
Narrative innovations predict symptom improvement: Studying innovative moments in narrative therapy...
12
This article was downloaded by: [37.189.127.36] On: 13 May 2015, At: 06:21 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Click for updates Psychotherapy Research Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/tpsr20 Narrative innovations predict symptom improvement: Studying innovative moments in narrative therapy of depression Miguel M. GonÇalves a , AntÓnio P. Ribeiro a , Joana R. Silva a , InÊs Mendes ab & Inês Sousa c a CIPsi – Psychology Research Center, Psychotherapy and Psychopathology, Research Unit, School of Psychology, University of Minho, Braga, Portugal b ISMAI, Avioso São Pedro, Portugal c Department of Mathematics and Applications, University of Minho, Braga, Portugal Published online: 13 May 2015. To cite this article: Miguel M. GonÇalves, AntÓnio P. Ribeiro, Joana R. Silva, InÊs Mendes & Inês Sousa (2015): Narrative innovations predict symptom improvement: Studying innovative moments in narrative therapy of depression, Psychotherapy Research, DOI: 10.1080/10503307.2015.1035355 To link to this article: http://dx.doi.org/10.1080/10503307.2015.1035355 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Narrative innovations predict symptom improvement: Studying innovative moments in narrative therapy...
This article was downloaded by: [37.189.127.36]On: 13 May 2015, At: 06:21Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Click for updates
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
Narrative innovations predict symptom improvement:Studying innovative moments in narrative therapy ofdepressionMiguel M. GonÇalvesa, AntÓnio P. Ribeiroa, Joana R. Silvaa, InÊs Mendesab & Inês Sousac
a CIPsi – Psychology Research Center, Psychotherapy and Psychopathology, Research Unit,School of Psychology, University of Minho, Braga, Portugalb ISMAI, Avioso São Pedro, Portugalc Department of Mathematics and Applications, University of Minho, Braga, PortugalPublished online: 13 May 2015.
To cite this article: Miguel M. GonÇalves, AntÓnio P. Ribeiro, Joana R. Silva, InÊs Mendes & Inês Sousa (2015): Narrativeinnovations predict symptom improvement: Studying innovative moments in narrative therapy of depression, PsychotherapyResearch, DOI: 10.1080/10503307.2015.1035355
To link to this article: http://dx.doi.org/10.1080/10503307.2015.1035355
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

EMPIRICAL PAPER
Narrative innovations predict symptom improvement: Studyinginnovative moments in narrative therapy of depression
MIGUEL M. GONÇALVES1*, ANTÓNIO P. RIBEIRO1, JOANA R. SILVA1, INÊS MENDES1,2,& INÊS SOUSA3
1CIPsi – Psychology Research Center, Psychotherapy and Psychopathology, Research Unit, School of Psychology, University ofMinho, Braga, Portugal; 2ISMAI, Avioso São Pedro, Portugal & 3Department of Mathematics and Applications, Universityof Minho, Braga, Portugal
(Received 21 July 2014; revised 21 November 2014; accepted 17 March 2015)
AbstractObjective: Innovative moments (IMs) are moments in the therapeutic dialog that constitute exceptions toward the client’sproblems. These narrative markers of meaning transformation are associated with change in different models of therapy anddiverse diagnoses. Our goal is to test if IMs precede symptoms change, or, on the contrary, are a mere consequence ofsymptomatic 15 change. Method: For this purpose, IMs and symptomatology (Outcome Questionnaire-10.2) wereassessed at every session in a sample of 10 cases of narrative therapy for depression. Hierarchical linear modeling wasconducted to explore whether (i) IMs in a given session predict patients’ symptoms in the following session and/or (ii)symptoms in a given session predict IMs in the next session. Results: Results suggested that IMs are better predictors ofsymptoms than the reverse. Conclusions: These results are discussed considering the contribution of meanings andnarrative processes’ changes to symptomatic improvement.
Keywords: narrative therapy; process of change; psychotherapy; depression
Over the last decade, a research program that aimed totrack how innovative moments (IMs) emerge in severalpsychotherapeutic modalities was developed. IMsmay be described as moments in the therapeuticdialog in which exceptions to the client’s problemsunfold and constitute narrative markers of meaningtransformation. Research was developed on the emer-gence of these narrative novelties in narrative therapy(NT; Matos, Santos, Gonçalves, & Martins, 2009),emotion-focused therapy (EFT;Mendes et al., 2010),client-centered therapy (CCT; Gonçalves et al.,2012), cognitive-behavior therapy (CBT) (Gonçalves,Silva, Ribeiro, Batista, & Sousa, 2015), and construct-ivist therapy (Alves et al., 2013), with patients suffer-ing from different complaints (domestic violence,depression, complicated grief, among others).
This line of research was built on the perspectivethat clinical problems result from the dominance of
an inflexible framework of understanding and experi-encing the world, which constrains the patients’behaviors, emotions, thoughts and relationships, thusgenerating psychological distress. For the sake ofsimplicity we use in this article the term maladaptiveframework, to describe this inflexible framework ofunderstanding and experiencing the world (in previ-ous publications we used this term interchangeablywith problematic self-narrative). It is proposed thatduring effective psychotherapy themaladaptive frame-work gets transformed and gives rise to a newemergent alternative framework. But for this trans-formation to take place, the emergence of exceptions(IMs) needs to repeatedly occur. This is akin to theproposal from Frank and Frank (1991), which sug-gests that clients need to transform their “maladaptiveassumptive systems” (p. 51) in order for change tooccur in psychotherapy. IMs are every time this
Correspondence concerning this article should be addressed toMiguelM.Gonçalves, CIPsi –PsychologyResearchCenter, Psychotherapy andPsychopathology, Research Unit, School of Psychology, University of Minho, 4710-057 Braga, Portugal. Email: [email protected]
Psychotherapy Research, 2015http://dx.doi.org/10.1080/10503307.2015.1035355
© 2015 Society for Psychotherapy Research
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

“maladaptive assumptive system” is revised during thetherapeutic dialog. The repetitions of IMs, as well as apattern that will be described below, make it morelikely that a new functional framework will occur.
For instance, if a depressive patient has a mala-daptive framework in which the theme “alwaysprioritize others’ wishes/needs/ideas and neglectyour own” is dominant, an IM would be any timethe patient asserts his or her own needs (Alves,Mendes, Gonçalves, & Neimeyer, 2012; Gonçalves,Ribeiro, Mendes, Matos, & Santos, 2011). Theseexceptions to the former maladaptive framework, orIMs, are suggested to constitute a new emergentframework of understanding and experiencing withthe potential for promoting change in psychotherapy(Gonçalves, Matos, & Santos, 2009; Gonçalves,Mendes, Ribeiro, Angus, & Greenberg, 2010). Thispotential for creating change is congruent with theidea that IMs may be a common change experienceacross psychotherapy, despite the different thera-peutic strategies that are used to elicit them (e.g.,Socratic questioning in CBT or chair work in EFT).That is, no matter the specific strategies used indifferent psychotherapies (Goldfried, 2012), innova-tion toward the previousmaladaptive framework needsto occur in the form of meaning transformation, inorder for change to take place, and for a new alternativeframework to develop at the end of treatment.
