
Molecular analysis of pancreatic cyst fluid: a comparative analysis with current practice of...
11
Molecular Analysis of Pancreatic Cyst Fluid A Comparative Analysis With Current Practice of Diagnosis Jian Shen, MD, PhD 1 ; William R. Brugge, MD 2 ; Christopher J. DiMaio, MD 2 ; and Martha B. Pitman, MD 1 BACKGROUND: The management of patients with pancreatic cysts is based on the preoperative distinction of nonmucinous and mucinous cysts in general and of benign and malignant cysts in particular. An accurate diagnosis is challenging, because endoscopic ultrasound (EUS) and cyst fluid analysis for carcinoembryonic antigen (CEA) and cytology have low sensitivity and specificity. Currently, molecular analysis is a commer- cially available test that promises an accurate diagnosis.The objective of the current study was to correlate a commercially provided molecular diagnosis (MDx) with a clinical consensus diagnosis (CCD) in the gen- eral categories of malignant, benign mucinous, and benign nonmucinous pancreatic cysts. METHODS: Pancreatic cysts that had aspirated fluid submitted for a commercially available molecular test (PathFin- derTG) were reviewed. The CCD, defined by histology, malignant cytology, or 2 concordant tests (such as EUS, cytology, or CEA 192 ng/mL for mucinous cysts), was categorized as malignant, benign mucinous, or benign nonmucinous cyst in 35 patients. Their MDx, based on the PathFinderTG report, including analysis of k-ras mutation, loss of heterozygosity, and quantity/quality of DNA, also was classified as malignant, benign mucinous, or benign nonmucinous cyst. These 2 diagnoses were compared and correlated. RESULTS: The concordance between CCD and MDx was 5 of 6 (83%), 13 of 15 (87%), and 13 of 14 (93%), respectively, for malignant, benign mucinous, and benign nonmucinous cysts, with an overall Cohen kappa statistic of 0.816.The sensitivity, specificity, and positive predictive value of the MDx were 83%, 100%, and 100%, respectively, for a malignant cyst and 86%, 93%, and 95%, respectively for a benign mucinous cyst. CONCLUSIONS: Molecular analysis of pancreatic cyst fluid adds diagnostic value to the preoperative diag- nosis with high sensitivity, specificity, and positive predictive value for the diagnosis of malignant and benign mucinous pancreatic cysts. Cancer (Cancer Cytopathol) 2009;117:217–27. V C 2009 American Cancer Society. KEY WORDS: pancreatic neoplastic mucinous cysts, mucinous cystic neoplasm, intraductal papillary mucinous neoplasm, k-ras gene, loss of heterozygosity, molecular diagnosis, clinical consensus diagnosis. Received: November 7, 2008; Revised: January 26, 2009; Accepted: January 27, 2009 Published online: May 4, 2009 V C 2009 American Cancer Society DOI: 10.1002/cncy.20027, www.interscience.wiley.com Corresponding author: Martha B. Pitman, MD, Department of Pathology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114; Fax: (617) 7260-7474; [email protected] 1 James Homer Wright Pathology Laboratories, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; 2 Department of Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts We thank Dr. Jingyun Yang from the Biostatistics Center at Massachusetts General Hospital, Boston, Massachusetts for help with the calculation of kappa statistics. Cancer Cytopathology June 25, 2009 217 Original Article
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Molecular analysis of pancreatic cyst fluid: a comparative analysis with current practice of...

Molecular Analysis of PancreaticCyst Fluid
A Comparative Analysis With Current Practice of Diagnosis
Jian Shen, MD, PhD1; William R. Brugge, MD2; Christopher J. DiMaio, MD2; and Martha B. Pitman, MD1
BACKGROUND: The management of patients with pancreatic cysts is based on the preoperative distinction
of nonmucinous and mucinous cysts in general and of benign and malignant cysts in particular. An accurate
diagnosis is challenging, because endoscopic ultrasound (EUS) and cyst fluid analysis for carcinoembryonic
antigen (CEA) and cytology have low sensitivity and specificity. Currently, molecular analysis is a commer-
cially available test that promises an accurate diagnosis. The objective of the current study was to correlate
a commercially provided molecular diagnosis (MDx) with a clinical consensus diagnosis (CCD) in the gen-
eral categories of malignant, benign mucinous, and benign nonmucinous pancreatic cysts. METHODS:
Pancreatic cysts that had aspirated fluid submitted for a commercially available molecular test (PathFin-
derTG) were reviewed. The CCD, defined by histology, malignant cytology, or 2 concordant tests (such as
EUS, cytology, or CEA �192 ng/mL for mucinous cysts), was categorized as malignant, benign mucinous, or
benign nonmucinous cyst in 35 patients. Their MDx, based on the PathFinderTG report, including analysis
of k-ras mutation, loss of heterozygosity, and quantity/quality of DNA, also was classified as malignant,
benign mucinous, or benign nonmucinous cyst. These 2 diagnoses were compared and correlated.
RESULTS: The concordance between CCD and MDx was 5 of 6 (83%), 13 of 15 (87%), and 13 of 14 (93%),
respectively, for malignant, benign mucinous, and benign nonmucinous cysts, with an overall Cohen kappa
statistic of 0.816. The sensitivity, specificity, and positive predictive value of the MDx were 83%, 100%, and
100%, respectively, for a malignant cyst and 86%, 93%, and 95%, respectively for a benign mucinous cyst.
CONCLUSIONS: Molecular analysis of pancreatic cyst fluid adds diagnostic value to the preoperative diag-
nosis with high sensitivity, specificity, and positive predictive value for the diagnosis of malignant and
benign mucinous pancreatic cysts. Cancer (Cancer Cytopathol) 2009;117:217–27. VC 2009 American Cancer
Society.
KEY WORDS: pancreatic neoplastic mucinous cysts, mucinous cystic neoplasm, intraductal papillary
mucinous neoplasm, k-ras gene, loss of heterozygosity, molecular diagnosis, clinical consensus diagnosis.
Received: November 7, 2008; Revised: January 26, 2009; Accepted: January 27, 2009
Published online: May 4, 2009 VC 2009 American Cancer Society
DOI: 10.1002/cncy.20027, www.interscience.wiley.com
Corresponding author: Martha B. Pitman, MD, Department of Pathology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114;
Fax: (617) 7260-7474; [email protected]
1James Homer Wright Pathology Laboratories, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; 2Department of
Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
We thank Dr. Jingyun Yang from the Biostatistics Center at Massachusetts General Hospital, Boston, Massachusetts for help with the calculation of
kappa statistics.
