
Localization of the Epileptogenic Zone by Ictal and Interictal SPECT with 99mTc-Ethyl Cysteinate...
10
Epilrp.sia, 40(6):693-702, 1999 Lippincotl Williams & Wilkins, Inc., Philadelphia 0 International League Against Epilephy Clinical Research Localization of the Epileptogenic Zone by Ictal and Interictal SPECT with Tc-Ethyl Cysteinate Dimer in Patients with 99m Medically Refractory Epilepsy Andrea J. Oliveira, Jaderson C. da Costa, "Lisiane N. Hilario, "0. Estrela Anselmi, and Andre Palmini Porto Alegre Epilepsy Surgery Program, Department of Internal Medicine, Division of Neurology, and *Service of Nuclear Medicine, Hospital Stio Lucas, Ponttjkia Universidade Catolica do Rio Grande do Sul (PUCRS), Porto Alegre, Brazil Summary: Purpose: To evaluate the accuracy, feasibility and clinical value of both ictal and interictal y9"Tc-ethyl cysteinate dimer (ECD) single photon emission computed tomography (SPECT) in patients with medically refractory epilepsy. Methods: The study included 75 consecutive patients, 48 with temporal lobe epilepsy (TLE group), and 27 with extra- temporal epilepsy (ExT group). The accuracy of SPECT was analyzed considering the final diagnosis reached by conver- gence of clinical, electrophysiologic, structural, pathologic and outcome data. Resulw Ictal SPECT correctly identified the epileptogenic zone in 21 (91.3%) of 23 patients, whereas interictal SPECTs could correctly identify the epileptogenic zone in only 41 (62.1%) of 66 patients (x' = 5.56, df = 1, p < 0.05). Results were similar when the two study groups were analyzed sepa- rately. Moreover, ictal studies had significantly higher speci- ficity (91.3 vs. 60.6%) and positive predictive value (91.3 vs. 66.2%) than interictal studies for the whole series of patients. Considering all tools used in the preoperative workup of these patients, ictal SPECT significantly contributed to the final to- pographic diagnosis in seven of 14 patients from TLE group and in six of nine patients from the ExT group. In these pa- tients, ictal SPECT either obviated the need for invasive EEG or helped to define where to concentrate the efforts of invasive investigation. Conclusions: These data demonstrate that ictal SPECT can be easily achieved by using 9'"'Tc-ECD and can accurately localize the epileptogenic zone in both temporal and extratem- poral epilepsies. Ictal ECD SPECT proved to be significantly more sensitive and specific than interictal ECD SPECT, and clinically useful in the definition of the epileptogenic zone. Key Words: Epilepsy-Single photon emission computed tomog- raphy-Ethyl cysteinate dimer-Seizures-Epilepsy surgery. Functional neuroimaging techniques, including singlc photon emission computed tomography (SPECT), have an established role in the preoperative workup of patients with refractory epilepsy (1-3). Indeed, ictal SPECT with an already well-known agent, hexamethyl propyl- eneamine oxime (HMPAO), has proved to be one of the most sensitive techniques for the localization of ictal onset zones (4-8). Conversely, the interictal modality of SPECT, although easier to obtain, has lower sensitivity (ranging from 30 to 80%) and specificity (from 36 to 95%) for the localization of the epileptogenic zone (3, 9-1 5). The latter figures are unacceptably low, consid- Accepted November 6, 1998. Address correspondenceand reprint requests to Dr. J. C. da Costa at Servip de Neurologia, Hospital SBo Lucas da PUC-RS, Av. Ipiranga, 6690, sala 322, 90610-000 Forto Alegre, RS, Brazil. ering the need for an accurate topographic diagnosis for resective surgery. One of the limitations of the use of ictal SPECT in the presurgical evaluation of patients with refractory epi- lepsy had been the low in vitro stability of HMPAO, which made ictal studies difficult to obtain routinely (3, 16,17). Some options have been developed as an attempt to overcome this problem. One is the use of ethyl cys- teinate dimer (ECD), a new agent for cerebral-blood- flow imaging, which has the advantage of high in vitro stability and more rapid clearance than HMPAO (18,19). It has now been used routinely for >3 years, and its use is already well established in the study of cerebrovascu- lar diseases (20,21). The pharmaceutic properties of ECD make it an excellent candidate for ictal imaging in epilepsy, but this issue has not been properly evaluated. There are few studies addressing this possibility, and 693
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Localization of the Epileptogenic Zone by Ictal and Interictal SPECT with 99mTc-Ethyl Cysteinate...

Epilrp.sia, 40(6):693-702, 1999 Lippincotl Williams & Wilkins, Inc., Philadelphia 0 International League Against Epilephy
Clinical Research
Localization of the Epileptogenic Zone by Ictal and Interictal SPECT with Tc-Ethyl Cysteinate Dimer in Patients with 99m
Medically Refractory Epilepsy
Andrea J . Oliveira, Jaderson C. da Costa, "Lisiane N. Hilario, "0. Estrela Anselmi, and Andre Palmini
Porto Alegre Epilepsy Surgery Program, Department of Internal Medicine, Division of Neurology, and *Service of Nuclear Medicine, Hospital Stio Lucas, Ponttjkia Universidade Catolica do Rio Grande do Sul (PUCRS), Porto Alegre, Brazil
Summary: Purpose: To evaluate the accuracy, feasibility and clinical value of both ictal and interictal y9"Tc-ethyl cysteinate dimer (ECD) single photon emission computed tomography (SPECT) in patients with medically refractory epilepsy.
Methods: The study included 75 consecutive patients, 48 with temporal lobe epilepsy (TLE group), and 27 with extra- temporal epilepsy (ExT group). The accuracy of SPECT was analyzed considering the final diagnosis reached by conver- gence of clinical, electrophysiologic, structural, pathologic and outcome data.
Resulw Ictal SPECT correctly identified the epileptogenic zone in 21 (91.3%) of 23 patients, whereas interictal SPECTs could correctly identify the epileptogenic zone in only 41 (62.1%) of 66 patients (x' = 5.56, df = 1, p < 0.05). Results were similar when the two study groups were analyzed sepa- rately. Moreover, ictal studies had significantly higher speci- ficity (91.3 vs. 60.6%) and positive predictive value (91.3 vs.
66.2%) than interictal studies for the whole series of patients. Considering all tools used in the preoperative workup of these patients, ictal SPECT significantly contributed to the final to- pographic diagnosis in seven of 14 patients from TLE group and in six of nine patients from the ExT group. In these pa- tients, ictal SPECT either obviated the need for invasive EEG or helped to define where to concentrate the efforts of invasive investigation.
Conclusions: These data demonstrate that ictal SPECT can be easily achieved by using 9'"'Tc-ECD and can accurately localize the epileptogenic zone in both temporal and extratem- poral epilepsies. Ictal ECD SPECT proved to be significantly more sensitive and specific than interictal ECD SPECT, and clinically useful in the definition of the epileptogenic zone. Key Words: Epilepsy-Single photon emission computed tomog- raphy-Ethyl cysteinate dimer-Seizures-Epilepsy surgery.
Functional neuroimaging techniques, including singlc photon emission computed tomography (SPECT), have an established role in the preoperative workup of patients with refractory epilepsy (1-3). Indeed, ictal SPECT with an already well-known agent, hexamethyl propyl- eneamine oxime (HMPAO), has proved to be one of the most sensitive techniques for the localization of ictal onset zones (4-8). Conversely, the interictal modality of SPECT, although easier to obtain, has lower sensitivity (ranging from 30 to 80%) and specificity (from 36 to 95%) for the localization of the epileptogenic zone (3, 9-1 5). The latter figures are unacceptably low, consid-
Accepted November 6, 1998. Address correspondence and reprint requests to Dr. J. C. da Costa at
S e r v i p de Neurologia, Hospital SBo Lucas da PUC-RS, Av. Ipiranga, 6690, sala 322, 90610-000 Forto Alegre, RS, Brazil.
ering the need for an accurate topographic diagnosis for resective surgery.