Empirical data collected, to date, have consistently(i) supported the idea that IMs may be reliablyidentified in therapy sessions using the InnovativeMoments Coding System (IMCS; Gonçalves et al.,2011); (ii) pointed to an association between IMsand psychotherapeutic change, that is, IMs aresignificantly more present in recovered than inunchanged cases; and (iii) suggested that IMs mayemerge in five different types: action, reflection,protest, reconceptualization, and performing change(Gonçalves et al., 2011). Table I provides additionaldescriptive details and several clinical illustrations ofthese different types of IMs. Hypothesis-testingstudies and case studies have also shown that at theinitial phase of treatment, there are no significantdifferences between recovered and unchanged casesin terms of the profile of IMs: both groups arecharacterized by the presence of action, reflection,and protest IMs (Alves et al., 2013; Matos et al.,2009; Mendes et al., 2010). However, from themiddle phase of treatment to the later treatmentstage, recovered and unchanged cases start to differ:reconceptualization (in several samples, also perform-ing change) IMs tend to increase from the middle tothe final stage of therapy in the recovered cases butnot in the unchanged cases, in which these IMsappear to be nearly or completely absent (Gonçalveset al., 2012; Matos et al., 2009; Mendes et al., 2010).
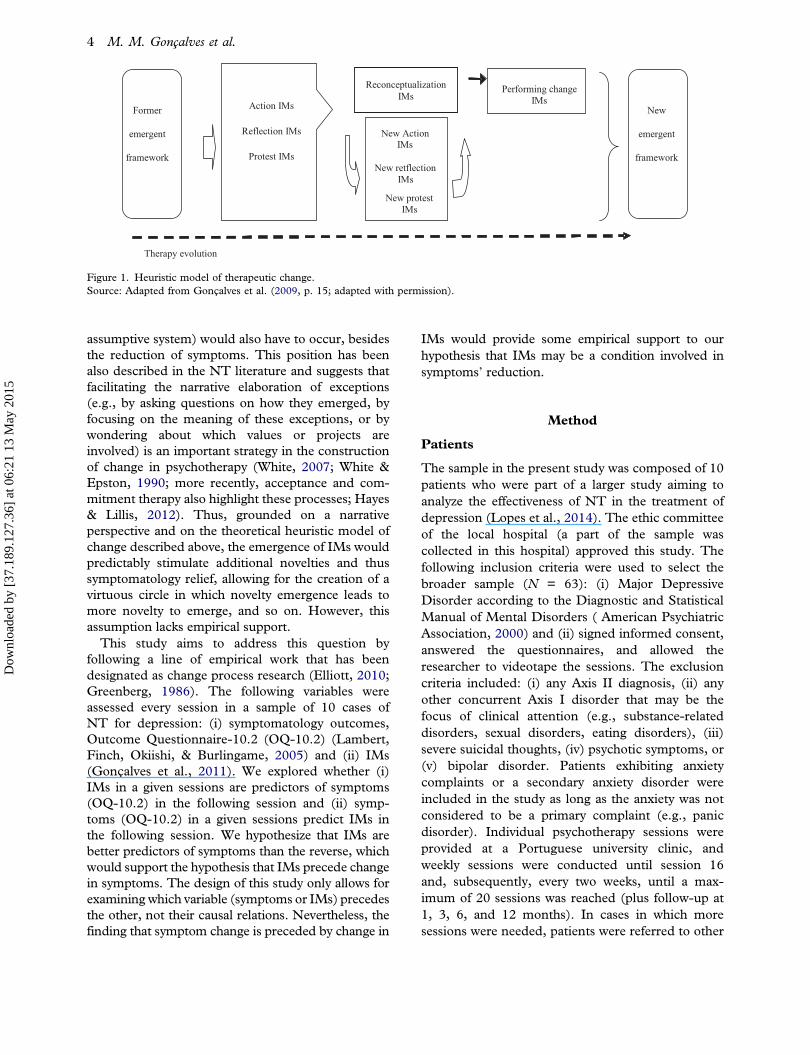
From these studies, a heuristic model of changewas proposed (Gonçalves et al., 2011) in whichreconceptualization IMs assume a central role insuccessful psychotherapy (Figure 1; for a furtherdescription on the role of reconceptualization fortherapeutic change, see Gonçalves et al., 2011;Mendes et al., 2010). According to this model,action, reflection, and protest IMs that are visiblefrom the early phases of therapy are elementarynarrative novelties that open the door to developingan alternative to the previous maladaptive frame-work. However, from the middle to the final phase oftherapy, the emergence of reconceptualization IMs iscrucial for the sustained development of significantchanges. Reconceptualization has two components:a contrast between a prior problematic aspect orposition of the self (“before I used to care moreabout what others thought about me”) and a (emer-gent) more adaptive one (“now I try putting myselffirst”) and an access to the processes that allowedthis transformation (“I’m doing this because Iunderstood that privileging others’ thoughts washarming myself”). Considering these two compo-nents, several processes were speculated to beinvolved in this type of IM (Gonçalves & Ribeiro,2012), which would account for its role in promotingchange in psychotherapy. First, reconceptualization,given its more developed narrative structure presentin the articulation between previous maladaptiveframework and a more adjusted one, has beensuggested to give meaning and structure to othermore elementary IMs (e.g., action and reflection). Inthe above example, understanding the relevance of“taking myself into consideration” may facilitate theorganization of actions, thoughts, and even relation-ships. Second, reconceptualization may operate as abridge between the maladaptive framework and themore adjusted one, thereby helping the patient tomake sense of this transformation. Our hypotheticalpatient understood that it was important to valueherself or himself and that this understanding couldbring a new meaning to life, thus providing a senseof continuity despite change. Third, as change isgradual, the repetition of reconceptualization IMsthroughout the treatment may facilitate the progress-ive identification with the emergent new framework,making it easier to integrate a new way of being.
