MCSP-MNCH Activity in Nigeria Quarterly Report - PDF Server
48
Jan – Mar 2018 www.mcsprogram.org MCSP-MNCH Activity in Nigeria Quarterly Report Quarter 2 – January 01 to March 31, 2018 Submission Date: April 30, 2018 Cooperative Agreement Number: AID-OAA-A-N-00028 Activity Start Date and End Date: OCTOBER 01, 2014 to DECEMBER 31, 2018 Activity Manager (Dr. Gertrude Odezugo) Submitted by: Dr. Oniyire Adetiloye, Project Director Jhpiego Corporation Plot 971, Reuben Okoya Crescent, Off Okonjo Iweala Street, Wuye District, Abuja Tel: +234-803-446-3508 Email: [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of MCSP-MNCH Activity in Nigeria Quarterly Report - PDF Server
Jan – Mar 2018 www.mcsprogram.org
MCSP-MNCH Activity in Nigeria Quarterly Report
Quarter 2 – January 01 to March 31, 2018
Submission Date: April 30, 2018 Cooperative Agreement Number: AID-OAA-A-N-00028 Activity Start Date and End Date: OCTOBER 01, 2014 to DECEMBER 31, 2018 Activity Manager (Dr. Gertrude Odezugo)
Submitted by: Dr. Oniyire Adetiloye, Project Director Jhpiego Corporation Plot 971, Reuben Okoya Crescent, Off Okonjo Iweala Street, Wuye District, Abuja Tel: +234-803-446-3508 Email: [email protected]
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Activity Manager: Dr. Gertrude Odezugo Submitted by: Dr.Oniyire Adetiloye, Project Director
Jhpiego Corporation Plot 971, Reuben Okoya Crescent, Off Okonjo Iweala Steet, Wuye District, Abuja Tel: +234-803-446-3508 Email: [email protected]
This document was produced for review by the United States Agency for International Development Nigeria (USAID/Nigeria). This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID) under the terms of the Cooperative Agreement AID-OAA-A-N-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Table of Contents
1.0 PROJECT OVERVIEW / SUMMARY ..................................................................................................................... 7
2.0 ACTIVITY IMPLEMENTATION PROGRESS .................................................................................................... 10
2.1. Progress Narrative................................................................................................................................................... 10
2.2. Implementation Status ............................................................................................................................................ 12
2.2.1. Maternal Health ........................................................................................................................................................ 12
2.2.2. Newborn Health ...................................................................................................................................................... 14
2.2.3. Child Health .............................................................................................................................................................. 17
2.2.4. Family Planning & Reproductive Health .............................................................................................................. 19
2.2.5. Adolescent Sexual and Reproductive Health (ASRH) ..................................................................................... 20
2.2.6. Health Systems Strengthening and Equity .......................................................................................................... 22
2.2.7. Pre-Service Education ............................................................................................................................................. 22
2.3. Monitoring and Evaluation ..................................................................................................................................... 23
2.4. Operations Research .............................................................................................................................................. 25
3.0 INTEGRATION OF CROSSCUTTING ISSUES AND USAID FORWARD PRIORITIES ...................... 26
4.0 STAKEHOLDERS PARTICIPATION / INVOLVEMENT ................................................................................ 29
4.1. Professional Associations ....................................................................................................................................... 29
5.0 MANAGEMENT AND ADMINISTRATIVE ISSUES ........................................................................................ 31
6.0 CHALLENGES / LESSONS LEARNED ............................................................................................................... 32
7.0 PLANNED ACTIVITIES FOR NEXT QUARTER INCLUDING UPCOMING EVENTS ........................ 33
8.0 HOW IMPLEMENTING PARTNER HAS ADDRESSED A/COR COMMENTS FROM THE LAST QUARTERLY OR SEMI-ANNUAL REPORT .................................................................................................... 36
9.0 FINANCIAL MANAGEMENT .............................................................................................................................. 37
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
ACRONYMS AND ABBREVIATIONS AAP American Academy of Pediatrics
ACCESS Access to Clinical and Community Maternal, Neonatal and Women’s Health Services
ACOG American College of Obstetrics and Gynecology
ACNM American College of Nurse-Midwives
AMTSL Active Management of the Third Stage of Labor
AMURT Ananda Marga Universal Relief Team
ANC Antenatal Care
AOR Activity Officer Representative
ARI Acute Respiratory Infection
ASRH Adolescent Sexual Reproductive Health
bCPAP Bubble Continuous Positive Airway Pressure
CAII Center for Accelerating Innovation and Impact
CG Clinical Governance
CH Child Health
CHAI Clinton Health Access Initiative
CHEW Community Health Extension Worker
CHO Community Health Officer
CHTWG CHX
Child Health Technical Working Group Chlorhexidine
CORPs Community Oriented Resource Persons
DHIS District Health Information System
ECEB Essential Care for Every Baby
ECSB Essential Care for Small Babies
EML Essential Medicine List
EmONC Emergency Obstetric and Newborn Care
ENC Essential Newborn Care
ENCC Essential Newborn Care Course
EPMCD Ending Preventable Maternal and Child Death
ETS Emergency Transport Scheme
FIGO Federation of International Gynecologists and Obstetricians
FMOH Federal Ministry of Health
FP Family Planning
FTYP First Time / Young Parent
FY Financial Year
GON Government of Nigeria
GSK Glaxo SmithKline
HBB Helping Babies Breathe
HFG Health Finance and Governance
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
HIV/AIDS Human Immunodeficiency Virus / Acquired Immune Deficiency Syndrome
HMIS Health Management Information System
HOD Head of Department
iCCM Integrated Community Case Management of Childhood Illnesses
JHU IRB Johns Hopkins University Institutional Review Board
KMC Kangaroo Mother Care
LGA Local Government Area
LOP Life of Project
LSS Life Saving Skills
MCHIP Maternal and Child Health Integrated Program
MCSP Maternal and Child Survival Program
M&E Monitoring and Evaluation
mENCC Modified Essential Newborn Care Course
MNCH Maternal, Neonatal and Child Health
MNH Maternal and Neonatal Health
MoWASD Ministry of Women Affairs and Social Development
MSLC Mothers’ Savings and Loans Clubs
NANNM NAPPMED
National Association of Nigerian Nurses and Midwives National Association of Patent and Propriety Medicine Dealers
NASG Non-Pneumatic Anti-Shock Garment
NHIS National Health Insurance Scheme
NiENAP Nigeria Every Newborn Action Plan
NISONM Nigerian Society of Neonatal Medicine
NPHCDA National Primary Health Care Development Agency
PAN Pediatric Association of Nigeria
PHC Primary Health Care
PMP Performance Monitoring Plan
PPFP Post-Partum Family Planning
PPH Post-Partum Hemorrhage
PPMV Patent Proprietary Medicine Vendors
PPUID Post-Partum Intra Uterine Device
PSE Pre-Service Education
PY Project Year
QIT Quality Improvement Team
QIC Quality Improvement Committee
QoC Quality of Care
R4D Results for Development
RH Reproductive Health
RMC Respectful Maternal Care
RMNCAH Reproductive, Maternal, Newborn, Child and Adolescent Health
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
SBM-R Standards-Based Management and Recognition
SCI Save the Children International
SDP Service Delivery Point
SIF Service Improvement Facilitator
SIO Strategic Information Officer
SMOH State Ministry of Health
SOGON Society of Gynecology and Obstetrics of Nigeria
SOML Saving One Million Lives
SPHCDA State Primary Health Care Development Agency
S&TGDA Survive and Thrive Global Development Alliance
SURE-P Subsidy Reinvestment and Empowerment Program
TOT Training of Trainers
TSHIP Targeted States High Impact Project
USAID United States Agency for International Development
USG United States Government
VOS Voluntary Obstetrics Scheme
VPSS Voluntary Pediatric Service Scheme
WHO World Health Organization
YFHS Youth-Friendly Health Services
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
1.0 PROJECT OVERVIEW / SUMMARY
Program Name: MCSP-MNCH Activity in Nigeria
Activity Start Date and End Date:
October 01, 2014 – December 31, 2018
Name of Prime Implementing Partner:
Jhpiego Corporation
[Contract/Agreement] Number:
AID-OAA-A-N-00028
Name of Subcontractors/ Sub-awardees:
Save The Children International (SCI) Results For Development (R4D) John Snow, Incorporated (JSI) Pediatric Association of Nigeria (PAN) Nigerian Society of Neonatal Medicine (NISONM) Society of Gynecology and Obstetrics of NIGERIA (SOGON) National Association of Nigerian Nurses and Midwives (NANNM)
Major Counterpart Organizations
State Ministries of Health
Geographic Coverage (cities and or countries)
Ebonyi and Kogi States
Reporting Period: January 1, 2018 – March 31, 2018
Approved MCSP Nigeria MNCH PY1-PY4 Budget
$30,179,317
Total expenditure this quarter (Jan-Mar, 2018)
$2,310,511
Accrued Expenditures $1,254,318
Total Estimated Expenditures to Date
$22,729,955
Workplan PY1-PY4 Budget Minus Expenditures to Date
$7,449,362
1.1. Program Description The Maternal and Child Survival Program (MSCP) is a global U.S. Agency for International Development (USAID) cooperative agreement to introduce and support high-impact health interventions in 25 priority countries with the ultimate goal of ending preventable child and maternal deaths (EPMCD) within a generation. MCSP engages governments, policymakers, private sector leaders, health care providers, and civil society organizations in adopting and accelerating proven approaches to address the major causes of maternal, newborn and child mortality. It aims to improve the quality of health services from the household to the hospital. MCSP’s Maternal, Newborn and Child Health (MNCH) project in Nigeria is working with the Government of Nigeria (GoN) to improve the quality and utilization of maternal, newborn and childcare services in public, private and faith-based facilities as well as in selected communities in Kogi and Ebonyi states. MCSP will be
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
implemented over five years, subject to available funds, and will build on the work of previous USAID global programs (ACCESS and MCHIP) in northern Nigeria. MCSP is being implemented in Nigeria by four consortium international partners – Jhpiego, John Snow, Inc. (JSI), Save the Children International (SCI) and Results for Development (R4D). The in-country partners include Federal Ministry of Health (FMOH), National Primary Health Care Development Agency (NPHCDA), and Ministry of Health and State Primary Health Care Development Agency (SPHCDA) in both Ebonyi and Kogi states. MCSP has sub-awards with four local professional associations – the Society of Gynecology and Obstetrics of Nigeria (SOGON), Pediatric Association of Nigeria (PAN), Nigerian Society of Neonatal Medicine (NISONM), and National Association of Nigerian Nurses and Midwives (NANNM). MCSP also collaborates with US-based professional associations including the American Academy of Pediatrics, American College of Obstetricians and Gynecologists, and American College of Nurse-Midwives, and with projects and partners like Saving One Million Lives (SOML) and Survive and Thrive Global Development Alliance partners (S&TGDA).
Project Objectives Life of Project (LOP) Expected Results
To improve quality of facility-based maternal, newborn and child health care (MNCH) services and community based child health services
To improve information systems to monitor & evaluate health outcomes
To increase use of life-saving innovations
80% of staff competent to provide quality maternal, newborn and postpartum family planning (PPFP) services in all program-supported facilities
80% of program-supported facilities recognized for achieving quality standards in maternal, newborn and family planning (FP) services
80% of program-supported facilities have a minimum package of essential equipment, commodities and supplies
Functional two-way referral systems within all program-supported clusters including pre-notification of patient transfers, use of emergency transport systems (ETS) that are enabled by savings and loans clubs as alternative financing systems
50% increase in percent of new graduates from nursing and midwifery schools and schools of health technology who can demonstrate competency in critical maternal, newborn and FP skills
Increase in the utilization of skilled birth attendance (SBA) for delivery by 10% in Kogi and 20% in Ebonyi
PPMVs recruited, trained and providing quality healthcare services to U5 children in focal LGAs, including referrals for sick children with danger signs or malnourished children.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
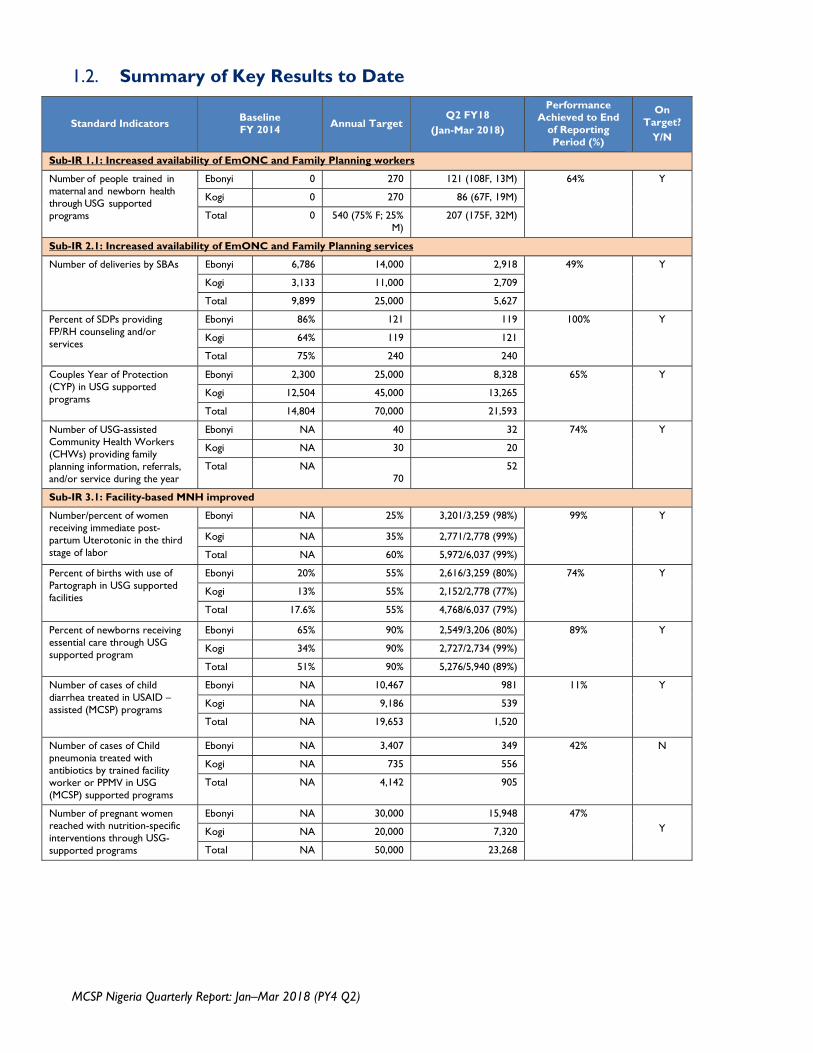
1.2. Summary of Key Results to Date
Standard Indicators Baseline FY 2014 Annual Target
Q2 FY18 (Jan-Mar 2018)
Performance Achieved to End
of Reporting Period (%)
On Target?
Y/N
Sub-IR 1.1: Increased availability of EmONC and Family Planning workers
Number of people trained in maternal and newborn health through USG supported programs
Ebonyi 0 270 121 (108F, 13M) 64% Y
Kogi 0 270 86 (67F, 19M)
Total 0 540 (75% F; 25% M)
207 (175F, 32M)
Sub-IR 2.1: Increased availability of EmONC and Family Planning services
Number of deliveries by SBAs Ebonyi 6,786 14,000 2,918 49% Y
Kogi 3,133 11,000 2,709
Total 9,899 25,000 5,627
Percent of SDPs providing FP/RH counseling and/or services
Ebonyi 86% 121 119 100% Y
Kogi 64% 119 121
Total 75% 240 240
Couples Year of Protection (CYP) in USG supported programs
Ebonyi 2,300 25,000 8,328 65% Y
Kogi 12,504 45,000 13,265
Total 14,804 70,000 21,593
Number of USG-assisted Community Health Workers (CHWs) providing family planning information, referrals, and/or service during the year
Ebonyi NA 40 32 74% Y
Kogi NA 30 20
Total NA 70
52
Sub-IR 3.1: Facility-based MNH improved
Number/percent of women receiving immediate post-partum Uterotonic in the third stage of labor
Ebonyi NA 25% 3,201/3,259 (98%) 99% Y
Kogi NA 35% 2,771/2,778 (99%)
Total NA 60% 5,972/6,037 (99%)
Percent of births with use of Partograph in USG supported facilities
Ebonyi 20% 55% 2,616/3,259 (80%) 74% Y
Kogi 13% 55% 2,152/2,778 (77%)
Total 17.6% 55% 4,768/6,037 (79%)
Percent of newborns receiving essential care through USG supported program
Ebonyi 65% 90% 2,549/3,206 (80%) 89% Y
Kogi 34% 90% 2,727/2,734 (99%)
Total 51% 90% 5,276/5,940 (89%)
Number of cases of child diarrhea treated in USAID –assisted (MCSP) programs
Ebonyi NA 10,467 981 11% Y
Kogi NA 9,186 539
Total NA 19,653 1,520
Number of cases of Child pneumonia treated with antibiotics by trained facility worker or PPMV in USG (MCSP) supported programs
Ebonyi NA 3,407 349 42% N
Kogi NA 735 556
Total NA 4,142 905
Number of pregnant women reached with nutrition-specific interventions through USG-supported programs
Ebonyi NA 30,000 15,948 47% Y Kogi NA 20,000 7,320
Total NA 50,000 23,268
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
2.0 ACTIVITY IMPLEMENTATION PROGRESS
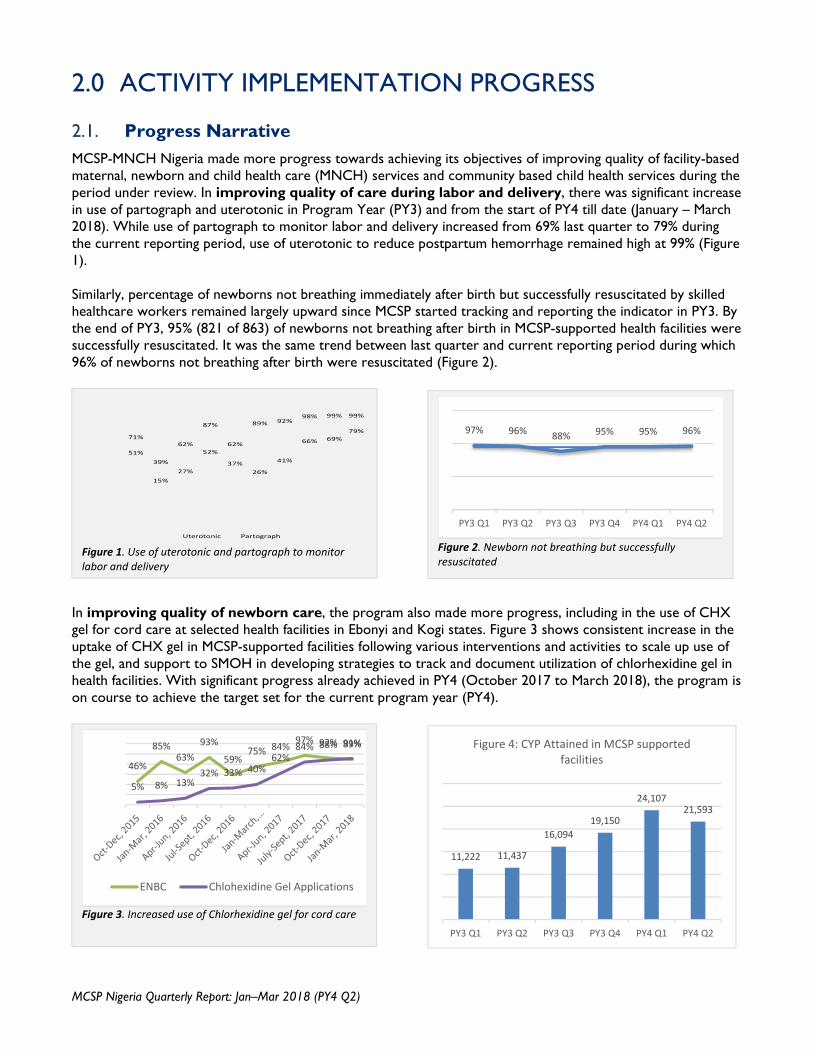
2.1. Progress Narrative MCSP-MNCH Nigeria made more progress towards achieving its objectives of improving quality of facility-based maternal, newborn and child health care (MNCH) services and community based child health services during the period under review. In improving quality of care during labor and delivery, there was significant increase in use of partograph and uterotonic in Program Year (PY3) and from the start of PY4 till date (January – March 2018). While use of partograph to monitor labor and delivery increased from 69% last quarter to 79% during the current reporting period, use of uterotonic to reduce postpartum hemorrhage remained high at 99% (Figure 1). Similarly, percentage of newborns not breathing immediately after birth but successfully resuscitated by skilled healthcare workers remained largely upward since MCSP started tracking and reporting the indicator in PY3. By the end of PY3, 95% (821 of 863) of newborns not breathing after birth in MCSP-supported health facilities were successfully resuscitated. It was the same trend between last quarter and current reporting period during which 96% of newborns not breathing after birth were resuscitated (Figure 2).
