
Oscillatory instabilities of intracellular fiber networks - eDiss
Upload
independentCategory
view
0download
0
Magnesium MetabolismA Review With Special Reference to theRelationship Between Intracellular Content and Serum LevelsRichard A. Reinhart, MD
\s=d\Magnesium (Mg++) is a ubiquitous element in nature,playing a role in photosynthesis and many metabolic functionsin humans. All enzymatic reactions that involve adenosinetriphosphate have an absolute requirement for Mg++. Levelsof Mg++ are controlled by the kidneys and gastrointestinaltract and appear closely linked to calcium, potassium, andsodium metabolism. The clinical manifestations and causesof abnormal Mg++ status are protean. Testing for altered Mg++homeostasis is problematic. Serum levels, which are thosegenerally measured, reflect only a small part of the total bodycontent of Mg++. The intracellular content can be low, despitenormal serum levels in a person with clinical Mg++ deficiency.Future directions in research related to intracellular contentof Mg++ are discussed. Treatment of altered Mg++ statusdepends on the clinical setting and may include the additionof a potassium/Mg++ \p=m-\sparingdrug to an existing diureticregimen. Guidelines for therapy are given.
(Arch Intern Med 1988;148:2415-2420)TV/Tagnesium (Mg++) is a ubiquitous element in nature, " * including in the human body. It forms an estimated
2.1% of the earth's crust,1 in the human body it is thesecond most abundant intracellular cation (second only topotassium), and it is the fourth most abundant total cation.Among the biologically important cations, Mg++ has thesmallest ionic radius; the smaller the relative size of an
atom, the greater the binding energies and the tendencyto form complex compounds. The formation of complexcompounds is one of the major metabolic roles of Mg+ +
.
The abundance and special properties of the Mg++ ionaccount for its key role in many metabolic functions in thebody.
Many clinical signs, symptoms, and disease states areattributed to altered Mg++ homeostasis. Determination ofserum Mg++ levels is generally the method used to detectthese problems, despite the fact that most Mg++ is con¬tained in the bone and soft tissue; only 1% of the totalbody content of this ion is found in the serum. Althoughoften correlated, serum concentration and intracellularcontent of Mg++ can be dissociated, and signs of Mg+ +
deficiency occur with normal or minimally low serum levels.
Accepted for publication May 3, 1988.From the Marshfield (Wis) Clinic.Reprint requests to 1000 N Oak Ave, Marshfield, WI54449 (Dr Reinhart).
In this article Mg++ is reviewed with regard to: (1) itsfunction in metabolic processes, (2) homeostasis and alteredhomeostasis, (3) the relationship of intracellular to serum
content, (4) the treatment of hypomagnesemia, and (5)future directions in research. The material reviewed wasderived from a MEDLINE search (1978 to present) andfrom selected references prior to 1978.
FUNCTION OF MAGNESIUM IN METABOLIC PROCESSESRole in the Evolutionary Process
Aikawa2 postulated that 3.5 billion years ago the Mg+ +
ion combined with porphyrin rings, owing to the chelatingproperties of Mg+ +, forming chlorophyll. Formation of thechlorophyll molecule made photosynthesis, and thereforean oxygen-rich environment, feasible. Magnesium in thechlorophyll molecule is essential for the process of captur¬ing photons from the sun and converting them to adenosinetriphosphate (ATP). The Mg-porphyrin complex, excitedby the sun, is capable of undergoing reversible photochem¬ical oxidation or reduction, ie, accepting or donatingelectrons between partner molecules. This process leadsto the formation of ATP and oxygen; both are necessaryfor the next higher step in the evolutionary process,oxidative phosphorylation.3
Geologic evidence suggests that as oxygen was formedby the photosynthetic process, the iron in the oceans,initially in the ferrous state, reacted with the oxygenformed by the photosynthetic process and precipitated inthe ferric state, forming rusty layers on the ocean floor.4As this process of precipitation was completed, oxygenwas released into the atmosphere, setting the stage foroxidative phosphorylation—a process that utilizes oxygenand a variety of substrates to produce ATP more efficientlythan can photosynthesis.
Role in Metabolic FunctionsIn addition to its central function in photosynthesis,
Mg+ * participates in many of the biochemical reactionsthat take place in the body, particularly in those processesinvolving the formation and utilization of ATP. Metals arecofactors required in approximately two thirds of allenzymatic reactions in the body. Magnesium participatesin such reactions through its ability to form a chelate, ie,an organometallic coordination complex. A variety of
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015

modes of this action have been identified: (1) alteration ofthe structural conformation of substrates, eg, allowingmore ready cleavage of the terminal phosphate of ATP andits attachment to other molecules; (2) coordination of asubstrate to the active enzyme site; (3) binding directly toan enzyme to stabilize it in its active conformation; and (4)binding catalytic subunits together to make an activeenzyme.5
All enzymatic reactions that involve ATP show an abso¬lute requirement for Mg+ +
. Magnesium coordinates withthe ATP molecule to form the true substrate and, inaddition, may labilize the terminal phosphate bond of ATPto facilitate transfer of phosphate to other molecules. Itmay also serve to neutralize the negative charge densityon the ATP molecule and facilitate its binding to theenzyme participating in a biochemical reaction.5
Mg HOMEOSTASISDistribution in the Body
The Mg+ + content of the human body ranges between22.7 and 35.0 mEq/kg of wet-weight tissue.6 The majority,approximately 60%, is found in bone. Muscle and othersoft tissue contain most of the remainder. Only about 1%is contained in the extracellular space; one third of this isnonspecifically bound to plasma protein, leaving the re¬mainder as the diffusible or ionized component.7 Results ofequilibrium studies8 using radioisotopes suggest that thelabile pool of Mg++ is primarily contained in connectivetissue, skin, and the soft tissues of the abdominal cavity;the Mg++ in bone, muscle, and red blood cells exchangesvery slowly.