Cancer Cytopathology June 25, 2009 217
Original Article
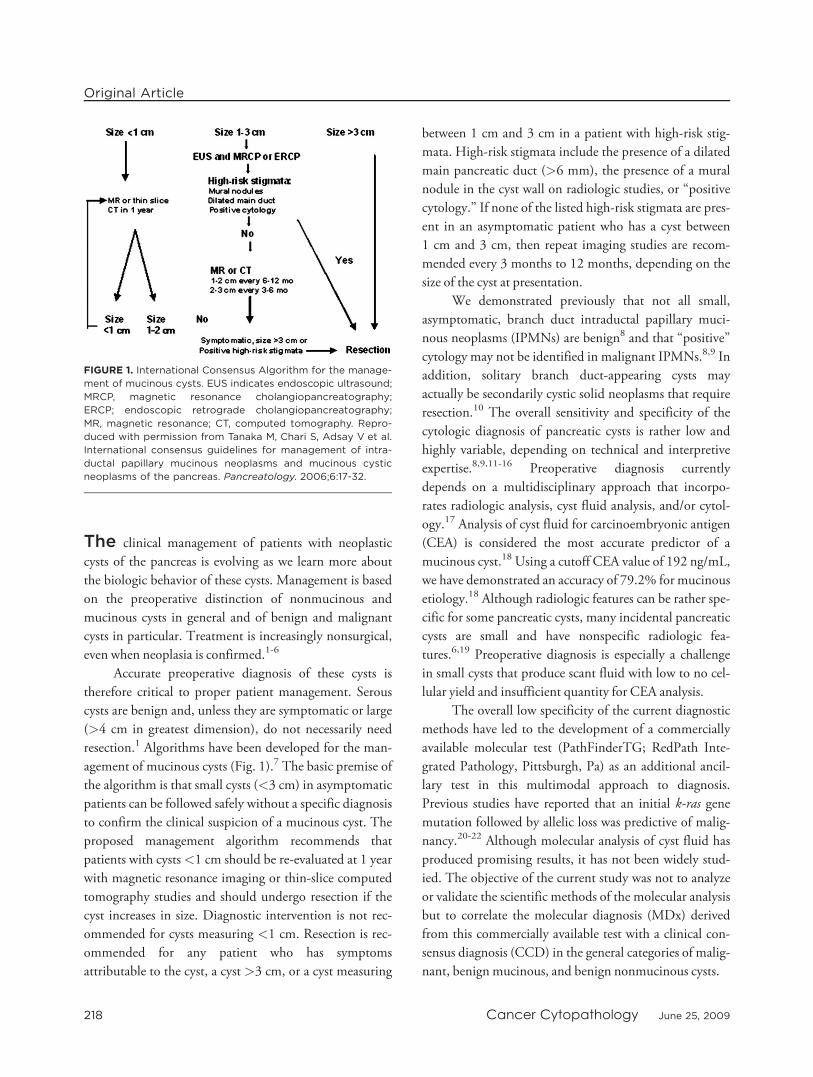
The clinical management of patients with neoplasticcysts of the pancreas is evolving as we learn more aboutthe biologic behavior of these cysts. Management is basedon the preoperative distinction of nonmucinous andmucinous cysts in general and of benign and malignantcysts in particular. Treatment is increasingly nonsurgical,even when neoplasia is confirmed.1-6
Accurate preoperative diagnosis of these cysts is
therefore critical to proper patient management. Serous
cysts are benign and, unless they are symptomatic or large
(>4 cm in greatest dimension), do not necessarily need
resection.1 Algorithms have been developed for the man-
agement of mucinous cysts (Fig. 1).7 The basic premise of
the algorithm is that small cysts (<3 cm) in asymptomatic
patients can be followed safely without a specific diagnosis
to confirm the clinical suspicion of a mucinous cyst. The
proposed management algorithm recommends that
patients with cysts<1 cm should be re-evaluated at 1 year
with magnetic resonance imaging or thin-slice computed
tomography studies and should undergo resection if the
cyst increases in size. Diagnostic intervention is not rec-
ommended for cysts measuring <1 cm. Resection is rec-
ommended for any patient who has symptoms
attributable to the cyst, a cyst >3 cm, or a cyst measuring
between 1 cm and 3 cm in a patient with high-risk stig-
mata. High-risk stigmata include the presence of a dilated
main pancreatic duct (>6 mm), the presence of a mural
nodule in the cyst wall on radiologic studies, or ‘‘positive
cytology.’’ If none of the listed high-risk stigmata are pres-
ent in an asymptomatic patient who has a cyst between
1 cm and 3 cm, then repeat imaging studies are recom-
mended every 3 months to 12 months, depending on the
size of the cyst at presentation.
We demonstrated previously that not all small,
asymptomatic, branch duct intraductal papillary muci-
nous neoplasms (IPMNs) are benign8 and that ‘‘positive’’
cytology may not be identified in malignant IPMNs.8,9 In
addition, solitary branch duct-appearing cysts may
actually be secondarily cystic solid neoplasms that require
resection.10 The overall sensitivity and specificity of the
cytologic diagnosis of pancreatic cysts is rather low and
highly variable, depending on technical and interpretive
expertise.8,9,11-16 Preoperative diagnosis currently
depends on a multidisciplinary approach that incorpo-
rates radiologic analysis, cyst fluid analysis, and/or cytol-
ogy.17 Analysis of cyst fluid for carcinoembryonic antigen
(CEA) is considered the most accurate predictor of a
mucinous cyst.18 Using a cutoff CEA value of 192 ng/mL,
we have demonstrated an accuracy of 79.2% for mucinous
etiology.18 Although radiologic features can be rather spe-
cific for some pancreatic cysts, many incidental pancreatic
cysts are small and have nonspecific radiologic fea-
tures.6,19 Preoperative diagnosis is especially a challenge
in small cysts that produce scant fluid with low to no cel-
lular yield and insufficient quantity for CEA analysis.
The overall low specificity of the current diagnostic
methods have led to the development of a commercially
available molecular test (PathFinderTG; RedPath Inte-
grated Pathology, Pittsburgh, Pa) as an additional ancil-
lary test in this multimodal approach to diagnosis.
