
Aftertreatment following syndesmotic screw placement; - CORE
Upload
independentCategory
view
0download
0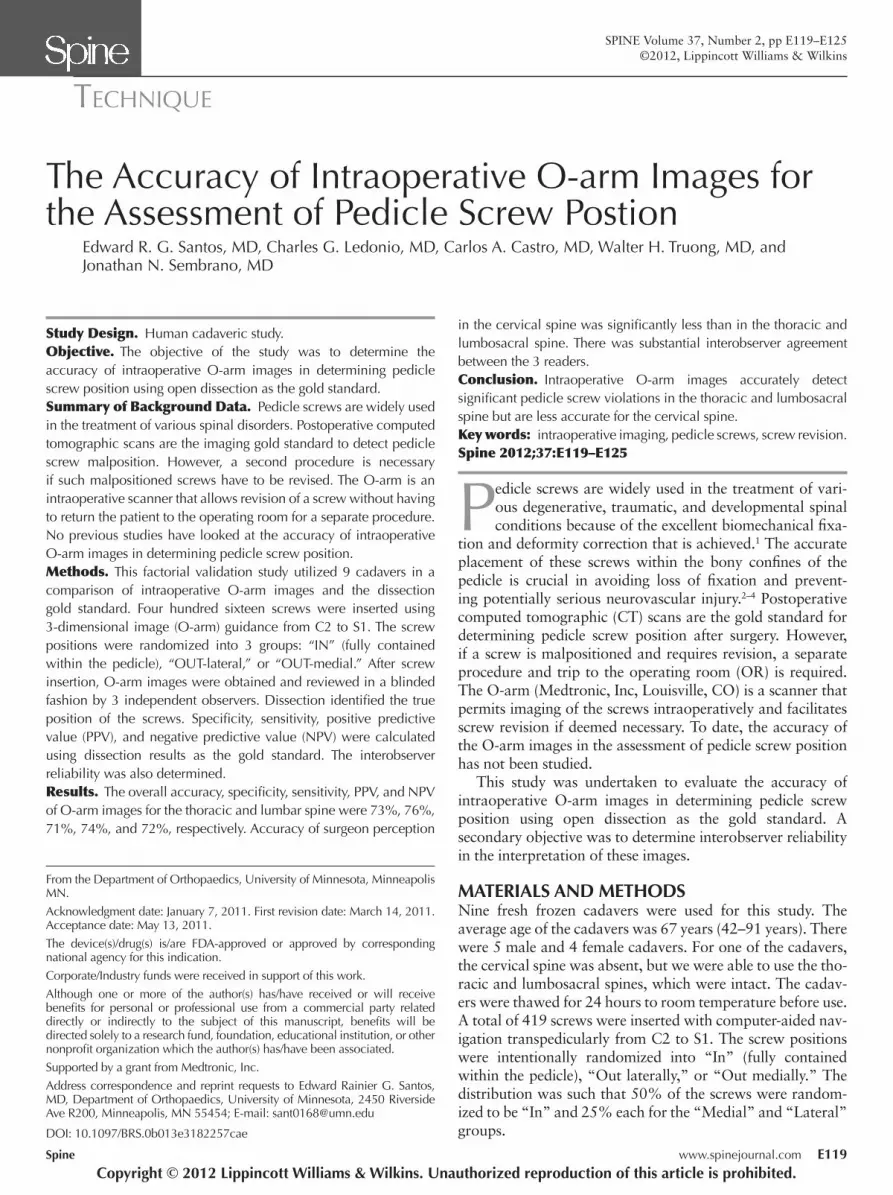
Spine www.spinejournal.com E119
TECHNIQUE
SPINE Volume 37, Number 2, pp E119–E125©2012, Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
The Accuracy of Intraoperative O-arm Images for the Assessment of Pedicle Screw Postion
Edward R. G. Santos , MD , Charles G. Ledonio , MD , Carlos A. Castro , MD , Walter H. Truong , MD , and Jonathan N. Sembrano , MD
Study Design. Human cadaveric study. Objective. The objective of the study was to determine the accuracy of intraoperative O-arm images in determining pedicle screw position using open dissection as the gold standard. Summary of Background Data. Pedicle screws are widely used in the treatment of various spinal disorders. Postoperative computed tomographic scans are the imaging gold standard to detect pedicle screw malposition. However, a second procedure is necessary if such malpositioned screws have to be revised. The O-arm is an intraoperative scanner that allows revision of a screw without having to return the patient to the operating room for a separate procedure. No previous studies have looked at the accuracy of intraoperative O-arm images in determining pedicle screw position. Methods. This factorial validation study utilized 9 cadavers in a comparison of intraoperative O-arm images and the dissection gold standard. Four hundred sixteen screws were inserted using 3-dimensional image (O-arm) guidance from C2 to S1. The screw positions were randomized into 3 groups: “IN” (fully contained within the pedicle), “OUT-lateral,” or “OUT-medial.” After screw insertion, O-arm images were obtained and reviewed in a blinded fashion by 3 independent observers. Dissection identifi ed the true position of the screws. Specifi city, sensitivity, positive predictive value (PPV), and negative predictive value (NPV) were calculated using dissection results as the gold standard. The interobserver reliability was also determined. Results. The overall accuracy, specifi city, sensitivity, PPV, and NPV of O-arm images for the thoracic and lumbar spine were 73%, 76%, 71%, 74%, and 72%, respectively. Accuracy of surgeon perception
Pedicle screws are widely used in the treatment of vari-ous degenerative, traumatic, and developmental spinal conditions because of the excellent biomechanical fi xa-