In sum, the research conducted with the IMCS hasprovided evidence that IMs emerge and can bereliably identified in the therapeutic dialog of differentmodels of therapy, that recovered cases tend topresent a higher proportion of IMs than the un-changed cases, and that reconceptualization tends toemerge in the middle of recovered cases and toincrease toward the end of treatment. Despite thesefindings, one question remained unanswered: are IMs
2 M. M. Gonçalves et al.
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

a consequence of symptomatic change or are IMs ameaning transformation outcome that precedes symp-tomatic change? In several previous papers, we sug-gested that IMs might depict the clients’ process ofmeaning transformation in different types of therapy
(Alves et al., 2013; Gonçalves et al., 2012, 2015;Matos et al., 2009; Mendes et al., 2010). The modelof Frank and Frank (1991) referred above wouldassume that for significant change to occur in psycho-therapy, changes in the meaning systems (the
Table I. Categories of innovative moments with examples.
Contents Examples
Action . New coping behaviors facing anticipated orexistent obstacles;
. Effective resolution of unsolved problem(s);
. Active exploration of solutions;
. Restoring autonomy and self-control;
. Searching for information about theproblem(s).
C: Yesterday, I went to the cinema for the first time in months!
Reflection Subtype I: Creating distance from the problem(s). Comprehension – Reconsidering problem(s)’
causes and/or awareness of its effects;. New problem(s) formulations;. Adaptive self-instructions and thoughts;. Intention to fight problem(s)’ demands,
references of self-worth, and/or feelings ofwell-being.
C: I realize that what I was doing was just, not humanly possiblebecause I was pushing myself and I never allowed myself anyfree time, uh, to myself … and it's more natural and morehealthy to let some of these extra activities go …
Subtype II: Centered on the change. Therapeutic process – Reflecting about the
therapeutic process;. Change process – Considering the process and
strategies;. implemented to overcome the problem(s);. references of self-worth and/or feelings of well-being
(as consequences of change);. New positions – References to new/emergent
identity versions in face of the problem(s).
C: I believe that our talks, our sessions have proven fruitful, I feltlike going back a bit to old times, it was good, I felt good, I feltit was worth it.
Protest Subtype I: Criticizing the problem(s). Repositioning oneself toward the problem(s).Subtype II: Emergence of new positions. Positions of assertiveness and empow‐
erment.
C: What am I becoming after all? Is this where I’ll be getting to?Am I going to stagnate here!?
C: I am an adult and I am responsible for my life, and I want toacknowledge these feelings and I’m going to let them out! I wantto experience life, I want to grow, and it feels good to be incharge of my own life.
Reconceptualization RC always involve two dimensions:. Description of the shift between two positions
(past and present);. The process underlying this transfor‐
mation.
C: You know …when I was there at the museum, I thought tomyself: you really are different… A year ago you wouldn’t beable to go to the supermarket! Ever since I started going out, Istarted feeling less depressed… it is also related to ourconversations and changing jobs …
T: How did you have this idea of going to the museum?C: I called my dad and told him: we’re going out today!T: This is new, isn’t it?C: Yes, it’s like I tell you … I sense that I’m different …
Performing change . Generalization into the future and other lifedimensions of good outcomes;
. Problematic experience as a resource to newsituations;
. Investment in new projects as a result of theprocess of change;
. Investment in new relationships as a result of theprocess of change;
. Performance of change: new skills;
. Re-emergence of neglected or forgottenself-versions.
T: You seem to have so many projects for the future now!C: Yes, you’re right. I want to do all the things that were
impossible for me to do while I was dominated by depression.I want to work again and to have the time to enjoy my life withmy children. I want to have friends again. The loss of all thefriendships of the past is something that still hurts me reallydeeply. I want to have friends again, to have people to talk to,to share experiences, and to feel the complicity in my life again.
RC, reconceptualization.Source: Adapted from Gonçalves et al. (2011, pp. 499–500; adapted with permission).
Psychotherapy Research 3
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015
assumptive system) would also have to occur, besidesthe reduction of symptoms. This position has beenalso described in the NT literature and suggests thatfacilitating the narrative elaboration of exceptions(e.g., by asking questions on how they emerged, byfocusing on the meaning of these exceptions, or bywondering about which values or projects areinvolved) is an important strategy in the constructionof change in psychotherapy (White, 2007; White &Epston, 1990; more recently, acceptance and com-mitment therapy also highlight these processes; Hayes& Lillis, 2012). Thus, grounded on a narrativeperspective and on the theoretical heuristic model ofchange described above, the emergence of IMs wouldpredictably stimulate additional novelties and thussymptomatology relief, allowing for the creation of avirtuous circle in which novelty emergence leads tomore novelty to emerge, and so on. However, thisassumption lacks empirical support.
This study aims to address this question byfollowing a line of empirical work that has beendesignated as change process research (Elliott, 2010;Greenberg, 1986). The following variables wereassessed every session in a sample of 10 cases ofNT for depression: (i) symptomatology outcomes,Outcome Questionnaire-10.2 (OQ-10.2) (Lambert,Finch, Okiishi, & Burlingame, 2005) and (ii) IMs(Gonçalves et al., 2011). We explored whether (i)IMs in a given sessions are predictors of symptoms(OQ-10.2) in the following session and (ii) symp-toms (OQ-10.2) in a given sessions predict IMs inthe following session. We hypothesize that IMs arebetter predictors of symptoms than the reverse, whichwould support the hypothesis that IMs precede changein symptoms. The design of this study only allows forexamining which variable (symptoms or IMs) precedesthe other, not their causal relations. Nevertheless, thefinding that symptom change is preceded by change in
IMs would provide some empirical support to ourhypothesis that IMs may be a condition involved insymptoms’ reduction.
Method
Patients
The sample in the present study was composed of 10patients who were part of a larger study aiming toanalyze the effectiveness of NT in the treatment ofdepression (Lopes et al., 2014). The ethic committeeof the local hospital (a part of the sample wascollected in this hospital) approved this study. Thefollowing inclusion criteria were used to select thebroader sample (N = 63): (i) Major DepressiveDisorder according to the Diagnostic and StatisticalManual of Mental Disorders ( American PsychiatricAssociation, 2000) and (ii) signed informed consent,answered the questionnaires, and allowed theresearcher to videotape the sessions. The exclusioncriteria included: (i) any Axis II diagnosis, (ii) anyother concurrent Axis I disorder that may be thefocus of clinical attention (e.g., substance-relateddisorders, sexual disorders, eating disorders), (iii)severe suicidal thoughts, (iv) psychotic symptoms, or(v) bipolar disorder. Patients exhibiting anxietycomplaints or a secondary anxiety disorder wereincluded in the study as long as the anxiety was notconsidered to be a primary complaint (e.g., panicdisorder). Individual psychotherapy sessions wereprovided at a Portuguese university clinic, andweekly sessions were conducted until session 16and, subsequently, every two weeks, until a max-imum of 20 sessions was reached (plus follow-up at1, 3, 6, and 12 months). In cases in which moresessions were needed, patients were referred to other
Action IMs
Reflection IMs
Protest IMs
ReconceptualizationIMs
New ActionIMs
New retflectionIMs
New protestIMs
Performing changeIMs
New
emergent
framework
Former
emergent
framework
Therapy evolution
Figure 1. Heuristic model of therapeutic change.Source: Adapted from Gonçalves et al. (2009, p. 15; adapted with permission).
