Superior intellectual ability in schizophrenia: Neuropsychological characteristics

Applied Ncurcpsychology2002, VoL 9, No. , 193-202
Copyright 2002 byLawrcocc Erlbaum Associates, Inc.
ARTICLES
Neuropsychological Performance of Patients Following Mold Exposure
Juliana v. BaldoVeterans Affairs Northern CalifornilJ Health Care System, Martinez. California, USA,
and San Francisco Clinical Neuroscknces, San Francisco, California, USA
Laeeq Ahmad and Ronald RuffSan Francisco Clinical Neuroscknces, San Francisco, California, USA
This study investigated the effects of mold exposure (ME) on human cognition by analyzingneurop.sychological data from patients who were exposed to mold in their homes or work-places. Compared to normative data, ME patients were impaired (.c( 10th percentile) on anumber of cognitive measures, with the most consistent deficits in visuospatiallearning, visuo-
spQlial memory, verbal learning, and p.sychomotor speed. We also examined emotionalfunc-tiomng and found that a number of ME patients showed evidence of both Axis and Axis II
patholOgy. Interestingly, there was a significant comlation among patients ' scores on theBeck Depression Inventory-Second Edition and the number oj neuropsychological testsfalling within the impaired range. Given the limited wukrstanding of ME and its effect on thehuman central nervous system, we provide a working model that attempts to capture the com-plex interactions of impaired cognition, psychosocial atressors, poor physical health, andemotional functioning in patients following ME.
KeywonJs: mold exposure, mild traumatic brain injury, toxic exposure
Adverse health effects due to mold exposure (ME)have been reported in humans for thousands of years(Sorenson, 1993; Ueno, 1980, 1983). Ergotism, asyndrome associated with ingestion of fungus-contaminated grains, involves symptoms such as convul-sions and gangrene and has been hypothesized as thebasis for unusual behavior that was interpreted as de-monic possession in medieval times (Donaldson, Ca-vanagh, & Rankin, 1997). In the late 1800s, a Japanesescientist showed that moldy rice contained toxins thatwere responsible for symptoms such as vomiting, con-vulsions, paralysis, and respiratory mest (Ueno, 1983).
We would 1iko to ttiInt Angelica 1. Isomura for her assistancewith data entIy CD !hi. project.
Requests for repriDtllhould be sent to 1uliana V. Baldo, Depart-meut of Psychology, Scripps Co\1eac. 1030 Columbia Ave., Clare-
/OOnt, CA 91711-3948, USA.
More rigorous research on ME bas taken place in thelast 100 years and has shown that certain toxic fungal(mold) metabolites, known as mycotoxins, are associ-ated with a number of health effects, including respira-tory disease, cardiac disease, cancer, and even death(Coulombe, 1993; Reijula, 1999; Sorenson, 1993;Ueno, 1980, 1983). In recent years, airborne mycotox-ins have been posited as the basis for adverse health ef-fects in water-damaged buildings (so-called sick build-ing syndrome), but documenting a causal link hasproven difficult (Fung, Clark, & Williams, 1998;Hodgson et aI., 1998).
Recently. it has been suggested that ME may also re-sult in central nervous system (CNS) changes (K. E.Gordon. Johanning, & Haddad, 1999; W. A. Gordon,Masotti, & Waddell, 1993; Johanning & Landsbergis1999; Sudakin, 1998). A recent case study reported thata teenage boy presented with tremorgenic encephalopa-thy following exposure to moldy fodder on his family
193
BALDO, AHMAD, & RUFF
farm (K. B. Gordon et al., 1993). The boy, in addition toother family members, experienced an acute illness ofheadache, fatigue, and flulike symptoms while clean-ing out a grain silo. Though the other family membersquickly recovered, the boy progressed, and at 48 hr fol-lowing exposure, be bad a severe tremor and displayedconfusion. Upon examination, be was found to be dis-oriented and slow to respond, and his attention capac-ity was reduced. BEG tests revealed a dysrhythmiaconsistent with a toxic encephalopathy
" (p. 238).He recovered 7 days postonset without significantresidua.
In a l81ger, retrospective study, Johanning andLandsbergis (1999) reviewed 151 cases that presentedat an occupational and environmental health clinic forevaluation following ME. Fungal exposure was as-sessed via environmental survey of the affected homeor workplace. Patients were given a symptom surveyand were tested for evidence of fungal reactions and al-tered immune system function. In addition to respira-tory symptoms, JohaDning and Landsbergis foundthat almost 80% of patients reported CNS-relatedsymptoms, with 52% endorsing three or more suchcomplaints. These symptoms included headaches, dif-ficulty concentrating, fatigue, dizziness, and nervous-ness. A follow-up survey revealed that a majority ofpatients (68%) bad a reduction in symptoms once theirexposure to mold ended or was reduced (e.g., due tomoving, repairs, etc.). A caveat of the study, however,was the finding that the correlation between CNSchanges and elevated immunoglobulin G (an indica-tion of allergic reactivity) was not significant. Further-more, approxiD1atcly SO% of a nonaffected, demo-
. graphically matched control group also experiencedCNS symptoms.
