
Clinimetrics in Parkinson's disease - LUMC
224
Clinimetrics in Parkinson's disease
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Clinimetrics in Parkinson's disease - LUMC

Clinimetrics in Parkinson's disease

Johan Marinus
Clinimetrics in Parkinson's disease
Thesis Leiden University, June 11, 2003
ISBN: 90-6734-265-3
© 2003, J. Marinus, except (parts of) the following chapters:
chapter 2: John Wiley & Sons, Ltd.
chapter 3: BMJ Publishing Group.
chapters 5 and 9: Lippincott Williams & Wilkins.
chapter 6: American Psychiatric Publishing, Inc.
chapter 11: Elsevier Science.
No part of this book may be reproduced, stored in a retrieval system of any nature, or
transmitted in any form or by any means, electronic, mechanical, photocopying, recording or
otherwise, without prior permission in writing of the copyright owner.
Printed by: [OPTIMA], grafische communicatie, Rotterdam
Cover illustration: Han Marinus & [OPTIMA]

Clinimetrics in Parkinson's disease
PROEFSCHRIFT
ter verkrijging van
de graad van Doctor aan de Universiteit Leiden,
op gezag van de Rector Magnificus Dr. D.D. Breimer,
hoogleraar in de faculteit der Wiskunde en
Natuurwetenschappen en die der Geneeskunde,
volgens besluit van het College voor Promoties
te verdedigen op woensdag 11 juni 2003
klokke 14.15 uur
door
Johan Marinus
geboren te Leiden
in 1954

Promotiecommissie
Promotor: Prof. Dr. R.A.C. Roos
Co-promotores: Dr. J.J. van Hilten
Dr. Ir. A.M. Stiggelbout
Referent: Prof. Dr. Ir. H.C.W. de Vet (Vrije Universiteit Amsterdam)
Lid: Prof. Dr. J.C. van Houwelingen
The studies described in this thesis were performed at the Department of Neurology of the
Leiden University Medical Center, Leiden, The Netherlands, and were financially supported
by the Netherlands Organization for Scientific Research (NWO, project no. 0940-33-021) and
the Leiden University Medical Center.
Financial support for this thesis has been provided by the Netherlands Organisation for
Scientific Research (Nederlandse Organisatie voor Wetenschappelijk Onderzoek: NWO),
Stichting Het Remmert Adriaan Laan Fonds, Boehringer Ingelheim BV, GlaxoSmithKline
BV, and Roche Nederland BV.

Aan mijn vader


Contents
1. Parkinson's disease, clinimetrics, and the 'disablement process': an introduction 9
2. Systematic evaluation of rating scales for impairment and disability in Parkinson's disease 15
C. Ramaker, J. Marinus, A.M. Stiggelbout, J.J. van Hilten
Mov Disord 2002;17:867-876
3. Health-related quality of life in Parkinson's disease: a systematic review of disease- 35
specific instruments
J. Marinus, C. Ramaker, J.J. van Hilten, A.M. Stiggelbout
J Neurol Neurosurg Psychiatry 2002;72:241-248
4. Development of an instrument for the assessment of cognition in Parkinson's disease 57
J. Marinus, M. Visser, N.A. Verwey, F.R.J. Verhey, H.A.M. Middelkoop, A.M. Stiggelbout,
J.J. van Hilten
Submitted for publication
5. Evaluation of the Hospital Anxiety and Depression Scale in patients with Parkinson's 85
disease
J. Marinus, A.F.G. Leentjens, M. Visser, A.M. Stiggelbout, J.J. van Hilten
Clin Neuropharmacol 2002;25:318-324
6. The contribution of somatic symptoms to the diagnosis of depressive disorder in 101
Parkinson's disease: a discriminant analytic approach
A.F.G. Leentjens, J. Marinus, J.J. van Hilten, R. Lousberg, F.R.J. Verhey
J Neuropsychiatry Clin Neurosci 2003;15:74-77
7. Development of a questionnaire for autonomic dysfunction in Parkinson's disease: 109
the SCOPA-AUT
M. Visser, J. Marinus, A.M. Stiggelbout, J.J. van Hilten
Submitted for publication

8. Development of a short scale for motor impairments and disabilities in Parkinson's disease: 125
the SPES/SCOPA
J. Marinus, M. Visser, A.M. Stiggelbout, J. M. Rabey, P. Martínez-Martín, U. Bonuccelli,
P.H. Kraus, J.J. van Hilten
Submitted for publication
9. Activity-based diary for Parkinson's disease 145
J. Marinus, M. Visser, A.M. Stiggelbout, J.M. Rabey, U. Bonuccelli, P.H. Kraus,
J.J. van Hilten
Clin Neuropharmacol 2002;25:43-50
10. Development of a questionnaire for sleep and sleepiness in Parkinson's disease 161
J. Marinus, M. Visser, J.J. van Hilten, G.J. Lammers, A.M. Stiggelbout
Submitted for publication
11. A short psychosocial questionnaire for patients with Parkinson's disease: the SCOPA-PS 179
J. Marinus, M. Visser, P. Martínez-Martín, J.J. van Hilten, A.M. Stiggelbout
J Clin Epidemiol 2003;56:61-67
12. Summary and conclusions 197
Samenvatting en conclusies 207
List of abbreviations 219
Nawoord 221
List of publications 222
Curriculum vitae 223

- 9 -
11 Parkinson's disease, clinimetrics, and the 'disablement
process': an introduction

Chapter 1
- 10 -
Parkinson's disease Parkinson's disease (PD) is a chronic, progressive, neurological disorder that affects almost
two percent of the population over 65 years.1 The disease is named after the London
physician James Parkinson, who reported on six patients with shaking palsy or paralysis
agitans.2 Parkinson described the disease as "involuntary tremulous motion, with lessened
muscle power, in parts not in action and even when supported; with a propensity to bend the
trunk forward, and to pass from a walking to a running pace: the senses and intellects being
uninjured."
The symptoms that accompany this disease are largely caused by a reduction of dopamine in
the striatum, resulting from the selective loss of dopaminergic neurons in the substantia nigra.
The first symptoms become apparent when approximately 70-80% of these neurons have
been destroyed, implying that the symptomatic phase of the disease is probably preceded by a
long asymptomatic phase. In PD not only the dopaminergic pathways are affected, but other
neurotransmitter systems, i.e., serotonergic, noradrenergic, and cholinergic, are also
involved.3 The cause of the disease is still unknown. Most researchers take the view that the
risk of developing PD is determined by genetic factors, environmental factors, or a
combination of both.
PD is characterized by tremor, rigidity, bradykinesia, and postural disturbances.4 Non-motor
features like autonomic dysfunctions, mood changes, and cognitive deterioration often
complicate the course of the disease.
The onset of the disease generally occurs between the ages of 50 and 65, and the incidence
increases with higher age. PD is associated with a two-fold higher relative risk of death,5,6
and a five-fold higher odds ratio of institutionalisation compared to age-matched controls.5
Patients die 3-6 years earlier than non-patients,7,8 after a mean disease duration of 11-15
years.6 Patients therefore spend a long time of their life with the disease.
Current knowledge on progression of PD is often not very accurate because assessment
instruments for the various involved domains are lacking or display clinimetric problems.
Furthermore, much of the information on disease progression is derived from clinical trials
that only include patients without other serious conditions. PD generally occurs at ages over
40 and patients may develop other conditions associated with ageing (comorbidity). Most
comorbid conditions are non-fatal, but add to the disease burden. Information on disease
progression in these ‘unselected’ patients is not available. Another problem is that the
longitudinal population studies that have been performed to date, have only included a

Introduction
- 11 -
limited number of endpoints. Better insight in the course of the disease may be obtained by
performing a longitudinal study, in which all relevant domains are addressed in unselected
patients with PD. A better understanding of the possible relations and interactions may, for
instance, allow physicians or other care providers to time their interventions better.
It is important to realise that the quality of the information that is obtained in such a
longitudinal study depends on the quality of the applied measurement instruments. The
discipline that is concerned with the quality of health measurement scales is called
clinimetrics.
Clinimetrics
The term clinimetrics was introduced by Alvan Feinstein, who defined it as the "domain
concerned with indexes, rating scales, and other expressions that are used to describe or
measure symptoms, physical signs, and other distinctly clinical phenomena in clinical
medicine."9 If instruments are used to quantify disease characteristics, it is essential that they
meet certain quality criteria in order to provide accurate answers. The most important criteria
are reliability, validity, and responsiveness. Reliability is the extent to which an instrument is
free of measurement error and is often defined as the proportion of variance that is
attributable to 'true' differences between individuals.10 The concept includes the idea of
reproducibility, but also refers to internal consistency or homogeneity of the components of
an index.9 Validity is commonly defined as the extent to which a test measures what it is
intended to measure.11 Responsiveness involves the ability of an instrument to reflect changes
in health status.12
Disablement Process
Many of the existing measurement scales in PD were developed without a clear framework to
guide the construction process, often resulting in heterogeneous scales that combine items
that evaluate impairments with those that assess disabilities. The use of a framework would
have facilitated the development of conceptually clear indices. Well-known frameworks are
the International Classification of Functioning, Disability, and Health (ICF, formerly
ICIDH),13 developed by the World Health Organization, and the model of the 'Disablement
Process', put forward by Verbrugge and Jette.14 In our research project we used the latter
framework to model our research. Verbrugge and Jette proposed a sociomedical model of

Chapter 1
- 12 -
disability, that is especially useful for epidemiological and clinical research. The model
describes the pathway that links pathology with impairments, functional limitations, and
disability and proposes bi-directional relations between these entities. Extra- and intra-
individual factors, and comorbidity as a special case of an intra-individual factor, may act
upon this pathway and modify the course of the disease and its impact on the individual.
Using this model may help to identify relevant aspects of the disease, to assign these aspects
to the appropriate domains, and to evaluate whether the instruments are of sufficient
clinimetric quality.
Aim of the study
This thesis reflects the first phase of a project that aims to provide data on disease progression
in patients with PD. This first phase is concerned with arriving at the appropriate instruments,
the second phase involves the use of these instruments in the longitudinal follow-up of
patients, stratified by disease duration and age at onset of the disease. The project is called
‘the assessment of the disablement process in Parkinson’s Disease’ and is financed by the
Netherlands Organization for Scientific Research (NWO; project 940-33-021) and the Leiden
University Medical Center.
The first phase of this project (called the SCOPA project, short for SCales for Outcomes in
PArkinson's disease) involves the selection or development of practical and clinimetric sound
instruments, intended for comparing groups of patients or for clinical use in individual
patients. Scales are considered clinimetric sound if they measure one single aspect of the
disease in a valid and reliable way, and practical if they can be administered swiftly, do not
demand special equipment or skills, and provide an index that can easily be obtained and
interpreted.
We followed a standard procedure for all scales. First we evaluated whether appropriate
instruments were available. Next we assessed whether these instruments had already been
tested in PD, and whether results of these studies justified the use of this scale in the
longitudinal phase. If a scale was available, but had not been tested in PD, we assessed its
clinimetric properties in this population. If appropriate scales were not available, we
developed them.
On the impairment level, modules for the following domains were selected or constructed:
cognition, mood, psychiatric complications, motor evaluation, motor complications, and

Introduction
- 13 -
autonomic dysfunction. On the disability level modules for psychosocial disability, activities
of daily living, and sleep were developed. Other modules that were evaluated or developed
included comorbidity and costs. Applying the concept of the disablement process to our
research project resulted in the model presented in figure 1. In this thesis, the clinimetric
evaluation of scales that involved impairment and disability levels, is described.
Figure 1. Model of the SCOPA project
Extra-individual factors:- medical care & rehabilitation- medication / external support
Intra-individual factors:- lifestyle, behaviour, coping- activity accomodations
Comorbidity
IMPAIRMENTS
cognition
mood
psychiatric dysfunction
motor
motor complications
autonomic
DISABILITY
sleep
physical
psychosocial
GLOBAL
global health
costs
utility
Extra-individual factors:- medical care & rehabilitation- medication / external support
Intra-individual factors:- lifestyle, behaviour, coping- activity accomodations
Extra-individual factors:- medical care & rehabilitation- medication / external support
Intra-individual factors:- lifestyle, behaviour, coping- activity accomodations
Comorbidity
IMPAIRMENTS
cognition
mood
psychiatric dysfunction
motor
motor complications
autonomic
DISABILITY
sleep
physical
psychosocialIMPAIRMENTS
cognition
mood
psychiatric dysfunction
motor
motor complications
autonomic
IMPAIRMENTS
cognition
mood
psychiatric dysfunction
motor
motor complications
autonomic
DISABILITY
sleep
physical
psychosocialDISABILITY
sleep
physical
psychosocial
GLOBAL
global health
costs
utility

Chapter 1
- 14 -
References
1. De Rijk MC, Launer LJ, Berger K, Breteler MM, Dartigues JF, Baldereschi M, et al. Prevalence of
Parkinson's disease in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in
the Elderly Research Group. Neurology 2000; 54(11 Suppl 5):S21-S23.
2. Parkinson J. An essay on the shaking palsy. London: Sherwood, Neely, and Jones, 1817.
3. Jellinger K. Overview of morphological changes in Parkinson's disease. Adv Neurol 1987; 45:1-18.
4. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's
disease. J Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
5. Berger K, Breteler MM, Helmer C, Inzitari D, Fratiglioni L, Trenkwalder C, et al. Prognosis with
Parkinson's disease in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in
the Elderly Research Group. Neurology 2000; 54(11 Suppl 5):S24-S27.
6. Di Rocco A, Molinari SP, Kollmeier B, Yahr MD. Parkinson's disease: Progression and Mortality in the
L-DOPA Era. In: Battistin L, Scarlato G, Caraceni T, Ruggieri S, editors. Parkinson's Disease.
Philadelphia: Lippincott - Raven, 1996: 3-11.
7. Wermuth L, Stenager EN, Stenager E, Boldsen J. Mortality in patients with Parkinson's disease. Acta
Neurol Scand 1995; 92(1):55-58.
8. Ben Shlomo Y, Marmot MG. Survival and cause of death in a cohort of patients with parkinsonism:
possible clues to aetiology? J Neurol Neurosurg Psychiatry 1995; 58(3):293-299.
9. Feinstein AR. Clinimetrics. 1 ed. New Haven: Yale University Press, 1987.
10. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use.
2 ed. Oxford: Oxford Medical Publications, 1995.
11. McDowell I, Newell C. Measuring Health: A Guide to Rating Scales and Questionnaires. 2 ed. New
York: Oxford University Press, 1996.
12. Kirshner B, Guyatt G. A methodological framework for assessing health indices. J Chronic Dis 1985;
38(1):27-36.
13. World Health Organization. The international classification of functioning, disability, and health. Internet
2002. http://www3.who.int/icf/onlinebrowser/icf.cfm
14. Verbrugge LM, Jette AM. The Disablement Process. Soc Sci Med 1994; 38(1):1-14.

- 15 -
22 Systematic evaluation of rating scales for impairment and
disability in Parkinson's disease
Claudia Ramaker1, Johan Marinus1, Anne M. Stiggelbout2, Jacobus J. van Hilten1
Departments of 1Neurology and 2Medical Decision Making, Leiden University Medical Center,
Leiden, The Netherlands
Parts of this chapter were published in Movement Disorders 2002;17:867-876

Chapter 2
- 16 -
Abstract We assessed the clinimetric characteristics of rating scales used for the evaluation of motor
impairments and disabilities of patients with Parkinson's disease (PD) by conducting a systematic
review of PD rating scales published from 1960 to the present. Thirty studies describing clinimetrics
of 11 rating scales used for PD were identified. Outcome measures included validity (including factor
structure), reliability (internal consistency, inter-rater, and intra-rater), and responsiveness. We found
three impairment scales (Webster, Columbia University Rating Scale [CURS], Parkinson's Disease
Impairment Scale), four disability scales (Schwab and England, Northwestern University Disability
Scale [NUDS], Intermediate Scale for Assessment of PD, Extensive Disability Scale), and four scales
evaluating both impairments and disabilities (New York University, University of California Los
Angeles, Unified Parkinson's Disease Rating Scale [UPDRS], Short Parkinson's Evaluation Scale).
The scales showed large differences in the extent of representation of items considered responsive to
dopaminergic treatment or to those symptoms that appear late in the disease course and lack
responsiveness to treatment. Irrespective of the scale, there was a lack of consistency concerning inter-
rater reliability of bradykinesia, tremor, and rigidity. Overall, disability items displayed moderate to
good inter-rater reliability. The available evidence indicated that the CURS, NUDS, and UPDRS have
moderate to good reliability and validity. The majority of instruments demonstrated clinimetric
shortcomings or had not been subjected to extensive clinimetric testing, despite their frequent use. The
CURS, NUDS, and UPDRS have been evaluated most often and these scales are also considered valid
and reliable.

Rating scales in Parkinson's diisease
- 17 -
Introduction Parkinson's disease (PD) is a progressive neurological disorder that gradually results in
accumulating disability. Because most of the motor features result from striatal dopamine
deficiency, the treatment of patients with PD has focussed on the administration of
dopaminergic drugs to alleviate symptoms. New insights in the pathophysiology of PD and an
increasing awareness of factors that contribute to levodopa-induced motor complications have
stimulated the development of not only new drugs, but also very promising surgical
techniques.1-3 Consequently, the increasing number of therapeutic interventions in PD has
highlighted the importance of measuring clinical outcomes. In 1981, Marsden and Schachter4
reviewed all methods for the assessment of extrapyramidal disorders and presented a
comprehensive summary of subjective and objective assessments, regardless of their validity
and reliability. Since the appearance of this review, the evaluation of patient outcomes,
clinimetrics, has developed in a science of its own. Information on validity, reliability, and
responsiveness is now considered as essential knowledge to assure the useful application of a
rating scale.5 We conducted a systematic review of the clinimetric aspects of scales that are
used by observers to evaluate the motor impairments and disabilities of patients with PD.
Methods
Studies were included if they evaluated clinimetric properties of a PD rating scale that
addressed motor impairments or disabilities, evaluated by an observer. Self-report scales and
quality-of-life measures were therefore excluded from this review.6 Scales that primarily
assessed dyskinesias or motor fluctuations were also excluded. Impairment is defined as an
abnormality in structure or function of a body organ or system, and disability as a reduction of
a person's ability to perform a basic task.7,8
Search Strategy
The following sources were used to identify studies of interest: computerized searches of
Medline and EMBase (using text words [rating] scale, impairment, disability, clinimetrics,
evaluation, and the individual scale names in combination with 'Parkinson' and related terms;
search conducted December 2001), reference lists of the reviews found by the Medline and
EMBase search-strategy, SCIsearch, the Cochrane Library,9 symposia reports, PD handbooks,

Chapter 2
- 18 -
and reference lists of all included publications. Searches were not restricted to the English
language.
Methods of Review
Two reviewers independently reviewed the identified publications according to a two-step
review process. First, abstracts were reviewed for eligibility. Eligible reports were judged
against a set of methodological criteria in which both thoroughness (methodological and
statistical) and results of studies evaluating validity, reliability, and responsiveness were
assessed. A checklist was used to record sample characteristics, outcome measures,
appropriateness of statistical analysis, and methodological quality. The method of presenting
the quality of scales was adopted from McDowell and Newell.10
In attempting to interpret the different indices of correlation and degrees of agreement, we
noticed that there was no general agreement about how high they should be. Because a new
rating scale is generally not designed to replicate exactly the existing method against which it
is compared, the expected correlation should not be perfect as this may indicate that the new
scale is redundant. Few studies, however, declare what levels of correlation are to be taken as
demonstrating adequate validity or reliability.
We interpreted the different correlations and degrees of agreement for validity and reliability
as follows: the Spearman's coefficient rs, Pearson's coefficient r, Kendall's coefficient W or T,
Eta coefficient, and Cramer's coefficient V with values of 0.70 and lower were considered
poor,11 whereas values over 0.70 were considered moderate to good. The values for kappa
(K), weighted kappa (Kw), and intra-class correlation coefficient (ICC) of 0.40 or lower were
considered to indicate poor agreement, 0.41-0.60 moderate, 0.61-0.80 substantial, and values
≥ 0.81 good to almost perfect agreement.12 Cronbach's α ≤ 0.70 was considered poor, whereas
values of 0.71-0.90 were considered moderate to good.10,13 If, however, α is too high (> 0.90),
this may reflect redundancy, indicating that some of the items are unnecessary.11
The thoroughness of the evidence was classified as follows. If the appropriate statistical
procedures were used, the sample size was considered large enough, and all circumstances
were optimal (i.e., the PD population), it was classified as good. If less preferable statistical
procedures were used or the circumstances were less optimal, it was classified as moderate. If
questionable statistical procedures were used or the circumstances were somewhat doubtful or
unclear, it was classified as fair, and if the statistical procedure or the circumstances were
inadequate, it was classified as poor.

Rating scales in Parkinson's diisease
- 19 -
Studies were eligible when they calculated the following clinimetric characteristics of disease
specific impairment and disability instruments in Parkinson's disease: validity (content
validity, criterion validity, and construct validity including factor structure), reliability
(internal consistency, inter-rater reliability, intra-rater reliability), or responsiveness.
Validity
Validity is the extent to which an instrument measures what it is supposed to measure and
does not measure what it is not supposed to measure. Three types of validity are frequently
discussed: content validity, criterion validity, and construct validity.
Content validity. Content validity consists of a judgment whether the instrument samples all
the relevant topics of a domain. It relies on expert opinions and reviews of the literature.
Criterion validity. This is the demonstration of the concordance of an assessment compared
with a particular standard, the criterion. It is assessed using correlation coefficients of
concordance, or percentages of agreement. The most commonly used correlation coefficients
of concordance are Spearman's coefficient rs, Pearson's coefficient r, Kendall's coefficient W,
and Cramer's coefficient V. Coefficients range from -1 (indicating an inverse linear
association) through 0 (indicating no association at all) to +1 (indicating perfect positive
linear association). This concept is particularly useful when an obvious gold standard exists
for use as a criterion.
Construct validity. Construct validity is commonly used instead of criterion validity, because
in most cases a gold standard is lacking. It is demonstrated by examining the relations among
a newly created test and another test to show that the new test measures the same construct.
Factor analysis. Factor analysis is commonly used to study the internal structure of a scale
that contains separate components, each reflecting a different aspect of the measured domain.
Using this technique, a large number of interrelated items are reduced to a smaller number of
common dimensions or factors (clusters of items). Unrelated items do not belong to the same
factor.
Reliability
Reliability is the extent to which an instrument is free of measurement error. Reliability
assessment aims to quantify the most important sources of measurement error, and includes
both consistency among scale items and reproducibility within and between observers.

Chapter 2
- 20 -
Internal consistency. Internal consistency estimates the extent to which all items are
measuring the same construct. Cronbach's coefficient α, the most frequently used indicator of
internal consistency, represents the average of all possible split-half reliabilities. Coefficient α
will be equal to zero, if there is no linear relationship between the items. If all items are
perfectly reliable and measure the same aspect (true score), then coefficient α is equal to 1.
For clinical applications at a group level the minimum value is 0.70, whereas for use at the
individual level, a minimum of 0.90 is desirable.11
Inter-rater reliability. Inter-rater reliability is the consistency among different observers
performing the same assessment on the same individual. Inter-rater reliability is best assessed
by ICC or K.14 The ICC is a parametric measure of agreement and represents the proportion
of variance among patients caused by true differences.15 Kappa, developed for the study of
nonparametric ratings by observers, measures agreement corrected for the extent of agreement
expected by chance alone. Where categories are ordered, it may be preferable to give different
weights to disagreements according to the magnitude of the discrepancy, Kw.16 If a squared
weighting scheme is used, Kw is equivalent to the ICC.
Intra-rater reliability. This measures the reproducibility of the assessment by the same
examiner during repeat assessment. The intra-rater reliability is also best assessed by the ICC
or the K statistics.
Responsiveness
Responsiveness or sensitivity to change is the ability of an instrument to reflect underlying
change over time. In contrast to the assessment of differences in change between individuals,
there is no clear consensus as to how this should be assessed for rating methods.15,17
Other information that was gathered included the type of scale, number of items, scoring
method, and administration time. Whenever information on studies or scales was unclear or
incomplete, we contacted the authors with the request to provide additional information.

Rating scales in Parkinson's diisease
- 21 -
Results
Description of Studies
Over the period of 1966 to December 2001, 30 studies were identified that described
clinimetric characteristics of 11 rating scales for patients with PD. We excluded a study by
Cutson et al.18 that dealt with the Duke University Parkinson's Rating Scale (DUPRS),
because the scale could not be retrieved. We were unable to trace studies that evaluated
responsiveness. Three impairment scales (Columbia University Rating Scale [CURS],
Webster rating scale [Webster], and Parkinson's Disease Impairment Scale [PDIS]), four
disability scales (Northwestern University Disability Scale [NUDS], Intermediate Scale for
Assessment of Parkinson's disease [ISAPD], Schwab and England, and Extensive Disability
Scale [EDS]), and four multimodular scales, containing both impairment and disability
sections (New York University Parkinson's disease evaluation [NYU], University of
California Los Angeles scale [UCLA], Short Parkinson's Evaluation Scale [SPES], and
Unified Parkinson's Disease Rating Scale [UPDRS]), were identified.
We report the clinimetric characteristics of individual impairment and disability items. Details
on individual scales are followed by a comparison of their clinimetric characteristics.
Impairment
Content validity. In evaluating the content of impairment scales and impairment sections of
multimodular scales, large differences emerged. Some impairment items were present in all
(tremor and bradykinesia) or in the majority (rigidity and gait) of scales. Some items were
unique for a particular scale (e.g., blepharospasm in the UCLA, short and extra steps in the
PDIS). As the core features are not equally represented and defined in the different rating
scales, the contribution of these symptoms to the total score varies from scale to scale (table
1). The contribution of items dealing with bradykinesia and hypokinesia (including finger and
foot taps, successive hand movements, facial expression, body bradykinesia, akinesia, and
arm swing) to the total impairment scores varies from 17% (SPES) to 40% (Webster). For
tremor these values vary from 10% (Webster) to 33% (SPES), for rigidity from 0% (PDIS) to
20% (CURS), and for postural stability from 0% (Webster, UCLA and NYU) to 10% (PDIS).

Chapter 2
- 22 -
Table 1. Contribution of type of symptoms to the total impairment score
WEBSTER UCLA CURS NYU UPDRS PDIS SPES
brady-/hypokinesia 40 23 28 16 37 30 17
tremor 10 11 20 14 26 20 33
rigidity 10 9 20 14 19 0 17
postural stability 0 0 4 0 4 10 8
other items 40 57 28 56 14 40 25
Values are percentages obtained by dividing the maximum score for that (group of) item(s) by the maximum
possible score for that scale.
Two scales used a weighting factor for each item. In the NYU, the maximum possible score
for each sign determines the weighting; in the UCLA, for example, 'akinesia' is weighted nine
times whereas ‘mask facies’ is weighted only once. Several studies repeatedly demonstrated
that tremor behaves independently from all other items, not significantly contributing to the
explained variance of a scale,19 nor to the construct validity (Hoehn and Yahr [H&Y]
staging).20,21 Postural instability, another major feature of PD occurring in the later stages of
the disease, is not evaluated in the Webster, the UCLA, and the NYU. Speech is present in
five impairment scales or sections (Webster, UCLA, CURS, and motor impairment sections
of UPDRS and SPES). Seborrhea and sialorrhea are evaluated in three (Webster, UCLA, and
CURS) and two impairment scales (UCLA and CURS), respectively.
Another problem that emerged concerned the applied methods of evaluation. This was
particularly noteworthy for bradykinesia.
Reliability. Nine studies reported inter-rater reliability of individual items, whereas only one
study evaluated intra-rater reliability.22 This latter study reported a moderate to good intra-
rater reliability for all items of the CURS, except for rigidity, which was not reported because
the study used video recordings.
Regardless of the scale, there was a lack of consistency among the findings (ranging from
poor to good) concerning inter-rater reliability of the core features bradykinesia, tremor, and
rigidity, as well as for the item speech (table 2). The majority of the studies found a good
inter-rater reliability for postural stability. Seborrhea and sialorrhea showed poor inter-rater
reliability in the CURS22,23 and moderate inter-rater reliability in the UCLA.24

Rating scales in Parkinson's diisease
- 23 -
Disability
Content validity. The Schwab and England activities-of-daily-living scale is a staging system,
in which 100% represents complete independency and 0% a vegetative state. The remaining
three disability scales and four disability sections of multimodular rating scales bear only
some resemblance in content of items. Dressing, walking, speech, hygiene, and feeding or
eating (swallowing), are included in all scales. Turning in or getting out of bed, and getting
out of a chair, are included in all scales except the NUDS. Handwriting is found in four scales
(UCLA, NYU, UPDRS Activities-of-Daily-Living [ADL] section and SPES ADL section)
and climbing stairs in three (UCLA, EDS, and ISAPD).
Reliability. Eight studies reported inter-rater reliability of separate items, in contrast to intra-
rater reliability, which was only evaluated in one study.20 This study reported a moderate to
good intra-rater reliability for all items of the PDIS.
Overall, the disability items displayed moderate to good inter-rater reliability, with a few
exceptions. Speech scored poor in two studies on the NUDS,23,34 and in one study on the
EDS.34 In the original publication of the UPDRS,27 Fahn et al. reported poor inter-rater
reliability for walking, in contrast to two later studies that found substantial to excellent
values for this item.21,34
Clinimetric characteristics of the included scales
Impairment scales. The three impairment scales (table 3), the Columbia University Rating
Scale (CURS), the Webster, and the Parkinson's Disease Impairment Scale (PDIS), vary in
number of items (25, 10, and 10, respectively) and response options (0-4, 0-3, and 0-3).
Parkinson's Disease Rating Scale by Webster. For a scale that has been used for a long time
by many investigators, surprisingly little evidence is published on its validity and reliability.
Notably, the Webster includes one disability item (self-care) and nine impairment items,
which makes this scale conceptually unclear. From a factor analysis assessed in one study,
three factors were derived, including: (I) arm swing, gait, self-care, and posture; (II) speech
and facies; (III) seborrhea.19 Four studies showed that the scale displays poor to moderate
inter-rater reliability.23-25,27,29,34

Chapter 2
- 24 -
Table 2. Interpretation of values for interrater reliability
WEBSTER UCLA CURS UPDRS SPES Brady-/hypokinesie finger tap +1
++22 +27 ++26 +++21,27,28
+++21
foot tap -23 ++22
+25,27 +++21,26,28
successive movements +29 ++23
-/+23 ++22
-27 ++25,28 ++/+++21,26
facial expression -23,24 -24 +22,23 -26,27 +25 ++21,28
body bradykinesia -23 ++22
+25,27 ++26 +++21,28
akinesia +24 arm swing -23
+24
Tremor rest and postural ++23
+24,29 +24 -/++23
+29 ++22
rest +25 ++/+++21,28 +++26,27
+++21
postural ++21 ++/+++21 action -28
+21,25 ++26,27
Rigidity -23 +24,29
++24 -29 -/+23
+26,27 ++/+++21 +++25
+++21
Postural stability +++22 +26,27 +++25,28,30
+++21
Posture -23 +24,29
+24 ++22 -27 +25,26 ++21 +++28
Speech -23 +24
+24 -23 +22
-26 +25 ++21,27 +++28
++21
Seborrhoea -23 +24 -22,23 Sialorrhoea +24 +24 -23 Numbers in superscript correspond with publications in the reference list. For the NYU and the PDIS, no
information on interrater reliability per item is available; - = poor; + = fair; ++ = moderate; +++ = good

Table 3. Results of validity and reliability, and thoroughness (strength of evidence) of validity and reliability testing
VALIDITY RELIABILITY
Scale typea N items Construct Factorb Inter-rater Intra-rater Internal
No of studiesc
CURS 1969 25 ++(+)/+++ /+++ ++/+++ +++/+++ +++/+++ 522,23,29,31,32
CURS-modified (Sydney) 1993 I 11 ++(+)/+++ 0 +++/+++ +++/+++ 0 122
CURS-modified 1985 8 0 /- +/+ 0 0 122
EDS 1991 D 21 +++/+++ 0 +++/+++ 0 0 129
ISAPD 1987 I,D 13 +++/+++ /+++ ++(+)/+++ 0 +++/+++ 133
NUDS 1980 D 6 ++(+)/+++ 0 ++(+)/+++ 0 0 62,19,23,24,29,34
NYU 1980 I,D 6 +++/+++ 0 0 0 0 135
PDIS 1987 I 10 -(+)/+ /- 0 ++(+)/++ 0 120
SPES 1997 I,D 25 +++/+++ /+++ +++/++(+) 0 0 121
UCLA 1981 I,D 21 0 0 ++(+)/+++ 0 0 224,34
UPDRS 1987 31 +++/+++ /+++ ++/+++ 0 +++/+++ 425-27,36
UPDRS ADL I,D 13 +++/+++ /+++ 0 0 +++/+++ 221,37
UPDRS ME 14 +(+)/+(++) /+++ ++/++ 0 +++/+++ 521,28,37-39
Webster I 10 ++/+ /++ -(+)/+++ 0 0 619,23,24,32,34,40
Signs before the slash refer to results of validity and reliability and signs behind the slash refer to thoroughness (strength of evidence) of validity and reliability testing.
Results of validity and reliability testing: 0 = no numerical results reported; ? = results not interpretable; - = poor results; + = fair results; ++ = moderate results; +++ =
good results. Thoroughness of validity and reliability testing: 0 = no reported evidence; ? = results not interpretable; - = poor evidence; + = fair evidence; ++ = moderate
evidence; +++ = good evidence a I, impairment scale; D, disability scale; b Thoroughness of testing only; c Superscript numbers correspond with the studies in Reference list.

Chapter 2
- 26 -
Columbia University Rating Scale. Although the Columbia University Rating Scale (CURS)
has been used frequently in clinical studies before the introduction of the UPDRS in 1981,
only a few studies have been published on the validity and/or reliability of this scale, mostly
in combination with other PD rating scales.22,23,32,34 The available evidence shows the CURS
to have moderate to good validity and reliability. The factor structure was evaluated in only
one study that included 95 patients with PD plus syndromes, and this therefore precludes a
conclusion on this issue in PD.31 A modified version of the CURS, the Sydney scale, appears
to be equally valid and reliable.22
Parkinson's Disease Impairment Scale. Only one study assessed validity and reliability of the
Parkinson's Disease Impairment Scale (PDIS). Due to an unclear factor analysis and the
subsequent assessment of the construct validity based on these factors, the validity of this
scale is questionable.20 The intra-rater reliability was moderate to good.
Disability Scales
Four disability scales, including the Northwestern University Disability Scale (NUDS), the
Intermediate Scale for Assessment of Parkinson's disease (ISAPD), the Schwab and England
scale, and the Extensive Disability Scale (EDS) are difficult to compare, because they vary
substantially in scoring, grading, number, and kind of items. Although the ISAPD is, among
others, based on the NUDS, its grading is different, 0 to 3 instead of 0 to 10.
Schwab and England. The Schwab and England scale has become a standard assessment tool
in PD and has been used in hundreds of studies. The clinimetric properties of this scale,
however, have never been established. The data available from studies with a primary aim to
investigate characteristics of other rating scales, suggest a moderate to substantial validity and
good reliability.33,34,38
Northwestern University Disability Scale. Two studies found a moderate to good construct
validity.19,34 These studies showed that the NUDS score correlates highly with the Webster
score (Kendall's W = 0.82)19 and with the CURS (Spearman's rs = -0.78),34 which are both
impairment scales. The inter-rater reliability of the NUDS was found excellent by its
designers,41 but only moderate by others.23,24,34 An explanation for the latter could be the
combined effect of the large number of severity gradations in this scale and the use of non-
weighted K’s. Although this scale is frequently used, no information is available on internal
consistency or intra-rater reliability.

Rating scales in Parkinson's disease
- 27 -
Intermediate Scale for Assessment of Parkinson's Disease. Evaluated only by its designers,
the Intermediate Scale for Assessment of Parkinson's disease (ISAPD) showed a moderate to
good correlation with the H&Y, with the UPDRS, and with the Schwab and England.33 In the
same study, the results were also excellent for internal consistency and good for inter-rater
reliability. The administration time was 7 (± 3.70) minutes.33
Extensive Disability Scale. The Extensive Disability Scale (EDS) is a modified version of the
Minimal Record of Disability (MRD),42,43 which is used in patients suffering from multiple
sclerosis. This scale has only been used and tested by its developers, who found a moderate to
good construct validity and inter-rater reliability.34 The administration time by a trained
reviewer was stated to be 15-20 minutes.34
Impairment and Disability Sections in Multimodular Scales
In comparing the four impairment and disability scales, the New York University Parkinson's
disease evaluation (NYU), the Short Parkinson's Evaluation Scale (SPES), the University of
California Los Angeles scale (UCLA), and the Unified Parkinson's Disease Rating Scale
(UPDRS), we noticed the similarity in content. All scales included items on bradykinesia,
tremor, rigidity, walking, eating, turning in bed, and handwriting.
New York University Parkinson's Disease Evaluation. For this scale only poor construct
validity with the H&Y was reported.35 The administration time by a trained examiner was
stated to be 10 minutes.35
University of California Los Angeles Scale. The UCLA scale was rarely used in clinical trials
and beyond the work of Martínez-Martín,24 who found a moderate to good inter-rater
reliability, no further evidence for reliability or validity of the scale has been published.
Unified Parkinson's Disease Rating Scale. The UPDRS has found broad acceptance for the
evaluation of PD and has been used in many trials.44 Nine studies extensively tested and
evaluated this scale. Like the Webster, the UPDRS ADL section is conceptually unclear since
it includes several impairment items (salivation, falling, freezing, tremor, and sensory
complaints). Nevertheless, the UPDRS demonstrates high internal consistency and inter-rater
reliability, shows moderate construct validity, and has a stable factor structure.21,26,28,34,36-39
Even across off- and on-state examinations, the motor examination (ME) section of this scale
has a stable factor structure and high internal consistency.38 The high internal consistency of
the ADL and motor section most likely indicates a redundancy of items. This was
underscored by a study that successfully reduced the ADL and motor section of the UPDRS

Chapter 2
- 28 -
to eight items each, without a loss in reliability or validity.37 The time to administer the
UPDRS was stated to be 10-20 minutes34 and assessed as 16.95 (± 7.98) minutes.34
Short Parkinson's Evaluation Scale. Evidence for construct validity and inter-rater reliability
of the SPES is good, but was only reported in an article by its original designers.21 An
advantage of the SPES is that it is short and easy to administer (7-10 minutes by
neurologists).21
Discussion
Compared to their widespread clinical use for assessment of impairment and disability in PD,
rating scales are seldom extensively evaluated for validity and reliability. The terms
impairment and disability are derived from the International Classification of Impairments,
Disabilities, and Handicaps of the WHO (ICIDH; http://www.who.int./icidh).7,8 The ICIDH-2
was developed recently, and introduces new terms, ‘body structures and function’ are handled
both positive (functional and structural integrity) and negative (impairment) and so are
activities (activity versus activity limitation).
Systematically searching the literature, we found 30 studies describing clinimetric issues of
11 scales for impairment and disability rating in PD. In general, a criticism could be made on
the frequent choice of the H&Y as the gold standard for testing other scales, because, to the
best of our knowledge, none have evaluated its clinimetric data. Nevertheless, the H&Y is the
most commonly used method of establishing the severity of PD.
In evaluating impairment items, the contribution of the core motor features of PD to the total
impairment score varies from scale to scale. For instance, items dealing with bradykinesia and
hypokinesia contribute almost 40% to the total score of the UPDRS ME section, resulting in a
strong effect on the sum scores of the impairment section and on the total score. There are
also large differences in the extent of representation of items considered responsive to
dopaminergic treatment (e.g., bradykinesia, rigidity) or to those symptoms that appear late in
the course of the disease and lack responsiveness to dopaminergic treatment (e.g., postural
instability, swallowing, speech, and freezing). Hence, these differences in content should be
taken into consideration when one has to select a scale for the evaluation of short-term
dopaminergic treatment or for long-term follow-up, in which the occurrence of symptoms not
responsive to dopaminergic treatment indicate disease progression. Generally, within the
framework of impairments, items as sialorrhea and seborrhea have limited clinical
significance. Irrespective of the scale, the findings concerning inter-rater reliability of the core

Rating scales in Parkinson's disease
- 29 -
features bradykinesia, tremor, and rigidity, as well as for the item speech, lacked consistency.
The majority of the studies, however, found a good inter-rater reliability for postural stability.
Clearer description of items may help to improve inter-rater reliability of items. To avoid the
problems with inter-rater reliability, objective measurements could be considered in assessing
impairments in PD.30,45-49 It is remarkable that only one study evaluated intra-rater reliability,
because it is a relevant issue in the case of longitudinal studies performed by one assessor.
Although there is general agreement on the definition of disability (i.e., experienced difficulty
in carrying out activities of daily living), there is no consensus on what should be measured.
All evaluated disability scales and sections included the items of the NUDS (dressing,
walking, speech, hygiene, feeding, and eating). Overall, disability items displayed moderate
to good inter-rater reliability. The low inter-rater reliability values repeatedly found for speech
and walking, suggest that these items are difficult to score or lack clear anchors.
The identified PD rating scales can be divided in three groups: impairment scales, disability
scales, and multimodular scales containing both impairment and disability sections. By
comparing the three impairment scales Webster, CURS, and PDIS, we found evidence for the
CURS to have strong validity, whereas there is insufficient data on validity available for the
Webster and the PDIS. As the overall reliability of the CURS is moderate to good, the inter-
rater reliability of the Webster is poor to moderate. Therefore, as a brief rating method the
Webster appears adequate, but the available clinimetric data on the CURS indicate that this
scale may be preferred. The PDIS was inadequately evaluated by its designers and due to a
lack of other information on clinimetric issues of the PDIS, no recommendations can be given
with respect to this scale. The four disability scales, NUDS, ISAPD, Schwab and England,
and EDS bear hardly any resemblance. Large differences between the scales are found in the
scoring and grading of items. The Schwab and England disability scale takes a unique
position, because it uses a different grading system and has never primarily been evaluated for
its clinimetric characteristics. The construct validity and inter-rater reliability of the NUDS,
ISAPD, and EDS were found to be moderate to good, indicating no particular preference.
Only the NUDS was evaluated independently. The ISAPD, evaluated only by its designers,
appears to be a very valid and reliable disability scale that may be useful as a tool for
evaluation of disability in PD. Independent verification of the clinimetric characteristics,
however, is recommended.
Of the scales containing both an impairment and a disability section, the UPDRS is the most
widely used and tested scale. The NYU, SPES, and UCLA have rarely been used and have

Chapter 2
- 30 -
only been evaluated by their designers. The construct validity of the UPDRS is satisfactory in
those studies that have used the H&Y for comparison. Important differences between these
scales include the scoring and the contribution of the individual items to the subtotal and total
score. In relation to the validity aspects of the UPDRS, some findings deserve comments. The
construct validity of the UPDRS has to be considered very satisfactory. The UPDRS ADL
section, however, is conceptually unclear as it includes several impairment items. With
respect to inter-rater reliability, the UPDRS, SPES, and UCLA should be considered reliable
scales. The SPES and UCLA, however, were evaluated only by the designers of the scales.
The UPDRS demonstrates a very high internal consistency, but the effects of redundancy
(several items focusing on the same aspect of the construct) should be kept in mind. Internal
consistency increases with the number of items and depends substantially on the homogeneity
of items and on the inter-item correlation.
Taken together, the evaluation of the impairment and disability sections as a whole, show that
the UPDRS is a reliable and valid scale, although these sections include some redundant and
unreliable items. The SPES appears to be a valid and reliable scale that might be considered
for evaluation of patients with PD. Nonetheless, independent verification of the clinimetric
characteristics is recommended. Because the UCLA and NYU lack thorough clinimetric
testing, no recommendations can be given.
Others have reviewed disease-specific PD scales,4,30,50,51 but only Mitchell and associates44
presented some clinimetric properties of the most commonly used scales (identified through a
Medline search conducted over the period from 1966 until August 1998). In this study the
UPDRS was found to be the most thoroughly studied scale with overall better clinimetric
properties compared to other scales. As indicated by the authors, one of the limitations of
their study concerned the main focus, which was not to summarize the clinimetrics of scales,
but to examine the pattern of utilization of disease-specific clinical scales used as endpoints in
PD trials. The summary of clinical properties they present is simple and intended to serve as a
guide.
In summary, this review underscores that the clinimetric soundness of the majority of PD
assessment scales is questionable. Moreover, as these scales are generally used in trials on PD
patients who lack serious comorbidity, there is no information on the clinimetric behaviour of
the scales in unselected PD populations.

Rating scales in Parkinson's disease
- 31 -
We emphasize the following critical notes regarding clinimetric issues:
1. The most important question in choosing a scale is how well it is suited to the task at
hand in terms of validity, reliability, and efficiency.
2. A greater number of items increases the internal consistency. Limiting the number of
items in a scale, however, contributes to simplicity and utility of the assessment, at the
expense of completeness, sensitivity, and reliability.
3. It is remarkable that none of the studies addressed differences in responsiveness
between scales, which is required to ensure the usefulness in the longitudinal evaluation
of PD. Responsiveness is an essential part of the statistical analysis since it involves the
ability of a measure to reflect change.
4. Video recordings may help to improve assessment of inter- and intra-rater reliability in
studies. These recordings have their limitations, however, for they can only be used to
score items that are clearly visible or audible. Rigidity, seborrhoea, and sialorrhea are
difficult to discern on tape and should not be included if a scale is used for video
assessments.
Acknowledgements
We thank Dr. F. Durif, Dr. M. Hely, Prof. L. Henderson, Prof. Dr. C. Kennard, Dr. P.
Martínez-Martín, Prof. Dr. J. Opara, Dr. J. M. Rabey, and Dr. N.C. Reynolds Jr. for providing
additional information. C.R. is funded by the Prinses Beatrix Fonds (project no. 97-0205) and
J.M. is funded by the Netherlands Organization for Scientific Research (project no. 0940-33-
021).
References
1. Rascol O, Brooks DJ, Korczyn AD, De Deyn PP, Clarke CE, Lang AE. A five-year study of the incidence
of dyskinesia in patients with early Parkinson's disease who were treated with ropinirole or levodopa. 056
Study Group. N Engl J Med 2000; 342(20):1484-1491.
2. Parkinson Study Group. Pramipexole vs levodopa as initial treatment for Parkinson disease: A
randomized controlled trial. JAMA 2000; 284(15):1931-1938.
3. Lang AE. Surgery for levodopa-induced dyskinesias. Ann Neurol 2000; 47(Suppl.):S193-S199.
4. Marsden CD, Schachter M. Assessment of extrapyramidal disorders. Br J Clin Pharmacol 1981;
11(2):129-151.
5. Handbook of neurological rating scales. New York: Demos Vermande, 1997.

Chapter 2
- 32 -
6. Marinus J, Ramaker C, Van Hilten JJ, Stiggelbout AM. Health related quality of life in Parkinson's
disease: a systematic review of disease specific instruments. J Neurol Neurosurg Psychiatry 2002;
72(2):241-248.
7. World Health Organization. International Classification of impairments, disabilities, and handicaps: a
manual of classifications relating to the consequences of diseases. Geneva: World Health Organization,
1980.
8. Simeonsson RJ, Lollar D, Hollowell J, Adams M. Revision of the International Classification of
Impairments, Disabilities, and Handicaps: developmental issues. J Clin Epidemiol 2000; 53(2):113-124.
9. The Cochrane Controlled Trials Register. The Cochrane Library 2001; Issue 3. Update Software. Internet:
http://.update-software.com/cochrane.
10. McDowell I, Newell C. Measuring Health: A Guide to Rating Scales and Questionnaires. 2 ed. New
York: Oxford University Press, 1996.
11. Nunnally JC, Bernstein IH. Psychometric Theory. 3 ed. New York: McGraw-Hill, Inc., 1994.
12. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;
33(1):159-174.
13. Feinstein AR. Clinimetrics. 1 ed. New Haven: Yale University Press, 1987.
14. Fleis JL. The measurement of inter-rater agreement. In: Statistical methods for rates and proportion. New
York: John Wiley, 1981: 212-236.
15. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use.
2 ed. Oxford: Oxford Medical Publications, 1995.
16. Cohen J. Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial
credit. Psychol Bull 1968; 70:213-220.
17. Husted JA, Cook RJ, Farewell VT, Gladman DD. Methods for assessing responsiveness: a critical review
and recommendations. J Clin Epidemiol 2000; 53(5):459-468.
18. Cutson TM, Sloane R, Schenkman M. Development of a clinical rating scale for persons with Parkinson's
disease. J Am Geriatr Soc 1999; 47(6):763-764.
19. Henderson L, Kennard C, Crawford TJ, Day S, Everitt BS, Goodrich S, et al. Scales for rating motor
impairment in Parkinson's disease: studies of reliability and convergent validity. J Neurol Neurosurg
Psychiatry 1991; 54:18-24.
20. Reynolds Jr. NC, Montgomery GK. Factor Analysis of Parkinson's Impairment: An Evaluation of the
Final Common Pathway. Arch Neurol 1987; 44:1013-1016.
21. Rabey JM, Bass H, Bonuccelli U, Brooks D, Klotz P, Korczyn AD, et al. Evaluation of the Short
Parkinson's Evaluation Scale: A New Friendly Scale for the Evaluation of Parkinson's Disease in Clinical
Drug Trials. Clin Neuropharmacol 1997; 20(4):322-337.
22. Hely MA, Wilson A, Williamson PM, O'Sullivan DJ, Rail D, Morris JGL. Reliability of the Columbia
Scale for Assessing Signs of Parkinson's Disease. Mov Disord 1993; 8(4):466-472.
23. Geminiani G, Cesana BM, Tamma F, Contri P, Pacchetti C, Carella F, et al. Interobserver Reliability
Between Neurologists in Training of Parkinson's Disease Rating Scales: A Multicenter Study. Mov
Disord 1991; 6(4):330-335.

Rating scales in Parkinson's disease
- 33 -
24. Martínez-Martín P, Carrasco de la Pena JL, Ramo C, Antiguedad AR, Bermejo F. [Study of inter-observer
reliability in the use of qualitative scales assessing Parkinson disease (II)]. Arch de Neurobiol 1988;
51(5):287-291.
25. Martínez-Martín P, Gil-Nagel A, Morlán Gracia L, Balseiro Gómez J, Martínez-Sarriés FJ, Bermejo F, et
al. Unified Parkinson's Disease Rating Scale Characteristic and Structure. Mov Disord 1994; 9(1):76-83.
26. Richards M, Marder K, Cote L, Mayeux R. Interrater Reliability of the Unified Parkinson's Disease
Rating Scale for Motor Examination. Mov Disord 1994; 9(1):89-91.
27. Fahn S, Elton RL, and members of the UPDRS Development Committee. Unified Parkinson's Disease
Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Clane DB, editors. Recent Developments in
Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information, 1987: 153-163.
28. Goetz CG, Stebbins GT, Chmura TA, Fahn S, Klawans HL, Marsden CD. Teaching Tape for the Motor
Section of the Unified Parkinson's Disease Rating Scale. Mov Disord 1995; 10(3):263-266.
29. Ginanneschi A, Degl'Innocenti F, Maurello MT, Magnolfi S, Marini P, Amaducci L. Evaluation of
Parkinson's Disease: A New Approach to Disability. Neuroepidemiology 1991; 10:282-287.
30. Tervainen H, Calne D. Quantitative assessment of parkinsonian deficit. In: Rinne K, Linger M, Stamm G,
editors. Parkinson's disease: current progress, problems, and management. New York: Elsevier
Biomedical Press, 1980.
31. Baas H, Stecker K, Fischer PA. Value and appropriate use of rating scales and apparative measurement in
quantification of disability in Parkinson's disease. J Neural Transm 1993; 5:45-61.
32. Ginanneschi A, Degl'Innocenti F, Magnolfi S, Maurello MT, Catarzi L, Marini P, et al. Evaluation of
Parkinson's Disease: Reliability of Three Rating Scales. Neuroepidemiology 1988; 7:38-41.
33. Martínez-Martín P, Gil-Nagel A, Morlán Gracia L, Balseiro Gómez J, Martínez-Sarriés FJ, Bermejo F, et
al. Intermediate Scale for Assessment of Parkinson's Disease: Characteristic and Structure. Parkinsonism
Relat Disord 1995; 1(2):97-102.
34. Martinez-Martin P, Carrasco de la Pena JL, Ramo C, Antiguedad AR, Bermejo F. [Inter-observer
reproducibility of qualitative scales in Parkinson disease (I)]. Arch de Neurobiol 1987; 50(5):309-314.
35. Lieberman A, Dziatolowki M, Gopinathan G, Kopersmith M, Neophytides A, Korein J. Evaluation of
Parkinson's disease. In: Goldstein M, editor. Ergot compounds and brain function: neuroendocrine and
neuropsychiatric aspects. New York: Raven Press, 1980: 277-286.
36. Nouzeilles MI, Merello M. Correlation Between Results of Motor Section of UPDRS and Webster Scale.
Mov Disord 1997; 12(4):613.
37. Van Hilten B, Van der Zwan AD, Zwinderman AH, Roos RAC. Rating Impairment and Disability in
Parkinson's Disease: Evaluation of the Unified Parkinson's Disease Rating Scale. Mov Disord 1994;
9(1):84-88.
38. Stebbins GT, Goetz CG. Factor structure of the Unified Parkinson's Disease Rating Scale: Motor
Examination section. Mov Disord 1998; 13(4):633-636.
39. Stebbins GT, Goetz CG, Lang AE, Cubo E. Factor Analysis of the Motor Section of the Unified
Parkinson's Disease Rating Scale During the Off-State. Movement Disorders 1999; 14(4):585-589.
40. Kennard C, Munro AJ, Park DM. The reliability of clinical assessment of Parkinson's disease. J Neurol
Neurosurg Psychiatry 1984; 47:322-323.

