Long-term Oncologic Outcomes Following Robot-assisted Radical Cystectomy: Results from the...
8
Bladder Cancer Long-term Oncologic Outcomes Following Robot-assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium Syed Johar Raza a , Timothy Wilson b , James O. Peabody c , Peter Wiklund d , Douglas S. Scherr e , Ali Al-Daghmin a , Shiva Dibaj a , Muhammad Shamim Khan f , Prokar Dasgupta f , Alex Mottrie g , Mani Menon c , Bertram Yuh b , Lee Richstone h , Matthias Saar i , Michael Stoeckle i , Abolfazl Hosseini d , Jihad Kaouk j , James L. Mohler a , Koon-Ho Rha k , Gregory Wilding a , Khurshid A. Guru a, * a Roswell Park Cancer Institute, Buffalo, NY, USA; b City of Hope and Beckman Research Institute, Duarte, CA, USA; c Henry Ford Health System, Detroit, MI, USA; d Karolinska University Hospital, Stockholm, Sweden; e Weill Cornell Medical College, New York, NY, USA; f Guy’s and St Thomas’s Hospital, London, UK; g Onze-Lieve-Vrouw Ziekenhuis, Aalst, Belgium; h Arthur Smith Institute for Urology, New Hyde Park, NY, USA; i University Clinics of Saarland, Homburg, Germany; j Cleveland Clinic Foundation, Cleveland, OH, USA; k Yonsei University Health Systems Severance Hospital, Seoul, Korea E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X ava ilable at www.sciencedirect.com journa l homepage: www.europea nurology.com Article info Article history: Accepted April 14, 2015 Associate Editor: James Catto Keywords: Robot-assisted Robotic Radical cystectomy Outcomes Survival Bladder cancer Recurrence Abstract Background: Long-term oncologic data on patients undergoing robot-assisted radical cystec- tomy (RARC) are limited and based largely on single-institution series. Objective: Report survival outcomes of patients who underwent RARC 5 yr ago. Design, setting, and participants: Retrospective review of the prospectively populated Inter- national Robotic Cystectomy Consortium multi-institutional database identified 743 patients with RARC performed 5 yr ago. Clinical, pathologic, and survival data at the latest follow-up were collected. Patients with palliative RARC were excluded. Final analysis was performed on 702 patients from 11 institutions in 6 countries. Intervention: RARC. Outcome measurements and statistical analysis: Outcomes of interest, recurrence-free sur- vival (RFS), cancer-specific survival (CSS), and overall survival (OS) were plotted using Kaplan- Meier survival curves. A Cox proportional hazards model was used to identify factors that predicted outcomes. Results and limitations: Pathologic organ-confined (OC) disease was found in 62% of patients. Soft tissue surgical margins (SMs) were positive in 8%. Median lymph node (LN) yield was 16, and 21% of patients had positive LNs. Median follow-up was 67 mo (interquartile range: 18–84 mo). Five-year RFS, CSS, and OS were 67%, 75%, and 50%, respectively. Non-OC disease and SMs were associated with poorer RFS, CSS, and OS on multivariable analysis. Age predicted poorer CSS and OS. Adjuvant chemotherapy and positive SMs were predictors of RFS (hazard ratio: 3.20 and 2.16; p < 0.001 and p < 0.005, respectively). Stratified survival curves demonstrated poorer outcomes for positive SM, LN, and non-OC disease. Retrospective interrogation and lack of contemporaneous comparison groups that underwent open radical cystectomy were major limitations. Conclusions: The largest multi-institutional series to date reported long-term survival out- comes after RARC. Patient summary: Patients who underwent robot-assisted radical cystectomy for bladder cancer have acceptable long-term survival. # 2015 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Department of Urology, Roswell Park Cancer Institute, Elm and Carlton Streets, Buffalo, NY 14263, USA. Tel. +1 716 845 3389; Fax: +1 716 845 3300. E-mail address: [email protected] (K.A. Guru). EURURO-6180; No. of Pages 8 Please cite this article in press as: Raza SJ, et al. Long-term Oncologic Outcomes Following Robot-assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. Eur Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021 http://dx.doi.org/10.1016/j.eururo.2015.04.021 0302-2838/# 2015 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Transcript of Long-term Oncologic Outcomes Following Robot-assisted Radical Cystectomy: Results from the...