To our knowledge, only one published study basconducted a detailed investigation of the neuropsycho-logical effects of ME. W. A. Gordon et al. (1999) studied20 patients who were exposed to
Stachybotrys. a toxicmold associated with adverse health effects (Pung etal., 1998). Patients were administered a standard bat-
tery of neuropsychological measures, and the followingimpairment criteria were used: Verbal IQ (VIQ) ~ Per-formance IQ (PIQ; by 10 points); visual memory ~verbal memory (by 10 points); general memory ~attention/concentration (by 10 points); verbal learningscores one standard score below the mean; and im-paired problem solving on the Booklet Category test.Although overall means on IQ and memory tests werein the normal range, all patients met at least one
of theaforementioned criteria. and 45% of the patients metthree of the criteria. W. A. Gordon et al. (1999) con-
194
eluded that long-term ME was associated with cognitiveimpairment, especially in the areas of visuospatial inte-
gration, verbal learning, attention, and set-shifting.However, film conclusions awaited further studies. In-terestingly, the authors noted that the pattern of impair-ment observed in these ME patients was similar
to thatobserved following mild traumatic brain injury(MTB I).
This study further explores the relationship betweenME and cognitive changes. We analyzed neuropsycho-logical data collected from a group of ME patients in-volved in litigation. An important question not ad-dressed by previous studies is the extent to whichemotional and psychosocial factors may playa role inthe presentation of ME patients. Therefore, in thisstudy, both cognitive and emotional functioning wereassessed using standardized neuropsychological and
psychological measures. As suggested by W. A. Gor-don et al. (1999), we compared ME patients to individ-ualS diagnosed with MTBI to directly compare thegroups' neuropsychological test performance. To con-trol for the effects of litigation, patients in the MTBI
group were chosen who were also involved in litiga-tion. The two main goals of this study were to (a) ex-plore the interaction of cognitive and emotionalchanges in the presentation of patients with ME; and(b) determine the specificity of test performance in MEpatients compared to another group of patients experi-encing mild cognitive symptomatology.
Method
Participants
We analyzed neuropsychological data from 10 pa-
tients who presented in a structured clinical interviewwith physical and cognitive changes following ME.Of these 10 patients, 7 were exposed to mold in theirhomes, and 3 were exposed at their workplaces. All
patients had been involved in litigation regardingtheir exposure. The type of mold varied across casesincluding, but not limited to, Stachybotrys alTa, Peni-cillium, and Aspergillus. The average duration of
was 2.3 years (range = 0. 0 years), estimated
from the time that patients fltSt reportcdbeing awareof the mold. The average duration
since onset
exposure to time of testing was 3. 17 years (range =years).
Common physical complaints in ME patients in-cluded fatigue, respiratory problems, recurringbloody noses, nausea, frequent sore throats, head-

COONmVl! .w"t'tiCIS OF MOLD EXPOSURE
aches, congestion, lung infections, chronic cough,
bronchitis, and skin rashes. These physical symp-toms were also generally documented in patients'medical records. Common cognitive complaints in-cluded difficulty concentrating, memory loss, de-creased attention span, difficulty following conversa-tions, and slowed mental processing. Many patientscomplained of emotional difficulties as well, includ-ing depressed mood, anxiety, and increased emotion-ality (e.g., increased anger, crying more often). At thetime of the evaluation, the majority (9 out of 10) ofME patients were no longer living or working in theME environment
The ME patients were compared to 10 gender-, age-,and education-matched patients who were diagnosedwith MTBI using the American Congress of Rehabili-tation Medicine criteria (Mild Traumatic Brain InjuryCommittee. 1993). They were also involved in litiga-tion. In this group, 3 of the patients' injuries were dueto a motor vehicle accident, 3 were due to blows to thehead, 3 were due to falls, and I was due to a pedestrianaccident At the time of testing, M'fBI patients were anaverage of 1.7 years postinjury(range = Z-2.years). In all MTBI patients, the time of loss of con-sciousness did not exceed 30 min, and the duration ofposttraumatic amnesia did not exceed 24 hr. Cognitiveand emotional complaints in the MTBI group over-lapped to ,a ~,pificant degree with symptoms de-scribed by the. . ME patients (previously discussed).Physical compWnts, however, were more distinct fromME patients and commonly included symptoms suchas headaches, chronic pain, and fatigue.
The ME and MTBI groups did not differ in terms of
gender (8 women and 2 men in each group); age(40.7 and 42.4 years, respectively), F(I, 19) = .17
= .
69; or education (15.1 and 14.4 years, respec-
tively), F(I, 19) = .53,
= .
48. Moreover, the ME andMTBI groups did not differ on an assessment of pre-morbid intclli,aence (the vocabulaI)' subtcst on theWechsler Adult Intelligence Scal~ Third Edition
(WArS-ill; Wechsler, 1997) = 70th vs. 69th per-centile , respectively), F(1, 19) = 04,
= .
85.Institutional Review Board approval was obtained for
the study at Ibe first author s primary setting, the Veter-ans Affairs Northern California Health Care System.
Procedure
All patients were evaluated with the San DiegoNeuropsychological Test Battery (Baser Ruff,1987), which has been used previously in the diagna-
sis of toxic encephalopathy (Trester & Ruff, 1990;Troster, Ruff, & Watson, 1991). The tests included inthis battery are listed in Table 1 and were adminis-tered according to standard procedures. The norma-tive data used for comparison were those published ineach of the individual tests as referenced in Table 1.To screen for poor motivation and malingering, theRey IS-Item Test and the Rey Dot Counting Testwere administered (Spreen & Strauss, 1998). On theformer, all participants recalled between 12 and 15items (within normal limits), and the two groups didnot differ on this measure, F(! 19) = . 11,
= .