One of the limitations of the use of ictal SPECT in the presurgical evaluation of patients with refractory epi- lepsy had been the low in vitro stability of HMPAO, which made ictal studies difficult to obtain routinely (3, 16,17). Some options have been developed as an attempt to overcome this problem. One is the use of ethyl cys- teinate dimer (ECD), a new agent for cerebral-blood- flow imaging, which has the advantage of high in vitro stability and more rapid clearance than HMPAO (18,19). It has now been used routinely for >3 years, and its use is already well established in the study of cerebrovascu- lar diseases (20,21). The pharmaceutic properties of ECD make it an excellent candidate for ictal imaging in epilepsy, but this issue has not been properly evaluated. There are few studies addressing this possibility, and
693
694 A. J. OLIVEIRA ET AL,
preliminary results have been encouraging, but the small number of patients precludes meaningful statistical analysis (16,17,22,23).
Our study aimed at evaluating the accuracy and fea- sibility of both ictal and interictal 99mTc-ECD SPECT in patients with medically refractory epilepsy. In addition, we correlated SPECT findings with those from other evaluation techniques, classically considered the major tools in the presurgical workup of patients with epilepsy: ictal scalp EEG and magnetic resonance imaging (MRI). Our ultimate goal was to establish the clinical value of SPECT for localizing the epileptogenic zone in patients undergoing evaluation for epilepsy surgery.
METHODS
Preoperative workup of epileptic patients The study included 75 consecutive patients with medi-
cally refractory partial epilepsy, evaluated with a view to surgical treatment at the Porto Alegre Epilepsy Surgery Program since March 1995. As part of the presurgical evaluation protocol, they all underwent a thorough clini- cal examination, multiple prolonged video-EEG record- ings with standard and sphenoidal electrodes, structural neuroimaging studies with 0.5 or 1.5 T MRI and neuro- psychological testing, including, whenever necessary, the Wada test. The protocol for the clinical trial was approved by the local ethics committee, and written in- formed consent was obtained from each patient or their parents or both. Women of reproductive age underwent pregnancy tests and were excluded from the study if these were positive. Also as part of the protocol for pre- surgical evaluation, all patients had their antiepileptic drug (AED) doses tapered during the period of investi- gation.
Forty-eight patients had temporal lobe epilepsy (TLE), and the other 27 had epilepsy of extratemporal origin (ExT group). This localization was determined by the convergence of clinical, electroencephalographic, MRI, neuropsychological, histopathologic data, and, eventu- ally, by the follow-up of surgical patients.
Preparation and injection of 9YmT~-ECD Venous access was secured previously, and injections
were performed during a daytime session of video-EEG monitoring.
Neurolite, a DuPont Pharma kit for the preparation of 99mTc-ECD, was labeled according to the information of the manufacturer. The radiopharmaceutical was reconsti- tuted with 100 mCi sterile, nonpyrogenic, oxidant-free sodium pertechnetate y y m T ~ in -2 ml. The mixture stood for 30 min for complete reaction. The reconstituted
Tc-ECD was then stored at room temperature at the monitoring room, and was always injected within 6 h of preparation.
The final dose of the radioisotope at preparation
Y 9 r n
ranged from 20 to 30 mCi, so that the total dose at injection would be -20 mCi.
For ictal SPECT, patients were injected as soon as a seizure was identified, both clinically and electroenceph- alographically . The time of seizure onset, the duration of the seizure, and the lapse between seizure onset and in- jection were recorded. Because all patients were receiv- ing reduced dosages of AEDs, they were medicated 20- 30 min after injection, before being transferred to the acquisition room. There were no cases of status epilep- ticus or seizures long enough to require immediate treat- ment.
For interictal SPECT, injection was also performed under video-EEG monitoring to assure that there were no subclinical seizures at the time of injection, and also for quantification of interictal epileptifom discharges. Dur- ing the injection of ”‘“Tc-ECD and for 210 min after- ward, patients were kept in a supine position, with their eyes open, in a room with dim light and little noise.
A slow, nonbolus flush of 5-10 ml saline solution followed each injection of the radiopharmaceutical, both ictally and interictally.
Image acquisition and interpretation In all patients, images were acquired within 1 4 h
from injection of the pharmaceutical and within 8 h of its preparation, by using a single-headed nondedicated y-camera (Starcam 3200i) with a low-energy, high- resolution collimator. Sixty-four images of 20 s each were acquired in a 64 x 64 matrix and 1.6 zoom over 360”. The tomographic resolution of the system was 12 mm, and the pixel size, 3.9 mm. Images were recon- structed on the axial, coronal, sagittal, and oblique (tem- poral) planes by filtered backprojection by using a But- tenvorth filter with cut-off frequency of 0.39 and power factor of 10, with an attenuation coefficient of 0.12km.
Images were analyzed separately by two of the authors (L.N.H. and O.E.A.), blind to the patient’s clinical, elec- trophysiologic, and MRI findings, but aware of whether the study was ictal or interictal.
Data analysis The epileptogenic zone was defined by the conver-
gence of clinical, electrophysiologic, structural, patho- logic, and outcome data.
When individually analyzed, EEG and MRI findings were considered “localizing” when they pointed to a clear-cut focal or lobar region of cortical abnormality, which eventually proved to be the correct localization of the epileptogenic zone.
In the single patient in whom the epileptogenic zone indeed proved to involve most cortical regions of one entire hemisphere, we considered as clear-cut localizing evidence the ictal EEG and MRI findings pointing to abnormalities of the whole involved hemisphere.
All other instances of diffuse unilateral or bilateral, as
Epilepsia. Vol. 40, No. 6, 1999
ICTAL AND INTERICTAL BRAIN SPECT IN EPILEPSY 695
well as focal bilateral abnormalities, were considered nonlocalizing. When a clear-cut focal abnormality pointed to a cortical region other than that eventually defined as the epileptogenic zone, the test was consid- ered as rnislocalizing.
