
Magmatic processes revealed by textural and compositional trends in Merapi dome lavas
Upload
independentCategory
view
3download
0
Ultrasound in Med. & Biol., Vol. 39, No. 1, pp. 54–61, 2013Copyright � 2013 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
/j.ultrasmedbio.2012.08.023
http://dx.doi.org/10.1016d Original Contribution
MYOCARDIAL ULTRASOUND TISSUE CHARACTERIZATION OF PATIENTSWITH PRIMARYALDOSTERONISM
HSIU-HAO LEE,*y CHI-SHENG HUNG,z XUE-MING WU,** VIN-CENT WU,z KAO-LANG LIU,x
SHUO-MENGWANG,k LUNG-CHUN LIN,z PAU-CHUNG CHEN,yYUE-LEON GUO,y SHIH-CHIEH CHUEH,kyy
YEN-HUNG LIN,z YI-LWUN HOz and KWAN-DUN WU
zAND THE TAIPAI STUDY GROUP
*Department of Internal Medicine, Taipei City Hospital, Zhongxing Branch; y Institution of Occupational Medicine andIndustrial Hygiene, National Taiwan University College of Public Health; zDepartment of Internal Medicine; xDepartmentof Radiology; kDepartment of Urology, National Taiwan University Hospital and National Taiwan University College of
Medicine, Taipei, Taiwan; **Department of Internal Medicine, Taoyuan General Hospital, Taoyuan, Taiwan; and yyDepartmentof Urology, Cleveland Clinic, Cleveland, Ohio, USA
(Received 20 May 2012; revised 29 July 2012; in final form 24 August 2012)
AInternaShan SYi-LwUniverE-mail
Abstract—Primary aldosteronism (PA), an underdiagnosed cause of hypertension, is associated with more signif-icant cardiac remodeling and myocardial fibrosis than is essential hypertension (EH). The aim of this study was tovalidate myocardial fibrosis and to evaluate factors associated with the degree of myocardial fibrosis in patientswith PA. We prospectively analyzed 62 patients with PA (including 46 patients with aldosterone-producingadenoma and 16 with bilateral hyperplasia) between October 2006 and October 2010, and we enrolled 17 patientswith EH as the control group. Echocardiography, including ultrasonic tissue characterization using cyclic varia-tion of integrated backscatter (CVIBS), was performed in individuals in both groups. Among patients with PA, thediastolic blood pressures and plasma aldosterone concentrations were significantly higher than those of patientswith EH. Moreover, the serum potassium levels and the plasma renin activities were significantly lower in patientswith EH. As observed by echocardiography, patients with PA had greater interventricular septal thickness, greaterleft ventricular posterior wall thickness, and higher left ventricular mass indexes than did patients with EH.Patients with PA had significantly lower CVIBS values than patients with EH (7.1 ± 2.2 vs. 8.7 ± 1.5 dB; p 5.005). In a correlation study that corrected for various clinical parameters, only log-transformed plasma reninactivity values correlated significantly with CVIBS values. Ultrasonic tissue characterization with CVIBS isa useful tool for determining the extent of myocardial fibrosis. Patients with PA exhibit a more severe degree ofmyocardial fibrosis, as detected by CVIBS, than do patients with EH.Moreover, the severity of fibrosis, as detectedby CVIBS, correlates with log-transformed plasma renin activity values. (E-mail: [email protected] [email protected]) � 2013 World Federation for Ultrasound in Medicine & Biology.
Key Words: Hypertension, Aldosterone, Primary aldosteronism, Myocardial fibrosis, Echocardiography, Cyclicvariation of integrated backscatter.
INTRODUCTION
Primary aldosteronism (PA), which is characterized byan inappropriate production of aldosterone, is an impor-tant cause of hypertension and affects between 5% and13% of patients with hypertension (Young 2003).Increasing evidence indicates that PA is much more
ddress correspondence to: Yen-Hung Lin, M.D., Department ofl Medicine, National Taiwan University Hospital, No. 7, Chung-. Road, Taipei 100, Taiwan. E-mail: [email protected] andun Ho, M.D., Department of Internal Medicine, National Taiwansity Hospital, No. 7, Chung-Shan S. Road, Taipei 100, Taiwan.: [email protected]
54
prevalent than previously believed, which makes thisdisease the most common cause of secondary hyperten-sion (Rossi et al. 2007).
Patients with PA experience more frequent cardio-vascular events and atrial fibrillation than do patientswho have essential hypertension (EH) (Milliez et al.2005). In terms of their cardiac structures, patients withPA were shown to have more prominent left ventricularmasses, which may be due to the high plasma aldosteronelevels in these patients (Rossi et al. 1996, 1997; Tanabeet al. 1997; Matsumura et al. 2006) because aldosteronecauses collagen deposition in the extracellular matrixand stimulates myocardial fibrosis (Weber and Brilla1991; Brilla et al. 1993). In animal studies, aldosterone

CVIBS in PA d H.-H. LEE et al. 55
infusion combined with a high salt intake induces notonly cardiac hypertrophy but also myocardial interstitialfibrosis and scarring in both the right and left ventricles(Brilla and Weber 1992). Furthermore, aldosterone infu-sion also induces increased interstitial fibrosis in the atriaand pulmonary artery (Sun et al. 1997), independently ofthe systemic blood pressure. Myocardial fibrosis isbelieved to reduce coronary vasodilator capacity andcause left ventricular diastolic dysfunction and heartfailure (Brilla and Janicki 1991). The disproportionateaccumulation of collagen is a characteristic feature ofhypertensive heart disease, although the extent ofmyocardial fibrosis may differ in various models ofhypertension (Kozakova et al. 2003). Interest in PA isincreasing and is currently focused on alterations to themyocardial extracellular matrix and collagen deposition,which have the potential to be measured early and non-invasively through an analysis involving ultrasoniccharacterization.