(ME = 14. 1 and MTBI = 14.3). In addition , allparticipants performed in the normal range on theDot Counting Test. These data suggested adequate
motivation, allowing the observed deficits to be inter-preted with reasonable certainty.
Results
ME Versus Normative Data
Neuropsychological data from patients with MEwere compared to normative data. Performancebelow the 10th percentile was considered an indica-tion of impairment. Between 1 and 5 ME patientsperformed below the 10th percentile on all but onecognitive measure, as shown in Table 1. A number ofmeasures revealed impaired performance in 4 or
more ME patients, including psychomotor speed(Ruff 2 & 7 Selective Attention Test), verbal learning(Selective Reminding Test), spatial span with a 20-sec delay, spatialleaming (Ruff-Light Trail LearningTest), and visuospatial memory (Rey Complex FigureTest, 3-min delay). The latter three tests all have incommon a reliance on visuospatial memory. How-ever, considerable variability existed within thegroup. For example, on the Rey Complex Figure Test(3-min delay), 4 patients scored at the 1st to 2nd per-centile, whereas 4 patients scored between the 69thand 88th percentiles. Mean percentiles across all testsare shown in Figure 1.
In contrast to the more specific cognitive measUIe$,
performance on the WArS-ill revealed very little impair-ment Only 1 patient with ME was impaired (.c( 10th per-centile) on a number of the WArS-ill subtests, scoring inthe impaired range on 10 out of 13 of the subtests given.One other ME patient scored at the 9th pen:entile onBlock Design. Otherwise, all ME patients scored in thelow to high average range on all subtests (lOth to 99th
percentile). As a group, ME patients' mean Full Scale IQ
19S

BALDO, AHMAD, &: RUFF
'I8b1e 1, NtIIlfJpsydtologlctll Deficits ill Mold Exponm Mild Tlrzumatic Brain Injury Patients
Measure
Finger 1ippiD1 Tel! (Ruff &: Parer, 1993)
Grooved Pegboard (Ruff It Parter, 1993)
Ruff 2 It 7 Selective Atlcntion Tc&a (Ruff It A11cD, 1996)Block-1Ipping Test Block- 'ntppiD1 (Baser It Ruff, 1987)
ThIt (2O-sec delay; Suer &: Ruff, 1987)
Selective RemiDdina ThIt (B\l8Chb &: Fu1d, 1974)Ruff-Light 'Inill.eImiDg Test (Ruff It AIIea, 1999)
WMS-m Lopc:a1 Memory I (Wccha1er, 1997b)WMS-JII Logical Manmy U (Wechsler, 1997b)
Rey Complex Figure, 3 min delay
Rey Complex Fiaure, 30 min delay
(Mitnaabioa, Boooc, &: D'Elia, 1999)Controlled Oral Word Association Test
(Ru1f, LiJbt, Parer, &: LeviD, 1996)Ru1fFigura1 FIucacy (Ruff. 1996)
Trai1makiug Test (Heatoa. Grant, &: Mat!bews, 1991)
WCST (Heaton, CIehmc, Ta11cy, Kay, It Curtis, 1993)
Stroop Color-Wold NIDIiDs (Spreen &: Strauss, 1998)
WAfS-W (Wechs1er, 1997a)
Number impairedoat 0110
FundI_(.) Assessed
Motor speed
Plychomotor speed and dexterity
PIycbomotor speed and accuracy, attentionSpatial immediate memory
SpItial short-term memoryVaballeaming
ViIuospatiallcaining
Verbal Memmy
Vaba11oDg-term memoty
Vaba1 Memory
Spada) long-termmcmory
MTBI
Verbal fluency
Nonverbal fluency
Copitive flexJ'bility
Copitive shifting and problem solviDgSe1cctive attention
VlQ 8Dd PIQ
Note: ME .. mold cxposwe; MTBI .. mild traumatic: brain injury; WMS-m .. Wechsler Memory Sc:a1e- Third edition; WCST = Wiscon-sin Card Sorting Test; WAlS-m .. Wechsler Adult IntcJljJel1U Sc:a1o- Third Edition; VIQ .. Verbal IQ; PIQ = Pedmmance lQ.
(FSIQ) was at the 62nd pctccntile, mean VIQ was at the65th percentile, and mean PlQ was at the S3rd percentile.
In sum, ME patients exhibited a number of weak-nesses on testing, most consistently on tests of visuo-spatial memory, but there was no single, consistentpattern of neuropsychological test performance acrosspatients. Also, the group was heterogeneous in thatsome patients scored in the impaired range on a num-ber of measures whereas other patients exhibited veryfew deficits.
ME Versus MTBI
To assess whether the observed effects of
were specific to this disorder, we compared theME group to a group of patients with MTBI. Acrossthe battery of tests, only one cognitive measure (theStroop Color Word Test) distinguished between thegroups when mean percentiles were compared (two-tailed tests, alpha set at
= .
05). That is, the ME andMTBI groups bad statistically comparable perfor-mance across neuropsychological measures when con-
196
sidering mean performance. Visual inspection of Fig-ure I shows that the ME and MTBI patients had anumber of similar strengths and weaknesses. Again,however, there was a broad range of perfortnancewithin both groups: Some individuals in each groupwere quite impaired whereas others perfonned in theaverage to high average range (see Table 1).
