
Mixoploidy in humans: Two surviving cases of diploid-tetraploid mixoploidy and comparison with...
7
American Journal of Medical Genetics 52:324-330 (1994) Mixoploidy in Humans: Two Surviving Cases of Diploid-Tetraploid Mixoploidy and Comparison With Diploid-Triploid Mixoploidy Matthew J. Edwards, Jonathan P. Park, Doris H. Wurster-Hill, and John M. Graham, Jr. Regional Medical Genetics Unit, The Hunter Area Health Service, Newcastle Western Suburbs Hospital, Waratah, New South Wales, Australia (M.J.E.); Department of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire (J.P.P., D.H. W.-H.), and Division of Clinical Genetics and Dysmorphology, Ahmanson Pediatric Center, Steuen Spielberg Pediatric Research Center, Medical Genetics Birth Defects Center, Cedars-Sinai Medical Center, UCLA School of Medicine, Los Angeles, California (J.M.G.) We report on 2 cases of diploidtetraploid (2d4n) mixoploidy in surviving females, 11 and 21 years old. Both individuals mani- fested severe mental retardation, reduced peripheral limb muscle bulk, asymmetric growth deficiency,seizure disorder, and skin pigmentary dysplasia. Previous lymphocyte karyotypes had been normal on 2 occasions, but when skin fibroblast karyotypes were done, 33% of the cells were tetraploid on the younger woman, and over 60% were tetraploid in the older woman (on 2 separate occasions). In both individuals, the distal limbs and digits were long and thin, with re- duced small muscle bulk. The similarity in distal limb findings prompted reexamina- tion of the younger woman’s chromosomal constitution in skin fibroblasts. We con- cluded that the clinical findings in these cases are unique and similar, and we caution clinicians about uniformly dismissing tetraploidy as artifactual in amniocytes from normal patients, especially since this phenotype would be very difficult to detect, even with directed prenatal ultrasonogra- phy. We compare the 2d4n phenotype with that in diploidtriploid (2d3n) mixoploidy and note subtle differences which might be detected postnatally. These findings should be useful in guiding clinicians on when to request skin fibroblast karyotypes in men- tally-deficient individuals with asymmetric growth deficiency and pigmentary skin vari- ation. 0 1994 Wiley-Liss, Inc. Received for publication November 15, 1993; revision received March 7, 1994. Address reprint requests to John M. Graham, Jr., M.D., Sc.D., Director of Clinical Genetics and Dysmorphology, Cedars-Sinai Medical Center, 444 South San Vicente Blvd., Suite 1001, Los Angeles, CA 90048. 0 1994 Wiley-Liss, Inc. KEY WORDS: triploidy, tetraploidy, mixo- ploidy, chromosome abnor- mality, mental retardation, growth asymmetry INTRODUCTION Mixoploidy refers to the coexistence of a normal diploid cell population with another that has 3 or more multiples of the haploid chromosome number. In (2n/3n) mixoploidy, the abnormal cell line has 69 chro- mosomes, whereas in (2d4n) mixoploidy the chromo- some complement of the abnormal line is 92. We review the literature on 2d4n mixoploidy and report 2 female long-term survivors who had mental retardation and minor anomalies, some being similar to those reported in 2d3n mixoploidy [Ferrier et al., 1964; Donnai et al., 1986; Jenkins et al., 1971; Graham et al., 1981; Tharapel et al., 1983; Wulfsberg et al., 19911. These anomalies include severe intellectual handicap, digital anomalies, reduced peripheral limb muscle bulk, growth asymmetry, truncal obesity, and skin pigmen- tary dysplasia. In each of our cases, peripheral leukocyte karyotypes had been repeatedly normal, 46,XX. Only cultured fibroblasts from skin biopsies showed the 4n cell line. Older 2d3n and 2d4n patients appeared to have simi- lar, recognizable clinical manifestations, but may have remained undiagnosed because cytogenetic investiga- tion ended when peripheral blood karyotypes were found to be normal. Polyploidy should be sought in cul- tured skin fibroblasts or an alternative tissue if mixo- ploidy is suspected even if the peripheral leukocyte karyotype is normal. Tetraploidy may be dismissed as an artifact induced by culture in amniocytes from nor- mal subjects lKohn and Robinson, 1970; Milunsky et al., 1971; Therkelson et al., 1972; Anneren, 19821, es- pecially if the culture is prolonged, but may be a signif- icant diagnostic finding when associated with the mixo- ploidy phenotype. This phenotype would be extremely
Transcript of Mixoploidy in humans: Two surviving cases of diploid-tetraploid mixoploidy and comparison with...
American Journal of Medical Genetics 52:324-330 (1994)
Mixoploidy in Humans: Two Surviving Cases of Diploid-Tetraploid Mixoploidy and Comparison With Diploid-Triploid Mixoploidy
Matthew J. Edwards, Jonathan P. Park, Doris H. Wurster-Hill, and John M. Graham, Jr. Regional Medical Genetics Unit, The Hunter Area Health Service, Newcastle Western Suburbs Hospital, Waratah, New South Wales, Australia (M.J.E.); Department of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire (J.P.P., D.H. W.-H.), and Division of Clinical Genetics and Dysmorphology, Ahmanson Pediatric Center, Steuen Spielberg Pediatric Research Center, Medical Genetics Birth Defects Center, Cedars-Sinai Medical Center, UCLA School of Medicine, Los Angeles, California (J.M.G.)
We report on 2 cases of diploidtetraploid (2d4n) mixoploidy in surviving females, 11 and 21 years old. Both individuals mani- fested severe mental retardation, reduced peripheral limb muscle bulk, asymmetric growth deficiency, seizure disorder, and skin pigmentary dysplasia. Previous lymphocyte karyotypes had been normal on 2 occasions, but when skin fibroblast karyotypes were done, 33% of the cells were tetraploid on the younger woman, and over 60% were tetraploid in the older woman (on 2 separate occasions). In both individuals, the distal limbs and digits were long and thin, with re- duced small muscle bulk. The similarity in distal limb findings prompted reexamina- tion of the younger woman’s chromosomal constitution in skin fibroblasts. We con- cluded that the clinical findings in these cases are unique and similar, and we caution clinicians about uniformly dismissing tetraploidy as artifactual in amniocytes from normal patients, especially since this phenotype would be very difficult to detect, even with directed prenatal ultrasonogra- phy. We compare the 2d4n phenotype with that in diploidtriploid (2d3n) mixoploidy and note subtle differences which might be detected postnatally. These findings should be useful in guiding clinicians on when to request skin fibroblast karyotypes in men- tally-deficient individuals with asymmetric growth deficiency and pigmentary skin vari- ation. 0 1994 Wiley-Liss, Inc.
