Visiting Associate Professor, Koç University, Istanbul, Turkey.
This research was supported by grant No. RO1-HS 13110 from the Agency forHealthcare Research and Quality (AHRQ). Dr. Kieckhefer’s work also was supported inpart by Project T 72 MC 00007 from the Maternal and Child Health Bureau (Title V,Social Security Act), Health Resources and Services Administration, Department ofHealth and Human Services.
Reprint requests: Jutta M. Joesch, PhD, Battelle Centers for Public Health Researchand Evaluation, 1100 Dexter Avenue N, Suite 400, Seattle, WA 98109-3598; e-mail:[email protected].
0891-5245/$32.00
Copyright © 2006 by the National Association of Pediatric Nurse Practitioners.
doi:10.1016/j.pedhc.2006.02.003
374 Volume 20 • Number 6
dence is examined in the report ofasthma for children, obtained in a sur-vey from the adult household membermost knowledgeable about householdhealth care (MKA).Method: MKA reports of asthma arecompared with pharmacy records ofprescriptions beneficial in asthmatreatment (“asthma medications”) forchildren 0 to 17 years old in the 1996Medical Expenditure Panel Survey.Results: “Asthma medications” werefilled for 6.5% of children, yet the MKAdid not report asthma for 47.3% ofthem. However, for 61.2% of thesechildren, the MKA reported plausiblealternative medical conditions. For9.0%, diagnosis information was miss-ing. Among children with an “asthmamedication,” the MKA was less likely toreport either asthma or a plausible al-ternative diagnosis for girls and forchildren 0 to 5 years of age. Reportingwas not statistically different by childrace/ethnicity, household income, ed-ucation level, and MKA English lan-guage proficiency.Discussion: Surveys do not overlookas many children with asthma as pre-viously reported. Among children with“asthma medications,” only sex andage appear to be different for childrenwhose MKA reported either asthma ora plausible alternative diagnosis versusthose whose MKA did not report ei-ther. J Pediatr Health Care. (2006) 20,374-383.
Asthma is one of the most com-mon chronic illnesses among chil-dren younger than 18 years in theUnited States (Adams, Hendershot,& Marano, 1999; American LungAssociation, 2004). The burden ofasthma for affected children andtheir families can be high, as arehealth care costs resulting fromasthma (National Heart, Lung, andBlood Institute [NHLBI], 2003;Smith et al., 1997). It is therefore ofinterest to know how many chil-dren have asthma and how theprevalence and impact of asthmachange over time.
Survey responses from parentsare an important source of infor-
mation about the prevalence andJournal of Pediatric Health Care

severity of pediatric asthma. Re-cently, the validity of household-reported asthma information forchildren living in the householdhas been questioned (Roberts,2003). The current article reportsresults from an analysis that exam-ines confidence in the report ofasthma for children, obtained in aninterview with the householdmember most knowledgeableabout household health care(MKA).
BACKGROUNDIn the United States, several na-
tional surveys collect data onasthma. For instance, informationon asthma prevalence and on dis-ability resulting from asthma is es-timated with data from the Na-tional Health Interview Survey(NHIS) and the National Healthand Nutrition Examination Survey(Lanphear & Gergen, 2003). Al-though standards of care forasthma have been published(NHLBI, 1997; 2003), universal sci-entific consensus is lacking on aclinical definition of asthma for usein surveys (Council of State andTerritorial Epidemiologists, 1998;Lanphear & Gergen). Surveys,therefore, rely on several differentapproaches to ascertain whether achild has the illness and how se-vere it is. For example, until 1996,the NHIS inquired whether anyonein the family had asthma duringthe past 12 months. Starting in1997, the NHIS switched to askingonly for a randomly chosen childin the family whether a health pro-fessional ever diagnosed asthmaand, if so, whether the child had anasthma episode or an asthma at-tack during the past 12 months.Since 2001, the asthma questionsin the NHIS core questionnaire askabout lifetime diagnosis, currentasthma, recent asthma attacks, andemergency room visits for asthma(Akinbami, Schoendorf, & Parker,2003).
The validity of measuring pedi-atric asthma prevalence by inter-
viewing parents has been ques-Journal of Pediatric Health Care
tioned in a recent study by Roberts(2003). Roberts’ study is based onthe following two hypotheses: (a)many children whose parents re-port that their child has asthma ob-tain asthma medications; and (b) ifa child obtains medications spe-cific to asthma, most parents willreport that their child has asthma.With respect to the first hypothesis,Roberts found that 64% of childrenwho were reported to have asthmadid not have any “asthma medica-tions” filled. Moreover, with re-spect to the second hypothesis, hefound that 45% of children whohad an “asthma medication” filledwere not reported to have asthma.“Asthma medications” are medica-tions that are considered beneficialin the treatment of asthma. Basedon these findings, Roberts con-cluded that surveys that ask par-ents about their children’s asthma“overlook many children with ac-tive disease” (p. 449).
To conduct his study, Roberts(2003) used data from the 1996Medical Expenditure Panel Survey(MEPS) and compared survey re-sponses regarding a child’s asthmafrom the adult household membermost knowledgeable about house-hold health care with the child’spharmacy records of prescriptionmedication often used in the treat-ment of asthma. The MEPS deter-mines the most knowledgeableadult household member as fol-lows: Before the first interview isconducted by the MEPS, each eli-gible household is contacted bythe MEPS via mail and telephone.The purpose of these contacts is toenlist the household respondentinto MEPS and to plan the deliveryof record-keeping materials beforethe study observation period be-gins (Cohen J., 1997). According toAgency for Healthcare Researchand Quality (AHRQ) staff, the pre-ferred MEPS respondent is the per-son who is most knowledgeableabout the family’s health care andwho has been keeping recordsabout health care use and ex-
penses, after MEPS providedrecord keeping materials to thehousehold (W. Carroll, Agency forHealthcare Research and Quality,personal communication, March22, 2002).