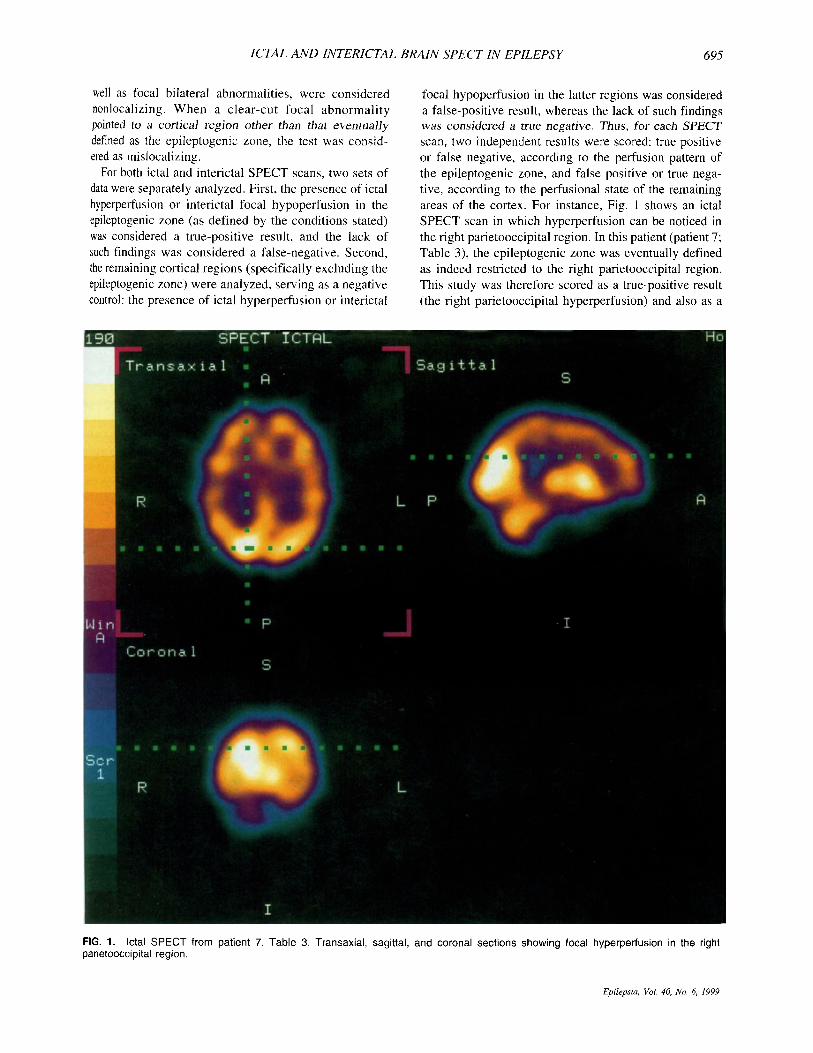
For both ictal and interictal SPECT scans, two sets of data were separately analyzed. First, the presence of ictal hyperperfusion or interictal focal hypoperfusion in the epileptogenic zone (as defined by the conditions stated) was considered a true-positive result, and the lack of such findings was considered a false-negative. Second, the remaining cortical regions (specifically excluding the epileptogenic zone) were analyzed, serving as a negative control: the presence of ictal hyperperfusion or interictal
focal hypoperfusion in the latter regions was considered a false-positive result, whereas the lack of such findings was considered a true negative. Thus, for each SPECT scan, two independent results were scored: true positive or false negative, according to the perfusion pattern of the epileptogenic zone, and false positive or true nega- tive, according to the perfusional state of the remaining areas of the cortex. For instance, Fig. 1 shows an ictal SPECT scan in which hyperperfusion can be noticed in the right parietooccipital region. In this patient (patient 7; Table 3), the epileptogenic zone was eventually defined as indeed restricted to the right parietooccipital region. This study was therefore scored as a true-positive result (the right parietooccipital hyperperfusion) and also as a
FIG. 1. lctal SPECT from patient 7, Table 3. Transaxial, sagittal, and coronal sections showing focal hyperperfusion in the right parietooccipital region.
Epilepsia, Vol. 40, No. 6, 1999
696 A. J. OLIVEIRA ET AL.
100
8o 1 0
2o I 1
0- TLE ExT TLE+ExT
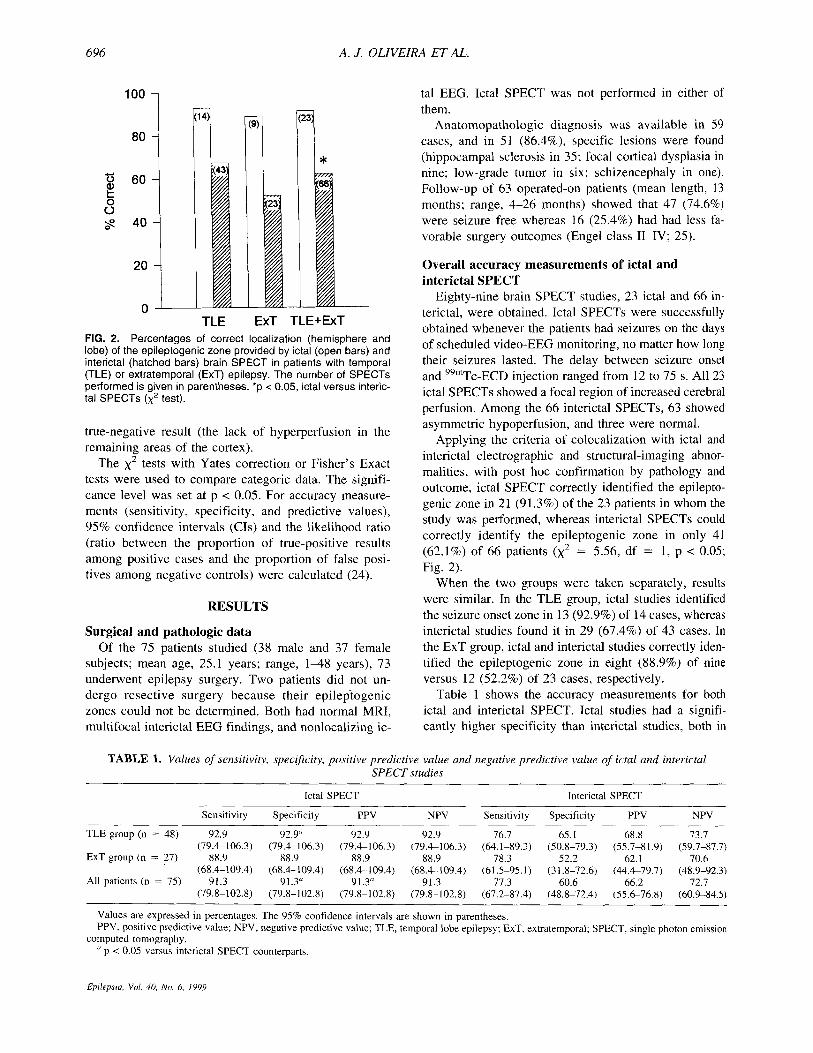
FIG. 2. Percentages of correct localization (hemisphere and lobe) of the epileptogenic zone provided by ictal (open bars) and interictal (hatched bars) brain SPECT in patients with temporal (TLE) or extratemporal (ExT) epilepsy. The number of SPECTs performed is given in parentheses. *p c 0.05, ictal versus interic- tal SPECTs (x' test).
true-negative result (the lack of hyperperfusion in the remaining areas of the cortex).
The x2 tests with Yates correction or Fisher's Exact tests were used to compare categoric data. The signifi- cance level was set at p < 0.05. For accuracy measure- ments (sensitivity, specificity, and predictive values), 95% confidence intervals (CIS) and the likelihood ratio (ratio between the proportion of true-positive results among positive cases and the proportion of false posi- tives among negative controls) were calculated (24).
RESULTS
Surgical and pathologic data Of the 75 patients studied (38 male and 37 female
subjects; mean age, 25.1 years; range, 1-48 years), 73 underwent epilepsy surgery. Two patients did not un- dergo resective surgery because their epileptogenic zones could not be determined. Both had normal MRI, multifocal interictal EEG findings, and nonlocalizing ic-
tal EEG. Ictal SPECT was not performed in either of them.
Anatornopathologic diagnosis was available in 59 cases, and in 51 (86.4%), specific lesions were found (hippocampal sclerosis in 35; focal cortical dysplasia in nine; low-grade tumor in six; schizencephaly in one). Follow-up of 63 operated-on patients (mean length, 13 months; range, 4-26 months) showed that 47 (74.6%) were seizure free whereas 16 (25.4%) had had less fa- vorable surgery outcomes (Engel class 11-IV; 25).