Chapter 2
- 34 -
41. Canter GJ, De La Torre R, Mier M. A method for evaluating disability in patients with Parkinson's
disease. J Nerv Ment Dis 1961; 133:143-147.
42. LaRocca NG. Statistical and Methodological Considerations in Scale Construction. In: Munsat TL, editor.
Quantification of Neurologic Deficit. Boston: Butterworths, 1989: 49-67.
43. Slater RJ, LaRocca NG, Scheinberg LC. Development and testing of a minimal record of disability in
multiple sclerosis. Ann N Y Acad Sci 1984; 436:453-468.
44. Mitchell SL, Harper DW, Lau A, Bhalla R. Patterns of outcome measurement in Parkinson's disease
clinical trials. Neuroepidemiology 2000; 19(2):100-108.
45. Potvin AR, Tourtellotte WW, Syndulko K, Potvin J. Quantitative methods in assessment of neurologic
function. CRC Crit Rev Bioeng 1981; 6(3):177-224.
46. Jankovic J. Pathophysiology and clinical assessment of motor symptoms in Parkinson's disease. In: Koller
WC, editor. Handbook of Parkinson's disease. New York: Marcel Dekker, 1992: 99-126.
47. Ringendahl H. Standardization of a test of fine motor functions (Motorische leistungsserie MLS) in
Parkinson's disease. Nervenarzt 1998; 69(6):507-515.
48. Lauk M, Chow CC, Lipsitz LA, Mitchell SL, Collins JJ. Assessing muscle stiffness from quiet stance in
Parkinson's disease. Muscle Nerve 1999; 22(5):635-639.
49. Caligiuri MP, Galasko DR. Quantifying drug-induced changes in parkinsonian rigidity using an
instrumental measure of activated stiffness. Clin Neuropharmacol 1992;15(1):1-12.
50. Lang AET, Fahn S. Assessment of Parkinson's Diseaese. In: Munsat TL, editor. Quantification of
Neurologic Deficit. Boston: Butterworths, 1989: 285-309.
51. Martínez-Martín P. Rating Scales in Parkinson's Disease. In: Jankovic J, Tolosa E, editors. Parkinson's
Disease and Movement Disorders. Baltimore: Williams and Wilkins, 1993: 281-292.

- 35 -
33 Health-related quality of life in Parkinson’s disease:
a systematic review of disease-specific instruments
Johan Marinus1, Claudia Ramaker1, Jacobus J. van Hilten1, Anne M. Stiggelbout2
Department of 1Neurology and 2Medical Decision Making, Leiden University Medical Center, Leiden,
The Netherlands
Published in the Journal of Neurology, Neurosurgery & Psychiatry 2002; 72:241-248

Chapter 3
- 36 -
Abstract Objective. To compare and contrast disease-specific quality of life instruments in Parkinson’s Disease
and assess their clinimetric properties. Methods. Two reviewers independently evaluated both
thoroughness and results of studies regarding clinimetric characteristics of identified scales. Results.
Twenty studies were found reporting on the clinimetric properties of four scales. The content validity
of the Parkinson’s Disease Questionnaire-39 item version (PDQ-39), the Parkinson’s Disease Quality
of Life questionnaire (PDQL), and the ‘Fragebogen Parkinson LebensQualität’ (Parkinson Quality of
Life questionnaire; PLQ) was adequate to good, but for the Parkinson’s Impact Scale (PIMS) it was
insufficient. Construct validity of both the PDQ-39 and the PDQL was good, but for the PLQ and the
PIMS this was insufficiently evaluated. Internal consistency of all scale totals and of subscale totals of
the PDQL were good, whereas for the social support subscale of the PDQ-39 and four subscales of the
PLQ this was inadequate. Test-retest reliability was not evaluated for the PDQL and was adequate in
the other scales. Responsiveness was partially established for the PDQ-39, and not assessed for the
other scales. The number of available translations, as well as the number of studies in which these
instruments were used, differed considerably. Conclusions. The selection of an instrument partially
depends on the goal of the study. In many situations however, the PDQ-39 will probably be the most
appropriate HRQoL instrument. The PDQL may be considered as an alternative, whereas the PLQ
may be considered in studies involving German speaking patients with Parkinson's disease. Use of the
PIMS should be considered only as a means of identifying areas of potential problems.

Health related quality of life in Parkinson's disease
- 37 -
Introduction Quality of life (QoL) is a multidimensional concept that reflects a subjective evaluation of a
person’s satisfaction with life and concerns, among others, the relationships with family or
relatives, a person’s own health, the health of another close person, finances, housing,
independence, religion, social life, and leisure activities.1 Health contributes to QoL, and this
domain is often referred to as ‘health-related quality of life’ (HRQoL). The World Health
Organization (WHO) describes health as a state of complete physical, mental, social, and
spiritual wellbeing, and not merely the absence of disease or infirmity.2 This indicates that
psychological and social factors are an integral part of health. Sometimes ‘role functioning’ is
added as a separate entity to the concept of HRQoL. Bowling3 takes several definitions of
HRQoL into account and defines the concept as optimum levels of mental, physical, role (e.g.
work, parent, carer etc.), and social functioning, including relationships, and perceptions of
health, fitness, life satisfaction, and wellbeing. HRQoL gained importance in the past three
decades and is considered to be an important outcome measure in studies involving patients
with chronic diseases. Although initially physician-based evaluations were chosen as primary
endpoints in clinical research, more recent studies often consider HRQoL as their main
outcome measure.
HRQoL can be assessed both with generic and disease-specific instruments. The generic
instruments (for example Medical Outcomes Study–Short Form 36, Sickness Impact Profile)
offer the possibility of comparing HRQoL across different diseases. These instruments
contain items of a more general nature, and therefore lack specificity. Disease specific
instruments generally tap the same domains, but the items are tailored to particular disease
characteristics and may also include items dealing with side effects of therapy. Consequently,
disease specific instruments better reflect the consequences of that disease to a particular
person and generally are more sensitive to change in perceived HRQoL.4
In Parkinson’s disease (PD), several disease-specific HRQoL instruments have become
available in the past few years. Investigators who want to use such an instrument are faced
with the choice between several scales, which differ in many respects. In the process of
selecting the appropriate instrument, a comparison of the quality of these scales can be
helpful. We therefore compared and contrasted HRQoL instruments in PD and evaluated their
clinimetric properties.
Chapter 3
- 38 -
Methods
Search strategy
We reviewed the literature from 1965 to 2000 and used the following sources to identify
studies of interest: Medline, Embase, SCIsearch, the Cochrane Library, symposia reports,
Parkinson's disease handbooks, and reference lists of included publications. We used the
following search terms: Parkinson Disease, quality of life, health status, PDQ39, PDQL,
Parkinson’s Disease Questionnaire, PIMS, Parkinson’s Impact Scale, PLQ, Fragebogen
Parkinson Lebensqualität, PDQUALIF. These terms were combined with the following terms:
clinimetric, psychometric, reliability, validity, internal consistency, factor analysis, factor
structure, responsiveness, and sensitivity to change. The list of publications regarding each
scale was sent to the developer, with the request to add references in the case of
incompleteness.
Methods of the review
Two reviewers independently reviewed the identified publications according to a two-step
review process. Firstly, abstracts were reviewed for eligibility. Thereafter, eligible reports
were judged against a set of methodological criteria, in which both thoroughness
(methodological and statistical) and results of studies testing validity, reliability, and
responsiveness were assessed. To this extent we used a checklist, evaluating sample
characteristics, outcome measures, appropriateness of statistical analysis, and methodological
quality. The method of presenting the quality of scales was adopted from McDowell and
Newell.5 For reliability, Cronbach’s α greater than 0.7 and intraclass correlation coefficients
(ICC) or kappa's (K) greater than 0.7 were considered a good result, and studies were judged
‘thorough’ if the appropriate statistical procedures were used and the sample size was
considered to be large enough. With respect to validity, the result of content validity was
considered ‘good’ if all relevant domains were covered and ‘thorough’ if unselected
(community based) PD patients were closely involved in both the generation and evaluation
of items. When only outpatient samples or samples from a Parkinson's disease society were
used in this phase, we considered thoroughness to be moderate and when the patients were not
involved at all, we considered thoroughness to be poor.
Discrepancies were registered and resolved by consensus with a third and fourth reviewer.

Health related quality of life in Parkinson's disease
- 39 -
Studies were eligible when they evaluated the following clinimetric characteristics of disease-
specific HRQoL instruments in PD: validity (content validity and construct validity, including
factor structure), reliability (internal consistency, test-retest reliability), and responsiveness.
Content validity reflects the extent to which a scale covers all important topics or domains.6
Construct validity is assessed by measuring the extent to which a scale correlates positively
with other measures that address the same construct (convergent validity), or negatively with
measures that address opposite constructs (divergent validity), in situations where a gold
standard is not available.
Another method of construct validation is the analysis of ‘known groups’ differences. In this
method patients are grouped on the basis of some characteristic, for example disease severity
or difficulties in performing activities. Patients with higher disease severity or patients
experiencing greater difficulty, are expected to have lower HRQoL.
In a factor analysis, items that correlate highly with each other group together in clusters
(factors), that are considered to reflect underlying common themes. Factor analysis may be
used to construct subscales, or to analyze the construct of an instrument.
Adequate internal consistency is a prerequisite for scales developed to measure one particular
construct. When all the items within a scale correlate highly with each other, the scale
demonstrates good internal consistency, and thus measures one underlying construct. Internal
consistency is calculated using Cronbach’s α. Values range from 0–1, with higher scores
reflecting higher internal consistency. For group comparisons in research situations, internal
consistency is considered adequate when α exceeds 0.7.7
Test-retest reliability is assessed by calculating the reproducibility of an instrument in stable
patients over a relatively short time period and is best calculated by means of the K
coefficient, or the ICC.
Responsiveness (or sensitivity to change) is the ability of an instrument to accurately detect
change when it has occurred. Responsiveness in HRQoL instruments is preferably
demonstrated with both internal indicators of change (correlation with patient’s own
evaluation of change) and external indicators of change (correlation with external measures).
Other information that was gathered included the procedure of item generation, type of scale,
number of items, response options, scoring method, available translations, availability of
instructions, conditions for use, administration time, and frequency of missing items.
Whenever information on studies or scales was unclear or incomplete, we contacted the
authors with the request to provide additional information.

Chapter 3
- 40 -
Results We found 21 studies addressing five scales. Five of these studies concerned translated
versions. One study, and consequently one scale (PDQUALIF)8, was excluded because
information on the format of this scale, as well as on the included items, was unavailable at
the time of our review. Therefore, 20 studies reporting on the clinimetric properties of four
scales were included in this review.
These scales were the Parkinson’s Disease Questionnaire-39 item version (PDQ-39),9 the
Parkinson’s Disease Quality of Life questionnaire (PDQL),10 the Parkinson’s Impact Scale
(PIMS),11 and the Parkinson LebensQualität (PLQ) (Parkinson QoL) questionnaire.12 Some
common characteristics of the scales are considered first. Details on individual scales are
discussed later, followed by a comparison of the clinimetric characteristics.
Disease-specific HRQoL scales
The four questionnaires were developed between 1995 and 1998. The scales can be self
completed by the patient, but can also easily be administered by an interviewer.
All scales can be used freely for scientific purposes, but in the case of the PDQL permission
for use must be granted from the developers. The PDQ-39 and the PDQL have a license fee
for commercial use. The administration time of these scales was never formally assessed, but
is expected to vary from 10 minutes (PIMS), to 15 or 20 minutes (PDQ-39, PDQL, PLQ).
All scales use a five point ordinal scoring system. The number of available translations differs
considerably between scales, ranging from one (PLQ) or two (PIMS), to 10 (PDQL) or 21
(PDQ-39). The number of studies in which these instruments have been used, range from one
(PLQ and PIMS) to at least five (PDQL) or 18 (PDQ-39). An instruction manual for scientific
users is only available for the PDQ-39 and the PLQ.
PDQ-39
The Parkinson’s Disease Questionnaire (PDQ-39) was designed by Peto et al.9 The scale has
39 items. Higher scores reflect lower HRQoL. The PDQ-39 has eight subscales: mobility (10
items), activities of daily living (six items), emotional well-being (six items), stigma (four
items), social support (three items), cognitions (four items), communication (three items), and
bodily discomfort (three items). Items in each subscale,13 as well as in the total scale,14 can be
summarized into an index and transformed linearly to a 0–100 scale. A shorter summary
index (PDQ-8 SI) can also be calculated.15

Health related quality of life in Parkinson's disease
- 41 -
The scale has been formally validated in United States English,16 United Kingdom English,9
German,17 and Spanish.18,19 A French version is currently being validated.20 Translations are
available in Australian English, Canadian English, Canadian French, Czech, Danish, Dutch,
Finnish, Hebrew, Italian, Polish, Portuguese, Russian, Swedish, Greek, Japanese, and Serbian.
PDQL
The PDQL was developed by de Boer et al.10 This scale has 37 items. Higher scores reflect
better HRQoL. Four subscales are discerned: parkinsonian symptoms (14 items), systemic
symptoms (seven items), social function (seven items), and emotional function (nine items).
The PDQL has been formally validated in Dutch,10 United Kingdom English,21 German,22 and
French.22 Translations are available in Argentinean Spanish, Belgian Dutch, Italian,
Portuguese, and Spanish.
PIMS
The PIMS was developed by Calne et al.11 The scale has 10 items and is completed three
times, one month apart. The items in the PIMS are broadly formulated and concern domains
rather than specific situations. Higher scores reflect lower HRQoL. Stable patients only score
each item once, whereas patients with fluctuations judge the negative impact for both 'on' and
'off' periods. The scale can be self completed, but the developers recommend that patients be
advised with respect to their disease state (stable or fluctuating). Guidelines for use by
physicians are available.
The scale is only available in Canadian English and Canadian French. The scale contains two
optional items (sexuality and financial security) that were left unanswered in 32% and 13% of
the questionnaires, respectively.
PLQ
The PLQ was designed by van den Berg.12 The scale has 44 items. Items in the scale are
grouped in nine domains: depression (five items), physical achievement (five items),
concentration (four items), leisure (five items), restlessness (four items), activity limitation
(six items), insecurity (five items), social integration (five items), and anxiety (five items).
There are five types of standard questions and four categories of responses, worded in two
directions. Responses can be recoded with a spreadsheet program that is available from the
author. The scale has been validated only in German.

Chapter 3
- 42 -
Scale development, scoring and time-frame
The method of item generation differed between scales. In the PIMS, items were decided
upon by consensus between 10 specialized nurses and tested in 167 patients. In the other three
scales, patients were directly involved in the generation and evaluation of items. Although the
PDQ-39 and the PLQ solely relied on patient information for item generation, items in the
PDQL were also obtained from interviews with neurologists, relatives of patients, and
studying the literature.
Items in the PDQ-39 were initially generated through interviews with 20 patients visiting an
outpatient neurology clinic. This resulted in a 65 item list that was reduced to 39 items on the
basis of a survey in 359 patients. Items in the PDQL were generated by means of interviews
with five patients and a relative, consulting neurologists, and reviewing the literature.
Seventy-three items were found and piloted in 13 inpatients and outpatients. Items endorsed
most often or rated as most important were selected for the final 37-item version, which was
tested in 384 patients. Items in the PLQ were generated by interviews with groups of patients.
This resulted in 113 items that subsequently were piloted in 61 inpatients and outpatients. The
questionnaire was then reduced to 44 items and tested in 405 patients (which constituted a
response rate of only 38%).
The PDQ-39 and the PDQL both assess the frequency with which patients experience
difficulties. The PIMS assesses the impact of the disease on patient’s lives, whereas the PLQ,
depending on the item of interest, assesses intensity, applicability, or quality.
Scales differ considerably in the period they refer to. The PIMS does not specify a time frame,
whereas the PDQL assesses the past three months, the PDQ-39 the past month, and the PLQ
the past week. The PDQL and PLQ assess the items ‘as is’, without asking the patient to
indicate whether this was due to PD, whereas the PDQ-39 and the PIMS relate the items to
having PD. In the PDQ-39 all items begin with: ‘Due to having PD, how much of the time did
you have trouble with…’. In the PIMS patients are asked to rate the negative impact of PD in
a particular domain.
Content validity
The content of the scales differs considerably. We grouped items thematically on the basis of
face value in domains reflecting physical, mental, and social or role functioning (table 1).
Whenever there was doubt regarding the correct allocation, items were assigned to domains
according to subscale allocation or factor structure as reported in the original studies. Table 2

Health related quality of life in Parkinson's disease
- 43 -
shows that about half of the items in the PDQ-39 and the PDQL concern physical features,
whereas the PIMS has only two items in this domain. In the PIMS, on the contrary, half of the
items deal with the social domain. In the PLQ almost half of the items involve mental
features.
In the physical domain, only transportation is addressed by all scales. In the PIMS, the only
other theme addressed in this domain concerns taking part in traffic. The PDQ-39, PDQL, and
PLQ share items on walking, motor features, and other disease features. Transfers are
addressed in detail in the PDQL, but are lacking in the PDQ-39 and PLQ. Items on self care
are assessed in detail in the PDQ-39, and as an overall item in the PLQ, but are lacking in the
PDQL. Many physical items in the PDQ-39 concern activities (‘disabilities’), whereas in the
PDQL and PLQ most items reflect impairments.
In the mental domain all scales include items on mood, feelings, and anxiousness. The PIMS
does not incorporate items on cognition, whereas the other scales address both concentration
and memory. The PLQ contains seven items addressing anxiousness.
In the social domain all scales address some aspect of relationships. Relationships with
partner, family, or friends are only addressed in the PDQ-39 and the PIMS. Sexuality is only
addressed in the PDQL and the PIMS. Social stigma is not assessed in the PIMS. Role
functioning is adequately assessed in the PIMS, but only marginally in the PDQ-39 and the
PLQ, whereas the PDQL does not address this theme at all.
Construct validity
Construct validity of both the PDQ-39 and the PDQL was thoroughly established using
generic HRQoL scales, disease specific instruments, ‘known groups’ comparisons, and other
health measures. The PLQ was less thoroughly assessed. Correlations with a generic HRQoL
scale and an ADL scale were adequate, but correlations with disease specific instruments
were poor, and known groups differences were not assessed. For the PIMS only known
groups comparisons were performed, demonstrating significant differences between stable
and fluctuating patients in their off situations (table 3).

Chapter 3
- 44 -
Table 1. Content HQoL-scales
ITEMS PDQ-39 PDQL PIMS PLQ
Physical
Walking
-problems getting around house 6
-walking 4,5 24 25
-shuffling; initiation / shuffling 11 7
Transfers
-turning in bed 35
-getting up 32
-turning around while walking 14
self care
-self care 23
-washing 11
-dressing 12
-cutting food 15
-holding drinks without spilling 16
-doing up buttons / shoe laces 13
daily activities
-looking after home* 1 2 (5) 40
-carrying bags / shopping 3
-doing leisure activities* 1 1 (8) 7 (38)
-getting around in public 7
Transportation
-take part in traffic 29 6 21
-needed company when going out 8
motor features
-mobility 27
-slowness 1
-rigidity 1 3
-dexterity 9 26
-shaking hands; tremor 6 4
-sudden uncontrolled movements 30 2
-on-off periods 20 14
-speech; talking 34 22
-writing 14 16
Other disease features
-generally unwell 2
-extreme exhaustion 13
-worn out 7 20

Health related quality of life in Parkinson's disease
- 45 -
ITEMS PDQ-39 PDQL PIMS PLQ
-painful cramps or spasms 37
-pain in joints or body 38 6
-unexpected falling asleep 30
-problems sleeping (at night) 19 5
-difficulty sitting still 27
-drooling 25
-incontinence / frequent urinating 28
-constipation 33
-feeling unpleasantly hot or cold 39
-feeling that body parts don’t belong to oneself 44
Mental
Cognition
-concentration 31 31 8
-adjusting to circumstances 32
-memory 32 34 28
Mood
-depression 17 26 2*2 11,30
-weepy or tearful 19
feelings (positive)
-feelings; confidence 1 41
-self worth 1 29
feelings (negative)
-being tense; stress 4 2 10
-angry or bitter 20
-unsure due physical limitations; trust body functions 5 34
-safety; doing what you want without harming yourself 8
-unsure around others 18
-feeling isolated / lonely 18
-feeling ignored 36
anxious / worry
-anxious 21 2
-worry loss cognitive capacity 18
-worry physical loss 19
-worry illness 42
-worry future; afraid progression 22 15 13,16,43
-worry operation 37
-fear side effects 17
-worry falling 9
Other features

Chapter 3
- 46 -
ITEMS PDQ-39 PDQL PIMS PLQ
-dependency on medication 15
-difficulty accepting illness 21
-confined to house more than liked 10
-distressing dreams / hallucinations 33 9
-disinterest/listnessless 12
Social and role functioning
Relationships
-problems with close relationships 27 3
-lacked support spouse / partner 28 3
-lacked support family / friends 29
-impact community relationships 4
-sexual relationship 36 10
-wanted to isolate oneself 35
-keeping up relationships 24
(fear of) social stigma
-embarrassed (in public) 25 10
-worried about other’s reaction 26
-felt had to conceal PD 23
-feeling that illness is noticed 36
-avoid eating / drinking in public 24
-signing name in public 23
role functioning
-work 5
-looking after home* 1 (2) 5
-financial security/support 9
-feeling dependent of others 31
social activities
-doing hobbies 3 39
-doing leisure activities* 1 (1) 8 (7) 38
-cancel social activities 12
-cancel important activities 33
-less able to go on holiday 17 37
-visit exhibitions 22
-problems with communication 35
Numbers correspond with number of the item in the scale; numbers in parentheses indicate that the item is
assessed, but was primarily allocated to another section * 1 ‘leisure activities’ and ‘looking after home’ present in physical and social domain because of differences in
subscale allocation among scales * 2 item numbers of the PIMS are sometimes presented more than once because of broad formulation.

Health related quality of life in Parkinson's disease
- 47 -
Table 2. Number of items per domain.
PDQ-39 PDQL PIMS PLQ
Physical 19 21 2 16
Mental 12 9 3 19
Social 8 7 5 9
Total number of items 39 37 10 44
Items are allocated to a domain on the basis of face value, or, in case of ambiguity, on the basis
of subscale allocation or factor structure, as presented by the scale developers in original study.
Internal consistency
Cronbach’s α’s for scale totals are all well over 0.8 (table 3). Alpha’s for subscales are higher
than 0.7, except for social support in the UK version of the PDQ-39,9 social support16,23 and
cognitions23 in the US version of the PDQ-39, for cognitions and bodily discomfort in the
Spanish version of the PDQ-39,19 and for mood, concentration, restlessness, and social
integration in the PLQ.12
Test-retest reliability
Test-retest reliability was not assessed for the PDQL. In the PIMS an ICC of 0.72 was
reported for the total score. Reproducibility of subscales was assessed for the PDQ-39 and the
PLQ. Subscales with correlations lower than 0.7 concerned the social support subscale in the
PDQ-39 and the anxiety subscale in the PLQ.
Responsiveness
Responsiveness was not established for either the PDQL or the PIMS. In the PLQ it was
assessed only in a small subset of 16 patients during a period in the hospital. Paired t-tests
were only significant for activity limitation and insecurity. When the tests were corrected for
multiple comparisons, all nine scale changes were non-significant. Two studies reported on
the responsiveness of the PDQ-39. Fitzpatrick et al.24 found moderate standardized response
means for the mobility and ADL subscales in 51 patients who indicated their situation had
worsened over a period of four months. Change in the PDQ-39 score was significantly
correlated with self reported change and change in the SF-36. In the other study, Harrison et
al.25 found that four subscales of the PDQ-39 (mobility, ADL, stigma, social support) were
responsive to deterioration in health state.

Table 3. Clinimetric characteristics of HQoL scales
scale reliability validity responsiveness intern consist test-retest content construct factorial
PDQ-39 α total scale:
0.84 - 0.9414,23,27
α subscales:
0.69 - 0.949 or
0.66 – 0.9527 or
0.57 – 0.9423
item-total correlation:
0.67 - 0.919
r = 0.68 - 0.949
(n=167; 3-6 days)
+++9 generic HRQoL scales:
• range subscales PDQ-39 and SF-36: r =- 0.34 - -0.809
• summary indices of PDQ-39 and EQ-5D: rs = -0.7528
disease-specific scales:
• H&Y: rs = 0.6028,29; vs PDQ subscales:rs = 0.16 – 0.7224,27
• SES: rs = -0.6628,29
• UPDRS-ME: rs = 0.4129
• Columbia, range subscales: rs = 0.08 – 0.5824,27
other measures:
• Beck DI with PDQ-39: rs = 0.6828, with PDQ-emotional: r = 0.7325
• Barthel Index with PDQ-39-ADL: rs = 0.325
• MMSE: rs = -0.3228,29
analysis of group differences:
• by self reported severity: s9
• by H&Y (clinic sample) : s (except social)27 or s (except
emotional, stigma, social, cognitions, body discomfort)23
• by H&Y (population sample): s30 (except social, stigma)
8 factoren9
• mobility
• ADL
• emotional
• stigma
• social support
• cognitions
• communication
• bodily discomfort
- SRM for mobility and ADL:
0.55 and 0.43, respectively
(n=51, 4 month interval)24
- change PDQ-39 compared to
change in24:
• Columbia: ns
• H&Y: ns
• SF-36: s
• self report change: s
- 4 subscales (mobility, ADL,
stigma, social support) show
significant deterioration
- PDQ-39 more responsive
than GHQ-28 and OPCS25
PDQL α total scale:
0.9410 – 0.9521
α subscales:
0.80 – 0.8710 or
0.77 – 0.8721
0 ++10 generic HRQoL scales:
• SF24, related domains: range r = 0.46 – 0.6610
disease-specific measures:
• ‘Webster contributes significant to QoL’21
other measures:
• CES-D vs PDQL-emotional: r = -0.7910
• MOS soc support survey vs PDQL-social: r = 0.1310
• ‘CAMCOG/GDS-15 contribute significant to QoL’21
analysis of group differences:
• by SES, 3 levels: s10
• by Webster, 3 levels: s (all, except emotional)21
4 factors10:
• parkinsonian
• systemic
• social
• emotional
0

scale reliability validity responsiveness
intern consist test-retest content construct factorial
PLQ α total scale: 0.9512
α subscales: 0.62 - 0.8712
correlation subscale - total
scale: r = 0.73 - 0.8612
(n = 405)
total scale:
r = 0.8712
subscales:
r = 0.69-0.8612
(n = 65; 14 days)
++12
generic HRQoL scales:
• EORTC-QLQ30: r = 0.67 (n = 111)12
disease-specific measures:
• H&Y: r = 0.27, ns (n = 21 – 29)12
• SES: r = -0.27, ns (n = 21 – 29)12
other measures:
• QoL-VAS: r = -0.28, ns (n = 21 – 29)12
• ADL–scale: r = 0.73 (n = 111)12
9 subscales, 1 or 2
factors per subscale,
>50% variance12
• depression
• physical.
achievement
• leisure
• concentration
• social integration
• insecurity
• restlessness
• activity limitation
• anxiety
2 week interval
no external criterion
(n=16)12
PIMS α total scale: 0.9011
correlation among factors:
r = 0.10 - 0.4611
ICC = 0.7211
(n= 149; 1 month)
-11
consensus
analysis of group differences:
• by self assessed fluctuations: s (only between stable patients and
fluctuating patients at their worst)11
4 factors, explaining
72% variance11:
• psychological
• social
• physical
• financial
0
n = number of patients; α = Cronbach’s α; r = Pearson; rs = Spearman;; ICC = Intraclass correlation coefficient; +++ = good; ++ = moderate; + = fair; - = poor; 0 = no
numerical results reported; ? = unclear; SES = Schwab and England scale; Beck’s DI = Beck Depression Inventory; s = significant; ns = not significant; SRM =
standardized response mean.

Table 4. Quality assessment table
SCALE RELIABILITY VALIDITY RESPONSIVENESS
internal consistency test-retest content construct
PDQ-39 +++ / +++ +++ / +++ ++ / +++ +++ / +++ ++ / +
PDQL +++ / +++ 0 ++ / ++ +++ / +++ 0
PIMS +++ / +++ +++ / +++ ? / - ? / - 0
PLQ +++ / +++ +++ / +++ ++ / +++ + / ++ - / -
+++ /+++: signs before the slash refer to results of validity, reliability, and responsiveness testing and signs behind the slash refer to thoroughness (‘strength of evidence’)
of validity, reliability, and responsiveness testing
Results of validity, reliability, and responsiveness testing: / Thoroughness of validity, reliability, and responsiveness testing:
0 no numerical results reported 0 no reported evidence
? results not interpretable ? results not interpretable
- poor results - poor evidence
+ fair results + fair evidence
++ moderate results ++ moderate evidence
+++ good results +++ good evidence

Health related quality of life in Parkinson's disease
- 51 -
Discussion Scales differed considerably in content. Probably this is largely the result of differences in the
ways the items were generated and reduced, and differences among the samples involved in
generating and evaluating the items may have added to the heterogeneity. In the PDQ-39 and
the PLQ items were only derived from interviews with patients, whereas in the PDQL also
information from neurologists, relatives, and the literature was used. Items in the PIMS were
obtained through consensus between specialized nurses.
To guarantee good content validity, patients should be closely involved in both item
generation and evaluation. For item generation other sources may be used as well. For the
evaluation of items, however, a large sample of patients should be involved. This sample
should ideally consist of patients attending a neurology clinic, patients living in nursing
homes, and of unselected patients living in the community. None of the scales applied this
method. The information on relevance of items in the item reduction phase was obtained from
patients who were members of a Parkinson’s disease society (PDQ-39), or from both
inpatients and outpatients of a neurology clinic (PDQL, PLQ). In the PDQL, only four
outpatients and one patient and a relative from the Parkinson’s disease society were involved
in the item generation process, whereas only thirteen inpatients and outpatients were involved
in the evaluation process. Both the small sample sizes as well as the fact that only a clinic-
based sample was involved, may have affected the final make-up considerably. For instance,
the item ‘feeling worried about a possible operation’ in the PDQL was not found in other
scales.
Different strategies with respect to the item reduction process – that is, psychometric or
clinimetric - affected the final content as well. In the first strategy, considerations of the
measurement properties of scales prevail, whereas in the second the completeness of the
assessment is considered more important. In the PDQ-39 and the PLQ, the developers used a
predominantly psychometric strategy. In the PDQ-39, items were omitted when they were
considered redundant, had low item scale correlations, or clustered in subscales that could not
be meaningfully interpreted. In the PLQ, items with low item scale correlations, non-normal
frequency distributions, often missing values, floor or ceiling effects, or items that could not
clearly be assigned to subscales, were removed. The developers of the PDQL, however,
followed a more clinimetric strategy and included all items patients considered important in
the final scale. Items that loaded on more than one subscale were assigned to subscales on the
basis of face validity.

Chapter 3
- 52 -
When the scales are compared in more detail, the differences in content become apparent. The
PDQ-39 lacks items addressing transfers and night-time sleep problems in the physical
domain, but covers all relevant themes in the mental domain. Role functioning is
insufficiently covered. Sexuality is not addressed in this scale.
The PDQL misses items on self care in the physical section, taps all items in the mental
domain, and lacks items on close relationships and role functioning in the social domain.
Our findings regarding the content validity of the PDQ-39 and the PDQL largely agree with
Damiano et al.26 However, their criterion list did not contain items explicitly addressing
transfers and hobbies.
The PIMS lacks items on walking, transfers, self-care, motor features, and other disease
features in the physical domain, on cognition and ‘other features’ in the mental domain, and
on social stigma in the social domain.
The PLQ lacks items on transfers and communication in the physical domain, but in the
mental domain all relevant themes are addressed. Role functioning and relationships are
insufficiently covered in the social domain. The PLQ is the only scale that explicitly asks for
the consequences of being dependent of others.
The construct validity of both the PDQ-39 and the PDQL are well established. For the PLQ
this was less thoroughly demonstrated, whereas for the PIMS construct validation with other
measures was not performed.
All scales share factors on physical, mental, and social functions. The other factors that
emerged in the scales were very different.
The internal consistency for scale totals is adequate for all scales. All subscales of the PDQL
demonstrate good internal consistency, whereas the social support subscale in the PDQ-39
and four subscales in the PLQ showed insufficient internal consistency. Test-retest reliability
was not assessed for the PDQL and was found to be adequate for the other scales, except for
the anxiety subscale in the PLQ and, again, the social support subscale in the PDQ-39.
Responsiveness was not assessed at all for either the PDQL or the PIMS. For the PLQ
responsiveness was inadequately evaluated. There are indications that the PDQ-39 is capable
of detecting deterioration, but for improvement this still needs to be established.
A comparison of the clinimetric qualities of the scales is presented in table 4.
Apart from methodological considerations, other issues may influence the selection of a
HRQoL instrument. For instance, the time frame is of importance. When short periods are
assessed (for example, one week in the PLQ), day to day differences may affect the total score

Health related quality of life in Parkinson's disease
- 53 -
considerably, resulting in lower comparability over time. Assessing longer periods may
therefore be preferred, as is done in both the PDQ-39 (one month) and the PDQL (three
months).
Another factor that may affect the selection of a scale is the framing of questions. The PDQL
and the PLQ evaluate health ‘as is’, regardless whether complaints were caused by PD or not.
Both other scales relate the health state to having PD. However, it may be difficult or even
impossible for patients to judge whether a particular situation (for example, sleep problems,
fatigue) is caused by PD, or is the result of aging or some comorbid condition.
Other considerations that may guide the selection of an appropriate HRQoL instrument for a
particular study may concern the language and the number of studies in which the instrument
has been used. In this respect the PDQL, and especially the PDQ-39, are attractive candidates.
The intended sample may also influence the selection. The PLQ was tested only in a sample
of patients that were members of a Parkinson’s disease society, whereas the PIMS was used
only in an outpatient clinic sample. The PDQL was evaluated both in a Parkinson's disease
society sample and a community based sample, whereas the PDQ-39 was evaluated in all the
aforementioned populations.
The number of items is not a useful criterion for selection, because the numbers hardly differ
between the PDQ-39, the PDQL and the PLQ, whereas insufficient clinimetric support exists
for the only short scale, the PIMS.
In most other respects the scales differed only marginally, and therefore these factors are not
expected to play a role in selecting a scale.
The selection of an instrument will partly be based on the goal of the study. For certain
interventions, some domains of HRQoL may be more important to assess than others and may
thus influence the selection of the instrument. In many situations, however, the PDQ-39 will
probably be the most appropriate HRQoL instrument, because this scale has been tested most
thoroughly, has adequate clinimetric characteristics, has been used in the largest number of
studies, and is available in many languages. However, responsiveness of this scale still needs
to be assessed more thoroughly, especially with respect to situations where patients are
expected to improve (for example, intervention studies). The PDQ-39 lacks items on self
image, night time sleep problems, sexual activity, and transfers. Reliability of the social
support subscale (test-retest and internal consistency) is inadequate. The PDQL may be
considered as an alternative. Information on test-retest reliability and responsiveness,
however, is still lacking and the scale does not include items on self-care, role functions, and

Chapter 3
- 54 -
close relationships. The PLQ may be considered in studies involving German-speaking
patients with PD. However, construct validity and responsiveness are insufficiently assessed,
and items concerning transfers and speech are missing, whereas relationships and role
functions are only scarcely addressed. Use of the PIMS should be considered only as a means
of identifying areas of potential problems. Items in this scale lack specificity, whereas the
content validity is insufficiently founded and construct validity and responsiveness have not
been assessed at all.
Acknowledgements
J.M. is supported by the Netherlands Organization for Scientific Research (project no. 0940-
33-021) and C.R. is supported by the Prinses Beatrix Fund (project no. 97-0205). We thank C.
Berne, S. Calne, A.G.E.M. de Boer, J.E. Harrison, V. Peto, M. van den Berg, and M.D. Welsh
for providing additional information.
References
1. Bowling A. What things are important in people's lives? A survey of the public's judgements to inform
scales of health related quality of life. Soc Sci Med 1995; 41(10):1447-1462.
2. World Health Organization. WHO-Constitution - the first two chapters. World Wide Web. 2001.
3. Bowling A. Health-related quality of life: a discussion of the concept, its use and measurement.
Measuring disease. Buckingham: Open University Press, 1995: 1-19.
4. Guyatt GH, Bombardier C, Tugwell PX. Measuring disease-specific quality of life in clinical trials.
CMAJ 1986; 134:889-895.
5. McDowell I, Newell C. Measuring Health: A Guide to Rating Scales and Questionnaires. 2 ed. New
York: Oxford University Press, 1996.
6. Kirshner B, Guyatt G. A methodological framework for assessing health indices. J Chronic Dis 1985;
38(1):27-36.
7. Bland JM, Altman DG. Cronbach's alpha. BMJ 1997; 314(7080):572.
8. Welsh M, McDermott M, Holloway R, Plumb S, Pfeiffer R, Hubble J. Development and Testing of the
Parkinson's Disease Quality of Life Scale: The PDQUALIF. Mov Disord 1997; 12(5):836.
9. Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and validation of a short measure of
functioning and well being for individuals with Parkinson's disease. Qual Life Res 1995; 4(3):241-248.
10. De Boer AG, Wijker W, Speelman JD, de Haes JC. Quality of life in patients with Parkinson's disease:
development of a questionnaire. J Neurol Neurosurg Psychiatry 1996; 61(1):70-74.
11. Calne S, Schulzer M, Mak E, Guyette C, Rohs G, Hatchard S, et al. Validating a quality of life rating
scale for idiopathic Parkinsonism: Parkinson's impact scale. Parkinsonism Relat Disord 1996; 2(2):55-61.

Health related quality of life in Parkinson's disease
- 55 -
12. Van den Berg M. Leben mit Parkinson - Entwicklung und psychometrische Testung des Fragenbogens
PLQ. Neurologie & Rehabilitation 1998; 4(5):221-226.
13. Peto V, Jenkinson C, Fitzpatrick R. PDQ-39: a review of the development, validation and application of a
Parkinson's disease quality of life questionnaire and its associated measures. J Neurol 1998; 245 Suppl
1:S10-S14.
14. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson's Disease Questionnaire
(PDQ-39): development and validation of a Parkinson's disease summary index score. Age Ageing 1997;
26(5):353-357.
15. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The PDQ-8: development and validation of a
short-form Parkinson's disease questionnaire. Psychol Health 1997; 12:805-814.
16. Bushnell DM, Martin ML. Quality of life and Parkinson's disease: Translation and validation of the US
Parkinson's Disease Questionnaire (PDQ-39). Qual Life Res 1999; 8(4):345-350.
17. Berger K, Broll S, Winkelmann J, Heberlein I, Muller T, Ries V. Untersuchung zur Reliabilität der
deutschen Version des PDQ-39: Ein krankheitsspezifischer Fragenbogen zur Erfassung der Lebensqualität
von Parkinson-Patienten. Aktuel Neurol 1999; 26(4):180-184.
18. Martinez-Martin P, Frades PB. Quality of life in Parkinson's disease: validation study of the PDQ-39
Spanish version. The Grupo Centro for Study of Movement Disorders. J Neurol 1998; 245 Suppl 1:S34-
S38.
19. Martinez-Martin P, Frades B, Jimenez Jimenez FJ, Pondal M, Lopez Lozano JJ, Vela L, et al. The PDQ-
39 Spanish version: reliability and correlation with the short- form health survey (SF-36). Neurologia
1999; 14(4):159-163.
20. Mauduit N, Schuck S, Allain H, Chaperon J. Échelles et questionnaires dans la maladie de Parkinson. Rev
Neurol (Paris) 2000; 156 Suppl 2Bis:63-69.
21. Hobson P, Holden A, Meara J. Measuring the impact of Parkinson's disease with the Parkinson's Disease
Quality of Life questionnaire. Age Ageing 1999; 28(4):341-346.
22. Marquis P, Girod I, Berdeaux G, Peyro Saint-Paul H, Cialdella P. Psychometric analysis of French and
German versions of the Parkinson's Disease Quality of Life Questionnaire (PDQL). Qual Life Res 1998;
7:632.
23. Damiano AM, McGrath MM, Willian MK, Snyder CF, LeWitt PA, Reyes PF, et al. Evaluation of a
measurement strategy for Parkinson's disease: assessing patient health-related quality of life. Qual Life
Res 2000; 9(1):87-100.
24. Fitzpatrick R, Peto V, Jenkinson C, Greenhall R, Hyman N. Health-related quality of life in Parkinson's
disease: a study of outpatient clinic attenders. Mov Disord 1997; 12(6):916-922.
25. Harrison JE, Preston S, Blunt SB. Measuring symptom change in patients with Parkinson's disease. Age
Ageing 2000; 29:41-45.
26. Damiano AM, Snyder C, Strausser B, Willian MK. A review of health-related quality-of-life concepts and
measures for Parkinson's disease. Qual Life Res 1999; 8(3):235-243.
27. Jenkinson C, Peto V, Fitzpatrick R, Greenhall R, Hyman N. Self-reported functioning and well-being in
patients with Parkinson's disease: comparison of the short-form health survey (SF-36) and the Parkinson's
Disease Questionnaire (PDQ-39). Age Ageing 1995; 24(6):505-509.

Chapter 3
- 56 -
28. Schrag A, Selai C, Jahanshahi M, Quinn NP. The EQ-5D-a generic quality of life measure-is a useful
instrument to measure quality of life in patients with Parkinson's disease. J Neurol Neurosurg Psychiatry
2000; 69(1):67-73.
29. Schrag A, Jahanshahi M, Quinn N. What contributes to quality of life in patients with Parkinson's disease?
J Neurol Neurosurg Psychiatry 2000; 69(3):308-312.
30. Schrag A, Jahanshahi M, Quinn N. How Does Parkinson's Disease Affect Quality of Life? A Comparison
With Quality of Life in the General Population. Mov Disord 2000; 15(6):1112-1118.

- 57 -
44 Development of an instrument for the assessment of
cognition in Parkinson's disease
Johan Marinus1, Martine Visser1, Nicolaas A. Verwey2, Frans R.J. Verhey3, Huub A.M.
Middelkoop4 5, Anne M. Stiggelbout6, Jacobus J. van Hilten1
Departments of 1Neurology, 4Neuropsychology, 6Medical Decision Making, Leiden University
Medical Center, Leiden, The Netherlands; 2Faculty of Medicine, Utrecht University, Utrecht, The
Netherlands; 3Department of Psychiatry, University Hospital of Maastricht, Maastricht, The
Netherlands; 5Department of Cognitive Psychology, Leiden University, Leiden, The Netherlands
Submitted

Chapter 4
- 58 -
Abstract
The cognitive deficits in Parkinson's disease (PD) may be underestimated if classical instruments for
cognition are used. These instruments generally put an emphasis on cortical functions. Some of these
functions are relatively spared in PD, whereas other cognitive functions that are frequently affected in
PD, are lacking. The objective of this study was to develop a short and practical instrument that is
sensitive to the specific cognitive deficits in PD, and is reliable and valid. We did not have the
objective to construct a screening tool or a diagnostic instrument. In stead, the instrument is intended
for comparing groups in research situations and for assessing change in individual functioning over
time. A literature search was conducted to identify the most frequently affected cognitive domains in
PD, and to select or develop candidate items from these domains for the initial scale. This scale was
next tested in 85 patients and 75 age-, education-, and sex-matched controls. Items that met predefined
criteria for data quality, reproducibility, and discriminative properties, were included in the final scale.
This scale, the SCOPA-COG, consists of 10 items with a maximum score of 43, with higher scores
reflecting better performance. The test-retest reliability of the sumscore was 0.78 (intraclass
correlation coefficient), and ranged from 0.40-0.75 for individual items (weighted kappa). Cronbach's
α was 0.83. Construct validity of the scale was supported by the expected correlations with the
CAMCOG and the MMSE, and by differences found between groups of participants classified by
dementia status, and between patients grouped by disease severity. The scale showed a clear trend
towards lower cognition scores for patients with more advanced PD. This trend was more pronounced
in the SCOPA-COG than in the CAMCOG and the MMSE and use of this scale may provide a better
insight into the longitudinal development of cognitive deficits in PD. The coefficient of variation of
the SCOPA-COG was higher than that of the CAMCOG or the MMSE, indicating a better ability to
detect differences between individuals. The SCOPA-COG is a short, reliable, and valid instrument that
is sensitive to the specific cognitive deficits in PD.

Assessment of cognition in Parkinson's disease
- 59 -
Introduction Patients with Parkinson’s disease (PD) generally perform less well on cognition tests than
age-, education-, and sex-matched controls.1-4 The reported prevalence of dementia in patients
with this condition varies widely between studies, with values ranging from 4 to 93 percent.1
This large difference is caused by differences in methodology, applied criteria for dementia,
and sample characteristics. The mean prevalence rate of 27 studies discussed in a review by
Cummings was 39.9%.1 More recent cross-sectional community studies also reported
prevalence rates of about 40 percent.5,6 The odds ratio for developing dementia compared
with controls was estimated 5.9 in a study by Aarsland et al.7 A longitudinal study by the
same authors found an 8-year prevalence of 78.7% in a large, representative community-
based cohort of patients with idiopathic PD.8
The pattern of cognitive decline in PD differs from that in Alzheimer’s disease (AD).1,9-11
According to the clinical diagnostic criteria of the fourth edition of the Diagnostic and
Statistical Manual of Mental Disorders (DSM-IV), the diagnosis of dementia is made if
memory is impaired, in combination with a decline in at least one of the four following
domains: language, gnosis, praxis, and executive functioning. The problems should be
sufficiently large to interfere with daily activities.12 The DSM-IV criteria are described in
qualitative terms. Patients with PD generally have normal or only slightly decreased
performance in language, gnosis, and praxis, whereas memory and executive functions are
more prominently affected.1,13 This pattern of cognitive decline is often referred to as
‘subcortical dementia’. Some authors state that the current definition of dementia is biased
towards the cortical type phenomenology.11,13 Therefore, applying the classical instruments
for dementia to patients with PD may lead to underestimation of the cognitive deficit in PD.
A quantitative instrument that would focus on the most vulnerable cognitive functions in PD
would provide important additional information. Such an instrument may allow finer
discrimination, detect changes earlier in the course of the disease, and serve as an 'index of
severity'. Items in this scale should be insensitive to the severity of the motor deficit.
The objective of this study was to develop a short and practical instrument, the SCOPA-COG,
that is sensitive to the specific cognitive deficits in PD, and is reliable and valid. We did not
have the objective to construct a screening tool or a diagnostic instrument. In stead, the
instrument is intended for comparing groups in research situations and for assessing change in
individual functioning over time. The development of the SCOPA-COG is part of a larger
research project, the SCales for Outcomes in PArkinson's disease (SCOPA), in which short,

Chapter 4
- 60 -
practical, and clinimetric sound instruments for all relevant domains in PD are selected or
developed.
Patients and methods
Scale development
We searched the literature on studies that dealt with cognitive functioning in PD. In selecting
candidate items from the literature we used the following procedure. First, the cognitive
domains that were affected most frequently were identified. Next, tests within those domains
that consistently yielded different scores for patients with PD and controls were selected,
provided they could easily be administered in a clinical setting and did not involve fine motor
activities, such as writing, drawing, and constructing. Multiple tests were selected for each
domain, allowing us to identify which item had the best characteristics with respect to data
quality, reproducibility, and sensitivity to discriminate between patients and controls.
We used the functional classification of Lezak14 and discerned the following cognitive
domains: attention, memory and learning, executive functions, visuospatial functions, verbal
functions, and thinking and reasoning. Findings from the literature are briefly reviewed and
the concept of bradyphrenia is discussed.
Attention. Attention deficits are often found in patients with PD,1,13,15 and hence addressed in
the scale.
Memory and learning. In PD, especially free recall (‘active memory’) is impaired, while cued
recall (‘passive memory’) is largely unimpaired.1,4,13,16-19 This pattern clearly differs from that
in AD, where both types are affected.19,20 This difference is found both for verbal and visual
memory.17 Thus, not memory function per se, but its functional use is hampered. Both
immediate and delayed recall were found to be impaired in demented and non-demented
patients with PD in a study by Richards et al.2 However, results from studies on immediate
recall are contradictory,17 whereas the results from studies on delayed recall show more
consistency, the vast majority of studies reporting impaired delayed recall. Patients with PD
also frequently display more problems with learning tasks.1,21-24 Orientation, on the other
hand, is typically intact.25 Taking these findings into account, we decided to include items on
free recall (both immediate and delayed, and visual and verbal) and learning, whereas cued
recall and orientation were not addressed.

Assessment of cognition in Parkinson's disease
- 61 -
Executive functions. Executive functions are defined as 'functions involved in the self-
regulation of problem solving strategies' or as 'mental processes involved in goal-directed
behaviour'.14 According to Lezak,14 executive functions can be conceptualised as having four
components: volition, planning, purposive action, and effective performance. However, the
concept is somewhat vague and consequently there is debate whether a particular function is
executive or not. Patients with PD especially show problems that involve internally guided
behaviour (spontaneous generation of task-specific planning), whereas externally guided
behaviour is normal.23,26-28 Both maintaining an attentional set and set-shifting may be
impaired.16,22 An attentional set is defined as a learned predisposition to attend to one
dimension of multidimensional stimuli in order to guide subsequent responding. Shifting
attentional set involves altering the rules which are currently guiding behaviour.29 Set shifting
may be impaired very early in the course of the disease.1,13,30-33 Other functions in this domain
concern concept formation, verbal fluency, and alternating tasks. The latter two are often
impaired in non-demented patients with PD. Concept formation, however, may be preserved.2
Therefore, items on motor planning, set shifting, alternating programs, and fluency tasks were
included in the initial scale.
Visuospatial functions. Assessment of visuospatial and visuoconstructive skills is difficult in
patients with profound motor impairment, but motor-free tasks suggest that patients with PD
have visuospatial deficits in excess of their motor abnormalities.1,26 According to Boller et
al.,26 a visuospatial deficit is characterized by difficulties in appreciating the relative position
of stimulus-objects in space, difficulties in integrating those objects into a coherent spatial
framework, and difficulties in performing mental operations involving spatial concepts. The
authors described the impairment of visuospatial function in PD and found that simple
visuospatial tests discriminated better between patients and controls than complex tests.26
Other problems that have been found include angle matching, figure rotation, figure-ground
discrimination, mental reconstruction of three-dimensional objects from line drawings, and
the perception of spatial positions, shape, and size.1,26 However, because not all of the
visuospatial functions are impaired and because some of these findings have not been
replicated in other studies, Brown and Marsden34 argue against a generalized visuospatial
deficit.16 We included two motor-free items in the visuospatial domain of the initial scale.
Verbal functions. Patients with PD often perform within the normal range of tests of verbal
functions. Patients without overt dementia have naming-test scores one standard deviation
below controls, but still perform within the normal range for the test. PD-patients with
dementia have more naming errors than non-demented patients, but scores remain within

Chapter 4
- 62 -
acceptable limits.1,2,35,36 In general, there is a clear tendency for verbal functions to remain
normal and hence verbal functions were not addressed in the scale.
Thinking and reasoning. Thinking and reasoning has not been assessed thoroughly in PD, but
the information that is available suggests that patients with PD tend to perform
normally.14,30,37 No items from this domain were included.
Bradyphrenia. Slowing of information processing has frequently been reported,21,38 but not
consistently found.21,22,28 It is imperative to differentiate cognitive slowing from depressive
and motor slowing, both of which are frequently present in PD. Mayeux et al.39 reported that
psychomotor retardation is an important component of depression, which is found in
approximately 40% of the patients with PD. Differentiating between 'cognitive slowing' and
'motor slowing' may be achieved by controlling for the motor demands of the task, while
increasing cognitive complexity. Thus prolongation of response time reflects cognitive
slowing as a function of task complexity. Studies using the choice reaction paradigm,
however, mostly failed to find evidence of cognitive slowing. One explanation for this is that
the cognitive demands may be too simple.22,28 Dubois et al.22 stated that cognitive slowing has
only been clearly demonstrated on tests that require a high level of processing (e.g. Tower of
London, Stroop task). However, these findings may indicate a disturbance in cognitive
strategy, rather than a true slowing of central processing.22 In a review on this subject, Dubois
et al.22 concluded that bradyphrenia, which they defined as a non-specific lengthening of
information-processing time, is not demonstrated in PD, although cognitive slowing may
result from impaired executive functioning. Brown and Marsden28 arrived at the same
conclusion and stated that "cognitive slowing is not a useful or valid general description of the
characteristics of cognitive dysfunction observed in PD". Taking these arguments into
consideration, we decided not to address this topic separately.
Taken together, the domains that were found to be affected most frequently concerned
attention, memory, executive functions, and visuospatial functions, and items from these
domains were included in the initial scale. Verbal functions and thinking and reasoning on the
other hand, tended to be normal and no items from these domains were included. Altogether
this resulted in an initial scale of 19 items (see Appendix).
Participants
Patients. Patients with idiopathic PD who gave informed consent and fulfilled the United
Kingdom Parkinson’s Disease Society Brain Bank criteria for idiopathic PD,40 were included.

