New perspectives on saw palmetto - UCL Discovery
241
New perspectives on saw palmetto {Serenoo repens): a medico historical/ analytical comparison of preparations derived from it and a clinical pilot trial in patients with benign prostatic hyperplasia and sexual dysfunctions Andy Suter Submitted for degree of Doctor of Philosophy Centre for Pharmacognosy and Phytotherapy The School of Pharmacy University of London
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of New perspectives on saw palmetto - UCL Discovery

New perspectives on saw palmetto
{Serenoo repens):
a medico historical/ analytical comparison
of preparations derived from it and a clinical
pilot trial in patients with benign prostatic
hyperplasia and sexual dysfunctions
Andy Suter
Submitted for degree of Doctor of Philosophy
Centre for Pharmacognosy and Phytotherapy
The School of Pharmacy
University of London
ProQuest Number: 10104226
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest.
ProQuest 10104226
Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States Code.
Microform Edition © ProQuest LLC.
ProQuest LLC 789 East Eisenhower Parkway
P.O. Box 1346 Ann Arbor, Ml 48106-1346

For my parents
and
Maja and Matthias
Andy Suter

This thesis describes research conducted in the School of Pharmacy, University of
London/University College of London between May 2008 and April 2012 under the
supervision of Professor Michael Heinrich.
I certify that the research described is original and that any parts of the work that have
been conducted by collaboration are clearly indicated. I also certify that I have written
all the text herein and have clearly indicated by suitable citation any part of this
dissertation that has already appeared in publication.
O c h é ^ '2 ^ ( 7 -
Signature Date
Anc/y Suter

Acknowledgements
Acknowledgements
I would like to express my gratitude to :
My supervisor Prof. Michael Heinrich for giving me the opportunity to carry out this
thesis, the interesting talks we had, his critical advice, and the entertaining group
meetings. I really enjoyed carrying out this phD in the good atmosphere of his research
group, it felt good being a student again!
A.Vogel Bioforce AG in RoggwiI, Switzerland and in particular Martin Tobler, Head of
Research and Quality, for enabling me to do this thesis and the financial funding.
Prof. Reinhard Sailer from the Department of Internal Medicine, Institute of Natural
Medicine, University Hospital of Zurich, for his advice on the study design and the
critical interpretation of the study results.
Roy Upton from the American Botanical Council and David Winston, head of the David
Winston's Center for Herbal Studies in New Jersey, U.S.A. for providing me documents
and sources on the first uses of saw palmetto by U.S. American physicians.
Monika Huber from the library of the Medical Historic Institute of the University of
Zurich for her help and support in finding historical medical literature.
Brigitte Strassel and Ana Krnjic from the Analytical département of A.Vogel Bioforce AG
for their great help with the analytical work of the saw palmetto preparations.
All the physicians and patients who attended in the clinical trial and invested a lot of
their time and efforts to make this a successful study.
Peter Klein, from d.s.h. statistical services GmbH, Rohrbach, Germany for helping in
solving statistical problems and his ideas for a proper analysis of the clinical trial.
All the people from the research group from Michael Heinrich for the inspiring and
enjoyable discussions at the group meetings.
And last but not least to Maja for her support, patience, and her great help to make this
thesis happen.
Andy Suter 4
/cù'e of CO/: (e/l
Table of contents
Abstract................................................................................................................................ 14
Aims..............................................................................................................................15
Thesis Layout...............................................................................................................16
1 Chapter 1; General Introduction..................................................................................... 18
1.1 Saw palmetto - the plant (Sabal serrulata, Serenoa repens)............................. 18
1.1.1 Discovery and taxonomic description............................................................. 18
1.1.2 Botanical Description..........................................................................................19
1.1.3 Distribution and Ecology.................................................................................... 20
1.1.4 Wildlife Use.......................................................................................................... 22
1.2 Pharmacological data of saw palmetto................................................................... 23
1.2.1 Constituents......................................................................................................... 23
1.2.2 Antiandrogenic properties.................................................................................25
1.2.3 Anti-inflammatory activity.................................................................................28
1.2.4 Muscle relaxation and vasodilatative effects................................................. 29
1.2.5 Interactions with P450 enzymes....................................................................... 30
1.3 lexicological assessment of saw palmetto............................................................ 31
1.3.1 Acute Toxicity..................................................................................................... 31
1.3.2 Repeat Dose Toxicity..........................................................................................31
1.3.3 Reproductive and developmental toxicity..................................................... 32
1.4 Clinical efficacy and safety of saw palmetto.......................................................... 33
1.4.1 Benign Prostatic Hyperplasia - the disease.................................................... 33
1.5 Clinical data from saw palmetto preparations.......................................................47
1.5.1 Monographs on saw palmetto, recommendedpreparations and daily dosages......................................................................47
1.5.2 Clinical studies with saw palmetto preparations.......................................... 48
1.6 Final remarks............................................................................................................... 49

Table o f conten i i
2 Chapter 2: Historical part.................................................................................................. 51
2.1 Introduction.................................................................................................................. 51
2.2 Research Strategy and Methods............................................................................... 52
2.2.1 Research strategy............................................................................................... 52
2.3 Results........................................................................................................................... 56
2.3.1 The history of benign prostatic hyperplasia and its treatment...................56
2.3.2 History of human use of saw palm etto...........................................................62
2.4 Discussion..................................................................................................................... 80
3 Chapter 3: Phytochemical analysis..................................................................................88
3.1 Introduction.................................................................................................................. 88
3.2 Material and Methods............................................................................................... 92
3.2.1 Reference samples..............................................................................................92
3.2.2 Thin layer chromatography (TLC) for identification..................................... 95
3.2.3 Gas chromatography for analysis of fatty acids............................................ 97
3.3 Results.........................................................................................................................103
3.3.1 Identification of the test samples with TLC..................................................103
3.3.2 Analysis of fatty acids...................................................................................... 110
3.4 Discussion................................................................................................................... 122
4 Chapter 4: Clinical pilot study........................................................................................ 135
4.1 Introduction................................................................................................................135
4.1.1 Epidemiological data of SDys in the elderly male population................... 136
4.1.2 Pathophysiology of sexual dysfunctions and BPH.......................................138
4.1.3 Sexual adverse events of BPH standard medication.................................. 139
4.1.4 Data from clinical studies on saw palmetto in SDys....................................140
4.1.5 Summary and Study Rationale.......................................................................141
4.2 Material and Methods............................................................................................. 142
4.2.1 Study design.......................................................................................................142
4.2.2 Investigators......................................................................................................144
4.2.3 Patients.............................................................................................................. 144
4.2.4 Study medication..............................................................................................145

/cù/c of con I erf:
4.2.5 Questionnaires.................................................................................................. 145
4.2.6 Assessment of adverse and serious adverse events.................................. 151
4.2.7 Assessed parameters....................................................................................... 152
4.2.8 Quality Standards and patient's safety......................................................... 152
4.2.9 Statistical analysis.............................................................................................153
4.3 Results.........................................................................................................................155
4.3.1 Patients and centres........................................................................................ 155
4.3.2 Efficacy............................................................................................................... 158
4.3.3 Acceptance and practice and policy questions...........................................164
4.3.4 Safety................................................................................................................. 165
4.3.5 Subgroup analyses........................................................................................... 166
4.3.6 Correlation analysis of changes and relationshipbetween bSFI and Urolife QoL-9 sex score.................................................. 167
4.4 Discussion...................................................................................................................170
5 Chapter 5: General discussion and conclusion...........................................................178
5.1 General discussion.....................................................................................................178
5.2 Final conclusion........................................................................................................183
6 Literature...........................................................................................................................184
7 Appendix........................................................................................................................... 215
7.1 Appendix 1................................................................................................................. 215
7.2 Appendix 2................................................................................................................. 221
7.3 Appendix 3................................................................................................................. 226
7.4 Publications................................................................................................................240
A no'/ Sivfcr
Figures
Figure 1: Saw palmetto plant with ripe berries (Source; A.Vogel Bioforce AG)..............20
Figure 2: The local distribution of Serenoa repens indicated with green colour,after United States Geological Survey USGS, 2006 (2)...................................... 21
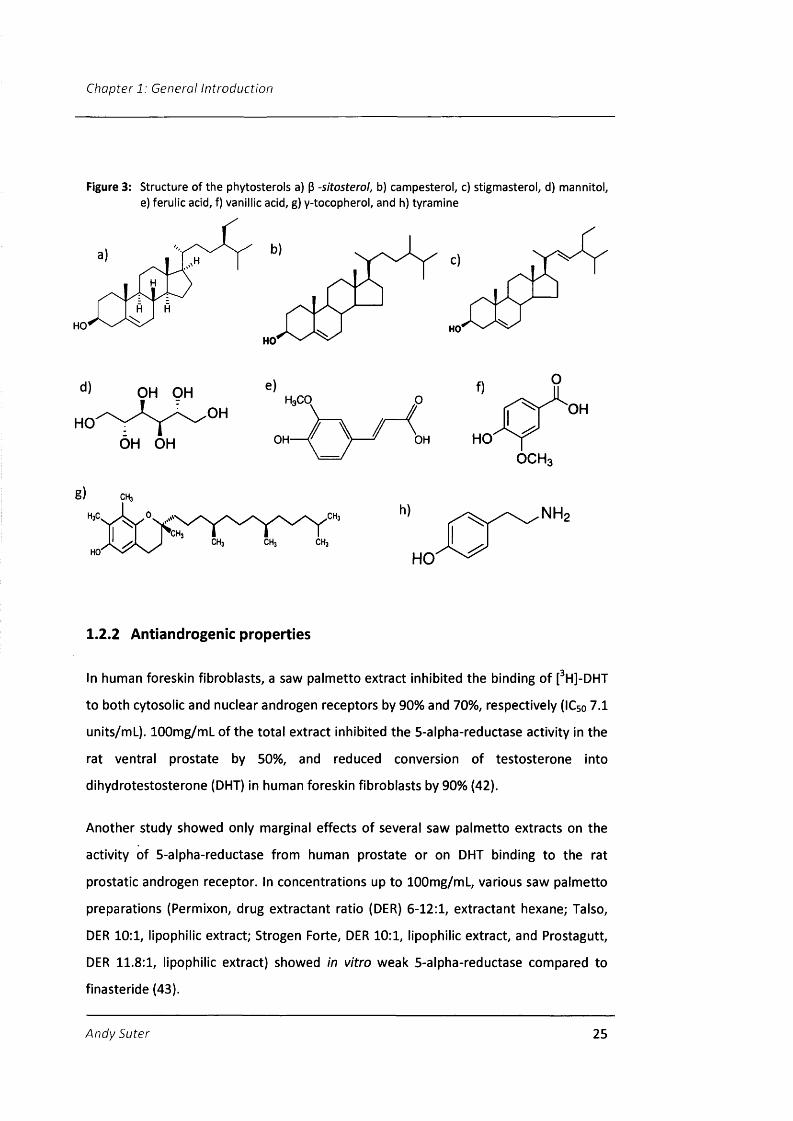
Figure 3: Structure of the phytosterols a) p -sitosterol, b) cam peste ro I, c) stigmasterol, d) mannitol, e) ferulic acid, f) vanillic acid, g) y-tocopherol, and h) tyramine.......................................................................... 25
Figure 4: Schematic drawing of prostate gland (1 )............................................................. 34
Figure 5: Presence of histologic BPH at autopsy by age group (3)....................................38
Figure 6: Chromatogram of a saw palmetto preparation with the identified peaks.. 102
Figure 7: TLC finger print profile of six different tablets.................................................. 103
Figure 8: TLC finger print profile of the tablet preparation SPSS...................................104
Figure 9: TLC fingerprints of nine products in hard gel capsules....................................105
Figure 10: TLC fingerprints of three hard gel capsules.......................................................105
Figure 11: TLC fingerprint of the six Swiss saw palmetto preparations........................... 106
Figure 12: TLC fingerprints of 14 different saw palmetto preparationswith soft gel capsules........................................................................................... 107
Figure 13: TLC fingerprints of two preparations made with soft gel capsules 108
Figure 14: TLC fingerprint of five saw palmetto preparations with soft gel capsules.. 108
Figure 15: Amount fatty acids per day of the lowest daily dosage givenon the package for each analysed product [mg/d] of all 46 investigated
commercial preparations...................................................................................... 112
Figure 16: Total amount of fatty acids per minimal daily dosage [mg/d]for mono products sorted by their country of origin.....................................113
Figure 17: Daily amount of total fatty acids for combination products accordingto the minimal dose of every preparation [mg/d], divided by country of origin........................................................................................................................ 114
Figure 18: Relative amount of the analysed single fatty acids compared to the total fatty acid content for each investigated combination product. (n=27).......................................................................................................117
Figure 19: Relative amount of the analysed single fatty acids compared to thetotal fatty acid content for each investigated mono product. (n=19).......... 119
Figure 20: Ellipse scores of saw palmetto soft extracts (SP25-37) versuscombination products (SP16-SP21) in chloroform...........................................121
Andv Suter 8
Figure 21: Urolife BPH QoL9-subscale 'patient's perceived sexual life' (from (446))... 149
Figure 22: The brief Sexual Function Inventory bSFI questionnaire (4 )........................... 150
Figure 23: Number of patients per study centre, the blue bars comprise theintention to treat- (n=84), the red bars the per protocol population which was used for the efficacy anaylsis (n=69)...............................................155
Figure 24: Change of International Prostate Symptom Score IPSS betweenthe start and end of treatment (Per Protocol population, n = 69)................ 158
Figure 25: Relative changes of the single IPSS items and the subscores fromvisit 2 to visit 3 (Per Protocol population, n=69).............................................. 159
Figure 26: Improvement of brief Sexual Function Inventory bSFI at start andend of therapy (Per Protocol population, n = 6 9 ).............................................160
Figure 27: Single item scores of the bSFI at the start and end of treatment, normalised to a scale of 0-10 (0 = worst state, 10 = best)(PP population, n = 69)..........................................................................................161
Figure 28: Relative improvements of the bSFI and Urolife QoL-9 total scores and single items between begin and end of treatment (PP-population, n=69)...........................................................................................163
Figure 29: Assessment of efficacy at end of treatment by patient andinvestigator for the PP-population (n=69).........................................................164
Figure 30: Assessment of tolerability at end of treatment by patient andinvestigator for the safety population (n=82)................................................... 165
Figure 31: Correlation between change in IPSS and changes in bSFI,compared between all visits. PP-population (n=69)........................................ 167
Figure 32: Correlation between change in IPSS and changes inUrolife QoL-9 for all visits, PP-population (n=69).............................................167
Figure 33: Correlation between IPSS and total Urolife QoL-9 for all visits,PP population (n=69)............................................................................................. 168
Figure 34: Correlation between total bSFI and total Urolife QoL-9 sex for all visits,PP population (n=69)............................................................................................. 168
:L:ier
Table:
Tables
Table 1: Treatment scheme for BPH patients with regard to their LUTS, prostate size, severity of symptoms, and complications after Issa, 2007 (100) with modifications regarding the use of saw palmetto after Geavlete (144) and Gregorin (145 )............................................................. 46
Table 2: Requirements on daily dosages and extractants from themonographs on saw palmetto...............................................................................48
Table 3: Libraries and online resources for the literature search..................................55
Table 4: Documented use of the whole plant of saw palmetto in historyin the United States and first mentioning in monographs and pharmacopoeia.........................................................................................................71
Table 5: Documented historical use of saw palmetto in Germanscientific literature.................................................................................................. 79
Table 6: Details of the 46 preparations containing saw palmetto whichwere included in the analytic comparison..........................................................94
Table 7: The elemental formula, lipid number, structure, and pharmacologicalactivities of the gaschromatographically analysed fatty acids...................... 110
Table 8: Differences between the amount of saw palmetto extract as statedon the package and the measured concentration of total fatty acids per tablet or capsule.....................................................................................................116
Table 9: The frequency of nine fatty acids in different saw palmettopreparations, the whole fruit, and extracts from Pygeum africanum, pumpkin seeds, olive, and coconut oil as comparison..................................... 125
Table 10: Mean content of the phytosterols campesterol, stigmasteroland ^-sitosterol in different preparations containing saw palmetto according to (340).................................................................................................. 130
Table 11: Study design of the pilot study with saw palmetto on SDysin BPH patients (Prostasan® Libido trial)............................................................143
Table 12: The International Prostate Symptom Score IPSS (99).....................................146
Table 13: Study procedure for a patient............................................................................ 154
Table 14: Demographic characteristics of the Intention to Treat andthe Per Protocol population.................................................................................157
Table 15: Single item scores of the bSFI and Urolife BPH QoL-9 at the startand end of treatment (n = 69)............................................................................. 160
A/io'y 10

Abbreviations
List of Abbreviations
AOAC
AP
ASEX
AST
AUASI
AUR
B.C.
BfArM
BPH
bSFI
bw
COX
CRF
CYP
DAN-PSSsex
DER
DMT
DISF/DISF-SR
ECso
ED
ESCOP
FAME
FDA
FID
GC
GCP
HPTLC
Association of Official Analytical Chemists
Sum of area of fatty acids in a sample
Arizona Sexual Experience Scale
Area of internal standard
American Urological Association Symptom Index
Acute urinary retention
Before Christ
Bundesinstitut für Arzneimittel und Medizinprodukte
Benign Prostatic Hyperplasia
Brief Sexual Function Inventory
Body weight
Cyclooxygenase
Case record form
Cytochrome
Danish Prostatic Symptom Score questionnaire for sexual dysfunction
Drug extractant ratio
Dihydrotestosterone
Derogatis Interview for Sexual Functioning
Half maximal effective concentration
Erectile dysfunctions
European Scientific Cooperative on Phytotherapy
Fatty acid methyl esters
Food and Drug Administration
Flame ionization detector
Gas chromatography
Good Clinical Practice
High performance thin layer chromatography
Andy Suter 11
Abbreviations
IC50
iD
IIEF
IIEF-5
IIEF-ED
IL
INF
IPSS
ITT
ITT
LNCaP
LOX
LUTS
kPa
MSHQ-EjD
MTOPS
NMR
NO
NSAID
PCA
PDE
PP
PRV
PSA
Q .m ax
QoL
RCT
Rf
Half maximal inhibitory concentration
Internal diameter
International Index of Erectile Function Questionnaire
Short version of the International Index of Erectile Function Questionnaire with only 5 questions
International Index of Erectile Function Questionnaire- erectile dysfunction subscale
Interleukine
Interferone
International Prostate Symptom Score
Intention to treat population
Intention to treat population
Human prostate adenocarcinoma cell line
Lipoxygenase
Lower urinary tract symptoms
kiloPascal
Male Sexual Health Questionnaire to assess ejaculatory dysfunction
Medical Therapy of Prostatic Symptoms study
Nuclear magnetic resonance
Nitric oxide
Non steroidal antiinflammatory drug
Principal component analysis
Phosphodiesterase
Per protocol population
Post-void residual urine
Prostatic specific antigen
Maximum Urinary Flow Rate
Quality of Life
Randomised clinical trial
Retardation factor
Andy Suter 12
Abbreviations
SDys
SHGB
SP
TID
TLC
Urolife QoL-9
Urolife QoL-9 sex
UV
Vklin
WHO
WIT
WS
Sexual dysfunctions
Sex hormone binding globulin
Sample (for the phytochemical analysis)
Three times daily
Thin layer chromatography
Urolife BPH Quality of Life 9-questionnaire
Urolife BPH Quality of Life 9-questionnaire subscale for 'patient's perceived sexual life'
Ultraviolet
Verordnung für klinische Studien
World Health Organisation
Weight of internal standard
Weight of sample
Andy Suter 13

Abstract
Saw palmetto berries {Serenoa repens) are used today for treatment of symptoms of
benign prostatic hyperplasia (BPH) which is an age dependent disease leading to lower
urinary tract symptoms (LUTS) and impacts negatively sexual functions.
I carried out the first clinical pilot trial to assess if a saw palmetto treatment in patients
with BPH and concomitant sexual dysfunctions (SDys) is effective and safe in both
groups of symptoms. After 8 weeks of treatment with 320mg saw palmetto extract
daily, BPH symptoms measured with the International Prostate Symptom Score IPSS
were reduced from 14.4 ± 4.7 to 6.9 ± 5.2 (p<0.0001). At the same time SDys measured
with the brief Sexual Function Inventory bSFI improved from 22.4 ± 7.2 to 31.4 ± 9.2
(p<0.0001), and with the Urolife BPH QoL-9 sex questionnaire from 137.3 ± 47.9 to
195.0 ± 56.3 (p<0.0001). The treatment was very well tolerated and accepted by the
patients.
Another subject of this thesis was to examine the quality of commercial preparations
from eight countries which contained saw palmetto and are sold as treatments for BPH
symptoms. For each of the 46 analysed products the amount of the main active
constituents, the fatty acids was determined using gas chromatography. The quantity of
fatty acids per daily dosage varied widely between the products and also the
composition of the samples was very heterogeneous.
A medico-historical investigation how saw palmetto was introduced firstly into U.S.
American medicine and how the plant became popular as a treatment in Germany was
the last aspect of the thesis. The eclectic physicians pioneered in using this plant in the
United States supported by homeopathic doctors and pharmacists. In Germany, mainly
the homeopaths favoured the use of saw palmetto and were the trailblazers making it a
popular treatment for BPH symptoms.
In conclusion, this thesis shows comprehensively how saw palmetto made its way into
medical practice in the United States and Germany, that preparations on the markets
containing saw palmetto differ widely in their content of the main active constituents,
the fatty acids, and thus higher quality demands from regulatory authorities are
warranted, and in a pilot trial it could be shown that saw palmetto is not only an
effective and safe treatment for BPH symptoms but also for concomitant SDys.
Andy Suter 14

Aims
Aims
In this thesis new data on historical, phytochemical, and clinical aspects of saw
palmetto as a medical treatment should be presented . This includes in more detail
• A historical review how saw palmetto became a popular treatment in the United
States and how the plant made it into the medical practice in Germany, this all
embedded in the historical context of treatment of benign prostatic hyperplasia
(BPH)
• A phytochemical analysis of 46 commercial preparations containing saw palmetto
on their amount of the main active constituents, the fatty acids
• A clinical pilot trial with a standardised saw palmetto product in patients with BPH
and sexual dysfunctions to assess if this treatment may improve not only urinary
symptoms but also concomitant sexual disorders
Andy Suter 15

Thesis Layout
Thesis Layout
The Chapter 1 presents a general introduction into botanical, pharmacological,
toxicological, and clinical particulars of saw palmetto and provides also an introduction
into the disease benign prostatic hyperplasia (BPH).
In Chapter 2 the history of treatments for BPH are laid out, followed by a
comprehensive review on the history of the use of saw palmetto. This includes the
traditional use by the indigenous population of the Florida region, the first mentioning
of the plant in Western literature and how the plant became a popular treatment in the
United States. The last part of this chapter depicts how saw palmetto was introduced
into the German scientific community and when the plant was acknowledged as a
medical treatment for BPH.
The Chapter 3 provides a phytochemical analysis of 46 commercial preparations which
contain saw palmetto and are sold as treatments for BPH.
Chapter 4 shows results from a clinical pilot trial in patients with BPH and concomitant
sexual dysfunctions.
Finally, Chapter 5 includes the final discussion and conclusions of all results gathered in
this phD thesis.
Andy Suter 16

Chapter 1
An introduction to saw paimetto, the plant, its pharmacology and efficacy
and
to benign prostatic hyperplasia BPH, the disease, its diagnosis, and treatments
Andy Suter 17
Chapter 1: General Introduction
1.1 Saw palmetto - the plant (Sabal serrulata, Serenoa
repens)
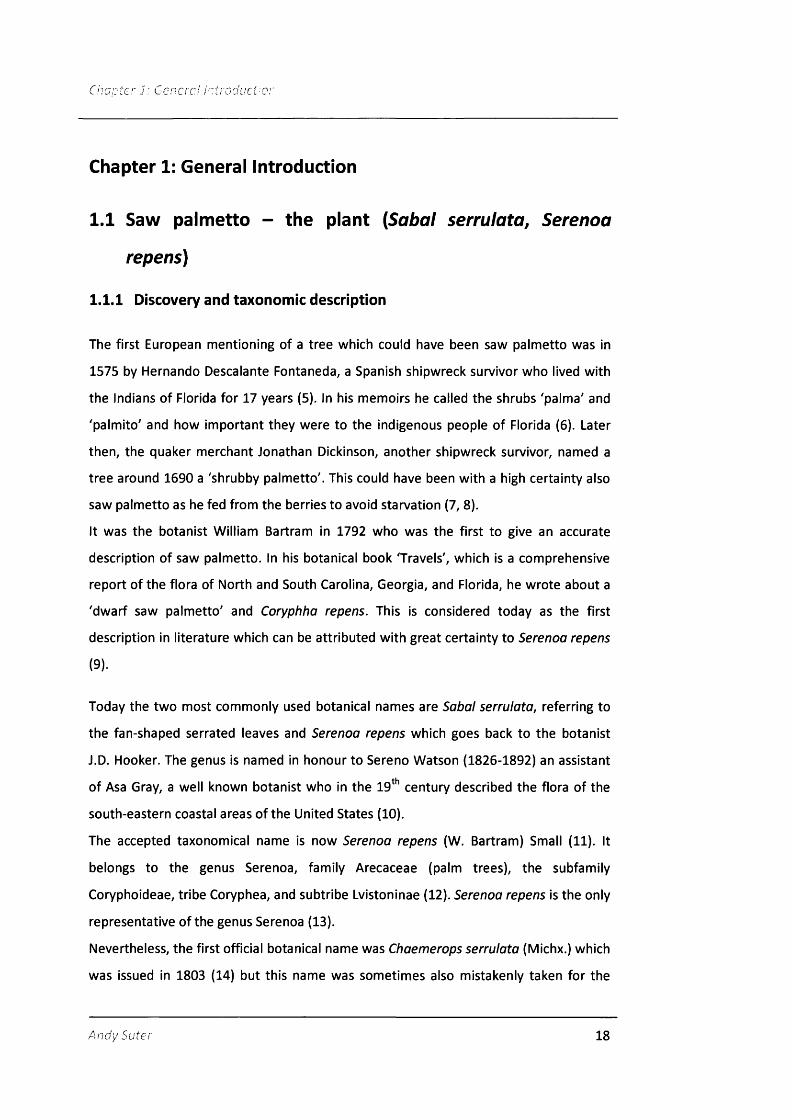
1.1.1 Discovery and taxonomie description
The first European mentioning of a tree which could have been saw palmetto was in
1575 by Hernando Descalante Fontaneda, a Spanish shipwreck survivor who lived with
the Indians of Florida for 17 years (5). In his memoirs he called the shrubs 'palma' and
'palmito' and how important they were to the indigenous people of Florida (6). Later
then, the quaker merchant Jonathan Dickinson, another shipwreck survivor, named a
tree around 1690 a 'shrubby palmetto'. This could have been with a high certainty also
saw palmetto as he fed from the berries to avoid starvation (7, 8).
It was the botanist William Bartram in 1792 who was the first to give an accurate
description of saw palmetto. In his botanical book 'Travels', which is a comprehensive
report of the flora of North and South Carolina, Georgia, and Florida, he wrote about a
'dwarf saw palmetto' and Coryphha repens. This is considered today as the first
description in literature which can be attributed with great certainty to Serenoa repens
(9).
Today the two most commonly used botanical names are Sabal serrulata, referring to
the fan-shaped serrated leaves and Serenoa repens which goes back to the botanist
J.D. Hooker. The genus is named in honour to Sereno Watson (1826-1892) an assistant
of Asa Gray, a well known botanist who in the 19 century described the flora of the
south-eastern coastal areas of the United States (10).
The accepted taxonomical name is now Serenoa repens (W. Bartram) Small (11). It
belongs to the genus Serenoa, family Arecaceae (palm trees), the subfamily
Coryphoideae, tribe Coryphea, and subtribe Lvistoninae (12). Serenoa repens is the only
representative of the genus Serenoa (13).
Nevertheless, the first official botanical name was Chaemerops serrulata (Michx.) which
was issued in 1803 (14) but this name was sometimes also mistakenly taken for the
Andy Suter 18
cabbage palm, a tree often to find in the same regions where saw palmetto grows (15).
Other common names for the plant are saw palmetto, in older literature the plant was
also often cited as dwarf palm (16) or Brahea serrulata (Michx.) or Digiossophyiium
serrulatum (Michx.) (14).
In the following only the term Serenoa repens will be used as it is the accepted name in
the botanical literature (17).
1.1.2 Botanical Description
The name of the saw palmetto is due to the saw-like leafs. These characteristic fan
shaped leaves are bright green and are up to one meter wide. Approximately three to
seven leaves are produced each year and remain alive on the plant for about two years.
The plant bears a densely cluster of white flowers, the so called spadix, which is shorter
than the leaves (18). The palm has a creeping and branching prostrate stem, which can
occasionally reach the height of two meters (Figure 1) (19, 20).
Saw-palmetto produces one to three prominent spadices during spring, and fruits
mature during summer. However, individual plants may flower throughout the year,
but fruit seldom matures outside the summer period.
The drupes are about the size of an olive, in its mature stages of green to orange colour
and harbour the pharmacologically active constituents. During ripening, the fruits turn
in colour from green (May-June) to yellow (mid-August), to orange (September), and to
bluish-black (September-October). Fruit production can be variable among years.
Annual average number of seeds per plant has been measured to vary between 100
and 500 in mid to late June, but decrease rapidly until mid-October when no fruits
remain on the plants (21).
Saw palmetto flowers are in densely-branched, interfoliar inflorescences, which are
about half a meter in size. The trees commonly produce one to three, at maximum five
inflorescences at the time whereas one contains several thousand individual flowers
(22).
Andv Suter 19

Chapter 1: General Introduction
By judging from their leaf scars and the length of their growing stems, it has been
estimated that the oldest saw palmetto plants in Southern Florida have an age of about
500 to 700 years (23).
Figure 1: Saw palm etto plant w ith ripe berries (Source: A.Vogel Bioforce AG)
1.1.3 Distribution and Ecology
Serenoa repens is one of the most abundant plants in the Southeastern United States. It
can be found in pine flatwoods, which are special soils formed from marine sediments,
prairies, and scrubs as well as in dunes and maritime forests but seems to be sensitive
to salt spray. Interestingly, saw palmetto is well adapted to fire and is one of the most
fire-tolerant among the pyric species (19).
Andy Suter 20

Chapter 1: General Introduction
The plant is endemic in Florida and according to the plant database of the United States
Department of Agriculture can be found also in the states of Texas, Louisiana,
Mississippi, Alabama, Indiana, Georgia, and South Carolina (24). In a similar database of
the United States Geological Survey, the same states as above are mentioned except
Texas. The map of the distribution shows that Serenoo repens occurs mainly in Florida
and in the other mentioned states mainly in the Southern coastal areas (2) (Figure 2).
Figure 2: The local distribution of Serenoa repens indicated w ith green colour, a fter United States Geological Survey USGS, 2006 (2).
A
«
— A-500 0 500 1000 1500 Kilometers ‘ X. A
EUSGS••V*
The Catalogo de las Plantas Vasculares de Panama describes the occurrence of Serenoo
repens also in Panama, which would be contradictory to the data above (25).
Generally, the plant grows best in regions with an average annual rainfall of 100-163 cm
and a minimum to maximum temperature range of -4° to 36°C. It seems to be
cultivated only in Northern America (13).
Andy Suter 21

j ; Gcncrc/
1.1.4 Wildlife Use
A wide variety of species use saw palmetto either as a source for food or for nesting or
protective cover.
Animals known to use it for nesting cover are the endangered Florida grasshopper
sparrow (Ammodramus savannarum), the Florida wood rat {Neotoma floridana), the
wild turkey {Meleagris gallopavo), the Florida panther {Felis concolor) (26), and the
Florida black bear {Ursus americanus ssp. floridanus) (19). As escape cover or bedding
cover during windy, cold days it is used by the white-tailed deer {Odocoileus
virginaniana) (27).
Not only the berries but also the apical meristem, the so-called heart of the plant are
eaten. It is physically extracted and eaten by black bears and feral pigs (Sus scrofa).
They usually eat on the freshly regrown plants after a fire (26). Cattle are known to
consume the leaves only if there is no better forage (28) or they consume the fronds
during winter (26).
However, generally, the herbal parts or the stem of the plant has little value as livestock
forage (29), in particular since the frond is less than 30% digestible even though its
phosphorous content is relatively high (26).
Over 300 species of insects have been observed visiting saw palmetto flowers. Some of
these flower visitors collect nectar and/or pollen, while others find mates or prey near
or on the flowers. The main visitors of the flowers and thus the primary pollinators
appear to be bees; the other most frequently observed insects were mostly dipterans
or hymenopterans (30).
The berries are the main source of food from saw palmetto for animals. A large variety
of animals have been observed consuming them, such as raccoons, foxes, rats, gopher
tortoises, white tail deer, black bears, feral hogs, and even fish and waterfowl (19). The
fruit or more precisely the drupe is an excellent source for carbohydrates and oils. In
late summer when the fruits are ripe, they are eaten extensively by black bears. A road
killed adult female bear was found to have more than 13,5 kg of saw palmetto fruit in
its stomach (26). White tailed deer favour the berries as an important late autumn and
Andy Suter 22

early-winter food, whilst given to cows it has been observed that they produce more
and better milk (19).
Generally, the animals eating the drupes serve as dispersal agents as the seeds are
distributed throughout the landscape in faeces (26). The fruit's endocarp and seed coat
are impermeable to oxygen and it takes four to six months for these tissues to
deteriorate (24).
In total, the plant itself provides food or cover for more than 100 bird, 27 mammal, 25
amphibian, and 61 reptile species (31).
1.2 Pharmacological data of saw palmetto
1.2.1 Constituents
The dried saw palmetto berries consist to about 36% of pericarp, 16% pulp, 10% testa
of the seed, and 38% of the seed. The pulp contains a highly active lipase which
dissociates triglycerides during ripening and drying to single fatty acids (32). The fruits
primarily contain free fatty acids such as capric, caproic, caprylic, lauric, myristic, oleic,
linoleic, linolenic, stearic, and palmitic acids (17) and their ethyl esters and glycerides
(33) which occur most likely during the extraction process (17). This process is catalysed
by an esterase which is to be found in the pulp (32). An analysis of 14 saw palmetto
berry extracts showed that up to 52.15 % of the total extract were methyl- or ethyl
esters and glycerides (34), while an investigation of the pressed juice of the berries
estimated that about one third of the oil were ethyl esters (32). Schantz et al. found in
an analysis of the saw palmetto fruit and a hexane/acetone (4:1 v/v) extract that the
ratio of triglycerides to free fatty acids in the fruit and the extract was about 2:1 (35). A
more extensive description of the fatty acids with the structure formulae is given in
chapter 3.3.2.
Further sterols (17) and specially the phytosterols such as ^-sitosterol and p-sitosterol
3-0-D-glucoside, (33) campesterol and stigmasterole can be found (Figure 3) (36). The
amount of phytosterols is rather low compared to the whole extract, the analyzed
amounts are in the range from 0.45 (35) to 0.1% of total mass in ripe fruits (37) to 1.9-
55.4mg campesterol, 4 -28 .6mg stigmasterol, and 6.9-174mg ^-sitosterol per lOOg in
Ar:dySi‘tcr 23

several investigated saw palmetto preparations like powdered berries, aquaeous,
ethanolic, and CO2 extracts (36).
An investigation on the substances of the hydrodistillate of saw palmetto berries
identified 144 compounds whereas lauric acid was with an amount of 40.4% the main
detected component (38).
Other constituents are carbohydrates such as mannitol and polysaccharides with
galactose and arabinose (33), triterpenes (17), aromatic acids like ferulic and vanillic
acid (33), |3-carotens, the vitamine E dérivâtes y-tocopherol and 6-tocopherols (35), and
the monoamine tyramine which was reported to be 0.72% of the total mass of an
ethanolic saw palmetto extract (Figure 3) (39).
In total, in lipophilic saw palmetto berry extracts, the fatty acids and its esters are
predomintant and comprise to about 75-95% of the total extract (40).
It is assumed that the fatty acids together with the phytosterols are the main active
principles of saw palmetto, particularly in treatment of prostate problems (41).
Since the main use of saw palmetto preparations is in benign prostatic hyperplasia
(BPH), the majority of the pharmacological experiments have been carried out targeting
this disease. These are primarily investigations on anti-androgenic, anti-inflammatory
and on muscle relaxation or vasodilatative effects where always lipophilic saw palmetto
berries extracts were used. They are abbreviated in the following as saw palmetto
extracts.
An civ Suter 24
Chapter 1: General Introduction
Figure 3: S tructure o f the phytosterols a) P -sitosterol, b) campesterol, c) stigm asterol, d) m annlto l, e) fe ru llc acid, f) vanillic acid, g) y-tocopherol, and h) tyram ine
HO'HO'
HO'
OH OH
OH OH
H3CO
OH
OH
1.2.2 Antiandrogenic properties
In human foreskin fibroblasts, a saw palmetto extract inhibited the binding of [^H]-DHT
to both cytosolic and nuclear androgen receptors by 90% and 70%, respectively (IC50 7.1
units/mL). lOOmg/mL of the total extract inhibited the 5-alpha-reductase activity in the
rat ventral prostate by 50%, and reduced conversion of testosterone into
dihydrotestosterone (DHT) in human foreskin fibroblasts by 90% (42).
Another study showed only marginal effects of several saw palmetto extracts on the
activity of 5-alpha-reductase from human prostate or on DHT binding to the rat
prostatic androgen receptor. In concentrations up to 100mg/mL, various saw palmetto
preparations (Permixon, drug extractant ratio (PER) 6-12:1, extractant hexane; Talso,
PER 10:1, lipophilic extract; Strogen Forte, PER 10:1, lipophilic extract, and Prostagutt,
PER 11.8:1, lipophilic extract) showed in vitro weak 5-alpha-reductase compared to
finasteride (43).
Andy Suter 25
i; Gr/ierc./ /r'r''cc/üTf'b.'i
The mode of action of saw palmetto and finasteride appears to be different. While the
addition of saw palmetto extract inhibited metabolism of [^H]-testosterone (0.1 pM) in
human prostate epithelial cells and fibroblasts to all metabolites (DHT, androst-4-ene-
3.17-dione, 5a-androstane-3,17-dione), finasteride blocked conversion of [^H]-
testosterone (0.1 pM) to DHT and 5a-androstane-3,17-dione, but not androst-4-ene-
3.17-dione. If this difference is relevant in the in vivo situation is questionable (44). The
inhibition of the two isoforms of 5-alpha-reductase by saw palmetto extract seems to
be non-competitive and less potent with a Ki level about ten times higher than
finasteride, which was a competitive inhibitor (45).
Of a fractioned saw palmetto extract - i) saponifiable, ii) non-saponifiable, and iii)
hydrophilic sub fractions - only the saponifiable sub-fraction (consisting mainly of lauric,
oleic, myristic and palmitic acids) was active in inhibiting 5-alpha-reductase.
Of the fatty acids investigated, lauric acid was the most active: It inhibited epithelial
and stromal 5-alpha-reductase activity by 51% and 42%, respectively, non-
competitively and dose dependently up to a concentration of O.2mmol/L. The non-
saponifiable fraction, consisting mainly of phytosterols, was weakly active, while the
hydrophilic sub fractions, containing carbohydrates, amino acids and polysaccharides,
were inactive (46). Raynaud, 2002 confirmed these findings, he showed that the dual
inhibitory activity of saw palmetto extract on 5-alpha-reductase type 1 and type 2 can
be attributed to its high content in free fatty acids (47). Also, lipophilic saw palmetto
extract effectively inhibited in LNCaP prostate cancer cell lines 5-alpha-reductase
activity (48).
A further confirmation of the in vitro results was seen in a rat model of prostate
hyperplasia induced by androgen stimulation. After oral administration of saw palmetto
extract, 200mg/d for six days, the hormone-induced increase in prostate weight was
stopped (49). Another trial showed similar findings : 50mg/kg bw/d saw palmetto
extract inhibited hormone-induced prostate weight as well. The maximum effect was
reached after 60 and 90 days for the dorsal and lateral regions of the rat prostate, and
for ventral region after 30 days and 60 days, respectively (50). Furthermore, in rats a
saw palmetto extract decreased testosterone-induced prostate weight by 38% (150mg
extract/d) or 76% (300mg extract/d) (51). Similar effects were reported by de Lourdes,
An dy Suter 26

2007 for 400mg/kg/d for 14 days, also in a rat model (52). The reduction of prostate
weight was 44%, while Jaipur, 2003 reported a reduction to the size of the control
group (53).
In dogs with asymptomatic mild to moderate prostate enlargement, a dose of 1,500
mg/d TID saw palmetto extract which is about five times of the human dose of 320mg
or 300mg/d TID for 90 days did not affect prostatic weight, volume or histology. In a
similar trial set up saw palmetto extract did not affect the prostate in the same way as
finasteride (54).
The in vitro results suggest that saw palmetto inhibits the 5-alpha-reductase due to its
content of fatty acids. But the interaction with the enzymes seems to be different from
that of finasteride. To which extent the inhibition is clinically relevant is still part of
discussion and needs further investigation but animal testing showed that this mode of
action could be of relevance for saw palmetto. In trials with biopsies of BPH patients no
clear confirmation of these findings could be observed. Di Silverio, 1992, saw small
antiandrogenic and antiestrogenic effects (55) and in removed prostate tissue after saw
palmetto berries treatment, effects on oestrogen, progesterone and androgen
receptors were seen in the nuclear, but not in the cytosolic fraction. In a subsequent
trial the decrease of DHT - as marker of 5-alpha-reductase activity in vivo - in that
region correlated with clinical improvements (56).
Andv Suter 27

C/73'/:f'cr ] Gc.ncrc,'
1.2.3 Anti-inflammatory activity
As will be shown below (Chapter 2), saw palmetto preparations were used traditionally
for diseases with a certain inflammatory component like cough or epididymitis. Even
though an anti-inflammatory activity could be of therapeutical relevance, only few
experimental data on this subject is available.
An older experiment showed moderate antiinflammatory activity. In a guinea pig model
lipophilic 1-5ml/kg bw saw palmetto extract one hour before exposure to UV light
inhibited erythema. But carrageenan induced rat paw oedema was not reduced, in line
with this that saw palmetto extract did not inhibit platelet cyclooxygenase (57).
Adult male Wistar rats, receiving 50 or 100mg/kg bw saw palmetto extract for 90 days
displayed a reduced accumulation of mast cells in proximal stroma in a dose dependent
manner (58) and Sabal extract prepared with supercritical carbon dioxide inhibited
cyclooxygenase and 5-lipoxygenase in vitro ( I C 5 0 28.1 and 18.0pg/mL, respectively) (59).
Further evidence of the antiinflammatory activity could be shown in vitro using LPS-
induced IL-12 formation with androgen-independent human prostate cancer PC-3 cells.
Saw palmetto extract 50pg/mL reduced this LPS-induced IL-12 formation by 40% (60).
Anti-inflammatory activity in vivo was investigated by Vela-Navarrete, 2005. The pilot
study showed a significant reduction of inflammatory parameters in prostatic tissues of
patients treated with saw palmetto extract. Interestingly, a correlation with clinical
improvement was observed (61).
AndvSulcr 28

1.2.4 Muscle relaxation and vasodilatative effects
The traditional use of saw palmetto particularly in bladder problems in women as will
be described in chapter 2, points to the possibility that extracts of the plant could also
interaction with specific receptors in the bladder. To some extent, positive results have
been seen but there is clear evidence yet lacking.
A saw palmetto extract inhibited specific binding of [H]-[N-methyl-H] scopolamine
methyl chloride (bladder) and [H]-prazosin (prostate) with IC50 values of 46.1 and 183
pg/ml, respectively (62). Another study showed that various saw palmetto extracts
inhibited radioligand binding to human prostatic alphal-adrenoceptors and agonist-
induced [^H]inositol phosphate formation in vitro noncompetitively (63). But the results
could not be confirmed in a subsequent clinical trial in 12 healthy volunteers (64).
In a series of in vitro experiments, saw palmetto extract inhibited the muscarinic M3
receptor with an I C 5 0 of 3-30pg/ml but not on the M l and M2 receptor. The M3
receptor is seen as the relevant receptor which needs to be inhibited to influence
overactive bladder syndrome (65).
Saw palmetto extract exerted significant binding activity on autonomic receptors in the
lower urinary tract under in vitro and in vivo conditions. Oral administration of saw
palmetto extract to rats significantly changed the maximal number of binding sites for
prostatic [^H]-prazosin binding and for bladder [^H]NMS binding. This alteration by saw
palmetto extract was selective to the receptors in the lower urinary tract (6 6 ).
A single dose of 60mg/kg saw palmetto extract caused in a hyperactive rat bladder
model a significant improvement of the micturition interval, micturition volume and
bladder capacity during intravesical saline infusion. Also, doses of 12 and 20mg/kg
significantly reversed the reduced micturition interval as well as the decreased
micturition volume and bladder capacity due to 0 .1 % acetic acid infusion dose
dependently. Repeated administration to conscious, freely moving rats of 6 mg/kg saw
palmetto extract daily constantly increased the micturition interval and concomitantly
decreased voiding frequency. These experiments showed that saw palmetto worked, at
least in the animal model, also in overactive bladder (62).
Andy Suter 29
1.2.5 Interactions with P450 enzymes
Based on in vitro and in vivo trials there are almost no signais for a relevant interaction
potential for saw palmetto. These findings correspond well with the clinical situation as
in patients so far no cases have been reported (17). The majority of BPH patients are
older than 60 years of age (67) and usually use more than only one medication (6 8 ).
The findings from the P450 studies imply that patients with concomitant medication
which is metabolised by P450 enzymes are not at risk of any interactions by taking
alongside a saw palmetto preparation.
Yale, 2005 reported a slight inhibition in vitro of CYP3A4, CYP2D6, and CYP2C9 with a
lipophilic saw palmetto extract which contained 85-95% fatty acids and sterols and 0.1-
0.3% d-sitosterol (producer PhytoPharmacia, Green Bay, U.S.A.). For the experiments
the extract was drained and diluted 1:10 in 2% methanol. The IC50 for the test items
were 0.8% of the enzyme activity for CYP2D6,0.14% or 0.24% for CYP3A4 depending on
substrate, and 0.43% for CYP2C9 calculated from the inhibitory concentrations of the
undiluted primary test samples (69). Budzinski, 2000 found only moderate inhibitory
potential on CYP3A4 when compared to the test substance 7-benzyloxyresorufin.
Among 21 investigated herbal products, the assessed saw palmetto preparation was
ranked 13 regarding its interaction potential, Hydrastis canadensis and Hypericum
perforatum had the lowest inhibitory concentrations. The tested saw palmetto product
was only described as a commercial product available in Canada. Echinacea purpurea
herb and ginkgo biloba, which were tested by both groups, had comparable results like
saw palmetto in both trials (69, 70).
An investigation on the ability of different herbal preparations to inhibit UDP-
glucuronosyltransferase showed a moderate inhibitory potential of 55.2 ± 9.2pg/ml for
a 96% ethanolic saw palmetto extract with more than 85% fatty acids and more than
0.1% sterols (Finzelberg and Co. KG, Andernach, Germany), but the clinical relevance of
this finding is unclear (71).
An dy Suter 30

C/ijprcr J. Gcnr.";?!/.'-!"'
In two clinical trials this topic was addressed in twelve healthy subjects of both sexes in
each trial. Markowitz, 2003 showed that 320mg saw palmetto extract four times daily
for 14 days did not change the enzyme activities of CYP2D6 and CYP3A4. There were no
significant differences between the mean ratios at baseline and after saw palmetto
exposure for dextrometorphane (CYP2D6 activity) and alprazolam (CYP3A4 activity).
The authors conclude that when taken at the recommended doses, saw palmetto
extracts are unlikely to lead to interaction with other medication which use the same
cytochromes for clearance (72).
Gurley, 2004 administered 320mg saw palmetto extract twice daily, containing
85 - 95 % of fatty acids, for 28 days. The extract had no influence on the activity of
CYP1A2, CYP2E1, CYP2D6 and CYP3A4. The authors stated as well that prolonged use of
saw palmetto poses a minimal risk of drug interactions related to interference with
these CYP enzymes (73).
1.3 Toxîcological assessment of saw palmetto
1.3.1 Acute Toxicity
In experiments to determine the anti-oedematous effect of a hexane extract of saw
palmetto maximum an oral dose of 10mI/kg exerted no 'toxic effects'. The calculated
LDso added up to 54mL/kg in male rats. However, no details were provided in support
of this statement. A dosage of 50mL/kg lead mice to no deaths after oral administration
of a saw palmetto extract (57).
1.3.2 Repeat Dose Toxicity
Following a report that a product containing a saw palmetto preparation caused
cholestatic hepatitis, the effect of saw palmetto on rat liver function was assessed.
Investigated were the effects of a saw palmetto extract on several enzymes and
formation of malondialdehyde (MDA), a by-product of lipid peroxidation. A significant
increase in these parameters is considered to be an indicator of liver toxicity. Thirty-six
rats were treated for two or four weeks with a placebo or saw palmetto at doses of
Andv Suter 31

9.14 or 22.86mg/kg/bw/day; that is, 2 x and 5 x the maximum recommended daily
human dosages. After two or four weeks, the results showed no significant difference in
animal body weight, enzyme activity, or MDA formation at either time or dosage level,
as compared to controls. The data indicate that saw palmetto is not involved in a
mechanism causing liver toxicity (74).
These results are in line with reports on animal toxicity. In male Wistar rats 50 and 100
mg/kg bw saw palmetto extract given by oral gavage, showed no toxicity. Also, no
changes in body and prostate weight at necropsy, and macroscopic examination of
prostate were noted (58).
No adverse effects were observed at higher levels for a shorter period of time. Rats
tolerated 100, 320 and 640mg/kg/d saw palmetto extract in 2.5% ethanol well for 30
days (75).
1.3.3 Reproductive and developmental toxicity
There is only limited data available on reproductive toxicity. In an in vitro study with
hamster oocytes and sperm, a lipophilic saw palmetto extract produced no significant
effect on sperm motility at doses of 0.9mg/mL. The extract had no inhibitory effect on
the penetration of oocytes by sperm nor were dénaturations or mutations of DNA
detected after prolonged exposure to this herb (76). Also, a newer study showed no
influence of saw palmetto in a mice model to induce DNA damage (77) nor did they
observe any mutagenic signals in Ames tests (78, 79).
Overall, saw palmetto extract appears to be safe for use in men with BPH in particular
in the recommended daily dosage of 320mg. In the period of January 2003 to
December 2007, 61.4 million daily dosages of Prostasan®, the preparation used in the
trial in this thesis, have been sold worldwide. During this time, only one minor case was
reported to the Pharmacovigilance Department of A.Vogel Bioforce AG (80).
A n d y Suter 32
i; Gcicrc.'
1.4 Clinical efficacy and safety of saw palmetto
More than 90 publications on clinical trials with saw palmetto extracts are available; all
were carried out in benign prostatic hyperplasia (BPH).
Thus, in the following the disease BPH will be explained before discussing the results of
the studies with saw palmetto. The next chapters will give information on the aetiology
and course of the disease, its diagnosis and the therapy options. A more detailed
description of the history of BPH and its treatments are given in chapter 2.
1.4.1 Benign Prostatic Hyperplasia - the disease
1.4.1.1 Aetiology of the disease
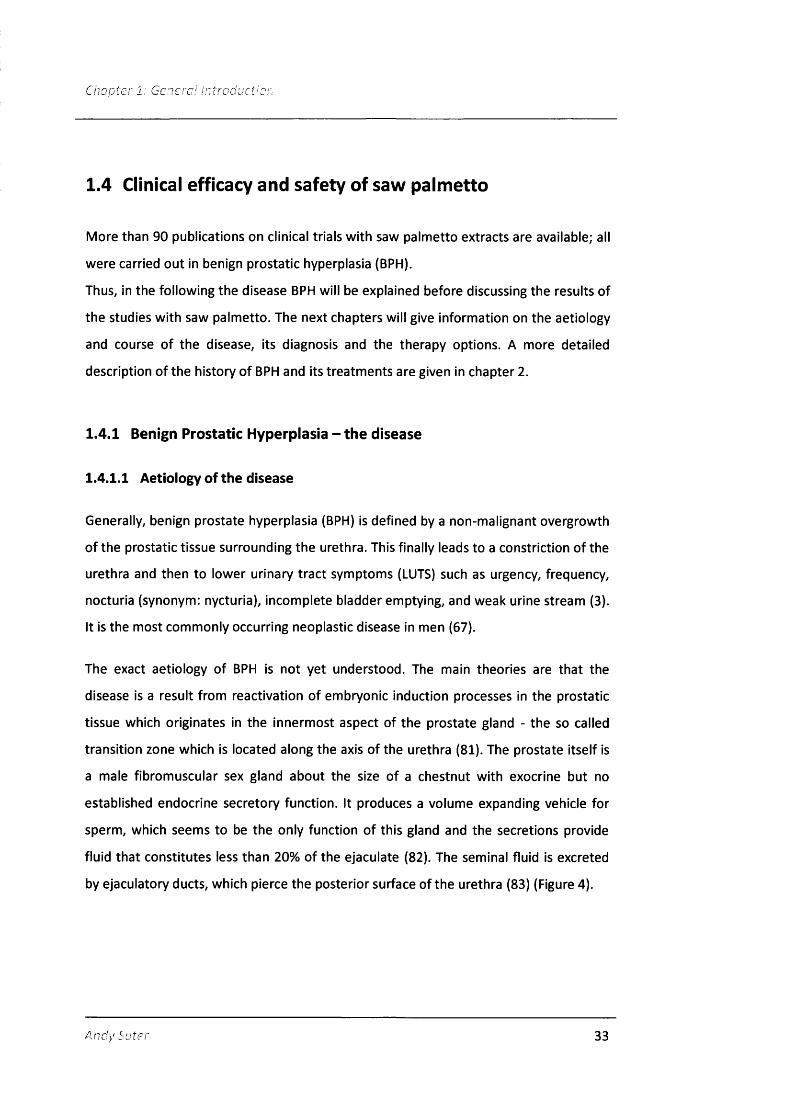
Generally, benign prostate hyperplasia (BPH) is defined by a non-malignant overgrowth
of the prostatic tissue surrounding the urethra. This finally leads to a constriction of the
urethra and then to lower urinary tract symptoms (LUTS) such as urgency, frequency,
nocturia (synonym: nycturia), incomplete bladder emptying, and weak urine stream (3).
It is the most commonly occurring neoplastic disease in men (67).
The exact aetiology of BPH is not yet understood. The main theories are that the
disease is a result from reactivation of embryonic induction processes in the prostatic
tissue which originates in the innermost aspect of the prostate gland - the so called
transition zone which is located along the axis of the urethra (81). The prostate itself is
a male fibromuscular sex gland about the size of a chestnut with exocrine but no
established endocrine secretory function. It produces a volume expanding vehicle for
sperm, which seems to be the only function of this gland and the secretions provide
fluid that constitutes less than 20% of the ejaculate (82). The seminal fluid is excreted
by ejaculatory ducts, which pierce the posterior surface of the urethra (83) (Figure 4).
Andy Suter 33

Chapter 1: General Introduction
Figure 4: Schematic drawing o f prostate gland (1)
Ureter opening
Bladder
Prostate
Opening of: Prostatic duct Ejaculatory
Sphincter
Verumontanum
Urethra
As mentioned the reason for the prostatic growth is not yet clearly understood. The
central factor is certainly age as it affects men above the age of 40 (67). There are some
theories for the reasons of the prostate growth postulated so far:
One is the hyperactivity of the membrane-bound 5-alpha-reductase, the enzyme that
converts testosterone to DHT, which in the end then leads to an increased cell
proliferation. Patients suffering from a 5-alpha-reductase deficiency show prostatic
volumes, which are approximately 1/10^ of age-matched normal controls highlighting
the importance of DHT for the normal formation of the prostate (84). On the other
hand, there is certainty that the development of BPH is exclusively dependent on
androgens since BPH does not occur in men castrated prior to puberty (85). The
reasons why the two isoforms of the 5-alpha-reductase should be overexpressed can
not be explained yet (86).
Andy Suter 34
Another influence on the prostate growth may be the shift in the balance of
testosterone to oestrogen, which tends towards oestrogen in the aging men. The
reason for this is that more testosterone is converted to DHT and bioavailable
testosterone levels decline due to decreased production by the testis and increased sex
hormone binding globulin (SHGB) levels which combine to lower free circulating
testosterone (87). However, circulating levels of free estradiol which is secreted mainly
by the adrenal gland remain constant in the aging male due to an age-related increase
in body weight and adipose cells which express high levels of aromatase and convert
androgens to oestrogens. The outcome is a significant increase in the
oestrogen/testosterone ratio allowing the balance of prostate growth to shift towards
oestrogen dominance. It has been proposed that increased estrogenic stimulation of
the prostate in the aging male may lead to reactivation of growth and subsequent
neoplastic transformation (88) mainly by activation of estrogenic receptors in the
prostatic tissue (89).
Another theory, which has received increasing attention postulates that BPH may be
triggered or at least catalysed by inflammatory conditions (90).
Histologically, the association of BPH and inflammation is well recognised. Already in
1979, it was noted that 98% in a series of 162 resected prostates had inflammatory
lesions (91). There is also clinical evidence for this hypothesis, two studies found a clear
correlation between inflammatory stages such as prostatitis and either the prostate
size (92) or symptom progression and prostate resection (93). A long term study carried
out between 1988 and 1994 in 2337 men in the United States revealed that those
having an increased C-reactive protein level of 3mg/l which acts as a marker of acute
inflammations were 1.47 times more likely to have more BPH symptoms than those
with lower values (94).
There are a lot of cytokines such as IL-2, IL-4, IL-6, IL-8, IL-15, IL-17 and INF-y involved in
inflammatory processes in BPH and have been found with rates of increased expression
and higher amounts at all in enlarged prostates. This lead to the hypothesis that BPH is
not only an inflammatory but as well an immuno-inflammatory disease since some of
the cytokines are not inflammatory at all but rather immune modulatory like IL-4 or
INF-y (95).
A ndy Suter 35

