
Punding in Parkinson's disease: The impact of patient's awareness on diagnosis
22
Letters to the Editor Related to New Topics Hiccups Associated with Non-Ergoline Dopamine Agonists in Parkinson’s Disease Hiccups can be an uncommon side effect of anti-parkinso- nian therapy, recently reported in the literature. In these reports, dopamine agonists (DAs) (pramipexole, piribedil, and pergolide) 1,2 seem to play a causative role as hiccups began increasing the dose and subsided when the drug was stopped. In the first case, 2 hiccups started with pramipexole 3 mg per day and ended after drug discontinuation; another patient had hiccups after piribedil 100 mg per day 2 which stopped after tapering the dose to 50 mg per day, whereas in another case pergolide was associated with hiccups at high and not at low doses. 3 Very recently also levodopa (L-dopa) intake 500 mg per day lead to severe hiccups in an old patient with de novo parkinsonism 1 and some cases were also described in the past in a French vigilance survey 4 after L-dopa therapy. Here we report a case of prominent hiccups after a first low-DAs dose intake. This 62-year-old man with a history of arterial hypertension developed a mild progressive tremor of the right arm and some months later a sense of heaviness of the right lower limb. One year later, resting tremor, brady- kinesia with rigidity, a stooped posture, and hypomimia became evident. Brain MRI scan was normal whereas DaTS- can Spect showed a mild left basal ganglia deficit. He was given a diagnosis of Parkinson’s disease (PD), Hoehn-Yahr stage I, and received as initial therapy pramipexole 0.18 mg tid. After few days he developed hiccups, which kept increas- ing in the next days with mild nausea that persisted almost 10 days even after discontinuation. He was then switched to ropinirole slow release 2 mg od but again hiccups developed immediately and the drug was stopped once again, while hiccups lasted 1 week. No symptomatic therapy was success- ful in treating these intractable hiccups. Finally, rasagiline 1 mg od was started and a few days later (L-dopa) 100 mg (levodopa-carbidopa) tid was added with no side effects seen. On therapy, both tremor and bradykinesia improved signifi- cantly and disappeared completely at next follow-up after 3 and 6 months and also stooped posture fully responded to (L-dopa) treatment. At 9 months follow-up he is still hiccups- free. In this case, a strict relationship between hiccups and DAs intake seems likely as hiccups disappeared after drugs were stopped. Hiccups are a common phenomenon but its physio- pathology still remains unclear. 5 Very probably a dopaminer- gic pathway could be involved even if both dopaminergic agonist (pramipexole) 6 and antagonist (neuroleptics) drugs are reported to be useful in its treatment or in having a caus- ative role. 7 A proposed hypothesis is that D3 dopamine receptors with an effective and prolonged stimulation by DAs can be involved in generating this symptom. 2,8 Another option could be via serotonergic pathways with a 5-HT1a or 5-HT1d receptors stimulation, as both ropinirole and prami- pexole share a mild agonist effect on these receptors 9 and this patient also had a mild nausea or finally, a combined effect of both the DAs and 5HT pathways in prone patients. To our knowledge, this case is the first report of both noner- goline oral DAs and ropinirole-induced intractable hiccups, indicating that in some parkinsonian patients this side effect seems to be related to the whole dopaminergic agents class and not merely to a given single DAs. In our patient, inter- estingly hiccups occurred in an early stage of PD and at the very beginning of the treatment even with a very low dose of two different DAs and were long-lasting after DA with- drawal, as if this patient had a sort of supersensitivity to this kind of medications. Financial Disclosure: nothing to disclose. Author’s Roles: Mario Coletti Moja wrote the paper and there was no other person involved. Mario Coletti Moja, MD* Department of Neurology University of Turin Turin, Italy *E-mail: [email protected] References 1. Sharma P, Morgan JC, Sethi KD. Hiccups associated with dopa- mine agonists in Parkinson’s disease. Neurology 2006;66:774. 2. Lester J, Raina GB, Uribe-Roca C, Micheli F. Hiccup secondary to dopamine agonists in Parkinson’s Disease. Mov Disord 2007; 22:1667–1668. 3. Gerschlager W, Bloem BR. Hiccups associated with L-dopa in Parkinson’s disease. Mov Disord 2009;24:621–622. 4. Bagheri H, Cismondo S, Montastruc JL. Drug-induced hiccup: a review of the France pharmacologic vigilance database. Therapie 1999;54:35–39. 5. Kahrilas PJ, Shi G. Why do we hiccup? Gut 1997;41:712–713. 6. Martinez-Ruiz M, Fernandez RFA, Quesada RR. Pramipexole for intractable hiccups. Med Clin 2004;123:679. 7. Miyaoka H, Kamijima K. Perphenazine-induced hiccups. Pharma- copsychiatry 1999;32:81. 8. Perachon S, Schwartz JC, Sokoloff P. Functional potencies of new antiparkinsonian drugs at recombinant human dopamine D1, D2 and D3 receptors. Eur J Pharmacol 1999;366:293–300. 9. Fox SH, Chuang R, Brotchie JM. Serotonin and Parkinson’s dis- ease: on movement, mood and madness. Mov Disord 2009;24: 1255 1266. Potential conflict of interest: Nothing to report. Published online 22 March 2010 in Wiley InterScience (www. interscience.wiley.com). DOI: 10.1002/mds.23056 1292 Movement Disorders Vol. 25, No. 9, 2010, pp. 1292–1313 Ó 2010 Movement Disorder Society
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Punding in Parkinson's disease: The impact of patient's awareness on diagnosis

Letters to the Editor Related to New Topics
Hiccups Associated with Non-Ergoline
Dopamine Agonists in Parkinson’s Disease
Hiccups can be an uncommon side effect of anti-parkinso-nian therapy, recently reported in the literature. In thesereports, dopamine agonists (DAs) (pramipexole, piribedil,and pergolide)1,2 seem to play a causative role as hiccupsbegan increasing the dose and subsided when the drug wasstopped. In the first case,2 hiccups started with pramipexole 3mg per day and ended after drug discontinuation; anotherpatient had hiccups after piribedil 100 mg per day2 whichstopped after tapering the dose to 50 mg per day, whereas inanother case pergolide was associated with hiccups at highand not at low doses.3 Very recently also levodopa (L-dopa)intake 500 mg per day lead to severe hiccups in an oldpatient with de novo parkinsonism 1 and some cases werealso described in the past in a French vigilance survey4 afterL-dopa therapy.
Here we report a case of prominent hiccups after a firstlow-DAs dose intake. This 62-year-old man with a history ofarterial hypertension developed a mild progressive tremorof the right arm and some months later a sense of heavinessof the right lower limb. One year later, resting tremor, brady-kinesia with rigidity, a stooped posture, and hypomimiabecame evident. Brain MRI scan was normal whereas DaTS-can Spect showed a mild left basal ganglia deficit. He wasgiven a diagnosis of Parkinson’s disease (PD), Hoehn-Yahrstage I, and received as initial therapy pramipexole 0.18 mgtid. After few days he developed hiccups, which kept increas-ing in the next days with mild nausea that persisted almost10 days even after discontinuation. He was then switched toropinirole slow release 2 mg od but again hiccups developedimmediately and the drug was stopped once again, whilehiccups lasted 1 week. No symptomatic therapy was success-ful in treating these intractable hiccups. Finally, rasagiline1 mg od was started and a few days later (L-dopa) 100 mg(levodopa-carbidopa) tid was added with no side effects seen.On therapy, both tremor and bradykinesia improved signifi-cantly and disappeared completely at next follow-up after3 and 6 months and also stooped posture fully responded to(L-dopa) treatment. At 9 months follow-up he is still hiccups-free.
In this case, a strict relationship between hiccups and DAsintake seems likely as hiccups disappeared after drugs werestopped. Hiccups are a common phenomenon but its physio-pathology still remains unclear.5 Very probably a dopaminer-gic pathway could be involved even if both dopaminergicagonist (pramipexole)6 and antagonist (neuroleptics) drugs
are reported to be useful in its treatment or in having a caus-ative role.7 A proposed hypothesis is that D3 dopaminereceptors with an effective and prolonged stimulation by DAscan be involved in generating this symptom.2,8 Anotheroption could be via serotonergic pathways with a 5-HT1a or5-HT1d receptors stimulation, as both ropinirole and prami-pexole share a mild agonist effect on these receptors9 andthis patient also had a mild nausea or finally, a combinedeffect of both the DAs and 5HT pathways in prone patients.To our knowledge, this case is the first report of both noner-goline oral DAs and ropinirole-induced intractable hiccups,indicating that in some parkinsonian patients this side effectseems to be related to the whole dopaminergic agents classand not merely to a given single DAs. In our patient, inter-estingly hiccups occurred in an early stage of PD and at thevery beginning of the treatment even with a very low dose oftwo different DAs and were long-lasting after DA with-drawal, as if this patient had a sort of supersensitivity to thiskind of medications.
Financial Disclosure: nothing to disclose.
Author’s Roles: Mario Coletti Moja wrote the paper andthere was no other person involved.
Mario Coletti Moja, MD*Department of Neurology
University of TurinTurin, Italy
*E-mail: [email protected]
References
1. Sharma P, Morgan JC, Sethi KD. Hiccups associated with dopa-mine agonists in Parkinson’s disease. Neurology 2006;66:774.
2. Lester J, Raina GB, Uribe-Roca C, Micheli F. Hiccup secondaryto dopamine agonists in Parkinson’s Disease. Mov Disord 2007;22:1667–1668.
3. Gerschlager W, Bloem BR. Hiccups associated with L-dopa inParkinson’s disease. Mov Disord 2009;24:621–622.
4. Bagheri H, Cismondo S, Montastruc JL. Drug-induced hiccup: areview of the France pharmacologic vigilance database. Therapie1999;54:35–39.
5. Kahrilas PJ, Shi G. Why do we hiccup? Gut 1997;41:712–713.6. Martinez-Ruiz M, Fernandez RFA, Quesada RR. Pramipexole for
intractable hiccups. Med Clin 2004;123:679.7. Miyaoka H, Kamijima K. Perphenazine-induced hiccups. Pharma-
copsychiatry 1999;32:81.8. Perachon S, Schwartz JC, Sokoloff P. Functional potencies of new
antiparkinsonian drugs at recombinant human dopamine D1, D2and D3 receptors. Eur J Pharmacol 1999;366:293–300.
9. Fox SH, Chuang R, Brotchie JM. Serotonin and Parkinson’s dis-ease: on movement, mood and madness. Mov Disord 2009;24:1255�1266.
Potential conflict of interest: Nothing to report.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23056
1292
Movement DisordersVol. 25, No. 9, 2010, pp. 1292–1313� 2010 Movement Disorder Society

Camptocormia Associated with an Expanded
Allele in the TATA Box-Binding Protein Gene
Video
Camptocormia may be associated with a variety of etiolo-gies, and movement disorders and neuromuscular diseasesare the most important from the neurological perspective.Camptocormia is most commonly found in association withidiopathic Parkinson’s disease or as a variant of idiopathicaxial dystonia. However, associations with other parkinsoniandisorders like Parkin-Parkinsonism (PARK2), atypical formssuch as multiple system atrophy and symptomatic Parkinson-ism such as postencephalitic Parkinsonism has been reported.Another miscellaneous group of associated conditions com-prises spine deformities, aging, strokes, hyperthyroidism,psychogenic causes, and conditions associated with certainneoplasias (Table 1).1,2 To our knowledge, camptocormia hasnot been associated with expansions in the TATA-bindingprotein (TBP) gene (OMIM *600075), causing spinocerebel-lar ataxia 17 (SCA17). We describe a patient with campto-cormia harboring an expanded TBP allele.
A 49-year-old male with an athletic lifestyle, complainingof progressive forward curvature of the upper body affectinghis gait, was referred to us for a second opinion. Onset hadoccurred 4 years previously, when he was training for a half-marathon, a distance he had run many times before. Accord-ing to the patient, the initial symptoms were pain in the rightthigh, and subsequent forward flexion in his trunk posture.The curvature gradually worsened, and abdominal musclespasms appeared, as did paresthesias in the upper limbs. Inthe past 2 years, he had also referred dysphagia and difficultyin miction control.
The most relevant findings in neurological examinationwere an abnormal forward-flexed posture when standing andwalking, which was more pronounced in the thoracic ratherthan the lumbar segments, and became more apparent in thelumbar spine after prolonged exertion and disappeared whenthe patient lay down (see Supporting Information Video).Other features included abolition of the gag reflex, gaze-evoked nystagmus, involuntary abdominal muscle move-ments, hyperactive tendon reflexes (except the Achillesreflex), and spasticity affecting the trunk (Grade 3, Ashworthscale) and left limbs (11). Muscle strength was normal, andother signs of cerebellar ataxia such as dysmetria, dysdiado-chokinesia, intention tremor, and dysarthria were absent.Chorea was not observed. No Babinski’s sign was present. Inthe retropulsion pull test, the patient would have fallen if notcaught. The ICARS score was 5/100. MMSE was 30/30, butneuropsychological evaluation revealed a mild cognitive dys-function manifesting as reduced visuospatial ability, impairedworking memory, and attention deficit.
Laboratory tests were normal, and included screening foracanthocytes, erythrocyte sedimentation rate, thyroid, PTH,CK, copper, ceruloplasmine, ANA, VDRL, anti-GAD65 andcalcium channel antibodies, HIV I/II and CSF analysis. Twoconsecutive EMG examinations (including anterior abdominalwall and paravertebral muscles) revealed no muscle abnor-mality or signs of continuous fiber activity. The electromyo-graphic activity of these contractions was normal. Somato-sensory and motor evoked potentials showed normal sensoryand motor central conduction times in the upper limbs.Brainstem auditory evoked potentials (BAEPs) showedabnormal delayed III–V and I–V interpeak latencies. Video-EEG and DaTSCAN showed no abnormalities. Brain MRIshowed putaminal rim hyperintensity and marked cerebellumatrophy. Spinal MRI was normal, with no paraspinal muscleatrophy. Molecular genetic screening for SCA17 confirmedthe presence of an expanded allele of 43 CAG repeats. Noclose relatives presented ataxia, dementia, dystonia, or camp-tocormia. Intravenous immunoglobulin, diazepam, trihexy-phenidyl, tizanidine, BTX-A (Dysport) injected in the lowerparaspinal muscles and rectus abdominis and baclofen ther-apy failed to relieve the symptoms.
The clinical spectrum of SCA17, which has only beendescribed in around 100 pedigrees, includes ataxia, dysarth-ria, dysphagia, dementia, personality change, seizures, oculo-motor abnormalities, bradykinesia, cogwheel rigidity,postural reflex disturbance, spasticity, and diverse forms ofdystonia.3–5 Affected individuals usually have more than 42repeats. However, carriers of 43 and 44 CAA/CAG repeatspresent a reduced penetrance, estimated at 50%, makinggenotype–phenotype correlations difficult.6,7 The presence ofcognitive deterioration, BAEPs abnormalities and MRI find-ings suggests that our patient belongs to this group of SCA17patients with small TBP allele expansions. BAEPs abnormal-ities are constant in SCA17, suggesting brainstem involve-ment.8 The short follow-up time for this patient (9 months)meant that it was impossible to establish the natural progres-sion of the disease. However, the patient continues to beclosely monitored. Although camptocormia has not yet beendescribed in SCA17, other hereditary ataxias have. A flexedposture has been described in a small subset of patients withSCA3/MJD.9 Camptocormia in SCA17 could be a form ofdystonia, as neuropathological and neuroimaging (18F-FDG)studies in SCA17 patients have shown basal ganglia lesions,especially in putamen.3,10,11 Furthermore, in our patient, nor-mal EMG findings at rest on two occasions, normal strengthof paravertebral muscles and the absence of paraspinal mus-cle atrophy in the MRI suggest that in our patient, campto-cormia is probably a result of dystonia. In conclusion, TBPgene analysis should be considered in patients with cerebellarabnormalities in clinical examination, especially when seenin conjunction with brainstem dysfunction. To our knowl-edge, this is the first description of camptocormia associatedwith an expanded trinucleotide (CAG) repeat in the encodingTBP gene, and with mild features of SCA17.
Legends to the Video
The patient presents an abnormal posture of the trunkwhile walking, with marked flexion of the thoraco-lumbarspine. Gait speed is slightly reduced and arm swing is lim-
Additional Supporting Information may be found in the onlineversion of this article.
Potential conflicts of interest: none.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23057
Movement Disorders, Vol. 25, No. 9, 2010
1293LETTERS TO THE EDITOR

