Effects of Anatomy and Particle Size on Nasal Sprays and Nebulizers
Upload
khangminh22Category
view
1download
0
1
NASAL CAVITY AND PARANASAL SINUSES1
EMBRYOLOGY, ANATOMY, AND HISTOLOGY OF THE NASAL CAVITY
Embryology
The facial prominences (frontonasal, max-illary, and mandibular) appear around the 4th week of gestation and give rise to the boundaries and structures of the face (1). The nasal placodes, bilateral thickenings of the surface ectoderm along the frontonasal prominence, form the nasal pits, which, by growth of the surrounding mesenchyme, become progressively depressed along their length, giving rise to the primitive nasal sacs, the forerunners of the nasal cavities. The anterior portion of the nasal cavity is the ves-tibule, the epithelium of which is ectodermally derived and represents the internal extension of the integument of the external nose (1). The epithelium lining the nasal cavities proper (Schneiderian membrane) is also ectodermally derived (1). The nasal septum develops from the merged medial nasal prominences.
The regions of continuity between the nasal and oral cavities following rupture of the oro-nasal membrane develop into the choanae. The conchae (turbinates) develop as elevations along the lateral wall of each nasal cavity. The olfactory epithelia develop in the superiposterior portion of each nasal cavity and differentiate from cells in the ectodermally derived nasal cavity epithelium.
Anatomic Borders
The nasal cavity is divided into right and left halves by the septum; each half opens onto the face via the nares, or nostrils, and communi-cates behind with the nasopharynx through the posterior nasal apertures, or the choanae (2,3). Each half of the nasal cavity has the following borders (walls) (figs. 1-1, 1-2): 1) the superior as-pect, or the roof, slopes downward in front and back and is horizontal in its middle; the frontal and nasal bones form the anterior sloping part; the cribriform plate of the ethmoid bone forms
the horizontal part and separates the nasal cav-ity from the anterior cranial fossa (medial part of floor). This area represents the deepest part of the cavity. The body of the sphenoid bone forms the posterior sloping part; 2) the inferior aspect (floor) is formed by the palatine processes of the maxillary bone, which represents the majority (75 percent) of the floor and, thereby, intervenes between the oral and nasal cavities; the remainder of the floor is formed by the hori-zontal process of the palatine bone; 3) the lateral aspect is formed mostly by the nasal surface of the maxilla below and in front, posteriorly by the perpendicular plate of the palatine bone, and above by the nasal surface of the ethmoidal labyrinth separating the nasal cavity from the orbit. Along the lateral wall of each nasal cavity are three horizontal bony projections: the su-perior, middle, and inferior conchae; occasion-ally a small fourth concha is identified above the superior concha and is called the supreme concha (3). The air spaces or meatuses (superior, middle, and inferior) lie beneath and lateral to the conchae and are named according to the concha immediately above it; and 4) the medial aspect is the bony nasal septum entirely formed by the vomer and the perpendicular plate of the ethmoid; the anterior portion of the nasal septum represents the septal cartilage (2).
Histology
The nasal vestibule is a cutaneous structure composed of keratinizing squamous epitheli-um and underlying subcutaneous tissue, with cutaneous adnexal structures (hair follicles, sebaceous glands, and sweat glands) (4). The mucocutaneous junction (limen nasi) is ap-proximately 1 to 2 cm posterior to the nares and represents the point at which the epithelial surface changes from keratinizing squamous epithelium to ciliated pseudostratified columnar (respiratory) epithelium, the latter lining the entire nasal cavity (fig. 1-3) and, as previously
By Dr. Bruce M. Wenig
Non-Neoplastic Diseases of the Head and Neck
2
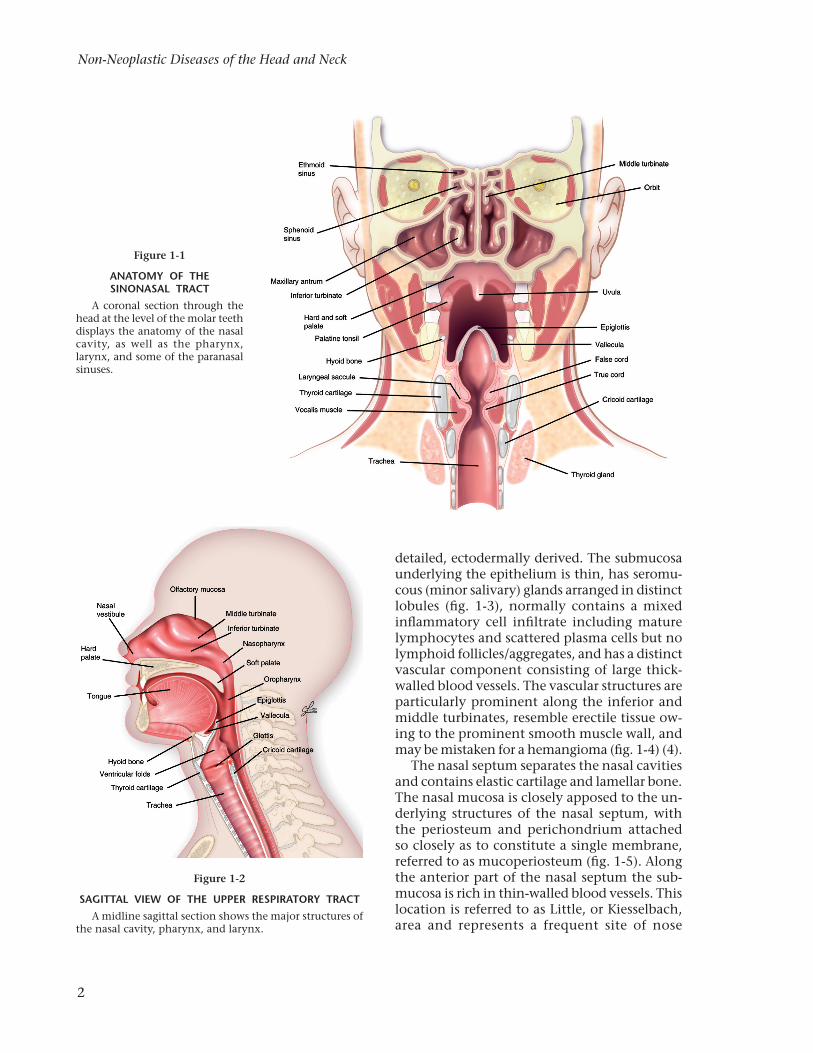
Figure 1-1
ANATOMY OF THE SINONASAL TRACT
A coronal section through the head at the level of the molar teeth displays the anatomy of the nasal cavity, as well as the pharynx, larynx, and some of the paranasal sinuses.
Figure 1-2
SAGITTAL VIEW OF THE UPPER RESPIRATORY TRACTA midline sagittal section shows the major structures of
the nasal cavity, pharynx, and larynx.
detailed, ectodermally derived. The submucosa underlying the epithelium is thin, has seromu-cous (minor salivary) glands arranged in distinct lobules (fig. 1-3), normally contains a mixed inflammatory cell infiltrate including mature lymphocytes and scattered plasma cells but no lymphoid follicles/aggregates, and has a distinct vascular component consisting of large thick-walled blood vessels. The vascular structures are particularly prominent along the inferior and middle turbinates, resemble erectile tissue ow-ing to the prominent smooth muscle wall, and may be mistaken for a hemangioma (fig. 1-4) (4).