Assessment of cognition in Parkinson's disease
- 63 -
Patients with a history of brain surgery or deep brain stimulation, patients with other diseases
of the central nervous system, and patients who were not able to read or understand Dutch,
were excluded. The patients were selected from the database of patients with idiopathic PD of
the outpatient clinic of the Department of Neurology of the Leiden University Medical
Center. We aimed to include 75 patients and 75 controls. Patients had to cover the whole
spectrum of the disease and we pursued to enrol at least 25 patients with mild, 25 with
moderate, and 25 with severe idiopathic PD.
Controls. Persons without idiopathic PD and without other diseases of the central nervous
system who had no history of brain surgery were included, provided that they gave informed
consent and were able to read and understand Dutch.
Recruitment. Eligible patients received a letter in advance, in which they were informed on
the goal of the study and the procedures at the time of assessment. The letter also stated that
an investigator would contact the patient and inquire whether s/he considered participating.
Patients were also requested to provide the names of two persons, one male and one female,
who consented to participate as a control subject. The age difference between the patient and
his or her controls was not to exceed 10 years. The introductory letter emphasised that only
the names of persons that explicitly expressed their willingness to participate were to be
provided. In recruiting the controls, a 'match-to-sample' procedure was followed, taking into
account that the distribution of age, sex, and education level in both groups had to be similar.
The study was approved by the institutional review board.
Other assessment instruments
The other scales that were used for comparison in this study were the Dutch version of the
CAMCOG,41 the Mini Mental State Examination (MMSE),42 and the Hoehn and Yahr (H&Y)
scale.43 The CAMCOG is part of the Cambridge Examination of Mental Disorders of the
Elderly (CAMDEX),44 and evaluates cognitive functioning. The CAMCOG is administered
by a trained interviewer and has 60 items with a maximum score of 107, with higher scores
reflecting better performance. Eight subscales are discerned, that is, orientation, language,
memory, attention, praxis, calculation, abstract thinking, and perception. In our study we used
59 items with a maximum score of 106. One item (recognition of person, function) was
excluded, because it was difficult to execute in our test situation. As advised by the
developers, a cut-off value of 79/80 was used to discriminate between demented and non-
demented individuals.41 The CAMCOG has good validity and reliability45 and has previously
been used to assess cognition in patients with PD.46 The MMSE is also included in the

Chapter 4
- 64 -
cognition section of the CAMDEX. The MMSE is administered by an interviewer and has 19
items with a maximum score of 30. Higher scores reflect better performance. There are five
subscales: orientation, registration, attention and calculation, recall, and language. For the
MMSE a cut-off point of 24/25 was used to separate demented from non-demented
participants. Fourteen items of the MMSE are included in the CAMCOG score. The H&Y
staging system was used to assess disease severity. H&Y 1 is the mildest stage with only
unilateral symptoms, whereas H&Y 5 represents the most severe stage, in which patients are
wheelchair-bound or bed-ridden. To discriminate between groups of patients with different
disease severity, we classified patients as mild (H&Y 1 and 2), moderate (H&Y 3), or severe
(H&Y 4 and 5). Because patients in H&Y stages 1 and 5 are usually underrepresented, stages
1 and 2 on the one hand, and 4 and 5 on the other hand, were collapsed. All the patients were
assessed when they had the full benefit of their medication (i.e., were 'on'). The participants
were examined by three trained investigators (JM, MV, NV).
Outcome measures and statistical analysis
Item reduction. Items were reduced in a two-step process. First, the quality of the data was
assessed and only items that had missing values in less than 5% of the patients and showed
adequate reproducibility (weighted kappa [Kw] ≥ 0.40; quadratic weights), were retained. The
second step was to select per domain those items that best discriminated between patients and
controls. To this extent the Mann-Whitney-U-test was used, with a significance level of 0.05.
Reliability. Test-retest reliability was assessed in 30 patients with an interval of six weeks.
Since test-retest reliability is preferably assessed in stable patients, an external criterion (i.e.,
outside the SCOPA-COG) was chosen to determine whether patients were stable or not.
Patients who had score changes in the MMSE of 5 or more points were considered unstable
and their scores were not used for reproducibility evaluation. For individual items Kw was
used, whereas an intraclass correlation coefficient (ICC) was used for the reproducibility of
sum scores. Since the kappa statistic is unstable in the case of limited variation,47 the
percentage agreement was calculated for tests where the chance expected agreement for a
particular response exceeded 0.85. Internal consistency was assessed with Cronbach's
coefficient α.
Validity. 'Known-groups' validity was assessed by comparing the SCOPA-COG scores of
participants grouped by CAMCOG scores (cut-off point 79/80) and MMSE scores (cut-off
point 24/25), using a t-test for independent samples. ‘Known-groups’ validity was also
Assessment of cognition in Parkinson's disease
- 65 -
examined by comparing the SCOPA-COG scores of patients grouped by modified H&Y
stages (mild, moderate, severe), using analysis of variance (ANOVA) and ordinal regression.
In order to assess the underlying structure, an explanatory factor analysis was performed on
the final version of the scale. In this analysis an extraction method with oblique rotation was
used, because factors were assumed to be correlated.
Discrimination. The proportion of the scale range that was used by patients was calculated to
evaluate the discriminative properties of the individual scales. The coefficients of variation
(CV) were also calculated and compared. In this coefficient the standard deviation is divided
by the mean. Higher values for CV reflect a greater ability to detect differences between
individuals and thus allows finer discrimination.
The data were analysed with the Statistical Package for the Social Sciences, release 10 (SPSS
Inc, Chicago, Illinois).
Results
Participants
Eighty-five patients and 75 controls were assessed between 1 January 2002 and 1 July 2002.
Demographic data of patients and controls were similar for male-female ratio, age, and
education (table 1). The required number of patients per disease category (mild, moderate,
severe) were included, although four patients with severe PD were recruited from another
hospital (Medical Center Haaglanden, The Hague, The Netherlands). This was necessary
because some of our patients with severe PD declined, whereas others had previously been
involved in pilot testing. Therefore, we were able to recruit only 21 patients with severe PD
from our outpatient clinic.
Item selection
The percentage of missing values was very low and ranged from 0-2.3%.
Three patients that participated in the retest assessments were considered unstable, since their
MMSE score differed 5 or more points between both assessments and their scores were
excluded from the reproducibility evaluation. Reproducibility was therefore assessed in 27
patients. Seven items (2,6,10,11,14,16,17) had weighted kappa values lower than 0.40 and
were removed (table 2). Of the remaining 12 items, two items (3,8) did not discriminate

Chapter 4
- 66 -
between patients and controls and were also excluded (table 2). All three executions of item 5
discriminated between patients and controls, but the score difference between the second and
third execution of this test and the previous ones, did not differ between these groups. Hence,
no difference between groups in the capacity to 'learn' from additional displays of these ten
words was found, and therefore we decided to administer this item only once in the final
version of the scale.
Table 1. Characteristics of participants
Patients Controls p-value
number of participants 85 75
% male 62 56 0.431
mean (SD) age (years) 69.7 (10.5) 69.4 (12.3) 0.852
mean (SD) years of education 10.6 (3.9) 11.0 (3.7) 0.552
median (IQ range)3 level of education4 3 (2,6) 4 (2,6) 0.085
Hoehn and Yahr stages
1 4 (4.7%)
2 23 (27.1%)
3 33 (38.8%)
4 19 (22.4%)
5 6 (7.1%)
mean (SD) disease duration (years) 9.5 (7.1)
number on levodopa 71 (84%)
mean (SD) dose of levodopa in mg 660 (298)
number on dopamine agonists 49 (58%)
number on other antiparkinsonian medication 46 (54%)
1 Chi-square; 2 t-tests for independent samples; 3 interquartile range (between 25th and 75th percentile); 4
assessed with ordinal scale, ranging from 1 (primary school) to 8 (university degree); 5 Mann-Whitney-U

Assessment of cognition in Parkinson's disease
- 67 -
Thus nine items were removed from the initial scale altogether. The remaining 10 items
fulfilled our criteria for eligibility and displayed good data quality, reproducibility, and
discriminative properties. An adequate content of the scale was guaranteed, because items of
sufficient quality were retained in all domains. In the memory domain, items addressed both
visual and verbal memory, whereas immediate and delayed recall was also assessed. In the
domain of executive functions, items were included that evaluated fluency, set-shifting, and
motor planning. Two items were included in the area of attention and one in the area of
visuospatial functions. The maximum score of the SCOPA-COG is 43, with higher scores
reflecting better cognitive performance. The SCOPA-COG is administered by an interviewer
and completed in 10-15 minutes.
Clinimetric characteristics of the SCOPA-COG
Reliability. Weighted kappa for individual items ranged from 0.40-0.75 (table 2), and the ICC
for the sum score was 0.78 (table 3). The reproducibility of the sumscore of the SCOPA-COG
was higher than that of the CAMCOG and that of the MMSE (0.72 and 0.66, respectively).
The internal consistency of the SCOPA-COG and the CAMCOG were similar, with
Cronbach's alphas of 0.83 and 0.84, respectively. These values were considerably higher than
that of the MMSE, which measured 0.62 (table 3). The corrected item-total correlations of the
SCOPA-COG ranged from 0.34 (counting down by threes) - 0.66 (delayed recall). None of
the items could be deleted without a decrease of Cronbach's α.
Validity. Thirteen subjects (10 patients and 3 controls) scored below the cut-off point of the
CAMCOG and were considered demented according to this criterion. The mean CAMCOG
score was 94.2 (SD 6.4) for the 147 non-demented participants, and 68.2 (SD 12.2) for the
demented subjects. The SCOPA-COG scores of these demented and non-demented persons
were 28.8 (SD 5.8) and 13.3 (SD 4.0), respectively, and differed significantly (p < 0.001).
Twenty-six individuals (21 patients and 5 controls) scored below the cut-off point of the
MMSE. The mean MMSE score for the 134 non-demented participants was 27.9 (SD 1.6),
and for the demented participants it was 21.5 (SD 3.5). Their SCOPA-COG scores differed
significantly (p < 0.001), and measured 29.0 (SD 6.1) and 20.2 (SD 7.3), respectively.
The mean SCOPA-COG score was 30.7 (SD 5.6) for controls and 24.8 (SD 7.1) for patients
(table 4). This score difference was significant (p < 0.001). The SCOPA-COG scores of
patients with mild, moderate, and severe disease status also differed significantly (ANOVA; p
< 0.001), and measured 28.5 (SD 5.5), 24.1 (SD 6.5), and 21.7 (SD 7.7), respectively (table 5,
figure 1).

Chapter 4
- 68 -
Table 2. Reproducibility and discrimination of SCOPA-COG scores
SCOPA item range significance1 Kw2
memory
1. cubes3 0-5 + 0.49
2. visual retention 0-5 + 0.23
3. digits forward 0-9 - 0.59
4. digits backward3 0-8 + 0.50
5. a. word recall3 0-5 + 0.40
b. word recall 0-5 +
c. word recall 0-5 +
attention
6. counting down by ones 0-2 - -0.02
7. counting down by threes3 0-2 + 0.54
8. serial sevens 0-5 - 0.52
9. months backward3 0-2 + 0.44
executive functions
10. tapping 0-3 + 0.29
11. go-no-go 0-3 + 0.39
12. fist-edge-palm3 0-3 + 0.46
13. dices3 0-3 + 0.50
14. letter-digit alternation 0-3 + 0.34
15. fluency animals3 0-6 + 0.70
16. odd-man-out 0-4 + 0.37
visuospatial functions
17. line orientation 0-4 - 0.38
18. figure assembly3 0-5 + 0.45
delayed recall
19. delayed word recall3 0-5 + 0.75
1 '+' indicates significant difference (p ≤ 0.05) between patients and controls
(Mann-Whitney-U); 2 weighted kappa assessed in 27 stable patients; 3 items in
italics are included in final version of the SCOPA-COG.
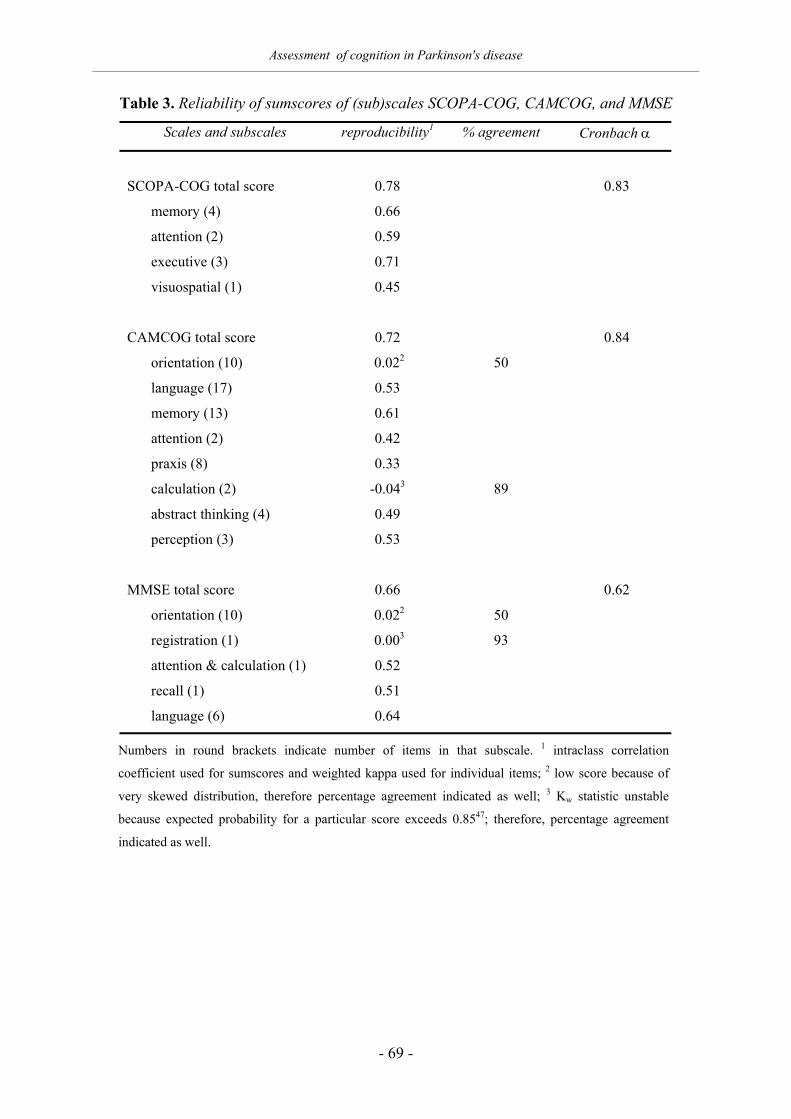
Assessment of cognition in Parkinson's disease
- 69 -
Table 3. Reliability of sumscores of (sub)scales SCOPA-COG, CAMCOG, and MMSE
Scales and subscales reproducibility1 % agreement Cronbach α
SCOPA-COG total score 0.78 0.83
memory (4) 0.66
attention (2) 0.59
executive (3) 0.71
visuospatial (1) 0.45
CAMCOG total score 0.72 0.84
orientation (10) 0.022 50
language (17) 0.53
memory (13) 0.61
attention (2) 0.42
praxis (8) 0.33
calculation (2) -0.043 89
abstract thinking (4) 0.49
perception (3) 0.53
MMSE total score 0.66 0.62
orientation (10) 0.022 50
registration (1) 0.003 93
attention & calculation (1) 0.52
recall (1) 0.51
language (6) 0.64
Numbers in round brackets indicate number of items in that subscale. 1 intraclass correlation
coefficient used for sumscores and weighted kappa used for individual items; 2 low score because of
very skewed distribution, therefore percentage agreement indicated as well; 3 Kw statistic unstable
because expected probability for a particular score exceeds 0.8547; therefore, percentage agreement
indicated as well.

Chapter 4
- 70 -
Table 4. SCOPA-COG, CAMCOG, and MMSE scores of patients and controls
maximum1 patients controls p-value % score2
Mean (SD) SCOPA sumscore 43 24.8 (7.1) 30.7 (5.6) < 0.001 0.81
SCOPA domain scores:
Mean (SD) memory 23 9.8 (3.8) 12.7 (3.6) < 0.001 0.77
Mean (SD) attention 4 2.9 (1.2) 3.5 (0.8) < 0.001 0.83
Mean (SD) executive 12 8.2 (2.2) 10.1 (1.9) < 0.001 0.81
Mean (SD) visuospatial 5 3.9 (1.2) 4.4 (0.8) 0.004 0.89
Mean (SD) CAMCOG sum 106 89.1 (11.2) 95.4 (7.0) < 0.001 0.94
CAMCOG domain scores:
Mean (SD) orientation 10 9.5 (1.1) 9.7 (0.5) 0.045 0.98
Mean (SD) language 30 26.1 (3.1) 27.8 (2.2) < 0.001 0.94
Mean (SD) memory 27 21.0 (3.4) 22.6 (2.8) 0.002 0.93
Mean (SD) attention 7 5.6 (1.7) 6.1 (1.2) 0.045 0.92
Mean (SD) praxis 12 10.4 (1.8) 11.4 (1.0) < 0.001 0.91
Mean (SD) calculation 2 1.9 (0.3) 1.9 (0.2) 0.324 1.00
Mean (SD) abstraction 8 6.3 (1.9) 6.9 (1.3) 0.023 0.91
Mean (SD) perception 10 8.2 (1.6) 9.1 (1.3) < 0.001 0.90
Mean (SD) MMSE sumscore 30 26.0 (3.7) 27.7 (2.0) < 0.001 0.94
MMSE domain scores:
Mean (SD) orientation 10 9.5 (1.1) 9.7 (0.5) 0.045 0.98
Mean (SD) registration 3 2.9 (0.4) 3.0 (0.1) 0.063 0.97
Mean (SD) attention 5 3.9 (1.0) 4.3 (1.4) 0.042 0.91
Mean (SD) recall 3 1.6 (1.0) 2.3 (0.9) < 0.001 0.70
Mean (SD) language 9 8.1 (1.3) 8.4 (0.7) 0.032 0.96
1 maximum score per (sub)scale; 2 scores of patients expressed as percentages of scores of controls
Ordinal regression analysis of the H&Y data on the SCOPA-COG score of all participants,
resulted in a good fitting model (p = 0.90) with a significant trend (p < 0.001), accounting for
29% of the variance. A regression analysis performed on the data of patients only, resulted in
a good fitting model (p = 0.71) with a significant trend (p < 0.001), accounting for 25% of the
variance (table 5). Including age as a covariate in this model, produced a model with good fit
and significant trend that explained 38% of the variance. Age was included because it

Assessment of cognition in Parkinson's disease
- 71 -
correlated significantly with the SCOPA-COG scores and differed significantly between
groups of patients with different disease severity. Significant trends were also obtained for all
domains of the SCOPA-COG (table 5). A similar analysis was performed on the data of the
CAMCOG (table 6).
The correlation between the SCOPA-COG score on the one hand and the CAMCOG and
MMSE scores on the other hand, was 0.83 and 0.72, respectively (table 7). The SCOPA and
CAMCOG correlated equally strong with the H&Y scores, whereas the correlation between
the MMSE and H&Y was somewhat lower.
The SCOPA-COG scores of male and female patients were not significantly different (table
8). Cognition scores generally correlated stronger with age than with education.
The factor analysis revealed two factors with an eigenvalue greater than 1, accounting for
50.5% of the variance (table 9). All memory items, and two of the three executive function
items (fist-edge-palm, animal fluency) loaded on the first factor, whereas the attention items
and the third executive function item (dices) loaded on the second factor. The visuospatial
task had equal loadings on both factors. The correlation between both factors was 0.37.
Discrimination. Scale scores in the patient group ranged from 10-30 for the MMSE, 38-105
for the CAMCOG, and 8-37 for the SCOPA-COG. The proportion of the scale range used by
patients was thus very similar, with values between 63 and 67%. If, however, the difference in
mean scores between patients and controls is expressed in percentages of the range of the
scale, the values differ considerably. These percentages are 6.5 for the MMSE, 7.1 for the
CAMCOG, and 23.7 for the SCOPA-COG. If the mean scores of controls and patients with
different disease severity are expressed as percentages of the maximum possible score, the
proportion of the scale range for these categories used by the participants is 12% for both the
MMSE and the CAMCOG, and 21% for the SCOPA-COG (figure 2). The CV, that reflects
the ability to detect differences between individuals, was calculated for the patient group and
measured 0.14 for the MMSE, 0.13 for the CAMCOG, and 0.29 for the SCOPA-COG.

Table 5. Comparisons of SCOPA-COG scores between controls and patients classified by modified Hoehn and Yahr stage
controls p-mild1 p-moderate1 p-severe1 fit2 trend3 pseudo R-sq4 adj pseudo R-sq 5
SCOPA-COG total 30.7 28.5 24.1 21.7 0.85 0.000 0.23 0.38
memory 12.7 11.8 9.2 8.5 0.84 0.000 0.18 0.37
attention 3.5 2.9 3.1 2.6 0.83 0.000 0.12 0.186
executive 10.1 9.3 7.8 7.5 0.37 0.000 0.23 0.34
visuospatial 4.4 4.6 3.9 3.3 0.77 0.000 0.14 0.20
1 refers to disease severity, classified by the modified Hoehn and Yahr (H&Y) stages, with H&Y 1 and 2 'mild', H&Y 3 'moderate', and H&Y 4 and 5 'severe' 2 goodness of fit: p > 0.05 indicates that the model does not differ significantly from a model with a good fit 3 p < 0.05 indicates that a trend is present (trend in the model is significantly different from zero); p > 0.05 indicates absence of trend 4 pseudo R2: part of the variance accounted for by the model 5 adj pseudo R2: proportion of the variance accounted for by the model with age included as a covariate 6 R square not informative because of insufficient fit.
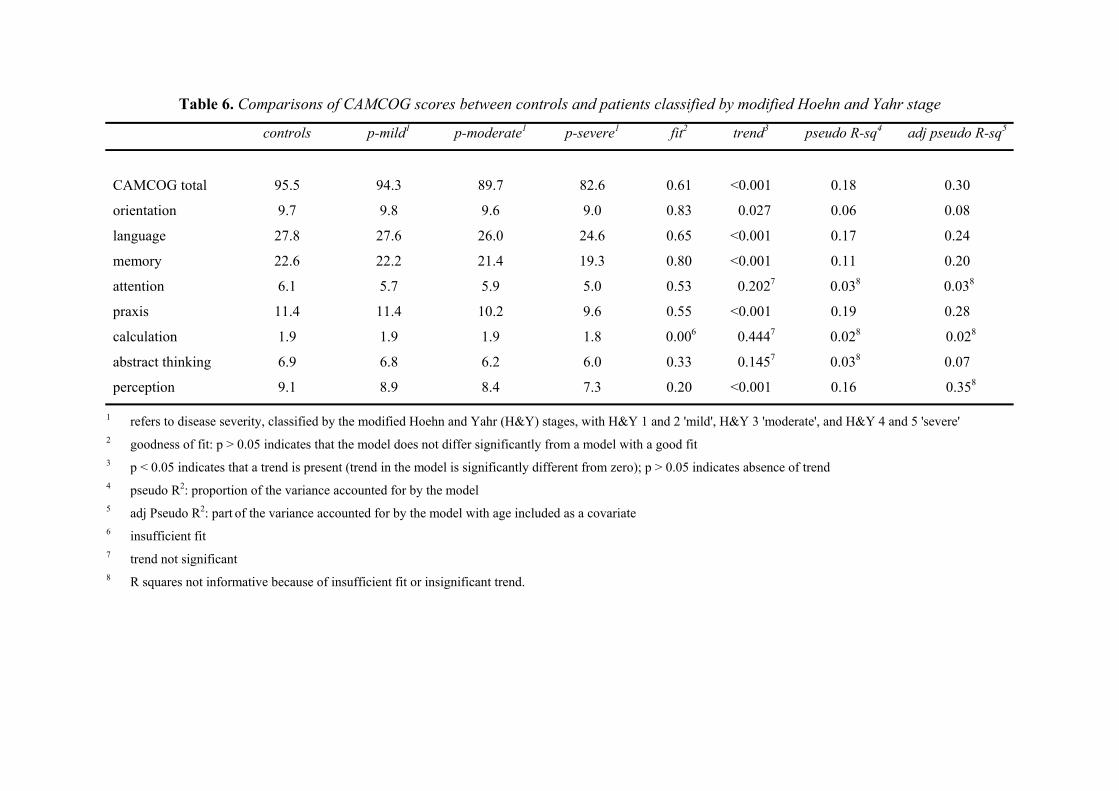
Table 6. Comparisons of CAMCOG scores between controls and patients classified by modified Hoehn and Yahr stage
controls p-mild1 p-moderate1 p-severe1 fit2 trend3 pseudo R-sq4 adj pseudo R-sq5
CAMCOG total 95.5 94.3 89.7 82.6 0.61 <0.001 0.18 0.30
orientation 9.7 9.8 9.6 9.0 0.83 0.027 0.06 0.08
language 27.8 27.6 26.0 24.6 0.65 <0.001 0.17 0.24
memory 22.6 22.2 21.4 19.3 0.80 <0.001 0.11 0.20
attention 6.1 5.7 5.9 5.0 0.53 0.2027 0.038 0.038
praxis 11.4 11.4 10.2 9.6 0.55 <0.001 0.19 0.28
calculation 1.9 1.9 1.9 1.8 0.006 0.4447 0.028 0.028
abstract thinking 6.9 6.8 6.2 6.0 0.33 0.1457 0.038 0.07
perception 9.1 8.9 8.4 7.3 0.20 <0.001 0.16 0.358
1 refers to disease severity, classified by the modified Hoehn and Yahr (H&Y) stages, with H&Y 1 and 2 'mild', H&Y 3 'moderate', and H&Y 4 and 5 'severe' 2 goodness of fit: p > 0.05 indicates that the model does not differ significantly from a model with a good fit 3 p < 0.05 indicates that a trend is present (trend in the model is significantly different from zero); p > 0.05 indicates absence of trend 4 pseudo R2: proportion of the variance accounted for by the model 5 adj Pseudo R2: part of the variance accounted for by the model with age included as a covariate 6 insufficient fit 7 trend not significant 8 R squares not informative because of insufficient fit or insignificant trend.

Chapter 4
- 74 -
Table 7. Correlations among scales in patient group
Hoehn and Yahr (rs)1 SCOPA-COG (r)2 CAMCOG (r)2
MMSE -0.283 0.72 0.83
CAMCOG -0.40 0.83
SCOPA-COG -0.39
1 Spearman's correlation coefficient (rho) 2 Pearson's product-moment correlation coefficient 3 correlation significant at p < 0.01; all other correlations significant at p < 0.001
Other findings
Linear regression analysis, using both the forward and backward stepwise method on the
scores of all three cognition scales, revealed that age, disease severity (i.e., H&Y), and level
of education were the variables that contributed most to the explanation of variance in scores
among participants. The adjusted R-squares of the constructed models were 0.23 in the
MMSE, 0.42 in the CAMCOG, and 0.47 in the SCOPA-COG. If this regression method was
applied to the data of the patients only, the same variables emerged, revealing adjusted R-
squares of 0.23 for the MMSE, 0.42 for the CAMCOG, and 0.34 for the SCOPA-COG.
Table 8. Relation between cognition and sex, age, and education in patients
mean (sd)
males
mean (sd)
females
p-value
m/f1
r age2
r years
educ2
rs level
educ3
MMSE 26.2 (3.6) 25.8 (3.9) 0.60 -0.45 0.20 (p = 0.072) 0.19 (p = 0.081)
CAMCOG 90.7 (9.6) 86.4 (13.2) 0.09 -0.50 0.33 (p = 0.002) 0.43 (p < 0.001)
SCOPA-COG 25.1 (7.1) 24.3 (7.3) 0.60 -0.54 0.20 (p = 0.069) 0.30 (p = 0.005)
1 p-value for differences in cognition scores between sexes 2 Pearson's correlation coefficient; all correlations with age significant (p < 0.001) 3 Spearman's correlation coefficient

Assessment of cognition in Parkinson's disease
- 75 -
Table 9. Factor analysis
factor 1 factor 2
1. cubes 0.51
2. digits backwards 0.61
3. word recall 0.71
4. counting by threes 0.64
5. months backwards 0.71
6. fist-edge-palm 0.79
7. dices 0.62
8. animal fluency 0.69
9. figure assembly 0.41 0.44
10. delayed recall words 0.63
Pattern matrix of explanatory factor analysis; extraction method:
oblique; data < 0.40 not shown. Two factors with eigenvalue > 1,
explaining 50.5% of the variance. Correlation between factors 0.37.
Figure 1. SCOPA-COG score and disease severity
Mean absolute SCOPA-COG scores of all participants. Controls included as
Hoehn and Yahr (H&Y) 0 (none, 'no signs of disease'; 75 persons). Disease
severity of patients categorised as mild (H&Y 1 and 2; 27 persons),
moderate (H&Y 3; 33 persons), or severe (H&Y 4 and 5; 25 persons).
Modified Hoehn and Yahr
severemoderatemildnone
SCO
PA-C
OG
sco
re
35
30
25
20
15
10
5
0

Chapter 4
- 76 -
Figure 2. Scores expressed in percentages of maximum score
Mean relative scores by modified H&Y stage, expressed as percentages of
maximum score. Controls included as H&Y 0 ('no signs of disease'; here 'none').
Discussion
We started this study with searching the literature for those cognitive functions that were
likely to be affected in PD, in order to select candidate items for a short, practical, and
sensitive scale that evaluates the specific cognitive deficits in PD. We found that especially
attention, active memory, executive functions, and visuospatial functions were impaired,
whereas verbal functions, and thinking and reasoning were relatively spared. The pattern that
thus emerged by following this strategy, is consistent with the concept of subcortical
dementia. It could therefore be argued that the SCOPA-COG is an instrument for assessing
subcortical functions in PD, although it was not our intention to create such an instrument. In
stead, we focussed on vulnerable functions, irrespective of whether these were considered
cortical or subcortical.
We developed a short and practical scale that displayed good clinimetric properties in this
study. Reproducibility and internal consistency were good, indicating adequate reliability.
The construct validity of the scale was supported by the expected correlations with other
scales, and by differences found between categories of participants grouped by dementia
modified Hoehn and Yahr
severemoderatemildnone
Scal
e sc
ores
in p
erce
ntag
es
100
90
80
70
60
50
40
30
20
10
0�����������������
���������������������������������� MMSE
CAMCOG
SCOPA-COG
���������
���������������������������������������������������������������
���������������������������������������������������������������
����������
����������������������������������������������������������������������
����������������������������������������������������������������������
������������
������������������������������������������������������������������������������������
������������������������������������������������������������������������������������
�������������
�������������������������������������������������������������������������������������������
�������������������������������������������������������������������������������������������
���������������
���������������������������������������������������������������������������������������������������������
���������������������������������������������������������������������������������������������������������
����������������
����������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������
����������������
����������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������
�����������������
�����������������������������������������������������������������������������������������������������������������������
�����������������������������������������������������������������������������������������������������������������������

Assessment of cognition in Parkinson's disease
- 77 -
status, and among patients grouped by disease severity. The higher CV in comparison with
the CAMCOG and the MMSE, indicates that the SCOPA-COG permits finer discrimination.
The scale shows a clear trend towards lower cognition scores for patients with more advanced
PD. This trend is more pronounced in the SCOPA-COG than in both other scales (figure 2).
Differences found in CAMCOG and MMSE scores between controls and patients with mild
PD are very small. In the SCOPA-COG these differences are larger, which may indicate that
this scale is more sensitive to the changes in cognitive performance that occur early in the
course of the disease. Male and female patients have similar scores, indicating that the
SCOPA is insensitive to the sex of the patient.
The SCOPA-COG correlates stronger with the CAMCOG than with the MMSE, but the latter
correlation is still substantial. Interestingly, the SCOPA-COG and MMSE correlate equally
strong with the CAMCOG, although the CAMCOG and SCOPA-COG share only one item,
whereas the CAMCOG and MMSE share 14 items.
The first group of items that emerged from the factor analysis, appears to reflect memory. All
memory items load on this factor. The loading of the 'fist-edge-palm' item on this factor may
be explained by the appeal that is made on memory to recall the sequence of movements. The
same explanation applies to the 'animal fluency task', in which memory must be activated to
produce correct responses. The second factor is best characterised by attention, since both
attention items load on this factor, whereas attention is also a prerequisite for correctly
executing the 'dices' task. The 'figure assembly' task loads only moderately on both factors,
which may indicate that this item is associated with an altogether different cognitive domain.
This is not surprising, given the nature of the task. The finding that the executive functions do
not emerge as a separate factor, indicates that these functions are somewhat heterogeneous,
which may be understood by the fact that functions within this domain, such as set-shifting,
fluency, and alternating motor programs, are rather different. Apparently the similarity with
other factors is stronger than the mutual resemblance among items in this domain.
Using a scale that selectively addresses some of the most often affected cognitive functions in
PD may add to our knowledge on cognitive difficulties that patients with this condition
experience. In general, the existing scales (such as the CAMCOG and MMSE), are based on a
more 'cortical' concept. Studying the CAMCOG scores in table 4, shows that seven of the
eight subscales of the CAMCOG differ significantly between patients and controls. This
indicates that these so-called 'cortical' functions are also affected in PD, albeit to a lesser
extent, as is apparent from the last column of this table. Some of the cortical functions, such

Chapter 4
- 78 -
as language and orientation, become affected later in the course of the disease (table 6). Using
both types of scales in longitudinal research may provide important information on the
interrelationship between these functions and may also shed light on several important topics.
Questions as to whether changes in 'cortical' and 'subcortical' functions occur simultaneously,
or whether one precedes the other, may be addressed. Other questions may concern the way
these changes interact, or whether changes in cortical and subcortical functions are related to
particular stages of the disease. These questions are all very relevant, even if the concept of
'subcortical dementia' as a distinctive entity is questioned.48,49 Arguments against this
distinction concern, among others, the overlap between the two dementias, the lack of a
consistent pattern among diseases that involve subcortical regions, the presence of subcortical
lesions in patients with cortical degeneration, and cortical lesions in patients with subcortical
lesions. Brown and Marsden50 argue that the dense pattern of neural interconnections between
cortical and subcortical regions suggests that the functional organisation of the brain does not
respect such convenient anatomical distinctions. Cummings and Benson,51 however,
emphasise that subcortical dementia is a clinical and not an anatomical concept. Advocates of
the dichotomy between cortical and subcortical functions refer to the consistent pattern of
spared and impaired functions, the neuropsychological differences between patients with AD
and PD, and to the association between subcortical gray matter lesions and the usual
presentations of subcortical dementias.25,52,53 Two prominent researchers in the area of
subcortical dementia provide somewhat different definitions of this concept. Dubois and
Pillon13 define subcortical dementia as a progressive dysexecutive syndrome with memory
deficits, in the absence of aphasia, apraxia, or agnosia. According to Cummings,1 subcortical
dementia is characterised by four cardinal features: memory impairment, decline in
intellectual function, psychomotor retardation, and mood abnormalities, whereas language
function is spared and motor disturbances coexist with the dementia. In a study by Korten et
al.,54 41 clinicians were asked to indicate which cognitive domains were affected in cortical,
subcortical, and frontal dementia. Agreement with respect to the latter two was disappointing.
This once again underlines the lack of a gold standard for subcortical dementia and indicates
that it is impossible to construct a screening or diagnostic instrument at this point in time.
After all, how should a cut-off point be determined? The SCOPA-COG is hence intended as
an index of severity and may be used to compare groups in research situations.
Although there is no consensus in this area, we tend to agree with Dubois et al.22 and Lezak,14
that the distinction between cortical and subcortical dementia still may be of heuristic value
and help research in this field. Our study should therefore be considered as a first attempt to
Assessment of cognition in Parkinson's disease
- 79 -
construct a cognitive scale that accounts for the typical phenomenology of subcortical
dementia.
It should be realised that the SCOPA-COG was constructed on the basis of differences in this
sample of participants and thus may reflect certain characteristics of this particular group.
Replication of the results in a different sample is needed to add further support to this scale.
In conclusion, the SCOPA-COG is a short and practical instrument with good clinimetric
properties that focuses on the most vulnerable cognitive functions in PD. The use of this scale
may provide a better insight into specific cognitive deficits that patients with PD experience.
Acknowledgements
This study was financed by the Netherlands Organization for Scientific Research (project no.
0940-33-021). The authors thank professor R.A.C. Roos for his helpful comments on the first
version of this manuscript. Doctors W.V.M. Perquin and J. van Rossum are gratefully
acknowledged for their help in the recruitment of patients.
References
1. Cummings JL. Intellectual impairment in Parkinson's disease: clinical, pathologic, and biochemical
correlates. J Geriatr Psychiatry Neurol 1988; 1(1):24-36.
2. Richards M, Stern Y, Marder K, Cote L, Mayeux R. Relationships between extrapyramidal signs and
cognitive function in a community-dwelling cohort of patients with Parkinson's disease and normal
elderly individuals. Ann Neurol 1993; 33(3):267-274.
3. Goldman WP, Baty JD, Buckles VD, Sahrmann S, Morris JC. Cognitive and motor functioning in
Parkinson disease: subjects with and without questionable dementia. Arch Neurol 1998; 55(5):674-680.
4. Katzen HL, Levin BE, Llabre ML. Age of disease onset influences cognition in Parkinson's disease. J Int
Neuropsychol Soc 1998; 1998 May;4(3):285-290.
5. Mayeux R, Denaro J, Hemenegildo N, Marder K, Tang MX, Cote LJ, et al. A population-based
investigation of Parkinson's disease with and without dementia. Relationship to age and gender. Arch
Neurol 1992; 49(5):492-497.
6. Sutcliffe RL, Meara JR. Parkinson's disease epidemiology in the Northampton District, England, 1992.
Acta Neurol Scand 1995; 92(6):443-450.
7. Aarsland D, Andersen K, Larsen JP, Lolk A, Nielsen H, Kragh-Sorensen P. Risk of dementia in
Parkinson's disease: A community-based, prospective study. Neurology 2001; 56(6):730-736.
8. Aarsland D, Andersen K, Larsen JP. 8-year prevalence of dementia in Parkinson's disease. Movement
Disorders 2001; 16 suppl 1:S57. Abstract.

Chapter 4
- 80 -
9. Stern Y, Richards M, Sano M, Mayeux R. Comparison of cognitive changes in patients with Alzheimer's
and Parkinson's disease. Arch Neurol 1993; 50(10):1040-1045.
10. Mahieux F, Fenelon G, Flahault A, Manifacier MJ, Michelet D, Boller F. Neuropsychological prediction
of dementia in Parkinson's disease. J Neurol Neurosurg Psychiatry 1998; 64(2):178-183.
11. Scheltens Ph. Dementia in Parkinson's disease: subclinical Alzheimer's disease? In: Wolters ECh,
Scheltens Ph, Berendse HW, editors. Mental Dysfunction in Parkinson's disease II. Utrecht: Academic
Pharmaceutical Productions, 1999: 189-193.
12. American Psychiatric Association. Delirium, Dementia, and Amnestic and Other Cognitive Disorders.
Diagnostic and Statistical Manual of Mental Disorders. Washington: American Psychiatric Association,
1994: 123-163.
13. Dubois B, Pillon B. Dementia in Parkinson's disease. In: Wolters ECh, Scheltens Ph, Berendse HW,
editors. Mental Dysfunction in Parkinson's Disease II. Utrecht: Academic Pharmaceutical Productions,
1999: 165-176.
14. Lezak MD. Neuropsychological Assessment. 3 ed. New York: Oxford University Press, 1995.
15. Brown GG, Rahill AA, Gorell JM, McDonald C, Brown SJ, Sillanpaa M, et al. Validity of the Dementia
Rating Scale in assessing cognitive function in Parkinson's disease. J Geriatr Psychiatry Neurol 1999;
12(4):180-188.
16. Brown RG, Marsden CD. Neuropsychology and cognitive function in Parkinson's disease: an overview.
In: Marsden CD, Fahn S, editors. Movement Disorders 2. London: Butterworths, 1987: 99-123.
17. Guillard A, Fenelon G, Mahieux F. Les altérations cognitives au cours de la maladie de Parkinson. Rev
Neurol (Paris) 1991; 147:337-355.
18. Pillon B, Deweer B, Agid Y, Dubois B. Explicit memory in Alzheimer's, Huntington's, and Parkinson's
diseases. Arch Neurol 1993; 50(4):374-379.
19. Barrett AM, Crucian GP, Schwartz RL, Heilman KM. Testing memory for self-generated items in
dementia: method makes a difference. Neurology 2000; 54(6):1258-1264.
20. Grober E, Buschke H, Crystal H, Bang S, Dresner R. Screening for dementia by memory testing.
Neurology 1988; 38(6):900-903.
21. Reid WG, Broe GA, Hely MA, Morris JG, Williamson PM, O'Sullivan DJ, et al. The neuropsychology of
de novo patients with idiopathic Parkinson's disease: the effects of age of onset. Int J Neurosci 1989;
48(3-4):205-217.
22. Dubois B, Boller F, Pillon B, Agid Y. Cognitive deficits in Parkinson's disease. In: Corkin S, Grafman J,
Boller F, editors. Handbook of Neuropsychology. Amsterdam: Elsevier Science Publishers, 1991: 195-
240.
23. Berger HJ, van Es NJ, Van Spaendonck KP, Teunisse JP, Horstink MW, 't Hof MA, et al. Relationship
between memory strategies and motor symptoms in Parkinson's disease. J Clin Exp Neuropsychol 1999;
21(5):677-684.
24. Faglioni P, Saetti MC, Botti C. Verbal learning strategies in Parkinson's disease. Neuropsychology 2000;
14(3):456-470.
25. Cummings JL. Subcortical dementia. Neuropsychology, neuropsychiatry, and pathophysiology. Br J
Psychiatry 1986; 149:682-697.

Assessment of cognition in Parkinson's disease
- 81 -
26. Boller F, Passafiume D, Keefe NC, Rogers K, Morrow L, Kim Y. Visuospatial impairment in Parkinson's
disease. Role of perceptual and motor factors. Arch Neurol 1984; 41(5):485-490.
27. Taylor AE, Saint-Cyr JA, Lang AE. Frontal lobe dysfunction in Parkinson's disease. The cortical focus of
neostriatal outflow. Brain 1986; 109 ( Pt 5):845-883.
28. Brown RG, Marsden CD. Cognitive function in Parkinson's disease: from description to theory. Trends
Neurosci 1990; 13(1):21-29.
29. Cools R, Swainson R, Owen AM, Robbins TW. Cognitive dysfunction in non-demented Parkinson's
disease. In: Wolters ECh, Scheltens Ph, Berendse HW, editors. Mental dysfunction in Parkinson's disease
2. Utrecht: Academic Pharmaceutical Productions, 1999: 142-164.
30. Flowers KA, Robertson C. The effect of Parkinson's disease on the ability to maintain a mental set. J
Neurol Neurosurg Psychiatry 1985; 48(6):517-529.
31. Gotham AM, Brown RG, Marsden CD. 'Frontal' cognitive function in patients with Parkinson's disease
'on' and 'off' levodopa. Brain 1988; 111 (Pt 2):299-321.
32. Van Spaendonck KP, Berger HJ, Horstink MW, Buytenhuijs EL, Cools AR. Executive functions and
disease characteristics in Parkinson's disease. Neuropsychologia 1996; 34(7):617-626.
33. Cools R, Barker RA, Sahakian BJ, Robbins TW. Mechanisms of cognitive set flexibility in Parkinson's
disease. Brain 2001; 124(Pt 12):2503-2512.
34. Brown RG, Marsden CD. Visuospatial function in Parkinson's disease. Brain 1986; 109(Pt 5):987-1002.
35. Maeshima S, Itakura T, Nakagawa M, Nakai K, Komai N. Visuospatial impairment and activities of daily
living in patients with Parkinson's disease: a quantitative assessment of the cube-copying task. Am J Phys
Med Rehabil 1997; 76(5):383-388.
36. Lee A, Harris J. Problems with perception of space in Parkinson's disease. Neuro-ophthalmology 1999;
22:1-15.
37. Brown RG, Marsden CD. How common is dementia in Parkinson's disease? Lancet 1984; 2(8414):1262-
1265.
38. Mayeux R, Stern Y, Sano M, Cote L, Williams JB. Clinical and biochemical correlates of bradyphrenia in
Parkinson's disease. Neurology 1987; 37(7):1130-1134.
39. Mayeux R, Stern Y, Rosen J, Leventhal J. Depression, intellectual impairment, and Parkinson disease.
Neurology 1981; 31(6):645-650.
40. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease.
J Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
41. Derix MMA, Teunisse S, Hijdra A, Wens L, Hofstede AB, Walstra GJM, et al. CAMDEX-N: De
Nederlandse versie van de Cambridge Examination for Mental Disorders of the Elderly. Lisse: Swets &
Zeitlinger, 1992.
42. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res 1975; 12(3):189-198.
43. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
44. Roth M, Tym E, Mountjoy CQ, Huppert FA, Hendrie H, Verma S, et al. CAMDEX. A standardised
instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection
of dementia. Br J Psychiatry 1986; 149:698-709.

Chapter 4
- 82 -
45. McDowell I, Newell C. Mental status testing. Measuring Health: A Guide to Rating Scales and
Questionnaires. New York: Oxford University Press, 1996: 287-334.
46. Hobson P, Meara J. The detection of dementia and cognitive impairment in a community population of
elderly people with Parkinson's disease by use of the CAMCOG neuropsychological test. Age Ageing
1999; 28(1):39-43.
47. Haas M. Statistical methodology for reliability studies. J Manipulative Physiol Ther 1991; 14(2):119-132.
48. Mayeux R, Stern Y, Rosen J, Benson F. Is "subcortical dementia" a recognizable clinical entity? Ann
Neurol 1983; 14(3):278-283.
49. Whitehouse PJ. The concept of subcortical and cortical dementia: another look. Ann Neurol 1986;
19(1):1-6.
50. Brown RG, Marsden CD. 'Subcortical dementia': the neuropsychological evidence. Neuroscience 1988;
25(2):363-387.
51. Cummings JL, Benson DF. Subcortical dementia. Review of an emerging concept. Arch Neurol 1984;
41(8):874-879.
52. Huber SJ, Shuttleworth EC, Paulson GW, Bellchambers MJ, Clapp LE. Cortical vs subcortical dementia.
Neuropsychological differences. Arch Neurol 1986; 43(4):392-394.
53. Cahn-Weiner DA, Grace J, Ott BR, Fernandez HH, Friedman JH. Cognitive and behavioral features
discriminate between Alzheimer's and Parkinson's disease. Neuropsychiatry Neuropsychol Behav Neurol
2002; 15(2):79-87.
54. Korten EC, Verhey FR, Derix MM, Klinkenberg EL, Jolles J. [Consensus on the concepts of cortical,
subcortical and frontal dementia. Research by national and international dementia experts]. Tijdschr
Gerontol Geriatr 2001; 32(3):109-116.
55. Benton AL. The Revised Visual Retention Test. 4 ed. New York: Psychological Corporation, 1974.
56. Luria AR. Higher cortical functions in man. 1 ed. London: Tavistock Publications, 1966.
57. Benton AL, Varney NR, Hamsher KD. Visuospatial judgment. A clinical test. Arch Neurol 1978;
35(6):364-367.

Assessment of cognition in Parkinson's disease
- 83 -
Appendix
Memory and learning
1. Cubes*
Copying the order in which four cubes are pointed; 5 series.
(Knox Cube Test from Arthur Point Scale of Performance Battery)
2. Visual retention test
Selecting the one figure (out of four resembling figures), that was shown previously; 5 series. (Selected
from Benton's visual retention test 55.)
3. Digit span forward
(3-9 digits); repeating a series of digits in the same direction they were presented.
4. Digit span backward*
(2-8 digits); as 3, but now in backward direction.
5. Verbal recall*
Reading and recalling 10 words. Series is performed three times. Differences between consecutive trials
reflect learning capacity.
Attention
6. Counting down by ones, 20 to 1
7. Counting down by threes, 30 to 0*
8. Serial sevens
Subtracting 7 from 100, and then again from the remaining total; repeat 5 times.42
9. Months backward*
Naming the months of the year in reverse order.
Executive functions
10. Tapping
"Tap twice when I tap once. Tap once when I tap twice"; series of 10.56
11. Go – No Go
"Tap once when I tap once. Do not tap when I tap twice"; series of 10.56
12. Fist-edge-palm*
Copying three consecutive hand movements; series of 10.56

Chapter 4
- 84 -
13. Dices*
Asking the subject to say "Yes" if the number on a dice that is printed on a card represents an even
number and "No" if it concerns an odd number. Correct if necessary. Then second trial is performed, in
which the subject is requested to say "Yes" if the number on the dice is higher than the one that was
shown previously, and "No", if the number is lower; series of 10. Only second trial is scored.
14. Letter-digit alternation
Showing 10 pairs of one letter and one digit. During the first series, only the letters should be read aloud.
Correct if necessary. During the second series, only digits are to be read aloud. Only the second trial is
scored.33
15. Fluency animals*
Naming as many animals as possible during one minute.
16. Odd-man-out
Have subject indicate and explain which figure is different from the other two. Then this explicated rule
has to be applied when answering the next three sets of three figures. Correct if necessary. Then the same
set is presented again, and another way in which one of the figures is differs from the other two should be
indicated and explained. Answers to the next set should be given according to this second rule.30
Differences concern size or shape of the figures.
Visuospatial functions
17. Angle matching
Indicating which of 12 lines have the same orientation as four presented line segments. (From visual
judgement of line orientation test57).
18. Figure assembly*
Indicating which figure parts are necessary to construct a presented figure; 5 series.
Memory
19. Verbal recall*
Delayed recall. Recalling the words of item 5.
* item included in final version of SCOPA-COG

- 85 -
55
Evaluation of the Hospital Anxiety and Depression Scale in patients with Parkinson’s disease
Johan Marinus1, Albert F.G. Leentjens2 3, Martine Visser1, Anne M. Stiggelbout4, Jacobus J.
van Hilten1
Departments of 1Neurology and 4Medical Decision Making, Leiden University Medical Center,
Leiden; 2Department of Psychiatry, Maastricht University Hospital, Maastricht; 3Institute for Brain and Behaviour, Maastricht University, Maastricht, The Netherlands
Published in Clinical Neuropharmacology 2002;25:318-324

Chapter 5
- 86 -
Abstract The purpose of this study was to evaluate the psychometric properties of the Hospital Anxiety and
Depression Scale (HADS) in patients with Parkinson's disease (PD), and to assess the prevalence of
symptoms of anxiety and depression in this population. The HADS was sent to 205 patients with PD,
together with three quality-of-life (QoL) instruments, i.e., the Parkinson’s Disease Questionnaire
(PDQ-39), the EQ-5D, and a visual analogue scale (VAS). HADS scores were also compared with
Hoehn and Yahr (H&Y) scores. Eighty-six percent of the patients returned the questionnaires. The
quality of the data was good. Cronbach’s α for the HADS was 0.88. Test-retest reliability over two
weeks was 0.84 for the sum score of the HADS (intraclass correlation coefficient), and ranged from
0.42-0.76 for individual items (weighted kappa). Factor analysis revealed two factors, accounting for
51.9% of the variance. One factor represented anxiety, the other depression. Correlations with PDQ-
39, EQ-5D, VAS, and H&Y were 0.72, -0.59, -0.59, and 0.32, respectively (p-values < 0.001).
Depression scores accounted for 52% of the variance in QoL, whereas disease severity explained
24%. Using the cut-off values proposed by the developers, indicated that possible and probable
anxiety were present in 28.9 and 19.8 percent of the patients, respectively. Percentages for possible
and probable depression were 21.6 and 16.5. The psychometric performance of the HADS in patients
with PD is satisfactory. In addition, almost 50% of the patients displayed symptoms of anxiety,
whereas nearly 40% showed signs of depression.
Keywords: Parkinson's disease, Hospital Anxiety and Depression Scale, anxiety, depression,
psychometrics.
Evaluation of the HADS in Parkinson's disease
- 87 -
Introduction
Depressive symptoms are common in patients with Parkinson’s disease (PD). The mean
prevalence of depressive symptomatology in 26 studies reviewed by Cummings was
estimated at 40%, with a range of 4-70%.1 Depression affects quality of life (QoL) in patients
with PD substantially2-4 and, therefore, evaluating depression is important. However, the
majority of rating scales for depression include somatic items that resemble somatic features
that are inherent to PD (e.g. psychomotor slowing, masked face, mental slowing,
concentration difficulties, sleep disturbances, fatigue). Application of these scales may lead to
overestimation of depressive symptoms in PD, and it may be more appropriate to use scales
without somatic items.
Anxiety is another common problem in PD, but this phenomenon has received much less
attention. Symptoms of anxiety may occur in up to 40% of the patients with PD,5 with two of
the largest studies reporting frequencies of about 20%.6,7 Several studies indicated that
anxiety and depression are related constructs.8,9 Just as in depression, anxiety may include
somatic symptoms that can be caused by PD as well (e.g. restlessness, being easily fatigued,
difficulty concentrating, irritability, muscle tension, sleep disturbance). Following the same
line of reasoning as in depression, scales without somatic symptoms may be preferred for use
in PD.
A scale that addresses both anxiety and depression and lacks somatic items, is the Hospital
Anxiety and Depression Scale (HADS).10 This scale is thus an attractive candidate to assess
these phenomena in PD. The HADS has 14 items, seven of which address depression and
seven that evaluate anxiety. Scores on individual items can either be summed to calculate a
total score or totalled per subscale to produce separate anxiety and depression scores. Each
item has four graded response options, scored 0 (absence) to 3 (present to extreme). Items are
phrased both indicative and contra-indicative. Scores on contra-indicative items are recoded
before adding up. Higher scores reflect greater problems.
Experience with this scale in PD is scarce.2,11 Therefore, we conducted a study with the
objective to both assess the psychometric properties of the HADS in patients with PD, and
evaluate the prevalence of symptoms of anxiety and depression in this population.

Chapter 5
- 88 -
Materials and Methods
Patients
Patients who visited the outpatient neurology clinic of the Leiden University Medical Center,
and who fulfilled the United Kingdom Parkinson’s Disease Society Brain Bank criteria for
idiopathic PD,12 were considered eligible. Patients with other diseases of the central nervous
system were excluded. The study was approved by the institutional review board.
Methods
Questionnaires were sent to 205 patients. The included instruments were the Parkinson’s
Disease Questionnaire (PDQ-39),13 the EQ-5D,14 and a visual analogue scale (VAS)
assessing quality of life with PD. The PDQ-39 is a disease-specific quality-of-life (QoL)
instrument with five ordinal response options that includes 39 items, clustered in eight
subscales (mobility, activities of daily living, emotional well-being, stigma, social support,
cognitions, communication, and bodily discomfort). Summary indices can be calculated both
for subscales and for the total scale. Higher scores reflect poorer QoL. The EQ-5D is a short
generic QoL instrument with three ordinal response options that includes five items
(mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). A summary
index with a maximum of 1.00 (reflecting the best health state) can be derived from the five
dimensions by conversion with a table of scores.15,16
Patients were requested to fill out the PDQ-39 first and subsequently put it in one of the two
enclosed return envelopes, which had to be sealed before the other scales were filled out. This
was done because some of the items in the PDQ-39 resembled items in other instruments, and
we wanted to ensure that patients did not look back at their previous responses in order to
avoid overestimation of the correlation between scales. Patients were asked to return the
completed questionnaires within one week. After two weeks we contacted all patients that
had not returned their questionnaires, and inquired whether they still wanted to participate.
Patients who returned their questionnaires within five days were asked to fill out the HADS a
second time two weeks later, in order to evaluate test-retest reliability.
Information from questionnaires was combined with information that was obtained from
patients records. This information concerned disease severity and disease duration. Disease
severity was evaluated at each control visit and assessed by the Hoehn and Yahr (H&Y)
staging system.17 H&Y 1 is the mildest stage with only unilateral symptoms, whereas H&Y 5
represents the most severe stage, in which patients are wheelchair-bound or bedridden.