Received for publication November 15, 1993; revision received March 7, 1994.
Address reprint requests to John M. Graham, Jr., M.D., Sc.D., Director of Clinical Genetics and Dysmorphology, Cedars-Sinai Medical Center, 444 South San Vicente Blvd., Suite 1001, Los Angeles, CA 90048.
0 1994 Wiley-Liss, Inc.
KEY WORDS: triploidy, tetraploidy, mixo- ploidy, chromosome abnor- mality, mental retardation, growth asymmetry
INTRODUCTION Mixoploidy refers to the coexistence of a normal
diploid cell population with another that has 3 or more multiples of the haploid chromosome number. In (2n/3n) mixoploidy, the abnormal cell line has 69 chro- mosomes, whereas in (2d4n) mixoploidy the chromo- some complement of the abnormal line is 92. We review the literature on 2d4n mixoploidy and report 2 female long-term survivors who had mental retardation and minor anomalies, some being similar to those reported in 2d3n mixoploidy [Ferrier et al., 1964; Donnai et al., 1986; Jenkins et al., 1971; Graham et al., 1981; Tharapel et al., 1983; Wulfsberg et al., 19911. These anomalies include severe intellectual handicap, digital anomalies, reduced peripheral limb muscle bulk, growth asymmetry, truncal obesity, and skin pigmen- tary dysplasia.
In each of our cases, peripheral leukocyte karyotypes had been repeatedly normal, 46,XX. Only cultured fibroblasts from skin biopsies showed the 4n cell line. Older 2d3n and 2d4n patients appeared to have simi- lar, recognizable clinical manifestations, but may have remained undiagnosed because cytogenetic investiga- tion ended when peripheral blood karyotypes were found to be normal. Polyploidy should be sought in cul- tured skin fibroblasts or an alternative tissue if mixo- ploidy is suspected even if the peripheral leukocyte karyotype is normal. Tetraploidy may be dismissed as an artifact induced by culture in amniocytes from nor- mal subjects lKohn and Robinson, 1970; Milunsky et al., 1971; Therkelson et al., 1972; Anneren, 19821, es- pecially if the culture is prolonged, but may be a signif- icant diagnostic finding when associated with the mixo- ploidy phenotype. This phenotype would be extremely
Mixoploidy: Two Cases of Mosaic Tetraploidy 325
difficult to detect prenatally, even with directed ultra- sonography. Our patients were 21 and 11 years old at the time we pursued skin fibroblast karyotypes and documented their true diagnoses. They had gone for many years with no diagnosis. Our patients’ clinical findings suggest that the phenotype of adult patients is recognizable and is similar to that of patients with either a 3n or 4n cell line. Other patients may remain undiagnosed because their parents abandoned pre- viously fruitless and distressing investigations.
CLINICAL REPORTS Patient 1
S.P., a 21-year-old woman with severe mental retar- dation and multiple congenital abnormalities, pre- sented for diagnosis and genetic counselling in 1987. She was born at 43 weeks gestation after an uncompli- cated pregnancy to a healthy 23-year-old primigravida and her 25-year-old husband, with an unremarkable family history. The patient’s birthweight was 2.41 kg (below the 3rd centile), with length 53.5 cm (50th cen- tile). There was little subcutaneous fat, esotropia, an abnormal nose, long thin hands and feet, equinovalgus foot deformities, and marked hypotonia in the neonatal period, and during infancy, severe developmental re- tardation, spastic paraparesis, and seizures were noted. An unusual central pattern of obesity developed and at age 12 years, weight was at the 75th centile, height at the 10th centile, and head circumference (OFC) at the 2nd centile. She required spinal fusion at age 12 years for thoracolumbar kyphoscoliosis, and a progressive valgus deformity of the ankles required bracing and then surgery. A 40-50 decibel sen- sorineural hearing loss was detected at age 15 years. The left kidney was not visible on intravenous pyelog- raphy, performed because of a history of recurrent uri- nary tract infection. Voiding cystourethrography was normal, and left retrograde pyelography disclosed an atretic left ureter. Results of numerous other investiga- tions including skull radiographs, urine metabolic pro- file, and cerebral CT scan, were not contributory. Two peripheral blood leukocyte karyotypes were normal in 1983, and in 1985 with 23 and 20 cells counted, respec- tively. No polyploidy was observed during the screening of metaphases from either analysis.
Without a diagnosis, the parents avoided further pregnancies because of the uncertain recurrence risk. They brought the patient for reassessment when she was 21 years old, at the suggestion of her group-home supervisors. Her weight, 64.9 kg, was between the 75th and 90th centile, height of 155 cm was on the 10th cen- tile, and OFC 54 cm was on the 2nd centile. There was marked obesity of the buttocks and thighs. We noted a disproportionately small face in relation to the cranium, and body asymmetry with the right face, mandible, ear, teeth, hand, and arm smaller than the left-sided structures. She had a prominent nasal tip and septum, small ears and mandible, hypoplastic thenar and hypothenar areas, proximal placement of the thumbs, long tapering fingers which were deviated to the ulnar side, minor camptodactyly, and partial syn- dactyly between fingers 3 and 4 (Fig. 1). The long sec-
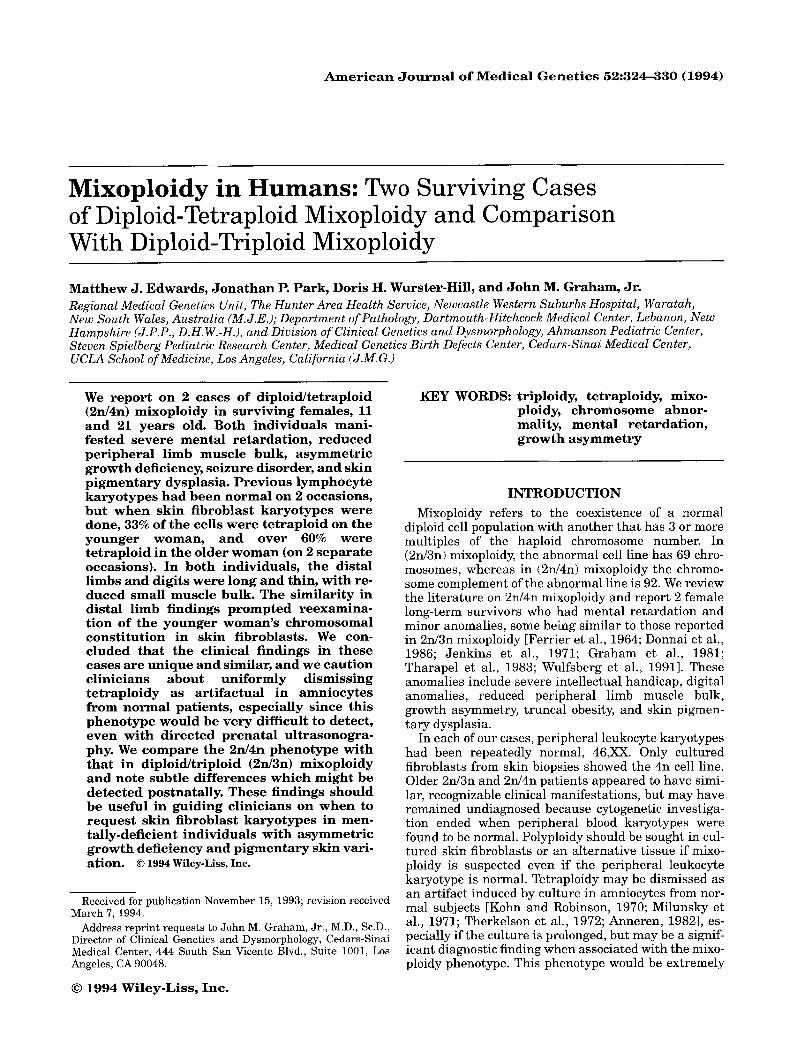
Fig. 1. This 21-year-old woman (Patient 1) with 2ni4n mixoploidy has minor anomaly features with irrcgular skin hyperpigmentation of axillae and trunk, and long, tapered digits with slender hands and feet.