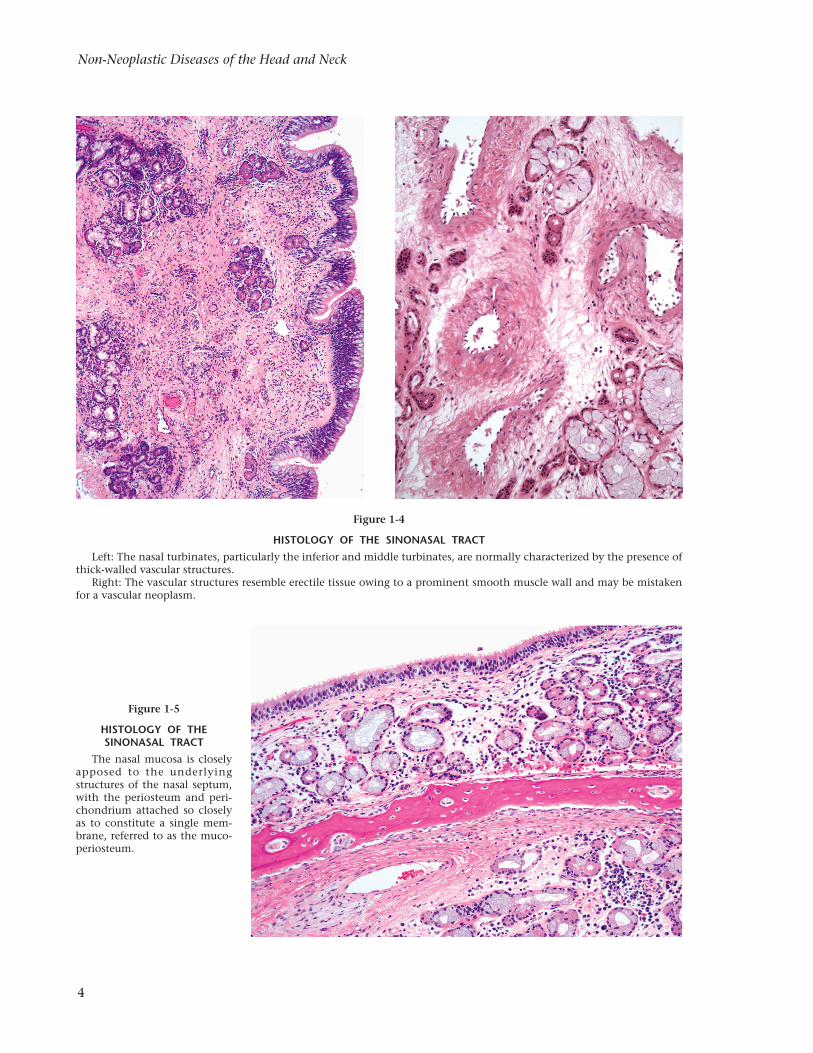
The nasal septum separates the nasal cavities and contains elastic cartilage and lamellar bone. The nasal mucosa is closely apposed to the un-derlying structures of the nasal septum, with the periosteum and perichondrium attached so closely as to constitute a single membrane, referred to as mucoperiosteum (fig. 1-5). Along the anterior part of the nasal septum the sub-mucosa is rich in thin-walled blood vessels. This location is referred to as Little, or Kiesselbach, area and represents a frequent site of nose
3
Nasal Cavity and Paranasal Sinuses
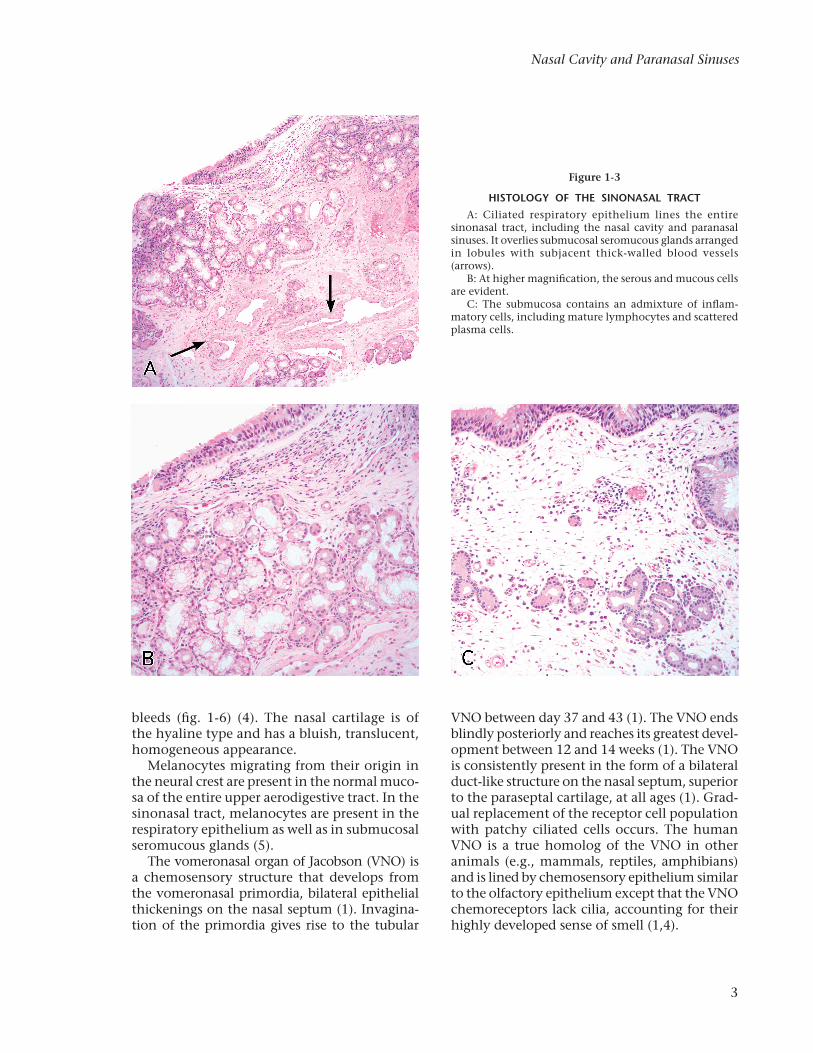
Figure 1-3
HISTOLOGY OF THE SINONASAL TRACTA: Ciliated respiratory epithelium lines the entire
sinonasal tract, including the nasal cavity and paranasal sinuses. It overlies submucosal seromucous glands arranged in lobules with subjacent thick-walled blood vessels (arrows).
B: At higher magnification, the serous and mucous cells are evident.
C: The submucosa contains an admixture of inflam-matory cells, including mature lymphocytes and scattered plasma cells.
bleeds (fig. 1-6) (4). The nasal cartilage is of the hyaline type and has a bluish, translucent, homogeneous appearance.
Melanocytes migrating from their origin in the neural crest are present in the normal muco-sa of the entire upper aerodigestive tract. In the sinonasal tract, melanocytes are present in the respiratory epithelium as well as in submucosal seromucous glands (5).
The vomeronasal organ of Jacobson (VNO) is a chemosensory structure that develops from the vomeronasal primordia, bilateral epithelial thickenings on the nasal septum (1). Invagina-tion of the primordia gives rise to the tubular
VNO between day 37 and 43 (1). The VNO ends blindly posteriorly and reaches its greatest devel-opment between 12 and 14 weeks (1). The VNO is consistently present in the form of a bilateral duct-like structure on the nasal septum, superior to the paraseptal cartilage, at all ages (1). Grad-ual replacement of the receptor cell population with patchy ciliated cells occurs. The human VNO is a true homolog of the VNO in other animals (e.g., mammals, reptiles, amphibians) and is lined by chemosensory epithelium similar to the olfactory epithelium except that the VNO chemoreceptors lack cilia, accounting for their highly developed sense of smell (1,4).
Non-Neoplastic Diseases of the Head and Neck
4
Figure 1-4
HISTOLOGY OF THE SINONASAL TRACTLeft: The nasal turbinates, particularly the inferior and middle turbinates, are normally characterized by the presence of
thick-walled vascular structures.Right: The vascular structures resemble erectile tissue owing to a prominent smooth muscle wall and may be mistaken
for a vascular neoplasm.
Figure 1-5
HISTOLOGY OF THE SINONASAL TRACT
The nasal mucosa is closely apposed to the underlying structures of the nasal septum, with the periosteum and peri-chon drium attached so closely as to constitute a single mem-brane, referred to as the muco-periosteum.
