Endovascular revascularization of renal artery stenosis in the solitary functioning kidney

Idiopathic Hypertrophic Subaortic Stenosis: Evaluation of
Angina1 Symptoms With Thallium-20 1 Myocardial Imaging
KENNETH A. RUBIN, MD* JOHN MORRISON, MD MARVIN B. PADNICK, MD ALAN J. BINDER, MD+ SALVATORE CHIARAMIDA, MD DONALD MARGOULEFF, MD VELLORE T. PADMANABHAN, MD STEPHEN J. GULOTTA, MD, FACC
Manhasset, New York
From the Division of Cardiology and the Division of Nuclear Medicine, Department of Medicine, North Shore University Hospital, Cornell University Medical College, New York, New York. Manuscript received January 8, 1979; revised manuscript received and accepted June 13, 1979
* Fellow, Westchester Heart Association, Port Chester, New York.
7 Fellow, Odd Fellows, John C. Sable Memorial Fund, Rochester, New York.
Address for reprints: Stephen J. Gulotta, MD, Division of Cardiology, North Shore University Hospital, Manhasset, New York 11030.
The evaluation of angina pectoris in patients with idiopathic hypertrophic subaortic stenosis is difficult in those in the age group prone to coronary artery disease. Ten patients with angina pectoris, normal coronary an- giograms and idiopathic hypertrophic subaortic stenosis were studied with thallium-201 myocardial imaging performed in conjunction with sub- maximal treadmill exercise testing. The resting electrocardiogram demonstrated left ventricular hypertrophy with S-T segment abnormalities in seven patients, thereby vitiating the further increase in S-T segment abnormalities that developed in these patients during exercise or in the postexercise period. Of the three patients with a normal resting electro- cardiogram, one had significant exercise-induced S-T segment depression. Thallium-201 myocardial imaging revealed no significant perfusion defects in 9 of the 10 patients (90 percent). In one patient with severe left ven- tricular hypertrophy significant perfusion defects developed afler exercise that were not present at rest. Stress thallium-201 myocardial perfusion imaging is a useful noninvasive technique that assists in ruling out the presence of significant coronary artery disease in patients with idiopathic hypertrophic subaortic stenosis.
The coexistence of idiopathic hypertrophic subaortic stenosis and cor- onary arterial disease has been well documented over the past 6 years.1-3 Although echocardiography has provided a reliable, noninvasive tech- nique for confirming the clinical diagnosis of idiopathic hypertrophic subaortic stenosis,4,5 the evaluation of angina1 symptoms in these pa- tients presents a diagnostic problem. Because resting electrocardio- graphic abnormalities, including left ventricular hypertrophy, are fre- quently present in these patients,s7 evaluation with exercise stress testing is often unreliab1e.s Cardiac catheterization and selective coro- nary angiography are usually necessary to establish the presence or ab- sence of coronary artery disease.
Recent data suggest that stress thallium-201 myocardial perfusion scanning allows the estimation of regional myocardial blood flow to areas supplied by critically narrowed coronary arteries.g-ll The present study was undertaken to evaluate the usefulness of stress myocardial perfusion imaging with thallium-201 in symptomatic patients with idiopathic hypertrophic subaortic stenosis and angina pectoris with angiographi- tally normal coronary arteries.
Methods
Patients. The study group consisted of eight consecutive patients with typical exertional angina and two with atypical chest pain in whom the diagnosis of idiopathic hypertrophic subaortic stenosis was established with clinical, he- modynamic and echocardiographic evaluation. All 10 patients had angio- graphically normal coronary arteries. There were seven men and three women with a mean age of 54.9 years (range 17 to 63 years). Clinical and laboratory data on the 10 patients are summarized in Table I. All patients had transseptal left heart catheterization with the catheter carefully placed in the inflow tract to avoid the entrapment phenomenon. Gradients were induced or increased across
1040 November 1979 The American Journal of CARDIOLOGY Volume 44

ANGINA AND IDIOPATHIC HYPERTROPHIC SUBAORTIC STENOSIS-RUBIN ET AL.
