
Novel insights targeting inflammation in CVD: the LoDoCo 2 trial
34
Novel insights targeting inflammation in CVD: the LoDoCo 2 trial Jan Hein Cornel, MD, PhD Professor of Cardiology Alkmaar, The Netherlands Nijmegen, The Netherlands
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Novel insights targeting inflammation in CVD: the LoDoCo 2 trial

Novel insights targeting inflammation in CVD: the LoDoCo 2 trial
Jan Hein Cornel, MD, PhDProfessor of Cardiology
Alkmaar, The NetherlandsNijmegen, The Netherlands

Grant from ZonMw and Dutch heart foundation.
Disclosures

Further LDL-C lowering reduces CV-risk… Large residual burden …
7-year event ratesCV, cardiovascular; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarctionCannon, et al. N Engl J Med 2015;372:2387-97
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
30
20
Even
t Rat
e (%
)
10
40
06543
Time since randomization (years)
Residual CV-risk
210 7
HR 0.936p=0.016
Simva 34.7%2742 events
SimvastatinSimvastatin–ezetimibe
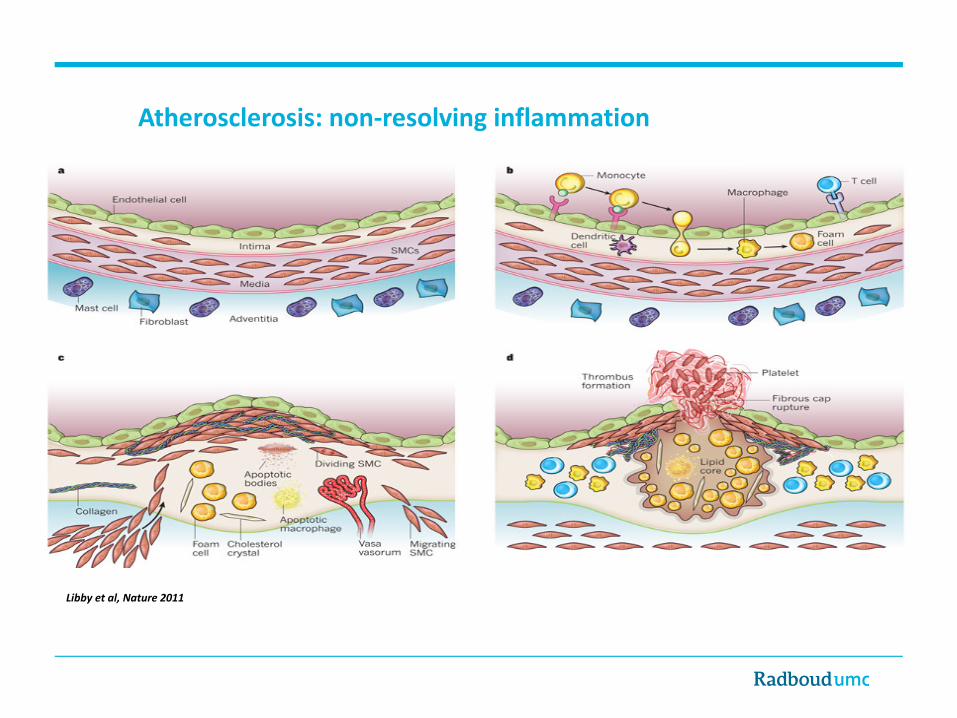
Atherosclerosis: non-resolving inflammation
Libby et al, Nature 2011
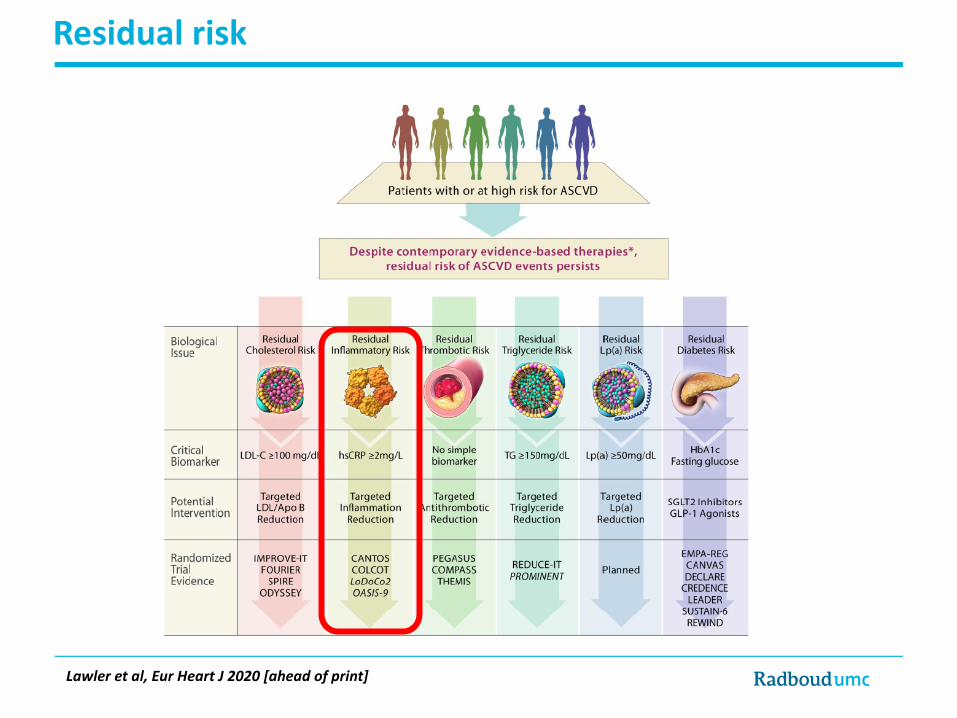
Residual risk
Lawler et al, Eur Heart J 2020 [ahead of print]