ond toes had bulbous tips and there was partial syn- dactyly between toes 2 and 3. The retina appeared nor- mal on direct fundoscopy and there were no focal neu- rological signs. There was irregular pigmentation of the axillai and trunk, which had been present for several years. No studies were performed to exclude a fungal infection as the basis for this pigmentation. We sus- pected 2d3n mixoploidy and, after considerable discus- sion with the parents about the merits of further inves- tigation, collected a skin biopsy for fibroblast culture and karyotype from an area of normal pigmentation over the flexor aspect of the forearm.
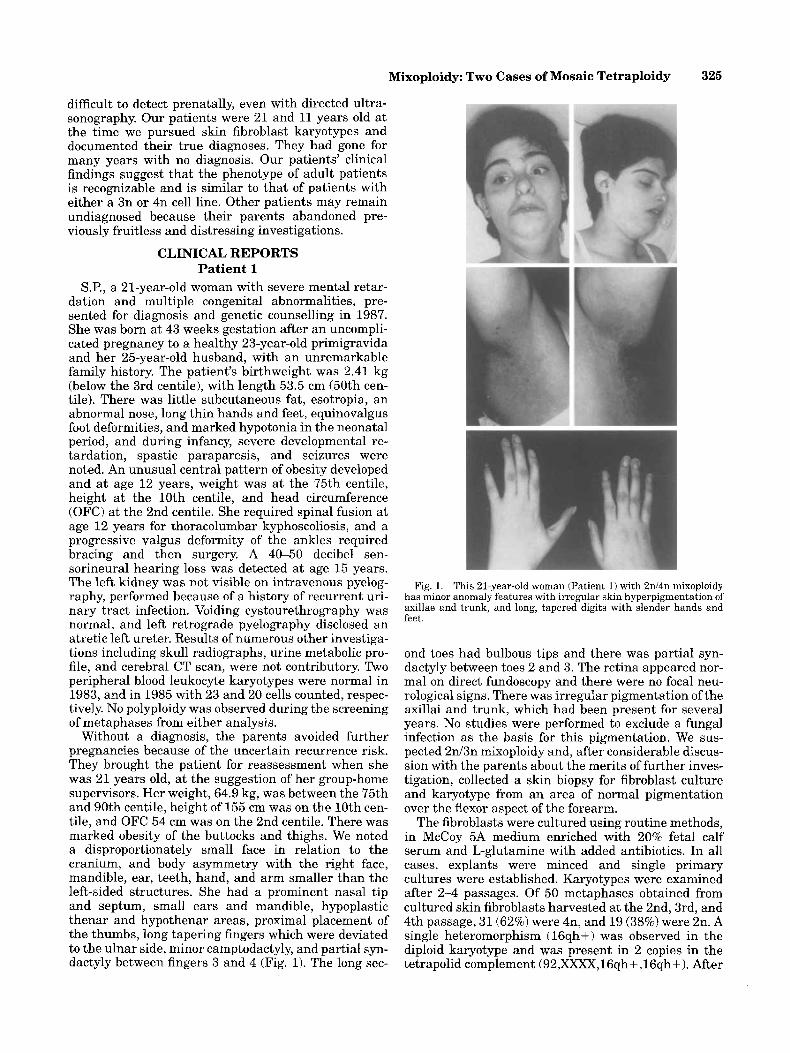
The fibroblasts were cultured using routine methods, in McCoy 5A medium enriched with 20% fetal calf serum and L-glutamine with added antibiotics. In all cases, explants were minced and single primary cultures were established. Karyotypes were examined after 2 4 passages. Of 50 metaphases obtained from cultured skin fibroblasts harvested at the 2nd, 3rd, and 4th passage, 31 (62%) were 4n, and 19 (38%) were 2n. A single heteromorphism (16qh+ ) was observed in the diploid karyotype and was present in 2 copies in the tetrapolid complement (92,XXXX,16qh+ ,16qh+). After
326 Edwards et al.
the results were available from the first study, a second skin biopsy was obtained and cultured in parallel with control fibroblasts to exclude a possible culture artifact. Of 200 metaphases from the third passage of cultured skin fibroblasts from the second biopsy, 61% were 4n and 39% were 2n. Of 100 cells from a third passage cul- ture of control skin fibroblasts, 13 were 4n and 87 were 2n (Fig. 2).
Patient 2 C.D., an 11-year-old girl with severe mental retarda-
tion, was first seen in 1992. She was born t o a healthy 26-year-old mother and 27-year-old father who had no significant family history. The pregnancy was compli- cated by influenza without severe fever at 6 weeks, and at 35 weeks gestation microcephaly was detected on an ultrasound scan. Birthweight was 2,635 g at term (3rd centile). There were early feeding problems requiring admission to an intensive care nursery, with associated failure to thrive. Absence-type seizures were noted from the age of one year, and a grand ma1 seizure ac- companied an illness diagnosed as meningoencephali- tis at age 3 years. No pathogen was isolated. The illness was followed by right hemiplegia and the loss of speech which had been previously limited to single words. The patient walked at age 5 years. Adrenarche, but not rnenarche, commenced at 11 years of age, and thoracic scoliosis (convex to the right) was also noted. She at- tends a special school for severely intellectually handi- capped children and has mixed seizures treated with valproate and carbamazepine. She has no speech but understands simple sentences.
