
Intraoperative arrhythmias and tissue damage during transmyocardial laser revascularization
11
1999;67:423-431 Ann Thorac Surg Clubb, Jr, Jeff L. Conger and O.H. Frazier Kamuran A. Kadipasaoglu, Michele Sartori, Takafumi Masai, Hasan B. Cihan, Fred J. revascularization Intraoperative arrhythmias and tissue damage during transmyocardial laser http://ats.ctsnetjournals.org/cgi/content/full/67/2/423 on the World Wide Web at: The online version of this article, along with updated information and services, is located Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1999 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 5, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Intraoperative arrhythmias and tissue damage during transmyocardial laser revascularization
1999;67:423-431 Ann Thorac SurgClubb, Jr, Jeff L. Conger and O.H. Frazier
Kamuran A. Kadipasaoglu, Michele Sartori, Takafumi Masai, Hasan B. Cihan, Fred J. revascularization
Intraoperative arrhythmias and tissue damage during transmyocardial laser
http://ats.ctsnetjournals.org/cgi/content/full/67/2/423on the World Wide Web at:
The online version of this article, along with updated information and services, is located
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1999 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from
Intraoperative Arrhythmias and Tissue DamageDuring Transmyocardial Laser RevascularizationKamuran A. Kadipasaoglu, PhD, Michele Sartori, MD, Takafumi Masai, MD,Hasan B. Cihan, MD, Fred J. Clubb, Jr, DVM, PhD, Jeff L. Conger, BS, andO. H. Frazier, MDCullen Cardiovascular Research Laboratories and Departments of Adult Cardiology, Cardiovascular Pathology, andCardiovascular Surgery, Texas Heart Institute, St. Luke’s Episcopal Hospital, Houston, Texas.
Background. Transmyocardial laser revascularizationcreates transmural channels to improve myocardial per-fusion. Different laser sources and ablation modalitieshave been proposed for transmyocardial laser revascular-ization. We investigated the incidence of cardiac arrhyth-mias and laser–tissue interactions during transmyocar-dial laser revascularization of normal porcinemyocardium with three different lasers.
Methods. We used a continuous-wave, chopped CO2
laser (20 J/pulse, 15 ms/pulse) synchronized with the Rwave; a holmium:yttrium aluminum garnet (Ho:YAG)laser (2 J/pulse, 250 ms/pulse, 5 Hz); and a xenon-chloride(excimer, Xe:Cl) laser (35 mJ/pulse, 20 ns/pulse, 30 Hz).Each laser was used 30 times as the sole modality in fourconsecutive pigs, yielding 120 channels.
Results. The average number of pulses needed to createa channel was 1, 11 6 4, and 37 6 8 for the CO2, Ho:YAG,and Xe:Cl lasers, respectively. All Ho:YAG and Xe:Clchannels had premature ventricular contractions. Ven-tricular tachycardia occurred in 70% of the Xe:Cl and 60%of the Ho:YAG channels. Only 36% of the CO2 channels
had premature ventricular contractions, and only 3% ofthe CO2 channels had ventricular tachycardia (p < 0.001versus Ho:YAG and Xe:Cl). Ho:YAG channels werehighly irregular: each had a 0.6-mm-wide central zonesurrounded by a ring of coagulation necrosis (diameter,1.84 6 0.67 mm) with effaced cellular architecture in athin hemorrhagic zone. The Xe:Cl sections exhibited thesame patterns on a smaller scale (diameter, 0.74 60.18 mm). The CO2 channels were straight and welldemarcated. The zone of structural and thermal damageextended over half the channel’s diameter, measuring0.52 6 0.25 mm.
Conclusions. During transmyocardial laser revascular-ization, the CO2 laser synchronized with the R wave issignificantly less arrhythmogenic than the Ho:YAG andXe:Cl lasers not synchronized with the R wave. In addi-tion, the interaction of the CO2 laser with porcine cardiactissue is significantly less traumatic than that of theHo:YAG and the Xe:Cl lasers.
(Ann Thorac Surg 1999;67:423–31)© 1999 by The Society of Thoracic Surgeons
Transmyocardial laser revascularization (TMLR) is arelatively new surgical technique in which transmu-
ral channels are created to increase myocardial perfu-sion. The technique is undergoing clinical investigationfor safety and long-term efficacy. In preliminary trials,TMLR with a high-energy carbon dioxide (CO2) laser(Heart Laser, PLC Medical Systems, Franklin, MA) hasbeen used as sole therapy for patients with refractoryangina. By July 1998, more than 500 such patients hadbeen enrolled in randomized and nonrandomized proto-cols, with encouraging results of clinical and cardiacperfusional improvement [1].
Despite the apparent clinical benefit of TMLR, someacute aspects of the technique, pertaining to its applica-tion and biologic tissue interaction, require further inves-tigation. First, the arrhythmogenicity associated withirradiation of cardiac tissue at various intervals duringthe cardiac cycle has not been systematically investi-
gated. Empirical observations during early animal exper-iments have suggested that if the laser is activated duringrepolarization of the myocardial cells (ie, during the Twave), the incidence of arrhythmic disturbances is in-creased, leading to an adverse outcome [2]. The arrhyth-mogenicity of the laser when fired during the T wavecould be relevant to the choice of the laser source and thelaser’s radiation pattern. Because the ablation speed incardiovascular tissue is directly proportional to the pulseenergy [3, 4], a laser with a sufficiently high pulse energycan create a channel with a single pulse. If this pulse issynchronized so as not to coincide with the T wave,arrhythmogenicity may be circumvented. At lower pulseenergies (lower ablation speeds), however, delivery ofmultiple continuous pulse trains becomes necessary tocreate a TMLR channel. Because a number of thesepulses will coincide with the T wave, arrhythmogenicitycould become important. Thus, researchers need to de-termine whether multiple-pulse TMLR without electro-cardiographic synchronization has a harmful effect on theelectrical activity of the ventricle.
Another aspect of TMLR involves the effect of laser-
Accepted for publication June 30, 1998.
Address reprint requests to Dr Kadipasaoglu, Texas Heart Institute, MC1-268, PO Box 20345, Houston, TX 77225-0345 (e-mail: [email protected]).
