
The EORTC treatment of early stages of hodgkin's disease: The role of radiotherapy
Upload
independentCategory
view
0download
0
Long-term follow-up of patients with diffuse large B-cell non-Hodgkin’s lymphoma receiving purged autografts after inductionfailure
JE Benjamin, GL Chen, TM Cao, PD Cao, RM Wong, K Sheehan, JA Shizuru, LJ Johnston,RS Negrin, R Lowsky, and GG LaportDivision of Blood and Marrow Transplantation, Stanford University, Stanford, CA, USA
AbstractPatients with diffuse large B-cell lymphoma (DLBCL) who do not achieve a complete response tofront-line combination chemotherapy are often offered high-dose therapy and autologoushematopoietic cell transplantation (AHCT). However, the efficacy of this therapy in this patientpopulation has been addressed in only a few published reports. We retrospectively analyzed theoutcomes of patients with a diagnosis of de novo DLBCL who underwent AHCT at our centerbetween 1988 and 2002, and identified 43 consecutive patients who had not achieved a CR beforeAHCT, although most showed at least a partial response (PR) to either induction or subsequentsalvage chemotherapy. A total of 15 patients received a conditioning regimen that included high-dose chemotherapy with fractionated TBI (FTBI), whereas 28 patients received high-dosechemotherapy only. All autografts were treated ex vivo with MoAbs and complement in an effort toremove any residual malignant B cells. A total of 33 (77%) patients achieved a CR after AHCT. Witha median follow-up of 7.3 years, the 5-year OS was 69% and EFS was 59%. Four patients died fromnon-relapse mortality. By univariate analyses, the following characteristics did not significantlyimpact OS: disease stage at diagnosis, age-adjusted IPI (International Prognostic Index) score, age≥40 years, earlier radiotherapy and the use of FTBI in the conditioning regimen. These results confirmthe long-term efficacy of AHCT for patients with DLBCL after induction failure.
Keywordslymphoma; large B-cell; diffuse; autologous transplantation
IntroductionApproximately 45% of patients with diffuse large B-cell non-Hodgkin’s lymphoma (DLBCL)with advanced disease at diagnosis achieve a CR with anthracycline-containing front-linechemotherapy, although this number has recently increased by approximately 25% since theintroduction of rituximab.1–3 An achievement of less than a CR to front-line chemotherapy,hereafter designated as induction failure, is associated with a median survival of <15 monthsif treated only with conventional chemotherapy.4,5
Correspondence: Dr JE Benjamin, Division of Blood and Marrow Transplantation, Stanford University Medical Center, 300 Pasteur Dr,Room H3249, Stanford, CA 94305-5623, USA. [email protected] of interestThe authors declare no conflict of interest.
NIH Public AccessAuthor ManuscriptBone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
Published in final edited form as:Bone Marrow Transplant. 2010 February ; 45(2): 303–309. doi:10.1038/bmt.2009.152.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The outcomes of DLBCL patients who fail induction therapy have been described previously.4,6–11 A majority of patients with induction failure will show chemosensitivity to platinum-containing salvage regimens, but few will experience long-term survival without autologoushematopoietic cell transplantation (AHCT).12,13 Similar to the observations with relapseddisease, the best outcomes are seen in those patients who show chemosensitivity to salvagechemotherapy before AHCT. However, an interpretation of these studies is limited by theinclusion of patients with heterogeneous lymphoma histologies, the use of varied responsecriteria and the inclusion of partial responders with truly chemorefractory patients. Earlierreports have also lacked long-term follow-up.
In this report, we describe the outcomes of 43 patients with de novo DLBCL who failed toachieve a CR in response to front-line anthracycline therapy and who underwent AHCT withB-cell-purged autografts. Most patients had disease that was deemed chemosensitive beforeAHCT.
Patients and methodsPatients
The Stanford Blood and Marrow Transplantation database was screened for patients with ahistological diagnosis of non-Hodgkin’s lymphoma (NHL), who underwent AHCT from theinception of the transplantation program in 1988 to December 2002, at which time ex vivo Aband complement purging was discontinued. Among the 591 consecutive patients fitting thesecriteria, we identified 156 patients who carried a diagnosis of de novo DLBCL. All patientshad biopsy specimens that were reviewed by the Pathology Department at Stanford University,Stanford, CA, USA and were classified according to the International Working Formulation(Group F), REAL (Revised European American Lymphoma) or WHO (World HealthOrganization) classification systems, and were without mixed histology or evidence oftransformation from a low-grade lymphoma. Stage of disease at diagnosis was assignedaccording to the Ann Arbor System. Age-adjusted IPI was assigned according to the methodof Shipp et al.14
Response to induction using anthracycline-containing chemotherapy was assessed by acomputed tomography (CT) scan with or without gallium scanning and BM biopsy. Positronemission tomography (PET) scanning was not widely available during the study period andwas thus not routinely used in the majority of patients described here. Response criteria wereas follows: complete response indicated an absence of all measurable disease, partial response(PR) indicated a >50% reduction in the sum of the product of diameters of all lesions withoutthe appearance of new lesions and stable disease indicated less than a partial response, butwithout evidence of progressive disease. From among the 156 patients with de novo DLBCL,46 (29%) patients were identified as having induction failure, that is, only achieving PR orstable disease. Of these 46 patients, 3 were not included in this analysis: one who was treatedwith high-dose sequential therapy and two who received post transplantation rituximab as partof a separate protocol.15,16 All patients were treated after providing a written informed consentunder a research protocol approved by the Stanford University Medical Center AdministrativePanel on Medical Human Subjects and according to the Declaration of Helsinki.