Previous studies have reported that an initial k-ras gene
mutation followed by allelic loss was predictive of malig-
nancy.20-22 Although molecular analysis of cyst fluid has
produced promising results, it has not been widely stud-
ied. The objective of the current study was not to analyze
or validate the scientific methods of the molecular analysis
but to correlate the molecular diagnosis (MDx) derived
from this commercially available test with a clinical con-
sensus diagnosis (CCD) in the general categories of malig-
nant, benign mucinous, and benign nonmucinous cysts.
FIGURE 1. International Consensus Algorithm for the manage-
ment of mucinous cysts. EUS indicates endoscopic ultrasound;
MRCP, magnetic resonance cholangiopancreatography;
ERCP; endoscopic retrograde cholangiopancreatography;
MR, magnetic resonance; CT, computed tomography. Repro-
duced with permission from Tanaka M, Chari S, Adsay V et al.
International consensus guidelines for management of intra-
ductal papillary mucinous neoplasms and mucinous cystic
neoplasms of the pancreas. Pancreatology. 2006;6:17-32.
Original Article
218 Cancer Cytopathology June 25, 2009

MATERIALS AND METHODS
Patient Cohort
Forty-five consecutive patients with pancreatic cysts who
underwent endoscopic ultrasound (EUS)-guided fine-
needle aspiration (FNA) biopsy between 2005 and 2007
at Massachusetts General Hospital (Boston, Mass) and
had aspirated fluid submitted for molecular analysis
(PathFinderTG) were evaluated. Patients’ electronic med-
ical records were reviewed for all follow-up information
and test values. Institutional Review Board approval was
obtained for this study.
Pancreatic cysts were identified and evaluated for
location, number, size, and characteristic features (wall
thickness, septations, associated mass lesions, calcifica-
tions, pancreatic duct communication, and/or dilation).
FNA was performed with a 22-gauge needle (Echotip;
Cook Medical, Winston-Salem, NC). The cysts were
evacuated until collapse was achieved. Fluid color, clarity,
and viscosity were recorded; and the samples were sent for
cytologic examination, CEA concentration, and molecu-
lar analysis (PathFinderTG). Of these 45 patients, 8 had
histologic follow-up, 29 had concurrent cytologic inter-
pretation, and 30 had CEA cyst fluid chemical analysis.
Clinical Consensus Diagnosis
All EUS findings and images were reviewed blindly by 2
separate endosonographers (W.R.B. and C.J.D.). The
cysts were categorized as malignant, mucinous (IPMN or
mucinous cystic neoplasm [MCN]) with or without ma-
lignant features, serous cystadenoma, pseudocyst, or
other, and the general features used for this classification
are listed in Table 1. Overall, the diagnosis was assigned
based primarily on cyst morphology and/or cyst fluid
characteristics; and cyst location, patient age, and patient
sex were used to differentiate competing diagnoses in
unclear cases (Table 1). Suspicion of malignancy was
determined by the presence of high-risk features, as listed
in Table 1. Large cyst size in the absence of any other
high-risk feature was not indicative of malignancy.
A CCD was established for each patient, and the
cyst was classified as malignant, benign mucinous, or
benign nonmucinous using either the histologic diagnosis
or a combination of 2 of 3 concordant characteristics:
1) EUS features, 2) cyst fluid CEA level, or 3) cytology
(Table 2). The following classification criteria were used.
1) Malignant cyst (invasive or in situ carcinoma):
required either histologic confirmation or positive
(malignant) cytology;
2) Benign mucinous cyst (nonmalignant): required histo-
logic confirmation of IPMN or MCN with low-grade
dysplasia (adenoma) or moderate dysplasia (borderline
malignancy) or 2 of the following: a) cyst fluid CEA
level �192 ng/mL; or b) cytology with thick, colloid-
like extracellular mucin with or without atypical epi-
thelial cells; or c) EUS features consistent with an
IPMN or MCN and the macroscopic appearance of
‘‘thick, viscous, mucoid cyst fluid’’; and
Table 1. Endoscopic Criteria for Pancreatic Cystic Lesions
CystType
Age,Decade
Sex Location Morphology FluidCharacteristics
MalignantFeatures
IPMN 7th Men ¼ women Head (or
multifocal,
diffuse)
Dilated pancreatic duct
(main duct or side
branch)
Viscous Dilated main pancreatic duct,
cyst size >3 cm, intramural
mass/nodules
MCN 5th-7th Women > men Body/tail Unilocular or multilocular,
thick wall, peripheral
calcifications
Viscous Cyst size >3 cm, thick wall,
intramural mass/nodules,
peripheral calcifications
Pseudocyst Any Men ¼ women Evenly
distributed
Unilocular, thick wall Low viscosity,
dark, opaque
SCA 7th Women > men Evenly
distributed
Microcystic/honeycomb
(less commonly
oligocystic, macrocystic);
central calcification
Low viscosity, clear
IPMN indicates intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; SCA, serous cystadenoma.
Molecular Analysis of Pancreatic Cysts/Shen et al
Cancer Cytopathology June 25, 2009 219

3) Benign nonmucinous cyst: required histologic confir-
mation or 2 of the following: a) cyst fluid CEA <5
ng/mL; or b) nonmucinous cytology (no extracellu-
lar mucin or mucinous or atypical epithelium); or c)
EUS features typical of a serous cyst and/or thin,
watery, and nonmucoid macroscopic cyst fluid.
A CCD was reached in 35 of 45 patients according
to the above criteria, and those 35 patients established the
study cohort. Ten cysts with molecular analysis did not
fulfill the above criteria, because they lacked either cyst
fluid analysis or cytology for a concordant clinical cyst
classification and were excluded from the final analysis.
Molecular Diagnosis
The MDx was taken directly from the PathFinderTG
report. It was not the purpose of this study to evaluate the
scientific methods or validity of this commercially avail-
able test. The molecular analyses developed by RedPath
Integrated Pathology include 3 tests: k-ras gene point
mutation, loss of heterozygosity (LOH) analysis using a
preselected panel of 15 genomic loci associated with tu-
mor suppressor genes, and determination of DNA quan-
tity/quality in cyst fluid.20-22 Each of the 3 tests is defined
as ‘‘abnormal’’ when the following are identified: 1) k-ras
gene point mutation, 2) LOH mutations present in �2
genomic loci, and, 3) a high quantity/quality of DNA
content. The cyst is consistent with a benign nonmuci-
nous cyst when none of the above-defined abnormalities
are present and with a benign mucinous cyst when 1 of 3
abnormal findings described above is identified. In addi-
tion to the criteria for a mucinous MDx, if the k-ras or
LOH mutation is present at high amplitude (>75% of
total DNA), suggesting a significant clonal expansion,
then a malignant diagnosis is rendered (Table 3).