Evaluation of the HADS in Parkinson's disease
- 89 -
Statistical analysis
Data were entered and analyzed with SPSS for windows 10.0 (SPSS Inc, Chicago, IL, USA).
The quality of the data was evaluated and items were considered to perform adequately if
they met the following criteria: missing values in less than 5% of the subjects, item-total
correlations of 0.20 or higher,18 and absence of floor and ceiling effects (endorsement rates
between 0.20 and 0.80).18
Reliability. Internal consistency was assessed using Cronbach’s α. Values higher than 0.7
were considered adequate for group comparisons, whereas values higher than 0.9 were
considered adequate for clinical application.19 The test-retest reliability for individual items
was assessed with a weighted kappa (Kw), whereas for the total score an intraclass correlation
coefficient (ICC) was used. Quadratic weights were used to calculate Kw, because with these
weights, kappa is equivalent to the ICC,20 which facilitates the interpretation of the results.
Validity. A principal component factor analysis was performed to explore the factor structure
of the HADS. An oblique rotation method was used because the factors were assumed to be
correlated. Construct validity with the PDQ-39, the EQ-5D, and the VAS was assessed using
Pearson’s correlation coefficient (r). For correlation with the H&Y scale, Spearman's rho (rs)
was used. Pearson's r was also used to assess the correlation between HADS scores and both
disease duration and age. An ordinal regression analysis was used to assess the relation
between HADS scores and H&Y scores. The significance threshold was set at 0.05.
Prevalence of symptoms
The cut-off values as proposed by the developers of the HADS10 were applied to our
population in order to determine the proportion of patients considered unimpaired (not
anxious or not depressed, scoring ≤ 7 on each subscale), possibly impaired (8-10 on each
subscale), or probably impaired (≥ 11 on each subscale).

Chapter 5
- 90 -
Results
Response rate and sample characteristics
One-hundred-and-seventy-seven questionnaires were returned, constituting a response rate of
86%. Sample characteristics are presented in table 1.
The first 59 patients were approached for the test-retest analysis. Fifty-four of these patients
(92%) returned the HADS the second time. Patient characteristics of the retest group were
similar to those of the total group.
Table 1. Patient characteristics
number of patients: 177
male / female ratio: 99 (56%) male / 78 (44%) female
mean (SD) age in years: 65.2 (11.1)
mean (SD) age at onset in years: 55.7 (11.6)
mean (SD) disease duration in years: 9.4 (5.6)
disease stage:
Hoehn &Yahr 1 and 2 (mild): 74 (41.8%)
Hoehn &Yahr 3 (moderate): 70 (39.5%)
Hoehn &Yahr 4 and 5 (severe): 33 (18.6%)
Clinimetric evaluation of the HADS
Data quality. The quality of the data was good. There were no missing values. All item-total
correlations exceeded 0.20 (table 2) and none of the items showed floor or ceiling effects.
Reliability. Cronbach’s α for the total HADS was 0.88. For the anxiety subscale and the
depression subscale this was 0.86 and 0.78, respectively. None of the anxiety items could be
deleted without a decrease of Cronbach’s α. Deletion of item 14 in the depression subscale
would have resulted in a slight increase of α to 0.80.
The test-retest reliability for sumscores, assessed with an ICC, was 0.84 for the total HADS,
and 0.86 and 0.84 for the anxiety and depression subscales, respectively. The test-retest
reliability for individual items (Kw) ranged from 0.42-0.76 (table 2).
Validity. Factor analysis with oblique rotation revealed three factors with an eigenvalue
greater than 1, together explaining 59.0% of the variance. Factor one included all the original
anxiety items, with the exception of item 5, which loaded slightly more on the second
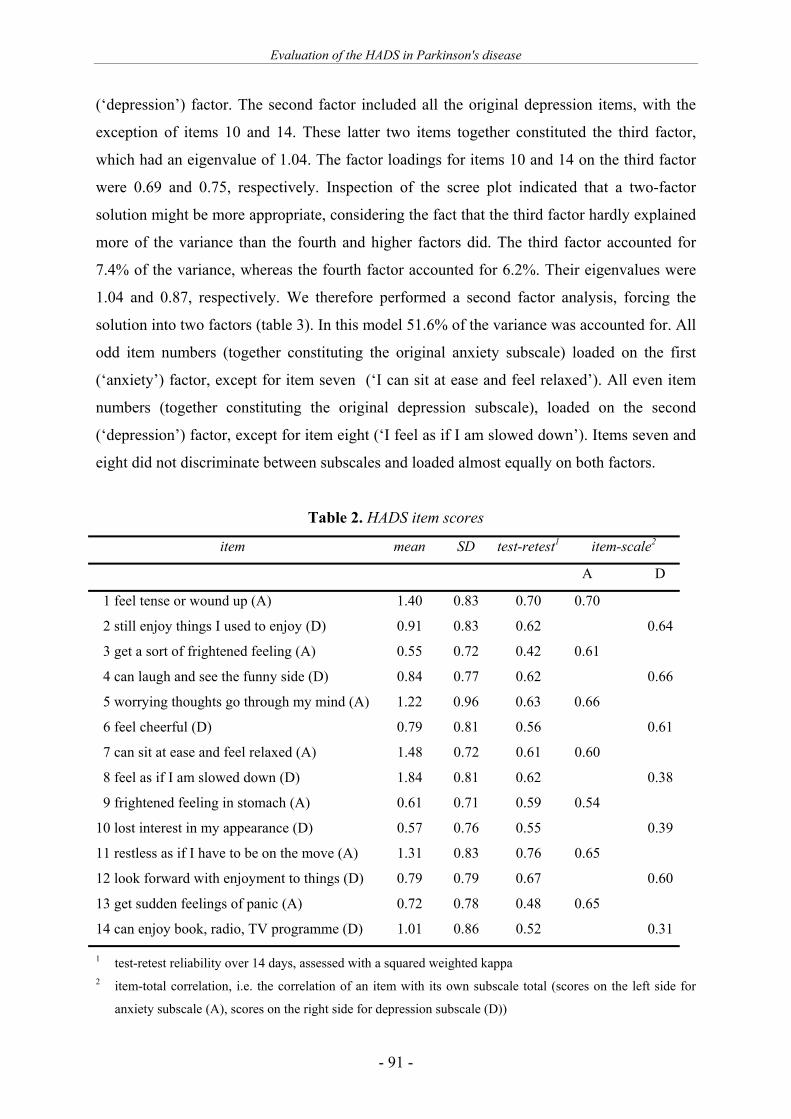
Evaluation of the HADS in Parkinson's disease
- 91 -
(‘depression’) factor. The second factor included all the original depression items, with the
exception of items 10 and 14. These latter two items together constituted the third factor,
which had an eigenvalue of 1.04. The factor loadings for items 10 and 14 on the third factor
were 0.69 and 0.75, respectively. Inspection of the scree plot indicated that a two-factor
solution might be more appropriate, considering the fact that the third factor hardly explained
more of the variance than the fourth and higher factors did. The third factor accounted for
7.4% of the variance, whereas the fourth factor accounted for 6.2%. Their eigenvalues were
1.04 and 0.87, respectively. We therefore performed a second factor analysis, forcing the
solution into two factors (table 3). In this model 51.6% of the variance was accounted for. All
odd item numbers (together constituting the original anxiety subscale) loaded on the first
(‘anxiety’) factor, except for item seven (‘I can sit at ease and feel relaxed’). All even item
numbers (together constituting the original depression subscale), loaded on the second
(‘depression’) factor, except for item eight (‘I feel as if I am slowed down’). Items seven and
eight did not discriminate between subscales and loaded almost equally on both factors.
Table 2. HADS item scores
item mean SD test-retest1 item-scale2
A D
1 feel tense or wound up (A) 1.40 0.83 0.70 0.70
2 still enjoy things I used to enjoy (D) 0.91 0.83 0.62 0.64
3 get a sort of frightened feeling (A) 0.55 0.72 0.42 0.61
4 can laugh and see the funny side (D) 0.84 0.77 0.62 0.66
5 worrying thoughts go through my mind (A) 1.22 0.96 0.63 0.66
6 feel cheerful (D) 0.79 0.81 0.56 0.61
7 can sit at ease and feel relaxed (A) 1.48 0.72 0.61 0.60
8 feel as if I am slowed down (D) 1.84 0.81 0.62 0.38
9 frightened feeling in stomach (A) 0.61 0.71 0.59 0.54
10 lost interest in my appearance (D) 0.57 0.76 0.55 0.39
11 restless as if I have to be on the move (A) 1.31 0.83 0.76 0.65
12 look forward with enjoyment to things (D) 0.79 0.79 0.67 0.60
13 get sudden feelings of panic (A) 0.72 0.78 0.48 0.65
14 can enjoy book, radio, TV programme (D) 1.01 0.86 0.52 0.31
1 test-retest reliability over 14 days, assessed with a squared weighted kappa 2 item-total correlation, i.e. the correlation of an item with its own subscale total (scores on the left side for
anxiety subscale (A), scores on the right side for depression subscale (D))

Chapter 5
- 92 -
Table 3. Factor analysis
item factor
1 2
1 feel tense or wound up 0.74
2 still enjoy things 0.70
3 sort of frightened feeling 0.81
4 can laugh and see funny side 0.26 0.64
5 worrying thoughts 0.61 0.29
6 feel cheerfull 0.68
7 sit at ease and feel relaxed 0.42 0.47
8 feel as if I am slowed down 0.35 0.29
9 frightened feeling in stomach 0.70
10 lost interest in appearance 0.70
11 restless as if I have to be on the move 0.72
12 look forward with enjoyment to things 0.62
13 sudden feelings of panic 0.81
14 enjoy book, radio, TV 0.55
• only scores higher than 0.25 are shown
• extraction method: principal component analysis
• rotation method: oblique rotation.
The distribution of the sumscore of the total HADS did not differ significantly from a normal
distribution (Kolmogorov Smirnov Z = 1.00, p = 0.27). The correlation among both subscales
of the HADS was 0.61. The total HADS correlated substantially (r > 0.60) with the PDQ-39
summary index, the PDQ emotional well-being subscale, and the ‘anxiety/depression item’ of
the EQ-5D, whereas correlations with the complete EQ-5D and the VAS were moderate
(table 4). The scores of the total HADS generally correlated higher with the subscales of the
PDQ-39 and the items of the EQ-5D, than the separate anxiety and depression scores did.
Patients in H&Y stages 1 and 5 were underrepresented and we therefore categorized patients
as mildly (H&Y 1 and 2, n = 74), moderately (H&Y 3, n = 70), and severely (H&Y 4 and 5, n
= 33) affected (table 1). The correlation between the H&Y stage and HADS total score was
0.32 (p < 0.001). Ordinal regression of HADS scores on modified H&Y data revealed a good
fitting model (Chi2 = 47.96, df = 58, p = 0.82), displaying a significant trend (p < 0.001).

Evaluation of the HADS in Parkinson's disease
- 93 -
The correlation between HADS total scores on the one hand and age and disease duration on
the other hand, were very low and non significant (-0.04 and 0.08, respectively). Correlation
between H&Y and the PDQ-39 summary index was 0.49 (rs).
Table 4. Correlation with other scales
HADS-total HADS-anxiety HADS-depression
PDQ-391 Summary Index 0.724 0.664 0.624
PDQ-39 subscales:
Mobility 0.53 0.47 0.48
activities of daily living 0.42 0.38 0.38
emotional well-being 0.734 0.724 0.59
Stigma 0.50 0.49 0.41
social support 0.39 0.36 0.33
cognitions 0.48 0.40 0.47
communication 0.34 0.26 0.36
bodily discomfort 0.47 0.52 0.32
Euroqol Summary Index 0.59 0.54 0.53
Euroqol items:
Mobility 0.22 0.20 0.193
daily activities 0.49 0.40 0.48
self-care 0.31 0.25 0.30
pain / discomfort 0.29 0.31 0.20
anxiety / depression 0.674 0.624 0.59
QoL VAS2 -0.59 -0.49 -0.58
1 PDQ-39: Parkinson’s Disease Questionnaire 2 QoL VAS: visual analogue scale assessing quality of life 3 correlation significant at 0.05 level; all other correlations significant at 0.01 level 4 substantial correlation (r > 0.60)

Chapter 5
- 94 -
Prevalence of anxiety and depression
When the cut-off scores as proposed by the developers were applied to our population, 61.9%
of the patients were considered not-depressed, whereas 21.6% were possibly, and 16.5% were
probably depressed. The distribution of anxiety scores indicated that 51.1% of the patients
were considered not-anxious, while 28.9% and 19.8% of the patients were regarded to
experience possible and probable anxiety, respectively (figure 1).
Differences in HADS total scores were not significant for male versus female patients (p =
0.64).
Figure 1. Percentage of patients with depression or anxiety for different cut-off values
vertical dashed lines indicate limits for non-cases (≤ 7), possible cases (8-10), and definite cases (≥ 11)
Subscale total
2520151050
Perc
enta
ge o
f 'ca
ses' 100
90
80
70
60
50
40
30
20
10
0
score HADS-D
score HADS-A

Evaluation of the HADS in Parkinson's disease
- 95 -
Discussion To date, sufficiently large studies addressing the psychometric properties of the HADS in a
population of patients with PD are lacking. The high response rate in our study supports the
notion that the reported data largely reflect the true scores of the target population.
The quality of the data in this study is high. The HADS shows adequate test-retest reliability
and sufficient internal consistency for group comparisons, with values resembling those
found in other populations.21-25 The internal consistency of 0.88 is just below the
recommended threshold of 0.90 and, consequently, using this scale for clinical evaluation
may be disputed. In this field the other depression rating scales generally do not perform
better than the HADS, however.26 The item-total correlations range from 0.31-0.70, which is
in accordance with results from other studies.10,23,25,27 If the factor solution is forced into two
factors, the factor structure is similar to that reported for other populations, that is, two factors
accounting for approximately 50% of the variance, with one factor representing anxiety and
the other depression.21-23,25,27,28 The correlation between the HADS and scores on QoL
instruments is consistent with the results of other studies that assessed the relation between
depression and quality of life in PD.2-4 In our study depression accounts for 52% of the
variance in QoL in patients with PD. Interestingly, this percentage is much higher than that
for disease severity, which accounts for only 24% of the variance in QoL. This underscores
the importance of assessing depression in PD. In clinical care disease severity is nearly
always routinely evaluated, but for depression this is far less common.
Disease duration does not affect the level of depression in our population. The relation
between depression and disease severity assessed by H&Y, shows a significant positive trend,
but the correlation is low. Neither age nor gender correlate with the HADS scores. These
findings are in line with results from the literature.1
Almost fifty percent of the patients shows symptoms of anxiety, with twenty percent
displaying probable anxiety. This latter percentage is in agreement with the prevalences
found by Aarsland et al.6 and Vasqeuz et al.7 Thirty-eight percent of the patients in our study
displays symptoms of depression, with 21 percent showing possible and 17 percent showing
probable depressive symptomatology. These results comply with the prevalences reported by
Cummings.1
Most of the rating scales for depression and anxiety were developed for use in psychiatric
populations and invariably include somatic items. Because the somatic features of depression
and anxiety show considerable overlap with those of PD, the prevalence of these symptoms

Chapter 5
- 96 -
may be overestimated if such scales are used in this population. Consequently, using scales
without somatic items may be more appropriate. Some researchers argue that scales including
somatic items may be used in physical diseases after all, provided that cut-off values are
adjusted to account for the presence of somatic symptoms.29,30 This argument holds only if
the severity of somatic symptoms co-vary in accordance with depressive symptoms. This
may be questioned however, as was demonstrated by Leentjens et al.,31 who found that non-
somatic items of the Hamilton Rating scale for Depression (HAM-D) and the Montgomery-
Åsberg Depression Rating Scale (MÅDRS) contributed more to the clinical diagnosis of
depression than individual somatic items did. This illustrates the differential importance of
these items with respect to depression in PD. The only somatic items that discriminated to
some extent, were ‘reduced appetite’ and ‘early morning wakening’, which is in agreement
with results of studies in other non-psychiatric populations.32,33
Despite this obvious advantage of the HADS for use in PD, the instrument has hardly been
used in this patient group. Hitherto, the HADS has only been used in PD for external
validation of another scale,2 or for describing baseline values for emotional state.11 Only
Leentjens et al.34 assessed the screening and diagnostic properties of the HADS in 55 non-
demented patients with idiopathic PD and concluded that the screening properties of this
scale seem adequate, but that the diagnosis of depression is better achieved with expert-
administered depression scales, such as the HAM-D and the MÅDRS.35 This is in line with
the intent of the developers, who aimed to construct a reliable screening test for psychiatric
disorder in the physically ill that could help the busy clinician. In the study by Leentjens et
al.34 maximum discrimination between depressed and non-depressed patients was obtained
when the total HADS was used with a cut-off of 18/19. However, as the sample size was
small relative to the number of items, this finding should be viewed with some caution.
The developers of the HADS consider the scale scores insensitive to somatic problems, and,
from their perspective, adjusting cut-off values for particular populations is unnecessary.10
This statement may be questioned with respect to items seven and eight in our population.
These items do not discriminate between subscales and the mean values are higher than those
found usually.25 This is most likely explained by a confounding effect of tremor and rigidity
on item 7 (‘I can sit at ease and feel relaxed’), and bradykinesia and rigidity on item 8 (‘I feel
as if I am slowed down’). Nevertheless, the item-total correlations of both items are quite
acceptable and deletion of these items would have resulted in a lower Cronbach’s alpha.

Evaluation of the HADS in Parkinson's disease
- 97 -
Consequently, there is no reason for deletion of these items in studies on patients with PD,
but our finding casts some doubt on the level of the cut-off value.
A disadvantage of this study was the lack of a gold standard, that is, psychiatric evaluation.
This would have enabled us to evaluate the diagnostic properties of the HADS. Looking
back, we regret that we did not include the Beck Depression Inventory in the survey as well.
A direct comparison of these frequently used self-administered depression scales would have
produced valuable information.
Although the absence of somatic items in scales that evaluate anxiety and depression in
patients with physical diseases has its advantages, it is important to realize that there is a
trade-off with face validity. After all, the concurrent validity with criteria for depression and
anxiety is decreased. For instance, five of the nine criteria for depression mentioned in the
fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)36
concern somatic items (insomnia, fatigue, reduced appetite, reduced concentration,
psychomotor slowing). Furthermore, since the HADS focuses on the core symptoms of
depression (mood and anhedonia), two of the other non-somatic items of the DSM-IV are not
addressed either (guilt, suicidal thoughts). In this respect, the Beck Depression Inventory
covers the domain of depression more thoroughly, since it addresses seven of the nine DSM
criteria for depression.
Taken together, the psychometric properties of the HADS in a large population of patients
with PD are satisfactory. Results regarding reliability and construct validity are adequate and
agree with results in other populations. The internal consistency is just below the desired
threshold for clinical evaluation, indicating that information on an individual level should be
interpreted with some caution. Although patients with PD may interpret two items
‘somatically’, removal of these items from this scale is unnecessary, although a slight rise of
the advised cut-off may increase the concurrent validity with the DSM criteria for depressive
disorder. Taking this into account, the HADS can adequately be used to assess anxiety and
depression in patients with PD. Although the screening properties of the HADS seem
adequate, the diagnostic properties may be questioned and it may be more appropriate to use
the scale scores as an ‘index of severity’. An additional advantage of this scale is that it can
be completed by patients without the help of an expert.

Chapter 5
- 98 -
Depression plays an important role and accounts for more than 50% of the variance in quality
of life in PD. This percentage is twice as high as that of disease severity and evaluating
depression should hence be part of the routine clinical assessment of patients with PD.
Acknowledgements
This study was financed by the Netherlands Organization for Scientific Research (project no.
0940-33-021). The authors thank Professor R.A.C. Roos for his helpful comments.
References
1. Cummings JL. Depression and Parkinson's disease: a review. Am J Psychiatry 1992; 149(4):443-454.
2. Martinez-Martin P, Frades PB. Quality of life in Parkinson's disease: validation study of the PDQ-39
Spanish version. The Grupo Centro for Study of Movement Disorders. J Neurol 1998; 245 Suppl 1:S34-
S38.
3. Schrag A, Jahanshahi M, Quinn N. What contributes to quality of life in patients with Parkinson's disease? J
Neurol Neurosurg Psychiatry 2000; 69(3):308-312.
4. Schrag A, Jahanshahi M, Quinn NP. What contributes to depression in Parkinson's disease? Psychol Med
2001; 31(1):65-73.
5. Richard IH, Schiffer RB, Kurlan R. Anxiety and Parkinson's disease. J Neuropsychiatry Clin Neurosci
1996; 8(4):383-392.
6. Aarsland D, Larsen JP, Lim NG, Janvin C, Karlsen K, Tandberg E, et al. Range of neuropsychiatric
disturbances in patients with Parkinson's disease. J Neurol Neurosurg Psychiatry 1999; 67(4):492-496.
7. Vazquez A, Jimenez-Jimenez FJ, Garcia-Ruiz P, Garcia-Urra D. "Panic attacks" in Parkinson's disease. A
long-term complication of levodopa therapy. Acta Neurol Scand 1993; 87(1):14-18.
8. Menza MA, Robertson-Hoffman DE, Bonapace AS. Parkinson's disease and anxiety: comorbidity with
depression. Biol Psychiatry 1993; 34(7):465-470.
9. Henderson R, Kurlan R, Kersun JM, Como P. Preliminary examination of the comorbidity of anxiety and
depression in Parkinson's disease. J Neuropsychiatry Clin Neurosci 1992; 4(3):257-264.
10. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983;
67(6):361-370.
11. Serra-Mestres J, Ring HA. Vulnerability to emotionally negative stimuli in Parkinson's disease: an
investigation using the Emotional Stroop task. Neuropsychiatry Neuropsychol Behav Neurol 1999;
12(1):52-57.
12. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease. J
Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
13. Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and validation of a short measure of
functioning and well being for individuals with Parkinson's disease. Qual Life Res 1995; 4(3):241-248.

Evaluation of the HADS in Parkinson's disease
- 99 -
14. Brazier J, Jones N, Kind P. Testing the validity of the Euroqol and comparing it with the SF-36 health
survey questionnaire. Qual Life Res 1993; 2(3):169-180.
15. Brooks R. EuroQol: the current state of play. Health Policy 1996; 37(1):53-72.
16. McDowell I, Newell C. Measuring Health: A Guide to Rating Scales and Questionnaires. 2 ed. New York:
Oxford University Press, 1996.
17. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
18. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use. 2
ed. Oxford: Oxford Medical Publications, 1995.
19. Bland JM, Altman DG. Cronbach's alpha. BMJ 1997; 314(7080):572.
20. Fleiss JL, Cohen J. The equivalence of weighted kappa and the intraclass correlation coefficient as
measures of reliability. Educational and Psychological Measurement 1973; 33:613-619.
21. Moorey S, Greer S, Watson M, Gorman C, Rowden L, Tunmore R, et al. The factor structure and factor
stability of the Hospital Anxiety and Depression Scale in patients with cancer. Br J Psychiatry 1991;
158:255-259.
22. Jack TM, Walker VA, Morley SJ, Hanks GW, Finlay-Mills BM. Depression, anxiety and chronic pain.
Anaesthesia 1987; 42(11):1235-1236.
23. Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, Van Hemert AM. A validation study of the
Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol Med 1997;
27(2):363-370.
24. Visser MC, Koudstaal PJ, Erdman RA, Deckers JW, Passchier J, van Gijn J, et al. Measuring quality of life
in patients with myocardial infarction or stroke: a feasibility study of four questionnaires in The
Netherlands. J Epidemiol Community Health 1995; 49(5):513-517.
25. Herrmann C. International experiences with the Hospital Anxiety and Depression Scale: a review of
validation data and clinical results. J Psychosom Res 1997; 42(1):17-41.
26. McDowell I, Newell C. Depression. In: McDowell I, Newell C. Measuring Health: A Guide to Rating
Scales and Questionnaires. New York: Oxford University Press, 1996: 238-286.
27. Fayers PM, Machin D. Factor analysis. In: Staquet MJ, Hays RD, Fayers PM, editors. Quality of Life
Assessment in Clinical Trials: Methods and Practice. Oxford: Oxford Univerity Press, 1998: 191-223.
28. Zesiewicz TA, Hauser RA. Depression in Patients with Parkinson's Disease: Epidemiology,
Pathophysiology and Treatment Options. CNS Drugs 2000; 13(4):253-264.
29. Lewis G, Wessely S. Comparison of the General Health Questionnaire and the Hospital Anxiety and
Depression Scale. Br J Psychiatry 1990; 157:860-864.
30. Bridges KW, Goldberg DP. The validation of the GHQ-28 and the use of the MMSE in neurological in-
patients. Br J Psychiatry 1986; 148:548-553.
31. Leentjens AFG, Marinus J, van Hilten JJ, Lousberg R, Verhey FRJ. The contribution of somatic symptoms
to the diagnosis of depressive disorder in Parkinson's disease: a discriminant analytic approach (accepted). J
Neuropsychiatry Clin Neurosci.
32. Moffic HS, Paykel ES. Depression in medical in-patients. Br J Psychiatry 1975; 126:346-353.
33. Clarke DC, Cavanaugh SA, Gibbons RD. The core symptoms of depression in medical and psychiatric
patients. J Nerv Ment Dis 1983; 171:705-713.

Chapter 5
- 100 -
34. Leentjens AFG, Lousberg R, Verhey FRJ. The psychometric properties of the Hospital Anxiety and
Depression Scale in patients with Parkinson's disease. Acta Neuropsychiatrica 2001; 13(4):83-85..
35. Leentjens AF, Verhey FR, Lousberg R, Spitsbergen H, Wilmink FW. The validity of the Hamilton and
Montgomery-Asberg depression rating scales as screening and diagnostic tools for depression in
Parkinson's disease. Int J Geriatr Psychiatry 2000; 15(7):644-649.
36. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4 ed.
Washington: American Psychiatric Association, 1994.

- 101 -
66 The contribution of somatic symptoms to the diagnosis of
depressive disorder in Parkinson’s disease: a discriminant analytic approach
Albert F.G. Leentjens1,2, Johan Marinus3, Jacobus J. van Hilten3, Richel Lousberg2, Frans
R.J. Verhey1,2
1 Department of Psychiatry, Maastricht University Hospital, Maastricht, The Netherlands; 2 Institute
for Brain and Behaviour, Maastricht University, Maastricht, The Netherlands; 3 Department of
Neurology, Leiden University Medical Center, Leiden, The Netherlands
Published in the Journal of Neuropsychiatry and Clinical Neurosciences 2003;15:74-77

Chapter 6
- 102 -
Abstract This study assessed the sensitivity of individual depressive symptoms and their relative contribution to the
diagnosis of depressive disorder in patients with Parkinson’s disease. The Structured Clinical Interview
for DSM-IV Depression and the Hamilton and the Montgomery-Åsberg Depression Rating Scales (Ham-
D, MADRS) were administered to 149 consecutive nondemented patients. The contribution of the
individual items of these scales to the diagnosis of “depressive disorder” was calculated by discriminant
analysis. The discriminant models based on the Ham-D and MADRS scores were both highly significant.
Nonsomatic core symptoms of depression had the highest correlation coefficient. Somatic items had
mostly low correlation coefficients, with the exception of reduced appetite and early morning wakening
(late insomnia). Nonsomatic symptoms of depression appear to be the most important for distinguishing
between depressed and nondepressed patients with Parkinson’s disease, along with reduced appetite and
early morning awakening.

Contribution of somatic symptoms to depression in Parkinson's disease
- 103 -
Introduction The diagnosis of depressive disorder in patients with somatic diseases, such as Parkinson’s
disease (PD), is often difficult because some of the physical symptoms of these diseases overlap
with the somatic symptoms of depressive disorder. In patients with PD, the “masked facies”,
psychomotor retardation, mental slowing, fatigue, and sleep disturbances may give the
appearance of depression in euthymic patients. A lot of research has been directed to the
specificity of depressive symptoms in these patients, that is, to the question whether a certain
symptom profile can be considered characteristic for depression in PD.1-4 Although there is some
evidence for a more prominent role of anxiety symptoms in depression in PD, the results of
different studies are not consistent.1-4 From a clinical point of view, however, the sensitivity of
depressive symptoms is more important. Clinicians are more interested in how to recognize
depressive disorder in a patient with known Parkinson’s disease, than in the way depressive
symptoms in PD patients differ from depressive symptoms in patients with other chronic
diseases, or in otherwise healthy individuals. This study analyzes the contribution of individual
depressive symptoms to the formal diagnosis of “depressive disorder” by using a discriminant
analytic approach.
Patients and methods
As part of an ongoing research project on psychopathology in PD, 169 consecutive patients with
primary PD, as defined by the clinical criteria of the United Kingdom Parkinson’s Disease
Society Brain Bank (UK-PDS-BB), were referred from the neurological outpatient department
for a protocolized mental status examination.5 This examination consisted of the Structured
Clinical Interview for DSM IV-Depression (SCID-D), to confirm or reject the diagnosis of
depressive disorder as defined by the DSM-IV criteria.6,7 The DSM IV diagnosis of depressive
disorder was considered the gold standard in this study. Patients fulfilling the DSM-IV criteria
for dementia were excluded in order to prevent unreliable answers due to recollection bias. All
patients completed the Hamilton Rating Scale for Depression (Ham-D),8 irrespective of the
presence or absence of depression. For 111 patients, the score on the Montgomery-Åsberg
Depression Rating Scale (MADRS)9 was also available. Thus, in this study, the Ham-D and
MADRS were used as symptom checklists and not as diagnostic scales. The physical disability
of patients was rated according to the Hoehn and Yahr staging system,10 which ranges from I

Chapter 6
- 104 -
(mild unilateral disease) to V (wheelchair bound or bedridden unless aided). The cognitive status
of the patients was assessed with the Mini-Mental State Examination (MMSE).11
On the basis of the individual items of the Ham-D and MADRS, a discriminant model was
calculated for both scales that would optimally predict whether patients would fall into the
depressed or nondepressed group according to the gold standard (i.e., DSM-IV criteria). Next, a
correlation coefficient with this discriminant function was obtained for each of the individual
items on these scales. These correlation coefficients reflect the relative strength of association of
each symptom with the discriminant function, and can thus be considered an indirect measure for
the contribution of these symptoms to the diagnosis of depressive disorder. Finally, the
individual items were grouped in order of descending correlation coefficients, that is, in order of
decreasing sensitivity. Wilks' lambda was calculated as a test of the discriminant function. As an
indicator of the prevalence of individual depressive symptoms, the percentage of nonzero scores
on each item of both scales is described. Means are accompanied by standard deviations. All
analyses were performed with the Statistical Package for the Social Sciences (SPSS) version 9.0.
Results
Of the 169 referred patients, 20 (11.8%) were excluded because of dementia. The other 149
patients participated in the analysis of the Ham-D items: 89 men and 60 women, with an average
age of 66.8 ± 10.2 years. Their average MMSE score was 27.4 ± 2.3. According to the Hoehn
and Yahr scale, 16 patients were classified as stage I, 81 as stage II, 24 as stage III, 9 as stage IV,
and none as stage V (19 patients not staged). Thirty-three patients met the criteria for depressive
disorder (22.1%). The average Ham-D score was 8.3 ± 3.9 for nondepressed patients and 16.9 ±
5.5 for depressed patients. The results of the discriminant analysis are shown in Table 1. Wilks’
lambda, as a test of the discriminant function in this model, was highly significant (λ = 0.438, χ2
= 108.502, df =17, P < 0.001). In this model 93.0% of the patients were correctly classified as
depressed or nondepressed. In this discriminant model of the Ham-D, suicidality was the best
discriminator between depressed and nondepressed patients. This item was followed, in
descending order, by feelings of guilt, psychic anxiety, reduced appetite, depressed mood, and
reduction of work and interest. Most somatic items, like psychomotor slowing, tiredness,
physical anxiety, and early and middle insomnia had low discriminative properties. The
exceptions were reduced appetite and early morning wakening (or late insomnia); these two
somatic items had relatively high discriminative properties.
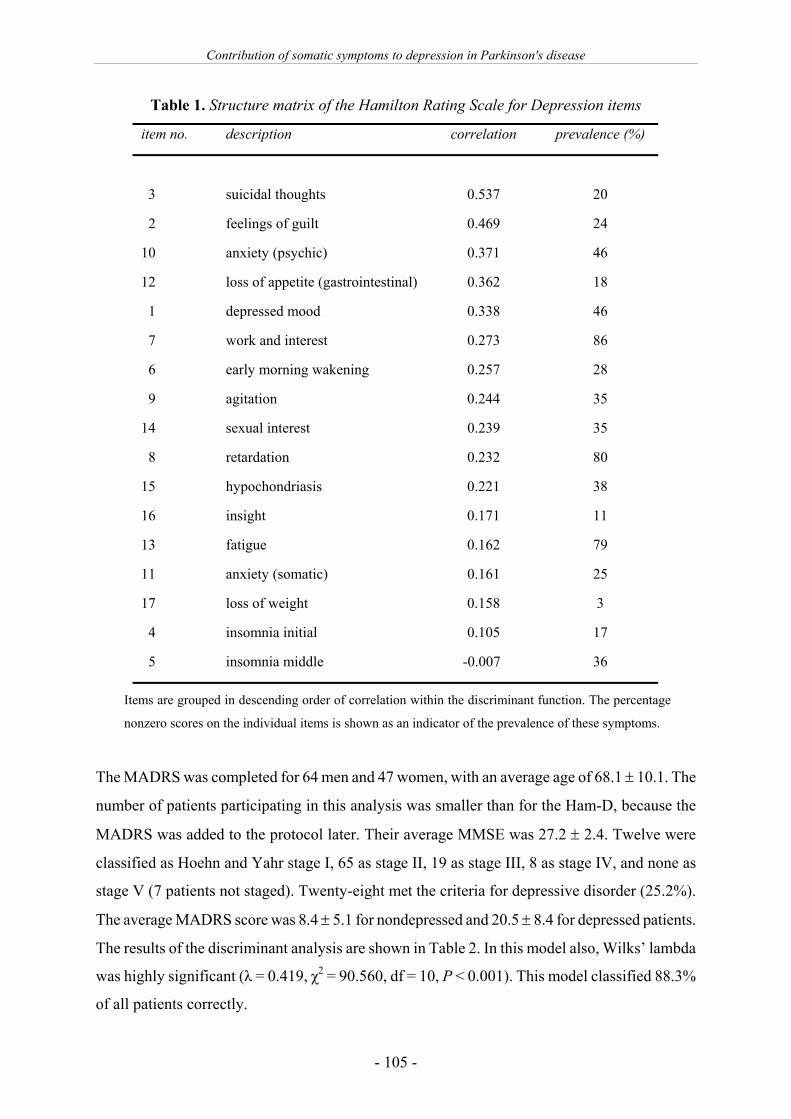
Contribution of somatic symptoms to depression in Parkinson's disease
- 105 -
Table 1. Structure matrix of the Hamilton Rating Scale for Depression items
item no. description correlation prevalence (%)
3 suicidal thoughts 0.537 20
2 feelings of guilt 0.469 24
10 anxiety (psychic) 0.371 46
12 loss of appetite (gastrointestinal) 0.362 18
1 depressed mood 0.338 46
7 work and interest 0.273 86
6 early morning wakening 0.257 28
9 agitation 0.244 35
14 sexual interest 0.239 35
8 retardation 0.232 80
15 hypochondriasis 0.221 38
16 insight 0.171 11
13 fatigue 0.162 79
11 anxiety (somatic) 0.161 25
17 loss of weight 0.158 3
4 insomnia initial 0.105 17
5 insomnia middle -0.007 36
Items are grouped in descending order of correlation within the discriminant function. The percentage
nonzero scores on the individual items is shown as an indicator of the prevalence of these symptoms.
The MADRS was completed for 64 men and 47 women, with an average age of 68.1 ± 10.1. The
number of patients participating in this analysis was smaller than for the Ham-D, because the
MADRS was added to the protocol later. Their average MMSE was 27.2 ± 2.4. Twelve were
classified as Hoehn and Yahr stage I, 65 as stage II, 19 as stage III, 8 as stage IV, and none as
stage V (7 patients not staged). Twenty-eight met the criteria for depressive disorder (25.2%).
The average MADRS score was 8.4 ± 5.1 for nondepressed and 20.5 ± 8.4 for depressed patients.
The results of the discriminant analysis are shown in Table 2. In this model also, Wilks’ lambda
was highly significant (λ = 0.419, χ2 = 90.560, df = 10, P < 0.001). This model classified 88.3%
of all patients correctly.

Chapter 6
- 106 -
In the discriminant model of the MADRS, the two “core” symptoms of depression, depressed
mood and anhedonia, had the highest correlation coefficients. In the MADRS, the clinician’s
judgment of “apparent sadness” was the item that distinguished the best between depressed and
nondepressed individuals. Somatic items of the MADRS had low correlation coefficients,
including the item “concentration difficulties”. However, as with the Ham-D, reduced appetite
was a relatively important indicator of depression.
.
Table 2. Structure matrix of the Montgomery-Åsberg Depression Rating Scale items
item no. description correlation prevalence (%)
1 observed depression 0.747 45
8 anhaedonia 0.739 47
2 reported depression 0.739 56
10 suicidal thoughts 0.435 29
9 feelings of guilt 0.388 53
5 reduced appetite 0.385 21
7 fatigue 0.292 81
3 tension 0.272 64
6 concentration 0.170 58
4 insomnia 0.082 52
Items are grouped in descending order of correlation within discriminant function. Percentage
of nonzero scores on the individual items shown as indicator of prevalence of these symptoms.
A post hoc analysis was performed for both the Ham-D and MADRS to discover in what way the
percentage of correctly classified patients would be affected when only nonsomatic symptoms of
depression would have been included in the analysis. After exclusion of the somatic items of the
Ham-D (items 4, 5, 6, 8, 11-14, and 16), 86.6% of the patients was correctly classified as
depressed or nondepressed. After exclusion of the somatic items of the MADRS (items 4-7),
88.3% of the patients was classified correctly

Contribution of somatic symptoms to depression in Parkinson's disease
- 107 -
Discussion We studied the sensitivity and discriminative properties of somatic and nonsomatic symptoms of
depression in a large sample of patients with PD. The prevalence of dementia and depressive
disorder in this population, as well as the scores of both depressed and nondepressed patients on
the Ham-D and MADRS, are comparable to that of other studies.12,13
The discriminant analyses showed that core symptoms and other nonsomatic symptoms of
depression were the most important symptoms for establishing the diagnosis of depressive
disorder in patients with PD, as was expected. The results also showed that most somatic items in
both depression rating scales do not contribute substantially to the discriminant model. This was
also illustrated by the post hoc analyses: the percentage of patients who were correctly classified
as depressed or nondepressed was hardly reduced by exclusion of the somatic items of the
model. However, in the case of PD, not all somatic symptoms should be considered of little
importance to the diagnosis of depression. Our analyses show that “reduced appetite” and “early
morning wakening” meaningfully contribute to the discriminant model, and thus to the diagnosis
of depressive disorder. In an attempt to prevent the inclusion of nonspecific symptoms in the
diagnosis of depression, some authors argue that all somatic symptoms should be eliminated.14-16
Our study does not support this often-advocated view. Instead, our study shows that somatic
symptoms differ among themselves in terms of diagnostic sensitivity and that a more refined
approach is warranted.
The discriminant analytic approach to the clinical problem of diagnosing depressive disorder in a
patient with PD has both its advantages and its limitations. Less prevalent depressive symptoms
may have a high discriminative power, whereas common symptoms may not have high
discriminative properties. This may limit the clinical applicability of our findings in the
individual patient. Furthermore, the correlation coefficients within the discriminant models do
not reflect absolute values, but only reflect the relative association of individual items with the
discriminant model. Therefore it is not possible to define cutoff values above which the
contribution of a symptom should be considered relevant. For the same reason, correlation
coefficients of the items of different discriminant models, such as those of the Ham-D and
MADRS, cannot be compared. The major advantage of discriminant analysis is that it looks at
the sensitivity, rather than the specificity, of individual symptoms for the diagnosis of
depression. Therefore it may help the physician to assign clinical importance to certain
symptoms if they are present. In this way discriminant analysis facilitates a more refined
approach to the diagnosis of depression in patients with physical disease, such as PD.

Chapter 6
- 108 -
In conclusion, the recognition of depressive disorder in PD is often difficult because of the
overlap of characteristic symptoms of this disease and the somatic symptoms of depression. The
present discriminant analyses show that the core symptoms and other nonsomatic symptoms of
depression are most important in distinguishing depressed and nondepressed PD patients. Most
somatic items only have low discriminatory properties, with the notable exception of two
symptoms that are relatively sensitive indicators of depression: reduced appetite and early
morning wakening.
References 1. Robins AH. Depression in patients with Parkinsonism. Br J Psychiatry 1976; 128:141-145.
2. Gotham AM, Brown RG, Marsden CD. Depression in Parkinson's disease: a quantitative and qualitative
analysis. J Neurol Neurosurg Psychiatry 1986; 49(4):381-389.
3. Huber SJ, Freidenberg DL, Paulson GW, Shuttleworth EC, Christy JA. The pattern of depressive symptoms
varies with progression of Parkinson's disease. J Neurol Neurosurg Psychiatry 1990; 53(4):275-278.
4. Ehmann TS, Beninger RJ, Gawel MJ, Riopelle RJ. Depressive symptoms in Parkinson's disease: a
comparison with disabled control subjects. J Geriatr Psychiatry Neurol 1990; 3(1):3-9.
5. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson's
disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992; 55(3):181-184.
6. Spitzer RL, Williams JBW, Gibbon M. Instruction manual for the Structured Clinical Interview for DSM-
III-R. New York: New York State Psychiatric Institute, 1987.
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4 ed.
Washington: American Psychiatric Association, 1994.
8. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56-62.
9. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry
1979; 134:382-389.
10. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
11. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res 1975; 12(3):189-198.
12. Cummings JL. Depression and Parkinson's disease: a review. Am J Psychiatry 1992; 149(4):443-454.
13. Leentjens AF, Verhey FR, Lousberg R, Spitsbergen H, Wilmink FW. The validity of the Hamilton and
Montgomery-Asberg depression rating scales as screening and diagnostic tools for depression in
Parkinson's disease. Int J Geriatr Psychiatry 2000; 15(7):644-649.
14. Endicott J. Measurement of depression in patients with cancer. Cancer 1984; 53(10 Suppl):2243-2249.
15. Rapp SR, Vrana S. Substituting nonsomatic for somatic symptoms in the diagnosis of depression in elderly
male medical patients. Am J Psychiatry 1989; 146(9):1197-1200.
16. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983;
67(6):361-370

- 109 -
77 Development of a questionnaire for autonomic dysfunction
in Parkinson's disease: the SCOPA-AUT
Martine Visser¹, Johan Marinus¹, Anne M. Stiggelbout², Jacobus J. van Hilten¹
Departments of Neurology¹ and Medical Decision Making², Leiden University Medical Center,
Leiden, The Netherlands.
Submitted

Chapter 7
- 110 -
Abstract Objectives. Autonomic symptoms are common in Parkinson's disease (PD), but there is no validated
questionnaire covering all relevant domains. The aim was to develop a disease-specific instrument, the
SCOPA-AUT, that evaluates autonomic symptoms in patients with PD and to assess its reliability and
validity. Methods. First, items were generated, based on an extensive literature search and expert
opinion. Based on the results of a postal survey among 46 patients with PD, 21 patients with multiple
system atrophy (MSA), and 8 movement disorders specialists, items were reduced according to the
frequency, burden, and clinical relevance of the symptoms. Evaluation of the validity of the
questionnaire was based on the results of a second postal survey in 140 patients with PD and 100
controls. Test-retest reliability was assessed in a subsample of 55 patients with PD, who received a
second questionnaire, two weeks after returning the first one. Results. The initial 45 items were
reduced to 25 items, that addressed the following domains: gastrointestinal (7 items), urinary (6
items), cardiovascular (3 items), thermoregulatory (4 items), pupillomotor (1 item), and sexual (2
items for men and 2 for women). Test-retest reliability of domain scores and individual items was
good, and each domain displayed high internal consistency. Most items and all domains, except sexual
dysfunction in men and women, differentiated between the PD and control group. Each domain had a
good content validity. A significant increase in autonomic problems was found for patients in the more
advanced stages of PD for all autonomic domains, except sexual dysfunction. Conclusions. The
SCOPA-AUT is a questionnaire that evaluates autonomic dysfunction in PD with good reliability and
validity.
Autonomic dysfunction in Parkinson's disease
- 111 -
Introduction Parkinson's disease (PD) has mainly been characterised in terms of motor impairments, but it
is increasingly recognized that the clinical spectrum of PD is more extensive and also affects
other areas such as cognition, mood, sleep, and autonomic functions. With respect to the
latter, a broad spectrum of autonomic features, involving gastrointestinal, urinary, sexual,
cardiovascular, thermoregulatory, respiratory, and pupillomotor functions, have been
described in PD.1-7 The overall prevalence of these autonomic features varies considerably,
ranging from 2% for urinary incontinence to 72% for constipation.8 In part, these autonomic
features have been related to disease duration, disease severity, or use of antiparkinsonian
drugs.9,10 For several autonomic symptoms, including gastrointestinal and urinary problems,
orthostatic hypotension, and erectile dysfunction, therapeutic interventions have become
available.11,12 The presence of autonomic dysfunction in patients with PD is associated with
depression and has an impact on daily functioning and patients' health-related quality of
life.13,14 Autonomic failure is also a frequent and prominent manifestation of multiple system
atrophy (MSA).15 Although MSA and PD are two distinct diseases, the profile of autonomic
features is quite similar.16
Despite the fact that a lot of research has been done, no reliable and valid instrument exists
that covers the full spectrum of autonomic problems in PD. Therefore, the primary aim of this
study was to develop a reliable and valid questionnaire for autonomic dysfunction in PD.
Additionally, because of the similarity in clinical presentation, the item generation and
reduction process was designed to account for the autonomic features of MSA as well.
The development of the SCOPA-AUT is part of a larger research project, the SCales for
Outcomes in PArkinson's disease (SCOPA), in which practical and clinimetric sound
instruments for all relevant domains in PD are selected or developed.
Methods
The SCOPA-AUT was developed in three stages: (1) item generation, based on a literature
search and expert opinion, (2) item reduction, based on the results of a postal survey, and (3)
clinimetric evaluation of the SCOPA-AUT, based on the results of a second postal survey.
The local medical ethical committee approved the study protocol.

Chapter 7
- 112 -
Item generation
The items were generated by conducting an extensive review of the literature on autonomic
symptoms in PD and MSA, including a review of questionnaires that evaluate specific
domains of autonomic dysfunction or address symptoms related to PD. Clinicians from the
areas of neurophysiology, gastro-enterology, gynaecology, urology, and sexology, who were
specialized in autonomic functions, were consulted regarding the generation of relevant items.
Patient functioning with respect to the selected items was addressed in two questions. The
first evaluated the frequency of the problem ("How often do you suffer from this problem?",
with response options ranging from 0 = 'never' to 3 = 'often'). This was followed by a second
question addressing the burden to the patient ("How much does this problem bother you?",
with response options ranging from 1 = 'not at all' to 4 = 'very much'). The time frame for all
questions was the past month, except for the item 'syncope' which addressed the past six
months. The questionnaire was first reviewed for content by the aforementioned professionals
and next piloted in 16 patients for intelligibility of questions and response options, after which
unclear questions were rephrased.
Item reduction
This initial questionnaire was sent to 55 patients with PD. All the patients were selected from
the database of the outpatient movement disorders clinic of the department of neurology of
the Leiden University Medical Center, in which clinical information is regularly updated. All
patients fulfilled the United Kingdom Parkinson's Disease Society Brain Bank (UKPDSBB)
criteria for idiopathic PD.17 Equal groups of patients with PD were selected from the different
Hoehn and Yahr (H&Y) stages,18 to cover the full spectrum of disease severity. The
questionnaire was also sent to 18 patients who fulfilled the criteria for MSA19 and were
registered at the same clinic. Additionally, 20 patients with MSA who attended a MSA
meeting organised by the Dutch Parkinson's Disease Society, were requested to complete the
questionnaire as well.
For both patient groups the mean, standard deviation, and frequency distribution of each item
was calculated for both the frequency and burden of the problem, as well as for the product of
frequency and burden. The aim was to select autonomic problems with a high frequency, a
high burden, or a combination of a high frequency and burden in patients with either PD or
MSA. Items were selected for the SCOPA-AUT if at least one of the following criteria was
fulfilled: (1) frequency: mean of 1 ('a little of the time') or higher, (2) burden: mean of 3
('quite a bit') or higher, or (3) product of frequency and burden: mean of 2 or higher. Items

Autonomic dysfunction in Parkinson's disease
- 113 -
were considered redundant and removed if the inter-item correlation exceeded 0.80. Items that
best covered the domain remained in the questionnaire. Items were not removed if it would
affect the content validity of the domain.
To ensure that uncommon problems with a high clinical relevance were not excluded, the
questionnaire was next sent to 10 movement disorder specialists, who rated the clinical
relevance of the items on a scale from 0 ('not at all') to 3 ('very high'). Items with a mean of 2
('rather important') or higher, were selected.
Evaluation of the SCOPA-AUT
The items that were thus selected, were rephrased into a single question evaluating the
frequency of the problem, with response options ranging from 0 ('never') to 3 ('often'). Extra
response options were added for questions in the urinary and sexual domain. In the urinary
domain, a response option anchored to the worst score of 3 was added, which allowed
subjects to indicate they used a catheter. In the domain of sexual dysfunction, an extra option
'not applicable' allowed subjects to indicate they had not been sexually active. This response
option was not included in the domain or total score. This second questionnaire was piloted
for intelligibility in 10 patients, and ambiguous or misleading items were rephrased.
A second postal survey was performed in 112 controls and 185 patients with PD, who were
selected from the SCOPA database and fulfilled the UKPDSBB criteria for idiopathic PD. To
ensure sufficient numbers of patients in all disease stages, 11 patients from H&Y stages 4 and
5, who participated in the first study, were again included in the second study. This was not
expected to bias the results, because all items had been rephrased and the time interval
between the two questionnaires was more than seven months. Each patient was asked to
provide, if possible, the names and addresses of one man and one woman of approximately
the same age (age difference less than 10 years), who agreed to participate in the control
group. Partners were not allowed as control subjects. The survey also included demographic
questions and a questionnaire on comorbid diseases, that addressed 20 common chronic
disorders.20 Each patient questionnaire was labelled to allow combination of the results with
information from patient records regarding disease severity, disease duration, and medication.
Non-responders were reminded by telephone after two weeks. A subsample, consisting of the
first 60 patients who returned the questionnaire, received a second mailing two weeks after
returning the first, to determine the test-retest reliability of the questionnaire.