4 M. M. Gonçalves et al.
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

therapists at the clinic or to alternative mental healthservices.
The present sample involved 14 dropouts (41.2%)and 20 completers (58.8%). From the 20 completers5 unchanged and 5 recovered cases were randomlyselected to integrate the current study’s sample.According to Jacobson and Truax’s criteria (1991)two conditions must be met at the end of thetreatment for a case to be considered recovered: (i)patients should move from a dysfunctional to afunctional range in a given outcome measure and(ii) the change should be reliable, that is, greaterthan the Reliable Change Index (RCI) for therespective measure. The unchanged cases wereselected when they did not comply with these twoconditions. The RCI analysis was conducted basedon the pre–post therapy scores in the Beck Depres-sion Inventory II (BDI-II; Beck, Steer, & Brown,1996) and the OQ-45.2 (Lambert et al., 1996; theRCI and cut-off values for each measure will bediscussed in detail in the subsection “Measures”).For considering the status of recovered or un-changed cases we considered the RCI and thecut-off criteria, regarding both the BDI-II andthe OQ-45.2, which means that recovered caseswere recovered in both measures and unchangedcases were unchanged in both measures. The reasonfor only selecting 10 out of 20 completers was thetime-consuming nature of the IMs’ coding (thecoding of each complete case takes approximatelyone month of full-time daily work, by two coders).
At the beginning of psychotherapy, the recoveredand the unchanged groups exhibited no significantdifferences in terms of the severity of symptoms,considering the BDI-II, t(8) = .61, p = .56 or theOQ-45.2 scores, t(8) = 1.79, p = .11. The groups didnot significantly differ in the number of therapysessions received throughout the treatment, t(8) =1.24, p = .24. The patients completed an average of18.70 (SD = 1.83) sessions.
From the 10 patients in this sample, 7 werewomen and 3 were men, ranging in age from 22years to 64 years (M = 41.00, SD = 14.97). Fourpatients were single, three were married, two weredivorced, and one was widowed. All the patientscompleted at least the 9th grade; however, somepatients had up to 24 years of academic education(M = 13.90, SD = 5.07). Regarding their profes-sional status, four patients were unemployed, twowere professionally active, two were students, andone was retired. Their socioeconomic level, assessedby the Graffar Index (Graffar, 1956), ranged from 8(Level I, high scale) to 16 (Level III, medium scale).These demographic characteristics were not signifi-cantly different for patients in both groups.
Therapist
All of the 10 patients comprising the sample weretreated by the same therapist, a Ph.D. student inclinical psychology with seven years of experience inpsychotherapy. The therapist was a male student inhis 30s that was selected for this three years researchproject, based on his interest and experience in NT.He had three years of experience in NT and receivedextensive training on a manual of narrative interven-tion based on the narrative model of White andEpston (1990). During the period of the samplecollection the therapist was practicing as a full-timetherapist, involved only in psychotherapy and super-vision activities.
NT Treatment
The manual (Gonçalves & Bento, 2008) involvedthree primary phases, which were sufficiently flexiblefor the therapist to attend to the patients’ idiosyn-cratic characteristics and individual progress withrespect to therapy: (i) deconstruction of the prob-lematic self-narrative (e.g., externalization, re-authoring conversations); (ii) reconstruction of thealternative/emergent self-narrative (e.g., working onthe expansion of unique outcomes); and (iii) con-solidation of the alternative/emergent self-narrativeand finalization (e.g., documenting the process ofchange, social validation, and ceremonies).
The first author of the manual served as asupervisor throughout the project, meeting weeklywith the therapist to ensure his adherence to thenarrative model of intervention. The therapist’sadherence to the narrative therapeutic model wasassessed according to the Adherence and Compet-ence Scale for Narrative and Cognitive-BehavioralTherapy (Gonçalves, Bento, Lopes, & Salgado,2009) and it proved to be adequate (for furtherdetails, see Lopes et al., 2014).
Measures
Pre-post Measures
Beck Depression Inventory II. The BDI-II,which is a 21-item self-report instrument, assessessymptoms of depression (Beck et al., 1996; Steer,Brown, Beck, & Sanderson, 2001), using a 4-pointLikert scale, in which the items are rated from 0 to 3;total scores range from 0 to 63. The BDI-II hasexhibited good internal consistency (α = .91; Steeret al., 2001; α = .89; see Lopes et al., 2014) andconstruct validity (Beck et al., 1996; Steer et al.,2001). Validation for the Portuguese population hasobtained results that were similar to the onesobserved in the American population (Campos &
Psychotherapy Research 5
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

Gonçalves, 2011; Coelho, Martins, & Barros, 2002).Because the RCI (Jacobson & Truax, 1991) couldnot be found across Portuguese studies, normativedata gathered from meta-analyses of diverse samples(Seggar, Lambert, & Hansen, 2002) were used tocalculate the proportion of clinical change (RCI =8.46; cut-off score = 14.29).
Outcome Questionnaire-45.2. The OQ-45.2,which is a widely used self-report questionnaire,allows for monitoring patients’ progress and clinicalconditions when the OQ-45.2 is administeredrepeatedly throughout therapy (Lambert et al.,1996). The OQ-45.2 is composed of 45 questionsconcerning not only psychological distress but alsointerpersonal relations and the social role of thepatients. Excellent values of internal consistencyhave been reported for Portuguese (α = .89;Machado & Fassnacht, 2014) and non-Portuguesesamples (de Jong et al., 2007; Lambert et al., 1996).A three-week test–retest reliability indicates a goodtemporal stability (Pearson’s r = .84; Lambert et al.,1996). The RCI calculated for the Portuguesepopulation was 15 points, and the cut-off was 62points (Machado & Fassnacht, 2014).
Session Measures
Outcome Questionnaire-10.2. The OQ-10.2,which is a brief version (with 10 items) of OQ-45.2(Lambert et al., 1996, 2005), is sensitive to changesin the patients’ symptomatic distress over short timeperiods. Empirical data have shown adequate valuesof internal consistency (α = .87; Goates-Jones &Hill, 2008) and test–retest reliability (Pearson’sr =.62; Lambert et al., 2005).