Ultrasound imaging of the heart has been exten-sively used to study hypertension-induced changes inleft ventricular geometry and function (Denolle et al.1993; Rossi et al. 1996; Yoshitomi et al. 1996; Rossiet al. 1998; Schlaich et al. 2000). Ultrasound signalsthat are reflected from the myocardium also contain infor-mation about myocardial texture that can be revealed byacoustic tissue characterization. Quantitative texturecharacterization can be performed through the videodensitometric analysis of standard echocardiographicimages or through the analysis of an ultrasonic back-scatter signal (Hoyt et al. 1984). In contrast to standardimaging techniques, whereby strong specular reflectionoccurs at tissue interfaces (such as the epicardium andendocardium), ultrasonic integrated backscatter signal(IBS) analysis examines low-amplitude, phase-sensitive,omnidirectional echoes arising from tissue heterogeneitywithin the myocardium (Hoyt and Skorton 1984). Theextracellular matrix represents an important source ofmyocardial IBS (Hall et al. 2000), and several experi-mental studies have demonstrated that IBS duringdiastole correlates with the collagen content of themyocardium (Mimbs et al. 1980; Hoyt and Skorton1984; Picano et al. 1990). Therefore, this technique isthought to provide noninvasively an estimation ofmyocardial fibrosis in humans. IBS values are greatestwhen the insonifying ultrasound beam is perpendicularto the predominant fiber orientation (Finch-Johnstonet al. 2000). Because fiber orientation changes withmyocardial contraction, myocardial IBS varies duringthe cardiac cycle. Ultrasonic tissue characterization bycyclic variation of integrated backscatter (CVIBS) isbelieved to reflect the contractile performance of themyocardium and is even more sensitive than absoluteIBS data (Maceira et al. 2002).
To our knowledge, CVIBS values in patients withPA have not been thoroughly investigated. Althoughadvancements in the diagnosis and treatment of primaryaldosteronism have improved its prognosis, interest inultrasonic tissue characterization by CVIBS for detectingthe extent of myocardial fibrosis is growing. As a result,more extensive experience regarding the use of thismethod for the detection of primary aldosteronism isneeded. The aim of this study was to assess the myocar-dial fibrosis caused by primary aldosteronism and to eval-uate the relationship between the CVIBS values and thebaseline clinical parameters of patients with PA.
MATERIALS AND METHODS
PatientsThis prospective study enrolled 62 patients diag-
nosed with PA between October 2006 and October 2010.These patients were registered in the Taiwan PrimaryAldosteronism Investigation (TAIPAI) database afterinitial evaluations. The database was constructed forquality assurance in 1 medical center (National TaiwanUniversity Hospital in Taipei, Taiwan) and its 3 branchhospitals in different cities (National Taiwan UniversityHospital Yun-Lin branch in Yun-Lin, southern Taiwan;Far-Eastern Memorial Hospital in Taipei; and Tao-YuanGeneral Hospital in Tao-Yuan, central Taiwan) (Kuo andWu 2011a,b; Lin et al. 2011a,b,c; Lin et al. 2012a; Wuet al. 2010; Wu et al. 2011; Lin et al. 2012b). Anadditional 17 patients with EH were enrolled as thecontrol group. The diagnosis of EH was made byexclusion, through appropriate clinical and biochemicalinvestigations of all detectable forms of secondaryhypertension, including a post captopril aldosterone-to-renin activity (ARR) level below 30. Patients with symp-toms of ischemic heart disease, impaired systolic function(left ventricular ejection fraction ,50%) or significantregional wall motion abnormality in echocardiographywere also excluded.
Serum biochemistry was assessed at the first patientevaluation at the National Taiwan University Hospital.Medical histories, including patient demographics andmedications, were carefully recorded. Plasma aldoste-rone concentrations (PACs) were measured usingcommercial radioimmune assay kits (Aldosterone MaiaKit, Adaltis Italia, Bologna, Italy), and plasma reninactivity (PRA) was measured as the generation of angio-tensin I in vitro using a commercially available radioim-mune assay kit (Cisbio, Bedford, MA, USA). This studywas approved by the Institutional Review Board ofNational Taiwan University Hospital, and all subjectsprovided informed consent. Report of this studyconforms to the STrengthening the Reporting of OBser-vational studies in Epidemiology (STROBE) statement,
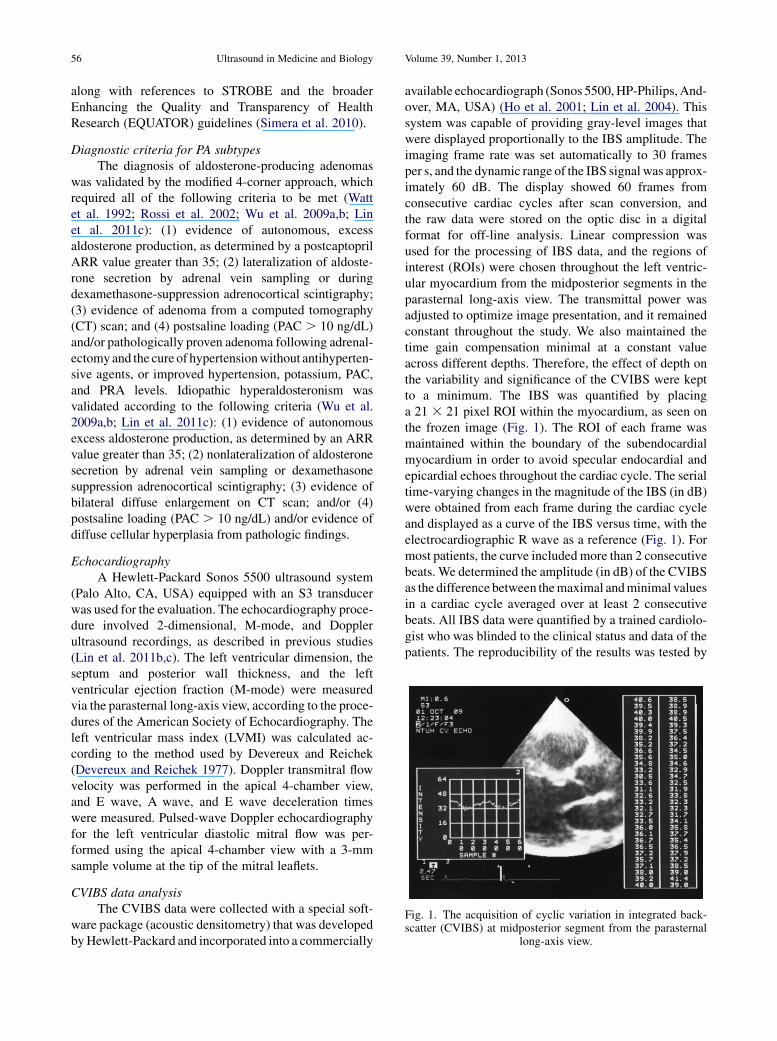
Fig. 1. The acquisition of cyclic variation in integrated back-scatter (CVIBS) at midposterior segment from the parasternal
long-axis view.
