Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations...
10
GASTROINTESTINAL Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting Regina G. H. Beets-Tan & Doenja M. J. Lambregts & Monique Maas & Shandra Bipat & Brunella Barbaro & Filipe Caseiro-Alves & Luís Curvo-Semedo & Helen M. Fenlon & Marc J. Gollub & Sofia Gourtsoyianni & Steve Halligan & Christine Hoeffel & Seung Ho Kim & Andrea Laghi & Andrea Maier & Søren R. Rafaelsen & Jaap Stoker & Stuart A. Taylor & Michael R. Torkzad & Lennart Blomqvist Received: 23 January 2013 / Revised: 12 March 2013 / Accepted: 30 March 2013 / Published online: 7 June 2013 # European Society of Radiology 2013 Abstract Objectives To develop guidelines describing a standardised approach regarding the acquisition, interpretation and reporting of magnetic resonance imaging (MRI) for clinical staging and restaging of rectal cancer. Methods A consensus meeting of 14 abdominal imaging ex- perts from the European Society of Gastrointestinal and Ab- dominal Radiology (ESGAR) was conducted following the RAND-UCLA Appropriateness Method. Two independent (non-voting) chairs facilitated the meeting. Two hundred and Electronic supplementary material The online version of this article (doi:10.1007/s00330-013-2864-4) contains supplementary material, which is available to authorized users. R. G. H. Beets-Tan : D. M. J. Lambregts : M. Maas Maastricht University Medical Centre+, Maastricht, The Netherlands S. Bipat : J. Stoker Academic Medical Centre, Amsterdam, The Netherlands B. Barbaro Catholic University School of Medicine, Rome, Italy F. Caseiro-Alves : L. Curvo-Semedo Coimbra University Hospitals, Coimbra, Portugal H. M. Fenlon Mater Misericordiae University Hospital, Dublin, Ireland M. J. Gollub Memorial Sloan-Kettering Cancer Center, New York, USA S. Gourtsoyianni University Hospital of Heraklion, Crete, Greece S. Gourtsoyianni Guy’ s & St. Thomas’ NHS FT, London, UK S. Halligan : S. A. Taylor Centre for Medical Imaging, University College London, London, United Kingdom C. Hoeffel Reims University Hospital, Reims, France S. H. Kim Inje University Haeundae Paik Hospital, Busan, South-Korea A. Laghi Sapienza - University of Rome, Rome, Italy A. Maier Medical University of Vienna, Vienna, Austria S. R. Rafaelsen Vejle Hospital, Vejle, Denmark M. R. Torkzad Uppsala University, Uppsala, Sweden L. Blomqvist Karolinska University Hospital and Karolinska Institutet, Stockholm, Sweden R. G. H. Beets-Tan (*) Department of Radiology, Maastricht University Medical Centre+, P.O. Box 5800, 6202 AZ Maastricht, The Netherlands e-mail: [email protected] Eur Radiol (2013) 23:2522–2531 DOI 10.1007/s00330-013-2864-4
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations...
GASTROINTESTINAL
Magnetic resonance imaging for the clinical managementof rectal cancer patients: recommendations from the 2012European Society of Gastrointestinal and AbdominalRadiology (ESGAR) consensus meeting
Regina G. H. Beets-Tan & Doenja M. J. Lambregts & Monique Maas & Shandra Bipat &Brunella Barbaro & Filipe Caseiro-Alves & Luís Curvo-Semedo & Helen M. Fenlon &
Marc J. Gollub & Sofia Gourtsoyianni & Steve Halligan & Christine Hoeffel &Seung Ho Kim & Andrea Laghi & Andrea Maier & Søren R. Rafaelsen &
Jaap Stoker & Stuart A. Taylor & Michael R. Torkzad & Lennart Blomqvist
Received: 23 January 2013 /Revised: 12 March 2013 /Accepted: 30 March 2013 /Published online: 7 June 2013# European Society of Radiology 2013
AbstractObjectives To develop guidelines describing a standardisedapproach regarding the acquisition, interpretation andreporting of magnetic resonance imaging (MRI) for clinicalstaging and restaging of rectal cancer.
Methods A consensus meeting of 14 abdominal imaging ex-perts from the European Society of Gastrointestinal and Ab-dominal Radiology (ESGAR) was conducted following theRAND-UCLA Appropriateness Method. Two independent(non-voting) chairs facilitated the meeting. Two hundred and
Electronic supplementary material The online version of this article(doi:10.1007/s00330-013-2864-4) contains supplementary material,which is available to authorized users.
R. G. H. Beets-Tan :D. M. J. Lambregts :M. MaasMaastricht UniversityMedical Centre+, Maastricht, The Netherlands
S. Bipat : J. StokerAcademic Medical Centre, Amsterdam, The Netherlands
B. BarbaroCatholic University School of Medicine, Rome, Italy
F. Caseiro-Alves : L. Curvo-SemedoCoimbra University Hospitals, Coimbra, Portugal
H. M. FenlonMater Misericordiae University Hospital, Dublin, Ireland
M. J. GollubMemorial Sloan-Kettering Cancer Center, New York, USA
S. GourtsoyianniUniversity Hospital of Heraklion, Crete, Greece
S. GourtsoyianniGuy’s & St. Thomas’ NHS FT, London, UK
S. Halligan : S. A. TaylorCentre for Medical Imaging, University College London,London, United Kingdom
C. HoeffelReims University Hospital, Reims, France
S. H. KimInje University Haeundae Paik Hospital, Busan, South-Korea
A. LaghiSapienza - University of Rome, Rome, Italy
A. MaierMedical University of Vienna, Vienna, Austria
S. R. RafaelsenVejle Hospital, Vejle, Denmark
M. R. TorkzadUppsala University, Uppsala, Sweden
L. BlomqvistKarolinska University Hospital and Karolinska Institutet,Stockholm, Sweden
R. G. H. Beets-Tan (*)Department of Radiology, Maastricht University Medical Centre+,P.O. Box 5800, 6202 AZ Maastricht, The Netherlandse-mail: [email protected]
Eur Radiol (2013) 23:2522–2531DOI 10.1007/s00330-013-2864-4

thirty-six items were scored by participants for appropriatenessand classified subsequently as appropriate or inappropriate (de-fined by ≥ 80 % consensus) or uncertain (defined by < 80 %consensus). Items not reaching 80 % consensus were noted.Results Consensus was reached for 88 % of items: recom-mendations regarding hardware, patient preparation, imagingsequences, angulation, criteria for MRI assessment and MRIreporting were constructed from these.Conclusions These expert consensus recommendations canbe used as clinical guidelines for primary staging andrestaging of rectal cancer using MRI.
Key Points• These guidelines recommend standardised imaging forstaging and restaging of rectal cancer.
• The guidelines were constructed through consensusamongst 14 abdominal imaging experts.
• Consensus was reached by in 88 % of 236 items discussed.
Keywords Rectal cancer . Consensus . Guideline .