Innovative Moments Coding System. TheIMCS allows for the identification of five majortypes of IMs: action, reflection, protest, reconcep-tualization, and performing change (for additionaldescriptions and illustrative clinical vignettes of eachtype, see Table I; Gonçalves et al., 2011). Inprevious studies, the IMCS (Gonçalves et al.,2011) proved to be reliable; Cohen’s k values of.89 were reported in the study on NT (Matos et al.,2009), .86 in the study on EFT (Mendes et al.2010), and .97 in the study on CCT (Gonçalveset al., 2012). In case studies, the values of Cohen’s kranged from .76 (Gonçalves et al., 2010) to .90(Ribeiro, Bento, Salgado, Stiles, & Gonçalves,2011), indicating an adequate inter-rater agreement(Hill & Lambert, 2004).
Procedures
Outcome measures. The outcome measureswere used at the beginning of each therapy session.The BDI-II and the OQ-45.2 were used at thebeginning and at the end of therapy and at eachfourth session and the OQ-10.2 was used in theother sessions. In the sessions in which the OQ-45.2was used (4th, 8th, 12th, and 16th) the items relativeto the OQ-10.2 were extracted for purposes ofcomparability with the other sessions, in which onlythe OQ-10.2 was used.
IM coding and reliability. All the therapeuticsessions of the 10 cases were transcribed andsubsequently analyzed according to the IMCS (Gon-çalves et al., 2011). Two independent coders (Ph.D.students), unaware of the outcome status of thecases and the hypothesis of the study, analyzed all ofthe transcripts intensively (N = 180 sessions). Thecoders were trained by the authors of the manual; atthe end of the training period, the reliability of thecoders was assessed by comparing their codes withthe codes of expert judges in a set of randomlyselected excerpts from the dialogs of therapeuticsessions of NT and EFT. The coders were consid-ered to be reliable and able to engage in coding ifthey achieved Cohen’s k values higher than .75. Theentire training procedure took several weeks ofintensive work; by the time coders started to workon the present sample, they already had considerableexpertise in applying IMCS. Three steps wereexecuted in the process of coding IMs: (i) a consen-sual definition of the facets of the maladaptiveframework by the two coders, (ii) identification ofeach IM and definition of its beginning and end, and(iii) categorization of previously identified IMs interms of type. The reliability between coders wascalculated on 100% of the material. Then codersidentified the disagreements emerging from thecoding process and these were resolved throughconsensus during regular discussion meetings. Thisinteractive and collaborative approach allowed thejudges to move on to integrating each other’sstrengths, which facilitated the coding of subsequentsessions (cf., Brinegar, Salvi, Stiles, & Greenberg,2006). Thus, all of the analyses presented werebased on the consensus between two judges.
IMCS allows for the identification of the type ofIM (e.g., action, reflection) and its proportion (inprevious papers we have used the term salience).Therefore, proportion is a measure of the IMs’length in the transcript. For each patient, theproportion of each type of IM for each session wascalculated as the percentage of words involved ineach type of IM per session. Since we take the
6 M. M. Gonçalves et al.
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

perspective that change is co-constructed betweentherapist and client (Angus, Levitt, & Hardtke,1999) each IM contained both client and therapistdialogs.
Reliability indexes were computed for the entiresample, resulting in a percentage of agreement onthe overall IMs’ proportion of 89.9%, which meansthat the judges agree on what portions of thetranscripts correspond to IMs in 89.9% of the text.Reliability in distinguishing IM types, assessed byCohen’s k, was .91. These values are highly satis-factory and comparable to the results noted inprevious samples (Gonçalves et al., 2012; Matoset al., 2009; Mendes et al., 2010).
HLM analyses. The data were analyzed usinghierarchical linear modeling (HLM), and the ana-lyses were performed using nonlinear mixed-effectsmodeling package for R (version 3.0.1, R Develop-ment Core Team, 2013). HLM is a useful techniquefor the analysis of nested or hierarchically structureddata (i.e., observations across time nested within-patients) because it accounts for the decompositionof variability within the data; that is, HLM allowsfor the simultaneous estimation of within- andbetween-patient effects. In the present study, anHLM was fitted to the data, allowing a regressionmodel for the fixed effects (predictors) and a patient-specific random effect. We can attribute a portion ofthe variability to differences between subjects. Thus,at Level 1 (within-patient), outcomes were estimatedto be a function of time; and at Level 2 (between-patients), variability in Level 1 coefficient wasmodeled as a function of patient-level time-invariantcovariates.
Two distinct sets of models were estimated to testthe hypothesis. The first set of models was estimatedwith different types of IMs in each session to bepredictors of patients’ symptomatology in the fol-lowing session (OQ-10.2 score), whereas a secondset of models was estimated with the patients’symptomatology in each session (OQ-10.2 score) tobe predictors of different types of IMs that emergedin the following session. We performed these ana-lyses for the five types of IMs.
Results
IMs as Predictors of Symptomatology (FirstSet of Models)
In the first set of HLM analyses (Table II), reflection(p = .018; R2
adj = .59), reconceptualization (p < .001;R2adj = .63), and performing change IMs (p = .003;
R2adj = .61) emerged as significant predictors of
patients’ symptomatology (OQ-10.2) in the next
session. These three models exhibited a similartendency of effects: the proportion of reflection,reconceptualization, and performing change IMs inone session tended to be negatively associated withpatients’ symptoms (OQ-10.2) in the next session.That is, higher levels in the proportion of reflection,reconceptualization, and performing change IMs in
Table II. HLM with the proportion of IMs as predictors ofsymptomatology (OQ-10.2 scores) in the following session.
Models and fixed effects Coefficient SE t p
Total IMs predicting OQ-10.2 ModelIntercept (β 00) 21.93 2.35 9.33 <.001Total IMs (β 01) –.04 .03 –1.21 .227
Action IMs predicting OQ-10.2 ModelIntercept (β 00) 20.99 2.30 9.12 <.001Action IMs (β 01) .01 .14 .04 .968
Reflection IMs predicting OQ-10.2 ModelIntercept (β 00) 22.53 2.31 9.77 <.001Reflection (β 01) –.09 .04 –2.39 .018
Protest IMs predicting OQ-10.2 ModelIntercept (β 00) 20.67 2.26 9.13 <.001Protest (β 01) .06 .10 .61 .541
RC IMs predicting OQ-10.2 ModelIntercept (β 00) 23.75 2.14 11.09 <.001RC (β 01) –1.88 .42 –4.54 <.001
PC IMs predicting OQ-10.2 ModelIntercept (β 00) 23.01 2.23 10.30 <.001PC IMs (β 01) –1.59 .53 –3.00 .003
RC, reconceptualization; PC, performing change.