© 1999 by The Society of Thoracic Surgeons 0003-4975/99/$20.00Published by Elsevier Science Inc PII S0003-4975(98)01135-7
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from

induced acute tissue damage on the long-term patency ofthe channels. Early experiments in which channels werebored by means of needle acupuncture suggested thatchannel occlusion by scar tissue was caused by an exten-sive fibrous reaction secondary to mechanical damage[5]. More recent research into basic laser–tissue interac-tions has shown that the mechanical component, mea-sured as acoustic tissue damage, increases in directproportion to the peak power of the laser source [6]. Thepeak power of the laser pulse, defined as the laser energydelivered per unit time, increases significantly with adecreasing pulse duration. Therefore, with short-pulselasers, the duration of the laser pulse may be one of themajor determinants of the degree of initial tissue traumaand, hence, of the long-term patency of the laserchannels.
Thus, an analysis of the relative arrhythmogenicity andtrauma-inducing potential of various laser sources cur-rently available for TMLR would be important, because itcould affect perioperative arrhythmic complications andincrease long-term efficacy. In the present study, weassessed the incidence of arrhythmias and the amount oftissue damage associated with three different lasers dur-ing TMLR in normal porcine hearts: the high-energy,long-pulse CO2 laser and the low-energy, short-pulseholmium:yttrium aluminum garnet (Ho:YAG) andxenon-chloride (excimer, Xe:Cl) lasers.
Material and Methods
All animals at the Texas Heart Institute receive humanecare in compliance with the Animal Welfare Act, the“Principles of Laboratory Animal Care,” formulated bythe National Society for Medical Research, and the“Guide for the Care and Use of Laboratory Animals”(NIH publication 85-23, revised 1996). All protocols re-lated to this program were approved by our hospital’sinstitutional animal care and use committee before thestudies were initiated.
Animal Preparation, Surgery, and InstrumentationDomestic pigs weighing approximately 56.2 to 67.5 kgwere acclimatized and quarantined for at least 1 weekbefore undergoing surgical intervention. After the ani-mals had fasted overnight, a preanesthetic regimen wasinduced with acepromazine maleate (0.11 to 0.22 mg/kgintramuscularly, not exceeding a total dose of 15 mg) andatropine sulfate (0.05 mg/kg intramuscularly, premixedin the syringe). An ear vein was catheterized, and generalanesthesia with ketamine hydrochloride (20 mg/kg intra-venously) was started 10 minutes after the preanestheticinjection. The animals were then intubated, and anesthe-sia was maintained throughout the operation by meansof an isoflurane and oxygen mixture.
Each animal was positioned on its right side on anelectrocoagulation electrode and a warming blanket tomaintain its body temperature at 41°C. The body tem-perature was monitored nasally. Surface electrocardio-graphic electrodes were applied, and the electrocardio-graphic waveform during and after the laser procedure
was recorded on a computerized data collection andanalysis system (Dataflow; Crystal Biotech, Northbor-ough, MA). Intravenous catheters were placed in the leftjugular vein for further infusion of medications and inthe carotid artery for monitoring the arterial pressure. Aleft thoracotomy was performed in the fourth intercostalspace. The pericardium was exposed and cut in a Tshape, and the heart was isolated in a pericardial cradle.To prevent muscle spasms, pancuronium bromide(0.1 mg/kg intravenously) was given for one time only.After creation of the laser channels, the experiment wasterminated by injecting the unconscious animal intrave-nously with a euthanizing agent (Beuthanasia solutionDelmarva Laboratories Inc, Midlothian, VA).
Transmyocardial Laser Revascularization ModalitiesWe used a high-energy CO2 laser (Heart Laser; PLCMedical Systems, Inc), a Ho:YAG laser (Laser Photonics,Sunnyvale, CA), and an Xe:Cl laser (Advanced Interven-tional Systems, Scottsdale, AZ).
Activation of the CO2 laser was adjusted to coincidewith the electrocardiographic R wave, and pulses weredelivered at 25 J. Because this laser’s average outputpower is fixed at 800 W, this pulse energy setting corre-sponded to a pulse duration of 31 ms. The pulses wereseparated from each other by at least 1 minute to achieveadequate hemostasis. In a separate set of experiments,CO2 laser emission was set to coincide with the T wave.The Ho:YAG laser was set to a pulse energy of 2 J/pulseand a pulsing frequency of 5 Hz. The Xe:Cl laser was setto an output energy of 0.035 J/pulse and a pulsingfrequency of 30 Hz. The pulse duration of the Ho:YAGand the Xe:Cl lasers was fixed at 250 3 1023 ms and 20 31029 ms, respectively. These settings corresponded topeak powers of 8,000 W for the Ho:YAG laser and 175 3103 W for the Xe:Cl laser. Both lasers were coupled to asilica fiber (outer diameter, 600 mm), and laser ablationwas continued with gentle forward pressure until the fullthickness of the myocardium was penetrated. In someadditional cases, the fiber was advanced without activat-ing the laser, to assess the arrhythmogenicity of the fiberalone. In other cases, the laser was activated during bothforward motion (toward the ventricular cavity) and back-ward motion of the fiber.
Histologic StudiesPorcine hearts subjected to TMLR in vivo were flushedwith 2 L of 4°C physiologic saline (retrograde through thecannulated thoracic aorta, at 40 mm Hg) and then with 1L of 10% buffered formalin. Each heart was removed andphotographed, and transmural sections of laser trackswere taken for microscopic evaluation. A minimum offour blocks from representative areas of each heart wereexamined grossly and microscopically. Sections for mi-croscopic studies were processed using standard paraf-fin-embedding techniques. Five-micrometer paraffin-embedded sections were stained with hematoxylin andeosin. Slides were coded and examined. After all sectionswere evaluated, the descriptions were collated by type oflaser.
424 KADIPASAOGLU ET AL Ann Thorac SurgINTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE 1999;67:423–31
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from

Experimental Design and Data AnalysisThe electrocardiographic and systemic arterial wave-forms during and after the lasing procedure were re-corded on the data analysis system. Each heart wastreated with a single laser modality, so that 30 channelswere created in the anterolateral aspect of the myocar-dium. To eliminate interanimal variability, the same lasermodality was used on 4 consecutive animals (total, 120channels for each laser modality). The experiments wereperformed in an acute setting.