ited. Attempts to straighten the body lead to oscillations anda tendency to fall forward with spontaneous recovery. Thecamptocormia disappears when the patient assumes a supineposition.
Financial Disclosures: Josep Gamez, Alba Sierra-Marcos,Margarita Gratacos, Laura de Jorge, Nuria Raguer, DulceMoncho-Rodriguez, Carlos Jacas, Juan Conejero, MerceBadia, Carlos Lorenzo-Bosquet, Victor Volpini, and JoanCastell-Conesa: none.
Author Roles: Josep Gamez was involved in conception,organization, and execution of research project; writing ofthe first draft and review and critique of manuscript. Alba Si-erra-Marcos was involved in conception, organization, andexecution of research project; writing of the first draft andreview and critique of manuscript. Margarita Gratacos wasinvolved in execution of research project. Laura de Jorgewas involved in execution of research project. Nuria Raguerwas involved in execution of research project. Dulce Mon-cho-Rodriguez was involved in execution of research project.Carlos Jacas was involved in execution of research project.Juan Conejero was involved in execution of researchproject. Merce Badia was involved in execution of researchproject. Carlos Lorenzo-Bosquet was involved in executionof research project. Victor Volpini was involved in executionof research project. Joan Castell-Conesa was involved inexecution of research project.
Josep Gamez, MD, PhD*Alba Sierra-Marcos, MDNeurology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain*E-mail: [email protected]
Margarita Gratacos, MDNeurophysiology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
TABLE 1. Causes of camptocormia
Movement disordersIdiopathic Parkinson DiseaseMultiple System AtrophyParkin MutationsPostencephalitic parkinsonismAtypical parkinsonismPrimary dystoniaSecondary dystoniaassociated with parkinsonism
Secondary dystonia associatedwith brain or spinal cord lesions
Vilyuisk encephalomyelitisTourette syndromeSCA3/MJDSCA17
Motor neurone disordersALSPLSPMASMABSMA (Kennedy disease)Benign focal amyotrophyof paraspinous muscles
Syringomielia/Arnold-Chiari malformationPPS
Muscle disordersLGMDFSHMDScapuloperoneal muscular dystrophyMyotonic dystrophies (types 1 and 2)OPMDBMD/DMDEDMDAxial myopathy-INEMWelander distal muscular dystrophyCongenital muscular dystrophiesQuadriceps myopathyGlycogenosis type IICongenital myopathies (nemaline, myotubular, etc)Carnitine deficiencyLOMM and other MMHypokaliemic myopathyEndocrine myopathies(Cushing, hypothyroidism,hyperparathyroidism )
Inflammatory myopathies(PM/DM/IBM/Focal myositis)
Peripheral nerve disordersCIDPBrachial neuritis with paraspinaldenervation (Parsonage-Turner syndrome)
Neuromuscular junction disordersAutoimmune Myasthenia GravisCongenital Myasthenic Syndromes (DOK-7)
Spine deformitiesOsteoporosisAnkylosing spondylitisVertebral fracturePott’s diseaseArnold-Chiari malformation
OthersStrokeAgingPsychogenicDrug induced (valproate, etc)
(Continued)
TABLE 1. (Continued)
HyperthyroidismParaneoplasticIdiopathic
Abbreviations: ALS, amyotrophic lateral sclerosis; BMD, Beckermuscular dystrophy; BSMA, bulbospinal muscular atrophy; CIDP,Chronic inflammatory demyelinating polyradiculoneuropathy; DM,dermatopolimyositis; DMD, Duchenne muscular dystrophy; EDMD,Emery-Dreifuss muscular dystrophy; FSHMD, facio-scapulo-humeralmuscular dystrophy; IBM, inclusion body myositis; INEM, isolatedneck extensor myopathy; LGMD, limb-girdle muscular dystrophies;LOMM, late onset mitochondrial myopathy; MJD, Machado-Josephdisease; MM, mitochondrial myopathy; OPMD, oculopharyngealmuscular dystrophy; PLS, Primary lateral sclerosis; PM, polymyosi-tis; PMA, progressive muscular amyotrophy; PPS, post-polio syn-drome; SCA, spinocerebellar ataxia; SMA, spinal muscular atrophy.
1294 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

Laurade Jorge, PhDCDGM-IDIBELL, Hospital Duran i Reynals
Hospitalet de LlobregatBarcelona, Spain
Nuria Raguer, MD, PhDNeurophysiology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Dulce Moncho-Rodriguez, MDNeurophysiology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Carlos Jacas, PhDPsychology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Juan Conejero, MD, PhDUrology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Merce Badia, RNNeurology Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Carlos Lorenzo-Bosquet, MD, PhDNuclear Medicine Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
Victor Volpini, PhDCDGM-IDIBELL
Hospital Duran i ReynalsHospitalet de Llobregat
Barcelona, Spain
Joan Castell-Conesa, MD, PhDNuclear Medicine Department
Hospital Universitari Vall d’HebronAutonomous University of Barcelona
Barcelona, Spain
References
1. Azher SN, Jankovic J. Camptocormia: pathogenesis, classifi-cation, and response to therapy. Neurology 2005;65:355–359.
2. Umapathi T, Chaudry V, Cornblath D, Drachman D, GriffinJ, Kunci R. Head drop and camptocormia. J Neurol Neuro-surg Psychiatry 2002;73:1–7.
3. Lasek K, Lencer R, Gaser C, et al. Morphological basis forthe spectrum of clinical deficits in spinocerebellar ataxia 17(SCA17). Brain 2006;129:2341–2352.
4. Mariotti C, Alpini D, Fancellu R, et al. Spinocerebellar ataxiatype 17 (SCA17): oculomotor phenotype and clinical charac-terization of 15 Italian patients. J Neurol 2007;254:1538–1546.
5. Zuhlke C, Hellenbroich Y, Dalski A, et al. Different types ofrepeat expansion in the TATA-binding protein gene are asso-ciated with a new form of inherited ataxia. Eur J Hum Genet2001;9:160–164.
6. Maltecca F, Filla A, Castaldo I, et al. Intergenerational insta-bility and marked anticipation in SCA-17. Neurology 2003;61:1441–1443.
7. Oda M, Maruyama H, Komure O, et al. Possible reducedpenetrance of expansion of 44 to 47 CAG/CAA repeats inthe TATA-binding protein gene in spinocerebellar ataxia type17. Arch Neurol 2004;61:209–212.
8. Manganelli F, Perretti A, Nolano M, et al. Electrophysiologiccharacterization in spinocerebellar ataxia 17. Neurology 2006;66:932–934.
9. Schols L, Peters S, Szymanski S, et al. Extrapyramidal motorsigns in degenerative ataxias. Arch Neurol 2000;57:1495–1500.
10. Rolfs A, Koeppen AH, Bauer I, et al. Clinical features andneuropathology of autosomal dominant spinocerebellar ataxia(SCA17). Ann Neurol 2003;54:367–375.
11. Minnerop M, Joe A, Lutz M, et al. Putamen dopamine trans-porter and glucose metabolism are reduced in SCA17. AnnNeurol 2005;58:490–491.
Pallidal Neuronal Activity in Diabetic
Hemichorea-Hemiballism
Diabetic hemichorea-hemiballism (DHH) is a unique syn-drome characterized by nonketotic hyperglycemia at onset,chorea-ballism and T1-MRI hyperintensity in the contralateralstriatum.1–3 We report on the firing pattern in the pallidal neu-rons and the effects of pallidotomy in a patient with DHH.
A 78-year-old woman with a history of poorly controlleddiabetes mellitus, acutely developed severe choreic and bal-listic movements in the left upper and lower limbs. Her bloodsugar was 455 mg/dL and glicosylated hemoglobin A1c(normal range 4.3–6.1%) was 14.4%. MRI demonstrated amarkedly high-intensity signal on T1-weighted images (Fig.1A) and slightly low-intensity signal on T2-weighted imagesin the bilateral striatum. Her blood sugar was controlledusing insulin after admission. Her choreic movements weretreated with oral administration of haloperidol, but were notwell-controlled.
To improve the intractable involuntary movements, a rightpallidotomy was performed with microelectrode guidance.We did not choose deep brain stimulation because of the dif-ficulty of her postoperative visiting of the hospital. No seda-tion was used in surgery, and all medications were withheldovernight and during surgery. Microrecording tracks weremade 58 from the parasagittal plane, proceeding from antero-dosal to posteroventral at an angle of 308 from the verticalline (Fig. 1B). Twenty- to 40-second samples of spontaneoussingle-cell activity were recorded from the external and inter-nal pallidum (GPe and GPi).
After coagulations in the GPi, her choreic movements dis-appeared and no recurrence of choreic movements was
Potential conflict of interest: Nothing to report.Published online 29 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23058
1295LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

observed for more than a 1-year period of follow-up. The ac-tivity of nine GPi cells and nine GPe cells was sampled (Fig.1C). The firing frequency of nine GPi cells (mean 6 SD,52.9 6 23.1 spikes/s) was significantly low (P < 0.002) com-pared with that in parkinsonian patients without dyskinesia(50 cells from 10 patients, 89.1 6 24.5 spikes/s), whereas thefrequency of nine GPe cells was not different (48.7 6 7.0spikes/s, P > 0.2) from that in parkinsonian patients (29 cellsfrom 10 patients, 59.3 6 18.7 spikes/s). The firing pattern ofthe GPi cells was generally irregular with relatively longpauses compared with that in parkinsonian patients.
The MRI lesions and involuntary movements usuallyappear unilaterally in DHH, but bilateral lesions and involun-
tary movements as observed in our patient can develop.3
Functional neurosurgery has been applied to treat chorea orballism of various etiologies, and the thalamus and the GPi arethe targets. Successful deep brain stimulation of the thalamushas been reported in a patient with this DHH,4 and successfulpallidotomy has been reported in a patient with chorea causedby striatal infarction.5 Our patient demonstrated the efficacy ofpallidal surgery for HDD, and these surgical results suggestthat pallidothalamocortical projection is the key for the devel-opment of chorea and ballism caused by striatal lesions.
Firing rates in the GPi were significantly lower thanthose in off-state Parkinson’s disease in the present patient.Firing rates in the GPe were not different from those in
FIG. A: T1-weighted axial MRI image obtained 20 days after onset showing markedly increased signal intensity in the bilateral lenticular nuclei.B: Reconstruction of the trajectories (Tracks 1, 2, and 3) through external and internal segments of the GPi and the recording sites (open circles)illustrated on the sagittal brain maps. The lateral location was measured by intraoperative computed tomography. The coagulation areas are shownas thick-lined demarcations. C: Raster display of neuronal firing of the GPi cells along microelectrode tracks with an inset of a typical firingexample of a parkinsonian patient on off-state, who was a 58-year-old man with Hohen & Yahr stage 4.9 GPi cells are numbered in the recordingorder. Spontaneous firing of the chorea-ballism patient showed reduced firing rates and irregular firing pattern in the GPi compared with that inthe parkinsonian patients.
Movement Disorders, Vol. 25, No. 9, 2010
1296 LETTERS TO THE EDITOR