56 Ultrasound in Medicine and Biology Volume 39, Number 1, 2013
along with references to STROBE and the broaderEnhancing the Quality and Transparency of HealthResearch (EQUATOR) guidelines (Simera et al. 2010).
Diagnostic criteria for PA subtypesThe diagnosis of aldosterone-producing adenomas
was validated by the modified 4-corner approach, whichrequired all of the following criteria to be met (Wattet al. 1992; Rossi et al. 2002; Wu et al. 2009a,b; Linet al. 2011c): (1) evidence of autonomous, excessaldosterone production, as determined by a postcaptoprilARR value greater than 35; (2) lateralization of aldoste-rone secretion by adrenal vein sampling or duringdexamethasone-suppression adrenocortical scintigraphy;(3) evidence of adenoma from a computed tomography(CT) scan; and (4) postsaline loading (PAC . 10 ng/dL)and/or pathologically proven adenoma following adrenal-ectomyand the cure of hypertensionwithout antihyperten-sive agents, or improved hypertension, potassium, PAC,and PRA levels. Idiopathic hyperaldosteronism wasvalidated according to the following criteria (Wu et al.2009a,b; Lin et al. 2011c): (1) evidence of autonomousexcess aldosterone production, as determined by an ARRvalue greater than 35; (2) nonlateralization of aldosteronesecretion by adrenal vein sampling or dexamethasonesuppression adrenocortical scintigraphy; (3) evidence ofbilateral diffuse enlargement on CT scan; and/or (4)postsaline loading (PAC . 10 ng/dL) and/or evidence ofdiffuse cellular hyperplasia from pathologic findings.
EchocardiographyA Hewlett-Packard Sonos 5500 ultrasound system
(Palo Alto, CA, USA) equipped with an S3 transducerwas used for the evaluation. The echocardiography proce-dure involved 2-dimensional, M-mode, and Dopplerultrasound recordings, as described in previous studies(Lin et al. 2011b,c). The left ventricular dimension, theseptum and posterior wall thickness, and the leftventricular ejection fraction (M-mode) were measuredvia the parasternal long-axis view, according to the proce-dures of the American Society of Echocardiography. Theleft ventricular mass index (LVMI) was calculated ac-cording to the method used by Devereux and Reichek(Devereux and Reichek 1977). Doppler transmitral flowvelocity was performed in the apical 4-chamber view,and E wave, A wave, and E wave deceleration timeswere measured. Pulsed-wave Doppler echocardiographyfor the left ventricular diastolic mitral flow was per-formed using the apical 4-chamber view with a 3-mmsample volume at the tip of the mitral leaflets.
CVIBS data analysisThe CVIBS data were collected with a special soft-
ware package (acoustic densitometry) that was developedbyHewlett-Packard and incorporated into a commercially
available echocardiograph (Sonos 5500,HP-Philips,And-over, MA, USA) (Ho et al. 2001; Lin et al. 2004). Thissystem was capable of providing gray-level images thatwere displayed proportionally to the IBS amplitude. Theimaging frame rate was set automatically to 30 framesper s, and the dynamic range of the IBS signal was approx-imately 60 dB. The display showed 60 frames fromconsecutive cardiac cycles after scan conversion, andthe raw data were stored on the optic disc in a digitalformat for off-line analysis. Linear compression wasused for the processing of IBS data, and the regions ofinterest (ROIs) were chosen throughout the left ventric-ular myocardium from the midposterior segments in theparasternal long-axis view. The transmittal power wasadjusted to optimize image presentation, and it remainedconstant throughout the study. We also maintained thetime gain compensation minimal at a constant valueacross different depths. Therefore, the effect of depth onthe variability and significance of the CVIBS were keptto a minimum. The IBS was quantified by placinga 21 3 21 pixel ROI within the myocardium, as seen onthe frozen image (Fig. 1). The ROI of each frame wasmaintained within the boundary of the subendocardialmyocardium in order to avoid specular endocardial andepicardial echoes throughout the cardiac cycle. The serialtime-varying changes in the magnitude of the IBS (in dB)were obtained from each frame during the cardiac cycleand displayed as a curve of the IBS versus time, with theelectrocardiographic R wave as a reference (Fig. 1). Formost patients, the curve included more than 2 consecutivebeats. We determined the amplitude (in dB) of the CVIBSas the difference between themaximal andminimal valuesin a cardiac cycle averaged over at least 2 consecutivebeats. All IBS data were quantified by a trained cardiolo-gist who was blinded to the clinical status and data of thepatients. The reproducibility of the results was tested by