To further assess the validity ofhousehold reported pediatricasthma, the study reported on hereexpands Roberts’ analysis in threeways. One, the current study ana-lyzes MEPS data that cover an en-tire calendar year. In contrast, Rob-erts’ study relied on MEPS data thatcovered only the first 5 to 6 monthsof 1996. Prescription data thatcover at most 6 months are likelyto underestimate how many chil-dren with asthma have an “asthmamedication” filled, because chil-dren whose asthma is well con-trolled may not need an “asthmamedication” filled during a6-month period. Thus, becauseRoberts (2003) restricted prescrip-tion data to no more than 6months, in his study children withasthma may be counted as nothaving a prescription filled, eventhough they do when a longer pe-riod is considered. Because mostasthma medications have a 1-yearexpiration date printed on them, itis reasonable to expect that an“asthma medication” is filled annu-ally when a child has asthma; thus,the current study analyzed datafrom an entire calendar year.
Two, the current study exam-ines in detail whether some MKAwere correct in not reporting anasthma diagnosis even thoughtheir child had an “asthma medica-tion” filled; this is possible if pro-viders prescribed “asthma medica-tions” for medical conditions otherthan asthma. Prescribing asthmamedications for nonasthma medi-cal conditions is likely and reason-able if symptoms common toasthma (e.g., wheeze and chesttightness) are present when a childis brought in for an evaluation, be-cause empiric treatment is oftenrecommended (Behrman, Klieg-man, & Arvin, 1996). In addition,some medications that are now
recommended exclusively for375November/December 2006

asthma were considered reason-able for other conditions in 1996,at the time the data analyzed byRoberts (2003) were collected. Forinstance, use of a bronchodilatorwas prescribed for bronchitis or re-current bronchitis then but is nolonger routinely recommended forthese conditions (National AsthmaEducation and Prevention Pro-gram, 1991; NHLBI, 1997;2003).Moreover, the 1991 ExecutiveSummary of the NHLBI NationalAsthma Education and PreventionProgram Diagnosis and Manage-ment of Asthma algorithm in useduring 1996 advocated using a trialof a bronchodilator prior to the di-agnosis of asthma to help make thedistinction between asthma andother possible conditions (Na-tional Asthma Education and Pre-vention Program). Likewise, al-though inhaled corticosteroids arecurrently the mainstay of manag-ing chronic pediatric asthma, theytoo were used for other conditionswhere inflammation of the airwayswas suspected (Hay, Groothuis,Hayward, & Levin, 1997). In addi-tion, some drugs (e.g., Flunisolide)come in both a nasal (Nasalide)and inhaled form (Aerobid), mak-ing their use for allergic rhinitisplausible, if the specific route ofadministration is unknown orlisted as “inhaled,” because “in-haled” may mean oral or nasal in-halation. Thus, some MKA mayhave been correct in not reportingasthma for their child, even thoughthey obtained for their child med-ications that are commonly associ-ated with a diagnosis of asthma.
Three, the current study furtherextends Roberts’ (2003) assess-ment of the validity of householdreports of pediatric asthma by ex-amining whether sociodemo-graphic differences exist betweenchildren whose MKA did or did notreport either asthma or a plausiblealternative medical conditionamong children who obtained
“asthma medications.”376 Volume 20 • Number 6
METHODStudy Population and Data
The analysis is based on datafrom the Medical ExpenditurePanel Survey, a survey of the civil-ian population living in U.S. com-munities. MEPS is designed to pro-vide person- and household-levelinformation on health care use,health care expenditures, sourcesof payment, and insurance cover-age for the U.S. civilian noninstitu-tionalized population. MEPS is co-sponsored by the AHRQ and theNational Center for Health Statis-tics (AHRQ, n.d.).
MEPS conducts three separatebut related surveys: the HouseholdComponent (HC), the Medical Pro-vider Component (MPC), and theInsurance Component. Data fromthe MEPS HC and MPC are used inthe current study. The samplingframe for the MEPS HC is drawnfrom households that respondedto the prior year’s NHIS (AHRQ,n.d.). The sample for the 1996MEPS Household Componentcomprised 10,500 households (Co-hen S. B., 1997), around one quar-ter of households responding tothe 1995 NHIS, including an over-sample of Hispanics and Blacks(Madans, 2002). The overall re-sponse rate for the 1996 MEPS HCis 70.2% (Madans, 2002). TheMEPS Medical Provider survey isused to supplement and validateinformation on medical care pro-vided in the HC. To this end, theMedical Provider survey is con-ducted with medical providers andpharmacies identified by respon-dents to the MEPS HouseholdComponent (AHRQ, n.d.). Thecurrent study uses data collectedfrom pharmacies with the MEPSMedical Provider survey.
The family member who identi-fied himself or herself as the onemost knowledgeable about familymedical care and who kept recordsabout family health care use andexpenses reported data for chil-dren 0 to 17 years of age. The sur-vey design specifies that each
survey respondent is to be inter-viewed five times to collect infor-mation for 2 consecutive calendaryears about the respondent,household members, and thehousehold. The interviews areconducted with computer-assistedpersonal interviewing (CAPI) tech-nology in the respondent’s home(Cohen J., 1997).
For the current study, child- andhousehold-level data records wereextracted from the MEPS HC andthe MEPS MPC after downloadingthe public use data sets from theofficial MEPS Web site (http://www.meps.ahrq.gov/). To be able tocompare the results from the currentstudy directly with those reported inRoberts (2003), data were extractedfrom the 1996 MEPS HC for all chil-dren 0 to 17 years of age for whomthere are data for the entire 1996calendar year: a total of 6789 differ-ent children. If a family had multiplechildren, data from all children wereincluded in the analysis.
