
Natural history of left ventricular thrombi: Their appearance and resolution in the...
11
790 CLINICALSTUDIES NaturalHistory Ventricular `' Thrombi-,TheirAppearanceand ResolutioninthePosthospitall i zationPeriodof AcuteMyocardialInfarction ANDRE KEREN,MD,SHMUELGOLDBERG,MD,SHMUELGOTTLIEB,MD, JACOBKLEIN,MD,CLAUDIOSCHUGER,MD,AHARONMEDINA,MD, DANTZIVONI,MD,FACC, SHLOMOSTERN,MD, FACC Jerusalem .Israel Aseriesof198consecutivepatientswithacutemyocardial infarctionwereprospectivelystudiedbeforehospitaldis- chargeandduring24 .0t8 .6monthsoffollow-up .A predischargeiirombuswasfoundIn38(31%)of124 patientswithanteriorInfarctionbutinnoneof74patients withinferiorinfarction(p<0 .001) .Earlythrombolytic therapyin34patientsdidnotdecreasetherateofthrombus occurrence .Acuteanteriorinfarction,ejectionfraction c35%andapicaldyskinesiaoraneurysm(butnotakinesia) weresignificantlyrelatedtotheappearanceofthrombus duringhospitalizationbystepwiselogisticregressionanal . ysis . Echocardiographicfollow-upof159patientsforatleast 6months(mean26 .6±8 .4)revealedthatthrombus disappearedin14(48%)of29 .Disappearanceofthrombus wasrelatedtopredischargeapicalakinesia(butnotdyski- nesla)andtowarfarintherapyduringthefollow-upperiod . Anewthrombusfirstappearedafterhospitaldischargein 13of130patients,andIn7ofthe13itresolvedduring furtherfollow-up .Thus,30%(13of42)ofthrombiinthese patientsappearedafterdischargefromthehospital . Leftventricularthrombusoccursfrequentlyinthecourseof acutemyocardialinfarctionandisassociatedwithincreased embolicrisk (1-6) . Acuteanteriorinfarctionandsevere apicalasynergyhavebeenuniformlycorrelatedwithforma- tionofthrombus (7-19) . Clinical(8-10,18-21)andlabora- tory(15-17)markersoftheextentofmyocardialdamageas wellasadministrationofanticoagulant(22-26)orfibrinolytic FromTheHeidenDepartmentofCardiology .BikurCholimHospitaland HebrewUniversityHadassah-MedicalSchool,Jerusalem .Israel . ManuscriptreceivedJuly5 .1989 :revisedmanuscriptreceivedOctober 18,1999 .acceptedOctober25 .1989. Address for reprints ; AndreKeren .MD.TheHeidenDar-rtmentof Cardiology,BikurCholimHospital .P.O.Box492.Jerusalem91000 .Israel . ®1990bytheAmericanCollegeofCardiology JACCVol .15,No .4 March15,1990 :790-800 Threefactorswererelatedtooccurrenceofnewthrombi duringthefollow-upperiod :deteriorationinleftventricu- larejectionfraction,predischargeejectionfractionX35% andventricularaneurysmordyskinesia.Systemicembo- lismoccurredinsixpatients,allwithap ischarge thrombusp<0 .001) .Mobilityofthethrombuswasthe onlyvariablesignificantlyrelatedtosubsequentembolic events(p=0 .001)bylogisticregressionanalysis .Thus,the predischargeechocardiogramidentifiespatientswith thrombusandthoseathighestriskofembolicevents .Itcan indicatepatientswhoarelikelytohavethrombusresolution andthoseatriskofdevelopinganewthrombusafter hospitaldischarge .Follow-upechocardiogramsmayhelpin guidingthelengthoflong-termanticoagulanttherapy . Fouradditionalpatientswithapredischargeapical mobilethrombus(notpartoftheconsecutiveseries)re- ceivedthrombolytictherapy .Intwoofthefour,lysisof thrombuswasachievedwithoutcomplications,butsystemic embolismoccurredintheothertwo,andprovedfatalin one. (JAmColl Cordial 1990;15 :790-800) (27-30)therapyduringtheacutephaseofinfarctionhave beenshowntohaveavariableinfluenceontheincidenceof thrombi .Athrombusdisappearanceraterangingfrom20% to71%(8,10,11,19,20,27,31-33)andfirstappearanceofleft ventricularthrombusafterhospitaldischarge(8,13,20)have beenreported .Factorsrelatedtothrombusappearancein theposthospitalizationperiodanditsembolicpotentialhave notbeensystematicallyevaluatedinprospectivestudies . Echocardiographyisbothsensitiveandspecificinthe detectionandmorphologiccharacterizationofventricular thrombus(21,34-37) .Protrusionandmobilityofthethrom- bushavebeenvariably(13%to83%)associatedwithin- creasedriskofembolization(12-18),butithasbeenclaimed (18)thatspontaneousvariabilityinthrombusshapeand 0735-10971901$3 .50
-
Upload
hadassah-med -
Category
Documents
-
view
0 -
download
0
Transcript of Natural history of left ventricular thrombi: Their appearance and resolution in the...

790
CLINICAL STUDIES
Natural History
Ventricular `'Thrombi-, Their Appearance andResolution in the Posthospitallization Period ofAcute Myocardial Infarction
ANDRE KEREN, MD, SHMUEL GOLDBERG, MD, SHMUEL GOTTLIEB, MD,
JACOB KLEIN, MD, CLAUDIO SCHUGER, MD, AHARON MEDINA, MD,
DAN TZIVONI, MD, FACC, SHLOMO STERN, MD, FACC
Jerusalem. Israel
A series of 198 consecutive patients with acute myocardialinfarction were prospectively studied before hospital dis-charge and during 24.0 t 8.6 months of follow-up. Apredischarge i irombus was found In 38 (31%) of 124patients with anterior Infarction but in none of 74 patientswith inferior infarction (p < 0 .001) . Early thrombolytictherapy in 34 patients did not decrease the rate of thrombusoccurrence. Acute anterior infarction, ejection fractionc35% and apical dyskinesia or aneurysm (but not akinesia)were significantly related to the appearance of thrombusduring hospitalization by stepwise logistic regression anal .ysis .
Echocardiographic follow-up of 159 patients for at least6 months (mean 26.6 ± 8.4) revealed that thrombusdisappeared in 14 (48%) of 29 . Disappearance of thrombuswas related to predischarge apical akinesia (but not dyski-nesla) and to warfarin therapy during the follow-up period .A new thrombus first appeared after hospital discharge in13 of 130 patients, and In 7 of the 13 it resolved duringfurther follow-up . Thus, 30% (13 of 42) of thrombi in thesepatients appeared after discharge from the hospital .
Left ventricular thrombus occurs frequently in the course ofacute myocardial infarction and is associated with increasedembolic risk (1-6) . Acute anterior infarction and severeapical asynergy have been uniformly correlated with forma-tion of thrombus (7-19) . Clinical (8-10,18-21) and labora-tory (15-17) markers of the extent of myocardial damage aswell as administration of anticoagulant (22-26) or fibrinolytic
From The Heiden Department of Cardiology . Bikur Cholim Hospital andHebrew University Hadassah-Medical School, Jerusalem . Israel .
Manuscript received July 5 . 1989 : revised manuscript received October18, 1999 . accepted October 25 . 1989.
Address for reprints; Andre Keren. MD. The Heiden Dar-rtment ofCardiology, Bikur Cholim Hospital . P.O. Box 492. Jerusalem 91000 . Israel .
®1990 by the American College of Cardiology
JACC Vol . 15, No . 4March 15,1990 :790-800
Three factors were related to occurrence of new thrombiduring the follow-up period: deterioration in left ventricu-lar ejection fraction, predischarge ejection fraction X35%and ventricular aneurysm or dyskinesia. Systemic embo-lism occurred in six patients, all with a p ischargethrombus p < 0.001) . Mobility of the thrombus was theonly variable significantly related to subsequent embolicevents (p = 0 .001) by logistic regression analysis. Thus, thepredischarge echocardiogram identifies patients withthrombus and those at highest risk of embolic events . It canindicate patients who are likely to have thrombus resolutionand those at risk of developing a new thrombus afterhospital discharge. Follow-up echocardiograms may help inguiding the length of long-term anticoagulant therapy .