The largest numeric differences between the MEand MTBI patients were observed on the Stroop ColorWord Test and the Rey Complex Figure Test. FourMTBI but no ME patients were impaired on the Strooptest, a measure of attention and executive functioning.Mean performance on this test differed significantlybetween the groups, F(l, 19) = 5. 38, .c( .05. In con.trast, 4 ME patients but only 2 MTBI patients were im-
paired on the Rey Complex Figure task (3-min delay),a test of visuospatial memory. However, the differencein mean performance on this test did not reach statisti-cal significance.
WAIS- scores also did not distinguish the MEfrom MTBI patients. tests comparing the groups onFSIQ, VIQ, PIQ, processing speed, working memory,
perceptual organization, and verbal comprehension reo

100
COGNmVE EFFECI'S OF MOLD EXPOSURE
.fO
.. "
II"
-+-
Mold Exp'
.......
MTBI
~ ; ~ ; ~ ~ ~, / / ~ ~ ~/ ~ ~ ~ ~
~/r/~
'/ ~ ~,/ #
IIIaure 1, Pat'onIumce almold apoaare (ME)'" mUd trauIIIIatIc bnID-lDJured (MTBI) pa8lenta on Yuious 1IIeIISURS In the nea.lOJII1eho1opC8l better'J. Motor nom .. FInpl'Tapplaa with damllwat hand; Motor Non :: FInger 'l8ppIDg with DODdolDlD8nt handjDext DoIn = Grooved Pepaud with dominant hand; . Dezt NOlI .. Grooved Pegboard w:Ith nODdominant Iumd; Speed 2&7 .. speedon the RIdr 2&7 tat; Aa:ur 2&7 .. aecaracy 011 the Raft 2&7 tat; LM I .. LogbI Memory I; LM U .. LoaIca1 Memory Uj Rey 3.. Rey Complex PJaure Test (3-mJD delay); Rey 30 = Key Complex FIpn Test (JO.min delay); Verbal Flu = verbal fluency; Desfpflu = deIIp DueDC)'; TndI B
.. part B of '('rIdIm..IrI "'I TeIt; WCST PH .. peneveratl,e errors 011 the WIscoasIn Card Sortlag Task.
vealed no significant group differences when compar-
ing mean performance between ME and MTBI pa.tients (all
:::-
OS; see Figure 2). V1SU8l inspection of
Figure 2, however, suggests a reladve weakness inperceptual-organization skiDs in ME patients.
Emotional Factors
In addition to cognitive functioning, we were alsointerested in assessing current emotional state, as wellas long-term personality features. To assess long-termpersonality style and emotional functioning, the MEand MTBI patients completed the Millon Clinical Mul-tiaxial Inventory-Third Edition (MCMI-UI). A num-ber of patients in both groups scored in the clinicallysignificant range (base rate :::- 85) on both MCMI AxisI and II categories. Specifically, 3 ME and 2 MTBI pa-
tients scored in the clinically significant range on atleast one MCMI Axis I category, and 4 ME and3 MTBI patients scored in the significant range on atleast one MCMI Axis II category. In the ME group,MCMI Axis I categories included anxiety, somatoformdisorder, and major depression, and MCMI Axis II cat-egories included hisbionic and compulsive personalitydisorders.
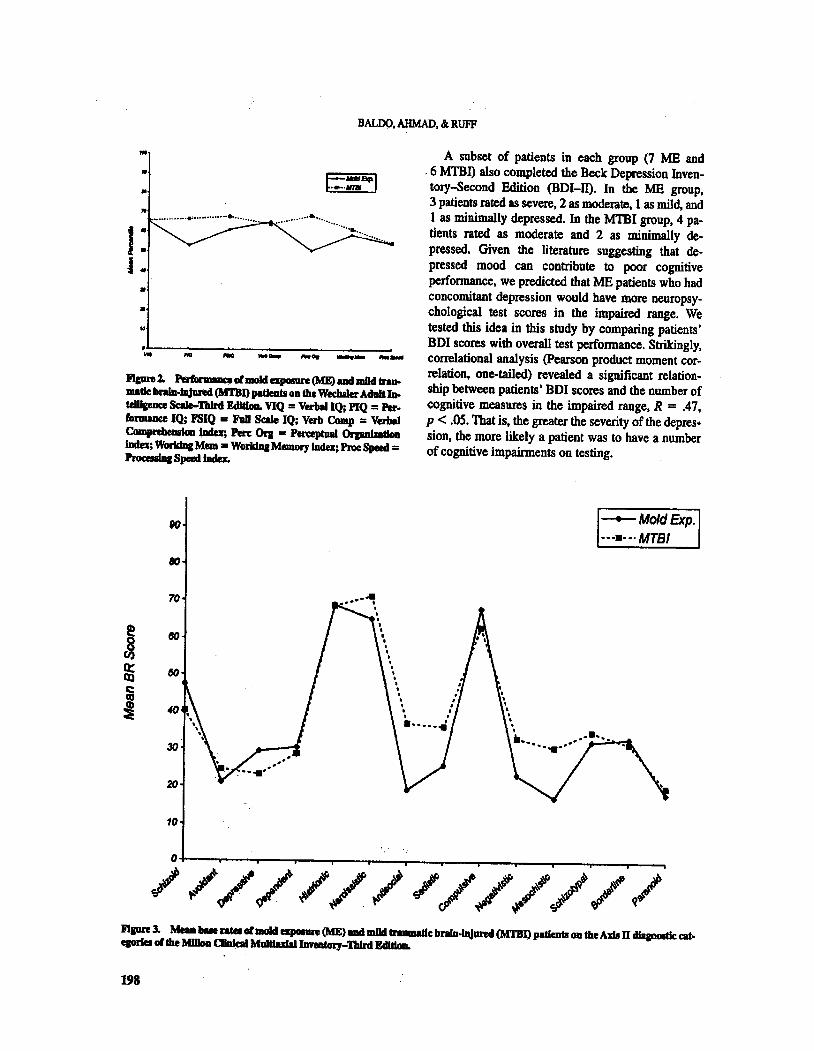
In terms of mean base rates, the ME and MTBI pa-tients had almost identical patterns of data across theMCMI Axjs n diagnostic categories, as shown in Fig-ure 3 (two-tailed tests, all
:::- .