Table III. HLM with symptomatology (OQ-10.2 scores) aspredictors of the proportion of IMs in the following session.
Models and fixed effects Coefficient SE t p
OQ-10.2 predicting Total IMs ModelIntercept (β 00) 18.93 3.25 5.83 <.001OQ-10.2 (β 01) .09 .13 .72 .471
OQ-10.2 predicting Action IMs ModelIntercept (β 00) 2.55 .96 2.66 .009OQ-10.2 (β 01) .10 .04 2.56 .011
OQ-10.2 predicting Reflection IMs ModelIntercept (β 00) 16.68 2.46 6.79 <.001OQ-10.2 (β 01) –.01 .11 –.12 .901
OQ-10.2 predicting Protest IMs ModelIntercept (β 00) 4.88 1.40 3.48 .001OQ-10.2 (β 01) .03 .05 .62 .535
OQ-10.2 predicting RC IMs ModelIntercept (β 00) 2.33 .23 10.29 <.001OQ-10.2 (β 01) –.04 .01 –4.09 .001
OQ-10.2 predicting PC IMs ModelIntercept (β 00) 1.72 .17 10.35 <.001OQ-10.2 (β 01) –.02 .01 –2.73 .007
RC, reconceptualization; PC, performing change.
Psychotherapy Research 7
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

one session are associated with a decrease in symp-toms in the next session.
Symptomatology as Predictors of IMs (SecondSet of Models)
Findings from the second set of HLM analyses (seeTable III) suggest that an increase in symptoms(OQ-10) predicts a higher proportion of action IMs(p = .011; R2
adj = .20) and a lower proportion ofreconceptualization (p = .001; R2
adj = .10) andperforming change IMs (p = .007; R2
adj = .10) inthe next session. Thus, when symptoms increase inone session, there appears to be an increase in theproportion of action IMs and a decrease in theproportion of reconceptualization and performingchange IMs in the next session. Interestingly, thesecond set of models explains a lower percentage ofvariance than the first set of models.
Discussion
The present study aimed to analyze whether IMs in agiven session are predictors of symptoms in the nextsession and conversely, whether symptoms in a givensession are predictors of IMs in the next session,testing our hypothesis that meaning changes wouldpredict symptom decrease. The results, particularlyin the first set of models tested, suggest that a higherproportion of reflection, reconceptualization, andperforming change IMs in a given session predict adecrease in symptoms in the next session.
According to the first set of findings, only theelaboration of reflection, reconceptualization, andperforming change IMs appears to have a facilitativefunction in the reduction of general symptoms.Specifically, when patients exhibit more of theseIMs in a given session, the level of symptoms tendsto decrease in the next session (according to the OQ-10.2). Conversely, when patients exhibit less of theseIMs in a given session, the level of symptoms tendsto increase in the next session. In general terms,these results provide support for the heuristic modelof change (Figure 1) and confirm previous findingsfrom the research conducted with IMCS (Gonçalveset al., 2011; Matos et al., 2009; Mendes et al., 2010)because reconceptualization and performing changeIMs were found to be particularly associated withsignificant therapeutic change. Reflection IMs werenot observed to differentiate recovered from un-changed patients in our previous studies; but in thisstudy reflection IMs were shown to predict adecrease in symptoms. Thus, what seems to beconsistent across studies is the distinctive roleassumed by reconceptualization in the constructionof change. The role of the other types of IMs is
probably dependent on the specific therapeuticmodality used and the target clients. For instance,protest has proved to be particularly high in EFT(Gonçalves et al., 2010) and it has been speculatedthat this type of IM can work as scaffolding forreconceptualization IMs to emerge (Mendes et al.,2011). However, in a sample of meaning reconstruc-tion in grief therapy, reflection emerged as the mostexpressive type of IM, which was attributed to thespecificity of the therapy and to the clients’ efforts tomake sense of their losses (Alves et al., 2013). In thepresent study reflection also emerged as the mostcommon form of innovation. Perhaps reflection ispredictive of symptom improvement as these IMsrepresented the major part of clients’ efforts toproduce innovations. Thus, we speculate that reflec-tion is herein working as a developmental precursorof reconceptualization, a more complex form ofinnovation.
These findings are congruent with recent studiesthat demonstrated the importance of narrative pro-cesses for therapeutic change. For instance, Boritz,Bryntwick, Angus, Greenberg, and Constantino(2013) investigated the narrative-emotion processesin three different therapeutic approaches (EFT,CCT, and cognitive therapy) and found significantlyhigher proportions of narrative-emotion processchange markers in recovered cases than in un-changed patients (Boritz et al., 2013) in threedifferent therapeutic models, namely, what theytermed “discovery storytelling markers,” whichmost likely overlaps with IMs. On the other hand,Adler and colleagues alluded to coherence andprocessing as two specific processes of narrativemeaning-making that have shown to be associatedwith sudden gains in psychotherapy (Adler, Harmel-ing, & Walder-Biesanz, 2013). Processing appears tobe related to reflection IMs, involving the elabora-tion of new manners of thinking and feeling that arenot predicted by the maladaptive framework. Coher-ence appears to be related to reconceptualizationIMs in which the patient narrates a contrast betweenan emergent new self-narrative and a problematicpast narrative as well as the description of how thischange was possible. According to these authors,when patients engage in these two processes, theyconsequently experience sudden gains in psycho-therapy (Adler et al., 2013). Finally, performingchange IMs entails the expansion of change intothe future, which predicts a decrease in symptoms inthe next session. Other researchers refer to therelevance of the future in clinical improvement(Habermas & Bluck, 2000).
Focusing on the second set of models explored inthis study, data suggest that an increase in symptomspredicts a higher proportion of action IMs and
8 M. M. Gonçalves et al.
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

decreases in reconceptualization and performingchange IMs in the next session. These decreases inthe latter two types of IMs are consistent with theresults of the first set of models. When patients do notexhibit reconceptualization and performing changeIMs, they appear to get worse in the next session. Onthe other hand, the positive association betweensymptom increase and action IMs is striking. In theabsence of significant and more profound narrativechanges and being aware of the strong therapeutic roleof behavioral activation for depression (Hopko,Lejuez, Ruggiero, & Eifert, 2003), the therapist mayhave focused more intensively on fostering patients’behavioral activity as an ultimate effort to help themchange. However, this argument is speculative andmust be addressed in future studies.
The predictive capacity and “goodness of fit” (R2adj)
found across the first set of models, that is, IMs aspredictors of symptomatology, proved to be consid-erably more satisfactory compared to the second set ofmodels tested, that is, symptomatology as predictor ofIMs, thus providing strong support in favor of theconceptualization of IMs as precursors of sympto-matic change, not merely an outcome of symptomchange. Obviously, despite the clinical and empiricalrelevance of these results for process research, thesedata do not prove that IMs are mechanisms of changebecause other variables can be involved. In fact,research emphasizes a diversity of mediator andmoderator variables that may account for the variancefound in the outcomes of patients (Kazdin, 2007).