Four additional patients with a predischarge apicalmobile thrombus (not part of the consecutive series) re-ceived thrombolytic therapy. In two of the four, lysis ofthrombus was achieved without complications, but systemicembolism occurred in the other two, and proved fatal inone.
(J Am Coll Cordial 1990;15:790-800)
(27-30) therapy during the acute phase of infarction havebeen shown to have a variable influence on the incidence ofthrombi. A thrombus disappearance rate ranging from 20%to 71% (8,10,11,19,20,27,31-33) and first appearance of leftventricular thrombus after hospital discharge (8,13,20) havebeen reported . Factors related to thrombus appearance inthe posthospitalization period and its embolic potential havenot been systematically evaluated in prospective studies .
Echocardiography is both sensitive and specific in thedetection and morphologic characterization of ventricularthrombus (21,34-37) . Protrusion and mobility of the throm-bus have been variably (13% to 83%) associated with in-creased risk of embolization (12-18), but it has been claimed(18) that spontaneous variability in thrombus shape and
0735-10971901$3 .50

JACC Vol, 15. No. 4March 15, 1990 :790-800
mobility significantly decreases the prognostic value of thesecharacteristics .
The present study prospectively investigated 198 consec-utive patients with acute transmural myocardial infarction .The patients had long-term clinical, echocardiographic andnuclear angiographic follow-up evaluations to attempt todefine 1) factors related to the formation of thrombus duringthe acute phase of infarction ; 2) factors related to disappear-ance of thrombus during the follow-up period ; 3) the fre-quency of and factors related to appearance of a newthrombus during the follow-up period-, and 4) the risk ofembolization of thrombus detected either before or afterhospital discharge. Pertinent experience is reported in fouradditional patients in whom fibrinolytic therapy was usedduring the late phase of acute infarction to achieve lysis of amobile thrombus .
MethodsStudy patients. The study group included 198 consecu-
tive patients who survived an acute transmural myocardialinfarction, had technically adequate predischarge echocar-diograms and had no additional cardiac or systemic illnessthat could affect left ventricular function or long-term prog-nosis. They represented 93% of the 212 patients with acuteinfarction discharged from the hospital between February1985 and January 1987 . Excluded were 2 patients withinadequate echocardiograms and 10 with primary myocar-dial or valvular heart disease, emergency surgery or coca .,-nary angioplasty during hospitalization or a systemic ilip-2ssthat could affect long-term prognosis . Two additional pa-tients with previous infarction and echocardiographic docu-mentation of left ventricular thrombus < 12 h after theirhospitalization were excluded because thrombus appearancecould not be attributed with certainty to the new infarction
CW the 198 patients included in the study, 168 were menand 30 were women ; the mean age was 62.3 ± 11 .8 years
(range 32 to 86) . Echocardiography was performed 10.6 ±4.1 days (range 7 to 21) after the acute event . Transmuralmyocardial infarction was diagnosed by typical history,characteristic increase in serum creatine kinase, glutamicoxaloacetic transaminase and lactic dehydrogenase enzyme
levels, and development of diagnostic Q waves on theelectrocardiogram (ECG) . The location of the infarction wasdefined from the ECG (38) . Patients with lateral and withcombined acute anterior and inferior infarction were in-cluded in the group with anterior infarction .
Six weeks after hospital discharge, the patients had theirfirst clinical and echocardiographic follow-up evaluation,and these examinations were repeated every 3 monthsduring the first year and every 6 months thereafter . Nuclearangiography was also performed before hospital discharge,every 6 months during the first year and every 12 monthsthereafter .
KEREN ET AL.
791NATURAL HISTORY OF THROMBI
Echocardiography. Two-dimensional echocardiographywas performed with use of a Hewlett Packard phased arrayultrasonograph and a medium and short focused 2 .5 or 3 .5MHz transducer, or both . Patients with previous infarctionand those who received streptokinase shortly after admis-sion had their first echocardiogram performed within 12 h ofhospitalization. Each study included all standard echocar-diographic views (36) . In assessing the apical area, imageswere recorded with different gain settings and angulations ofthe transducer, and a short focused transducer was used ineach patient to minimize near field artifacts and to differen-tiate muscular trabeculae and aberrant bands from thrombus(21,34,36) .
Left ventricular thrombus was defined as an echo-densemass, contiguous but distinct from the endocardium, locatedin an area of asyne .,-gy that was seen in both systole anddiastole in at least two echucardiographic views (8,21,34-36). The agreement of two independent reviewers was re-quired for diagnosis of thrombus and other echocardio-graphic variables . Theri-, was 96% interobserver agreementfor thrombus and 92% agreement for characteristics of wallmotion abnormalities adjacent to the cardiac mass . In casesof disagreemem, a decision was reached by joint review ofthe case .
A thrombus was classified as either mural (if the freemargin of the mass was concave following the curvature ofthe endocardial surface) or protruding (if the free margin wasconvex in relation to the adjacent endocardium) ; it wasconsidered mobile if any portion of it moved independent ofthe underlying myocardium (6,12-15) . The area of the throm-bus was defined by tracing its contour on a still frame image(16) using the built-in calibrated measurement system of theechocardiographic machine . During follow-up evaluations, a?50% change in thrombus area was considered to be asignificant change in thrombus size . Left ventricular aneu-rysm was defined as a localized area of akinesia or dyskine-sia that deformed the ventricular contour in both systole anddiastole 16,15 .20) .
Wall inotion of the apical area, where most of thethrombi predictably (6-16) occurred, was qualitativelygraded as normal . hypokinetic, akinetic or dyskinetic ; 90%of dyskinetic segments were: located in the area of an apicalaneurysm. Therefore, apical dyskinesia and left ventricularaneurysm (the latter associated in some cases with apicalakinesia) were analyzed as a single category for statisticalcorrelations. Akinesia without aneurysm was separatelyevaluated. Changes from hypokinesia to akinesia or fromakinesia to dyskinesia were defined as deterioration in wallmotion, and improvement was diagnosed when the oppositechanges occurred .
Nuclear angiography . Left ventricular ejection fractionwas evaluated using multiple gated technetium blood poolscans on an Elscint 400 Apex gamma camera . A change of

792
KEREN ET AL.NATURAL HISTORY OF THROMBI
>5% in ejection fraction was defined as deterioration orimprovement in global ventricular contractility (39) .
Early fibrinolytic and long-term anticoagulant therapy .Thirty-four patients admitted to the emergency room within4 h of the onset of typical chest pain, with ST segmentelevation in at least two ECG leads and lack of response tosublingual nitrates received fibrinolytic therapy (27) . Afterintravenous irnfusk i of hydrocortisone (100 mg), streptoki-nase (1 .5 million U) and heparin (15 IU/kg per h) were alsogiven intravenously . The hematologic effect of the medica-tion was assessed by repeat fibs inogen level and partialthromboplastin time measurements . After 24 h, the heparindose was adjusted to maintain the partial thromboplastintime in the therapeutic range (70 to 140 s) . Successfulreperfusion was defined using clinical and angiugraphiccriteria (30) . Patency of the infarct-related artery was eval-uated in each case on coronary arteriograms obtained 5 to 10days after hospitalization . Before hospital discharge, oralwarfarin was started, and neparin administration wasstopped when the prothrombin time reached the therapeuticrange (20% to 30%). Changes in the warfarin regimen andbleeding complications were recorded .
