association of patient's characteristics on patient's satisfaction ...

International Journal of Cardiology 182 (2015) 141–147
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Low socioeconomic status of a patient's residential area is associatedwithworse prognosis after acute myocardial infarction in Sweden☆
Göran Bergström c,1, Björn Redfors a,1, Oskar Angerås a, Christian Dworeck a, Yangzhen Shao a,Inger Haraldsson a, Petur Petursson a, Davor Milicic b, Hans Wedel c, Per Albertsson a, Truls Råmunddal a,Annika Rosengren c, Elmir Omerovic a,⁎a Department of Cardiology, Sahlgrenska University Hospital, Gothenburg, Swedenb Department of Cardiology, University Hospital Centre, Zagreb, Croatiac Department of Molecular and Clinical Medicine, Institute of Medicine, Gothenburg University, Gothenburg, Sweden
☆ Socioeconomic status and prognosis post-myocardial⁎ Corresponding author.
E-mail address: [email protected] (E. Omerovic).1 Contributed equally.
http://dx.doi.org/10.1016/j.ijcard.2014.12.0600167-5273/© 2014 Elsevier Ireland Ltd. All rights reserved
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 31 October 2014Accepted 21 December 2014Available online 23 December 2014Keywords:Myocardial infarctionMortalitySocioeconomic statusInequalities in health
Introduction: Previous studies have established a relationshipbetween socioeconomic status (SES) and survival incoronary heart disease. Acute cardiac care in Sweden is considered to be excellent and independent of SES. Westudied the influence of area-level socioeconomic status on mortality after hospitalization for acute myocardialinfarction (AMI) between 1995 and 2013 in the Gothenburg metropolitan area, which has little over 800,000 in-habitants and includes three city hospitals.Methods: Data were obtained from the SWEDEHEART registry (Swedish Websystem for Enhancement ofEvidence-Based Care inHeart Disease EvaluatedAccording to Recommended Therapies) and the Swedish CentralBureau of Statistics for patients hospitalized for ST-elevationmyocardial infarction (STEMI) and non-STEMI in thecity of Gothenburg in Western Sweden. The groups were compared using Cox proportional hazards regression
and logistic regression.Results: 10,895 (36% female) patients were hospitalized due to AMI during the study period. Patients residingin areas with lower SES had higher rates of smoking and diabetes (P b 0.001), and were also at increasedrisk of developing complications, including heart failure and cardiogenic shock (P b 0.05). Living in an areawith lower SES associated with increased risk of dying after an AMI also in models adjusted for risk factors(P b 0.05).Conclusion: Also in a country with strong egalitarian traditions, lower SES associates with worse prognosis afterAMI, an association that persists after adjustments for differences in traditional cardiovascular risk factors.© 2014 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Previous studies have established a relationship between socioeco-nomic status (SES) and incidence of coronary heart disease, and alsothat SES influences prognosis after myocardial infarction [1]. Both indi-vidual and area-level socioeconomic indices influence the risk of devel-oping coronary heart disease [2–4]. The area-level effect has beendescribed both for larger area units, e.g., different economic regionsand counties, and for smaller area units such as different neighborhoodswithin the same city [3,5–7]. Despite some discrepancies between stud-ies, lower individual and/or area-level SES consistently associate withincreased risk of death [3,5,6].
infarction.
.
Lower SES is associated with a higher burden of cardiovascular riskfactors, and may therefore influence prognosis indirectly through aworse risk factor profile [8,9]. However, most studies to date have notconsidered mediating effects of for instance socioeconomic differencesin risk factors [6].
Cardiovascular mortality in Sweden has decreased by 60% over thepast decade and cardiac care in Sweden is considered to be excellent[10]. Sweden is one of the most egalitarian countries in the worldwith an express ambition to provide equal healthcare to its citizens re-gardless of SES [11]. The country has national medical and health carequality registries, which contain individualized data concerning diagno-ses, interventions and outcome. This allows data to be obtained on areaand individual SES for each patient treated at a Swedish hospital, aswellas a traditional risk-factor profile.
So far, no previous study has addressed the impact of SES onmortal-ity after acute myocardial infarction (AMI) in Sweden, while simulta-neously also considering socioeconomic differences in risk factors.Therefore, we studied the influence of area-level SES on mortality

142 G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
after hospitalization for AMI between 1995 and 2013 in the Gothenburgmetropolitan area in western Sweden, with just over 800,000 inhabi-tants and three city hospitals.
2. Methods
Data were obtained from the SWEDEHEART registry (Swedish Websystem for En-hancement of Evidence-Based Care in Heart Disease Evaluated According to Recommend-ed Therapies) and the Swedish Central Bureau of Statistics for patients hospitalized for ST-elevationmyocardial infarction (STEMI) and non-STEMI in the city of Gothenburg inwestSweden. Between 1995 and 2013, 41,825 patients (43% female) were hospitalized in thethree city hospitals. Of these, 10,895 (36% female) were diagnosed with acute myocardialinfarction (AMI) based on guidelines from the European Society of Cardiology/AmericanCollege of Cardiology/American Heart Association [12]. Each postal code area within thecity was ranked according to the average SES of its residents, where SES was calculatedas combined income and education [13]. Patients were subsequently divided into tertilesbased on the SES of the postal code area in which they reside, i.e., into low (n = 4280),middle (n = 3570) and high (n = 3048) SES groups.