In improving quality of newborn care, the program also made more progress, including in the use of CHX gel for cord care at selected health facilities in Ebonyi and Kogi states. Figure 3 shows consistent increase in the uptake of CHX gel in MCSP-supported facilities following various interventions and activities to scale up use of the gel, and support to SMOH in developing strategies to track and document utilization of chlorhexidine gel in health facilities. With significant progress already achieved in PY4 (October 2017 to March 2018), the program is on course to achieve the target set for the current program year (PY4).
11,222 11,437
16,094
19,150
24,10721,593
PY3 Q1 PY3 Q2 PY3 Q3 PY3 Q4 PY4 Q1 PY4 Q2
Figure 4: CYP Attained in MCSP supported facilities
71%
39%
62%
87%
62%
89% 92%98% 99% 99%
51%
15%
27%
52%
37%
26%
41%
66% 69%
79%
Uterotonic Partograph
Figure 1. Use of uterotonic and partograph to monitor labor and delivery
Figure 2. Newborn not breathing but successfully resuscitated
97% 96% 88% 95% 95% 96%
PY3 Q1 PY3 Q2 PY3 Q3 PY3 Q4 PY4 Q1 PY4 Q2
Figure 3. Increased use of Chlorhexidine gel for cord care
46%
85%63%
93%
59%75% 84%
97% 92% 89%
5% 8% 13%32% 33% 40%
62%84% 88% 91%
ENBC Chlohexidine Gel Applications
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Other progress of note include the annual Couple Years of Protection (CYP), the estimated protection provided by contraceptive methods during a one-year period, which has been rising in Ebonyi and Kogi states since the inception of the program. Figure 4 above shows the increasing trend of CYP from PY1 to PY3 and current status for PY4 (i.e. first and second quarters), which by inference implies continuation of the rising trend. MCSP uses USAID conversion factors to calculate amount of family planning methods dispensed to clients by service providers in MCSP-supported health facilities to arrive at the CYP figures. Overall, the results mentioned above are largely attributable to frontline healthcare workers whose capacity to deliver lifesaving services had been enhanced through MCSP interventions, and who were able to apply their new knowledge and skills to prevent needless deaths of women and newborns in Ebonyi and Kogi states.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
2.2. Implementation Status
2.2.1. Maternal Health
MCSP's strategy for maternal health emphasizes an integrated, systems-oriented approach to reducing direct and indirect causes of maternal morbidity and mortality. The interventions in the maternal health technical area include building capacity of health workers on basic emergency, obstetric and newborn care (BEmONC) and comprehensive obstetric and newborn care (CEmONC), and increasing access to affordable quality care for pregnant women.
2.2.1.1. Updates on BEmONC and CEmONC Support
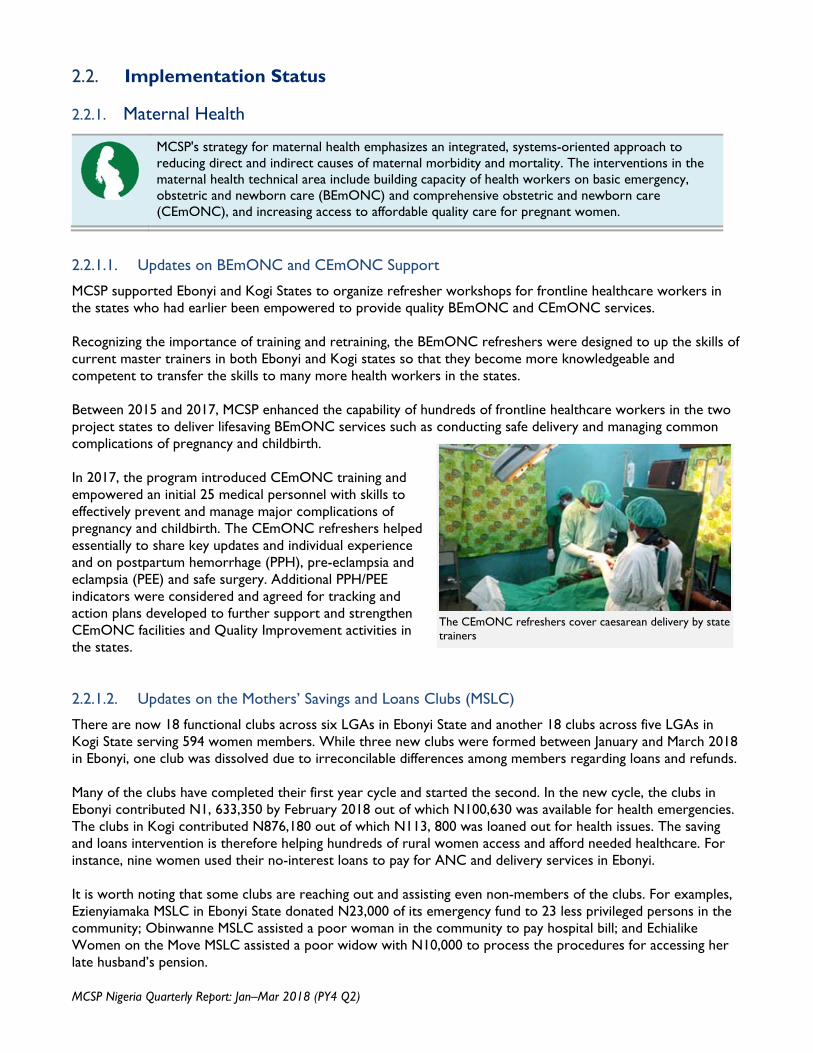
MCSP supported Ebonyi and Kogi States to organize refresher workshops for frontline healthcare workers in the states who had earlier been empowered to provide quality BEmONC and CEmONC services. Recognizing the importance of training and retraining, the BEmONC refreshers were designed to up the skills of current master trainers in both Ebonyi and Kogi states so that they become more knowledgeable and competent to transfer the skills to many more health workers in the states. Between 2015 and 2017, MCSP enhanced the capability of hundreds of frontline healthcare workers in the two project states to deliver lifesaving BEmONC services such as conducting safe delivery and managing common complications of pregnancy and childbirth. In 2017, the program introduced CEmONC training and empowered an initial 25 medical personnel with skills to effectively prevent and manage major complications of pregnancy and childbirth. The CEmONC refreshers helped essentially to share key updates and individual experience and on postpartum hemorrhage (PPH), pre-eclampsia and eclampsia (PEE) and safe surgery. Additional PPH/PEE indicators were considered and agreed for tracking and action plans developed to further support and strengthen CEmONC facilities and Quality Improvement activities in the states. 2.2.1.2. Updates on the Mothers’ Savings and Loans Clubs (MSLC)
There are now 18 functional clubs across six LGAs in Ebonyi State and another 18 clubs across five LGAs in Kogi State serving 594 women members. While three new clubs were formed between January and March 2018 in Ebonyi, one club was dissolved due to irreconcilable differences among members regarding loans and refunds. Many of the clubs have completed their first year cycle and started the second. In the new cycle, the clubs in Ebonyi contributed N1, 633,350 by February 2018 out of which N100,630 was available for health emergencies. The clubs in Kogi contributed N876,180 out of which N113, 800 was loaned out for health issues. The saving and loans intervention is therefore helping hundreds of rural women access and afford needed healthcare. For instance, nine women used their no-interest loans to pay for ANC and delivery services in Ebonyi. It is worth noting that some clubs are reaching out and assisting even non-members of the clubs. For examples, Ezienyiamaka MSLC in Ebonyi State donated N23,000 of its emergency fund to 23 less privileged persons in the community; Obinwanne MSLC assisted a poor woman in the community to pay hospital bill; and Echialike Women on the Move MSLC assisted a poor widow with N10,000 to process the procedures for accessing her late husband’s pension.
The CEmONC refreshers cover caesarean delivery by state trainers
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
The apparatus for managing the clubs are also becoming well established. In Ebonyi, the Ministry of Women Affairs and Social Development (MoWASD) is firmly coordinating the activities of the clubs and has instituted a quarterly meeting of all mothers’ savings and loans clubs in the state. The meeting serves as a forum for exchanging ideas, experiences and good practices, and for addressing challenges. The first quarterly meeting of the clubs was held in January 2018. Furthermore, MCSP collaborated with MoWASD in both project states to hold a five-day training and review meeting to empower new women members of the clubs and review the progress, achievements and challenges of the existing 33 clubs. One of the main highlights of the meeting was having the women display several items that each of the clubs embarked on collectively to improve their economic and social wellbeing. 2.2.1.3. Updates on Emergency Transport Scheme (ETS) for strengthening referral system
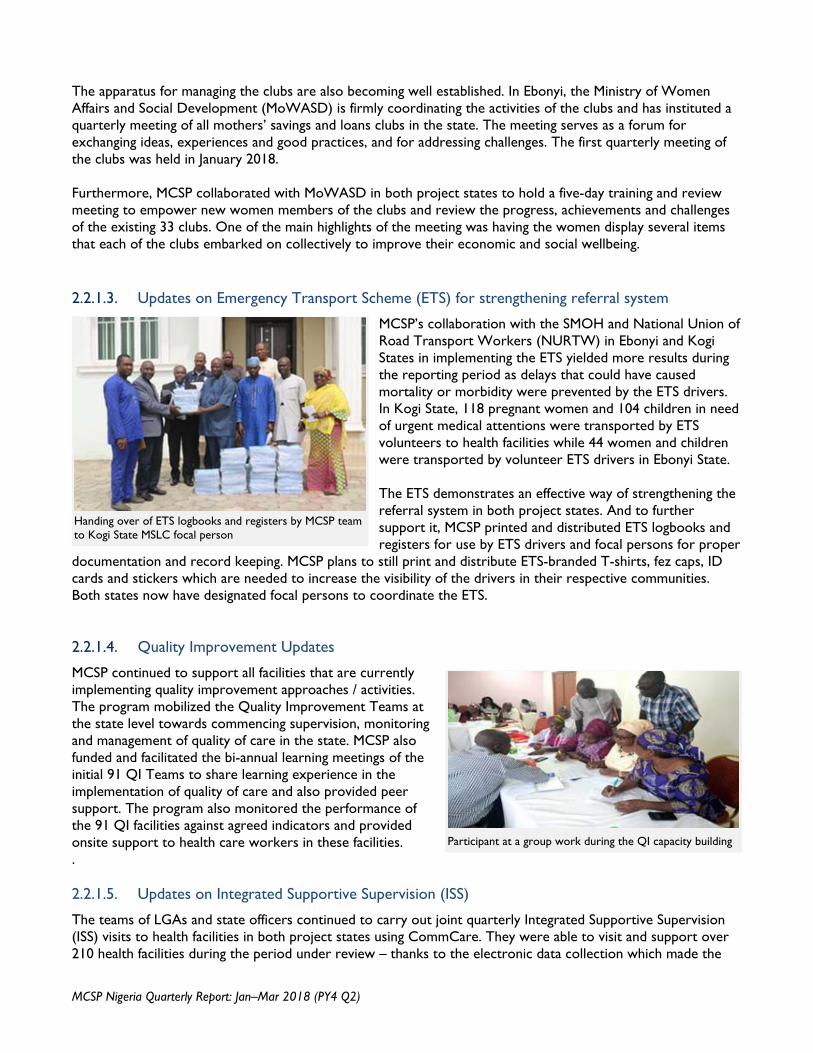
MCSP’s collaboration with the SMOH and National Union of Road Transport Workers (NURTW) in Ebonyi and Kogi States in implementing the ETS yielded more results during the reporting period as delays that could have caused mortality or morbidity were prevented by the ETS drivers. In Kogi State, 118 pregnant women and 104 children in need of urgent medical attentions were transported by ETS volunteers to health facilities while 44 women and children were transported by volunteer ETS drivers in Ebonyi State. The ETS demonstrates an effective way of strengthening the referral system in both project states. And to further support it, MCSP printed and distributed ETS logbooks and registers for use by ETS drivers and focal persons for proper
documentation and record keeping. MCSP plans to still print and distribute ETS-branded T-shirts, fez caps, ID cards and stickers which are needed to increase the visibility of the drivers in their respective communities. Both states now have designated focal persons to coordinate the ETS. 2.2.1.4. Quality Improvement Updates MCSP continued to support all facilities that are currently implementing quality improvement approaches / activities. The program mobilized the Quality Improvement Teams at the state level towards commencing supervision, monitoring and management of quality of care in the state. MCSP also funded and facilitated the bi-annual learning meetings of the initial 91 QI Teams to share learning experience in the implementation of quality of care and also provided peer support. The program also monitored the performance of the 91 QI facilities against agreed indicators and provided onsite support to health care workers in these facilities. . 2.2.1.5. Updates on Integrated Supportive Supervision (ISS) The teams of LGAs and state officers continued to carry out joint quarterly Integrated Supportive Supervision (ISS) visits to health facilities in both project states using CommCare. They were able to visit and support over 210 health facilities during the period under review – thanks to the electronic data collection which made the
Handing over of ETS logbooks and registers by MCSP team to Kogi State MSLC focal person
Participant at a group work during the QI capacity building
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
supervision process more efficient. The contact between the ISS teams and the health workers remains a motivation for the health workers and an opportunity for immediate feedback to them on ways to improve service delivery in the facilities.
2.2.2. Newborn Health
The newborn health technical area focuses on interventions that address the three major causes of mortality in newborns in Nigeria – prematurity (29%), birth asphyxia (26%) and sepsis (23%). The intervention areas are essential newborn care; care of preterm babies and babies with respiratory distress through the use of (bCPAP) where applicable; prevention and management of birth asphyxia; scale-up of use of chlorhexidine for cord care and prevention and management of newborn sepsis.
2.2.2.1. Updates on Newborn Health Capacity Building
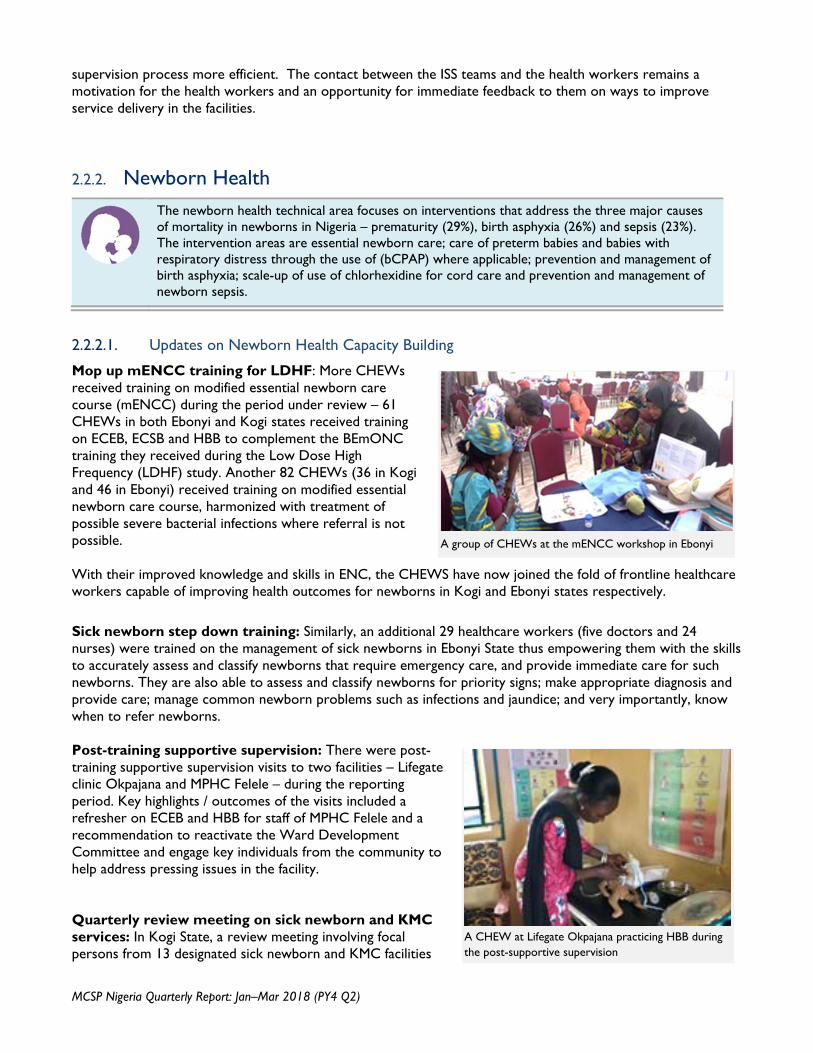
Mop up mENCC training for LDHF: More CHEWs received training on modified essential newborn care course (mENCC) during the period under review – 61 CHEWs in both Ebonyi and Kogi states received training on ECEB, ECSB and HBB to complement the BEmONC training they received during the Low Dose High Frequency (LDHF) study. Another 82 CHEWs (36 in Kogi and 46 in Ebonyi) received training on modified essential newborn care course, harmonized with treatment of possible severe bacterial infections where referral is not possible. With their improved knowledge and skills in ENC, the CHEWS have now joined the fold of frontline healthcare workers capable of improving health outcomes for newborns in Kogi and Ebonyi states respectively. Sick newborn step down training: Similarly, an additional 29 healthcare workers (five doctors and 24 nurses) were trained on the management of sick newborns in Ebonyi State thus empowering them with the skills to accurately assess and classify newborns that require emergency care, and provide immediate care for such newborns. They are also able to assess and classify newborns for priority signs; make appropriate diagnosis and provide care; manage common newborn problems such as infections and jaundice; and very importantly, know when to refer newborns. Post-training supportive supervision: There were post-training supportive supervision visits to two facilities – Lifegate clinic Okpajana and MPHC Felele – during the reporting period. Key highlights / outcomes of the visits included a refresher on ECEB and HBB for staff of MPHC Felele and a recommendation to reactivate the Ward Development Committee and engage key individuals from the community to help address pressing issues in the facility. Quarterly review meeting on sick newborn and KMC services: In Kogi State, a review meeting involving focal persons from 13 designated sick newborn and KMC facilities
A group of CHEWs at the mENCC workshop in Ebonyi
A CHEW at Lifegate Okpajana practicing HBB during the post-supportive supervision
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
and PAN/NISONM was held to reiterate the need for quality sick newborn and KMC service provision that is geared towards reducing neonatal mortality in the state. The review meeting was also an opportunity to assess the status of sick newborn and KMC services in the state with focus on identifying and addressing challenges encountered by health workers in providing KMC and sick newborn services. The meeting also served as an opportunity to distribute sick newborn guidelines, KMC guidelines and registers, and breast feeding and vital signs charts produced with support from MCSP. 2.2.2.2. Updates on use of bCPAP as a lifesaving innovation
Activities carried out with respect to the promotion and use of bCPAP during the period under review include: step down training on bCPAP for two doctors and 11 nurses working in the SCBU of General Hospital Calabar; mentoring visit to the Special Care Baby Unit of the hospital; visit to in-born and out-born SCBU at the University of Calabar Teaching Hospital; and evaluation of Pumani bCPAP services in the three centers in Ebonyi State by a visiting AAP member. The activities brought to light the various challenges associated with the use of bCPAP in Nigeria. MCSP team and partners helped to address some of the issues, such as repair of malfunctioning bCPAP devices, mentoring facility staff on techniques for routinely maintaining the device, and presentation of job aids to help the health workers effectively use the machine. 2.2.2.3. Updates on Possible Severe Bacterial Infection (PSBI)
Pre-testing or Field testing of Harmonized PSBI/ENCC Curriculum: MCSP worked with FMOH and PAN/NISONM to pre-test the harmonized, PSBI-integrated curriculum for essential newborn care course. Thirty-two ENCC trainers from both Kogi and Ebonyi states were involved in the pre-testing, which covered action plans for ECEB and ECSB (including the new additions), and ‘Where referral is not possible’. The pre-testing is an important step before the curriculum is finalized. Action Media workshop: MCSP organized an action media workshop to gain insight into values, practices and behaviors that community members in Kogi and Ebonyi states consider as the ‘right behaviors’ to promoting newborn health. Participants at the workshop discussed the major challenges affecting care seeking for sick newborns in their communities. The information elicited from the participants was used to develop draft posters and BCC/IEC materials for demand creation activities for PSBI intervention. PSBI ToT for Community Oriented Resource Persons (CORPs): Thirty-three (33) persons including SMOH officials and SOML volunteers were trained to counsel pregnant women, mothers, newborns and young infants using counselling cards adapted from WHO. The participants were trained to assess and identify danger signs in mothers and newborns and the importance of care seeking in the health facility. They were also introduced to the CORPS training materials, counselling cards and proposed CORPS register. 2.2.2.4. Updates on support for national scale-up of Chlorhexidine Engagement with manufacturers of CHX and erythromycin eye ointment: MCSP organized a visit to the facilities of three CHX manufacturers – Drugfield Pharmaceuticals, Emzor Pharmaceuticals and Jawa
One of the poster designs conceptualized by participants at the workshop
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Industries – as part of efforts to enhance demands for CHX at state level, and to support the manufacturers in attaining global GMP certification. The visit to the manufacturers was an opportunity to stimulate the involvement of the private sector in scaling up chlorhexidine use and in generating accurate data on production and distribution of chlorhexidine in Nigeria. Such data will provide a picture of states that are actively scaling up chlorhexidine, which can be used for targeted support, and to understand other stakeholders driving scale up in the country, which can inform basis for collaboration and synergy. Tracking implementation progress using tools and national dashboard: In January 2018, MCSP supported FMOH to convene a stakeholders meeting of state Reproductive Health (RH) Coordinators tasked in the national strategy to lead the capturing and reporting of non-routine indicators at the state level. States used the meeting to share experience in capturing CHX utilization. As CHX utilization is not captured presently in the national register, they adopted MCSP model (ruling a column in the labor and delivery register) pending the completion of the ongoing review of the national HMIS registers. MCSP utilized the workshop to update RH Coordinators on policy recommendations for CHX scale-up and the actions they are expected to take as RH Coordinators. Partnership with implementing partners: MCSP also engaged implementing partners to seek areas of
collaboration for the scale up of CHX in Nigeria. The partners include Maternal, Newborn and Child Health II project (MNCH2), Plan International, Pact Nigeria, Society for Family Health, United Nations International Children’s Fund, Health Communication Capacity Collaborative (HC3) and Clinton Health Access Initiative (CHAI). The meetings with the partners revealed that most partners are only tracking distribution of CHX to facility or program level, not its utilization. The engagement with the partners also showed that while progress on integrating CHX indicators in routine systems is being made, collecting CHX data would require direct outreach to a range of stakeholders including FMOH, SMOH, implementing partners, and manufacturers.