Collection and processing of hematopoietic cellsThe patients who underwent AHCT before 1 April 1994 received BM as the hematopoieticcell source, whereas patients transplanted after this date received mobilized peripheral bloodhematopoietic cells. This shift reflected the change in practice at that time within the field ofHCT (hematopoietic cell transplantation). Those who received peripheral blood graftsunderwent mobilization with CY (4 gm/m2) or VP-16 (2 gm/m2) and G-CSF (10 mcg/kg/day).
Benjamin et al. Page 2
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
The autografts were purged as previously described.17 Briefly, nucleated cells were isolatedby discontinuous Percoll gradients, washed and resuspended in media containing 1% humanalbumin. The washed cells were incubated for 30 min at 4 °C in a cocktail of MoAbs directedagainst B-cell Ags, including anti-CD9 (clone J9), anti-CD10 (clone 4–35), anti-CD19 (cloneJ149) and anti-CD20 (clone 1F5). DNAse was added at a concentration of 100 U/ml. Rabbitcomplement was then added at a dilution of 1:8 or 1:16. After an incubation of 45 min at 37 °C, the cells were pelleted by centrifugation, resuspended in media and the process was repeated.The cells were then resuspended in 70% autologous plasma supplemented with 10% dimethylsulfoxide and frozen in a controlled-rate freezing chamber.
Conditioning regimenPatients were treated with fractionated TBI (FTBI) in 10 equal fractions to a total dose of 1200cGy, VP-16 (60 mg/kg) and with CY (100 mg/kg). BCNU (15 mg/kg up to a maximum of 550mg/m2) or CCNU (15 mg/kg orally) was substituted for FTBI in those patients who hadreceived earlier radiotherapy to the chest or pelvis, or if excessive morbidity with FTBI wasanticipated on the basis of age >50 years or poor performance status. Chemotherapy doseswere determined according to the adjusted ideal body weight, defined as ideal body weightplus 50% of the difference between ideal body weight and actual body weight.
Engraftment criteriaNeutrophil engraftment was defined as the first of three consecutive days after transplantationwith an absolute neutrophil count (ANC) of ≥500/mm3. Platelet engraftment was defined asthe first day with a platelet count of ≥20 000/mm3 and no platelet transfusions within theprevious five days.
Response evaluationRestaging CT scans and BM biopsies were performed at 3, 6 and 12 months after AHCT, andthen annually.
Statistical analysisOutcome was analyzed with respect to response, OS, EFS and freedom from progression (FFP).Time to an OS event was defined as time from HCT to death from any cause. The EFS eventtime was defined as time from HCT to death from any cause or progression of disease. In FFPanalysis, disease progression was defined as an event with censoring at the time of death,without disease progression. Two patients who achieved CR after AHCT subsequently relapsedand proceeded to non-myeloablative allogeneic transplantation. These patients were censoredfrom analysis of OS, EFS and FFP at the time of second HCT. The Kaplan–Meier method wasused to estimate actuarial OS, EFS and FFP. Cox proportional hazards regression models wereused to identify the predictors of survival. Significance (P≤0.05) was determined from theWald χ2-test.
