Lesionectomy in epileptogenic gangliogliomas: Seizure outcome and surgical results
7
Clinical study Lesionectomy in epileptogenic gangliogliomas: Seizure outcome and surgical results Marco Giulioni a, * , Elena Gardella b , Guido Rubboli b , Federico Roncaroli d , Mino Zucchelli a , Bruno Bernardi c , Carlo Alberto Tassinari b , Fabio Calbucci a a Divisions of Neurosurgery, Department of Neurosciences, Bellaria Hospital, Via Attura 3, 40139 Bologna, Italy b Divisions of Neurology, Department of Neurosciences, Bellaria Hospital, Bologna, Italy c Divisions of Neuroradiology, Department of Neurosciences, Bellaria Hospital, Bologna, Italy d Department of Oncology, Bellaria Hospital, Bologna, Italy Received 27 April 2005; accepted 6 July 2005 Abstract We retrospectively analysed seizure outcome and surgical results in a series of 21 patients with ganglioglioma treated with lesionec- tomy. The 21 patients (13 males, eight females) had a history of epilepsy longer than 1 year and post-operative follow up of at least 1 year. Information on the duration of the seizures, type and frequency was retrieved from medical records. In all patients, surgery was limited to the tumour. The interval between onset of seizures and surgery ranged from 1 to 35 years (mean 11). Patient age ranged from 6 to 61 years (mean 27.5). Fifteen patients (71.4%) had complex partial seizures and six had simple partial seizures. Secondary generalisa- tion was present in 10 patients (47.6%). Seizure frequency varied from several per day to one per month. Sixteen tumours were temporal (76.1%; 11 temporo-mesial, five temporo-lateral), and five were extratemporal (23.8%). The mean follow-up period was 5.4 years (range: 1.25–10 years). No tumour progression was observed. No patient died during surgery or the post-operative course. Fourteen patients (66.6%) were Engel class I (five temporo-mesial, five temporo-lateral, four extratemporal) and seven (33.3%) were Engel class II. Post-operative complications were observed in six patients (28.6%), two of whom had cerebellar haemorrhage, possibly due to increased transmural venous pressure. In our patients with temporal neocortical and extratemporal ganglioglioma, lesionectomy allowed good sei- zure control. The unsatisfactory outcome for mesiotemporal gangliogliomas might indicate the need for extensive neurophysiological presurgical evaluation in order to perform tailored surgery. To avoid cerebellar haemorrhage, attention should be paid to those factors involved in transmural venous pressure increases. Ó 2006 Elsevier Ltd. All rights reserved. Keywords: Ganglioglioma; Lesionectomy; Epilepsy surgery; Complication; Cerebellar haemorrhage 1. Introduction Ganglioglioma (GG) is the most common neoplasm causing chronic focal epileptic disorders, accounting for approximately 40% of all epileptogenic tumours. 1–9 GG are usually located in the temporal lobe. 1,2,9–12 Their asso- ciation with dysplasia of the adjacent cortex has also been noted. 3,13–15 The optimal surgical treatment for epileptogenic GG has not been fully established. Previous studies of seizure outcome evaluated GG together with other tumours, 16–19 or grouped together different surgical strategies. 3,4,13,14,20– 22 To our knowledge, no study has previously investigated the seizure outcome of a homogeneous series of patients with GG, all treated with lesionectomy alone. In the pres- ent study, we retrospectively analysed the results of pure lesionectomy for 21 patients with epileptogenic GG. 0967-5868/$ - see front matter Ó 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.jocn.2005.07.017 * Corresponding author. Tel.: +39 051 6225111; fax: +39 051 6225344. E-mail address: [email protected] (M. Giulioni). www.elsevier.com/locate/jocn Journal of Clinical Neuroscience 13 (2006) 529–535
Transcript of Lesionectomy in epileptogenic gangliogliomas: Seizure outcome and surgical results

www.elsevier.com/locate/jocn
Journal of Clinical Neuroscience 13 (2006) 529–535
Clinical study
Lesionectomy in epileptogenic gangliogliomas: Seizure outcomeand surgical results
Marco Giulioni a,*, Elena Gardella b, Guido Rubboli b, Federico Roncaroli d,Mino Zucchelli a, Bruno Bernardi c, Carlo Alberto Tassinari b, Fabio Calbucci a
a Divisions of Neurosurgery, Department of Neurosciences, Bellaria Hospital, Via Attura 3, 40139 Bologna, Italyb Divisions of Neurology, Department of Neurosciences, Bellaria Hospital, Bologna, Italy
c Divisions of Neuroradiology, Department of Neurosciences, Bellaria Hospital, Bologna, Italyd Department of Oncology, Bellaria Hospital, Bologna, Italy
Received 27 April 2005; accepted 6 July 2005
Abstract