2.1. Ethics statement
The study was approved by the ethics committee at Gothenburg University. In accor-dancewith Swedish legislation and due to the fact that datawere anonymizedbefore anal-ysis the regional ethical review board waived the need for written informed consent fromthe participants.
2.2. Endpoint
The primary endpoint of the studywas all-causemortality. Personal unique identifierswere used to link patients with the National Death Registry in Sweden. All patients werefollowed up until March 5 2013. Mean follow-up time was 1720 days. We also studiedthe likelihood of patients receiving the recommended treatment, the risk of sufferingpre-hospital cardiac arrest or arriving at the hospital in cardiogenic shock and the risk ofdeveloping in-hospital heart failure. The patient was considered to have suffered from di-abetes, hypertension, hyperlipidemia, previousmyocardial infarction, previouspercutane-ous coronary intervention (PCI), previous stroke, cardiogenic shock or heart failure if theyhad been discharged with the respective International Classification of Diseases (ICD)codes (including subcategories) [14].
Table 1Patient characteristics and treatment.
Variable SESLown = 4280
SESIntermediaten = 3570
Age mean (SD) 70 ± 13 72 ± 13Female gender n (%) 1613 (38) 1321 (37)BMI mean (±SD) 26.7 (5.1) 26.2 (4.3)Smoker, n (%) 1284 (32) 719 (22)Diabetes n (%) 900 (21) 625 (18)Hypertension n (%) 1771 (42) 1433 (41)Hyperlipidemia n (%) 705 (17) 479 (14)Serum creatinine mean (SD) 97 (60) 97 (52)LV function n (%) 2585 1921
N50% 1420 (55) 1123 (58)40–49% 636 (25) 421 (22)30–39% 328 (13) 228 (12)b30% 201 (8) 149 (8)
Previous myocardial infarction n (%) 760 (18) 546 (16)Previous PCI n (%) 119 (3) 81 (2)Previous cardiac surgery n (%) 188 (4) 164 (5)Previous stroke n (%) 290 (11) 180 (9)Pacemaker n (%) 65 (2) 49 (1)Reperfusion n (%) 1457 (34) 1178 (33)ASA after discharge n (%) 3561 (85) 2927 (85)Other antiplatelet at discharge n (%) 2035 (48) 1537 (44)Beta blocker at discharge n (%) 3489 (83) 2829 (82)ACEI or ARB at discharge n (%) 2354 (56) 1850 (53)Oral anticoagulants at discharge n (%) 323 (8) 267 (8)Statins at discharge n (%) 2686 (64) 2077 (60)I.v. diuretics during hospitalization n (%) 1342 (32) 1005 (28)I.v. inotropes during hospitalization n (%) 254 (6) 216 (6)CPAP during hospitalization n (%) 388 (9) 255 (7)Pre-hospital cardiogenic shock n (%) 213 (5) 197 (6)Pre-hospital cardiac arrest; n (%) 85 (2) 92 (3)ST-elevation; n (%) 1560 (37) 1279 (36)In-hospital heart failure n (%) 1554 (38) 1161 (34)
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; ASA, acetyventricle; SES, socioeconomic status.
2.3. Statistics
Continuous variables are presented as mean ± SD and categorical variables are re-ported as frequencies. Normal distribution of variables was assessed by inspecting the dis-tribution of values on histograms. Differences between the SES tertiles in continuousvariableswere testedwith ANOVA andmodified Student's t test. Differences in categoricalvariables were tested by the chi-square test.
Missing data and observations in the database were imputed using multiple imputa-tion using the chain-equation method [15] with 20 data sets. This was applied to each ofthe variables listed in Table 1, together with an event indicator [16] for subsequent logisticregression models. The imputation procedure and subsequent analyses were performedaccording to Rubin's protocol [17] under the assumption that missing data are missingat random.
The three SES groups were compared using Cox proportional hazards regression, lo-gistic or multiple linear regression. The analyses were performed on patients with com-plete data and using the multiple imputation method. Differences in patientcharacteristics were accounted for by adjusting for covariates or by propensity scores[18]. Multilevel models accounting for calendar year and/or clustering of patients withindifferent hospitals were fitted and compared to single-level models. A Cox proportionalhazards model adjusted for age; gender; smoking habits; hypertension; diabetes; hyper-lipidaemia; previous myocardial infarction; previous cardiac surgery; previous PCI;revascularisation treatment; STEMI and calendar year fitted on imputed data was pre-defined as the primarymodel. These covariates were entered into themodel as a main ef-fect only and were used in all adjusted models, unless otherwise specified.
In addition to the primary analysiswith traditional multivariablemodeling of risk fac-tors, weusedpropensity scores to adjust for differences in patient characteristics aswell asmedical treatment at discharge (Suppl. Table 1) [18]. To generate the propensity scores foreach patient, multinomial logistic regression was used to calculate the likelihood of livingin an area with a specific SES. The covariates used were the same as inmultivariable logis-tic regression with the addition of BMI; left ventricular function; number of diagnoses;pre-hospital cardiac arrest; pre-hospital cardiogenic shock; in-hospital heart failure;whether the patient was discharged with beta blocker, aspirin, angiotensin enzymeconverting enzyme inhibitor (ACEI)/angiotensin receptor blockers (ARB), antiplatelettherapy, oral anticoagulant, and/or statin; employment status; and pacemaker. The calcu-latedpropensity scorewas entered in theCox regressionmodel as a continuous variable orfactor based on quintiles of propensity scores.