100
80
60
YO 40
20
0
0 Diploid Tetrapiold
Fig. 2. Results of lymphocyte and skin fibroblast cultures for cyto- genetic analysis are shown here graphically for Patient 1.
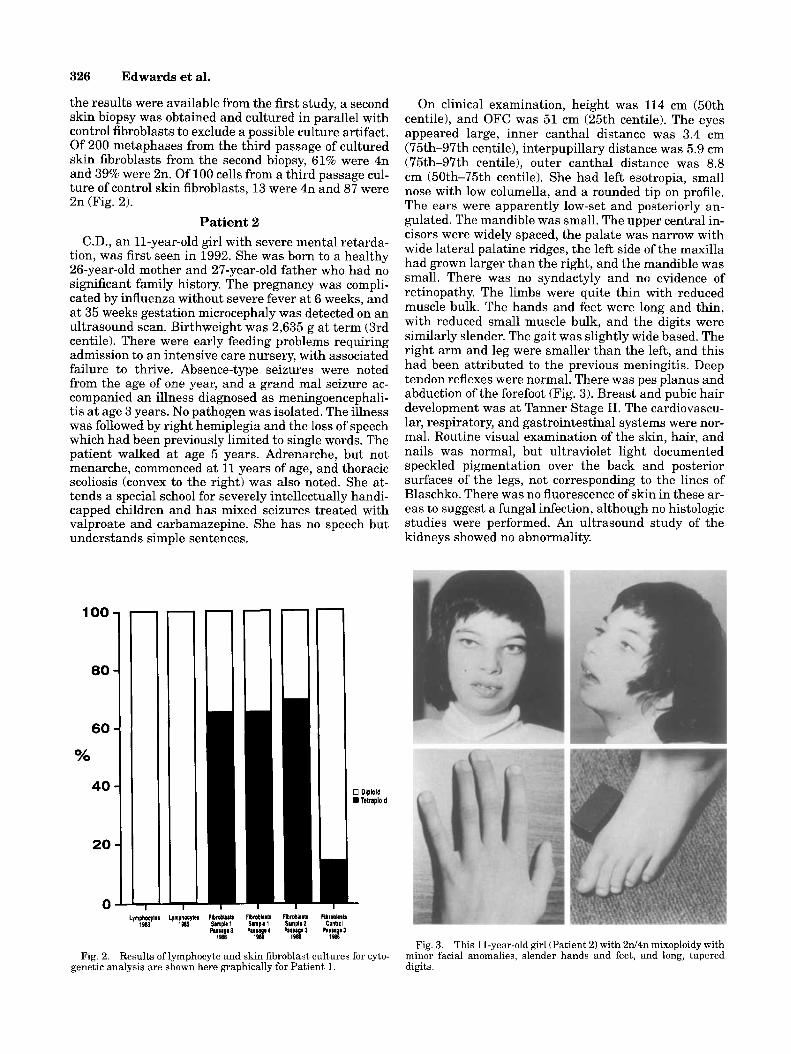
On clinical examination, height was 114 cm (50th centile), and OFC was 51 cm (25th centile). The eyes appeared large, inner canthal distance was 3.4 cm (75th-97th centile), interpupillary distance was 5.9 cm (75th-97th centile), outer canthal distance was 8.8 cm (50th-75th centile). She had left esotropia, small nose with low columella, and a rounded tip on profile. The ears were apparently low-set and posteriorly an- gulated. The mandible was small. The upper central in- cisors were widely spaced, the palate was narrow with wide lateral palatine ridges, the left side of the maxilla had grown larger than the right, and the mandible was small. There was no syndactyly and no evidence of retinopathy. The limbs were quite thin with reduced muscle bulk. The hands and feet were long and thin, with reduced small muscle bulk, and the digits were similarly slender. The gait was slightly wide based. The right arm and leg were smaller than the left, and this had been attributed to the previous meningitis. Deep tendon reflexes were normal. There was pes planus and abduction ofthe forefoot (Fig. 3). Breast and pubic hair development was at Tanner Stage 11. The cardiovascu- lar, respiratory, and gastrointestinal systems were nor- mal. Routine visual examination of the skin, hair, and nails was normal, but ultraviolet light documented speckled pigmentation over the back and posterior surfaces of the legs, not corresponding to the lines of Blaschko. There was no fluorescence of skin in these ar- eas to suggest a fungal infection, although no histologic studies were performed. An ultrasound study of the kidneys showed no abnormality.
Fig. 3. This 11-year-old girl (Patient 2) with 2d4n mixoploidy with minor facial anomalies, slender hands and feet, and long, tapered digits.
Mixoploidy: Two Cases of Mosaic Tetraploidy 327
fro previous peripheral blood lymphocyte kary- otypes had been normal, 46,XX (20 cells counted). Be- cause of clinical similarities with Patient 1, skin from a normally pigmented area was collected for fibroblast karyotype. Skin fibroblasts were cultured for one pas- sage without controls, and 15 of 45 cells counted (33%) were 4n (92,XXXX). Although there was no parallel control, no other cultures of skin fibroblasts in this cytogenetics lab had ever exceeded 15% tetraploidy. About 1 patient in every 20 has had a few tetraploid fi- broblasts, which have been attributed to culture arti- fact in this laboratory. Rare artifactual tetraploid cells in otherwise diploid cell cultures are thought t o arise by in vitro duplication of the chromosome complement without subsequent cytokinesis.
DISCUSSION Mixoploidy may arise by a number of theoretical
mechanisms [Niebuhr, 1974; Van Den Berghe et al., 1970; Chambon et al., 19751, but is usually due to mo- saicism (populations of cells with different genetic com- position arising from a single zygote). The mechanisms of 2 d 3 n mixoploidy formation implicated by studies of genetic or chromosomal polymorphisms have been re- viewed previously [Donnai et al., 19881, and include dispermy with incorporation of the second sperm to an early diploid nucleus of the embryo [Dewald et al., 19751, incorporation of the second polar body into a daughter nucleus of the zygote [Schmid and Vischer, 1967; Ellis e t al., 19631, or chimera formation by union of triploid and diploid embryos [Lejeune et al., 19671.
The occurrence of 2d3n mixoploidy in one pair of monochorionic diamniotic twin females suggests that mixoploidy can arise between 3 and 8 days of embryonic development [Wulfsberg et al., 19911. Recently, tetraploidy was noted by CVS following death of one twin in early pregnancy. Amniocentesis and ultrasound evaluation were normal. After delivery of an appar- ently normal boy, 2d4n mixoploidy was demonstrated in placental tissues, but no long-term follow-up or cyto- genetic evaluation of the child was reported [Rudnicki et al., 19911. A similar vanishing twin phenomenon has been demonstrated after the prenatal diagnosis of trisomy 16 mosaicism in direct and cultured CVS, with normal amniocentesis and cord blood karyotype [Tharapel e t al., 19891.