C/iGcrc," G cnerov
So far there is one clinical trial available which has investigated the influence of an anti
inflammatory drug on BPH symptoms. Patients suffering from BPH taking the COX-2
inhibitor celecoxib had, after only one month of treatment, significantly less nocturia
and a significantly lower score in the International Prostate Symptom Score IPSS than
those taking placebo (96). This trial indicated that the inhibition of the inflammatory
component of the BPH may lead to fast symptom relief for the patients.
The latest theory postulates that the prostate growth is a secondary condition caused
by insufficient veins in the testicles. Because of the inadequate transport of blood from
the testicular veins to the upper body, the prostate which is penetrated by this vein, is
exposed to blood which contains up to 130-fold the serum level of testosterone. This
testosterone is then converted to DHT and leads subsequently to prostatic cell
proliferation (97). This theory is plausible as it is the only one explaining why and how
an increased amount testosterone is available in the prostate as in elderly men the
serum levels of this hormone are decreasing (98). First results from 28 patients where
the insufficient veins were obliterated showed good treatment results in reducing their
BPH symptoms (97).
1.4.1.2 Course of the disease and diagnosis
BPH symptoms occur in men over the age of 40 who have testosterone-producing
testes, whereas morphologically it can already be detected in men over 30 years of age
(99). The main symptoms which have static and dynamic components (100) are
increased frequency of urination with nocturia, difficulty starting and stopping
urination, weak urine stream, feeling that the bladder has not emptied completely with
residual urine and in later stages urinary retention and painful urination (101).
The symptoms may not progress over time. Studies have shown that in populations
over a period of three years about 25% of all patients who had primary symptoms of
BPH respectively lower urinary tract symptoms (LUTS) had an improvement in their
symptoms without treatment (99).
Andy Suter 36
i; Ge/iem/ /nfroc-'ucf;,:
BPH is not a life threatening disease except when urinary retention is not treated since
this could lead to renal failure (102). Nevertheless, it may affect the quality of life of
patients in many ways be it by causing lack of sleep by nocturia, pressure to visit the
toilet very frequently or fear of urine smell due to terminal dribbling.
The disease is mainly diagnosed by assessment of the symptoms. The standard
instrument is a validated questionnaire, the International Prostate Symptom Score IPSS
(99) or the American Urological Association (AUA) symptom score (103). The difference
to the IPSS is that there is an additional quality of life question amended (99).
The severity of the disease is furthermore defined in two classifications, one from
Aiken, 1955 (104) and the other from Vahlensieck, 1985 (105), which are mostly used in
Germany. Whereas Aiken defines the three stages mild, moderate and severe as the
irritative, the residual urine and the decompensation-stages, in the definition of
Vahlensieck there are four stages with the first three being similar to the Aiken
definition, but he adds an initial stage where no symptoms occur at all.
A common diagnosis of BPH is via rectal examination, but it is important to note that
enlargement does not correlate with the severity of symptoms (106). With the physical
exam prostatic cancer can be excluded since cancerous tissue is different at palpation
than smooth BPH-tissue. A marker for prostatic cancer is additionally the measurement
of the prostate-specific antigen PSA, even though its values may be influenced by other
conditions like for example inflammations (107).
Optional tests for the evaluation of the BPH or LUTS include urinary flow rate
measurements, post void residual urine measurements, pressure flow studies and
ultrasonography to determine the size of the prostate (106).
Andy Suter 37

Chapter 1: General Introduction
1.4.1.3 Epidemiology
Histologically BPH is shown in 8% of men aged 31 to 40 years. This number rises
progressively with age and can be distinguished in the 9 decade in about 90% of all
men. Figure 5 shows the frequency of histologic BPH in different age groups (3).
Figure 5: Presence of histologic BPH at autopsy by age group (3)
100 ^90
60 - *
0
31-40 51-60 61-70 81-90
Age Group (y)
Prostatic enlargement is a necessary but not sufficient condition for the development
of LUTS. This means that not all men having an enlarged prostate finally also suffer
from the symptoms of a BPH as mentioned previously (67).
Epidemiological studies have shown that nearly 50% of all men of age 80-90 suffer from
symptoms (108). The prostate size nevertheless seems to be the main factor for
inducing the symptoms; The odds to develop moderate to severe symptoms after the
age of 50 were 3.5 higher in men with a prostate volume >50mL than those with
smaller prostate volume (109).
Andy Suter 38

Comparison of data for development of microscopic BPH from the USA, England,
Denmark, Austria, India, and Japan showed that there is almost no difference in
frequency related to age group (67). Another large epidemiological study indicated that
black and Hispanic men were at higher risk of having BPH symptoms (110) whereas in a
large survey in the United States no difference in frequencies for BPH surgery between
Black, Asian and White males could be found (111).
In the study of Kristal with 5667 BPH patients obesity, particularly abdominal obesity,
was one of the main risk factors leading to BPH symptoms (110). Another survey
detailed that in addition intake of alcohol, lack of physical activity, and diabetes were
risk factors, it could not be established if smoking, diet, hypertension, and
environmental factors were connected to increased BPH symptoms (112). Genetic
factors and diet may nevertheless have an important influence on the progression of
BPH. The occurrence of BPH is less frequent in Asian countries as compared to the
United States. However, on entering the USA, Asians immigrants develop BPH mirroring
the rates of US American men (101).
Because of its high prevalence in the older male population, BPH is an increasing
burden for the health systems.
It is the fourth most diagnosed disease in men older than 50 years with a prevalence
rate of 13.5%, which is in the same range as osteoarthritis (113). For the U.S.A., the
direct costs of medical services for treatment of BPH are estimated to about
1.1 billion $ per year (114) whereas a Spanish study assessed the costs for only
medicine for one BPH patient per year to about 300 Euro (115).
Ai i c ' yS.uter 39
CAcp i?.'' j. Ge/icrc' A'lr.' ooyc Vc.".
1.4.1.4 Treatment of BPH
1.4.1.4.1 Watchful waiting
The first treatment option for patients with an IPSS up the total score of seven points is
watchful waiting (106). Studies have shown that for these patients medical treatments
are not better than placebo. The patient needs to be monitored during this phase as
well as spontaneous exacerbations and remissions of BPH may occur (116).
1.4.1.4.2 Medical treatments
1.4.1.4.2.1 Herbal preparations
Even though not stated in any of the actual treatment guidelines on BPH such as the
U.S. American, British, Australian, European, and Canadian guidelines (117)
phytomedicinal products are often applied as first line treatments to reduce BPH
symptoms.
The main used herbal products are saw palmetto preparations or combinations of saw
palmetto with stinging nettle which provide good treatment results in patients with
mild to moderate symptoms of BPH also showing good tolerability (118). Since there is
a strong patient demand for saw palmetto it is stated in one treatment guideline that
doctors nevertheless should become familiar with this treatment (106).
There are further herbal treatments available for the treatment of BPH.
Preparations made from African plum (Pygeum africanum) showed positive effects on
the symptoms of BPH. The authors of a Cochrane analysis including 18 controlled
clinical trials concluded that despite of weak methodologies, small number of patients
in the trials, and the short study durations a small but significant improvement
compared to placebo could be observed. In these studies lipophilic extracts containing
mainly fatty acids with a daily amount of lOOmg were applied (119,120).
Andy Suter 40

Since men in Asia suffer less from BPH it is assumed that probably a soy-rich diet may
be a treatment option for BPH or its prevention. A short term clinical trial (one month)
with an isoflavone product derived from red clover ('Trinovin') showed in dosages of 40
mg and 80mg per day a rapid relief of BPH symptoms with a very good safety profile
(121).
In several placebo controlled studies ^-sitosterol exerted promising effects in patients
with BPH (122-126). A shortcoming of these trials is their big heterogeneity regarding
the investigated products and the number of participants which ranged from 62 (122)
to 200 (124). The used preparations contained pure ^-sitosterol or ^-sitosterol-
glucoside of diverse origin, with different daily dosages. In the trial of Berges 60mg p-
s/tostero/from Cucurbita pepo were applied daily which were described as 'containing a
variety of phytosterols' (124), Kadow used 0.3mg of a ^-sitosterol glucoside (122) and
Fischer 195mg ^-sitosterol (126) per day, and Klippel 130mg free ^-sitosterol from
Hypoxis rooperi, Pinus pinaster, and Picea abies (125). Except for the lowest dose of
0.3mg ^-sitosterol glucoside, the trials showed good efficacy and safety. A Cochrane
analysis (2000) carried out on the use of ^-sitosterol in the treatment of BPH symptoms
based on these few trials suggested that the use of non-glucosidic ^-sitosterol could
improve urinary symptoms and flow measurements but gave no recommendation on
the daily dosage (127).
Three placebo controlled clinical trials have been carried out with a rye grass pollen
extract. The available evidence suggests that rye pollen extract was well tolerated and
modestly improved overall urological symptoms, including nocturia. In one trial rye
grass pollen was superior in its efficacy to a Pygeum africanum preparation. Since the
trials were mostly not carried out with state of the art parameters and were of short
treatment duration, currently a conclusive statement if rye-grass pollen extract is a
reasonable treatment option cannot be made (128).
\nc'y Suter 41

j . Ccnerj,'
1.4.1.4.2.2 Alpha blockers
For patients with an IPSS > 7 or bothersome symptoms, the main treatment prescribed
are a-blockers. This therapy is based on the concept that LUTS are partly caused by
al-adrenergic-mediated contraction of prostatic smooth muscle and bladder neck
(129). The main substances used are doxazosin, tamsulosin, alfuzosin, and terazosin.
They all have been widely studied in the treatment of BPH and LUTS (117).
The most selective of these four substances is tamsulosin since it targets the
a -lA adrenoreceptor subtype which accounts for 70% of all adrenoreceptors in the
prostate and is 13 times more specific in targeting these prostatic receptors than those
in the urethra (130).
Meta-analytical data on alpha-blockers derived from the AUA guideline showed that all
four substances have about the same efficacy whereas tamsulosin was slightly better
leading to an improvement of 4 to 6 points on the IPSS. The main advantage of a-
blockers is the fast onset of activity (131).
Side effects of these medications may differ; orthostatic hypotension, dizziness,
weakness, nasal congestion and abnormal or retrograde ejaculation were reported
most frequently (132).
1.4.1.4.2.3 5-alpha-reductase inhibitors
Currently, there are two 5-alpha-reductase inhibitors available, finasteride and
dutasteride. Dutasteride is selective for both isoforms of the 5-alpha-reductase
whereas finasteride more selectively blocks the isoform type 2 (133). Both treatments
lead to a symptom relief after 6-9 months of therapy and to a shrinking of the prostate
size by about 20% (106). The advantage of these therapies is that they significantly
prevent the incidence for surgery and urinary retention whereas alpha-blockers can
only lead to a delay of 2-2.5 years of these two items (134). The disadvantages are the
long onset of action, the efficacy seen on BPH symptoms are lower than with a-blockers
or surgery (116), and that PSA values are decreased by about 50% (135).
A:idy Suter 42
j ; Gc;:e,''c/ /ruTOo'c/cf/o.":
If long term use of 5-alpha-reductase inhibitors is favourable for chemoprevention
(prevention of prostatic cancer in particular) is still a topic for discussion. The Prostate
Cancer prevention trial with 19'000 men receiving either placebo or finasteride
revealed a significantly lower frequency of cancers in the finasteride groups but the
tumours were more aggressive than those found in the placebo group (136).
Which of the two Sa-reductase inhibitors is more efficacious is still a matter of
discussion. A large study with 5090 patients found a significant difference regarding
acute urinary retention (AUR) and prostate-related surgeries in favour of dutasteride.
Even though the differences were statistically significant they may not have been
clinically relevant as they were quite low (12% for dutasteride vs. 14.7% for finasteride)
(137).
Most often cited side effects were ejaculatory dysfunction, erectile dysfunction, and
decreased libido (138).
Regarding the choice for the right medication to treat BPH it seems that finasteride and
dutasteride are most favourable for patients with a large prostate (>50mL) whereas
a-blockers can be used in patients with all kind of prostate sizes (106).
1.4.1.4.2.4 Combination therapy
The largest trial, evaluating if a combination of an alpha blocker with a 5-alpha-
reductase inhibitor is useful in the treatment of BPH was the Medical Therapy of
Prostatic Symptoms (MTOPS) study. More than 3000 men received either placebo,
doxazosin, finasteride, and a combination of doxazosin and finasteride. After 4.5 years,
in the placebo group the AUA score had declined to a median value of 4, with doxazosin
to six points, with finasteride five points and with the combination seven points were
reached (p<0.05). With the combination the risk of progression was reduced by 66%
compared to a 39% reduction with doxazosin and 34% with finasteride (134).
An dy Suter 43
The overall outcome from this study was that the combination was more effective not
only in treatment but also in terms of a favourable progression of the BPH. The
combined use of 5-alpha-reductase inhibitors and a-blockers is generally used in every
day practice (106).
1.4.1.4.3 Surgical treatments
1.4.1.43.1 Open prostatectomy
This is the oldest and most effective treatment for relieving BPH symptoms (106). It is
still performed and recommended for large prostates (138) and the symptomatic
improvement occurs in 98% of all patients (106).
1.4.1.4.3.2 Transurethral resection of the prostate (TURP)
The method was developed in the 1920's (106) and is still the gold standard for surgical
treatment of BPH. It is a surgical procedure in which portions of the prostate gland are
removed through the urethra with a unipolar wire loop-electrocautery device. Sterile
glycine irrigation fluid is used to distend the bladder and urethra during the procedure.
After the surgery, which lasts about one hour, a catheter is placed for about one day
(138).
TURP reduces symptoms of BPH by 88% (116) and is the most effective treatment for
BPH with respect to the improvement of symptoms and flow rates (138) but morbidity
associated with the procedure is still an important issue (139). Immediate post
operative side effects include bleeding, and urinary tract infections (139), whereas long
term complications comprise retrograde ejaculation (70% of the treated patients),
impotence (14%; range 3-32%), partial incontinence (6%) and total incontinence (1%)
(140). About one in ten patients needs retreatment within five years after surgery
(116).
Andy Suter 44

C/Tcpf-E/' ' Genera/ //i/roa'ac/Vcr.
1.4.1.4.4 Other surgical treatment options
Since many elderly patients are poor surgical candidates and younger patients find the
risk of sexual dysfunction unacceptable, 'minimally invasive' surgical techniques have
been developed (106).
The transurethral microwave thermotherapy is a method where by insertion of a device
the temperature within the prostate (via the urethra) is increased to above 45“C, which
leads to necrosis of the prostatic tissue (139). The advantage of this method is that long
term complications such as impotence and retrograde ejaculation occur much less
frequently than with TURP (141) and the surgery can be performed in an ambulatory
setting (138). However, only a small patient population is eligible for this treatment
(139).
Transurethral needle ablation is a further non-invasive method where low-level
radiofrequency is delivered via a needle into the prostatic tissue. The results of this
treatment may be limited since the bladder neck and the median prostate lobe cannot
be treated but it is safe and generally well tolerated without further long term side
effects (106).
Instead of using a electrocautery device to resect the prostate tissue, laser is also
applied (laser prostatectomy). This method seems to be as effective as TURP (142) by
leading to less long term side effects but the method is not easy to apply and needs
'significant endoscopic skills' (139).
The latest minimally surgical intervention is the above mentioned so called Gat-Goren
method which aims at sclerosing insufficient testicular veins and reduces thus the
venular hypertension in the prostatic tissue and subsequently the extensive
testosterone concentration. This method is still in a pilot phase and should be
established with larger clinical trials (97).
In summary, the medical treatments fall short of achieving a patient perception of more
than fair to good improvement in most cases. The awareness of very good to excellent
improvement is reserved for surgical interventions. Patients, who are dissatisfied with
An dy Suter 45
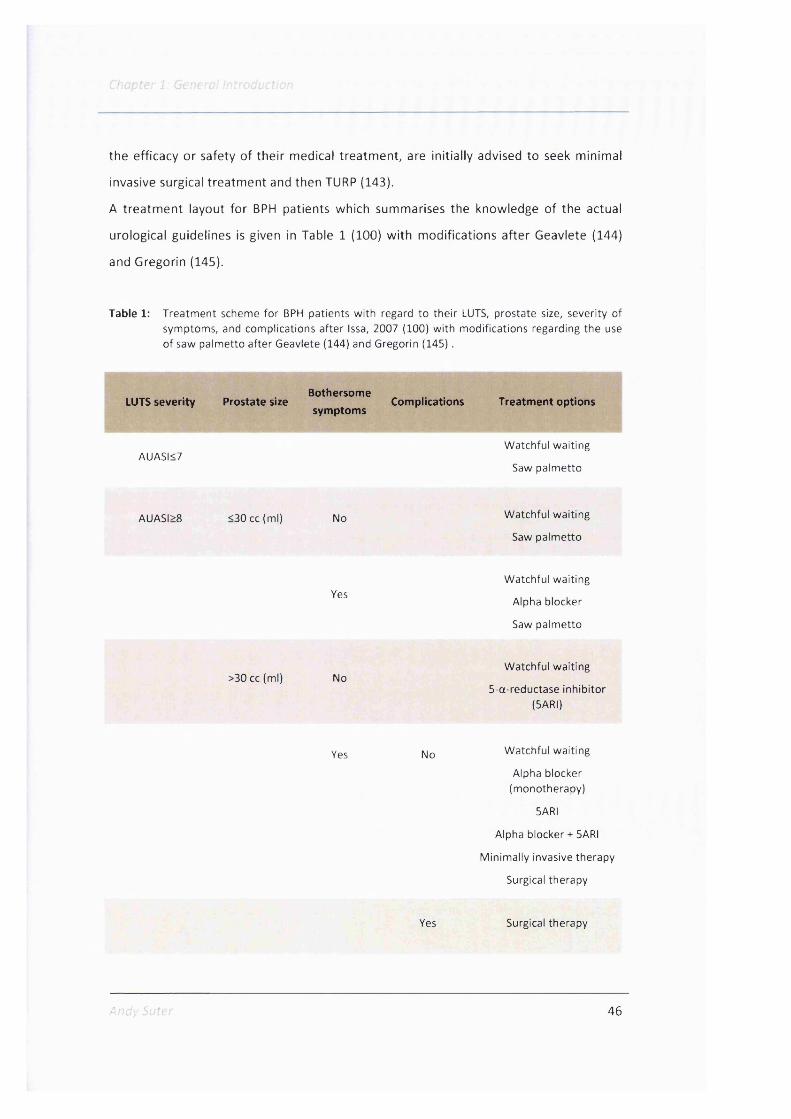
the efficacy or safety of their medical treatment, are initially advised to seek minimal
invasive surgical treatment and then TURP (143).
A treatment layout for BPH patients which summarises the knowledge of the actual
urological guidelines is given in Table 1 (100) with modifications after Geavlete (144)
and Gregorin (145).
Table 1: Treatm ent scheme fo r BPH patients w ith regard to the ir LUTS, prostate size, severity ofsymptoms, and complications after Issa, 2007 (100) w ith m odifications regarding the use o f saw palm etto a fter Geavlete (144) and Gregorin (145).
BothersomeLUTS severity Prostate size Complications Treatment options
symptoms
AUASI<7W atchful waiting
Saw palm etto
AUASI>8 <30 cc(m l) No W atchful waiting
Saw palm etto
YesW atchful waiting
Alpha blocker
Saw palm etto
>30 cc (ml) NoW atchful waiting
5-a-reductase inh ib ito r (SARI)
Yes |yjQ W atchful waiting
Alpha blocker (monotherapy)
SARI
Alpha blocker + SARI
M inim ally invasive therapy
Surgical therapy
Yes Surgical therapy
A c'v 46

C/'iuCf-c/' J, Gc/icm.''
1.5 Clinical data from saw palmetto preparations
Monographs and meta analyses are the two major sources which give an assessment
on the clinical efficacy and safety of a treatment. The main difference between these
two documents is that monographs for herbal medicines consider also the traditional
use of a plant, whereas meta analyses rely only on published clinical data.
In the following, a short summary on the present monographs on saw palmetto and the
most recent important reviews is given.
1.5.1 Monographs on saw palmetto, recommended preparations and daily
dosages
Currently, there are four monographs available on saw palmetto, an older German
Commission E monograph (146), a WHO (147) and an ESCOP monograph (17) and one
from the Canadian health authority (40). They all recommend the use of saw palmetto
in mild to moderate forms of BPH. As side effects stomach problems, nausea, diarrhoea
or other minor gastrointestinal complaints are cited. No interaction with other
medications are quoted nor any restrictions of use or contraindications.
As daily dosage 320mg of a lipophilic saw palmetto berry extract are recommended in
all monographs, the WHO monograph advices to apply this dosage as a single dose or
twice daily at ISOmg (147). The monographs advise to use extractants such as hexane
(40, 146, 147), ethanol 90% (40, 146, 147), supercritical CO2 (147) or equivalent agents
(17, 40, 146, 147). Only the Canadian monograph addresses further requirements on
the extract quality i.e. it should contain between 70-95% free fatty acids and
corresponding ethyl esters (40). Table 2 summarises the data from the monographs on
the different extractants and recommended daily dosages.
Andv Suter 47
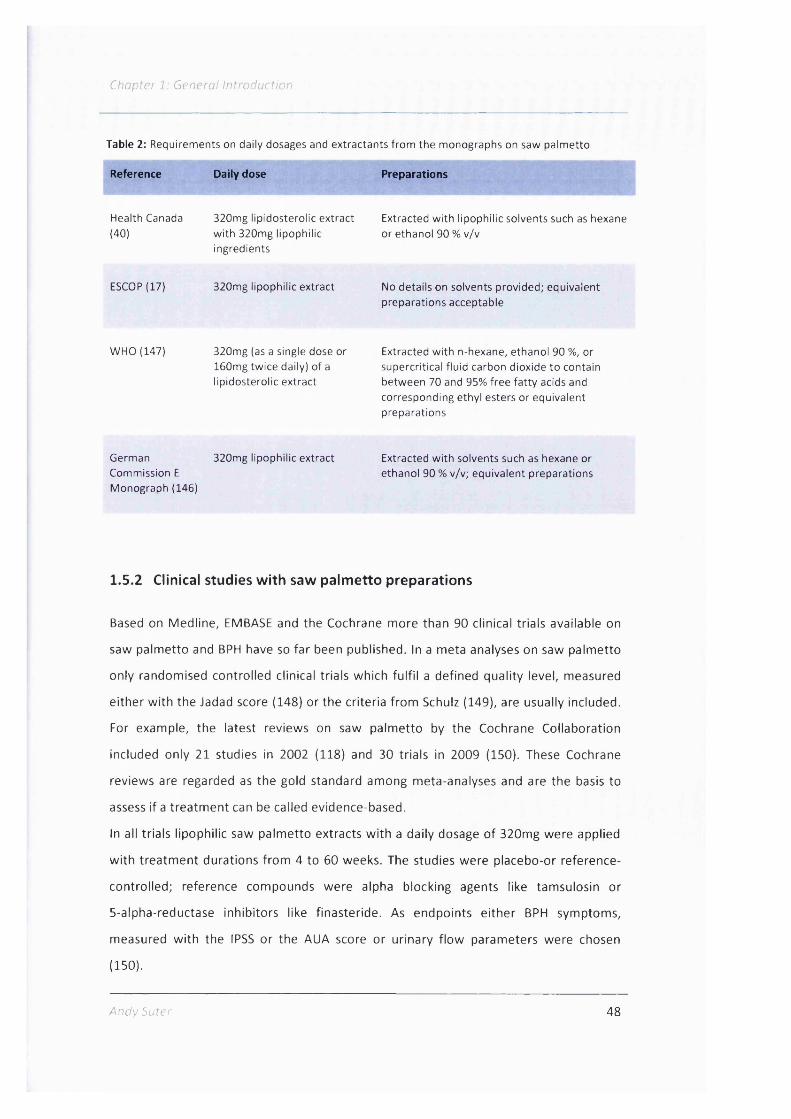
Chapter 1 General Introduction
Table 2: Requirements on daily dosages and extractants from the monographs on saw palm etto
Reference Daily dose Preparations
Health Canada (40)
ESCOP (17)
320mg lipidosterolic extract w ith 320mg lipophilic ingredients
320mg lipophilic extract
Extracted w ith lipophilic solvents such as hexane or ethanol 90 % v/v
No details on solvents provided; equivalent preparations acceptable
WHO (147) 320mg (as a single dose or160mg tw ice daily) of a lipidosterolic extract
Extracted w ith n-hexane, ethanol 90 %, or supercritical fluid carbon dioxide to contain between 70 and 95% free fa tty acids and corresponding ethyl esters or equivalent preparations
German Commission E Monograph (146)
320mg lipophilic extract Extracted w ith solvents such as hexane or ethanol 90 % v/v; equivalent preparations
1.5.2 Clinical studies w ith saw palm etto preparations
Based on Medline, EMBASE and the Cochrane more than 90 clinical trials available on
saw palmetto and BPH have so far been published. In a meta analyses on saw palmetto
only randomised controlled clinical trials which fulfil a defined quality level, measured
either with the Jadad score (148) or the criteria from Schulz (149), are usually included.
For example, the latest reviews on saw palmetto by the Cochrane Collaboration
included only 21 studies in 2002 (118) and 30 trials in 2009 (150). These Cochrane
reviews are regarded as the gold standard among meta-analyses and are the basis to
assess if a treatment can be called evidence-based.
In all trials lipophilic saw palmetto extracts with a daily dosage of 320mg were applied
with treatment durations from 4 to 60 weeks. The studies were placebo-or reference-
controlled; reference compounds were alpha blocking agents like tamsulosin or
5-alpha-reductase inhibitors like finasteride. As endpoints either BPH symptoms,
measured with the IPSS or the AUA score or urinary flow parameters were chosen
(150).
Andy Suter 48

In 2000 and 2002 the reviews from the Cochrane Collaboration gave a positive
statement on the efficacy and safety of saw palmetto in treatment of BPH symptoms.
LUTS and flow parameters were assessed as having improved significantly compared to
placebo and were as good as under finasteride treatment (118,151).
After a large placebo controlled clinical trial, carried out in the United States, with
negative outcome was published (152), the next Cochrane review in 2009 regarded the
efficacy of saw palmetto as doubtful but paradoxically still as good as finasteride or an
alpha blocking agent in longer term treatment of more than 16 weeks (150).
The findings from this review are thus often cited to question the efficacy of saw
palmetto like in the latest BPH treatment guideline from the American Urological
Association (153). In all trials, the safety of the saw palmetto preparations was
excellent, the treatments were very well tolerated and no severe side effect occurred
(154).
The conclusions from the Cochrane analyses are debatable since these reviews had a
restricted view on a treatment. They neglected not only the traditional use of the plant
but also personal experiences from urologists which regard saw palmetto as a good
symptomatic first line treatment for BPH patients (144,145). Also the trials which were
chosen in the analyses may have shortcomings as well. It is for instance not explainable
why trials from France (155-157), Italy (158, 159) or Germany (160, 161) yielded
positive results but why the latest U.S. American studies on saw palmetto in BPH
produced only negative outcomes (152,162).
1.6 Final remarks
In conclusion, there is sufficient scientific evidence from in vitro testings and animal
experiments to explain the mode of action of saw palmetto in patients with BPH.
Furthermore, there are plenty of clinical trials and personal experiences showing that
saw palmetto acts as a very well tolerated and efficacious treatment in patients with
mild to moderate BPH symptoms; this is also widely accepted and used in the
recommendations by four respected monographs.
A ndy Suter 49

Chapter 2
A short history o f the treatments fo r BPH, the use o f saw palmetto in the United
States until the 1930's and the introduction o f saw palmetto into Germany
Andy Suter 50

Chapter 2: Historical part
A short history of the treatments for BPH, the use of saw
palmetto in the United States until the 1930's and the
introduction of saw palmetto to Germany
2.1 Introduction
Today saw palmetto is a well known treatment option for mild to moderate symptoms
of BPH. In the United States, Saba I ranks third among the food supplements with an
annual sales volume of 200 million dollars (163) and an estimated number of 2.5 million
users (164). The worldwide turnover is likely to be 700 million dollars per annum (163)
reaching almost blockbuster status in pharmaceutical terms and in Germany half of the
urologists prescribe herbal treatments for BPH symptoms with saw palmetto being the
favourite one (164). The same situation is reported for France (165) and Italy where five
times more saw palmetto products are prescribed than alpha antagonists for treatment
of BPH symptoms (166).
Surprisingly, despite of the status as being one of the most popular phytomedicines
little is known about the origins of saw palmetto as a treatment for BPH. Only two
publications dealt so far to some extent with the history of the use of saw palmetto.
The book by David Winston (167) and the review by Bennett (19) give some details on
how the plant was applied by the indigenous population of the Florida region as well as
the first medical uses of saw palmetto among white settlers in the United States.
Bennett gives a good and comprehensive description of the indications where saw
palmetto was used traditionally but lacked historical data on when, how and by whom
the species was used nor did it assess the timeline of its introduction into medical
practice. Winston quotes interesting sources documenting the first use of saw palmetto
among white settlers but the historical part in his book is rather short and is not the
main scope of the book which lies in the medical use of the plant.
Andy Suter 51

C/iOjCfer 2; H / s po/i'
A coherent review on how saw palmetto made its way to become an acknowledged
treatment in the United States is lacking. The same applies also for Germany where the
plant has a special status as it is not a traditional European medicinal plant but was
introduced from the United States. There are no data who introduced saw palmetto
into Germany, how it became known and who used it first as a medical treatment or as
a food. Additionally there is no literature available which puts saw palmetto as a
treatment for BPH into the context to available and generally applied cures for this
disease until 1930.
With the medical historic part of my thesis I aimed to provide new insights about these
topics. The goal was to find out how saw palmetto was used among the Indians of the
Florida region, then how the white settlers gained knowledge about the plant, for
which indications they used it and how it was described in literature. One main interest
was further to assess if a group of practitioners favoured the use of saw palmetto and
then how this treatment became popular and made its way into the official U.S.
American compendiums.
In a last step I wanted then to find out how saw palmetto made its way over the
Atlantic and became known in Germany. The goal was to show how the knowledge
grew about saw palmetto in Germany over time, how was the plant used and who were
the first practitioners to use it as a remedy.
2.2 Research Strategy and Methods
2.2.1 Research strategy
In order to understand how the disease BPH evolved in medical literature first I
searched for publications on the history of BPH and checked all available medical
standard textbooks from 1870 to 1930 on the treatment of the prostate disorders in
the Wellcome Library in London as well as in the library of the Medical Historic Institute
of the University of Zurich.
Andv Suter 52

2; h'lStcr/cc;
Secondly, literature searches on when saw palmetto was first mentioned in the
medicinal literature of English language allowed an understanding of how it was
introduced into medical or alternative practice. The timeframe 1870 to 1930 was
chosen as saw palmetto was apparently first mentioned in American medical literature
in the period after the American civil war, i.e. post 1870 (167) and in 1926 it was
included in the official U.S. formulary, showing that the plant had an official status as
medical agent (19).
In a third step, the relevant literature was assessed to determine how and when saw
palmetto appeared for the first time in popular, medicinal or scientific German
literature. This country was chosen as subject of research as I am of German mother
tongue and since saw palmetto is today an important herbal remedy in this country.
I also preferred Germany to the other German speaking countries Austria or
Switzerland as it is the biggest country and the majority of literature was assumingly
published there.
As a framework how to find historical sources I used the methodology and
considerations given by Brundage in his book 'Going to the Sources' (168).
He divides the most important research material, the primary sources in two classes.
The first are manuscript sources like handwritten records which were not intended for
publication, the others published sources. These encompass two categories, manuscript
materials such as letters, diaries which were later published and materials that were
intended to be made public like newspaper articles, annual reports, books or the like
(168).
For this research I used almost only published sources like journal articles and books
but no manuscript sources or archive material. Like this, my work is a comprehensive
medico-historical collection of published material on saw palmetto covering how the
plant was used first in the United States by indigenous people and physicians and its
introduction into German medical society.
A nd y Suter 53

To assess the quality of a source I used the guidance given for source criticism in the
book of Howell and Prevenier, 'From reliable sources - an introduction to historical
methods' (169). This involves the evaluation of the genealogy, genesis, originality, and
interpretation of a document as well as the authority of its author and his or her
competence and trustworthiness. Regarding the genealogy, genesis, and originality I
tried to find out if the document was an original or copy and where, by whom and
when the source was produced. In a second step I interpreted the document by
understanding its intended meaning, for example was it a research article to inform the
scientific community or rather intended to promote a commercial product.
At last I assessed the authorial authority of a document by finding out who was its
writer and what was the competence and trustworthiness of the author regarding the
content of the article or document. For these evaluations I carried out in the majority
internet searches by using the name or institution of the author as search term, which
often provided good background information.
All literature searches were carried out either online or in the named libraries from
January 2010 until January 2012. A literature was marked as a hit when it provided
sufficient evidence for the use of saw palmetto as a medicinal treatment or as a hint
that the saw palmetto was known but not used as a medicinal treatment (but for
example as a garden plant).
Table 3 lists the libraries or resources I used for my searches with the search terms,
limitations in year of publication and the hits. When a hit was of special interest or
needed further clarification, then the biggest historical U.S. online library, Hathi Trust
(170) or in case of a German reference, the 'Karlsruhe virtual catalog' (171), the biggest
German library resource were searched or individual libraries where a certain reference
was kept in original.
In the end I had assessed more than 1700 documents for use in this medico-historical
overview.
Andy Suter 54

> hnr :P:
Table 3: Libraries and online resources fo r the literature search from January 2010 until January 2012 w ith search terms, lim its on publication dates, num ber o f hits, and the hits which could be used fo r the analysis.
Library/Resource
ZVAB (Zentrales Verzeichnis Antiquarischer Bûcher [central register of antiquarian books]) zvab.com
Google books (books.google.com)
Google books (books.google.com)
Google books (books.google.com)
Medical historic library university of Zurich
The Wellcome library, London
Swissbib.ch (all Swiss libraries)
Zentralbibliothek Zürich (central library Zurich, it combines the libraries of the ETH Zurich, University of Zurich and the Canton of Zurich
PubMed Medline(h t tp : / /w w w .n c b i .n lm .n ih .g O v /p
ubmed/)
American Botanical Council ABC
Google books (books.google.com)
Search terms1
Period Number of j hits
Usable hits
Serenoa ; Sabal ; Sagepalme 1870-1920 None None
Sagepalme 1870-1930 53 15
Serenoa 1870-1930342 german hits
13
Sabal 1870-19306750 german hits, viewed around 1000
14
Serenoa, Sabal, Sagepalme 1870-1930 50 50
Prostate, prostatic hyperplasia ; saw palmetto
1870-1930 200 15
Sabal, Sagepalme, Serenoa, Hagers Handbuch, Homoopathisches Arzneibuch, Homoopathische Arzneibücher
1870-1930 80 ca. 20
Hagers Handbuch, Homoopathisches Arzneibuch, Sagepalme, Prostata
1870-1930 50 15
Saw palmetto AND historic; prostate AND history; benign prostatic hyperplasia AND historic; historical AND prostate
No limits 517 10
Literature on traditional use of saw palmetto, sent on request by Roy Upton, president of the American Herbal Pharma - copoeia and David Winston, American Botanical Council
10
Chaemerops serrulata, Brahea serrulata, Diglossophyllum 1800-1930 200 10serrulatum
55

Cnc/;Z'e,''2 ' H/s ter,'ce; pa,';
2.3 Results
2.3.1 The history of benign prostatic hyperplasia and its treatment
2.3.1.1 The discovery of the prostate and benign prostatic hyperplasia
The first mentioning of the prostate in medicinal literature is credited to Herophilus of
Alexandria (ca. 300 B.C.) but it is questionable if the organ he described as 'parastates'
(172) or as 'prostatae glandulosae' and 'prostatae cirsoides' was really the prostate and
were not the seminal vesicles and the ampulae of the ductus deferens (173).
Erasistratos, a Greek anatomist living from 320-250 B.C., wrote about the prostate in
the same manner several years later as Herophilus. It was then Rufus of Ephesos, a
physician who lived between the 2" and the 1* century B.C. who was apparently the
first author to give a good description of the glandular nature of the prostate. He was
followed by the dominant medical doctor of this era, Galen (131-201 B.C.) who gave in
his explanations of anatomical procedures an account of the prostate as ,spongy flesh
at the side of the neck of the urinary bladder' (174). Interestingly, benign prostatic
hyperplasia as a disease was not mentioned by earlier ancient authors, be it by
Hippocrates (ca. 406-377 B.C.) who was considered to be first urologist nor by ancient
Egypt authors (172).
Surprisingly from the Hippocratic period to the 16 century, the prostate or prostatic
hyperplasia were only vaguely portrayed in medical literature (175). The famous
anatomist Vesalius (1514-1564) reported the existence of the prostate only in very
general terms and Leonardo da Vinci (1452-1519) ignored the prostate in his drawings
of the male urogenital tract completely (173).
Nicolo Massa of Padua is believed to be the author who around 1550 'rediscovered' the
prostate as an organ (175) and in 1648 Jean Riolan, the younger (1577-1657), was the
first person to find the relationship between an enlarged prostate and urinary problems
(176). Previously the French surgeon Ambroise Paré (1510-1590) had observed that
male urinary problems occurred more frequently in the elderly and that these LUTS
arose age-dependently (172).
A'rc'y Sutci ' 56

2; H.'sfc/vcû/' /:jr:
That the prostate or BPH symptoms were not more frequently a topic in medical books
during the 16 * to the 17 century may be attributed to only few men reaching the
'prostate-age of sixty years' as the historian Shelley names it and the average life-span
of forty years at that time (173). But there is evidence that BPH was apparent in
medieval times as could be shown with the autopsy of the mummy from one of the
leading figures of the Italian Renaissance, Pandolfo III Malatesta (1370-1427).
Macroscopic and histological findings showed that he suffered from an enlarged
prostate which is the first paleopathological record (177).
Even though several physicians and anatomists like Thomas Bartholin (1616-1680),
Pierre Dionis (1650-1718) or Giovanni Domenico Santorini (1681-1737) tried to dissolve
the mechanism behind BPH it was until 1761 that the Italian anatomist Giovanni
Battista Morgagni gave in his comprehensive work 'De sedibus et causis morborum per
anatomen indagatis' a proper account of prostatic hypertrophy and he realised the
relationship between retention symptoms and pathological findings.
His mechanical view on the disease that an enlarged prostate leads to urinary problems
was a breakthrough since until then it was believed that urinary symptoms in elderly
men were caused by a paralysis of the bladder or leniency of the urinary tract (176).
Although several anatomists tried thereafter to explain the real nature of prostatic
growth, it was in 1862 Rudolf Virchow who established that prostatic hypertrophy was
a hyperplastic disease (178). In 1911 Lendorf set a milestone in BPH research
confirming the concept that the hyperplastic growth was in fact a growth in the
periurethral glands (176) which is the actual understanding of the disease (3).
Andy Suter 57

2.3.1.2 The history of BPH treatments
2.3.1.2.1 Catheterisations and surgical interventions in BPH in history until 1930
Not many treatments for patients suffering from BPH symptoms have been reported
until the beginning of the 20 century. Mainly catheterisations or needle punctuations
of the distended bladder were recommended indicating that only patients with
moderate to severe obstructive symptoms were treated (173).
Already in ancient Greek catheterisations were carried out, Erasistratos was the first to
describe one with an S-shaped catheter. In the 16 to the 19 century catheterisations
became popular again and different catheters and methods were developed and tried
out (175). Major milestones were then the invention of the gum-elastic catheter in
1777 by Theden (179), around 1840 the bladder catheter of Mercier called the ,cathéter
condé' and in 1853 the balloon catheters by Reybard (176). At the end of the 18 and
until the begin of the 20 century catheterisation was the general accepted treatment
for prostatic problems; for one patient in the early nineteenth century even the
number of 6892 catheterisations is documented (173).
The first operative procedure on the prostate was performed by the French surgeon
Ambrose Paré in 1575 using a genius punch-type instrument to cut out tissue. His
method of inserting a hollow tube with a cutting or crushing implement into the
urethra to remove prostate tissue was the same construction as is used today in
endoscopes for prostatic surgery (175). On the principle of the Pa re's method different
approaches with dilating, compressing or cutting the prostate were exercised until the
end of the 19 * century (176).
In the last quarter of the 19 century bladder puncture was carried out often where a
coarse needle was inserted via the transrectal, perineal, or suprapubic route and the
bladder was then emptied through the punctuation (173). A further development was
open adectomy which was performed from the end of the 19 century when
anaesthetics and antiseptic surgery were established. The transurethral procedures
were further developed, leading to the method of transurethral resection of the
A ndy Su 1er 58

C/7cp"c/- 2; Hfsfcntcz;'
prostate (TURP) with an electrocautery device. This surgery first was tried out in 1926
and is the gold standard for prostatic surgery today (175).
In the late 19* century castration was also advocated as a treatment because of
observations made with animals and the apparent similarity of prostatic adenoma and
uterine myoma which decreased in volume after oophorectomy (175). This treatment
attained a ,short and hectic period of glory' (176) but soon disappeared as method of
choice because of the lack of efficacy and the obvious mental and aesthetic burden for
the patients (175).
2.3.1.2.2 Medication used for BPH from 1820 until 1930
Non-surgical therapies for BPH were rarely ever mentioned in medicinal literature. The
leading opinion at the end of the 19 century was that BPH was an ,incurable disease'
(180) and earlier, in 1874 it was stated by the doctors van Buren and Keys that ,ln the
present state of our knowledge, hypertrophy of the prostate is not curable by any
means that have yet been used' (181).
The main medical books on genitourinary diseases in the period of 1870 to 1930
recommended in the majority catheterisations or surgical interventions as efficacious
treatments particularly for moderate to severe BPH symptoms (181-190).
In 1810 Hunter advocated sea bath cures, blistering to the perineum, opiate blisters
against pain, and drugs such as hemlock (most probably Conium maculatum) or
mezereon (Daphne mezerum) which was often used as powder or decoction to treat
syphillis (191). The British surgeon Henry Thompson described in his book 'The enlarged
prostate' a holistic treatment regimen for the patients affected by BPH which included
moderate and well digestible food and beverages, sufficient physical activity, modest
sexual behaviour, and a positive mind-set. He also discussed the use of hemlock as
proposed by Hunter but was more sceptical about the efficacy of the plant in BPH as it
was then used successfully 'in enlargements of the lymphatic and mammary glands'.
Furthermore, he opposed the use of mercury in BPH patients, a treatment which was
obviously administered quite often these days. He also promoted the use of ,the
An d y Suter 59

r/7cpücr 2; H.'rro.'Vcn,'
hydrochlorate of ammonia' which was a treatment administered in Germany and
France where 4-12 grams had to be taken for a duration of 4-8 weeks (192).
A further treatment was the application of iodine either as suppository, orally or as
topical treatment on th e ,urethral surface of the prostate'. Thompson cited the findings
of Stafford, who reported good efficacy in treatment of enlarged prostates (193) but
also advocated the use of bromine but both, iodine and bromine should only be
administered cautiously (192). He was impressed by the waters of the springs of
Kreuznach in Germany which were rich in iodine and bromine. He had visited the baths
and subsequently, recommended hip baths to British patients suffering from BPH using
the Kreuznach waters from the Elizabeth-Quelle which could be bought then in the
United Kingdom. The spring water contained also other minerals such as sodium,
calcium and carbonic acid gas (192).
The treatment with iodine and bromide was also described later by the physician
William T. Belfield and he proposed further an injection to the bladder containing a
solution of tannin in glycerine and water with 0.5-1% zinc citrate as treatment of BPH
(185). Van Buren and Keys regarded the treatment with iodine and bromide as not
efficacious and wrote that ,the advocates of these and other methods have failed to
establish their claims' (181).
The U.S. American urologist Eugene Fuller recommended for BPH patients as
medicamentous treatments mild diuretics such as ,sweet spirits of nitro, terpentine,
and juniper' where citrate of potash, buchu (Barosma betulina) and a fluid extract of
corn silk (Stigmatis maidis) should be added for best efficacy (187).
Another American urologist, Robert W. Taylor endorsed only few non-surgical
treatments, aside from hot bathes and lifestyle changes like a balanced diet or enough
physical activity. He suggested 'strychnine, quinine, and tonics ... in run down and
debilitated subjects' (188). The American urologist Hugh Cabot advised not to use
'palliative measures' but promoted catheterisation or operations (189). Abrahams and
Morson, two American urologists, were even stricter by declaring that 'the correct
treatment for this disease is removal of the whole gland by operation' (194).
Andy Su ter 60

C/: o;: tc /' / . /-f.': Cc; ,Tc / c/'^
Among German urologists medications or palliative treatment, as it was called, was not
highly regarded as method of choice. This is also shown in the standard work of
Schlagintweit, 1921 who recommended catheterisation and then surgery but no
medicamentous or other treatments (190).
In summary, until 1930 no standard medications for BPH patients were available and
saw palmetto was never mentioned in the standard books on urology.
Catheterisation and surgery were the methods of choice and the medicamentous
breakthrough was achieved in the late 1970's after the discovery that alpha blocking
agents like phenoxybenzamine, a nonselective a-adrenoreceptor antagonist, were
effective in treating BPH symptoms (195). In 1992, then the first 5-alpha-reductase
inhibitor, finasteride, was granted marketing authorisation by the U.S. Food and Drug
Administration for treatment of BPH symptoms (196).
These two classes of drugs are at the time the main synthetical drugs for BPH
symptoms (197). Further details of current treatments of BPH were already given in
chapter I.4 .I.4 .
A n d y Suter 51
C/fOptc/ 2. H.'r -c.n'co.'pc.''-
2.3.2 History of human use of saw palmetto
2.3.2.1 Use as material and wax
The fibres were important to Florida's indigenous people, the Seminole. Since saw
palmetto leaves and stems are rich in fibres, they were used to fabricate brushes (19),
served as basic material for the production of paper (7), and in some specialised cases
during World War II even for cartridge plugs and wallboards (198). The Seminole made
thatches for their houses and constructed huts and used the fibre to braid fruit
collecting, corn sifting and ritual baskets (7) either for their own use or these days
mainly as souvenirs for tourists (199). Further use of the fibres of saw palmetto was
made for production of fire fans and ceremonial dance fans. Even baby rattles were
produced from the leaves by producing a little closed basket, which held pieces of
charcoal (19) and with the fibres also mattresses and straw hats were manufactured
(20).
Palmetto leaves may also be a source of wax. Wilder and Kitzke described a yield of 1.4
to 2.7g of the free flaking wax per lOOg of leafs. But as most of the palm wax of other
species is also free flaking and easy to collect, the costs for collecting and processing
saw palmetto wax is economically questionable (28).
2.3.2 2 Use as food
Since saw palmetto berries are rich in oils, they formed an important part of the diet of
Florida's indigenous people and the berries are ubiquitous in archaeological sites in
Florida. In the 1990's older Seminole Indians still ate the fruit raw but they advised not
to eat more than five fruits per day since they are bitter and moreover it is
recommended not to eat them with hot liquids as this may burn the mouth (19). The
Indians also prepare a sweetened traditional drink with the berries, which is called
'shiopee sofkee' (33).
An dy Suter 62

C/'jprcr 2/ jCC.'T
The use among non-indigenous residents was detected in settlements from the
16 * century from Spanish Florida (200) and there in particular at Lake Okeechobee (8 ).
Generally, records of the plant have been found among the indigenous groups of the
Timucua and Apalachee, the Cochtaw living near the Mississippi river who used the
dried berries for winter use, and also among the Sioux Indians (8 ).
The known first record of non-indigenous habitants of America eating saw palmetto
fruit was by a young Quaker merchant, Jonathan Dickinson, who wrote in a book 1796
about the misadventures of a boat full of Quakers shipwrecked on August 23, 1696 on
Florida's east coast. They were captured by indigenous people and kept as prisoners for
several weeks. They almost starved and all they could eat were fish and saw palmetto
berries. He describes this often cited experience of eating saw palmetto fruits: 'We
tasted them, but not one among us could suffer them to stay in our mouths, for we
could compare the taste of them to nothing else but rotten cheese steeped in tobacco
juice.'(7).
The botanist Bartram to the other hand, wrote in 1792 that the berries were 'delicious
and nourishing food' but as he interviewed later the Creek Indians about the berries
they defined them as 'bitterish and stinging on the palate, at first using it, but soon
become familiar and desirable' (8 , 9).
The mentioning of the species' use as a beverage by white settlers or in later centuries
by the inhabitants of Florida is firstly as a soft drink, which in the early 1900's was sold
by Miami pioneers. This drink was called 'metto' and was a mixture of saw palmetto
berries with carbonated water (201). Secondly, it was tried as an aromatic in cognac
(202).
In 1866, a German book already mentioned that the saw palmetto tree was used to get
a starch flour (203). In 1888, the same was described in detail in an article where the
production of a flour used by the Seminole Indians made from the root of saw palmetto
was detailed (204). A newer source, the book 'Field Guide to Edible Wild Plants'
explained further that the palm heart is 'tender and makes an excellent salad or cooked
vegetable' (205).
A nd y Suter 63

C/7Cprc." 2; H/sic/Vcr;,'' pcr/T
23.2.3 Use as a medicine
2.3.2.3.1 Medical uses by indigenous people
The indigenous people of Florida knew saw palmetto as a medication with diuretic,
sedative and aphrodisiac properties. The steam from cooking fruits was inhaled as a
treatment for bronchitis, as expectorant and to soothe irritated mucous membranes
(206). Infusions of the leaves and roots were taken to treat dysentery and stomach
pains by 'Gulf Coast Indians' (most probably referring to the Seminole Indians) and they
applied the inner trunk bark as a dressing or poultice for insect and snakebites and skin
ulcers. The indigenous group of the Houma (Louisiana) administered a decoction of the
root for sore eyes, high blood pressure, and kidney problems (207).
2.3.2.3 2 Use in U.S. American, Non-indigenous medicine
The first mentioning of the use of saw palmetto in Western medicine appeared in an
article published in the journal 'The Medical Brief from St. Louis by Dr. J. B. (James
Bond) Reed of Savannah, Georgia in 1877 (208). Despite of an extensive search, I could
not find the original literature as the first issues available in the largest American library
catalogue, Hathi Trust from this journal are from 1882 on onwards (209) and libraries in
St. Louis hold no old issues of this journal either. His real name was actually James B.
Read and he was from 1878 to 1879 president of the Georgia Medical Society (210), in
the following he will be named as 'Read' and not Reed.
The article from Read was cited in the journal 'New Preparations' under the title 'a new
remedy-Sobo/ serrulata-Savj palmetto' in 1879. He wrote that 'settlers of the South'
observed that animals feeding from the berries 'grew sleek and fat' and noticed that
the animals were in a 'marked health'. The settlers seemingly prepared a decoction of
the fruits for medical purposes. In his neighbourhood several people tried preparations
of the berry and obviously Read tried them also in humans and reported that the
berries improved digestion, increased 'flesh, strength and weight' and relieved
irritations of the mucous tissues, in particular of the airways and were a good remedy
for bronchial coughs and common colds (211). In 1911, the same article was also cited
AndyS i : t e r 64

C/?i7pLp/' 2." /JOff
in a publication called 'History of the vegetable drugs of the pharmacopeia of the
United States' by John Uri Lloyd. He was an influential pharmacist and follower of the
eclectic philosophy of that time and owned together with his brothers one of the
biggest factories for production of herbal medicines, the Lloyd Brothers, Pharmacists,
Inc. in Cincinatti, Ohio (212). He confirmed the cited data from 'Reed' in his article and
also mentioned that saw palmetto was before 1879 practically unknown in medicine
(213).
'Reed' was later often cited correctly as J.B. Read and appears like this in the Archiv der
Pharmazie, 1879 (214), in the Materia Medica, 1900 (215) and the books of Madaus,
1938 (216); Read is regarded as the first person bringing saw palmetto into the U.S.
medical society of these days.
In the same year, 1879, a description of saw palmetto berries of J.B. Read was given in
the American Journal of Pharmacy (217) and in 'The Planter's Gazette' (218) with a
broad description of the plant, its appearance, where it grows. He reported that he
observed three imiscible phases as the expressed liquid from the fresh fruits settled: A
volatile yello essential oil, a brown lipidic oily phase, and an aqueous yellowish phase
with sugary taste. The articles cite the medical use, adding that indigenous people like
the berries as food and that even fish ate the berries greedily once the fell into the
water. The article cited here is not the original article but a German translation which
was published the same year in a German journal (219).
Further reports of medicinal uses of saw palmetto were mainly from eclectic doctors.
Eclectic medicine combined herbal medicine with physical therapy practices and was a
direct reaction to the academic medicine of that time which, as described above,
involved a lot of harmful therapies like the application of mercury-based remedies or
excessive bloodletting (220). The term eclectic was first used by Constantine Samuel
Rafinesque (1783-1840), a French polymath who lived among native Northern
American Indians and observed their use of medicinal herbs (221). The word 'eclectic'
was derived from the Greek word 'ekiego' meaning 'to choose from' and should refer
to physicians who chose anything beneficial to help their patients (2 2 0 ).
An d y Suter 65

In 1829, a medical doctor called Wooster Beach founded in New York the 'Reformed
Medical College' to teach eclectic medicine. This school was soon followed by about a
dozen other privately funded eclectic medical schools, generally located in the
Midwestern United States. The best known college was the 'Eclectic Medical Institute'
in Worthington, Ohio, which later moved to Cincinnati; this was also the last eclectic
institution to teach students and closed in 1939.
Eclectic medicine expanded during the 1840's and peaked in the 1880's and 1890's and
was described as a 'large populistic, anti-regular medical movement in North America'
(222 ).
The eclectic schools failed to gain approvement by the 'Flexner Report' in 1910, which
was used to decide on accreditation of medical schools in the United States (223). This
forced the eclectic colleges either to change their curriculum and to become 'normal'
medical schools or they had sooner or later to close down (2 2 0 ).
In 1879, saw palmetto was introduced to the eclectic community by a doctor called
I.J.M. Goss of Marietta, Georgia (220, 224). He recommended the use of the plant for
the same indications previously mentioned by Read.
In the Kings dispensatory, the main book of the eclectic doctors the plant was already
mentioned in 1894 demonstrating its wide spread recognition and semi-official use
(225). Saw palmetto was indicated for irritated mucous membranes, such as caused by
coughs, pertussis, sore throats, acute catarrh, and asthma. For genitourinary
conditions, it was found to be effective for irritations associated with gonorrhoea,
epididimytis, and ovarian pain. It was also recommended for the treatment of enlarged
prostates as well as for atrophied breasts, testes, and ovaries (225, 226).
Other eclectic physicians such as Herbert T. Webster from California gave details about
the use of saw palmetto berries for an indication called 'the relaxation of the urinary
organs of the nervous system' which included frequent urination and vesical irritation
with BPH. He also mentioned administration of Sabal for female reproductive problems
such as 'dragging sensation in the pelvis and abdominal tenderness' (227). A further
eclectic physician, Eli G. Jones, later well known for his books on herbal medicines and
Andv Su te r 66
Chapter 2. Histcr'ca! p
cancer (228) wrote that he considered palmetto useful for 'deficient sexual
performance/drive, loss of libido, infertility due to overwork, exhaustion and excessive
childbearing' (229).
Around 1895 Dr. A. L. Davidson from Mount Pleasant, Utah, also an eclectic physician
wrote an article describing a single case of a man of 51 years who had lost his sexual
potency (given the description of the symptoms most probably due to BPH) and that he
could not satisfy his 'wife, a buxom blonde, several years his junior' any longer. Having
prescribed him 15 drops of a saw palmetto tincture four times daily, the patient noticed
within two weeks an improvement of his urine flow, an increase of his testicle size and
his 'vigor of life' had returned (230). In 1896, Dr. William. E. Bloyer, a professor at the
Eclectic Medical Institute in Cincinnati wrote in the Eclectic Medical Journal an article
on saw palmetto describing its medical uses ranging from bronchitis to treatment of
BPH (231).
An interesting view on the use of saw palmetto can also be found in the Journal of the
North American Eclectic Materia Medica Association (around 1895 to 1900, edition
unknown). Here the tonsils and the prostate were described as being similar in tissues
and therefore, saw palmetto was recommended not only for genitourinary ailments but
also for the treatment of tonsillitis, croup, for snoring, and chronic sore throat (167). In
the book of Winston, a J.W. Fyfe is cited who advocated the use of saw palmetto also
for respiratory tract symptoms and a J.D. Hatton published in 1897 in the 'Medical
Gleaner', an eclectic medical journal, on saw palmetto recommending it for 'prostatic
troubles of old men' and for symptoms of chronic gonorrhoea (232).
But it was not only among the eclectic community that saw palmetto gained already
soon after the publication of Read attention. A pharmacist, J.M. Dixon made around
1880 the first mention of saw palmetto as a treatment for disorders of the genito
urinary tract. He described a special effect of the fluid extract on the reproductive
glands, the ovaries, prostate, and testes, for 'sexual debility' but said that 'the remedy
seems to have a special affinity to the prostate, and a specific effect upon it' (167, 233).
Andy Suter 67