Unadjusted and adjustedmultivariate analyseswere fitted, using both complete casesand imputedmodels, to detect the difference in risk between presenting to the hospital incardiogenic shock and the risk of developing in-hospital heart failure. The same covariates
SESHighn = 3048
Missingn (%)
P-value P-valuepropensity scores
70 ± 13 5 (b1) b0.001 0.946999 (33) 3 (b1) b0.001 0.92326.0 (4.7) 4507 (41) b0.001 0.930581 (20) 779 (7) b0.001 0.966397 (13) 85 (b1) b0.001 0.9151212 (40) 171 (2) 0.339 0.909443 (15) 151 (1) 0.001 0.928100 (61) 4243 (39) 0.256 0.4711800 4592 (42) b0.001 0.9111146 (64) n/a n/a n/a364 (20) n/a n/a n/a182 (10) n/a n/a n/a108 (6) n/a n/a n/a410 (14) 154 (1) b0.001 0.96869 (2) 157 (1) 0.250 0.939124 (4) 128 (1) 0.567 0.988158 (9) 4430 (41) 0.025 0.12340 (1) 63 (b1) 0.747 0.9291085 (36) 67 (b1) 0.090 0.8562596 (87) 242 (2) 0.032 0.9611454 (49) 240 (2) b0.001 0.9852480 (83) 245 (2) 0.283 0.9651625 (54) 246 (2) 0.063 0.988222 (7) 247 (2) 0.881 0.9691895 (63) 247 (2) 0.001 0.583700 (23) 74 (b1) b0.001 0.161147 (5) 76 (b1) 0.056 0.139183 (6) 72 (b1) b0.001 0.297122 (4) 528 (5) 0.015 0.94167 (2) 556 (5) 0.243 0.8611154 (38) 183 (2) 0.260 0.818840 (30) 615 (5) b0.001 0.986
lsalicylic acid; BMI, body-mass-index; CPAP, continuous positive airway pressure; LV, left

143G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
used in the other adjusted Cox models were included. However, revascularization treat-ment was excluded from the models predicting risk of pre-hospital cardiac arrest or riskof presenting with cardiogenic shock. Multivariate adjusted models fitted on imputeddata were considered the primary analysis for predicting the risk of presenting with car-diogenic shock or risk of developing in-hospital heart failure.
A multivariate logistic regression model containing the same covariates as the multi-variate Cox regression was fitted on imputed data to detect differences between SESgroups in the likelihood of receiving reperfusion treatment and prescriptions for recom-mended long-term medications at discharge.
Subgroup analyses were performed, by inclusion of interaction terms in Cox propor-tional hazards models, to detect associations between area-level SES and calendar year;gender; age; or presence of ST-elevation, respectively.
Time from symptom onset to PCI was analyzed by unadjusted and adjusted ordinaryleast squares (OLS) regression with complete case and imputed models. Patients diag-nosed with AMI prior to 2005 were excluded from this analysis since the time-between-symptom-onset-to-reperfusion variable was not included in the SWEDEHEART registrybefore this date. Missing values for time-between-symptom-onset-to-reperfusion wereimputed for patients with STEMI. A separate imputation model was used for this analysiswith time-between-symptom-onset-to-reperfusion included as an additional variable.
Goodness-of-fit (calibration) for the models was assessed with Hosmer–Lemeshowtest. Multicollinearity between the variables in the model was assessed by calculation ofthe variance inflation factor. Cox proportional hazardsmodels were tested for proportion-ality of hazards by visual inspection of the log–log plots. Balancing properties of the calcu-lated propensity scores were evaluated using multivariate linear and logistic regressions.All statistical analyseswere performedusing Stata® software (version 13.1, StataSorp, Col-lege Station, Texas, USA). All tests were two-tailed and a P b 0.05 was considered statisti-cally significant. Because ofmultiple analyses P b 0.05was expected to occur accidently in1 out of 20 analyses.
3. Results
3.1. Patient characteristics and treatments
During the study period, 41,825 patients (43% female) were hospi-talized in the three city hospitals. Of these, 10,895 (36% female)were di-agnosed with AMI and lived within the Gothenburg metropolitan area.The three SES tertiles contained 4280 (low), 3570 (middle), and 3048
Fig. 1. Flow chart and geographical distribution of different SES areas within Gothenburg city. Aareas. AMI, acute myocardial infarction; SES, socioeconomic status.
(high) patients, respectively (see Fig. 1). Patients living in areas withlower SES had on average higher BMI, were more likely to smoke andwere more likely to have hyperlipidaemia or diabetes. However, SEShad no impact on the prevalence of hypertension. Baseline characteris-tics of the three groups are presented in Table 1 andwerewell balancedafter adjustment with propensity scores.