We retrospectively analysed seizure outcome and surgical results in a series of 21 patients with ganglioglioma treated with lesionec-tomy. The 21 patients (13 males, eight females) had a history of epilepsy longer than 1 year and post-operative follow up of at least 1year. Information on the duration of the seizures, type and frequency was retrieved from medical records. In all patients, surgery waslimited to the tumour. The interval between onset of seizures and surgery ranged from 1 to 35 years (mean 11). Patient age ranged from 6to 61 years (mean 27.5). Fifteen patients (71.4%) had complex partial seizures and six had simple partial seizures. Secondary generalisa-tion was present in 10 patients (47.6%). Seizure frequency varied from several per day to one per month. Sixteen tumours were temporal(76.1%; 11 temporo-mesial, five temporo-lateral), and five were extratemporal (23.8%). The mean follow-up period was 5.4 years (range:1.25–10 years). No tumour progression was observed. No patient died during surgery or the post-operative course. Fourteen patients(66.6%) were Engel class I (five temporo-mesial, five temporo-lateral, four extratemporal) and seven (33.3%) were Engel class II.Post-operative complications were observed in six patients (28.6%), two of whom had cerebellar haemorrhage, possibly due to increasedtransmural venous pressure. In our patients with temporal neocortical and extratemporal ganglioglioma, lesionectomy allowed good sei-zure control. The unsatisfactory outcome for mesiotemporal gangliogliomas might indicate the need for extensive neurophysiologicalpresurgical evaluation in order to perform tailored surgery. To avoid cerebellar haemorrhage, attention should be paid to those factorsinvolved in transmural venous pressure increases.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Ganglioglioma; Lesionectomy; Epilepsy surgery; Complication; Cerebellar haemorrhage
1. Introduction
Ganglioglioma (GG) is the most common neoplasmcausing chronic focal epileptic disorders, accounting forapproximately 40% of all epileptogenic tumours.1–9 GGare usually located in the temporal lobe.1,2,9–12 Their asso-
0967-5868/$ - see front matter � 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jocn.2005.07.017
* Corresponding author. Tel.: +39 051 6225111; fax: +39 051 6225344.E-mail address: [email protected] (M. Giulioni).
ciation with dysplasia of the adjacent cortex has also beennoted.3,13–15
The optimal surgical treatment for epileptogenic GGhas not been fully established. Previous studies of seizureoutcome evaluated GG together with other tumours,16–19
or grouped together different surgical strategies.3,4,13,14,20–
22 To our knowledge, no study has previously investigatedthe seizure outcome of a homogeneous series of patientswith GG, all treated with lesionectomy alone. In the pres-ent study, we retrospectively analysed the results of purelesionectomy for 21 patients with epileptogenic GG.

530 M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535
2. Materials and methods
2.1. Patient selection
We selected all patients operated on for the removal ofGG at the Division of Neurosurgery, Bellaria Hospital,Bologna, Italy, over the period January 1991–December2001. Of the 33 patients, 24 (73%) presented with seizuresand 21 had a history longer than 1 year and a follow-upperiod of at least 1 year. Information on the type and fre-quency of seizures was obtained from medical records. Oneor more pre-operative electroencephalography recordingswere performed in all patients. At the time of surgery, allpatients were receiving anti-epileptic therapy. All patientspresented with seizures that were uncontrolled by full dosesof at least two major antiepileptic drugs. In particular, 17out of 21 subjects presented with seizures not controlledby two or more major antiepileptic drugs for a period ofat least 2 years. Four patients had seizures that were notcontrolled by two major antiepileptic drugs, but the presur-gical duration of epilepsy was shorter than 2 years.
Some patients had reported variability in seizure fre-quency, especially those with longer presurgical epilepsydurations and on occasions when the drug regimen wasmodified, but none of them had seizure-free periods longerthan a few months. Presurgical invasive monitoring for epi-lepsy surgery was not performed. Presurgical evaluation inthis group of patients was limited to basic neurophysiologi-cal exams to confirm the diagnosis of focal epilepsy topo-graphically related to the site of the lesion. Preoperativemagnetic resonance imaging (MRI) was performed for 20patients and computed tomography (CT) scanning for one.
2.2. Surgical treatment
In all patients the surgical treatment was limited to re-moval of the GG. Temporo-mesial tumours were resectedwith fronto-temporo-pterional craniotomy using a trans-sylvian approach. For other tumours, the surgical ap-proach was chosen depending on the site of the lesion.The extent of the resection was evaluated using post-oper-ative MRI.