Systemic embolism . The c iteria for systemic emboliza-tion were similar with those described in previous studies(11,15-17) . The diagnosis of embolism to a limb required thepresence of sudden circulatory compromise and pathologicconfirmation. A cerebrovasculat embolic event was diag-nosed in the presence of a sudden neurologic deficit in theabsence of a previous transient ischemic attack and a carotidartery bruit, normal carotid Doppler recording and indepen-dent confirmation of the embolic; nature of the event by aneurologist. In patients with hypertension, nonlacunar cere-bral infarction had to be demonstrated by computed tomog-raphy .
Statistical analysis . Clinical, echocardiographic and nu-clear angiographic variables were evaluated by univariateand multivariate analysis . Continuous variables were ex-pressed as mean values ± SD. Differences between twomean values were evaluated by a paired or unpaired two-tailed Student t test . Differences among three mean valueswere evaluated with one-way analysis of variance . Categoricvariables were tested by chi-square test or Fisher's exacttest where indicated .
Stepwise logistic regression analysis (40) was used todefine explanatory variables for four major events ("riskgroups") . 1) The risk of thrombus formation during hospi-talization was evaluated in the original 198 patients ; 2) therisk of systemic embolization was evaluated in 189 patients(9 patients were lost to follow-up) who had a clinical follow-up period of 24.0 ± 8.6 months (range I to 48) ; 3) factorsrelated to the disappearance of thrombus ; and 4) the risk ofnew thrombus appearance during the follow-up period wereevaluated in 159 patients with s6 months of echocardio-graphic follow-up study (range 6 to 48 months, mean 26 .6 ±
m134
n-74
at-86
n-94
0-0
0066
Tt-
LM
n-11(43!5)
m37(36%)
n∎0
Figure 1 . Myocardial infarction (Ml) location, therapy and presenceof left ventricular thrombus (LVT+) during initial hospitalization of98 patients . Ant = anterior; Inf = inferior ; STK + = streptakinaseadministered within 3 h of chest pain ; STK - = no streptokinaseadministered .
8.4) . Thus, patients who had an echocardiographic follow-upperiod of <6 months because of death, cardiac surgery orcoronary angioplasty performed before that time periodwere excluded from this analysis .
The stepwise regression analysis defined the beta coeffi-cient and its standard error as well as the corrected oddsratio (comparing the risk and reference groups) for eachexplanatory variable selected (40) .
Attempt to lyre left ventricular thrombi . After conclusionof our study, four additional patients had a large protrudingmobile ventricular thrombus . Each received intravenousstreptokinase or urokinase in an attempt to achieve lysis oftee thrombus. Streptokinase was given in doses usuallyemployed in patients with a thrombosed prosthetic valve(41,42), namely, a 375,000IU bolus followed by 70,000 IU/hand heparin, 1,000 U/h . Urokinase was given as previouslydescribed by Kremer et al . (43), as a 250,000 IU bolusfollowed by 75,000 IU/h and heparin, 1,000 U/h . After this,warfarin therapy was started . Two of these patients havebeen previously described (44,45), but the complicationsnoted and the relevance of these cases to those described inthe consecutive series warrant inclusion of this experience .
ResultsIncidence and factors related to ventricular thrombus
before hospital discharge (Fig . 1) . A left ventricular throm-bus was found on predischarge echocardiograms in 38 (31%)of 124 patients with anterior and none of 74 patients withinferior infarction (p < 0.001). Of the 38 thrombi, 18 (47%)were mural and 20 (53%) were protruding . Six (16%) of the
JACC Vol. 15, No. 4March 15, 1990:790-800

JACC Vol . t5 . No . 4March 15, 1990:790-800
Table 1 . Predischarge Clii cal and Echocaruiographicf virrelations in 124 Patients With Anterior Wall MyocardialInfarction (univariate analysis)
*Multiples of upper normai limit of creatie kinase (CK) level . tAtrialfibrillation, ventricular tachycardia or fibrillation, complete heart block . Ant= anterior ; CHF = congestive heart failure : CPR = cardiopulmonary resus-tation ; echo = echocarliography : int' = inferior; LVEF = left ventricular
ejection fraction ; MI = myocardial infarction .
38 thrombi were mobile ; a,) 6 were of the protruding type .Mean thrombus size was 3.2 ± 1 .6 cm 2 (range 0 .5 to 7.1) .
Comparison of clinical and laboratory data in patientswith anterior infarction with and i ;-ithout thro®nbaac (Table 1)
Table 2 . Results of Stepwise Logistic Itegre,s .,ion Analysis
showed similar findings in the two groups, except thatpatients with a thrombus were younger (p = 0 .02) and had ahigher prevalence of left ventricular ejection fraction <35%(p = 0.01) . The incidence of hypokinetic apical contractilitywas higher in patients without a thrombus (p = 0 .01),whereas dyskinesia or left ventricular aneurysm, or both,were more frequently found in patients with a thrombus (p =0.006) .
Stepwise logistic regression analysis (Table 2) showedthat anterior location of the infarct, decreased left ventricu-lar ejection fraction (35%) and apical dyskinesia or aneurysmhad the highest association with left ventricular thrombusduring hospitalization .
Effect of early throw holytic therapy . Streptokinase wasgiven to 34 patients (Fig . 1) ; 26 had anterior infarction and 11(42%) of these had an apical thrombus . Six (55%) of the 11thrombi were mural, 4 (36%®) were protruding and 1(9%®) wasmobile. The mean thrombus size was 2 .7 ± 1 .9 cm' . None ofthese patients had evidenced thrombus on the first echocar-diogram performed within 12 h of hospitalization . Amongthese 26 patients, thrombus was found in 5 (63%) of 8patients without and in 6 (33%) of 18 patients with reperfu-sion (p = NS) . Among the 98 patients with anterior infarc .Lion and no streptokinase therapy, 27 (28%) had a leftventricular thrombus (p = NS compared with treated pa-tients) . No significant differences were found among clinicalfeatures, ejection fraction, type of thrombus or apical wallmotion between patients with and without streptokinasetherapy .
KEREN ET AL .
793NATURAL HISTORY OF THROMBI
*Because follow-up and predischarge left ventricular ejection fraction (LVEF) =_35% showed a high correlationcoefficient (r = 0.79), the model arbitrarily included one of these variables . because follow-up and predischargeventricular aneurysm showed a high correlation coefficient (r = 0 .81), the model arbitrarily also included one of these
variables . #Apical aneurysm during follow-up showed a negative correlation coefficient (r = -0 .98) with apical
akinesia and could replace it in the model . §Presence of presdischarge left ventricular thrombus showed a highcorrelation coefficient (r = 0.89) with thrombus mobility. FU = follow-up; LV = left ventricular; Pre = predischarge ;
other abbreviations as in Table 1 .
Variable BetaStandardError Odds Ratio p Valu.