5
Nasal Cavity and Paranasal Sinuses
The olfactory mucosa is located in the most superior portion of the nasal cavity, involving the superior portion of the superior turbinate (cribriform plate) and approximately a third of the superior nasal septum (fig. 1-7). The olfacto-ry epithelium consists of bipolar, spindle-shaped olfactory neural (receptor) cells composed of myelinated axons that penetrate the basal lam-ina to protrude from the mucosal surface and nonmyelinated proximal processes that traverse the cribriform plate, columnar sustentacular or supporting cells, rounded basal cells that lie on basal lamina, and olfactory or Bowman glands in the lamina propria that represent purely se-rous type glands (fig. 1-8) (3,4). The olfactory epithelial cells are reactive for neuron-specific enolase (NSE) (fig. 1-8).
EMBRYOLOGY, ANATOMY, AND HISTOLOGY OF THE PARANASAL SINUSES
Embryology
The paranasal sinuses (maxillary, ethmoid, sphenoid, and frontal) develop as outgrowths of the walls of the nasal cavities and become air-filled extensions of the nasal cavities (fig. 1-9). Some of the nasal sinuses (the maxillary and portions of the ethmoidal sinuses) develop during late fetal life and others (frontal and sphenoid sinuses) are not present at birth but develop during the early years of life.
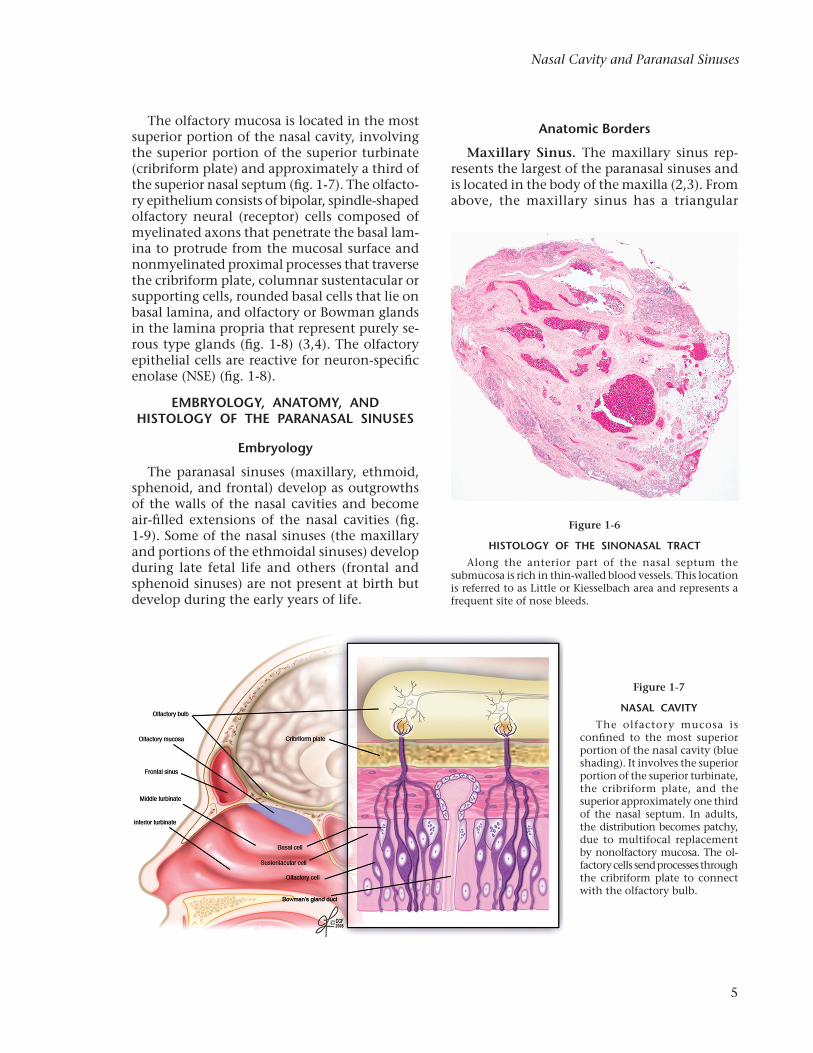
Figure 1-6
HISTOLOGY OF THE SINONASAL TRACTAlong the anterior part of the nasal septum the
submucosa is rich in thin-walled blood vessels. This location is referred to as Little or Kiesselbach area and represents a frequent site of nose bleeds.
Figure 1-7
NASAL CAVITYThe olfactory mucosa is
confined to the most superior portion of the nasal cavity (blue shading). It involves the superior portion of the superior turbinate, the cribriform plate, and the superior approximately one third of the nasal septum. In adults, the distribution becomes patchy, due to multifocal replacement by nonolfactory mucosa. The ol-factory cells send processes through the cribriform plate to connect with the olfactory bulb.
Anatomic Borders
Maxillary Sinus. The maxillary sinus rep-resents the largest of the paranasal sinuses and is located in the body of the maxilla (2,3). From above, the maxillary sinus has a triangular
Non-Neoplastic Diseases of the Head and Neck
6
shape, with the base formed by the lateral wall of the nasal cavity and the apex projecting into the zygomatic arch. Its borders include: 1) the superior aspect (roof) composed of the orbital surface of the maxilla (floor of the orbit); 2) the inferior aspect (floor), composed of the alveolar and palatine process of the maxilla; 3) the anterolateral aspect, composed of the facial surface of the maxilla; 4) the posterior
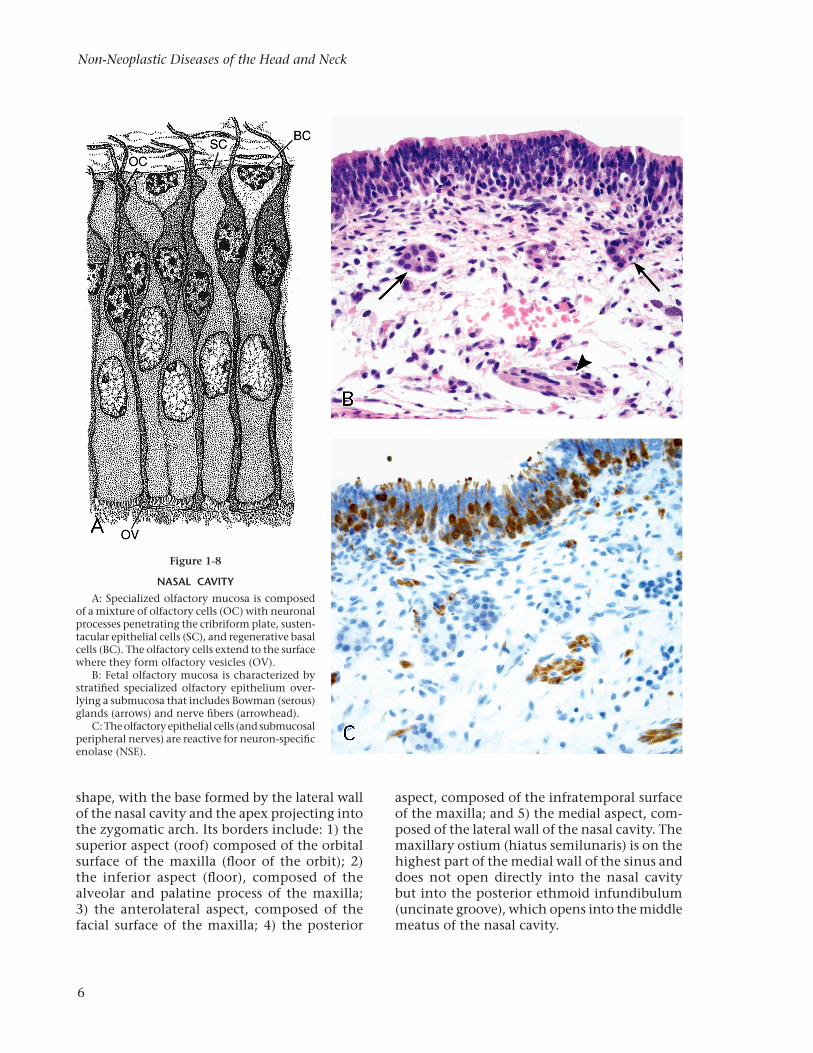
Figure 1-8
NASAL CAVITYA: Specialized olfactory mucosa is composed
of a mixture of olfactory cells (OC) with neuronal processes penetrating the cribriform plate, susten-tacular epithelial cells (SC), and regenerative basal cells (BC). The olfactory cells extend to the surface where they form olfactory vesicles (OV).