2.3. Pathological examination
The tumour tissue was fixed in 10% buffered formalinand processed routinely. Five-micrometre sections werestained with hematoxylin and eosin. Immunohistochemis-try was performed using the avidin-biotin-peroxidasemethod with antisera raised against glial fibrillary antigenprotein (Dako, Carpinteria, CA, USA; monoclonal1:1200), neurofilament proteins (Biogenex, San Ramon,CA, USA; monoclonal 1:30), and synaptophysin (Neomar-kers, Freemont, CA, USA; polyclonal 1:40). The Ki67(Dako; polyclonal 1:50) labelling index was calculated asthe percentage positive cells per high power (·400) field.Twenty fields were manually measured in each case.
2.4. Follow up
Seizure outcome was assessed with periodic evaluationat the outpatient service. Telephone interviews with pa-tients and their families were also used. Post-operative sei-zure outcome was graded according to the method of Engelet al.23 Evaluation of the influence of quantitative variables(age of epilepsy onset, age at surgery and duration of epi-lepsy) on seizure outcome was based on the two-tailed Stu-dent’s t-test or the Wilcoxon test, depending on the normalor non-normal distribution of the data. Non-parametricfactors (seizure type, seizure frequency, secondary general-isation, total/subtotal resection, GG localisation) werecompared by means of a v2 test or the two-sided Fisher’sexact test, depending on the sample size. A P value lessthan 0.01 was considered significant.
3. Results
3.1. Clinical findings
The ages of the patients ranged from 6 to 61 years (mean27.6). Eight patients were female. Fifteen patients sufferedfrom complex partial seizures (71.4%), and six from simplepartial seizures (28.5%) (patients 2, 3, 8, 9, 11, and 18). Tenpatients (47%) had a history of seizures that was longerthan 10 years (patients 2, 4, 5, 7, 9, 11, and 16–18). The fre-quency of seizures ranged from several per day to one permonth. The mean interval between the onset of seizuresand surgery was 11 years (range 1–35). Secondary general-ization occurred in 10 patients (47.6%; patients 2–4, 8–11,14, 16, and 18). Sixteen tumours were temporal (76.1%;nine left temporal), two were left frontal (patients 8 and11), one left parieto-occipital (patient 2), one right occip-ito-mesial (patient 3), and one left parietal (patient 12). Ele-ven temporal lesions were temporo-mesial, and fiveinvolved the temporal neocortex (patients 1, 4, 9, 13 and20). Mass effect and peritumoural oedema were minimalor absent. No infiltration of the surrounding brain wasnoted. Neuroimaging showed no cortical dysplasia adja-cent to GG.
3.2. Surgical results
Gross total removal was achieved in 18 patients (85.7%;Fig. 1) and subtotal removal in three (patients 4, 5 and 15).Two subtotally resected tumours were temporo-mesial andone was adjacent to the left Wernicke area. No tumourrecurrence or progression was observed during the fol-low-up period.
3.3. Pathological findings
All tumours showed features of World Health Organiza-tion grade 1 GG. They consisted of a mixture of bland neo-plastic astrocytes and clusters of large, ganglion-likeneurons. Granular bodies were a common finding. Mitoses,

Fig. 1. Sagittal T1-weighted MRI after contrast agent administration shows a homogenously enhanced tumour of the uncal region (A). Sagittal post-operative T1-weighted image (B) shows gross total removal (Patient 19).
M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535 531
necrosis and proliferation of vessels as well as of endothe-lial cells were absent.
3.4. Seizure outcome
After a mean follow up of 5.4 years (range 1–10), 14patients (66.6%) were seizure free (Engel class I) (patients1–6, 8, 9, 12, 13, and 18–21) and seven (33.3%; patients7, 10, 11, and 14–17) experienced marked reduction ofseizure frequency (Engel class II). Two patients (patients4 and 5) treated with subtotal tumourectomy were Engelclass I. All patients with temporal neocortical GG (pa-tients 1, 4, 9, 13, and 20) and all (patients 2, 3, 8, and12) but one (patient 11) with extratemporal tumours
Table 1Clinical findings for the 21 patients with epileptogenic ganglioglioma
Patient Sex/age Seizure type Generalisation Frequency Durat
1 F/21 Partial complex Monthly 12 M/47 Partial Yes Several/week 353 M/14 Partial Yes Several/day 14 M/24 Partial complex Yes Several/day 135 M/17 Partial complex Several/day 166 M/18 Partial complex Several/day 57 F/29 Partial complex Several/day 168 M/12 Partial Yes Monthly 19 M/18 Partial Yes Several/day 14
10 M/23 Partial complex Yes Several/week 411 F/29 Partial Yes Weekly 1912 F/48 Partial complex Several/week 213 F/55 Partial complex Monthly 114 F/20 Partial complex Yes Weekly 215 F/61 Partial complex Weekly 316 M/48 Partial complex Yes Several/week 3317 M/31 Partial complex Weekly 2218 M/20 Partial Yes Monthly 1919 M/6 Partial complex Several/day 620 F/15 Partial complex Several/day 1421 M/23 Partial complex Monthly 4
M, male; F, female.
were seizure free. This result was achieved only in five(patients 5, 6, 18, 19, and 21) out of 11 patients withtemporo-mesial lesions. This finding suggests that presur-gical neurophysiological assessment may be useful in pa-tients with temporo-mesial GG to define theepileptogenic area and its relationship with the lesion,in order to evaluate the possibility of tailored surgery.The clinical findings and surgical outcome are reportedin Tables 1 and 2.