Chapter 7
- 114 -
The following properties were examined for each item: mean, standard deviation, and
frequency distribution of the responses. Test-retest reliability for items was assessed with a
weighted kappa (quadratic weights). Differences in item scores between the two groups were
analysed using the Mann-Whitney-U test. Items that did not differentiate between the PD and
control group were removed, provided that an adequate content validity of the domain was
preserved. Means and standard deviations were calculated for the total score and for each
domain, and differences between groups were analysed using a t-test. Test-retest reliability of
domains and total score were analysed with an intraclass correlation coefficient (ICC) and the
internal consistency of the domains with Cronbach's alpha. 'Known-groups' analyses, using
Kruskal-Wallis or ANOVA with post-hoc t-tests and Bonferoni correction, were performed to
examine domain and total scores of controls and patients grouped by disease severity.
Results
Item generation and item reduction
Forty-five items in the following domains were selected for the initial questionnaire: gastro-
intestinal (14 items), urinary (8 items), cardiovascular (5 items), thermoregulatory (6 items),
pupillomotor (1 item), skin (1 item), respiratory (1 item), and sexual dysfunction (6 items for
men, 3 for women). An additional item assessed the use of medication in the aforementioned
domains. Forty-six of the 55 patients with PD (84%) returned the questionnaire in the first
postal survey. The mean age of these patients was 64.9 (SD 9.2) years and the disease
duration 10.6 (SD 5.9) years (table 1). Twenty-one patients with MSA (53%) returned the
questionnaire. The mean age of the MSA patients was 63.9 (SD 8.0) years and their disease
duration 6.8 (SD 2.7) years. Eight of the 10 movement disorder specialists returned the
questionnaire. Based on the results in patients with PD, 23 items fulfilled the criteria of
frequency, burden, and product of both. Two items were additionally included based on
information from patients with MSA. The specialists indicated clinical relevance of another
10 items, resulting in a total of 35 items. The item 'problems with orgasm', that did not meet
the criteria in the female group, was preserved to obtain a similar coverage of the sexual
domain in both sexes. Two items in the urinary domain, two items involving orthostatic
hypotension, and three items concerning sexual dysfunction in men, were removed because of
redundancy. The item on medication was modified to match the selected items. Overall, the
item reduction process resulted in a total of 28 items, with one additional question on the use

Autonomic dysfunction in Parkinson's disease
- 115 -
of relevant medication. The selected items assessed the following domains: gastro-intestinal
(10 items), urinary (6 items), cardiovascular (3 items), thermoregulatory (4 items),
pupillomotor (1 item), and sexual dysfunction (2 items for men and 2 for women).
Evaluation of the SCOPA-AUT
In the second postal survey, 143 of the 185 patients (77%) returned the questionnaire. Three
patients were excluded from the analyses because more than 20% of their data was missing.
The response rate in the test-retest assessment was 92%. Data from two patients were
removed from this analysis because they had more than 20% missing values. In the control
group 100 of the 108 subjects (93%) returned the questionnaire. There were no differences
between the characteristics of the total PD group and the subsample used for test-retest
reliability. Compared to the PD group, subjects in the control group were younger and
included more females (table 1), and the analyses were therefore adjusted for age and sex.
Table 1. Characteristics of PD / MSA group in first, and PD / control group in second survey
postal survey 1 postal survey 2
variable PD-1 MSA PD-2 controls p
N 46 21 140 100 -
Mean (SD) age (years) 64.9 (9.2) 63.9 (8.0) 65.6 (10.9) 61.4 (11.2) 0.0051
Gender (M/F) 26/19 12/9 84/56 48/52 0.0662
Mean (SD) disease duration (years) 10.6 (5.9) 6.8 (2.7) 9.9 (5.2)
Hoehn and Yahr stage (n)
1
2
3
4
5
missing
3
15
15
10
1
2
NA3
4
55
52
26
3
0
NA3
1T-test 2Chi-square test of the subjects in the second postal survey 3Not applicable

Chapter 7
- 116 -
Missing data was low, namely 0-1% per item in the control group and 0-4% in the PD group,
except for questions regarding sexual functioning. These four questions had the most missing
values, especially in female patients (11-13%). In total 46-50% of the women with PD and
39-40% of the female controls indicated 'not applicable' on these two items, compared to 21-
24% in male patients and 10-17% in male controls. Women who had missing values or scored
'not applicable', were significantly older, both in the PD and the control group.
Table 2. Frequency distribution and item characteristics of PD group in second survey
Item 0 1 2 3 extra valid¹ Kw²
swallowing 55 75 9 1 - 140 0.69
salivation 34 63 31 12 - 140 0.86
dysphagia 83 52 4 0 - 139 0.74
gastric emptying 68 50 17 5 - 140 0.73
constipation 64 46 19 11 - 140 0.75
straining 24 66 29 21 - 140 0.74
faecal incontinence 120 17 2 1 - 140 0.56
urgency 44 58 19 14 4³ 139 0.79
urinary incontinence 72 42 13 8 4³ 139 0.84
incomplete emptying 62 49 15 9 4³ 139 0.69
weak stream of urine 48 55 21 8 4³ 136 0.87
frequency of urination 14 56 46 20 3³ 139 0.45
nocturia 13 24 55 43 5³ 140 0.76
light-headed when standing up 68 55 12 3 - 138 0.75
light-headed when standing for some time 84 38 12 1 - 135 0.69
syncope 133 6 1 0 - 140 0.85
hyperhidrosis during the day 67 49 17 7 - 140 0.73
hyperhidrosis during the night 52 52 22 14 - 140 0.80
cold intolerance 77 39 17 4 - 137 0.74
heat intolerance 63 39 27 6 - 135 0.74
over-sensitive to bright light 54 58 20 8 - 140 0.74
Men: impotence 25 15 14 8 184 80 0.87
Men: ejaculation problem 26 17 11 6 204 80 0.73
Women: vaginal dryness 12 7 1 3 264 49 0.77
Women: orgasm problem 7 9 4 2 284 50 0.61
¹number of valid responses; ² weighted Kappa; ³extra response option (catheter); 4extra option (not applicable).

Autonomic dysfunction in Parkinson's disease
- 117 -
Test-retest reliability for individual items was high with weighted kappa's ranging from 0.45-
0.90 (table 2). According to the criteria of Landis and Koch,21 only two items had moderate
agreement (i.e., between 0.41-0.60): 'frequency of urination' (0.45) and 'faecal incontinence'
(0.56). Compared to controls, patients had significantly higher scores on all items (p < 0.05),
except for 'heart burn', 'diarrhoea', 'flatulence', and 'syncope'. Similar results emerged when
the scores were corrected for age, or analysed separately for men and women. In men the
items 'incomplete emptying', 'impotence', and 'ejaculation problem', and in women the items
'faecal incontinence', 'vaginal lubrication', and 'problems with orgasm', did not differentiate
between patients and controls. Compared to controls, patients reported significantly higher
use of medication for constipation (23% versus 4%). No differences in the use of medication
were reported for other domains. After removal of the items 'heartburn', 'diarrhoea', and
'flatulence', the remaining 7 items still adequately covered the gastrointestinal domain. The
final version of the questionnaire includes 23 items for each sex (appendix). The scale has a
score range of 0-69, with higher scores reflecting worse autonomic functioning.
The test-retest reliability of the domain scores was good, with ICCs ranging from 0.67-0.90.
The ICC for the total score was 0.87 (table 3). The internal consistency was calculated in the
PD group and was high for most domains, with Cronbach's alpha ranging from 0.56-0.86
(table 3). The internal consistency of the pupillomotor domain could not be calculated, since it
includes only one item.
Patients had significantly higher scores than controls in all domains (p < 0.05), except for
sexual dysfunction in men and women (table 3). We compared the scores of controls with
those of patients, classified into groups according to their H&Y stages as: mild (H&Y 1 and
2), moderate (H&Y 3), or severe (H&Y 4 and 5). The total score and the domain scores
showed significant differences between groups, except for the sexual dysfunction domain in
women (table 4). A significant trend, with more autonomic problems in groups with higher
disease severity, was present in all domains, except sexual dysfunction. There were no
differences in domain scores of patients with severe PD who participated in both the first and
second postal survey, and patients who only participated in the second postal survey.
Patients with PD recorded more comorbid diseases than subjects in the control group. Some
of these comorbidities, however, are inherent to PD, i.e., dizziness, urinary incontinence, and
bowel dysfunction. After the removal of these symptoms from the comorbidity questionnaire,
no differences between the groups were found.

Chapter 7
- 118 -
Table 3. Means (SD) of the domains in patients and controls, and reliability in patients
Domain PD controls p Cronbach's α ICC¹
Gastrointestinal (7 items) 5.3 (3.1) 1.4 (1.6) 0.000² 0.66 0.90
Urinary (6 items) 7.1 (4.2) 3.9 (2.4) 0.000² 0.84 0.83
Cardiovascular (3 items) 1.2 (1.3) 0.3 (0.6) 0.000² 0.57 0.83
Thermoregulatory (4 items) 1.8 (2.0) 3.1 (2.4) 0.000² 0.68 0.82
Pupillomotor (1 item) 0.9 (0.9) 0.4 (0.7) 0.000³ - 0.744
Sexual combined (2+2 items) 1.9 (1.8) 1.3 (1.6) 0.035² - -
Sexual men (2 items) 2.0 (1.9) 1.3 (1.7) 0.055² 0.88 0.84
Sexual women (2 items) 1.7 (1.5) 1.4 (1.5) 0.440² 0.56 0.68
Total autonomic score (25 items) 18.8 (8.5) 8.8 (5.4) 0.000² - 0.87
¹intraclass correlation coefficient; ²T-test; ³Mann-Whitney-U test; 4Weighted kappa statistic
Table 4. Comparisons between controls and patients grouped by Hoehn & Yahr stages
Domain controls patients p fit4 trend5
1¹ 2¹ 3¹
Gastrointestinal 1.4 4.4 5.7 6.9 <0.001² 0.71 <0.001
Urinary 3.9 6.2 7.5 8.1 <0.001² 0.38 <0.001
Cardiovascular 0.27 1.0 1.2 1.1 <0.001² 0.18 <0.001
Thermoregulatory 1.8 3.1 3.1 3.9 <0.001² 0.85 <0.001
Pupillomotor 0.4 0.8 0.9 0.8 <0.001³ 0.75 <0.001
Sexual (combined) 1.3 1.6 2.3 1.5 0.055² 0.07 0.060
Sexual (men) 1.3 1.6 2.6 1.5 0.062² 0.40 0.065
Sexual (women) 1.4 1.4 1.8 1.6 0.890² 0.14 0.748
Total autonomic score 8.8 16.5 19.8 21.4 <0.001² 0.52 <0.001
¹modified Hoehn & Yahr stages: 1 = mild (H&Y 1+2), 2 = moderate (H&Y 3), 3 = severe (H&Y 4+5);
²ANOVA; ³Kruskal Wallis test; 4Goodness of fit: p > 0.05 indicates the model does not differ significantly from
a model with good fit; 5Trend: p < 0.05 indicates that a trend is present and differs significantly from zero.

Autonomic dysfunction in Parkinson's disease
- 119 -
Discussion
This study was designed to develop and evaluate a questionnaire for autonomic dysfunction in
patients with PD and indicates that autonomic dysfunction is a prominent aspect of PD, being
present early in the disease and increasing with advancing H&Y stages. Although some
studies have used a questionnaire to assess autonomic dysfunction, these instruments were
never thoroughly validated.22 The items in the SCOPA-AUT were selected because they were
common, had a high patient burden, were clinically relevant, and were more frequently
present in patients with PD than in controls. The response rate in both surveys was high,
which ensures that the characteristics of the intended sample are adequately reflected and it
may also indicate that these aspects are relevant to patients.
The evaluation of the validity of the SCOPA-AUT is based on content validity and 'known-
groups' comparisons. No gold standard or validated questionnaire exists against which the
SCOPA-AUT can be compared. Urodynamic tests,23 cardiovascular reflex measurements,24 or
anorectal manometry,25 are autonomic function tests that have been used in patients with PD.
These tests are useful in obtaining insight in specific aspects of autonomic failure, but cannot
be used for validation of this questionnaire. The presence of clinical symptoms as indicated
by the patients, does not necessarily reflect the result of a laboratory test, or vice versa. In the
process of developing the SCOPA-AUT, we focussed on the content and clinical applicability
of the questionnaire. Therefore infrequent but serious symptoms, like syncope, remained in
the questionnaire because of the clinical relevance of this problem. Taken together, the
content validity of the SCOPA-AUT is good and based on both experts' and patients'
opinions, therewith capturing all relevant features of the different autonomic domains. The
instrument also shows adequate known-groups validity, as the instrument discriminates
between patients and controls, and between patients in mild, moderate, and severe stages. The
test-retest reliability of items, domains, and the total score is high. These are important
characteristics, especially for use in longitudinal studies and clinical trials. In the clinical
management of patients, the questionnaire can be used to identify problematic autonomic
areas that require attention or treatment.
To capture the spectrum of autonomic dysfunction in PD adequately, we aimed to include
sufficient numbers of patients from each H&Y stage. As patients from H&Y stages 4 and 5
were underrepresented, 11 patients who participated in the first survey were re-included in the
second survey. Potential bias in the final results is considered small, as all items were
rephrased and the interval between both surveys was more than seven months. This was

Chapter 7
- 120 -
confirmed by a post-hoc analysis, which showed no differences between patients who
participated both times and those who participated in the second survey only.
Although PD and MSA are pathologically distinct diseases, the clinical spectrum of
dysautonomia overlaps.16 Severe autonomic dysfunction is often associated with MSA, but
Riley et al.26 found no differences between PD and MSA patients in five different tests of
autonomic function. Therefore, in the item selection and reduction process, the SCOPA-AUT
was designed to cover the relevant domains of autonomic dysfunction of both diseases,
allowing this instrument to be used in both patient groups. Patients with MSA were not
included in the final evaluation of the SCOPA-AUT, because our main objective was to
evaluate its use in PD. In the near future we aim to evaluate the SCOPA-AUT in a sample of
patients with MSA, to determine the reliability and validity of this instrument in patients with
this condition.
The domain scores are the sum of the individual item scores in that particular domain and
reflect the degree of dysfunction. The items evaluate different functions within these domains
and can even represent the extremes of a continuum, e.g., heat and cold intolerance. We
therefore were somewhat surprised that the internal consistencies of the domains, measured
with Cronbach's alpha, were still fairly high.
In agreement with other studies,27 the questions in the domain of sexual dysfunction displayed
the most missing values, viz., 13% in female patients, in addition to 50% answering 'not
applicable'. Only the data of a small subsample of women was therefore available for analysis
and this revealed no differences in sexual dysfunction between patients and controls. Women
who did not answer these questions were significantly older than women who responded.
Different results may be found in a younger sample.
Patients with PD had significantly higher scores than controls in most items, most domains,
and the total score. These results differ from findings in previous studies, where only some of
these symptoms differed significantly between patients and controls.22,28 This discrepancy
may be explained by the comparatively large sample in our study. The aforementioned studies
included 48 patients and 32 controls, and 44 patients and 24 controls, respectively.
Additionally, patients in our study covered a broad range of disease severity and disease
duration. Within the PD group, patients with more advanced disease stages had higher domain
scores, except for sexual dysfunction. This indicates that the questionnaire may have the
ability to measure change, although responsiveness of this questionnaire still needs to
evaluated.

Autonomic dysfunction in Parkinson's disease
- 121 -
Acknowledgements
The authors thank Prof. J.G. van Dijk, Dr. A.A.M. Masclee, Dr. P.T.M. Wijenborg, and Dr.
A.A.B. Lycklama à Nijeholt for their help in generating relevant items. We like to thank Prof.
R.A.C. Roos for reviewing the manuscript.
References
1. Edwards LL, Pfeiffer RF, Quigley EM, Hofman R, Balluff M. Gastrointestinal symptoms in Parkinson's
disease. Mov Disord 1991; 6(2):151-156.
2. Lemack GE, Dewey Jr RB, Roehrborn CG, O'Suilleabhain PE, Zimmern PE. Questionnaire-based
assessment of bladder dysfunction in patients with mild to moderate Parkinson's disease. Urology 2000;
56(2):250-254.
3. Brown RG, Jahanshahi M, Quinn N, Marsden CD. Sexual function in patients with Parkinson's disease and
their partners. J Neurol Neurosurg Psychiatry 1990; 53(6):480-486.
4. Senard JM, Rai S, Lapeyre MM, Brefel C, Rascol O, Rascol A, et al. Prevalence of orthostatic hypotension
in Parkinson's disease. J Neurol Neurosurg Psychiatry 1997; 63(5):584-589.
5. Fischer M, Gemende I, Marsch WC, Fischer PA. Skin function and skin disorders in Parkinson's disease. J
Neural Transm 2001; 108(2):205-213.
6. Shill H, Stacy M. Respiratory function in Parkinson's disease. Clin Neurosci 1998; 5(2):131-135.
7. Armstrong RA. Parkinson's disease and the eye. Ophthalmic Physiol Opt 1997; 17 Suppl 2:S9-16.
8. Martignoni E, Pacchetti C, Godi L, Micieli G, Nappi G. Autonomic disorders in Parkinson's disease. J
Neural Transm Suppl 1995; 45:11-19.
9. Turkka JT. Correlation of the severity of autonomic dysfunction to cardiovascular reflexes and to plasma
noradrenaline levels in Parkinson's disease. Eur Neurol 1987; 26(4):203-210.
10. Kujawa K, Leurgans S, Raman R, Blasucci L, Goetz CG. Acute Orthostatic Hypotension When Starting
Dopamine Agonists in Parkinson's Disease. Arch Neurol 2000; 57(10):1461-1463.
11. Task force Movement Disorders Society. Drugs to treat autonomic dysfunction in Parkinson's disease. Mov
Disord 2002; 17 Suppl 4:S103-S111. Abstract.
12. Hussain IF, Brady CM, Swinn MJ, Mathias CJ, Fowler CJ. Treatment of erectile dysfunction with sildenafil
citrate (Viagra) in parkinsonism due to Parkinson's disease or multiple system atrophy with observations on
orthostatic hypotension. J Neurol Neurosurg Psychiatry 2001; 71(3):371-374.
13. Berrios GE, Campbell C, Politynska BE. Autonomic failure, depression and anxiety in Parkinson's disease.
Br J Psychiatry 1995; 166(6):789-792.
14. Damiano AM, Snyder C, Strausser B, Willian MK. A review of health-related quality-of-life concepts and
measures for Parkinson's disease. Qual Life Res 1999; 8(3):235-243.
15. Chaudhuri KR. Autonomic dysfunction in movement disorders. Curr Opin Neurol 2001; 14(4):505-511.
16. Magalhaes M, Wenning GK, Daniel SE, Quinn NP. Autonomic dysfunction in pathologically confirmed
multiple system atrophy and idiopathic Parkinson's disease--a retrospective comparison. Acta Neurol Scand
1995; 91(2):98-102.

Chapter 7
- 122 -
17. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease. J
Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
18. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
19. Gilman S, Low PA, Quinn N, Albanese A, Ben Shlomo Y, Fowler CJ, et al. Consensus statement on the
diagnosis of multiple system atrophy. J Neurol Sci 1999; 163(1):94-98.
20. Van der Velden J, Abrahamse HPhH, Donker G, Van der Steen J, Van Sonsbeek JLA, Van den Bos GAM.
What do health interview surveys tell us about the prevalences of somatic chronic diseases? : A study into
concurrent validity. Eur J Public Health 1998; 8:52-58.
21. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;
33(1):159-174.
22. Siddiqui MF, Rast S, Lynn MJ, Auchus AP, Pfeiffer RF. Autonomic dysfunction in Parkinson's disease: a
comprehensive symptom survey. Parkinsonism Relat Disord 2002; 8(4):277-284.
23. Araki I, Kitahara M, Oida T, Kuno S. Voiding dysfunction and Parkinson's disease: urodynamic
abnormalities and urinary symptoms. J Urol 2000; 164(5):1640-1643.
24. Turkka JT, Tolonen U, Myllyla VV. Cardiovascular reflexes in Parkinson's disease. Eur Neurol 1987;
26(2):104-112.
25. Stocchi F, Badiali D, Vacca L, D'Alba L, Bracci F, Ruggieri S, et al. Anorectal function in multiple system
atrophy and Parkinson's disease. Mov Disord 2000; 15(1):71-76.
26. Riley DE, Chelimsky TC. Autonomic nervous system testing may not distinguish multiple system atrophy
from Parkinson's disease. J Neurol Neurosurg Psychiatry 2003; 74(1):56-60.
27. Sakakibara R, Shinotoh H, Uchiyama T, Sakuma M, Kashiwado M, Yoshiyama M, et al. Questionnaire-
based assessment of pelvic organ dysfunction in Parkinson's disease. Auton Neurosci 2001; 92(1-2):76-85.
28. Singer C, Weiner WJ, Sanchez-Ramos JR. Autonomic dysfunction in men with Parkinson's disease. Eur
Neurol 1992; 32(3):134-140.

Autonomic dysfunction in Parkinson's disease
- 123 -
Appendix
SCOPA-AUT
The response options for all questions are: never, sometimes, regularly, often. In some domains extra response
options are added. The questions concerning medication have the response options: no and yes.
1. In the past month, have you had difficulty swallowing or have you choked?
2. In the past month, has saliva dribbled out of your mouth?
3. In the past month, has food ever become stuck in your throat?
4. In the past month, did you ever have the feeling during a meal that you were full very quickly?
5. Constipation is a blockage of the bowel, a condition in which someone has a bowel movement twice a
week or less. In the past month, have you had problems with constipation?
6. In the past month, did you have to strain hard to pass stools?
7. In the past month, have you had involuntary loss of stools?
8. In the past month, have you had difficulty retaining urine? (extra: use catheter)
9. In the past month, have you had involuntary loss of urine? (extra: use catheter)
10. In the past month, have you had the feeling that after passing urine your bladder was not completely
empty? (extra: use catheter)
11. In the past month, has the stream of urine been weak? (extra: use catheter)
12. In the past month, have you had to pass urine again within 2 hours of the previous time? (extra: use
catheter)
13. In the past month, have you had to pass urine at night? (extra: use catheter)
14. In the past month, when standing up have you had the feeling of becoming either light-headed, or no
longer being able to see properly or no longer being able to think clearly?
15. In the past month, did you become light-headed after standing for some time?
16. Have you fainted in the past 6 months?
17. In the past month, have you ever perspired excessively during the day?
18. In the past month, have you ever perspired excessively during the night?
19. In the past month, have your eyes ever been over-sensitive to bright light?
20. In the past month, how often have you had trouble tolerating cold?
21. In the past month, how often have you had trouble tolerating heat?
The following 3 questions are only for men:
22. In the past month, have you been impotent (unable to have or maintain an erection)? (extra: not
applicable)
23. In the past month, how often have you been unable to ejaculate?
(extra: not applicable)
23a. In the past month, have you taken medication for an erection disorder? (If so, which medicine?) (no;
yes: _______)

Chapter 7
- 124 -
The following 2 questions are only for women:
24. In the past month, was your vagina too dry during sexual activity? (extra: not applicable)
25. In the past month, have you had difficulty reaching an orgasm? (extra: not applicable)
The following questions are for everyone:
26. In the past month, have you used medication for:
a. constipation? b. urinary problems?c. blood pressure? d. other symptoms (no; yes: _______)

- 125 -
88 Development of a short scale for motor impairments and
disabilities in Parkinson's disease: the SPES/SCOPA
Johan Marinus1, Martine Visser1, Anne M. Stiggelbout2, Jose Martin Rabey3, Pablo Martínez-
Martín4, Ubaldo Bonuccelli5, Peter H. Kraus6, Jacobus J. van Hilten1
Department of 1Neurology and 2Medical Decision Making, Leiden University Medical Center, Leiden,
The Netherlands; 3Department of Neurology, Assaf Harofeh Medical Center, Zerefin, Israel; 4Neuroepidemiology Unit, Department of Applied Epidemiology, National Center for Epidemiology
I.S. Carlos III, Madrid, Spain; 5Department of Neurology, University Hospital, Pisa, Italy; 6Department of Neurology, St. Josef University Hospital, Bochum, Germany
Submitted

Chapter 8
- 126 -
Abstract Objective. To evaluate the reliability and validity of the SPES/SCOPA, a short scale developed to
assess motor function in patients with Parkinson’s disease (PD). Methods. Eighty-five patients with
PD were assessed with the SPES/SCOPA, Unified Parkinson’s Disease Rating Scale (UPDRS), Hoehn
and Yahr (H&Y) scale, and Schwab and England (S&E) scale. Thirty-four patients were examined
twice by two different assessors, who were blind to each other’s scores and test executions ('clinical
assessment situation'). Additionally, six items of the motor section of the SPES/SCOPA were assessed
in nine patients and recorded on videotape, to evaluate inter-rater and intra-rater reliability for this
situation ('video assessment situation'). Results. The reproducibility of the sumscores in the clinical
assessments was high for all subscales of the SPES/SCOPA. Inter-rater reliability of individual items
ranged from 0.27-0.83 in the motor impairment section, from 0.58-0.82 in the activities-of-daily-living
section, and from 0.65-0.92 in the motor complications section. Inter-rater reliability of the motor
items in the video assessments ranged from 0.69-0.87, and intra-rater reliability from 0.81-0.95. The
correlation between related subscales of the SPES/SCOPA and UPDRS were all higher than 0.85 and
both scales revealed similar correlations with other measures of disease severity. The mean time to
complete the scales was 8.1 (SD 1.9) minutes for the SPES/SCOPA and 15.6 (SD 3.6) minutes for the
UPDRS. Conclusions. The SPES/SCOPA is a short, reliable, and valid scale that can adequately be
used in both research and clinical practice.

Motor impairments and disabilities in Parkinson’s disease
- 127 -
Introduction
Over the last 15 years the Unified Parkinson's Disease Rating Scale (UPDRS) has become a
standard tool in the clinical evaluation of patients with Parkinson's Disease (PD). The UPDRS
is the most frequently used scale in trials in PD1 and has acceptable inter- and intra-rater
reliability for most items.2,3 The construct validity with other scales is adequate, but the
content validity has been questioned, especially with respect to its conceptual clearness and
balance between items that represent symptoms responsive to dopaminergic therapy and those
more resistant to this intervention.2 Other critiques include the length of the scale4 and the
redundancy of items.5 The mean time to complete the scale is approximately 17 minutes for
experienced users,4 which makes it less suitable for clinical application. Van Hilten et al.5
demonstrated that the UPDRS can be shortened by removing redundant items from the motor
section and conceptually unclear items from the activities-of-daily-living (ADL) section,
without negative consequences for reliability or validity. Obviously, a shorter scale with
similar clinimetric properties may have advantages for patients, clinicians, and researchers.
As a result of the aforementioned considerations, the Short Parkinson's Evaluation Scale
(SPES) was developed.6 The scale is short, conceptually clear, and has good reliability and
validity.2,6 The instrument is considered easy to use by its evaluators,6 but has only been used
in a few studies.7,8
Careful inspection of the SPES, however, indicates that the consistency in the framing of
response options may be improved, and that the item 'swallowing' represents an impairment
and should be moved from the disability (ADL) section to the motor impairment (MI) section,
in order to be consistent with current methodological concepts of scale construction.9,10
Additionally, some clinimetric aspects of the SPES have not been addressed to date. These
involve intra-rater reliability and inter-rater reliability between two assessors who perform the
clinical assessments separately. Hence, we first modified the SPES according to the
aforementioned considerations and subsequently evaluated this scale, the SPES/SCOPA. The
development of this scale is part of a larger research project on SCales for Outcomes in
PArkinson’s disease (SCOPA),11 in which short, practical, and clinimetric sound scales for all
relevant domains in PD are selected or developed.
The objective of this study was to evaluate the reliability (intra- and inter-rater reliability,
internal consistency) and construct validity (correlation with related scales, 'known-groups'
comparisons) of the SPES/SCOPA.

Chapter 8
- 128 -
Methods
Development of the SPES/SCOPA
The SPES/SCOPA consists of three sections: motor impairments (MI), activities-of-daily-
living (ADL), and motor complications (MC). There are four response options, ranging from
0 (normal) to 3 (severe). In comparison with the original SPES, some modifications to the
three sections were made based on findings in the literature and empirical testing of some of
the items. The mental section was removed altogether, because we felt that these important
functions could not be assessed in a reliable and valid way by a few single questions. As a
part of the SCOPA project, we tested and developed separate instruments to evaluate these
functions.11
Motor impairments. Tremor. Pooled data of several studies8,12-15 (together including 1361
patients) revealed that in less than 4% of the patients the tremor score of the legs was higher
than that of the arms, and that in only 2% of the patients a tremor in the legs was present
while it was absent in the arms. For reasons of efficiency we decided to evaluate tremor only
in the upper extremities. Additionally, in the response options we linked the amplitude of the
tremor to a displacement in centimetres to improve the quantification of 'small', 'moderate',
and 'severe'. Bradykinesia. 'Finger tapping' was replaced by 'rapid alternating movements' on
the basis of the results of a study in which we compared five different tests for bradykinesia.16
This study revealed that this test had the highest intra- and inter-rater reliability and the
highest correlation with measures of disease severity. Both tremor and bradykinesia were
assessed during 20 seconds. A time window was not indicated in the original SPES. Rigidity.
The phrase 'detectable only on activation of the contralateral arm' was removed from the
response options, since a pilot study showed that the muscle tone in the ipsilateral arm also
increased in many healthy individuals if the contralateral arm was raised. Rigidity was now
evaluated by the 'perceived difficulty in trying to reach the end positions in elbow or wrist',
which proved to be a useful criterion in a pilot study we held in 17 patients with PD. Postural
stability. This item was modified on the basis of a study, in which we compared six tests for
postural stability.17 The word 'retropulsion' was removed from the response options, and the
scoring was now determined by the number of steps patients took to restore balance, and by
whether a patient would fall or not. Arising from chair, gait and speech. These items only
underwent minimal changes compared with the original SPES and do not need detailed
discussion. Two other impairments were added and evaluated historically, viz., swallowing
and freezing during 'on'. We considered it more important to assign items to the appropriate

Motor impairments and disabilities in Parkinson’s disease
- 129 -
section, than to assign items to sections on the basis of the way they are elicited (examination
versus history). 'Swallowing' was therefore moved from the ADL section to the MI section.
'Freezing during on' was added because it was considered a useful progression marker of PD
that is less responsive to dopaminergic interventions. We expected to achieve a better balance
between more dopamine-responsive and more dopamine-resistant features if this item was
added. The maximum score in the MI section is 42.
Activities of daily living. The response options were framed as uniformly as possible.
Responses reflected no difficulty (normal), some difficulty (no assistance needed),
considerable difficulty (possibly needing assistance), and unable (or needing complete or
almost complete assistance). As stated before, the item 'swallowing' (previously addressed
under 'eating') was removed from this section. 'Turning and getting out of bed', was extended
to 'changing positions', to include all important transfers of daily life. The maximum score in
this section is 21.
Motor complications. The original section on complications of therapy was modified and
now evaluated both presence and severity of dyskinesias and motor fluctuations. Freezing and
dystonia were removed, because these phenomena cannot solely be attributed to dopaminergic
therapy and hence do not purely reflect complications of therapy. Items were framed to
address the impairment level. The maximum score for both dyskinesias and motor
fluctuations is 6.
Patients
Eighty-five consecutive patients who visited the outpatient clinic of the Department of
Neurology of the Leiden University Medical Center, and who fulfilled the United Kingdom
Parkinson’s Disease Society Brain Bank criteria for idiopathic PD,18 were included in the
clinical assessments. Patients were excluded if they also had other diseases of the central
nervous system or were not able to understand Dutch. Nine patients that met the same
eligibility criteria were included in video assessments. The study was approved by the
medical ethics committee of the Leiden University Medical Center.
Assessment procedures
The patients were evaluated with the SPES/SCOPA (appendix), UPDRS parts II - IV,19 the
Hoehn and Yahr (H&Y) scale,20 and the Schwab and England (S&E) scale.21 The latter three

Chapter 8
- 130 -
scales were included to evaluate the construct validity of the SPES/SCOPA. One global
question evaluated overall ADL functioning and patients were asked to indicate on a seven-
point-scale (ranging from very good to very bad) how well they had been able to carry out
various daily activities in the past month. Patients also had to indicate whether they were 'on'
or 'off' at the time of assessment. Additional information that was gathered involved
medication, disease duration, and comorbidity.
Reproducibility of the SPES/SCOPA was assessed in three different ways, i.e., inter-rater
reliability of clinical assessments, inter-rater reliability of video assessments, and intra-rater
reliability of video assessments. In the clinical assessments, 34 patients were assessed twice
by the investigators (JM, MV), who assessed patients separately and were blind to each
other's scores and test executions. Reproducibility was calculated in those patients who had a
stable response to medication over this period (i.e., who had no 'on-off' transitions). In the
video assessments, inter-rater reliability was assessed by an international panel of movement
disorders specialists (from Italy, Israel, Spain, Germany, and The Netherlands), who rated
nine videotaped patients who had a stable response to medication during the time the
recordings were made. The panel rated the patients twice with an interval of 7-14 days. In the
video recordings, six items from the MI section of the SPES/SCOPA were included. The
other four items of this section were not appropriate for video scoring, i.e., rigidity, speech,
and the two historic items. Rigidity could not be evaluated from video for obvious reasons,
the other three items were not included because patients and raters spoke different languages.
Statistical analysis
Reproducibility was assessed with the intra-class correlation coefficient (ICC; one-way
random effects model) if two ratings were compared (inter-rater reliability in clinical
assessments and intra-rater reliability in video assessments), and with Kendall's coefficient of
concordance W if it concerned agreement between more than two raters (inter-rater reliability
in video assessments). The ICC is equivalent to weighted kappa if quadratic weights are
used,22 and we therefore used the 'strength-of-agreement' classification as proposed by Landis
and Koch.23 These authors classified strength of agreement as slight (0.00-0.20), fair (0.21-
0.40), moderate (0.41-0.60), substantial (0.61-0.80), or almost perfect (0.81-1.00). Internal
consistency of subscales was evaluated with Cronbach's alpha. Construct validity was
evaluated by determining the correlation between scales, using Pearson's r for the correlation
of SPES/SCOPA with UPDRS and S&E, and Spearman's rs for the correlation with H&Y and

Motor impairments and disabilities in Parkinson’s disease
- 131 -
'global functioning'. 'Known-groups' validity was assessed by comparing scores of patients
with different disease severity (by H&Y), using analysis of variance and ordinal regression.
Results
Characteristics of patients that participated in the clinical assessment are presented in table 1.
The nine patients that were recorded on video involved five men and four women, with a
mean age of 62.4 and a mean disease duration of 12.4 years. Three of these patients were in
H&Y stage 2, three in H&Y 3, and three in H&Y 4 (data not shown).
Table 1. Patient characteristics
n1 85
mean (SD) age (years) 65.4 (10.4)
number (%) males 52 (61.2%)
mean (SD) disease duration (years) 10.5 (5.8)
Hoehn & Yahr stages:
1 0
2 25
3 42
4 18
5 0
mean (SD) SPES/SCOPA-Motor impairments 13.8 (5.1)
mean (SD) SPES/SCOPA-ADL 8.5 (3.2)
mean (SD) UPDRS-Motor evaluation 32.6 (10.9)
mean (SD) UPDRS-ADL 15.9 (6.0)
mean (SD) Schwab & England 75.7 (12.4)
n assessed while 'on' / 'off' / missing 78 / 5 / 2
n (%) on levodopa 72 (84.7%)
mean (SD) levodopa dose in users (mg) 535 (407)
n (%) on dopamine agonists 63 (74.1%)
1 number of patients

Chapter 8
- 132 -
Practicality. The mean time necessary to complete the scales was 8.1 (SD 1.9) minutes for the
SPES/SCOPA and 15.6 (SD 3.6) minutes for the UPDRS.
Reliability of clinical assessments. One patient changed from 'on' to 'off' between both clinical
assessments and was removed from the analysis. Inter-rater reliability was hence assessed in
33 patients. Inter-rater reliability coefficients of the motor sections of the clinical assessments
were all at least 'moderate' according to the Landis & Koch criteria, except for two items in
the SPES/SCOPA ('postural tremor right hand', 'rigidity right arm') and eight items in the
UPDRS (table 2). The latter eight items also included the two items that had 'fair' reliability in
the SPES/SCOPA. The mean reliability coefficient calculated over the items that were shared
by both scales, was 0.56 for both. The mean ICC calculated over all the items of the motor
sections was 0.58 for the SPES/SCOPA and 0.50 for the UPDRS. Two items in the UPDRS
(rest tremor left and right leg) could not reliably be calculated as a result of insufficient
dispersion. However, percentage agreement for these items was high (table 2). Results for the
ADL section are presented in table 3. All agreements were at least 'substantial', except
'changing positions' in the SPES/SCOPA. The mean reliability coefficient calculated over the
shared items of the ADL sections was 0.69 for the SPES/SCOPA and 0.71 for the UPDRS.
The mean ICC over all items of the ADL section of the UPDRS was 0.76. The MC sections of
both scales (table 4) shared only one item in both the dyskinesia and the motor fluctuation
section. The mean ICC for the items in the dyskinesia section was 0.83 for the SPES/SCOPA
and 0.75 for the UPDRS. The mean ICC for items in the motor fluctuation sections was 0.67
for the SPES/SCOPA and 0.60 for the UPDRS. The ICCs of the sumscores of the UPDRS
were generally somewhat higher than those of the SPES/SCOPA (table 5).
Reliability of video assessments. The inter-rater reliability coefficients for all items in the
video assessments were at least 'substantial' (> 0.60; table 6). Intra-rater reliability coefficients
were higher, with all items above 0.80 ('almost perfect').
Internal consistency. The internal consistencies of the SPES/SCOPA scales were higher than
those of the UPDRS, with the exception of the MI scale (table 5). 'Sensory symptoms' in the
UPDRS-ADL even had a negative corrected item-total correlation (-0.02). Other items with
corrected correlations below 0.20 involved rest tremor of the right hand (0.15) and
swallowing (0.18) in the SPES/SCOPA scales, and rest tremor of head, right hand, left hand,
and right leg (0.03, 0.11, 0.16, and 0.18, respectively) in the UPDRS motor section, and
tremor (0.05) in the UPDRS ADL section. The corrected item-total correlation of the tremor
of the left hand was considerably higher in both scales (0.40 in the SPES/SCOPA and 0.31 in
the UPDRS).

Motor impairments and disabilities in Parkinson’s disease
- 133 -
Table 2. Inter-rater reliability (ICC) of motor impairment items in clinical assessment
Shared items SPES/SCOPA UPDRS Non-shared items
Rest tremor R 0.63 0.53
Rest tremor L 0.67 0.45
Postural tremor R 0.34* 0.34*
Postural tremor L 0.64 0.58
Rapid alternating movements R 0.58 0.59
Rapid alternating movements L 0.45 0.50
Rigidity R 0.27* 0.38*
Rigidity L 0.61 0.64
Rise from chair 0.83 0.83
Postural instability 0.60 0.59
Gait 0.60 0.63
Speech 0.55 0.68
0.57 Freezing during ‘on’
0.79 Swallowing
0.36* Facial expression
0.21* Rest tremor head
0.00** Rest tremor R leg
0.00** Rest tremor L leg
0.59 Rigidity head
0.29* Rigidity R leg
0.44 Rigidity L Leg
0.46 Finger tap R
0.39* Finger tap L
0.28* Hand movements R
0.67 Hand movements L
0.53 Leg agility R
0.61 Leg agility L
0.66 Posture
0.23* Body bradykinesia
* all agreements at least 'moderate' (> 0.40), except *, where agreement is fair (ICC = 0.21-0.40)23
** estimates unreliable due to insufficient dispersion; % agreement 97.1 (R leg) and 91.2 (L leg)
NB: 8 items in UPDRS (U) and 2 items in SPES/SCOPA (S) with poor agreement (≤ 0.40)

Chapter 8
- 134 -
Table 3. Inter-rater reliability (ICC) of ADL items in clinical assessment
Shared items SPES/SCOPA UPDRS Non-shared items
Speech 0.66 0.68
Feeding 0.63 0.61
Dressing 0.80 0.76
Hygiene 0.70 0.71
Changing positions 0.58* 0.73
Walking 0.61 0.66
Handwriting 0.82 0.85
0.91 Salivation
0.90 Swallowing
0.73 Falling (unrelated to freezing)
0.77 Freezing when walking
0.83 Tremor
0.68 Sensory complaints
* all agreements 'substantial' (> 0.60), except changing positions (S15), where agreement is 'moderate'
Table 4. Inter-rater reliability (ICC) of motor complication items in clinical assessment
Shared items SPES/SCOPA UPDRS Non-shared items
Dyskinesias
Presence dyskinesias 0.92 0.96
0.74 Severity dyskinesias
0.94 How disabling dyskinesias?
0.71 How painful dyskinesias?
0.39* Early morning dystonia?
Motor Fluctuations
Presence 'off' periods 0.69 0.65
0.65 Severity 'off' periods
0.71 Off periods predictable?
0.41** Off periods unpredictable?
0.62 Sudden offs?
NB: all agreements 'substantial', except for * U35 ('fair') and ** U37 ('moderate')

Motor impairments and disabilities in Parkinson’s disease
- 135 -
Table 5. Inter-rater reliability and internal consistency of SPES/SCOPA and UPDRS
ICC sumscores ICC items Cronbach alpha item-total1
SPES/SCOPA Motor 0.86 0.27 - 0.83 0.74 0.15 – 0.65
UPDRS Motor 0.90 0.002 - 0.83 0.88 0.03 – 0.65
SPES/SCOPA ADL 0.89 0.58 - 0.82 0.81 0.38 – 0.72
UPDRS ADL 0.93 0.61 - 0.91 0.75 -0.023 – 0.65
SPES/SCOPA Dyskinesias 0.89 0.74 – 0.92 0.92 NA4
UPDRS Dyskinesias 0.94 0.39 - 0.96 0.58 0.11 - 0.63
SPES/SCOPA Fluctuations 0.72 0.65 – 0.69 0.95 NA4
UPDRS Fluctuations 0.75 0.41 – 0.71 0.74 0.48 - 0.66
NB: Values obtained by clinical assessment in 85 patients. 1 corrected item-total correlation; 2 tremor R and L
leg; estimates unreliable due to insufficient dispersion; 3 sensory symptoms; 4 not applicable (only two items)
Table 6. Reliability of SPES/SCOPA items assessed by video
intra-rater1 inter-rater2
rest tremor R 0.95 0.83
rest tremor L 0.87 0.71
postural tremor R 0.91 0.71
postural tremor L 0.93 0.87
rapid alt mov R 0.85 0.82
rapid alt mov L 0.81 0.69
rise from chair 0.86 0.72
postural instability 0.87 0.87
gait 0.84 0.70
1 assessed by weighted kappa (quadratic weights); 14 raters 2 assessed by Kendall's coefficient of concordance W; 14 raters

Chapter 8
- 136 -
Validity. Correlations between related sections of the SPES/SCOPA and the UPDRS were
0.88 for motor impairments, 0.86 for ADL, 0.86 for dyskinesias, and 0.95 for motor
fluctuations. The correlations of these sections with the H&Y and S&E scale were all very
similar (table 7). The correlation between these sections and disease duration also bore strong
resemblance, with coefficients of 0.38 (SPES/SCOPA) and 0.23 (UPDRS) for the motor
sections, and 0.29 (SPES/SCOPA) and 0.36 (UPDRS) for the ADL sections. The correlation
with global ADL functioning was 0.49 for SPES/SCOPA ADL and 0.48 for the UPDRS
ADL.
Table 7. Correlations with Hoehn &Yahr and Schwab & England (Spearman’s rho)
Hoehn & Yahr Schwab & England
SPES/SCOPA Motor 0.50 -0.58
UPDRS Motor 0.47 -0.53
SPES/SCOPA ADL 0.47 -0.66
UPDRS ADL 0.45 -0.62
SPES/SCOPA complications1 0.26 -0.31
UPDRS IV complications1 0.26 -0.41
1 sum of dyskinesia and fluctuation scores
Mean scores of patients grouped by their H&Y stages (table 8) indicated significant
differences between groups for both the motor and ADL sections (ANOVA; p < 0.001). Post-
hoc t-tests showed no significant differences between patients in H&Y 2 and H&Y 3 in both
scales, but differences between stages 2 and 4, and between stages 3 and 4, were significant.
A significant trend was present in both sections of the scales, with higher scores for patients
with more advanced PD.

Motor impairments and disabilities in Parkinson’s disease
- 137 -
Table 8. Scale scores grouped by Hoehn and Yahr stages ('known-groups' comparisons)
Hoehn & Yahr ANOVA post-hoc t-tests1 ordinal regression
2 3 4 2-3 3-4 2-4 trend2 fit3 R-sq4
SPES/SCOPA motor 11.1 13.4 18.7 <0.001 0.11 <0.001 <0.001 <0.001 0.57 0.26
UPDRS motor 27.7 31.0 43.1 <0.001 0.51 <0.001 <0.001 <0.001 0.78 0.25
SPES/SCOPA ADL 7.2 7.9 11.8 <0.001 0.84 <0.001 <0.001 <0.001 0.33 0.30
UPDRS ADL 13.4 15.0 21.6 <0.001 0.72 <0.001 <0.001 <0.001 0.44 0.26
1 numbers in the columns are p-values of differences in scores of patients in different Hoehn and Yahr stages 2 a significant trend indicates that the trend differs significant from zero (i.e., no trend) 3 goodness of fit: p > 0.05 indicates that the model does not differ significantly from a model with a good fit 4 R-square: proportion of the variance accounted for by the model.
Discussion
We evaluated several aspects of the clinimetric performance of the SPES/SCOPA. Inter-rater
reliability and internal consistency obtained by clinical assessment in 85 patients, were very
similar for the SPES/SCOPA and the UPDRS. The reproducibility of the sumscores of the
SPES/SCOPA was high. Two items in the motor section displayed less than moderate
agreement, i.e., 'postural tremor' and 'rigidity', both of the right arm. The same items on the
same side also performed only fairly in the UPDRS, and previous studies on this scale have
also found lower scores for these items.4,24,25 Inter-rater reliability of the SPES/SCOPA MI
section assessed from video, showed higher scores than the clinical assessments with all
values higher than 0.60. Intra-rater reliability is even higher, with all reliability coefficients
above 0.80. Items in the ADL section were only evaluated historically in the clinical
assessment situation and all displayed at least 'substantial agreement', with the exception of
'changing positions'. Items in the MC section all showed at least 'substantial' reproducibility.
The results from our study comply with previous findings in which the SPES and UPDRS
were compared,6 with comparable items displaying similar reliability.
Internal consistency of all SPES/SCOPA scales were above 0.70, which is considered the
minimum for group comparisons.26 Item-total correlations of the tremor items were low,
indicating that these items behave rather independently, an observation was previously
reported by Martínez-Martín et al.4

Chapter 8
- 138 -
The correlation between the SPES/SCOPA and UPDRS is high, indicating that these scales
largely measure the same constructs. Moreover, the similarity of the correlations between the
SPES/SCOPA and UPDRS on the one hand, and measures of disease severity, such as H&Y,
S&E, global ADL functioning, and disease duration on the other hand, is striking. This further
endorses the impression that the scales capture the same phenomena. Differences between
patients grouped by their H&Y stages also display very similar results for both scales.
Although the SPES/SCOPA contains only half the number of items and uses four response
options instead of five, reliability and validity are apparently preserved.
Inter-rater reliability in our study was generally lower than that seen in other studies. This is
not surprising, given that most previous studies have used either video recordings, or a design
where several raters assess patients simultaneously, therewith excluding potential biases
caused by changes in the patient's state and differences in test executions. Video assessments
are useful since they provide information on reproducibility in standardised situations, thus
presenting the opportunity to locate weaker items that may benefit from clearer instructions
and descriptions. However, knowledge on the degree of reliability if patients are assessed at
separate occasions, either by the same or by different assessors, provides additional
information, since it reflects the routine of studies and clinical practice. To the best of our
knowledge, only one study has assessed reproducibility of the UPDRS over separate clinical
examinations.3 That study has evaluated intra-rater reliability over a two-week interval,
whereas we have assessed inter-rater reliability in immediate succession. Compared with our
data, that study found somewhat higher values for reproducibility of items in the motor
section and somewhat lower values for ADL items. This may seem somewhat surprising since
usually reliability scores are higher for intra- than for inter-rater reliability, and higher for
shorter than for longer intervals. One may have expected that both their scores would either
have been higher, because intra-rater reliability was assessed, or lower, because of the longer
interval. A possible explanation for this apparent discrepancy is that descriptions of ADL
items generally leave less room for interpretation bias than the description of motor items.
To summarise, the SPES/SCOPA is a reliable, valid, and conceptually clear scale that is
completed in half the time it takes to administer the UPDRS. Additionally, the SPES/SCOPA
has a better balance between early and late features of the disease and between items that are
more responsive to dopaminergic interventions and those that are more resistant. Altogether,
these advantages may favour the use of the SPES/SCOPA in evaluating motor function in
patients with PD.

Motor impairments and disabilities in Parkinson’s disease
- 139 -
Acknowledgements
Professor R.A.C. Roos is gratefully acknowledged for reviewing the manuscript. The authors
thank the following persons for their participation in evaluating the videotapes: Dr. S.
Agostini, Dr. S. Bernardini, Dr. C. Berti, Dr. D. Canteparo, Dr. E. Cubo, Dr. G. Gambacchi,
Dr. C. Klein, Dr. T. van Laar, Dr. C. Lucetti, and Dr. T. Prokhorov.
References
1. Mitchell SL, Harper DW, Lau A, Bhalla R. Patterns of outcome measurement in Parkinson's disease
clinical trials. Neuroepidemiology 2000; 19(2):100-108.
2. Ramaker C, Marinus J, Stiggelbout AM, Van Hilten BJ. Systematic evaluation of rating scales for
impairment and disability in Parkinson's disease. Mov Disord 2002; 17(5):867-876.
3. Siderowf A, McDermott M, Kieburtz K, Blindauer K, Plumb S, Shoulson I. Test-Retest reliability of the
Unified Parkinson's Disease Rating Scale in patients with early Parkinson's disease: Results from a
multicenter clinical trial. Mov Disord 2002; 17(4):758-763.
4. Martínez-Martin P, Gil-Nagel A, Morlán Gracia L, Balseiro Gómez J, Martínez-Sarriés FJ, Bermejo F, et
al. Unified Parkinson's Disease Rating Scale Characteristic and Structure. Mov Disord 1994; 9(1):76-83.
5. Van Hilten B, Van der Zwan AD, Zwinderman AH, Roos RAC. Rating Impairment and Disability in
Parkinson's Disease: Evaluation of the Unified Parkinson's Disease Rating Scale. Mov Disord 1994;
9(1):84-88.
6. Rabey JM, Bass H, Bonuccelli U, Brooks D, Klotz P, Korczyn AD, et al. Evaluation of the Short
Parkinson's Evaluation Scale: A New Friendly Scale for the Evaluation of Parkinson's Disease in Clinical
Drug Trials. Clin Neuropharmacol 1997; 20(4):322-337.
7. Werber EA, Rabey JM. The beneficial effect of cholinesterase inhibitors on patients suffering from
Parkinson's disease and dementia. J Neural Transm 2001; 108(11):1319-1325.
8. Reichmann H, Brecht HM, Kraus PH, Lemke MR. [Pramipexole in Parkinson disease. Results of a
treatment observation]. Nervenarzt 2002; 73(8):745-750.
9. World Health Organization. The international classification of functioning, disability, and health. Internet
2002. http://www3.who.int/icf/onlinebrowser/icf.cfm
10. Verbrugge LM, Jette AM. The Disablement Process. Soc Sci Med 1994; 38(1):1-14.
11. SCOPA homepage. Internet 2002. http://www.lumc.nl/2050/research/scopa_homepage.html
12. Guttman M. Double-blind comparison of pramipexole and bromocriptine treatment with placebo in
advanced Parkinson's disease. International Pramipexole- Bromocriptine Study Group. Neurology 1997;
49(4):1060-1065.
13. Hubble JP, Koller WC, Cutler NR, Sramek JJ, Friedman J, Goetz C, et al. Pramipexole in patients with
early Parkinson's disease. Clin Neuropharmacol 1995; 18(4):338-347.
14. Lieberman A, Ranhosky A, Korts D. Clinical evaluation of pramipexole in advanced Parkinson's disease:
results of a double-blind, placebo-controlled, parallel-group study. Neurology 1997; 49(1):162-168.

Chapter 8
- 140 -
15. Pinter MM, Pogarell O, Oertel WH. Efficacy, safety, and tolerance of the non-ergoline dopamine agonist
pramipexole in the treatment of advanced Parkinson's disease: a double blind, placebo controlled,
randomised, multicentre study. J Neurol Neurosurg Psychiatry 1999; 66(4):436-441.
16. Gruber RA, Marinus J, Visser M, Van Hilten JJ. Inter- and intra-rater reliability and discriminative ability
of five measures of bradykinesia in subjects with and without Parkinson's disease. Mov Disord 2002;
17(supplement 5):S119. Abstract.
17. Visser M, Marinus J, Bloem BR, Kisjes H, Van den Berg BM, Van Hilten JJ. Clinical tests for postural
instability in patients with Parkinson's disease. Mov Disord 2002; 17(supplement 5):S120. Abstract.
18. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease.
J Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
19. Fahn S, Elton RL, and members of the UPDRS Development Committee. Unified Parkinson's Disease
Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Clane DB, editors. Recent Developments in
Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information, 1987: 153-163.
20. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
21. Schwab RS, England AC, Jr. Projection technique for evaluting surgery in Parkinson's disease. In:
Gilingham FJ, Donaldson IML, editors. Third symposium on Parkinson's disease. Edinburgh: E. & S.
Livingstone, 1969: 152-157.
22. Fleiss JL, Cohen J. The equivalence of weighted kappa and the intraclass correlation coefficient as
measures of reliability. Educational and Psychological Measurement 1973; 33: 613-619.
23. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;
33(1):159-174.
24. Prochazka A, Bennett DJ, Stephens MJ, Patrick SK, Sears-Duru R, Roberts T, et al. Measurement of
rigidity in Parkinson's disease. Mov Disord 1997; 12(1):24-32.
25. Richards M, Marder K, Cote L, Mayeux R. Interrater Reliability of the Unified Parkinson's Disease
Rating Scale for Motor Examination. Mov Disord 1994; 9(1):89-91.
26. Bland JM, Altman DG. Cronbach's alpha. BMJ 1997; 314(7080):572.

Motor impairments and disabilities in Parkinson’s disease
- 141 -
Appendix
SPES/SCOPA scale
A. Motor evaluation Clinical examination 1. Rest tremor
assess each arm separately during 20 seconds; hands rest on thighs; if tremor is not evident at rest, try to keep the patient attentive, e.g. by having him/her count backwards with eyes closed
0 = absent 1 = small amplitude (< 1 cm) occurring spontaneously, or obtained only while keeping patient attentive (any amplitude) 2 = moderate amplitude (1-4 cm), occurring spontaneously 3 = large amplitude (≥ 4 cm), occurring spontaneously. 2. Postural tremor
check with arms outstretched, pronated and semipronated, and with index fingers of both hands almost touching each other (elbows flexed); assess each position during 20 seconds
0 = absent 1 = small amplitude (< 1cm) 2 = moderate amplitude (1-4 cm) 3 = large amplitude (≥ 4 cm). 3. Rapid alternating movements of hands
rapid alternating pronation/supination movements of upper hand, each time slapping the palm of the horizontally held lower hand during 20 seconds; each hand separately 0 = normal 1 = slow execution, or mild slowing and/or reduction in amplitude; may have occasional arrests 2 = moderate slowing and/or reduction in amplitude or hesitations in initiating movements or frequent
arrests in ongoing movements 3 = can barely perform task.
4. Rigidity
assess passive movements of elbow and wrist over full range, with the patient relaxed in sitting position; ignore cogwheeling; check each arm separately
0 = absent 1 = mild rigidity over full range, no difficulty reaching end positions
2 = moderate rigidity, some difficulties reaching end positions 3 = severe rigidity, considerable difficulties reaching end positions. 5. Rise from chair patient is instructed to fold arms across chest; use straight back chair 0 = normal 1 = slowly; does not need arms to get up 2 = needs arms to get up (can get up without help) 3 = unable to rise (without help). 6. Postural stability stand behind the patient and pull patient backwards, while s/he is standing erect with eyes open and feet
spaced slightly apart; patient is not prepared 0 = normal, may take up to 2 steps to recover 1 = takes 3 or more steps; recovers unaided 2 = would fall if not caught 3 = spontaneous tendency to fall or unable to stand unaided.

