
MRI of the Hip for the evaluation of femoroacetabular impingement; past, present, and future
15
CME Article MRI of the Hip for the Evaluation of Femoroacetabular Impingement; Past, Present, and Future Geoffrey M. Riley, MD, 1 Emily J. McWalter, PhD, 1 Kathryn J. Stevens, MD, 1 Marc R. Safran, MD, 2 Riccardo Lattanzi, PhD, 3 and Garry E. Gold, MD 1 * This article is accredited as a journal-based CME activity. If you wish to receive credit for this activity, please refer to the website: www.wileyhealthlearning.com/jmri ACCREDITATION AND DESIGNATION STATEMENT Blackwell Futura Media Services designates this journal based CME activity for a maximum of 1 AMA PRA Category 1 Credit TM . Physicians should only claim credit commensurate with the extent of their participation in the activity. Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to pro- vide continuing medical education for physicians. EDUCATIONAL OBJECTIVES Upon completion of this educational activity, participants will have an understanding of the evolution of the diagnosis of FAI, be better able to interpret MRI examinations of the hip with regard to FAI, and have a better understanding of the state of advanced MRI techniques for the evaluation of FAI. ACTIVITY DISCLOSURES No commercial support has been accepted related to the development or publication of this activity. Faculty Disclosures: Editor-in-Chief: Mark E. Schweitzer, MD, discloses DSMB con- sulting fees from Paradigm Spine and HistoGeneX, and con- sulting fees from MMI. CME Editor: Scott B. Reeder, MD, PhD discloses research sup- port to his institution from GE Healthcare and Bracco Diag- nostics; and personal stock in Novelos, Inc, and NeuWave, Inc. CME Committee: Shreyas Vasanawala, MD, PhD, discloses research collabora- tion with GE Healthcare and co-founder equity in Morpheus Medical. Frank Korosec, PhD, discloses research support to his institu- tion from GE Healthcare. Scott K. Nagle, MD, PhD, discloses personal stock in GE Healthcare. Mustafa R. Bashir, MD, discloses research support and con- sulting fees from Siemens Healthcare and Bayer Healthcare. Tim Leiner, MD, PhD, discloses speaker fees and grant funding from Phillips, and grant funding from Bracco and Bayer. Bonnie Joe, MD, PhD, has no relevant financial relationships to disclose. Authors: Geoffrey M. Riley, MD, Kathryn J. Stevens, MD, and Riccardo Lattanzi, PhD, have no relevant financial relation- ships to disclose. Marc R. Safran, MD discloses consulting fees from ConMed Linvatec, Cool Systems, Biomimedica, and Eleven Blade Solu- tions; and publishing royalties from Stryker, DJO, Elsevier, and Lippincott. Garry E. Gold, MD discloses research support from GE Health- care and consulting fees from Boston Scientific. Emily J. McWalter, PhD discloses research support from GE Healthcare. This manuscript underwent peer review in line with the stand- ards of editorial integrity and publication ethics maintained by Journal of Magnetic Resonance Imaging. The peer reviewers have no relevant financial relationships. The peer review pro- cess for Journal of Magnetic Resonance Imaging is double- blinded. As such, the identities of the reviewers are not dis- closed in line with the standard accepted practices of medical journal peer review. Conflicts of interest have been identified and resolved in accordance with Blackwell Futura Media Services’ Policy on Activity Disclosure and Conflict of Interest. INSTRUCTIONS ON RECEIVING CREDIT For information on applicability and acceptance of CME credit for this activity, please consult your professional licensing board. This activity is designed to be completed within an hour; physi- cians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, partic- ipants must complete the activity during the valid credit period. Follow these steps to earn credit: • Log on to www.wileyhealthlearning.com • Read the target audience, educational objectives, and activity disclosures. • Read the article in print or online format. • Reflect on the article. • Access the CME Exam, and choose the best answer to each question. • Complete the required evaluation component of the activity. This activity will be available for CME credit for twelve months following its publication date. At that time, it will be reviewed and potentially updated and extended for an additional period. JOURNAL OF MAGNETIC RESONANCE IMAGING 00:00–00 (2014) CME V C 2014 Wiley Periodicals, Inc. 1
Transcript of MRI of the Hip for the evaluation of femoroacetabular impingement; past, present, and future

CME Article
MRI of the Hip for the Evaluation ofFemoroacetabular Impingement; Past,Present, and Future
Geoffrey M. Riley, MD,1 Emily J. McWalter, PhD,1 Kathryn J. Stevens, MD,1
Marc R. Safran, MD,2 Riccardo Lattanzi, PhD,3 and Garry E. Gold, MD1*
This article is accredited as a journal-based CME activity. Ifyou wish to receive credit for this activity, please refer to thewebsite: www.wileyhealthlearning.com/jmri
ACCREDITATION AND DESIGNATION STATEMENT
Blackwell Futura Media Services designates this journalbased CME activity for a maximum of 1 AMA PRA Category 1
CreditTM. Physicians should only claim credit commensuratewith the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by theAccreditation Council for Continuing Medical Education to pro-vide continuing medical education for physicians.
EDUCATIONAL OBJECTIVES
Upon completion of this educational activity, participants willhave an understanding of the evolution of the diagnosis ofFAI, be better able to interpret MRI examinations of the hipwith regard to FAI, and have a better understanding of thestate of advanced MRI techniques for the evaluation of FAI.
ACTIVITY DISCLOSURES
No commercial support has been accepted related to thedevelopment or publication of this activity.
Faculty Disclosures:
Editor-in-Chief: Mark E. Schweitzer, MD, discloses DSMB con-sulting fees from Paradigm Spine and HistoGeneX, and con-sulting fees from MMI.
CME Editor: Scott B. Reeder, MD, PhD discloses research sup-port to his institution from GE Healthcare and Bracco Diag-nostics; and personal stock in Novelos, Inc, and NeuWave, Inc.
CME Committee:Shreyas Vasanawala, MD, PhD, discloses research collabora-tion with GE Healthcare and co-founder equity in MorpheusMedical.
Frank Korosec, PhD, discloses research support to his institu-tion from GE Healthcare.
Scott K. Nagle, MD, PhD, discloses personal stock in GEHealthcare.
Mustafa R. Bashir, MD, discloses research support and con-sulting fees from Siemens Healthcare and Bayer Healthcare.
Tim Leiner, MD, PhD, discloses speaker fees and grant fundingfrom Phillips, and grant funding from Bracco and Bayer.
Bonnie Joe, MD, PhD, has no relevant financial relationships todisclose.
Authors: Geoffrey M. Riley, MD, Kathryn J. Stevens, MD, andRiccardo Lattanzi, PhD, have no relevant financial relation-ships to disclose.
Marc R. Safran, MD discloses consulting fees from ConMedLinvatec, Cool Systems, Biomimedica, and Eleven Blade Solu-tions; and publishing royalties from Stryker, DJO, Elsevier,and Lippincott.
Garry E. Gold, MD discloses research support from GE Health-care and consulting fees from Boston Scientific.
Emily J. McWalter, PhD discloses research support from GEHealthcare.
This manuscript underwent peer review in line with the stand-ards of editorial integrity and publication ethics maintained byJournal of Magnetic Resonance Imaging. The peer reviewershave no relevant financial relationships. The peer review pro-cess for Journal of Magnetic Resonance Imaging is double-blinded. As such, the identities of the reviewers are not dis-closed in line with the standard accepted practices of medicaljournal peer review.
Conflicts of interest have been identified and resolved inaccordance with Blackwell Futura Media Services’ Policy onActivity Disclosure and Conflict of Interest.
INSTRUCTIONS ON RECEIVING CREDIT
For information on applicability and acceptance of CME creditfor this activity, please consult your professional licensing board.
This activity is designed to be completed within an hour; physi-cians should claim only those credits that reflect the timeactually spent in the activity. To successfully earn credit, partic-ipants must complete the activity during the valid credit period.
Follow these steps to earn credit:
• Log on to www.wileyhealthlearning.com
• Read the target audience, educational objectives, and
activity disclosures.
• Read the article in print or online format.
• Reflect on the article.
• Access the CME Exam, and choose the best answer to
each question.
• Complete the required evaluation component of the
activity.
This activity will be available for CME credit for twelve monthsfollowing its publication date. At that time, it will be reviewedand potentially updated and extended for an additional period.
JOURNAL OF MAGNETIC RESONANCE IMAGING 00:00–00 (2014)
CME
VC 2014 Wiley Periodicals, Inc. 1

The concept of femoroacetabular impingement (FAI) has,in a relatively short time, come to the forefront of orthope-dic imaging. In just a few short years MRI findings thatwere in the past ascribed to degenerative change, normalvariation, or other pathologies must now be describedand included in radiology reports, as they have beenshown, or are suspected to be related to, FAI. Crucialquestions have come up in this time, including: what isthe relationship of bony morphology to subsequent carti-lage and labral damage, and most importantly, how isthis morphology related to the development of osteoarthri-tis? In this review, we attempt to place a historical per-spective on the controversy, provide guidelines forinterpretation of MRI examinations of patients with sus-pected FAI, and offer a glimpse into the future of MRI ofthis complex condition.
Key Words: magnetic resonance imaging; femoroacetabu-lar impingement; acetabular labrum; hip cartilage; carti-lage mapping
J. Magn. Reson. Imaging 2014;00:000–000.VC 2014 Wiley Periodicals, Inc.
FEMOROACETABULAR IMPINGEMENT (FAI) hasbecome a controversial topic in the radiology andorthopedic literature in a relatively short time. In thisarticle, we review the history of the concept thatabnormal femoral morphology results in the clinicalentity known as FAI which can in turn lead to primaryosteoarthritis (OA) of the hip. Following a discussionof the historical perspective, we discuss the patho-physiology and the magnetic resonance imaging (MRI)findings of FAI. Finally we review the latest literatureon advanced MRI techniques for the evaluation of FAI.
HISTORICAL PERSPECTIVE
Relationship of FAI to Osteoarthritis
In a meta-analysis of 970 cases Ng et al concludedthat surgical treatment for FAI reliably improvessymptoms in patients without OA but that additionalstudies are needed to confirm if surgery can delay OA(1). Although the underlying cause of OA of the hip isknown in many patients, there are numerous cases ofunexplained hip OA. In a recent review, Rubin pointsout that radiologists frequently come across anatomicmorphology thought to be associated with FAI (2). Yet
if FAI truly leads to OA, as many authors contend,then one would expect a much higher incidence of OAamongst the general population. Rubin also pointsout that imaging findings are not sufficient for thediagnosis of FAI without the appropriate clinical signsand symptoms (2,3). MRI, with its sensitivity to softtissue and bony anatomy, may be able to answer thequestion of whether FAI anatomy leads to OA.