Parkinson’s disease in our patient, suggesting that theincreased activity in the direct striatum-GPi inhibitory path-ways may be primarily responsible for the low-firing rate inthe GPi. Decreased firing rate in the GPi has been com-monly observed in chorea and ballism caused by striatal orsubthalamic lesions in humans.5–7 In the pathogenesis ofchorea and ballism, low-firing rate in the GPi may lead todisinhibition of the thlamocortical projection resulting inchoreic excessive movements; however, abolition of chorea-ballism after further reduction of GPi activity by pallidot-omy is contradictory to this theory. An irregular firing pat-tern with pauses was another characteristic in GPi firing inour patient as well as in other choreic or ballistic disor-ders.5–7 The synchronous pauses following bursts of GPi firingare expected to drive ballistic excitation of the thalamo-corticalprojection leading to chorea or ballism. Actually, correlationbetween GPi neuronal firing and chorea or ballism electromyo-grams has been observed in a patient with hemiballism causedby subthalamic hemorrhage7 and one with chorea caused bystriatal infarction.5 Therefore, irregular firing with pauses inthe GPi, more than a low-firing rate, is assumed to be responsi-ble for the pathogenesis of chorea in DHH, and pallidotomyand GPi DBS abolish chorea or ballism probably by blockingthe irregular choreogenic neuronal firing in the GPi.
Financial Disclosure: All authors report no financialdisclosure.
Author’s Roles: Tetsuya Goto: writing of the first draft;Takao Hashimoto: analysis of neuronal data, supervision; allauthors: acquisition of data.
Tetsuya Goto, MD, PhDDepartment of Neurosurgery
Shinshu University School of MedicineMatsumoto, Japan
Takao Hashimoto, MD, PhDCenter for Neurological Diseases
Aizawa Hospital, Matsumoto, Japan
Shuichi Hirayama, MDKazuo Kitazawa, MD, PhD
Department of Neurosurgery,Aizawa Hospital, Matsumoto, Japan
References
1. Yahikozawa H, Hanyu N, Yamamoto K, et al. Hemiballism withstriatal hyperintensity on T1-weighted MRI in diabetic patients: aunique syndrome. J Neurol Sci 1994;124:208–214.
2. Lee BC, Hwang SH, Chang GY. Hemiballismus-hemichorea inolder diabetic women: a clinical syndrome with MRI correlation.Neurology 1999;52:646–648.
3. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion onT1-weighted brain MRI study: a meta-analysis of 53 cases includ-ing four present cases. J Neurol Sci 2002;200:57–62.
4. Nakano N, Uchiyama T, Okuda T, Kitano M, Taneda M. Successfullong-term deep brain stimulation for hemichorea-hemiballism in apatient with diabetes. J Neurosurg 2005;102:1137–1141.
5. Hashimoto T, Morita H, Tada T, Maruyama T, Yamada Y, Ikeda S.Neuronal activity in the globus pallidus in chorea caused by striatallacunar infarction. Ann Neurol 2001;50:528–531.
6. Suarez JI, Metnum LV, Reich SG, et al. Pallidotomy for hemiballis-mus: efficacy and characteristics of neuronal activity. Ann Neurol1997;42:807–811.
7. Vitek JL, Chockkan V, Zhang JY, et al. Neuronal activity in the ba-sal ganglia in patients with generalized dystonia and hemiballismus.Ann Neurol 1999;46:22–35.
Punding in Parkinson’s Disease: The Impact of
Patient’s Awareness on Diagnosis
Punding is a peculiar stereotyped behavior characterizedby an intense fascination with complex, excessive, nongoaloriented, repetitive activities such as manipulation of techni-cal equipment, handling, examining or sorting through com-mon objects, grooming, hoarding, or engagement in extendedmonologes devoid of content.1,2 Nowadays, the most com-mon cause of punding is dopaminergic replacement therapyin patients affected by Parkinson’s disease (PD).3 Patients’awareness of punding might be poor, so that they underreportit. As a consequence, albeit described in the seventies,4 onlyrecently the medical and scientific community has focused onthe relevance of this side effect.5
We investigated the patients’ awareness of pundingthrough an anonymous questionnaire administered to 20 PDpatients (six women, mean age 68.9 6 9.5 years, disease du-ration 14.3 6 9.3 years) before and after attending a confer-ence on the matter. Patients were first asked whether theyhad cultivated any hobby, if this activity had ever been trou-blesome, and in this case if they had reported it to medicalattention. The majority of patients (17) reported to have atleast one hobby (five of them developed it after PD onset); 2patients felt it as troublesome. Three patients reported it tothe medical attention but only one of them was taken intoconsideration by the treating physician.
Following this first part, a neurologist expert on pundinggave a 20-minute talk on this topic. Afterwards the PundingRating Scale (PRS)3,6 was administered. Three patients over20 (two women, 47, 52, and 68 years old, disease duration:10, 11, 13 years) answered ‘‘Yes’’ to six over seven ques-tions, revealing an underlying punding, unrecognized by thepatients till that moment. Severity score was 20.3 6 10according to severity section of the PRS (maximum score36).3,6 These patients had no awareness of this phenomenonbefore attending the conference (Fig. 1), as they neverreported a ‘‘troublesome hobby’’ to their physicians. Interest-ingly, in two of them (66.7%) the repetitive behavior devel-oped after PD onset whereas only 11.8% of nonpundersreported a hobby beginning after disease onset (P 5 0.03,chi-square test). There were no significant differencesbetween punders and nonpunders in terms of age or diseaseduration.
Although uncommon, punding is a challenge for bothpatients and treating physicians. Punders can recognize thattime and money spent on their behaviors is excessive and
Potential conflict of interest: The authors neither have conflict ofinterest nor financial disclosures.
Published online 14 May 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23061
1297LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

inappropriate however, in spite of the consequent self-injury,they do not stop the behavior which can lead to devastatingpsychosocial consequences.1,2 However, patients’ insightcould be impaired, as punding commonly occurs without sub-jective distress and is frequently hidden or unnoticed becauseit is experienced as being internally consistent with one’sthoughts and behavioral repertoires. Therefore, physiciansmust actively screen for punding, highlighting the importanceof the information on patient’s daily activities collected byspouses or other family members. Key questions includewhether the behavior is excessive (missing meals, medicationdosages, sleep, proper hygiene, and interaction with familymembers) or disruptive (leftover pieces, incompleted tasks)and whether interruption results in irritability or anger.2
A study on cocaine addicts indicated that a repetitivebehavior started before cocaine use but it was enhanced bythe drug.6 This underlines the relationship between habitand the development of punding according to the so-called‘‘habit theory.’’3 By contrast, in our survey two over threepunders were engaged in a repetitive behavior not presentbefore disease onset: the occurrence of this repetitivebehavior after PD onset could represent a red flag in thediagnosis of punding although further investigations areneeded. Remarkably, in 2 cases the repetitive action wasrepresented by computer use, as already described in aprevious report.7
In this small survey the prevalence of punding is 15%.Due to low reporting, the exact prevalence is still unknown.Miyasaki et al. found a prevalence of 1.4% using a patient-rated questionnaire,8 whereas Evans et al. directly inter-viewed patients and found a prevalence of 14%.1 Anotherstudy not specifically designed to detect punding reported aprevalence of 3%.9 This disparity has been attributed to thedifferences in the study populations but it could also beexplained by the contrasting referral and assessment proce-dures used. A selection bias could limit our approach as weenrolled patients belonging to a local patients association,then more likely to be affected by a more severe disease. Inaddition, due to the anonymity of the questionnaire diagnosiscould not have been confirmed through a psychiatric counseling.
In conclusion, we argue that punding, albeit with differentdegrees of severity, is more common than previously described.Both physicians and patients should be well informed on thefeatures of the phenomenon because the boundary between nor-mal and pathological behavior is difficult to define. To improvethe diagnosis accuracy on a larger scale, the phenomenology ofpunding should be more widely promoted and every patientshould be routinely screened during the control visit by focusingon aspects of daily life. Failure to recognize punding in theearly stages may be the cause of personal, familial, and socialdifficulties for the patient and caregivers, whereas early diagno-sis can lead to prompt and efficacious intervention.
Acknowledgments: The authors are grateful to the patientsparticipating in this study and to Mrs Laura Horn—‘‘AzioneParkinson Onlus.’’
Author Roles: A. Fasano—research project: conceptionand execution; statistical analysis: execution; manuscript: writ-ing of the first draft. M. Pettorruso—research project: organi-zation and execution; statistical analysis: execution. L. Ric-ciardi—research project: organization and execution; manu-script: writing of the first draft. G. L. Conte—manuscript:review and critique. A. R. Bentivoglio—statistical analysis:review and critique; manuscript: review and critique.
Financial Disclosure: A. Fasano—stock ownership inmedically related fields, intellectual property rights, consul-tancies, expert testimony, advisory boards, employment, part-nerships, contracts, honoraria, royalties, and others: none;grants—Neureca–Onlus, Milan. M. Pettorruso, L. Ricciardi,and G.L. Conte—stock ownership in medically related fields,intellectual property rights, consultancies, expert testimony,advisory boards, employment, partnerships, contracts, honora-ria, royalties, grants, and others: none. A.R. Bentivoglio—stock ownership in medically related fields, intellectual prop-erty rights, consultancies, expert testimony, advisory boardsUCB-pharma, employment, partnerships, contracts, honora-ria—Allergan, Ipsen, Novartis, Medtronic, Boheringer-Inghe-leim, UCB-Pharma, and Glaxo, royalties, and others: none;grants—Allergan, Ipsen, Chiesi, and Medtronic.
FIG. 1. Patients’ awareness of punding before and after attending a conference on the topic. The table lists the clinical features of three pundersrecognized after administering the PRS.3,6
1298 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

Alfonso Fasano, MD*Department of Neurology
Catholic University of Sacred HeartRome, Italy
Neuromed InstitutePozzilli (IS), Italy
E-mail: [email protected]
Mauro Pettorruso, MDDepartment of Psychiatry
Catholic University of Sacred HeartRome, Italy
Lucia Ricciardi, MDDepartment of Neurosciences, Psychiatry
and Anaesthesiological ScienceUniversity of Messina
Messina, Italy
Gianluigi Conte, MDDepartment of Psychiatry
Catholic University of Sacred HeartRome, Italy
Anna Rita Bentivoglio, MD, PhDDepartment of Neurology
Catholic University of Sacred HeartRome, Italy
References
1. Evans AH, Katzenschlager R, Paviour D, et al. Punding in Parkin-son’s disease: its relation to the dopamine dysregulation syn-drome. Mov Disord 2004;19:397–405.
2. Voon V. Repetition, repetition, and repetition: compulsive andpunding behaviors in Parkinson’s disease. Mov Disord 2004;19:367–370.
3. Fasano A, Petrovic I. Insights into pathophysiology of pundingreveal possible treatment strategies. Mol Psychiatr (in press).
4. Rylander G. Psychoses and the punding and choreiform syn-dromes in addiction to central stimulant drugs. Psychiatr NeurolNeurochir 1972;75:203–212.
5. Friedman JH. Punding on levodopa. Biol Psychiatry 1994;36:350–351.
6. Fasano A, Barra A, Nicosia P, et al. Cocaine addiction: from hab-its to stereotypical-repetitive behaviors and punding. Drug AlcoholDepend 2008;96:178–182.
7. Fasano A, Elia AE, Soleti F, Guidubaldi A, Bentivoglio AR.Punding and computer addiction in Parkinson’s disease. Mov Dis-ord 2006;21:1217�1218.
8. Miyasaki JM, Al Hassan K, Lang AE, Voon V. Punding preva-lence in Parkinson’s disease. Mov Disord 2007;22:1179�1181.
9. Pontone G, Williams JR, Bassett SS, Marsh L. Clinical featuresassociated with impulse control disorders in Parkinson disease.Neurology 2006;67:1258�1261.
Pyridostigmine-Induced Dystonic
Blepharospasm in a Patient With Ocular
Myasthenia Gravis
A previously healthy 40-year-old housewife presentedwith a 2-month history of droopy eyelids, which worsenedtoward the evening. There was no diplopia, bulbar symp-toms, or recent stressful events. Family history was unre-markable. Examination revealed bilateral partial ptosis withmarked fatigability and the patient was blinking frequently.The visual acuity and the extraocular movements were nor-mal. The ice-pack test was positive, and there was reversalof the ptosis with the first 2 mg of edrophonium. Repetitivenerve stimulation showed decremental response of >20% inthe CMAP of the anconeus. SFEMG of the orbicularis oculishowed prolonged jitter in 3 of 20 pairs of single fiber actionpotentials. Anti-AchR and antistriated muscle antibodieswere not detected. Screening for connective tissue diseasesand thyroid disorders were negative. CT scan of the thoraxwas normal.
She was diagnosed with ocular MG, and pyridostigmine(60 mg) thrice daily was started. A week later, the patientwent to another center with worsening of symptoms. She hadcomplained of ‘difficulty in keeping her eyes open’ and gen-eralized body weakness, abdominal cramps, and diarrhea.Prednisolone (20 mg) daily was added to her treatment pre-sumably treating for myasthenic crisis. Upon review by us 2weeks later, she had sustained contractions of both orbicula-ris oculi and could not open her eyes voluntarily. She alsocomplained of diarrhea and abdominal cramps. There wereno signs of myasthenic crisis. The forced vital capacity wasnormal. EMG study of the obicularis oculi revealed spas-modic contractions of both orbicularis oculi, during the ‘‘eye-closing’’ episodes (Fig. 1).
A diagnosis of pyridostigmine-induced blepharospasmwith cholinergic overactivity was made. Both prednisoloneand pyridostigmine were stopped. Three days after with-drawal of medication, the diarrhea and generalized bodyweakness resolved. Her eye-closing episodes improved dramat-ically, and she was able to open her eyes, with ease, withmild residual blepharospasm. There was bilateral partial ptosiswith sustained upgaze. When rechallenged with pyridostigmine(30 mg) daily, she again developed blepharospasm and sys-temic signs of cholinergic overactivity again. The pyridostig-mine was withheld, and she was given a trial of clonazepamand subsequently her blepharospasm resolved.
The spasmodic blinking in dystonic blepharospasm is adifferent entity when compared with fatigable weakness ofthe levator palpebrae muscle in MG. Although our patientpresented initially with frequent eye-blinks mimicking thepresentation of blepharospasm, she had demonstrable fatig-ability of the eyelids and all investigations including elec-trophysiological tests and the edrophonium test confirmedthe diagnosis of MG. However, she developed symptoms ofexcessive cholinergic activity even with small doses of pyri-dostigmine, and severe blepharospasm, with higher doses.The blepharospasm resolved with discontinuation of pyridos-
Potential conflict of interest: Nothing to report.Published online in 17 May 2010 Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.22931
Movement Disorders, Vol. 25, No. 9, 2010
1299LETTERS TO THE EDITOR