The results of the experiments were evaluated sepa-rately for each laser modality. Premature ventricularcontractions (PVCs), ventricular tachycardia (VT), andother changes in cardiac rhythm, as recorded by contin-uous electrocardiography, were classified as events. Pre-mature ventricular contractions were differentiated fromother changes by the accompanying compensatorypause. Runs of three or more PVCs in a row wereclassified as a VT episode. The number of events perchannel was analyzed from analog and digital tracingsrecorded during TMLR. Table 1 shows the total numberof events per channel and the classification of theseevents for each laser modality.
Statistical AnalysisWith each laser modality, the onset of arrhythmias asso-ciated with channel creation was considered the endpoint of the experiment. The nature of each arrhythmia,as well as the time of occurrence of the arrhythmia(measured from the time of activation of the laser), wasalso recorded. We adopted the worst-case value of 0.5 forthe standard deviation, s [s 5 p (1 2 p)], of the binomialdistribution of the outcomes (arrhythmia or no arrhyth-mia) with each laser modality. For an acceptable standarderror of 10% around the mean proportion, p, of occur-rence of arrhythmias with each laser modality, the min-imum number, n, of laser pulses that should be deliveredwith each laser modality was calculated with the follow-ing formula:
1.96Î p~1 2 p!
n5 0.10
where 1.96 is the Z value for a confidence limit of 95% (a5 0.05). Carrying on the calculation gives n 5 96, which
means that to detect a significant difference between thearrhythmic effects of each laser modality, at least 96channels should be created with each modality.
To preserve regional myocardial structural integrity,we refrained from creating more than 30 channels peranimal. Because each laser modality was used on 4different animals to account for interanimal variability, atotal of 120 channels were created with each laser mo-dality in a total of 4 animals. This arrangement gave us anadditional margin of safety of 120/96 5 1.25, or 25% abovethe minimum number of channels required for statisticalsignificance.
Results
No animals died of arrhythmia during the procedures.The average number of pulses needed to create a singlechannel was 1 for the CO2, 11 6 4 for the Ho:YAG, and37 6 8 for the Xe:Cl. The specimens obtained from eachanimal’s heart were preserved in paraffin blocks andsubjected to histopathologic examination.
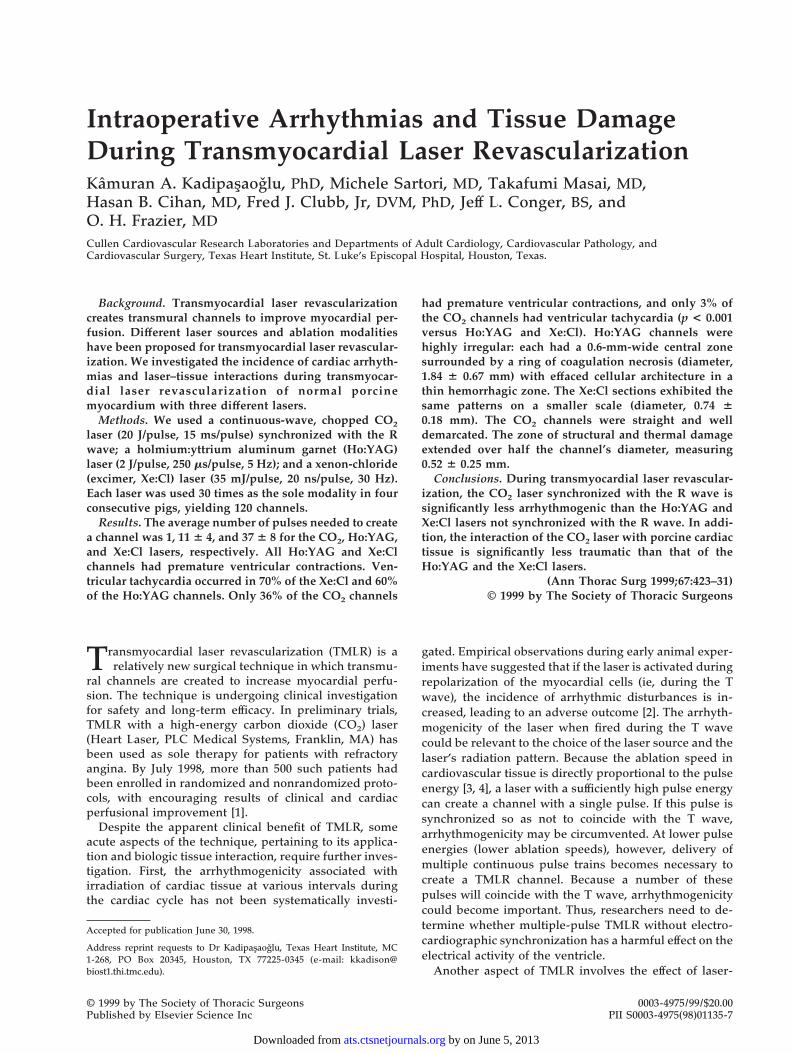
Arrhythmia ExperimentsDuring creation of the 120 channels with the Ho:YAGlaser, a total of 431 events were recorded in 117 channels(98%), at an average rate of 3.68 events per channel (Table1). All but one of the events were PVCs, occurring in 116channels (97%). In 74 cases, distributed among 68 chan-nels (60%), the PVCs occurred in runs of three or more,qualifying for classification as VT. The PVCs and VTepisodes consistently occurred when the laser was acti-vated, regardless of the direction of motion of the cath-eter, as long as the fiber was in contact with the myocar-dial tissue (Fig 1A). A brief pause in the generation ofarrhythmias occurred when the fiber tip was fired intothe blood within the ventricular cavity (Fig 1A). The laserfiber itself was also arrhythmogenic: by simply pokingthe transmural channel without firing the laser, we elic-ited arrhythmias in some cases (Fig 1B).
When the Xe:Cl laser was used, 426 events wererecorded in 120 channels, no channels being free ofarrhythmic events (Table 1). Therefore, an average of 3.55events occurred per channel. In all cases, the morphologywas PVC-like (Fig 1C). A total of 81 VT-type arrhythmias
Table 1. Arrhythmias Associated With Channel Formation During TMLR
LaserModality
Total No. ofEventsa
Events perChannel
% ChannelsWith an Event
Total No. ofPVCsa
% ChannelsWith PVCs
Total No.of VTsa
% ChannelsWith VT
Ho:YAG 431 3.68 98 430 97 74 60Xe:Cl 426 3.55 100 426 100 81 70CO2 (R) 164b 2.34b 60b 77b 36b 4b 3b
CO2 (T) 332 3.22 86 325 81 26c 15c
a Recorded in 120 channels. b p , 0.01 versus all other laser modalities. c p , 0.01 versus Xe:Cl and Ho:YAG laser modalities.