Therefore, the serum measurements of Mg++ that are
routinely made in the clinical setting assess only a smallpart of the total body content. Atomic-absorption spectro-photometry, the most common method of routine clinicaldetermination, gives normal serum values of 0.7 to 1.0mmol/L. No difference on the basis of sex or age was shownin one study,9 while some difference on the basis of age,sex, and race was shown in another.10
Absorption and EliminationEvidence from studies in animals shows Mg++ to be
absorbed from the small intestine.11 Studies using the 28Mgradioisotope indicate that Mg++ absorption from the gas¬trointestinal tract is influenced by the load presented: thesmaller the load, the greater the percentage of absorption(ranging between 24% and 76%). There is no evidence thatMg+ + is actively transported across the intestinal mucosa.Absorption begins within one hour of ingestion and contin¬ues at a steady rate uniformly throughout the smallintestine for two to eight hours. Little or no absorptionoccurs in the large bowel.12
The kidney is the main regulator of serum concentrationand total body content of Mg+ +
. The diffusible fraction ofMg++ is filtered by the glomerulus and reabsorbed in thetubules, 60% to 75% in the thick ascending limb. Sustainedhypermagnesemia is difficult to maintain in the presenceof normal renal function because renal excretion increasesin proportion to the load presented to the kidney.13 Thekidney conserves Mg++ in response to a deficiency. In a
study of experimental Mg+ + deficiency in humans, urinaryexcretion decreased to less than 1 mEq/d.14 Those factorsthat lead to abnormal urinary excretion do so by inhibitingtubular reabsorption.
There is no convincing evidence of tubular secretion ofMg*+ by the kidney.13 There is some evidence to supportthe hypothesis that parathyroid hormone (PTH) plays a
role in Mg*+ homeostasis by way of a negative feedback
mechanism1415; hypomagnesemia, unless severe, may en¬hance PTH production, while PTH may enhance tubularreabsorption of Mg**.13
Hypomagnesemia is often associated with hypocalcemia.The mechanisms postulated to result in the hypocalcemiaassociated with hypomagnesemia remain controversial.They include (1) impaired functioning of the parathyroidglands due to abnormal release16 or synthesis15 of PTH; (2)unresponsiveness of the peripheral tissues to PTH, possi¬bly related to inactivity ofadenyl cyclase, a Mg+ +-requiringenzyme1718; (3) decreased heteroionic exchange of Mg+ +
and calcium*+ at the bone surface, independent of PTHinitially but perpetuated by lack of appropriate increase inPTH levels19; and (4) reduction of Ca+ + release from thebone, independent of PTH.20
Rude and colleagues21 reported low serum concentrationsof calcitriol (1,25-dihydroxyvitamin D3) in Mg+ + deficiency,possibly due to impaired I- hydroxylation of vitamin D.The data in that study suggested that vitamin D metabo¬lism may be more sensitive to Mg++ deficiency than isPTH secretion.
Magnesium loss also occurs through perspiration.22 Whenthe body is exposed to high temperatures, as much as 10%to 15% of the total output of Mg+ + can be recovered in thesweat. Furthermore, unlike that of sodium and potassium,excretion of Mg+ * in sweat does not decrease appreciablyduring acclimatization.23
Dietary Sources and RequirementThe average daily intake of Mg++ is 20 to 40 mEq.
Common dietary sources are listed in Table l.24 Therecommended daily allowance of Mg++ varies according toage and sex and is listed in Table 2.26
Dietary intake of Mg* + in the United States may be lessthan the recommended amount,26 leading to a frank orborderline state of hypomagnesemia in much of our popu¬lation.27 This reduced intake may be due to an increaseduse of refined or processed cereals and carbohydrates fromwhich the majority of Mg** has been removed. Thesoftening of "hard" water removes variable quantities ofMg+ * and may also contribute to reduced intake of Mg+ +.
ALTERED Mg HOMEOSTASISHypomagnesemia
The causes of hypomagnesemia are many (Table 3)2730and the clinical manifestations are varied (Table 4).14·31-33 Ina survey performed in a community hospital, hypomagne¬semia was the most common electrolyte abnormality inpatients entering the intensive care unit, being present in20%.34 In a similar study, 65% of patients with serumcreatinine concentrations of 97 µ /L or less were hypo-magnesemic.35
The timing of sampling for Mg** determinations shouldbe taken into consideration in evaluating such findings. Inpatients with acute myocardial infarction, the serum Mg**level fluctuates as a function of time from the onset ofinfarction. One study showed the lowest serum Mg+ +
concentrations 12 to 20 hours after patients were admittedto the hospital.36 A sharp increase in the plasma level offree fatty acids occurred concomitantly with the decreasein levels of serum Mg**.37 Transient hypomagnesemia inthese patients may be caused by Mg+ * migration from theextracellular to the intracellular space due to a drop in theintracellular concentration of ionized Mg+ ; catecholamine-induced lipolysis causes intracellular precipitation of Mg*+as an insoluble soap.