Community of practice to oversee coordination and reporting on CHX scale up: In January 2018, MCSP initiated the setting up of a WhatsApp group – CHX-RH Coordinators – to engage key stakeholders and coordinate scale up implementation in Nigeria. While the WhatsApp group was initially meant to coordinate attendance of RHC at a workshop, it has now evolved to a reporting platform where states share their activities and progress in implementing their action plans. The social media platform has also helped to address some of the challenges of having a national scale up management team. This technological approach is helping to facilitate national and state coordination structures and active participation by stakeholders. Updates on operationalizing CHX scale up in Kogi and Ebonyi states: At the state-level, MCSP supported a wide range of activities in Kogi and Ebonyi states leading to the design, development and pretesting of IEC materials on CHX for umbilical cord care and newborn health danger signs. Following these activities, stakeholders involved such as LGA health educators and Social Mobilization Officers were able to demonstrate better understanding of newborn health terminologies and interventions. They demonstrated more confidence to carry out community sensitization and communication using SBCC-centered approach. They also developed state specific costed work plans for sensitization activities on newborn health. CHX Scale-up Management Team: The CHX Scale up Management Team at the state level continued to meet to share knowledge and improve better coordination in the state and provide updates on ongoing plans and activities, such as the present need to expand state-wide CHX tracking and reporting.
Representatives of implementing partners at a panel discussion
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
2.2.2.5. Updates on WASH / Sepsis
Activities carried out during the reporting period and in line with the implementation of Phase III of the WASH study include the meeting of the WASH consultant with key state actors on IPC in Ebonyi and Kogi states respectively. The meetings focused on disseminating and discussing the findings of the WASH III study. The consultant also carried out an assessment of WASH pilot sites in both Ebonyi and Kogi states. Some of the findings include: availability of some form of running water (all centers); limited availability of liquid hand washing soap available (all centers); inadequate IEC materials on IPC (all centers); inadequate color-coded waste bins (all centers); lack of separation of IPC commodities between highly infectious and less infectious areas (all centers); and fair but limited knowledge of IPC protocol (all centers).
2.2.3. Child Health
The broad objectives of the child health technical area are to (i) advance federal policies supportive of Integrated Community Case Management of Childhood Illness (iCCM) and its well-coordinated roll out across the states; (ii) improve the coverage and quality of evidence-based, high-impact child health interventions in Kogi and Ebonyi states; and (iii) improve preventive and care-seeking behavior for childhood illnesses among communities in Kogi and Ebonyi states.
2.2.3.1. Updates on Enhancing Quality iCCM through PPMVs and Partnership Approach
The Enhancing Quality iCCM through PPMVs and Partnership (EQuiPP) is MCSP’s revised private sector iCCM approach and study. Activities relating to the approach in the quarter include the Knowledge, Practice and Coverage (KPC), care seeking, and quality of care studies; consultative meeting of stakeholders on EQuiPP; capacity assessment of Community-based Organizations (CBOs) involved in the studies; and support to Pharmaceutical Council of Nigeria (PCN) to increase availability and access to quality and affordable child health commodities at PPMV shops. KPC, Care-seeking and Quality of Care studies: During the reporting period, MCSP facilitated the training of data collectors in Ebonyi and Kogi for both KPC and care-seeking studies. For the KPC’s household survey, data collection has been completed and data analysis is ongoing. Similarly, for the Quality of Care (QoC) of PPMV services assessment, a central level training on survey tools, survey CTO, research ethics and informed consent was conducted for MCSP M&E team and LGA supervisors from Kogi and Ebonyi states. This was followed by a step down training for study evaluators and supervisors at the state level. Data collection started in Q2 and will be completed early in Q3. Training of LGA iCCM Trainers: MCSP collaborated with Kogi and Ebonyi SMOH, SPHCDA and PCN to conduct iCCM training for LGA Trainers ahead of the start of Proprietary and Patent Medicine Vendor (PPMV) training for the EQuiPP study. The training prepared the LGA personnel with the knowledge, clinical and facilitation skills to cascade iCCM training to PPMVs in two intervention LGAs. In Ebonyi and Kogi, participants drawn from health institutions, CBOs and PCN were trained using the FMOH training manuals and the iCCM addenda (CHMIS and Inventory Management of Childhood Medicines for PPMVs). Newly developed iCCM training addenda for PPMVs were successfully field tested during the training and found to be very informative, useful and relevant to PPMV service delivery.
A health worker assesses a sick child at OPD during LGA TOT

MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
The main emphasis was on how to identify, classify and treat sick children with malaria, pneumonia, diarrhea and malnutrition, and how to identify danger signs and refer sick newborns and children with danger signs to health facilities. At the end, 59 participants (30 in Kogi, 29 in Ebonyi) were certified as trainers to facilitate the iCCM training course for the PPMVs in both states. Consultative meetings of stakeholders on EQuiPP: MCSP facilitated consultative meetings in Kogi and Ebonyi states for key stakeholders including SMOH, SPHCDA, PCN and National Association of Patent and Proprietary Medicines (NAPPMED) to conclude discussions on EQuiPP strategy, build consensus on roles and responsibilities of each stakeholder, and finalize EQuiPP letter of understanding. These objectives were achieved at the end of the meetings. Ebonyi stakeholders have signed the letter of understanding and it is expected that Kogi stakeholders will sign same letter of understanding next quarter. Capacity assessment of CBOs: MCSP facilitated a participatory capacity assessment of eight CBOs in order to find out their capacity to provide demand creation activities for the EQuiPP intervention. The CBOs were assessed in the areas of technical capacity, experience in demand creation, organizational structure/relevant policies, reporting/documentation, administrative and financial procedure, and conduciveness of physical structure (office space). Based on the findings of the assessment, two CBOs in Kogi and three in Ebonyi states respectively were recommended for engagement. The selection and engagement of the CBOs will be concluded next quarter. Support to PCN to increase availability and access to quality and affordable child health commodities at PPMV shops: MCSP worked with PCN to identify registered pharmaceutical wholesalers in Kogi and Ebonyi states. The premises of the wholesalers were inspected and key informant interviews were scheduled with Superintendent Pharmacists to assure willingness to procure quality essential medicines of relevance to the EQuiPP study. With the support of USP, local manufacturers of childhood commodities were engaged for willingness to produce Amoxicillin Dispersible tablets, Low Osm. ORS, Zinc and anti-malaria medicines. Strengthening the linkages between local manufacturers, wholesalers, SMOH and NAPPMED will improve availability of quality and affordable medicines to manage malaria, diarrhea and pneumonia at the community level. 2.2.3.2. Updates on Integrated Management of Childhood Illnesses (IMCI) activities
Capacity building on IMCI: MCSP supported Kogi SMOH to conduct IMCI case management step-down training for 15 PHC workers drawn mainly from scale-up PHCs in Idah and Okehi. The training resulted in the entire coverage of the LGAs (one PHC per ward) and will ensure availability of referral PHCs for sick children who would be referred from PPMV outlets under the EQuiPP study. Participants used the IMCI Nigeria adaptation (December 2017) revised training modules. Post-training evaluation showed significant improvement in participants’ knowledge of IMCI. Similarly, MCSP conducted a two-day orientation on PSBI for PHC workers and IMCI supervisors previously trained on IMCI in 2017. This became necessary as a result of the update in the in-service IMCI module on Management of the Sick Young Infant. Additionally, participants were trained on how to use PSBI data reporting tool, which
A group of IMCI evaluators during PSBI orientation
Stakeholders at the EQuiPP consultative meeting in Kogi State
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
comprises of both the cohort register and monthly summary form. In total, 227 persons (116 Kogi, 111 Ebonyi) were trained. Post-training follow-up visits: MCSP supported state trainers and supervisors to conduct follow-up visits to health care workers already trained on IMCI. The team visited 18 facilities and reached at least 22 healthcare workers. The visits enabled the team to identify and proffer solutions to problems affecting IMCI implementation in the states. One of the key challenges observed was unavailability of Amoxicillin DT in Ebonyi but which is expected to be addressed after the distribution of child health commodities procured by Ebonyi SOML. National iCCM Symposium in Abuja: MCSP joined other stakeholders to participate in the National iCCM Symposium in Abuja organized to share experiences and lessons learned in the implementation of iCCM in Nigeria. MCSP presented updates on the EQuiPP study, highlighting implementation framework and sustainability approach. Recommendations made during the symposium included the need to strengthen CORPs supervision; need to advocate for government and community ownership of iCCM; development of iCCM sustainability roadmap at project inception; exploring other funding sources outside of donor funding; independent QoC assessment of practice of CORPs; and strengthening of community-health facility referral services. It is worth noting that 11 states are currently implementing iCCM in Nigeria with over 2 million sick children already treated. Other important child-health related activities carried out during the reporting period include:
Training of 267 (Kogi 137, Ebonyi 130) service providers and staff of LMCU from 12 LGAs in Kogi and Ebonyi states during which the trainees were re-introduced to sick child recording forms, data collation monthly summary form, and HMIS and LMIS tools relevant for child health data reporting
Review of the draft National Child Health Policy (2017) during the National Child Health Technical Working Group (NCHTWG) meeting in March 2018
2.2.4. Family Planning & Reproductive Health
MCSP is supporting Kogi and Ebonyi states to increase access to and uptake of postpartum contraceptives towards actualizing Nigeria’s commitment to achieving the global contraceptive prevalence rate (CPR) of 36% by 2020.
2.2.4.1. Updates on family planning capacity building intervention
PP-LARC training: Sixty-five (65) healthcare workers – comprising nurses, midwives and doctors from postnatal, ANC and labor units of 43 health facilities in Ebonyi and Kogi States – joined the ranks of health workers capable of providing postpartum Long Acting Reversible Contraceptives (PP-LARC), following their participation in PP-LARC training organized by MCSP and SMOH in Ebonyi and Kogi states. This brings the total of facilities MCSP is currently supporting to offer immediate PPFP to 195 To ensure that the benefiting healthcare workers promptly initiate postpartum family planning counseling and services at their facilities, MCSP donated essential PP-LARC tools and materials such as PPIUD insertion kit, interval IUD insertion kits, implant removal kits, BCS counseling card, family planning posters, counseling flip books and seed stock of family planning commodities to all 43 health facilities.
One of the trained providers offers PPFP counselling to a woman at a facility in Kogi State
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Post training follow up and supportive supervision: The focus of the post-training follow-up and supportive supervision during the reporting period was on ensuring that health workers trained on mini laparotomy in September-October, 2017 are delivering quality services. The supervision team visited four hospitals (FETHA and General Hospital Iboko in Ebonyi State, and Federal Medical Center and Okene Zonal Hospital in Kogi State). They reviewed plans and actions taken to implement mini laparotomy in the facilities, which showed that consent forms for minilap have been adapted and printed, minilap included in theatre register, minilap service cost reviewed and pegged at N5,000 per case, and private areas identified for counseling in some facilities. Forty-six (46) minilap procedures have been carried out by trained health workers since the training. 2.2.4.2. Provider networking and experience sharing workshop To encourage knowledge sharing through peer learning, MCSP conducted a provider networking and experience sharing workshop for postpartum family planning providers in Ebonyi State. The activity brought together providers from high and low performing health facilities who were encouraged to work together for three days to learn from one another. Participants were supported to generate data from their registers and compare number of facility deliveries with PPFP uptake. This approach was an eye opener to many of the service providers. It created a healthy competition among them and helped them to learn from their peers’ ways to address any identified gaps in their practice.
2.2.5. Adolescent Sexual and Reproductive Health (ASRH)
MCSP’s ASRH work aims to improve the quality of health services for adolescents and young mothers/parents by building knowledge and skills necessary to delay early childbearing, care for pregnancy, birth, and the postpartum period, including access to postnatal care, PPFP, and CH services
The main activities for the reporting period were the facility-based orientation to advance quality ASRH services; commencement of first time mother / parent (FTM/P) implementation activities using Our First Baby approach to strengthen the skills of FTM/P on pregnancy, delivery and baby care; and preparatory activities for end line documentation. Orientation of non-health ad-hoc facility staff on youth friendly services in Kogi and Ebonyi state: MCSP organized this activity to introduce the concept of ASRH and FTM/P to the ad-hoc staff at pilot sites and to motivate them to direct ASRH and FTM/P to the service points thereby providing greater visibility to “adolescent corners’ at pilot sites. Ninety-six ad-hoc staff of three facilities were reached. At one of the facilities, four teachers and three students of two nearby schools participated in the orientation. At the end of the orientation, the ad-hoc staff from the three facilities developed plans to reach adolescents in their communities and direct those who came for services to the adolescent corners. Quarterly supportive supervision visits: MCSP supported Ebonyi SMOH to conduct supportive supervision to three ASRH pilot sites in Ebonyi State – MCH Onueke, MCH Nwofe and Abakaliki YDC – during the
Facility registers were reviewed to ensure proper documentation during the supportive supervision visits
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
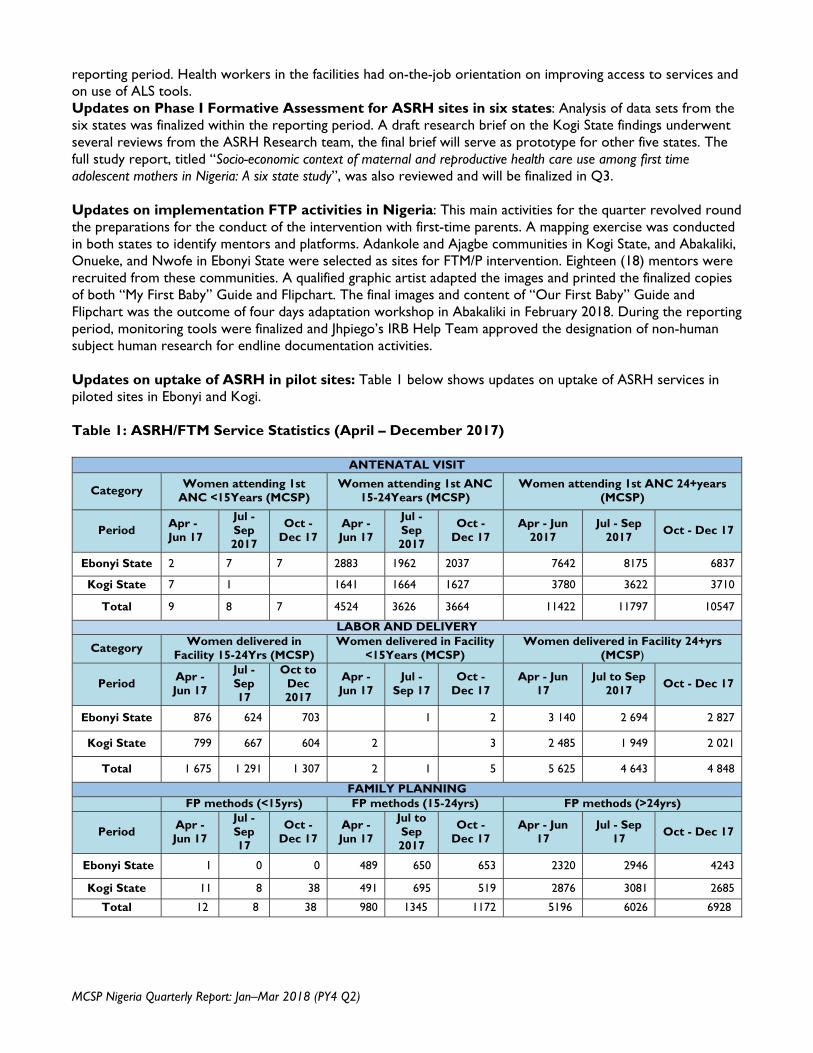
reporting period. Health workers in the facilities had on-the-job orientation on improving access to services and on use of ALS tools. Updates on Phase I Formative Assessment for ASRH sites in six states: Analysis of data sets from the six states was finalized within the reporting period. A draft research brief on the Kogi State findings underwent several reviews from the ASRH Research team, the final brief will serve as prototype for other five states. The full study report, titled “Socio-economic context of maternal and reproductive health care use among first time adolescent mothers in Nigeria: A six state study”, was also reviewed and will be finalized in Q3. Updates on implementation FTP activities in Nigeria: This main activities for the quarter revolved round the preparations for the conduct of the intervention with first-time parents. A mapping exercise was conducted in both states to identify mentors and platforms. Adankole and Ajagbe communities in Kogi State, and Abakaliki, Onueke, and Nwofe in Ebonyi State were selected as sites for FTM/P intervention. Eighteen (18) mentors were recruited from these communities. A qualified graphic artist adapted the images and printed the finalized copies of both “My First Baby” Guide and Flipchart. The final images and content of “Our First Baby” Guide and Flipchart was the outcome of four days adaptation workshop in Abakaliki in February 2018. During the reporting period, monitoring tools were finalized and Jhpiego’s IRB Help Team approved the designation of non-human subject human research for endline documentation activities. Updates on uptake of ASRH in pilot sites: Table 1 below shows updates on uptake of ASRH services in piloted sites in Ebonyi and Kogi. Table 1: ASRH/FTM Service Statistics (April – December 2017)
ANTENATAL VISIT
Category Women attending 1st
ANC <15Years (MCSP) Women attending 1st ANC
15-24Years (MCSP) Women attending 1st ANC 24+years
(MCSP)
Period Apr - Jun 17
Jul - Sep 2017
Oct - Dec 17
Apr - Jun 17
Jul - Sep 2017
Oct - Dec 17
Apr - Jun 2017
Jul - Sep 2017
Oct - Dec 17
Ebonyi State 2 7 7 2883 1962 2037 7642 8175 6837
Kogi State 7 1 1641 1664 1627 3780 3622 3710
Total 9 8 7 4524 3626 3664 11422 11797 10547
LABOR AND DELIVERY
Category Women delivered in
Facility 15-24Yrs (MCSP) Women delivered in Facility
<15Years (MCSP) Women delivered in Facility 24+yrs
(MCSP)
Period Apr - Jun 17
Jul - Sep 17
Oct to Dec 2017
Apr - Jun 17
Jul - Sep 17
Oct - Dec 17
Apr - Jun 17
Jul to Sep 2017
Oct - Dec 17
Ebonyi State 876 624 703 1 2 3 140 2 694 2 827
Kogi State 799 667 604 2 3 2 485 1 949 2 021
Total 1 675 1 291 1 307 2 1 5 5 625 4 643 4 848
FAMILY PLANNING FP methods (<15yrs) FP methods (15-24yrs) FP methods (>24yrs)
Period Apr - Jun 17
Jul - Sep 17
Oct - Dec 17
Apr - Jun 17
Jul to Sep 2017
Oct - Dec 17
Apr - Jun 17
Jul - Sep 17
Oct - Dec 17
Ebonyi State 1 0 0 489 650 653 2320 2946 4243
Kogi State 11 8 38 491 695 519 2876 3081 2685
Total 12 8 38 980 1345 1172 5196 6026 6928
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
2.2.6. Health Systems Strengthening and Equity
MCSP’s health systems strengthening and equity (HSS/E) work aims to address systems-level barriers that directly affect service delivery for high-quality, equitable RMNCH.