CO2 (R) 5 CO2 laser synchronized to fire on the R wave; CO2 (T) 5 CO2 laser synchronized to fire on the T wave; Ho:YAG 5 holmium:yttriumaluminum garnet laser; PVCs 5 premature ventricular contractions; TMLR 5 transmyocardial laser revascularization; VT 5 ventriculartachycardia; Xe:Cl 5 xenon-chloride laser.
425Ann Thorac Surg KADIPASAOLU ET AL1999;67:423–31 INTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from
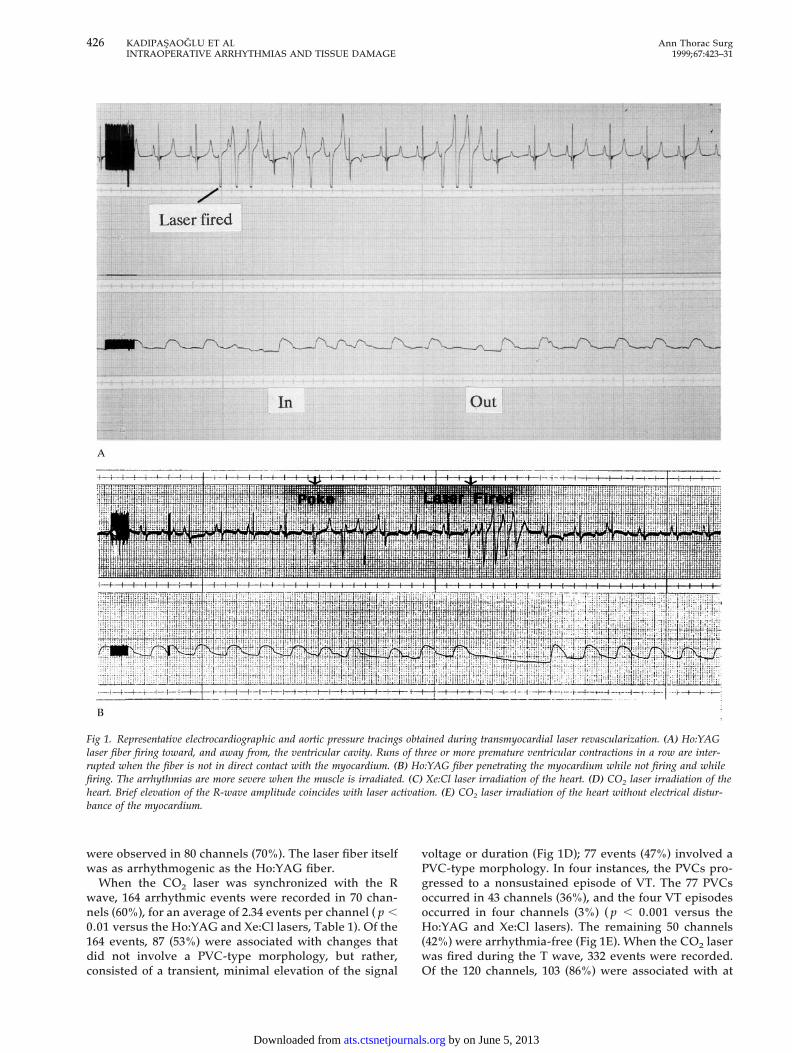
were observed in 80 channels (70%). The laser fiber itselfwas as arrhythmogenic as the Ho:YAG fiber.
When the CO2 laser was synchronized with the Rwave, 164 arrhythmic events were recorded in 70 chan-nels (60%), for an average of 2.34 events per channel ( p ,0.01 versus the Ho:YAG and Xe:Cl lasers, Table 1). Of the164 events, 87 (53%) were associated with changes thatdid not involve a PVC-type morphology, but rather,consisted of a transient, minimal elevation of the signal
voltage or duration (Fig 1D); 77 events (47%) involved aPVC-type morphology. In four instances, the PVCs pro-gressed to a nonsustained episode of VT. The 77 PVCsoccurred in 43 channels (36%), and the four VT episodesoccurred in four channels (3%) ( p , 0.001 versus theHo:YAG and Xe:Cl lasers). The remaining 50 channels(42%) were arrhythmia-free (Fig 1E). When the CO2 laserwas fired during the T wave, 332 events were recorded.Of the 120 channels, 103 (86%) were associated with at
Fig 1. Representative electrocardiographic and aortic pressure tracings obtained during transmyocardial laser revascularization. (A) Ho:YAGlaser fiber firing toward, and away from, the ventricular cavity. Runs of three or more premature ventricular contractions in a row are inter-rupted when the fiber is not in direct contact with the myocardium. (B) Ho:YAG fiber penetrating the myocardium while not firing and whilefiring. The arrhythmias are more severe when the muscle is irradiated. (C) Xe:Cl laser irradiation of the heart. (D) CO2 laser irradiation of theheart. Brief elevation of the R-wave amplitude coincides with laser activation. (E) CO2 laser irradiation of the heart without electrical distur-bance of the myocardium.
426 KADIPASAOGLU ET AL Ann Thorac SurgINTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE 1999;67:423–31
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from
least one event, and the average number of events perchannel was 3.22 ( p , 0.001 versus the CO2 laser firedduring the R wave). Of the 332 events, 325 (98%), occur-ring in 97 channels (81%), involved PVC-type morphol-ogy ( p , 0.01 versus the CO2 fired during the R wave).A total of 26 VT episodes were observed in 18 channels
(15%). This was significantly less compared with theHo:YAG- and Xe:Cl-induced VT episodes ( p , 0.01).
In Figure 2, the results of the arrhythmia experimentsare presented in graphic form with respect to the numberof events per channel (Fig 2A) and the percentage ofchannels that had an event (Fig 2B).
Fig. 1. Continued.