How common is residual inflammatory risk?
PROVE-IT
29%
13%
14%
44%
IMPROVE-IT
33%
14%14%
39%
Residual Inflammatory Risk
hsCRP > 2 mg/LLDLC < 70 mg/dL
Residual Cholesterol Risk
hsCRP < 2 mg/LLDLC > 70 mg/dL
Both
hsCRP > 2 mg/LLDLC > 70 mg/dL
Neither
hsCRP < 2 mg/LLDLC < 70 mg/dL
Ridker. Circulation Res 2017;120:617-9
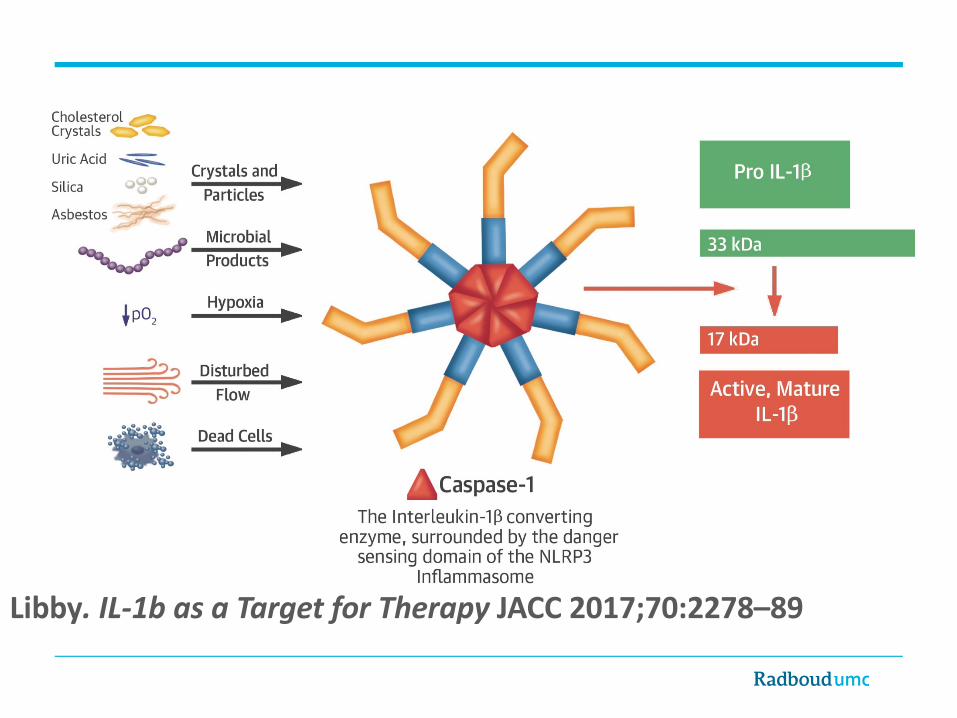
Libby. IL-1b as a Target for Therapy JACC 2017;70:2278–89