Overall accuracy measurements of ictal and interictal SPECT
Eighty-nine brain SPECT studies, 23 ictal and 66 in- terictal, were obtained. Ictal SPECTs were successfully obtained whenever the patients had seizures on the days of scheduled video-EEG monitoring, no matter how long their seizures lasted. The delay between seizure onset and 99mTc-ECD injection ranged from 12 to 75 s. All 23 ictal SPECTs showed a focal region of increased cerebral perfusion. Among the 66 interictal SPECTs, 63 showed asymmetric hypoperfusion, and three were normal.
Applying the criteria of colocalization with ictal and interictal electrographic and structural-imaging abnor- malities, with post hoc confirmation by pathology and outcome, ictal SPECT correctly identified the epilepto- genic zone in 21 (91.3%) of the 23 patients in whom the study was performed, whereas interictal SPECTs could correctly identify the epileptogenic zone in only 41 (62.1 %) of 66 patients (x2 = 5.56, df = 1, p < 0.05; Fig. 2).
When the two groups were taken separately, results were similar. In the TLE group, ictal studies identified the seizure onset zone in 13 (92.9%) of 14 cases, whereas interictal studies found it in 29 (67.4%) of 43 cases. In the ExT group, ictal and interictal studies correctly iden- tified the epileptogenic zone in eight (88.9%) of nine versus 12 (52.2%) of 23 cases, respectively.
Table 1 shows the accuracy measurements for both ictal and interictal SPECT. Ictal studies had a signifi- cantly higher specificity than interictal studies, both in
TABLE 1. Values of sensitivity, specifcity, positive predictive value and negative predictive value of ictal and interictal SPECT studies
Ictal SPECT Interictal SPECT
Sensitivity Specificity PPV NPV Sensitivity Specificity PPV NPV
TLE group (n = 48) 92.9 92.9" 92.9 92.9 76.7 65.1 68.8 73.7 (79.4-106.3) (79.4-106.3) (79.4-106.3) (79.4-106.3) (64.1-89.3) (50.8-79.3) (55.7-81.9) (59.7-87.7)
(68.4-1 09.4) (68.4- 109.4) (68.4- 1 09.4) (68.4- 109.4) (6 1.5-95. I ) (3 1.8-72.6) (44.4-79.7) (48.9-92.3)
(79.8-102.8) (79.8-102.8) (79.8-102.8) (79.8-102.8) (67.2-87.4) (48.8-72.4) (55.6-76.8) (60.9-84.5)
ExT group (n = 27) 88.9 88.9 88.9 88.9 78.3 52.2 62.1 70.6
All patients (n = 75) 91.3 91.3" 91.3" 91.3 77.3 60.6 66.2 72.7
Values are expressed in percentages. The 95% confidence intervals are shown in parentheses. PPV, positive predictive value; NPV, negative predictive value; TLE, temporal lobe epilepsy; ExT, extratemporal; SPECT, single photon emission
" p < 0.05 versus interictal SPECT counterparts. computed tomography.
Epilepsia, Vul. 40, Nu. 6. 1999

ICTAL AND INTERICTAL BRA" SPECT IN EPILEPSY 697
m
*
TLE ExT TLE+ExT FIG. 3. Likelihood ratios (&5% GI) calculated for topographic diagnosis of the epileptogenic zone provided by ictal (open bars) and interictal (hatched bars) brain SPECTs in patients with tem- poral (TLE) or extratemporal (ExT) epilepsy. *Statistically signifi- cant difference between ictal and interictal SPECT.
the TLE group (92.9 vs. 65.1%) and in the group of all patients together (91.3 vs. 60.6%), as well as an also significantly higher positive predictive value (91.3 vs. 66.2%) for the whole series of patients.
Ictal SPECT had a likelihood ratio of 10.5 (95% CI, 2.78-39.7), which was significantly higher than the like- lihood ratio of interictal studies (1.96; 95% C1, 1.42- 2.72; Fig. 3).
Correlation between SPECT findings and other key methods of evaluation
Ictal SPECT versus ictal EEG in patients with temporal lobe epilepsy (TLE group)
Thirty-nine of the 48 patients with TLE had ictal scalp EEGs. In the remaining nine, seizures were not recorded, but interictal EEG and MRI were congruent. In 26
(66.7%) of the 39 patients who had ictal scalp EEGs, this method correctly localized the epileptogenic zone. In the remaining 13 (33.3%), in whom ictal scalp EEGs were nonlocalizing, five had and eight did not have intracra- nial EEG investigation.
Two of the five patients in whom intracranial EEG investigation was performed also had ictal SPECT. In both, the latter colocalized with ictal intracranial EEG findings (patients 6 and 8; Table 2). Of the other eight patients in whom interictal scalp EEG and MRI provided sufficient localizing information to obviate the need for intracranial EEG, ictal SPECT was obtained in four. In all of them, ictal SPECT provided localizing information congruent with unilateral hippocampal atrophy by MRI. From a clinical standpoint, these SPECT findings sup- ported the decision to proceed with surgery irrespective of the lack of ictal EEG data (patients 2, 5 , 10, and 11; Table 2).
The other eight patients from this TLE group who had ictal SPECT belong to the subgroup of 26 patients whose ictal scalp EEGs were localizing. In seven of the eight, ictal SPECT was concordant with the ictal scalp EEGs.
Finally, in one patient, ictal SPECT mislocalized the epileptogenic zone, the latter being lateralized to the con- tralateral temporal lobe, as demonstrated by ictal scalp EEG, MRI, and surgical outcome (patient 3; Table 2).
Ictal SPECT versus ictal EEG in patients with epilepsy from extratemporal origin (ExT group)
All 27 patients with extratemporal epilepsy (ExT group) had ictal scalp EEGs. In only seven (25.9%), the latter correctly indicated the epileptogenic zone eventu- ally determined.
From the 20 (74.1%) patients whose ictal scalp EEGs were nonlocalizing, seven underwent invasive record- ings, which were able to demonstrate the epileptogenic
TABLE 2. Patients with temporal lobe epilepsy who had ictal SPECT
Patient no.
Interictal scalp EEG
1 2 3
4 5 6 1 8
9 10 I 1 12 13 14
Bi-T LT Bi-T
LT LT Bi-T Normal Bi-FT
RT LT Bi-T RT RT RT
Ictal scalp EEG
LT Nonlocalizing RT
LT Nonlocalizing Nonlocalizing LT Nonlocalizing,
RT Nonlocalizing Nonlocalizing RT RT RT
left hemisphere
MRI
Normal LT tumor RT (HA)
LT (HA) LT (HA) LT tumor + RT HA LT (HA) Normal
RT (HA) RT (HA) RT (HA) RT (HA) RT (HA) RT (HA)
Ictal SPECT
LT LT LT
LT LT LT LT LT
RT RT RT RT RT RT
Final localization (epileptogenic
zone)
LT LT RT
LT LT LT LT LT
RT RT RT RT RT RT
Putative role of SPECT htudies
Contributory contributory Unnecessary
Unnecessary Contributory Mandatory Unnecessary Mandatory
Unnecessary Contributory Contributory Unnecessary Unnecessary Unnecessary
(and discordant)
~~~~~
R, right; L, left; T, temporal lobe; F, frontal lobe; Bi, bilateral; HA, hippocampal atrophy. ~~~ ~
E p r l e p w Vol 40, NO 6, 1999
698 A. J . OLIVEIRA ET AL.
zone in six. Only two of these seven patients also had ictal SPECT, which colocalized with intracranial EEGs in both (patients 3 and 5 ; Table 3). Of clinical relevance, in these two patients, placement of intracranial electrodes was mostly guided by the SPECT findings, because MRI was either normal or mislocalizing. Seven other patients had ictal SPECT, but did not have intracranial EEG.