427Ann Thorac Surg KADIPASAOGLU ET AL1999;67:423–31 INTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from
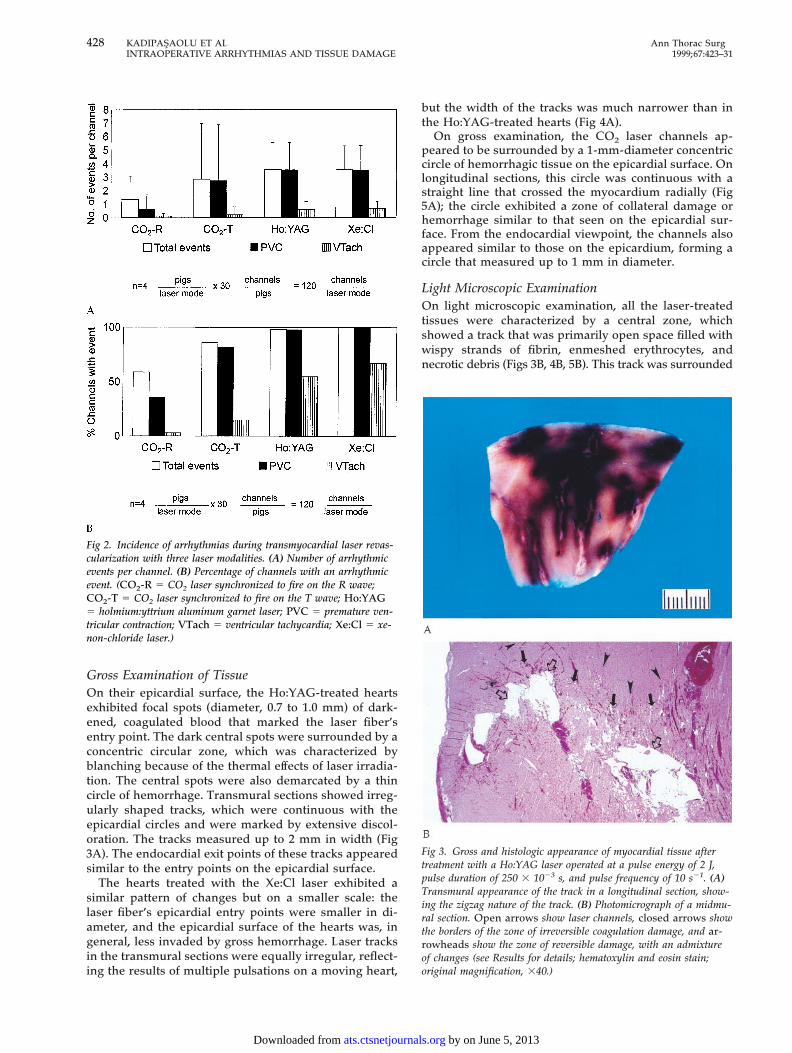
Gross Examination of TissueOn their epicardial surface, the Ho:YAG-treated heartsexhibited focal spots (diameter, 0.7 to 1.0 mm) of dark-ened, coagulated blood that marked the laser fiber’sentry point. The dark central spots were surrounded by aconcentric circular zone, which was characterized byblanching because of the thermal effects of laser irradia-tion. The central spots were also demarcated by a thincircle of hemorrhage. Transmural sections showed irreg-ularly shaped tracks, which were continuous with theepicardial circles and were marked by extensive discol-oration. The tracks measured up to 2 mm in width (Fig3A). The endocardial exit points of these tracks appearedsimilar to the entry points on the epicardial surface.
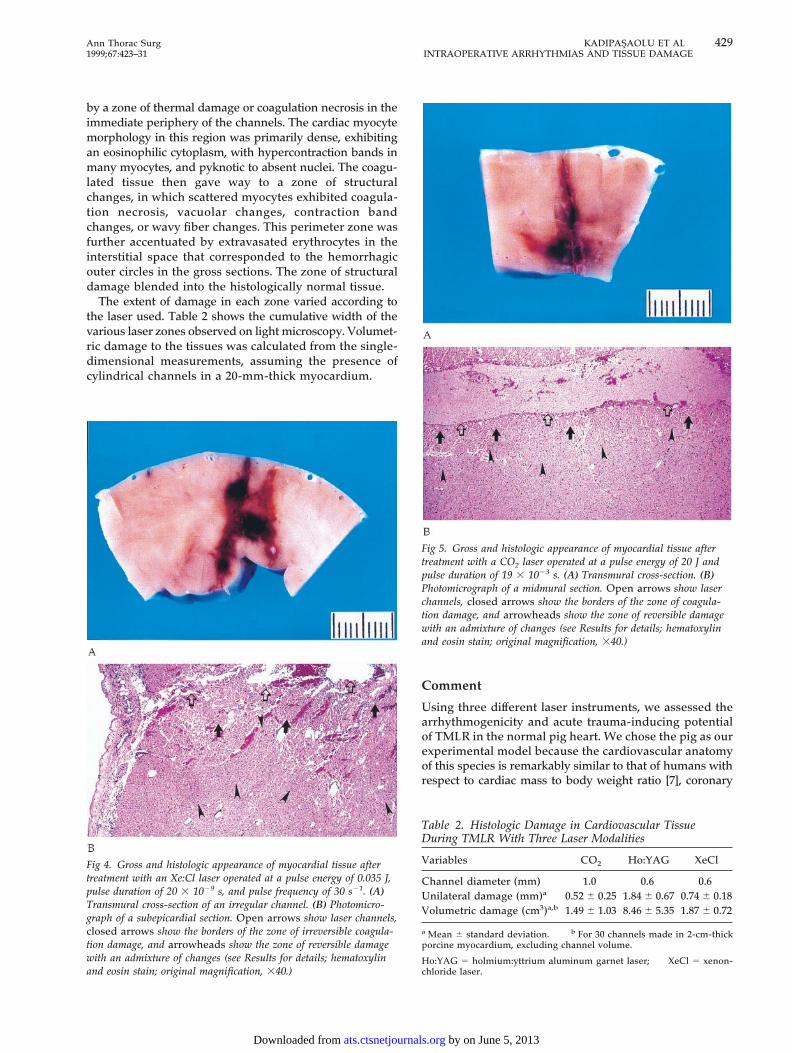
The hearts treated with the Xe:Cl laser exhibited asimilar pattern of changes but on a smaller scale: thelaser fiber’s epicardial entry points were smaller in di-ameter, and the epicardial surface of the hearts was, ingeneral, less invaded by gross hemorrhage. Laser tracksin the transmural sections were equally irregular, reflect-ing the results of multiple pulsations on a moving heart,
but the width of the tracks was much narrower than inthe Ho:YAG-treated hearts (Fig 4A).