Also in 1880 a physician, Stephen F.Dupore of Savannah, Georgia wrote that saw
palmetto worked well in affections of the throat, bronchial tubes, lungs, and even in
haemorrhage of the lungs (234).
Around 1885 a doctor F.A. Evans wrote in the journal The Medical Brief that he found
approximately 15 drops of the fluid extract to be effective against paroxysms of
migraine. In addition to the already mentioned effects on the genitourinary system, he
also promoted saw palmetto for 'all cases of wasting of the testes' which in his view
was often a cause for impotence. Even though he favoured also the use in
gynaecological practice to promote the ,use of the mammae', he believed that the best
effects were generally seen on enlarged prostates (167). The same indications were
also reported in an article in the Western Druggist by Dr. H. Knapp who thought it had
the action of a 'great vitalized (235).
In the same year, 1895, in the 'Proceedings of the American Pharmaceutical
Association' a pharmaceutical chemist gave a comprehensive description of saw
palmetto, the plant, the chemistry of different extracts of the drug as well as different
accounts of medical use citing Read, Dixon, the below mentioned Evans and a Dr.
Kinnicut who had published in 1892 in the New York Medical Journal that saw palmetto
was in his view a good remedy for patients suffering from tuberculosis and in laryngitis
(236). Two years later in the same journal, saw palmetto berries were discussed with an
extensive description of the appearance of the fruit and some data on its chemistry
(237).
Interestingly, some of the medicinal standard text books of the United States of that
time such as Drugs And Medicines of North America by Lloyd, 1884 (238) and the
Specific Medication and Specific Medicines, 1870 (239) made no notice yet of saw
palmetto nor did the earlier works from Jonathan Pereira in 1842 and 1852 about the
'Elements of the Materia medica and Therapeutics' (240, 241) which described the
plants in use in the United States.
An dy Suter 68

By the late 1890's, the use of saw palmetto in eclectic, homeopathic, and allopathic
medicine in the United States became widespread. Pharmaceutical companies like
Wyeth Laboratories, Lilly, Squibb, and Merck all produced saw palmetto preparations
(242).
In 1898, the homeopathic physician Edwin Moses Hale from Chicago published his
standard book on saw palmetto which was a milestone as this was a comprehensive
compendium on the history, the use and the preparations of saw palmetto which were
available in the United States. They included the whole range of watery to oily
preparations of the berries such as tinctures, fluid extracts, pure oil, saccharated oil,
malto-sabal (saw palmetto oil mixed with maltose), aqua oleum sabal, and
suppositories (7).
The most detailed portrayal those days on the use of Sabal serrulata in a standard book
was given soon after the book of Hale, in 1900, in the 'Dictionary of Materia Medica' by
J.H. Clarke. He referred mainly to the book of Hale, but also discussed several cases in
women where overactive bladder, kidney problems, irregular menses and breast
atrophies and peritonitis were treated successfully with saw palmetto. He described a
wide variety of indications for saw palmetto with main emphasis on urinary problems
but recommended it also as a remedy to improve sexual dysfunctions, such as erectile
dysfunction and lack of drive in men, as well as to increase libido in women and as a
treatment for ovarian pain (215).
The homeopath William Boericke issued in 1901 his own 'Boericke's Materia Medica
(Materia medica: the Tinctures)' where he described the use of saw palmetto mainly for
'irritability of the genito-urinary organs' and in particular for 'prostatic troubles' but
indicated the plant also for various disorders like a 'confused, full head; makes her
angry' (243).
In 1903 John William Fyfe gave in an eclectic manual of a modern materia medica for
saw palmetto the dosage recommendation of 10-30 drops thrice daily in water, mainly
for treatment of BPH and 'functional inactivity of the reproductive system' (244).
Ai : c ' y Suter 69

The journal 'Kew Bulletin' reported 1899 that in this year 250 tons of liquid extracts of
saw palmetto berries were consumed in the United States as a remedy (245).
The widespread use of saw palmetto found at the begin of the 20 century recognition
by the U.S. American health authorities and the plant gained an official status as a
remedy: From 1906 onwards it was listed and then mentioned in the United States
Pharmacopeia (1916) and then in the National Formulary from 1926 until 1950 (19).
These official records were a milestone for saw palmetto as a treatment in the United
States. The plant was not any further a treatment solely favoured by a special and
marginal group of physicians like the eclectics but were an officially accepted
medication of that time.
A n d v Suter 70
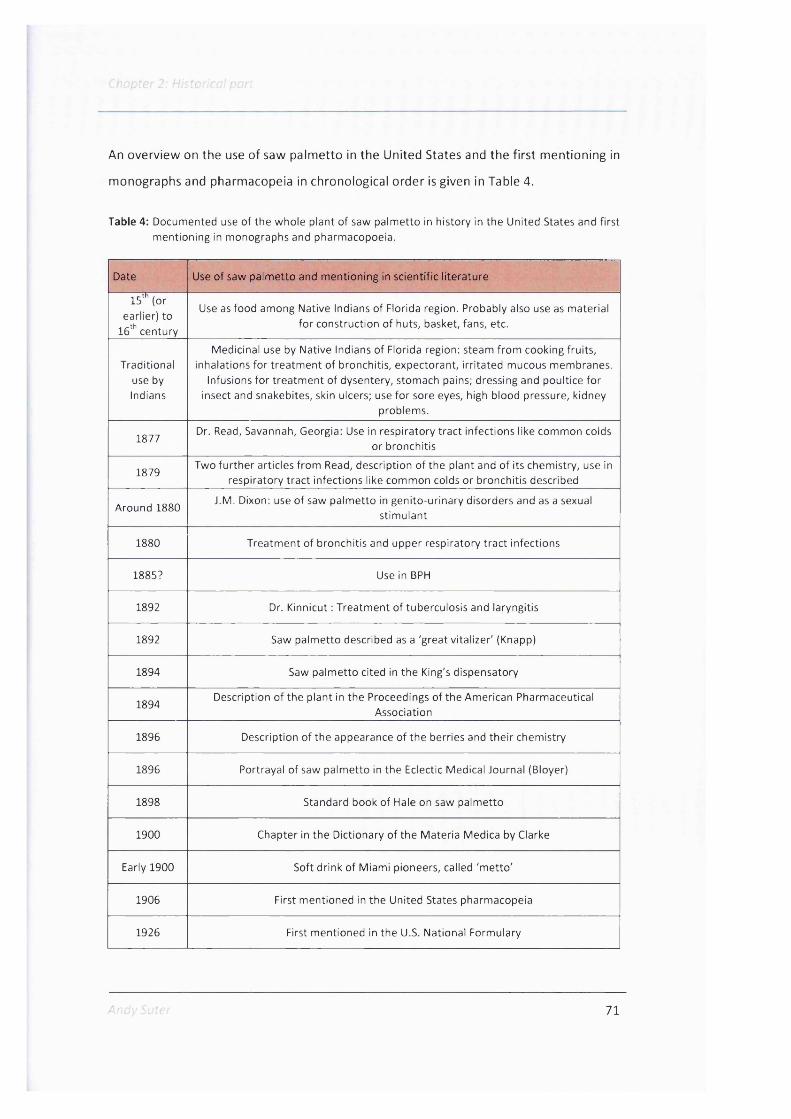
An overview on the use of saw palmetto in the United States and the first mentioning in
monographs and pharmacopeia in chronological order is given in Table 4.
Table 4: Documented use o f the whole plant of saw palm etto in history in the United States and first m entioning in monographs and pharmacopoeia.
Date Use o f saw palm etto and m entioning in scientific lite rature
15'^ (or earlier) to
16^ century
Use as food among Native Indians of Florida region. Probably also use as material fo r construction o f huts, basket, fans, etc.
Traditional use by Indians
Medicinal use by Native Indians of Florida region: steam from cooking fruits, inhalations fo r trea tm ent o f bronchitis, expectorant, irrita ted mucous membranes.
Infusions fo r trea tm ent of dysentery, stomach pains; dressing and poultice fo r insect and snakebites, skin ulcers; use fo r sore eyes, high blood pressure, kidney
problems.
1877Dr. Read, Savannah, Georgia: Use in respiratory tract infections like common colds
or bronchitis
1879Two fu rthe r articles from Read, description o f the plant and o f its chemistry, use in
respiratory tract infections like common colds or bronchitis described
Around 1880J.M. Dixon: use o f saw palm etto in genito-urinary disorders and as a sexual
stim ulant
1880 Treatm ent o f bronchitis and upper respiratory tract infections
1885? Use in BPH
1892 Dr. Kinnicut : Treatm ent o f tuberculosis and laryngitis
1892 Saw palm etto described as a 'great vitalizer' (Knapp)
1894 Saw palm etto cited in the King's dispensatory
1894Description o f the plant in the Proceedings of the American Pharmaceutical
Association
1896 Description o f the appearance o f the berries and the ir chemistry
1896 Portrayal of saw palm etto in the Eclectic Medical Journal (Bloyer)
1898 Standard book of Hale on saw palm etto
1900 Chapter in the Dictionary o f the Materia Medica by Clarke
Early 1900 Soft drink of Miami pioneers, called 'm etto '
1906 First mentioned in the United States pharmacopeia
1926 First mentioned in the U.S. National Formulary
71
2.3.2.33 The appearance of saw palmetto in German scientific literature
In 1835, a plant was described in a German book on general botany under the name
'Chaemerops palmetto' as an example for a palm tree without thorns but it is not clear
if really saw palmetto was meant (246). In the 'Nomenclator botanicus hortensis', an
enumeration of 'European cultivated plants' from 1840, Chaemerops was named
'Zwergpalme' [dwarf palm] and 'Chaemerops serrulate' as the finely serrulated
[feingesagt] dwarf palm tree, growing in Georgia, USA (247). In a story about the
garden show 1850 in Gent, Belgium, the same palm tree, 'Chaemerops serrulata' was
mentioned as being one of the objects in a special exhibition on palm trees (248).
The first mentioning of saw palmetto in German literature as 'Sagepalme' is from a
description of a Journey to Effingham County in Georgia, U.S.A, in 1862 (249). The
author mentioned that 'the ground is covered for hours with saw palmetto
(Chaemerops serrulata)' ['..der Boden stundenweit mit Sage-Palme, Chaemerops
serrulata, als Unterholz bedeckt']. And in a book on Northern-American agriculture,
'Sagepalme Chaemerops serrulata' was cited as a tree used from Indians to gain a
starch flour from it (203).
'Sabal serrulata' appeared around the same time also in a book on palm trees, the
origins of the plant were stated as Georgia and Florida (250). Later, the plant was
described in an account of the flora of Northern America as 'Sabal palmetto, serrulata'
(251).
In 1879 the first citation of saw palmetto in non botanical but medicinal German
literature appeared. In the journal 'Archiv der Pharmazie', a journal for German
pharmacists, the article from the above mentioned American Journal of Pharmacy on
saw palmetto was published as a German translation (219).
In 1890, the plant 'Sabal serrulata' was quoted in the 'Real-encyclopadie der
gesammten pharmacie', a dictionary for pharmacists and physicians (252).
'^,ndy Suter 72
2; H/sfcnra/ /rcr/
A year later, in 1891, the medical use of saw palmetto was described for the first time:
Brestowski cited in his book 'Die neueren und neusten Arzneimittel' a plant he called
'Sabiana serrulata'. He referred in the description of the drug to Dixon, meaning by this
maybe not only the pharmacist named from the article of Davis, 1892 (233), but
probably 'Dixon's saw palmetto', a saw palmetto preparation sold those days by the
Dixon saw palmetto medicine company from Jacksonville, Florida (253). Brestowski
wrote that the berries were 'calming, sleep-inducing and at the same time diuretic' and
that they had a positive effect on the digestion and a 'specific action' on the glands of
the sexual organs. The fluid should be used in weakness of the sexual organs, muscle
atony, nervous disorders which leads to digestive complaints, male impotence and
vaginal balls made with cocoa butter and saw palmetto fluid should be applied in
proplapsus uteri, leucorrheoa, exhaustion caused by frequent parturation or sexual
excesses (254).
In 1897, the well known German chemist and pharmacognost Carl Hartwich gave
details on 'Sabal serrulata'. He described the appearance of the fruits and that they
could be used for phthisis and diseases of the lung and that they may have a diuretic
effect (255).
In his posthumously published standard work on healing plants Dragendorff mentioned
1898 also 'Sabal serrulatum' shortly and wrote about the medical use of the 'fruit
nutrititvum [Frucht nutritivum] by phthisis, bronchitis, etc.' and to use a as a 'diurectic,
sedativum and stimulant remedy for the glands of the genitals' (256).
Aside from the three cited sources cited, until 1900 no other German pharmaceutical
standard book mentioned saw palmetto nor gave an account on its medical use.
'Hagers Handbuch', 1878, 1883 (257, 258), 'Die neueren Arzneimittel für Apotheker,
Aerzte und Drogisten ', 1888 (259), the 'Handbuch der allgemeinen und speciellen
Arzneiverordnungs-Lehre', 1873 (260), 'die wichtigsten Arzneimittel', 1886 (261),
'Compendium der Arzneimittelverdordnung', 1891 (262), the ,Pharmacopoea
Helvetica', 1891 (263) or the 'Vergleichende Arzneimittellehre', 1892 (264) made no
citation of the plant.
A n d y Suter 73

C/icprer 2; H/stor/cc?,'
Also homeopathic standard books of that time from two of the German opinion leaders
in homeopathy, Carl Heinigke and Arthur Lutze (265) the 'Handbuch der
homoopathischen Arzneiwirkungslehre', 1880 by Heinigke (266) or ,Dr. Lutze's
Lehrbuch der Homoopathie', 1860,1878,1887 (267-269) did not quote Sabal nor was it
included in the 'Arzneibuch für das deutsche Reich', the German pharmacopoeia, of the
years 1891 and 1900 (270, 271) or on a pharmacognostic map of the world of 1899
(272).
For a short period of time, the stem of saw palmetto gained some interest as a tanning
agent in German literature. In 1896, 'palmetto extract from Serenoa serrulata' was
described as a new tanning agent in a German chemical technical repertory with
reference to an U.S. American publication (273), in 1898 the content of tannins of
'Serenoa serrulata' was discussed in another scientific publication (274), and in 1899 a
botanical annual report detailed the tannin content of the stem and roots of 'Serenoa
serrulata' (275). Later, the use of saw palmetto for tanning appeared no longer in
literature.
In 1900, in the ,Zeitschrift des Berliner Vereines Homoopathischer Aerzte' the journal of
the homeopathic doctors of Berlin cited under the chapter ,Lesefrüchte aus
homoopathischen Zeitungen' [News from (literally 'reading fruits') homeopathic
Journals] a lecture given on the 7 of December 1899 by a Dr. E. M. Madden at the
British Homeopathic Society on saw palmetto (the article was entitled as 'Sabal
serrulata oder Saw palmetto'). He gave a description of the fruits and recommended
the use for enlargement of the prostate, explained one case of successful treatment of
enuresis in a boy and cited then some cases from the book of Hale (276). In the
meantime, the book from Hale had seemingly been translated to German by F.G.
Oehnme, then a well known homepathic scientist. I could not find the book itself but
only a citation that he had translated the book and used himself saw palmetto with
success (277).
Andy Su te r 74
C/icTCler 2; H/;
A year later, in 1901, saw palmetto was to be found in the German homeopathic
dispensatory (Homoopathisches Arzneibuch) issued by the Association of German
Pharmacists. Under 'Sabal serrulata' a description of the fruits was given and the
receipt for the preparation of a mother tincture : one part of the fruit and two parts
'spirit of wine' [Weingeist] (278). In the 'Pharmacopoea homoeopathica polyglotta' by
Willmar Schwa be which came out in the same year, saw palmetto was interestingly not
mentioned (279).
At the same time, in a book on homeopathic remedies, ‘Sabal serrulata' was discussed
using mainly Hale, 1898 as source, for urinary problems as well as a therapy causing
'a curious juvenilisation with return of the potency and increase of the vitality'. The
author recommended silicea as an antidote in 'excited states' under saw palmetto
(280).
In 1903 the book 'Deutsche homoopathische Arzneimittellehre' stated that a catheter
may not be used any longer after having taken a saw palmetto remedy (281).
Later on in the book 'Handbuch der homoopathischen Arzneiwirkungslehre' of 1905 by
the homeopath Karl Heinigke the medical use of 'Sabal serrulata' was explained in
detail with reference to the existing Northern American knowledge of Hale. Heinigke
recommended five drops of a mother tincture in water taken several times daily for
treatment of prostate disorders, lack of drive, testicular inflammations in men and in
women for ovarian inflammations, urethritis, mastitis, and dysmenorrhea; furthermore
for venereal diseases, enuresis, and inflammations of the bladder in men and women
(282).
The journal of the customs of the Germany ('Reichszollblatt') demanded 1906 for
1 deciliter of 'saw palmetto fruits drenched in wine spirit ' [mit Weingeist getrankte
Früchte der Sagepalme] a duty rate of 80 German mark indicating that saw palmetto
fruits had been imported on a regular basis (283).
Anc'yS'Jtcr 75
2; pa;
In 1908, saw palmetto was described as a remedy for nycturia in a homeopathic book
which was published by the homeopathic doctors of Berlin (284) and in 1909 the plant
was cited as an aphrodisiac in a journal of German pharmacists (285). Sabal was also
briefly quoted that it appeared in Northern America in a book on pharmacognosy by
Tschirch but no further information on the plant or its use was given (286).
In 1914 saw palmetto was mentioned in an article about an exam in a university or
school [Lehranstalt] in Hamburg where fruit kernels had to be determined and saw
palmetto was among one of those (287).
During World War I, saw palmetto was several times a topic in German scientific
literature; at a time when no saw palmetto could be delivered from the United States
because of the British naval blockade (288). In 1916 the 'Chemisches Zentralblatt'
described the fluid extract of saw palmetto, its appearance and main constituents
(289), and in 1917 the berries and the plant were characterised in the ,Zeitschrift für
angewandte Chemie' (290), in the ,Therapeutische Monatshefte' a short description of
Sabal was alluded (291), the ,Zeitschrift für Untersuchung der Nahrungs- und
Genussmittel' gave a morphological description of the berries (292), and ,the
Hygienische Rundschau' gave details on the plant (293). In 1918 saw palmetto was
depicted in the 'Jahresbericht der Pharmazie' as a , little known preparation which was
mentioned in literature as an aphrodisiac' (294).
In 1922, Rosenberg cited saw palmetto in a guide to the different official compendiums
(295) and in 1924 Sabal serrulatum was quoted in Dr. Wilmar Schwabe's homeopathic
compendium for the first time but only in the appendix under 'seldomly used
homeopathic remedies' very shortly with name and that with ripe fresh berries an
essence with 90% ethanol should be prepared (296).
In 1928, the use of saw palmetto berries to aromatise cognac could be found in a book
on etheric oils (297).
A n d y S u t e r 76

These citations show that saw palmetto between 1901 to 1930 was known among
homeopathic doctors, pharmacists, chemists, and nutrition scientists in Germany.
However, the use may not been that wide spread as several homeopathic standard
books of that time make no reference to saw palmetto, like the 'Arzneiwirkungslehre
neuerer homoopathischer Heilmittel by Voorhoeve', 1910 (298), the , Kurze Anieitung
zum richtigen Gebrauch der wichtigsten homoopathischen Arzneimittel' in 1913 (299),
the 'Lehrbuch der homoopathischen Therapie' in 1914 (300), 'Ottinger's Homoopathie'
in 1921 (301) or the ,Handbuch der homoopathischen Arzneiwirkungslehre' from 1922
(302), and 1927 the 'Lehrbuch der Homoopathie' (303).
The plant was also not too well known among herbalists and in the pharmacognostic
society since most pharmacognostic or herbal books of that time make no quote of saw
palmetto such as 1909 the 'Vergleichende Volksmedizin' (304), 1911 'Schroters
Schatzkastlein der Pfianzenheilkunde' (305), 1914 the book 'Volkstümliche Namen der
Arzneimittel, Drogen und Chemikalien' (300), 1920 ,Schreibers kleiner Atlas der
wichtigeren Heilpflanzen' (306) and 1924 ,Pharmakognosie als Vademecum für Aerzte'
(307).
Also until 1930 in academic medicine, among general practitioners or medicinal
authorities saw palmetto was not well known and accepted generally as a treatment.
Books on new pharmaceutical drugs like 'Die neueren Arzneimittel in der arztlichen
Praxis', 1908 (308), the 'Arzneimittel der heutigen Medizin', 1919 (309), and 'Neue
Arzneimittel und pharmazeutische Spezialitaten', 1926 (310) make no mentioning of
the plant nor does the official German Pharmacopeia, the 'Arzneibuch für das deutsche
Reich', 1910 (311), its supplement 1916 (312) and the issue of the Arzneibuch of 1926
(313).
A n d y S u t e r 77
In 1938, Madaus described saw palmetto in his work on 'biological remedies' as a good
treatment for BPH and that homeopaths used the plant mainly for this indication. He
showed the results of a survey he had carried out among 'outstanding adepts of
medicinal plants' [hervorragende Heilpflanzenkenner] which included not more than
hundred persons but also 'heads of clinics and sanatoria'. Of them, 41.2% stated that
they used saw palmetto for the treatment of BPH as the primary treatment, followed
by Populus tremulus with 12.4% and Pareira brava with 9.4%. This survey showed that
among at least a certain group of German doctors saw palmetto was broadly applied in
patients with BPH (216).
The most comprehensive German book on herbal drugs and medications, 'Hagers
Handbuch' also reflected the status of saw palmetto as a well known treatment as the
plant was first mentioned in the issue of 1944 (314) whereas it was not cited in any
previous editions of the book in 1903 (315), 1913 (316), 1925 (317), 1927 (318), and
1930 (319).
The chapter on saw palmetto gives a description of the partially dried, ripe berries and
their use as a 'diureticum, sedativum, stimulant; and a fluid extract for lung disorders'
with reference to the National Formulary, sixth edition, 1938 of the United States. The
chapter cites the production of an essence according to the homeopathic dispensatory
('Homoopathisches Arzneibuch'), the production of an elixir with sandalwood and of a
fluid extract of saw palmetto also according to the National Formulary (314).
I regard this first mentioning of saw palmetto in Hagers Handbuch as the breakthrough
of the plant as a remedy in Germany. A quotation in this standard book reflects that
saw palmetto was used as a treatment in Germany and an acceptance as an important
medication. This might have also been the trailblazer for its general introduction and
recognition to the pharmaceutical and medical community in Germany after World
War II until today.
A chronological description of the citations of saw palmetto in German literature is
given in Table 5.
A n d v S u t e r 78

Table 5: Documented historical use of saw palmetto in German scientific literature
Time Reference of saw palmetto in German literature
1835 First m entioning of'Chaem erops pa lm etto ' in a book on general botany
1840, 1850,1862, 1866, 1863, 1878
Botanical description o f saw palm etto and its habita t as 'Chaemerops serrulata' or 'Sagepalme'
1879First citation o f saw palm etto in a pharmaceutical journal, translation o f an U.S. American article
1890 'Sabal serru lata ' cited in a dictionary fo r pharmacists and physicians
1891First description o f medical use of saw palm etto ('Sabiana serrulata') as a calming, sleep inducing, d iuretic trea tm ent w ith effects on the sexual organs in men and women, and as therapy fo r prolapsus uteri and others in women
1897M entioning by a pharmacognost, Carl Hartwich fo r phthisis and diseases o f the lung, w ith d iuretic properties
1898Quotation by Dragendorff, same indications as Hartwich and as a' stim ulatory remedy' fo r the genitals
1896, 1898, 1899 Discussion in literature of saw palm etto as a tanning agent
1900Article on the use of saw palm etto in a homeopathic journal of homeopaths from Berlin
1900 German translation o f the book of Hale
1901'Sabalserru la ta ' in the German homeopathic dispensatory, issued by pharmacists
1901Description of 'Sabalserrulata ' in a book on homeopathic remedies. Silicea recommended as antidote in excited states from saw palm etto
1903 Saw palm etto cited in a book on homeopathic drugs, w ith use in BPH
1905Detailed in form ation on saw palmetto, use as mentioned in Hale but also fo r enuresis, venereal diseases and bladder inflammations
1906 M entioning o f saw palm etto in the journal o f the customs o f Germany
1908Saw palm etto fo r nycturia described in a homeopathic book from homeopaths from Berlin
1909Quoting of saw palm etto as an aphrodisiac drug in a journal o f German pharmacists
1914 Article on the an exam in Hamburg where saw palm etto had to be determ ined
1916 Inform ation in a chemistry journal on saw palm etto and the flu id extract
1917, 1918Details about saw palm etto in medical, food, and pharmaceutical scientific journals
1924 Saw palm etto in W illm ar Schwabe's homeopathic compendium
1938 Chapter on saw palm etto in Madaus' book on biological remedies
1944 Hagers Handbuch cites saw palm etto fo r the firs t tim e
79

CAr p : HA t c . 'Vc r . ' pc/'
2.4 Discussion
Being a patient suffering from BPH at the end of the 19 century in the Western world
was a miserable thing. The disease itself was quite new, it was not well understood nor
was properly known how it developed. As medicamentous treatments baths, some
herbal medicines or iodine, bromide or even mercury were applied which in the end
might have done more harm than being any good at all. The standard treatment were
catheterisations, an often painful procedure and if it was not carried out under sterile
conditions secondary infections of the bladder or prostate regularly occurred (320). This
again impaired the quality of life of a patient, not to talk about the mental burden of
this intervention.
As a final procedure surgeries were carried out but the operation techniques were not
very advanced and involved castration or the total resection of the prostate. Severe
side effects must have occurred frequently regarding the still high rate of side effects in
TURP these days (81).
Regarding the circumstances a BPH patient was in around 1870, it was no surprise that
saw palmetto soon was tested in this patient group. Interestingly, it was not the
traditional knowledge of the Indians on saw palmetto that was copied by practitioners
but the observation of settlers that the berries had a positive effect on animals feeding
them. Thanks to the settlers and Dr. Reads curiosity, openness and attention, saw
palmetto was tried out as a new remedy which soon spread among the eclectic medical
community.
And it is no wonder that the eclectic doctors were the ones trying out saw palmetto and
evaluating whether it worked best in common colds, bronchitis, in BPH, in urogenital
inflammations and disorders for men and women, and that the plant had vitalizing and
aphrodisiac properties. The eclectic philosophy based on the use of herbal medicine
and physical therapy with the goal to find new treatments in alignment with nature
which were well tolerated and in a way 'softer' than the existing often harming
medication and surgical treatments (220). Therefore the eclectic doctors were open to
try out new herbal treatments and since they were well connected, had their own
journals and even medical schools, they could teach and spread their knowledge widely
A n d y S u t e r 80
and rapidly (222). It is thanks to them and also the coincidence that the eclectics were
most popular in the time saw palmetto was rediscovered that within 2 0 years saw
palmetto became a broadly used treatment in the United States. The number of 250
tons of saw palmetto tincture produced in the U.S.A. in 1900, which equals to 50 million
daily dosages of 5ml and this in a population of then of 76 million people shows this
clearly.
The second group of practitioners which helped saw palmetto to become a well known
treatment in the United States were the homeopaths. Their medication consisted
mainly of herbal medicines and as they were not part of academic medicine they were
by their nature more open to new therapies. By having their own journals and medical
schools, the homeopaths, too, could spread the knowledge on saw palmetto effectively
like the eclectics. Hale for example, who wrote the standard book on saw palmetto was
a homeopath himself, teaching at the Hahnemann Medical College of Chicago (321).
And the third group of groundbreakers for saw palmetto in the United States were the
pharmacists as they occupied themselves as early as 1879 with saw palmetto. They
were experts on the production and quality of saw palmetto preparations and played
thus an important role that the plant was soon mentioned in the official U.S.
pharmacopeia and then in the National Formulary.
So, in short, the combination of the eclectics as the discoverers and pioneers on saw
palmetto, the homeopaths as the catalysts, and the pharmacists as the ones who had
the pharmaceutical quality and production of the tincture in their scope made saw
palmetto an officially acknowledged treatment.
In Germany in the meantime, it took some years longer until saw palmetto became a
well known remedy. The plant was known in German literature in botanical terms and
some scientific knowledge was summarised soon after its publication in the United
States. However, it was not until the turn of the century that the scientific community
showed a wider interest in the plant. Until 1900 the use of saw palmetto was not
widespread and the knowledge about the plant confined to some experts as shown by
the fact that it was only rarely mentioned in scientific books and articles.
81

( 2 ' H /f for.'To/ pn / "
In the time from 1900 to 1910 saw palmetto was mainly included in homeopathic
books. It looks thus as if the homeopaths were the ones giving saw palmetto a special
attention as a remedy but that the pharmacists knew already earlier about the plant.
Both together then were the ones making saw palmetto known and popular as a
treatment. This is corroborated by the fact that in 1901 the German Homeopathic
Dispensatory issued by the Association of German Pharmacists mentioned saw
palmetto but that the Homeopathic Pharmacopoeia (also 1901) by Schwabe, an
enthusiastic homeopath himself, did not mention saw palmetto.
However, by the end of World War I the plant was known and investigated in Germany
also by chemists and nutritional scientists. It looks that they became interested in saw
palmetto as German practitioners used it more frequently and it was more often a topic
in U.S. scientific journals. Taken as a whole, by the 1920's there were plenty of people
in the scientific community who had worked on saw palmetto and there was sufficient
knowledge on the plant available in Germany. I suppose this assisted saw palmetto
further to become an acknowledged treatment.
To which extent saw palmetto was used in medical practice as a remedy between 1920
and the 1930's is difficult to assess with the public sources available. In 1924 Schwabe
cited saw palmetto in the chapter of 'seldomly used remedies' (296), but Madaus
showed in his survey in 1938 that saw palmetto was the favourite herbal treatment for
BPH at least among practitioners he had asked (216). It seems that between 1920 and
1930 saw palmetto became popular resulting in the mid 1940's in the standard book on
German drugs and pharmaceutical preparations, the Hagers Handbuch (314).
Nevertheless, I could not identify a single brand, company or a practitioner which was
the main promoter of saw palmetto in Germany. I had asked several German
phytomedical companies like Schwabe for data on their product portfolio between
1900 to the 1930's but none had any archive material available (322). The only saw
palmetto preparation I found was a fresh plant trituration of saw palmetto berries from
Madaus in 1938, one of his so called 'Teep' products which were a mixture between a
homeopathic and a herbal remedy containing 0.025 g Sabal fruits per tablet.
A n d y S u t e r 82

The reason why not more saw palmetto brands were identified could be because the
available public sources were limited in its number and content or that due to the
volatile economic situation in Germany after World War I with several phases of
hyperinflation (323) it was difficult to market sustainably a saw palmetto product and
create a strong Sabal brand. To verify these hypotheses searches in archives are
mandatory.
What made saw palmetto as a treatment popular in the end is difficult to say but it
must have been primarily the same reasons as in the United States : There was no
medication for BPH, by the standards of the period saw palmetto was obviously
efficacious and safe - and probably also that it was a remedy from another continent
piquing people's curiosity might have helped as well. The strong interest in Germany
that time for foreign plants is reflected by the fact that in 1933 for more than 20 million
Reichsmark different herbal drugs were imported (324).
Further, German homeopathy was significantly influenced at least until 1900 by the
American homeopaths and their publications. Like this, knowledge about treatments
was extensively exchanged between the two homeopathic communities and it is highly
likely that a new therapy like the use of saw palmetto was promoted by this channel
(265).
The success of saw palmetto in treating BPH could not have been foreseen. The Indians
used inhalations from the berries for infections of the respiratory tract such as
bronchitis and for treatment of irritated mucous membranes (206). Further, external
treatments made from the inner trunk bark against insect or snake bites or skin ulcers
were applied or teas from the leaves and roots for treatment of gastrointestinal
disorders. From one Indian tribe even the treatment of sore eyes or kidney problems
were reported (207). The settlers trying out saw palmetto concentrated themselves
only on the use of the berries. There were no records that parts of the stem or the
leaves were applied by the settlers, thus confirming the story of Read.
Andy Sutei 83

2; H/sfoncny pg/i'
One major difference between the preparations used by the Indians and those by the
settlers were that the latter used alcohol as an extractant. Therefore the tinctures were
rich In lipophilic substances which are today considered as the main active constituents
(41). These tinctures were certainly more potent than watery preparations as they
contain substances with good antl-lnflammatory (59), antl-gonadotropic (48), muscle
relaxating (62) and vasodilating effects (6 6 ).
Interestingly, the settlers used preparations from the berries like the Indians firstly for
treatment of Infections of the respiratory tract, even though some positive effects on
digestive function were observed as well (208). It was already three years later, 1880,
that the first mention of saw palmetto as a therapy of genitourinary ailments appeared:
Its effects on ovaries, the prostate and testes were described and the aphrodisiac
properties of the plant. Remarkably, already In this publication It was noted that the
best effect was seen In BPH (167, 233). But from then on until the 1920's, saw palmetto
was seen as a remedy for three main Indications: Severe Infections of the respiratory
tract like bronchitis, genitourinary diseases In women and men like prostate problems
or Inflammations of the ovaries, and, finally, sexual dysfunctions like erectile
dysfunctions or testicular atrophy In men. Infertility and breast atrophy In women and
as a sexual stimulant for both, men and women (7 ,19,167, 215, 226).
Why saw palmetto In the end became a treatment Indicated today only for mild to
moderate stages of BPH (17) Is obvious. The plant showed In this Indication a very good
efficacy and at the same time almost no other medicamentous treatments were
available. Moreover, BPH Is a disease where Improvements can be observed well and
fast (99), contrarlly to other Indications where the plants was used for example like
Inflammations of the genitourinary tract (325).
But nevertheless, looking at the successful use of saw palmetto In other Indications
than BPH, further or new research Is warranted to confirm the reported findings.
Therefore, I carried out a clinical pilot trial In BPH patients with sexual dysfunctions to
assess If saw palmetto Is efficacious In this Indication and to see If old knowledge could
thus be confirmed.
A n d v S u t e r 84
C/ÿGpCc/' 2;
Even though I presented in this chapter a wealth of data, this historical part has several
shortcomings.
First of all, I have no training in historical research nor any education in historical
sciences. My searches were carried out and assessed according to my best knowledge,
helped by two standard books (168, 169) and sometimes with tips from the people
from the medical historic library in Zurich.
Secondly, I carried out the majority of the searches and views of the literature via the
internet using public online resources. Even though historians recommend the use of
internet searches as they are faster, more comprehensive and lead in the end to same
results as visiting libraries and looking at original literature (326, 327), it still not seen as
state of the art in historical research (168). Furthermore, the view of original literature
is due to copyright problems and fraudulent behaviour of users issuing reprints form
online books more and more limited to so called snippet views where only parts of the
literature can be viewed (328).
Thirdly, this use of only public material is a further important limitation of the whole
medico-historical part. For almost any aspect of this investigation, like which were in
the U.S.A. or in Germany the most important saw palmetto products, who were the key
promoters of Sabal or where and how many preparations of the plant were sold in both
countries until 1930, deeper research using archive material is warranted. Since this
historical investigation forms only a third of this thesis and time was limited, I could not
address all these additional questions.
Fourthly, it was difficult for me sometimes to assess the importance of a single
reference and to carry out a proper source criticism. How far spread was a journal for
example, who read it and how did it influence practicioners or how important was the
opinion of a certain author is difficult to judge and would need also further and deeper
research, mainly in archives.
A n d v S u t e r 85

C/:rrptc,'
Yet, with this research I could show for the first time, embedded in the treatment
context for BPH until the beginning of the 20 * century, at least trends which groups of
practitioners pioneered in using saw palmetto in the United States and in Germany and
how it became a popular treatment.
And, finally, that saw palmetto was quoted for the first time in Hagers Handbuch in
1944, at a time when Germany was at war with the United States, gives this research
chapter an almost political or maybe at least a philosophical final twist. The boldness of
the authors to include saw palmetto with reference to the U.S. National Formulary
shows that on one hand the plant must have been a really good remedy but to the
other hand that scientific evidence is in the end stronger than political ideology.
A n d y S u t e r 86

Chapter 3The phytochemical analysis of 46 commercial preparations containing saw palmetto by
using thin iayer and gas chromatography
AndySuter 87

Chapter 3: Phytochemical analysis
The phytochemical analysis of 46 commercial preparations
containing saw palmetto by using thin layer and gas
chromatography
3.1 Introduction
As described in the previous chapters, saw palmetto preparations are the most popular
herbal therapies for treatment of BPH. In general, they are produced by using a
lipophilic extractant like N-hexane, 90-96% V/V ethanol or supercritical carbon dioxide
(17, 40). For example, a common extraction procedure using ethanol is to crush the
fruits in a mill, then macerate them for 1-2 days in the extractant. After this an
exhaustive extraction for 4-5 hours is performed using percolation and hot ethanol at a
temperature of about 55“C. In the end, the percolate is concentrated to an ethanolic
spissum extract which will be encapsulated (329).
For supercritical fluid with carbon dioxide conditions which equal or exceed its critical
temperature of 31.1° C and its critical pressure of 73.8 bar (330) are used. Therefore,
extraction conditions like, for example, of at least about SOObar and a temperature of
less than 80° C are used (331).
The majority of these products are at the time sold worldwide as food supplements
(332, 333) and only in a few countries like Germany or Switzerland they are registered
and have to fulfil high quality requirements regarding the amount of active constituents
and their stability (334). Therefore, I intended to assess the composition and quality of
different preparations containing saw palmetto which are marketed for treatment of
BPH symptoms.
Currently, there are only a few publications available which address the quality of
different saw palmetto products even though in 2 0 0 0 a consultation paper on
treatments for BPH demanded further research on this topic (335).
A; ic'y SLiter 88

C/7(7p 'e.'' S; Pr'/rcc/'c.'ii'cr''' r r
The four monographs on saw palmetto all demand a daily amount of 320mg lipophilic
saw palmetto extract (17, 40, 146, 147). As the main active constituents of these
extracts free fatty acids and their ethyl esters are seen as well as phytosterols (17, 40,
62,146,147, 336). The only official quality marker so far for saw palmetto preparations
is to be found in the European Pharmacopeia which requires lauric acid to be at least
20% of the total fatty acid (336). Thus, the quantity of fatty acids in saw palmetto
preparations may serve as an important good quality marker. A more detailed
description of the fatty acids in saw palmetto are given in chapter 3.3.2.
Feifer et al. examined six commercial preparations analytically and compared the
amount of total fatty acids per unit with the information given on the package. They
could show that there were large differences for three of the products between the
stated information and the quantity of fatty acids determined in this analysis (337).In
another publication, fourteen Sabal products were compared regarding their content of
free fatty acids, methyl, ethyl, and long chain esters, triglycerides, and unsaponified
matter. The results indicated large differences in the proportion of free fatty acids and
their esters and the authors concluded that only those products with sound clinical data
can be seen as effective (34).
In two further series of experiments the difference on bioactivity of different saw
palmetto preparations was investigated. Scaglione et al. tested eight commercially
available saw palmetto products on their ability to inhibit the two isoforms of the
5-alpha-reductase in vitro. The EC50 for both isoforms differed widely for the products
and in the majority also between different batches of a product. Nevertheless, the
authors were cautious to relate these data to clinical efficacy (338).
In 2004 the German authority BfArM initiated a comparison of the bioactivity of three
different saw palmetto extracts produced with ethanol 90%, ethanol 96% and hexane.
The three preparations were similar in this in vitro setting in their activity to inhibit the
5-alpha-reductase (339).
The cited investigations focussed always on products from one country and the sample
number was at all times small. Therefore, I wanted to carry out a broader investigation
which included many test products from different countries to assess the daily amount
of fatty acids and the composition of fatty acids in each product.
A n d y S u t e r 89
I collected 46 preparations containing saw palmetto from eight countries worldwide,
with 19 of these products containing saw palmetto only as active constituent (mono
preparations) and the other 27 where combined with other components such as
vitamins, herbal extracts or minerals (combi preparations).
As quality reference, in each preparation the amount of the fatty acids lauric acid,
capric acid, caprylic acid, myristic acid, palmitic acid, linolenic acid, oleic/linoleic acid,
and stearic acid was determined using gas chromatography.
With this investigation I wanted to evaluate if the analysed products varied in their
daily amount of total fatty acids and if these differences were country-specific or
related to the regulatory status of a product.
Of further interest was, if the preparations differed in their proportion of fatty acids
and if there were general differences between mono and combination products
regarding their composition of fatty acids.
An additional goal was to assess how conform the measured fatty acid values were with
the requirement of the monographs, the European Pharmacopeia, and the information
given on the package.
In total, an overview on the quality of commercial preparations containing saw
palmetto from different countries should be presented in the end.
The method of choice for this assessment was gas chromatography. This is a robust and
uncomplicated method but the outcome is limited to the determination of nine fatty
acids.
A n d y S u t e r 90

C/Y:7,c:L' 5 F /:;T c r/7 c r7 ,'c c /(/n j'} '5 .'':
Even though the fatty acids are the group of the active constituents to be found in the
highest amount in saw palmetto extracts (40) there are also other active constituents in
the extract like the phytosterols ^-sitosterol, campesterol or stigmasterol, (340)
polysaccharides (17) (3-carotens, tocopherols (35) or the monoamine tyramine (39).
As it was not possible, due to lack of time and too few available test samples to carry
out further analysis to quantify other active constituents, a further analytical
investigation was carried out on the same samples using proton-NMR-spectroscopy in a
Master thesis with a metabolomic approach using Principal Component Analysis (PGA)
as statistical method (341). The goal of this thesis was to establish a fast and
reproducible method to analyse saw palmetto products which should give a
comprehensive answer on the characteristics of the products by using PGA (342).
The results from the NMR-analysis are compared in the end with the gas-
chromatographic analysis.
Anc'y ^U ic r 91

C/iuOfcr j; F/ntcc/'cnT.'Cc/ r.'TC.'iT.:
3.2 Material and Methods
3.2.1 Reference samples
Forty-six commercial products containing saw palmetto, indicated for treatment of BPH
and which were known to sell well in their country were obtained from retail outlets or
pharmacies. The preparations came from eight different countries, namely Canada,
Finland, Germany, the Netherlands, the United Kingdom, South Korea, Spain,
Switzerland, and the United States. Only the products from Switzerland were registered
herbal products which needed to fulfil quality standards as demanded in the ESCOP
monograph (17) and the European Pharmacopeia (336). The samples from Finland and
Canada were also registered but no strict quality requirements have to be fulfilled, the
registration acts rather as an official sales license.
The 46 products were tablets, soft gel or hard gel capsules, and the combination
partners in combi products were mostly pumpkin seed oil [Cucurbita pepo),
preparations from Pygeum africanum or stinging nettle {Urtica dioica) or single plant-
derived substances like \i-sitosterol or lycopene. Further from vitamins in the majority
vitamins D and E and as minerals selenium or zinc were supplemented.
The daily dosages of all preparations were heterogeneous. Regarding the minimal daily
dosage this was one unit per day for 2 0 products, for 2 1 products twice and for one
preparation thrice daily, for three products there was a 4 x daily and for one product
even a six times daily consumption. From the products containing only saw palmetto as
active constituent only eight products were dosed once daily and six brands twice daily.
Also the amount of saw palmetto extract declared for one tablet or capsule varied
widely reaching from 2.5mg to SOOmg per unit.
The extracts were in the majority not well declared on the packages or package leaflets,
so only for a few products proper drug extractant ratios (DER) and the extractant were
available. The given declarations showed that the greater number of the saw palmetto
extracts were highly lipophilic, at least one (SP 14) contained also crude saw palmetto
berry powder. None of the investigated products had reached expiry date.
A n d y i L ' t c r 92

C/icpfcr 3; P/:yfoc,^er:.'cc.' r.io /y j/i
Table 6 gives details on the test products, a more comprehensive description of each
item including additionally the brand name, manufacturer, drug-extractant ratio, other
active substances, and batch number is given in Appendix 1.
In the following the test samples can be identified with their reference number given in
Table 6 , abbreviated as SP and the number whereas SP stands for specimen.
A n d y S u t e r 93
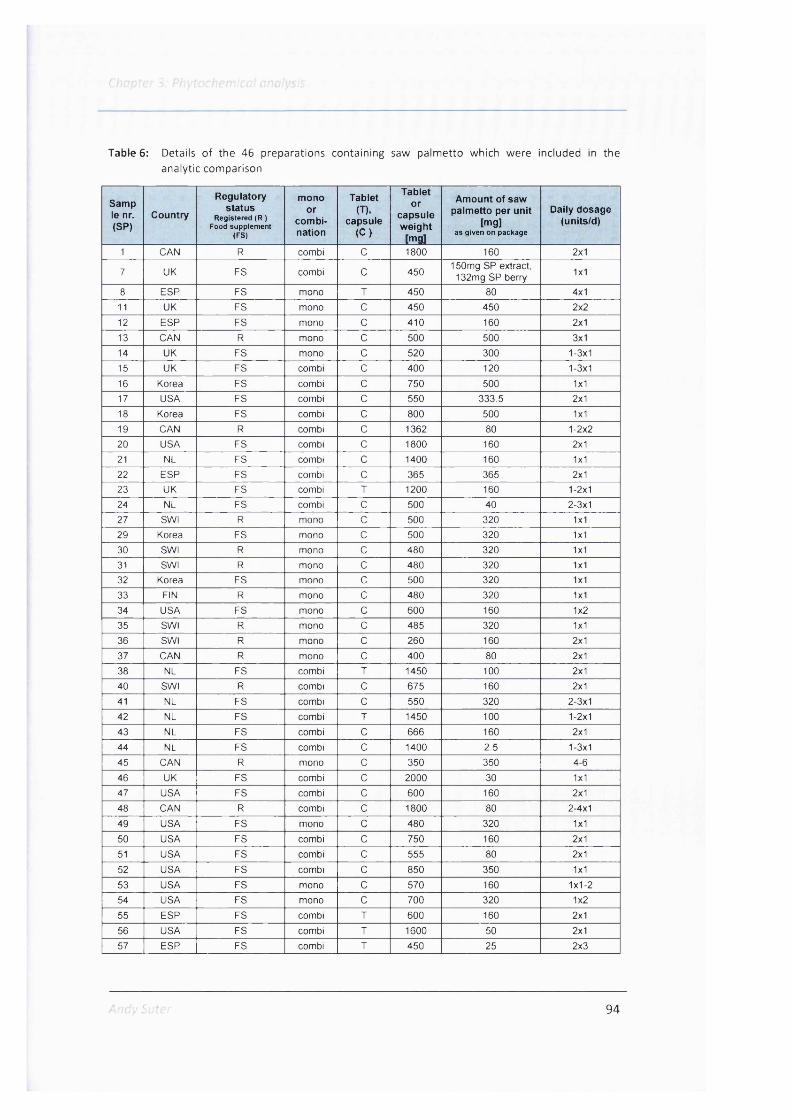
Table 6: Details o f the 46 preparations containing saw palm etto which were included in theanalytic comparison
Samp le nr. (SP)
Country
Regulatorystatus
Registered (R ) Food supplement
(PS)
monoor
combination
Tablet(T).
capsule(C)
Tabletor
capsuleweight
[mg]
Amount of saw palmetto per unit
[mg]as given on package
Daily dosage (units/d)
1 CAN R combi C 1800 160 2x1
7 UK FS combi C 450150mg SP extract,
132mg SP berry 1x1
8 ESP FS mono I 450 80 4x1
11 UK FS mono c 450 450 2x2
12 ESP FS mono c 410 160 2x1
13 CAN R mono c 500 500 3x114 UK FS mono c 520 300 1-3x1
15 UK FS combi c 400 120 1-3x1
16 Korea FS combi c 750 500 1x117 USA FS combi c 550 333.5 2x1
18 Korea FS combi c 800 500 1x1
19 CAN R combi c 1362 80 1-2x220 USA FS combi c 1800 160 2x121 NL FS combi c 1400 160 1x1
22 ESP FS combi c 365 365 2x123 UK FS combi T 1200 160 1-2x124 NL FS combi c 500 40 2-3x127 SWI R mono c 500 320 1x1
29 Korea FS mono c 500 320 1x1
30 SWI R mono c 480 320 1x1
31 SWI R mono c 480 320 1x132 Korea FS mono c 500 320 1x1
33 FIN R mono c 480 320 1x1
34 USA FS mono c 600 160 1x2
35 SWI R mono c 485 320 1x1
36 SWI R mono c 260 160 2x1
37 CAN R mono c 400 80 2x1
38 NL FS combi T 1450 100 2x1
40 SWI R combi c 675 160 2x1
41 NL FS combi c 550 320 2-3x1
42 NL FS combi I 1450 100 1-2x1
43 NL FS combi c 666 160 2x1
44 NL FS combi c 1400 2.5 1-3x1
45 CAN R mono c 350 350 4-6
46 UK FS combi c 2000 30 1x147 USA FS combi c 600 160 2x1
48 CAN R combi c 1800 80 2-4x1
49 USA FS mono c 480 320 1x1
50 USA FS combi c 750 160 2x1
51 USA FS combi c 555 80 2x1
52 USA FS combi c 850 350 1x1
53 USA FS mono c 570 160 1x1-254 USA FS mono c 700 320 1x2
55 ESP FS combi I 600 160 2x1
56 USA FS combi I 1600 50 2x1
57 ESP FS combi T 450 25 2x3
94

3.2.2 Thin layer chromatography (TLC) for identification
3.2.2.1 Main principle
TLC is a simple and well known chromatographic technique to analyse drugs quickly and
with great certainty (343) and is known to be 'the workhorse' for screening tests in
laboratories (344). The method was first established by Izmailov and Sraiber in 1938
who separated galenic formulations using loose layers of aluminium oxide on glass
plates by continuously dropping a solvent on the point of application. The breakthrough
for TLC was achieved when Stahl in 1958 developed high quality equipment for
preparation and separation together with a standardised fine-grained silica gel. He was
also the first person to propose the name TLC for this analytic method (345).
The method is based on the principle that the flat layer of the material serves as a
stationary phase and that the mobile liquid phase is moved by capillary forces across
this layer. Like this, compounds in mixtures are separated by their migration speed on
the plate. The distance they migrate per time depends on the adsorption of the specific
molecule to the stationary phase and, therefore, depends on its distribution between
the two phases. The more a substance is adsorbed, the slower it moves (343,344).
The detection is carried out by locating the spots on the plate and identifying the
substances (344). Several methods are available to locate the spots on the plate. This
can be by exploiting the luminescence characteristics of the analyte either by a
fluorescence or phosphorescence or by impregnating the layer bed with a fluorescent
indicator substance and afterwards inspection under UV light. Furthermore the layer
can be sprayed with a nonspecific strong oxidant or with a group - or substance specific
reagent solution (344, 346). A substance is much easier to identify when an authentic
reference substance is applied as well and the separated spots can be compared to it
(344).
Like this, TLC is the standard method for identification of herbal drugs which can also
give answers on the quality and even on the quantity of certain compounds (343).
Furthermore, the procedures and results are documented in pharmacopoeias (336,
343) and are easy to reproduce.
A n d y S u t e r 95

3.2 2.2 Protocol for analytical TLC
The method applied was in accordance with the requirements of the European
Pharmacopoeia on thin layer chromatography, chapter 2.2.27 and the monograph on
saw palmetto fruit (336). The principle of this TLC method was that with an a polar,
acidic mobile phase the lipophilic substances of the saw palmetto preparation were
separated on a silica gel layer. After spraying with anisaldehyde reagent and heated to
llO 'C , the zones were analysed at daylight.
This TLC method was already used routinely at A.Vogel Bioforce AG quality assurance
for identification of the saw palmetto preparation Prostasan®. This is a registered
product containing 320mg saw palmetto extract per capsule extracted with ethanol
96% V/V and fulfils the requirements of the European pharmacopoeia and the
monographs (17, 40,146 ,147, 336). The amount of each test preparations for TLC was
calculated using a modified formula after having carried out previous experiments.
The formula for Prostasan® is as follows :
0.25x320 ^ = 0.16
485 =[g]
0.25 = [g] necessary Prostasan® content
320 = [mg] Saw Palmetto extract per Prostasan® capsule
485 = [mg] Prostasan® capsule weight
The adjusted formula for soft gel capsules and tablets was :
0.16x bCalculation formula: x =
a
X = [g] necessary capsules (tablets) content
a = [mg] Saw Palmetto per capsule (tablet) as given on the package
b = [mg] capsule (tablet) weight
for hard eel capsules the formula was adjusted to
0.4x bX —
a
A n d y S u t e r 96

C/7(7jTLC.' z'
The amount of a capsule content or tablet was dissolved in 4ml toluol. As reference
substances lOmg ^-sitosterol and 4mg p-amyrin were separately dissolved in 10ml
ethanol (96%). 4pl of the saw palmetto preparation, which was a clear yellow solution
as well as 2pl each of the reference solutions and additionally also Prostasan® as a
reference saw palmetto product were applied to a silica gel F254 HPTLC plate with SOnm
pore size from Merck.
As mobile phase acted a mixture of toluene, ethlyacetate and acetic acid mixed in the
ratio of 70:30:1 V/V. The runtime was about 20 minutes and the dried plate was
thereafter sprayed with anisaldehyde reagent. After heating the plate up for 5-10
minutes to 1 1 0 ”, the zones were visible and the plate could be analysed.
The method applied here serves only for the identification and not for quantification of
substances.
3.2.3 Gas chromatography for analysis of fatty acids
3.2.3.1 Main principle
In gas chromatography (GC), the mobile phase is an inert carrier gas which is generally
helium, argon, or nitrogen which has no significant interactions with the analyte. The
main function of the carrier gas is to transport the compounds to be analysed from the
injector to the detector. The stationary phase is either solid or liquid where the
constituents to be separated can be adsorbed (344).
GC is applicable to substances or their derivatives which can be volatilised under the
temperatures which are applied (336), mainly organic and anorganic materials with
molecular weight ranging from 2 to 1000 Daltons and is the premier technique to
separate and analyse volatile compounds (347). The method is based on the works of
Prior and Cremer who were the first to develop a solid gas chromatography method in
1947 which was published officially in 1951 (348).
A n d y S u t e r 97

Chapter 3: Fhy iochcnCcal anolys i r
The basic principle of a gas chromatograph is quite simple and the differences in gas
chromatographic systems lay generally in the use of the carrier gases. The system is
that gas is directed through the injector to the column and the sample is injected either
into a special injector or to the column itself. The analytes are then separated in the
column which is heated by an oven and usually temperature gradients are used to
improve the separation. The separated compounds are then recognised in the detector
(344, 349).
The choice of the gas is often important, even though it is inert, as it determines by its
molar mass, density, and viscosity how long the analytes stay in the column. A longer
diffusion time leads in the end to a better peak broadening and a better resolution
(344).
Also, there are several injection systems used but the oldest and most popular is split
injection. Here, a small proportion of the sample is transferred to the column with a
standard syringe on the heated injection port which contains a deactivated glass liner.
The sample is rapidly evaporised and the major part is discharged as waste through the
split which is an opening right at the top of the column (347).
There are a wide variety of columns in use for GC like packed columns where the
stationary phase is coated on a granular support material or capillary columns with a
liquid stationary phase deposed on the column wall. Depending on the type of column
they differentiate in their diameter and length, whereas capillary columns are generally
narrower and much longer, up to 100 m, than the packed ones (344).
More than 60 detectors have been tried out in GC (347) but most often flame ionization
detectors (FID) are used. The principle of this detection system is the measurement of
the electric conductivity of a hydrogen flame between two electrodes. When an organic
compound enters the flame the substance is ionised causing an electric current and this
allows to detect this compound (344, 350).
The advantages of GC is that it is a fast, efficient, and sensitive analysis providing a high
resolution. Further the method is non destructive making it possible for online-coupling
for example to a mass spectrometer and is easy to apply, reliable and inexpensive
(347).
A n d y S u t e r 98