tigmine and recurred when rechallenged with even smalldoses of pyridostigmine, which makes the treatment difficultfor this patient. It is most probable that our patient wassomewhat predisposed to developing dystonic blepharo-spasm, despite the negative family history, as even withsmall doses of pyridostigmine, the previously asymptomatic(but observable) blepharospasm became apparent. The initialdiagnosis of MG had masked the presentation of blepharo-spasm, leading to a delay in its diagnosis, especially, as thefrequent eye-blinks were initially attributed to insufficientdosage of pyridostigmine. The diagnosis of dystonic ble-pharospasm was considered only after the patient continuedto complain of other cholinergic symptoms, and later con-firmed by EMG.
There are few reported cases of blepharospasm occurringconcomitantly in patients with autoimmune diseases, such asMG and systemic lupus erythematous.1 Blepharospasmoccurred during exacerbation of the autoimmune disordersand resolved spontaneously with disease remission.1 Thereare also reports of ocular MG presenting with frequent eye-blinks mimicking the clinical presentation of blepharo-spasm.2,3 However, unlike our patient, the ‘‘eye-blinking epi-sodes’’ resolved with pyridostigmine therapy, as the patientsdid not have true blepharospasm.2
In summary, this case highlights the diagnostic and man-agement difficulties in a patient who had both ocular MGand blepharospasm. Therefore, persistent eye-blinks despitetreatment in a patient with ocular MG should alert to the pos-sible diagnosis of concomitant blepharospasm.
Author Roles: C.V. Yew: Conception, organization, andexecution of research project, writing of the first draft andreview and critique of the manuscript; Norlinah: Conception,organization, and execution of research project, review andcritique of the manuscript; Nafisah: Conception and execu-tion of research project; Shariful: Conception and executionof research project.
Yew Chien Voon, MDDepartment of Ophthalmology
Hospital Kuala LumpurKuala Lumpur, Malaysia
Wan Nur Nafisah Wan Yahya MMed, MDShariful Hasan, MBBS
Norlinah Mohamed Ibrahim, MRCP*Department of Medicine
Faculty of Medicine, UKM Medical CenterKuala Lumpur, Malaysia
*E-mail: [email protected] or [email protected]
References
1. Jankovic J, Pattern BM. Blepharospasm and autoimmune diseases.Mov Disord 1987;2:159–163.
2. Funakawa I, Yasuda T, Katoh H, Hara K, Terao A. A case ofbilateral blepharospasm responsive to edrophonium. Rinsho Shin-keigaku 1992;32:527–531 (Japanese).
3. Kurlan R, Jankovic J, Rubin A, Patten B, Griggs R, Shoulson I.Coexistent Meige’s syndrome and myasthenia gravis. A relation-ship between blinking and extraocular muscle fatigue? Arch Neu-rol 1987;44:1057–1060.
4. Jankovic J. Clinical features, differential diagnosis, and pathogene-sis of blepharospasm and cranial-cervical dystonia. In: BosniakSL, editors. Blepharospasm, Advances Ophthalmic and PlasticReconstructive Surgery. Vol. 4. New York: Pergamon Press;1985. p 67–82.
5. Roberts ME, Steiger MJ, Hart IK. Presentation of myastheniagravis mimicking blepharospasm. Neurology 2002;58:150–151.
6. Tsuda H, Kamei S, Mizutani T, Saito N, Ishikawa H, Omori K.Blepharospasm in a patient with thymoma and positive anti-ace-tylcholine receptor antibody. Rinsho Shinkeigaku 2003;43:500–502 (Japanese).
7. Jankovic J, Ford J. Blepharospasm and orofacial-cervical dystonia:clinical and pharmacological findings in 100 patients. Ann Neurol1983;13:402–411.
FIG. 1. Needle EMG of the right orbicularis oculi at rest showing MUAPs occurring at regular intervals in keeping with blepharospasm.
1300 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

Dementia with Lewy Bodies Associated with
Ataxia, Myoclonus, and Cortical Blindness
The differential diagnosis of Creutzfeldt-Jakob disease(CJD) includes dementia with Lewy bodies (DLB) and Alz-heimer’s disease (AD).1 CJD presents with a rapidly progres-sive dementia associated with a minimum of two of the fouradditional symptoms of myoclonus, visual or cerebellar dis-turbances, pyramidal or other extrapyramidal dysfunction,and akinetic mutism (Table 1). Movement disturbances maygive rise to confusion in the differential diagnosis of CJD.Edler et al.2 reported in this journal that ataxia was relativelymore common in CJD and myoclonus to be common in CJD,AD, and DLB. The presence of visual disturbances may alsogive rise to diagnostic confusion. We present a case of DLBwith rapidly progressive dementia with both ataxia and myo-clonus together with cortical blindness associated with Lewybody pathology in the visual cortex.
A 67-year-old male was diagnosed AD early in 2007 withgeneralized atrophy on CT brain scan. He was admitted in De-cember 2007 with unsteadiness. He had a Mini Mental StateExamination of 10/30 but no visual hallucinations. His cogni-tive impairment progressed quickly and he became agitated.He was not treated with neuroleptics. He developed ataxia,myoclonic jerks, and pyramidal signs in his legs but no Parkin-sonism. A CT brain showed mild periventricular white matterchange with sulcal prominence consistent with age. He wasunable to tolerate MRI. He developed bilateral cortical blind-ness, deteriorated rapidly and became mute. EEG in January2008 showed symmetrical generalized irregular rhythmicaltheta activity at 5–6 Hz, with posterior intermittent rhythmic 7Hz theta activity. Two weeks later the repeated EEG showeddeterioration but no features of CJD. The CJD surveillance unitclassified him as possible CJD based on rapidly progressing de-mentia over <2 years combined with ataxia, blindness, andmyoclonus (Table 1). His family declined a lumbar puncturebut consented to postmortem. He died late January 2008.
On neuropathology there was a mild atrophy all regionsexcept occipital lobes. In hematoxylin and eosin–stained sec-tions there were cortical Lewy bodies in frontal, parietal,occipital (visual, striate) and entorhinal cortices and temporalneocortex. Immunohistochemistry for alpha-synuclein showedfrequent cortical Lewy bodies (Fig. 1a) and in addition prom-inent Lewy neurites. Lewy body scores were the highest pos-sible in all regions. Immunohistochemistry for Ab proteinshowed extensive senile plaques in frontal, parietal, occipitaland entorhinal cortices and temporal neocortex. Immunohis-tochemistry for tau showed neurofibrillary tangles in the hip-pocampus, subiculum, and entorhinal cortex. There was nospongiform change (including in the medial temporal lobes)and immunohistochemistry for prion protein was negative inall brain regions. Midbrain showed mild depigmentation andfrequent Lewy bodies in the substantia nigra (Fig. 1b), mod-erate neuronal loss, pigment-laden macrophages with Lewybodies and Lewy neurites in the tegmentum of the pons andmedulla. The pathology was in keeping with a diagnosis ofDLB of the neocortical category with no evidence of CJD.
The most common differential pathological diagnoses ofCJD are AD and DLB which can mimic CJD clinically.1
Ataxia and dysmetria are more frequent in CJD than in ADor DLB, whereas hypokinesia is more frequent in AD orDLB.2 Myoclonus is common in DLB and associated with amore aggressive progression.2 Cortical blindness is commonin CJD and may be the main feature in the Heidenhain vari-ant which predominantly involves the occipitoparietalregion.3 Cortical blindness can sometimes be associated withneurodegenerative disorders such as the posterior variant ofAD or corticobasal degeneration. There is functional disturb-ance of the occipital lobes in DLB, which was not related tothe presence of Lewy bodies in previous studies.4,5 The occi-pital cortex is affected by Lewy body pathology in late Par-kinson’s disease and cases with visual hallucinations mayhave frequent CLB in the temporal lobes.6 There are onlytwo reported cases with DLB and blindness.7,8 In one case,cortical blindness was not associated with frequent Lewybodies in the visual cortex.7 In the other case, there was hem-ianopia associated with severe neurofibrillary tangle (tau) pa-thology in the contra lateral occipital lobe.8
This case of DLB appears unique in which the corticalblindness was associated with frequent Lewy bodies in the vis-ual cortex. It was also unusual for the history of dementia with-out hypokinesia (despite Lewy body pathology in the substan-tia nigra) and the subacute final illness masquerading as CJD.
Myoclonus is a common feature of DLB with ataxia occur-ring less common. Blindness can rarely be a feature of DLB.
Potential conflict of interest: none.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23074
TABLE Sporadic CJD
DefiniteNeuropathologically/immunocytochemically confirmed
ProbableI 1 2 of II 1 IIIPossible 1 positive 14-3-3
PossibleI 1 2 of II 1 duration <2 years
I. Rapidly progressive dementia.II. (A) Myoclonus. (B) Visual or cerbellar problems. (C) Pyrami-
dal or extrapyramidal features. (D) Akinetic mutism.III. Typical EEG.
FIG. 1 (a) Cortical Lewy body in the visual cortex. Immunohisto-chemistry for alpha-synuclein. (b) Classical Lewy body in the sub-stantia nigra. Haematoxylin and eosin.
Movement Disorders, Vol. 25, No. 9, 2010
1301LETTERS TO THE EDITOR

Acknowledgments: We thank Prof. J. W. Ironside, Direc-tor of the National CJD Surveillance Unit, for assisting thiswork. The National CJD Surveillance Unit is funded by theUK Department of Health and the Scottish Executive. TheBrain Bank in the National CJD Surveillance Unit is sup-ported by the Medical Research Council (Grant NumberG0600953).
Financial Disclosures: J.V. Hindle: Honoraria—Honorariafor lectures and participation at educational events—receivedfrom Teva pharma, Glaxo Smith Klein, UCB, and BoehringerIngelheim; Grants—Research funding—Parkinson’s diseaseSociety UK (PDS), Economic and Social Research Council(ESRC), Biotechnology and Biological Sciences ResearchCouncil (BBSRC); Employment—Betsi Cadwaladr UniversityHealth Board. L. Bridges: Employment—St Georges HealthCare Trust. G. Chohan: Employment—Department of Health.
Author Roles: J.V. Hindle: Clinical assessment, Manu-script—Writing first; L. Bridges: Neuropathology, Manu-script—Review and Critique; G. Chohan: Clinical Assess-ment, Manuscript—Review and Critique.
John V. Hindle, MBBS, FRCP, FRCPsych*Department of Care of the Elderly
School of Medical SciencesBangor University
Bangor, United KingdomLlandudno Hospital
Conwy, United Kingdom*E-mail: [email protected]
Leslie Bridges, BSc, MBBS, MD,FRCPath, FRCPA, FHEADepartment of Pathology
St. George’s HospitalLondon, United Kingdom
Gurjit Chohan, MBChB, MRCPNational CJD Surveillance Unit
Western General HospitalEdinburgh, United Kingdom
References
1. Van Everbroeck B, Dobbeleir I, De Waele M, De Deyn P, MartinJ, Cras P. Differential diagnosis of 201 possible Creutzfeldt-Jakobdisease patients. J Neurol 2004;251:298–304.
2. Edler J, Mollenhauer B, Heinemann U, et al. Movement disturban-ces in the differential diagnosis of Creutzfeldt-Jakob disease. MovDisord 2009;24:350–356.
3. Proulx AA, Strong MJ, Nicoille DA. Creutzfeld-Jakob disease pre-senting with visual manifestations. Can J Opthalmol 2008;43:591–595.
4. Mosimann UP, Mather G, Wesnes KA, O’Brien JT, Burn DJ,McKeith IG. Visual perception in Parkinson disease dementia anddementia with Lewy bodies. Neurology 2004;63:2091–2096.
5. Harding AJ, Broe GA, Halliday GM. Visual hallucinations inLewy body disease relate to Lewy bodies in the temporal lobe.Brain 2002;125:391–403.
6. Braak H, Del Tredici K, Rub U, De Vos RAI, Steur ENHJ, BraakE. Staging of brain pathology related to sporadic Parkinson’s dis-ease. Neurobiol Aging 2003;24:197–211.
7. Schultz DW, Lennox GG, Ironside JW, Warlow CP. Behaviouraldisturbance and visual hallucinations in a 78 year old man. J Neu-rol Neurosurg Psychiatry 1998;65:933–938.
8. Bashir K, Elble RJ, Ghobrial M, Struble RG. Hemianopsia in de-mentia with Lewy Bodies. Arch Neurol 1998;55:1132–1135.
Paradoxical Kinesia in Parkinsonian Patients
Surviving Earthquake
The region where our Movement Disorders Clinic is sitedwas stricken by a major earthquake (6.0 points Richter scale)on April 6, 2009 causing 309 victims and destruction ofmany historical buildings in the town of L’Aquila (70 Kmfrom our clinic).
Thirty-one patients with Parkinson’s disease (PD) inhabit-ing the epicenter area had been regularly followed in ourClinic for about 3–9 years before the event, with regularassessments by independent raters with Unified Parkinson’sDisease Rating Scale (UPDRS),1 Freezing of Gait question-naire (FOG),2 and Mini-Mental State Examination(MMSE)3every 2–3 months.
Seventeen patients were in Hoehn/Yahr (H/Y)4 stage 1–2(and therefore were not considered in the present report), 14were in stage 3–5. We interviewed and examined the 14patients in H/Y stage 3–5 and their relatives after the earth-quake to understand whether paradoxical kinesia (PK) hadoccurred. PK describes ‘‘a sudden and a brief period of mo-bility following emotional or physical stress,’’ often causedby unique life-threatening situations5–7 in patients withadvanced PD.
Three mechanisms are proposed to explain PK: noradren-ergic augmentation, compensatory activation of cerebellarcircuitry, and activation of basal ganglia reserves.7
Prior to the earthquake, 13 of the 14 patients were in H/Ystage 3–4, one was bedridden in stage 5. Ten were affectedby severe freezing episodes, all presented motor fluctuationsand moderate dyskinesias. All patients received optimal levelof treatments. Ten patients had severe nighttime akinesia,requiring assistance for turning in bed. Table 1 reports theassessment scores and demographics. MMSE was <24 in allpatients, Rapid Eye Movements (REM) sleep behavior disor-der (RBD) was present in 12 patients; fluctuating cognition(FC) in 13; visual hallucinations (VH) in 10.
All the 14 patients could escape during or immediately af-ter the earthquake, which occurred at 3.30 a.m. Caregivers of11 patients reported that patients were the first ones in thehouse to be alerted by the quake, to help or alert relativesand to run out of collapsing buildings, probably saving theirlives, as collapse of centuries old buildings followed theearthquake by minutes to hours. According to caregiverreports (e.g., ‘‘jumped out of bed and ran out of the buildingyelling to relatives to follow’’), six patients ran out of thirdto fourth floor apartments, four ran out of the second floor,and three escaped from first floor (12–24 steps). Nine care-givers reported to have been helped by patients (e.g., ‘‘hepractically lifted me up through the collapsing three floorbuilding’’).
Potential conflict of interest: Nothing to report.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23075
1302 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