05). There was also agreat deal of concordance across MCMI Axis I diag-nostic categories, except for a numerically higher baserate on dysthymia and lower base rates on drug depen-dence and delusional disorder in the ME patients (seeFigure 4). Only delusional disorder differed signifi.cantly between the groups F(l, 18) = 10.61, .c( .01.
197
BALDO, AHMAD, &: RUFF
==B90
...._.n......""""""'.""
J :
... ...
-Go
-- --
FIpre 2. vi mold GpIIIIIre (ME) 8Dd mBd trau-matic: braID-1D,Jand (MTBI) pldea.ts om the Wechsler Adult JD.telUpace Sale-1bIrd Edldoa. VIQ = Verb8lIQ; PlQ = Per-fDrmmce IQ; FSIQ a FaD Scale IQ; Verb Camp = Verb8IComprebeDllGa
~;
Pen: 0rI = Perceptual Orpnl_"'"iDda; WorIdaa MelD . WorIdaa Memory Index; Proc Speed =ProcessIa& Speed Inda.
A subset of patients in each group (7 ME and. 6 MTBI) also completed the Beck Depression Inven-tory-Second Edition (BDI-U). In the ME group,3 patients rated as severe, 2 as moderate, 1 as mild, and1 as minimally depressed. In the MTBI group, 4 pa-tients rated as moderate and 2 as minimally de-pressed. Given the literature suggesting that de-pressed mood can contribute to poor cognitiveperfonnance, we predicted that ME patients who hadconcomitant depression would have more neuropsy-chological test scores in the impaired range. tested this idea in this study by comparing patients'BDI scores with overall test performance. Strikingly,colTelational analysis (pearson product moment cor-relation, one-tailed) revealed a significant relation-ship between patients' BOI scores and the number ofcognitive measures in the impaired range,
= .
47,.c( .05. That is, the greater the severity of the depres-
sion, the more likely a patient was to have a numberof cognitive impairments on testing.
-+-
Mold Exp.
.......
MTBI
////// ///////
Flpre 3. Meu bue nteI of mold apGIIIR (ME) ad mild 8nI8utIc brain-"" (M1'B1) patients oa the AxIs D diapJostk: alt.eprfes oIlhe MfIIoD ~ MaItIuIalllmatory-1bIrd EdI8IoD.
198

COONITIVB EfFECTS OF MOLD EXPOSURE
100
I:t
.I ll'
-+-
Mold Exp.
.......
MTBI
.....
JI.
.. ... .
t;f'
/ /#'.
i1aun 4. Meaa ... rates of maid apoIIII'e (ME) IDd mild trumatk: b~1IRd (MI'BI) patients on the AxIs I d1agDostIc cat-e,orIeI of the MIIIoa CJIDIc:al MulClu:l8lIJmatGry- TIdnI Edldaa. AJcoboJ Dep. = alcolaoJ clependeuce; Drug Dep. = drug depenodeDCe; FI'SD = poIUnumatIe Itre8 disorder; MaJ. DepftlldOD ... major clepnssloa.
DJseussiOD
This study presents preliminary findings docu-menting a number of cognitive imPairments in pa-tients following ME, Areas that were most consis-tently affected in ME patients included psychomotorspeed, verbal learning, visuospatialleaming, and vi-suospatial memory. These findings are in part consis-tent with those ofW. A. Gordon et a!. (1999) who reo.
ported impaired visuospatial integration in patientsfollowing ME, As in that study, we also found that asubset of patients were impaired on verballeaming.This study s results are also similar to a recent studyof solvent-cxposcd individuals that found reducedperformance in the same cognitive domains (MOITOW,
Stein, Bagovich, Condray, & Scott, 2001). It shouldbe noted, however, that a great deal of variability ex-isted in this study, such that on any given measure,some ME patients were very impaired whereas otherswere in the average to high average range. Thus, wedid not find evidence of a single, consistent pattern ofneuropsychological performance in patients exposedto mold.