EURURO-6180; No. of Pages 8
Bladder Cancer
Long-term Oncologic Outcomes Following Robot-assisted Radical
Cystectomy: Results from the International Robotic Cystectomy
Consortium
Syed Johar Raza a, Timothy Wilson b, James O. Peabody c, Peter Wiklund d, Douglas S. Scherr e,Ali Al-Daghmin a, Shiva Dibaj a, Muhammad Shamim Khan f, Prokar Dasgupta f,Alex Mottrie g, Mani Menon c, Bertram Yuh b, Lee Richstone h, Matthias Saar i, Michael Stoeckle i,Abolfazl Hosseini d, Jihad Kaouk j, James L. Mohler a, Koon-Ho Rha k, Gregory Wilding a,Khurshid A. Guru a,*
a Roswell Park Cancer Institute, Buffalo, NY, USA; b City of Hope and Beckman Research Institute, Duarte, CA, USA; c Henry Ford Health System, Detroit, MI,
USA; d Karolinska University Hospital, Stockholm, Sweden; e Weill Cornell Medical College, New York, NY, USA; f Guy’s and St Thomas’s Hospital, London, UK;g Onze-Lieve-Vrouw Ziekenhuis, Aalst, Belgium; h Arthur Smith Institute for Urology, New Hyde Park, NY, USA; i University Clinics of Saarland, Homburg,
Germany; j Cleveland Clinic Foundation, Cleveland, OH, USA; k Yonsei University Health Systems Severance Hospital, Seoul, Korea
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X
ava i lable at www.sc iencedirect .com
journa l homepage: www.europea nurology.com
Article info
Article history:Accepted April 14, 2015Associate Editor:James Catto
Keywords:
Robot-assisted
Robotic
Radical cystectomy
Outcomes
Survival
Bladder cancer
Recurrence
Abstract
Background: Long-term oncologic data on patients undergoing robot-assisted radical cystec-tomy (RARC) are limited and based largely on single-institution series.Objective: Report survival outcomes of patients who underwent RARC �5 yr ago.Design, setting, and participants: Retrospective review of the prospectively populated Inter-national Robotic Cystectomy Consortium multi-institutional database identified 743 patientswith RARC performed �5 yr ago. Clinical, pathologic, and survival data at the latest follow-upwere collected. Patients with palliative RARC were excluded. Final analysis was performed on702 patients from 11 institutions in 6 countries.Intervention: RARC.Outcome measurements and statistical analysis: Outcomes of interest, recurrence-free sur-vival (RFS), cancer-specific survival (CSS), and overall survival (OS) were plotted using Kaplan-Meier survival curves. A Cox proportional hazards model was used to identify factors thatpredicted outcomes.Results and limitations: Pathologic organ-confined (OC) disease was found in 62% of patients.Soft tissue surgical margins (SMs) were positive in 8%. Median lymph node (LN) yield was 16,and 21% of patients had positive LNs. Median follow-up was 67 mo (interquartile range: 18–84mo). Five-year RFS, CSS, and OS were 67%, 75%, and 50%, respectively. Non-OC disease and SMswere associated with poorer RFS, CSS, and OS on multivariable analysis. Age predicted poorerCSS and OS. Adjuvant chemotherapy and positive SMs were predictors of RFS (hazard ratio:3.20 and 2.16; p < 0.001 and p < 0.005, respectively). Stratified survival curves demonstratedpoorer outcomes for positive SM, LN, and non-OC disease. Retrospective interrogation and lackof contemporaneous comparison groups that underwent open radical cystectomy were majorlimitations.Conclusions: The largest multi-institutional series to date reported long-term survival out-comes after RARC.Patient summary: Patients who underwent robot-assisted radical cystectomy for bladdercancer have acceptable long-term survival.
soc
. Department of Urology, Roswell Park Cancer Institute, Elm and Carlton63, USA. Tel. +1 716 845 3389; Fax: +1 716 845 3300.
# 2015 European As
* Corresponding authorStreets, Buffalo, NY 142
E-mail address: khurshid.guPlease cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
http://dx.doi.org/10.1016/j.eururo.2015.04.0210302-2838/# 2015 European Association of Urology. Published by Elsevier
iation of Urology. Published by Elsevier B.V. All rights reserved.
[email protected] (K.A. Guru).
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021
B.V. All rights reserved.

Table 1 – Patient characteristics and operative and pathologicfindings
Characteristic Result
Patient characteristics
Age, yr, median (IQR) 69 (61–76)
Gender, male, n (%) 569 (82)
BMI, median (IQR) 26.6 (24–30)
ASA score >2, n (%) 273 (47)
Neoadjuvant chemotherapy, yes, n (%) 94 (15)
Operative data
Overall operative time, median (IQR) 438 (360–515)
Estimated blood loss, median (IQR) 400 (250–600)
Pathologic data
Positive soft tissue margins, yes, n (%) 55 (8)
LN yield, median (IQR) 16 (10–24)
Positive LNs, yes, n (%) 137 (21)
pT stage, n (%)*
pT0 116 (17)
pIS 78 (11)
pT1 80 (12)
pT2 148 (22)
pT3 197 (29)
pT4 60 (9)
pN stage, n (%)
N0 484 (75)
N1 54 (8)
N2–3 83 (13)
Nx 27 (4)
Adjuvant chemotherapy, yes, n (%) 134 (24)
Histology, n (%)
Transitional cell 349 (68)
Squamous cell 133 (26)
Adenocarcinoma 21 (4)
Small cell 7 (1)
Sarcomatoid 4 (1)
Extent of LN dissection, n (%)
Standard 30 (4)
Extended 507 (72)
Unknown 138 (20)
None 27 (4)
ASA = American Society of Anesthesiology; BMI = body mass index;
IQR = interquartile range; LN = lymph node.* Percentages may not add up to a total of 100, due to rounding off or due to
missing values.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X2
EURURO-6180; No. of Pages 8
1. Introduction
Recent technological advancements in minimally invasive
surgery have increased the diversity of options for surgical
management of oncologic diseases. Robot-assisted radical
cystectomy (RARC) has been compared with open radical
cystectomy (ORC) in randomized and prospective studies
and appears to reduce operative blood loss and complica-
tions while providing similar early oncologic outcomes [1–
4]. However, ORC and pelvic lymph node dissection (PLND)
remain the gold standard for muscle-invasive or recurrent
noninvasive bladder cancer, since open operation provides
>60% 10-yr recurrence-free survival (RFS) [5,6].