3.2. Data analysis and post-estimation diagnostics
Most variables had negligible missing information (b5%), except foremployment status (35%), BMI (41%), smoking status (7%), serumcreat-inine levels (39%), LV function (42%), previous stroke (41%) and pre-hospital cardiac arrest (5%).
Proportionality of hazards was verified by inspection of Schoenfeldresiduals on − ln(− ln(survival)) plots for each Cox proportional haz-ards model. Post-estimation analysis for the logistic regression models,including propensity scores estimation, by Hosmer–Lemeshow testshowed adequate goodness of fit for the models (P N 0.05). After intro-duction of propensity scores as a covariate in the regression model, nostatistical differences in baseline characteristics between the groupswere found (Table 1). Average variance inflation factor was below4.58 for the adjusted models and 4.47 for the propensity scores models,demonstrating that there was no significant multicollinearity betweenthe variables in the models. Multi-level modeling that attempted to ac-count for potential clustering of patients between different calendaryears or between different hospitals did not improve the predictivepower of the models and was therefore abandoned.
3.3. Primary endpoint
Our pre-specified primary analysis, i.e., an adjusted Cox proportionalhazards regression model on imputed data, revealed a significant effect
. Patient selection and number of patients. B. Geographical distribution of the different SES
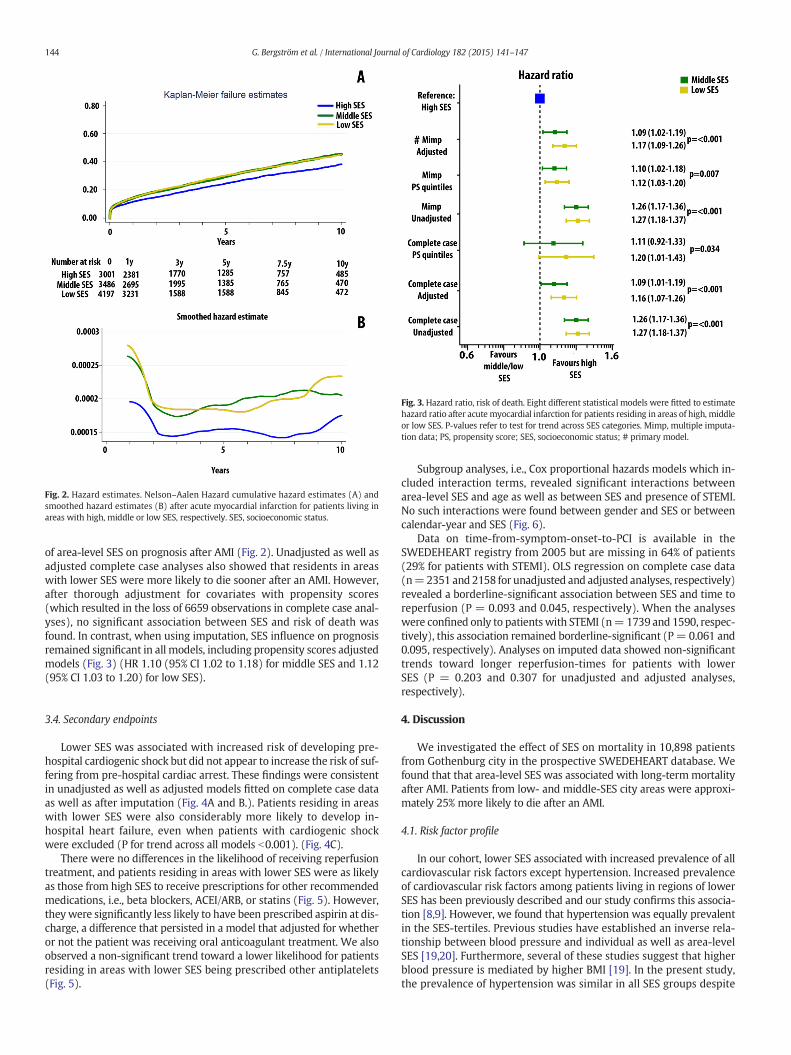
Fig. 2. Hazard estimates. Nelson–Aalen Hazard cumulative hazard estimates (A) andsmoothed hazard estimates (B) after acute myocardial infarction for patients living inareas with high, middle or low SES, respectively. SES, socioeconomic status.
Fig. 3. Hazard ratio, risk of death. Eight different statistical models were fitted to estimatehazard ratio after acute myocardial infarction for patients residing in areas of high, middleor low SES. P-values refer to test for trend across SES categories. Mimp, multiple imputa-tion data; PS, propensity score; SES, socioeconomic status; # primary model.
144 G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
of area-level SES on prognosis after AMI (Fig. 2). Unadjusted as well asadjusted complete case analyses also showed that residents in areaswith lower SES were more likely to die sooner after an AMI. However,after thorough adjustment for covariates with propensity scores(which resulted in the loss of 6659 observations in complete case anal-yses), no significant association between SES and risk of death wasfound. In contrast, when using imputation, SES influence on prognosisremained significant in all models, including propensity scores adjustedmodels (Fig. 3) (HR 1.10 (95% CI 1.02 to 1.18) for middle SES and 1.12(95% CI 1.03 to 1.20) for low SES).
