National AIDS Control Council - World Bank Group
41
Building on our Experiences: Lessons Learnt and Future Direction of the Community Programme Kenya National AIDS Control Council Office of the President September 2003
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of National AIDS Control Council - World Bank Group
Building on our experiences1
National AIDS Control Council
Building on our Experiences:Lessons Learnt and Future Direction
of the Community Programme
Kenya
National AIDS Control CouncilOffice of the President
September 2003

Building on our experiences 2
National AIDS Control Council
Technical assistance in compiling and producing this report provided by Apex Communications Ltd.,
P.O Box 12313-00400 Nairobi, Tel: 2716890, Tel/Fax: 2719478 Email: [email protected]
Acknowledgments
The National AIDS Control Council would like to express their sincere gratitude to all
those people whose time and effort went into the production of this report. We particularly
recognise the contribution of the community based, faiths based and non-governmental
organisations for their effort in preparing project reports and ensuring that the projects which form
the basis of this report are implemented.
We also extend our gratitude to the Provincial, District and Constituency AIDs Control
Committees for organising and coordinating the regional experience-sharing meetings both in
Nairobi and Eldoret. Special thanks to the Kenya AIDs NGO’s Consortium (KANCO) for
accepting to assist in facilitation during the first meeting.
Profound appreciation goes to the World Bank and the United Nations Development
Programme (UNDP), without whose financial support the regional-experience sharing meetings as
well as this report would not have been undertaken.

Building on our experiences3
National AIDS Control Council
Contents
Acronyms and Abbreviations ..................................................................................................................................................... 4
Foreword ................................................................................................................................................................................................ 5
Summary ................................................................................................................................................................................................ 7
Background .......................................................................................................................................................................................... 9
Accomplishments ........................................................................................................................................................................... 13
Emerging Issues and Challenges ............................................................................................................................................ 25
Emerging Lessons and Future Direction ............................................................................................................................. 31
Appendix
List of Participants ............................................................................................................................................................. 34
Workshop Programme ..................................................................................................................................................... 37

Building on our experiences 4
National AIDS Control Council
Acronyms and AbbreviationsACUs AIDS Control Units
AIDS Acquired Immune Deficiency Syndrome
AMREF African Medical Research Foundation
ARVs Antiretrovirals
CACC Constituency AIDS Control Committee
CBO Community Based Organisation
CIA Community Initiative Account
COCC Community Orphans Care Committee
DACC District AIDS Control Committee
FBO Faith Based Organisation
FGM Female Genital Mutilation
FMA Financial Management Agency
FONI Friends of Nomads International
HIV Human Immunodeficiency Virus
IEC Information, Education & Communication
IFC International Fellowship Centre
IGAs Income Generating Activities
KANCO Kenya AIDS NGO’s Consortium
KAPC Kenya Association of Professional Counselors
KHADREP Kenya HIV/AIDS Disaster Response Project
MADICAA Makadara Division Campaign Against AIDS
MOCASO Mother/Child with AIDS Support Organisation
NACC National AIDS Control Council
NASCOP National AIDS and STDs Control Programme
NCC Nairobi City Council
NGO Non-Governmental Organization
NOPE The National Organisation of Peer Educators
OIs Opportunistic Infections
OVC Orphans and Vulnerable Children
PACC Provincial AIDS Control Committee
PAIDO Participatory Approaches for Integral Development Organization
PLWD People Living With Disabilities
PLWHA People Living With HIV/AIDS
RICOAN Riruta Community Against AIDS Network
SDA Seventh Day Adventist
SSM Stepping Stones Methodology
STDs Sexually Transmitted Diseases
UCC Ukamba Christian Community
UN United Nations
USAID United States Agency for International Development
VCT Voluntary Counseling and Testing
WEMIHS WEM Integrated Health Services

Building on our experiences5
National AIDS Control Council
Foreword
Over the years, HIV/AIDS has emerged as the greatest development challenge facing our
country. By 2001, approximately 2.2 million Kenyans were infected with HIV/AIDS while 1.5
million Kenyans are estimated to have died from AIDS related illnesses.
To meet the challenges posed by the HIV/AIDS pandemic, the Kenya Government declared
HIV/AIDS a national disaster in 1999 and set up the National AIDS Control Council. Declaring
AIDS a national disaster and setting up NACC, marked the beginning of the road to a strong
multisectoral coordination mechanism to tap the full potential of all sectors in the fight against
HIV/AIDS.
The Kenya HIV/AIDS Disaster Response Project (KHADREP), funded to the tune of US$ 50
million by the World Bank provides the framework for involving all government ministries and
departments, civil society, private sector, and faith-based organizations among other stakeholders
in the response towards the epidemic. This project is to run from year 2001 to 2004.
A key component of KHADREP is to support community driven local initiatives through capac-
ity building, financial and human resources through the Community Initiative Account (CIA) with
a budget of US$ 30 million out of the US$ 50 million. The CIA component was operationalized in
June 2002 and by June 2003, over Ksh 816 million from this Account had been approved for dis-
bursement to CBOs, FBOs and NGOs to support community based interventions that they are
spearheading throughout the country.
To tap the “emerging wisdom” over the short period of implementing these interventions,
NACC organized two experience-sharing workshops in May and June 2003 not only to document
the accomplishments and emerging issues but more importantly to draw lessons on the effective-
ness, successes or problems faced in the course of implementing these interventions.
This report is the outcome of those two workshops. It has many inspiring examples of how
communities are organizing themselves to address the challenges posed by HIV/AIDS. These
include the challenges of setting up a community VCT centre, taking care of orphans or increasing
knowledge among specific groups. The report has examples of challenges that need to be ad-
dressed in order for Kenya to face up to the HIV/AIDS challenge with increasing effectiveness.
The report also provides insight on the future direction of the community based interventions
and also points out areas that require action. This report is an important resource for those imple-
menting or planning to implement community based interventions in different parts of the country.
Prof. Miriam Were
Chairman
National AIDS Control Council

Building on our experiences 6
National AIDS Control Council

Building on our experiences7
National AIDS Control Council
Summary
As the world enters the third decade of the AIDS epidemic, the evidence of its tragic impact is
undeniable. According to UNAIDS, sub-Saharan Africa is by far the worst affected region. By
2002, the region was home to 29.4 million people living with HIV/AIDS. Approximately 3.5 million
new infections occurred there in 2002.
The epidemic claimed the lives of an estimated 2.4 million Africans in the past year. Ten million
young people aged 15-24 years and almost 3 million children under 15 years are living with HIV.
The situation in Kenya reflects this continental pattern.
The government is however determined to stem the epidemic and reduce the impact on Kenyan
society and economy. The popular version of the Kenya National HIV/AIDS Strategic Plan pro-
vides the roadmap to address priority areas for the control of HIV/AIDS as well as mechanisms for
the mitigation of the social economic impacts at individual, family community, sectoral and na-
tional levels.
This report is the outcome of two workshops held in May and June 2003 that brought together
community based, faiths based and non-governmental organisations funded by NACC. It
documents their experiences, accomplishments, challenges and successes in implementing
community initiatives in response to the HIV/AIDS epidemic and points to the future direction of
these initiatives.
The report is divided into three major parts:
Part one gives an outline of the key accomplishments under three thematic areas namely preven-
tion and advocacy, treatment, continuum of care and support and mitigation of the socio-economic
impact.
Prevention and advocacy activities undertaken by the implementers are focused on increasing
knowledge on HIV/AIDS, modes of transmission and measures that would lead to attitudinal and
behavioural change on sexual matters.
In the area of prevention, creating awareness was the key focus. Several methods have been
used ranging from workshops and seminars to sports forums. The implementers are also working
with priority groups for HIV/AIDS interventions.
Activities carried out under treatment, continuum of care and support include treatment of
opportunistic infections by traditional medical practitioners, counseling, homebased care and
refferals to conventional health facilities.
Under mitigation of social and economic impact, effort is geared towards income generating
activities and care and support of orphans.
Part two of the report documents the emerging issues and the challenges associated with imple-
menting the HIV/AIDS projects at the community level. Key issues and challenges emerged from
discussions that followed presentations and plenary discussions.

Building on our experiences 8
National AIDS Control Council
Issues that require action range from increasing community participation, easing procedures for
proposal approval and disbursement of funds, to building capacity and developing guidelines on
information and education materials. There were also crosscutting issues that emerged which
includes networks for People Living With HIV/AIDS, lack of capacity and the fate of equipment in
use after the expiry of projects.
Part three discusses the emerging lessons and proposed future direction of the community initia-
tives.
Community participation was found inadequate in some cases and needs to be addressed by the
implementers. Participants also called for the establishment of a central body to coordinate preven-
tive efforts addressing the youth, who form the largest case load of new HIV infection.
Other issues related to capacity building, dissemination of guidelines on home based care and
development of appropriate IEC materials. Action is also required on strengthening the link among
the different structures of NACC on the one hand and the community based implementers to
enhance the supervisory role of these structures.
Another emerging issue relates to monitoring and evaluation. As the project moves on, it will be
important to establish and integrate monitoring and evaluation mechanism for programme activi-
ties in order to capture its successes and challenges more systematically and effectively.