Ridker et al., EHJ 2019
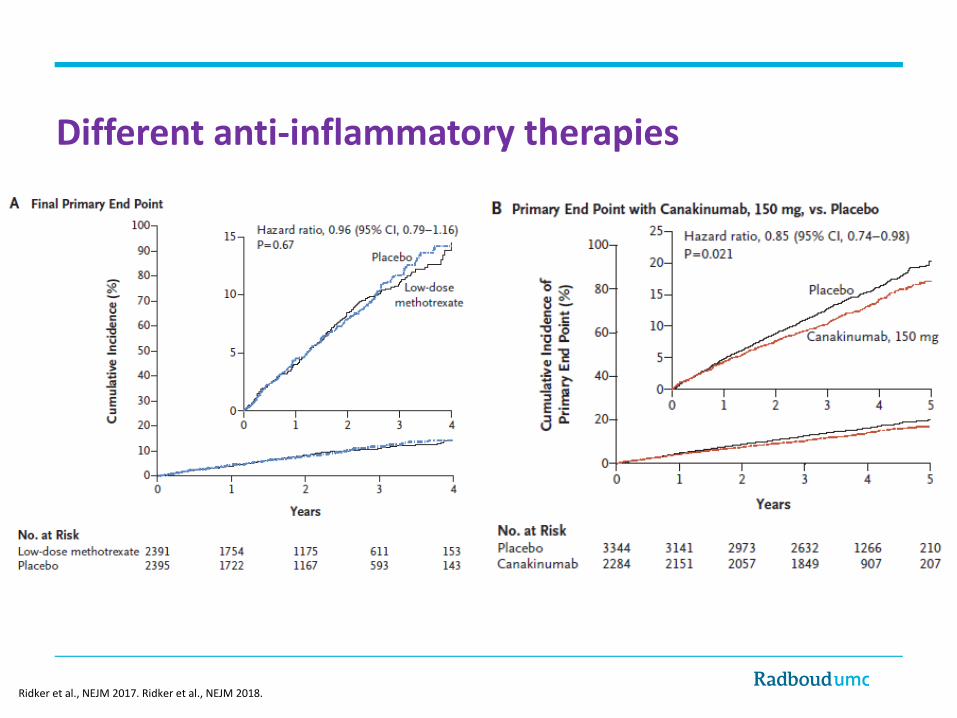
Different anti-inflammatory therapies
Ridker et al., NEJM 2017. Ridker et al., NEJM 2018.

The inflammatory process in atherosclerosis is primarily driven by the formation of cholesterol crystals (CCs) within atheroma
Atherosclerosis is a crystallopathy
Nidorf et.al. Viewing atherosclerosis through a crystal lens https://doi.org/10.1016/j.jacl.2020.07.003
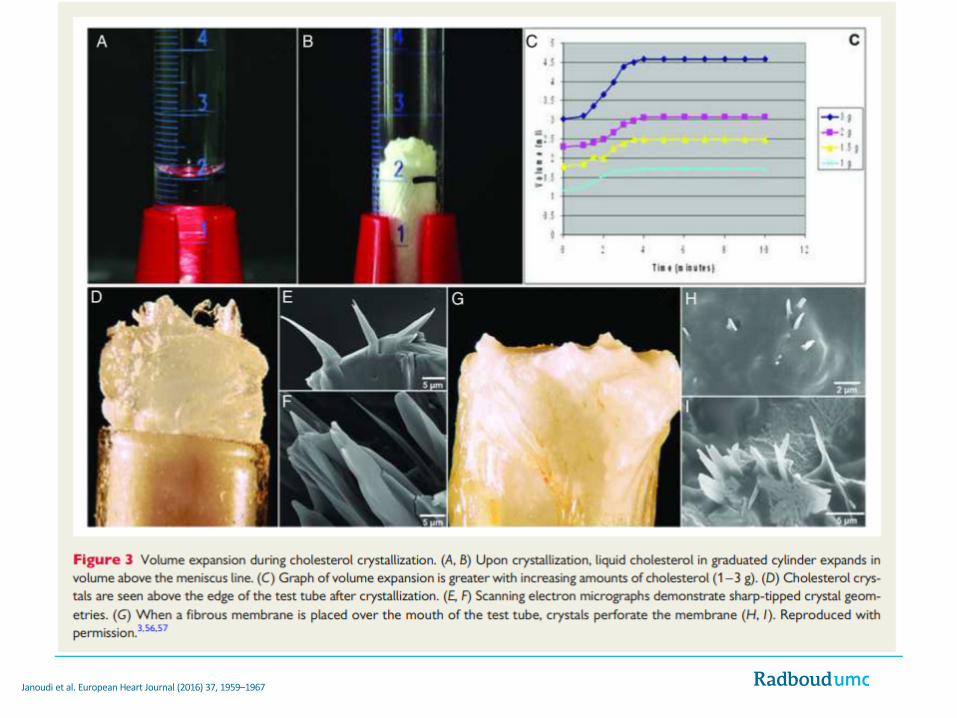
Janoudi et al. European Heart Journal (2016) 37, 1959–1967

Mulay et al. N Engl J Med 2016;374:2465-76.