The most plausible mechanism for 2d4n mixoploidy is failure of cytokinesis a t some time after the first mi- totic division of the zygote, resulting in a mosaic. Alter- natively, a 2n zygote and a 4n zygote may unite to form a chimera. An initially 4n zygote could arise by several mechanisms which include trispermy [Sheppart et al., 19821, but suppression of cytokinesis is the most likely explanation for tetraploid cells with equal numbers of maternal and paternal chromosomes [Kajii and Niikawa, 1977; Pitt et al., 19811. Fertilization of a 2n ovum by 3 spermatoza is less likely. The mechanisms of origin have been deduced by studying parental chro- mosome polymorphisms, although some doubt has recently been cast on the accuracy of this technique in the study of parental origin and meiotic stage of origin of trisomy 21 [Peterson et al., 19911.
Stillborn or miscarried fetuses, and a smaller num- ber of surviving newborn infants with complete triploidy or tetraploidy, may have several manifesta- tions in common with mixoploid patients, although abnormalities are often less severe in mixoploidy. A greater degree of genetic imbalance and a more severe phenotype may intuitively be expected in 4n vs. 3n in- dividuals, but a “dosage effect” is not clearly apparent [Wilson et al., 19881. The percentage of polyploid cells in affected tissues, and the tissue distribution of poly- ploidy, could influence the severity of phenotypic ex- pression, as well as the sensitivity of karyotypic diag- nosis in both forms of mixoploidy. The ratio of paternal to maternal genetic material, which is always unbal- anced in triploid cells, may also be important. Also, fail- ure of X inactivation occurs in triploidy, and this may contribute to the phenotypic alterations in this disorder [Jacobs et al., 1979; Graham et al., 1981; Maraschio et al., 19841. The relative rarity of 4n mixoploidy com- pared with 3n mixoploidy may reflect a relatively in- frequent etiological mechanism, a greater likelihood of early pregnancy loss, relative difficulty of diagnosis, or failure to recognize tetraploidy as pathological.
There have been 8 neonates reported with complete tetraploidy [Golbus et al., 1976; Pitt e t al., 1981; Scar- brough et al., 1984; Lafer and Neu, 1988; Shiono et al., 1988; Lopez-Pajaves et al., 19901. They have demon- strated intrauterine growth deficiency, hypotonia, microcephaly with prominent forehead, small pinched nose, cleft lip and/or palate, small palpebral fissures, microphthalmia and/or coloboma, apparently low-set “dysplastic” ears with occasional preauricular tags, long slender limbs and digits with positional deforma- tion, and occasional CNS, heart, and genitourinary de- fects. Only 2 of the cases survived the first year to be alive a t 15 and 22 months, with a third surviving child alive at 3 months.
Thirteen cases of 2d4n mixoploidy have been re- ported, including the 2 cases described herein [Kohn et al., 1967; Kelly and Rary, 1974; Reddy et al., 1977; Veenema et al., 1982; Quiroz et al., 1985; Wittwer and Wittwer, 1985; Wilson et al., 1988; Aughton et al., 1988; Morris and Lustgarten, 1989; Urioste et al., 1990; Wullich et al., 19911. The two sisters reported by Rojanasakul et al. 119851 were excluded because of the low level of mosaicism in blood and fibroblasts and the lack of morphological or developmental changes. The case of Atnip and Summit [19711 was excluded because he also had trisomy 18 mosaicism. Postnatal features of another patient detected antenatally, who also had a 14/21 translocation, have not been published to our knowledge [Mitter e t al., 19881.
As shown in Table I, the phenotype for 2d4n mixo- ploidy is similar to full tetraploidy but milder. As demonstrated by our 2 cases, the facial changes and limb findings are distinct and unusual when combined with asymmetric growth deficiency and mental retar- dation.
Most reports of 2d4n mixoploidy have only involved young children [Aughton et al., 1988; Wilson et al., 1988 Urioste e t al., 1990; Wullich et al., 19911. We de- scribe the phenotype in older patients, and it bears
328 Edwards et al.
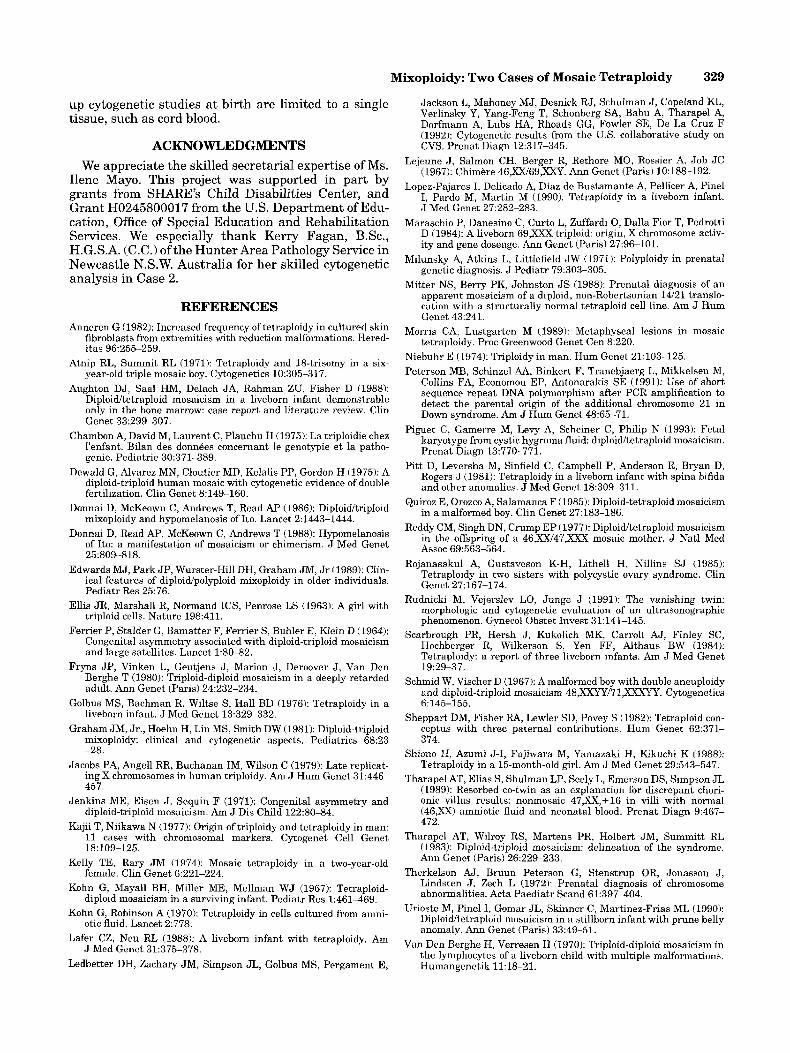
TABLE I . Manifestations of Polvploidv in Humans'
Diploidyltriploidy Diploidyltetraploidy Distinguishing manifestations 2d3n 2d4n Triploidy 3n Tetraploidy 4n
Asymmetry 11/17 4/10 2/44 015 Irregular skin pigmentation 5/13 3/9 Lethal 015 Tivncal obesity after 6 yrs. 618 113 Lethal Lethal Microlanophthalmia 2/12 118 10144 516 Ocular coloboma 1/12 119 11/44 013 Epicanthus 1/12 016 14144 013 Cleft liplpalate 2/12 119 8/44 516 Finger syndactyly 6112 219 27/44 116 Toe syndactyly 6/12 4f8 15/44 216 Genital abnormalities 5/10 1/11 2012 1 3/51 Common findings: Mental retardation 10114 919 Lethal 515
External ear anomalies 411 2 811 0 15/22 414 Prominent nose, broad root 3/12 819 10144 213 Micrognathia 5/12 711 0 13/44 314 Contractures 611 2 3/10 10144 5/5 Failure to thrive 12/15 711 0 Lethal Lethal IUGR Frequent Frequent Frequent 516 Urological anomalies ? 3/12 23/38 115 Congenital heart disease 216 411 1 16/38 113
*Modified from Wilson et al., 1988, with additional data from Donnai et al., 1988; Aughton et al., 1988; Shiono et al., 1988; Lopes-Pajares et al., 1990; Lafer and Neu., 1988; Morris and Lustgarten, 1988; Wullich et al., 1991; Urioste et al., 1990.