Predischarge LV thrombusAnterior MI (Pre) 2 .22 1 .08 9 .20 0.04
LVEF s35% (Pre) 1 .49 0 .52 4 .42 0 .005
Aneurysm (Pre) 1 .00 0.45 2 .73 0.03
Follow-up: new LV thrombusDeterioration iii LV contractility (FU) 2 .46 0 .90 1) .80 0.006
LVEF <_35% (Pre)* 1 .54 0.69 4 .69 0 .02
Aneurysm (Pre)t 1.46 0.90 4 .31 0.05
Follow-up; disappearance of LV thrombusNo dyskinesialaneurysm (Pre)* 1 .59 0.80 4 .90 0 .03
Long-term anticoagulant therapy (FU) 1 .38 0 .92 ? .00 0 .04
Systemic embolismLV thrombus mobility (Pre)§ 6 .80 0.43 6 .10 0.001
Left VentricularThr,>mbus
Present(n = 38)
Absent(n = 86) p Value
Age (yr) 59
13 64 ± 11 0 .02Male 36(95%) 71 (83%) NSPrevious MI 30%) 22(26%) NSAnt + inf MI 4(11%) 1002%) NSMaximal CK* 7.4 ± 3 .9 7.0 ± 4 .6 NSCHF 14(37%) 43150%) NSArrhythmiast 10 (26%) 21 (24%) NSCardiogenic shock or CPR 4 (11°( t 14(16%x) NSLVEF (%) 32 ± 11 40 ± 12 NSLVEF =_?5% 34 189x) 57(66%) 0 .01Apical wall motion (echo)
Hypokinesia 0 18 (21 1/c) 0 .01Akincsia 2-1 (587() 52 46fff) NSDyskinesia/aueurys n 16(421/(, ) 16,19%) 0 .1N16
794 KEREN ET AL .NATURAL HISTORY OF THROMBI
FQLt2W-1110 6E611111110 LYr MM LOCATION OF ANI
n-159
Nat<..et
inf In
n∎95
n-64
Is 1i
6YL
1~
n-29
n-66
n-64
nuam-
L1
it
LIE
n-14
n-10
no 3
1~xti Lwrtn• 2
13/130(106)
sF
LYr-
LYT+
14/29(46%)
6/130(4.60
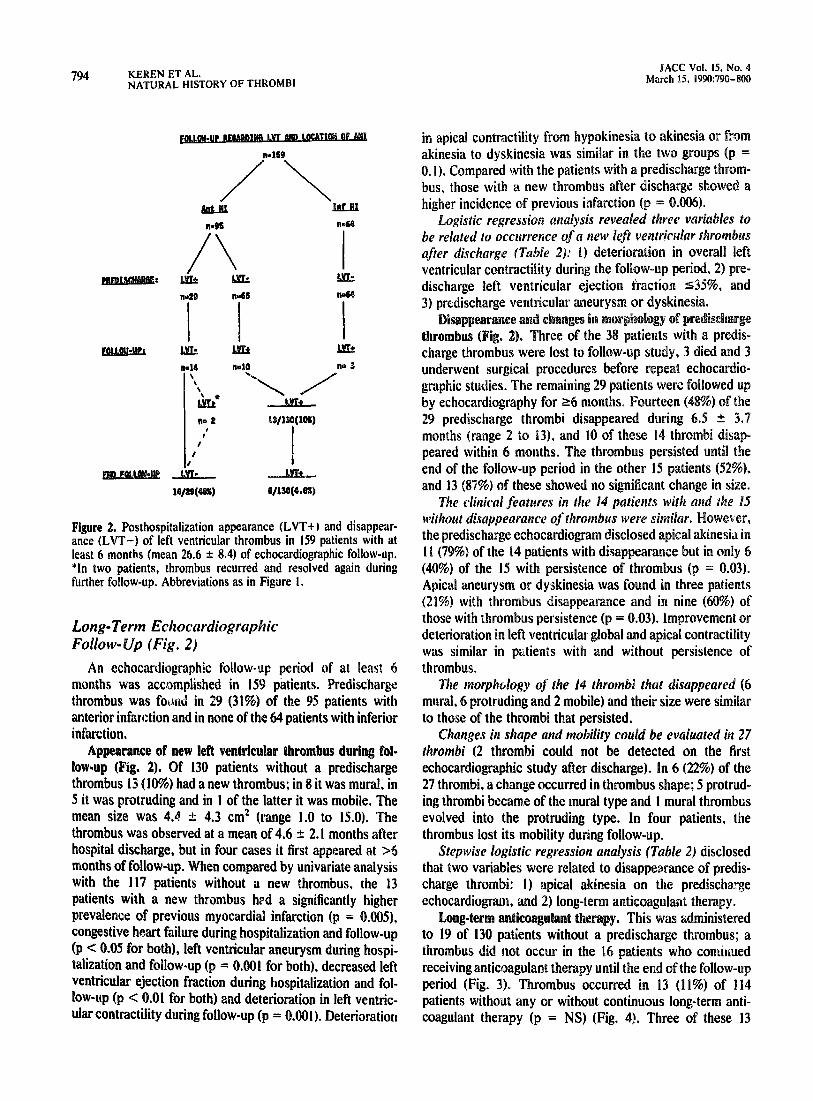
Figure 2 . Posthospitalization appearance (LVT+) and disappear-ance (LVT-) of left ventricular thrombus in 159 patients with atleast 6 months (mean 26 .6 ± 8.4) of echocardiographic follow-up .*In two patients, thrombus recurred and resolved again duringfurther follow-up . Abbreviations as in Figure I .
Long-Term EchocardiographicFollow-Up (Fig. 2)
An echocardiographic follow-up period of at least 6months was accomplished in 159 patients . Predischargethrombus was foorid in 29 (31%) of the 95 patients withanterior infarction and in none of the 64 patients with inferiorinfarction .
Appearance of new left ventricular thrombus during fol-low-up (Fig. 2). Of 130 patients without a predischargethrombus 13 (10%) had a new thrombus ; in 8 it was mural, in5 it was protruding and in I of the latter it was mobile . Themean size was 4.4 ± 4.3 cm 2 (range 1 .0 to 15 .0). Thethrombus was observed at a mean of 4 .6 ± 2.1 months afterhospital discharge, but in four cases it first appeared at >6months of follow-up. When compared by univariate analysiswith the 117 patients without a new thrombus, the 13patients with a new thrombus hed a significantly higherprevalence of previous myocardial infarction (p = 0.005),congestive heart failure during hospitalization and follow-up(p < 0.05 for both), left ventricular aneurysm during hospi-talization and follow-up (p = 0.001 for both), decreased leftventricular ejection fraction during hospitalization and fol-low-up (p < 0 .01 for both) and deterioration in left ventric-ular contractility during follow-up (p = 0 .001). Deterioration
JACC Vol . 15, No. 4March 15, 1990:790-800
in apical contractility from hypokinesia to akinesia or fromakinesia to dyskinesia was similar in the two groups (p =0.1) . Compared with the patients with a predischarge throm-bus, those with a new thrombus after discharge showed ahigher incidence of previous infarction (p = 0 .006) .
Logistic regression analysis revealed three variables tobe related to occurrence of a new left ventricular thrombusafter discharge (Table 2) : 1) deterioration in overall leftventricular contractility during the follow-up period, 2) pre-discharge left ventricular ejection fraction <_35%®, and3) predischarge ventricular aneurysm or dyskinesia .
Disappearance and changes in morphology of predischargethrombus (Fig. 2). Three of the 38 patients with a predis-charge thrombus were lost to follow-up study, 3 died and 3underwent surgical procedures before repeat echocardio-graphic studies . The remaining 29 patients were followed upby echocardiography for ~6 months . Fourteen (48%) of the29 predischarge thrombi disappeared during 6 .5 ± 3.7months (range 2 to 13), and 10 of these 14 thrombi disap-peared within 6 months . The thrombus persisted until theend of the follow-up period in the other 15 patients (52%) .and 13 (87%) of these showed no significant change in size .
The clinical features in the 14 patients with and the 15without disappearance of thrombus were similar. However,the predischarge echocardiogram disclosed apical akinesia in11 (79%) of the 14 patients with disappearance but in only 6(40%) of the 15 with persistence of thrombus (p = 0 .03) .Apical aneurysm or dyskinesia was found in three patients(21%) with thrombus disappearance and in nine (60%) ofthose with thrombus persistence (p = 0 .03). Improvement ordeterioration in left ventricular global and apical contractilitywas similar in patients with and without persistence ofthrombus .
The morphology of the 14 thrombi that disappeared (6mural, 6 protruding and 2 mobile) and their size were similarto those of the thrombi that persisted .
Changes in shape and mobility could be evaluated in 27thrombi (2 thrombi could not be detected on the firstechocardiographic study after discharge) . In 6 (22%) of the27 thrombi, a change occurred in thrombus shape ; 5 protrud-ing thrombi became of the mural type and I mural thrombusevolved into the protruding type. In four patients, thethrombus lost its mobility during follow-up .
Stepwise logistic regression analysis (Table 2) disclosedthat two variables were related to disappearance of predis-charge thrombi: 1) apical akinesia on the predischargeechocardiogram, and 2) long-term anticoagulant therapy .