Building on our experiences9
National AIDS Control Council
Background
The magnitude and impact of HIV/AIDS in Kenya is a major development and public health
challenge that is increasingly creating severe negative socio-economic impact. More than one
million people have developed AIDS and died since 1984. At the end of June 2000, more than two
million Kenyans were living with HIV. In 1998 alone, over 200,000 new infections occurred while 70
per cent of those already infected live in the rural areas. The majority are young people aged
between 15-39 years.
In order to meet the challenges posed by the HIV/AIDS pandemic, the Kenyan government
declared HIV/AIDS a national disaster in 1999, and set the stage for the setting up of the National
AIDS Control Council vide a Gazette Notice No. 170 of 1999. This marked the beginning of a strong
multisectoral coordination mechanism to tap the full potential and participation of all sectors and
stakeholders to deal with the numerous challenges presented by the HIV/AIDS epidemic.
The aim is to mount a successful multisectoral response to the epidemic in accordance with
provisions and objectives of the Sessional Paper No.4 of 1997 on HIV/AIDS in Kenya.
The mandate of the National AIDS Control Council is divided into three broad categories which
include to coordinate and manage the implementation of a national multisectoral HIV/AIDS
programme, provide policy directions for the national multisectoral HIV/AIDS programme and
mobilise resources for the national HIV/AIDS programme.
The setting up of NACC was followed by the development of the Kenya National HIV/AIDS
strategic plan for the year 2002-2005, to guide the national multisectoral approach to HIV/AIDS
control and prevention.
The overarching theme of the plan is social transformation to reduce HIV/AIDS and poverty.
The Plan’s principle objective is to stop the epidemic and reduce its impact on Kenyan society and
economy by:
■ Reducing HIV prevalence in Kenya by 20 to 30 per cent among people aged 15 to 24 years
by 2005;
■ Increasing access to care and support for people infected and affected by HIV/AIDS in
Kenya; and
■ Strengthening response capacity and coordination at all levels.
Priority areas include:
■ Prevention and advocacy;
■ Treatment, continuum of care and support;
■ Mitigation of the socio-economic impact;
■ Monitoring and evaluation and research; and
■ Management and coordination.

Building on our experiences 10
National AIDS Control Council
Within these agreed priority areas, a variety of interventions are being implemented to achieve
defined objectives for each priority area. In the absence of a cure for HIV/AIDS, the Kenya Na-
tional HIV/AIDS strategic plan for year 2002-2005 weights resources more heavily towards preven-
tive activities within the priority areas and on the communities.
Implementation of the strategic plan capitalises on existing infrastructure and strengths to
increase coverage and quality of service provision through key stakeholders, mainly non-govern-
mental organisations, community based organisations, public and private sectors and religious
organizations. The structural arrangements may be adjusted for greater effectiveness.
For the specific purpose of involving the above stakeholders in the national response to the
HIV/AIDS epidemic and making financial resources available to these organisations, NACC has
established an HIV/AIDS Community Initiative Account (CIA), funded to the tune of US$ 30
million, out of a total of US$ 50 million for the entire Kenya HIV/AIDS Disaster Response Project
(KHADREP).
This component constitutes the largest fund allocation of this project, highlighting the high
priority that is being given to the expansion of community-driven local initiatives. Other compo-
nents are the AIDS Control Units (ACUs) established within government ministries and depart-
ments for US$ 10.3 million and coordination and management of AIDS program by NACC and its
structures for US$ 12.1 million.
The CIA will contribute to the improvement of the welfare of communities by increasing their
access to financial and human resources to assist them to limit further spread of HIV and address
the impact of the epidemic on individuals and households.
It will respond to demands for sub-projects, which aim to address the prevention of HIV infec-
tion or the issues related to the impact of HIV/AIDS on those infected or affected by the disease.
These may include activities aimed at behaviour change, social support to those infected and
affected by HIV/AIDS, training programmes for community volunteers and care-givers, as well as
seed funding to start income generating activities. These sub-projects will be identified, designed,
implemented, managed and maintained by the beneficiary communities.
Disbursement of the funds started in June 2002. As of June 20, 2003, a total of 982 projects had
been appproved for funding to the tune of Ksh 816,661,080 out of which Ksh 487,144,980 has
already been disbursed.
As of June 20, 2003, priority areas which had either been partly or fully funded since the incep-
tion of the programme include prevention and advocacy to the tune of Ksh 522,456,993 and treat-
ment, continuum of care and support to the tune of Ksh 94,242,354 . Others are mitigation of socio-
economic impact to the tune of Ksh 116,339,151 support to orphans to the tune of Ksh 76,122,582
and monitoring, evaluation and research to the tune of Ksh 7.5 million.
The implementation of the KHADREP project of which the Community Initiative Account is a
component is slated to lapse in December 2004. However there are indications that the project will
be extended beyond 2004.
This report is the product of two regional experience sharing workshops which brought together
community based, faith based and non-governmental organisations funded by NACC from the

Building on our experiences11
National AIDS Control Council
Community Initiative Account. Organisations made presentations on the activities they had carried
out, the challenges they faced and the lessons they learnt.
The specific objectives of the workshops were to:
■ Identify and discuss what worked and what did not work in project development and
implementation;
■ Identify and discuss the challenges and problems encountered in project development and
implementation; and
■ Identify and document the lessons learnt.

Building on our experiences 12
National AIDS Control Council
Building on our experiences13
National AIDS Control Council
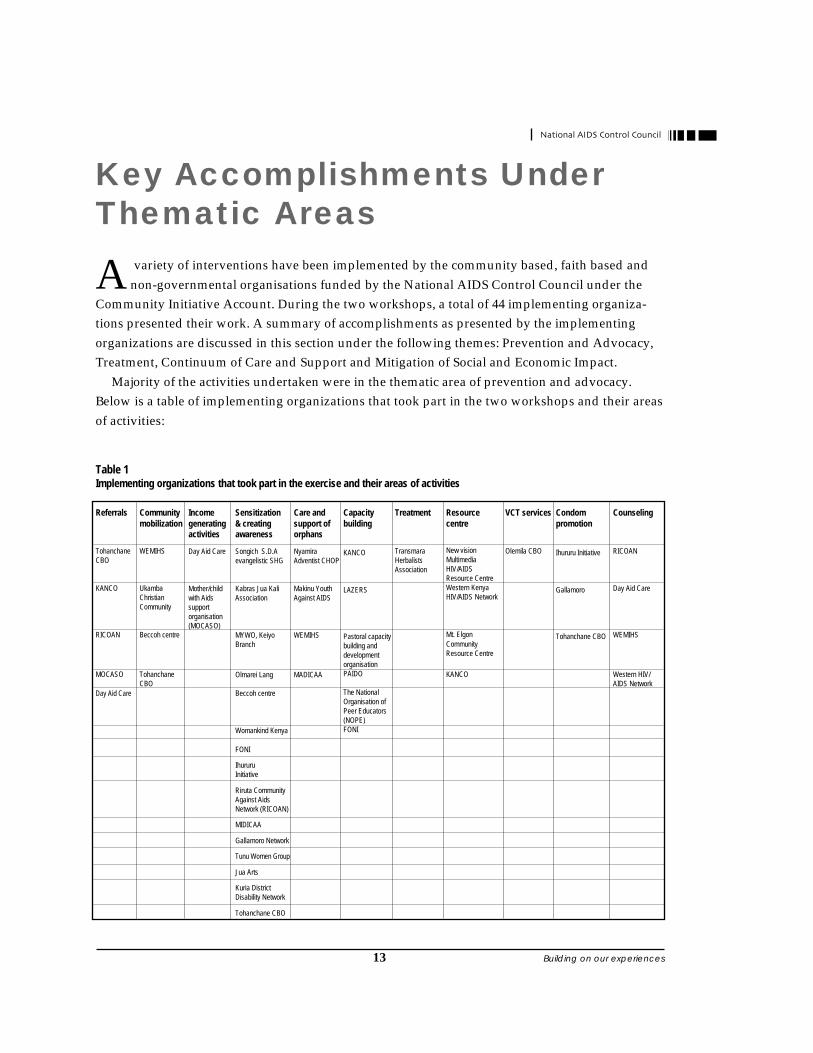
Key Accomplishments UnderThematic Areas
A variety of interventions have been implemented by the community based, faith based and
non-governmental organisations funded by the National AIDS Control Council under the
Community Initiative Account. During the two workshops, a total of 44 implementing organiza-
tions presented their work. A summary of accomplishments as presented by the implementing
organizations are discussed in this section under the following themes: Prevention and Advocacy,
Treatment, Continuum of Care and Support and Mitigation of Social and Economic Impact.
Majority of the activities undertaken were in the thematic area of prevention and advocacy.
Below is a table of implementing organizations that took part in the two workshops and their areas
of activities:
Table 1Implementing organizations that took part in the exercise and their areas of activities
Referrals
TohanchaneCBO
KANCO
RICOAN
MOCASO
Day Aid Care
Communitymobilization
WEMIHS
UkambaChristianCommunity
Beccoh centre
TohanchaneCBO
Incomegeneratingactivities
Day Aid Care
Mother/childwith Aidssupportorganisation(MOCASO)
Sensitization& creatingawareness
Songich S.D.Aevangelistic SHG
Kabras Jua KaliAssociation
MYWO, KeiyoBranch
Olmarei Lang
Beccoh centre
Womankind Kenya
FONI
IhururuInitiative
Riruta CommunityAgainst AidsNetwork (RICOAN)
MIDICAA
Gallamoro Network
Tunu Women Group
Jua Arts
Kuria DistrictDisability Network
Tohanchane CBO
Care andsupport oforphans
NyamiraAdventist CHOP
Makinu YouthAgainst AIDS
WEMIHS
MADICAA
Capacitybuilding
KANCO
LAZERS
Pastoral capacitybuilding anddevelopmentorganisationPAIDO
The NationalOrganisation ofPeer Educators(NOPE)FONI
Treatment
TransmaraHerbalistsAssociation
Resourcecentre
New visionMultimediaHIV/AIDSResource CentreWestern KenyaHIV/AIDS Network
Mt. Elgon
CommunityResource Centre
KANCO
VCT services
Olemila CBO
Condompromotion
Ihururu Initiative
Gallamoro
Tohanchane CBO
Counseling
RICOAN
Day Aid Care
WEMIHS
Western HIV/AIDS Network

