
Noninvasive assessment of left ventricular diastolic function by pulsed doppler echocardiography in...
10
lACC VoL 10, NO.4 October I'.lH7:7H-42 CLINICAL STUDIES Noninvasive Assessment of Left Ventricular Diastolic Function by Pulsed Doppler Echocardiography in Patients With Hypertrophic Cardiomyopathy BARRY J. MARON, MD, FACC, PAOLOSPIRITO, MD, KIMBERLY J. GREEN, MA, YVONNE E. WESLEY, ROBERT O. BONOW, MD, FACe, JAVIER ARCE, MD Bethesda, Maryland 733 Hypertrophic cardiomyopathy is a primary myocardial disease in which symptoms may frequently result from impaired left ventricular relaxation, filling and compli- ance. In the present investigation, Doppler echocardi- ography was utilized to measure transmitral flow veloc- ity and thereby assess left ventricular diastolic performance noninvasively in a group of III patients representative of the broad clinical spectrum of hyper- trophic cardiomyopathy. In patients with hypertrophic cardiomyopathy, all Doppler indexes of diastolic relax- ation and filling differed significantly (p < 0.001) from those obtained in 86 control subjects without heart dis- ease, namely, prolongation of isovolumic relaxation (94 ± 24 versus 78 ± 12 ms) and of the early diastolic peak of flow velocity (244 ± 55 versus 220 ± 28 ms), as well as slower deceleration (3.4 ± 1.4 versus 4.9 ± 1.3 m/s 2 ) and reduced maximal flow velocity in early diastole (0.5 ± 0.2 versus 0.6 ± 0.1 m/s). As an apparent compen- sation for impaired relaxation and early diastolic filling, the atrial contribution to left ventricular filling was in- creased, as shown by increased late diastolic flow velocity (0.4 ± 0.3 versus 0.3 ± 0.1 m/s) and reduced ratio of maximal flow velocity in early diastole to that in late diastole (1.4 ± 0.8 versus 2.1 ± 0.9). Hypertrophic cardiomyopathy is a primary cardiac disease characterized by an increase in left ventricular wall thickness ( 1-7) and a diverse clinical and functional spectrum that includes patients with or without cardiac symptoms, ob- struction to left ventricular outflow or impaired diastolic function (8-1 I). From the Echocardiography Laboratory, Cardiology Branch, National Heart, Lung, and Blood Institute. National Institutes of Health, Bethesda, Maryland. Manuscript received January 20, 1987; revised manuscript received March 17, 1987, accepted April 3, 1987. Address ")r reprints: Barry J. Maron. MD. National Institutes of Health, Building 10, Room 7B-15, Bethesda, Maryland 20Xn. (0 by the American College of Cardiology The vast majority of patients with hypertrophic car- diomyopathy (91 [82%) of Ill) showed evidence of im- paired left ventricular diastolic performance, as assessed from the Doppler waveform. Abnormal Doppler dia- stolic indexes were identified with similar frequency in patients with (78%) or without (83%) left ventricular outflow obstruction, as well as in patients with (84%) or without (80%) cardiac symptoms. However, patients with nonobstruetive hypertrophic cardiomyopathy showed more severe alterations in the Doppler indexes of dia- stolic function than did patients with obstruction. Thus, abnormal diastolic performance as assessed by Doppler echocardiography was apparent in the vast ma- jority of the study patients with hypertrophic cardio- myopathy, independent of the presence or absence of cardiac symptoms or a subaortic pressure gradient. The high frequency with which diastolic abnormalities are identified in asymptomatic patients with hypertrophic cardiomyopathy suggests that impaired diastolic per- formance may be present at a time in the natural history of the disease when functional limitation is not yet evi- dent. (J Am Coil Cardiol 1987;10:733-42) Abnormalities of left ventricular relaxation, filling and compliance are particularly common in patients with hy- pertrophic cardiomyopathy and are generally considered to be responsible for symptoms of cardiac failure (1,9.12-31). However, the frequency with which left ventricular diastolic dysfunction occurs among patients within the broad clinical spectrum of hypertrophic cardiomyopathy (particularly those who are asymptomatic or mildly symptomatic) and the re- lation between diastolic dysfunction and obstruction to left ventricular outflow have not been well defined. Several recent investigations (32-39) have suggested that the assessment of transmitral flow velocity with pulsed Doppler echocardiography provides a noninvasive and c1in- 0735-IO,)7/X7/$3.50
Transcript of Noninvasive assessment of left ventricular diastolic function by pulsed doppler echocardiography in...

lACC VoL 10, NO.4October I'.lH7:7H-42
CLINICAL STUDIES
Noninvasive Assessment of Left Ventricular Diastolic Function byPulsed Doppler Echocardiography in Patients With HypertrophicCardiomyopathy
BARRY J. MARON, MD, FACC, PAOLO SPIRITO, MD, KIMBERLY J. GREEN, MA,
YVONNE E. WESLEY, ROBERT O. BONOW, MD, FACe, JAVIER ARCE, MD
Bethesda, Maryland
733
Hypertrophic cardiomyopathy is a primary myocardialdisease in which symptoms may frequently result fromimpaired left ventricular relaxation, filling and compliance. In the present investigation, Doppler echocardiography was utilized to measure transmitral flow velocity and thereby assess left ventricular diastolicperformance noninvasively in a group of III patientsrepresentative of the broad clinical spectrum of hypertrophic cardiomyopathy. In patients with hypertrophiccardiomyopathy, all Doppler indexes of diastolic relaxation and filling differed significantly (p < 0.001) fromthose obtained in 86 control subjects without heart disease, namely, prolongation of isovolumic relaxation (94± 24 versus 78 ± 12 ms) and of the early diastolic peakof flow velocity (244 ± 55 versus 220 ± 28 ms), as wellas slower deceleration (3.4 ± 1.4 versus 4.9 ± 1.3 m/s2
)
and reduced maximal flow velocity in early diastole (0.5± 0.2 versus 0.6 ± 0.1 m/s). As an apparent compensation for impaired relaxation and early diastolic filling,the atrial contribution to left ventricular filling was increased, as shown by increased late diastolic flowvelocity(0.4 ± 0.3 versus 0.3 ± 0.1 m/s) and reduced ratio ofmaximal flow velocity in early diastole to that in latediastole (1.4 ± 0.8 versus 2.1 ± 0.9).
Hypertrophic cardiomyopathy is a primary cardiac diseasecharacterized by an increase in left ventricular wall thickness(1-7) and a diverse clinical and functional spectrum thatincludes patients with or without cardiac symptoms, obstruction to left ventricular outflow or impaired diastolicfunction (8-1 I).
From the Echocardiography Laboratory, Cardiology Branch, NationalHeart, Lung, and Blood Institute. National Institutes of Health, Bethesda,Maryland.
Manuscript received January 20, 1987; revised manuscript receivedMarch 17, 1987, accepted April 3, 1987.
Address ")r reprints: Barry J. Maron. MD. National Institutes of Health,Building 10, Room 7B-15, Bethesda, Maryland 20Xn.
(0 19~7 by the American College of Cardiology
The vast majority of patients with hypertrophic cardiomyopathy (91 [82%) of Ill) showed evidence of impaired left ventricular diastolic performance, as assessedfrom the Doppler waveform. Abnormal Doppler diastolic indexes were identified with similar frequency inpatients with (78%) or without (83%) left ventricularoutflow obstruction, as well as in patients with (84%) orwithout (80%) cardiac symptoms. However, patients withnonobstruetive hypertrophic cardiomyopathy showedmore severe alterations in the Doppler indexes of diastolic function than did patients with obstruction.