RARC has been criticized for limited reports of long-term
oncologic outcomes [7]. Published series report outcomes
from individual institutions with smaller numbers of
patients, representative of selected patient cohorts [8–
10]. The International Robotic Cystectomy Consortium
(IRCC) has a prospectively populated quality-assurance
database that contains >2000 RARC patients. The IRCC has
reported on learning curve, margin status, lymph node (LN)
yield, and complications [11–14]. The IRCC database was
queried to report the long-term oncologic outcomes for a
large series of patients who underwent RARC.
2. Patients and methods
The study is a retrospective review of the prospectively populated and
maintained, institutional review board–approved (I97906) database.
The IRCC database comprises 2187 patients from 37 institutions in
17 countries who were treated with RARC for clinically localized bladder
cancer from 2003 to date. Overall, 743 patients underwent RARC �5 yr
earlier. Patients with missing pathologic information or palliative RARC
were excluded at the time of analysis.
Primary outcome measures included RFS, cancer-specific survival
(CSS), and overall survival (OS). OS was defined as time from date of
cystectomy to death due to any cause. CSS was defined as the time to
death due to bladder cancer, whereas RFS was defined as time from date
of cystectomy to local and or metastatic recurrence, based on histologic
or radiologic evidence. Patients who were still alive without experienc-
ing the event of interest at their last follow-up date were considered
censored in analyses. Univariable and multivariable analyses were
performed to determine the influence of perioperative factors on the
primary outcome. Considered predictors included age, gender, patho-
logic tumor stage, pelvic LN (PLN) status, soft tissue surgical margins
(SMs), adjuvant chemotherapy, and histology. Tumor grade and
pathologic stage were determined using, respectively, the 2002 Ameri-
can Joint Committee on Cancer TNM staging system and the 2004 World
Health Organization/International Society of Urologic Pathologists
classification of papillary urothelial neoplasms [15]. Positive SM
(PSM) included radial bladder soft tissue margins. Pathologic specimens
were not reviewed at a central pathology facility.
Patients were followed using clinical, radiologic, and pathologic
evaluation, at the treating physician’s discretion. Follow-up data were
entered prospectively in the centralized database, using preset
parameters. Any missing information from any institution was acquired
to generate the most recent and thorough data set possible for this
analysis.
Descriptive analyses consisted of frequencies and relative frequen-
cies for all categorical variables. Numeric variables were summarized
using median and interquartile range (IQR). The estimated distributions
of RSF, CSS, and OS were obtained using the product limit–based
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
Kaplan-Meier method. The comparison of time-to-event distributions
for groups defined by categorical predictors was done using the log-rank
test. The univariable statistical assessment of numeric predictors was
done using the Cox proportional hazards model. Furthermore, the Cox
proportional hazards model was used in examining the multivariable
associations among RFS, CSS, and OS and considered predictors. Because
the predictive nature of each variable in the presence of the other
considered predictors was of interest, all variables were included in the
multivariable model regardless of univariable results. A nominal
significance level of 0.05 was used throughout, and all analyses were
conducted using SAS version 9.3 (SAS Institute, Cary, NC, USA).
3. Results
Overall, 702 patients were included in the analysis. The
median age was 69 yr (IQR: 61–76 yr), and 569 patients
(82%) were male. Median operative time was 438 min (IQR:
360–515 min). Most of the patients (62%) had pathologic
organ-confined (OC) disease. SMs were positive in 8%.
Median PLN yield was 16 (IQR: 10–24 nodes), and 21% of
PLNs were positive (Table 1).
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

Table 2 – Recurrence, survival, and follow-up data
Variable Result
Follow-up, mo, median (IQR) 67 (18–84)
Local recurrence, yes, n (%)* 79 (11)
Metastatic recurrence, yes, n (%)* 154 (22)
Time to recurrence, mo, median (IQR) 24 (8–60)
Survival status, alive, n (%) 383 (55)
Time to cancer-specific death, mo, median (IQR) 14 (8–28)
Time to non–cancer-specific death, mo, median (IQR) 10 (4–33)
Time to death, mo, median (IQR) 15 (7–33)
5-yr survival, %
Recurrence-free 67
Cancer-specific 75
Overall 50
IQR = interquartile range.* Includes combined local and metastatic recurrences.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X 3
EURURO-6180; No. of Pages 8
Median follow-up was 67 mo (IQR: 18–84 mo) from the
date of RARC until the time of analysis (Table 2). The overall
recurrence rate was 29%, which included an 11% local
recurrence rate. The median time to cancer-specific and
non–cancer-specific death was 14 and 10 mo, respectively.