Fifteen days to 1 month after the earthquake and twice inthe following 6 months, UPDRS and FOG scores wereassessed in these 14 patients in ‘‘on’’ state by five differentraters (interrater reliability reached 97%). Statistical compari-sons were based on mixed models analysis of covariance.The study was complied with the declaration of Helsinki andrevisions.8
Table 1 shows the scale score comparison before theearthquake and during the follow-up. No differences wereobserved for mentation and depression UPDRS scores. Noneof the patients required therapy adjustments. Patients, as con-firmed by relatives, reported transient improvement of theirmobility lasting some days after the earthquake. In fivepatients, motor improvement were observed during the fol-low-up visit at 2 and 5 months [UPDRS mean (SD)—37.0(15.1) before the earthquake, 21.0 (10.9) 2 months after theearthquake, FOG mean (SD)—19.8 (3.2) before the earth-quake, 5.8 (2.0) after the earthquake]. Beyond the time inter-action (before/after the earthquake, P < 0.05, five patientsvs. nine patients), no differences could be evidenced in allother items of UPDRS or treatments between the five patientswho experienced persistent benefit after PK and the ninepatients who did not.
The meaning of our report is that we could collect evi-dence of PK in a large group of patients whose disability hadbeen regularly documented in our clinic. The relevant findingwas that all parkinsonian patients with H/Y stage 3–5 experi-enced PK according to caregivers and to the undebatable evi-dence that all survived.
The PD population evaluated in our study was of 31patients, for a total of 67,000 inhabitants in the epicenter
area. According to point prevalence estimates,9 the PD popu-lation regularly followed in our clinic represents more than20% of the expected total PD population in this area (prob-ably more for severe PD). Thus, it is conceivable that ourobservations were not simply linked to chance, and suggestthat PK in a life-threatening situation is not uncommon.
Cognitive decline and the presence of RBD, VH, FC hadbeen observed prior to the occurrence of PK in almost all ourpatients in H/Y stage 3–5. This finding suggests that PK mayoccur in patients classifiable as PD–dementia or dementiawith Lewy bodies. Cognitive or mental activity scores hadsurprisingly not been worsened after the earthquake. Butmore surprising was the finding of transient motor benefit infive patients.
None of our patients underwent treatment changes duringthe period of prolonged benefit, so it is likely that PK itselfinduced the benefit. The disappearance/reduction of freezingwas one of the major effects of PK.
The weak part of our observation is that, despite all ourattempts (raters unaware of the purpose of the study, randomassignment to raters), biases could not be avoided. We couldnot be confident that the joy of surviving conveyed bypatients and caregivers was not forcing our interpretations.Yet, the setting of adequate scientific methods is impossiblein life-threatening situations. Only one prior study attempteda systematic evaluation of PK, but with an artificial reproduc-tion of a war-like threat.7
Author Roles: L. Bonanni: research project—execution;statistical analysis—design and execution; manuscript—writ-ing of the first draft. A. Thomas: research project—organiza-tion and execution. M. Onofrj: research project—conceptionand organization; statistical analysis—design; manuscript—writing of the first draft, review and critique.
Financial Disclosure: M. Onofrj was a member of Advi-sory boards for GSK, Novartis, Medtronic, Newron; receivedgrants as adviser on Parkinson’s disease and dementia;received grants from the Italian National Institute of Healthand from the Italian Ministry of Education for research onDementia, epilepsy, parkinsonism, and multiple sclerosis. L.Bonanni received a grant from the Italian Ministry of Health.A. Thomas received grants as adviser on Parkinson’s diseasefrom GSK, UCB, and Newron.
Laura Bonanni, MD, PhDAstrid Thomas, MD, PhD
Marco Onofrj, MD*Department of Neurology
University G.D’Annunzio of Chieti-PescaraItaly and Aging Research Center, Ce.S.I.
‘‘Gabriele d’Annunzio’’ University FoundationChieti-Pescara, Chieti, Italy
*E-mail: [email protected]
References
1. Fahn S, Elton RL. Members of the Unified Parkinson’s DiseaseRating Scale Development Committee. Unified Parkinson’s diseaserating scale. In: Fahn S, Marsden CD, Calne DB, Goldstein M, edi-tors. Recent development in Parkinson’s disease, Vol. 2. FlorhamPark, NJ: Macmillan Healthcare Information; 1987. p 153–164.
2. Giladi N, Tal J, Azulay T, et al. Validation of the freezing of gaitquestionnaire in patients with Parkinson’s disease. Mov Disord2009;24:655–661.
TABLE 1. Demographics and clinical characteristicsof patients
Number of patients 14Age 70.6 (10.0)Gender 4 F/10 MDisease duration 6.1 (2.7)H/Y 3.4 (0.5)RBD 86%FC 93%MMSE 21.9 (2.3)UPDRS mentation B: 3.2 (0.7)
2: 3.2 (0.7)5: 3.2 (0.7)
UPDRS motor score B: 37.4 (14.5)2: 31.6 (15.7)5: 36.1 (15.1)
UPDRS freezing B: 2.4 (1.7)2: 1.3 (1.4)5: 2.1 (1.6)
FOGa B:19.6 (2.8)2:12.7 (7.6)5:17.6 (5.6)
When not differently stated data are presented as mean (SD). H/Y,Hoehn/Yahr staging; RBD, REM sleep behavior disorder; FC, fluctu-ating cognition; MMSE, mini-mental state examination; UPDRS, unifiedParkinson’s disease rating scale; B, before earthquake; 2 and 5 state scalescores evaluations respectively at 2 and 5 months after the earthquake.
aFOG were evaluated only in patients presenting with freezing ofgait at UPDRS (10 patients).
Movement Disorders, Vol. 25, No. 9, 2010
1303LETTERS TO THE EDITOR

3. Folstein NF, Folstein SE, McHugh PR. Mini-mental state: a practi-cal method for grading the cognitive state of patients for clinician.J Psychiatry Res 1975;12:189–198.
4. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mor-tality. Neurology 1967;17:427–442.
5. Souques AA. Kinesie paradoxicale. Rev Neurol 1921;37:559–560.6. Robottom BJ, Weiner WJ, Asmus F, Huber H, Gasser T, Schols L.
Kick and rush: paradoxical kinesia in Parkinson disease. Neurology2009;73:328; author reply 328–329.
7. Schlesinger I, Erikh I, Yarnitsky D. Paradoxical kinesia at war.Mov Disord 2007;22:2394–2397.
8. Declaration of Helsinki. Recommendations guiding physicians in bio-medical research involving human subjects. JAMA 1997;277:925–926.
9. Beghi E, Monticelli ML, Sessa A, Simone P, The Italian GeneralPractitioner Study Group (IGPSG). The prevalence of parkinsonismin Italy: an epidemiological survey of the disease in general practice.Mov Disord 1994;9:403–408.
Dysphagia in Symptomatic Palatal Tremor
Video
Palatal tremor (PT) is characterized by rhythmic involun-tary movements of the soft palate and occasionally othermuscles innervated by cranial or spinal nerves.1,2 PT is sub-divided in the essential (EPT) and the symptomatic form(SPT). EPT patients often suffer from a compromising ear-click. Underlying diseases and characteristic brain imagingabnormalities are lacking in these patients.1 Various etiolo-gies have been related to SPT, which is supposed to arisefrom brainstem or cerebellar lesions in the Guillain-Mollarettriangle. Examples for underlying brain diseases are cerebralischemia, hemorrhage, infection, Whipple’s and Wilson’s dis-ease or neurodegenerative disorders (progressive ataxia andPT, spinocerebellar ataxia, SCA 20).3,4 In most cases, SPT isassociated with a hypertrophic degeneration of the inferiorolive in brain magnetic resonance imaging (MRI).5 Gait andextremity ataxia, dysarthria, nystagmus, and abnormal brain-stem reflexes are often observed in SPT depending on theextent of the primary brain lesion. The involvement of thelarynx is rare and shows breathing abnormalities as the mostprominent clinical symptom.3,6,7
We report on a 59-year-old man presenting with a historyof slowly progressive speech and swallowing difficultiessince about 3 years. He complained of repetitive short inter-ruptions of his voice and of incidental choking, but he didnot report ear-click. The initial neurological examinationshowed a reduced phonation duration and phonation capacitywith intermittent tremulous voice arrest and mild dysarthria.Visual inspection disclosed rhythmic movement of the exter-nally visible laryngeal cartilages and PT with permanentrhythmic contractions of the soft palate and the digastricusand stylohyoideus muscles. At a follow-up visit 6 monthslater, a horizontal and vertical rotational nystagmus, hyper-
metric saccades, a pathologic VOR test (Halmagyi) and adisturbed fixation-suppression were additionally found. BrainMRI showed asymmetric signal hyperintensities of the infe-rior olives (Fig. 1). Vascular ischemia, hemorrhage, CNSinfection as well as autoimmune and metabolic causes (i.e.,Whipples disease) were ruled out. Regarding the slow pro-gression of symptoms and the age of onset, we assume thatour patient might suffer from a neurodegenerative disease,such as sporadic progressive ataxia and palatal tremor(PAPT) or SCA 20.4,8
Although clinical examination revealed no signs of severepenetration or aspiration, fiberoptic endoscopy showed leak-ing in the valleculae during liquid swallowing (see Video).Aspiration occurred before and during swallowing followedby delayed but effective clearing (penetration aspiration score5 PAS 7). Moreover, the musculature of the soft palate andlarynx (Mm. cricothyroideus lateralis, thyroarytaenoideus,arytaenoideus obliquus, and arytaenoideus transversus)revealed permanent rhythmic myoclonic movements, whichwere shortly suppressed during phonation. Penetration andaspiration could be avoided by using the compensatory supra-glottic swallowing technique: the patient was told to take abreath, hold it during swallowing and then cough afterward.Moreover, the patient learned to prevent choking by notstretching his neck too much backward during the swallow-ing procedure. A repeated endoscopy at the 6 months follow-up visit did not show signs of aspiration anymore.
This case demonstrates severe laryngeal involvement withclinically relevant penetration and aspiration in a patient withSPT. Dysphagia has been rarely reported in PT6,7 and usuallynot been paid major attention to in these patients. Our reportclearly shows that SPT patients have a high risk for dysphagiaand aspiration even if they are clinically virtually asymptom-
Additional Supporting Information may be found in the onlineversion of this article.
Potential conflict of interest: None to report.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23076
FIG. 1. T2-weighted MRI showing bilateral hyperechogenicity ofthe inferior olives in the patient with SPT.
1304 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

atic. Dysphagia in SPT results from a poor bolus controlcaused by an inconstant glosso-velar occlusion due to invol-untary contractions of the veli palatini muscle.3 In addition,the timing of the laryngeal closure including adduction of thevocal folds is impaired by the tremulous hyperkinesias. Froma clinical point of view, we suggest to extend the neurologicalwork-up in these patients with a clinical swallowing examina-tion by a specialized speech therapist along with a technicalinvestigation of the swallowing procedure if available. In thisparticular case, we regarded clinical observation and directendoscopy suitable to generate a diagnostic and treatmentstrategy. However, it has to be pointed out that video fluoros-copy provides unique and additional information in the over-all functional status of the swallowing function and should,therefore, be also considered in patients with PT. Speech ther-apy and the acquisition of compensatory swallowing techni-ques are useful to avoid aspiration in SPT patients.
LEGENDS TO THE VIDEO
Segment 1. Initial clinical examination showing rhythmicmovements of the ventral neck muscles, the soft palate (vis-ual inspection and fiberendoscopic view) and a mild slurredspeech.
Segment 2. Initial fiberoptic endoscopy showing rhythmicinvoluntary movements of the soft palate and the laryngealmuscles at rest and during phonation and laryngeal aspirationwhile swallowing of liquids.
Segment 3. Clinical examination at 6 months follow-upvisit revealing horizontal and vertical rotational nystagmus,hyper- and hypometric saccades and a disturbed fixation-sup-pression of the VOR.
Segment 4. Fiberoptic endoscopy at 6 months follow-upvisit demonstrating progressive symptom severity of palataland laryngeal tremor.
Author Roles: S. van de Loo: Research project: concep-tion, organization, and execution; manuscript: writing of thefirst draft and review and critique. S. Somasundaram:Research project: conception, organization, and execution;manuscript: writing of the first draft and review and critique.M. Wagner: Research project: execution; manuscript: reviewand critique. O. C. Singer: manuscript: review and critique.H. Steinmetz: manuscript: review and critique. R. Hilker:Research project: conception; manuscript: writing of the firstdraft and review and critique.
Financial Disclosures: R. Hilker, Advisory Boards: Ceph-alon; Honoraria: Medtronic and Orion; Grants: ClaxoSmith-Kline, Teva, Cephalon, Desitin, Boehringer Ingelheim(speaker honoraria), Medtronic, Cephalon (travel grants),Deutsche Parkinson Vereinigung (research funding). H. Stein-metz: Consultancies: PhotoThera, USA; Honoraria: Boeh-ringer, GlaxoSmithKline, SanofiAventis.
Simone van de Loo, MDSriramya SomasundaramDepartment of Neurology
Goethe UniversityFrankfurt am Main
Germany
Marlies Wagner, MDInstitute of Neuroradiology
Goethe UniversityFrankfurt am Main
Germany
Oliver C. Singer, MDHelmuth Steinmetz, MD
Rudiger Hilker, MD*Department of Neurology
Goethe UniversityFrankfurt am Main
Germany*E-mail: [email protected]
References
1. Deuschl G, Wilms H. Clinical spectrum and physiology of palataltremor. Mov Disord 2002;17(Suppl 2):S63–S66.
2. Pearce JM. Palatal myoclonus (syn. palatal tremor). Eur Neurol2008;60:312–315.
3. Deuschl G, Toro C, Valls-Sole J, Zeffiro T, Zee DS, Hallett M.Symptomatic and essential palatal tremor. I. Clinical, physiologi-cal and MRI analysis. Brain 1994;117:775–788.
4. Samuel M, Torun N, Tuite PJ, Sharpe JA, Lang AE. Progressiveataxia and palatal tremor (PAPT): clinical and MRI assessmentwith review of palatal tremors. Brain 2004;127:1252–1268.
5. Goyal M, Versnick E, Tuite P, et al. Hypertrophic olivary degen-eration: metaanalysis of the temporal evolution of MR findings.Am J Neuroradiol 2000;21:1073–1077.
6. Sumer M. Symptomatic palatal myoclonus: an unusual cause ofrespiratory difficulty. Acta neurologica Belgica 2001;101:113–115.
7. Drysdale AJ, Ansell J, Adeley J. Palato-pharyngo-laryngeal myo-clonus: an unusual cause of dysphagia and dysarthria. J LaryngolOtol 1993;107:746�747.
8. Storey E, Knight MA, Forrest SM, Gardner RJ. Spinocerebellarataxia type 20. Cerebellum 2005;4:55�57.
Paroxysmal Kinesigenic Dyskinesia sans
Dyskinesia or Paroxysmal Kinesigenic
Dysesthesia?
Since being first described in 19401 and undergoing chang-ing nosology, paroxysmal kinesigenic dyskinesia (PKD) hasbeen well characterized.2 Prodromal feelings of pins and nee-dles and numbness have been recognized3 and are common.4
This case presented with strikingly similar characteristics, yetlacked dyskinesia. Here is presented a possible variant notpreviously reported.
A 19-year-old women student presented in 2003 concernedher episodic symptoms over the preceding 5 months might bedue to multiple sclerosis.
The first episode was noted as walking after an exam.Symptom onset consisted of numbness in the left foot, whichthen ascended to the hip. The left leg muscles felt differentyet still moved normally. The right leg was then affectedreaching a climax and resolving within less than a minute.
Potential conflict of interest: Nothing to report.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23077
Movement Disorders, Vol. 25, No. 9, 2010
1305LETTERS TO THE EDITOR