Thus, abnormal diastolic performance as assessed byDoppler echocardiography was apparent in the vast majority of the study patients with hypertrophic cardiomyopathy, independent of the presence or absence ofcardiac symptoms or a subaortic pressure gradient. Thehigh frequency with which diastolic abnormalities areidentified in asymptomatic patients with hypertrophiccardiomyopathy suggests that impaired diastolic performance may be present at a time in the natural historyof the disease when functional limitation is not yet evident.
(J Am Coil Cardiol 1987;10:733-42)
Abnormalities of left ventricular relaxation, filling andcompliance are particularly common in patients with hypertrophic cardiomyopathy and are generally considered tobe responsible for symptoms of cardiac failure (1,9.12-31).However, the frequency with which left ventricular diastolicdysfunction occurs among patients within the broad clinicalspectrum of hypertrophic cardiomyopathy (particularly thosewho are asymptomatic or mildly symptomatic) and the relation between diastolic dysfunction and obstruction to leftventricular outflow have not been well defined.
Several recent investigations (32-39) have suggested thatthe assessment of transmitral flow velocity with pulsedDoppler echocardiography provides a noninvasive and c1in-
0735-IO,)7/X7/$3.50

734 MARON ET ALDIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
JACC Vol. 10. No.4October 1987:733-42
ically useful expressionof left ventriculardiastolicperformance. Indexes of diastolic function obtained with this technique have been shown to correlate well with thoseobtainedat cardiac catheterization (35,36) or with radionuclide angiography (37) and also to have satisfactory intraobserverand interobserver reproducibility (37). Therefore, in thepresent investigation, we utilizedpulsed Dopplerechocardiography to characterize left ventricular diastolic performance noninvasively in a large group of patients representative of the pathophysiologic spectrum of hypertrophiccardiomyopathy.
MethodsSelection of patients. The study group comprises III
patientswithhypertrophic cardiomyopathy whowerestudiedprospectively between January 1983 and April 1986 at theNational Institutes of Health and met the following criteria:I) patients who were not taking cardioactive medications(primarily beta-adrenergic blocking or calcium channelblocking agents) or who could have the drugs safely withdrawn at least48 hours before the Dopplerstudy; 2) patientswho had technically satisfactory diastolic waveforms thatcould be obtained with Doppler echocardiography from theleft ventricular inflow area (as described in detail later); 3)patients with normal sinus rhythm and a heart rate < 90beats/min at the time of the Doppler study, ensuring thatthe early and late diastolic peaks of flow velocity wereseparated and that flow velocity returned to baseline afterthe early peak; and 4) patients with no evidenceof moderateor severe mitral regurgitation, as determined by clinicalexamination, contrast angiography or pulsed Dopplerechocardiography (40) in those patients who did not undergocardiac catheterization.
The diagnosis of hypertrophic cardiomyopathy was confirmed in each patient by the echocardiographic demonstration of a hypertrophied nondilated left ventricle in theabsence of any other cardiac or systemic disease capable ofproducing left ventricular hypertrophy (2). Significant narrowing of the extramuralcoronary arteries was excluded bycoronary arteriography in 58 of the study patients. Coronaryartery disease was considered unlikely in the other 53 patients who did not undergo cardiac catheterization; 37 ofthese 53 patients were < 40 years old, and 15 of the 16patients who were 2:40 years of age were asymptomatic (ormildly symptomatic) or had no history of chest pain. Fourof the study patients had relatively mild systemic hypertension, which itself was not considered to be of sufficientseverity to produce left ventricular hypertrophy of the magnitude that was present (41). The control group comprised86 subjects without clinical or echocardiographic evidenceof cardiovascular disease.
Demographic and clinical profiles. Patients with hypertrophic cardiomyopathy. The 111 patientsranged in agefrom 10 to 62 years (mean 34); 81 (73%) were male. Of
the III patients, 54 were asymptomatic (or had minimaltransient symptoms), 21 had mild symptoms (New YorkHeart Association functional class II) and 36 had moderateto severe symptoms (functional classes III and IV). Thelatter group includes five patients who survived a cardiacarrest. Patientsexperienceda wide range of symptoms. Themost common limiting symptoms were dyspnea or fatigue.or both, which occurred in 53 patients. Other less frequentfindings were chest pain (43 patients), presyncope (34patients) and syncope or cardiac arrest (18 patients).
Patients were also classified as having obstructive (23patients) or nonobstructive (88 patients) hypertrophic cardiomyopathy. dependingon whetheror not a left ventricularoutflow tract gradient 2:30 mm Hg was present under basalconditions (42). In 58 patients, this assessment was madeat cardiac catheterization (performed within 18 months ofthe Doppler echocardiographic study). In the other 53 patients who did not undergo catheterization, the subaorticpressure gradient was estimated from the magnitude andduration of systolic anterior motion of the mitral valve onM-mode echocardiography (43.44).
Control subjects . The 86 control subjects without heartdisease ranged in age from 20 to 74 years (mean 36); 48(55%) were male. These control subjects and the patientswith hypertrophic cardiomyopathy did not differ significantly with respect to mean age or their distribution intoage subgroups(that is, :::::29, 30 to 49 and 2:50 years) (TableI) .
Doppler echocardiography. An AdvancedTechnologyLaboratory Mark 500 ultrasound system was utilized to perform the Doppler echocardiographic studies. This instrument combines a pulsed Doppler flow analyzer with a 3MHz, two-dimensional wide angle (90°) mechanical sectorscanner, as previously described (37). The system has amovable cursor that allows positioning of the Doppler sample volume anywhere in the two-dimensional sector plane.Doppler shift was detected only in that region occupied bythe sample volume. Left ventricular diastolic flow velocitywas measured at depths ranging from 9 to 13 cm. Doppleroutput of diastolic flow velocity was available as an audiosignal and as a spectral display. The spectral display wasdevelopedby subjectingthe Dopplersignal to electronic fastFourier transform analysis, with sampling at 5 ms intervalsand division of the signal into 128 frequency bins. Flowvelocity profiles appeared as a waveform composition ofsmall individual gray and black blocks and were displayedon a monitorsimultaneously witha lead II electrocardiogramand phonocardiogram, and recordedon a strip chart recorderat 100 mm/s.
Each subject was examined in the left lateral decubitusposition with the transducer at or slightly to the left of theapical impulse. The transducer was oriented to obtain anapical four chamber view of the heart that provided goodvisualization of the left ventricular cavity and maximal ex-

lACC Vol. 10, No.4October 1987:733-42
MARON ET AL.DIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
Table 1. Comparison of Age in Patients With Hypertrophic Cardiomyopathy and inControl Subjects
Patients WithHypertrophic Cardiomyopathy Control Subjects
Age Group No. of Mean No. of Mean(yr) Patients '!c Age (yr) Patients ?r Age (yr)
:529 46 41 19 :+: 5* 35 41 22 :+: 3*30 to 49 44 39 39 :+: 5 33 38 40 :+: 5
2':50 21 20 57 :+: 4 18 21 57 :+: 6All patients III 34 :+: 15 86 36 :+: 14
*Comparison achieved statistical significance (p < 0.005); none of the other comparisons were statisticallysignificant.