Building on our experiences 14
National AIDS Control Council
Prevention and AdvocacyAccording to the strategic plan, the objectives of efforts in prevention and advocacy is to reduce
HIV/AIDS prevalence by 10 per cent per year through promotion of behaviour change, prevention
of transmission of HIV from mother to child, reducing prevalence of sexually transmitted
infections and ensuring safe blood transfusions and blood products.
The high risk priority groups for interventions are:
■ Adolescents and youth (in and out of school);
■ Women and girls;
■ Security forces;
■ Populations in certain locations such as slums and border towns;
■ Populations who are difficult to reach such as nomads and beach communities; and
■ High-risk groups such as commercial sex workers and long distance drivers.
The following activities have been undertaken under the prevention and advocacy thematic area.
■ Creating awareness on HIV/AIDS;
■ Capacity building;
■ Establishment of resource centres on HIV/AIDS;
■ Condom promotion;
■ Community mobilisation; and
■ Voluntary counseling and testing.
Intended Audiences for Prevention EffortsPresentations by organizations implementing activities under the CIA demonstrated that they are
reaching or working with priority groups for HIV/AIDS interventions. Below is a summary of
groups being reached by different organizations.
YouthOrganisations like Songich Evangelistic Group of Eldoret, RICOAN of Nairobi, Jua Arts of Kilifi,
Olmarei Lang of Narok, Ihururu Initiative of Nyeri, Gallamoro of Nairobi, Womankind of Garissa,
Tunu Women Group of Lamu, Foni of Isiolo and Tohanchane CBO of Kuria District have activities
directed at both in and out of school youth. Indeed a group such as Jua Arts was set up by the
youth themselves as a vehicle for reaching their peers.
Women GroupsOrganisations like RICOAN of Nairobi, Olmarei Lang of Narok and Tohanchane in Kuria Districts
respectively are examples of women groups which mainstream HIV/AIDS to their agenda.

Building on our experiences15
National AIDS Control Council
Local and Religious LeadersIn some areas, activities geared towards awareness creation have been directed at local leaders as
agents of change. In this category, are organisations like FONI, Maendeleo ya Wanawake, Keiyo
Branch, Kuria District Disability Network and Tohanchane CBO. FONI of Isiolo District have
trained councillors and chiefs on HIV/AIDS while Maendeleo ya Wanawake, Keiyo Branch has
trained divisional women leaders and other leaders to create awareness on HIV/AIDS at the
grassroots.
FONI and WomanKind who operate in predominantly Muslim communities involve religious
leaders by conducting workshops for Imams and preachers.
Matatu FraternityThe Ihururu Initiative of Nyeri has organized seminars and workshops for matatu drivers and
touts on HIV/AIDS issues. From their report, the workshops were so successful that they had more
willing participants than they could accommodate. Majority of the participants were out of school
youth.
House helps, out of schoolgirls and single mothersBeccoh Centre of Mombasa is involved in educational programmes for house helps, out of school
girls and single mothers. It has organized educational seminars for the above categories in Mom-
basa.
Nomadic HerdersWomankind has conducted awareness sessions at water points in Garissa District targeting no-
mads. The area is characterised by high illiteracy levels.
The physically challengedThe Kuria District Disability Network which brings together 23 disability self help groups in Kuria
District works to reduce the spread of HIV/AIDS among the physically challenged through
sensitization among other activities.
Creating Awareness and Increasing Knowledge on HIV/AIDSA quarter of the organizations that participated at the two workshops are involved in activities
geared towards creating awareness and increasing knowledge on HIV/AIDS. Their activities focus
on increasing knowledge on HIV/AIDS, modes of transmission and preventive measures that
would lead to attitudinal and behavioural change on sexual matters.
In creating awareness, several methods have been used to pass HIV/AIDS messages as de-
scribed below.
Building on our experiences 16
National AIDS Control Council
Workshops and seminarsWorkshops and seminars are popular with groups like Olmarei Lang Self Help Group, The Ihururu
Initiative, WomanKind Kenya, Beccoh Centre, Kuria District Disability Network and Tohanchane
CBO. In most of these seminars and workshops, facilitators are hired to educate the people on
issues related to HIV/AIDS.
Video ShowsVideo Shows are also popular with the groups in creating awareness. Organisations like Jua Arts of
Kilifi, MADICAA of Nairobi, the Ihururu Initiative and the Tunu Women Group sensitize people
on the dangers of HIV/AIDS and STDs through video shows. Some of the video tapes used include
the Yellow Card and The Silent Epidemic. Most of the video tapes are donations from organisations
engaged in HIV/AIDS activities like AMREF and Church organisations.
Visits to leisure spotsVisits to leisure spots have been used as an entry point in creating awareness on HIV/AIDS. Such
spots include disco halls, pool and darts clubs. The Ihururu Initiative visits such premises where
they conduct talks with the youth on drug abuse and alcoholism in relation to HIIV/AIDS.
Schools and churchesOrganisations like Olmarei Lang of Narok, Jua Arts of Kilifi, MADICAA, Gallamoro and RICOAN
of Nairobi, Ihururu Initiative of Nyeri, Tunu Women Group in Lamu District and Maendeleo ya
Wanawake in Keiyo District makes visits to schools and churches to talk to the youth. Topics
covered in such sessions include common STDs and their relationship with HIV/AIDS, facts on
HIV/AIDS, modes of transmission and the ABCs of prevention.
Alternative mediaUse of alternative media like drama, theatre, song and dance is another way through which the
organisations create awareness. In this category, we have Jua Arts, MADICAA and the Ihururu
Initiative who are into drama. Gallamoro has been able to enhance and encourage drama groups in
schools. They have organised and registered a drama group with the Ministry of Home Affairs and
Office of the President called the Gallamoro Films and Drama Group.
Gallamoro is also into song and dance where they organise schools to create dances, poems,
plays and music extravaganza on HIV/AIDS. Songich S.D.A Evangelistic self help group of Eldoret
South constituency preach the gospel and sing gospel songs on HIV/AIDS. The group which
operates in Eldoret has visited different places in Eldoret Constituency to sensitize the people
through songs.

Building on our experiences17
National AIDS Control Council
Distribution of IEC materialsIn the course of creating awareness, organistaions like RICOAN, Gallamoro and MADICAA of
Nairobi have distributed information, education and communication materials on HIV/AIDS to
their audience. Such
materials are sourced
from Kenya AIDS
NGOs Consortium
(KANCO), Pathfinder,
and National AIDS and
STDs Control Pro-
gramme (NASCOP)
among other organiza-
tions.
Sports ForumsSports is another
method used by the
implementers in
creating awareness.
Gallamoro and
MIDICAA, both of
Nairobi organizes
sports activities like
football matches and
tug of war around
which they create a
platform for dissemi-
nating information on
HIV/AIDS.
Capacity BuildingCapacity building is
another component of
the advocacy and
prevention activities
undertaken by the
implementers. Organi-
sations in this area
include KANCO
branch of Nakuru,
Case Study 1
Reaching the physically challenged in thecampaign against HIV/AIDS
The Kuria District Disability Network ExperienceKuria District Disability Network is an established Community Based Organization (CBO), comprising of the
physically challenged from Kuria District of Nyanza Province. The Network is an umbrella organization of 23
self help groups in the district.
The group is led by Abednego Maroa Mwita, the elected Executive Coordinator of the Network, who
resigned from his teaching job at the district primary school to play an active role in the campaign against HIV/
AIDS among his people.
“The overall goal of the Network is to bring together people who are physically challenged to chart the
way forward in reducing HIV/AIDS among themselves,” says the 35 year old Abednego, who has been physically
challenged since birth.
Contrary to popular belief that the physically challenged are not involved in promiscuous sex, Abednego
says that they are more vulnerable to HIV/AIDS because of the limiting nature of their lifestyles.
“Our mission is to ensure the prevalence of HIV/AIDS among PLWD is reduced by 20 per cent by the year
2005,” says Abednego.
Despite the high HIV/AIDS awareness levels among Kenyans, Abednego says that PLWDs have no access
to such information. Due to various challenges like deafness, blindness, mental problems and those who
have a combination of all the above, PLWDs have completely been left out of the HIV/AIDS campaign in
Kenya, explains the network coordinator.
Abednego, one of the few educated physically challenged people in Kuria, has one motto that drives him:
disability is not inability. He has done what was initially perceived as impossible and organized workshops
and seminars for PLWD to train them on HIV/AIDS related issues.
“Our greatest challenge is the high rate of illiteracy among PLWDs,” explains Abednego, because many
parents do not take their disabled children to school, they lack basic sign language skills, making it very
difficult to communicate with them, he adds.
In response to this challenge, the Kuria Disability Network has discovered that in the process of socialization,
PLWDs have developed their own mode of communication, which suits them. Although it is not the standard
mode of sign language, it is the most effective mode of communication between the Network officials and its
members.
Through this new approach, PLWD in Kuria District have slowly begun to change their sexual behaviour.
However, Abednego says that the best way to reach his fellow brothers and sisters who are physically challenged
has been by way of example.
After several years of campaigning for people to take the HIV test, Abednego, a husband and father of four
daughters, finally decided to take the VCT test, to determine his serostatus. Like anyone else, he was scared,
but resolved to be a role model whatever the outcome. If he were positive, he would become even louder as
an advocate to ensure that HIV/AIDS levels drop among his people and especially among the physically
challenged in Kuria district.