ResultsClinical characteristics at diagnosis
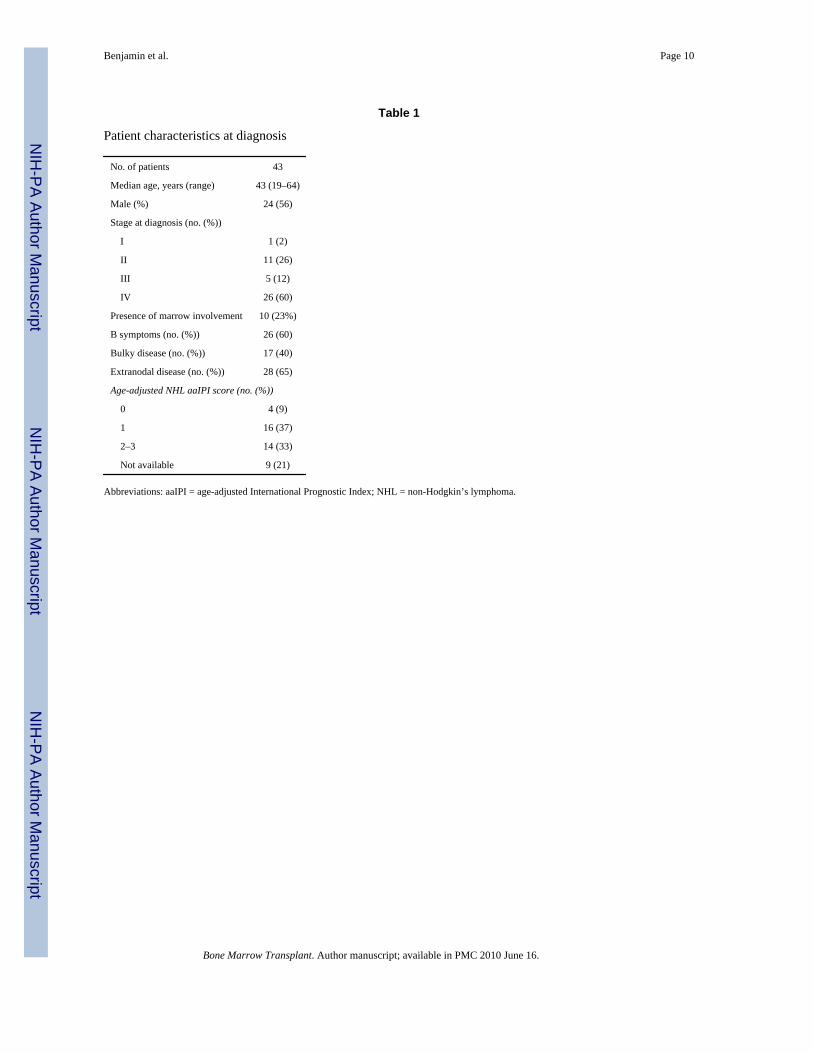
Patient characteristics are listed in Table 1. There were 24 men and 19 women, ranging in agefrom 19 to 64 years, with a median of 43 years. A total of 12 (28%) patients had stage I–IIdisease, 5 (12%) had stage III disease and 26 (60%) had stage IV disease. A total of 28 (65%)of 43 patients had extranodal disease, 11 of whom had more than one extranodal site ofinvolvement. A total of 10 (23%) patients had BM involvement, 17 (40%) had bulky diseaseand 26 (60%) experienced B symptoms. The age-adjusted NHL IPI score was low risk in 20(47%) patients, high risk in 14 (32%) patients and not available in 9 (21%) patients.
Benjamin et al. Page 3
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Induction and salvage regimens before AHCTTreatment characteristics are presented in Table 2. All patients were initially treated with ananthracycline-containing regimen: 29 (70%) patients received CHOP, 6 (14%) receivedrituximab–CHOP and 8 (16%) received other regimens. A total of 22 of 43 patients achieveda PR with a median of six cycles (range 2–12 cycles). The remaining 21 patients had stabledisease after a median of six cycles of chemotherapy (range 2–8 cycles). A total of 13 patientsdid not receive salvage chemotherapy, and proceeded directly to BM harvest (n=2) ormobilization chemotherapy (n=11) and AHCT, including four patients with stable disease. Ofthe 30 patients who received salvage chemotherapy, 25 received a platinum-containingregimen. One patient who did not receive rituximab as a part of induction therapy receivedrituximab as a part of salvage therapy. All patients who received salvage chemotherapyachieved a PR. The median time from mobilization chemotherapy to transplantation was 32days (range 27–42 days). Patients were not routinely restaged after mobilization. A total of 10(23%) of the original 43 induction failure patients required involved field radiation therapy fordisease control before mobilization chemotherapy.
Conditioning regimen and AHCTThe median time from diagnosis until AHCT was 8.8 months (range, 2.3–15.3 months). Themajority of patients (n = 26, 60%) received BCNU, CY and VP-16, whereas the remainderreceived FTBI (n = 15, 35%), or CCNU, CY and VP-16 (n = 2, 5%) as the preparative regimen.Six patients (14%) received a BM graft. Of the 37 patients who received a peripheral bloodgraft, 32 received CY as mobilization chemotherapy and 5 received VP-16. All patientsreceived B-cell-purged products. A total of 10 (23%) of the 43 patients received involved fieldradiation therapy after AHCT. Of these, eight had consolidative radiotherapy that had beenplanned before AHCT to sites of earlier bulky disease. The remaining two patients receivedradiotherapy as a component of a non-myeloablative conditioning regimen for salvageallogeneic HCT.