Long-term anticoagulant therapy . This was administeredto 19 of 130 patients without a predischarge thrombus ; athrombus did not occur in the 16 patients who continuedreceiving anticoagulant therapy until the end of the follow-upperiod (Fig. 3). Thrombus occurred in 13 (11%) of 114patients without any or without continuous long-term anti-coagulant therapy (p = NS) (Fig. 4). Three of these 13

JACC Vol . VS, No . 4March 15, 1990 :790-800
PREDISCUMSE
kmnQ9
EQL
GAPME-Nn-AN-An469
FOLLOW-UP
Aft-
j1q__
k&-
_&__
9
R-20
n-16
n-114
-11
To-719(78%)
7/20(36%)
0/16(0%)
Figure 4 . Formation of a left ventricular thrombus after hospital--AU-
n-13 L91°4
discharge . Upper panel : A, Patient with apical dyskinesia withoutpredischarge thrombus . B . Protruding thrombus (T) found 3 months
-Lifft-
later. C. Resolution of the thrombus after 5 months of warfarin6/114(5%)
therapy . Lower panel : A, Patient with left ventricular (LV) aneu-rysm (an) . Thrombus was not found before discharge and during 12
Figure 3. Correlation between changes in echocardiographic incin months of echocardiographic follow-up study while warfarin wasdence of left ventricular thrombus and long-term anticoagulant administered . B, A mobile thrombus (1) detected 3 months aftertherapy during follow-up . Ac+ = long-term anticoagulants admin- cessation of anticoagulant therapy, which resolved (C) within 2istered ; Ac- = no anticoagulant therapy given, other abbreviations months of renewed anticoagulant therapy. LA = left atrium ; RAas in Figure 2 .
right atrium : RV = right v ;mtricie .
KEREN ET AL .
795NAB ORAL HISTORY OF THROMBI
patients had aneurysm and no thrombus while receivinganticoagulant therapy for 3 to 21 months, but a thrombus didoccur 1 .5 to 3 months after cessation of anticoagulanttherapy . After diagnosis of a new thrombus, treatment withwarfarin was begun in all 13 patients, and the thrombusresolved in I during a further follow-up period of 3 to 18months (mean 6 .8 ± 4.9) (Fig . 3 and 4) .
Among the 29 patients with a predischarge thrombus,long-term anticoagulant therapy was administered to 9 (Fig .3). The thrombus disappeared in 7 (7890 of the 9 patients

796
KEREN ET AL .NATURAL HISTORY OF THROMBI
Table 3. Use of Thrombolytic Agents for Lysis of Apical Mobile Thrombus During AcuteMyocardial Infarction in Four Patients
with and 7 (3517,)) of we 20 patients without anticoagulanttherapy (p < 0 .05). In five patients (three with aneurysm andtwo with apical akinesia), warfarin therapy was stopped 3 to12 months after resolution of the thrombus. However,thrombus recurred in two patients with aneurysm and dis-appeared again after renewal of anticoagulant therapy . Innone of the seven patients with thrombus resolution withoutlong-term anticoagulant therapy was recurrence of a throm-bus seen .
Systemic embolism . Six (17%) of the 35 patients with athrombus on the predischarge evaluation had systemic em-bolism during the follow-up period . None of the 154 patientswithout a thrombus had systemic embolism (p < 0 .001) .Among the 13 patients who developed a new thrombusduring the follow-up period and received long-term anti-coagulant therapy thereafter, none had systemic embolism .The time interval between hospital discharge and emboliza-tion was 10 .9 ± 14.0 months (range I to 36), but four patientshad embolism within 6 months . Two, emboli were to a limband organized thrombus was retrieved at surgery . In fourpatients, an ischemic type cerebrovascular accident wasdiagnosed, and two of these patients died . Systemic embo-lism occurred in I (7%) of 14 patients with a predischargemural thrombus, 1 (7%) of 15 with a protruding nonmobilethrombus and 4 (66%) of the 6 with a protracting mobilethrombus (p < 0 .001) .
Long-term anticoagulant therapy . Twenty-one patients(9 with thrombus on the predischarge echocardiogram and 13with a new thrombus during follow-up period) receivedlong-term anticoagulant therapy and none had systemicembolism. Of the 26 patients with a thrombus withoutanticoagulant treatment, 6 (23%) had an emboik' event (p <0.02). Stepwise logistic regression analysis (Table ?) relatedsubsequent embolic events to presence of a protrudingmobile thrombus (p = 0.001).
Prognostic significance of a left ventricular thrombus .Twenty-nine patients (15%) died among the 189 patientsobserved during the 2 year follow-up period . Cause of deathwas congestive heart failure in 12, recurrent myocardialinfarction in 5, sudden cardiac death in 8, cerebrovascularaccident in 2 and unknown in 2 . The mortality rate was 23%
Thrombolytic Therapy
*Fifteen percent of the original thrombus persisted and embolized. M = male ; STK = streptokinase ; UK =urokinase : other abbreviations as in Table I .
JACC Vol . 15, No. 4March 15, 1990:790-800
(8 of 35) in those with anterior infarction associated with apredischarge thrombus, 15% (13 of 84) in those with anteriorinfarction without a thrombus and I 1 % (8 of 70) in those withinferior infarction (p = NS) . There were no significantcomplications related to warfarin therapy .
Thrombolytic therapy for apical mobile thrombus (Table3). Urokinase or streptokinase was used in four patientswho were not part of the consecutive series described here ;Data on patients I and 2 have been previously published(44,45) . All four patients had anterior infarction with apicalakinesia or dyskinesia, and the diagnosis of thrombus wasmade on days 5 to 16 . Ejection fraction ranged from 28% to46%. After diagnosis of thrombus, systemic heparinizationwas applied for 48 to 72 h . During heparin therapy, Patient Ihad a transient ischemic attack, with disappearance of thesmallest of three apical thrombi originally found. Becauseheparin therapy did not change thrombus size or mobility,urokinase or streptokinase was started . In all four cases, asignificant decrease in size of the thrombus, together with amarked increase in its mobility was seen 8 to 12 h later . InPatients I and 2, the thrombus disappeared without compli-cations . In Patient 3, diplopia occurred 9 h after the start ofstreptokinase infusion . Heparin infusion was continued, butstreptokinase administration was stopped for 24 h untilcomplete resolution of diplopia. The renewed streptokinaseinfusion led to complication-free resolution of the thrombus .
Patient 4 had a large protruding mobile apical thrombusthat decreased significantly in size after 52 h of uncompli-cated infusion of streptokinase . One hour later, the patientsuddenly lost consciousness and developed signs of a righthemispheric stroke . Disappearance of the apical thrombuswas documented by immediate echocardiography ; computedtomography excluded cerebral hemorrhage and showed thepresence of extensive right hemispheric infarction (Fig . 5) .The p.Atient died a few days later .
Patients 1, 2 and 3 were discharged on long-term anti-coagulant treatment . During 20 to 32 months of follow-up,thrombus recurred in one patient after cessation of warfarin,but disappeared again after renewal of anticoagulant ther-apy .
Patient No .Age (yr)/Gender
Day PostMl Type
DurationIh) Outcome
I 41/M 23 UK 36 Successful, no complications
2 451M 10 STK 14 Successful. no complications3 591M 8 STK 64 Successful, transient diplopia4 541M 8 STK 54 Stroke,* death

JACC Vol, 15, No . 4March 15 . 1990:790- 800
Figure 5. Fatal cerebral embolism in a patient with a mobile apicalthrombus who received streptokinase . A, Echocardiogram showinga large apical thrombus (T) (arrows) with a mobile protrudingportion . B, The thrombus after 52 h of uncomplicated sti optokinasetherapy . C, One hour later, signs of right hemispheric strokeoccurred and the thrombus disappeared . D, Computed tomographyshowed extensive right hemispheric cerebral infarction (Cl) occu-pying the territory of the right middle cerebral artery . L = left ;my = mitral valve ; R = right ; tv = tricuspid valve .