735
cursion of the mitral valve leaflets, The cursor line waspositioned through a plane traversing the left ventricle fromapex to mitral valve anulus. Care was taken to attain thesmallest possible angle between the presumed direction ofdiastolic blood flow and the orientation of the ultrasoundbeam (cursor); this angle was estimated to be zero or <200
in each subject. The sample volume was positioned in theinflow area of the left ventricle approximately I ern belowthe mitral anulus (Fig, I), and its position along the cursor
Figure 1. Stop-frame two-dimensional echocardiogram showinglocation of the Doppler sample volume (enclosed within the broken circle) utilized to obtain leftventricular diastolic flow velocitywaveforms. Sample volume is positioned just below the mitralvalve anulus within the inflow area of the left ventricle, VSventricular septum, (Reproduced from Spirito et al. [37],)
line was adjusted until the highest early and late peaks ofdiastolic flow velocity were recorded and the graphic qualityof the Doppler waveform was optimal,
Quantitative assessment of diastolic flow velocitywaveforms. In each subject, the three recorded waveformswith the highest diastolic flow velocity and the steepestdescent of early diastolic flow velocity, as well as the bestsignal to noise ratio, were chosen for analysis, Each of thethree waveforms was individually characterized quantitatively, and these values were averaged,
The following measurements were obtained (Fig, 2): I)the time interval from the aortic closing component of thesecond heart sound to the onset of diastolic flow velocity(ArO), a measure of duration of isovolumic relaxation(45); 2) duration of the early diastolic peak of flow velocity,defined as the time interval from its onset to the point whereflow velocity returned to baseline (D-F); 3) rate of decrease(or deceleration) of flow velocity in early diastole (EF); 4)maximal early diastolic flow velocity, measured as the heightof the early peak (E); 5) maximal late diastolic flowvelocity,measured as the height of the late peak (A), which is dueto atrial contraction; and 6) the ratio of maximal flow velocity in early diastole to that in late diastole (E/A), ameasure of the relative contributions of early and late diastolic flow velocity to left ventricular filling,
Points D. E andA on the flow velocity waveform wereidentified as the mid points of the gray-scale spectrum.Deceleration of early diastolic flow velocity was defined asthe slope of a straight line (EF slope) passing through themid portion of the gray-scale spectrum from the peak ofearly diastolic flow velocity (at point E) to point F, In thoseinstances in which the EF slope was a curved rather than astraight line. EF was constructed as the line identifying themaximal incline of the slope. Because flow velocity waveforms may demonstrate wide spectral spread at the end ofthe descent of early flow velocity, point F was identified asthe intersection between the line of the descent of the earlydiastolic peak and the baseline.
In the individual patient analyses, a variable was considered abnormal if the value exceeded the upper or lower
736 MARON ET AL.DIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
lACC Vol. 10, No.4October 1987:733-42
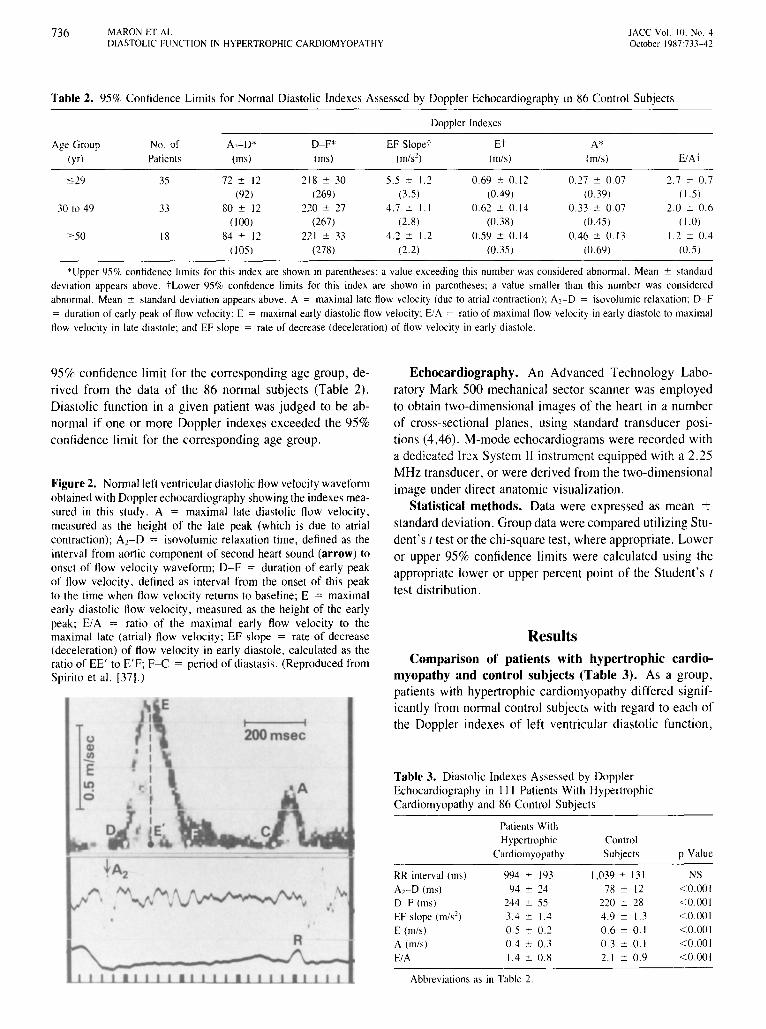
Table 2. 95% Confidence Limits for Normal Diastolic Indexes Assessed by Doppler Echocardiography in 86 Control Subjects
Doppler Indexes
Age Group No. of A,-D* D-F* EFSlopet Et A*(yr) Patients (ms) (ms) (m/s') (m/s) (m/s) E/AT
529 35 72 ± 12 218 ± 30 5.5 ± 1.2 0.69 ± 0.12 0.27 ± 007 2.7 ± 0.7(92) (269) (3.5) (0.49) (0.39) ( 1.5)
30 to 49 33 80 ± 12 220 ± 27 4.7 ± 1.1 0.62 ± 0.14 0.33 ± 0.07 2.0 ± 0.6(100) (267) (2.8) (0.38) (0.45) (1.0)
2'50 18 84 ± 12 221 ± 33 4.2 ± 1.2 0.59 ± 0.14 0.46 ± 0.13 1.2 ± 0.4(105) (278) (2.2) (0.35) (0.69) (0.5)
*Upper 95% confidence limits for this index are shown in parentheses; a value exceeding this number was considered abnormal. Mean ± standarddeviation appears above. tLower 95% confidence limits for this index are shown in parentheses; a value smaller than this number was consideredabnormal. Mean ± standard deviation appears above. A = maximal late flow velocity (due to atrial contraction); A1-D = isovolurnic relaxation; D-F= duration of early peak of flow velocity; E = maximal early diastolic flow velocity; E/A = ratio of maximal flow velocity in early diastole to maximalflow velocity in late diastole; and EF slope = rate of decrease (deceleration) of flow velocity in early diastole.
ResultsComparison of patients with hypertrophic cardio
myopathy and control subjects (Table 3). As a group,patients with hypertrophic cardiomyopathy differed significantly from normal control subjects with regard to each ofthe Doppler indexes of left ventricular diastolic function,
Echocardiography. An Advanced Technology Laboratory Mark 500 mechanical sector scanner was employedto obtain two-dimensional images of the heart in a numberof cross-sectional planes, using standard transducer positions (4,46). M-mode echocardiograms were recorded witha dedicated Irex System II instrument equipped with a 2.25MHz transducer, or were derived from the two-dimensionalimage under direct anatomic visualization.
Statistical methods. Data were expressed as mean ±standard deviation. Group data were compared utilizing Student's t test or the chi-square test, where appropriate, Loweror upper 95% confidence limits were calculated using theappropriate lower or upper percent point of the Student's t
test distribution,
Table 3. Diastolic Indexes Assessed by DopplerEchocardiography in III Patients With HypertrophicCardiomyopathy and 86 Control Subjects
NS<0.001<0.001<0.001<0.001<0.001<0.001
p ValueControlSubjects
1,039 ± 13178 ± 12
220 ± 284.9 ± U0.6 ± 0.10.3 ± 0.12.1 ± 0.9
994 ± 19394 ± 24
244 ± 553.4 ± 1.40.5 ± 0.20.4 ± 0.31.4 ± 0.8
Patients WithHypertrophic
Cardiomyopathy
Abbreviations as in Table 2.
RR interval (rns)
ArD (rns)
D~F (rns)
EF slope (m/s')E (m/s)
A (m/s)
E/A
."