B: Fetal olfactory mucosa is characterized by stratified specialized olfactory epithelium over-lying a submucosa that includes Bowman (serous) glands (arrows) and nerve fibers (arrow head).
C: The olfactory epithelial cells (and submucosal peripheral nerves) are reactive for neuron-specific enolase (NSE).
aspect, composed of the infratemporal surface of the maxilla; and 5) the medial aspect, com-posed of the lateral wall of the nasal cavity. The maxillary ostium (hiatus semilunaris) is on the highest part of the medial wall of the sinus and does not open directly into the nasal cavity but into the posterior ethmoid infundibulum (uncinate groove), which opens into the middle meatus of the nasal cavity.
7
Nasal Cavity and Paranasal Sinuses
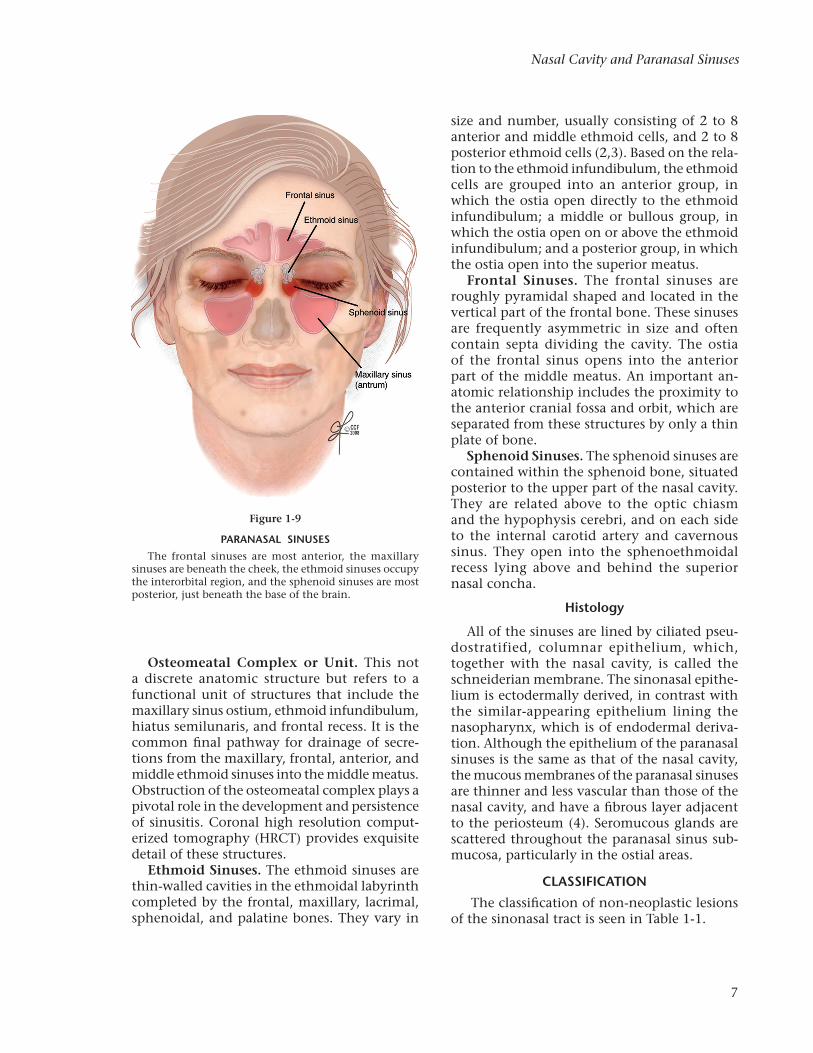
Figure 1-9
PARANASAL SINUSESThe frontal sinuses are most anterior, the maxillary
sinuses are beneath the cheek, the ethmoid sinuses occupy the interorbital region, and the sphenoid sinuses are most posterior, just beneath the base of the brain.
Osteomeatal Complex or Unit. This not a discrete anatomic structure but refers to a functional unit of structures that include the maxillary sinus ostium, ethmoid infundibulum, hiatus semilunaris, and frontal recess. It is the common final pathway for drainage of secre-tions from the maxillary, frontal, anterior, and middle ethmoid sinuses into the middle meatus. Obstruction of the osteomeatal complex plays a pivotal role in the development and persistence of sinusitis. Coronal high resolution comput-erized tomography (HRCT) provides exquisite detail of these structures.
Ethmoid Sinuses. The ethmoid sinuses are thin-walled cavities in the ethmoidal labyrinth completed by the frontal, maxillary, lacrimal, sphenoidal, and palatine bones. They vary in
size and number, usually consisting of 2 to 8 anterior and middle ethmoid cells, and 2 to 8 posterior ethmoid cells (2,3). Based on the rela-tion to the ethmoid infundibulum, the ethmoid cells are grouped into an anterior group, in which the ostia open directly to the ethmoid infundibulum; a middle or bullous group, in which the ostia open on or above the ethmoid infundibulum; and a posterior group, in which the ostia open into the superior meatus.
Frontal Sinuses. The frontal sinuses are roughly pyramidal shaped and located in the vertical part of the frontal bone. These sinuses are frequently asymmetric in size and often contain septa dividing the cavity. The ostia of the frontal sinus opens into the anterior part of the middle meatus. An important an-atomic relationship includes the proximity to the anterior cranial fossa and orbit, which are separated from these structures by only a thin plate of bone.
Sphenoid Sinuses. The sphenoid sinuses are contained within the sphenoid bone, situated posterior to the upper part of the nasal cavity. They are related above to the optic chiasm and the hypophysis cerebri, and on each side to the internal carotid artery and cavernous sinus. They open into the sphenoethmoidal recess lying above and behind the superior nasal concha.
Histology
All of the sinuses are lined by ciliated pseu-dostratified, columnar epithelium, which, together with the nasal cavity, is called the schneiderian membrane. The sinonasal epithe-lium is ectodermally derived, in contrast with the similar-appearing epithelium lining the nasopharynx, which is of endodermal deriva-tion. Although the epithelium of the paranasal sinuses is the same as that of the nasal cavity, the mucous membranes of the paranasal sinuses are thinner and less vascular than those of the nasal cavity, and have a fibrous layer adjacent to the periosteum (4). Seromucous glands are scattered throughout the paranasal sinus sub-mucosa, particularly in the ostial areas.
CLASSIFICATION
The classification of non-neoplastic lesions of the sinonasal tract is seen in Table 1-1.

Non-Neoplastic Diseases of the Head and Neck
8
DEVELOPMENTAL LESIONS
Heterotopic Central Nervous System (Glial) Tissue
Definition. Heterotopic central nervous system (glial) tissue (HCNST) is a midline congenital developmental error composed of altered brain tissue that occurs in or near the bridge of the nose, but without a patent connection to the cranial cavity. It is commonly referred to as nasal glioma, but “glioma” is more appropriately used for glial neoplasms. It is also referred to as glial heterotopia.
Embryogenesis. HCNST seems to be sporadic, and is only rarely found with other congenital ab-normalities (fig. 1-10). Such rare associations may be coincidental and the abnormality is not part of a congenital “syndrome” or a constellation of developmental abnormalities. There is, however, some embryologic association with nasal dermoids and encephaloceles (see below). In early embryo-genesis, the prenasal space contains a projection of dura that transiently contacts the overlying ectoderm (6). An abnormal persistence of this contact could produce an effect that would result in some embryonic CNS tissue being abnormally positioned toward the ectodermal area.