3.5. Statistical analysis
No statistically significant correlation was observed be-tween seizure outcome and age of patients at the time of
ion (years) Tumour site Surgery Follow-up(years)
Engel class
Left temporo-lateral Total 5 ILeft Parieto-occipital Total 5 IRight occipito-mesial Total 1.7 ILeft temporo-lateral Subtotal 7 ILeft temporo-mesial Subtotal 9 IRight temporo-mesial Total 9 ILeft temporo-mesial Total 9 IILeft frontal Total 8 ILeft temporo-lateral Total 6 ILeft temporo-mesial Total 4 IILeft frontal Total 5 IILeft parietal Total 3 ILeft temporo-lateral Total 5 IRight temporo-mesial Subtotal 4 IIRight temporo-mesial Total 9 IILeft temporo-mesial Total 3 IILeft temporo-mesial Total 1.25 IILeft temporo-mesial Total 1.5 IRight temporo-mesial Total 1.5 IRight temporo-lateral Total 7 IRight temporo-mesial Total 10 I
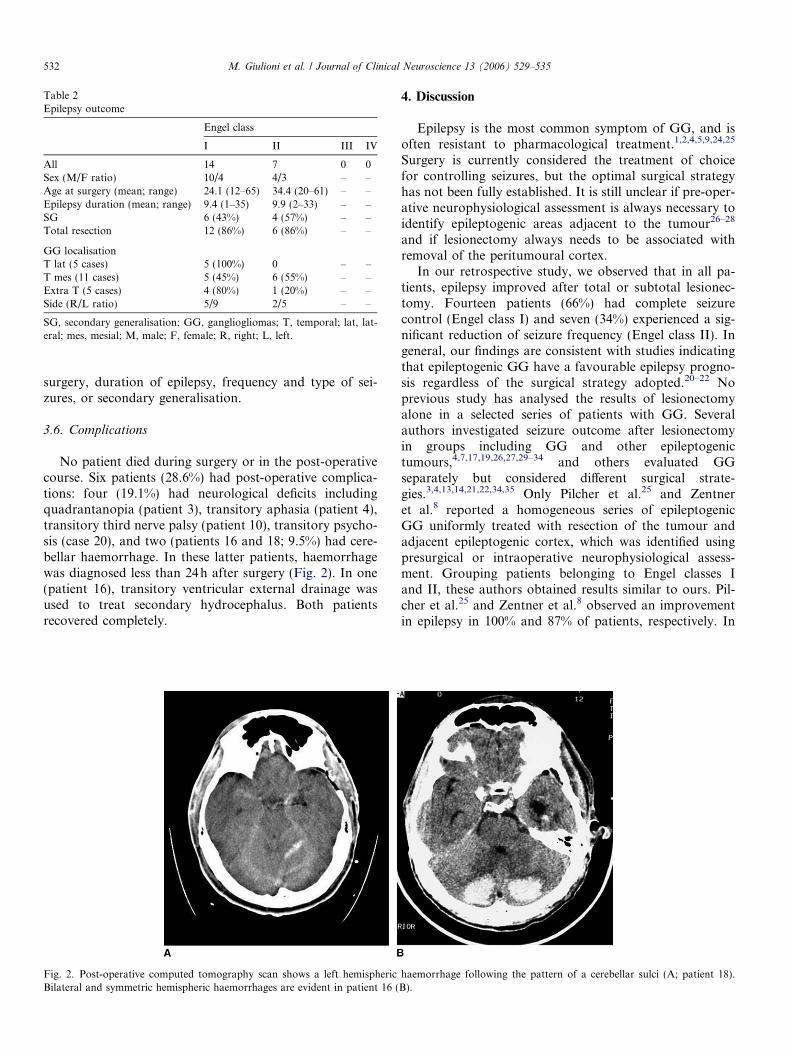
Table 2Epilepsy outcome
Engel class
I II III IV
All 14 7 0 0Sex (M/F ratio) 10/4 4/3 – –Age at surgery (mean; range) 24.1 (12–65) 34.4 (20–61) – –Epilepsy duration (mean; range) 9.4 (1–35) 9.9 (2–33) – –SG 6 (43%) 4 (57%) – –Total resection 12 (86%) 6 (86%) – –
GG localisationT lat (5 cases) 5 (100%) 0 – –T mes (11 cases) 5 (45%) 6 (55%) – –Extra T (5 cases) 4 (80%) 1 (20%) – –Side (R/L ratio) 5/9 2/5 – –
SG, secondary generalisation; GG, gangliogliomas; T, temporal; lat, lat-eral; mes, mesial; M, male; F, female; R, right; L, left.