The MEPS MPC includes phar-macy-provided records of filledprescriptions with up to threehousehold-reported medical con-dition codes (ICD-9-CM) per phar-macy record. For the current study,the pharmacy records were ex-tracted for all children in the sam-ple who were reported to have“asthma medications” filled, butwhose MKA did not report that thechild has asthma: 381 differentpharmacy records from 183 differ-ent children. Because the MEPSpublic use data sets do not includedirect identifiers, the study proto-col was determined to be exemptfrom Institutional Review Boardapproval by the Battelle Centersfor Public Health Research andEvaluation Institutional ReviewBoard.
MeasuresAsthma. The MEPS data in-
clude information about children’smedical conditions. The MEPS ob-tains this information as follows:When the MEPS interviews areconducted, respondents are asked
for each child: (a) whether thereJournal of Pediatric Health Care

are medical conditions that both-ered the child during the periodcovered by the interview; and (b)whether the child has medical con-ditions that resulted in missedschool days, in bed days, or inmedical events (e.g., health carevisit, prescription fill/refill) duringthe period covered by the inter-view. The MEPS interviewersrecord medical conditions re-ported by the respondents verba-tim. Professional coders subse-quently create ICD-9-CM medicalcondition and V codes from themedical conditions reported by therespondents for each child. Thus,the MEPS identifies children ashaving asthma when the MKA re-ports either that the child wasbothered by asthma and/or thatasthma was the reason for a bedday, a school absence, a prescrip-tion fill/refill, or a medical visitduring the time period covered bythe interview.
Prescribed Medications. TheMEPS respondents also are askedto provide the name of any pre-scribed medication they or theirfamily members had purchased orotherwise obtained during the pe-riod covered by the interview andthe name(s) of any health prob-lems for which the medication wasprescribed. “If the respondent withthe prescription gave written per-mission to release his or her phar-macy records, pharmacy providersidentified by the household werecontacted by mail for the phar-macy follow-back component.
Each establishment was in-formed of all persons participatingin the survey who had prescrip-tions filled at their place of busi-ness, and a computerized printoutof all prescriptions filled for eachperson was sought. For each med-ication listed, the following infor-mation was requested: date filled;national drug code (NDC); medi-cation name; strength of medicine(amount and unit); quantity (pack-age size/amount dispensed); totalcharge; and payments by source”
(AHRQ, 2001). As noted, for theJournal of Pediatric Health Care
current study, these data were ex-tracted for sample children fromthe MEPS MPC. If written permis-sion was not given to release phar-macy records, respondents werekept in the analysis sample, usingtheir personally provided data.
Asthma Medications. To beconsistent with the approach usedby Roberts (2003), the followingfilled prescriptions were consid-ered medications beneficial toasthma: long- and short-actingbronchodilators, mast cell stabiliz-ers, methylxanthines, leukotrienereceptor inhibitors, and inhaledcorticosteroids.
Sociodemographic Charac-teristics. Data on each child’srace/ethnicity, sex, age, maternaleducation level, household income,and whether the MEPS interviewwas conducted in English or in an-other language were extracted fromthe MEPS HC. The racial and ethniccategories are defined as non-His-panic Black, non-Hispanic White,Hispanic, and non-Hispanic “other.”The “other” category combinesAsian, Pacific Islander, Native Amer-ican or American Indian, and Es-kimo groups, because of the smallnumber of sample children withasthma medications in these racialgroups. The child’s age is repre-sented with the following four cate-gories: 2 years old or younger, be-tween 3 and 5 years, between 6 and12 years, and between 13 and 17years. Maternal education is repre-sented with three categories:whether the mother had at most 12years of education, between 13 and15 years of education, or 16 or moreyears of education.
The MEPS adjusts family incomelevels for family size and survey yearto create an index of total familyincome over the calendar year rela-tive to federal poverty thresholds.This index was used to group chil-dren into three income categories:below or near poverty (�125% fed-eral poverty level [FPL]), poor (125-199% FPL), and moderate to highincome level (�200% FPL).
MEPS interviews are conducted
in an alternate language by bilingualinterviewers, if the respondent doesnot have sufficient English languageproficiency to understand and re-spond to questions in English. Ameasure indicates whether the inter-view was conducted in a languageother than English. Nearly all re-spondents who were interviewed inan alternate language were inter-viewed in Spanish.
Statistical AnalysisThe MEPS sample design in-
cludes stratification, clustering,multiple stages of selection, anddisproportionate sampling to gen-erate national estimates of the U.S.civilian noninstitutionalized popu-lation. Given the complex sampledesign, MEPS recommends usingweights to obtain accurate esti-mates and appropriate standard er-rors from MEPS survey data (Mach-lin, Yu, & Zodet, 2005). For thecurrent study, weighted percent-ages were estimated of children re-ported to have: (a) asthma and (b)“asthma medications” filled. In ad-dition, for each child in the samplewho had an “asthma medication”prescription filled, but whose MKAdid not report that the child hasasthma (N � 183), each “asthmamedication” (N � 381) and its as-sociated ICD-9-CM codes were ex-amined. The purpose of this exam-ination was to see whether themedication was reasonable for thenonasthmatic medical conditionreported by the MKA. After thisexamination, weighted percent-ages were estimated of: (a) chil-dren with an MKA report of eitherasthma or a plausible alternativemedical condition; and (b) chil-dren without an MKA report ofasthma/plausible alternative medi-cal condition. Pearson chi-squarestatistics were used to examinewhether sociodemographic differ-ences exist between children whohave a report of asthma/plausiblealternative medical condition ver-sus children who do not have sucha report, among the children with
“asthma medications.” All esti-377November/December 2006
ondi
ast c recep
ondi
mates were derived with Stata sta-tistical software version 9 modulefor survey data (StataCorp, 2005).