Treatment outcomesThe median time to neutrophil and plt engraftment was 10 days (range 8–30 days) and 14 days(range 11–33 days), respectively. There were two deaths (4.7%) within 100 days after AHCT:one from interstitial pneumonitis and the other from hepatic failure. These patients were notevaluated for disease response. Eight patients failed to achieve a CR with a median time todisease progression of 144 days (range 81–189 days). A total of 33 patients (77%) achieved aCR after AHCT. Of these, seven had a relapse of disease with a median time to relapse of 1363days (range 307–2416 days). With a median follow-up of 7.3 years (range 0.1–16.3 years), the5-year OS was 69% (95% CI 55–83%) and EFS was 59% (95% CI 42–74%), with a medianEFS of 6.7 years. The median OS has not been reached. The 5-year FFP rate was 63% (95%CI 48–78%) (see Figure 1). Causes of death after AHCT were related to relapse in 10 patientsand 5 patients died from non-relapse mortality due to hepatic, cardiac or respiratory failure.One patient died of unknown causes. Two patients developed treatment-relatedmyelodysplasia, including one patient who was diagnosed 16 years after transplantation and10 years after salvage chemotherapy for recurrent disease after AHCT.
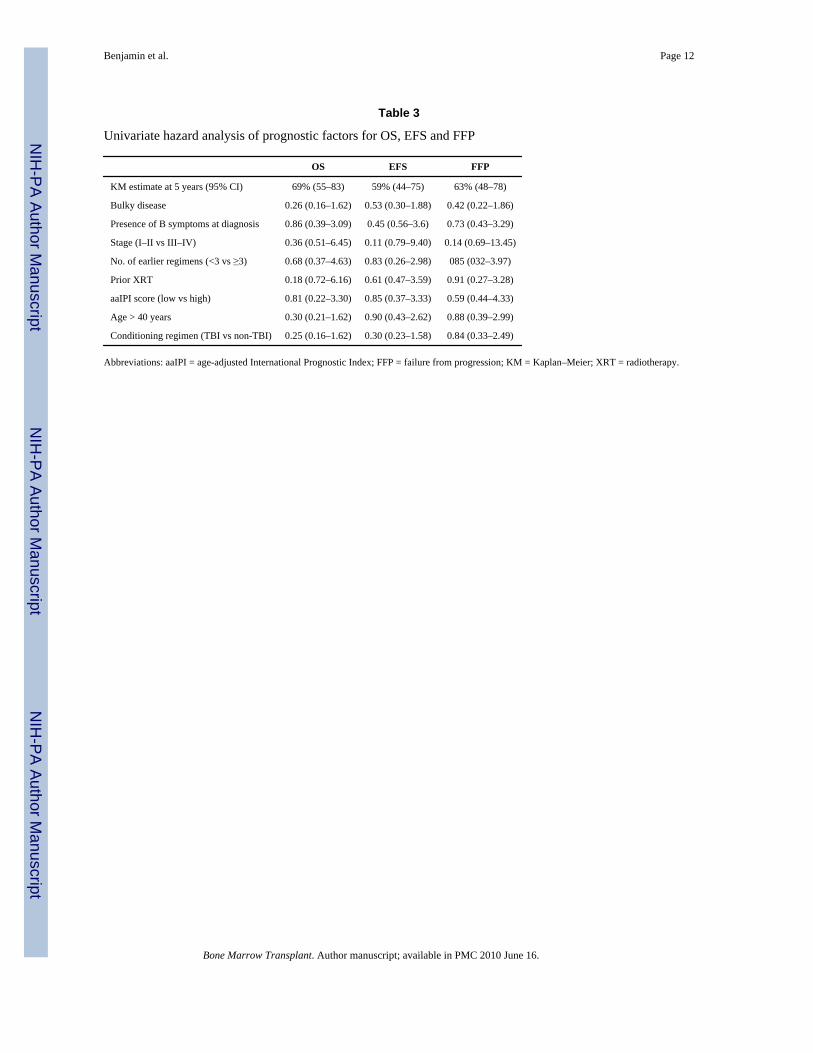
Prognostic factorsUnivariate analysis for prognostic factors is presented in Table 3. Stage at diagnosis, beforeAHCT irradiation, age-adjusted IPI, number of earlier regimens before AHCT (≤3 vs 3), age≥40 years and the use of FTBI in the preparative regimen were not significantly associatedwith worse outcomes.
Benjamin et al. Page 4
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
DiscussionIn this report, we describe the efficacy of AHCT in patients with de novo DLBCL who failedto achieve a CR to front-line conventional chemotherapy. With a lengthy follow-up, we showan OS of 69% and an EFS of 59%, which compares favorably with earlier published reportsof the outcomes of patients with induction failure, provided chemosensitivity is established.