TABLE I
Clinical Features and Diagnostic Results in 10 Patients
Case no. Age (yr) & Sex Symptoms
Echocardiogram IVS:LPW
SAM Ratio
Cardiac Catheterization Resting LVOF Provoked LVOF
Gradient Gradient (mm Hg) (mm Hg)
1 17M Atypical chest pain
3’ 39F Exertional chest pain; dizziness :
1.51 6 3.5:1 t ;
50F Chest pressure with shortness of breath T
1.2:1 3: 180
2 63M Chest pressure; fatigue 1.8:1 60 45M Exertional chest pain + 2.5: 1
6 48F Exertional chest pain; shortness of breath :
2:l 3: !:: NA
: 53M Exertional chest pain 1.8:1 62M Exertional fatigue; chest pressure
:: Zl A:
50 192
9 63M Chest pressure with shortness of breath 16 90 10 49M Atypical chest pain; fatigue 0 1:5:1 0 20
IVS = interventricular septal thickness; LPW = left posterior wall thickness; LVOF = left ventricular outflow tract; NA = not attempted; SAM = systolic anterior movement of anterior mitral leaflet.
the left ventricular outflow tract in seven patients by inducing ventricular premature beats and recording the postextrasys- tolic beats or by having the patient perform the Valsalva maneuver or inhale amyl nitrite. Simultaneous left ventricular inflow and ascending aortic pressures were recorded to eval- uate the change in pressure gradient across the left ventricular outflow tract. Simultaneous left ventricular inflow and outflow pressures demonstrated the obstruction to be subvalvular.
The echocardiographic criteria used for diagnosis of idio- pathic hypertrophic subaortic stenosis were a septal-free wall index equal or greater than to 1.3, systolic anterior motion of the mitral valve, or both.
Coronary arteriography: Selective coronary arteriogra- phy was performed using the Sones technique. Exposures were made on 35 mm double-X negative Kodak film at 60 frames/ set using a GE DXS-550 9 inch (23 cm) and 6 inch (14 cm) single plane image intensifier system. Arteriograms were ob- tained in the anteroposterior and left and right anterior oblique views with hemiaxial views obtained for better visu- alization of the proximal left coronary system. Each study was reviewed by three independent observers.
Exercise testing: Treadmill exercise testing was performed in all 10 patients using a modified Balke technique. A scalp vein needle was inserted percutaneously into a forearm vein to facilitate injection of thallium-201 during exercise. Stan- dard 12 lead electrocardiograms were recorded at rest and in the postexercise period using a Marquette 3000 Automatic Electrocardiograph. During exercise, leads V4 to Vs were re- corded using an Avionics 3070 Electrocardiocharter with linear response characteristics throughout the range of 0.05 to 150 hertz which was fitted with a low noise stress cable.
After an initial warm-up period of 2 minutes during which the patient walked on the treadmill at a speed of 3 miles/hour and zero grade, the grade was increased by 2.5O every 2 min- utes whereas the speed remained constant at 3 miles/hour. Exercise was terminated when the patient complained of chest pain or fatigue or when the preselected submaximal heart rata (85 percent of the maximal heart rate for age) was achieved. Thallium-201 chloride was injected at peak exercise, and pa- tients were encouraged to maintain that level of exercise for an additional minute after administration of the radionu- elide.
Myocardial perfusion imaging: Thallium-201 chloride was administered intravenously in a dose of 2 to 3 mCi during peak exercise. Myocardial perfusion imaging was begun within 10 minutes in all but one patient in whom imaging was begun
within 20 minutes (Patient 2). Myocardial images were re- corded in the anterior view, 15’ and 45” left anterior oblique views, and left lateral view. A gamma scintillation camera (Searle Pho/Gamma LEM) interfaced with a DEC (Digital Equipment Corporation) PDP 1 l/35 computer was equipped with a low energy, high resolution converging collimator and images were recorded with a 20 percent window centered on the mercury X-ray peaks (69 to 80 kev). In each view 300,000 to 400,000 counts were collected and the data stored on a 64 by 64 matrix. The perfusion scintigrams were enhanced with a nine point computer smoothing technique before data analysis. With algorithms, the perimeter of the myocardial image was circumscribed in a regular region, and all cells outside of this region were changed to zero counts. The min- imal count within the regular region circumscribing the left ventricle was considered as background and thus subtracted from each cell in the matrix.