MCSP’s HSS/E work focuses on addressing the availability of essential commodities in Primary Health Centers (PHCs) through the establishment of a sustainable commodity financing scheme in Ebonyi State. The new commodity financing scheme will be based on a drug revolving fund (DRF) model, using lessons learned from other DRF models in the country. During the reporting period, MCSP agreed on an action plan for the PHC-DRF strategy design process with key Ebonyi State government counterparts, including the SMOH and SPHCDA, and led a one-day sensitization meeting with all proposed DRF operators at the State, LGA, and facility levels. Action plan consensus with Ebonyi State government: MCSP held one-on-one and small group meetings with key representatives from the Ebonyi State government, including the Honorable Commissioner of Health, the newly appointed SMOH DRF Pharmacist, the Director of the Central Medical Store, the Director of Pharmaceutical Services, and the Executive Secretary of the SPHCDA, to discuss an action plan for the design and implementation of the PHC-DRF. Partners agreed to collaborate for the strategy design, financial analysis for decision-making, development of a Logistics Management and Information System (LMIS), and relevant capacity building for State, LGA, and facility-level staff. One-day sensitization meeting: On March 21, MCSP facilitated a meeting convened by the Ebonyi State government in Abakaliki with all proposed DRF operators from the State, LGA, and facility levels. Participants included the Honorable Commissioner of Health, Executive Secretary of the SPHCDA, the DRF Pharmacist, the Director of Pharmaceutical Services, the Administrative Secretaries from all 13 LGAs in the State, as well as Officers In-Charge (OIC) and Pharmacy Technicians from the targeted PHCs. The purpose of this meeting was to orient key stakeholders on the purpose of the new commodity financing approach, to revisit past DRF schemes and lessons learned, and to discuss the roles and responsibilities of all stakeholders in the scheme. It was agreed that more in-depth orientations would be necessary to address outstanding questions related to financing, administration, and governance, and to provide capacity building for implementation. The first of the in-depth meetings was scheduled for early Q3
2.2.7. Pre-Service Education
During the reporting period, MCSP facilitated pre-service education stakeholders’ meetings in Ebonyi and Kogi states to identify outstanding interventions needed to improve quality of training in health-related PSE institutions in the two project states. At the meetings, findings and recommendations from baseline assessments of 14 PSE institutions in the states were shared. The extent of the implementation of activities sponsored by MCSP to bridge identified gaps was also reviewed and discussed. Other pertinent gaps were unrooted, their causes analyzed, and action gaps developed by each institution to bridge the gaps. One of the major gaps identified in Kogi State was lack of collaboration and coordination of training programs between the Schools of Nursing and Midwifery at ECWA Hospital in Egbe and the Hospital Management. In order to address this, a committee headed by the Director Nursing Services, Kogi State Ministry of Health was
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
setup to visit the schools and the hospital management, followed up on the issue and liaise with the appropriate persons to address the issue. MCSP also supported the setting up of clinical skills laboratories in five additional PSE institutions – in Kogi State, College of Health Technology, Idah and Grimard School of Midwifery, Anyigba, and in Ebonyi State, Schools of Health Technology Izzi, Ngbo and Ezzangbo. MCSP has thus helped to set up 10 clinical skills laboratories in both states till date. MCSP also supported the states to set up Education Development Committees both at the institutional and state levels. These committees are responsible for continuous quality improvement activities both within the schools and at the state levels. They are also responsible for ensuring sustainability of all ongoing MCSP interventions in the PSE institutions. 2.3. Monitoring and Evaluation
At the country level, MCSP’s monitoring and evaluation (M&E) activities support governments in their use of improved metrics and methodologies to effectively collect data for assessing the coverage, quality and equity of RMNCH interventions.
Indicator Testing: MCSP, Department of Planning Research and Statistics (DPRS) of FMOH, and Ebonyi and Kogi SMOH tested 11 RMNCAH indicators (Table 2) to, among other objectives, understand if the indicators are useful for making decisions to improve quality of care, and understand the level of health system at which the indicators are useful. The outcomes of the assessment, which was carried out in 24 health facilities in Ebonyi and Kogi states, will inform the ongoing review of the NHMIS. MCSP will share the report of the meeting with the DPRS of the FMoH and discuss the implications of the findings for developing training manual to be used in training service providers and HMIS officers when the revised HMIS is ready Preliminary findings from the indicator testing showed that majority of the facilities (80%) documented data on the selected indicators; only a few service providers (33%) had basic understanding of the numerators and denominators of the indicators; and use of collected data for decision making was low among service providers (42%). Findings of the assessment will be shared with the DPRS of the FMoH and other IPs with the aim of using the information in re-designing the NHMIS which is currently being revised. It is also expected that the results will inform the process of training service providers and LGA M&E officers on indicators calculation the he second round will be conducted in June Table 2: RMNCAH indicators tested to inform review of NHMIS Maternal Health Newborn Health Child Health % of women receiving Uterotonic
immediately after birth of the baby
% of women that received a FP method pre-discharge after delivery
% of antenatal care visits at which blood pressure was measured
% of women with severe preeclampsia or eclampsia treated with magnesium sulfate injection
% of newborns not breathing/crying at birth resuscitated by stimulation or with bag & mask ventilation
# of newborns receiving essential newborn care
# of babies for whom Chlorhexidine was applied to the umbilical cord at birth
Number of cases of diarrhea treated
Number of cases of pneumonia treated with antibiotics
Proportion of uder-5 children with confirmed uncomplicated Malaria treated with ACT
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Institutional maternal mortality ratio
Meetings with USAID: During the reporting period, MCSP attended two meetings organized by USAID on Monitoring and Evaluation. The meetings were the regular HPN monthly meeting with all implementing partners while the second meeting was with only MCSP to discuss the program indicators and the Mission standard indicators within the context of the indicator reference sheets. For the monthly HPN IPs meeting, the discussion centered on the volume of standard indicators that IPs are presently tracking vis-à-vis the expectations of the Mission. It was noted that IPs are presently tracking and reporting more of custom indicators (397) than standards indicators (19). Yet, the latter are USAID’s priorities. IPs were encouraged wherever possible to track more standards indicators relating to their project.. MCSP will be able to track and report data on two of the new standard indicators which are number of CHEWs providing family planning services and number of pregnant women that received folic acid in USG supported programs. Data on these indicators are included in the current report Data Visualization: To encourage use of data for decision making at facility, LGA and state levels, MCSP supported Ebonyi SMOH to conduct a training session on the use of data for decision making for LGA M&E officers, state HIMS officers, and personnel drawn from MCSP-supported health facilities in the state. Participants were introduced to the concepts of data, strategies of using data for decision making, and data visualization. Emphasis was placed on data visualization using the laminated cardboard which MCSP printed and supplied to the facilities. MCSP produced the laminated dashboards for facilities with selected Quality of Care indicators to regularly display routine data. The health facilities Have started displaying data on selected indicators after the training and this has provided opportunity for data review and use if data for decision making at facility level. Updates on use of scorecards: Follow-up meetings and orientations were held during the reporting period on use of scorecards in Ebonyi and Kogi states. For Ebonyi, the inability of the state to officially launch the scorecards necessitated the follow-up meeting, during which stakeholders were tasked to expedite action in launching and using the scorecards. Going forward, the Commissioner for Health will take the leadership role of launching and using the scorecards. Similarly, in Kogi State, MCSP provided technical support for the development of QI scorecard for the state. Although the Commissioner for Health had launched the scorecard, the state has not maximize its use. The follow-up meeting was therefore used to advocate for the use of the scorecards. Record Keeping and Training for IMCI Health Facilities: MCSP supported SMOH and SPHCDA during the reporting period to train 273 (136 in Ebonyi and 137 in Kogi) health workers and officers from Logistic Management and Commodity Units on Health Management Information System and Logistic Management Information System. The training helped to build the competencies of participants on data recording for IMCI using NHMIS tools and child health logistics data collection tools. It was an opportunity to discuss strategies for improving child health data reporting and data quality in the states. Participation in Community Health Data and Use of DHIS2 Workshop in Senegal: MCSP assisted in the coordination of the Nigerian delegation and participated in the workshop in March 2018, which aimed to provide insights into the building of a CHIS while considering, in a holistic manner, the work context of a community health worker, and the particular complexities of their information needs. The workshop also aimed at helping countries adopt an architecture approach to enable viewing the challenge of building a sustainable and well-governed CHIS. For Nigeria, CHIS tools have been developed and presently hosted on a staging server. Some partners in conjunction with FMOH DHPRS would be piloting the tools to support and build the system. MCSP plans to use the iCCM tools and the Monthly Summary Forms with the PPMV outlets serving as the primary organization units and hierarchical levels for data entry and this experience
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
and learning will inform the FMOH DHPRS’s efforts. MCSP will continue to support all national efforts in this regard. 2.4. Operations Research
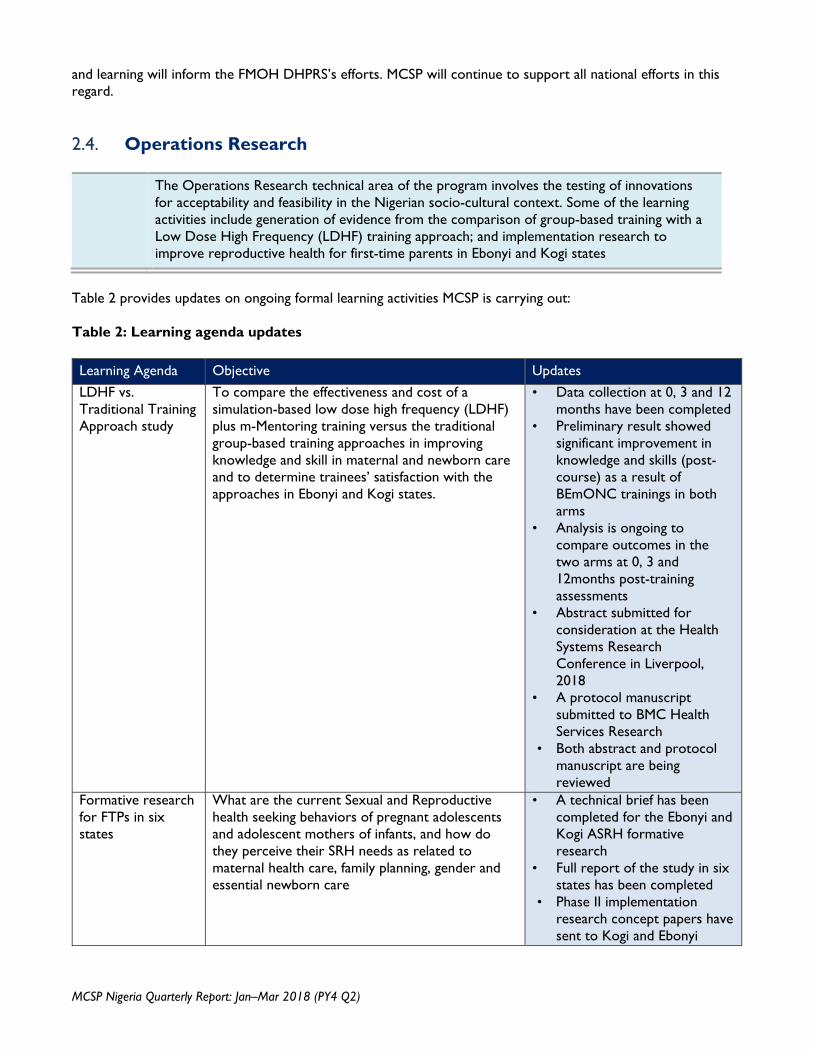
The Operations Research technical area of the program involves the testing of innovations for acceptability and feasibility in the Nigerian socio-cultural context. Some of the learning activities include generation of evidence from the comparison of group-based training with a Low Dose High Frequency (LDHF) training approach; and implementation research to improve reproductive health for first-time parents in Ebonyi and Kogi states
Table 2 provides updates on ongoing formal learning activities MCSP is carrying out: Table 2: Learning agenda updates
Learning Agenda Objective Updates
LDHF vs. Traditional Training Approach study
To compare the effectiveness and cost of a simulation-based low dose high frequency (LDHF) plus m-Mentoring training versus the traditional group-based training approaches in improving knowledge and skill in maternal and newborn care and to determine trainees’ satisfaction with the approaches in Ebonyi and Kogi states.
• Data collection at 0, 3 and 12 months have been completed
• Preliminary result showed significant improvement in knowledge and skills (post-course) as a result of BEmONC trainings in both arms
• Analysis is ongoing to compare outcomes in the two arms at 0, 3 and 12months post-training assessments
• Abstract submitted for consideration at the Health Systems Research Conference in Liverpool, 2018
• A protocol manuscript submitted to BMC Health Services Research
• Both abstract and protocol manuscript are being reviewed
Formative research for FTPs in six states
What are the current Sexual and Reproductive health seeking behaviors of pregnant adolescents and adolescent mothers of infants, and how do they perceive their SRH needs as related to maternal health care, family planning, gender and essential newborn care
• A technical brief has been completed for the Ebonyi and Kogi ASRH formative research
• Full report of the study in six states has been completed
• Phase II implementation research concept papers have sent to Kogi and Ebonyi
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
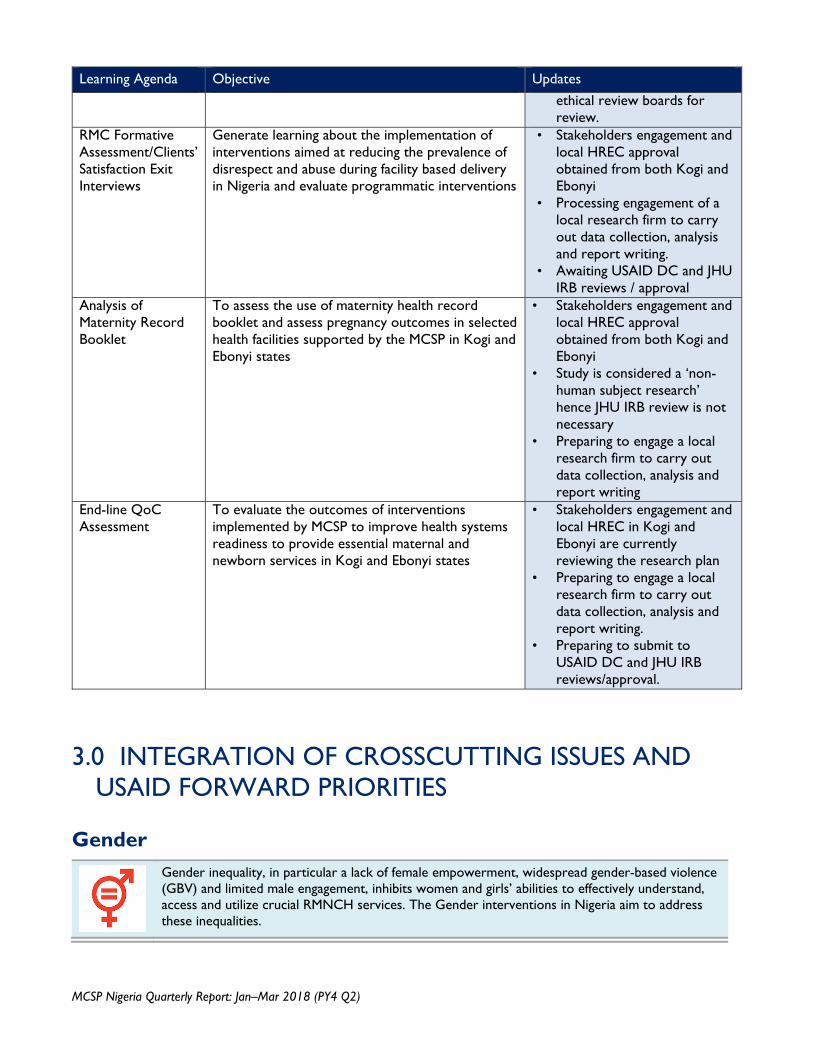
Learning Agenda Objective Updates
ethical review boards for review.
RMC Formative Assessment/Clients’ Satisfaction Exit Interviews
Generate learning about the implementation of interventions aimed at reducing the prevalence of disrespect and abuse during facility based delivery in Nigeria and evaluate programmatic interventions
• Stakeholders engagement and local HREC approval obtained from both Kogi and Ebonyi
• Processing engagement of a local research firm to carry out data collection, analysis and report writing.
• Awaiting USAID DC and JHU IRB reviews / approval
Analysis of Maternity Record Booklet
To assess the use of maternity health record booklet and assess pregnancy outcomes in selected health facilities supported by the MCSP in Kogi and Ebonyi states
• Stakeholders engagement and local HREC approval obtained from both Kogi and Ebonyi
• Study is considered a ‘non-human subject research’ hence JHU IRB review is not necessary
• Preparing to engage a local research firm to carry out data collection, analysis and report writing
End-line QoC Assessment
To evaluate the outcomes of interventions implemented by MCSP to improve health systems readiness to provide essential maternal and newborn services in Kogi and Ebonyi states
• Stakeholders engagement and local HREC in Kogi and Ebonyi are currently reviewing the research plan
• Preparing to engage a local research firm to carry out data collection, analysis and report writing.
• Preparing to submit to USAID DC and JHU IRB reviews/approval.
3.0 INTEGRATION OF CROSSCUTTING ISSUES AND USAID FORWARD PRIORITIES
Gender
Gender inequality, in particular a lack of female empowerment, widespread gender-based violence (GBV) and limited male engagement, inhibits women and girls’ abilities to effectively understand, access and utilize crucial RMNCH services. The Gender interventions in Nigeria aim to address these inequalities.