Early Evidence that Hip OA Occurs Secondary toUnderlying Morphological Alterations of the Hip.
If the current rationale for treating abnormal mor-phology that results in FAI is to prevent OA, then itmust be established that the abnormal morphologydoes indeed result in OA if untreated. To understandthe evidence favoring this concept, it is beneficial tobriefly review the historical literature around thisconcept. In 1933, Elmslie described a coxa planadeformity of the femoral head, now known asLegg-Calve-Perthes disease, leading to OA. He con-cluded that “many patients who develop osteoarthritisat a comparatively early age—for example from 40 to50—will be found to have a pre-existing deformity ofthe joint” (4). This was the beginning of many investi-gations to determine the cause of hip OA that con-tinue to this day.
Murray, in 1965, introduced the concept that sec-ondary OA not only occurs with severe developmentalor acquired deformities, but also in cases of moresubtle morphologic abnormalities of the hip. Hedescribed OA as secondary to the “tilt deformity” com-prising abnormal varus tilting of the femoral headwith respect to the neck. In this study, OA wasdescribed as secondary if its development was relatedto a pre-existing symptomatic abnormality (5). Usingprior reports he determined that more than half (65%)of the OA cases could be considered secondary usingthis criterion, and the remainder was considered idio-pathic or primary. The purpose of Murray’s study wasto suggest an explanation for the development of theseprimary OA cases. He posited that a more criticalreview of radiographs reveals minimal anatomic varia-tions, that can be so subtle that they can be inter-preted as normal, but that are sufficient to cause OAin the long term. Stulberg et al, in 1975, introducedthe term “pistol grip deformity” to describe a findingresembling the “tilt deformity” described above (6),including a flattened lateral femoral neck with loss ofheight and widening of the femoral neck (Fig. 1). Withthe advent of MRI, attention turned to the soft tissuefindings related to FAI, including labral tears and car-tilage damage. This has in turn lead to the develop-ment of new promising quantitative MRI techniquesfor improved detection of early cartilage damage.These techniques are discussed at the end of thisarticle.
Early Studies of FAI with MRI
The predominant theory of the origin of morphologicalterations of the femoral neck, with loss of femoral
1Department of Radiology, Stanford University, Stanford, California,USA.2Department of Orthopaedic Surgery, Stanford University, RedwoodCity, California, USA.3Department of Radiology, The Bernard and Irene Schwartz Centerfor Biomedical Imaging, New York University School of Medicine, NewYork, New York, USA.
Contract grant sponsor: NIH; Contract grant numbers: EB002524,AR062068, CA159992, R01 EB002568, R01 EB000447, EB002524,AR062068, CA159992.
*Address reprint requests to: G.E.G., Stanford University, Depart-ment of Radiology, Lucas Center P-271, Stanford, CA 94305.E-mail: [email protected]
Received April 14, 2014; Accepted July 21, 2014.
DOI 10.1002/jmri.24725View this article online at wileyonlinelibrary.com.
2 Riley et al.
head–neck offset, was that it resulted from a mild orsubclinical slipped capital epiphysis. While FAI can besecondary to pediatric hip disease or trauma, mostcases are considered to be “primary FAI.” To thispoint, Siebenrock et al in 2004 attempted to clarifythe association of a superior and laterally bowed,extended femoral capital physis with a nonsphericalfemoral head and decreased offset anterosuperiorly.Using MRI examinations, they noted that none of thepatients they studied had a posterior tilt of the epiph-ysis, as would be expected with a prior slipped capitalfemoral epiphysis. They concluded that these“findings suggest a growth abnormality of the capitalphysis as one probable underlying cause for a non-spherical femoral head” (7). This article also pointedout the association between a laterally extended capi-tal physis on AP radiographs and a decreased femoralhead–neck offset anterosuperiorly. Because the femo-ral head and greater trochanter share a common
physis until age 4, delayed separation due to traumaor infection could potentially result in the head neckdeformity.
Role of Labral Pathology in Development of FAI
With the advent of advanced imaging and arthro-scopy, attention turned to the role of the injured lab-rum in hip pathology and early literature focused ontraumatic labral tears (8). In 2001 McCarthy et al setout to establish that labral disruption, includingdegeneration and tears, contributes to early OA. Theyused arthroscopic data to show an associationbetween the progression of labral pathology and theprogression of articular cartilage lesions, and demon-strated that “the frequency and severity of acetabularcartilage degeneration was dramatically higher inpatients with labral pathology” (9). They also pointedout that the cartilage damage was directly adjacent to
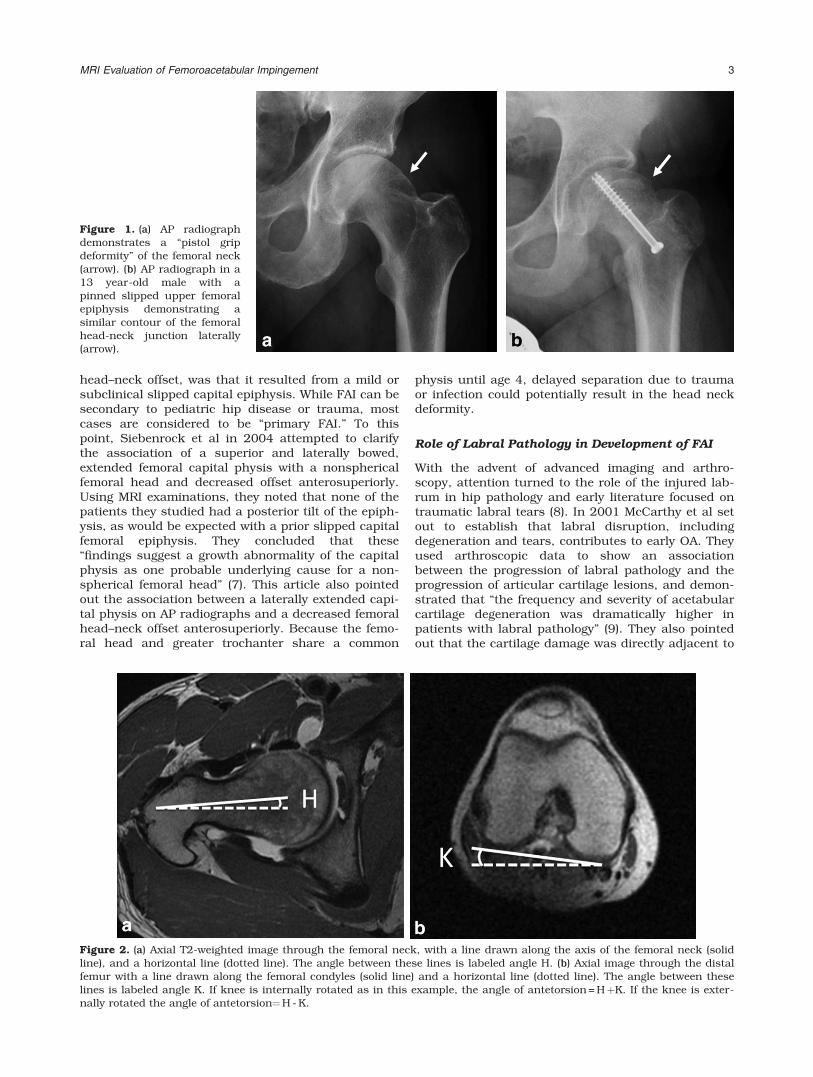
Figure 2. (a) Axial T2-weighted image through the femoral neck, with a line drawn along the axis of the femoral neck (solidline), and a horizontal line (dotted line). The angle between these lines is labeled angle H. (b) Axial image through the distalfemur with a line drawn along the femoral condyles (solid line) and a horizontal line (dotted line). The angle between theselines is labeled angle K. If knee is internally rotated as in this example, the angle of antetorsion = HþK. If the knee is exter-nally rotated the angle of antetorsion¼H - K.
Figure 1. (a) AP radiographdemonstrates a “pistol gripdeformity” of the femoral neck(arrow). (b) AP radiograph in a13 year-old male with apinned slipped upper femoralepiphysis demonstrating asimilar contour of the femoralhead-neck junction laterally(arrow).
MRI Evaluation of Femoroacetabular Impingement 3

the labral lesions, strengthening the case for a trueassociation rather than a coincidental association.They concluded that labral injury, through traction orimpingement at the extremes of motion, leads to aseries of progressive events including labral fraying,tearing, cartilage delamination, and finally global lab-ral and cartilage degeneration.
PATHOPHYSIOLOGY OF FEMORACETABULARIMPINGEMENT
Two Patterns of FAI
While FAI has been generally divided into two distincttypes, based on the whether the inciting causeinvolves the acetabular side (pincer-type) or the femo-ral side (cam-type), this breakdown may be artificialas many cases reportedly involve both (10). However,it is useful to consider the two patterns separately tobetter understand the pathophysiology, as well as theimaging findings of cam and pincer-type FAI.
In pincer-type FAI, acetabular morphological abnor-malities result in excessive bony coverage of the femo-ral head, and can be generalized or focal. In trueacetabular retroversion, the anterior wall of the acetab-ulum is lateral to the posterior wall, resulting in ante-rior bony over-coverage of the femoral head. In cranialacetabular retroversion the anterior acetabular wall islateral to the posterior wall superiorly causing focalbony over-coverage of the femoral head. General bonyover-coverage of the femoral head is less common (10)and occurs with coxa profunda and protrusio aceta-buli. While both of these can result in a more general-ized pattern of disruption, most of the lesions arelocated along the anterosuperior acetabular rim,because flexion is the principle movement of the hip(10). Coxa profunda has been considered a risk factorin the development of pincer-type FAI, but recently thishas been called into question by Nepple et al (11) whonoted that coxa profunda is commonly seen in asymp-tomatic individuals and in those with other hip pathol-ogy. This also has implications for the assertion thatmost cases of FAI are of mixed cam- and pincer-types,because if one uses coxa profunda as an indication ofpincer type FAI, the number of cases demonstratingmixed morphology will be falsely inflated. This studyalso underlines the contention that FAI morphologydoes not necessarily equate to symptomatic FAI.
The focus of damage in pincer FAI is the acetabularlabrum, which gets compressed between the femoralneck and acetabulum resulting in labral disruption.With repetitive compression, the labrum may ossify,which compounds the problem.