With a regular region of interest algorithm, the left ven- tricular scintigrams were divided into seven equal squares drawn to fit the left ventricle on each view. Regions were not necessarily representative of a specific myocardial area but were chosen to evaluate possible subsegmental areas of di- minished myocardial perfusion.
In each view, the region with the highest count density was used as a relative index of normal to compare with the other six regions. Counts in each region were subtracted from the region with the highest count density and the percent of dif- fuse perfusion in each region was determined. A (highest) - B (another region) X 100/A = percent diffuse perfusion. Deficits greater than 25 percent diffuse perfusion, if present in one or more regions in two or more views, were considered abnormal.
Interpretation of resting and exercise electrocardio- grams: Resting and exercise electrocardiograms were inter- preted by two independent observers without knowledge of the clinical diagnosis or angiographic findings. Seven patients whose resting electrocardiograms demonstrated voltage cri- teria for left ventricular hypertrophy with ST-T wave ab- normalities were considered to have uninterpretable exercise electrocardiograms because of the known high incidence rate of false-positive tests in these patients. Exercise electrocar- diograms in the remaining three patients were considered positive for ischemia if horizontal or downsloping S-T segment depression equal to or greater than 1 mm 0.08 second after the J point developed in the monitoring leads during exercise or in the postexercise tracings.
November 1979 The American Journal of CARDIOLOGY Volume 44 1041

ANGINA AND IDIOPATHIC HYPERTROPHIC SUBAORTIC STENOSIS-RUBIN ET AL.
TABLE II
Results of Electrocardiogram, Treadmill Exercise Test and Thallium-201 Scan
Case no.
Resting S-T Depression on Achieved Heart Rate Exercise Perfusion Electrocardiogram Stress Test (% max.) Reason for Stopping Scintigram
1
3’ 4
NSR, LVH 2mm NSR, LVH 1 mm NSR, LVH 1 mm NSR, LVH 2mm NSR, normal 2mm NSR, LVH 2mm NSR, normal Normal NSR, LVH 1 mm NSR, LVH 1.5 mm NSR, normal Normal
85
iA 65
6”: 85 54 85 a5
LVH = left ventricular hypertrophy; max. = maximal; NSR = normal sinus rhythm
Results
Table II lists the results of electrocardiography, stress tests and perfusion scintigraphy in each patient. All patients had normal coronary anatomy documented angiographically.
Resting electrocardiograms: All patients had normal sinus rhythm. Seven of 10 patients had evidence of left ventricular hypertrophy with accompanying S-T segment depressions or T wave inversions, or both, in the resting electrocardiogram. Three patients had a normal resting electrocardiogram.
Exercise tests: In the seven patients with an ab- normal resting electrocardiogram due to the presence of left ventricular hypertrophy, treadmill testing re- sulted in further increases in S-T segment depressions of at least 1 mm during exercise or in the postexercise
FIGURE 1. Patient 5 with a normal resting electrocardiogram. a, ex- ercise monitoring lead Vs demonstrating 3-mm S-T segment depression. b, 2 minute postexercise electrocardiogram demonstrating horizontal and downsloping S-T segments in limb and precordial leads. F = lead aVF.
1042 November 1979 The American Journal of CARDIOLOGY
Target rate achieved Chest pain: S-T depression Chest pain; S-T depression Chest pain; S-T depression Target rate achieved Chest pain; S-T depression Target rate achieved Chest pain; S-T depression Target rate achieved Target rate achieved -~
Normal Normal Normal Normal Normal Abnormal Normal Normal Normal Normal
period. In five of the seven patients, substernal chest pain developed necessitating termination of exercise.
Of the three patients with a normal resting electro- cardiogram, two had normal results on the exercise stress test. The remaining patient had markedly ab- normal results on the treadmill test with 2 mm hori- zontal S-T segment depressions in leads II, III, aVF and Vs to Vs. No patient had chest pain during exercise testing.