3 2.3.2 Protocol for fatty acids analysis with GC
The method used was based on the principle that the lipophilic constituents of the saw
palmetto preparations were extracted with hexane, then saponified with sodium-
hydroxide and finally esterified to fatty acid methyl esters (FAME) with boron
trifluoride-methanol complex. The FAME were then separated with GC and analysed
using heptadecanoic acid as internal standard. Like this the esters and free fatty acids
are determined together, counted as free fatty acids.
This was a modified standard method of the German Society for Fat Science for fatty
acid methyl esters (351) which is in alignment with the recommendations of the
European Pharmacopoeia for gas chromatography and for determination of fatty acids
in saw palmetto products (336). Tablets, soft and hard gel capsules had each to be
prepared with different protocol for GC as will be shown in the following.
a) Preparation of tablets
For tablets this formula was applied to determine the amount needed for analysis:
1000x0.16x6x = -----------------
a
X = [mg] necessary tablet content
a = [mg] Saw Palmetto extract per tablet as given on the package
b = [mg] tablet weight as given on the package
1 0 0 0 = coefficient on mg
0.16 = calculations coefficient based on preliminary experiments
The corresponding amount of tablets were pulverised and combined with 4ml ethanol
40%, 8 ml water and 5ml internal standard solution in a 40ml centrifuge tube.
Afterwards the mixture was extracted with 3 times with 15ml hexane. The hexane
phases were then combined and dried with sodium sulphate and then concentrated in
a rotary evaporator.
A n d y S u t e r 99

b) Preparation of soft gel capsules
The amount of the content of soft gel capsules needed for the analysis was calculated
as follows:
1000x0.13xZ?x = ------------------
a
X = [mg] necessary capsule content
a = [mg] Saw Palmetto per capsule as given on the package
b = [mg] capsule weight as given on the package
1 0 0 0 = coefficient in mg
0.13 = calculations coefficient based on preliminary experiments
From each soft gel capsule the calculated capsule content was added to a 50ml
centrifuge tube and mixed with 5ml of the internal standard solution (BOOmg
heptadecanoic acid dissolved in 50ml petroleum ether) and then dissolved in 10ml
petroleum ether. After addition of Ig water-free sodium sulphate the tube was
centrifuged for 5 minutes at 3000U/min. Of the supernatant, 10ml were then
concentrated to dryness in a rotary evaporator.
c) Hard gel capsules
The quantity from the content of hard gel capsules mandatory for the GC analysis was
calculated using the following formula :
1000x6x = ----------
a
X = [mg] necessary capsule content
a = [mg] Saw Palmetto extract per capsule as given on the package
b = [mg] capsule weight as given on the package
1 0 0 0 = [g] amount of herb for the analysis
An dy SLiter 100
5; P/7'/foc/7cni,'cc/ nnoâ/f/:
The calculated amount of the capsule content was transferred to a Soxhlet extraction
thimble, covered with wool and extracted for 45 minutes with 70ml hexane and 5ml
internal standard solution. The extraction solution was thereafter concentrated on the
rotary evaporator to ca. 2ml and then dried with water-free sodium sulphate. The clear
solution was then evaporated until dry on the rotary evaporator.
The next preparatory steps were the same for all investigated galenic forms.
Six ml of 2% methanolic sodium hydroxide-solution were added to the residue and
heated up to the boiling point for 10 minutes, then 5ml boron trifluoride-methanol
complex were added and the whole mixture was boiled for another 2 minutes. Finally,
2 0 ml heptane were added, stirred and cooled down.
Afterwards saturated sodium chloride solution was added until the heptane phase
ascended into the flask neck. About 1ml of the resulting heptane phase was dried in a
centrifuge tube with water-free sodium sulphate; the clear yellowish green solution
was used for the chemical analysis.
The analysis was performed twice for each test preparation with a gas chromatograph
(Trace GC ultra. Thermo electro-cooperation) using an Optima 5 capillary column, 25m
X 0.32mm ID with 0.25pm layer thickness.
The column was held isothermally at 100°C, then the temperature was programmed to
increase at a rate of 5°C /min to 190“C where it was kept for 5 minutes. The injector
was set to 250°C and an amount of Ip l solution was injected using the split mode with
hydrogen as carrier gas at a constant pressure of 40 kPa.
The system suitability was given when in the chromatogram the resolution between the
main peak lauric acid and myristic acid amounted to at last ten. The single fatty acids
which were assigned according to the retention time of the peaks and were calculated
in reference to the area of heptadecanoic acid. The areas were integrated by using
Chromcard software. The methods precision is 0.9% and the correlation in linearity
0.998.
Fig. 6 shows a typical chromatogram of an analysis with the identification of the peaks.
Andy Safer 101

Chapter 3; Phytochemical analysis
Figure 6: Chromatogram of a saw palm etto preparation w ith the identified peaks
900-
800-
700-
500-mV
400-
min
For capric acid, caprylic acid, lauric acid, myristic acid, palmitic acid, linolenic acid,
oleic/linoleic acid, and stearic acid the amount was calculated in reference to
heptadecanoid acid as follows:
Fatty acid [mg/unit] =AP WIT 320
AST 10 WS
AP = sum of area of fatty acids in a sample
AST = area of internal standard
WIT = weight of internal standard [mg]
1 0 = dilution of internal standard
WS = weight of sample [mg]
320 = standard weight of capsule content
Each test preparations was analysed twice. The corresponding mean value of every
product was used for the analysis. All analyses were carried in the analytical
laboratories of A.Vogel Bioforce AG, RoggwiI, Switzerland with the assistance of
laboratory technicians.
Andy Suter 102

Chapter 3: Phytochemical analysis
3.3 Results
3.3.1 Identification of the test samples with TLC
The products were applied grouped together according to their galenic form, means
tablets, soft and hard gel capsules on separate silica gel plates.
On Figure 7 and 8 are the TLC fingerprints of the tablet samples. Except for the
preparation on position 2 in Figure 7 and the reference substance Prostasan® on
position 7, these were all combination products. The two products on lane 5 and 6 were
sold by different manufacturers but had the same composition given on the package
containing a large variety of herbal substances, vitamins and minerals. The fingerprint
identifies them as similar products.
Figure 7: TLC finger print profile o f six d iffe rent tablets on band 1-6, band 7 is the reference product Prostasan capsules, band 8 are the reference substances P-sitosterol (upper band) and p-amvrin (lower band)
f f
#; - e # #
1= SP 57, Spasmo-Urgenin, Madaus, Spain 5 = SP 38, Prostaat, Phital, Netherland2 = SP 8, Sereprostat, Robapharm Espaha S.A., Spain 6 = SP 42, Prosta Totaal, Distributie care bv, NL3 = SP 55, Prosta-Fort, GSN, Spain 7 = SP 10, Prostasan, Bioforce AG, Switzerland4 = SP 23, Saw Palmetto Complex, Natures Aid Ltd., UK 8 = Reference solution: p-Sitosterol; P-Amyrin
Andy Suter 103

Chapter 3: Phytochemical analysis
Figure 8: TLC finger prin t profile of the tab le t preparation SP56 on band 1, band 2 is the reference product Prostasan capsules, band 3 are the reference substances (3-sitosterol (upper band) and p-am yrin (lower band, barly visible)
9 ##
Among the hard gel capsule products, Figure 9 shows that all the mono preparations
presented almost the same TLC fingerprint (lane 1, 3, 4, 5, 7). The fingerprints of the
two Dutch products in Figure 9 on lane 8 and 9 indicated that they were combination
products. The products in lane 2 and 6 were also combinations but they were for this
assay maybe not sufficiently concentrated. The three further hard capsule preparations
in Figure 10 were all combination products whereas the product on lane 2, a
combination product with vitamin D and minerals showed almost the same pattern like
the reference product Prostasan.
Andy Suter 104

Chapter 3: Phytochemical analysis
Figure 9: TLC fingerprints o f nine products in hard gel capsules, on position 10 is the reference product Prostasan capsules, on position 11 are the reference substances p-sitosterol (upper band) and p-amyrin (lower band)
1 = SP 12 Permlxon, Pierre Fabre Iberica S.A., Spain 7 =2 = SP 22 Biprostat, Dietéticos Intersa S.A., Spain 8 =3 = SP 13 Saw Palmetto Berries, , Natural Factors, 9 =
Canada 10 =4 = SP 45 Saw Palmetto, Homeocan, Canada 11 =5 = SP 14 Saw Palmetto Berries, Solgar Vitamin and
Herb, UK
SP 11 Saw Palmetto, Holland and Barret, UK SP 24, ProstaFleur Extra Forte, Bloem Natupr. NL SP 41, Prostalife, Bloem Natuurprodukten NL SP 35, Prostasan, Bioforce AG, Switzerland Reference solution: p-Sitosterol; p-Amyrin
Figure 10: TLC fingerprints o f three hard gel capsules on lane 1-3 , the reference substance Prostasan on lane 4 and on lane 5 ^-sitostero l (upper band) sand p-am yrin (lower band)
1 = SP 15, Saw Palmetto & Pygeum Bark, Higher Nature, UK 2= SP 17, Prostate Health, Schiff Nutrition Group Inc, USA3 = SP 47, Saw Palmetto & Pygeum Extract, Country Life,
USA4 = SP 10, Prostasan, Bioforce AG, Switzerland5 = Reference solution: P-Sitosterol; p-Amyrin
Andy Suter 105

Chapter 3: Phytochemical analysis
The majority (n=29) of the commercial preparations were made with soft gel capsules.
Figure 11 shows the fingerprints of the six saw palmetto brands from Switzerland.
All except the sample on position 4 which contained also an Urtica dioica extract were
mono preparations. They displayed an almost uniform TLC fingerprint and could
evidently be identified as a lipophilic saw palmetto preparation when compared to the
reference product Prostasan® (Figure 11).
Figure 11: TLC fingerprin t o f the six Swiss saw palm etto preparations which were all made w ith soft gel capsules. On lane 7 are the reference substances ^-sitoste ro l (upper band) and P- amyrin (lower band)
14^
s g g
5 6
1 = SP 30, Prosta Urgenin, Max Zeller Sdhne AG, CH2 = SP 31, SabCaps, Vifor SA, CH3 = SP 27, Prostagutt Uno, Schwabe Pharma AG, CH
4 = SP 40, Prostagutt F, Schwabe Pharma AG, CH5 = SP 36, Prostadyn, Dr. Dünner AG, CH6 = SP 10, Prostasan, Bioforce AG, CH7 = Reference solution: ^-Sitosterol; p-Amyrin
Andy Suter 106
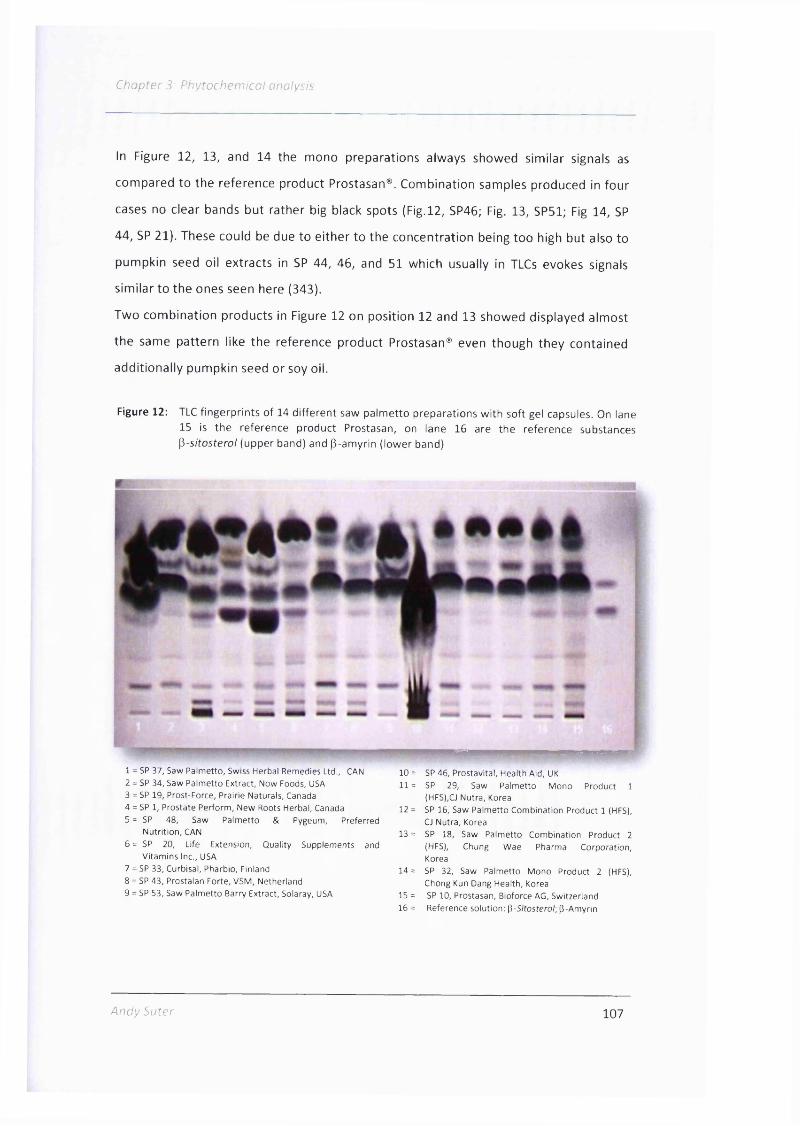
Chapter 3: Phytochemical analysis
In Figure 12, 13, and 14 the mono preparations always showed similar signals as
compared to the reference product Prostasan®. Combination samples produced in four
cases no clear bands but rather big black spots (Fig.l2, SP46; Fig. 13, SP51; Fig 14, SP
44, SP 21). These could be due to either to the concentration being too high but also to
pumpkin seed oil extracts in SP 44, 46, and 51 which usually in TLCs evokes signals
similar to the ones seen here (343).
Two combination products in Figure 12 on position 12 and 13 showed displayed almost
the same pattern like the reference product Prostasan® even though they contained
additionally pumpkin seed or soy oil.
Figure 12: TLC fingerprints o f 14 d iffe rent saw palm etto preparations w ith soft gel capsules. On lane 15 is the reference product Prostasan, on lane 16 are the reference substances ^-s itoste ro l (upper band) and P-amyrin (lower band)
1 = SP 3 7 , S aw P a lm e tto , Swiss H e rb a l R em ed ies Ltd., CAN
2 = SP 3 4 , S aw P a lm e tto E xtrac t, N o w Foods, USA
3 = SP 1 9 , P rost-Force , P ra irie N a tu ra ls , Canada
4 = SP 1, P ro s ta te P e rfo rm , N e w Roots H e rb a l, C anada
5 = SP 4 8 , S aw P a lm e tto & P ygeum , P re fe rre dN u tr it io n , CAN
6 = SP 2 0 , Life E xtens ion , Q u a lity S u p p lem e n ts and
V ita m in s Inc., USA
7 = SP 3 3 , C urb isal, P harb io , Fin land
8 = SP 4 3 , P rostalan F o rte , V S M , N e th e rla n d
9 = SP 5 3 , S aw P a lm e tto B arry E xtract, S o laray, USA
10 = SP 4 6 , P ro stav ita l, H e a lth A id , UK
11 = SP 2 9 , Saw P a lm e tto M o n o P ro d u ct 1
(HFS),CJ N u tra , Korea
12 = SP 16, S aw P a lm e tto C o m b in a tio n P roduct 1 (HFS),
CJ N u tra , Korea
13 = SP 18, S aw P a lm e tto C o m b in a tio n P roduct 2
(HFS), C hung W a e P h arm a C o rp o ra tio n ,
Korea
1 4 = SP 3 2 , S aw P a lm e tto M o n o P ro d u ct 2 (HFS),
C hong Kun D ang H e a lth , Korea
15 = SP 1 0 , P rostasan , B io force AG , S w itze rlan d
1 6 = R e fe ren c e s o lu tion : p -S ;tosfero /; P -A m y rin
Andy Suter 107

Chapter 3: Phytochemical analysis
Figure 13: TLC fingerprin ts o f tw o preparations made w ith soft gel capsules. On lane 3 is the reference product Prostasan, on lane 4 are the reference substances ^-sitosterol (upper band) and g-am yrin (lower band)
1 = SP 44, Prostavit, Bional, Netherland2 = SP 21, Prostavit Forte, Bional, Netherlands3 = SP 10, Prostasan, Bioforce AG, Switzerland4 = Reference solution: [i-Sitosterol-, p-Amyrin
1 2 3 4
Figure 14: TLC fingerp rin t of fiye saw palm etto preparations w ith soft gel capsules. On lane 6 is the reference product Prostasan, on lane 7 are the reference substances ^-sitoste ro l (upper band) and p-am yrin (lower band)
: r n m # •
1 = SP 4 9 , P rostA ctive , N a tu re 's W a y , USA
2 = SP 5 0 , P ro s ta te 5LX, N e w C h a p te r Inc., USA
3 = SP 5 1 , P ro state A d v a n ta g e , E nzym atic T h e r., USA
4 = SP 5 2 , Saw P a lm e tto & P ygeum , N a tu re 's W a y , USA
5 = SP 5 4 , S aw P a lm e tto E xtrac t, Source N a t., USA
6 = SP 1 0 , P rostasan , B io force AG, S w itze rlan d
7 = R e fe ren c e so lu tion : P -S /tosfero /; P -A m y rin
Andy Suter 108

5" r,'10 ,
In conclusion, the results show that the applied concentrations were sufficient to cause
a good signal strength. The TLC fingerprints displayed that the saw palmetto mono
preparations could well be identified when compared to the reference product
Prostasan® no matter the galenic form of a product. Also, in general the mono
preparations could be differed from the combination products. Answers on quantity of
the saw palmetto extracts or which were the components in a combination product
could not be given with this TLC methodology.
Methodological aspects, how ^-sitosterol could be determined qualitatively and
quantitatively by also using TLC are presented in the discussion section.
Andy Suter 109

Chapter 3: Phytochemical analysis
3.3.2 Analysis of fatty acids
For each of the tested products the amount of the fatty acids lauric acid, capric acid,
caprylic acid, myristic acid, palmitic acid, linolenic acid, oleic acid, linoleic acid, and
stearic acid were determined whereas for oleic and linoleic acid the sum for both were
assessed since the resolution of the peak was not satisfactory. The chosen fatty acids
are known to form the majority of lipophilic constituents of saw palmetto fruits and are
thus a good marker for the botanical drug's active constituents (352). A detailed
description of the fatty acids analysed is given in Table 7.
Table 7: The elemental form ula, lipid number, structure, and pharmacological activities o f thegaschromatographically analysed fa tty acids
Fatty acid (lUPAC name)
Elemental formula/
lipid numberStructure Pharmacologically known activities
C aprylic acid
(o c ta n o ic ac id )CsHieOî
C 8:0
0
HQ
A n tib a c te r ia l (3 5 3 -3 5 7 )
C apric acid
(d ecan o ic a c id )
C10H 20O 2
C 10:0
0A n tiv ira l (3 5 8 )
Lauric acid
(d o d ec an o ic acid )C12H 24O 2
C 12:0
0A n tib a c te r ia l (3 5 9 ), in su lin o tro p ic (3 6 0 ),
increasing high d en sity lip o p ro te in
(H DL) (3 6 1 ), an tim u sc a rin ic ,
a n tia n d ro g e n ic (4 1 , 4 6 , 4 7 )
M y ris tic acid
(te tra d e c a n o ic acid )
C14H 28O 2
C 1 4:0
0 A n tib a c te r ia l (3 6 2 ), a n tip a ra s itic (3 6 3 ),
H y p e rc h o le s te ro la e m ic (3 6 4 )
P a lm itic acid
(h e x ad e c an o ic acid )C16H 32O 2
C 1 6:0
0H y p e rc h o le s te ro la e m ic (3 6 4 , 3 6 5 )
S te aric acid
(o c ta d e c a n o ic acid)
C18H 36O 2
1 8 :0
0
a n ti-a d ip o g e n ic (3 6 6 -3 6 8 )
O le ic acid
((9Z ) o c ta d e c -9 -e n o ic
a c id )
Cj8H3402
18:1
0 A ntic a rc in o g e n ic (3 6 9 ), hy p o te n siv e
(3 7 0 ) an tim u sc a rin ic , a n tia n d ro g e n ic
(4 1 )
L inoleic acid
(cis, c is -9 ,1 2 -
o c ta d e c a d ie n o ic acid )
C18H 32O 2
1 8 :2 HO
a n ti-a d ip o g e n ic (3 7 1 ), in fla m m a to ry (?)
( 3 7 2 ,3 7 3 )
c t-lino len ic acid
((9 Z ,1 2 Z ,1 5 Z )-
o c ta d e c a -9 ,1 2 ,1 5 -
tr ie n o ic a c id )
C18H 30O 2
1 8 :3' ---------------------------------—
A n tiin f la m m a to ry , im m u n e m o d u la to ry ,
a n ti-a d ip o g e n ic , radical scavenger,
increasing lip o p ro te in p e ro x id a tio n ,
an tica rc in o g en ic (3 7 4 )
Andy Suter 110

3.3.2.1 Total daily amount of fatty acids per preparation
The test samples varied widely in their amount of saw palmetto extract as declared by
the producer, the capsule or tablet weight, and the daily dosages (Table 6). Thus in the
following the results of the fatty acid analysis will be shown for the lowest daily dosage
as given on the package as this is the amount of tablets or capsules which the
manufacturer of the product still considers to be efficacious.
The results showed there great heterogeneity between the products in the amount of
fatty acids per day as can be seen in Figure 15 for the lowest daily dosage per
preparation. The concentrations were in the range between 8.43mg for the product
with the lowest daily amount of fatty acids to 1473mg for the item with the highest
value. The mean reached 372.4 ± 333.7mg fatty acids per day and the median value
was 283.5mg/d.
Mono and combination products differed slightly in the average when looking at all test
items regarding the content of fatty acids but the combinations displayed a larger
variability. Products containing only saw palmetto result in 230.5 ± 127.2mg fatty acids
per day with values ranging from 30.89 to 1473.2mg, combination products in 261.0 ±
247.5mg with a range from 8.34 to 1173.02mg daily; the corresponding median values
were 271.9mg for mono preparations, respectively 239.3mg per day for combinations
(Figure 15).
Andv Suter 111

Chapter 3: Phytochemical analysis
Figure 15 : Am ount fa tty acids per day o f the lowest daily dosage given on the package fo r each analysed product [m g/d] of all 46 investigated commercial preparations. W hite bars indicate mono preparations containing only saw palm etto as active constituent, red bars combination oroducts.
w. ^ i > =0f BJWf,
200 400 600 800 1000 1200
mg fatty acids/day
1400 1600
Andy Suter 112

Chapter 3: Phytochemical analysis
The differences in the daily amount of fatty acids per product were more pronounced
when looking at the country of origin. The mono preparations from Switzerland and
South Korea showed all similar concentrations while the highest dosed U.S. American
product contained 2.7 times the amount of the preparation with lowest dose, for
Canada this ratio was 3.0, and for Spain even 13.3 (Figure 16).
Figure 16: Total am ount o f fa tty acids per minimal daily dosage [m g/d] fo r mono products sorted by the ir country o f origin
>- 800
600
SP SP SP SP32 29 8 12
SP SP SP SP37 45 13 33
Canada Finland Korea Spain
SP SP SP SP SP 36 35 27 31 30
Switzerland
SP SP 11 14
UK
SP SP SP SP 34 54 53 49
U.S.A
Combination products when analysed by their country of origin showed an even more
ambiguous picture regarding the amount of total fatty acids. The mean values were
highest for the Canadian products (n=3) with 1008.5 ± 219.6mg/d, followed
preparations from the U.S.A (n=7) with 378.3 ± 288.6mg/d, and South Korea (n=2) with
358.7 ± 61.1mg/d. The lowest average value for the total fatty acid content displayed
the Spanish products (n=3) with 129.2 ± 193.7mg/d.
The enormous standard deviations highlight that there was a large variability between
the daily amount of fatty acids between the preparations within one country. The
highest dosed brand in Spain contained 42.3 times more fatty acids than the lowest
dosed, for the products from the United Kingdom this factor was 27.9, for those from
the Netherlands 14.4, from the U.S.A. 9.0, from Canada 1.6, and from South Korea 1.3.
Andy Suter 113

Chapter 3: Phytochemical analysis
The total amount of fatty acids in combination products cannot be explained by other
botanical drugs included in a preparation. Samples containing one or both of these
extracts could contain high amounts of fatty acids like for example for the Canadian
SP19 with 1173.02mg/d but also very low daily concentrations like 26.64mg of the
Spanish sample SP 15 (Figure 17).
Figure 17: Daily am ount o f to ta l fa tty acids fo r combination products according to the minimal dose of every preparation [m g/d], divided by country o f origin. The darker bar indicates fo r each country the mean value w ith standard deviation.
1400
r . 600
(T3 CM LT) LD
l/> LO I /) CO t/> LO UO
Canada Korea Netherlands Spain Switz. United Kingdom U.S.A
Andy Suter 114
Chapter 3: Fhytocheni ical cnciys:
3.3.2 2 Comparison of measured fatty acid quantities to the amounts given on
the packages of mono preparations
The differences in the total amount of fatty acids between the products might not be
that relevant for a customer when the quantities of extract are declared correctly. Thus
for the mono preparations I compared the measured quantities of fatty acids to the
amounts given on the packages or the package leaflet. For the calculation of the
difference between the stated and measured amount I assumed that an extract would
consist of 100% fatty acids.
There were large dissimilarities between the measured values and the package
information ranging from about 10 times less fatty acids up to 4.6 more fatty acids than
what was stated by the manufacturer.
Usually lipophilic saw palmetto extracts contain 70-95% fatty acids (147, 352). Only for
eight of the analysed 19 preparations a percentage of fatty acids per capsule or tablet
in this range could be calculated by comparing the measured amount of fatty acids to
the written quantity of extract by the manufacturer. Interestingly, all registered Swiss
products were among these eight products as well as the also registered Finnish
product and one Korean product. The only U.S. American preparation (SP49) which was
in the calculated range is actually a German preparation similar to SP 27 as both are
produced by the same manufacturer, Schwabe Pharma in Germany (375).
Surprisingly, for SP12, Permixon®, a saw palmetto product with a good preclinical and
clinical background and known to be a reputed product (34, 338) only a value of 34.8%
fatty acids of the extract could be determined (Table 8).
A ndy Suter 115

Table 8: Differences between the am ount of saw palm etto extract as stated on the package and the measured concentration o f to ta l fa tty acids per tab le t or capsule assuming the extract consists o f 100% o f fa tty acids.
Samplenr. Country
Unit: Tablet (t)
orcapsule (c)
Amount of saw palmetto
extract per unit [mg]
asdeclared on
package
Total fatty acids [mg] per unit
measured
Difference in % of information on package vs. measurement
SP8 ESP t 80 368.3 460.4%
SP 37 CAN c 80 253.06 316.3%
SP 34 USA c 160 378.2 236.4%
SP 53 USA c 160 354.61 221.6%
SP 54 USA c 320 444.31 138.8%
SP 36 SWI c 160 151.56 94.7%
SP 33 FIN c 320 290.24 90.7%
SP 49 USA c 320 285.68 89.3%
SP 35 SWI c 320 281.34 87.9%
SP 27 SWI c 320 274.53 85.8%
SP31 SWI c 320 274.45 85.8%
SP 32 Korea c 320 271.9 85.0%
SP 30 SWI c 320 271.82 84.9%
SP 29 Korea c 320 237.74 74.3%
SP 12 ESP c 160 55.68 34.8%
SP 45 CAN c 350 51.01 14.6%
SP 14 UK c 300 34.5 11.5%
SP 13 CAN c 500 56.8 11.4%
SP 11 UK c 450* 44.57 9.9%
♦Contains also saw palmetto powder
116

Chapter 3: Phytochemical analysis
3.3.2.3 The relative amount of the single fatty acids per preparations giving and
indicator for their inner composition
a) Combination products
For each of the analysed products the relative amount of every single fatty acid was
assessed compared to the total amount of fatty acids. Like this, a fingerprint on the
composition for each product can be produced.
For the combination preparations, the relative amount of fatty acids and the resulting
pattern varied widely. For example, only eleven products had a lauric acid content of
more than 20% of the total fatty acids, three test items, SP44, SP46, and SP56
contained almost none at all. To link the amount of certain fatty acids to extracts like
Pygeum africanum, soy, or pumpkin seeds which were part of the combinations was
not possible (Figure 18).
Figure 18: Relative amount o f the analysed single fa tty acids compared to the tota l fa tty acidcontent fo r each investigated com bination product. The bar at the very right shows the average value of all investigated combi products (n=27).
100%
90%
80%
70%
M 60%
50%
° 40%
è 30%
20%
10%
f N p v r H r ^ f N L n ^ L n k D r ^ r ^ n n o o o r o o r ^ r M t H ^ - i r s o o o ^ o o t D ^ û ^ o;
Û - t / ) Û . Û . Q . Û . Û . Q . C L C L Q . Q . a . a . Û . Q . Q . C L t / ) Q . Û . Q . Q . Q . Q . O . Û . 2 00 L O L O L O L O L O L O L O t / ) ( / ) l / l L O ( / l L O L O O O U O L O L O L / I L O L O L O O O O O Qj
■ Lauric acid■ Myristic acid■ Oleic+/Linoleic acid
I Caprylic acid I Palmitic acid I Stearic acid
I Capric acid I Linolenic acid
Andy Suter 117

r S . - Fny(or/i(?nj'rr/ o.no,'ys.''r
b) Mono products
The composition of the saw palmetto mono extracts was in the majority comparable as
can be seen in Figure 19. The percentage of the eight different single fatty acids was
more or less comparable in about 14 of the mono preparations, the samples SP54, 34,
53, 8, and 37 differed the most from the average values.
Saw palmetto fruits contain high amounts of oleic and lauric acid, each is present with
around 30-40% of the total fatty acids (352), the above mentioned 14 preparations
showed high concentrations of lauric and oleic/linoleic acid as well. The amount of 20%
lauric acid per saw palmetto extract as demanded in the European Pharmacopeia (336)
was reached by all but four mono preparations. Three of these four products, SP34,
SP54, and SP8 had larger amounts of oleic and linoleic acid and one item, SP37,
contained a very high concentration of linolenic acid which is unusual for saw palmetto
berries and gave raise to a suspected adulteration with another plant oil.
In general the pulp of the saw palmetto fruit contains more myristic acid compared to
the whole drupe (352). None of the test items had increased values of this fatty acid
which indicates that in all cases the whole fruits were extracted.
The extractant was available from the package or patient information leaflet for SP27,
30, 31, 33, 35, and 36; either 90% or 96% ethanol was used and all these products had
comparable drug extractant ratios. These ethanolic preparations showed the same
relative amount of the fatty acids compared to the only product extracted with hexane,
SP12 (Figure 19).
Andy Suter 118
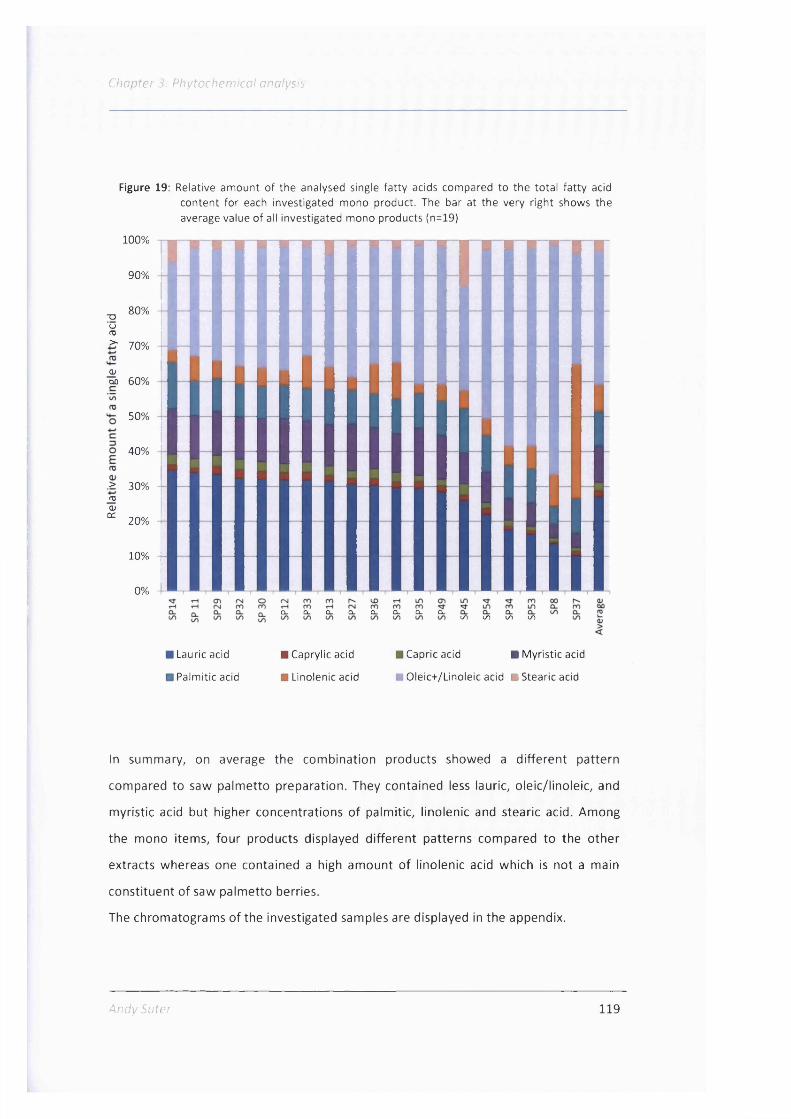
Chapter 3: Phytochemical analysis
Figure 19: Relative am ount o f the analysed single fa tty acids compared to the to ta l fa tty acid content fo r each investigated mono product. The bar at the very right shows the average value o f all investigated mono products (n=19)
100%
90%
T3Uns>-
80%
70%
djM 60%
50%
40%
> 30%mO)oc 20%
10% -
0%
Q - Û - Q u a - Q - Q - Q - Q - (✓) 1/1 I/) I/)
Lauric acid ■ Caprylic acid ■ Capric acid ■ M yristic acid
Palmitic acid ■ Linolenic acid mOleic+/Linoleic acid ■ Stearic acid
In summary, on average the combination products showed a different pattern
compared to saw palmetto preparation. They contained less lauric, oleic/linoleic, and
myristic acid but higher concentrations of palmitic, linolenic and stearic acid. Among
the mono items, four products displayed different patterns compared to the other
extracts whereas one contained a high amount of linolenic acid which is not a main
constituent of saw palmetto berries.
The chromatograms of the investigated samples are displayed in the appendix.
Andy Suter 119
C/iopfer 3; Pnytcc/iFni.co,' o/io-ys;
3.3.2 4 Main results from proton-NMR-analysis from the master thesis of Tony
Booker(2010)
In the NMR analysis the test items SPl to SP37, except SP8 were analysed and
additionally four saw palmetto mono tinctures and one German lipophilic mono extract
(Prostess uno, TAD Pharma) and a British product from Chapmans which contained saw
palmetto powder extract.
For better comparison of the two analytical methods, GC and NMR-spectroscopy,
I focus in the following only on products which were analysed using both techniques.
For sample preparation, the test items were first extracted with methanol and then
analysed, but as with this extraction method the soft extracts dissolved insufficiently,
deuterated chloroform was used thereafter as extractant.
With the NMR analysis the compounds gallic acid, absorbic acid, galactose, sitosterol,
stigmasterol, caproic acid ethyl ester, and oleic acid could be analysed. The latter two
substances could be positively identified from the spectra of the methanolic sub
extracts from the saw palmetto products and could be used for quantitative work.
In general, the analysis showed that tinctures and preparations containing dried saw
palmetto powder could be differentiated with the principal component analysis (PCA)
from powder extracts.
Among the soft gel extracts, the hexane extract Permixon (SP12) presented a different
metabolomic fingerprint than the others which partly might be due to the excipient
polyoxethylene glycol but it contained also more methyl and ethyl esters.
Three other preparations, SP26, SP34, and SP37 were different from the main group of
soft gel extracts.
Andy Satcr 120

Further small differences between the test items, also between combination and mono
products could not be detected with NMR nor were at this stage any quantifications of
constituents in the extracts possible. But the NMR-method, here used for the first time
for a metabolomic approach for different saw palmetto preparations proved to be
robust and reproducible and the clustering allowed well to identify outliers.
A good example for a PCA is shown in Figure 20 for soft extracts in chloroform. The saw
palmetto mono extracts build in the majority one cluster whereas combi preparations
deviated from it (Figure 20).
Figure 20: Ellipse scores of saw palm etto soft extracts (SP25-37) versus com bination products (SP16-SP21) in chloroform .
Scores0.3
0,2
0.1
-0 1
-0.2
SP20
1 SF 18 IY mê6 ' J
SP19 /
SP37
-0.6 -0.5 -0.4 -0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 0.5 0.6PC-1 (82%)
121

5 ' r . r c f / f
3.4 Discussion
This phytochemical analysis of 46 commercial preparations from eight different
countries which contain saw palmetto is at the time the most comprehensive
investigation of saw palmetto products carried out so far.
The study showed that with the TLC methodology lipophilic saw palmetto mono
extracts could be identified well and that the total amounts of fatty acids measured
with GC were very heterogeneous between all analysed products. The relative amounts
of the nine investigated fatty acids were similar in ethanolic mono preparations but
rather different in combinations. Furthermore, this investigation provided evidence
that the mono preparations sold as food supplements displayed large differences
between the declared and the measured amount of fatty acids.
The analysis confirmed that the TLC method of the European Pharmacopoeia (336)
showed good results in identifying saw palmetto mono products.
With this TLC method saw palmetto preparations with different extractants could be
distinguished since SP12, the only investigated hexane-based extract, showed a
different TLC fingerprint than the ethanolic mono extracts. More test samples with
hexane as extractant for comparison would be needed to confirm this finding.
Otherwise, the TLC fingerprints were very heterogeneous and only in some cases the
saw palmetto component was to some extent identifiable. Also for preparations
containing same combination partners like Pygeum africanum- or pumpkin seed
extracts no uniform fingerprints which could be related to one of the components could
be observed. Thus, this TLC method is best applied in saw palmetto mono preparations
and solely for identification and not for quantification or qualitative determination of
substances like ^-sitosterol.
A better method to evaluate the quality of a product with Saba I is the analysis of its
amount of fatty acids which are seen as the main active constituents in saw palmetto
preparations (17, 40) and are known to influence positively pathological mechanisms of
BPH (41, 48, 52, 376).
With the applied GC standard method nine fatty acids were analysed which comprise
more than 95% of the fatty acids of saw palmetto berries. Other fatty acids not
Andy Suter 122

Cncptcr 3; P/iyfoc/iEni/cc/ rnaf/i.':
determined in this analysis like tridecanoic acid, pentadecanoic acid, arachic acid,
behenic acid, and lignoric acid are only to be found in very low quantities in saw
palmetto extracts of less than 0.2% each (35). Caproic acid which also could not be
analysed with the applied GC methodology, accounts for about 3% of all fatty acids in
saw palmetto (352, 377).
The analysis demonstrated that the total amount of these nine fatty acids per lowest
daily dosage were very heterogeneous between the test samples and that they varied
widely with a factor of about 177 between the minimum and maximum concentration
in mono products, respectively with a factor of 38 for combinations.
In general saw palmetto monographs recommend a daily dosage of 320mg lipophilic
berry extract with 70-95% fatty acids (17, 40,146, 147). When this daily dosage of 224-
304 mg fatty acids is taken as an acceptable quality standard, then only nine mono
preparations were in this range. Sixteen combinations and five saw palmetto only
brands displayed higher daily fatty acid values, five mono and eleven combination items
lower quantities.
A too low daily amount of fatty acids may lead to a lack of efficacy, too high
concentrations may not results in immediate health hazards as these fatty acids have a
very low toxicity (378) and higher dosages of saw palmetto extract for example were
still very well tolerated (162) but it makes it impossible to compare these products in
terms of their efficacy. If a higher daily dosage of these fatty acids would result in
improved efficacy in BPH patients is unclear as clinical data is lacking.
In general there is no need to exceed the recommended dosages for these fatty acids as
with 320mg lipophilic saw palmetto extract and with lOOmg lipophilic Pygeum
africanum extract satisfying results in BPH patients were achieved (17, 40, 119, 146,
147).
A higher dosed long term supplementation with some fatty acids may have negative
health effects. Palmitic acid and myristic acid are suspected to be a risk factor for
cardiovascular disease (364) and linoleic acid as it is a precursor of arachidonic acid
which is converted to prostaglandins can also be pro-inflammatory (372, 373).
A n d y Suter 123

Cnrpte/ 3; Fn)for/ip,'?' TC,'G.'?G.Y5.:
Whether increasing the amount of fatty acids by combining saw palmetto with another
herbal extract like Pygeum africanum or Urtica dioica or by fortifying it with vitamins
and mineral leads to a better efficacy in treatment of BPH symptoms is doubtful.
Studies of products containing saw palmetto and urtica, saw palmetto and Pygeum
africanum or even a combination of saw palmetto with cernitin, 3 -sitosterol, and
vitamin E showed no better efficacy in reducing BPH symptoms than what is known
from saw palmetto mono-preparations (379-381).
The total daily amount of fatty acids is one important quality marker to assess the
investigated products. Another one is the relative concentration of each investigated
fatty acid to know about the composition of the total fatty acids.
The only quality requirement for the composition of saw palmetto extracts is the
demand of the European Pharmacopoeia that saw palmetto extracts must contain at
least 20% lauric acid (336). The majority of the evaluated mono preparations fulfilled
this criterion, from the combination products only twelve did. There was no clear
differentiation between registered and unregistered brands concerning the amount of
lauric acid; two food supplements from the UK, SP14 and S P ll, presented the highest
relative concentrations of lauric acid, one licensed product from Canada, SP37, the
lowest ones.
The composition of fatty acids acts like a fingerprint for a preparation and can thus be
compared to other products. In Table 9 the mean frequency of the single fatty acids are
given for seven ethanolic saw palmetto mono products who fulfilled the criteria of the
monographs (SP27, SP30, SP31, SP33, SP35, SP36, SP49; Table 9)(17, 40, 146, 147). For
comparison further fatty acid compositions for saw palmetto fruits, other saw palmetto
extracts, the average values of all combination products, and other herbal extracts are
listed as well.
124

Chapter 3: Phytochemical analysis
Table 9: The frequency o f nine fa tty acids in d iffe rent saw palm etto preparations, the whole fru it, and extracts from Pygeum africanum, pumpkin seeds, olive, and coconut oil as comparison.
%Capric
acidCapryMc
acidLaurieacid
Myristicacid
Palmiticacid
Linolenicacid
O le ic+ /Unoleic
acid
Stearicacid
Average monographed saw palm etto mono products (n=7)
2.4 1.93 30.41 12.37 9.76 6.28 35.16 1.69
Average all saw palm etto m ono products (n=19) 2.28 1.69 27.2 10.52 9.92 7.64 37.83 2.91
Saw pa lm etto whole fru it (352) (n=143 sites) 2.7 2.7 31.7 12.86 9.79 3.92 34.41 1.83
Saw pa lm etto ethanolic extract (382)( Indena)
1.82 2.11 30.86 13.68 10.06 0.92 39.04 1.51
Saw pa lm etto CO2 extract (382)(lndena) 2.78 2.36 33.3 12.51 9.26 0.99 36.89 1.9
Permixon SP12 2.59 1.99 32.04 12.97 9.64 4.2 34.99 1.69
Permixon (hexane) (47) ? ? 30 11 ? ? 40 ?
Hexane/acetone saw pa lm etto extract 4:1 (v/v) (35)
- 1.2 11.9 10.6 13.5 1.5 59.4 1.9
Average all combination products (n=27) 2.34 2.55 16.61 6.32 16.05 13.93 31.35 10.85
Pygeum africanum(382) - - 0.38 0.94 28.3 4.3 55.5 10.58
Cucurbita(382) - - - - 20.24 - 79.76 -
Cucurbita (383) - - - - 4 14 -0:21-47
1:35-595-6
Coconut oil (383) 6.4 8.0 48.5 17.5 8.4 1.5 6.5 2.5
Olive oil (383) - - - - 12.2 0.9 84.5 2.2
Andy Suter 125
C/lopf-e/' S; P/iyfoc/iP/iT/'cc/ ano/ys'f
Interestingly, the average fatty acid frequencies of the seven mono products comply
almost exactly with the values given for the whole fruit by Bubrick et al. (352) who
investigated saw palmetto berries collected from 143 sites in Florida. An ethanolic and
a CO2 saw palmetto extract analysed by Ganzera et al. also showed similar results like
the average frequencies of the seven mono preparations only with a smaller linolenic
acid content (382).
The hexane extract Permixon® displayed in our analysis an almost congruent fatty acid
pattern compared to the seven ethanolic extracts and similar values for lauric, myristic,
oleic, and linoleic acid as reported in literature (47).
Only a hexane/acetone standard extract which was developed by the U.S. American
National Institute of Standards and Technology in cooperation with the Food and Drug
Administration FDA presented a different fingerprint than the mentioned extracts. It
had almost threefold less lauric acid than the ethanolic extracts but almost twice as
much oleic and linoleic acids and more palmitic acid (35).
Mature saw palmetto fruits yield twice as much lauric acid than immature fruits, very
mature fruits contain more oleic acid than lauric acid (377). The pattern from the eight
ethanolic preparations showed that the majority of the manufacturers of the extracts
obviously used the same mixture of immature and mature fruits and that they were a
mixture from all regions of Florida as the fatty acid pattern varies significantly between
the different regions in Florida (352). The only samples that differed from the average
fatty acid content were SP34, SP54, and SP8 which contained more oleic/linoleic acid
than the other test items. This could be due to using more very mature fruits and/or
that they were from one cultivation where the berries contain more oleic acid. In an
unpublished report Berries from central Florida displayed a twice as high laureate to
oleate ratio compared to samples from northern Florida (377). Bubrick et al. found also
geographic variation in the content of oleic to lauric acid throughout Florida, they
observed the highest ratio in a cultivations towards central Florida but the lowest ratio
in a plantation on the East coast of Florida. Interestingly, the amount of ^-sitosterol,
cam peste ro I, and stigmasterol remained throughout the saw palmetto berries samples
of 143 investigated sites in Florida almost the same (352).
Andy Suter 126

C/fCpZer r - F / . o / i n . ' y s . ' r
One test item, SP37, showed a very high concentration of linolenic acid which is
unusual for saw palmetto berries, this product was suspected to be adultered with
another plant oil (383). A later inspection of the package showed that it contained soy
bean oil which was mentioned as an excipient but not as an active, this oil is rich
linolenic acid (384).
With this fingerprint, the mono preparations could well be distinguished from
combination products as they offered in the average a different fatty acid pattern. In
general combination products had lower amounts of lauric and myristic acid but higher
amounts of palmitic, linolenic, and stearic acid. These differences could be mainly
contributed to fatty oils from Pygeum africanum and Cucurbita pepo extracts which are
known to contain more linolenic and stearic acid than saw palmetto extracts.
Saw palmetto is unique in its composition of fatty acids if one compares it for example
with the amount of fatty acids of coconut and olive oils (Table 9).
In summary, an extract can well be characterised by its composition of fatty acids which
acts like a fingerprint for a product.
Thus, to guarantee a good extract quality I would propose that not only the minimum
percentage of lauric acid should be recommended by the pharmacopoeia but also
minimum relative amounts from other important fatty acids like oleic and myristic acid.
A broader analysis of saw palmetto mono preparations with known extraction
conditions could define where the margin would lie. This analysis and data from
literature in Table 9 show that for ethanolic extracts an amount of at last 30% oleic and
1 0 % myristic acid could be suitable.
Nevertheless, the GC method applied is limited as only fatty acids could be analysed.
Other substances like ii-sitosteroi (127, 385) or 8 -carotene (386) which influence
symptoms associated with BPH positively should also be determined in these extracts
and a certain amount could be required as quality marker as well. In particular
\i-sitosterol which exerted in vitro a positive influence on several mechanism associated
with BPH as showing antiandrogenic (385), apoptotic (387), and antiinflammatory (388)
A n d y Suter 127

activity and for which at least in higher dosages also clinically significant improvements
of BPH symptoms could be shown (127) is a good further quality marker besides the
fatty acids. As a clinical trial with 0.3mg H-sitosterol per day showed no clinical efficacy
in BPH patients (122) the amount of about Im g \i-sitosterol/g which can be found in
saw palmetto extracts (340) is obviously not the main active principle of a berry extract
but may have an positive supportive role in improving LUTS.
Whether ^-sitosterol was present in the test items could not have been detected using
our TLC-system, the method used in this thesis was solely for the identification of saw
palmetto preparations. The majority of the preparations showed a signal with similar Rf
of the ^-sitosterol reference but they were often rather large dark spots in contrast to
the the violet-pink zone which is characteristic for H-sitosterol (336), they contained
most probably fatty acids and their esters.
A more precise way by using TLC to determine the presence of H-sitosterol would be to
quantify its amount densitrometrically. Numerous validated TLC methods are described
in literature but mainly for plants containing only a small amount of fatty acids or
triglycerides. To use one of these methods, our test items must have been prepared
previously to omit the fatty acids and its esters for example by extraction with hexane.
These prepared test items could be applied on silica gel plates (F254 HPTLC plate with
60Â pore size) using toluene:chloroform:methanol (4:4:1 [v/v/v]) as mobile phase with
ii-sitosterol as control. After derivatisation with anisaldehyde-sulphuric acid reagent
Murthy et al. could quantify the amount of H-sitosterol from the Indian medical plant
Mucuna pruriens densitographically at 527nm by comparing it to a calibration curve
with i^-sitosterol (389). A similar technique was described by Sparzak et al. who showed
a robust and validated method for identification and quantification of {i-sitosterol in
Phyllanthus species by using the same plates as mentioned above with a mobile phase
consisting of chloroform:hexane:methanol (65:30:5 [v/v/v]) and subsequent deri -
vatisation with vanillin reagent. Compared to a calibration curve with different
\i-sitosterol concentrations densitrometrically at 525nm wavelength they determined
the amount of ii-sitosterol in each test item (390).
Andy Suter 128
S' P/iyfoc/icm/co/ ano/yffs
Also, various HPLC (391, 392) and gas chromatographic methods are available for the
separation, identification, and quantification of phytosterols whereas GC, often
combined with mass spectrometry is the method of choice these days to determine
phytosterols. There are several standardized GC methods for phytosterol analysis
available which are approved by for example the German government (393), the
Association of Official Analytical Chemists (AOAC)(394) or the International
Organisation for Standardisation (ISO)(395). A common principle for the analysis of
phytosterols is that the test samples are saponified at high temperature with ethanolic
KOH solution to obtain the free sterols. The unsaponifiable fraction containing
phytosterols is then extracted with toluene, reduced and the phytosterols are
derivatized to trimethylsilyl (TMS) ethers so they become volatile. They are then
quantified by gas chromatography (GC) with hydrogen flame ionization detection (FID)
(36). Samples that contain 50-150pg of a mixture of phytosterols can well be analysed
(396).
A survey on the concentration of the phytosterols campesterol, stigmasterol, and
^-sitosterol in different preparations containing saw palmetto has already been carried
out by Sorenson et al. in 2006 (340). Since the amount of these three phytosterols is
similar in saw palmetto berries from all over Florida (352) the major influencing factor
in saw palmetto mono-preparations is the extraction method used (Table 10). An
alcohol-free extract and a liquid extract had the lowest phytosterol quantities, a CO2
extract the highest amounts. Two ethanolic extracts, Prostasan and ProstActive
capsules, also investigated in our survey, exerted similar phytosterol values. The
combination with pygeum increases the amount of \i-sitosterol but seemingly not of
campesterol and stigmasterol (340).
Andy Suter 129

Table 10: Mean content of the phytosterols campesterol, stigmasterol and \i-sitosterol In d iffe rent preparations containing saw palm etto according to (340).
Mean phytosterol content, mg/g
Campesterol Stigmasterol H-sitosterol
Saw palmetto 45% powdered extract 0.35 0.17 1.09
Alcohol-free saw palmetto 0.025 0.013 0.069
Liquid herbal extract: saw palmetto 0.019 0.014 0.076
ProstActive once daily ( A SP49) 0.363 0.193 1.07
ProstActive Plus saw palmetto with stinging nettle 0.334 0.099 1.22
Prostasan capsules ( A SPIO) 0.395 0.201 1.12
Pygeum and saw palmetto 0.223 0.087 2.73
Saw palmetto pygeum lycopene complex tablets 1.17 1.04 2.76
Saw palmetto CO2 extract 0.554 0.286 1.74
Saw palmetto berry 0.054 0.040 0.322
Even though the quantification of another active substance like H-sitosterol in the test
samples would have given additional information, we decided to use a different
approach for further assessment of the preparations.
Our method of choice was proton-NMR-spectroscopy and PCA for statistical evaluation.
This allows not only to focus on one or two substance groups like fatty acids or
phytosterols but on all with NMR detectable constituents. By using the statistical
procedure of PCA, preparations with similar characteristics can be grouped in clusters.
In the Master thesis of Tony Booker which was the first to use this methodology to
evaluate different products containing saw palmetto, he could arrange preparations
with similar compositions and could identify outliers. He showed that SP12, SP26, SP34,
and SP37 did not belong to a cluster. The difference to other extracts was most
probably explicable as SP12 contained polyoxethylene glycol as excipient, SP26 used
super critical fluid extraction, SP34 had added extra, glycerine, carob, and zinc oxide.
130

3; P/?yror/7(:.m;'crT' o/ia.Y:':
and SP37 additionally to the saw palmetto extract soy bean oil and glycerine as was
already discussed in the fatty acid analysis.
For a broad analysis of saw palmetto products the method is superior to GC-analysis as
it is not only robust, easy to apply but has the asset that with PCA a statistical method is
applicable with which in short time relationships between different preparations can be
assessed.
To compare the results from the NMR-analysis from single substances with the ones
from the GC analysis is difficult as one identified substance, caproic acid ethyl ester was
not determined with GC. However, in general, the ethanolic mono-preparations which
were similar in the GC analysis were also related in the PCA of the proton-NMR-
analysis.
Further work on the NMR-methodology is thus recommended with more products to
have more data to form more and clearer clusters to differentiate the various products
on the markets as well as outliers.
However, whether an extract with a certain composition is efficacious can in the end
only be shown in a clinical trial. In vitro testing of preparations, focussing mostly on one
assay only like inhibition of the 5-alpha-reductase may give an idea about the clinical
efficacy but can not exclude nor predict a clinical outcome (34, 338).
Looking at it from a patient's perspective, the results of this phytochemical study are
even of greater importance. A BPH patient buying an unregistered food supplement
containing saw palmetto which is marketed for treatment of prostate problems has no
certainty what kind of quality or quantity of active constituents he receives as they are
mostly not declared on the package. And when they are stated, then in case of the saw
palmetto mono preparations sold as food supplements they were in the majority faulty.
This finding is in accordance with the analysis of Feifer et al. (337) who showed that
only three of six investigated saw palmetto preparations from the U.S.A. presented the
amount of fatty acids correctly. Another survey published in the American journal
'Consumer Reports' reported that of 13 assessed brands containing saw palmetto only
eight complied with the declared amount (397).
Andy Suter 131

C/;C7/:re.'' S. n.'io.'y-
Saw palmetto serves consequently as a good example for discussion if herbal
preparations should be on the market as unregulated food supplements or as
registered medicinal products.
From a legal perspective, in Europe food supplements are defined as 'concentrated
sources of nutrients or other substances with a nutritional or physiological effect,
whose purpose is to supplement the normal diet' (398), they are not intended for
treatment of diseases but to maintain 'functions of the organism or to support health'
(399). Medicinal products are by definition of the European Union 'substances or
combination of substances for treating or preventing disease in human beings or which
may be used in or administered to human beings either with a view to restoring,
correcting or modifying physiological functions'(400).
Saw palmetto preparations are used to treat symptoms of BPH which is a disease (401)
and therefore should be regarded at least from a legislative point of view as medicinal
products and be registered. This regulatory framework applies not only for prescription
but also for non-prescription medication, the over-the-counter (OTC) products to which
herbal medicines belong (402).
Nevertheless, one could still argue that food supplements and herbal products are both
moderately efficacious and well tolerated and for that reason phytomedical
preparations should be available as food supplements. This would reflect for example
the U.S. American or Dutch situation for herbal medicinal products.
Regarding the heterogeneous results from this phytochemical analysis of saw palmetto
products I favour the approach to register these preparations also based on the
following considerations.
A registration allows not only to use an herbal product in a certain indication but
demands from the manufacturers to adhere to high quality requirements. The quality
part of a registration dossier for a traditional herbal medicinal product demands the
same data on quality as for any synthetical medication. This includes not only validated
production processes but also that a manufacturer has to provide stable products with
same uniformity of dose (402).
Andy Suter 132

Like this, the customer is protected from incorrect declarations on the packages and is
assured to obtain a good quality product for his or her disease. With the situation
present in many countries where herbal products are unregulated, patients are often
mislead regarding the amount of active constituents and declarations as could be
shown in this phytochemical analysis.
An often heard argument from opponents of a regulation for herbal medicinal products
is that this would confine the patient's freedom of choice for natural medicines and
that rather the public needs to be educated to differentiate between good and low
quality products instead of registrating them (403). These arguments are in reality
nothing more than excuses from companies which cannot provide good quality nor
clinical data for their preparations. A registration would answer the question about the
quality of a product and is much easier to carry out than a public education of
consumers.
Another reason why I advocate the registration of Sabal preparations and herbal
medicinal products is that they show generally moderate efficacy with a very good
safety profile. To guarantee this at least mite efficacy a good product quality is
mandatory, this can be reached best by registrations.
With this good benefit/risk ratio, herbal medicinal products could become at least in
Europe an interesting treatment alternative to synthetical drugs for several mild to
moderate disorders. It would be a pity if patients could not profit from this therapy
option - due to lack of quality.
Ar,dv 133

Chapter 4A clinical pilot study with saw palmetto in patients with BPH and concomitant sexual dysfunctions
Andy Suter 134

