
Role of dietary fatty acids and acute hyperglycemia in modulating cardiac cell death
Upload
independentCategory
view
2download
0
Acta Neuropsychiatrica 2007: 19: 92–103All rights reservedDOI: 10.1111/j.1601-5215.2007.00189.x
# 2007 The AuthorsJournal compilation # 2007 Blackwell Munksgaard
ACTA NEUROPSYCHIATRICA
Review article
Long chain omega-3 polyunsaturated fattyacids in the treatment of psychiatric illnessesin children and adolescents
Clayton EH, Hanstock TL, Garg ML, Hazell PL. Long chain omega-3polyunsaturated fatty acids in the treatment of psychiatric illnesses inchildren and adolescents.
Objective: Long chain omega-3 polyunsaturated fatty acids (LCn-3PUFA) are in increasing use in the general population to treat healthproblems. The objective of the current article is to review the evidencefor the rationale and benefit of LCn-3PUFA in the treatment ofcommon psychiatric disorders in children and adolescents.Methods: A search of Psychlit, PubMed and Cochrane Databases wasconducted using the terms child, adolescent, bipolar, depression,psychosis, first-episode psychosis, schizophrenia, attention deficithyperactivity disorder (ADHD), autism, psychiatric, omega-3, n-3,docosahexaenoic acid and eicosapentaenoic acid. Further studies wereidentified from the bibliographies of published reviews.Results: One small randomized controlled trial with LCn-3PUFAsupplementation in depression in children found a small beneficial effectover placebo. Four placebo-controlled trials showed uncertain benefit ofLCn-3PUFA for ADHD. Single placebo-controlled trials showed nobenefit in autism or bipolar disorder. There is an absence of studiesexamining benefit for first-episode psychosis or schizophrenia in childrenand adolescents.Conclusions: While children and adolescents are receiving LCn-3PUFAfor a range of psychiatric indications, there is only evidence of likelybenefit for unipolar depression.
Edward H. Clayton1,Tanya L. Hanstock2,3,Manohar L. Garg1,Philip L. Hazell4,51Nutraceuticals Research Group, University ofNewcastle, Callaghan, NSW, Australia; 2The BipolarProgram, Hunter New England Area Health Service,Newcastle, NSW, Australia; 3Department ofPsychology, University of Newcastle, Callaghan, NSW,Australia; 4Central Clinical School, University ofSydney, NSW, Australia; and 5Discipline of Psychiatry,School of Medical Practice and Population Health,University of Newcastle, Callaghan, NSW, Australia
Keywords: ADHD; adolescents; autism; bipolar;children; depression; DHA; EPA; omega-3;psychiatry; schizophrenia
Dr Edward Clayton, Research Fellow, NutraceuticalsResearch Group, Room 305B, Medical SciencesBuilding, University of Newcastle, Callaghan,NSW 2305, Australia.Tel: 161 249 215 343;Fax: 161 249 212 028;E-mail: [email protected]
Introduction
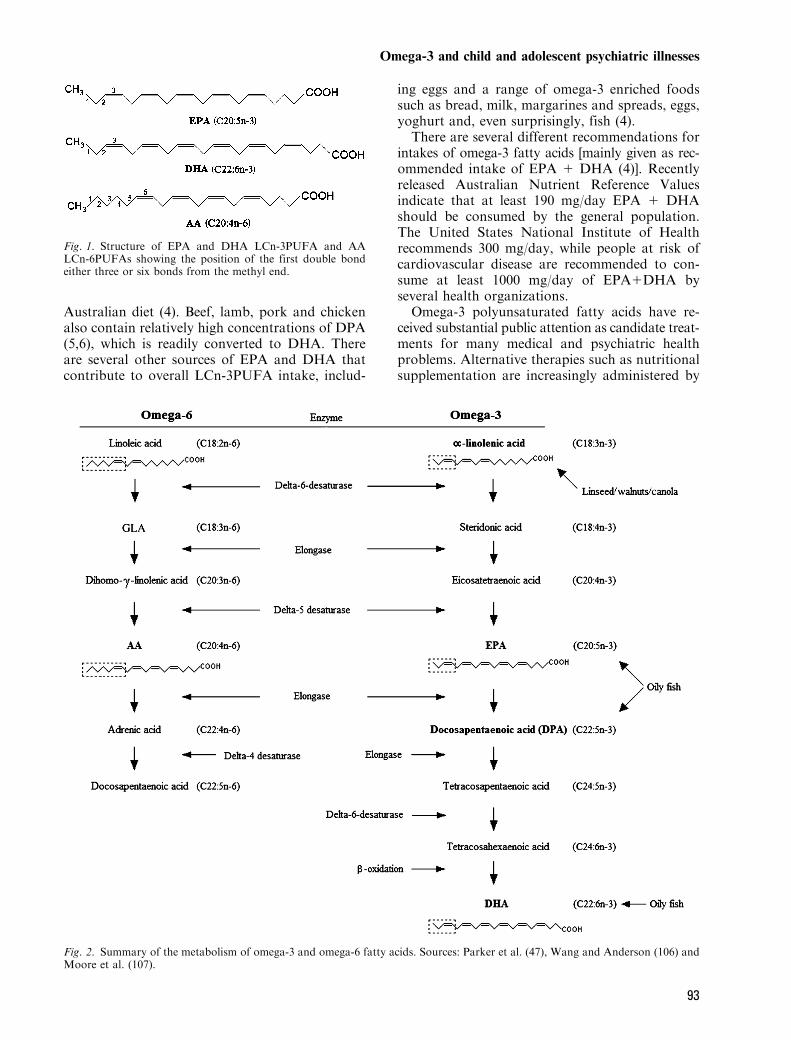
Omega-3 fatty acids (long chain omega-3 poly-unsaturated fatty acids, LCn-3PUFA) is becomingan increasingly used term in the lay public andmedia as well as in the health profession. LCn-3PUFA are long chain fatty acids with more thanone double bond in their structure, with the firstdouble bond occurring three bonds from themethyl end of the chain. LCn-6PUFA containsmore than one double bond with the first doublebond occurring six bonds from the methyl end(Fig. 1). LCn-3PUFAs are consumed from twomain dietary sources, plants and marine life.The plant form of omega-3, a-linolenic acid
(C18:3n-3), found in high quantities in linseed oil
for example, is an essential fatty acid that can beconverted to eicosapentaenoic acid (C20:5n-3; EPA)and docosahexaenoic acid (C22:6n-3; DHA) (1)(Fig. 2). The conversion from a-linolenic acid toEPA and DHA is very inefficient though withestimates of only 0.2% (2) to 6% (3) of consumeda-linolenic acid being converted to EPA and onlyapproximately 63% of EPA being converted toDHA (3). Furthermore, increased intake of linoleicacid (C18:2n-6) also decreases the conversion ofa-linolenic acid to EPA (3) through competitiveinhibition.
The highest concentrations of EPA and DHALCn-3PUFA are found in seafood, which contrib-utes around 70% of LCn-3PUFA intake in the
92
Australian diet (4). Beef, lamb, pork and chickenalso contain relatively high concentrations of DPA(5,6), which is readily converted to DHA. Thereare several other sources of EPA and DHA thatcontribute to overall LCn-3PUFA intake, includ-
ing eggs and a range of omega-3 enriched foodssuch as bread, milk, margarines and spreads, eggs,yoghurt and, even surprisingly, fish (4).There are several different recommendations for
intakes of omega-3 fatty acids [mainly given as rec-ommended intake of EPA 1 DHA (4)]. Recentlyreleased Australian Nutrient Reference Valuesindicate that at least 190 mg/day EPA 1 DHAshould be consumed by the general population.The United States National Institute of Healthrecommends 300 mg/day, while people at risk ofcardiovascular disease are recommended to con-sume at least 1000 mg/day of EPA1DHA byseveral health organizations.Omega-3 polyunsaturated fatty acids have re-
ceived substantial public attention as candidate treat-ments for many medical and psychiatric healthproblems. Alternative therapies such as nutritionalsupplementation are increasingly administered by
Fig. 1. Structure of EPA and DHA LCn-3PUFA and AALCn-6PUFAs showing the position of the first double bondeither three or six bonds from the methyl end.