On gross examination, the CO2 laser channels ap-peared to be surrounded by a 1-mm-diameter concentriccircle of hemorrhagic tissue on the epicardial surface. Onlongitudinal sections, this circle was continuous with astraight line that crossed the myocardium radially (Fig5A); the circle exhibited a zone of collateral damage orhemorrhage similar to that seen on the epicardial sur-face. From the endocardial viewpoint, the channels alsoappeared similar to those on the epicardium, forming acircle that measured up to 1 mm in diameter.
Light Microscopic ExaminationOn light microscopic examination, all the laser-treatedtissues were characterized by a central zone, whichshowed a track that was primarily open space filled withwispy strands of fibrin, enmeshed erythrocytes, andnecrotic debris (Figs 3B, 4B, 5B). This track was surrounded
Fig 2. Incidence of arrhythmias during transmyocardial laser revas-cularization with three laser modalities. (A) Number of arrhythmicevents per channel. (B) Percentage of channels with an arrhythmicevent. (CO2-R 5 CO2 laser synchronized to fire on the R wave;CO2-T 5 CO2 laser synchronized to fire on the T wave; Ho:YAG5 holmium:yttrium aluminum garnet laser; PVC 5 premature ven-tricular contraction; VTach 5 ventricular tachycardia; Xe:Cl 5 xe-non-chloride laser.)
Fig 3. Gross and histologic appearance of myocardial tissue aftertreatment with a Ho:YAG laser operated at a pulse energy of 2 J,pulse duration of 250 3 1023 s, and pulse frequency of 10 s21. (A)Transmural appearance of the track in a longitudinal section, show-ing the zigzag nature of the track. (B) Photomicrograph of a midmu-ral section. Open arrows show laser channels, closed arrows showthe borders of the zone of irreversible coagulation damage, and ar-rowheads show the zone of reversible damage, with an admixtureof changes (see Results for details; hematoxylin and eosin stain;original magnification, 340.)
428 KADIPASAOLU ET AL Ann Thorac SurgINTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE 1999;67:423–31
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from
by a zone of thermal damage or coagulation necrosis in theimmediate periphery of the channels. The cardiac myocytemorphology in this region was primarily dense, exhibitingan eosinophilic cytoplasm, with hypercontraction bands inmany myocytes, and pyknotic to absent nuclei. The coagu-lated tissue then gave way to a zone of structuralchanges, in which scattered myocytes exhibited coagula-tion necrosis, vacuolar changes, contraction bandchanges, or wavy fiber changes. This perimeter zone wasfurther accentuated by extravasated erythrocytes in theinterstitial space that corresponded to the hemorrhagicouter circles in the gross sections. The zone of structuraldamage blended into the histologically normal tissue.
The extent of damage in each zone varied according tothe laser used. Table 2 shows the cumulative width of thevarious laser zones observed on light microscopy. Volumet-ric damage to the tissues was calculated from the single-dimensional measurements, assuming the presence ofcylindrical channels in a 20-mm-thick myocardium.
Comment
Using three different laser instruments, we assessed thearrhythmogenicity and acute trauma-inducing potentialof TMLR in the normal pig heart. We chose the pig as ourexperimental model because the cardiovascular anatomyof this species is remarkably similar to that of humans withrespect to cardiac mass to body weight ratio [7], coronary
Fig 4. Gross and histologic appearance of myocardial tissue aftertreatment with an Xe:Cl laser operated at a pulse energy of 0.035 J,pulse duration of 20 3 1029 s, and pulse frequency of 30 s21. (A)Transmural cross-section of an irregular channel. (B) Photomicro-graph of a subepicardial section. Open arrows show laser channels,closed arrows show the borders of the zone of irreversible coagula-tion damage, and arrowheads show the zone of reversible damagewith an admixture of changes (see Results for details; hematoxylinand eosin stain; original magnification, 340.)
Fig 5. Gross and histologic appearance of myocardial tissue aftertreatment with a CO2 laser operated at a pulse energy of 20 J andpulse duration of 19 3 1023 s. (A) Transmural cross-section. (B)Photomicrograph of a midmural section. Open arrows show laserchannels, closed arrows show the borders of the zone of coagula-tion damage, and arrowheads show the zone of reversible damagewith an admixture of changes (see Results for details; hematoxylinand eosin stain; original magnification, 340.)
Table 2. Histologic Damage in Cardiovascular TissueDuring TMLR With Three Laser Modalities
Variables CO2 Ho:YAG XeCl
Channel diameter (mm) 1.0 0.6 0.6Unilateral damage (mm)a 0.52 6 0.25 1.84 6 0.67 0.74 6 0.18Volumetric damage (cm3)a,b 1.49 6 1.03 8.46 6 5.35 1.87 6 0.72
a Mean 6 standard deviation. b For 30 channels made in 2-cm-thickporcine myocardium, excluding channel volume.
Ho:YAG 5 holmium:yttrium aluminum garnet laser; XeCl 5 xenon-chloride laser.
429Ann Thorac Surg KADIPASAOLU ET AL1999;67:423–31 INTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from

anatomy [8], and collateral formation [9]. Moreover, ourprevious experience with this model suggested that it ishighly susceptible to the induction of arrhythmias, evenunder conditions of normal perfusion. In our earlier porcineexperiments, we had observed that attempts to createregional ischemia by ligating the left anterior descendingcoronary artery were incompatible with survival in mostcases unless prophylactic antiarrhythmic therapy was insti-tuted. Such therapy, however, would have interfered withthe experimental design of the present study, because itwould have affected the primary dependent variable, ie,the number of arrhythmic events observed per channel.The typical clinical scenario would have best been rep-resented by an ischemic model, particularly that of achronically hibernating myocardium as described byBolukoglu and coworkers [10]. Nevertheless, the presentstudy was conducted on porcine hearts under conditionsof normal coronary artery blood flow. We believe thatthis model was appropriate for assessing the arrhythmo-genicity and trauma-inducing potential of TMLR, whichwas the specific purpose of our study.