Chapter 4: Clinical pilot study
A clinical pilot study with saw palmetto in patients with BPH
and concomitant sexual dysfunctions
4.1 Introduction
The first U.S. American physicians using saw palmetto discovered that the plant was not
only efficacious in respiratory tract infections and genitourinary disorders but also as
treatment for sexual dysfunctions (SDys).
As outlined in chapter 2.3.2.3.2, already in 1880 the pharmacist Dixon indicated the use
of Sabal for 'sexual debility' (233), in 1885 a doctor Evans wrote that the plant had a
good effect on 'wasting of the testes', in his view the reason for impotence (167), and
Knapp in 1892 (235) and Davidson in 1895 (230) substantiated Sabal as treatment of
male SDys such as impotence or lack of drive. Also in current literature saw palmetto is
often cited as a herbal treatment for testicular atrophy (404, 405) and for erectile
dysfunctions (406) or as an aphrodisiac (407).
Nevertheless, even though the properties of saw palmetto on SDys are known only a
few clinical studies assessed this topic. Therefore I carried out a clinical pilot trial in BPH
patients with concomitant SDys to evaluate if a saw palmetto treatment could improve
BPH and SDys symptoms as well.
In the following, an overview is given about the epidemiology of male SDys, their
relation to BPH, the possible underlying pathophysiology, the detrimental effect of BPH
standard medication on SDys, and clinical data of saw palmetto in SDys.
A ndv Suter 135
C/.n.rCf'
4.1.1 Epidemiological data of SDys in the elderly male population
Generally, sexual functions are divided into the four domains desire (libido), erection
(arousal), ejaculation (force, volume) and orgasm/satisfaction (408). Until the begin of
the new millennium, it was assumed that SDys, meaning dysfunctions of one of the
above mentioned four domains in men are a natural consequence of the ageing
process. Recent studies showed that a decrease in sexual functions is not inevitably a
consequence of ageing (409). A variety of large-scale epidemiological studies showed
that BPH in particular is an important factor for SDys.
In a large epidemiological survey with 15'496 men aged between 40-69 years a clear
correlation between age and erectile dysfunctions and lack of libido was shown.
Whereas more than 60% of men aged 40 stated no erectile problems, only about 10%
of all men in the age group of 65-69 years were in the identical situation. The same
went for libido where 60% of all around 40 year old faced no problems but only around
18% of all men aged 65-69 years had still a good libido. The study did not investigate
the prevalence of LUTS as well but acts as a good marker for the general prevalence of
SDys. Interestingly, men with moderate to severe sexual problems were up to three
times more frequently seeing a doctor than those with none or light symptoms (410).
The most comprehensive trial to date which investigated LUTS and SDys was the
Multinational Survey of the Ageing Male (MSAM-7) study in 2003 with 12'815 men
aged between 50 and 80 years from the USA and six European countries. About 49% of
all men experienced erectile dysfunctions with a higher proportion in the USA (55%)
compared to Europe (45%) and around 45% of all patients suffered from ejaculatory
dysfunctions. LUTS were prevalent in around 90% of all patients. The more severe the
symptoms of LUTS, the more frequent and more severe the mentioned SDys occurred.
Age and LUTS were stronger risk factors for erectile dysfunction and ejaculatory
disorders than diabetes, hypertension, heart disease, or hyperlipidaemia (411).
A n d y S i ' t e r 136
In a large study carried out in Germany, the Cologne Male Survey, which examined
4489 men between 30 to 80 years, the overall prevalence of erectile dysfunctions was
19%. Interestingly, the incidence of LUTS was 72% in patients with erectile dysfunctions
versus 38% in those without erectile dysfunctions. In addition to age, diabetes,
hypertension, and pelvic surgery, LUTS was seen as an independent risk factor for
erectile dysfunction (412).
The same findings were observed in the UrEpik study which assessed the relationship
between erectile dysfunction and LUTS in 4800 men from the United Kingdom, the
Netherlands, France, and Korea. Erectile disorders were present in 21% of all men
which was significantly associated with age (p>0.001) and LUTS was seen as an
important co-factor for erectile dysfunctions and lack of libido (413).
LUTS as an important and independent comorbidity for erectile dysfunction was also
shown in a survey investigating 2476 men between 25-70 years in Spain (414) and a
study with 2412 men from Brazil, Italy, Japan and Malaysia aged 50 to 78 years also
reported that LUTS were the most significant predictor of moderate to severe erectile
dysfunctions (415).
Overall, the epidemiological studies presented a clinically significant association
between LUTS and various types of SDys in ageing men worldwide.
Rosen assumed from the epidemiological data that the relative risk of developing
erectile dysfunction is 3.7 higher in patients with BPH-symptoms than those without
symptoms in a time period of two years after first reporting them (409).
Andy Suter 137

4.1.2 Pathophysiology of sexual dysfunctions and BPH
The pathophysiologic mechanisms which lead to erectile dysfunction, ejaculatory
disorders, and lack of libido after enlargement of the prostate are still not clear and yet
not very well investigated.
There are several hypotheses on possible mechanisms of action for SDys caused by
BPH. One theory assumes that an imbalance in the autonomic control of smooth
muscle contraction may lead to SDys. The main reason for this might be an over
presence of al-adrenergic receptors in patients with LUTS in the prostatic capsule and
the bladder neck which results in an increased smooth muscle tone (416).
Noradrenaline is involved in the contraction of the penile tissues, in particular the
corpus cavernosum smooth muscle, via activation of al-adrenergic receptors which are
most probably regulated by androgens (417). Any impairment of these receptors may
therefore lead to erectile dysfunctions and ejaculatory disorders (409), also since
contraction and growth of vascular smooth muscle cells are mediated by al-adrenergic
receptors (418).
Another hypothesis states that endothelial dysfunction is a possible mechanism which
refers to impaired endothelium dependent relaxation (i.e. vasodilatation) due to
decreased activity of nitric oxide (NO) (419). Noardrenaline acts as the major
sympathetic neurotransmitter, whereas NO is the major parasympathetic
neurotransmitter. To produce an erection, the balance has to change: The
noradrenaline effect must be minimised and the NO effect increased (420).
In prostatic tissue from men with BPH, the innervation which leads to NO secretion
(nitrergic innervation) is decreased compared to normal prostatic tissue assuming that
this change in the endothelium leads to erectile dysfunctions (421).
A further risk factor to decrease endothelial function is chronic inflammations (422).
Since low grade systematic inflammations seem to be the connection between
metabolic syndrome, coronary artery diseases and erectile dysfunctions, anti
inflammatory therapy might be an additional treatment option for erectile problems
(423).
A n d / S u t e r 138
CA'n/rc/
Another theory assumes that a change in sex hormones impacts sexual functions. Data
from a longitudinal study, the Massachusetts Male Aging Study, with 1290 men
aged 40 to 70 years, showed that the serum levels of total testosterone,
dehydroepiandrosteron, cortisol, and oestrone decreased, whilst the levels of DHT, sex
hormone binding globuline, luteinizing hormone and prolactin increased during an
observation period of seven to ten years (424). Since hormones itself are produced and
secreted in one tissue but have the ability to regulate or induce signal cascades in their
target tissues either by enzyme activities or by the receptors (425) it is assumed that a
change in the concentration of these hormones may have an influence in the
pathophysiology of BPH and sexual dysfunctions (409).
If it is correct, that LUTS/BPH and SDys share a common mechanism, the optimal
treatment strategy would be a single agent which improves both conditions (411). Our
pilot study with saw palmetto tried to assess if saw palmetto could be one of these
desired therapies.
4.1.3 Sexual adverse events of BPH standard medication
As outlined in chapter 1.4.1.4, the main medical treatments for BPH symptoms include
alpha blockers such as tamsulosin, doxazosin, and alfuzosin (117) which provide fast
relief of LUTS symptoms (131) or the 5-alpha-reductase-inhibitors finasteride and
dutasteride, which lead to symptom relief after 6-9 months and are most favourable in
patients with large prostates (106). Both treatment options show beneficial effects on
BPH symptoms; however, they also each have a significant negative impact on sexual
functions.
The main SDys reported under alpha blocker therapy were retrograde or abnormal
ejaculation, which occurred in 4-18% of patients taking tamsulosin, with rise to 30%
during long term use (426), under silodosin treatment a rate of ejaculatory disorders of
28% ensued (427). Studies on 5-alpha-reductase inhibitors stated SDys with a frequency
of 2.1% to 38%, with erectile dysfunctions being most prominent, followed by
decreased libido and ejaculatory disorders (428). SDys were the most often observed
Andy Suter 139

adverse events under 5-alpha-reductase-inhibition, with similar frequencies reported
for finasteride and dutasteride (429).
The latest American Urological Association guideline on treatment of BPH
recommended the combination of an alpha blocking agent with a 5-alpha-reductase-
inhibitor for better efficacy but neglecting safety (197). Two trials assessing
combination treatments, one with dutasteride and tamsulosin (430), the other with
finasteride and doxazosin (134) showed that the incidence of sexual adverse events was
higher in the combinations than with monotherapy alone.
Summarised, a BPH patient is at a significant risk to cause or deteriorate existing SDys
by taking one or a combination of these standard therapies for prostate problems.
4.1.4 Data from clinical studies on saw palmetto in SDys
Five previous clinical trials of saw palmetto treatment for BPH also evaluated changes in
SDys as a secondary parameter, with mixed results. However, patients in these trials
had mainly BPH symptoms, not necessarily SDys as well. Using the International Index
of Erectile Function (IIEF), Willetts, 2003 observed a trend of improvement, with an
increase from 51.5 to 55.1 after 12 weeks of saw palmetto treatment compared to a
small decrease from 49.4 to 48.7 with placebo (431), and Sinescu et al. reported under
saw palmetto a significant improvement of the IIEF from 44.4 to 50.8 after 24 months
of treatment (432). In the trial conducted by Gerber (2001) patients had to fill out a
non-specified "sexual function questionnaire" which did not change either with placebo
or saw palmetto (433). In an open study, Bauer (1999) asked if the treatment had an
influence on patient's "sexual activity"; responses indicated that it mostly remained
unchanged with two patients reporting an increase (160). The placebo controlled Sabal
study from Barry et al. observed after 72 weeks of treatment no change in IPSS and
urinary flow rates and also not in the IIEF erectile function subscale (p=0.29) and in the
Male Sexual Health Questionnaire to assess ejaculatory dysfunction MSHQ-EJD (p=0.16)
(162).
Taken together, data from these trials is insufficient to show convincingly that saw
palmetto had a positive influence on BPH-related SDys.
Andy Suter 140

C/iGC'TEr CA'.'i.c o.' j ' u C i
4.1.5 Summary and Study Rationale
Epidemiological studies gave evidence that BPH is one of the strongest co-factors to
cause SDys in the ageing male population. Standard therapies for BPH symptoms like
alpha-blockers or 5-alpha-reductase inhibitors cause frequently sexual adverse events
and may so deteriorate existing SDys. Thus, therapies are sought which are efficacious
and safe in the treatment of BPH symptoms and SDys as well.
Historically saw palmetto was also used as treatment of male SDys but clinical trials
could not confirm efficacy in this indication so far for Sabal. In all the above discussed
saw palmetto studies, BPH symptoms were always the primary parameter which means
the patients could have suffered from SDys but they were never mandatory an
inclusion criterion.
Thus, the pilot trial presented here is the first study ever to investigate if saw palmetto
is efficacious and safe as treatment of SDys in BPH patients.
Andy Suter 141
C/?opfe/' 4; C//Vi/cn,' pA'ot
4.2 Material and Methods
4.2.1 Study design
The trial was initiated by the urologist Dr. Eugen Riedi, then head of the urology
department at the Kantonsspital Chur, Switzerland. He observed that BPH patients he
had prescribed a saw palmetto treatment often reported an improvement in their
concomitant SDys. Together with him and Prof. Reinhard Sailer, head of the Institute of
Complementary Medicine of the University hospital of Zurich, the study design was set
up (Table 11).
As this was a pilot trial to gain data for generation of hypotheses for a larger study an
uncontrolled study design was chosen. This open design was in accordance with other
pilot studies on SDys in BPH patients, for example from alpha blocking agents (434,
435).
The study period for our trial consisted of a one-week untreated run-in phase and a
subsequent treatment period of eight weeks. At each visit, efficacy parameters were
recorded as detailed below. The run-in phase was carried out to observe if BPH
symptoms and SDys remained stable. The treatment duration of eight week was chosen
since in other saw palmetto trials after this period already good results were observed
(118,436).
Andy Suter 142

Table 11: Study design of the p ilo t study w ith saw palm etto on SDys in BPH patients (Prostasan" Libido tria l)
Title Clinical p ilo t tria l to investigate the influence o f a saw palm etto berry preparation (Prostasan®) on sexual functions in patients w ith benign prostatic hyperplasia (Prostasan® Libido trial)
Phase IV (lllb )
Study number 920'136
Principal investigator Dr.med. Eugen Riedi, urologist, Chur, Switzerland
Other study centres About ten GPs or urologists in the cantons of Zurich, Berne, Grisons, St. Gallen and Zug in Switzerland
Reimbursement For each investigator: 500 Swiss franks/patient; fo r each patient: 100 Swiss franks/patient
Study duration per patient 1 week untreated, run-in phase; 8 weeks w ith trea tm ent (56 ± 5 days), to ta l 9 weeks
Number of patients At least 40 patients
Medication, dosage 1x1 capsule Prostasan® daily (320mg extract per capsule, 96%V/V ethanolic Serenoo repens berries extract)
Study design Open m ulticentric clinical tria l(planned to generate hypothesis fo r a larger tria l, thus a p ilo t tria l)
Inclusion criteria Patients w ith BPH and sexual dysfunctions (erectile dysfunction and/or decrease of libido) which existed fo r at least tw o months and are defined by:
• Age 18-80 years old• International Prostate Symptom Score IPSS Score >7• Sexual drive from bSFI (brie f Sexual Function Inventory) <5• Patient is not satisfied w ith his sexual performance• Notion and possibility to practise his sexuality (masturbation,
intercourse)• No organ-dependent damages which rule out the performance
of sexual activities.• Willingness to answer honestly to questions on sexuality• W ritten informed consent
Exclusion criteria Lack of libido which is due to a psychiatric disease or a depressive moodLack of libido in the judgm ent o f the investigator w ith in the last tw o monthsPatients w ith severe vascular disorders (microangiopathies)Severe diabetes mellitusPatients w ith hypertension who are on a stableantihypertensive medication fo r less than tw o monthsKnown neuropathiesKnown bad compliance o f the patientParticipation in a clinical tria l w ith in the last 2 month beforestudy startAlcohol-, drugs-abusePlanned surgeries w ith in the observation tim e
A S X 143

Not allowed concom itant medication:with the exception of stable application since at least 3 months:Application of 5-alpha-reductase inhib itorsApplication of alpha-antagonistsLong-term application of NSAIDs (synthetics andphytochemicals) and paracetamolApplication of synthetic antidepressive agentsRegularly application (>1 un it/2 weeks) o f phosphodiesteraseinhibitorsApplication of phosphodiesterase inhib itors less than 4 days prior to the study visit_____________________________________
Illicit concomitant medication
All of the following medication is not permitted if it has not been taken stable for at least during three months:5-alpha-reductase-inhibitorsalpha-blockerslong term intake of synthetical and herbal NSAID and paracetamol as well as synthetical antidepressants
Continuous intake o f phosphodiesterase-inhibitors, defined as more than one u n it/ tw o weeks, and intake of a phosphodiesterase-inhibitor less than four days prior to the first study visit
4.2.2 Investigators
More than 50 physicians in Switzerland were asked with a letter to participate in the
trial and followed up with a personal contact, in the end nine doctors agreed to take
part. Together with the main investigator, the urologist Dr. Eugen Riedi, a total of three
urologists and seven general practitioners were the study centres.
4.2.3 Patients
Eligible were ambulatory patients with a confirmed BPH diagnosis with at least
moderate symptoms measured with an IPSS>7 and not older than 80 years. They had to
fulfil the inclusion and the exclusion criteria as given in Table 11 and sign the informed
consent form after having read the detailed patient information on the study. The
participants were recruited by their physician, in each practice leaflets and a poster
about the trial were displayed to attract study participants.
144

C/iopfer 4; C/zVnro/ cfù'c')
4.2.4 Study medication
The patients received at the second visit a brown glass with 90 capsules of Prostasan®.
One capsule contained 320mg saw palmetto berry extract (batch: 025070) which was
extracted with 96% ethanol (V/V) and had a DER of 9.0-12.0 : 1. The berries were from
A.Vogel Bioforce's own organic certified cultivation in Florida, USA.
Patients had to take one capsule daily after eating, the time point for intake was not
defined. The compliance was checked by counting the remaining tablets at the final
study visit.
4.2.5 Questionnaires
4.2.5.1 Questionnaire for BPH symptoms
The main symptoms of BPH, which include static and dynamic components (100), are
increased frequency of urination with nocturia, difficulty starting and stopping
urination, weak urine stream, feeling that the bladder has not emptied completely with
residual urine, and in later stages urinary retention and painful urination (101). The
International Prostate Symptom Score IPSS is the validated standard instrument to
measure the severity of these symptoms (99) (Table 12). The investigator needed to fill
it out with the patient which takes about 10-15 minutes time. A validated German
version was available and used in this trial (437).
Andy Suter 145
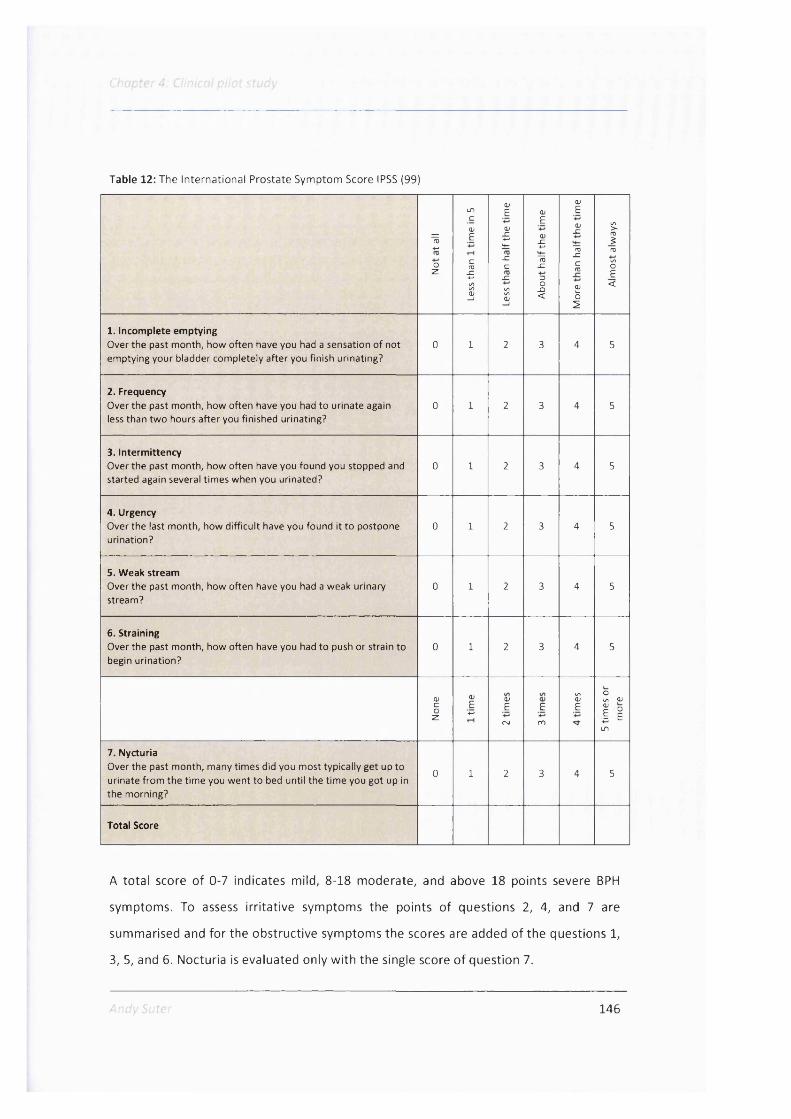
Table 12: The International Prostate Symptom Score IPSS (99)
Ï
oz
If)cQ)g
CfU_c
1
(VEOJ
g
x:c_c
1
(VE<u-C4-*IE-C3O_Q<
OJEOJ-C
IEx:croÏo2
1rosE<
1. Incomplete emptyingOver the past month, how often have you had a sensation of not 0 1 2 3 4 5emptying your bladder completely after you finish urinating?
2. FrequencyOver the past month, how often have you had to urinate again 0 1 2 3 4 5less than two hours after you finished urinating?
3. IntermittencyOver the past month, how often have you found you stopped and 0 1 2 3 4 5started again several times when you urinated?
4. UrgencyOver the last month, how difficult have you found it to postpone 0 1 2 3 4 5urination?
5. Weak streamOver the past month, how often have you had a weak urinary 0 1 2 3 4 5stream?
6. StrainingOver the past month, how often have you had to push or strain to 0 1 2 3 4 5begin urination?
OJ Q) w soun 0)c
oz
E+-• E
rst
Ero
E| iI f )
7. NycturiaOver the past month, many times did you most typically get up to 0 1 2 3 4 5urinate from the time you went to bed until the time you got up inthe morning?
Total Score
A total score of 0-7 indicates mild, 8-18 moderate, and above 18 points severe BPH
symptoms. To assess irritative symptoms the points of questions 2, 4, and 7 are
summarised and for the obstructive symptoms the scores are added of the questions 1,
3, 5, and 6. Nocturia is evaluated only with the single score of question 7.
146

Cnnpfer ' C/ n/i 0/ r.'.'or ; ;
4 2.5.2 Questionnaires for sexual dysfunctions
Attempts to measure human sexual functions appeared first in literature in the early
1960's (438). The central problem lied first in the definition of a SDys since sexual
functioning, hypoactive sexual desire disorder, and sexual satisfaction are merely
hypothetical constructs. Therefore the measurement of these parameters and the
instruments used are generally not as powerful as those used in physical sciences (439).
The current instruments, namely questionnaires, are mostly a product of the thinking of
Masters and Johnson (440, 441), a team which pioneered in the research of diagnosis
and treatment of SDys, and Helen Kaplan who examined hypoactive sexual desire and
so called 'inhibited sexual desire' (442). With their knowledge the sexual response cycle
was defined which strongly emphasized on the above mentioned phases of desire,
arousal, orgasm, and resolution (408). In this model a dysfunction or disturbance may
occur in any or multiple phases of the cycle and the diagnosis is usually made without
statement of the aetiology (439).
For setting up the design of this clinical trial, I investigated and compared available
validated questionnaires for male SDys which are discussed in the following.
4.2.5.2.1 The Derogatis Interview for Sexual Functioning (DISF/DISF-SR)
The Derogatis Interview for Sexual Functioning (DISF/DISF-SR) is an instrument
designed to assess an individual current sexual functioning. It consists of 25 questions
and is available for men and women as separate issues and covers five separate
domains which are sexual cognition/fantasy, sexual arousal, sexual
behaviour/experience, orgasm and sexual drive (443). As this score is also dedicated to
areas such as relationship and behaviour but not mainly on male SDys and is with 25
questions too long to apply, it was not selected for the planned clinical trial.
Andv Suter 147

Chapter 4: Chnical pi lot study
4.2.5.2 2 The Arizona Sexual Experience Scale (ASEX)
The Arizona Sexual Experience Scale (ASEX) is a self reporting inventory to evaluate
SDys in men and women covering the items drive, arousal, penile erection/vaginal
lubrication, ability to reach orgasm, and satisfaction with orgasm (444). The limitations
of this instrument are that it was developed for patients taking psychotropic drugs and
not many epidemiological data is available.
4.2.5 2.3 The International Index of Erectile Function (IIEF)
The International Index of Erectile Function (IIEF) has become the standard
questionnaire in assessing erectile dysfunctions and was used so far in more than 50
clinical trials (439). Patients have to fill out 15 questions covering erectile function,
orgasmic function, sexual desire and satisfaction, and overall satisfaction (445). Even
though this instrument is sensitive, highly reliable and also very well available, it was
not selected for this trial as it only focuses on erectile functions.
4.2.5.2.4 Urolife BPH QoL9-questionnaire
A simple, reliable instrument for the measurement of SDys related to BPH is the
subscale for 'patient's perceived sexual life' of the Urolife BPH Quality of Life 9-
questionnaire (Figure 21). The total score consists of nine questions covering quality of
life items, the subscore on SDys consists of three questions covering sexual desire,
satisfaction with erections, and satisfaction with sex life which have to be answered on
a 10 cm visual analogue scale (446). The score ranges from 0 to 300 or from 0 to 30.
The Urolife BPH QoL-9 'patient's perceived sexual life' subscale is recommended for the
evaluation of SDys in BPH (447), easy to apply, and validated patient data from a large
trial with 2289 men with BPH are available (448).
Due to its validity and easy application, I decided to use this instrument in this pilot trial
with saw palmetto. In the following, this 'patient's perceived sexual life' subscale will be
abbreviated as 'Urolife BPH QoL-9 sex'.
Andy Suter 148
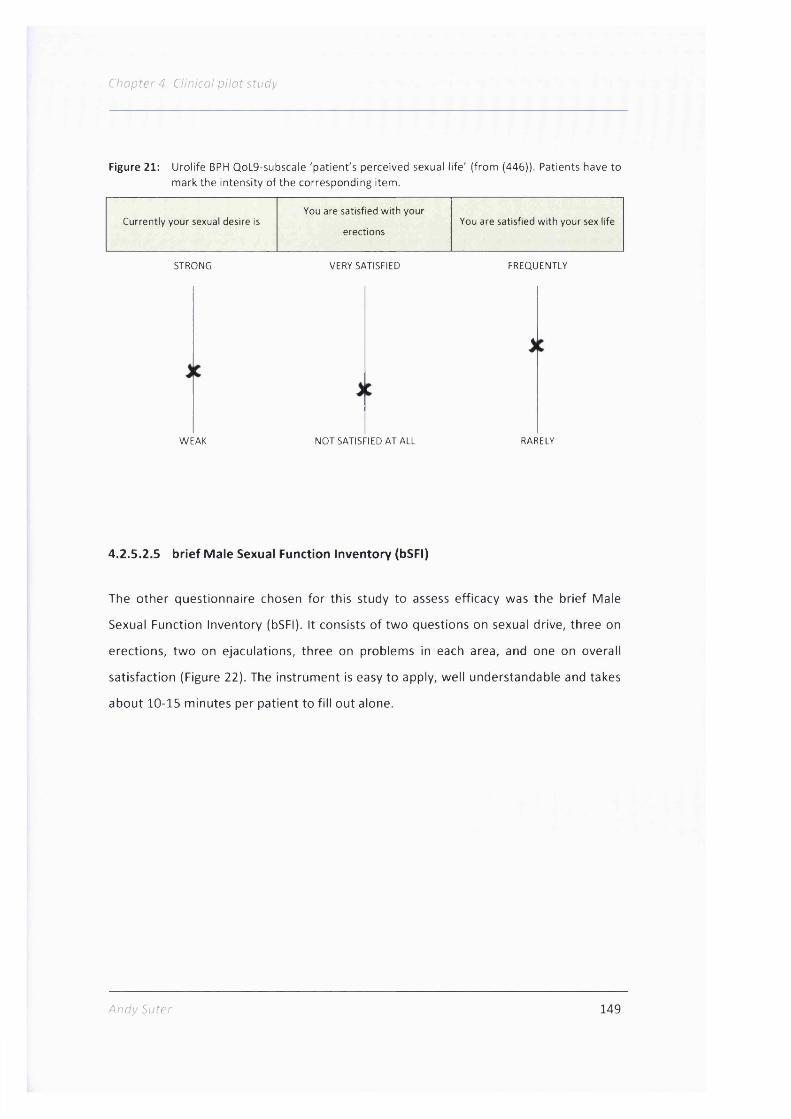
Chapter 4: Clinical pilot study
Figure 21: Urolife BPH QoL9-subscale 'patient's perceived sexual life ' (from (446)). Patients have to mark the intensity of the corresponding item.
You are satisfied with yourCurrently your sexual desire is
erectionsYou are satisfied with your sex life
STRONG
WEAK
VERY SATISFIED
NOT SATISFIED AT ALL
FREQUENTLY
RARELY
4.2.5.2 5 brief Male Sexual Function Inventory (bSFI)
The other questionnaire chosen for this study to assess efficacy was the brief Male
Sexual Function Inventory (bSFI). It consists of two questions on sexual drive, three on
erections, two on ejaculations, three on problems in each area, and one on overall
satisfaction (Figure 22). The instrument is easy to apply, well understandable and takes
about 10-15 minutes per patient to fill out alone.
Andy Suter 149

Chapter 4: Clinical p ilo t study
Figure 22: The brief Sexual Function Inventory bSFI questionnaire (4)
Sexual Drive
Let’s define sexual drive as a feeling that may include wanting to have a sexual experience (masturbation or intercourse), thinking about having sex, or feeling frustrated because of lack of sex.
No days Only a few days
Some days Most days Almost every day
1. During the past 30 days, on how many days have you felt sexual drive? B 0 1 1 B
None at all Low Medium Medium high High
2. During the past 30 days, how would you rate your level of sexual drive? B 0 1 1 BErections Not at all A few times Fairly often usually always
3. Over the past 30 days, how often have you had partial or full sexual erections when you were sexually stimulated in any way?
B 0 1 1 B
4. Over the past 30 days, when you had erections, how often were they firm enough to have sexual intercourse?
B 0 1 B BDid not get erections at
all
A lot of difficulty
Somedifficulty Little difficulty No difficulty
5. How much difficulty did you have getting an erection during the past 30 days?
B 0 1 1 B
EjaculationHave had no
sexual stimulation in past month
A lot of difficulty
Somedifficulty Little difficulty No difficulty
6. In the past 30 days, how much difficulty have you had ejaculating when you have been sexually stimulated?
B 0 1 B BDid not climax
Big problem Mediumproblem
Smallproblem
No problem
7. In the past 30 days, how much did you consider the amount of semen you ejaculate to be a problem?
B 0 B B
Problem Assessment Big problem Mediumproblem
Smallproblem
Very small problem No problem
8. In the past 30 days, to what extent have you considered a lack of sex drive to be a problem?
B 0 I B B9. In the past 30 days, to what extent have you considered your ability to get and keep erections to be a problem?
B 0 I B B10. In the past 30 days, to what extent have you considered your ejaculation to be a problem?
B 0 § B BOverall satisfaction Very
dissatisfiedMostly
dissatisfiedNeutral or
mixedMostly
satisfiedVery satisfied
11. Overall, during the past 30 days, how satisfied have you been with your sex life?
a 1 a
Andy Suter 150
Chapter 4: Ci inicai p i i c t s tudy
It is a thoroughly validated instrument which evolved in the validation process from a
41-item questionnaire to a score with 11 questions (4).
An advantage of using the bSFI in this pilot trial is that it was already used in two large
epidemiological studies. O'Leary and his colleagues tested 2'115 men aged 40 to 79
years (449) and a survey investigated in Norway 1185 men between 20 to 79 years
(450) both with the bSFI and thus good epidemiological data for comparison is
available.
Two questionnaires, the bSFI and the Urolife BPH QoL-9 sex were used instead of only
one to achieve a better soundness of changes in SDys. No validated German version
was available for the Urolife BPH QoL-9 sex - and the bSFI questionnaire, and thus they
were first translated to German by two independent translators. From these two
translated versions, one German version was compiled, which was then re-translated to
English by two other translators, to be compared to the original version. The German
version was then corrected and used by a German speaking doctor in his daily practice.
Based on his experiences, further corrections were made and final versions of the
German scores completed.
4.2.6 Assessment of adverse and serious adverse events
An adverse event is defined as any untoward medical occurrence in a patient and does
not need to have a causal relationship to the treatment (451). Any occurring adverse
event needed to be documented on a special form in the case record form where the
following items were noted: Nature of the adverse event, seriousness, date of onset,
severity (light, medium, severe), relationship to treatment, measures taken, outcome,
end of the adverse event, and if a concomitant medication had been given for
treatment of the adverse event.
A serious adverse event is any adverse event which is lethal, life threatening, leads to
hospitalisation or prolongs a hospitalisation, causes continuous damages, as well as any
malignant deformation or congenital anomaly (451).
Serious adverse events had to be reported within one workday on a special form by fax
to A.Vogel Bioforce AG and the responsible ethical committee.
Andy Suter 151
4.2.7 Assessed parameters
Changes in BPH symptoms were evaluated using the IPSS, SDys with the bSFI and the
Urolife BPH QoL-9 sex questionnaire. At end of the treatment, global assessment of
efficacy by patient and investigator was given on a four point scale (very good, good,
moderate, or unchanged). Additionally, it was examined if the patient observed the
best effect of the treatment on libido, erections or both and about the patients' daily
routines. Patients were asked the practice and policy questions if they would take the
medication again, how important it was for them to use a herbal treatment, and
whether they would prefer a herbal remedy over a synthetic compound. Investigators
were addressed if they would use the test medication again and were asked to provide
reasons if they answered affirmatively.
Safety parameters included the occurrence of adverse events and the global
assessment of safety by patient and investigator at the end of the treatment as very
good, good, moderate, or poor.
4.2.8 Quality Standards and patient's safety
The study was carried out according to the provisions of Good Clinical Practice GCP
(452) which is a legally binding law for Switzerland written down in the regulations for
clinical trials, the 'Verordnung für klinische Studien, VKlin' (453) and the ethical
obligations of the Declaration of Helsinki were also respected (454).
The trial was approved by the cantonal ethical committees of the cantons St. Gallen on
the 13 of May 2009, from Zurich and Grisons on the 30 * of June 2009, from Zug on
the of August 2009, and from Berne on the 27 of August. The Swiss regulatory
authority Swissmedic notified the study on the 6 of August 2009, the trial is registered
in the international clinical trial registry ClinicalTrials.gov, identifier number
NCT01021267. The School of Pharmacy Research Ethics Working Group was informed
about the trial on the 16 of July 2009, they confirmed the acceptance of the
information on the 5 of August 2009.
Andy Suter 152
C/iopfe/- 4; CAn/co/ p.Vcf' j Tuc')
Each study participant was covered by an insurance (Gerling, Policy Nr. 01050561-
14042) against any potential harmful event, which could have taken place throughout
the whole study. The whole trial was insured for the sum of 10 million Swiss franks and
one single patient for personal harm up to 1 million Swiss franks.
Furthermore, A.Vogel Bioforce guaranteed that damages which would exceed the sum
of 1 million per patient would be covered by the company itself and its liability
insurance.
The study could be terminated at any time by a single patient without giving details or
reasons why.
During the trial I visited each physician thrice for monitoring of the data quality and to
assure the study procedure was carried out as outlined in the study protocol.
4.2.9 Statistical anaiysis
All variables measured in the study, were described descriptively using Excel and SAS
Version 9.2. For continuous variables, the following descriptive statistics were
calculated: mean, standard deviation, number non-missing, median, 25 percentile,
75 percentile, minimum, and maximum. For categorical or binary variables, absolute
and relative frequencies were displayed.
For the outcome measures IPSS, bSFI and Urolife BPH QoL-9 sex within group
comparisons of changes from visit 1 to visit 2, from visit 1 to visit 3 and from visit 2 to
visit 3 were performed using the Wilcoxon test for paired differences. Correlation of
changes between IPSS and bSFI, between IPSS and Urolife BPH QoL-9 sex and between
bSFI and Urolife BPH QoL-9 sex were analysed calculating Pearson's coefficient of
correlation.
All statistical analyses were checked for correctness by Peter Klein from the d.s.h.
statistical services GmbH, Rohrbach, Germany.
An outline on the study procedure for every patient is given in Table 13.
Andy Suter 153

Table 13: Study procedure for a patient
Patient in form ation and informed consent
Check o f inclusion and exclusion criteria
Documentation o f diagnostic criteria
Documentation o f concom itant therapies
Documentation o f concom itant medication
Filling out o f IPSS
Filling out o f bSFI
Filling out o f Urolife BPH QoL-9 sex
Handing out of study medication
Assessment of efficacy by investigator and patient
Assessment o f to le rab ility by investigator and patient
Documentation o f adverse events
Questions fo r practice
Return of test medication
Reimbursement fo r travel costs and study participation
Run in phase
Treatment phase
Visit 1
(d a y -7 )
X
X
X
X
X
X
X
X
Visit 2 Visit 3
(dayO) (day 56±5)
A nd y Suter 154

Chapter 4: Clinical pilot study
4.3 Results
4.3.1 Patients and centres
Eighty two patients were included in the trial between June 24 2009 and October 29 '
2010. This was the period from inclusion of the first patient until final visit of the last
study participant. Only six of the ten study centres recruited participants, whereas
centre 7, a practice specialised in complementary medicine in the centre of Zurich
recruited the majority of the patients (Figure 23). The baseline characteristics of the
patients from this one centre did not differ significantly from those form the other
centres.
Figure 23: Number o f patients per study centre, the blue bars comprise the in tention to trea t- (n=84), the red bars the per protocol population which was used fo r the efficacy anaylsis (n=69)
7 0 1
ro 4 0
^ 30
C e n tre 1, u ro log ist C e n tre 3, GP C e n tre 5, u ro log ist C e n tre 7, GP C e n tre 8, GP C e n tre 9 , GP
The patient population was separated for the analysis in three sub-populations. The
safety population which was used for safety analysis comprised all patients who were
included and treated once, the intention to treat (ITT) - population those patients who
had additionally at least one efficacy assessment, and in the Per Protocol (PP)-
population were all patients which completed the study without one major protocol
violation which was defined as use of less than 80% or more than 120% of the study
Andy Suter 155
CAn/'co/
medication, treatment duration less than 51 days or longer than 63 days, and violation
of an exclusion or inclusion criterion. The safety and the ITT population were identical
with the totally recruited 84 patients.
Thirteen patients had at least one major protocol deviation and were excluded from
the PP population which was used for final analysis with 69 patients. Deviations
included one patient with IPSS <7 at inclusion, one with sexual drive component of bSFI
>5 at inclusion, four patients with disallowed concomitant medication, and seven
patients who did not return to the participating practice after the first visit. Reasons for
discontinuation of treatment included one instance of the death of a patients wife, two
adverse events (nausea that was seen as related to the study medication and an
unrelated transient ischemic attack), and in four cases patients did not show up at all to
the follow-up visits.
The demographic parameters of the ITT- and the PP-population were comparable thus
to take the PP as the population for efficacy analysis was justified (Table 14).
Andy Suter 156
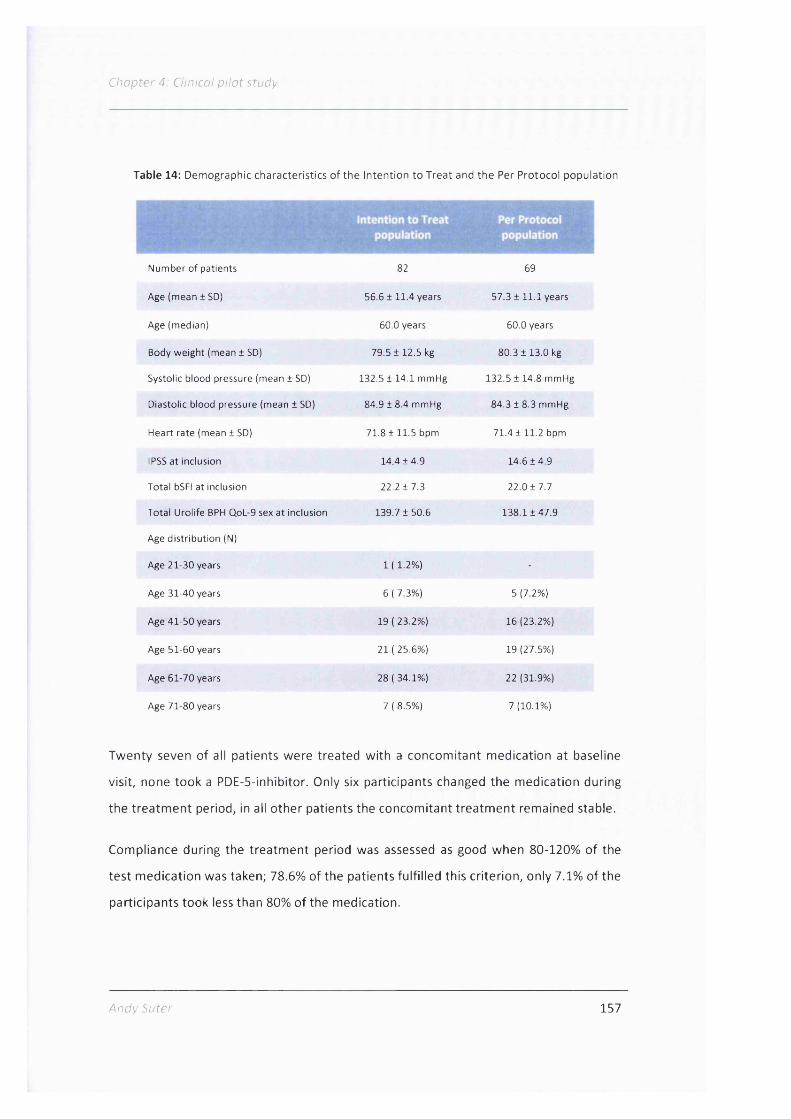
Chapter 4: Clinical p ilo t study
Table 14: Demographic characteristics of the Intention to Treat and the Per Protocol population
Number of patients 82 69
Age (mean ± SD) 56.6 ± 11.4 years 5 7 .3 1 1 1 .1 years
Age (median) 60.0 years 60.0 years
Body weight (mean ± SD) 79.5 ± 1 2 .5 kg 8 0 .3 1 1 3 .0 kg
Systolic blood pressure (mean ± SD) 132.5 ± 14.1 mmHg 132.5 1 1 4 .8 mmHg
Diastolic blood pressure (mean ± SD) 84.9 ± 8.4 mmHg 84.3 1 8 .3 mmHg
Heart rate (mean ± SD) 7 1 .8 1 1 1 .5 bpm 71.4 11 1 .2 bpm
IPSS at inclusion 1 4 .4 1 4 .9 1 4 .6 1 4 .9
Total bSFI at inclusion 2 2 .2 1 7 .3 2 2 .0 1 7 .7
Total Urolife BPH QoL-9 sex at inclusion 139.7 1 50.6 1 3 8 .1 1 4 7 .9
Age distribution (N)
Age 21-30 years 1 ( 1.2%) -
Age 31-40 years 6 ( 7.3%) 5 (7.2%)
Age 41-50 years 19 ( 23.2%) 16 (23.2%)
Age 51-60 years 21 ( 25.6%) 19 (27.5%)
Age 61-70 years 28 ( 34.1%) 22 (31.9%)
Age 71-80 years 7 ( 8.5%) 7 (10.1%)
Twenty seven of all patients were treated with a concomitant medication at baseline
visit, none took a PDE-5-inhibitor. Only six participants changed the medication during
the treatment period, in all other patients the concomitant treatment remained stable.
Compliance during the treatment period was assessed as good when 80-120% of the
test medication was taken; 78.6% of the patients fulfilled this criterion, only 7.1% of the
participants took less than 80% of the medication.
Andy Suter 157

Chapter 4: Clinical p ilo t study
4.3 .2 Efficacy
For all efficacy parameters there was no statistically significant difference between the
first and the second visit showing that the symptoms were stable in the treatment free
run-in week. In the following only efficacy data from the treatment phase, means from
visit 2 to visit 3 will be shown.
4.3.2.1 International Prostate Symptom Score IPSS
The IPSS was reduced by 51%, from 14.4 ± 4.7 to 6.9 ± 5.2, after 8 weeks of treatment
(P< 0.0001) (Figure 24).
Figure 24: Change o f International Prostate Symptom Score IPSS between the start and end o f treatm ent (Per Protocol population, n = 69; P < 0.0001)
COCOo_
20 1
16 -
12 -
8 -
4 -
day 0
day 56
0
A score between 0-7 is defined as mild, 8-19 as moderate, and 20-35 as severe BPH
symptoms. At the beginning of the treatment, 18.8% of all patients had severe and
78.3% had moderate symptoms; by the final visit, this shifted to 63.8% patients with
mild, 31.9% with moderate, and only 4.3% with severe symptoms.
Looking at the single items contributing to the score, they were all significantly
improved to the same extent except for nycturia which had the lowest relative change.
Andy Suter 158
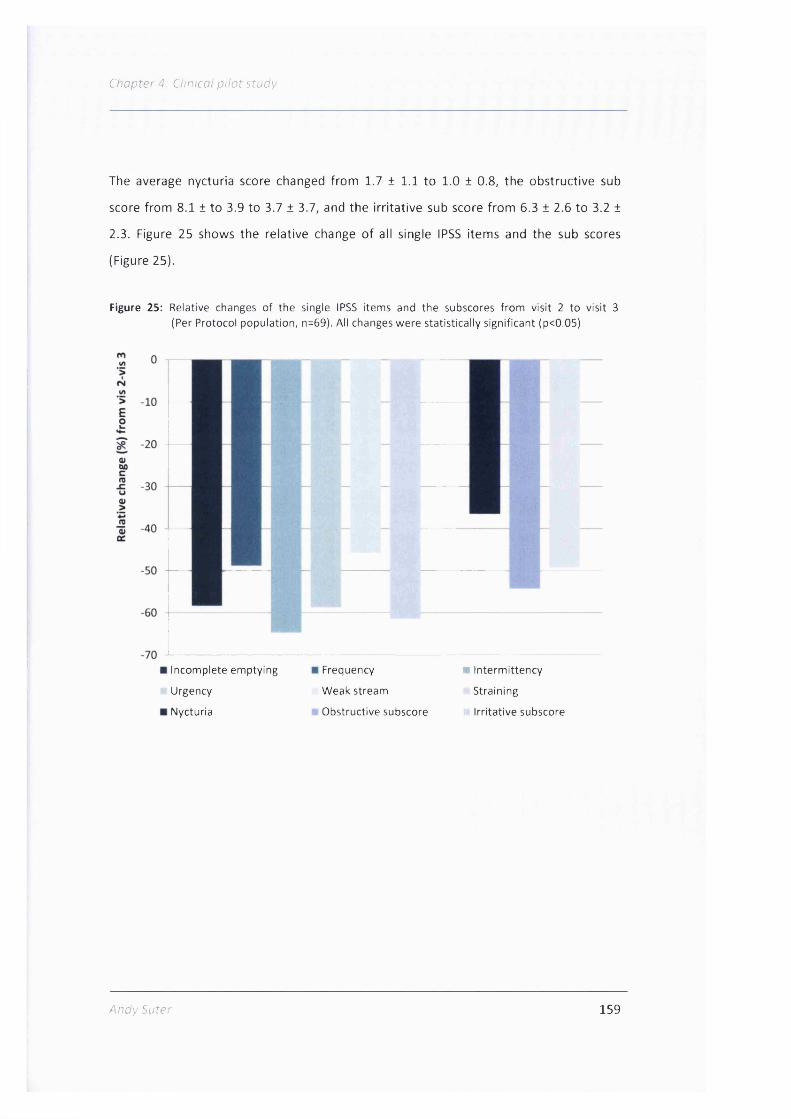
Chapter 4: Clinical pilot study
The average nycturia score changed from 1.7 ± 1.1 to 1.0 ± 0.8, the obstructive sub
score from 8.1 ± to 3.9 to 3.7 ± 3.7, and the irritative sub score from 6.3 ± 2.6 to 3.2 ±
2.3. Figure 25 shows the relative change of all single IPSS items and the sub scores
(Figure 25).
Figure 25: Relative changes o f the single IPSS items and the subscores from visit 2 to visit 3 (Per Protocol population, n=69). All changes were statistically significant (p<0.05)
I
Incomplete emptying
Urgency
Nycturia
Frequency
Weak stream
Obstructive subscore
■ Interm ittency
Straining
ir Irrita tive subscore
Andy Suter 159

Chapter 4: Clinical pilo t study
4.3.2.2 Brief Sexual Function Inventory (bSFI)
The total bSFI score improved from 22.4 ± 7.2 to 31.4 ± 9.2 (P < 0.0001) (Figure 26).
Figure 26: Improvem ent o f brief Sexual Function Inventory bSFI at start and end of therapy (Per Protocol population, n = 69; P < 0.0001)
40 -
30 -
.o 20 -
10 -
0
day 0 day 56
The single item scores for sexual drive, erectile function, ejaculatory function, problem
assessment, and sexual satisfaction were each also significantly improved (P < 0.0001)
(Table 15).
Table 15: Single item scores of the bSFI and Urolife BPH QoL-9 sex at the start and end o f trea tm ent (n = 69)
Score item w ith range (min-max)Start o f treatm ent
day 0End o f trea tm ent
day 56P-value
bSFI
Sexual drive (0-8) 2.0 ±0 .8 2.9 ±0 .9 <0.0001
Erectile function (0-12) 6.2 ±3 .0 8.5 ±3 .5 <0.0001
Ejaculatory function (0-8) 5.0 ±2 .0 6.3 ±2 .4 <0.0001
Sexual problem assessment (0-12) 5.8 ±2 .4 9.2 ±3 .0 <0.0001
Sexual satisfaction (0-4) 2.0 ±0 .8 2.9 ±0 .9 <0.0001
Urolife BPH QoL-9 sex
Sexual drive (0-100) 48.7 ±20.6 66.1 ±20.0 <0.0001
Erections (0-100) 45.0 ±21.0 65.2 ±24.2 <0.0001
Sexual satisfaction (0-100) 43.6 ± 19.7 63.7 ±22.4 <0.0001
* Wilcoxon signed rank test
Andy Suter 160

Chapter 4: Clinical pilot study
The biggest relative improvements in single questions were seen in the problem
assessment domain, where "getting and keeping an erection" improved by 64%, and
"having problems with lack of drive" and "ejaculation" each increased by 54%. "Feeling
sexual drive within the last 30 days" progressed by 47% and "having an erection firm
enough to have sexual intercourse" was scored as 42% better, which, in absolute
values, is a change from below "fairly often" to "usually"(Figure 27).
Figure 27: Single item scores o f the bSFI at the start and end o f treatm ent, normalised to a scale o f 0-10 (0 = worst state, 10 = best) (PP population, n = 69)
Sexual drive •start of treatm ent
end of treatm ent
Sexualsatisfaction
V Erectile / function
Sexualproblem
Ejaculatoryfunction
assessment
There was a centre effect, as mean values of the centre with the most patients
exhibited a significant improvement, whereas the other 15 patients pooled together
from the other centres only exhibited a trend (P = 0.12). Of these 15 patients, eight saw
an improvement, four no change, and three a worsening of their state, whereas the
vast majority of the patients from the single centre experienced at least some
improvement of their SDys.
Andy Suter 161
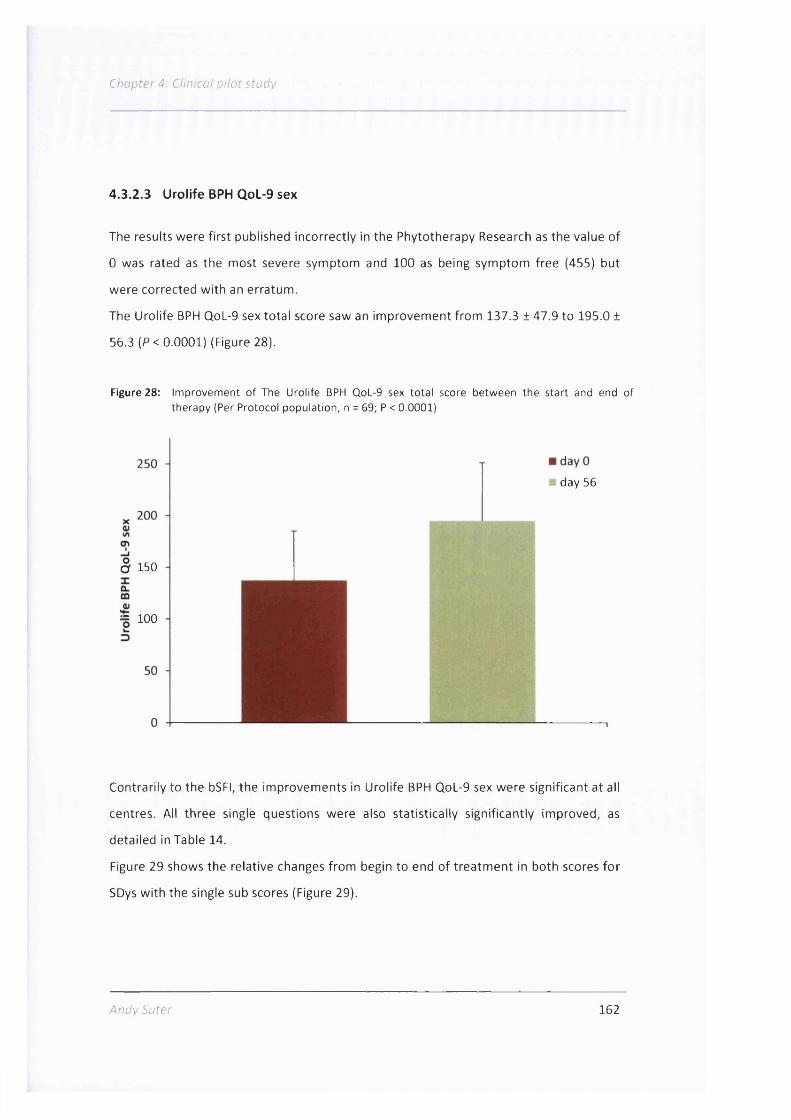
Chapter 4: Clinical pilot study
4.3.2.3 Urolife BPH QoL-9 sex
The results were first published incorrectly in the Phytotherapy Research as the value of
0 was rated as the most severe symptom and 100 as being symptom free (455) but
were corrected with an erratum.
The Urolife BPH QoL-9 sex total score saw an improvement from 137.3 ± 47.9 to 195.0 ±
56.3 (P< 0.0001) (Figure 28).
Figure 28: Improvement o f The Urolife BPH QoL-9 sex to ta l score between the start and end of therapy (Per Protocol population, n = 69; P < 0.0001)
day 56
O' 150
= 100
Contrarily to the bSFI, the improvements in Urolife BPH QoL-9 sex were significant at all
centres. All three single questions were also statistically significantly improved, as
detailed in Table 14.
Figure 29 shows the relative changes from begin to end of treatment in both scores for
SDys with the single sub scores (Figure 29).
Andy Suter 162

Chapter 4: Clinical pilot study
Figure 29: Relative im provem ents of the bSFI and Urolife QoL-9 sex to ta l scores and single items between begin and end of trea tm ent (PP-population, n=69)
70
60
50
40
30
20
10
Urolife QoL-9 sex
Andy Suter 163

Chapter 4: Clinical pilot study
4.3.2.4 Global assessment of efficacy
The majority of the patients rated the efficacy as very good (22%) or good (54%) and
only 15% saw a small effect. The investigators assessed efficacy more favourably,
reporting 38% of the cases as being very good, 44% good, and only 7% patients with
unchanged condition (Figure 30).
Figure 30: Assessment of efficacy at end of trea tm ent by patient and investigator fo r the PP- population (n=69)
unchanged
■ moderate■ good■ very good
60 n
50 -
40 -
^ 30 -
20 -
10 - - '.,1" ': i..
0 - * 1Patient Investigator
When asked on what parameters the study medication had the best effect, 8% of the
patients indicated erectile function, 26% libido, and 66% erectile function and libido
together.
4.3.3 Acceptance and practice and policy questions
Of the total 82 patients, 62 patients would take the capsules again (data are missing
from six patients) and in 91% of all cases the investigators would use the medication
again.
For 61% of the patients, it was very important that the medication was of herbal origin
and 97% of them would, given the same efficacy and safety, prefer a herbal to a
synthetic drug. Investigators stated that the most important reason to apply this saw
Andy Suter 164

Chapter 4: Clinical pilot study
palmetto preparation was the good safety assessed in 95% of all cases, followed by the
efficacy observed in 93% of patients.
4 .3 .4 Safety
Five patients reported six adverse events, including nausea, eructation, and acid
regurgitation, all of which were mild in nature and seen as related to the study
medication, and two incidents of a transient ischemic attack in the same patient and a
mild pruritus, which were not related to the study medication. From the total 82
patients, data from six patients were missing on the safety assessment; from the
remaining patients, 89.5% rated tolerability as very good and 6.6% as good. Similarly,
investigators regarded tolerability in 90.8% of the cases as very good and 5.3% as good
(Figure 31).
Figure 31: Assessment o f to le rab ility at end o f trea tm ent by patient and investigator fo r the safety population (n=82), values from six patients are missing
80
70 -
60 -
40
E 30 -
20 -
10
bad moderate
good ■ very good
Patient Investigator
Andy Suter 165