Fig. 2. Summary of the metabolism of omega-3 and omega-6 fatty acids. Sources: Parker et al. (47), Wang and Anderson (106) andMoore et al. (107).
Omega-3 and child and adolescent psychiatric illnesses
93

parents to their children as an adjunct to mainstreamtreatment (7,8), of which the LCn-3PUFA supple-ments appear to be the most popular. Many brandsof omega-3 supplements are promoted in themedia, and these supplements are readily availablefrom retail outlets and through the Internet. Ad-vertisements claim benefits for a wide range ofsymptoms and disorders. LCn-3PUFA supplementshave been used in the treatment of childhoodmedical conditions such as asthma (9), Crohn’s dis-ease (10,11) and eczema [for review, see Horrobin(12)], and one study has reported the benefits ofomega-3 supplementation in reducing the frequencyof seizures in epilepsy (13).Clinicians in the field of child and adolescent
mental health will likely encounter patients who arereceiving LCn-3PUFA supplements and may beasked questions about efficacy and safety in psychi-atric conditions. The following paper will examinethe rationale for treating psychiatric problems withLCn-3PUFA supplementation and review the evi-dence for efficacy in common psychiatric disordersaffecting children and adolescents.
Background evidence linking LCn-3PUFA to psychiatricillness
There are several lines of evidence that suggest thatLCn-3PUFA may be involved with the aetiology ofpsychiatric illness in adults. First, epidemiologicalstudies linking fish consumption with rates of psy-chiatric disease, second, comparative studies exam-ining deficiencies of LCn-3PUFA in the plasma ofpeople with psychiatric conditions compared withhealthy controls and, last, evidence from interven-tion studies examining the effectiveness of LCn-3PUFA either as monotherapy or as adjunct therapyin several illnesses.Early evidence of the role of LCn-3PUFA came
from the treatment of mental disorders with flax-seed oil (14). Since that time, Western Europeandiets have often been referred to as being largelydeficient in LCn-3PUFA (15), which may be asso-ciated with increasing rates of several psychiatricillnesses, including affective disorders (16). There isepidemiological evidence relating fish consumptionto the incidence of several psychiatric diseasesincluding depression (17,18), post-natal depression(19), bipolar disorder (20) and schizophrenia (21).Many studies have been conducted examining
both deficiencies of LCn-3PUFA in the blood ofindividuals with psychiatric illness compared withhealthy controls and supplementation studies inseveral diseases. This evidence will be examined indetail in relation to psychiatric illness of childrenand adolescents throughout this review.
Omega-3 in brain development
LCn-3PUFA plays a vital role in brain develop-ment. DHA is a major structural component of cellmembranes throughout the body, particularly inbrain neurones (22). DHA is predominantly foundin phospholipids, while EPA is found primarily incholesterol esters, triglycerides and phospholipids.DHA is the most abundant unsaturated fatty acidfound in the brain (23), particularly in the cerebralcortex accounting for approximately 14% of totalfatty acids (24). DHA is also found in large con-centrations in the retina, testes and sperm (25).Normal brain growth and development in infantsand children require dietary intake of LCn-3PUFAas the major structural components of neural cellmembranes (26,27), and DHA, in particular,appears to be involved in the development ofcognition in infants [for review, see Willatts andForsyth (28)].
Proposed mechanisms of action of omega-3 fatty acids
A number of possible mechanisms may linkimprovement in psychiatric illness symptoms withLCn-3PUFA supplementation. LCn-3PUFA sup-plementation is associated with increased mem-brane fluidity in patients with bipolar disorder(29), which is believed to be associated witha general dampening of signal transduction path-ways associated with phosphatidylinositol, arach-idonic acid (AA) and other systems (30).
Increased EPA and DHA concentrations alsoinhibit the activity of rat protein kinase C in vitro(31,32), similar to the actions of lithium andvalproate. Altering the ratio of LCn-6PUFA toLCn-3PUFA by supplementation, in conjunctionwith standard pharmacotherapy (33), may furtherimprove membrane function. It is recommended,therefore, that LCn-3PUFAs are used as an adjunctto standard pharmacotherapy for the treatment ofbipolar disorder (34).
LCn-3PUFA and LCn-6PUFA are believed tohave opposing biological effects (34), and, ingeneral, the LCn-6PUFA AA (20:4 n-6) is believedto be proinflammatory and associated with upre-gulation of cytokines, while the LCn-3PUFAsEPA and DHA are anti-inflammatory (35). WhileEPA is not found in neuronal cell membranes, it isan important precursor for eicosanoids and isa modulator of inflammation [for review, see Peetand Stokes (36)]. Increased circulating proinflam-matory cytokines have been proposed to beinvolved with the aetiology of depression [forreview, see Charlton (37) and Raison et al. (38)].Higher concentrations of LCn-3PUFA in brain
Clayton et al.
94

may lead to decreased cytokine production (andinflammation) via alterations to the tumournecrosis factor-a receptor for example (30), therebyproviding a further possible link between LCn-3PUFA and the treatment of depression.Further evidence linking LCn-3PUFA to psy-
chiatric disorders comes from the effect of com-monly used psychiatric medications on fatty acidmetabolism. Lithium and valproate treatmentdecrease the turnover of brain AA, withoutaltering concentrations of DHA (39,40) or increas-ing the turnover of DHA in brain phospholipids inrats (41).Low intakes of DHA are associated with lower
concentrations of dopamine and serotonin in thefrontal cortex of pigs (42) and rats (43). Lowomega-3 is also associated with reduced serotoner-gic transmission in rats (44).
LCn-3PUFA in child and adolescent psychiatry
Several comprehensive reviews have been con-ducted over recent years relating LCn-3PUFA topsychiatric illness in adults (24,36,45–48). Thecurrent review will not try to re-present much ofthe information contained in these reviews butrather examine what evidence from psychiatricresearch indicates the effectiveness of LCn-3PUFA, particularly in children and adolescents.
Depression
Studies of adult patients with major depressionhave found a depletion in LCn-3PUFA, includinga-linolenic acid (C18:3 n-3), EPA (C20:5n-3) andDHA (C22:6 n-3), in plasma cholesteryl esters (49)and DHA compared with AA in red blood cell(RBC) membrane phospholipids (50) than healthycontrols. Plasma total DHA is also found to bereduced in depressed patients who attempt suicidecompared with those who do not attempt suicide(51). LCn-3PUFAs are depleted and monounsat-urated fatty acids increased in plasma phospholi-pids of adult patients with major depressioncompared with non-psychiatric controls (52,53).Preliminary clinical studies, however, suggest thatsupplementation with LCn-3PUFA is of equivocalbenefit for depression in adults (54–56).There are no studies comparing blood LCn-
3PUFA concentrations between patients withdepression compared with controls in children oradolescents. A negative relationship betweensymptoms of depression and adipose tissue fattyacid ratios in an adolescent population (57) hasbeen reported; however, there is no relationship
between adipose LCn-3PUFA concentration anddepression severity, and no studies have beenconducted examining whether there is a deficiencyin adipose tissue LCn-3PUFA concentrations inadolescent patients diagnosed with depressioncompared with controls.Nemets et al. (58) conducted a controlled,
double-blind pilot study investigating LCn-3PUFA supplementation in the treatment ofchildren aged 8–12 years with a first episode ofdepression. Ratings were performed at baselineas well as at 2, 4, 8, 12 and 16 weeks using theChildren’s Depression Ratings Scale (CDRS),Children’s Depression Inventory (CDI) and Clin-ical Global Impressions (CGI). Subjects wererandomized to receive LCn-3PUFA (380 mgEPA and 180 mg DHA/day) or placebo (oliveoil or safflower oil) as monotherapy. Twenty-eight subjects were randomized to the treatment,of whom 20 returned ratings for at least 1 month.Seven of 10 children receiving active treatmentachieved response criteria (50% reduction frombaseline score on the CDRS) compared with noneof 10 children receiving placebo (P , 0.01,Fischer’s exact test). More children receivingactive treatment (4 of 10) achieved remission(defined as a score of 29 or less on the CDRS)than did children receiving placebo (0 of 10), butthe difference was not statistically significant.Conclusions that may be drawn from the study
by Nemets et al. (58) are limited by the lack ofintention to treat analyses that should be con-ducted for all randomized controlled trials (59).Participant disposition at least should be shownusing a flow diagram as outlined in the CONSORTguidelines (60). In addition, blood LCn-3PUFAconcentrations were not measured and, therefore,changes in blood LCn-3PUFA could not becorrelated to severity or improvement in symp-toms. Finally, the placebo capsule contained eitherolive or safflower depending on whether partic-ipants could swallow 500 or 1000 mg capsules,respectively. This highlights the importance ofchoosing a placebo, as safflower oil containsapproximately 74% linoleic acid (C18:2n-6), whichis known to compete with conversion of a-linolenicacid to EPA.In summary, there is evidence that LCn-3PUFA
may be involved with the aetiology of depression inadults, but to date, there are no large controlledstudies examining this relationship in children oradolescents. One small randomized control trialhas shown LCn-3PUFA to be of likely benefit inreducing depressive symptoms in pre-pubertalchildren with major depression but not in achievingremission. The study warrants replication.