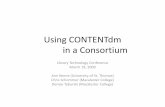
RFS, CSS, and OS were 67%, 75%, and 50%, respectively
(Table 2; Fig. 1).
Non–organ-confined (NOC) disease and positive PLNs
predicted RFS, CSS, and OS on multivariate analysis
(Table 3). PSM was associated with RFS only, on multivari-
able analysis. Age affected CSS and OS, whereas adjuvant
chemotherapy was associated with RFS only. The log-rank
test demonstrated better RFS, CSS, and OS for patients with
OC, PLN-negative, and SM-negative disease (Figs. 2 and 3).
4. Discussion
RARC is used increasingly for muscle-invasive and high-
grade recurrent bladder cancer because of consistent
applicability and acceptable perioperative morbidity
[2]. Despite a paucity of long-term oncologic outcomes,
retrospective reports of short- and intermediate-term
outcomes appear to show that RARC provides results
similar to ORC; however, selection bias has been considered
limiting [8–10]. The IRCC database was used to evaluate
whether 5-yr oncologic outcomes for RARC appeared
similar to those reported by many for ORC.
Fig. 1 – Kaplan-Meier recurrence-free, c
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
The IRCC data demonstrated that 38% patients had NOC
disease, 21% had positive PLNs, and 8% had PSM. At median
follow-up of 67 mo, 11% of patients had developed local
recurrence. The 5-yr CSS was 75%, with median time to
cancer-specific death of 14 mo. Oncologic outcomes of RARC
have been reported but with smaller numbers of patients in
selected cohorts [16]. Recently, a few studies have reported
intermediate- to long-term oncologic outcomes of RARC.
Raza et al [8] reported long-term oncologic outcomes of
99 consecutive RARC patients from a single institution. The
OS was 42% at median follow-up of 73 mo, and 52% patients
had NOC disease. The study reported 8% with PSM, with 5-yr
RFS and CSS of 53% and 68%, respectively. Yuh et al [9]
reported intermediate-term outcomes for 162 RARC
patients over a median follow-up of 52 mo. The study
included a higher number of patients with OC disease (67%)
and lower PSMs and positive PLNs (4.3% and 22%,
respectively). The 5-yr OS, RFS, and CSS were 54%, 74%,
and 80%, respectively. Xylinas et al [10] reported outcomes
for 175 RARC patients over a relatively shorter follow-up of
37 mo. They reported 65% of patients with OC disease, and
5% had PSM. The 5-yr RFS and CSS were 63% and 66%,
respectively. Long-term data from a multicenter European
database of 503 patients undergoing laparoscopic radical
cystectomy (RC) was reported by Albisinni et al [17]. Five-
year RFS, CSS, and OS rates were 66%, 75%, and 62%,
respectively. This study reported poorer outcomes associ-
ated with advanced stage, margin status, and LN involve-
ment; however, the study did not relate preoperative
variables with survival outcomes. The better OS may have
been related to selection of a younger and healthier cohort
(median age: 68 yr; American Society of Anesthesiologists
score <2 in 71% of patients).
Long-term oncologic efficacy of ORC has been well
reported [5,6,18]. Table 4 summarizes and compares the
IRCC results with the key ORC and RARC series results. Stein
et al reported outcomes of 1054 patients in a large single-
institution series and found 68% and 60% 5-yr RFS and OS,
respectively [5]. Non-OC disease and LN metastases were
37% and 23%, respectively. Ghoneim et al reported RFS of
56% at 5 yr in patients with transitional cell carcinoma
[6]. Shariat et al [19] reported outcomes of 888 consecutive
patents with transitional cell carcinoma after ORC in a
ancer-specific, and overall survival.
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

Table 3 – Univariable and Multi variable analysis of factors associated with recurrence-free, cancer-specific, and overall survival
Variable Univariable Multivariable
Hazard ratio Confidence interval p value Hazard ratio Confidence interval p value
Proportional hazard model for recurrence-free survival
Age 1.01 (1.00–1.02) 0.2 1.00 (0.98–1.02) 0.8
Gender (male vs female) 0.83 (0.58–1.17) 0.29 0.74 (0.50–1.11) 0.1
pT stage (>2 vs � 2) 3.74 (2.77–5.05) <0.001 2.12 (1.43–3.13) 0.0002
LN (positive vs negative) 1.13 (1.10–1.17) <0.001 1.08 (1.02–1.13) 0.003
Margins (positive vs negative) 2.96 (1.93–4.56) <0.001 2.16 (1.27–3.68) 0.005
Adjuvant chemotherapy (yes vs no) 4.59 (3.37–6.25) <0.001 3.20 (2.20–4.66) <0.001