Statistical Analysis
The data were analyzed using Fisher exact tests, and the
differences were considered statistically significant when
P < .05. A kappa statistic was calculated using MatLab
(release 2008a; The MathWorks, Natick, Mass) for the
concordance between CCD andMDx.
RESULTS
The 35 patients included 27 women and 8 men who
ranged in age from 31 years to 85 years (mean age,
65 years). On the basis of our criteria for CCD, there were
6 malignant cysts, 15 benign mucinous cysts, and 14
benign nonmucinous cysts (Table 4). Malignant cysts
were located in the head (5 of 6 cysts) and body (1 of 6
cysts) and ranged in size from 1.6 cm to 5 cm (mean size,
3.1 cm). Benign mucinous cysts were located in the head
or uncinate process (8 of 15 cysts), body (5 of 16 cysts),
and tail (2 of 15 cysts) and ranged in size from 0.6 cm to
4.5 cm (mean size, 2.2 cm). Benign nonmucinous cysts
were located in the head or uncinate process (5 of 14 cysts),
body (7 of 14 cysts), and tail (2 of 14 cysts) and ranged in
size from 0.3 to 7.6 cm (mean size, 3.7 cm).
Comparison of Molecular Analysis
(PathFinderTG) Among Cyst Types
The cyst fluid contained high DNA quantity and quality
in 5 of 6 (83%) malignant cysts, which was significantly
different (P < .01) from benign mucinous cysts (2 of 15
cysts; 13%) and benign nonmucinous cysts (0 of 14 cysts;
Table 2. Criteria for Clinical Consensus Diagnosis
Clinical Consensus Diagnosis Criteria
Malignant (in situ or invasive carcinoma) Histology: invasive or in situ adenocarcinoma arising from IPMN or MCN OR cytology positive for
adenocarcinoma (in situ or invasive carcinoma) with abundant extracellular mucin and radiologic
evidence of cystic lesion
Benign mucinous Histology: IPMN or MCN with low-to-moderate grade dysplasia OR 2 of the following: 1) cyst fluid
CEA �192 ng/mL, 2) EUS consistent with IPMN or MCN, 3) cytology consistent with mucinous cyst
Benign nonmucinous Histology: nonmucinous cyst OR 2 of the following: 1) cyst fluid CEA <5ng/mL, 2) EUS consistent with
nonmucinous cyst, 3) cytology consistent with nonmucinous cyst
IPMN indicates intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; CEA, carcinoembryonic antigen; EUS, endoscopic ultrasound.
Original Article
220 Cancer Cytopathology June 25, 2009

0%) (Table 5). There was no difference in DNA quantity/
quality between benign mucinous and nonmucinous
cysts. k-ras gene mutation was present in 5 of 6 (83%) ma-
lignant cysts compared with 7 of 15 (47%) benign muci-
nous cysts and 0 of 14 (0%) benign nonmucinous cysts
(Table 5), a finding that was identified more frequently in
both malignant cysts (P < .01) and mucinous cysts (P <
.05) compared with nonmucinous cysts, but there was no
significant difference between malignant and benign
mucinous cysts. LOHmutations in�2 genomic loci were
identified in 5 of 6 (83%) malignant cysts, 4 of 15 (27%)
benign mucinous cysts, and 1 of 14 (7%) benign nonmu-
cinous cysts (Table 5), an abnormality that occurred more
frequently in malignant cysts than in benign mucinous
and benign nonmucinous cysts (P < .05), but no signifi-
cant difference was observed between benign mucinous
and benign nonmucinous cysts.
Correlation Between Clinical Consensus
Diagnosis and Molecular Diagnosis
(PathFinderTG)
Malignant cysts
Of 6 patients who had a malignant CCD diagnosis,
5 had positive cytology, 3 had histologic confirmation, 3
demonstrated clinically or pathologically proven meta-
static disease, and 2 died of disease within 2 years from the
initial diagnosis (Table 4). Within this group, 83% had
molecular changes consistent with malignancy, specifi-
cally, k-ras gene point mutation, a high quantity/quality
of DNA content in fluid samples, and LOH mutations in
�2 genomic loci (Table 5).
The concordance rate between the CCD and the
MDx was 83% in this group, and the overall Cohen kappa
statistic was 0.816 (95% confidence interval [95% CI],
0.6464-0.9857), indicating perfect agreement (Table 6).
The 1 false-negative MDx (Patient 6, who had an IPMN
with carcinoma in situ) (Table 4) was a 1.6-cm cyst
located in the head of the pancreas with indeterminate cy-
tology and EUS features of a low-grade IPMN. This
patient eventually underwent a Whipple resection after 1
year because of a strong family history of pancreatic cancer
and detection of BRCA2mutation.
Benign mucinous cysts
Fifteen patients had their cysts classified as benign
mucinous based on the CCD: Three patients had histo-
logic follow-up (an MCN with low-grade dysplasia and 2
IPMNs with moderate dysplasia), 4 patients had muci-
nous cysts according to cytology, and CEA levels were
available in 14 of 15 patients and were elevated (�192 ng/
mL) in 13 of 14 patients. The concordance rate between
the CCD and the MDx was 87%, and the overall Cohen
kappa statistic was 0.816 (95% CI, 0.6464-0.9857) (Ta-
ble 6). In this group, 47% (7 of 15 patients) had k-ras
gene point mutations, 27% (4 of 15 patients) had LOH
mutations present in �2 genomic loci, and 13% (2 of 15
patients) had high DNA content (Table 5). The 2 non-
concordant cases included the following.
1. Patient 21 (Table 4) had a 4.2-cm, thinly septated
cyst located in the tail of pancreas with 3 associated
mural nodules that ranged in size from 0.3 cm to
0.8 cm on EUS. Cytology demonstrated extracellular
mucin that was positive on alcian blue stain and
contained atypical epithelial cells consistent with at
least moderate dysplasia (Fig. 2). The cyst fluid was
macroscopically viscous, but the CEA level was only
71.6 ng/mL. The overall clinical impression was side
branch IPMN or MCN. Molecular analysis (Path-
FinderTG) revealed low quantity/quality DNA with
no k-ras point mutation or LOH identified, consist-
ent with benign nonmucinous cyst. The patient
remained alive and well at 18 months.