4 .3 .5 Subgroup analyses
The mean total bSFI improved significantly in centre 7, the general practice recruiting
the majority of study participants, but not in the average in all the other study centres.
Therefore, sub analyses were carried out to assess if the patient population of centre 7
was different than that of all the other centres.
Baseline characteristics for age, body weight, blood pressure, heart rate, as well as for
initial IPSS, total bSFI, and total Urolife QoL-9 sex score were not significantly different
between the 54 patients from centre 7 compared to the other 15 patients. The IPSS
decreased in participants from centre 7 in the average by 8.43 points, in all the other
centres by 4.33 points. The total bSFI improved in almost all patients in centre 7 (98.1%)
and in 53.3% of all other study participants, but a big part of these patients (40%)
experienced already an improvement in the treatment free run in-phase. Thus when
compared the total bSFI between visit 1 and visit 3, for 73.3% of these patients an
improvement was observed. Also the administration of co-medication was not different
between the study participants from centre 7 compared to all the other patients.
The main difference was that centre 7 was a well known practice in Zurich specialised
on complementary medicine and it was easy for the physician to recruit patients. The
other investigators reported that they barely found patients who were eager to
participate in the trial.
Because of the small patient numbers per centre, no distinct pattern or parameters
could be elucidated why some of them showed not the same improvement in the bSFI
than those from centre 7.
Additional subgroup analyses were performed for all patients by using age, symptom
severity, and concomitant medication as co-factors for efficacy.
They showed that patients with a higher IPSS at inclusion (IPSS 20-35) exhibited better
improvements in their bSFI (P = 0.029) and in their Urolife QoL-9 sex (P = 0.031) values
than did patients with lower IPSS (8-19). Comparing younger patients (21-50 years) to
older patients (51-80 years) did not reveal a significant difference regarding changes of
IPSS, bSFI, and Urolife QoL-9 sex, nor did concomitant medication have an influence on
these parameters.
Anc'v Suter 166

Chapter 4: Clinical pilot study
4.3 .6 Correlation analysis o f changes and relationship betw een bSFI and
Urolife QoL-9 sex score
In cooperation with the statistician Peter Klein, I carried out correlation analyses to
assess if changes in IPSS, bSFI, and Urolife Q.oL-9 sex were associated. Reason was to
see firstly, if the known influence of BPH symptoms on SDys was linearly related and
secondly, if for an assessment of total SDys symptoms rather the easier to fill out
Urolife QoL-9 sex score than the bSFI could be used.
There was a negative correlation between changes from visit 2 to visit 3 in the IPSS
score and the bSFI (Pearson's rho = -0.366; P = 0.002) (Figure 32) and between changes
in the IPSS and the Urolife QoL-9 sex (Pearson's rho = -0.365; P = 0.002) (Figure 33),
indicating that less urinary problems were associated with better assessment of sexual
function. Both correlations were statistically significant but of rather moderate extent.
Correlation between change in IPSS and changes in bSFI - Per-Protocol population
30A Change V1 vs. V2 (N = 69)• Change V1 vs. V3 (N = 69)■ Change V2 vs. V3 (N = 69)
20
Li_CO-Q0)O)c05x:O
-10-20 -15 -10 5 0 5
Change IPSS
Andy Suter 167

Chapter 4: Clinical p ilot study
Figure 33: Correlation between change in IPSS and changes in Urolife QoL-9 fo r all visits. PP-population (n=69)
OO
&TOÜ
200
150
100
50
0
-50 Change V I vs. V2 (N = 69) Change V I vs. V3 (N = 69) Change V2 vs. V3 (N = 69)
-100-20 15 -10 5 0 5
Change IPSS
Furthermore, there was a more pronounced positive correlation between the bSFI and
Urolife QoL-9 sex, showing that both questionnaires were valid for evaluating SDys and
consequently assessed changes to the same degree (Pearson's rho = 0.607; P < 0.0001)
(Figure 34)
F Correlation between change in bSFI and changes in UQol - Per-Protocol population
200
150
100—I
83500)D)cTO
s zÜ
-50 Change V I vs. V2 (N = 69) Change V I vs. V3 (N = 69) Change V2 vs. V3 (N = 69)
-1005 0 5 15 20 2510
Change bSFI
Andy Suter 168

C.'.'i.'rrN?
A further regression analyses of the subdomains of the bSFI and Urolife QoL-9 sex
based of actual scores showed that the erection sub scores of both questionnaires were
correlated best at visit 3 (Pearson's rho = 0.806; P < 0.0001). A good correlation is given
with a Pearson's rho of > 10.7 [ (456).
The sexual drive subscale of the bSFI and Urolife QoL-9 sex score (Pearson's rho =
0.645; P<0.0001) and the Urolife satisfaction and the bSFI satisfaction subscale
(Pearson's rho = 0.657; P<0.0001) were thus comparatively weaker correlated
compared to the total score and the erection sub scores, showing a rather moderate
but still significant correlation.
The Urolife QoL-9 sex satisfaction question was less prominently correlated to the bSFI
problem assessment sub score (Pearson's rho = 0.559; P<0.0001).
An analysis using the Spearman coefficient which is used in non-normally distributed
data yielded about the same results as with the Pearson's coefficient.
Summarised, the analysis showed a good correlation of BPH symptoms and SDys
measured either with the bSFI or the Urolife QoL-9 sex score. The two total scores for
SDys correlated well and also the sub scores for erection, sexual drive, and satisfaction.
5:;r 169
Chapter 4: Ctinical p i l o t r t u c y
4.4 Discussion
In this pilot trial we wanted to assess if a saw palmetto berry preparation had an
influence on both, prostate symptoms and SDys. We first examined the improvement in
BPH symptoms as measured with the IPSS, which is the standard instrument to quantify
severity of BPH symptoms (99). We saw a greater than 50% reduction, indicating a good
treatment response that was in the range observed for saw palmetto treatments in
other trials on BPH and larger than the effect of placebo. A survey of seven clinical trials
for a lipophilic saw palmetto preparation with a total of 2555 patients described an
average treatment duration of 300 days and a mean initial IPSS value of 14.72. At the
end of the treatment, IPSS was reduced on average by 31.2% (457). In two other clinical
trials, 320mg lipophilic saw palmetto berry extract was used daily and, after 6 months,
the IPSS was reduced by 26.3% (433) and 37% (160) with respective reductions under
placebo of 13.9% and 13.6%.
Secondly and more importantly, we assessed whether the treatment had a positive
influence on concomitant SDys.
To determine this, it was important to confirm at inclusion that the patients in our trial
definitely suffered from SDys; all patients here had obvious SDys, based on
comparisons of the initial values from the bSFI and the Urolife QoL-9 sex in our trial
with epidemiological data.
O'Leary (2003) observed an average total bSFI score of 27.7 in a population of 1883,
>50-year-old men in the United States (449), whereas in our study the same age group
had a lower initial value of 20.1. In another study the patients with ages of 36.9 ± 12.0
years displayed an average total bSFI of 33.5 ± 2.2 (458) compared to the total initial
bSFI of 26.3 ± 6.6 observed in our 21-50-year-old patients. A large study of 2829 LUTS
patients with an average age of 65.9 years evaluated Urolife QoL-9 scores and found an
for the Urolife QoL-9 sex an initial total value of 8.8 ± 0.1 (scale 0-30) (448), while in our
study an initial score of 130.0 ± 47.0 (scale 0-300) was recorded for the 51-80 year
patient group.
Andy Suter 170

Saw palmetto showed a significant improvement of SDys in this study population. Both
scores for SDys changed significantly, the bSFI by 41% and the Urolife QoL-9 sex by
42.0%.
Looking at the sub scores "sexual drive" and "erectile function", almost the same
degree of improvement was seen for both scores, with 35.3% and 37% in the bSFI and
35.7% and 44.9% in the Urolife QoL-9 sex, respectively. The major difference between
these two scores is caused by the more weighted problem assessment domain of the
bSFI. It has been shown that both questionnaires are equally sensitive in assessing
sexual dysfunctions, which was also substantiated by the correlation analysis.
Interestingly, we observed that it was almost impossible for patients to fill out the bSFI
without a doctor's help, whereas the Urolife QoL-9 sex was quite easy for patients to fill
out alone.
In summary, we have shown for the first time that a saw palmetto intervention in
patients with BPH and SDys had a beneficial influence on both BPH symptoms and on
SDys.
Our efficacy results are of further importance when considering the other available
options for simultaneous treatment of LUTS and SDys. It is currently debated whether
alpha blockers or phosphodiesterase (PDE) inhibitors may be beneficial for treating
symptoms of both disorders. Experimental models showed that al-adrenergic agents
may improve erectile dysfunctions by influencing the balance between contraction and
relaxation of the corpus cavernosum smooth muscle, of which, relaxation leads to an
erection (459). On the other hand, experimental data also indicates that NO synthase
and NO could play important roles in tissue from the urethra, corpus cavernosum,
prostate, vas deferens, and bladder neck (460). Reduced concentrations of NOS/NO in
the prostate and bladder increase smooth muscle tone and may improve prostatic cell
proliferation (461), indicating that PDE-5-inhibitors, which increase the NO
concentration, may have positive effects on LUTS.
Andy Suter 171

C/7Qpfe'' 4'
Initial clinical trials were carried out with alpha blockers or PDE-5-inhibitors (462).
Clinical data with alpha blockers, however, showed a good treatment effect on BPH
symptoms but only a small positive influence on SDys. In a clinical trial where patients
with moderate to severe BPH symptoms took lOmg alfuzosin for six months, the IPSS
decreased from 18.93 to 9.59 points and the Male Sexual Health Questionnaire MSHQ
ejaculation sub score improved from 23.09 to 21.54; this was statistically significant,
but the clinical relevance remains doubtful with an improvement only of about 7%. The
overall number of patients with moderate to severe erectile dysfunctions decreased
from 35% to 22% (434).
These results were not confirmed in another trial where patients with BPH symptoms
took lOmg alfuzosin daily for 12 weeks. Results of this trial showed that IPSS decreased
significantly from 17.92 to 12.07, but the MSHQ ejaculatory subdomain worsened
significantly from 24.9 to 27.14 and subdomains for erection and satisfaction did not
change significantly (463).
In a large open trial with 839 enrolled patients suffering from LUTS caused by BPH,
lOmg alfuzosin was taken daily for two years. The initial IPSS of 15.5 was reduced by 7
points, while the total initial bSFI value of 21.5 improved only slightly during the
treatment period, leading to the assessment by the authors that the treatment at least
"did not have any deleterious effect on sexual functions" (435).
A further open clinical trial with lOmg alfuzosin showed, besides a significant
improvement of the IPSS after 1 year of treatment, a significant improvement of the
bother score of the Danish Prostatic Symptom Score questionnaire for sexual
dysfunction (DAN-PSSsex) (464) while a study comparing tamsulosin/solifenacin either
alone or in combination in patients with LUTS also saw improved IPSS, but observed no
significant changes in the IIEF (465).
The IPSS reductions of about 6 to 7 points found in these studies with alpha-blockers
were similar to those observed in placebo-controlled trials (466,467). This is in line with
the trials of Debruyne (2004) and Zlotta (2005), which showed similar IPSS reductions
following treatment with a saw palmetto preparation and tamsulosin (468,469).
It also remains doubtful whether PDE-5 inhibitors are a good treatment for both LUTS
and SDys together. Clinical data for PDE-5 inhibitors showed a good improvement on
An CIV Suter 172

Chapter 4: Ciinicai pi lot stud}.
erectile dysfunctions, but a small effect on BPH symptoms.
McVary (2007) saw a significant decrease in the IPSS following 12 weeks of treatment
with lOOmg sildenafil, with an IPSS change of -6.3 vs. -1 .9 with placebo, as well as a
significant improvement of the IIEF erectile function domain (470).
In the trial of Roehrborn et al. (2008), the application of different dosages of tadalafil
demonstrated that an increased dosage correlated with increased IPSS improvement,
from +3.9 at 2.5mg to +5.2 at 20mg, with a dose of Smg showing the best benefit/risk
ratio. After a treatment period of 12 weeks, improvement was also seen in the IIEF
erectile function subdomain (471).
Vardenafil (20mg) taken twice daily for 8 weeks improved the IPSS by 5.9 points,
compared to placebo with 3.6 points; significant changes were also seen in the IIEF-ED,
and the Urolife QoL-9 sex improved by 62.6% compared to 17.2% under placebo (472).
While IPSS was improved in these trials, interestingly, changes in flow rates were never
reported.
In total, clinical data for PDE-5-inhibitors showed a moderate improvement in LUTS
from 2.3 to 4.4 IPSS-points compared to placebo even though sildenafil and vardenafil
were used at the highest applicable daily dosage, meanwhile the SDys improved in all
studies significantly.
One solution discussed in the literature for concomitant reduction of BPH symptoms
and ED is the combination of an alpha blocker with a PDE-5-inhibitor. Data from three
such clinical studies are presently available.
One small trial investigated alfuzosin, sildenafil, or the combination on LUTS and
erectile dysfunctions. After 12 weeks of treatment, initial values of IPSS, which were
between 16.9 and 17.8, were reduced significantly in all treatment groups with the
largest reduction (24.1%) in the combination group. The IIEF erectile function score was
significantly improved by the combination and sildenafil, but not in the alfuzosin group
(473).
Another combination trial with sildenafil or tamsulosin showed comparable results,
with the largest IPSS improvement observed with the combination (-40.1%), followed
by tamsulosin (-36.2%), and sildenafil (-28.2%); the IIEF improved significantly with
sildenafil and the combination but not with tamsulosin (474).
Andy Suter 173

In a further trial, lOOmg udenafil was added to a stable alpha-blocking therapy in
patients with BPH and erectile dysfunction for 8 weeks. The IPSS was reduced by 2.8
points and the IIEF-5 improved by more than 5 points, indicating that a combination or
add-on therapy of udenafil may be beneficial (475).
PDE-5-inhibitors are expensive treatments; therefore, a cost-benefit assessment is
warranted for a further extensive PDE-prescription. In the USA, a single dose of 25mg
sildenafil costs about 8 times as much as an alpha-blocking agent like Im g doxazosin
(476) or 30 times more than 0.4mg tamsulosin in Germany (477), whereas the cost for a
daily dosage of Prostasan® is in the lower range of an alpha blocker. These differences
in price, in addition to the only moderate efficacy, make it doubtful if PDE-5-inhibitors
should be advocated as a standard treatments for BPH symptoms.
When looking at safety and tolerability, our data was in accordance with previous
findings and indicated that saw palmetto was very well tolerated, in contrast to the
standard treatments for LUTS. A major problem for patients taking an alpha blocker
and/or a 5-alpha-reductase inhibitor is the occurrence of sexual adverse effects that
cause many men to discontinue treatment (478).
Study data show that 2-16% of all patients under alpha reductase inhibitor therapy
experience erectile dysfunctions, decreased libido, and decreased volume of ejaculate
(twice the frequency seen with placebo), whereas alpha-blocking agents, particularly
tamsulosin, have been frequently linked with ejaculatory disorders in around 10% of all
patients (479).
In daily practice, the incidence rates may even be higher than in clinical trials. In a large
epidemiological study carried out with urologists and internal medicine physicians in
the United States, doctors estimated that 18-27% of the patients taking an alpha-
blocking medication suffer from ejaculatory disorders and 16-22% of men taking a
5-alpha-reductase-inhibitor suffer from erectile dysfunctions (480). Nevertheless, the
latest American Urology Association guideline for treatment of BPH symptoms also
advocates using a combination of alpha-blockers and 5-alpha-reductase inhibitors
(197), a protocol designed to achieve better efficacy, but without fully considering the
additive side effect rates of these two drugs as shown in combination trials (461).
Andy S'j 1er 174

O'lopte/'4; C/.n.To/ p/'/o::' iTL/c'y
This trial has some limitations; it was designed as an uncontrolled pilot trial to elucidate
if an effect of a saw palmetto treatment could be observed. Consequently, the size of
the placebo effect can only be estimated.
A review on the placebo effect in studies with alpha blockers and 5-alpha-reductase
inhibitors in BPH found a reduction in LUTS under placebo ranging from 9-34% (481).
Considering this effect size, that the reductions in IPSS seen in our trial were similar to
those of other controlled saw palmetto trials it can be assumed that our Sabal
treatment was probably efficacious in reducing BPH symptoms.
To assess the placebo effect in reducing SDys in this trial is more difficult and no clear
statement can be made as our observed improvement of SDys was about 40%.
A review on treatments for erectile dysfunction showed an average placebo effect
when looking at improvement of erectile function in nine clinical trials of 28.0% (482),
another review taking the intercourse success rate as main measure found a placebo
effect of 31.4% as mean from 19 sildenafil trials, 32% from twelve tadalafil studies, and
35.1% from eleven vardenafil trials (483).
Furthermore, there was a strong centre effect in our trial, as one centre recruited
substantially more patients than the others and these other centres did have fewer
responders than the main centre. Subgroup analysis did not unveil any significant
differences in patient characteristics between these centres; however, these analyses
were limited by the low number of patients in the other five centres together.
Nevertheless, a strong influence by the treating physician on the outcome of SDys could
not be confirmed with the data available as there was a positive correlation between
the bSFI which was filled out by the investigator and the Urolife sex QoL-9 score which
was completed by patients. Further, during the treatment-free run in period the values
for SDys and IPSS remained in the majority stable.
Nevertheless, the results of this uncontrolled pilot trial showed that the applied saw
palmetto treatment exerted a good benefit/risk ratio in reducing BPH symptoms and at
least not negatively affecting SDys at the same time. When considering also the low
treatment costs, the very good acceptance and compliance by the patients it can be
nonetheless assumed that this trial showed promising results for the effectiveness,
which describes the degree of a beneficial effect in a real world clinical settings (484) of
saw palmetto in treating BPH symptoms and concomitant SDys.
A ndy Su te i 175

Based on our findings here, a further placebo-controlled clinical trial with a more
balanced patient distribution in the centres would be the next step to prove the
efficacy.
Conclusions
This is the first trial ever to observe that a saw palmetto treatment could have a
positive effect in reducing BPH symptoms and in concomitant SDys. The applied
medication was very well tolerated, safe, highly accepted and the compliance was very
good. Further, the cost of daily treatment with saw palmetto is much cheaper than with
many other medications, for example, in Switzerland the cost would be 0.75 Swiss
franks for saw palmetto vs. 22.30 Swiss franks for lOOmg sildenafil (485).
The results from our pilot trial let assume that due to the positive benefit/risk ratio of
saw palmetto in treating BPH symptoms and at least not deteriorating SDys, there is a
good chance for a good effectiveness of this treatment.
Based on these promising results, a further, larger placebo-controlled clinical trial
should be carried out to confirm the findings and answer questions on the efficacy of
saw palmetto in treating BPH symptoms and SDys.
An dy Suter 176

Chapter 5General discussion and conciusion
Andy Suter 177

5/ Gene'-o,' cc.'?dL/F,r'
5 Chapter 5: General discussion and conclusion
5.1 General discussion
In the last 150 years saw palmetto has made a fascinating journey as a medical plant:
Starting with the first use by the Indians of Florida, then discovered by white settlers
and made popular within 20 years in the United States, soon after in Europe to become
today's world favourite herbal treatment for BPH with a turnover of an estimated 700
million dollars (163) which is equivalent to the worldwide annual combined sales of the
5-alpha-reductase inhibitor top brands Proscar® (486) and Avodart® (487).
This thesis followed important aspects of this path and gained new data on the past,
present and future of saw palmetto as a medical therapy.
In terms of the past the aim was to show who first made medical use of saw palmetto
among the U.S. American physicians and how the plant became popular in the United
States and later in Germany.
I identified the first written record of saw palmetto as a medical treatment in 1877 by
J.B. Read of Savannah, Georgia (208). One can speculate that his description of the use
of the plant was lead by commercial interests as Dr. Read was to become president of
the Georgia Medical Society (210) and a large manufacturer of medical products, the
A.A. Solomons Drug Co. was situated in his hometown (488). It was the time of the so
called 'Gilded Age' in the United States, an exciting era of economic growth - also for
venturers in the medical field and quacks. This is well documented in the 1880's, for
example, in case of Echinacea - made popular in the U.S.A. also as a product called
'Meyer's Blood Purifier'. Its producer, H.C.F. Meyer proposed to a medical board to
prove the efficacy of his product by letting himself bite by a rattlesnake and then take
the 'Blood Purifier' as a treatment (489).
But saw palmetto was more than quackery - it proved to be a good remedy which is
demonstrated by the broad acceptance and use firstly among the eclectic physicians,
followed soon by homeopathic doctors. A comprehensive collection of various sources
documenting the wide spread use of the plant indicate that the first experiences with
Andy Suter 178

C f Gene' of r/fCL/ss/cn ono' conc/L/s.'c.'-
Sabal were gathered in respiratory tract infections (208) but soon after in genito
urinary problems and as a sexual stimulant (253). The important medical role of eclectic
medicine in this period contributed to the plant becoming a popular therapy. The 'gold
standards' of available therapies for BPH symptoms in the second half 19 century like
catheterisations or use of mercury, iodine, and bromine were generally harmful.
Consequently, saw palmetto could fill a gap as a safe and also efficacious new therapy
which proved to be best for prostatic problems.
To show how saw palmetto was introduced as a medical treatment in Europe, I chose
Germany as a model. In this country mainly the homeopaths were the first to use saw
palmetto and they had strong ties to the American homeopathic society (265). Soon
afterwards the pharmacists, too and then food scientists and chemists became
interested in the plant and until the beginning of the Second World War the species
must have been known and also used at least by a certain group of practitioners in
Germany.
Further botanico-historical studies especially in archives need to focus on
How the plant became popular in Germany,
Who were its main promoters and
Which were the main brands being used.
Nevertheless, this is at the time the most comprehensive medico-historical evaluation
of the first use on saw palmetto in the U.S.A. and Germany from publicly available
sources.
Regarding the present, the largest phytochemical analysis so far of 46 products from
nine different countries containing Sabal was carried out. The advantage of saw
palmetto is that in clinical trials 320mg berry extract with 70-95% fatty acids proved to
be efficacious and safe in treating BPH symptoms demonstrating that the fatty acids are
most probably one of the main active constituent of saw palmetto preparations (17,
A n d v S i J t c r 179

n .'jp r fr 5; Gf/ifro.' n.no' (onr/û/s/o/
151). Like this a good reference standard is given to measure the product quality of saw
palmetto preparations.
There was an unexpectedly large difference in the amount of fatty acids per daily dose
among saw palmetto mono preparations: The highest dosed product contained 177
times more fatty acids than the lowest dosed. When compared to the proposed dosage
of the monographs of 320mg extract (17, 40, 146, 147), unregistered Sabal
preparations contained in the majority either too low or too high daily amounts of fatty
acids and these were further often wrongly declared, casting serious doubts on the
usefulness of these products as therapeutic agents, especially since extensive
preclinical and clinical research with more than 90 publicly available clinical trials
provided sound evidence for this dose range (151). The analysis also showed that on
average registered products contained an amount of 320mg lipophilic saw palmetto
extract and the declarations were correct. The capsule sizes of unregistered
preparations were in average also bigger than those of registered products, indicating
that manufacturers wanted to profit from the fact that patients regard larger capsules
as more efficacious than smaller ones (490).
Additionally, the ethanolic mono-extracts showed a characteristic pattern in their
composition of nine fatty acids and, consequently, a saw palmetto extract can be
distinguished easily from other herbal extracts containing fatty acids. Based on this
study the proposed amount of 20% lauric acid for a saw palmetto extract proposed by
the European Pharmacopoeia (336) may not be sufficient to characterise the quality of
a Sabal extract; in the future minimum concentrations of oleic or myristic acids should
be recommended as well.
Even though fatty acids are an important marker, further investigations should focus
also on other active constituents as well. This could be phytosterols like ^-sitosterol,
cam peste ro I or stigmasterol which showed to have a positive effect on mechanisms
associated with the BPH pathology (385, 387, 388). These compounds were also shown
to be efficacious in improving BPH symptoms (127). However, they had to be taken in
dosages at least 60 times higher than generally found in saw palmetto mono
preparations (127, 340).
A n d y S u te r 180

C/7(7prer5; Gerem/ nVsci'fs-o.'i nrn ronc/ur.'c.':
To assess the characteristics of the different test samples, we used a different method
than just to determine a further marker substance. For the first time a metabolomic
approach to characterise saw palmetto preparations using proton-NMR was carried out
in the MSc-thesis of Anthony Booker (341). His results emphasise that in the future this
could become the method of choice for a characterisation of saw palmetto products. It
is fast and reliable, straightforward to set up a library of products and their
characteristics and with PCA a good statistical method is available to analyse the
different preparations. With the applied clustering, preparations which are similar in
their characteristics could be grouped together and outliers can well be identified.
In general, this phytochemical analysis showed that what is sold on the markets under
the label 'saw palmetto' varies widely in its amount of active constituents highlighting
that the registration of herbal medicinal products would be the best measure for
quality assurance on the markets.
The last part of my thesis addressed the future of saw palmetto with a clinical pilot trial
in patients with BPH and concomitant SDys.
I stated in the discussion of the historical part that being a BPH patient at the end of the
19 *’ century was a miserable thing. At the begin of the 21® century, the situation looks
brighter for a patient but it is far from being shiny.
The disease is better understood but why it evolves is still unclear; the latest hypothesis
that BPH could be caused by a venous insufficiency in the testicular veins (97) still
needs to be substantiated. There are only two classes of medication available for
treatment of BPH symptoms, alpha-blockers and 5-alpha-reductase inhibitors but both
cause frequently side effects like ejaculatory disorders (426) or erectile problems (428).
The last treatment option is surgery and the golden standard, TURP is a surgical method
which is about hundred years old (175) and also causes a lot of side effects (139).
It is also known today that a BPH patient is at a greater risk of experiencing SDys. Large
epidemiological studies carried out about 10 years ago corrected the existing paradigm
that SDys in the elderly male population were simply age related. The results of these
Andy Suter 181
oVscL fS'cn cndconc/us,'o.'
trials showed that BPH is besides age the most important factor causing SDys - which
could be worsened significantly with the mentioned therapy options to treat BPH.
Therefore, additional treatment solutions are intensively sought which are efficacious
and safe in treating BPH and SDys together (411).
Saw palmetto with its clinically proven efficacy in BPH and the traditional use as a
therapy for SDys was predestined to be a good treatment for these disorders. Our
clinical pilot trial which was designed to be a pragmatic study (491) showed a tendency
that after a treatment duration of eight weeks, saw palmetto could reduce BPH
symptoms and at the same time improve SDys.
Our results are of considerable interest in particular in the context of improved
compliance, good acceptance, the low treatment costs of the saw palmetto treatment,
and the good benefit/risk ratio for one patient. Consequently, a good effectiveness of
saw palmetto in treating BPH symptoms and concomitant SDys can be assumed.
Nevertheless, the study has several limitations and its level of evidence is ll-b according
to the rating in Evidence Based Medicine where level I stands for a well designed
randomised clinical trial and level III are case reports or opinions from expert
authorities (492). There was no placebo control involved in our study and the amount
of the placebo effect could only be estimated. Further, a strong centre effect was noted
as one centre recruited the majority of the patients and since this study was designed
as a pilot study to generate hypotheses for a further controlled study, the sample size
was also rather small with 69 analysable patients.
To confirm the promising findings from our pilot trial, next a placebo controlled study
needs to be carried out. The results from our trial can be taken to estimate the effect
size of the saw palmetto treatment and the needed sample size.
Probably even better results could be obtained when combining Sabal with another
plant which proved to be efficacious in SDys like Panax ginseng where a review on six
placebo controlled trials reported efficacy in treating ED (493) or maca (Lepidium
meyenii) which in two placebo controlled studies improved SDys (494). Existing
combinations of saw palmetto with an additional herbal extract were mainly developed
182

rrn'conc/cvs/o'
to improve uroflow or BPH symptoms like with Urtica dioica (150) but none to improve
concomitant SDys.
A further topic of interest relates to the mechanisms underlying these effects. It could
be that in our trial the reduction of BPH symptoms leads to the improvement of SDys or
that saw palmetto itself has aphrodisiac properties. A trial with BPH-free patients
suffering from SDys could answer this question.
In summary, our trial gave interesting hints that saw palmetto has also a positive effect
on concomitant SDys. Given, this the plant has now even more the potential to become
the first line treatment for mild to moderate BPH symptoms.
5.2 Final conclusion
Saw palmetto is one of the best known and investigated herbal treatments worldwide.
This thesis contributes new historical, analytical and clinical knowledge on the plant.
Overall, good quality products which are manufactured in accordance with the existing
monographs on saw palmetto have a bright future - they could become a well
tolerated and cost effective therapeutic option for patients suffering from mild to
moderate BPH symptoms with concomitant SDys. More clinical research and maybe a
combination with another plant which is efficacious in improving SDys is warranted to
secure saw palmetto its place as a more widely recognised treatment for BPH and other
urogenital conditions.
183
L i te ra t u rc
6 Literature
1. yoursurgery.com. Transurethral resection of the prostate 2010 [cited 2012 Feb. 5]; Available from:http://www.voursurgerv.com/ProcedurePetails.cfm?BR=7&Proc=55.
2. United States Geological Service. Saw palmetto, distribution. 2006 [cited 2009 August 23rd]; Available from: http://esp.cr.usgs.gov/data/atlas/little/2006.
3. Berry SJ, Coffey PS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132(3):474-9.
4. O'Leary MP, Fowler FJ, Lenderking WR, Barber B, Sagnier PP, Guess HA, et al. A brief male sexual function inventory for urology. Urology. 1995;46(5):697-706.
5. Wikipedia. Hernando de Escalante Fontaneda. 2012; Available from: http://en.wikipedia.org/wiki/Hernando de Escalante Fontaneda.
6. P'Escalante Fontaneda H. Memoir of Hernando P'Escalante Fontaneda on the country and ancient Indian tribes of Florida. 1575 [cited 2012 25st of January]; Available from: http://www.treasurelore.com/florida/fontaneda.htm.
7. Hale EM. Saw palmetto (Sabal serrulata, Serenoa repens): Its history, botany, chemistry, pharmacology, provings, clinical experience and therapeutic applications. Philadelphia: Boericke and Taffel; 1898.103 p.
8. Austin P. Florida ethnobotany. Boca Raton, FL: CRC Press; 2004.
9. Bertram W. Travels through North and South Carolina, Georgia, East and WestFlorida: the Cherokee country, the extensive territories of the Muscogulges or Creek cenfederacy, and the country of the Chactaws ... embellished with copper plates: Johnson; 1792. 520 p.
10. Zona S. The genera of Palmae (Arecaceae) in the southeastern United States.. Harv pap bot. 1997;11:89-125.
11. Lawrence KS. Saw palmetto. Jour New York Bot Garden. 1926;27(321):197.
12. Uhl N, Pransfield J. Genera Palmarum: a classification of palms based on the workof Harold E. Moore, Jr. L. H. Bailey Hortorium and the international palm society Ithaca, New York. Lawrence, Kansas: Allen Press; 1987.
13. Bolli R. Floridas Sagepalme. Phytother. 2001;4:23-6.
14. Govaerts R. Serenoa repens (W.Bartram) Small. 2012 [cited 2012 12th of March]; Available from: http://apps.kew.org/wcsp/namedetail.do7name id=24036.
15. Kew Garden. Chamaerops serrulata. 2012; Available from: http://apps.kew.org/wcsp/namedetail.do:isessionid=10570B804089A142335F58BA 76AF4703?name id=37820.
16. Oshims. Saw palmetto. 1999; Available from: http://www.oshims.com/herb- d i recto rv/s/sa w-pa I metto.
A ndy Suter 184
/ ercrf L/,'r
17. ESCOP. Serenoae repentis fructus. 2nd ed. Monographs E, editor. Stuttgart; Thieme Verlag; 2003.
18. Baker MF. Florida wild flowers; an introduction to the flora of the Florida peninsula. New York: The Macmillan company; 1926.
19. Bennett BC, Flicklin J. Uses of saw palmetto (Serenoa repens, Arecaceae) in Florida. Economic Botany 1998;52:381-93.
20. Kress H. Saw Palmetto. Serenoa serrulata. 2011 [cited 2012 2.1.2012]; Available from: www.henriettesherbal.com.
21. Hilmon JB. Autecology of saw palmetto, [Serenoa repens (Bartr.) Small]. Durham, NC: Duke University; 1968.
22. Godfrey RK. Trees, shrubs, and woody vines of northern Florida and adjacent Georgia and Alabama. Athens, GA, USA: University of Georgia Press; 1988.
23. Hobbs C, Brown S. Saw palmetto. The herb for prostate health. Loveland, Colorado, USA: Interweave Press; 1997. 96 p.
24. Van Deelen TR. Serenoa repens. 1991 [cited 2009 May 23]; Available from: http://www.fs.fed.us/database/feis.
25. Correa A, Galdames C, de Stapf MS. Catalogo de las plantas vasculares de Panama , catalogo de las plantas vasculares de Panama. Panama: Smithsonian Tropical Research Institute City., 2004.
26. Tanner G, Mullahey JJ, Maehr D. Saw palmetto: an ecologically and economically important native palm. I FAS Circular WEC-109.1996:1-4.
27. Fults GA. Florida ranchers manage for deer. Rangelands. 1991;13(l):28-30.
28. Wilder EA, Kitzke ED. Waxy saw palmetto - a chemurgic opportunity. Chermurgic Digest. 1954;13:18-9.
29. Hendricks RG. Burn-chop-rest on flatwoods/bluestem range. Rangeland J. 1983;5(l):ll-2.
30. Carrington ME, Gottfried TD, Mullahey JF. Pollination biology of Saw Palmetto (Serenoa repens) in Southwestern Florida. Int Palm Soc. 2003;47:23-7.
31. Maehr DS, Layne JN. Florida's all purpouse plant the saw palmetto. The Palmetto. 1996;6(15):22.
32. Harnischfeger G, Stolze H. Serenoa repens - Die Sagezahnpalme. Z Phytother. 1989;10:71-6.
33. Expert Committee. United States pharmacopeial forum: (DSB) dietary supplement. Saw palmetto extract.Rockville, Md.: Pharmacopeial Convention, botanicals. 2005;28(2).
34. Habib FK, Wyllie MG. Not all brands are created equal: a comparison of selected components of different brands of Serenoa repens extract. Prostate Cancer Prostatic Dis. 2004;7(3):195-200.
An dy Suter 185

Literoiwc
35. Schantz MM, Bedner M, Long SE, Molloy JL, Murphy KE, Porter BJ, et al. Development of saw palmetto (Serenoa repens) fruit and extract standard reference materials. Anal Bioanal Chem. 2008;392(3):427-38.
36. Sorenson WR, Sullivan D. Determination of campesterol, stigmasterol, and beta- sitosterol in saw palmetto raw materials and dietary supplements by gas chromatography: collaborative study. J AOAC Int. 2007;90(3):670-8.
37. Weber A, Catch pole 0, Eltringham W. Supercritical fluid assisted, integrated process for the synthesis and separation of different lipid derivatives. J Sep Sci. 2008;31(8):1346-51.
38. Rosier TW, Matusch R, Weber B, Schwarze B. Analysis of the hydrodistillate from the fruits of Serenoa repens. Planta Med. 2009;75(2):184-6.
39. Chua T, Simpson JS, Ventura S. Ethanol extracts of saw palmetto contain the indirectly acting sympathomimetic: tyramine. Prostate. 2011;71(l):71-80.
40. Health Canada. Saw palmetto. Compendium of Monographs 2008.
41. Abe M, Ito Y, Oyunzul L, Oki-Fujino T, Yamada S. Pharmacologically relevant receptor binding characteristics and Salpha-reductase inhibitory activity of free fatty acids contained in saw palmetto extract. Biol Pharm Bull. 2009;32(4):646-50.
42. Sultan C, Terraza A, Devillier C, Carilla E, Briley M, Loire C, et al. Inhibition of androgen metabolism and binding by a liposterolic extract of "Serenoa repens B" in human foreskin fibroblasts. J Steroid Biochem. 1984;20(l):515-9.
43. Rhodes L, Primka RL, Berman C, Vergult G, Gabriel M, Pierre-Malice M, et al. Comparison of finasteride (Proscar), a 5 alpha reductase inhibitor, and various commercial plant extracts in in vitro and in vivo 5 alpha reductase inhibition. Prostate. 1993;22(1):43-51.
44. Delos S, Carsol JL, Ghazarossian E, Raynaud JP, Martin PM. Testosterone metabolism in primary cultures of human prostate epithelial cells and fibroblasts. J Steroid Biochem Mol Biol. 1995;5S(3-4):375-83.
45. lehle C, Delos S, Guirou 0, Tate R, Raynaud JP, Martin PM. Human prostatic steroid 5 alpha-reductase isoforms-a comparative study of selective inhibitors. J Steroid Biochem Mol Biol. 1995;54(5-6):273-9.
46. Weisser H, Tunn S, Behnke B, Krieg M. Effects of the sabal serrulata extract IDS 89 and its subfractions on 5 alpha-reductase activity in human benign prostatic hyperplasia. Prostate. 1996;28(5):300-6.
47. Raynaud JP, Cousse H, Martin PM. Inhibition of type 1 and type 2 Salpha-reductase activity by free fatty acids, active ingredients of Permixon. J Steroid Biochem Mol Biol. 2002;82(2-3):233-9.
48. Habib FK, Ross M, Ho CK, Lyons V, Chapman K. Serenoa repens (Permixon) inhibits the Salpha-reductase activity of human prostate cancer cell lines without interfering with PSA expression. Int J Cancer. 2005;114(2):190-4.
Andv Suter 186

49. Stenger A, Tarayre i, Carilla E, Delhon A, Charveron M, Morre M, et al. Pharmacology and biochemistry of hexane extract of Serenoa repens (PA-109). Gaz Med Fr. 1982;89(2041-48).
50. Paubert-Braquet M, Richardson FO, Servent-Saez N, Gordon WC, Monge MG, Bazan NG, et al. Effect of Serenoa repens extract (Permixon) on estradiol/testosterone- induced experimental prostate enlargement in the rat. Pharmacol Res. 1996;34(3- 4):171-9.
51. Cristoni A, Morazzoni P, Bombardelli E. Chemical and pharmacological study on hypercritical C02 extracts of Serenoa repens fruits. Fitoterapia 1997;68:355-58.
52. de Lourdes Arruzazabala M, Molina V, Mas R, Carbajal D, Marrero D, Gonzalez V, et al. Effects of coconut oil on testosterone-induced prostatic hyperplasia in Sprague- Dawley rats. J Pharm Pharmacol. 2007;59(7):995-9.
53. Talpur N, Echard B, Bagchi D, Bagchi M, Preuss HG. Comparison of Saw Palmetto (extract and whole berry) and Cernitin on prostate growth in rats. Mol Cell Biochem. 2003;250(l-2):21-6.
54. Barsanti JA, Finco DR, Mahaffey MM, Fayrer-Hosken RA, Crowell WA, Thompson FN, Jr., et al. Effects of an extract of Serenoa repens on dogs with hyperplasia of the prostate gland. Am J Vet Res. 2000;61(8):880-5.
55. Di Silverio F, D'Eramo G, Lubrano C, Flammia GP, Sciarra A, Palma E, et al. Evidence that Serenoa repens extract displays an antiestrogenic activity in prostatic tissue of benign prostatic hypertrophy patients. Eur Urol. 1992;21(4):309-14.
56. Ravenna L, Di Silverio F, Russo MA, Salvatori L, Morgante E, Morrone S, et al. Effects of the lipidosterolic extract of Serenoa repens (Permixon) on human prostatic cell lines. Prostate. 1996;29(4):219-30.
57. Tarayre JP, Delhon A, Lauressergues H, Stenger A, Barbara M, Bru M, et al. [Anti- edematous action of a hexane extract of the stone fruit of Serenoa repens Bartr] Action anti-oedemateuse d'un extrait hexanique de drupes de Serenoa repens Bartr. Ann Pharm Fr. 1983;41(6):559-70.
58. Mitropoulos D, Kyroudi A, Zervas A, Papadoukakis S, Giannopoulos A, Kittas C, et al. In vivo effect of the lipido sterolic extract of Serenoa repens (Permixon) on mast cell accumulation and glandular epithelium trophism in the rat prostate. World J Urol. 2002;19(6):457-61.
59. Breu W, Hagenlocher M, RedI K, Tittel G, Stadler F, Wagner H. [Anti-inflammatory activity of sabal fruit extracts prepared with supercritical carbon dioxide. In vitro antagonists of cyclooxygenase and 5-lipoxygenase metabolism] Antiphlogistische Wirkung eines mit hyperkritischem Kohlencfioxid gewonnenen Sabalfrucht- Extraktes. In-vitro-Hemmung des Cyclooxygenase- und 5-Lipoxygenase- Metabolismus. Arzneimittelforschung. 1992;42(4):547-51.
60. Iglesias-Gato D, Carsten T, Vesterlund M, Pousette A, Schoop R, Norstedt G. Androgen-independent Effects of Serenoa repens extract (Prostasan(R)) on prostatic epithelial cell proliferation and inflammation. Phytother Res. 2011; 26(2):259-64
Andy Suter 187
61. Vela-Navarrete R, Escribano-Burgos M, Farre AL, Garcia-Cardoso J, Manzarbeitia F, Carrasco C. Serenoa repens treatment modifies bax/bcl-2 index expression and caspase-3 activity in prostatic tissue from patients with benign prostatic hyperplasia. J Urol. 2005;173(2):507-10.
62. Oki T, Suzuki M, Nishioka Y, Yasuda A, Umegaki K, Yamada S. Effects of saw palmetto extract on micturition reflex of rats and its autonomic receptor binding activity. J Urol. 2005;173(4):1395-9.
63. Goepel M, Hecker U, Krege S, Rubben H, Michel MG. Saw palmetto extracts potently and noncompetitively inhibit human alphal-adrenoceptors in vitro. Prostate. 1999;38(3):208-15.
64. Goepel M, Dinh L, Mitchell A, Schafers RF, Rubben H, Michel MG. Do saw palmetto extracts block human alphal-adrenoceptor subtypes in vivo? Prostate. 2001;46(3):226-32.
65. Suter A, Bommer S. Effects of saw palmetto extract in vitro on receptors and enzymes which are relevant in incontinence. International Congress and 54th Annual Meeting of the Society for Medicinal Plant Research Aug 29 - Sept 2; Helsinki 2006.
66. Suzuki M, Oki T, Sugiyama T, Umegaki K, Uchida S, Yamada S. Muscarinic and alpha 1-adrenergic receptor binding characteristics of saw palmetto extract in rat lower urinary tract. Urology. 2007;69(6):1216-20.
67. Isaacs JT, Coffey DS. Etiology and disease process of benign prostatic hyperplasia. Prostate Suppl. 1989;2:33-50.
68. Sergi G, De Rui M, Sarti S, Manzato E. Polypharmacy in the elderly: can comprehensive geriatric assessment reduce inappropriate medication use? Drugs Aging. 2011;28(7):509-18.
69. Yale SH, Glurich I. Analysis of the inhibitory potential of Ginkgo biloba, Echinacea purpurea, and Serenoa repens on the metabolic activity of cytochrome P450 3A4, 2D6, and 2C9. J Altern Complement Med. 2005;ll(3):433-9.
70. Budzinski JW, Foster BC, Vandenhoek S, Arnason JT. An in vitro evaluation of human cytochrome P450 3A4 inhibition by selected commercial herbal extracts and tinctures. Phytomedicine. 2000;7(4):273-82.
71. Mohamed ME, Frye RF. Inhibitory effects of commonly used herbal extracts on UDP-glucuronosyltransferase 1A4, 1A6, and 1A9 enzyme activities. Drug Metab Dispos. 2011;39(9):1522-8.
72. Markowitz JS, Donovan JL, Devane CL, Taylor RM, Ruan Y, Wang JS, et al. Multiple doses of saw palmetto (Serenoa repens) did not alter cytochrome P450 2D6 and 3A4 activity in normal volunteers. Clin Pharmacol Ther. 2003;74(6):536-42.
73. Gurley BJ, Gardner SF, Hubbard MA, Williams DK, Gentry WB, Carrier J, et al. In vivo assessment of botanical supplementation on human cytochrome P450 phenotypes: Citrus aurantium, echinacea purpurea, milk thistle, and saw palmetto. Clin Pharmacol Ther. 2004;76(5):428-40.
’ter 188

[ il e rature-
74. Singh YN, Devkota AK, Sneeden DC, Singh KK, Halaweish F. Hepatotoxicity potential of saw palmetto (Serenoa repens) in rats. Phytomedicine. 2007;14(2-3):204-8.
75. Van Coppenolle F, Le Bourhis X, Carpentier F, Delaby G, Cousse H, Raynaud JP, et al. Pharmacological effects of the lipidosterolic extract of Serenoa repens (Permixon) on rat prostate hyperplasia induced by hyperprolactinemia: comparison with finasteride. Prostate. 2000;43(l):49-58.
76. Ondrizek RR, Chan PJ, Patton WC, King A. Inhibition of human sperm motility by specific herbs used in alternative medicine. J Assist Reprod Genet. 1999;16(2):87-91.
77. Trinachartvanit W, Francis BM, Rayburn AL. Saw palmetto extract induces nuclear heterogeneity in mice. Environ Toxicol Pharmacol. 2009;27(l):149-54.
78. Medicines and Healthcare products Regulatory Agency M. Prostasan saw palmetto capsules. 2007. p. 27.
79. Medicines and Healthcare products Regulatory Agency MHRA. PhytoCon sabal fortecapsules. 2011. p. 23.
80. Bioforce AG. PSU0878.e01, Periodic safety update report for Prostasan (capsules). 2008.
81. Oesterling JE. Benign prostatic hyperplasia: a review of its histogenesis and naturalhistory. Prostate Suppl. 1996;6:67-73.
82. McVary KT. Clinical evaluation of benign prostatic hyperplasia. Rev Urol. 2003;5Suppl 5:S3-S11.
83. Elbadawi A, Mathews R, Light JK, Wheeler TM. Immunohistochemical andultrastructural study of rhabdosphincter component of the prostatic capsule. J Urol. 1997;158(5):1819-28.
84. Imperato-McGinley J, Sanchez RS, Spencer JR, Yee B, Vaughan ED. Comparison ofthe effects of the 5 alpha-reductase inhibitor finasteride and the antiandrogenflutamide on prostate and genital differentiation: dose-response studies.Endocrinology. 1992;131(3):1149-56.
85. Huggins C, Stevens R. The effect of castration on benign hypertrophy of theprostate in man. J Urol. 1940;43:705-7.
86. Zhu YS, Sun GH. Salpha-Reductase isozymes in the prostate. J Med Sci.2005;25(1):1-12.
87. Kaufman JM, Vermeulen A. The decline of androgen levels in elderly men and itsclinical and therapeutic implications. Endocr Rev. 2005;26(6):833-76.
88. Prins GS, Korach KS. The role of estrogens and estrogen receptors in normalprostate growth and disease. Steroids. 2008;73(3):233-44.
89. Prins GS, Huang L, Birch L, Pu Y. The role of estrogens in normal and abnormaldevelopment of the prostate gland. Ann N Y Acad Sci. 2006;1089:1-13.
90. Wang L, Yang JR, Yang LY, Liu ZT. Chronic inflammation in benign prostatichyperplasia: implications for therapy. Med Hypotheses. 2008;70(5):1021-3.
A ndy Suter 189

/ /'Otü'/'C
91. Kohnen PW, Drach GW. Patterns of inflammation in prostatic hyperplasia: ahistologic and bactériologie study. J Urol. 1979;121(6):755-60.
92. Gerstenbluth RE, Seftel AD, MacLennan GT, Rao RN, Corty EW, Ferguson K, et al. Distribution of chronic prostatitis in radical prostatectomy specimens with up- regulation of bcl-2 in areas of inflammation. J Urol. 2002;167(5):2267-70.
93. Roehrborn C, Kaplan SA, Noble WD. The impact of acute and chronic inflammation in baseline biopsy on the risk of clinical progression of BPH: Results from the MTOPS study. AUA Meeting; San Antonio, Texas2005.
94. Rohrmann S, De Marzo AM, Smit E, Giovannucci E, Platz EA. Serum C-reactiveprotein concentration and lower urinary tract symptoms in older men in the ThirdNational Health and Nutrition Examination Survey (NHANES III). Prostate.2005;62(l):27-33.
95. Kramer G, Mitteregger D, Marberger M. Is benign prostatic hyperplasia (BPH) an immune inflammatory disease? Eur Urol. 2007;51(5):1202-16.
96. Falahatkar S, Mokhtari G, Pourreza F, Asgari SA, Kamran AN. Celecoxib for treatment of nocturia caused by benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled study. Urology. 2008;72(4):813-6.
97. Gat Y, Gornish M, Heiblum M, Joshua S. Reversal of benign prostate hyperplasia by selective occlusion of impaired venous drainage in the male reproductive system: novel mechanism, new treatment. Andrologia. 2008;40(5):273-81.
98. van den Beld AW, de Jong FH, Grobbee DE, Pols HA, Lamberts SW. Measures of bioavailable serum testosterone and estradiol and their relationships with muscle strength, bone density, and body composition in elderly men. J Clin Endocrinol Metab. 2000;85(9):3276-82.
99. Simpson RJ. Benign prostatic hyperplasia. Br J Gen Pract. 1997;47(417):235-40.
100. Issa MM, Regan TS. Medical therapy for benign prostatic hyperplasia-present andfuture impact. Am J Manag Care. 2007; 13 Suppl l:S4-9.
101. Tim iras PS. Physiological Basis of Aging and Geriatrics. 4 ed. Boca Raton, FL: CRC Press; 2007. 464 p.
102. McVary KT. BPH: epidemiology and comorbidities. Am J Manag Care. 2006;12(S Suppl):S122-8.
103. Barry MJ, Fowler FJ, Jr., O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American urological association symptom index for benign prostatic hyperplasia. J Urol. 1992;148(S):1S49-S7; discussion 64.
104. Aiken CE. Leitfaden der Urologie. Suttgart: Thieme-Verlag; 19SS.
105. Vahlensieck EW. Die Prostata. Frankfurt: Pmi-Verlag; 198S.
106. Dull P, Reagan RW, Jr., Bahnson RR. Managing benign prostatic hyperplasia. AmFam Physician. 2002;66(l):77-84.
Andy Suter 190

107. Schroeder RP, van Weerden WM, Bangma C, Krenning EP, de Jong M. Peptide receptor imaging of prostate cancer with radiolabelled bombesin analogues. Methods. 2009;48(2):200-4.
108. Wei JT, Calhoun E, Jacobsen SJ. Urologie diseases in america project: benign prostatic hyperplasia. J Urol. 2008;179(5 ):S75-80.
109. Wei JT, Calhoun E, Jacobsen SJ. Urologie diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173(4):1256-61.
110. Krista I AR, Arnold KB, Schenk JM, Neuhouser ML, Weiss N, Goodman P, et al. Race/ethnicity, obesity, health related behaviors and the risk of symptomatic benign prostatic hyperplasia: results from the prostate cancer prevention trial. J Urol. 2007;177(4):1395-400; quiz 591.
111. Platz EA, Kawachi I, Rimm EB, Willett WC, Giovannucci E. Race, ethnicity and benign prostatic hyperplasia in the health professionals follow-up study. J Urol. 2000;163(2):490-5.
112. Parsons JK. Modifiable risk factors for benign prostatic hyperplasia and lower urinary tract symptoms: new approaches to old problems. J Urol. 2007;178(2):395-401.
113. Issa MM, Renter TC, Black L, Grogg AL, Kruep EJ. An assessment of the diagnosed prevalence of diseases in men 50 years of age or older. Am J Manag Care. 2006; 12 (4):83-9.
114. Nickel JC. BPH: costs and treatment outcomes. Am J Manag Care. 2006;12(5 ):141- 8.
115. Carballido J, Ruiz-Cerda JL, Unda M, Baena V, Campoy P, Manasanch J, et al. [Economic evaluation of medical treatment of benign prostatic hyperplasia (BPH) in the specialised care setting in Spain. Application to the cost-effectiveness of two drugs frequently used in its treatment). Actas Urol Esp. 2008;32(9):916-25.
116. McConnell JD. Benign prostatic hyperplasia: diagnosisand treatment. Benign prostatic hyperplasia guideline panel. AHCPR publication no. 8 edl994.
117. Novara G, G alfa no A, Ficarra V, Artibani W. Anticholinergic drugs in patients with bladder outlet obstruction and lower urinary tract symptoms: A systematic review. Eur Urol. 2006;50(4):675-83.
118. Wilt T, Ishani A, Mac Donald R. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002(3):CD001423.
119. Ishani A, MacDonald R, Nelson D, Rutks I, Wilt TJ. Pygeum africanum for the treatment of patients with benign prostatic hyperplasia: a systematic review and quantitative meta-analysis. Am J Med. 2000;109(8):654-64.
120. Pygeum africanum (Prunus africanus) (African plum tree). Monograph. Altern Med Rev. 2002;7(l):71-4.
121. Gerber C, Lowe PC, Spigelman S. The use of standardized extract of red clover isoflavones for the alleviation of BPH symptoms [French]. The Endocrine Society's 82nd Annual Meeting; June 21-24; Toronto2000.
Z' ' ir ' : ; 191

122. Kadow C, Abrams PH. A double-blind trial of the effect of beta-sitosteryl glucoside (WA184) in the treatment of benign prostatic hyperplasia. Eur Urol. 1986;12(3):187- 9.
123. Berges RR, Kassen A, Senge T. Treatment of symptomatic benign prostatic hyperplasia with beta-sitosterol: an 18-month follow-up. BJU Int. 2000;85(7):842-6.
124. Berges RR, Windeler J, Trampisch HJ, Senge T. Randomised, placebo-controlled, double-blind clinical trial of beta-sitosterol in patients with benign prostatic hyperplasia. Beta-sitosterol Study Group. Lancet. 1995;345(8964):1529-32.
125. Klippel KF, HiltI DM, Schipp B. A multicentric, placebo-controlled, double-blind clinical trial of beta-sitosterol (phytosterol) for the treatment of benign prostatic hyperplasia. German BPH-Phyto Study group. Br J Urol. 1997;80(3):427-32.
126. Fischer A, Jurincic CD, Klippel KF. Conservative treatment of benign prostatic hyperplasia with high-dosage b-sitosterol (SSmg): results of a placebo-controlled double-blind study. Uroscop. 1993;1:12-20.
127. Wilt T, Ishani A, MacDonald R, Stark G, Mulrow C, Lau J. Beta-sitosterols for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2000(2):CD001043.
128. MacDonald R, Ishani A, Rutks I, Wilt TJ. A systematic review of Cernilton for the treatment of benign prostatic hyperplasia. BJU Int. 2000;85(7):836-41.
129. Roehrborn CG, Prajsner A, Kirby R, Andersen M, Quinn S, Malien S. A double-blind placebo-controlled study evaluating the onset of action of doxazosin gastrointestinal therapeutic system in the treatment of benign prostatic hyperplasia. Eur Urol. 2005;48(3):44S-52; discussion 52.
130. Roehrborn CG, Van Kerrebroeck P, Nordling J. Safety and efficacy of alfuzosin 10 mg once-daily in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a pooled analysis of three dOuble-blind, placebo-controlled studies. BJU Int. 2003;92(3):257-61.
131. Kaplan SA. AUA guidelines and their impact on the management of BPH: an update. Rev Urol. 2004;6 (9):46-52.
132. Narayan P, Tewari A. Overview of alpha-blocker therapy for benign prostatic hyperplasia. Urology. 1998;51(4A ):38-45.
133. Tindall DJ, Rittmaster RS. The rationale for inhibiting Salpha-reductase isoenzymes in the prevention and treatment of prostate cancer. J Urol. 2008;179(4):1235-42.
134. McConnell JD, Roehrborn CG, Bautista CM, Andriole GL, Jr., Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349(25):2387-98.
135. Guess HA, Gormley GJ, Stoner E, Oesterling JE. The effect of finasteride on prostate specific antigen: review of available data. J Urol. 1996;155(l):3-9.
136. Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349(3):215-24.
Andy Suter 192