Considering all nine patients of this ExT group who had ictal SPECT (Table 3), in three (33.3%), it was en- tirely concordant with ictal scalp EEG findings. In five additional patients, ictal SPECT successfully pointed to the epileptogenic zone, whereas ictal scalp EEGs failed to provide such information. In two of these patients, depth EEG studies were performed, and ictal findings entirely agreed with those previously shown by ictal SPECT. In the other three, intracranial EEG was not deemed necessary, because the other localizing tools (in- cluding ictal SPECT) were thought to provide sufficient information. In a single patient of these nine for whom ictal SPECT was available, the latter did not provide correct localizing information. Actually, in this patient, ictal SPECT pointed to an anterior temporal seizure on- set, whereas both ictal scalp EEG and MRI clearly de- fined an epileptogenic zone in the ipsilateral parietooc- cipital cortex.
lctal SPECT versus MRI in patients with TLE Thirty-two (66.7%) of the 48 patients in this group had
MRI evidence of hippocampal atrophy ipsilateral to the epileptogenic zone, as eventually determined. In I 1 (22.9%), MRI scans were normal, and in the remaining five ( 1 0.4%), it was abnormal but either nonlocalizing or mislocalizing: Two patients had bilateral neocortical at- rophy or polymicrogyria, one had a neocortical tumor on one side and hippocampal atrophy on the other, and the other two had unilateral hippocampal atrophy. This, however, was proven to be contralateral to the epilepto- genic zone.
Considering the 14 patients of this group who under- went ictal SPECT (Table 2), in 1 1 (78.6%), MRI showed a focal abnormality congruent with the epileptogenic
zone (hippocampal atrophy or tumor). I n 10 (89%) of these, ictal SPECT findings agreed with the MRI local- ization. In one patient, however, the localizing data de- rived from the two imaging studies were discordant (pa- tient 3; Table 2). In this patient, MRI was congruent with the ictal EEG findings, thus defining the epileptogenic zone, as confirmed by pathology and a favorable surgical outcome.
In the three remaining patients, MRI was either normal or nonlocalizing. The single patient in whom MRI was considered nonlocalizing (patient 6; Table 2) had imag- ing evidence for a dual lesion, consisting of a right hip- pocampal atrophy and a left temporal lobe neocortical tumor. Ictal SPECT showed focal hyperperfusion on the left temporal lobe, which agreed with the localizing in- formation provided by intracranial EEG. The patient un- derwent left anterior temporal lobectomy, with resection of the tumor (an oligodendroglioma) and has been sei- zure free for 26 months.
In the two patients in whom MRI was normal (patients 1 and 8; Table 2), ictal SPECT was of localizing value. In one, the latter was congruent with scalp EEG, both suggesting a left temporal lobe seizure onset, which al- lowed a surgical decision on the basis of noninvasive data. The patient underwent left anterior temporal lobec- tomy and amygdalohippocampectomy and has been sei- zure free for 13 months. Pathology revealed hippocampal sclerosis. In the other patient with normal MRI, ictal scalp EEG also was nonlocalizing, showing a possible left hemisphere seizure onset, undefined between the frontal and temporal lobes. Ictal SPECT pointed to the temporal lobe on the basis of a left temporal hyperper- fusion. This was further confirmed by invasive EEG with subdural strips and grids.
Ictal SPECT versus MRI in patients with extratemporal lobe epilepsy (ExT group)
Fourteen ( 5 I .9%) of the 27 patients in this ExT group had a well-localized epileptogenic lesion identified by MRI. Three other patients had abnormal but nonlocaliz-
TABLE 3. Patients with epilepsy f rom extratemporal origin who had ictal SPECT
Patient no.
lnterictal scalp EEG
Ictal scalp EEG
Bi-F + LPO
Left hemisphere LT LCTP LFC t RT RCP RPO Bi-FT Bi-PO
LPO
Nonlocalizing Nonlocal izing Nonlocalizing Nonlocalizing RCP RPO Nonlocalizing €3-PO
Invasive EEG
(ECoG) MRI
- LPO atrophy
- Normal LTO Normal
RFT RT (HA) - Nonlocalizing - RPO
- Bi-PO
LP atrophy -
RF -
Ictal SPECT
Final localization (epileptogenic
zone) Putative role of SPECT studies
LT
LFP LTO LP RFT RCP RPO RF Bi-PO
LPO
LFP LTO LP RF RP RPO RF Bi-PO
Unnecessary
Mandatory Mandatory Contributory Contributory Contribumy Unnecessary Contributory Unnecessary
(and discordant)
L, left; R, right; B, bilateral; T, temporal lobe; F, frontal lobe; P, parietal lobe; 0, occlpital lobe; C, central region; HA, hippocampal atrophy.
Eprlepsiu, Vol. 40. No. 6, 1999
ICTAL AND INTEUICTAL BRAIN SPECT IN EPILEPSY 699
ing imaging findings, and the remaining 10 (37%) had normal MRI scans.
Five of the 14 patients in whom MRI detected a well- localized structural lesion also underwent ictal SPECT studies. In four (go%), the latter were strikingly colocal- ized with the structural imaging findings, whereas in one (patient 1 ; Table 3) ictal SPECT and MRI pointed to abnormalities in the same hemisphere but were discor- dant for the affected lobes: MRI showed left parietooc- cipital atrophy, whereas ictal SPECT displayed a left temporal hyperperfusion. The MRI findings were sup- ported by ictal EEG studies, and by the resolution of the epileptic seizures on resection of the gliotic parietooc- cipital cortex.
Ictal SPECT was available in only one of the 10 pa- tients in whom MRI was normal, and both interictal scalp EEG and ictal SPECT agreed with subdural recordings in suggesting seizure onset from the left temporooccipital region. Unfortunately, because no resective surgery was performed, the underlying putative structural pathology could not be verified.
In two (7.4%) of the 27 patients of this ExT group, MRI proved to be misleading. In one it showed a right hippocampal atrophy, but seizures were unequivocally identified as originating from the ipsilateral frontal lobe (patient 5; Table 3), and in the other patient, bilateral laminar heterotopia was identified by MRI in both cen- trotemporoparietal regions, although seizures were con- sistently recorded from the right centroparietal region (patient 6; Table 3). These two patients underwent ictal SPECT, and ictal hyperperfusion was remarkably colo- calized with the neurophysiologically determined ictal- onset zones, either by scalp (patient 6) or invasive (pa- tient 5) EEGs.
In the last patient, the structural abnormalities as shown by MRI involved most of the right hemisphere in the form of a multilobar dysplastic lesion. Seizures were recorded on scalp, and likewise, had a diffuse, hemi- spherical distribution. Ictal SPECT was not available.
DISCUSSION The results of this study clearly demonstrate that
Y"T~-ECD SPECT is fairly comparable to '"Tc- HMPO SPECT in accuracy measurements for the local- ization of the epileptogenic zone in epileptic patients undergoing preoperative evaluation. Sensitivity ranged from 88.9% (ExT group) to 92.9% (TLE group) for ictal studies and from 76.7% (TLE group) to 78.3% (ExT group) for interictal studies, which is comparable to re- ported results for HMPAO SPECT (3-8,10,13,26-30). Also, specificity values of "mTc-ECD SPECT, ranging from 52.2% (ExT group, interictal studies) to 92.9% (TLE group, ictal studies), are similar to those found by Spencer (3) in a comprehensive meta-analysis of brain SPECT in epilepsy.