Histology (TCC vs variant) 0.79 (0.55–1.13) 0.2 0.55 (0.37–0.80) 0.002
Proportional hazard model for cancer-specific survival
Age 1.01 (1.00–1.03) 0.09 1.02 (1.00–1.04) 0.03
Gender (male vs female) 0.84 (0.55–1.27) 0.4 0.83 (0.52–1.35) 0.5
pT stage (>2 vs � 2) 4.87 (3.34–7.09) <0.001 4.78 (2.91 – 7.86) <0.001
LN (positive vs negative) 1.12 (1.08–1.15) <0.001 1.11 (1.05–1.17) <0.001
Margins (positive vs negative) 3.62 (0.18–0.55) <0.001 1.52 (0.81–2.82) 0.2
Adjuvant chemotherapy (yes vs no) 2.75 (1.90–4.00) <0.001 1.23 (0.77–1.95) 0.4
Histology (TCC vs variant) 1.36 (0.92–2.00) 0.1 1.07 (0.70–1.63) 0.7
Proportional hazard model for overall survival
Age 1.02 (1.01–1.03) 0.002 1.02 (1.01–1.04) 0.002
Gender (male vs female) 1.06 (0.80–1.41) 0.7 1.12 (0.78–1.62) 0.5
pT stage (>2 vs � 2) 3.40 (2.70–4.27) <0.001 3.60 (2.60–4.98) <0.001
LN (positive vs negative) 1.10 (1.07–1.13) <0.001 1.07 (1.02–1.12) 0.003
Margins (positive vs negative) 2.81 (1.98–3.99) <0.001 1.51 (0.96–2.39) 0.07
Adjuvant chemotherapy (yes vs no) 2.31 (1.78–2.98) <0.001 1.12 (0.80–1.55) 0.5
Histology (TCC vs variant) 1.05 (0.79–1.39) 0.7 0.82 (0.61–1.11) 0.2
LN = lymph node; TCC = transitional cell carcinoma.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X4
EURURO-6180; No. of Pages 8
multi-institutional series. Overall, 43% of patients had NOC
disease and 20% had positive PLNs, with 5-yr RFS and CSS of
58% and 66%, respectively.
The negative impact of tumor stage on oncologic outcome
has been demonstrated by several studies [20,21]. Stein et al
Fig. 2 – Kaplan-Meier (a) recurrence-free and (b) cancer-specific survival estimmargins.
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
reported 5-yr RFS and OS of 68% and 66%, respectively.
However, substratified analysis of patients with pT3b and
pT4 were associated with 47% and 37% 5-yr RFS, respectively
[5]. In addition to surgical approach, OS and RFS differences
between series could be confounded by many factors like age,
ates, stratified according to pT stage, pN stage, and soft tissue surgical
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

Fig. 3 – Kaplan-Meier overall survival estimates, stratified according to pT stage, pN stage, and soft tissue surgical margins.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X 5
EURURO-6180; No. of Pages 8
preoperative surgical risks, and thoroughness of the follow-
up protocol seen with current advances in imaging.
A significant body of evidence suggests that an extended
PLND (ePLND) may improve staging, better identify patients
for adjuvant chemotherapy, control micrometastasis, and
improve survival. Abol-Enein et al [21] reported the
beneficial effect of ePLND on survival. The ePLND group,
with a median of 49 LNs removed, had 66% 5-yr CSS
compared with the standard PLND group. The difference in
survival was noted even for patients with LN-positive disease
(node positive in 24%). In the present study, 21% patients had
LN metastasis and a median nodal yield of 16 LNs. Negative
impact of LN metastasis on survival has been well
documented [22]. Shariat et al [19] found that patients with
LN-negative disease had 7-yr RFS and CSS of 66% and 72%,
respectively. Similarly, RFS is negatively affected by LN
metastasis, with 5-yr RFS of only 27% versus 62% for patients
with and without LN metastasis, respectively [6].
Meticulous tumor resection with negative SM is a key
predictor of oncologic outcomes in bladder cancer [23]. The
standards reported by collaborative groups remain the
main criteria for adequate cancer control following
ORC [24]. The IRCC reported outcomes based on these
Table 4 – Comparison of long-term oncologic outcomes among histori
Study Number Duration Follow-up, mo,mean (range)
OCdisease, %
Ghoneim
et al, 2008 [6]
2720/O 1970–2000 66 (0–410) 74
Stein et al, 2001 [5] 1054/O 1971–1997 120 (1–336) 63^
Hautmann
et al, 2012 [18]
1100/O 1986–2009 38 (0–282) 67
Shariat
et al, 2006 [19]
888/O 1984–2003 39* (0.4–183) 57
Xylinas
et al, 2013 [10]
175/R 2004–2011 37 (21–53) 65
Yuh
et al, 2014 [9]
162/R 2004–2010 52* (NR) 67
Raza
et al, 2014 [8]
99/R 2005–2009 40* (12.7–70.8) 49
Current study 702/R 2003–2009 67* (18–84) 62
CSS = cancer-specific survival; NR = not reported; O = open radical cystectomy; OC
assisted radical cystectomy; RFS = recurrence-free survival; TCC = transitional cel* Median.^ Includes pT3a as organ confined.