Table 1. Clinical and laboratory characteristics ofpatients with primary aldosteronism and essential
hypertension
PAn 5 62
EHn 5 17 p value
Age 47 6 12 43 6 16 0.332Male sex 7 (41) 31 (50) 0.591Weight, kg 68 6 15 64 6 13 0.138Height, cm 161 6 8.7 165 6 9.4 0.293Body mass index, kg/m2 26 6 4.1 23 6 2.7 0.011Duration of HTN, years 6.5 6 6.7 3.7 6 5.2 0.126SBP, mm Hg 153 6 22 145 6 17 0.140DBP, mm Hg 95 6 13 86 6 11 0.012Number of HTN medications 1.9 6 1.0 1.5 6 0.8 0.153Plasma potassium, mmol/L 3.5 6 0.6 4.1 6 0.4 ,0.001PRA, ng/dL 0.7 6 0.9 4.1 6 4.9 ,0.001PAC, ng/mL/hr 44 6 25 26 6 13 0.006Creatinine, mg/dL 0.9 6 0.2 1.0 6 0.2 0.774HTN medicationCCB 42 (68) 8 (47) 0.157ACE-I 0 (0) 2 (12) 0.044ARB 17 (27) 8 (47) 0.147Thiazide 4 (6) 1 (6) 1.000Alpha-blocker 23 (37) 2 (12) 0.075Beta-blocker 32 (52) 5 (29) 0.169Spironolactone 33 (53) 0 (0) ,0.001
ACE-I 5 angiotensin-converting enzyme inhibitor; ARB 5 angio-tensin receptor blocker; CCB 5 calcium channel blocker; DBP 5diastolic blood pressure; EH5 essential hypertension;HTN5 hyperten-sion; PA 5 primary aldosteronism; PAC 5 plasma aldosterone concen-tration; PRA5 plasma renin activity; SBP5 systolic blood pressure.Values are expressed as the mean6 SD or as a number (percentage),
as indicated by the format in the table.
Table 2. Left ventricular geometric characteristics inpatients with primary aldosteronism and essential
hypertension
PAn 5 62
EHn 5 17 p value
LVST, mm 12.3 6 2.4 10.7 6 2.2 0.012LVPWT, mm 11.3 6 1.9 9.7 6 1.5 0.002LVEDD, mm 46.0 6 5.3 46.4 6 5.0 0.775LVESD, mm 28.2 6 4.3 27.2 6 4.4 0.420LVMI, g/m2 140.2 6 47.1 114.7 6 35.7 0.042LVEF, % 68.2 6 6.9 71.1 6 7.5 0.130E wave, cm/s 77.0 6 19.7 76.5 6 16.1 0.923A wave, cm/s 72.2 6 14.3 67.8 6 18.5 0.297DT, ms 191.8 6 42.9 193.6 6 40.3 0.876E integral, cm 12.7 6 3.0 12.8 6 2.1 0.894A integral, cm 7.6 6 1.9 7.5 6 3.3 0.872E integral/A integral 1.8 6 0.5 2.0 6 0.2 0.239CVIBS (dB) 7.1 6 2.2 8.7 6 1.5 0.005
CVIBS 5 cyclic variation of integrated backscatter; DT 5 decelera-tion time; EH 5 essential hypertension; IVST 5 interventricular septalthickness; LVEDD 5 left ventricular end-diastolic diameter; LVEF 5left ventricular ejection fraction; LVESD 5 left ventricular end-systolic diameter; LVPWT 5 left ventricular posterior wall thickness;LVMI 5 left ventricular mass index; PA 5 Primary aldosteronism.
Values are expressed as the mean 6 SD.
CVIBS in PA d H.-H. LEE et al. 57
the assessment of the CVIBS from 2 different acquisitionsof 15 randomly selected segments by a single observer.The mean difference in the CVIBS amplitude betweengroups was 0.456 0.31 dB, and the coefficients of varia-tion averaged 5% (Lin et al. 2011b).
Statistical analysisThe data were expressed as the mean 6 standard
deviation (SD).Comparisons for continuous data collectedfrom PA and EH patients were made using the Mann-Whitney U test. Differences between proportions wereassessed using the chi-square or Fisher exact test. ThePearson correlation test was used to analyze the associa-tionbetween theCVIBSvalue and its determinants.Valuesfor PAC and PRAwere log-transformed prior to the corre-lation analysis because of their non-normality, as assessedusing the Kolmogorov-Smirnov test. Prior to subsequentanalysis, the log-transformed data were reassessed toensure a normal distribution. The p values less than 0.05were considered to indicate statistical significance.
RESULTS
Patient characteristicsWe enrolled 62 patients with PA (including 46
patients with aldosterone-producing adenomas, 16 with
idiopathic hyperaldosteronism, and 17 patients withEH) in the study. The baseline characteristics and clinicaldata of the PA patients and EH controls are listed inTable 1. Patients with PA had significantly higher bodymass indexes, higher diastolic blood pressure and PACvalues but lower serum potassium levels and PRA valuesthan patients with EH. There were no significant differ-ences between PA patients and EH controls regardingage, sex, weight, height, duration of hypertension,systolic blood pressure, number of hypertension medi-cations taken, or serum creatinine levels. In terms ofmedication usage, a higher percentage of patients withPA were actively receiving spironolactone, and a lowerpercentage of these patients were receiving angiotensin-converting enzyme inhibitors.