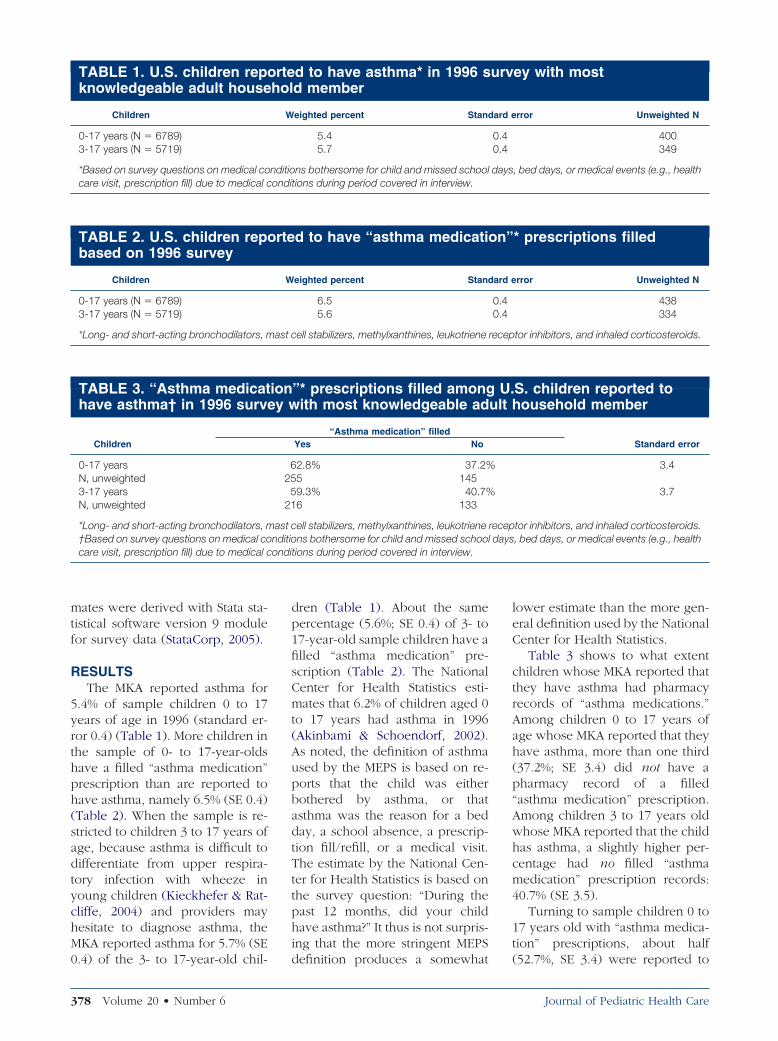
RESULTSThe MKA reported asthma for
5.4% of sample children 0 to 17years of age in 1996 (standard er-ror 0.4) (Table 1). More children inthe sample of 0- to 17-year-oldshave a filled “asthma medication”prescription than are reported tohave asthma, namely 6.5% (SE 0.4)(Table 2). When the sample is re-stricted to children 3 to 17 years ofage, because asthma is difficult todifferentiate from upper respira-tory infection with wheeze inyoung children (Kieckhefer & Rat-cliffe, 2004) and providers mayhesitate to diagnose asthma, theMKA reported asthma for 5.7% (SE
TABLE 1. U.S. children repoknowledgeable adult house
Children
0-17 years (N � 6789)3-17 years (N � 5719)
*Based on survey questions on medical cocare visit, prescription fill) due to medical c
TABLE 2. U.S. children repobased on 1996 survey
Children
0-17 years (N � 6789)3-17 years (N � 5719)
*Long- and short-acting bronchodilators, m
TABLE 3. “Asthma medicathave asthma† in 1996 surve
Children
0-17 yearsN, unweighted3-17 yearsN, unweighted
*Long- and short-acting bronchodilators, m†Based on survey questions on medical cocare visit, prescription fill) due to medical c
0.4) of the 3- to 17-year-old chil-
378 Volume 20 • Number 6
dren (Table 1). About the samepercentage (5.6%; SE 0.4) of 3- to17-year-old sample children have afilled “asthma medication” pre-scription (Table 2). The NationalCenter for Health Statistics esti-mates that 6.2% of children aged 0to 17 years had asthma in 1996(Akinbami & Schoendorf, 2002).As noted, the definition of asthmaused by the MEPS is based on re-ports that the child was eitherbothered by asthma, or thatasthma was the reason for a bedday, a school absence, a prescrip-tion fill/refill, or a medical visit.The estimate by the National Cen-ter for Health Statistics is based onthe survey question: “During thepast 12 months, did your childhave asthma?” It thus is not surpris-ing that the more stringent MEPS
d to have asthma* in 1996 sd member
eighted percent Stand
5.45.7
ns bothersome for child and missed schooltions during period covered in interview.
d to have “asthma medicati
eighted percent Stand
6.55.6
ell stabilizers, methylxanthines, leukotriene
”* prescriptions filled amongith most knowledgeable ad
“Asthma medication” filledYes No
2.8% 37.2%5 1459.3% 40.7%6 133
ell stabilizers, methylxanthines, leukotrienens bothersome for child and missed schoo
tions during period covered in interview.
definition produces a somewhat
lower estimate than the more gen-eral definition used by the NationalCenter for Health Statistics.
Table 3 shows to what extentchildren whose MKA reported thatthey have asthma had pharmacyrecords of “asthma medications.”Among children 0 to 17 years ofage whose MKA reported that theyhave asthma, more than one third(37.2%; SE 3.4) did not have apharmacy record of a filled“asthma medication” prescription.Among children 3 to 17 years oldwhose MKA reported that the childhas asthma, a slightly higher per-centage had no filled “asthmamedication” prescription records:40.7% (SE 3.5).