3.4. Secondary endpoints
Lower SES was associated with increased risk of developing pre-hospital cardiogenic shock but did not appear to increase the risk of suf-fering from pre-hospital cardiac arrest. These findings were consistentin unadjusted as well as adjusted models fitted on complete case dataas well as after imputation (Fig. 4A and B.). Patients residing in areaswith lower SES were also considerably more likely to develop in-hospital heart failure, even when patients with cardiogenic shockwere excluded (P for trend across all models b0.001). (Fig. 4C).
There were no differences in the likelihood of receiving reperfusiontreatment, and patients residing in areas with lower SES were as likelyas those from high SES to receive prescriptions for other recommendedmedications, i.e., beta blockers, ACEI/ARB, or statins (Fig. 5). However,theywere significantly less likely to have been prescribed aspirin at dis-charge, a difference that persisted in a model that adjusted for whetheror not the patient was receiving oral anticoagulant treatment. We alsoobserved a non-significant trend toward a lower likelihood for patientsresiding in areas with lower SES being prescribed other antiplatelets(Fig. 5).
Subgroup analyses, i.e., Cox proportional hazards models which in-cluded interaction terms, revealed significant interactions betweenarea-level SES and age as well as between SES and presence of STEMI.No such interactions were found between gender and SES or betweencalendar-year and SES (Fig. 6).
Data on time-from-symptom-onset-to-PCI is available in theSWEDEHEART registry from 2005 but are missing in 64% of patients(29% for patients with STEMI). OLS regression on complete case data(n=2351 and 2158 for unadjusted and adjusted analyses, respectively)revealed a borderline-significant association between SES and time toreperfusion (P = 0.093 and 0.045, respectively). When the analyseswere confined only to patientswith STEMI (n=1739 and 1590, respec-tively), this association remained borderline-significant (P= 0.061 and0.095, respectively). Analyses on imputed data showed non-significanttrends toward longer reperfusion-times for patients with lowerSES (P = 0.203 and 0.307 for unadjusted and adjusted analyses,respectively).
4. Discussion
We investigated the effect of SES on mortality in 10,898 patientsfrom Gothenburg city in the prospective SWEDEHEART database. Wefound that that area-level SES was associated with long-termmortalityafter AMI. Patients from low- and middle-SES city areas were approxi-mately 25% more likely to die after an AMI.
4.1. Risk factor profile
In our cohort, lower SES associated with increased prevalence of allcardiovascular risk factors except hypertension. Increased prevalenceof cardiovascular risk factors among patients living in regions of lowerSES has been previously described and our study confirms this associa-tion [8,9]. However, we found that hypertension was equally prevalentin the SES-tertiles. Previous studies have established an inverse rela-tionship between blood pressure and individual as well as area-levelSES [19,20]. Furthermore, several of these studies suggest that higherblood pressure is mediated by higher BMI [19]. In the present study,the prevalence of hypertension was similar in all SES groups despite
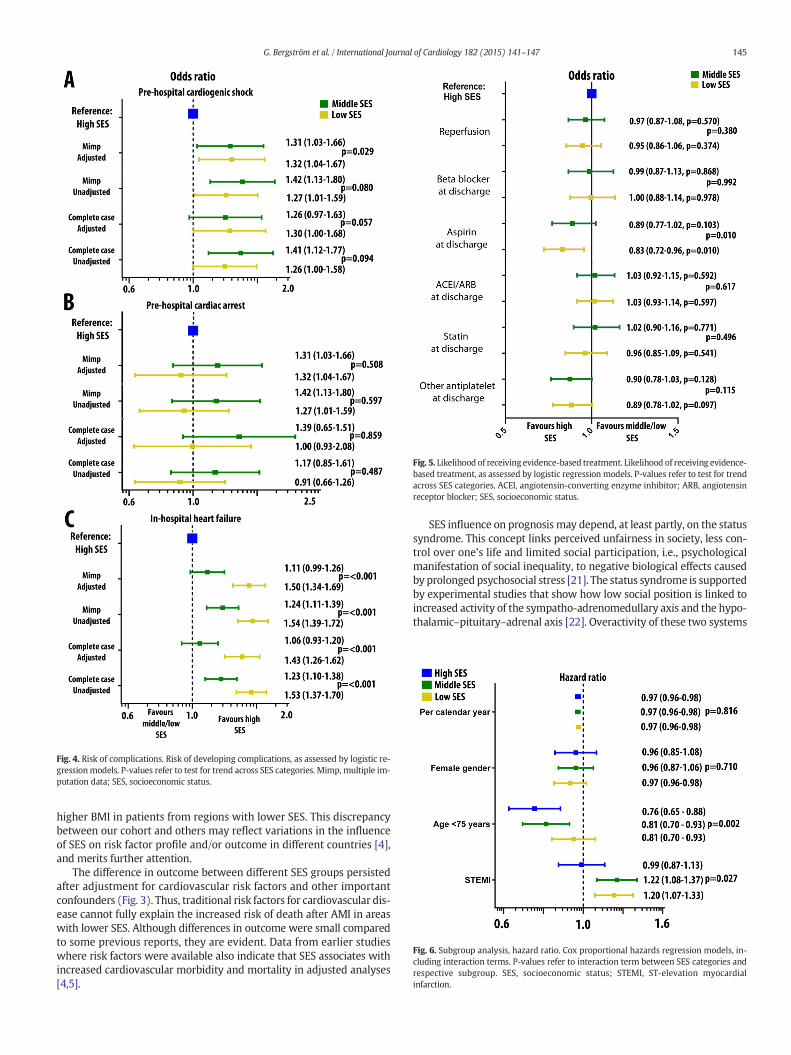
Fig. 4. Risk of complications. Risk of developing complications, as assessed by logistic re-gressionmodels. P-values refer to test for trend across SES categories. Mimp, multiple im-putation data; SES, socioeconomic status.