Another typical feature of pincer-type FAI occurs asa consequence of the constrained morphology of thehip. With hip impingement, further hip flexion posteri-orly subluxes the femoral head resulting in pressureon the posteroinferior acetabulum. This has beentermed a countrecoup lesion and can affect both thefemoral head cartilage and acetabular cartilage (10).
Femoral antetorsion is defined as the angle betweenthe axis of the femoral neck and a line drawn alongthe femoral condyles (Fig. 2). A reduced femoral ante-
torsion may lead to increased impaction of the femuron the anterior acetabular rim during internal rota-tion. With increased femoral antetorsion there ispotential for impaction of the femur on the posterioracetabulum with external rotation. The method ofmeasurement on MRI is elucidated by Sutter et al,who found that femoral antetorsion was significantlyincreased in pincer-type FAI compared with cam-type(12). They postulated that this could result in directmechanical impact of the femoral head–neck junctionagainst the posterior and posteroinferior aspect of thehip joint during external rotation, possible accountingfor characteristic posteroinferior cartilage defects.They concluded by suggesting that rapid axial imagesperformed through the femoral neck and femoral con-dyles to calculate femoral antetorsion, be routinelyincluded in MRI examinations for FAI.
On the femoral side, cam-type FAI is related toa nonspherical femoral head, referred to as“asphericity.” Most cases involve an osseous bumpalong the femoral head–neck junction anterosuper-iorly or laterally resulting in the so-called “pistol grip”deformity (Fig. 1). The osseous bump, or cam defor-mity, results in a loss of the normal femoral headneck junction concavity or “offset.” The lack of offsethas also been referred to as “absent waisting” of thefemoral head neck junction (10). The osseous bumpabuts the anterosuperior acetabulum during flexionand results in compression of the chondrolabral junc-tion. Adding internal rotation to flexion compoundsthe problem. This can result in detachment of the lab-rum from the adjacent articular cartilage, termedchondrolabral separation, although the labrum itselfmay remain attached to the acetabular rim.
On the other hand, several investigations have dem-onstrated that not all hips with abnormal morphologysuffer from FAI. Gosvig et al identified a cam defor-mity in 17% of males and found that there was no sig-nificant correlation between hip or groin pain andcam malformations in either gender (13). Similarly,Laborie et al reported that radiographic findings ofFAI were “quite common” in a population of healthyyoung adults, especially males (3). They reported camfeatures in 35% of males and 10% of females and pin-cer features in 34% of males and 17% of females.Studies in Japan showed that impingement of thefemoral head and acetabulum in certain positionsdoes not correlate with symptomatic FAI. These stud-ies also point out the rarity of primary OA in Japan, acountry where postures that would contribute to thisimpingement are common in everyday living (14,15).
CURRENT ROLE OF IMAGING OF FAI
While MRI has the dominant role in the evaluation ofhip abnormalities other modalities do still play animportant role.
Radiography
The work up of FAI should begin with radiographs,which are useful to assess for OA in the hip, including
4 Riley et al.
joint space narrowing and marginal osteophytosis,and to exclude other hip pathology such as osteonec-rosis. Radiographs should include a low anteroposte-rior (AP) view of the pelvis and a cross table lateralview of the affected hip. The radiograph is the initialassessment of bony morphology that predisposes toFAI (16–18). The low AP radiograph of the pelvisallows comparison of the affected hip to the asymp-tomatic side for detection of subtle bony morphologi-cal changes predisposing to FAI, and affordsvisualization of other bony structures that can resultin hip symptoms including the pubic symphysis, sac-rum, sacroiliac joints, ilium, and ischium (19,20).
Arthrography, Ultrasound, and ComputedTomography
Conventional arthrography has been superseded bymagnetic resonance arthrography (MRA). However,the intra-articular injection of local anesthetic is help-ful to confirm that the hip joint is the source of pain.Concurrent corticosteroid administration can be bene-ficial in cases of arthritis and may be used to delaysurgery in the setting of symptomatic labral tears.
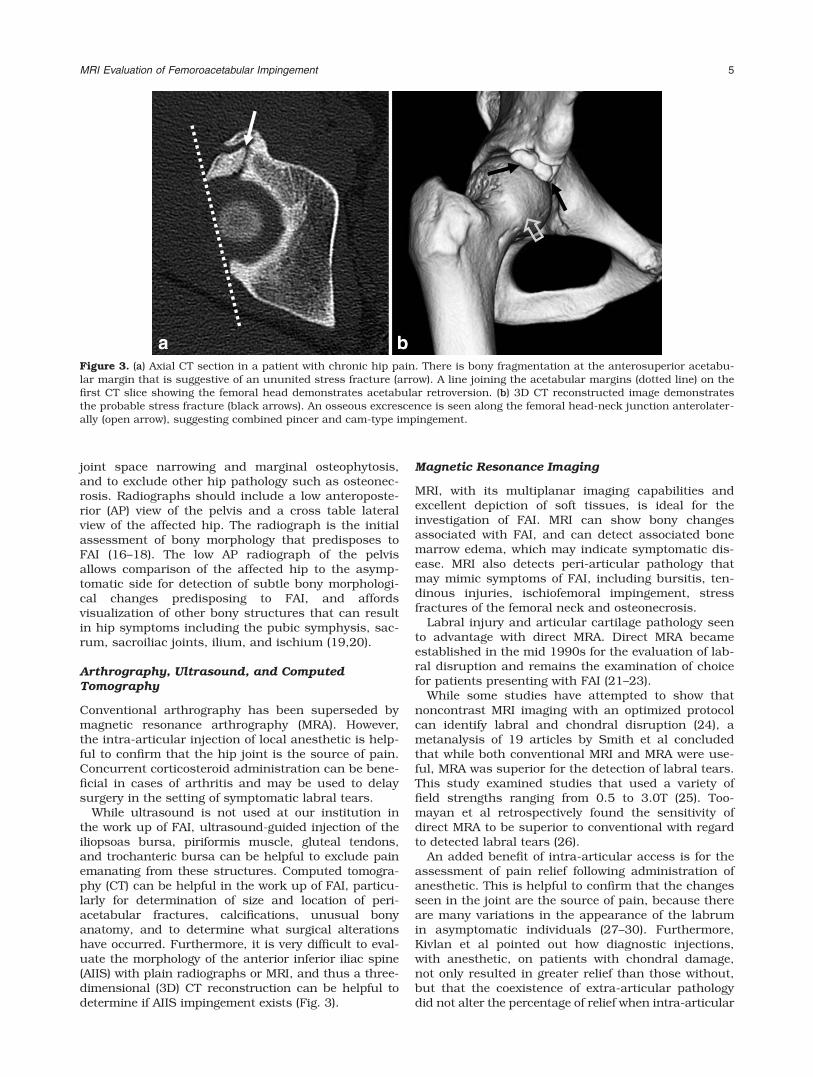
While ultrasound is not used at our institution inthe work up of FAI, ultrasound-guided injection of theiliopsoas bursa, piriformis muscle, gluteal tendons,and trochanteric bursa can be helpful to exclude painemanating from these structures. Computed tomogra-phy (CT) can be helpful in the work up of FAI, particu-larly for determination of size and location of peri-acetabular fractures, calcifications, unusual bonyanatomy, and to determine what surgical alterationshave occurred. Furthermore, it is very difficult to eval-uate the morphology of the anterior inferior iliac spine(AIIS) with plain radiographs or MRI, and thus a three-dimensional (3D) CT reconstruction can be helpful todetermine if AIIS impingement exists (Fig. 3).
Magnetic Resonance Imaging
MRI, with its multiplanar imaging capabilities andexcellent depiction of soft tissues, is ideal for theinvestigation of FAI. MRI can show bony changesassociated with FAI, and can detect associated bonemarrow edema, which may indicate symptomatic dis-ease. MRI also detects peri-articular pathology thatmay mimic symptoms of FAI, including bursitis, ten-dinous injuries, ischiofemoral impingement, stressfractures of the femoral neck and osteonecrosis.
Labral injury and articular cartilage pathology seento advantage with direct MRA. Direct MRA becameestablished in the mid 1990s for the evaluation of lab-ral disruption and remains the examination of choicefor patients presenting with FAI (21–23).
While some studies have attempted to show thatnoncontrast MRI imaging with an optimized protocolcan identify labral and chondral disruption (24), ametanalysis of 19 articles by Smith et al concludedthat while both conventional MRI and MRA were use-ful, MRA was superior for the detection of labral tears.This study examined studies that used a variety offield strengths ranging from 0.5 to 3.0T (25). Too-mayan et al retrospectively found the sensitivity ofdirect MRA to be superior to conventional with regardto detected labral tears (26).
An added benefit of intra-articular access is for theassessment of pain relief following administration ofanesthetic. This is helpful to confirm that the changesseen in the joint are the source of pain, because thereare many variations in the appearance of the labrumin asymptomatic individuals (27–30). Furthermore,Kivlan et al pointed out how diagnostic injections,with anesthetic, on patients with chondral damage,not only resulted in greater relief than those without,but that the coexistence of extra-articular pathologydid not alter the percentage of relief when intra-articular
Figure 3. (a) Axial CT section in a patient with chronic hip pain. There is bony fragmentation at the anterosuperior acetabu-lar margin that is suggestive of an ununited stress fracture (arrow). A line joining the acetabular margins (dotted line) on thefirst CT slice showing the femoral head demonstrates acetabular retroversion. (b) 3D CT reconstructed image demonstratesthe probable stress fracture (black arrows). An osseous excrescence is seen along the femoral head-neck junction anterolater-ally (open arrow), suggesting combined pincer and cam-type impingement.
MRI Evaluation of Femoroacetabular Impingement 5
pathology was present (30). A concern about the use ofdirect arthrography is pain related to the procedure. Gia-coni et al prospectively surveyed patients between 3 and7 days following a joint injections (including but not lim-ited to hips) and found that more than half of patientsexperienced pain following the procedure, some of whichwas relieved by anti-inflammatory drugs and ice. Thissuggests that the pain may be an inflammatory responseto the injection (31,32).
Indirect arthrography has also been shown to beuseful for evaluation of labral tears, however, it is notas useful to detect cartilage injury (33) and we do notcurrently perform this study at our institution.
We perform direct MR arthrography on a 3 Tesla (T)system using the following protocol:
� In a 20 mL syringe, the following solution is mixed:
� 5 mL Lidocaine 1%,� 5 mL Ropivacaine 0.5%� 1 mL Omnipaque 240� 0.1 mL Gd-DTPA (Magnevist)� 5 to 10 mL is injected into the hip joint.