Table 3. Molecular Criteria (PathFinderTG) Developed by RedPath Integrated Pathology
Molecular Diagnosis Criteria
Benign nonmucinous 1) DNA quantity/quality low to moderate; AND 2) k-ras gene point mutation not present; AND 3) LOH,
<2 genomic loci present
Benign mucinous 1) DNA quantity/quality: high; OR 2) k-ras gene point mutation present; OR 3) LOH, �2 genomic loci present
Malignant (in situ or invasive carcinoma) 1) k-ras gene point mutation, high amplitude (>75%); OR 2) �2 more LOH, high amplitude (>75%)
LOH indicates loss of heterozygosity.
Molecular Analysis of Pancreatic Cysts/Shen et al
Cancer Cytopathology June 25, 2009 221

Table
4.PatientList
CCD
Patient
No.
Age,
ySex
Cyst(s)
Size,cm
Cyst(s)
Location
EUS
CEA,
ng/m
LCytology
Histology/
Clinical
follow-up
MDx
Malig
nant
171
Woman
5Head
ACA
NA
MA
NR
MA
260
Woman
2Body
MCN-m
alig
nant
4151.5
MA
IPMN-A
CA
MA
365
Woman
2Head
IPMN-m
alig
nant
NA
MA
IPMN-A
CA
MA
472
Woman
4Head
IPMN-m
alig
nant
320,099
MA
DOD
MA
585
Woman
4Head
MCN-m
alig
nant
NA
MA
DOD
MA
665
Woman
1.6
Head
IPMN-low
grade
NA
IND
IPMN-C
ISNM
Benign
mucinous
755
Man
1.8
Head
IPMN-low
grade
378.4
NA
AWD
at12mo
MU
831
Woman
4.5
Tail
MCN-m
oderate
927.4
IND
MCN-low
grade
MU
976
Man
3.7
Uncinate
IPMN-m
oderate
4602
IND
NA
MU
10
63
Man
2Body
IPMN-low
grade
213.7
NA
IPMN-m
oderate
MU
11
66
Woman
0.6
Head
IPMN-low
grade
NA
MU
NA
MU
12
69
Woman
1.8
Body
MCN-low
grade
6860
MU
NA
MU
13
61F
Woman
1.2
Head
IPMN-low
grade
�37,900
IND
AWD
at60mo
NM
14
81
Woman
2Head
IPMN-low
grade
200.3
IND
AWD
at15mo
MU
15
73
Woman
1.7
Body(m
ultiple)
IPMN-low
grade
604
IND
NA
MU
16
68
Woman
2.4
Head
IPMN-low
grade
4514
MU
IPMN-low
grade
MU
17
70
Man
2.5
Head
IPMN-low
grade
6827
NA
AWD
at17mo
MU
18
85
Woman
1Head
IPMN-m
alig
nant
392-528
IND
AWD
at36mo
MU
19
81
Woman
1.7
Body
IPMN-low
grade
>50,000
NA
NA
MU
20
68
Woman
1Body
MCN-low
grade
22,720
NA
AWD
at36mo
MU
21
75
Man
4.2
Tail
MCN-m
alig
nant
71.6
MU
AWD
at18mo.
NM
Benign
nonmucinous
22
76
Woman
3Neck
SCA
3.3-4.6
NM
AWD
at31mo
NM
23
54
Woman
2.5
Tail
MCN-m
oderate
>5000
IND
Entericduplication
cyst
NM
24
80
Woman
3.5
Head
SCA
0.7
NM
NA
MU
25
44
Woman
5Head
Pseudocyst
176.5
NM
Pseudocyst
NM
26
49
Man
2.5
Body
SCA
0.2
IND
NA
NM
27
56
Woman
0.3
Head
SCA
0.2
NM
NA
NM
28
76
Woman
5Head
SCA
0.4
NA
AWD
at60mo
NM
29
70
Woman
2.5
Uncinate
SCA
0.2
IND
NA
NM
30
48
Woman
2-2.4
Body
SCA
0.6
IND
AWD
at14mo
NM
31
53
Woman
1.7
Body
SCA
1.4
IND
NA
NM
32
64
Man
5.7
Body
Pseudocyst
2.3
NM
NA
NM
33
50
Woman
7.6
Tail
Gastric
duplicationcyst
2.4
IND
NA
NM
34
36
Man
4.3
Body
Gastric
duplicationcyst
0.2
NM
NA
NM
35
71
Woman
3.7
Body
SCA
NA
NM
AWD
at13mo
NM
CCD
indicatesclinicalconsensusdiagnosis;EUS,endoscopic
ultrasound;CEA,carcinoembryonic
antigen;MDx,moleculardiagnosis;ACA,adenocarcinoma;NA,notavailable;MA,malig
nant;NR,notresect-
able;MCN,mucinouscysticneoplasm;IPMN,intraductalpapillary
mucinousneoplasm;DOD,diedofdisease;IND,indeterm
inate;CIS,carcinomain
situ;AWD,alivewithdisease;MU,benignmucinous;NM,
benignnonmucinous;SCA;seruscystadenoma.
Original Article
222 Cancer Cytopathology June 25, 2009

2. Patient 13 (Table 4) had a 2.5-cm cyst in the pan-
creatic head with indeterminate cytology but a CEA
value that ranged from 27.6 ng/mL, 962 ng/mL,
1184 ng/mL, and 37,900 ng/mL between 2001 and
2004. The patient underwent ethanol ablation,
which resulted in a reduction of the cyst size from
2.5 cm to 1.2 cm. The MDx obtained 2 years after
ethanol ablation was nonmucinous based on low
DNA quality and quantity and only 1 LOH muta-
tion. The patient remained alive and disease free >5
years.
Benign nonmucinous cysts
Fourteen patients had their cysts classified as benign
nonmucinous according to CCD criteria. Thirteen of 14
cyst fluid samples were tested for CEA, and all but 2 sam-
ples demonstrated levels <5 ng/mL. Only 1 sample dem-
onstrated a CEA level >192 ng/mL. Cytology was
deemed nonmucinous in 7 of 13 cysts and indeterminate
in 6 of 13 cysts. Histologic follow-up was available in 2
patients, including 1 patient who had an enteric duplica-
tion cyst and 1 patient who had a pseudocyst. In this
group, none of the cyst fluids had k-ras point mutations
or high DNA content, and 7% (1 of 14 cysts) had LOH
mutations detected in >2 genomic loci (Table 5). The
concordance rate between the CCD and the MDx (Path-
FinderTG) was 93%, and the overall Cohen kappa sta-
tistic was 0.816 (95% CI, 0.6464-0.9857). The 1
discordant case (Patient 24) (Table 4) had thin, clear cyst
fluid with a CEA level of 0.7 ng/mL, nonmucinous cytol-
ogy, and EUS features consistent with a serous cystade-
noma. Molecular analysis revealed 3 LOH at loci of 10q,
21q, and 17q, leading to a mucinous MDx. No follow-up
was available on this patient at the time of this writing.