Jan – Mar 2018 www.mcsprogram.org
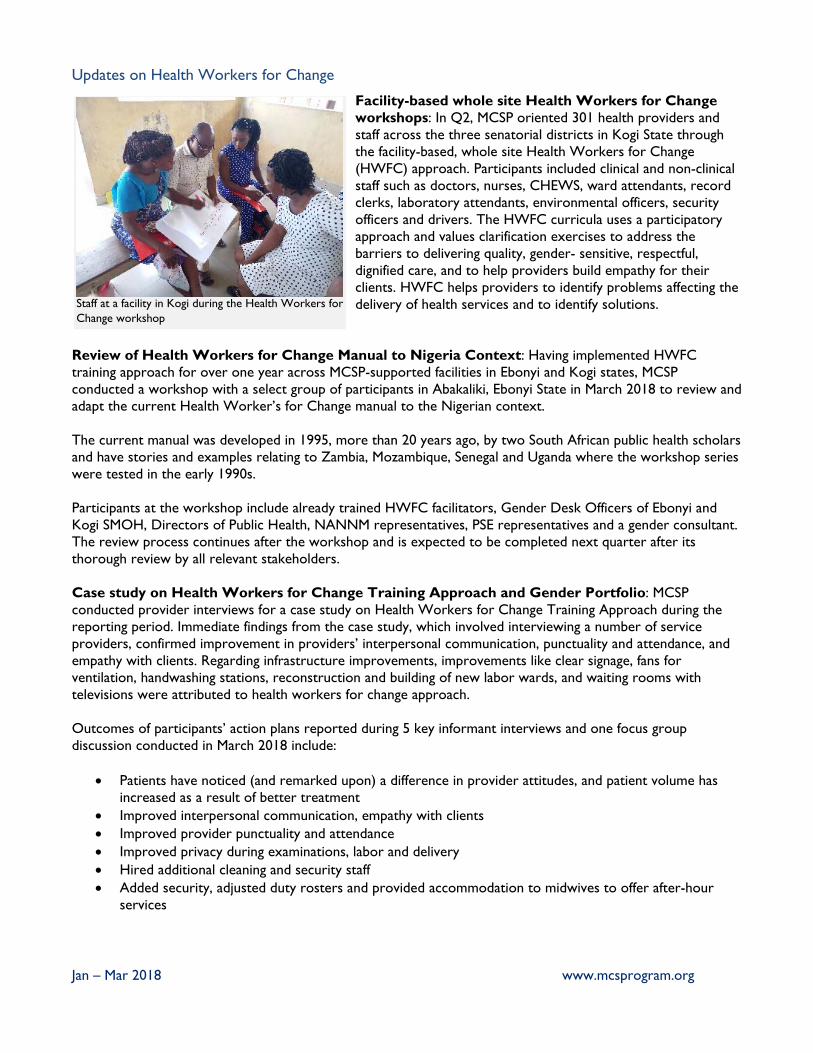
Updates on Health Workers for Change
Facility-based whole site Health Workers for Change workshops: In Q2, MCSP oriented 301 health providers and staff across the three senatorial districts in Kogi State through the facility-based, whole site Health Workers for Change (HWFC) approach. Participants included clinical and non-clinical staff such as doctors, nurses, CHEWS, ward attendants, record clerks, laboratory attendants, environmental officers, security officers and drivers. The HWFC curricula uses a participatory approach and values clarification exercises to address the barriers to delivering quality, gender- sensitive, respectful, dignified care, and to help providers build empathy for their clients. HWFC helps providers to identify problems affecting the delivery of health services and to identify solutions.
Review of Health Workers for Change Manual to Nigeria Context: Having implemented HWFC training approach for over one year across MCSP-supported facilities in Ebonyi and Kogi states, MCSP conducted a workshop with a select group of participants in Abakaliki, Ebonyi State in March 2018 to review and adapt the current Health Worker’s for Change manual to the Nigerian context. The current manual was developed in 1995, more than 20 years ago, by two South African public health scholars and have stories and examples relating to Zambia, Mozambique, Senegal and Uganda where the workshop series were tested in the early 1990s. Participants at the workshop include already trained HWFC facilitators, Gender Desk Officers of Ebonyi and Kogi SMOH, Directors of Public Health, NANNM representatives, PSE representatives and a gender consultant. The review process continues after the workshop and is expected to be completed next quarter after its thorough review by all relevant stakeholders. Case study on Health Workers for Change Training Approach and Gender Portfolio: MCSP conducted provider interviews for a case study on Health Workers for Change Training Approach during the reporting period. Immediate findings from the case study, which involved interviewing a number of service providers, confirmed improvement in providers’ interpersonal communication, punctuality and attendance, and empathy with clients. Regarding infrastructure improvements, improvements like clear signage, fans for ventilation, handwashing stations, reconstruction and building of new labor wards, and waiting rooms with televisions were attributed to health workers for change approach. Outcomes of participants’ action plans reported during 5 key informant interviews and one focus group discussion conducted in March 2018 include:
Patients have noticed (and remarked upon) a difference in provider attitudes, and patient volume has increased as a result of better treatment
Improved interpersonal communication, empathy with clients Improved provider punctuality and attendance Improved privacy during examinations, labor and delivery Hired additional cleaning and security staff Added security, adjusted duty rosters and provided accommodation to midwives to offer after-hour
services
Staff at a facility in Kogi during the Health Workers for Change workshop
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Infrastructure improvements: clear signage, fans for ventilation, handwashing stations, reconstructed and built new labor wards to allow for supportive companions to have space to attend L&D, waiting room televisions.
Providers and the State Ministries of Health gave MCSP highly positive feedback about the training. One provider remarked, “When I get back to my facility, I will allow pregnant women to choose their preferred position during delivery with respect and politeness, encourage men to be involved during ANC and delivery and explain every procedure to the client before commencing”
- Bilkisu Adagiri from PHC Nagagi, Kogi State
Updates on male engagement support
Training of facilitators on gender-based violence (GBV) first line support and basic clinical care: MCSP built the capacity of 41 service providers from pre-service institutions and in-service health facilities as facilitators on basic post-GBV care. The 2.5 day training was adapted from the forthcoming WHO training curricula, and included empathetic counseling using the LIVES model (Listen, Inquire, Validate, Ensure Safety and Support through referrals) and basic clinical care (treating acute injuries, offering HIV post-exposure prophylaxis and emergency contraception). Participants conducted role plays of simulated counseling sessions, allowing them to differentiate between effective approaches for child survivors, intimate partner violence survivors, and sexual assault survivors. The training was based on the baseline Quality of Care Assessment finding that 0% of providers offered GBV information or services. Pre-testing of GBV Referral Directories with Service Providers
Draft copies of GBV Referral Directories developed for both Kogi and Ebonyi states were pre-tested with participants at the Training of Facilitators on Male Engagement in RMNCAH in March in Ebonyi State. The directories provide contact information for support services for post-GBV care. Valuable feedback was received during the pre-test and will be incorporated before the final production and dissemination of the GBV Referral Directories in the both Kogi and Ebonyi states. Training of facilitators on male engagement: MCSP built the capacity of 41 service providers from pre-service institutions and in-service health facilities as facilitators on male engagement approaches in RMNCAH and on providing first-line support to survivors of GBV. The 2.5 day training focused on promoting male engagement in RMNCAH as well as providing post-GBV care. The workshop helped to improve the interpersonal communication, counselling, and facilitation skills (including emotional and social intelligence) of the participants. Development of male engagement job aids and IEC materials: Draft copies of male engagement job aids for providers and information, education and communication (IEC) posters and pamphlets designed by MCSP were pre-tested during the trainings of facilitators on male engagement in RMNCAH and GBV in Afikpo, Ebonyi State. The job aids and IEC materials were also pre-tested with service providers and clients at different health facilities in both Kogi and Ebonyi states.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
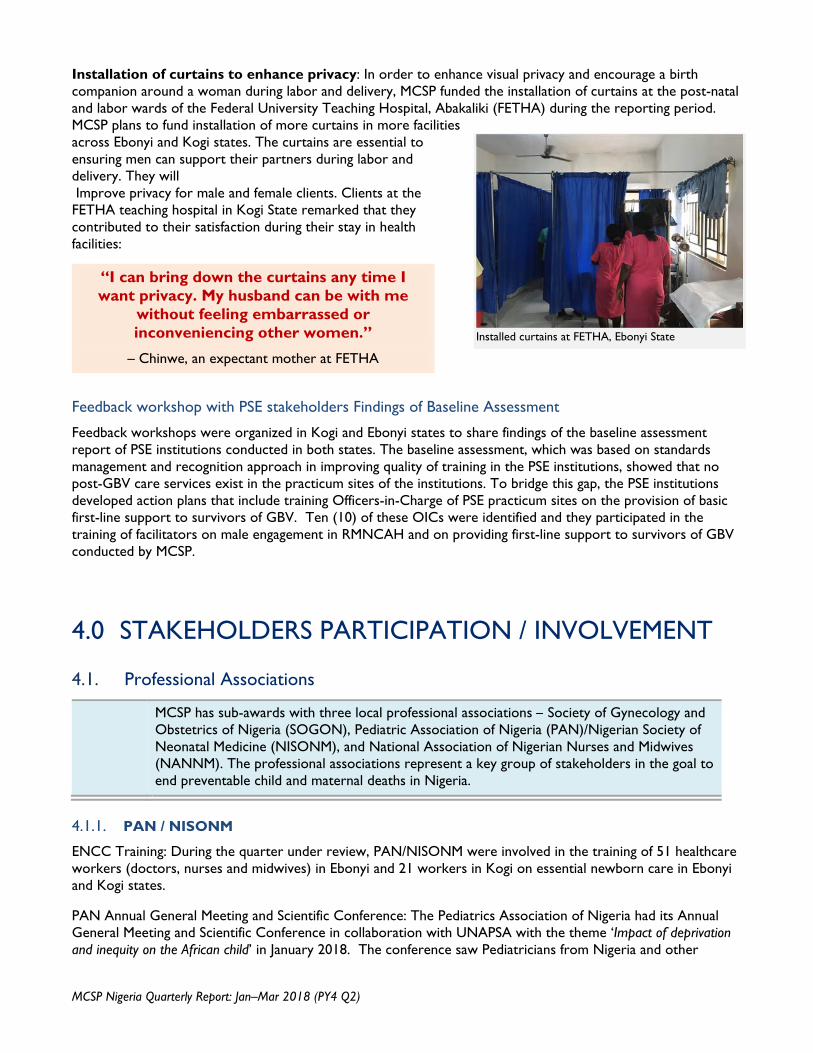
Installation of curtains to enhance privacy: In order to enhance visual privacy and encourage a birth companion around a woman during labor and delivery, MCSP funded the installation of curtains at the post-natal and labor wards of the Federal University Teaching Hospital, Abakaliki (FETHA) during the reporting period. MCSP plans to fund installation of more curtains in more facilities across Ebonyi and Kogi states. The curtains are essential to ensuring men can support their partners during labor and delivery. They will Improve privacy for male and female clients. Clients at the FETHA teaching hospital in Kogi State remarked that they contributed to their satisfaction during their stay in health facilities:
Feedback workshop with PSE stakeholders Findings of Baseline Assessment
Feedback workshops were organized in Kogi and Ebonyi states to share findings of the baseline assessment report of PSE institutions conducted in both states. The baseline assessment, which was based on standards management and recognition approach in improving quality of training in the PSE institutions, showed that no post-GBV care services exist in the practicum sites of the institutions. To bridge this gap, the PSE institutions developed action plans that include training Officers-in-Charge of PSE practicum sites on the provision of basic first-line support to survivors of GBV. Ten (10) of these OICs were identified and they participated in the training of facilitators on male engagement in RMNCAH and on providing first-line support to survivors of GBV conducted by MCSP.
4.0 STAKEHOLDERS PARTICIPATION / INVOLVEMENT 4.1. Professional Associations
MCSP has sub-awards with three local professional associations – Society of Gynecology and Obstetrics of Nigeria (SOGON), Pediatric Association of Nigeria (PAN)/Nigerian Society of Neonatal Medicine (NISONM), and National Association of Nigerian Nurses and Midwives (NANNM). The professional associations represent a key group of stakeholders in the goal to end preventable child and maternal deaths in Nigeria.
4.1.1. PAN / NISONM
ENCC Training: During the quarter under review, PAN/NISONM were involved in the training of 51 healthcare workers (doctors, nurses and midwives) in Ebonyi and 21 workers in Kogi on essential newborn care in Ebonyi and Kogi states.
PAN Annual General Meeting and Scientific Conference: The Pediatrics Association of Nigeria had its Annual General Meeting and Scientific Conference in collaboration with UNAPSA with the theme ‘Impact of deprivation and inequity on the African child’ in January 2018. The conference saw Pediatricians from Nigeria and other
Installed curtains at FETHA, Ebonyi State
“I can bring down the curtains any time I want privacy. My husband can be with me
without feeling embarrassed or inconveniencing other women.”
– Chinwe, an expectant mother at FETHA
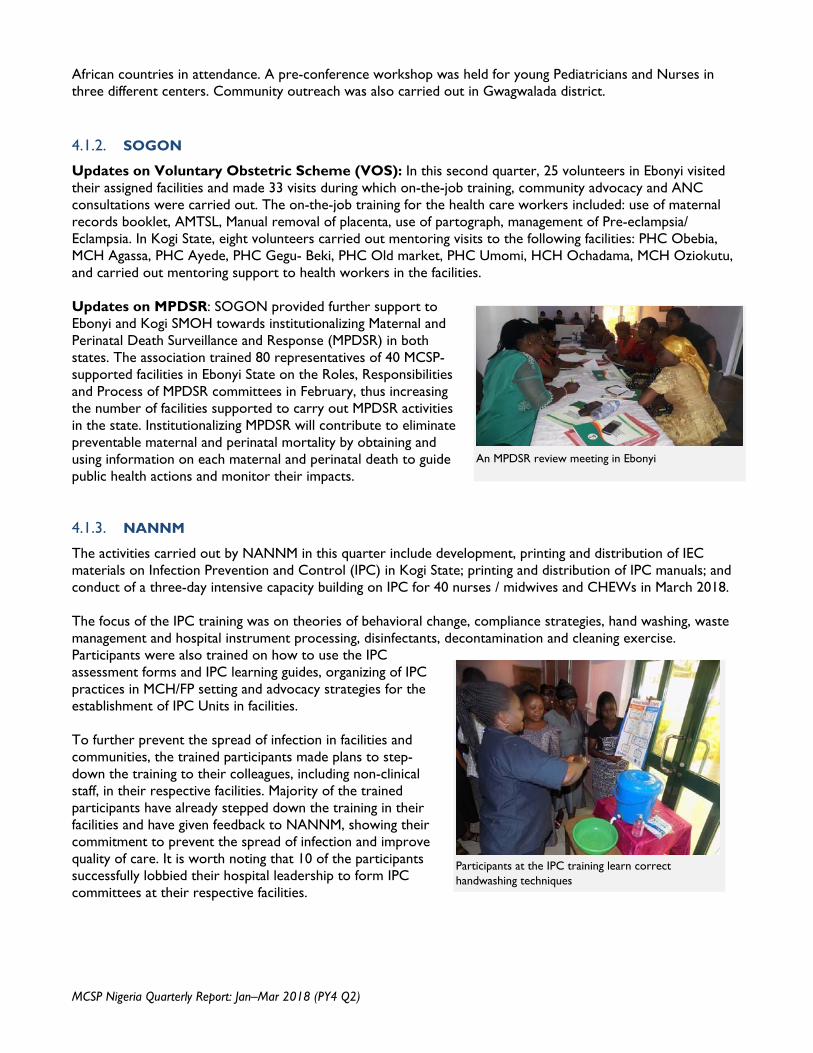
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
African countries in attendance. A pre-conference workshop was held for young Pediatricians and Nurses in three different centers. Community outreach was also carried out in Gwagwalada district. 4.1.2. SOGON
Updates on Voluntary Obstetric Scheme (VOS): In this second quarter, 25 volunteers in Ebonyi visited their assigned facilities and made 33 visits during which on-the-job training, community advocacy and ANC consultations were carried out. The on-the-job training for the health care workers included: use of maternal records booklet, AMTSL, Manual removal of placenta, use of partograph, management of Pre-eclampsia/ Eclampsia. In Kogi State, eight volunteers carried out mentoring visits to the following facilities: PHC Obebia, MCH Agassa, PHC Ayede, PHC Gegu- Beki, PHC Old market, PHC Umomi, HCH Ochadama, MCH Oziokutu, and carried out mentoring support to health workers in the facilities. Updates on MPDSR: SOGON provided further support to Ebonyi and Kogi SMOH towards institutionalizing Maternal and Perinatal Death Surveillance and Response (MPDSR) in both states. The association trained 80 representatives of 40 MCSP-supported facilities in Ebonyi State on the Roles, Responsibilities and Process of MPDSR committees in February, thus increasing the number of facilities supported to carry out MPDSR activities in the state. Institutionalizing MPDSR will contribute to eliminate preventable maternal and perinatal mortality by obtaining and using information on each maternal and perinatal death to guide public health actions and monitor their impacts.
4.1.3. NANNM
The activities carried out by NANNM in this quarter include development, printing and distribution of IEC materials on Infection Prevention and Control (IPC) in Kogi State; printing and distribution of IPC manuals; and conduct of a three-day intensive capacity building on IPC for 40 nurses / midwives and CHEWs in March 2018. The focus of the IPC training was on theories of behavioral change, compliance strategies, hand washing, waste management and hospital instrument processing, disinfectants, decontamination and cleaning exercise. Participants were also trained on how to use the IPC assessment forms and IPC learning guides, organizing of IPC practices in MCH/FP setting and advocacy strategies for the establishment of IPC Units in facilities. To further prevent the spread of infection in facilities and communities, the trained participants made plans to step-down the training to their colleagues, including non-clinical staff, in their respective facilities. Majority of the trained participants have already stepped down the training in their facilities and have given feedback to NANNM, showing their commitment to prevent the spread of infection and improve quality of care. It is worth noting that 10 of the participants successfully lobbied their hospital leadership to form IPC committees at their respective facilities.
An MPDSR review meeting in Ebonyi
Participants at the IPC training learn correct handwashing techniques
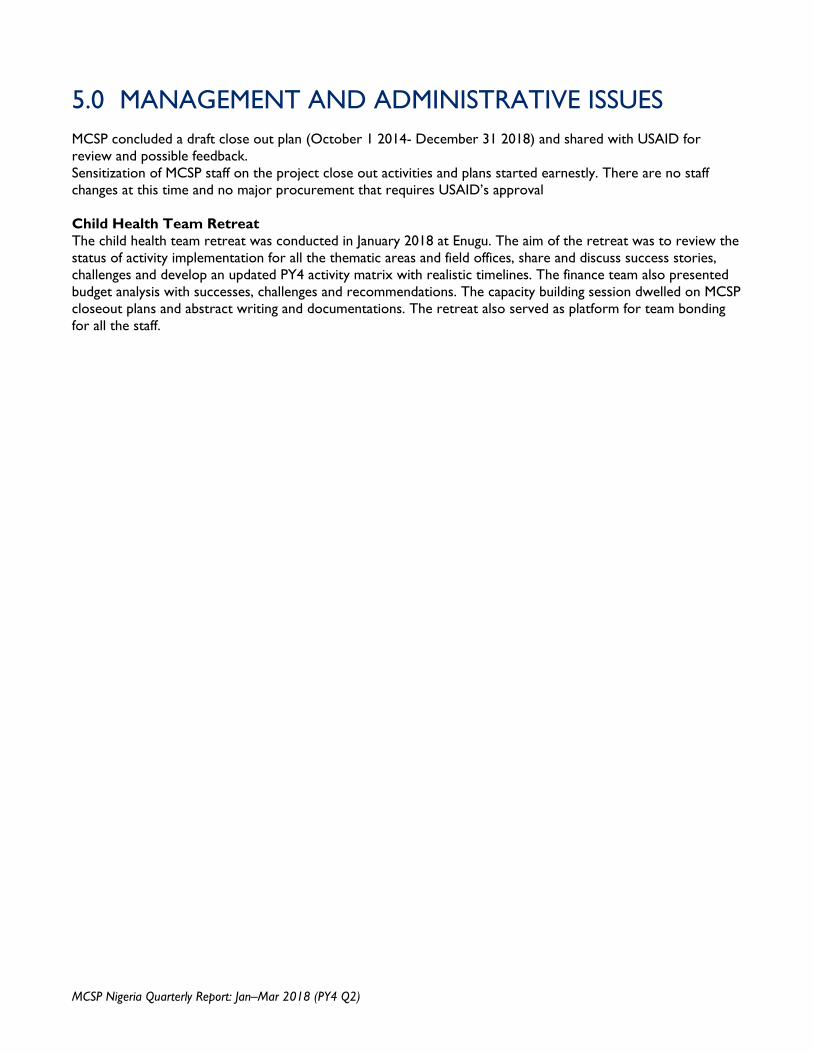
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
5.0 MANAGEMENT AND ADMINISTRATIVE ISSUES MCSP concluded a draft close out plan (October 1 2014- December 31 2018) and shared with USAID for review and possible feedback. Sensitization of MCSP staff on the project close out activities and plans started earnestly. There are no staff changes at this time and no major procurement that requires USAID’s approval Child Health Team Retreat The child health team retreat was conducted in January 2018 at Enugu. The aim of the retreat was to review the status of activity implementation for all the thematic areas and field offices, share and discuss success stories, challenges and develop an updated PY4 activity matrix with realistic timelines. The finance team also presented budget analysis with successes, challenges and recommendations. The capacity building session dwelled on MCSP closeout plans and abstract writing and documentations. The retreat also served as platform for team bonding for all the staff.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
6.0 CHALLENGES / LESSONS LEARNED 6.1. Implementation Challenges
Below are some of the challenges – programmatic (internal) and external – that impacted the implementation of interventions and activities of the Program during the period under review, and the strategies adopted to address the challenges.