Echocardiographic dataThe echocardiographic data of the PA and EH
patients are shown in Table 2. Patients with PA demon-strated greater interventricular septal thickness (12.3 62.4 vs. 10.76 2.2 mm, p5 0.012); greater left ventricularposterior wall thickness (11.3 6 1.9 vs. 9.7 6 1.5 mm,p 5 0.002); and higher LVMI values (140.2 6 47.1 vs.114.7 6 35.7 g/m2, p 5 0.042) than did patients withEH. Moreover, patients with PA had significantly lowerCVIBS values than patients with EH (7.16 2.2 vs. 8.761.5 dB, p5 0.005). There were no significant differencesbetween patient groups with respect to left ventricularend-diastolic diameter, left ventricular end-systolicdiameter, left ventricular ejection fraction, E velocity, A

Table 3. Clinical parameters associated with baselineCVIBS values (N 5 79)
Pearson correlationcoefficient p value
Age, year 20.037 0.744Male sex 0.021 0.856Duration of HTN, years 0.018 0.879Number of HTN medications 20.101 0.109Body mass index, kg/m2 20.182 0.109Log PAC 20.064 0.574Log PRA 0.239 0.034
58 Ultrasound in Medicine and Biology Volume 39, Number 1, 2013
velocity, or deceleration time. There were also no signif-icant differences in terms of the E integral, the A integral,or the E/A integral ratio between the 2 groups.
The analyses regarding the correlation betweenCVIBS values and various clinical parameters are shownin Table 3 (all study patients, N 5 79). Of all the param-eters studied in these patients, only the log-transformedPRA values correlated positively with the CVIBS valuesto a significant degree (Pearson correlation coefficient 50.239, p 5 0.034).
SBP, mm Hg 20.013 0.907DBP, mm Hg 20.064 0.573
DBP5 diastolic blood pressure;HTN5 hypertension; PAC5 plasmaaldosterone concentration; PRA5 plasma renin activity; SBP5 systolicblood pressure.
DISCUSSION
In this prospective case-controlled study, we usedechocardiography to compare left ventricular geometryand function in patients with PA and EH. The majorfndings of this study were as follows: (1) patients withPA exhibited a higher degree of left ventricular hyper-trophy, including greater interventricular septal thick-ness, greater left ventricular posterior wall thickness,and higher left ventricular mass indexes than patientswith EH; (2) patients with PA had significantly lowerCVIBS values than did patients with EH (7.1 6 2.2 vs.8.7 6 1.5 dB, p 5 0.005); and (3) of the various clinicalparameters, only the log-transformed values for plasmarenin activity correlated significantly with the CVIBSvalues.
Patients with PA typically exhibited a more severedegree of myocardial fibrosis, as detected by CVIBS.When studying myocardial fibrosis, myocardial biopsyis the gold standard for the detection of fibrosis, butthis technique is limited by its invasiveness. Severalechocardiographic methods can be employed to definemyocardial fibrosis quantitatively, and IBS is amongthe methods used most often to detect myocardialfibrosis (Di Bello et al. 2004; Wang et al. 2009).Scatter is produced when the ultrasound beam interactswith material that has a diameter smaller than theultrasound wavelength. A portion of this scatter isdirected back toward the probe (i.e., backscatter) andcan therefore be detected by the probe. The extracel-lular matrix represents an important source of myocar-dial IBS (Hall et al. 2000) because excess extracellularcollagen deposition may change the myocardial watercontent and the myofibril orientation relative to theincident ultrasound beam (Holland et al. 1998). Inanimal studies, quantitative assessments of the IBSsignal have been used as a direct method of evaluatingcollagen content morphometrically (Mimbs et al. 1980;O’Donnell et al. 1981; Di Bello et al. 2004; Wanget al. 2009). Furthermore, in a study by Di Belloet al. (Di Bello et al. 2004), the CVIBS value wasfound to negatively correlate, to a significant degree,with the ratio of myocyte to fibrosis area within
myocardial biopsy specimens. Therefore, IBS canprovide a method to investigate myocardial changesnoninvasively in various cardiac diseases, includingischemic heart disease (Lin et al. 1998a,b), hearttransplantation (Ho et al. 2001), and hypertensive heartdisease (Maceira et al. 2002; Di Bello et al. 2003; Linet al. 2004). IBS studies have also been useful forstudying collagen content in the hypertensive myocar-dium (Maceira, Barba 2002; Lin et al. 2004) and themyocardium of PA patients (Maceira et al. 2002;Kozakova et al. 2003). PA patients tend to have moresevere myocardial fibrosis, and as a result, thesepatients also tend to have increased IBS values anddecreased CVIBS values compared with patientswith EH (Kozakova et al. 2003). In support of thisconcept, the results of our study demonstrated thesame phenomena.
The method of acquiring CVIBS data was basicallythe same as the method used by Kozakva (Kozakovaet al. 2003), except for 1 difference, which was thesampling position. We used the midposterior segmentsin the parasternal long axis view as the sampling posi-tion. In contrast, the midportion of the interventricularseptum was used in the study by Kozakova andcolleagues (2003). Because integrated backscatter isangle dependent, only signals from structures that areperpendicular to the path of the ultrasound beam areusually analyzed. Both midposterior segments and themidportion of the interventricular septum fit the criteriaand can be used in analysis. In our previous study, thevalues of CVIBS obtained from midposterior segmentswere larger than those obtained from the midportionof the interventricular septum (Lin et al. 2004). So theposition of measurement may explain the value differ-ence between our study and Kozakova’s study(Kozakova et al. 2003).
In this study, we chose to study CVIBS valuesrather than absolute integrated backscatter values, and

CVIBS in PA d H.-H. LEE et al. 59
we chose the left ventricular posterior wall in the para-sternal long-axis view for the detection of CVIBS.This analysis of the dynamic portion of the integratedbackscatter signal is able to minimize the influence ofextracardiac tissue, and it is more sensitive to the detec-tion of fibrotic change in the hypertensive myocardiumthan an analysis of the absolute integrated backscattervalue (Di Bello et al. 2003). In our previous study, theanalysis of CVIBS at the midposterior in the parasternallong-axis view was more sensitive for detecting fibrosisof the hypertensive myocardium (Lin et al. 2004).Therefore, in this study, we chose this region for detect-ing myocardial fibrosis rather than the septum in theparasternal short-axis view. Most remarkably, theseverity of fibrosis detected by CVIBS correlated withlog-transformed PRA values. The PRA values were notnormally distributed and were thus log-transformedprior to the correlation study to ensure a normal distribu-tion, as assessed by the Kolmogorov-Smirnov test.Similar results were also found in a similar study byRossi et al. (2002).