Omega-3 and child and adolescent psychiatric illnesses
95

Bipolar disorder
There is typically a 10–15 year delay from firstonset of symptoms of bipolar disorder untildiagnosis, such that many affected individuals willhave active but untreated disorder through adoles-cence (61). Early treatment is warranted, as eachmanic episode is associated with an incrementaldecrease in cognitive functioning (62), and there isa 20% lifetime risk of mortality because of suicide(63,64). Bipolar disorder is associated with a highlevel of impairment, ranking as the 6th mostdebilitating disorder in the world (65).The percentage of DHA in erythrocyte mem-
brane phospholipids is depleted in adults withbipolar disorder compared with healthy controls(66). Some authors (67) have reported a beneficialeffect of LCn-3PUFA supplementation in treatingsymptoms of bipolar disorder in adults, whereasother authors have not found any benefit ofsupplementation, particularly when using ethylEPA alone as the supplement [for example, seeKeck et al. (68), Post et al. (69)]. No publishedstudies have examined the LCn-3PUFA status ofchildren or adolescents with bipolar disorder com-pared with healthy controls.In a pilot study, children and adolescents aged
6–17 years with currently symptomatic bipolar I orII disorder were randomized to either flax-seed oilor an olive oil placebo adjunctively or as mono-
therapy (70). Primary outcome measures includingKaplan-Meier survival analysis, Young ManiaRating Scale, Children’s Depression RatingScale-Revised (CDRS-R) and Clinical GlobalImpressions-Bipolar (CGI-BP) ratings were notsignificantly different between treatment groups.The lack of treatment effect could have beenbecause of low conversion of a-linolenic acid toEPA and DHA (Fig. 2), the main active forms ofLCn-3PUFA. Analysis of RBC membrane LCn-3PUFA would be necessary to confirm anyproposed changes. To date, no studies examiningthe effectiveness of EPA or DHA LCn-3PUFA inchild and adolescent bipolar disorder have beenpublished. Evidence from studies in adults, how-ever, suggests that studies with EPA and DHAmay be warranted in this patient population.
Attention-deficit hyperactivity disorder
Fatty acid deficiency was first proposed as apossible cause for the development of attentiondeficit hyperactivity disorder (ADHD) more than25 years ago (71). Results from a number of studiesindicate lower concentrations of LCn-3PUFA inthe blood of children with hyperactive difficultiescompared with matched healthy controls (72–75).
Five randomized control trials have examinedthe efficacy of LCn-3PUFA supplementation for
Table 1. Clinical randomized controlled trials examining the effectiveness of LCn-3PUFA supplementation in psychiatric illnesses in children and adolescents
Psychiatric illness Population age* Clinical trial Supplement Number of participants analysed Symptom improvement with PUFAs
Bipolar disorder Children andadolescents
Gracious (70) a-linolenic (flax-seed – plant) 22, placebo, 22 flax-seed oil No significant improvement
Depression Children Nemets et al. (58) EPA ¼ 380 mg/day,DHA ¼ 180 mg/day
10, placebo; 10, PUFA Significant improvement onCDRS and CDI
Adolescents None reportedSchizophrenia orfirst-episodepsychosis
Children oradolescents
None reported
ADHD Children Voigt et al. (76) DHA ¼ 345 mg/day 31, placebo; 32, DHA No improvementRichardson and
Puri (77)EPA ¼ 186 mg/day,DHA ¼ 480 mg/day,
GLA† ¼ 96 mg/day
14, placebo; 15, PUFA Significant improvement on twoof seven ADHD measures onlycompared with placebo
Stevens et al. (79) EPA ¼ 80 mg/day,DHA ¼ 480 mg/day,
GLA ¼ 96 mg/day
25, placebo; 25, PUFA Significant improvement on 1 of16 ADHD measures only comparedwith placebo
Hirayama et al. (80) EPA ¼ 100 mg/day,DHA ¼ 514 mg/day
20, placebo; 20 PUFA No improvement. Controls higherin visual short-term memory
Sinn and Bryan (81) EPA ¼ 558 mg/day,DHA ¼ 174 mg/day,
GLA ¼ 60 mg/day
27 placebo; 36, PUFA; 41,PUFA 1 MN
Significant improvement in 9 of 14Conners' Parent ratings but not inteacher ratings
Adolescents None ReportedAutism Children and
adolescentsAmminger et al. (92) EPA ¼ 840 mg/day,
DHA ¼ 700 mg/day7, fish oil; 5, placebo No significant effect
CDI, Child Depression Inventory (patient self-administered); CDRS, Children's Depression Rating Scale (clinician administered); MN, micronutrients.*Children, 5–12 years and adolescents, 12–17 years.†GLA (C18:3n-6).
Clayton et al.