DiscussionDeterminants of ventricular thrombus appearance before
hospital discharge. Logistic regression analysis showed thatanterior location of the infarction, left ventricular ejectionfraction :s35% and apical dyskinesia or aneurysm were themajor variables related to thrombus formation . The 31%incidence rate of left ventricular thrombus in anterior infarc-tion and its absence in inferior infarction are in agreementwith previous reports (8-14) . In anterior infarction, furt.`erclinical variables (such as previous infarction, congestiveheart failure, cardiogeaic shock, maximal serum enzymelevels) did not separate patients with and without predis-charge thrombus . Thus, on the basis of clinical criteria, allpatients with anterior infarction should be considered at highrisk of thrombus formatio .j . Decreased ejection fraction wasan independent predictor of (46) but not a prerequisite for(11) thrombus formation . Thrombus is rare in the presence of
a preserved or only mildly decreased left ventricular ejectionfraction, but may occur in patients with an apical aneurysm,as seen in four patients in this series . Similar to find-ngs inother studies (8,46), apical dyskinesia or aneurysm corre-lated better with thrombus occurrence by univariate (p =UK (Table 1) or multivariate (p = (103) (Table 2) analysisthan did akinesia (p = NS) .
Effect of early fibrinolyfic therapy. This study did notdemonstrate a benefic;al effect of early fibrinolytic therapyon left ventricular ejection fraction and the incidence ofthrombus. Sharma et al . (29) observed thrombus within 24 hof streptokinase administration . In the present study, throm-bus was found only after the lytic phase, while patients werefully anticoagulated. The unusually high incidence of throm-bus (42%) found in our patients with anterior infarctionreceiving streptokinase may be related to the small numberof patients evaluated. However, two randomized (28,30) andone uncontrolled (29) study showed an incidence of 26% to55% of thrombus in similar patients . In contrast, Eigler et al .(27) compared 12 patients treated with and 10 patientswithout early thrombolytic therapy and found a significantimprovement in both ejection fraction and thrombus inci-dence in the treated group . Our present study and a previousstudy (30) showed a statistically nonsignificant trend towardfewer thrombi in patients with successful reperfusion .
Appearance of ventricular thromLns during follow-up .Prospective echocardiographic studies have shown that 33%to 62% of thrombi detected during hospitalization arepresent within 48 h of the acute event (18,20,24,27) and somemay be found at admission (20) . Few data (8, 18,20) areavailable concerning the appearance of thrombi after hospi-talization . In 13 (1017c) of our 130 patients. a thrombus firstdeveloped during the follow-up period . This was found in15% of patients with anterior and 5% of those with inferiorinfarction . All patients with inferior infarction had either alarge inferior wall aneurysm or severe inferoapical asynergy .The new thrombus occurred within 6 months of the infarc-tion in 69% of cases, and in 38% of the cases, it was of theprotruding type (Fig . 4) . None of the 16 patients on contin-uous anticoagulant therapy developed a thrombus during thefollow-up period compared with 11% of patients withoutanticoagulant therapy (p = NS) .
Logistic regression analysis showed three factors to berelated to the occurrence of thrombus after hospital dis-charge : 1) deterioration in left ventricular ejection fractionduring the f P,:r;-J . '.) iniiiall,' low ejection fraction,and 3) ventricular aneurysm or dyskinesia during hospital-ization or follow-up . Previous infarction and congestiveheart failure showed a significant correlation with the occur-rence of thrombus by univariate but not by stepwise logisticregression analysis .
Disappearance of thrombus during follow-up. Logisticregression analysis revealed that the type of apical wallmotion before and warfarin therapy after hospital discharge
KEREN ET AL .
797NATURAL HISTORY OF THROMBI
798
KEREN ET AL .NATURAL HISTORY OF THROMBI
were the major factors associated with disappearance ofthrombus in 48% of the patients with a predischarge throm-bus. Thrombus disappeared in 65% of patients with apicalakinesia but in only 25% of those with apical aneurysm ordyskinesia (p = 0 .03). Seven of the 13 new thrombi foundafter hospital discharge disappeared during further follow-up(Fig. 4). Improvement in wall motion adjacent to the throm-bus has been suggested as a possible mechanism for throm-bus resolution (10) . The current study and others (20,22) donot support this observation .
Thrombus disappeared in 78% of patients wcomparedw t only 35% of those without long-term anticoagulantt erapy (p < 0 .05). A randomized study (32) of warfarintherapy in patients with thrombus after acute myocardialinfarction demonstrated 88% versus 24°j~ disappearancerates in treated and untreated patients, respectively . Innonrandomized studies (8,10,11,18 .20,27,33) thrombus dis-appearance rates have ranged from 42% to 84% with and14% to 40% without long-term anticoagulant therapy . Thebeneficial effect of long-term anticoagulant therapy has beensupported by indium-Ill platelet imaging, which showedprolonged (months to years) surface activity of thrombi withactive platelet deposition (47,48) and inhibition of this activ-ity by warfarin in some cases (48) . Furthermore, there arereports (8,20) of thrombus reappearance after cessation ofanticoagulation therapy . to this study and another study(20), thrombus recurred after cessation of anticoagulantsonly in patients with aneursym or dyskinesia, not in thosewith apical akinesia.
Systemic embolism . Previous studies (8-21,25,26,33)have demonstrated systemic embolism in 147 (20%) of 746patients (range 4% to 63%) with echocardiographically doc-umented ventricular thrombus, but in only 16 of 785 patients(2%, range 0 to 4%) without thrombus . In this study,systemic embolism occurred in 6 (17%) of 35 patients with athrombus, but in none of the 154 patients without a predis-charge thrombus (p < 0.001) . Clinical and nuclear angio-graphic variables were not predictive of embolic events .Although most embolic events occur within 6 months ofinfarction, ventricular thrombus continued to represent anincreased risk for systemic embolism in the current andprevious (12-15) reports .
Thrombus mobility on predischarge echocardiographvshowed the best correlation with subsequent embolic events(p < 0 .001), The incidence of embolism in patients with amobile thrombus has ranged from 13% to 83% (11-17) and, inmost cases, mobile thrombi were of the protruding type(13-20). The reported average rates of systemic embolismwere 55% (47 of 86) in protruding mobile, 18% (18 of 102) inprotruding nonmobile and 10% (25 of 255) in mural thrombi(11-16,18). Changes in thrombus shape and mobility werecommon when evaluated from the first day of infarction (18),but were rare in patients evaluated ?3 months after the acuteevent (33) . In the present study, the morphologic character-
JACC Vol . 15, No . 4March 15, 1990 :790-800
istics of persistent thrombus defined before hospital dis-charge remained relatively stable and were predictive ofsubsequent embolic events. A thrombus formed after hospi-tal discharge was not associated with systemic embolism .However, in this group, there was only one patient with amobile thrombus, and long-term anticoagulant therapy wasgiven to all patients immediately after detection of thrombus .Further studies are needed to evaluate the embolic potentialof thrombi formed during follow-up .
It has been suggested that long-term anticoagulant ther-apy is not indicated in patients with ventricular aneurysmbecause of a low incidence of embolism (6,49-51) . In thecurrent series, three of six emboli occurred in patients witha ventricular aneurysm . Moreover, cessation of anticoagu-lant therapy after periods of up to 2 years was associatedwith either recurrence or first appearance of a new thrombusonly in patients with aneurysm . Similar to our results, otherinvestigators (12,15,17) found the same incidence of embo-lism in patients with and without aneurysm, and Reeder etal. (52) demonstrated that in patients with aneurysm, thefrequency of systemic embolism decreased significantly withlonger periods of anticoagulant therapy.