Prominent forehead 7/15 5/9 Frequent 3/5
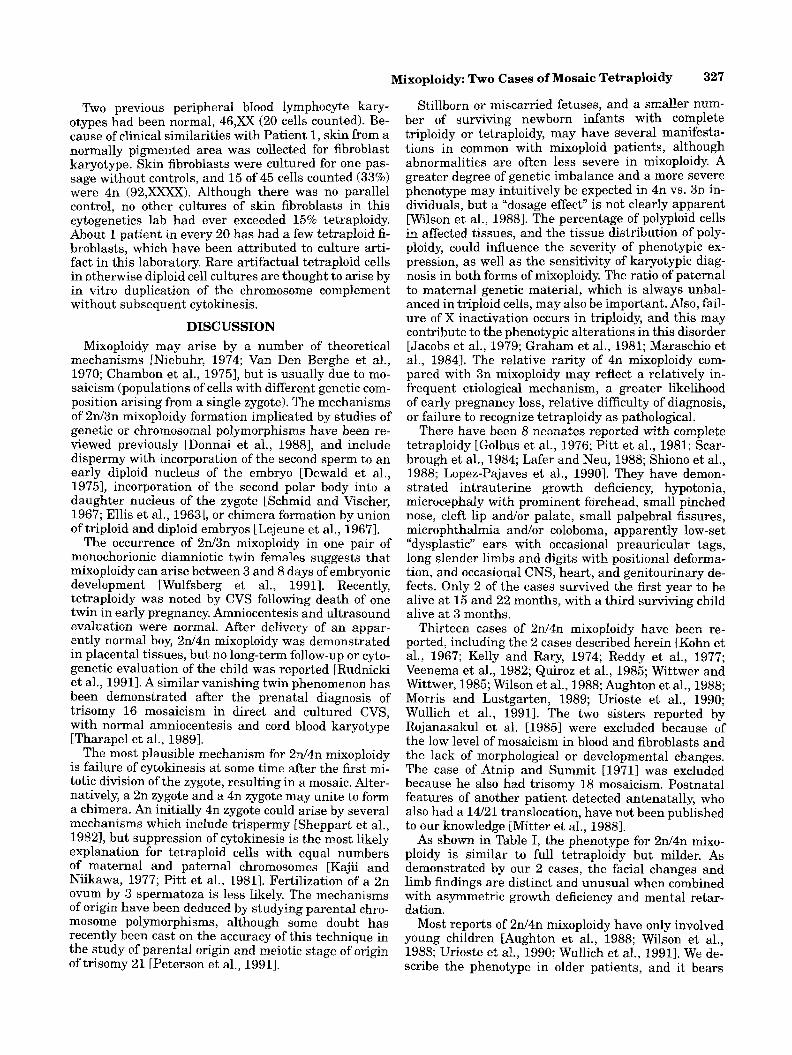
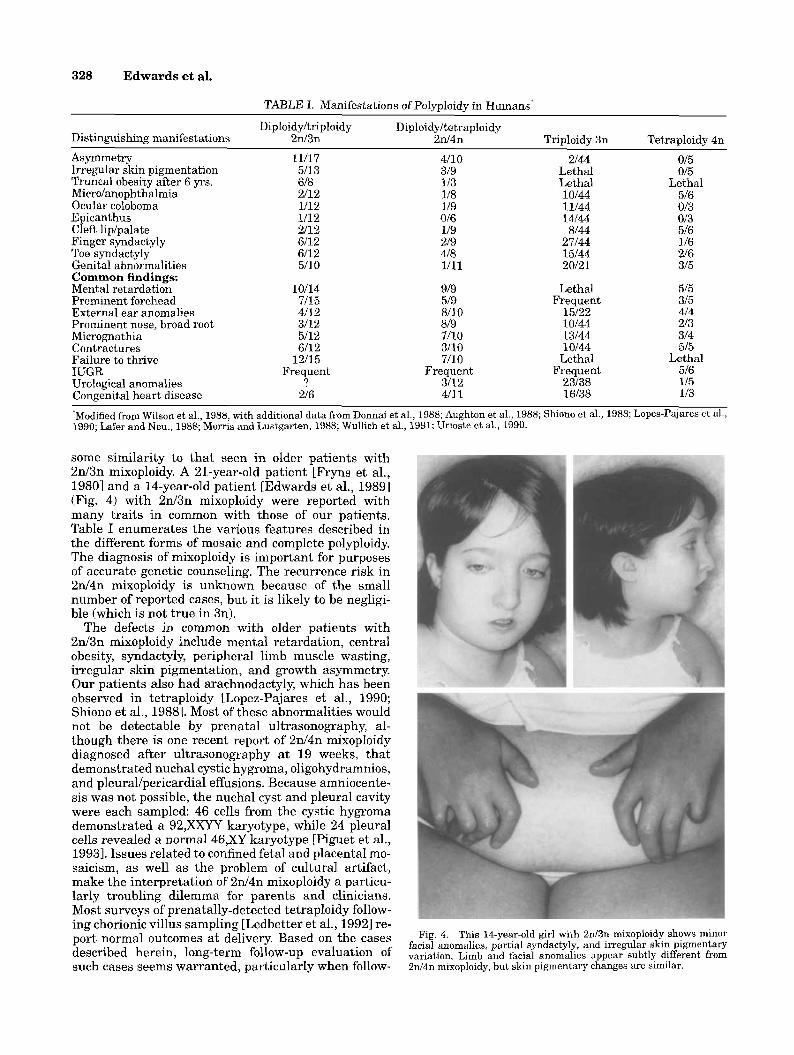
some similarity to that seen in older patients with 2d3n mixoploidy. A 21-year-old patient [Fryns et al., 19801 and a 14-year-old patient [Edwards et al., 19891 (Fig. 4) with 2d3n mixoploidy were reported with many traits in common with those of our patients. Table I enumerates the various features described in the different forms of mosaic and complete polyploidy. The diagnosis of mixoploidy is important for purposes of accurate genetic counseling. The recurrence risk in 2d4n mixoploidy is unknown because of the small number of reported cases, but it is likely to be negligi- ble (which is not true in 3n).
