
The spatial range of contour integration deficits in schizophrenia

BRAIN AND COGNITION 9, 191-200 (1989)
Memory Deficits before and after Temporal Lobectomy: Effect of Laterality and Age of Onset
ANDREW J. SAYKIN, RUBEN C. GUR, NEIL M. SUSSMAN, MICHAEL J. O’CONNOR, AND RAQUEL E. GUR
Brain-Behavior Laboratory, Departments of Psychiatry and Neurology, University of Pennsyhunia, and the Comprehensive Epilepsy Center, Graduate Hospital
Laterality and age of onset effects on semantic and figural memory were evaluated in 30 right-handed, left speech dominant (amobarbital test) patients with epilepsy before and after temporal lobectomy. There were no effects of focus on WAIS-R IQ scores. Early onset (~5 years) was associated with lower IQ and memory (WMS). Left Temporal (LT) patients showed worse semantic than figural memory preoperatively. Unexpectedly, early onset LT had marked postoperative decline of figural memory, whereas late onset LT patients showed the previously reported worsening of semantic memory. Right Temporal (RT) lobectomy patients, in contrast, improved in both semantic and figural memory regardless of age of onset. A “crowding effect” was suggested by the decline in figural memory following surgery in the early onset LT patients who remained stable or improved in semantic memory. Results indicate the need to incorporate age of onset of seizures into laterality models of memory function following unilateral temporal-hippocampal resection. 0 1989 Academic Press, 1~.
The temporal lobes and adjacent subcortical structures have long been implicated in memory (Squire & Butters, 1984, for review), in part on the basis of reports of memory deficits in temporal lobe epilepsy and temporal lobectomy (TL) (Milner, 1975, for summary). Hemispheric effects further have suggested a laterality model of semantic and figural memory, with semantic memory localized to the left temporal-hippocampal complex and figural memory to the homotopic right hemispheric region. Left temporal lobectomy (LTL) has been associated with decline in semantic
We thank Barbara Malamut, Susan McGroarty, Joanne McMahon, and Dr. Barbara Watson for their help. An earlier version of this paper was presented at the International Neuropsychological Society meeting in Denver, February 1986. Dr. Sussman is now at the Mid-Atlantic Regional Epilepsy Center, Department of Neurology, Medical College of Pennsylvania. Address correspondence and reprint requests to Dr. Andrew J. Saykin, Department of Psychiatry, Brain-Behavior Laboratory, 205 Piersol Building, University of Pennsylvania, Philadelphia, PA 19104.
191 027%2626/89 $3.00
Copyright Q 1989 by Academic Press, Inc. All rights of reproduction in any form reserved.

192 SAYKIN ET AL.
memory while right temporal lobectomy (RTL) has been associated with a decrease in figural memory (Kimura, 1963; Milner, 1968).
Mimer (1975) has also observed that LT focus patients show preoperative semantic memory impairment, but that deficits in figural memory are usually detected only after RTL. This suggests that the left hemisphere can partially compensate for figural memory deficits, and that lateralized effects of seizure focus are more pronounced after surgery. Others have likewise noted that the relationship between side of focus and pattern of memory impairment is not as clear preoperatively as postoperatively (Mateer & Dodrill, 1985). Thus, the laterality model may require adjustment to account for the preoperative pattern of memory deficits. Its modified form introduces a hemispheric asymmetry factor, with less pronounced effects of right focus on figural memory than of left focus on semantic memory.
The adequacy of the simple laterality model has also been challenged by evidence of improved memory following TL resection both for neoplasm (Cavazzuti, et al., 1980) and seizure control (Novelly et al., 1984). This suggests the effects of relief of the intact temporal lobe from the pathological influence of the diseased hemisphere, such as proposed by the concept of diaschisis (Von Monakow, 1960). A model incorporating this evidence would predict that TL, while still lowering memory functions associated with the operated hemisphere, will improve memory functions associated with the contralateral hemisphere.