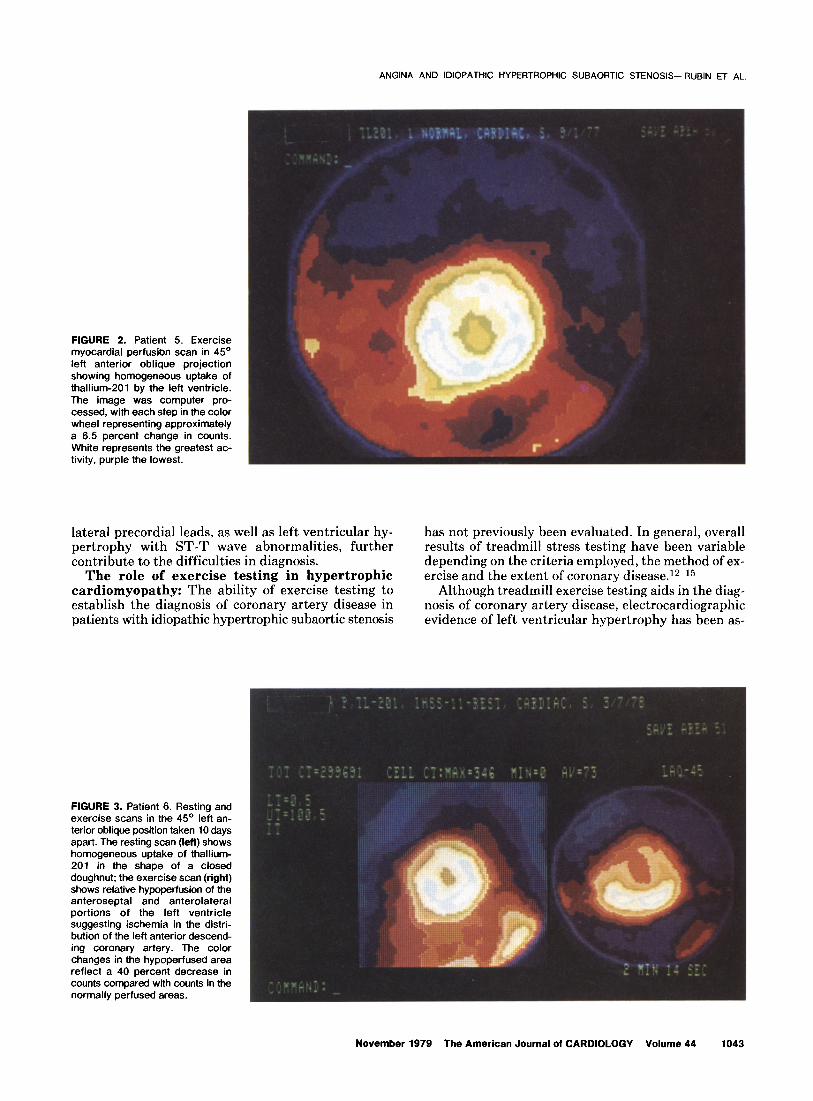
Myocardial perfusion scintigrams: Nine of 10 patients had normal stress perfusion scintigrams as judged by both unenhanced analog images and com- puter-enhanced images. Of particular interest was Pa- tient 5, a 45 year old white man, who had previously undergone two cardiac catheterizations because of persistent, severe exertional chest pain. Coronary an- giography gave normal results on both occasions, and the presence of idiopathic hypertrophic subaortic ste- nosis was not diagnosed. Figures 1 and 2 display the stress electrocardiogram and scintigrams of this patient. The resting electrocardiogram was normal; however, stress electrocardiograms revealed significant S-T segment depressions in leads II, III, aVF and Vs to Vs. Myocardial perfusion imaging was normal. Echocardi- ography revealed the presence of systolic anterior mo- tion of the anterior leaflet of the mitral valve with septal hypertrophy.
One patient had a normal resting myocardial perfu- sion scintigram but a markedly abnormal stress scan with diminished thallium-201 uptake in the anterior, anteroseptal and anterolateral portions of the left ventricle (Fig. 3).
Discussion
The occurrence of chest pain, with or without asso- ciated coronary artery disease, in patients with idio- pathic hypertrophic subaortic stenosis is well recog- nized. Clinical evaluation combined with echocardiog- raphy has proved to be highly reliable in establishing the diagnosis of idiopathic hypertrophic subaortic ste- nosis4g5; however, the evaluation of angina1 chest pain in these patients has continued to present a diagnostic problem. Abnormalities of the resting electrocardio- gram, including abnormal Q waves in the inferior and
Volume 44
ANGINA AND IDIOPATHIC HYPERTROPHIC SUBAORTIC STENOSIS-RUBIN ET AL.