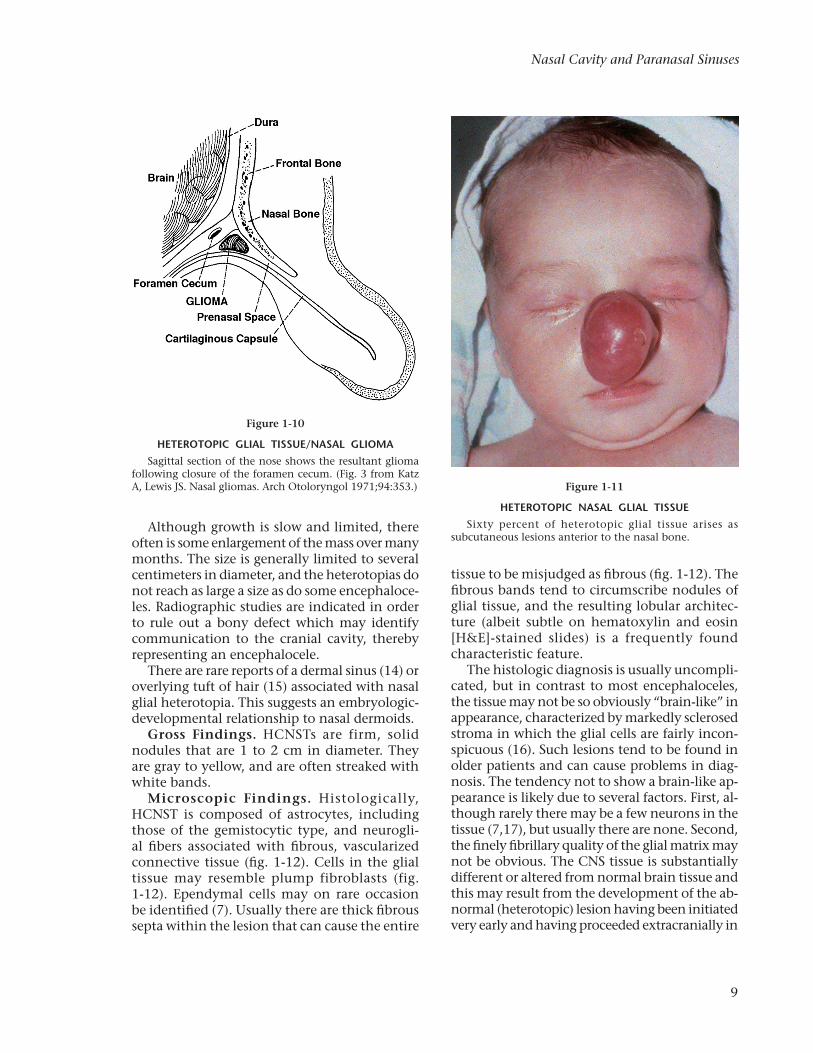
Clinical Features. HCNST have been estimat-ed to occur in approximately 1 of 4,000 births. There is no familial association and the gender incidence is roughly equal. The heterotopias usually present within the first year of life, al-though occurrence in adults has been reported (7). HCNST most commonly occurs in and around the nasal cavity, usually associated with the septum; a midline location with swelling in the nasal bridge area is common (fig. 1-11). The lesion is usually not always midline but may occur more laterally (paramidline), toward or near the inner canthus of the eye. Other sites of involvement include the ethmoid sinus, palate, middle ear, tonsil, and pharyngeal area.
HCNST may be extranasal, intranasal, or mixed. Extranasal lesions make up approxi-mately 60 percent of cases (8). Such lesions present as a subcutaneous blue or red mass along the bridge of the nose; the skin overlying the swelling or mass may be slightly erythematous. This appearance may clinically simulate the appearance of a hemangioma (9), however, the lesion is usually firmer than a hemangioma, as well as an encephalocele (10).
Intranasal lesions represent approximately 30 percent of cases (8) and present with obstruction and/or septal deviation (11,12). Intranasal le-sions are clinically confused with nasal polyps. Nasal attachment occurs high within the nasal vault, along the lateral wall of the nasal fossa or middle turbinate. Rare reports of visual loss in adults have been attributed to HCNST (13).
Mixed extranasal and intranasal lesions represent approximately 10 percent of cases. Communication occurs through a defect in the nasal bone. Patients with HCNST have a negative Furstenberg test, which is the absence of swelling or a pulsating lesion following pres-sure on the ipsilateral jugular vein; typically patients with a positive Furstenberg test have an encephalocele.
Table 1-1
CLASSIFICATION OF NON-NEOPLASTIC LESIONS OF THE SINONASAL TRACT
Developmental Heterotopic central nervous system tissue and encephalocele Nasal dermoid sinus and cyst Primary ciliary dyskinesia
Noninfectious Inflammatory and Tumor-like Sinonasal inflammatory polyps Paranasal sinus mucocele Sinonasal hamartomas Respiratory epithelial adenomatoid hamartoma (REAH) Seromucinous hamartoma Chondro-osseous and respiratory epithelial (CORE) hamartoma Nasal chondromesenchymal hamartoma Granulomatosis with polyangiitis (formerly referred as Wegener granulomatosis) Myospherulosis Extranodal sinus histiocytosis with massive lymph- adenopathy (Rosai-Dorfman disease) Necrotizing sialometaplasia Eosinophilic angiocentric fibroma Sarcoidosis Rhinophyma Relapsing polychondritis
Infectious Fungi (noninvasive and invasive fungal sinusitis, others) Bacteria (rhinoscleroma, others) Protozoa (leishmaniasis, amebiasis) Viruses Rhinosinusitis
9
Nasal Cavity and Paranasal Sinuses
Figure 1-10
HETEROTOPIC GLIAL TISSUE/NASAL GLIOMASagittal section of the nose shows the resultant glioma
following closure of the foramen cecum. (Fig. 3 from Katz A, Lewis JS. Nasal gliomas. Arch Otoloryngol 1971;94:353.) Figure 1-11
HETEROTOPIC NASAL GLIAL TISSUESixty percent of heterotopic glial tissue arises as
subcutaneous lesions anterior to the nasal bone.Although growth is slow and limited, there
often is some enlargement of the mass over many months. The size is generally limited to several centimeters in diameter, and the heterotopias do not reach as large a size as do some encephaloce-les. Radiographic studies are indicated in order to rule out a bony defect which may identify communication to the cranial cavity, thereby representing an encephalocele.
There are rare reports of a dermal sinus (14) or overlying tuft of hair (15) associated with nasal glial heterotopia. This suggests an embryologic-developmental relationship to nasal dermoids.
Gross Findings. HCNSTs are firm, solid nodules that are 1 to 2 cm in diameter. They are gray to yellow, and are often streaked with white bands.
Microscopic Findings. Histologically, HCNST is composed of astrocytes, including those of the gemistocytic type, and neurogli-al fibers associated with fibrous, vascularized connective tissue (fig. 1-12). Cells in the glial tissue may resemble plump fibroblasts (fig. 1-12). Ependymal cells may on rare occasion be identified (7). Usually there are thick fibrous septa within the lesion that can cause the entire
tissue to be misjudged as fibrous (fig. 1-12). The fibrous bands tend to circumscribe nodules of glial tissue, and the resulting lobular architec-ture (albeit subtle on hematoxylin and eosin [H&E]-stained slides) is a frequently found characteristic feature.