The landmark Parma trial established the role of AHCT in patients with chemosensitive,relapsed disease, but the value of AHCT for patients with aggressive NHL who failed inductionchemotherapy is less well defined.5 Previous studies have shown a poor prognosis for thisparticular population, with salvage therapy yielding an EFS of only <15% and a median OSof <15 months.4,5 In a randomized study, a prospective Italian multicenter study attempted toestablish the optimal regimen for NHL patients who were induction failures.8 Patients wererestaged after receiving four of six planned cycles of front-line therapy. Those who achieveda PR were randomized to receive salvage chemotherapy (n=27) or AHCT (n=22). The 3-yearOS was 59% for the salvage group vs 73% for the AHCT group, with the corresponding PFSbeing 52 and 73%. Owing to the small sample size and lack of power, these differences werenot statistically significant.
In an analysis from the Autologous Blood and Marrow Transplant Registry, Vose et al.11
identified 184 patients with diffuse aggressive NHL who never achieved a CR withconventional chemotherapy. A total of 96% of patients received subsequent salvagechemotherapy, with 60% being deemed chemosensitive and 28% being chemotherapy resistantbefore AHCT. A total of 12% were not assessable. For all patients, the 5-year OS and PFSwere 37% and 41%, respectively, but patients who were chemoresistant at the time of AHCThad a 2.44-fold higher relative risk of death from relapse than chemosensitive patients (P =<0.0001), thus confirming the unequivocal prognosticator of chemosensitivity. Response aftertransplantation also affected survival, as OS was 61% for patients who obtained a CR afterAHCT compared with only 11% for PR patients and non-responders. These data are similarto a report from the GEL-TAMO (Grupo de Espanol de Linformas/Trasplante Autologo deMedula Osea) registry of 114 DLBCL patients who did not achieve a CR after induction.18
The 5-year OS was 43% for all patients. For patients who were truly chemoresistant and whodid not respond to salvage therapy, OS and EFS were 10 and 0%, respectively, compared with61 and 71%, respectively, for PR patients. Unlike our analyses, both of these registry studiesincluded chemoresistant patients, which may explain our superior survival incidences.
In a single institution retrospective analysis, the Memorial Sloan Kettering group reported theoutcome of 85 patients with aggressive NHL who achieved less than a CR after front-linechemotherapy.4 All patients subsequently received ICE (ifosfamide–carboplatin–etoposide)salvage chemotherapy. In an intent-to-treat analysis, the 3-year OS and EFS were 25 and 22%,respectively, but when the patients who actually proceeded to AHCT (n=42) were analyzedseparately, the 3-year OS and EFS were 52 and 44%, respectively. The patients who did notproceed to AHCT had a median OS of only 3.7 months. Thus, these results also validate therole of AHCT for this challenging patient population. The investigators note that the outcomesof their chemosensitive patients who proceeded to AHCT were similar to the Parma results,which confirm that once chemosensitivity is established, there is no significant difference inoutcome after AHCT in patients who were induction failures or who had relapsed disease.
As previously mentioned, our results compare favorably with the above mentioned studies andshow the long-term success of this treatment approach. In contrast to those reports, our studywas limited to patients with histologically confirmed DLBCL. Previous similar studiesincluded diverse NHL subtypes, including transformed indolent disease, high-grade disease orT-cell histologies.4,8,11 Another distinct feature of our study is the lengthy follow-up of 7.3
Benjamin et al. Page 5
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

years as other similar published studies only reach a follow-up duration of up to 4 years. Despitethe long follow-up duration, our favorable outcomes have remained durable over time.
All of our patients received ex vivo purged autografts, which is another distinct feature of ourstudy and also may have contributed to our notable outcomes. Our method of purging with apanel of MoAbs and complement has been shown to reduce the lymphoma tumor burden fromperipheral blood autografts.17 Purging had no impact on the time to neutrophil and pltengraftment. A comparison of this with subsequent protocols at our institution using unpurgedautografts showed comparable times to engraftment.
The impact of purging on survival after AHCT for NHL is controversial.19 Randomized trialsthat aimed at assessing the value of in vitro purging have shown no benefit, although some ofthese studies were limited by the inclusion of diverse lymphoma histologies and a variety ofpurging techniques.19 Of patients with DLBCL in CR mobilized with chemotherapy and G-CSF, approximately 50% will have apheresis products that show a PCR evidence ofcontamination with tumor cells.20 Vose et al.21 also reported that patients with DLBCL whoreceived unpurged BM with PCR evidence of contamination by lymphoma had an inferior EFScompared with patients whose grafts were PCR negative for tumor cells. There are norandomized studies evaluating the impact of B-cell purging of autografts in DLBCL, and it isunlikely that such studies will ever be conducted given the labor and cost of producing clinical-grade antibodies, as well as the increasing use of rituximab for the purposes of in vivo purging.22
In addition, with rare exception, DLBCL patients are currently treated with rituximab as partof front-line therapy, salvage therapy or both. Rituximab has also been used for purposes ofin vivo purging and has yielded PCR-negative grafts primarily in patients with follicular andmantle cell NHL.22–24 Thus, the advent of rituximab has nearly eliminated the need or interestin pursuing ex vivo purging with MoAbs or immunomagnetic columns, both of which are quitelabor intensive. Only seven patients in our cohort received rituximab before AHCT, and thusthe impact of rituximab in our cohort cannot be accurately assessed. A recent publication byAlousi et al.25 has shown that patients with metabolically active disease and who receiverituximab as a component of the mobilization regimen have a 5-year PFS of 46%. In contrast,similar patients who did not receive rituximab had a 5-year PFS of 10%.