Chapter 8
- 142 -
7. Gait
assess gait pattern; use walking aid or offer assistance, if necessary 0 = normal 1 = mild slowing and/or reduction of step height or length; does not shuffle
2 = severe slowing, or shuffles or has festination 3 = unable to walk.
8. Speech 0 = normal 1 = slight loss of expression, diction and/or volume 2 = slurred; not always intelligible 3 = unintelligible always or most of the time. Historical information 9. Freezing during 'on'
Freezing is characterized by hesitation when trying to start walking or 'gluing' to the ground while walking. 0 = absent 1 = start hesitation only, occasionally present 2 = frequently present, may have freezing when walking 3 = severe freezing when walking.
10. Swallowing 0 = normal 1 = some difficulty or slow; does not choke; normal diet 2 = sometimes chokes; may require soft food 3 = chokes frequently; may require soft food or alternative method of food intake.
B. Activities of Daily Living 11. Speech 0 = normal 1 = some difficulty; may sometimes be asked to repeat sentences 2 = considerable difficulty; frequently asked to repeat sentences 3 = unintelligible most of the time. 12. Feeding (cutting, filling cup, etc.) 0 = normal 1 = some difficulty or slow; does not need assistance 2 = considerable difficulty; may need some assistance 3 = needs almost complete or complete assistance. 13. Dressing 0 = normal 1 = some difficulty or slow; does not need assistance 2 = considerable difficulty; may need some assistance (e.g. buttoning, getting arms into sleeves) 3 = needs almost complete or complete assistance. 14. Hygiene (washing, combing hair, shaving, brushing teeth, using toilet) 0 = normal 1 = some difficulty or slow; does not need assistance 2 = considerable difficulty; may need some assistance 3 = needs almost complete or complete assistance.

Motor impairments and disabilities in Parkinson’s disease
- 143 -
15. Changing position (turning over in bed, getting up out of bed, getting up out of a chair, turning
around when standing) 0 = normal 1 = some difficulty or slow; does not need assistance with any change of position 2 = considerable difficulty; may need assistance with one or more changes of position 3 = needs almost complete or complete assistance with one or more changes of position. 16. Walking 0 = normal 1 = some difficulty or slow; does not need assistance or walking aid 2 = considerable difficulty; may need assistance or walking aid 3 = unable to walk, or walks only with assistance and great effort. 17. Handwriting 0 = normal 1 = some difficulty (e.g. slow, small letters); all words legible 2 = considerable difficulty; not all words legible; may need to use block letters 3 = majority of words are illegible.
C. Motor Complications 18. Dyskinesias (presence)
0 = absent 1 = present some of the time 2 = present a considerable part of the time 3 = present most or all of the time.
19. Dyskinesias (severity) 0 = absent 1 = small amplitude 2 = moderate amplitude 3 = large amplitude 20. Motor fluctuations (presence of 'off' periods)
What proportion of the waking day is patient 'off' on average? 0 = none 1 = some of the time 2 = a considerable part of the time 3 = most or all of the time.
21. Motor fluctuations (severity of 'off' periods)
0 = absent 1 = mild end-of-dose fluctuations 2 = moderate end-of-dose fluctuations; unpredictable fluctuations may occur occasionally 3 = severe end-of-dose fluctuations; unpredictable on-off oscillations occur frequently.


- 145 -
99 Activity-based diary for Parkinson’s disease
Johan Marinus1, Martine Visser1, Anne M. Stiggelbout2, Jose Martin Rabey3, Ubaldo
Bonuccelli4, Peter H. Kraus5, Jacobus J. van Hilten1
Department of 1Neurology and 2Medical Decision Making, Leiden University Medical Center,
Leiden, The Netherlands; 3Department of Neurology, Assaf Harofeh Medical Center, Zerefin, Israel; 4Department of Neurology, University Hospital, Pisa, Italy; 5Department of Neurology, St. Josef
University Hospital, Bochum, Germany
Published in Clinical Neuropharmacology 2002;25:43-50

Chapter 9
- 146 -
Abstract The objective of this study was to develop a Parkinson's disease (PD) diary that evaluates a patient’s
difficulties in performing activities, as a substitute for the amount of 'on'- and 'off'-time, and to assess
its clinimetric qualities. In this study 84 PD-patients kept a diary for two or three periods of five days.
Daily, five items were recorded across 11 time periods. Patients simultaneously recorded ‘on-off’ in
the traditional way. The diary was easily understood and median recording time was 5-10 minutes a
day. Clinimetric analysis showed that the diary could successfully be reduced to three days, in which
five items (walking, transfers, manual activities, dyskinesias, and sleep) with four response options
were assessed seven times daily. Sumscores of the first three items accurately predicted being 'on' or
'off' in 93% of the cases, making separate scoring of 'on' and 'off' unnecessary. The diary was
internally consistent and showed good reproducibility. Construct validity with external measures was
adequate, and comparisons between patients grouped by disease severity and by degree of fluctuations
revealed significant differences in the expected directions. Taken together, this PD diary has a sound
clinimetric basis and provides information on the extent of perceived disability, thereby accurately
reflecting both the severity of off-periods and the variability of motor fluctuations.

Activity-based diary for Parkinson’s disease
- 147 -
Introduction Rating scales offer the possibility to record the clinical status of patients. However, they
provide a momentary impression that will generally describe the situation of stable patients
more accurately than that of patients with a fluctuating disease pattern. Information gathered
over a longer period of time will reflect the status of the latter patients more accurately, and
therefore diaries are especially useful in clinical evaluation and research involving fluctuating
patients.
Most patients with Parkinson’s disease (PD) experience motor fluctuations (‘wearing off’,
‘on-off’ fluctuations) after a number of years of levodopa use. Therapy in this situation is
often aimed at reducing the amount of ‘off-time’, which is usually evaluated by recording the
amount of time spent in ‘on’ and ‘off’ over a number of days. However, clinimetric
characteristics of these ‘on-off diaries’ have never been reported. Further, there are several
disadvantages of this assessment method. Firstly, some patients have difficulties establishing
whether they are ‘on’ or ‘off’.1 Secondly, considering ‘on-off’ in terms of a dichotomy may
be too simplistic, since different gradations of ‘off’ exist, and transitions from ‘on’ to ‘off’
and vice versa may occur gradually. Thirdly, since patients usually have to make hourly or
half-hourly recordings during several days, the method is time-consuming and the large
number of evaluations may affect compliance.
Therefore, constructing a diary that lacks these shortcomings is of considerable importance.
We hypothesized that being ‘on’ or ‘off’ will affect the ability to perform activities and that
this ability could successfully replace ‘on-off’ evaluations. We decided to focus on activities
(‘disabilities’), rather than on signs and symptoms (‘impairments’), because studies
evaluating reliability of self-reports of disabilities have shown good results,2,3 whereas for
impairments poor results were found.4 We therefore aimed to construct a diary that reflects
‘on’ and ‘off’ time, that has a low respondent burden, and is nevertheless valid, reliable, and
responsive.
Materials and Methods
Patients
Consecutive, cognitively unimpaired PD-patients (MMSE ≥ 24), who visited the outpatient
neurology clinic of the Leiden University Medical Center, who were willing to co-operate,
and who fulfilled the United Kingdom Parkinson’s Disease Society Brain Bank criteria for

Chapter 9
- 148 -
idiopathic PD,5 entered the study. Patients with other central neurological conditions were
excluded.
Diary Card
The development of the diary card (DC) is part of a larger research project, the SCOPA-
project (SCales for Outcomes in PArkinson’s disease). The SCOPA-DC has five items that
concern walking, the ability to make transfers, manual activities, dyskinesias, and quality of
sleep (appendix C). Patients simultaneously recorded whether they were ‘on’ or ‘off’. The
SCOPA-DC was filled out during five consecutive days, and items were evaluated 11 times
daily (after wakening, at breakfast, after breakfast, before lunch, at lunch, after lunch, before
dinner, at dinner, after dinner, while going to bed, at night). In this way each day was split
into time periods, anchored to specific parts of the day, rather than to separate hours. At
awakening patients recorded both the quality of sleep and the actual number of hours asleep
during the previous night. The number of minutes of sleep during daytime was also recorded.
There were four response options. Patients were asked to take an average over the previous
time period. Each day a new DC was completed. Instructions were given on the back of the
card (Appendix B).
Methods of assessment
Patients made diary recordings during five consecutive days and brought their DC’s to the
clinic on the sixth day. On that day the patients were first asked to fill out a questionnaire,
evaluating the experiences with the use of the DC. Hereafter, patients were interviewed by an
investigator, who gathered information from both the patient and, if present, the partner. The
investigator evaluated the same DC-items and recorded, on the basis of the obtained historical
information, which response option best reflected the patient’s average situation over the past
week. The partner was interviewed on the actual performance of a patient’s activities. The
investigator also administered the Mini-Mental State Examination (MMSE),6 the Hoehn and
Yahr scale (H&Y),7 and the Activities of Daily Living sections of both the Unified
Parkinson’s Disease Rating Scale (UPDRS-ADL),8 and the Short Parkinson’s Evaluation
Scale (SPES-ADL).9 This latter scale has four response options and was developed by a
group of European neurologists with the intent to simplify scoring of patients with PD. The
investigator was blind to the patient’s diary recordings at the time these scales were
administered. A neurologist independently assessed whether the patient suffered from motor
fluctuations. Patients not experiencing motor fluctuations were considered stable. Stable

Activity-based diary for Parkinson’s disease
- 149 -
patients were asked to fill out the DC during another period of five consecutive days two
weeks later, and once again three months later. Fluctuating patients were only asked to fill
out the DC’s three months later.
Statistical analysis
Data were entered and analyzed with SPSS for windows (release 9.0). The feasibility and
acceptability of the DC was assessed using the percentages of patients who expressed
difficulties with the DC. We assessed whether we could reduce both the number of recording
days as well as the number of daily evaluations without substantial changes in item means,
standard deviations, and test-retest reliability.
Reliability. Internal consistency was assessed using Cronbach’s α. Values higher than 0.7
were considered to reflect adequate internal consistency for group comparisons.10 For each
patient an activity score was calculated, based on the sum of the scores on walking, transfers
and manual activities across five days. This score was linearly transformed to a 0-100 scale
and labeled ‘DCsum’ (Appendix D). Higher values of DCsum reflect greater difficulties with
activities, while the complement of DCsum represents a percentage of ‘good functioning’.
Test-retest reliability was established by computing intraclass correlation coefficients (ICC)
for stable patients, both for a two-week and a three-month interval. Both the investigator’s
ratings of item scores over the last week and the partner’s ratings of the actual performance of
a patient’s activities, were compared with the patient’s own diary recordings, using Pearson’s
correlation coefficient (r). These ratings were considered to reflect inter-observer reliability.
Validity. Construct validity with external measures (H&Y, UPDRS-ADL, SPES-ADL) was
established using Pearson’s correlation coefficient. Construct validity using ‘known-groups’
comparisons based on disease severity (H&Y) was assessed with analysis of variance
(ANOVA), whereas patients with and without motor fluctuations were compared using an
independent samples t-test. The significance level was set at 0.05 and corrected for multiple
comparisons (Bonferroni) whenever appropriate.
Responsiveness. Within-person standard deviations of the aggregated first three items of
stable patients were compared with those of fluctuating patients, using a t-test for
independent samples. Smaller within-persons standard deviations of stable patients compared
to fluctuating patients, may be indicative for responsiveness. An independent samples t-test
was also used to compare the within-subjects coefficients of variation (CV) of stable and
fluctuating patients. In the CV the standard deviation of an item mean is expressed as a

Chapter 9
- 150 -
percentage of this item mean. Higher CV’s indicate greater variability and consequently,
fluctuating patients are expected to show significantly higher CV’s than stable patients.
Prediction of ‘on’ and ‘off’. Logistic regression was used to assess whether DCsum could
adequately predict whether patients were ‘on’ or ‘off’.
Results
Eighty-four eligible patients entered the study (table 1). Because patients in H&Y stages 1
and 5 were underrepresented, disease severity was categorized as mild (H&Y 1 and 2),
moderate (H&Y 3), or severe (H&Y 4 and 5). Thirty-four patients had a stable disease
pattern, whereas 47 patients had motor fluctuations. Three patients could not unequivocally
be assigned to one of both categories.
Eighty-three percent of the patients indicated that the DC was easily understood, while
another 69% considered the DC easy to use. Seventy-nine percent indicated that completing
the DC did not take much time. The median recording time was 5-10 minutes a day.
Data reduction
The DC was successfully reduced. Item means, standard deviations, and test-retest reliability
did not substantially change when the number of days was reduced from five to three and the
number of daily evaluations from 11 to seven, neither for stable patients, nor for fluctuating
patients (table 2). We made no efforts to further reduce the number of days in order to avoid
the risk that ‘day-to-day’ fluctuations would seriously affect the results. Nor did we attempt
to further reduce the number of daily evaluations, as this would have resulted in too large
gaps in the distribution of evaluations across the day.
Clinimetrics of the SCOPA Diary Card
The summary score DCsum was calculated and used as an index of severity, because it
reflects the level of difficulties in performing activities. Items 4 (dyskinesias) and 5 (sleep)
were considered separately, because they do not necessarily reflect disease severity.
Dyskinesias and quality of sleep were significantly correlated with DCsum (r = 0.46 and
0.32, respectively; p < 0.01). DCsum was normally distributed (Kolmogorov-Smirnov Z =
0.59; p = 0.87).

Activity-based diary for Parkinson’s disease
- 151 -
Table 1. Patient characteristics
number of patients 84 (50 male, 34 female)
modified Hoehn and Yahr
mild (H&Y 1 and 2)
moderate (H&Y 3)
severe (H&Y 4 and 5)
n = 26 (H&Y 1: n = 6; H&Y 2: n = 20)
n = 37
n = 21 (H&Y 4: n = 21; H&Y 5: n = 0)
mean (SD) age in years 63.06 (8.05)
mean (SD) age at onset in years 54.02 (9.92)
mean (SD) disease duration in years 8.91 (5.26)
number of patients on levodopa 68 (81%)
mean (SD) years on levodopa (n=68)
mean (SD) levodopa dose in mg (n=68)
6.67 (4.92)
631 (367)
number of patients on dopamine agonists 69 (84%)
number on other antiparkinsonian medication 49 (60%)
mean (SD) MMSE
mean (SD) SPES-ADL
mean (SD) UPDRS-ADL
27.04 (2.21)
9.68 (3.77)
16.49 (6.52)
Reliability. Cronbach’s α, calculated over the first three items, was 0.80. Test-retest
reliability, evaluated using sumscores per item across three days, was assessed in 34 stable
patients. The mean ICC was 0.91 for a two week interval (range items: 0.84-0.95; table 3)
and 0.68 for a three month interval (range items: 0.53-0.76). The mean reproducibility over a
three month interval in 33 fluctuating patients was 0.37 (range items: 0.30-0.44). The
correlation between investigator’s ratings and patient’s ratings was 0.81, while the correlation
between partner’s ratings and patient’s ratings was 0.70 (r).
Validity. Construct validity of DCsum with external measures was 0.46 for the H&Y stage,
0.57 for the SPES-ADL, and 0.62 for the UPDRS-ADL. Diary recordings of patients grouped
by disease severity revealed significant differences between groups (ANOVA, p < 0.001).
Post hoc comparisons between the three groups indicated that differences between mildly and
moderately affected patients just failed to reach significance (p = 0.08), whereas both other
differences (mild versus severe, moderate versus severe) were significant at the 0.001 level.

Chapter 9
- 152 -
Table 2. Comparison long and short version of the SCOPA Diary Card
parameter long version
(5 days, 11 evaluations)
short version
(3 days, 7 evaluations)
mean (SD) aggregated items 1-3 0.84 (0.44) 0.86 (0.44)
mean (SD) item 4 (dyskinesias) 0.49 (0.60) 0.49 (0.60)
mean (SD) item 5 (sleep) 1.06 (0.55) 1.04 (0.57)
mean (SD) of hours sleep night 6.43 (1.52) 6.40 (1.55)
mean (SD) of minutes sleep day 0.62 (0.66) 0.65 (0.70)
ICC1 aggregated items 1-3 0.93 0.93
ICC 4 (dyskinesia) 0.93 0.94
ICC 5 (sleep) 0.84 0.84
ICC hours slept at night 0.89 0.89
ICC hours slept during day 0.86 0.86
1 ICC: intraclass correlation coefficient
‘Known-groups’-comparisons between stable and fluctuating patients revealed significant
differences in DCsum (23.88 ± 13.05 versus 30.81 ± 14.28, respectively; p < 0.05).
Responsiveness. Within-person standard deviations of stable patients, calculated over the first
three items of three consecutive days, differed significantly from those of fluctuating patients
(1.58 ± 1.42 versus 2.81 ± 1.59, respectively; p < 0.001). Coefficients of variation of
fluctuating patients were significantly higher than those of stable patients (0.39 versus 0.17, p
< 0.001).
Prediction of ‘on’ and ‘off’. The mean correlation (r) between DCsum and the patient’s own
estimation of ‘on’ and ‘off’ was 0.75. Binary logistic regression analysis revealed that being
‘on’ or ‘off’ was accurately predicted by DCsum in 93% of the cases, making separate
evaluation of this characteristic unnecessary. This indicated that we could remove the ‘on-
off’-item from the final version of the DC. This resulted in a DC with five items, to be
assessed seven times daily during three consecutive days (Appendix A).

Activity-based diary for Parkinson’s disease
- 153 -
Table 3. Test-retest reliability Diary Card
stable patients 2 weeks 3 months
item 1 (walking) ICC1 = 0.95 ICC = 0.76
item 2 (transfers) ICC = 0.95 ICC = 0.70
item 3 (manual activities) ICC = 0.89 ICC = 0.53
item 4 (dyskinesias)
item 5 (sleep)
number of hours sleep at night
number of hours sleep in daytime
DCsum2
ICC = 0.94
ICC = 0.84
ICC = 0.89
ICC = 0.86
ICC = 0.88
ICC = 0.73
ICC = 0.66
ICC = 0.79
ICC = 0.44
ICC = 0.73
1 ICC: intraclass correlation coefficient 2 DCsum: scores aggregated over first three items of three days, linearly
transformed to 0-100 scale
Discussion
Despite the general use of ‘on-off’ diaries in drug trials involving PD-patients with motor
fluctuations, no information is available on the clinimetric characteristics of such diaries.
Information on other forms of self-report in PD is also sparse. The available studies indicate
that self-assessment of ‘disabilities’ (i.e., difficulties performing activities such as walking,
dressing, and eating) in PD-patients can produce reliable2,3 and valid2 results. Reliability and
validity of ‘impairments’ (signs and symptoms) in PD, however, is less favorable.4 Diaries
should therefore focus on disabilities rather than on impairments. Another reason for
preferring disabilities over impairments is that disabilities generally are more meaningful to
patients.11
We decided to select three key activities: walking, transfers, and manual activities. These
activities were chosen because they are important to people, are difficult to avoid, and occur
frequently during the day. Additional support for these activities is provided by four factor
analysis studies that addressed ADL and disability in PD patients.12-15 These studies revealed
a general pattern of one factor concerned with functions on the whole body level (gait and
mobility, ADL functions), and one factor predominantly dealing with manual activities. We
therefore decided to focus on these factors. In our study the first factor (‘gross mobility’) was
split into two items, one concerning walking, the other the ability to make transfers. Manual
activities was the third item. Dyskinesias were included as the fourth item as they reflect

Chapter 9
- 154 -
another important motor complication, and this item was also addressed at the disability
level. Although dyskinesias may affect the performance of activities, the item was not
included in the sumscore because there is no clear-cut relation with the extent of disability.
After all, on the one hand dyskinesias may aggravate disabilities, while on the other hand
dyskinesias frequently occur during ‘on’, when patients benefit from medication and are
better capable of performing activities. The fifth item concerned the quality of night-time
sleep and was assessed once a day. The actual amount of sleep time, both during night and
day, was included in the diary as well.
We selected seven evaluation moments, anchored to usual breaks in the day, for the final
version of the DC. The time points ‘mid-morning’ and ‘mid-afternoon’ can be linked to
coffee and tea breaks, or be combined with other breaks, given the cultural setting. The
natural pauses make moments of reflection possible and patients are asked to take an average
over the previous period. This is less burdensome for patients than hourly evaluations that
may affect compliance. For people with other schedules, or whenever considered appropriate,
an alternative time table may be adopted, provided that an equal spread over the day is taken
into account.
The clinimetric analysis of the DC shows good results. Both the internal consistency and the
reproducibility in stable patients over two weeks are good. As can be expected, the
reproducibility decreases over longer time intervals, especially in fluctuating patients. The
lower values for reproducibility of fluctuating patients are in fact a favorable outcome, as this
may indicate that the DC is potentially responsive. After all, stable patients should produce
consistent scores on the outcome measure and thus reveal high reproducibility, whereas
fluctuating patients should display lower results, given the fact that changes occur.
The DC correlates adequately with external measures (scales, investigator, partner), which
gives evidence to the construct validity of this assessment method. Construct validity is also
confirmed by group comparisons, showing differences in the expected directions between
patients with different disease severity, and between stable and fluctuating patients.
This study had some potential shortcomings. Firstly, the accuracy of patients’ own ratings of
‘on’ and ‘off’ was not independently established and therefore may lack validity. Secondly,
the responsiveness of the SCOPA-DC still needs to be established more thoroughly, for
instance in a study with an intervention of known efficacy.

Activity-based diary for Parkinson’s disease
- 155 -
It may be hypothesized that this DC produces indices that do not seem to be as clear-cut as
the reduction in ‘off-time’. However, the complement of DCsum represents a percentage of
‘good functioning’, and changes in this percentage reflect treatment efficacy. Additionally, as
we outlined before, it is too simplistic to consider ‘on-off’ as a dichotomy, since there are
gradual differences in off-state, which are not accounted for in the traditional on-off diaries.
This study is the first thorough attempt to evaluate the clinimetric characteristics of a PD
diary. Additionally, pre-post comparisons of row scores and DCsum scores, can be used to
evaluate the efficacy of interventions. Correspondingly, column totals can be used to assess
the stability of performance over time. To this end, standard deviations of the column totals
are expressed in a percentage of the means of the column totals, in a ‘coefficient of variation’.
Fluctuating patients will display greater variability in performance, resulting in a larger
coefficient of variation. Consequently, a decrease of the coefficient of variation after an
intervention indicates treatment efficacy, as it reflects a reduction of fluctuations.
Statistical analysis indicates that seven daily evaluations suffice, and for that reason the
SCOPA Diary Card in the form outlined here, is an appropriate outcome measure in both
research and clinical practice. With respect to the management of motor complications in
daily practice, a more frequent sampling is desirable. In this situation an alternative form with
separate hourly intervals (but with the same items and response options), is more appropriate.
Acknowledgements
Financial support for this study was granted from the Netherlands Organization for Scientific
Research (NWO, project number 0940-33-021). The authors thank Prof. R.A.C. Roos and Dr.
A.H. Zwinderman for their help with the manuscript.
References 1. Goetz CG, Stebbins GT, Blasucci LM, Grobman MS. Efficacy of a patient-training videotape on motor
fluctuations for on-off diaries in Parkinson's disease. Mov Disord 1997; 12(6):1039-1041.
2. Brown RG, MacCarthy B, Jahanshahi M, Marsden CD. Accuracy of self-reported disability in patients
with parkinsonism. Arch Neurol 1989; 46(9):955-959.
3. Louis ED, Lynch T, Marder K, Fahn S. Reliability of Patient Completion of the Historical Section of the
Unified Parkinson's Disease Rating Scale. Mov Disord 1996; 11(2):185-192.

Chapter 9
- 156 -
4. Golbe LI, Pae J. Validity of a Mailed Epidemiological Questionnaire and Physical Self-Assessment in
Parkinson's Disease. Mov Disord 1988; 3(3):245-254.
5. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's
disease. J Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
6. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the
cognitive state of patients for the clinician. J Psychiatr Res 1975; 12(3):189-198.
7. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
8. Fahn S, Elton RL, and members of the UPDRS Development Committee. Unified Parkinson's Disease
Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Clane DB, editors. Recent Developments in
Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information, 1987: 153-163.
9. Rabey JM, Bass H, Bonuccelli U, Brooks D, Klotz P, Korczyn AD, et al. Evaluation of the Short
Parkinson's Evaluation Scale: A New Friendly Scale for the Evaluation of Parkinson's Disease in Clinical
Drug Trials. Clin Neuropharmacol 1997; 20(4):322-337.
10. Bland JM, Altman DG. Cronbach's alpha. BMJ 1997; 314(7080):572.
11. Hogan T, Grimaldi R, Dingemanse J, Martin M, Lyons K, Koller W. The Parkinson's disease symptom
inventory (PDSI): a comprehensive and sensitive instrument to measure disease symptoms and treatment
side-effects. Parkinsonism Relat Disord 1999; 5:93-98.
12. Baas H, Stecker K, Fischer PA. Value and appropriate use of rating scales and apparative measurement
in quantification of disability in Parkinson's disease. J Neural Transm 1993; 5:45-61.
13. Henderson L, Kennard C, Crawford TJ, Day S, Everitt BS, Goodrich S, et al. Scales for rating motor
impairment in Parkinson's disease: studies of reliability and convergent validity. J Neurol Neurosurg
Psychiatry 1991; 54:18-24.
14. Martínez-Martin P, Gil-Nagel A, Morlán Gracia L, Balseiro Gómez J, Martínez-Sarriés FJ, Bermejo F, et
al. Intermediate Scale for Assessment of Parkinson's Disease. Characteristic and Structure. Parkinsonism
& Related Disorders 1995; 1(2):97-102.
15. Van Hilten B, Van der Zwan AD, Zwinderman AH, Roos RAC. Rating Impairment and Disability in
Parkinson's Disease: Evaluation of the Unified Parkinson's Disease Rating Scale. Mov Disord 1994;
9(1):84-88.

QUESTIONSprevious
nightbreakfast
(or until 7.00)
mid-morning
(7.00 - 10.00)
lunch(10.00 - 13.00)
mid-afternoon
(13.00 – 16.00)
dinner
(16.00 – 19.00)
bed time(19.00 - 22.00)
sum
Slept greater part?
1. Walking
2. Changing position
3. Using your hands
4. Uncontrollablemovements
5. SleepNumber of hours sleep in previous night:
(to the nearest half hour)
Number of minutes sleep during the day:
(to the nearest 15 minutes)
sum 1-3
Date: Name: IDno:
Place a cross in the box which best reflects your situation over the previous time period.
For ‘walking’, ‘changing position’ and ‘using your hands’: For ‘uncontrollable movements’: For ‘sleep’:
0 = no difficulty 0 = absent or do not bother me 0 = slept very well
1 = slight difficulty (somewhat slow, no help required) 1 = bother me slightly 1 = slept rather well
2 = moderate difficulty (rather slow, some help required) 2 = bother me moderately 2 = slept rather badly
3 = severe difficulty (impossible or only with a lot of help) 3 = bother me a lot 3 = slept very badly
0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 30 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 3
0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
yesyes yes yes yes yes
QUESTIONSprevious
nightbreakfast
(or until 7.00)
mid-morning
(7.00 - 10.00)
lunch(10.00 - 13.00)
mid-afternoon
(13.00 – 16.00)
dinner
(16.00 – 19.00)
bed time(19.00 - 22.00)
sum
Slept greater part?
1. Walking
QUESTIONSprevious
nightbreakfast
(or until 7.00)
mid-morning
(7.00 - 10.00)
lunch(10.00 - 13.00)
mid-afternoon
(13.00 – 16.00)
dinner
(16.00 – 19.00)
bed time(19.00 - 22.00)
sum
Slept greater part?
1. Walking
2. Changing position
3. Using your hands
2. Changing position
3. Using your hands
4. Uncontrollablemovements
5. SleepNumber of hours sleep in previous night:
(to the nearest half hour)
Number of minutes sleep during the day:
(to the nearest 15 minutes)
sum 1-3
4. Uncontrollablemovements
5. SleepNumber of hours sleep in previous night:
(to the nearest half hour)
Number of minutes sleep during the day:
(to the nearest 15 minutes)
sum 1-3
Date: Name: IDno:
Place a cross in the box which best reflects your situation over the previous time period.
For ‘walking’, ‘changing position’ and ‘using your hands’: For ‘uncontrollable movements’: For ‘sleep’:
0 = no difficulty 0 = absent or do not bother me 0 = slept very well
1 = slight difficulty (somewhat slow, no help required) 1 = bother me slightly 1 = slept rather well
2 = moderate difficulty (rather slow, some help required) 2 = bother me moderately 2 = slept rather badly
3 = severe difficulty (impossible or only with a lot of help) 3 = bother me a lot 3 = slept very badly
0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 30 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
0 1 2 3
0 1 2 3
0 1 2 3
0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3
yesyes yes yes yes yes
Appendix A. SCOPA Diary Card

Chapter 9
- 158 -
Appendix B. Patient instruction
How to complete the SCOPA Diary Card?
• Fill in one Diary Card each day and indicate name and date.
• Indicate at each time point, by means of a cross, which description best reflects your situation over the
previous time period. For example: if you experienced slight difficulty walking during the period from
waking up until breakfast, place a cross in box ‘1’ in the row ‘walking’ under the heading ‘breakfast’.
Always estimate an average over the relevant time period. At ‘mid-morning’, place a cross in the box that
on average best reflects the period from breakfast until mid-morning.
• On waking in the morning, fill in the column ‘previous night’. You may not be able to assess some
categories in the column ‘previous night’ (e.g. walking). In that case, do not fill anything in. If you went to
the toilet, then you can assess this.
• Also on waking, record in the category ‘Sleep’ how well you slept (by means of a cross in the appropriate
box), as well as the number of hours you slept the previous night. This means the number of hours you
actually slept and not the number of hours you spent in bed. At the end of the day (at ‘bed time’) record the
total number of minutes you slept during that day.
• In the other columns always indicate first whether you slept the greater part of the relevant time period. If
you slept during the greater part of a particular time period during the day, then do not place a cross in any
of the categories, but place a cross in the box ‘yes’ in the row ‘slept greater part?’. If you did not sleep
during the relevant time period, or only during the lesser part of the time, then fill in the categories 1 to 4
and do not place a cross in the row ‘slept greater part?’.
• If your daily time table is very different, e.g. because you do not eat breakfast in the morning, use the times
specified under the column headings.
• Do not write in the row labelled ‘sum 1-3’ or in the column labelled ‘sum’.

Activity-based diary for Parkinson’s disease
- 159 -
Appendix C. Item descriptions
WALKING
Which of the following descriptions of walking best reflects your situation?
0. No difficulty walking.
1. Slight difficulty walking (no help required).
2. Moderate difficulty walking (some help required).
3. Severe difficulty walking (impossible or only with a lot of help).
CHANGING POSITION
Which of the following descriptions of turning over in bed, getting up out of bed, getting up out of a chair and
turning around when standing best reflects your situation?
0. No difficulty with any of these actions.
1. Slight difficulty with one or more of these actions (somewhat slow, no help required).
2. Moderate difficulty with one or more of these actions (rather slow, some help required).
3. Severe difficulty with one or more of these actions (impossible or only with a lot of help).
USING YOUR HANDS
Which of the following descriptions of using your hands when eating, drinking, getting dressed, washing,
shaving, combing your hair and brushing your teeth best reflects your situation?
0. No difficulty with any of these actions.
1. Slight difficulty with one or more of these actions (somewhat slow, no help required).
2. Moderate difficulty with one or more of these actions (rather slow, some help required).
3. Severe difficulty with one or more of these actions (impossible or only with a lot of help).
UNCONTROLLABLE (SUPERFLUOUS) MOVEMENTS*
* These so-called ‘dyskinesias’ involve irregular, abrupt, jerking movements of arms, legs, trunk or head that
occur involuntarily. It does not include shaking or trembling.
Which of the following statements about uncontrollable movements best reflects your situation?
0. Absent or does not bother me.
1. Present and bothers me slightly.
2. Present and bothers me moderately.
3. Present and bothers me a lot.
SLEEP
Which of the following statements about sleep best reflects your situation?
0. I have slept very well.
1. I have slept rather well.
2. I have slept rather badly.
3. I have slept very badly.
Chapter 9
- 160 -
Appendix D. Guidelines for scientific use of the SCOPA Diary Card 1. The SCOPA Diary Card is recorded for a period of three consecutive days, e.g. three at baseline and three
days at follow-up assessments.
2. Per item a total score is calculated over these three days and this score is transformed to a 0-100 scale
(dividing by 63, multiplication by 100; subtract 3 from 63 for each missing value). Do not calculate row
scores for days where two or more time points are missing.
3. A sumscore (DCsum) is calculated over the aggregated first three items and transformed to a 0-100 scale.
To this end, first the score on each item (as computed in 2) is divided by 3, after which these scores are
summed. Higher scores of DCsum indicate greater difficulty, while its complement reflects the percentage
of ‘good functioning’.
4. Scores on dyskinesia and sleep are not included in the sumscore DCsum, but are evaluated separately.
Calculate as in 2.
5. In order to explore the stability of performance, calculate co lumn totals over the first three items of each
time point of each day. Then calculate the mean column total (over all 21 columns, or less in the case of
missing values) and the standard deviation of this column total. Divide the standard deviation by the mean.
This yields the ‘coefficient of variation’ (CV). Stable patients are not expected to show large variations and
will have a small CV, while fluctuating patients will have higher CV’s. CV’s greater than 0.30 are regarded
to reflect a fluctuating disease pattern. In order to calculate a column total, no scores should be missing in
that particular column.
The CV becomes unstable in the case of very low means, and therefore this parameter should not be
computed if the mean column total is lower than 1 (as these values are only found in patients without
disabilities and without fluctuations this presents no problem, because the DC was not meant to be used in
these patients).

- 161 -
1100 Development of a questionnaire for sleep and sleepiness in
Parkinson's disease
Johan Marinus1, Martine Visser1, Jacobus J. van Hilten1, Gert Jan Lammers1 Anne M.
Stiggelbout2
Departments of Neurology1 and Medical Decision Making2, Leiden University Medical Center,
Leiden, The Netherlands.
Submitted

Chapter 10
- 162 -
Abstract
Objective. To develop a valid, reliable, and short questionnaire (SCOPA-SLEEP) that assesses night-
time sleep (NS) and daytime sleepiness (DS) in patients with Parkinson's disease (PD). Methods. A
postal survey including four instruments, the SCOPA-SLEEP NS (5 items) and DS (6 items), the
Pittsburgh Sleep Quality Index (PSQI), and the Epworth Sleepiness Scale (ESS) was completed by
142 patients with PD and 100 controls. Results. Reliability of the scale was high: internal consistency
of the NS and DS scales were 0.88 and 0.91, respectively (Cronbach alpha), and test-retest reliabilities
were 0.94 and 0.89, respectively (intraclass correlation coefficient). Scale scores differed significantly
between patients and controls (p < 0.001). Construct validity was assessed by correlations with scales
that addressed similar constructs. Correlation between the NS scale and the PSQI was 0.83 (p <
0.001), and the correlation between the DS scale and the ESS was 0.81 (p < 0.001). Factor analysis
revealed one factor each for both scales, indicating that the scales measure one construct, which
justifies the calculation of sumscores. The coefficient of variation of both the NS and the DS scale was
higher than that of the PSQI and the ESS, indicating a better ability to detect differences between
individuals. Conclusions. The SCOPA-SLEEP is a reliable, valid, and practical instrument for
assessing both night-time sleep and daytime sleepiness in patients with PD.

Sleep and sleepiness in Parkinson’s disease
- 163 -
Introduction Insomnia and hypersomnia occur frequently in the general population and increase with
higher age. Several studies found even higher prevalences of both types of sleep problems in
patients with Parkinson's disease (PD).1-3 Poor night-time sleep is associated with lower
quality of life of patients and their spouses,4-6 while excessive daytime sleepiness may be
bothersome or even dangerous. A few studies reported the occurrence of 'sleep attacks' among
patients with PD, potentially causing hazardous situations.7-9 Sleep problems therefore merit
particular attention and this raises the question how these should be evaluated.
Within the scope of selecting appropriate instruments for a longitudinal study of patients with
PD, we were interested in a concise, practical, and clinimetric sound instrument to assess both
night-time sleep problems and daytime sleepiness in PD. The questionnaire should be
appropriate for both research and clinical practice. However, none of the existing sleep scales
matched our objective. Some scales lacked conceptual clarity and combined scores on items
addressing different constructs into a sumscore (e.g., Pittsburgh Sleep Quality Index,10
Parkinson's Disease Sleep Scale11). Other scales had potential problems with face validity and
were either too short (Stanford Sleepiness Scale,12 Karolinska Sleepiness Scale13), lacked
relevant items (Sleep Problems Scale14), or asked patient to indicate the chance of falling
asleep in situations they possibly did not experience (Epworth Sleepiness Scale15). Still other
scales were not suitable for clinical use, because they were too long, the calculation of
sumscores was complex (Pittsburgh Sleep Quality Index), or combined continuous and
categorical responses (St. Mary's Hospital Sleep Questionnaire16). Additionally a number of
scales were not appropriate because they involved diagnostic instruments (Sleep Disorders
Questionnaire17), or were intended for particular patient groups (e.g., narcolepsy) or particular
interventions (e.g., pharmacological in the Leeds Sleep Evaluation Questionnaire18).
We therefore decided to develop and validate a new scale, the SCOPA-SLEEP, that evaluates
both night-time sleep (NS) and daytime sleepiness (DS) in patients with PD. The scale is
intended for comparing groups in research situations and for clinical use in individual
patients. The development of this scale is part of a larger project on SCales for Outcomes in
PArkinson’s disease (SCOPA; http://www.lumc.nl/2050/research/scopa_homepage.html), in
which short, practical, and clinimetric sound scales for all relevant domains in PD are selected
or developed.

Chapter 10
- 164 -
Methods
Scale development
Items in the NS scale were selected from the literature and evaluated whether patients
experienced problems with respect to their nocturnal sleep. It was hypothesized that together
these items would reflect a patient's perceived sleep quality. The items were judged by experts
and piloted among patients regarding comprehensibility and clarity. Testing was continued
until no further problems were encountered and patients understood all items well. The DS
scale was developed similarly and evaluated how often patients had fallen asleep in daytime,
had experienced difficulty staying awake, and whether falling asleep in daytime was
considered a problem. The SCOPA-SLEEP thus consists of two parts. The NS subscale
addresses night-time sleep problems in the past month and includes five items with four
response options. Patients have to indicate how much they were bothered by particular sleep
problems, ranging from 0 (not at all) to 3 (a lot). The five items address sleep initiation, sleep
fragmentation, sleep efficiency, sleep duration, and early wakening. The maximum score of
this scale is 15, with higher scores reflecting more severe sleep problems. One additional
question evaluates overall sleep quality on a seven-point scale (ranging from 'slept very well'
to 'slept very badly'). The score on this item is not included in the sumscore of NS, but used
separately as a global measure of sleep quality. The DS subscale evaluates daytime sleepiness
in the past month and includes six items with four response options, ranging from 0 (never) to
3 (often). Subjects indicate how often they fell asleep unexpectedly, fell asleep in particular
situations (while sitting peacefully, while watching TV or reading, or while talking to
someone), how often they had difficulty staying awake, and whether falling asleep in daytime
was considered a problem. The maximum score is 18, with higher scores reflecting more
severe sleepiness.
Participants
Since patients with PD reported more sleep problems than controls in almost all previous
studies, the scales would have to be able to detect these differences, and therefore subjects
without PD were included as a control group.
Patients. Patients who visited the outpatient clinic of the Department of Neurology of the
Leiden University Medical Center and fulfilled the United Kingdom Parkinson’s Disease
Society Brain Bank criteria for idiopathic PD,19 were included. Patients were excluded if they
Sleep and sleepiness in Parkinson’s disease
- 165 -
also had other diseases of the central nervous system or were not able to read or understand
Dutch.
Controls. Subjects without PD who were able to read or understand Dutch were eligible as
controls, provided that they had no history of diseases of the central nervous system.
Recruitment. Questionnaires were sent to eligible patients. An introductory letter provided
information on the goal of the study and requested patients to provide the names of two
persons, one man and one woman, who consented to participate as a control subject. The age
difference between the patient and his or her controls was not to exceed 10 years. The
introductory letter emphasized that only the names of persons that explicitly expressed their
willingness to participate were to be provided. Partners were not eligible as controls, since
nocturnal sleep problems of patients could affect the partner’s sleep pattern.6,20 Response was
interpreted as consent to participate. The study was approved by the medical ethics committee
of the Leiden University Medical Center.
Scale evaluation
A postal survey was sent to potential participants. The included questionnaires were the
SCOPA-SLEEP (appendix), the Pittsburgh Sleep Quality Index (PSQI),10 and the Epworth
Sleepiness Scale (ESS).15 Eight additional questions were used to evaluate use of sleep
medication, sleep initiation time (minutes), time awake per night (hours), actual duration of
night-time sleep (hours), duration of daytime sleep (minutes), and how often subjects had
'planned naps', 'unplanned naps', or 'fallen asleep quite unexpectedly' in the past month.
Response options for the latter three questions ranged from ‘not at all’ to ‘every day’. The
PSQI, ESS, and the eight additional questions were included to assess the construct validity of
the SCOPA-SLEEP. The PSQI and the ESS were included because they are frequently used
and have previously been used in studies involving patients with PD. The PSQI evaluates
several aspects of night-time sleep and consists of 19 self-rated questions and five questions
rated by the bedpartner or roommate.10 The latter five questions are used for clinical
information only and are not tabulated in the scoring of the PSQI. Scores are first grouped in
seven domains and next recoded to a 0-3 scale. The seven domains include subjective sleep
quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of
sleep medication, and daytime dysfunction. Both the total score and the subscale scores can
be used. The total score has a maximum of 21, with higher scores reflecting greater problems.
The developers advise a cut-off score of 5/6 to separate good from bad sleepers.10

Chapter 10
- 166 -
The ESS evaluates daytime sleepiness. In this scale, the individual is asked to rate the chance
of dozing off for eight different situations.15 There are four response options, ranging from 0
(would never doze) to 3 (high chance of dozing). The maximum score is 24, with higher
scores reflecting more severe sleepiness. Healthy controls usually have scores ≤ 10. Scores ≥
11 are considered indicative for excessive sleepiness.21 Scores ≥ 16 indicate a high level of
daytime sleepiness, but are by themselves not diagnostic of a particular sleep disorder.15
Participants were asked to complete the questionnaires within one week. After two weeks
non-responders were contacted by telephone and the investigator inquired whether the subject
still considered participating. Patients who returned their questionnaires within one week were
asked to complete the SCOPA-SLEEP a second time two weeks later, for the evaluation of
the test-retest reliability. Information from the questionnaires of participating patients was
combined with information from patient records, i.e., disease severity, disease duration, and
medication, to assess 'known-groups' validity. Disease severity was evaluated at each control
visit and assessed by the Hoehn and Yahr (H&Y) staging system.22 H&Y 1 is the mildest
stage with only unilateral symptoms, whereas H&Y 5 is the most severe stage in which
patients are wheelchair-bound or bedridden.
Statistical analysis
Data were entered and analyzed with SPSS for Windows 10.0 (SPSS Inc, Chicago, IL, USA).
Questionnaires were excluded if they had more than 20% missing values.
Data quality and score distribution. The quality of the data was considered acceptable if item
scores were missing in less than 10% of the patients23 and item-total correlations in the patient
group exceeded 0.20.24
Reliability. Internal consistency of the scales was assessed with Cronbach α. Test-retest
reliability for individual items was assessed with a weighted kappa (Kw; quadratic weights),
whereas for the total score an intraclass correlation coefficient (ICC) was used.
Validity. Age, disease severity, and male-female ratio of responders were compared with
those of non-responders, using t-tests, Mann-Whitney-U tests, and Chi-square tests,
respectively. Independent samples t-tests were used to compare scores of patients and
controls, and scores of patients that were on medication (levodopa, dopamine agonists, or
sleep medication) versus those who were not. The significance threshold was set at 0.05.
Construct validity of the SCOPA-SLEEP was assessed by calculating the correlation between
this scales and scales that addressed similar constructs, using Pearson's correlation coefficient

Sleep and sleepiness in Parkinson’s disease
- 167 -
(r). This coefficient was also used to explore the relation with disease duration. Spearman’s
correlation coefficient (rs) was used if the correlation involved subscales of the PSQI and the
‘global sleep quality’ item. Known-groups validity was assessed by comparing the NS and DS
scores of patients with different disease severity, using analysis of variance (ANOVA). To
discriminate groups of patients with different disease severity, patients were classified as mild
(H&Y 1 and 2), moderate (H&Y 3), or severe (H&Y 4 and 5). Stages 1 and 2 on the one
hand, and 4 and 5 on the other hand, were collapsed because patients in H&Y stages 1 and 5
were underrepresented, a common finding in studies involving patients with PD. A principal
component factor analysis with orthogonal rotation was performed to explore the underlying
structure of the scales. Coefficients of variation (CV) were calculated to assess the
discriminative properties of the scale. The CV is calculated by dividing the standard deviation
of the score by the mean of the score. Higher values for CV indicate a better ability to detect
differences between individuals.
Results
Response rate and sample characteristics
A postal survey was sent to 185 patients with PD and 112 controls. One-hundred-forty-three
patients returned their questionnaires. One questionnaire had more than 20% missing data and
was excluded. Thus 142 usable questionnaires remained, constituting a response rate of
76.7%. One-hundred-and-four controls returned their questionnaires. Four questionnaires
were excluded because the age difference with the corresponding patient was more than 10
years. Therefore, 100 usable questionnaires (89.3%) were available for analysis. Fifty-six of
the 60 patients that returned their questionnaire within one week, completed the SCOPA-
SLEEP a second time. One questionnaire was subsequently removed from the analysis
because too much data were missing, leaving a response rate of 91.7%.
Differences between responders and non-responders in the patient group were not significant
for disease severity and age, but the proportion of women among the non-responders was
significantly higher (p < 0.05). The mean disease duration of the patients was 9.9 years (table
1). Disease severity was mild in 61 patients (43.0%), moderate in 52 patients (36.6%), and
severe in 29 patients (20.4%). The male-female ratio did not differ significantly between
patients and controls (p = 0.053), but controls were significantly younger.

Chapter 10
- 168 -
Table 1. Characteristics of participants
Patients Controls p
n 142 100
% male 60.5 48.0 0.0531
mean (SD) age (years) 65.6 (10.8) 61.4 (11.2) 0.0042
H&Y 1 4 (2.8%)
H&Y 2 57 (40.1%)
H&Y 3 52 (36.6%)
H&Y 4 26 (18.3%)
H&Y 5 3 (2.1%)
mean (SD) disease duration (years) 9.9 (5.4)
n on levodopa 73 (51%)
mean (SD) levodopa dose in users (mg) 665 (361)
n on dopamine agonists 60 (42%)
n on levodopa + dopamine agonists 54 (38%)
n on sleep medication 27 (19%) 7 (7%) < 0.0011
1 Chi-square test 2 t-test
Scale evaluation
Data quality and score distribution. The quality of the data was good. None of the items had
missing values in more than 10% of the patients, indicating good acceptability. All item-total
correlations exceeded 0.20. Patients used the full score range in both scales. Twenty-five
patients (17.7%) had a sumscore of 0 in the NS scale, whereas 2 patients (1.4%) scored 15.
Seventeen patients (12.1%) had a sumscore of 0 in the DS scale, whereas one patient (0.7%)
scored 18.
Reliability. Cronbach α for the NS subscale was 0.88, with corrected item-scale correlations
ranging from 0.48-0.85 (table 2). Test-retest reliability for the sumscore of this scale was 0.94
(ICC), whereas Kw for items ranged from 0.82-0.90. Cronbach α for the DS subscale was
0.91, with corrected item-scale correlations between 0.55 and 0.88. The ICC for the sumscore
of DS was 0.89, with Kw for items ranging from 0.49-0.82.

Sleep and sleepiness in Parkinson’s disease
- 169 -
Table 2. Reliability of SCOPA-SLEEP scales in patient group
Cronbach α item-total1 ICC sum2 Kw items3
SCOPA-NS (night-time sleep) 0.88 0.48-0.85 0.94 0.82-0.94
1: difficulty falling asleep 0.48 0.90
2: been awake too often 0.77 0.82
3: lying awake too long 0.85 0.86
4: waking too early 0.72 0.83
5: had too little sleep 0.77 0.90
Overall sleep quality N/A N/A N/A 0.91
Pittsburgh Sleep Quality Iindex 0.77 0.27-0.71 * *
SCOPA-DS (daytime sleepiness) 0.91 0.55-0.88 0.89 0.49-0.82
1: falling asleep unexpectedly 0.88 0.79
2: falling asleep while sitting 0.86 0.78
3: falling asleep while watching TV 0.82 0.81
4: falling asleep while talking 0.55 0.78
5: difficulty staying awake 0.76 0.82
6: falling asleep considered a problem 0.64 0.49
Epworth Sleepiness Scale 0.86 0.56-0.71 * *
1 corrected item-total correlations; 2 intraclass correlation coefficient for the sumscore (calculated over 2 week
interval); 3 weighted kappa of items, calculated over 2 week interval; * reproducibility not assessed for this scale;
N/A = not applicable
Validity. The scores on all items of both parts of the SCOPA-SLEEP differed significantly
between patients and controls, with the exception of item NS1 (difficulty falling asleep) (table
3). Responses to seven of the eight additional questions also differed significantly between
patients and controls (all p-values < 0.001). The one exception again concerned sleep
initiation, with both groups indicating similar amounts of time before falling asleep.
Sumscores of patients and controls differed significantly on all included sleep scales (table 4).
The correlation between NS and the PSQI sumscore in the patient group was 0.83 (p < 0.001)
and the correlation with the separate subscales of the PSQI ranged from 0.38–0.73 (all p-
values < 0.001). The correlation between NS and the 'global sleep quality score' was 0.85 (p <
0.001), whereas this was 0.78 (p < 0.001) for the PSQI with the global score. The correlation
between the DS scale and the ESS in the patient group was 0.81 (p < 0.001). No significant
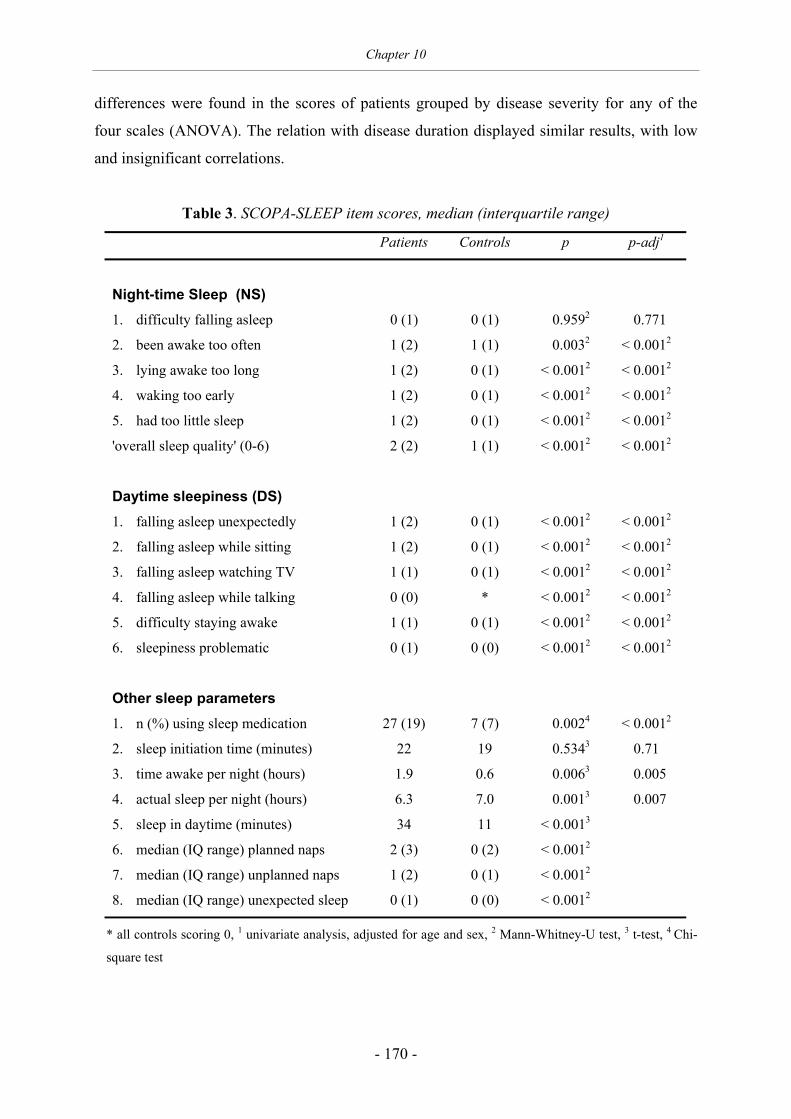
Chapter 10
- 170 -
differences were found in the scores of patients grouped by disease severity for any of the
four scales (ANOVA). The relation with disease duration displayed similar results, with low
and insignificant correlations.
Table 3. SCOPA-SLEEP item scores, median (interquartile range)
Patients Controls p p-adj1
Night-time Sleep (NS)
1. difficulty falling asleep 0 (1) 0 (1) 0.9592 0.771
2. been awake too often 1 (2) 1 (1) 0.0032 < 0.0012
3. lying awake too long 1 (2) 0 (1) < 0.0012 < 0.0012
4. waking too early 1 (2) 0 (1) < 0.0012 < 0.0012
5. had too little sleep 1 (2) 0 (1) < 0.0012 < 0.0012
'overall sleep quality' (0-6) 2 (2) 1 (1) < 0.0012 < 0.0012
Daytime sleepiness (DS)
1. falling asleep unexpectedly 1 (2) 0 (1) < 0.0012 < 0.0012
2. falling asleep while sitting 1 (2) 0 (1) < 0.0012 < 0.0012
3. falling asleep watching TV 1 (1) 0 (1) < 0.0012 < 0.0012
4. falling asleep while talking 0 (0) * < 0.0012 < 0.0012
5. difficulty staying awake 1 (1) 0 (1) < 0.0012 < 0.0012
6. sleepiness problematic 0 (1) 0 (0) < 0.0012 < 0.0012
Other sleep parameters
1. n (%) using sleep medication 27 (19) 7 (7) 0.0024 < 0.0012
2. sleep initiation time (minutes) 22 19 0.5343 0.71
3. time awake per night (hours) 1.9 0.6 0.0063 0.005
4. actual sleep per night (hours) 6.3 7.0 0.0013 0.007
5. sleep in daytime (minutes) 34 11 < 0.0013
6. median (IQ range) planned naps 2 (3) 0 (2) < 0.0012
7. median (IQ range) unplanned naps 1 (2) 0 (1) < 0.0012
8. median (IQ range) unexpected sleep 0 (1) 0 (0) < 0.0012
* all controls scoring 0, 1 univariate analysis, adjusted for age and sex, 2 Mann-Whitney-U test, 3 t-test, 4 Chi-
square test

Sleep and sleepiness in Parkinson’s disease
- 171 -
There were no significant differences in any of the four scale scores between patients who
used levodopa and those who did not. We also found no significant correlation between the
levodopa dose and any of the scale scores in those patients that took levodopa. Scores on both
scales that evaluated daytime sleepiness were higher for patients taking dopamine agonists,
with differences reaching significance in the ESS (8.8 versus 5.9; p = 0.04), but not in the DS
(5.9 versus 4.1; p = 0.07). Subjects who used sleep medication had significantly higher NS
and PSQI scores in both the patient and the control group (p < 0.001), but differences in DS
and ESS scores were not significant.
If the proposed PSQI cut-off value (5/6) was used to discriminate between good and bad
sleepers, 106 subjects (29 controls and 77 patients, i.e., 43.8% of the total sample) were
considered poor sleepers. Using this PSQI cut-off as an external criterion for the NS subscale,
resulted in an area under the receiver operating characteristic (ROC) of 0.90, with an optimal
cut-off at 3/4, yielding a sensitivity of 0.82 and specificity of 0.84. Since we considered the
proportion of subjects with poor sleep by this criterion in both groups exceptionally high, we
also used responses to the 'global sleep quality' item as a criterion. This learned that only 32
subjects (3 controls, 29 patients) actually considered themselves poor sleepers, a finding that
agrees better with the literature.1,25,26 If this global item was used to separate patients who
slept badly (scores 4-6) from those who did not (scores 0-3), the best cut-off point for the NS
subscale was 6/7, with an area under the ROC curve in patients of 0.94. This cut-off value
showed a sensitivity of 0.97 and a specificity of 0.80. Using this same 'global sleep quality
criterion' for the PSQI, suggested that a cut-off of 8/9 would be more appropriate, both in
patients and in all subjects, resulting in an area under the ROC curve of 0.91, with a
sensitivity of 0.93 and a specificity of 0.76.
Three controls and 38 patients had an ESS score ≥ 11, whereas none of the controls and 16 of
the patients scored ≥ 16. Using the cut-off value of 10/11 to separate persons with excessive
daytime sleepiness from those without, indicated an optimal cut-off value of 4/5 for the
SCOPA-DS. The area under the ROC curve was 0.93, with a sensitivity of 0.90 and a
specificity of 0.82.