Building on our experiences 18
National AIDS Control Council
Lazers of Eldama Ravine, Pastoral Capacity Building and Development Organisation of Garissa,
PAIDO of Kitui, The National Organisation of Peer Educators (NOPE) based in Mombasa and
FONI of Isiolo.
Lazers management team trains the various sectoral leaders in every location of Eldama Ravine
Division who in turn train group leaders and representatives. The group leaders and representa-
tives are expected to play a leading role in sensitizing the general public.
KANCO in Nakuru trains organisations in HIV/AIDS activities on technical aspects like pro-
posal writing , programme design and management and resource mobilisation. Examples of
organisations trained by the Nakuru branch of KANCO include Yoseh 2000 Youth Group, Born
Ministries and Love and Hope Centre, all of Nakuru. PAIDO on the other hand trains facilitators
through Stepping Stones Methodology (SSM) workshops in Yatta Division of Kitui District. Such
facilitators are expected to drive the process of behaviour change.
Pastoral Capacity Building and Development Organisation and FONI build capacity in Garissa
and Isiolo Districts respectively. The former has developed a training manual for the youth as well
as training youth groups while the latter has empowered the marginalised pastoralists communi-
ties living in Isiolo District through education and other means in order to influence the attitude
and behaviour change of the residents.
A unique organisation in this category is NOPE of Mombasa, which is a professional body
comprising of peer educators, trainers of peer educators and trainer of trainers in the community
and work places. It was formed to respond to the growing demand for HIV and AIDS prevention
programmes especially in the work places. The group has trained more than 23 organisations on
peer education throughout the country.
Condom PromotionStrengthening condom promotion is another activity carried out by organisations as per the work-
shop proceedings. Organizations in this category include the Ihururu Initiative, Gallamoro Net-
work and Tohanchane CBO. However, what the organisations have done is to distribute the con-
doms and demonstrate their proper use and disposal. There is no feedback to determine the effec-
tiveness of such promotion.
Resource CentresSome of the participating organisations have set up resource centres to provide IEC materials and
information on HIV/AIDS. Such organisations include New Vision Multimedia, HIV/AIDS
Resource Centre in Matayos Division, Busia District, Mt. Elgon Community Resource Centre,
Western Kenya HIV/AIDS Network of Kakamega and KANCO in Nakuru.
Most of the resource centres are situated at central locations and more so at district headquarters
such as Western Kenya Network HQ in Kakamega and KANCO in Nakuru. While some like Mt.
Elgon Community Resource Centre are stand-alone resource centres. A few supplement the re-

Building on our experiences19
National AIDS Control Council
source centres through outreach programmes.
The resource centres offer a reading room, audio and videotapes, published materials and
books. KANCO offers information through CD-ROMS and Internet Services. Most of the published
materials are either in English or Kiswahili and therefore of limited use to the users especially in
the rural areas, where majority are less proficient in English and Kiswahili. Because of their central
locations, the resource centres are not readily accessible to all community members.
Community mobilizationOrganisations which have undertaken community mobilisation include WEM Integrated Health
Services (WEMIHS) of Thika, Ukamba Christian Community (UCC), a development arm of the
Anglican Church, Dioceses of Machakos and Kitui Districts, Beccoh Centre of Mombasa and
Tohanchane CBO in Kuria District.
WEMIHS which is guided by a shared vision of empowering communities to effectively re-
spond to the HIV/AIDS has been able to mobilise the community in its area of operation to
strengthen community orphan support interventions which include a day care centre, a school
feeding programme, education support and vocational skills training. Such services are facilitated
by the Community Orphan Care Committees (COCCs), which have been formed by the organisa-
tion in collaboration with the community members.
Community mobilisation activities by the Ukamba Christian Community has led to the forma-
tion of divisional and locational HIV/AIDS committees and the selection of trainers to work as
volunteers to run the HIV/AIDS activities in selected divisions in the three Ukambani districts of
Machakos, Kitui and Makueni.
Beccoh which caters for house helps, out of school girls and single mothers in Mombasa has
facilitated community participation through identification of community based pillars that are
easily acceptable to both employers and house helps.
Tohanchane CBO on the other hand has facilitated formation of Home Based Care committees
per division in Kuria District as a result of involving the office of social services.
Voluntary Counseling and TestingIn voluntary testing and counseling for HIV, a person receives the counseling necessary to make an
informed choice on whether to undergo confidential testing. Such testing and counseling has been
shown to have a role in preventing HIV infection. For people living with HIV, it is a gateway to
care.
Olemila Community Based Organisation offers voluntary counseling and testing in Kapsabet,
Nandi District of the Rift Valley Province to empower the community members to take control of
their lives.
With the assistance from USAID, Olemila counselors have undertaken a one-week training
course in basic counseling conducted by the Kenya Association of Professional Counselors (KAPC).
Six of their members have undergone further VCT specific training with the Liverpool School of
Tropical Medicine VCT project.

Building on our experiences 20
National AIDS Control Council
Case Study 2:
VCT’s do make a difference – the Olemila ExperienceWhen Michael Otieno came for counseling at the Olemila VCT centre in Kapsabet town, Nandi District, he was scared. Only
25, Michael had led a highly promiscuous life, and was proud of it. Then one day, Michael watched both of his parents’ die one
after the other of a strange incurable disease.
Before he had time to recover from the tragedy, his closest friends began to pass away almost simultaneously including his
most recent girlfriend Anna. The cause? HIV/AIDS. That’s when Michael walked in to the Olemila VCT centre, half trembling,
to prepare for his death. He was certain that he had only a few months to live and wanted to know how he would cope.
The main objective of Olemila is to reduce the HIV/AIDS prevalence by offering Voluntary Counseling and Testing services
for HIV/AIDS in Nandi District. Voluntary HIV counseling and testing is the process by which an individual undergoes counseling
to enable him/her to make an informed choice about being tested for HIV. This decision must be entirely the choice of the
individual and he or she must be assured that the process will be confidential.
The project has eleven members strategically recruited from various socio-economic and professional fields including
health, education, youth and women groups, municipal council, administration and People Living with HIV/AIDS. With this
approach, the Olemila volunteers have been able to reach every aspect of life in the community. The volunteers have also
undergone the Kenya Association of Professional Counselors (KAPC) training course to enable them provide quality services.
At a VCT centre, pre-test counseling is the first step an individual will go through. Pre-test counseling is done to ensure that
the individual understands the basics about HIV/AIDS, the HIV test, and what the results mean. The counselor explains the
risks and benefits of knowing one’s status and discusses the fears, worries and anxieties with each individual client.
When the counselor was sure that Michael was ready to have his test taken, he performed an on-site rapid test which
means results are available within an hour. In all VCT clinics, the protocol is the same; the first screening test is done, if it is
negative, the counselor completes the HIV register and then informs the client his result during post-test counseling. If the
results are positive, a confirmatory test is performed immediately. If the positive result is confirmed, the test results are given
to the client during post-test counseling.
Members of the Olemila VCT centre have established post-test clubs for their clients; for those who are positive and
negative, where they provide support for clients who return to the centre for regular counseling. For those who are positive,
Olemila provides an opportunity to learn about nutrition from their demonstration kitchen garden so that they can learn how to
enhance their bodies’ immunity.
When the test proved Michael negative, it motivated him to stay negative by practicing total abstinence. Michael also
decided that if he had a partner, he would ensure she is counseled in a VCT clinic.
The Olemila project has been successful because of implementing two main strategies which are ensuring that the community
plays a role in establishing the VCT centre and learning best practices from similar centres in the area on the requirements of
establishing a VCT centre.
“After one year of counseling at the VCT centre, we have learned that we still have a long way to go in teaching the
community the truth about HIV/AIDS,” says Godfrey Kutwa, the youth counselor at the Olemila VCT centre.
The stand-alone VCT facility also provides first hand information on HIV/AIDS through videos
and pamphlets, facilitates joining of post-test clubs for the positive and the negative. There is also
counseling as well as education on nutrition from the demonstration garden.
Building on our experiences21
National AIDS Control Council
Treatment, Continuum of Care and SupportThe strategic plan defines the objective of the treatment, continuum of care and support for the
infected and affected as to promote quality health life for people infected and affected.
To achieve the above objectives, the following strategies have been identified:
■ Strengthen clinical management and nursing care of opportunistic infections;
■ Prevent spread of infection through infection control guidelines and measures;
■ Reduce social stigma and discrimination;
■ Develop guiding framework on implementation of youth-friendly treatment, care and
support services;
■ Strengthen institutional capacity for providing continuum of care; and
■ Provide social support through NGOs, CBOs and families.
The following activities have been undertaken under the treatment, continuum of care and support
for the infected and affected priority area:
■ Treatment of opportunistic diseases;
■ Counseling; and
■ Referrals.
Treatment of opportunistic infectionsTransmara Herbalists Association in Transmara District of the Rift Valley Province has been treat-
ing Opportunistic Infections (OIs) using herbal medicine since it was established in 2000. Its activi-
ties have not been documented to determine their effectiveness.
With a membership of 35 people, the Association’s goal is to ensure HIV/AIDS patients are free
of opportunistic infections. They have partnered with the Kenya National Museum to analyse and
quantify the chemical ingredients in the herbs they use.
Treatment is based on assumptions of the ailment since the patients come to them as a last resort
after failing to get well from use of modern medicine. Availability of herbs is however threatened
by the loss of forest cover in the surrounding forests.
CounselingOrganizations that offer counseling include RICOAN of Nairobi, Day Aid Care of Kisumu,
WEMIHS of Thika and Western HIV/AIDS Network of Kakamega.
Day Aid Care is a grouping of People Living with HIV/AIDS. Counseling has played a major
role in encouraging them to live positively with the virus. Western HIV/AIDS Network on the
other hand has two trained counselors who offer the services to their clients.
There is no uniformity on the training of the counselors. While some have undergone a two-
week training conducted by the Kenya Association of Professional Counselors, the duration of the
training differs from one organization to another.