Magnetic resonance imaging . Tumour staging
Introduction
In many countries magnetic resonance imaging (MRI) is nowcentral to the investigation and management of rectal cancer.International guidelines for the management of rectal cancerrecommend MRI as pivotal for staging the primary tumour [1,2]. MRI accurately identifies prognostic markers for risk of localrecurrence and helps to stratify patients into those needing pre-operative chemoradiotherapy [3, 4]. Recently the role ofMRI hasexpanded to encompass assessment of response to preoperative(chemoradiotherapy) treatment. For example, patients exhibitinga good response can be directed towards less extensive surgery orminimally invasive alternatives [5, 6]. In order to best achieve allthese objectives,MRI should be performed according to state-of-the-art principles and reported in a structured fashion so thatimportant findings impacting directly on therapeutic decisionmaking are not omitted. Although experts in the field generallyregard MRI as invaluable, there is some professional disagree-ment relating to its accuracy and the generalisability of resultsobtained from specialist centres. These concerns relate partly tothe wide range of different available MR protocols and a lack ofstandardisation that serves to increase variation between differentcentres. In particular, the minimal requirements for an optimalMR protocol are unclear. There is, therefore, a need for recom-mendations from an expert panel regarding the performance andinterpretation of state-of-the-art rectal MRI.
This paper reports the recommendations of a panel of expertradiologists from leading colorectal cancer centres – an initia-tive of the European Society of Gastrointestinal and AbdominalRadiology (ESGAR). These experts participated in a formal
consensus process aimed at defining a state-of-the-art MRprotocol for rectal cancer, how it should be performed, andhow the imaging findings should be interpreted and reported.
Materials and methods
The consensus method
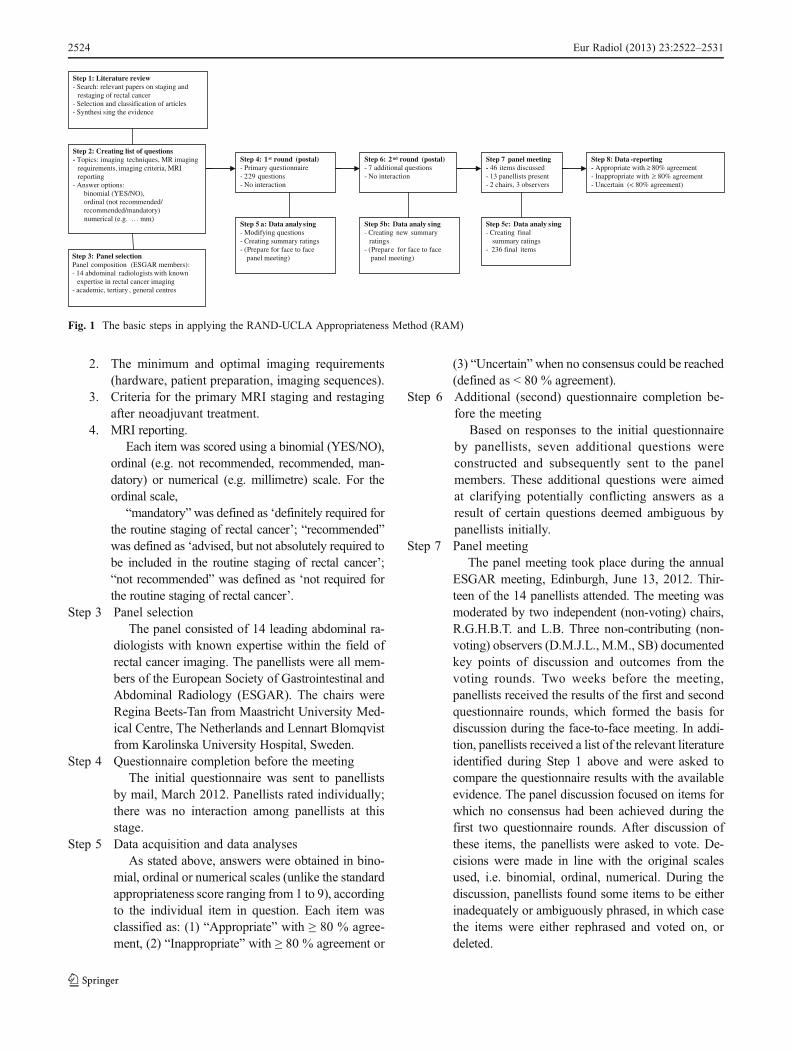
The RAND-UCLA Appropriateness Method (RAM) was cho-sen as it combines all available evidence (unlike CochraneReviews, which summarise the best available evidence follow-ing application of inclusion and exclusion criteria) with thecollective judgement of experts to yield a statement regardingthe appropriateness of a specific question [7]. The RAM is amodified Delphi method that, unlike the original Delphi, pro-vides panellists with the opportunity to discuss their judgementsduring a face-to-face meeting, which appears to additionallymotivate panellists to participate. In summary, RAM combinespostal and face-to-face rounds, and panellists rate each questiontwice, in a two-round “modified Delphi” process. The basicsteps for applying the RAM are shown in Fig. 1.
Step 1 Literature reviewTwo of the organising members (D.M.J.L., M.M.)
in consensus performed a literature review tosynthesise the available scientific evidence regardingthe imaging of rectal cancer. They searched thePubMed and Medline databases for all relevant En-glish language original articles, systematic reviews andmeta-analyses published between 1990 and October2011 using the following search terms: “imaging”,“magnetic resonance imaging or MRI”, “rectal neo-plasms”, “staging”, “restaging”, “response evaluation”and “chemoradiation, chemoradiotherapy, chemother-apy and/or radiotherapy”. Additional studies weretraced by tracking the reference lists of the retrievedstudies. The collected evidence was primarily used toextract the relevant topics which should be addressedby the panel in order to construct the questionnaire.
Step 2 Construct of the questionnaireA questionnaire consisting of 229 items was
constructed in November 2011. The first draft wasproduced by three of the organising members(R.G.H.B.T., D.M.J.L., M.M.). Refinements weremade in consultation with two separate advisingorganising members (L.B., S.B.). The questionnairewas designed to address:
1. The role of MRI in relation to alternative techniquesfor primary staging and restaging of rectal cancer(i.e. non-mucinous type adenocarcinoma) afterneoadjuvant treatment.
Eur Radiol (2013) 23:2522–2531 2523
2. The minimum and optimal imaging requirements(hardware, patient preparation, imaging sequences).
3. Criteria for the primary MRI staging and restagingafter neoadjuvant treatment.
4. MRI reporting.Each item was scored using a binomial (YES/NO),
ordinal (e.g. not recommended, recommended, man-datory) or numerical (e.g. millimetre) scale. For theordinal scale,
“mandatory”was defined as ‘definitely required forthe routine staging of rectal cancer’; “recommended”was defined as ‘advised, but not absolutely required tobe included in the routine staging of rectal cancer’;“not recommended” was defined as ‘not required forthe routine staging of rectal cancer’.