Another possible explanation for our notable results is that our patients were assessed by CTand not by metabolic imaging with [18F] fluorodeoxyglucose PET scanning, which may haveled to an underestimation of a true CR rate. CT scanning is unable to distinguish viable tumorfrom fibrotic or necrotic tissue, and is therefore likely to overestimate the presence of viabletumor. Juweid et al.26 compared the response assessment by CT with PET–CT in 54 patientswith aggressive NHL, including 47 with DLBCL. A total of 31% of patients evaluated withCT achieved a CR, whereas restaging with PET–CT increased the CR rate to 65%. PET–CTeliminated the category of Cru (complete response, unconfirmed) and also reduced thepercentage of PR from 35 to 22%. The 3-year PFS was significantly lower in patients scoredas PR by CT–PET compared with those scored as PR by CT alone. Thus, it is possible that apercentage of our patients were actually in a CR after front-line therapy and thus were alreadyin a favorable prognostic group.
In summary, we conclude that for de novo DLBCL patients, failure to achieve a CR to upfrontcombination chemotherapy does not necessarily confer a poor prognosis. Our favorableoutcomes may partially be attributed to our homogenous population of DLBCL patients andto the use of B-cell purging. Our results showed that over half of such patients can be curedwith AHCT, provided chemosensitivity is established either with induction and/or with salvagechemotherapy. The impact of our B-cell purging technique cannot be definitively assessed as
Benjamin et al. Page 6
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

this was not a randomized trial, but the current widespread use of rituximab during induction,salvage and/or mobilization is most likely to reduce risk of tumor cell contamination inmobilized autografts and may ultimately improve outcomes of this patient population. Thus,our results show the long-term benefit of this treatment strategy for patients with DLBCL whodo not achieve a CR with induction chemotherapy.
AcknowledgmentsThis study was supported in part by grant, P01-CA 49605, from the National Institutes of Health, Bethesda, MD, USA.
References1. Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, et al. Comparison of a standard
regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin’slymphoma. N Engl J Med 1993;328:1002–1006. [PubMed: 7680764]
2. Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, et al. CHOP chemotherapy plusrituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N EnglJ Med 2002;346:235–242. [PubMed: 11807147]
3. Pfreundschuh M, Trumper L, Osterborg A, Pettengell R, Trneny M, Imrie K, et al. CHOP-likechemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera InternationalTrial (MInT) Group. Lancet Oncol 2006;7:379–391. [PubMed: 16648042]
4. Kewalramani T, Zelenetz AD, Hedrick EE, Donnelly GB, Hunte S, Priovolos AC, et al. High-dosechemoradiotherapy and autologous stem cell transplantation for patients with primary refractoryaggressive non-Hodgkin lymphoma: an intention-to-treat analysis. Blood 2000;96:2399–2404.[PubMed: 11001890]
5. Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, et al. Autologous bonemarrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitivenon-Hodgkin’s lymphoma. N Engl J Med 1995;333:1540–1545. [PubMed: 7477169]
6. Philip T, Hartmann O, Biron P, Cahn JY, Pein F, Bordigoni P, et al. High-dose therapy and autologousbone marrow transplantation in partial remission after first-line induction therapy for diffuse non-Hodgkin’s lymphoma. J Clin Oncol 1988;6:1118–1124. [PubMed: 3292712]
7. Verdonck LF, Dekker AW, de Gast GC, van Kempen ML, Lokhorst HM, Nieuwenhuis HK. Salvagetherapy with ProMACE-MOPP followed by intensive chemoradiotherapy and autologous bonemarrow transplantation for patients with non-Hodgkin’s lymphoma who failed to respond to first-lineCHOP. J Clin Oncol 1992;10:1949–1954. [PubMed: 1453209]
8. Martelli M, Vignetti M, Zinzani PL, Gherlinzoni F, Meloni G, Fiacchini M, et al. High-dosechemotherapy followed by autologous bone marrow transplantation versus dexamethasone, cisplatin,and cytarabine in aggressive non-Hodgkin’s lymphoma with partial response to front-linechemotherapy: a prospective randomized Italian multicenter study. J Clin Oncol 1996;14:534–542.[PubMed: 8636768]
9. Prince HM, Crump M, Imrie K, Stewart AK, Girouard C, Brandwein JM, et al. Intensive therapy andautotransplant for patients with an incomplete response to front-line therapy for lymphoma. Ann Oncol1996;7:1043–1049. [PubMed: 9037363]
10. Sharp JG, Kessinger A, Mann S, Crouse DA, Armitage JO, Bierman P, et al. Outcome of high-dosetherapy and autologous transplantation in non-Hodgkin’s lymphoma based on the presence of tumorin the marrow or infused hematopoietic harvest. J Clin Oncol 1996;14:214–219. [PubMed: 8558200]