Challenges MCSP Response
1. Insecurity (characterized mostly by communal clashes, kidnapping and herdsmen attacks) hinders program implementation and activities
To continue to fast track activities whenever there is a window of opportunity in the areas of insecurity
2. Frequent transfer of trained staff from MCSP-supported facilities to non-supported facilities hinders service delivery by affected workers and post-training follow-up and supportive supervision
Stepped up subsisting advocacy to SPHCDA to reverse some transfers, and be more strategic in any future transfers; Nonetheless, new staff transferred to MCSP-supported facilities were and will continue to be mentored
3. Continued delay or non-payment of salaries of affected healthcare workers, especially in Kogi State, demotivated them and limited their level of commitments
Continuous advocacy on staff welfare to Kogi State government at any given opportunity
4. The measles vaccine campaign conducted in Ebonyi State delayed the implementation of some planned activities.
Keep collaborating closely with State Ministries of Health to avoid delay in implementation of MCSP activities.
5. Delay to the implementation of formal learning activities due to long process of protocol reviews and approval from both local HREC and JHU IRB
To work simultaneously on other aspects of the research project not affected by JHU IRB approval
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
7.0 PLANNED ACTIVITIES FOR NEXT QUARTER INCLUDING UPCOMING EVENTS
# Thematic Areas Planned Activities Notes
1 Maternal Health Conduct 3-day onsite refresher training on PPH, PEE, infection control and ANC (Maternity Health Records) for 160 MCSP facilities utilizing clinical skills laboratory as training sites where appropriate.
Strengthen CEmONC service delivery for 10 Doctors in Ebonyi State. Program efforts will focus on remaining HFs not trained previously and key officers from SMOH that are medical doctors
Support State and LGA Supervisors to conduct joint quarterly ISS visits to MCSP-supported sites in Kogi and Ebonyi states
Support monitoring and data collection on a monthly basis for all MSLCs Support 91 QI teams in Kogi and Ebonyi States to close critical MNCH
quality gaps and to routinely collect and analyze prioritized quality measures using QI/MPDSR reporting template.
In collaboration with trainers, and relevant Professional Associations, develop post training follow up visit schedule to 241 HFs
Support printing and distribution of IEC materials – 1500 copies each (ANC, Safe Motherhood, Early Detection of Danger Signs, BPCR, Malaria in Pregnancy, IPT, MSLC) and 100,000 copies of Maternal Health Records Booklets and BPCR cards
2 Newborn Health
PSBI orientation for WDC Members in Ikwo and Abakaliki LGAs, Ebonyi and LGA HODs in Kogi State
WASH Orientation for Heads of Facilities in Abakaliki, Ebonyi Support for the implementation of the chlorhexidine operational plan in
Kogi and Ebonyi states Post-Training Supportive Supervisory Visits/Monitoring visit in Kogi and
Ebonyi states Harmonized mENCC/PSBI Training of CHEWs in Ebonyi Participation in AGPMPN Conference, Kogi Pretesting of PSBI IEC materials with community actors in Kogi and
Ebonyi states KMC Orientation for KMC Centre Facilities in Onicha, Ivo, & Ohaozara
LGAs, Ebonyi Sick Newborn/KMC Quarterly Review Meeting in Kogi and Ebonyi
states Mentorship of CHEWS trained on PSBI in Kogi and Ebonyi states
3 Child Health Ongoing technical support to FMOH Child Health Division to advocate for increased availability of essential child health commodities
Support SMOH to address funding gaps and advocate for support for procurement and distribution of child health commodities
Work with SMOH, relevant partners and LMCU to facilitate last mile distribution of key child health commodities
Stakeholder engagements with national programs and partners to advocate for improved coordination
Support State CMS and HF staff to improve stock-keeping and storage practices for CH commodities
Improve capacity of LGA IMCI focal persons and LMCU to monitor inventory management of CH commodities at health facilities
Work with LMCU to integrate CH commodities into monitoring and supportive supervision visits
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
# Thematic Areas Planned Activities Notes
Strengthen SMOH capacity to lead quantification and distribution planning for CH commodities
Support SMOH, PCN, SPHCDA, LGAs and NAPPMED to increase availability and access to quality and affordable frontline child health commodities at PPMV shops
Train PPMVs and PPMV supervisors in selected LGAs in Kogi and Ebonyi states
Provide on-the-job capacity building and mentoring to supported facilities on IMCI/PSBI
Selection and training of PHC mentors on Tertiary Health Institutions (THIs) mentorship program
Post-training mentorship visits to facilities Monthly supervision of PPMVs implementation of EQuiPP in the outlets Host 1st Quality Improvement meeting for PPMV supervisors Participate at PPMV monthly meetings and conduct refresher training on
identified gaps. 4 Family Planning Conduct PP-LARC Training for 40 health care workers
Facilitate post-training supportive follow-up visits to health workers trained on PPLARC in Kogi and Ebonyi states
Conduct one day FP/Abortion legislative policy compliance training for 40 health care workers
Conduct post MLLA mentorship and follow up visit Support Kogi Ministry of health and FP Advocacy working group
meetings for development of FP costed implementation plan Conduct dedicated counselors program progress evaluation Conduct whole-site orientation on PPFP in 24 health facilities in Kogi
and Ebonyi state
5 ASRH Support and participate in bi-annual national NAHDWG meetings Continue to support and participate in Kogi and Ebonyi state ASRH
Technical Working Groups Conduct quarterly supportive supervision visits to follow up with facility
based providers Finalize Phase I formative research report and briefs for FTPs in 6 states Hold workshop with key stakeholders to disseminate ASRH Phase 1
formative research findings in 6 states Implement Our First Baby discussion groups Train Our First Baby and Age & Life-Stage Counseling tools endline
documentation team. Printing FTM Savings and loans club membership cards, T-shirts, Bags
and fez caps
6 Gender Support the Federal Ministry of Health in the development of a national gender policy on health in Nigeria.
Finalize male engagement IEC materials following feedback from pre-testing and disseminate same
Cascade the training on the provision of basic first-line support for GBV survivors to reach up to 500 service providers
Cascade the training on effective male engagement in RMNCAH to reach up to 500 service providers
Print and disseminate GBV Referral Directories/Maps to health facilities Follow-up with the integration of the Gender Service Delivery
Standards, into MCSP Quality improvement approaches Finalize the Nigeria adaptation of the HWfC manual, print and
disseminate.
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
# Thematic Areas Planned Activities Notes
Scale up HWFC to additional skilled and unskilled providers etc. to sustain health worker’s participatory engagement to change negative attitudes and improve provider-client relations
7 Pre-Service Education
Conduct first follow-up biannual SBMR assessments in all PSE training institutions and practicum sites
Set up additional clinical skills laboratories in remaining PSE institutions in both project states
8 SOGON Continue support of SOGON members under VOS for supportive visits to MCSP supported health facilities (to include 33 QI facilities (PHCs) and post training supervision (use of partograph, MgSO4, PE/E and maternal health booklet etc.)
Conduct 3-day training for 2 Facility Representatives on Maternal Perinatal Death Surveillance and Response (MPDSR) from 40 facilities (2 sets) in Kogi State
Quarterly Supportive Supervision to QI Facilities [Secondary, Primary (community)] and on-site post-training supervision on MPDSR
Support State Technical Committee to conduct Maternal and Perinatal Death reviews
Quarterly Review meetings for VOS volunteers Quarterly MPDSR Committee Meetings for review, action and
dissemination of MPDSR processes Advocacy and engagement for passage of MPDSR bill Sensitization workshop for Adoption of MPDSR code (ICD-MM-PM)
9 PAN/NISONM Conduct full ENCC in-service HCW Participate in NISONM conference Continue mentoring and supportive supervision by the VPSS
10 HSS/E Conduct financial analysis and literature review to inform PHC-DRF strategy development
Develop first draft of PHC-DRF strategy Gather and synthesize lessons learned related to LMIS Convene second high-level meeting for PHC-DRF operators and agree on
way forward for capacity building
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
8.0 HOW IMPLEMENTING PARTNER HAS ADDRESSED A/COR COMMENTS FROM THE LAST QUARTERLY OR SEMI-ANNUAL REPORT
This is not applicable at this time
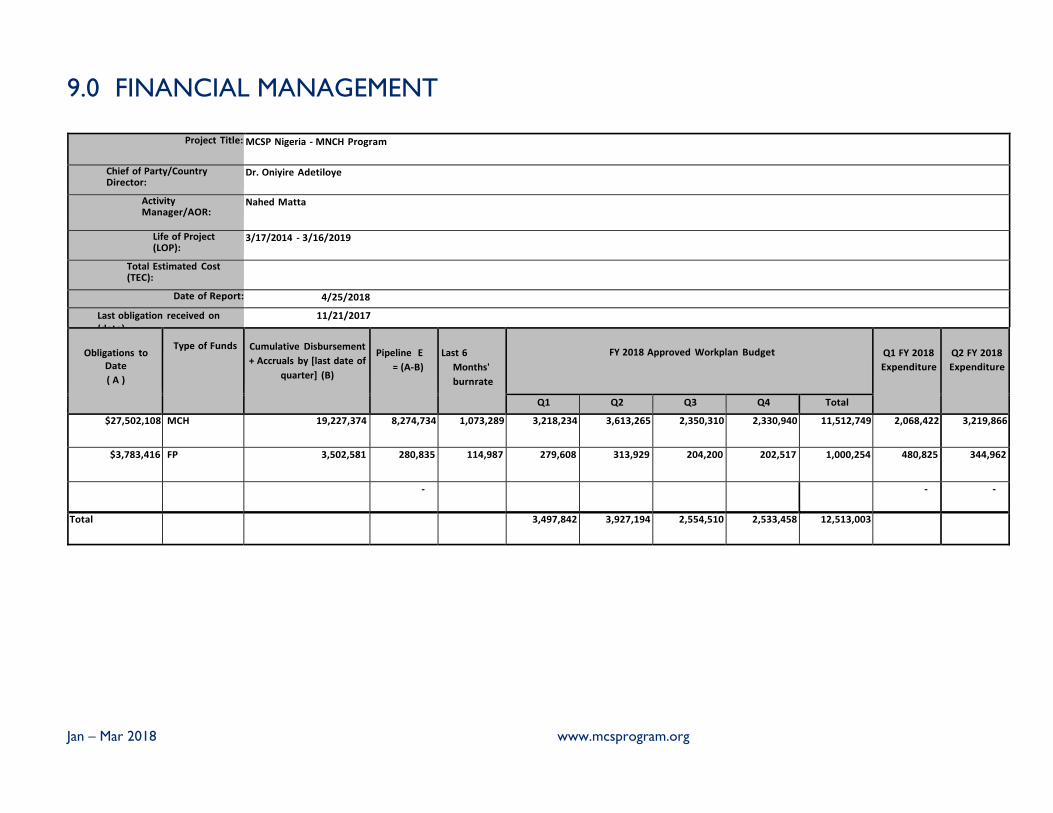
Jan – Mar 2018 www.mcsprogram.org
9.0 FINANCIAL MANAGEMENT
Project Title: MCSP Nigeria ‐ MNCH Program
Chief of Party/Country Director:
Dr. Oniyire Adetiloye
Activity Manager/AOR:
Nahed Matta
Life of Project (LOP):
3/17/2014 ‐ 3/16/2019
Total Estimated Cost (TEC):
Date of Report: 4/25/2018
Last obligation received on (date):
11/21/2017
Obligations to
Date
( A )
Type of Funds
Cumulative Disbursement
+ Accruals by [last date of
quarter] (B)
Pipeline E
= (A‐B)
Last 6
Months'
burnrate
FY 2018 Approved Workplan Budget
Q1 FY 2018
Expenditure
Q2 FY 2018
Expenditure
Q1 Q2 Q3 Q4 Total
$27,502,108 MCH 19,227,374 8,274,734 1,073,289 3,218,234 3,613,265 2,350,310 2,330,940 11,512,749 2,068,422 3,219,866
$3,783,416 FP 3,502,581 280,835 114,987 279,608 313,929 204,200 202,517 1,000,254 480,825 344,962
‐ ‐ ‐
Total 3,497,842 3,927,194 2,554,510 2,533,458 12,513,003
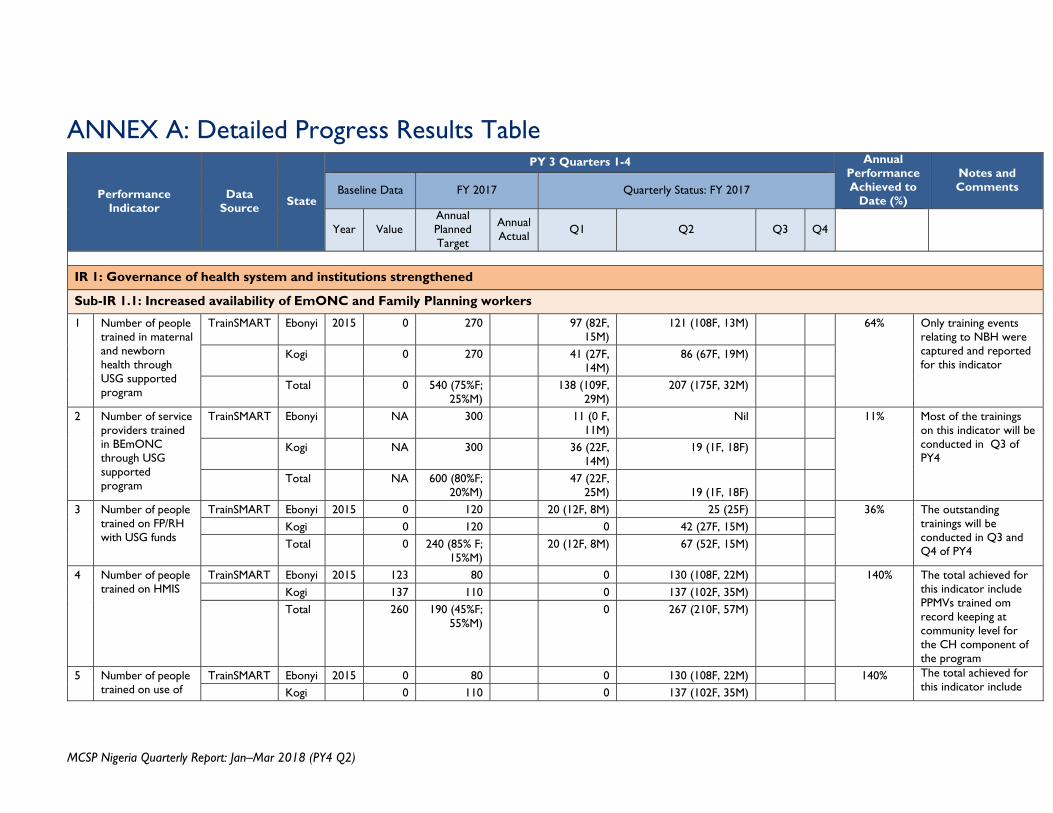
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
ANNEX A: Detailed Progress Results Table
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
IR 1: Governance of health system and institutions strengthened
Sub-IR 1.1: Increased availability of EmONC and Family Planning workers
1 Number of people trained in maternal and newborn health through USG supported program
TrainSMART Ebonyi 2015 0 270 97 (82F, 15M)
121 (108F, 13M) 64% Only training events relating to NBH were captured and reported for this indicator
Kogi 0 270 41 (27F, 14M)
86 (67F, 19M)
Total 0 540 (75%F; 25%M)
138 (109F, 29M)
207 (175F, 32M)
2 Number of service providers trained in BEmONC through USG supported program
TrainSMART Ebonyi NA 300 11 (0 F, 11M)
Nil 11% Most of the trainings on this indicator will be conducted in Q3 of PY4
Kogi NA 300 36 (22F, 14M)
19 (1F, 18F)
Total NA 600 (80%F; 20%M)
47 (22F, 25M)
19 (1F, 18F)
3 Number of people trained on FP/RH with USG funds
TrainSMART Ebonyi 2015 0 120 20 (12F, 8M) 25 (25F) 36% The outstanding trainings will be conducted in Q3 and Q4 of PY4
Kogi 0 120 0 42 (27F, 15M) Total 0 240 (85% F;
15%M) 20 (12F, 8M) 67 (52F, 15M)
4 Number of people trained on HMIS
TrainSMART Ebonyi 2015 123 80 0 130 (108F, 22M) 140% The total achieved for this indicator include PPMVs trained om record keeping at community level for the CH component of the program
Kogi 137 110 0 137 (102F, 35M) Total 260 190 (45%F;
55%M) 0 267 (210F, 57M)
5 Number of people trained on use of
TrainSMART Ebonyi 2015 0 80 0 130 (108F, 22M) 140% The total achieved for this indicator include Kogi 0 110 0 137 (102F, 35M)
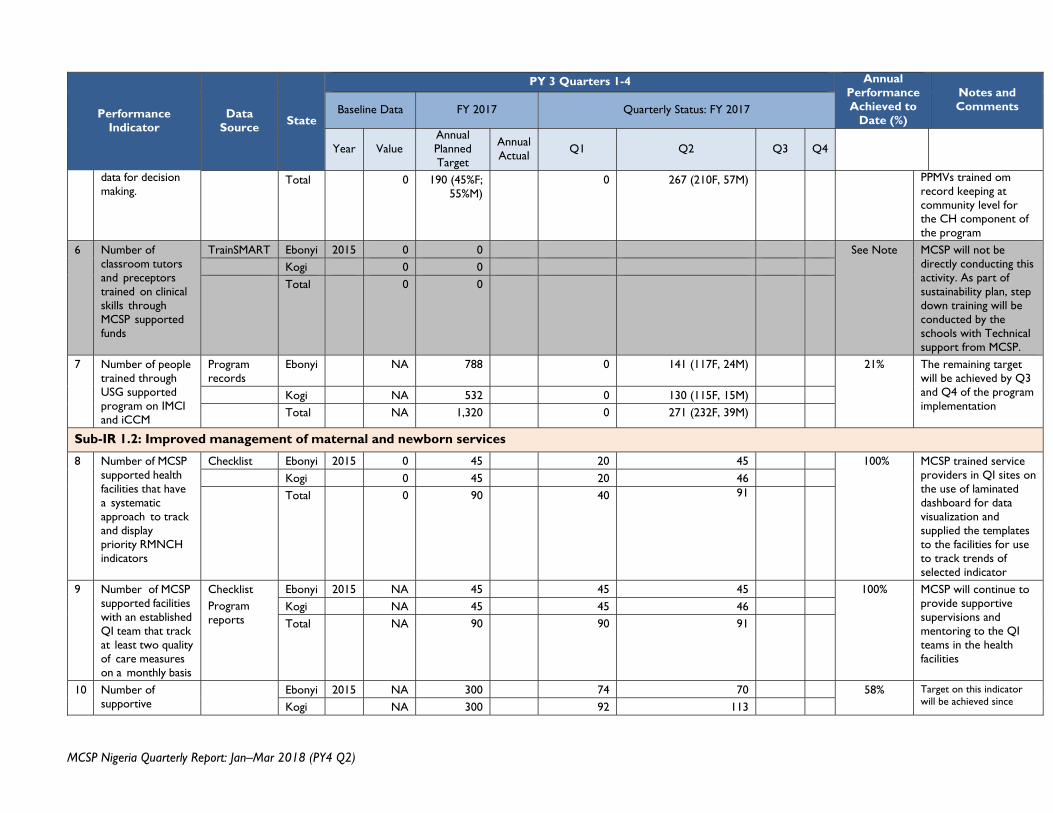
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
data for decision making.
Total 0 190 (45%F; 55%M)
0 267 (210F, 57M) PPMVs trained om record keeping at community level for the CH component of the program
6 Number of classroom tutors and preceptors trained on clinical skills through MCSP supported funds
TrainSMART Ebonyi 2015 0 0 See Note MCSP will not be directly conducting this activity. As part of sustainability plan, step down training will be conducted by the schools with Technical support from MCSP.