Step 3 Panel selectionThe panel consisted of 14 leading abdominal ra-
diologists with known expertise within the field ofrectal cancer imaging. The panellists were all mem-bers of the European Society of Gastrointestinal andAbdominal Radiology (ESGAR). The chairs wereRegina Beets-Tan from Maastricht University Med-ical Centre, The Netherlands and Lennart Blomqvistfrom Karolinska University Hospital, Sweden.
Step 4 Questionnaire completion before the meetingThe initial questionnaire was sent to panellists
by mail, March 2012. Panellists rated individually;there was no interaction among panellists at thisstage.
Step 5 Data acquisition and data analysesAs stated above, answers were obtained in bino-
mial, ordinal or numerical scales (unlike the standardappropriateness score ranging from 1 to 9), accordingto the individual item in question. Each item wasclassified as: (1) “Appropriate” with ≥ 80 % agree-ment, (2) “Inappropriate” with ≥ 80 % agreement or
(3) “Uncertain”when no consensus could be reached(defined as < 80 % agreement).
Step 6 Additional (second) questionnaire completion be-fore the meeting
Based on responses to the initial questionnaireby panellists, seven additional questions wereconstructed and subsequently sent to the panelmembers. These additional questions were aimedat clarifying potentially conflicting answers as aresult of certain questions deemed ambiguous bypanellists initially.
Step 7 Panel meetingThe panel meeting took place during the annual
ESGAR meeting, Edinburgh, June 13, 2012. Thir-teen of the 14 panellists attended. The meeting wasmoderated by two independent (non-voting) chairs,R.G.H.B.T. and L.B. Three non-contributing (non-voting) observers (D.M.J.L., M.M., SB) documentedkey points of discussion and outcomes from thevoting rounds. Two weeks before the meeting,panellists received the results of the first and secondquestionnaire rounds, which formed the basis fordiscussion during the face-to-face meeting. In addi-tion, panellists received a list of the relevant literatureidentified during Step 1 above and were asked tocompare the questionnaire results with the availableevidence. The panel discussion focused on items forwhich no consensus had been achieved during thefirst two questionnaire rounds. After discussion ofthese items, the panellists were asked to vote. De-cisions were made in line with the original scalesused, i.e. binomial, ordinal, numerical. During thediscussion, panellists found some items to be eitherinadequately or ambiguously phrased, in which casethe items were either rephrased and voted on, ordeleted.
Step 1: Literature review- Search: relevant papers on staging and
restaging of rectal cancer- Selection and classification of articles- Synthesi sing the evidence
Step 4: 1st round (postal)- Primary questionnaire- 229 questions- No interaction
Step 8: Data -reporting - Appropriate with ≥ 80% agreement- Inappropriate with ≥ 80% agreement- Uncertain (< 80% agreement)
Step 2: Creating list of questions- Topics: imaging techniques, MR imaging
requirements, imaging criteria, MRI reporting
- Answer options: binomial (YES/NO), ordinal (not recommended/recommended/mandatory)numerical (e.g. … mm)
Step 5 a: Data analysing - Modifying questions- Creating summary ratings- (Prepare for face to face
panel meeting)Step 3: Panel selectionPanel composition (ESGAR members): - 14 abdominal radiologists with known
expertise in rectal cancer imaging- academic, tertiary , general centres
Step 6: 2nd round (postal)- 7 additional questions- No interaction
Step 7 panel meeting- 46 items discussed- 13 panellists present- 2 chairs, 3 observers
Step 5b: Data analy sing - Creating new summary
ratings- (Prepare for face to face
panel meeting)
Step 5c: Data analy sing - Creating final
summary ratings- 236 final items
Fig. 1 The basic steps in applying the RAND-UCLA Appropriateness Method (RAM)
2524 Eur Radiol (2013) 23:2522–2531

Step 8 Data-reportingData from the initial questionnaire, second
round, and face-to-face meeting were collectedand descriptive metrics calculated by D.M.J.L.and M.M. Each item was ultimately classifiedas: (1) “appropriate” with ≥ 80 % agreement,(2) “Inappropriate” with ≥ 80 % agreement or(3) “Uncertain” (no consensus, i.e. < 80 %agreement).
Results
Demographic data of panellists’ base hospitals aresummarised in Table 1. The initial pre-meeting ques-tionnaire comprised 229 items. The second questionnaireround added a further seven, for a total of 236. Duringthe face-to-face meeting the items on which no consen-sus had been reached during the first two rounds werediscussed. Two additional items were added, two itemswere deleted, and wording was rephrased in three items.Hence, the final number of items was 236. The finalresults from the consensus procedure for these 236items are given in electronic supplementary materialAppendix 1.
Areas of consensus
In the pre-meeting questionnaires, consensus was reached in190/236 of items (81 %). This number increased to 208/236(88 %) after the panel meeting. The main recommendationsbased on the items on which ≥ 80 % consensus was reachedare listed in Table 2.
Areas lacking consensus
After the panel meeting, lack of consensus remained in 28 ofthe items (12 %). The main issues on which no consensuswas reached are summarised in Table 3.
Discussion
Using the RAM method, we ultimately achieved consensusfor 88 % of the individual items. Although a consensus of80 % or more was not achieved for 12 % of items, reasonableagreement (60–79 %) was obtained in 7 % out of these 12 %.