� Dedicated phased-array surface coil, unilateralsmall (16-20 cm) field of view
� Axial oblique fat suppressed T1 weighted sequenceparallel to the long axis of the femoral neck
� Axial T1 weighted sequence� Axial fat suppressed proton density weighted
sequence� Coronal fat suppressed T1 weighted sequence� Coronal fat suppressed T2 weighted sequence� Sagittal fat suppressed T1 weighted sequence� Sagittal fat suppressed T2 weighted sequence� Radial proton density weighted sequences perpen-
dicular to the long axis of the femoral neck� Optional: T1 localizer of the knee and hip to obtain
femoral antetorsion
MRI Findings of FAI
When evaluating an MRI study for FAI, it is importantto use an organized search pattern. The followingitems should be routinely evaluated (34,35).
Bony Morphology
Assessment of bony morphology includes a detailedanalysis of the acetabulum and femoral head–neckjunction. Acetabular retroversion, while more easilydetermined radiographically, can also be detected onaxial MRI images. The most cranial image thatincludes the femoral head is used to determine if theanterior rim of the acetabulum is located medial(anteversion) or lateral (retroversion) to the posterioracetabular rim.
The acetabular depth is also well depicted radio-graphically but can be determined using the axialoblique MRI images through the medial femoral neck.A line is drawn between the anterior and posterioracetabular rims and the distance between the lineand the center of the femoral head determines acetab-ular depth (36).
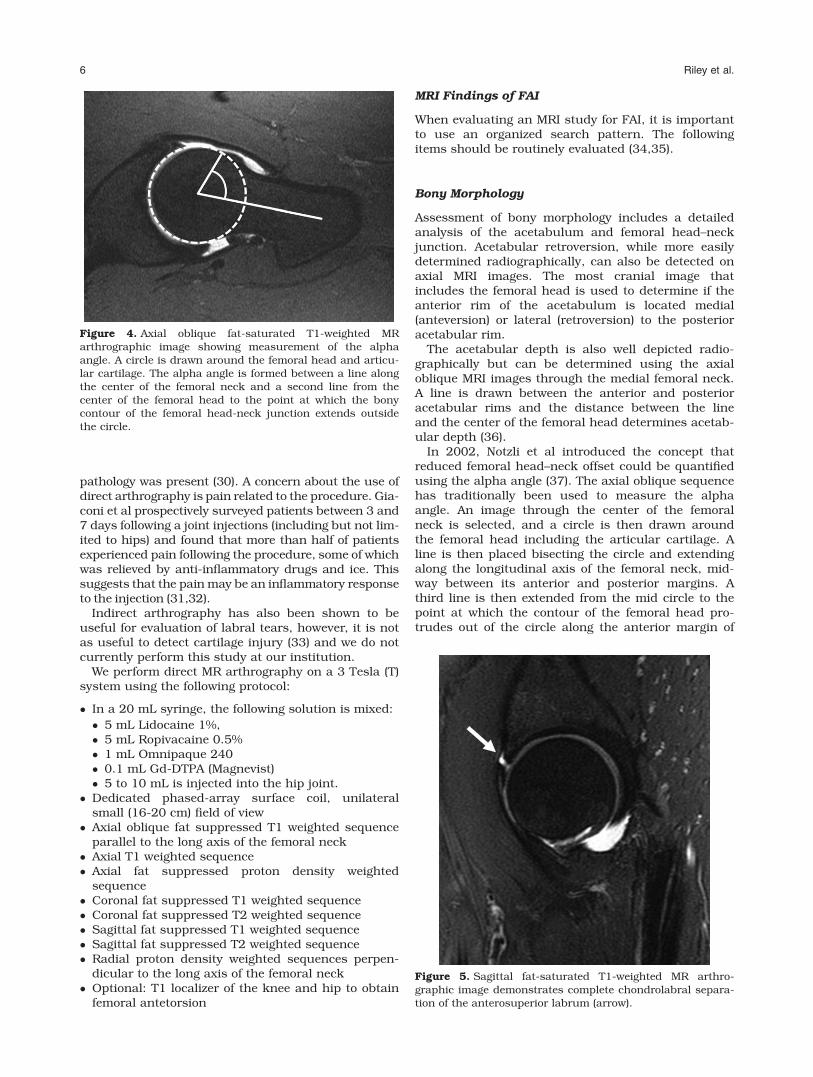
In 2002, Notzli et al introduced the concept thatreduced femoral head–neck offset could be quantifiedusing the alpha angle (37). The axial oblique sequencehas traditionally been used to measure the alphaangle. An image through the center of the femoralneck is selected, and a circle is then drawn aroundthe femoral head including the articular cartilage. Aline is then placed bisecting the circle and extendingalong the longitudinal axis of the femoral neck, mid-way between its anterior and posterior margins. Athird line is then extended from the mid circle to thepoint at which the contour of the femoral head pro-trudes out of the circle along the anterior margin of
Figure 5. Sagittal fat-saturated T1-weighted MR arthro-graphic image demonstrates complete chondrolabral separa-tion of the anterosuperior labrum (arrow).
Figure 4. Axial oblique fat-saturated T1-weighted MRarthrographic image showing measurement of the alphaangle. A circle is drawn around the femoral head and articu-lar cartilage. The alpha angle is formed between a line alongthe center of the femoral neck and a second line from thecenter of the femoral head to the point at which the bonycontour of the femoral head-neck junction extends outsidethe circle.
6 Riley et al.

the femur (Fig. 4). Cam-type deformities are mostcommon in the anterosuperior head neck junction.While radiography is often adequate to detect acetab-ular sided causes of FAI, it is less reliable for the fem-oral side (38,39). While the alpha angle has been inuse since its introduction, several studies show bothinterobserver variation and overlap in alpha anglemeasurements between asymptomatic and sympto-matic individuals (40,41).
In a retrospective study using symptomatic andasymptomatic individuals, Sutter et al attempted todiscover a reliable threshold for the alpha angle todistinguish asymptomatic from symptomatic camdeformities. They found that using the radial planeincreased sensitivity to detect cam deformities. This isnot a surprise considering that most cam deformitiesare most pronounced at the anterosuperior femoralneck (40). This is in accordance with a retrospectivestudy by Rakhra et al found that radial images yieldedhigher alpha angle values than oblique axial images(42).
Values used in both orthopedic and radiologic litera-ture to indicate abnormal morphology include both 50and 55 degrees (36,40,43). While we routinely reportthe alpha angle, we also include a subjective descrip-tion of the femoral head neck junction morphology.
Femoral head–neck offset is measured by compar-ing the maximal radius of the femoral head with themaximal radius of the femoral neck (44). Femoralantetorsion is also included in the assessment of bonymorphology and is described in detail above. Femoralhead–neck offset is measured by comparing the maxi-mal radius of the femoral head with the maximalradius of the femoral neck (44).
Cartilage
Cam impingement generally leads to cartilage damagefrom shearing caused by the osseous bump. Damageoccurs at the anterosuperior acetabular cartilage withresultant chondrolabral separation (Fig. 5).
Pincer impingement generally leads to labral dam-age due to crushing between the acetabular rim andthe femoral neck. The damage tends to be circumfer-ential comprising a narrow 5 mm strip around theacetabular margin. Another finding unique to pincer-type FAI is the “countrecoup” lesion of the posteroinfe-rior joint, described above (Fig. 6).
Beaule et al, in 2004, described the imaging find-ings of four cases of arthroscopically proven cartilagedelamination. Using MR arthrography, they describedthe lesions as a low signal intensity curvilinear intra-
Figure 6. (a) Sagittal fat-saturated T2-weighted MR arthrographic image in a patient with pincer-type impingement demon-strating a complex tear of the anterosuperior labrum (arrow), with cartilage thinning and bone marrow edema along the pos-terior acetabulum (open arrow). (b) Axial oblique fat-saturated T2-weighted image demonstrates the typical countrecoupcartilage injury of the posteroinferior acetabulum (open arrow), with peripheral chondral thinning and irregularity, and sub-chondral cystic change.
Figure 7. Coronal fat-saturated T2-weighted image in apatient with cam-type femoroacetabular impingement dem-onstrates delamination of the superior acetabular cartilage(arrow). Bone marrow edema is seen along the lateral femoralhead-neck junction (open arrow). In addition there is non-specific edema between the iliotibial tract and greater tro-chanter (arrowhead).
MRI Evaluation of Femoroacetabular Impingement 7

articular flap with bright signal deep to the flap. Theysurmised that the lesion represented an advancedstage of articular cartilage degeneration, with impor-tant implications for prognosis (45) (Fig. 7).
In 2008, a retrospective study by Pfirrmann et alsought to assess the performance of MRI to detectchondral delamination. The acetabular cartilage dam-age is thought to result from shearing forces betweenthe femoral head and acetabular cartilage leading todetachment of the cartilage from the subchondralbone. This is referred to as “detachment” and canoccur with or without the disruption extending to thecartilage surface. Delamination without disruption ofthe cartilage surface is referred to as “carpet likedelamination” because of its conceptual similarity to acarpet on a slippery floor. When, on the other hand,the disruption extends to the articular cartilage sur-face, it creates a flap tear. While the identification ofincreased signal deep to a flap is very specific findingfor delamination, it is not often seen. This may be dueto the lack of communication with the joint space orcould be of the tight nature of the joint, resulting inthe femoral head exerting pressure on the cartilagepreventing fluid from entering the tear.
Pfirrmann et al found delamination in 52% ofpatients requiring surgery for cam-type impingement.Hypointensity of the articular cartilage onintermediate-weighted fat-saturated or MRA T1-weighted images was considered a useful finding toidentify delamination. This study used 1.5T systemsand the findings would be expected to be more clearlydepicted using 3T systems with higher signal to noiseratios (46). In our experience confident identificationof delamination remains a challenge.
Acetabular Labrum
While the acetabular labrum generally has a sharp,diffusely dark, triangular appearance, many varia-tions exist in asymptomatic individuals. Alterations inlabral morphology and signal are seen with a higherfrequency among older individuals and are frequentlyasymptomatic (27,47). The fact that these alterationsincrease in frequency with age, suggests that someare degenerative. Anatomic variations also add to thedifficulty in interpretation of labral pathology.