ECD could therefore be chosen as a suitable pharma- ceutical for brain imaging in patients with partial epi- lepsy refractory to medical treatment. Interictal SPECT, however, both with HMPAO and with ECD, is of limited value in the localization of the epileptogenic zone for surgical decision (3,9-12,15,3 I) , as indicated by its rela- tively low positive predictive value (66.2%, 95% CI 55.6-76.8%). In contrast, ictal studies have been shown to be a highly effective and reliable method for determi- nation of the seizure-onset zone in patients undergoing evaluation for epilepsy surgery, both in TLE (5,6,30) and in epilepsy of extratemporal origin (4,7,8). In our study, ictal SPECT with ECD has confirmed its significantly higher positive predictive value (91.3%) as compared with interictal ECD SPECT (66.2%).
Thus ictal SPECT could be a useful noninvasive tool in the presurgical evaluation of patients with refractory epilepsy. The major limitation for its widespread use has been the methodologic difficulties imposed by in vitro unstable agents, which could no longer be used after 30 min from preparation (3,16). To overcome this limita- tion, special techniques to shorten time of injection have been described (32,33), and a new form of stabilized HMPAO was recently developed (34). As we observed here, ictal SPECTs with ECD are perfectly feasible and require no special or expensive techniques, because the higher in vitro stability of ECD allows previous recon- stitution and instant availability at the time of seizure occurrence. Therefore ECD could be a useful alternate agent for performing ictal brain SPECTs.
It is important to remember that, when resective sur- gery for treatment of epilepsy is being considered, one must identify with precision the patient's seizure-onset zone, rather than the less precise cortical dysfunctional zone or the "irritative" zone (35). The former can be defined only by functional methods that can be applied at the moment of seizure occurrence (i.e., ictal EEG and ictal SPECT). Ictal EEG is considered the gold-standard method for this purpose, but EEG has its own accuracy limitations, which sometimes determine the need for in- vasive electrophysiologic studies (3,36). In our series, ictal scalp EEG was nonlocalizing in 13 (27%) patients from the TLE group and in 18 (67%) patients from the ExT group.
Furthermore, even intracranial EEG may be unhelpful or even misleading because it is entirely dependent on the correctness of the choice of the cortical regions to be probed by the electrodes. This limitation has been widely recognized, particularly when MRI does not show struc- tural abnormalities (4,37-39). In such cases, functional imaging studies can be particularly helpful in identifying candidate cortical regions to be invasively recorded.
In our series, ictal SPECT proved to be effective in the evaluation of both temporal and extratemporal epilep- sies, dissenting from the belief that this technique would
Epilepsia, Vol. 40, No. 6, 19Y9
700 A. J. OLIVEIRA ET AL.
be less sensitive and specific in the latter due to the propagation of extratemporal seizures. In our patients with extratemporal epilepsy, ictal SPECT had a sensitiv- ity of 88.9%, and identical specificity, as well as positive and negative predictive values. It follows that in most patients ictal hyperperfusion was restricted to a localized cortical region, usually corresponding to the epilepto- genic zone. This high accuracy could be explained in part by the early injection of ECD, which was made possible by its prompt availability at the moment of the seizure, as discussed previously.
A second point to be considered is that seizure spread from a seizure-onset zone outside the temporal lobe is probably less frequent or slower or both than from the temporal lobe (4,7,8). If we consider that it is precisely in these extratemporal epilepsies that EEG limitations are certainly more relevant, ictal SPECT may play a pivotal role in the identification of the epileptogenic zone.
Ictal SPECT as a determinant of evaluation and surgical strategies
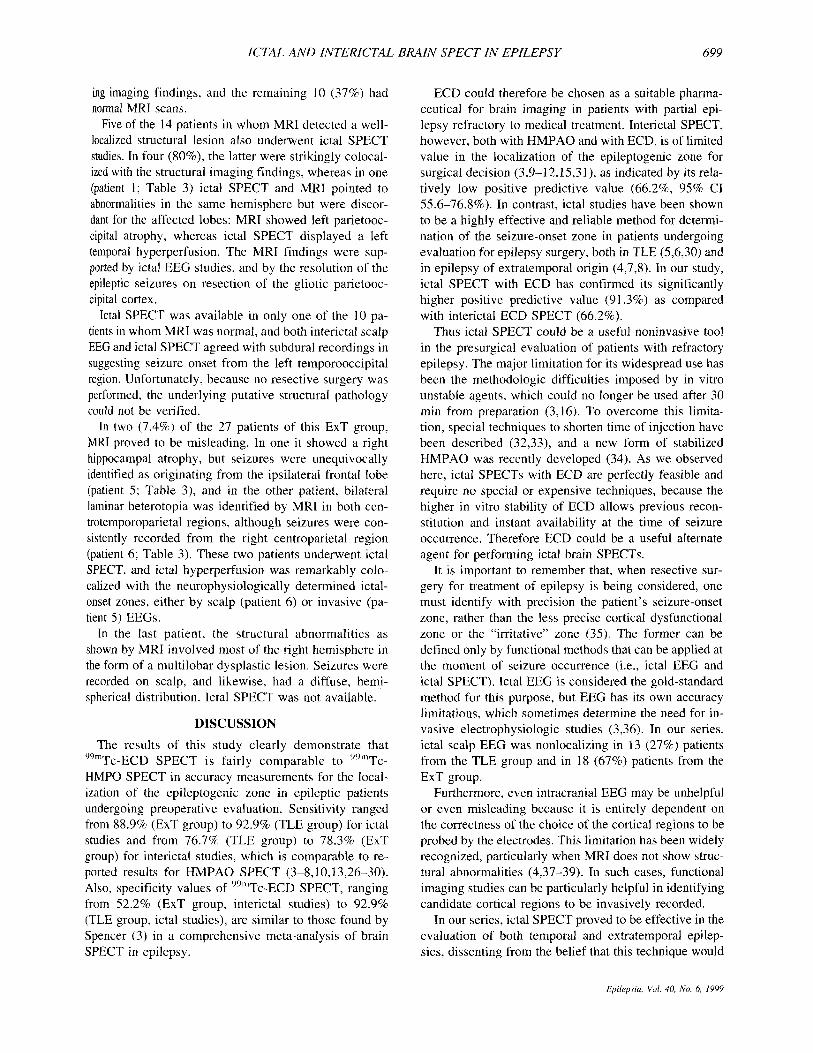
Our results have shown that ictal SPECT has a role in the presurgical evaluation and surgical strategies in pa- tients with refractory epilepsy, not only in those with extratemporal epilepsies, in whom it is frequently diffi- cult to localize the epileptogenic zone, but also in pa- tients with TLE. Based on the examples supplied by our study groups, we herein propose different scenarios in which ictal SPECT is confirmatory, contributory, or mandatory (Fig. 4). The real value of ictal SPECT in the presurgical workup of patients with partial epilepsy will eventually rest on the reliability of the localizing infor- mation to be provided noninvasively by this method. The usefulness of ictal SPECT in the evaluation protocol should be viewed in the context of the data already pro- vided by other relevant noninvasive tools, mostly ictal scalplsphenoidal EEG and MRI. Whether ictal SPECT will be merely confirmatory, contributory, or absolutely mandatory for a successful localization of the epilepto- genic zone will depend on the data already provided by EEG and MRI.