Our study has several limitations. First, the numberof patients included in this study was small, which mayhave limited the ability to detect a relationship betweenthe degree of myocardial fibrosis and various clinical orbiochemical parameters. However, the results of thecurrent study will likely stimulate additional researchin this area, and a large-scale follow-up study is neededto confirm these results. Second, CVIBS values aredependent on the angle between the fiber orientationand the ultrasonic beam, which is called anisotropy(Holland et al. 1998). To avoid the phenomenon ofanisotropy, we used midposterior segments for whichthe myocardial fibers were kept perpendicular to theincident ultrasound beam. However, individual variationin heart position occasionally impedes the positioningof the myocardial segments absolutely perpendicularto the ultrasonic beam. Third, because we could detectCVIBS values only of midposterior segments, we de-tected only alterations limited to these segments. Alter-nations in other segments could not be detected in thisstudy setting. Fourth, we did not perform endomyocar-dial biopsy to document the fibrotic process because itis unethical to perform routine endomyocardial biopsyin patients with PA or EH. Fifth, the diastolic bloodpressure (DBP) and body mass indexes (BMIs) werehigher in patients with PA and could therefore representsources of bias. However, because the CVIBS valuesdid not correlate with the DBPs and BMIs, the influenceof DBP and BMI on the results of this study were prob-ably minimal. Sixth, the prevalence of usage of spirono-lactone and angiotensin-converting enzyme inhibitorswas different in the 2 groups and could therefore repre-sent a source of bias. Seventh, the duration of hyperten-
sion in patients with PA is insignificantly higher than inpatients with EH, and that is also a potential bias of thisstudy.
In conclusion, patients with PA had significantlyaltered left ventricular geometry and myocardial textureas compared with demographically and hemodynami-cally similar patients with EH. Moreover, ultrasonictissue characterization with CVIBS was shown to bea useful tool for detecting the extent of myocardialfibrosis. These findings support the hypothesis that aldo-sterone can induce hemodynamic alterations indepen-dently of changes to myocardial texture caused by anincreased collagen content in the myocardium.
Acknowledgments—This study was supported by the National TaiwanUniversity Hospital (NTUH 101-001974), National Taiwan University(National Taiwan University Cutting-Edge Steering Research); NTU-NTUH MediaTek Innovative Medical Electronics Research Center(PC851); Taiwan National Science Council (NSC 100-2314-B-002-139); and Taiwan National Science Council support for the Center forDynamical Biomarkers and Translational Medicine, National CentralUniversity (NSC 100-2911-I-008-001). We thank Fen-Fun Hsien formedical technologic support and the staff of the Second Core Lab ofthe Department of Medical Research of the National Taiwan UniversityHospital for technical assistance.
REFERENCES
Brilla CG, Janicki JS, Weber KT. Impaired diastolic function and coro-nary reserve in genetic hypertension: Role of interstitial fibrosis andmedial thickening of intramyocardial coronary arteries. Circ Res1991;69:107–115.
Brilla CG, Matsubara LS, Weber KT. Antifibrotic effects of spironolac-tone in preventing myocardial fibrosis in systemic arterial hyperten-sion. Am J Cardiol 1993;71:12A–16A.
Brilla CG, Weber KT. Reactive and reparative myocardial fibrosisin arterial hypertension in the rat. Cardiovasc Res 1992;26:671–677.
Denolle T, Chatellier G, Julien J, Battaglia C, Luo P, Plouin PF.Left ventricular mass and geometry before and after etiologictreatment in renovascular hypertension, aldosterone-producingadenoma, and pheochromocytoma. Am J Hypertens 1993;6:907–913.
Devereux RB, Reichek N. Echocardiographic determination of leftventricular mass in man: Anatomic validation of the method. Circu-lation 1977;55:613–618.
Di Bello V, Giorgi D, Talini E, Dell’Omo G, Palagi C, Romano MF,Pedrinelli R, Mariani M. Incremental value of ultrasonic tissue char-acterization (backscatter) in the evaluation of left ventricularmyocardial structure and mechanics in essential arterial hyperten-sion. Circulation 2003;107:74–80.
Di Bello V, Giorgi D, Viacava P, Enrica T, Nardi C, Palagi C, GraziaDelle Donne M, Verunelli F, Mariani MA, Grandjean J,Dell’Anna R, Di Cori A, Zucchelli G, Romano MF, Mariani M.Severe aortic stenosis and myocardial function: Diagnostic andprognostic usefulness of ultrasonic integrated backscatter analysis.Circulation 2004;110:849–855.
Finch-Johnston AE, Gussak HM, Mobley J, Holland MR, Petrovic O,Perez JE, Miller JG. Cyclic variation of integrated backscatter:Dependence of time delay on the echocardiographic view usedand the myocardial segment analyzed. J Am Soc Echocardiogr2000;13:9–17.
Hall CS, Scott MJ, Lanza GM, Miller JG, Wickline SA. The extracel-lular matrix is an important source of ultrasound backscatter frommyocardium. J Acoust Soc Am 2000;107:612–619.