Spells continued approximately once per week, only triggeredby brisk walking. These novel, odd sensations were associ-ated with anxiety and a need to sit down.
The symptom was not triggered by heat, and she had noother complaints. Her arms were never involved, and therewas no leg weakness, abnormal movement, bladder or bowelsymptoms, headache, and back pain. Her past medical historywas unremarkable. She was on oral contraception. There wasno family history of similar symptoms, multiple sclerosis orinvoluntary movements.
Neurologic exam was unremarkable. On sensory testing,there was a subtle sensitivity to temperature and pin prickbetween T6 and T10 bilaterally, which seemed to be withinthe spectrum of a ticklish response. Superficial abdominalreflexes were normal.
ESR, CPK, ANA, antiphospholipid antibodies, and MRI ofthe brain and spinal cord showed no abnormality. There wasa minor central disk bulge at T6–7 without cord involvement.Auditory, visual, and somatosensory evoked potentials werenormal.
By 2004, symptoms increased to daily. Discontinuing thebirth control pill did not change the symptoms. Despite theincreased frequency of the spells, she became quite accus-tomed to them and was not seeking treatment.
She was next seen in 2009. Episodic symptoms persisted,now occurring many times every day, triggered by walkingor jogging, but also with rising quickly from a chair. The du-ration characteristically was 30 to 60 seconds. The paroxys-mal symptoms continued in the same sensory disturbance butthe left arm was also sometimes affected. There was no lossof power, coordination, or movement disorder. When symp-toms occurred with jogging, she continued as it wouldresolve despite ongoing exercise. Her examination wasunchanged. During the visit, subsequent to rising from herchair, she indicated the symptoms were occurring. There wasno evidence of any involuntary movement, cramping, or ab-normality on tone testing. The spell did not last long enoughto enable a sensory exam when symptomatic.
A repeat spine MRI demonstrated no significantabnormality. A 24-hour ambulatory EEG was normal duringfour captured events. Two occurred while jogging and twowhile walking. The patient agreed to a therapeutic trial ofcontinuous release carbamazepine, 200 milligram once a day.This completely resolved the symptoms within a few daysfor the first time in 5 years. The patient discontinued the car-bamazepine after experiencing 2 weeks completely free ofspells, due to her preference to avoid medications and thenonlimiting nature of her symptoms. The spells returnedwithin a few days.
The kinesigenic trigger, short duration, lack of loss of con-sciousness or pain, control of attacks with carbamazepine,age of onset, together with the negative investigations andexam, fulfill the diagnostic criteria for PKD.4 Interestingly,these authors do not mention dyskinesia within their pub-lished diagnostic criteria list, although it was implied withinthe text of their publication. The history of sensory symptomin this patient is reminiscent of the auras described in 94%of their sporadic cases.
A psychogenic disorder is in the differential diagnosis ofPKD, but this women did not meet the minimal criteriarequired for a ‘‘possible psychogenic movement disorder.’’5
She had no psychiatric history or other systemic complaints.
She had not stopped any life activity nor was she seekingcompensation.
To my knowledge, there are no reported cases of a parox-ysmal, non epileptic, purely sensory symptom complex, trig-gered by movement, without associated dyskinesia. Neitherhave family members of typical PKD cases been reported tohave symptoms restricted to an ‘‘aura.’’ Given the strikingsimilarities between this case and PKD, this perhaps couldbe described as a ‘‘PKD equivalent’’ in the same manner asa migraine aura without headache (migraine equivalent).Alternatively, this case could be labelled as paroxysmal kine-sigenic dysesthesia. Investigators should screen family mem-bers of cases of PKD in search of other similar cases as Isuspect this is not an isolated one.
Douglas E.Hobson, BSc, FRCP(C)*Movement Disorder Program
Deer Lodge CentreUniversity of Manitoba
Winnipeg, Canada*E-mail:[email protected]
References
1. Mount I, Reback S. Familial paroxysmal choreoathetosis; Prelimi-nary report on a hitherto undescribed clinical syndrome. ArchNeurol Psychiatry 1940;44:841–847.
2. Lance J. Familial paroxysmal dystonic choreoathetosis and its dif-ferentiation from related syndromes. Ann Neurol 1977;2:285–293.
3. Mehta S, Morgan J, Sethi K. Paroxysmal dyskinesias. Curr TreatOptions Neurol 2009;11:170–178.
4. Bruno M, Hallet M, Gwinn-Hardy K, et al. Clinical evaluation ofidiopathic paroxysmal kinesigenic dyskinesia; new diagnostic cri-teria. Neurology 2004;12:2280–2287.
5. Shill H, Gerber P. Evaluation of clinical diagnostic criteria for psy-chogenic movement disorders. Mov Disord 2006;21:1163–1168.
Adult-Onset Leg Dystonia Due to a Missense
Mutation in THAP1
Video
THAP1 encodes a transcription factor that contains an atypi-cal zinc finger domain and regulates cell proliferation in thecontext of cell cycle progression.1 An Exon 2 insertion/deletionframeshift mutation in THAP 1 produces DYT 6 dystonia inAmish-Mennonites.1 Two early, follow-up studies identified 11additional sequence variants in familial, primarily early-onset,primary dystonia.2 More recently, a heterogeneous collection ofTHAP1 sequence variants has been associated with varied ana-tomical distributions and onset ages of both familial and spo-radic primary dystonia. Adult-onset dystonia characteristicallybegins in the craniocervical or brachial areas and tends toremain confined to these regions, whereas dystonia manifesting
Additional Supporting Information may be found in the onlineversion of this article.
Potential conflict of interest: None.Published online 13 April 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23086
1306 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

before the age of 30 usually starts in a leg or arm and thenbecomes more generalized.3 Peripheral trauma and other senso-rimotor perturbations may induce dystonia in genetically pre-disposed individuals.4,5 Adult-onset focal lower extremity dys-tonia usually involves foot inversion.6
A 63-year-old, right-handed American man of Danish ances-try, and without known Amish-Mennonite roots, presented witha 12-year history of gait difficulties, initially manifesting asintermittent ‘‘flopping’’ of his left foot and paresthesias overthe lateral aspect of his left leg. He had not undergone lumbo-sacral spine surgery. Over time, the patient began to notice thathis left leg would feel ‘‘tight, like a bow’’ while ambulating.He also found that he would ‘‘need to walk quicker to feelmore stable.’’ Indeed, his wife has noticed that he seems towalk at a ‘‘double-step’’ now. He has not found other gaitadaptations that will alleviate his problem nor is a diurnal vari-ation apparent; the feeling of ‘‘tightness’’ in his leg is onlyapparent while ambulating. A couple of years before presenta-tion, the patient retired from the post office, because of deterio-ration in his handwriting, associated with ‘‘shaking’’ and a feel-ing of ‘‘tightness’’ in his forearm and hand. The latter has notbeen alleviated by alcohol consumption or writing in differentpositions. The patient does not have much difficulty with tasks,such as eating, pouring, or dressing. His deceased father wasdiagnosed with ‘‘torticollis’’ after sustaining a neck injury atage 16, and a living, paternal aunt developed ‘‘neck shakingand twitching,’’ allegedly after undergoing thyroid surgery inher 20s. The patient’s examination was notable for mild, leftL5/S1 distribution weakness. His gait revealed excessive con-traction of his left hamstrings and gastrocnemius as he made astep with his left leg; having him walk backward and run didnot alleviate his gait dysfunction notably (see video, segment1). The patient had a severe writing tremor, yet only a subtlepostural and action upper limb tremor, and no action tremor onpouring (see video, segments 2 and 3), suggesting that his writ-ing tremor is likely dystonic. No adventitial neck movementsor abnormal cervical or upper limb postures were evident.Electromyography revealed evidence of a relatively mild, qui-escent, left L5/S1 radiculopathy. Sequencing of THAP1 in theforward and reverse directions revealed a c.446T>C sequencevariant, producing substitution of a strongly hydrophobic iso-leucine residue with a threonine (l149T) in the nuclear localiza-tion signal domain of THAP1. The patient’s paternal aunt,alluded to above, was found to harbor the same c.446T>Csequence variant. The patient has not responded to a levodopatrial and has not been interested in pursuing other treatmentoptions, such as botulinum toxin injections.
Our patient’s history of present illness, family history,neurologic and neurophysiologic examinations, and THAP1mutation demonstrate that adult-onset, primary dystonia maybegin in a lower extremity, may not be associated with footinversion, and reinforces that the anatomic site of onset of aprimary dystonia may be influenced by trauma and/or a struc-tural lesion, potentially producing a multifocal dystonic state.
LEGENDS TO THE VIDEO
Segment 1. Ambulating, the patient has excessive contrac-tion of his left gastrocnemius and hamstrings, but no inver-sion of his foot. Walking backward does not significantlyaffect his gait abnormalities.
Segment 2. Excessive contraction is noted in the patient’sright hand and forearm as he writes, producing tremulous writing.
Segment 3. Holding two glasses of water outstretched andpouring one into the other, no significant tremor is present.
Acknowledgments: Dr. Wszolek and Dr. Van Gerpenreceive research support from the NIH through Udall GrantNS40256-09CCJ. We are grateful to Audrey Strongosky forher superb video editing and clerical assistance.
Financial Disclosures: Dr. LeDoux has received supportfrom the Neuroscience Institute at the University of Tennes-see Health Science Center, Dystonia Medical Research Foun-dation, NIH (ROIN5048458), and Bachman-Strauss Dystonia& Parkinson’s Foundation.
Author Roles: Jay Van Gerpen contributed to conceptionand design, data acquisition/analysis, drafting and editing ofthe text. Mark LeDoux contributed to conception and design,data analysis, editing of text. Zbigniew W. Szolek contrib-uted to conception and design, data acquisition, editing oftext.
Jay A. Van Gerpen, MD*Section of Movement Disorders
Department of NeurologyMayo Clinic
Jacksonville, Florida, USA*E-mail: [email protected]
Mark S. LeDoux, MD, PhDDivision of Movement Disorders
Department of NeurologyUniversity of Tennessee Health Sciences Center
Memphis, Tennessee, USA
Zbigniew K. Wszolek, MDSection of Movement Disorders
Department of NeurologyMayo Clinic
Jacksonville, Florida, USA
References
1. Fuchs T, Gavarini S, Saunders-Pullman R, et al. Mutations in theTHAP1 gene are responsible for DYT6 primary torsion dystonia.Nat Genet 2009;41:286–288.
2. Bressman SB, Raymond D, Fuchs T, Heiman GA, Ozelius LJ,Saunders-Pullman R. Mutations in THAP1 (DYT6) in early-onsetdystonia: a genetic screening study. Lancet Neurol 2009;8:441–446.
3. Albanese A. Dystonia: clinical approach. Parkinsonism Relat Dis-ord 2007;13 (Suppl 3):S356–S361.
4. Conti AM, Pullman S, Frucht SJ. The hand that has forgotten itscunning—lessons from musicians’ hand dystonia. Mov Disord2008;23:1398–1406.
5. Jankovic J. Can peripheral trauma induce dystonia and other move-ment disorders? Yes! Mov Disord 2001;16:7–12.
6. McKeon A, Matsumoto JY, Bower JH, Ahlskog JE. The spectrumof disorders presenting as adult-onset focal lower extremity dysto-nia. Parkinsonism Relat Disord 2008;14:613–619.
Movement Disorders, Vol. 25, No. 9, 2010
1307LETTERS TO THE EDITOR

Reversible Hyperkinetic Movement Disorder
Associated with Quetiapine Withdrawal
Video
In recent years, the atypical antipsychotics (AAs) are morefavorably used for long-term treatment of schizophrenia andbipolar disorders when compared to conventional agents. AAshave less adverse effects, particularly in regards to extrapyra-midal symptoms.1 Among the AAs, quetiapine is a potentserotonergic receptor antagonist and a moderate dopaminergicantagonist. It is commonly used in the treatment of not onlyschizoaffective and bipolar disorders but also psychosis in Par-kinson’s disease. Neurological complications of this drug andpsychotic decompensation during quetiapine withdrawal arenot uncommon.2,3 Reports of movement disorders followingabrupt quetiapine withdrawal, however, are limited.
We report a rare case of acute quetiapine withdrawal-related movement disorder.
A 30-year-old male tourist was discovered by hotel staffin a state of confusion with abnormal limb movements. Hehad appeared well on the night before upon checking into thehotel. On arrival at the Emergency Department he was foundto be agitated, profusely sweating, tachycardic (pulse rate110 beats per min), and blood pressure was 130/72. He hadincoherent speech and was not able to give any relevant his-tory. He had traveled alone, and there were no relatives orfriends to contact for further history. He had involuntary,irregular jerky movements of his head and facial grimacing.There were also purposeless, asynchronous, tremulous move-ments of his hands which were almost continuous (Sup-porting Information Video). Gait was mildly ataxic. Theremainder of the neurologic examination was nonfocalincluding reflexes, with flexor plantar responses.
Routine investigations included infectious, inflammatory,and metabolic screening, which were negative. Electroence-phalography and CT scan of the brain were also normal. Hewas initially diagnosed with delirium tremens and treatedwith benzodiazepines, but there was little improvement. Sub-sequently, his urine toxicology screen returned as unremark-able except for traces of quetiapine. He was started on que-tiapine 12.5 mg bid with gradual increment to 100 mg perday. Three days after the introduction of quetiapine, he wasspeaking coherently and the involuntary movements wereless pronounced. He informed us that he carried a diagnosisof schizophrenia and had been on long-term quetiapine treat-ment, with total dose 400 mg per day. He had run out of themedication 2 days before arriving to Singapore. His symp-toms resolved completely 4 days after restarting quetiapine,and he was discharged in a stable state.
Quetiapine withdrawal-related psychotic decompensationhas been previously reported in the literature.3,4 However, toour knowledge, there are limited descriptions of abnormalmovements following abrupt withdrawal of quetiapine. A sin-gle case report described a patient with bipolar disorder onquetiapine, lithium, and divalproex who developed chorei-
form movements after discontinuation of his medications;however, in this case, the contributions of the other medica-tions to the acute movement disorder could not be separatedfrom those of quetiapine.5 Our patient had long-standingschizoaffective disorder and was solely on high-dose quetia-pine when he developed a complex hyperkinetic movementdisorder 2 days after discontinuation of the drug. The com-plete symptom resolution when quetiapine was restarted sup-ports a primary role for quetiapine in the patient’s movementdisorder.
There are several potential explanations for the role ofquetiapine in the generation of patient’s movement disorder.Quetiapine is a serotonin 5-HT1A and dopamine D2 receptorantagonist. As with other tardive syndromes, chronic block-ade of these receptors may have caused a compensatory up-regulation of central neurotransmitter production as well asreceptor binding sites and affinity.6,7 Other factors that mayhave influenced the severity of symptoms include the highdoses of drug, long duration of use, and the abrupt with-drawal of the drug. The dramatic therapeutic improvementwithin a short period of time also raises the possibility thatthis individual patient may be highly sensitive to the pharma-cological effects of quetiapine.
The use of AAs such as quetiapine is rapidly increasing asresult of a widening number of therapeutic indications andless severe side effects as compared to the conventionalagents. Therefore, it is expected that withdrawal symptomsdue to these agents may become more commonly observedin the future. Our experience with this patient emphasizes theimportance of having a high index of suspicion for possibleantipsychotic withdrawal-related symptoms as patients maynot be able to give a relevant history of antipsychotic use atpresentation. In these situations, toxicology tests may behelpful in detecting traces of the withdrawn medication.Finally, when initiating treatment with antipsychotic agents,patients and their caregivers need to be warned against thepossible risks of sudden discontinuation of these drugs.
Legends to the Video
The patient has involuntary, irregular, jerky movements ofhis head, facial grimacing, and purposeless, asynchronous,tremulous movements of his hands (right more pronouncedthan left as he suffered brachial plexopathy on left side inrecent past).
Financial Disclosures: Nothing to disclose.
Author Roles: Mohammed T. Ahmad was involved in thewriting of the first draft, patient assessment, followup, andvideo filming. Kumar M. Prakash was involved in reviewand critique, writing of the final draft, patient and videoassessment, and video editing.
Mohammed T. Ahmad, MD*Kumar M. Prakash, MD
Department of NeurologyNational Neuroscience Institute (SGH campus)
Singapore*E-mail: [email protected]
Potential conflict of interest: None to report.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23089
1308 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