To control for a number of factors, such as involve-ment in litigation and psychosocial stress, we com-
pared patients with ME to a neurologic comparisongroup ofMTBI patients who were also involved in liti-gation, We did not find any evidence of attempts to ex-aggerate deficits in either the ME or MTBI group. Allpatients appeared to exert full effort, and, in fact, many
199
BALDO, AHMAD. &: RUFF
scored in the average to high average range on a num-ber of measures. As predicted by Gordon et al. (1999),we found that the ME and MTBI patients had a numberof similar strengths and weaknesses across a broadrange of cogoi,tjve and psychological measures. Com-mon wea~'~' : included deficits in visuospatiallearning andDlClDOl)', as well as in psychomotor speed.This concordanc:c suggests potential CNS involvementin ME and a comparable comOIbid complexity c0m-
prised of medical. cognitive, and emotional residua inboth disorders. In future studies, we hope to tease apartthe effects of litiption .in ME by comparing litigants tononlitigants. addition, future studies should includea more comprehensive assessment of motivation andmalingering.
As documented in this study, significant emotionalsymptomatology was present in many of theME pa-tients. Five out of7 ME patients rated as moderately toseverely depressed on the BDI-ll. There were also anumber of ME patients who rated in the clinically sig-nificant range for Axis I and Axis IT pathology on theMCMI-ill. These findings were compatible with ourclinical impressions as well. Based on patients' clinicalhistories, it appeared as though chronic physical illness(e.g., chronic respiratory problems) and psychosocialstressors contributed significantly to depressed moodand increased anxiety. Psychosocial stressors includedhaving to relocate, bankruptcy, undergoing majorhome renovations, disputes with insurance companiesregarding coverage, and a reduced capacity to work:with a concomitant loss of income.
The interpretation of cognitive deficits in the MEgroup is complicated by the presence of these emo-tional and psychosocial factors. As has been shown ina number of swdies. depression in and of itself can af-fect memory and attention performance (Austin,Mitchell, & Goodwin, 2001; Elliot & GRen, 1992;King, Caine, Conwell, & Cox, 1991; Massman, Delis,Butters, Dupont, & Gillin, 1992). Indeed, in this study,we found a significant relationship between severity ofdepI'ession and the number of tests on which ME andMTBI patients were impaired. This finding suggeststhat accompanying depression may have played a rolein the presentation of cognitive deficits in our group of
patie$. 'Ideally, future studies with larger samplesizes will be able to statistically control for these fac-tOrs, 80 that ~c;ognitive effects of ME can be deter-mined.moJ:e ~Y.
The mitigatillg role of emotional factors, however,docs not negate tbescriousness or impact of ME. Thatis, ME may have a detrimental impact on cognition in-directly via its impact on physical and emotional
200
MOLD EXPOSURE
CNS PHYSICALALTERATIONS SYMPTOMS
COON111VE EMOTIONALDEFICITS SYMPTOMS
PSYCHOSOCIAL AND FINANCIALPROBLEMS
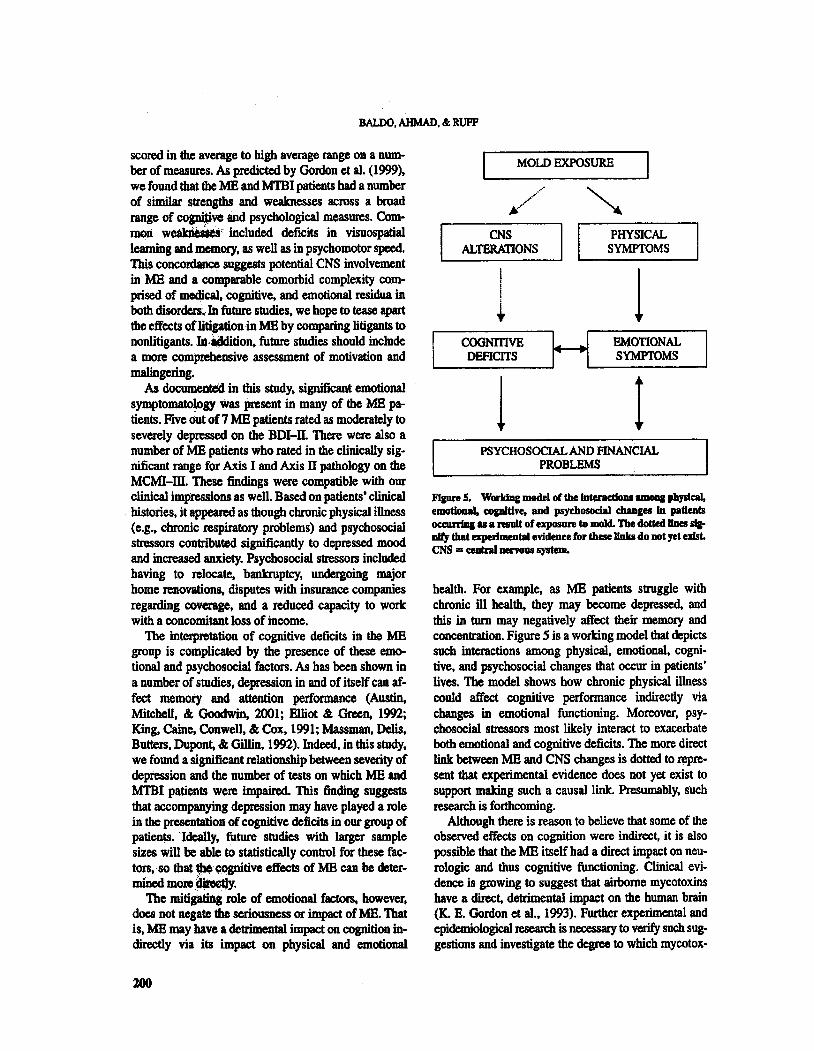
Flpre 5, WorIdn& model of the JuteracdoDi 8IDOIII physical,
emotloa8J. copItive, and psychosoclal chanle& Ju patients0CCIII'I'iq as a result of exposure to mokL The doUed IDes sJa-DIfy that eqJeriment81 evidence for these lInkII do not yet ufst.CNS = c:eatraI nenous system.