Turning to sample children 0 to17 years old with “asthma medica-tion” prescriptions, about half
ey with most
rror Unweighted N
400349
, bed days, or medical events (e.g., health
* prescriptions filled
rror Unweighted N
438334
tor inhibitors, and inhaled corticosteroids.
S. children reported toousehold member
Standard error
3.4
3.7
tor inhibitors, and inhaled corticosteroids., bed days, or medical events (e.g., health
rte urvhol
W ard e
0.40.4
nditio days
rte on”
W ard e
0.40.4
ion U.y w ult h
6255
21
ast c recepnditio l days
(52.7%, SE 3.4) were reported to
Journal of Pediatric Health Care

mast recep
have asthma by their MKA (Table4). The percentage increases to60.4% (SE 3.7) among the 3- to17-year-old sample children with“asthma prescriptions.” Taken atface value, these figures, like Rob-erts’ (2003) study, would suggestthat a considerable number of chil-dren with asthma are not reportedto have the condition when theMKA is interviewed in a survey. Toexamine whether this is indeed thecase, Table 5 lists the names of all“asthma medications” for whichprescriptions were filled for chil-dren 0 to 17 years old and whoseMKA did not report that the childhas asthma. Next to each “asthmamedication” is a list of the ICD-9-CM codes for which the medica-tion was prescribed according tothe MKA. For nonhighlighted med-ical conditions we were able tocreate a scenario where the child’spresenting symptoms could haveincluded those for which a pro-vider might have attempted acourse of the listed “asthma medi-cation” (plausible alternative med-ical condition). Medical conditionsare highlighted grey if the corre-
TABLE 4. Children reportedadult household member amprescriptions
Children
0-17 yearsN, unweighted3-17 yearsN, unweighted
*Based on survey questions on medical cocare visit, prescription fill) due to medical c†Long- and short-acting bronchodilators,
It is crucial to know wwith parents provid
information regardinbeen diagnose
sponding medication cannot rea-
Journal of Pediatric Health Care
sonably have been expected tomanage the medical condition un-der circumstances we know of,given medical practice in 1996(less plausible alternative medicalcondition). Based on the classifica-tion of medical conditions intoplausible and less plausible condi-tions, the MKA reported a plausi-ble alternative medical conditionfor 61.2% (SE 4.4) of children 0 to17 years old with a filled “asthmamedication” prescription but noMKA report of asthma (figures notpresented in tables). Thus, forthese children, it appears that theMKA was correct to not report anasthma diagnosis. For an addi-tional 9.0% (SE 3.5) of children 0 to17 years old, ICD-9-CM informa-tion was missing for the filled“asthma medications.” Only the re-maining 29.7% (SE 3.9) of children0 to 17 years old had medical con-ditions for which the prescribed“asthma medications” would notbe expected to have desirable ther-apeutic effects.
When the sample is restricted tochildren 3 to 17 years old withfilled “asthma medication” pre-
have asthma* in 1996 surveg U.S. children with filled “a
Asthma reportedYes No
2.7% 47.3%5 1830.4% 39.6%6 118
ns bothersome for child and missed schooltions during period covered in interview.cell stabilizers, methylxanthines, leukotriene
her surveys conductedvalid and reliablewhether a child haswith asthma.
scriptions but no MKA-reported
asthma, 63.1% (SE 4.8) had medi-cal conditions other than asthmafor which the “asthma medica-tions” might reasonably have beenprescribed. Again, it appears thatfor these children the MKA wascorrect to not report that the childhas asthma. For an additional 4.3%(SE 0.2) of children 3 to 17 yearsold, ICD-9-CM information wasmissing. For the remaining 32.6%(SE 4.6) of these older children, theICD-9-CM codes represent medicalconditions for which the “asthmamedications” are unlikely to havehad desirable therapeutic effects.
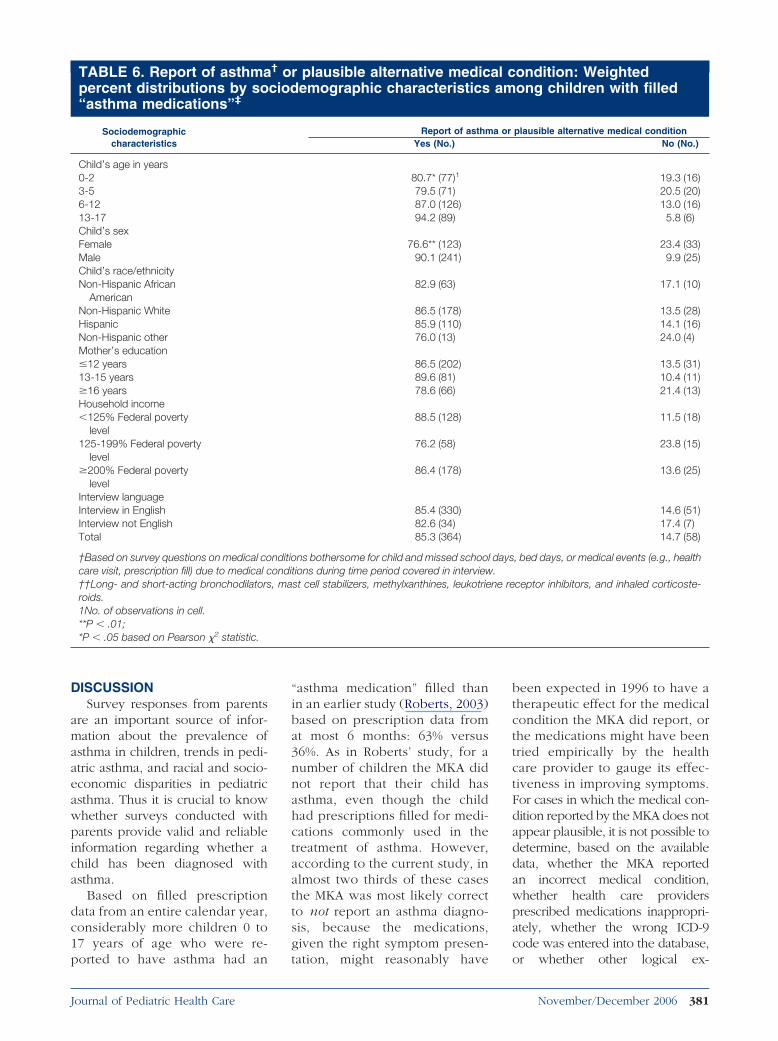
Table 6 provides additional in-formation about the children forwhom “asthma medications” werefilled. Children younger than 6years and girls are more likely tohave no MKA report of asthma/plausible alternative medical con-dition than are older children andboys. Specifically, the MKA did notreport asthma/plausible alternativemedical condition for 9.9% of boysand for 23.4% of girls. Further, theMKA did not report asthma/plausi-ble alternative diagnosis for about20% of children between 0 and 5years old, compared with 13% ofchildren 6 to 12 years, and 5.8% ofchildren 13 to 17 years of age. Dif-ferences in reporting asthma/plau-sible alternative medical conditionwere not statistically significantlydifferent by child race/ethnicity,household income, and educationlevel and English language profi-
ith most knowledgeablema medicationӠ
Standard error
3.4
3.7
, bed days, or medical events (e.g., health
tor inhibitors, and inhaled corticosteroids.