The histologic diagnosis is usually uncompli-cated, but in contrast to most encephaloceles, the tissue may not be so obviously “brain-like” in appearance, characterized by markedly sclerosed stroma in which the glial cells are fairly incon-spicuous (16). Such lesions tend to be found in older patients and can cause problems in diag-nosis. The tendency not to show a brain-like ap-pearance is likely due to several factors. First, al-though rarely there may be a few neurons in the tissue (7,17), but usually there are none. Second, the finely fibrillary quality of the glial matrix may not be obvious. The CNS tissue is substantially different or altered from normal brain tissue and this may result from the development of the ab-normal (heterotopic) lesion having been initiated very early and having proceeded extracranially in
Non-Neoplastic Diseases of the Head and Neck
10
Figure 1-12
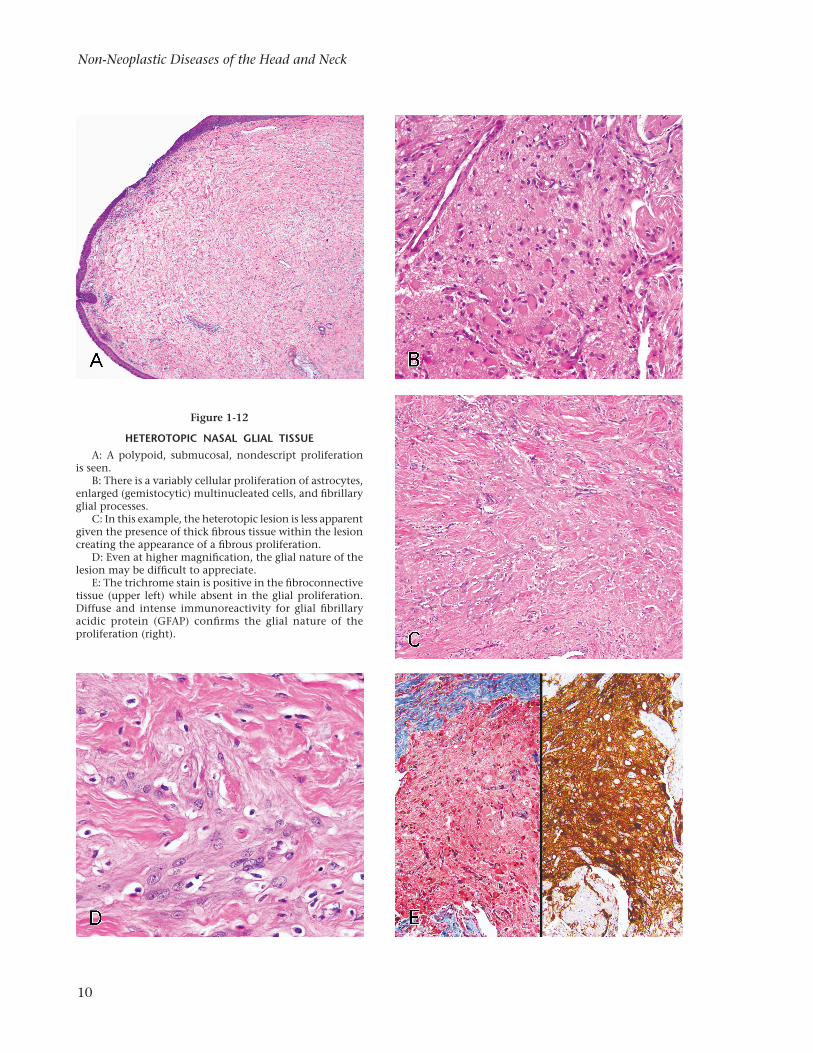
HETEROTOPIC NASAL GLIAL TISSUEA: A polypoid, submucosal, nondescript proliferation
is seen.B: There is a variably cellular proliferation of astrocytes,
enlarged (gemistocytic) multinucleated cells, and fibrillary glial processes.
C: In this example, the heterotopic lesion is less apparent given the presence of thick fibrous tissue within the lesion creating the appearance of a fibrous proliferation.
D: Even at higher magnification, the glial nature of the lesion may be difficult to appreciate.
E: The trichrome stain is positive in the fibrocon nective tissue (upper left) while absent in the glial pro liferation. Diffuse and intense immunoreactivity for glial fibrillary acidic protein (GFAP) confirms the glial nature of the proliferation (right).

11
Nasal Cavity and Paranasal Sinuses
a fibrous microenvironment. If the diagnosis is suspected, however, the difference between the fibrous tissue and the glial tissue can be striking-ly highlighted by a trichrome stain (fig. 1-12) and more definitively by immunoreactivity for glial fibrillary acidic protein (GFAP) (fig. 1-12) as well as S-100 protein (7,16).
Differential Diagnosis. Distinction from an encephalocele is important because of the definite communication of the latter with the cerebrospinal fluid (CSF) space. Since some glial HCNSTs have a fibrous stalk projecting to the cranial base and since some encephalo-celes have only a meager cranial base defect, a feasible inference is that the heterotopias and encephaloceles may be manifestations of a similar developmental defect (18), with the heterotopias being the more meager or more “arrested” manifestation of the defect. In any event, distinction between the two may be dif-ficult. Although radiographic features and sur-gical operative findings are the most definitive features of differentiation, the histopathologic features are important for diagnosis. The lobular architecture formed by circumscribing fibrous septa is more characteristic of a heterotopia. The finding of neurons favors an encephalocele but the absence of definite neurons, however, does not exclude an encephalocele. In general, an encephalocele is composed of tissue that is more obviously brain-like than is the case with the heterotopias.
If the glial nature of the tissue is overlooked, an intranasal glial heterotopia may be misinter-preted as an inflammatory polyp, especially if the child is older than an infant (with inflam-matory nasal polyps being virtually absent in infants). The tissue of the heterotopia should be less edematous and less inflammatory than is expected in an inflammatory polyp.
Careful scrutiny of the tissue should allow distinction from a neurofibroma. The latter tends to have more spindled and elongated cells than a heterotopia.
Astrocytes within the glial tissue can some-times be very gemistocytic and occasionally can cause some concern about a malignant lesion (19). Awareness of this phenomenon in this set-ting obviates the error of a malignant diagnosis.
When the glial nature of the lesion is dis-cerned, the possibility of olfactory neuroblas-
toma may be considered, particularly since olfactory neuroblastomas are well known to occur mostly in young children. Olfactory neu-roblastomas, however, although they certainly occur in pediatric patients, are not a primarily pediatric tumor; occurrence in an infant is not expected. Histologically, an olfactory neu-roblastoma is distinctly more cellular than a congenital HCNST.
Treatment and Prognosis. Left untreated, the HCNSTs do not spontaneously regress. There is a small tendency for enlargement (20), perhaps via increased accumulation of reactive fibrous tissue (21), so operative removal is gener-ally indicated. Every reasonable effort should be made to preoperatively judge the likelihood of a CSF communication (i.e., an encephalocele) so that the requirement of repair can be planned. If the lesion is indeed a heterotopia, the prog-nosis is excellent; these lesions do not produce a deforming hypertelorism (22) and operative removal produces no risk of CNS infection.
Encephaloceles
Definition. Encephaloceles are herniations of brain tissue beyond the confines of the cranial cavity. The abnormality is associated with a congenital developmental skull defect or an acquired condition, often related to some inju-ry that results in a skull defect. The condition is called a meningoencephalocele when the meninges are present, but the shortened form of encephalocele is often understood to imply that the meninges are probably also involved in the formation of the lesion.
Encephaloceles are sincipital, occipital, and basal (23,24). A sincipital encephalocele is situated in the anterior part of the skull and is interfrontal (cranial defect lies between the two frontal bones) or frontoethmoidal (nasofrontal, nasoethmoidal, nasoorbital). Occipital enceph-aloceles are cervico-occipital, low occipital in-volving the foramen magnum, or high occipital above the intact rim of the foramen magnum. Basal encephaloceles are rare and are categorized by their point of passage through the skull and the area where they extend to: midline basal encephaloceles (transsphenoidal type, sphen-oethmoidal type, transethmoidal type) and lateral basal encephaloceles (sphenorbital and sphenomaxillary types) (23).
Non-Neoplastic Diseases of the Head and Neck
12
Embryogenesis. Almost all encephaloceles seem to be sporadic and not related to recog-nized genetic syndromes (fig. 1-13). Occipital encephaloceles may be associated with other neural tube closure defects such as myelome-ningocele; associated anomalies include cleft lip, cleft palate, nasal tip malformation, ocular abnormalities, and craniosynostosis (23,25,26). While occipital encephaloceles may be asso-ciated with other neural tube closure defects, anterior (sincipital or nasofrontal and basal) encephaloceles are seldom so associated.