In this context, from the 14 patients with TLE in whom ictal SPECTs were performed, in six it merely confirmed the localization already defined by MRI and ictal scalp EEG. In all these, MRI and ictal scalp EEG were both localizing and congruent. Therefore, in those patients, we could retrospectively propose that ictal SPECT was unnecessary. However, in five patients, ictal SPECT indeed contributed to the final topographic diag- nosis, because either ictal scalp EEG or MRI did not provide localizing data: in one, ictal SPECT agreed with ictal scalp EEG localization, whereas MRI was normal, and in the other four, ictal scalp EEGs were nonlocaliz- ing, but ictal SPECTs always agreed with the localizing information provided by MRI. We think these five pa-
1 MRI and lctal Scalp EEG 1
pJp----&J Unnecessa Contributo Mandato
FIG. 4. Proposal of an algorithm of clinical indications for ictal SPECT studies on the basis of our data. The findings of the major evaluation methods, ictal scalp/sphenoidal EEG and MRI, will determine the putative role of ictal SPECT studies.
tients illustrate situations in which ictal SPECT should be considered a contributory step in the presurgical evaluation. Furthermore, in two other patients, ictal SPECTs were definitely important in the determination of the epileptogenic zone, because both ictal scalp EEG and MRI were nonlocalizing (patients 6 and 8; Table 2). In this context, we believe ictal SPECT is mandatory. The ultimate localization of the epileptogenic zone in these two patients was further defined by invasive EEG studies, histologic analysis of the resected tissue, and surgical results (both patients are seizure free).
The findings regarding the usefulness of ictal SPECT in the context of normal MRI should be viewed with caution because only qualitative methods of MRI inter- pretation were applied to our patients. Admittedly, some of these patients might have had an adequate localization on the basis of structural findings if quantitative MRI methods (volumetrics of T, relaxometry) were applied (40-43).
Finally, there was one patient with TLE (patient 3; Table 2) in whom ictal SPECT mislocalized the epilep- togenic zone, yielding information incongruent with that provided by both ictal scalp EEG and MRI. However, because these latter were clearly localizing and congm- ent, ictal SPECT in this patient could retrospectively be regarded as unnecessary. Two possibilities could explain this discrepancy between ictal SPECT, which showed a clear and well-defined zone of hyperperfusion in the left temporal lobe, and the EEG and MRI data, both pointing to the contralateral temporal lobe, which was eventually confirmed as the actual epileptogenic zone. First, pa- tients with TLE occasionally do have hitemporal inde- pendent seizures (4446) . Thus one cannot exclude the possibility that the particular ictal episode registered by the ictal SPECT could have originated in the contralat- era1 temporal lobe. The fact that this patient is com- pletely seizure free, 26 months after right anterior tem- poral lobectomy, does not exclude that possibility (44- 46). A second possibility would be seizure spread to the
Epilepsic[, Vol. 40. No. 6, I999

ICTAL AND INTERICTAL>
contralateral temporal lobe. Because the injection of the radiopharmaceutical occurred 69 s after seizure onset (in contrast to a mean of 23 s in this group), this possibility, although rarely observed, should not be discarded (28,47).
In the context of extratemporal epilepsy, we found ictal SPECT even more useful. In six of the nine patients in whom it was performed, ictal SPECT definitely played a role in the final localization of the epileptogenic zone. In four of these, ictal SPECT was highly contributory because either MRI or ictal scalp EEG was nonlocaliz- ing, and SPECT was congruent with the test providing localization. In the other two, it was even mandatory, because both had normal MRI and ictal scalp EEGs were nonlocalizing.
However, in two of these nine patients with extratem- poral epilepsy in whom ictal SPECT was obtained, it was merely confirmatory of the localization of the epilepto- genic zone, because ictal scalp EEG and MRI were al- ready localizing and congruent. Finally, in a single pa- tient, ictal SPECT was misleading, displaying focal hy- perperfusion over the left temporal lobe, whereas MRI and ictal EEG yielded congruent data, which pointed to an epileptogenic zone in the left parietooccipital region (patient 1; Table 3). Retrospectively, for the same rea- sons described earlier, ictal SPECT in this patient was unnecessary and could have been skipped.
In conclusion, these data demonstrate that ictal SPECT can be easily obtained by using 99"Tc-ECD and can accurately localize the epileptogenic zone in patients with both temporal and extratemporal epilepsies. As al- ready previously demonstrated for HMPAO SPECT studies, ictal ECD SPECT proved to be significantly more sensitive and specific than interictal ECD SPECT. In addition, the results of this study clearly support the contention that ictal ECD SPECT is a valuable tool in the presurgical evaluation of patients with medically refrac- tory partial epilepsies. However, its rational use should be regarded in the context of the whole constellation of findings provided by clinical, electrographic, and struc- tural imaging methods.
Acknowledgment: We are thankful to Dr. Fernando M. dos Reis for his helpful comments and statistical advice. We ac- knowledge the outstanding suggestions made by the anony- mous reviewers. This study was supported in part by a grant from Funda@o de Amparo B Pesquisa do Estado do Rio Grande do Sul (FAPERGS), protocol 94/60996-9.
REFERENCES
Devous MD. The role of SPECT brain imaging in epilepsy. J Nucl Med 1994;35: 1094-6. Holman BL, Devous MD. Functional brain SPECT: the emergence of a powerful clinical method. J Nucl Med 1992;33:1888-904. Spencer SS. The relative contributions of MRI, SPECT, and PET imaging in epilepsy. Epilepsiu 199435(suppl 6):S72-89. Ho SS, Berkovic SF, Newton MR, Austin MC, McKay WJ, Bladin
BRAIN SPECT IN EPILEPSY 701
PF. Parietal lobe epilepsy: clinical features and seizure localization by ictal SPECT. Neurologj! 1994;442277-84.
5. Ho SS, Berkovic SF, Berlangieri SU, et al. Comparison of ictal SPECT and interictal PET in the presurgical evaluation of temporal lobe epilepsy. Ann Neurol 1995;37:73845.
6. Harvey AS, Bowe JM, Hopkins IJ, Shield LK, Cook DJ, Berkovic SF. Ictal yymTc-HMPAO single photon emission computed tomog- raphy in children with temporal lobe epilepsy. Epilepsia 1993;34: 869-77.
7. Harvey AS, Hopkins IJ, Bowe JM, Cook DJ, Shield LK, Berkovic SF. Frontal lobe epilepsy: clinical seizure characteristics and lo- calization with ictal """Tc-HMPAO SPECT. Neurology I993;43: 196680.
8. Marks DA, Katz A, Hoffer P, Spencer SS. Localization of extra- temporal epileptic foci during ictal single photon emission com- puted tomography. An= Neurol I992;3 1 :250-5.
9. Rowe CC, Berkovic SF, Austin MC, et al. Visual and quantitative analysis of interictal SPECT with technetium-99m-HMPAO in temporal lobe epilepsy. J Nucl Med 199132: 1688-94.
10. Menzel C, Hufnagel A, Grunwald F, et al. The relevance of in- terictal rCBF brain SPECT in temporal lobe epilepsy: diagnostical value and effects of spatial resolution. Ann Nucl Med 1995;9:215- 23.
1 1 . Duncan R, Patterson J, Hadley DM, Roberts R, Bone I. Interictal temporal hypoperfusion is related to early-onset temporal lobe epi- lepsy. Epilepsia I996;37: 13440.
12. Ryvlin P, Garcia-Larrea L, Philippon B, et al. High signal intensity on T,-weighted MRI correlates with hypoperfusion in temporal lobe epilepsy. Epilepsici 1992;33:28-35.
13. Lauoes J, Iivanainen M, Salmi T, Nikkinen P, Lindroth L, Lie- wend'ahl K. lnterictal brain 9911-Tc-HMPAO SPECT hypoperfu- sion in patients with unstable partial epilepsy and normal CT. Acra Neurol Scand 1992;86:558-62.
14. Carrilho PG, Yacubian EMT, Cukiert A, et al. MRI and brain SPECT findings in patients with unilateral temporal lobe epilepsy and normal CT scan. Arq Neuropsiquiatr 1994;52: 149-52.