Schmitz et al, in a prospective study of military per-sonnel, showed that asymptomatic labral tears, as
Figure 8. (a) Coronal fat-sat-urated T1-weighted MRarthrographic image shows apartial thickness tear of thesuperior labrum (arrow). (b)Coronal fat-saturated T2-weighted MR arthrographicimage demonstrates a well-defined fluid-filled cleft at thechondrolabral junction in theposterosuperior labrum,compatible with a sublabralrecess (arrow). (c) Axialoblique fat-saturated T1-weighted image through theinferior acetabulum demon-strates a pseudo-tear formedby a cleft of fluid between theinferior labrum and trans-verse acetabular ligament(arrow).
8 Riley et al.

indicated by linear increased signal extending to anarticular surface, occur in up to 83% of younger indi-viduals (age range, 27–43 years) (48). They alsorecorded the presence of paralabral cysts in upto 26% asymptomatic individuals. The concludedthat labral tears and paralabral cysts are not an indi-cation alone for arthroscopy, but that the findingsmust be correlated with symptoms and that otherpotential sources of intra-articular pain must beconsidered.
It is important to point out that labral tears alsooccur in pathologic conditions aside from FAI, includ-ing trauma, capsular laxity/hip hypermobility, acetab-ular dysplasia, and OA. These causes were describedin various studies from the late 1990s (8,49,50). Thisis supported by the presence of traumatic tears in hipswithout FAI morphology.
Lage et al have proposed an arthroscopic classifica-tion of labral tears by prospectively performing arthro-scopy on 367 patients (50). Tears were considereddegenerative if there was also evidence of cartilagedegeneration or if degeneration was seen in the lab-rum. Labral tears were considered traumatic if therewas a clear history of trauma and there were no signsof cartilage or labral degeneration. They classified lab-ral tears as radial flaps, radial fibrillation, longitudi-nal peripheral, or unstable. However, as Blankenbakerand Tuite pointed out, it is often difficult to differentiatethese on MRA (51). In a separate study, Blankenbakeret al compared findings of labral tears on MRA, asdefined by Czerny et al in 1996, with the Lage’s arthro-scopic classification (52,53). This (arthrographic) sys-tem assesses labral morphology, intralabral signal,presence of a tear or detachment, and the presence orabsence of an adjacent perilabral recess. The compari-son showed no correlation between the systems andBlankenbaker proposed a new classification system.This includes “fraying” to indicate free edge irregularity,partial-thickness tear, full thickness tear, and complextear. A full thickness tear at the labral base may be
more accurately described as “chondral labral separa-tion” or labral “detachment” (8) (Fig. 5).
When assessing the acetabular labrum, the presenceof normal anatomic variations such as a sublabral sul-cus, acetabular cleft, and labral absence needs to beconsidered. Sulci have been the source of much con-troversy as to their existence and location (Fig. 8).
Dinauer et al, in 2004, retrospectively found a post-eroinferior sublabral sulcus or groove in 23% ofpatients undergoing arthroscopy (54). Saddik et al in2006 retrospectively examined 27 hip MRI studiesand defined sulci arthroscopically as a well definedcleft between the labrum and articular cartilage withsmooth edges, no signs of attempted healing, and nolabral detachment on probing (55). This study foundsulci in all anatomic positions of the labrum.
Figure 9. (a) AP radiograph and (b) Coronal fat-saturated T2-weighted MR arthrographic image shows prominent fibrocysticchange in the femoral neck laterally (arrow).
Figure 10. Coronal fat-saturated T1-weighted MR arthro-graphic image shows a partial tear of the ligamentum teresat the foveal attachment (arrow).
MRI Evaluation of Femoroacetabular Impingement 9
Studler et al in 2008 retrospectively looked at MRarthrograms of 57 patients who subsequently went onto surgery. They found what they termed a sublabral“recess” at the anteroinferior labrum but no tears in thislocation. They also found that labral tears were morecommon than recesses in the anterosuperior labrumand suggested that interposition of contrast at the baseof the labrum in this location should be considered atear. Furthermore, they pointed out that in contrast totears labral recesses do not extend through the entirelabral base (56). The absence of cartilage damage, bonylesions, or peralabral cysts are additional factors sug-gesting a labral variant instead of a peralabral tear.
DeBois aptly summarized the situation by stating thata normal sublabral sulcus likely exists posteroinferiorly,but that a similar finding in the anterior or anterosupe-rior labrum should be viewed with higher suspicion for alabral tear. Furthermore, sulci do not involve more thana third of the labral thickness, are wider than they aredeep, and are without adjacent cartilage damage (57).
In addition to a sublabral sulcus, clefts at the ante-rior and posteroinferior acetabulum can be seen atthe labral-ligamentous junction, where the transverseacetabular ligament joins the acetabular rim to com-plete a ring around the acetabulum (54,57) (Fig. 8).
The anterosuperior labrum has been reported to beabsent in up to 10% of asymptomatic volunteers (29).Lecouvet et al found labral absence in up to 14% ofasymptomatic volunteers, which increased with age(27). These studies were both performed in the late1990s before refinements of imaging had improvedconspicuity of the labrum and adjacent capsule and,as DuBois and Omar point out, until further evidencesupports absence as a normal variant, focal absenceshould be considered abnormal (57).
Fibrocystic Change at the Anterosuperior FemoralNeck
Fibrocystic change at the anterosuperior femoral neckrepresent synovial herniation pits and are thought toresult from repetitive mechanical contact of the femo-ral head neck junction with the acetabular rim. Leu-nig et al retrospectively showed these to be present in33% of hip radiographs of patients with FAI and nonein patients with developmental dysplasia (58) (Fig. 9).
PARALABRAL OSSIFICATIONS
Bony fragments adjacent to the superior acetabularrim can be a source of confusion. While these havebeen traditionally termed “os acetabuli” suggesting adevelopmental origin, other causes include incompletehealing of an acetabular rim fracture and ossificationof the acetabular labrum (59) (Fig. 3).
Ligamentum Teres
The ligamentum teres arises from the transverse ace-tabular ligament across the inferior acetabular notch.Two fascicles also attach to the acetabular notch(60,61). Proximally the ligamentum teres attaches tothe fovea capitis of the femoral head. The MRI appear-ance generally consists of two or three bundles with astriated appearance. Blankenbaker et al sought out toestablish reliable MRA imaging findings that repre-sented ligamentum teres injury. Partial tears wereconsidered when there was thickening and focal par-tial loss of continuity. Degeneration of the ligamentumwas considered when there was thickening and highto intermediate signal on all pulse sequences. Con-firming an injury arthroscopically is limited becausethe surface of the ligament may remain intact in thepresence of degeneration and thereby be undetectableby the surgeon. This study concluded that findings ofthe intact and partially torn ligamentum teres over-lapped on MRA (62) (Fig. 10).
Miscellaneous
Synovial membrane infoldings, known as synovial pli-cae, can be villous or flat. The purpose of these plicaeis to form synovial fluid, transmit neurovascularstructures, and to help stabilize the joint (63,64).While first described in anatomic literature, theirimportance was later recognized with regard to trans-ferring arterial blood supply to the femoral head (65).The presence of plicae is important for two primaryreasons. One is as a mimicker of pathology on MRIstudies and the other is as a potential source of symp-toms. A cause of symptoms, however, is not based onspecific imaging findings, but based on their presencewith no other identifiable abnormality to explain thepatient’s symptoms.
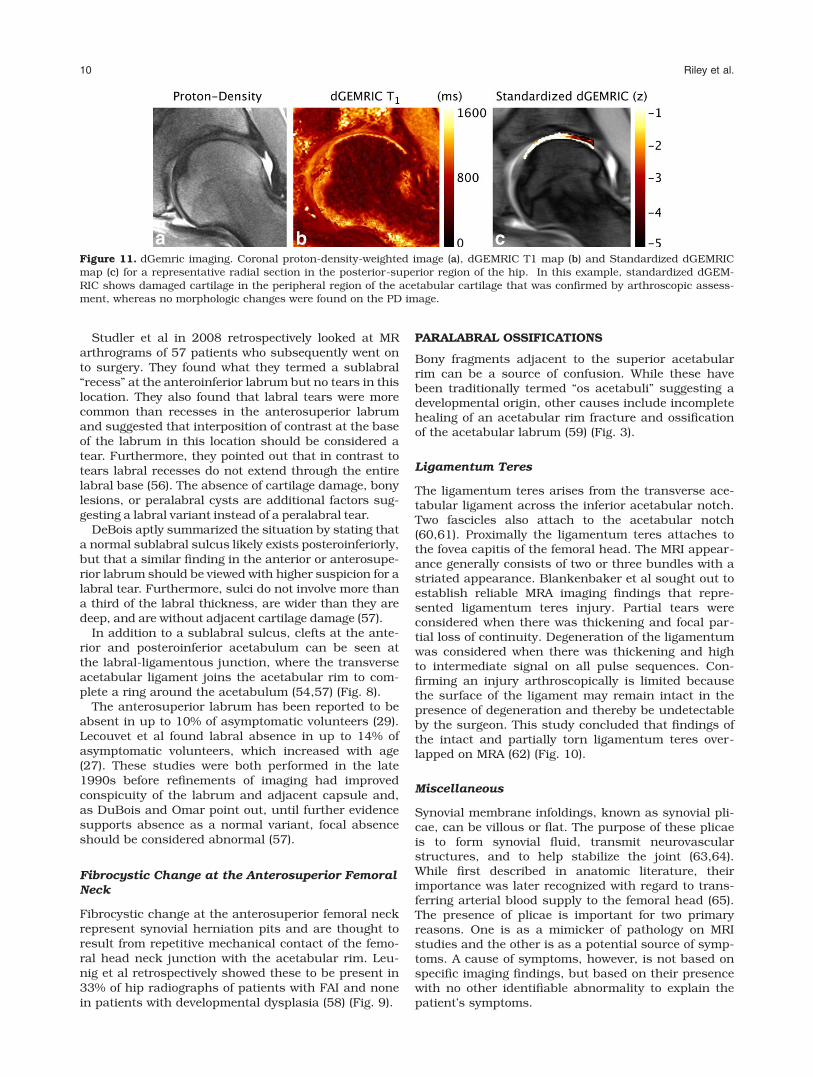
Figure 11. dGemric imaging. Coronal proton-density-weighted image (a), dGEMRIC T1 map (b) and Standardized dGEMRICmap (c) for a representative radial section in the posterior-superior region of the hip. In this example, standardized dGEM-RIC shows damaged cartilage in the peripheral region of the acetabular cartilage that was confirmed by arthroscopic assess-ment, whereas no morphologic changes were found on the PD image.