Imaging techniques
The panel reached consensus that MRI is the imaging tech-nique of first choice for primary staging of rectal cancer.There was a 100 % agreement that endorectal ultrasound(EUS) remains the imaging method of first choice to differ-entiate between T1 and T2 tumours if local resection isbeing considered [3]. Discussion regarding the best imagingtechnique to differentiate between T2 and T3 tumoursreached 67 % agreement that either EUS or MRI can beused. Panellists could not agree which technique is best forprimary staging in the absence of access to MRI. Bothcomputed tomography (CT) and EUS were voted for equal-ly. Positron emission tomography (PET) or PET/CT was notan option for most (92 %) of the panellists. For restagingafter a long course of chemoradiotherapy (CRT), it wasagreed that MRI should be performed routinely. Three quar-ters (75 %) agreed that the combination of endoscopy withMRI is the best approach to confirming a complete response
Table 1 Demographic datafrom the hospitals of thepanellists
Median (range) number of patients diagnosed with rectal cancer per year 50 (20–250)
MRI used as a standard staging tecnique for rectal cancer 100 %
Restaging after chemoradiation performed routinely 77 %
MRI used since 2004-2007
MR vendors Siemens 42 %
Philips 17 %
GE 25 %
Multiple 17 %
Field strength 1.5 T 77 %
3.0 T 8 %
1.5 T and 3.0 T 15 %
Use of a surface coil 100 %
Use of an endorectal coil 0 %
Use of spasmolytics (buscopan or glucagon) 38 %
Use of endorectal filling 23 %
Use of intravenous contrast material 15 %
Eur Radiol (2013) 23:2522–2531 2525
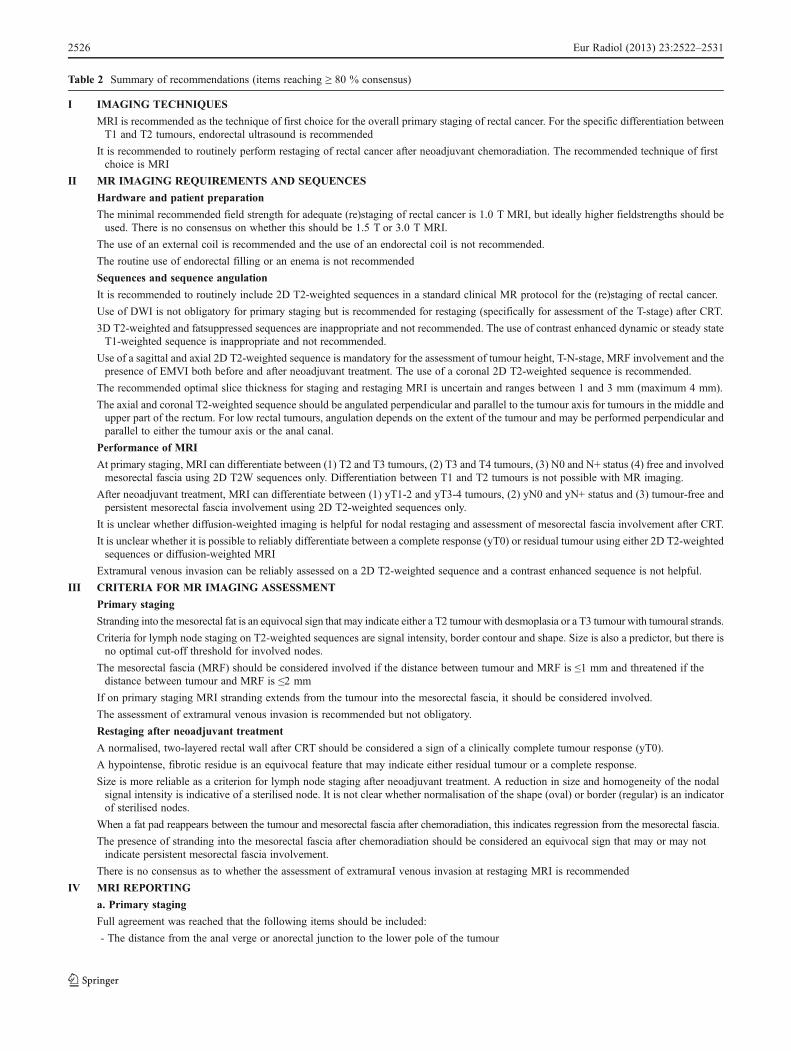
Table 2 Summary of recommendations (items reaching ≥ 80 % consensus)
I IMAGING TECHNIQUES
MRI is recommended as the technique of first choice for the overall primary staging of rectal cancer. For the specific differentiation betweenT1 and T2 tumours, endorectal ultrasound is recommended
It is recommended to routinely perform restaging of rectal cancer after neoadjuvant chemoradiation. The recommended technique of firstchoice is MRI
II MR IMAGING REQUIREMENTS AND SEQUENCES
Hardware and patient preparation
The minimal recommended field strength for adequate (re)staging of rectal cancer is 1.0 T MRI, but ideally higher fieldstrengths should beused. There is no consensus on whether this should be 1.5 T or 3.0 T MRI.
The use of an external coil is recommended and the use of an endorectal coil is not recommended.
The routine use of endorectal filling or an enema is not recommended
Sequences and sequence angulation
It is recommended to routinely include 2D T2-weighted sequences in a standard clinical MR protocol for the (re)staging of rectal cancer.
Use of DWI is not obligatory for primary staging but is recommended for restaging (specifically for assessment of the T-stage) after CRT.
3D T2-weighted and fatsuppressed sequences are inappropriate and not recommended. The use of contrast enhanced dynamic or steady stateT1-weighted sequence is inappropriate and not recommended.
Use of a sagittal and axial 2D T2-weighted sequence is mandatory for the assessment of tumour height, T-N-stage, MRF involvement and thepresence of EMVI both before and after neoadjuvant treatment. The use of a coronal 2D T2-weighted sequence is recommended.
The recommended optimal slice thickness for staging and restaging MRI is uncertain and ranges between 1 and 3 mm (maximum 4 mm).
The axial and coronal T2-weighted sequence should be angulated perpendicular and parallel to the tumour axis for tumours in the middle andupper part of the rectum. For low rectal tumours, angulation depends on the extent of the tumour and may be performed perpendicular andparallel to either the tumour axis or the anal canal.
Performance of MRI
At primary staging, MRI can differentiate between (1) T2 and T3 tumours, (2) T3 and T4 tumours, (3) N0 and N+ status (4) free and involvedmesorectal fascia using 2D T2W sequences only. Differentiation between T1 and T2 tumours is not possible with MR imaging.
After neoadjuvant treatment, MRI can differentiate between (1) yT1-2 and yT3-4 tumours, (2) yN0 and yN+ status and (3) tumour-free andpersistent mesorectal fascia involvement using 2D T2-weighted sequences only.
It is unclear whether diffusion-weighted imaging is helpful for nodal restaging and assessment of mesorectal fascia involvement after CRT.
It is unclear whether it is possible to reliably differentiate between a complete response (yT0) or residual tumour using either 2D T2-weightedsequences or diffusion-weighted MRI
Extramural venous invasion can be reliably assessed on a 2D T2-weighted sequence and a contrast enhanced sequence is not helpful.
III CRITERIA FOR MR IMAGING ASSESSMENT
Primary staging
Stranding into the mesorectal fat is an equivocal sign that may indicate either a T2 tumour with desmoplasia or a T3 tumour with tumoural strands.
Criteria for lymph node staging on T2-weighted sequences are signal intensity, border contour and shape. Size is also a predictor, but there isno optimal cut-off threshold for involved nodes.
The mesorectal fascia (MRF) should be considered involved if the distance between tumour and MRF is ≤1 mm and threatened if thedistance between tumour and MRF is ≤2 mm
If on primary staging MRI stranding extends from the tumour into the mesorectal fascia, it should be considered involved.
The assessment of extramural venous invasion is recommended but not obligatory.
Restaging after neoadjuvant treatment
A normalised, two-layered rectal wall after CRT should be considered a sign of a clinically complete tumour response (yT0).
A hypointense, fibrotic residue is an equivocal feature that may indicate either residual tumour or a complete response.
Size is more reliable as a criterion for lymph node staging after neoadjuvant treatment. A reduction in size and homogeneity of the nodalsignal intensity is indicative of a sterilised node. It is not clear whether normalisation of the shape (oval) or border (regular) is an indicatorof sterilised nodes.
When a fat pad reappears between the tumour and mesorectal fascia after chemoradiation, this indicates regression from the mesorectal fascia.
The presence of stranding into the mesorectal fascia after chemoradiation should be considered an equivocal sign that may or may notindicate persistent mesorectal fascia involvement.