The defects in common with older patients with 2d3n mixoploidy include mental retardation, central obesity, syndactyly, peripheral limb muscle wasting, irregular skin pigmentation, and growth asymmetry. Our patients also had arachnodactyly, which has been observed in tetraploidy [Lopez-Pajares et al., 1990; Shiono et al., 19881. Most of these abnormalities would not be detectable by prenatal ultrasonography, al- though there is one recent report of 2d4n mixoploidy diagnosed after ultrasonography at 19 weeks, that demonstrated nuchal cystic hygroma, oligohydramnios, and pleuraVpericardia1 effusions. Because amniocente- sis was not possible, the nuchal cyst and pleural cavity were each sampled: 46 cells from the cystic hygroma demonstrated a 92,XXYY karyotype, while 24 pleural cells revealed a normal 46,XY karyotype [Piguet et al., 19931. Issues related to confined fetal and placental mo- saicism, as well as the problem of cultural artifact, make the interpretation of 2d4n mixoploidy a particu- larly troubling dilemma for parents and clinicians. Most surveys of prenatally-detected tetraploidv follow- ing chorionic villus sampling [Ledbetter e t al., i9921 re-
Fig. 4. This 14-year-old girl with 2d3n mixoploidy shows minor facial anomalies, partial syndactyly, and irregular skin pigmentary variation. Limb and facial anomalies appear subtly different from
outcomes at Based On the described herein, follow-~P evaluation of such cases seems warranted, particularly when follow- 2d4n mixoploidy, but skin pigmentary changes arc similar.
Mixoploidy: Two Cases of Mosaic Tetraploidy 329
Jackson L, Mahoney MJ, Desnick RJ, Schulnlan J , Copeland KL, Verlinsky Y, Yang-Feng T, Schonberg SA, Babu A, Tharapel A, Dorfmann A, Lubs HA, Rhoads GG, Fowler SE, De La Cruz F (1992): Cytogenetic results from the US . collaborative study on CVS. Prenat Diagn 12:317-345.
Lejeune J , Salmon CH, Berger R, Rethore MO, Rossier A, Job J C (1967): Chimere 46,xXi69,XXY. Ann Genct (Paris) 10:188-192.
Lopez-Pajares I, Delicado A, Diaz de Bustamante A, Pellicer A, Pinel I, Pardo M, Martin M (1990): Tetraploidy in a liveborn infant. J Med Genet 27:282-283.
Maraschio P, Danesino C; Curto L, Zuffardi 0 , Dalla Fior T, Pedrotti D (1984): A liveborn 69 , Iwr triploid: origin, X chromosome activ- ity and gene doseage. Ann Genet (Paris) 27:96-101.
Milunsky A, Atkins L, Littlefield JW (1971): Polyploidy in prenatal genetic diagnosis. J Pediatr 79:303-305.
Mitter NS, Berry PK, Johnston JS (1988): Prenatal diagnosis of an apparent mosaicism of a diploid, non-Robertsonian 14/21 translo- cation with a structurally normal tetraploid cell line. Am J Hum Genct 43:241.
Morris CA, Lustgarten M (1989): Metaphyseal lesions in mosaic tetraploidy. Proc Greenwood Genet Cen 8:220.
Niebuhr E (1974): Triploidy in man. Hum Genet 21:103-125. Peterson ME, Schinzel AA, Binkert F, Tranebjaerg L, Mikkelsen M,
Collins FA, Economou EP, Antonarakis SE (1991): Use of short sequence repeat DNA polymorphism after PCR amplification to detect the parental origin of the additional chromosome 21 in Down syndrome. Am J Hum Genet 48:65-71.
Piguet C, Gamerre M, Levy A, Scheiner C, Philip N (1993): Fetal karyotype from cystic hygroma fluid: diploidketraploid mosaicism. Prenat Diagn 13:770-771.
Pitt D, Leversha M, Sinfield C, Campbell P, Anderson R, Bryan D, Rogers J (1981): Tetraploidy in a liveborn infant with spina bifida and other anomalics. J Mcd Genct 18:309-311.
Quiroz E, Orozco A; Salamanca F (1985): Diploid-tetraploid mosaicism in a malformed boy. Clin Genet 27:183-186.
Reddy CM, Singh DN, Crump E P (1977): Diploidketraploid mosaicism in the offspring of a 46,XX/47,XXX mosaic mother. J Natl Med A~soc 69:563-564.
Rojanasakul A, Gustavcson K-H, Lithell H, Nillins SJ (1985): Tetraploidy in two sisters with polycystic ovary syndromc. Clin Genet 27:167-174.
Rudnicki M, Vejerslev LO, Junge J (1991): The vanishing twin: morphologic and cytogenetic evaluation of an ultrasonographic phenomenon. Gynecol Obstet Invest 31:141-145.
Scarbrough PR, Hersh J, Kukolich MK, Carroll AJ, Finley SC, Hochberger R, Wilkerson S, Yen FF, Althaus BW (1984): Tetraploidy: a report of three liveborn infants. Am J Med Genet 19:29-37.
Schmid W, Vischer D (1967): A malformcd boy with double aneuploidy and diploid-triploid mosaicism 48,xxYY:71 ,xXXYY. Cytogenetics 6:145-155.
Sheppart DM, Fisher RA, Lewler SD, Povey S (1982): Tetraploid con- ccptus with thrcc paternal contributions. Hum Genet 62:371- 374.