Fig. 5. Likelihood of receiving evidence-based treatment. Likelihood of receiving evidence-based treatment, as assessed by logistic regression models. P-values refer to test for trendacross SES categories. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensinreceptor blocker; SES, socioeconomic status.
Fig. 6. Subgroup analysis, hazard ratio. Cox proportional hazards regression models, in-cluding interaction terms. P-values refer to interaction term between SES categories andrespective subgroup. SES, socioeconomic status; STEMI, ST-elevation myocardialinfarction.
145G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
higher BMI in patients from regions with lower SES. This discrepancybetween our cohort and others may reflect variations in the influenceof SES on risk factor profile and/or outcome in different countries [4],and merits further attention.
The difference in outcome between different SES groups persistedafter adjustment for cardiovascular risk factors and other importantconfounders (Fig. 3). Thus, traditional risk factors for cardiovascular dis-ease cannot fully explain the increased risk of death after AMI in areaswith lower SES. Although differences in outcome were small comparedto some previous reports, they are evident. Data from earlier studieswhere risk factors were available also indicate that SES associates withincreased cardiovascular morbidity and mortality in adjusted analyses[4,5].
SES influence on prognosis may depend, at least partly, on the statussyndrome. This concept links perceived unfairness in society, less con-trol over one's life and limited social participation, i.e., psychologicalmanifestation of social inequality, to negative biological effects causedby prolonged psychosocial stress [21]. The status syndrome is supportedby experimental studies that show how low social position is linked toincreased activity of the sympatho-adrenomedullary axis and the hypo-thalamic–pituitary–adrenal axis [22]. Overactivity of these two systems

146 G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
after AMI could be expected to increase the risk for newmyocardial in-farction, sudden death and/or heart failure [22].
4.2. Adherence to recommended therapies
SES did not influence whether the patients received revasculariza-tion treatment or were prescribed other recommended medical thera-pies at discharge, i.e., a beta blocker, ACEI, ARB, or statin. However,residents in areas with lower SES were less likely to receive prescrip-tions for aspirin at discharge (Fig. 4). We also observed a trend towarda lower likelihood of these patients receiving prescriptions for other an-tiplatelet drugs. This is of concern given that several large clinical trialshave shown that antiplatelet treatment significantly improves progno-sis after AMI [23]. Compliance to prescribed medications is a well-known problem [24,25], and previous studies have reported an associa-tion between SES and adherence to prescribed therapies in patientswith cardiovascular disease [26]. In this study we were unable to ad-dress patient compliance.
4.3. Time-to-reperfusion, post-infarct heart failure and cardiogenic shock
Living in an areawith lower SES increased the risk of developing car-diogenic shock before reaching the hospital. Furthermore, when pa-tients who had developed pre-hospital cardiogenic shock wereexcluded from the analysis, lower SES still associated with increasedrisk of in-hospital heart failure. The incidence of cardiogenic shock andheart failure after AMI has declined over the past decades, attributedprimarily to timely reperfusion [27]. Time-to-reperfusion is considereda major determinant of outcome after AMI and large resources arebeing devoted to ensure effective transfer of patients with AMI, particu-larly STEMI, for emergent angiography and PCI [28]. An association be-tween SES and increased risk of cardiogenic shock and heart failurecould potentially reflect delayed reperfusion in these patients. However,incidence of cardiac arrest, another important complication of AMIwhich has a weaker relationship with time-to-reperfusion, did not ap-pear to differ across SES tertiles. The complete case analysis of time-from-symptom-onset-to-PCI revealed a trend toward increasing timeto reperfusion in patients residing in areas with lower SES. Hence, de-lays in reperfusion for patients residing in areas with lower SES are aplausible explanation for the association between SES and cardiogenicshock. Future studies should address whether lower SES systemicallyassociates with delays in reperfusion and, if that is the case, whichpatient-, society- and/or healthcare-related factors explain such delays.
4.4. Focus on subgroups
In our study, SES had particularly strong influence on prognosis bothin younger patients and in patientswhopresentedwith STEMI. Our dataindicate that particular efforts need to be directed toward these sub-groups. STEMI is a diagnosis for which standardized treatment recom-mendations and a particularly well-defined chain of care exist. Thefinding that SES has a stronger influence on prognosis in patients withSTEMI compared with patients with non-STEMI suggests that thischain of care may be less efficient for patients residing in areaswith lower SES. This observation fits well with delays in time-to-reperfusion and the higher incidence of cardiogenic shock and post-infarct heart failure for these patients. These are complications thatcould be expected if timely reperfusion in STEMI is delayed. We foundno interaction between the influence of SES and calendar year, i.e., notrend toward decreasing SES-related differences in cardiovascularhealth over the past decade. These findings were consistent when weconfined the analysis to patients with STEMI or to patients b75 yearsold.