137. Renter TC, Davis EA, Shah MB, Lin PJ. Dutasteride vs finasteride: assessment ofdifferences in acute urinary retention rates and surgical risk outcomes in an elderlypopulation aged > or =65 years. Am J Manag Care. 2008;14(5):154-9.
138. Gjertson CK, Walmsley K, Kaplan SA. Benign prostatic hyperplasia: now we can begin to tailor treatment. Cleve Clin J Med. 2004;71(11):857, 60, 63-5 passim.
139. Miano R, De Nunzio C, Asimakopoulos AD, Germani S, Tubaro A. Treatment options for benign prostatic hyperplasia in older men. Med Sci Monit. 2008;14(7):RA94-102.
140. Oesterling JE. Benign prostatic hyperplasia. Medical and minimally invasivetreatment options. N Engl J Med. 1995;332(2):99-109.
141. Norby B, Frimodt-Moller PC. Development of a urethrorectal fistula aftertransurethral microwave thermotherapy for benign prostatic hyperplasia. BJU Int. 2000;85{4):554-5.
142. Ahyai SA, Lehrich K, Kuntz RM. Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow-up results of a randomized clinical trial. Eur Urol. 2007;52(5):1456-63.
143. Roehrborn CG. Current medical therapies for men with lower urinary tract symptoms and benign prostatic hyperplasia: achievements and limitations. Rev Urol. 2008;10(l):14-25.
144. Geavlete P, Multescu R, Geavlete B. Serenoa repens extract in the treatment of benign prostatic hyperplasia. Ther Adv Urol. 2011;3(4):193-8.
145. Gregorin JP. Eine probatorische Therapie 1st verantwortbar. Ars Med. 2012;2:62-3.
146. Commission E. Saw Palmetto berry. The Complete German Commission E Monographs: American Botanical Council Blumenthal M, editorl998.
147. WHO. Fructus Serenoae Repentis. WHO monographs on selected medicinal plants. 2002. 285-99 p.
148. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1-12.
149. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA. 1995;273(5):408-12.
150. Tacklind J, MacDonald R, Rutks I, Wilt TJ. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2009(2):CD001423.
151. Wilt T, Ishani A, Stark G, MacDonald R, Mulrow C, Lau J. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2000(2):CD001423.
152. Bent S, Kane C, Shinohara K, Neuhaus J, Hudes ES, Goldberg H, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-66.
153. McVary KT, Roehrborn C. American Urological Association guideline:management of benign prostatic hyperplasia (BPH), revised 2010. American Urological Association; 2010 [cited 2012 12th of January]; Available from:
Andv Suter 193
http://www.auanet.org/content/clinical-practice-guidelines/clinical-guidelines/main-reports/bph-management/authors.pdf.
154. Agbabiaka TB, Pittler MH, Wider B, Ernst E. Serenoa repens (saw palmetto): a systematic review of adverse events. Drug Saf. 2009;32(8):637-47.
155. Debruyne F, Koch G, Boyle P, Da Silva PC, Gillenwater JG, Hamdy PC, et al. [Comparison of a phytotherapeutic agent (Permixon) with an alpha-blocker (Tamsulosin) in the treatment of benign prostatic hyperplasia: a 1-year randomized international study]. Prog Urol. 2002;12(3):384-92; discussion 94-4.
156. Champault G, Bonnard AM, Cauquil J, Patel JC. [Medical treatment of prostatic adenoma. Controlled trial: PA 109 vs placebo in 110 patients]. Ann Urol (Paris). 1984;18(6):407-10.
157. Carraro JC, Raynaud JP, Koch G, Chisholm GD, Di Silverio P, Teillac P, et al. Comparison of phytotherapy (Permixon) with finasteride in the treatment of benign prostate hyperplasia: a randomized international study of 1,098 patients. Prostate. 1996;29(4):231-40; discussion 41-2.
158. Mattei S, Capone M, Acconcia A. Drug therapy of benign prostate hyperplasia with Serenoa repens extract. Tw Urologie Néphrologie. 1990;2:346-50.
159. Tasca A, Barulli M, Cavazzana A, Zattoni P, Artibani W, Pagano P. [Treatment of obstructive symptomatology caused by prostatic adenoma with an extract of Serenoa repens. Double-blind clinical study vs. placebo]. Minerva Urol Nefrol. 1985;37(1):87-91.
160. Bauer HW, Casarosa C, Cosci M, Pratta M, Blessmann G. [Saw palmetto fruit extract for treatment of benign prostatic hyperplasia. Results of a placebo-controlled double-blind study]. MMW Portschr Med. 1999;141(25):62.
161. Lobelenz J. Extractum Sabal fructus bei benigner prostatahyperplasie (BPH). Thera peutikon. 1992;6:34-7.
162. Barry MJ, Meleth S, Lee JY, Kreder KJ, Avins AL, Nickel JC, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306(12):1344-51.
163. Moerck ER. Leading saw palmetto producer reports that consumers may be using saw palmetto incorrectly in support of prostate health Valensa International; 2012 [cited 2012 15th of January]; Available from: httD://www.prnewswire.com/news- releases/leading-saw-palmetto-producer-reports-that-consumers-mav-be-using- saw-palmetto-incorrectlv-in-support-of-prostate-health-100342039.html.
164. Daniells S. Saw palmetto 'does not improve' prostate problems. 2006 [cited 2012 12th of January]; Available from: http://www.nutraingredients.com/Research/Saw- palmetto-does-not-improve-prostate-problem.
165. Levin RM, Das AK. A scientific basis for the therapeutic effects of Pygeum africanum and Serenoa repens. Urol Res. 2000;28(3):201-9.
166. Lowe PC, Ku JC. Phytotherapy in treatment of benign prostatic hyperplasia: a critical review. Urology. 1996;48(l):12-20.
<y Suter 194

L i te ra t i r c
167. Winston D. Saw palmetto for men & women: herbal healing for the prostate, urinary tract, immune system and more Massachuttes: Storey Publishing, LLC; 1999.
168. Brundage A. Going to the sources: A guide to historical research and writing. 3 ed: Harlan Davidson; 2002.107 p.
169. Howell MC, Prevenier W. From Reliable Sources: An Introduction to Historical Methodology. Ithaca: Cornell University Press; 2001. 207 p.
170. Hathi Trust. Hathi trust digital library. 2012; Available from: http://www.hathitrust.org/.
171. Karlsruher Institut für Technologie. Karlsruher Virtueller Katalog (Karlsruhe Virtual Catalog). 2012; Available from: http://www.ubka.uni-karlsruhe.de/kvk.html.
172. Rognon LM, Raymond G. Historique de I'hyperplasie bénigne de la prostate (A historical overview of benign prostatic hyperplasia). . Ann Urol (Paris). 1992;26(3):167-87.
173. Shelley HS. The enlarged prostate. A brief history of its treatment. J Hist Med Allied Sci. 1969;24(4):452-73.
174. Galen. Galen on anatomical procedures. The later books. Cambridge: Cambridge University Press; 2010. 304 p.
175. Herr HW. The enlarged prostate: a brief history of its surgical treatment. BJU Int. 2006;98(5):947-52.
176. Lauridsen L. From the history of prostatic hypertrophy. A medico-historical investigation of its pathology and palliative surgical treatment up to the beginning of the 20th century. Appendix: from the history of lithotomy. A short survey of the development of the different methods. Dan Med Bull. 1969;16(3):77-82.
177. Ciranni R, Giusti L, Fornaciari G. Prostatic hyperplasia in the mummy of an italian renaissance prince. Prostate. 2000;45(4):320-2.
178. Franks LM. Benign nodular hyperplasia of the prostate; a review. Ann R Coll Surg Engl. 1953;14(2):92-106.
179. Kirkup J. The evolution of surgical instruments: an illustrated history from ancient times to the twentieth century. Novato: The evolution of surgical instruments: an illustrated history from ancient ;2005. 510 p.
180. Jones D. Diseases of the bladder and prostate, and obscure affections of the urinary organs. London: Simpkin, Marshall& Co.; 1890. 235 p.
181. van Buren WH, Keyes EL. A practical treatise on the surgical diseases of the genitourinary organs, including syphilis, designed as a manual for students and practitioners. New York: D. Appleton and Company; 1874. 672 p.
182. Portner E. Genitourinary diagnosis and therapy for urologists and general practitioners. London: Henry Kimpton; 1913. 221 p.
183. Ebstein W, Lebert H, Curschmann H. Handbuch der Krankheiten des Harnapparates. 2nd ed. Leipzig: Verlag von F.C.W Vogel; 1878. 360 p.
Andy Suter 195

L l i c r r t i r c
184. Gant FJ. Diseases of the bladder prostate gland, and urethra. 2nd ed. Philadelphia: Lindsay and Blakiston; 1876. 468 p.
185. Belfield WT. Diseases of the urinary and male sexual organs. New York: William Wood & Company; 1884. 351 p.
186. Young HH, Davis DM. Young's practice of urology, based on a study of 12,500 cases Philadelphia: W.B. Saunder Company; 1926.
187. Fuller E. Diseases of the genito-urinary system. London: The Macmillan company;1900.
188. Taylor RW. A practical treatise on genito-urinary and veneral diseases and syphilis. 3rd ed. London: Henry Kimpton; 1905. 757 p.
189. Cabot H. Modern urology. Philadelphia: Lea & Febiger; 1918. 744 p.
190. Schlagintweit F. Urologie des praktischen Arztes. München: J. F. Lehmanns Verlag; 1921.135 p.
191. Hunter J. A Treatise on the venereal disease. London: Nicol G. and W.; 1810. 429 p.
192. Thompson H. The enlarged prostate, its pathology and treatment. London: John Churchill; 1858. 320 p.
193. Stafford RA. An essay on the treatment of some affections of the prostate gland. London: John Churchill; 1840. 86 p.
194. Abrahams A, Morson AC. A guide to urinary diseases: Edward Arnold & Co.; 1921.120 p.
195. Caine M, Perl berg 5, Meretyk S. A placebo-controlled double-blind study of the effect of phenoxybenzamine in benign prostatic obstruction. Br J Urol. 1978;50(7):551-4.
196. Wikipedia. Finasteride. 2012; Available from: http://en.wikipedia.org/wiki/Finasteride.
197. McVary KT, Roehrborn CG, Avins AL, Barry MJ, Bruskewitz RC, Donnell RF, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185(5):1793-803.
198. Robinson RB. Minor fiber industries. Economic botany 1947;1:4-56.
199. Porter FW. The art of native basketry: a living legacy Conneticut: Pp. Greenwood Publishing Group; 1990.
200. Reitz DJ, Scarry CM. Reconstructing historical subsistence with an example from sixteenth-century Spanish Florida. Hist Archaeol. 1985;3:1-150.
201. Morton JF. Wild plants for survival in south Florida. 4 ed. Coral Gables, FL: Fairchild Tropical Garden; 1977.
202. Duke JA. CRC handbook of botanical herbs. Boca Raton, FL: CRC press; 1985.
203. Pfiaume K. Einleitung zur KenntniR der Nord-Amerikanischen Landwirthschaft: Zunachst für Auswanderer. Leipzig: Georg Wigand; 1866.189 p.
A n d y S i ; t c r 196

204. Roberts C Fecula of the saw-palmetto, used by Indians as food. Am J Pharm. 1888;4:256-7.
205. Peterson LA. Field guide to edible wild plants Boston: Houghton Mifflin Co.; 1977.
206. Gruenwald J. History of saw palmetto and its use. American Herbal Products Association, International Saw Palmetto Symposium; August 1998; Naples, Florida. 1998.
207. Krochmal A. A guide to medicinal plants of the United States New York: The New York Times Book Company; 1973.
208. Reed JB. A new remedy - Sabal serrulata - saw palmetto. Medical Brief. 1877:unknown.
209. Hathi Trust. The Medical brief. A monthly journal of scientific medicine and surgery. 2012 [cited 2012 12th of January]; Available from: http://catalog.hathitrust.Org/Record/000061076.
210. Delorme RH. Catholic doctors faced yellow fever in 1854. Southern Cross, The Diocesan Newspaper. 2010(May 13):S.
211. Reed JB. A New Remedy - Sabal Serrulata - Saw Palmetto. New Preparations. 1879;3(7):181-2.
212. Flannery MA. John Uri Lloyd: The great American eclectic. Carbondale, IL: SlU Press; 1998.
213. Lloyd JU. History of the vegetable drugs of the pharmacopeia of the United States.Bulletin of the Lloyd library of botany, pharmacy and materia medica.1911;4(18):97.
214. Deutsche Pharmazeutische Gesellschaft, Deutscher Apotheker-Verein. Archiv der Pharmazie. 1879. 548-9 p.
215. Clarke JH. A dictionary of pratical materia medica: The homoeopathic publishing company; 1900.
216. Madaus G. Lehrbuch der biologischen Heilmittel. Leipzig: Georg Thieme Verlag; 1938.
217. Read JB. The saw palmetto (Sabal serrulata). Am J Pharm. 1879;51:169-71.
218. Read JB. The saw palmetto (Sabal serrulata), Sabal levistona? Feay.). The Planter'sGazette. 1879:123-4.
219. Anonymous. Sabal serrulata. Archiv der Pharmazie. 1879;215(6):548-51.
220. Haller JS. A profile in alternative medicine: the eclectic medical college of Cincinnati. Kent State: Kent State University Press; 1999.
221. Wikipedia. Constantine Samuel Rafinesque. 2012 [cited 2012 lis t of April]; Available from: http://en.wikipedia.org/wiki/Constantine Samuel Rafinesque.
222. Moore M. Plant monographs extracted from the eclectic materia medica, pharmacology and therapeutics. 2008 [cited 2012 l is t of April]; Available from: http://www.swsbm.com/FelterMM/Felters.html.
Andv Suter 197
Lite roture
223. Flexner A, Medical education in the United States and Canada. New York City: The Carnegie Foundation for the Advancement of Teaching, 1910.
224. Goss IJM. New preparations; 1879.
225. Wood GB, Bache F. The dispensatory of the United States of America. 17 ed. Philadelphia: Wood, Remington and Sadtler; 1894.
226. Felter HW, Lloyd JU. King's American dispensatory. 18th ed l898 .1750-2 p.
227. Webster HJ. Dynamical therapeutics. San Francisco: H.J.Webster; 1898.
228. Jones EG. Cancer: its causes, symptoms and treatment, giving the results of over forty years' experience in the medical treatment of this disease. Boston: Therapeutic publishing company; 1911.
229. Jones E. Definite medication. Boston: Therapeutic Publishing Company; 1911.
230. Davidson AL, in Clarke, H.J. A Dictionary of practical materia medica HomeopathicPub. Co.; 1895 (1900).
231. Bloyer WE. Saw palmetto. Eclectic Medical Journal. 1896;56(12):581-2.
232. Hatton JD. Saw palmetto Eclectic medical gleaner. 1897;8(11):331.
233. Davis GS. The pharmacology of the newer materia medica. Detroit: Geo. Davis; 1892.
234. Dupore SF. Therapeutic Gazette. 1880:243.
235. Knapp H. Saw palmetto. The Western Druggist. 1892:355-6.
236. Sherrard CC. Saw palmetto (Sabal serrulata). A P A Proc. 1894(Bd. 42).
237. Rusby H. Saw palmetto - pharmacology. Proceedings of the American Pharmaceutical Association. 1896;44:534-7.
238. Lloyd JU, Lloyd CG. Drugs and medicines of North America. Cincinnati: Robert Clark & Co.; 1884.
239. Scudder JM. Specific medication and specific medicines. Cincinnatti: Wilstach, Baldwin & Co.; 1870.
240. Pereira J. The elements of materia medica and therapeutics v.l, 1852. Philadelphia: Blanchard and Lea; 1852. 836 p.
241. Pereira J, Carson J. The elements of materia medica and therapeutics. London: Longman, Brown, Green, and Longmans; 1842.1126 p.
242. Winston D. Saw palmetto use by Wyeth Laboratories, Lilly, Squibb and Merck. 2012.
243. Boericke W. Boerickes materia medica: the tinctures. San Franciscol901.
244. Fyfe JW. The essentials of the modern materia medica and therapeutics. Cincinatti: The Scudder Brothers Company; 1903.
245. Sargent CS. Serenoa serrulata as a remedy. Kew Bull. 1899:55-6.
An dy Suter 198

/.'iF.'T'ii'/r
246. Roemer MJ. Handbuch der allgemeinen Botanik: zum Selbststudium auf der Grundlage des natürlichen Systems, Band 1. München: Fleischmann; 1835. 426 p.
247. Heynhold G. Nomenclator botanicus hortensis: oder alphabetische und synonymische aufzahlung der in den garten Europa's cultlvirten gewachse, nebst angabe ihres autors, ihres vaterlandes, ihrer dauer und cultur: In der Arnoldischen Buchhandlung; 1840. 888 p.
248. Kegel H. Chaemerops serrulata. Botanische Zeitung. 1850;8.
249. Anonymous. Das Ausland: Wochenschrift für Lander- u. Volkerkunde: Cotta; 1862.
250. Seemann B, Bolle C. Die Palmen: populare Naturgeschichte derselben : nebst Verzeichnisse aller bekannten und in Garten eingeführten Arten: W. Engelmann; 1863. 368 p.
251. Petermann A, Behm E, Supan AG, Langhans PMH, Creutzburg N, Haack H. Petermanns Geographische Mitteilungen: H. Haack; 1878.
252. Geissler E, Moeller J. Real-encyclopadie der gesammten pharmacie:Handworterbuch für apotheker, arzte und medicinalbeamte: Urban &Schwarzenberg; 1890.
253. Anonymous. Dixons Saw palmetto. Meyer Brothers druggist. 1907.
254. Brestowski A. Die neueren und neuesten Arzneimittel, ihre Zusammensetzung, Darstellung, Eigenschaften, Anwendung und Dosirung: Verlag von H. Hassel; 1891. 547 p.
255. Hartwich C. Die neuen Arzneidrogen aus dem Pfianzenreiche: J. Springer; 1897. 469 p.
256. Dragendorff G. Die Heilpflanzen der verschiedenen Volker und Zeiten: IhreAnwendung, wesentlichen Bestandtheile und Geschichte. Ein Handbuch für Arzte, Apotheker, Botaniker und Droguisten. Stuttgart: F. Enke; 1898.
257. Hager H. Handbuch der pharmaceutischen Praxis für Apotheker, Arzte, Drogisten und Medicinalbeamte: Springer; 1878.1460 p.
258. Hager H. Handbuch der pharmaceutischen Praxis für Apotheker, Arzte, Drogisten und Medicinalbeamte: Erganzungsband: J. Springer; 1883.1326 p.
259. Fischer B. Die Neueren Arzneimittel für Apotheker, Aerzte und Drogisten. Berlin: Verlag Julius Springer; 1888.
260. Waldenburg L, Simon CE. Handbuch der allgemeinen und speciellenArzneiverdordnungs-Lehre. Berlin: Verlag Ausgust Hirschwald; 1873.
261. Plugge PC. Die wichtigsten Heilmittel in ihrer wechselnden chemischenZusammensetzung und pharmkodynamischen Wirkung. Jena: Verlag Gustav Fischer; 1886.
262. Liebreich 0, Langgard A. Compendium der Arzneiverordnung. 3 ed. Berlin: Fischer's Medicinische Buchhandlung; 1891.
263. Pharmacopoea helvetica. Pharmacopoea helvetica. Zurich: Orell Füssii; 1898. 398 p.
An d yS i : : e r 199

[ i i e ra t Lüf
264. Gross H, Hering C. Vergleichende Arzneiwirkungslehre. Leipzig: A. Margraafs Homôopathische Offizin; 1892.
265. Doerries LS. Die Ausbildung homôopathischer Àrzte in Deutschland und inFrankreich, 1860-1900. Freiburg im Breisgau: Albert-Ludwigs-Universitat; 2007.
266. Heinigke C. Handbuch der homoopathischen Arzneiwirkungslehre. Leipzig: Dr. Willmar Schwabe; 1880.
267. Lutze A. Lehrbuch der Homoeopathie. Coethen: Arthur Lutze; 1860.
268. Lutze A. Lehrbuch der Homoepathie. Coethen: Paul Schettlers Verlag; 1878.
269. Lutze P. Lehrbuch der Homoopathie. 11 ed. Koethen: Verlag der Lutzeschen Heilanstalt; 1887.
270. Arzneibuch für das deutsche Reich. Arzneibuch für das deutsche Reich (Pharmacopoea Germanica, editio III). Ausgabe D, editor. Berling: G. Schenck, R. V. Decker Verlag; 1890.432 p.
271. Germany Reichsgesundheitsamt, Pharmacopoea Germanica. Arzneibuch für das Deutsche Reich. Berlin: R.V Decker Verlag; 1900.
272. Schelenz HE. Pharmacognostische Karte für die Arzneibücher Europas und der Vereinigten Staaten von Amerika: G. Freytag & Berndt; 1899.
273. Hardy, Brownsward, Bradley. Chemisch-technisches repertorium. 1896(Bd. 34).
274. Anonymous. Jahresbericht über die Fortschritte der Pharmacognosie, Pharmacie und Toxicologie: Vandenhoeck & Ruprecht.; 1898.
275. Just L, Koehne E. Just's botanischer Jahresbericht: Systematisch geordnetes Repertorium der botanischen Literatur aller Lander: Gebr. Borntraeger; 1899.
276. Berliner Verein Homôopathischer Aerzte. Zeitschrift des Berliner Vereines Homôopathischer Aerzte: 0. Janke; 1900.
277. Allgemeine homôopathische Zeitung. Allgemeine homôopathische Zeitung: W. Schwabe; 1900.
278. Deutscher Apotheker-Verein. Deutsches homôopathisches Arzneibuch: Selbstverlag des Deutschen apotheker-vereins; 1901. 266 p.
279. Schwabe W. Pharmacopoea homoeopathica polyglotta: homôopathischeNormalpharmakopôe. Leipzig: Dr. Willmar Schwabe; 1901. 364 p.
280. Scharff W. Charakteristik der wichtigaten homôopathischen mittel: A. Strauch;1901. 59-60 p.
281. Faulwasser E. Deutsche homôopathische Arzneimittellehre: Im Auftrage des homôopathischen Central-Vereins Deutschlands herausgegeben von Dr. E. Faulwasser,... und Dr. R. Windelband: B. Behr; 1903.
282. Heinigke C. Karl Heinigke's Handbuch der homôopathischen Arzneiwirkungslehre. 2 ed. Leipzig: Schwabe; 1905. 658 p.
283. Germany. Reichsfinanzministerium. Reichszollblatt; 1906.
A n d y S i i t e r 200
284. Berliner Verein homôopathischer Àrzte. Handbuch der homoopathischen Heillehre: Im Auftrage des Berliner Vereins homôopathischer Àrzte herausgegeben: B. Behr; 1908.
285. Deutscher Apotheker-Verein. Vierteljahresschrift für praktische Pharmazie: Deutschen apotheker-vereins.; 1909.
286. Tschirch A, Remy E. Handbuch der pharmakognosie: bd. Allgemeinepharmakognosie. 2 v. Leipzig: C.H. Tauchnitz; 1909.
287. Hamburger Oberschulbehôrde Sektion für die Wissenschaftlichen Anstalten. Jahrbuch der hamburgischen wissenschaftlichen Anstalten: L. Grafe & Sillem; 1914.
288. Keegan J. Der erste Weltkrieg, eine europaische Tragôdie. Reinbek bei Hamburg: Rowohit Taschenbuch Verlag; 2001.
289. Griebel C. Chemisches Zentralblatt. Gesellschaft DC, Chemiker VD, editors: L. Voss; 1916.
290. Verein Deutscher Chemiker, Deutsche Gesellschaft für Angewandte Chemie. Zeitschrift für angewandte Chemie: Verlag Springer; 1917.
291. Langstein L, v. Noorden C, Loewe S. Therapeutische Monatshefte: J. Springer.; 1917.
292. Marcussen J, Schilling H. Pflanzenôlnachweis in Tierfetten. Zeitschrift für Untersuchung der Nahrungs- und Genussmittel. 1917(Bd. 33).
293. Fraenkel C. Hygienische Rundschau. 1917.
294. Unknown. Jahresbericht der Pharmazie. 1918;76:178.
295. Rosenberg H. Pharmakompendium: ein Führer durch die offiziellen Arzneibücher: Urban & Schwarzenberg; 1922. 665 p.
296. Schwabe W. Willmar Schwabe's Homôopathisches Arzneibuch: Aufzahlung und Beschreibung der homôopathischen Arzneimittel nebst Vorschrift für ihre Bereitung, Prüfung und Wertbestimmung. Leipzig: Dr. Willmar Schwabe; 1924. 410 p.
297. Gildemeister E, Hoffmann F. Die atherischen Ole: Schimmel & Co.Aktiengesellschaft, für den Buchhandel: L. Staackmann; 1928.
298. Voorhoeve J. Arzneiwirkungslehre neuerer homôopathischer Heilmittel Leipzig: Schwabe; 1910.
299. Bruckner T. Kurze Anieitung zum richtigen Gebrauch der wichtigsten Arzneimittel in den alltaglichen leichteren Erkrankungsfallen. Leipzig: Verlag Dr. Willmar Schwabe; 1913.
300. Holfert J. Volkstümliche Namen der Arzneimittel, Drogen und Chemikalien. 7 ed. Berlin: Verlag Julius Springer; 1914.
301. Ottinger HU. Ottinger's Homôopathie: diese vereinfachte, zusammengesetzte Homôopathie ist das Résultat einer sehr grossen Heilpraxis und bewahrte sich in tausenden von Krankheitsfallen. Berlin: Linser-verlag, g.m.b.h.; 1921.133 p.
A n d y S u t e r 201
302. Heinigke C, Klien P. Handbuch der homôopathischen Arzneiwirkungslehre Bed. Leipzig: W. Schwabe; 1922. 758 p.
303. Leeser 0. Lehrbuch der Homôopathie Stuttgart: Hippokrates-Verlag; 1927.
304. Hovorka D, Kronfeld A. Vergleichende Volksmedizin. Stuttgart: Verlag Strecker & Schrôder; 1909.
305. Schrôter. Schrôters Schatzkastlein der Pflanzenheilkunde: kurze und übersichtiiche Beschreibung der bedeutendsten Heilpflanzen. Basel: Schrôter; 1911. 235 p.
306. Schreiber JF. Schreibers kleiner Atlas der wichtigeren Heilpflanzen. Essiingen: J. F. Schreiber; 1920.16 p.
307. Schlickum 0. Pharmakognosie als vademecum für Àrzte, Apotheker, Studierende der Medizin und Pharmazie.cksichtigung ihrer wichtigsten theoretischen Grundiagen. Ed. 3 ed. Leipzig: J.A. Barth; 1924.
308. Skutetzky A. Die neueren Arzneimittel in der arztlichen Praxis. Berlin: Verlag Julius Springer; 1908.
309. Dornblüth 0. Arzneimittel der heutigen Medizin. Leipzig and Würzburg: Verlag Curt Kabitzsch; 1919.
310. Arends G. Neue Arzneimittel und pharmazeutische Spezialitaten 7ed. Berlin: J. Springer; 1926. 648 p.
311. Reichsgesundheitsamt. Arzneibuch für das deutsche Reich. 5 ed. Berlin: G. v. Schenk Verlag; 1910.
312. Deutscher Apotheker-Verein. Erganzungsbuch zum Arzneibuch für das Deutsche Reich: (Arzneimittel, welche in dem Arzneibuch für das Deutsche Reich nicht enthalten sind): Deutscher Apotheker-Verein; 1916.
313. Reichsgesundheitsamt. Arzneibuch für das deutsche Reich. 6 ed. Berlin: R.v.Deckers Verlag; 1926.
314. Reichert B, Frerichs G, Arends G, Zôrnig H. Hagers Handbuch der pharmazeutischen Praxis. Berlin: Springer-Verlag; 1944.
315. Fischer B, Hartwich C. Hagers Handbuch der pharmaceutischen Praxis. Berlin: Verlag Julius Springer; 1903.
316. Lenz W, Arends G. Hagers Handbuch der pharmazeutischen Praxis. Ergânzungsband. Berlin: Verlag Julius Springer; 1913.
317. Hager H, Frerichs G. Hagers Handbuch der pharmazeutischen Praxis für Apotheker, Aerzte, Drogisten und Medizinalbeamte. Berlin: J. Springer; 1925.
318. Frerichs G, Arends G, Zôrnig H. Hagers Handbuch der pharmazeutischen Praxis. Berlin: Verlag Julius Springer; 1927.
319. Frerichs G, Arends G, Zôrnig H. Hagers Handbuch der pharmazeutischen Praxis für Apotheker, Àrzte, Drogisten u. Medizinalbeamte. Berlin: Julius Springer; 1930.1573 p.
; fr: 202
L i terature
320. Siracusano S, Ciciliato S, Ollandini G, Visalli F, Catheters and infections. Clinical management of complicated urinary tract infection: InTech; 2011. p. 83-98.
321. Homéopathe International. Dr Edwin Moses Hale (1829-1899). 2009 [cited 2012 l is t of January]; Available from: http://h0 me0 int.0 rg/ph0 t0 /h/haleedwi.htm.
322. Kaddour H. Information from Schwabe. In: Suter A, editor. 2012.
323. Castillo D. German Economy in the 1920s. Santa Barbara. 2003 [cited 2012 12th of January ]; Available from:http://www.historv.ucsb.edu/facultv/marcuse/classes/33d/proiects/1920s/Econ20s.htm.
324. Schroder G. Die Wiederbelebung der Phytothérapie im Zusammenhang mit denRef o r m best re bu nge n der NS-Pharmazie. In: Hickel E, Schroder G, editors. Neue Be it rage zur Arzneimittelgeschichte. Stuttgart:: WissenschaftlicheVerlagsgesellschaft; 1982. p. 122.
325. Bjorling DE, Wang ZY, Bushman W. Models of inflammation of the lower urinary tract. Neurourol Urodyn. 2011;30(5):673-82.
326. Cohen D. Is google good for history? 2010 [updated 7th of January 2010; cited 2012 10th of January]; Available from: http://www.dancohen.org/2010/01/07/is-google- good-for-historv/.
327. Clements Library Chronicles. Five ways to use google books for historical research. 2009 [cited 2010 5th of August ]; Available from: http://theclementslibrarv.blogspot.eom/2009/08/five-wavs-to-use-google-books- for.html.
328. Erkkisan. The end of google books as a tool for historical research ? google groups. 2011.
329. A.Vogel Bioforce AG. Prostasan capsules, pharmaceutical development, CTD Module 2.3 2011.
330. Castor TP, inventor; Compositions and methods for inhibiting 5-a reductase. United States2008.
331. Gregg FB, inventor; Saw palmetto composition and associated methods. United States of America2003.
332. European Parliament and Council. Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the approximation of the laws of the Member States relating to food supplements. Official Journal 2002. p. 51-7.
333. U.S. Food and Drug Administration FDA. Dietary supplement health and educationact of 1994. 1994 [cited 2012 Jan 3rd]; Available from:http://www.fda.gov/Regulatorvlnformation/Legislation/FederalFoodDrugandCosm eticActFDCAct/SignificantAmendmentstotheFDCAct/ucml48003.htm.
334. Swissmedic SH. Anieitung zum Einreichen von Zulassungsgesuchen für pfianzliche Arzneimittel der Humanmedizin (Phyto-Anleitung) Berne; 2006. p. 18.
A n d y S u t e r 203
I of i//e
335. Khoury S, Cockett A, Aso Y, Chatelain C, Andersson L, Abrams P, et al. International consultation on urological diseases: a decade of progress. Prostate. 2000;45(2):194-9.
336. European Directorate for the Quality of Medicines & Healthcare. European pharmacopoeia. 7th ed. Strasbourg: Council of Europe; 2005.
337. Feifer AH, Fleshner NE, Klotz L. Analytical accuracy and reliability of commonly used nutritional supplements in prostate disease. J Urol. 2002;168(l):150-4; discussion 4.
338. Scaglione F, Lucini V, Pannacci M, Caronno A, Leone C. Comparison of the potency of different brands of Serenoa repens extract on Salpha-reductase types I and II in prostatic co-cultured epithelial and fibroblast cells. Pharmacology. 2008;82(4):270-5.
339. Romalo G, Schweikert HU. Inhibition of Sa-reductase activity by Sabal serrulata extract 2002.
340. Sorenson WR, Sullivan D. Determination of campesterol, stigmasterol, and beta- sitosterol in saw palmetto raw materials and dietary supplements by gas chromatography: single-laboratory validation. J AOAC Int. 2006;89(l):22-34.
341. Booker AJ. Assessment of proton NMR spectroscopy and principal component analysis as techniques for the metabolomic profiling of commercial saw palmetto products. London: University of London; 2010.
342. Hall R, Beale M, Fiehn 0, Hardy N, Sumner L, Bino R. Plant metabolomics: the missing link in functional genomics strategies. Plant Cell. 2002;14(7):1437-40.
343. Wagner H, Bladt S, Zgainski EM. Drogenanalyse. Dünnschichtchromatographische Analyse von Arzneidrogen. Berlin Heidelberg New York: Springer-Verlag; 1983.
344. Kellner R, Mermet JM, Otto M, Valcarcel M, Widmer HM. Analytical Chemistry. Weinheim: Wiley-VCH Verlag; 2004.1181 p.
345. Frey HP, Zieloff K. Qualitative und quantitative Diinnschichtchromatography. Weinheim New York Basel Cambridge: VHC Verlagsgesellschaft; 1992.
346. Jork H, Funk W, Fischer W, Wimmer H. Dünnschichtchromatographie: Reagenzien und Nachweismethoden. Weinheim New York Basel Cambridge Tokyo: VCH Verlag; 1993. 499 p.
347. McNair HM, Miller JM. Basic Gas Chromatography. 2nd ed. Hoboken, New Jersey: John Wiley & Sons; 2009.
348. Cremer E. Discussion remarks. Z Elektrochem. 1951;55:65.
349. Bobleter 0. Exhibition of the first gas chromatographic work of Erika Cremer and Fritz Prior. Chromatographia. 1996;43(7-8):444-6.
350. Stuart B, Prichard E. Practical laboratory skills, training guides. Gas Chromatography. Cambridge: Royal Society of Chemistry; 2003.
351. Fiebig HJ, Deutsche Gesellschaft für Fettwissenschaft. DGF-Einheitsmethoden, Deutsche Einheitsmethoden zur Untersuchung von Fetten, Fettprodukten, Tensiden
A n d y S u t e r 204

und verwandten Stoffen. Stuttgart: Wissenschaftliche Verlagsgesellschaft mbH Stuttgart; 2011.
352. Bubrick P, Johnson P, Stonebrook K. Saw palmetto: Critical Review, Chemistry, and Application. In: Bidlack W, Omaye ST, Meskin MS, Topham DKW, editors. Phytochemicals as bioactive agents. Lancaster, Pennsilvania: Technomic Publishing Company 2000. p. 189-97.
353. Valipe SR, Nadeau JA, Annamali I , Venkitanarayanan K, Hoagland T. In vitro antimicrobial properties of caprylic acid, monocaprylin, and sodium caprylate against Dermatophilus congolensis. Am J Vet Res. 2011;72(3):331-5.
354. Nair MK, Joy J, Vasudevan P, Hinckley L, Hoagland TA, Venkitanarayanan KS. Antibacterial effect of caprylic acid and monocaprylin on major bacterial mastitis pathogens. J Dairy Sci. 2005;88(10):3488-95.
355. Omura Y, O'Young B, Jones M, Pallos A, Duvvi H, Shimotsuura Y. Caprylic acid in the effective treatment of intractable medical problems of frequent urination, incontinence, chronic upper respiratory infection, root canalled tooth infection, ALS, etc., caused by asbestos & mixed infections of Candida albicans, helicobacter pylori & cytomegalovirus with or without other microorganisms & mercury. Acupunct Electrother Res. 2011;36(l-2):19-64.
356. Skrivanova E, Molatova Z, Marounek M. Effects of caprylic acid and triacylglycerols of both caprylic and capric acid in rabbits experimentally infected with enteropathogenic Escherichia coli 0103. Vet Microbiol. 2008;126(4):372-6.
357. Chang SS, Redondo-Solano M, Thippareddi H. Inactivation of Escherichia coli 0157:H7 and Salmonella spp. on alfalfa seeds by caprylic acid and monocaprylin. Int J Food Microbiol. 2010;144(l):141-6.
358. Skulason S, Holbrook WP, Thormar H, Gunnarsson GB, Kristmundsdottir T. A study of the clinical activity of a gel combining monocaprin and doxycycline: a novel treatment for herpes labialis. J Oral Pathol Med. 2012;41(l):61-7.
359. Nakatsuji T, Kao MG, Fang JY, Zouboulis CC, Zhang L, Gallo RL, et al. Antimicrobial property of lauric acid against Propionibacterium acnes: its therapeutic potential for inflammatory acne vulgaris. J Invest Dermatol. 2009;129(10):2480-8.
360. Garfinkel M, Lee S, Opara EC, Akwari OE. Insulinotropic potency of lauric acid: a metabolic rationale for medium chain fatty acids (MCF) in TPN formulation. J Surg Res. 1992;52(4):328-33.
361. Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr. 2003;77(5):1146-55.
362. Narasimhan B, Mourya V, Dhake A. Design, synthesis, antibacterial, and QSAR studies of myristic acid derivatives. Bioorg Med Chem Lett. 2006;16(ll):3023-9.
363. Doering TL, Lu T, Werbovetz KA, Gokel GW, Hart GW, Gordon Jl, et al. Toxicity of myristic acid analogs toward African trypanosomes. Proc Natl Acad Sci U S A . 1994;91(21):9735-9.
A n d v S i : t c r 205

i i teratu' c
364. World Health Organisation WHO, Diet, nutrition and the prevention of chronic diseases Geneva2003, p. 160.
365. French MA, Sundram K, Clandinin MT. Cholesterolaemic effect of palmitic acid in relation to other dietary fatty acids. Asia Pac J Clin Nutr. 2002;11 SuppI 7:5401-7.
366. Sampath H, Ntambi JM. The fate and intermediary metabolism of stearic acid. Lipids. 2005;40(12):1187-91.
367. Berry SE. Triacylglycerol structure and interesterification of palmitic and stearic acid-rich fats: an overview and implications for cardiovascular disease. Nutr Res Rev. 2009;22(1):3-17.
368. Kris-Etherton PM, Griel AE, Psota TL, Gebauer SK, Zhang J, Etherton TD. Dietary stearic acid and risk of cardiovascular disease: intake, sources, digestion, and absorption. Lipids. 2005;40(12):1193-200.
369. Menendez JA, Lu pu R. Mediterranean dietary traditions for the moleculartreatment of human cancer: anti-oncogenic actions of the main olive oil's monounsaturated fatty acid oleic acid (18:ln-9). Curr Pharm Biotechnol.2006;7(6):495-502.
370. Teres S, Barcelo-Coblijn G, Benet M, Alvarez R, Bressani R, Halver JE, et al. Oleic acidcontent is responsible for the reduction in blood pressure induced by olive oil. Proc Natl Acad Sci USA. 2008;105(37):13811-6.
371. Kennedy A, Martinez K, Schmidt S, Mandrup S, LaPoint K, McIntosh M. Antiobesity mechanisms of action of conjugated linoleic acid. J Nutr Biochem. 2010;21(3):171-9.
372. Patwardhan AM, Scotland PE, Akopian AN, Hargreaves KM. Activation of TRPVl in the spinal cord by oxidized linoleic acid metabolites contributes to inflammatory hyperalgesia. Proc Natl Acad Sci USA. 2009; 106(44): 18820-4.
373. Hennig B, Lei W, Arzuaga X, Ghosh DD, Saraswathi V, Toborek M. Linoleic acid induces proinflammatory events in vascular endothelial cells via activation of PI3K/Akt and ERKl/2 signaling. J Nutr Biochem. 2006;17(ll):766-72.
374. Hennessy AA, Ross RP, Devery R, Stanton C. The health promoting properties of the conjugated isomers of alpha-linolenic acid. Lipids. 2011;46(2):10S-19.
375. Nature's Way. Nature's way - about us. 2008 [cited 2012 February 1]; Available from: http://www.natureswav.com/About-Us.aspx.
376. Bravi F, Bosetti C, Dal Maso L, Talamini R, Montella M, Negri E, et al. Macronutrients, fatty acids, cholesterol, and risk of benign prostatic hyperplasia. Urology. 2006;67(6):120S-11.
377. Bennett BC. Variation in the fatty acid composition of saw palmetto (Serenoa repens) and comparison of field collected-hexane extracts with ethanolic extracts. 2006.
378. Lima TM, Kanunfre CC, Pompeia C, Verlengia R, Curi R. Ranking the toxicity of fatty acids on Jurkat and Raji cells by flow cytometric analysis. Toxicol In Vitro. 2002;16(6):741-7.
AndySuter 206

/ lier
379. Preuss HG, Marcusen C, Regan J, Klimberg IW, Welebir TA, Jones WA. Randomized trial of a combination of natural products (cernitin, saw palmetto, B-sitosterol, vitamin E) on symptoms of benign prostatic hyperplasia (BPH). Int Urol Nephrol. 2001;33(2):217-25.
380. Lopatkin N, Sivkov A, Schlafke S, Funk P, Medvedev A, Engelmann U. Efficacy and safety of a combination of Sabal and Urtica extract in lower urinary tract symptoms- -long-term follow-up of a placebo-controlled, double-blind, multicenter trial. Int Urol Nephrol. 2007;39(4):1137-46.
381. Mantovani F. Serenoa repens in benign prostatic hypertrophy: analysis of 2 Italian studies. Minerva Urol Nefrol. 2010;62(4):335-40.
382. Ganzera M, Croom EM, Khan lA. Determination of the Fatty Acid content of pumpkin seed, pygeum, and saw palmetto. J Med Food. 1999;2{l):21-7.
383. Gunstone FD, Harwood JL, Padley FB. The Lipid Handbook. 3rd ed. Boca Raton, FL: CRC Press; 2007.
384. Gao Y. Synthesis and Evaluation of Vegetable (soybean) Oil Based Epoxy Resin for beverage can coating and enzymatic synthesis and characterization of tailored n&c end protected oliopeptides. Missouri: Missouri university of science and technology; 2008.
385. Cabeza M, Bratoeff E, Heuze I, Ramirez E, Sanchez M, Flores E. Effect of beta- sitosterol as inhibitor of 5 alpha-reductase in hamster prostate. Proc West Pharmacol Soc. 2003;46:153-5.
386. Rohrmann S, Giovannucci E, Willett WC, Platz EA. Fruit and vegetable consumption, intake of micronutrients, and benign prostatic hyperplasia in US men. Am J Clin Nutr. 2007;85(2):523-9.
387. von Holtz RL, Fink CS, Awad AB. beta-Sitosterol activates the sphingomyelin cycle and induces apoptosis in LNCaP human prostate cancer cells. Nutr Cancer. 1998;32(1):8-12.
388. Loizou S, Lekakis I, Chrousos GP, Moutsatsou P. Beta-sitosterol exhibits antiinflammatory activity in human aortic endothelial cells. Mol Nutr Food Res. 2010;54(4):551-8.
389. Murthy K, Mishra S. Quantification of beta -sitosterol from Mucuna pruriens by TLC. Chromatographia. 2009;69:183-6.
390. Sparzak B, Krauze-Baranowska M, Pobiocka-Olech L. High-performance thin-layer chromatography densitometric determination of beta-sitosterol in Phyllanthus species. J AOAC Int. 2009;92(5):1343-8.
391. Moreau RA, Whitaker BD, Hicks KB. Phytosterols, phytostanols, and their conjugates in foods: structural diversity, quantitative analysis, and health- promoting uses. Prog Lipid Res. 2002;41(6):457-500.
392. Abidi SL. Chromatographic analysis of plant sterols in foods and vegetable oils. J Chromatogr A. 2001;935(1-2):173-201.
AndvS' jtcr 207
L iief'otu'c
393. Aitzetmüller K, Brühl L, Fiebig HJ. Analysis of sterol content and composition in fats and oils by capillary-gas liquid chromatography using an internal standard. Comments on the German sterol method. Fett/Lipid. 1998;100:429-35.
394. Horwitz W, Latimer G. Cholesterol in foods, and Approved Method 2007.03 Campesterol, stigmasterol, and beta-sitosterol in saw palmetto raw materials and dietary supplements. In: International A, editor. Official Methods of Analysis of AOAC International. 18th ed. Gaithersburg, MD2010.
395. International Organization for Standardization I. Animal and vegetable fats and oils- determination of individual and total sterols content-gas chromatographic method. Geneva: ISO; 1999.
396. Winkler JK, Rennick KA, Eller FJ, Vaughn SF. Phytosterol and tocopherol components in extracts of corn distiller's dried grain. J Agric Food Chem. 2007;55(16):6482-6.
397. No Author. Herbal Rx for prostate problems. Consum Rep. 2000;65(9):60-2.
398. European Food Safety Authority EFSA. Directive 2002/46/EC of the European parliament and of the council. Luxemburg: European Union; 2002.
399. Hahn A. Nahrungserganzungsmittel: Fakten und Oaten der zur Nahrungserganzung meistverwendeten Stoffe. Stuttgart: Wissenschaftliche Verlagsgesellschaft; 2001.
400. EU commission. Directive 2001/83/EC of the European parliament and of the Council on the community code relating to medicinal products for human use. 2001.
401. ICD9Data.com. 2011 ICD-9-CM diagnosis code 600, hyperplasia of prostate. 2012 [cited 2012 24th of March ]; Available from: http://www.icd9data.eom/2011/Volumel/580-629/600-608/600/600.htm.
402. European Parliament and Council. Directive 2004/24/EC, directive on traditional herbal medicinal products. Brussels: European Parliament and Council; 2004. p. 85-90.
403. Alliance for natural health E. Consumers kept in the dark as EU directive looks set to ban majority of high street herbal remedies. 2012 [cited 2012 24th of March]; Available from: http://www.anh-europe.org/news/anh-intl-press-release-eu-herb- directive-keeps-consumers-in-the-dark.
404. Barnes J, Anderson LA, Philipson JD. Herbal medicines: a guide for health-care professionals. London: Pharmaceutical Press; 1996.
405. British Herbal Medicine Association. British herbal pharmacopoeia. Surrey: BMHA Publishing; 1996.
406. Bonnard M. Saw palmetto. The viagra alternative: the complete guide to overcoming erectile dysfunction naturally. Rochester, Vermont: Inner Traditions / Bear & Co; 1999. p. 102.
407. Stark R. Saw palmetto. The book of aphrodisiacs: Methuen Publications; 1999. p.84.
408. Hellstrom WJ. Benign prostatic hyperplasia, sexual function, and overall evaluation of the male patient. J Am Osteopath Assoc. 2004; 104(2 ):5-10.
Ar .dv SutC! 208

Litem turc
409. Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH). Eur Urol. 2005;47(6):824-37.
410. Makinen Jl, Perheentupa A, Raitakari 01, Koskenvuo M, Pollanen P, Makinen J, et al. Sexual symptoms in aging men indicate poor life satisfaction and increased health service consumption. Urology. 2007;70(6):1194-9.
411. Rosen R, Altwein J, Boyle P, Kirby RS, Lukacs B, Meuleman E, et al. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol. 2003;44(6):637-49.
412. Braun MH, Sommer F, Haupt G, Mathers MJ, Reifenrath B, Engelmann UN. Lower urinary tract symptoms and erectile dysfunction: co-morbidity or typical "Aging Male" symptoms? Results of the "Cologne Male Survey". Eur Urol. 2003;44(5):588-94.
413. Boyle P, Robertson C, Mazzetta C, Keech M, Hobbs R, Fourcade R, et al. The association between lower urinary tract symptoms and erectile dysfunction in four centres: the UrEpik study. BJU Int. 2003;92(7):719-25.
414. Martin-Morales A, Sanchez-Cruz JJ, Saenz de Tejada I, Rodriguez-Vela L, Jimenez- Cruz JF, Burgos-Rodriguez R. Prevalence and independent risk factors for erectile dysfunction in Spain: results of the Epidemiologia de la Disfuncion Erectil Masculina Study. J Urol. 2001;166(2):569-74; discussion 74-5.
415. Nicolosi A, Moreira ED, Jr., Shirai M, Bin Mohd Tambi Ml, Glasser DB. Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Urology. 2003;61(l):201-6.
416. Medina JJ, Parra RO, Moore RG. Benign prostatic hyperplasia (the aging prostate). Med Clin North Am. 1999;83(5):1213-29.
417. Reilly CM, Stopper VS, Mills TM. Androgens modulate the alpha-adrenergic responsiveness of vascular smooth muscle in the corpus cavernosum. J Androl. 1997;18(1):26-31.
418. Rudner XL, Berkowitz DE, Booth JV, Funk BL, Cozart KL, D'Amico EB, et al. Subtype specific regulation of human vascular alpha(l)-adrenergic receptors by vessel bed and age. Circulation. 1999;100(23):2336-43.
419. Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ Res. 2000;87(10):840-4.
420. Stief CG. Is there a common pathophysiology of erectile dysfunction and how does this relate to new pharmacotherapies? Int J Impôt Res. 2002; 14 SuppI l:S ll-6 .
421. Bloch W, Klotz T, Loch C, Schmidt G, Engelmann U, Addicks K. Distribution of nitric oxide synthase implies a regulation of circulation, smooth muscle tone, and secretory function in the human prostate by nitric oxide. Prostate. 1997;33(l):l-8.
422. Jackson G. The importance of risk factor reduction in erectile dysfunction. Curr Urol Rep. 2007;8(6):463-6.
AndySuter 209
/ . ÏF.' OTu'C
423. Vlachopoulos C, Rokkas K, loakeimidis N, Stefanadis C. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: common links. Eur Urol. 2007;52(6):1590-600.
424. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and itsmedical and psychosocial correlates: results of the Massachusetts Male AgingStudy. J Urol. 1994;151{1):54-61.
425. Bauman DR, Steckelbroeck S, Peehl DM, Penning TM. Transcript profiling of the androgen signal in normal prostate, benign prostatic hyperplasia, and prostate cancer. Endocrinology. 2006;147(12):5806-16.
426. Carbone DJ, Jr., Hodges S. Medical therapy for benign prostatic hyperplasia: sexualdysfunction and impact on quality of life. Int J Impôt Res. 2003;15(4):299-306.
427. Marks LS, Gittelman MG, Hill LA, Volinn W, Hoel G. Rapid efficacy of the highly selective alphalA-adrenoceptor antagonist silodosin in men with signs and symptoms of benign prostatic hyperplasia: pooled results of 2 phase 3 studies. J Urol. 2009;181(6):2634-40.
428. Erdemir F, Harbin A, Hellstrom WJ. 5-alpha reductase inhibitors and erectiledysfunction: the connection. J Sex Med. 2008;5(12):2917-24.
429. Naslund MJ, Miner M. A review of the clinical efficacy and safety of Salpha-reductase inhibitors for the enlarged prostate. Clin Then 2007;29(l):17-25.
430. Roehrborn CG, Siami P, Barkin J, Damiao R, Major-Walker K, Nandy I, et al. The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the CombAT study. Eur Urol. 2010;57(1):123-31.
431. Willetts KE, Clements MS, Champion S, Ehsman S, Eden JA. Serenoa repens extract for benign prostate hyperplasia: a randomized controlled trial. BJU Int. 2003;92(3):267-70.
432. Sinescu I, Geavlete P, Multescu R, Gangu C, Miclea F, Coman I, et al. Long-term efficacy of Serenoa repens treatment in patients with mild and moderate symptomatic benign prostatic hyperplasia. Urol Int. 2011;86(3):284-9.
433. Gerber GS, Kuznetsov D, Johnson BC, Burstein JD. Randomized, double-blind, placebo-controlled trial of saw palmetto in men with lower urinary tract symptoms. Urology. 2001;58(6):960-4; discussion 4-5.
434. Leungwattanakij S, Watanachote D, Noppakulsatit P, Petchpaibuol T, Choeypunt N, Tongbai T, et al. Sexuality and management of benign prostatic hyperplasia with alfuzosin: SAMBA Thailand. J Sex Med. 2010;7(9):3115-26.
435. Elhilali M, Emberton M, Matzkin H, van Moorselaar RJ, Hartung R, Harving N, et al. Long-term efficacy and safety of alfuzosin 10 mg once daily: a 2-year experience in 'real-life' practice. BJU Int. 2006;97(3):513-9.
436. Riedi E, Schoop R, Suter A. BPH natürlich behandeln. Ein Praxiserfahrungsbericht zu ProstaMed. Ars Medici. 2005;2:1-3.
Andy Sl'te r 210
L i t f r a t u ’ C
437. Madersbacher S, Haidinger G, TemmI C, Schmidbauer CP. Prevalence of lower urinary tract symptoms in Austria as assessed by an open survey of 2,096 men. Eur Urol. 1998;34(2):136-41.
438. Harrison D, Westhuis DJ. Rating scales for sexual adjustment. J Soc Ser Res. 1990;3(3):85-100.
439. DeRogatis LR. Assessment of sexual function/dysfunction via patient reported outcomes. Int J Impôt Res. 2008;20(l):35-44.
440. Masters WH, Johnson VE. Human Sexual Response. Toronto, New York: Bantam Books; 1966.
441. Masters WH, Johnson VE. Human Sexual Inadequacy. Toronto, New York: Bantam Books; 1970.
442. Kaplan HS. Disorders of sexual desire. New York: Brunner/Mazel; 1979.
443. Derogatis LR. The Derogatis Interview for Sexual Functioning (DISF/DISF-SR): an introductory report. J Sex Marital Ther. 1997;23(4):291-304.
444. McGahuey CA, Gelenberg AJ, Laukes CA, Moreno FA, Delgado PL, McKnight KM, et al. The Arizona sexual experience scale (ASEX): reliability and validity. J Sex Marital Ther. 2000;26(l):25-40.
445. Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49(6):822-30.
446. Lukacs B, Comet D, Grange JC, Thibault P. Construction and validation of a short- form benign prostatic hypertrophy health-related quality-of-life questionnaire. BPH Group in General Practice. Br J Urol. 1997;80(5):722-30.
447. O'Leary MP. Quality of life and sexuality: methodological aspects. Eur Urol. 2001;40 SuppI 3:13-8.
448. Lukacs B, Grange JC, Comet D. One-year follow-up of 2829 patients with moderate to severe lower urinary tract symptoms treated with alfuzosin in general practice according to IPSS and a health-related quality-of-life questionnaire. BPM Group in General Practice. Urology. 2000;55(4):540-6.
449. O'Leary MP, Rhodes T, Girman CJ, Jacobson DJ, Roberts RO, Lieber MM, et al. Distribution of the brief male sexual inventory in community men. Int J Impôt Res. 2003;15(3):185-91.
450. Mykletun A, Dahl AA, O'Leary MP, Fossa SD. Assessment of male sexual function by the brief sexual function inventory. BJU Int. 2006;97{2):316-23.
451. World Health Organisation WHO. International statistical classification of diseases and related health problems. Geneval992.
452. International Conference on Harmonisation ICH. International conference on harmonisation of technical requirements for registration of pharmaceuticals for human use. ICH tripartite guideline. Guideline for Good Clinical Practice E6(R1). 1996 [cited 2012 12th of January]; Available from: http://www.ich.org/LOB/media/MEDIA482.pdf.
211

L i terature
453. Schweizerische Eidgenosenschaft. SR 812.214.2, Verordnung vom 17. Oktober 2001 über klinische Versuche mit Heilmittein (VKlin). 2001.
454. The world medical association. The world medical association declaration ofHelsinki. Ethical principles for medical research involving human subjects. 59thWMA General Assembly, Seoul2008.
455. Suter A, Sailer R, Riedi E, Heinrich M. Improving BPH symptoms and sexual dysfunctions with a saw palmetto preparation? Results from a pilot trial. Phytother Res. 2012. DOI: 10.1002/ptr.4696
456. Sachs L. Angewandte Statistik. Berlin: Springer Verlag; 2004.
457. Boyle P, Robertson C, Lowe F, Roehrborn C. Updated meta-analysis of clinical trialsof Serenoa repens extract in the treatment of symptomatic benign prostatic hyperplasia. BJU Int. 2004;93(6):751-6.
458. Collins 5, Upshaw J, Rutchik S, Ohannessian C, Ortenberg J, Albertsen P. Effects of circumcision on male sexual function: debunking a myth? J Urol. 2002;167(5):2111- 2.
459. Hellstrom WJ, Kendirci M. Type 5 phosphodiesterase inhibitors: curing erectile dysfunction. Eur Urol. 2006;49(6):942-5.
460. Ehren I, Adolfsson J, Wiklund NP. Nitric oxide synthase activity in the human urogenital tract. Urol Res. 1994;22(5):287-90.
461. Mirone V, Sessa A, Giuliano F, Berges R, Kirby M, Moncada I. Current benign prostatic hyperplasia treatment: impact on sexual function and management of related sexual adverse events. Int J Clin Pract. 2011;65(9):1005-13.
462. Kami nets ky J. Comorbid LUTS and erectile dysfunction: optimizing their management. Curr Med Res Opin. 2006;22(12):2497-506.
463. Kim MK, Cheon J, Lee KS, Chung MK, Lee JY, Lee SW, et al. An open, noncomparative, multicentre study on the impact of alfuzosin on sexual function using the Male Sexual Health Questionnaire in patients with benign prostate hyperplasia. Int J Clin Pract. 2010;64(3):345-50.
464. van Moorselaar RJ, Hartung R, Emberton M, Harving N, Matzkin H, Elhilali M, et al. Alfuzosin 10 mg once daily improves sexual function in men with lower urinary tract symptoms and concomitant sexual dysfunction. BJU Int. 2005;95(4):603-8.
465. Seo DH, Kam SC, Hyun JS. Impact of lower urinary tract symptoms/benign prostatic hyperplasia treatment with tamsulosin and solifenacin combination therapy on erectile function. Korean J Urol. 2011;52(l):49-54.
466. van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. Efficacy and safety of a new prolonged release formulation of alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily and placebo in patients with symptomatic benign prostatic hyperplasia. ALFORTI Study Group. Eur Urol. 2000;37(3):306-13.
467. Nordling J. Efficacy and safety of two doses (10 and 15 mg) of alfuzosin or tamsulosin (0.4 mg) once daily for treating symptomatic benign prostatic hyperplasia. BJU Int. 2005;95(7):1006-12.
A n d y S u t e r 212