11. Vose JM, Zhang MJ, Rowlings PA, Lazarus HM, Bolwell BJ, Freytes CO, et al. Autologoustransplantation for diffuse aggressive non-Hodgkin’s lymphoma in patients never achievingremission: a report from the Autologous Blood and Marrow Transplant Registry. J Clin Oncol2001;19:406–413. [PubMed: 11208832]
12. Press OW, Livingston R, Mortimer J, Collins C, Appelbaum F. Treatment of relapsed non-Hodgkin’slymphomas with dexamethasone, high-dose cytarabine, and cisplatin before marrow transplantation.J Clin Oncol 1991;9:423–431. [PubMed: 1999711]
Benjamin et al. Page 7
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

13. Velasquez WS, McLaughlin P, Tucker S, Hagemeister FB, Swan F, Rodriguez MA, et al. ESHAP–an effective chemotherapy regimen in refractory and relapsing lymphoma: a 4–year follow-up study.J Clin Oncol 1994;12:1169–1176. [PubMed: 8201379]
14. The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model foraggressive non-Hodgkin’s lymphoma. N Engl J Med 1993;329:987–994. [PubMed: 8141877]
15. Johnston LJ, Stockerl-Goldstein KE, Hu WW, Negrin RS, Hoppe RT, Blume KG, et al. Toxicity ofhigh-dose sequential chemotherapy and purged autologous hematopoietic cell transplantationprecludes its use in refractory/recurrent non-Hodgkin’s lymphoma. Biol Blood Marrow Transplant2000;6 (5A):555–562. [PubMed: 11071261]
16. Horwitz SM, Negrin RS, Blume KG, Breslin S, Stuart MJ, Stockerl-Goldstein KE, et al. Rituximabas adjuvant to high-dose therapy and autologous hematopoietic cell transplantation for aggressivenon-Hodgkin lymphoma. Blood 2004;103:777–783. [PubMed: 12907446]
17. Negrin RS, Kusnierz-Glaz CR, Still BJ, Schriber JR, Chao NJ, Long GD, et al. Transplantation ofenriched and purged peripheral blood progenitor cells from a single apheresis product in patientswith non-Hodgkin’s lymphoma. Blood 1995;85:3334–3341. [PubMed: 7538824]
18. Rodriguez J, Caballero MD, Gutierrez A, Solano C, Arranz R, Lahuerta JJ, et al. Autologous stem-cell transplantation in diffuse large B-cell non-Hodgkin’s lymphoma not achieving completeresponse after induction chemotherapy: the GEL/TAMO experience. Ann Oncol 2004;15:1504–1509. [PubMed: 15367411]
19. Jacobsen E, Freedman A. B-cell purging in autologous stem-cell transplantation for non-Hodgkinlymphoma. Lancet Oncol 2004;5:711–717. [PubMed: 15581541]
20. Jacquy C, Soree A, Lambert F, Bosly A, Ferrant A, Andre M, et al. A quantitative study of peripheralblood stem cell contamination in diffuse large-cell non-Hodgkin’s lymphoma: one-half of patientssignificantly mobilize malignant cells. Br J Haematol 2000;110:631–637. [PubMed: 10997975]
21. Vose JM, Sharp G, Chan WC, Nichols C, Loh K, Inwards D, et al. Autologous transplantation foraggressive non-Hodgkin’s lymphoma: results of a randomized trial evaluating graft source andminimal residual disease. J Clin Oncol 2002;20:2344–2352. [PubMed: 11981006]
22. Magni M, Di Nicola M, Devizzi L, Matteucci P, Lombardi F, Gandola L, et al. Successful in vivopurging of CD34-containing peripheral blood harvests in mantle cell and indolent lymphoma:evidence for a role of both chemotherapy and rituximab infusion. Blood 2000;96:864–869. [PubMed:10910898]
23. Gianni AM, Magni M, Martelli M, Di Nicola M, Carlo-Stella C, Pilotti S, et al. Long-term remissionin mantle cell lymphoma following high-dose sequential chemotherapy and in vivo rituximab-purgedstem cell autografting (R-HDS regimen). Blood 2003;102:749–755. [PubMed: 12663455]
24. Lazzarino M, Arcaini L, Bernasconi P, Alessandrino EP, Gargantini L, Cairoli R, et al. A sequenceof immunochemotherapy with Rituximab, mobilization of in vivo purged stem cells, high-dosechemotherapy and autotransplant is an effective and non-toxic treatment for advanced follicular andmantle cell lymphoma. Br J Haematol 2002;116:229–235. [PubMed: 11841421]
25. Alousi AM, Saliba RM, Okoroji GJ, Macapinlac HA, Hosing C, Korbling M, et al. Disease stagingwith positron emission tomography or gallium scanning and use of rituximab predict outcome forpatients with diffuse large B-cell lymphoma treated with autologous stem cell transplantation. Br JHaematol 2008;142:786–792. [PubMed: 18564354]
26. Juweid ME, Wiseman GA, Vose JM, Ritchie JM, Menda Y, Wooldridge JE, et al. Responseassessment of aggressive non-Hodgkin’s lymphoma by integrated International Workshop Criteriaand fluorine-18–fluorodeoxyglucose positron emission tomography. J Clin Oncol 2005;23:4652–4661. [PubMed: 15837965]
Benjamin et al. Page 8
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Kaplan–Meier estimates of OS and EFS for all patients.