health. For example, as ME patients struggle withchronic ill health, they may become depressed, and
this in turn may negatively affect their memory andconcentration. Figure 5 is a working model that depictssuch interactions among physical, emotional, cogni-tive, and psychosocial changes that occur in patientslives. The model shows how chronic physical illnesscould affect cognitive performance indirectly viachanges in emotional functioning. Moreover, psy-chosocial stressors most likely interact to exacerbateboth emotional and cognitive deficits. The more directlink between ME and CNS changes is dotted to repre-sent that experimental evidence does not yet exist tosupport making such a causal link. Presumably, suchresearch is forthcoming.
Although there is reason to believe that some of theobserved effects on cognition were indirect, it is also
possible that the ME itself had a direct impact on neu-rologic and thus cognitive functioning. Clinical evi-dence is growing to suggest that airborne mycotoxinshave a direct, detrimental impact on the human brain(K. E. Gordon et al., 1993). Further experimental andepidemiological research is necessary to verify such sug-gestions and investigate the degree to which mycotox-

COONmVE EPFBCTS OF MOLD EXPOSURE
ins have a significant and direct impact on cognition.Also, we await further studies in epidemiology aDdtoxicology that will provide more objective and quan-tifiable indicators of toxic ME in humans (Johanning& Landsbergis, 1999).
In summary, this study showed that (a) patientswith ME are impaired on a number of measures ofcognitive functioning, (b) the pattern of cognitive andpsychological impairment following ME bears somesimilarity to that following MTBI, and (c) mitigatingfactors such as depression and psychosocial stressplaya role in the presentation of patients followingME. This study was limited by its small sample sizeand the fact that we were able to assess only those pa-tients in litigation who had a number of other compli-cating factors. Also. the patient group used in thisstudy was not homogeneous, as they bad been ex-posed to different molds, were exposed in differentsettings. and were exposed for varying lengths oftime. We await studies that will further elucidate thecomplex issue of neurocognitive changes associatedwith toxic ME, Such future studies should includeconsideration of all aspects of patients' functioning,namely, the interaction among physical, emotional,
psychosocial, and cognitive changes.
Referenca
Austin, M., Mitcbcl1. P., &: Goodwin, G. M. (2001). Cognitivedeficits in dcpIeuioa: Possible implicalioDS for fuucliODBl ncu-ropaIbolollY. BriliIlt JDII17IIIl 0/ PsychitJtry. 178, 200-206.
Baser, C. A, &: Ruff, R. M. (1987). Coosttuct validity of die SanDiego Neuropsychological Test Battery. ArdIlves 0/ CUnical
NeuroPlJC1wlogy, 2, U-32.Buschke, H., &: PuJd, P. A (1974). Evaluation of 8toJI&e, raeatioD,
and mrieval in dison:Iaed memmy and lcamina. Newology,11, 1019-1025.
CCWombe, R. A. (1993). Biological action of mycotoxins. JOIU7UIlo/DaJry Sc:lmce. 76. 880-891.
DcJaaJdaoo, L. J., cavanap, J., &: Rankin, J. (1997).1110 dancinap1aaue: A public bea1Ih COIIWIdrum. Public H eoldJ, 11 J, 20 1-204.
Elliot, C., &: R. L. (1992). Clinic:a1 depression and implicitmenlOI)'. Jt1IImal of Almormsl psychology, 101, 572-574.
Fung, p., C\ark, R., &: Williams, S. (1998). Stachybotryl,
mycotoxin-producios fungus of increasins toxicologic: impor-tance. Journal ofToxic%gy, Clinical TO.J:ic%gy, 36. 79-86.
Gordon, K. Eo, Masotti, R. Eo, &: Waddell, W. R. (1993). 'ftemor-
geuic eoccpba1opltby: A role of mycotoxins in die productiooof CNS cIiaeue in humaDs? Cmodian JollT7llll oj NeurologicScienc" 20 237-239.
Gmdon, W. A. lo1wmiDg, B., &: Haddad, L. (1999). Cognitive im-
pairmad 8SIOCiatecI with cxpollUJ'C to toJdgenic: fuoai. In Joban-Ding, E. (Ed), Bioaerosols. fungi and mycotoDu: Health ef-fects, lUSUlII/nII, pTrHlllioft and controL New York: EasternNew York Occupationalllld Environmental Health Centc&
Heaton, R. It , Chelune, G. J., Talley, 1. L., Kay, G. G., &: Curtis, G.(1993). WUconsin Card Sorting Test (WCST) mtl1IIIlII mlisedand e:qHI1Idul. Odessa, Fl.: Psychologk:al s-~tResources.
Heaton, R., Grant, L, &: Matthews, C. (1991). Comprehensive Mmzsform an expt11Uhd Halstead.Reilan neuropsychological battery:Demogmphic comctions. rt!searchjindings. and clinical appli.cations. Odessa, FL: Psycbological A:isessment Resources.