tion and deformity correction that is achieved. 1 The accurate placement of these screws within the bony confi nes of the pedicle is crucial in avoiding loss of fi xation and prevent-ing potentially serious neurovascular injury. 2 – 4 Postoperative computed tomographic (CT) scans are the gold standard for determining pedicle screw position after surgery. However, if a screw is malpositioned and requires revision, a separate procedure and trip to the operating room (OR) is required. The O-arm (Medtronic, Inc, Louisville, CO) is a scanner that permits imaging of the screws intraoperatively and facilitates screw revision if deemed necessary. To date, the accuracy of the O-arm images in the assessment of pedicle screw position has not been studied.
This study was undertaken to evaluate the accuracy of intraoperative O-arm images in determining pedicle screw position using open dissection as the gold standard. A secondary objective was to determine interobserver reliability in the interpretation of these images.
MATERIALS AND METHODS Nine fresh frozen cadavers were used for this study. The average age of the cadavers was 67 years (42–91 years). There were 5 male and 4 female cadavers. For one of the cadavers, the cervical spine was absent, but we were able to use the tho-racic and lumbosacral spines, which were intact. The cadav-ers were thawed for 24 hours to room temperature before use. A total of 419 screws were inserted with computer-aided nav-igation transpedicularly from C2 to S1. The screw positions were intentionally randomized into “In” (fully contained within the pedicle), “Out laterally,” or “Out medially.” The distribution was such that 50% of the screws were random-ized to be “In” and 25% each for the “Medial” and “Lateral” groups.
From the Department of Orthopaedics, University of Minnesota, Minneapolis MN .
Acknowledgment date: January 7, 2011. First revision date: March 14, 2011. Acceptance date: May 13, 2011.
The device(s)/drug(s) is/are FDA-approved or approved by corresponding national agency for this indication.
Corporate/Industry funds were received in support of this work.
Although one or more of the author(s) has/have received or will receive benefi ts for personal or professional use from a commercial party related directly or indirectly to the subject of this manuscript, benefi ts will be directed solely to a research fund, foundation, educational institution, or other nonprofi t organization which the author(s) has/have been associated.
Supported by a grant from Medtronic, Inc.