FIGURE 2. Patient 5. Exercise myocardial perfusion scan in 45” left anterior oblique projection showing homogeneous uptake of thallium-201 by the left ventricle. The image was computer pro- cessed, with each step in the color wheel representing approximately a 6.5 percent change in counts. White represents the greatest ac- tivity, purple the lowest.
lateral precordial leads, as well as left ventricular hy- has not previously been evaluated. In general, overall pertrophy with ST-T wave abnormalities, further results of treadmill stress testing have been variable contribute to the difficulties in diagnosis. depending on the criteria employed, the method of ex-
The role of exercise testing in hypertrophic ercise and the extent of coronary disease.12-l5 cardiomyopathy: The ability of exercise testing to Although treadmill exercise testing aids in the diag- establish the diagnosis of coronary artery disease in nosis of coronary artery disease, electrocardiographic patients with idiopathic hypertrophic subaortic stenosis evidence of left ventricular hypertrophy has been as-
FIGURE 3. Patient 6. Resting and exercise scans in the 45O left an- terior oblique position taken 10 days apart. The resting scan (left) shows homogeneous uptake of thallium- 201 in the shape of a closed doughnut; the exercise scan (right) shows relative hypoperfusion of the anteroseptal and anterolateral portions of the left ventricle suggesting ischemia in the distri- bution of the left anterior descend- ing coronary artery. The color changes in the hypoperfused area reflect a 40 percent decrease in counts compared with counts in the normally perfused areas.
November 1979 The American Journal of CARDIOLOGY Volume 44 1043
ANGINA AND IDIOPATHIC HYPERTROPHIC SUBAORTIC STENOSIS-RUBIN ET AL.
sociated with wide variability in treadmill response, rendering the test uninterpretable. Harris et a1.8 per- formed treadmill exercise tests in 16 patients with left ventricular hypertrophy. In 14 patients, worsening S-T segment depressions were noted whereas in 2 patients there were no changes in the S-T segments. In both groups, 50 percent of patients had coronary artery dis- ease whereas the other 50 percent had normal coronary arteries. In our patients with idiopathic hypertrophic subaortic stenosis, all seven patients with electrocar- diographic evidence of left ventricular hypertrophy had worsening S-T segment depressions during exercise whereas one of three with a normal resting electrocar- diogram had an abnormal treadmill response. Because every patient had normal coronary arteries, stress testing was not helpful in identifying those patients with normal arteries.
Role of myocardial perfusion imaging versus electrocardiographic exercise testing: The devel- opment of techniques for myocardial perfusion imaging has provided a useful, noninvasive method for assessing relative myocardial hypoperfusion.16-lg Although the sensitivity of myocardial perfusion imaging varies with the number and location of vessels involved, several studies suggest it is more sensitive than treadmill ex- ercise testing alone.17-I9 When abnormalities in both exercise electrocardiograms and myocardial perfusion images are present, the sensitivity and specificity ap- proach 90 percent. 18~ls Thus, stress myocardial perfu- sion imaging might play an extremely important role in ferreting out true false-positive stress test results as well as aid in the interpretation of test results in patients with preexisting electrocardiographic abnormali- ties.lgm21
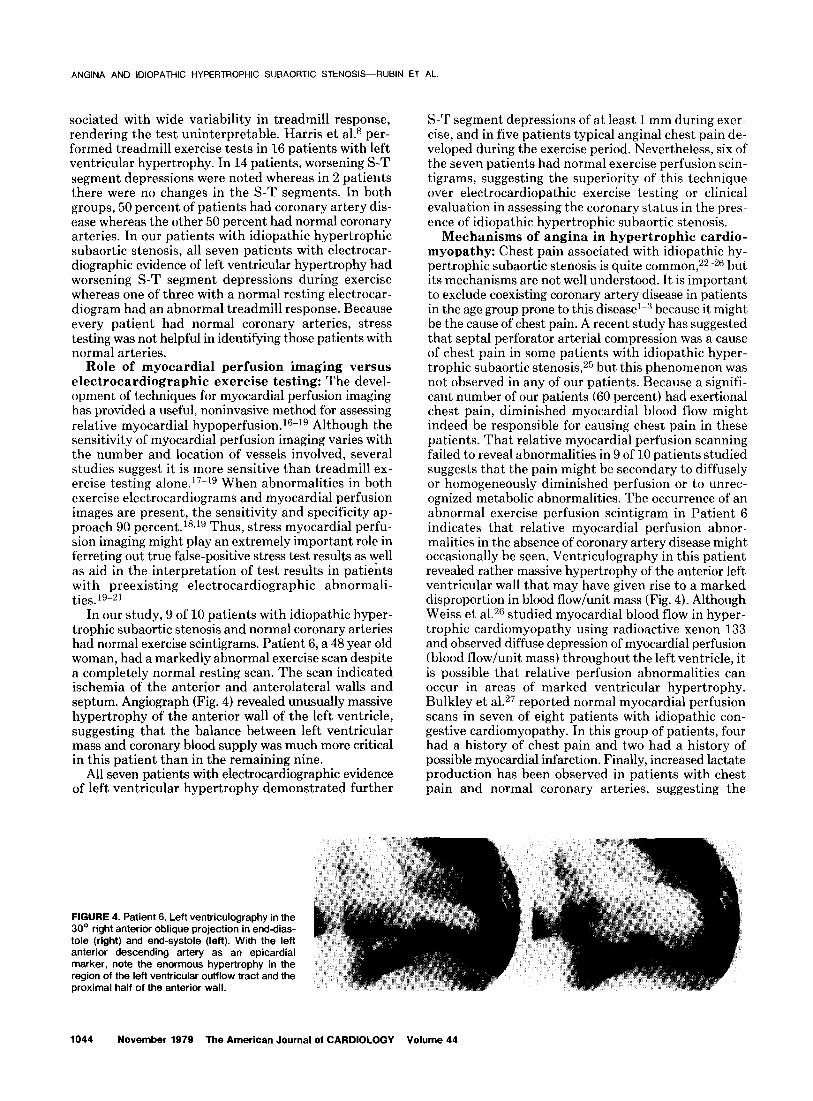