Fibrinolytic therapy in patients with a mobile apical throm-bus. Kremer et al . (43) reported lysis of a protruding throm-bus in 10 of 16 patients after acute myocardial infarction . Atleast three of their patients had a mobile thrombus . Thetreatment was successful in eight of nine patients within 4weeks of the acute infarction . None of the patients hadclinical embolism, and only in one was therapy discontinuedbecause of hematuria . Shenoy et al . (53) reported successfullysis of an apical mural thrombus with streptokinase . Con-sidering the foregoing discussion, we selectively applied thistherapy to four patients with a protruding mobile thrombus .In the first two previously reported cases (44,45), lysis ofthrombus was achieved without complication . In the lattertwo cases, however, systemic embolism occurred, withtransient diplopia in one and stroke followed by death in theother. This experience confirms that fibrinolytic agents arecapable of lysing ventricular thrombi but suggests that therisks of this therapy may be higher than previously assumed .
Limitations of the study. This was an observational studyin which anticoagulant and fibrinolytic therapies were notcontrolled and were applied to a small number of patients .Therefore, the results regarding these therapies are notconclusive. The data regarding resolution and appearance ofa new thrombus during the follow-up period can be appliedonly to long-term survivors on medical therapy becauseechocardiographic follow-up of ?6 months was not availablein approximately 20% of the patients, mostly because ofdeath or operative interventions during that time period . Theresults of univar9 .ate statistical .analysis should be consideredwith caution given the multiple comparisons made . How-ever, we also used logistic regression analysis, which elim-inated fortuitous statistical significance .

JACC Vol . 15, No. 4March 15,1990 :790-800
Clinical implications. The results of this study supportthe view that echocardiography should be routinely per-formed before hospital discharge in all patients with acuteanterior myocardial infarction (54,55) to 1) diagnose patientswith ventricuiar thrombus and those with a protrudingmobile thrombus who are at especially high risk of embo-lization ; 2) define patients at risk of developing thrombusafter hospital discharge ; and 3) identify patients who mayundergo resolution of thrombus during follow-up . We did notdemonstrate a reduction in incidence of lentricular throm-bus by early fib inoytiQ therapy and a full dose of anticoag-ulants during the acute phase of infarct'an . However, long-term anticoagulant therapy applied to a relatively smallnumber of patients in the posthospitalization period wasassociated with an increased resolution rate of thrombus andwith prevention of systemic embolism in patients with doc-umented thrombus . Long-term anticoagulant therapy underechocardiographic guidance is probably indicated until res-olution of the thrombus is seen on the follow-up echocardio-gram. 1A eighing the risk-benefit ratio, long-term anticoagu-lant therapy may be given indefinitely to selected patientswith left ventricular aneurysm, decreased or deterioratingleft ventricular ejection fraction (that is, in the presence ofthe factors that predispose to occurrence of a new thrombusduring the follow-up period) . Lysis of fresh thrombi withthrombolytic agents is feasible, but may be associated withdeath. More data are needed before thrombolysis is accepteaas the therapy of choice in patients with a mobile thrombus(56) .
We thank Richard L. Popp, MD of Stanford . California for reviewing themanuscript and his valuable editorial comments . We thank Shaul Yalon fortechnical help, and Hanna Sebag for preparation of the manuscript .
References
1 . Wright IS, Marple CD, Beck DF . Report of the Committee for theEvaluation of Anticoagulants in the Treatment of Coronary ThrombosisWith Myocardial Infarction . Am Heart J 1948 ;36 :801-15 .
2 . Arnott WM, Bigs R, Gilchrist AR, et al . Assessment of short-termanticoagulation administration after cardiac infarction : report of theWorking Party on Anticoagulant Therapy in Coronary Thrombosis to theMedical Research Council . Br Med J 1969:1 :335-42 .
3 . Veterans Administration Cooperative Study . Anticoagulants in acutemyocardial infarction : results of a cooperative clinical trial . JAMA1973 ;225 :724-9 .
4 . Hellerstein HK, Martin JW . Incidence of thromboembolic lesions accom-panying myocardial infarction . Am Heart 3 1947 :33 :443-52 .
5, Jordan RA, Miller RD, Edwards JE, Parker RL. Thromboembolism inacute and healed myocardial infarction . Circulation 1952 :6 :1-6 .
6. Cabin HS, Roberts WC. Left ventricular aneurysm . intraaneurysmalthrombus and systemic embolus in coronary heart disease . Chest 1980;77 :585-90.
7 . DeMaria AN, Bommer W, Neumann A, et al . Left ventricular thrombiidentified by cross-sectional echocardiography . Ann Intern Med 1979 :90:14-8.
KEREN ET AL .
799NATURAL HISTORY OF THROMBI
8 . singer RW . Mikell FL. Elsperger J . Hodges M . Incidence of left-vmoricular thrombosis after acute transmural myocardial infarction :serial Avaluwion by two-dimensional echocardiography . N Engl I Med198130:197-302 .
9 . Friedman 011 ('srlson K . Marcus Fl . WcAfenden JM . Clinical correla-tions in patient, with acute myocardial infarction and left ventricularthrombus detected by two-dimensional echocardiography . Am J Med1982 :72 :894-8 .
10 . Keating EC . Gross SA, Schlamowitz RA, et al . Mural thrombi inmyocardial infarctions : prospective evaluation by two-dimensional echo-cardiography . Am J Med 19,93,74 :989-95 .
11 . Weinreich DJ . Burke JF, Pauletto FJ . Left ventricular mural thrombicomplicating acute myocardial infarction: long-term follow-up with serialechocardiography . Ann intern Med 1984 :100 :789-94 .
12 . Haugland JM, Asinger RW, Mikell FL, Elspergcr J, Hodges M . Embolicpotential of left ventricular thrombi detected by two-dimensional echo-cardiography . Circulation 1984 :70 :588-98 .
13 . Meltzer RS, Visser CA, Kan G, Roelandt J . Two-dimensional echocar-diographic appearance of left ventricular thrombi with systemic emboliafter myocardial infarction . Am J Cardiol 1984 :53 :1511-3 .
14 . Visser CA, Kan G, Meltzer RS, et al . Embolic potential of left ventricularthrombus after myocardial infarction : a two-dimensional echocardio-graphic study of 119 patients . J Am Coll Cardiol 1985 :5 :1276-80 .
15 . Stratton JR . Resnick AD . Increased embolic risk in patients with leftventricular thrombi . Circulation 1987 :75 :1004--11 .
16. Johannessen KA, Nordrehaug JE, von der Lippe G, Vollset SE . Riskfactors for embolisation in patients with left ventricular thrombi and acutemyocardial infarction . Br Heart J 1988 :60 :104-10 .
17 . Jugdutt BI . Sivaram CA, Wortman C, Trudell C . Penner P . Prospectivetwo-dimensional echocardiographic evaluation of left ventricular throm-bus and embolism after acute myocardial infarction . J Am Coll Cardiol1989 :13 :554-64 .
18. Domenicucci S, Bellotti P . Chiarella F . Lupi G . Vecchio C . Spontaneousmorphologic changes in left ventricular thrombi : a prospective two-dimensional echocardiographic study . Circulation 1987 :75 :737-43 .
19. Spirito P, Bellotti P. Chiarella F, Domenicucci S . Sementa A . Vecc 'iio CPrognostic significance and natural history of left ventricular thromft titpatients with acute myocardial infarction : a two-dimensional echuc> -'graphic study . Circulation 1985 -.72 :774-80,
20. Visser CA . Kan G . Meltzer RS, Liek 1, Durrer D . Long-term follow-au, o•;.left ventricular thrombus after acute myocardial infarction : a 'ovo-dimensional echocardiographic study in 96 patients . Chest 1984 ;86 :532-~ .
21 . Stratton JR, Lighty GW . Pearlman AS, Ritchie JL . Detection of I&ventricular thrombus by two-dimensional echocardiography : sensitivity,specificity, and causes of uncertainty . Circulation 1982 :66 :156-66 .