96
ADHD (Table 1). Voigt et al. (76) randomized 63children aged 6–12 years with ADHD to receiveLCn-3PUFA capsules containing 345 mg DHA/day (n ¼ 32) or placebo (type not specified, n ¼ 31)for 12 weeks as an adjunct to established treat-ment with stimulant medication. Stimulant medi-cation was withheld from participants for 24 hprior to completing pre- and post-laboratorymeasures for inattention and impulsivity usingthe Test of Variables of Attention and the Child-ren’s Color Trails. Secondary outcome measureswere parent ratings of ADHD symptoms using theChild Behavior Checklist and the Conners ParentRating Scale. Blood samples were also collectedfor the measurement of long chain fatty acid con-centrations.Twenty-seven participants from each treatment
arm completed the study. Plasma phospholipidDHA percentage of total fatty acids increasedsignificantly (1.89 � 0.45% to 4.85 � 1.35%) overthe treatment period in children receiving DHAcompared with those receiving the placebo; how-ever, there were no significant correlations betweenplasma phospholipid DHA concentrations andany behavioural measures. There were no statisti-cally significant improvements in any measures(laboratory measures or parent ratings of ADHDsymptoms) in children receiving DHA comparedwith children receiving placebo. An important limi-tation of the study was continuation of stimulanttreatment, which may have caused a ceiling effect.In addition, one of the behavioural rating scalesused in the study is not sensitive to treatmenteffects.Richardson and Puri (77) randomized 41
children aged 8–12 years with specific learningdisorder and ADHD symptoms to receive capsu-les containing 186 mg EPA, 480 mg DHA, 96 mgg-linolenic acid (GLA), 864 mg linoleic acid and42 mg AA/day (n ¼ 22) or placebo capsules(containing olive oil, n ¼ 19) for 12 weeks.Analysable data from the Conners Parent RatingScale were available for 17 participants in theactive treatment arm and 14 participants in theplacebo arm. Improvements in parent-reportedsymptoms (change in score over 12 weeks) weresignificantly greater for children receiving activetreatment than for those receiving placebo foronly two of seven ADHD subscales [CognitiveProblems: mean � standard deviation (SD) ¼ 62.1� 9.6 to 57.0 � 10.4 for active treatment vs. 63.4� 7.6 to 63.5 � 9.3 for placebo, P ¼ 0.01; andAnxious/Shy: mean � SD ¼ 61.1 � 13.1 to 53.9 �14.6 for active treatment vs. 61.9 � 13.6 to 62.1 �11.8 for placebo, P ¼ 0.04] and for one of sevenGlobal subscales (Global Conners Index: mean �
SD ¼ 64.9 � 10.2 to 59.7 � 6.9 for activetreatment vs. 65.1 � 10.7 to 65.2 � 10.51 forplacebo, P ¼ 0.02). Overall, this study failed toshow any clear advantage of the LCn-3PUFAsupplement over placebo for symptoms of ADHDin this participant population. Limitations of thestudy include that the supplements contained highdoses of LCn-6PUFA as well as LCn-3PUFA andthe absence of an intent-to-treat analysis. Addi-tionally, the statistical methods do not allow anaccurate comparison of the change in symptomsbetween treatment groups over time and a MIXEDmodel repeated measures analysis using the SASstatistical program for example, could be used toshow the interaction between treatment and timefor each treatment (78).Stevens et al. (79) randomized 50 children with
ADHD-like symptoms to receive either placebo(olive oil, n ¼ 25) or 480 mg DHA, 80 mg EPA, 96mg GLA, 40 mg AA and 24 mg vitamin E/day (n ¼25) for 4 months. Using an intent-to-treat analysis,only attention symptoms rated by teachers weresignificantly improved in children receiving LCn-3PUFA supplements compared with placebo(214.8 vs. 13.4% respectively, P ¼ 0.03). Changesin RBC membrane EPA as a percentage of totalfatty acids were significantly and negatively corre-lated with changes in disruptive behaviour asassessed by the Abbreviated Symptom Question-naire rated by parents and teachers and DisruptiveBehavior Disorders (DBD) Rating Scale, subscalefor Attention rated by teachers. Changes in RBCmembrane vitamin E concentrations were alsosignificantly negatively correlated with changes inhyperactivity, attention, conduct and oppositionaldefiant disorder subscales of the teachers DBDRating Scale. Although the children in this studyhad symptoms of ADHD, they did not havea formal diagnosis of ADHD. Therefore, theseresults should be treated with caution and needreplication in a clinical population.Hirayama et al. (80) randomized 32 children
with a definite ADHD diagnosis and 8 witha probable ADHD diagnosis to receive wholefoods fortified with fish oil containing 514 mgDHA and 100 mg EPA/day (n ¼ 20) or wholefoods containing placebo (olive oil; n ¼ 20). Twochildren receiving LCn-3PUFA and four childrenreceiving placebo were receiving concurrent stim-ulant medication. The study measured the meannumber of attention deficit, hyperactivity andimpulsivity symptoms according to the DSM-IVand performance on a continuous performancetask (CPT). No ADHD-related measures weresignificantly improved in participants receivingLCn-3PUFA compared with participants receiving
Omega-3 and child and adolescent psychiatric illnesses
97
placebo. Performance was significantly improvedin children receiving the placebo compared withthose receiving active treatment for two measuresincluding visual short-term memory (median,25th–75th percentile ¼ 0 (0–2) to 0 (0–0.3) forplacebo vs. 0.5 (0–1) to 1 (0–2) for active treatment,P ¼ 0.001) and commission errors on the CPT[median (25th–75th percentile) ¼ 3.5 (2–6) to5 (3–7) for placebo vs. 2.5 (1–6) to 3 (2–4) foractive treatment, P ¼ 0.02]. In summary, supple-mentation with LCn-3PUFA did not improvesymptoms of ADHD in this study population. Alimitation of the study was the absence of an ob-jective measure of compliance with the study diet.Sinn and Bryan (81) randomized 167 children
aged 7–12 years using Conners ADHD Indexscores greater than 2 SDs from the populationaverage to receive capsules containing LCn-3PUFA including 558 mg EPA, 174 mg DHAand 60 mg GLA/day or capsules containing LCn-3PUFA and a range of micronutrients or placebo(palm oil) for 15 weeks. Data were available for104 children over the first 15 weeks of treatment(placebo, n ¼ 27; LCn-3PUFA, n ¼ 36 and LCn-3PUFA 1 micronutrients, n ¼ 41). Improvementswere reported for 9 of 14 subscales on the ConnorsParent Rating Scale, mostly in the inattention andhyperactivity/impulsivity subscales in both treat-ment groups receiving LCn-3PUFA comparedwith placebo after 15 weeks of treatment (P ,
0.01 for Cognitive Problems/Inattention, ADHDindex, Global:Restless/Impulsive, Global Total,DSM-IV Inattentive, DSM-IV Hyperactive/Impul-sive, DSM-IV Total and Oppositional, and P ,
0.05 for Hyperactivity). No significant differenceswere reported for ratings from children receivingthe LCn-3PUFA alone compared with thosereceiving LCn-3PUFA and micronutrients. Limi-tations of the study include a high drop out rate,no assessment of dietary intake of LCn-3PUFA orsupplement compliance and no clinical confirma-tion of the ADHD diagnosis.In summary, clinical trials demonstrate uncer-
tain benefit of LCn-3PUFA supplementation inchildren with ADHD. As other authors havehighlighted (81,82), the inconsistent findings maybe because of the variation in the design of thesestudies such as in sample sizes, inclusion/exclusioncriteria, dosage levels of PUFAs, period ofsupplementation, baseline PUFA status, type ofoutcome measures, lack of measurement of com-pliance and a lack of control of comorbid diag-noses or medications. While several studies havebeen conducted with children, no studies have yetbeen published examining the effects of LCn-3PUFA in adolescents.
Schizophrenia and first-episode psychosis
Epidemiology studies have indicated that adultpatients with schizophrenia have a better outcomeif they live in countries where people consumea diet rich in fats from vegetable and marinesources that are rich in LCn-3PUFA (83). Lowerconcentrations of LCn-3PUFA are reported inRBC membranes of patients with schizophrenia[for example, see Reddy et al. (84)] and first-episode psychosis (85,86) and in cultured skinfibroblasts of patients with first-episode psychosis(87) compared with healthy controls. Althougha confirmed diagnosis of schizophrenia is difficultto make in child and adolescent patients, first-episode psychosis often occurs in the adolescentpopulation. No studies have been conductedexamining deficiencies of LCn-3PUFA or theefficacy of supplementation with LCn-3PUFA inchildren and adolescents with schizophrenia orfirst-episode psychosis.
One of the difficulties in determining whypatients with schizophrenia or first-episode psy-chosis have lower levels of essential fatty acids isthat RBC membrane concentrations of LCn-3PUFA are significantly affected by cigarettesmoking, poor diet and even the long-term effectof taking psychiatric medications (88,89). Thesefactors are very common in people with mentalillness, especially schizophrenia and first-episodepsychosis. Only one clinical trial examining the ef-fectiveness of LCn-3PUFA in schizophrenia reportsto participants who have included were aged 18years (88); however, no studies have been publishedincluding participants younger than 18 years.
Autism
Bell et al. (90) reported lower percentages of DHAand AA in erythrocyte membrane phospholipidsin a patient with autism compared with controlsbut gave no information about the patient’s age,gender or dietary intake. The percentage of LCn-3PUFA in plasma phospholipids was reported tobe lower in 15 children and adolescents with autismcompared with 15 children and adolescents withintellectual delay without autism (91).
Amminger et al. (92) randomized 13 childrenand adolescents diagnosed with autism accordingto the Autism Diagnostic Interview Revised andthe Autism Diagnosis Observational Schedule, withhigh baseline scores on the Aberrant BehaviourChecklist (ABC), to receive capsules containingeither 840 mg EPA and 700 mg DHA/day (n ¼ 7)or placebo (coconut oil; n ¼ 6) for 6 weeks. Datawere analysed by repeated measures analysis of
Clayton et al.