Early onset of seizure disorder may lead to atypical hemispheric rep- resentation of function (Milner, 1975; McGlone, 1985; Mateer and Dodrill 1985), and thus the neuropsychological presentation of TL patients could be related to the age at which the cerebral damage is sustained. Many studies have associated early age of onset of seizures with lower IQ (e.g., Sullivan & Gahagan, 1935; Klove & Matthews, 1974; Dikmen, Matthews, & Harley, 1975; Woods, 1980). Lower neuropsychological functioning in general (motoric, attentional, memory, and cognitive) was found in a sample of children with tonic-clonic seizures with onset prior to age 5 (O’Leary, Seidenberg, Berent, & Boll, 1981). There has been a paucity of prospective data, but one study by Bourgeois, Prensky, Palkes, Talent, and Busch (1983) found that age at onset of seizures in children was one of the two best predictors of IQ on 4-year follow-up.
In cases of early dominant left hemispherectomy, language development can be shifted to the right hemisphere with relatively normal outcome (Smith, 1981, for review). However, verbal intellectual ability is usually spared at some expense to nonverbal cognitive function (Sperry, 1974; Teuber, 1974), which Milner (1974) has attributed to “crowding.” Laterality models have been suggested for language development (e.g., Moscovitch, 1976), but there has been disagreement regarding the “critical period” for language acquisition. Lenneberg (1967) suggested that normal later-
MEMORY AND TEMPORAL LOBECTOMY 193
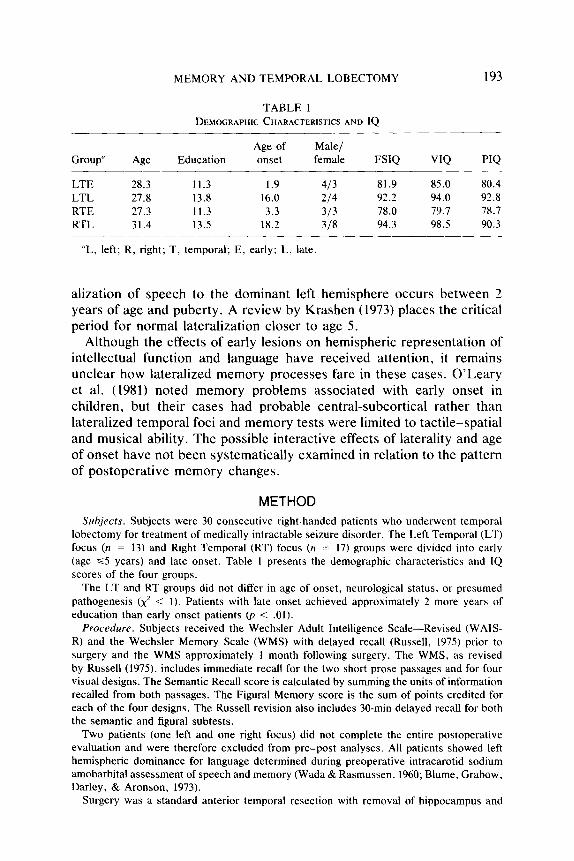
TABLE 1 DEMOGRAPHIC CHARACTERISTICS AND IQ
Group“ Age Education Age of onset
Male/ female FSIQ VIQ
LTE 28.3 11.3 1.9 413 81.9 85.0 80.4 LTL 27.8 13.8 16.0 214 92.2 94.0 92.8 RTE 27.3 11.3 3.3 313 78.0 79.7 78.7 RTL 31.4 13.5 18.2 318 94.3 98.5 90.3
“L, left; R, right; T, temporal; E, early; L, late.
alization of speech to the dominant left hemisphere occurs between 2 years of age and puberty. A review by Krashen (1973) places the critical period for normal lateralization closer to age 5.
Although the effects of early lesions on hemispheric representation of intellectual function and language have received attention, it remains unclear how lateralized memory processes fare in these cases. O’Leary et al. (1981) noted memory problems associated with early onset in children, but their cases had probable central-subcortical rather than lateralized temporal foci and memory tests were limited to tactile-spatial and musical ability. The possible interactive effects of laterality and age of onset have not been systematically examined in relation to the pattern of postoperative memory changes.
METHOD Subjects. Subjects were 30 consecutive right-handed patients who underwent temporal
lobectomy for treatment of medically intractable seizure disorder. The Left Temporal (LT) focus (n = 13) and Right Temporal (RT) focus (n = 17) groups were divided into early (age ~5 years) and late onset. Table I presents the demographic characteristics and IQ scores of the four groups.