15. Jack CR Jr, Mullan BP, Sharbrough FW, et al. Intractable nonle- sional epilepsy of temporal lobe origin: lateralization by interictal SPECT versus MRI. Neurology 1994;44:829-36.
16. Grunwald F, Menzel C, Pavics L, et al. Ictal and interictal brain SPECT imaging in epilepsy using technetium-99m-ECD. J Nucl Med 1994;35:1896901.
17. Lancman ME, Morris 111 HH, Raja S, Sullivan MJ, Saha G, Go R. Usefulness of ictal and inteiictal 99m-Tc ethyl cysteinate dimer single photon emission computed tomography in patients with re- fractory partial epilepsy. Epilepsia 1997;38:466-7 1 .
18. Walovitch RC, Hill TC, Garrity ST, et al. Characterization of technetium-99m-L-L-ECD for brain perfusion imaging, part I: pharmacology of technetium 99-m ECD in nonhuman primates. J Nucl Med 1989;30: 1892-901.
19. Leveille J, Demonceau G, Walovitch RC. Intrasubject comparison between technetium-99m-ECD and technetium-99m-HMPAO in healthy human subjects. J Nucl Med 1992;33:4804.
20. Tsuchida T, Nishizawa S, Yonekura Y, et al. SPECT images of technetium-99n-ethyl cysteinate dimer in cerebrovascular dis- eases: comparison with other cerebral perfusion tracers and PET. J NucI Med 1994;35:27-31.
21. Matsuda H, Li YM, Higashi S, et al. Comparative SPECT study of stroke using Tc-99m ECD, 1-123 IMP, and Tc-99m HMPAO. Clin Nucl Med 1993;18:754-8.
22. Packard AB, Roach PJ, Davis RT, et al. Ictal and interictal tech- netium-99m-bicisate brain SPECT in children with refractory epi- lepsy. J Nucl Med 1996;37: I101-6.
23. Ahmann P, Musser C, Veluvolu P, et al. Correlation of ictal SPECT using technetium 99m bicisate (Neurolite) with video EEG and MRI [Abstract]. Epilepsia 1997;38(suppl 3 ) : 10.
24. Fletcher RH, Fletcher SW, Wagner EH. Clinical epidemiology: the essentials. 3rd ed. Baltimore: Williams & Wilkins, 1996.
25. Engel J Jr, Van Ness PC, Rasmussen TB, Ojemann LM. Outcome with respect to epileptic seizures. In: Engel J Jr, ed. Surgical rreuf- menf of the epilepsies. New York: Raven Press, 1993:609-21.
26. Stefan H, Bauer J, Feistel H, et al. Regional cerebral blood flow
Epilepsia, Vul. 40, No. 6, 1999

702 A. J. OLIVEIRA ET AL.
27.
28.
29.
30
31.
32
33
34
35
36
during focal seizures of temporal and frontocentral onset. Ann Neurol 1990;27: 162-6. Markand 0, Salanova V, Worth RM, Park HM, Wellmann HH. Ictal brain imaging in presurgical evaluation of patients with medi- cally intractable complex partial seizures. Acta Neurol Scand
Weis M, Feistel H, Stefan H. Utility of ictal SPECT: peri-ictal, post-ictal. Acta Neurol Scand 1994;suppl 152: 145-7. Kuzniecky R, Mountz JM, Wheatley G, Morawetz R. Ictal single- photon emission computed tomography demonstrates localized epileptogenesis in cortical dyaplasia. Ann Neurol 1993;34:627-3 1. Newton MR, Berkovic SF, Austin MC, Reutens DC, McKay WJ, Bladin PF. Dystonia, clinical lateralization, and regional blood flow changes in temporal lobe seizures. Neurology 1992;42:37 1-7. Vattimo A, Burroni L, Bertelli P, Volterrani D, Vella A. Cerebral perfusion abnormalities in therapy-resistant epilepsy in childhood: comparison between EEG, MRI and ""'Tc-ECD brain SPET. Nucl Med Commun 1996;17:48-53. Newton MR, Austin MC, Chan JG, McKay WJ, Rowe CC, Berk- ovic SF. Ictal SPECT using technetium-99m-HMPAO: methods for rapid preparation and optimal deployment of tracer during spontaneous seizures. J Nucl Med 1993;34:666-70. Alksne JF, Tecoma E, Iragui-Madoz V, et al. Development of a device to facilitate routine ictal SPECT studies [Abstract]. Epilep via 1993;34(suppl 6): 139. Manglera KO, Vanbilloen HP, Schiepers CW, Verbruggen AM. Stabilisation of high-activity """'Tc-d,f-HMPAO preparations with cobalt chloride and their biological hehaviour. Eur J Nucl Med 1995;22: I 163-72. Luders H, Awad I. Conceptual considerations. In: Luders H, ed. Epileps). surgery. New York: Raven Press, 1991:Sl-62. Sammaritano M, Lothiniere A, Andermann F, Olivier A, Gloor P, Queaney LF. False lateralization by surfdce EEG of seizure onset
1994;suppl 152: 13744.
37.
38.
39.
40.
41 42
43
44
45
46
47
in patients with temporal lobe epilepsy and gross focal cerebral lesions. Ann Neurol 1987;21:361-9. Williamson PD, Boon PA, Thadani VM, et al. Parietal lobe epi- lepsy: diagnostic considerations and results of surgery. Ann Neurol 1992;31:193-201. Spencer S S , So NK, Engel J Jr, Williamson PD, Levesque MF, Spencer DD. Depth electrodes. In: Engel J Jr, ed. Surgical treat- ment qf the epilepsies. New York: Raven Press, 1993:359-76. Arroyo S, Lesser RP, Awad IA, Goldring S, Sutherling WW, Resnick TJ. Subdural and epidural grids and strips. In: Engel J Jr, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1993:377-97. Cendes F, Andermann F, Gloor P. MRI volumetric measurement of amygdala and hippocampus in temporal lobe epilepsy. Neurol- ogy 1993;43:7 19-25. Duncan JS. lmaging and epilepsy. Brain 1997;120:339-77. Palmini A, Sam M, Cascino GD. MRI in the evaluation of epilepsy surgery. In: Wyllie E, ed. The treatment of epilepsy: principles und practice. Baltimore: Williams & Wilkins, 1996: 1006-16. Jack CR. Magnetic resonance imaging in epilepsy. Mayo Clin Proc 1996;71:695-7 1 1 . Hirsch LJ, Spencer SS, Spencer DD, Williamson PD, Mattson RH. Temporal lobectomy in patients with bitemporal epilepsy defined by depth electroencephalography. Ann Neurol 1991 ;30:347-56. Sirven JI, Malamut B, Liporace JD, O'Connor MJ, Sperling MR. Ontcoine after temporal lobectomy in bilateral temporal lobe epi- lepsy. Ann Neurol 1997;42:873-8. Sperling MR, O'Connor MJ, Saykin AJ, Plummer C. Temporal lobectomy for refractory epilepsy. JAMA 1996;276:470-5. Stefan H, Bauer J, Feistel H, et al. Regional cerebral blood flow during focal seizures of temporal and frontocentral onset. Ann Neurol 1990:27: 162-6.
Epilepsiu. Vul. 40, N o . 6, 1999


![Accuracy of distinguishing between dysembryoplastic neuroepithelial tumors and other epileptogenic brain neoplasms with [11C]methionine PET](https://static.fdokumen.com/doc/165x107/63360da5cd4bf2402c0b568c/accuracy-of-distinguishing-between-dysembryoplastic-neuroepithelial-tumors-and-other.jpg)