Riksen & Netea, Mol Aspects Med 2020
Metabolic – Epigenetic crosstalk

The Low Dose Colchicine(LoDoCo) trials
Jan Hein Cornel
Dit project wordt mogelijk gemaakt door:

Herfsttijloos (Colchicum autumnale)
• used by the ancient Greeks and Egyptians• broad cellular effects that include inhibition of tubulin
polymerization
M1
M2
Core
CoreF
Ost
Macro CCs
Micro CCs
Circulating LeucocytesS
C3b
IL-1β Expression
CC ClearanceIL 10, TGFβ
EndothelialDisruption
EndothelialDisruptionS
1 2 653
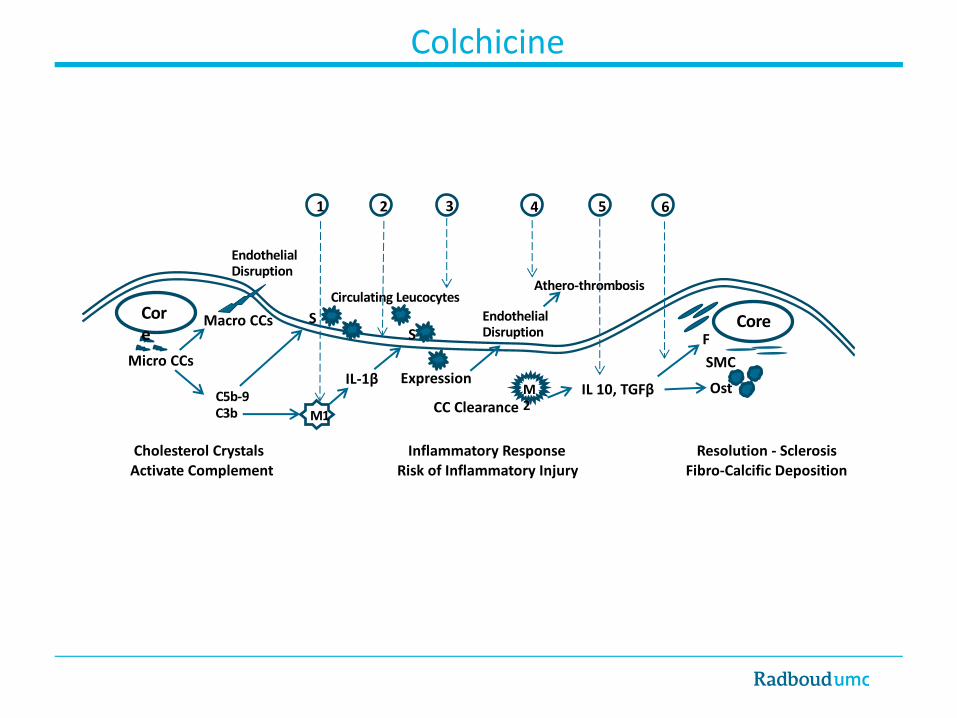
Cholesterol Crystals Activate Complement
Inflammatory ResponseRisk of Inflammatory Injury
Resolution - SclerosisFibro-Calcific Deposition
SMC
Athero-thrombosis
4
C5b-9
Colchicine

Proteomic analysis LoDoCo2 (run-in period)
• 176 patients post-ACS patients selected from LoDoCO2 study
• Serum drawn at baseline and after 30 days run-in; all patients treated with
colchicine 0.5mg daily, paired samples
• Olink proteomic analysis: Panels: CV-II and CV-III; 184 serum proteins
• High sensitive C-reactive protein available from previous analysis