In our study, 9 of 10 patients with idiopathic hyper- trophic subaortic stenosis and normal coronary arteries had normal exercise scintigrams. Patient 6, a 48 year old woman, had a markedly abnormal exercise scan despite a completely normal resting scan. The scan indicated ischemia of the anterior and anterolateral walls and septum. Angiograph (Fig. 4) revealed unusually massive hypertrophy of the anterior wall of the left ventricle, suggesting that the balance between left ventricular mass and coronary blood supply was much more critical in this patient than in the remaining nine.
All seven patients with electrocardiographic evidence of left ventricular hypertrophy demonstrated further
S-T segment depressions of at least 1 mm during exer- cise, and in five patients typical angina1 chest pain de- veloped during the exercise period. Nevertheless, six of the seven patients had normal exercise perfusion scin- tigrams, suggesting the superiority of this technique over electrocardiopathic exercise testing or clinical evaluation in assessing the coronary status in the pres- ence of idiopathic hypertrophic subaortic stenosis.
Mechanisms of angina in hypertrophic cardio- myopathy: Chest pain associated with idiopathic hy- pertrophic subaortic stenosis is quite common,22-26 but its mechanisms are not well understood. It is important to exclude coexisting coronary artery disease in patients in the age group prone to this disease’-” because it might be the cause of chest pain. A recent study has suggested that septal perforator arterial compression was a cause of chest pain in some patients with idiopathic hyper- trophic subaortic stenosis, 25 but this phenomenon was not observed in any of our patients. Because a signifi- cant number of our patients (60 percent) had exertional chest pain, diminished myocardial blood flow might indeed be responsible for causing chest pain in these patients. That relative myocardial perfusion scanning failed to reveal abnormalities in 9 of 10 patients studied suggests that the pain might be secondary to diffusely or homogeneously diminished perfusion or to unrec- ognized metabolic abnormalities. The occurrence of an abnormal exercise perfusion scintigram in Patient 6 indicates that relative myocardial perfusion abnor- malities in the absence of coronary artery disease might occasionally be seen. Ventriculography in this patient revealed rather massive hypertrophy of the anterior left ventricular wall that may have given rise to a marked disproportion in blood flow/unit mass (Fig. 4). Although Weiss et a1.26 studied myocardial blood flow in hyper- trophic cardiomyopathy using radioactive xenon 133 and observed diffuse depression of myocardial perfusion (blood flow/unit mass) throughout the left ventricle, it is possible that relative perfusion abnormalities can occur in areas of marked ventricular hypertrophy. Bulkley et a1.27 reported normal myocardial perfusion scans in seven of eight patients with idiopathic con- gestive cardiomyopathy. In this group of patients, four had a history of chest pain and two had a history of possible myocardial infarction. Finally, increased lactate production has been observed in patients with chest pain and normal coronary arteries, suggesting the
FIGURE 4. Patient 6. Left ventriculography in the 30’ right anterior oblique projection in end-dias- tole (right) and end-systole (left). With the left anterior descending artery as an epicardial marker, note the enormous hypertrophy in the region of the left ventricular outflow tract and the proximal half of the anterior wall.