Table 5. Molecular Data in Different Categories of Clinical Consensus Diagnosis
Clinical Consensus Diagnosis: No (%)
Molecular Data Status Malignant,n56
Benign Mucinous,n515
Benign Nonmucinous,n514
DNA quantity/quality High/good 5 (83) 2 (13) 0 (0)
k-ras point mutation Present 5 (83) 7 (47) 0 (0)
No. of LOH present �2 Genomic loci 5 (83) 4 (27) 1 (7)
LOH indicates loss of heterozygosity.
Table 6. Correlation Between Clinical Consensus Diagnosis and Molecular Diagnosis (PathFinderTG)
Clinical Consensus Diagnosis: No. (%)
BenignMolecular Diagnosis Malignant Mucinous Nonmucinous Sensitivity, % Specificity, % PPV, %
Malignant 5 (83)* 0 0 83 100 100
Benign mucinous 0 13 (87)* 1 86 93 95
Benign nonmucinous 1 2 13 (93%)* 93 86 81
PPV indicates positive predictive value.
* Agreement (kappa statistic, 0.816).
FIGURE 2. A single, atypical epithelial cell cluster with cyto-
plasmic mucin is noted in the mucinous cyst fluid of an intra-
ductal papillary mucinous neoplasm with moderate dysplasia
(Papanicolaou stain; high-power view).
Molecular Analysis of Pancreatic Cysts/Shen et al
Cancer Cytopathology June 25, 2009 223

DISCUSSION
We evaluated the diagnostic concordance of a commer-
cially available molecular test for the diagnosis of pancre-
atic cysts (PathFinderTG) with the current method of
diagnosing pancreatic cysts, either by histology after resec-
tion or preoperatively using a combination of cytology,
cyst fluid analysis, and radiologic features. Our data pro-
duced 83% concordance for malignant cysts, 87% con-
cordance for benign mucinous cysts, 93% concordance
for benign nonmucinous cysts, and an overall Cohen
kappa statistic of 0.816 (95% CI, 0.6464-0.9857), indi-
cating perfect agreement (Table 6). The sensitivity, speci-
ficity, and positive predictive value for a malignant MDx
with PathFinderTG were 83%, 100%, and 100%, res-
pectively; and the same rates for a mucinous MDx with
PathFinderTG were 86%, 93%, and 95%, respectively
(Table 6). There were no false-positive results for a
malignant MDx.
The accuracy and validity of the commercially avail-
able molecular test PathFinderTG are controversial,
because to our knowledge there have been few published
reports20-22 and no validation studies outside of studies
that were sponsored by RedPath Integrated Pathology. It
was not the purpose of this study to delve into the accu-
racy of the scientific or proprietary techniques offered in
their molecular analysis of pancreatic cyst fluid. The basic
principals outlined above highlight the MDx criteria. Ma-
lignant cysts require either k-ras gene point mutation,
LOH mutations present in �2 genomic loci, or a high
quantity/quality of DNA with k-ras or LOH mutations
present at high amplitude (>75% of total DNA), suggest-
ing significant clonal expansion. Benign mucinous cysts
require either k-ras gene point mutation, LOH present in
�2 genomic loci, or a high quantity/quality of DNA; and
benign nonmucinous cysts do not have any of these mo-
lecular changes and have little or poor-quality DNA. We
abstracted the MDx directly from the PathFinderTG
report on each patient in this study and categorized the
cyst as either malignant, benign mucinous, or benign
nonmucinous.
On the basis of our CCD criteria, k-ras gene muta-
tion appears to be the best discriminator between muci-
nous cysts and nonmucinous cysts (P < .05). High DNA
quantity/quality and accumulation of LOH occurred more
frequently in malignant cysts but did not differ signifi-
cantly between benign mucinous cysts and nonmucinous
cysts (P > .05) (Table 5). These observations suggest that
k-ras gene mutation is a rather early event for a mucinous
cyst, whereas the accumulation of LOH and increased
DNA quantity/quality occur more commonly later during
malignant transformation. This is consistent with the pre-
vious findings, which suggested that an initial hit of k-ras
mutation followed by allelic loss is most predictive of the
presence of malignancy in pancreatic cyst fluid.20
In the current study, we compared the MDx (Path-
FinderTG) with our CCD, a diagnosis that was deter-
mined from either the histology from resection or from 2
of 3 concordant preoperative tests (EUS features, CEA
cyst fluid analysis, and cytology) that supported the same
clinical cyst classification. The weakness of the study rests
here, but the weakness in our ability to accurately diag-
nose pancreatic cysts in current practice also rests here,
hence the need for additional ancillary tests that will help
classify these often small cysts with nonspecific and non-
diagnostic features.
Five of the 6 malignant cysts in this study were sus-
pected of being malignant by EUS because of complex
features and/or direct invasion of surrounding structures,
and all 5 of those cysts were confirmed as malignant by cy-
tology and MDx. CEA analysis was performed in 2 cysts,
and both had markedly elevated CEA levels (Table 4).
There was no false-positive cytology result, but there was
1 false-negative cytology and MDx result. One small cyst
(1.6 cm) located in the pancreatic head in a woman aged
65 years (a low-grade IPMN by EUS without CEA analy-
sis and with indeterminate cytology) proved to be a malig-
nant IPMN on histology (moderate dysplasia with focal
carcinoma in situ). The MDx on this cyst fluid was non-
mucinous. It is highly likely that there was a complete
sampling error in this case, which is not surprising given
the small size of the cyst.
All remaining 29 cysts except 1 (Patient 18) (Table
4) did not demonstrate malignant EUS features and ini-
tially were categorized as mucinous (IPMN or MCN) or
nonmucinous by EUS (outlined in Table 1), and EUS-
FNA was performed either to support the EUS diagnosis
or to refine it. The triage of cyst fluid for analysis from our
institution generally is based on cyst fluid volume. Cyst
fluid with a volume �1 mL is submitted for cytology and
cyst fluid analysis. Molecular analysis is obtained at the
discretion of the gastroenterologist and usually is
Original Article
224 Cancer Cytopathology June 25, 2009

requested because of previous nondiagnostic cytology or
because of an amount of fluid that is too scant for both cy-
tology and/or cyst fluid analysis. In the current study, 6
cyst fluid samples were not tested for CEA or cytologic
analysis because of insufficient fluid sample. Of the 29
specimens that were examined cytologically, 13 of 29
samples (45%) were indeterminate or nondiagnostic.