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
recommendations, with PSMs of 8% and LN yield of
16. Urologic oncologists are more likely to perform a PLND
in comparison to general urologists while performing RC
(62% vs 23%) [25]. In our series, 72% had an ePLND. Based on
previous study, a majority of IRCC members do not perform
PLND above the inferior mesenteric artery and presacral
regions [13]. PSM rates should be <15% for locally advanced
tumors and <20% for salvage RC. IRCC results compare
favorably with a multi-institutional study for 4410 patients
by Novara et al [23], who reported PSM rates of 4.1% for OC
disease and 12% for NOC disease (7.7% and 24% for pT3 and
pT4, respectively). In IRCC data, PSM did not independently
predict CSS and OS. On the contrary, Dotan et al [26]
demonstrated PSM as an independent predictor of local
disease relapse, distant metastasis, and CSS. In IRCC data,
5-yr RFS for NOC and PLN-negative disease and for
SM-negative patients was approximately 80% and 70%,
respectively (Fig. 2). Similar benefit was noted for CSS and
OS (Figs. 2 and 3). These findings reiterate that pathologic
factors drive outcomes for both RARC and ORC.
SWOG emphasizes the need for good surgical technique
and the benefits of favorable pathology for better outcomes
[25]. In this study of muscle-invasive disease only, 9% had
cal open and robot-assisted radical cystectomy series
Non-TCC,%
PLNyield
pN+,%
Neoadjuvantchemotherapy, %
RFS,%
CSS,%
OS,%
64 NR 20 NR 56 NR NR
0 NR 23 5 68 NR 66
0 18 18 Excluded 70 71 58
0 20 23 5 58 66 NR
4 19 17 23 63 66 NR
0 28 22 23 74 80 54
NR 21 30 6 53 68 42
32 16 21 15 67 75 50
= organ confined; OS = overall survival; PLN = pelvic lymph node; R = robot-
l carcinoma.
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

Table 5 – Site of recurrence and related pathologic findings
Recurrence site * n (%) Mean time to recurrence. d �pT2, % SM, % LN positive, %
Local 38 (19) 356 85 12 26
Pelvis 23 421 86 14 33
Vagina 4 634 100 0 0
Rectum 2 364 50 0 0
Perineum 5 140 80 0 0
Incision/port site 1 88 100 100 100
Multiple local recurrences 1 230 100 0 0
Other+ 2 153 100 0 50
Distant 121 (63) 458 78 9 46
LNs 27 537 68 8 56
Lung 27 534 73 0 31
Liver 11 506 64 18 36
Bone 23 323 83 4 48
Peritoneum 7 178 100 0 60
Multiple distant recurrences 15 390 85 23 54
Other^ 11 492 100 18 45
GU tract 17 (8) 593 53 0 21
Renal pelvis/ureter 6 736 60 0 0
Urethra 7 490 29 0 29
Anastomotic site 4 434 100 0 50
Combined (local and distant) 18 (10) 422 83 11 44
GU = genitourinary; LN = lymph node; SM = soft tissue surgical margins.* Total recurrences in 200, information on site of recurrence unavailable for 6 patients. In case of overlap, site of first recurrence is reported.** Other: Pubis and penis.^ Other: Cause not mentioned in database for 9, adrenal for 1, mesentery for 1.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X6
EURURO-6180; No. of Pages 8
no PLND, 37% had node sampling, and 54% had a standard
bilateral PLND. Only 26% had >15 nodes removed. The
recurrence risks reported for patients with disease higher
than pT3, with PSM, and with PLND were 32%, 68%, and 29%,
respectively. A group at the University of Bern found that
only 4% of LNs were situated above the aorta and vena cava
as high as the inferior mesenteric artery [27]. These findings
were based on the use of single photon emission computed
tomography. The authors postulated that only 1 in 100 cys-
tectomy patients may benefit from a superextended LN
dissection up to the inferior mesenteric artery.
The IRCC data showed a higher percentage of distant
metastasis than local recurrences (63% vs 19%), whereas
only seven patients (3.5%) were found to have peritoneal
carcinomatosis (Table 5). Nguyen et al reported their
recurrence experience for RARC and ORC [28]. Extra PLN
metastases (23% vs 15%) and peritoneal carcinomatosis
were more frequent in RARC than in ORC (21% vs 8%),
Table 6 – Number of procedures per year from participating Internati
Year Instituti
A B C D E F
2002 0 0 0 0 0 2
2003 0 0 0 0 0 1
2004 0 0 8 0 3 3
2005 0 2 12 0 5 3
2006 0 16 16 0 4 5
2007 4 1 12 1 11 15
2008 7 2 21 8 16 9
2009 12 11 12 10 19 3
Total 23 32 81 19 58 41
* Alphabetical arrangement, not arranged based on volume, author, or institution
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
respectively, and were attributed to possible cancer biology
(eight of nine RARC patients with peritoneal carcinomatosis
had disease higher than pT3). Our study included patients
from this group, but these patients may not have been
included in the current analysis, as our last date of
cystectomy was in 2009. The IRCC previously reported its
findings of early oncologic failure and found that 0.4% of
1586 patients had rapid local and port-site metastases
[29]. All of these patients had disease higher than pT2, and
two patients had positive PLNs.