Shils14 reported the clinical and biochemical abnormali¬ties that occurred in experimental Mg** deficiency in
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015

Table 1.—Dietary Sources of Magnesium*Magnesium Content,
Source mg 100 g Edible PortionNuts 200Unprocessed cereal 66Legumes 20Vegetables 14Dairy products 15Drinking water 30-90tMeats 14-30
*Data from Robinson24 and Pennington and Church.59tMeasured in milligrams per liter.
Table 2.—Recommended Daily Dietary Allowance ofMagnesium*
Age, y Magnesium, mg/dInfants
0.0-0.5 500.5-1.0 70
Children1-3 1504-6 2007-10 250
Adolescents/adultsMales
11-14 35015-18 400>18 350
Femalesfell 300
Pregnant femalesand lactating mothers 450
*Data from Munro.25
seven human subjects. Plasma Mg** levels decreasedprogressively to levels that were 10% to 30% of those incontrol periods. Urine and fecal Mg** decreased to ex¬
tremely low levels within seven days. Hypocalcemia oc¬curred in six of the subjects despite adequate calciumintake. In the majority of the Mg**-deficient subjects,hypokalemia and negative potassium balance developed;serum sodium levels remained normal, but a positivesodium balance developed. Neurologic signs occurred infive of the seven subjects; the most common manifestationwas a positive Trousseau sign. Other neurologic abnormal¬ities included personality change, tremor, fasciculations,and generalized spasticity. Hypomagnesemia, hypocalce¬mia, and hypokalemia were consistently present in allsymptomatic patients. All abnormalities reverted to normalwith reinstitution of Mg* +
.
In an investigation of patients admitted to a coronarycare unit, Dyckner38 studied the relationship of serumMg* * levels to cardiac arrhythmias. Among patients withacute myocardial infarction, the incidence of serious ven¬tricular arrhythmias (multifocal, repetitive, >5/min, cou¬pled, and R-on-T phenomenon) was significantly greaterin the presence of hypomagnesemia. The incidence ofventricular tachycardia and ventricular fibrillation, as wellas of atrial fibrillation and supraventricular tachycardia,was also significantly greater in patients with hypomag¬nesemia. The author hypothesized that a reduction ofmembrane adenosine triphosphatase (ATPase) activity iscaused by reduced levels of Mg+*. In turn, this results ina loss of potassium from the intracellular space, causing a
change in the ratio of intracellular to extracellular potas¬sium. Since this ratio largely determines the restingmembrane electrical potential, the consequences of analteration are increased cellular electrical excitability anda greater tendency to arrhythmias.
Table 3.—Causes of Hypomagnesemia*Reduced Intake
StarvationProlonged intravenous therapy without magnesium* * supplement
Impaired intestinal absorptionChronic diarrheaMalabsorption syndromes, including Mg+ +-specificFamilial
_______________
Renal lossDiabetes mellitus and diabetic ketoacidosisDiuretics (with the exception of potassium+-sparing agents)Antibiotics (gentamicin sulfate, carbenicillin disodium, and ticar¬
cillin disodium)Osmotic agents (including hyperglycemia)AlcoholCisplatinCyclosporineHyperparathyroidism (and other causes of hypercalcémie)Renal tubular acidosisPostobstructive diuresis
MiscellaneousIdiopathicAcute myocardial infarction (intracellular shift)Excessive sweatingDigitalis toxicityCongestive heart failure
*Data from Whang,27 Wacker and Parisi,26 Agus et al,29 Ryan,54 and Bartonet al.60
Table 4.—Clinical Manifestations of Hypomagnesemia*Neuromuscular
Muscle weaknessMuscle twitching and tremorPositive Chvostek's signDeliriumHyperreflexiaConvulsionsComa
_______________________________
CardiacElectrocardiographic
Premature ventricular contractionsProlongation of PR and QT intervalsT-wave flatteningAtrial fibrillationTorsades de pointes
MiscellaneousPossible coronary artery spasmEnhanced sensitivity to digitalis intoxicationPossible greater size of myocardial infarctionPossible enhanced susceptibility to ventricular fibrillation and
sudden death in ischemie heart disease
Refractory hypokalemiaHypocalcemia
*Data from Shils,14 Kingston et al,31 Juan,32 and Vallee et al.33
Serum Mg** levels in patients with symptomatic atrialfibrillation and the relationship of the levels to rhythmcontrol by intravenous digoxin were the subject of a studyby DeCarli et al.39 Of 45 consecutive patients with atrialfibrillation, 20% were hypomagnesemic and required twicethe amount of intravenous digoxin to control the ventricularresponse to atrial fibrillation as did the patients withnormal serum Mg** levels.