The LT and RT groups did not differ in age of onset, neurological status, or presumed pathogenesis (x’ < 1). Patients with late onset achieved approximately 2 more years of education than early onset patients (p < .Ol).
Procedure. Subjects received the Wechsler Adult Intelligence Scale-Revised (WAIS- R) and the Wechsler Memory Scale (WMS) with delayed recall (Russell, 1975) prior to surgery and the WMS approximately 1 month following surgery. The WMS, as revised by Russell (1975), includes immediate recall for the two short prose passages and for four visual designs. The Semantic Recall score is calculated by summing the units of information recalled from both passages. The Figural Memory score is the sum of points credited for each of the four designs. The Russell revision also includes 30-min delayed recall for both the semantic and figural subtests.
Two patients (one left and one right focus) did not complete the entire postoperative evaluation and were therefore excluded from pre-post analyses. All patients showed left hemispheric dominance for language determined during preoperative intracarotid sodium amobarbital assessment of speech and memory (Wada &Rasmussen, 1960; Blume, Grabow. Darley, & Aronson, 1973).
Surgery was a standard anterior temporal resection with removal of hippocampus and
194 SAYKIN ET AL.
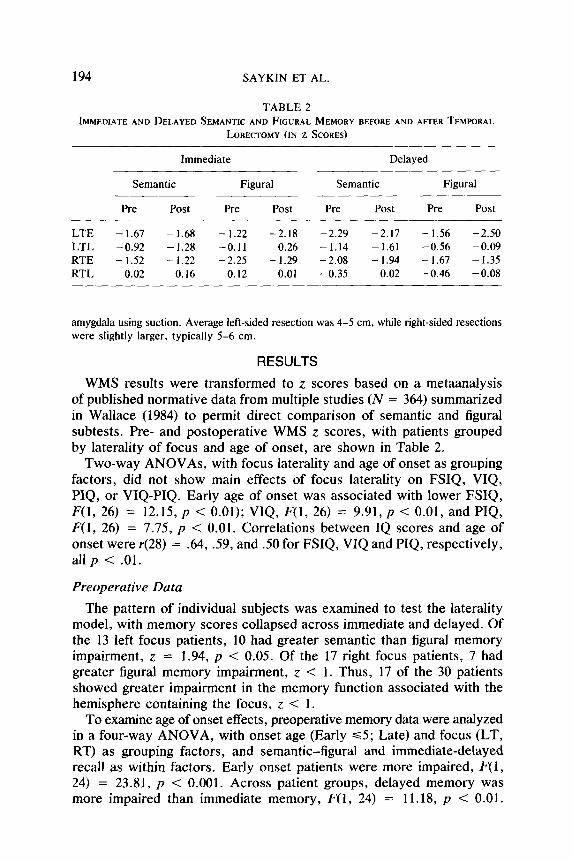
TABLE 2 IMMEDIATE AND DELAYED SEMANTIC AND FIGURAL MEMORY BEFORE AND AFTER TEMPORAL
LOBECTOMY (IN z SCORES)
LTE LTL RTE RTL
Immediate Delayed
Semantic Figural Semantic Figural
Pre Post Pre Post Pre Post Pre Post
-1.67 - 1.68 -1.22 -2.18 -2.29 -2.17 - 1.56 - 2.50 -0.92 -1.28 -0.11 0.26 -1.14 -1.61 -0.56 -0.09 - 1.52 - 1.22 -2.25 -1.29 - 2.08 - 1.94 - 1.67 - 1.35
0.02 0.16 0.12 0.01 -0.35 -0.02 -0.46 -0.08
amygdala using suction. Average left-sided resection was 4-5 cm, while right-sided resections were slightly larger, typically 5-6 cm.
RESULTS
WMS results were transformed to z. scores based on a metaanalysis of published normative data from multiple studies (N = 364) summarized in Wallace (1984) to permit direct comparison of semantic and figural subtests. Pre- and postoperative WMS z scores, with patients grouped by laterality of focus and age of onset, are shown in Table 2.