Although thick and viscous extracellular mucin is a
helpful clue in the diagnosis on cytology, its sensitivity
remains suboptimal.9 In fact, extracellular mucin is not
always observed in neoplastic mucinous cysts, and MCN
and IPMN can produce thin, clear fluid that resembles se-
rous cysts as well as thin, brown fluid that mimics a pseu-
docyst.9 CEA cyst fluid analysis has provided an objective
test to determine whether the cyst fluid is mucinous or
nonmucinous and is considered the most accurate predic-
tor for the diagnosis of a mucinous cyst with 79.2% accu-
racy using a threshold CEA level of 192 ng/mL.18 Various
studies have produced different CEA cutoff values for a
mucinous cyst.23 Increasing the required value for CEA to
support the diagnosis of a mucinous cyst increases the
specificity but decreases the sensitivity of the test.18,23 It is
preferable to have a more sensitive and less specific value
for CEA given the malignant potential of all mucinous
cysts and the tendency for cytology to underestimate the
grade of the neoplasm because of the heterogeneity of the
cyst lining epithelium.9 Of the 14 cysts in the nonmuci-
nous category, only 1 case of an enteric duplication cyst
produced a CEA value >192 ng/mL (>5000 ng/mL); 1
other cyst, a pseudocyst, produced a CEA value >5 ng/mL
(176 ng/mL) but less than our 192 ng/mL threshold for a
mucinous cyst. The etiology for both of those cysts was
confirmed as benign nonmucinous on MDx. The median
value for CEA in the benign nonmucinous category was
0.7 ng/mL. Of the 14 benign mucinous cysts that had
CEA analysis, all but 1 produced a CEA value >192 ng/
mL. The range of CEA values for benign mucinous cysts
was from 71.6 ng/mL to 50,000 ng/mL (median, 4514
ng/mL). Only 2 malignant cysts were tested for CEA: One
had a CEA level >4000 ng/mL, and the other had a CEA
level >320,000 ng/mL.
Discordant findings in the benign mucinous cate-
gory included Patients 13 and 21 (Table 4). Patient 13, a
woman aged 61 years with a 1.2-cm cyst in the pancre-
atic head that had EUS features consistent with a branch
duct IPMN, produced cyst fluid with nondiagnostic cy-
tology, but her previous CEA level was elevated up to
37,900 ng/mL. Although the MDx was nonmucinous
based on no k-ras mutation and only 1 LOH mutation,
it was made 2 years after she underwent ethanol abla-
tion/lavage of the cyst, a process that denudes the cyst
lining from cell necrosis.24,25 No doubt such instrumen-
tation and treatment had a directly impact on the cytol-
ogy results, CEA analysis, and molecular analysis in this
patient. Patient 21 (Table 4) was a man aged 75 years
who had a 4.2-cm, malignant-appearing cyst located in
the pancreatic tail by EUS that had benign mucinous cy-
tology but a CEA level of only 71.6 ng/mL, which was
elevated but well below our cutoff level of 192 ng/mL for
supporting a diagnosis of mucinous cyst. The MDx in
this patient also was nonmucinous. Although no histol-
ogy was available in this patient, he remained alive and
well at 18 months.
In the benign nonmucinous group of cysts, accord-
ing to the CCD, there was 1 false mucinous MDx. Patient
24 (Table 4), who had a CCD of a serous cystadenoma
because of EUS features, a 0.7 ng/mL CEA analysis, and
nonmucinous cytology, had molecular analysis indicating
3 LOH mutations, including loci of 10q, 21q, and 17q.
No k-ras mutation was identified in this patient. The rea-
son for this discrepancy between the CCD and the MDx
is unclear. Although the presence of >2 LOH mutations
was used as 1 of the criteria for mucinous etiology by Red-
Path Integrated Pathology, as discussed above, this is less
specific for mucinous etiology than for k-ras mutation,
which was absent in this case.
Accurate diagnosis is essential for proper patient
management, which is evolving as we learn more about
the biologic behavior of neoplastic cysts in the pancreas.1-
6 Historically, treatment has been surgical excision of all
pancreatic cysts suspected of being neoplastic, but studies
of both serous cysts1 and mucinous cysts indicate that
not all cysts require resection,7,26 especially small (�3
cm) branch duct IPMNs,7,8 given the typical older age of
this often asymptomatic patient population, which is
fraught with comorbid conditions that increase surgical
risk, in addition to the likelihood that the patient with
not outlive the time to malignant progression of the cyst.
Nonsurgical therapies, such as ethanol ablation, also are
under investigation.24,25,27
International consensus guidelines recently were
proposed to address the diagnosis and treatment of
Molecular Analysis of Pancreatic Cysts/Shen et al
Cancer Cytopathology June 25, 2009 225

neoplastic mucinous cysts of the pancreas in general and
branch duct IPMNs in particular.7 An algorithm for the
preoperative evaluation of branch duct IPMNs to assist in
determining which patients should be offered surgical
resection was proposed (Fig. 1). We have demonstrated
that not all small cysts in asymptomatic patients are be-
nign and that not all cysts>3 cm are malignant.8 We also
demonstrated that ‘‘positive cytology’’ may not be
observed in IPMNs with malignancy.8,9 Therefore, add-
ing molecular analysis as an additional ancillary test to the
current multimodal approach offers improved sensitivity
and specificity for the major cyst classifications of malig-
nant, benign mucinous, and benign nonmucinous. A
combination of different ancillary tests is critical for a
more accurate diagnosis.
In summary, the results of the current study demon-
strate that there is significant agreement between the cur-
rent multimodal approach to pancreatic cyst diagnosis
and MDx of cyst fluid provided by PathFinderTG. The
current multimodal approach is achieved by the combina-
tion of routine clinical tests, such as EUS features, CEA
levels, and (most important) cytologic examination. How-
ever, a significant proportion of cases fall into the clinical
gray zone between benign mucinous and nonmucinous
cysts. Molecular analysis of k-ras gene mutation and LOH
can provide diagnostic information with minimal sample
volume, which may be the only information available
for clinical management when aspirated cyst fluid is
insufficient for chemical and cytologic analyses. The
current study provides valuable outcome data on molec-
ular testing of pancreatic cyst fluid. A large study with
validation of PathFinderTG molecular testing of pan-
creatic cyst fluid will be needed before we can draw a
firm conclusion.