Address correspondence and reprint requests to Edward Rainier G. Santos, MD, Department of Orthopaedics, University of Minnesota, 2450 Riverside Ave R200, Minneapolis, MN 55454; E-mail: [email protected]
in the cervical spine was signifi cantly less than in the thoracic and lumbosacral spine. There was substantial interobserver agreement between the 3 readers. Conclusion. Intraoperative O-arm images accurately detect signifi cant pedicle screw violations in the thoracic and lumbosacral spine but are less accurate for the cervical spine. Key words: intraoperative imaging , pedicle screws , screw revision . Spine 2012 ; 37 : E119 – E125
DOI: 10.1097/BRS.0b013e3182257cae
BRS204584.indd E119BRS204584.indd E119 19/12/11 4:04 PM19/12/11 4:04 PM
E120 www.spinejournal.com January 2012
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
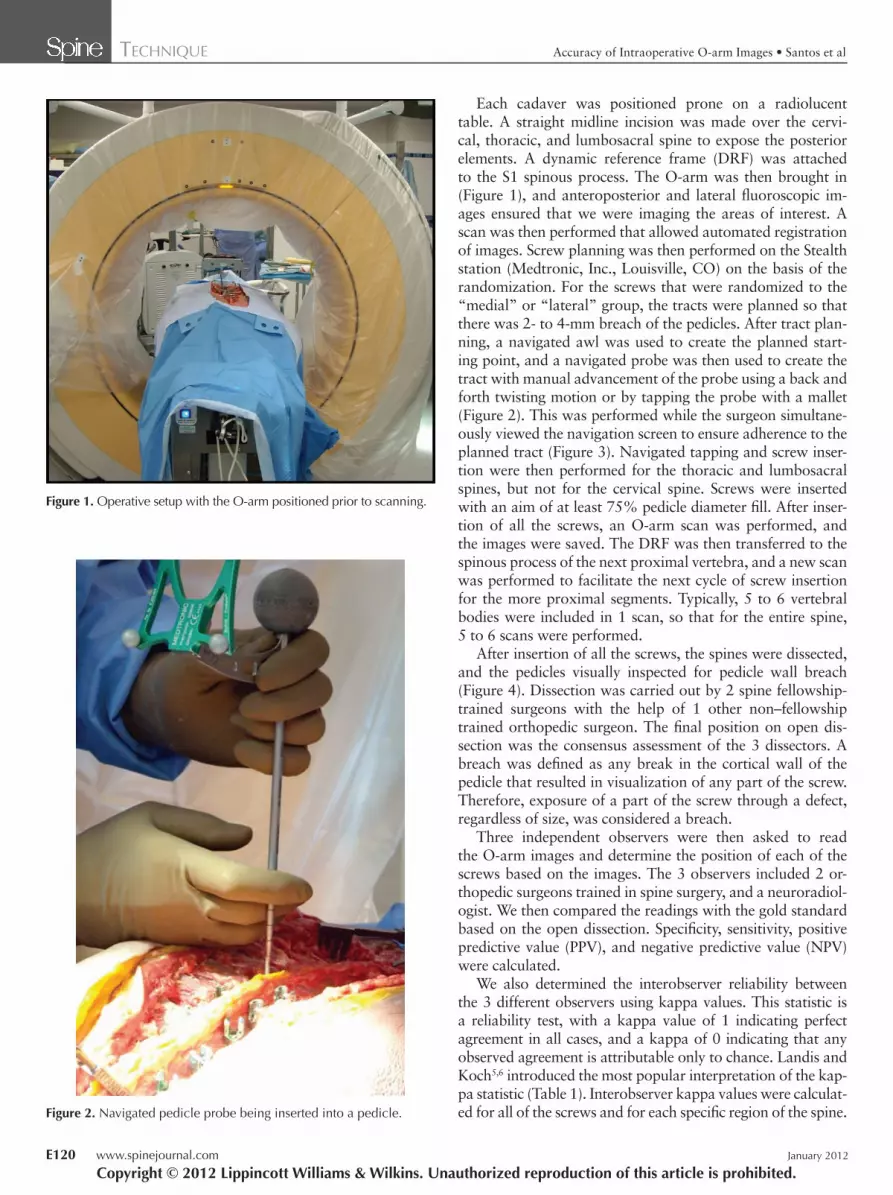
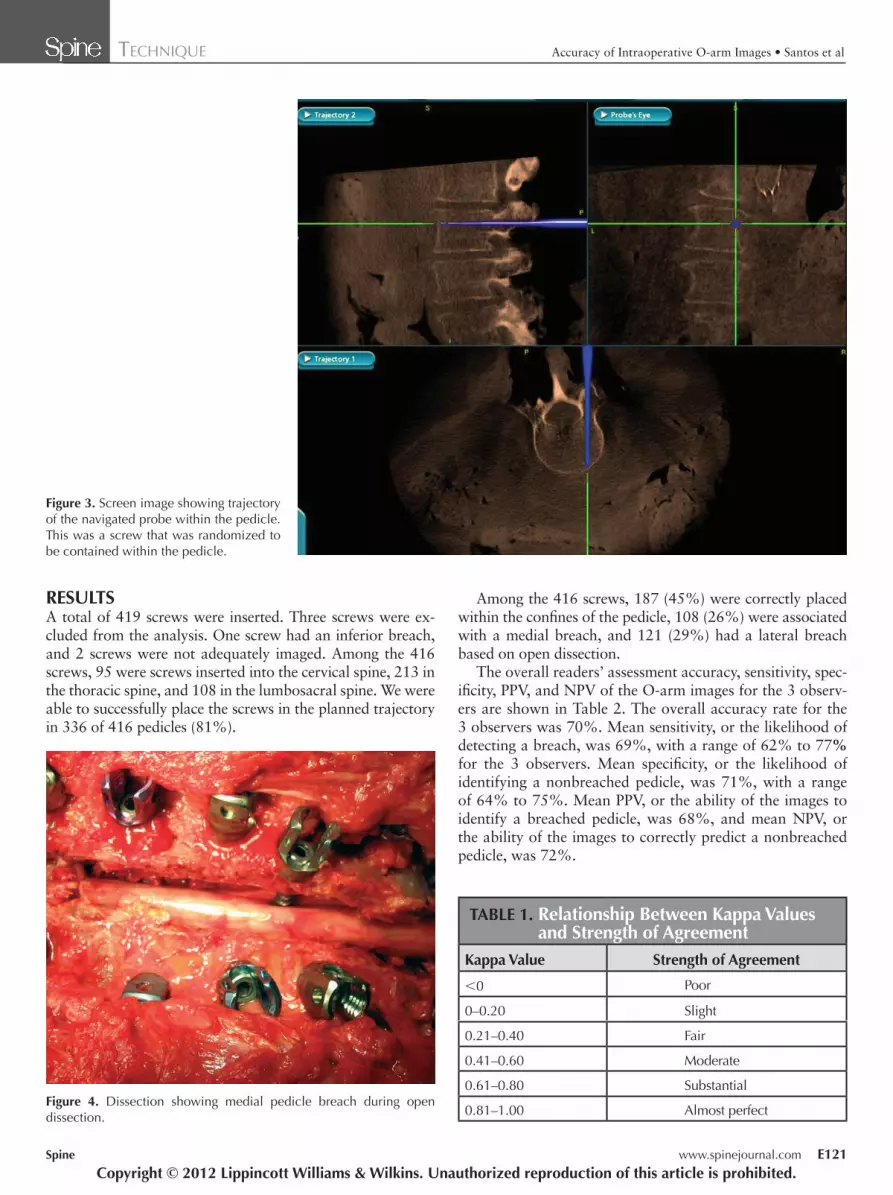
Each cadaver was positioned prone on a radiolucent table. A straight midline incision was made over the cervi-cal, thoracic, and lumbosacral spine to expose the posterior elements. A dynamic reference frame (DRF) was attached to the S1 spinous process. The O-arm was then brought in ( Figure 1 ), and anteroposterior and lateral fl uoroscopic im-ages ensured that we were imaging the areas of interest. A scan was then performed that allowed automated registration of images. Screw planning was then performed on the Stealth station (Medtronic, Inc., Louisville, CO) on the basis of the randomization. For the screws that were randomized to the “medial” or “lateral” group, the tracts were planned so that there was 2- to 4-mm breach of the pedicles. After tract plan-ning, a navigated awl was used to create the planned start-ing point, and a navigated probe was then used to create the tract with manual advancement of the probe using a back and forth twisting motion or by tapping the probe with a mallet ( Figure 2 ). This was performed while the surgeon simultane-ously viewed the navigation screen to ensure adherence to the planned tract ( Figure 3 ). Navigated tapping and screw inser-tion were then performed for the thoracic and lumbosacral spines, but not for the cervical spine. Screws were inserted with an aim of at least 75% pedicle diameter fi ll. After inser-tion of all the screws, an O-arm scan was performed, and the images were saved. The DRF was then transferred to the spinous process of the next proximal vertebra, and a new scan was performed to facilitate the next cycle of screw insertion for the more proximal segments. Typically, 5 to 6 vertebral bodies were included in 1 scan, so that for the entire spine, 5 to 6 scans were performed.