Shiono H, Azumi J-I, Fujiwara 111, Yamazaki H, Kikuchi K (1988): Tetraploidy in a 15-month-old girl. Am J Med Genet 29543-547.
Tharapel AT, Elias S, Shulman LP, Seely L, Emerson DS, Simpson JL (1989): Resorbed co-twin as an explanation for discrepant chori- onic villus results: nonmosaic 47,XX,+16 in villi with normal (46,XX) amniotic fluid and neonatal blood. Prenat Diagn 9467- 472.
Tharapel AT, Wilroy RS, Martens PR, Holbert JM, Summitt RL (1983): Diploid-triploid mosaicism: delineation of the syndrome. Ann Genet (Paris) 26:229-233.
Therkelson AJ, Bruun Peterson G, Stenstrup OR, Jonasson J, Lindsten J , Zech L (1972): Prenatal diagnosis of chromosome abnormalities. Acta Paediatr Scand 6L397-404.
Urioste M, Pinel I, Gomar JL, Skinner C, Martinez-Frias ML (1990): Diploid'tetraploid mosaicism in a stillborn infant with prune belly anomaly. Ann Genet (Paris) 33:49-51.
Van Den Berghe H, Verresen H (1970): Triploid-diploid mosaicism in the lymphocytes of a liveborn child with multiple malformations. Humangenctik 11: 18-21,
up cytogenetic studies at birth are limited to a single tissue, such as cord blood.
ACKNOWLEDGMENTS We appreciate the skilled secretarial expertise of Ms.
Ilene Mayo. This project was supported in part by grants from SHARE'S Child Disabilities Center, and Grant H0245800017 from the U.S. Department of Edu- cation, Office of Special Education and Rehabilitation Services. We especially thank Kerry Fagan, B.Sc., H.G.S.A. (C.C.) of the Hunter Area Pathology Service in Newcastle N.S.W. Australia for her skilled cytogenetic analysis in Case 2.
REFERENCES Anneren G (1982): Increased frequency of tetraploidy in cultured skin
fibroblasts from extremities with reduction malformations. Hered- itas 96:255-259.
Atnip RL, Summit RL (1971): Tetraploidy and 18-trisomy in a six- year-old triple mosaic boy. Cytogenetics 10:305-317.
Aughton DJ, Saal HM, Delach JA, Rahman ZU, Fisher D (1988): Diploidhtraploid mosaicism in a liveborn infant demonstrable only in the bnne marrow: case report and literature review. Clin Genet 33:299-307.
Chambon A, David M, Laurent C, Plauchu €1 (1975): La triploidie chez l'enfant. Bilan des donnees concernant le genotypie et la patho- genie. Pediatrie 30571-389.
Dewald G, Alvarez MN, Cloutier MD, Kelalis PP, Gordon H (1975): A diploid-triploid human mosaic with cytogenetic evidence of double fertilization. Clin Genet 8:149-160.
Donnai D, McKeown C, Andrews T, Read AP (1986): Diploiditriploid mixoploidy and hypomelanosis of Ito. Lancet 2:1443-1444.
Donnai D, Read AP, McKeown C, Andrews T (1988): Hypomelanosis of Ito: a manifestation of mosaicism or chimerism. J Med Genet 25:809-818.
Edwards MJ, Park JP, Wurster-Hill DH, Graham JM, Jr (1989): Clin- ical features of diploid/polyploid mixoploidy in older individuals. Pediatr Res 25:76.
Ellis JR, Marshall R, Normand ICS, Penrose LS (1963): A girl with triploid cells. Nature 198:411.
Ferrier P, Stalder G, Bamatter F, Ferrier S, Buhler E, Klein D (1964): Congenital asymmetry associated with diploid-triploid mosaicism and large satellites. Lancet 1:80-82.
Fryns JP, Vinken L, Geutjens J, Marion J , Deroover J , Van Den Berghe T (1980): Triploid-diploid mosaicism in a deeply retarded adult. Ann Genet (Paris) 24:232-234.
Golbus MS, Bachman R, Wiltse S , Hall BL) (1976): Tetraploidy in a liveborn infant. J Med Genet 13:329-332.
Graham JM, Jr., Hoehn H, Lin MS, Smith DW (1981): Diploid-triploid mixoploidy: clinical and cytogenetic aspects. Pediatrics 68:23 -28.
Jacobs PA, Angel1 RR, Buchanan IM, Wilson C (1979): Late replicat- ing X chromosomes in human triploidy. Am J Hum Genet 31:446- 457.
Jenkins ME, Eisen J, Sequin F (1971): Congenital asymmetry and diploid-triploid mosaicism. Am J Dis Child 122230-84.
Kajii T, Niikawa N (1977): Origin of triploidy and tetraploidy in man: 11 cases with chromosomal markers. Cytogenet Cell Genet 18:109-125.
Kelly TE, Rary JM (1974): Mosaic tetraploidy in a two-year-old female. Clin Genet 6:221-224.
Kohn G, Mayall BH, Miller ME, Mellman WJ (1967): Tetraploid- diploid mosaicism in a surviving infant. Pediatr Res 1:461469.
Kohn G, Robinson A (1970): Tctraploidy in cells cultured from amni- otic fluid. Lancet 2:778.
Lafer CZ, Neu RL (1988): A liveborn infant with tetraploidy. Am J Med Genet 31:375-378.
Ledbetter DH, Zachary JM, Simpson JL, Ckdbus MS, Pergament E,

330 Edwards et al.
Veenema H, Tasseron EWK, Geraedts J P M (1982): Mosaic tetraploidy
Wilson GN, Vekemans MJJ, Kaplan P (1988): MCA/MR syndrome in
Wulfsberg EA, Wassel WC, Polo CA (1991): Monozygotic twin girls with diploidhriploid chromosome mosaicism and cutaneous pig- mentary dyplasia. Clin Genet 39:370-375.
Mosaic tetraploidy in a liveborn infant with features of the DiGeorge anomaly. Clin Genet 40:353-357.
Ym0ffM, h r k e LB (1973): 0c.u and central newous system find- ings in tetraploid-diploid mosaicism. Am J Ophthalmol 76:1036-
in a male neonate. Clin Genet 22295-298.
a female infant with tetraploidy mosai~sm: review ofthe human Wullich B, Henn W, eoterath E, Emis A, Fuchs S, Zankl M (1991): polyploidy phenotype. Am J Med Genet 30953-961.
Wither BB, wittwer HB (1985): Letter to the Editor: Information about diploid-tetraploid mosaicism in a six-year-old male. Clin Genet 28567468. 1042.




