There is no consensus as to whether the assessment of extramuraI venous invasion at restaging MRI is recommended
IV MRI REPORTING
a. Primary staging
Full agreement was reached that the following items should be included:
- The distance from the anal verge or anorectal junction to the lower pole of the tumour
2526 Eur Radiol (2013) 23:2522–2531
after CRT. There was no agreement on the optimal fieldstrength, although most believed that 1.5 T is preferable to3 T (75 % vs 33 %). The panel agreed that 1.0-T MRIshould only be used if there is no access to a 1.5-T or 3.0-T system. Hypothetically, it is also feasible to performstaging at 1.0 Tesla, although the panel believes that it isimportant to assess whether the diagnostic performance is at asufficient level—which depends on factors such as equipment(e.g. outdated versus modern magnet, closed versus open MRsystem).
MR imaging requirements
No consensus was reached regarding the use of spasmo-lytic agents (e.g. Buscopan or Glucagon). Routine admin-istration was advised by 50 % of the panel. Argumentsfor their use were the presence of bowel movementartefacts on the (sagittal) planning scan. Furthermore,
spasmolytics may be advised when imaging is performedat 3 T, because movement artefacts tend to be moresignificant. Panellists agreed that routine rectal filling(e.g. with ultrasonography gel) is not recommended.The main argument against routine endorectal fillingwas that the primary goal of staging with MRI is notto assess the endoluminal part of the tumour as this isachieved at endoscopy; rather, the aim of MRI is toassess the extent of transmural tumour growth and itsrelationship to the mesorectal structures. Distension ofthe rectum by endoluminal contrast agents can compressthe mesorectal fat, which may overestimate fascial in-volvement and hamper evaluation of mesorectal nodes[8]. Some, however, suggested that filling might be help-ful in specific cases; for example, to facilitate tumourdetection for readers with limited experience in readingrectal MRI or to reduce susceptibility artefacts ondiffusion-weighted acquisitions.
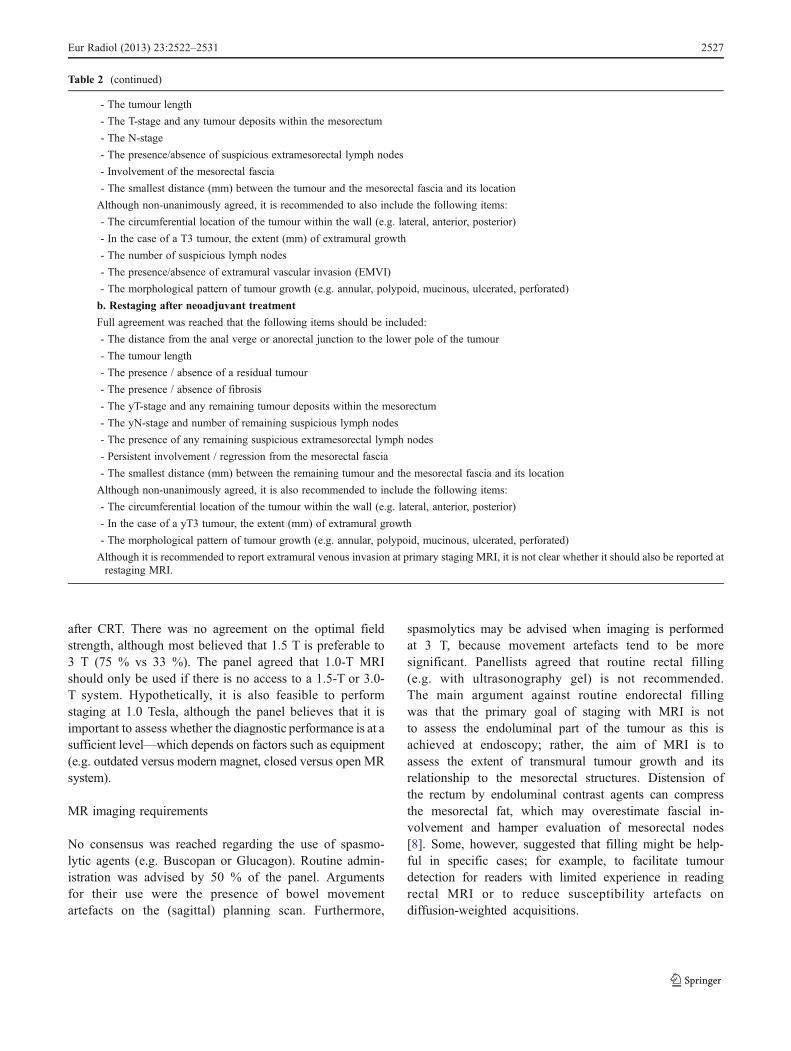
- The tumour length
- The T-stage and any tumour deposits within the mesorectum
- The N-stage
- The presence/absence of suspicious extramesorectal lymph nodes
- Involvement of the mesorectal fascia
- The smallest distance (mm) between the tumour and the mesorectal fascia and its location
Although non-unanimously agreed, it is recommended to also include the following items:
- The circumferential location of the tumour within the wall (e.g. lateral, anterior, posterior)
- In the case of a T3 tumour, the extent (mm) of extramural growth
- The number of suspicious lymph nodes
- The presence/absence of extramural vascular invasion (EMVI)
- The morphological pattern of tumour growth (e.g. annular, polypoid, mucinous, ulcerated, perforated)
b. Restaging after neoadjuvant treatment
Full agreement was reached that the following items should be included:
- The distance from the anal verge or anorectal junction to the lower pole of the tumour
- The tumour length
- The presence / absence of a residual tumour
- The presence / absence of fibrosis
- The yT-stage and any remaining tumour deposits within the mesorectum
- The yN-stage and number of remaining suspicious lymph nodes
- The presence of any remaining suspicious extramesorectal lymph nodes
- Persistent involvement / regression from the mesorectal fascia
- The smallest distance (mm) between the remaining tumour and the mesorectal fascia and its location
Although non-unanimously agreed, it is also recommended to include the following items:
- The circumferential location of the tumour within the wall (e.g. lateral, anterior, posterior)
- In the case of a yT3 tumour, the extent (mm) of extramural growth
- The morphological pattern of tumour growth (e.g. annular, polypoid, mucinous, ulcerated, perforated)
Although it is recommended to report extramural venous invasion at primary staging MRI, it is not clear whether it should also be reported atrestaging MRI.