After insertion of all the screws, the spines were dissected, and the pedicles visually inspected for pedicle wall breach ( Figure 4 ). Dissection was carried out by 2 spine fellowship-trained surgeons with the help of 1 other non–fellowship trained orthopedic surgeon. The fi nal position on open dis-section was the consensus assessment of the 3 dissectors. A breach was defi ned as any break in the cortical wall of the pedicle that resulted in visualization of any part of the screw. Therefore, exposure of a part of the screw through a defect, regardless of size, was considered a breach.
Three independent observers were then asked to read the O-arm images and determine the position of each of the screws based on the images. The 3 observers included 2 or-thopedic surgeons trained in spine surgery, and a neuroradiol-ogist. We then compared the readings with the gold standard based on the open dissection. Specifi city, sensitivity, positive predictive value (PPV), and negative predictive value (NPV) were calculated.
We also determined the interobserver reliability between the 3 different observers using kappa values. This statistic is a reliability test, with a kappa value of 1 indicating perfect agreement in all cases, and a kappa of 0 indicating that any observed agreement is attributable only to chance. Landis and Koch 5 , 6 introduced the most popular interpretation of the kap-pa statistic ( Table 1 ). Interobserver kappa values were calculat-ed for all of the screws and for each specifi c region of the spine.
Figure 1. Operative setup with the O-arm positioned prior to scanning.
Figure 2. Navigated pedicle probe being inserted into a pedicle.
BRS204584.indd E120BRS204584.indd E120 19/12/11 4:05 PM19/12/11 4:05 PM
Spine www.spinejournal.com E121
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
RESULTS A total of 419 screws were inserted. Three screws were ex-cluded from the analysis. One screw had an inferior breach, and 2 screws were not adequately imaged. Among the 416 screws, 95 were screws inserted into the cervical spine, 213 in the thoracic spine, and 108 in the lumbosacral spine. We were able to successfully place the screws in the planned trajectory in 336 of 416 pedicles (81%).
Among the 416 screws, 187 (45%) were correctly placed within the confi nes of the pedicle, 108 (26%) were associated with a medial breach, and 121 (29%) had a lateral breach based on open dissection.
The overall readers’ assessment accuracy, sensitivity, spec-ifi city, PPV, and NPV of the O-arm images for the 3 observ-ers are shown in Table 2 . The overall accuracy rate for the 3 observers was 70%. Mean sensitivity, or the likelihood of detecting a breach, was 69%, with a range of 62% to 77 % for the 3 observers. Mean specifi city, or the likelihood of identifying a nonbreached pedicle, was 71%, with a range of 64% to 75%. Mean PPV, or the ability of the images to identify a breached pedicle, was 68%, and mean NPV, or the ability of the images to correctly predict a nonbreached pedicle, was 72%.
TABLE 1. Relationship Between Kappa Values and Strength of Agreement
Kappa Value Strength of Agreement
< 0 Poor
0–0.20 Slight
0.21–0.40 Fair
0.41–0.60 Moderate
0.61–0.80 Substantial
0.81–1.00 Almost perfect Figure 4. Dissection showing medial pedicle breach during open dissection.
Figure 3. Screen image showing trajectory of the navigated probe within the pedicle. This was a screw that was randomized to be contained within the pedicle.
BRS204584.indd E121BRS204584.indd E121 19/12/11 4:05 PM19/12/11 4:05 PM

E122 www.spinejournal.com January 2012
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
38 in the lumbosacral spine). There were a total of 189 false-positive readings (43 cervical, 110 thoracic, 36 lumbosacral).