4.5. International perspective
Sweden is considered to be one of the most egalitarian countries inthe world [11]. Despite well-developed social support for all citizensand a low poverty rate, prognosis after AMI is directly influenced bythe SES of the area in which a patient resides. Thus, for patients withAMI, equity in health is not achieved by the Swedish health-care system[29]. Furthermore, the situation does not appear to have improved overthe past decade. Data obtained during the last part of the twentieth cen-tury indicated that Sweden and other Nordic countries, despite havinglong histories of egalitarian politics and low poverty rates, sufferedfrom larger inequalities in cardiovascularmortality comparedwith cen-tral European countries [30]. Almost twenty years later, these health in-equalities persist. It is possible that status syndrome ismore detrimentalin more egalitarian societies than in less egalitarian societies.
Although additional studies are needed to establish which factorsmediate the negative influence of area-level SES on prognosis afterAMI, the findings in our study indicate that reducing socioeconomic dis-parities should be an important goal for national health care policy inorder to improve prognosis after AMI in the future. Other importantmeasures should be: (1) targeting cardiovascular risk factors in patientswith low SES, (2) minimizing post-AMI complications, e.g., by ade-quately educating residents in areas with lower SES about symptomsand signsof AMI andprovidingefficient access to cardiac care, (3) ensur-ing that physicians prescribe evidence-based recommended treatmentto all patients, and (4) improvement of patient's compliance to the pre-scribe evidence-based treatment.
4.6. Limitations
There are several limitations that need to be addressed. First, this isan observational retrospective study and as such it provides only asso-ciative evidence, not causative and we cannot exclude selection biasand residual confounding. However, the observational nature of ourstudy provides real-world data on a large cohort of patients. Second,we do not have data on cause-specific mortality. Third, a proportion ofpatients hadmissing data for at least some variable, and this was partic-ularly high for the variable time-from-symptom-onset-to-PCI. Exclusionof patients from the analysis who had missing data might have pro-duced biased results. However, results from the multiple imputationmodel were congruent with the data from the complete case analysis.Fourth, data on individual SES were not available. The relationship be-tween individual- and area-level SES and prognosis after AMI couldtherefore not be studied. Lastly, we performedmany analyses using sev-eral different statistical models. Therefore, we cannot exclude the possi-bility that some of the discovered associations occurred by chance.
5. Conclusion
This report shows that even in a country with strong egalitarian tra-ditions, lower SES associates with worse prognosis after AMI, and thishas not improved over thepast decade. The association persists after ad-justments for differences in traditional cardiovascular risk factors andfor differences in received treatment.
Funding
This work was supported by AFA Insurance [AFA 110115]; SwedishHeart and Lung Foundation [HLF 20120670]; Swedish Scientific Re-search Council [VR 2008-2487]; ALF Västra Götaland; and Universityof Gothenburg, Sweden [ALFGBG 141131].
Conflict of interest
The authors report no relationships that could be construed as a con-flict of interest.
147G. Bergström et al. / International Journal of Cardiology 182 (2015) 141–147
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ijcard.2014.12.060.
References
[1] J.Y.Wang, C.Y.Wang, S.Y. Juang, K.Y. Huang, P. Chou, C.W. Chen, et al., Low socioeco-nomic status increases short-term mortality of acute myocardial infarction despiteuniversal health coverage, Int. J. Cardiol. 172 (2014) 82–87.
[2] V. Salomaa, M. Niemela, H. Miettinen, M. Ketonen, P. Immonen-Raiha, S. Koskinen,et al., Relationship of socioeconomic status to the incidence and prehospital, 28-day, and 1-year mortality rates of acute coronary events in the FINMONICA myocar-dial infarction register study, Circulation 101 (2000) 1913–1918.
[3] S.Wing, M. Casper, W. Riggan, C. Hayes, H.A. Tyroler, Socioenvironmental character-istics associated with the onset of decline of ischemic heart disease mortality in theUnited States, Am. J. Public Health 78 (1988) 923–926.
[4] A. Rosengren, S.V. Subramanian, S. Islam, C.K. Chow, A. Avezum, K. Kazmi, et al., Ed-ucation and risk for acute myocardial infarction in 52 high, middle and low-incomecountries: INTERHEART case–control study, Heart 95 (2009) 2014–2022.
[5] A.V. Diez Roux, S.S. Merkin, D. Arnett, L. Chambless, M. Massing, F.J. Nieto, et al.,Neighborhood of residence and incidence of coronary heart disease, N. Engl. J.Med. 345 (2001) 99–106.
[6] K. Sundquist, M. Winkleby, H. Ahlen, S.E. Johansson, Neighborhood socioeconomicenvironment and incidence of coronary heart disease: a follow-up study of 25,319women and men in Sweden, Am. J. Epidemiol. 159 (2004) 655–662.
[7] M. Rosvall, S. Gerward, G. Engstrom, B. Hedblad, Income and short-term case fatalityafter myocardial infarction in thewholemiddle-aged population ofMalmo, Sweden,Eur. J. Pub. Health 18 (2008) 533–538.