Chapter 10
- 172 -
Table 4. Sumscores of patients and controls
Patients Controls p-adj1 CV2
mean (SD) SCOPA-NS (night-time sleep) 4.9 (4.0) 2.8 (2.7) < 0.001 0.82
mean (SD) Pittsburgh Sleep Quality Index 7.2 (4.3) 4.5 (3.3) < 0.001 0.70
mean (SD) SCOPA-DS (daytime sleepiness) 5.2 (4.1) 2.1 (2.0) < 0.001 0.79
mean (SD) Epworth Sleepiness Scale 7.9 (5.3) 4.1 (3.2) < 0.001 0.67
1 univariate analysis of variance, adjusted for age and sex 2 Coefficient of Variation, i.e., the standard deviation of the score divided by the mean of the score; higher
values of CV indicate better ability to detect differences between individuals
Factor analysis of the SCOPA-NS revealed one factor, accounting for 68.1% of the variance.
For the DS subscale also one factor emerged, explaining 69.1% of the variance. The factor
analysis of the PSQI was performed on the seven subscales, which produced two factors
accounting for 58.7% of the variance, with the sleep pattern related items (quality, duration,
efficiency, and latency) loading on one factor, and daytime dysfunction and sleep
disturbances loading on the other. The ESS also revealed two factors, together explaining 63.4
%. Items that addressed the more private situations at home (items 1, 2, 5, and 7) loaded on
one factor, whereas items that evaluated more 'public' situations (car, public places, talking to
someone; items 3, 4, 6, and 8) loaded on the other.
The CV of both the NS and the DS scales were higher than those of the PSQI and the ESS
(table 4).
Discussion
We developed a short questionnaire for the assessment of sleep problems in patients with PD,
consisting of two scales, one that evaluates night-time sleep (NS) and one that assesses
daytime sleepiness (DS). The scales displayed good acceptability, and substantial floor and
ceiling effects were absent. Both scales revealed good internal consistency and
reproducibility, indicating reliability for both scales. Patients with PD had significantly higher
scores than controls on both scales. Correlation with other scales that address similar
constructs was high, giving support to the construct validity of the SCOPA-SLEEP. The
factor analysis revealed one factor for each SCOPA scale, indicating that the scales each
measure one construct, therewith justifying the calculation of sumscores. The coefficient of

Sleep and sleepiness in Parkinson’s disease
- 173 -
variation of both SCOPA scales was higher than that of the PSQI and the ESS, indicating a
better ability to detect differences between individuals. Responsiveness of the SCOPA scales
remains to be evaluated.
Assessment of night-time sleep. Studies in other populations showed that the PSQI has
adequate reliability and validity.10,27-30 For internal consistency this was confirmed by the
results of our study. The scale has previously been used in PD.31-33 Some comments regarding
the PSQI are in order, however. First, the content validity of the PSQI may be questioned,
especially with respect to use in PD. The PSQI evaluates daytime dysfunction, but problems
in this area can often be explained by symptoms of PD. The score on the 'daytime
dysfunction' subscale is made up of two items, i.e., 'enthusiasm to get things done' (which
could be affected by PD or by depression, present in approximately 25% of the patients with
PD34) and 'trouble staying awake' (which could be caused by PD or by the effect of
antiparkinsonian medication). Second, the incorporation of 'trouble staying awake' and taking
sleep medication' in the sumscore is questionable. These items address a clearly different
construct than the other items, that evaluate aspects of sleep pattern. This is partially
confirmed by the factor analysis, in which daytime dysfunction (together with sleep
disturbances) loads on one factor, whereas the other, sleep pattern related items (quality,
duration, efficiency, and latency) load on the other. Third, calculating the sumscore of the
PSQI is time-consuming, which makes it less suitable for clinical application. These
arguments favor the use of the SCOPA-NS in patients with PD. Additionally, if the PSQI is
used in patients with PD, a higher cut-off may be more appropriate.
Assessment of daytime sleepiness. Studies in other populations have shown that the test-retest
reliability and internal consistency of the ESS are adequate.15,35-37 The scale has shown to
discriminate successfully between healthy controls and patients with sleep disorders. The ESS
has frequently been used in PD.8,9,31,38-45 Two comments regarding the use of the ESS are in
place. First, patients are asked to rate the chance of dozing, without actually having to have
had the experience of dozing off in that particular situation. Three of the situations described
in the ESS (sitting inactive in a public place, as a passenger in a car for an hour without a
break, and in a car while stopped for a few minutes) may actually be experienced infrequently
by the more severely affected or older patients, which may further compromise the patient's
appraisal of the situation. Second, both in the patient and the control group two factors
emerged, suggesting that the scale does not measure one construct. The SCOPA-DS may
therefore be preferred in this population, since it does not have the aforementioned objections.

Chapter 10
- 174 -
The first disease-specific sleep scale in PD, the Parkinson's Disease Sleep Scale (PDSS),11
was published very recently and evaluates various aspects of nocturnal sleep problems.
Unfortunately, this publication appeared after we finished our data collection and hence this
scale was not included in our study. A direct comparison of these two disease-specific scales
would have produced valuable information. The PDSS includes 15 items that evaluate overall
sleep quality (1 item), insomnia (2 items), potential reasons of sleep disturbances (6 items),
motor symptoms (4 items), sleep refreshment (1 item), and daytime dozing (1 item). Patients
indicate on a 10 cm visual analogue scale (VAS) how well they slept or how often the
described items applied to them, based on their experience during the past week. On face
value, the scale appears to measure various constructs. A thorough clinimetric evaluation has
not been published yet. Internal consistency and factor analysis were not reported, therewith
ruling out the possibility to judge whether the calculation of sumscores is justified. The
reproducibility of this scale seems adequate, but was only assessed in 15 patients. The relation
with other scales was only assessed by calculating the correlation between one item of this
scale (unexpectedly falling asleep during the day) and a scale that addresses daytime
sleepiness (ESS), but not with scales that evaluate nocturnal sleep problems.
In conclusion, sleep problems occur frequently in PD and deserve appropriate attention.
However, patients with PD may experience problems in many domains that all may have to
be considered and, consequently, short and practical instruments have considerable
advantages. These instruments allow rapid detection of areas that need further attention. It is
nevertheless essential that these instruments have good clinimetric properties. The SCOPA-
SLEEP scale fulfils these criteria, and may therefore be included in the assessment schedule
of patients with this condition.
Acknowledgements Professor R.A.C. Roos is gratefully acknowledged for reviewing the manuscript. This study
was financed by the Netherlands Organization for Scientific Research (project number 0940-
33-021).

Sleep and sleepiness in Parkinson’s disease
- 175 -
References
1. Tandberg E, Larsen JP, Karlsen K. A community-based study of sleep disorders in patients with
Parkinson's disease. Mov Disord 1998;13:895-899.
2. Tandberg E, Larsen JP, Karlsen K. Excessive daytime sleepiness and sleep benefit in Parkinson's disease:
a community-based study. Mov Disord 1999;14:922-927.
3. Factor SA, McAlarney T, Sanchez-Ramos JR, Weiner WJ. Sleep disorders and sleep effect in Parkinson's
disease. Mov Disord 1990;5:280-285.
4. Caap-Ahlgren M, Dehlin O. Insomnia and depressive symptoms in patients with Parkinson's disease.
Relationship to health-related quality of life. An interview study of patients living at home. Arch Gerontol
Geriatr 2001;32:23-33.
5. Pal PK, Calne S, Samii A, Fleming JAE. A review of normal sleep and its disturbances in Parkinson's
disease. Parkinsonism Relat Disord 1999;5:1-17.
6. Smith MC, Ellgring H, Oertel WH. Sleep disturbances in Parkinson's disease patients and spouses. J Am
Geriatr Soc 1997;45:194-199.
7. Frucht S, Rogers JD, Greene PE, Gordon MF, Fahn S. Falling asleep at the wheel: motor vehicle mishaps
in persons taking pramipexole and ropinirole. Neurology 1999;52:1908-1910.
8. Chaudhuri KR, Pal S, Brefel-Courbon C. 'Sleep attacks' or 'unintended sleep episodes' occur with
dopamine agonists: is this a class effect? Drug Saf 2002;25:473-483.
9. Hobson DE, Lang AE, Martin WR, Razmy A, Rivest J, Fleming J. Excessive daytime sleepiness and
sudden-onset sleep in Parkinson disease: a survey by the Canadian Movement Disorders Group. JAMA
2002;287:455-463.
10. Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a
new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193-213.
11. Chaudhuri KR, Pal S, DiMarco A, Whately-Smith C, Bridgman K, Mathew R, et al. The Parkinson's
disease sleep scale: a new instrument for assessing sleep and nocturnal disability in Parkinson's disease. J
Neurol Neurosurg Psychiatry 2002;73:629-635.
12. Hoddes E, Zarcone V, Smythe H, Phillips R, Dement WC. Quantification of sleepiness: a new approach.
Psychophysiology 1973;10:431-436.
13. Gillberg M, Kecklund G, Akerstedt T. Relations between performance and subjective ratings of sleepiness
during a night awake. Sleep 1994;17:236-241.
14. Jenkins CD, Stanton BA, Niemcryk SJ, Rose RM. A scale for the estimation of sleep problems in clinical
research. J Clin Epidemiol 1988;41:313-321.
15. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep
1991;14:540-545.
16. Ellis BW, Johns MW, Lancaster R, Raptopoulos P, Angelopoulos N, Priest RG. The St. Mary's Hospital
sleep questionnaire: a study of reliability. Sleep 1981;4:93-97.
17. Douglass AB, Bornstein R, Nino-Murcia G, Keenan S, Miles L, Zarcone Jr VP, et al. The Sleep Disorders
Questionnaire. I: Creation and multivariate structure of SDQ. Sleep 1994;17:160-167.
18. Parrott AC, Hindmarch I. The Leeds Sleep Evaluation Questionnaire in psychopharmacological
investigations - a review. Psychopharmacology (Berl) 1980;71:173-179.
Chapter 10
- 176 -
19. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease.
J Neurol Neurosurg Psychiatry 1988;51:745-752.
20. Thommessen B, Aarsland D, Braekhus A, Oksengaard AR, Engedal K, Laake K. The psychosocial
burden on spouses of the elderly with stroke, dementia and Parkinson's disease. Int J Geriatr Psychiatry
2002;17:78-84.
21. Johns MW. Sensitivity and specificity of the multiple sleep latency test (MSLT), the maintenance of
wakefulness test and the Epworth Sleepiness Scale: failure of the MSLT as a gold standard. J Sleep Res
2000;9:5-11.
22. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17:427-442.
23. The World Health Organization Quality of Life Assessment (WHOQOL): development and general
psychometric properties. Soc Sci Med 1998;46:1569-1585.
24. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use.
2 ed. Oxford: Oxford Medical Publications, 1995.
25. Lees AJ, Blackburn NA, Campbell VL. The nighttime problems of Parkinson's disease. Clin
Neuropharmacol 1988;11:512-519.
26. Nausieda PA, Weiner WJ, Kaplan LR, Weber S, Klawans HL. Sleep disruption in the course of chronic
levodopa therapy: an early feature of the levodopa psychosis. Clin Neuropharmacol 1982;5:183-194.
27. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the
Pittsburgh Sleep Quality Index in primary insomnia. J Psychosom Res 2002;53:737.
28. Carpenter JS, Andrykowski MA. Psychometric evaluation of the Pittsburgh Sleep Quality Index. J
Psychosom Res 1998;45(1 Spec No):5-13.
29. Fictenberg NL, Putnam SH, Mann NR, Zafonte RD, Millard AE. Insomnia screening in postacute
traumatic brain injury: utility and validity of the Pittsburgh Sleep Quality Index. Am J Phys Med Rehabil
2001;80:339-345.
30. Gentili A, Weiner DK, Kuchibhatla M, Edinger JD. Test-retest reliability of the Pittsburgh sleep quality
index in nursing home residents. J Am Geriatr Soc 1995;43:1317-1318. Letter.
31. Fabbrini G, Barbanti P, Aurilia C, Vanacore N, Pauletti C, Meco G. Excessive daytime sleepiness in de
novo and treated Parkinson's disease. Mov Disord 2002;17:1026-1030.
32. Iranzo A, Valldeoriola F, Santamaria J, Tolosa E, Rumia J. Sleep symptoms and polysomnographic
architecture in advanced Parkinson's disease after chronic bilateral subthalamic stimulation. J Neurol
Neurosurg Psychiatry 2002;72:661-664.
33. Shulman LM, Taback RL, Bean J, Weiner WJ. Comorbidity of the nonmotor symptoms of Parkinson's
disease. Mov Disord 2001;16:507-510.
34. Cummings JL. Depression and Parkinson's disease: a review. Am J Psychiatry 1992;149:443-454.
35. Bloch KE, Schoch OD, Zhang JN, Russi EW. German version of the Epworth Sleepiness Scale.
Respiration 1999;66:440-447.
36. Johns MW. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 1992;15:376-381.
37. Johns MW. Sleepiness in different situations measured by the Epworth Sleepiness Scale. Sleep
1994;17:703-710.

Sleep and sleepiness in Parkinson’s disease
- 177 -
38. Ondo WG, Dat VK, Khan H, Atassi F, Kwak C, Jankovic J. Daytime sleepiness and other sleep disorders
in Parkinson's disease. Neurology 2001;57:1392-1396.
39. Tan EK, Lum SY, Fook-Chong SM, Teoh ML, Yih Y, Tan L, et al. Evaluation of somnolence in
Parkinson's disease: Comparison with age- and sex-matched controls. Neurology 2002;58:465-468.
40. Arnulf I, Konofal E, Merino-Andreu M, Houeto JL, Mesnage V, Welter ML, et al. Parkinson's disease and
sleepiness: An integral part of PD. Neurology 2002;58:1019-1024.
41. Pal S, Bhattacharya KF, Agapito C, Chaudhuri KR. A study of excessive daytime sleepiness and its
clinical significance in three groups of Parkinson's disease patients taking pramipexole, cabergoline and
levodopa mono and combination therapy. J Neural Transm 2001;108:71-77.
42. Ondo WG, Vuong KD, Jankovic J. Exploring the relationship between Parkinson disease and restless legs
syndrome. Arch Neurol 2002;59:421-424.
43. Nieves AV, Lang AE. Treatment of excessive daytime sleepiness in patients with Parkinson's disease with
modafinil. Clin Neuropharmacol 2002;25:111-114.
44. O'Suilleabhain PE, Dewey Jr RB. Contributions of dopaminergic drugs and disease severity to daytime
sleepiness in Parkinson disease. Arch Neurol 2002;59:986-989.
45. Moller JC, Stiasny K, Hargutt V, Cassel W, Tietze H, Peter JH, et al. Evaluation of sleep and driving
performance in six patients with Parkinson's disease reporting sudden onset of sleep under dopaminergic
medication: a pilot study. Mov Disord 2002;17:474-481.

Chapter 10
- 178 -
APPENDIX
SCOPA-SLEEP scale
Aim of the questionnaire
By means of this questionnaire, we would like to find out to what extent in the past month you have had
problems with sleeping. Some of the questions are about problems with sleeping at night, such as, for example,
not being able to fall asleep or not managing to sleep on. Another set of questions is about problems with
sleeping during the day, such as dozing off (too) easily and having trouble staying awake.
First read these instructions before you answer the questions!
Place a cross in the box above the answer which best reflects your situation. If you wish to change an answer, fill
in the ‘wrong’ box and place a cross in the correct one. If you have been using sleeping tablets, then the answer
should reflect how you have slept while taking these tablets.
NS: Night-time sleep problems
response options: not at all – a little – quite a bit – a lot
In the past month, … 1. … have you had trouble falling asleep when you went to bed at night?
2. … to what extent do you feel that you have woken too often?
3. … to what extent do you feel that you have been lying awake for too long at night?
4. … to what extent do you feel that you have woken up too early in the morning?
5. … to what extent do you feel you have had too little sleep at night?
Overall, how well have you slept at night during the past month?
response options: very well – well – rather well – not well but not badly - rather badly – badly - very badly
DS: Daytime sleepiness
response options: never – sometimes – regularly – often
1. How often in the past month have you fallen asleep unexpectedly either during the day or in the evening?
2. How often in the past month have you fallen asleep while sitting peacefully?
3. How often in the past month have you fallen asleep while watching TV or reading?
4. How often in the past month have you fallen asleep while talking to someone?
5. In the past month, have you had trouble staying awake during the day or in the evening?
6. In the past month, have you experienced falling asleep during the day as a problem?

- 179 -
1111 A short psychosocial questionnaire for patients with
Parkinson’s disease: the SCOPA-PS
Johan Marinus1, Martine Visser1, Pablo Martínez-Martín2, Jacobus J. van Hilten1, Anne M.
Stiggelbout3
Departments of 1Neurology and 3Medical Decision Making, Leiden University Medical Center,
Leiden, The Netherlands; 2Neuroepidemiology Unit, Department of Applied Epidemiology, National
Center for Epidemiology I.S. Carlos III, Madrid, Spain
Published in the Journal of Clinical Epidemiology 2003;56:61-67

Chapter 11
- 180 -
Abstract Purpose. To develop a short questionnaire for psychosocial functioning in patients with Parkinson’s
Disease (PD). Methods. The SCales for Outcomes in PArkinson's disease - PsychoSocial
questionnaire (SCOPA-PS) was tested in a survey and compared with other instruments and with
medical information. This survey was sent to 205 patents with idiopathic PD. Results. Eighty-six
percent of the questionnaires were returned. Cronbach’s α was 0.83. Two-week test-retest reliability
was 0.85 (intraclass correlation coefficient). Construct validity with other scales (Spearman's rho) was
0.82 for the Parkinson’s Disease Questionnaire - 39 item version (PDQ-39), 0.76 for the PDQ-8, 0.69
for the Hospital Anxiety and Depression Scale, -0.61 for the Euroqol, and -0.60 for a visual analogue
scale evaluating Quality-of-Life. The summary index revealed a significant increase with increasing
disease severity. Conclusions. The SCOPA-PS is a new, short psychosocial questionnaire for patients
with PD with good clinimetric properties.
Keywords: Parkinson disease, Quality of Life, Clinimetrics, Psychosocial, SCOPA

Psychosocial questionnaire for Parkinson’s disease
- 181 -
Introduction Parkinson's disease (PD) is a chronic, progressive, neurological disorder that affects almost
two percent of the population over 65 years of age.1 The onset of the disease generally occurs
between the ages of 50 and 65, and the incidence increases with higher age. PD is
characterized by tremor, rigidity, slowness of movement, and abnormalities of posture. Non-
motor features like autonomic dysfunctions, mood changes, and cognitive deterioration often
complicate the course of the disease.
Chronic progressive illnesses like PD can have a considerable impact on the psychosocial
functioning of patients. Yet in PD, this impact is seldom evaluated separately. The
psychosocial consequences of PD are usually assessed with generic or disease-specific
health-related quality-of-life (HRQoL) instruments that include physical items in addition to
items that address psychosocial functioning. HRQoL is generally considered to consist of
physical, mental, and social (including 'role') aspects of a disease.2 Item selection in HRQoL
scales is usually based on interviews with patients, in which patients are asked to rate the
importance of certain features of the disease, and where the most relevant items are retained
for the final version of the scale. Consequently, HRQoL instruments consist of a mixture of
items that only have in common that patients consider them important, and that either
physical, mental, or social aspects are evaluated. Additionally, these instruments often
include items that address impairment levels and items that address disability levels, which
further adds to the heterogeneity. It is often far from clear whether patients interpret certain
impairments as being 'physical' or 'psychosocial'. If, for instance, a patient indicates that he
often has trouble with the shaking of his hands, this could mean he experiences trouble with
dressing (physical), feels ashamed (psychosocial), or both. Therefore, including items that
evaluate the extent to which patients are bothered by impairments, provides no direct insight
in the impact this impairment has upon the level of psychosocial functioning. However, the
distinction between physical and psychosocial is important. First, separate information on the
psychosocial consequences may provide a better understanding of the different consequences
of the disease to an individual. Second, neurologists may, because of their professional focus
on physical consequences of the disease, interpret particular problems somatically and hence
overlook psychosocial difficulties. Third, the distinction between physical and psychosocial
consequences may have implications for the choice of an intervention. After all, if the
difficulties are predominantly experienced at the physical level, this may call for
interventions that aim to improve motor functions, e.g., pharmacotherapy or physical therapy.
Although people with psychosocial difficulties will also benefit from optimally controlled

Chapter 11
- 182 -
motor symptoms, additional support from other healthcare providers, such as psychologists or
social workers, may be indicated. To quantify the psychosocial impact of PD, an instrument
that only includes items that directly address perceived emotions and experienced difficulties
in social situations is needed.
To date, a short, clinimetrically sound scale that evaluates this psychosocial impact of PD is
not available. We therefore conducted a study with the objective to develop a short
psychosocial instrument for patients with PD, and to evaluate its reliability (internal
consistency, test-retest reliability) and validity (construct validity, 'known-groups
comparisons').
The development of the SCOPA psychosocial questionnaire (SCOPA-PS) is part of a larger
research project, the SCales for Outcomes in PArkinson’s disease (SCOPA), in which short,
practical, and clinimetric sound scales for all relevant domains in PD are selected or
developed.
Methods
Scale construction
Information on topics that were relevant for inclusion in the SCOPA-PS was derived from
two studies that evaluated the content validity of disease-specific HRQoL instruments in
PD.3,4 Next, articles that included information on the relevance of items to patients with PD
(frequency of occurrence, severity of problems, frequency-severity products, item-total
correlations) were studied.5-7 Items were included in the SCOPA-PS if they concerned social
or emotional consequences of PD, were comprehensive, and were important to patients. In
order for a short scale to have good content validity, items had to cover a broad area. This
was achieved by a less specific formulation of items, or by combining more than one element
into an item. The items were written to address the disability or handicap level. Together the
items aimed to cover the psychosocial domain in PD. The initial scale was piloted until no
further problems were encountered and patients understood all items well. This resulted in a
scale of 11 items, which evaluated the severity of a particular problem during the past month
on a scale from 0 (not at all) to 3 (very much). The scale was developed in Dutch, but an
English translation is also available (appendix). The scale can be used free of charge and is
available from the first author.

Psychosocial questionnaire for Parkinson’s disease
- 183 -
Patients
All patients that were registered at the outpatient neurology clinic of the Leiden University
Medical Center on 1 January 2001, and who fulfilled the United Kingdom Parkinson's
Disease Society Brain Bank criteria for idiopathic PD,8 were considered eligible. Patients
with other disorders of the central nervous system, and patients that were not capable of
reading or understanding Dutch, were excluded. Response was interpreted as consent to
participate.
Methods
A postal survey was sent to the 205 patients that fulfilled the aforementioned criteria. The
survey included the SCOPA-PS, the Parkinson’s Disease Questionnaire (PDQ-39),6 the PDQ-
8,9 the Euroqol (EQ-5D),10 the Hospital Anxiety and Depression Scale (HADS),11 and a
visual analogue scale (VAS) assessing HRQoL with PD. The PDQ-39 is a disease-specific
HRQoL instrument with five ordinal response options that includes 39 items, clustered in
eight subscales (mobility, activities of daily living, emotional well-being, stigma, social
support, cognitions, communication, and bodily discomfort). Summary indices can be
calculated both for the subscales and for the total scale. The scale addresses a conceptually
related (though not identical) construct. The PDQ-8 is the short version of the PDQ-39,
constructed by the developers by selecting the items with the highest item-total correlation
from each of the eight subscales. The EQ-5D is a short generic HRQoL instrument that
consists of five items (mobility, self-care, usual activities, pain/discomfort, and
anxiety/depression) with three ordinal response options. A summary index with a maximum
score of 1.00 (reflecting the best health state) can be derived from the five dimensions by
conversion with a table of scores.10,12 The scale was previously shown to perform well in a
population of patients with PD.13 The HADS was included because patients with PD show
elevated levels of anxiety and depression, and because depression accounts for approximately
50 percent of the variance in HRQoL in this patient group.14-16 The HADS has fourteen items,
with seven items addressing depression and seven anxiety. Scores on individual items can
either be summed to calculate a total score, or summed per subscale to produce separate
anxiety and depression scores. Each item has four graded response options, scored 0
(absence) to 3 (present to extreme).
Patients were requested to fill out the PDQ-39 first and to seal it into one of the two enclosed
return envelopes, before completing the other scales. This was done because some of the
items in the PDQ-39 resembled items in other instruments, and we wanted to ensure that
Chapter 11
- 184 -
patients did not check their previous responses, in order to avoid overestimation of the
correlation between scales. Patients were asked to return the completed questionnaires within
one week. After two weeks we contacted those patients that had not returned their
questionnaires, and inquired whether they still considered participating. All patients that
returned the questionnaires within five days, were asked to fill out the SCOPA-PS a second
time two weeks later, in order to assess test-retest reliability.
Information from the questionnaires was combined with information on disease duration and
disease severity obtained by chart review. Disease severity was evaluated with the Hoehn and
Yahr (H&Y) staging system17 at each control visit. H&Y 1 is the mildest stage with only
unilateral symptoms, whereas H&Y 5 represents the most severe stage, in which patients are
wheelchair-bound or bed-ridden.
The study protocol was approved by the institutional review board.
Statistical analysis
Data quality. Items were considered to perform adequately when they met the following
criteria: missing values in less than 5% of the patients, item-total correlation of 0.20 or
higher,18 and absence of floor and ceiling effects of individual items (endorsement rates
between 0.20 and 0.80).18
First a sum score was computed by adding the scores on the individual items, and then a
summary index (SI) was calculated by transformation of this sum score to a 0-100 scale.
Higher scores reflected greater psychosocial difficulties.
Reliability. Internal consistency was assessed using Cronbach’s α. The test-retest reliability
for individual items over a two-week interval was assessed with a weighted kappa (Kw;
quadratic weights), whereas for the total score an intraclass correlation coefficient (ICC) was
calculated.
Validity. Construct validity with other scales was assessed using Spearman's correlation
coefficient (rs). This coefficient was also used to assess the correlation between the SCOPA-
PS SI and both disease duration and age. T-tests for independent samples were used to
compare the SCOPA-PS SI of male patients with those of female patients, and to compare the
mean age and disease duration of responders and non-responders. The differences in male-
female ratio and disease severity among responders and non-responders, were assessed using
a Chi-square test and a Mann-Whitney-U test, respectively. The significance threshold was
set at 0.05. 'Known-groups' validity was assessed by comparing the SCOPA-PS SI of patients

Psychosocial questionnaire for Parkinson’s disease
- 185 -
with different disease severities and different levels of anxiety and depression (assessed by
item 5 of the EQ-5D), using ordinal regression.
Results
One-hundred-seventy-seven questionnaires (86%) were returned. The characteristics of the
patients are presented in table 1. Mean age and male-female ratio did not differ between
responders and non-responders. However, non-responders had significantly higher H&Y
stages (p = 0.008) and longer disease duration (12.7 versus 9.4; p = 0.017). The first 59
patients were approached for the test-retest analysis. Fifty-four of these patients (92%)
returned the SCOPA-PS the second time. The patient characteristics of the retest group were
similar to those of the total group.
Table 1. Patient characteristics
number of patients: 177
male / female ratio 99 (56%) / 78 (44%)
mean age (SD) in years: 65.2 (11.1)
mean age at onset (SD) in years: 55.7 (11.6)
mean disease duration (SD) in years: 9.4 (5.6)
Modified Hoehn and Yahr stage: mild (H&Y1 1: 10, H&Y 2: 64): 74 (41.8%)
moderate (H&Y 3): 70 (39.5%)
severe (H&Y 4: 31, H&Y 5: 2): 33 (18.6%)
1 Hoehn and Yahr stage
Data quality. None of the items had missing values in more than 5% of the subjects. There
were no floor or ceiling effects and all item-total correlations exceeded 0.20 (table 2).
Reliability. The internal consistency of the scale, calculated by Cronbach’s α, was 0.83. Item-
total correlations ranged from 0.24 (problems with sexuality) – 0.67 (asking others for help
too often) (table 2). The test-retest reliability (ICC) of the total scale was 0.85. For individual
items the test-retest reliability, measured as a weighted kappa, ranged from 0.46 (problems
getting along with partner, family, or good friends) - 0.83 (problems with sexuality).

Table 2. Frequency distribution and item characteristics
item no. frequency of responses valid1 item-total2 Kw3
0 1 2 3
During the past month, have you ..
1 ..had difficulty with work, household, or other chores? 22 67 60 28 177 0.61 0.69
2 ..had difficulty with hobbies, sport, or leisure activities? 20 72 56 29 177 0.59 0.73
3 ..felt uncertain in your contact with others? 64 79 30 4 177 0.58 0.50
4 ..had problems getting along with your partner, family, or good friends? 122 42 11 2 177 0.34 0.46
5 ..had problems in the area of sexuality? 69 44 36 20 169 0.24 0.83
6 ..felt more house-bound than you would wish to be? 44 62 47 22 175 0.63 0.73
7 ..had the feeling you have had to ask others for help too often? 57 62 40 17 176 0.67 0.61
8 ..felt isolated and lonely? 85 64 21 6 176 0.61 0.71
9 ..had difficulty when having a conversation? 61 77 30 8 176 0.49 0.55
10 ..felt ashamed of your disease? 125 35 12 3 175 0.28 0.65
11 ..been concerned about the future? 30 76 51 20 177 0.49 0.68
1 number of valid responses 2 item-total correlations 3 weighted kappa (quadratic weights) for test-retest reliability of individual items

Psychosocial questionnaire for Parkinson’s disease
- 187 -
Validity. Correlations between the SCOPA-PS SI on the one hand, and the PDQ-39 SI and
PDQ-8 SI on the other hand, were 0.82 and 0.76, respectively. Correlations of the SCOPA-PS
with the HADS, the EQ-5D and the VAS were somewhat lower and remarkably similar to the
correlation of the PDQ-39 with these scales (table 3). The correlation of the SCOPA-PS SI
with the subscales of the PDQ-39 ranged from 0.42 (with the bodily discomfort subscale) to
0.68 (with the emotional well-being subscale). The correlation between both versions of the
PDQ was high, which might be expected since the PDQ-8 was derived from the PDQ-39.
Table 3. Correlation between SCOPA-PS and other scales (Spearman's rho)
PDQ39 SI1 PDQ8 SI1 HADS2 HADS-A3 HADS-D4 EQ-5D SI5 VAS6
SCOPA-PS SI 0.82 0.76 0.69 0.61 0.62 -0.61 -0.60
PDQ39 SI 0.91 0.74 0.69 0.65 -0.69 -0.54
PDQ8 SI 0.74 0.69 0.64 -0.59 -0.46
HADS 0.92 0.88 -0.63 -0.58
HADS-A 0.64 -0.55 -0.49
HADS-D -0.58 -0.56
EQ-5D SI 0.41
NB: all correlations significant (p < 0.001); 1 Parkinson’s Disease Questionnaire Summary Index, 39 and 8 item
version; 2 Hospital Anxiety and Depression Scale; 3 HADS anxiety subscale; 4 HADS depression subscale; 5
Euroqol summary index; 6 Visual analogue scale assessing quality of life.
The mean duration between the H&Y assessments and the time of the survey was 3.5 months.
Because patients in H&Y stages 1 and 5 were underrepresented (10 and 2 patients,
respectively), disease severity was categorised as mild (H&Y 1 and 2), moderate (H&Y 3), or
severe (H&Y 4 and 5). Ordinal regression yielded a good fitting model (Chi-square 45.9,
degrees of freedom 46; p = 0.48) displaying a significant increase in psychosocial disability
with increasing H&Y stages (p < 0.001). The mean SCOPA SI of mildly affected patients
was 25.7 (SD 12.7), whereas for moderately and severely affected patients this was 37.2 (SD
18.7) and 45.1 (SD 18.5), respectively. Ordinal regression of the SCOPA-PS SI on the scores
of the anxiety/depression item of the EQ-5D also displayed a good fitting model (Chi-square

Chapter 11
- 188 -
37.5, degrees of freedom 48; p = 0.86) indicating a significant increase in psychosocial
disability with higher anxiety/depression scores (p < 0.001). The mean SCOPA-SI of patients
scoring 1 (no problem), 2 (some difficulty), or 3 (extreme difficulty) on this item of the EQ-
5D were 26.5 (SD 14.6), 41.1 (SD 17.0), and 63.0 (SD 9.2), respectively.
The SCOPA-PS SI correlated significantly with disease duration (rs = 0.20; p < 0.01), but not
with age (rs = 0.02; p = 0.78). No significant difference in SCOPA-PS SI was observed
between male and female patients.
Discussion
We have developed a short questionnaire that evaluates psychosocial functioning in patients
with PD. The response rate in this study was high and the quality of the data was good.
Patients that participated in this study attended an outpatient movement disorders clinic in the
western part of The Netherlands. This clinic has a regional function and serves patients with a
wide range of disease severities in PD.
The internal consistency and retest reliability of the SCOPA-PS SI were good, and
convergent validity with other scales agreed with our expectations. ‘Known-groups’
comparisons indicated that patients with longer disease duration, higher disease severity, and
elevated levels of anxiety and depression had significantly higher SCOPA-PS scores. Age
and sex were not related to worse outcomes. Although the non-response rate in our study was
low, the SCOPA-PS scores may actually have been somewhat higher, since non-responders
had higher disease severity and longer disease duration and both of these variables were
associated with higher SCOPA-PS scores.
The use of this scale on an individual level is somewhat disputable. The minimum threshold
for reliability in group comparisons is often set at 0.70, whereas for use on the individual
level, generally more stringent demands are made. Nunnally and Bernstein19 state that for
important decisions on an individual level, a reliability of 0.90 is the minimum. Helmstadter20
quotes variable reliability values for various types of psychological tests intended for
individuals, the median for personality tests being 0.85, that for ability tests being 0.90, and
for attitude tests, 0.79. Hays et al.21 state that the 0.90 criterion for individual assessment may
be too stringent and that many highly regarded instruments fail to meet this standard. Since
the SCOPA-PS is not intended for diagnostic purposes (that could involve important
decisions for individuals based on the patient’s score in relation to a cut-off level), the

Psychosocial questionnaire for Parkinson’s disease
- 189 -
demands for internal consistency may be somewhat less stringent. We believe that the scale
can adequately be used for monitoring psychosocial functioning over time, and may serve as
an indicator of areas of potential problems.
All items of the scale had item-total correlations that exceeded the predefined criterion.
However, some items had moderate item-total correlations and will be discussed in more
detail. This concerned item 4 ('getting along with partner, family, or good friends'), item 5
('problems with sexuality') and item 10 ('felt ashamed') with values of 0.32, 0.24, and 0.28,
respectively. We did not consider to remove one or more of these items, because in our view
test characteristics of items should not dominate the item selection process at the expense of
content validity. In this so-called clinimetric approach, it is important that all relevant
attributes of the construct are measured, and hence, content validity and reproducibility are
the most important parameters.22
The moderate item-total correlation for item 4 ('getting along with partner, family, or good
friends') is most likely explained by the low endorsement of this item. To examine whether
this may have been the result of the way this item was framed, we evaluated five different
versions of this item in 30 patients after the postal survey had been completed. However, no
differences between these versions were found, and we therefore decided to retain the
original description. Our findings regarding this item are supported by observations from
various studies on the PDQ-39, in which the 'social support' subscale consistently has been
found to produce the lowest mean score, both in clinic and non-clinic samples, and across
populations from different countries.6,9,14,23,24 This subscale also showed the lowest
correlations with measures of disease severity,6,9,14,25 indicating that progression of the
disease does not greatly affect the quality of close relationships.
The pattern of correlations and endorsement frequencies of item 10 ('felt ashamed') is very
similar to that of item 4 ('problems getting along with partner, family, or good friends').
Seventy-one percent of the patients indicated no problems with respect to this item. In several
studies this item showed low item means,6,14,23,24,26 and its correlation with measures of
disease severity were also moderate (range 0.29-0.33).6,14,23,24,26
The moderate item-total correlation of the item on sexuality may be explained by physical
features of the disease, especially with respect to male patients. Problems with erectile
function may affect up to 60% of males,27 while on the other hand antiparkinsonian
medication may increase libido. Female patients more often report vaginal tightness and
involuntary urination, which may affect the quality of the sexual relationship.28 Evidently,

Chapter 11
- 190 -
these physical problems do not necessarily correlate highly with other psychosocial
consequences of the disease. Although the origin of the problems may be physical, the
consequences for the psychosocial level are considerable and, consequently, an item
addressing this topic should be present in a psychosocial instrument. A large proportion of
our patients (59%) indicated problems in this area. Men had significantly higher scores than
women (item means 1.40 versus 0.56, respectively; p < 0.001), but the severity of the sexual
problems did not correlate significantly with disease severity or age.
Several disease-specific HRQoL instruments have become available in PD in the past few
years.5-7,9,29,30 These scales include items on physical, mental, and social aspects of the
disease. The instruments usually inquire how often patients had difficulty with certain aspects
of the disease, and often include both impairments and disabilities. As far as the impairments
are concerned, it is not always clear whether these difficulties are of a physical or a
psychosocial nature. We therefore propose to disentangle these levels by using separate
instruments to assess physical and psychosocial functions. These separate measures may
produce more meaningful and conceptually clear indices. Instruments that assess physical
disabilities in PD already exist,31-33 but to date a short scale that evaluates the psychosocial
consequences of PD was not available.
One could argue that the separate subscales of the two most frequently used disease-specific
HRQoL scales in PD, the PDQ-396 and the Parkinson's Disease Quality-of-Life questionnaire
(PDQL),5 may be used, since the PDQ-39 has subscales on emotional well-being, stigma,
social support, and communication, while the PDQL has both a social and an emotional
subscale. Apart from the fact that it is unusual to use only subscales of an instrument and that
the involved subscales of both instruments would still consist of 16 items each, other
arguments favour the use of the SCOPA-PS. As far as the PDQ-39 is concerned, both internal
consistency and test-retest reliability of the social support subscale have been found to be low
(Cronbach’s α and Pearson’s r < 0.70) in some studies,6,34 whereas role functioning is only
marginally addressed and sexuality is not addressed at all in this scale.3 The PDQL on the
other hand, provides no information on two important psychosocial items, viz. close
relationships and role functioning.
If the basic assumption is to select a short disease-specific instrument, the SCOPA-PS may be
preferred over the other currently available short HRQoL instruments, the Parkinson’s Impact
Scale (PIMS, 10 items)29 and the PDQ-8,9 because of the potential problems with respect to

Psychosocial questionnaire for Parkinson’s disease
- 191 -
content validity of these scales. The items in the PIMS were obtained by consensus between
specialised nurses and did not involve patients in the item generation phase. The PDQ-8 was
obtained through statistical procedures in which the item with the highest item-total
correlation in each of the eight subscales of the PDQ-39 was selected for the short version.
This approach may lead to a scale that does not reflect the content of the original scale
adequately. In the PDQ-8 engagement in work, household, and leisure activities is not
assessed, while items on sexuality and role functioning are also lacking. Furthermore, the
internal consistency of the PDQ-8 was somewhat low in our study (Cronbach's α 0.74).
Taken together, the SCOPA-PS fills the need for a short, clinimetrically sound scale. It
addresses the difficulties patients experience in social and emotional spheres. The scale can
adequately be used in research situations, whereas the use in clinical practice may be argued.
The internal consistency is, however, similar to that of comparable subscales of other disease-
specific HRQoL instruments in PD. The distinction between physical difficulties on the one
hand and emotional and social difficulties on the other hand, provides a clear insight in the
difficulties patients perceive in the two distinct domains.
Acknowledgements
This study was financed by the Netherlands Organization for Scientific Research (project no.
0940-33-021). The authors thank professor R.A.C. Roos for his helpful comments.
References
1. De Rijk MC, Launer LJ, Berger K, Breteler MM, Dartigues JF, Baldereschi M, et al. Prevalence of
Parkinson's disease in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in
the Elderly Research Group. Neurology 2000; 54(11 Suppl 5):S21-S23.
2. Bowling A. Health-related quality of life: a discussion of the concept, its use and measurement.
Measuring disease. Buckingham: Open University Press, 1995: 1-19.
3. Marinus J, Ramaker C, Van Hilten JJ, Stiggelbout AM. Health related quality of life in Parkinson's
disease: a systematic review of disease specific instruments. J Neurol Neurosurg Psychiatry 2002;
72(2):241-248.
4. Damiano AM, Snyder C, Strausser B, Willian MK. A review of health-related quality-of-life concepts
and measures for Parkinson's disease. Qual Life Res 1999; 8(3):235-243.

Chapter 11
- 192 -
5. De Boer AG, Wijker W, Speelman JD, De Haes JC. Quality of life in patients with Parkinson's disease:
development of a questionnaire. J Neurol Neurosurg Psychiatry 1996; 61(1):70-74.
6. Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and validation of a short measure of
functioning and well being for individuals with Parkinson's disease. Qual Life Res 1995; 4(3):241-248.
7. Van den Berg M. Leben mit Parkinson - Entwicklung und psychometrische Testung des Fragenbogens
PLQ. Neurol Rehabil 1998; 4(5):221-226.
8. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's
disease. J Neurol Neurosurg Psychiatry 1988; 51(6):745-752.
9. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The PDQ-8: development and validation of a
short-form Parkinson's disease questionnaire. Psychol Health 1997; 12:805-814.
10. Brooks R. EuroQol: the current state of play. Health Policy 1996; 37(1):53-72.
11. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983;
67(6):361-370.
12. McDowell I, Newell C. Measuring Health: A Guide to Rating Scales and Questionnaires. 2 ed. New
York: Oxford University Press, 1996.
13. Schrag A, Selai C, Jahanshahi M, Quinn NP. The EQ-5D-a generic quality of life measure-is a useful
instrument to measure quality of life in patients with Parkinson's disease. J Neurol Neurosurg Psychiatry
2000; 69(1):67-73.
14. Martinez-Martin P, Frades PB. Quality of life in Parkinson's disease: validation study of the PDQ-39
Spanish version. The Grupo Centro for Study of Movement Disorders. J Neurol 1998; 245 Suppl 1:S34-
S38.
15. Schrag A, Jahanshahi M, Quinn N. What contributes to quality of life in patients with Parkinson's
disease? J Neurol Neurosurg Psychiatry 2000; 69(3):308-312.
16. Schrag A, Jahanshahi M, Quinn NP. What contributes to depression in Parkinson's disease? Psychol Med
2001; 31(1):65-73.
17. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967; 17(5):427-442.
18. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use.
2 ed. Oxford: Oxford Medical Publications, 1995.
19. Nunnally JC, Bernstein IH. Psychometric Theory. 3 ed. New York: McGraw-Hill, Inc., 1994.
20. Helmstadter GC. Evaluation of tests - reliability. Principles of psychological measurement. London:
Methuen & Co Ltd, 1966: 58-86.
21. Hays RD, Anderson RT, Revicki D. Assessing reliability and validity of measurement in clinial trials. In:
Staquet MJ, Hays RD, Fayers PM, editors. Quality of Life Assessment in Clinical Trials. Oxford: Oxford
University Press, 1998: 169-182.
22. Wright JG, Feinstein AR. A comparative contrast of clinimetric and psychometric methods for
constructing indexes and rating scales. J Clin Epidemiol 1992; 45(11):1201-1218.
23. Berger K, Broll S, Winkelmann J, Heberlein I, Muller T, Ries V. Untersuchung zur Reliabilität der
deutschen Version des PDQ-39: Ein krankheitsspezifischer Fragenbogen zur Erfassung der
Lebensqualität von Parkinson-Patienten. Aktuel Neurol 1999; 26(4):180-184.
Psychosocial questionnaire for Parkinson’s disease
- 193 -
24. Fitzpatrick R, Peto V, Jenkinson C, Greenhall R, Hyman N. Health-related quality of life in Parkinson's
disease: a study of outpatient clinic attenders. Mov Disord 1997; 12(6):916-922.
25. Jenkinson C, Peto V, Fitzpatrick R, Greenhall R, Hyman N. Self-reported functioning and well-being in
patients with Parkinson's disease: comparison of the short-form health survey (SF-36) and the
Parkinson's Disease Questionnaire (PDQ-39). Age Ageing 1995; 24(6):505-509.
26. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson's Disease Questionnaire
(PDQ-39): development and validation of a Parkinson's disease summary index score. Age Ageing 1997;
26(5):353-357.
27. Brown RG, Jahanshahi M, Quinn N, Marsden CD. Sexual function in patients with Parkinson's disease
and their partners. J Neurol Neurosurg Psychiatry 1990; 53(6):480-486.
28. Welsh M, Hung L, Waters CH. Sexuality in women with Parkinson's disease. Mov Disord 1997;
12(6):923-927.
29. Calne S, Schulzer M, Mak E, Guyette C, Rohs G, Hatchard S, et al. Validating a quality of life rating
scale for idiopathic Parkinsonism: Parkinson's impact scale. Parkinsonism Relat Disord 1996; 2(2):55-61.
30. Welsh M, McDermott M, Holloway R, Plumb S, Pfeiffer R, Hubble J. Development and Testing of the
Parkinson's Disease Quality of Life Scale: The PDQUALIF. Mov Disord 1997; 12(5):836-836. Abstract.
31. Fahn S, Elton RL, and members of the UPDRS Development Committee. Unified Parkinson's Disease
Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Clane DB, editors. Recent Developments in
Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information, 1987: 153-163.
32. Martínez-Martin P, Gil-Nagel A, Morlán Gracia L, Balseiro Gómez J, Martínez-Sarriés FJ, Bermejo F, et
al. Intermediate Scale for Assessment of Parkinson's Disease. Characteristic and Structure. Parkinsonism
Relat Disord 1995; 1(2):97-102.
33. Rabey JM, Bass H, Bonuccelli U, Brooks D, Klotz P, Korczyn AD, et al. Evaluation of the Short
Parkinson's Evaluation Scale: A New Friendly Scale for the Evaluation of Parkinson's Disease in Clinical
Drug Trials. Clin Neuropharmacol 1997; 20(4):322-337.
34. Bushnell DM, Martin ML. Quality of life and parkinson's disease: Translation and validation of the US
Parkinson's Disease Questionnaire (PDQ-39). Qual Life Res 1999; 8(4):345-350.

Chapter 11
- 194 -
Appendix: SCOPA – PS
Questionnaire on the psychosocial consequences of Parkinson’s Disease
In this questionnaire, we inquire about problems which you may encounter as a result of your illness in the areas
of (social) activities, contact with other people, and on an emotional level. When answering the following
questions, please think carefully about your personal situation during the past month, and consider to what
extent the situation described actually posed a problem for you. Tick the box above the answer which best
reflects your situation.
1. During the past month, have you had difficulty with work, household or other chores?
2. During the past month, have you had difficulty with hobbies, sport or leisure activities?
3. During the past month, have you felt uncertain in your contact with others?
4. During the past month, have you had problems getting along with your partner, family
or good friends?
5. During the past month, have you had problems in the area of sexuality?
6. During the past month, have you felt more house-bound than you would wish to be?
7. To what extent have you had the feeling that you have had to ask others for help too often during the past
month?
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much

Psychosocial questionnaire for Parkinson’s disease
- 195 -
8. To what extent have you felt isolated and lonely during the past month?
9. During the past month, have you had difficulty when having a conversation?
10. To what extent have you felt ashamed of your disease during the past month?
11. During the past month, have you been concerned about the future?
© This questionnaire is made available free of charge, with the permission of the authors, to all those
undertaking non-profit and profit making research. The authors may be requested to share data for psychometric
purposes. Use of this questionnaire in studies should be communicated to the developers. No changes may be
made to the questionnaire without written permission. For further information, please contact
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much
not at all a little quite a bit very much


- 197 -
1122 Summary and conclusions

Chapter 12
- 198 -
This thesis reflects the first phase of the project called ‘The assessment of the disablement
process in Parkinson’s Disease’, that aims to provide data on disease progression in patients
with Parkinson's disease (PD). This first phase (called the SCOPA project, short for SCales
for Outcomes in PArkinson's disease) is concerned with arriving at the appropriate
instruments, the second phase involves the use of these instruments in the longitudinal follow-
up of patients, stratified by disease duration and age at onset of the disease.
Chapter 1 is the introduction to this thesis and poses the problem that in many relevant
domains in PD good instruments, that allow clinicians and researchers to quantify the extent
of a particular problem, are lacking. We use the framework of the Disablement Process1, to
test already existing instruments for their use in PD or to develop new instruments that are
valid, reliable, and clinimetrically sound. This framework proposes a sociomedical model of
disability, describing a pathway that links pathology with impairments, functional limitations,
and disability and acknowledges bi-directional relations between these entities. Extra- and
intra-individual factors, and comorbidity as a special case of an intra-individual factor, may
act upon this pathway and modify the course of the disease and the extent to which an
individual is affected. The following domains on the impairment level were considered of
such relevance that it justifies separate evaluation: cognition, mood, psychiatric
complications, motor function, motor complications, and autonomic dysfunction (discussed in
chapters 4-8). On the disability level, modules for psychosocial disability, activities-of-daily-
living (ADL), and sleep were developed (chapters 8-11). Other modules that have been tested
or developed, but not presented in this thesis, involve comorbidity and costs.
Chapter 2 presents an overview of the clinimetric characteristics of existing rating scales that
evaluate impairments and disabilities in PD. The study involves a systematic review of 30
studies that report on the clinimetric characteristics of 11 rating scales. Outcome measures
included validity, reliability, and responsiveness. We found three impairment scales (Webster,
Columbia University Rating Scale [CURS], Parkinson's Disease Impairment Scale), four
disability scales (Schwab and England, Northwestern University Disability Scale [NUDS],
Intermediate Scale for Assessment of Parkinson's Disease, Extensive Disability Scale), and
another four scales that evaluated both impairments and disabilities (New York University
Parkinson's Disease Rating Scale, University of California Los Angeles Scale, Unified
Parkinson's Disease Rating Scale [UPDRS], Short Parkinson Evaluation Scale). The scales
showed large differences in their representation of items considered responsive to

Summary and conclusions
- 199 -
dopaminergic treatment or of symptoms that appear late in the course of the disease and lack
responsiveness to treatment. Irrespective of the scale, there was a lack of consistency in the
inter-rater reliability of items addressing bradykinesia, tremor, and rigidity. Overall, disability
items displayed moderate to good inter-rater reliability. The available evidence indicates that
the CURS, NUDS, and UPDRS have moderate to good reliability and validity. The majority
of instruments demonstrated clinimetric shortcomings or had not been subjected to extensive
clinimetric testing, despite their frequent use. The CURS, NUDS, and UPDRS are the scales
that have been evaluated most often, and are considered valid and reliable.
In chapter 3 we compared and contrasted disease-specific quality-of-life instruments in PD
and assessed their clinimetric properties. Two reviewers independently evaluated both
thoroughness and results of 20 studies that reported clinimetric properties of four scales. The
content validity of the Parkinson’s Disease Questionnaire-39 item version (PDQ-39), the
Parkinson’s Disease Quality of Life questionnaire (PDQL), and the ‘Fragebogen Parkinson
LebensQualität’ (Parkinson Quality of Life questionnaire; PLQ) was found to be adequate to
good, but for the Parkinson’s Impact Scale (PIMS) it was insufficient. Construct validity of
both the PDQ-39 and the PDQL was good, but for the PLQ and the PIMS this was
insufficiently evaluated. Internal consistency of all scale totals and of subscale totals of the
PDQL was good, whereas for the social support subscale of the PDQ-39 and four subscales of
the PLQ this was inadequate. Test-retest reliability was not evaluated for the PDQL and was
adequate in other scales. Responsiveness was partially established for the PDQ-39, and not
assessed for the other scales. The number of available translations, as well as the number of
studies in which these instruments are used, differed considerably. The conclusion of our
study was that the selection of an instrument obviously depends on the goal of the study, but
that in most situations the PDQ-39 probably will be the most appropriate HRQoL instrument
currently available. The PDQL may be considered an alternative, whereas the PLQ may be
considered in studies involving German speaking patients with PD. Use of the PIMS should
be considered only as a means of identifying areas of potential problems.
Chapter 4 involves the assessment of cognition in PD. We argue that cognitive deficits in
Parkinson's disease (PD) may be underestimated if classical instruments for cognition are
used. These instruments generally put an emphasis on cortical functions. Some of these
functions are relatively spared in PD, whereas other cognitive functions that are frequently
affected in PD, are lacking. The objective of this study was to develop a short and practical

Chapter 12
- 200 -
instrument that is sensitive to the specific cognitive deficits in PD, and is valid and reliable. It
was not our objective to construct a screening tool or a diagnostic instrument. In stead, the
instrument is intended for comparing groups in research situations and for assessing change in
individual functioning over time. First we searched the literature to identify the most
frequently affected cognitive domains in PD, and to select or develop candidate items from
these domains for the initial scale. This scale was next tested in 85 patients with PD and 75
age-, education-, and sex-matched controls. Items that met predefined criteria for data quality,
reproducibility, and discriminative properties, were included in the final scale. This scale, the
SCOPA-COG, consists of 10 items with a maximum score of 43, with higher scores reflecting
better performance. The test-retest reliability of the sumscore was 0.78 (intraclass correlation
coefficient), and ranged from 0.40-0.75 for individual items (weighted kappa). Cronbach's α
was 0.83. Construct validity of the scale was supported by the expected correlations with the
CAMCOG and the MMSE, and by differences found between groups of participants
classified by dementia status, and between patients grouped by disease severity. The scale
showed a clear trend towards lower cognition scores for patients with more advanced PD.
This trend was more pronounced in the SCOPA-COG than in the CAMCOG and the MMSE
and use of this scale could provide a better insight into the longitudinal development of
cognitive deficits in PD. The coefficient of variation of the SCOPA-COG was higher than that
of the CAMCOG or the MMSE, indicating a better ability to detect differences between
individuals. The SCOPA-COG is a short, reliable, and valid instrument that is sensitive to the
specific cognitive deficits in PD and suitable for comparing groups in research situations.
The purpose of the study presented in chapter 5 was to evaluate the psychometric properties
of the Hospital Anxiety and Depression Scale (HADS) in patients with Parkinson's disease
(PD), and to assess the prevalence of symptoms of anxiety and depression in this population.
The HADS was sent to 205 patients with PD, together with three quality-of-life (QoL)
instruments, i.e., the Parkinson’s Disease Questionnaire (PDQ-39), the EQ-5D, and a visual
analogue scale (VAS). HADS scores were also compared with Hoehn and Yahr (H&Y)
scores. Eighty-six percent of the patients returned the questionnaires. Cronbach’s α for the
HADS was 0.88. Test-retest reliability over two weeks was 0.84 for the sum score of the
HADS (intraclass correlation coefficient), and ranged from 0.42-0.76 for individual items
(weighted kappa). Factor analysis revealed two factors, accounting for 51.9% of the variance.
One factor represented anxiety, the other depression. Correlations with the PDQ-39, EQ-5D,
VAS, and H&Y were 0.72, -0.59, -0.59, and 0.32, respectively (all p-values < 0.001).