60 Ultrasound in Medicine and Biology Volume 39, Number 1, 2013
Ho YL, Chen CL, Hsu RB, Lin LC, Yen RF, Lee CM, Chen MF,Huang PJ. Assessment of the myocardial changes in heart transplantrecipients without evident acute myocardial rejection by integratedbackscatter: Comparison with simultaneous dobutamine stress echo-cardiography and (201)thallium spect. Ultrasound Med Biol 2001;27:171–179.
Holland MR, Wilkenshoff UM, Finch-Johnston AE, Handley SM,Perez JE, Miller JG. Effects of myocardial fiber orientation inechocardiography: Quantitative measurements and computer simu-lation of the regional dependence of backscattered ultrasound inthe parasternal short-axis view. J Am Soc Echocardiogr 1998;11:929–937.
Hoyt RM, SkortonDJ, Collins SM,Melton HE Jr. Ultrasonic backscatterand collagen in normal ventricular myocardium. Circulation 1984;69:775–782.
Kozakova M, Buralli S, Palombo C, Bernini G, Moretti A, Favilla S,Taddei S, Salvetti A. Myocardial ultrasonic backscatter in hyperten-sion: Relation to aldosterone and endothelin. Hypertension 2003;41:230–236.
Kuo CC, Wu VC, Huang KH, Wang SM, Chang CC, Lu CC, Yang WS,Tsai CW, Lai CF, Lee TY, Lin WC, Wu MS, Lin YH, Chu TS,Lin CY, Chang HW, Wang WJ, Kao TW, Chueh SC, Wu KD. TaipaiStudy Group. Verification and evaluation of aldosteronism demo-graphics in the Taiwan Primary Aldosteronism Investigation Group(TAIPAI Group). J Renin Angiotensin Aldosterone Syst 2011a;12:348–357.
Kuo CC, Wu VC, Tsai CW, Wu KD. Relative kidney hyperfiltration inprimary aldosteronism: A meta-analysis. J Renin Angiotensin Aldo-sterone Syst 2011b;12:113–122.
Lin LC, Wu CC, Ho YL, Chen MF, Liau CS, Lee YT. Ultrasonic tissuecharacterization in predicting residual ischemia and myocardialviability for patients with acute myocardial infarction. UltrasoundMed Biol 1998a;24:1107–1120.
Lin LC,Wu CC, Ho YL, Lin CW, ChenWJ, ChenMF, Liau CS, Lee YT.Ultrasonic tissue characterization for coronary care unit patientswith acute myocardial infarction. Ultrasound Med Biol 1998b;24:187–196.
Lin YH, Huang KH, Lee JK, Wang SM, Yen RF, Wu VC, Chung SD,Liu KL, Chueh SC, Lin LY, Ho YL, ChenMF,WuKD. Factors influ-encing left ventricular mass regression in patients with primary aldo-steronism post adrenalectomy. JRAAS 2011a;12:48–53.
Lin YH, Lee HH, Liu KL, Lee JK, Shih SR, Chueh SC, LinWC, Lin LC,Lin LY, Chung SD, Wu VC, Kuo CC, Ho YL, Chen MF, Wu KD.Reversal of myocardial fibrosis in patients with unilateralhyperaldosteronism receiving adrenalectomy. Surgery 2011b;150:526–533.
Lin YH, Wang SM, Wu VC, Lee JK, Kuo CC, Yen RF, Liu KL,Huang KH, Chueh SC, Wang WJ, Lin LY, Chien KL, Ho YL,Chen MF, Wu KD. The association of serum potassium level withleft ventricular mass in patients with primary aldosteronism. Eur JClin Invest 2011c;41:743–750.
Lin YH, Lin LY, Chen A, Wu XM, Lee JK, Su TC, Wu VC, Chueh SC,Lin WC, Lo MT, Wang PC, Ho YL, Wu KD. Adrenalectomyimproves increased carotid intima-media thickness and arterial stiff-ness in patients with aldosterone-producing adenoma. Atheroscle-rosis 2012a;221:154–159.
Lin YH,WuXM, LeeHH, Lee JK, Liu YC, ChangHW, Lin CY,WuVC,Chueh SC, Lin LC, Lo MT, Ho YL, Wu KD. Adrenalectomyreverses myocardial fibrosis in patients with primary aldosteronism.J Hypertens 2012b;30:1606–1613.
Lin YH, Shiau YC, Yen RF, Lin LC, Wu CC, Ho YL, Huang PJ.The relation between myocardial cyclic variation of integratedbackscatter and serum concentrations of procollagen propepti-des in hypertensive patients. Ultrasound Med Biol 2004;30:885–891.
Maceira AM, Barba J, Varo N, Beloqui O, Diez J. Ultrasonic backscatterand serum marker of cardiac fibrosis in hypertensives. Hypertension2002;39:923–928.
Matsumura K, Fujii K, Oniki H, Oka M, Iida M. Role of aldosterone inleft ventricular hypertrophy in hypertension. Am J Hypertens 2006;19:13–18.
Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ.Evidence for an increased rate of cardiovascular events in patientswith primary aldosteronism. J Am Coll Cardiol 2005;45:1243–1248.
Mimbs JW, O’Donnell M, Bauwens D,Miller JW, Sobel BE. The depen-dence of ultrasonic attenuation and backscatter on collagen contentin dog and rabbit hearts. Circ Res 1980;47:49–58.
O’DonnellM,Mimbs JW,Miller JG. Relationship between collagen andultrasonic backscatter in myocardial tissue. J Acoust Soc Am 1981;69:580–588.
Picano E, Pelosi G, Marzilli M, Lattanzi F, Benassi A, Landini L,L’Abbate A. In vivo quantitative ultrasonic evaluation of myocardialfibrosis in humans. Circulation 1990;81:58–64.
Rossi GP, Di Bello V, Ganzaroli C, Sacchetto A, Cesari M, Bertini A,Giorgi D, Scognamiglio R, Mariani M, Pessina AC. Excess aldoste-rone is associated with alterations of myocardial texture in primaryaldosteronism. Hypertension 2002;40:23–27.