10 Riley et al.

Supra-acetabular Fossa and the Stellate Lesion
The supra-acetabular fossa is a normal indentation ofthe superior acetabulum, often filled with fibrous tis-sue. The stellate lesion (or crease) is a normal focus ofabsent cartilage in the superomedial acetabulum.located medial to the supra-acetabular fossa (57).
MRI AND THE FUTURE
While many of the changes associated with FAI,including bony morphology, are well depicted withcurrent imaging techniques, comprehensive assess-ment of cartilage lesions and the acetabular labrumremains elusive. This is paramount because extensivecartilage damage renders surgical correction lesseffective (66–69).
MRI of cartilage within the hip is challenging for avariety of reasons, including the relatively thin carti-lage layer, the curved shape of the hip (making partialvolume effects an issue), limited signal to noise due tothe depth of the structure, and a lack of hip-specificcoils. Current clinical MRI techniques are capable ofdetecting cartilage damage only once gross morpho-logic changes have already occurred. Damage at a bio-chemical level, however, may have preceded thesemorphological changes (68).
New quantitative MRI techniques have great poten-tial to detect early degenerative changes to cartilageand the labrum. In particular, these techniques canprobe changes in cartilage thickness and volume, aswell as proteoglycan, collagen, and water content, all ofwhich are early indications of degenerative disease.While these techniques have been more readily appliedin the knee (70), one study has shown that reproduci-bility of cartilage thickness, volume, T1r and T2 relaxa-tion times are sufficient to study clinical hip patientpopulations (71). In this section we will discuss theadvanced MRI techniques that have been used in thehip and those showing promise for use future.
Quantitative MRI of Cartilage Morphology
Quantitative assessment of cartilage morphology, suchas thickness, volume and surface area, has long beenused in the knee; however, very few studies have appliedthese techniques in the hip. While studies have shownthat it is possible to reproducibly assess femoral andacetabular cartilage thickness (71,72), few have appliedthe technique in patient populations. One study didshow increases in cartilage thickness in patients withdysplastic hips as compared to healthy individuals (73).Quantitative changes in cartilage morphology have beenshown to discriminate between patient groups in theknee and have potential to also be useful in the hip.
MRI of Cartilage Proteoglycan Content
Degenerative diseases, such as OA, result in a deple-tion of proteoglycan content and there are severalquantitative MRI techniques that probe this macro-molecule. These include delayed gadolinium enhancedMRI of cartilage (dGEMRIC), T1r relaxation time map-
ping, sodium MRI and glycosaminoglycan chemicalexchange saturation transfer imaging (gagCEST).Again, these techniques have been successfully usedin the knee and are increasingly being used in thehip.
Of all the techniques that probe proteoglycan con-tent, dGEMRIC has been used most frequently in thehip (Fig. 11). It is based on the detection of a relativeabsence of negatively charged glycosaminoglycan(GAG) side chain of the proteoglycan macromoleculewithin articular cartilage. The technique consists ofinjecting an intravenous double dose of gadolinium-diethylene triamine pentaacetic acid (Gd-DTPA�2).This negatively Gd-DTPA�2 anion distributes inverselyto the negatively charged GAG content within carti-lage. With cartilage degeneration, there will be anincrease in the concentration of Gd-DPTA�2. This inturn will cause a decrease the T1 relaxation time ofthe cartilage that can be measured to assess glycos-aminoglycan loss (74).
Most often, the output of dGEMRIC is a T1d relaxationtime color map, however, one group recently attemptedto create a standardized color map which displays thedata with respect to known ranges of healthy cartilageand other confounding factors (age, size, sex, and diffu-sion of gadolinium contrast) (68,75). They applied thisstandardized technique to an FAI population and foundit can increase the sensitivity of detecting cartilagedegeneration. Other groups have studied whetherintra-articular, instead of intravenous, injection can beused for dGEMRIC (76,77). This technique would offerthe benefits of both MRA and cartilage mapping. Bothstudies found that intra-articular results were similarto those of the intravenous technique.
Several other studies have used dGEMRIC to studyFAI patients. One study revealed that patterns of car-tilage damage were dependent on the type of FAI.Cam-type FAI patients had evidence of cartilage dam-age anterosuperiorly while pincer-type FAI patientshad damage circumferentially (76). Another studysuggested the use of radial images for the assessmentof the anterosuperior quadrant cartilage, an area fre-quently affected by cam-type FAI but difficult toassess on routine coronal MR imaging slices. Theyretrospectively looked at 20 patients and concludedthat radial imaging did offer a benefit over 2D imagingin these patients because radial imaging is able toassess the entire hip (78). dGEMRIC has also beenshown to detect cartilage damage in asymptomatic
Figure 12. T1-rho map (a) and T2-map (b) in a subject withFAI performed at 3T with a 3D fast spin echo method.Patients with FAI showed greater variability in relaxationtimes than healthy volunteers.
MRI Evaluation of Femoroacetabular Impingement 11

patients with cam deformities, identified on radio-graphs, but no radiographic joint space narrowing.Furthermore, the damage was found to correlate withthe severity of cam deformities (79). Together, thesefindings suggest that dGEMRIC is a useful tool forassessing early degeneration of cartilage as a result ofFAI.
T1r relaxation time mapping is another promisingtechnique for detection of early cartilage degeneration(Fig. 12). Correlations have been observed betweenGAG content of cartilage and T1r relaxation times,with increased T1r values indicating GAG loss (80).T1r, or spin lattice relaxation in the rotating frame,assesses the transverse relaxation of spins after theyhave been ‘locked’ in the transverse plane. Briefly,when the magnetization is tipped into the transverseplane an additional RF field is applied effectively“locking” the spin for differing amounts of time, allow-ing for quantitative relaxation time mapping. Earlyinvestigations of T1r relaxation time mapping in sub-jects with FAI have shown degenerative changes inacetabular and femoral cartilage before gross tissueloss (81,82). It has also shown that FAI patients dis-play differences in distribution patterns across thethickness of the tissue (82), increases in T1r in theanterosuperior region (81) and increased heterogene-ity in T1r (83,84).
Sodium MRI has been used to study knee cartilagebut likely requires high field strengths. As its namesuggest, sodium MRI measures the positive sodiumions in cartilage that distribute inversely to the nega-tively charged GAG (85). Wang et al recently describedrapid isotropic 3D-Sodium MRI using a 7T system forthe evaluation of knee cartilage. They concluded thatthis technique is a feasible alternative for evaluatingOA (86). Unfortunately, due to the depth of the hipcartilage and the low sodium concentration relative toprotons in the body, this method is limited at the cur-rent time in evaluation of hip cartilage.
gagCEST is perhaps the only technique that directlymeasures GAG concentration and has shown promise inknee cartilage (87). It is based on an asymmetry in the z-spectrum of cartilage created by hydroxyl groups in theglycosaminoglycan molecule. Application of this methodin the hip or to patients with FAI has not yet been dem-onstrated but, as with sodium MRI, will likely need to betested at high field strengths (7T) and will be challengingdue to low SNR and a lack of a hip specific coil.
MRI of Cartilage Collagen and Water Content
The depletion and disorganization of collagen isanother indicator of cartilage degeneration in degener-ative tissue diseases such as OA. T2 relaxation timemapping is a quantitative measure of the transverserelaxation time that occurs due to dephasing of spinsas a result of spin–spin interactions. It has been shownto correlate with cartilage matrix hydration and colla-gen fiber integrity (88). Degeneration induced changesin water content and cartilage arrangement could thenbe detected by this technique giving important infor-mation as to the presence of early degeneration. Wata-nabe et al performed T2 relaxation time mapping of
hips in 12 healthy volunteers and noted topographicvariation likely due to factors including cartilagematrix composition and magic angle phenomenon (88).These findings are important to consider before attrib-uting changes to early degeneration. Another studyhas also showed that T2 relaxation time mapping issufficiently sensitive and specific to study hip cartilagedamage (89). Studies of T2 relaxation times in FAIpatients have shown increased heterogeneity in theanterior acetabular region (84) and increased relaxa-tion times as compared to controls (81). Conversely,another study that measured T2* relaxation time inhips of FAI patients undergoing hip arthroscopy (a met-ric similar to T2 relaxation time, but includes dephasingdue to field inhomogeneities and susceptibility, as wellas spin–spin interactions) found decreases in T2* relax-ation times in hips with increasing modified Beck score(a measure of degeneration) (90). Although, T2 and T2*relaxation times are slightly different metrics, theseconflicting results indicate a need to explore quantita-tive MRI in the hip further in the FAI population,because the mechanism of degenerative changes maybe different than those of knee cartilage which has con-sistently shown increases in T2 and T2* relaxation timeswith osteoarthritic degeneration (81). Newer quantita-tive methods, such as quantitaitve double echo steadystate (DESS) sequences (91,92), have the potential toprovide measures of cartilage T2 relaxation time and dif-fusion in the femoral and acetabular cartilage, and mayprove useful in elucidating this the differences observedthus far because these sequences are faster and there-fore more practical for patient studies.
Short T2 Tissues: Labrum and Deep CartilageLayer
Advanced imaging of the acetabular labrum and deepcartilage layer may benefit from techniques such asultra-short echo time (uTE) MRI (93–95). These tis-sues appear dark on conventional MRI images due totheir short T2 relaxation times; with uTE techniquessignal can be observed and thus quantitative mappingis possible. uTE can be used to measure T2 or T2*relaxation time mapping and may provide informationabout early degeneration of these difficult to imagetissues. For example, it may be possible to detectdegeneration before labral tears occur. Many of thesemethods have been applied to the knee meniscus (96)and the zone of calcified cartilage in the knee, but asof yet not adapted for imaging hip cartilage.
CONCLUSIONS
In conclusion, subtle morphological changes to the hiphave been revealed to be causes of FAI and OA. How-ever, there are many unanswered questions in regardsto the diagnosis, evaluation, and treatment of FAI.Morphological MRI plays a central role in the evalua-tion of FAI and special attention to how the imagingstudies are performed and interpreted is required.Advanced MRI of the composition of cartilage and thelabrum in patients with FAI may provide evidence of
12 Riley et al.
early degenerative changes in these tissues before car-tilage delamination and labral tears occur. Detectionand monitoring of tissue changes in FAI is an impor-tant research goal that could lead to evidence of rever-sal of the disease with drug or surgical treatment.Improvements in the speed, resolution, and sensitivityof new MRI techniques may lead to widespread adop-tion of these methods for monitoring FAI treatment.