532 M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535
surgery, duration of epilepsy, frequency and type of sei-zures, or secondary generalisation.
3.6. Complications
No patient died during surgery or in the post-operativecourse. Six patients (28.6%) had post-operative complica-tions: four (19.1%) had neurological deficits includingquadrantanopia (patient 3), transitory aphasia (patient 4),transitory third nerve palsy (patient 10), transitory psycho-sis (case 20), and two (patients 16 and 18; 9.5%) had cere-bellar haemorrhage. In these latter patients, haemorrhagewas diagnosed less than 24h after surgery (Fig. 2). In one(patient 16), transitory ventricular external drainage wasused to treat secondary hydrocephalus. Both patientsrecovered completely.
Fig. 2. Post-operative computed tomography scan shows a left hemisphericBilateral and symmetric hemispheric haemorrhages are evident in patient 16 (
4. Discussion
Epilepsy is the most common symptom of GG, and isoften resistant to pharmacological treatment.1,2,4,5,9,24,25
Surgery is currently considered the treatment of choicefor controlling seizures, but the optimal surgical strategyhas not been fully established. It is still unclear if pre-oper-ative neurophysiological assessment is always necessary toidentify epileptogenic areas adjacent to the tumour26–28
and if lesionectomy always needs to be associated withremoval of the peritumoural cortex.
In our retrospective study, we observed that in all pa-tients, epilepsy improved after total or subtotal lesionec-tomy. Fourteen patients (66%) had complete seizurecontrol (Engel class I) and seven (34%) experienced a sig-nificant reduction of seizure frequency (Engel class II). Ingeneral, our findings are consistent with studies indicatingthat epileptogenic GG have a favourable epilepsy progno-sis regardless of the surgical strategy adopted.20–22 Noprevious study has analysed the results of lesionectomyalone in a selected series of patients with GG. Severalauthors investigated seizure outcome after lesionectomyin groups including GG and other epileptogenictumours,4,7,17,19,26,27,29–34 and others evaluated GGseparately but considered different surgical strate-gies.3,4,13,14,21,22,34,35 Only Pilcher et al.25 and Zentneret al.8 reported a homogeneous series of epileptogenicGG uniformly treated with resection of the tumour andadjacent epileptogenic cortex, which was identified usingpresurgical or intraoperative neurophysiological assess-ment. Grouping patients belonging to Engel classes Iand II, these authors obtained results similar to ours. Pil-cher et al.25 and Zentner et al.8 observed an improvementin epilepsy in 100% and 87% of patients, respectively. In
haemorrhage following the pattern of a cerebellar sulci (A; patient 18).B).

M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535 533
these two studies, there was no mention of cortical dys-plasia of the non-tumoural epileptogenic cortex.
All lesions included in the present study were radiologi-cally consistent with GG in that they involved both thecortex and the subcortical white matter, were well-circum-scribed from the surrounding brain, and lacked peritumo-ural oedema, mass effect and features of infiltration.2,9,24
No cortical dysplasia of the peritumoural brain was detect-able at pre-operative neuroimaging, and its presence or ab-sence was not confirmed pathologically, given thatresection was limited to the tumour. Approximately 40%of GG may be associated with dysplastic cortex.14,15
Although a clear relationship between epilepsy and dyspla-sia of the cortex adjacent to GG has not yet been estab-lished, it has been claimed that such an association maydetermine a less effective control of seizures after surgery.3
We cannot exclude the possibility that our patients whoexperienced only a reduction in seizures had areas ofmicroscopic dysplasia in the peritumoural brain.