Building on our experiences 22
National AIDS Control Council
Home Based CareHome Based Care is the care of persons infected and affected by HIV/AIDS that is extended from
the hospital or the health facility to their homes through family participation and community
involvement, with available resources and in collaboration with health workers.
Day Aid Care in Kisumu and MOCASO of Nairobi whose members are People Living with
HIV/AIDS provides Home Based Care for their members. Day Aid Care for instance has trained
40 members with HIV/AIDS on practical and psychological issues in relation to Home Based Care.
These trainees in turn provide immediate care and support to their terminally ill-relatives.
The Nyamira Adventist Community Health and Outreach Programme, based in Nyamira
District trains PLWHAs to develop self-reliance skills to enable them cope depending on their
situation.
MADICAA is taking care of a grandmother who is infected and a girl who deliberately went to
live with a man who was already infected. They are also engaged in the Home Based Care pro-
gramme run by the Nairobi City Council (NCC).
Referral servicesImplementers offering referral services include Tohanchane CBO in Kuria District, Day Aid Care of
Kisumu, KANCO in Nakuru, RICOAN and MOCASO, both of Nairobi.
Most members of Day Aid Care and MOCASO are People Living with HIV/AIDS. Both organi-
zations refer their members to hospitals for treatment for opportunistic infections. KANCO,
RICOAN and Tohanchane on their part refer those who come to them for any assistance to relevant
organizations.
Mitigation of Social and Economic ImpactThe strategic plan defines the objective of the mitigation of social and economic impact as to
reduce the negative social and economic impacts of the HIV/AIDS epidemic.
Consequently, the following activities have been identified in this priority area:
■ Empower NACC to coordinate mobilisation of resources from individuals, communities,
UN agencies, development partners and the private sector;
■ Pass legislation in support of orphans, the infected and the affected;
■ Develop training plans in all sectors, to provide assistance to the infected, and to enable
survivors and the affected to cope with their loss;
■ Develop strategies for resource mobilisation for HIV/AIDS prevention; and
■ Develop and implement a coordinated, multisectoral approach to combat HIV/AIDS and
its impact.
Activities undertaken by implementers under this priority area include:
Building on our experiences23
National AIDS Control Council
■ Income generating activities; and
■ Care and support of orphans
Income Generating ActivitiesOrganisations that have engaged in income generating activities include the Day Aid Care of
Kisumu, MOCASO of Nairobi and Olemila in Nandi District. Both Day Aid Care and MOCASO
were formed by People Living With HIV/AIDS. Most of the income generated by the two organisa-
tions is used to support the members.
Day Aid Care is currently engaged in soap and candle making, tailoring and training of other
community based organisa-
tions on soap making. The
income generated is used by
the members for nutritional
support, buying of ARVs and
assisting orphans left behind
by their members, most of
whom are PLWHAs.
The organization has
started a revolving fund
where members borrow
money and return it at a fee.
The organisation is working
with microfinance organiza-
tions like Jamii Bora of
Kisumu to access funds to
facilitate members to start
income generating activities.
Members of MOCASO are
mostly single mothers who
were initially commercial sex
workers in Pumwani area of
Nairobi. Being the sole
breadwinners for their fami-
lies, they lived in low-income
areas of Nairobi and engaged
in petty trades like brewing of
illicit drinks like changaa. A
number of them have died as
a result of HIV/AIDS, living
behind orphans.
To cushion the members,
the organisation has em-
Case Study 3:
The family’s contribution to the fightagainst HIV/AIDSOlmarei Lang self-help group is made up of fifteen closely related members, who have lost their
relatives to HIV/AIDS. The group, which started in 1998, has one major goal; to reduce the
spread of HIV/AIDS in Narok District, Mau Division, by addressing retrogressive cultural practices
that accelerate the spread of the disease.
Simei Ole Sankei, one of the pioneers of the group explains that in the Masaai community, the
family is a very important component, thus the deliberate decision to call their group “Olmarei
Lang,” which simply means family in the Maasai language.
With this approach, Sankei says that they have been able to penetrate core cultures of the
community like Moranism and Female Genital Mutilation, which excerbates the spread of HIV/
AIDS among the Maasai.
In Moranism, for example, young Maasai warriors are encouraged to indulge in casual sex as
a rite of passage. This high-risk kind of behaviour has been condemned severally by many
groups claiming to create awareness on HIV/AIDS in the region. However, due to the wrong
approach, the cultural practice continues every year, raising mortality rates in Narok by significanly
because HIV/AIDS is directly influenced by social behaviour that is part of their local culture.
“Olmarei Lang, focuses on educating the local leaders on the dangers of encouraging sexual
activity during the rites of passage without condemning the culture as a whole,” says Ole Sankei.
The group also recognizes the importance of educating mothers on issues regarding HIV/AIDS
because they believe they are centrally placed to pass on pertinent information that can impact
the community positively.
“Once educated, mothers have great potential to influence the desired behavioural change in
their families,” explains Ole Sankei.
Olmarei Lang has made great progress in creating role models out of respectable families in
the community who have rejected retrogressive aspects of their culture in an effort to reduce the
infection rate of HIV/AIDS in Narok. However, Ole Sankei says that it is a long process that
needs patience.
The Olmarei Lang group has succeeded because they have shifted from project strategies to
people strategies, where partnerships have been formed with the ordinary mwananchi and
ownership of the problem and its solutions created from within at the local level by the community.

Building on our experiences 24
National AIDS Control Council
barked on income generating activities which include tie and dye, batik, bar and powder soaps
processing and hand weaving.
The most successful has been powder soap processing, resulting in quality soap products which
have been certified by the Kenya Bureau of Standards. The income generated has enabled members
to abstain from commercial sex activities.
Olemila on its part charges a fee to those who visit their VCT centre. They also make beaded red
ribbons for sale.
Care and Support of OrphansOne of the worst consequences of AIDS death is an increase in the number of orphans. There were
an estimated one million orphans as a result of HIV/AIDS deaths in Kenya in 2002.
Organisations that deal with orphans include MOCASO of Nairobi, Day Aid Care of Kisumu,
Olmarei Lang Self Help Group in Narok District, Makinu Youth Against AIDS in Nyando District,
WEMIHS of Thika and Nyamira Adventist Community Health and Outreach Programme in
Nyamira District.
MOCASO whose members have died of AIDS have left behind 400 orphans. Such orphans are
forced to move to the rural areas to stay with their relatives. MOCASO follows them up to ensure
they are coping with life.
Nyamira Adventist Community Health and Outreach Programme is currently supporting 3,100
orphans and empower them on self-reliance through training on how to mobilise and utilise the
available resources. They also contribute to school levies, clothing and medical costs for school
going orphans.
Olemarei Lang works with female members in the organisation to identify the orphans to be
assisted. The group is currently providing books and uniforms to school going orphans.
Makinu Youth Against AIDS is providing 39 orphans with uniforms. The community contrib-
utes food which they distribute to the orphans.
Day Aid Care in partnership with International Fellowship Centre (IFC) of Norway is taking
care of 25 school going orphans whose parents died of AIDS. It has organized mini harambees to
raise money for the orphans upkeep. The organisation provides for all the needs of the orphans
who stay with their relatives.
Lastly WEMIHS provides all the basic needs for orphans and vulnerable children under their
care. They have set up a day care centre for children aged between 3-6 years. Services offered in the
day care centre include informal learning, nutrition and feeding programme, paediatric counseling
and clinical care.
For children between 6-15 years, WEMIHS in partnership with the community offers education
support in terms of uniforms, books, tuition, counseling and a school-feeding programme. Those
between 13-15 years are offered quality life skills training, peer education and better interaction for
behaviour change and vocational training.
The organisation has entered into collaboration with schools, teachers, the government and
church based organisations in assisting the orphans. This has led to the formation of Community
Orphan Care Committees (COCCs) that oversees the orphans programme.
Building on our experiences25
National AIDS Control Council
Emerging Issues andChallenges
Participants at the two workshops identified the following emerging issues and the challenges
associated with implementing the HIV/AIDS projects at the community level from the presen-
tations and the plenary discussions. There was consensus on the following issues:
Community ParticipationSome implementers complained of lack of support for their activities on HIV/AIDS by politicians.
After discussions, there was general consensus that political and community support can be
strengthened by ensuring continous involvement of politicians and community leaders in all
aspects of project planning and implemention. There was general agreement that involvement of
community members right from the beginning of the project fosters ownership and ensures
sustainability of the projects.
Proposals and Disbursement of FundsParticipants expressed concern over the delay in approval of proposals, which in turn delays the
commencement of projects. In such cases, by the time funds are disbursed, the situation on the
ground may have changed.
On accountability of the funds, NACC made it clear that disbursements will continue to be
made to ongoing projects only after the project implementers’ account for what they had received.
Participants complained about the complex documentation requirements. They gave an example of
the North Eastern region where a section of the population involved in implementing HIV/AIDS
projects is illiterate, and therefore finds it difficult to meet the documentation requirements.
The FMA officials however clarified that the documentation requirements had been simplified
and promised to make it even simpler, to facilitate the documentation process. Participants were
encouraged to network closely with the NACC structures to hasten the approval proposals and
disbursment of funds.
Participants were informed that NACC regional structures are mandated to forward any infor-
mation on misappropriation of funds by the implementers to the headquarters for action.
Educational Materials, Awareness Creation onPreventive Measures and Community MobilizationSeveral issues emerged during discussions covering information and educational materials, creat-
ing awareness on preventive measures and behaviour change, cultural practices that hinder pre-
ventive efforts and mobilizing different community groups.