to y won sth
5256
21
nditio daysondi
hetegd
ciency of the MKA.
379November/December 2006

TABLE 5. Medications commonly prescribed for asthma and additional medicalconditions for which prescriptions were filled for U.S. children in 1996 according tomost knowledgeable adult household member
Generic medication name(brand name) Plausible alternative medical conditions Less plausible alternative medical conditions
Albuterol sulfate (Albuterol,Proventil, Ventolin)
079 – Viral and chlamydial infection inconditions classified elsewhere and ofunspecified site
465 – Acute upper respiratory infections ofmultiple or unspecified sites
466 – Acute bronchitis and bronchiolitis478 – Other diseases of upper respiratory
tract486 – Pneumonia, organism unspecified487 – Influenza490 – Bronchitis, not specified as acute or
chronic518 – Other diseases of lung519 – Other diseases of respiratory system786 – Symptoms involving respiratory
system and other chest symptoms
008 –Intestinal infections due to other organisms135 – Sarcoidosis136 – Other and unspecified infectious and parasitic
diseases382 – Suppurative and unspecified otitis media386 – Vertiginous syndromes and other disorders of
vestibular system429 – Ill-defined descriptions and complications of
heart disease460 – Acute nasopharyngitis464 – Acute laryngitis and tracheitis473 – Chronic sinusitis477 – Allergic rhinitis514 – Pulmonary congestion and hypostasis747 – Other congenital anomalies of circulatory
system780 – General symptoms
BeclomethasoneDipropionate, nasal orinhaled (Beclovent,Vanceril)
473 – Chronic sinusitis477 – Allergic rhinitis490 – Bronchitis, not specified as acute or
chronic
519 – Other diseases of respiratory system
Cromolyn sodium, nasal orinhaled (Intal)
473 – Chronic sinusitis477 – Allergic rhinitis482 – Other bacterial pneumonia486 – Pneumonia, organism unspecified490 – Bronchitis, not specified as acute or
chronic491 – Chronic bronchitis518 – Other diseases of lung786 – Symptoms involving respiratory
system and other chest symptoms
583 – Nephritis and nephropathy, not specified asacute, chronic
610 – Benign mammary dysplasias719 – Other and unspecified disorders of joint728 – Disorders of muscle, ligament, and fascia847 – Sprains and strains of other and unspecified
parts of back
Diprophylline, Guaifenesin(Dilor-G)
460 – Acute nasopharyngitis987 – Toxic effects of other gases, fumes, or
vaporsFlunisolide, nasal or inhaled
(Aerobid, Nasalide)477 – Allergic rhinitis
Guaifenesin,Pseudoephedrine(Hydrophed Exp)
388 – Other disorders of ear490 – Bronchitis, not specified as acute or
chronicIpratropium bromide
(Atrovent)460 –Acute nasopharyngitis466 – Acute bronchitis and bronchiolitis482 – Other bacterial pneumonia
Metaproterenol sulfate(Alupent, Metaproterenol)
490 – Bronchitis, not specified as acute orchronic
786 – Symptoms involving respiratorysystem and other chest symptoms
Pirbuterol acetate (Maxair) 518 – Other diseases of lungSodium chloride (Broncho
Saline*)490 – Bronchitis, not specified as acute orchronic
Triamcinolone acetonide,nasal or inhaled(Nasacort, Azmacort)
477 – Allergic rhinitis490 – Bronchitis, not specified as acute or
chronic987 – Toxic effects of other gases, fumes, or
vapors
787 – Symptoms involving digestive system
*Used as administration medium.
380 Volume 20 • Number 6 Journal of Pediatric Health Care
DISCUSSIONSurvey responses from parents
are an important source of infor-mation about the prevalence ofasthma in children, trends in pedi-atric asthma, and racial and socio-economic disparities in pediatricasthma. Thus it is crucial to knowwhether surveys conducted withparents provide valid and reliableinformation regarding whether achild has been diagnosed withasthma.