We have been using the CO2 laser in clinical trials sinceJune 1993. We therefore had access to it for experimentalstudies. However, despite our requests, we were not able toobtain the Ho:YAG or the Xe:Cl laser hardware directlyfrom the manufacturer of a clinically used model. There-fore, we substituted alternative commercial models forthese laser modalities. Our understanding was that thenature of the laser–tissue interactions would not be affectedso long as the clinically important variables, ie, the respec-tive wavelengths (308 nm and 2,010 nm), delivery systems(600-mm optical silica fibers), and settings for pulse energyand repetition rate (see Methods) were kept identical tocurrent clinical specifications. It should be noted, how-ever, that there is at least one manufactured Ho:YAGmodality that is undergoing clinical evaluation and that isgated to the R wave. Therefore, the conclusions drawnfrom the present results may not apply to this modality.
The first factor of interest in this study was the rate ofgeneration of complex arrhythmias associated with thecreation of a single channel using the three different lasermodalities. When the CO2, Ho:YAG, and Xe:Cl laserswere fired during the cardiac repolarization period (ie,during the T wave), all three lasers caused a high inci-dence of PVC arrhythmias (98%, 100%, and 100%, respec-tively). The incidence of VT, however, was significantlyhigher with the Ho:YAG (60%) and Xe:Cl (70%) instru-ments than with the CO2 laser (15%). This finding sug-gests that complex ventricular arrhythmias may be influ-enced by the type of laser when firing of the laser is notsynchronized to occur away from the T wave. The inci-dence of VT with the CO2 laser was further reducedwhen that laser was fired during the depolarizationperiod (R wave). This fact supports our initial hypothesisthat arrhythmias during ablation are influenced by thetime of lasing with respect to the cardiac cycle.
The hearts of patients undergoing TMLR are vulnerableto arrhythmias [11]. The presence of scar tissue or periin-farct ischemia is a well-known risk factor for reentrantventricular tachyarrhythmias [12]. Because extracorporealcardiopulmonary support is not used, the duration ofTMLR is shortened; nevertheless, left-side volume overload
and circumferential ventricular stress, which often ac-company ischemic cardiomyopathy, predispose these pa-tients to ventricular and supraventricular arrhythmias.
In the initial 35-patient series treated at our hospital(which reflects our early experience in using TMLR witha CO2 laser [13, 14] either as sole therapy or as an adjunctto coronary artery bypass grafting between July 1993 andJuly 1995), 28 patients had a history of major arrhythmiassuch as frequent PVCs and runs of VT, pacemaker-dependent syncope, or cardiac arrest at baseline. AfterTMLR, 17 (61%) of these patients had one or morearrhythmic sequelae, 7 of which proved fatal despite theaggressive use of various antiarrhythmic agents. Only 3(11%) of the 28 patients had no arrhythmias postopera-tively. In 9 (32%) of the 28 patients with a history of majorarrhythmias, the postoperative arrhythmias were similarto those seen at baseline. The 7 patients without a historyof arrhythmias at baseline had no postoperative compli-cations. The increased perioperative incidence of ar-rhythmic complications in patients predisposed to ar-rhythmia suggests that TMLR exacerbates the electricalvulnerability of the myocardium, even when the opera-tion is performed with the least arrhythmogenic modality(the CO2 laser synchronized with the R wave). Thus, thethreat of arrhythmias is a major limitation to the morewidespread application of TMLR. Use of optimal laserablation parameters and synchronization with the car-diac cycle are highly important. In light of our findings,TMLR should be done with extreme caution when thenonsynchronized laser modalities are used. In the cur-rent randomized phase of the clinical TMLR trials, pa-tients with a history of major arrhythmias are excluded.
The second factor of interest in our study was therelative extent of the tissue damage caused by the cur-rently available TMLR laser modalities. The thermal andacoustic damage that surrounded the transmyocardialchannel was significantly greater with the Ho:YAG andXe:Cl lasers than with the CO2 laser. It is important tonote that we did not test to determine whether thedifference in arrhythmogenic effect with the three laserswas causally related to the different amount of tissuedamage that each laser created in our heart model.However, as discussed below, the trauma-inducing ca-pacity may arguably govern the long-term patency of thelaser channels. The damage imparted to the target tissuewas considerably less with the CO2 laser than with theother two laser modalities. The damage was predomi-nantly thermal in the immediate vicinity of the channelsand structural in the outlying layers. The gross appear-ance of the channels closely reflected the geometry ofchannels created in tissue phantoms observed under fastvideo cinegrams [15]. The extent of the damage was also inagreement with the acute effects that Fisher and associates[16] observed in CO2- and Ho:YAG-treated cardiac tissue.
Ablation of cardiovascular tissue with laser energy isgoverned not only by the thermal- and light-distributioncharacteristics of the tissue but also by the nonadjustablesettings of the laser pulse. The important parameters ofthe laser pulse are its energy, duration, and frequency.For a given amount of energy delivered per laser pulse,the peak power (energy over time) will increase with adecrease in the pulse duration. Therefore, with ultrashort
430 KADIPASAOLU ET AL Ann Thorac SurgINTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE 1999;67:423–31
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from

pulses, the peak power will be very high, even at arelatively low pulse energy. The higher the peak power,the faster the rate at which the pulse energy is deliveredto the tissue. Any excess energy not used for activeablation is used to heat the tissue, and that heat shouldeventually dissipate by means of conductive processes. Ifa high pulse frequency, however, causes heat to build upwithin a confined tissue space faster than it can bedissipated, water vapor bubbles will form. The explosivecollapse of these bubbles will send shock waves throughthe adjacent tissue layers. As this acoustic effect radiatesfrom the ablation site in all directions, it will rip the tissueapart and superimpose a considerable structural compo-nent on the already existing thermal damage [6].