98

variance for seven children receiving LCn-3PUFAand five children receiving placebo after drop outs.In the primary analysis, no significant differencesin any subscale scores on the ABC betweenparticipants receiving either LCn-3PUFA or pla-cebo were reported. In a secondary intent-to-treatanalysis using hot-deck imputation to replacemissing scores, there was a significant interactionbetween treatment and time (P ¼ 0.046). Limi-tations of the study include no assessment ofcompliance and the small sample size. In conclu-sion, LCn-3PUFA supplementation is of uncertainbenefit in children and adolescents with autism.
Safety of omega-3 use
LCn-3PUFAs have been shown to be very safeeven when used in relatively high doses (67). LCn-3PUFAs do not generally affect bleeding time;however, LCn-3PUFA may reduce platelet activa-tion (93–95) and should be used cautiously inpatients with pre-existing haematological condi-tions and, when high doses are used, any unusualsymptoms of bleeding should be carefully moni-tored and reported.Side-effects of omega-3 include nausea, fishy
eructation and loose stools [for review, see Peetand Stokes (36)], which may mean that patients arenot blind to treatment. There are currently novalidated questionnaires suitable for the assess-ment of gastrointestinal symptoms in the contextof treatment with LCn-3PUFA. Most question-naires measuring abnormal gastrointestinal symp-toms have been designed for use in InflammatoryBowel Disease or Irritable Bowel Syndrome (96). Agastrointestinal symptom evaluation record de-signed specifically for the monitoring of symptomsbefore and following treatment with LCn-3PUFAis needed.
Discussion
There are few well-designed studies that showpositive results for using LCn-3PUFA as adjunctor monotherapy treatments for children andadolescents with psychiatric illness. One study inchildren with unipolar depression has shownpromising results (58); however, studies in ADHD,the area in which the majority of research has beenconducted and autism, have shown equivocalbenefit. There is no published evidence for theeffectiveness of LCn-3PUFA in the treatment ofbipolar disorder, schizophrenia or first-episodepsychosis. The lack of large randomized controlledstudies is a problem that has been previously
highlighted in the adult population (97). Based onavailable evidence, claims for the benefit of LCn-3PUFA for psychiatric disorders in children andadolescents are currently overstated.Parents and children and adolescents are often
interested in using alternative therapies in thetreatment of their psychiatric illness, either asadjunct treatment or as monotherapy (7). LCn-3PUFA supplements are commonly used in a rangeof psychiatric illnesses in young people; however, itappears as though many people may be takingthese supplements without knowing which is thebest source (marine vs. plant) and what doses totake and may not know what improvements tolook for. For some individuals, LCn-3PUFAsupplements may provide effective treatment, withless harmful side-effects than pharmacologicaltreatments. In particular, the effectiveness ofLCn-3PUFA in unipolar depression in childrenand adolescents should be further explored.
Methodological issues in omega-3 research
The media coverage of LCn-3PUFA has led tomany parents encouraging their children to takethese supplements. Studying the efficacy of LCn-3PUFA is, therefore, difficult because of the youngpeople already receiving different strengths andtypes of LCn-3PUFA supplements and for varyingduration.Studies need to investigate more clearly the
reason as to why people with psychiatric illnesshave lower plasma levels of LCn-3PUFA. Thisincludes investigating whether the reduced level ofLCn-3PUFA in psychiatric illness is a state or traitproblem (such as because of a specific metabolicproblem). Studies need to take into account socio-economic status and dietary intake of foods high inLCn-3PUFA such as fish, meat and vegetables.Epidemiological studies linking diet, blood LCn-3PUFA status and incidence of psychiatric illnessin children and adolescents are also needed.A Food Frequency Questionnaire specific for
LCn-3PUFA in children and adolescents is neededin order to estimate the intake of LCn-3PUFA toallow an examination of whether differences inintake or metabolism underlie the relationshipbetween LCn-3PUFA and severity of illness orresponse to treatment. Additionally, owing to theknown effects alcohol and nicotine on LCn-3PUFA metabolism (89), the effects of comorbidsubstance/alcohol abuse and cigarette smoking inpeople with a mental illness on LCn-3PUFA needto be addressed.As mentioned above, the importance of choosing
an effective placebo that enables patients and
Omega-3 and child and adolescent psychiatric illnesses
99

researchers to be blind to treatment in randomisedcontrolled trials studies is very important. Thechoice of placebo is also important, as olive oil,which is high in oleic acid, may affect eicosanoidproduction for example (98). The choice of LCn-3PUFA is also important, with EPA and DHAoffering most promise of benefit compared withthe shorter chain a-linoleic acid.Treatment studies testing the efficacy of LCn-
3PUFA should also be conducted according to theInternational Committee for Harmonisation GoodClinical Practice guidelines (99,100), thereby treat-ing LCn-3PUFA in the same way as any otherpharmacotherapy. Studies of these types are harderto conduct than those normally conducted in nutri-tion; however, the benefits of these well-designed,conducted, recorded and reported studies wouldoutweigh the initial cost of conducting the study.
Future directions
Research with LCn-3PUFA in psychiatric illnessesin younger populations may help in determiningwhether abnormalities in LCn-3PUFA metabolismare associated with the onset and progression ofthese illnesses. Long-term studies of effectivesupplementation will also determine whether theseverity of these illnesses can be reduced over time.While the studies reviewed have examined single
axis I diagnoses in children and adolescents, it ismore common for young people to have comorbidaxis I diagnoses than a single axis I diagnoses.Future studies would be helpful in examiningchildren and adolescents with comorbid axis Idisorders such as ADHD and bipolar disorder,ADHD and depression as well as schizoaffectivedisorder.The efficacy of LCn-3PUFA supplementation
has not been studied in number of child andadolescent psychiatric populations (Table 1). Iffuture studies show more convincing evidence forthe effectiveness of LCn-3PUFA supplementationin children and adolescent psychiatric illness, thenpreventative studies with at risk populationsshould be undertaken.LCn-3PUFA may also be helpful in reducing
side-effects of medications in certain psychiatricconditions. Some commonly prescribed antipsy-chotic medication such as clozapine and olanza-pine are associated with increased plasmatriglycerides (101). Omega-3 fatty acids are knownto reduce plasma triglyceride concentrations (4)and may, therefore, also be beneficial when used asan adjunct therapy even without concomitantreduction in psychotic symptoms.
While measuring the plasma and RBC levels ofLCn-3PUFA and symptoms before and aftertreatment is important, there is also a need toinvestigate cognitive and brain changes because ofLCn-3PUFA adjunctive or monotherapy treat-ment. Pre- and post-cognitive testing would beuseful in studies examining LCn-3PUFA supple-mentation in children and adolescent psychiatricillness to determine whether abilities such as atten-tion and concentration can improve. Richardsonand Montgomery (102) included assessments ofacademic abilities in their study of supplementa-tion with EPA and DHA on improvements inreading, spelling and symptoms of behaviour inchildren with developmental coordination disor-der. Further studies combining neuropsychologicaltesting with blood levels of LCn-3PUFA andbehaviour and symptom ratings may be beneficialto use in children and psychiatric patient popula-tions.
Finally, neuroimaging has been used to studychanges in brain size and function in adults [forexample, see Drevets et al. (103)], children andadolescents [for reviews, see Biederman and James(104), Kowatch et al. (105)] experiencing severaldisorders including bipolar disorder. Similar stud-ies examining changes in brain function followingsupplementation with LCn-3PUFA would provideimproved insight into the possible mechanisms ofaction of LCn-3PUFA in psychiatric illness.
Conclusions
Omega-3 from fish oil is a common supplementused for children and adolescents, especially thosesuffering from a psychiatric illness. However, thepublished evidence to date for its effectiveness inthis population does not match its commercialpopularity. There is growing evidence that LCn-3PUFA may be effective in the treatment and,possibly, in the prevention of child and adolescentpsychiatric illness; however, good quality, well-controlled research is greatly needed in this area.