1644 November 1979 The American Journal of CARDIOLOGY Volume 44

ANGINA AND IDIOPATHIC HYPERTROPHIC SUBAORTIC STENOSIS-RUBIN ET AL.
presence of metabolic derangements with tissue hypoxia in the absence of major coronary artery disease.2s None of our patients were studied to evaluate this possi- bility.
Clinical implications: Since the initiation of our investigation, we have not had the opportunity to study patients with coexisting idiopathic hypertrophic sub- aortic stenosis and coronary artery disease. However, the use of myocardial perfusion imaging in the detection of exercise-induced myocardial ischemia in coronary artery disease has been well documenteds-11Js-21 and
our own experience parallels the published data. We
would expect that the results in patients having both idiopathic hypertrophic subaortic stenosis and coronary artery disease would be comparable. The presence of asymmetric septal thickening in itself did not produce abnormal scans.
Although the cause of chest pain in patients with id- iopathic hypertrophic subaortic stenosis and normal coronary anatomy continues to be obscure, relative myocardial perfusion scintigraphy with thallium-201 appears to be a useful noninvasive technique that assists in ruling out significant coronary artery disease in these patients.
References
1. Gufotta SJ, Hamby RI, Arenson AL, Ewing K: Coexistent idiopathic hypertrophic subaortic stenosis and coronary arterial disease. Circulation 46:690-896, 1972
2. Marcus GB, Popp RL, Stinson EB: Coronary artery disease with idiopathic hypertrophic subaortic stenosis. Lancet 1:901-903, 1974
3. Waiston A, Behan V: Spectrum of coronary artery disease in id- iopathic hypertrophic subaortic stenosis. Am J Cardioi 36:12-16, 1976
4. Shah PM: Echocardiography in the diagnosis of hypertrophic cardiomyopathy. Am J Med 62:630-835, 1977
5. Henry WL, Clark CE, Epstein SE: Asymmetric septai hype&trophy. Echocardiographic identification of the pathognomonic abnormaitty in IHSS. Circulation 47:225-233. 1973
6. Bahi OP, Walsh TJ, Ma&e E: Electrocardiography and vector- cardiography in idiopathic hypertrophic subaortic stenosis. Am J bled Sci 259:262-271, 1970
7. Prescott R, Guinn JS, Llttman D: Electrocardiographic changes in idiopathic hypertrophic subaortic stenosis which simulate myocardiai infarction. Am Heart J 66:43-48, 1963
6. Harris CW, Aronow WS, Parker DP, Kaplan MA: Treadmill stress test in left ventricular hypertrophy. Chest 63:353-357, 1973
9. Strauss HW, Harrison K, Langan JK, Lebowitz E, PM B: Thal- lium-201 for myocardiai imaging. Relation of thallium-201 to re- gional myocardial perfusion. Circulation 5 1:64 l-645, 1975
10. Rouieau J, Griffith L, Strauss HW, PM B: Detection of diffuse coronary artery disease by quantification of thallium-201 myo- cardiai images (abstr). Circulation 51, 52:Suppl ii:ii-3, 1975
11. Bailey IK, Griffith LSC, Strauss HW, PIE B: Detection of coronary artery disease and myocardiai ischemia by electrocardiography and myocardiai perfusion scanning with thallium-201 (abstr). Am J Cardioi 37:118, 1976
12. Goidschiager N, Seizer A, Cohn K: Treadmill stress test as indi- cators of presence and severity of coronary artery disease. Ann intern Med 85:277-286, 1976
13. Rosing DR, Relcheck N, Perioff JK: The exercise test as a diag- nostic and therapeutic aid. Am Heart J 87:584-596, 1974