References
1. Stanniland C, Taylor D. Tolerability of atypical antipsychotics.Drug Saf 2000;22:195–214.
2. Graver DL. Review of quetiapine side effects. J Clin Psychiatry2000;61:31–33.
3. Thurstone CC, Alahi P. A possible case of quetiapine withdrawalsyndrome. J Clin Psychiatry 2000;61:602–603.
4. Kim DR, Staab JP. Quetiapine discontinuation syndrome. Am JPsychiatry 2005;162:1020.
5. Michaelides C, Thakore-James M. Reversible withdrawal dyskine-sia associated with quetiapine. Mov Disord 2005;20:769–770.
6. Burt DR, Creese I, Snyder SH. Antischizophrenic drugs: chronictreatment elevates dopamine receptor binding in brain. Science1977;196:326–328.
7. Hitri A, Weiner WJ, Borison RL, Diamond BI, Nausieda PA,Klawans HL. Dopamine binding following prolonged haloperidolpretreatment. Ann Neurol 1978;3:134–140.
Isolated Continuous Lingual Myoclonus:
Unusual Presentation of Amyotrophic
Lateral Sclerosis
Video
Continuous lingual myoclonus is a rare disorder frequentlyassociated with similar palatal, facial, or cervical move-ments.1,2 Isolated myoclonus of the tongue is an exceptionalpoorly documented and understood entity. We recentlyobserved a case of isolated continuous myoclonus of thetongue as a presentation of amyotrophic lateral sclerosis(ALS).
A 45-year-old woman noted a continuous involuntarymovement of the tongue and impairment of speech. Neuro-logical examination revealed bilateral symmetric contractionof the tongue that produced a narrowing of its anterior por-tion. The movements were continuous, apparently rhythmic,observed both when the tongue was protruded and at rest(Video, Segments 1 and 2), unresponsive to placebo drugs,distraction, and suggestion. Speech was mildly dysarthric,with impaired rate, intelligibility and prosody (Video, Seg-ment 3). No other neurological signs were manifested at theonset. Brain MRI and electroencephalography evoked poten-tials and transcranial magnetic stimulation (TMS) fromtongue and hand muscles were normal. Cortical excitabilitytest (relaxed motor threshold, central silent period, and intra-cortical inhibition and facilitation) were also normal. Exten-sive electromyography (EMG) of bulbar, trunk, and limbmuscles was also normal. Multichannel-EMG recordings(Fig. 1) showed a bilateral continuous, low frequency (1–2Hz), long duration (<400 milliseconds), synchronous, andpseudorhythmic bursts only in genioglossus muscles. Endos-copy did not reveal palatal or pharyngeal involvement. Clo-
nazepam slightly affected in amplitude and frequency myo-clonus. Six months later, she developed a progressive bulbarand motor palsy. Neurological examination showed: swallow-ing problems, fasciculations of the tongue; exaggerated pha-ryngeal, jaw, and facial reflexes; mild weakness on neckflexor muscles; weakness and atrophy in the right thenarmuscles; increased tendon jerks in upper and lower limbs.EMG showed diffused involvement of lower motor neuronlimbs and bulbar muscles. Electroneurography was normal.TMS detected a delay of the central motor conduction timein tongue, upper limb, and lower limb.
MRI of brain and spinal cord, serological, and cerebrospi-nal fluid (CSF) examination, also for tropheryma whippleipolymerase chain reaction, were normal. According to the ElEscorial revised criteria,3 other condition that can mimicALS (e.g., Paraneoplastic) were excluded. She was finallydiagnosed as clinically definite ALS.3 Lingual myoclonuscontinued till she died after 2 years from the onset becauseof respiratory failure.
Different etiological conditions that involves inferior olivenuclei (ION)/dentate-olivary pathway4 can cause involuntarymovements of the tongue and sometime of other branchialmuscles.1,2,4 Two forms of isolated lingual myoclonus hasbeen described: symptomatic and spontaneous.1,2 In sympto-matic,2 movements typically occur in episodes beginning asposterior midline depression of the tongue, also referred to as‘‘galloping tongue.’’
In spontaneous form of lingual myoclonus, patients experi-ence continuous bilateral and symmetric involuntary contrac-tions of the tongue that produce narrowing of its anterior por-tion, not be influenced or stopped by any action often with dys-arthric speech.1 Our patient exactly reflected this description.
ALS is a complex and multifactorials disease; the hallmarkis represented by motor neuron loss in cortex, brainstem, andspinal cord.3 Up to 35% of new ALS patients show orolin-gual motor deficit as an early sign of the disease.3
In our patient, isolated continuous lingual myoclonus pre-ceded the clinical onset of ALS.
Additional Supporting Information may be found in the onlineversion of this article.
Potential conflict of interest: Nothing to report.Published online 13 April 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23099
FIG. 1 . Multichannel surface and needle electromyography showeda bilateral continuous, low frequency (1–2 Hz), long duration (<400milliseconds), synchronous, and rhythmic bursts in genioglossusmuscles. No EMG activity was recorded in orbicularis oris and mass-eter muscles.
Movement Disorders, Vol. 25, No. 9, 2010
1309LETTERS TO THE EDITOR

Neuronal loss and increase of excitatory neurotransmissionare the main mechanisms of ALS; its unbalance of neuro-transmission may act on the modulatory effects of dentate-ol-ivary pathway, that is, dynamically organized around the os-cillatory (1–10 Hz) membrane potential properties of IONneurons and on their connectivity.5 In our patient, MRI didnot show ION/dentate-olivary lesions nor early TMS findingspoint to cortico-bulbar involvement. In conclusion, wehypothesize that in our patient the unbalance of neurotrans-mission, proper of ALS, acts on dentate-olivary tracts andconsequently on ION property discharges causing myoclonus.To our knowledge, this is the first case of isolated continuouslingual myoclonus as a first sign of presentation of ALS.
Legends to the Video
Neurological examination revealed bilateral symmetriccontraction of the tongue that produced a narrowing of its an-terior portion. The movements were continuous, apparentlyrhythmic, observed both when the tongue was at rest (Seg-ment 1) and protruded (Segment 2), unresponsive to placebodrugs, distraction, and suggestion. Speech was mildlydysarthric, with impaired rate, intelligibility and prosody(Segment 3).
Financial Disclosure: Nothing to disclose.Author Roles: C. Civardi: Conception, organization, and
execution of research project; design, execution, and reviewand critique of statistical analysis; writing of the first draftand review and critique of the manuscript. A. Collini: Execu-tion of research project; design, execution, and review andcritique of statistical analysis; review and critique of themanuscript. L. Mazzini: Organization of research project;review and critique of statistical analysis; review and critiqueof the manuscript. L. Testa: Execution of research project;review and critique of statistical analysis; review and critiqueof the manuscript. F. Monaco: Review and critique of statisti-cal analysis; review and critique of the manuscript.
Carlo Civardi, MD*Alessandra Collini, MD
Letizia Mazzini, MDLucia Testa, MD
Francesco Monaco, MDDepartment of Neurology
Universita del Piemonte Orientale‘‘A. Avogadro’’, Novara, Italy
*E-mail: [email protected]
References
1. Gobernado JM, Galarreta M, De Blas G, Jimenez-Escrig A, Her-nandez A. Isolated continuous rhythmic lingual myoclonus. MovDisord 1992;7:367–369.
2. Kulisevsky J, Avila A, Grau-Veciana JM. Isolated lingual myoclo-nus associated with an Arnold-Chiari malformation. J Neurol Neu-rosurg Psychiatry 1994;57:660–661.
3. Brooks BR, Miller RG, Swash M, Munsat TL,World Federationof Neurology Research Group on Motor Neuron Diseases. ElEscorial revisited: revised criteria for the diagnosis of amyotrophiclateral sclerosis. Amyotroph Lateral Scler Other Motor NeuronDisord 2000;1:293–299.
4. Silverdale MA, Schneider SA, Bhatia KP, Lang AE. The spectrumof orolingual tremor-a proposed classification system. Mov Disord2008;23:159–167.
5. De Zeeuw CI, Simpson JI, Hoogenraad CC, Galjart N, KoekkoekSK, Ruigrok TJ. Microcircuitry and function of the inferior olive.Trends Neurosci 1998;21:391–400.
Reduced Facial Nerve Hyperexcitability
from Contralateral Cerebral Stroke in
Hemifacial Spasm
There are several theories regarding the cause of hemifa-cial spasm. Support for the theory that hemifacial spasm isdue to compression of the facial nerve comes from neuroi-maging studies which frequently show contact between thenerve and offending vessel, and histological evidence of de-myelination or nerve degeneration at the root exit zone. Sur-gical relief of compression usually results in relief of the dis-order. The synkinesis of hemifacial spasm has been postu-lated to result from ephaptic transmission and axonalexcitability studies suggest that the facial nerve may have apropensity to develop ectopic impulse activity.1
In contrast, there is also evidence of hyperexcitability ofthe facial nerve motor nucleus,2 suggesting the abnormal ac-tivity may be generated central to the exit zone. In additionto its peripheral effects, botulinum toxin acts on the centralnervous system and may alter cortical excitability.3
We report a patient with right hemifacial spasm, whichpartially resolved following a left middle cerebral arterystroke.
A woman with a history of hypertension developed righthemifacial spasm at the age of 68 years. Onset of the spasmswas in the periorbital region which then gradually spread toinvolve other muscles supplied by the right facial nerve.Magnetic resonance imaging (MRI) brain showed some tortu-osity of the right vertebral artery, with kinking posteriorlycausing compression on the brainstem in the region of theright facial nerve exit zone. She began treatment with 3monthly botulinum toxin injections, usually receiving a totaldose of 14 units (BotoxTM, Allergan, Irvine, CA) into ninesites including the right orbicularis oculi, orbicularis oris, andmentalis. She obtained a good response to this treatment withsome recurrence of spasm reliably and predictably within 3weeks prior to the next dose.
At the age of 75 years, the patient suffered an ischemicsubcortical stroke involving the left middle and posterior cer-ebral artery territories resulting in expressive and receptivedysphasia, right lower quadrant facial droop, and right armand leg weakness (diffusion weighted MRI, Fig. 1A,B).Investigations showed paroxysmal atrial fibrillation. After 6months, the dysphasia and right facial droop had improvedbut mild right arm and leg weakness persisted. She wasfound to be clinically free of hemifacial spasm until 5 monthsafter her stroke and 7 months after her last botulinum toxininjection, when there was a very mild recurrence of right fa-cial twitch. Hemifacial spasm remained mild 18 months afterthe event, not requiring further toxin injections.
A post-stroke facial blink study was within normal limits.Facial muscle F-wave studies were performed (Table 1) using
Potential conflict of interest: None reported.Published online 22 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23094
1310 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010
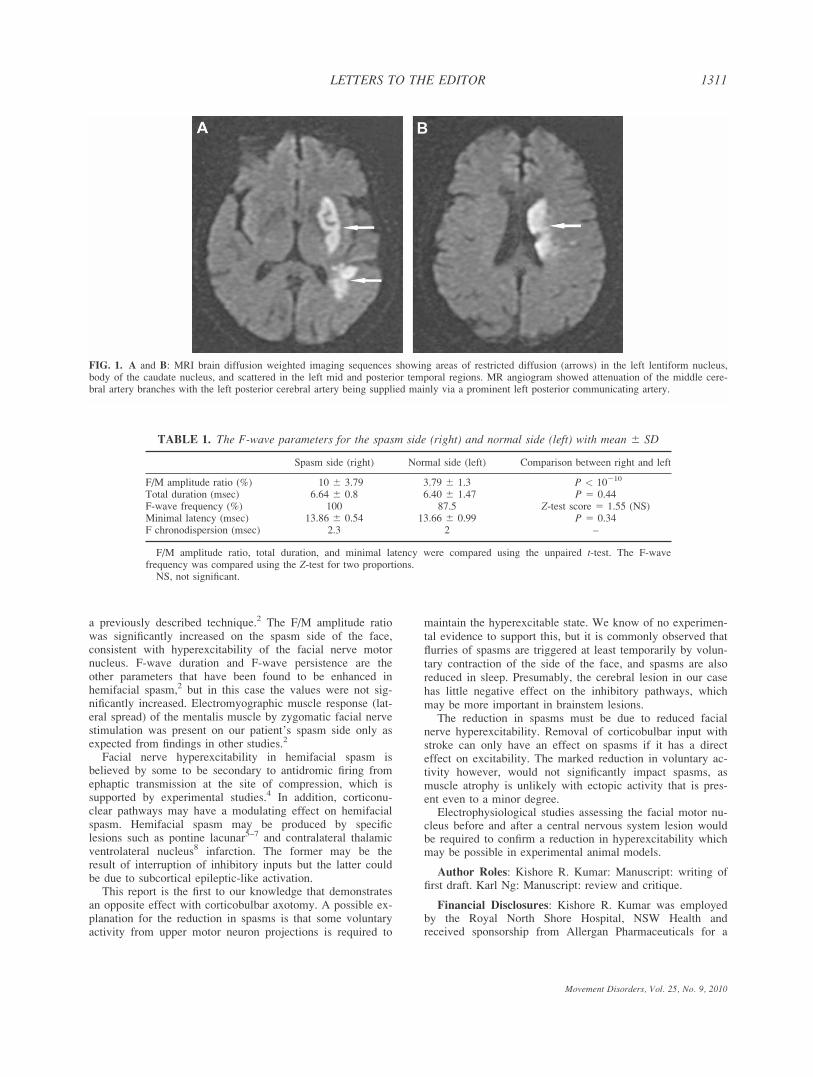
a previously described technique.2 The F/M amplitude ratiowas significantly increased on the spasm side of the face,consistent with hyperexcitability of the facial nerve motornucleus. F-wave duration and F-wave persistence are theother parameters that have been found to be enhanced inhemifacial spasm,2 but in this case the values were not sig-nificantly increased. Electromyographic muscle response (lat-eral spread) of the mentalis muscle by zygomatic facial nervestimulation was present on our patient’s spasm side only asexpected from findings in other studies.2
Facial nerve hyperexcitability in hemifacial spasm isbelieved by some to be secondary to antidromic firing fromephaptic transmission at the site of compression, which issupported by experimental studies.4 In addition, corticonu-clear pathways may have a modulating effect on hemifacialspasm. Hemifacial spasm may be produced by specificlesions such as pontine lacunar5–7 and contralateral thalamicventrolateral nucleus8 infarction. The former may be theresult of interruption of inhibitory inputs but the latter couldbe due to subcortical epileptic-like activation.
This report is the first to our knowledge that demonstratesan opposite effect with corticobulbar axotomy. A possible ex-planation for the reduction in spasms is that some voluntaryactivity from upper motor neuron projections is required to
maintain the hyperexcitable state. We know of no experimen-tal evidence to support this, but it is commonly observed thatflurries of spasms are triggered at least temporarily by volun-tary contraction of the side of the face, and spasms are alsoreduced in sleep. Presumably, the cerebral lesion in our casehas little negative effect on the inhibitory pathways, whichmay be more important in brainstem lesions.
The reduction in spasms must be due to reduced facialnerve hyperexcitability. Removal of corticobulbar input withstroke can only have an effect on spasms if it has a directeffect on excitability. The marked reduction in voluntary ac-tivity however, would not significantly impact spasms, asmuscle atrophy is unlikely with ectopic activity that is pres-ent even to a minor degree.
Electrophysiological studies assessing the facial motor nu-cleus before and after a central nervous system lesion wouldbe required to confirm a reduction in hyperexcitability whichmay be possible in experimental animal models.
Author Roles: Kishore R. Kumar: Manuscript: writing offirst draft. Karl Ng: Manuscript: review and critique.
Financial Disclosures: Kishore R. Kumar was employedby the Royal North Shore Hospital, NSW Health andreceived sponsorship from Allergan Pharmaceuticals for a
TABLE 1. The F-wave parameters for the spasm side (right) and normal side (left) with mean 6 SD
Spasm side (right) Normal side (left) Comparison between right and left
F/M amplitude ratio (%) 10 6 3.79 3.79 6 1.3 P < 10210
Total duration (msec) 6.64 6 0.8 6.40 6 1.47 P 5 0.44F-wave frequency (%) 100 87.5 Z-test score 5 1.55 (NS)Minimal latency (msec) 13.86 6 0.54 13.66 6 0.99 P 5 0.34F chronodispersion (msec) 2.3 2 –
F/M amplitude ratio, total duration, and minimal latency were compared using the unpaired t-test. The F-wavefrequency was compared using the Z-test for two proportions.
NS, not significant.
FIG. 1. A and B: MRI brain diffusion weighted imaging sequences showing areas of restricted diffusion (arrows) in the left lentiform nucleus,body of the caudate nucleus, and scattered in the left mid and posterior temporal regions. MR angiogram showed attenuation of the middle cere-bral artery branches with the left posterior cerebral artery being supplied mainly via a prominent left posterior communicating artery.
Movement Disorders, Vol. 25, No. 9, 2010
1311LETTERS TO THE EDITOR