References
1. SIMOPOULOS AP. Essential fatty acids in health andchronic disease. Am J Clin Nutr 1999;70:S560–S569.
2. PAWLOSKY RJ, HIBBELN JR, NOVOTNY JA, SALEM N Jr.Physiological compartmental analysis of alpha-linolenicacid metabolism in adult humans. J Lipid Res 2001;42:1257–1265.
3. EMKEN EA, ADLOF RO, GULLEY RM. Dietary linoleic acidinfluences desaturation and acylation of deuterium-labeled linoleic and linolenic acids in young adult males.Biochim Biophys Acta 1994;1213:277–288.
Clayton et al.
100
4. GARG ML, WOOD LG, SINGH H, MOUGHAN PJ. Means ofdelivering recommended levels of long chain n-3 poly-unsaturated fatty acids in human diets. J Food Sci 2006;71:R66–R71.
5. OLLIS TE, MEYER BJ, HOWE PR. Australian food sourcesand intakes of omega-6 and omega-3 polyunsaturatedfatty acids. Ann Nutr Metab 1999;43:346–355.
6. HOWE P, MEYER B, RECORD S, BAGHURST K. Dietaryintake of long-chain omega-3 polyunsaturated fatty acids:contribution of meat sources. Nutrition 2006;22:47–53.
7. KEMPER KJ. Dietary supplements for attention-deficit/hyperactivity disorder – a fishy business? J Pediatr 2001;139:173–174.
8. JORM AF, ALLEN NB, O’DONNELL CP, PARSLOW RA,PURCELL R, MORGAN AJ. Effectiveness of complementaryand self-help treatments for depression in children andadolescents. Med J Aust 2006;185:368–372.
9. DAS UN. Perinatal supplementation of long-chain poly-unsaturated fatty acids, immune response and adultdiseases. Med Sci Monit 2004;10:HY19–HY25.
10. ROMANO C, CUCCHIARA S, BARABINO A, ANNESE V,SFERLAZZAS C. Usefulness of omega-3 fatty acid supple-mentation in addition to mesalazine in maintainingremission in pediatric Crohn’s disease: a double-blind,randomized, placebo-controlled study. World J Gastro-enterol 2005;11:7118–7121.
11. BELLUZZI A, BOSCHI S, BRIGNOLA C, MUNARINI A, CARIANI
G, MIGLIO F. Polyunsaturated fatty acids and inflamma-tory bowel disease. Am J Clin Nutr 2000;71:S339–S342.
12. HORROBIN DF. Essential fatty acid metabolism and itsmodification in atopic eczema. Am J Clin Nutr 2000;71:S367–S372.
13. SCHLANGER S, SHINITZKY M, YAM D. Diet enriched withomega-3 fatty acids alleviates convulsion symptoms inepilepsy patients. Epilepsia 2002;43:103–104.
14. RUDIN DO. The major psychoses and neuroses as omega-3 essential fatty acid deficiency syndrome: substratepellagra. Biol Psychiatry 1981;16:837–850.
15. LEAF A, WEBER PC. A new era for science in nutrition.Am J Clin Nutr 1987;45:1048–1053.
16. WEISSMAN MM, BLAND RC, CANINO GJ et al. Cross-national epidemiology of major depression and bipolardisorder. JAMA 1996;276:293–299.
17. HIBBELN JR. Fish consumption and major depression.Lancet 1998;351:1213.
18. EDWARDS R, PEET M, SHAY J, HORROBIN D. Omega-3polyunsaturated fatty acid levels in the diet and in redblood cell membranes of depressed patients. J AffectDisord 1998;48:149–155.
19. HIBBELN JR. Seafood consumption, the DHA contentof mothers’ milk and prevalence rates of postpartumdepression: a cross-national, ecological analysis. J AffectDisord 2002;69:15–29.
20. NOAGHIUL S, HIBBELN JR. Cross-national comparisonsof seafood consumption and rates of bipolar disorders.Am J Psychiatry 2003;160:2222–2227.
21. PEET M. International variations in the outcome ofschizophrenia and the prevalence of depression in relationto national dietary practices: an ecological analysis. Br JPsychiatry 2004;184:404–408.
22. HORROBIN DF, MANKU MS, HILLMAN H, IAIN A, GLEN M.Fatty acid levels in the brains of schizophrenics andnormal controls. Biol Psychiatry 1991;30:795–805.
23. SASTRY PS. Lipids of nervous tissue: composition andmetabolism. Prog Lipid Res 1985;24:69–176.
24. MCNAMARA RK, CARLSON SE. Role of omega-3 fattyacids in brain development and function: potential
implications for the pathogenesis and prevention ofpsychopathology. Prostaglandins Leukot Essent FattyAcids 2006;75:329–349.
25. SIMOPOULOS AP. Omega-3 fatty acids in health and diseaseand in growth and development. Am J Clin Nutr 1991;54:438–463.
26. FARQUHARSON J, COCKBURN F, PATRICK WA, JAMIESON
EC, LOGAN RW. Infant cerebral cortex phospholipidfatty-acid composition and diet. Lancet 1992;340:810–813.
27. INNIS SM. Perinatal biochemistry and physiology of long-chain polyunsaturated fatty acids. J Pediatr 2003;143:S1–S8.
28. WILLATTS P, FORSYTH JS. The role of long-chain poly-unsaturated fatty acids in infant cognitive development.Prostaglandins Leukot Essent Fatty Acids 2000;63:95–100.
29. HIRASHIMA F, PAROW AM, STOLL AL et al. Omega-3 fattyacid treatment and t2 whole brain relaxation times inbipolar disorder. Am J Psychiatry 2004;161:1922–1924.
30. TAPPIA PS, LADHA S, CLARK DC, GRIMBLE RF. Theinfluence of membrane fluidity, TNF receptor binding,cAMP production and GTPase activity on macrophagecytokine production in rats fed a variety of fat diets.Mol Cell Biochem 1997;166:135–143.
31. MIRNIKJOO B, BROWN SW, SEUNG KIM HF, MARANGELL
LB, SWEATT JD, WEEBER EJ. Protein kinase inhibition byw-3 fatty acids. J Biol Chem 2001;276:10888–10896.
32. SEUNG KIM HF, WEEBER EJ, SWEATT JD, STOLL AL,MARANGELL LB. Inhibitory effects of omega-3 fatty acidson protein kinase C activity in vitro. Mol Psychiatry 2001;6:246–248.
33. CHANG MC, CONTRERAS MA, ROSENBERGER TA, RINTALA
JJ, BELL JM, RAPOPORT SI. Chronic valproate treatmentdecreases the in vivo turnover of arachidonic acid in brainphospholipids: a possible common effect of moodstabilizers. J Neurochem 2001;77:796–803.
34. STOLL AL, LOCKE CA, MARANGELL LB, SEVERUS WE.Omega-3 fatty acids in bipolar disorder: a review.Prostaglandins Leukot Essent Fatty Acids 1999;60:329–337.
35. HORROBIN DF, BENNETT CN. Depression and bipolardisorder: relationships to impaired fatty acid andphospholipid metabolism and to diabetes, cardiovasculardisease, immunological abnormalities, cancer, ageing andosteoporosis. Possible candidate genes. ProstaglandinsLeukot Essent Fatty Acids 1999;60:217–234.
36. PEET M, STOKES C. Omega-3 fatty acids in the treatmentof psychiatric disorders. Drugs 2005;65:1051–1059.
37. CHARLTON BG. The malaise theory of depression: majordepressive disorder is sickness behavior and antidepres-sants are analgesic. Med Hypotheses 2000;54:126–130.
38. RAISON CL, CAPURON L, MILLER AH. Cytokines sing theblues: inflammation and the pathogenesis of depression.Trends Immunol 2006;27:24–31.
39. CHANG MC, GRANGE E, RABIN O, BELL JM, ALLEN DD,RAPOPORT SI. Lithium decreases turnover of arachidonatein several brain phospholipids. Neurosci Lett 1996;220:171–174.