HypermagnesemiaElevation of the serum Mg** level above 2.0 mmol/L is
usually accompanied by symptoms. The effects of a pro¬gressive rise in serum Mg** levels include hypotension(1.5 to 2.5 mmol/L); electrocardiographic changes of PRinterval and QRS-duration prolongation and peaked waves (2.5 to 5.0 mmol/L); areflexia (5.0 mmol/L); respi¬ratory paralysis (7.5 mmol/L); and cardiac arrest (12.5
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015

mmol/L).28 The most common cause of hypermagnesemiais renal insufficiency, particularly when Mg**-containingmedications such as antacids or laxatives are used. It isdifficult to induce sustained hypermagnesemia in a patientwith normal renal function, a fact demonstrated in treatingeclampsia with magnesium sulfate.40 In this setting, a
loading dose of 4 g as a 20% solution is given intravenouslyat a rate of 1 g/min, followed by a 10-g intramuscular dose,and then 5 g given intramuscularly every four hours. Thisamount is required to maintain serum Mg* * levels between2 and 3.5 mmol/L.
The initial treatment of hypermagnesemia is cessationof Mg++ administration. Calcium is a direct antagonist ofMg**; administration of gluconate calcium, 1 g intrave¬nously, may reverse the effects of hypermagnesemia. Sincethe Mg** ion is readily diffusible, peritoneal dialysis orhemodialysis is effective and may be required.29
RELATIONSHIP OF INTRACELLULAR TO SERUM Mg LEVELMeasurement of Mg** levels in the serum is the usual
method for determining Mg* * homeostasis. However, theremay be a dissociation between serum and intracellularlevels of Mg**,4142 and intracellular levels may betterreflect homeostasis. Furthermore, it is not clear whichtissue level best reflects overall homeostasis and whethersome specific subcellular compartment levels of Mg* * havemore clinical significance than others. Subcellular com¬
partments can be separated and the levels of Mg* * in someof these can be measured, but the degree of laboratorysophistication necessary to do this is not yet widelyavailable.43
In a group of seven patients receiving digitalis therapywith digitalis-induced arrhythmias, Cohen and Kitzes41demonstrated that cellular Mg* * depletion with or withouthypomagnesemia seems to predispose patients to thesearrhythmias. Cellular potassium depletion also appearedto be associated with Mg** deficiency. As the authorspointed out, such a state of Mg*+ deficiency and secondarypotassium deficiency can be difficult to diagnose, sinceconcomitant serum levels of both ions may be normal.These conclusions were substantiated by the finding ofdecreased lymphocyte levels of Mg** and potassium andresolution of the arrhythmias with intravenous administra¬tion of magnesium sulfate in patients with normal serumlevels of Mg+*.
Other studies refer to intracellular electrolyte levels invarious tissues and their relationship to serum levels.Tzivoni et al44 reported successful magnesium sulfate treat¬ment of torsades de pointes in three consecutive patients,all of whom had normal serum Mg** levels. However,intracellular levels were not measured and the authorsstated that they could not rule out the possibility that theselevels were reduced. Dyckner and Wester42 demonstratedby findings from percutaneous muscle biopsies that no
relationship exists between extracellular and intracellularelectrolyte levels in humans. Ryan and Ryan45 showed thatduring Mg* + deficiency in the rat, the losses of intracellularMg* * from the lymphocytes paralleled losses from cardiacand skeletal muscle and from serum.
Although Ryan and Ryan45 showed that in the Mg**-deficient rat losses of intracellular Mg* * from lymphocytes(9%) were similar to losses from cardiac muscle (10%) andskeletal muscle (6%), the magnitude of loss was less thanthat from serum (71%) and red blood cells (33%). In thatstudy during the Mg++ deficient state, lymphocyte levelsof sodium and calcium increased. In a study by Chang andBloom46 of the Mg* +-deficient hamster, no reduction inlevels of intracellular myocardial Mg** was found, despite
a fall in serum Mg** levels to about half of the controlvalue. These authors did find an increase in myocardialsodium and calcium levels. In a study of Mg*+ deficiencyand myocardial infarct size in the dog, Chang et al47 foundsimilar increases in myocardial sodium and calcium levels.The myocardial Mg* * content was unaltered.
Comparing the results of these three studies,4"7 thedifferences found in intracellular Mg** levels could beexplained by differences in species-specific metabolic pat¬terns, or may reflect a difference among the studies in thedegree or rate of development of Mg*+ deficiency. Acommon denominator appears to be the increase of intra¬cellular sodium and calcium levels induced by Mg** defi¬ciency. Possibly due to its influence on the cellular mem¬brane via the (Na*-K*)-ATPase system, Mg** directlyalters intracellular levels of sodium and indirectly altersthose of calcium.48 Do the intracellular levels of sodium andcalcium actually represent a more sensitive index of theeffects of Mg* * deficiency than the Mg* + content itself?The answer to this awaits further study.