On histomorphometric analysis of our CO2 laser-treated tissues, the combined thermal and structuralcomponents of the laser-induced damage extendedthrough a zone of 0.52 6 0.25 mm on each side of thechannel in planar cross-sections (Table 2). Assuming thatthe laser channels had a cylindrical geometry in a 20-mm-thick porcine myocardium, the volume of damagedmyocardium was calculated as 1.49 6 1.03 cm3, excludingthe channel volume itself. The total volume of damagedtissue was calculated as 1.87 6 0.72 cm3 for the Xe:Cl laserand 8.46 6 5.35 cm3 for the Ho:YAG laser. Therefore,these two lasers respectively produced 25% and 568%more volumetric damage than did the CO2 laser. If theintensity of the fibrous repair process is indeed propor-tional to the extent of the damage, the tissue reaction toHo:YAG and Xe:Cl laser ablation will be that muchgreater than the reaction to CO2 laser ablation. There-fore, unlike TMLR with the CO2 laser [17], TMLR withthe Ho:YAG and Xe:Cl lasers may not be compatible withlong-term channel patency; according to one untestedtheory, however, it may enhance angiogenesis [18].
In conclusion, compared with the high-energy CO2
laser, the lower energy Ho:YAG and Xe:Cl lasers thatwere not synchronized to the subject’s electrocardiogramwere more arrhythmogenic owing to the necessity ofdelivering multiple pulses per TMLR channel. Also, theHo:YAG and Xe:Cl lasers, which have a shorter pulseduration than the CO2 device, were more traumatic tocardiovascular tissue, possibly owing to the developmentof high peak powers. One way to minimize these adversereactions may be to synchronize activation of the Ho:YAG and Xe:Cl lasers with the subject’s electrocardio-graphic waveform. Whether the comparative effects ob-served in our animal model can be extrapolated to theclinical setting is a question that should be evaluated incontrolled, multicenter, clinical trials.
We thank Ms. Virginia Fairchild, senior medical editor andwriter, for her assistance in editing the manuscript. We alsoappreciate the technical help of Daniel Tamez in conductingsome of the experiments and Sheila Moore in reducing the data.
This work was partially supported by PLC Systems, Inc., Frank-lin, MA.
References
1. Horvath KA, Cohn LH, Cooley DA, et al. Transmyocardiallaser revascularization: results of a multicenter trial withtransmyocardial laser revascularization used as sole therapyfor end-stage coronary artery disease. J Thorac CardiovascSurg 1997;113:645–54.
2. Mirhoseini M, Muckerheide M, Cayton MM. Transventricu-lar revascularization by laser. Lasers Surg Med 1982;2:187–98.
3. Kadipasaoglu KA, Restagar S, Sartori M, et al. In vitroablation of human aorta under saline and blood with theholmium:YAG laser. Lasers Life Sci 1992;5:95–112.
4. Deckelbaum LI, Isner JN, Donaldson RF, Laliberte SM,Clarke RH, Saleem DN. Use of pulsed energy delivery tominimize tissue injury resulting from carbon dioxide laserirradiation of cardiovascular tissues. J Am Coll Cardiol1986;7:898–908.
5. Pifarre R, Jasuja ML, Lynch RD, Neville WE. Myocardialrevascularization by transmyocardial acupuncture. J ThoracCardiovasc Surg 1969;58:424–31.
6. Rastegar S, Motamadi M, Welch AJ. Moses effect producedby Ho:YAG laser. Lasers Surg Med 1990;(Suppl 2):62A.
7. White FC, Roth DM, Bloor CM. The pig as a model formyocardial ischemia and exercise. Lab Animal Sci 1986;36:351–6.
8. White FC, Bloor CM. Coronary collateral circulation in thepig: correlation of coronary collateral flow to end coronarybed size. Basic Res Cardiol 1981;767:189–96.
9. Millard RW. Induction of functional coronary collaterals inthe swine heart. Basic Res Cardiol 1991;76:468–73.
10. Bolukoglu H, Ledtke AJ, Nellis SH, Eggleston AM, Subra-manian R, Renstrom B. An animal model of chronic stenosisresulting in hibernating myocardium. Am J Physiol 1992;263:H20–9.
11. Moss AJ, Hall WJ, Cannom DS, et al. Improved survival withan implanted defibrillator in patients with coronary diseaseat high risk for ventricular arrhythmia. Multicenter Auto-matic Defibrillator Implantation Trial Investigators. N EnglJ Med 1996;335:1933–40.
12. Autschbach R, Falk V, Gonska BD, Dalichau M. The effect ofCABG surgery for the prevention of sudden cardiac death:recurrent episodes after ICD implantation and review ofliterature. Pacing Clin Electrophysiol 1994;17:552–8.
13. Frazier OH, Cooley DA, Kadipasaoglu KKA, et al. Myocar-dial revascularization with laser. Preliminary findings. Cir-culation 1995;92:58–65.
14. Cooley DA, Frazier OH, Kadipasaoglu KA, et al. Transmyo-cardial laser revascularization: clinical experience with twelve-month follow-up. J Thorac Cardiovasc Surg 1996;111:791–9.
15. Jansen ED, Frenz M, Kadipasaoglu KA, et al. Laser-tissueinteraction during transmyocardial laser revascularization.Ann Thoras Surg 1997;63:640–7.
16. Fisher PE, Khomoto T, DeRosa CM, Spotnitz HM, Smith CR,Burkhoff D. Histologic analysis of transmyocardial channels:comparison of CO2 and holmium:YAG lasers. Ann ThoracSurg 1997;64:466–72.
17. Cooley DA, Frazier OH, Kadipasaoglu KA, Pehlivanoglu S,Shannon RL, Angelini P. Transmyocardial laser revascular-ization. Anatomic evidence of long-term channel patency.Tex Heart Inst J 1994;21:220–4.
18. Almanza O, Wassmer P, Morenoc A, et al. Laser TMRimproves myocardial blood flow via collaterals. J Am CollCardiol 1977;29(Suppl A):99A.
431Ann Thorac Surg KADIPASAOLU ET AL1999;67:423–31 INTRAOPERATIVE ARRHYTHMIAS AND TISSUE DAMAGE
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from

1999;67:423-431 Ann Thorac SurgClubb, Jr, Jeff L. Conger and O.H. Frazier
Kamuran A. Kadipasaoglu, Michele Sartori, Takafumi Masai, Hasan B. Cihan, Fred J. revascularization
Intraoperative arrhythmias and tissue damage during transmyocardial laser
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/67/2/423including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/67/2/423#BIBL
This article cites 15 articles, 6 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/67/2/423#otherarticles
This article has been cited by 4 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 5, 2013 ats.ctsnetjournals.orgDownloaded from




