[8] A.V. Diez-Roux, F.J. Nieto, C. Muntaner, H.A. Tyroler, G.W. Comstock, E. Shahar, et al.,Neighborhood environments and coronary heart disease: a multilevel analysis, Am.J. Epidemiol. 146 (1997) 48–63.
[9] G.D. Smith, C. Hart, G. Watt, D. Hole, V. Hawthorne, Individual social class, area-based deprivation, cardiovascular disease risk factors, and mortality: the Renfrewand Paisley study, J. Epidemiol. Community Health 52 (1998) 399–405.
[10] S.C. Chung, R. Gedeborg, O. Nicholas, S. James, A. Jeppsson, C. Wolfe, et al., Acutemyocardial infarction: a comparison of short-term survival in national outcome reg-istries in Sweden and the UK, Lancet 383 (2014) 1305–1312.
[11] M. Jantti, L. Nordberg, The Gini coefficient and international comparisons, Ekon.Samfundets Tidskr. 60 (2007) (123-+).
[12] K. Thygesen, J.S. Alpert, H.D. White, Universal definition of myocardial infarction,Eur. Heart J. 28 (2007) 2525–2538.
[13] J. Cundiff, B. Uchino, T. Smith,W. Birmingham, Socioeconomic status and health: ed-ucation and income are independent and joint predictors of ambulatory blood pres-sure, J. Behav. Med. 1–8 (2013).
[14] O. Frobert, B. Lagerqvist, G.K. Olivecrona, E. Omerovic, T. Gudnason, M. Maeng, et al.,Thrombus aspiration during ST-segment elevation myocardial infarction, N. Engl. J.Med. 369 (2013) 1587–1597.
[15] S. van Buuren, Multiple imputation of discrete and continuous data by fully condi-tional specification, Stat. Methods Med. Res. 16 (2007) 219–242.
[16] I.R. White, P. Royston, Imputing missing covariate values for the Cox model, Stat.Med. 28 (2009) 1982–1998.
[17] D.B. Rubin, Inference and missing data, Biometrika 63 (1976) 581–590.[18] P.R. Rosenbaum, D.B. Rubin, The central role of the propensity score in observational
studies for causal effects, Biometrika 70 (1983) 41–55.[19] B. Chaix, K. Bean, C. Leal, F. Thomas, S. Havard, D. Evans, et al., Individual/neighbor-
hood social factors and blood pressure in the RECORD Cohort Study: which risk fac-tors explain the associations? Hypertension 55 (2010) (769-U97).
[20] I. Grotto, M. Huerta, Y. Sharabi, Hypertension and socioeconomic status, Curr. Opin.Cardiol. 23 (2008) 335–339.
[21] M.G. Marmot, Status syndrome — a challenge to medicine, JAMA 295 (2006)1304–1307.
[22] E. Brunner, Stress and the biology of inequality, BMJ (Clin. Res. Ed.) 314 (1997)1472–1476.
[23] F.G. Kushner, M. Hand, S.C. Smith Jr., S.B. King III, J.L. Anderson, E.M. Antman, et al.,2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients WithST-Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 FocusedUpdate) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention(updating the 2005 Guideline and 2007 Focused Update): a report of theAmerican College of Cardiology Foundation/American Heart Association TaskForce on Practice Guidelines, Circulation 120 (2009) 2271–2306.
[24] L. Tang, C. Patao, J. Chuang, N.D. Wong, Cardiovascular risk factor control and adher-ence to recommended lifestyle and medical therapies in persons with coronaryheart disease (from the National Health and Nutrition Examination Survey 2007–2010), Am. J. Cardiol. 112 (2013) 1126–1132.
[25] S. Yusuf, S. Islam, C.K. Chow, S. Rangarajan, G. Dagenais, R. Diaz, et al., Use of second-ary prevention drugs for cardiovascular disease in the community in high-income,middle-income, and low-income countries (the PURE Study): a prospective epide-miological survey, Lancet 378 (2011) 1231–1243.
[26] S.P. Kulkarni, K.P. Alexander, B. Lytle, G. Heiss, E.D. Peterson, Long-term adherencewith cardiovascular drug regimens, Am. Heart J. 151 (2006) 185–191.
[27] J.P. Hellermann, T.Y. Goraya, S.J. Jacobsen, S.A. Weston, G.S. Reeder, B.J. Gersh, et al.,Incidence of heart failure after myocardial infarction: is it changing over time? Am. J.Epidemiol. 157 (2003) 1101–1107.
[28] K.A. Reimer, J.E. Lowe, M.M. Rasmussen, R.B. Jennings, The wavefront phenomenonof ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion indogs, Circulation 56 (1977) 786–794.
[29] P. Braveman, S. Gruskin, Defining equity in health, J. Epidemiol. Community Health57 (2003) 254–258.
[30] J.P. Mackenbach, I. Stirbu, A.J. Roskam, M.M. Schaap, G. Menvielle, M. Leinsalu, et al.,Socioeconomic inequalities in health in 22 European countries, N. Engl. J. Med. 358(2008) 2468–2481.
Copyright © 2022 FDOKUMEN