There was unanimous agreement in assessment in 320 of 416 screws (77%). Overall interobserver reliability was sub-stantial among the 3 observers, with a kappa value of 0.77. This is also more reliable in the thoracic and lumbosacral
When analyzed according to the specifi c regions of the spine, the accuracy rates, sensitivity, and PPV were signifi cant-ly higher in the thoracic and lumbosacral spines when com-pared with the cervical spine ( P = 0.0001) ( Tables 3 – 6 ). There were a total of 184 false-negative readings of the total 1248 readings (57 in the cervical spine, 89 in the thoracic spine, and
TABLE 4. Interpretation of Images for the Cervical Spine According to the Different Raters Rater Accuracy Sensitivity Specifi city PPV NPV Kappa Ratio
Rater 1 70% 35% 83% 43% 77% 0.67
Rater 2 67% 24% 85% 41% 72%
Rater 3 59% 38% 69% 34% 72%
PPV indicates positive predictive value; NPV, negative predictive value.
TABLE 6. Interpretation of Images for the Lumbosacral Spine According to the Different Raters Rater Accuracy Sensitivity Specifi city PPV NPV Kappa Ratio
Rater 1 80% 86% 73% 79% 82% 0.84
Rater 2 75% 73% 75% 80% 69%
Rater 3 75% 77% 73% 80% 70%
PPV indicates positive predictive value; NPV, negative predictive value.
TABLE 5. Interpretation of Images for the Thoracic Spine According to the Different Raters Rater Accuracy Sensitivity Specifi city PPV NPV Kappa Ratio
Rater 1 75% 82% 69% 72% 80% 0.80
Rater 2 67% 66% 76% 69% 66%
Rater 3 64% 71% 57% 65% 64%
PPV indicates positive predictive value; NPV, negative predictive value.
TABLE 2. Accuracy of O-arm Images Compared With Anatomic Dissection Accuracy Sensitivity Specifi city PPV NPV
Overall 70% 69% 71% 68% 72%
Cervical 65% 32% 79% 40% 74%
Thoracic, lumbosacral 73% 76% 71% 74% 72%
PPV indicates positive predictive value; NPV, negative predictive value.
TABLE 3. Interpretation of Images (Combined Cervical, Thoracic, and Lumbosacral Spine) by the Different Readers
Rater Accuracy Sensitivity Specifi city PPV NPV Kappa Ratio
Rater 1 75% 77% 74% 71% 79% 0.77
Rater 2 69% 62% 75% 70% 69%
Rater 3 66% 68% 64% 65% 68%
PPV indicates positive predictive value; NPV, negative predictive value.
BRS204584.indd E122BRS204584.indd E122 19/12/11 4:05 PM19/12/11 4:05 PM

Spine www.spinejournal.com E123
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
radiographs alone are unreliable in determining pedicle screw position. 7 – 9
The gold standard for assessment of pedicle screw posi-tion is postoperative CT scans. Previous reports looking at the use of CT scans in detecting pedicle wall breaches show an accuracy rate of 68% to 84% as compared with open dis-section, 10 – 12 with sensitivity rates ranging from 67% to 94%. A previous study has also shown how CT scan images tend to overestimate screw malpositions 13 ; the study’s authors at-tributed this to the plastic deformation of the pedicle that can lead to an apparent perforation on CT scan images. The main disadvantage of imaging postoperatively is that it does not permit correction of a malpositioned screw within the same surgical procedure.
Our study results for the intraoperative O-arm images are consistent with previous studies using postoperative CT scans for the thoracic and lumbar spine, with an over-all accuracy rate of 73% and a sensitivity rate of 76%. The O-arm was noted to have the ability to generate images that allow accurate detection of pedicle screws in the majority of pedicles. Figure 5 shows screws that are clearly within the bony confi nes of the pedicle, which was confi rmed with direct visualization. Figure 6 , on the contrary, illustrates screws with a medial violation on 1 side and a lateral breach on the other. The advantage of the O-arm images lies in the ability of the surgeon to reposition the screw as necessary instead of having to bring the patient back to the OR for revision.