Summary and conclusions
- 201 -
Depression scores accounted for 52% of the variance in QoL, whereas disease severity
explained 24%. Using the cut-off values proposed by the developers indicated that possible
and probable anxiety was present in 28.9 and 19.8 percent of the patients, respectively.
Percentages for possible and probable depression were 21.6 and 16.5. We conclude that the
psychometric performance of the HADS in patients with PD is satisfactory. In addition,
almost 50% of the patients display symptoms of anxiety, whereas nearly 40% show signs of
depression.
In chapter 6 we assessed the sensitivity of individual depressive symptoms and their relative
contribution to the diagnosis of depressive disorder in patients with PD. This study was
conducted because there is a considerable overlap between the somatic symptoms of PD and
those of depression, which makes it particularly difficult to diagnose depression in patients
with PD. The significance of the somatic symptoms of depression in patients with PD is
therefore unclear. To evaluate this, the Structured Clinical Interview for DSM-IV Depression
and the Hamilton and the Montgomery-Åsberg Depression Rating Scales (Ham-D, MADRS)
were administered to 149 consecutive nondemented patients. The contribution of the
individual items of these scales to the diagnosis of “depressive disorder” was calculated by
discriminant analysis. The discriminant models based on the Ham-D and MADRS scores
were both highly significant. Nonsomatic core symptoms of depression (anhedonia and mood)
had the highest correlation coefficient. Somatic items had mostly low correlation coefficients,
with the exception of reduced appetite and early morning wakening. The conclusion of the
study was that nonsomatic symptoms of depression appear to be the most important for
distinguishing between depressed and nondepressed patients with PD, along with reduced
appetite and early morning awakening.
The objective of the study presented in chapter 7 was to develop and test a questionnaire for
autonomic symptoms in PD, the SCOPA-AUT. First, items were generated by an extensive
literature search and by consulting experts. Based on the results of a postal survey in 46
patients with PD, 21 patients with multiple system atrophy (MSA), and 8 movement disorders
specialists, items were reduced according to frequency, burden, and clinical relevance of
symptoms. Evaluation of the validity of the questionnaire was based on the results of a second
postal survey in 140 PD patients and 100 controls. Medication was assessed in an additional
question. The test-retest reliability was established in a subsample of 55 PD patients, who
received the questionnaire twice. The initial 45 items were reduced to 25 items addressing the

Chapter 12
- 202 -
following domains: gastrointestinal (7 items), urinary (6 items), cardiovascular (3 items),
thermoregulatory (4 items), pupillomotor (1 item), and sexual dysfunction (2 items for men
and 2 for women). Test-retest reliability was good for all items and domain scores, and all
domains demonstrated high internal consistency. Each domain had a good content validity.
All domains and most items differentiated between the PD and control groups. A significant
increase in autonomic problems was found in patients in the more advanced disease stages for
all autonomic domains, except sexual dysfunction. We conclude that the SCOPA-AUT is a
reliable and valid questionnaire that accurately evaluates autonomic disturbances in patients
with PD.
In chapter 8 we evaluated the reliability and construct validity of the SPES/SCOPA, a short
scale developed to assess motor function in patients with PD. Eighty-five patients with PD
were assessed with the SPES/SCOPA, Unified Parkinson’s Disease Rating Scale (UPDRS),
Hoehn and Yahr (H&Y) scale, and Schwab and England (S&E) scale. Thirty-four patients
were examined twice by two different assessors, who were blinded to each other’s scores and
test executions ('clinical assessment situation'). Additionally, six items of the motor section of
the SPES/SCOPA were assessed in nine patients and recorded on videotape, to evaluate inter-
rater and intra-rater reliability for this situation ('video assessment situation'). The
reproducibility of the sumscores in the clinical assessments was high for all subscales of the
SPES/SCOPA. Inter-rater reliability of individual items ranged from 0.27-0.83 in the motor
impairment section, from 0.58-0.82 in the Activities-of-Daily-Living section, and from 0.65-
0.92 in the motor complications section. Inter-rater reliability of the motor items in the video
assessments ranged from 0.69-0.87, and intra-rater reliability from 0.81-0.95. The correlation
between related subscales of the SPES/SCOPA and UPDRS were all over 0.85 and both
scales revealed similar correlations with other measures of disease severity. The mean time to
complete the scales was 8.1 (SD1.9) minutes for the SPES/SCOPA and 15.6 (SD 3.6) minutes
for the UPDRS. We conclude that the SPES/SCOPA is a reliable, valid, and short scale that
can adequately be used in both research and clinical practice.
The objective of the study in chapter 9 was to develop a PD diary that evaluates a patient’s
difficulties in performing activities, as a substitute for the amount of 'on'- and 'off'-time, and
to assess its clinimetric qualities. In this study 84 patients with PD kept a diary for two or
three periods of five days. Daily, five items were recorded across 11 time periods. Patients
simultaneously recorded being ‘on' or 'off’ in the traditional way. The diary was easily

Summary and conclusions
- 203 -
understood and median recording time was 5-10 minutes a day. Clinimetric analysis showed
that the diary could successfully be reduced to three days, in which five items (walking,
transfers, manual activities, dyskinesias, and sleep) with four response options were assessed
seven times daily. Sumscores of the first three items accurately predicted being 'on' or 'off' in
93% of the cases, therewith making separate scoring of 'on' and 'off' unnecessary. The diary
was internally consistent and showed good reproducibility. Construct validity with external
measures was adequate, and comparisons between patients grouped by disease severity and
by degree of fluctuations, revealed significant differences in the expected directions. Our
conclusion is that the SCOPA Diary Card has a sound clinimetric basis and provides
information on the extent of perceived disability, therewith accurately reflecting both the
severity of off-periods and the variability of motor fluctuations.
Chapter 10 describes a study that had the objective to develop a valid, reliable, and short
questionnaire (SCOPA-SLEEP) that assesses nighttime sleep (NS) and daytime sleepiness
(DS) in patients with PD. A postal survey including four instruments, the SCOPA-SLEEP NS
(5 items) and DS (6 items), the Pittsburgh Sleep Quality Index (PSQI), and the Epworth
Sleepiness Scale (ESS) was completed by 142 patients with PD and 100 controls. We found
that the reliability of the questionnaire was high: internal consistency of the NS and DS scales
was 0.88 and 0.91, respectively (Cronbach's alpha), and test-retest reliability was 0.94 and
0.89, respectively (intraclass correlation coefficient). Scale scores differed significantly
between patients and controls. Construct validity was assessed by correlations with scales that
addressed similar constructs. Correlation between the NS scale and the PSQI was 0.83, and
the correlation between the DS scale and the ESS was 0.81. Factor analysis revealed one
factor each for both scales, indicating that the scales measure one construct, which justifies
the calculation of sumscores. The coefficient of variation of both the NS and the DS scale was
higher than that of the PSQI and the ESS, indicating a better ability to detect differences
between individuals. Our conclusion is that the SCOPA-SLEEP is a practical, reliable, and
valid instrument for assessing nighttime sleep and daytime sleepiness in patients with PD.
The purpose of the study presented in chapter 11 was to develop a short questionnaire for
psychosocial functioning in patients with PD. The SCOPA-PS was tested in a survey and
compared with other instruments and with medical information. This survey was sent to 205
patients with idiopathic PD. Eighty-six percent of the questionnaires were returned. Internal
consistency and test-retest reliability were high, indicating good reliability. Construct validity

Chapter 12
- 204 -
with other diseases-specific QoL instruments (PDQ-39, PDQ-8) was also high and
correlations with other scales (HADS, EQ-5D) were as expected. The summary index
revealed a significant increase with increasing disease severity. The conclusion of this study is
that the SCOPA-PS is a new, short psychosocial questionnaire for patients with PD with good
clinimetric properties.
Concluding remarks
Looking back on this study there are a few points that need further clarification. At the
conception of this study in 1997, a choice had to be made between two research frameworks,
i.e., the International Classification of Impairments, Disabilities, and Handicaps, version I
(ICIDH-1)2 and the Disablement Process of Verbrugge and Jette.1 The latter model was
chosen, because it allowed better insight in the course of the disease. The disablement process
proposes bi-directional relations between domains and acknowledges the influence of extra-
and intra-individual factors that may modify the course of the disease and its impact on the
individual. These influences were not accounted for in the ICIDH-1. Other disadvantages of
this latter model were the supposed linear and causal relationships, and the lack of mutual
exclusiveness between domains.3 For instance, is experienced difficulty with household work
a disability (difficulty with performing basic tasks) or a handicap (experienced disadvantage
to fulfil social roles)? The updated version of the ICIDH-1, known as the ICF (International
Classification of Functioning, disability, and health),4 now also includes personal and
environmental influences and bi-directional relationships between domains, and differences
between the two models have become much smaller. Choosing between these models would
now have been more difficult, because of the smaller differences, but also less essential,
because these differences are less fundamental.
One impairment scale that is still being tested and hence not present in this thesis, is the
Parkinson Psychosis Rating Scale (PPRS). This scale evaluates psychiatric complications.
The reason for the delay is that we encountered some shortcomings of this scale later in the
course of the evaluation process. The scale has now been modified in co-operation with the
developers, and the modified version is currently being assessed. Two other scales, addressing
costs of PD and comorbidity, have already been tested, but will be presented in another thesis.
For the calculation of costs, a questionnaire has been developed and for the assessment of
comorbidity an existing instrument, the Cumulative Illness Rating Scale–Geriatric (CIRS-G)
will be used.

Summary and conclusions
- 205 -
We have selected and developed instruments that met our initial criteria of practicality (short
and easy to administer) and quality (valid and reliable). These scales will be used in the
longitudinal phase of the study. An overview of the instruments is presented in table 1. Six
instruments included in the SCOPA are completed by patients, that is, the HADS (mood),
SCOPA-AUT (autonomic disturbances), SCOPA Diary Card (motor complications), SCOPA-
SLEEP (evaluation of night-time sleep and daytime sleepiness), SCOPA-PS (psychosocial
disability), and costs. The other six instruments are administered by researchers or physicians:
the SPES/SCOPA (with scales on motor impairments, ADL, and motor complications), the
SCOPA-COG (cognition), the PPRS (psychiatric complications), and the CIRS-G
(comorbidity). The time to complete the full set of scales is approximately one hour for
patients and 45 minutes for investigators. We are currently comparing a self-administered
version of the ADL scale of the SPES/SCOPA with the physician-administered version, to
evaluate whether the potential loss of information outweighs the reduction in research burden
for physicians or researchers.
Table 1. Scales for the longitudinal phase of the SCOPA project
Completed by Domain Scale items minutes
Patient mood HADS 21 10
autonomic disturbances SCOPA-AUT 23 10
sleep SCOPA-SLEEP 14 8
psychosocial disability SCOPA-PS 11 6
costs Questionnaire on costs 18 20
motor complications SCOPA Diary Card 5 8
Neurologist motor evaluation SPES/SCOPA-motor impairments 10 6
or Activities of Daily Living SPES/SCOPA-ADL 7 5
Researcher motor complications SPES/SCOPA-motor complications 4 2
cognition SCOPA-COG 10 10
psychiatric complications PPRS 6 10
comorbidity CIRS-G 14 10

Chapter 12
- 206 -
Looking to the future we hope that our multi-modular scale, the SCOPA, will fulfil the
expectations we have for this instrument. The primary objective of this study has been to
develop a toolbox that includes modules that can be used either separately or as a whole. The
full scale will be used in the annual follow-up of a group of patients with PD, stratified by
disease duration and age at onset of the disease. This allows a more thorough assessment of
relations between various variables, such as personal characteristics, social and environmental
influences, comorbidity, and disease parameters. Some of the previously supposed relations
may be confirmed or rejected, while new associations may be found. Additionally, the
complete assessment will give a more accurate description of the phenotype of patients and
may allow a more detailed assessment of the relation with genetic make-up. However, the
most important hope we have for this instrument is that it will lead to a better understanding
of PD and will help to indicate new directions for research and therapy, thus improving the
future prognosis of patients with Parkinson's disease.
References
1. Verbrugge LM, Jette AM. The Disablement Process. Soc Sci Med 1994; 38(1):1-14.
2. World Health Organization. International Classification of impairments, disabilities, and handicaps: a
manual of classifications relating to the consequences of diseases. Geneva: World Health Organization,
1980.
3. Simeonsson RJ, Lollar D, Hollowell J, Adams M. Revision of the International Classification of
Impairments, Disabilities, and Handicaps: developmental issues. J Clin Epidemiol 2000; 53(2):113-124.
4. World Health Organization. The international classification of functioning, disability, and health. Internet
2002. http://www3.who.int/icf/onlinebrowser/icf.cfm

- 207 -
Samenvatting en conclusies

Samenvatting en conclusies
- 208 -
In dit proefschrift wordt de eerste fase beschreven van een onderzoek naar het 'disablement
proces' van de ziekte van Parkinson (ZvP). Het doel van dit project is gegevens te verschaffen
over de gevolgen van het ziekteproces voor patiënten met de ZvP. Deze eerste fase (genaamd
het SCOPA project, een afkorting van SCales for Outcomes in PArkinson's disease, ofwel
schalen voor uitkomstmaten bij de ZvP) houdt zich bezig met het bijeenbrengen van de goede
instrumenten, de tweede fase behelst het gebruik van deze instrumenten in het longitudinale
onderzoek van patiënten.
Hoofdstuk 1 is de inleiding van dit proefschrift waarin wordt beschreven dat op vele
relevante domeinen van de ZvP goede meetinstrumenten ontbreken. We gebruiken het model
van het 'disablement process'1 om reeds bestaande instrumenten voor gebruik bij de ZvP te
testen óf om nieuwe instrumenten te ontwikkelen, die valide, betrouwbaar en conceptueel
helder zijn. 'Disability' is een Angelsaksisch begrip voor de mate van verlies van menselijke
activiteiten binnen een relevante sociaal-culturele en maatschappelijke context.2 'Disability'
ontstaat als een persoon als gevolg van een medische conditie niet kan beantwoorden aan de
sociaal-maatschappelijke taakstelling. Het raamwerk van het 'disablement process' beschrijft
een pad dat pathologie verbindt met stoornissen ('impairments'), beperkingen in vaardigheden
of bewegen ('functional limitations') en beperkingen in activiteiten, bezigheden of participatie
('disablities'). Het model gaat uit van wederzijdse relaties tussen deze entiteiten. Extra- en
intra-individuele factoren, en co-morbiditeit als een bijzonder geval van een intra-individuele
factor, werken op dit pad en kunnen het ziektebeloop modificeren en de mate waarin iemand
beperkt wordt, beïnvloeden.
De volgende domeinen op stoornisniveau werden dermate belangrijk geacht dat er apart
aandacht aan diende te worden besteed: cognitie, stemming, motorische functies, motorische
complicaties en autonome functies (hoofdstukken 4 tot en met 8). Op beperkingniveau
werden modules ontwikkeld voor de psychosociale gevolgen van de ZvP, activiteiten van het
dagelijks leven (ADL) en slaapproblemen (hoofdstukken 8 tot en met 11). Andere modules
die werden getest of ontwikkeld, maar die niet in dit proefschrift worden beschreven,
betreffen comorbiditeit en kosten.
In hoofdstuk 2 wordt een overzicht gegeven van de klinimetrische karakteristieken van
schalen, die gebruikt worden om de motorische stoornissen en beperkingen van de ZvP te
beoordelen. Het artikel omvat een literatuuroverzicht van 30 studies, die tezamen inzicht
geven in de klinimetrische karakteristieken van 11 verschillende schalen. De uitkomstmaten

Samenvatting en conclusies
- 209 -
waren validiteit, betrouwbaarheid en responsiviteit. We vonden drie schalen op stoornisniveau
(Webster, Columbia University Rating Scale [CURS], Parkinson's Disease Impairment Scale),
vier op beperkingniveau (Schwab and England, Northwestern University Disability Scale
[NUDS], Intermediate Scale for Assessment of Parkinson's Disease, Extensive Disability
Scale) en nog eens vier schalen die zowel stoornissen als beperkingen evalueerden (New York
University Parkinson's Disease Rating Scale, University of California Los Angeles Scale,
Unified Parkinson's Disease Rating Scale [UPDRS], Short Parkinson Evaluation Scale). De
schalen lieten grote onderlinge verschillen zien in de verhouding tussen het aantal items dat
beschouwd wordt gevoelig te zijn voor dopaminerge behandeling (dopa-responsief) en items
die pas later in de ziekte optreden en juist minder goed op deze behandeling reageren (dopa-
resistent). Ongeacht om welke schaal het ging, was er weinig consistentie te ontdekken in de
interbeoordelaarsbetrouwbaarheid van items die bradykinesie, tremor en rigiditeit
beoordeelden. Over het algemeen genomen vertoonden de items een matige tot goede
interbeoordelaarsbetrouwbaarheid. De beschikbare informatie toonde aan dat de CURS, de
NUDS en de UPDRS een matig tot goede betrouwbaarheid en validiteit hebben. De meeste
instrumenten vertoonden klinimetrische tekortkomingen of waren niet grondig getest,
ondanks hun veelal frequente gebruik. De CURS, NUDS en UPDRS werden het meest
geëvalueerd en kunnen als betrouwbaar en valide worden beschouwd.
In hoofdstuk 3 vergeleken we vier ziektespecifieke kwaliteit-van-leven (KvL) instrumenten
en evalueerden hun klinimetrische eigenschappen. Twee reviewers beoordeelden,
onafhankelijk van elkaar, de grondigheid en de resultaten van 20 studies. De inhoudsvaliditeit
van de Parkinson’s Disease Questionnaire-39 (PDQ-39), de Parkinson’s Disease Quality of
Life vragenlijst (PDQL) en de ‘Fragebogen Parkinson LebensQualität’ (PLQ) was voldoende
tot goed, maar die van de Parkinson’s Impact Scale (PIMS) was onvoldoende. De
constructvaliditeit van zowel de PDQ-39 als de PDQL was goed, maar voor de PLQ en de
PIMS was dit onvoldoende onderzocht. De interne consistentie van alle vier de volledige
schalen en van alle subschalen van de PDQL was goed, terwijl dit voor de 'sociale steun'
subschaal van de PDQ-39 en voor vier subschalen van de PDQL onvoldoende was. De test-
hertestbetrouwbaarheid van de PDQL bleek niet onderzocht te zijn, maar in het geval van de
overige schalen was deze voldoende. De responsiviteit van de PDQ-39 was gedeeltelijk
onderzocht, maar voor de overige schalen was dit nog niet geëvalueerd. Het aantal
beschikbare vertalingen, alsmede het aantal studies waarin de instrumenten gebruikt werden,
verschilde aanzienlijk. De conclusie van onze studie was dat de selectie van het

Samenvatting en conclusies
- 210 -
meetinstrument natuurlijk afhangt van het doel van de studie, maar dat in de meeste gevallen
de PDQ-39 het meest geschikte meetinstrument is dat op dit moment voorhanden is. De
PDQL kan als een alternatief worden beschouwd, terwijl het gebruik van de PLQ in een
Duitssprekende populatie kan worden overwogen. Gebruik van de PIMS moet hooguit
worden overwogen als methode om mogelijke probleemgebieden op te sporen.
Hoofdstuk 4 gaat over het onderzoek naar de cognitie bij patiënten met de ZvP. We stellen
dat de cognitieve problemen bij de ZvP mogelijk worden onderschat als de klassieke cognitie-
instrumenten worden gebruikt. Deze instrumenten leggen in het algemeen de nadruk op de
corticale functies. Sommige van deze functies blijven bij Parkinson echter gespaard, terwijl
andere cognitieve functies, die bij deze aandoening vaak zijn aangedaan, in deze schalen juist
ontbreken. Het doel van de in dit hoofdstuk beschreven studie was om een korte, praktische
schaal te ontwikkelen, die gevoelig is voor de specifieke cognitieve problemen van de ZvP, en
die valide en betrouwbaar is. Het was niet de bedoeling een screeningsinstrument of een
diagnostisch instrument te ontwikkelen. De schaal is bedoeld om in onderzoekssituaties
groepen met elkaar te vergelijken en om veranderingen in individueel functioneren in de tijd
te onderzoeken.
Allereerst hebben we de literatuur bestudeerd om na te gaan welke cognitieve domeinen bij de
ZvP het vaakst zijn aangedaan en om kandidaat-items uit deze domeinen te selecteren voor de
initiële schaal. Deze schaal werd vervolgens getest bij 85 patiënten met de ZvP en 75
controlepersonen, die wat betreft leeftijd, opleiding en geslacht vergelijkbaar waren. Items die
voldeden aan vantevoren vastgestelde criteria voor datakwaliteit, reproduceerbaarheid en
discriminatieve eigenschappen, werden opgenomen in de uiteindelijke schaal. Deze schaal, de
SCOPA-COG, bestaat uit 10 items met een maximumscore van 43. Een hogere score duidt op
een betere prestatie. De test-hertestbetrouwbaarheid van de somscore was 0.78 (intraclass
correlatiecoëfficiënt), die van de afzonderlijke items lag tussen 0.40 en 0.75 (gewogen kappa).
Cronbach's α bedroeg 0.83. De constructvaliditeit van de schaal werd ondersteund door de
verwachte relaties met de CAMCOG en de MMSE, alsmede door de verschillen die werden
gevonden tussen groepen deelnemers die waren ingedeeld naar het al of niet aanwezig zijn
van dementie én tussen groepen patiënten die op grond van hun ziekte-ernst werden
onderscheiden. De schaal liet een duidelijke trend zien naar lagere cognitiescores voor
patiënten in een meer gevorderd ziektestadium. Deze trend was meer uitsproken bij de
SCOPA-COG dan bij de CAMCOG en de MMSE. De variatiecoëfficiënt van de SCOPA-
COG was groter dan die van de CAMCOG en de MMSE, hetgeen duidt op een groter

Samenvatting en conclusies
- 211 -
discriminerend vermogen. De conclusie van dit onderzoek was dat de SCOPA-COG een kort,
betrouwbaar en valide instrument is dat gevoelig is voor de specifieke cognitieve stoornissen
van de ZvP en gebruikt kan worden om in onderzoekssituaties groepen patiënten met elkaar te
vergelijken.
Het doel van de in hoofdstuk 5 beschreven studie was om de psychometrische eigenschappen
van de Hospital Anxiety and Depression Scale (HADS) bij patiënten met de ZvP te
onderzoeken én om de prevalentie van symptomen van angst en depressie in deze populatie te
bepalen. De HADS werd verstuurd naar 205 patiënten met de ZvP, tezamen met drie KvL
instrumenten, te weten de PDQ-39, de EuroQol (EQ-5D) en een visueel analoge schaal
(VAS). De HADS scores werden tevens vergeleken met de Hoehn en Yahr (H&Y) scores.
Zesentachtig procent van de patiënten stuurde de vragenlijsten terug. De Cronbach’s α van de
HADS was 0.88. De test-hertestbetrouwbaarheid over twee weken was 0.84 voor de somscore
van de HADS (intraclass correlatiecoëfficiënt) en bedroeg 0.42-0.76 voor de afzonderlijke
items (gewogen kappa). De factoranalyse liet twee factoren zien, die 51.9% van de variantie
bepaalden. De ene factor vertegenwoordigde angst, de andere depressie. De correlaties met de
PDQ-39, EQ-5D, VAS en H&Y waren respectievelijk 0.72, -0.59, -0.59 en 0.32 (alle p-
waarden < 0.001). Depressie bepaalde 52% van de variantie in KvL, terwijl ziekte-ernst 24%
ervan bepaalde. De door de ontwikkelaars van de schaal voorgestelde afkappunten werden
aangehouden en hierbij bleek er van 'mogelijke' en 'waarschijnlijke' angst sprake te zijn bij
respectievelijk 28.9 en 19.8% van de patiënten. De percentages voor mogelijke en
waarschijnlijke depressie bedroegen 21.6 en 16.5. De conclusie was dat de psychometrische
eigenschappen van de HADS in een populatie van patiënten met de ZvP bevredigend waren.
Daarnaast vertoonde bijna 50% van de patiënten tekenen van angst en bijna 40% tekenen van
depressie.
In hoofdstuk 6 onderzochten we de sensitiviteit van de afzonderlijke depressieve symptomen
en hun relatieve bijdrage aan de diagnose van depressie bij patiënten met de ZvP. Deze studie
werd uitgevoerd omdat er een aanzienlijke overlap bestaat tussen de somatische
verschijnselen van de ZvP en die van depressie, hetgeen het bijzonder lastig maakt om
depressie te diagnosticeren bij patiënten met de ZvP. De betekenis van deze somatische
symptomen van depressie is bij mensen met de ZvP daarom onduidelijk. Om deze betekenis
nader te onderzoeken, werd het gestructureerde klinische interview voor DSM-IV Depressie
en de Hamilton en Montgomery-Åsberg depressieschalen (Ham-D, MADRS) afgenomen bij

Samenvatting en conclusies
- 212 -
149 opeenvolgende niet-demente patiënten. De bijdrage van de afzonderlijke items van deze
schalen aan de diagnose 'depressie' werd bepaald met behulp van discriminantanalyse.
De discriminantmodellen gebaseerd op de scores van de Ham-D en de MADRS waren beide
zeer significant. De niet-somatische kernsymptomen van depressie (anhedonie en stemming)
hadden de hoogste correlatiecoëfficiënt. De somatische items hadden meestal lage
correlatiecoëfficiënten, met uitzondering van 'verminderde eetlust' en 'vroeg ontwaken'. De
conclusie van de studie was dat de niet-somatische symptomen van depressie het belangrijkste
lijken te zijn bij het onderscheiden van depressieve en niet-depressieve patiënten, tezamen
met 'verminderde eetlust' en 'vroeg ontwaken'.
Het doel van de in hoofdstuk 7 beschreven studie was om een vragenlijst te ontwikkelen voor
de stoornissen van de autonome functies bij de ZvP, de SCOPA-AUT. Eerst werden, door
middel van literatuuronderzoek en het raadplegen van experts, items gegenereerd. Op basis
van de resultaten van een postenquête onder 46 patiënten met de ZvP, 21 patiënten met
multiple systeem atrofie (MSA) en 8 specialisten in bewegingsstoornissen, werden de items
vervolgens gereduceerd. Frequentie van voorkomen, ervaren hinder en klinische relevantie
bepaalden of items al dan niet werden behouden. De validiteit van de aldus verkregen
vragenlijst werd onderzocht in een tweede postenquête onder 140 patiënten met de ZvP en
100 controlepersonen. De test-hertestbetrouwbaarheid werd bepaald in subgroep van 55
patiënten die de vragenlijst twee keer ontvingen. De aanvankelijke 45 items werden
gereduceerd tot 25 items en bestreken de volgende gebieden: gastro-intestinaal (7 items),
urogenitaal (6 items), cardiovasculair (3 items), thermoregulatoir (4 items), pupillomotorisch
(1 item) en seksuele disfunctie (2 items voor mannen en 2 voor vrouwen). Medicatie werd in
een apart item uitgevraagd. De test-hertest betrouwbaarheid van de domeinscores en de
afzonderlijke items was goed en alle domeinen lieten een hoge interne consistentie zien. Elk
domein had een goede inhoudsvaliditeit. Alle domeinen en het merendeel van de items
differentieerden tussen patiënten en controles. We vonden een significante toename van
autonome problemen bij toenemende ziekte-ernst in alle domeinen, met uitzondering van
seksuele disfunctie. Onze conclusie was dat de SCOPA-AUT een betrouwbare en valide
vragenlijst is, die het mogelijk maakt op accurate wijze de autonome stoornissen bij de ZvP te
evalueren.

Samenvatting en conclusies
- 213 -
In hoofdstuk 8 onderzochten we de betrouwbaarheid en constructvaliditeit van de
SPES/SCOPA, een schaal die ontworpen is om de motorische functie van patiënten met de
ZvP te onderzoeken. Vijfentachtig patiënten met de ZvP werden onderzocht met de
SPES/SCOPA, de Unified Parkinson’s Disease Rating Scale (UPDRS), de Hoehn en Yahr
schaal (H&Y) en de Schwab en England schaal (S&E). Vierendertig patiënten werden twee
maal onderzocht door twee verschillende onderzoekers, die geblindeerd waren voor elkaar's
scores en testuitvoering. Daarnaast werden er van negen patiënten video-opnamen gemaakt,
teneinde de inter- en intrabeoordelaarsbetrouwbaarheid voor deze situatie vast te stellen.
De reproduceerbaarheid van de somscores in het klinisch onderzoek, berekend met behulp
van een intraclass-correlatiecoëfficiënt (ICC), was hoog voor alle subschalen van de
SPES/SCOPA. De interbeoordelaarsbetrouwbaarheid van de afzonderlijke items van de
motore sectie liep van 0.27-0.83, van de ADL-sectie van 0.58-0.82 en van de sectie
motorische complicaties van 0.65-0.92. De interbeoordelaarsbetrouwbaarheid van de
afzonderlijke items van de motorsectie in het video-onderzoek liep van 0.69-0.87 en voor de
intrabeoordelaarsbetrouwbaarheid van 0.81-0.95. De correlatie tussen gerelateerde subschalen
van de SPES/SCOPA en de UPDRS was, met alle coëfficiënten boven 0.85, hoog. Beide
schalen lieten vergelijkbare correlaties zien met de diverse maten voor ziekte-ernst. De tijd
benodigd voor het invullen van de SPES/SCOPA was 8 minuten, die voor de UPDRS 16
minuten. Wij concludeerden dat de SPES/SCOPA een korte, betrouwbare en valide schaal is,
met goede eigenschappen voor onderzoek en klinische praktijk.
Het doel van de in hoofdstuk 9 beschreven studie was om een Parkinsondagboek voor
patiënten met motorische fluctuaties te ontwikkelen. Dit dagboek ging niet uit van de
hoeveelheid 'on'- en 'off'-tijd, maar nam de moeilijkheden die een patiënt ervaart bij het
uitvoeren van activiteiten als uitgangspunt. In deze studie hielden 84 patiënten met de ZvP
gedurende twee of drie periodes van vijf dagen een dagboek bij. Per dag werden er over 11
periodes steeds vijf items beoordeeld. Patiënten hielden tegelijkertijd op de gebruikelijke
manier bij of zij ‘on' dan wel 'off’ waren. Patiënten hadden er geen moeite mee om het
dagboek te begrijpen. De mediane invultijd bedroeg 5-10 minuten per dag. Statistische
analyses maakten duidelijk dat het dagboek teruggebracht kon worden naar drie dagen,
waarbij er zeven maal daags vijf verschillende items (lopen, positieveranderingen, manuele
activiteiten, dyskinesieën en slaap) met elk vier responsopties moesten worden beoordeeld.
Op basis van de somscores over de eerste drie items, kon in 93% van de gevallen het 'on' dan
wel 'off' zijn correct worden voorspeld. Een aparte evaluatie hiervan wordt daarmee

Samenvatting en conclusies
- 214 -
overbodig. Het dagboek bleek intern consistent en had een goede reproduceerbaarheid. De
constructvaliditeit met externe maten kwam overeen met de verwachtingen. Ook de
vergelijkingen tussen patiënten ingedeeld naar hun ziekte-ernst en naar de ernst van hun
fluctuaties lieten significante verschillen in de verwachte richtingen zien. Onze conclusie was
dat de SCOPA Dagboekkaart een goede klinimetrische basis heeft en informatie verschaft
over de ervaren problemen met het uitvoeren van activiteiten, waarbij zowel de ernst van de
'off'-periodes als de variabiliteit van de motorische fluctuaties goed worden weerspiegeld.
In Hoofdstuk 10 wordt een studie beschreven die tot doel had om een korte, betrouwbare en
valide vragenlijst, de SCOPA-SLEEP, te ontwikkelen. Deze lijst informeerde bij patiënten
met de ZvP zowel naar het slapen 's nachts (NS) als naar slaperigheid overdag (DS). Een
postenquête met vier meetinstrumenten, de SCOPA-SLEEP NS (5 items) en DS (6 items), de
Pittsburgh Sleep Quality Index (PSQI) en de Epworth Sleepiness Scale (ESS), werd ingevuld
door 142 patiënten met de ZvP en 100 controlepersonen. Wij vonden een hoge
betrouwbaarheid voor deze vragenlijst: de interne consistentie van de NS en DS schalen was
respectievelijk 0.88 en 0.91 (Cronbach's alpha) en de test-hertestbetrouwbaarheid was
respectievelijk 0.94 en 0.89 (ICC). De somscores op de schalen verschilden significant tussen
patiënten en controles. De constructvaliditeit werd bepaald aan de hand van correlaties met
schalen die gerelateerde constructen evalueerden. De correlatie tussen de NS schaal en de
PSQI was 0.83 en de correlatie tussen de DS schaal en de ESS was 0.81. Een factoranalyse
liet een factor zien voor elke SCOPA-schaal. Dit geeft aan dat de schalen een enkel construct
meten, hetgeen het berekenen van somscores rechtvaardigt. De variatiecoëfficiënt van zowel
de NS- als de DS-schaal was hoger dan die van de PSQI en de ESS, hetgeen duidt op een
groter vermogen om verschillen tussen individuen te ontdekken. Wij oordeelden dat de
SCOPA-SLEEP een betrouwbaar, valide en praktisch instrument is om zowel het slapen 's
nachts als slaperigheid overdag bij patiënten met de ZvP te onderzoeken.
Het doel van de studie die in hoofdstuk 11 wordt beschreven, was om een korte vragenlijst te
ontwikkelen voor het psychosociaal functioneren van patiënten met de ZvP. De SCOPA-PS
werd getest in een enquête en werd vergeleken met andere instrumenten en met informatie uit
medische dossiers. De enquête werd verzonden naar 205 patiënten met idiopathische
Parkinson. Zesentachtig procent van de vragenlijsten werd teruggestuurd. De interne
consistentie en de test-hertestbetrouwbaarheid waren hoog, hetgeen duidt op een goede
betrouwbaarheid. De constructvaliditeit met andere ziektespecifieke KvL-instrumenten (PDQ-

Samenvatting en conclusies
- 215 -
39, PDQ-8) was eveneens hoog en de correlaties met andere schalen (HADS, EQ-5D)
kwamen overeen met onze verwachtingen. De somscore liet een significante toename zien bij
toenemende ziekte-ernst. De conclusie van de studie was dat de SCOPA-PS een nieuwe,
korte, psychosociale vragenlijst voor patiënten met de ZvP is, die goede klinimetrische
eigenschappen heeft.
Tot besluit
Terugkijkend op deze studie zijn er een aantal punten die een nadere uitleg behoeven. Toen in
1997 het idee voor deze studie ontstond, moest er een keuze gemaakt worden tussen twee
onderzoeksmodellen, namelijk die van de internationale classificatie van stoornissen,
beperkingen en handicaps versie I (ICIDH-1; International Classification of Impairments,
Disabilities, and Handicaps)3 en het model van het Disablement Process van Verbrugge en
Jette.1 Het laatste model werd gekozen, omdat het een beter inzicht verschafte in het beloop
van de ziekte. Het 'disablement process' gaat uit van wederzijdse relaties tussen domeinen en
erkent de invloed van extra- en intra-individuele factoren die het verloop van de ziekte en de
invloed die dit op het individu heeft, kunnen wijzigen. Met deze invloeden werd geen
rekening gehouden in de ICIDH-1. Andere nadelen van dit laatstgenoemde model waren de
veronderstelde lineaire en causale relaties, en het gebrek aan wederzijdse uitsluiting tussen
domeinen.4 Zijn bijvoorbeeld problemen die bij het huishouden worden ervaren, nu een
beperking (moeilijkheid met het uitvoeren van een basale taak) of een handicap (ervaren
nadeel om een sociale rol te vervullen)? De vernieuwde versie van de ICIDH-1, die bekend
staat als de ICF (International Classification of Functioning, disability, and health),5 erkent
inmiddels ook persoons- en omgevingsinvloeden, en gaat nu ook uit van wederzijdse relaties
tussen domeinen. De verschillen tussen beide modellen zijn nu dan ook veel kleiner
geworden. Kiezen tussen deze twee modellen zou nu, vanwege deze kleinere verschillen,
moeilijker zijn geweest, maar tevens minder essentieel, omdat de verschillen minder
fundamenteel zijn.
Een schaal die nog steeds getest wordt en daarom ontbreekt in dit proefschrift is de Parkinson
Psychosis Rating Scale (PPRS). Met deze schaal worden de psychiatrische complicaties
onderzocht. De reden van de vertraging is dat wij enkele tekortkomingen van deze schaal pas
later in het evaluatieproces tegenkwamen. De schaal is inmiddels in samenwerking met de
oorspronkelijke ontwikkelaars aangepast en de gemodificeerde versie wordt nu onderzocht.

Samenvatting en conclusies
- 216 -
Twee andere schalen, over comorbiditeit en de kosten van de ZvP, zijn al getest, maar zullen
in een ander proefschrift worden beschreven. Voor het berekenen van de kosten is een
vragenlijst ontwikkeld en voor comorbiditeit zal een bestaand meetinstrument, de Cumulative
Illness Rating Scale–Geriatric (CIRS-G) worden gebruikt.
Wij hebben meetinstrumenten geselecteerd en ontwikkeld die voldoen aan onze bij aanvang
gestelde criteria voor bruikbaarheid (kort en eenvoudig af te nemen) en kwaliteit
(betrouwbaar en valide). Deze schalen zullen worden gebruikt in de longitudinale fase van de
studie. Een overzicht van de instrumenten is weergegeven in tabel 1.
Tabel 1. Instrumenten voor de longitudinale fase van het SCOPA-project
Invullen door Domein Schaal items minuten
Patient stemming HADS 21 10
autonome stoornissen SCOPA-AUT 23 10
slaap SCOPA-SLEEP 14 8
psychosociale beperkingen SCOPA-PS 11 6
kosten Kostenvragenijst ZvP 18 20
motorische complicaties SCOPA Dagboekkaart 5 8
Neuroloog motorisch onderzoek SPES/SCOPA-motor sectie 10 6
of Activiteiten dagelijks leven SPES/SCOPA-ADL 7 5
Onderzoeker motorische complicaties SPES/SCOPA-motor complications 4 2
cognitie SCOPA-COG 10 10
psychiatrische complicaties PPRS 6 10
comorbiditeit CIRS-G 14 10
Zes instrumenten die in SCOPA zijn opgenomen, worden door patiënten zelf ingevuld, te
weten de HADS (stemming), de SCOPA-AUT (autonome stoornissen), de SCOPA
dagboekkaart (motorische complicaties), de SCOPA-SLEEP (slaapstoonissen), de SCOPA-PS
(psychosociale beperkingen) en de kostenvragenlijst. De overige zes instrumenten worden
afgenomen door een arts of onderzoeker: de SPES/SCOPA (met schalen over motorische
stoornissen, ADL en motorische complicaties), de SCOPA-COG (cognitie), de PPRS
(psychiatrische complicaties) en de CIRS-G (comorbiditeit). De tijd die nodig is om de

Samenvatting en conclusies
- 217 -
volledige set schalen in te vullen bedraagt circa een uur voor patiënten en 45 minuten voor
onderzoekers. Momenteel vergelijken wij een door patiënten zelf ingevulde versie van de
ADL schaal met de door de arts ingevulde versie, om na te gaan in hoeverre het mogelijke
verlies aan informatie opweegt tegen de reductie in onderzoekslast voor artsen en
onderzoekers.
Kijkend naar de toekomst hopen wij dat dit multi-modulaire instrument, de SCOPA, aan onze
verwachtingen zal voldoen. Het belangrijkste doel van de studie was om een gereedschapkist
te ontwikkelen, die modules bevat die zowel afzonderlijk als in hun geheel kunnen worden
gebruikt. De volledige set schalen zal worden gebruikt bij de jaarlijkse follow-up van een
groep patiënten met de ZvP, die worden gestratificeerd naar ziekteduur en leeftijd bij aanvang
van de ziekte. Dit maakt een grondig onderzoek mogelijk naar de relaties tussen verschillende
variabelen, zoals persoonskenmerken, maatschappelijke factoren en omgevingsinvloeden,
comorbiditeit en ziekteparameters. Sommige van de eerder veronderstelde relaties kunnen dan
geverifieerd of gefalsifieerd worden, terwijl mogelijk weer andere relaties worden gevonden.
Tevens zal het volledige onderzoek een meer accurate beschrijving van het fenotype van
patiënten geven, en kan daarmee een meer gedetailleerd onderzoek naar de relatie met
genetische opmaak mogelijk maken. Wij hopen echter vooral dat het gebruik van dit
instrument zal leiden tot een beter begrip van de ZvP en op deze wijze zal helpen bij het
vinden van nieuwe richtingen voor onderzoek en behandeling, waardoor in de toekomst de
prognose van patiënten met de ZvP zal worden verbeterd.
Referenties
1. Verbrugge LM, Jette AM. The Disablement Process. Soc Sci Med 1994; 38(1):1-14.
2. Helders PJM, Van der Net J, Engelbert RHH. Functionele diagnostiek en spreekkamerwerkelijkheid.
Fysiopraxis 1999;(3):20-23.
3. World Health Organization. International Classification of impairments, disabilities, and handicaps: a
manual of classifications relating to the consequences of diseases. Geneva: World Health Organization,
1980.
4. Simeonsson RJ, Lollar D, Hollowell J, Adams M. Revision of the International Classification of
Impairments, Disabilities, and Handicaps: developmental issues. J Clin Epidemiol 2000; 53(2):113-124.
5. World Health Organization. The international classification of functioning, disability, and health. Internet .
2002. http://www3.who.int/icf/onlinebrowser/icf.cfm


- 219 -
List of Abbreviations
AD Alzheimer's Disease
ADL Activities of Daily Living / Activiteiten van het Dagelijks Leven
ANOVA Analysis of variance
CAMCOG Cognition section of the Cambridge Examination of Mental Disorders of the Elderly
CAMDEX Cambridge Examination of Mental Disorders of the Elderly
CIRS-G Cumulative Illness Rating Scale - Geriatric
CURS Columbia University Rating Scale
CV Coefficient of Variation
DC Diary Card
DS scale Daytime Sleepiness subscale of the SCOPA-SLEEP questionnaire
DSM-IV Diagnostic and Statistical Manual of Mental Disorders, fourth edition
DUPRS Duke University Parkinson's Disease Rating Scale
EDS Extensive Disability Scale
EQ-5D EuroQol (five dimensions)
ESS Epworth Sleepiness Scale
H&Y Hoehn and Yahr scale
HADS Hospital Anxiety and Depression Scale
HAM-D Hamilton rating scale for depression
HRQoL Health-Related Quality of Life
ICC Intraclass Correlation Coefficient
ICF International Classification of Functioning, disability, and health
ICIDH International Classification of Impairments, Disabilities and Handicaps
ISAPD Intermediate Scale for Assessment of Parkinson's Disease
K Kappa
KvL Kwaliteit van Leven
Kw weighted Kappa
MADRS Montgomery-Åsberg Depression Rating Scale
MC Motor Complications
ME Motor Evaluation
MI Motor Impairments
MMSE Minimental State Examination
MRD Minimal Record of Disability
MSA Multiple System Atrophy
NS scale Night-time Sleep subscale of the SCOPA-SLEEP questionnaire
NUDS Northwestern University Disability Scale

- 220 -
NWO Nederlandse organisatie voor Wetenschappelijk Onderzoek; the Netherlands
Organization for scientific research
NYU New York University Parkinson's disease rating scale
PD Parkinson's disease
PDIS Parkinson's Disease Impairment Scale
PDQ-39, PDQ-8 Parkinson's Disease Questionnaire – 39 item version, 8 item version
PDQL Parkinson's Disease Quality of Life questionnaire
PDQUALIF Parkinson's Disease Quality of Life questionnaire
PIMS Parkinson's disease Impact Scale
PLQ Parkinson's disease 'LebensQualität Fragebogen' (Quality of Life questionnaire)
PPRS Parkinson Psychosis Rating Scale
PSQI Pittsburgh Sleep Quality Index
QoL Quality of Life
r Pearson's product moment correlation coefficient
ROC receiver operating characteristic
rs Spearman's rank correlation coefficient
S&E Schwab and England Scale
SCID-D Structural Clinical Interview for DSM-IV Depression
SCOPA SCale for Outcomes in PArkinson's disease
SCOPA-AUT SCale for Outcomes in PArkinson's disease, autonomic module
SCOPA-COG SCale for Outcomes in PArkinson's disease, cognition module
SCOPA-DC SCale for Outcomes in PArkinson's disease Diary Card
SCOPA-PS SCale for Outcomes in PArkinson's disease, psychosocial module
SCOPA-SLEEP SCale for Outcomes in PArkinson's disease, sleep questionnaire
SD Standard Deviation
SI Summary Index
SPES Short Parkinson's Evaluation Scale
SPES/SCOPA Short Parkinson's Evaluation Scale / SCale for Outcomes in PArkinson's disease
SPSS Statistical Package for the Social Sciences
SRM Standardized Response Mean
UCLA University of Columbia Los Angelos Parkinson's disease rating scale
UKPDSBB United Kingdom Parkinson's Disease Society Brain Bank
UPDRS Unified Parkinson's Disease Rating Scale
VAS Visual Analogue Scale
WHO World Health Organization
ZvP Ziekte van Parkinson

- 221 -
Nawoord
Dit proefschrift is mogelijk gemaakt doordat heel veel patiënten, hun partners en soms zelfs
hun familieleden, vrienden en kennissen, bereid waren om mee te werken aan de hier
beschreven onderzoeken. Daarnaast ben ik veel dank verschuldigd aan mensen die als
controlepersoon aan dit onderzoek hebben meegedaan.

- 222 -
List of publications
• Marinus J, Niël CG, De Bie RA, Wiggenraad RG, Schoppink EM, Beukema LH. Measuring
radiation fibrosis: the interobserver reliability of two methods of determining the degree of
radiation fibrosis. Int J Radiat Oncol Biol Phys 2000; 47(5):1209-1217.
• Marinus J. Bestralingsfibrose: ontstaan, onderzoek en behandeling. Oedeminus 2000;3(1):18-25.
• Dijkstra PU, Van Wilgen PC, Buijs RP, Brendeke W, De Goede CJ, Kerst A, Koolstra M, Marinus
J, Schoppink EM, Stuiver MM, Van der Velde CF, Roodenburg JLN. Incidence of shoulder pain
after neck dissection: a clinical explorative study for risk factors. Head Neck 2001; 23(11):947-
953.
• Marinus J, Ramaker C, Van Hilten JJ, Stiggelbout AM. Health related quality of life in Parkinson's
disease: a systematic review of disease specific instruments. J Neurol Neurosurg Psychiatry 2002;
72(2):241-248.
• Marinus J, Visser M, Stiggelbout AM, Rabey JM, Bonuccelli U, Kraus PH, Van Hilten JJ.
Activity-based diary for Parkinson's disease. Clin Neuropharmacol 2002; 25(1):43-50.
• Marinus J, Leentjens AFG, Visser M, Stiggelbout AM, Van Hilten JJ. Evaluation of the hospital
anxiety and depression scale in patients with Parkinson's disease. Clin Neuropharmacol 2002;
25(6):318-324.
• Ramaker C, Marinus J, Stiggelbout AM, Van Hilten BJ. Systematic evaluation of rating scales for
impairment and disability in Parkinson's disease. Mov Disord 2002; 17(5):867-876.
• Leentjens AFG, Marinus J, Van Hilten JJ, Lousberg R, Verhey FRJ. The Contribution of Somatic
Symptoms to the Diagnosis of Depressive Disorder in Parkinson's Disease: A Discriminant
Analytic Approach. J Neuropsychiatry Clin Neurosci 2003; 15(1):74-77.
• Marinus J, Visser M, Martínez-Martín P, Van Hilten JJ, Stiggelbout AM. A short psychosocial
questionnaire for patients with Parkinson's disease. the SCOPA-PS. J Clin Epidemiol 2003;
56(1):61-67.
• Visser M, Marinus J, Bloem BR, Kisjes H, Van den Berg B, Van Hilten JJ. Clinical tests for the
evaluation of postural instability in patients with Parkinson's disease. Arch Phys Med Rehabil
(accepted).

- 223 -
Curriculum vitae
Johan Marinus werd op 7 februari 1954 in Leiden geboren. Na de HBS-A te hebben
doorlopen, studeerde hij fysiotherapie aan de Haagse Academie voor Fysiotherapie. Na het
behalen van het diploma van deze opleiding in 1977, is hij gaan werken op de afdeling
Fysiotherapie van het Westeinde Ziekenhuis te Den Haag (thans Medisch Centrum
Haaglanden). In 1994 werd hij teamleider van deze afdeling. Tussen 1983 en 1991 was hij
tevens docent aan de Haagse Academie voor Fysiotherapie. In 1995 begon hij met de studie
Bewegingswetenschappen aan de Faculteit der Gezondheidswetenschappen van de
Universiteit Maastricht. In 1999 studeerde hij cum laude af. Het afstudeeronderzoek betrof
een vergelijking van de interbeoordelaarsbetrouwbaarheid van twee verschillende methoden
om de stugheid van bestraald borstweefsel te meten. Na afronding van de studie begon hij aan
een baan als onderzoeker in opleiding op de afdeling Neurologie van het Leids Universitair
Medisch Centrum. Het promotieonderzoek had als thema de klinimetrie bij de ziekte van
Parkinson, en de resultaten hiervan zijn in dit proefschrift beschreven. Het onderzoek werd
gefinancierd door de Nederlandse Organisatie voor Wetenschappelijk Onderzoek (NWO) en
het Leids Universitair Medisch Centrum. Gedurende deze periode volgde hij diverse
cursussen op het gebied van epidemiologie en biostatistiek. Het opleidingsprogramma
epidemiologie werd door de Vereniging voor Epidemiologie in 2002 goedgekeurd, zodat na
de promotie de registratie als Wetenschappelijk onderzoeker Epidemiologie kan plaatsvinden.
Sinds 2001 is de auteur als docent betrokken bij het post-HBO onderwijs van de opleiding
Fysiotherapie van de Leidse Hogeschool. Op 1 april 2003 is hij begonnen aan een baan als
onderzoeker op de afdeling Reumatologie van het Erasmus Medisch Centrum te Rotterdam.





