468. Debruyne F, Boyle P, Calais Da Silva F, Gillenwater JG, Hamdy FC, Perrin P, et al. Evaluation of the clinical benefit of permixon and tamsulosin in severe BPH patients-PERMAL study subset analysis. Eur Urol. 2004;45(6):773-9; disucssion 9-80.
469. Zlotta AR, Teillac P, Raynaud JP, Schulman CC. Evaluation of male sexual function in patients with lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) treated with a phytotherapeutic agent (Permixon), tamsulosin or finasteride. Eur Urol. 2005;48(2):269-76.
470. McVary KT, Monnig W, Camps JL, Jr., Young JM, Tseng U, van den Ende G. Sildenafil citrate improves erectile function and urinary symptoms in men with erectile dysfunction and lower urinary tract symptoms associated with benign prostatic hyperplasia: a randomized, double-blind trial. J Urol. 2007; 177(3): 1071-7.
471. Roehrborn CG, McVary KT, Elion-Mboussa A, Viktrup L. Tadalafil administered once daily for lower urinary tract symptoms secondary to benign prostatic hyperplasia: a dose finding study. J Urol. 2008;180(4):1228-34.
472. Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. A randomised, placebo-controlled study to assess the efficacy of twice-daily vardenafil in the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. Eur Urol. 2008;53(6):1236-44.
473. Kaplan SA, Gonzalez RR, Te AE. Combination of alfuzosin and sildenafil is superior to monotherapy in treating lower urinary tract symptoms and erectile dysfunction. Eur Urol. 2007;51(6):1717-23.
474. Tuncel A, Nalcacioglu V, Ener K, Aslan V, Aydin 0, Atan A. Sildenafil citrate and tamsulosin combination is not superior to monotherapy in treating lower urinary tract symptoms and erectile dysfunction. World J Urol. 2010;28(l):17-22.
475. Chung BH, Lee JY, Lee SH, Yoo SJ, Lee SW, Oh CY. Safety and efficacy of the simultaneous administration of udenafil and an alpha-blocker in men with erectile dysfunction concomitant with BPH/LUTS. Int J Impôt Res. 2009;21(2):122-8.
476. Stafford RS, Radley DC. The potential of pill splitting to achieve cost savings. Am J Manag Care. 2002;8(8):706-12.
477. Schneider D RF. Checkliste Arzneimittel. Stuttgart: Georg Thieme Verlag; 2008.
478. Roehrborn CG. Lower urinary tract symptoms, benign prostatic hyperplasia, erectile dysfunction, and phosphodiesterase-5 inhibitors. Rev Urol. 2004;6(3):121-7.
479. Gacci M, Eardley I, Giuliano F, Hatzichristou D, Kaplan SA, Maggi M, et al. Critical analysis of the relationship between sexual dysfunctions and lower urinary tract symptoms due to benign prostatic hyperplasia. Eur Urol. 2011;60(4):809-25.
480. Seftel A, Rosen R, Kuritzky L. Physician perceptions of sexual dysfunction related to benign prostatic hyperplasia (BPH) symptoms and sexual side effects related to BPH medications. Int J Impôt Res. 2007;19(4):386-92.
481. van Leeuwen JH, Castro R, Busse M, Bemelmans BL. The placebo effect in the pharmacologic treatment of patients with lower urinary tract symptoms. Eur Urol. 2006;50(3):440-52; discussion 53.
A n d ] ' S u t e r 213

Li t e<ot U! c
482. Campbell HE. Clinical monograph for drug formulary review: erectile dysfunction agents. J Manag Care Pharm. 2005;11(2):151-71.
483. Eardley I. Oral therapy for erectile dysfunction. Arch Esp Urol. 2010;63(8):703-14.
484. Gartlehner G, Hansen RA, Nissman D, Lohr KN, Carey TS. Criteria for distinguishing effectiveness from efficacy trials in systematic reviews. Rockville (MD)2006.
485. Stebler T. Viagra® (Sildenafil). Goldene Engel Apotheke Basel; 2009 [cited 2011 12nd of November]; Available from: http://www.engelapo.ch/medis/viagra.htm.
486. Wikipedia. Annual pharmaceutical drug sales. 2011 [cited 2012 19th of April]; Available from: http://en.wikipedia.org/wiki/Annual pharmaceutical drug sales.
487. Drugpatentwatch. Avodart. 2012 [cited 2012 19th of April]; Available from: http://www.drugpatentwatch.com/ultimate/preview/tradename/index.php7querv =AVODART.
488. Wilson RC. Drugs and pharmacy in the life of Georgia, 1733-1959. Athens, Georgia: University of Georgia Press; 2010.
489. Bauer R, Wagner H. Echinacea, Handbuch für Àrzte, Apotheker und andere Naturwissenschaftler. Stuttgart: Wissenschaftliche Verlagsgesellschaft mbH; 1990.
490. Buckalew LW, Ross S. Relationship of perceptual characteristics to efficacy of placebos. Psychol Rep. 1981;49(3):955-61.
491. Macpherson H. Pragmatic clinical trials. Complement Ther Med. 2004;12(2-3):136- 40.
492. U.S. Preventive Services Task Force. Guide to clinical preventive services: report of the U.S. preventive services task force: DIANE Publishing; 1989.
493. Jang DJ, Lee MS, Shin BC, Lee YC, Ernst E. Red ginseng for treating erectile dysfunction: a systematic review. Br J Clin Pharmacol. 2008;66(4):444-50.
494. Shin BC, Lee MS, Yang EJ, Lim HS, Ernst E. Maca (L. meyenii) for improving sexual function: a systematic review. BMC Complement Altern Med. 2010;10:44.
A n d y S u t e r 214

7 Appendix
7.1 Appendix 1
Data on reference samples for analytic investigations including sample number, country
of origin, brand name, producer, galenic form, tablet or capsule weight, amount of saw
palmetto per unit, daily dosage, drug extractant ratio DER, active constituents, and
batch numbers
Andy Suter 215
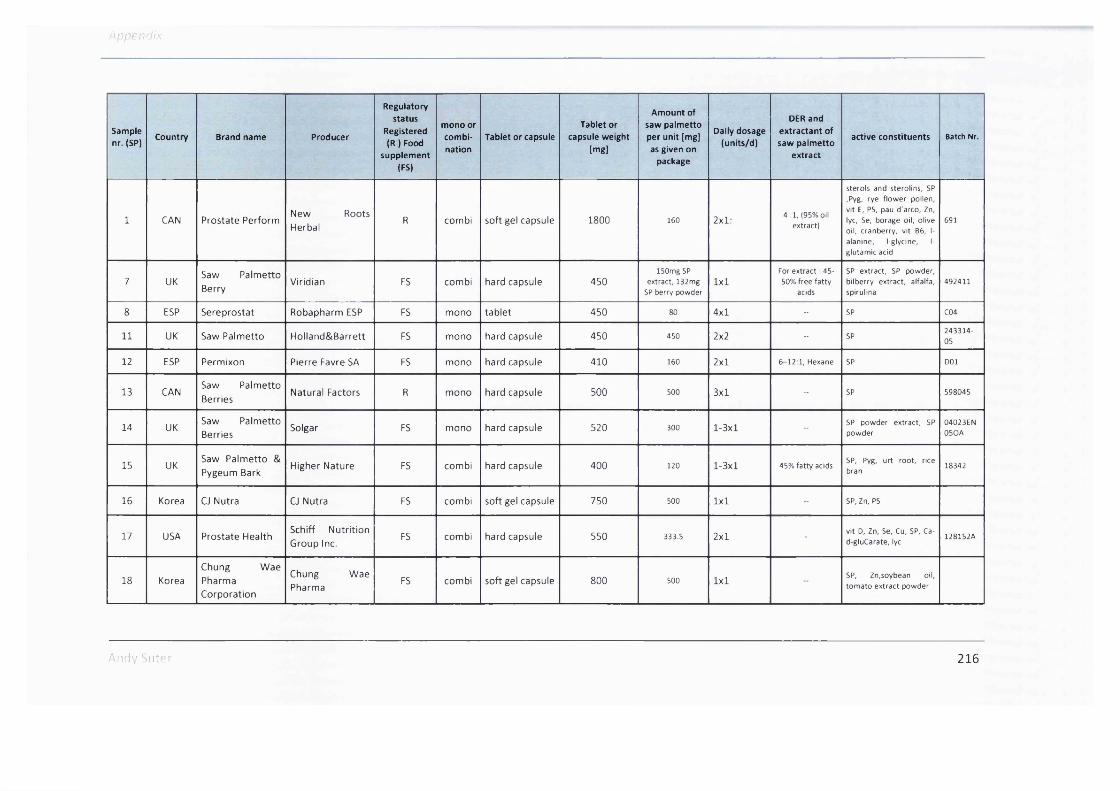
Appendix
Sample nr. (SP)
Country Brand name Producer
Regulatory status
Registered (R ) Food
supplement |FS)
mono or combination
Tablet or capsuleTablet or
capsule weight[mg]
Amount of saw palmetto per unit [mg] as given on
package
Daily dosage (units/d)
DER and extractant of saw palmetto
extract
active constituents Batch Nr.
1 CAN Prostate PerformNew Roots Herbal
R combi soft gel capsule 1800 160 2x1: 4 :1 , (95% oil extract)
sterols and sterolins, 5P ,Pyg, rye flower pollen, vit E, P5, pau d'arco, Zn, lyc, 5e, borage oil, olive oil, cranberry, vit 86, 1- alanine, l-glycine, 1- glutamic acid
691
7 UKSaw Palmetto Berry
Viridian FS combi hard capsule 450ISOmg SP
extract, 132mg SP berry powder
1x1For extract : 45- 50% free fatty
acids
5P extract, 5P powder, bilberry extract, alfalfa, spirulina
492411
8 ESP Sereprostat Robapharm ESP FS mono tablet 450 80 4x1 - 5P C04
11 UK Saw Palmetto Holland&Barrett FS mono hard capsule 450 450 2x2 - 5P243314-05
12 ESP Permixon Pierre Favre SA FS mono hard capsule 410 160 2x1 6-12:1 , Hexane 5P DOI
13 CANSaw Palmetto Berries
Natural Factors R mono hard capsule 500 500 3x1 - 5P 598045
14 UKSaw Palmetto Berries
Solgar FS mono hard capsule 520 300 1-3x1 -5P powder extract, 5P powder
04023EN05OA
15 UKSaw Palmetto & Pygeum Bark
Higher Nature FS combi hard capsule 400 120 1-3x1 45% fatty acids5P, Pyg, urt root, rice bran
18342
16 Korea CJ Nutra CJ Nutra FS combi soft gel capsule 750 500 1x1 - 5P, Zn, P5
17 USA Prostate HealthSchiff Nutrition Group Inc.
FS combi hard capsule 550 333.5 2x1 vit D, Zn, 5e, Cu, 5P, Ca- d-gluCarate, lyc
128152A
18 KoreaChung WaePharmaCorporation
Chung Wae Pharma
FS combi soft gel capsule 800 500 1x15P, Zn,soybean oil, tom ato extract powder
Andy Siitcr 216

Appendix
Sample nr. (SP)
Country Brand name Producer
Regulatory status
Registered (R ) Food
supplement (FS)
mono or combination
Tablet or capsuleTablet or
capsule weight [mg]
Amount of saw palmetto per unit [mg] as given on
package
Daily dosage (units/d)
DER and extractant of saw palmetto
extract
active constituents Batch Nr.
19 CAN Frost - Force Prairie Naturals R combi soft gel capsule 1362 80 1-2x2 -vit B6, Zn, SP, Pyg, lyc, urt, PS, lecithin
20907146
20 USA Life ExtensionQualitySupplements and Vitamins Inc.
FS combi soft gel capsule 1800 160 2x1
CO2, Standardized to
85-95% fatty acids
SP, flower pollen extract, boswellia serrata extract, urt, Pyg, lyc, phytosterols, enterolactone,B, rosemary
2410110
21 NL Prostavit Forte Bional FS combi soft gel capsule 1400 160 1x1 -PS oil, urt, SP, Zn, Se, yeast, tomatoes extract, vitE
09E0404
22 ESP BiprostatDietéticos Intersa S.A.
FS combi hard capsule 365 365 2x1 -SP, PS, Pyg, bearberry, Zn, vit B6
9HE7
23 UKSaw Palmetto Complex
Natures aid FS combi tablet 1200 160 1-2x1 1 :10, 72mg fatty acids per tab!.
SP, PS211D0117
24 NLProstaFleur Extra Forte
BloemNatuurprodukte n Winschoten bv
FS combi hard capsule 500 40 2-3x1 4 :1SP, PS, Epilobium
p a rv iflo ru m , b-sit. Se, Zn, vit E, lyc
80S1447S
27 SW! Prostagutt UnoSchwabe Pharma AG
R mono soft gel capsule 500 320 1x110-14.3 :1,
ethanol 90% m /m
SP 1470S10
29 KoreaCJ Nutra Saw Palmetto
CJ Nutra FS mono soft gel capsule 500 320 1x1 - SP
30 SW! Prosta UrgeninMax Zeller AG
( Schwabe Pharma AG)
R mono soft gel capsule 480 320 1x1 8-9.52 :1, ethanol 90% V /V
SPB090168S
31 SW! SabCaps Vifor SA R mono soft gel capsule 480 320 1x1 9 -1 1 :1, ethanol 96% V /V
SP6S4760100
ndy Suter 217

Sample nr. (SP)
Country Brand name Producer
Regulatory status
Registered (R I Food
supplement (FS)
mono or combination
Tablet or capsuleTablet or
capsule weight [mg]
Amount of saw palmetto per unit [mg] as given on
package
Daily dosage (units/d)
DER and extractant of saw palmetto
extract
active constituents Batch Nr.
32 KoreaChong Kun Dang HealthSaw Palmetto
Chong Kun Dang Health
FS mono soft gel capsule soo 320 1x1 - 5P
33 FIN Curbisal Pharbio R mono soft gel capsule 480 320 1x1 9 -1 1 :1, ethanol 5P 220181
34 USASaw Palmetto Extract
Now Foods FS mono soft gel capsule 600 160 1x2standardized to
85-95% fatty acids
5P12147060239
35 SWI ProstasanA. Vogel Bioforce AG
R mono soft gel capsule 48S 320 1x19 ,0 -12 ,0 :1 ,
ethanol 96% (V/V).
SP L030S618
36 SW! Prostadyn Dr. Diinner AG R mono soft gel capsule 260 160 2x110-14 :1, ethanol
90% m /mSP E090276
37 CAN Saw PalmettoSwiss Herbal Remedies Ltd
R mono soft gel capsule 400 80 2x110:1 extract,
85%-95% fatty acids
SP 34426
38 NL Prostaat Phital FS combi tablet 14S0 100 2x1 -
lyc, Pyg, phytosterols, urt, SP, provit A, vit A, vit E, 81, vit 82, vit 83, vit 85, vit 86, vit 88, vit 811, vit 812, vit C, vit D3, vit K, choline, inositol, paba, lutein, b- sit, Ca, Cr, Fe, 1, Na, Cu, Mg, Mn, Se, Mo, Se, Si, Zn, g rap e seed, ginseng, ginkgo b ilo b a , green tea
07J08C
40 SWI Prostagutt FSchwabe Pharma AG
R combi soft gel capsule 67S 160 2x110-14.3 :1,
ethanol 90% m /m
SP, urt 6760910
41 NL ProstalifeBloemNatuurprodukte n Winschoten bv
FS combi hard capsule SSO 320 2-3x1 4 :1SP, urt root, Epim ed ium ,
M u ira p u a m a , b-sit. Se, Zn, vit 86, vit E, lyc
91019829
!y Sut" : 218

Appendix
Sample nr. (SP)
Country Brand name Producer
Regulatory status
Registered (R ) Food
supplement (FS)
mono or combination
Tablet or capsuleTablet or
capsule weight [mg]
Amount of saw palmetto per unit [mg] as given on
package
Daily dosage (units/d)
DER and extractant of saw palmetto
extract
active constituents Batch Nr.
42 NL Prosta TotaalDistributie care bv
FS combi tablet 1450 100 1-2x1
lyc, Pyg, phytosterols, urt, 5P, provit A, vit A, vit E, 81, vit 82, vit 83, vit 85, vit 86, vit 88, vit 811, vit 812, vit C, vit D3, vit K, choline, inositol, paba, lutein, b- sit, Ca, Cr, Fe, 1, Na, Cu, Mg, Mn, 5e, Mo, 5e, 5i, Zn, g ra p e seed, ginseng,
ginkgo b iloba, green tea
08818E
43 NL Prostalan Forte VSM FS combi soft gel capsule 666 160 2x1 -SP, urt, saturated fatty acids
71221
44 NL Prostavit Bional FS combi soft gel capsule 1400 2.5 1-3x1SP, PS oil, urt, echinacea pallida, b-sit. Mg, vit E, Zn
0910202
45 CAN Saw Palmetto Homeocan R mono hard capsule 350 350 04. Jun12:1,
standardised to 25% fatty acids
5P 0 0034
46 UK Prostavital Health Aid FS combi soft gel capsule 2000 30 1x1 12 :1
vit E, vit C, vit 86, Mg, Zn, Cr, Cu, Se, lyc, 1- alanine, l-glutamic acid, wheat germ oil, PS oil, lecithin, urt, SP, Pyg
710
47 USASaw Palmetto & Pygeum Extract
Country Life FS combi soft gel capsule 600 160 2x1
9 :1 , standardised to
45% fatty acids=72mg/caps
SP, Pyg, plant sterol complex, soy phosphatides (soy lecithin), lipase
10A996A
48 CANSaw Palmetto & Pygeum
PreferredNutrition
R combi soft gel capsule 1800 80 2-4x1 85% fatty acids
b-sit, PS oil, flower pollen extract, SP, urt, Pyg, Zn, hydrangea root, lyc, Cu SP
616880
49 USA ProstActiveNature's Way
(Schwabe Pharma AG)
FS mono soft gel capsule 480 320 1x1 12:01SP, Se, probiotic nutrients, green tea , PS, ginger, urt, rosemary
589696
50 USA Prostate 5LX New Chapter Inc. FS combi soft gel capsule 750 160 2x1 Supercritical extract, 136mg
SP, Se, probiotic nutrients, green tea , PS,
40503009A
Andy Siit'-r 219
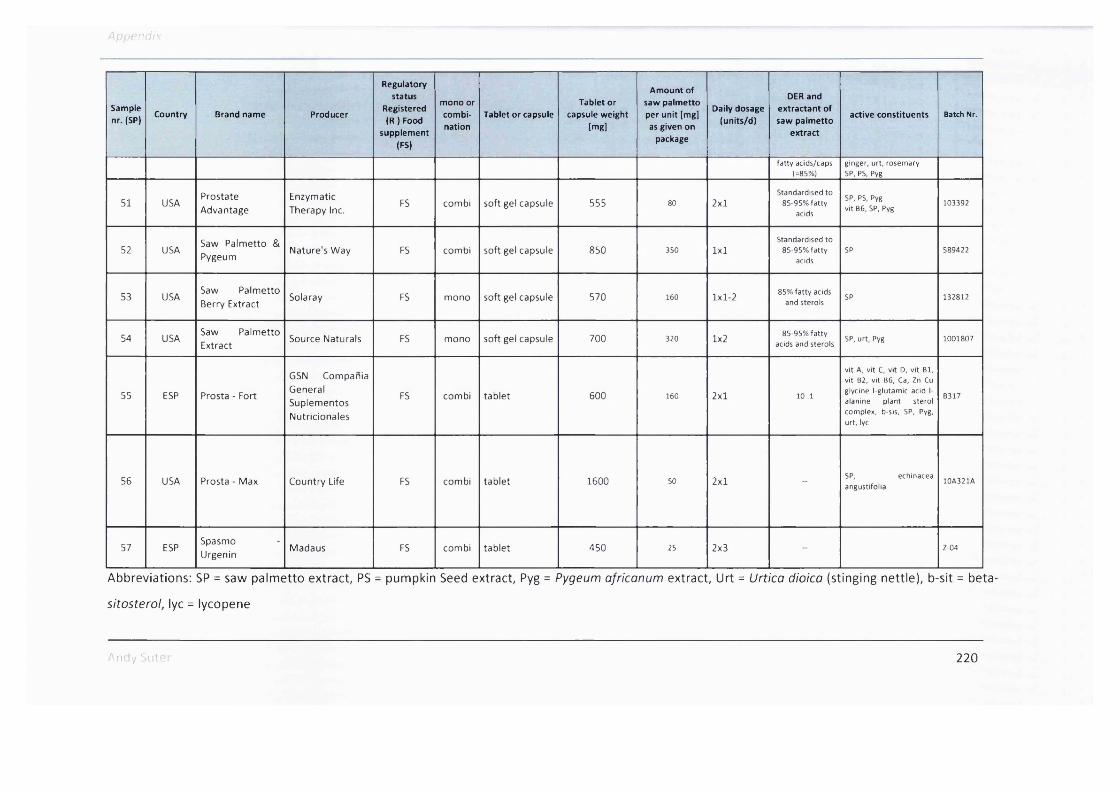
Appendix
Sample nr. (SP)
Country Brand name Producer
Regulatory status
Registered (R I Food
supplement (FS)
mono or combination
Tablet or capsuleTablet or
capsule weight [mg]
Amount of saw palmetto per unit [mg] as given on
package
Daily dosage (units/d)
DER and extractant of saw palmetto
extract
active constituents Batch Nr.
fatty acids/caps (=85%)
ginger, urt, rosemary SP, P5, Pyg
51 USAProstateAdvantage
Enzymatic Therapy Inc.
FS combi soft gel capsule 555 80 2x1Standardised to
85-95% fatty acids
SP, PS, Pyg vit 86, 5P, Pyg
103392
52 USASaw Palmetto & Pygeum
Nature's Way FS combi soft gel capsule 850 350 1x1Standardised to
85-95% fatty acids
5P 589422
53 USASaw Palmetto Berry Extract
Solaray FS mono soft gel capsule 570 160 1x1-2 85% fatty acids and sterols
SP 132812
54 USASaw Palmetto Extract
Source Naturals FS mono soft gel capsule 700 320 1x285-95% fatty
acids and sterolsSP, urt, Pyg 1001807
55 ESP Prosta - Fort
GSN Compania General Suplementos Nutricionales
FS combi tablet 600 160 2x1 10 ;1
vit A, vit C, vit D, vit 81, vit 82, vit 86, Ca, Zn Cu glycine l-glutamic acid 1- alanine plant sterol complex, b-sis, SP, Pyg, urt, lyc
8317
56 USA Prosta - Max Country Life FS combi tablet 1600 50 2x1SP, echinacea angustifolia
10A321A
57 ESPSpasmoUrgenin
Madaus FS combi tablet 450 25 2x3 Z-04
Abbreviations: SP = saw palmetto extract, PS = pumpkin Seed extract, Pyg = Pygeum ofricanum extract, Urt = Urtica dioica (stinging nettle), b-sit = beta-
sitosterol, lyc = lycopene
An ‘y '-L't- 2 2 0

7.2 Appendix 2
Total fatty acid content per capsule or tablet of each tested preparation and of the single fatty acids lauric acid, capric acid, caprylic acid, myristic acid,
palmitic acid, linolenic acid, oleic/linoleic acid and stearic acid
Andy Suter 221

Appendix
Mono or
combin
ation
Brand name Producer Country SP Nr.
Total fatty
acid
[m g /ta b le t o r
capsule]
Lauric acid
[m g /ta b le t o r
capsule]
Caprylic acid
[m g /ta b le t o r
capsule]
Capric acid
[m g /ta b le t o r
capsule]
Myristic
acid
[m g /ta b le t o r
capsule]
Palmitic acid
[m g /ta b le t o r
capsule]
Linolenic
acid
[m g /ta b le t o r
capsule]
Oleic+/
Linoleic acid
[m g /ta b le t o r
capsule]
Stearic acid
[m g /ta b le t o r
capsule]
m o n oSaw Palmetto
ExtractSource
Naturals Inc.USA SP 5 4 4 4 4 .3 1 9 7 .7 8 7 .8 8 7 .0 5 3 9 .1 5 4 6 .9 9 2 1 .2 1 2 1 2 .9 6 1 1 .2 7
m o n o Curbisal Pharbio F in land S P 3 3 2 9 0 .2 4 9 2 .9 4 6 8 .6 1 34 2 7 .6 2 6 .6 7 8 9 .6 4 .8
m o n oSawpalmetto
Mono Product 2 (HFS)
Chong Kun
Dang HealthKorea SP32 2 7 1 .9 8 8 .1 6 6 .5 6 8 .2 1 3 3 .1 7 2 5 .2 5 14 .1 9 0 .0 2 6 .4 5
m o n o Prosta UrgeninM ax Zeller
Sohne AGS w itzerlan d S P 3 0 2 7 1 .8 2 8 7 .4 1 5 .7 8 7 .7 6 3 3 .5 7 2 5 .4 7 1 4 .1 9 2 .5 3 5 .2
m o n o Prostagutt UnoSchwabe
Phram a AGS w itzerlan d S P 2 7 2 7 4 .5 3 8 4 .4 2 4 .6 4 5 .6 3 6 .6 4 2 7 .1 5 9 .6 1 0 1 .9 7 4 .5 1
m o n o Prostasan Bioforce S w itzerlan d S P 3 5 2 8 1 .3 4 8 3 .0 1 5 .7 4 .7 3 8 .1 2 8 .1 1 7 .5 1 1 0 .4 3 .8 7
m o n o ProstActive Nature 's W ay USA S P 4 9 2 8 5 .6 8 8 1 .3 6 4 .8 6 5 .6 3 6 .0 2 2 8 .3 5 1 3 .3 6 1 1 1 .5 7 4 .5 8
m o n o SabCaps V ifo r SA S w itzerlan d S P 3 1 2 7 4 .4 5 8 1 .2 5 5 .0 6 7 .1 4 3 0 .8 6 2 7 .1 2 2 8 .2 7 8 9 .3 4 5 .4 1
m o n oSawpalmetto
Mono Product 1 (HFS)
CJ Nutra Korea SP 29 2 3 7 .7 4 7 9 .8 1 5 .3 9 7 .1 4 2 9 .9 8 2 2 .5 9 1 2 .1 6 7 5 .3 1 5 .3 9
m o n oSaw Palmetto
ExtractN ow Foods USA S P 3 4 3 7 8 .2 6 6 .4 5 4 .3 6 .0 4 2 3 .4 8 3 6 .7 5 2 0 .9 9 2 1 1 .3 5 8 .8 3
m o n oSaw Palmetto Berry Extract
Solaray USA S P 5 3 3 5 4 .6 1 5 7 .8 3 3 .8 9 4 .4 9 2 3 .2 3 5 .3 4 2 3 .3 7 1 9 8 .7 5 7 .7 5
m o n o SereoprostatRobapharm
Espana S.A.Spain S P 8 3 6 8 .3 5 0 .2 1 .9 4 4 .3 7 1 4 .3 8 1 9 .0 4 3 3 .8 2 2 4 0 .1 2 4 .4 8
m o n o ProstadynDr. D iinner
AGS w itzerlan d SP 3 6 1 5 1 .5 6 4 5 .9 7 3 .1 1 4 .0 7 1 7 .8 5 1 4 .8 1 1 2 .7 6 5 0 .4 1 2 .5 8
Andy Suter 222

Aro ! -/
Mono or
combin
ation
Brand name Producer Country SP Nr.
Total fatty
acid
[m g /ta b le t o r
capsule]
Lauric acid
[m g /ta b le t o r
capsule]
Caprylic acid
[m g /ta b le t o r
capsule]
Capric acid
[m g /ta b le t o r
capsule]
Myristic
acid
[m g /ta b le t o r
capsule]
Palmitic acid
[m g /ta b le t o r
capsule]
Linolenic
acid
[m g /ta b le t o r
capsule]
Oleic+/
Linoleic acid
(m g /ta b le t o r
capsule]
Stearic acid
[m g /ta b le t o r
capsule]
m o n o Saw PalmettoSwiss Herbal Rem edies Ltd
C anada S P 3 7 2 S 3 .0 6 2S .94 2 .9 7 2 .8 lO.OS 2 S .7 9 9 6 .9 4 7 9 .1 3 9 .4S
m o n oSaw Palmetto
BerriesNaturalFactors
C anada S P 1 3 S 6.8 17.9S 0 .9 l.S S 6 .6 8 S .7 8 3 .6 3 1 8 .0 3 2 .2S
m o n o PermixonPierre Fabre
Iberica S.A.Spain SP 12 S S.68 1 7 .8 4 1 .11 1 .4 4 7 .2 2 S .37 2 .3 4 1 9 .4 8 0 .9 4
m o n o Saw PalmettoHolland &
BarretUK SP 11 4 4 .S 7 I S . 17 0 .S 4 1 .1 7 S .S 6 4 .4 1 3 .2 13.SS 0 .9 S
m o n o Saw Palmetto Hom eocan C anada SP 4 5 S l.O l 1 3 .2 1 0 .8 9 1 .S9 4.S 3 6 .4 6 2 .6 4 IS .O S 6 .6
m o n oSaw Palmetto
Berries
Solgar
V itam in and Herb
UK SP 14 34.S 1 1 .9 6 0 .6 0 .9 6 4.S 4 .6 3 1 .2 8 .S 8 2 .1 1
com bi Life ExtensionQuality
Supplements and Vitamins
USA SP 20 402 .S S S .94 6 .7 7 S 8 .9 8 2 1 .2 1 4 4 .4 9 1 4 0 .3 1 0 9 .3 6 IS .S
com bi Prost - ForcePrairie
NaturalsC anada SP 19 S 86.S1 6.S 2 6 .3 4 2 4 .4 1 9.7S 6 8 .7 3 2 1 7 .9 2 2 2 S .7 4 2 7 .0 1
com bi Prosta - FortGSN Compania
General Suplementos
Spain SPS S 1 7 6 .3 1 2 .0 1 4 .8 4 6 .6 2 1 4 .8 2 1 1 .6 1 1 0 .7 1 80.SS S .16
com bi Prosta - Max Country Life USA S P S 6 4 4 .8 8 0 0 0 .1 6 0 .4 2 S .6 8 0 .8 8 0 .7 2 1 7 .0 4
com bi Prosta TotaalD istributie
care bvN e th e rla n d SP 4 2 S 9 .2 3 0 .7 3 0 .7 3 6 .0 2 2 .6 8 1 4 .2 8 1 .3 1 7 .1 8 2 6 .3 2
com bi Prostaat Phital N e th e rla n d SP 38 S 2 .9 3 O .S l 0 .S 8 4 .2 1 1 .8 9 1 6 .1 7 0 .S 8 4 .4 2 24.S 1
com biProstaFleur Extra
Forte
Bloem
N atuurprodukten
N e th e rla n d SP 24 2 8 .6 3 0 .3 3 0 .S 3 7.4S 2 .6 8 3 .1 8 S .18 8 .S 3 0 .7 S
com bi Prostalan Forte VSM N e th e rla n d S P 4 3 2 3 9 .3 3 1 .0 6 2 2 .6 7 3 8 .6 3 17.S 4 3 3 .3 6 S.S3 4 6 .8 4 3 .6 8
ndv Su'T 223
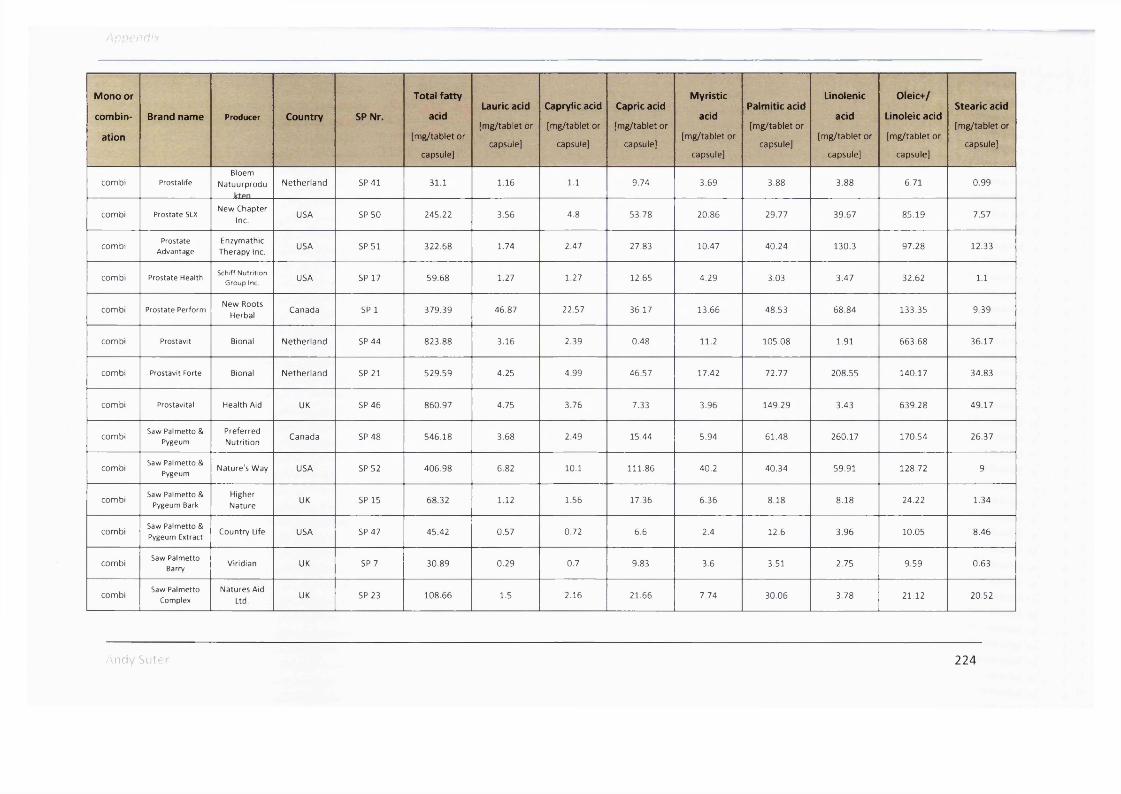
App en d i x
Mono or
combin
ation
Brand name Producer Country SP Nr.
Total fatty
acid
[m g /ta b le t o r
capsule]
Lauric acid
[m g /ta b le t or
capsule]
Caprylic acid
[m g /ta b le t or
capsule]
Capric acid
[m g /ta b le t o r
capsule]
Myristic
acid
[m g /ta b le t o r
capsule]
Palmitic acid
[m g /ta b le t o r
capsule]
Linolenic
acid
(m g /ta b le t o r
capsule]
Oleic+/
Linoleic acid
(m g /ta b le t o r
capsule]
Stearic acid
[m g /ta b le t o r
capsule]
com bi ProstalifeBloem
N atuurprodu N e th e rla n d S P 4 1 3 1 .1 1 .1 6 1 .1 9 .7 4 3 .6 9 3 .8 8 3 .8 8 6 .7 1 0 .9 9
com bi Prostate 5LXN ew Chapter
Inc.USA SP 5 0 2 4 5 .2 2 3 .5 6 4 .8 5 3 .7 8 2 0 .8 6 2 9 .7 7 3 9 .6 7 8 5 .1 9 7 .5 7
com biProstate
AdvantageEnzym athic
Therapy Inc.USA S P 5 1 3 2 2 .6 8 1 .7 4 2 .4 7 2 7 .8 3 1 0 .4 7 4 0 .2 4 1 3 0 .3 9 7 .2 8 1 2 .3 3
com bi Prostate HealthSchiff Nutrition
Group Inc. USA SP 17 5 9 .6 8 1 .2 7 1 .2 7 1 2 .6 5 4 .2 9 3 .0 3 3 .4 7 3 2 .6 2 1.1
com bi Prostate PerformN ew Roots
HerbalC anada SP 1 3 7 9 .3 9 4 6 .8 7 2 2 .5 7 3 6 .1 7 1 3 .6 6 4 8 .5 3 6 8 .8 4 1 3 3 .3 5 9 .3 9
com bi Prostavit Bional N e th e rla n d SP 4 4 8 2 3 .8 8 3 .1 6 2 .3 9 0 .4 8 1 1 .2 1 0 5 .0 8 1 .9 1 6 6 3 .6 8 3 6 .1 7
com bi Prostavit Forte Bional N e th e rla n d SP 21 5 2 9 .5 9 4 .2 5 4 .9 9 4 6 .5 7 1 7 .4 2 7 2 .7 7 2 0 8 .5 5 1 4 0 .1 7 3 4 .8 3
com bi Prostavital Health Aid UK SP 4 6 8 6 0 .9 7 4 .7 5 3 .7 6 7 .3 3 3 .9 6 1 4 9 .2 9 3 .4 3 6 3 9 .2 8 4 9 .1 7
com biSaw Palmetto &
PygeumPreferredN utrition
C anada SP 4 8 5 4 6 .1 8 3 .6 8 2 .4 9 1 5 .4 4 5 .9 4 6 1 .4 8 2 6 0 .1 7 1 7 0 .5 4 2 6 .3 7
com biSaw Palmetto &
PygeumNature 's W ay USA S P 5 2 4 0 6 .9 8 6 .8 2 10 .1 1 1 1 .8 6 4 0 .2 4 0 .3 4 5 9 .9 1 1 2 8 .7 2 9
com biSaw Palmetto &
Pygeum BarkHigher
N atureUK SP 15 6 8 .3 2 1 .1 2 1 .5 6 1 7 .3 6 6 .3 6 8 .1 8 8 .1 8 2 4 .2 2 1 .3 4
com biSaw Palmetto & Pygeum Extract
Country Life USA SP 4 7 4 5 .4 2 0 .5 7 0 .7 2 6 .6 2 .4 1 2 .6 3 .9 6 1 0 .0 5 8 .4 6
com biSaw Palmetto
BarryViridian UK S P 7 3 0 .8 9 0 .2 9 0 .7 9 .8 3 3 .6 3 .5 1 2 .7 5 9 .5 9 0 .6 3
com biSaw Palmetto
ComplexNatures Aid
Ltd.UK S P 2 3 1 0 8 .6 6 1 .5 2 .1 6 2 1 .6 6 7 .7 4 3 0 .0 6 3 .7 8 2 1 .1 2 2 0 .5 2
Andy Sutrr 224

Appi ndix
Mono or
combin
ation
Brand name Producer Country SP Nr.
Total fatty
acid
[mg/tablet or
capsule]
Laurie acid
[mg/tablet or
capsule]
Caprylic acid
[mg/tablet or
capsule]
Capric acid
[mg/tablet or
capsule]
Myristic
acid
(mg/tablet or
capsule]
Palmitic acid
[mg/tablet or
capsule]
Linolenic
acid
[mg/tablet or
capsule]
Olelc+/
Linoleic acid
[mg/tablet or
capsule]
Stearic acid
(mg/tablet or
capsule]
c om biSawpatmetto Combination
Product 1 (HFS)CJ Nutra Korea SP 16 4 0 1 .8 7 8 .0 9 8 .9 3 8 7 .4 4 3 3 .7 8 4 1 .9 6 6 .2 1 1 4 0 .4 1 1 5 .0 5
c om biSawpatmetto Combination
Product 2 (HFS)
Chung Wae Pharma
CorporationKorea SP 18 3 1 5 .4 5 6 .7 6 5 .5 4 5 4 .7 3 2 0 .4 9 3 1 .2 3 8 1 .1 5 1 0 3 .9 9 1 1 .5 1
c om bi Prostagutt FSchwabe
Phram a AGSwitzerlancJ SP 27 2 6 5 .5 9 3 8 .1 3 2 5 .2 9 4 3 .5 7 1 9 .2 7 3 6 .6 2 5 .6 2 4 8 .7 7 4 8 .3 2
c om biSpasmo - Urgenin
IVladaus Spain S P 5 7 1 .3 9 0 0 .0 2 0 .2 9 0 .0 9 0 .2 3 0 .0 9 0 .4 7 0 .2
Andy buter 225

7.3 Appendix 3
Chromatograms of GC analytic of each investigated preparation from chapter 2
And /S u te r 226
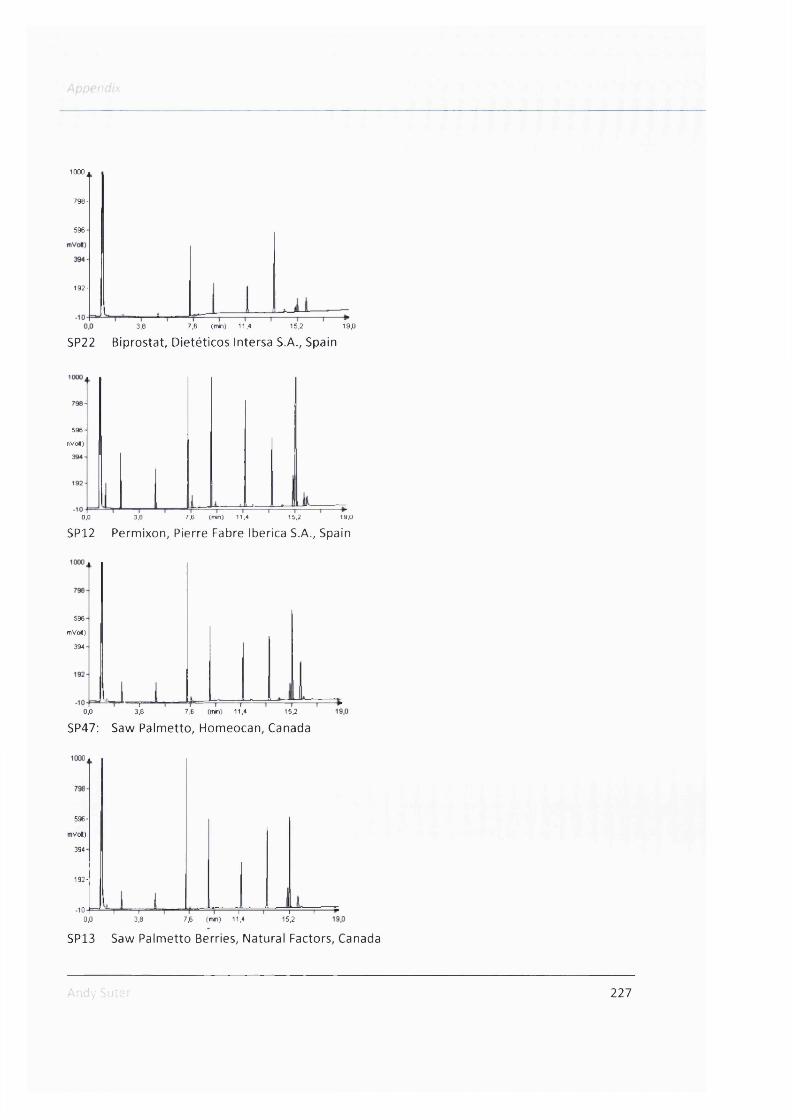
1000
798-
596
192-
3,8 7,6 (min) 11,4 15,2 19,0
SP22 Biprostat, Dietéticos Intersa S.A., Spain
596
nVo«)
15,20,0 3,8 7,6 (mm) 11,4 19,0
SP12 Permixon, Pierre Fabre Iberica S.A., Spain
596
mVoK)
394
- r -0,0 3,8 7,6 (min) 11,4 15,2
SP47: Saw Palmetto, Homeocan, Canada
596-
mVol)
394
192-
-100,0
I ‘ I 3,8
1----------1----------1----------r15,27,6 (min) 11,4
SP13 Saw Palmetto Berries, Natural Factors, Canada
'■ - .^y Sul. 227

Appendix
596
nVoH)
394-1
Ja-0,0 3,8 7,6 (tnin) 11,4 15,2 19,0
S P ll Saw Palmetto, Holland & Barret, UK
596
mVol)
394
0,0=F
3,8 7,6 (min) 11,4 15,2 19,0
SP15 Saw Palmetto & Pygeum Bark, Higher Nature, UK
596
mVol)
394-
.10-t=J =*Tl----1 * 1 ' »‘l"“0,0 3,8 7,6 (mh) 11,4 15,2
SP7 Saw Palmetto Berry, Viridian, UK19,0
596-
nVo«)
394-
0,0J___ L
3,8 7,6 (min) 11,4 15,2 19,0
SP14 Saw Palmetto Berries, Solgar Vitamin and Herb, UK
Andy Suter 228

•P/
mVoft)
1.0,0 3,8 7,6 (min) 11,4 15,2 19,0
SP41 Prostaiife, Bloem Natuurprodukten Winschoten bv, Netherland
1 0 0 0 a
596-
nVolt)
394-1
0,0— t—
3,8 7.6 (min) 11,4 15,2 19,0
SP24 ProstaFleur Extra Forte, Bloem Natuurprodukten Winschoten bv, Netherland
1000
798
596
iVol)
394-
192
-107,6 (min) 11,4 15,2 19,00,0 3,8
SP17 Prostate Health, Schiff Nutrition Group, USA
596
;mVol)
394
Li0,0
i .3,8 7,6 (min) 11,4 15,2 19,0
SP47 Saw Palmetto & Pygeum Extract, Country Life, USA
Andv Su:6! 229

1000^
798
596-
mVolt)
394
-100,0 3,8 7,6 (min) 11,4 15,2 19,0
SP55 Prosta - Fort, GSN Compania General Suplementos Nutricionales, Spain
1000
795
590
385
180
-253,8 7,8 (min) 11,4 15,2 19,00,0
SP8 Sereprostat, Robapharm Espana S.A., Spain
1000 a
798-
596
nVo«)
394
-100,0
■| ' I 3,8
I I---------------1---------------r7,6 (min) 11,4
Î ' I 15.2 19,0
SP57 Spasmo - Urgenin, Madaus, Spain
Andy Sut: 230

A p n r : . d :
596-
iVoK)
394-
4 : I ^0,0 3.8 7,8 (min) 11,4 18,2 19,0
SP23 Saw Palmetto Complex, Natures Aid Ltd. UK
596
mVo»)
394
L u0,0
SP42
—1—3,8 7,6 (min) 11,4 15,2 19,0
Prosta Totaal, Distributie care bv, Netherland
596
iVo«)
394
0,0 3,8 7,6 (min) 11,4
SP38 Prostaat, Phital, Netherland15,2 19,0
596
■nVoi)
394
0,0
SP56
-T-3,8 7,6 (min) 11,4 15,2
Prosta - Max, Country Life, USA19,0
Andy Suter 231
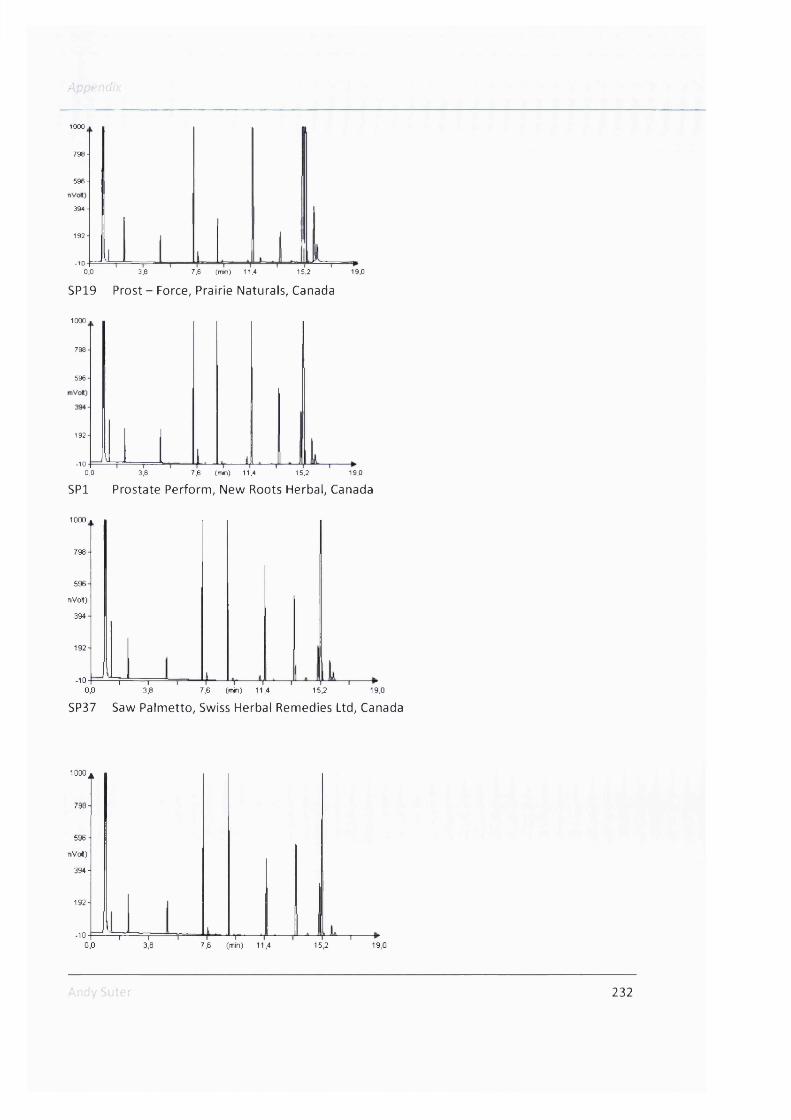
û n ; .-: Q
1000
798-
596-
394-
192-
-100,0 3,8 7,6 (tnin) 11,4 15,2 19,0
SP19 Prost - Force, Prairie Naturals, Canada
1000
798
596
192
-100,0 3,1,8 7,6 (min) 11,4 15,2 19,0
SPl Prostate Perform, New Roots Herbal, Canada
1000
798
596
nVolt)
394
192
-10 “1 r~0.0 3,8 7,6 (tnin) 11,4 15,2 19,0
SP37 Saw Palmetto, Swiss Herbal Remedies Ltd, Canada
1000^
798-
596 -
n V d )
394 -
192
-100,0
1 r3,8 7,6 (min) 11,4 15,2 19,0
232

SP48 Saw Palmetto & Pygeum, Preferred Nutrition, Canada
596-
nVolt)
394-
3,8 7,6 (min) 11,4 15,2 19 ,0
SP20 Life Extension, Quality Supplements and Vitamins Inc., USA
1 0 0 0 a
mVolt)
0,0 3,8 7,6 (tnin) 11,4 15,2
SP49 ProstActive, Nature's Way, USA
798-
596-
iVolt)
394-
0,0 3,8 7,6 (min) 11,4 15,2
SP50 Prostate 5LX, New Chapter Inc., USA19,0
Ar-' 233

Appendix
0,0 3,8 7,8 (min) 11,4 15,2 19,0
SP51 Prostate Advantage, Enzymatic Therapy Inc., USA
1 000.
596-
(mVo*)
394
f0,0 3,8 7,6 (min) 11,4 15,2 19,0
SP52 Saw Palmetto & Pygeum, Nature's Way, USA
596
mVo»)
394
-10 L L _ l0,0 3,8 7,6 (min) 11,4 15,2
SP53 Saw Palmetto Barry Extract, Solaray, USA
1000^
798
5961
nVo»)
394
-100,0 3,8 7,6 (min) 11,4
L15,2 19,0
Andy Suter 234

SP34 Saw Palmetto Extract, Now Foods, USA
798-
596-
(rnVoH)
394-
192-
0,01 r—
3,8 7,6 (min) 11,4 15,2 19,0
SP54 Saw Palmetto Extract, Source Naturals Inc., USA
1000
796-
596 -
(mVoK)
394-
J0.0 3.8 7,6 (min) 11,
SP33 Curbisal, Pharbio, Finland15,2 19,0
1000
798
596
;mVo»)
394
192
-100,0
-n—3,8
47,6 (min) 11,4 15,2 19,0
SP43 Prostalan Forte, VSM, Netherland
596-
(mVo«)
394-
0,0 3,8-V ^ — H7,6 (min) 11,4 15,2 19,0
235

ive'
SP44 Prostavit, Bional, Netherland
1000
798
596 4 (mVolt)
394 4
192
lJ0,0
I3,8 7,6 (min) 11,4 15,2
SP21 Prostavit Forte, Bional, Netherland
19,0
7981
598
mVol)
394
-10 —T"0,0 3,8 7,6 (min) 11,4
SP46 Prostavital, Health Aid, UK
15,2 19,0
798
596-
mVolt)
394
192-
-100,0 3,8 7,6 (mh) 11,4 15,2 19,0
SP16 Sawpalmetto Combination Product 1 (HFS), CJ Nutra, Korea
Andy Sutei 236
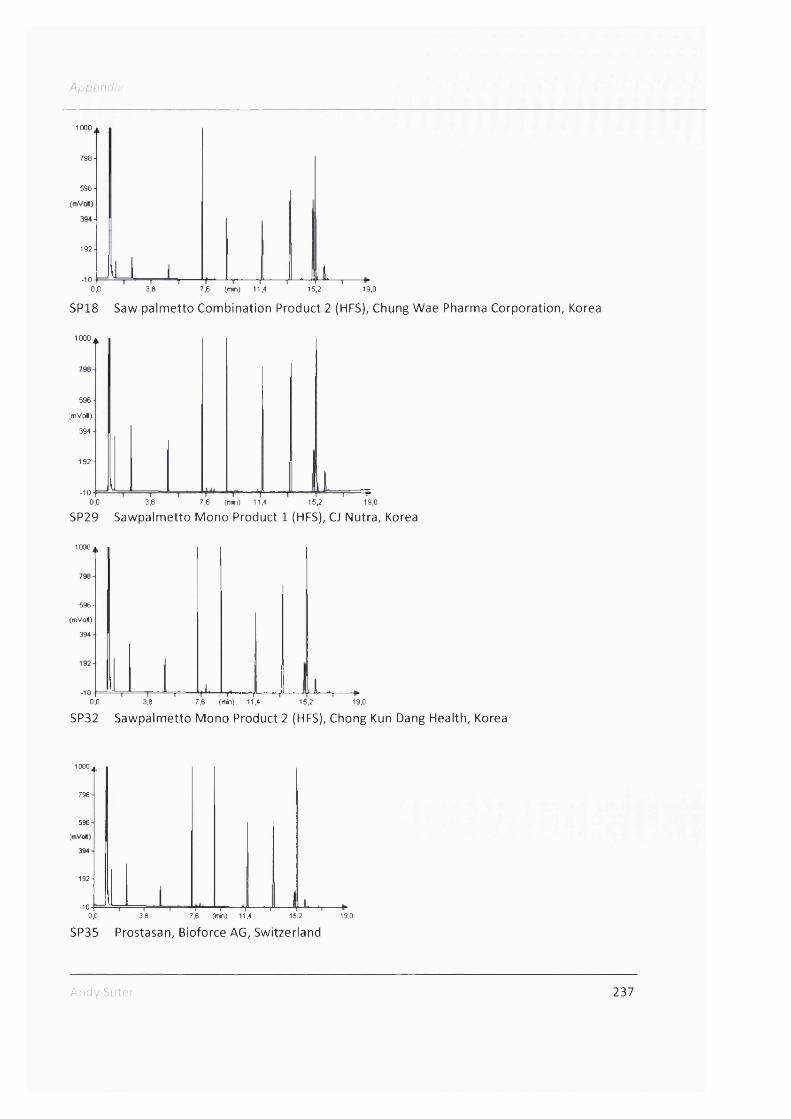
Appendix
1000
798-
596-
192-
-103,8 7,6 (min) 11,40,0 15.2 19,0
SP18 Saw palmetto Combination Product 2 (HFS), Chung Wae Pharma Corporation, Korea
1000 .
596 -
;mVo»)
394
1 92-
-100,0 3,8 7,6 (min) 11,4 15,2 19,0
SP29 Sawpalmetto Mono Product 1 (HFS), CJ Nutra, Korea
1000 *
596-
(mVo«)
394
0,0 3,8 7,6 (min) 11,4 15,2 19,0
SP32 Sawpalmetto Mono Product 2 (HFS), Chong Kun Dang Health, Korea
1000
798-
596
192-
-100,0 3,8 7,6 (tnin) 11,4 15,2 19,0
SP35 Prostasan, Bioforce AG, Switzerland
Andy Suter 237

5 3 0 -
(mVol)
385-
-25-0,0
SP30
-I 1--------------1--------------r3,8 7,6 (min) 11,4 15,2
Prosta Urgenin, Zeller, Switzerland19,0
590
(m V o l)
-250,0 3,8 7,6 (min) 11,4 15,2 19,0
SP31 SabCaps, Vifor, Switzerland
7 9 5 -
590-
180-
-250.0 3,8 7,6 Cmh) 11,4 15,2 19,0
SP27 Prostagutt Uno, Schwabe, Switzerland
795
590
(mva)
385 ■
180
0,0-| 1—
3,8 7,6 (min) 11,4— I---------- r
15,2
SP40 Prostagutt F, Schwabe, Switzerland
19,0
238

Anper
(mvol)
0,0 3,8 7,6 (min) 11,4 15,2
SP36 Prostadyn, Dr.Dünner, Switzerland19,0
Andy Suter 239

7.4 Publications
Publications
Suter A, Sailer R, Riedi E, Heinrich M. Improving BPH symptoms and sexual dysfunctions with a
saw palmetto preparation? Results from a pilot trial. Phytother Res. DOI: 10.1002/ptr.4696,
Published online, 23 * of April 2012
Poster presentations
Suter A, Sailer R, Heinrich M. A new View on Saw Palmetto - Results from an Analytical
Comparison and of a Clinical Pilot Trial. PhD Research Day, Internal Symposium at the School of
Pharmacy, 15.04.2011, London, United Kingdom.
Suter A, Sailer R, Riedi E, Heinrich M. Improving BPH symptoms and sexual dysfunctions with a
saw palmetto prepare
St. Petersburg, Russia.
saw palmetto preparation? XVI International Congress "PHYTOPHARM 2012" 9-11.07.2012,
Booker AJ, Zloh M, Said M, Suter A, Heinrich M. Metabolomic profiling of saw palmetto products
using proton-NMR spectroscopy and multi-variate analysis. 59 International Congress and
Annual Meeting of the Society for Medicinal Plant and Natural Product Research. 4-9.09.2011,
Antalya, Turkey.
Talks
Suter A, Sailer R, Riedi E, Heinrich M. The quality of different saw palmetto products on the
market and a pilot trial with saw palmetto in treatment of benign prostatic hyperplasia and
sexual dysfunctions. PhD Research Day, Internal Symposium at the School of Pharmacy,
29.09.2011, London, United Kingdom. Awarded with first price for best presentation.
Andy Suter 240