Honma et al [30] found higher T stage (higher than T3–4)
and positive PLNs to be predictors of recurrence while
analyzing recurrence and distant metastasis; however,
concomitant squamous cell carcinoma was the only inde-
pendent predictor of local recurrence. Squamous cell
carcinoma was seen in 26% of our patients, but multivariable
analysis did not predict variant histology as a predictor for
recurrence.
onal Robotic Cystectomy Consortium institutions in the study
on* Total
G H I J K L
0 0 0 0 0 0 2
1 3 0 0 0 0 5
6 1 0 0 1 0 22
1 11 3 0 0 0 37
5 8 32 0 23 0 109
2 13 33 12 35 6 145
8 12 51 13 39 8 194
17 3 39 28 27 7 188
40 51 158 53 125 21 702
authorship.
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X 7
EURURO-6180; No. of Pages 8
The present IRCC report is the largest multi-institutional,
multinational series of RARC and reports long-term
oncologic outcomes. The IRCC reports suffer from limita-
tions inherent to retrospective analysis. The IRCC database
is standardized and populates multiple surgeons with
variable experience, institutional operative volume, patient
selection, and reporting bias (Table 6). The majority of
surgeons participating in the IRCC are experienced robotic
surgeons, so IRCC results should not be applied to all
urologic surgeons. Oncologic outcomes from the largest
series of RARC add to the current body of evidence, which
suggests similarity between RARC and ORC.
5. Conclusions
The largest multi-institutional cohort of RARC presents
long-term oncologic outcomes that appear similar to
historical ORC data, which support the need for randomized
trials comparing RARC and ORC.
Author contributions: Khurshid A. Guru had full access to all the data in
the study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Guru, Wilson, Wiklund, Menon, Peabody.
Acquisition of data: Raza, Saar, Stoeckle, Mottrie, Dasgupta, Scherr, Yuh,
Richstone, Kaouk, Hosseini, Rha, Khan.
Analysis and interpretation of data: Raza, Wilding, Guru.
Drafting of the manuscript: Raza, Al-Daghmin, Guru, Mohler.
Critical revision of the manuscript for important intellectual content:
Menon, Wilson, Wiklund, Peabody, Yuh.
Statistical analysis: Dibaj, Wilding.
Obtaining funding: Guru.
Administrative, technical, or material support: Raza.
Supervision: Guru.
Other (specify): None.
Financial disclosures: Khurshid A. Guru certifies that all conflicts of
interest, including specific financial interests and relationships and
affiliations relevant to the subject matter or materials discussed in the
manuscript (eg, employment/affiliation, grants or funding, consultan-
cies, honoraria, stock ownership or options, expert testimony, royalties,
or patents filed, received, or pending), are the following: None.
Funding/Support and role of the sponsor: Funding support was received
from the Vattikuti Foundation Collective Quality Initiative and the
Roswell Park Alliance Foundation. P.D. acknowledges support from the
Medical Research Council Centre for Transplantation, National Institute
for Health Research Biomedical Research Centre, King’s College London-
Vattikuti Institute of Robotic Surgery, Guy’s Hospital, King’s Health
Partners, the Guy’s and St. Thomas’ Charity, and European Union 7th
Framework Programme (EU-FP7), Sponsors were involved in the
collection of the data.
Acknowledgments: The authors acknowledge Lindsay A. Amico for
administrative support.
References
[1] Yuh B, Wilson T, Bochner B, et al. Systematic review and cumulative
analysis of oncologic and functional outcomes after robot-assisted
radical cystectomy. Eur Urol 2015;67:402–22.
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
[2] Wilson TG, Guru K, Rosen RC, et al. Best practices in robot-assisted
radical cystectomy and urinary reconstruction: recommendations
of the Pasadena Consensus Panel. Eur Urol 2015;67:363–75.
[3] Parekh DJ, Messer J, Fitzgerald J, Ercole B, Svatek R. Perioperative
outcomes and oncologic efficacy from a pilot prospective random-
ized clinical trial of open versus robotic assisted radical cystectomy.
J Urol 2013;189:474–9.
[4] Bochner BH, Dalbagni G, Sjoberg DD, et al. Comparing open radical
cystectomy and robot-assisted laparoscopic radical cystectomy: a
randomized clinical trial. Eur Urol 2015;67:1042–50.
[5] Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the
treatment of invasive bladder cancer: long-term results in 1,054
patients. J Clin Oncol 2001;19:666–75.
[6] Ghoneim MA, Abdel-Latif M, el-Mekresh M, et al. Radical cystec-
tomy for carcinoma of the bladder: 2,720 consecutive cases 5 years
later. J Urol 2008;180:121–7.
[7] Novara G, Catto JW, Wilson T, et al. Systematic review and cumu-
lative analysis of perioperative outcomes and complications after
robot-assisted radical cystectomy. Eur Urol 2015;67:376–401.
[8] Raza SJ, Al-Daghmin A, Zhuo S, et al. Oncologic outcomes following
robot-assisted radical cystectomy with minimum 5-year follow-up:
the Roswell Park Cancer Institute experience. Eur Urol 2014;66:
920–8.
[9] Yuh B, Torrey RR, Ruel NH, et al. Intermediate-term oncologic
outcomes of robot-assisted radical cystectomy for urothelial carci-
noma. J Endourol 2014;28:939–45.
[10] Xylinas E, Green DA, Otto B, et al. Robotic-assisted radical cystec-
tomy with extracorporeal urinary diversion for urothelial carcino-
ma of the bladder: analysis of complications and oncologic
outcomes in 175 patients with a median follow-up of 3 years.