Building on our experiences 26
National AIDS Control Council
One cross-cutting issue emerging from the discussions revolved around lack of guidelines or a
strategy for developing communication approaches to motivate different groups to change their
behaviour.
Other issues are summarized below.
IEC materialsTwo key issues were identified concerning the IEC materials that were available for use in project
areas. The first was the relevance of the message carried by these materials such as Crush AIDS
which participants said was inappropriate and of little relevance. The second issue was the lan-
guage barrier as most materials were in either English or Kiswahili. There was consensus that IEC
materials would have greater impact at the community level if they were translated into local
languages and had messages that were relevant to the intended audience. The messages should
also be personalised to facilitate behaviour change.
NACC undertook to offer technical assistance in the development and production of IEC
materials appropriate for different communities.
Based on experiences shared by participants using educational videos on HIV/AIDS in their
work, there was agreement that these videos serve as a powerful tool to stimulate discussion and
their use should be encouraged. One such video cited is the Yellow Card available free of charge to
project implementers from AMREF.
Resource centersSome implementers such as the New Vision Theatre Group supplements their outreach pro-
grammes with a resource centre, which makes materials on HIV/AIDS accesible to its target
audiences. Resource centres located in centralized locations such as district headquarters were
found to be of limited benefit since they are removed from the community. Further, most of the
materials available are in either English or Kiswahili, languages that grassroots populations are less
proficient in. To address this need, the theatre group plans to shoot educational videos in local
languages.
Materials on HIV/AIDS for schoolsParticipants were informed that NACC and the Ministry of Education, Science and Technology are
developing an HIV/AIDS training manual for teachers. This is to build capacity of the teachers for
the introduction of HIV/AIDS school curriculum.
CondomsParticipants emphasized the importance of promoting condoms as a preventive measure alongside
other control methods in response to concerns that some implementers gave a lot of emphasis to a
single preventive measure such as condoms instead of adopting a wholistic approach in response
to HIV/AIDS.
Building on our experiences27
National AIDS Control Council
On the acceptability of condoms by faith based organizations, a secretary from one of the Con-
stituency AIDS Control Committees in Coast Province said that Muslims are not against use of the
condoms as a protective measure against HIV and urged projects implementers to educate people
on its correct use.
Youth Mobilization in the prevention of HIV/AIDSParticipants expressed concern over lack of an umbrella body that brings the youth together to
empower them to address HIV/AIDS, yet they make the largest case load of new HIV infection as
a group.
Participants proposed that a directory on youth programmes or youth networks dealing with
HIV/AIDS be compiled as a step towards forming a National Youth Network. They requested
NACC to provide assistance in identifying youth organizations at the constituency, district and
provincial level and help them mainstream HIV/AIDS issues to their core activities.
A national forum for Kenyan youth took place in July 2003 to jumpstart the process of bringing
the youth together to chart their national agenda that could be supported by NACC for implemen-
tation.
Home Based CareThere were concerns over the technical capacity of individuals and organizations providing Home
Based Care. Projects implementers said that they found it necessary to engage in Home Based Care
to fill the void since those with AIDS require it.
NACC, the meeting recommended should facilitate wide dissemination of the national guide-
lines on Home Based Care to guide the project implementers.
Cultural Practices and TraditionsThe meeting encouraged participants to use African traditions such as those that provide for
counseling of girls by their aunts on sexuality in HIV/AIDS prevention efforts. However there
were other cultural practices such as wife inheritance that perpetuate the spread of HIV that should
be discouraged.
Voluntary Counseling and TestingOne implementer has a programme on Voluntary Counseling and Testing. Results from project
experiences have identified the fear of stigma, rejection and discrimination for those who test
positive for HIV especially in situations where there is no follow up support services or treatment.
Participants considered counseling in VCT a good entry point for tackling stigma.
Other issues:
■ Unqualified service providers offering counseling; and

Building on our experiences 28
National AIDS Control Council
■ People preferring VCT services located away from where they live due to fear of stigma
and breach of confidentiality.
NACC informed the participants that the Ministry of Health has developed guidelines on VCT and
those engaged in counseling should follow those guidelines.
During discussions, it emerged that clients prefer VCT services that are far from their area of
residence. Mobile VCT clinics were preferred even more because they are considered more confi-
dential. The meeting agreed that implementers should offer VCT services that are acceptable to the
people they serve which may range from integrated services, mobile or stand-alone VCT services.
Cross-cutting IssuesNetworks for PLWHAsExperience from implementers showed that majority of the people who test positive are shy of
publicly declaring their sero-status. One way of overcoming this fear is through facilitating setting
up of networks for people living with HIV/AIDS to create a forum where those who declare their
status publicly can get support.
Capacity of CBOs, FBOs and NGOs to implement activitiesParticipants heard that implementers in some regions lacked the capacity to implement their HIV/
AIDS related programmes due to several reasons, one of them being political interference. The
other reason cited was the lack of capacity to plan and implement programmes. The meeting
agreed that DACC and PACC should spearhead capacity building in such regions.
On KANCO’s role in supporting implementers in capacity building, a representative explained
that their services are provided free of charge to organizations implementing HIV/AIDS activities.
Implementers were encouraged to seek the services of KANCO in building their capacity.
Fate of equipment after lapse of KHADREPParticipants wanted to know the fate of equipment such as generators and television sets bought
with project funds after the lapse of the project. There was consensus that since HIV/AIDS is a
long-term problem, the equipment could be used to generate income to sustain the project after the
Community Initiative Account lapses.
In the event the group disintegrates in the process of implementing the project, the NACC
structures should keep an inventory of the equipment bought at each level and retrieve them for
reissuing to other implementers.
Multiplicity of CBOs/NGOs/FBOsParticipants expressed concern over the mushrooming of organizations claiming to be undertaking
work on HIV/AIDS. NACC structures were asked to vet proposals at every level from such organi-
zations and reject those which in their opinion were not genuine. In addition, the communities
Building on our experiences29
National AIDS Control Council
should be in a position to identify and flush out organisations that are not genuine.
Income generating activitiesIn response to a question on whether NACC supports income generating activities (IGAs), partici-
pants were informed that IGAs are considered an important component in mitigating the social
impact of HIV/AIDS. Project implementers can use funds from NACC to start IGAs so long as they
are outlined in their work plans.
Such projects are likely to succeed when the beneficiaries are trained on micro enterprise man-
agement and then linked up with micro enterprise credit organizations that can help them with
initial capital.
Day Aid Care is an example of an implementer supporting IGAs. It is involved in soap making,
tailoring and training to generate income to support its members, most of who are PLWHA’s. The
money generated is shared among the members for nutritional support, buying of ARV’s and
assisting orphans.
The members have also started a revolving fund where money is lent out to members and paid
back with interest. The organization is also working with micro finance institutions like Jamii Bora
to access funds for starting small businesses.
Lack of support by medical personnel in the regionTohanchane CBO told the participants that they lack support from the medical practitioners in the
area since the medical practitioners feel that other people are encroaching into their profession. To
overcome this, a clinical officer has been attached to the group as a resource person to advice the
members on care giving.
VolunteersThe meeting heard of difficulties faced by implementers relying on volunteers. The WEMIHS
representative, whose project is fully run by volunteers, shared how they have overcome this. They
have built shared expectations by outlining what volunteers should expect right at the onset by
signing contracts with the volunteers. However, it was agreed that an implementing organization
should employ adequate staff to handle the technical aspects of the project at a reasonable pay
while volunteers should be given incentives to sustain their morale and meet their basic needs.
Transport for project activitiesMost implementers complained of difficulties in transporting their resource persons and equip-
ment during project activities and wanted to know if NACC could provide them with efficient
means of transport.
NACC explained that implementors should build in transport costs in their proposed budget
from the beginning.