40. CHANG MC, BELL JM, PURDON AD, CHIKHALE EG,GRANGE E. Dynamics of docosahexaenoic acid metabo-lism in the central nervous system: lack of effect ofchronic lithium treatment. Neurochem Res 1999;24:399–406.
41. RAPOPORT SI, BOSETTI F. Do lithium and anticonvulsantstarget the brain arachidonic acid cascade in bipolardisorder? Arch Gen Psychiatry 2002;59:592–596.
Omega-3 and child and adolescent psychiatric illnesses
101
42. DE LA PRESA OWENS S, INNIS SM. Docosahexaenoicand arachidonic acid prevent a decrease in dopaminer-gic and serotoninergic neurotransmitters in frontalcortex caused by a linoleic and alpha-linolenic aciddeficient diet in formula-fed piglets. J Nutr 1999;129:2088–2093.
43. ZIMMER L, DELPAL S, GUILLOTEAU D, AIOUN J, DURAND
G, CHALON S. Chronic n-3 polyunsaturated fatty aciddeficiency alters dopamine vesicle density in the ratfrontal cortex. Neurosci Lett 2000;284:25–28.
44. KODAS E, GALINEAU L, BODARD S et al. Serotoninergicneurotransmission is affected by n-3 polyunsaturatedfatty acids in the rat. J Neurochem 2004;89:695–702.
45. YOUNG G, CONQUER J. Omega-3 fatty acids and neuro-psychiatric disorders. Reprod Nutr Dev 2005;45:1–28.
46. FREEMANMP. Omega-3 fatty acids in psychiatry: a review.Ann Clin Psychiatry 2000;12:159–165.
47. PARKER G, GIBSON NA, BROTCHIE H, HERUC G, REES
AM, HADZI-PAVLOVIC D. Omega-3 fatty acids and mooddisorders. Am J Psychiatry 2006;163:969–978.
48. MCNAMARA RK. The emerging role of omega-3 fattyacids in psychiatry. Prostaglandins Leukot Essent FattyAcids 2006;75:223–225.
49. MAES M, SMITH R, CHRISTOPHE A, COSYNS P, DESNYDER
R, MELTZER H. Fatty acid composition in majordepression: decreased omega 3 fractions in cholesterylesters and increased C20: 4 omega 6/C20:5 omega 3 ratioin cholesteryl esters and phospholipids. J Affect Disord1996;38:35–46.
50. PEET M, MURPHY B, SHAY J, HORROBIN D. Depletion ofomega-3 fatty acid levels in red blood cell membranes ofdepressive patients. Biol Psychiatry 1998;43:315–319.
51. SUBLETTE ME, HIBBELN JR, GALFALVY H, OQUENDO MA,MANN JJ. Omega-3 polyunsaturated essential fatty acidstatus as a predictor of future suicide risk. Am JPsychiatry 2006;163:1100–1102.
52. ADAMS PB, LAWSON S, SANIGORSKI A, SINCLAIR AJ.Arachidonic acid to eicosapentaenoic acid ratio in bloodcorrelates positively with clinical symptoms of depression.Lipids 1996;31:S157–S161.
53. MAES M, CHRISTOPHE A, DELANGHE J, ALTAMURA C,NEELS H, MELTZER HY. Lowered omega-3 polyunsatu-rated fatty acids in serum phospholipids and cholesterylesters of depressed patients. Psychiatry Res 1999;85:275–291.
54. SU KP, HUANG SY, CHIU CC, SHEN WW. Omega-3 fattyacids in major depressive disorder. A preliminary double-blind, placebo-controlled trial. Eur Neuropsychopharma-col 2003;13:267–271.
55. MARANGELL LB, MARTINEZ JM, ZBOYAN HA, KERTZ B,KIM HF, PURYEAR LJ. A double-blind, placebo-controlledstudy of the omega-3 fatty acid docosahexaenoic acid inthe treatment of major depression. Am J Psychiatry 2003;160:996–998.
56. SILVERS KM, WOOLLEY CC, HAMILTON FC, WATTS PM,WATSON RA. Randomised double-blind placebo-controlled trial of fish oil in the treatment of depression.Prostaglandins Leukot Essent Fatty Acids 2005;72:211–218.
57. MAMALAKIS G, KIRIAKAKIS M, TSIBINOS G, KAFATOS A.Depression and adipose polyunsaturated fatty acids in anadolescent group. Prostaglandins Leukot Essent FattyAcids 2004;71:289–294.
58. NEMETS H, NEMETS B, APTER A, BRACHA Z, BELMAKER
RH. Omega-3 treatment of childhood depression: a con-trolled, double-blind pilot study. Am J Psychiatry 2006;163:1098–1100.
59. HOLLIS S, CAMPBELL F. What is meant by intention totreat analysis? Survey of published randomised controlledtrials. BMJ 1999;319:670–674.
60. MOHER D, SCHULZ KF, ALTMAN D. The CONSORTstatement: revised recommendations for improving thequality of reports of parallel-group randomized trials.JAMA 2001;285:1987–1991.
61. LISH JD, DIME-MEENAN S, WHYBROW PC, PRICE RA,HIRSCHFELD RM. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar mem-bers. J Affect Disord 1994;31:281–294.
62. VIETA E, BENABARRE A, MARTINEZ-ARAN A. Brainimaging correlates of cognitive dysfunctions in bipolardisorder. Bipolar Disord 2004;6:19.
63. GOODWIN F, JAMISON KR. Manic-depressive illness. NewYork: Oxford University Press, 1990.
64. GOODWIN FK, FIREMAN B, SIMON GE, HUNKELER EM,LEE J, REVICKI D. Suicide risk in bipolar disorder duringtreatment with lithium and divalproex. JAMA 2003;290:1467–1473.
65. WHO, World Bank. The global burden of disease:summary. Cambridge, MA: The Harvard School ofPublic Health Harvard University Press, 1996.
66. CHIU CC, HUANG SY, SU KP et al. Polyunsaturated fattyacid deficit in patients with bipolar mania. Eur Neuro-psychopharmacol 2003;13:99–103.
67. STOLL AL, SEVERUS WE, FREEMAN MP et al. Omega 3fatty acids in bipolar disorder: a preliminary double-blindplacebo-controlled trial. Arch Gen Psychiatry 1999;56:407–412.
68. KECK PE Jr, MINTZ J, MCELROY SL et al. Double-blind,randomized, placebo-controlled trials of ethyl-eicosa-pentanoate in the treatment of bipolar depression andrapid cycling bipolar disorder. Biol Psychiatry 2006;60:1020–1022.
69. POST RM, LEVERICH GS, ALTSHULER LL et al. An over-view of recent findings of the Stanley Foundation BipolarNetwork (Part I). Bipolar Disord 2003;5:310–319.
70. GRACIOUS BL. An RCT of flax oil in children andadolescents with bipolar. National Institute of MentalHealth (NIMH) Pediatric Bipolar Conference. Chicago,IL, April 2006.
71. COLQUHOUN I, BUNDAY S. A lack of essential fatty acidsas a possible cause of hyperactivity in children. MedHypotheses 1981;7:673–679.
72. MITCHELL EA, AMAN MG, TURBOTT SH, MANKU M.Clinical characteristics and serum essential fatty acidlevels in hyperactive children. Clin Pediatr (Phila) 1987;26:406–411.
73. STEVENS LJ, ZENTALL SS, DECK JL et al. Essential fattyacid metabolism in boys with attention-deficit hyperac-tivity disorder. Am J Clin Nutr 1995;62:761–768.
74. BURGESS JR, STEVENS L, ZHANG W, PECK L. Long-chainpolyunsaturated fatty acids in children with attention-deficit hyperactivity disorder. Am J Clin Nutr 2000;71:S327–S330.
75. CHEN JR, HSU SF, HSU CD, HWANG LH, YANG SC.Dietary patterns and blood fatty acid composition inchildren with attention-deficit hyperactivity disorder inTaiwan. J Nutr Biochem 2004;15:467–472.