Benjamin et al. Page 9
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Benjamin et al. Page 10
Table 1
Patient characteristics at diagnosis
No. of patients 43
Median age, years (range) 43 (19–64)
Male (%) 24 (56)
Stage at diagnosis (no. (%))
I 1 (2)
II 11 (26)
III 5 (12)
IV 26 (60)
Presence of marrow involvement 10 (23%)
B symptoms (no. (%)) 26 (60)
Bulky disease (no. (%)) 17 (40)
Extranodal disease (no. (%)) 28 (65)
Age-adjusted NHL aaIPI score (no. (%))
0 4 (9)
1 16 (37)
2–3 14 (33)
Not available 9 (21)
Abbreviations: aaIPI = age-adjusted International Prognostic Index; NHL = non-Hodgkin’s lymphoma.
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Benjamin et al. Page 11
Table 2
Treatment characteristics
Response to induction therapy n
CHOP (%) 29 (67)
PR 15
SD 14
R–CHOP (%) 6 (14)
PR 0
SD 6
Others (%) 8 (19)
PR 7
SD 1
Salvage chemotherapy (%) 28 (65)
ESHAP 7
DHAP 13
ICE 3
Other 5
Best response after salvage chemotherapy 28
PR 27
SD 1
Pre-transplant IF radiotherapy (%) 10 (23)
Mobilization chemotherapy
CY 32
VP-16 5
Conditioning regimen
BCNU/VP16/CY (%) 26 (60)
FTBI/VP-16/CY (%) 15 (35)
CCNU/VP-16/CY (%) 2 (5)
Hematopoietic cell source
BM 6 (14%)
Peripheral blood 37 (86%)
Post-AHCT IF radiotherapy (%) 10 (23)
Abbreviations: BCNU = carmustine; CCNU = lomustine; ESHAP = etoposide, methylprednisolone, cytarabine and cisplatin; FTBI = fractionatedTBI; ICE = ifosfamide, carboplatin and etoposide; IF = involved field; PR = partial response; R = rituximab; SD = stable disease; VP-16 = etoposide.
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Benjamin et al. Page 12
Table 3
Univariate hazard analysis of prognostic factors for OS, EFS and FFP
OS EFS FFP
KM estimate at 5 years (95% CI) 69% (55–83) 59% (44–75) 63% (48–78)
Bulky disease 0.26 (0.16–1.62) 0.53 (0.30–1.88) 0.42 (0.22–1.86)
Presence of B symptoms at diagnosis 0.86 (0.39–3.09) 0.45 (0.56–3.6) 0.73 (0.43–3.29)
Stage (I–II vs III–IV) 0.36 (0.51–6.45) 0.11 (0.79–9.40) 0.14 (0.69–13.45)
No. of earlier regimens (<3 vs ≥3) 0.68 (0.37–4.63) 0.83 (0.26–2.98) 085 (032–3.97)
Prior XRT 0.18 (0.72–6.16) 0.61 (0.47–3.59) 0.91 (0.27–3.28)
aaIPI score (low vs high) 0.81 (0.22–3.30) 0.85 (0.37–3.33) 0.59 (0.44–4.33)
Age > 40 years 0.30 (0.21–1.62) 0.90 (0.43–2.62) 0.88 (0.39–2.99)
Conditioning regimen (TBI vs non-TBI) 0.25 (0.16–1.62) 0.30 (0.23–1.58) 0.84 (0.33–2.49)
Abbreviations: aaIPI = age-adjusted International Prognostic Index; FFP = failure from progression; KM = Kaplan–Meier; XRT = radiotherapy.
Bone Marrow Transplant. Author manuscript; available in PMC 2010 June 16.
Copyright © 2022 FDOKUMEN




