The intracellular Mg** content of mononuclear cellsfrom the venous blood of clinically normal subjects hasbeen determined by our center9 and in normal volunteersby Elin and Hosseini.30 In our study, the mean mononuclearcell (lymphocyte and monocyte) Mg++ content was 67.8 fg/cell (SD, 13.8 fg/cell) and in the study by Elin and Hosseini,it was 70.7 fg/cell (SD, 14.1 fg/cell). No correlation wasfound between the intracellular content and simultaneouslymeasured serum levels of Mg* * in both studies, nor were
any differences found on the basis of sex or age in our
study.Studies have shown the superiority of measuring the
intracellular content of Mg* * over measuring serum levelsin determining the Mg+* status of patients. Ryzen et al,49in a study of patients in an intensive care unit, showed alow mononuclear blood cell content of Mg** in 53% ofunselected patients. There was no correlation found withserum levels of Mg** simultaneously measured in thesepatients. It was concluded by those authors that theincidence of intracellular Mg** deficiency in patients withcardiovascular disease is much higher than the serum
Mg** determinations would indicate. Elin et al50 studiedserum, mononuclear blood cell, and erythrocyte Mg* +
levels in hyperparathyroid and hypoparathyroid patients.The results suggested that high blood concentrations ofPTH reduced the cellular Mg** content of erythrocytesand mononuclear blood cells but did not alter plasmaconcentrations. Finally, in patients with digitalis-inducedarrhythmias, Cohen and Kitzes41 showed that measuringthe Mg* * content of mononuclear blood cells was a betterindicator of altered Mg** status than determining theserum levels of Mg* +
.
Magnesium balance studies also give valuable informa¬tion regarding the Mg*+ status of an individual patient.One practical method is that described by Ryzen et al,51which uses a calculation of the percentage of retention of a
single intravenous dose of a Mg** salt administered on ashort-term basis. Those authors concluded that this test isa more sensitive index of Mg* * deficiency than is measure¬ment of the serum Mg* * concentrations.
Treatment of HypomagnesemiaThe conditions that benefit from Mg** supplementation
are listed in Table 5. * A patient with one of these conditionsmay benefit from Mg** supplementation despite normalserum levels of Mg* *.
*References 28, 31, 33, 36, 38, 39, 41, 44, 52-55.
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015
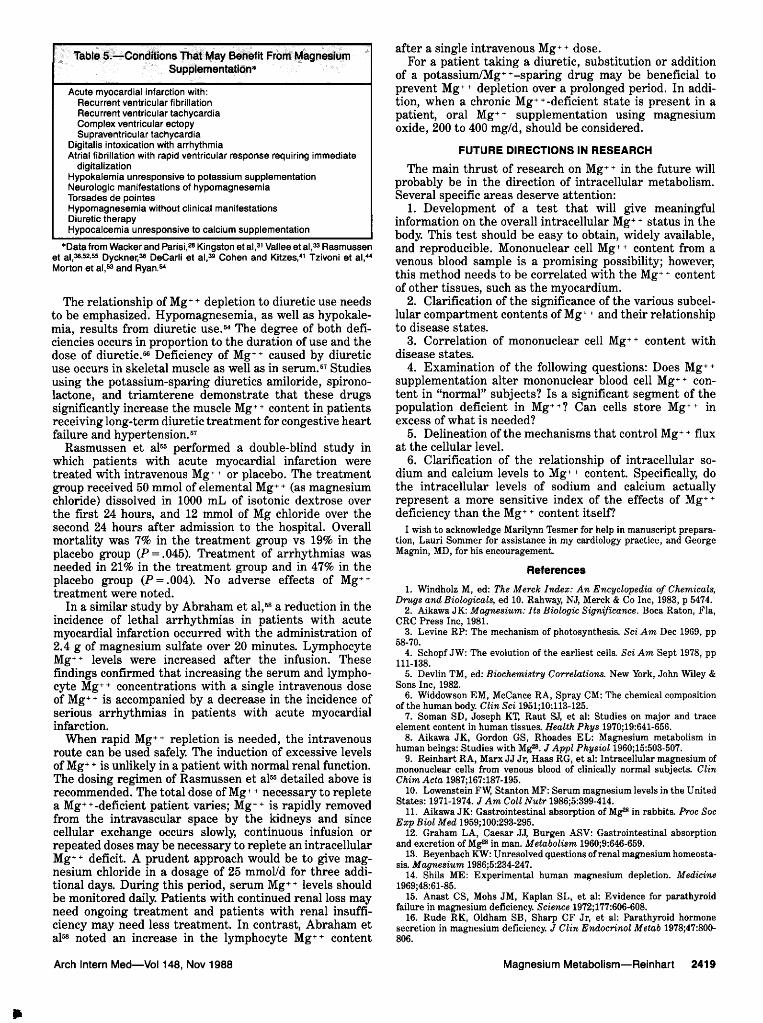
Table 5.—Conditions That May Benefit From MagnesiumSupplementation*
Acute myocardial infarction with:Recurrent ventricular fibrillationRecurrent ventricular tachycardiaComplex ventricular ectopySupraventricular tachycardia
Digitalis intoxication with arrhythmiaAtrial fibrillation with rapid ventricular response requiring immediate
digitalizationHypokalemia unresponsive to potassium supplementationNeurologic manifestations of hypomagnesemiaTorsades de pointesHypomagnesemia without clinical manifestationsDiuretic therapyHypocalcemia unresponsive to calcium supplementation
*Data from Wacker and Parisi,28 Kingston et al,31 Vallee et al,33 Rasmussenet al,36·52·55 Dyckner,36 DeCarli et al,39 Cohen and Kitzes,4' Tzivoni et al,44Morton et al,53 and Ryan.54
The relationship of Mg* * depletion to diuretic use needsto be emphasized. Hypomagnesemia, as well as hypokale¬mia, results from diuretic use.54 The degree of both defi¬ciencies occurs in proportion to the duration of use and thedose of diuretic.56 Deficiency of Mg** caused by diureticuse occurs in skeletal muscle as well as in serum.57 Studiesusing the potassium-sparing diuretics amiloride, spirono-lactone, and triamterene demonstrate that these drugssignificantly increase the muscle Mg** content in patientsreceiving long-term diuretic treatment for congestive heartfailure and hypertension.57