R
I I200msec
Figure 2. Nonnalleft ventriculardiastolicflowvelocitywaveformobtainedwith Dopplerechocardiography showingthe indexesmeasured in this study. A = maximal late diastolic flow velocity,measured as the height of the late peak (which is due to atrialcontraction); Az-D = isovolumic relaxation time, defined as theinterval from aortic component of second heart sound (arrow) toonset of flow velocity waveform; D-F = duration of early peakof flow velocity, defined as interval from the onset of this peakto the time when flow velocity returns to baseline; E = maximalearly diastolic flow velocity, measured as the height of the earlypeak; E/A = ratio of the maximal early flow velocity to themaximal late (atrial) flow velocity; EF slope = rate of decrease(deceleration) of flow velocity in early diastole, calculated as theratio of EE' to E'F; F-C = period of diastasis. (Reproduced fromSpirito et al. [37].)
95% confidence limit for the corresponding age group, derived from the data of the 86 normal subjects (Table 2),Diastolic function in a given patient was judged to be abnormal if one or more Doppler indexes exceeded the 95%confidence limit for the corresponding age group,
lACC Vol. 10. NO.4October 1987:733-42
MARON ET AL.DIASTOLIC ('UNCTION IN HYPERTROPHIC CARDIOMYOPATHY
737
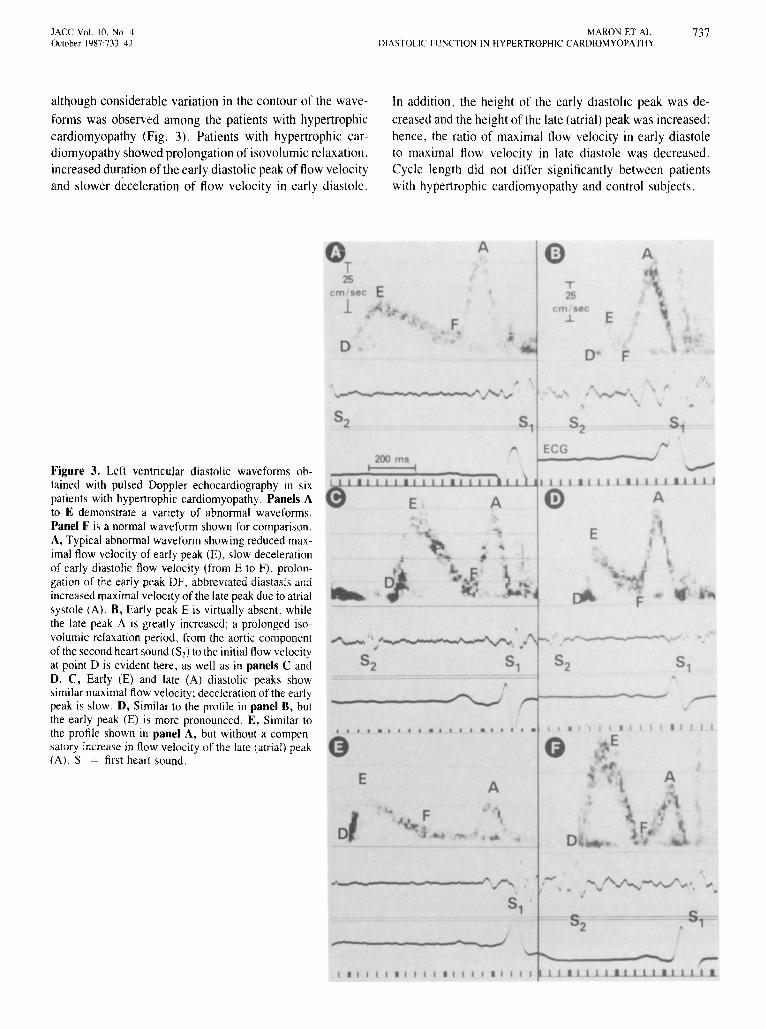
although considerable variation in the contour of the wave
forms was observed among the patients with hypertrophiccardiomyopathy (Fig. 3). Patients with hypertrophic cardiomyopathy showed prolongation of isovolumic relaxation.increased duration of the early diastolic peak of flow velocityand slower deceleration of flow velocity in early diastole.
In addition. the height of the early diastolic peak was de
creased and the height of the late (atrial) peak was increased;hence, the ratio of maximal flow velocity in early diastole10 maximal flow velocity in late diastole was decreased.Cycle length did not differ significantly between patientswith hypertrophic cardiomyopathy and control subjects.
Figure 3. Left ventricular diastolic waveforms obtained with pulsed Doppler echocardiography in sixpatients with hypertrophic cardiomyopathy. Panels Ato E demonstrate a van ely of abnormal waveforms.PanelF is a normal waveform shown for comparison.A, Typical abnormal waveform showing reduced maximal flow velocity of early peak (E), slow decelerationof early diastolic flow velocity (from E to F). prolongation of the early peak DF. abbreviated diastasis andincreased maximal velocity of the late peak due to atrialsystole (A). B, Early peak E is virtually absent. whilethe late peak A is greatly increased; a prolonged isovolumic relaxation period, from the aortic componentof the second heart sound (S2l to the initial flow velocityat point D is evident here. as well as in panels C andD. C, Early (E) and late (A) diastolic peaks showsimilar maximal flow velocity; deceleration of the earlypeak is slow. D, Similar to the profile in panel B, butthe early peak (E) is more pronounced. E, Similar tothe profile shown in panel A, but without a compensatory increase in flow velocity of the late (atrial) peak(A). S, = first heart sound.
EA
A
DF
FD
,... ,/"'-. -- ..... " ~./\-..."-v../' .,.- '"S1
S152----.-;
rr:I • I I I I • I I I I • I I I I • I I I I I 1 . 1 I 11 .. 1.1 1 1 111 J.
738 MARON ET AL.DIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
No . Patients
LV Diastolic----- Function -----
NoSymptoms
l ACC Vol. 10, No. 4October 1987:733-42
Nonobstructive Obstructive Nonobstructive Obstructive Nonobstructive
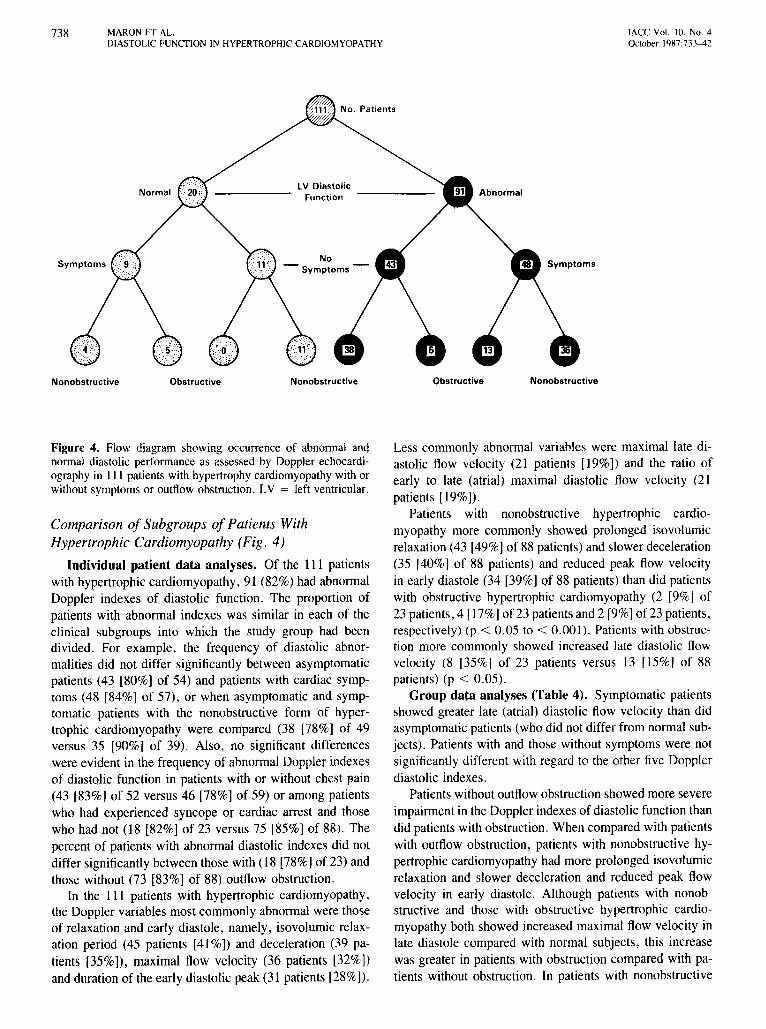
Figure 4. Flow diagram showing occurrence of abnormal andnormal diastolic performance as assessed by Doppler echocardiography in III patients with hypertrophy cardiomyopathy with orwithout symptoms or outflow obstruction. LV = left ventricular.