14. Mason RE, Likar I, Biern RO, Ross RS: Multiple-lead exercise electrocardiography: experience in 107 normal subjects and 67 patients with angina pectoris, and comparison with coronary cin- eangiography in 84 patients. Circulation 36:517-525, 1967
15. Redwood DR, Epstein SE: Uses and limitations of stress testing in the evaluation of ischemic heart disease. Circulation 46: 1115-1131,1972
16. Zaret BL, Strauss HW, Martin WD, Welts HP, Fianun MD: Non- invasive regional myocardial perfusion with radioactive potassium.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
N Engi J Med 286:809-812, 1973 Berman DS, Sabei AF, DeNardo GL, Mason DT: Non-invasive detection of regional myocardiai ischemia using Rb-81 and the scintillation camera: comparison with stress electrocardiography in patients with arteriographicaiiy documented coronary stenosis. Circulation 52:619-626, 1975 Botvinick EH, Shames DM, Gershengom KN, Cartson E, Ratshin RA, Parmiey WW: The clinical advantages of myocardiai stress perfusion scintigraphy with rubidium 81 over stress eiectrocardi- ography. Am J Cardioi 39:364-371, 1971 Bailey IK, Griff’h CSL, Ronieau J, Strauss HW, Pitt B: Thailium- 201 myocardiai perfusion imaging at rest and during exercise: comparative sensitivity to electrocardiography in coronary artery disease.,Circuiation 55: 79-87, 1977 Tardash M, Botvinick E, Shames D, Parmiey W: Thallium-201 myocardiai perfusion imaging for the clinical clarification of normal, abnormal and equivocal stress tests (abstr). Circulation 53, 54: Suppi ii:li-217, 1976 Zaret BL, Stenson RE, Martin ND, Strauss HW, Welts HP, McGowan RL, Fianun MD: Potassium 43 myocardiai perfusion scanning for the noninvasive evaluation of patients with false positive exercise tests. Circulation 48:1234-1241, 1973 Frank S, Braunwaid E: idiopathic hypertrophic subaortic stenosis. Clinical analysis of 126 patients with emphasis on the natural history. Circulation 37:759-788, 1968 Parker BM: The course in idiopathic hypertrophic muscular sub- aortic stenosis. Ann intern Med 70:903-911, 1969 Shah PM, Adeiman .AG, Wigie ED, Gobei FL, Burcheii HB, Hendarson T, Curiei R, de la Caigada C, Oakley CM, Goodwin JF: The natural (and unnatural) history of hypertrophic obstructive cardiomyopathy. Circ Res 34, 35:Suppi ii:ii-179-11-195, 1974 Pjchard AD, Metier J, Teichhoiz LE, Lipnik S, Goriin R, Herman MV: 6eptai perforator compression (narrowing) in idiopathic hy- pertrophic subaortic stenosis. Am J Cardioi 40:310-314, 1977 Weiss MB, Ellis K, Sciacca RR, Johnson LL, Schmidt DH, Cannon PJ: Myocardial blood flow in congestive and hypertrophic cardio- myopathy. Relationship to peak wail stress and mean velocity of circumferential fiber shortening. Circulation 54:484-495, 1976 Buikiey BH, Hutchins GM, Bailey I, Strauss HW, Pitt B: Thai- iium-201 imaging and gated cardiac blood pool scans in patients with ischemic and idiopathic congestive cardiomyopathy. A clinical and pathologic study. Circulation 55:753-760. 1977 Parker JO, Chiong MA, West RO, Case RB: Sequential alterations in myocardiai lactate metabolism, ST-segments, and left ventricular function during angina induced by atrial pacing. Circulation 40: 113-131. 1969
November 1979 The American Journal of CARDIOLOGY Volume 44 1045
Copyright © 2022 FDOKUMEN