Rasmussen et al55 performed a double-blind study inwhich patients with acute myocardial infarction weretreated with intravenous Mg* * or placebo. The treatmentgroup received 50 mmol of elemental Mg* + (as magnesiumchloride) dissolved in 1000 mL of isotonic dextrose overthe first 24 hours, and 12 mmol of Mg chloride over thesecond 24 hours after admission to the hospital. Overallmortality was 7% in the treatment group vs 19% in theplacebo group (P = .045). Treatment of arrhythmias wasneeded in 21% in the treatment group and in 47% in theplacebo group (P = .004). No adverse effects of Mg**treatment were noted.
In a similar study by Abraham et al,58 a reduction in theincidence of lethal arrhythmias in patients with acutemyocardial infarction occurred with the administration of2.4 g of magnesium sulfate over 20 minutes. LymphocyteMg++ levels were increased after the infusion. Thesefindings confirmed that increasing the serum and lympho¬cyte Mg** concentrations with a single intravenous doseof Mg* * is accompanied by a decrease in the incidence ofserious arrhythmias in patients with acute myocardialinfarction.
When rapid Mg** repletion is needed, the intravenousroute can be used safely. The induction of excessive levelsof Mg* * is unlikely in a patient with normal renal function.The dosing regimen of Rasmussen et al56 detailed above isrecommended. The total dose of Mg* * necessary to repletea Mg**-deficient patient varies; Mg** is rapidly removedfrom the intravascular space by the kidneys and sincecellular exchange occurs slowly, continuous infusion or
repeated doses may be necessary to replete an intracellularMg* + deficit. A prudent approach would be to give mag¬nesium chloride in a dosage of 25 mmol/d for three addi¬tional days. During this period, serum Mg*+ levels shouldbe monitored daily. Patients with continued renal loss mayneed ongoing treatment and patients with renal insuffi¬ciency may need less treatment. In contrast, Abraham etal58 noted an increase in the lymphocyte Mg** content
after a single intravenous Mg++ dose.For a patient taking a diuretic, substitution or addition
of a potassium/Mg*+-sparing drug may be beneficial toprevent Mg** depletion over a prolonged period. In addi¬tion, when a chronic Mg**-deficient state is present in a
patient, oral Mg** supplementation using magnesiumoxide, 200 to 400 mg/d, should be considered.
FUTURE DIRECTIONS IN RESEARCHThe main thrust of research on Mg** in the future will
probably be in the direction of intracellular metabolism.Several specific areas deserve attention:
1. Development of a test that will give meaningfulinformation on the overall intracellular Mg* * status in thebody. This test should be easy to obtain, widely available,and reproducible. Mononuclear cell Mg** content from avenous blood sample is a promising possibility; however,this method needs to be correlated with the Mg* * contentof other tissues, such as the myocardium.
2. Clarification of the significance of the various subcel¬lular compartment contents of Mg* + and their relationshipto disease states.
3. Correlation of mononuclear cell Mg** content withdisease states.
4. Examination of the following questions: Does Mg* *
supplementation alter mononuclear blood cell Mg*+ con¬tent in "normal" subjects? Is a significant segment of thepopulation deficient in Mg*+? Can cells store Mg** inexcess of what is needed?
5. Delineation of the mechanisms that control Mg* * fluxat the cellular level.
6. Clarification of the relationship of intracellular so¬dium and calcium levels to Mg* * content. Specifically, dothe intracellular levels of sodium and calcium actuallyrepresent a more sensitive index of the effects of Mg* *
deficiency than the Mg* * content itself?I wish to acknowledge Marilynn Tesmer for help in manuscript prepara¬
tion, Lauri Sommer for assistance in my cardiology practice, and GeorgeMagnin, MD, for his encouragement.