Table 2 (continued)
Eur Radiol (2013) 23:2522–2531 2527

MR imaging sequences
A consensus was reached that the minimum requirement fora standard MR rectal protocol is 2D T2-weighted sequencesin sagittal, axial and oblique coronal planes. The sagittalsequence should be used to determine the longitudinaltumour axis in order to angle the axial and coronalplanes as perpendicular and parallel to the tumour axisas possible, respectively. For low tumours, coronal planesshould be angled parallel to the anal canal so that therelation of the tumour’s lower pole to the anal sphinctermuscles and its relationship to the adjacent pelvic floorcan be evaluated, as this will determine the surgicalapproach. Armed with this knowledge, surgeons wouldopt to perform a total mesorectal excision (TME) withlow anastomosis or modified TME with wider excisionmargins [9]. Because the mesorectum and its fascia tapercaudally as they funnel towards the pelvis floor, thisregion (including the anterior pelvic organs, such asthe prostate/seminal vesicles in male patients anduterus/vagina in female patients) is at increased risk ofinvolvement by low tumours and angulation of axialplanes here is crucial. Despite the higher performanceof MRI compared with CT for assessment of an-terior invasion into the prostate/seminal vesicles orvagina/uterus this remains very difficult to assess onMRI [10]. Radiographic technicians should be thoroughly
trained to perform angulation properly. While use of a3D T2-weighted sequence could theoretically avoid thesedifficulties, available evidence is lacking and the paneldid not recommend this approach as a replacement formultiplanar 2D T2-weighted sequences.
In addition to T2-weighted sequences, the panel rec-ommends that a diffusion-weighted sequence should beincluded in the restaging MR protocol. There is noevident benefit for diffusion-weighted imaging (DWI)at primary staging but there is growing evidence thatDWI improves the diagnostic performance of MRIwhen evaluating response (the yT-stage) after CRT.DWI is of additional value to T2-weighted fast-spinecho (FSE) sequences to differentiate between the pa-tients whose response is “good” versus “poor” [11–13].The panel did not reach consensus regarding whetherDWI is valuable for assessment of a complete responseafter CRT, although three quarters (75 %) recommendedit in this specific setting. There was no consensusregarding any benefit of DWI at restaging for assess-ment of yN-stage and/or mesorectal fascia involvementafter CRT. So far, only a limited number of studiessupport the use of DWI to evaluate lymph node[14–16] and mesorectal fascia status [17], but no clearevidence is available regarding these specific applica-tions. Around 70 % agreement was reached for the useof DWI for nodal (re)staging. DWI, although probably
Table 3 Items lacking consensus
I MR IMAGING REQUIREMENTS
It is unclear what the technique of second choice for rectal cancer staging is.
The most frequently suggested techniques of second choice are CT (46 %) and endorectal ultrasound (31 %).
There is no consensus on the optimal field strength for adequate rectal cancer staging.
It should be at least 1.0 T, but 75 % indicate that 1.5 T and 33 % indicate that 3 T is the optimal field strength.
There is no consensus on the benefit of using a 3D T2-weighted sequence. It may be used as an alternative to 2D T2-weighted sequences inthree directions.
There is agreement that dynamic or steady state contrast enhanced T1-weighted imaging is not helpful, but there is no consensus on the benefitof using unenhanced T1-weighted imaging.
There is no consensus on the routine use of spasmolytics.
Although axial and coronal images are recommended for low rectal tumours, it is unclear how its angulation should ideally be performed.
There was only 54 % agreement that the anal canal should be taken as an anatomical landmark for angulation.
A diffusion-weighted sequence is only recommended at restaging MRI after CRT and is beneficial for the evaluation of yT stage. Currently,there is insufficient evidence for the use of DWI at primary staging, nor is there sufficient evidence for its use in lymph nodes and mesorectalfascia (MRF) assessment.
II CRITERIA FOR MR IMAGING ASSESSMENT
There is no consensus on whether normalisation in shape and border contour are appropriate criteria for sterilisation of lymph nodes afterchemoradiation.
III MR IMAGING REPORTING
There is no consensus on whether after CRT the tumour volume, the circumferential growth and the presence/absence of EMVI should beroutinely reported.
2528 Eur Radiol (2013) 23:2522–2531

not accurate for nodal characterisation, may be usefulfor locating nodes, which is supported by the literature[15, 18].
Fat-suppressed sequences were considered inappropriatebecause the mesorectal fascia is not well visualised. The useof contrast-enhanced dynamic or steady state T1-weightedsequences is not recommended either. While some studieshave investigated dynamic contrast-enhanced MRI for tu-mour response evaluation [19] or lymph-node-specific con-trast agents [20, 21] for nodal staging, the available evidenceis limited and consensus was reached that at present there isno role for contrast-enhanced MR sequences in either theprimary MR staging or restaging of rectal cancer. The use ofadditional unenhanced T1-weighted sequences to T2-weighted FSE was supported by 25 % of the panelists,mainly to characterise coincidental findings in other pelvicorgans.
Criteria for MRI assessment
A clear consensus was reached for most of the imagingcriteria. The main discussion items for which no agreementwas achieved were related to size criteria for diagnosis ofinvolved lymph nodes and the evaluation of extramuralvenous invasion (EMVI). Regarding nodal assessment,panellists all recommend that size should remain the primecriterion for malignancy. The panel was aware that in clin-ical practice size thresholds in the range of 5–8 mm are oftenadvocated. Available evidence, however, indicates that nosingle diameter threshold is sufficiently accurate to differ-entiate benign from malignant nodes, and that the choice ofa threshold is contingent upon the desired balance betweensensitivity and specificity, which varies per clinical set-ting. Accordingly, panellists chose not to recommend asingle threshold and possible cut-off points ranging be-tween 1 mm (i.e. any visible node) and 6 mm weresuggested. Other criteria such as margin irregularity,heterogeneity of nodal texture and shape, are also occa-sionally beneficial for differentiation [22], although onlyaround 70–75 % consensus was reached regarding theuse of these criteria as predictive markers for nodalmetastases on restaging MRI.
Regarding the assessment of EMVI as a routine com-ponent of MR evaluation, 25 % of the panellists con-sider it mandatory for primary staging, while 67 %considered it not obligatory but useful. Evidence existsthat EMVI assessed by MRI correlates with the pres-ence of EMVI at histology, and that its presence isassociated with subsequent relapse and poor survival[23]. For restaging following CRT, there was no agree-ment as to whether evaluation of EMVI remains bene-ficial. This lack of consensus probably reflects a paucityof evidence for the benefit of EMVI assessment after
preoperative CRT. In currently available publications,EMVI was mainly assessed in patients undergoing im-mediate surgery (without preoperative treatment). Instudies where the whole cohort was investigated, nosubset analyses were performed comparing patients un-dergoing immediate surgery with those undergoing pre-operative CRT [23, 24].
MRI reporting
Overall, panellists reached excellent consensus regardingthose items that should be included routinely in clinicalreports, for both primary staging and restaging after CRT(see Table 2). The only items without agreement werewhether or not tumour volume and—specifically in therestaging setting—the extent of circumferential tumourgrowth and the presence or absence of EMVI should beincluded in the report.