Comparison of Subgroup s of Patients WithHypertrophic Cardiomyopathy (Fig, 4)
Individual patient data analyses. Of the III patientswith hypertrophic cardiomyopathy, 91 (82%) had abnorm alDoppler indexes of diastolic function. The proportion ofpatients with abnormal indexes was similar in each of theclinical subgroups into which the study group had beendivided. For example, the frequency of diastolic abnormalities did not differ significantly between asymptomaticpatient s (43 [80%] of 54) and patients with cardiac symptoms (48 [84%] of 57), or when asymptomatic and symptomatic patients with the nonobstruct ive form of hypertrophic cardiomyopathy were compared (38 [78%] of 49versus 35 [90%] of 39). Also, no significant differenceswere evident in the frequen cy of abnormal Doppler indexe sof diastolic function in patients with or without chest pain(43 [83%] of 52 versus 46 [78%] of 59) or among patientswho had experienced syncope or cardiac arrest and thosewho had not (18 [82%] of 23 versus 75 [85%] of 88) , Thepercent of patients with abnormal diastolic indexes did notdiffer significantly between those with (18 [78%] of 23) andthose without (73 [83%] of 88) outflow obstruction .
In the I I I patients with hypertrophic cardiomyopathy,the Doppler variables most commonly abnormal were thoseof relaxation and early diastole , namely , isovolumi c relaxation period (45 patients [41%]) and decelerat ion (39 patients [35%J), maximal flow velocity (36 patients [32%])and duration of the early diastolic peak (31 patients [28%]),
Less comm only abnormal variables were maximal late diastolic flow velocity (21 patients [19%]) and the ratio ofearly to late (atrial) maximal diastolic flow velocity (2 1patients [19%]),
Patien ts with nonobstructive hypertrophic cardiomyopathy more commonly showed prolonged isovolumicrelaxation (43 [49%] of88 patients) and slower deceleration(35 [40%) of 88 patients) and reduced peak flow velocityin early diastole (34 [39%] of 88 patients) than did patientswith obstructive hypertrophic cardiomyopathy (2 [9%) of23 patients, 4 [17%) of 23 patients and 2 [9%1of 23 patients,respecti vely) (p < 0.05 to < 0.001). Patients with obstruction more commonly showed increased late diastolic flowvelocity (8 [35%] of 23 patients versus 13 [15%] of 88patients) (p < 0,05),
Group data analyses (Table 4). Symptomatic patient sshowed greater late (atrial) diastoli c flow velocity than didasymptomatic patient s (who did not diffe r from normal subjects). Patient s with and those without symptoms were notsignificantly different with regard to the other five Dopplerdiastolic indexes,
Patients without outflow obstruction showed more severeimpairment in the Doppler indexes of diastolic function thandid patient s with obstruction . When comp ared with patientswith outflow obstruction, patients with nonobstructive hypertrophic cardiomyopathy had more prolonged isovolumi crelaxation and slower deceleration and reduced peak flowvelocity in early diastole . Although patients with nonob structive and those with obstructive hypertrophic cardiomyopathy both showed increased maximal flow velocity inlate diastole compared with normal subjec ts, this increasewas greater in patient s with obstruction compared with patients without obstruction . In patients with nonobstructive
l ACC Vol. 10, No.4October 1987:733- 42
MARON ET AL.DIA STOLIC FUNCTION IN HYPERTROPHIC CARf)(O MYOPATHY
739
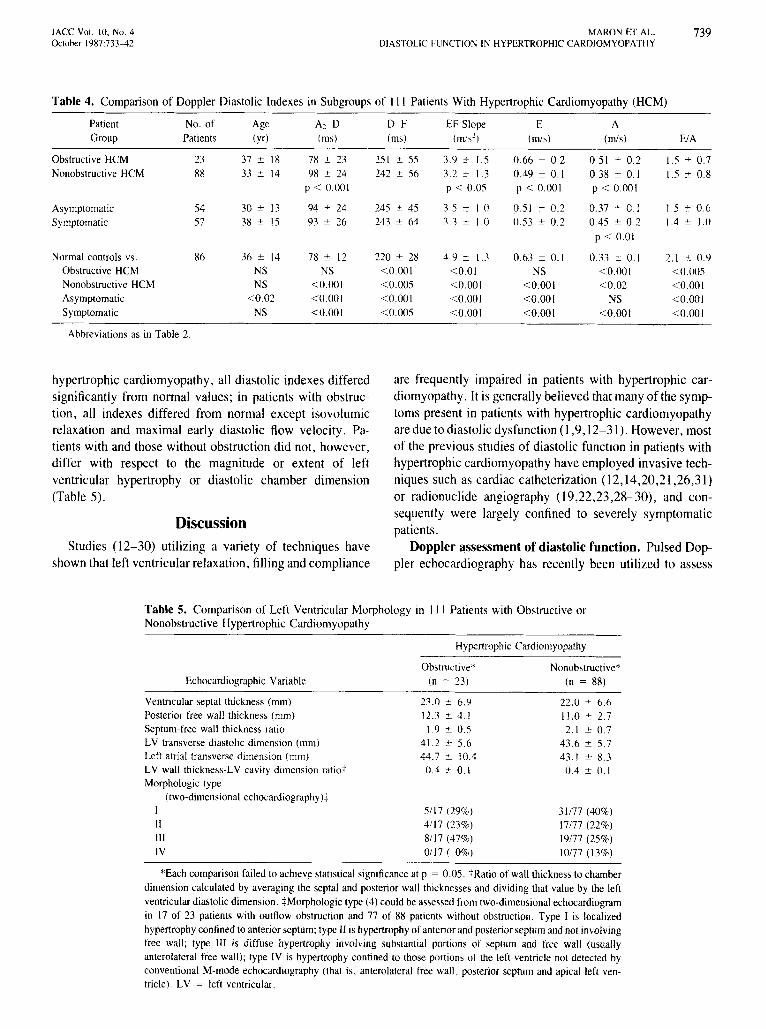
T able 4. Com pariso n of Doppler Diastoli c Ind exe s in Subgroup s o f II I Pati ents W ith Hy pe rt ro phic Card io m yo pathy (H CM)
Patient No. of Age A2-D D-F EF Slope E A
Group Patients (yr) (ms) (rns) (rn/s'') (mls) (mls) EtA
Obstructive HCM 23 37 ::: 18 7H ::: 23 25 l ::: 55 3.9 ::: 1.5 0 .66 ::: 0 .2 0 .5 1 ± 0 .2 1.5 ::: 0 .7
Nonobstructive HCM 88 33 =: 14 9H ± 24 242 ± 56 3.2 =: 1.3 OA9 ± 0. 1 0 .3H ± 0. 1 1.5 ± 0.8p < 0.00 1 P < 0.05 P < 0.00 1 P < 0.00 1
Asymptomatic 54 30 ::: 13 94 ::: 24 245 :t 45 3.5 ::: 1.0 0 .5 1 ::: 0 .2 0 .37 ± 0. 1 1.5 ::: 0.6Symptomatic 57 38 ::: 15 93 ::: 26 243 ::: 64 .1.3 :t 1.0 0.53 ::: 0. 2 OA5 ± 0.2 1.4 ::: 1.0
p < 0.01
Normal controls vs, 86 36 ::: 14 78 ::: 12 220 ::: 28 4.9 ± 1.3 0 .63 ± 0 . 1 0.33 ± 0. 1 2. 1 ± 0.9Obstructive HCM NS NS < 0.00 1 < 0.0 1 NS < 0.00 1 < 0.005Nonobstructive HCM NS < 0.00 1 < 0.005 < 0.00 1 < 0.00 1 < 0.02 < 0.00 1Asymptomatic < 0 .02 <0.001 < 0.00 1 < 0.00 1 < 0.00 1 NS < 0.00 1Symptomatic NS < 0.00 1 < 0.005 < 0.001 < 0.00 1 < 0.00 1 < 0.00 1
Abbreviations as in Table 2.