In our study, no correlation was noted between seizureoutcome and age at the time of surgery, duration of epi-lepsy, seizure frequency, secondary generalisation or extentof removal. Some authors observed an improvement in sei-zure outcome in young patients,13,14 whereas others foundno correlation with age at the time of surgery.3 The dura-tion of epilepsy prior to surgery did not affect seizure con-trol. Six out of 10 of our patients with a history longer than10 years were seizure-free. This finding is supported by thestudies of Him et al.3 and Morris et al.,14 who achieved sei-zure-free outcomes after about 10 years of intractable epi-lepsy. Unlike Aronica et al.13 and Morris et al.,14 we foundno correlation with secondary generalisation. This differ-ence remains unexplained and likely depends on the limitednumber of patients included in our study. Two out of threepatients treated with subtotal resection were seizure-free 7and 9 years after surgery. This indicates that subtotal resec-tion may not necessarily imply a worse epilepsy outcome.Similar findings have been observed in otherstudies.3,14,36,37
To our knowledge only a few studies20–22 have comparedseizure outcome with lesion site in temporal low-grade tu-mours, including GG (that is mesial versus neocortical),but the surgical treatment consisted of the removal of theepileptogenic focus, including the lesion (tailored surgery).We evaluated the effects on epilepsy outcome of only pureGG lesionectomy. Our patients with extra-temporal andneocortical temporal GG benefited from lesionectomy morethan those with temporo-mesial GG. Six of these latter wereEngel class II, five of whom had gross total removal. Thisfinding suggests that, to further improve seizure outcome,presurgical neurophysiological assessment may be usefulin patients with temporo-mesial GG to define the epilepto-genic area and its relationship with the lesion, in order toevaluate the possibility of tailored surgery.
Six patients (28.6%) had post-operative complications.Three patients had focal neurological deficits, one, withright temporo-lateral GG, had a psychotic episode, and
two had cerebellar haemorrhage. Likely the consequenceof forced normalisation, psychotic episodes are an uncom-mon complication after resection of epileptogenic GG, asreported by Andermann et al.38
Cerebellar haemorrhage occurred in two patients withleft temporo-mesial GG, who were treated with a standardpterional craniotomy and trans-sylvian approach. In bothinstances, there was intraoperative (from arachnoid cisternand/or temporal horn) as well as post-operative (from sub-galeal drainage) cerebrospinal fluid withdrawal. Our pa-tients had normal intracranial pressure and lackedcerebral oedema or mass effects. Cerebellar haemorrhageafter supratentorial craniotomy has been reported in0.6% of all supratentorial craniotomies,39 and particularlyafter surgery for unruptured aneurysms39–41 and epi-lepsy.39,42–44 Although its venous origin has been recogni-sed, the pathogenesis of cerebellar haemorrhage isunclear.42–46 We suggest that the increase in transmural ve-nous pressure (intravascular venous pressure minus extra-vascular pressure; that is intracranial pressure) associatedwith normal intracranial pressure is the critical factor. Asin patients operated on for unruptured aneurysms ordrug-resistant epilepsy, our patients had normal intracra-nial pressure. We suggest that the most critical situationsfor this complication are the surgical procedures requiringa pterional or temporal approach and some degree of cere-brospinal fluid withdrawal, in conditions of normal intra-cranial pressure. In our opinion, cerebellar haemorrhagemight be caused by an increase in transmural venous pres-sure related either to venous pressure increase favoured byhead position, or to intracranial pressure decrease deter-mined by cerebrospinal fluid withdrawal, or to a combina-tion of both factors. The rare occurrence of cerebellarhaemorrhage when surgery is performed in conditions ofhigh intracranial pressure, such as in ruptured aneurysms,may support our point of view.
5. Conclusion
In our patients lesionectomy provided good seizure con-trol in temporal neocortical and extratemporal GG,whereas in mesiotemporal GG seizure outcome was lesssatisfactory. In this latter condition, extensive presurgicalneurophysiological investigation to define the epileptogeniccortex seems to be important to yield better results leadingto tailored surgery. The outcome was unrelated to patientage at the time of surgery, duration of epilepsy, type or fre-quency of seizures, or secondary generalisation. Severaltopics need to be clarified, in particular the intrinsic epilep-togenesis of GGs and predicting their association with epi-leptogenic cortical dysplasia. Prospective randomisedstudies comparing epilepsy outcome after lesionectomyonly and lesionectomy plus resection of the surroundingtissues are necessary to clarify the best surgical approachto epileptogenic GGs. In order to avoid cerebellar haemor-rhage, attention should be paid to the factors related to anincrease in transmural venous pressure such as head posi-

534 M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535
tion, cerebrospinal fluid withdrawal, and drugs that reduceintracranial pressure.
Acknowledgement
A special thanks to Prof. Mauro Ursino, Department ofElectronics, Computer Science and Systems, University ofBologna, for his assistance with statistical analysis of thedata.