Attenuation of inflammasome related proteins• hsCRP: 1.52 mg/l (IQR 0.66 – 3.43 mg/l) to 1.00 mg/l (IQR 0.37 – 2.28 mg/l, p <0.001)
• Reduction of IL-18 by -4.8%• NLRP3 inflammasome produced caspase-1 cleaves pro-IL-18 into IL-18
• Reduction of IL-1 receptor antagonist by -8.6%• Reflects reduced levels of IL-1β, caspase-1 cleaves pro-IL-1β into IL-1β
• Reduction of IL-6 by -9.7%• Production of IL-6 strongly induced by IL-1
• However: • Reduction of NF-κB essential modulator, activator of NF-κB, which is necessary for NLRP3
inflammasome activation -> more upstream attenuation?• Strongest attenuation in proteins not directly related to inflammasome• More important role for neutrophils?
Conclusions ProLoDoCo analysis
Treatment with colchicine in subjects with chronic CAD resulted in a significant reduction in thirty-seven serum proteins, underscoring a marked anti-inflammatory effect stretching
beyond the NLRP3 inflammasome pathway, and suggesting an important role of neutrophil inhibition.
The effect of colchicine on the measured circulating proteins is independent of baseline hsCRP levels and largely independent of change in hsCRP levels, which questions the ability of CRP
measurements to assess the efficacy of colchicine treatment.
Objective: To determine whether colchicine 0.5mg once daily prevents cardiovascular events in patients with chronic coronary disease.Design: Investigator-initiated, double-blind, placebo-controlled, event-driven trial.Enrolment: Began in Australia (GenesisCare) in August 2014. Expanded to The Netherlands, Dutch Network for Cardiovascular Research (WCN) in October 2016. Last enrolment: November 4, 2018.
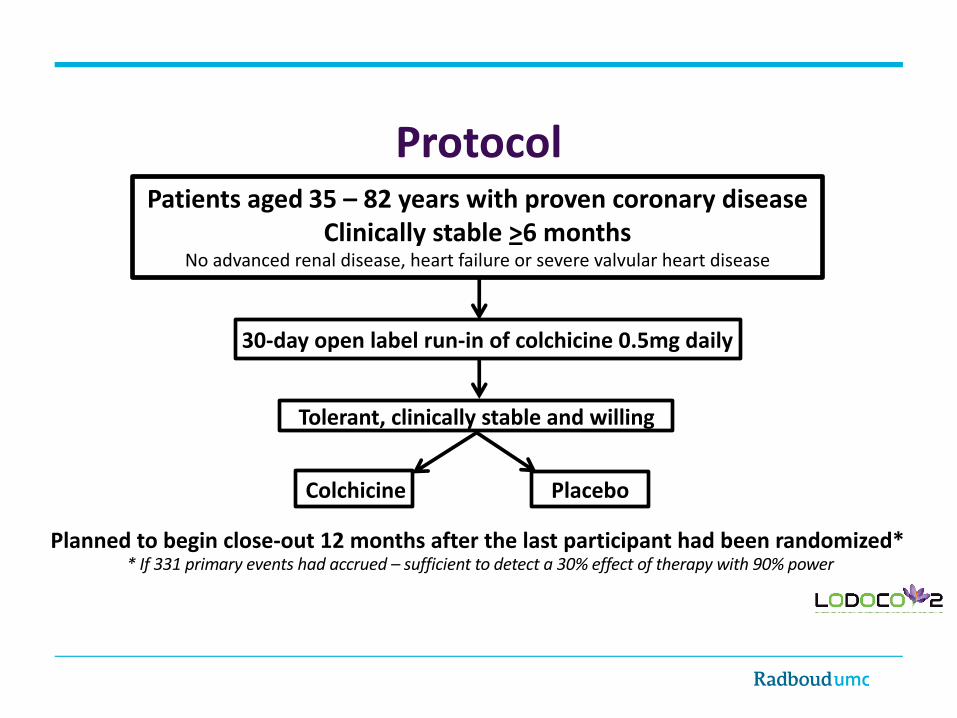
ProtocolPatients aged 35 – 82 years with proven coronary disease
Clinically stable >6 monthsNo advanced renal disease, heart failure or severe valvular heart disease
30-day open label run-in of colchicine 0.5mg daily
Colchicine
Tolerant, clinically stable and willing
Placebo
Planned to begin close-out 12 months after the last participant had been randomized** If 331 primary events had accrued – sufficient to detect a 30% effect of therapy with 90% power

Primary end pointThe composite of Cardiovascular death Myocardial infarction Ischemic stroke Ischemia-driven coronary revascularization

6528
5522
Enrolled91.3% Tolerated open label therapy
RandomizedFollowed for a median of 29 months (12-64 months)90.3% in each arm continued their trial medication
3.4% in each arm ceased due to perceived effects
Close-out Began on December 4, 2019; Ended February 17, 2020 99.9% Final, end point status known
55215521