22. Nordrehaug JE . Johannessen KA, von der Lippe G . Usefulness ofhigh-dose anticoagulants in preventing left ventricular thrombus in acutemyocardial infarction . Am J Cardiol 1985 :55 :1491-3 .
23 . Davis MJ . Ireland MA . Effect of early anticongulation on the frequency ofleft ventricular thrombi after anterior wall acute myocardial infarction .Am J Cardiol 1986 :57 :1244-7 .
24 . Gueret P. Dubourg 0 . Ferrier A, Farcot JC, Rigaud M, Bourdarias JP .Effects of full-dose heparin anticoagulation on the development of leftventricular thrombosis in acute transmural myocardial infarction . J AmCoil Cardio! 1986 :8 :419-26 .
25. Aryan S, Boscha K . Prophylactic anticoagulation for left ventricularthrombi after acute myocardial infarctior : a prospective randomized tri(4 .Am Heart J 1987 :113 :688-93 .
26. Turpie AGG . Robinson JG, Doyle DJ, et al . Comparison of high-dosewith low-dose subcoatmous heparin to prevent left ventricular muralthrombosis in patients w I acute transmural anterior myocardial infarc-tion . N Engl J Med 1989 ;320 :352-7 .

800
KL:tEN ET AL .NATURAL HISTORY OF THROMBI
27 . Eigler N. Maurer G . Shah PK . Effect of early systemic thrombolytictherapy on left ventricular thrombus formation in acute anterior myocar-dial infarction . Am J Cardiol 1984 ;54:261-3 .
28 . Stratton JR. Speck SM. Caldwell JH, et al . Late effects of intracoronarystreptokinase on regional wall motion, ventricular aneurysm ind leftventricular thrombus in myocardial infarction : results from the WesternWashington Randomized Trial . J Am Coll Cardiol 1985 :5 :1023-8 .
29. Sharma B, Carvalho A, Wyeth R . Franciosa JA . Left ventricular thrombidiagnosed by echocardiography in patients with acute myocardial infarc-tion treated with intracoronary streptokinase followed by intravenot ;heparin. Am J Cardiol 1985 ;56 :422-5.
30. Held AC, Gore JM, Paraskos J, et al . Impact of thrombolytic therapy onleft ventricular mural thrombi in acute myocardial infarction . Am JCardiol 1988 ;62 :310-1 .
31 . Meltzer RS . Guthaner D. Rakowski H . Popp RL . Martin RP. Diagnosis ofleft ventricular thrombi by two-dimensional echocardiography . Br HeartJ 1979 ;42 :261-5 .
32 . Tramarin R, Pozzoli M . Febo O. et al . Two-dimensional echocardio-graphic assessment of anticoagulant therapy in left ventricular thrombosisearly after acute myocardial infarction . Eur Heart J 1986-.7 :482-92,
33 . Stratton JR . Nemanich JW. Johannessen KA . Resnick AD . Fate of leftventricular thrombi in patients with remote myocardial infarction oridiopathic cardiomyopathy . Circulation 1988 ;78 :1388-93 .
34 . Asinger RW, Mikell FL, Sharma B, Hodges M . Observations on detectingleft ventricular thrombus with two-dimensional echocardiography : em-phasis on avoidance of false positive diagnoses. Am J Cardiol 1981 ;47 :145-56.
35 . Visser CA, Kan G. David GK, Lie K1, Duffer D. Two-dimensionalechocardiography in the diagnosis of left ventricular thrombus : a prospec-tive study of 67 patients with anatomic validation. Chest 1983 ;83:228-32 .
36 . Keren A, Billingham ME . Popp RL . Echocardiographic recognition andimplications of ventricular hypertrophic trabeculations and aberrantbands . Circulation 1984 :70:836-42 .
37 . Keren A, Takamoto T . Harrison DC . Popp RL. Left ventricular apicalmasses : noninvasive differentiation of rare from common ones . Am JCardiol 1985 ;58:697-9.
38. Criteria Committee of the New York Heart Association . Nomet;ciaturcand Criteria for Diagnosis of Disease of the Heart and Great Vessels . 7thed . Boston: Little .3rown, ±O73 :959.
39. Wackers FJT, Berger HJ . Jehnstone DE, et al . Multiple gated cardiacblood pool imaging for left ventricular ejection fraction : validation of thetechnique and assessment of variability . Am J Cardiol 1979 ;43 :1159-66.
40. Pregibond D. Logistic regression diagnostics . Ann Statist 1981 :9:705-24 .
41. Ledain LD. Ohayon JP, Co!te JP. Lorient-Roudaut FM . Roudaut RP .
JACC Vol . 15 . No . 4March 15 . 1990 :790-800
Besse PM . Acute thrombotic obstruction with disc valve prostheses :diagnostic considerations and fibrinolytic treatment . J Am Coll Cardiol1986 :7 :743-51 .
42 . Kurzrok S . Singh AK. Most AS, Williams DO. Thrombolytic therapy forprosthetic cardiac valve thrombosis . J Am Coll Cardiol 1987 ;9 :592-8 .
43 . Kremer P. Fiebig R, Tilsner V . Bleifeld W . Mathey DG . Lysis of leftventricular thrombi with urokinase . Circulation 1985 ;72:112-8.
44. Keren A, M,dina A, Gottlieb S. Banai S, Stern S . Lysis of mobile leftventricular thrombi during acute myocardial infarction with urokinase .Am J Cardiol 1987 ;60 :1180-I .
45 . Keren A. Mazouz B. Moriel M . Tzivoni D, Stern S. Use of streptokinasefor lysis of a mobile left ventricular thrombus . report of a case and reviewof the literature . Cardiology 1988;75 :444-7.
46. Lamas GA, Vaughan DE . Pfeffer MA . Left ventricular thrombus forma .tion after first anterior wall acute myocardial infarction . Am J Cardiol1988 :62:31-5 .
47 . Ezekowitz MD, Wilson DA . Smith EO, el al . Comparison of indium- l I Iplatelet scintigraphy and two-dimensional echocardiography in the diag-nosis of left ventricular thrombi . N Engl J Med 1982 ;306 :1509-13 .
48 . Stratton JR. Ritchie JL. The effects of antithrombotic drugs in patientswith left ventricular thrombi : assessment with indium- I I I platelet imagingand two-dimensional echocardiography . Circulation 1984 ;69:561-8.
49 . Fuster V . Halperin JL . Left ventricular thrombi and cerebral embolism .N EnglJ Med 1989;320:392-4.
50. Simpson MT. Oberman A . Kouchoukos NT, Rogers WJ . Prevalence ofmural thrombi and systemic embolization with left ventricular aneurysm :effect of anticoagulation therapy . Chest 1980 ;77 :463-9.
51 . Lapeyre AC . Steele PM . Kazmier FJ, Chesebro JH, Vlietstra RE, FusterV. Systemic embolism in chronic left ventricular aneurysm : incidence andthe role of anticoagulation . J Am Coll Cardiol 1985 ;6:534-8 .
52. Reeder GS, Lengyel M, Tgjik AJ, Seward JB, Smith HC, Danielson GK .Mural thrombus in left ventricular aneurysm : incidence, role of angiog-raphy, and relation between anticoagulation and embolization . Mayo ClinProc 1981 ;56:77-81 .
53 . Shenoy MM. Friedman SA . Dhar S . Berman P . Streptokinase lysis ofintraventricular thrombus and pulmonary emboli with resolution of ac-quired intracardiac shunt . Ann Intern Med 1985 :103:65-6.
54 . Nixon JV . Left ventricular mural thrombus . Arch Intern Med 1983 ;143 :1567-71 .
55. Kaplan K. Prophylactic anticoagulation following acute myocardial in-farction. Arch Intern Med 1986 ;146:593-7.
56 . Gutt,:rman DD . Characterization of the acute left ventricular thrombus :hermit or nomad? J Am Coll Cardiol 1989:13 :565-6.




