Kogi 0 0 Total 0 0
7 Number of people trained through USG supported program on IMCI and iCCM
Program records
Ebonyi NA 788 0 141 (117F, 24M) 21% The remaining target will be achieved by Q3 and Q4 of the program implementation
Kogi NA 532 0 130 (115F, 15M) Total NA 1,320 0 271 (232F, 39M)
Sub-IR 1.2: Improved management of maternal and newborn services
8 Number of MCSP supported health facilities that have a systematic approach to track and display priority RMNCH indicators
Checklist Ebonyi 2015 0 45 20 45 100% MCSP trained service providers in QI sites on the use of laminated dashboard for data visualization and supplied the templates to the facilities for use to track trends of selected indicator
Kogi 0 45 20 46 Total 0 90 40 91
9 Number of MCSP supported facilities with an established QI team that track at least two quality of care measures on a monthly basis
Checklist Program reports
Ebonyi 2015 NA 45 45 45 100% MCSP will continue to provide supportive supervisions and mentoring to the QI teams in the health facilities
Kogi NA 45 45 46 Total NA 90 90 91
10 Number of supportive
Ebonyi 2015 NA 300 74 70 58% Target on this indicator will be achieved since Kogi NA 300 92 113
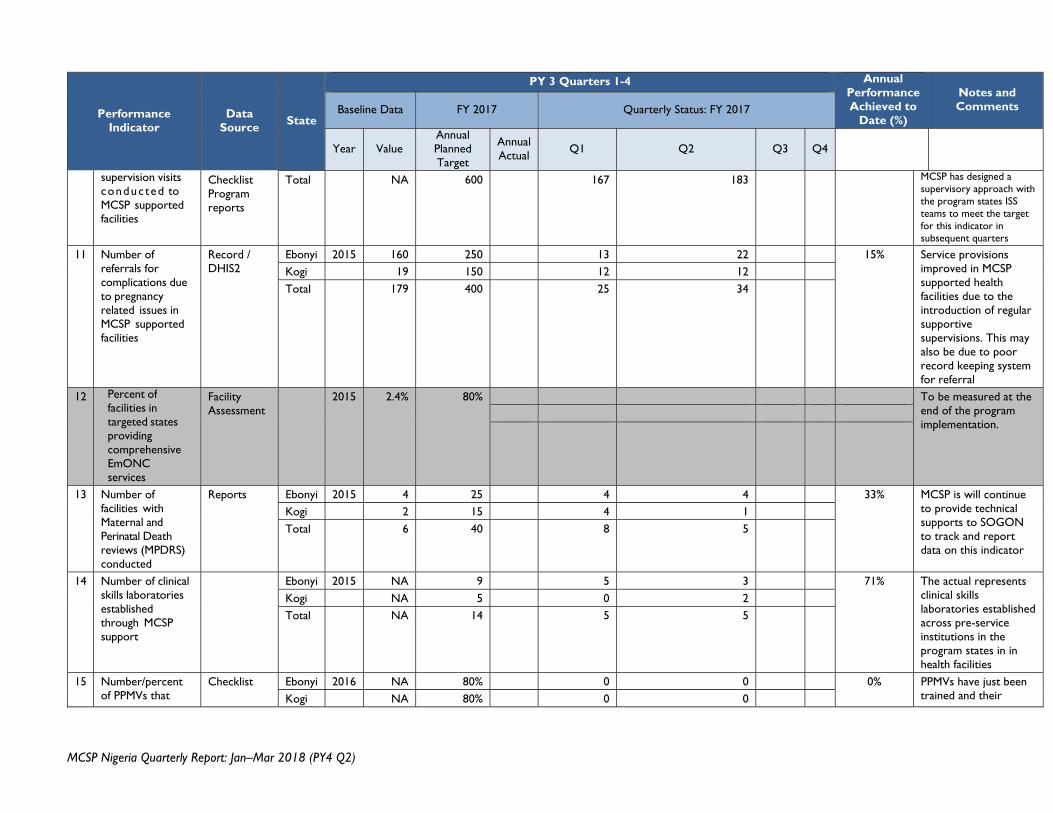
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
supervision visits conduc ted to MCSP supported facilities
Checklist Program reports
Total NA 600 167 183 MCSP has designed a supervisory approach with the program states ISS teams to meet the target for this indicator in subsequent quarters
11 Number of referrals for complications due to pregnancy related issues in MCSP supported facilities
Record / DHIS2
Ebonyi 2015 160 250 13 22 15% Service provisions improved in MCSP supported health facilities due to the introduction of regular supportive supervisions. This may also be due to poor record keeping system for referral
Kogi 19 150 12 12 Total 179 400 25 34
12
Percent of facilities in targeted states providing comprehensive EmONC services
Facility Assessment
2015
2.4%
80%
To be measured at the end of the program implementation.
13 Number of facilities with Maternal and Perinatal Death reviews (MPDRS) conducted
Reports Ebonyi 2015 4 25 4 4 33% MCSP is will continue to provide technical supports to SOGON to track and report data on this indicator
Kogi 2 15 4 1 Total 6 40 8 5
14 Number of clinical skills laboratories established through MCSP support
Ebonyi 2015 NA 9 5 3 71% The actual represents clinical skills laboratories established across pre-service institutions in the program states in in health facilities
Kogi NA 5 0 2 Total NA 14 5 5
15 Number/percent of PPMVs that
Checklist Ebonyi 2016 NA 80% 0 0 0% PPMVs have just been trained and their Kogi NA 80% 0 0
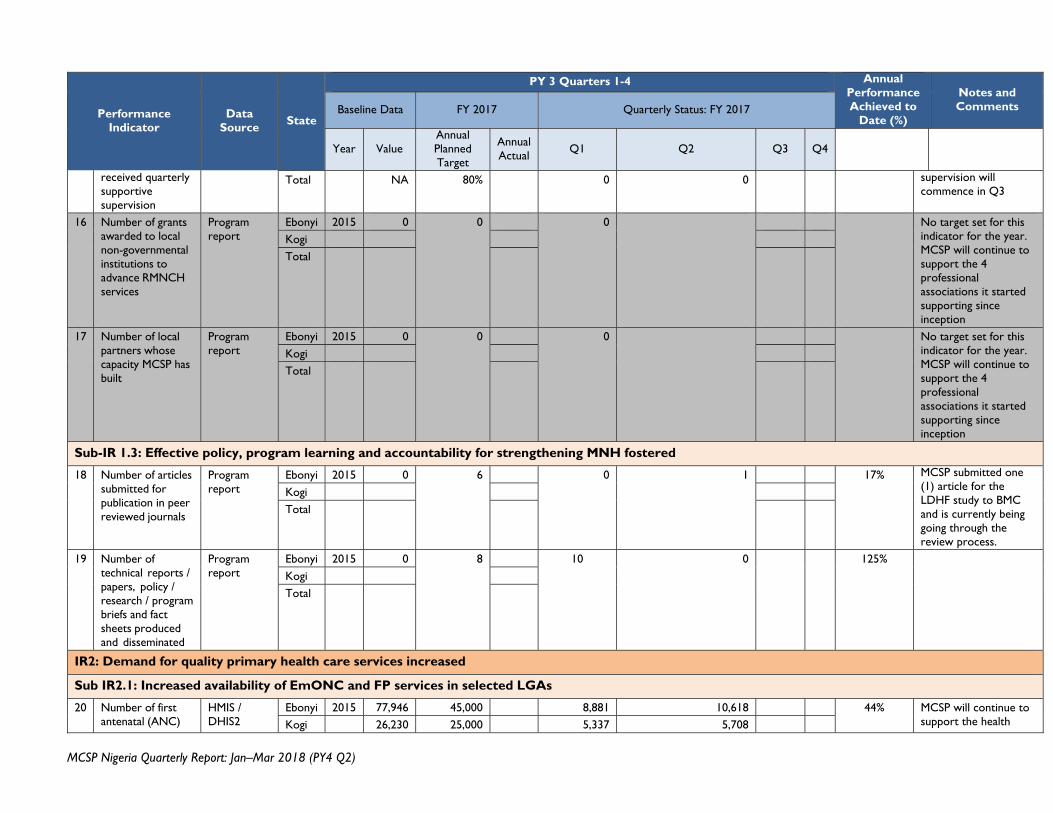
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
received quarterly supportive supervision
Total NA 80% 0 0 supervision will commence in Q3
16 Number of grants awarded to local non-governmental institutions to advance RMNCH services
Program report
Ebonyi 2015 0 0 0 No target set for this indicator for the year. MCSP will continue to support the 4 professional associations it started supporting since inception
Kogi Total
17 Number of local partners whose capacity MCSP has built
Program report
Ebonyi 2015 0 0 0 No target set for this indicator for the year. MCSP will continue to support the 4 professional associations it started supporting since inception
Kogi Total
Sub-IR 1.3: Effective policy, program learning and accountability for strengthening MNH fostered
18 Number of articles submitted for publication in peer reviewed journals
Program report
Ebonyi 2015 0 6 0 1 17% MCSP submitted one (1) article for the LDHF study to BMC and is currently being going through the review process.
Kogi Total
19 Number of technical reports / papers, policy / research / program briefs and fact sheets produced and disseminated
Program report
Ebonyi 2015 0 8 10 0 125% Kogi Total
IR2: Demand for quality primary health care services increased
Sub IR2.1: Increased availability of EmONC and FP services in selected LGAs
20 Number of first antenatal (ANC)
HMIS / DHIS2
Ebonyi 2015 77,946 45,000 8,881 10,618 44% MCSP will continue to support the health Kogi 26,230 25,000 5,337 5,708
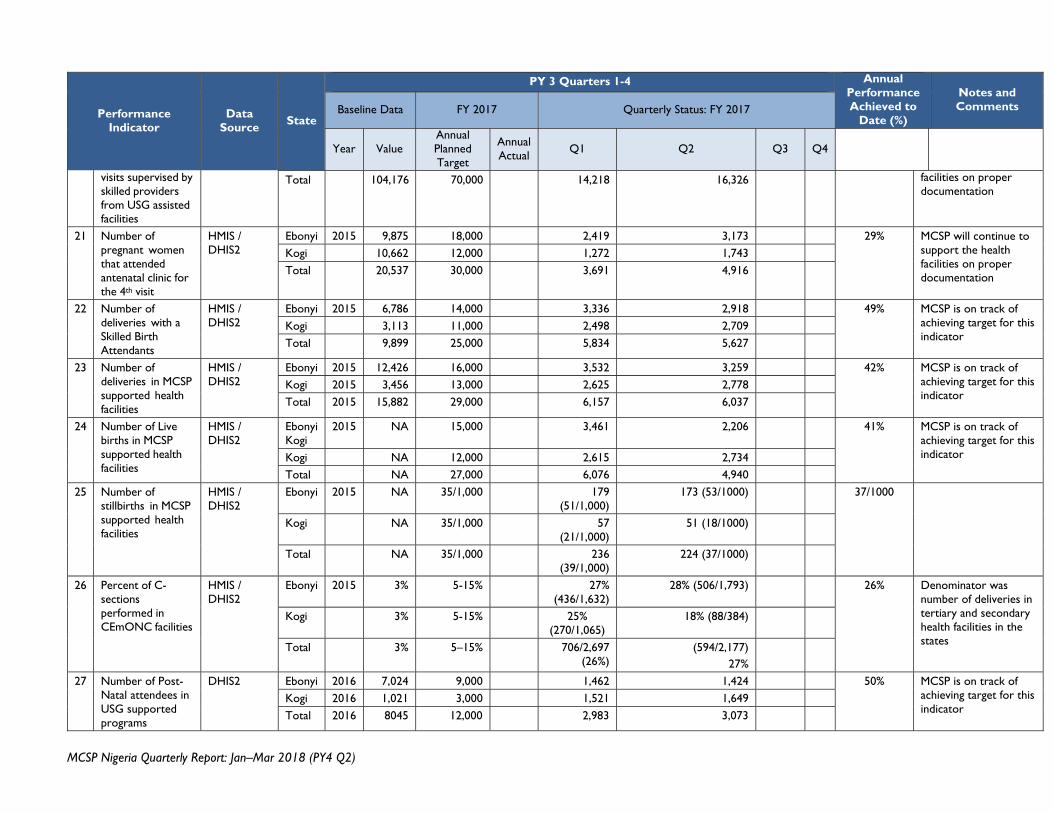
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
visits supervised by skilled providers from USG assisted facilities
Total 104,176 70,000 14,218 16,326 facilities on proper documentation
21 Number of pregnant women that attended antenatal clinic for the 4th visit
HMIS / DHIS2
Ebonyi 2015 9,875 18,000 2,419 3,173 29% MCSP will continue to support the health facilities on proper documentation
Kogi 10,662 12,000 1,272 1,743 Total 20,537 30,000 3,691 4,916
22 Number of deliveries with a Skilled Birth Attendants
HMIS / DHIS2
Ebonyi 2015 6,786 14,000 3,336 2,918 49% MCSP is on track of achieving target for this indicator
Kogi 3,113 11,000 2,498 2,709 Total 9,899 25,000 5,834 5,627
23 Number of deliveries in MCSP supported health facilities
HMIS / DHIS2
Ebonyi 2015 12,426 16,000 3,532 3,259 42% MCSP is on track of achieving target for this indicator
Kogi 2015 3,456 13,000 2,625 2,778 Total 2015 15,882 29,000 6,157 6,037
24 Number of Live births in MCSP supported health facilities
HMIS / DHIS2
Ebonyi Kogi
2015 NA 15,000 3,461 2,206 41% MCSP is on track of achieving target for this indicator Kogi NA 12,000 2,615 2,734
Total NA 27,000 6,076 4,940 25 Number of
stillbirths in MCSP supported health facilities
HMIS / DHIS2
Ebonyi 2015 NA 35/1,000 179 (51/1,000)
173 (53/1000) 37/1000
Kogi NA 35/1,000 57 (21/1,000)
51 (18/1000)
Total NA 35/1,000 236 (39/1,000)
224 (37/1000)
26 Percent of C-sections performed in CEmONC facilities
HMIS / DHIS2
Ebonyi 2015 3% 5-15% 27% (436/1,632)
28% (506/1,793) 26% Denominator was number of deliveries in tertiary and secondary health facilities in the states
Kogi 3% 5-15% 25% (270/1,065)
18% (88/384)
Total 3% 5–15% 706/2,697 (26%)
(594/2,177) 27%
27 Number of Post-Natal attendees in USG supported programs
DHIS2 Ebonyi 2016 7,024 9,000 1,462 1,424 50% MCSP is on track of achieving target for this indicator
Kogi 2016 1,021 3,000 1,521 1,649 Total 2016 8045 12,000 2,983 3,073
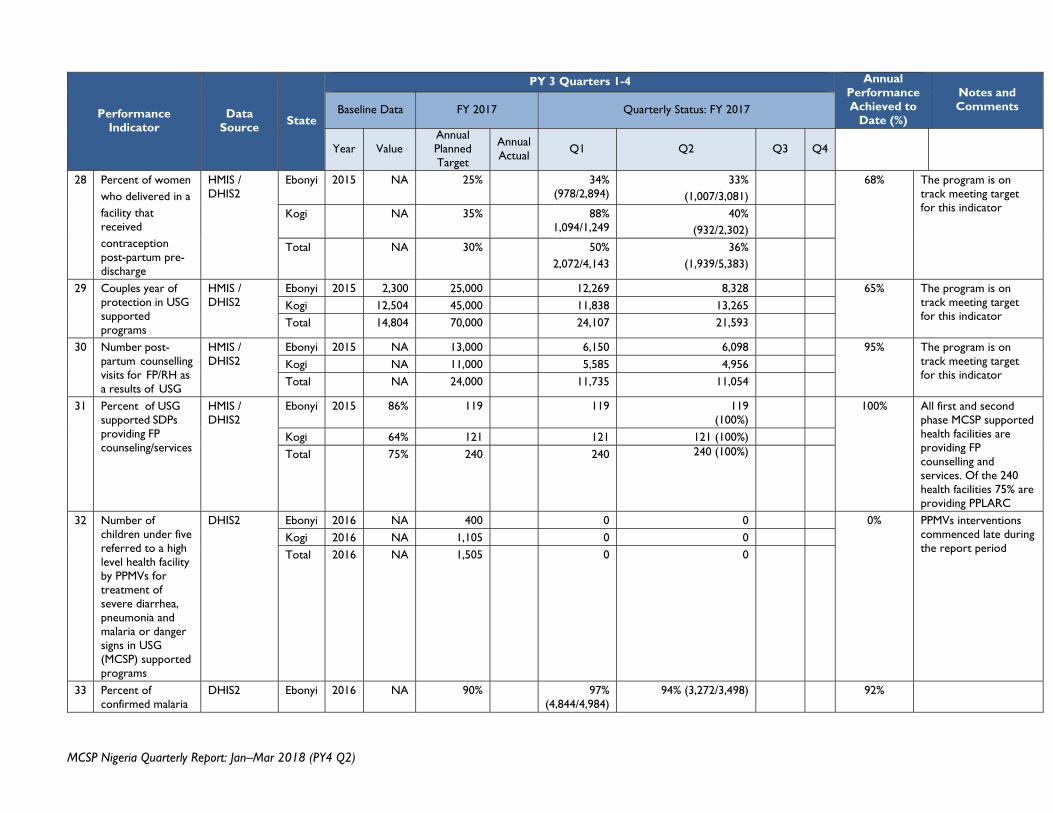
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
28 Percent of women who delivered in a facility that received contraception post-partum pre-discharge
HMIS / DHIS2
Ebonyi 2015 NA 25% 34% (978/2,894)
33% (1,007/3,081)
68% The program is on track meeting target for this indicator Kogi NA 35% 88%
1,094/1,249 40%
(932/2,302)
Total NA 30% 50% 2,072/4,143
36% (1,939/5,383)
29 Couples year of protection in USG supported programs
HMIS / DHIS2
Ebonyi 2015 2,300 25,000 12,269 8,328 65% The program is on track meeting target for this indicator
Kogi 12,504 45,000 11,838 13,265 Total 14,804 70,000 24,107 21,593
30 Number post-partum counselling visits for FP/RH as a results of USG
HMIS / DHIS2
Ebonyi 2015 NA 13,000 6,150 6,098 95% The program is on track meeting target for this indicator
Kogi NA 11,000 5,585 4,956 Total NA 24,000 11,735 11,054
31 Percent of USG supported SDPs providing FP counseling/services
HMIS / DHIS2
Ebonyi 2015 86% 119 119 119 (100%)
100% All first and second phase MCSP supported health facilities are providing FP counselling and services. Of the 240 health facilities 75% are providing PPLARC
Kogi 64% 121 121 121 (100%) Total 75% 240 240 240 (100%)
32 Number of children under five referred to a high level health facility by PPMVs for treatment of severe diarrhea, pneumonia and malaria or danger signs in USG (MCSP) supported programs
DHIS2 Ebonyi 2016 NA 400 0 0 0% PPMVs interventions commenced late during the report period