However, we did encounter instances when the accurate determination of screw position was diffi cult. There were a total of 184 false-negative readings of the 1248 readings. The occurrence of false negatives when using these intraop-erative O-arm images may be explained by several factors. First, in cadavers that had osteoporotic spines, it was diffi -cult to identify the medial and lateral cortices of the pedicles, thus making it diffi cult to identify the presence of a breach. Figure 7 shows an example of such a case. Secondly, it was also diffi cult to accurately determine the presence of a breach in smaller pedicles, where the screw artifact obscured clear visualization ( Figure 8 ). The potential clinical scenarios where this may be encountered include revision settings, where one
spines (kappa of 0.80 and 0.84, respectively) than in the cervi-cal spine (kappa of 0.67) ( Tables 3 –6).
When stratifi ed according to direction of breach, the ac-curacy was higher in detecting medial breaches than lateral breaches (74.4% vs. 62.8%). There were a total of 108 ped-icles with a medial breach based on open dissection: 34 in the cervical, 46 in the thoracic, and 28 in the lumbar spine. Of these, 76 (70.4%) had less than 2-mm breach and 32 (29.6%) had breaches greater than 2 mm. In the cervical, tho-racic, and lumbar spine, all of the medial breaches that were missed were less than 2-mm breaches and would not have required repositioning. None of the breaches more than 2 to 4 mm (which could potentially have required repositioning) were missed.
DISCUSSION Pedicle screws are commonly used for the treatment of vari-ous spinal disorders. The effectiveness and safety of pedicle screws depend on accurate placement, and screw malposi-tion can have potentially serious neurovascular complications and lead to loss of fi xation. Studies have shown that plain
Figure 5. There was a unanimous reading that the right-sided screw was in the pedicle, and this was confi rmed with open dissection.
Figure 6. Image of cervical spine where there was a unanimous read-ing of a medial breach on the left side and a lateral breach on the right side.
Figure 7. Image where the poor bony defi nition made it diffi cult to determine the position of the screws accurately.
BRS204584.indd E123BRS204584.indd E123 19/12/11 4:05 PM19/12/11 4:05 PM

E124 www.spinejournal.com January 2012
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
The data show that the O-arm images are not as reliable in the cervical spine. Although the observers were able to iden-tify breaches in the majority of cases, the sensitivity and ac-curacy rates were signifi cantly lower when compared with the thoracic and lumbosacral spines. The low accuracy rates in the cervical spine may be attributed to several factors. First, as was mentioned previously, the cervical spine pedicles are gen-erally smaller and, therefore, more affected by artifact. Also, dissection of the pedicles in the cervical spine was challenging, and in spines that were osteoporotic, inadvertent breaches may have been created despite careful dissection, leading to a falsely positive gold standard reading.
The kappa values for the 3 different observers showed that there was substantial agreement with the readings. This indi-cates that the utility of the O-arm images in assessing pedicle screw position is reproducible across different observers.
In the past 3 years, we have used intraoperative images to determine screw position in thoracic and lumbar pedicles, and we have had no reoperations for screw malposition in 166 cases and more than 2000 screws.
In conclusion, intraoperative O-arm images are accurate in determining pedicle screw position in the thoracic and lumbo-sacral spine, but not in the cervical spine. There was substan-tial interobserver agreement when these images were used to assess pedicle screw position.
would have to place larger screws to get adequate purchase, and also in the midthoracic spine and in dysplastic pedicles in certain conditions such as scoliosis, where the pedicle-to-screw diameter ratio is small. This would also partly account for the lower accuracy rates in the cervical spine, where ped-icles are generally smaller and where we had limited pedicle screw diameters. However, we also noted that all the false-negative readings in the thoracic and lumbar spines involved pedicles where the breach was less than 2 mm. There were no false-negative readings where the breach was more than 4 mm. This shows that screws that are grossly malpositioned are accurately picked up by the O-arm images, and those that were missed are minor ( < 2 mm) breaches, which are often inconsequential clinically. In a situation where a postoperative scan demonstrates a signifi cant breach which correlates with clinical symptoms, we feel that revision of the screw is the preferred option regardless of what the intraoperative scans had shown. However, on the basis of our results, we think that this scenario where a clinically relevant breach will be missed is very unlikely.