ACKNOWLEDGMENTS
Grant support and disclosures are as follows: GeoffreyM. Riley, MD: None. Emily J. McWalter, PhD: NIHEB002524, AR062068, and CA159992. GE Health-care. Kathryn J. Stevens, MD. None. Marc R. Safran,MD: Safran MR, Villar R: Can PreOperative 3D Com-puter Simulation Improve Clinical Outcomes ofArthroscopic Surgery for FAI: An International Pro-spective Randomized Controlled Trial. Submitted tothe ISAKOS – OREF MultiCenter InternationalResearch Grant. March 2013, $100,000. RiccardoLattanzi, PhD: NIH grants R01 EB002568 and R01EB000447. Garry E. Gold, MD: NIH EB002524,AR062068, and CA159992. GE Healthcare. E.J.M.,R.L., and G.E.G. were funded by the NIH.
REFERENCES
1. Ng VY, Arora N, Best TM, Pan X, Ellis TJ. Efficacy of surgery forfemoroacetabular impingement: a systematic review. Am J SportsMed 2010;38:2337–2345.
2. Rubin DA. Femoroacetabular impingement: fact, fiction, or fan-tasy? AJR Am J Roentgenol 2013;201:526–534.
3. Laborie LB, Lehmann TG, Engesaeter IO, Engesaeter LB,Rosendahl K. Is a positive femoroacetabular impingement test acommon finding in healthy young adults? Clin Orthop Relat Res2013;471:2267–2277.
4. Elmslie RC. Remarks on aetiological factors in osteo-arthritis ofthe hip-joint. Br Med J 1933;1:1–46.
5. Murray RO. The aetiology of primary osteoarthritis of the hip. BrJ Radiol 1965;38:810–824.
6. Stulberg SD, Cordell LD, Harris WH, Ramesey PL, MacEwan GD.Unrecognized childhood hip disease: a major cause of idiopathicosteoarthritis of the hip. In: Proceedings of the Third Open Scien-tific Meeting of The Hip Society, St. Louis, MO, USA. C.V. Mosby;1975.
7. Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, GanzR. Abnormal extension of the femoral head epiphysis as a causeof cam impingement. Clin Orthop Relat Res 2004:54–60.
8. Fitzgerald RH, Jr. Acetabular labrum tears. Diagnosis and treat-ment. Clin Orthop Relat Res 1995:60–68.
9. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. The water-shed labral lesion: its relationship to early arthritis of the hip.J Arthroplast 2001;16(Suppl 1):81–87.
10. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influencesthe pattern of damage to the acetabular cartilage: femoroacetabu-lar impingement as a cause of early osteoarthritis of the hip.J Bone Joint Surg Br 2005;87:1012–1018.
11. Nepple JJ, Lehmann CL, Ross JR, Schoenecker PL, Clohisy JC.Coxa profunda is not a useful radiographic parameter for diag-nosing pincer-type femoroacetabular impingement. J Bone JointSurg Br Am 2013;95:417–423.
12. Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW. Femoral antetor-sion: comparing asymptomatic volunteers and patients with fem-oroacetabular impingement. Radiology 2012;263:475–483.
13. Gosvig KK, Jacobsen S, Sonne-Holm S, Gebuhr P. The prevalenceof cam-type deformity of the hip joint: a survey of 4151 subjectsof the Copenhagen Osteoarthritis Study. Acta Radiol 2008;49:436–441.
14. Yamamura M, Miki H, Nakamura N, Murai M, Yoshikawa H,Sugano N. Open-configuration MRI study of femoro-acetabularimpingement. J Orthop Res 2007;25:1582–1588.
15. Takeyama A, Naito M, Shiramizu K, Kiyama T. Prevalence of fem-oroacetabular impingement in Asian patients with osteoarthritisof the hip. Int orthopaed 2009;33:1229–1232.
16. Beall DP, Sweet CF, Martin HD, et al. Imaging findings of femo-roacetabular impingement syndrome. Skeletal Radiol 2005;34:691–701.
17. Boykin RE, Anz AW, Bushnell BD, Kocher MS, Stubbs AJ,Philippon MJ. Hip instability. J Am Acad Orthop Surg 2011;19:340–349.
18. Philippon MJ, Kuppersmith DA, Wolff AB, Briggs KK. Arthro-scopic findings following traumatic hip dislocation in 14 profes-sional athletes. Arthroscopy 2009;25:169–174.
19. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabularimpingement: radiographic diagnosis–what the radiologist shouldknow. AJR Am J Roentgenol 2007;188:1540–1552.
20. Safran MR. Evaluation of the hip: History, physical examination,and imaging. Oper Tech Sports Med 2005;13:2–12.
21. Hodler J, Yu JS, Goodwin D, Haghighi P, Trudell D, Resnick D.MR arthrography of the hip: improved imaging of the acetabularlabrum with histologic correlation in cadavers. AJR Am J Roent-genol 1995;165:887–891.
22. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, LiebermanJM, Buly R. Acetabular labral tears: evaluation with MR arthrog-raphy. Radiology 1996;200:231–235.
23. Freedman BA, Potter BK, Dinauer PA, Giuliani JR, Kuklo TR,Murphy KP. Prognostic value of magnetic resonance arthrographyfor Czerny stage II and III acetabular labral tears. Arthroscopy2006;22:742–747.
24. Mintz DN, Hooper T, Connell D, Buly R, Padgett DE, Potter HG.Magnetic resonance imaging of the hip: detection of labral andchondral abnormalities using noncontrast imaging. Arthroscopy2005;21:385–393.
25. Smith TO, Hilton G, Toms AP, Donell ST, Hing CB. The diagnosticaccuracy of acetabular labral tears using magnetic resonanceimaging and magnetic resonance arthrography: a meta-analysis.Eur Radiol 2011;21:863–874.
26. Toomayan GA, Holman WR, Major NM, Kozlowicz SM, Vail TP.Sensitivity of MR arthrography in the evaluation of acetabularlabral tears. AJR Am J Roentgenol 2006;186:449–453.
27. Lecouvet FE, Vande Berg BC, Malghem J, et al. MR imaging ofthe acetabular labrum: variations in 200 asymptomatic hips. AJRAm J Roentgenol 1996;167:1025–1028.
28. Aydingoz U, Ozturk MH. MR imaging of the acetabular labrum: acomparative study of both hips in 180 asymptomatic volunteers.Eur Radiol 2001;11:567–574.
29. Cotten A, Boutry N, Demondion X, et al. Acetabular labrum: MRIin asymptomatic volunteers. J Comput Assist Tomogr 1998;22:1–7.
30. Kivlan BR, Martin RL, Sekiya JK. Response to diagnostic injec-tion in patients with femoroacetabular impingement, labral tears,chondral lesions, and extra-articular pathology. Arthroscopy2011;27:619–627.
31. Giaconi JC, Link TM, Vail TP, et al. Morbidity of direct MRarthrography. AJR Am J Roentgenol 2011;196:868–874.
32. Saupe N, Zanetti M, Pfirrmann CW, Wels T, Schwenke C, HodlerJ. Pain and other side effects after MR arthrography: prospectiveevaluation in 1085 patients. Radiology 2009;250:830–838.
33. Zlatkin MB, Pevsner D, Sanders TG, Hancock CR, Ceballos CE,Herrera MF. Acetabular labral tears and cartilage lesions of thehip: indirect MR arthrographic correlation with arthroscopy–apreliminary study. AJR Am J Roentgenol 2010;194:709–714.
34. Ilizaliturri VM Jr, Byrd JW, Sampson TG, et al. A geographic zonemethod to describe intra-articular pathology in hip arthroscopy:cadaveric study and preliminary report. Arthroscopy 2008;24:534–539.
35. Sampson TG. Arthroscopic treatment for chondral lesions of thehip. Clin Sports Med 2011;30:331–348.
36. Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M,Hodler J. Cam and pincer femoroacetabular impingement: char-acteristic MR arthrographic findings in 50 patients. Radiology2006;240:778–785.
37. Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, HodlerJ. The contour of the femoral head-neck junction as a predictor
MRI Evaluation of Femoroacetabular Impingement 13

for the risk of anterior impingement. J Bone Joint Surg Br 2002;84:556–560.
38. Dudda M, Albers C, Mamisch TC, Werlen S, Beck M. Do normalradiographs exclude asphericity of the femoral head-neck junc-tion? Clin Orthop Relat Res 2009;467:651–659.
39. Siebenrock KA, Kalbermatten DF, Ganz R. Effect of pelvic tilt onacetabular retroversion: a study of pelves from cadavers. ClinOrthop Relat Res 2003:241–248.
40. Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW. How useful is thealpha angle for discriminating between symptomatic patientswith cam-type femoroacetabular impingement and asymptomaticvolunteers? Radiology 2012;264:514–521.
41. Nouh MR, Schweitzer ME, Rybak L, Cohen J. Femoroacetabularimpingement: can the alpha angle be estimated? AJR Am JRoentgenol 2008;190:1260–1262.
42. Rakhra KS, Sheikh AM, Allen D, Beaule PE. Comparison of MRIalpha angle measurement planes in femoroacetabular impinge-ment. Clin Orthop Relat Res 2009;467:660–665.
43. Barton C, Salineros MJ, Rakhra KS, Beaule PE. Validity of thealpha angle measurement on plain radiographs in the evaluationof cam-type femoroacetabular impingement. Clin Orthop RelatRes 2011;469:464–469.
44. Dimmick S, Stevens KJ, Brazier D, Anderson SE. Femoroacetabu-lar impingement. Radiol Clin North Am 2013;51:337–352.
45. Beaule PE, O’Neill M, Rakhra K. Acetabular labral tears. J BoneJoint Surg Am 2009;91:701–710.
46. Pfirrmann CW, Duc SR, Zanetti M, Dora C, Hodler J. MR arthrog-raphy of acetabular cartilage delamination in femoroacetabularcam impingement. Radiology 2008;249:236–241.
47. Abe I, Harada Y, Oinuma K, et al. Acetabular labrum: abnormalfindings at MR imaging in asymptomatic hips. Radiology 2000;216:576–581.
48. Schmitz MR, Campbell SE, Fajardo RS, Kadrmas WR. Identifica-tion of acetabular labral pathological changes in asymptomaticvolunteers using optimized, noncontrast 1.5-T magnetic reso-nance imaging. Am J Sports Med 2012;40:1337–1341.
49. Hase T, Ueo T. Acetabular labral tear: arthroscopic diagnosis andtreatment. Arthroscopy 1999;15:138–141.
50. Lage LA, Patel JV, Villar RN. The acetabular labral tear: anarthroscopic classification. Arthroscopy 1996;12:269–272.