References
1. Blumcke I, Wiestler OD. Gangliogliomas: an intriguing tumor entityassociated with focal epilepsies. J Neuropathol Exp Neurol
2002;61:575–84.2. Haddad SF, Moore SA, Menezes AH, VanGildere JC. Gangliogli-
oma: 13 years of experience. Neurosurgery 1992;31:171–8.3. Him SH, Chung CK, Cho BK, Lee K. Supratentorial gangliogliomas
and epilepsy: postoperative seizures outcome. J Neurooncol
2002;57:59–66.4. Khajavi K, Comair YG, Prayson RA, et al. Childhood ganglioglioma
and medically intractable epilepsy: a clinicopathological study of 15patients and a review of the literature. Pediatr Neurosurg
1995;22:181–8.5. Silver JM, Rawlings III CE, Rossitch Jr E, Zeidman SM, Friedman
AH. Ganglioglioma: a clinical study with long-term follow-up. Surg
Neurol 1991;35:261–6.6. Sutton LN, Packer RJ, Rorke LB, Bruce DA, Schut L. Cerebral
gangliogliomas during childhood. Neurosurgery 1983;13:124–8.7. Weber JP, Silbergeld DL, Winn HR. Surgical resection of epilepto-
genic cortex associated with structural lesions. Neurosurg Clin North
Am 1993;4:327–36.8. Zentner J, Hufnagel A, Wolf HK, et al. Surgical treatment of
neoplasms associated with medically intractable epilepsy. Neurosur-
gery 1997;41:378–87.9. Zentner J, Wolf HK, Ostertun B, et al. Gangliogliomas: clinical,
radiological, and histopathological findings in 51 patients. J Neurol
Neurosurg Psychiatry 1994;57:1497–502.10. Johnson Jr JH, Hariharan S, Berman J, et al. Clinical outcome of
pediatric gangliogliomas: ninety-nine cases over 20 years. Pediatr
Neurosurg 1997;27:203–7.11. Mickle JP. Ganglioglioma in children: a review of 32 cases at the
University of Florida. Pediatr Neurosurg 1992;18:310–4.12. Nelson JS, Bruner JM, Wiestler OD, Vandenberg SR. Ganglioglioma
and gangliocytoma. In: Kleihues P, Cavenee WK, editors. Pathology
and Genetics of Tumours of the Nervous System. Lyon: IARC Press;2000. p. 96–8.
13. Aronica E, Leenstra S, van Veelen CWM, et al. Glioneuronal tumorsand medically intractable epilepsy: a clinical study with long-termfollow-up of seizure outcome after surgery. Epilepsy Res
2001;43:179–91.14. Morris HH, Matkovic Z, Estes ML, et al. Ganglioglioma and
intractable epilepsy: clinical and neurophysiologic features andpredictors of outcome after surgery. Epilepsia 1998;39:307–13.
15. Prayson RA, Khajavi K, Comair YG. Cortical architectural abnor-malities and MIB1 immunoreactivity in gangliogliomas: A study of 60patients with intracranial tumors. J Neuropathol Exp Neurol
1995;54:513–20.16. Berger MS, Ghatan S, Haglund MM, Dobbins J, Ojemann GA. Low-
grade gliomas associated with intractable epilepsy: seizure outcomeutilizing electrocorticography during tumor resection. J Neurosurg
1993;79:62–9.17. Kim SK, Wang KC, Hwang YS, Kim KJ, Cho BK. Intractable
epilepsy associated with brain tumors in children: surgical modalityand outcome. Childs Nerv Syst 2001;17:445–52.
18. Montes JL, Rosenblatt B, Farmer JP, et al. Lesionectomy of MRIdetected lesions in children with epilepsy. Pediatr Neurosurg
1995;22:167–73.19. Packer RJ, Sutton LN, Patel KM, et al. Seizure control following
tumor surgery for childhood cortical low-grade gliomas. J Neurosurg
1994;80:998–1003.20. Clussman H, Schramm J, Kral T, et al. Prognostic factors and
outcome after different types of resection for temporal lobe epilepsy. J
Neurosurg 2002;97:1131–41.21. Luyken C, Blumke I, Fimmers R, et al. The spectrum of long-term
epilepsy associated tumors: Long-term seizure and tumor outcomeand neurosurgical aspects. Epilepsia 2003;44:822–33.
22. Schramm J, Kral T, Grunwald T, Blumke I. Surgical treatment forneocortical temporal lobe epilepsy: clinical and surgical aspects andseizure outcome. J Neurosurg 2001;94:33–42.
23. Engel Jr J, Van Ness P, Rasmussen TB, Ojemann LM. Outcome withrespect to epileptic seizures. In: Engel Jr J, editor. Surgical Treatment
of the Epilepsies. New York: Raven Press; 1993. p. 609–21.24. Kalyan-Raman UP, Olivero WC. Ganglioglioma: a correlative
clinicopathological and radiological study of ten surgically treatedcases with follow-up. Neurosurgery 1987;20:428–33.
25. Pilcher WH, Silbergeld DL, Berger MS, Ojemann GA. Intraoperativeelectrocorticography during tumor resection: impact on seizureoutcome in patients with gangliogliomas. J Neurosurg
1993;78:891–902.26. Catatelpe O, Comair YG. Strategies in operating on patients with
tumor-related epilepsy. In: Kotagal P, Luders HO, editors. The
Epilepsies: Etiologies and Prevention. Burlington: Academic Press;1999. p. 365–70.