Building on our experiences 30
National AIDS Control Council
Disinheritance of OrphansParticipants were informed that orphans are losing property to relatives when their parents die of
HIV/AIDS. In some communities, cultural beliefs dictate that homesteads in which parents have
died be demolished or be burnt to ashes thereby depriving orphans of shelter. Participants wanted
advice on the course of action in such cases since the Taskforce on legal issues related to HIV/AIDS
has not made public its findings.
After discussions, it was agreed that Kenyan laws can competently address the problem of
orphans and participants were advised to channel such grievances through the children’s depart-
ment for guidance.
NACC would soon disseminate an Orphans and Vulnerable Children (OVC) National Action
Plan developed following a recent international HIV/AIDS meeting in Namibia on orphans while
the bill on legal issues related to HIV/AIDS was already in parliament awaiting debate.
Building on our experiences31
National AIDS Control Council
Emerging Lessons and FutureDirectionBelow are the emerging lessons and areas that require action based on discussions at the two
workshops:
1. A good number of the implementing organisations were recruited as a result of mobilization
through the NACC structures from the year 2002. The NACC structures are therefore the best
placed to recruit the implementers.
2. Participants acknowledged and valued the existing linkages working with NACC viz PACC and
DACC. There are however problems with the linkage between DACC , CACC on one hand
and organizations implementing activities at the local level which needs to be enhanced.
3. Some of the implementers do not involve the community during the planning and implementa-
tion of the HIV/AIDS projects. It is important for implementers to deliberately involve the
community in the projects right from the planning stage all the way to monitoring and evalu-
ation. This will build ownership and sustainability of the projects.
4. Majority of organizations that participated at the workshops are involved in preventive activi-
ties. Most of the activities revolve around creating awareness and increasing knowledge on
HIV/AIDS. Many of the organizations lack the capacity to go beyond creating awareness to
implementing programmes that can motivate individuals to change their behaviour. Their work
is hampered by lack of skills and capacity to implement preventive activities systematically.
There is need to assist the implementers build capacity to design and implement preventive
programmes using methodologies that are likely to bring about behaviour change.
5. Educational materials used lack uniformity on key messages on HIV/AIDS. Majority of them are
in English or Kiswahili, languages that people at community level are not proficient in. Imple-
menters should develop the materials based on key thematic messages suitable for their
audiences and in a language they can understand.
6. Preventive activities undertaken by implementing organizations are not well integrated within
existing structures. A deliberate effort is necessary to help implementing organizations add on
HIV/AIDS behaviour change communication to the work of such structures to make it sus-
tainable. Working with established structures such as churches or schools will make it easy to
monitor the interventions.

Building on our experiences 32
National AIDS Control Council
7. The procedures for disbursing funds are lengthy and result in delays of commencement of
projects. There is need to simplify the procedures and the documentation as well as to con-
tinuously educate applicants on the process. Implementers at the local level should familiar-
ize themselves with proposal writing and financial procedures set out by NACC.
8. Mechanisms for supervising implementation of activities at the community level are weak due to
poor linkages with CACCs, some of which are dormant. There is need to strengthen the capac-
ity of CACC, DACC and PACC to supervise and monitor the work of implementing organiza-
tions. Implementers on the other hand should proactively learn from organizations that have
succeeded through networking. This can be strengthened through establishment of regular
networking forums at district and provincial levels coordinated by NACC structures.
9. Some implementers who were successful in obtaining funds had difficulties implementing
activities they had set out to undertake due to lack of skills to plan and deliver programmes.
Implementers should liaise with NACC structures at the provincial and district level to
facilitate capacity building. There is also the need to identify lead NGOs, FBOs or CBOs with
capacity to provide a resource based for district level capacity building activities for both
existing and newly emerging CBOs.
10. There are multiple guidelines from different organizations on an area such as home based care
which at times is confusing to the implementers. The national guidelines need to be dissemi-
nated and implemented to make training and delivery of services easy.
11. The youth present the largest case load of new HIV infection as a group but lack a central body
to coordinate preventive efforts. Structures within NACC, community groups and NGOs
should facilitate developing of a network that can serve as a platform for bringing the
various youth organizations together.
Building on our experiences33
National AIDS Control Council
Appendix- List of participants
- List of organizations that participated
- Workshop programmes

Building on our experiences 34
National AIDS Control Council
List of Participants1. Ezekiel Omanwa Mouko,
Chairman, NACHOP
2. James K. Leitich,
Secretary, CACC Eldoret South
3. Annabel Kihuha,
Field Officer, NACC-FMA
4. Dominic T. Ngechu,
Training/Resource Officer,
NACC-FMA
5. Phillip K. Koitelel,
UNV, South Rift
6. Nelson C. Chepkech,
CACC Chairman, Mt. Elgon
7. Zachariah A. Muyokani,
Project Coordinator,
Western HIV/AIDS Network
8. Kefa Gekonde,
DDO/DACC, Narok
9. Fred I. Amudavi,
CACC Secretary, Kakamega
10. Simeon I. Salach,
Chairman
Mt. Elgon Community Resource
Centre
11. Bathsheba Osoro,
PACC, Western Province
12. Bramwel Amondo,
Coordinator,
Kabras Jua Kali Association
13. Rebecca Koech,
Secretary,
Songich SDA Evangelistic
S.H.G.
14. Lawrence Okudo,
PACC, Nyanza Province
15. Joseph Chacha,
Chairman, Tohanchane C.B.O.
16. Eunice E. Odongi,
PACC Member, Kakamega
17. Mathew M. Mudenyu,
Secretary, CACC
Kitutu Masaba
18. Peter John Akhonya,
DDO, Busia
19. Godfery Kutwa,
Secretary,
Olemila CBO
20. Andrew M. Karanja,
KANCO - Nakuru Branch
21. Timothy J. Ogwang,
DACC, Mt. Elgon
22. Boniface O. Otwani,
CACC Secretary, Nambale
23. Ngota Ephraem,
Coordinator,
New Vision Theatre Group
24. Brigit A. Omondi,
CACC Secretary,
Kwanza
25. Paul Ole Ntaiyin,
Chairman,
Transmara Herbal Association
26. Agnes Nkuyayu,
CACC Secretary,
Narok North
27. Wilfred A. Omari,
DDO, Nandi
28. Oluoch C. Obiero,
CACC Secretary,
Kisumu Town West
29. Tissia John,
Secretary, Lasers
30. M. Maroa Abednego,
Chairman,
Kuria District - Disability
Network
31. Simel Ole Sankei,
Secretary,
Olmarei Lang S.H.G.
32. Joseph L. Ololngojine,
CACC Secretary,
Kilgoris
33. Martin Wekesa,
DDO,
Iten
34. Ruth Sialala,
CACC Secretary,
Eldama Ravine
35. Anne Suter,
Chairperson,
MYWO-Keiyo District
36. Aloyce M. Ratemo,
DDO/DACCO,
Nyamira
37. Joel K.K. Meto,
DDO/DACCO, Koibatek
38. Peter A. Nyakwara
NCPD, Kakamega

Building on our experiences35
National AIDS Control Council
39. William C. Kendagor,
CACC Secretary,
Marakwet West
40. Mary Elsie Amolo,
Coordinator, Day Aid Care
S.H.G.
41. Maureen A. Omollo,
Secretary, Makinu Youth
Against AIDS
42. Joshua L. Silingi,
DACC, Marakwet
43. Boniface M. Kariuki,
DACC, Kilgoris
44. George O. Ayoma,
DDO, Kuria
45. Grace Chebii,
MYWO, Keiyo Branch
46. Simon Korir,
DDO, Kisumu
47. Margaret Janet Kariuki,
CACC Treasurer, LARI
48. Rukiya Lali,
Chairperson, Tunu Women
Group
49. Mahmoud Ahmed Abdulalkadir
CACC Chairman, Lamu West
50. Joseph J. Olita,
Programme Director,
Gallamoro Network Nairobi
51. Hassan Mohamud M.,
Field Coordinator, Handicap
International,
Garissa
52. Micah K. Kisoo,
Programme Officer,
National AIDS Control Council
53. John Ochako,
DACC Member, Garissa
54. Amos Ndenge,
CACC Secretary,
Bahari CACC-Kilifi
55. Abdikadir Dokata Guyo,
Project Officer, FONI, Isiolo
56. Nicholas Wambua Kitua,
DDO/DACC, Lamu
57. Michael Kyalo,
DACC/DDO, Kitui
58. James Mwanzia,
PACC, Eastern Province
59. Japhet Shadrack,
Secretary, Jua-Arts Kilifi
60. Dr. Esther Getambu,
PACC, Mombasa
61. Agisu Adangah,
Programme Officer,
NACC, Nairobi
62. Abdullah Hersi,
Project Officer,
Nomadic Heritage Aid, Garissa
63. Job Akuno,
Youth Programme & Special
Events Coordinator,
National Organization of Peer
Educators (NOPE),
Mombasa
64. Mohamed A. Hirey,
Volunteer, HAMADOWR, Garissa
65. Philip Osoro,
CACC Secretary, Nairobi
66. Hassan Osman Shurie
PACC Member, North Eastern
Province
67. Abdi Dagane,
Vice Chairman, IYAP Youth
Group,
Isiolo
68. Abdullahi Adon Diis,
CACC Secretary, Dujis, Garissa
69. Agnes Muthanje,
CACC Secretary,
Maragua, Makuyu
70. Dr. Mtana Lewa,
Chairman,
Coast HIV/AIDS Consortium,
Kilifi
71. Joyce Kamondo,
Coordinator,
Mother/Child with AIDS Support
Organisation,
Nairobi
72. Diriye Ibrahim Maalim,
Coordinator,
Pastrol Capacity Building and
Development Organisation,
Garissa
73. Anthony Maina
Program Manager,
Womankind Kenya,
Garissa
74. Sirat Kithye Abdi
Chairman, Ramagab Wildlife
Conservation Group,
Ijara District