hypertrophic cardiomyopathy, all diastolic indexes differedsignificantly from normal values; in patients with obstruction, all indexes differed from normal except isovolumicrelaxation and maximal early diastolic flow velocity. Patients with and those without obstruction did not, however,differ with respect to the magnitude or extent of leftventricular hypertrophy or diastolic chamber dimension(Table 5).
Discussion
Studies (12-30) utilizing a variety of techniques haveshown that left ventricular relaxation, fill ing and compliance
are frequently impaired in patients with hypertrophic cardiomyopathy. It is generally believed that many of the symptoms present in patients with hypertrophic cardiomyopathyaredue to diastolicdysfunction(1,9, 12- 31). However, mostof the previous studies of diastolic function in patients withhypertrophic cardiomyopathy have employed invasive techniques such as cardiac catheterization (l 2,14,20 ,21,26,31)or radionuclide angiography (19,22,23,28- 30), and consequently were largely confined to severely symptomaticpatients.
Doppler assessment of diastolic function. Pulsed Doppler cchocardiography has recently been utilized to assess
Table 5. Compari son of Left Ventricular Morphol ogy in 111 Patients with Obstruct ive orNonobstru ctive Hypert rophic Card io myopathy
Hypertrophic Card iomyopathy
Echocardiographic Variable
Ventricular septal thickness (mm)Posterior free wall thickness (mm)Septum-free wall thickness ratioLV transverse diastolic dimension (rnm)Left atrial transverse dimension (mm)LV wall thickness-LV cavity dimension ratiot
Morphologic type(two-dimensional echocardiographyjt
IIIIIIIV
Obstructive*
(n "" 23)
23.0 :::: 6 .912.3 :::: 4 . 11.9 =: 0.5
41.2 ::: 5.644.7 ::: 10.4
OA :t O. I
5/17 (29%)411 7 (230/c)8117 (47%)0117 ( 0%)
Nonobstructive*(n = 88)
22.0 ::: 6 .611.0 :t 2.72.1 :::: 0 .7
43.6 =: 5.743. 1 :t 8.3OA ± 0 . 1
31/77 (40%)17/77 (22%)19/77 (25%)10177 (13%)
*Each comparison failed to achieve statistical significance at p = 0 .05. t Ralio of wall thickness to chamberdimension calculated by averaging the septal and posterior wall thicknesses and dividing that value by the leftventricular diastolic dimen sion . :j: Morphologic type (4) could be assessed from two-dimensional echocardiogramin 17 of 23 patients with outflow obstruction and 77 of 88 patients without obstruction. Type I is localizedhypertroph y confined to anterior septum; type II is hypertrophy of anterior and posterior septum and not involvingfree wall; type III is diffuse hypertrop hy involving substantial portions of septum and free wall (usuallyanterolateral free wall); type IV is hypertroph y confined to those portions of the left ventricle not detected byconventional M-mode echocardiography (that is, anterolateral free wall. posterior septum and apical left ventricle) . LV = left ventricular.

740 MARON ET AL.DIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
lACC Vol. 10. No.4October J987:733-42
left ventricular diastolic function in normal subjects andpatients with heart disease (32-39). Doppler echocardiographic assessment of diastolic function has the advantagesof being noninvasive, easily performed and probably notadversely affected by the small size and abnormal geometrythat characterize the left ventricle in hypertrophic cardiomyopathy. Therefore, it seemed to us that Doppler echocardiography is a technique that is particularly applicableto the study of diastolic function in a large group of patientsrepresentative of the broad clinical spectrum of hypertrophiccardiomyopathy, including a substantial number of asymptomatic patients.
Diastolic function in hypertrophic cardiomyopathy.In our overall group of patients with hypertrophic cardiomyopathy, we observed a variety of alterations in the leftventricular diastolic waveform. The most typical pattern forthe group included prolongation of the isovolumic relaxationperiod and abnormalities of both the early and late diastolicphases (that is, prolongation, slowed deceleration and reduced flow velocity of the early diastolic peak and increasedflow velocity of the late diastolic peak resulting from atrialcontraction, with a reduced ratio of the early to the latemaximal diastolic flow velocity). As a group, patients withhypertrophic cardiomyopathy differed significantly fromcontrol subjects without heart disease with respect to eachof the Doppler indexes of diastolic function assessed. However, although these differences were statistically significantfor the intergroup comparison of mean values, the absolutedifferences may not always have been of sufficient magnitude to distinguish individual patients with hypertrophiccardiomyopathy from normal subjects.
The results of the present study also show that diastolicdysfunction, as assessed by Doppler echocardiography, isparticularly common in patients with hypertrophic cardiomyopathy whether or not symptoms are present. Over 80%of our patients had impaired isovolumic relaxation or anabnormal Doppler filling pattern. However, an unexpectedfinding of our study was that 80% of those patients withoutcardiac symptoms also had evidence of diastolic dysfunctiondetectable by Doppler study. Although the clinical significance of this finding is unclear at this time, it may indicatethat many patients with hypertrophic cardiomyopathy havesubclinical impairment of diastolic function (under basalconditions) at a time in the natural history of their diseasewhen functional limitation is not yet evident. Alternatively,it is possible that such alterations in the Doppler waveformdo not reflect a true diastolic abnormality that will ultimatelybecome clinically relevant to that individual patient, butrather represent an intrinsic feature of the primary underlying cardiomyopathic process in hypertrophic cardiomyopathy. Whether symptoms will subsequently becomeclinically overt in such patients remains to be determined,and longitudinal follow-up studies will be required to definethe clinical relevance and long-term significance of abnor-
mal Doppler waveforms in asymptomatic patients with hypertrophic cardiomyopathy.
Diastolic function in patients with and patients without outflow obstruction. Our data also show that mostpatients with hypertrophic cardiomyopathy and basal obstruction to left ventricular outflow had associated abnormalities in Doppler indexes of diastolic function; indeed,diastolic abnormalities occurred with similar frequency inpatients with and patients without outflow obstruction. Thisobservation suggests that diastolic dysfunction is a pathophysiologic feature of hypertrophic cardiomyopathy that isnot confined to those patients with the nonobstructive formof the disease, but rather may be characteristic of the overalldisease process. Hence, cardiac symptoms and functionallimitation in patients with subaortic obstruction may resultfrom the consequences of the subaortic pressure gradient(and elevated intraventricular systolic pressure), and alsofrom impaired diastolic function.