27. Jooma R, Yeh HS, Privitera MD, Gartner M. Lesionectomy versuselectrophysiologically guided resection for temporal lobe tumorsmanifesting with complex partial seizures. J Neurosurg
1995;83:231–6.28. Morris III HH. Lesionectomy as a treatment for chronic epilepsy: is it
sufficient for a good outcome? In: Luders HO, Comair YG, editors.Epilepsy Surgery. Philadelphia: Lippincott Williams and Wilkins;2001. p. 967–71.
29. Britton JW, Cascino GD, Sharbrough FW, Kelly PJ. Low-grade glialneoplasms and intractable partial epilepsy: efficacy of surgicaltreatment. Epilepsia 1994;35:1130–5.
30. Casazza M, Avanzini G, Ciceri E, Spreafico R, Broggi G. Lesionec-tomy in epileptogenic temporal lobe lesions: preoperative seizurecourse and post-operative outcome. Acta Neurochir Suppl (Wien)
1997;68:64–9.31. Lombardi D, Marsch R, de Tribolet N. Low grade glioma in
intractable epilepsy: lesionectomy versus epilepsy surgery. Acta
Neurochir Suppl (Wien) 1997;68:70–4.32. Moore JL, Cascino GD, Trenerry MR, Kelly PJ, Marsh VR. A
comparative study of lesionectomy versus corticectomy inpatients with temporal lobe lesional epilepsy. J Epilepsy
1993;6:239–42.33. Rassi-Neto A, Ferraz FP, Campos CR, Braga FM. Patients with
epileptic seizures and cerebral lesion who underwent lesionectomyrestricted or associated with the adjacent irritative area. Epilepsia
1999;40:856–64.34. Rossi GF, Pompucci A, Colicchio G, Scerrati M. Factors of surgical
outcome in tumoural epilepsy. Acta Neurochir (Wien)
1999;41:819–24.35. Otsubo H, Hoffmann H, Humphreys RP, et al. Evaluation, surgical
approach and outcome of seizure patients with gangliogliomas.Pediatr Neurosurg 1990–1991;16:208–12.
36. Celli P, Scarpinati M, Nardacci B, Cervoni L, Cantore GP. Ganglio-gliomas of the cerebral hemispheres: Report of 14 cases with long-term follow-up and review of the literature. Acta Neurochir (Wien)
1993;125:52–7.37. Kirkpatrick PJ, Honavar M, Janota I, Polkey CE. Control of
temporal lobe epilepsy following en bloc resection of low-gradetumors. J Neurosurg 1993;78:19–25.

M. Giulioni et al. / Journal of Clinical Neuroscience 13 (2006) 529–535 535
38. Andermann LF, Savard G, Meeke HJ, McLachlan R, Moshe S,Andermann F. Psychosis after resection of ganglioglioma or DNET:evidence for an association. Epilepsia 1999;40:83–7.
39. Friedman JA, Piepgras DG, Duke DA, et al. Remote cerebellarhemorrhage after supratentorial surgery. Neurosurgery
2001;49:1327–40.40. Cloft HJ, Matsumoto JA, Lanzino G, Cail WS. Posterior fossa
hemorrhage after supratentorial craniotomy. Am J Neuroradiol
1997;18:1573–80.41. Papanastassiou V, Kerr R, Adams C. Controlateral cerebellar
hemorrhagic infarction after pterional craniotomy: report offive cases and review of the literature. Neurosurgery
1996;39:841–52.42. Honegger J, Zentner J, Spreer J, Carmona H, Schulze-Bonage A.
Cerebellar hemorrhage arising postoperatively as a complication of
supratentorial surgery: a retrospective study. J Neurosurg
2002;96:248–54.43. Toczec MT, Morrel MJ, Silverberg GA, Lowe GM. Cerebellar
hemorrhage complicating temporal lobectomy. Report of four cases. J
Neurosurg 1996;85:718–22.44. Yacubian EM, de Andrade MM, Jorge CL, Valerio RM. Cerebellar
hemorrhage after supratentorial surgery for treatment of epilepsy:report of three cases. Neurosurgery 1999;45:159–62.
45. Konig A, Laas R, Hermann HD. Cerebellar hemorrhage as acomplication after supratentorial craniotomy. Acta Neurochir (Wien)
1987;88:184–8.46. Seoane E, Rhoton AL. Compression of the internal jugular vein by
the transverse process of the atlas as the cause of cerebellarhemorrhage after supratentorial craniotomy. Surg Neurol
1999;51:500–5.