Methodological limitations
Our study has a few limitations. A single panellist wasabsent during the face-to-face meeting. For the items thatwere discussed and voted upon during the panel meeting,we therefore calculated the percentage of agreement basedon the forms for those panellists who were present. Second,most of the panel members were experts mainly working inthe field of MRI, which may have introduced some bias intothe imaging techniques advised. Third, the recommenda-tions in this paper mainly concern the staging of non-mucinous type adenocarcinoma. No specific recommenda-tions regarding the assessment of mucinous tumours areprovided. Also, the paper does not include any recommen-dations regarding the assessment of rectal tumours withrelation to peritoneal reflection. Although in many Europeancentres peritoneal reflection is not routinely used for treat-ment stratification, in the USA it is often an importantlandmark that influences the treatment decision whether (iftumour is below the peritoneal reflection) or not (if thetumour is above it) patients should receive neoadjuvanttreatment. In these cases there is evidence that radiologistscan accurately determine the level of the peritoneal reflec-tion using MRI [25, 26].
A final limitation, inherent to a face-to-face method-ology, is that bias might be introduced by the undueinfluence of any panellists whose personality was proneto “dominate” during discussions. Nevertheless, we feelthat this potential drawback does not outweigh the ben-efits of the face-to-face design, which provides an op-portunity to identify and clarify questions that had beenobscure during previous rounds. Moreover, two non-voting chairs presided over the meeting to ensure thatdiscussions were structured and well-balanced.
Eur Radiol (2013) 23:2522–2531 2529
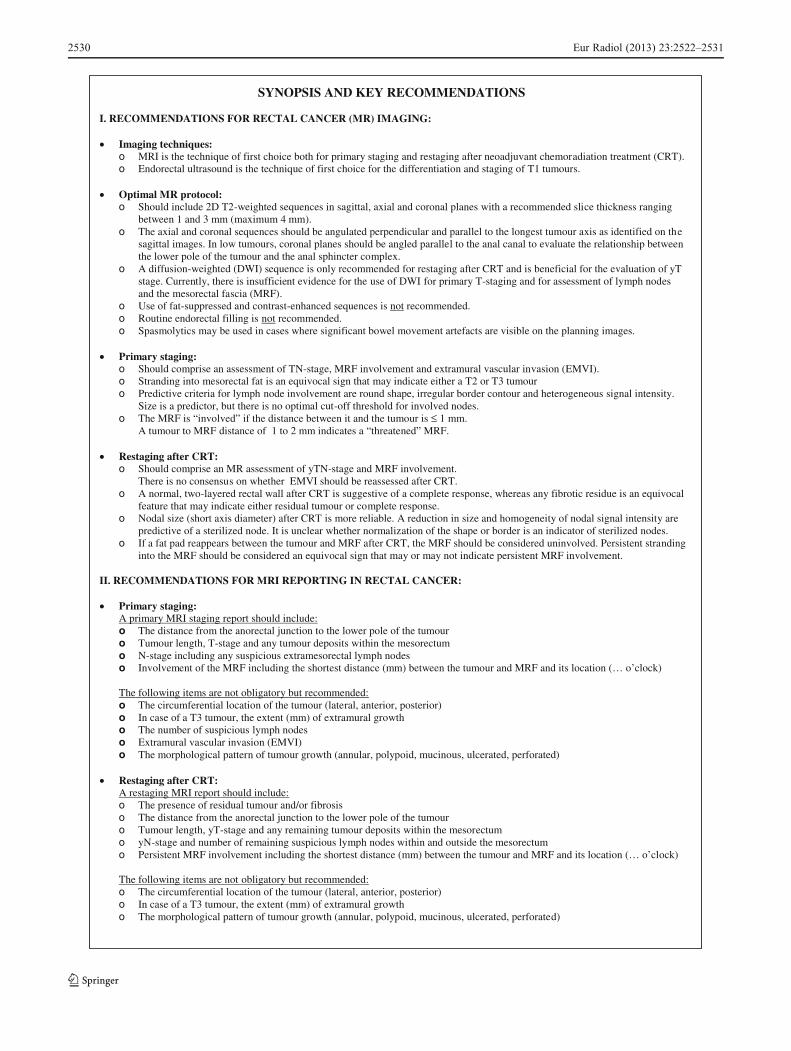
SYNOPSIS AND KEY RECOMMENDATIONS
I. RECOMMENDATIONS FOR RECTAL CANCER (MR) IMAGING:
Imaging techniques:o MRI is the technique of first choice both for primary staging and restaging after neoadjuvant chemoradiation treatment (CRT). o Endorectal ultrasound is the technique of first choice for the differentiation and staging of T1 tumours.
Optimal MR protocol: o Should include 2D T2-weighted sequences in sagittal, axial and coronal planes with a recommended slice thickness ranging
between 1 and 3 mm (maximum 4 mm). o The axial and coronal sequences should be angulated perpendicular and parallel to the longest tumour axis as identified on the
sagittal images. In low tumours, coronal planes should be angled parallel to the anal canal to evaluate the relationship between the lower pole of the tumour and the anal sphincter complex.
o A diffusion-weighted (DWI) sequence is only recommended for restaging after CRT and is beneficial for the evaluation of yT stage. Currently, there is insufficient evidence for the use of DWI for primary T-staging and for assessment of lymph nodes and the mesorectal fascia (MRF).
o Use of fat-suppressed and contrast-enhanced sequences is not recommended.o Routine endorectal filling is not recommended. o Spasmolytics may be used in cases where significant bowel movement artefacts are visible on the planning images.
Primary staging:o Should comprise an assessment of TN-stage, MRF involvement and extramural vascular invasion (EMVI).o Stranding into mesorectal fat is an equivocal sign that may indicate either a T2 or T3 tumouro Predictive criteria for lymph node involvement are round shape, irregular border contour and heterogeneous signal intensity.
Size is a predictor, but there is no optimal cut-off threshold for involved nodes. o The MRF is “involved” if the distance between it and the tumour is ≤ 1 mm.
A tumour to MRF distance of 1 to 2 mm indicates a “threatened” MRF.
Restaging after CRT:o Should comprise an MR assessment of yTN-stage and MRF involvement.
There is no consensus on whether EMVI should be reassessed after CRT. o A normal, two-layered rectal wall after CRT is suggestive of a complete response, whereas any fibrotic residue is an equivocal
feature that may indicate either residual tumour or complete response.o Nodal size (short axis diameter) after CRT is more reliable. A reduction in size and homogeneity of nodal signal intensity are
predictive of a sterilized node. It is unclear whether normalization of the shape or border is an indicator of sterilized nodes.o If a fat pad reappears between the tumour and MRF after CRT, the MRF should be considered uninvolved. Persistent stranding
into the MRF should be considered an equivocal sign that may or may not indicate persistent MRF involvement.