Kogi 2016 NA 1,105 0 0 Total 2016 NA 1,505 0 0
33 Percent of confirmed malaria
DHIS2 Ebonyi 2016 NA 90% 97% (4,844/4,984)
94% (3,272/3,498) 92%
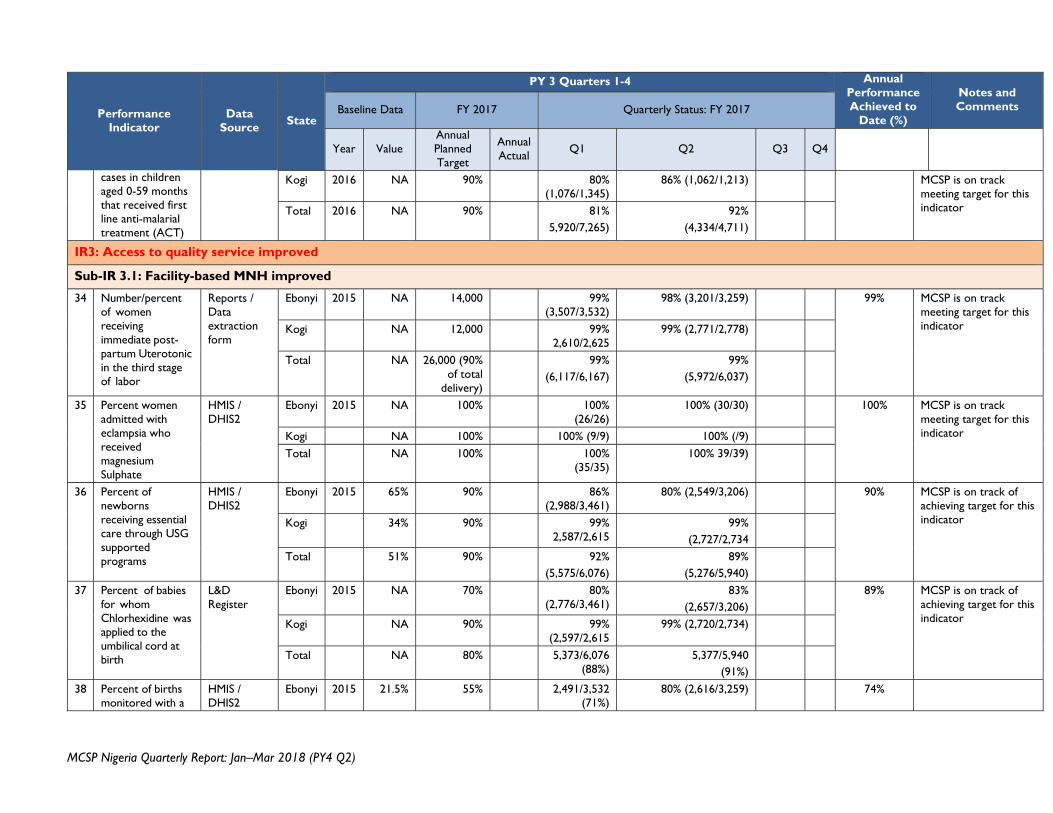
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
cases in children aged 0-59 months that received first line anti-malarial treatment (ACT)
Kogi 2016 NA 90% 80% (1,076/1,345)
86% (1,062/1,213) MCSP is on track meeting target for this indicator Total 2016 NA 90% 81%
5,920/7,265) 92%
(4,334/4,711)
IR3: Access to quality service improved
Sub-IR 3.1: Facility-based MNH improved
34 Number/percent of women receiving immediate post- partum Uterotonic in the third stage of labor
Reports / Data extraction form
Ebonyi 2015 NA 14,000 99% (3,507/3,532)
98% (3,201/3,259) 99% MCSP is on track meeting target for this indicator Kogi NA 12,000 99%
2,610/2,625 99% (2,771/2,778)
Total NA 26,000 (90% of total
delivery)
99% (6,117/6,167)
99% (5,972/6,037)
35 Percent women admitted with eclampsia who received magnesium Sulphate
HMIS / DHIS2
Ebonyi 2015 NA 100% 100% (26/26)
100% (30/30) 100% MCSP is on track meeting target for this indicator Kogi NA 100% 100% (9/9) 100% (/9)
Total NA 100% 100% (35/35)
100% 39/39)
36 Percent of newborns receiving essential care through USG supported programs
HMIS / DHIS2
Ebonyi 2015 65% 90% 86% (2,988/3,461)
80% (2,549/3,206) 90% MCSP is on track of achieving target for this indicator Kogi 34% 90% 99%
2,587/2,615 99%
(2,727/2,734
Total 51% 90% 92% (5,575/6,076)
89% (5,276/5,940)
37 Percent of babies for whom Chlorhexidine was applied to the umbilical cord at birth
L&D Register
Ebonyi 2015 NA 70% 80% (2,776/3,461)
83% (2,657/3,206)
89% MCSP is on track of achieving target for this indicator Kogi NA 90% 99%
(2,597/2,615 99% (2,720/2,734)
Total NA 80% 5,373/6,076 (88%)
5,377/5,940 (91%)
38 Percent of births monitored with a
HMIS / DHIS2
Ebonyi 2015 21.5% 55% 2,491/3,532 (71%)
80% (2,616/3,259) 74%
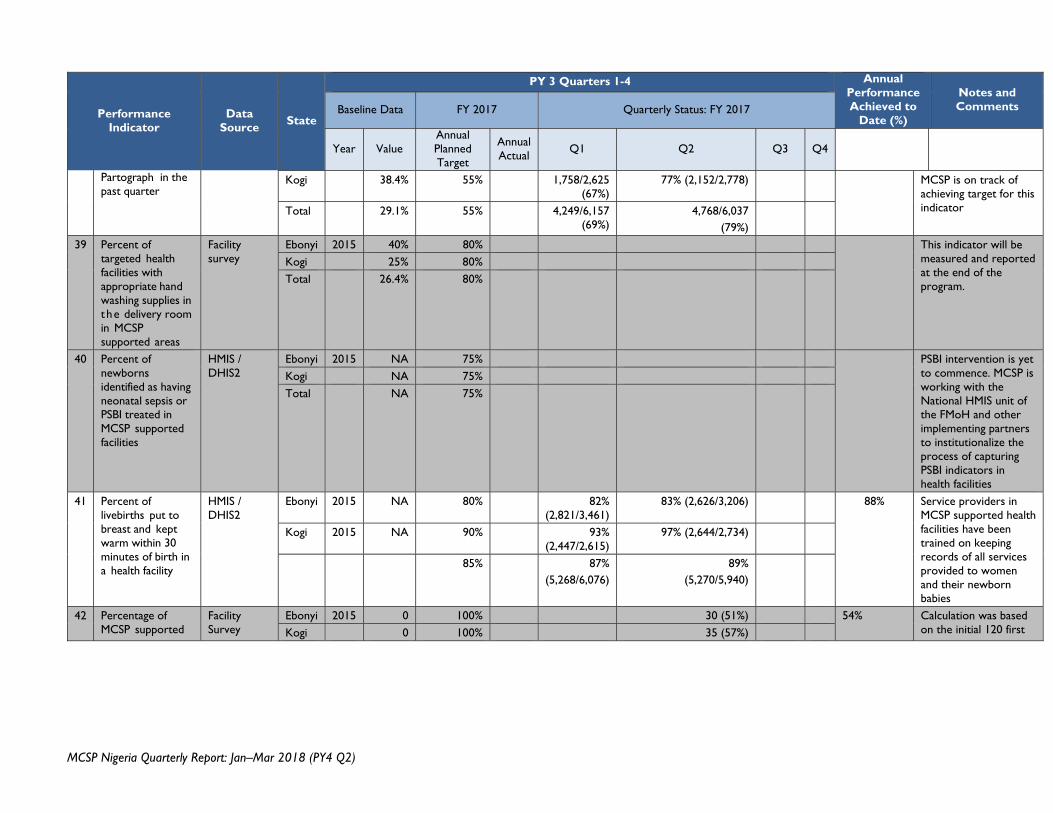
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
Partograph in the past quarter
Kogi 38.4% 55% 1,758/2,625 (67%)
77% (2,152/2,778) MCSP is on track of achieving target for this indicator Total 29.1% 55% 4,249/6,157
(69%) 4,768/6,037
(79%)
39 Percent of targeted health facilities with appropriate hand washing supplies in the delivery room in MCSP supported areas
Facility survey
Ebonyi 2015 40% 80% This indicator will be measured and reported at the end of the program.
Kogi 25% 80% Total 26.4% 80%
40 Percent of newborns identified as having neonatal sepsis or PSBI treated in MCSP supported facilities
HMIS / DHIS2
Ebonyi 2015 NA 75% PSBI intervention is yet to commence. MCSP is working with the National HMIS unit of the FMoH and other implementing partners to institutionalize the process of capturing PSBI indicators in health facilities
Kogi NA 75% Total NA 75%
41 Percent of livebirths put to breast and kept warm within 30 minutes of birth in a health facility
HMIS / DHIS2
Ebonyi 2015 NA 80% 82% (2,821/3,461)
83% (2,626/3,206) 88% Service providers in MCSP supported health facilities have been trained on keeping records of all services provided to women and their newborn babies
Kogi 2015 NA 90% 93% (2,447/2,615)
97% (2,644/2,734)
85% 87% (5,268/6,076)
89% (5,270/5,940)
42 Percentage of MCSP supported
Facility Survey
Ebonyi 2015 0 100% 30 (51%) 54% Calculation was based on the initial 120 first Kogi 0 100% 35 (57%)
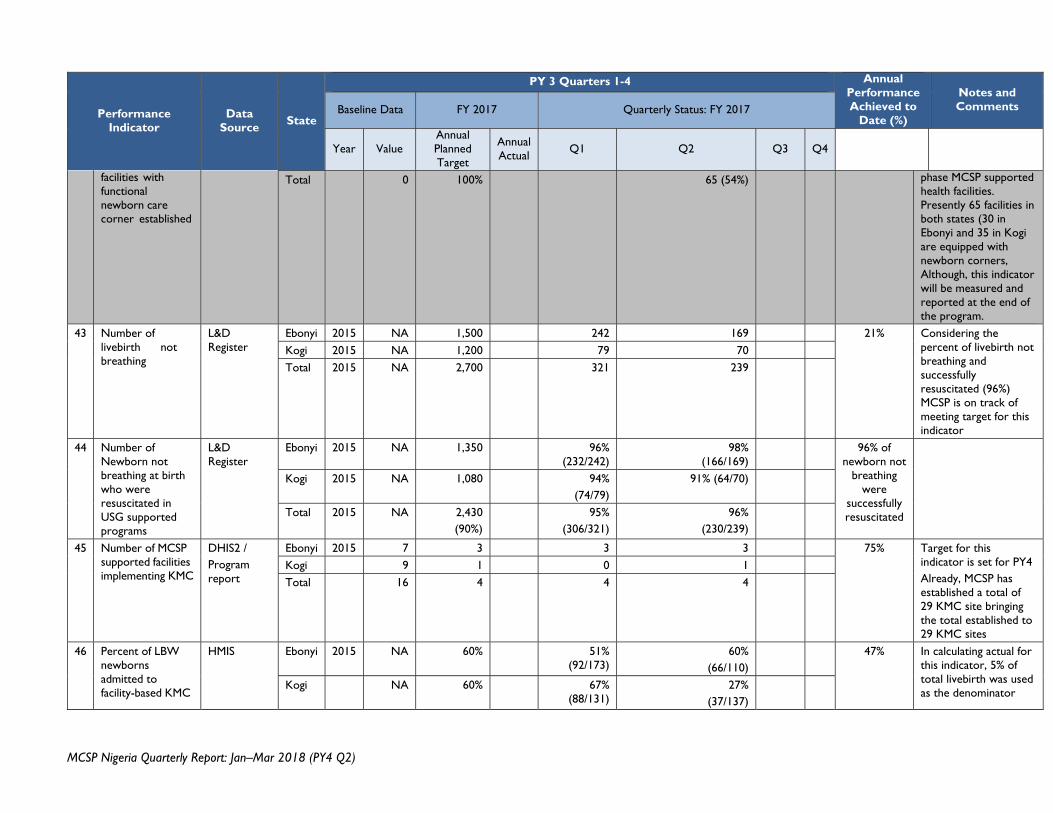
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
facilities with functional newborn care corner established
Total 0 100% 65 (54%) phase MCSP supported health facilities. Presently 65 facilities in both states (30 in Ebonyi and 35 in Kogi are equipped with newborn corners, Although, this indicator will be measured and reported at the end of the program.
43 Number of livebirth not breathing
L&D Register
Ebonyi 2015 NA 1,500 242 169 21% Considering the percent of livebirth not breathing and successfully resuscitated (96%) MCSP is on track of meeting target for this indicator
Kogi 2015 NA 1,200 79 70 Total 2015 NA 2,700 321 239
44 Number of Newborn not breathing at birth who were resuscitated in USG supported programs
L&D Register
Ebonyi 2015 NA 1,350 96% (232/242)
98% (166/169)
96% of newborn not
breathing were
successfully resuscitated
Kogi 2015 NA 1,080 94% (74/79)
91% (64/70)
Total 2015 NA 2,430 (90%)
95% (306/321)
96% (230/239)
45 Number of MCSP supported facilities implementing KMC
DHIS2 / Program report
Ebonyi 2015 7 3 3 3 75% Target for this indicator is set for PY4 Already, MCSP has established a total of 29 KMC site bringing the total established to 29 KMC sites
Kogi 9 1 0 1 Total 16 4 4 4
46 Percent of LBW newborns admitted to facility-based KMC
HMIS Ebonyi 2015 NA 60% 51% (92/173)
60% (66/110)
47% In calculating actual for this indicator, 5% of total livebirth was used as the denominator
Kogi NA 60% 67% (88/131)
27% (37/137)
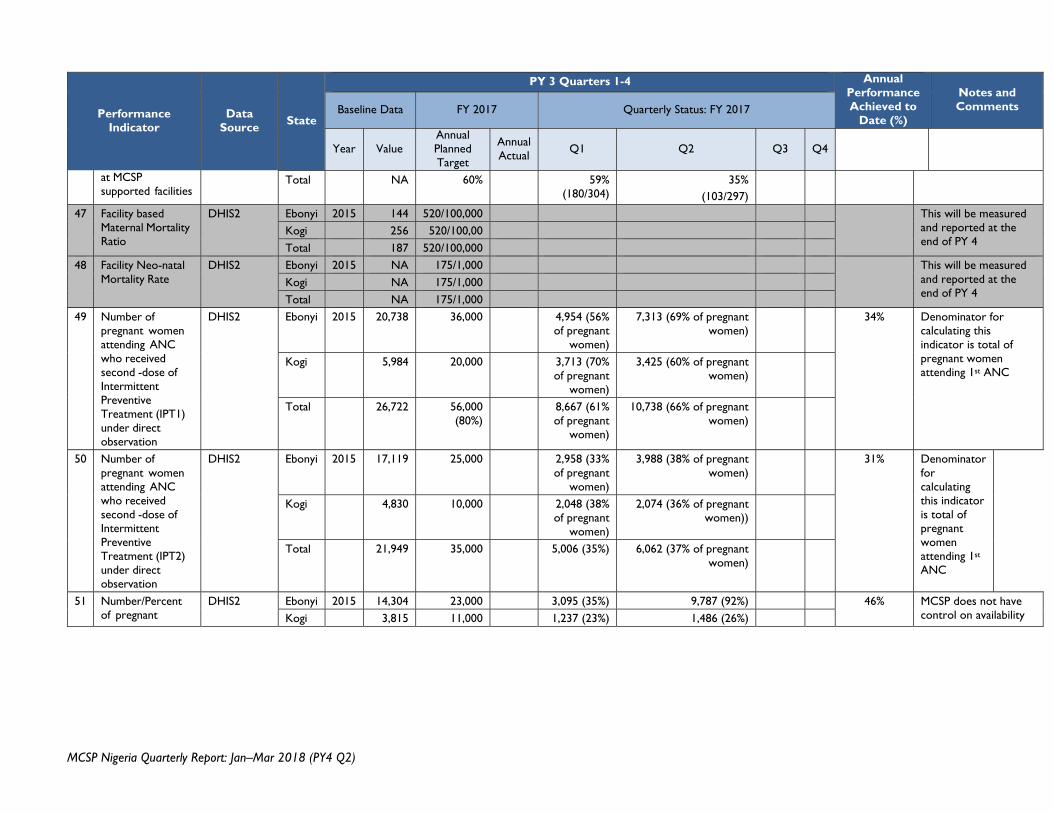
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
at MCSP supported facilities
Total NA 60% 59% (180/304)
35% (103/297)
47 Facility based Maternal Mortality Ratio
DHIS2 Ebonyi 2015 144 520/100,000 This will be measured and reported at the end of PY 4
Kogi 256 520/100,00 Total 187 520/100,000
48 Facility Neo-natal Mortality Rate
DHIS2 Ebonyi 2015 NA 175/1,000 This will be measured and reported at the end of PY 4
Kogi NA 175/1,000 Total NA 175/1,000
49 Number of pregnant women attending ANC who received second -dose of Intermittent Preventive Treatment (IPT1) under direct observation
DHIS2 Ebonyi 2015 20,738 36,000 4,954 (56% of pregnant
women)
7,313 (69% of pregnant women)
34% Denominator for calculating this indicator is total of pregnant women attending 1st ANC
Kogi 5,984 20,000 3,713 (70% of pregnant
women)
3,425 (60% of pregnant women)
Total 26,722 56,000 (80%)
8,667 (61% of pregnant
women)
10,738 (66% of pregnant women)
50 Number of pregnant women attending ANC who received second -dose of Intermittent Preventive Treatment (IPT2) under direct observation
DHIS2 Ebonyi 2015 17,119 25,000 2,958 (33% of pregnant
women)
3,988 (38% of pregnant women)
31% Denominator for calculating this indicator is total of pregnant women attending 1st ANC
Kogi 4,830 10,000 2,048 (38% of pregnant
women)
2,074 (36% of pregnant women))
Total 21,949 35,000 5,006 (35%) 6,062 (37% of pregnant women)
51 Number/Percent of pregnant
DHIS2 Ebonyi 2015 14,304 23,000 3,095 (35%) 9,787 (92%) 46% MCSP does not have control on availability Kogi 3,815 11,000 1,237 (23%) 1,486 (26%)
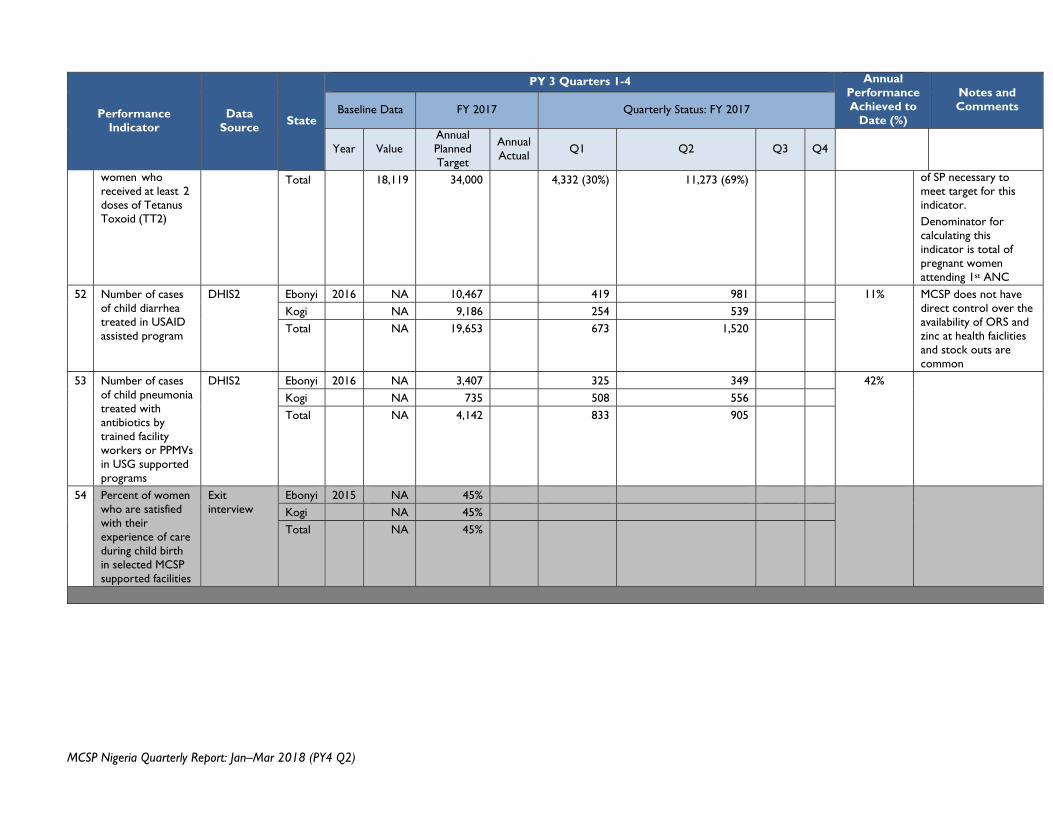
MCSP Nigeria Quarterly Report: Jan–Mar 2018 (PY4 Q2)
Performance Indicator
Data Source
State
PY 3 Quarters 1-4 Annual Performance Achieved to
Date (%)
Notes and Comments Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual
Q1 Q2 Q3 Q4
women who received at least 2 doses of Tetanus Toxoid (TT2)
Total 18,119 34,000 4,332 (30%) 11,273 (69%) of SP necessary to meet target for this indicator. Denominator for calculating this indicator is total of pregnant women attending 1st ANC
52 Number of cases of child diarrhea treated in USAID assisted program
DHIS2 Ebonyi 2016 NA 10,467 419 981 11% MCSP does not have direct control over the availability of ORS and zinc at health faiclities and stock outs are common
Kogi NA 9,186 254 539 Total NA 19,653 673 1,520
53 Number of cases of child pneumonia treated with antibiotics by trained facility workers or PPMVs in USG supported programs
DHIS2 Ebonyi 2016 NA 3,407 325 349 42% Kogi NA 735 508 556 Total NA 4,142 833 905
54 Percent of women who are satisfied with their experience of care during child birth in selected MCSP supported facilities
Exit interview
Ebonyi 2015 NA 45% Kogi NA 45% Total NA 45%