Hodgson, M. I., Morey, P., Leung, W-Y., Morrow, L., Miller, D.,Iarvis, B. B., et al. (1998). Building-associated pulmonary dis.ease from exposure to Staclrybotrys cIuutlI1'um and Aspergillusversicolor. JolU7lQl 0/ OccupaticnoJ and Environmental Medi.ciM, 40, 241-249.
Johanning, E., &: Landsbergis, P. (1999). CHnica1 findings rclated
to indoor fungal exposur&--review of clinic data of a specialtyclinic. In lohanning, E. (Ed.
),
BioaeroUJls, fungi and mycotox-ins: Health effects, lUsessment, pmlention and controL NewYork: Eastern New York Occupational 8Dd EnvironmentalHealth Center.
King, D. A. , Caine, E. D., Conwell, Y., &: Cox, C. (1991). The DCU-
ropsychology of depression in the elderly: A comparative studywith normal aging and Alzheimer's disease. Journal of Neu-
ropsychilJlry and Clinical Neurosciences, 3, Massman, P. J" Delis, D. C., Butters, N., Dupont, R. M., &: Gillin,
1. C. (1992). The subcortical dysfunction hypothesis of memorydeficits in depression: Neuropsychological validation in a sub-
group of patients. JollT7llll of Clinical and Experimental Neu-
ropsychology, 14, 687-706.Mild Tnlumatic Brain Injwy Committee of the Head lnjwy IDter-
disciplilwy SpeciallDterest Group of the American Congressof Rehabi6tation Medicine (1993). Definition of mild traumaticbrain injury. Journal of Head 7rauma RMabUitatioll, 8, 86-87.
MitrushiDa, M. N., Boone, It B., &: D'Elia, L. P. (1999). Hand-book o/normative data/or neuropsyc:Jwlogical assessmentNew York: Oxford University Press.
Morrow, L. A., Stein, L., Bagovich. G. R., Condray, R., &:Scott, A. (2001). Neuropsychological assessment, depression, andpast exposure to organic solvents.
Applied Neuropsychology,
65-73.Rcijula, K. (1999). Occupational exposure to molds. diseases and
diagnosis. In 10hanning, E. (Ed.
),
Biooerosols. fungi and nryco-toxins: Health effects. assessment. pmention and controL NewYork: Eastern New York Occupational and EnvironmentalHealth Center.
Ruff, R. M. (1996). Ruff figural jhIency test. Odessa, FL: Psycho-logical Assessment Resources.
Ruff, R. M., &: A11cn, C. C. (1996). Ruff and smCfive tlI1entiontest Odessa, Fl.: Psyc:holoaical Assessment Resources.
Ruff, R. M., &: Allen, C. C. (1999). Ruff-Light traillemning tut.
Odessa, FL: Psychological Assessment ResolUtes.Ruff. R. M., Ught, R. H.. Parker, S. B., &: Levin, H. S. (1996). Ben-
ton Controlled Oral Word Association Test: Re1iabDity .andupdated norms. Archivu of Clinical Ne/lropsychology. II,329-338.
Ruff, R. M., &: Parker, S. B. (1993). Gerder and age.specificchanges in motor speed and eye-hand coordination in adults:Nonnative values for the F"mger Tapping and Grooved Peg-board tcIU. Perceptual and Motor Skills. 76, 1219-1230.
Sorensen, W. G. (1993). Mycotoxins: Toxic metabolites of fungi.In 1. MUJphy, H. Friedman, &: M. Bendinelli (Eds.
),
Fungal in.fections and immune msponses (pp. 469-491). New York:Plenum.
201

BALDO, AHMAD, &: RUFF
Spreen, M., &: Stnu8I, O. (1998). A compendium ofMUropsydtO-loglcDl tuts. adIribtiI~n, /lOmas. and commentary (2nd eel).New York: Oxton!Uuivcnity Press.
SUdakin, D. L. (1998). Toxigenic fungi in a water-damaged build-ing: An inte:rveatim study. AmeriCCDI JoUl7IQ1 of IndvstrltJlMtdJclM. 34, 183-190.
Trostel', A. L, &: Ruff, R. M. (1990). Neuropsychological sequelae
of exposwe to the chlorinated hydrocarbon solvents 1Ii-ch10J0dby1eue and trichloroethane. Ardtivu of ClinaIl NeII-
ro~ S, 31-47.Troster, A. L, RuJr, R. M., &: Watson, D. P. (1991). Dementia as a
neuroJIIYcholoaical couequence of chronic occupadooa1 ezpo-sure to polycb1orWted bipbeoyb (PCBs). An:hivu oj ClinicalNeuropsychology. 6, 301-318.
202
Ueno, Y. (1980). Trichothecenes, myootoxicology, mycology, chem-istry and toxicology. AdvlW:ed Nutrition Science. 3. 301-353.
Ucno, Y. (1983). Trichothecmes: ChemkaJ, biological and toxico-logical aspects. New York: Elsevier.
Wechsler, D. (l997a). Wechsler AtbJt /nlt:lligmce Scuie-ThirrJ
Edition. San Antonio, TX: Psychological COIpOration.
Wechsler, D. (1mb). Wech.rltr Memory Scale-Third Edition. SanAntonio, TX: The Psychological Corpontion.
Original submission March 29, 2002Accepted July 16, 2002
Copyright © 2022 FDOKUMEN