51. Blankenbaker DG, Tuite MJ. Acetabular labrum. Magn ResonImaging Clin North Am 2013;21:21–33.
52. Czerny C, Hofmann S, Neuhold A, et al. Lesions of the acetabularlabrum: accuracy of MR imaging and MR arthrography in detec-tion and staging. Radiology 1996;200:225–230.
53. Blankenbaker DG, De Smet AA, Keene JS, Fine JP. Classificationand localization of acetabular labral tears. Skeletal Radiol 2007;36:391–397.
54. Dinauer PA, Murphy KP, Carroll JF. Sublabral sulcus at the post-eroinferior acetabulum: a potential pitfall in MR arthrographydiagnosis of acetabular labral tears. AJR Am J Roentgenol 2004;183:1745–1753.
55. Saddik D, Troupis J, Tirman P, O’Donnell J, Howells R. Preva-lence and location of acetabular sublabral sulci at hip arthro-scopy with retrospective MRI review. AJR Am J Roentgenol 2006;187:W507–W511.
56. Studler U, Kalberer F, Leunig M, et al. MR arthrography of thehip: differentiation between an anterior sublabral recess as a nor-mal variant and a labral tear. Radiology 2008;249:947–954.
57. DuBois DF, Omar IM. MR imaging of the hip: normal anatomicvariants and imaging pitfalls. Magn Reson Imaging Clin NorthAm 2010;18:663–674.
58. Leunig M, Beck M, Kalhor M, Kim YJ, Werlen S, Ganz R. Fibro-cystic changes at anterosuperior femoral neck: prevalence in hipswith femoroacetabular impingement. Radiology 2005;236:237–246.
59. Martinez AE, Li SM, Ganz R, Beck M. Os acetabuli in femoro-acetabular impingement: stress fracture or unfused secondaryossification centre of the acetabular rim? Hip Int 2006;16:281–286.
60. Cerezal L, Kassarjian A, Canga A, et al. Anatomy, biomechanics,imaging, and management of ligamentum teres injuries. Radio-graphics 2010;30:1637–1651.
61. Gray AJ, Villar RN. The ligamentum teres of the hip: an arthro-scopic classification of its pathology. Arthroscopy 1997;13:575–578.
62. Blankenbaker DG, De Smet AA, Keene JS, Del Rio AM. Imagingappearance of the normal and partially torn ligamentum teres onhip MR arthrography. AJR Am J Roentgenol 2012;199:1093–1098.
63. Fu Z, Peng M, Peng Q. Anatomical study of the synovial plicae ofthe hip joint. Clin Anat 1997;10:235–238.
64. Bencardino JT, Kassarjian A, Vieira RL, Schwartz R, Mellado JM,Kocher M. Synovial plicae of the hip: evaluation using MRarthrography in patients with hip pain. Skeletal Radiol 2011;40:415–421.
65. Gojda J, Bartonicek J. The retinacula of Weitbrecht in the adulthip. Surg Radiol Anat 2012;34:31–38.
66. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anteriorfemoroacetabular impingement: part II. Midterm results of surgi-cal treatment. Clin Orthop Relat Res 2004:67–73.
67. Byrd JW, Jones KS. Arthroscopic management of femoroacetabu-lar impingement in athletes. Am J Sports Med 2011;39(Suppl):7S–13S.
68. Lattanzi R, Petchprapa C, Glaser C, et al. A new method to ana-lyze dGEMRIC measurements in femoroacetabular impingement:preliminary validation against arthroscopic findings. Osteoarthri-tis cartilage 2012;20:1127–1133.
69. Sambandam SN, Hull J, Jiranek WA. Factors predicting the fail-ure of Bernese periacetabular osteotomy: a meta-regression anal-ysis. Int Orthop 2009;33:1483–1488.
70. Matzat SJ, van Tiel J, Gold GE, Oei EH. Quantitative MRI techni-ques of cartilage composition. Quantit Imaging Med Surg 2013;3:162–174.
71. Carballido-Gamio J, Link TM, Li X, et al. Feasibility and reprodu-cibility of relaxometry, morphometric, and geometrical measure-ments of the hip joint with magnetic resonance imaging at 3T.J Magn Reson Imaging 2008;28:227–235.
72. Li W, Abram F, Beaudoin G, Berthiaume MJ, Pelletier JP, Martel-Pelletier J. Human hip joint cartilage: MRI quantitative thicknessand volume measurements discriminating acetabulum and femo-ral head. IEEE Trans Biomed Eng 2008;55:2731–2740.
73. Nishii T, Sugano N, Sato Y, Tanaka H, Miki H, Yoshikawa H. Three-dimensional distribution of acetabular cartilage thickness inpatients with hip dysplasia: a fully automated computational anal-ysis of MR imaging. Osteoarthritis Cartilage 2004;12:650–657.
74. Bashir A, Gray ML, Boutin RD, Burstein D. Glycosaminoglycan inarticular cartilage: in vivo assessment with delayed Gd(DTPA)(2-)-enhanced MR imaging. Radiology 1997;205:551–558.
75. Lattanzi R, Petchprapa C, Ascani D, et al. Detection of cartilagedamage in femoroacetabular impingement with standardizeddGEMRIC at 3 T. Osteoarthritis Cartilage 2014;22:447–456.
76. Zilkens C, Miese F, Kim YJ, et al. Direct comparison of intra-articular versus intravenous delayed gadolinium-enhanced MRIof hip joint cartilage. J Magn Reson Imaging 2014;39:94–102.
77. Bittersohl B, Hosalkar HS, Werlen S, Trattnig S, Siebenrock KA,Mamisch TC. Intravenous versus intra-articular delayedgadolinium-enhanced magnetic resonance imaging in the hipjoint: a comparative analysis. Invest Radiol 2010;45:538–542.
78. Domayer SE, Mamisch TC, Kress I, Chan J, Kim YJ. RadialdGEMRIC in developmental dysplasia of the hip and in femoroa-cetabular impingement: preliminary results. Osteoarthritis Carti-lage 2010;18:1421–1428.
79. Pollard TC, McNally EG, Wilson DC, et al. Localized cartilageassessment with three-dimensional dGEMRIC in asymptomatichips with normal morphology and cam deformity. J Bone JointSurg Am 2010;92:2557–2569.
80. Wheaton AJ, Casey FL, Gougoutas AJ, et al. Correlation of T1rhowith fixed charge density in cartilage. J Magn Reson Imaging2004;20:519–525.
81. Subburaj K, Valentinitsch A, Dillon AB, et al. Regional analysis ofhip cartilage MR relaxation times in subjects with and withoutfemoroacetabular impingement. In: Proceedings of the 21stAnnual Meeting of ISMRM, Salt Lake City, 2013. (abstract 430).
82. Rakhra KS, Lattanzio PJ, Cardenas-Blanco A, Cameron IG,Beaule PE. Can T1-rho MRI detect acetabular cartilage degenera-tion in femoroacetabular impingement?: a pilot study. J BoneJoint Surg Br 2012;94:1187–1192.
83. Blumenkrantz G, Majumdar S. Quantitative magnetic resonanceimaging of articular cartilage in osteoarthritis. Eur Cell Mater2007;13:76–86.
14 Riley et al.

84. Matzat SJ, McWalter EJ, Chen W, Safran MR, Gold GE. Standarddeviation of T1r and T2 relaxation times show regional changesin hip articular cartilage of patients with FAI. In: Proceedings ofthe 21st Annual Meeting of ISMRM, Salt Lake City, 2013.(abstract 3548).
85. Staroswiecki E, Bangerter NK, Gurney PT, Grafendorfer T, GoldGE, Hargreaves BA. In vivo sodium imaging of human patellarcartilage with a 3D cones sequence at 3 T and 7 T. J Magn ResonImaging 2010;32:446–451.
86. Wang L, Wu Y, Chang G, et al. Rapid isotropic 3D-sodium MRI ofthe knee joint in vivo at 7T. J Magn Reson Imaging 2009;30:606–614.
87. Ling W, Regatte RR, Navon G, Jerschow A. Assessment of glycos-aminoglycan concentration in vivo by chemical exchange-dependent saturation transfer (gagCEST). Proc Natl Acad Sci U SA 2008;105:2266–2270.
88. Watanabe A, Boesch C, Siebenrock K, Obata T, Anderson SE. T2mapping of hip articular cartilage in healthy volunteers at 3T: astudy of topographic variation. J Magn Reson Imaging 2007;26:165–171.
89. Ascani D, Petchprapa C, Babb JS, Recht M, Lattanzi R. Detectionand staging of acetabular cartilage damage in femoroacetabularimpingement using dGEMRIC and T2 mapping. In: Proceedingsof the 21st Annual Meeting of ISMRM, Salt Lake City, 2013.(abstract 634).
90. Ellermann J, Ziegler C, Nissi MJ, et al. Acetabular cartilageassessment in patients with femoroacetabular impingement byusing T2* mapping with arthroscopic verification. Radiology2014;271:512–523.
91. Staroswiecki E, Granlund KL, Alley MT, Gold GE, Hargreaves BA.Simultaneous estimation of T(2) and apparent diffusion coeffi-cient in human articular cartilage in vivo with a modified three-dimensional double echo steady state (DESS) sequence at 3 T.Magn Reson Med 2012;67:1086–1096.
92. Bieri O, Ganter C, Scheffler K. Quantitative in vivo diffusionimaging of cartilage using double echo steady-state free preces-sion. Magn Reson Med 2012;68:720–729.
93. Gold GE, Pauly JM, Macovski A, Herfkens RJ. MR spectroscopicimaging of collagen: tendons and knee menisci. Magn Reson Med1995;34:647–654.
94. Gatehouse PD, Thomas RW, Robson MD, Hamilton G, HerlihyAH, Bydder GM. Magnetic resonance imaging of the knee withultrashort TE pulse sequences. Magn Reson Imaging 2004;22:1061–1067.
95. Williams A, Qian Y, Chu CR. UTE-T2* mapping of human articu-lar cartilage in vivo: a repeatability assessment. OsteoarthritisCartilage 2011;19:84–88.
96. McWalter EJ, Gold GE, Alley MT, Hargreaves BA. T2 and T2*Relaxometry in the meniscus using a novel, rapid multi-echosteady state sequence. In: Proceedings of the 21st Annual Meet-ing of ISMRM, Salt Lake City, 2013. (abstract 686).
MRI Evaluation of Femoroacetabular Impingement 15




