Furthermore, the question of which specific thera-peutic techniques are associated with IMs remainsunanswered. So, one of the future directions we wantto pursuit regards the hypothesis that therapeuticinterventions, as mechanisms of change, would facil-itate meaning transformation (IMs) and subsequentlyIMs would promote symptom reduction. Activeingredients may be described as therapeutic processeswithin the treatment that predicts favorable outcomes(Magill & Longabaugh, 2013). Specifically, consider-ing that reflection, reconceptualization and perform-ing change IMs can work as predictors and potentialfacilitators of change, it would be interesting forfuture studies to identify particular therapeutic strat-egies that are capable of promoting these narrativenovelties. As Frank and Frank (1991) suggestedhumans have an intrinsic need of making sense ofthe world and for that purpose an assumptive systemis constructed. In this construction individuals trans-form their problematic meanings into new ones andIMs could be a form to measure this meaningtransformation. As meaning transformation is acommon factor in psychotherapy, we assume IMs as
a potential mediator between model-specific inter-vention strategies and therapeutic change.
The size of this sample, the participation of asingle therapist, the specificity of the problem(depression), and the therapeutic model (NT) limitthe generalizability of this study. The results of thepresent study may reveal more about NT (elaborat-ing IMs produce change) than about IMs andtherapeutic change in general. However, previousstudies suggested that IMs are not specific to NT;the proportion of IMs differentiates recovered fromunchanged cases in several therapeutic modalitieslike CBT, EFT, or CCT. Also, EFT, which is atherapeutic model that focuses on emotional prob-lem markers and not on narrative novelties, haspresented a higher proportion of IMs (Mendes et al.,2010) than NT (Matos et al., 2009). Only futureresearch with other samples can clarify this issue.
Disclosure statement
No potential conflict of interest was reported by theauthors.
Funding
This research was supported by the Portuguese Founda-tion for Science and Technology (Ambivalence andunsuccessful psychotherapy) [grant number PTDC/PSI-PCL/121525/2010]; the Post-doctoral [grant numberSFRH/BPD/84157/2012], [grant number SFRH/BPD/98196/2013].
References
Adler, J. M., Harmeling, L. H., & Walder-Biesanz, I. (2013).Narrative meaning making is associated with sudden gains inpsychotherapy clients’ mental health under routine clinicalconditions. Journal of Consulting and Clinical Psychology, 81,839–845. doi:10.1037/a0033774
Alves, D., Fernández-Navarro, P., Baptista, J., Ribeiro, E., Sousa, I.,& Gonçalves, M.M. (2013). Innovative moments in grief therapy:The meaning reconstruction approach and the processes of self-narrative transformation. Psychotherapy Research. Advance onlinepublication. doi:10.1080/10503307.2013.814927
Alves, D., Mendes, I., Gonçalves, M. M., & Neimeyer, R. A.(2012). Innovative moments in grief therapy: Reconstructingmeaning following perinatal death. Death Studies, 36, 795–818.doi:10.1080/07481187.2011.608291
American Psychiatric Association. 2000. DSM-IV-TR: Diagnosticand statistical manual of mental disorders (4th rev. ed.). Wash-ington, DC: Author.
Angus, L., Levitt, H., & Hardtke, K. (1999). The narrativeprocesses coding system: Research applications and implica-tions for psychotherapy practice. Journal of Clinical Psychology,55, 1255–1270. doi:10.1002/(SICI)1097-4679(199910)55:10<1255::AID-JCLP7>3.0.CO;2-F
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for theBeck Depression Inventory-II (BDI-II). San Antonio, TX: Psy-chological Corporation.
Boritz, T., Bryntwick, E., Angus, L., Greenberg, L. S., &Constantino, M. J. (2013). Narrative and emotion process in
Psychotherapy Research 9
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

psychotherapy:An empirical test of theNarrative-EmotionProcessCoding System (NEPCS).PsychotherapyResearch. Advance onlinepublication. doi:10.1080/10503307.2013.851426
Brinegar, M. G., Salvi, L. M., Stiles, W. B., & Greenberg, L. S.(2006). Building a meaning bridge: Therapeutic progress fromproblem formulation to understanding. Journal of CounselingPsychology, 53, 165–180. doi:10.1037/0022-0167.53.2.165
Campos, R. C., & Gonçalves, B. (2011). The Portuguese Version ofthe Beck Depression Inventory-II (BDI-II) preliminary psycho-metric data with two nonclinical samples. European Journal ofPsychological Assessment, 27, 258–264. doi:10.1027/1015-5759/a000072
Coelho, R., Martins, A., & Barros, H. (2002). Clinical profilesrelating gender and depressive symptoms among adolescentsascertained by the Beck Depression Inventory II. EuropeanPsychiatry, 17, 222–226. doi:10.1016/S0924-9338(02)00663-6
de Jong, K., Nugter, M. A., Polak, M. G., Wagenborg, J. E. A.,Spinhoven, P., & Heiser, W. J. (2007). The outcome Ques-tionnaire (OQ-45) in a Dutch population: A cross-culturalvalidation. Clinical Psychology & Psychotherapy, 14, 288–301.doi:10.1002/cpp.529
Elliott, R. (2010). Psychotherapy change process research: Real-izing the promise. Psychotherapy Research, 20, 123–135.doi:10.1080/10503300903470743
Frank, J. D., & Frank, J. (1991). Persuasion and healing: Acomparative study of psychotherapy (3rd ed.). Baltimore, MD:Johns Hopkins University Press.
Goates-Jones, M., & Hill, C. E. (2008). Treatment preference,treatment-preference match, and psychotherapist credibility:Influence of session outcome and preference shift. Psychotherapy:Theory, Research, Practice, Training, 45, 61–74. doi:10.1037/0033-3204.45.1.61
Goldfried, M. R. (2012). On entering and remaining in psycho-therapy. Clinical Psychology: Science and Practice, 19(2), 125–128. doi:10.1111/j.1468-2850.2012.01278.x
Gonçalves, M. M., & Bento, T. (2008). Manual terapêuticopsicoterapia narrativa de re-autoria [Re-authoring NarrativeTherapy Manual]. Unpublished manuscript.
Gonçalves, M. M., Bento, T., Lopes, R., & Salgado, J. (2009).Manual da Escala de Adesão e Competência [Therapy Adherenceand Competence Scale Manual]. Unpublished manuscript.