Conflict of Interest Disclosures
This article was not supported financially by RedPath IP or anyother entity.
References
1. Tseng JF, Warshaw AL, Sahani DV, et al. Serous cystade-noma of the pancreas: tumor growth rates and recommenda-tions for treatment. Ann Surg. 2005;242:413-419; discussion419-421.
2. Matthes K, Mino–Kenudson M, Sahani DV, Holalkere N,Brugge WR. Concentration-dependent ablation of pancre-
atic tissue by EUS-guided ethanol injection. GastrointestEndosc. 2007;65:272-277.
3. Garcea G, Ong SL, Rajesh A, et al. Cystic lesions of thepancreas. A diagnostic and management dilemma. Pancrea-tology. 2008;8:236-251.
4. Allen PJ, Brennan MF. The management of cystic lesionsof the pancreas. Adv Surg. 2007;41:211-228.
5. Farnell MB. Surgical management of intraductal papillarymucinous neoplasm (IPMN) of the pancreas. J GastrointestSurg. 2008;12:414-416.
6. Lahav M, Maor Y, Avidan B, Novis B, Bar-Meir S. Non-surgical management of asymptomatic incidental pancreaticcysts. Clin Gastroenterol Hepatol. 2007;5:813-817.
7. Tanaka M, Chari S, Adsay V, et al. International consensusguidelines for management of intraductal papillary muci-nous neoplasms and mucinous cystic neoplasms of the pan-creas. Pancreatology. 2006;6:17-32.
8. Pitman MB, Michaels PJ, Deshpande V, Brugge WR,Bounds BC. Cytological and cyst fluid analysis of small(�3 cm) branch duct intraductal papillary mucinous neo-plasms adds value to patient management decisions. Pan-creatology. 2008;8:277-284.
9. Michaels PJ, Brachtel EF, Bounds BC, Brugge WR, PitmanMB. Intraductal papillary mucinous neoplasm (IPMN) ofthe pancreas: cytohistologic analysis and correlation withhistologic grade. Cancer (Cancer Cytopathol). 2006;108:163-173.
10. Deshpande V, Lauwers GY. Cystic pancreatic endocrine tu-mor: a variant commonly confused with cystic adenocarci-noma. Cancer (Cancer Cytopathol). 2007;111:47-53.
11. Vignesh S, Brugge WR. Endoscopic diagnosis and treat-ment of pancreatic cysts. J Clin Gastroenterol. 2008;42:493-506.
12. Jhala NC, Jhala D, Eltoum I, et al. Endoscopic ultrasound-guided fine needle aspiration biopsy: a powerful tool toobtain samples from small lesions. Cancer (Cancer Cytopa-thol). 2004;102:239-246.
13. Layfield LJ, Cramer H. Fine-needle aspiration cytology ofintraductal papillary-mucinous tumors: a retrospective anal-ysis. Diagn Cytopathol. 2005;32:16-20.
14. Recine M, Kaw M, Evans DB, Krishnamurthy S. Fine-nee-dle aspiration cytology of mucinous tumors of the pancreas.Cancer (Cancer Cytopathol). 2004;102:92-99.
15. Stelow EB, Stanley MW, Bardales RH, et al. Intraductalpapillary-mucinous neoplasm of the pancreas. The findingsand limitations of cytologic samples obtained by endoscopicultrasound-guided fine needle aspiration. Am J Clin Pathol.2003;120:398-404.
16. Shin HJ, Lahoti S, Sneige N. Endoscopic ultrasound-guided fine-needle aspiration in 179 cases: the M. D.Anderson Cancer Center experience. Cancer (Cancer Cyto-pathol). 2002;96:174-180.
17. Pitman MB, Deshpande V. Endoscopic ultrasound-guidedfine needle aspiration cytology of the pancreas: a
Original Article
226 Cancer Cytopathology June 25, 2009

morphological and multimodal approach to the diagnosisof solid and cystic mass lesions. Cytopathology. 2007;18:331-347.
18. Brugge WR, Lewandrowski K, Lee-Lewandrowski E, et al.Diagnosis of pancreatic cystic neoplasms: a report of theCooperative Pancreatic Cyst Study. Gastroenterology. 2004;126:1330-1336.
19. Brugge WR. Cystic pancreatic lesions: can we diagnosethem accurately what to look for? FNA marker molecularanalysis resection, surveillance, or endoscopic treatment?Endoscopy. 2006;38(suppl 1):S40-S47.
20. Khalid A, McGrath KM, Zahid M, et al. The role of pan-creatic cyst fluid molecular analysis in predicting cyst pa-thology. Clin Gastroenterol Hepatol. 2005;3:967-973.
21. Khalid A, Finkelstein S, McGrath K. Molecular diagnosisof solid and cystic lesions of the pancreas. GastroenterolClin North Am. 2004;33:891-906.
22. Schoedel KE, Finkelstein SD, Ohori NP. K-Ras and micro-satellite marker analysis of fine-needle aspirates from intra-ductal papillary mucinous neoplasms of the pancreas. DiagnCytopathol. 2006;34:605-608.
23. van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluidanalysis in the differential diagnosis of pancreatic cystic lesions:a pooled analysis. Gastrointest Endosc. 2005;62:383-389.
24. Gan SI, Thompson CC, Lauwers GY, Bounds BC, BruggeWR. Ethanol lavage of pancreatic cystic lesions: initial pilotstudy. Gastrointest Endosc. 2005;61:746-752.
25. Oh HC, Seo DW, Lee TY, et al. New treatment for cystictumors of the pancreas: EUS-guided ethanol lavage withpaclitaxel injection. Gastrointest Endosc. 2008;67:636-642.
26. Walsh RM, Vogt DP, Henderson JM, et al. Managementof suspected pancreatic cystic neoplasms based on cyst size.Surgery. 20008;144:677-684; discussion 684-5.
27. Brugge WR. Management and outcomes of pancreaticcystic lesions. Dig Liver Dis. 2008;40:854-859.
Molecular Analysis of Pancreatic Cysts/Shen et al
Cancer Cytopathology June 25, 2009 227




