Nevertheless, the magnitude of the abnormalities in Doppler diastolic indexes was greater in those patients withoutoutflow obstruction than in those with obstruction. Suchdifferences in diastolic performance (as assessed with Doppler ultrasound) between these two groups of patients didnot appear to be caused by differences in left ventricularmorphology, including the distribution and pattern of hypertrophy (4). It is possible, however, that the presence ofrelatively mild mitral regurgitation, so common in patientswith outflow obstruction (47,48), may have increased leftventricular filling velocity and, conceivably, partially maskedabnormalities of the early filling phase. Our observation thatthe isovolumic relaxation period is longer in nonobstructivecompared with obstructive hypertrophic cardiomyopathy isconsistent with previous radionuclide angiographic data (28),and may reflect the differences between these subgroups ofpatients with respect to left ventricular systolic pressure andejection time (which are load-dependent determinants of leftventricular relaxation (49,50). Thus, the higher systolicpressure and greater ejection time (51-53) in patients withoutflow obstruction could contribute to a shorter durationof left ventricular relaxation.
Our observations differ substantially in several respectsfrom those of Takenaka et al. (38), who assessed mitralflow velocity by Doppler ultrasound in 17 patients withhypertrophic cardiomyopathy. These investigators reportedthat Doppler variables of diastolic function are frequentlynormal in patients with hypertrophic cardiomyopathy, particularly those without evidence of obstruction. Discrepancies between the present study and that of Takenaka etal. (38) could be due to the fact that they studied particularlysmall subgroups of patients (11 with evidence of obstructionand only 6 without) and just 16 normal subjects for comparison. In addition, the methodology utilized by those investigators (in which Doppler assessment of diastolic function was based on an analysis of only one cardiac cycle for

l ACC Vol. 10. No. 4October 1987:733-42
MAR ON lOT AL.DIASTOLIC fUNCTION IN HYPERTROPHIC CARDIOMYOPATH Y
741
but rather reflect in large measure intrinsic cycle to cyclevariability of the Doppler method.
We should also emphasize that left ventricular diastolicfunction is a complex phenomenon,determinedby multiplefactors including the intrinsic properties of the cardiac muscle, left ventricular systolic function and loading conditionsof the ventricle (49,54-56). Hence, diastolic indexes obtained from the Doppler flow velocity waveform cannot beconsidered a puremeasureof diastolicfunction because theymay be influenced by such variables. Therefore, althoughour Doppler echocardiographic findings show that patientswith hypertrophic cardiomyopathy usually have alterationsin relaxation and diastolic filling patterns, we cannot becertain that these alterations are solely attributable to abnormalities in the primary intrinsic properties of cardiacmuscle itself.
Conclusions. Using Doppler echocardiography, alterations in isovolumic relaxation or in Doppler indexes of diastolic filling were identified noninvasively in the vast majority of the III study patients with hypertrophiccardiomyopathy whetheror not cardiac symptoms or a subaortic pressure gradient was present. The high prevalenceof Dopplerabnormalities in asymptomatic patientswith hypertrophic cardiomyopathy implies that diastolic performance may be altered at a time in the natural history of thedisease when functional limitation is not yet evident.
We recognize the quality technical assistance of Judith S. Merrill. SRNand acknowledge the superb secretarial support of Imogene Surrey.
ReferencesI. Wigle ED. Sasson Z. Henderson MA. et al. Hypertrophic cardio
myopathy. The importance of the site and the extent of hypertrophy.A review. Prog Cardiovasc Dis 1985;28:1- 83.
2. Maron BJ. Epstein SE. Hypertrophic cardiomyopathy: a discussionof nomenclature. Am 1 Cardiol 1979;43:1242-4 .
3. Shapiro LM. McKenna Wl. Distribution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a two-dimensional echocardiographic study. 1 Am Coli Cardiol 1983;2:437-44 .
4. Maron B1. Gottdiener lS . Epstein SE. Patterns and significance ofdistribution of left ventricular hypertrophy in hypertrophic cardiomyopathy. A wide angle, two-dimensional echocardiographic studyof 125 patients. Am 1 Cardiol 1981;48:418-28.
5. Abbasi AS. MacAlpin RN. Eber LM. Pearce ML. Echocardiographicdiagnosis of idiopathic hypertrophic cardiomyopathy without outflowobstruction. Circulation 1972;46:897- 904.
6. Henry WL. Clark CEo Epstein SEc Asymmetric septal hypertrophy(ASH):echocardiographic identification of the pathogonomic anatomicabnormality of tHSS. Circulation IlJ73;47:225- 33.
7. Martin RP. Rakowski H, French 1. Popp RL. Idiopathic hypertrophicsubaortic stenosis viewed by wide-angle. phased-array echocardiography. Circulation 1979;59:1200-1 7.
8. Braunwald E, Lambrew CT, Rockoff SO. Ross 1 Jr, Morrow AG.Idiopathic hypertrophic subaortic stenosis. I. A description of the
disease based upon an analysisof 64 patients. Circulation 1964;30(supplI V ) :I V · ~-2 13 .
9. Goodwin IF. Congestive and hypertrophic cardiomyopathies. A decadeof study. Lancet 1970; I:731- 9.
10. Epstein SE. Henry WL, Clark CE, et al. Asymmetric septal hypertrophy. Ann Intern Med 1974;8I:650- 80.
II . McKenna W. Deanfield1. Faruqui A, England D, Oakley C. Goodwin1. Prognosis in hypertrophic cardiomyopathy: role of age and clinical.electrocardiographic and hemodynamic features. Am J Cardiel 1981:47:532-8.
12. Stewart S. Mason DT. Braunwald E. Impaired rate of left ventricularfilling in idiopathic hypertrophic subaortic stenosis and valvular aorticstenosis. Circulation 1968;37:8-1 4.
13. Goodwin JF. Oakley CM. The cardiomyopathies. Br Heart 1 1972;34:545- 52.
14. Sanderson lE . Gibson DG, Brown 01, Goodwin IF. Left ventricularfilling in hypertrophic cardiomyopathy. An angiographic study. BrHeart 1 1977;39:661-70 .
15. Sanderson JE. Traill TA. 51. lohn Sutton MG. Brown OJ. GibsonDG. GoodwinJF. Left ventricular relaxation and tilling in hypertrophiccardiomyopathy: an echocardiographic study. Br Heart 1 1978;40:596- 601.
16. SI. lohn Sutton MG. Tajik Al . Gibson DG. Brown Cl , Seward JB.Giuliani ER. Echocardiographic assessment of left ventricular tillingand septal and posterior wall dynamics in idiopathic hypertrophicsubaortic stenosis. Circulation 1978;57:512-20 .
17. Hanrath P. Mathey DG. Kremer P, Sonntag F. Bleifeld W Effect ofveraparnil on left ventricular isovolumic relaxation time and regionalleft ventricular tilling in hypertrophic cardiomyopathy. Am 1 Cardiel19110;45:12511-64.
18. Hanrath P. Mathey DG. Siegert R. Bleifeld W. Left ventricular relaxation and tilling pattern in different forms of left ventricular hypertrophy: an echocardiographic study. Am 1 Cardiel 1980:45:15- 23.
19. Bonow RO. Rosing DR. Bacharach SL. et al. Effects of verapamilon left ventricular systolic function and diastolic tilling in patientswith hypertrophic cardiomyopathy. Circulation 1981;64:787- 96.
20. Lorell BH. Paulus W1. Grossman W, Wynne 1. Cohn PF. Modificationof abnormal left ventricular diastolic properties by nifedipine in patients with hypertrophic cardiomyopathy. Circulation 1982;65:499-507.
21. ten CalCFJ. Serruys PW. Simon M, Roelandl J . Effects of short-termadministration of verapamil on left ventricular relaxation and fillingdynamics measured by a combined hemodynamic-ultrasonic techniquein patients with hypertrophic cardiomyopathy. Circulation 148.'\ ;68:1274-9.
22. Bonnw RO. Frederick TM. Bacharach SL. et al. Atrial systole andleft ventricular tilling in patients with hypertrophic cardiomyopathy:effect of verapamil. Am 1 Cardiol 1983:5 1:1386- 91.