There were a total of 189 false-positive readings of the 1248 readings. We looked at the screws where a false-positive reading was made, and most relate to screw artifact that ob-scures the cortices and also can lead to an overestimation of the margins of the screw, resulting in a false-positive reading, a fi nding noted in a previous study. 11 The penalty for a false-positive reading may not be as signifi cant in the setting of in-traoperative scans, as you can simply remove the screw and repalpate the pedicle walls, vs. a return to OR if the imaging was based on postoperative CT scans.
Both medial and lateral breaches greater than 2 mm were detected accurately, with a slightly greater accuracy for detect-ing medial breaches. This may be explained by the fact that the observers may have been biased by the knowledge that medial breaches are more signifi cant than lateral breaches in terms of neural element injury or impingement, thus poten-tially lowering the threshold for calling a breach through the medial wall as opposed to the lateral wall.
➢ Key Points
Intraoperative O-arm images are accurate in deter-mining pedicle screw position in the thoracic and lumbar spine.
Intraoperative O-arm images are less accurate for assessing pedicle screw position in the cervical spine.
There is good interobserver agreement in the inter-pretation of the O-arm images.
References 1. Gaines RW Jr . The use of pedicle-screw internal fi xation for the
operative treatment of spinal disorders . J Bone Joint Surg Am 2000 ; 82 : 1458 – 76 .
2. Davne SH , Myers DL . Complications of lumbar spinal fusion with transpedicular instrumentation . Spine 1992 ; 17 : S184 – 9 .
3. Esses SI , Sachs BL , Dreyzin V . Complications associated with the technique of pedicle screw fi xation. A selected survey of ABS mem-bers . Spine 1993 ; 18 : 2231 – 9 .
4. O’Brien JR , Krushinski E , Zarro CM , et al. Esophageal injury from thoracic pedicle screw placement in a polytrauma patient: a case report and literature review . J Orthop Trauma 2006 ; 20 : 431 – 4 .
5. Landis JR , Koch GG . An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers . Biometrics 1977 ; 33 : 363 – 74 .
6. Landis JR , Koch GG . The measurement of observer agreement for categorical data . Biometrics 1977 ; 33 : 159 – 74 .
7. Weinstein JN , Spratt KF , Spengler D , et al. Spinal pedicle fi xation: reliability and validity of roentgenogram-based assessment and sur-gical factors on successful screw placement . Spine 1988 ; 13 : 1012 – 8 .
8. Ferrick MR , Kowalski JM , Simmons ED Jr . Reliability of roentgen-ogram evaluation of pedicle screw position . Spine 1997 ; 22 : 1249 – 52 ; discussion 1253.
Figure 8. Image showing good bony defi nition, but where the artifact created by titanium screw made accurate assessment of screw position diffi cult.
BRS204584.indd E124BRS204584.indd E124 19/12/11 4:05 PM19/12/11 4:05 PM

Spine www.spinejournal.com E125
TECHNIQUE Accuracy of Intraoperative O-arm Images • Santos et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
tomography: a proposed systematic approach to improve accuracy of interpretation . Spine 2004 ; 29 : 767 – 73 .
12. Yoo JU , Ghanayem A , Petersilge C , et al. Accuracy of using com-puted tomography to identify pedicle screw placement in cadaveric human lumbar spine . Spine 1997 ; 22 : 2668 – 71 .
13. Rao G , Brodke DS , Rondina M , et al. Comparison of computer-ized tomography and direct visualization in thoracic pedicle screw placement . J Neurosurg 2002 ; 97 : 223 – 6 .
9. Laine T , Makitalo K , Schlenzka D , et al. Accuracy of pedicle screw insertion: a prospective CT study in 30 low back patients . Eur Spine J 1997 ; 6 : 402 – 5 .
10. Brooks D , Eskander M , Balsis S , et al. Imaging assessment of lum-bar pedicle screw placement: sensitivity and specifi city of plain ra-diographs and computer axial tomography . Spine 2007 ; 32 : 1450 – 3 .
11. Learch TJ , Massie JB , Pathria MN , et al. Assessment of pedicle screw placement utilizing conventional radiography and computed
BRS204584.indd E125BRS204584.indd E125 19/12/11 4:05 PM19/12/11 4:05 PM
Copyright © 2022 FDOKUMEN




