Colchicine PlaceboN=2762
N=2760Age, years 65.8 +8.4 65.9 +8.7 Male 2305 (83.5) 2352 (85.9)
Risk Factors and HistoryCurrent Smoker 318 (11.5) 330 (12.0)Hypertension 1421 (51.4) 1387 (50.3)Diabetes 492 (17.8) 515 (18.7)Prior Revascularization 2419 (83.4) 2468 (84.0)Prior ACS 2323 (84.1) 2335 (84.6) - Last ACS >24m 1570 (67.6) 1609 (68.9)
Baseline characteristics
Colchicine PlaceboN= 2762 N= 2760
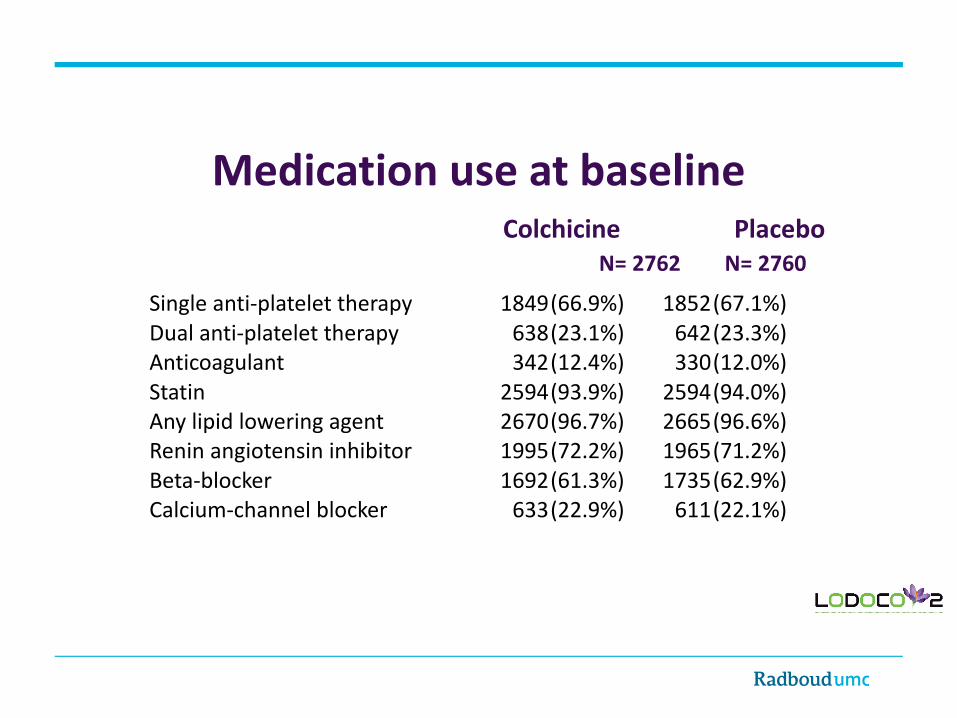
Medication use at baseline
Single anti-platelet therapy 1849(66.9%) 1852(67.1%)Dual anti-platelet therapy 638(23.1%) 642(23.3%)Anticoagulant 342(12.4%) 330(12.0%)Statin 2594(93.9%) 2594(94.0%)Any lipid lowering agent 2670(96.7%) 2665(96.6%)Renin angiotensin inhibitor 1995(72.2%) 1965(71.2%)Beta-blocker 1692(61.3%) 1735(62.9%)Calcium-channel blocker 633(22.9%) 611(22.1%)
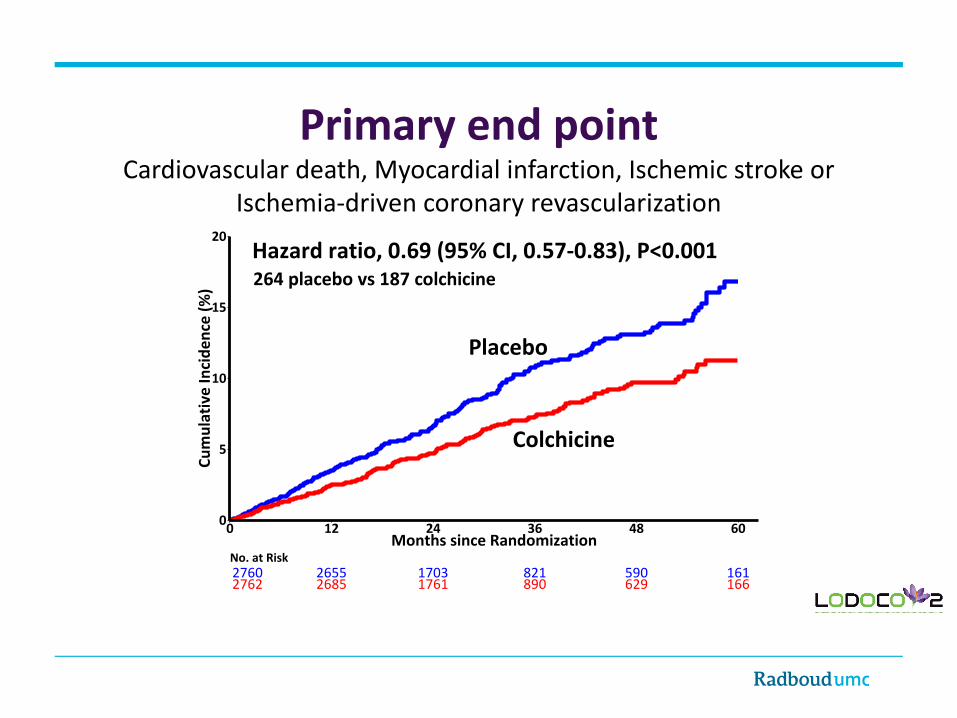
Hazard ratio, 0.69 (95% CI, 0.57-0.83), P<0.001
Placebo
Colchicine
0
5
10
15
20
0 12 24 36 48 60Months since Randomization
Cum
ulat
ive
Inci
denc
e (%
)
2760 2655 1703 821 590 1612762 2685 1761 890 629 166
No. at Risk
Primary end point Cardiovascular death, Myocardial infarction, Ischemic stroke or
Ischemia-driven coronary revascularization
264 placebo vs 187 colchicine