Two-way ANOVAs, with focus laterality and age of onset as grouping factors, did not show main effects of focus laterality on FSIQ, VIQ, PIQ, or VIQ-PIQ. Early age of onset was associated with lower FSIQ, F(1, 26) = 12.15, p < 0.01); VIQ, F(1, 26) = 9.91, p < 0.01, and PIQ, F(1, 26) = 7.75, p < 0.01. Correlations between IQ scores and age of onset were r(28) = .64, 59, and 50 for FSIQ, VIQ and PIQ, respectively, all p < .Ol.
Preoperative Data
The pattern of individual subjects was examined to test the laterality model, with memory scores collapsed across immediate and delayed. Of the 13 left focus patients, 10 had greater semantic than figural memory impairment, z = 1.94, p < 0.05. Of the 17 right focus patients, 7 had greater figural memory impairment, z < 1. Thus, 17 of the 30 patients showed greater impairment in the memory function associated with the hemisphere containing the focus, z < 1.
To examine age of onset effects, preoperative memory data were analyzed in a four-way ANOVA, with onset age (Early ~5; Late) and focus (LT, RT) as grouping factors, and semantic-figural and immediate-delayed recall as within factors. Early onset patients were more impaired, F(1, 24) = 23.81, p < 0.001. Across patient groups, delayed memory was more impaired than immediate memory, F(1, 24) = 11.18, p -=c 0.01.

MEMORY AND TEMPORAL LOBECTOMY
IMPAIRMENT IZ-SCORE)
r--
IMM DEL IMM DEL
EARLY ONSET LATE ONSET
195
FIG. 1. Preoperative memory function in temporal lobectomy patients: Effects of semantic (solid lines) vs. figural (dashed lines) material, immediate (IMM) vs. delayed (DEL) recall, and early vs. late age of onset.
There was a Semantic-figural x Onset age x Immediate-delayed in- teraction, F(1, 24) = 5.04, p < 0.05. This interaction is illustrated in Fig. 1.
Whereas for early onset patients delayed recall was worse than immediate recall for semantic and slightly better than immediate recall for figural, in late onset patients delayed recall was worse for both, with a steeper gradient for figural.
The Effects of Lobectomy
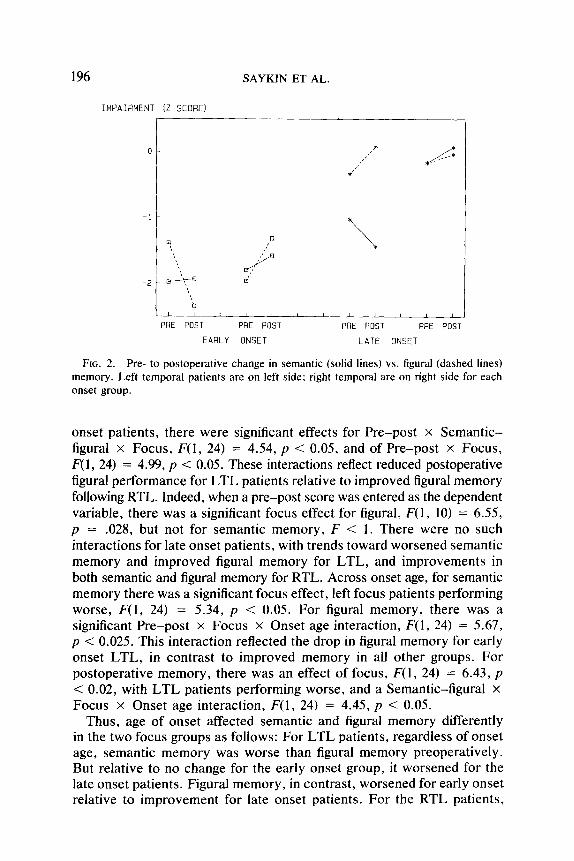
To examine age of onset effects on memory changes, a preoperative- postoperative factor was added to the ANOVA design applied to the preoperative data. This factor did not have a significant main effect, F < 1, indicating no overall change in memory functioning following lo- bectomy. The effects of onset age and immediate-delayed which were significant for the preoperative scores remained significant when post- operative scores were added. Early onset patients performed worse than late onset patients for every cell included in the ANOVA (all p < 0.001). The only new effect of surgery was a Pre-post x Onset age x Focus x Semantic-figural interaction, F(1, 24) = 6.98, p < 0.01. This interaction is illustrated in Fig. 2. The same main effects and interactions were obtained when FSIQ was entered as a covariate.