Based on filled prescriptiondata from an entire calendar year,considerably more children 0 to17 years of age who were re-
TABLE 6. Report of asthmapercent distributions by so“asthma medications”‡
Sociodemographiccharacteristics
Child’s age in years0-23-56-1213-17Child’s sexFemaleMaleChild’s race/ethnicityNon-Hispanic African
AmericanNon-Hispanic WhiteHispanicNon-Hispanic otherMother’s education�12 years13-15 years�16 yearsHousehold income�125% Federal poverty
level125-199% Federal poverty
level�200% Federal poverty
levelInterview languageInterview in EnglishInterview not EnglishTotal
†Based on survey questions on medical cocare visit, prescription fill) due to medical c††Long- and short-acting bronchodilatorsroids.1No. of observations in cell.**P � .01;*P � .05 based on Pearson �2 statistic.
ported to have asthma had an
Journal of Pediatric Health Care
“asthma medication” filled thanin an earlier study (Roberts, 2003)based on prescription data fromat most 6 months: 63% versus36%. As in Roberts’ study, for anumber of children the MKA didnot report that their child hasasthma, even though the childhad prescriptions filled for medi-cations commonly used in thetreatment of asthma. However,according to the current study, inalmost two thirds of these casesthe MKA was most likely correctto not report an asthma diagno-sis, because the medications,given the right symptom presen-
r plausible alternative medicemographic characteristics
Report of asthmYes (No.)
80.7* (77)1
79.5 (71)87.0 (126)94.2 (89)
76.6** (123)90.1 (241)
82.9 (63)
86.5 (178)85.9 (110)76.0 (13)
86.5 (202)89.6 (81)78.6 (66)
88.5 (128)
76.2 (58)
86.4 (178)
85.4 (330)82.6 (34)85.3 (364)
ns bothersome for child and missed schootions during time period covered in interviewst cell stabilizers, methylxanthines, leukotrie
tation, might reasonably have
been expected in 1996 to have atherapeutic effect for the medicalcondition the MKA did report, orthe medications might have beentried empirically by the healthcare provider to gauge its effec-tiveness in improving symptoms.For cases in which the medical con-dition reported by the MKA does notappear plausible, it is not possible todetermine, based on the availabledata, whether the MKA reportedan incorrect medical condition,whether health care providersprescribed medications inappropri-ately, whether the wrong ICD-9code was entered into the database,
ondition: Weightedong children with filled
plausible alternative medical conditionNo (No.)
19.3 (16)20.5 (20)13.0 (16)5.8 (6)
23.4 (33)9.9 (25)
17.1 (10)
13.5 (28)14.1 (16)24.0 (4)
13.5 (31)10.4 (11)21.4 (13)
11.5 (18)
23.8 (15)
13.6 (25)
14.6 (51)17.4 (7)14.7 (58)
, bed days, or medical events (e.g., health
ceptor inhibitors, and inhaled corticoste-
† o al cciod am
a or
nditio l daysondi ., ma ne re
or whether other logical ex-
381November/December 2006

planations would explain thediscrepancy.
Because there may be less cer-tainty about a child’s asthma diag-nosis in an intermittent, chroniccondition like asthma when chil-dren are young, it is reasonablethat the current study finds moreuncertainty in the MKA report ofeither asthma or a plausible alter-native medical condition for chil-dren who are younger than 6years. However, there is no obvi-ous explanation for the findingthat girls with an “asthma medica-tion” are less likely than boys withsuch a medication to have an MKAreport of either asthma or a plau-sible alternative medical condition.
It is important to keep in mindthat the sociodemographic differ-ences reported here are based on arelatively small number of obser-vations. It is thus important to rep-licate the analysis reported in thisarticle with a larger sample of chil-dren with medications beneficialto asthma before definite conclu-sions can be drawn about the con-fidence in the report of pediatricasthma based on surveys withadult household members.
CONCLUSIONSIn summary, it seems to us that
there is insufficient evidence toconclude that “surveys of parentalreports of asthma overlook manychildren with active disease” (Rob-erts, 2003, p.449). The intermittentnature of asthma symptoms re-quires a sufficiently long time win-dow for data review. Survey ques-tions need to be more focused anddetailed to include the prescriber’s
Providers must make cfor their treatment c
diagnosis is in questioor the treatm
rationale for specific conditions to
382 Volume 20 • Number 6
get the breadth of informationneeded to make judgments, butthat does not in and of itself meanthat the household member mostknowledgeable about householdhealth care does not accurately re-port their children’s medicalconditions.
Although the purpose of thisstudy was to evaluate the validityof MKA reports of asthma in survey
data, clinical implications may bedrawn. First, making sure provid-ers keep up with the latest recom-mended treatments for asthma iscritical. The 1997 and 2002 NHLBItreatment Guides (NHLBI, 1997;2003) have each refined care, andfuture Guides will do the same.Providers must keep informed toprovide best-practice, evidence-based, appropriate care in linewith the emerging understandingof asthma’s underlying pathophys-iology rather than rely on outdatedtreatments. Second, the resultsfrom the current study emphasizethe importance of provider-parentcommunication. A recent studyfound that providers and familiesdiffer in how they report symp-toms of asthma (Yoos et al., 2005).
r the specific reasonsices, even when thethe treatment empiric,t “off label.”
At this point we conevidence exists to inferreports of asthma over
active
These communication differences
may extend to communicationabout diagnosis and treatment aswell. Thus, providers must makeclear the specific reasons for theirtreatment choices, even when thediagnosis is in question, the treat-ment empiric, or the treatment “offlabel.” This is the foundation fortrue informed consent for care.Third, families are considered themost central member of theirchild’s health care team (Instituteof Medicine, 2001). They cannoteffectively take on this role un-less they are given accurate andunderstandable information fromthe child’s provider. In an envi-ronment where the family maychange providers multiple timesin the child’s life and the transferof medical records is less thanideal, a correctly informed parent
is critical so the next provider re-ceives accurate information fromthe parent and care can besmoothly transitioned withoutunnecessary discontinuities andcostly repetitive diagnostic work.