Hazard ratio, 0.72 (95% CI, 0.57-0.92), P=0.007
Placebo
Colchicine0
5
10
15
20
0 12 24 36 48 60Months since Randomization
Cum
ulat
ive
Inci
denc
e (%
)
2760 2694 1760 863 625 1742762 2714 1787 913 651 176
No. at Risk
Key secondary end point Cardiovascular death, Myocardial infarction or Ischemic stroke
157 placebo vs 115 colchicine

Ranked secondary end points Colchicine (N = 2762)
Placebo(N = 2760)
Hazard Ratio (95% CI) P Value
1. Cardiovascular death, Myocardial infarction,or Ischemic stroke
115(4.2) 157(5.7) 0.72(0.57-0.92) 0.007
2. Myocardial infarction or Ischemia-driven coronary revascularization
155(5.6) 224(8.1) 0.67 (0.55-0.83) <0.001
3. Cardiovascular death or Myocardial infarction
100(3.6) 138(5.0) 0.71(0.55-0.92) 0.010
4. Ischemia-driven coronary revascularization 135(4.9) 177(6.4) 0.75(0.60-0.94) 0.0125. Myocardial infarction 83(3.0) 116(4.2) 0.70 (0.53-0.93) 0.0146. Ischemic stroke 16(0.6) 24(0.9) 0.66(0.35-1.25) 0.1987. Death from any cause 73(2.6) 60(2.2) 1.21(0.86-1.71)8. Cardiovascular death 20(0.7) 25(0.9) 0.80(0.44-1.44)
Colchicine Placebo(N = 2762) (N = 2760)
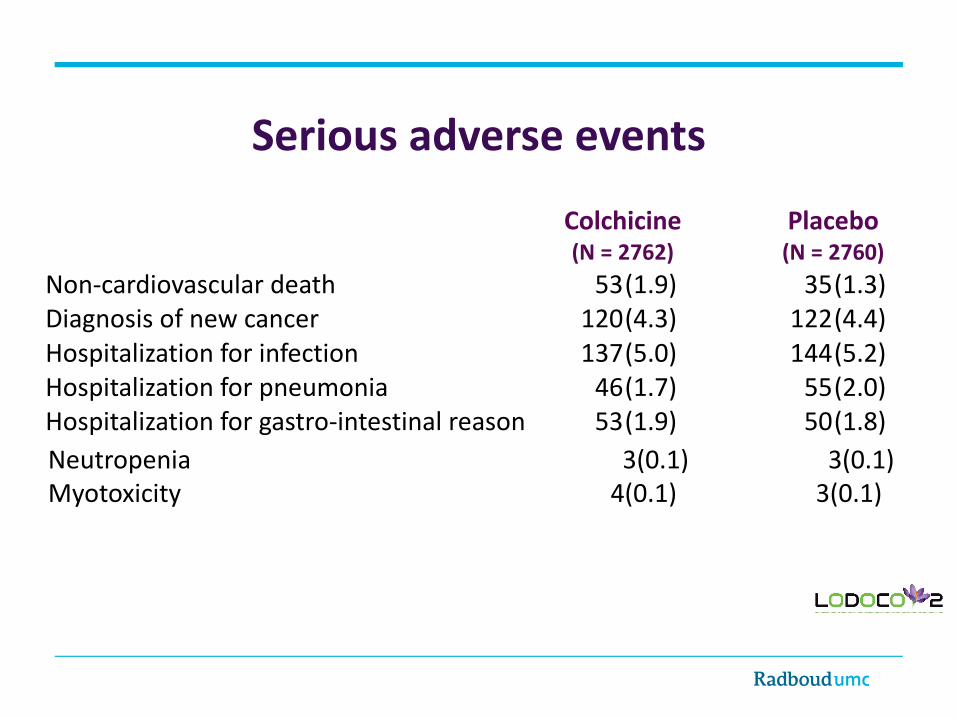
Non-cardiovascular death 53(1.9) 35(1.3)Diagnosis of new cancer 120(4.3) 122(4.4)Hospitalization for infection 137(5.0) 144(5.2)Hospitalization for pneumonia 46(1.7) 55(2.0)Hospitalization for gastro-intestinal reason 53(1.9) 50(1.8)
Serious adverse events
Neutropenia 3(0.1) 3(0.1)Myotoxicity 4(0.1) 3(0.1)
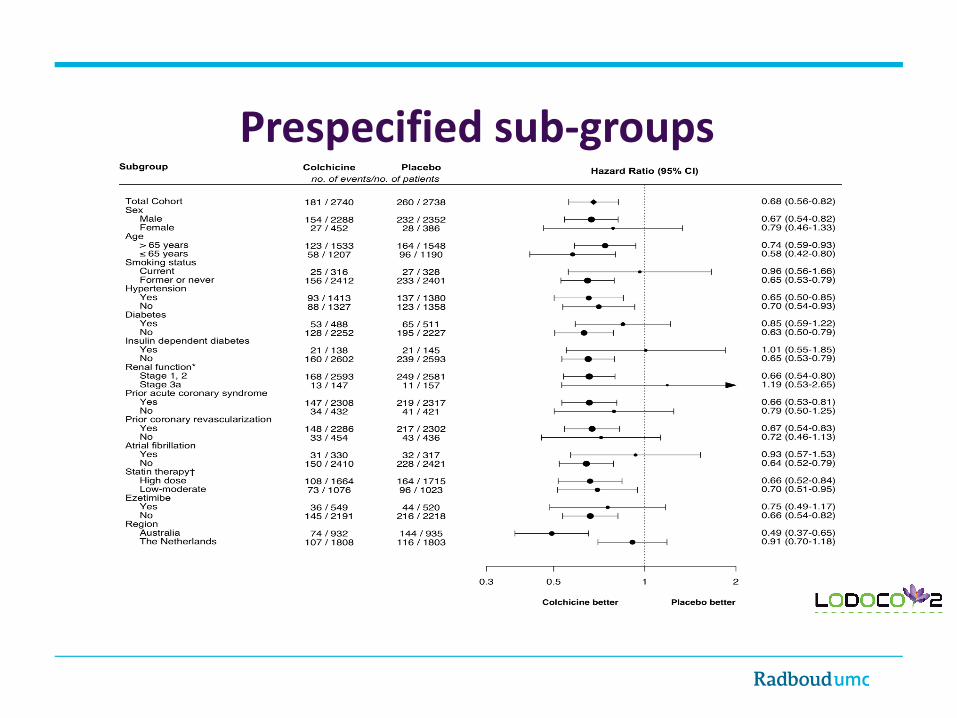
Prespecified sub-groups