Neuromuscular Fellowship. Karl Ng is employed by theRoyal North Shore Hospital, NSW Health and receives fund-ing from the National Health and Medical Research Councilof Australia.
Kishore R. Kumar, MBBS, FRACP*Karl Ng, MBBS (Hons 1), MRCP, FRCAP
Department of Neurology and NeurophysiologyRoyal North Shore Hospital, St Leonards
New South Wales, Australia*E-mail: [email protected]
References
1. Krishnan AV, Hayes M, Kiernan MC. Axonal excitability proper-ties in hemifacial spasm. Mov Disord 2007;22:1293–1298.
2. Ishikawa M, Ohira T, Namiki J, Gotoh K, Takase M, Toya S.Electrophysiological investigation of hemifacial spasm: F-wavesof the facial muscles. Acta Neurochir (Wien) 1996;138:24–32.
3. Curra A, Trompetto C, Abbruzzese G, Berardelli A. Centraleffects of botulinum toxin type A: evidence and supposition. MovDisord 2004;19 (Suppl 8):S60–S64.
4. Vermersch P, Petit H, Marion MH, Montagne B. Hemifacialspasm due to pontine infarction. J Neurol Neurosurg Psychiatry1991;54:1018.
5. Kawakami M, Sato T, Tochigi S, Ito T. Lacunar pontine infarctionwith hemifacial spasm as the initial symptom. Stroke 1990;21:1236.
6. Ambrosetto P, Forlani S. Lacunar pontine infarction presenting asisolated facial spasm. Stroke 1988;19:784–785.
7. Toda T, Matsumura K. Facial spasm from lacunar infarction ofthe thalamic ventrolateral nucleus. Stroke 1989;20:1289–1290.
8. Sen CN, Moller AR. Signs of hemifacial spasm created by chronicperiodic stimulation of the facial nerve in the rat. Exp Neurol1987;98:336–349.
‘‘Sensory Trick’’ in Hemichorea-Hemiballism
and in Parkinson’s Disease Tremor
Video
A puzzling clinical feature of several involuntary move-ment disorders is a phenomenon commonly known as‘‘sensory trick’’ (ST) and also termed ‘‘trick maneuver,’’‘‘geste antagonistique,’’ or ‘‘Gegendruckphanomen’’ in theinternational neurology literature. This terminology designa-tes a temporary reprieve from muscle contractions accom-plished by a specific gesture or touch (generally made inproximity to the involuntary movements). STs, which arecharacteristic occurrences for some patients with dystoniaaffecting cervical and cranial regions, add to a wide range ofevidence for sensory interactions with dystonic pathophysiol-ogy.1 Though STs also can occur with tics, they have notbeen described in hemichorea-hemiballism or in Parkinson’sdisease (PD), as in the following cases:
1. A 68 year-old man suddenly developed involuntary re-petitive movements of the tongue, face, and trunk alongwith twisting and flinging motions of the left arm andleg. Occasional oculogyric deviations occurred upwardsand to the right. The severity of this near-constantmovement disorder increased with voluntary activitiesand during a levodopa (L-dopa) trial. Review of systems,family history, and neurological examination were non-contributory apart from impaired fine motor control inthe left hand and a clumsy gait due to left-sided invol-untary movements. As illustrated in the video, thepatient eventually discovered a ST involving forcefulpressure applied at the midline posterior base of theskull. This maneuver consistently produced marked(though transient) improvement in the involuntary move-ments and also could be conducted by another person.When the ST was stopped, the involuntary movementsrecurred within 15 seconds. The patient was subsequentlystarted on tetrabenazine, 75 mg/day, with benefit for theinvoluntary movements. Head MRI revealed a localizedlow intensity signal change consistent with a right sub-thalamic infarct (see Fig. 1), accounting for the contra-lateral hemichorea-hemiballism.
2. A 54 year-old woman experienced the gradual onset ofright-sided resting tremor, cogwheel rigidity, and slowedmovement. Beyond typical features of PD, her neurologi-cal examination revealed no other motor impairments apartfrom mild right arm action tremor. She had a family his-tory of essential tremor. Her parkinsonism and actiontremor responded to L-dopa, but not to amantadine. AnMRI study of the head was normal. Five years after onsetof symptoms, her chiropractor discovered a ST thatpromptly halted resting and action tremor. This maneuverinvolved forceful, nonpainful pressure applied to the terri-
FIG. 1. In Case report 1, T2-weighted FLAIR MRI brain scan car-ried out 5 months after sudden onset of left hemichorea-hemiballism,demonstrating an old infarct within the right subthalamic nucleus(open arrow) and not evident in the first MRI scan a few days afteronset of the movement disorder. Other old infarcts are seen in theregion of the left subthalamic nucleus (solid arrow) and in the pon-tine tegmentum.
Additional Supporting Information may be found in the onlineversion of this article.
Potential conflict of interest: None reported.Published online 29 March 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23104
1312 LETTERS TO THE EDITOR
Movement Disorders, Vol. 25, No. 9, 2010

tory of the right rhomboid muscles. Relief of tremor con-tinued as long as the contact was maintained (by anotherperson), and repeated applications did not diminish itseffectiveness. This ST did not affect her right-sided brady-kinesia or rigidity.
STs add to the complexity of understanding dystonia andother movement disorders. Demonstration of a ST can leadto suspicion of ‘‘functionality’’ (and STs have been describedwith psychogenic movement disorders2). However, genuineSTs provide patients with a frustrating experience of normalmotor function lurking beneath their movement disorder.Although tics can be suppressed by mental efforts, STs donot lend themselves to simplistic explanations such as dis-tracted attention.
Most commonly, STs are simple gestures involving con-tact within the sensory territory linked to the abnormal move-ments. The sensory feedback that patients use to abort cervi-cal dystonia or tremor does not necessarily require physicaltouch, as indicated by patients whose ST consists of a gesturemade without contact.3 Blepharospasm, which can be respon-sive to sensory input around the eyes, has also beendescribed to improve from STs involving speech, coughing,eating, deviating gaze, or reading.4
Insight into the brain circuitry by which STs producesymptom relief has come from H2(
15O) positron emission to-mography investigations in cases of ST-responsive cervicaldystonia.5 Initiation of the STs led to multiple regionalchanges in the brain, including activation of bilateral occipi-tal cortices and the inferior and superior parietal regions ipsi-lateral to the direction of head turning, and decreased meta-bolic activity in supplementary motor area and primary sen-sorimotor cortex contralateral to the direction of headturning. These findings in STs emphasize the large poly-synaptic fields of brain involvement and the complexity ofsensorimotor integration in these phenomena.6
In the cases of PD and hemichorea-hemiballism presentedhere, the basis for improvements from midline back or necktactile stimulation awaits further explanation. While restingtremor in PD can be modulated by mental activity or volun-tary movement, responsiveness to a tactile ST has not beendescribed previously. Hemichorea-hemiballism can improvewith dopaminergic blockade or depletion, or with contralat-eral lesioning of the globus pallidus. Several pathways ofsensory input to the subthalamic nucleus are known by whichthe somatosensory modulation of involuntary movementsmight be enacted7 as in the present case.
Legends to the Video
In Case report 1, the typical appearance of the patient’soro-lingual, facial, and truncal dyskinesia and left-sidedlimb hemichorea-hemiballism are demonstrated at 3 monthsafter onset. There is also intermittent choreic involuntary
movement of the right upper extremity (possibly from theinfarct affecting the left subthalamic nucleus). At the end ofthe first video sequence, the patient’s ST (applying pressurewith his hand at the base of the skull) produced, within afew seconds, a marked reduction in the left-sided involun-tary movements. Next, an assistant achieved a similarresult.
Financial Disclosures: Dr. LeWitt reports receiving lec-ture fees from Boehringer Ingelheim, Glaxo SmithKline,Teva, and Novartis; consulting fees from Boehringer Ingel-heim, Impax, Ipsen, Novartis, Santhera Pharmaceuticals,Schering-Plough, and XenoPort, and grant support fromBoehringer Ingelheim, Chelsea Therapeutics, Neurologix,Novartis, Santhera Pharmaceuticals, Schering-Plough, and UCB(previously, Schwarz Pharma). Dr. Gostkowski has nothing todisclose.
Author Roles: Peter A. Lewitt and Michal T. Gostkowski:writing of the manuscript drafts, review and critique, andcompletion of the report.
Peter A. Lewitt, MD*Department of NeurologyWayne State University
School of MedicineDetroit, Michigan, USA
Department of NeurologyHenry Ford Hospital
Southfield, Michigan, USA*E-mail: [email protected]
Michal T. Gostkowski, DOCleveland Clinic Foundation
Cleveland, Ohio, USA
References
1. Tinazzi M, Rosso T, Fiaschi A. Role of the somatosensory sys-tem in primary dystonia. Mov Disord 2003;18:605–622.
2. Munhoz RP, Lang AE. Gestes antagonistiques in psychogenic dys-tonia. Mov Disord 2004;19:331–332.
3. Wissel J, Muller J, Ebersbach G, Poewe W. Trick maneuvers incervical dystonia: investigation of movement- and touch-relatedchanges in polymyographic activity. Mov Disord 1999;14:994–999.
4. Jimenez-Jimenez FJ, Garcıa-Albea E, Vaquero-Ruiperez JA,Tejeiro J, Cabrera-Valdivia F, Ayuso-Peralta L. Reading as a‘‘trick’’ for relieving blepharospasm. Mov Disord 1992;7:186.
5. Naumann M, Magvar-Lehmann S, Reiners K, Erbguth F, LeendersKL. Sensory tricks in cervical dystonia: perceptual dysbalance ofparietal cortex modulates frontal motor programming. Ann Neurol2000;47:322–328.
6. Abbruzzese G, Berardelli A. Sensorimotor integration in move-ment disorders. Mov Disord 2003;18:231–240.
7. Postuma RB, Lang AE. Hemiballism: revisiting a classic disorder.Lancet Neurol 2003;2:661–668.
Movement Disorders, Vol. 25, No. 9, 2010
1313LETTERS TO THE EDITOR




