Gonçalves, M. M., Matos, M., & Santos, A. (2009). Narrativetherapy and the nature of “innovative moments” in theconstruction of change. Journal of Constructivist Psychology, 22,1–23. doi:10.1080/10720530802500748
Gonçalves, M. M., Mendes, I., Cruz, G., Ribeiro, A. P., Sousa, I.,Angus, L., & Greenberg, L. (2012). Innovative moments andchange in client-centered therapy. Psychotherapy Research, 22,389–401. doi:10.1080/10503307.2012.662605
Gonçalves, M. M., Mendes, I., Ribeiro, A. P., Angus, L., &Greenberg, L. (2010). Innovative moments and change in emo-tion-focused therapy: The case of Lisa. Journal of ConstructivistPsychology, 23, 267–294. doi:10.1080/10720537.2010.489758
Gonçalves, M. M., & Ribeiro, A. P. (2012). Therapeutic change,innovative moments, and the reconceptualization of the self: Adialogical account. International Journal for Dialogical Science, 6,81–98.
Gonçalves,M.M., Ribeiro, A. P.,Mendes, I.,Matos,M., & Santos,A. (2011) Tracking novelties in psychotherapy process research:The innovative moments coding system. Psychotherapy Research,21, 497–509. doi:10.1080/10503307.2011.560207
Gonçalves, M. M., Silva, J. R., Ribeiro, A. P., Batista, J., & Sousa,I. (2015). Innovative moments in cognitive behavioral therapy.Manuscript in preparation.
Graffar, M. (1956). Une méthode de classification socialed’echantillons de population [A method to score social level].Courrier, 6, 455–459.
Greenberg, L. S. (1986). Change process research. Journal ofConsulting and Clinical Psychology, 54, 4–9. doi:10.1037/0022-006X.54.1.4
Habermas, T., & Bluck, S. (2000). Getting a life: The emergenceof the life story in adolescence. Psychological Bulletin, 126, 748–769. doi:10.1037/0033-2909.126.5.748
Hayes, S. C., & Lillis, J. (2012). Acceptance and commitment therapy(1st ed.). Washington, DC: American Psychological Association.
Hill, C. E., & Lambert, M. J. (2004). Methodological issues instudying psychotherapy processes and outcomes. In M. J.Lambert (Ed.), Handbook of psychotherapy and behavior change(5th ed., pp. 84–135). New York, NY: Wiley.
Hopko, D. R., Lejuez, C. W., Ruggiero, K. J., & Eifert, G. H.(2003). Contemporary behavioral activation treatments fordepression: Procedures, principles and progress. Clinical Psy-chology Review, 23, 699–717. doi:10.1016/S0272-7358(03)00070-9
Jacobson, N. S., & Truax, P. (1991). Clinical significance: Astatistical approach to defining meaningful change in psycho-therapy research. Journal of Consulting and Clinical Psychology,59, 12–19. doi:10.1037/0022-006X.59.1.1
Kazdin, A. E. (2007). Mediators and mechanisms of change inpsychotherapy research. Annual Review of Clinical Psychology, 3,1–27. doi:10.1146/annurev.clinpsy.3.022806.091432
Lambert, M. J., Burlingame, G. M., Umphress, V., Hansen, N.B., Vermeersch, D. A., Clouse, G. C., & Yanchar, S. C.(1996). The reliability and validity of the Outcome Question-naire. Clinical Psychology & Psychotherapy, 3, 249–258.doi:10.1002/(SICI)1099-0879(199612)
Lambert, M. J., Finch, A. M., Okiishi, J., & Burlingame, G. M.(2005). Administration and scoring manual for the OQ-30.2.Orem: American Professional Credentialing Services, LLC.
Lopes, R., Gonçalves, M., Machado, P. P., Sinai, D., Bento, T., &Salgado, J. (2014). Narrative Therapy vs. Cognitive-BehavioralTherapy for moderate depression: Empirical evidence from acontrolled clinical trial. Psychotherapy Research, 24, 662–674.doi:10.1080/10503307.2013.874052
Machado, P. P., & Fassnacht, D. (2014). The Portuguese version ofthe Outcome Questionnaire (OQ-45): Normative data, reliabil-ity, and clinical significance cut-offs scores. Psychology andPsychotherapy: Theory, Research and Practice. doi:10.1111/papt.12048
Magill, M., & Longabaugh, R. (2013). Efficacy combined withspecified ingredients: A new direction for empirically supportedaddiction treatment. Addiction, 108, 874–881. doi:10.1111/add.12013
Matos, M., Santos, A., Gonçalves, M. M., & Martins, C.(2009). Innovative moments and change in narrative therapy.Psychotherapy Research, 19, 68–80. doi:10.1080/10503300802430657
Mendes, I., Ribeiro, A., Angus, L., Greenberg, L. S., Sousa, I., &Gonçalves, M. M. (2010). Narrative change in emotion-focused therapy: How is change constructed through the lensof the Innovative Moments Coding System? PsychotherapyResearch, 20, 692–701. doi:10.1080/10503307.2010.514960
Mendes, I., Ribeiro, A., Angus, L., Greenberg, L., Sousa, I., &Gonçalves, M. M. (2011). Narrative change in emotion-focused psychotherapy: A study on the evolution of reflectionand protest innovative moments. Psychotherapy Research, 21,304–315. doi:10.1080/10503307.2011.565489
R Development Core Team. (2013). The R Foundation forstatistical computing. Retrieved from www.Rproject.org
Ribeiro, A. P., Bento, T., Salgado, J., Stiles, W. B., & Gonçalves,M. M. (2011). A dynamic look at narrative change inpsychotherapy: A case-study tracking innovative moments andprotonarratives using state-space grids. Psychotherapy Research,21, 34–69. doi:10.1080/10503307.2010.504241
10 M. M. Gonçalves et al.
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015

Seggar, L. B., Lambert, M. J., & Hansen, N. B. (2002). Assessingclinical significance: Application to the Beck DepressionInventory. Behavior Therapy, 33, 253–269. doi:10.1016/S0005-7894(02)80028-4
Steer, R. A., Brown, G. K., Beck, A. T., & Sanderson, W. C.(2001). Mean Beck Depression Inventory-II scores by severity
of major depressive episode. Psychological Reports, 88, 1075–1076. doi:10.2466/pr0.2001.88.3c.1075
White, M. (2007). Maps of narrative practice. New York, NY:Norton.
White, M., & Epston, D. (1990). Narrative means to therapeuticends. New York, NY: Norton.
Psychotherapy Research 11
Dow
nloa
ded
by [
37.1
89.1
27.3
6] a
t 06:
21 1
3 M
ay 2
015




