23. Bonow RO. Dilsizian V, Rosing DR, Maron 81, Bacharach SL. GreenMV. Vcrapamil-induced improvement in left ventricular diastolic tilling and increased exercise tolerance in hypertrophic cardiomyopathy:short-term and long-term effects. Circulation 1985;72:853- 04.
24. Alvares RF. Shaver lA , Gamble WHo Goodwin IF. Isovolumic relaxation period in hypertrophic cardiomyopathy. 1 Am Coil Cardiol1984:3:71- 81.
25. Gamble WHoShaver JA, Alvares RF. Salemi R. Reddy PS. A criticalappraisal of diastolic time intervals as a measure of relaxation in leftventricular hypertrophy. Circulation 1983;68:76-87.
26. Newman H. Sugrue D. Oakley CM. Goodwin 11'. McKenna Wl .Relation of left ventricular function and prognosis in hypertrophiccardiomyopathy: an angiographic study. J Am Coli Carriinl 141\5:5:1004-74 .
27. Spirito P. Maron BJ, Chiarella F. et al. Diastolic abnormalities inpatients with hypertrophic cardiomyopathy: relation to magnitude ofleft ventricular hypertrophy. Circulation 1985;72:310-6.
28. Betocchi S. Bonow RO. Bacharach SL. Rosing DR. Maron Bl. Green
742 MARON ET AL.DIASTOLIC FUNCTION IN HYPERTROPHIC CARDIOMYOPATHY
MV. lsovolurnic relaxation period in hypertrophic cardiomyopathy:assessment by radionuclide angiography. J Am Coli Card iol 1986;7:74- lIl .
2'.J . Honow RO. Ostrow HG. Rosing DR. er al. Verapamil effects on leftventricular systolic and diastolic function in patients with hypertrophiccardiomyopathy: pressure-volume analysis with a non-imaging scintillation probe. Circulation 1983;6l1: 1062-73 .
30. Betocch i S. Cannon RO. Watson RM. el al. Effects of sublingualnifedipine on hemodynamics and systolic and diastolic function inpatients with hypertrophic cardiomyopathy. Circulation 1985;72: 1001- 7.
31 . Hirota Y. A clinical study of left ventricular relaxation. Circulation19l10;62 :756-63.
32 . Miyatake K. Okamoto M. Kinoshita N. et al. Augmentation of atrialcontribution to left ventricular inflow with aging as assessed by intracardiac Doppler flowmetry . Am J Cardiol 1984;53:586-9.
.13. Snider RA. Gidding SS. Rocchini AI'. et al. Doppler evaluation ofleft ventricular diastolic filling in children with systemichypertension.Am J Cardiol 1985;56:921-6.
34 . Fujii 1. Yoshizumi Y. Sawada H, Aizawa T, Watanabe H, Kato K.Noninvasive assessment of left and right ventricular filling in myocardial infarction with a two-dimensional Doppler echocardiograph icmethod. J Am Coli Cardiol 1985 ;5: 1155-60.
35 . Charmer KS. Culling W. Wilde P. Jones JV. Estimation of left ventricular end-diastolic pressure by pulsed Doppler ultrasound , Lancet19l16: I : 1005-7 .
.'0. Rokey R. Kuo LC, Zoghbi WA. Limacher Me. Quinones MA. Determinationof parameters of left ventricular diastolic filling with pulsedDoppler echocardiography: comparison with cineangiography. Circulation 1985:71:543- 50.
37 . Spirito 1'. Maron B1. Bonow RO. Noninvasive assessment of leftventricular diastolic function: comparative analysis of Doppler echocardiographic and radionuclide angiographic techniques. J Am ColiCardiol 1986;7:5111-26.
3l1. Takenaka K. Dabesiani A. Gardin JM. et al. Left ventricular fillingin hypertrophic cardiomyopathy: a pulsed Doppler echocardiographicstudy. J Am Coli Cardiol 1986;7:1203-7 1.
J':l . Kitabatake A, Inoue M. Asao M, et al. Transmitral blood flow reflecting diastolic behaviour of the left ventricle in health and disease:a study by pulsed Doppler technique. Jpn Circ J 1982;46:92-102.
40 . Abbassi A. Allen M. DeCristofaro D. Ungar U. Detection and estimation of the degree of mitral regurgitation by range-gated pulsedDoppler echocardiography. Circulation I9110;6 I:143-7.
41 . Savage DD, Drayer JIM. Henry WL. et al. Echocardiographic assessment of cardiac anatomy and function in hypertensive subjects.Circulation 1979 ;59:623-32 .
42 . Spirito P. Maron BJ. Significance of left ventricular outflow tract
l ACC Vol. 10. No.4October 1987:733-42
cross-sectional area in hypertrophic cardiomyopathy: a two-dimensional echocard iographic assessment. Circulation 19113;67 : 1100- 8 .
43 . Pollick C, Rakowski H. Wigle ED. Muscular subao rtic stenosis: thequantitative relationship betweensystolic anterior motion and the pressure gradient. Circulation 19114;69:43-9 .
44 . Henry WL. Clark CE, Glancy DL. Epstein SE. Echocardiographicmeasurement of left ventricular outflow gradient in idiopathic hypertrophic subaortic stenosis. N Engl J Med I973;2R8:989- 93.
45 . Spirito P. Maron BJ. Belloui P. Chiarella F. Vecchio C. Noninvasiveassessment of left ventricular diastolic function: comparative analysisof pulsed Doppler ultrasound and digitized M-mode ech oc ard iography .Am J Cardiol 1986;58:837- 43.
46 . Tajik AJ, Seward JB. Hagler DJ, Mair DO. Lie JT. Two-dimensionalrealtime ultrasoundimaging of the heart and great vessels. Technique.image orientation, structure identification and validation. Mayo ClinProc 1978:53:271-303 .
47. Wigle ED, Adelman AG. Auger P, Marquis Y. Mitral regurgitationin muscular subaortic stenosis. Am J Cardiol 1969;24:698-706.
48. Kinoshita N. Nimura Y, Okamoto M. Miyatake K. Nagata S. Sakakibara H. Mitral regurgitation in hypertrophic cardiomyopathy. Noninvasive study by two-dimensional Doppler echocardiography. Br HeartJ I983A9:574-113.
49 . Brutsaert DL. Housmans PR. Goethals MA. Dual control of relaxation. Its role in the ventricular function in the mammalian heart. CircRes 1980;47:637-52.
50 . Hori M, Inoue M. Kitakaze M. et al. Ejection liming as a majordeterminant of left ventricular relaxation rate in isolated perfused canine heart. Circ Res 1984;55:31-8 .
51 . Wigle ED. Auger P. Marquis Y. Muscular subaortic stenosis. Thedirect relation between the intraventricular pressure difference and theleft ventricular ejection time. Circulation 1967;36 :36-44.
52. Maron B1. Gottdiener JS. Arce 1. Rosing DR. Wesley YEo EpsteinSE. Dynamic subaortic obstruction in hypertrophic cardiomyopathy:analysis by pulsed Doppler echocardiography. J Am Coli Cardiol1985;6:1-15.
53. Gardin JM. Dabestani A. Glasgow GA. Butman S. Bum CS. HenryWL. Echocardiographic and Doppler flow observations in obstructedand nonobstructed hypertrophic cardiomyopathy. Am J Cardiol 1985;56:6 14- 2 1.
54 . Gaasch WHo Cole JS. Quinones MA. Alexander JK. Dynamic determinants of left ventricular diastolic pressure-volume relations inman. Circulation 1975;51:317-23.
55 . Grossman W. McLaurin LP. Diastolic properties of the left ventricle.Ann Intern Med 1976;84 :316-26 .
56 . Grossman W. Barry WHoDiastolic pressure-volume relations in thediseased heart. Fed Proc 1980 ;39: 148-55 .




