76. VOIGT RG, LLORENTE AM, JENSEN CL, FRALEY JK,BERRETTA MC, HEIRD WC. A randomized, double-blind,placebo-controlled trial of docosahexaenoic acid supple-mentation in children with attention-deficit/hyperactivitydisorder. J Pediatr 2001;139:189–196.
77. RICHARDSON AJ, PURI BK. A randomized double-blind,placebo-controlled study of the effects of supplementation
Clayton et al.
102

with highly unsaturated fatty acids on ADHD-relatedsymptoms in children with specific learning difficulties.Prog Neuropsychopharmacol Biol Psychiatry 2002;26:233–239.
78. LITTELL RC, HENRY PR, AMMERMAN CB. Statisticalanalysis of repeated measures data using SAS procedures.J Anim Sci 1998;76:1216–1231.
79. STEVENS L, ZHANG W, PECK L et al. EFA supplementationin children with inattention, hyperactivity, and otherdisruptive behaviors. Lipids 2003;38:1007–1021.
80. HIRAYAMA S, HAMAZAKI T, TERASAWA K. Effect ofdocosahexaenoic acid-containing food administration onsymptoms of attention-deficit/hyperactivity disorder – aplacebo-controlled double-blind study. Eur J Clin Nutr2004;58:467–473.
81. SINN N, BRYAN J. Effect of supplementation with poly-unsaturated fatty acids and micronutrients on attentionand behavior problems associated with child ADHD.J Dev Behav Pediatr 2007 (in press).
82. RICHARDSON AJ. Clinical trials of fatty acid supplemen-tation in ADHD. In: GLEN AIM, PEET M, HORROBIN DF,eds. Phospholipid spectrum disorders in psychiatry andneurology. Carnforth: Marius Press, 2003: 529–541.
83. CHRISTENSEN O, CHRISTENSEN E. Fat consumption andschizophrenia. Acta Psychiatr Scand 1988;78:587–591.
84. REDDY RD, KESHAVAN MS, YAO JK. Reduced red bloodcell membrane essential polyunsaturated fatty acids infirst episode schizophrenia at neuroleptic-naive baseline.Schizophr Bull 2004;30:901–911.
85. KHAN MM, EVANS DR, GUNNA V, SCHEFFER RE, PARIKH
VV, MAHADIK SP. Reduced erythrocyte membraneessential fatty acids and increased lipid peroxides inschizophrenia at the never-medicated first-episode ofpsychosis and after years of treatment with antipsy-chotics. Schizophr Res 2002;58:1–10.
86. EVANS DR, PARIKH VV, KHAN MM, COUSSONS C,BUCKLEY PF, MAHADIK SP. Red blood cell membraneessential fatty acid metabolism in early psychotic patientsfollowing antipsychotic drug treatment. ProstaglandinsLeukot Essent Fatty Acids 2003;69:393–399.
87. MAHADIK SP, MUKHERJEE S. Cultured skin fibroblasts asa cell model for investigating schizophrenia. J PsychiatrRes 1996;30:421–439.
88. HIBBELN JR, MAKINO KK, MARTIN CE, DICKERSON F,BORONOW J, FENTON WS. Smoking, gender, and dietaryinfluences on erythrocyte essential fatty acid compositionamong patients with schizophrenia or schizoaffectivedisorder. Biol Psychiatry 2003;53:431–441.
89. PEET M. The metabolic syndrome, omega-3 fatty acidsand inflammatory processes in relation to schizophrenia.Prostaglandins Leukot Essent Fatty Acids 2006;75:323–327.
90. BELL JG, SARGENT JR, TOCHER DR, DICK JR. Red bloodcell fatty acid compositions in a patient with autisticspectrum disorder: a characteristic abnormality in neuro-developmental disorders? Prostaglandins Leukot EssentFatty Acids 2000;63:21–25.
91. VANCASSEL S, DURAND G, BARTHELEMY C et al. Plasmafatty acid levels in autistic children. ProstaglandinsLeukot Essent Fatty Acids 2001;65:1–7.
92. AMMINGER GP, BERGER GE, SCHAFER MR, KLIER C,FRIEDRICH MH, FEUCHT M. Omega-3 fatty acids supple-
mentation in children with autism: a double-blindrandomized, placebo-controlled pilot study. Biol Psychi-atry 2006;61:551–553.
93. GOODNIGHT SH Jr, HARRIS WS, CONNOR WE. The effectsof dietary omega 3 fatty acids on platelet composition andfunction in man: a prospective, controlled study. Blood1981;58:880–885.
94. WENSING AG, MENSINK RP, HORNSTRA G. Effects ofdietary n-3 polyunsaturated fatty acids from plant andmarine origin on platelet aggregation in healthy elderlysubjects. Br J Nutr 1999;82:183–191.
95. WOODMAN RJ, MORI TA, BURKE V et al. Effects ofpurified eicosapentaenoic acid and docosahexaenoic acidon platelet, fibrinolytic and vascular function in hyper-sensitive type 2 diabetic patients. Atherosclerosis 2002;166:85–93.
96. VELDHUYZEN VAN ZANTEN SJOV, TALLEY NJ, BYTZER P,KLEIN KB, WHORWELL PJ, ZINSMEISTER AR. Design oftreatment trials for functional gastrointestinal disorders.Gut 1999;45:69–77.
97. CALABRESE JR, RAPPORT DJ, SHELTON MD. Fish oils andbipolar disorder. A promising but untested treatment.Arch Gen Psychiatry 1999;56:413–414.
98. PURI BK, RICHARDSON AD. The effects of olive oil onomega-3 fatty acids and mood disorders. Arch GenPsychiatry 2000;57:715.
99. BROUWER IA, ZOCK PL, WEVER EF et al. Rationale anddesign of a randomised controlled clinical trial onsupplemental intake of n-3 fatty acids and incidence ofcardiac arrhythmia: SOFA. Eur J Clin Nutr 2003;57:1323–1330.
100. International Conference on Harmonisation of TechnicalRequirements for Registration of Pharmaceuticals forHuman Use (ICH). E6 Good Clinical Practice: Consol-idated Guidance. April 1996: Available at: www.tga.gov.au/docs/html/ich13595.htm
101. PEET M, HORROBIN DF. A dose-ranging study of theeffects of ethyl-eicosapentaenoate in patients with ongo-ing depression despite apparently adequate treatmentwith standard drugs. Arch Gen Psychiatry 2002;59:913–919.
102. RICHARDSON AJ, MONTGOMERY P. The Oxford-Durhamstudy: a randomized, controlled trial of dietary supple-mentation with fatty acids in children with developmentalcoordination disorder. Pediatrics 2005;115:1360–1366.
103. DREVETS WC, PRICE JL, SIMPSON JR Jr et al. Subgenualprefrontal cortex abnormalities in mood disorders.Nature 1997;386:824–827.
104. BIEDERMAN J, JAMES RS. Advances in the neurobiologyof pediatric bipolar disorder. Biol Psychiatry 2005;58:515–516.
105. KOWATCH R, DAVANZO PA, EMSLIE G. Pediatric mooddisorders and neuroimaging. In: ERNST M, RUMSEY JM,eds. Functional neuroimaging in child psychiatry. Cam-bridge: Cambridge University Press, 2000: 205–223.
106. WANG N, ANDERSON RE. Synthesis of docosahexaenoicacid by retina and retinal pigment epithelium. Bio-chemistry 1993;32:13703–13709.
107. MOORE SA, YODER E, MURPHY S, DUTTON GR, SPECTOR
AA. Astrocytes, not neurons, produce docosahexaenoicacid (22:6 omega-3) and arachidonic acid (20:4 omega-6).J Neurochem 1991;56:518–524.
Omega-3 and child and adolescent psychiatric illnesses
103
Copyright © 2022 FDOKUMEN







![Effects of Fatty Acids on Benzo[a]pyrene Uptake and Metabolism in Human Lung Adenocarcinoma A549 Cells](https://static.fdokumen.com/doc/165x107/63334a02a290d455630a124b/effects-of-fatty-acids-on-benzoapyrene-uptake-and-metabolism-in-human-lung-adenocarcinoma.jpg)