Building on our experiences 36
National AIDS Control Council
75. Suleiman Mohamed Laag,
CACC Secretary Fafi, Garissa
76. Mustafa K. Wachu
CACC Secretary,
Isiolo North
77. Chege W. Jenipher
Programme Manager,
RICOAN, Nairobi
78. Mureithi Oscar Kingori,
Chairman, The Ihururu Initiative,
Nyeri
79. Rev. Wamathai Bildad,
Church Minister,
Presbyterian Church, Nyeri
80. William K. Mahinda
PACC, Central Province
81. Mutie Lawrence
CACC Secretary Kasarani,
Nairobi
82. Gertrude Openda
Chairperson, MADICAA,
Nairobi
83. Rev. Amos Mumu Mbithi
Pastor Coordinator,
Thome Baptist Dev Group,
Nairobi
84. Kasaya Edward Kisaka,
PACC, Nairobi
85. Lawrence Nyamwaya
DDO/DACCO, Isiolo
86. Mailu Gideon Makundi
PACC member,
Nyeri
87. Mutava Johnrick
Chairman, Beccoh Centre,
Mombasa
88. John Kimanthi Mainga
Team Leader, PAIDO,
Kitui
89. Esther Musili
Director, UCCS/ACK,
Machakos
90. Benson Kimani
DDO/DACCO,
Maua
91. Mboroki Jackson Kiogora
CACC Secretary, Igembe,
Maua
92. Mutinda Kithuku
Member, DACC,
Garissa
93. Shakuntala Haraksinsh Thilsted
Consultant, The World Bank,
Nairobi
94. Loise Muriuki
Support Programme Officer,
WEMIHS,
Thika.
95. Beatrice Manyonge
DACC, Kiambu
96. Michael Oyalo
DACC, Nairobi
97. Patrick M. Wambua
UNV/NACC,
Nairobi
98. Wairimu Mungai
Program Director,
WEMIHS, Thika
99. Michael Musili
Project Volunteer,
Beccoh Centre,
Mombasa
100. Daniel M. Kairu
Aids Control Coordinator
Maragwa DACC, Makuyu
101. Nyambura Githagui
World Bank, Nairobi
102. Wacuka Ikua
Operations Officer, World Bank
103. Yusuf Mbuno,
DACC,
Kilifi
104. Mohamud M. Asan
Field Coordinator
Handicap International,
Garissa
105. Dr. Bert Voetberg
World Bank, Nairobi
106. Diriye I. Maalim
Coordinator
Pastrol Capacity Building &
Department Organisation
107. Abdikadir Dokata,
Project Officer
Friends of Nomads
International (FONI)
Isiolo
108. Dr. Magaret Makumi
Field Co-ordinator/Facilitator
National Aids Control Council,
Nairobi
109. Esther Gatua
Facilitator,
KANCO, Nairobi

Building on our experiences37
National AIDS Control Council
Regional Experience Sharing Meeting forNGOs/CBOs/FBOs from Selected Districts27th - 28th May 2003, Silver Springs Hotel - Nairobi
Programme
DATE
26th May 2003
27th May 2003
28th May 2003
TIME
5.00pm - 6.00pm
8.30am - 9.00am
9.00am - 10.00am
10.00am - 10.30am
10.30am - 11.00am
11.00am - 12.00pm
1.00pm - 2.00pm
2.00pm - 4.30pm
4.30pm - 5.00pm
8.30am - 9.00am
9.00am - 10.30am
10.30am - 11.00am
11.00am - 12.00pm
12.00pm - 1.00pm
1.00pm - 2.00pm
2.00pm
ACTIVITY
Arrival
Registration
■ Climate Setting
- Introduction
- Participants Expectations
- Workshops Objectives
- Administrative Issues
Official Opening
Tea Break
■ KHADREP, Overview of Community
Initiative Account
■ Roles and Responsibilities of Civil
Societies, FBOs, Private Sector and
Development Partners
■ Accountability
Lunch Break
Experience Sharing in Plenary
■ Central Province
■ Eastern Province
■ Coast Province
Tea Break
Re-cap previous day
Experience Sharing in Plenary
■ North Eastern Province
Tea Break
Nairobi Province
Discussion of Emerging Issues and Way
Forward
Lunch Break
Departure
FACILITATOR
NACC
KANCO
Dr. Margaret Makumi
Director NACC
Dr. Margaret Makumi
KANCO
FMA
PACC
Nairobi
Participant
PACC
Eastern/KANCO
PACC
CENTRAL
Deputy Director (T)/
Deputy Director (F&A)
Workshop Programme
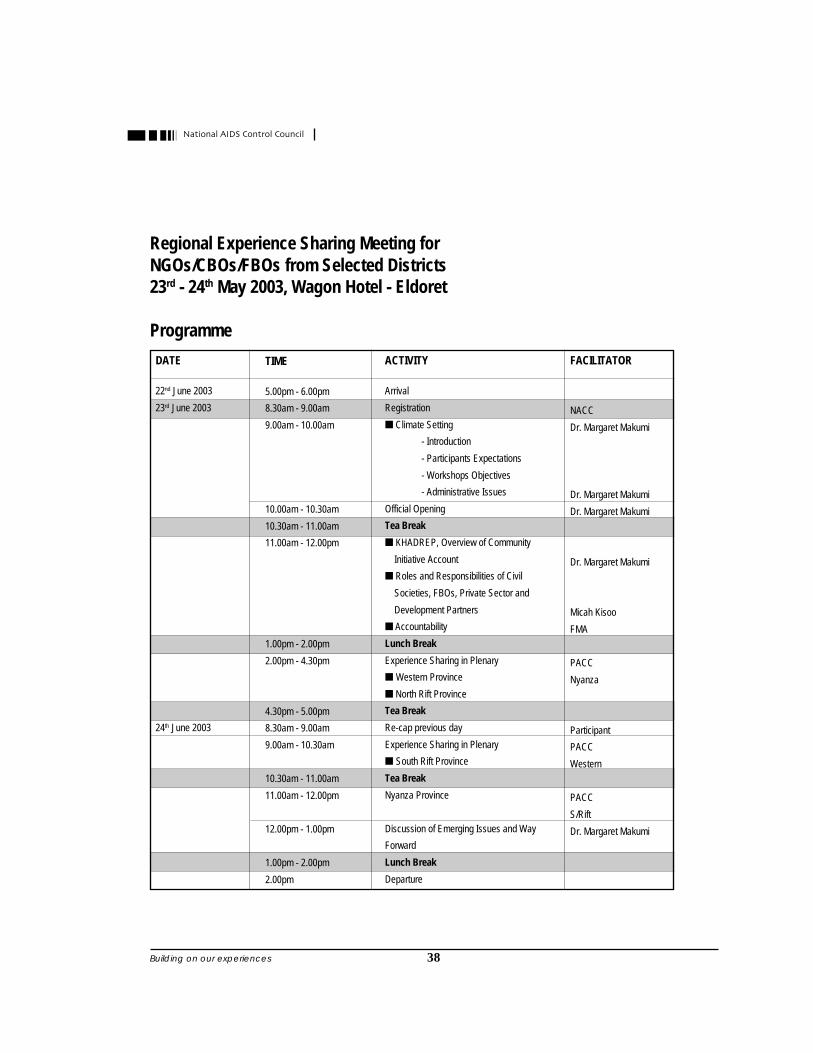
Building on our experiences 38
National AIDS Control Council
Regional Experience Sharing Meeting forNGOs/CBOs/FBOs from Selected Districts23rd - 24th May 2003, Wagon Hotel - Eldoret
Programme
DATE
22nd June 2003
23rd June 2003
24th June 2003
TIME
5.00pm - 6.00pm
8.30am - 9.00am
9.00am - 10.00am
10.00am - 10.30am
10.30am - 11.00am
11.00am - 12.00pm
1.00pm - 2.00pm
2.00pm - 4.30pm
4.30pm - 5.00pm
8.30am - 9.00am
9.00am - 10.30am
10.30am - 11.00am
11.00am - 12.00pm
12.00pm - 1.00pm
1.00pm - 2.00pm
2.00pm
ACTIVITY
Arrival
Registration
■ Climate Setting
- Introduction
- Participants Expectations
- Workshops Objectives
- Administrative Issues
Official Opening
Tea Break
■ KHADREP, Overview of Community
Initiative Account
■ Roles and Responsibilities of Civil
Societies, FBOs, Private Sector and
Development Partners
■ Accountability
Lunch Break
Experience Sharing in Plenary
■ Western Province
■ North Rift Province
Tea Break
Re-cap previous day
Experience Sharing in Plenary
■ South Rift Province
Tea Break
Nyanza Province
Discussion of Emerging Issues and Way
Forward
Lunch Break
Departure
FACILITATOR
NACC
Dr. Margaret Makumi
Dr. Margaret Makumi
Dr. Margaret Makumi
Dr. Margaret Makumi
Micah Kisoo
FMA
PACC
Nyanza
Participant
PACC
Western
PACC
S/Rift
Dr. Margaret Makumi

Building on our experiences39
National AIDS Control Council
Notes

Building on our experiences 40
National AIDS Control Council
Notes

Building on our experiences41
National AIDS Control Council
Dear Reader,
BUILDING ON OUR EXPERIENCES: Lessons learnt and Future Direction of the Community Programme.
The National AIDS Control Council would like to know if this publication is of interest to you, and whetheryou will use its information in your work. Please take a moment to complete this questionnaire by tickingthat which applies to each question. It will guide future publication decisions. Thank you!
Is this publication relevant to your work?
Very relevant
Somewhat relevant
Not relevant but of personal interest
Neither relevant nor of personal interest
How would you use this publication in your work?
Programme planning
Reference purposes
Share with colleagues
Library
Other
Is the way the information is presented in this publication useful to you?
Yes
No - I would prefer to see this information .......................................................................................................................................................
Who else would you recommend this publication to and why?
..................................................................................................................................................................................................................................................................................................
Other comments
..................................................................................................................................................................................................................................................................................................
Please mail the completed questionnaire directly to:
The Field CoordinatorThe National AIDS Control CouncilP.O. Box 61307Nairobi
Or your respective PACC or DACC.