References1. Windholz M, ed: The Merck Index: An Encyclopedia of Chemicals,
Drugs and Biologicals, ed 10. Rahway, NJ, Merck & Co Inc, 1983, p 5474.2. Aikawa JK: Magnesium: Its Biologic Significance. Boca Raton, Fla,
CRC Press Inc, 1981.3. Levine RP: The mechanism of photosynthesis. Sci Am Dec 1969, pp
58-70.4. Schopf JW: The evolution of the earliest cells. Sci Am Sept 1978, pp
111-138.5. Devlin TM, ed: Biochemistry Correlations. New York, John Wiley &
Sons Inc, 1982.6. Widdowson EM, McCance RA, Spray CM: The chemical composition
of the human body. Clin Sci 1951;10:113-125.7. Soman SD, Joseph KT, Raut SJ, et al: Studies on major and trace
element content in human tissues. Health Phys 1970;19:641-656.8. Aikawa JK, Gordon GS, Rhoades EL: Magnesium metabolism in
human beings: Studies with Mg28. J Appl Physiol 1960;15:503-507.9. Reinhart RA, Marx JJ Jr, Haas RG, et al: Intracellular magnesium of
mononuclear cells from venous blood of clinically normal subjects. ClinChim Acta 1987;167:187-195.
10. Lowenstein FW, Stanton MF: Serum magnesium levels in the UnitedStates: 1971-1974. J Am Coll Nutr 1986;5:399-414.
11. Aikawa JK: Gastrointestinal absorption of Mg28 in rabbits. Proc SocExp Biol Med 1959;100:293-295.
12. Graham LA, Caesar JJ, Burgen ASV: Gastrointestinal absorptionand excretion of Mg28 in man. Metabolism 1960;9:646-659.
13. Beyenbach KW: Unresolved questions of renal magnesium homeosta-sis. Magnesium 1986;5:234-247.
14. Shils ME: Experimental human magnesium depletion. Medicine1969;48:61-85.
15. Anast CS, Mohs JM, Kaplan SL, et al: Evidence for parathyroidfailure in magnesium deficiency. Science 1972;177:606-608.
16. Rude RK, Oldham SB, Sharp CF Jr, et al: Parathyroid hormonesecretion in magnesium deficiency. J Clin Endocrinol Metab 1978;47:800\x=req-\806.
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015

17. Estep H, Shaw WA, Watlington C, et al: Hypocalcemia due tohypomagnesemia and reversible parathyroid hormone unresponsiveness.J Clin Endocrinol Metab 1969;29:842-848.
18. MacManus J, Heaton FW, Lucas PW: A decreased response toparathyroid hormone in magnesium deficiency. J Endocrinol 1971;49:253\x=req-\258.
19. Chase LR, Slatopolsky E: Secretion and metabolic efficacy of para-thyroid hormone in patients with severe hypomagnesemia. J Clin Endocri-nol Metab 1974;38:363-371.
20. Graber ML, Schulman G: Hypomagnesemic hypocalcemia independ-ent of parathyroid hormone. Ann Intern Med 1986;104:804-805.
21. Rude RK, Adams JS, Ryzen E, et al: Low serum concentrations of1,25-dihydroxyvitamin D in human magnesium deficiency. J Clin Endocri-nol Metab 1985;61:933-940.
22. Beller GA, Maher JT, Hartley LH, et al: Changes in serum and sweatmagnesium levels during work in the heat. Aviat Space Environ Med1975;46:709-712.
23. Consolazio CF, Matoush LO, Nelson RA, et al: Excretion of sodium,potassium, magnesium and iron in human sweat and the relation of each tobalance and requirements. J Nutr 1963;79:407-415.
24. Robinson CH: Normal and Therapeutic Nutrition. London, CollierMcMillan, 1972, pp 669-685.
25. Munro HN: Recommended Dietary Allowances, ed 9. Washington,DC, National Academy of Sciences, 1980, pp 134-136.
26. Marier JR: Magnesium content of the food supply in the modern-dayworld. Magnesium 1986;5:1-8.
27. Whang R: Magnesium deficiency: Pathogenesis, prevalence, andclinical implications. Am J Med 1987;82(suppl 3A):24-29.
28. Wacker WEC, Parisi AF: Magnesium metabolism. N Engl J Med1968;278:658-663, 712-717, 772-776.
29. Agus ZS, Wasserstein A, Goldfarb S: Disorders of calcium andmagnesium homeostasis. Am J Med 1982;72:473-488.
30. Elin RJ, Hosseini JM: Magnesium content of mononuclearblood cells.Clin Chem 1985;31:377-380.
31. Kingston ME, Al-Siba'I MB, Skooge WC: Clinical manifestations ofhypomagnesemia. Crit Care Med 1986;14:950-954.
32. Juan D: Clinical review: The clinical importance of hypomagnesemia.Surgery 1982;91:510-517.
33. Vallee BL, Wacker WEC, Ulmer DD: The magnesium-deficiencytetany syndrome in man. N Engl J Med 1960;262:155-161.
34. Reinhart RA, Desbiens NA: Hypomagnesemia in patients enteringthe ICU. Crit Care Med 1985;13:506-507.
35. Ryzen E, Wagers PW, Singer FR, et al: Magnesium deficiency in amedical ICU population. Crit Care Med 1985;13:19-21.
36. Rasmussen HS, Aurup P, Hojberg S, et al: Magnesium and acutemyocardial infarction. Arch Intern Med 1986;146:872-874.
37. Flink EB, Brick JE, Shane SR: Alterations of long-chain free fattyacid and magnesium concentrations in acute myocardial infarction. ArchIntern Med 1981;141:441-443.