II. RECOMMENDATIONS FOR MRI REPORTING IN RECTAL CANCER:
Primary staging:A primary MRI staging report should include:o The distance from the anorectal junction to the lower pole of the tumouro Tumour length, T-stage and any tumour deposits within the mesorectumo N-stage including any suspicious extramesorectal lymph nodeso Involvement of the MRF including the shortest distance (mm) between the tumour and MRF and its location (… o’clock)
The following items are not obligatory but recommended:o The circumferential location of the tumour (lateral, anterior, posterior)o In case of a T3 tumour, the extent (mm) of extramural growtho The number of suspicious lymph nodeso Extramural vascular invasion (EMVI)o The morphological pattern of tumour growth (annular, polypoid, mucinous, ulcerated, perforated)
Restaging after CRT:A restaging MRI report should include:o The presence of residual tumour and/or fibrosiso The distance from the anorectal junction to the lower pole of the tumouro Tumour length, yT-stage and any remaining tumour deposits within the mesorectum o yN-stage and number of remaining suspicious lymph nodes within and outside the mesorectumo Persistent MRF involvement including the shortest distance (mm) between the tumour and MRF and its location (… o’clock)
The following items are not obligatory but recommended:o The circumferential location of the tumour (lateral, anterior, posterior)o In case of a T3 tumour, the extent (mm) of extramural growtho The morphological pattern of tumour growth (annular, polypoid, mucinous, ulcerated, perforated)
2530 Eur Radiol (2013) 23:2522–2531

References
1. Valentini V, Aristei C, Glimelius B et al (2009) Multidisciplinaryrectal cancer management: 2nd European Rectal CancerConsensus Conference (EURECA-CC2). Radiother Oncol92:148–163
2. Glimelius B, Pahlman L, Cervantes A (2010) Rectal cancer:ESMO clinical practice guidelines for diagnosis, treatment andfollow-up. Ann Oncol 2:v82–v86
3. Bipat S, Glas AS, Slors FJ, Zwinderman AH, Bossuyt PM, StokerJ (2004) Rectal cancer: local staging and assessment of lymphnode involvement with endoluminal US, CT, and MR imaging—ameta-analysis. Radiology 232:773–783
4. Lahaye MJ, Engelen SM, Nelemans PJ et al (2005) Imaging forpredicting the risk factors—the circumferential resection marginand nodal disease—of local recurrence in rectal cancer: a meta-analysis. Semin Ultrasound CT MR 26:259–268
5. Maas M, Beets-Tan RG, Lambregts DM et al (2011) Wait-and-seepolicy for clinical complete responders after chemoradiation forrectal cancer. J Clin Oncol 29:4633–4640
6. Lezoche G, Baldarelli M, Guerrieri M et al (2008) A prospectiverandomized study with a 5-year minimum follow-up evaluation oftransanal endoscopic microsurgery versus laparoscopic totalmesorectal excision after neoadjuvant therapy. Surg Endosc22:352–358
7. Fitch K, Bernstein S, Aguilar M et al (2001) The RAND/UCLAappropriateness method user’s manual. AHCPR Pub. No. 95–0009. Public Health Service, US Department of Health and HumanService, Rockville
8. Slater A, Halligan S, Taylor SA, Marshall M (2006) Distancebetween the rectal wall and mesorectal fascia measured by MRI:effect of rectal distension and implications for preoperative pre-diction of a tumour-free circumferential resection margin. ClinRadiol 61:65–70
9. Shihab OC, Moran BJ, Heald RJ, Quirke P, Brown G (2009) MRIstaging of low rectal cancer. Eur Radiol 19:643–650
10. Torkzad MR, Suzuki C, Tanaka S, Palmer G, Holm T, Blomqvist L(2008) Morphological assessment of the interface between tumorand neighboring tissues, by magnetic resonance imaging, beforeand after radiotherapy in patients with locally advanced rectalcancer. Acta Radiol 49:1099–1103
11. Kim SH, Lee JM, Hong SH et al (2009) Locally advanced rectalcancer: added value of diffusion-weighted MR imaging in theevaluation of tumor response to neoadjuvant chemo- and radiationtherapy. Radiology 253:116–125
12. Lambregts DM, Vandecaveye V, Barbaro B et al (2011) Diffusion-weighted MRI for selection of complete responders afterchemoradiation for locally advanced rectal cancer: a multicenterstudy. Ann Surg Oncol 18:2224–2231
13. Song I, Kim SH, Lee SJ, Choi JY, Kim MJ, Rhim H (2012) Valueof diffusion-weighted imaging in the detection of viable tumourafter neoadjuvant chemoradiation therapy in patients with locallyadvanced rectal cancer: comparison with T2-weighted and PET/CT imaging. Br J Radiol 85:577–586
14. Kim SH, Lee JM, Moon SK et al (2012) Evaluation of lymph nodemetastases: comparison of gadofluorine M-enhanced MRI anddiffusion-weighted MRI in a rabbit VX2 rectal cancer model. JMagn Reson Imaging 35:1179–1186
15. Lambregts DM, Maas M, Riedl RG et al (2011) Value of ADCmeasurements for nodal staging after chemoradiation in locallyadvanced rectal cancer-a per lesion validation study. Eur Radiol21:265–273
16. Mizukami Y, Ueda S, Mizumoto A et al (2011) Diffusion-weightedmagnetic resonance imaging for detecting lymph node metastasisof rectal cancer. World J Surg 35:895–899
17. Park MJ, Kim SH, Lee SJ, Jang KM, Rhim H (2011) Locallyadvanced rectal cancer: added value of diffusion-weighted MRimaging for predicting tumor clearance of the mesorectal fasciaafter neoadjuvant chemotherapy and radiation therapy. Radiology260:771–780
18. Mir N, Sohaib SA, Collins D, Koh DM (2010) Fusion of high b-value diffusion-weighted and T2-weighted MR images improvesidentification of lymph nodes in the pelvis. J Med Imaging RadiatOncol 54:358–364
19. Gollub MJ, Gultekin DH, Akin O et al (2012) Dynamic contrastenhanced-MRI for the detection of pathological complete responseto neoadjuvant chemotherapy for locally advanced rectal cancer.Eur Radiol 22:821–831
20. Koh DM, Brown G, Collins DJ (2009) Nanoparticles in rectalcancer imaging. Cancer Biomark 5:89–98
21. Lambregts DM, Beets GL, Maas M et al (2011) Accuracy ofgadofosveset-enhanced MRI for nodal staging and restaging inrectal cancer. Ann Surg 253:539–545
22. Brown G, Richards CJ, Bourne MW et al (2003) Morphologicpredictors of lymph node status in rectal cancer with use of high-spatial-resolution MR imaging with histopathologic comparison.Radiology 227:371–377
23. SmithNJ, BarbachanoY,NormanAR, Swift RI, Abulafi AM,BrownG(2008) Prognostic significance of magnetic resonance imaging-detectedextramural vascular invasion in rectal cancer. Br J Surg 95:229–236
24. Koh DM, Smith NJ, Swift RI, Brown G (2008) The relationshipbetween mr demonstration of extramural venous invasion andnodal disease in rectal cancer. Clin Med Oncol 2:267–273
25. Brown G, Kirkham A, Williams GT et al (2004) High-resolutionMRI of the anatomy important in total mesorectal excision of therectum. AJR Am J Roentgenol 182:431–439
26. Gollub MJ, Maas M, Weiser M et al (2013) Recognition of theanterior peritoneal reflection at rectal MRI. AJR Am J Roentgenol200:97–101
Eur Radiol (2013) 23:2522–2531 2531