Decomposition of this four-way interaction by separate ANOVAs in- dicated that the Pre-post x Semantic-figural x Onset age was significant for LTL, F(1, 24) = 7.54, p < 0.01, but not for RTL, F < 1. For early
196 SAYKIN ET AL.
IMPAIAMENT (Z-SCORE1 -
PRE POST PRE POST PRE POST PRE POST
EARLY ONSET LATE ONSET
FIG. 2. Pre- to postoperative change in semantic (solid lines) vs. figural (dashed lines) memory. Left temporal patients are on left side; right temporal are on right side for each onset group.
onset patients, there were significant effects for Pre-post x Semantic- figural x Focus, F(1, 24) = 4.54, p < 0.05, and of Pre-post x Focus, F(l, 24) = 4.99, p < 0.05. These interactions reflect reduced postoperative figural performance for LTL patients relative to improved figural memory following RTL. Indeed, when a pre-post score was entered as the dependent variable, there was a significant focus effect for figural, F(1, 10) = 6.55, p = .028, but not for semantic memory, F < 1. There were no such interactions for late onset patients, with trends toward worsened semantic memory and improved figural memory for LTL, and improvements in both semantic and figural memory for RTL. Across onset age, for semantic memory there was a significant focus effect, left focus patients performing worse, F(1, 24) = 5.34, p < 0.05. For figural memory, there was a significant Pre-post x Focus x Onset age interaction, F( 1, 24) = 5.67, p < 0.025. This interaction reflected the drop in figural memory for early onset LTL, in contrast to improved memory in all other groups. For postoperative memory, there was an effect of focus, F(1, 24) = 6.43, p < 0.02, with LTL patients performing worse, and a Semantic-figural X Focus x Onset age interaction, F(1, 24) = 4.45, p < 0.05.
Thus, age of onset affected semantic and figural memory differently in the two focus groups as follows: For LTL patients, regardless of onset age, semantic memory was worse than figural memory preoperatively. But relative to no change for the early onset group, it worsened for the late onset patients. Figural memory, in contrast, worsened for early onset relative to improvement for late onset patients. For the RTL patients,
MEMORY AND TEMPORAL LOBECTOMY 197
in both onset groups, there was no difference between semantic and figural memory, preoperatively or postoperatively, and both showed post- operative improvement.
Age, Onset Age, and Duration of Illness
Analyses were performed to tease apart the effects of onset age from age at surgery and illness duration. Age and duration, defined as AGE- ONSET AGE, were entered as covariates in the Focus x Onset age ANOVAs. This did not influence the significant effects. Subjects were then grouped by median age into younger (range 13-29) and older (range 30-44) age, and by median duration score into shorter (range 3- 19 years) and longer (range 21-36 years) duration. A Focus x Age x
Pre-post ANOVA showed no age effects. A Focus x Duration x Pre- post ANOVA showed a main effect for duration, F(1, 24) = 6.68, p < 0.025, but when onset age was entered as a covariate, this effect dis- appeared, F < 1. Thus, neither age nor illness duration can account for the onset age findings.
DISCUSSION
The results do not support the stringent laterality model for the effects of temporal lobectomy on semantic and figural memory. This model was adequate for predicting preoperative pattern of deficits for the left focus patients only, as the majority of them had greater impairment in semantic memory. There was not a preponderance of figural memory impairment in right focus patients consistent with earlier reports (Milner, 1975; Mateer & Dodrill, 1985). The model was inadequate for predicting the effects of surgery in either group; the majority of left lobectomy patients did not show a drop in semantic memory, nor did the majority of right lobectomy patients show a drop in figural memory.
A model incorporating the hypothesis that relief from pathologic effects of the diseased hemisphere may cause memory improvement did not enhance the ability to predict surgery effects. There was not an increased frequency of improvement for figural memory following left and semantic memory following right lobectomy. Left lobectomy either improved figural memory at the expense of semantic memory, or improved semantic at the expense of figural memory. Right lobectomy seemed to improve semantic memory without causing a decline in figural memory. This is consistent with evidence for greater ability of the left hemisphere to cope with “crowding” of semantic and figural memory. Since all of our patients showed left hemisphere speech dominance on the amobarbital procedure, transfer of speech to the right hemisphere does not appear to be a prerequisite for crowding in the memory system.