Whether post-1996 improve-ments in provider education, com-munication skills, or acceptance ofthe National Asthma TreatmentGuidelines would show greater ac-curacy in MKA reports of child-hood asthma remains to be deter-mined. At this point we concludethat insufficient evidence exists toinfer that surveys of parental re-ports of asthma overlook manychildren with active disease.
REFERENCESAdams, P. F., Hendershot, G. E., & Marano,
M. A. (1999). Current estimates from
de that insufficientat surveys of parentalk many children withsease.
leahon,en
cluth
loodi
the National Health Interview Survey,
Journal of Pediatric Health Care
1996 (Vital and Health Statistics, Series10: Data from the National HealthInterview Survey, No. 200) (DHHSpublication no. (PHS) 99-1528) (GPOno 017-01471-8). Hyattsville, MD:National Center for Health Statistics,1999.
Agency for Healthcare Research and Qual-ity. (n.d.). Medical Expenditure PanelSurvey (MEPS). Retrieved February 8,2006, from http://www.ahrq.gov/data/mepsweb.htm
Agency for Healthcare Research and Qual-ity. (2001). MEPS HC-010A: 1996 Pre-scribed Medicines. Retrieved March 3,2004, from http://www.meps.ahrq.go,v/Pubdoc/HC010a/HC10ADoc.htm
Akinbami, L. J., & Schoendorf, K. C. (2002).Trends in childhood asthma preva-lence, health care utilization, and mor-tality. Pediatrics, 110(2 Pt. 1), 315-322.
Akinbami, L. J., Schoendorf, K. C., &Parker, J. (2003). US childhood asthmaprevalence estimates: The impact ofthe 1997 National Health Interview Sur-vey redesign. American Journal of Epi-demiology, 158, 99-104.
American Lung Association. (2004). Asthmaand children fact sheet. Retrieved Jan-uary 14, 2006, from http://www.lungusa.org/site/apps/s/content.asp?c�dvLUK9O0E&b�34706&ct�67462
Behrman, R., Kliegman, R., & Arvin, A.(1996). Nelson textbook of pediatrics.Philadelphia: W.B. Saunders.
Cohen, J. (1997). Design and methods ofthe Medical Expenditure Panel SurveyHousehold Component (MEPS Meth-odology Report No. 1. AHCPR publica-tion No. 97-0026). Rockville, MD:Agency for Health Care Policy and Re-search.
Cohen, S. B. (1997). Sample design of the
1996 Medical Expenditure Panel Sur-Journal of Pediatric Health Care
vey Household Component (MEPSMethodology Report No. 2. AHCPRpublication No. 97-0027). Rockville,MD: Agency for Health Care Policy andResearch.
Council of State and Territorial Epidemiolo-gists. Position statement 1998-EH/CD1. Retrieved April 12, 2005, fromhttp://www.cste.org/ps/1998/1998-eh-cd-01.htm
Hay, W., Groothuis, J., Hayward, A., &Levin, M. (1997). Current pediatric di-agnosis and treatment (13th ed.).Stamford, CT: Appleton & Lang.
Institute of Medicine, Committee on Qualityof Health Care in America. (2001).Crossing the quality chasm: A newhealth system for the 21st century.Washington, DC: National AcademyPress.
Kieckhefer, G., & Ratcliffe, M. (2004).Asthma. In P. Jackson & J. Vessey(Eds.), Primary care of children withchronic conditions (4th ed.) (pp. 174-198). St. Louis, MO: Mosby.
Lanphear, B. P., & Gergen, P. J. (2003).Invited commentary: Asthma surveil-lance in children. American Journal ofEpidemiology, 158, 105-107.
Machlin, S., Yu, W., & Zodet, M. (2005).Computing standard errors for MEPSestimates. Agency for Healthcare Re-search and Quality, Rockville, MD. Re-trieved January 28, 2006, fromhttp://www.meps.ahrq.gov/factsheets/FS_StandardErrors.htm
Madans, J. (2002). Achieving efficiencythrough survey integration (ICIS August25-28, 2002 Papers). Retrieved Febru-ary 8, 2006, from http://www.icis.dk/ICIS_papers/E_3_3.pdf
National Asthma Education and PreventionProgram. (1991). Expert panel report:
Guidelines for the diagnosis and man-agement of asthma (Publication No91-3642). Bethesda, MD: NationalInstitutes of Health.
National Heart, Lung, and Blood Institute.(1997). National Asthma Education andPrevention Program Expert Panel Re-port 2: Guidelines for the diagnosis andmanagement of asthma (Publication No97-4051A). Bethesda, MD: U.S. De-partment of Health and Human Ser-vices.
National Heart, Lung, and Blood Institute.(2003). National Asthma Education andPrevention Program Expert Panel Re-port: Guidelines for the diagnosis andmanagement of asthma—update onselected topics 2002 (Publication No02-5074). Bethesda, MD: U.S. Depart-ment of Health and Human Services.
Roberts, E. M. (2003). Does your child haveasthma? Parent reports and medica-tion use for pediatric asthma. Archivesof Pediatrics & Adolescent Medicine,157, 449-455.
Smith, D. H., Malone, D. C., Lawson,K. A., Okamoto, L. J., Battista, C., &Saunders, W. B. (1997). A nationalestimate of the economic costs ofasthma. American Journal of Respira-tory and Critical Care Medicine, 156,787-793.
StataCorp. (2005). Stata Statistical Soft-ware: Release 9.0. College Station, TX:Stata Corporation.
Yoos, H. L., Kitzman, H., McMullen, A.,Sidora-Arcoleo, K., & Anson, E. (2005).The language of breathlessness: Dofamilies and health care providersspeak the same language whendescribing asthma symptoms?,Journal of Pediatric Health Care, 19,
197-205.383November/December 2006