SummaryIn patients with chronic coronary disease, low-dose colchicine Reduced the risk of; - The primary composite end point
Cardiovascular death, myocardial infarction, ischemic stroke or ischemia-driven coronary revascularization.
- Key secondary composite end pointsCardiovascular death, myocardial infarction or ischemic stroke.
- Individual secondary end pointsMyocardial infarction & Ischemia-driven coronary revascularization.… with broadly consistent effects across a range of clinical subgroups
Was well tolerated and appeared safeThe incidence of premature discontinuation & serious adverse events were both low & equivalent to placebo.
Our co-investigatorsTjerk S.J. Opstal, Salem H.K. The, Xiao-Fang Xu, Mark A. Ireland, Timo Lenderink, Donald Latchem,Pieter Hoogslag, Jeroen Schaap, Anastazia Jerzewski,Peter Nierop, Alan Whelan, Randall Hendriks, Henk Swart, Aaf F.M. Kuijper, Maarten W.J. van Hessen, Pradyot Saklani, Isabel Tan, Angus G Thompson, Allison Morton, Chris Judkins, Willem A. Bax, Maurits Dirksen, Marco M.W. Alings, Graeme J. Hankey
The trial coordinatorsTrial monitors and staff from GenesisCareand the Heart and Vascular Research Institute of Sir Charles Gairdner Hospital Perth WA, including Penny Buczec, Denny Craig, Karen Doherty, Louise Nidorf, and Karen Youl, and from theDutch Network for Cardiovascular Research (WCN), including Marjelle van Leeuwen as project manager, Ingrid Groenenberg and Glentino Rodriguez for data management, Erik Stroes, Max Silvis, & Tim de Vries for medical review, Petra Bunschoten & Wendy Tousain for site monitoring
Organizational supportThe National Health Medical Research Council of Australia, The Sir Charles Gairdner Research Advisory Committee Grant, The Withering Foundation The Netherlands, The Netherlands Heart Foundation, The Netherlands Organization for Health Research and Development, and The Dutch Pharma consortium;Teva, Disphar and Tiofarma. Both the active and placebo tablets were supplied at no cost by; Tiofarma in The Netherlands and Aspen Pharmacare in AustraliaNeither the funders nor pharma had any role in the design of the study, the collection or management of the data, the statistical analyses, or presentation of the results
We would like to acknowledge Every participant in the trial
an investigator-initiated trial, of an old drug in an ancient disease

Research Publication“ Authors Name”
Article NameJOURNAL NAME ,
Volume XX, Issue XX, Date , Page Refhttps://doi.org/XXX/yyj/zzzz




