Hemispheric differences in the ability to cope with crowding have been reported in hemispherectomy studies (Smith, 1981) and are of relevance

198 SAYKIN ET AL.
to theories concerning the underlying dimensions of hemispheric spe- cialization. For example, it has been proposed that hemispheric spe- cialization is a necessary sacrifice for the sake of achieving higher levels of specialized cognitive organization (Levy, 1969). This asymmetry may also relate to the hypothesis of more “diffuse” organization of functions in the right, relative to “focal” representation in the left hemisphere (Semmes, 1968). This latter hypothesis was supported by data on hemi- spheric asymmetry in the percentage of gray matter (Gur et al., 1980), measured by the 133-Xenon inhalation technique (Obrist, Thompson, Wang, & Wilkinson, 1975).
Age of onset was examined as a potential moderating factor, and the results indicate its importance. We replicated prior reports of lower IQ associated with early onset (e.g., Sullivan & Gahagan, 1935; Klove & Matthews, 1974) and also obtained similar effects for memory, controlling for duration of seizures. Our findings suggest that age of onset affects not only the level, but the pattern of memory changes produced by temporal lobectomy, and that the effects depend on the side of focus. For patients with left temporal lobe epilepsy, early onset may be associated with worsening of figural memory following lobectomy, whereas late onset portends improvement in figural and worsening in semantic memory. Larger samples will be required to evaluate whether a model incorporating this evidence will enable better specification of surgery outcome in relation to figural and semantic memory. Since the present study was limited to short term postoperative effects, further research is needed to determine the long term postoperative course of these patterns of memory impairment.
The effect of age of onset persisted across groups and was pronounced both for memory and IQ. It indicates that a longer history of temporal lobe epilepsy is associated with greater memory impairment. In light of evidence that uncontrolled seizures produce tissue loss (Engel, 1983), this finding supports the role of the temporal-hippocampal complex in memory. The more general effects of early brain damage need further clarification, particularly in relation to irritative lesions. It is known that early structural lesions or hemispheric resection can lead to anomalous representation of function, but the role of unilateral epileptic discharges in altered representation of cerebral function deserves further study. In this regard, it is important to note that age of onset of seizures may be later than onset of the original underlying pathology.
The slightly larger resections in the right temporal patients could also be a factor in the pattern of test results. However, there was no main effect of side of focus, only interactions. Although the LT patients had smaller lesions, they showed a general trend toward worse performance.
The inability to predict the side of focus in right temporal lobe patients could reflect inadequacies in the figural memory measure of the Wechsler Memory Scale, as was pointed out by Milner (1975). In the present study
MEMORY AND TEMPORAL LOBECTOMY 199
the scale appeared to be of some validity, since there were significant relationships with side of focus and onset age. However, it would be important to examine other measures of nonverbal memory in relation to age of onset.
REFERENCES Blume, W., Grabow, J., Dailey, F., & Aronson, A. 1973. Intracarotid amobarbital test of
language and memory before temporal lobectomy for seizure control. Neurology, 23, 812-819.
Bourgeois, B., Prensky, A., Palkes, H., Talent, B., & Busch, S. 1983. Intelligence in epilepsy: A prospective study in children. Annuls of Neurology, 14(4), 438-444.
Cavazzuti, V., Winston, K., Baker, R., et al. 1980. Psychological changes following surgery for tumors in the temporal lobe. Journal of Neurosurgery, 53, 618-626.
Dikmen, S., Matthews, C., & Harley, J. P. 1975. The effect of early versus late onset of major motor epilepsy upon cognitive-intellectual performance. Epilepsia, 16, 73-81.
Engel, J. 1983. Epileptic brain damage: How much excitement can a limbic neuron take. Trends in Neuroscience, September, 1983.
Gur, R. C., Packer, I. K., Hungerbuhler, J. P., Reivich, M., Obrist, W. D., Amamek. W. S., & Sackeim, H. A. 1980. Differences in the distribution of gray and white matter in human cerebral hemispheres. Science, 207, 1226-1228.