One theory of genesis is a hypothetical failure of anterior neuropore closure. Since anterior encephaloceles are not associated with other neural tube closure defects, however, and there is no dysraphism of the brain underlying such an encephalocele, this seems to be an unlikely explanation. Also, the postembryonic site of anterior neuropore closure is in the area of the sphenoid sinus and this theory would not ex-plain sincipital encephaloceles.
Another theory is a failure of ossification at foci in the anterior skull base. At the outset, this would seem to be a feasible theory, but embryo-logic-anatomic studies have indicated that the
meningeal-neural protrusions that eventuate in an encephalocele are present quite early, and be-fore ossification normally occurs, i.e., the failure of bone formation occurs around the protrusion defect as a secondary effect.
Perhaps the most likely explanation is that after the neural tube fissure closes, there may be connections (“adhesions”) between the neural tissue and the overlying cutaneous ectodermal structures. If such a connection persists abnor-mally, then this could explain both the neural protrusion or herniation and the associated skull defect (the latter being a result of the former). In the sincipital area, this explanation has the appealing added capacity of explaining the for-mation of the dermoids that occur in the fron-tonasal area. The traction produced by the neural tube-ectodermal connection (adhesion) could either “pull out” neural tissue, resulting in glial heterotopia or encephalocele, or it could “pull in” cutaneous ectoderm, resulting in a dermoid. This common mechanism of genesis for both the frontonasal neural anomalies and dermoids is supported by a few reports suggesting that in rare instances there is evidence of both lesions in the same patient, i.e, a tuft of hair associated with a glial heterotopia (27) or some neural elements associated with a dermoid (28).
Clinical Features. The prevalence of congen-ital encephaloceles varies in different parts of the world from about 0.8 to 4.0 per 10,000 live births (25). They are more common in Asia than in the western hemisphere. The ratio of sincipital to occipital lesions also varies geographically. Sincipital encephaloceles are about nine times more frequent than occipital ones in Southeast Asia, but in Europe and North America, occipital lesions are more common. Basal encephaloceles are rare (2 to 10 percent of cases) in all geograph-ic regions. The incidence of acquired sinonasal encephaloceles in adults is difficult to ascertain. Since some of these are postsurgical complica-tions, they are seldom reported or catalogued. Also, many of these lesions are probably misdiag-nosed as “heterotopias,” with their true nature and genesis unrecognized.
Some acquired encephaloceles are probably related to head trauma other than a surgical cause. The cause of others is not clear. Such lesions conceivably develop from arachnoid granulations projecting into thinner areas of the
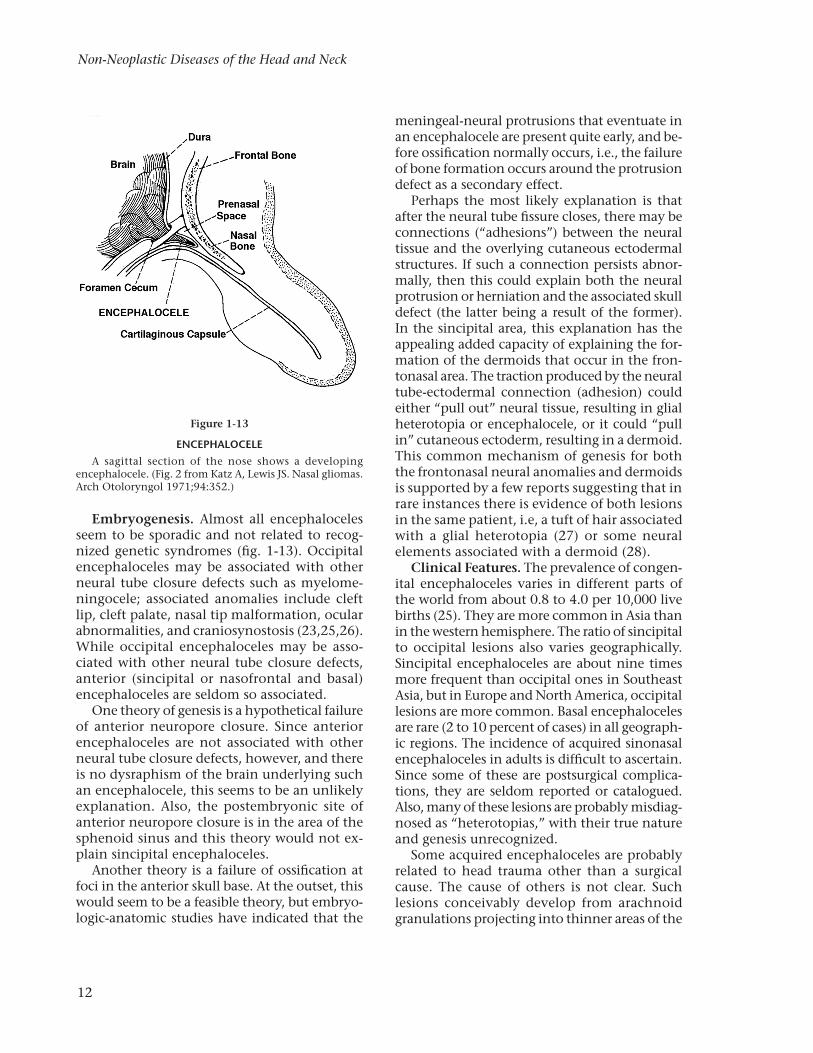
Figure 1-13
ENCEPHALOCELEA sagittal section of the nose shows a developing
encephalocele. (Fig. 2 from Katz A, Lewis JS. Nasal gliomas. Arch Otoloryngol 1971;94:352.)

13
Nasal Cavity and Paranasal Sinuses
skull base. Slowly, over many years, such pro-jections can eventuate in resorbtive increased thinning (“remodeling”) of the bone focally and occasionally cause an acquired encephalocele. Although not congenital, this cause of acquired encephalocele could be thought of as develop-mental in the broadest sense of the term.
Sincipital congenital encephaloceles usually form a visible midline or paramidline mass in the region of the bridge (root) of the nose and glabella, and are almost always evident at birth. Often these lesions are much larger than the glial heterotopias and are more compressible than the heterotopias. Hypertelorism may often be associated.
Basal encephaloceles do not produce a visible facial mass but rather are masses in the nasal or nasopharyngeal cavities (traversing the sphen-oethmoid sinus areas), the posterior orbital region, or the sphenomaxillary fossa. The basal (internal) lesions may not be evident during infancy and may not present until the patient is significantly older, accounting for a “second peak” of encephalocele incidence around the age of 5 to 10 years (29). Likely the lesions slow-ly enlarge and thus tend to eventually become
Figure 1-14
SPHENOETHMOIDAL ENCEPHALOCELEAxial spin echo T1- (left) and coronal FSE T2-weighted (right) images demonstrate a defect in the sphenoid bone. A
meningocele containing cerebrospinal fluid (CSF) and meninges extends through the sphenoid sinus into the posterior nasal cavity. (Courtesy of Dr. A. Khorsandi, New York, NY.)
more symptomatic. Sometimes these lesions are clinically mistaken for an inflammatory nasal polyp, a potentially important error. For both the sincipital and basal lesions, it is important to search radiographically for evidence of a CNS (CSF) connection (fig. 1-14) so that the lesion is known not to be a heterotopia and the proper operative repair can be planned.
Gross Findings. Encephaloceles may be small but often are impressively large masses. The masses are moderately firm and pinkish, and surrounded by a pseudocapsule. They are usually solid, although there may be small cys-tic areas or collapsed spaces. These latter areas represent either extensions from the ventricular system (meningoencephalocystocele) or areas of degeneration of the brain tissue. The lesions are seldom recognizable as brain tissue grossly.