Rossi GP, Sacchetto A, Pavan E, Palatini P, Graniero GR, Canali C,Pessina AC. Remodeling of the left ventricle in primaryaldosteronism due to Conn’s adenoma. Circulation 1997;95:1471–1478.
Rossi GP, Sacchetto A, Pavan E, Scognamiglio R, Pietra M, Pessina AC.Left ventricular systolic function in primary aldosteronism andhypertension. J Hyperten 1998;16:2075–2077.
Rossi GP, Sacchetto A, Visentin P, Canali C, Graniero GR, Palatini P,Pessina AC. Changes in left ventricular anatomy and function inhypertension and primary aldosteronism. Hypertension 1996;27:1039–1045.
Rossi GP, Seccia TM, Pessina AC. Clinical use of laboratory tests for theidentification of secondary forms of arterial hypertension. Crit RevClin Lab Sci 2007;44:1–85.
Schlaich MP, Schobel HP, Hilgers K, Schmieder RE. Impact of aldoste-rone on left ventricular structure and function in young normoten-sive and mildly hypertensive subjects. Am J Cardiol 2000;85:1199–1206.
Simera I, Moher D, Hoey J, Schulz KF, Altman DG. A catalogue of re-porting guidelines for health research. Eur J Clin Invest 2010;40:35–53.
Sun Y, Ramires FJ, Weber KT. Fibrosis of atria and great vessels inresponse to angiotensin II or aldosterone infusion. Cardiovasc Res1997;35:138–147.
Tanabe A, Naruse M, Naruse K, Hase M, Yoshimoto T, Tanaka M,Seki T, Demura R, Demura H. Left ventricular hypertrophy ismore prominent in patients with primary aldosteronism than inpatients with other types of secondary hypertension. HypertensRes 1997;20:85–90.
Wang GD, Shen LH, Wang L, Li HW, Zhang YC, Chen H. Relationshipbetween integrated backscatter and atrial fibrosis in patients withand without atrial fibrillation who are undergoing coronary bypasssurgery. Clin Cardiol 2009;32:E56–E61.
Watt GC, Harrap SB, Foy CJ, Holton DW, Edwards HV, Davidson HR,Connor JM, Lever AF, Fraser R. Abnormalities of glucocorticoidmetabolism and the renin-angiotensin system: A four-cornersapproach to the identification of genetic determinants of blood pres-sure. J Hypertens 1992;10:473–482.
Weber KT, Brilla CG. Pathological hypertrophy and cardiac intersti-tium: Fibrosis and renin-angiotensin-aldosterone system. Circula-tion 1991;83:1849–1865.
Wu VC, Chang HW, Liu KL, Lin YH, Chueh SC, Lin WC, Ho YL,Huang JW, Chiang CK, Yang SY, Chen YM, Wang SM,Huang KH, Hsieh BS, Wu KD. Primary aldosteronism: Diagnosticaccuracy of the losartan and captopril tests. Am J Hypertens2009a;22:821–827.
Wu VC, Chueh SC, Chang HW, Lin LY, Liu KL, Lin YH, Ho YL,Lin WC, Wang SM, Huang KH, Hung KY, Kao TW, Lin SL,Yen RF, Chen YM, Hsieh BS, Wu KD. Association of kidneyfunction with residual hypertension after treatment ofaldosterone-producing adenoma. Am J Kidney Dis 2009b;54:665–673.
Wu VC, Kuo CC, Chang HW, Tsai CT, Lin CY, Lin LY, Lin YH,Wang SM, Huang KH, Fang CC, Ho YL, Liu KL, Chang CC,

CVIBS in PA d H.-H. LEE et al. 61
Chueh SC, Lin SL, Yen RF, Wu KD. Diagnosis of primary aldo-steronism: Comparison of post-captopril active renin concentra-tion and plasma renin activity. Clin Chim Acta 2010;411:657–663.
Wu VC, Yang SY, Lin JW, Cheng BW, Kuo CC, Tsai CT, Chu TS,Huang KH, Wang SM, Lin YH, Chiang CK, Chang HW, Lin CY,Lin LY, Chiu JS, Hu FC, Chueh SC, Ho YL, Liu KL, Lin SL,Yen RF, Wu KD. Kidney impairment in primary aldosteronism.Clin Chim Acta 2011;412:1319–1325.
Yoshitomi Y, Nishikimi T, Abe H, Yoshiwara F, Suzuki T, Ashizawa A,Nagata S, Kuramochi M, Matsuoka H, Omae T. Comparison ofchanges in cardiac structure after treatment in secondary hyperten-sion. Hypertension 1996;27:319–323.
Young WF Jr. Minireview: primary aldosteronism: Changing conceptsin diagnosis and treatment. Endocrinology 2003;144:2208–2213.
APPENDIX
The Taiwan Primary Aldosteronism Investigation (TAIPAI) StudyGroup: Vin-CentWu,MD, PhD; Yen-Hung Lin, MD, PhD; Yi-Luwn Ho,MD, PhD; Hung-Wei Chang, MD, PhD; Lian-Yu Lin, MD, PhD; Fu-Chang Hu, MS, ScD; Kao-Lang Liu, MD; Shuo-Meng Wang, MD;Kuo-How Huang, MD, PhD; Yung-Ming Chen, MD; Chin-Chi Kuo,MD;Shih-ChiehChueh,MD,PhD;Ching-ChuLu,MD;Fang-ChiChang,MD; Shih-Cheng Liao, MD; Ruoh-Fang Yen, MD, PhD; Wei-Chou Lin,MD, PhD; Bor-Sen Hsieh, MD, PhD; and Kwan-Dun Wu, MD, PhD.
Copyright © 2022 FDOKUMEN




