Kimura, D. 1963. Right temporal lobe damage. Archives of Neurology, 8, 264-271. Klove, H., & Matthews, C. 1974. Neuropsychological studies of patients with epilepsy.
In. R. Reitan and J. Davidson (Eds.), Clinical neuropsychology. Washington, DC: Winston.
Krashen, S. 1973. Lateralization, language learning and the critical period: Some new evidence. Language Learning, 23, 63-74.
Lenneberg, E. 1967. Biological foundations of language. New York: Wiley. Levy, J. 1969. Possible basis for the evolution of lateral specialization of the human brain,
Nature (London), 224, 614-615. Mateer, C. A., & Dodrill, C. 1985. Atypical language dominance. Presented at International
Neuropsychological Society, 13th Annual Meeting, San Diego, California, Symposium on the Sodium Amytal Procedure.
M&lone, J. 1985. Presentation at International Neuropsychological Society, 13th Annual Meeting, San Diego, California, Symposium on the Sodium Amytal Procedure.
Milner, B. 1968. Visual recognition and recall after right temporal lobe excision in man. Neuropsychologia, 6, 191-209.
Milner, B. 1974. Sparing of language functions after early unilateral brain damage. In E. Eidelberg and D. Stein (Eds.), Functional recovery after lesions of the nervous system. Neuroscience research program bulletin, 12, 213-216.
Milner, B. 1975. Psychological aspects of epilepsy and its neurosurgical management. In Advances in neurology. New York: Raven Press. Vol. 8.
Moscovitch, M. 1976. On the representation of language in the right hemisphere of right handed people. Brain and Language, 3, 47-71.
Novelly, R., Augustine, E., Mattson, R., Glaser, G., Williamson, P., Spencer, D., & Spencer, S. 1984. Selective memory improvement and impairment in temporal lobectomy for epilepsy. Annals of Neurology, 15, 64-67.
Obtist, W. D., Thompson, W. K., Wang, H. S., & Wilkinson, W. D. 1975. Regional cerebral blood flow estimated by 133-Xe inhalation. Stroke, 6, 245-256.
O’Leary, D. S., Seidenberg, M., Berent, S., & Boll, T. 1981. Effects of age of onset of tonic-clonic seizures on neuropsychological performance in children. Epilepsia, 22, 197-204.

200 SAYKIN ET AL.
Russell, E. 1975. A multiple scoring method for complex memory functions. Journal of Consulting and Clinical Psychology, 43, 800-809.
Semmes, J. 1968. Hemispheric specialization: A possible clue to mechanism. Neuropsy- chologia, 6, 11-26.
Smith, A. 1981. Principles underlying human brain functions in neuropsychological sequelae of different neuropathological processes. In S. Filskov and T. Boll (Eds.), Handbook of clinical neuropsychology. New York: Wiley. Vol. 1, pp. 175-226.
Sperry, R. 1974. Lateral specialization in the surgically separated hemispheres. In F. Schmitt and F. Worden (Eds.), The neurosciences: Third study program. Boston: MIT Press.
Squire, L., & Butters, N. 1984. Neuropsychology of memory. New York: Guilford. Sullivan, E. B., & Gahagan, L. 1935. On intelligence of epileptic children. Generic Psychology
Monographs, 17, 309-376. Teuber, H.-L. 1974. Why two brains? In F. Schmitt and F. Worden (Eds.), The neurosciences:
third study program. Boston: MIT Press. Von Monakow, C. 1960. Localization of brain functions [German]. (G. Von Bonin, Trans.)
In Some papers on the cerebral cortex. Springfield, IL: Thomas. (Original work published in 1911)
Wada, J., & Rasmussen, T. 1960. Intracarotid injection of sodium amytal for the lateralization of cerebral speech dominance. Journal of Neurosurgery, 17, 266-282.
Wallace, J. L. 1984. Wechsler Memory Scale. International Journal of Clinical Neuro- psychology, 6(3, Suppl.), 216-226.
Woods, B. T. 1980. The restricted effects of right hemisphere lesions after age one: Wechsler test data. Neuropsychologia, 18, 65-70.
Copyright © 2022 FDOKUMEN




