Microscopic Findings. Because of the nutri-tional impairment of the herniated brain tissue that constitutes an encephalocele, the tissue has degenerative-reactive alterations (of varying de-grees and of variable chronicity). Neurons may disappear and gliosis may be prominent. Chang-es secondary to congestion or hemorrhage also contribute to the appearance. Even if neurons
Non-Neoplastic Diseases of the Head and Neck
14
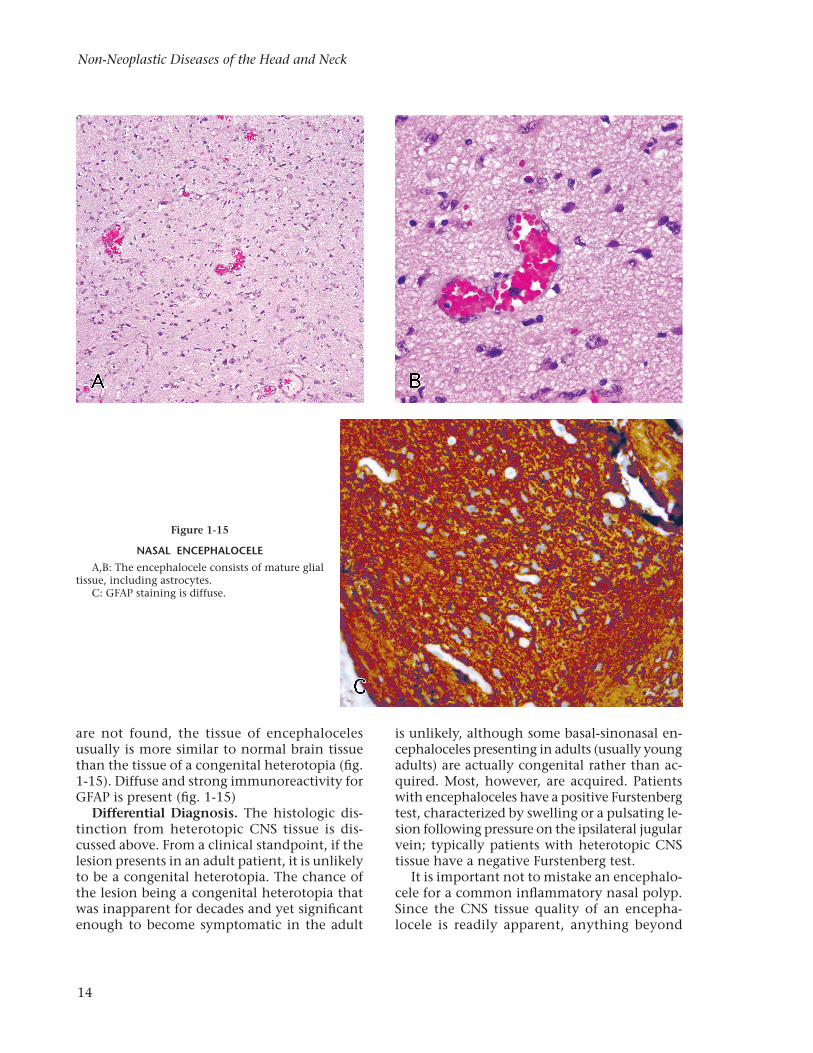
are not found, the tissue of encephaloceles usually is more similar to normal brain tissue than the tissue of a congenital heterotopia (fig. 1-15). Diffuse and strong immunoreactivity for GFAP is present (fig. 1-15)
Differential Diagnosis. The histologic dis-tinction from heterotopic CNS tissue is dis-cussed above. From a clinical standpoint, if the lesion presents in an adult patient, it is unlikely to be a congenital heterotopia. The chance of the lesion being a congenital heterotopia that was inapparent for decades and yet significant enough to become symptomatic in the adult
Figure 1-15
NASAL ENCEPHALOCELEA,B: The encephalocele consists of mature glial
tissue, including astrocytes.C: GFAP staining is diffuse.
is unlikely, although some basal-sinonasal en-cephaloceles presenting in adults (usually young adults) are actually congenital rather than ac-quired. Most, however, are acquired. Patients with encephaloceles have a positive Furstenberg test, characterized by swelling or a pulsating le-sion following pressure on the ipsilateral jugular vein; typically patients with heterotopic CNS tissue have a negative Furstenberg test.
It is important not to mistake an encephalo-cele for a common inflammatory nasal polyp. Since the CNS tissue quality of an encepha-locele is readily apparent, anything beyond

15
Nasal Cavity and Paranasal Sinuses
a cursory examination of the tissue should obviate this error.
The histologic appearance may suggest a pos-sible low-grade astrocytoma or other intracra-nial neoplasm. Clinical considerations should resolve the issue: a low-grade CNS neoplasm arising within the cranial cavity and presenting within the sinonasal tract, without an obvious intracranial origin, does not seem feasible.
Treatment and Prognosis. Congenital sin-cipital-basal encephaloceles require transcranial resection (30,31). If gross hypertelorism has de-veloped, orbital translocation may be required. The developmental outcome has been normal in approximately 60 percent of cases (25). In adults, acquired encephaloceles may not be very large and the most important part of surgical removal may entail repair of a CNS leak and prevention of infection. The prognosis generally is good.
Nasal Dermoid Sinus and Cyst
Definition. Nasal dermoid cyst is a congenital developmental lesion that is virtually identical to dermoid cysts found in other anatomic lo-cations. A congenital developmental origin is usually obvious for these nasal cysts since they usually present in infants or young children. A distinction should be made between nasal der-moids and so-called nasopharyngeal dermoids; the latter are not cysts and are considered to be ectopic accessory auricles (32). Craniofacial dermoid cyst is a synonym.
Embryogenesis. Although a few nasal der-moids are found in the lower and lateral regions (e.g., near the ala) of the nose, most are midline structures in the nasal bridge. As such, they are in the same location as glial heterotopias. The development of these two lesions seems related. It is useful to think of both as resulting from the cutaneous-neural connection or synechium in this location (33), with the glial tissue result-ing from neural tissue being “pulled out” and the dermoid formed when cutaneous tissue is “pulled in” (although this may not quite liter-ally describe the developmental dynamics).
Clinical Features. There is no gender pre-dilection. Nasal dermoid cysts usually present in infants or young children, but may occur in adults (34). They are usually midline swellings at the root of the nose and make up approximately 10 percent of all dermoids in the cervicofacial
region (35). Small lesions or deeply seated cysts may not be apparent until after they become infected and inflamed. A sinus tract with an epidermal opening may be present. Intracranial extension may occur (36–38). Rarely, patients present with a median upper lip fistula (37). Coexistence of a dermal sinus tract, dermoid cyst, and encephalocele has been reported in a patient presenting with nasal cellulitis (40).
Preoperative radiologic evaluation is essential to rule out intracranial extension. Computer-ized tomography (CT) and magnetic resonance imaging (MRI) are indicated to delineate deep tissue involvement and to exclude possible as-sociated intracranial extension.
Nasal dermoid cysts and sinuses may be as-sociated with or coexist with other congenital developmental malformations such as Gorlin syndrome (41). They may be familial (42).
Gross and Microscopic Findings. The mac-roscopic and microscopic findings are similar to those of dermoid cysts in more common locations. Grossly, these cysts vary in size from a few millimeters to several centimeters. On cut section, skin and hair are often readily identifi-able and the contents of the cyst may include grumous and greasy material. Histologically, the cyst is lined by keratinized squamous epitheli-um; sebaceous glands, hair follicles, and sweat glands are typically identified. The wall of the cyst is thick with fibrovascular tissue. Respira-tory epithelium may be identified. Endodermal and mesodermal elements are not found.
Differential Diagnosis. The histologic ap-pearance usually is diagnostic. Problems can arise, however, if the tissue is mistaken for portions of the normal skin surface or if the features are obscured because of marked alter-ations secondary to infection. These potential problems should be kept in mind when exam-ining a specimen from this anatomic location.
Treatment and Prognosis. Complete surgi-cal resection is the treatment of choice and is usually curative (43–45). The most important treatment concern is the possibility of the associated existence of a deeply seated cyst or its related sinus tract involving the anterior midline skull base (46). Radiographic examina-tion to judge the deep extent of the lesion is important in planning operative removal. Good cosmetic results and only a low recurrence rate
Copyright © 2022 FDOKUMEN