38. Dyckner T: Serum magnesium in acute myocardial infarction. ActaMed Scand 1980;207:59-66.
39. DeCarli C, Sprouse G, LaRosa JC: Serum magnesium levels insymptomatic atrial fibrillation and their relation to rhythm control by
intravenous digoxin. Am J Cardiol 1986;57:956-959.40. Pritchard JA, MacDonald PC, Gant NF, eds: Williams Obstetrics, ed
17. East Norwalk, Conn, Appleton-Century-Crofts, 1985, pp 525-560.41. Cohen L, Kitzes R: Magnesium sulfate and digitalis-toxic arrhyth-
mias. JAMA 1983;249:2808-2810.42. Dyckner T, Wester PO: The relation between extra- and intracellular
electrolytes in patients with hypokalemia and/or diuretic treatment. ActaMed Scand 1978;204:269-282.
43. Polimeni PI, Page E: Magnesium in heart muscle. Circ Res1973;33:367-374.
44. Tzivoni D, Keren A, Cohen AM, et al: Magnesium therapy fortorsades de pointes. Am J Cardiol 1984;53:528-530.
45. Ryan MF, Ryan MP: Lymphocyte electrolyte alterations duringmagnesium deficiency in the rat. Ir J Med Sci 1979;148:108-109.
46. Chang C, Bloom S: Interrelationship of dietary Mg intake andelectrolyte homeostasis in hamsters: I. Severe Mg deficiency, electrolytehomeostasis, and myocardial necrosis. J Am Coll Nutr 1985;4:173-185.
47. Chang C, Varghese PJ, Downey J, et al: Magnesium deficiency andmyocardial infarct size in the dog. J Am Coll Cardiol 1985;5:280-289.
48. Skou JS: Further investigations on a Mg++ + Na+ -activated adeno-sintriphosphatase, possibly related to the active, linked transport of Na+and K+ across the nerve membrane. Biochim Biophys Acta 1960;42:6-23.
49. Ryzen E, Elkayam U, Rude RK: Low blood mononuclear cellmagnesium in intensive cardiac care unit patients. Am HeartJ1986;111:475\x=req-\480.
50. Elin RJ, Hosseini JM, Fitzpatrick L, et al: Magnesium status ofpatients with parathyroid disease. Clin Chem 1986;32:1087.
51. Ryzen E, Elbaum N, Singer FR, et al: Parenteral magnesiumtolerance testing in the evaluation of magnesium deficiency. Magnesium1985;4:137-147.
52. Rasmussen HS, Norregard P, Lindeneg O, et al: Intravenous mag-nesium in acute myocardial infarction. Lancet 1986;1:234-236.
53. Morton BC, Nair RC, Smith FM, et al: Magnesium therapy in acutemyocardial infarction: A double-blind study. Magnesium 1984;3:346-352.
54. Ryan MP: Diuretics and potassium/magnesium depletion: Directionsfor treatment. Am J Med 1987;82(suppl 3A):38-47.
55. Rasmussen HS, Svenson M, McNair P, et al: Magnesium infusionreduces the incidence of arrhythmias in acute myocardial infarction: Adouble-blind placebo-controlled study. Clin Cardiol 1987;10:351-356.
56. Hollifield JW: Magnesium depletion, diuretics and arrhythmia. AmJ Med 1987;82(suppl 3A):30-37.
57. Dyckner T, Wester PO: Intracellular magnesium loss after diureticadministration. Drugs 1984;28(suppl 1):161-166.
58. Abraham AS, Rosenmann D, Kramer M, et al: Magnesium in theprevention of lethal arrhythmias in acute myocardial infarction. Arch InternMed 1987;147:753-755.
59. Pennington JAT, Church HN: Bowe's and Church's Food Values ofPortions Commonly Used, ed 14. Philadelphia, JB Lippincott, 1985, pp XV,99-109.
60. Barton CH, Vaziri ND, Martin DC, et al: Hypomagnesemia and renalmagnesium wasting in renal transplant recipients receiving cyclosporine.Am J Med 1983;83:693-699.
Incorrect Data. \p=m-\In the article entitled "Effect of Army Basic Training inSickle-Cell Trait," published in the May 1988 issue of the Archives(1988;148:1140-1144), errors appeared in Tables 2 and 3, page 1142. In Table 2,the values for hemoglobin (Hb) should have read as follows: 152 (15.2) \m=+-\3;146(14.6)\m=+-\2;147 (14.7)\m=+-\3;and 141 (14.1)\m=+-\3+,respectively. Under hematocrit(Hct), the value in the third column should have read 0.45\m=+-\0.008(45.2). Thevalues for MCHC should have read as follows: 336 (33.6)\m=+-\3;330 (33.0)\m=+-\3;326(32.6)\m=+-\2;and 324 (32.4)\m=+-\2,respectively. In Table 3, the last entry undercreatinine should have had a dagger following it and should have read as follows:106(1.2)\m=+-\6+.
Downloaded From: http://archinte.jamanetwork.com/ by a East Carolina University User on 08/08/2015
Copyright © 2022 FDOKUMEN




