Urology 2013;82:1323–9.
[11] Hayn MH, Hussain A, Mansour AM, et al. The learning curve of
robot-assisted radical cystectomy: results from the International
Robotic Cystectomy Consortium. Eur Urol 2010;58:197–202.
[12] Hellenthal NJ, Hussain A, Andrews PE, et al. Surgical margin
status after robot assisted radical cystectomy: results from the
International Robotic Cystectomy Consortium. J Urol 2010;184:
87–91.
[13] Marshall SJ, Hayn MH, Stegemann AP, et al. Impact of surgeon and
volume on extended lymphadenectomy at the time of robot-
assisted radical cystectomy: results from the International Robotic
Cystectomy Consortium (IRCC). BJU Int 2013;111:1075–80.
[14] Johar RS, Hayn MH, Stegemann AP, et al. Complications after robot-
assisted radical cystectomy: results from the International Robotic
Cystectomy Consortium. Eur Urol 2013;64:52–7.
[15] Montironi R, Lopez-Beltran A. The 2004 WHO classification of
bladder tumors: a summary and commentary. Int J Surg Pathol
2005;13:143–53.
[16] Khan MS, Elhage O, Challacombe B, et al. Long-term outcomes of
robot-assisted radical cystectomy for bladder cancer. Eur Urol
2013;64:219–24.
[17] Albisinni S, Rassweiler J, Abbou C, et al. Long-term analysis of
oncological outcomes after laparoscopic radical cystectomy in
Europe: results from a multicentre study by the European Associa-
tion of Urology (EAU) section of Uro-technology. BJU Int. In press.
http://dx.doi.org/10.1111/bju.12947
[18] Hautmann RE, de Petriconi RC, Pfeiffer C, Volkmer BG. Radical
cystectomy for urothelial carcinoma of the bladder without neoad-
juvant or adjuvant therapy: long-term results in 1100 patients. Eur
Urol 2012;61:1039–47.
[19] Shariat SF, Karakiewicz PI, Palapattu GS, et al. Outcomes of radical
cystectomy for transitional cell carcinoma of the bladder: a con-
temporary series from the Bladder Cancer Research Consortium. J
Urol 2006;176:2414–22, discussion 2422.
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021

E U R O P E A N U R O L O G Y X X X ( 2 0 1 5 ) X X X – X X X8
EURURO-6180; No. of Pages 8
[20] Madersbacher S, Hochreiter W, Burkhard F, et al. Radical cystec-
tomy for bladder cancer today–a homogeneous series without
neoadjuvant therapy. J Clin Oncol 2003;21:690–6.
[21] Abol-Enein H, Tilki D, Mosbah A, et al. Does the extent of
lymphadenectomy in radical cystectomy for bladder cancer influ-
ence disease-free survival? A prospective single-center study. Eur
Urol 2011;60:572–7.
[22] Karl A, Carroll PR, Gschwend JE, et al. The impact of lympha-
denectomy and lymph node metastasis on the outcomes of
radical cystectomy for bladder cancer. Eur Urol 2009;55:
826–35.
[23] Novara G, Svatek RS, Karakiewicz PI, et al. Soft tissue surgical
margin status is a powerful predictor of outcomes after radical
cystectomy: a multicenter study of more than 4,400 patients. J Urol
2010;183:2165–70.
[24] Herr H, Lee C, Chang S, Lerner S. Standardization of radical cystec-
tomy and pelvic lymph node dissection for bladder cancer: a
collaborative group report. J Urol 2004;171:1823–8, discussion
1827-8.
Please cite this article in press as: Raza SJ, et al. Long-term OncolResults from the International Robotic Cystectomy Consortium. Eu
[25] Herr HW, Faulkner JR, Grossman HB, et al. Surgical factors influence
bladder cancer outcomes: a cooperative group report. J Clin Oncol
2004;22:2781–9.
[26] Dotan ZA, Kavanagh K, Yossepowitch O, et al. Positive surgical
margins in soft tissue following radical cystectomy for bladder
cancer and cancer specific survival. J Urol 2007;178:2308–12,
discussion 2313.
[27] Roth B, Wissmeyer MP, Zehnder P, et al. A new multimodality
technique accurately maps the primary lymphatic landing sites of
the bladder. Eur Urol 2010;57:205–11.
[28] Nguyen DP, Al Hussein Al Awamlh B, Wu X, et al. Recurrence patterns
after open and robot-assisted radical cystectomy for bladder cancer.
Eur Urol. In press. http://dx.doi.org/10.1016/j.eururo.2015.02.003
[29] Saar M, Syed J, Guru KA. Early oncologic failure after robot-assisted
radical cystectomy: results from the International Robotic Cystec-
tomy Consortium. Eur Urol Suppl 2014;13:41.
[30] Honma I, Masumori N, Sato E, et al. Local recurrence after radical
cystectomy for invasive bladder cancer: an analysis of predictive
factors. Urology 2004;64:744–8.
ogic Outcomes Following Robot-assisted Radical Cystectomy:r Urol (2015), http://dx.doi.org/10.1016/j.eururo.2015.04.021